User login
Obesity and Pregnancy
Do Artificial Sweeteners Really Help People With Diabetes?
It seems intuitive that, because people with type 2 diabetes (T2D) generally need to avoid sugar, clinicians should recommend eating foods and using recipes containing artificial sweeteners such as sucralose instead.
Splenda, which produces sucralose and other non-sugar sweeteners (NSS), is a sponsor of the American Diabetes Association (ADA) Diabetes Food Hub. Earlier in 2024, the ADA settled a lawsuit regarding its former director of nutrition’s refusal to approve recipes containing sucralose (Splenda), which she believed “flew in the face of the ADA’s mission.”
“There’s not a lot of evidence that sweeteners like sucralose provide significant benefits, especially over the long term,” said Susan Swithers, PhD, professor, department of psychological sciences and associate dean for faculty affairs at Purdue University, West Lafayette, Indiana.
Dr. Swithers authored an article several years ago cautioning that consuming nonnutritive sweeteners in beverages not only fails to prevent disease but also is associated with an increase in risks for the same health outcomes associated with sugar-sweetened beverages, including T2D, cardiovascular disease, hypertension, and stroke.
“At this point, we have pretty good evidence that these chemicals that were once touted as being completely inert are, in fact, not inert,” she said. “We know that they’re unlikely to be toxic in the short term, but they are not benign, and they have consequences. Right now, we have little understanding of the outcomes of consumption of these products chronically.”
What the Science Says
In 2023, the World Health Organization (WHO) released a guideline on NSS that recommended against their use for weight control or to reduce the risk for noncommunicable diseases.
The systematic review and meta-analysis upon which the guideline is based found that high intakes of NSS were associated with increases in body mass index and, as Dr. Swithers found, risks of developing T2D, cardiovascular events, and any type of stroke, as well as hypertension, bladder cancer, and all-cause mortality.
In a press release announcing the guideline, Francesco Branca, WHO director for Nutrition and Food Safety, said, “NSS are not essential dietary factors and have no nutritional value. People should reduce the sweetness of the diet altogether, starting early in life, to improve their health.”
The “common” NSS named by WHO included sucralose, as well as acesulfame K, aspartame, advantame, cyclamates, neotame, saccharin, stevia, and stevia derivatives.
If NSS consumption can increase T2D risk, what about people who already have T2D?
Some research suggests that NSS may affect people with and without T2D differently, said Dr. Swithers. For example, one small study showed that sucralose enhanced glucagon-like peptide 1 release and lowered blood glucose in healthy patients but not in patients with newly diagnosed T2D.
Similarly, Jotham Suez, PhD, an assistant professor in the department of molecular microbiology and immunology at Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland, said in an interview that his group “showed for the first time in 2014 that disruption of the microbiome by artificial sweeteners is causally linked to disrupted glycemic control.”
Recently, the team studied the impact of sucralose, aspartame, saccharin, and stevia in healthy adults and “were surprised to discover that all four sweeteners altered gut bacteria and the molecules they secrete,” he said. However, subsequent glucose tolerance tests in healthy humans showed varying results, “suggesting that human microbiome responses to the nonnutritive sweeteners we assessed are highly personalized and may lead to glycemic alterations in some, but not all, consumers depending on their microbes and the sweeteners they consume.”
Nevertheless, a recent review led by researchers in Mexico concluded that sucralose consumption “is associated with various adverse health effects. Despite being considered safe following previous studies, recent research suggests possible links to systemic inflammation, metabolic diseases, disruptions in gut microbiota, liver damage, and toxic effects at the cellular level.”
In addition, they wrote, “it is crucial to highlight the persistence of sucralose in the body, its ability to cross the placenta, and its presence in breast milk, raising concerns about prenatal and neonatal exposure.”
Sabyasachi Sen, MD, a professor of biochemistry and molecular medicine at George Washington School of Medicine & Health Sciences, Washington, DC, has led and coauthored preclinical and clinical studies demonstrating the potential ill effects of sucralose and other artificial sweeteners. One showed that sucralose and acesulfame potassium–containing diet soda altered microbial taxa in two pilot studies in healthy young adults; another showed a connection between artificial sweeteners and inflammation.
But Dr. Sen’s current work is directed at his team’s finding that sucralose promotes the accumulation of reactive oxygen species and adipogenesis in human stem cells, he said in an interview. “It is essentially an additive that is clearly harmful to cells. Our concern is that stem cells are going to remain in the system for a long period of time. If it is causing inflammation in these cells, then that may lead to adverse outcomes.”
Ruchi Mathur, MD, director of the Diabetes Outpatient Treatment & Education Center at Cedars-Sinai in Los Angeles, California, is the principal investigator of a recent study suggesting that non-aspartame NSS and aspartame alone may alter the structure and function of the stool and duodenal microbiomes. Levels of circulating inflammatory markers were also altered in participants who consumed artificial sweeteners, compared with control participants who did not.
In addition to these potential adverse effects, “we have to think about the fact that patients with diabetes often have other comorbidities like obesity and are at higher risk for cardiovascular disease and other conditions,” she said in an interview. “If you’re taking a patient who’s already at risk for those things and you don’t have a detailed discussion with them about pros and cons, you’re doing them a disservice.”
Industry Interests
Addressing the largely negative but varying findings, Dr. Swithers said, “one of the difficulties with getting clear answers about the science is that the food and beverage industry has an interest in confusing the picture. If people are selling or using a product, the best thing is for them not have a clear reason to change their behavior. All that needs to happen is for them to be able say, ‘well, it’s not clear, and we don’t really know what’s going on, so I’m just going to keep doing what I’m doing.’ Then the producers and sellers of that product have won.”
“As Upton Sinclair said,” she added, “‘It is difficult to get a man to understand something when his salary depends on his not understanding it.’ When organizations like ADA appear to be promoting a product like sucralose, and they’re not always being clear about disclosing the funding, I think that’s problematic.”
In fact, some recipes in the ADA’s hub that contain Splenda are marked sponsored, such as the four-ingredient peanut butter cookies; others, such as gluten-free brownies, are not — even though the latter contains “1/4 cup plus 1 tbsp” of Splenda Sugar Blend (Splenda produces several nonnutritive sweeteners, not all of which contain sucralose). Splenda is a sponsor of the ADA’s hub.
Consume in Moderation?
Regarding the use of Splenda products, Robert Gabbay, MD, PhD, the ADA’s chief scientific and medical officer, said in an interview that “some people with diabetes are accustomed to regularly consuming sugar-sweetened products, which can make management of their diabetes more challenging. As highlighted in the ADA’s Standards of Care, nonnutritive sweeteners (containing few or no calories) may be an acceptable substitute for sweeteners that contain sugar and calories when consumed in moderation. By providing a diabetes-friendly way to prepare foods people are used to eating, we can meet people where they are in offering support to effectively manage their diabetes.”
Of course, “moderation” means different things to different people. “With sucralose in particular, you can bake with it, you can cook with it, and beverages and packaged foods contain it, so it’s easy to end up overconsuming foods that may be fine if they’re occasional treats but aren’t healthy choices to have every single day,” Dr. Swithers said. “If you’re having a cookie containing sucralose once a week, it’s not a big deal, but if you’re having a cookie or a brownie every day, that’s something different.”
“I think ‘everything in moderation’ is a very reasonable approach here,” Dr. Mathur said. “Anything too much is probably not good, and that includes sweeteners like sucralose and others.”
Dr. Suez, whose team is currently exploring the mechanisms through which gut bacteria interact with nonnutritive sweeteners in the pathogenesis of cardiometabolic diseases, was more circumspect.
“We believe that additional, long-term, and non–industry-sponsored studies in humans are needed before we can make a recommendation in favor or against the use of nonnutritive sweeteners,” he said.
“However, our results demonstrating that nonnutritive sweeteners are not inert, when taken together with a growing body of evidence on potential harms of these sweeteners, merit caution until additional studies are completed,” he added. “Our findings do not imply in any way that sugar consumption, shown to be harmful to human health in many studies, is superior to nonnutritive sweeteners. Sugar consumption should be minimized, especially in individuals with obesity or diabetes. Of all the options, unsweetened beverages, specifically water, seem to be the safest and best options.”
Dr. Sen, who also “tries to convince patients to have sparkling or cold bottled water,” instead of artificially sweetened soda, agreed. “If a diabetes patient is trying to choose between sugar and sucralose, I’m not sure which one is worse.”
Dr. Swithers, Dr. Mathur, Dr. Sen, and Dr. Suez declared no competing interests.
A version of this article first appeared on Medscape.com.
It seems intuitive that, because people with type 2 diabetes (T2D) generally need to avoid sugar, clinicians should recommend eating foods and using recipes containing artificial sweeteners such as sucralose instead.
Splenda, which produces sucralose and other non-sugar sweeteners (NSS), is a sponsor of the American Diabetes Association (ADA) Diabetes Food Hub. Earlier in 2024, the ADA settled a lawsuit regarding its former director of nutrition’s refusal to approve recipes containing sucralose (Splenda), which she believed “flew in the face of the ADA’s mission.”
“There’s not a lot of evidence that sweeteners like sucralose provide significant benefits, especially over the long term,” said Susan Swithers, PhD, professor, department of psychological sciences and associate dean for faculty affairs at Purdue University, West Lafayette, Indiana.
Dr. Swithers authored an article several years ago cautioning that consuming nonnutritive sweeteners in beverages not only fails to prevent disease but also is associated with an increase in risks for the same health outcomes associated with sugar-sweetened beverages, including T2D, cardiovascular disease, hypertension, and stroke.
“At this point, we have pretty good evidence that these chemicals that were once touted as being completely inert are, in fact, not inert,” she said. “We know that they’re unlikely to be toxic in the short term, but they are not benign, and they have consequences. Right now, we have little understanding of the outcomes of consumption of these products chronically.”
