User login
Are you sure your patient is alive?
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.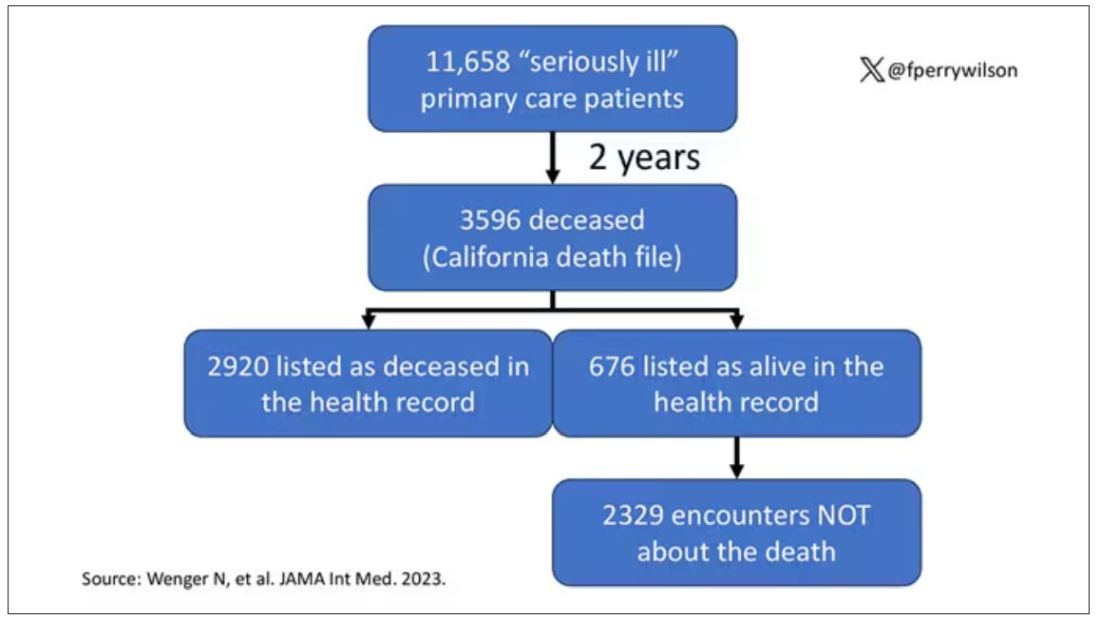
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.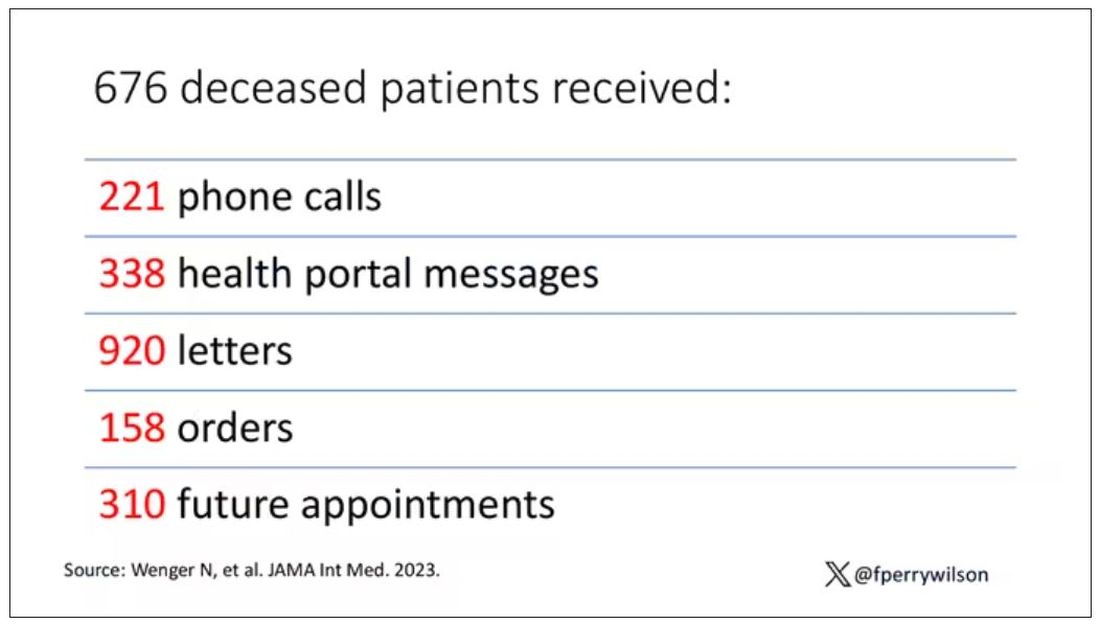
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
Meet the newest acronym in primary care: CKM
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
FROM CIRCULATION
Hematology is in the Brodsky family’s blood
In interviews, Robert and Max Brodsky spoke about the appeal of hematology and the threads that unite them with family members who came before. The elder Brodsky also talked about the work that’s made him the proudest during his year-long presidency at ASH.

Robert A. Brodsky is professor of medicine and director of hematology at Johns Hopkins University, Baltimore. He is stepping down as ASH president at its annual meeting in San Diego, December 9-12. Here are excerpts from our conversation:
Q: What drew your dad into medicine?
Dr. Robert A. Brodsky: He was going through his medical training at the University of Pennsylvania, then the Vietnam War came, and he served at the National Institutes of Health in what they referred to as the Yellow Berets. He got very interested in retroviruses and viruses that lead to cancer, which was a foreign idea at the time. This led him into hematology, stem cells, and myeloproliferative disorders.
He had a very successful career in hematology and just loved it. He performed the first bone marrow transplant in the tristate area of Pennsylvania, Delaware, and New Jersey.
Q: What did he like about hematology specifically?
Dr. Robert A. Brodsky: It’s a fascinating field, probably the most scientific area of medicine. It’s so easy to access blood and bone marrow. You can grow it, you can look at it, you can see it. It’s hard to do that with a lung, heart, kidney, or brain. Even back then, they could translate some of the science. What really drew him to hematology — and me, for that matter — was looking at a blood smear or bone marrow and being able to make a diagnosis. The other thing is the personal aspect. Hematologists tend to like the long-term relationships that they develop with their patients over the years.
Q: What were the biggest transformations in hematology during his career?
Dr. Robert A. Brodsky: Bone marrow transplant had the biggest impact, and it’s an area he really pioneered. He was very much involved in some of the early bone marrow transplants and was very close with Dr. George W. Santos, who was at Johns Hopkins and one of the big pioneers in that area as well. To be able to take marrow from related donors, get it to grow without the patient rejecting it, and cure a disease, was really huge. When he started doing this, patients had no other option. To see patients be cured was incredibly satisfying to him.
Q: How did you end up following your father into hematology?
Dr. Robert A. Brodsky: My brother Jeff, who’s a surgeon and older than me, knew he was going into medicine — probably about 3 hours after he was born. I came to it late. I was a political science major as an undergrad and really trying to figure out what I wanted to do. In my sophomore year, I decided I wanted to give this a shot. My dad worked very hard, long hours, but you could tell he loved what he did. And he was never absent, always involved in our lives and still made time for everyone. At some level, that must have had an influence on me.
Q: What has changed in hematology over your 30-plus years in medicine?
A: When I look back at when I was a fellow, it’s just mind-boggling how many lethal or life-threatening diseases are now pretty easy to treat. I studied disorders like aplastic anemia, which was very fatal. Without treatment, patients would die within a year. Now, over 95% are cured. Another classic examples is chronic myeloid leukemia disorder. Back when I was a fellow, the median survival for CML was maybe 4 to 6 years. Now, Kareem Abdul Jabbar has had this[for about 15 years]. Also a lot of hematologic malignancies are being cured with immunotherapy approaches. We’ve figured out the pathophysiology of a lot of diseases, and there are incredible genetic diagnostic assays.
Q: What was your father’s relationship with ASH?
Dr. Robert A. Brodsky: The first ASH meeting was 1958 in Atlantic City, New Jersey. There were 300 hematologists there, and my dad was one of them. We’re going to have over 30,000 people in San Diego, which is a record, and another 5,000 or 6,000 virtually.
Q: As ASH president, what are your biggest accomplishments when it comes to addressing the shortage of hematologists and other issues?
Dr. Robert A. Brodsky: ASH is investing $19 million to develop fellowships with a focus on hematology.* This is going to put lots of new hematologists into the workforce over the next 5 to 10 years. We’ve also been working on the Maintenance of Certification [MOC] process to make it less onerous on physicians. It’s really a bad process, and it’s not just ASH [that’s complaining], it’s all of medicine. We’re hearing this from GI, endocrine, renal and the general internists.
[In a September 2023 letter to the American Board of Internal Medicine’s president and chief officer, Dr. Brodsky wrote that “ASH continues to support the importance of lifelong learning for hematologists via a program that is evidence-based, relevant to one’s practice, and transparent; however, these three basic requirements are not met by the current ABIM MOC program.” ASH is calling for a new and reformed MOC program.]
Q: What convinced ASH to expand its journals by adding Blood Neoplasia and Blood Vessels, Thrombosis & Hemostasis?
Dr. Robert A. Brodsky: ASH has two flagship journals right now, Blood and Blood Advances, and they’re both very competitive, high-impact journals. It turns out there’s not enough room to publish all the new science, and they end up rejecting the majority of the submissions that come to them. We decided to keep these journals in the ASH family because there’s some fantastic clinical trials and science that would be going elsewhere.
Dr. Brodsky’s sons both have medical degrees: Brett Brodsky, DO, is a resident at Virginia Commonwealth University who plans to become a sports medicine specialist, and Max Brodsky, MD, is a second-year fellow in hematology at Johns Hopkins University.
In an interview, Max Brodsky, MD, talked about the roots of his family’s dedication to caring for others.
Q: What drew you to hematology?
Dr. Max Brodsky: I’ve watched both my dad and my grandfather be leaders in the field as both physicians and scientists, and that was very inspirational for me to see. And I went to a medical school [Drexel University College of Medicine] that my dad went to and where my grandfather was on faculty. That was like walking in their footsteps in a major way.
Q: What do you hope to focus on as a hematologist?
Dr. Max Brodsky: I’m still working through that, but I am really interested in thrombotic thrombocytopenic purpura. Patients used to not be able to survive their initial episodes, but now we have good treatments and are able to follow them as outpatients. With this whole cohort of patients that are surviving, we’re seeing that they have more health problems — more heart disease, more strokes and kidney disease. There’s a whole growing field exploring how to treat these patients for their lifespan.
