User login
Commentary: Predicting Migraine Treatment Outcomes, July 2024

Medications classified as anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAb), a relatively new category of migraine therapy, have shown strong evidence of efficacy for migraine treatment and prevention. However, as these medications — which include Aimovig (erenumab), Emgality (galcanezumab), Ajovy (fremanezumab), and Vyepti (eptinezumab) — are new, their long-term outcomes are not known; in addition, they are expensive and they do not work for everyone. Patients who are doing relatively well on other medications might ask about switching to one of the anti-CGRP mAb so that they can experience the better outcomes and low side-effect profile that they've been hearing about. New research is showing some prognostic indicators that can help identify which patients might experience a better response to anti-CGRP mAb.
A prospective real-world study published in the May 2024 issue of Journal of Neurology, Neurosurgery, and Psychiatry included 5818 patients who had been treated with an anti-CGRP mAb for high-frequency episodic or chronic migraine. The researchers assessed responses after 6 months of use, defining a good response as ≥50% reduction in monthly headache days and excellent response as ≥75% reduction in monthly headache days. They found that several pretreatment baseline factors were predictors of a good or excellent 6-month response: older age, the presence of unilateral pain, the absence of depression, fewer monthly migraine days, and lower Migraine Disability Assessment (MIDAS) score. Notably, men and women experienced comparable outcomes. While it's not completely clear why these factors were associated with better responses to anti-CGRP mAb, the results could help in selecting patients who might or might not benefit from this new medication class.
Results of a prospective study published in the May 2024 in The Journal of Headache and Pain demonstrated that patients treated with eptinezumab for 3 months experienced a reduction of monthly headaches, migraines, and the use of acute medication. The patients who had previously had an inadequate response to or were unable to tolerate other anti-CGRP mAb (erenumab, galcanezumab, fremanezumab) were less likely to experience improvement with eptinezumab than patients who had not had previous unsuccessful attempts with anti-CGRP mAb. This suggests that it might not be beneficial for patents to try multiple medications in this category if they have had an inadequate response or intolerability to others in the same drug class.
Lifestyle factors can play a role in migraine outcomes and may reduce the need for medication. A study published in The Journal of Headache and Pain in May 2024 examined the relationship between migraine and the American Heart Association (AHA) Guidelines for Cardiovascular Health recommended lifestyle factors. The study included 332,895 participants, with a median follow-up of 13.58 years. Researchers found that maintaining targeted or recommended body mass index (BMI), physical activity, sleep duration, sleep pattern, and sedentary time were associated with substantial reductions in migraine risk.
Diet, another lifestyle factor, can also have an effect on migraine. Avoiding dietary triggers is a well-known adjustment that many patients are advised to make. Overall diet quality can play a role in migraine outcomes as well. According to a study published in the May 2024 issue of Nutritional Neuroscience, participants who followed a diet that qualified as having a high Carbohydrate Quality Index (CQI) had lower migraine severity and duration than participants whose diets did not qualify as high CQI. The study included 266 women (age 18-45 years), using a 147-item food frequency questionnaire to assess CQI. The CQI, a relatively new index for measuring carbohydrate quality, includes four components: glycemic index, dietary fiber intake, ratio of whole grain to total grain, ratio of solid carbohydrates to total (solid + liquid) carbohydrates.1 A low glycemic index and higher scores for the other three factors translates to a high CQI.
While the results of the AHA/migraine study and the CQI/migraine study are interesting, the physiologic reasons for the outcomes and validation of the results need further investigation. It's not clear whether the decrease in migraines that's associated with optimal carbohydrate intake is associated with outcomes such as low BMI or better sleep, or whether carbohydrate metabolism could be an independent factor.
Predictive factors can be beneficial in making migraine treatment decisions. While trial and error will always remain part of optimal migraine therapy, customizing treatment on the basis of an individual patient's characteristics can help in reaching an effective treatment and better quality of life sooner.
Additional References
1. Sawicki CM, Lichtenstein AH, Rogers GT, et al. Comparison of indices of carbohydrate quality and food sources of dietary fiber on longitudinal changes in waist circumference in the Framingham Offspring Cohort. Nutrients. 2021;13:997. Source
Medications classified as anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAb), a relatively new category of migraine therapy, have shown strong evidence of efficacy for migraine treatment and prevention. However, as these medications — which include Aimovig (erenumab), Emgality (galcanezumab), Ajovy (fremanezumab), and Vyepti (eptinezumab) — are new, their long-term outcomes are not known; in addition, they are expensive and they do not work for everyone. Patients who are doing relatively well on other medications might ask about switching to one of the anti-CGRP mAb so that they can experience the better outcomes and low side-effect profile that they've been hearing about. New research is showing some prognostic indicators that can help identify which patients might experience a better response to anti-CGRP mAb.
A prospective real-world study published in the May 2024 issue of Journal of Neurology, Neurosurgery, and Psychiatry included 5818 patients who had been treated with an anti-CGRP mAb for high-frequency episodic or chronic migraine. The researchers assessed responses after 6 months of use, defining a good response as ≥50% reduction in monthly headache days and excellent response as ≥75% reduction in monthly headache days. They found that several pretreatment baseline factors were predictors of a good or excellent 6-month response: older age, the presence of unilateral pain, the absence of depression, fewer monthly migraine days, and lower Migraine Disability Assessment (MIDAS) score. Notably, men and women experienced comparable outcomes. While it's not completely clear why these factors were associated with better responses to anti-CGRP mAb, the results could help in selecting patients who might or might not benefit from this new medication class.
Results of a prospective study published in the May 2024 in The Journal of Headache and Pain demonstrated that patients treated with eptinezumab for 3 months experienced a reduction of monthly headaches, migraines, and the use of acute medication. The patients who had previously had an inadequate response to or were unable to tolerate other anti-CGRP mAb (erenumab, galcanezumab, fremanezumab) were less likely to experience improvement with eptinezumab than patients who had not had previous unsuccessful attempts with anti-CGRP mAb. This suggests that it might not be beneficial for patents to try multiple medications in this category if they have had an inadequate response or intolerability to others in the same drug class.
Lifestyle factors can play a role in migraine outcomes and may reduce the need for medication. A study published in The Journal of Headache and Pain in May 2024 examined the relationship between migraine and the American Heart Association (AHA) Guidelines for Cardiovascular Health recommended lifestyle factors. The study included 332,895 participants, with a median follow-up of 13.58 years. Researchers found that maintaining targeted or recommended body mass index (BMI), physical activity, sleep duration, sleep pattern, and sedentary time were associated with substantial reductions in migraine risk.
Diet, another lifestyle factor, can also have an effect on migraine. Avoiding dietary triggers is a well-known adjustment that many patients are advised to make. Overall diet quality can play a role in migraine outcomes as well. According to a study published in the May 2024 issue of Nutritional Neuroscience, participants who followed a diet that qualified as having a high Carbohydrate Quality Index (CQI) had lower migraine severity and duration than participants whose diets did not qualify as high CQI. The study included 266 women (age 18-45 years), using a 147-item food frequency questionnaire to assess CQI. The CQI, a relatively new index for measuring carbohydrate quality, includes four components: glycemic index, dietary fiber intake, ratio of whole grain to total grain, ratio of solid carbohydrates to total (solid + liquid) carbohydrates.1 A low glycemic index and higher scores for the other three factors translates to a high CQI.
While the results of the AHA/migraine study and the CQI/migraine study are interesting, the physiologic reasons for the outcomes and validation of the results need further investigation. It's not clear whether the decrease in migraines that's associated with optimal carbohydrate intake is associated with outcomes such as low BMI or better sleep, or whether carbohydrate metabolism could be an independent factor.
Predictive factors can be beneficial in making migraine treatment decisions. While trial and error will always remain part of optimal migraine therapy, customizing treatment on the basis of an individual patient's characteristics can help in reaching an effective treatment and better quality of life sooner.
Additional References
1. Sawicki CM, Lichtenstein AH, Rogers GT, et al. Comparison of indices of carbohydrate quality and food sources of dietary fiber on longitudinal changes in waist circumference in the Framingham Offspring Cohort. Nutrients. 2021;13:997. Source
Medications classified as anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAb), a relatively new category of migraine therapy, have shown strong evidence of efficacy for migraine treatment and prevention. However, as these medications — which include Aimovig (erenumab), Emgality (galcanezumab), Ajovy (fremanezumab), and Vyepti (eptinezumab) — are new, their long-term outcomes are not known; in addition, they are expensive and they do not work for everyone. Patients who are doing relatively well on other medications might ask about switching to one of the anti-CGRP mAb so that they can experience the better outcomes and low side-effect profile that they've been hearing about. New research is showing some prognostic indicators that can help identify which patients might experience a better response to anti-CGRP mAb.
A prospective real-world study published in the May 2024 issue of Journal of Neurology, Neurosurgery, and Psychiatry included 5818 patients who had been treated with an anti-CGRP mAb for high-frequency episodic or chronic migraine. The researchers assessed responses after 6 months of use, defining a good response as ≥50% reduction in monthly headache days and excellent response as ≥75% reduction in monthly headache days. They found that several pretreatment baseline factors were predictors of a good or excellent 6-month response: older age, the presence of unilateral pain, the absence of depression, fewer monthly migraine days, and lower Migraine Disability Assessment (MIDAS) score. Notably, men and women experienced comparable outcomes. While it's not completely clear why these factors were associated with better responses to anti-CGRP mAb, the results could help in selecting patients who might or might not benefit from this new medication class.
Results of a prospective study published in the May 2024 in The Journal of Headache and Pain demonstrated that patients treated with eptinezumab for 3 months experienced a reduction of monthly headaches, migraines, and the use of acute medication. The patients who had previously had an inadequate response to or were unable to tolerate other anti-CGRP mAb (erenumab, galcanezumab, fremanezumab) were less likely to experience improvement with eptinezumab than patients who had not had previous unsuccessful attempts with anti-CGRP mAb. This suggests that it might not be beneficial for patents to try multiple medications in this category if they have had an inadequate response or intolerability to others in the same drug class.
Lifestyle factors can play a role in migraine outcomes and may reduce the need for medication. A study published in The Journal of Headache and Pain in May 2024 examined the relationship between migraine and the American Heart Association (AHA) Guidelines for Cardiovascular Health recommended lifestyle factors. The study included 332,895 participants, with a median follow-up of 13.58 years. Researchers found that maintaining targeted or recommended body mass index (BMI), physical activity, sleep duration, sleep pattern, and sedentary time were associated with substantial reductions in migraine risk.
Diet, another lifestyle factor, can also have an effect on migraine. Avoiding dietary triggers is a well-known adjustment that many patients are advised to make. Overall diet quality can play a role in migraine outcomes as well. According to a study published in the May 2024 issue of Nutritional Neuroscience, participants who followed a diet that qualified as having a high Carbohydrate Quality Index (CQI) had lower migraine severity and duration than participants whose diets did not qualify as high CQI. The study included 266 women (age 18-45 years), using a 147-item food frequency questionnaire to assess CQI. The CQI, a relatively new index for measuring carbohydrate quality, includes four components: glycemic index, dietary fiber intake, ratio of whole grain to total grain, ratio of solid carbohydrates to total (solid + liquid) carbohydrates.1 A low glycemic index and higher scores for the other three factors translates to a high CQI.