What the Science Says
In 2023, the World Health Organization (WHO) released a guideline on NSS that recommended against their use for weight control or to reduce the risk for noncommunicable diseases.
The systematic review and meta-analysis upon which the guideline is based found that high intakes of NSS were associated with increases in body mass index and, as Dr. Swithers found, risks of developing T2D, cardiovascular events, and any type of stroke, as well as hypertension, bladder cancer, and all-cause mortality.
In a press release announcing the guideline, Francesco Branca, WHO director for Nutrition and Food Safety, said, “NSS are not essential dietary factors and have no nutritional value. People should reduce the sweetness of the diet altogether, starting early in life, to improve their health.”
The “common” NSS named by WHO included sucralose, as well as acesulfame K, aspartame, advantame, cyclamates, neotame, saccharin, stevia, and stevia derivatives.
If NSS consumption can increase T2D risk, what about people who already have T2D?
Some research suggests that NSS may affect people with and without T2D differently, said Dr. Swithers. For example, one small study showed that sucralose enhanced glucagon-like peptide 1 release and lowered blood glucose in healthy patients but not in patients with newly diagnosed T2D.
Similarly, Jotham Suez, PhD, an assistant professor in the department of molecular microbiology and immunology at Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland, said in an interview that his group “showed for the first time in 2014 that disruption of the microbiome by artificial sweeteners is causally linked to disrupted glycemic control.”
Recently, the team studied the impact of sucralose, aspartame, saccharin, and stevia in healthy adults and “were surprised to discover that all four sweeteners altered gut bacteria and the molecules they secrete,” he said. However, subsequent glucose tolerance tests in healthy humans showed varying results, “suggesting that human microbiome responses to the nonnutritive sweeteners we assessed are highly personalized and may lead to glycemic alterations in some, but not all, consumers depending on their microbes and the sweeteners they consume.”
Nevertheless, a recent review led by researchers in Mexico concluded that sucralose consumption “is associated with various adverse health effects. Despite being considered safe following previous studies, recent research suggests possible links to systemic inflammation, metabolic diseases, disruptions in gut microbiota, liver damage, and toxic effects at the cellular level.”
In addition, they wrote, “it is crucial to highlight the persistence of sucralose in the body, its ability to cross the placenta, and its presence in breast milk, raising concerns about prenatal and neonatal exposure.”
Sabyasachi Sen, MD, a professor of biochemistry and molecular medicine at George Washington School of Medicine & Health Sciences, Washington, DC, has led and coauthored preclinical and clinical studies demonstrating the potential ill effects of sucralose and other artificial sweeteners. One showed that sucralose and acesulfame potassium–containing diet soda altered microbial taxa in two pilot studies in healthy young adults; another showed a connection between artificial sweeteners and inflammation.
But Dr. Sen’s current work is directed at his team’s finding that sucralose promotes the accumulation of reactive oxygen species and adipogenesis in human stem cells, he said in an interview. “It is essentially an additive that is clearly harmful to cells. Our concern is that stem cells are going to remain in the system for a long period of time. If it is causing inflammation in these cells, then that may lead to adverse outcomes.”
Ruchi Mathur, MD, director of the Diabetes Outpatient Treatment & Education Center at Cedars-Sinai in Los Angeles, California, is the principal investigator of a recent study suggesting that non-aspartame NSS and aspartame alone may alter the structure and function of the stool and duodenal microbiomes. Levels of circulating inflammatory markers were also altered in participants who consumed artificial sweeteners, compared with control participants who did not.
In addition to these potential adverse effects, “we have to think about the fact that patients with diabetes often have other comorbidities like obesity and are at higher risk for cardiovascular disease and other conditions,” she said in an interview. “If you’re taking a patient who’s already at risk for those things and you don’t have a detailed discussion with them about pros and cons, you’re doing them a disservice.”
Industry Interests
Addressing the largely negative but varying findings, Dr. Swithers said, “one of the difficulties with getting clear answers about the science is that the food and beverage industry has an interest in confusing the picture. If people are selling or using a product, the best thing is for them not have a clear reason to change their behavior. All that needs to happen is for them to be able say, ‘well, it’s not clear, and we don’t really know what’s going on, so I’m just going to keep doing what I’m doing.’ Then the producers and sellers of that product have won.”
“As Upton Sinclair said,” she added, “‘It is difficult to get a man to understand something when his salary depends on his not understanding it.’ When organizations like ADA appear to be promoting a product like sucralose, and they’re not always being clear about disclosing the funding, I think that’s problematic.”
In fact, some recipes in the ADA’s hub that contain Splenda are marked sponsored, such as the four-ingredient peanut butter cookies; others, such as gluten-free brownies, are not — even though the latter contains “1/4 cup plus 1 tbsp” of Splenda Sugar Blend (Splenda produces several nonnutritive sweeteners, not all of which contain sucralose). Splenda is a sponsor of the ADA’s hub.
Consume in Moderation?
Regarding the use of Splenda products, Robert Gabbay, MD, PhD, the ADA’s chief scientific and medical officer, said in an interview that “some people with diabetes are accustomed to regularly consuming sugar-sweetened products, which can make management of their diabetes more challenging. As highlighted in the ADA’s Standards of Care, nonnutritive sweeteners (containing few or no calories) may be an acceptable substitute for sweeteners that contain sugar and calories when consumed in moderation. By providing a diabetes-friendly way to prepare foods people are used to eating, we can meet people where they are in offering support to effectively manage their diabetes.”
Of course, “moderation” means different things to different people. “With sucralose in particular, you can bake with it, you can cook with it, and beverages and packaged foods contain it, so it’s easy to end up overconsuming foods that may be fine if they’re occasional treats but aren’t healthy choices to have every single day,” Dr. Swithers said. “If you’re having a cookie containing sucralose once a week, it’s not a big deal, but if you’re having a cookie or a brownie every day, that’s something different.”
“I think ‘everything in moderation’ is a very reasonable approach here,” Dr. Mathur said. “Anything too much is probably not good, and that includes sweeteners like sucralose and others.”
Dr. Suez, whose team is currently exploring the mechanisms through which gut bacteria interact with nonnutritive sweeteners in the pathogenesis of cardiometabolic diseases, was more circumspect.
“We believe that additional, long-term, and non–industry-sponsored studies in humans are needed before we can make a recommendation in favor or against the use of nonnutritive sweeteners,” he said.
“However, our results demonstrating that nonnutritive sweeteners are not inert, when taken together with a growing body of evidence on potential harms of these sweeteners, merit caution until additional studies are completed,” he added. “Our findings do not imply in any way that sugar consumption, shown to be harmful to human health in many studies, is superior to nonnutritive sweeteners. Sugar consumption should be minimized, especially in individuals with obesity or diabetes. Of all the options, unsweetened beverages, specifically water, seem to be the safest and best options.”
Dr. Sen, who also “tries to convince patients to have sparkling or cold bottled water,” instead of artificially sweetened soda, agreed. “If a diabetes patient is trying to choose between sugar and sucralose, I’m not sure which one is worse.”
Dr. Swithers, Dr. Mathur, Dr. Sen, and Dr. Suez declared no competing interests.
A version of this article first appeared on Medscape.com.
It seems intuitive that, because people with type 2 diabetes (T2D) generally need to avoid sugar, clinicians should recommend eating foods and using recipes containing artificial sweeteners such as sucralose instead.
Splenda, which produces sucralose and other non-sugar sweeteners (NSS), is a sponsor of the American Diabetes Association (ADA) Diabetes Food Hub. Earlier in 2024, the ADA settled a lawsuit regarding its former director of nutrition’s refusal to approve recipes containing sucralose (Splenda), which she believed “flew in the face of the ADA’s mission.”
“There’s not a lot of evidence that sweeteners like sucralose provide significant benefits, especially over the long term,” said Susan Swithers, PhD, professor, department of psychological sciences and associate dean for faculty affairs at Purdue University, West Lafayette, Indiana.
Dr. Swithers authored an article several years ago cautioning that consuming nonnutritive sweeteners in beverages not only fails to prevent disease but also is associated with an increase in risks for the same health outcomes associated with sugar-sweetened beverages, including T2D, cardiovascular disease, hypertension, and stroke.
“At this point, we have pretty good evidence that these chemicals that were once touted as being completely inert are, in fact, not inert,” she said. “We know that they’re unlikely to be toxic in the short term, but they are not benign, and they have consequences. Right now, we have little understanding of the outcomes of consumption of these products chronically.”
What the Science Says
In 2023, the World Health Organization (WHO) released a guideline on NSS that recommended against their use for weight control or to reduce the risk for noncommunicable diseases.
The systematic review and meta-analysis upon which the guideline is based found that high intakes of NSS were associated with increases in body mass index and, as Dr. Swithers found, risks of developing T2D, cardiovascular events, and any type of stroke, as well as hypertension, bladder cancer, and all-cause mortality.
In a press release announcing the guideline, Francesco Branca, WHO director for Nutrition and Food Safety, said, “NSS are not essential dietary factors and have no nutritional value. People should reduce the sweetness of the diet altogether, starting early in life, to improve their health.”
The “common” NSS named by WHO included sucralose, as well as acesulfame K, aspartame, advantame, cyclamates, neotame, saccharin, stevia, and stevia derivatives.
If NSS consumption can increase T2D risk, what about people who already have T2D?
Some research suggests that NSS may affect people with and without T2D differently, said Dr. Swithers. For example, one small study showed that sucralose enhanced glucagon-like peptide 1 release and lowered blood glucose in healthy patients but not in patients with newly diagnosed T2D.
Similarly, Jotham Suez, PhD, an assistant professor in the department of molecular microbiology and immunology at Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland, said in an interview that his group “showed for the first time in 2014 that disruption of the microbiome by artificial sweeteners is causally linked to disrupted glycemic control.”