Q: How do you deal with the reality that more of your patients will die than in some other medical fields?
Dr. Max Brodsky: It is challenging, but I also see those moments as opportunities to support patients and families. I’m good at connecting to patients and families who are in scary situations. I’ve always had that skill of putting people at ease, making people feel calm, knowing that they can trust me, and I have their best interests in mind.
Q: Why do you think your family is so committed to medicine?
Dr. Max Brodsky: We’re Jewish, and looking to help the world is one of the main core values of Judaism. The Torah expects us to make this world better. Actually, my great-grandfather Max, whom I’m named after, used to dig tunnels to help people escape Ukraine and get to freedom. He was always looking to help others as well. My great-grandmother was shot crossing the border escaping from Ukraine, and he carried her the whole way to the boat. They lived in very poor West Philadelphia and poured everything into my grandfather. He became a great doctor, and his sons and his grandchildren are in medicine today.
*Correction, 12/11: A previous version of this story misstated the amount of ASH’s $19 million investment in developing fellowships with a focus on hematology.
In interviews, Robert and Max Brodsky spoke about the appeal of hematology and the threads that unite them with family members who came before. The elder Brodsky also talked about the work that’s made him the proudest during his year-long presidency at ASH.
Robert A. Brodsky is professor of medicine and director of hematology at Johns Hopkins University, Baltimore. He is stepping down as ASH president at its annual meeting in San Diego, December 9-12. Here are excerpts from our conversation:
Q: What drew your dad into medicine?
Dr. Robert A. Brodsky: He was going through his medical training at the University of Pennsylvania, then the Vietnam War came, and he served at the National Institutes of Health in what they referred to as the Yellow Berets. He got very interested in retroviruses and viruses that lead to cancer, which was a foreign idea at the time. This led him into hematology, stem cells, and myeloproliferative disorders.
He had a very successful career in hematology and just loved it. He performed the first bone marrow transplant in the tristate area of Pennsylvania, Delaware, and New Jersey.
Q: What did he like about hematology specifically?
Dr. Robert A. Brodsky: It’s a fascinating field, probably the most scientific area of medicine. It’s so easy to access blood and bone marrow. You can grow it, you can look at it, you can see it. It’s hard to do that with a lung, heart, kidney, or brain. Even back then, they could translate some of the science. What really drew him to hematology — and me, for that matter — was looking at a blood smear or bone marrow and being able to make a diagnosis. The other thing is the personal aspect. Hematologists tend to like the long-term relationships that they develop with their patients over the years.
Q: What were the biggest transformations in hematology during his career?
Dr. Robert A. Brodsky: Bone marrow transplant had the biggest impact, and it’s an area he really pioneered. He was very much involved in some of the early bone marrow transplants and was very close with Dr. George W. Santos, who was at Johns Hopkins and one of the big pioneers in that area as well. To be able to take marrow from related donors, get it to grow without the patient rejecting it, and cure a disease, was really huge. When he started doing this, patients had no other option. To see patients be cured was incredibly satisfying to him.
Q: How did you end up following your father into hematology?
Dr. Robert A. Brodsky: My brother Jeff, who’s a surgeon and older than me, knew he was going into medicine — probably about 3 hours after he was born. I came to it late. I was a political science major as an undergrad and really trying to figure out what I wanted to do. In my sophomore year, I decided I wanted to give this a shot. My dad worked very hard, long hours, but you could tell he loved what he did. And he was never absent, always involved in our lives and still made time for everyone. At some level, that must have had an influence on me.
Q: What has changed in hematology over your 30-plus years in medicine?
A: When I look back at when I was a fellow, it’s just mind-boggling how many lethal or life-threatening diseases are now pretty easy to treat. I studied disorders like aplastic anemia, which was very fatal. Without treatment, patients would die within a year. Now, over 95% are cured. Another classic examples is chronic myeloid leukemia disorder. Back when I was a fellow, the median survival for CML was maybe 4 to 6 years. Now, Kareem Abdul Jabbar has had this[for about 15 years]. Also a lot of hematologic malignancies are being cured with immunotherapy approaches. We’ve figured out the pathophysiology of a lot of diseases, and there are incredible genetic diagnostic assays.
Q: What was your father’s relationship with ASH?
Dr. Robert A. Brodsky: The first ASH meeting was 1958 in Atlantic City, New Jersey. There were 300 hematologists there, and my dad was one of them. We’re going to have over 30,000 people in San Diego, which is a record, and another 5,000 or 6,000 virtually.
Q: As ASH president, what are your biggest accomplishments when it comes to addressing the shortage of hematologists and other issues?
Dr. Robert A. Brodsky: ASH is investing $19 million to develop fellowships with a focus on hematology.* This is going to put lots of new hematologists into the workforce over the next 5 to 10 years. We’ve also been working on the Maintenance of Certification [MOC] process to make it less onerous on physicians. It’s really a bad process, and it’s not just ASH [that’s complaining], it’s all of medicine. We’re hearing this from GI, endocrine, renal and the general internists.
[In a September 2023 letter to the American Board of Internal Medicine’s president and chief officer, Dr. Brodsky wrote that “ASH continues to support the importance of lifelong learning for hematologists via a program that is evidence-based, relevant to one’s practice, and transparent; however, these three basic requirements are not met by the current ABIM MOC program.” ASH is calling for a new and reformed MOC program.]
Q: What convinced ASH to expand its journals by adding Blood Neoplasia and Blood Vessels, Thrombosis & Hemostasis?
Dr. Robert A. Brodsky: ASH has two flagship journals right now, Blood and Blood Advances, and they’re both very competitive, high-impact journals. It turns out there’s not enough room to publish all the new science, and they end up rejecting the majority of the submissions that come to them. We decided to keep these journals in the ASH family because there’s some fantastic clinical trials and science that would be going elsewhere.
Dr. Brodsky’s sons both have medical degrees: Brett Brodsky, DO, is a resident at Virginia Commonwealth University who plans to become a sports medicine specialist, and Max Brodsky, MD, is a second-year fellow in hematology at Johns Hopkins University.
In an interview, Max Brodsky, MD, talked about the roots of his family’s dedication to caring for others.
Q: What drew you to hematology?
Dr. Max Brodsky: I’ve watched both my dad and my grandfather be leaders in the field as both physicians and scientists, and that was very inspirational for me to see. And I went to a medical school [Drexel University College of Medicine] that my dad went to and where my grandfather was on faculty. That was like walking in their footsteps in a major way.
Q: What do you hope to focus on as a hematologist?
Dr. Max Brodsky: I’m still working through that, but I am really interested in thrombotic thrombocytopenic purpura. Patients used to not be able to survive their initial episodes, but now we have good treatments and are able to follow them as outpatients. With this whole cohort of patients that are surviving, we’re seeing that they have more health problems — more heart disease, more strokes and kidney disease. There’s a whole growing field exploring how to treat these patients for their lifespan.
Q: How do you deal with the reality that more of your patients will die than in some other medical fields?
Dr. Max Brodsky: It is challenging, but I also see those moments as opportunities to support patients and families. I’m good at connecting to patients and families who are in scary situations. I’ve always had that skill of putting people at ease, making people feel calm, knowing that they can trust me, and I have their best interests in mind.
Q: Why do you think your family is so committed to medicine?
Dr. Max Brodsky: We’re Jewish, and looking to help the world is one of the main core values of Judaism. The Torah expects us to make this world better. Actually, my great-grandfather Max, whom I’m named after, used to dig tunnels to help people escape Ukraine and get to freedom. He was always looking to help others as well. My great-grandmother was shot crossing the border escaping from Ukraine, and he carried her the whole way to the boat. They lived in very poor West Philadelphia and poured everything into my grandfather. He became a great doctor, and his sons and his grandchildren are in medicine today.
*Correction, 12/11: A previous version of this story misstated the amount of ASH’s $19 million investment in developing fellowships with a focus on hematology.
In interviews, Robert and Max Brodsky spoke about the appeal of hematology and the threads that unite them with family members who came before. The elder Brodsky also talked about the work that’s made him the proudest during his year-long presidency at ASH.
Robert A. Brodsky is professor of medicine and director of hematology at Johns Hopkins University, Baltimore. He is stepping down as ASH president at its annual meeting in San Diego, December 9-12. Here are excerpts from our conversation:
Q: What drew your dad into medicine?
Dr. Robert A. Brodsky: He was going through his medical training at the University of Pennsylvania, then the Vietnam War came, and he served at the National Institutes of Health in what they referred to as the Yellow Berets. He got very interested in retroviruses and viruses that lead to cancer, which was a foreign idea at the time. This led him into hematology, stem cells, and myeloproliferative disorders.
He had a very successful career in hematology and just loved it. He performed the first bone marrow transplant in the tristate area of Pennsylvania, Delaware, and New Jersey.
Q: What did he like about hematology specifically?
Dr. Robert A. Brodsky: It’s a fascinating field, probably the most scientific area of medicine. It’s so easy to access blood and bone marrow. You can grow it, you can look at it, you can see it. It’s hard to do that with a lung, heart, kidney, or brain. Even back then, they could translate some of the science. What really drew him to hematology — and me, for that matter — was looking at a blood smear or bone marrow and being able to make a diagnosis. The other thing is the personal aspect. Hematologists tend to like the long-term relationships that they develop with their patients over the years.
Q: What were the biggest transformations in hematology during his career?
Dr. Robert A. Brodsky: Bone marrow transplant had the biggest impact, and it’s an area he really pioneered. He was very much involved in some of the early bone marrow transplants and was very close with Dr. George W. Santos, who was at Johns Hopkins and one of the big pioneers in that area as well. To be able to take marrow from related donors, get it to grow without the patient rejecting it, and cure a disease, was really huge. When he started doing this, patients had no other option. To see patients be cured was incredibly satisfying to him.
Q: How did you end up following your father into hematology?
Dr. Robert A. Brodsky: My brother Jeff, who’s a surgeon and older than me, knew he was going into medicine — probably about 3 hours after he was born. I came to it late. I was a political science major as an undergrad and really trying to figure out what I wanted to do. In my sophomore year, I decided I wanted to give this a shot. My dad worked very hard, long hours, but you could tell he loved what he did. And he was never absent, always involved in our lives and still made time for everyone. At some level, that must have had an influence on me.
Q: What has changed in hematology over your 30-plus years in medicine?
