User login
Discharge Planning
Hospitalized patients are often debilitated, either from their admitting illness or from the deconditioning that occurs with inactivity. Functional decline, which appears to progress in a hierarchical pattern,1 occurs in 24% to 50% of geriatric patients during hospitalization and is poorly documented.2 Such a decline is associated not only with longer hospital stays and increased health care costs but also with higher mortality.3 The American College of Physicians, through its Assessing Care of Vulnerable Elders project, expressly endorsed gait and mobility evaluation as a quality indicator, and examination insufficiency is well documented.4
Of the several existing mobility assessment tools, few are used routinely in hospital. Some require complex scoring; others require timing and/or a trained occupational therapist.5 We created a simplified tool named Independent Mobility Validation Examination (I‐MOVE) for use by bedside caregivers. We evaluated the tool's face validity and interobserver agreement.
I‐MOVE
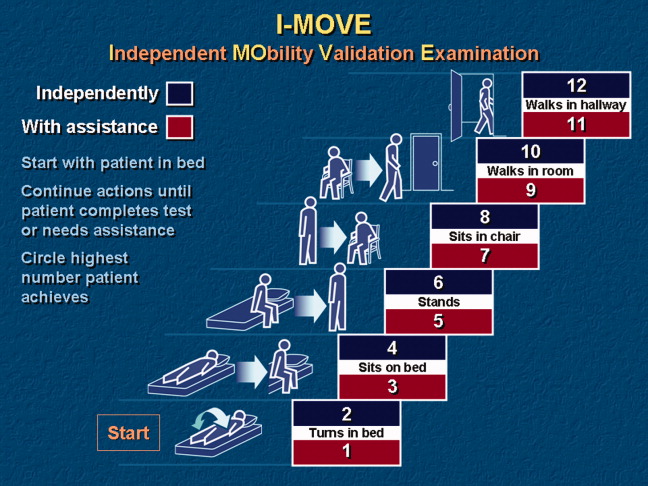
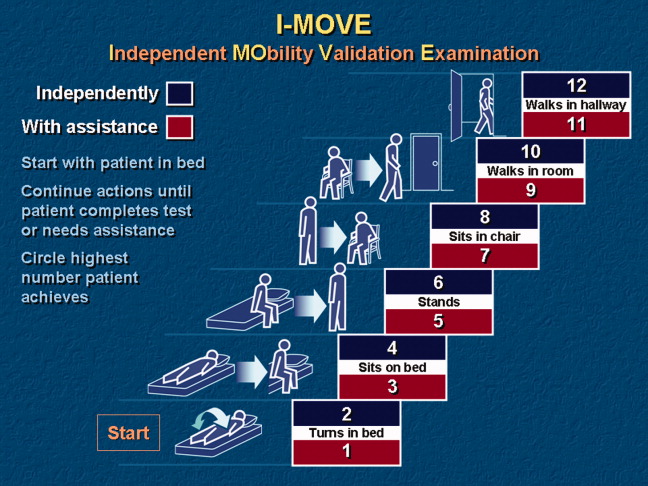
I‐MOVE, represented schematically in Figure 1, is a performance test that assesses the patient's ability to perform a sequence of 6 basic tasks: rolling over in bed, sitting up, standing, transferring to a chair, walking in the room, and walking in the hallway. Most motor functions can be assumed to be hierarchical in nature; any patient who can perform at the highest level, such as walking safely, also would be expected to perform at the lowest level.
Instructions for administering I‐MOVE are as follows:
-
Review current orders. Exclude patients ordered on bed rest or non‐weight‐bearing or other orders precluding any of the 6 requested actions.
-
Prepare environment.
-
Chair at bedside.
-
Lower side bed rail closest to chair.
-
Clear path for patient to ambulate.
-
Ensure patient dons slippers.
-
Flatten bed.
-
Ensure any gait assistive device, if generally used by the patient, is within reach from the bedside.
-
Requests for patient action (for steps c through f, make available and within reach any appropriate gait‐assistance device such as walker or cane, if such is customarily used at home or newly prescribed):
-
With patient lying supine in bed, with close supervision, ask patient to turn from side to side in bed (request when both bed rails are up).
-
Lower side rail closer to chair and ask the patient to rise up to a sitting position and turn to sit up with legs dangling off the bed.
-
Ask the patient to stand.
-
Ask the patient to take a seat in the chair next to the bed.
-
Ask the patient to ambulate in the room.
-
Ask the patient to ambulate in the hallway.
-
At any point if the patient seems incapable, unsteady, or unsafe to accomplish the requested task, render hands‐on assistance and immediately end the test.
-
Document, by number (1‐12), the activity level successfully accomplished independently by the patient (even number levels) or accomplished with assistance (odd number levels).
-
Patient may be considered independent if able to perform the activity with a normal assistive device (cane, walker, brace, or crutches) but not using furniture.
-
Assistance is defined as any physical contact with the patient.
Findings
Face Validity
We sent surveys to 6 experienced practicing clinicians at our hospital: a geriatrician, a physiatrist, an exercise physiologist, an occupational therapist, a physical therapist, and a registered nurse. We asked each clinician to rate the 6 I‐MOVE elements (requested actions) for clinical relevance to mobility independence. Relevance of each element was measured on an ordinal scale with scores ranging from 1 to 4, with: 1 not relevant; 2 somewhat relevant; 3 quite relevant; and 4 very relevant. From the 5 responses we received, 4 evaluators ranked all 6 I‐MOVE requested actions as very relevant. The fifth evaluator ranked 5 of the 6 actions as very relevant and 1 action (walking in the room) as quite relevant. These results demonstrate general agreement that I‐MOVE is, at face value, a reasonable measure of independent mobility.
Interrater Reliability
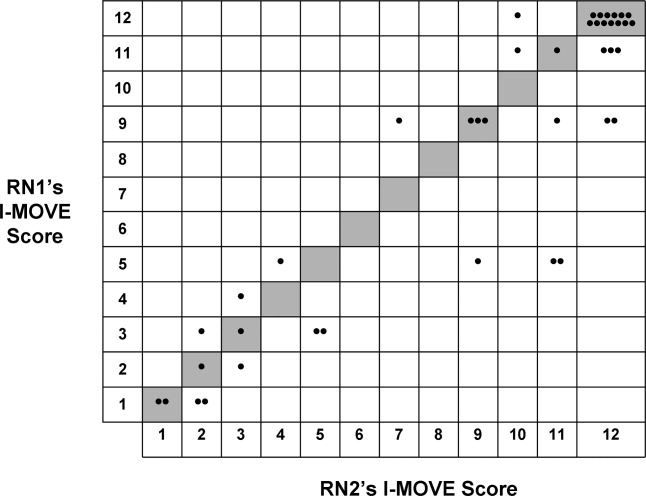
The protocol was approved by the hospital's institutional review board. On a general medical unita non‐electrocardiographic telemetry, nonsurgical unit of an acute care hospital, where patients are assigned the primary service of an internal medicine physicianwe instructed 2 registered nurse (RN) volunteers (RN1 and RN2) in the I‐MOVE protocol. Each RN administered I‐MOVE independently to 41 consecutive, cognitively intact patients in a blinded fashion (ie, neither nurse was aware of the other's scoring of each patient) and within 1 hour of each other's assessment.
After administering I‐MOVE to each patient, the nurse judged and scored the patient's performance using the 12‐level I‐MOVE ordinal scale, ranging from a low value of 1, complete dependence, to the highest value of 12, complete independence. The patients' I‐MOVE score pairs recorded by RN1 and RN2 were statistically compared. Interrater reliability, a comparison of the 41 patients' score pairs, is graphically represented in Figure 2. The calculated intraclass correlation coefficient (r) was 0.90, indicating excellent agreement (r > 0.75).
Discussion
Traditional physical examinations by physicians and assessments by nurses do not routinely extend to standardized mobility testing and may fail to recognize disability. Of the existing mobility assessment tools, we believe that most are not suited to patients hospitalized on general medical units. I‐MOVE has been designed to address this need, with an emphasis on practicality and brevity to allow repetition at appropriate intervals (tracking), as is done for vital signs. In this initial study, I‐MOVE was found to have face‐valid content and excellent interrater agreement.
Our study had several limitations. Only 1 pair of test administrators was involved; the sample population was chosen by convenience; clustering of outcomes occurred at level 12, which may have augmented the agreement; and the study was limited to cognitively intact patients. Note that we chose to use the intraclass correlation coefficient rather than the statistic because the weighting between the ordinal I‐MOVE scores has not yet been studied and defined. Also, the weighted is asymptotically equivalent to the intraclass correlation coefficient.
I‐MOVE is intended to aid caregivers in the recognition of debility so that appropriate interventions such as physical therapy may be prescribed. It was designed to complement, not replace, specialized evaluations such as those performed by physical therapists, occupational therapists, or comprehensive geriatric assessments. This practical assessment of basic functioning may enhance communication among caregivers, patients, and patients' family members, especially with regard to discharge planning. Further study is needed to validate I‐MOVE against existing tools, evaluate I‐MOVE's utility as a vital sign, and discern whether a sharp or unexpected decline portends a medical complication.
- .Health status and physical capacity. In:Osterweil D,Brummel‐Smith K,Beck JC, eds.Comprehensive Geriatric Assessment.New York:McGraw‐Hill;2000:41–66.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8(12):645–652.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52(8):1263–1270.
- ,,, et al.Detection and management of falls and instability in vulnerable elders by community physicians.J Am Geriatr Soc.2004;52(9):1527–1531.
- ,,.Exercising body and mind: an integrated approach to functional independence in hospitalized older people.J Am Geriatr Soc.2008;56(4):630–635.
Hospitalized patients are often debilitated, either from their admitting illness or from the deconditioning that occurs with inactivity. Functional decline, which appears to progress in a hierarchical pattern,1 occurs in 24% to 50% of geriatric patients during hospitalization and is poorly documented.2 Such a decline is associated not only with longer hospital stays and increased health care costs but also with higher mortality.3 The American College of Physicians, through its Assessing Care of Vulnerable Elders project, expressly endorsed gait and mobility evaluation as a quality indicator, and examination insufficiency is well documented.4
Of the several existing mobility assessment tools, few are used routinely in hospital. Some require complex scoring; others require timing and/or a trained occupational therapist.5 We created a simplified tool named Independent Mobility Validation Examination (I‐MOVE) for use by bedside caregivers. We evaluated the tool's face validity and interobserver agreement.
I‐MOVE
I‐MOVE, represented schematically in Figure 1, is a performance test that assesses the patient's ability to perform a sequence of 6 basic tasks: rolling over in bed, sitting up, standing, transferring to a chair, walking in the room, and walking in the hallway. Most motor functions can be assumed to be hierarchical in nature; any patient who can perform at the highest level, such as walking safely, also would be expected to perform at the lowest level.
Instructions for administering I‐MOVE are as follows:
-
Review current orders. Exclude patients ordered on bed rest or non‐weight‐bearing or other orders precluding any of the 6 requested actions.
-
Prepare environment.
-
Chair at bedside.
-
Lower side bed rail closest to chair.
-
Clear path for patient to ambulate.
-
Ensure patient dons slippers.
-
Flatten bed.
-
Ensure any gait assistive device, if generally used by the patient, is within reach from the bedside.
-
Requests for patient action (for steps c through f, make available and within reach any appropriate gait‐assistance device such as walker or cane, if such is customarily used at home or newly prescribed):
-
With patient lying supine in bed, with close supervision, ask patient to turn from side to side in bed (request when both bed rails are up).
-
Lower side rail closer to chair and ask the patient to rise up to a sitting position and turn to sit up with legs dangling off the bed.
-
Ask the patient to stand.
-
Ask the patient to take a seat in the chair next to the bed.
-
Ask the patient to ambulate in the room.
-
Ask the patient to ambulate in the hallway.
-
At any point if the patient seems incapable, unsteady, or unsafe to accomplish the requested task, render hands‐on assistance and immediately end the test.
-
Document, by number (1‐12), the activity level successfully accomplished independently by the patient (even number levels) or accomplished with assistance (odd number levels).
-
Patient may be considered independent if able to perform the activity with a normal assistive device (cane, walker, brace, or crutches) but not using furniture.
-
Assistance is defined as any physical contact with the patient.
Findings
Face Validity
We sent surveys to 6 experienced practicing clinicians at our hospital: a geriatrician, a physiatrist, an exercise physiologist, an occupational therapist, a physical therapist, and a registered nurse. We asked each clinician to rate the 6 I‐MOVE elements (requested actions) for clinical relevance to mobility independence. Relevance of each element was measured on an ordinal scale with scores ranging from 1 to 4, with: 1 not relevant; 2 somewhat relevant; 3 quite relevant; and 4 very relevant. From the 5 responses we received, 4 evaluators ranked all 6 I‐MOVE requested actions as very relevant. The fifth evaluator ranked 5 of the 6 actions as very relevant and 1 action (walking in the room) as quite relevant. These results demonstrate general agreement that I‐MOVE is, at face value, a reasonable measure of independent mobility.
Interrater Reliability
The protocol was approved by the hospital's institutional review board. On a general medical unita non‐electrocardiographic telemetry, nonsurgical unit of an acute care hospital, where patients are assigned the primary service of an internal medicine physicianwe instructed 2 registered nurse (RN) volunteers (RN1 and RN2) in the I‐MOVE protocol. Each RN administered I‐MOVE independently to 41 consecutive, cognitively intact patients in a blinded fashion (ie, neither nurse was aware of the other's scoring of each patient) and within 1 hour of each other's assessment.
After administering I‐MOVE to each patient, the nurse judged and scored the patient's performance using the 12‐level I‐MOVE ordinal scale, ranging from a low value of 1, complete dependence, to the highest value of 12, complete independence. The patients' I‐MOVE score pairs recorded by RN1 and RN2 were statistically compared. Interrater reliability, a comparison of the 41 patients' score pairs, is graphically represented in Figure 2. The calculated intraclass correlation coefficient (r) was 0.90, indicating excellent agreement (r > 0.75).
Discussion
Traditional physical examinations by physicians and assessments by nurses do not routinely extend to standardized mobility testing and may fail to recognize disability. Of the existing mobility assessment tools, we believe that most are not suited to patients hospitalized on general medical units. I‐MOVE has been designed to address this need, with an emphasis on practicality and brevity to allow repetition at appropriate intervals (tracking), as is done for vital signs. In this initial study, I‐MOVE was found to have face‐valid content and excellent interrater agreement.
Our study had several limitations. Only 1 pair of test administrators was involved; the sample population was chosen by convenience; clustering of outcomes occurred at level 12, which may have augmented the agreement; and the study was limited to cognitively intact patients. Note that we chose to use the intraclass correlation coefficient rather than the statistic because the weighting between the ordinal I‐MOVE scores has not yet been studied and defined. Also, the weighted is asymptotically equivalent to the intraclass correlation coefficient.
I‐MOVE is intended to aid caregivers in the recognition of debility so that appropriate interventions such as physical therapy may be prescribed. It was designed to complement, not replace, specialized evaluations such as those performed by physical therapists, occupational therapists, or comprehensive geriatric assessments. This practical assessment of basic functioning may enhance communication among caregivers, patients, and patients' family members, especially with regard to discharge planning. Further study is needed to validate I‐MOVE against existing tools, evaluate I‐MOVE's utility as a vital sign, and discern whether a sharp or unexpected decline portends a medical complication.
Hospitalized patients are often debilitated, either from their admitting illness or from the deconditioning that occurs with inactivity. Functional decline, which appears to progress in a hierarchical pattern,1 occurs in 24% to 50% of geriatric patients during hospitalization and is poorly documented.2 Such a decline is associated not only with longer hospital stays and increased health care costs but also with higher mortality.3 The American College of Physicians, through its Assessing Care of Vulnerable Elders project, expressly endorsed gait and mobility evaluation as a quality indicator, and examination insufficiency is well documented.4
Of the several existing mobility assessment tools, few are used routinely in hospital. Some require complex scoring; others require timing and/or a trained occupational therapist.5 We created a simplified tool named Independent Mobility Validation Examination (I‐MOVE) for use by bedside caregivers. We evaluated the tool's face validity and interobserver agreement.
I‐MOVE
I‐MOVE, represented schematically in Figure 1, is a performance test that assesses the patient's ability to perform a sequence of 6 basic tasks: rolling over in bed, sitting up, standing, transferring to a chair, walking in the room, and walking in the hallway. Most motor functions can be assumed to be hierarchical in nature; any patient who can perform at the highest level, such as walking safely, also would be expected to perform at the lowest level.
Instructions for administering I‐MOVE are as follows:
-
Review current orders. Exclude patients ordered on bed rest or non‐weight‐bearing or other orders precluding any of the 6 requested actions.
-
Prepare environment.
-
Chair at bedside.
-
Lower side bed rail closest to chair.
-
Clear path for patient to ambulate.
-
Ensure patient dons slippers.
-
Flatten bed.
-
Ensure any gait assistive device, if generally used by the patient, is within reach from the bedside.
-
Requests for patient action (for steps c through f, make available and within reach any appropriate gait‐assistance device such as walker or cane, if such is customarily used at home or newly prescribed):
-
With patient lying supine in bed, with close supervision, ask patient to turn from side to side in bed (request when both bed rails are up).
-
Lower side rail closer to chair and ask the patient to rise up to a sitting position and turn to sit up with legs dangling off the bed.
-
Ask the patient to stand.
-
Ask the patient to take a seat in the chair next to the bed.
-
Ask the patient to ambulate in the room.
-
Ask the patient to ambulate in the hallway.
-
At any point if the patient seems incapable, unsteady, or unsafe to accomplish the requested task, render hands‐on assistance and immediately end the test.
-
Document, by number (1‐12), the activity level successfully accomplished independently by the patient (even number levels) or accomplished with assistance (odd number levels).
-
Patient may be considered independent if able to perform the activity with a normal assistive device (cane, walker, brace, or crutches) but not using furniture.
-
Assistance is defined as any physical contact with the patient.
Findings
Face Validity
We sent surveys to 6 experienced practicing clinicians at our hospital: a geriatrician, a physiatrist, an exercise physiologist, an occupational therapist, a physical therapist, and a registered nurse. We asked each clinician to rate the 6 I‐MOVE elements (requested actions) for clinical relevance to mobility independence. Relevance of each element was measured on an ordinal scale with scores ranging from 1 to 4, with: 1 not relevant; 2 somewhat relevant; 3 quite relevant; and 4 very relevant. From the 5 responses we received, 4 evaluators ranked all 6 I‐MOVE requested actions as very relevant. The fifth evaluator ranked 5 of the 6 actions as very relevant and 1 action (walking in the room) as quite relevant. These results demonstrate general agreement that I‐MOVE is, at face value, a reasonable measure of independent mobility.
Interrater Reliability
The protocol was approved by the hospital's institutional review board. On a general medical unita non‐electrocardiographic telemetry, nonsurgical unit of an acute care hospital, where patients are assigned the primary service of an internal medicine physicianwe instructed 2 registered nurse (RN) volunteers (RN1 and RN2) in the I‐MOVE protocol. Each RN administered I‐MOVE independently to 41 consecutive, cognitively intact patients in a blinded fashion (ie, neither nurse was aware of the other's scoring of each patient) and within 1 hour of each other's assessment.
After administering I‐MOVE to each patient, the nurse judged and scored the patient's performance using the 12‐level I‐MOVE ordinal scale, ranging from a low value of 1, complete dependence, to the highest value of 12, complete independence. The patients' I‐MOVE score pairs recorded by RN1 and RN2 were statistically compared. Interrater reliability, a comparison of the 41 patients' score pairs, is graphically represented in Figure 2. The calculated intraclass correlation coefficient (r) was 0.90, indicating excellent agreement (r > 0.75).
Discussion
Traditional physical examinations by physicians and assessments by nurses do not routinely extend to standardized mobility testing and may fail to recognize disability. Of the existing mobility assessment tools, we believe that most are not suited to patients hospitalized on general medical units. I‐MOVE has been designed to address this need, with an emphasis on practicality and brevity to allow repetition at appropriate intervals (tracking), as is done for vital signs. In this initial study, I‐MOVE was found to have face‐valid content and excellent interrater agreement.
Our study had several limitations. Only 1 pair of test administrators was involved; the sample population was chosen by convenience; clustering of outcomes occurred at level 12, which may have augmented the agreement; and the study was limited to cognitively intact patients. Note that we chose to use the intraclass correlation coefficient rather than the statistic because the weighting between the ordinal I‐MOVE scores has not yet been studied and defined. Also, the weighted is asymptotically equivalent to the intraclass correlation coefficient.
I‐MOVE is intended to aid caregivers in the recognition of debility so that appropriate interventions such as physical therapy may be prescribed. It was designed to complement, not replace, specialized evaluations such as those performed by physical therapists, occupational therapists, or comprehensive geriatric assessments. This practical assessment of basic functioning may enhance communication among caregivers, patients, and patients' family members, especially with regard to discharge planning. Further study is needed to validate I‐MOVE against existing tools, evaluate I‐MOVE's utility as a vital sign, and discern whether a sharp or unexpected decline portends a medical complication.
- .Health status and physical capacity. In:Osterweil D,Brummel‐Smith K,Beck JC, eds.Comprehensive Geriatric Assessment.New York:McGraw‐Hill;2000:41–66.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8(12):645–652.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52(8):1263–1270.
- ,,, et al.Detection and management of falls and instability in vulnerable elders by community physicians.J Am Geriatr Soc.2004;52(9):1527–1531.
- ,,.Exercising body and mind: an integrated approach to functional independence in hospitalized older people.J Am Geriatr Soc.2008;56(4):630–635.
- .Health status and physical capacity. In:Osterweil D,Brummel‐Smith K,Beck JC, eds.Comprehensive Geriatric Assessment.New York:McGraw‐Hill;2000:41–66.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8(12):645–652.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52(8):1263–1270.
- ,,, et al.Detection and management of falls and instability in vulnerable elders by community physicians.J Am Geriatr Soc.2004;52(9):1527–1531.
- ,,.Exercising body and mind: an integrated approach to functional independence in hospitalized older people.J Am Geriatr Soc.2008;56(4):630–635.
A New Narrative for Hospitalists
The hospitalist is not typically the hero in contemporary narratives about medical practice. More often, the hospitalist is portrayed as an interloper, a doctor who works for the hospital and not the patient, an employee focused on efficiency and rapid discharge rather than continuous medical care. Elsewhere in this issue, Mai Pham1 offers an updated story in which a hospitalist organizes the loose ends of a patient's medical history and contributes significantly to healthcare coordination.
Hospitalists acknowledge that an admission to the hospital disrupts established outpatient continuity and that discharge can be a perilous event, with potential for medical errors. The Society of Hospital Medicine has recognized discontinuity as enough of a concern that care transitions are considered a core competency for hospital physicians.2 This competency requires hospitalists to be able to move a patient safely from the outpatient setting through the hospital wards and back home again.
As our specialty approaches two decades of practice experience, the work that we do in coordinating medical care and ensuring continuity has evolved and deepened. Initial efforts to coordinate care from the inpatient setting focused on how key hospital events could be best communicated to the patient's primary physician.3, 4 Communication at admission and at critical junctures was encouraged, and research demonstrated that a timely discharge summary sent to the primary care office could decrease hospital readmission.5
Experienced hospitalists recognize, however, that not every inpatient can identify a primary care doctor; sometimes, it is this very lack of established outpatient care that triggers a patient's admission. Reasons for discontinuous prehospital care include disrupted outpatient relationships, particularly as provider networks and insurance status are re‐evaluated, as well as cultural and social barriers. Complex, overcrowded outpatient health systems can be challenging to navigate even for the savviest of patients.
These concerns have helped us to focus on the hospital as a critical setting for delivering continuity of care. The mechanisms for ensuring continuity include, harnessing the inpatient capability for real‐time diagnosis and treatment synthesis, which, in Mai Pham's case,1 enabled decision‐making and timely care coordination for her dying grandmother. Hospitals typically offer an array of tools needed to assist physicians in coordinating a patient's care, including rapid diagnostic testing and simultaneous multidisciplinary evaluation with consulting physicians; nurses; case managers; physical, occupational, and speech therapists; pharmacists; nutritionists; social workers; and palliative care teams. The patient's family members and friends are frequently present in the inpatient setting and can provide additional data points that are not always available in a timely manner in the ambulatory setting. Each of these inpatient interactions can help patients to develop routes of access to healthcare after they are discharged from the hospital.
Despite the advantages of the hospital setting, however, the knock on hospitalists is that we are just on the clock. Frequent handoffs, both when physician shifts change and when a fresh hospitalist rotates on service, present a significant concern to seamless care.6 Increasing fragmentation in hospital staffing may correlate with lengthened hospital stay and increased difficulty in receiving follow‐up outpatient care.7 A new narrative for hospitalists, one focused on enhancing continuity, requires mindfulness toward schedule fragmentation and balances personal desires with the need to maintain a continued presence and availability for patients.
Enhancing continuity and care coordination in the hospital also means continually working to improve provider‐to‐provider communications. Solutions may include well‐executed chart documentation, with active concerns flagged for the oncoming physician, and an electronic medical record that is easy to access from various locations. Computerized templates may enable more thorough handoffs in certain settings.8 As the use of systems and checklists gains traction for their ability to reduce iatrogenic complications and save money,9 hospitalists may come to rely more widely on systems that improve continuity, especially for aspects of inpatient care such as medication reconciliation.10
We believe that the most critical way in which hospitalists can ensure continuous care involves increasing physician efforts to engage with patients during their hospitalization. Hospitalists meet patients at particularly intense and vulnerable times of life, and we have all observed how patients can lose autonomy simply by being hospitalized. In the hospital, things happen to patients, sometimes because of the sheer size and force of the inpatient team and the momentum of a hospital stay.
Yet hospitalists can quickly develop a rapport with their patients through the number and intensity of their patient interactions. The free‐form structure of the inpatient schedule means a flexibility to be present with patients on short notice, to respond to acute events in real time, and to be available to talk with family members and other caregivers at their convenience. Hospitalists can take part in multiple bedside interactions in a single day and on consecutive days. Because of this flexibility, hospitalists can bond with their patients in a short time frame11 as they access critical social and clinical contexts, often more efficiently than possible elsewhere. As one primary care physician wrote when she gave up caring for her hospitalized patients, I know what happened to my patient, but I didn't really experience it with my patient.12 Hospitalists do get to share in this drama.
The medical community has been slow to recognize that hospitalists, as much as any generalist physician, can and do engage patients actively in their medical care. The hospital can be an ideal setting to ensure continuity through real‐time diagnostics and therapeutics and even more so through the intense bonding that can happen between physicians and patients on the wards. The old story of an outpatient provider single‐handedly managing a patient's care is rapidly disappearing in many locales. However, the story of the hospitalist is more than that of the hero in waiting. The story is a cautionary tale, one in which the relationship between the hospitalist and his or her patients is still under development, a tale for which much work remains. As hospitalists, we must continue to refine our skills and systems to deliver continuous care for patients in transition. We must also continue to focus on experiences with our patients and their families and, when called upon, to engage in those challenging conversations that Mai Pham1 says force us to align our expectations of one another. Forging this human connection will always be part of seamless healthcare for every physician, not least for the hospitalist.
Acknowledgements
The authors acknowledge Andrew Auerbach, MD, and John Choe, MD, MPH, for their comments on this article.
- .Dismantling Rube Goldberg: Cutting through chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- Transitions of care.J Hosp Med.2006;1(suppl 1):95.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- ,.Care transitions for hospitalized patients.Med Clin North Am.2008;92(2):315–324, viii.
- ,,,,.Impact of fragmentation of hospitalist care on length of stay and postdischarge issues. Abstract presented at: Society of Hospital Medicine 2008 Annual Meeting; April 2008; San Diego, CA.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200(4):538–545.
- .The checklist.New Yorker. December 10, 2007.
- ,,, et al.Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists.J Hosp Med.2006;1(6):354–360.
- ,.The hospitalist's story.JAMA.2006;296(17):2067–2068.
- .Satisfaction?JAMA.2005;293(18):2193.
The hospitalist is not typically the hero in contemporary narratives about medical practice. More often, the hospitalist is portrayed as an interloper, a doctor who works for the hospital and not the patient, an employee focused on efficiency and rapid discharge rather than continuous medical care. Elsewhere in this issue, Mai Pham1 offers an updated story in which a hospitalist organizes the loose ends of a patient's medical history and contributes significantly to healthcare coordination.
Hospitalists acknowledge that an admission to the hospital disrupts established outpatient continuity and that discharge can be a perilous event, with potential for medical errors. The Society of Hospital Medicine has recognized discontinuity as enough of a concern that care transitions are considered a core competency for hospital physicians.2 This competency requires hospitalists to be able to move a patient safely from the outpatient setting through the hospital wards and back home again.
As our specialty approaches two decades of practice experience, the work that we do in coordinating medical care and ensuring continuity has evolved and deepened. Initial efforts to coordinate care from the inpatient setting focused on how key hospital events could be best communicated to the patient's primary physician.3, 4 Communication at admission and at critical junctures was encouraged, and research demonstrated that a timely discharge summary sent to the primary care office could decrease hospital readmission.5
Experienced hospitalists recognize, however, that not every inpatient can identify a primary care doctor; sometimes, it is this very lack of established outpatient care that triggers a patient's admission. Reasons for discontinuous prehospital care include disrupted outpatient relationships, particularly as provider networks and insurance status are re‐evaluated, as well as cultural and social barriers. Complex, overcrowded outpatient health systems can be challenging to navigate even for the savviest of patients.
These concerns have helped us to focus on the hospital as a critical setting for delivering continuity of care. The mechanisms for ensuring continuity include, harnessing the inpatient capability for real‐time diagnosis and treatment synthesis, which, in Mai Pham's case,1 enabled decision‐making and timely care coordination for her dying grandmother. Hospitals typically offer an array of tools needed to assist physicians in coordinating a patient's care, including rapid diagnostic testing and simultaneous multidisciplinary evaluation with consulting physicians; nurses; case managers; physical, occupational, and speech therapists; pharmacists; nutritionists; social workers; and palliative care teams. The patient's family members and friends are frequently present in the inpatient setting and can provide additional data points that are not always available in a timely manner in the ambulatory setting. Each of these inpatient interactions can help patients to develop routes of access to healthcare after they are discharged from the hospital.
Despite the advantages of the hospital setting, however, the knock on hospitalists is that we are just on the clock. Frequent handoffs, both when physician shifts change and when a fresh hospitalist rotates on service, present a significant concern to seamless care.6 Increasing fragmentation in hospital staffing may correlate with lengthened hospital stay and increased difficulty in receiving follow‐up outpatient care.7 A new narrative for hospitalists, one focused on enhancing continuity, requires mindfulness toward schedule fragmentation and balances personal desires with the need to maintain a continued presence and availability for patients.
Enhancing continuity and care coordination in the hospital also means continually working to improve provider‐to‐provider communications. Solutions may include well‐executed chart documentation, with active concerns flagged for the oncoming physician, and an electronic medical record that is easy to access from various locations. Computerized templates may enable more thorough handoffs in certain settings.8 As the use of systems and checklists gains traction for their ability to reduce iatrogenic complications and save money,9 hospitalists may come to rely more widely on systems that improve continuity, especially for aspects of inpatient care such as medication reconciliation.10
We believe that the most critical way in which hospitalists can ensure continuous care involves increasing physician efforts to engage with patients during their hospitalization. Hospitalists meet patients at particularly intense and vulnerable times of life, and we have all observed how patients can lose autonomy simply by being hospitalized. In the hospital, things happen to patients, sometimes because of the sheer size and force of the inpatient team and the momentum of a hospital stay.
Yet hospitalists can quickly develop a rapport with their patients through the number and intensity of their patient interactions. The free‐form structure of the inpatient schedule means a flexibility to be present with patients on short notice, to respond to acute events in real time, and to be available to talk with family members and other caregivers at their convenience. Hospitalists can take part in multiple bedside interactions in a single day and on consecutive days. Because of this flexibility, hospitalists can bond with their patients in a short time frame11 as they access critical social and clinical contexts, often more efficiently than possible elsewhere. As one primary care physician wrote when she gave up caring for her hospitalized patients, I know what happened to my patient, but I didn't really experience it with my patient.12 Hospitalists do get to share in this drama.
The medical community has been slow to recognize that hospitalists, as much as any generalist physician, can and do engage patients actively in their medical care. The hospital can be an ideal setting to ensure continuity through real‐time diagnostics and therapeutics and even more so through the intense bonding that can happen between physicians and patients on the wards. The old story of an outpatient provider single‐handedly managing a patient's care is rapidly disappearing in many locales. However, the story of the hospitalist is more than that of the hero in waiting. The story is a cautionary tale, one in which the relationship between the hospitalist and his or her patients is still under development, a tale for which much work remains. As hospitalists, we must continue to refine our skills and systems to deliver continuous care for patients in transition. We must also continue to focus on experiences with our patients and their families and, when called upon, to engage in those challenging conversations that Mai Pham1 says force us to align our expectations of one another. Forging this human connection will always be part of seamless healthcare for every physician, not least for the hospitalist.
Acknowledgements
The authors acknowledge Andrew Auerbach, MD, and John Choe, MD, MPH, for their comments on this article.
The hospitalist is not typically the hero in contemporary narratives about medical practice. More often, the hospitalist is portrayed as an interloper, a doctor who works for the hospital and not the patient, an employee focused on efficiency and rapid discharge rather than continuous medical care. Elsewhere in this issue, Mai Pham1 offers an updated story in which a hospitalist organizes the loose ends of a patient's medical history and contributes significantly to healthcare coordination.
Hospitalists acknowledge that an admission to the hospital disrupts established outpatient continuity and that discharge can be a perilous event, with potential for medical errors. The Society of Hospital Medicine has recognized discontinuity as enough of a concern that care transitions are considered a core competency for hospital physicians.2 This competency requires hospitalists to be able to move a patient safely from the outpatient setting through the hospital wards and back home again.
As our specialty approaches two decades of practice experience, the work that we do in coordinating medical care and ensuring continuity has evolved and deepened. Initial efforts to coordinate care from the inpatient setting focused on how key hospital events could be best communicated to the patient's primary physician.3, 4 Communication at admission and at critical junctures was encouraged, and research demonstrated that a timely discharge summary sent to the primary care office could decrease hospital readmission.5
Experienced hospitalists recognize, however, that not every inpatient can identify a primary care doctor; sometimes, it is this very lack of established outpatient care that triggers a patient's admission. Reasons for discontinuous prehospital care include disrupted outpatient relationships, particularly as provider networks and insurance status are re‐evaluated, as well as cultural and social barriers. Complex, overcrowded outpatient health systems can be challenging to navigate even for the savviest of patients.
These concerns have helped us to focus on the hospital as a critical setting for delivering continuity of care. The mechanisms for ensuring continuity include, harnessing the inpatient capability for real‐time diagnosis and treatment synthesis, which, in Mai Pham's case,1 enabled decision‐making and timely care coordination for her dying grandmother. Hospitals typically offer an array of tools needed to assist physicians in coordinating a patient's care, including rapid diagnostic testing and simultaneous multidisciplinary evaluation with consulting physicians; nurses; case managers; physical, occupational, and speech therapists; pharmacists; nutritionists; social workers; and palliative care teams. The patient's family members and friends are frequently present in the inpatient setting and can provide additional data points that are not always available in a timely manner in the ambulatory setting. Each of these inpatient interactions can help patients to develop routes of access to healthcare after they are discharged from the hospital.
Despite the advantages of the hospital setting, however, the knock on hospitalists is that we are just on the clock. Frequent handoffs, both when physician shifts change and when a fresh hospitalist rotates on service, present a significant concern to seamless care.6 Increasing fragmentation in hospital staffing may correlate with lengthened hospital stay and increased difficulty in receiving follow‐up outpatient care.7 A new narrative for hospitalists, one focused on enhancing continuity, requires mindfulness toward schedule fragmentation and balances personal desires with the need to maintain a continued presence and availability for patients.
Enhancing continuity and care coordination in the hospital also means continually working to improve provider‐to‐provider communications. Solutions may include well‐executed chart documentation, with active concerns flagged for the oncoming physician, and an electronic medical record that is easy to access from various locations. Computerized templates may enable more thorough handoffs in certain settings.8 As the use of systems and checklists gains traction for their ability to reduce iatrogenic complications and save money,9 hospitalists may come to rely more widely on systems that improve continuity, especially for aspects of inpatient care such as medication reconciliation.10
We believe that the most critical way in which hospitalists can ensure continuous care involves increasing physician efforts to engage with patients during their hospitalization. Hospitalists meet patients at particularly intense and vulnerable times of life, and we have all observed how patients can lose autonomy simply by being hospitalized. In the hospital, things happen to patients, sometimes because of the sheer size and force of the inpatient team and the momentum of a hospital stay.