Recently, the team studied the impact of sucralose, aspartame, saccharin, and stevia in healthy adults and “were surprised to discover that all four sweeteners altered gut bacteria and the molecules they secrete,” he said. However, subsequent glucose tolerance tests in healthy humans showed varying results, “suggesting that human microbiome responses to the nonnutritive sweeteners we assessed are highly personalized and may lead to glycemic alterations in some, but not all, consumers depending on their microbes and the sweeteners they consume.”
Nevertheless, a recent review led by researchers in Mexico concluded that sucralose consumption “is associated with various adverse health effects. Despite being considered safe following previous studies, recent research suggests possible links to systemic inflammation, metabolic diseases, disruptions in gut microbiota, liver damage, and toxic effects at the cellular level.”
In addition, they wrote, “it is crucial to highlight the persistence of sucralose in the body, its ability to cross the placenta, and its presence in breast milk, raising concerns about prenatal and neonatal exposure.”
Sabyasachi Sen, MD, a professor of biochemistry and molecular medicine at George Washington School of Medicine & Health Sciences, Washington, DC, has led and coauthored preclinical and clinical studies demonstrating the potential ill effects of sucralose and other artificial sweeteners. One showed that sucralose and acesulfame potassium–containing diet soda altered microbial taxa in two pilot studies in healthy young adults; another showed a connection between artificial sweeteners and inflammation.
But Dr. Sen’s current work is directed at his team’s finding that sucralose promotes the accumulation of reactive oxygen species and adipogenesis in human stem cells, he said in an interview. “It is essentially an additive that is clearly harmful to cells. Our concern is that stem cells are going to remain in the system for a long period of time. If it is causing inflammation in these cells, then that may lead to adverse outcomes.”
Ruchi Mathur, MD, director of the Diabetes Outpatient Treatment & Education Center at Cedars-Sinai in Los Angeles, California, is the principal investigator of a recent study suggesting that non-aspartame NSS and aspartame alone may alter the structure and function of the stool and duodenal microbiomes. Levels of circulating inflammatory markers were also altered in participants who consumed artificial sweeteners, compared with control participants who did not.
In addition to these potential adverse effects, “we have to think about the fact that patients with diabetes often have other comorbidities like obesity and are at higher risk for cardiovascular disease and other conditions,” she said in an interview. “If you’re taking a patient who’s already at risk for those things and you don’t have a detailed discussion with them about pros and cons, you’re doing them a disservice.”
Industry Interests
Addressing the largely negative but varying findings, Dr. Swithers said, “one of the difficulties with getting clear answers about the science is that the food and beverage industry has an interest in confusing the picture. If people are selling or using a product, the best thing is for them not have a clear reason to change their behavior. All that needs to happen is for them to be able say, ‘well, it’s not clear, and we don’t really know what’s going on, so I’m just going to keep doing what I’m doing.’ Then the producers and sellers of that product have won.”
“As Upton Sinclair said,” she added, “‘It is difficult to get a man to understand something when his salary depends on his not understanding it.’ When organizations like ADA appear to be promoting a product like sucralose, and they’re not always being clear about disclosing the funding, I think that’s problematic.”
In fact, some recipes in the ADA’s hub that contain Splenda are marked sponsored, such as the four-ingredient peanut butter cookies; others, such as gluten-free brownies, are not — even though the latter contains “1/4 cup plus 1 tbsp” of Splenda Sugar Blend (Splenda produces several nonnutritive sweeteners, not all of which contain sucralose). Splenda is a sponsor of the ADA’s hub.
Consume in Moderation?
Regarding the use of Splenda products, Robert Gabbay, MD, PhD, the ADA’s chief scientific and medical officer, said in an interview that “some people with diabetes are accustomed to regularly consuming sugar-sweetened products, which can make management of their diabetes more challenging. As highlighted in the ADA’s Standards of Care, nonnutritive sweeteners (containing few or no calories) may be an acceptable substitute for sweeteners that contain sugar and calories when consumed in moderation. By providing a diabetes-friendly way to prepare foods people are used to eating, we can meet people where they are in offering support to effectively manage their diabetes.”
Of course, “moderation” means different things to different people. “With sucralose in particular, you can bake with it, you can cook with it, and beverages and packaged foods contain it, so it’s easy to end up overconsuming foods that may be fine if they’re occasional treats but aren’t healthy choices to have every single day,” Dr. Swithers said. “If you’re having a cookie containing sucralose once a week, it’s not a big deal, but if you’re having a cookie or a brownie every day, that’s something different.”
“I think ‘everything in moderation’ is a very reasonable approach here,” Dr. Mathur said. “Anything too much is probably not good, and that includes sweeteners like sucralose and others.”
Dr. Suez, whose team is currently exploring the mechanisms through which gut bacteria interact with nonnutritive sweeteners in the pathogenesis of cardiometabolic diseases, was more circumspect.
“We believe that additional, long-term, and non–industry-sponsored studies in humans are needed before we can make a recommendation in favor or against the use of nonnutritive sweeteners,” he said.
“However, our results demonstrating that nonnutritive sweeteners are not inert, when taken together with a growing body of evidence on potential harms of these sweeteners, merit caution until additional studies are completed,” he added. “Our findings do not imply in any way that sugar consumption, shown to be harmful to human health in many studies, is superior to nonnutritive sweeteners. Sugar consumption should be minimized, especially in individuals with obesity or diabetes. Of all the options, unsweetened beverages, specifically water, seem to be the safest and best options.”
Dr. Sen, who also “tries to convince patients to have sparkling or cold bottled water,” instead of artificially sweetened soda, agreed. “If a diabetes patient is trying to choose between sugar and sucralose, I’m not sure which one is worse.”
Dr. Swithers, Dr. Mathur, Dr. Sen, and Dr. Suez declared no competing interests.
A version of this article first appeared on Medscape.com.
Ultraprocessed Food Linked to Constipation
TOPLINE:
METHODOLOGY:
- Excess consumption of UPF has been linked to disturbed intestinal motility.
- Using data from the National Health and Nutrition Examination Survey (2005-2010), researchers performed a cross-sectional study to assess the association between UPF and MPF intake and bowel habits.
- They used two 24-hour dietary recalls to capture the participants’ dietary intake and subsequently categorized food items into MPF, processed culinary ingredients, processed food, and UPF, according to the Nova classification.
- The Bowel Health Questionnaire was used to assess bowel habits, with constipation and diarrhea being defined according to the Bristol Stool Form Scale and stool frequency.
- The odds ratios for constipation and diarrhea were calculated by comparing the quartiles of UPF and MPF consumption using survey-weighted logistic regressions adjusted for potential confounding factors.
TAKEAWAY:
- Researchers included 12,716 US adults, of whom 1290 and 1067 had constipation and diarrhea, respectively.
- Increased consumption of UPF was associated with more than two times increased odds of constipation; the association held after adjusting for diet quality, water intake, and fiber intake.
- Conversely, increased intake of MPF was associated with reduced odds of constipation; the association held after adjustment.
- Substituting 10% of UPF with an equivalent proportion of MPF was associated with 10% lower odds of constipation.
- Neither MPF nor UPF consumption was associated with increased odds of diarrhea.
IN PRACTICE:
“The persistently strong associations with [UPF] and MPF consumption despite adjustment for diet quality suggest that food processing plays a unique role in constipation,” the authors wrote.
SOURCE:
The study, led by Chun-Han Lo, MD, MPH, Department of Internal Medicine, Kirk Kerkorian School of Medicine at the University of Nevada, Las Vegas, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The evaluation of dietary intake using two 24-hour dietary recalls did not allow for the assessment of dietary changes over time. Misclassification bias could be present due to varying degrees of food processing across different brands. The authors could not fully account for unmeasured confounders owing to the observational nature of this study.
DISCLOSURES:
This study did not receive any funding. Some authors declared serving as consultants, being on advisory boards, or receiving research funding from various sources.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Excess consumption of UPF has been linked to disturbed intestinal motility.
- Using data from the National Health and Nutrition Examination Survey (2005-2010), researchers performed a cross-sectional study to assess the association between UPF and MPF intake and bowel habits.
- They used two 24-hour dietary recalls to capture the participants’ dietary intake and subsequently categorized food items into MPF, processed culinary ingredients, processed food, and UPF, according to the Nova classification.
- The Bowel Health Questionnaire was used to assess bowel habits, with constipation and diarrhea being defined according to the Bristol Stool Form Scale and stool frequency.
- The odds ratios for constipation and diarrhea were calculated by comparing the quartiles of UPF and MPF consumption using survey-weighted logistic regressions adjusted for potential confounding factors.
TAKEAWAY:
- Researchers included 12,716 US adults, of whom 1290 and 1067 had constipation and diarrhea, respectively.
- Increased consumption of UPF was associated with more than two times increased odds of constipation; the association held after adjusting for diet quality, water intake, and fiber intake.
- Conversely, increased intake of MPF was associated with reduced odds of constipation; the association held after adjustment.
- Substituting 10% of UPF with an equivalent proportion of MPF was associated with 10% lower odds of constipation.
- Neither MPF nor UPF consumption was associated with increased odds of diarrhea.
IN PRACTICE:
“The persistently strong associations with [UPF] and MPF consumption despite adjustment for diet quality suggest that food processing plays a unique role in constipation,” the authors wrote.
SOURCE:
The study, led by Chun-Han Lo, MD, MPH, Department of Internal Medicine, Kirk Kerkorian School of Medicine at the University of Nevada, Las Vegas, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The evaluation of dietary intake using two 24-hour dietary recalls did not allow for the assessment of dietary changes over time. Misclassification bias could be present due to varying degrees of food processing across different brands. The authors could not fully account for unmeasured confounders owing to the observational nature of this study.
DISCLOSURES:
This study did not receive any funding. Some authors declared serving as consultants, being on advisory boards, or receiving research funding from various sources.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Excess consumption of UPF has been linked to disturbed intestinal motility.