While the results of the AHA/migraine study and the CQI/migraine study are interesting, the physiologic reasons for the outcomes and validation of the results need further investigation. It's not clear whether the decrease in migraines that's associated with optimal carbohydrate intake is associated with outcomes such as low BMI or better sleep, or whether carbohydrate metabolism could be an independent factor.
Predictive factors can be beneficial in making migraine treatment decisions. While trial and error will always remain part of optimal migraine therapy, customizing treatment on the basis of an individual patient's characteristics can help in reaching an effective treatment and better quality of life sooner.
Additional References
1. Sawicki CM, Lichtenstein AH, Rogers GT, et al. Comparison of indices of carbohydrate quality and food sources of dietary fiber on longitudinal changes in waist circumference in the Framingham Offspring Cohort. Nutrients. 2021;13:997. Source
A New Psychotherapeutic ‘Gold Standard’ for Chronic Pain?
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
, the current psychotherapeutic gold standard, a new study suggested.
Two thirds of the patients who received EAET reported at least a 30% reduction in pain compared with 17% of those who received CBT. The randomized clinical trial also showed that individuals with depression and anxiety responded more favorably to EAET, a novel finding.
The study is one of only a few to directly compare EAET with CBT.
“Most people with chronic pain don’t consider psychotherapy at all,” said study investigator Brandon C. Yarns, MD, a staff psychiatrist at the VA Greater Los Angeles Healthcare System, and clinical professor of health sciences at the Department of Psychiatry and Biobehavioral Sciences, UCLA Health.
Although patients were allowed to continue medication for pain and other comorbidities during the study, those who received EAET “had larger improvements in pain, depression, and anxiety,” Dr. Yarns said. “That suggests that the effect was due to the EAET.”
The findings were published online in JAMA Network Open.
‘Gold Standard’
EAET was first used in the early 2010s. In the therapy, patients are asked to recall a difficult or traumatic memory, engage in experiencing how the related emotions feel in the body, express those feelings in words, and release or let them go. They are taught that the brain’s perception of pain is strongly influenced by the evasion of grief, fear, rage, or guilt, Dr. Yarns said.
This contrasts with CBT — considered the current gold standard for chronic pain — which teaches patients to improve the ability to tolerate pain though guided imagery, muscle relaxation, and other exercises and to adapt their thinking to change how they think about pain.
Although prior studies suggested EAET is effective in reducing pain in fibromyalgia and chronic musculoskeletal, pelvic, and head pain, most included primarily younger, female patients.
The research is the “first full-scale evaluation of EAET, to our knowledge, in a medically or psychiatrically complex, racially and ethnically diverse, older sample comprising predominantly men,” investigators wrote.
The trial enrolled 126 veterans (92% men; 55% Black or African American) aged 60-95 years with at least 3 months of musculoskeletal pain. More than two thirds of patients had a psychiatric diagnosis, with about one third having posttraumatic stress disorder (PTSD). Almost all had back pain, and many had pain in multiple locations.
All services were delivered in-person at the US Department of Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles. Half underwent CBT, while the other half received EAET.
Each patient had one 90-minute individual session and eight additional 90-minute group sessions.
Patients were asked to rate their pain using a 0-10 scale in the Brief Pain Inventory (BPI) before starting treatment, at the end of the nine sessions (at week 10), and 6 months after the sessions ended. Baseline BPI score for both groups was a mean of around 6.
Post treatment, people in the EAET versus CBT group had a mean two-point reduction versus 0.60 reduction, respectively, on the BPI scale. A clinically significant reduction in pain — defined as ≥ 30% decrease — was reported in 63% of EAET patients versus 17% of CBT patients (odds ratio [OR], 21.54; P < .001).
At 6 months, the mean reduction was 1.2 for the EAET group compared with 0.25 for the CBT group, and 40% of the EAET group reported a clinically significant reduction in pain.
A little more than a third (35%) of veterans receiving EAET reported at least a 50% reduction in pain at 10 weeks compared with 7% of those receiving CBT. At 6 months, 16% of the EAET arm reported a halving of their pain.
EAET was also superior to CBT in reducing anxiety, depression, and PTSD symptoms at the 10-week mark.
More Work Needed
In an accompanying editorial, Matthias Karst, MD, PhD, a clinician with the Pain Clinic, Hannover Medical School, in Hannover, Germany, noted that EAET’s effects “are significantly superior to those of CBT in almost all dimensions, even after 6 months.”
EAET “assigns a special place to the integration of the body into the emotional experience,” he wrote.
The study demonstrated that “the evocation and expression of emotions is superior to the mere cognitive discussion of these emotions in therapy of patients with chronic pain.”
Commenting on the findings, Traci J. Speed, MD, PhD, assistant professor of psychiatry and behavioral sciences and an attending psychiatrist of the Johns Hopkins Pain Treatment Program at Johns Hopkins University, Baltimore, called the study “ground-breaking” because it showed effectiveness in people with high rates of PTSD, anxiety, and depression.
“It is a little bit surprising how impressive the study outcomes are in terms of maintaining the effects at the end of the treatment and sustaining some of the effects on pain sensitivity even at the 6-month follow-up,” said Dr. Speed, who was not part of the study.
However, she continued, “I don’t think it changes the current standard of practice yet. CBT has decades of research and evidence that it is effective for chronic pain and that will I think continue to be the standard of care.”