Yet hospitalists can quickly develop a rapport with their patients through the number and intensity of their patient interactions. The free‐form structure of the inpatient schedule means a flexibility to be present with patients on short notice, to respond to acute events in real time, and to be available to talk with family members and other caregivers at their convenience. Hospitalists can take part in multiple bedside interactions in a single day and on consecutive days. Because of this flexibility, hospitalists can bond with their patients in a short time frame11 as they access critical social and clinical contexts, often more efficiently than possible elsewhere. As one primary care physician wrote when she gave up caring for her hospitalized patients, I know what happened to my patient, but I didn't really experience it with my patient.12 Hospitalists do get to share in this drama.
The medical community has been slow to recognize that hospitalists, as much as any generalist physician, can and do engage patients actively in their medical care. The hospital can be an ideal setting to ensure continuity through real‐time diagnostics and therapeutics and even more so through the intense bonding that can happen between physicians and patients on the wards. The old story of an outpatient provider single‐handedly managing a patient's care is rapidly disappearing in many locales. However, the story of the hospitalist is more than that of the hero in waiting. The story is a cautionary tale, one in which the relationship between the hospitalist and his or her patients is still under development, a tale for which much work remains. As hospitalists, we must continue to refine our skills and systems to deliver continuous care for patients in transition. We must also continue to focus on experiences with our patients and their families and, when called upon, to engage in those challenging conversations that Mai Pham1 says force us to align our expectations of one another. Forging this human connection will always be part of seamless healthcare for every physician, not least for the hospitalist.
Acknowledgements
The authors acknowledge Andrew Auerbach, MD, and John Choe, MD, MPH, for their comments on this article.
- .Dismantling Rube Goldberg: Cutting through chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- Transitions of care.J Hosp Med.2006;1(suppl 1):95.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- ,.Care transitions for hospitalized patients.Med Clin North Am.2008;92(2):315–324, viii.
- ,,,,.Impact of fragmentation of hospitalist care on length of stay and postdischarge issues. Abstract presented at: Society of Hospital Medicine 2008 Annual Meeting; April 2008; San Diego, CA.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200(4):538–545.
- .The checklist.New Yorker. December 10, 2007.
- ,,, et al.Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists.J Hosp Med.2006;1(6):354–360.
- ,.The hospitalist's story.JAMA.2006;296(17):2067–2068.
- .Satisfaction?JAMA.2005;293(18):2193.
- .Dismantling Rube Goldberg: Cutting through chaos to achieve coordinated care.J Hosp Med.2009;4(4):259–260.
- Transitions of care.J Hosp Med.2006;1(suppl 1):95.
- ,,,,,.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care.JAMA.2007;297(8):831–841.
- ,,,.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists.J Hosp Med.2007;2(5):314–323.
- ,,,.Effect of discharge summary availability during post‐discharge visits on hospital readmission.J Gen Intern Med.2002;17(3):186–192.
- ,.Care transitions for hospitalized patients.Med Clin North Am.2008;92(2):315–324, viii.
- ,,,,.Impact of fragmentation of hospitalist care on length of stay and postdischarge issues. Abstract presented at: Society of Hospital Medicine 2008 Annual Meeting; April 2008; San Diego, CA.
- ,,,,.A randomized, controlled trial evaluating the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200(4):538–545.
- .The checklist.New Yorker. December 10, 2007.
- ,,, et al.Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists.J Hosp Med.2006;1(6):354–360.
- ,.The hospitalist's story.JAMA.2006;296(17):2067–2068.
- .Satisfaction?JAMA.2005;293(18):2193.
Impact of Elderly Inpatient Care Bundle
Elderly patients (aged 65 years and older) consume a disproportionate amount of acute health care resources, composing up to 20% of emergency department (ED) visits,1, 2 having a 2‐fold to 5‐fold increase in likelihood of hospital admission,1 and frequently incurring lengths of hospital stay (LOS) approximately 15% higher than the national averages.3 In addition, they are at increased risk for hospital readmission in the 90‐day interval following hospital discharge.1, 4, 5 Specific risk factors for readmission include age above 80 years, discharge within the previous 30 days, the presence of 3 or more comorbid diagnoses, use of 5 or more prescription medications, difficulty with at least 1 activity of daily living (ADL), and lack of discharge education.6 These risk factors can translate into adverse drug events,79 exacerbations of chronic diseases,10 or functional decline4, 5 that can trigger ED visits or hospital readmission.
Hospital‐based care coordinationdefined as a multidisciplinary interaction between inpatients and providers that focuses on education, communication, and discharge planning with the primary aim of improving outcomeshas demonstrated inconsistent results as a mechanism to reduce LOS, postdischarge ED visits, or hospital readmission rates. While disease‐specific care coordination programs for congestive heart failure and chronic obstructive pulmonary disease have been effective in reducing rehospitalization rates,1015 the benefits of comprehensive care coordination for elderly general medical inpatients with a broader range of diagnoses are less clear. In a group of 750 elderly patients with 1 of 11 common inpatient diagnoses (such as stroke or hip fracture) likely to ultimately require a high level of home support, Coleman et al.16 found that a structured transitional care program centered on a personal coach decreased rehospitalization rates at 30 and 90 days. Preen et al.17 found improved patient involvement and perceived quality of life with care coordination focused on discharge planning, but no impact on LOS. Likewise, a recent meta‐analysis18 failed to demonstrate statistically significant differences in mortality, LOS, or readmission rates in hospitalized patients who received intensive care coordination versus usual care; however, variation in the components of the care coordination intervention and reported outcomes restricted the ability to pool data in this study.
Care coordination programs demonstrating efficacy in reducing health care utilization in elderly medical patients have generally included an outpatient transitional component with out‐of‐hospital postacute care visits by health care personnel such as a nurse, pharmacist, or physician.1923 These offsite interventions generate additional expenses and resource demands that may not be practical for smaller hospitals to implement.24, 25 In contrast, hospital‐based care coordination programs have clear ownership and thus may be more practical to disseminate. Individual elements of hospital‐based care coordination such as pharmacist counseling, discharge education, and telephone follow‐up have been shown to reduce ED visitation and readmission rates in high‐risk elderly patients. Less information is available regarding the impact of these interventions delivered in an aggregate bundle by hospital staff in the absence of bridging transitional visits.2629
The objective of this pilot study was to determine whether a supplemental elderly care bundle, targeted to high‐risk inpatients by hospital staff as an enhancement to existing care coordination, would affect postdischarge readmission and ED visit rates. The intervention was designed to capitalize on existing resources, and focused specifically on elderly inpatients who were hospitalized with diagnoses commonly encountered in a general medical unit and predisposed to recidivism.
Patients and Methods
Patient Selection and Enrollment
The screening population consisted of elderly patients admitted to 1 of 2 hospital‐medicine groups (MedProvider Inpatient Care Unit or Texas Primary Care) at the 900‐bed Baylor University Medical Center (BUMC, Dallas, TX) between March and June 2007 with a diagnosis likely to fall within 1 of 20 frequent Medicare medical diagnosis reimbursement groups (DRGs) at BUMC, as listed in Table 1. Study personnel performed daily chart review to establish eligibility criteria, which included age 70 years, use of 5 medications regularly, 3 chronic comorbid conditions, requirement for assistance with 1 ADL, and preadmission residence at home or assisted living with a reasonable expectation of disposition back to that domicile. These criteria were based on factors found in the literature to be associated with extended LOS and postdischarge readmission/ED visit events.5, 6, 3032 Potential enrollees needed to be conversant in English (a multilingual staff was not feasible due to limited resources for this pilot project) and have reliable phone contact, or have a proxy caregiver who could speak English and be reached by phone. Predefined exclusion criteria were admission primarily for a surgical procedure, terminal diagnosis with life expectancy 6 months, residence in a long‐term care facility (long‐term acute care [LTAC], skilled nursing facility [SNF], or nursing home) prior to hospitalization with anticipated discharge back to that facility, and patient/family refusal to participate. Additionally, with an average LOS between 5 and 6 days in BUMC's Medicare population for the DRGs of interest, it was felt that the effects of the care bundle intervention would be obscured unless initiated early in the hospitalization. Thus, patients who could not be enrolled within 72 hours following admission were subsequently excluded. The Baylor Health Care System (BHCS) Institutional Review Board (IRB) approved this study, and written informed consent was obtained from all patients or their surrogates.
| DRG | DRG Name |
|---|---|
| |
| 127 | Heart failure and shock |
| 14 | Intracranial hemorrhage or cerebral infarction |
| 89 | Simple pneumonia/pleurisy |
| 416 | Septicemia |
| 316 | Renal failure |
| 182 | Esophagitis/gastroenterological/miscellaneous digestive disorders with complications |
| 174 | Gastrointestinal hemorrhage with complications |
| 88 | Chronic obstructive pulmonary disease |
| 320 | Kidney/urinary tract infection with complications |
| 144 | Other circulatory diagnoses with complications |
| 138 | Arrhythmia/conduction disorders with complications |
| 277 | Cellulitis with complications |
| 124 | Circulatory disorders except acute myocardial infarction with cardiac catheterization and complex diagnosis |
| 430 | Psychoses |
| 188 | Other digestive diagnoses with complications |
| 395 | Red blood cell disorders |
| 79 | Respiratory infections and inflammations with complications |
| 524 | Transient ischemia |
| 143 | Chest pain |
| 141 | Syncope and collapse with complications |
Patients meeting eligibility criteria were approached within 72 hours of admission for study participation. After consent and enrollment, patients were randomized to intervention or usual care arms in permuted blocks of 8 via a random number generator and sealed opaque envelopes. Nursing and care coordination staff providing usual care to patients (independent of the research team) were blinded to the treatment group status of enrollees; trial design precluded blinding of study personnel and patients.
Delivery of the Supplemental Care Bundle
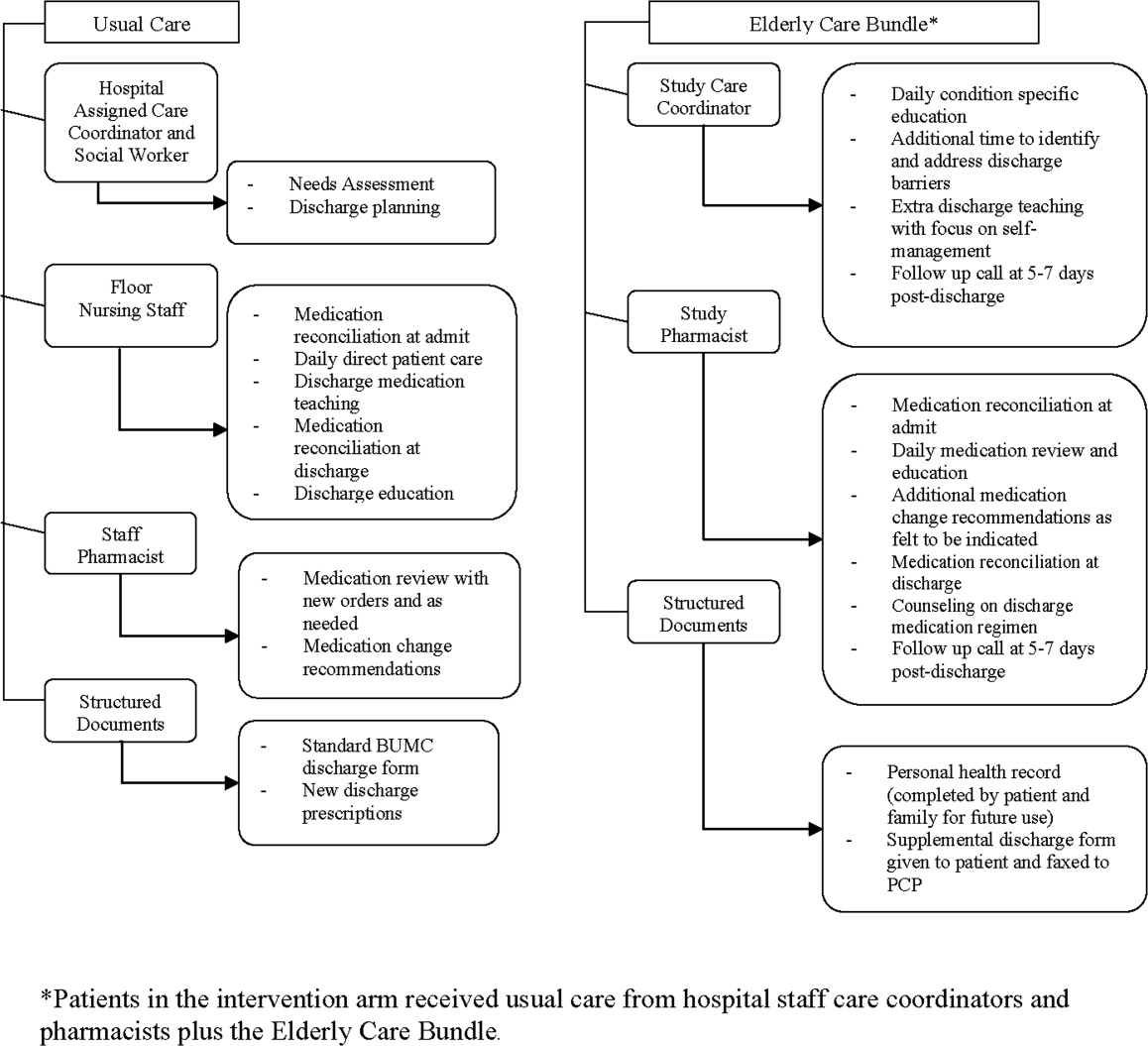
Starting no later than 24 hours after enrollment and continuing up to 1 week following hospital discharge, intervention group patients received a targeted care bundle provided by 1 of 3 care coordinators (CCs) and 1 of 4 clinical pharmacists (CPs) working with the study team. The care bundle was designed as an intensive patient‐centered educational program that would augment BUMC's existing care coordination processes (delivered to all patients regardless of study participation); specific elements are displayed in Figure 1. Study CCs saw patients daily throughout their hospital stay, and instructed patients on specific health conditions, with an emphasis on optimizing home self‐care and contingency plans if problems arose. CP visits focused on medication reconciliation and education regarding any new agents started during the hospitalization. The personal health record (PHR) provided a tool to engage patients in self‐care, and as discussed by Coleman et al.,7, 16, 33 promoted information transfer from the hospital to outpatient settings. During the postdischarge phone call, CCs followed a basic script to confirm receipt of medical equipment, medications, home health arrangements, and scheduling of follow‐up appointments. They also used this contact as an opportunity to reinforce patient education on managing their conditions. CPs reviewed medication use (type, schedule, dose), and spoke with patients about any symptoms they may have experienced as medication side effects. If indicated based on their phone discussions, both CCs and CPs could recommend an action plan to the patient.
The study CCs and CPs were existing hospital staff and performed their research activities in addition to their usual duties. Study CCs were highly experienced (averaging 8 years of inpatient floor nursing plus 10 years as CCs) and all had advanced nursing certifications (ACM, BSN, or MSN). The CPs were upper‐level pharmacy residents completing their inpatient clinical rotations. Additional training for both study CCs and CPs was limited to a series of 3 meetings (each 45 minutes in duration) regarding the intent and delivery of the supplemental care bundle, including use of study forms.
At the time of the trial, the particular CCs and CPs chosen to deliver the supplemental care bundle had work assignments ensuring that crossover between intervention and usual care groups would not occur. For example, 1 of the study CCs normally covered a surgical floor such that her normal scope of responsibilities would not influence the medical patients in the study (their baseline care coordination was provided by nonstudy personnel). Medication reconciliation and medication education is generally performed by floor nursing staff rather than CPs at BUMC.
Data Collection and Outcomes Measurement
Following enrollment, demographic information and a basic medical history were documented by research staff. Inaccuracies in medication lists discovered by pharmacists during the medication reconciliation process were entered directly into the universal medication list on the hospital chart. CPs also kept a log of the medication education given to patients (and recommendations for changes to patients' regimens given to physicians) throughout their hospital stay. Study CCs recorded their assessments of patient needs and associated responses. Furthermore, the research team CC prepared an enhanced discharge form that was given to intervention patients in addition to BUMC's standard form. Data on LOS, illness severity (APR‐DRGs), and unplanned hospital readmission or ED visitation at 30 and 60 days postdischarge were collected via BUMC's electronic reporting systems. All patient follow‐up was completed as of September 1, 2007.
Statistical Analyses
Resource and time constraints necessitated a sample size that would allow implementation of the intervention despite a limited number of study CCs and pharmacists. To accommodate these conditions while still generating pilot data, an a priori decision was made to enroll up to 80 patients. Continuous data variables were normally distributed. Differences between groups for continuous variables were assessed with the Student t‐test; differences in proportions between groups were compared with Fisher's exact tests. Time to readmission events between the groups were evaluated in a post hoc manner using the log‐rank test. Data were analyzed using Prism version 5 for Windows (GraphPad Software, Inc., San Diego, CA) and SPSS version 15 for Windows (SPSS Inc., Chicago, IL). P values < 0.05 were considered statistically significant.
Results
The final sample size for this pilot was small, with 41 total patients (21 controls, 20 interventions). The main reason for enrollment failure of patients meeting study criteria was an inability to obtain informed consent. Sixty patients declined participation after being approached, and another 56 patients were unable to give their informed consent due to impairments (poor cognition, medication induced sedation, severity of illness) with lack of an available proxy to give written consent during the 72‐hour postadmission recruitment window. There were no statistically significant differences in the baseline characteristics of the intervention and control groups (Table 2). A similar proportion of patients (23% in the intervention, 15% in controls; P = 0.70) had preexisting diagnoses of dementia or depression. However, on APR‐DRG measures relating to acuity of illness and mortality risk, patients in the intervention group trended toward higher severity (Table 2). Likewise, although it was not a statistically significant difference, 13 of 20 patients in the intervention group were taking medications from 2 drug classes commonly implicated in adverse drug events (warfarin, insulin, diuretics, sedating agents) as part of their discharge medication regimen compared to 10 of 21 patients in the control group.
| Control (n = 21) | Intervention (n = 20) | P Value | |
|---|---|---|---|
| Age in years (mean SD) | 79.8 5.6 | 77.2 5.3 | 0.14 |
| Males, n (%) | 8 (38) | 3 (15) | 0.10 |
| Females, n (%) | 13 (62) | 17 (85) | 0.10 |
| Race, n (%) | |||
| African‐American | 3 (14) | 5 (25) | 0.45 |
| Asian | 0 (0) | 1 (5) | 0.49 |
| Caucasian | 17 (81) | 14 (70) | 0.48 |
| Hispanic | 1 (5) | 0 | 1.0 |
| Preadmission living status, n (%) | |||
| Alone | 6 (29) | 4 (20) | 0.72 |
| With spouse or other family | 11 (52) | 15 (75) | 0.20 |
| Assisted living | 4 (19) | 1 (5) | 0.34 |
| Inpatient medications (mean SD) | 11 3 | 12 5 | 0.18 |
| Charlson score (mean, SD) | 3.2 1.3 | 3.7 1.1 | 0.21 |
| % with APR DRG severity rating 3 | 57.5 | 83.3 | 0.12 |
| % with APR DRG mortality rating 3 | 20.0 | 55.6 | 0.07 |
| Primary admission diagnoses (n cases, in order of frequency) | 3 pneumonia | 3 pneumonia | |
| 3 CHF | 3 syncope | ||
| 2 syncope | 2 CHF | ||
| 2 COPD | 2 COPD | ||
| 2 cellulitis | 2 cellulitis | ||
| 2 GI disorder (nonbleed) | 2 GI disorder (nonbleed) | ||
| 2 GI bleed | 1 GI bleed | ||
| 2 UTI | 1 atrial fibrillation | ||
| 1 atrial fibrillation | 1 encephalopathy | ||
| 1 stroke | 1 TIA | ||
| 1 renal failure | 1 renal failure | ||
| 1 volume depletion |
Study outcomes are displayed in Table 3. Mean LOS is reported as a descriptive finding; there was insufficient power to compare this outcome statistically between groups. The majority of patients were discharged to home. A similar proportion of patients in the intervention (20%) and control groups (22%) who had lived at home immediately prior to admission were discharged from the hospital to skilled care facilities (P = 0.87). The number of readmissions/ED visits (taken as a composite measure of unplanned healthcare utilization) within 30 days of discharge was lower in the intervention group; by 60 days, there was no longer a statistically significant difference in readmission/ED visit rates between groups. For those patients who had a readmission or ED visit following hospital discharge, the intervention group had a longer time interval to first event compared to controls (36.2 versus 15.7 days, P = 0.05). Of the patients discharged to skilled care, 1 in the intervention group (at 53 days) and 1 in the control group (at 16 days) had a readmission/ED visit event. Figure 2 shows time‐to‐first readmission or ED visit event curves at 30 and 60 days for both intervention and control groups. For patients who had a readmission/ED visit event, LOS for this episode was 2.2 2.1 days in controls and 3.7 2.1 days in the intervention group (insufficient power for statistical comparison). The study's small sample size prevented development of a meaningful regression model.
| Outcome Measure | Control (n = 21) | Intervention (n = 20) | P Value |
|---|---|---|---|
| |||
| Length of stay for index hospitalization (days)* | 4.7 3.7 | 6.2 4.1 | |
| 0‐30 day postdischarge readmissions/ED visits | 8 (38%) | 2 (10%) | 0.03 |
| 31‐60 day postdischarge readmissions/ED visits | 1 (5%) | 4 (20%) | 0.18 |
| Total postdischarge readmissions/ED visits at 60 days | 9 | 6 | 0.52 |
Resource utilization and the specifics of patient‐study personnel interaction associated with the intervention were tracked. Research assistants spent an average of 50 minutes daily screening charts for potential candidates. For the 20 patients who received the supplemental elderly care bundle, study CCs averaged 20 to 25 minutes per patient daily of additional time counseling patients and families, identifying and attending to discharge barriers, filling out documentation, and faxing the supplemental study discharge form to the patient's primary care physician. Any residual home care needs or issues unresolved at discharge were addressed with the patient in the 5 to 7 day follow‐up phone call. Similarly, study CPs expended approximately 20 minutes daily per patient providing medication education, reconciliation, and optimization of drug therapy. Study pharmacists recommended a change to the medication regimens of 10 patients in the intervention group; physicians acted upon these recommendations for 7 of the patients. The changes included dosage adjustment, discontinuation of medications due to possible drug interaction or duplication of drugs with the same pharmacologic effect, and addition of medications as indicated by patient condition or to reconcile with patients' at‐home medication regimens. Patients contacted via phone by the study pharmacist within 1 week after discharge were able to describe proper use of new medications started in the hospital and confirm that they obtained or had the means to obtain the prescribed drugs.
Discussion
This pilot study examined the effects of a supplemental care bundle involving patient education and discharge planning delivered by hospital‐based CCs and CPs on the rate of readmission/ED visitation in 41 elderly (70 years of age) patients. The study was not adequately powered to detect an impact of the intervention on index LOS. The care bundle did lead to significantly fewer readmissions or ED visits 30 days postdischarge and appeared to increase the time interval to first unplanned readmission or ED visit compared to usual care. This effect was no longer present at 60 days postdischarge. Resource allocations and scope of duties for CCs and CPs (an average of 20 minutes per patient per day) related to delivering the intervention were realistic for broader implementation in the hospitalized elderly population at high risk for readmission or ED visitation following discharge.
Length of stay for the initial hospitalization associated with the care bundle was an original outcome of interest to the study team. However, with the final enrollment of 41 patients and a power of 0.8, the between group difference would have needed to be 2.6 days to be statistically significant. It is likely that any change in LOS related to the care bundle would be much smaller, particularly since 2 key determinants of LOS, severity of illness and physician behavior, were beyond this patient education‐oriented intervention's scope of influence.3437 Furthermore, the diverse range of eligible diagnoses limited the study CCs' ability to reduce variability through use of clinical care pathways. One approach in leveraging an elderly care bundle to reduce LOS may be to focus on a specific disease that has well‐established inpatient benchmarks and treatment algorithms. For example, in patients with community‐acquired pneumonia, the use of care coordination in combination with standardized order sets decreased LOS without compromising safety, mainly by shortening the time from clinical stability to discharge.38
On separation of the readmission/ED visit outcome into 30 and 60 day postdischarge time frames, the intervention group had a lower rate of unplanned acute health care use within 30 days postdischarge; the difference between groups had dissipated by 60 days postdischarge. This convergence suggests that a hospital‐based intervention's influence is strongest closer to the time of the initial hospital stay, and wanes as more time has elapsed. Indeed, interventions that have successfully maintained lower readmission rates beyond 60 and 90 days postdischarge in a high‐risk elderly population (such as the program advocated by Coleman et al.16) have included a transitional care provider engaging patients during the hospitalization and performing subsequent visits to the home or nursing facility.33 An optimal intervention would capitalize on the hospital‐based staff's ability to improve short‐term readmission/ED visit rates while linking patients to longer‐term transitional care to extend these outcomes. Electronic health records could potentially facilitate these care transitions, beginning with an automated screening process for identification of high‐risk inpatients and continuing through postdischarge follow‐up. How to develop these resources in settings where outpatient practices are independent or only loosely affiliated with hospitals is an area for continued investigation.
In a group of elderly patients with multiple comorbidities and complex pharmacotherapy regimens, the study bundle component targeting medication management appears to be a high‐yield intervention to reduce unplanned health care utilization following hospital discharge. These patients are more susceptible to nonadherence and drug‐related adverse events, which may contribute to hospital readmission or ED visitation.7, 9, 39 Consistent with findings at other sites,28, 40 a heightened level of CP involvement in the care of high‐risk elderly patients may have helped reduce these undesirable outcomes. Of the 9 readmission/ED visit events in the control group, 3 were attributable to medication related complications (2 from sedatives, 1 from a diuretic). None of the readmission/ED visit events in intervention group patients stemmed from medication effects.
Correspondingly, the research CCs' provision of daily condition‐specific education, additional time to more thoroughly investigate discharge needs, engagement of patients' families as active partners in self‐care, and the use of a structured discharge form along with follow‐up phone calls may have better prepared patients to manage their health problems once released from the hospital.26, 28, 29 For example, 1 patient in the control group was readmitted less than 24 hours after initial discharge due to inability to perform self‐care at home. Given the study power issues described previously, data on LOS for the second hospitalization for patients who had a readmission event are difficult to interpret, but could suggest the occurrence of some shorter, preventable readmissions in the control group. Conversely, the readmission/ED visit events in intervention patients appeared to be associated with a specific medical condition (eg, failure of diabetic cellulitis to respond to appropriate outpatient treatment) rather than problems that would have been corrected with an educational/self‐management program such as this targeted care bundle.
This pilot study had several limitations. The main issue was a small patient sample size that was primarily due to an inability to obtain informed consent. Design of the study as a randomized controlled trial and plans to disseminate study findings beyond BHCS necessitated IRB approval rather than delivery of the supplemental care bundle as a quality improvement (QI) project. Placing QI initiatives under research regulations can lead to project delays, higher costs, and patient frustrations with the process.41, 42 This tension was evident during study screening and enrollment, as many patients who otherwise met criteria and would potentially benefit from the intervention were hesitant to participate in a research study or refused to sign a multipage consent document. The difficulties of enrolling elderly patients in clinical trials have been well‐described.43, 44 Further research involving a minimal‐risk, educational intervention such as this elderly care‐bundle would likely better fit under the category of expedited IRB review with waiver or modification of the informed consent process.45
Incomplete blinding could have potentially affected our results. At the study site, the team members delivering the care bundle were a regular part of the hospital staff (as opposed to external researchers), and it is not unusual for a CC or a pharmacist to enter a patient's room (eg, to confirm a drug allergy history). In view of this, the impact of imperfect blinding on 30‐day outcomes would likely be minimal. Furthermore, a floor staff perception that a specific patient was being taken care of by the study team resulting in a lower than usual level of care, would tend to bias the result of the intervention toward the null effect.
vThe study cohort did not have enough subjects to perform analyses (ie, modeling or examination of subgroups) beyond basic comparative findings. Issues such as preadmission living situation and the presence of depression or cognitive impairment (Mini‐Mental Status Exams were not performed on these patients) may potentially influence postdischarge recidivism; their effects can not be reliably ascertained from these data. Additionally, to prevent study personnel from engaging patients who would soon be going home, it was felt that the benefits from the care bundle would be recognized only if the intervention could be initiated within 72 hours of admission and delivered in full, a requirement that further reduced the enrollment pool. The intent of this pilot work was to guide future investigations surrounding hospital‐to‐home transitional care. The next phase of research in this area will need an enhanced sample size with more extensive baseline data collection so that potential confounding factors or outcomes in specific populations can be explored.
Another problem restricting applicability of study findings was the use of only 3 different CCs and 3 pharmacists on the research team to deliver the components of patient education, discharge planning, and medication counseling in the elderly care bundle. Personnel for the trial were chosen for their experience and interest in the area of care transitions. To distinguish the benefit of the elderly care bundle in general versus the expertise of these particular CCs and study pharmacists, a larger‐scale, multisite trial would be necessary. Lastly, due to resource constraints, patients who resided in long‐term care (either LTAC, SNFs, or nursing homes) prior to admission with anticipated return to those sites were not eligible for the study. Similar to the patients whose comorbidities or acute severity of illness prevented informed consent, this segment of the elderly population may have derived even more benefit from receipt of the elderly care bundle.10, 15, 46 Despite exclusion of this group (which would be expected to lessen the impact of the intervention), a difference in readmission/ED visits rates at 30 days following discharge was observed.
Conclusions
This pilot randomized clinical trial (RCT) evaluated the effects of a supplemental, aggregate care bundle centered on patient education, discharge planning, and medication counseling and reconciliation compared to usual care in a group of elderly patients at high risk of readmission or ED visitation following an index hospitalization. The intervention was designed to be reproducible and make use of existing hospital resources. Probably through facilitation of patient self‐care and home management, the elderly care bundle reduced the composite outcome of readmission/ED visits at 30 days postdischarge. By 60 days, this effect had waned, demonstrating the short‐term benefit of a hospital‐based educational intervention and stressing the need to incorporate additional outpatient transitional care support to sustain favorable outcomes. The study was not powered to detect small differences (which would be more likely than a change of multiple days) in length of index hospital stay related to the care bundle. There were important study limitations (primarily associated with small sample size), and this work should be viewed as hypothesis‐generating. Future trials should assess the impact of a standardized targeted care bundle delivered across multiple healthcare systems on a larger cohort of high‐risk elderly patients, including analysis of financial and personnel allocations relative to the benefits of the intervention.
Acknowledgements
The authors thank study pharmacists Kristen Hesch (PharmD), Renee Danysh (PharmD), Rema Thyagarajan (PharmD), and Betina Thomas (PharmD) for providing patients with medication education and conducting medication reconciliation. They also thank Jeanne Bradbury (RN, ACM), Diana Davis (RN, BSN), and Gail McVea (RN, MSN) for their involvement as care coordinators; Veronica Odom (RN) for her contributions as a research nurse; and Marilyn Callies (RN, MBA) for her role as project advisor.
- ,.Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions.Ann Emerg Med.2002;39(3):238–247.
- ,,,,,.Emergency department utilization by the elderly: analysis of the National Hospital Ambulatory Medical Care Survey.Acad Emerg Med.1996;3(7):694–699.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007(385):1–19.
- ,,,,.Short‐term outcomes of elderly patients discharged from an emergency department.J Am Geriatr Soc.1989;37(10):937–943.
- ,,,,.The discharge of elderly patients from an accident and emergency department: functional changes and risk of readmission.Age Ageing.1990;19(6):415–418.
- ,,,,,.Factors associated with unplanned hospital readmission among patients 65 years of age and older in a Medicare managed care plan.Am J Med.1999;107(1):13–17.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165(16):1842–1847.
- ,.From the emergency department to home.J Clin Nurs.2005;14(6):776–785.
- ,,.Adverse drug events in elderly patients receiving home health services following hospital discharge.Ann Pharmacother.1999;33(11):1147–1153.
- ,,, et al.A randomized trial of the efficacy of multidisciplinary care in heart failure outpatients at high risk of hospital readmission.J Am Coll Cardiol.2002;39(3):471–480.
- ,,,.A systematic review of randomized trials of disease management programs in heart failure.Am J Med.2001;110(5):378–384.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291(11):1358–1367.
- ,,,.Case management may reduce length of hospital stay in patients with recurrent admissions for chronic obstructive pulmonary disease.Respirology.2001;6(1):37–42.
- ,,,,,.A chronic disease management programme can reduce days in hospital for patients with chronic obstructive pulmonary disease.Intern Med J.2004;34(11):608–614.
- ,,.Disease management programmes for older people with heart failure: crucial characteristics which improve post‐discharge outcomes.Eur Heart J.2006;27(5):596–612.
- ,,,.The care transitions intervention: results of a randomized controlled trial.Arch Intern Med.2006;166(17):1822–1828.
- ,,, et al.Effects of a multidisciplinary, post‐discharge continuance of care intervention on quality of life, discharge satisfaction, and hospital length of stay: a randomized controlled trial.Int J Qual Health Care.2005;17(1):43–51.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004(1):CD000313.
- ,.A systematic review of interventions to improve outcomes for elders discharged from the emergency department.Acad Emerg Med.2005;12(10):978–986.
- .Transitional care for older adults: a cost‐effective model.LDI Issue Brief.2004;9(6):1–4.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281(7):613–620.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,.Home‐based intervention in congestive heart failure: long‐term implications on readmission and survival.Circulation.2002;105(24):2861–2866.
- ,,, et al.Effectiveness of team‐managed home‐based primary care: a randomized multicenter trial.JAMA.2000;284(22):2877–2885.
- ,,,.Home‐based medication review in older people: is it cost effective?Pharmacoeconomics.2007;25(2):171–180.
- ,,,,.The value of inpatient pharmaceutical counselling to elderly patients prior to discharge.Br J Clin Pharmacol.2002;54(6):657–664.
- ,,,,.Does the addition of a pharmacist transition coordinator improve evidence‐based medication management and health outcomes in older adults moving from the hospital to a long‐term care facility? Results of a randomized, controlled trial.Am J Geriatr Pharmacother.2004;2(4):257–264.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166(5):565–571.
- ,,,,,.An investigation of hospital generated pharmaceutical care when patients are discharged home from hospital.Br J Clin Pharmacol.1997;44(2):163–165.
- ,,.The community assessment risk screen (CARS): identifying elderly persons at risk for hospitalization or emergency department visit.Am J Manag Care.2000;6(8):925–933.
- ,,.“Risk” factors affecting readmission of the elderly into the health care system.Med Care.1986;24(5):429–437.
- ,,.Re‐admission to intensive care: identification of risk factors.Physiother Res Int.2005;10(3):154–163.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,,,.Impact of the rapid diagnosis of influenza on physician decision‐making and patient management in the pediatric emergency department: results of a randomized, prospective, controlled trial.Pediatrics.2003;112(2):363–367.
- ,,,,.A survey on hospitalised community‐acquired pneumonia in Italy.Monaldi Arch Chest Dis.2006;65(2):82–88.
- ,,,,.Determinants of the length of stay in intensive care and in hospital after coronary artery surgery.Br Heart J.1995;73(1):92–98.
- ,,.Variation in duration of hospital stay between hospitals and between doctors within hospitals.Soc Sci Med.1993;37(6):833–839.
- ,,, et al.The impact of standardized order sets and intensive clinical case management on outcomes in community‐acquired pneumonia.Arch Intern Med.2007;167(15):1664–1669.
- ,,.Compliance with medication orders among the elderly after hospital discharge.Hosp Formul.1992;27(7):720–724.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166(9):955–964.
- .Quality improvement and ethical oversight.Ann Intern Med.2007;146(9):680–681.
- ,,, et al.The ethics of using quality improvement methods in health care.Ann Intern Med.2007;146(9):666–673.
- ,,.Enrollment of elderly patients in clinical trials for cancer drug registration: a 7‐year experience by the US Food and Drug Administration.J Clin Oncol.2004;22(22):4626–4631.
- ,,,.Striving to recruit: the difficulties of conducting clinical research on elderly care home residents.J R Soc Med.2007;100(6):258–261.
- ,.Quality‐improvement research and informed consent.N Engl J Med.2008;358(8):765–767.
- ,,,.An evaluation of the impact of the ventilator care bundle.Nurs Crit Care.2005;10(5):242–246.