A: When I look back at when I was a fellow, it’s just mind-boggling how many lethal or life-threatening diseases are now pretty easy to treat. I studied disorders like aplastic anemia, which was very fatal. Without treatment, patients would die within a year. Now, over 95% are cured. Another classic examples is chronic myeloid leukemia disorder. Back when I was a fellow, the median survival for CML was maybe 4 to 6 years. Now, Kareem Abdul Jabbar has had this[for about 15 years]. Also a lot of hematologic malignancies are being cured with immunotherapy approaches. We’ve figured out the pathophysiology of a lot of diseases, and there are incredible genetic diagnostic assays.
Q: What was your father’s relationship with ASH?
Dr. Robert A. Brodsky: The first ASH meeting was 1958 in Atlantic City, New Jersey. There were 300 hematologists there, and my dad was one of them. We’re going to have over 30,000 people in San Diego, which is a record, and another 5,000 or 6,000 virtually.
Q: As ASH president, what are your biggest accomplishments when it comes to addressing the shortage of hematologists and other issues?
Dr. Robert A. Brodsky: ASH is investing $19 million to develop fellowships with a focus on hematology.* This is going to put lots of new hematologists into the workforce over the next 5 to 10 years. We’ve also been working on the Maintenance of Certification [MOC] process to make it less onerous on physicians. It’s really a bad process, and it’s not just ASH [that’s complaining], it’s all of medicine. We’re hearing this from GI, endocrine, renal and the general internists.
[In a September 2023 letter to the American Board of Internal Medicine’s president and chief officer, Dr. Brodsky wrote that “ASH continues to support the importance of lifelong learning for hematologists via a program that is evidence-based, relevant to one’s practice, and transparent; however, these three basic requirements are not met by the current ABIM MOC program.” ASH is calling for a new and reformed MOC program.]
Q: What convinced ASH to expand its journals by adding Blood Neoplasia and Blood Vessels, Thrombosis & Hemostasis?
Dr. Robert A. Brodsky: ASH has two flagship journals right now, Blood and Blood Advances, and they’re both very competitive, high-impact journals. It turns out there’s not enough room to publish all the new science, and they end up rejecting the majority of the submissions that come to them. We decided to keep these journals in the ASH family because there’s some fantastic clinical trials and science that would be going elsewhere.
Dr. Brodsky’s sons both have medical degrees: Brett Brodsky, DO, is a resident at Virginia Commonwealth University who plans to become a sports medicine specialist, and Max Brodsky, MD, is a second-year fellow in hematology at Johns Hopkins University.
In an interview, Max Brodsky, MD, talked about the roots of his family’s dedication to caring for others.
Q: What drew you to hematology?
Dr. Max Brodsky: I’ve watched both my dad and my grandfather be leaders in the field as both physicians and scientists, and that was very inspirational for me to see. And I went to a medical school [Drexel University College of Medicine] that my dad went to and where my grandfather was on faculty. That was like walking in their footsteps in a major way.
Q: What do you hope to focus on as a hematologist?
Dr. Max Brodsky: I’m still working through that, but I am really interested in thrombotic thrombocytopenic purpura. Patients used to not be able to survive their initial episodes, but now we have good treatments and are able to follow them as outpatients. With this whole cohort of patients that are surviving, we’re seeing that they have more health problems — more heart disease, more strokes and kidney disease. There’s a whole growing field exploring how to treat these patients for their lifespan.
Q: How do you deal with the reality that more of your patients will die than in some other medical fields?
Dr. Max Brodsky: It is challenging, but I also see those moments as opportunities to support patients and families. I’m good at connecting to patients and families who are in scary situations. I’ve always had that skill of putting people at ease, making people feel calm, knowing that they can trust me, and I have their best interests in mind.
Q: Why do you think your family is so committed to medicine?
Dr. Max Brodsky: We’re Jewish, and looking to help the world is one of the main core values of Judaism. The Torah expects us to make this world better. Actually, my great-grandfather Max, whom I’m named after, used to dig tunnels to help people escape Ukraine and get to freedom. He was always looking to help others as well. My great-grandmother was shot crossing the border escaping from Ukraine, and he carried her the whole way to the boat. They lived in very poor West Philadelphia and poured everything into my grandfather. He became a great doctor, and his sons and his grandchildren are in medicine today.
*Correction, 12/11: A previous version of this story misstated the amount of ASH’s $19 million investment in developing fellowships with a focus on hematology.
FROM ASH 2023
The prospect of a medication to treat OSA is getting closer
For researchers involved with sleep disorders, developing a pharmacologic treatment for obstructive sleep apnea (OSA) is a bit like searching for the holy grail. P K Schweitzer and colleagues have published the results of the randomized MARIPOSA study assessing a combination of two medicinal products known as AD109, one of the products having an antimuscarinic effect (aroxybutynin), and the other a noradrenergic effect (atomoxetine), in treating this condition.
MARIPOSA Methodology
The trial included 209 patients, 176 of whom completed the 4-week protocol. The trial was double-blinded according to four parallel arms: participants in the first and second arms received AD109 containing doses of 2.5 mg/75 mg and 5 mg/75 mg of aroxybutynin and atomoxetine, respectively. The third arm received atomoxetine alone (75 mg), and the fourth arm was given a placebo.
Two polysomnograms (PSGs) were carried out at the start and end of the trial, allowing researchers to calculate the apnea-hypopnea index (AHI) and to quantify nocturnal desaturation. The impact of these variables are now being deemed as the primary marker of the risk for cardiovascular complications secondary to OSA. Finally, questionnaires that evaluated excessive daytime sleepiness, fatigue, and sleep quality were completed.
The median age varied from 5 to 57 years, depending on the arm of the study, and body mass index varied between 31.2 and 34.5. Inclusion criteria comprised an AHI between 10 and 45 events per hour, of which, at least 75% were described as obstructive. Where continuous positive airway pressure (CPAP) was used (21%-30% of cases), it was abandoned during the trial (in a time frame that is perhaps too short to consider these patients as treatment naive).
Combination Brought Improvements
After the 4 weeks of treatment, the AHI measured via follow-up PSG went from a median of 20.5 to 10.8 (in arm one and from 19.4 to 9.5 in arm two (P < .0001 vs placebo in these two arms). For participants in arm three, AHI went from 19.0 to 11.8 (P < .01 vs placebo).
The rate of nocturnal desaturation (in percentage per hour) declined from -12.7 in arm one (P = .03), from -16.6 in arm two (P = .005), and from -5.2 in arm three (P = .003) compared with the placebo. The fatigue score was significantly improved by AD109 2.5 mg/75 mg. The use of atomoxetine alone slightly worsened the sleep disturbance score.
The main side effects were dry mouth sensation (which was markedly more common with AD109 5 mg/75 mg), difficulty passing urine in 7%-22% of cases, tachycardia in all trial arms, and increased diastolic blood pressure at the 2.5-mg/75-mg dose. The authors concluded that AD109, a combination of noradrenergic and antimuscarinic molecules, is effective in correcting mild to severe OSA.
The 2.5-mg/75-mg dose was as effective as the 5-mg/75-mg dose. Atomoxetine alone is less effective, has more side effects, and is associated with lower quality sleep. Finally, it is reported that compliance with oral treatment was not checked, yet the argument of patient noncompliance with CPAP is largely used by the authors in their presentation of their study. A phase 3 trial is underway.
Nevertheless, these results herald important scientific benefits if we consider that Colin Sullivan’s original 1981 research paper, which ushered in the CPAP era, presented the results of just five participants.
This article was translated from JIM, which is part of the Medscape professional network.
A version of this article appeared on Medscape.com.
For researchers involved with sleep disorders, developing a pharmacologic treatment for obstructive sleep apnea (OSA) is a bit like searching for the holy grail. P K Schweitzer and colleagues have published the results of the randomized MARIPOSA study assessing a combination of two medicinal products known as AD109, one of the products having an antimuscarinic effect (aroxybutynin), and the other a noradrenergic effect (atomoxetine), in treating this condition.
MARIPOSA Methodology
The trial included 209 patients, 176 of whom completed the 4-week protocol. The trial was double-blinded according to four parallel arms: participants in the first and second arms received AD109 containing doses of 2.5 mg/75 mg and 5 mg/75 mg of aroxybutynin and atomoxetine, respectively. The third arm received atomoxetine alone (75 mg), and the fourth arm was given a placebo.
Two polysomnograms (PSGs) were carried out at the start and end of the trial, allowing researchers to calculate the apnea-hypopnea index (AHI) and to quantify nocturnal desaturation. The impact of these variables are now being deemed as the primary marker of the risk for cardiovascular complications secondary to OSA. Finally, questionnaires that evaluated excessive daytime sleepiness, fatigue, and sleep quality were completed.
The median age varied from 5 to 57 years, depending on the arm of the study, and body mass index varied between 31.2 and 34.5. Inclusion criteria comprised an AHI between 10 and 45 events per hour, of which, at least 75% were described as obstructive. Where continuous positive airway pressure (CPAP) was used (21%-30% of cases), it was abandoned during the trial (in a time frame that is perhaps too short to consider these patients as treatment naive).
Combination Brought Improvements
After the 4 weeks of treatment, the AHI measured via follow-up PSG went from a median of 20.5 to 10.8 (in arm one and from 19.4 to 9.5 in arm two (P < .0001 vs placebo in these two arms). For participants in arm three, AHI went from 19.0 to 11.8 (P < .01 vs placebo).
The rate of nocturnal desaturation (in percentage per hour) declined from -12.7 in arm one (P = .03), from -16.6 in arm two (P = .005), and from -5.2 in arm three (P = .003) compared with the placebo. The fatigue score was significantly improved by AD109 2.5 mg/75 mg. The use of atomoxetine alone slightly worsened the sleep disturbance score.
The main side effects were dry mouth sensation (which was markedly more common with AD109 5 mg/75 mg), difficulty passing urine in 7%-22% of cases, tachycardia in all trial arms, and increased diastolic blood pressure at the 2.5-mg/75-mg dose. The authors concluded that AD109, a combination of noradrenergic and antimuscarinic molecules, is effective in correcting mild to severe OSA.
The 2.5-mg/75-mg dose was as effective as the 5-mg/75-mg dose. Atomoxetine alone is less effective, has more side effects, and is associated with lower quality sleep. Finally, it is reported that compliance with oral treatment was not checked, yet the argument of patient noncompliance with CPAP is largely used by the authors in their presentation of their study. A phase 3 trial is underway.
Nevertheless, these results herald important scientific benefits if we consider that Colin Sullivan’s original 1981 research paper, which ushered in the CPAP era, presented the results of just five participants.
This article was translated from JIM, which is part of the Medscape professional network.
A version of this article appeared on Medscape.com.