Although EAET is in its infancy, chronic pain experts are interested in learning more about the therapy, Dr. Speed added.
“It blends well with the current techniques and extends the current gold standard treatment approaches,” she said. “We are starting to really appreciate the role that emotions play in pain sensitivity.”
Both Dr. Karst and Dr. Speed noted that more study is needed to determine the sustainability of treatment effects.
Dr. Yarns agreed. “We need more research on what the appropriate dose is and perhaps how one might go about personalizing that for the patient,” he said.
The study was funded by a career development award to Dr. Yarns from the VA Clinical Science Research and Development Service. Dr. Yarns reported receiving grants from the US Department of Veterans Affairs during the study. Other authors’ disclosures are in the original article. Dr. Speed reported no conflicts.
A version of this article appeared on Medscape.com.
‘Just Be Prepared’: MD Finds Overdose Victim in an Alley
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Long COVID Can’t Be Solved Until We Decide What It Is
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.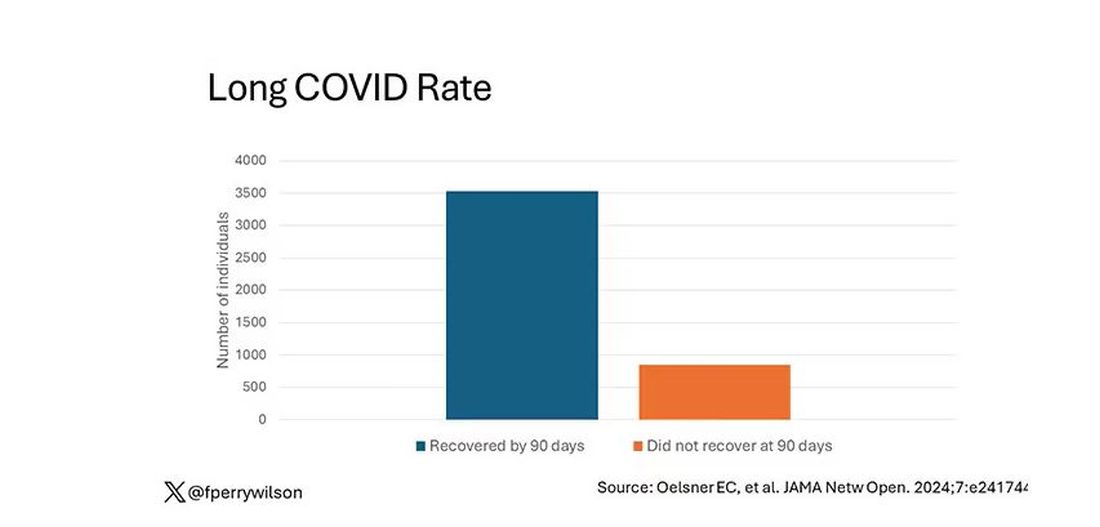
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.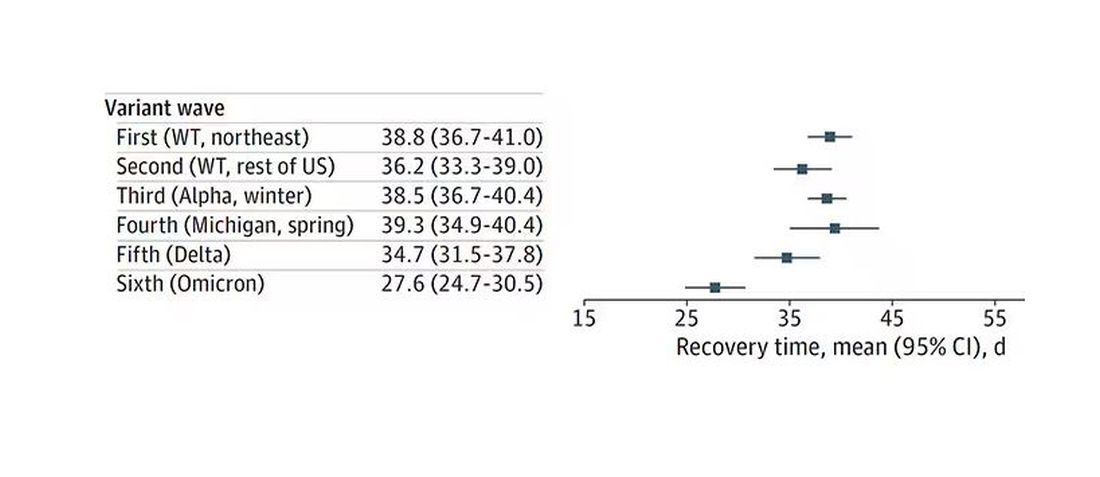
Recovery times were longer for smokers, those with diabetes, and those who were obese.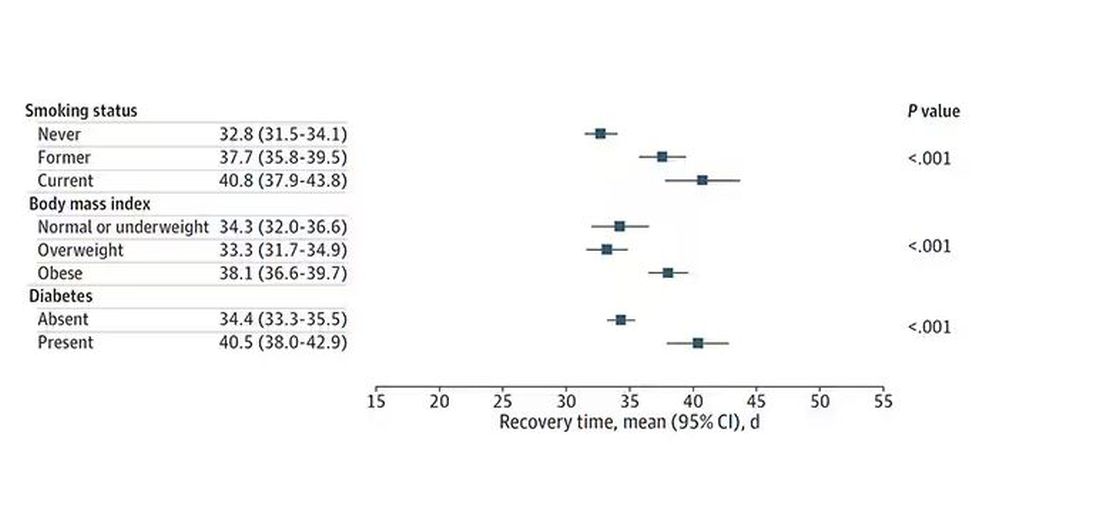
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.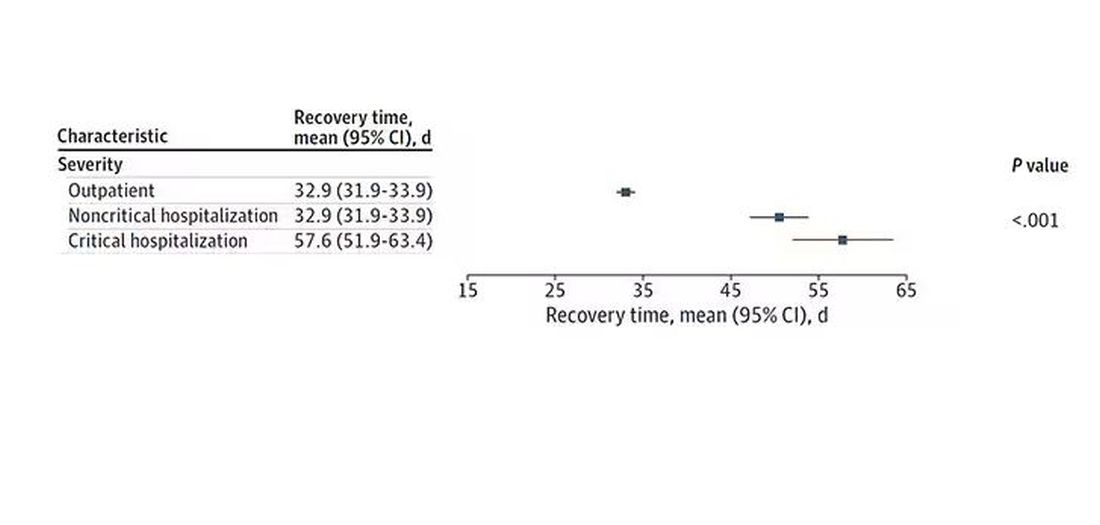
Vaccination was associated with shorter recovery times, as you can see here. 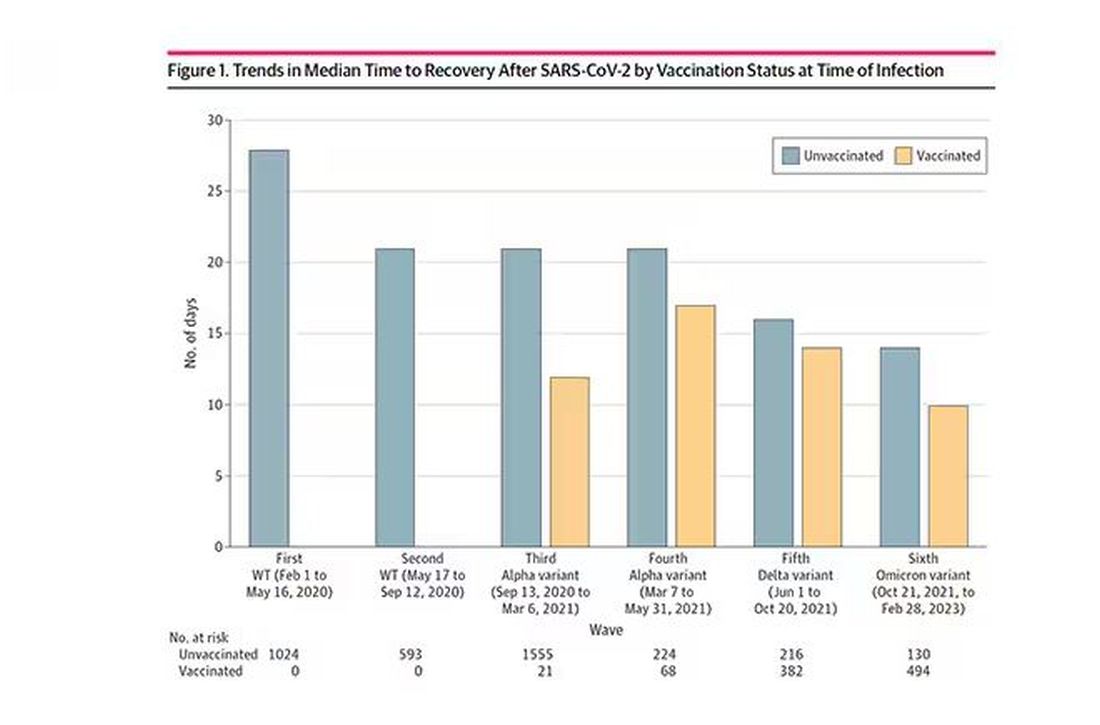
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.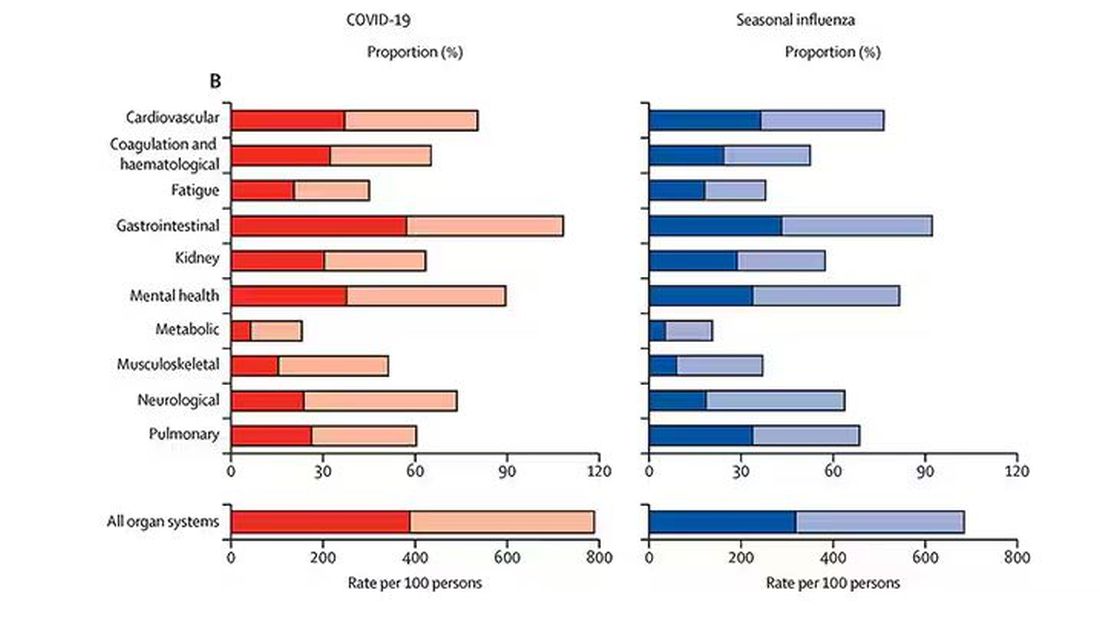
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.
Recovery times were longer for smokers, those with diabetes, and those who were obese.
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.
Vaccination was associated with shorter recovery times, as you can see here.
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.
Recovery times were longer for smokers, those with diabetes, and those who were obese.
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.
Vaccination was associated with shorter recovery times, as you can see here.
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FDA Approves New Pneumococcal Vaccine
A new vaccine to prevent invasive pneumococcal disease and pneumococcal pneumonia in adults has been approved by the Food and Drug Administration.
The injectable drug, Capvaxive (Pneumococcal 21-valent Conjugate Vaccine), protects against 22 serotypes that cause invasive pneumococcal disease in adults, the company said in a news release. These strains account for about 84% of invasive pneumococcal disease cases among adults aged 50 years or older and about 85% of these cases in adults aged 65 years or older.
The drug company said about 150,000 adults in the United States are hospitalized annually because of pneumococcal pneumonia.
“Many cases of adult disease are caused by serotypes not included in other approved pneumococcal conjugate vaccines,” Walter Orenstein, MD, a professor emeritus of medicine, epidemiology, global health, and pediatrics at Emory University, Atlanta, Georgia, and a member of Merck’s Scientific Advisory Committee, said in the release.
A draft agenda shows a Centers for Disease Control and Prevention (CDC) advisory panel will meet on June 27 to discuss the vaccine. If the committee votes to approve Capvaxive, the CDC director will decide whether to make it available across the country.
Testing showed that Capvaxive was well tolerated by people it was tested on, with the main reports being pain where they got the shot, fatigue, headaches, and muscle aches, Merck said.
The eight unique serotypes included in CAPVAXIVE will protect against invasive pneumococcal disease and pneumococcal pneumonia, not just pneumonia.
According to Reuters, Merck said Capvaxive has a wholesale acquisition price of $287 per dose, but most people will probably have access to it at no cost if the drug receives a routine CDC recommendation. Capvaxive’s main competition is expected to be Pfizer’s shot, Prevnar 20, which was approved in 2021 for use in adults aged 18 years or older, Reuters reported.
A version of this article appeared on Medscape.com.
A new vaccine to prevent invasive pneumococcal disease and pneumococcal pneumonia in adults has been approved by the Food and Drug Administration.
The injectable drug, Capvaxive (Pneumococcal 21-valent Conjugate Vaccine), protects against 22 serotypes that cause invasive pneumococcal disease in adults, the company said in a news release. These strains account for about 84% of invasive pneumococcal disease cases among adults aged 50 years or older and about 85% of these cases in adults aged 65 years or older.
The drug company said about 150,000 adults in the United States are hospitalized annually because of pneumococcal pneumonia.
“Many cases of adult disease are caused by serotypes not included in other approved pneumococcal conjugate vaccines,” Walter Orenstein, MD, a professor emeritus of medicine, epidemiology, global health, and pediatrics at Emory University, Atlanta, Georgia, and a member of Merck’s Scientific Advisory Committee, said in the release.
A draft agenda shows a Centers for Disease Control and Prevention (CDC) advisory panel will meet on June 27 to discuss the vaccine. If the committee votes to approve Capvaxive, the CDC director will decide whether to make it available across the country.
Testing showed that Capvaxive was well tolerated by people it was tested on, with the main reports being pain where they got the shot, fatigue, headaches, and muscle aches, Merck said.
The eight unique serotypes included in CAPVAXIVE will protect against invasive pneumococcal disease and pneumococcal pneumonia, not just pneumonia.
According to Reuters, Merck said Capvaxive has a wholesale acquisition price of $287 per dose, but most people will probably have access to it at no cost if the drug receives a routine CDC recommendation. Capvaxive’s main competition is expected to be Pfizer’s shot, Prevnar 20, which was approved in 2021 for use in adults aged 18 years or older, Reuters reported.