Elderly patients (aged 65 years and older) consume a disproportionate amount of acute health care resources, composing up to 20% of emergency department (ED) visits,1, 2 having a 2‐fold to 5‐fold increase in likelihood of hospital admission,1 and frequently incurring lengths of hospital stay (LOS) approximately 15% higher than the national averages.3 In addition, they are at increased risk for hospital readmission in the 90‐day interval following hospital discharge.1, 4, 5 Specific risk factors for readmission include age above 80 years, discharge within the previous 30 days, the presence of 3 or more comorbid diagnoses, use of 5 or more prescription medications, difficulty with at least 1 activity of daily living (ADL), and lack of discharge education.6 These risk factors can translate into adverse drug events,79 exacerbations of chronic diseases,10 or functional decline4, 5 that can trigger ED visits or hospital readmission.
Hospital‐based care coordinationdefined as a multidisciplinary interaction between inpatients and providers that focuses on education, communication, and discharge planning with the primary aim of improving outcomeshas demonstrated inconsistent results as a mechanism to reduce LOS, postdischarge ED visits, or hospital readmission rates. While disease‐specific care coordination programs for congestive heart failure and chronic obstructive pulmonary disease have been effective in reducing rehospitalization rates,1015 the benefits of comprehensive care coordination for elderly general medical inpatients with a broader range of diagnoses are less clear. In a group of 750 elderly patients with 1 of 11 common inpatient diagnoses (such as stroke or hip fracture) likely to ultimately require a high level of home support, Coleman et al.16 found that a structured transitional care program centered on a personal coach decreased rehospitalization rates at 30 and 90 days. Preen et al.17 found improved patient involvement and perceived quality of life with care coordination focused on discharge planning, but no impact on LOS. Likewise, a recent meta‐analysis18 failed to demonstrate statistically significant differences in mortality, LOS, or readmission rates in hospitalized patients who received intensive care coordination versus usual care; however, variation in the components of the care coordination intervention and reported outcomes restricted the ability to pool data in this study.
Care coordination programs demonstrating efficacy in reducing health care utilization in elderly medical patients have generally included an outpatient transitional component with out‐of‐hospital postacute care visits by health care personnel such as a nurse, pharmacist, or physician.1923 These offsite interventions generate additional expenses and resource demands that may not be practical for smaller hospitals to implement.24, 25 In contrast, hospital‐based care coordination programs have clear ownership and thus may be more practical to disseminate. Individual elements of hospital‐based care coordination such as pharmacist counseling, discharge education, and telephone follow‐up have been shown to reduce ED visitation and readmission rates in high‐risk elderly patients. Less information is available regarding the impact of these interventions delivered in an aggregate bundle by hospital staff in the absence of bridging transitional visits.2629
The objective of this pilot study was to determine whether a supplemental elderly care bundle, targeted to high‐risk inpatients by hospital staff as an enhancement to existing care coordination, would affect postdischarge readmission and ED visit rates. The intervention was designed to capitalize on existing resources, and focused specifically on elderly inpatients who were hospitalized with diagnoses commonly encountered in a general medical unit and predisposed to recidivism.
Patients and Methods
Patient Selection and Enrollment
The screening population consisted of elderly patients admitted to 1 of 2 hospital‐medicine groups (MedProvider Inpatient Care Unit or Texas Primary Care) at the 900‐bed Baylor University Medical Center (BUMC, Dallas, TX) between March and June 2007 with a diagnosis likely to fall within 1 of 20 frequent Medicare medical diagnosis reimbursement groups (DRGs) at BUMC, as listed in Table 1. Study personnel performed daily chart review to establish eligibility criteria, which included age 70 years, use of 5 medications regularly, 3 chronic comorbid conditions, requirement for assistance with 1 ADL, and preadmission residence at home or assisted living with a reasonable expectation of disposition back to that domicile. These criteria were based on factors found in the literature to be associated with extended LOS and postdischarge readmission/ED visit events.5, 6, 3032 Potential enrollees needed to be conversant in English (a multilingual staff was not feasible due to limited resources for this pilot project) and have reliable phone contact, or have a proxy caregiver who could speak English and be reached by phone. Predefined exclusion criteria were admission primarily for a surgical procedure, terminal diagnosis with life expectancy 6 months, residence in a long‐term care facility (long‐term acute care [LTAC], skilled nursing facility [SNF], or nursing home) prior to hospitalization with anticipated discharge back to that facility, and patient/family refusal to participate. Additionally, with an average LOS between 5 and 6 days in BUMC's Medicare population for the DRGs of interest, it was felt that the effects of the care bundle intervention would be obscured unless initiated early in the hospitalization. Thus, patients who could not be enrolled within 72 hours following admission were subsequently excluded. The Baylor Health Care System (BHCS) Institutional Review Board (IRB) approved this study, and written informed consent was obtained from all patients or their surrogates.
| DRG | DRG Name |
|---|---|
| |
| 127 | Heart failure and shock |
| 14 | Intracranial hemorrhage or cerebral infarction |
| 89 | Simple pneumonia/pleurisy |
| 416 | Septicemia |
| 316 | Renal failure |
| 182 | Esophagitis/gastroenterological/miscellaneous digestive disorders with complications |
| 174 | Gastrointestinal hemorrhage with complications |
| 88 | Chronic obstructive pulmonary disease |
| 320 | Kidney/urinary tract infection with complications |
| 144 | Other circulatory diagnoses with complications |
| 138 | Arrhythmia/conduction disorders with complications |
| 277 | Cellulitis with complications |
| 124 | Circulatory disorders except acute myocardial infarction with cardiac catheterization and complex diagnosis |
| 430 | Psychoses |
| 188 | Other digestive diagnoses with complications |
| 395 | Red blood cell disorders |
| 79 | Respiratory infections and inflammations with complications |
| 524 | Transient ischemia |
| 143 | Chest pain |
| 141 | Syncope and collapse with complications |
Patients meeting eligibility criteria were approached within 72 hours of admission for study participation. After consent and enrollment, patients were randomized to intervention or usual care arms in permuted blocks of 8 via a random number generator and sealed opaque envelopes. Nursing and care coordination staff providing usual care to patients (independent of the research team) were blinded to the treatment group status of enrollees; trial design precluded blinding of study personnel and patients.
Delivery of the Supplemental Care Bundle
Starting no later than 24 hours after enrollment and continuing up to 1 week following hospital discharge, intervention group patients received a targeted care bundle provided by 1 of 3 care coordinators (CCs) and 1 of 4 clinical pharmacists (CPs) working with the study team. The care bundle was designed as an intensive patient‐centered educational program that would augment BUMC's existing care coordination processes (delivered to all patients regardless of study participation); specific elements are displayed in Figure 1. Study CCs saw patients daily throughout their hospital stay, and instructed patients on specific health conditions, with an emphasis on optimizing home self‐care and contingency plans if problems arose. CP visits focused on medication reconciliation and education regarding any new agents started during the hospitalization. The personal health record (PHR) provided a tool to engage patients in self‐care, and as discussed by Coleman et al.,7, 16, 33 promoted information transfer from the hospital to outpatient settings. During the postdischarge phone call, CCs followed a basic script to confirm receipt of medical equipment, medications, home health arrangements, and scheduling of follow‐up appointments. They also used this contact as an opportunity to reinforce patient education on managing their conditions. CPs reviewed medication use (type, schedule, dose), and spoke with patients about any symptoms they may have experienced as medication side effects. If indicated based on their phone discussions, both CCs and CPs could recommend an action plan to the patient.
The study CCs and CPs were existing hospital staff and performed their research activities in addition to their usual duties. Study CCs were highly experienced (averaging 8 years of inpatient floor nursing plus 10 years as CCs) and all had advanced nursing certifications (ACM, BSN, or MSN). The CPs were upper‐level pharmacy residents completing their inpatient clinical rotations. Additional training for both study CCs and CPs was limited to a series of 3 meetings (each 45 minutes in duration) regarding the intent and delivery of the supplemental care bundle, including use of study forms.
At the time of the trial, the particular CCs and CPs chosen to deliver the supplemental care bundle had work assignments ensuring that crossover between intervention and usual care groups would not occur. For example, 1 of the study CCs normally covered a surgical floor such that her normal scope of responsibilities would not influence the medical patients in the study (their baseline care coordination was provided by nonstudy personnel). Medication reconciliation and medication education is generally performed by floor nursing staff rather than CPs at BUMC.
Data Collection and Outcomes Measurement
Following enrollment, demographic information and a basic medical history were documented by research staff. Inaccuracies in medication lists discovered by pharmacists during the medication reconciliation process were entered directly into the universal medication list on the hospital chart. CPs also kept a log of the medication education given to patients (and recommendations for changes to patients' regimens given to physicians) throughout their hospital stay. Study CCs recorded their assessments of patient needs and associated responses. Furthermore, the research team CC prepared an enhanced discharge form that was given to intervention patients in addition to BUMC's standard form. Data on LOS, illness severity (APR‐DRGs), and unplanned hospital readmission or ED visitation at 30 and 60 days postdischarge were collected via BUMC's electronic reporting systems. All patient follow‐up was completed as of September 1, 2007.
Statistical Analyses
Resource and time constraints necessitated a sample size that would allow implementation of the intervention despite a limited number of study CCs and pharmacists. To accommodate these conditions while still generating pilot data, an a priori decision was made to enroll up to 80 patients. Continuous data variables were normally distributed. Differences between groups for continuous variables were assessed with the Student t‐test; differences in proportions between groups were compared with Fisher's exact tests. Time to readmission events between the groups were evaluated in a post hoc manner using the log‐rank test. Data were analyzed using Prism version 5 for Windows (GraphPad Software, Inc., San Diego, CA) and SPSS version 15 for Windows (SPSS Inc., Chicago, IL). P values < 0.05 were considered statistically significant.
Results
The final sample size for this pilot was small, with 41 total patients (21 controls, 20 interventions). The main reason for enrollment failure of patients meeting study criteria was an inability to obtain informed consent. Sixty patients declined participation after being approached, and another 56 patients were unable to give their informed consent due to impairments (poor cognition, medication induced sedation, severity of illness) with lack of an available proxy to give written consent during the 72‐hour postadmission recruitment window. There were no statistically significant differences in the baseline characteristics of the intervention and control groups (Table 2). A similar proportion of patients (23% in the intervention, 15% in controls; P = 0.70) had preexisting diagnoses of dementia or depression. However, on APR‐DRG measures relating to acuity of illness and mortality risk, patients in the intervention group trended toward higher severity (Table 2). Likewise, although it was not a statistically significant difference, 13 of 20 patients in the intervention group were taking medications from 2 drug classes commonly implicated in adverse drug events (warfarin, insulin, diuretics, sedating agents) as part of their discharge medication regimen compared to 10 of 21 patients in the control group.
| Control (n = 21) | Intervention (n = 20) | P Value | |
|---|---|---|---|
| Age in years (mean SD) | 79.8 5.6 | 77.2 5.3 | 0.14 |
| Males, n (%) | 8 (38) | 3 (15) | 0.10 |
| Females, n (%) | 13 (62) | 17 (85) | 0.10 |
| Race, n (%) | |||
| African‐American | 3 (14) | 5 (25) | 0.45 |
| Asian | 0 (0) | 1 (5) | 0.49 |
| Caucasian | 17 (81) | 14 (70) | 0.48 |
| Hispanic | 1 (5) | 0 | 1.0 |
| Preadmission living status, n (%) | |||
| Alone | 6 (29) | 4 (20) | 0.72 |
| With spouse or other family | 11 (52) | 15 (75) | 0.20 |
| Assisted living | 4 (19) | 1 (5) | 0.34 |
| Inpatient medications (mean SD) | 11 3 | 12 5 | 0.18 |
| Charlson score (mean, SD) | 3.2 1.3 | 3.7 1.1 | 0.21 |
| % with APR DRG severity rating 3 | 57.5 | 83.3 | 0.12 |
| % with APR DRG mortality rating 3 | 20.0 | 55.6 | 0.07 |
| Primary admission diagnoses (n cases, in order of frequency) | 3 pneumonia | 3 pneumonia | |
| 3 CHF | 3 syncope | ||
| 2 syncope | 2 CHF | ||
| 2 COPD | 2 COPD | ||
| 2 cellulitis | 2 cellulitis | ||
| 2 GI disorder (nonbleed) | 2 GI disorder (nonbleed) | ||
| 2 GI bleed | 1 GI bleed | ||
| 2 UTI | 1 atrial fibrillation | ||
| 1 atrial fibrillation | 1 encephalopathy | ||
| 1 stroke | 1 TIA | ||
| 1 renal failure | 1 renal failure | ||
| 1 volume depletion |
Study outcomes are displayed in Table 3. Mean LOS is reported as a descriptive finding; there was insufficient power to compare this outcome statistically between groups. The majority of patients were discharged to home. A similar proportion of patients in the intervention (20%) and control groups (22%) who had lived at home immediately prior to admission were discharged from the hospital to skilled care facilities (P = 0.87). The number of readmissions/ED visits (taken as a composite measure of unplanned healthcare utilization) within 30 days of discharge was lower in the intervention group; by 60 days, there was no longer a statistically significant difference in readmission/ED visit rates between groups. For those patients who had a readmission or ED visit following hospital discharge, the intervention group had a longer time interval to first event compared to controls (36.2 versus 15.7 days, P = 0.05). Of the patients discharged to skilled care, 1 in the intervention group (at 53 days) and 1 in the control group (at 16 days) had a readmission/ED visit event. Figure 2 shows time‐to‐first readmission or ED visit event curves at 30 and 60 days for both intervention and control groups. For patients who had a readmission/ED visit event, LOS for this episode was 2.2 2.1 days in controls and 3.7 2.1 days in the intervention group (insufficient power for statistical comparison). The study's small sample size prevented development of a meaningful regression model.
| Outcome Measure | Control (n = 21) | Intervention (n = 20) | P Value |
|---|---|---|---|
| |||
| Length of stay for index hospitalization (days)* | 4.7 3.7 | 6.2 4.1 | |
| 0‐30 day postdischarge readmissions/ED visits | 8 (38%) | 2 (10%) | 0.03 |
| 31‐60 day postdischarge readmissions/ED visits | 1 (5%) | 4 (20%) | 0.18 |
| Total postdischarge readmissions/ED visits at 60 days | 9 | 6 | 0.52 |
Resource utilization and the specifics of patient‐study personnel interaction associated with the intervention were tracked. Research assistants spent an average of 50 minutes daily screening charts for potential candidates. For the 20 patients who received the supplemental elderly care bundle, study CCs averaged 20 to 25 minutes per patient daily of additional time counseling patients and families, identifying and attending to discharge barriers, filling out documentation, and faxing the supplemental study discharge form to the patient's primary care physician. Any residual home care needs or issues unresolved at discharge were addressed with the patient in the 5 to 7 day follow‐up phone call. Similarly, study CPs expended approximately 20 minutes daily per patient providing medication education, reconciliation, and optimization of drug therapy. Study pharmacists recommended a change to the medication regimens of 10 patients in the intervention group; physicians acted upon these recommendations for 7 of the patients. The changes included dosage adjustment, discontinuation of medications due to possible drug interaction or duplication of drugs with the same pharmacologic effect, and addition of medications as indicated by patient condition or to reconcile with patients' at‐home medication regimens. Patients contacted via phone by the study pharmacist within 1 week after discharge were able to describe proper use of new medications started in the hospital and confirm that they obtained or had the means to obtain the prescribed drugs.
Discussion
This pilot study examined the effects of a supplemental care bundle involving patient education and discharge planning delivered by hospital‐based CCs and CPs on the rate of readmission/ED visitation in 41 elderly (70 years of age) patients. The study was not adequately powered to detect an impact of the intervention on index LOS. The care bundle did lead to significantly fewer readmissions or ED visits 30 days postdischarge and appeared to increase the time interval to first unplanned readmission or ED visit compared to usual care. This effect was no longer present at 60 days postdischarge. Resource allocations and scope of duties for CCs and CPs (an average of 20 minutes per patient per day) related to delivering the intervention were realistic for broader implementation in the hospitalized elderly population at high risk for readmission or ED visitation following discharge.
Length of stay for the initial hospitalization associated with the care bundle was an original outcome of interest to the study team. However, with the final enrollment of 41 patients and a power of 0.8, the between group difference would have needed to be 2.6 days to be statistically significant. It is likely that any change in LOS related to the care bundle would be much smaller, particularly since 2 key determinants of LOS, severity of illness and physician behavior, were beyond this patient education‐oriented intervention's scope of influence.3437 Furthermore, the diverse range of eligible diagnoses limited the study CCs' ability to reduce variability through use of clinical care pathways. One approach in leveraging an elderly care bundle to reduce LOS may be to focus on a specific disease that has well‐established inpatient benchmarks and treatment algorithms. For example, in patients with community‐acquired pneumonia, the use of care coordination in combination with standardized order sets decreased LOS without compromising safety, mainly by shortening the time from clinical stability to discharge.38
On separation of the readmission/ED visit outcome into 30 and 60 day postdischarge time frames, the intervention group had a lower rate of unplanned acute health care use within 30 days postdischarge; the difference between groups had dissipated by 60 days postdischarge. This convergence suggests that a hospital‐based intervention's influence is strongest closer to the time of the initial hospital stay, and wanes as more time has elapsed. Indeed, interventions that have successfully maintained lower readmission rates beyond 60 and 90 days postdischarge in a high‐risk elderly population (such as the program advocated by Coleman et al.16) have included a transitional care provider engaging patients during the hospitalization and performing subsequent visits to the home or nursing facility.33 An optimal intervention would capitalize on the hospital‐based staff's ability to improve short‐term readmission/ED visit rates while linking patients to longer‐term transitional care to extend these outcomes. Electronic health records could potentially facilitate these care transitions, beginning with an automated screening process for identification of high‐risk inpatients and continuing through postdischarge follow‐up. How to develop these resources in settings where outpatient practices are independent or only loosely affiliated with hospitals is an area for continued investigation.
In a group of elderly patients with multiple comorbidities and complex pharmacotherapy regimens, the study bundle component targeting medication management appears to be a high‐yield intervention to reduce unplanned health care utilization following hospital discharge. These patients are more susceptible to nonadherence and drug‐related adverse events, which may contribute to hospital readmission or ED visitation.7, 9, 39 Consistent with findings at other sites,28, 40 a heightened level of CP involvement in the care of high‐risk elderly patients may have helped reduce these undesirable outcomes. Of the 9 readmission/ED visit events in the control group, 3 were attributable to medication related complications (2 from sedatives, 1 from a diuretic). None of the readmission/ED visit events in intervention group patients stemmed from medication effects.
Correspondingly, the research CCs' provision of daily condition‐specific education, additional time to more thoroughly investigate discharge needs, engagement of patients' families as active partners in self‐care, and the use of a structured discharge form along with follow‐up phone calls may have better prepared patients to manage their health problems once released from the hospital.26, 28, 29 For example, 1 patient in the control group was readmitted less than 24 hours after initial discharge due to inability to perform self‐care at home. Given the study power issues described previously, data on LOS for the second hospitalization for patients who had a readmission event are difficult to interpret, but could suggest the occurrence of some shorter, preventable readmissions in the control group. Conversely, the readmission/ED visit events in intervention patients appeared to be associated with a specific medical condition (eg, failure of diabetic cellulitis to respond to appropriate outpatient treatment) rather than problems that would have been corrected with an educational/self‐management program such as this targeted care bundle.
This pilot study had several limitations. The main issue was a small patient sample size that was primarily due to an inability to obtain informed consent. Design of the study as a randomized controlled trial and plans to disseminate study findings beyond BHCS necessitated IRB approval rather than delivery of the supplemental care bundle as a quality improvement (QI) project. Placing QI initiatives under research regulations can lead to project delays, higher costs, and patient frustrations with the process.41, 42 This tension was evident during study screening and enrollment, as many patients who otherwise met criteria and would potentially benefit from the intervention were hesitant to participate in a research study or refused to sign a multipage consent document. The difficulties of enrolling elderly patients in clinical trials have been well‐described.43, 44 Further research involving a minimal‐risk, educational intervention such as this elderly care‐bundle would likely better fit under the category of expedited IRB review with waiver or modification of the informed consent process.45
Incomplete blinding could have potentially affected our results. At the study site, the team members delivering the care bundle were a regular part of the hospital staff (as opposed to external researchers), and it is not unusual for a CC or a pharmacist to enter a patient's room (eg, to confirm a drug allergy history). In view of this, the impact of imperfect blinding on 30‐day outcomes would likely be minimal. Furthermore, a floor staff perception that a specific patient was being taken care of by the study team resulting in a lower than usual level of care, would tend to bias the result of the intervention toward the null effect.
vThe study cohort did not have enough subjects to perform analyses (ie, modeling or examination of subgroups) beyond basic comparative findings. Issues such as preadmission living situation and the presence of depression or cognitive impairment (Mini‐Mental Status Exams were not performed on these patients) may potentially influence postdischarge recidivism; their effects can not be reliably ascertained from these data. Additionally, to prevent study personnel from engaging patients who would soon be going home, it was felt that the benefits from the care bundle would be recognized only if the intervention could be initiated within 72 hours of admission and delivered in full, a requirement that further reduced the enrollment pool. The intent of this pilot work was to guide future investigations surrounding hospital‐to‐home transitional care. The next phase of research in this area will need an enhanced sample size with more extensive baseline data collection so that potential confounding factors or outcomes in specific populations can be explored.
Another problem restricting applicability of study findings was the use of only 3 different CCs and 3 pharmacists on the research team to deliver the components of patient education, discharge planning, and medication counseling in the elderly care bundle. Personnel for the trial were chosen for their experience and interest in the area of care transitions. To distinguish the benefit of the elderly care bundle in general versus the expertise of these particular CCs and study pharmacists, a larger‐scale, multisite trial would be necessary. Lastly, due to resource constraints, patients who resided in long‐term care (either LTAC, SNFs, or nursing homes) prior to admission with anticipated return to those sites were not eligible for the study. Similar to the patients whose comorbidities or acute severity of illness prevented informed consent, this segment of the elderly population may have derived even more benefit from receipt of the elderly care bundle.10, 15, 46 Despite exclusion of this group (which would be expected to lessen the impact of the intervention), a difference in readmission/ED visits rates at 30 days following discharge was observed.
Conclusions
This pilot randomized clinical trial (RCT) evaluated the effects of a supplemental, aggregate care bundle centered on patient education, discharge planning, and medication counseling and reconciliation compared to usual care in a group of elderly patients at high risk of readmission or ED visitation following an index hospitalization. The intervention was designed to be reproducible and make use of existing hospital resources. Probably through facilitation of patient self‐care and home management, the elderly care bundle reduced the composite outcome of readmission/ED visits at 30 days postdischarge. By 60 days, this effect had waned, demonstrating the short‐term benefit of a hospital‐based educational intervention and stressing the need to incorporate additional outpatient transitional care support to sustain favorable outcomes. The study was not powered to detect small differences (which would be more likely than a change of multiple days) in length of index hospital stay related to the care bundle. There were important study limitations (primarily associated with small sample size), and this work should be viewed as hypothesis‐generating. Future trials should assess the impact of a standardized targeted care bundle delivered across multiple healthcare systems on a larger cohort of high‐risk elderly patients, including analysis of financial and personnel allocations relative to the benefits of the intervention.
Acknowledgements
The authors thank study pharmacists Kristen Hesch (PharmD), Renee Danysh (PharmD), Rema Thyagarajan (PharmD), and Betina Thomas (PharmD) for providing patients with medication education and conducting medication reconciliation. They also thank Jeanne Bradbury (RN, ACM), Diana Davis (RN, BSN), and Gail McVea (RN, MSN) for their involvement as care coordinators; Veronica Odom (RN) for her contributions as a research nurse; and Marilyn Callies (RN, MBA) for her role as project advisor.
Elderly patients (aged 65 years and older) consume a disproportionate amount of acute health care resources, composing up to 20% of emergency department (ED) visits,1, 2 having a 2‐fold to 5‐fold increase in likelihood of hospital admission,1 and frequently incurring lengths of hospital stay (LOS) approximately 15% higher than the national averages.3 In addition, they are at increased risk for hospital readmission in the 90‐day interval following hospital discharge.1, 4, 5 Specific risk factors for readmission include age above 80 years, discharge within the previous 30 days, the presence of 3 or more comorbid diagnoses, use of 5 or more prescription medications, difficulty with at least 1 activity of daily living (ADL), and lack of discharge education.6 These risk factors can translate into adverse drug events,79 exacerbations of chronic diseases,10 or functional decline4, 5 that can trigger ED visits or hospital readmission.
Hospital‐based care coordinationdefined as a multidisciplinary interaction between inpatients and providers that focuses on education, communication, and discharge planning with the primary aim of improving outcomeshas demonstrated inconsistent results as a mechanism to reduce LOS, postdischarge ED visits, or hospital readmission rates. While disease‐specific care coordination programs for congestive heart failure and chronic obstructive pulmonary disease have been effective in reducing rehospitalization rates,1015 the benefits of comprehensive care coordination for elderly general medical inpatients with a broader range of diagnoses are less clear. In a group of 750 elderly patients with 1 of 11 common inpatient diagnoses (such as stroke or hip fracture) likely to ultimately require a high level of home support, Coleman et al.16 found that a structured transitional care program centered on a personal coach decreased rehospitalization rates at 30 and 90 days. Preen et al.17 found improved patient involvement and perceived quality of life with care coordination focused on discharge planning, but no impact on LOS. Likewise, a recent meta‐analysis18 failed to demonstrate statistically significant differences in mortality, LOS, or readmission rates in hospitalized patients who received intensive care coordination versus usual care; however, variation in the components of the care coordination intervention and reported outcomes restricted the ability to pool data in this study.
Care coordination programs demonstrating efficacy in reducing health care utilization in elderly medical patients have generally included an outpatient transitional component with out‐of‐hospital postacute care visits by health care personnel such as a nurse, pharmacist, or physician.1923 These offsite interventions generate additional expenses and resource demands that may not be practical for smaller hospitals to implement.24, 25 In contrast, hospital‐based care coordination programs have clear ownership and thus may be more practical to disseminate. Individual elements of hospital‐based care coordination such as pharmacist counseling, discharge education, and telephone follow‐up have been shown to reduce ED visitation and readmission rates in high‐risk elderly patients. Less information is available regarding the impact of these interventions delivered in an aggregate bundle by hospital staff in the absence of bridging transitional visits.2629
The objective of this pilot study was to determine whether a supplemental elderly care bundle, targeted to high‐risk inpatients by hospital staff as an enhancement to existing care coordination, would affect postdischarge readmission and ED visit rates. The intervention was designed to capitalize on existing resources, and focused specifically on elderly inpatients who were hospitalized with diagnoses commonly encountered in a general medical unit and predisposed to recidivism.
Patients and Methods
Patient Selection and Enrollment
The screening population consisted of elderly patients admitted to 1 of 2 hospital‐medicine groups (MedProvider Inpatient Care Unit or Texas Primary Care) at the 900‐bed Baylor University Medical Center (BUMC, Dallas, TX) between March and June 2007 with a diagnosis likely to fall within 1 of 20 frequent Medicare medical diagnosis reimbursement groups (DRGs) at BUMC, as listed in Table 1. Study personnel performed daily chart review to establish eligibility criteria, which included age 70 years, use of 5 medications regularly, 3 chronic comorbid conditions, requirement for assistance with 1 ADL, and preadmission residence at home or assisted living with a reasonable expectation of disposition back to that domicile. These criteria were based on factors found in the literature to be associated with extended LOS and postdischarge readmission/ED visit events.5, 6, 3032 Potential enrollees needed to be conversant in English (a multilingual staff was not feasible due to limited resources for this pilot project) and have reliable phone contact, or have a proxy caregiver who could speak English and be reached by phone. Predefined exclusion criteria were admission primarily for a surgical procedure, terminal diagnosis with life expectancy 6 months, residence in a long‐term care facility (long‐term acute care [LTAC], skilled nursing facility [SNF], or nursing home) prior to hospitalization with anticipated discharge back to that facility, and patient/family refusal to participate. Additionally, with an average LOS between 5 and 6 days in BUMC's Medicare population for the DRGs of interest, it was felt that the effects of the care bundle intervention would be obscured unless initiated early in the hospitalization. Thus, patients who could not be enrolled within 72 hours following admission were subsequently excluded. The Baylor Health Care System (BHCS) Institutional Review Board (IRB) approved this study, and written informed consent was obtained from all patients or their surrogates.
| DRG | DRG Name |
|---|---|
| |
| 127 | Heart failure and shock |
| 14 | Intracranial hemorrhage or cerebral infarction |
| 89 | Simple pneumonia/pleurisy |
| 416 | Septicemia |
| 316 | Renal failure |
| 182 | Esophagitis/gastroenterological/miscellaneous digestive disorders with complications |
| 174 | Gastrointestinal hemorrhage with complications |
| 88 | Chronic obstructive pulmonary disease |
| 320 | Kidney/urinary tract infection with complications |
| 144 | Other circulatory diagnoses with complications |
| 138 | Arrhythmia/conduction disorders with complications |
| 277 | Cellulitis with complications |
| 124 | Circulatory disorders except acute myocardial infarction with cardiac catheterization and complex diagnosis |
| 430 | Psychoses |
| 188 | Other digestive diagnoses with complications |
| 395 | Red blood cell disorders |
| 79 | Respiratory infections and inflammations with complications |
| 524 | Transient ischemia |
| 143 | Chest pain |
| 141 | Syncope and collapse with complications |
Patients meeting eligibility criteria were approached within 72 hours of admission for study participation. After consent and enrollment, patients were randomized to intervention or usual care arms in permuted blocks of 8 via a random number generator and sealed opaque envelopes. Nursing and care coordination staff providing usual care to patients (independent of the research team) were blinded to the treatment group status of enrollees; trial design precluded blinding of study personnel and patients.
Delivery of the Supplemental Care Bundle
Starting no later than 24 hours after enrollment and continuing up to 1 week following hospital discharge, intervention group patients received a targeted care bundle provided by 1 of 3 care coordinators (CCs) and 1 of 4 clinical pharmacists (CPs) working with the study team. The care bundle was designed as an intensive patient‐centered educational program that would augment BUMC's existing care coordination processes (delivered to all patients regardless of study participation); specific elements are displayed in Figure 1. Study CCs saw patients daily throughout their hospital stay, and instructed patients on specific health conditions, with an emphasis on optimizing home self‐care and contingency plans if problems arose. CP visits focused on medication reconciliation and education regarding any new agents started during the hospitalization. The personal health record (PHR) provided a tool to engage patients in self‐care, and as discussed by Coleman et al.,7, 16, 33 promoted information transfer from the hospital to outpatient settings. During the postdischarge phone call, CCs followed a basic script to confirm receipt of medical equipment, medications, home health arrangements, and scheduling of follow‐up appointments. They also used this contact as an opportunity to reinforce patient education on managing their conditions. CPs reviewed medication use (type, schedule, dose), and spoke with patients about any symptoms they may have experienced as medication side effects. If indicated based on their phone discussions, both CCs and CPs could recommend an action plan to the patient.
The study CCs and CPs were existing hospital staff and performed their research activities in addition to their usual duties. Study CCs were highly experienced (averaging 8 years of inpatient floor nursing plus 10 years as CCs) and all had advanced nursing certifications (ACM, BSN, or MSN). The CPs were upper‐level pharmacy residents completing their inpatient clinical rotations. Additional training for both study CCs and CPs was limited to a series of 3 meetings (each 45 minutes in duration) regarding the intent and delivery of the supplemental care bundle, including use of study forms.
At the time of the trial, the particular CCs and CPs chosen to deliver the supplemental care bundle had work assignments ensuring that crossover between intervention and usual care groups would not occur. For example, 1 of the study CCs normally covered a surgical floor such that her normal scope of responsibilities would not influence the medical patients in the study (their baseline care coordination was provided by nonstudy personnel). Medication reconciliation and medication education is generally performed by floor nursing staff rather than CPs at BUMC.
Data Collection and Outcomes Measurement
Following enrollment, demographic information and a basic medical history were documented by research staff. Inaccuracies in medication lists discovered by pharmacists during the medication reconciliation process were entered directly into the universal medication list on the hospital chart. CPs also kept a log of the medication education given to patients (and recommendations for changes to patients' regimens given to physicians) throughout their hospital stay. Study CCs recorded their assessments of patient needs and associated responses. Furthermore, the research team CC prepared an enhanced discharge form that was given to intervention patients in addition to BUMC's standard form. Data on LOS, illness severity (APR‐DRGs), and unplanned hospital readmission or ED visitation at 30 and 60 days postdischarge were collected via BUMC's electronic reporting systems. All patient follow‐up was completed as of September 1, 2007.
Statistical Analyses
Resource and time constraints necessitated a sample size that would allow implementation of the intervention despite a limited number of study CCs and pharmacists. To accommodate these conditions while still generating pilot data, an a priori decision was made to enroll up to 80 patients. Continuous data variables were normally distributed. Differences between groups for continuous variables were assessed with the Student t‐test; differences in proportions between groups were compared with Fisher's exact tests. Time to readmission events between the groups were evaluated in a post hoc manner using the log‐rank test. Data were analyzed using Prism version 5 for Windows (GraphPad Software, Inc., San Diego, CA) and SPSS version 15 for Windows (SPSS Inc., Chicago, IL). P values < 0.05 were considered statistically significant.
Results
The final sample size for this pilot was small, with 41 total patients (21 controls, 20 interventions). The main reason for enrollment failure of patients meeting study criteria was an inability to obtain informed consent. Sixty patients declined participation after being approached, and another 56 patients were unable to give their informed consent due to impairments (poor cognition, medication induced sedation, severity of illness) with lack of an available proxy to give written consent during the 72‐hour postadmission recruitment window. There were no statistically significant differences in the baseline characteristics of the intervention and control groups (Table 2). A similar proportion of patients (23% in the intervention, 15% in controls; P = 0.70) had preexisting diagnoses of dementia or depression. However, on APR‐DRG measures relating to acuity of illness and mortality risk, patients in the intervention group trended toward higher severity (Table 2). Likewise, although it was not a statistically significant difference, 13 of 20 patients in the intervention group were taking medications from 2 drug classes commonly implicated in adverse drug events (warfarin, insulin, diuretics, sedating agents) as part of their discharge medication regimen compared to 10 of 21 patients in the control group.
| Control (n = 21) | Intervention (n = 20) | P Value | |
|---|---|---|---|
| Age in years (mean SD) | 79.8 5.6 | 77.2 5.3 | 0.14 |
| Males, n (%) | 8 (38) | 3 (15) | 0.10 |
| Females, n (%) | 13 (62) | 17 (85) | 0.10 |
| Race, n (%) | |||
| African‐American | 3 (14) | 5 (25) | 0.45 |
| Asian | 0 (0) | 1 (5) | 0.49 |
| Caucasian | 17 (81) | 14 (70) | 0.48 |
| Hispanic | 1 (5) | 0 | 1.0 |
| Preadmission living status, n (%) | |||
| Alone | 6 (29) | 4 (20) | 0.72 |
| With spouse or other family | 11 (52) | 15 (75) | 0.20 |
| Assisted living | 4 (19) | 1 (5) | 0.34 |
| Inpatient medications (mean SD) | 11 3 | 12 5 | 0.18 |
| Charlson score (mean, SD) | 3.2 1.3 | 3.7 1.1 | 0.21 |
| % with APR DRG severity rating 3 | 57.5 | 83.3 | 0.12 |
| % with APR DRG mortality rating 3 | 20.0 | 55.6 | 0.07 |
| Primary admission diagnoses (n cases, in order of frequency) | 3 pneumonia | 3 pneumonia | |
| 3 CHF | 3 syncope | ||
| 2 syncope | 2 CHF | ||
| 2 COPD | 2 COPD | ||
| 2 cellulitis | 2 cellulitis | ||
| 2 GI disorder (nonbleed) | 2 GI disorder (nonbleed) | ||
| 2 GI bleed | 1 GI bleed | ||
| 2 UTI | 1 atrial fibrillation | ||
| 1 atrial fibrillation | 1 encephalopathy | ||
| 1 stroke | 1 TIA | ||
| 1 renal failure | 1 renal failure | ||
| 1 volume depletion |
Study outcomes are displayed in Table 3. Mean LOS is reported as a descriptive finding; there was insufficient power to compare this outcome statistically between groups. The majority of patients were discharged to home. A similar proportion of patients in the intervention (20%) and control groups (22%) who had lived at home immediately prior to admission were discharged from the hospital to skilled care facilities (P = 0.87). The number of readmissions/ED visits (taken as a composite measure of unplanned healthcare utilization) within 30 days of discharge was lower in the intervention group; by 60 days, there was no longer a statistically significant difference in readmission/ED visit rates between groups. For those patients who had a readmission or ED visit following hospital discharge, the intervention group had a longer time interval to first event compared to controls (36.2 versus 15.7 days, P = 0.05). Of the patients discharged to skilled care, 1 in the intervention group (at 53 days) and 1 in the control group (at 16 days) had a readmission/ED visit event. Figure 2 shows time‐to‐first readmission or ED visit event curves at 30 and 60 days for both intervention and control groups. For patients who had a readmission/ED visit event, LOS for this episode was 2.2 2.1 days in controls and 3.7 2.1 days in the intervention group (insufficient power for statistical comparison). The study's small sample size prevented development of a meaningful regression model.
| Outcome Measure | Control (n = 21) | Intervention (n = 20) | P Value |
|---|---|---|---|
| |||
| Length of stay for index hospitalization (days)* | 4.7 3.7 | 6.2 4.1 | |
| 0‐30 day postdischarge readmissions/ED visits | 8 (38%) | 2 (10%) | 0.03 |
| 31‐60 day postdischarge readmissions/ED visits | 1 (5%) | 4 (20%) | 0.18 |
| Total postdischarge readmissions/ED visits at 60 days | 9 | 6 | 0.52 |
Resource utilization and the specifics of patient‐study personnel interaction associated with the intervention were tracked. Research assistants spent an average of 50 minutes daily screening charts for potential candidates. For the 20 patients who received the supplemental elderly care bundle, study CCs averaged 20 to 25 minutes per patient daily of additional time counseling patients and families, identifying and attending to discharge barriers, filling out documentation, and faxing the supplemental study discharge form to the patient's primary care physician. Any residual home care needs or issues unresolved at discharge were addressed with the patient in the 5 to 7 day follow‐up phone call. Similarly, study CPs expended approximately 20 minutes daily per patient providing medication education, reconciliation, and optimization of drug therapy. Study pharmacists recommended a change to the medication regimens of 10 patients in the intervention group; physicians acted upon these recommendations for 7 of the patients. The changes included dosage adjustment, discontinuation of medications due to possible drug interaction or duplication of drugs with the same pharmacologic effect, and addition of medications as indicated by patient condition or to reconcile with patients' at‐home medication regimens. Patients contacted via phone by the study pharmacist within 1 week after discharge were able to describe proper use of new medications started in the hospital and confirm that they obtained or had the means to obtain the prescribed drugs.