For researchers involved with sleep disorders, developing a pharmacologic treatment for obstructive sleep apnea (OSA) is a bit like searching for the holy grail. P K Schweitzer and colleagues have published the results of the randomized MARIPOSA study assessing a combination of two medicinal products known as AD109, one of the products having an antimuscarinic effect (aroxybutynin), and the other a noradrenergic effect (atomoxetine), in treating this condition.
MARIPOSA Methodology
The trial included 209 patients, 176 of whom completed the 4-week protocol. The trial was double-blinded according to four parallel arms: participants in the first and second arms received AD109 containing doses of 2.5 mg/75 mg and 5 mg/75 mg of aroxybutynin and atomoxetine, respectively. The third arm received atomoxetine alone (75 mg), and the fourth arm was given a placebo.
Two polysomnograms (PSGs) were carried out at the start and end of the trial, allowing researchers to calculate the apnea-hypopnea index (AHI) and to quantify nocturnal desaturation. The impact of these variables are now being deemed as the primary marker of the risk for cardiovascular complications secondary to OSA. Finally, questionnaires that evaluated excessive daytime sleepiness, fatigue, and sleep quality were completed.
The median age varied from 5 to 57 years, depending on the arm of the study, and body mass index varied between 31.2 and 34.5. Inclusion criteria comprised an AHI between 10 and 45 events per hour, of which, at least 75% were described as obstructive. Where continuous positive airway pressure (CPAP) was used (21%-30% of cases), it was abandoned during the trial (in a time frame that is perhaps too short to consider these patients as treatment naive).
Combination Brought Improvements
After the 4 weeks of treatment, the AHI measured via follow-up PSG went from a median of 20.5 to 10.8 (in arm one and from 19.4 to 9.5 in arm two (P < .0001 vs placebo in these two arms). For participants in arm three, AHI went from 19.0 to 11.8 (P < .01 vs placebo).
The rate of nocturnal desaturation (in percentage per hour) declined from -12.7 in arm one (P = .03), from -16.6 in arm two (P = .005), and from -5.2 in arm three (P = .003) compared with the placebo. The fatigue score was significantly improved by AD109 2.5 mg/75 mg. The use of atomoxetine alone slightly worsened the sleep disturbance score.
The main side effects were dry mouth sensation (which was markedly more common with AD109 5 mg/75 mg), difficulty passing urine in 7%-22% of cases, tachycardia in all trial arms, and increased diastolic blood pressure at the 2.5-mg/75-mg dose. The authors concluded that AD109, a combination of noradrenergic and antimuscarinic molecules, is effective in correcting mild to severe OSA.
The 2.5-mg/75-mg dose was as effective as the 5-mg/75-mg dose. Atomoxetine alone is less effective, has more side effects, and is associated with lower quality sleep. Finally, it is reported that compliance with oral treatment was not checked, yet the argument of patient noncompliance with CPAP is largely used by the authors in their presentation of their study. A phase 3 trial is underway.
Nevertheless, these results herald important scientific benefits if we consider that Colin Sullivan’s original 1981 research paper, which ushered in the CPAP era, presented the results of just five participants.
This article was translated from JIM, which is part of the Medscape professional network.
A version of this article appeared on Medscape.com.
Early age at first period raises type 2 diabetes risk
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
TOPLINE:
, a retrospective study of US women under age 65 found.
METHODOLOGY:
- Researchers analyzed data from 17,377 women who were aged 20-65 years when they participated in a National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 and reported their age at first menstruation, which was classified as ≤ 10, 11, 12, 13, 14, or ≥ 15 years of age.
- In total, 0.2% of the women (1773) had type 2 diabetes; of these, 11.5% (205) had cardiovascular disease (CVD), defined as coronary heart disease (CHD), myocardial infarction, or stroke.
- Compared with women who had their first menstrual period at age 13 (the mean age in this population), those who had their period at age ≤ 10 had a significantly greater risk of having type 2 diabetes, after adjustment for age, race/ethnicity, education, parity, menopause status, family history of diabetes, smoking status, physical activity, alcohol consumption, and body mass index (odds ratio, 1.32; 95% CI, 1.03-1.69; P trend = .03).
- Among the women with diabetes, compared with those who had their first menstrual period at age 13, those who had it at age ≤ 10 had a significantly greater risk of having stroke (OR, 2.66; 95% CI, 1.07-6.64; P trend = .02), but not CVD or CHD, after adjustment for these multiple variables.
TAKEAWAY:
- In a racially and ethnically diverse national sample of US women younger than 65, “extremely early” age at first menstrual period was associated with significantly increased risk for type 2 diabetes; among the women with type 2 diabetes, it was associated with significantly increased risk for stroke but not CVD or CHD, after adjustment for multiple variables.
- Early age at menarche may be an early indicator of the cardiometabolic disease trajectory in women.
IN PRACTICE:
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for progression of diabetes complications,” the study authors write.
SOURCE:
The authors, mainly from Tulane University School of Public Health and Tropical Medicine, New Orleans, Louisiana, and also from Harvard Medical School, Boston, Massachusetts, published their findings in BMJ Nutrition, Prevention & Health.
LIMITATIONS:
- The women who participated in NHANES may not be representative of all women in the United States (selection bias).
- The study only included women who reported the age when they had their first menstrual period (selection bias).
- This was a cross-sectional, observational study, so it cannot show causality.
- The women may have reported the wrong age at which they had their first period (recall bias and social desirability bias).
- The women may have inaccurately reported CVD and type 2 diabetes (recall bias and social desirability bias).
DISCLOSURES:
The researchers were supported by grants from the National Heart, Lung, and Blood Institute and from the National Institute of General Medical Sciences of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
‘Hidden hearing loss’ may cause tinnitus: Study
Scientists know that tinnitus, or ringing in the ears, affects 10% of adults worldwide. But they’re not exactly sure what causes the condition.
The traditional belief is that tinnitus happens in people who had already lost hearing. But some people who have tinnitus are still able to perform well on standard hearing tests, according to researchers at the Massachusetts Eye and Ear Infirmary. That happens because the tests don’t pick up auditory nerve loss, sometimes called “hidden hearing loss.”
Stéphane F. Maison, PhD, the lead author of a new study on tinnitus, said in a news release about the study.
Tinnitus is sometimes compared to phantom limb syndrome, in which people feel pain in limbs they no longer have. While the study published in Scientific Reports doesn’t refer to phantom limb syndrome, it does talk about “phantom sound.”
“In other words, the brain tries to compensate for the loss of hearing by increasing its activity, resulting in the perception of a phantom sound, tinnitus. Until recently though, this idea was disputed as some tinnitus sufferers have normal hearing tests,” the researchers explained in the news release.
Annoyed by the ringing in your ears? What causes tinnitus, and how can you get the sound to buzz off?
The study included 294 adults — 201 who had never reported having tinnitus, 64 who had reported having temporary tinnitus, and 29 who had reported having constant tinnitus for 6 months or more.
All 294 had performed normally on a pure tone test, in which subjects raise their hands when they hear beeps to measure the quietest sounds they can detect.
In a different kind of test, electrodes measured responses to clicking sounds in the inner ear, the auditory nerve, and the brain. The second test found reduced response in the auditory nerves and increased activity in the brainstem activity among those who had tinnitus.
Dr Maison, a principal investigator at Eaton-Peabody Laboratories at Mass Eye and Ear/Harvard Medical School, called the study “a first step toward our ultimate goal of silencing tinnitus.”
“Beyond the nuisance of having persistent ringing or other sounds in the ears, tinnitus symptoms are debilitating in many patients, causing sleep deprivation, social isolation, anxiety and depression, adversely affecting work performance, and reducing significantly their quality of life,” he said in the news release. “We won’t be able to cure tinnitus until we fully understand the mechanisms underlying its genesis.”
A version of this article appeared on WebMD.com.
Scientists know that tinnitus, or ringing in the ears, affects 10% of adults worldwide. But they’re not exactly sure what causes the condition.
The traditional belief is that tinnitus happens in people who had already lost hearing. But some people who have tinnitus are still able to perform well on standard hearing tests, according to researchers at the Massachusetts Eye and Ear Infirmary. That happens because the tests don’t pick up auditory nerve loss, sometimes called “hidden hearing loss.”
Stéphane F. Maison, PhD, the lead author of a new study on tinnitus, said in a news release about the study.
Tinnitus is sometimes compared to phantom limb syndrome, in which people feel pain in limbs they no longer have. While the study published in Scientific Reports doesn’t refer to phantom limb syndrome, it does talk about “phantom sound.”
“In other words, the brain tries to compensate for the loss of hearing by increasing its activity, resulting in the perception of a phantom sound, tinnitus. Until recently though, this idea was disputed as some tinnitus sufferers have normal hearing tests,” the researchers explained in the news release.
Annoyed by the ringing in your ears? What causes tinnitus, and how can you get the sound to buzz off?
The study included 294 adults — 201 who had never reported having tinnitus, 64 who had reported having temporary tinnitus, and 29 who had reported having constant tinnitus for 6 months or more.
All 294 had performed normally on a pure tone test, in which subjects raise their hands when they hear beeps to measure the quietest sounds they can detect.
In a different kind of test, electrodes measured responses to clicking sounds in the inner ear, the auditory nerve, and the brain. The second test found reduced response in the auditory nerves and increased activity in the brainstem activity among those who had tinnitus.
Dr Maison, a principal investigator at Eaton-Peabody Laboratories at Mass Eye and Ear/Harvard Medical School, called the study “a first step toward our ultimate goal of silencing tinnitus.”
“Beyond the nuisance of having persistent ringing or other sounds in the ears, tinnitus symptoms are debilitating in many patients, causing sleep deprivation, social isolation, anxiety and depression, adversely affecting work performance, and reducing significantly their quality of life,” he said in the news release. “We won’t be able to cure tinnitus until we fully understand the mechanisms underlying its genesis.”
A version of this article appeared on WebMD.com.
Scientists know that tinnitus, or ringing in the ears, affects 10% of adults worldwide. But they’re not exactly sure what causes the condition.
The traditional belief is that tinnitus happens in people who had already lost hearing. But some people who have tinnitus are still able to perform well on standard hearing tests, according to researchers at the Massachusetts Eye and Ear Infirmary. That happens because the tests don’t pick up auditory nerve loss, sometimes called “hidden hearing loss.”
Stéphane F. Maison, PhD, the lead author of a new study on tinnitus, said in a news release about the study.
Tinnitus is sometimes compared to phantom limb syndrome, in which people feel pain in limbs they no longer have. While the study published in Scientific Reports doesn’t refer to phantom limb syndrome, it does talk about “phantom sound.”