A version of this article appeared on Medscape.com.
A new vaccine to prevent invasive pneumococcal disease and pneumococcal pneumonia in adults has been approved by the Food and Drug Administration.
The injectable drug, Capvaxive (Pneumococcal 21-valent Conjugate Vaccine), protects against 22 serotypes that cause invasive pneumococcal disease in adults, the company said in a news release. These strains account for about 84% of invasive pneumococcal disease cases among adults aged 50 years or older and about 85% of these cases in adults aged 65 years or older.
The drug company said about 150,000 adults in the United States are hospitalized annually because of pneumococcal pneumonia.
“Many cases of adult disease are caused by serotypes not included in other approved pneumococcal conjugate vaccines,” Walter Orenstein, MD, a professor emeritus of medicine, epidemiology, global health, and pediatrics at Emory University, Atlanta, Georgia, and a member of Merck’s Scientific Advisory Committee, said in the release.
A draft agenda shows a Centers for Disease Control and Prevention (CDC) advisory panel will meet on June 27 to discuss the vaccine. If the committee votes to approve Capvaxive, the CDC director will decide whether to make it available across the country.
Testing showed that Capvaxive was well tolerated by people it was tested on, with the main reports being pain where they got the shot, fatigue, headaches, and muscle aches, Merck said.
The eight unique serotypes included in CAPVAXIVE will protect against invasive pneumococcal disease and pneumococcal pneumonia, not just pneumonia.
According to Reuters, Merck said Capvaxive has a wholesale acquisition price of $287 per dose, but most people will probably have access to it at no cost if the drug receives a routine CDC recommendation. Capvaxive’s main competition is expected to be Pfizer’s shot, Prevnar 20, which was approved in 2021 for use in adults aged 18 years or older, Reuters reported.
A version of this article appeared on Medscape.com.
Why Don’t Migraine Patients Seek Treatment?
SAN DIEGO — results of a recent survey showed.
Participants cited concerns that their complaints would be dismissed, a belief that healthcare providers could offer no additional help, and a prior unsuccessful clinician visit as reasons for not seeking care. Survey respondents saw an average of four clinicians before finally receiving a diagnosis.
“I was shocked that a third of patients were reluctant to seek care,” said study investigator Elizabeth K. Seng, PhD, associate professor, Ferkauf Graduate School of Psychology, Yeshiva University, and research associate professor, department of neurology, Albert Einstein College of Medicine, both in New York City. “That just shows a much higher level of medical distress than I expected from this community of people who are obviously suffering from this significant neurologic disease.”
The findings were presented at the annual meeting of the American Headache Society.
‘Significant Disease’
The study included 500 adults with migraine (mean age, 40 years) who signed up for a patient support group sponsored by Eli Lilly and completed a comprehensive survey. Respondents were mostly female, White, non-Hispanic, and well-educated individuals.
Half of participants had episodic migraines, and half had chronic migraines; 46% reported experiencing anxiety and 33% reported depression.
Almost all respondents had initiated treatment with a first calcitonin gene-related peptide (CGRP) monoclonal antibody.
“These are people who have significant enough disease that eventually they needed our top-tier preventive medication,” Dr. Seng said.
Participants answered a variety of questions pertaining to disease factors and treatment seeking. Just over 70% said they suspected they had migraine prior to diagnosis, “which means for almost 30%, it was a surprise when they received the diagnosis,” said Dr. Seng.
Nearly 40% reported that a relative first suggested they may have migraine, and 33% suspected it themselves. Only 17.4% said a healthcare provider suggested they may have the condition.
Almost a third of respondents (30.5%) reported they were reluctant to seek medical help.
“Some said they didn’t think their physician could do anything more than they were already doing for themselves, or that they’d be taken seriously, or they had had talked to doctors before and this wasn’t helpful,” said Dr. Seng.
These responses speak to the need for better public health messaging, she said. “People have this idea that migraine attacks aren’t a big deal when, in fact, these attacks area big deal and certainly deserve treatment.”
Family and friends were participants’ most common source of information on migraine, followed by the Internet. “This highlights the importance of getting migraine-related information out there so that when people talk to their friends and family, they’re receiving accurate information,” said Dr. Seng.
When asked about the path to a diagnosis, respondents reported consulting an average of four providers before receiving an accurate diagnosis. “That’s pretty remarkable,” Dr. Seng said.
An increase in frequency or severity of migraine attacks or attacks that interfered with work or school “pushed people over the threshold to seek care,” Dr. Seng said.
A subset of patients was asked about the factors they believed could help with migraine attacks. Of these, 80% cited diet and 70% stress reduction. Supplements, exercise, and relaxation techniques were cited much less frequently, said Dr. Seng.
The mean age of respondents’ migraine diagnosis was 26 years, so there was about 18 years from the time of diagnosis to participation in the survey, which could introduce recall bias. Other potential limitations included the fact that the survey had no open-ended questions, and men and ethnic minorities were underrepresented.
Useful Data
Commenting on the study findings, Nina Riggins, MD, PhD, president, Brain Performance Center and Research Institute, and director of the Headache Center at The Neuron Clinic, San Diego, California, said the survey findings are “very useful” and highlight “significant opportunities for improvement in migraine education for clinicians and people living with migraine disease.”
The fact that participants reported consulting an average of four healthcare providers before receiving an accurate diagnosis underscores the importance of providing clinicians with tools to identify migraine, she said.
This is especially relevant as new migraine therapies that may improve efficacy and have fewer side effects become available, she added.
“It would be interesting to see in future studies if migraine recognition by non-headache specialists improved after CGRP-blocking medications for migraine management became available,” said Dr. Riggins, who is cochair of the AHS First Contact program which is aimed at improving headache management in primary care.
She added that she and her colleagues will keep these survey results in mind when creating future educational materials for clinicians.
The study was supported by Eli Lily. Dr. Seng is a consultant for GlaxoSmithKline, Theranica, and Abbvie, and receives research support from the National Institutes of Health, National Center for Complementary and Integrative Health, National Institute of Neurological Disorders and Stroke, Veterans Health Administration, Cystic Fibrosis Foundation, and the American Heart Association. Dr. Riggins reported no relevant conflicts.
A version of this article appeared on Medscape.com.
SAN DIEGO — results of a recent survey showed.
Participants cited concerns that their complaints would be dismissed, a belief that healthcare providers could offer no additional help, and a prior unsuccessful clinician visit as reasons for not seeking care. Survey respondents saw an average of four clinicians before finally receiving a diagnosis.
“I was shocked that a third of patients were reluctant to seek care,” said study investigator Elizabeth K. Seng, PhD, associate professor, Ferkauf Graduate School of Psychology, Yeshiva University, and research associate professor, department of neurology, Albert Einstein College of Medicine, both in New York City. “That just shows a much higher level of medical distress than I expected from this community of people who are obviously suffering from this significant neurologic disease.”
The findings were presented at the annual meeting of the American Headache Society.
‘Significant Disease’
The study included 500 adults with migraine (mean age, 40 years) who signed up for a patient support group sponsored by Eli Lilly and completed a comprehensive survey. Respondents were mostly female, White, non-Hispanic, and well-educated individuals.
Half of participants had episodic migraines, and half had chronic migraines; 46% reported experiencing anxiety and 33% reported depression.
Almost all respondents had initiated treatment with a first calcitonin gene-related peptide (CGRP) monoclonal antibody.
“These are people who have significant enough disease that eventually they needed our top-tier preventive medication,” Dr. Seng said.
Participants answered a variety of questions pertaining to disease factors and treatment seeking. Just over 70% said they suspected they had migraine prior to diagnosis, “which means for almost 30%, it was a surprise when they received the diagnosis,” said Dr. Seng.
Nearly 40% reported that a relative first suggested they may have migraine, and 33% suspected it themselves. Only 17.4% said a healthcare provider suggested they may have the condition.
Almost a third of respondents (30.5%) reported they were reluctant to seek medical help.
“Some said they didn’t think their physician could do anything more than they were already doing for themselves, or that they’d be taken seriously, or they had had talked to doctors before and this wasn’t helpful,” said Dr. Seng.
These responses speak to the need for better public health messaging, she said. “People have this idea that migraine attacks aren’t a big deal when, in fact, these attacks area big deal and certainly deserve treatment.”
Family and friends were participants’ most common source of information on migraine, followed by the Internet. “This highlights the importance of getting migraine-related information out there so that when people talk to their friends and family, they’re receiving accurate information,” said Dr. Seng.
When asked about the path to a diagnosis, respondents reported consulting an average of four providers before receiving an accurate diagnosis. “That’s pretty remarkable,” Dr. Seng said.
An increase in frequency or severity of migraine attacks or attacks that interfered with work or school “pushed people over the threshold to seek care,” Dr. Seng said.
A subset of patients was asked about the factors they believed could help with migraine attacks. Of these, 80% cited diet and 70% stress reduction. Supplements, exercise, and relaxation techniques were cited much less frequently, said Dr. Seng.
The mean age of respondents’ migraine diagnosis was 26 years, so there was about 18 years from the time of diagnosis to participation in the survey, which could introduce recall bias. Other potential limitations included the fact that the survey had no open-ended questions, and men and ethnic minorities were underrepresented.
Useful Data
Commenting on the study findings, Nina Riggins, MD, PhD, president, Brain Performance Center and Research Institute, and director of the Headache Center at The Neuron Clinic, San Diego, California, said the survey findings are “very useful” and highlight “significant opportunities for improvement in migraine education for clinicians and people living with migraine disease.”
The fact that participants reported consulting an average of four healthcare providers before receiving an accurate diagnosis underscores the importance of providing clinicians with tools to identify migraine, she said.
This is especially relevant as new migraine therapies that may improve efficacy and have fewer side effects become available, she added.
“It would be interesting to see in future studies if migraine recognition by non-headache specialists improved after CGRP-blocking medications for migraine management became available,” said Dr. Riggins, who is cochair of the AHS First Contact program which is aimed at improving headache management in primary care.
She added that she and her colleagues will keep these survey results in mind when creating future educational materials for clinicians.
The study was supported by Eli Lily. Dr. Seng is a consultant for GlaxoSmithKline, Theranica, and Abbvie, and receives research support from the National Institutes of Health, National Center for Complementary and Integrative Health, National Institute of Neurological Disorders and Stroke, Veterans Health Administration, Cystic Fibrosis Foundation, and the American Heart Association. Dr. Riggins reported no relevant conflicts.
A version of this article appeared on Medscape.com.
SAN DIEGO — results of a recent survey showed.
Participants cited concerns that their complaints would be dismissed, a belief that healthcare providers could offer no additional help, and a prior unsuccessful clinician visit as reasons for not seeking care. Survey respondents saw an average of four clinicians before finally receiving a diagnosis.
“I was shocked that a third of patients were reluctant to seek care,” said study investigator Elizabeth K. Seng, PhD, associate professor, Ferkauf Graduate School of Psychology, Yeshiva University, and research associate professor, department of neurology, Albert Einstein College of Medicine, both in New York City. “That just shows a much higher level of medical distress than I expected from this community of people who are obviously suffering from this significant neurologic disease.”