- Using data from the National Health and Nutrition Examination Survey (2005-2010), researchers performed a cross-sectional study to assess the association between UPF and MPF intake and bowel habits.
- They used two 24-hour dietary recalls to capture the participants’ dietary intake and subsequently categorized food items into MPF, processed culinary ingredients, processed food, and UPF, according to the Nova classification.
- The Bowel Health Questionnaire was used to assess bowel habits, with constipation and diarrhea being defined according to the Bristol Stool Form Scale and stool frequency.
- The odds ratios for constipation and diarrhea were calculated by comparing the quartiles of UPF and MPF consumption using survey-weighted logistic regressions adjusted for potential confounding factors.
TAKEAWAY:
- Researchers included 12,716 US adults, of whom 1290 and 1067 had constipation and diarrhea, respectively.
- Increased consumption of UPF was associated with more than two times increased odds of constipation; the association held after adjusting for diet quality, water intake, and fiber intake.
- Conversely, increased intake of MPF was associated with reduced odds of constipation; the association held after adjustment.
- Substituting 10% of UPF with an equivalent proportion of MPF was associated with 10% lower odds of constipation.
- Neither MPF nor UPF consumption was associated with increased odds of diarrhea.
IN PRACTICE:
“The persistently strong associations with [UPF] and MPF consumption despite adjustment for diet quality suggest that food processing plays a unique role in constipation,” the authors wrote.
SOURCE:
The study, led by Chun-Han Lo, MD, MPH, Department of Internal Medicine, Kirk Kerkorian School of Medicine at the University of Nevada, Las Vegas, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The evaluation of dietary intake using two 24-hour dietary recalls did not allow for the assessment of dietary changes over time. Misclassification bias could be present due to varying degrees of food processing across different brands. The authors could not fully account for unmeasured confounders owing to the observational nature of this study.
DISCLOSURES:
This study did not receive any funding. Some authors declared serving as consultants, being on advisory boards, or receiving research funding from various sources.
A version of this article first appeared on Medscape.com.
Experts Expect New Human Cases of Avian Flu
With avian influenza spreading quickly around the globe, the virus has more opportunities to mutate and cause problems for people. By some calculations, H5N1 bird flu is still at least two mutations away from widespread human infections, but experts warn that new flu symptoms in individuals at high risk are likely to start turning up in health systems this summer.
“Some of this will not be obvious or at the forefront of our minds.”
Dr. Dugan is leading the team of CDC scientists that is working with partners from the US Department of Agriculture, the US Food and Drug Administration (FDA), and state and local health departments to track and respond to the H5N1 bird flu outbreak currently sweeping through the United States.
Since 2022, avian influenza A viruses have been detected in more than 9300 wild birds in 50 states and territories and in commercial and backyard flocks.
“It’s a bad situation,” said Florian Krammer, PhD, professor of vaccinology at the Icahn School of Medicine at Mount Sinai in New York. “Globally, we’ve seen tons of exposure in cities around the world and even in the birds here in New York City where I am.”
Birds shed the virus in their saliva, mucous, and feces, so people or other animals with close, unprotected contact with infected birds or their contaminated environments can be infected.
And for the first time in March 2024, H5N1 bird flu was reported in dairy cows. The US Department of Agriculture said that at last count, 101 dairy herds in 12 states had been infected, with several cases also found in dairy workers.
From Birds to Cattle and Farm Workers
The National Veterinary Services Laboratories confirmed the infections were highly pathogenic avian influenza H5N1 clade 2.3.4.4b of Eurasian lineage. Also known as the goose, Guangdong clade from China, phylogenetic analysis and epidemiology suggests a single introduction into cows followed by onward transmission.
“I was surprised when H5 was introduced to dairy cattle in this way,” Dr. Dugan said. “Influenza viruses are always surprising us and it reminds me to stay humble and keep an open mind when dealing with them.”
People rarely inhale or get sufficient virus in their eyes or mouth to get sick, Dr. Dugan said, but those in close contact with animals are still at risk for infection, which could lead to upper respiratory tract symptoms such as shortness of breath, cough, sore throat, or runny or stuffy nose.
Like with other viruses, people can also experience muscle or body aches, headache, fatigue, fever or, as was seen in farm workers, conjunctivitis.
But there are less-common symptoms too like diarrhea, nausea, and vomiting — and sometimes, even seizures.
The risk to the general public is still low, Dr. Dugan said, but authorities recommend that people working with animals wash their hands with soap and water and wear personal protective equipment that includes fluid-resistant coveralls, a waterproof apron, a safety-approved respirator, properly fitted goggles or face shield, a head or hair cover, gloves, and boots.
Dr. Dugan said that health care providers often don’t take a history of occupational exposures when a patient presents with flu. But with rising rates of bird flu in new animal hosts, “this will be an important next step.”
Asking Unusual Questions
This approach is not standardized on most electronic health records, so these are questions that clinicians will need to initiate themselves.
“Physicians should ask about work,” said Meghan Davis, PhD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “If it’s not already on the radar, asking about any direct contact with dairy cows, poultry, pigs, wild birds, or wild mammals is important.”
Dr. Davis says she’s worried about a new study tracking risk factors for farm-to-farm transmission because it shows that farms testing positive for avian influenza often have workers with a family member also employed on another farm. “This suggests that we might need to be on the lookout for possible transmission within families,” she said. Now, we have to ask “not just if the person with symptoms has contact with or works on a dairy farm, milk processing plant, or slaughterhouse, but also if any family member does.”
Dr. Davis said that it’s important to bear in mind when taking these histories that there may be younger workers on farms and in slaughter and processing facilities due to exemptions or illegal work.
What is important now is to get the situation under control this season in dairy cattle, Dr. Krammer said. “This will be easier to stop in cows than humans, so this is the time to stop moving dairy cattle and start vaccinating them.”
Spotting New Cases
Since April 2024, there have been three human cases of avian influenza after exposure to dairy cows reported. “And what we don’t want to see this summer is an unusual human cluster of influenza. It’s important we keep a close, watchful eye for this,” Dr. Krammer said.
“Influenza viruses do very interesting things and as we head into fall and winter flu season, we don’t want new human co-infections that could cause major problems for us,” he said.
If people become mixing vessels of a seasonal cocktail of multiple viruses, that could empower H5N1 to mutate again into something more dangerous, sparking a new pandemic.
“It wasn’t all that long ago that we were asking China difficult questions about the steps Chinese authorities took to protect human lives from SARS-CoV-2 in the COVID pandemic. Now, we must ask ourselves many of these questions,” Dr. Krammer said. “We are at a crucial crossroad where we will either elude a new pandemic or see one take off, risking 10 to 20 million lives.”
There is a precedent for safely evading more trouble, Dr. Krammer pointed out. Government agencies have already been working with the poultry industry for a couple of years now. “And here, we have successfully stopped H5N1 with new regulations and policies.”
But moving from poultry farms to cattle has not been an easy transition, Dr. Dugan said. Cattle farms have no experience with bird flu or tactics to contain it with regulations, and officials too are working in new, unfamiliar terrain.
“What we have now isn’t a science problem, it’s a policy issue, and it hasn’t always been clear who is in charge,” Dr. Krammer said.
“Agencies are working together at the state, federal, and global level,” said Dr. Dugan. “We are increasing our transparency and are working to share what we know, when we know it.”
The infrastructure built during the COVID pandemic has helped teams prepare for this new crisis, Dr. Dugan said. Year-round, layered monitoring has clinical labs reporting seasonal influenza and novel cases.
“Laboratories are ready to help with testing,” Dr. Dugan said.
Specimens should be collected as soon as possible from patients with flu symptoms. A nasopharyngeal swab is recommended with a nasal swab combined with an oropharyngeal swab. If a patient has conjunctivitis with or without respiratory symptoms, both a conjunctival swab and a nasopharyngeal swab should be collected.
People with severe respiratory disease should also have lower respiratory tract specimens collected.
Standard, contact, and airborne precautions are recommended for patients presenting for medical care who have illness consistent with influenza and recent exposure to birds or other animals.
Antiviral Drugs
There are four FDA-approved antivirals for influenza: Oseltamivir phosphate (available as a generic drug or by the trade name Tamiflu), zanamivir (Relenza), peramivir (Rapivab) , and baloxavir (Xofluza).
For people with suspected or confirmed avian influenza, treatment is recommended as soon as possible.
There are no clinical trials measuring the outcome of antivirals in people infected with avian influenza. However, data from animal models and human observational studies suggest a benefit.
“We can’t afford to wait this summer,” Dr. Krammer said. “We have an opportunity right now to stop this in cows before we risk infecting more people. I hope we do.”
A version of this article first appeared on Medscape.com.
With avian influenza spreading quickly around the globe, the virus has more opportunities to mutate and cause problems for people. By some calculations, H5N1 bird flu is still at least two mutations away from widespread human infections, but experts warn that new flu symptoms in individuals at high risk are likely to start turning up in health systems this summer.
“Some of this will not be obvious or at the forefront of our minds.”
Dr. Dugan is leading the team of CDC scientists that is working with partners from the US Department of Agriculture, the US Food and Drug Administration (FDA), and state and local health departments to track and respond to the H5N1 bird flu outbreak currently sweeping through the United States.
Since 2022, avian influenza A viruses have been detected in more than 9300 wild birds in 50 states and territories and in commercial and backyard flocks.
“It’s a bad situation,” said Florian Krammer, PhD, professor of vaccinology at the Icahn School of Medicine at Mount Sinai in New York. “Globally, we’ve seen tons of exposure in cities around the world and even in the birds here in New York City where I am.”
Birds shed the virus in their saliva, mucous, and feces, so people or other animals with close, unprotected contact with infected birds or their contaminated environments can be infected.
And for the first time in March 2024, H5N1 bird flu was reported in dairy cows. The US Department of Agriculture said that at last count, 101 dairy herds in 12 states had been infected, with several cases also found in dairy workers.