“In other words, the brain tries to compensate for the loss of hearing by increasing its activity, resulting in the perception of a phantom sound, tinnitus. Until recently though, this idea was disputed as some tinnitus sufferers have normal hearing tests,” the researchers explained in the news release.
Annoyed by the ringing in your ears? What causes tinnitus, and how can you get the sound to buzz off?
The study included 294 adults — 201 who had never reported having tinnitus, 64 who had reported having temporary tinnitus, and 29 who had reported having constant tinnitus for 6 months or more.
All 294 had performed normally on a pure tone test, in which subjects raise their hands when they hear beeps to measure the quietest sounds they can detect.
In a different kind of test, electrodes measured responses to clicking sounds in the inner ear, the auditory nerve, and the brain. The second test found reduced response in the auditory nerves and increased activity in the brainstem activity among those who had tinnitus.
Dr Maison, a principal investigator at Eaton-Peabody Laboratories at Mass Eye and Ear/Harvard Medical School, called the study “a first step toward our ultimate goal of silencing tinnitus.”
“Beyond the nuisance of having persistent ringing or other sounds in the ears, tinnitus symptoms are debilitating in many patients, causing sleep deprivation, social isolation, anxiety and depression, adversely affecting work performance, and reducing significantly their quality of life,” he said in the news release. “We won’t be able to cure tinnitus until we fully understand the mechanisms underlying its genesis.”
A version of this article appeared on WebMD.com.
FROM SCIENTIFIC REPORTS
MDMA therapy for loneliness? Researchers say it could work
Some call the drug “ecstasy” or “molly.” Researchers are calling it a potential tool to help treat loneliness.
As public health experts sound the alarm on a rising loneliness epidemic in the United States and across the globe,
In the latest study, MDMA “led to a robust increase in feelings of connection” among people socializing in a controlled setting. Participants were dosed with either MDMA or a placebo and asked to chat with a stranger. Afterward, those who took MDMA said their companion was more responsive and attentive, and that they had plenty in common. The drug also “increased participants’ ratings of liking their partners, feeling connected and finding the conversation enjoyable and meaningful.”
The study was small — just 18 participants — but its results “have implications for MDMA-assisted therapy,” the authors wrote. “This feeling of connectedness could help patients feel safe and trusting, thereby facilitating deeper emotional exploration.”
MDMA “really does seem to make people want to interact more with other people,” says Harriet de Wit, PhD, a neuropharmacologist at the University of Chicago and one of the study’s authors. The results echo those of earlier research using psychedelics like LSD or psilocybin.
It’s important to note that any intervention involving MDMA or psychedelics would be a drug-assisted therapy — that is, used in conjunction with the appropriate therapy and in a therapeutic setting. MDMA-assisted therapy has already drawn popular and scientific attention, as it recently cleared clinical trials for treating posttraumatic stress disorder (PTSD) and may be nearing approval by the US Food and Drug Administration (FDA).
According to Friederike Holze, PhD, psychopharmacologist at the University of Basel, in Switzerland, “there could be a place” for MDMA and psychedelics in treating chronic loneliness, but only under professional supervision.
There would have to be clear guidelines too, says Joshua Woolley, MD, PhD, a psychiatrist at the University of California, San Francisco.
MDMA and psychedelics “induce this plastic state, a state where people can change. They feel open, they feel like things are possible,” Dr. Woolley says. Then, with therapy, “you can help them change.”
Loneliness Can Impact Our Health
On top of the mental health ramifications, the physiologic effects of loneliness could have grave consequences over time. In observational studies, loneliness has been linked to higher risks for cancer and heart disease, and shorter lifespan. One third of Americans over 45 say they are chronically lonely.
Chronic loneliness changes how we think and behave, research shows. It makes us fear contact with others and see them in a more negative light, as more threatening and less trustworthy. Lonely people prefer to stand farther apart from strangers and avoid touch.
This is where MDMA-assisted therapies could potentially help, by easing these defensive tendencies, according to Dr. Woolley.
MDMA, Psychedelics, and Social Behavior
MDMA, or 3,4-methylenedioxymethamphetamine, is a hybrid between a stimulant and a psychedelic. In Dr. de Wit’s earlier experiments, volunteers given MDMA engaged more in communal activities, chatting, and playing games. They used more positive words during social encounters than those who had received a placebo. And after MDMA, people felt less rejected if they were slighted in Cyberball — a virtual ball-tossing game commonly used to measure the effects of social exclusion.
MDMA has been shown to reduce people’s response to other’s negative emotions, diminishing activation of the amygdala (the brain’s fear center) while looking at pictures of angry faces.
This could be helpful. “If you perceive a person’s natural expression as being a little bit angry, if that disappears, then you might be more inclined to interact,” de Wit says.
However, there may be downsides, too. If a drug makes people more trusting and willing to connect, they could be taken advantage of. This is why, Dr. Woolley says, “psychedelics have been used in cults.”
MDMA may also make the experience of touch more pleasant. In a series of experiments in 2019, researchers gently stroked volunteers ’ arms with a goat-hair brush, mimicking the comforting gestures one may receive from a loved one. At the same time, the scientists monitored the volunteers’ facial muscles. People on MDMA perceived gentle touch as more pleasant than those on placebo, and their smile muscles activated more.
MDMA and psychedelics boost social behaviors in animals, too — suggesting that their effects on relationships have a biological basis. Rats on MDMA are more likely to lie next to each other, and mice become more resilient to social stress. Even octopuses become more outgoing after a dose of MDMA, choosing to spend more time with other octopuses instead of a new toy. Classic psychedelics show similar effects — LSD, for example, makes mice more social.
Psychedelics can induce a sense of a “dissolution of the self-other boundary,” Dr. Woolley says. People who take them often say it’s “helped them feel more connected to themselves and other people.” LSD, first synthesized in 1938, may help increase empathy in some people.
Psilocybin, a compound found in over 200 species of mushrooms and used for centuries in Mesoamerican rituals, also seems to boost empathy, with effects persisting for at least seven days. In Cyberball, the online ball-throwing game, people who took psilocybin felt less socially rejected, an outcome reflected in their brain activation patterns in one study — the areas responsible for social-pain processing appeared to dim after a dose.
Making It Legal and Putting It to Use
In 2020, Oregon became the first state to establish a regulatory framework for psilocybin for therapeutic use, and Colorado followed suit in 2022. Such therapeutic applications of psilocybin could help fight loneliness as well, Dr. Woolley believes, because a “ common symptom of depression is that people feel socially withdrawn and lack motivation, ” he says. As mentioned above, MDMA-assisted therapy is also nearing FDA approval for PTSD.
What remain unclear are the exact mechanisms at play.
“MDMA releases oxytocin, and it does that through serotonin receptors,” Dr. de Wit says. Serotonin activates 5-HT1A receptors in the hypothalamus, releasing oxytocin into the bloodstream. In Dr. de Wit’s recent experiments, the more people felt connected after taking MDMA, the more oxytocin was found circulating in their bodies. (Another drug, methamphetamine, also upped the levels of oxytocin but did not increase feelings of connectedness.)
“It’s likely that both something in the serotonin system independent of oxytocin, and oxytocin itself, contribute,” Dr. de Wit says. Dopamine, a neurotransmitter responsible for motivation, appears to increase as well.
The empathy-boosting effects of LSD also seem to be at least partly driven by oxytocin, experiments published in 2021 revealed. Studies in mice, meanwhile, suggest that glutamate, a chemical messenger in the brain, may be behind some of LSD’s prosocial effects.
Scientists are fairly certain which receptors these drugs bind to and which neurotransmitters they affect. “How that gets translated into these higher-order things like empathy and feeling connected to the world, we don’t totally understand,” Dr. Woolley says.
Challenges and the Future
Although MDMA and psychedelics are largely considered safe when taken in a legal, medically controlled setting, there is reason to be cautious.
“They have relatively low impact on the body, like heart rate increase or blood pressure increase. But they might leave some disturbing psychological effects,” says Dr. Holze. Scientists routinely screen experiment volunteers for their risk for psychiatric disorders.
Although risk for addiction is low with both MDMA and psychedelics, there is always some risk for misuse. MDMA “ can produce feelings of well-being, and then people might use it repeatedly, ” Dr. de Wit says. “ That doesn ’ t seem to be a problem for really a lot of people, but it could easily happen. ”
Still, possibilities remain for MDMA in the fight against loneliness.
“[People] feel open, they feel like things are possible, they feel like they’re unstuck,” Dr. Woolley says. “You can harness that in psychotherapy.”
A version of this article appeared on Medscape.com.
Some call the drug “ecstasy” or “molly.” Researchers are calling it a potential tool to help treat loneliness.
As public health experts sound the alarm on a rising loneliness epidemic in the United States and across the globe,
In the latest study, MDMA “led to a robust increase in feelings of connection” among people socializing in a controlled setting. Participants were dosed with either MDMA or a placebo and asked to chat with a stranger. Afterward, those who took MDMA said their companion was more responsive and attentive, and that they had plenty in common. The drug also “increased participants’ ratings of liking their partners, feeling connected and finding the conversation enjoyable and meaningful.”
The study was small — just 18 participants — but its results “have implications for MDMA-assisted therapy,” the authors wrote. “This feeling of connectedness could help patients feel safe and trusting, thereby facilitating deeper emotional exploration.”
MDMA “really does seem to make people want to interact more with other people,” says Harriet de Wit, PhD, a neuropharmacologist at the University of Chicago and one of the study’s authors. The results echo those of earlier research using psychedelics like LSD or psilocybin.
It’s important to note that any intervention involving MDMA or psychedelics would be a drug-assisted therapy — that is, used in conjunction with the appropriate therapy and in a therapeutic setting. MDMA-assisted therapy has already drawn popular and scientific attention, as it recently cleared clinical trials for treating posttraumatic stress disorder (PTSD) and may be nearing approval by the US Food and Drug Administration (FDA).
According to Friederike Holze, PhD, psychopharmacologist at the University of Basel, in Switzerland, “there could be a place” for MDMA and psychedelics in treating chronic loneliness, but only under professional supervision.
There would have to be clear guidelines too, says Joshua Woolley, MD, PhD, a psychiatrist at the University of California, San Francisco.
MDMA and psychedelics “induce this plastic state, a state where people can change. They feel open, they feel like things are possible,” Dr. Woolley says. Then, with therapy, “you can help them change.”
Loneliness Can Impact Our Health
On top of the mental health ramifications, the physiologic effects of loneliness could have grave consequences over time. In observational studies, loneliness has been linked to higher risks for cancer and heart disease, and shorter lifespan. One third of Americans over 45 say they are chronically lonely.