Discussion
This pilot study examined the effects of a supplemental care bundle involving patient education and discharge planning delivered by hospital‐based CCs and CPs on the rate of readmission/ED visitation in 41 elderly (70 years of age) patients. The study was not adequately powered to detect an impact of the intervention on index LOS. The care bundle did lead to significantly fewer readmissions or ED visits 30 days postdischarge and appeared to increase the time interval to first unplanned readmission or ED visit compared to usual care. This effect was no longer present at 60 days postdischarge. Resource allocations and scope of duties for CCs and CPs (an average of 20 minutes per patient per day) related to delivering the intervention were realistic for broader implementation in the hospitalized elderly population at high risk for readmission or ED visitation following discharge.
Length of stay for the initial hospitalization associated with the care bundle was an original outcome of interest to the study team. However, with the final enrollment of 41 patients and a power of 0.8, the between group difference would have needed to be 2.6 days to be statistically significant. It is likely that any change in LOS related to the care bundle would be much smaller, particularly since 2 key determinants of LOS, severity of illness and physician behavior, were beyond this patient education‐oriented intervention's scope of influence.3437 Furthermore, the diverse range of eligible diagnoses limited the study CCs' ability to reduce variability through use of clinical care pathways. One approach in leveraging an elderly care bundle to reduce LOS may be to focus on a specific disease that has well‐established inpatient benchmarks and treatment algorithms. For example, in patients with community‐acquired pneumonia, the use of care coordination in combination with standardized order sets decreased LOS without compromising safety, mainly by shortening the time from clinical stability to discharge.38
On separation of the readmission/ED visit outcome into 30 and 60 day postdischarge time frames, the intervention group had a lower rate of unplanned acute health care use within 30 days postdischarge; the difference between groups had dissipated by 60 days postdischarge. This convergence suggests that a hospital‐based intervention's influence is strongest closer to the time of the initial hospital stay, and wanes as more time has elapsed. Indeed, interventions that have successfully maintained lower readmission rates beyond 60 and 90 days postdischarge in a high‐risk elderly population (such as the program advocated by Coleman et al.16) have included a transitional care provider engaging patients during the hospitalization and performing subsequent visits to the home or nursing facility.33 An optimal intervention would capitalize on the hospital‐based staff's ability to improve short‐term readmission/ED visit rates while linking patients to longer‐term transitional care to extend these outcomes. Electronic health records could potentially facilitate these care transitions, beginning with an automated screening process for identification of high‐risk inpatients and continuing through postdischarge follow‐up. How to develop these resources in settings where outpatient practices are independent or only loosely affiliated with hospitals is an area for continued investigation.
In a group of elderly patients with multiple comorbidities and complex pharmacotherapy regimens, the study bundle component targeting medication management appears to be a high‐yield intervention to reduce unplanned health care utilization following hospital discharge. These patients are more susceptible to nonadherence and drug‐related adverse events, which may contribute to hospital readmission or ED visitation.7, 9, 39 Consistent with findings at other sites,28, 40 a heightened level of CP involvement in the care of high‐risk elderly patients may have helped reduce these undesirable outcomes. Of the 9 readmission/ED visit events in the control group, 3 were attributable to medication related complications (2 from sedatives, 1 from a diuretic). None of the readmission/ED visit events in intervention group patients stemmed from medication effects.
Correspondingly, the research CCs' provision of daily condition‐specific education, additional time to more thoroughly investigate discharge needs, engagement of patients' families as active partners in self‐care, and the use of a structured discharge form along with follow‐up phone calls may have better prepared patients to manage their health problems once released from the hospital.26, 28, 29 For example, 1 patient in the control group was readmitted less than 24 hours after initial discharge due to inability to perform self‐care at home. Given the study power issues described previously, data on LOS for the second hospitalization for patients who had a readmission event are difficult to interpret, but could suggest the occurrence of some shorter, preventable readmissions in the control group. Conversely, the readmission/ED visit events in intervention patients appeared to be associated with a specific medical condition (eg, failure of diabetic cellulitis to respond to appropriate outpatient treatment) rather than problems that would have been corrected with an educational/self‐management program such as this targeted care bundle.
This pilot study had several limitations. The main issue was a small patient sample size that was primarily due to an inability to obtain informed consent. Design of the study as a randomized controlled trial and plans to disseminate study findings beyond BHCS necessitated IRB approval rather than delivery of the supplemental care bundle as a quality improvement (QI) project. Placing QI initiatives under research regulations can lead to project delays, higher costs, and patient frustrations with the process.41, 42 This tension was evident during study screening and enrollment, as many patients who otherwise met criteria and would potentially benefit from the intervention were hesitant to participate in a research study or refused to sign a multipage consent document. The difficulties of enrolling elderly patients in clinical trials have been well‐described.43, 44 Further research involving a minimal‐risk, educational intervention such as this elderly care‐bundle would likely better fit under the category of expedited IRB review with waiver or modification of the informed consent process.45
Incomplete blinding could have potentially affected our results. At the study site, the team members delivering the care bundle were a regular part of the hospital staff (as opposed to external researchers), and it is not unusual for a CC or a pharmacist to enter a patient's room (eg, to confirm a drug allergy history). In view of this, the impact of imperfect blinding on 30‐day outcomes would likely be minimal. Furthermore, a floor staff perception that a specific patient was being taken care of by the study team resulting in a lower than usual level of care, would tend to bias the result of the intervention toward the null effect.
vThe study cohort did not have enough subjects to perform analyses (ie, modeling or examination of subgroups) beyond basic comparative findings. Issues such as preadmission living situation and the presence of depression or cognitive impairment (Mini‐Mental Status Exams were not performed on these patients) may potentially influence postdischarge recidivism; their effects can not be reliably ascertained from these data. Additionally, to prevent study personnel from engaging patients who would soon be going home, it was felt that the benefits from the care bundle would be recognized only if the intervention could be initiated within 72 hours of admission and delivered in full, a requirement that further reduced the enrollment pool. The intent of this pilot work was to guide future investigations surrounding hospital‐to‐home transitional care. The next phase of research in this area will need an enhanced sample size with more extensive baseline data collection so that potential confounding factors or outcomes in specific populations can be explored.
Another problem restricting applicability of study findings was the use of only 3 different CCs and 3 pharmacists on the research team to deliver the components of patient education, discharge planning, and medication counseling in the elderly care bundle. Personnel for the trial were chosen for their experience and interest in the area of care transitions. To distinguish the benefit of the elderly care bundle in general versus the expertise of these particular CCs and study pharmacists, a larger‐scale, multisite trial would be necessary. Lastly, due to resource constraints, patients who resided in long‐term care (either LTAC, SNFs, or nursing homes) prior to admission with anticipated return to those sites were not eligible for the study. Similar to the patients whose comorbidities or acute severity of illness prevented informed consent, this segment of the elderly population may have derived even more benefit from receipt of the elderly care bundle.10, 15, 46 Despite exclusion of this group (which would be expected to lessen the impact of the intervention), a difference in readmission/ED visits rates at 30 days following discharge was observed.
Conclusions
This pilot randomized clinical trial (RCT) evaluated the effects of a supplemental, aggregate care bundle centered on patient education, discharge planning, and medication counseling and reconciliation compared to usual care in a group of elderly patients at high risk of readmission or ED visitation following an index hospitalization. The intervention was designed to be reproducible and make use of existing hospital resources. Probably through facilitation of patient self‐care and home management, the elderly care bundle reduced the composite outcome of readmission/ED visits at 30 days postdischarge. By 60 days, this effect had waned, demonstrating the short‐term benefit of a hospital‐based educational intervention and stressing the need to incorporate additional outpatient transitional care support to sustain favorable outcomes. The study was not powered to detect small differences (which would be more likely than a change of multiple days) in length of index hospital stay related to the care bundle. There were important study limitations (primarily associated with small sample size), and this work should be viewed as hypothesis‐generating. Future trials should assess the impact of a standardized targeted care bundle delivered across multiple healthcare systems on a larger cohort of high‐risk elderly patients, including analysis of financial and personnel allocations relative to the benefits of the intervention.
Acknowledgements
The authors thank study pharmacists Kristen Hesch (PharmD), Renee Danysh (PharmD), Rema Thyagarajan (PharmD), and Betina Thomas (PharmD) for providing patients with medication education and conducting medication reconciliation. They also thank Jeanne Bradbury (RN, ACM), Diana Davis (RN, BSN), and Gail McVea (RN, MSN) for their involvement as care coordinators; Veronica Odom (RN) for her contributions as a research nurse; and Marilyn Callies (RN, MBA) for her role as project advisor.
- ,.Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions.Ann Emerg Med.2002;39(3):238–247.
- ,,,,,.Emergency department utilization by the elderly: analysis of the National Hospital Ambulatory Medical Care Survey.Acad Emerg Med.1996;3(7):694–699.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007(385):1–19.
- ,,,,.Short‐term outcomes of elderly patients discharged from an emergency department.J Am Geriatr Soc.1989;37(10):937–943.
- ,,,,.The discharge of elderly patients from an accident and emergency department: functional changes and risk of readmission.Age Ageing.1990;19(6):415–418.
- ,,,,,.Factors associated with unplanned hospital readmission among patients 65 years of age and older in a Medicare managed care plan.Am J Med.1999;107(1):13–17.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165(16):1842–1847.
- ,.From the emergency department to home.J Clin Nurs.2005;14(6):776–785.
- ,,.Adverse drug events in elderly patients receiving home health services following hospital discharge.Ann Pharmacother.1999;33(11):1147–1153.
- ,,, et al.A randomized trial of the efficacy of multidisciplinary care in heart failure outpatients at high risk of hospital readmission.J Am Coll Cardiol.2002;39(3):471–480.
- ,,,.A systematic review of randomized trials of disease management programs in heart failure.Am J Med.2001;110(5):378–384.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291(11):1358–1367.
- ,,,.Case management may reduce length of hospital stay in patients with recurrent admissions for chronic obstructive pulmonary disease.Respirology.2001;6(1):37–42.
- ,,,,,.A chronic disease management programme can reduce days in hospital for patients with chronic obstructive pulmonary disease.Intern Med J.2004;34(11):608–614.
- ,,.Disease management programmes for older people with heart failure: crucial characteristics which improve post‐discharge outcomes.Eur Heart J.2006;27(5):596–612.
- ,,,.The care transitions intervention: results of a randomized controlled trial.Arch Intern Med.2006;166(17):1822–1828.
- ,,, et al.Effects of a multidisciplinary, post‐discharge continuance of care intervention on quality of life, discharge satisfaction, and hospital length of stay: a randomized controlled trial.Int J Qual Health Care.2005;17(1):43–51.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004(1):CD000313.
- ,.A systematic review of interventions to improve outcomes for elders discharged from the emergency department.Acad Emerg Med.2005;12(10):978–986.
- .Transitional care for older adults: a cost‐effective model.LDI Issue Brief.2004;9(6):1–4.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281(7):613–620.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,.Home‐based intervention in congestive heart failure: long‐term implications on readmission and survival.Circulation.2002;105(24):2861–2866.
- ,,, et al.Effectiveness of team‐managed home‐based primary care: a randomized multicenter trial.JAMA.2000;284(22):2877–2885.
- ,,,.Home‐based medication review in older people: is it cost effective?Pharmacoeconomics.2007;25(2):171–180.
- ,,,,.The value of inpatient pharmaceutical counselling to elderly patients prior to discharge.Br J Clin Pharmacol.2002;54(6):657–664.
- ,,,,.Does the addition of a pharmacist transition coordinator improve evidence‐based medication management and health outcomes in older adults moving from the hospital to a long‐term care facility? Results of a randomized, controlled trial.Am J Geriatr Pharmacother.2004;2(4):257–264.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166(5):565–571.
- ,,,,,.An investigation of hospital generated pharmaceutical care when patients are discharged home from hospital.Br J Clin Pharmacol.1997;44(2):163–165.
- ,,.The community assessment risk screen (CARS): identifying elderly persons at risk for hospitalization or emergency department visit.Am J Manag Care.2000;6(8):925–933.
- ,,.“Risk” factors affecting readmission of the elderly into the health care system.Med Care.1986;24(5):429–437.
- ,,.Re‐admission to intensive care: identification of risk factors.Physiother Res Int.2005;10(3):154–163.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,,,.Impact of the rapid diagnosis of influenza on physician decision‐making and patient management in the pediatric emergency department: results of a randomized, prospective, controlled trial.Pediatrics.2003;112(2):363–367.
- ,,,,.A survey on hospitalised community‐acquired pneumonia in Italy.Monaldi Arch Chest Dis.2006;65(2):82–88.
- ,,,,.Determinants of the length of stay in intensive care and in hospital after coronary artery surgery.Br Heart J.1995;73(1):92–98.
- ,,.Variation in duration of hospital stay between hospitals and between doctors within hospitals.Soc Sci Med.1993;37(6):833–839.
- ,,, et al.The impact of standardized order sets and intensive clinical case management on outcomes in community‐acquired pneumonia.Arch Intern Med.2007;167(15):1664–1669.
- ,,.Compliance with medication orders among the elderly after hospital discharge.Hosp Formul.1992;27(7):720–724.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166(9):955–964.
- .Quality improvement and ethical oversight.Ann Intern Med.2007;146(9):680–681.
- ,,, et al.The ethics of using quality improvement methods in health care.Ann Intern Med.2007;146(9):666–673.
- ,,.Enrollment of elderly patients in clinical trials for cancer drug registration: a 7‐year experience by the US Food and Drug Administration.J Clin Oncol.2004;22(22):4626–4631.
- ,,,.Striving to recruit: the difficulties of conducting clinical research on elderly care home residents.J R Soc Med.2007;100(6):258–261.
- ,.Quality‐improvement research and informed consent.N Engl J Med.2008;358(8):765–767.
- ,,,.An evaluation of the impact of the ventilator care bundle.Nurs Crit Care.2005;10(5):242–246.
- ,.Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions.Ann Emerg Med.2002;39(3):238–247.
- ,,,,,.Emergency department utilization by the elderly: analysis of the National Hospital Ambulatory Medical Care Survey.Acad Emerg Med.1996;3(7):694–699.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007(385):1–19.
- ,,,,.Short‐term outcomes of elderly patients discharged from an emergency department.J Am Geriatr Soc.1989;37(10):937–943.
- ,,,,.The discharge of elderly patients from an accident and emergency department: functional changes and risk of readmission.Age Ageing.1990;19(6):415–418.
- ,,,,,.Factors associated with unplanned hospital readmission among patients 65 years of age and older in a Medicare managed care plan.Am J Med.1999;107(1):13–17.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165(16):1842–1847.
- ,.From the emergency department to home.J Clin Nurs.2005;14(6):776–785.
- ,,.Adverse drug events in elderly patients receiving home health services following hospital discharge.Ann Pharmacother.1999;33(11):1147–1153.
- ,,, et al.A randomized trial of the efficacy of multidisciplinary care in heart failure outpatients at high risk of hospital readmission.J Am Coll Cardiol.2002;39(3):471–480.
- ,,,.A systematic review of randomized trials of disease management programs in heart failure.Am J Med.2001;110(5):378–384.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291(11):1358–1367.
- ,,,.Case management may reduce length of hospital stay in patients with recurrent admissions for chronic obstructive pulmonary disease.Respirology.2001;6(1):37–42.
- ,,,,,.A chronic disease management programme can reduce days in hospital for patients with chronic obstructive pulmonary disease.Intern Med J.2004;34(11):608–614.
- ,,.Disease management programmes for older people with heart failure: crucial characteristics which improve post‐discharge outcomes.Eur Heart J.2006;27(5):596–612.
- ,,,.The care transitions intervention: results of a randomized controlled trial.Arch Intern Med.2006;166(17):1822–1828.
- ,,, et al.Effects of a multidisciplinary, post‐discharge continuance of care intervention on quality of life, discharge satisfaction, and hospital length of stay: a randomized controlled trial.Int J Qual Health Care.2005;17(1):43–51.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004(1):CD000313.
- ,.A systematic review of interventions to improve outcomes for elders discharged from the emergency department.Acad Emerg Med.2005;12(10):978–986.
- .Transitional care for older adults: a cost‐effective model.LDI Issue Brief.2004;9(6):1–4.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial.JAMA.1999;281(7):613–620.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,.Home‐based intervention in congestive heart failure: long‐term implications on readmission and survival.Circulation.2002;105(24):2861–2866.
- ,,, et al.Effectiveness of team‐managed home‐based primary care: a randomized multicenter trial.JAMA.2000;284(22):2877–2885.
- ,,,.Home‐based medication review in older people: is it cost effective?Pharmacoeconomics.2007;25(2):171–180.
- ,,,,.The value of inpatient pharmaceutical counselling to elderly patients prior to discharge.Br J Clin Pharmacol.2002;54(6):657–664.
- ,,,,.Does the addition of a pharmacist transition coordinator improve evidence‐based medication management and health outcomes in older adults moving from the hospital to a long‐term care facility? Results of a randomized, controlled trial.Am J Geriatr Pharmacother.2004;2(4):257–264.
- ,,, et al.Role of pharmacist counseling in preventing adverse drug events after hospitalization.Arch Intern Med.2006;166(5):565–571.
- ,,,,,.An investigation of hospital generated pharmaceutical care when patients are discharged home from hospital.Br J Clin Pharmacol.1997;44(2):163–165.
- ,,.The community assessment risk screen (CARS): identifying elderly persons at risk for hospitalization or emergency department visit.Am J Manag Care.2000;6(8):925–933.
- ,,.“Risk” factors affecting readmission of the elderly into the health care system.Med Care.1986;24(5):429–437.
- ,,.Re‐admission to intensive care: identification of risk factors.Physiother Res Int.2005;10(3):154–163.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,,,.Impact of the rapid diagnosis of influenza on physician decision‐making and patient management in the pediatric emergency department: results of a randomized, prospective, controlled trial.Pediatrics.2003;112(2):363–367.
- ,,,,.A survey on hospitalised community‐acquired pneumonia in Italy.Monaldi Arch Chest Dis.2006;65(2):82–88.
- ,,,,.Determinants of the length of stay in intensive care and in hospital after coronary artery surgery.Br Heart J.1995;73(1):92–98.
- ,,.Variation in duration of hospital stay between hospitals and between doctors within hospitals.Soc Sci Med.1993;37(6):833–839.
- ,,, et al.The impact of standardized order sets and intensive clinical case management on outcomes in community‐acquired pneumonia.Arch Intern Med.2007;167(15):1664–1669.
- ,,.Compliance with medication orders among the elderly after hospital discharge.Hosp Formul.1992;27(7):720–724.
- ,,,.Clinical pharmacists and inpatient medical care: a systematic review.Arch Intern Med.2006;166(9):955–964.
- .Quality improvement and ethical oversight.Ann Intern Med.2007;146(9):680–681.
- ,,, et al.The ethics of using quality improvement methods in health care.Ann Intern Med.2007;146(9):666–673.
- ,,.Enrollment of elderly patients in clinical trials for cancer drug registration: a 7‐year experience by the US Food and Drug Administration.J Clin Oncol.2004;22(22):4626–4631.
- ,,,.Striving to recruit: the difficulties of conducting clinical research on elderly care home residents.J R Soc Med.2007;100(6):258–261.
- ,.Quality‐improvement research and informed consent.N Engl J Med.2008;358(8):765–767.
- ,,,.An evaluation of the impact of the ventilator care bundle.Nurs Crit Care.2005;10(5):242–246.
Copyright © 2009 Society of Hospital Medicine
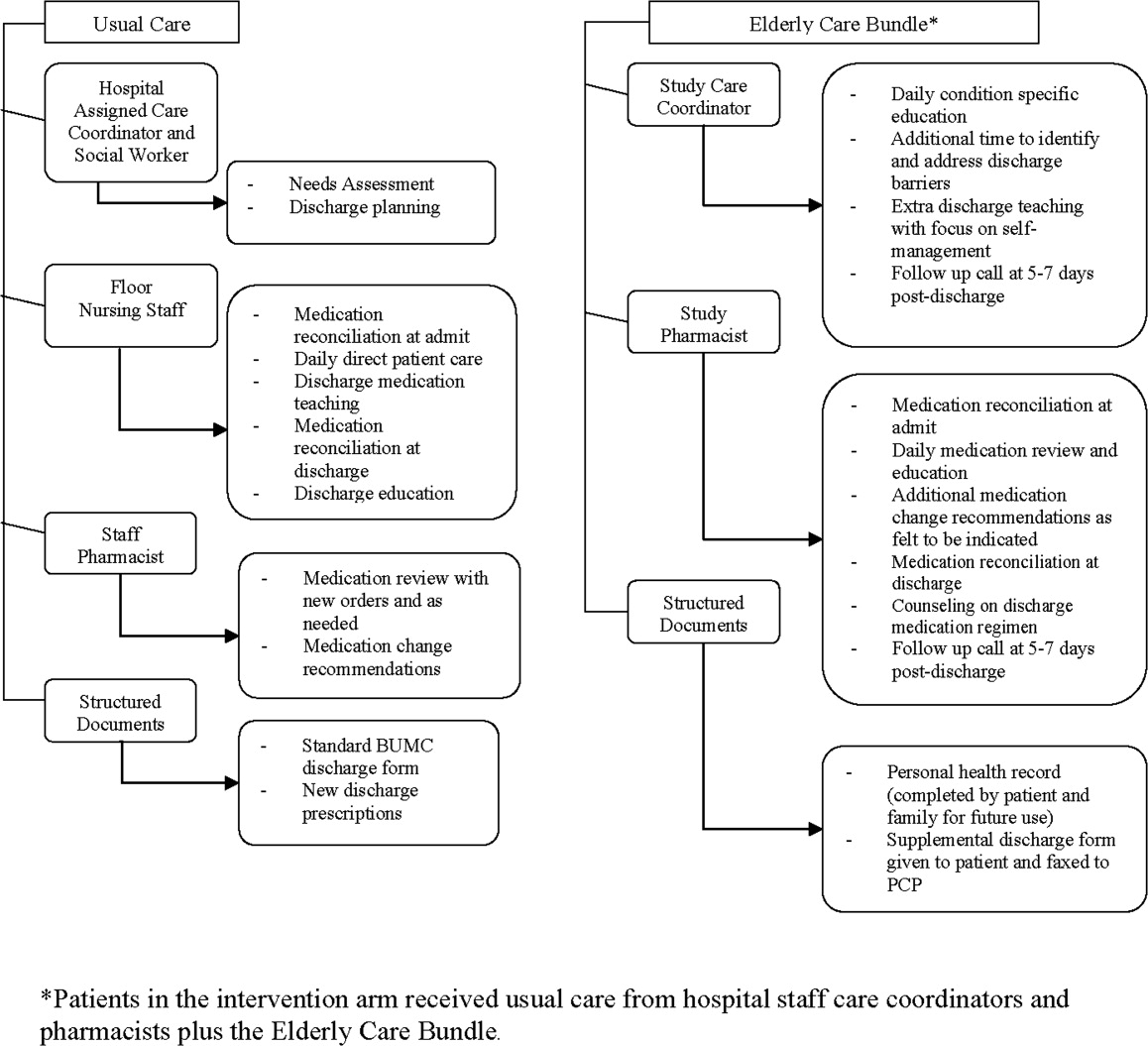
Late Discharges from a Medical Ward
In the past 2 decades, emergency department (ED) overcrowding has become an issue large enough to receive coverage in the popular press, and to spawn research around its causes and effects.116 At the same time, nurses and physicians on the inpatient wards have been urged to shorten the length of stay for patients as health system leaders face an aging population but limited capital to build new beds or hire additional clinical staff. Capacity managementencompassing the flow of patients from ED triage to inpatient dischargehas become a shared concern of clinicians and hospital administrators alike.
How to achieve the goals of diagnosing and healing while ushering patients ever more quickly through the modern hospital is not yet entirely clear. Past research and work by business groups suggests that demand for inpatient beds starts early in the day, but discharges typically occur in the late afternoon.17 This creates a potential bottleneck in patient flow. Many hospitals have implemented measures to improve patient throughput.1821 However, formal research has focused on factors leading to an additional inpatient day.2226 We have found no peer‐reviewed publications that address the problem of same‐day delays by describing hour of day for each step in the discharge process and variables associated with late‐day discharges. To fill this gap, we conducted a prospective cohort study of 209 consecutive discharges from a general medical ward to: (1) describe the natural history of hospital discharge, (2) measure time of day and duration for each step, and (3) identify factors associated with discharges that occur later in the day. We hypothesized that time and duration of discharge would be associated with 5 factors: patient demographics and clinical characteristics, departmental occupancy, type of inpatient testing done immediately prior to discharge, and discharge characteristics such as discharge to a location other than home.
Patients and Methods
Setting
The setting was the Hospitalist Unit of a single teaching hospital in Baltimore (The Johns Hopkins Hospital) from January 1, 2005 to April 30, 2005. Patients entered the cohort upon initiation of the discharge process by the hospitalist team on the Hospitalist Unit, and were followed until they were discharged alive from the hospital.
There were no published data on which to base firm a priori sample size calculations. Based on pilot data, we estimated that a sample size of about 170 would yield precise estimates for means and standard deviations, giving us 80% to 90% power to determine differences in time intervals across categories, with alpha set to 0.05. We estimated that we would need 4 months of data collection to achieve this sample size.
During the period of study, the 16‐bed unit was staffed with in‐house hospitalist attending physicians without house‐staff, from 7 AM (weekdays) or 8 AM (weekends) to 10 PM (Monday to Thursday) or 8 PM (Friday to Sunday). The hospitalist unit had 24‐hour physician coverage, but attending physicians provided overnight coverage from home (backed up by in‐house residents for patient care emergencies). Handoffs of patient care from one attending physician to another typically occurred on Friday afternoon or Monday morning. The unit had 1 dedicated social worker and a nurse clinician who provided part‐time assistance with discharge planning.
Outcome Measurements
We defined the start of the discharge process as the time the patient's last medically necessary test was needed by his or her attending physician. Specifically, physicians were asked when the results of this test first would have been useful in clearing the patient for discharge. In the remainder of this work, we will refer to the start of the discharge process as time decisive test needed.
The end of the discharge process was called the discharge time, and defined as the time the unit clerk saw the patient leave the unit. We defined early discharges as those occurring before the median hour of discharge (3:00 PM), and late discharges as those occurring at or after this hour.
A focus group composed of nurses, physicians, social worker, unit clerks, and support associates (group responsible for cleaning patient rooms) volunteered to map out the discharge process. Based on these discussions, durations in the discharge process were defined as follows: (1) duration 1: time decisive test needed, until time the attending physician was aware of test results; (2) duration 2: time the physician was aware of test results until discharge paperwork was complete; (3) duration 3: time discharge paperwork complete until patient leaves unit; and (4) total discharge duration: time decisive test needed until patient leaves unit.
Exposure Measurements
We categorized exposures into 5 groups: (1) demographics (age, gender, race, source of patient such as outside hospital versus emergency department versus other, and payer on discharge); (2) clinical characteristics (length of stay, any psychiatric diagnosis, any substance abuse diagnosis, and severity of illness); (3) system characteristics (departmental occupancy defined as proportion of hospital beds designated for Department of Medicine patients that were occupied on the day of discharge); (4) last test characteristics (physical exam, laboratory test, procedure, and consult); and (5) discharge characteristics (discharged to home versus not discharged to home, prescriptions filled in hospital pharmacy prior to discharge, and ambulance required for transport).
Psychiatric diagnosis was defined as the presence of any of the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) codes: 290319 (any fourth or fifth digits).27 Substance abuse diagnosis was defined as the presence of any of the following ICD‐9‐CM codes: 303305 (any fourth or fifth digits). Substance abuse codes encompassed drug dependence and abuse, including alcohol dependence and abuse.
The all patient refined diagnosis related group relative weight (APRDRGwt) is a unitless number that estimates the total cost of care for inpatients, based on clinical and demographic characteristics.28 A patient with a relative APRDRGwt of 1 is predicted to have the same cost of care as the national average for inpatients. A patient with a score of 2 is predicted to be twice as costly as the average. In this study, we used APRDRGwt as a gross proxy for severity of illness.
Adjusted length of stay was measured as length of stay minus discharge duration. This adjustment was made to avoid including the exposure (length of stay) in the outcome (discharge duration). Unadjusted length of stay was used when the outcome was discharge time.
Data Sources
We created a separate 4‐item to 9‐item paper questionnaire (included in the Appendix) for each of 4 functional groups participating directly in the discharge process: nurses, physicians, social worker, and unit clerks. Questions were based on staff feedback about the sequence of steps in the discharge process, and potential reasons for delay. The surveys were piloted for several weeks to further refine the wording of questions, and to ensure that the length and location of the surveys minimized workflow interruptions. The questionnaires captured information about the timing of routine events not recorded in existing databases.
Physicians were asked to identify the last test/procedure/consult needed prior to the patient being medically ready for discharge. They were asked when the test results first could have cleared the patient for discharge (time decisive test needed), and when they actually received the test results (time test results back). Nursing and social work surveys provided information on whether or not prescriptions were filled prior to discharge, and the type of transportation used on discharge. Unit clerks documented when the patient left the unit.
Response rates were: nurses (97%), physicians (97%), social worker (99%), and unit clerks (94%). All 4 surveys were completed for 88% of the 209 included patients (prior to 8 exclusions for missing data or extreme outlier observations). Group response rates were tallied at the end of each month and posted on the unit. We did not track how soon after discharge the surveys were completed. However, we reviewed survey responses frequently (often daily, at most every 4 days) and if surveys were incomplete we personally approached staff members to complete the survey.
We supplemented and cross‐checked data from the questionnaire with information from existing hospital databases. These databases were: (1) the patient's medical record for time patient arrived on the floor, and completion time for consults/procedures; (2) the Electronic Bedboard (EBB) for time patient left the unit (as recorded by unit clerk); (3) the Patient Order Entry System for time discharge papers were completed by the physician, and ordering time for select tests; (4) the Electronic Patient Record for demographic information and completion time for select tests; and (5) Datamart, the hospital's administrative/billing database, for information such as length of stay, diagnosis, patient demographics, and insurance status.
Cross‐checking of data and calculation of durations 1, 2, and 3 identified areas of disagreement that were addressed in the following way. Discharge time was provided by 3 sources: social worker and nurses as an ad hoc addition to each of their surveys, unit clerks as a mandatory question on their survey, and unit clerks as entered in the EBB. We used EBB data for discharge time, as this was the most complete and accurate single source of data. However, survey results and knowledge about the sequential process for discharge, suggested that in 20 cases EBB data did not provide the most accurate time. In these cases, discharge time was provided by the unit clerk survey (16 cases), the social work survey (3 cases), and the nursing survey (1 case).
In 28 cases (14%), discharge paperwork was completed before decisive test results were back. And in 8 cases (4%) test results were received earlier than needed. As these were a minority of cases, these negative durations were converted to zero for analysis.
Statistical Analysis
The unit of analysis was the unique hospital discharge. For patients who were discharged from the Hospitalist Unit more than once during the 4‐month study period, each discharge was treated as a separate unit of analysis.
We defined patients discharged before the median discharge time as early discharges, and all others as late discharges. We then categorized patients with discharge durations less than 24 hours as short discharges, and all others as long discharges.
We described the characteristics of 2 groups of patients: early and short discharges versus all others. We used the chi square statistic and Fisher's exact test (when frequency 5 in 1 or both groups) to test the null hypothesis that there was no association between the 2 groups and select patient characteristics. When comparing medians, we used the nonparametric equality of medians test.
For each step in the discharge process, we identified a median time of occurrence. For the first point in the processtime decisive test neededwe also used 1‐way analysis of variance and the F‐test to assess whether or not timing varied significantly by physician.
Because our primary goal was to quantify in hours the association between various factors and discharge time or duration, we used bivariate linear regression models to identify factors associated with time of discharge (primary analysis) and total duration of the discharge process (secondary analysis). We then used multivariate linear regression to identify factors associated with both outcomes. We used forward and backward selection methods to choose the final models for the multivariate analyses, after forcing in the variables for race, sex, and age. Both methods of selection produced identical results. We assessed for colinearity using variance inflation factors.29
Sensitivity Analyses
For both discharge time and discharge duration, we performed regression diagnostics including leverage, Studentized residuals, and influence. Excluding outliers for influence slightly altered the results of our multivariate analyses. However, all variables that were significant at the P < 0.05 level remained significant in the models without outliers.
We chose to include outliers for influence in our final data set after verifying the data as accurate. For discharge time, the number of outliers (3; 1.5%) for influence was in the range expected for a normally distributed data set.
We also tested for normality of the 2 outcome variables. Discharge time was normally distributed, but discharge duration was not. Because of this, we used 2 additional methods to assess the robustness of our results for discharge duration.
First, we log‐transformed the outcome and repeated the analysis. Variables significant in the non‐log‐transformed model remained significant after log‐transformation. Second, we applied bootstrapping30 with 1,000 repetitions for the bivariate and multivariate analyses. The 95% confidence intervals (CIs) (using the bias‐corrected confidence intervals) were modestly altered (some narrowed, some widened), but our conclusions remained the same except for a single variable with borderline significance (payer on discharge) in bivariate analysis. The final reported confidence intervals for discharge duration are based on our analysis without bootstrapping.
Results
Data were collected on 216 patients. Seven patients were excluded from the study, because they were discharged against medical advice. Since these patients left before their decisive test was completed, there was no way to assess duration of the discharge process. Of the remaining 209 patients, 6 patients lacked necessary data to complete analysis (5 without survey data; 1 without administrative data). Two additional patients were eliminated from the final analysis because they bypassed the normal discharge process and were extreme outliers in either discharge time (1 discharged at 1 AM), or discharge duration (1 with discharge duration of 400+ hours). A total of 201 patients were included in the final analyses.