From Birds to Cattle and Farm Workers
The National Veterinary Services Laboratories confirmed the infections were highly pathogenic avian influenza H5N1 clade 2.3.4.4b of Eurasian lineage. Also known as the goose, Guangdong clade from China, phylogenetic analysis and epidemiology suggests a single introduction into cows followed by onward transmission.
“I was surprised when H5 was introduced to dairy cattle in this way,” Dr. Dugan said. “Influenza viruses are always surprising us and it reminds me to stay humble and keep an open mind when dealing with them.”
People rarely inhale or get sufficient virus in their eyes or mouth to get sick, Dr. Dugan said, but those in close contact with animals are still at risk for infection, which could lead to upper respiratory tract symptoms such as shortness of breath, cough, sore throat, or runny or stuffy nose.
Like with other viruses, people can also experience muscle or body aches, headache, fatigue, fever or, as was seen in farm workers, conjunctivitis.
But there are less-common symptoms too like diarrhea, nausea, and vomiting — and sometimes, even seizures.
The risk to the general public is still low, Dr. Dugan said, but authorities recommend that people working with animals wash their hands with soap and water and wear personal protective equipment that includes fluid-resistant coveralls, a waterproof apron, a safety-approved respirator, properly fitted goggles or face shield, a head or hair cover, gloves, and boots.
Dr. Dugan said that health care providers often don’t take a history of occupational exposures when a patient presents with flu. But with rising rates of bird flu in new animal hosts, “this will be an important next step.”
Asking Unusual Questions
This approach is not standardized on most electronic health records, so these are questions that clinicians will need to initiate themselves.
“Physicians should ask about work,” said Meghan Davis, PhD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “If it’s not already on the radar, asking about any direct contact with dairy cows, poultry, pigs, wild birds, or wild mammals is important.”
Dr. Davis says she’s worried about a new study tracking risk factors for farm-to-farm transmission because it shows that farms testing positive for avian influenza often have workers with a family member also employed on another farm. “This suggests that we might need to be on the lookout for possible transmission within families,” she said. Now, we have to ask “not just if the person with symptoms has contact with or works on a dairy farm, milk processing plant, or slaughterhouse, but also if any family member does.”
Dr. Davis said that it’s important to bear in mind when taking these histories that there may be younger workers on farms and in slaughter and processing facilities due to exemptions or illegal work.
What is important now is to get the situation under control this season in dairy cattle, Dr. Krammer said. “This will be easier to stop in cows than humans, so this is the time to stop moving dairy cattle and start vaccinating them.”
Spotting New Cases
Since April 2024, there have been three human cases of avian influenza after exposure to dairy cows reported. “And what we don’t want to see this summer is an unusual human cluster of influenza. It’s important we keep a close, watchful eye for this,” Dr. Krammer said.
“Influenza viruses do very interesting things and as we head into fall and winter flu season, we don’t want new human co-infections that could cause major problems for us,” he said.
If people become mixing vessels of a seasonal cocktail of multiple viruses, that could empower H5N1 to mutate again into something more dangerous, sparking a new pandemic.
“It wasn’t all that long ago that we were asking China difficult questions about the steps Chinese authorities took to protect human lives from SARS-CoV-2 in the COVID pandemic. Now, we must ask ourselves many of these questions,” Dr. Krammer said. “We are at a crucial crossroad where we will either elude a new pandemic or see one take off, risking 10 to 20 million lives.”
There is a precedent for safely evading more trouble, Dr. Krammer pointed out. Government agencies have already been working with the poultry industry for a couple of years now. “And here, we have successfully stopped H5N1 with new regulations and policies.”
But moving from poultry farms to cattle has not been an easy transition, Dr. Dugan said. Cattle farms have no experience with bird flu or tactics to contain it with regulations, and officials too are working in new, unfamiliar terrain.
“What we have now isn’t a science problem, it’s a policy issue, and it hasn’t always been clear who is in charge,” Dr. Krammer said.
“Agencies are working together at the state, federal, and global level,” said Dr. Dugan. “We are increasing our transparency and are working to share what we know, when we know it.”
The infrastructure built during the COVID pandemic has helped teams prepare for this new crisis, Dr. Dugan said. Year-round, layered monitoring has clinical labs reporting seasonal influenza and novel cases.
“Laboratories are ready to help with testing,” Dr. Dugan said.
Specimens should be collected as soon as possible from patients with flu symptoms. A nasopharyngeal swab is recommended with a nasal swab combined with an oropharyngeal swab. If a patient has conjunctivitis with or without respiratory symptoms, both a conjunctival swab and a nasopharyngeal swab should be collected.
People with severe respiratory disease should also have lower respiratory tract specimens collected.
Standard, contact, and airborne precautions are recommended for patients presenting for medical care who have illness consistent with influenza and recent exposure to birds or other animals.
Antiviral Drugs
There are four FDA-approved antivirals for influenza: Oseltamivir phosphate (available as a generic drug or by the trade name Tamiflu), zanamivir (Relenza), peramivir (Rapivab) , and baloxavir (Xofluza).
For people with suspected or confirmed avian influenza, treatment is recommended as soon as possible.
There are no clinical trials measuring the outcome of antivirals in people infected with avian influenza. However, data from animal models and human observational studies suggest a benefit.
“We can’t afford to wait this summer,” Dr. Krammer said. “We have an opportunity right now to stop this in cows before we risk infecting more people. I hope we do.”
A version of this article first appeared on Medscape.com.
With avian influenza spreading quickly around the globe, the virus has more opportunities to mutate and cause problems for people. By some calculations, H5N1 bird flu is still at least two mutations away from widespread human infections, but experts warn that new flu symptoms in individuals at high risk are likely to start turning up in health systems this summer.
“Some of this will not be obvious or at the forefront of our minds.”
Dr. Dugan is leading the team of CDC scientists that is working with partners from the US Department of Agriculture, the US Food and Drug Administration (FDA), and state and local health departments to track and respond to the H5N1 bird flu outbreak currently sweeping through the United States.
Since 2022, avian influenza A viruses have been detected in more than 9300 wild birds in 50 states and territories and in commercial and backyard flocks.
“It’s a bad situation,” said Florian Krammer, PhD, professor of vaccinology at the Icahn School of Medicine at Mount Sinai in New York. “Globally, we’ve seen tons of exposure in cities around the world and even in the birds here in New York City where I am.”
Birds shed the virus in their saliva, mucous, and feces, so people or other animals with close, unprotected contact with infected birds or their contaminated environments can be infected.
And for the first time in March 2024, H5N1 bird flu was reported in dairy cows. The US Department of Agriculture said that at last count, 101 dairy herds in 12 states had been infected, with several cases also found in dairy workers.
From Birds to Cattle and Farm Workers
The National Veterinary Services Laboratories confirmed the infections were highly pathogenic avian influenza H5N1 clade 2.3.4.4b of Eurasian lineage. Also known as the goose, Guangdong clade from China, phylogenetic analysis and epidemiology suggests a single introduction into cows followed by onward transmission.
“I was surprised when H5 was introduced to dairy cattle in this way,” Dr. Dugan said. “Influenza viruses are always surprising us and it reminds me to stay humble and keep an open mind when dealing with them.”
People rarely inhale or get sufficient virus in their eyes or mouth to get sick, Dr. Dugan said, but those in close contact with animals are still at risk for infection, which could lead to upper respiratory tract symptoms such as shortness of breath, cough, sore throat, or runny or stuffy nose.
Like with other viruses, people can also experience muscle or body aches, headache, fatigue, fever or, as was seen in farm workers, conjunctivitis.
But there are less-common symptoms too like diarrhea, nausea, and vomiting — and sometimes, even seizures.
The risk to the general public is still low, Dr. Dugan said, but authorities recommend that people working with animals wash their hands with soap and water and wear personal protective equipment that includes fluid-resistant coveralls, a waterproof apron, a safety-approved respirator, properly fitted goggles or face shield, a head or hair cover, gloves, and boots.
Dr. Dugan said that health care providers often don’t take a history of occupational exposures when a patient presents with flu. But with rising rates of bird flu in new animal hosts, “this will be an important next step.”
Asking Unusual Questions
This approach is not standardized on most electronic health records, so these are questions that clinicians will need to initiate themselves.
“Physicians should ask about work,” said Meghan Davis, PhD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “If it’s not already on the radar, asking about any direct contact with dairy cows, poultry, pigs, wild birds, or wild mammals is important.”
Dr. Davis says she’s worried about a new study tracking risk factors for farm-to-farm transmission because it shows that farms testing positive for avian influenza often have workers with a family member also employed on another farm. “This suggests that we might need to be on the lookout for possible transmission within families,” she said. Now, we have to ask “not just if the person with symptoms has contact with or works on a dairy farm, milk processing plant, or slaughterhouse, but also if any family member does.”
Dr. Davis said that it’s important to bear in mind when taking these histories that there may be younger workers on farms and in slaughter and processing facilities due to exemptions or illegal work.
What is important now is to get the situation under control this season in dairy cattle, Dr. Krammer said. “This will be easier to stop in cows than humans, so this is the time to stop moving dairy cattle and start vaccinating them.”
Spotting New Cases
Since April 2024, there have been three human cases of avian influenza after exposure to dairy cows reported. “And what we don’t want to see this summer is an unusual human cluster of influenza. It’s important we keep a close, watchful eye for this,” Dr. Krammer said.
“Influenza viruses do very interesting things and as we head into fall and winter flu season, we don’t want new human co-infections that could cause major problems for us,” he said.
If people become mixing vessels of a seasonal cocktail of multiple viruses, that could empower H5N1 to mutate again into something more dangerous, sparking a new pandemic.