Chronic loneliness changes how we think and behave, research shows. It makes us fear contact with others and see them in a more negative light, as more threatening and less trustworthy. Lonely people prefer to stand farther apart from strangers and avoid touch.
This is where MDMA-assisted therapies could potentially help, by easing these defensive tendencies, according to Dr. Woolley.
MDMA, Psychedelics, and Social Behavior
MDMA, or 3,4-methylenedioxymethamphetamine, is a hybrid between a stimulant and a psychedelic. In Dr. de Wit’s earlier experiments, volunteers given MDMA engaged more in communal activities, chatting, and playing games. They used more positive words during social encounters than those who had received a placebo. And after MDMA, people felt less rejected if they were slighted in Cyberball — a virtual ball-tossing game commonly used to measure the effects of social exclusion.
MDMA has been shown to reduce people’s response to other’s negative emotions, diminishing activation of the amygdala (the brain’s fear center) while looking at pictures of angry faces.
This could be helpful. “If you perceive a person’s natural expression as being a little bit angry, if that disappears, then you might be more inclined to interact,” de Wit says.
However, there may be downsides, too. If a drug makes people more trusting and willing to connect, they could be taken advantage of. This is why, Dr. Woolley says, “psychedelics have been used in cults.”
MDMA may also make the experience of touch more pleasant. In a series of experiments in 2019, researchers gently stroked volunteers ’ arms with a goat-hair brush, mimicking the comforting gestures one may receive from a loved one. At the same time, the scientists monitored the volunteers’ facial muscles. People on MDMA perceived gentle touch as more pleasant than those on placebo, and their smile muscles activated more.
MDMA and psychedelics boost social behaviors in animals, too — suggesting that their effects on relationships have a biological basis. Rats on MDMA are more likely to lie next to each other, and mice become more resilient to social stress. Even octopuses become more outgoing after a dose of MDMA, choosing to spend more time with other octopuses instead of a new toy. Classic psychedelics show similar effects — LSD, for example, makes mice more social.
Psychedelics can induce a sense of a “dissolution of the self-other boundary,” Dr. Woolley says. People who take them often say it’s “helped them feel more connected to themselves and other people.” LSD, first synthesized in 1938, may help increase empathy in some people.
Psilocybin, a compound found in over 200 species of mushrooms and used for centuries in Mesoamerican rituals, also seems to boost empathy, with effects persisting for at least seven days. In Cyberball, the online ball-throwing game, people who took psilocybin felt less socially rejected, an outcome reflected in their brain activation patterns in one study — the areas responsible for social-pain processing appeared to dim after a dose.
Making It Legal and Putting It to Use
In 2020, Oregon became the first state to establish a regulatory framework for psilocybin for therapeutic use, and Colorado followed suit in 2022. Such therapeutic applications of psilocybin could help fight loneliness as well, Dr. Woolley believes, because a “ common symptom of depression is that people feel socially withdrawn and lack motivation, ” he says. As mentioned above, MDMA-assisted therapy is also nearing FDA approval for PTSD.
What remain unclear are the exact mechanisms at play.
“MDMA releases oxytocin, and it does that through serotonin receptors,” Dr. de Wit says. Serotonin activates 5-HT1A receptors in the hypothalamus, releasing oxytocin into the bloodstream. In Dr. de Wit’s recent experiments, the more people felt connected after taking MDMA, the more oxytocin was found circulating in their bodies. (Another drug, methamphetamine, also upped the levels of oxytocin but did not increase feelings of connectedness.)
“It’s likely that both something in the serotonin system independent of oxytocin, and oxytocin itself, contribute,” Dr. de Wit says. Dopamine, a neurotransmitter responsible for motivation, appears to increase as well.
The empathy-boosting effects of LSD also seem to be at least partly driven by oxytocin, experiments published in 2021 revealed. Studies in mice, meanwhile, suggest that glutamate, a chemical messenger in the brain, may be behind some of LSD’s prosocial effects.
Scientists are fairly certain which receptors these drugs bind to and which neurotransmitters they affect. “How that gets translated into these higher-order things like empathy and feeling connected to the world, we don’t totally understand,” Dr. Woolley says.
Challenges and the Future
Although MDMA and psychedelics are largely considered safe when taken in a legal, medically controlled setting, there is reason to be cautious.
“They have relatively low impact on the body, like heart rate increase or blood pressure increase. But they might leave some disturbing psychological effects,” says Dr. Holze. Scientists routinely screen experiment volunteers for their risk for psychiatric disorders.
Although risk for addiction is low with both MDMA and psychedelics, there is always some risk for misuse. MDMA “ can produce feelings of well-being, and then people might use it repeatedly, ” Dr. de Wit says. “ That doesn ’ t seem to be a problem for really a lot of people, but it could easily happen. ”
Still, possibilities remain for MDMA in the fight against loneliness.
“[People] feel open, they feel like things are possible, they feel like they’re unstuck,” Dr. Woolley says. “You can harness that in psychotherapy.”
A version of this article appeared on Medscape.com.
Some call the drug “ecstasy” or “molly.” Researchers are calling it a potential tool to help treat loneliness.
As public health experts sound the alarm on a rising loneliness epidemic in the United States and across the globe,
In the latest study, MDMA “led to a robust increase in feelings of connection” among people socializing in a controlled setting. Participants were dosed with either MDMA or a placebo and asked to chat with a stranger. Afterward, those who took MDMA said their companion was more responsive and attentive, and that they had plenty in common. The drug also “increased participants’ ratings of liking their partners, feeling connected and finding the conversation enjoyable and meaningful.”
The study was small — just 18 participants — but its results “have implications for MDMA-assisted therapy,” the authors wrote. “This feeling of connectedness could help patients feel safe and trusting, thereby facilitating deeper emotional exploration.”
MDMA “really does seem to make people want to interact more with other people,” says Harriet de Wit, PhD, a neuropharmacologist at the University of Chicago and one of the study’s authors. The results echo those of earlier research using psychedelics like LSD or psilocybin.
It’s important to note that any intervention involving MDMA or psychedelics would be a drug-assisted therapy — that is, used in conjunction with the appropriate therapy and in a therapeutic setting. MDMA-assisted therapy has already drawn popular and scientific attention, as it recently cleared clinical trials for treating posttraumatic stress disorder (PTSD) and may be nearing approval by the US Food and Drug Administration (FDA).
According to Friederike Holze, PhD, psychopharmacologist at the University of Basel, in Switzerland, “there could be a place” for MDMA and psychedelics in treating chronic loneliness, but only under professional supervision.
There would have to be clear guidelines too, says Joshua Woolley, MD, PhD, a psychiatrist at the University of California, San Francisco.
MDMA and psychedelics “induce this plastic state, a state where people can change. They feel open, they feel like things are possible,” Dr. Woolley says. Then, with therapy, “you can help them change.”
Loneliness Can Impact Our Health
On top of the mental health ramifications, the physiologic effects of loneliness could have grave consequences over time. In observational studies, loneliness has been linked to higher risks for cancer and heart disease, and shorter lifespan. One third of Americans over 45 say they are chronically lonely.
Chronic loneliness changes how we think and behave, research shows. It makes us fear contact with others and see them in a more negative light, as more threatening and less trustworthy. Lonely people prefer to stand farther apart from strangers and avoid touch.
This is where MDMA-assisted therapies could potentially help, by easing these defensive tendencies, according to Dr. Woolley.
MDMA, Psychedelics, and Social Behavior
MDMA, or 3,4-methylenedioxymethamphetamine, is a hybrid between a stimulant and a psychedelic. In Dr. de Wit’s earlier experiments, volunteers given MDMA engaged more in communal activities, chatting, and playing games. They used more positive words during social encounters than those who had received a placebo. And after MDMA, people felt less rejected if they were slighted in Cyberball — a virtual ball-tossing game commonly used to measure the effects of social exclusion.
MDMA has been shown to reduce people’s response to other’s negative emotions, diminishing activation of the amygdala (the brain’s fear center) while looking at pictures of angry faces.
This could be helpful. “If you perceive a person’s natural expression as being a little bit angry, if that disappears, then you might be more inclined to interact,” de Wit says.
However, there may be downsides, too. If a drug makes people more trusting and willing to connect, they could be taken advantage of. This is why, Dr. Woolley says, “psychedelics have been used in cults.”
MDMA may also make the experience of touch more pleasant. In a series of experiments in 2019, researchers gently stroked volunteers ’ arms with a goat-hair brush, mimicking the comforting gestures one may receive from a loved one. At the same time, the scientists monitored the volunteers’ facial muscles. People on MDMA perceived gentle touch as more pleasant than those on placebo, and their smile muscles activated more.
MDMA and psychedelics boost social behaviors in animals, too — suggesting that their effects on relationships have a biological basis. Rats on MDMA are more likely to lie next to each other, and mice become more resilient to social stress. Even octopuses become more outgoing after a dose of MDMA, choosing to spend more time with other octopuses instead of a new toy. Classic psychedelics show similar effects — LSD, for example, makes mice more social.
Psychedelics can induce a sense of a “dissolution of the self-other boundary,” Dr. Woolley says. People who take them often say it’s “helped them feel more connected to themselves and other people.” LSD, first synthesized in 1938, may help increase empathy in some people.
Psilocybin, a compound found in over 200 species of mushrooms and used for centuries in Mesoamerican rituals, also seems to boost empathy, with effects persisting for at least seven days. In Cyberball, the online ball-throwing game, people who took psilocybin felt less socially rejected, an outcome reflected in their brain activation patterns in one study — the areas responsible for social-pain processing appeared to dim after a dose.
Making It Legal and Putting It to Use
In 2020, Oregon became the first state to establish a regulatory framework for psilocybin for therapeutic use, and Colorado followed suit in 2022. Such therapeutic applications of psilocybin could help fight loneliness as well, Dr. Woolley believes, because a “ common symptom of depression is that people feel socially withdrawn and lack motivation, ” he says. As mentioned above, MDMA-assisted therapy is also nearing FDA approval for PTSD.
What remain unclear are the exact mechanisms at play.
“MDMA releases oxytocin, and it does that through serotonin receptors,” Dr. de Wit says. Serotonin activates 5-HT1A receptors in the hypothalamus, releasing oxytocin into the bloodstream. In Dr. de Wit’s recent experiments, the more people felt connected after taking MDMA, the more oxytocin was found circulating in their bodies. (Another drug, methamphetamine, also upped the levels of oxytocin but did not increase feelings of connectedness.)
“It’s likely that both something in the serotonin system independent of oxytocin, and oxytocin itself, contribute,” Dr. de Wit says. Dopamine, a neurotransmitter responsible for motivation, appears to increase as well.