The findings were presented at the annual meeting of the American Headache Society.
‘Significant Disease’
The study included 500 adults with migraine (mean age, 40 years) who signed up for a patient support group sponsored by Eli Lilly and completed a comprehensive survey. Respondents were mostly female, White, non-Hispanic, and well-educated individuals.
Half of participants had episodic migraines, and half had chronic migraines; 46% reported experiencing anxiety and 33% reported depression.
Almost all respondents had initiated treatment with a first calcitonin gene-related peptide (CGRP) monoclonal antibody.
“These are people who have significant enough disease that eventually they needed our top-tier preventive medication,” Dr. Seng said.
Participants answered a variety of questions pertaining to disease factors and treatment seeking. Just over 70% said they suspected they had migraine prior to diagnosis, “which means for almost 30%, it was a surprise when they received the diagnosis,” said Dr. Seng.
Nearly 40% reported that a relative first suggested they may have migraine, and 33% suspected it themselves. Only 17.4% said a healthcare provider suggested they may have the condition.
Almost a third of respondents (30.5%) reported they were reluctant to seek medical help.
“Some said they didn’t think their physician could do anything more than they were already doing for themselves, or that they’d be taken seriously, or they had had talked to doctors before and this wasn’t helpful,” said Dr. Seng.
These responses speak to the need for better public health messaging, she said. “People have this idea that migraine attacks aren’t a big deal when, in fact, these attacks area big deal and certainly deserve treatment.”
Family and friends were participants’ most common source of information on migraine, followed by the Internet. “This highlights the importance of getting migraine-related information out there so that when people talk to their friends and family, they’re receiving accurate information,” said Dr. Seng.
When asked about the path to a diagnosis, respondents reported consulting an average of four providers before receiving an accurate diagnosis. “That’s pretty remarkable,” Dr. Seng said.
An increase in frequency or severity of migraine attacks or attacks that interfered with work or school “pushed people over the threshold to seek care,” Dr. Seng said.
A subset of patients was asked about the factors they believed could help with migraine attacks. Of these, 80% cited diet and 70% stress reduction. Supplements, exercise, and relaxation techniques were cited much less frequently, said Dr. Seng.
The mean age of respondents’ migraine diagnosis was 26 years, so there was about 18 years from the time of diagnosis to participation in the survey, which could introduce recall bias. Other potential limitations included the fact that the survey had no open-ended questions, and men and ethnic minorities were underrepresented.
Useful Data
Commenting on the study findings, Nina Riggins, MD, PhD, president, Brain Performance Center and Research Institute, and director of the Headache Center at The Neuron Clinic, San Diego, California, said the survey findings are “very useful” and highlight “significant opportunities for improvement in migraine education for clinicians and people living with migraine disease.”
The fact that participants reported consulting an average of four healthcare providers before receiving an accurate diagnosis underscores the importance of providing clinicians with tools to identify migraine, she said.
This is especially relevant as new migraine therapies that may improve efficacy and have fewer side effects become available, she added.
“It would be interesting to see in future studies if migraine recognition by non-headache specialists improved after CGRP-blocking medications for migraine management became available,” said Dr. Riggins, who is cochair of the AHS First Contact program which is aimed at improving headache management in primary care.
She added that she and her colleagues will keep these survey results in mind when creating future educational materials for clinicians.
The study was supported by Eli Lily. Dr. Seng is a consultant for GlaxoSmithKline, Theranica, and Abbvie, and receives research support from the National Institutes of Health, National Center for Complementary and Integrative Health, National Institute of Neurological Disorders and Stroke, Veterans Health Administration, Cystic Fibrosis Foundation, and the American Heart Association. Dr. Riggins reported no relevant conflicts.
A version of this article appeared on Medscape.com.
FROM AHS 2024
Women with Autoimmune Liver Diseases Still Face Increased CVD Risks
WASHINGTON – , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, women with autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) appear to have higher risks than women without AIH or PBC. Those with primary sclerosing cholangitis (PSC) don’t seem to have increased risks.
“We know that cardiovascular disease remains the number one cause of death, but the mortality rate for women over the last decade has plateaued, whereas in men it’s actually declining due to interventions,” said lead author Rachel Redfield, MD, a transplant hepatology fellow at Thomas Jefferson University Hospital in Philadelphia.
“This is likely because we don’t have adequate risk stratification, especially for women,” she said. “We know that immune-mediated diseases — such as rheumatoid arthritis and psoriasis — carry a higher risk of cardiovascular disease, but there’s not a lot of data on our autoimmune liver disease patients.”

Although being a female can offer protection against some CVD risks, the atherosclerotic cardiovascular disease (ASCVD) 10-year risk score calculator recommended by the American College of Cardiology doesn’t include chronic inflammatory diseases associated with increased CVD risk, including AILD.
Dr. Redfield and colleagues conducted a multicenter, retrospective cohort study of patients with AIH, PBC, and PSC from 1999-2019. Using TriNetX data, the researchers looked at women with AILD who also had diabetes mellitus, hypertension, and hyperlipidemia, as well as a control group of men and women with these same disorders, excluding those who used biologics, immune modulators, and steroids or had other autoimmune disorders.
The research team used 1:1 propensity-score matching for women in the study group and in the control group based on age, race, ethnicity, ASCVD risk factors, and tobacco use. Women in the study group and men in the control group were matched for age, race, ethnicity, and tobacco use.
The primary outcome was summative cardiovascular risk, including unstable angina, acute myocardial infarction, presence of coronary angioplasty implant, coronary artery bypass, percutaneous coronary intervention, and cerebral infarction.
Overall, women with AIH had a significantly higher cardiovascular risk compared to women without AIH, at 25.4% versus 20.6% (P = .0007).
Specifically, women with PBC had a significantly higher cardiovascular risk compared to women without PBC, at 27.05% versus 20.9% (P < .0001).
There wasn’t a significant difference in risk between women with and without PSC, at 27.5% versus 21.8% (P = .27).
When compared to men without disease, women with AIH didn’t have a statistically significant higher risk, at 25.3% versus 24.2% (P = .44). Similarly, there didn’t appear to be a significant difference between women with PBC and men without PBC, at 26.9% versus 25.9% (P = .52), or between women with PSC and men without PSC, at 27.7% versus 26.2% (P = .78).
Dr. Redfield and colleagues then compared the ASCVD-calculated risk versus database risk, finding that in each group of women with AILD — including AIH, PBC, and PSC — the ASCVD-calculated risk was around 11%, compared with database risk scores of 25% for AIH, 27% for PBC, and 28% for PSC. These database risks appeared similar to both the ASCVD and database risk percentages for men.
“So potentially there’s an oversight in women with any kind of inflammatory disease, but specifically here, autoimmune liver diseases,” she said. “We really need to enhance our risk assessment strategies to take into account their risk and optimize patient outcomes.”
Dr. Redfield noted the limitations with using TriNetX data, including coding consistency among providers and healthcare organizations, unknown patient follow-up dates, and the inability to capture various inflammatory disease phenotypes, such as autoimmune hepatitis with multiple flares, which may be associated with higher cardiovascular risks.
As an attendee of the DDW session, Kenneth Kelson, MD, a gastroenterologist with Fremont Medical Group and Washington Hospital Healthcare System in Fremont, California, noted the importance of investigating the effects of different types of statins in these patients. Although the research team looked at top-level differences among statin users, finding that women with AILD were more likely to be on a statin, they didn’t incorporate statin therapy in the propensity-score matching model.
“Lipid-soluble statins are known to cause more liver trouble, even though it’s pretty low,” Dr. Kelson said. “Whereas the water-soluble statins have a lower incidence of liver issues.”
Dr. Redfield and Dr. Kelson reported no relevant disclosures.
WASHINGTON – , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, women with autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) appear to have higher risks than women without AIH or PBC. Those with primary sclerosing cholangitis (PSC) don’t seem to have increased risks.
“We know that cardiovascular disease remains the number one cause of death, but the mortality rate for women over the last decade has plateaued, whereas in men it’s actually declining due to interventions,” said lead author Rachel Redfield, MD, a transplant hepatology fellow at Thomas Jefferson University Hospital in Philadelphia.
“This is likely because we don’t have adequate risk stratification, especially for women,” she said. “We know that immune-mediated diseases — such as rheumatoid arthritis and psoriasis — carry a higher risk of cardiovascular disease, but there’s not a lot of data on our autoimmune liver disease patients.”
Although being a female can offer protection against some CVD risks, the atherosclerotic cardiovascular disease (ASCVD) 10-year risk score calculator recommended by the American College of Cardiology doesn’t include chronic inflammatory diseases associated with increased CVD risk, including AILD.
Dr. Redfield and colleagues conducted a multicenter, retrospective cohort study of patients with AIH, PBC, and PSC from 1999-2019. Using TriNetX data, the researchers looked at women with AILD who also had diabetes mellitus, hypertension, and hyperlipidemia, as well as a control group of men and women with these same disorders, excluding those who used biologics, immune modulators, and steroids or had other autoimmune disorders.
The research team used 1:1 propensity-score matching for women in the study group and in the control group based on age, race, ethnicity, ASCVD risk factors, and tobacco use. Women in the study group and men in the control group were matched for age, race, ethnicity, and tobacco use.
The primary outcome was summative cardiovascular risk, including unstable angina, acute myocardial infarction, presence of coronary angioplasty implant, coronary artery bypass, percutaneous coronary intervention, and cerebral infarction.
Overall, women with AIH had a significantly higher cardiovascular risk compared to women without AIH, at 25.4% versus 20.6% (P = .0007).
Specifically, women with PBC had a significantly higher cardiovascular risk compared to women without PBC, at 27.05% versus 20.9% (P < .0001).
There wasn’t a significant difference in risk between women with and without PSC, at 27.5% versus 21.8% (P = .27).
When compared to men without disease, women with AIH didn’t have a statistically significant higher risk, at 25.3% versus 24.2% (P = .44). Similarly, there didn’t appear to be a significant difference between women with PBC and men without PBC, at 26.9% versus 25.9% (P = .52), or between women with PSC and men without PSC, at 27.7% versus 26.2% (P = .78).
Dr. Redfield and colleagues then compared the ASCVD-calculated risk versus database risk, finding that in each group of women with AILD — including AIH, PBC, and PSC — the ASCVD-calculated risk was around 11%, compared with database risk scores of 25% for AIH, 27% for PBC, and 28% for PSC. These database risks appeared similar to both the ASCVD and database risk percentages for men.
“So potentially there’s an oversight in women with any kind of inflammatory disease, but specifically here, autoimmune liver diseases,” she said. “We really need to enhance our risk assessment strategies to take into account their risk and optimize patient outcomes.”
Dr. Redfield noted the limitations with using TriNetX data, including coding consistency among providers and healthcare organizations, unknown patient follow-up dates, and the inability to capture various inflammatory disease phenotypes, such as autoimmune hepatitis with multiple flares, which may be associated with higher cardiovascular risks.
As an attendee of the DDW session, Kenneth Kelson, MD, a gastroenterologist with Fremont Medical Group and Washington Hospital Healthcare System in Fremont, California, noted the importance of investigating the effects of different types of statins in these patients. Although the research team looked at top-level differences among statin users, finding that women with AILD were more likely to be on a statin, they didn’t incorporate statin therapy in the propensity-score matching model.