“It wasn’t all that long ago that we were asking China difficult questions about the steps Chinese authorities took to protect human lives from SARS-CoV-2 in the COVID pandemic. Now, we must ask ourselves many of these questions,” Dr. Krammer said. “We are at a crucial crossroad where we will either elude a new pandemic or see one take off, risking 10 to 20 million lives.”
There is a precedent for safely evading more trouble, Dr. Krammer pointed out. Government agencies have already been working with the poultry industry for a couple of years now. “And here, we have successfully stopped H5N1 with new regulations and policies.”
But moving from poultry farms to cattle has not been an easy transition, Dr. Dugan said. Cattle farms have no experience with bird flu or tactics to contain it with regulations, and officials too are working in new, unfamiliar terrain.
“What we have now isn’t a science problem, it’s a policy issue, and it hasn’t always been clear who is in charge,” Dr. Krammer said.
“Agencies are working together at the state, federal, and global level,” said Dr. Dugan. “We are increasing our transparency and are working to share what we know, when we know it.”
The infrastructure built during the COVID pandemic has helped teams prepare for this new crisis, Dr. Dugan said. Year-round, layered monitoring has clinical labs reporting seasonal influenza and novel cases.
“Laboratories are ready to help with testing,” Dr. Dugan said.
Specimens should be collected as soon as possible from patients with flu symptoms. A nasopharyngeal swab is recommended with a nasal swab combined with an oropharyngeal swab. If a patient has conjunctivitis with or without respiratory symptoms, both a conjunctival swab and a nasopharyngeal swab should be collected.
People with severe respiratory disease should also have lower respiratory tract specimens collected.
Standard, contact, and airborne precautions are recommended for patients presenting for medical care who have illness consistent with influenza and recent exposure to birds or other animals.
Antiviral Drugs
There are four FDA-approved antivirals for influenza: Oseltamivir phosphate (available as a generic drug or by the trade name Tamiflu), zanamivir (Relenza), peramivir (Rapivab) , and baloxavir (Xofluza).
For people with suspected or confirmed avian influenza, treatment is recommended as soon as possible.
There are no clinical trials measuring the outcome of antivirals in people infected with avian influenza. However, data from animal models and human observational studies suggest a benefit.
“We can’t afford to wait this summer,” Dr. Krammer said. “We have an opportunity right now to stop this in cows before we risk infecting more people. I hope we do.”
A version of this article first appeared on Medscape.com.
Migraine Differential Diagnosis
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
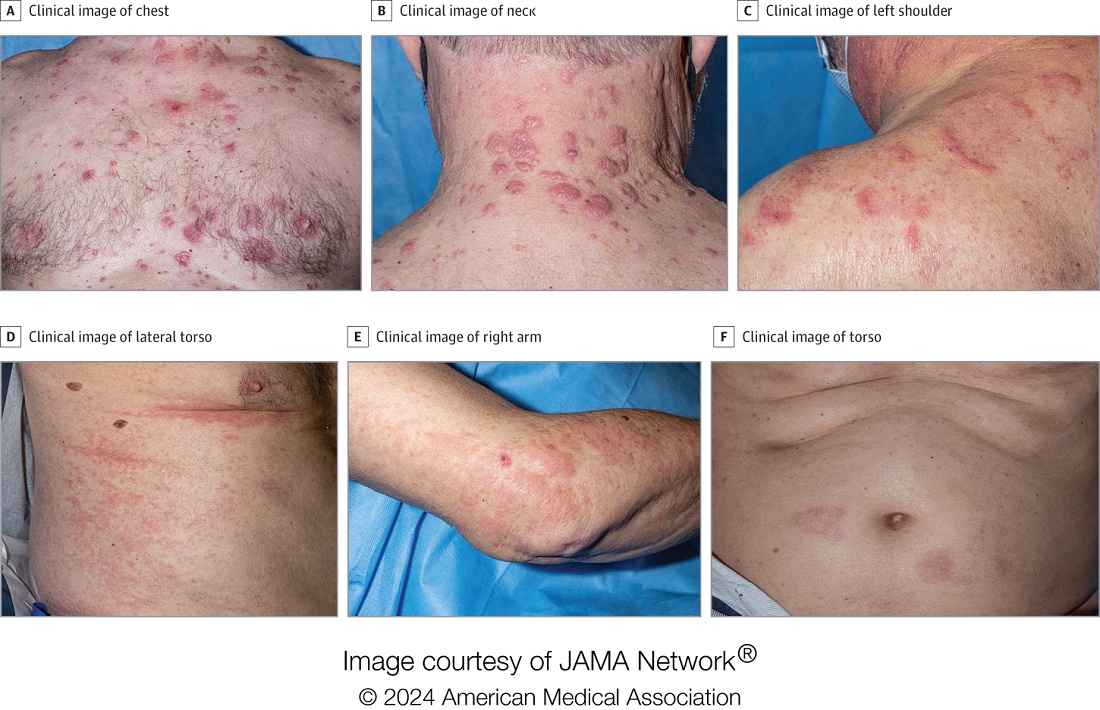
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
Pruritic, violaceous papules in a patient with renal cell carcinoma
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.

The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.

Shift Needed in Research, Treatment, Care for Aging MS Population
NASHVILLE, TENNESSEE — a phenomenon that’s driving a shift in priorities including the creation of MS aging centers and a push for more clinical trials aimed at this growing patient population.
Given typical patterns of MS onset and its rate of progression, disease duration has long been thought to be the key variable driving disability, but Jennifer Graves, MD, PhD, director of the neuroimmunology research program at the University of California, San Diego, said she now believes that “patient age is actually more important.”

Speaking at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC), Dr. Graves noted that it is well known that key MS symptoms increase over time, particularly during the transition from a relapsing to a progressive phenotype.
However, she maintains that, independent of disease progression, the impact of aging on MS has been underappreciated. She cited research showing that, relative to chronological age, biologic age is more robustly correlated with MS outcomes.
In studies evaluating variables such as telomere length, various markers of senescence, and DNA methylation patterns, Dr. Graves and others have shown that biologic versus chronological aging is more rapid in patients with MS than those without the disease. In addition, within the population with MS, there are also data supporting the premise that disease progression is slower in those with a younger versus older biologic age.
“This raises the question of whether biologic age is a driver of MS and whether we can slow the disease trajectory if we slow [biologic] aging,” Dr. Graves said. While she acknowledged that genetics play an important role in the aging process, she pointed to evidence showing exposure to toxins and other biological stressors, as well as poor lifestyle choices, such as lack of exercise and smoking, are modifiable aging variables.
There are already many avenues of research regarding aging processes and their interaction with MS. Dr. Graves spoke briefly about current research into the relationship between declining ovarian function, declining telomere length, and how this might relate to the transition to progressive MS and advancing disability. To date, her research has revealed a correlation between declining ovarian function and increasing MS disability.
Shifting Priorities
The rapid aging of the population with MS in the United States makes research into slowing biologic aging a priority, said Robert Motl, PhD, professor in the department of physical therapy, University of Alabama at Birmingham Multiple Sclerosis Center. He reported he was able to secure funding from the National MS Society for the Healthy Aging through LifesTyle MS Research Center 10 years ago.
“We are the first and, so far, the only research center devoted to the study of aging in MS,” said Dr. Motl, another participant in the CMSC aging symposium. Dr. Motl said he and a colleague have been evaluating specific strategies to meet the varied needs of aging patients with MS with a key focus on physical therapy and preserving function.
Yinan Zhang, MD, an assistant professor of neurology at the Ohio State University Wexner Medical Center in Columbus, recently started a multidisciplinary clinic for the management of older patients with MS and said he hopes these types of clinics will help shed light on the unmet needs of older adults with MS — particularly the need for better therapies to address common types of neurodegeneration in this population.
“We need to move away from immunomodulatory agents [in older patients],” Dr. Zhang said. Older patients are typically excluded from therapeutic MS trials for a number of reasons, not least because trials have been traditionally targeted at relapsing disease, which is less common in older patients with MS. He believes older patients are particularly appropriate candidates for MS therapy trials aimed at progressive neurodegeneration, which is characteristic of late-stage disease. Therapies with the potential to slow, or even reverse, demyelination are among the novel strategies being pursued in progressive MS.
Multidisciplinary Approach
Dr. Zhang acknowledged that his recently established MS clinic is still in the early phases and is largely focused on comprehensive care designed to meet the diverse needs of older individuals who often have advanced disabilities and comorbidities.
Currently, each patient that attends the clinic consults with six different types of providers, including a psychologist, a pharmacist, and a physical therapist — all in a single appointment.
Dr. Zhang said his decision to open a clinic was motivated by the increased volume of older patients with MS and was inspired by similar clinics for other disease states in older individuals.
“The need is already strong and growing,” said Dr. Zhang, who speculated that these types of clinics will become widespread as the need for this care is more broadly recognized and accepted.
As the clinic evolves and matures, Dr. Zhang anticipates there will be a research component to better characterize cell senescence and aging processes that might eventually be modifiable or even reversible. He also speculated that aging in MS might eventually become a subspecialty.
Dr. Graves reported financial relationships with Horizon Therapeutics. Dr. Zhang reported no potential conflicts of interest. Dr. Motl reported financial relationships with Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
NASHVILLE, TENNESSEE — a phenomenon that’s driving a shift in priorities including the creation of MS aging centers and a push for more clinical trials aimed at this growing patient population.
Given typical patterns of MS onset and its rate of progression, disease duration has long been thought to be the key variable driving disability, but Jennifer Graves, MD, PhD, director of the neuroimmunology research program at the University of California, San Diego, said she now believes that “patient age is actually more important.”
Speaking at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC), Dr. Graves noted that it is well known that key MS symptoms increase over time, particularly during the transition from a relapsing to a progressive phenotype.
However, she maintains that, independent of disease progression, the impact of aging on MS has been underappreciated. She cited research showing that, relative to chronological age, biologic age is more robustly correlated with MS outcomes.