The empathy-boosting effects of LSD also seem to be at least partly driven by oxytocin, experiments published in 2021 revealed. Studies in mice, meanwhile, suggest that glutamate, a chemical messenger in the brain, may be behind some of LSD’s prosocial effects.
Scientists are fairly certain which receptors these drugs bind to and which neurotransmitters they affect. “How that gets translated into these higher-order things like empathy and feeling connected to the world, we don’t totally understand,” Dr. Woolley says.
Challenges and the Future
Although MDMA and psychedelics are largely considered safe when taken in a legal, medically controlled setting, there is reason to be cautious.
“They have relatively low impact on the body, like heart rate increase or blood pressure increase. But they might leave some disturbing psychological effects,” says Dr. Holze. Scientists routinely screen experiment volunteers for their risk for psychiatric disorders.
Although risk for addiction is low with both MDMA and psychedelics, there is always some risk for misuse. MDMA “ can produce feelings of well-being, and then people might use it repeatedly, ” Dr. de Wit says. “ That doesn ’ t seem to be a problem for really a lot of people, but it could easily happen. ”
Still, possibilities remain for MDMA in the fight against loneliness.
“[People] feel open, they feel like things are possible, they feel like they’re unstuck,” Dr. Woolley says. “You can harness that in psychotherapy.”
A version of this article appeared on Medscape.com.
2023 AGA Innovation Conference on the Advances in Endosurgery
WASHINGTON, DC — (formerly Consensus Conference) on the Advances in Endosurgery, November 10 – 11. It was organized and chaired by Amrita Sethi, MD, Columbia University Irving Medical Center—NYP and Sri Komanduri, MD, MS, Feinberg School of Medicine, Northwestern University, Chicago.
The conference brought together gastroenterologists (GIs), surgeons, and industry partners to explore what further collaboration and clinical adoption is needed to advance endosurgical applications. Both GIs and surgeons welcomed potential collaboration especially in developing strategies to promote education and training initiatives, including defining what procedures and techniques are to be included in the endosurgery arena. Jeffrey Potkul, Medtronic Endoscopy, noted that this was a “great forum, format, and discussions — it will take novel approaches such as this conference and new collaboration models to ensure technology innovation in the endoluminal space can reach patients and empower improved outcomes in Gastroenterology.”

Topics discussed included third space endoscopy, endobariatric and metabolic endoscopy, and endoscopy related to transluminal access. Exciting new developments in robotic endoscopy were also highlighted with an attempt to understand the value proposition of this innovation in the endoscopy space, as well as successes and failures of past efforts to help guide success going forward. Other issues raised were methods for device development including initiating research studies, how to navigate regulatory processes for Food and Drug Administration approval of new devices, and ongoing issues related to billing and reimbursement. There was consensus around the need for collaboration between all stakeholders to drive innovation and its adoption in the field of endosurgery. This meeting is one of the first of its kind to bring innovators across multiple disciplines together with the intention of moving the entire field of endosurgery forward and encouraging creative solutions.
We would like to thank the members of the AGA Center for GI Innovation and Technology Committee and attendees who made this year’s conference a success. The conference was supported by independent grants from Boston Scientific Corporation, Cook Medical Inc., Endo Tools Therapeutics, Fujifilm Healthcare Americas Corporation, Intuitive Surgical, Olympus Corporation, and Medtronic.
WASHINGTON, DC — (formerly Consensus Conference) on the Advances in Endosurgery, November 10 – 11. It was organized and chaired by Amrita Sethi, MD, Columbia University Irving Medical Center—NYP and Sri Komanduri, MD, MS, Feinberg School of Medicine, Northwestern University, Chicago.
The conference brought together gastroenterologists (GIs), surgeons, and industry partners to explore what further collaboration and clinical adoption is needed to advance endosurgical applications. Both GIs and surgeons welcomed potential collaboration especially in developing strategies to promote education and training initiatives, including defining what procedures and techniques are to be included in the endosurgery arena. Jeffrey Potkul, Medtronic Endoscopy, noted that this was a “great forum, format, and discussions — it will take novel approaches such as this conference and new collaboration models to ensure technology innovation in the endoluminal space can reach patients and empower improved outcomes in Gastroenterology.”
Topics discussed included third space endoscopy, endobariatric and metabolic endoscopy, and endoscopy related to transluminal access. Exciting new developments in robotic endoscopy were also highlighted with an attempt to understand the value proposition of this innovation in the endoscopy space, as well as successes and failures of past efforts to help guide success going forward. Other issues raised were methods for device development including initiating research studies, how to navigate regulatory processes for Food and Drug Administration approval of new devices, and ongoing issues related to billing and reimbursement. There was consensus around the need for collaboration between all stakeholders to drive innovation and its adoption in the field of endosurgery. This meeting is one of the first of its kind to bring innovators across multiple disciplines together with the intention of moving the entire field of endosurgery forward and encouraging creative solutions.
We would like to thank the members of the AGA Center for GI Innovation and Technology Committee and attendees who made this year’s conference a success. The conference was supported by independent grants from Boston Scientific Corporation, Cook Medical Inc., Endo Tools Therapeutics, Fujifilm Healthcare Americas Corporation, Intuitive Surgical, Olympus Corporation, and Medtronic.
WASHINGTON, DC — (formerly Consensus Conference) on the Advances in Endosurgery, November 10 – 11. It was organized and chaired by Amrita Sethi, MD, Columbia University Irving Medical Center—NYP and Sri Komanduri, MD, MS, Feinberg School of Medicine, Northwestern University, Chicago.
The conference brought together gastroenterologists (GIs), surgeons, and industry partners to explore what further collaboration and clinical adoption is needed to advance endosurgical applications. Both GIs and surgeons welcomed potential collaboration especially in developing strategies to promote education and training initiatives, including defining what procedures and techniques are to be included in the endosurgery arena. Jeffrey Potkul, Medtronic Endoscopy, noted that this was a “great forum, format, and discussions — it will take novel approaches such as this conference and new collaboration models to ensure technology innovation in the endoluminal space can reach patients and empower improved outcomes in Gastroenterology.”
Topics discussed included third space endoscopy, endobariatric and metabolic endoscopy, and endoscopy related to transluminal access. Exciting new developments in robotic endoscopy were also highlighted with an attempt to understand the value proposition of this innovation in the endoscopy space, as well as successes and failures of past efforts to help guide success going forward. Other issues raised were methods for device development including initiating research studies, how to navigate regulatory processes for Food and Drug Administration approval of new devices, and ongoing issues related to billing and reimbursement. There was consensus around the need for collaboration between all stakeholders to drive innovation and its adoption in the field of endosurgery. This meeting is one of the first of its kind to bring innovators across multiple disciplines together with the intention of moving the entire field of endosurgery forward and encouraging creative solutions.
We would like to thank the members of the AGA Center for GI Innovation and Technology Committee and attendees who made this year’s conference a success. The conference was supported by independent grants from Boston Scientific Corporation, Cook Medical Inc., Endo Tools Therapeutics, Fujifilm Healthcare Americas Corporation, Intuitive Surgical, Olympus Corporation, and Medtronic.
Statins and the liver: Not harmful and perhaps beneficial
, including glucose intolerance and hyperlipidemia. A lingering concern about potential hepatotoxicity has resulted in widespread reluctance to prescribe statins to treat hyperlipidemia in patients with liver disease; however, their safety in this setting has been documented in the literature as well as in clinical practice. Therefore, statins should not be withheld in patients with liver disease when indicated — with a few caveats. Baseline liver chemistries should be obtained. After initiation of statin therapy, a modest rise in serum aminotransferase levels may occur but is not an indication to discontinue the drug. In fact, monitoring of liver biochemical tests more frequently than is appropriate for any patient with chronic liver disease is unnecessary. The role of statins in cirrhosis may even expand, as recent reports suggest that statin use in patients with cirrhosis may slow the progression of liver disease and reduce the frequency of complications, such as hepatocellular carcinoma. These observations, however, require confirmation before statins can be suggested for any indication other than treating hyperlipidemia in patients with chronic liver disease, and statins are generally not appropriate in patients with decompensated cirrhosis.


Pearls from the Pros was published in Gastro Hep Advances .
Dr. Friedman is the Anton R. Fried, MD, Chair of the Department of Medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University, Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
, including glucose intolerance and hyperlipidemia. A lingering concern about potential hepatotoxicity has resulted in widespread reluctance to prescribe statins to treat hyperlipidemia in patients with liver disease; however, their safety in this setting has been documented in the literature as well as in clinical practice. Therefore, statins should not be withheld in patients with liver disease when indicated — with a few caveats. Baseline liver chemistries should be obtained. After initiation of statin therapy, a modest rise in serum aminotransferase levels may occur but is not an indication to discontinue the drug. In fact, monitoring of liver biochemical tests more frequently than is appropriate for any patient with chronic liver disease is unnecessary. The role of statins in cirrhosis may even expand, as recent reports suggest that statin use in patients with cirrhosis may slow the progression of liver disease and reduce the frequency of complications, such as hepatocellular carcinoma. These observations, however, require confirmation before statins can be suggested for any indication other than treating hyperlipidemia in patients with chronic liver disease, and statins are generally not appropriate in patients with decompensated cirrhosis.
Pearls from the Pros was published in Gastro Hep Advances .
Dr. Friedman is the Anton R. Fried, MD, Chair of the Department of Medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University, Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
, including glucose intolerance and hyperlipidemia. A lingering concern about potential hepatotoxicity has resulted in widespread reluctance to prescribe statins to treat hyperlipidemia in patients with liver disease; however, their safety in this setting has been documented in the literature as well as in clinical practice. Therefore, statins should not be withheld in patients with liver disease when indicated — with a few caveats. Baseline liver chemistries should be obtained. After initiation of statin therapy, a modest rise in serum aminotransferase levels may occur but is not an indication to discontinue the drug. In fact, monitoring of liver biochemical tests more frequently than is appropriate for any patient with chronic liver disease is unnecessary. The role of statins in cirrhosis may even expand, as recent reports suggest that statin use in patients with cirrhosis may slow the progression of liver disease and reduce the frequency of complications, such as hepatocellular carcinoma. These observations, however, require confirmation before statins can be suggested for any indication other than treating hyperlipidemia in patients with chronic liver disease, and statins are generally not appropriate in patients with decompensated cirrhosis.
Pearls from the Pros was published in Gastro Hep Advances .
Dr. Friedman is the Anton R. Fried, MD, Chair of the Department of Medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University, Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
AGA clinical practice guideline affirms role of biomarkers in Crohn’s disease management
, offering the most specific evidence-based recommendations yet for the use of fecal calprotectin (FCP) and serum C-reactive protein (CRP) in assessing disease activity.