“Lipid-soluble statins are known to cause more liver trouble, even though it’s pretty low,” Dr. Kelson said. “Whereas the water-soluble statins have a lower incidence of liver issues.”
Dr. Redfield and Dr. Kelson reported no relevant disclosures.
WASHINGTON – , according to a study presented at the annual Digestive Disease Week® (DDW).
In particular, women with autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) appear to have higher risks than women without AIH or PBC. Those with primary sclerosing cholangitis (PSC) don’t seem to have increased risks.
“We know that cardiovascular disease remains the number one cause of death, but the mortality rate for women over the last decade has plateaued, whereas in men it’s actually declining due to interventions,” said lead author Rachel Redfield, MD, a transplant hepatology fellow at Thomas Jefferson University Hospital in Philadelphia.
“This is likely because we don’t have adequate risk stratification, especially for women,” she said. “We know that immune-mediated diseases — such as rheumatoid arthritis and psoriasis — carry a higher risk of cardiovascular disease, but there’s not a lot of data on our autoimmune liver disease patients.”
Although being a female can offer protection against some CVD risks, the atherosclerotic cardiovascular disease (ASCVD) 10-year risk score calculator recommended by the American College of Cardiology doesn’t include chronic inflammatory diseases associated with increased CVD risk, including AILD.
Dr. Redfield and colleagues conducted a multicenter, retrospective cohort study of patients with AIH, PBC, and PSC from 1999-2019. Using TriNetX data, the researchers looked at women with AILD who also had diabetes mellitus, hypertension, and hyperlipidemia, as well as a control group of men and women with these same disorders, excluding those who used biologics, immune modulators, and steroids or had other autoimmune disorders.
The research team used 1:1 propensity-score matching for women in the study group and in the control group based on age, race, ethnicity, ASCVD risk factors, and tobacco use. Women in the study group and men in the control group were matched for age, race, ethnicity, and tobacco use.
The primary outcome was summative cardiovascular risk, including unstable angina, acute myocardial infarction, presence of coronary angioplasty implant, coronary artery bypass, percutaneous coronary intervention, and cerebral infarction.
Overall, women with AIH had a significantly higher cardiovascular risk compared to women without AIH, at 25.4% versus 20.6% (P = .0007).
Specifically, women with PBC had a significantly higher cardiovascular risk compared to women without PBC, at 27.05% versus 20.9% (P < .0001).
There wasn’t a significant difference in risk between women with and without PSC, at 27.5% versus 21.8% (P = .27).
When compared to men without disease, women with AIH didn’t have a statistically significant higher risk, at 25.3% versus 24.2% (P = .44). Similarly, there didn’t appear to be a significant difference between women with PBC and men without PBC, at 26.9% versus 25.9% (P = .52), or between women with PSC and men without PSC, at 27.7% versus 26.2% (P = .78).
Dr. Redfield and colleagues then compared the ASCVD-calculated risk versus database risk, finding that in each group of women with AILD — including AIH, PBC, and PSC — the ASCVD-calculated risk was around 11%, compared with database risk scores of 25% for AIH, 27% for PBC, and 28% for PSC. These database risks appeared similar to both the ASCVD and database risk percentages for men.
“So potentially there’s an oversight in women with any kind of inflammatory disease, but specifically here, autoimmune liver diseases,” she said. “We really need to enhance our risk assessment strategies to take into account their risk and optimize patient outcomes.”
Dr. Redfield noted the limitations with using TriNetX data, including coding consistency among providers and healthcare organizations, unknown patient follow-up dates, and the inability to capture various inflammatory disease phenotypes, such as autoimmune hepatitis with multiple flares, which may be associated with higher cardiovascular risks.
As an attendee of the DDW session, Kenneth Kelson, MD, a gastroenterologist with Fremont Medical Group and Washington Hospital Healthcare System in Fremont, California, noted the importance of investigating the effects of different types of statins in these patients. Although the research team looked at top-level differences among statin users, finding that women with AILD were more likely to be on a statin, they didn’t incorporate statin therapy in the propensity-score matching model.
“Lipid-soluble statins are known to cause more liver trouble, even though it’s pretty low,” Dr. Kelson said. “Whereas the water-soluble statins have a lower incidence of liver issues.”
Dr. Redfield and Dr. Kelson reported no relevant disclosures.
FROM DDW 2024
Number of FPs, Procedures They Perform Dropping
At the same time the Medicare population is growing, the number of family practice (FP) physicians and the number of procedures they perform are decreasing, according to a new analysis in Annals of Family Medicine.
“The reasons might represent a changing scope of family practice, increasing referrals, shifting tasks to [physician assistants] and [nurse practitioners], or some combination,” wrote the authors, led by Robert McKenna, DMSc, MPH, PA-C, with Marshall B. Ketchum University, Fullerton, California. But understanding the reasons may be important to improve training programs.
The Council of Academic Family Medicine (CAFM) in 2014 addressed variability in how FPs perform procedures with a consensus statement on 44 procedures FPs should be competent to perform after a family medicine residency and 24 more for which residency programs should offer training.
Researchers wanted to see how often the procedures were being done so they performed a retrospective, observational study of the Medicare Part B cohort to understand how often FPs report CAFM-recommended procedures in an outpatient setting. They used data from 2014 to 2021, the most recent years for which data were available, and modified the list of procedures for Medicare beneficiaries to match with Current Procedural Terminology codes.
Procedures Dropped by a Third in 8 Years
For the 8 years ending in 2021, there was a 33% decrease in outpatient procedures filed and a 36% decrease in the number of FPs who filed them, according to the paper. However, the number of FPs who treat Medicare beneficiaries has remained relatively stable. Almost all procedures performed were for the skin; musculoskeletal; eyes, ears, nose, and throat; and pulmonary categories.
There was a 17% decrease in every category of modified CAFM procedures between 2014 and 2019 before the pandemic.
Concurrently, the U.S. Bureau of Labor Statistics reported a 7% decrease in clinically active FPs from 2013 to 2022; 100,940 FPs were employed clinically in 2022. The Association of American Medical Colleges estimates a shortage of 17,800-48,000 primary care physicians by 2034.
“In 2021, the number of Medicare Part B claims by FPs for all [modified] CAFM outpatient procedures was reported by 12% of these clinicians and represented less than 1% of all CPT claims submitted,” the researchers wrote.
“Meanwhile, the 17% of Americans aged [at least] 65 years is projected to represent 20% of the U.S. population by 2030,” the authors pointed out.
The reasons for the decrease in procedures need further study, the authors said. From 2010 to 2020, there was a 30% and 47% increase in the employment of PAs and NPs, respectively, across all specialties, many employed in primary care. And 42% and 56% of family physicians reported working with PAs and NPs, respectively, from 2014 to 2018, according to the paper.
One explanation is a shifting of roles. “NPs and PAs might increasingly serve as proceduralists, freeing FPs to focus on other aspects of their practice such as complex chronic disease management or annual wellness visits,” the authors wrote.
It’s also possible that more Medicare-eligible Americans are being referred to various specialists such as urologists, gynecologists, and cardiologists, they speculated, adding that, “because demographic trends show an increasingly older population, family medicine training programs might need to adjust to meet this change.”
Among the limitations of the data are that publicly available Medicare data are limited to the approximately 60% of beneficiaries who are traditional Part B enrollees. Those enrolled in Medicare Advantage plans were excluded.
The work was supported in part by a Small Research Grant from the American Academy of Physician Associates in 2022. The authors reported no relevant financial relationships.
At the same time the Medicare population is growing, the number of family practice (FP) physicians and the number of procedures they perform are decreasing, according to a new analysis in Annals of Family Medicine.
“The reasons might represent a changing scope of family practice, increasing referrals, shifting tasks to [physician assistants] and [nurse practitioners], or some combination,” wrote the authors, led by Robert McKenna, DMSc, MPH, PA-C, with Marshall B. Ketchum University, Fullerton, California. But understanding the reasons may be important to improve training programs.
The Council of Academic Family Medicine (CAFM) in 2014 addressed variability in how FPs perform procedures with a consensus statement on 44 procedures FPs should be competent to perform after a family medicine residency and 24 more for which residency programs should offer training.
Researchers wanted to see how often the procedures were being done so they performed a retrospective, observational study of the Medicare Part B cohort to understand how often FPs report CAFM-recommended procedures in an outpatient setting. They used data from 2014 to 2021, the most recent years for which data were available, and modified the list of procedures for Medicare beneficiaries to match with Current Procedural Terminology codes.
Procedures Dropped by a Third in 8 Years
For the 8 years ending in 2021, there was a 33% decrease in outpatient procedures filed and a 36% decrease in the number of FPs who filed them, according to the paper. However, the number of FPs who treat Medicare beneficiaries has remained relatively stable. Almost all procedures performed were for the skin; musculoskeletal; eyes, ears, nose, and throat; and pulmonary categories.
There was a 17% decrease in every category of modified CAFM procedures between 2014 and 2019 before the pandemic.
Concurrently, the U.S. Bureau of Labor Statistics reported a 7% decrease in clinically active FPs from 2013 to 2022; 100,940 FPs were employed clinically in 2022. The Association of American Medical Colleges estimates a shortage of 17,800-48,000 primary care physicians by 2034.
“In 2021, the number of Medicare Part B claims by FPs for all [modified] CAFM outpatient procedures was reported by 12% of these clinicians and represented less than 1% of all CPT claims submitted,” the researchers wrote.
“Meanwhile, the 17% of Americans aged [at least] 65 years is projected to represent 20% of the U.S. population by 2030,” the authors pointed out.
The reasons for the decrease in procedures need further study, the authors said. From 2010 to 2020, there was a 30% and 47% increase in the employment of PAs and NPs, respectively, across all specialties, many employed in primary care. And 42% and 56% of family physicians reported working with PAs and NPs, respectively, from 2014 to 2018, according to the paper.
One explanation is a shifting of roles. “NPs and PAs might increasingly serve as proceduralists, freeing FPs to focus on other aspects of their practice such as complex chronic disease management or annual wellness visits,” the authors wrote.
It’s also possible that more Medicare-eligible Americans are being referred to various specialists such as urologists, gynecologists, and cardiologists, they speculated, adding that, “because demographic trends show an increasingly older population, family medicine training programs might need to adjust to meet this change.”
Among the limitations of the data are that publicly available Medicare data are limited to the approximately 60% of beneficiaries who are traditional Part B enrollees. Those enrolled in Medicare Advantage plans were excluded.
The work was supported in part by a Small Research Grant from the American Academy of Physician Associates in 2022. The authors reported no relevant financial relationships.
At the same time the Medicare population is growing, the number of family practice (FP) physicians and the number of procedures they perform are decreasing, according to a new analysis in Annals of Family Medicine.
“The reasons might represent a changing scope of family practice, increasing referrals, shifting tasks to [physician assistants] and [nurse practitioners], or some combination,” wrote the authors, led by Robert McKenna, DMSc, MPH, PA-C, with Marshall B. Ketchum University, Fullerton, California. But understanding the reasons may be important to improve training programs.