In studies evaluating variables such as telomere length, various markers of senescence, and DNA methylation patterns, Dr. Graves and others have shown that biologic versus chronological aging is more rapid in patients with MS than those without the disease. In addition, within the population with MS, there are also data supporting the premise that disease progression is slower in those with a younger versus older biologic age.
“This raises the question of whether biologic age is a driver of MS and whether we can slow the disease trajectory if we slow [biologic] aging,” Dr. Graves said. While she acknowledged that genetics play an important role in the aging process, she pointed to evidence showing exposure to toxins and other biological stressors, as well as poor lifestyle choices, such as lack of exercise and smoking, are modifiable aging variables.
There are already many avenues of research regarding aging processes and their interaction with MS. Dr. Graves spoke briefly about current research into the relationship between declining ovarian function, declining telomere length, and how this might relate to the transition to progressive MS and advancing disability. To date, her research has revealed a correlation between declining ovarian function and increasing MS disability.
Shifting Priorities
The rapid aging of the population with MS in the United States makes research into slowing biologic aging a priority, said Robert Motl, PhD, professor in the department of physical therapy, University of Alabama at Birmingham Multiple Sclerosis Center. He reported he was able to secure funding from the National MS Society for the Healthy Aging through LifesTyle MS Research Center 10 years ago.
“We are the first and, so far, the only research center devoted to the study of aging in MS,” said Dr. Motl, another participant in the CMSC aging symposium. Dr. Motl said he and a colleague have been evaluating specific strategies to meet the varied needs of aging patients with MS with a key focus on physical therapy and preserving function.
Yinan Zhang, MD, an assistant professor of neurology at the Ohio State University Wexner Medical Center in Columbus, recently started a multidisciplinary clinic for the management of older patients with MS and said he hopes these types of clinics will help shed light on the unmet needs of older adults with MS — particularly the need for better therapies to address common types of neurodegeneration in this population.
“We need to move away from immunomodulatory agents [in older patients],” Dr. Zhang said. Older patients are typically excluded from therapeutic MS trials for a number of reasons, not least because trials have been traditionally targeted at relapsing disease, which is less common in older patients with MS. He believes older patients are particularly appropriate candidates for MS therapy trials aimed at progressive neurodegeneration, which is characteristic of late-stage disease. Therapies with the potential to slow, or even reverse, demyelination are among the novel strategies being pursued in progressive MS.
Multidisciplinary Approach
Dr. Zhang acknowledged that his recently established MS clinic is still in the early phases and is largely focused on comprehensive care designed to meet the diverse needs of older individuals who often have advanced disabilities and comorbidities.
Currently, each patient that attends the clinic consults with six different types of providers, including a psychologist, a pharmacist, and a physical therapist — all in a single appointment.
Dr. Zhang said his decision to open a clinic was motivated by the increased volume of older patients with MS and was inspired by similar clinics for other disease states in older individuals.
“The need is already strong and growing,” said Dr. Zhang, who speculated that these types of clinics will become widespread as the need for this care is more broadly recognized and accepted.
As the clinic evolves and matures, Dr. Zhang anticipates there will be a research component to better characterize cell senescence and aging processes that might eventually be modifiable or even reversible. He also speculated that aging in MS might eventually become a subspecialty.
Dr. Graves reported financial relationships with Horizon Therapeutics. Dr. Zhang reported no potential conflicts of interest. Dr. Motl reported financial relationships with Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
NASHVILLE, TENNESSEE — a phenomenon that’s driving a shift in priorities including the creation of MS aging centers and a push for more clinical trials aimed at this growing patient population.
Given typical patterns of MS onset and its rate of progression, disease duration has long been thought to be the key variable driving disability, but Jennifer Graves, MD, PhD, director of the neuroimmunology research program at the University of California, San Diego, said she now believes that “patient age is actually more important.”
Speaking at the annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC), Dr. Graves noted that it is well known that key MS symptoms increase over time, particularly during the transition from a relapsing to a progressive phenotype.
However, she maintains that, independent of disease progression, the impact of aging on MS has been underappreciated. She cited research showing that, relative to chronological age, biologic age is more robustly correlated with MS outcomes.
In studies evaluating variables such as telomere length, various markers of senescence, and DNA methylation patterns, Dr. Graves and others have shown that biologic versus chronological aging is more rapid in patients with MS than those without the disease. In addition, within the population with MS, there are also data supporting the premise that disease progression is slower in those with a younger versus older biologic age.
“This raises the question of whether biologic age is a driver of MS and whether we can slow the disease trajectory if we slow [biologic] aging,” Dr. Graves said. While she acknowledged that genetics play an important role in the aging process, she pointed to evidence showing exposure to toxins and other biological stressors, as well as poor lifestyle choices, such as lack of exercise and smoking, are modifiable aging variables.
There are already many avenues of research regarding aging processes and their interaction with MS. Dr. Graves spoke briefly about current research into the relationship between declining ovarian function, declining telomere length, and how this might relate to the transition to progressive MS and advancing disability. To date, her research has revealed a correlation between declining ovarian function and increasing MS disability.
Shifting Priorities
The rapid aging of the population with MS in the United States makes research into slowing biologic aging a priority, said Robert Motl, PhD, professor in the department of physical therapy, University of Alabama at Birmingham Multiple Sclerosis Center. He reported he was able to secure funding from the National MS Society for the Healthy Aging through LifesTyle MS Research Center 10 years ago.
“We are the first and, so far, the only research center devoted to the study of aging in MS,” said Dr. Motl, another participant in the CMSC aging symposium. Dr. Motl said he and a colleague have been evaluating specific strategies to meet the varied needs of aging patients with MS with a key focus on physical therapy and preserving function.
Yinan Zhang, MD, an assistant professor of neurology at the Ohio State University Wexner Medical Center in Columbus, recently started a multidisciplinary clinic for the management of older patients with MS and said he hopes these types of clinics will help shed light on the unmet needs of older adults with MS — particularly the need for better therapies to address common types of neurodegeneration in this population.
“We need to move away from immunomodulatory agents [in older patients],” Dr. Zhang said. Older patients are typically excluded from therapeutic MS trials for a number of reasons, not least because trials have been traditionally targeted at relapsing disease, which is less common in older patients with MS. He believes older patients are particularly appropriate candidates for MS therapy trials aimed at progressive neurodegeneration, which is characteristic of late-stage disease. Therapies with the potential to slow, or even reverse, demyelination are among the novel strategies being pursued in progressive MS.
Multidisciplinary Approach
Dr. Zhang acknowledged that his recently established MS clinic is still in the early phases and is largely focused on comprehensive care designed to meet the diverse needs of older individuals who often have advanced disabilities and comorbidities.
Currently, each patient that attends the clinic consults with six different types of providers, including a psychologist, a pharmacist, and a physical therapist — all in a single appointment.
Dr. Zhang said his decision to open a clinic was motivated by the increased volume of older patients with MS and was inspired by similar clinics for other disease states in older individuals.
“The need is already strong and growing,” said Dr. Zhang, who speculated that these types of clinics will become widespread as the need for this care is more broadly recognized and accepted.
As the clinic evolves and matures, Dr. Zhang anticipates there will be a research component to better characterize cell senescence and aging processes that might eventually be modifiable or even reversible. He also speculated that aging in MS might eventually become a subspecialty.
Dr. Graves reported financial relationships with Horizon Therapeutics. Dr. Zhang reported no potential conflicts of interest. Dr. Motl reported financial relationships with Bristol-Myers Squibb.
A version of this article appeared on Medscape.com.
FROM CMSC 2024
Managing Heart Failure in Women: Key Differences and Clinical Tips
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
Mediterranean Diet Lowers Tachyarrhythmia in Paroxysmal AF
BOSTON — A Mediterranean diet with extra virgin olive oil (EVOO) significantly reduced the risk for tachyarrhythmia recurrence after atrial fibrillation (AF) ablation in patients with paroxysmal disease, but the diet had less of an impact on patients with persistent AF, a new study showed.
“An intervention with the Mediterranean diet with EVOO produced a nonsignificant reduction in any atrial tachycardia in a selected population after undergoing atrial fibrillation ablation, but this intervention produced a significant reduction in any atrial tachyarrhythmias in patients with paroxysmal AF,” said Maria Teresa Barrio-Lopez, MD, PhD, an electrophysiologist at University Hospital HM Monteprincipe in Madrid, Spain, who presented results from the PREDIMAR trial at the Heart Rhythm Society (HRS) 2024 annual meeting.
The PREDIMAR study enrolled 720 patients from the larger PREDIMED study, which showed that patients without AF at enrollment and who followed a Mediterranean diet enriched with EVOO had a 38% lower rate of incidental AF than control individuals.
PREDIMAR evaluated the impact of the diet on arrhythmia recurrence in patients after ablation. The patients were randomized in a 1:1 ratio to either the dietary intervention group or the control group.
PREDIMAR Study Results
However, among the 431 patients with paroxysmal AF, 25.2% in the diet group and 34.7% in the control group had no tachyarrhythmia recurrence, which translates into a 31% lower risk in the diet group.
In this study, the diet was rich in fish, nuts, fruits, and vegetables and was complemented with EVOO. Participants were also permitted moderate wine consumption.
The intervention involved dietitians who remotely followed patients and made periodic telephone calls to encourage them to stay on the diet. Participants had weight and body measurements taken at baseline and at 3, 6, 12, and 18 months and underwent an ECG at 6, 12, and 18 months. Labs were obtained at baseline and at 12 months. Participants were also given educational materials throughout the intervention.
Average scores, based on a scale of 0-13, excluding an item for wine intake, were 7.8 in the diet group and 7.2 in the control group.
Daily average alcohol intake was higher in the diet group than in the control group (9.8 vs 8.2 g), but “the weight of the patient during the study didn’t change in any group,” Dr. Barrio-Lopez reported.
Baseline characteristics were similar in the two groups. About 60% were taking antiarrhythmic drugs, and about 84% were taking anticoagulants.