The hospitalist program primarily serves an indigent, local adult population with general medical problems, and this is reflected in the patient characteristics (Table 1). We compared the characteristics of patients discharged early and quickly (discharged prior to median hour of 3:00 PM, and discharge process lasting less than 24 hours) to all other discharges, to identify factors associated with later and longer discharges.
| Early and Short Discharges (n = 75)* | All Other Discharges (n = 126) | P Value | |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | |||
| Median | 55 | 55 | 0.73 |
| Range | (19, 94) | (20, 90) | |
| Gender (%) | |||
| Female | 61.3 | 61.1 | 0.98 |
| Race (%) | 0.08 | ||
| African American | 76.0 | 60.3 | |
| Caucasian | 21.3 | 34.9 | |
| Other | 2.7 | 4.8 | |
| Payor on discharge (%) | 0.29 | ||
| Medicaid | 32.0 | 20.6 | |
| Medicare | 32.0 | 38.9 | |
| Self‐pay | 12.0 | 16.7 | |
| Other | 24.0 | 23.8 | |
| Clinical characteristics | |||
| Adjusted length of stay (days) | |||
| Median | 3 | 3 | 0.19 |
| Range | (<1, 20) | (<1, 138) | |
| Substance abuse (%) | 41.3 | 37.3 | 0.57 |
| Psychiatric diagnosis (%) | 20.0 | 25.4 | 0.38 |
| Last test characteristics | |||
| Test type (%) | <0.001 | ||
| Exam | 42.7 | 26.2 | |
| Laboratory test | 38.7 | 13.5 | |
| Procedure | 10.7 | 35.7 | |
| Consult | 8.0 | 24.6 | |
| Discharge characteristics | |||
| Discharged to home (%) | 93.3 | 71.4 | <0.001 |
| Prescriptions filled prior to discharge (%) | 10.7 | 19.8 | 0.09 |
| Ambulance required for transport (%) | 8.0 | 21.4 | 0.01 |
Overall, 81% of patients were admitted from the ED, and 40% of all patients were insured by Medicaid or were self‐pay at time of discharge. Median expected charges were similar to the national average, as demonstrated by the median APRDRGwt of 1.0. Patients stayed an average of 6 days (median = 3 days). Patients with the longest adjusted lengths of stay (>20 days) were never early and short discharges. The most common discharge diagnoses were: congestive heart failure, chest pain or myocardial infarction, pneumonia, asthma/chronic obstructive pulmonary disease, and sickle‐cell disease. Thirty‐nine percent of all patients carried the diagnosis of alcohol or drug dependence or abuse, although for most this was not their discharge diagnosis. None of these demographic or clinical factors were associated with a late or long discharge.
The types of tests patients required on discharge were categorized into 4 groups: consults (18.4%), laboratory tests (22.9%), procedures (26.4%), and physical exam (32.3%). Distribution differed significantly between early and short discharges, and all other discharges (P < 0.001). Procedures and consults were less frequent among early and short discharges (procedures: 10.7% versus 35.7%; consults: 8.0% versus 24.6%).
For all patients, there was fragmentation within the consult and procedure categories. Within the consult group, there were 12 different types of consults ordered, with the dominant category (35.1%) being other. The next highest volume consult was physical/occupational therapy (27.0%). Within the procedure group, there were 11 different types of procedures, with the most common being stress echocardiograms (28.3%). Non‐MRI radiology procedures made up the next largest category (20.8%) and the third was other (18.9%).
Many patients had immediate postdischarge needs, as demonstrated by the 20% of patients not discharged home. The majority (66%) of those who were discharged to a facility required an ambulance. Early and short discharges were less likely to use an ambulance to leave the hospital (8.0% versus 21.4%; P = 0.01), and more likely to be discharged directly to home (99.3% versus 71.4%; P < 0.001).
Based on process mapping, we defined a 4‐step sequential discharge process for all patients (Figure 1). The first step was: decisive test needed by physician to discharge patient. Subgroup analysis demonstrated no significant difference in the timing of this step by individual physician (P = 0.44). The remaining 3 steps were as follows: physician aware of test results, discharge paperwork complete by physician, and patient leaves the unit. Each of the 4 steps showed wide variability in hour of occurrence.

Total discharge duration showed even more variability than the time of day when steps were likely to occur (Figure 2). Median duration of the discharge process was 7.6 hours (25th% to 75th%: 4 to 22 hours). Median duration from decisive test needed until resulted (duration 1) was 2 hours (25th% to 75th%: 0 to 8 hours); between test resulted until discharge paperwork complete (duration 2) was 1.4 hours (25th% to 75th%: 0.3 to 4.2 hours); and between discharge paperwork complete and patient leaving the unit (duration 3) was 2.0 hours (25th% to 75th%: 1.1 to 3.1 hours). All durations were skewed to the right, with durations 1 and 2 each taking at least 24 hours to occur in 10% of patients.
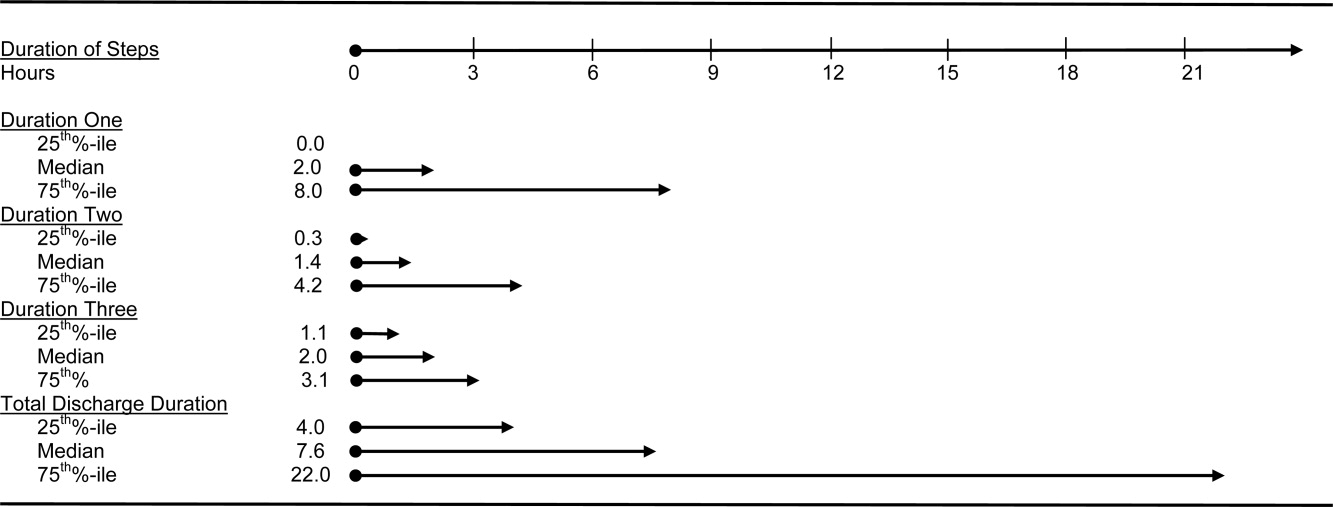
The final multivariate model for time of discharge contained 6 covariates: age, sex, race, test type, prescriptions filled prior to discharge, and need for an ambulance on discharge (Table 2). Special discharge needs continued to be associated with later discharges. Those patients who required an ambulance for transport had mean discharge times that were later by 1.5 hours (95% CI, 0.42.5). If staff obtained discharge medications for patients, these patients left 1.4 hours later than those patients who filled their prescriptions on their own (95% CI, 0.32.4). Patients requiring a consult or procedure also had significantly later discharges (1.2 hours for consults, 95% CI, 0.12.4; 1.1 hours for procedures, 95% CI, 0.12.1) than those needing a bedside exam. Age, sex, and race remained insignificant at the P 0.05 level in the final multivariate model. Length of stay was significantly associated with discharge time in crude analysis, but this variable dropped out of the final multivariate model.
| Adjusted Coefficient, Discharge Time as Outcome in Hours (95% CI)* | P Value | Adjusted Coefficient, Discharge Duration as Outcome in Hours (95% CI) | P Value | |
|---|---|---|---|---|
| ||||
| Demographics | ||||
| Age in quartiles (years) | ||||
| 7294 | 0.5 (0.5, 1.6) | 0.33 | 0.6 (8.3, 7.2) | 0.88 |
| 5671 | 0.5 (0.6, 1.6) | 0.41 | 1.3 (9.2, 6.6) | 0.75 |
| 4455 | 0.2 (0.9, 1.3) | 0.74 | 1.2 (9.0, 6.5) | 0.76 |
| Male gender | 0.0 (0.8, 0.8) | 0.97 | 1.2 (6.8, 4.5) | 0.69 |
| African American race | 0.1 (0.7, 0.9) | 0.80 | 0.3 (5.6, 6.1) | 0.93 |
| Last test characteristics | ||||
| Test type | ||||
| Consult | 1.2 (0.1, 2.4) | 0.04 | 14.8 (6.5, 23.1) | 0.001 |
| Procedure | 1.1 (0.1, 2.1) | 0.03 | 13.4 (6.0, 20.7) | <0.001 |
| Laboratory test | 0.8 (1.8, 0.3) | 0.14 | 0.9 (8.4, 6.6) | 0.82 |
| Exam (reference) | ||||
| Discharge needs | ||||
| Prescriptions filled prior to discharge | 1.4 (0.3, 2.4) | 0.02 | ||
| Not discharged to home | 28.9 (21.9, 35.9) | <0.001 | ||
| Ambulance required for transport | 1.5 (0.4, 2.5) | 0.007 | ||
We used duration of discharge as a secondary outcome measure. The final multivariate model for discharge duration included: age, sex, race, test type, and discharge to a facility (Table 2). Those who went to a facility on average left 28.9 hours (95% CI, 21.935.9) later than those who went home. Test type continued to show a significant association with discharge duration, although the estimates were slightly lower in the adjusted model. Need for a consult was associated with a discharge that was on average 14.8 hours (95% CI, 6.523.1) longer than discharges contingent on a physical exam. Similarly, those patients who had procedures had discharges that were on average 13.4 hours (95% CI, 6.020.7) longer than those whose last test was an exam. Several factors that were significantly associated with discharge duration in unadjusted analyses dropped out of the final multivariate model. These included: need for an ambulance, length of stay, insurance status, and medical complexity as estimated by APRDRGwt.
Conclusions
We found that discharge time and duration had wide variability and that certain factors were associated with only one outcome variabledischarge time or duration. Two factorsneed for an ambulance and filling of prescriptions prior to dischargewere associated with later hour of discharge. Discharge to a location other than home was associated with prolonged discharge duration. Test characteristicsin particular need for a procedure and consultwere significantly associated with both longer and later discharges.
In bivariate analysis, several factors were not associated with discharge time or duration. These were: African‐American race, sex, age, Department of Medicine occupancy on day of discharge, source of admission, psychiatric comorbidity, and substance abuse comorbidity. We had expected higher occupancy to delay discharge as demand exceeded capacity for tests, consults, etc. Our findings suggest that even though our study was conducted during the winter months when hospital occupancy is typically at its peak, supply of staff was still adequate enough to meet high demand. We had also expected that psychiatric and substance abuse comorbidities would prolong discharge as prior studies have found some of these diagnoses to be associated with longer lengths of stay.3134 However, our results do not support such an association, and may reflect our decision to group all psychiatric diagnoses together due to limited sample size.
The main strength of our study is the use of 2 outcome variablestime and durationto define delayed discharges. Our findings demonstrate that few factors are associated with both later and longer discharges. In an era when avoiding emergency room walkouts through early morning hospital discharges can be as important as managing overall length of stay, identifying factors associated with both duration and timing of discharges addresses actual challenges faced by hospitals with limited resources. Prior studies have rarely addressed both outcomes. An additional strength of our study is our use of an interdisciplinary survey. The discharge process is a key component of the inpatient stay, but it is also one for which no group is entirely responsible. Through the development and administration of an interdisciplinary survey, our study adds detail to existing descriptions of this fragmented process, and identifies potential areas for improvement.
Several limitations of our study deserve comment. First, we examined patients discharged from a hospitalist unit without house‐staff at an urban tertiary care hospital. Our findings may need additional interpretation prior to their application in dissimilar settings such as: (1) resident‐covered units in which workflow is shaped by teaching rounds, and (2) nonacademic hospitals in which incentives to provide rapid consults and procedures may be different. Second, we relied on self‐reporting for certain variables such as time decisive test needed. This may be subject to recall bias, as we did not have staff to independently verify recalled times. However, since the discharge process is generally a linear one, we were able to verify the general scope of recalled times with times date‐stamped by the computer during the discharge process (eg, checking that time decisive test needed did not occur after the discharge worksheet had been finalized in the electronic order‐entry system). Third, our sample size was not large enough to control for disease‐specific quality measures. Of note, prior studies have not identified a consistently positive or negative relationship between quality of care and efficiency.3538
Past work has used administrative and survey data to analyze the effect of discharge planning interventions on financial or quality outcomes. Outcomes have included readmissions, mortality, patient satisfaction, length of stay, and inappropriate bed days.22, 3845 However, as capacity management has become a more pressing issue for hospitals, greater focus is being placed on the mismatch between supply and demand of patients at each hour of the day. The relevant unit of measure for efficient discharges has become hour of day, in addition to total length of stay. Some hospital improvement projects have already addressed this shift in thinking.20, 21 Our study adds to this work by formally describing the precise timing and duration of steps in the discharge process, and identifying factors associated with both time and duration.
We believe the results of our study have several implications for hospital administrators and patients interested in more timely care. First, the methods used provide a tangible framework for addressing problems that cross disciplines (eg, nursing, physician, social work) and departments (eg, medicine and radiology), and have a multitude of potential causes and confounders. The survey results offer guidance on where to focus resources, provide a shared baseline metric for improvement, and suggest the cross‐functional team that should be involved in change efforts. Such an approach may be useful for addressing common system‐based challenges in inpatient quality and safety.
Second, with specific regard to discharge planning, our study supports the notion that modifiable factors are associated with discharge time and duration. However, we also describe a fragmented discharge process, with no single bottleneck or department responsible for the majority of late and long discharges. Although procedures and consults were both associated with longer and later discharges, only 26% of patients required a procedure prior to discharge, and 18% required a consult. Moreover, among procedures, different people and events are needed to carry out the 2 most popular procedures: stress echocardiograms, and non‐MRI radiology procedures. Hospital leadership at the highest levels will be required to improve efficiency based on local usage patterns, and to increase coordination among the multiple interdepartmental processes that make up the more general categories of procedure and consult.
Acknowledgements
The authors thank the patients and staff of the Hospitalist Unit for their participation in this study. In addition, they sincerely thank Paul X. Allen, Richard O. Davis, Ronald R. Peterson, and Shuai Shao. They also thank the anonymous reviewers for their thoughtful comments.
- ,,,,.Emergency departments and crowding in United States teaching hospitals.Ann Emerg Med.1991;20:980–986.
- ,,,,,.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- ,,.Frequent overcrowding in U.S. emergency departments.Acad Emerg Med.2001;8:151–155.
- ,,,,.The effect of hospital occupancy on emergency department length of stay and patient disposition.Acad Emerg Med.2003;10:127–133.
- .Calculus, chaos, and other models of emergency department crowding.Ann Emerg Med.2003;42:181–184.
- ,.Increased health care costs associated with ED overcrowding.Am J Emerg Med.1994;12:265–266.
- ,,, et al.Decreased health care quality associated with emergency department overcrowding.Eur J Emerg Med.1999;6:105–107.
- ,,.Can good bed management solve the overcrowding in accident and emergency departments?Emerg Med J.2003;20:149–155.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- General Accounting Office. Hospital emergency departments: crowded conditions vary among hospitals and communities. 2003:GAO‐03–460. Available at: http://www.gao.gov/new.items/d03460.pdf. Accessed October.
- ,.Do you want to die?Time.1990;135:58–60+
- .The ER crisis.Ladies Home J.2001;118:70–79.
- .Placing emergency department crowding on the decision agenda.Nurs Econ.2005;23:14–24.
- .Crisis seen in nation's ER care. Washington Post. June 15,2006;A01.
- Committee on the Future of Emergency Care in the United States Health System.Hospital‐based Emergency Care: at the Breaking Point.Washington DC:National Academies Press;2006.
- ,,, et al.Waits to see an emergency department physician: U.S. trends and predictors, 1997–2004.Health Aff.2008;27:w84–w95.
- Advisory Board.Maximizing Hospital Capacity: Expediting Throughput in an Era of Shortage. Health Care Advisory Board research study.Washington DC:Advisory Board; September 12,2002.
- ,,,.Does U.S. hospital capacity need to be expanded?Health Aff.2003;22:40–54.
- Institute for Healthcare Improvement.Optimizing Patient Flow: Moving Patients Smoothly Through Acute Care Settings.Cambridge, MA:Institute for Healthcare Improvement;2003.
- ,. Leveraging six sigma to improve hospital bed availability. Available at: http://healthcare.isixsigma.com/library/content/c030708a.asp. Accessed October2008.
- University Health System Consortium. Managing patient flow implementation: 2005 benchmarking project field brief. Available at: http://www.musc.edu/medcenter/UHC‐CCP/PFMgmtFldBk.pdf.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004;1:CD000313.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
- ,,.Utilisation of hospital beds by the elderly—a cohort study of admissions to a teaching hospital.Ir Med J.1995;88:124–126.
- ,,,,,.Demographic and clinical characteristics as predictors of length of hospitalization and readmission.J Clin Psychol.1977;33:1093–1099.
- ,,,.The epidemiology of delays in a teaching hospital: the development and use of a tool that detects unnecessary hospital days.Med Care.1989;27:112–129.
- American Medical Association.AMA Physician ICD‐9‐CM 2004, Vols 1 and 2.Eden Prairie, MN:Ingenix;2003.
- 3M Health Information Systems and the Maryland Health Care Payment System: frequently asked questions.2004. Available at: http://multimedia.mmm.com/mws/mediawebserver.dyn?6666660Zjcf6lVs6EVs66S7wwCOrrrrQ‐.
- .Statistics with STATA.Belmont, CA:Duxbury Press;2004.
- ,.Statistical data analysis in the computer age.Science.1991;253:390–395.
- ,,,,.Psychological comorbidity and length of stay in the general hospital.Am J Psychiatry.1991;148(3):324–329.
- ,,,,,.Psychiatric comorbidity and greater hospitalization risk, longer length of stay, and higher hospitalization costs in older adults with heart failure.J Am Geriatr Soc.2007;55:1585–1591.
- ,,,.Does psychiatric comorbidity increase the length of stay in general hospitals?Gen Hosp Psychiatry.2001;23:8–14.
- ,,.The impact of psychiatric comorbidity on length of stay of medical inpatients.Gen Hosp Psychiatry.2003;25:14–19.
- ,,,,,.The implications of regional variations in Medicare spending. Part 1: The content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,,,,.The implications of regional variations in Medicare spending. Part 2: Health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,,, et al.Is early too early? Effect of shorter stays after bypass surgery.Ann Thorac Surg.2007;83:100–107.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders, a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,,,.Comprehensive discharge planning for the hospitalized elderly, a randomized clinical trial.Ann Intern Med.1994;120:999–1006.
- ,.Evaluating hospital discharge planning: a randomized clinical trial.Med Care.1993;31:358–370.
- ,,,,.Does a dedicated discharge coordinator improve the quality of hospital discharge?Qual Health Care.1996;5:89–96.
- ,,, et al.The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital.Am J Med.2001;111:627–632.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,.Does increased access to primary care reduce hospital readmissions?N Engl J Med.1996;334:1441–1447.
In the past 2 decades, emergency department (ED) overcrowding has become an issue large enough to receive coverage in the popular press, and to spawn research around its causes and effects.116 At the same time, nurses and physicians on the inpatient wards have been urged to shorten the length of stay for patients as health system leaders face an aging population but limited capital to build new beds or hire additional clinical staff. Capacity managementencompassing the flow of patients from ED triage to inpatient dischargehas become a shared concern of clinicians and hospital administrators alike.
How to achieve the goals of diagnosing and healing while ushering patients ever more quickly through the modern hospital is not yet entirely clear. Past research and work by business groups suggests that demand for inpatient beds starts early in the day, but discharges typically occur in the late afternoon.17 This creates a potential bottleneck in patient flow. Many hospitals have implemented measures to improve patient throughput.1821 However, formal research has focused on factors leading to an additional inpatient day.2226 We have found no peer‐reviewed publications that address the problem of same‐day delays by describing hour of day for each step in the discharge process and variables associated with late‐day discharges. To fill this gap, we conducted a prospective cohort study of 209 consecutive discharges from a general medical ward to: (1) describe the natural history of hospital discharge, (2) measure time of day and duration for each step, and (3) identify factors associated with discharges that occur later in the day. We hypothesized that time and duration of discharge would be associated with 5 factors: patient demographics and clinical characteristics, departmental occupancy, type of inpatient testing done immediately prior to discharge, and discharge characteristics such as discharge to a location other than home.
Patients and Methods
Setting
The setting was the Hospitalist Unit of a single teaching hospital in Baltimore (The Johns Hopkins Hospital) from January 1, 2005 to April 30, 2005. Patients entered the cohort upon initiation of the discharge process by the hospitalist team on the Hospitalist Unit, and were followed until they were discharged alive from the hospital.
There were no published data on which to base firm a priori sample size calculations. Based on pilot data, we estimated that a sample size of about 170 would yield precise estimates for means and standard deviations, giving us 80% to 90% power to determine differences in time intervals across categories, with alpha set to 0.05. We estimated that we would need 4 months of data collection to achieve this sample size.
During the period of study, the 16‐bed unit was staffed with in‐house hospitalist attending physicians without house‐staff, from 7 AM (weekdays) or 8 AM (weekends) to 10 PM (Monday to Thursday) or 8 PM (Friday to Sunday). The hospitalist unit had 24‐hour physician coverage, but attending physicians provided overnight coverage from home (backed up by in‐house residents for patient care emergencies). Handoffs of patient care from one attending physician to another typically occurred on Friday afternoon or Monday morning. The unit had 1 dedicated social worker and a nurse clinician who provided part‐time assistance with discharge planning.
Outcome Measurements
We defined the start of the discharge process as the time the patient's last medically necessary test was needed by his or her attending physician. Specifically, physicians were asked when the results of this test first would have been useful in clearing the patient for discharge. In the remainder of this work, we will refer to the start of the discharge process as time decisive test needed.
The end of the discharge process was called the discharge time, and defined as the time the unit clerk saw the patient leave the unit. We defined early discharges as those occurring before the median hour of discharge (3:00 PM), and late discharges as those occurring at or after this hour.
A focus group composed of nurses, physicians, social worker, unit clerks, and support associates (group responsible for cleaning patient rooms) volunteered to map out the discharge process. Based on these discussions, durations in the discharge process were defined as follows: (1) duration 1: time decisive test needed, until time the attending physician was aware of test results; (2) duration 2: time the physician was aware of test results until discharge paperwork was complete; (3) duration 3: time discharge paperwork complete until patient leaves unit; and (4) total discharge duration: time decisive test needed until patient leaves unit.
Exposure Measurements
We categorized exposures into 5 groups: (1) demographics (age, gender, race, source of patient such as outside hospital versus emergency department versus other, and payer on discharge); (2) clinical characteristics (length of stay, any psychiatric diagnosis, any substance abuse diagnosis, and severity of illness); (3) system characteristics (departmental occupancy defined as proportion of hospital beds designated for Department of Medicine patients that were occupied on the day of discharge); (4) last test characteristics (physical exam, laboratory test, procedure, and consult); and (5) discharge characteristics (discharged to home versus not discharged to home, prescriptions filled in hospital pharmacy prior to discharge, and ambulance required for transport).
Psychiatric diagnosis was defined as the presence of any of the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) codes: 290319 (any fourth or fifth digits).27 Substance abuse diagnosis was defined as the presence of any of the following ICD‐9‐CM codes: 303305 (any fourth or fifth digits). Substance abuse codes encompassed drug dependence and abuse, including alcohol dependence and abuse.
The all patient refined diagnosis related group relative weight (APRDRGwt) is a unitless number that estimates the total cost of care for inpatients, based on clinical and demographic characteristics.28 A patient with a relative APRDRGwt of 1 is predicted to have the same cost of care as the national average for inpatients. A patient with a score of 2 is predicted to be twice as costly as the average. In this study, we used APRDRGwt as a gross proxy for severity of illness.
Adjusted length of stay was measured as length of stay minus discharge duration. This adjustment was made to avoid including the exposure (length of stay) in the outcome (discharge duration). Unadjusted length of stay was used when the outcome was discharge time.
Data Sources
We created a separate 4‐item to 9‐item paper questionnaire (included in the Appendix) for each of 4 functional groups participating directly in the discharge process: nurses, physicians, social worker, and unit clerks. Questions were based on staff feedback about the sequence of steps in the discharge process, and potential reasons for delay. The surveys were piloted for several weeks to further refine the wording of questions, and to ensure that the length and location of the surveys minimized workflow interruptions. The questionnaires captured information about the timing of routine events not recorded in existing databases.
Physicians were asked to identify the last test/procedure/consult needed prior to the patient being medically ready for discharge. They were asked when the test results first could have cleared the patient for discharge (time decisive test needed), and when they actually received the test results (time test results back). Nursing and social work surveys provided information on whether or not prescriptions were filled prior to discharge, and the type of transportation used on discharge. Unit clerks documented when the patient left the unit.
Response rates were: nurses (97%), physicians (97%), social worker (99%), and unit clerks (94%). All 4 surveys were completed for 88% of the 209 included patients (prior to 8 exclusions for missing data or extreme outlier observations). Group response rates were tallied at the end of each month and posted on the unit. We did not track how soon after discharge the surveys were completed. However, we reviewed survey responses frequently (often daily, at most every 4 days) and if surveys were incomplete we personally approached staff members to complete the survey.
We supplemented and cross‐checked data from the questionnaire with information from existing hospital databases. These databases were: (1) the patient's medical record for time patient arrived on the floor, and completion time for consults/procedures; (2) the Electronic Bedboard (EBB) for time patient left the unit (as recorded by unit clerk); (3) the Patient Order Entry System for time discharge papers were completed by the physician, and ordering time for select tests; (4) the Electronic Patient Record for demographic information and completion time for select tests; and (5) Datamart, the hospital's administrative/billing database, for information such as length of stay, diagnosis, patient demographics, and insurance status.
Cross‐checking of data and calculation of durations 1, 2, and 3 identified areas of disagreement that were addressed in the following way. Discharge time was provided by 3 sources: social worker and nurses as an ad hoc addition to each of their surveys, unit clerks as a mandatory question on their survey, and unit clerks as entered in the EBB. We used EBB data for discharge time, as this was the most complete and accurate single source of data. However, survey results and knowledge about the sequential process for discharge, suggested that in 20 cases EBB data did not provide the most accurate time. In these cases, discharge time was provided by the unit clerk survey (16 cases), the social work survey (3 cases), and the nursing survey (1 case).
In 28 cases (14%), discharge paperwork was completed before decisive test results were back. And in 8 cases (4%) test results were received earlier than needed. As these were a minority of cases, these negative durations were converted to zero for analysis.
Statistical Analysis
The unit of analysis was the unique hospital discharge. For patients who were discharged from the Hospitalist Unit more than once during the 4‐month study period, each discharge was treated as a separate unit of analysis.
We defined patients discharged before the median discharge time as early discharges, and all others as late discharges. We then categorized patients with discharge durations less than 24 hours as short discharges, and all others as long discharges.
We described the characteristics of 2 groups of patients: early and short discharges versus all others. We used the chi square statistic and Fisher's exact test (when frequency 5 in 1 or both groups) to test the null hypothesis that there was no association between the 2 groups and select patient characteristics. When comparing medians, we used the nonparametric equality of medians test.
For each step in the discharge process, we identified a median time of occurrence. For the first point in the processtime decisive test neededwe also used 1‐way analysis of variance and the F‐test to assess whether or not timing varied significantly by physician.
Because our primary goal was to quantify in hours the association between various factors and discharge time or duration, we used bivariate linear regression models to identify factors associated with time of discharge (primary analysis) and total duration of the discharge process (secondary analysis). We then used multivariate linear regression to identify factors associated with both outcomes. We used forward and backward selection methods to choose the final models for the multivariate analyses, after forcing in the variables for race, sex, and age. Both methods of selection produced identical results. We assessed for colinearity using variance inflation factors.29
Sensitivity Analyses
For both discharge time and discharge duration, we performed regression diagnostics including leverage, Studentized residuals, and influence. Excluding outliers for influence slightly altered the results of our multivariate analyses. However, all variables that were significant at the P < 0.05 level remained significant in the models without outliers.
We chose to include outliers for influence in our final data set after verifying the data as accurate. For discharge time, the number of outliers (3; 1.5%) for influence was in the range expected for a normally distributed data set.
We also tested for normality of the 2 outcome variables. Discharge time was normally distributed, but discharge duration was not. Because of this, we used 2 additional methods to assess the robustness of our results for discharge duration.
First, we log‐transformed the outcome and repeated the analysis. Variables significant in the non‐log‐transformed model remained significant after log‐transformation. Second, we applied bootstrapping30 with 1,000 repetitions for the bivariate and multivariate analyses. The 95% confidence intervals (CIs) (using the bias‐corrected confidence intervals) were modestly altered (some narrowed, some widened), but our conclusions remained the same except for a single variable with borderline significance (payer on discharge) in bivariate analysis. The final reported confidence intervals for discharge duration are based on our analysis without bootstrapping.
Results
Data were collected on 216 patients. Seven patients were excluded from the study, because they were discharged against medical advice. Since these patients left before their decisive test was completed, there was no way to assess duration of the discharge process. Of the remaining 209 patients, 6 patients lacked necessary data to complete analysis (5 without survey data; 1 without administrative data). Two additional patients were eliminated from the final analysis because they bypassed the normal discharge process and were extreme outliers in either discharge time (1 discharged at 1 AM), or discharge duration (1 with discharge duration of 400+ hours). A total of 201 patients were included in the final analyses.
The hospitalist program primarily serves an indigent, local adult population with general medical problems, and this is reflected in the patient characteristics (Table 1). We compared the characteristics of patients discharged early and quickly (discharged prior to median hour of 3:00 PM, and discharge process lasting less than 24 hours) to all other discharges, to identify factors associated with later and longer discharges.
| Early and Short Discharges (n = 75)* | All Other Discharges (n = 126) | P Value | |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | |||
| Median | 55 | 55 | 0.73 |
| Range | (19, 94) | (20, 90) | |
| Gender (%) | |||
| Female | 61.3 | 61.1 | 0.98 |
| Race (%) | 0.08 | ||
| African American | 76.0 | 60.3 | |
| Caucasian | 21.3 | 34.9 | |
| Other | 2.7 | 4.8 | |
| Payor on discharge (%) | 0.29 | ||
| Medicaid | 32.0 | 20.6 | |
| Medicare | 32.0 | 38.9 | |
| Self‐pay | 12.0 | 16.7 | |
| Other | 24.0 | 23.8 | |
| Clinical characteristics | |||
| Adjusted length of stay (days) | |||
| Median | 3 | 3 | 0.19 |
| Range | (<1, 20) | (<1, 138) | |
| Substance abuse (%) | 41.3 | 37.3 | 0.57 |
| Psychiatric diagnosis (%) | 20.0 | 25.4 | 0.38 |
| Last test characteristics | |||
| Test type (%) | <0.001 | ||
| Exam | 42.7 | 26.2 | |
| Laboratory test | 38.7 | 13.5 | |
| Procedure | 10.7 | 35.7 | |
| Consult | 8.0 | 24.6 | |
| Discharge characteristics | |||
| Discharged to home (%) | 93.3 | 71.4 | <0.001 |
| Prescriptions filled prior to discharge (%) | 10.7 | 19.8 | 0.09 |
| Ambulance required for transport (%) | 8.0 | 21.4 | 0.01 |
Overall, 81% of patients were admitted from the ED, and 40% of all patients were insured by Medicaid or were self‐pay at time of discharge. Median expected charges were similar to the national average, as demonstrated by the median APRDRGwt of 1.0. Patients stayed an average of 6 days (median = 3 days). Patients with the longest adjusted lengths of stay (>20 days) were never early and short discharges. The most common discharge diagnoses were: congestive heart failure, chest pain or myocardial infarction, pneumonia, asthma/chronic obstructive pulmonary disease, and sickle‐cell disease. Thirty‐nine percent of all patients carried the diagnosis of alcohol or drug dependence or abuse, although for most this was not their discharge diagnosis. None of these demographic or clinical factors were associated with a late or long discharge.
The types of tests patients required on discharge were categorized into 4 groups: consults (18.4%), laboratory tests (22.9%), procedures (26.4%), and physical exam (32.3%). Distribution differed significantly between early and short discharges, and all other discharges (P < 0.001). Procedures and consults were less frequent among early and short discharges (procedures: 10.7% versus 35.7%; consults: 8.0% versus 24.6%).
For all patients, there was fragmentation within the consult and procedure categories. Within the consult group, there were 12 different types of consults ordered, with the dominant category (35.1%) being other. The next highest volume consult was physical/occupational therapy (27.0%). Within the procedure group, there were 11 different types of procedures, with the most common being stress echocardiograms (28.3%). Non‐MRI radiology procedures made up the next largest category (20.8%) and the third was other (18.9%).
Many patients had immediate postdischarge needs, as demonstrated by the 20% of patients not discharged home. The majority (66%) of those who were discharged to a facility required an ambulance. Early and short discharges were less likely to use an ambulance to leave the hospital (8.0% versus 21.4%; P = 0.01), and more likely to be discharged directly to home (99.3% versus 71.4%; P < 0.001).
Based on process mapping, we defined a 4‐step sequential discharge process for all patients (Figure 1). The first step was: decisive test needed by physician to discharge patient. Subgroup analysis demonstrated no significant difference in the timing of this step by individual physician (P = 0.44). The remaining 3 steps were as follows: physician aware of test results, discharge paperwork complete by physician, and patient leaves the unit. Each of the 4 steps showed wide variability in hour of occurrence.
Total discharge duration showed even more variability than the time of day when steps were likely to occur (Figure 2). Median duration of the discharge process was 7.6 hours (25th% to 75th%: 4 to 22 hours). Median duration from decisive test needed until resulted (duration 1) was 2 hours (25th% to 75th%: 0 to 8 hours); between test resulted until discharge paperwork complete (duration 2) was 1.4 hours (25th% to 75th%: 0.3 to 4.2 hours); and between discharge paperwork complete and patient leaving the unit (duration 3) was 2.0 hours (25th% to 75th%: 1.1 to 3.1 hours). All durations were skewed to the right, with durations 1 and 2 each taking at least 24 hours to occur in 10% of patients.
The final multivariate model for time of discharge contained 6 covariates: age, sex, race, test type, prescriptions filled prior to discharge, and need for an ambulance on discharge (Table 2). Special discharge needs continued to be associated with later discharges. Those patients who required an ambulance for transport had mean discharge times that were later by 1.5 hours (95% CI, 0.42.5). If staff obtained discharge medications for patients, these patients left 1.4 hours later than those patients who filled their prescriptions on their own (95% CI, 0.32.4). Patients requiring a consult or procedure also had significantly later discharges (1.2 hours for consults, 95% CI, 0.12.4; 1.1 hours for procedures, 95% CI, 0.12.1) than those needing a bedside exam. Age, sex, and race remained insignificant at the P 0.05 level in the final multivariate model. Length of stay was significantly associated with discharge time in crude analysis, but this variable dropped out of the final multivariate model.
| Adjusted Coefficient, Discharge Time as Outcome in Hours (95% CI)* | P Value | Adjusted Coefficient, Discharge Duration as Outcome in Hours (95% CI) | P Value | |
|---|---|---|---|---|
| ||||
| Demographics | ||||
| Age in quartiles (years) | ||||
| 7294 | 0.5 (0.5, 1.6) | 0.33 | 0.6 (8.3, 7.2) | 0.88 |
| 5671 | 0.5 (0.6, 1.6) | 0.41 | 1.3 (9.2, 6.6) | 0.75 |
| 4455 | 0.2 (0.9, 1.3) | 0.74 | 1.2 (9.0, 6.5) | 0.76 |
| Male gender | 0.0 (0.8, 0.8) | 0.97 | 1.2 (6.8, 4.5) | 0.69 |
| African American race | 0.1 (0.7, 0.9) | 0.80 | 0.3 (5.6, 6.1) | 0.93 |
| Last test characteristics | ||||
| Test type | ||||
| Consult | 1.2 (0.1, 2.4) | 0.04 | 14.8 (6.5, 23.1) | 0.001 |
| Procedure | 1.1 (0.1, 2.1) | 0.03 | 13.4 (6.0, 20.7) | <0.001 |
| Laboratory test | 0.8 (1.8, 0.3) | 0.14 | 0.9 (8.4, 6.6) | 0.82 |
| Exam (reference) | ||||
| Discharge needs | ||||
| Prescriptions filled prior to discharge | 1.4 (0.3, 2.4) | 0.02 | ||
| Not discharged to home | 28.9 (21.9, 35.9) | <0.001 | ||
| Ambulance required for transport | 1.5 (0.4, 2.5) | 0.007 | ||
We used duration of discharge as a secondary outcome measure. The final multivariate model for discharge duration included: age, sex, race, test type, and discharge to a facility (Table 2). Those who went to a facility on average left 28.9 hours (95% CI, 21.935.9) later than those who went home. Test type continued to show a significant association with discharge duration, although the estimates were slightly lower in the adjusted model. Need for a consult was associated with a discharge that was on average 14.8 hours (95% CI, 6.523.1) longer than discharges contingent on a physical exam. Similarly, those patients who had procedures had discharges that were on average 13.4 hours (95% CI, 6.020.7) longer than those whose last test was an exam. Several factors that were significantly associated with discharge duration in unadjusted analyses dropped out of the final multivariate model. These included: need for an ambulance, length of stay, insurance status, and medical complexity as estimated by APRDRGwt.