The Council of Academic Family Medicine (CAFM) in 2014 addressed variability in how FPs perform procedures with a consensus statement on 44 procedures FPs should be competent to perform after a family medicine residency and 24 more for which residency programs should offer training.
Researchers wanted to see how often the procedures were being done so they performed a retrospective, observational study of the Medicare Part B cohort to understand how often FPs report CAFM-recommended procedures in an outpatient setting. They used data from 2014 to 2021, the most recent years for which data were available, and modified the list of procedures for Medicare beneficiaries to match with Current Procedural Terminology codes.
Procedures Dropped by a Third in 8 Years
For the 8 years ending in 2021, there was a 33% decrease in outpatient procedures filed and a 36% decrease in the number of FPs who filed them, according to the paper. However, the number of FPs who treat Medicare beneficiaries has remained relatively stable. Almost all procedures performed were for the skin; musculoskeletal; eyes, ears, nose, and throat; and pulmonary categories.
There was a 17% decrease in every category of modified CAFM procedures between 2014 and 2019 before the pandemic.
Concurrently, the U.S. Bureau of Labor Statistics reported a 7% decrease in clinically active FPs from 2013 to 2022; 100,940 FPs were employed clinically in 2022. The Association of American Medical Colleges estimates a shortage of 17,800-48,000 primary care physicians by 2034.
“In 2021, the number of Medicare Part B claims by FPs for all [modified] CAFM outpatient procedures was reported by 12% of these clinicians and represented less than 1% of all CPT claims submitted,” the researchers wrote.
“Meanwhile, the 17% of Americans aged [at least] 65 years is projected to represent 20% of the U.S. population by 2030,” the authors pointed out.
The reasons for the decrease in procedures need further study, the authors said. From 2010 to 2020, there was a 30% and 47% increase in the employment of PAs and NPs, respectively, across all specialties, many employed in primary care. And 42% and 56% of family physicians reported working with PAs and NPs, respectively, from 2014 to 2018, according to the paper.
One explanation is a shifting of roles. “NPs and PAs might increasingly serve as proceduralists, freeing FPs to focus on other aspects of their practice such as complex chronic disease management or annual wellness visits,” the authors wrote.
It’s also possible that more Medicare-eligible Americans are being referred to various specialists such as urologists, gynecologists, and cardiologists, they speculated, adding that, “because demographic trends show an increasingly older population, family medicine training programs might need to adjust to meet this change.”
Among the limitations of the data are that publicly available Medicare data are limited to the approximately 60% of beneficiaries who are traditional Part B enrollees. Those enrolled in Medicare Advantage plans were excluded.
The work was supported in part by a Small Research Grant from the American Academy of Physician Associates in 2022. The authors reported no relevant financial relationships.
FROM ANNALS OF FAMILY MEDICINE
Inavolisib Added to Standard Tx Shows Sustained Benefit in Advanced BC
The U.S. Food and Drug Administration (FDA) recently granted Breakthrough Therapy Designation for inavolisib in combination with palbociclib and fulvestrant based on initial results of the study presented at a December 2023 meeting. The phase 3 results showed the inavolisib-based regimen more than doubled progression-free survival (PFS) compared with the two other drugs alone as first-line treatment, researchers reported.
The expanded analysis of the trial, which was presented at the annual meeting of the American Society of Clinical Oncology, looked at additional endpoints, including PFS2 (defined as time from randomization to end of next-line treatment), time to first chemotherapy, key adverse events (AEs) and patient-reported outcomes (PROs).
“Triple combination of inavolisib, a novel PI3K inhibitor, with palbociclib and fulvestrant, resulted in significant and clinically meaningful improvement in PFS (15.0 vs 7.3 months, hazard ratio [HR] 0.43, P less than .0001),” lead investigator Dejan Juric, MD, reported at the meeting, referring to the initial results.
In additional endpoints, the inavolisib-based triplet also “sustained benefit beyond disease progression, delay in chemotherapy initiation, a manageable safety profile, prolonged time to deterioration in pain severity, and maintained quality of life, supporting the overall conclusion that this triple combination is a promising new treatment option for patients with PIK3CA-mutated HR-positive, HER2-negative metastatic breast cancer,” said the oncologist, of Massachusetts General Hospital Cancer Center and assistant professor at Harvard Medical School in Boston.
Methods and Results
The trial enrolled 325 patients whose disease had progressed during or within 12 months of adjuvant endocrine therapy (ET) with an aromatase inhibitor or tamoxifen and who had not received prior systemic therapy for recurrent LA/mBC. Patients were enrolled from December 2019 to September 2023 and randomized to either the triplet combination of inavolisib with palbociclib and fulvestrant (n = 161) or the doublet therapy of placebo with palbociclib and fulvestrant (n = 164) until discontinuation due to progressive disease or toxicity.
At the analysis cutoff date at the end of September, 57.8% of patients in the experimental triple therapy arm and 70.1% in the doublet arm had discontinued treatment. In addition, “7.5% versus 11.6% of patients died without subsequent therapy,” said Dr. Juric, and 40.4% of those in the triplet arm, and 50% in the doublet arm received subsequent therapy.
In the expanded analysis, at a median follow-up of 21.3 months, the triplet combination was associated with a PFS2 benefit of 8.9 months over the doublet – meaning patients had 24 months versus 15.1 months from randomization to end of next-line treatment (HR = 0.54). There was a similar benefit in time to first chemotherapy.
Hyperglycemia, diarrhea, rash, and mucosal effects are a known toxicity of PI3K inhibition and were experienced more frequently in the inavolisib arm compared with the placebo arm: (59% vs 9%; 48% vs 16%; 25% vs 17%; and 51% vs 27% respectively). However, “in the vast majority of patients these AEs were experienced in a grade 1 or grade 2 level,” and had resolved by the cutoff date, said Dr. Juric.
There was a 6.2% rate of inavolisib discontinuation due to AEs, but most AEs could be managed with “common approaches” such as metformin for hyperglycemia, loperamide for diarrhea, topical hydrocortisone for rash, and steroid mouthwash for stomatitis/mucosal inflammation, he added.
Patients in the triple treatment arm experienced a longer interval before pain worsened, a median of 30.9 versus 18.1 months, and patient-reported outcomes and health-related quality of life measures showed no decrease with the addition of inavolisib, Dr. Juric reported.
Rationale for Using PFS2 as Endpoint
The PFS2 endpoint has emerged with studies of targeted cancer therapies, Kevin Kalinsky, MD, director of the Glenn Family Breast Center at Winship Cancer Institute of Emory University, in Atlanta, said in an interview.
“Presenting PFS2 is not a new thing — we’ve been doing this in other breast cancer studies (of CDK4/6 inhibitors),” said Dr. Kalinsky, a coauthor of the study. “The concern is that you give a drug, and then, after that, things grow so rapidly that then you’re actually not benefiting the patient.
“If you’re giving a targeted agent in the first-line, then the biology changes after that first-line, are you really even making a difference? Or is the drug so toxic that they’re not able to tolerate a next line of treatment?” Dr. Kalinsky continued. “So that’s really the intent of PFS2. The PFS2 included the next line of treatment, so it’s really a first, and second-line representation of treatment. The study presented at ASCO was really about toxicity.”
The study was funded by F. Hoffmann-La Roche Ltd. Dr. Juric disclosed having stock and other ownership interests in PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; consulting or advisory roles with AstraZeneca, Eisai, Genentech, Lilly, MapKure, Novartis, Pfizer, PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; and research funding from Amgen, Arvinas, AstraZeneca, Blueprint Medicines, Eisai, Genentech, Infinity Pharmaceuticals, InventisBio, Novartis, Pfizer, Ribon Therapeutics, Scorpion Therapeutics, Syros Pharmaceuticals, and Takeda.
The U.S. Food and Drug Administration (FDA) recently granted Breakthrough Therapy Designation for inavolisib in combination with palbociclib and fulvestrant based on initial results of the study presented at a December 2023 meeting. The phase 3 results showed the inavolisib-based regimen more than doubled progression-free survival (PFS) compared with the two other drugs alone as first-line treatment, researchers reported.
The expanded analysis of the trial, which was presented at the annual meeting of the American Society of Clinical Oncology, looked at additional endpoints, including PFS2 (defined as time from randomization to end of next-line treatment), time to first chemotherapy, key adverse events (AEs) and patient-reported outcomes (PROs).
“Triple combination of inavolisib, a novel PI3K inhibitor, with palbociclib and fulvestrant, resulted in significant and clinically meaningful improvement in PFS (15.0 vs 7.3 months, hazard ratio [HR] 0.43, P less than .0001),” lead investigator Dejan Juric, MD, reported at the meeting, referring to the initial results.
In additional endpoints, the inavolisib-based triplet also “sustained benefit beyond disease progression, delay in chemotherapy initiation, a manageable safety profile, prolonged time to deterioration in pain severity, and maintained quality of life, supporting the overall conclusion that this triple combination is a promising new treatment option for patients with PIK3CA-mutated HR-positive, HER2-negative metastatic breast cancer,” said the oncologist, of Massachusetts General Hospital Cancer Center and assistant professor at Harvard Medical School in Boston.
Methods and Results
The trial enrolled 325 patients whose disease had progressed during or within 12 months of adjuvant endocrine therapy (ET) with an aromatase inhibitor or tamoxifen and who had not received prior systemic therapy for recurrent LA/mBC. Patients were enrolled from December 2019 to September 2023 and randomized to either the triplet combination of inavolisib with palbociclib and fulvestrant (n = 161) or the doublet therapy of placebo with palbociclib and fulvestrant (n = 164) until discontinuation due to progressive disease or toxicity.
At the analysis cutoff date at the end of September, 57.8% of patients in the experimental triple therapy arm and 70.1% in the doublet arm had discontinued treatment. In addition, “7.5% versus 11.6% of patients died without subsequent therapy,” said Dr. Juric, and 40.4% of those in the triplet arm, and 50% in the doublet arm received subsequent therapy.
In the expanded analysis, at a median follow-up of 21.3 months, the triplet combination was associated with a PFS2 benefit of 8.9 months over the doublet – meaning patients had 24 months versus 15.1 months from randomization to end of next-line treatment (HR = 0.54). There was a similar benefit in time to first chemotherapy.
Hyperglycemia, diarrhea, rash, and mucosal effects are a known toxicity of PI3K inhibition and were experienced more frequently in the inavolisib arm compared with the placebo arm: (59% vs 9%; 48% vs 16%; 25% vs 17%; and 51% vs 27% respectively). However, “in the vast majority of patients these AEs were experienced in a grade 1 or grade 2 level,” and had resolved by the cutoff date, said Dr. Juric.
There was a 6.2% rate of inavolisib discontinuation due to AEs, but most AEs could be managed with “common approaches” such as metformin for hyperglycemia, loperamide for diarrhea, topical hydrocortisone for rash, and steroid mouthwash for stomatitis/mucosal inflammation, he added.
Patients in the triple treatment arm experienced a longer interval before pain worsened, a median of 30.9 versus 18.1 months, and patient-reported outcomes and health-related quality of life measures showed no decrease with the addition of inavolisib, Dr. Juric reported.