‘A Tour de Force’
PREDIMAR was “really a tour de force,” Christine Albert, MD, MPH, chair of cardiology at the Smidt Heart Institute at the Cedars-Sinai Medical Center in Los Angeles, California, said during a commentary presented at HRS. “We talk about how we’re going to do these dietary interventions and weight loss and all the risk-factor reduction, and they pulled it off with 700 individuals and also did it in a way that was very novel.”
This is the first large-scale dietary intervention trial of patients with AF. However, Dr. Albert noted later in an interview, the Mediterranean diet poses potential challenges for some people with AF.
“The Mediterranean diet recommends that people drink wine, but then there’s clear evidence that abstinence from alcohol actually reduces recurrences of atrial fibrillation, so even though there are a lot of things about the Mediterranean diet that are probably healthy and good for atrial fibrillation, that aspect of it might be working against the patient,” she explained.
The finding that patients in the Mediterranean diet group experienced no significant weight loss could be counterintuitive when it comes to preventing AF. But “you could adapt the diet for AF,” Dr. Albert said. You could “leave out the wine and focus more on weight loss if the patient is obese because those are also the pillars of what we’ve learned for patients with atrial fibrillation.”
Making weight loss a key component of the study could be significant for the American population. “At least in the United States, that’s a huge part of the risk factors for atrial fibrillation after ablation,” she said.
The remote follow-up component of the PREDIMAR study is also intriguing. “I think what’s most exciting about what they did is, they showed they can do all these things remotely,” Dr. Albert added.
Dr. Barrio-Lopez had no relevant financial relationships. Dr. Albert disclosed relationships with Abbott, Roche Diagnostics, St. Jude Medical, Boston Scientific, Medtronic, and Element Science.
A version of this article appeared on Medscape.com.
BOSTON — A Mediterranean diet with extra virgin olive oil (EVOO) significantly reduced the risk for tachyarrhythmia recurrence after atrial fibrillation (AF) ablation in patients with paroxysmal disease, but the diet had less of an impact on patients with persistent AF, a new study showed.
“An intervention with the Mediterranean diet with EVOO produced a nonsignificant reduction in any atrial tachycardia in a selected population after undergoing atrial fibrillation ablation, but this intervention produced a significant reduction in any atrial tachyarrhythmias in patients with paroxysmal AF,” said Maria Teresa Barrio-Lopez, MD, PhD, an electrophysiologist at University Hospital HM Monteprincipe in Madrid, Spain, who presented results from the PREDIMAR trial at the Heart Rhythm Society (HRS) 2024 annual meeting.
The PREDIMAR study enrolled 720 patients from the larger PREDIMED study, which showed that patients without AF at enrollment and who followed a Mediterranean diet enriched with EVOO had a 38% lower rate of incidental AF than control individuals.
PREDIMAR evaluated the impact of the diet on arrhythmia recurrence in patients after ablation. The patients were randomized in a 1:1 ratio to either the dietary intervention group or the control group.
PREDIMAR Study Results
However, among the 431 patients with paroxysmal AF, 25.2% in the diet group and 34.7% in the control group had no tachyarrhythmia recurrence, which translates into a 31% lower risk in the diet group.
In this study, the diet was rich in fish, nuts, fruits, and vegetables and was complemented with EVOO. Participants were also permitted moderate wine consumption.
The intervention involved dietitians who remotely followed patients and made periodic telephone calls to encourage them to stay on the diet. Participants had weight and body measurements taken at baseline and at 3, 6, 12, and 18 months and underwent an ECG at 6, 12, and 18 months. Labs were obtained at baseline and at 12 months. Participants were also given educational materials throughout the intervention.
Average scores, based on a scale of 0-13, excluding an item for wine intake, were 7.8 in the diet group and 7.2 in the control group.
Daily average alcohol intake was higher in the diet group than in the control group (9.8 vs 8.2 g), but “the weight of the patient during the study didn’t change in any group,” Dr. Barrio-Lopez reported.
Baseline characteristics were similar in the two groups. About 60% were taking antiarrhythmic drugs, and about 84% were taking anticoagulants.
‘A Tour de Force’
PREDIMAR was “really a tour de force,” Christine Albert, MD, MPH, chair of cardiology at the Smidt Heart Institute at the Cedars-Sinai Medical Center in Los Angeles, California, said during a commentary presented at HRS. “We talk about how we’re going to do these dietary interventions and weight loss and all the risk-factor reduction, and they pulled it off with 700 individuals and also did it in a way that was very novel.”
This is the first large-scale dietary intervention trial of patients with AF. However, Dr. Albert noted later in an interview, the Mediterranean diet poses potential challenges for some people with AF.
“The Mediterranean diet recommends that people drink wine, but then there’s clear evidence that abstinence from alcohol actually reduces recurrences of atrial fibrillation, so even though there are a lot of things about the Mediterranean diet that are probably healthy and good for atrial fibrillation, that aspect of it might be working against the patient,” she explained.
The finding that patients in the Mediterranean diet group experienced no significant weight loss could be counterintuitive when it comes to preventing AF. But “you could adapt the diet for AF,” Dr. Albert said. You could “leave out the wine and focus more on weight loss if the patient is obese because those are also the pillars of what we’ve learned for patients with atrial fibrillation.”
Making weight loss a key component of the study could be significant for the American population. “At least in the United States, that’s a huge part of the risk factors for atrial fibrillation after ablation,” she said.
The remote follow-up component of the PREDIMAR study is also intriguing. “I think what’s most exciting about what they did is, they showed they can do all these things remotely,” Dr. Albert added.
Dr. Barrio-Lopez had no relevant financial relationships. Dr. Albert disclosed relationships with Abbott, Roche Diagnostics, St. Jude Medical, Boston Scientific, Medtronic, and Element Science.
A version of this article appeared on Medscape.com.
BOSTON — A Mediterranean diet with extra virgin olive oil (EVOO) significantly reduced the risk for tachyarrhythmia recurrence after atrial fibrillation (AF) ablation in patients with paroxysmal disease, but the diet had less of an impact on patients with persistent AF, a new study showed.
“An intervention with the Mediterranean diet with EVOO produced a nonsignificant reduction in any atrial tachycardia in a selected population after undergoing atrial fibrillation ablation, but this intervention produced a significant reduction in any atrial tachyarrhythmias in patients with paroxysmal AF,” said Maria Teresa Barrio-Lopez, MD, PhD, an electrophysiologist at University Hospital HM Monteprincipe in Madrid, Spain, who presented results from the PREDIMAR trial at the Heart Rhythm Society (HRS) 2024 annual meeting.
The PREDIMAR study enrolled 720 patients from the larger PREDIMED study, which showed that patients without AF at enrollment and who followed a Mediterranean diet enriched with EVOO had a 38% lower rate of incidental AF than control individuals.
PREDIMAR evaluated the impact of the diet on arrhythmia recurrence in patients after ablation. The patients were randomized in a 1:1 ratio to either the dietary intervention group or the control group.
PREDIMAR Study Results
However, among the 431 patients with paroxysmal AF, 25.2% in the diet group and 34.7% in the control group had no tachyarrhythmia recurrence, which translates into a 31% lower risk in the diet group.
In this study, the diet was rich in fish, nuts, fruits, and vegetables and was complemented with EVOO. Participants were also permitted moderate wine consumption.
The intervention involved dietitians who remotely followed patients and made periodic telephone calls to encourage them to stay on the diet. Participants had weight and body measurements taken at baseline and at 3, 6, 12, and 18 months and underwent an ECG at 6, 12, and 18 months. Labs were obtained at baseline and at 12 months. Participants were also given educational materials throughout the intervention.
Average scores, based on a scale of 0-13, excluding an item for wine intake, were 7.8 in the diet group and 7.2 in the control group.
Daily average alcohol intake was higher in the diet group than in the control group (9.8 vs 8.2 g), but “the weight of the patient during the study didn’t change in any group,” Dr. Barrio-Lopez reported.
Baseline characteristics were similar in the two groups. About 60% were taking antiarrhythmic drugs, and about 84% were taking anticoagulants.
‘A Tour de Force’
PREDIMAR was “really a tour de force,” Christine Albert, MD, MPH, chair of cardiology at the Smidt Heart Institute at the Cedars-Sinai Medical Center in Los Angeles, California, said during a commentary presented at HRS. “We talk about how we’re going to do these dietary interventions and weight loss and all the risk-factor reduction, and they pulled it off with 700 individuals and also did it in a way that was very novel.”
This is the first large-scale dietary intervention trial of patients with AF. However, Dr. Albert noted later in an interview, the Mediterranean diet poses potential challenges for some people with AF.
“The Mediterranean diet recommends that people drink wine, but then there’s clear evidence that abstinence from alcohol actually reduces recurrences of atrial fibrillation, so even though there are a lot of things about the Mediterranean diet that are probably healthy and good for atrial fibrillation, that aspect of it might be working against the patient,” she explained.
The finding that patients in the Mediterranean diet group experienced no significant weight loss could be counterintuitive when it comes to preventing AF. But “you could adapt the diet for AF,” Dr. Albert said. You could “leave out the wine and focus more on weight loss if the patient is obese because those are also the pillars of what we’ve learned for patients with atrial fibrillation.”
Making weight loss a key component of the study could be significant for the American population. “At least in the United States, that’s a huge part of the risk factors for atrial fibrillation after ablation,” she said.
The remote follow-up component of the PREDIMAR study is also intriguing. “I think what’s most exciting about what they did is, they showed they can do all these things remotely,” Dr. Albert added.
Dr. Barrio-Lopez had no relevant financial relationships. Dr. Albert disclosed relationships with Abbott, Roche Diagnostics, St. Jude Medical, Boston Scientific, Medtronic, and Element Science.
A version of this article appeared on Medscape.com.
FROM HRS 2024