Conclusions
We found that discharge time and duration had wide variability and that certain factors were associated with only one outcome variabledischarge time or duration. Two factorsneed for an ambulance and filling of prescriptions prior to dischargewere associated with later hour of discharge. Discharge to a location other than home was associated with prolonged discharge duration. Test characteristicsin particular need for a procedure and consultwere significantly associated with both longer and later discharges.
In bivariate analysis, several factors were not associated with discharge time or duration. These were: African‐American race, sex, age, Department of Medicine occupancy on day of discharge, source of admission, psychiatric comorbidity, and substance abuse comorbidity. We had expected higher occupancy to delay discharge as demand exceeded capacity for tests, consults, etc. Our findings suggest that even though our study was conducted during the winter months when hospital occupancy is typically at its peak, supply of staff was still adequate enough to meet high demand. We had also expected that psychiatric and substance abuse comorbidities would prolong discharge as prior studies have found some of these diagnoses to be associated with longer lengths of stay.3134 However, our results do not support such an association, and may reflect our decision to group all psychiatric diagnoses together due to limited sample size.
The main strength of our study is the use of 2 outcome variablestime and durationto define delayed discharges. Our findings demonstrate that few factors are associated with both later and longer discharges. In an era when avoiding emergency room walkouts through early morning hospital discharges can be as important as managing overall length of stay, identifying factors associated with both duration and timing of discharges addresses actual challenges faced by hospitals with limited resources. Prior studies have rarely addressed both outcomes. An additional strength of our study is our use of an interdisciplinary survey. The discharge process is a key component of the inpatient stay, but it is also one for which no group is entirely responsible. Through the development and administration of an interdisciplinary survey, our study adds detail to existing descriptions of this fragmented process, and identifies potential areas for improvement.
Several limitations of our study deserve comment. First, we examined patients discharged from a hospitalist unit without house‐staff at an urban tertiary care hospital. Our findings may need additional interpretation prior to their application in dissimilar settings such as: (1) resident‐covered units in which workflow is shaped by teaching rounds, and (2) nonacademic hospitals in which incentives to provide rapid consults and procedures may be different. Second, we relied on self‐reporting for certain variables such as time decisive test needed. This may be subject to recall bias, as we did not have staff to independently verify recalled times. However, since the discharge process is generally a linear one, we were able to verify the general scope of recalled times with times date‐stamped by the computer during the discharge process (eg, checking that time decisive test needed did not occur after the discharge worksheet had been finalized in the electronic order‐entry system). Third, our sample size was not large enough to control for disease‐specific quality measures. Of note, prior studies have not identified a consistently positive or negative relationship between quality of care and efficiency.3538
Past work has used administrative and survey data to analyze the effect of discharge planning interventions on financial or quality outcomes. Outcomes have included readmissions, mortality, patient satisfaction, length of stay, and inappropriate bed days.22, 3845 However, as capacity management has become a more pressing issue for hospitals, greater focus is being placed on the mismatch between supply and demand of patients at each hour of the day. The relevant unit of measure for efficient discharges has become hour of day, in addition to total length of stay. Some hospital improvement projects have already addressed this shift in thinking.20, 21 Our study adds to this work by formally describing the precise timing and duration of steps in the discharge process, and identifying factors associated with both time and duration.
We believe the results of our study have several implications for hospital administrators and patients interested in more timely care. First, the methods used provide a tangible framework for addressing problems that cross disciplines (eg, nursing, physician, social work) and departments (eg, medicine and radiology), and have a multitude of potential causes and confounders. The survey results offer guidance on where to focus resources, provide a shared baseline metric for improvement, and suggest the cross‐functional team that should be involved in change efforts. Such an approach may be useful for addressing common system‐based challenges in inpatient quality and safety.
Second, with specific regard to discharge planning, our study supports the notion that modifiable factors are associated with discharge time and duration. However, we also describe a fragmented discharge process, with no single bottleneck or department responsible for the majority of late and long discharges. Although procedures and consults were both associated with longer and later discharges, only 26% of patients required a procedure prior to discharge, and 18% required a consult. Moreover, among procedures, different people and events are needed to carry out the 2 most popular procedures: stress echocardiograms, and non‐MRI radiology procedures. Hospital leadership at the highest levels will be required to improve efficiency based on local usage patterns, and to increase coordination among the multiple interdepartmental processes that make up the more general categories of procedure and consult.
Acknowledgements
The authors thank the patients and staff of the Hospitalist Unit for their participation in this study. In addition, they sincerely thank Paul X. Allen, Richard O. Davis, Ronald R. Peterson, and Shuai Shao. They also thank the anonymous reviewers for their thoughtful comments.
In the past 2 decades, emergency department (ED) overcrowding has become an issue large enough to receive coverage in the popular press, and to spawn research around its causes and effects.116 At the same time, nurses and physicians on the inpatient wards have been urged to shorten the length of stay for patients as health system leaders face an aging population but limited capital to build new beds or hire additional clinical staff. Capacity managementencompassing the flow of patients from ED triage to inpatient dischargehas become a shared concern of clinicians and hospital administrators alike.
How to achieve the goals of diagnosing and healing while ushering patients ever more quickly through the modern hospital is not yet entirely clear. Past research and work by business groups suggests that demand for inpatient beds starts early in the day, but discharges typically occur in the late afternoon.17 This creates a potential bottleneck in patient flow. Many hospitals have implemented measures to improve patient throughput.1821 However, formal research has focused on factors leading to an additional inpatient day.2226 We have found no peer‐reviewed publications that address the problem of same‐day delays by describing hour of day for each step in the discharge process and variables associated with late‐day discharges. To fill this gap, we conducted a prospective cohort study of 209 consecutive discharges from a general medical ward to: (1) describe the natural history of hospital discharge, (2) measure time of day and duration for each step, and (3) identify factors associated with discharges that occur later in the day. We hypothesized that time and duration of discharge would be associated with 5 factors: patient demographics and clinical characteristics, departmental occupancy, type of inpatient testing done immediately prior to discharge, and discharge characteristics such as discharge to a location other than home.
Patients and Methods
Setting
The setting was the Hospitalist Unit of a single teaching hospital in Baltimore (The Johns Hopkins Hospital) from January 1, 2005 to April 30, 2005. Patients entered the cohort upon initiation of the discharge process by the hospitalist team on the Hospitalist Unit, and were followed until they were discharged alive from the hospital.
There were no published data on which to base firm a priori sample size calculations. Based on pilot data, we estimated that a sample size of about 170 would yield precise estimates for means and standard deviations, giving us 80% to 90% power to determine differences in time intervals across categories, with alpha set to 0.05. We estimated that we would need 4 months of data collection to achieve this sample size.
During the period of study, the 16‐bed unit was staffed with in‐house hospitalist attending physicians without house‐staff, from 7 AM (weekdays) or 8 AM (weekends) to 10 PM (Monday to Thursday) or 8 PM (Friday to Sunday). The hospitalist unit had 24‐hour physician coverage, but attending physicians provided overnight coverage from home (backed up by in‐house residents for patient care emergencies). Handoffs of patient care from one attending physician to another typically occurred on Friday afternoon or Monday morning. The unit had 1 dedicated social worker and a nurse clinician who provided part‐time assistance with discharge planning.
Outcome Measurements
We defined the start of the discharge process as the time the patient's last medically necessary test was needed by his or her attending physician. Specifically, physicians were asked when the results of this test first would have been useful in clearing the patient for discharge. In the remainder of this work, we will refer to the start of the discharge process as time decisive test needed.
The end of the discharge process was called the discharge time, and defined as the time the unit clerk saw the patient leave the unit. We defined early discharges as those occurring before the median hour of discharge (3:00 PM), and late discharges as those occurring at or after this hour.
A focus group composed of nurses, physicians, social worker, unit clerks, and support associates (group responsible for cleaning patient rooms) volunteered to map out the discharge process. Based on these discussions, durations in the discharge process were defined as follows: (1) duration 1: time decisive test needed, until time the attending physician was aware of test results; (2) duration 2: time the physician was aware of test results until discharge paperwork was complete; (3) duration 3: time discharge paperwork complete until patient leaves unit; and (4) total discharge duration: time decisive test needed until patient leaves unit.
Exposure Measurements
We categorized exposures into 5 groups: (1) demographics (age, gender, race, source of patient such as outside hospital versus emergency department versus other, and payer on discharge); (2) clinical characteristics (length of stay, any psychiatric diagnosis, any substance abuse diagnosis, and severity of illness); (3) system characteristics (departmental occupancy defined as proportion of hospital beds designated for Department of Medicine patients that were occupied on the day of discharge); (4) last test characteristics (physical exam, laboratory test, procedure, and consult); and (5) discharge characteristics (discharged to home versus not discharged to home, prescriptions filled in hospital pharmacy prior to discharge, and ambulance required for transport).
Psychiatric diagnosis was defined as the presence of any of the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) codes: 290319 (any fourth or fifth digits).27 Substance abuse diagnosis was defined as the presence of any of the following ICD‐9‐CM codes: 303305 (any fourth or fifth digits). Substance abuse codes encompassed drug dependence and abuse, including alcohol dependence and abuse.
The all patient refined diagnosis related group relative weight (APRDRGwt) is a unitless number that estimates the total cost of care for inpatients, based on clinical and demographic characteristics.28 A patient with a relative APRDRGwt of 1 is predicted to have the same cost of care as the national average for inpatients. A patient with a score of 2 is predicted to be twice as costly as the average. In this study, we used APRDRGwt as a gross proxy for severity of illness.
Adjusted length of stay was measured as length of stay minus discharge duration. This adjustment was made to avoid including the exposure (length of stay) in the outcome (discharge duration). Unadjusted length of stay was used when the outcome was discharge time.
Data Sources
We created a separate 4‐item to 9‐item paper questionnaire (included in the Appendix) for each of 4 functional groups participating directly in the discharge process: nurses, physicians, social worker, and unit clerks. Questions were based on staff feedback about the sequence of steps in the discharge process, and potential reasons for delay. The surveys were piloted for several weeks to further refine the wording of questions, and to ensure that the length and location of the surveys minimized workflow interruptions. The questionnaires captured information about the timing of routine events not recorded in existing databases.
Physicians were asked to identify the last test/procedure/consult needed prior to the patient being medically ready for discharge. They were asked when the test results first could have cleared the patient for discharge (time decisive test needed), and when they actually received the test results (time test results back). Nursing and social work surveys provided information on whether or not prescriptions were filled prior to discharge, and the type of transportation used on discharge. Unit clerks documented when the patient left the unit.
Response rates were: nurses (97%), physicians (97%), social worker (99%), and unit clerks (94%). All 4 surveys were completed for 88% of the 209 included patients (prior to 8 exclusions for missing data or extreme outlier observations). Group response rates were tallied at the end of each month and posted on the unit. We did not track how soon after discharge the surveys were completed. However, we reviewed survey responses frequently (often daily, at most every 4 days) and if surveys were incomplete we personally approached staff members to complete the survey.
We supplemented and cross‐checked data from the questionnaire with information from existing hospital databases. These databases were: (1) the patient's medical record for time patient arrived on the floor, and completion time for consults/procedures; (2) the Electronic Bedboard (EBB) for time patient left the unit (as recorded by unit clerk); (3) the Patient Order Entry System for time discharge papers were completed by the physician, and ordering time for select tests; (4) the Electronic Patient Record for demographic information and completion time for select tests; and (5) Datamart, the hospital's administrative/billing database, for information such as length of stay, diagnosis, patient demographics, and insurance status.
Cross‐checking of data and calculation of durations 1, 2, and 3 identified areas of disagreement that were addressed in the following way. Discharge time was provided by 3 sources: social worker and nurses as an ad hoc addition to each of their surveys, unit clerks as a mandatory question on their survey, and unit clerks as entered in the EBB. We used EBB data for discharge time, as this was the most complete and accurate single source of data. However, survey results and knowledge about the sequential process for discharge, suggested that in 20 cases EBB data did not provide the most accurate time. In these cases, discharge time was provided by the unit clerk survey (16 cases), the social work survey (3 cases), and the nursing survey (1 case).
In 28 cases (14%), discharge paperwork was completed before decisive test results were back. And in 8 cases (4%) test results were received earlier than needed. As these were a minority of cases, these negative durations were converted to zero for analysis.
Statistical Analysis
The unit of analysis was the unique hospital discharge. For patients who were discharged from the Hospitalist Unit more than once during the 4‐month study period, each discharge was treated as a separate unit of analysis.
We defined patients discharged before the median discharge time as early discharges, and all others as late discharges. We then categorized patients with discharge durations less than 24 hours as short discharges, and all others as long discharges.
We described the characteristics of 2 groups of patients: early and short discharges versus all others. We used the chi square statistic and Fisher's exact test (when frequency 5 in 1 or both groups) to test the null hypothesis that there was no association between the 2 groups and select patient characteristics. When comparing medians, we used the nonparametric equality of medians test.
For each step in the discharge process, we identified a median time of occurrence. For the first point in the processtime decisive test neededwe also used 1‐way analysis of variance and the F‐test to assess whether or not timing varied significantly by physician.
Because our primary goal was to quantify in hours the association between various factors and discharge time or duration, we used bivariate linear regression models to identify factors associated with time of discharge (primary analysis) and total duration of the discharge process (secondary analysis). We then used multivariate linear regression to identify factors associated with both outcomes. We used forward and backward selection methods to choose the final models for the multivariate analyses, after forcing in the variables for race, sex, and age. Both methods of selection produced identical results. We assessed for colinearity using variance inflation factors.29
Sensitivity Analyses
For both discharge time and discharge duration, we performed regression diagnostics including leverage, Studentized residuals, and influence. Excluding outliers for influence slightly altered the results of our multivariate analyses. However, all variables that were significant at the P < 0.05 level remained significant in the models without outliers.
We chose to include outliers for influence in our final data set after verifying the data as accurate. For discharge time, the number of outliers (3; 1.5%) for influence was in the range expected for a normally distributed data set.
We also tested for normality of the 2 outcome variables. Discharge time was normally distributed, but discharge duration was not. Because of this, we used 2 additional methods to assess the robustness of our results for discharge duration.
First, we log‐transformed the outcome and repeated the analysis. Variables significant in the non‐log‐transformed model remained significant after log‐transformation. Second, we applied bootstrapping30 with 1,000 repetitions for the bivariate and multivariate analyses. The 95% confidence intervals (CIs) (using the bias‐corrected confidence intervals) were modestly altered (some narrowed, some widened), but our conclusions remained the same except for a single variable with borderline significance (payer on discharge) in bivariate analysis. The final reported confidence intervals for discharge duration are based on our analysis without bootstrapping.
Results
Data were collected on 216 patients. Seven patients were excluded from the study, because they were discharged against medical advice. Since these patients left before their decisive test was completed, there was no way to assess duration of the discharge process. Of the remaining 209 patients, 6 patients lacked necessary data to complete analysis (5 without survey data; 1 without administrative data). Two additional patients were eliminated from the final analysis because they bypassed the normal discharge process and were extreme outliers in either discharge time (1 discharged at 1 AM), or discharge duration (1 with discharge duration of 400+ hours). A total of 201 patients were included in the final analyses.
The hospitalist program primarily serves an indigent, local adult population with general medical problems, and this is reflected in the patient characteristics (Table 1). We compared the characteristics of patients discharged early and quickly (discharged prior to median hour of 3:00 PM, and discharge process lasting less than 24 hours) to all other discharges, to identify factors associated with later and longer discharges.
| Early and Short Discharges (n = 75)* | All Other Discharges (n = 126) | P Value | |
|---|---|---|---|
| |||
| Demographics | |||
| Age (years) | |||
| Median | 55 | 55 | 0.73 |
| Range | (19, 94) | (20, 90) | |
| Gender (%) | |||
| Female | 61.3 | 61.1 | 0.98 |
| Race (%) | 0.08 | ||
| African American | 76.0 | 60.3 | |
| Caucasian | 21.3 | 34.9 | |
| Other | 2.7 | 4.8 | |
| Payor on discharge (%) | 0.29 | ||
| Medicaid | 32.0 | 20.6 | |
| Medicare | 32.0 | 38.9 | |
| Self‐pay | 12.0 | 16.7 | |
| Other | 24.0 | 23.8 | |
| Clinical characteristics | |||
| Adjusted length of stay (days) | |||
| Median | 3 | 3 | 0.19 |
| Range | (<1, 20) | (<1, 138) | |
| Substance abuse (%) | 41.3 | 37.3 | 0.57 |
| Psychiatric diagnosis (%) | 20.0 | 25.4 | 0.38 |
| Last test characteristics | |||
| Test type (%) | <0.001 | ||
| Exam | 42.7 | 26.2 | |
| Laboratory test | 38.7 | 13.5 | |
| Procedure | 10.7 | 35.7 | |
| Consult | 8.0 | 24.6 | |
| Discharge characteristics | |||
| Discharged to home (%) | 93.3 | 71.4 | <0.001 |
| Prescriptions filled prior to discharge (%) | 10.7 | 19.8 | 0.09 |
| Ambulance required for transport (%) | 8.0 | 21.4 | 0.01 |
Overall, 81% of patients were admitted from the ED, and 40% of all patients were insured by Medicaid or were self‐pay at time of discharge. Median expected charges were similar to the national average, as demonstrated by the median APRDRGwt of 1.0. Patients stayed an average of 6 days (median = 3 days). Patients with the longest adjusted lengths of stay (>20 days) were never early and short discharges. The most common discharge diagnoses were: congestive heart failure, chest pain or myocardial infarction, pneumonia, asthma/chronic obstructive pulmonary disease, and sickle‐cell disease. Thirty‐nine percent of all patients carried the diagnosis of alcohol or drug dependence or abuse, although for most this was not their discharge diagnosis. None of these demographic or clinical factors were associated with a late or long discharge.
The types of tests patients required on discharge were categorized into 4 groups: consults (18.4%), laboratory tests (22.9%), procedures (26.4%), and physical exam (32.3%). Distribution differed significantly between early and short discharges, and all other discharges (P < 0.001). Procedures and consults were less frequent among early and short discharges (procedures: 10.7% versus 35.7%; consults: 8.0% versus 24.6%).
For all patients, there was fragmentation within the consult and procedure categories. Within the consult group, there were 12 different types of consults ordered, with the dominant category (35.1%) being other. The next highest volume consult was physical/occupational therapy (27.0%). Within the procedure group, there were 11 different types of procedures, with the most common being stress echocardiograms (28.3%). Non‐MRI radiology procedures made up the next largest category (20.8%) and the third was other (18.9%).
Many patients had immediate postdischarge needs, as demonstrated by the 20% of patients not discharged home. The majority (66%) of those who were discharged to a facility required an ambulance. Early and short discharges were less likely to use an ambulance to leave the hospital (8.0% versus 21.4%; P = 0.01), and more likely to be discharged directly to home (99.3% versus 71.4%; P < 0.001).
Based on process mapping, we defined a 4‐step sequential discharge process for all patients (Figure 1). The first step was: decisive test needed by physician to discharge patient. Subgroup analysis demonstrated no significant difference in the timing of this step by individual physician (P = 0.44). The remaining 3 steps were as follows: physician aware of test results, discharge paperwork complete by physician, and patient leaves the unit. Each of the 4 steps showed wide variability in hour of occurrence.
Total discharge duration showed even more variability than the time of day when steps were likely to occur (Figure 2). Median duration of the discharge process was 7.6 hours (25th% to 75th%: 4 to 22 hours). Median duration from decisive test needed until resulted (duration 1) was 2 hours (25th% to 75th%: 0 to 8 hours); between test resulted until discharge paperwork complete (duration 2) was 1.4 hours (25th% to 75th%: 0.3 to 4.2 hours); and between discharge paperwork complete and patient leaving the unit (duration 3) was 2.0 hours (25th% to 75th%: 1.1 to 3.1 hours). All durations were skewed to the right, with durations 1 and 2 each taking at least 24 hours to occur in 10% of patients.
The final multivariate model for time of discharge contained 6 covariates: age, sex, race, test type, prescriptions filled prior to discharge, and need for an ambulance on discharge (Table 2). Special discharge needs continued to be associated with later discharges. Those patients who required an ambulance for transport had mean discharge times that were later by 1.5 hours (95% CI, 0.42.5). If staff obtained discharge medications for patients, these patients left 1.4 hours later than those patients who filled their prescriptions on their own (95% CI, 0.32.4). Patients requiring a consult or procedure also had significantly later discharges (1.2 hours for consults, 95% CI, 0.12.4; 1.1 hours for procedures, 95% CI, 0.12.1) than those needing a bedside exam. Age, sex, and race remained insignificant at the P 0.05 level in the final multivariate model. Length of stay was significantly associated with discharge time in crude analysis, but this variable dropped out of the final multivariate model.
| Adjusted Coefficient, Discharge Time as Outcome in Hours (95% CI)* | P Value | Adjusted Coefficient, Discharge Duration as Outcome in Hours (95% CI) | P Value | |
|---|---|---|---|---|
| ||||
| Demographics | ||||
| Age in quartiles (years) | ||||
| 7294 | 0.5 (0.5, 1.6) | 0.33 | 0.6 (8.3, 7.2) | 0.88 |
| 5671 | 0.5 (0.6, 1.6) | 0.41 | 1.3 (9.2, 6.6) | 0.75 |
| 4455 | 0.2 (0.9, 1.3) | 0.74 | 1.2 (9.0, 6.5) | 0.76 |
| Male gender | 0.0 (0.8, 0.8) | 0.97 | 1.2 (6.8, 4.5) | 0.69 |
| African American race | 0.1 (0.7, 0.9) | 0.80 | 0.3 (5.6, 6.1) | 0.93 |
| Last test characteristics | ||||
| Test type | ||||
| Consult | 1.2 (0.1, 2.4) | 0.04 | 14.8 (6.5, 23.1) | 0.001 |
| Procedure | 1.1 (0.1, 2.1) | 0.03 | 13.4 (6.0, 20.7) | <0.001 |
| Laboratory test | 0.8 (1.8, 0.3) | 0.14 | 0.9 (8.4, 6.6) | 0.82 |
| Exam (reference) | ||||
| Discharge needs | ||||
| Prescriptions filled prior to discharge | 1.4 (0.3, 2.4) | 0.02 | ||
| Not discharged to home | 28.9 (21.9, 35.9) | <0.001 | ||
| Ambulance required for transport | 1.5 (0.4, 2.5) | 0.007 | ||
We used duration of discharge as a secondary outcome measure. The final multivariate model for discharge duration included: age, sex, race, test type, and discharge to a facility (Table 2). Those who went to a facility on average left 28.9 hours (95% CI, 21.935.9) later than those who went home. Test type continued to show a significant association with discharge duration, although the estimates were slightly lower in the adjusted model. Need for a consult was associated with a discharge that was on average 14.8 hours (95% CI, 6.523.1) longer than discharges contingent on a physical exam. Similarly, those patients who had procedures had discharges that were on average 13.4 hours (95% CI, 6.020.7) longer than those whose last test was an exam. Several factors that were significantly associated with discharge duration in unadjusted analyses dropped out of the final multivariate model. These included: need for an ambulance, length of stay, insurance status, and medical complexity as estimated by APRDRGwt.
Conclusions
We found that discharge time and duration had wide variability and that certain factors were associated with only one outcome variabledischarge time or duration. Two factorsneed for an ambulance and filling of prescriptions prior to dischargewere associated with later hour of discharge. Discharge to a location other than home was associated with prolonged discharge duration. Test characteristicsin particular need for a procedure and consultwere significantly associated with both longer and later discharges.
In bivariate analysis, several factors were not associated with discharge time or duration. These were: African‐American race, sex, age, Department of Medicine occupancy on day of discharge, source of admission, psychiatric comorbidity, and substance abuse comorbidity. We had expected higher occupancy to delay discharge as demand exceeded capacity for tests, consults, etc. Our findings suggest that even though our study was conducted during the winter months when hospital occupancy is typically at its peak, supply of staff was still adequate enough to meet high demand. We had also expected that psychiatric and substance abuse comorbidities would prolong discharge as prior studies have found some of these diagnoses to be associated with longer lengths of stay.3134 However, our results do not support such an association, and may reflect our decision to group all psychiatric diagnoses together due to limited sample size.
The main strength of our study is the use of 2 outcome variablestime and durationto define delayed discharges. Our findings demonstrate that few factors are associated with both later and longer discharges. In an era when avoiding emergency room walkouts through early morning hospital discharges can be as important as managing overall length of stay, identifying factors associated with both duration and timing of discharges addresses actual challenges faced by hospitals with limited resources. Prior studies have rarely addressed both outcomes. An additional strength of our study is our use of an interdisciplinary survey. The discharge process is a key component of the inpatient stay, but it is also one for which no group is entirely responsible. Through the development and administration of an interdisciplinary survey, our study adds detail to existing descriptions of this fragmented process, and identifies potential areas for improvement.
Several limitations of our study deserve comment. First, we examined patients discharged from a hospitalist unit without house‐staff at an urban tertiary care hospital. Our findings may need additional interpretation prior to their application in dissimilar settings such as: (1) resident‐covered units in which workflow is shaped by teaching rounds, and (2) nonacademic hospitals in which incentives to provide rapid consults and procedures may be different. Second, we relied on self‐reporting for certain variables such as time decisive test needed. This may be subject to recall bias, as we did not have staff to independently verify recalled times. However, since the discharge process is generally a linear one, we were able to verify the general scope of recalled times with times date‐stamped by the computer during the discharge process (eg, checking that time decisive test needed did not occur after the discharge worksheet had been finalized in the electronic order‐entry system). Third, our sample size was not large enough to control for disease‐specific quality measures. Of note, prior studies have not identified a consistently positive or negative relationship between quality of care and efficiency.3538
Past work has used administrative and survey data to analyze the effect of discharge planning interventions on financial or quality outcomes. Outcomes have included readmissions, mortality, patient satisfaction, length of stay, and inappropriate bed days.22, 3845 However, as capacity management has become a more pressing issue for hospitals, greater focus is being placed on the mismatch between supply and demand of patients at each hour of the day. The relevant unit of measure for efficient discharges has become hour of day, in addition to total length of stay. Some hospital improvement projects have already addressed this shift in thinking.20, 21 Our study adds to this work by formally describing the precise timing and duration of steps in the discharge process, and identifying factors associated with both time and duration.
We believe the results of our study have several implications for hospital administrators and patients interested in more timely care. First, the methods used provide a tangible framework for addressing problems that cross disciplines (eg, nursing, physician, social work) and departments (eg, medicine and radiology), and have a multitude of potential causes and confounders. The survey results offer guidance on where to focus resources, provide a shared baseline metric for improvement, and suggest the cross‐functional team that should be involved in change efforts. Such an approach may be useful for addressing common system‐based challenges in inpatient quality and safety.
Second, with specific regard to discharge planning, our study supports the notion that modifiable factors are associated with discharge time and duration. However, we also describe a fragmented discharge process, with no single bottleneck or department responsible for the majority of late and long discharges. Although procedures and consults were both associated with longer and later discharges, only 26% of patients required a procedure prior to discharge, and 18% required a consult. Moreover, among procedures, different people and events are needed to carry out the 2 most popular procedures: stress echocardiograms, and non‐MRI radiology procedures. Hospital leadership at the highest levels will be required to improve efficiency based on local usage patterns, and to increase coordination among the multiple interdepartmental processes that make up the more general categories of procedure and consult.
Acknowledgements
The authors thank the patients and staff of the Hospitalist Unit for their participation in this study. In addition, they sincerely thank Paul X. Allen, Richard O. Davis, Ronald R. Peterson, and Shuai Shao. They also thank the anonymous reviewers for their thoughtful comments.
- ,,,,.Emergency departments and crowding in United States teaching hospitals.Ann Emerg Med.1991;20:980–986.
- ,,,,,.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- ,,.Frequent overcrowding in U.S. emergency departments.Acad Emerg Med.2001;8:151–155.
- ,,,,.The effect of hospital occupancy on emergency department length of stay and patient disposition.Acad Emerg Med.2003;10:127–133.
- .Calculus, chaos, and other models of emergency department crowding.Ann Emerg Med.2003;42:181–184.
- ,.Increased health care costs associated with ED overcrowding.Am J Emerg Med.1994;12:265–266.
- ,,, et al.Decreased health care quality associated with emergency department overcrowding.Eur J Emerg Med.1999;6:105–107.
- ,,.Can good bed management solve the overcrowding in accident and emergency departments?Emerg Med J.2003;20:149–155.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- General Accounting Office. Hospital emergency departments: crowded conditions vary among hospitals and communities. 2003:GAO‐03–460. Available at: http://www.gao.gov/new.items/d03460.pdf. Accessed October.
- ,.Do you want to die?Time.1990;135:58–60+
- .The ER crisis.Ladies Home J.2001;118:70–79.
- .Placing emergency department crowding on the decision agenda.Nurs Econ.2005;23:14–24.
- .Crisis seen in nation's ER care. Washington Post. June 15,2006;A01.
- Committee on the Future of Emergency Care in the United States Health System.Hospital‐based Emergency Care: at the Breaking Point.Washington DC:National Academies Press;2006.
- ,,, et al.Waits to see an emergency department physician: U.S. trends and predictors, 1997–2004.Health Aff.2008;27:w84–w95.
- Advisory Board.Maximizing Hospital Capacity: Expediting Throughput in an Era of Shortage. Health Care Advisory Board research study.Washington DC:Advisory Board; September 12,2002.
- ,,,.Does U.S. hospital capacity need to be expanded?Health Aff.2003;22:40–54.
- Institute for Healthcare Improvement.Optimizing Patient Flow: Moving Patients Smoothly Through Acute Care Settings.Cambridge, MA:Institute for Healthcare Improvement;2003.
- ,. Leveraging six sigma to improve hospital bed availability. Available at: http://healthcare.isixsigma.com/library/content/c030708a.asp. Accessed October2008.
- University Health System Consortium. Managing patient flow implementation: 2005 benchmarking project field brief. Available at: http://www.musc.edu/medcenter/UHC‐CCP/PFMgmtFldBk.pdf.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004;1:CD000313.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
- ,,.Utilisation of hospital beds by the elderly—a cohort study of admissions to a teaching hospital.Ir Med J.1995;88:124–126.
- ,,,,,.Demographic and clinical characteristics as predictors of length of hospitalization and readmission.J Clin Psychol.1977;33:1093–1099.
- ,,,.The epidemiology of delays in a teaching hospital: the development and use of a tool that detects unnecessary hospital days.Med Care.1989;27:112–129.
- American Medical Association.AMA Physician ICD‐9‐CM 2004, Vols 1 and 2.Eden Prairie, MN:Ingenix;2003.
- 3M Health Information Systems and the Maryland Health Care Payment System: frequently asked questions.2004. Available at: http://multimedia.mmm.com/mws/mediawebserver.dyn?6666660Zjcf6lVs6EVs66S7wwCOrrrrQ‐.
- .Statistics with STATA.Belmont, CA:Duxbury Press;2004.
- ,.Statistical data analysis in the computer age.Science.1991;253:390–395.
- ,,,,.Psychological comorbidity and length of stay in the general hospital.Am J Psychiatry.1991;148(3):324–329.
- ,,,,,.Psychiatric comorbidity and greater hospitalization risk, longer length of stay, and higher hospitalization costs in older adults with heart failure.J Am Geriatr Soc.2007;55:1585–1591.
- ,,,.Does psychiatric comorbidity increase the length of stay in general hospitals?Gen Hosp Psychiatry.2001;23:8–14.
- ,,.The impact of psychiatric comorbidity on length of stay of medical inpatients.Gen Hosp Psychiatry.2003;25:14–19.
- ,,,,,.The implications of regional variations in Medicare spending. Part 1: The content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,,,,.The implications of regional variations in Medicare spending. Part 2: Health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,,, et al.Is early too early? Effect of shorter stays after bypass surgery.Ann Thorac Surg.2007;83:100–107.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders, a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,,,.Comprehensive discharge planning for the hospitalized elderly, a randomized clinical trial.Ann Intern Med.1994;120:999–1006.
- ,.Evaluating hospital discharge planning: a randomized clinical trial.Med Care.1993;31:358–370.
- ,,,,.Does a dedicated discharge coordinator improve the quality of hospital discharge?Qual Health Care.1996;5:89–96.
- ,,, et al.The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital.Am J Med.2001;111:627–632.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,.Does increased access to primary care reduce hospital readmissions?N Engl J Med.1996;334:1441–1447.
- ,,,,.Emergency departments and crowding in United States teaching hospitals.Ann Emerg Med.1991;20:980–986.
- ,,,,,.A conceptual model of emergency department crowding.Ann Emerg Med.2003;42:173–180.
- ,,.Frequent overcrowding in U.S. emergency departments.Acad Emerg Med.2001;8:151–155.
- ,,,,.The effect of hospital occupancy on emergency department length of stay and patient disposition.Acad Emerg Med.2003;10:127–133.
- .Calculus, chaos, and other models of emergency department crowding.Ann Emerg Med.2003;42:181–184.
- ,.Increased health care costs associated with ED overcrowding.Am J Emerg Med.1994;12:265–266.
- ,,, et al.Decreased health care quality associated with emergency department overcrowding.Eur J Emerg Med.1999;6:105–107.
- ,,.Can good bed management solve the overcrowding in accident and emergency departments?Emerg Med J.2003;20:149–155.
- ,.Emergency department overcrowding in the United States: an emerging threat to patient safety and public health.Emerg Med J.2003;20:402–405.
- General Accounting Office. Hospital emergency departments: crowded conditions vary among hospitals and communities. 2003:GAO‐03–460. Available at: http://www.gao.gov/new.items/d03460.pdf. Accessed October.
- ,.Do you want to die?Time.1990;135:58–60+
- .The ER crisis.Ladies Home J.2001;118:70–79.
- .Placing emergency department crowding on the decision agenda.Nurs Econ.2005;23:14–24.
- .Crisis seen in nation's ER care. Washington Post. June 15,2006;A01.
- Committee on the Future of Emergency Care in the United States Health System.Hospital‐based Emergency Care: at the Breaking Point.Washington DC:National Academies Press;2006.
- ,,, et al.Waits to see an emergency department physician: U.S. trends and predictors, 1997–2004.Health Aff.2008;27:w84–w95.
- Advisory Board.Maximizing Hospital Capacity: Expediting Throughput in an Era of Shortage. Health Care Advisory Board research study.Washington DC:Advisory Board; September 12,2002.
- ,,,.Does U.S. hospital capacity need to be expanded?Health Aff.2003;22:40–54.
- Institute for Healthcare Improvement.Optimizing Patient Flow: Moving Patients Smoothly Through Acute Care Settings.Cambridge, MA:Institute for Healthcare Improvement;2003.
- ,. Leveraging six sigma to improve hospital bed availability. Available at: http://healthcare.isixsigma.com/library/content/c030708a.asp. Accessed October2008.
- University Health System Consortium. Managing patient flow implementation: 2005 benchmarking project field brief. Available at: http://www.musc.edu/medcenter/UHC‐CCP/PFMgmtFldBk.pdf.
- ,,,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2004;1:CD000313.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
- ,,.Utilisation of hospital beds by the elderly—a cohort study of admissions to a teaching hospital.Ir Med J.1995;88:124–126.
- ,,,,,.Demographic and clinical characteristics as predictors of length of hospitalization and readmission.J Clin Psychol.1977;33:1093–1099.
- ,,,.The epidemiology of delays in a teaching hospital: the development and use of a tool that detects unnecessary hospital days.Med Care.1989;27:112–129.
- American Medical Association.AMA Physician ICD‐9‐CM 2004, Vols 1 and 2.Eden Prairie, MN:Ingenix;2003.
- 3M Health Information Systems and the Maryland Health Care Payment System: frequently asked questions.2004. Available at: http://multimedia.mmm.com/mws/mediawebserver.dyn?6666660Zjcf6lVs6EVs66S7wwCOrrrrQ‐.
- .Statistics with STATA.Belmont, CA:Duxbury Press;2004.
- ,.Statistical data analysis in the computer age.Science.1991;253:390–395.
- ,,,,.Psychological comorbidity and length of stay in the general hospital.Am J Psychiatry.1991;148(3):324–329.
- ,,,,,.Psychiatric comorbidity and greater hospitalization risk, longer length of stay, and higher hospitalization costs in older adults with heart failure.J Am Geriatr Soc.2007;55:1585–1591.