Repeated monitoring with endoscopy allows for an objective assessment of inflammation and mucosal healing compared with symptoms alone. However, relying solely on endoscopy to guide management is an approach “limited by cost and resource utilization, invasiveness, and reduced patient acceptability,” wrote guideline authors on behalf of the AGA Clinical Guidelines Committee. The guideline was published online Nov. 17 in Gastroenterology.
“Use of biomarkers is no longer considered experimental and should be an integral part of IBD care and monitoring,” said Ashwin Ananthakrishnan, MBBS, MPH, a gastroenterologist with Massachusetts General Hospital in Boston and first author of the guideline. “We need further studies to define their optimal longitudinal use, but at a given time point, there is now abundant evidence that biomarkers provide significant incremental benefit over symptoms alone in assessing a patient’s status.”
Using evidence from randomized controlled trials and observational studies, and applying it to common clinical scenarios, there are conditional recommendations on the use of biomarkers in patients with established, diagnosed disease who were asymptomatic, symptomatic, or in surgically induced remission. Those recommendations, laid out in a detailed Clinical Decision Support Tool, include the following:
For asymptomatic patients: Check CRP and FCP every 6-12 months. Patients with normal levels, and who have endoscopically confirmed remission within the last 3 years without any subsequent change in symptoms or treatment, need not undergo endoscopy and can be followed with biomarker and clinical checks alone. If CRP or FCP are elevated (defined as CRP ≥ 5 mg/L, FCP ≥ 150 mcg/g), consider repeating biomarkers and/or performing endoscopic assessment of disease activity before adjusting treatment.
For mildly symptomatic patients: Role of biomarker testing may be limited and endoscopic or radiologic assessment may be required to assess active inflammation given the higher rate of false positive and false negative results with biomarkers in this population.
For patients with more severe symptoms: Elevated CRP or FCP can be used to guide treatment adjustment without endoscopic confirmation in certain situations. Normal levels may be false negative and should be confirmed by endoscopic assessment of disease activity.
For patients in surgically induced remission with a low likelihood of recurrence: FCP levels below 50 mcg/g can be used in lieu of routine endoscopic assessment within the first year after surgery. Higher FCP levels should prompt endoscopic assessment.
For patients in surgically induced remission with a high risk of recurrence: Do not rely on biomarkers. Perform endoscopic assessment.
All recommendations were deemed of low to moderate certainty based on results from randomized clinical trials and observational studies that utilized these biomarkers in patients with Crohn’s disease. Citing a dearth of quality evidence, the guideline authors determined they could not make recommendations on the use of a third proprietary biomarker — the endoscopic healing index (EHI).
Recent AGA Clinical Practice Guidelines on the role of biomarkers in ulcerative colitis, published in March, also support a strong role for fecal and blood biomarkers, determining when these can be used to avoid unneeded endoscopic assessments. However, in patients with Crohn’s disease, symptoms correlate less well with endoscopic activity.
As a result, “biomarker performance was acceptable only in asymptomatic individuals who had recently confirmed endoscopic remission; in those without recent endoscopic assessment, test performance was suboptimal.” In addition, the weaker correlation between symptoms and endoscopic activity in Crohn’s “reduced the utility of biomarker measurement to infer disease activity in those with mild symptoms.”
The guidelines were fully funded by the AGA Institute. The authors disclosed a number of potential conflicts of interest, including receiving research grants, as well as consulting and speaking fees, from pharmaceutical companies.
, offering the most specific evidence-based recommendations yet for the use of fecal calprotectin (FCP) and serum C-reactive protein (CRP) in assessing disease activity.
Repeated monitoring with endoscopy allows for an objective assessment of inflammation and mucosal healing compared with symptoms alone. However, relying solely on endoscopy to guide management is an approach “limited by cost and resource utilization, invasiveness, and reduced patient acceptability,” wrote guideline authors on behalf of the AGA Clinical Guidelines Committee. The guideline was published online Nov. 17 in Gastroenterology.
“Use of biomarkers is no longer considered experimental and should be an integral part of IBD care and monitoring,” said Ashwin Ananthakrishnan, MBBS, MPH, a gastroenterologist with Massachusetts General Hospital in Boston and first author of the guideline. “We need further studies to define their optimal longitudinal use, but at a given time point, there is now abundant evidence that biomarkers provide significant incremental benefit over symptoms alone in assessing a patient’s status.”
Using evidence from randomized controlled trials and observational studies, and applying it to common clinical scenarios, there are conditional recommendations on the use of biomarkers in patients with established, diagnosed disease who were asymptomatic, symptomatic, or in surgically induced remission. Those recommendations, laid out in a detailed Clinical Decision Support Tool, include the following:
For asymptomatic patients: Check CRP and FCP every 6-12 months. Patients with normal levels, and who have endoscopically confirmed remission within the last 3 years without any subsequent change in symptoms or treatment, need not undergo endoscopy and can be followed with biomarker and clinical checks alone. If CRP or FCP are elevated (defined as CRP ≥ 5 mg/L, FCP ≥ 150 mcg/g), consider repeating biomarkers and/or performing endoscopic assessment of disease activity before adjusting treatment.
For mildly symptomatic patients: Role of biomarker testing may be limited and endoscopic or radiologic assessment may be required to assess active inflammation given the higher rate of false positive and false negative results with biomarkers in this population.
For patients with more severe symptoms: Elevated CRP or FCP can be used to guide treatment adjustment without endoscopic confirmation in certain situations. Normal levels may be false negative and should be confirmed by endoscopic assessment of disease activity.
For patients in surgically induced remission with a low likelihood of recurrence: FCP levels below 50 mcg/g can be used in lieu of routine endoscopic assessment within the first year after surgery. Higher FCP levels should prompt endoscopic assessment.
For patients in surgically induced remission with a high risk of recurrence: Do not rely on biomarkers. Perform endoscopic assessment.
All recommendations were deemed of low to moderate certainty based on results from randomized clinical trials and observational studies that utilized these biomarkers in patients with Crohn’s disease. Citing a dearth of quality evidence, the guideline authors determined they could not make recommendations on the use of a third proprietary biomarker — the endoscopic healing index (EHI).
Recent AGA Clinical Practice Guidelines on the role of biomarkers in ulcerative colitis, published in March, also support a strong role for fecal and blood biomarkers, determining when these can be used to avoid unneeded endoscopic assessments. However, in patients with Crohn’s disease, symptoms correlate less well with endoscopic activity.
As a result, “biomarker performance was acceptable only in asymptomatic individuals who had recently confirmed endoscopic remission; in those without recent endoscopic assessment, test performance was suboptimal.” In addition, the weaker correlation between symptoms and endoscopic activity in Crohn’s “reduced the utility of biomarker measurement to infer disease activity in those with mild symptoms.”
The guidelines were fully funded by the AGA Institute. The authors disclosed a number of potential conflicts of interest, including receiving research grants, as well as consulting and speaking fees, from pharmaceutical companies.
, offering the most specific evidence-based recommendations yet for the use of fecal calprotectin (FCP) and serum C-reactive protein (CRP) in assessing disease activity.
Repeated monitoring with endoscopy allows for an objective assessment of inflammation and mucosal healing compared with symptoms alone. However, relying solely on endoscopy to guide management is an approach “limited by cost and resource utilization, invasiveness, and reduced patient acceptability,” wrote guideline authors on behalf of the AGA Clinical Guidelines Committee. The guideline was published online Nov. 17 in Gastroenterology.
“Use of biomarkers is no longer considered experimental and should be an integral part of IBD care and monitoring,” said Ashwin Ananthakrishnan, MBBS, MPH, a gastroenterologist with Massachusetts General Hospital in Boston and first author of the guideline. “We need further studies to define their optimal longitudinal use, but at a given time point, there is now abundant evidence that biomarkers provide significant incremental benefit over symptoms alone in assessing a patient’s status.”
Using evidence from randomized controlled trials and observational studies, and applying it to common clinical scenarios, there are conditional recommendations on the use of biomarkers in patients with established, diagnosed disease who were asymptomatic, symptomatic, or in surgically induced remission. Those recommendations, laid out in a detailed Clinical Decision Support Tool, include the following:
For asymptomatic patients: Check CRP and FCP every 6-12 months. Patients with normal levels, and who have endoscopically confirmed remission within the last 3 years without any subsequent change in symptoms or treatment, need not undergo endoscopy and can be followed with biomarker and clinical checks alone. If CRP or FCP are elevated (defined as CRP ≥ 5 mg/L, FCP ≥ 150 mcg/g), consider repeating biomarkers and/or performing endoscopic assessment of disease activity before adjusting treatment.
For mildly symptomatic patients: Role of biomarker testing may be limited and endoscopic or radiologic assessment may be required to assess active inflammation given the higher rate of false positive and false negative results with biomarkers in this population.
For patients with more severe symptoms: Elevated CRP or FCP can be used to guide treatment adjustment without endoscopic confirmation in certain situations. Normal levels may be false negative and should be confirmed by endoscopic assessment of disease activity.
For patients in surgically induced remission with a low likelihood of recurrence: FCP levels below 50 mcg/g can be used in lieu of routine endoscopic assessment within the first year after surgery. Higher FCP levels should prompt endoscopic assessment.
For patients in surgically induced remission with a high risk of recurrence: Do not rely on biomarkers. Perform endoscopic assessment.
All recommendations were deemed of low to moderate certainty based on results from randomized clinical trials and observational studies that utilized these biomarkers in patients with Crohn’s disease. Citing a dearth of quality evidence, the guideline authors determined they could not make recommendations on the use of a third proprietary biomarker — the endoscopic healing index (EHI).
Recent AGA Clinical Practice Guidelines on the role of biomarkers in ulcerative colitis, published in March, also support a strong role for fecal and blood biomarkers, determining when these can be used to avoid unneeded endoscopic assessments. However, in patients with Crohn’s disease, symptoms correlate less well with endoscopic activity.
As a result, “biomarker performance was acceptable only in asymptomatic individuals who had recently confirmed endoscopic remission; in those without recent endoscopic assessment, test performance was suboptimal.” In addition, the weaker correlation between symptoms and endoscopic activity in Crohn’s “reduced the utility of biomarker measurement to infer disease activity in those with mild symptoms.”
The guidelines were fully funded by the AGA Institute. The authors disclosed a number of potential conflicts of interest, including receiving research grants, as well as consulting and speaking fees, from pharmaceutical companies.
FROM GASTROENTEROLOGY