Rationale for Using PFS2 as Endpoint
The PFS2 endpoint has emerged with studies of targeted cancer therapies, Kevin Kalinsky, MD, director of the Glenn Family Breast Center at Winship Cancer Institute of Emory University, in Atlanta, said in an interview.
“Presenting PFS2 is not a new thing — we’ve been doing this in other breast cancer studies (of CDK4/6 inhibitors),” said Dr. Kalinsky, a coauthor of the study. “The concern is that you give a drug, and then, after that, things grow so rapidly that then you’re actually not benefiting the patient.
“If you’re giving a targeted agent in the first-line, then the biology changes after that first-line, are you really even making a difference? Or is the drug so toxic that they’re not able to tolerate a next line of treatment?” Dr. Kalinsky continued. “So that’s really the intent of PFS2. The PFS2 included the next line of treatment, so it’s really a first, and second-line representation of treatment. The study presented at ASCO was really about toxicity.”
The study was funded by F. Hoffmann-La Roche Ltd. Dr. Juric disclosed having stock and other ownership interests in PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; consulting or advisory roles with AstraZeneca, Eisai, Genentech, Lilly, MapKure, Novartis, Pfizer, PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; and research funding from Amgen, Arvinas, AstraZeneca, Blueprint Medicines, Eisai, Genentech, Infinity Pharmaceuticals, InventisBio, Novartis, Pfizer, Ribon Therapeutics, Scorpion Therapeutics, Syros Pharmaceuticals, and Takeda.
The U.S. Food and Drug Administration (FDA) recently granted Breakthrough Therapy Designation for inavolisib in combination with palbociclib and fulvestrant based on initial results of the study presented at a December 2023 meeting. The phase 3 results showed the inavolisib-based regimen more than doubled progression-free survival (PFS) compared with the two other drugs alone as first-line treatment, researchers reported.
The expanded analysis of the trial, which was presented at the annual meeting of the American Society of Clinical Oncology, looked at additional endpoints, including PFS2 (defined as time from randomization to end of next-line treatment), time to first chemotherapy, key adverse events (AEs) and patient-reported outcomes (PROs).
“Triple combination of inavolisib, a novel PI3K inhibitor, with palbociclib and fulvestrant, resulted in significant and clinically meaningful improvement in PFS (15.0 vs 7.3 months, hazard ratio [HR] 0.43, P less than .0001),” lead investigator Dejan Juric, MD, reported at the meeting, referring to the initial results.
In additional endpoints, the inavolisib-based triplet also “sustained benefit beyond disease progression, delay in chemotherapy initiation, a manageable safety profile, prolonged time to deterioration in pain severity, and maintained quality of life, supporting the overall conclusion that this triple combination is a promising new treatment option for patients with PIK3CA-mutated HR-positive, HER2-negative metastatic breast cancer,” said the oncologist, of Massachusetts General Hospital Cancer Center and assistant professor at Harvard Medical School in Boston.
Methods and Results
The trial enrolled 325 patients whose disease had progressed during or within 12 months of adjuvant endocrine therapy (ET) with an aromatase inhibitor or tamoxifen and who had not received prior systemic therapy for recurrent LA/mBC. Patients were enrolled from December 2019 to September 2023 and randomized to either the triplet combination of inavolisib with palbociclib and fulvestrant (n = 161) or the doublet therapy of placebo with palbociclib and fulvestrant (n = 164) until discontinuation due to progressive disease or toxicity.
At the analysis cutoff date at the end of September, 57.8% of patients in the experimental triple therapy arm and 70.1% in the doublet arm had discontinued treatment. In addition, “7.5% versus 11.6% of patients died without subsequent therapy,” said Dr. Juric, and 40.4% of those in the triplet arm, and 50% in the doublet arm received subsequent therapy.
In the expanded analysis, at a median follow-up of 21.3 months, the triplet combination was associated with a PFS2 benefit of 8.9 months over the doublet – meaning patients had 24 months versus 15.1 months from randomization to end of next-line treatment (HR = 0.54). There was a similar benefit in time to first chemotherapy.
Hyperglycemia, diarrhea, rash, and mucosal effects are a known toxicity of PI3K inhibition and were experienced more frequently in the inavolisib arm compared with the placebo arm: (59% vs 9%; 48% vs 16%; 25% vs 17%; and 51% vs 27% respectively). However, “in the vast majority of patients these AEs were experienced in a grade 1 or grade 2 level,” and had resolved by the cutoff date, said Dr. Juric.
There was a 6.2% rate of inavolisib discontinuation due to AEs, but most AEs could be managed with “common approaches” such as metformin for hyperglycemia, loperamide for diarrhea, topical hydrocortisone for rash, and steroid mouthwash for stomatitis/mucosal inflammation, he added.
Patients in the triple treatment arm experienced a longer interval before pain worsened, a median of 30.9 versus 18.1 months, and patient-reported outcomes and health-related quality of life measures showed no decrease with the addition of inavolisib, Dr. Juric reported.
Rationale for Using PFS2 as Endpoint
The PFS2 endpoint has emerged with studies of targeted cancer therapies, Kevin Kalinsky, MD, director of the Glenn Family Breast Center at Winship Cancer Institute of Emory University, in Atlanta, said in an interview.
“Presenting PFS2 is not a new thing — we’ve been doing this in other breast cancer studies (of CDK4/6 inhibitors),” said Dr. Kalinsky, a coauthor of the study. “The concern is that you give a drug, and then, after that, things grow so rapidly that then you’re actually not benefiting the patient.
“If you’re giving a targeted agent in the first-line, then the biology changes after that first-line, are you really even making a difference? Or is the drug so toxic that they’re not able to tolerate a next line of treatment?” Dr. Kalinsky continued. “So that’s really the intent of PFS2. The PFS2 included the next line of treatment, so it’s really a first, and second-line representation of treatment. The study presented at ASCO was really about toxicity.”
The study was funded by F. Hoffmann-La Roche Ltd. Dr. Juric disclosed having stock and other ownership interests in PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; consulting or advisory roles with AstraZeneca, Eisai, Genentech, Lilly, MapKure, Novartis, Pfizer, PIC Therapeutics, Relay Therapeutics, and Vibliome Therapeutics; and research funding from Amgen, Arvinas, AstraZeneca, Blueprint Medicines, Eisai, Genentech, Infinity Pharmaceuticals, InventisBio, Novartis, Pfizer, Ribon Therapeutics, Scorpion Therapeutics, Syros Pharmaceuticals, and Takeda.
FROM ASCO 2024
FDA Expands Pembrolizumab Approval for Endometrial Cancer
The Food and Drug Administration has expanded the indication for pembrolizumab (Keytruda, Merck) to include the use of the targeted immunotherapy agent plus chemotherapy followed by single-agent pembrolizumab in adults with primary advanced or recurrent endometrial cancer.
Approval in this setting was granted following priority review and was based on efficacy demonstrated in the randomized, placebo-controlled, phase 3 KEYNOTE-868/NRG-GY018 trial. The multicenter trial showed improved progression-free survival (PFS) with chemotherapy plus pembrolizumab versus chemotherapy plus placebo in patients with stage 3 or 4 disease or stage IVB recurrent disease in two cohorts: 222 patients with mismatch repair (MMR) deficiency, and 588 patients with MMR proficiency.
Among the MMR-deficient patients, median PFS was not reached in the treatment arm and was 6.5 months in the control arm (hazard ratio, 0.30). Among the MMR-proficient patients, the median PFS was 11.1 versus 8.5 months in the study arms, respectively (HR, 0.60), according to an FDA press release.
Patients in both cohorts were randomized 1:1 to receive 200 mg of either pembrolizumab or placebo every 3 weeks, followed by paclitaxel at a dose of 175 mg/m2 and carboplatin at a dose of AUC 5 mg/mL/min for six cycles and then 400 mg of pembrolizumab or placebo every 6 weeks for up to 14 cycles.
“Adverse reactions associated with pembrolizumab and chemotherapy were generally similar to those previously reported for pembrolizumab or chemotherapy with the exception of a higher incidence of rash,” the FDA noted.
According to the full prescribing information for pembrolizumab, the recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or for up to 24 months.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has expanded the indication for pembrolizumab (Keytruda, Merck) to include the use of the targeted immunotherapy agent plus chemotherapy followed by single-agent pembrolizumab in adults with primary advanced or recurrent endometrial cancer.
Approval in this setting was granted following priority review and was based on efficacy demonstrated in the randomized, placebo-controlled, phase 3 KEYNOTE-868/NRG-GY018 trial. The multicenter trial showed improved progression-free survival (PFS) with chemotherapy plus pembrolizumab versus chemotherapy plus placebo in patients with stage 3 or 4 disease or stage IVB recurrent disease in two cohorts: 222 patients with mismatch repair (MMR) deficiency, and 588 patients with MMR proficiency.
Among the MMR-deficient patients, median PFS was not reached in the treatment arm and was 6.5 months in the control arm (hazard ratio, 0.30). Among the MMR-proficient patients, the median PFS was 11.1 versus 8.5 months in the study arms, respectively (HR, 0.60), according to an FDA press release.
Patients in both cohorts were randomized 1:1 to receive 200 mg of either pembrolizumab or placebo every 3 weeks, followed by paclitaxel at a dose of 175 mg/m2 and carboplatin at a dose of AUC 5 mg/mL/min for six cycles and then 400 mg of pembrolizumab or placebo every 6 weeks for up to 14 cycles.
“Adverse reactions associated with pembrolizumab and chemotherapy were generally similar to those previously reported for pembrolizumab or chemotherapy with the exception of a higher incidence of rash,” the FDA noted.
According to the full prescribing information for pembrolizumab, the recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or for up to 24 months.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has expanded the indication for pembrolizumab (Keytruda, Merck) to include the use of the targeted immunotherapy agent plus chemotherapy followed by single-agent pembrolizumab in adults with primary advanced or recurrent endometrial cancer.
Approval in this setting was granted following priority review and was based on efficacy demonstrated in the randomized, placebo-controlled, phase 3 KEYNOTE-868/NRG-GY018 trial. The multicenter trial showed improved progression-free survival (PFS) with chemotherapy plus pembrolizumab versus chemotherapy plus placebo in patients with stage 3 or 4 disease or stage IVB recurrent disease in two cohorts: 222 patients with mismatch repair (MMR) deficiency, and 588 patients with MMR proficiency.
Among the MMR-deficient patients, median PFS was not reached in the treatment arm and was 6.5 months in the control arm (hazard ratio, 0.30). Among the MMR-proficient patients, the median PFS was 11.1 versus 8.5 months in the study arms, respectively (HR, 0.60), according to an FDA press release.
Patients in both cohorts were randomized 1:1 to receive 200 mg of either pembrolizumab or placebo every 3 weeks, followed by paclitaxel at a dose of 175 mg/m2 and carboplatin at a dose of AUC 5 mg/mL/min for six cycles and then 400 mg of pembrolizumab or placebo every 6 weeks for up to 14 cycles.
“Adverse reactions associated with pembrolizumab and chemotherapy were generally similar to those previously reported for pembrolizumab or chemotherapy with the exception of a higher incidence of rash,” the FDA noted.
According to the full prescribing information for pembrolizumab, the recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or for up to 24 months.
A version of this article first appeared on Medscape.com.