- ,,,.Does psychiatric comorbidity increase the length of stay in general hospitals?Gen Hosp Psychiatry.2001;23:8–14.
- ,,.The impact of psychiatric comorbidity on length of stay of medical inpatients.Gen Hosp Psychiatry.2003;25:14–19.
- ,,,,,.The implications of regional variations in Medicare spending. Part 1: The content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,,,,.The implications of regional variations in Medicare spending. Part 2: Health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,,, et al.Is early too early? Effect of shorter stays after bypass surgery.Ann Thorac Surg.2007;83:100–107.
- ,.Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization.JAMA.2003;290:1868–1874.
- ,,, et al.Comprehensive discharge planning and home follow‐up of hospitalized elders, a randomized clinical trial.JAMA.1999;281:613–620.
- ,,,,,.Comprehensive discharge planning for the hospitalized elderly, a randomized clinical trial.Ann Intern Med.1994;120:999–1006.
- ,.Evaluating hospital discharge planning: a randomized clinical trial.Med Care.1993;31:358–370.
- ,,,,.Does a dedicated discharge coordinator improve the quality of hospital discharge?Qual Health Care.1996;5:89–96.
- ,,, et al.The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital.Am J Med.2001;111:627–632.
- ,,,,,.Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta‐analysis.JAMA.2004;291:1358–1367.
- ,,.Does increased access to primary care reduce hospital readmissions?N Engl J Med.1996;334:1441–1447.
Copyright © 2009 Society of Hospital Medicine

Caught in the Web: e‐Diagnosis
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 52‐year‐old woman presented with a 3‐month history of progressive bilateral leg edema and dyspnea while climbing a flight of stairs or while walking up a steep slope. She also complained of a tingling sensation in both hands and fingers, which started about 2 months prior to the onset of edema. She did not describe sensory problems in the lower extremities and did not have any other neurological complaints. She denied fever, cough, chest pain, palpitations, orthopnea, paroxysmal nocturnal dyspnea, and dark stools. She had no history of hypertension, diabetes, dyslipidemia, or asthma and had never been hospitalized. She did not smoke or consume alcohol and used no medications, including over‐the‐counter drugs or dietary supplements. The patient was born in Japan and had not traveled outside the country since her birth. She was a homemaker and had worked occasionally as a manual laborer in sugar cane agriculture. A review of systems revealed no history of polydipsia, polyuria, or cold or heat intolerance but did identify new hair growth, especially on the extremities.
This middle‐aged woman shows progressive changes in her general health status that are characterized by edema and dyspnea on effort. The differential diagnosis of edema includes a broad spectrum of illnesses, such as cardiac, lung, renal, endocrine, and hepatic diseases. Because of the life‐threatening potential, my first concern is cardiac disease, although the patient is not experiencing typical symptoms of ischemic heart disease or congestive failure. Bilateral and distal distribution of neuropathic symptoms is likely due to diseases of peripheral nerves rather than those of the central nervous system. Her complaint of a bilateral tingling sensation in the hands may suggest carpal tunnel syndrome as a result of her long‐term agricultural work. Other possible causes include radiculopathy of the cervical spine or polyneuropathy. Clues in the physical examination may help narrow the differential diagnosis to a cardiac, hepatic, or endocrine disorder.
The patient appeared ill. Her weight had increased from 48 to 61 kg since she was last weighed 6 months previously. Her blood pressure was 140/78 mm Hg, her heart rate was 72 beats/minute with a regular rhythm, her respiratory rate was 18/minute, and her temperature was 37.5C. The jugular venous pressure was elevated at 10 cm above the sternal angle. A grade III/VI systolic ejection murmur was evident at the second interspace along the left sternal border. The second heart sound was fixed and split. There were decreased breath sounds and complete dullness to percussion over both lower lung fields. Shifting dullness was noted on abdominal examination. There was pitting edema from the feet to the thighs, with slow pit‐recovery time in both legs, and she exhibited generalized hirsutism on the face, body, and extremities. There was no lymphadenopathy. On neurological examination, her mental status was normal. The cranial nerves were normal, as was coordination. There was mild generalized distal‐dominant motor weakness with generalized hyporeflexia. Sensory testing demonstrated glove‐and‐stocking type loss of sensation to pinpricks as well as dysesthesia in all extremities. Phalen and Tinel tests were negative.
The elevated venous pressure and pitting edema with slow recovery suggest high venous pressure edema rather than hypoproteinemic edema. Complete bilateral dullness of the chest and shifting dullness of the abdomen indicate the presence of bilateral pleural effusion and ascites. Edema from high venous pressure is usually caused by right, left, or biventricular cardiac failure. A fixed splitting of the second heart sound suggests an atrial septal defect, which is a rare cause of progressive right heart failure in adults. I recommend checking the patient's thyroid function to investigate the possibility of hypothyroidism, which is a common illness among middle‐aged women and could contribute to her edema as well as hirsutism. The neurological findings suggest a generalized polyneuropathy. The unusual combination of high venous pressure edema and polyneuropathy may indicate a rare multisystem disorder such as amyloidosis. Alternatively, the patient might have developed multiple diseases during the same time period. For instance, diabetic polyneuropathy is the most common cause of polyneuropathy among the middle‐aged. Finally, the differential diagnosis of hirsutism includes ovarian, adrenal, or pituitary sources of hyperandrogenism in addition to hypothyroidism. I would first evaluate for diabetes, thyroid disease, and cardiac disease and would like to see the results of laboratory tests for thyrotropin and plasma glucose as well as chest radiography and electrocardiography.
The white‐cell count was 5400/mm3 with a normal differential. Hemoglobin was 10.7 g/dL with normal red‐cell indices, and the platelet count was 276,000/mm3. The erythrocyte sedimentation rate was 29 mm/hour. Other laboratory tests revealed the following values: total protein, 6.2 g/dL; albumin, 3.3 g/dL; blood urea nitrogen, 12 mg/dL; creatinine, 0.7 mg/dL; aspartate aminotransferase, 6 U/L; alanine aminotransferase, 2 U/L; lactate dehydrogenase, 96 U/L; alkaline phosphatase, 115 U/L; creatine phosphokinase, 60 U/L; total bilirubin, 0.9 mg/dL; glucose, 96 mg/dL; hemoglobin A1c, 4.6%; total cholesterol, 111 mg/dL; and thyrotropin, 6.32 mIU/mL (normal range, 0.50‐5.00 mIU/mL). Serum free thyroxine, triiodothyronine, and urine testosterone were normal. Serum dehydroepiandrosterone sulfate was mildly elevated for her age (864 ng/mL: normal range, 180‐750 ng/mL). Serological studies for human immunodeficiency virus, human T‐lymphotrophic virus type 1, and syphilis were negative. Urinalysis was weakly positive for protein but negative for casts and occult blood. The stool was negative for occult blood.
A chest radiograph showed bilateral pleural effusions. Computed tomography demonstrated bilateral pleural effusions, ascites, mild hepatomegaly, and small, multiple, mediastinal lymph nodes. Her electrocardiogram was normal. A transesophageal echocardiogram with agitated saline contrast demonstrated normal ventricular systolic and diastolic function and no atrial septal defect. The inferior vena cava did not collapse with inspiration, and there was no evidence of infiltrative cardiomyopathy.
These laboratory results rule out diabetes as the cause of the polyneuropathy. The subclinical hypothyroidism would not explain profound edema and hirsutism. A serum albumin level of 3.3 g/dL confirms high venous pressure edema rather than hypoproteinemic edema. Normochromic, normocytic anemia and a mildly elevated sedimentation rate point to a chronic illness or inflammatory state. The mediastinal lymphadenopathy may reflect congestion as a result of the high venous pressure or reflect a systemic disease involving lymph nodes. Normal ventricular function with high venous pressure is suggestive of heart failure from diastolic dysfunction, although the patient does not have risk factors for diastolic dysfunction, such as hypertension, and has no other echocardiographic features of diastolic impairment. The combination of hyperandrogenism and neuropathy points to a systemic process, such as a paraneoplastic syndrome. I would next investigate the source of the excess androgens.
Because serum dehydroepiandrosterone sulfate was mildly elevated, I‐131 aldosterol scintigraphy was performed, and it was negative. Electromyography showed a pattern of generalized sensorimotor polyneuropathy.
At this point, it appears that cardiac, endocrine, hepatic, and renal diseases have been largely ruled out as a cause of her symptoms. Reframing and unifying the important clinical problems for this patient may be useful in resolving this diagnostic puzzle. They include (1) systemic high venous pressure edema; (2) generalized sensorimotor polyneuropathy; (3) hirsutism; (4) normocytic, normochromic anemia; (5) an elevated erythrocyte sedimentation rate; (6) mediastinal lymphadenopathy; and (7) subclinical hypothyroidism. At this point, I cannot unify these pieces of information into a single diagnosis. I would search the medical literature, focusing on these terms.
A general internist consultant performed MEDLINE and Google Scholar searches using the key words edema, polyneuropathy, and hirsutism. This search suggested the diagnosis of Crow‐Fukase syndrome, also known as POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) syndrome. Subsequent evaluations were performed. First, serum protein electrophoresis revealed the presence of monoclonal proteins, although hypergammaglobulinemia was not present. Second, a bone marrow examination demonstrated increased abnormal plasma cell proliferation (7%), although a radiographic skeletal survey found no lesions suggestive of plasmacytoma. Third, cerebrospinal fluid analysis showed normal cell counts but increased protein concentration (202 mg/dL). Fourth, a blood sample referred to an outside laboratory demonstrated elevated levels of vascular endothelial growth factor (3902 pg/mL: normal range, 150‐500 pg/mL). On the basis of these findings, the diagnosis of POEMS syndrome was made. After oral prednisolone (40 mg/day) was initiated, the systemic edema improved gradually, and she did well during the 2‐year follow‐up period.
Commentary
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder first described by Crow in 1956.1, 2 It is characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes, as indicated by the acronym. The diagnosis of POEMS syndrome is difficult as this syndrome is rare and requires high clinical suspicion. According to a nationwide cross‐sectional survey in Japan, the prevalence of POEMS syndrome is very low (about 3 patients per 1,000,000 persons),3 and its prevalence in Western countries is considered even lower than that in Japan. The average age at onset is around 45 to 50 years old, and men are twice as likely to have this syndrome as women.46 Table 1 shows the diagnostic criteria of POEMS syndrome, based on research by Dispenzieri and others at the Mayo Clinic, and Table 2 presents the relative frequency of these clinical features.6, 7 The initial symptomatology generally includes polyneuropathy, skin changes, and generalized edema, which are nonspecific symptoms, as are other well‐recognized associated conditions such as clubbing, weight loss, thrombocytosis, polycythemia, and hyperhidrosis. Thus, it is important to consider this syndrome when one is facing an undiagnosed illness involving multiple organ systems and to distinguish it from other conditions such as multiple myeloma, amyloidosis, and monoclonal gammopathy of undetermined significance. Vascular endothelial growth factor is thought to be involved in the edema of POEMS syndrome, as massive release from aggregated platelets increases vascular permeability and venous pressure.710
| |
| Major criteria | Polyneuropathy |
| Monoclonal plasma cell‐proliferative disorder | |
| Minor criteria | Sclerotic bone lesions |
| Castleman disease | |
| Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy) | |
| Edema (peripheral edema, pleural effusion, or ascites) | |
| Endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, or pancreatic) | |
| Skin changes (hyperpigmentation, hirsutism, plethora, hemangiomata, and white nails) | |
| Papilledema | |
| Characteristic | % |
|---|---|
| |
| Peripheral neuropathy | 100 |
| Monoclonal plasma cell dyscrasia | 100 |
| Sclerotic bone lesions | 97 |
| Endocrinopathy | 71 |
| Skin changes | 68 |
| Organomegaly | 46 |
| Extravascular volume overload | 39 |
| Papilledema | 29 |
| Castleman disease | 11 |
Data regarding treatment and survival are largely observational. Overall mean survival from diagnosis in the 2003 Dispenzieri cohort was 13.7 years, with death often due to infection or cardiorespiratory failure.6 When a solitary plasmacytoma or osteosclerotic myeloma is present, radiation to the lesion can often lead to clinical remission. Other treatment options include alkylating agents and/or high‐dose chemotherapy with peripheral stem‐cell transplantation, corticosteroids, and supportive care.7
Clinicians frequently use the internet to aid in the clinical decision process. In a survey of the Royal New Zealand College of General Practitioners,11 half reported that they used the Internet to search for clinical information. Two well‐known resources are MEDLINE, which contains over 11 million references dating back to the 1960s, and internet search engines such as Google (and a more recent product, Google Scholar, which attempts to sort search results by including factors such as the author, the publication in which the article appears, and how often the article has been cited).
MEDLINE searches a well‐defined set of journals and uses the Medical Subject Headings (MeSH) vocabulary, which consists of sets of descriptive terms organized in a hierarchical structure to allow searching with various levels of specificity. For instance, entering the term heart attack will map to the MeSH term myocardial infarction and will also include more specific terms such as myocardial stunning and cardiogenic shock.
Google, in comparison, explores resources beyond journals without any clear boundary to its scope, and its advanced search functions can be occasionally unreliable. For instance, search results are occasionally marred by outdated citation information and may include materials that are not truly scholarly. However, search engines can search through the actual text of manuscripts and access the gray literature, which includes open‐source material that is usually original but not widely distributed or often easily available, such as technical reports and dissertations. A direct study comparing the results of searches in PubMed (one of the MEDLINE search engines) and Google Scholar is difficult, but the critical characteristics of each can be compared and contrasted (Table 3).
| Google Scholar | PubMed |
|---|---|
| 1. Database selection is clumped under subject areas, and it cannot be searched with unique identifiers: Con | 1. It allows one to choose a database at the outset and can search with a unique identifier (PubMed identifier): Pro |
| 2. Results cannot be filtered (ie, it does not allow multiple article selection): Con | 2. The single citation matcher allows retrieval of articles with pieces of information: Pro |
| 3. A search for related articles or similar pages is not available: Con | 3. It allows article selection by checkbox to reduce the number of articles relevant to the search query and to append the filter to search box: Pro |
| 4. It allows one to search by without words to exclude unwanted and confusing retrieved data: Pro | 4. It provides unique identifier (PubMed identifier) for each retrieved article for easy communicability: Pro |
| 5. It allows one to search a single journal/publication of interest: Pro | 5. Search are limited to journals only; it does not include the grey area of literature: Con |
| 6. Initial search results are those articles that are most cited by journals that themselves are the most cited: Pro | 6. It lists search results in chronological order and not by relevance: Con |
Internet searches may also suggest diagnoses from a compilation of clinical features, such as in this case. To be successful, such a search must complement the cognitive process; a search engine cannot completely replace clinical judgment. Clinicians must be able to identify salient clinical features and generate high‐yield search terms and then exercise skill in sifting through the citations to arrive at the appropriate diagnosis. A recent study found that Google searches revealed the correct diagnosis in 58% of the case records of the New England Journal of Medicine,12 although each search query resulted in many results, which then had to be manually reviewed for appropriateness within the case's context.
Like a traditional diagnostic test, a search can be described by sensitivity, specificity, and the number of articles needed to read.13 For example, in a study comparing the performance of search strategies to identify clinical practice guidelines in Google Scholar and SUMSearch (another freely accessible search engine), using the term guideline yielded the highest sensitivity, and using the term practice guideline generated the highest specificity and the lowest number of articles needed to read (Table 4).14
| Search Strategy | Sensitivity (%) | Specificity (%) | NNR |
|---|---|---|---|
| |||
| SUMSearch | |||
| Guideline* | 81.51 (74.5388.49) | 74.29 (72.6475.94) | 8.18 (6.9010.05) |
| Recommendation* | 60.50 (51.7269.28) | 76.28 (74.6777.89) | 9.93 (8.1412.72) |
| Practice guideline* | 40.34 (31.5249.16) | 89.45 (88.2990.61) | 6.96 (5.529.43) |
| Google Scholar | |||
| Guideline/s | 31.93 (23.5640.30) | 78.05 (76.5079.60) | 16.67 (12.7624.04) |
| Recommendation/s | 8.40 (3.4213.38) | 92.11 (91.0993.13) | 22.42 (13.9756.82) |
| Practice guideline/s | 11.76 (5.9817.54) | 95.72 (94.9696.48) | 9.29 (6.2118.38) |
Although there are several other popular hosts of web‐based search engines, a more robust decision‐support program may help physicians more efficiently consider relevant diagnoses. One program, named Isabel, has been developed through the indexing of a database of more than 11,000 diseases according to word patterns in journal articles associated with each disease, and it is updated as new and relevant articles emerge. One recent study demonstrated that the correct diagnosis was made in 48 of 50 cases (96%) with specific, key findings as search terms but in only 37 of the same 50 cases (74%) if the entire case history was simply pasted in, again emphasizing the importance of specific search terms.15
POEMS syndrome is a rare entity occasionally seen in middle‐aged individuals and marked by a multitude of nonspecific findings, particularly polyneuropathy and plasma cell dyscrasia. In this case, the diagnostic test was an internet search based on the most prominent clinical symptoms. Such a strategy can provide a powerful addition to traditional literature and MEDLINE resources. However, the efficiency of this process is heavily dependent on the quality of the search strategy and, therefore, the cognitive faculties of the treating physician to avoid the predictable shortcoming of low specificity. Garbage in, garbage out still applies whether the computer in question is the human mind or the desktop PC.
Teaching Points
-
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes.
-
Internet‐based searches, including Google and MEDLINE, are being used more frequently because they are widely available, quick, and freely accessed.
-
Internet searches appear most useful as adjuncts to PubMed and clinical reasoning in identifying case reports when a well‐constructed collection of symptoms and signs is used for searches.
- .Peripheral neuritis in myelomatosis.Br Med J.1956;2(4996):802–804.
- ,,,,,.Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature.Medicine (Baltimore).1980;59(4):311–322.
- .Nationwide Epidemiologic Survey of Crow‐Fukase Syndrome in 2004.Tokyo, Japan:Japanese Ministry of Health and Welfare Government Report, 2004.
- ,,, et al.The Crow‐Fukase syndrome: a study of 102 cases in Japan.Neurology.1984;34(6):712–720.
- ,,.POEMS syndrome: a study of 25 cases and a review of the literature. French Study Group on POEMS Syndrome.Am J Med.1994;97(6):543–553.
- ,,, et al.POEMS syndrome: definitions and long‐term outcome.Blood.2003;101(7):2496–2506.
- .POEMS syndrome.Hematology.2005;1(1):360–367.
- ,,,,.Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome.Lancet.1996;347(9002):702.
- ,.Assessment of hypoproteinaemic oedema: a simple physical sign.Br Med J.1978;1(6117):890–891.
- ,,, et al.Ratio of serum vascular endothelial growth factor to platelet count correlates with disease activity in a patient with POEMS syndrome.Eur J Intern Med.2002;13(1):70–74.
- .In search of evidence: family practitioners' use of the Internet for clinical information.J Med Libr Assoc.2002;90(4):370–379.
- ,.Googling for a diagnosis—use of Google as a diagnostic aid: internet based study.BMJ.2006;333(7579):1143–5114.
- ,,.The number needed to read—a new measure of journal value.Health Info Libr J.2005;22(2):81–82.
- ,,,.Developing search strategies for clinical practice guidelines in SUMSearch and Google Scholar and assessing their retrieval performance.BMC Med Res Methodol.2007;7:28.
- ,.Performance of a web‐based clinical diagnosis support system for internists.J Gen Intern Med.2008;23(suppl 1):37–40.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 52‐year‐old woman presented with a 3‐month history of progressive bilateral leg edema and dyspnea while climbing a flight of stairs or while walking up a steep slope. She also complained of a tingling sensation in both hands and fingers, which started about 2 months prior to the onset of edema. She did not describe sensory problems in the lower extremities and did not have any other neurological complaints. She denied fever, cough, chest pain, palpitations, orthopnea, paroxysmal nocturnal dyspnea, and dark stools. She had no history of hypertension, diabetes, dyslipidemia, or asthma and had never been hospitalized. She did not smoke or consume alcohol and used no medications, including over‐the‐counter drugs or dietary supplements. The patient was born in Japan and had not traveled outside the country since her birth. She was a homemaker and had worked occasionally as a manual laborer in sugar cane agriculture. A review of systems revealed no history of polydipsia, polyuria, or cold or heat intolerance but did identify new hair growth, especially on the extremities.
This middle‐aged woman shows progressive changes in her general health status that are characterized by edema and dyspnea on effort. The differential diagnosis of edema includes a broad spectrum of illnesses, such as cardiac, lung, renal, endocrine, and hepatic diseases. Because of the life‐threatening potential, my first concern is cardiac disease, although the patient is not experiencing typical symptoms of ischemic heart disease or congestive failure. Bilateral and distal distribution of neuropathic symptoms is likely due to diseases of peripheral nerves rather than those of the central nervous system. Her complaint of a bilateral tingling sensation in the hands may suggest carpal tunnel syndrome as a result of her long‐term agricultural work. Other possible causes include radiculopathy of the cervical spine or polyneuropathy. Clues in the physical examination may help narrow the differential diagnosis to a cardiac, hepatic, or endocrine disorder.
The patient appeared ill. Her weight had increased from 48 to 61 kg since she was last weighed 6 months previously. Her blood pressure was 140/78 mm Hg, her heart rate was 72 beats/minute with a regular rhythm, her respiratory rate was 18/minute, and her temperature was 37.5C. The jugular venous pressure was elevated at 10 cm above the sternal angle. A grade III/VI systolic ejection murmur was evident at the second interspace along the left sternal border. The second heart sound was fixed and split. There were decreased breath sounds and complete dullness to percussion over both lower lung fields. Shifting dullness was noted on abdominal examination. There was pitting edema from the feet to the thighs, with slow pit‐recovery time in both legs, and she exhibited generalized hirsutism on the face, body, and extremities. There was no lymphadenopathy. On neurological examination, her mental status was normal. The cranial nerves were normal, as was coordination. There was mild generalized distal‐dominant motor weakness with generalized hyporeflexia. Sensory testing demonstrated glove‐and‐stocking type loss of sensation to pinpricks as well as dysesthesia in all extremities. Phalen and Tinel tests were negative.
The elevated venous pressure and pitting edema with slow recovery suggest high venous pressure edema rather than hypoproteinemic edema. Complete bilateral dullness of the chest and shifting dullness of the abdomen indicate the presence of bilateral pleural effusion and ascites. Edema from high venous pressure is usually caused by right, left, or biventricular cardiac failure. A fixed splitting of the second heart sound suggests an atrial septal defect, which is a rare cause of progressive right heart failure in adults. I recommend checking the patient's thyroid function to investigate the possibility of hypothyroidism, which is a common illness among middle‐aged women and could contribute to her edema as well as hirsutism. The neurological findings suggest a generalized polyneuropathy. The unusual combination of high venous pressure edema and polyneuropathy may indicate a rare multisystem disorder such as amyloidosis. Alternatively, the patient might have developed multiple diseases during the same time period. For instance, diabetic polyneuropathy is the most common cause of polyneuropathy among the middle‐aged. Finally, the differential diagnosis of hirsutism includes ovarian, adrenal, or pituitary sources of hyperandrogenism in addition to hypothyroidism. I would first evaluate for diabetes, thyroid disease, and cardiac disease and would like to see the results of laboratory tests for thyrotropin and plasma glucose as well as chest radiography and electrocardiography.
The white‐cell count was 5400/mm3 with a normal differential. Hemoglobin was 10.7 g/dL with normal red‐cell indices, and the platelet count was 276,000/mm3. The erythrocyte sedimentation rate was 29 mm/hour. Other laboratory tests revealed the following values: total protein, 6.2 g/dL; albumin, 3.3 g/dL; blood urea nitrogen, 12 mg/dL; creatinine, 0.7 mg/dL; aspartate aminotransferase, 6 U/L; alanine aminotransferase, 2 U/L; lactate dehydrogenase, 96 U/L; alkaline phosphatase, 115 U/L; creatine phosphokinase, 60 U/L; total bilirubin, 0.9 mg/dL; glucose, 96 mg/dL; hemoglobin A1c, 4.6%; total cholesterol, 111 mg/dL; and thyrotropin, 6.32 mIU/mL (normal range, 0.50‐5.00 mIU/mL). Serum free thyroxine, triiodothyronine, and urine testosterone were normal. Serum dehydroepiandrosterone sulfate was mildly elevated for her age (864 ng/mL: normal range, 180‐750 ng/mL). Serological studies for human immunodeficiency virus, human T‐lymphotrophic virus type 1, and syphilis were negative. Urinalysis was weakly positive for protein but negative for casts and occult blood. The stool was negative for occult blood.
A chest radiograph showed bilateral pleural effusions. Computed tomography demonstrated bilateral pleural effusions, ascites, mild hepatomegaly, and small, multiple, mediastinal lymph nodes. Her electrocardiogram was normal. A transesophageal echocardiogram with agitated saline contrast demonstrated normal ventricular systolic and diastolic function and no atrial septal defect. The inferior vena cava did not collapse with inspiration, and there was no evidence of infiltrative cardiomyopathy.
These laboratory results rule out diabetes as the cause of the polyneuropathy. The subclinical hypothyroidism would not explain profound edema and hirsutism. A serum albumin level of 3.3 g/dL confirms high venous pressure edema rather than hypoproteinemic edema. Normochromic, normocytic anemia and a mildly elevated sedimentation rate point to a chronic illness or inflammatory state. The mediastinal lymphadenopathy may reflect congestion as a result of the high venous pressure or reflect a systemic disease involving lymph nodes. Normal ventricular function with high venous pressure is suggestive of heart failure from diastolic dysfunction, although the patient does not have risk factors for diastolic dysfunction, such as hypertension, and has no other echocardiographic features of diastolic impairment. The combination of hyperandrogenism and neuropathy points to a systemic process, such as a paraneoplastic syndrome. I would next investigate the source of the excess androgens.
Because serum dehydroepiandrosterone sulfate was mildly elevated, I‐131 aldosterol scintigraphy was performed, and it was negative. Electromyography showed a pattern of generalized sensorimotor polyneuropathy.
At this point, it appears that cardiac, endocrine, hepatic, and renal diseases have been largely ruled out as a cause of her symptoms. Reframing and unifying the important clinical problems for this patient may be useful in resolving this diagnostic puzzle. They include (1) systemic high venous pressure edema; (2) generalized sensorimotor polyneuropathy; (3) hirsutism; (4) normocytic, normochromic anemia; (5) an elevated erythrocyte sedimentation rate; (6) mediastinal lymphadenopathy; and (7) subclinical hypothyroidism. At this point, I cannot unify these pieces of information into a single diagnosis. I would search the medical literature, focusing on these terms.
A general internist consultant performed MEDLINE and Google Scholar searches using the key words edema, polyneuropathy, and hirsutism. This search suggested the diagnosis of Crow‐Fukase syndrome, also known as POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) syndrome. Subsequent evaluations were performed. First, serum protein electrophoresis revealed the presence of monoclonal proteins, although hypergammaglobulinemia was not present. Second, a bone marrow examination demonstrated increased abnormal plasma cell proliferation (7%), although a radiographic skeletal survey found no lesions suggestive of plasmacytoma. Third, cerebrospinal fluid analysis showed normal cell counts but increased protein concentration (202 mg/dL). Fourth, a blood sample referred to an outside laboratory demonstrated elevated levels of vascular endothelial growth factor (3902 pg/mL: normal range, 150‐500 pg/mL). On the basis of these findings, the diagnosis of POEMS syndrome was made. After oral prednisolone (40 mg/day) was initiated, the systemic edema improved gradually, and she did well during the 2‐year follow‐up period.
Commentary
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder first described by Crow in 1956.1, 2 It is characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes, as indicated by the acronym. The diagnosis of POEMS syndrome is difficult as this syndrome is rare and requires high clinical suspicion. According to a nationwide cross‐sectional survey in Japan, the prevalence of POEMS syndrome is very low (about 3 patients per 1,000,000 persons),3 and its prevalence in Western countries is considered even lower than that in Japan. The average age at onset is around 45 to 50 years old, and men are twice as likely to have this syndrome as women.46 Table 1 shows the diagnostic criteria of POEMS syndrome, based on research by Dispenzieri and others at the Mayo Clinic, and Table 2 presents the relative frequency of these clinical features.6, 7 The initial symptomatology generally includes polyneuropathy, skin changes, and generalized edema, which are nonspecific symptoms, as are other well‐recognized associated conditions such as clubbing, weight loss, thrombocytosis, polycythemia, and hyperhidrosis. Thus, it is important to consider this syndrome when one is facing an undiagnosed illness involving multiple organ systems and to distinguish it from other conditions such as multiple myeloma, amyloidosis, and monoclonal gammopathy of undetermined significance. Vascular endothelial growth factor is thought to be involved in the edema of POEMS syndrome, as massive release from aggregated platelets increases vascular permeability and venous pressure.710
| |
| Major criteria | Polyneuropathy |
| Monoclonal plasma cell‐proliferative disorder | |
| Minor criteria | Sclerotic bone lesions |
| Castleman disease | |
| Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy) | |
| Edema (peripheral edema, pleural effusion, or ascites) | |
| Endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, or pancreatic) | |
| Skin changes (hyperpigmentation, hirsutism, plethora, hemangiomata, and white nails) | |
| Papilledema | |
| Characteristic | % |
|---|---|
| |
| Peripheral neuropathy | 100 |
| Monoclonal plasma cell dyscrasia | 100 |
| Sclerotic bone lesions | 97 |
| Endocrinopathy | 71 |
| Skin changes | 68 |
| Organomegaly | 46 |
| Extravascular volume overload | 39 |
| Papilledema | 29 |
| Castleman disease | 11 |
Data regarding treatment and survival are largely observational. Overall mean survival from diagnosis in the 2003 Dispenzieri cohort was 13.7 years, with death often due to infection or cardiorespiratory failure.6 When a solitary plasmacytoma or osteosclerotic myeloma is present, radiation to the lesion can often lead to clinical remission. Other treatment options include alkylating agents and/or high‐dose chemotherapy with peripheral stem‐cell transplantation, corticosteroids, and supportive care.7
Clinicians frequently use the internet to aid in the clinical decision process. In a survey of the Royal New Zealand College of General Practitioners,11 half reported that they used the Internet to search for clinical information. Two well‐known resources are MEDLINE, which contains over 11 million references dating back to the 1960s, and internet search engines such as Google (and a more recent product, Google Scholar, which attempts to sort search results by including factors such as the author, the publication in which the article appears, and how often the article has been cited).
MEDLINE searches a well‐defined set of journals and uses the Medical Subject Headings (MeSH) vocabulary, which consists of sets of descriptive terms organized in a hierarchical structure to allow searching with various levels of specificity. For instance, entering the term heart attack will map to the MeSH term myocardial infarction and will also include more specific terms such as myocardial stunning and cardiogenic shock.
Google, in comparison, explores resources beyond journals without any clear boundary to its scope, and its advanced search functions can be occasionally unreliable. For instance, search results are occasionally marred by outdated citation information and may include materials that are not truly scholarly. However, search engines can search through the actual text of manuscripts and access the gray literature, which includes open‐source material that is usually original but not widely distributed or often easily available, such as technical reports and dissertations. A direct study comparing the results of searches in PubMed (one of the MEDLINE search engines) and Google Scholar is difficult, but the critical characteristics of each can be compared and contrasted (Table 3).
| Google Scholar | PubMed |
|---|---|
| 1. Database selection is clumped under subject areas, and it cannot be searched with unique identifiers: Con | 1. It allows one to choose a database at the outset and can search with a unique identifier (PubMed identifier): Pro |
| 2. Results cannot be filtered (ie, it does not allow multiple article selection): Con | 2. The single citation matcher allows retrieval of articles with pieces of information: Pro |
| 3. A search for related articles or similar pages is not available: Con | 3. It allows article selection by checkbox to reduce the number of articles relevant to the search query and to append the filter to search box: Pro |
| 4. It allows one to search by without words to exclude unwanted and confusing retrieved data: Pro | 4. It provides unique identifier (PubMed identifier) for each retrieved article for easy communicability: Pro |
| 5. It allows one to search a single journal/publication of interest: Pro | 5. Search are limited to journals only; it does not include the grey area of literature: Con |
| 6. Initial search results are those articles that are most cited by journals that themselves are the most cited: Pro | 6. It lists search results in chronological order and not by relevance: Con |
Internet searches may also suggest diagnoses from a compilation of clinical features, such as in this case. To be successful, such a search must complement the cognitive process; a search engine cannot completely replace clinical judgment. Clinicians must be able to identify salient clinical features and generate high‐yield search terms and then exercise skill in sifting through the citations to arrive at the appropriate diagnosis. A recent study found that Google searches revealed the correct diagnosis in 58% of the case records of the New England Journal of Medicine,12 although each search query resulted in many results, which then had to be manually reviewed for appropriateness within the case's context.
Like a traditional diagnostic test, a search can be described by sensitivity, specificity, and the number of articles needed to read.13 For example, in a study comparing the performance of search strategies to identify clinical practice guidelines in Google Scholar and SUMSearch (another freely accessible search engine), using the term guideline yielded the highest sensitivity, and using the term practice guideline generated the highest specificity and the lowest number of articles needed to read (Table 4).14
| Search Strategy | Sensitivity (%) | Specificity (%) | NNR |
|---|---|---|---|
| |||
| SUMSearch | |||
| Guideline* | 81.51 (74.5388.49) | 74.29 (72.6475.94) | 8.18 (6.9010.05) |
| Recommendation* | 60.50 (51.7269.28) | 76.28 (74.6777.89) | 9.93 (8.1412.72) |
| Practice guideline* | 40.34 (31.5249.16) | 89.45 (88.2990.61) | 6.96 (5.529.43) |
| Google Scholar | |||
| Guideline/s | 31.93 (23.5640.30) | 78.05 (76.5079.60) | 16.67 (12.7624.04) |
| Recommendation/s | 8.40 (3.4213.38) | 92.11 (91.0993.13) | 22.42 (13.9756.82) |
| Practice guideline/s | 11.76 (5.9817.54) | 95.72 (94.9696.48) | 9.29 (6.2118.38) |
Although there are several other popular hosts of web‐based search engines, a more robust decision‐support program may help physicians more efficiently consider relevant diagnoses. One program, named Isabel, has been developed through the indexing of a database of more than 11,000 diseases according to word patterns in journal articles associated with each disease, and it is updated as new and relevant articles emerge. One recent study demonstrated that the correct diagnosis was made in 48 of 50 cases (96%) with specific, key findings as search terms but in only 37 of the same 50 cases (74%) if the entire case history was simply pasted in, again emphasizing the importance of specific search terms.15
POEMS syndrome is a rare entity occasionally seen in middle‐aged individuals and marked by a multitude of nonspecific findings, particularly polyneuropathy and plasma cell dyscrasia. In this case, the diagnostic test was an internet search based on the most prominent clinical symptoms. Such a strategy can provide a powerful addition to traditional literature and MEDLINE resources. However, the efficiency of this process is heavily dependent on the quality of the search strategy and, therefore, the cognitive faculties of the treating physician to avoid the predictable shortcoming of low specificity. Garbage in, garbage out still applies whether the computer in question is the human mind or the desktop PC.
Teaching Points
-
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes.
-
Internet‐based searches, including Google and MEDLINE, are being used more frequently because they are widely available, quick, and freely accessed.
-
Internet searches appear most useful as adjuncts to PubMed and clinical reasoning in identifying case reports when a well‐constructed collection of symptoms and signs is used for searches.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 52‐year‐old woman presented with a 3‐month history of progressive bilateral leg edema and dyspnea while climbing a flight of stairs or while walking up a steep slope. She also complained of a tingling sensation in both hands and fingers, which started about 2 months prior to the onset of edema. She did not describe sensory problems in the lower extremities and did not have any other neurological complaints. She denied fever, cough, chest pain, palpitations, orthopnea, paroxysmal nocturnal dyspnea, and dark stools. She had no history of hypertension, diabetes, dyslipidemia, or asthma and had never been hospitalized. She did not smoke or consume alcohol and used no medications, including over‐the‐counter drugs or dietary supplements. The patient was born in Japan and had not traveled outside the country since her birth. She was a homemaker and had worked occasionally as a manual laborer in sugar cane agriculture. A review of systems revealed no history of polydipsia, polyuria, or cold or heat intolerance but did identify new hair growth, especially on the extremities.
This middle‐aged woman shows progressive changes in her general health status that are characterized by edema and dyspnea on effort. The differential diagnosis of edema includes a broad spectrum of illnesses, such as cardiac, lung, renal, endocrine, and hepatic diseases. Because of the life‐threatening potential, my first concern is cardiac disease, although the patient is not experiencing typical symptoms of ischemic heart disease or congestive failure. Bilateral and distal distribution of neuropathic symptoms is likely due to diseases of peripheral nerves rather than those of the central nervous system. Her complaint of a bilateral tingling sensation in the hands may suggest carpal tunnel syndrome as a result of her long‐term agricultural work. Other possible causes include radiculopathy of the cervical spine or polyneuropathy. Clues in the physical examination may help narrow the differential diagnosis to a cardiac, hepatic, or endocrine disorder.
The patient appeared ill. Her weight had increased from 48 to 61 kg since she was last weighed 6 months previously. Her blood pressure was 140/78 mm Hg, her heart rate was 72 beats/minute with a regular rhythm, her respiratory rate was 18/minute, and her temperature was 37.5C. The jugular venous pressure was elevated at 10 cm above the sternal angle. A grade III/VI systolic ejection murmur was evident at the second interspace along the left sternal border. The second heart sound was fixed and split. There were decreased breath sounds and complete dullness to percussion over both lower lung fields. Shifting dullness was noted on abdominal examination. There was pitting edema from the feet to the thighs, with slow pit‐recovery time in both legs, and she exhibited generalized hirsutism on the face, body, and extremities. There was no lymphadenopathy. On neurological examination, her mental status was normal. The cranial nerves were normal, as was coordination. There was mild generalized distal‐dominant motor weakness with generalized hyporeflexia. Sensory testing demonstrated glove‐and‐stocking type loss of sensation to pinpricks as well as dysesthesia in all extremities. Phalen and Tinel tests were negative.
The elevated venous pressure and pitting edema with slow recovery suggest high venous pressure edema rather than hypoproteinemic edema. Complete bilateral dullness of the chest and shifting dullness of the abdomen indicate the presence of bilateral pleural effusion and ascites. Edema from high venous pressure is usually caused by right, left, or biventricular cardiac failure. A fixed splitting of the second heart sound suggests an atrial septal defect, which is a rare cause of progressive right heart failure in adults. I recommend checking the patient's thyroid function to investigate the possibility of hypothyroidism, which is a common illness among middle‐aged women and could contribute to her edema as well as hirsutism. The neurological findings suggest a generalized polyneuropathy. The unusual combination of high venous pressure edema and polyneuropathy may indicate a rare multisystem disorder such as amyloidosis. Alternatively, the patient might have developed multiple diseases during the same time period. For instance, diabetic polyneuropathy is the most common cause of polyneuropathy among the middle‐aged. Finally, the differential diagnosis of hirsutism includes ovarian, adrenal, or pituitary sources of hyperandrogenism in addition to hypothyroidism. I would first evaluate for diabetes, thyroid disease, and cardiac disease and would like to see the results of laboratory tests for thyrotropin and plasma glucose as well as chest radiography and electrocardiography.
The white‐cell count was 5400/mm3 with a normal differential. Hemoglobin was 10.7 g/dL with normal red‐cell indices, and the platelet count was 276,000/mm3. The erythrocyte sedimentation rate was 29 mm/hour. Other laboratory tests revealed the following values: total protein, 6.2 g/dL; albumin, 3.3 g/dL; blood urea nitrogen, 12 mg/dL; creatinine, 0.7 mg/dL; aspartate aminotransferase, 6 U/L; alanine aminotransferase, 2 U/L; lactate dehydrogenase, 96 U/L; alkaline phosphatase, 115 U/L; creatine phosphokinase, 60 U/L; total bilirubin, 0.9 mg/dL; glucose, 96 mg/dL; hemoglobin A1c, 4.6%; total cholesterol, 111 mg/dL; and thyrotropin, 6.32 mIU/mL (normal range, 0.50‐5.00 mIU/mL). Serum free thyroxine, triiodothyronine, and urine testosterone were normal. Serum dehydroepiandrosterone sulfate was mildly elevated for her age (864 ng/mL: normal range, 180‐750 ng/mL). Serological studies for human immunodeficiency virus, human T‐lymphotrophic virus type 1, and syphilis were negative. Urinalysis was weakly positive for protein but negative for casts and occult blood. The stool was negative for occult blood.
A chest radiograph showed bilateral pleural effusions. Computed tomography demonstrated bilateral pleural effusions, ascites, mild hepatomegaly, and small, multiple, mediastinal lymph nodes. Her electrocardiogram was normal. A transesophageal echocardiogram with agitated saline contrast demonstrated normal ventricular systolic and diastolic function and no atrial septal defect. The inferior vena cava did not collapse with inspiration, and there was no evidence of infiltrative cardiomyopathy.
These laboratory results rule out diabetes as the cause of the polyneuropathy. The subclinical hypothyroidism would not explain profound edema and hirsutism. A serum albumin level of 3.3 g/dL confirms high venous pressure edema rather than hypoproteinemic edema. Normochromic, normocytic anemia and a mildly elevated sedimentation rate point to a chronic illness or inflammatory state. The mediastinal lymphadenopathy may reflect congestion as a result of the high venous pressure or reflect a systemic disease involving lymph nodes. Normal ventricular function with high venous pressure is suggestive of heart failure from diastolic dysfunction, although the patient does not have risk factors for diastolic dysfunction, such as hypertension, and has no other echocardiographic features of diastolic impairment. The combination of hyperandrogenism and neuropathy points to a systemic process, such as a paraneoplastic syndrome. I would next investigate the source of the excess androgens.
Because serum dehydroepiandrosterone sulfate was mildly elevated, I‐131 aldosterol scintigraphy was performed, and it was negative. Electromyography showed a pattern of generalized sensorimotor polyneuropathy.
At this point, it appears that cardiac, endocrine, hepatic, and renal diseases have been largely ruled out as a cause of her symptoms. Reframing and unifying the important clinical problems for this patient may be useful in resolving this diagnostic puzzle. They include (1) systemic high venous pressure edema; (2) generalized sensorimotor polyneuropathy; (3) hirsutism; (4) normocytic, normochromic anemia; (5) an elevated erythrocyte sedimentation rate; (6) mediastinal lymphadenopathy; and (7) subclinical hypothyroidism. At this point, I cannot unify these pieces of information into a single diagnosis. I would search the medical literature, focusing on these terms.
A general internist consultant performed MEDLINE and Google Scholar searches using the key words edema, polyneuropathy, and hirsutism. This search suggested the diagnosis of Crow‐Fukase syndrome, also known as POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) syndrome. Subsequent evaluations were performed. First, serum protein electrophoresis revealed the presence of monoclonal proteins, although hypergammaglobulinemia was not present. Second, a bone marrow examination demonstrated increased abnormal plasma cell proliferation (7%), although a radiographic skeletal survey found no lesions suggestive of plasmacytoma. Third, cerebrospinal fluid analysis showed normal cell counts but increased protein concentration (202 mg/dL). Fourth, a blood sample referred to an outside laboratory demonstrated elevated levels of vascular endothelial growth factor (3902 pg/mL: normal range, 150‐500 pg/mL). On the basis of these findings, the diagnosis of POEMS syndrome was made. After oral prednisolone (40 mg/day) was initiated, the systemic edema improved gradually, and she did well during the 2‐year follow‐up period.
Commentary
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder first described by Crow in 1956.1, 2 It is characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes, as indicated by the acronym. The diagnosis of POEMS syndrome is difficult as this syndrome is rare and requires high clinical suspicion. According to a nationwide cross‐sectional survey in Japan, the prevalence of POEMS syndrome is very low (about 3 patients per 1,000,000 persons),3 and its prevalence in Western countries is considered even lower than that in Japan. The average age at onset is around 45 to 50 years old, and men are twice as likely to have this syndrome as women.46 Table 1 shows the diagnostic criteria of POEMS syndrome, based on research by Dispenzieri and others at the Mayo Clinic, and Table 2 presents the relative frequency of these clinical features.6, 7 The initial symptomatology generally includes polyneuropathy, skin changes, and generalized edema, which are nonspecific symptoms, as are other well‐recognized associated conditions such as clubbing, weight loss, thrombocytosis, polycythemia, and hyperhidrosis. Thus, it is important to consider this syndrome when one is facing an undiagnosed illness involving multiple organ systems and to distinguish it from other conditions such as multiple myeloma, amyloidosis, and monoclonal gammopathy of undetermined significance. Vascular endothelial growth factor is thought to be involved in the edema of POEMS syndrome, as massive release from aggregated platelets increases vascular permeability and venous pressure.710
| |
| Major criteria | Polyneuropathy |
| Monoclonal plasma cell‐proliferative disorder | |
| Minor criteria | Sclerotic bone lesions |
| Castleman disease | |
| Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy) | |
| Edema (peripheral edema, pleural effusion, or ascites) | |
| Endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, or pancreatic) | |
| Skin changes (hyperpigmentation, hirsutism, plethora, hemangiomata, and white nails) | |
| Papilledema | |
| Characteristic | % |
|---|---|
| |
| Peripheral neuropathy | 100 |
| Monoclonal plasma cell dyscrasia | 100 |
| Sclerotic bone lesions | 97 |
| Endocrinopathy | 71 |
| Skin changes | 68 |
| Organomegaly | 46 |
| Extravascular volume overload | 39 |
| Papilledema | 29 |
| Castleman disease | 11 |
Data regarding treatment and survival are largely observational. Overall mean survival from diagnosis in the 2003 Dispenzieri cohort was 13.7 years, with death often due to infection or cardiorespiratory failure.6 When a solitary plasmacytoma or osteosclerotic myeloma is present, radiation to the lesion can often lead to clinical remission. Other treatment options include alkylating agents and/or high‐dose chemotherapy with peripheral stem‐cell transplantation, corticosteroids, and supportive care.7
Clinicians frequently use the internet to aid in the clinical decision process. In a survey of the Royal New Zealand College of General Practitioners,11 half reported that they used the Internet to search for clinical information. Two well‐known resources are MEDLINE, which contains over 11 million references dating back to the 1960s, and internet search engines such as Google (and a more recent product, Google Scholar, which attempts to sort search results by including factors such as the author, the publication in which the article appears, and how often the article has been cited).
MEDLINE searches a well‐defined set of journals and uses the Medical Subject Headings (MeSH) vocabulary, which consists of sets of descriptive terms organized in a hierarchical structure to allow searching with various levels of specificity. For instance, entering the term heart attack will map to the MeSH term myocardial infarction and will also include more specific terms such as myocardial stunning and cardiogenic shock.
Google, in comparison, explores resources beyond journals without any clear boundary to its scope, and its advanced search functions can be occasionally unreliable. For instance, search results are occasionally marred by outdated citation information and may include materials that are not truly scholarly. However, search engines can search through the actual text of manuscripts and access the gray literature, which includes open‐source material that is usually original but not widely distributed or often easily available, such as technical reports and dissertations. A direct study comparing the results of searches in PubMed (one of the MEDLINE search engines) and Google Scholar is difficult, but the critical characteristics of each can be compared and contrasted (Table 3).
| Google Scholar | PubMed |
|---|---|
| 1. Database selection is clumped under subject areas, and it cannot be searched with unique identifiers: Con | 1. It allows one to choose a database at the outset and can search with a unique identifier (PubMed identifier): Pro |
| 2. Results cannot be filtered (ie, it does not allow multiple article selection): Con | 2. The single citation matcher allows retrieval of articles with pieces of information: Pro |
| 3. A search for related articles or similar pages is not available: Con | 3. It allows article selection by checkbox to reduce the number of articles relevant to the search query and to append the filter to search box: Pro |
| 4. It allows one to search by without words to exclude unwanted and confusing retrieved data: Pro | 4. It provides unique identifier (PubMed identifier) for each retrieved article for easy communicability: Pro |
| 5. It allows one to search a single journal/publication of interest: Pro | 5. Search are limited to journals only; it does not include the grey area of literature: Con |
| 6. Initial search results are those articles that are most cited by journals that themselves are the most cited: Pro | 6. It lists search results in chronological order and not by relevance: Con |
Internet searches may also suggest diagnoses from a compilation of clinical features, such as in this case. To be successful, such a search must complement the cognitive process; a search engine cannot completely replace clinical judgment. Clinicians must be able to identify salient clinical features and generate high‐yield search terms and then exercise skill in sifting through the citations to arrive at the appropriate diagnosis. A recent study found that Google searches revealed the correct diagnosis in 58% of the case records of the New England Journal of Medicine,12 although each search query resulted in many results, which then had to be manually reviewed for appropriateness within the case's context.
Like a traditional diagnostic test, a search can be described by sensitivity, specificity, and the number of articles needed to read.13 For example, in a study comparing the performance of search strategies to identify clinical practice guidelines in Google Scholar and SUMSearch (another freely accessible search engine), using the term guideline yielded the highest sensitivity, and using the term practice guideline generated the highest specificity and the lowest number of articles needed to read (Table 4).14
| Search Strategy | Sensitivity (%) | Specificity (%) | NNR |
|---|---|---|---|
| |||
| SUMSearch | |||
| Guideline* | 81.51 (74.5388.49) | 74.29 (72.6475.94) | 8.18 (6.9010.05) |
| Recommendation* | 60.50 (51.7269.28) | 76.28 (74.6777.89) | 9.93 (8.1412.72) |
| Practice guideline* | 40.34 (31.5249.16) | 89.45 (88.2990.61) | 6.96 (5.529.43) |
| Google Scholar | |||
| Guideline/s | 31.93 (23.5640.30) | 78.05 (76.5079.60) | 16.67 (12.7624.04) |
| Recommendation/s | 8.40 (3.4213.38) | 92.11 (91.0993.13) | 22.42 (13.9756.82) |
| Practice guideline/s | 11.76 (5.9817.54) | 95.72 (94.9696.48) | 9.29 (6.2118.38) |
Although there are several other popular hosts of web‐based search engines, a more robust decision‐support program may help physicians more efficiently consider relevant diagnoses. One program, named Isabel, has been developed through the indexing of a database of more than 11,000 diseases according to word patterns in journal articles associated with each disease, and it is updated as new and relevant articles emerge. One recent study demonstrated that the correct diagnosis was made in 48 of 50 cases (96%) with specific, key findings as search terms but in only 37 of the same 50 cases (74%) if the entire case history was simply pasted in, again emphasizing the importance of specific search terms.15
POEMS syndrome is a rare entity occasionally seen in middle‐aged individuals and marked by a multitude of nonspecific findings, particularly polyneuropathy and plasma cell dyscrasia. In this case, the diagnostic test was an internet search based on the most prominent clinical symptoms. Such a strategy can provide a powerful addition to traditional literature and MEDLINE resources. However, the efficiency of this process is heavily dependent on the quality of the search strategy and, therefore, the cognitive faculties of the treating physician to avoid the predictable shortcoming of low specificity. Garbage in, garbage out still applies whether the computer in question is the human mind or the desktop PC.
Teaching Points
-
POEMS syndrome, also known as Crow‐Fukase syndrome, is a rare multisystem disorder characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes.
-
Internet‐based searches, including Google and MEDLINE, are being used more frequently because they are widely available, quick, and freely accessed.
-
Internet searches appear most useful as adjuncts to PubMed and clinical reasoning in identifying case reports when a well‐constructed collection of symptoms and signs is used for searches.
- .Peripheral neuritis in myelomatosis.Br Med J.1956;2(4996):802–804.
- ,,,,,.Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature.Medicine (Baltimore).1980;59(4):311–322.
- .Nationwide Epidemiologic Survey of Crow‐Fukase Syndrome in 2004.Tokyo, Japan:Japanese Ministry of Health and Welfare Government Report, 2004.
- ,,, et al.The Crow‐Fukase syndrome: a study of 102 cases in Japan.Neurology.1984;34(6):712–720.
- ,,.POEMS syndrome: a study of 25 cases and a review of the literature. French Study Group on POEMS Syndrome.Am J Med.1994;97(6):543–553.
- ,,, et al.POEMS syndrome: definitions and long‐term outcome.Blood.2003;101(7):2496–2506.
- .POEMS syndrome.Hematology.2005;1(1):360–367.
- ,,,,.Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome.Lancet.1996;347(9002):702.
- ,.Assessment of hypoproteinaemic oedema: a simple physical sign.Br Med J.1978;1(6117):890–891.
- ,,, et al.Ratio of serum vascular endothelial growth factor to platelet count correlates with disease activity in a patient with POEMS syndrome.Eur J Intern Med.2002;13(1):70–74.
- .In search of evidence: family practitioners' use of the Internet for clinical information.J Med Libr Assoc.2002;90(4):370–379.
- ,.Googling for a diagnosis—use of Google as a diagnostic aid: internet based study.BMJ.2006;333(7579):1143–5114.
- ,,.The number needed to read—a new measure of journal value.Health Info Libr J.2005;22(2):81–82.
- ,,,.Developing search strategies for clinical practice guidelines in SUMSearch and Google Scholar and assessing their retrieval performance.BMC Med Res Methodol.2007;7:28.
- ,.Performance of a web‐based clinical diagnosis support system for internists.J Gen Intern Med.2008;23(suppl 1):37–40.
- .Peripheral neuritis in myelomatosis.Br Med J.1956;2(4996):802–804.
- ,,,,,.Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature.Medicine (Baltimore).1980;59(4):311–322.
- .Nationwide Epidemiologic Survey of Crow‐Fukase Syndrome in 2004.Tokyo, Japan:Japanese Ministry of Health and Welfare Government Report, 2004.
- ,,, et al.The Crow‐Fukase syndrome: a study of 102 cases in Japan.Neurology.1984;34(6):712–720.
- ,,.POEMS syndrome: a study of 25 cases and a review of the literature. French Study Group on POEMS Syndrome.Am J Med.1994;97(6):543–553.
- ,,, et al.POEMS syndrome: definitions and long‐term outcome.Blood.2003;101(7):2496–2506.
- .POEMS syndrome.Hematology.2005;1(1):360–367.
- ,,,,.Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome.Lancet.1996;347(9002):702.
- ,.Assessment of hypoproteinaemic oedema: a simple physical sign.Br Med J.1978;1(6117):890–891.
- ,,, et al.Ratio of serum vascular endothelial growth factor to platelet count correlates with disease activity in a patient with POEMS syndrome.Eur J Intern Med.2002;13(1):70–74.
- .In search of evidence: family practitioners' use of the Internet for clinical information.J Med Libr Assoc.2002;90(4):370–379.
- ,.Googling for a diagnosis—use of Google as a diagnostic aid: internet based study.BMJ.2006;333(7579):1143–5114.
- ,,.The number needed to read—a new measure of journal value.Health Info Libr J.2005;22(2):81–82.
- ,,,.Developing search strategies for clinical practice guidelines in SUMSearch and Google Scholar and assessing their retrieval performance.BMC Med Res Methodol.2007;7:28.
- ,.Performance of a web‐based clinical diagnosis support system for internists.J Gen Intern Med.2008;23(suppl 1):37–40.
Genesis and exodus of the healthcare industry
He looked upon the earth so filled with misery and pox
On Cro‐Magnon Neurosurgeons taking tumors out with rocks
With the blood banks run by leeches and their pterodactyl nursing
And observed This can't be healthcare these mere creatures are rehearsing
What shall we do when their lifespan will exceed eleven years?
When they no longer drink from toilet pits or make hearts from used pig ears?
There will need to be a better way to care for newer ills
A time when broadband wireless will be cheaper than their pills
He came up with a brilliant plan to revolutionize the health
To advance all medical outcomes and thereby spread the wealth
But for some strange combination of wisdom, luck, and quirk
He devised sufficient stakeholders to ensure this could not work
So a King might hire a knight to wipe out enemies with his lance
Then buy a plan to pay the cost of repairing his chain mail pants
Then along will come men with crosses of Blue who can manage that so much smarter
By inventing rules that convert poor fools from heroic docs to martyrs
He made tiny things that hide in meat and cause nasty cramps and rashes
That leave only the fittest alive to run in the royal 50 yard dashes
He made plants with spikes and purple leaves that can make one very sick
Then companies who turn green goop to gold that can flow thru a needle stick
He made medical schools to teach more tools, taking 10 years from students' lives
Then ruined careers with malpractice fears if they forget to wash their knives.
He made men whose pockets are filled with stuff from frivolous medical suits
When the experts forget the proper dosing of Peruvian medicinal fruits
He made routine birth a hazardous game between midwife, mom, and fetus
He made people who dress in masks and gloves to bravely retrieve and greet us
Then if anything goes wrong because one more time he throws snake eyes on the dice
He made lawyers to ensure that at least someone benefits while everyone else paid the price
Then along came the buildings with gadgets and learning, to find things we can't hope to fix
And those who get paid to know how NOT to pay the providers of care to the sick
He made organized giants that make tablets and gizmos from the minds of the cream of the crop
And made multiple races with all different faces whose subjective complaints will not stop
But alas came the gadgets, the photons and diodes, the software, the web and the data
Then the standards, the knowledge bases, multiuser interfaces, all in perpetual BETA
To automate the arcane, declare real what is feigned, and make INPUT like losing a toe
Then the last fatal strawhe made privacy laws to ensure they can't share what they know
Oh what have I done, this is really no fun, they now live to one hundred and thirty
But there's no more MDs and the few with degrees refuse to get their hands dirty
Next time when I try to take research to practice I'll start with a real I.O.M.
Evidence galore, so when we screw up once more I can put all the blame right on them
He looked upon the earth so filled with misery and pox
On Cro‐Magnon Neurosurgeons taking tumors out with rocks
With the blood banks run by leeches and their pterodactyl nursing
And observed This can't be healthcare these mere creatures are rehearsing
What shall we do when their lifespan will exceed eleven years?
When they no longer drink from toilet pits or make hearts from used pig ears?
There will need to be a better way to care for newer ills
A time when broadband wireless will be cheaper than their pills
He came up with a brilliant plan to revolutionize the health
To advance all medical outcomes and thereby spread the wealth
But for some strange combination of wisdom, luck, and quirk
He devised sufficient stakeholders to ensure this could not work
So a King might hire a knight to wipe out enemies with his lance
Then buy a plan to pay the cost of repairing his chain mail pants
Then along will come men with crosses of Blue who can manage that so much smarter
By inventing rules that convert poor fools from heroic docs to martyrs
He made tiny things that hide in meat and cause nasty cramps and rashes
That leave only the fittest alive to run in the royal 50 yard dashes
He made plants with spikes and purple leaves that can make one very sick
Then companies who turn green goop to gold that can flow thru a needle stick
He made medical schools to teach more tools, taking 10 years from students' lives
Then ruined careers with malpractice fears if they forget to wash their knives.
He made men whose pockets are filled with stuff from frivolous medical suits
When the experts forget the proper dosing of Peruvian medicinal fruits
He made routine birth a hazardous game between midwife, mom, and fetus
He made people who dress in masks and gloves to bravely retrieve and greet us
Then if anything goes wrong because one more time he throws snake eyes on the dice
He made lawyers to ensure that at least someone benefits while everyone else paid the price
Then along came the buildings with gadgets and learning, to find things we can't hope to fix
And those who get paid to know how NOT to pay the providers of care to the sick
He made organized giants that make tablets and gizmos from the minds of the cream of the crop
And made multiple races with all different faces whose subjective complaints will not stop
But alas came the gadgets, the photons and diodes, the software, the web and the data
Then the standards, the knowledge bases, multiuser interfaces, all in perpetual BETA
To automate the arcane, declare real what is feigned, and make INPUT like losing a toe
Then the last fatal strawhe made privacy laws to ensure they can't share what they know
Oh what have I done, this is really no fun, they now live to one hundred and thirty
But there's no more MDs and the few with degrees refuse to get their hands dirty
Next time when I try to take research to practice I'll start with a real I.O.M.
Evidence galore, so when we screw up once more I can put all the blame right on them
He looked upon the earth so filled with misery and pox
On Cro‐Magnon Neurosurgeons taking tumors out with rocks
With the blood banks run by leeches and their pterodactyl nursing
And observed This can't be healthcare these mere creatures are rehearsing
What shall we do when their lifespan will exceed eleven years?
When they no longer drink from toilet pits or make hearts from used pig ears?
There will need to be a better way to care for newer ills
A time when broadband wireless will be cheaper than their pills
He came up with a brilliant plan to revolutionize the health
To advance all medical outcomes and thereby spread the wealth
But for some strange combination of wisdom, luck, and quirk
He devised sufficient stakeholders to ensure this could not work
So a King might hire a knight to wipe out enemies with his lance
Then buy a plan to pay the cost of repairing his chain mail pants
Then along will come men with crosses of Blue who can manage that so much smarter
By inventing rules that convert poor fools from heroic docs to martyrs
He made tiny things that hide in meat and cause nasty cramps and rashes
That leave only the fittest alive to run in the royal 50 yard dashes
He made plants with spikes and purple leaves that can make one very sick
Then companies who turn green goop to gold that can flow thru a needle stick
He made medical schools to teach more tools, taking 10 years from students' lives
Then ruined careers with malpractice fears if they forget to wash their knives.
He made men whose pockets are filled with stuff from frivolous medical suits
When the experts forget the proper dosing of Peruvian medicinal fruits
He made routine birth a hazardous game between midwife, mom, and fetus
He made people who dress in masks and gloves to bravely retrieve and greet us
Then if anything goes wrong because one more time he throws snake eyes on the dice
He made lawyers to ensure that at least someone benefits while everyone else paid the price
Then along came the buildings with gadgets and learning, to find things we can't hope to fix
And those who get paid to know how NOT to pay the providers of care to the sick
He made organized giants that make tablets and gizmos from the minds of the cream of the crop
And made multiple races with all different faces whose subjective complaints will not stop
But alas came the gadgets, the photons and diodes, the software, the web and the data
Then the standards, the knowledge bases, multiuser interfaces, all in perpetual BETA
To automate the arcane, declare real what is feigned, and make INPUT like losing a toe
Then the last fatal strawhe made privacy laws to ensure they can't share what they know
Oh what have I done, this is really no fun, they now live to one hundred and thirty
But there's no more MDs and the few with degrees refuse to get their hands dirty
Next time when I try to take research to practice I'll start with a real I.O.M.
Evidence galore, so when we screw up once more I can put all the blame right on them
Rapid Response: A QI Conundrum
Many in‐hospital cardiac arrests and other adverse events are heralded by warning signs that are evident in the preceding 6 to 8 hours.1 By promptly intervening before further deterioration occurs, rapid response teams (RRTs) are designed to decrease unexpected intensive care unit (ICU) transfers, cardiac arrests, and inpatient mortality. While implementing RRTs is 1 of the 6 initiatives recommended by the Institute for Healthcare Improvement,2 data supporting their effectiveness is equivocal.3, 4
In October 2006, at Denver Health Medical Center, an academic, safety net hospital, we initiated a rapid response systemclinical triggers program (RRS‐CTP).5 In our RRS‐CTP, an abrupt change in patient status (Figure 1) triggers a mandatory call by the patient's nurse to the primary team, which is then required to perform an immediate bedside evaluation. By incorporating the primary team into the RRT‐CTP, we sought to preserve as much continuity of care as possible. Also, since the same house staff compose our cardiopulmonary arrest or cor team, and staff the ICUs and non‐ICU hospital wards, we did not feel that creating a separate RRT was an efficient use of resources. Our nurses have undergone extensive education about the necessity of a prompt bedside evaluation and have been instructed and empowered to escalate concerns to senior physicians if needed. We present a case that illustrates challenges to both implementing an RRS and measuring its potential benefits.
Case
A 59‐year‐old woman with a history of bipolar mood disorder was admitted for altered mental status. At presentation, she had signs of acute mania with normal vital signs. After initial laboratory workup, her altered mental status was felt to be multifactorial due to urinary tract infection, hypernatremia (attributed to lithium‐induced nephrogenic diabetes insipidus), and acute mania (attributed to medication discontinuation). Because she was slow to recover from the acute mania, her hospital stay was prolonged. From admission, the patient was treated with heparin 5000 units subcutaneously twice daily for venous thromboembolism prophylaxis.
On hospital day 7, at 21:32, the patient was noted to have asymptomatic tachycardia at 149 beats per minute and a new oxygen requirement of 3 L/minute. The cross‐cover team was called; however, although criteria were met, the RRS‐CTP was not activated and a bedside evaluation was not performed. A chest X‐ray was found to be normal and, with the exception of the oxygen requirement, her vital signs normalized by 23:45. No further diagnostic testing was performed at the time.
The next morning, at 11:58, the patient was found to have a blood pressure of 60/40 mmHg and heart rate of 42 beats per minute. The RRS‐CTP was activated. The primary team arrived at the bedside at 12:00 and found the patient to be alert, oriented, and without complaints. Her respiratory rate was 30/minute, and her oxygen saturation was 86% on 3 L/minute. An arterial blood gas analysis demonstrated acute respiratory alkalosis with hypoxemia and an electrocardiogram showed sinus tachycardia with a new S1Q3T3 pattern. A computed tomography angiogram revealed a large, nearly occlusive pulmonary embolus (PE) filling an enlarged right pulmonary artery, as well as thrombus within the left main pulmonary artery. She was transferred to the medical ICU and alteplase was administered. The patient survived and was discharged in good clinical condition.
Discussion
Despite the strong theoretical benefit of the RRT concept, a recent review by Ranji et al.4 concluded that RRTs had not yet been shown to improve patient outcomes. In contrast to dedicated RRTs, this case illustrates a different type of RRS that was designed to address abrupt changes in patient status, while maintaining continuity of care and efficiently utilizing resources.
If one considers an RRS to have both afferent (criteria recognition) and efferent (RRT or primary team response) limbs, the afferent limb must be consistently activated in order to obtain the efferent limb's response.6 The greatest opportunities to improve RRSs are thought to lie in the afferent limb.3 Our RRS‐CTP was not triggered in 1 of 2 instances in which criteria for mandatory initiation of the system were met. This is consistent with the findings of the Medical Early Response Intervention and Therapy (MERIT) trial, in which RRTs were called in only 41% of the patients meeting criteria and subsequently having adverse events,7 and with the ongoing monitoring of the use of the system at our hospital. Had the cross‐covering team seen the patient at the bedside initially, the PE might have been diagnosed while the patient was hemodynamically stable, giving the patient nearly a 3‐fold lower relative mortality.8 When the RRS‐CTP was activated, a prompt bedside evaluation occurred, allowing for lytic therapy to be administered before cardiopulmonary arrest (attendant mortality of 90%).9
While rapid response criteria were originally based upon published sensitivity analyses, more recent studies suggest that these criteria lack diagnostic accuracy. As demonstrated by Cretikos et al,10 to reach a sensitivity of 70%, the corresponding specificity would be only 86%. Given that the prevalence of adverse events in the MERIT trial was only 0.6%, the resulting positive predictive value (PPV) of rapid response call criteria is 3%. Accordingly, 33 calls would be needed to prevent 1 unplanned ICU transfer, cardiac arrest, or death. Nurses' attempts to minimize false‐positive calls may help explain the low call rates for patients meeting RRT criteria. The 2 avenues to increase the PPV of criteria are:
-
Increase the prevalence of disease in the population screened by risk factor stratification.
-
Increase the specificity of the call criteria, which has been limited by the associated decrease in sensitivity.10
Regarding the efferent response limb of RRS, our case demonstrates that the primary team (rather than a separate group of caregivers), when alerted appropriately, can effectively respond to critical changes in patient status. Accordingly, our data show that since the inception of the program, cardiopulmonary arrests have decreased from a mean of 4.1 per month to 2.3 per month (P = 0.03).
Many clinical trials of RRTs would not capture the success demonstrated in this case. For example, due to the low prevalence of events, the MERIT trial used a composite endpoint that included unplanned ICU transfers, cardiac arrests, and mortality. Because our patient still required an unplanned ICU transfer after being evaluated by the responding team, she would have been counted as a system failure.
Conclusion
While local needs should inform the type of RRS implemented, this case illustrates one of the major obstacles ubiquitous to RRS implementation: failure of system activation. With appropriate activation, an RRS‐CTP can meet RRS goals while maintaining continuity of care and maximizing existing resources. This case also illustrates the difficulty of achieving a statistically relevant outcome, while demonstrating the potential benefits of evolving RRSs.
- ,,,,.Rapid response teams—do they make a difference.Dimens Crit Care Nurs.2007;26(6):253–260.
- Institute for Healthcare Improvement. 5 Million Lives Campaign. Available at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId=1IHI. Accessed February2009.
- .The rapid response team paradox: why doesn't anyone call for help?Crit Care Med.2008;36(2):634–636.
- ,,,,.Effects of rapid response systems on clinical outcomes: review and meta‐analyses.J Hosp Med.2007;2:422–432.
- ,,.Clinical triggers and rapid response escalation criteria.Patient Saf Qual Healthc.2007;4(2):12–13. Available at: http://www.psqh.com/archives.html. Accessed February 2009.
- ,,, et al.Use of medical emergency team responses to reduce hospital cardiopulmonary arrest.Qual Saf Health Care.2004;13:251–254.
- MERIT Study Investigators.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,.Acute pulmonary embolism: clinical outcomes in the international cooperative pulmonary embolism registry (ICOPER).Lancet.1999;353(9162):1386–1389.
- ,,,.Early predictors of mortality for hospitalized patients suffering cardiopulmonary arrest.Chest.1990;97(2):413–419.
- ,,,,,.The objective medical emergency team activation criteria: a case–control study.Resuscitation.2007;73:62–72.
Many in‐hospital cardiac arrests and other adverse events are heralded by warning signs that are evident in the preceding 6 to 8 hours.1 By promptly intervening before further deterioration occurs, rapid response teams (RRTs) are designed to decrease unexpected intensive care unit (ICU) transfers, cardiac arrests, and inpatient mortality. While implementing RRTs is 1 of the 6 initiatives recommended by the Institute for Healthcare Improvement,2 data supporting their effectiveness is equivocal.3, 4
In October 2006, at Denver Health Medical Center, an academic, safety net hospital, we initiated a rapid response systemclinical triggers program (RRS‐CTP).5 In our RRS‐CTP, an abrupt change in patient status (Figure 1) triggers a mandatory call by the patient's nurse to the primary team, which is then required to perform an immediate bedside evaluation. By incorporating the primary team into the RRT‐CTP, we sought to preserve as much continuity of care as possible. Also, since the same house staff compose our cardiopulmonary arrest or cor team, and staff the ICUs and non‐ICU hospital wards, we did not feel that creating a separate RRT was an efficient use of resources. Our nurses have undergone extensive education about the necessity of a prompt bedside evaluation and have been instructed and empowered to escalate concerns to senior physicians if needed. We present a case that illustrates challenges to both implementing an RRS and measuring its potential benefits.
Case
A 59‐year‐old woman with a history of bipolar mood disorder was admitted for altered mental status. At presentation, she had signs of acute mania with normal vital signs. After initial laboratory workup, her altered mental status was felt to be multifactorial due to urinary tract infection, hypernatremia (attributed to lithium‐induced nephrogenic diabetes insipidus), and acute mania (attributed to medication discontinuation). Because she was slow to recover from the acute mania, her hospital stay was prolonged. From admission, the patient was treated with heparin 5000 units subcutaneously twice daily for venous thromboembolism prophylaxis.
On hospital day 7, at 21:32, the patient was noted to have asymptomatic tachycardia at 149 beats per minute and a new oxygen requirement of 3 L/minute. The cross‐cover team was called; however, although criteria were met, the RRS‐CTP was not activated and a bedside evaluation was not performed. A chest X‐ray was found to be normal and, with the exception of the oxygen requirement, her vital signs normalized by 23:45. No further diagnostic testing was performed at the time.
The next morning, at 11:58, the patient was found to have a blood pressure of 60/40 mmHg and heart rate of 42 beats per minute. The RRS‐CTP was activated. The primary team arrived at the bedside at 12:00 and found the patient to be alert, oriented, and without complaints. Her respiratory rate was 30/minute, and her oxygen saturation was 86% on 3 L/minute. An arterial blood gas analysis demonstrated acute respiratory alkalosis with hypoxemia and an electrocardiogram showed sinus tachycardia with a new S1Q3T3 pattern. A computed tomography angiogram revealed a large, nearly occlusive pulmonary embolus (PE) filling an enlarged right pulmonary artery, as well as thrombus within the left main pulmonary artery. She was transferred to the medical ICU and alteplase was administered. The patient survived and was discharged in good clinical condition.
Discussion
Despite the strong theoretical benefit of the RRT concept, a recent review by Ranji et al.4 concluded that RRTs had not yet been shown to improve patient outcomes. In contrast to dedicated RRTs, this case illustrates a different type of RRS that was designed to address abrupt changes in patient status, while maintaining continuity of care and efficiently utilizing resources.
If one considers an RRS to have both afferent (criteria recognition) and efferent (RRT or primary team response) limbs, the afferent limb must be consistently activated in order to obtain the efferent limb's response.6 The greatest opportunities to improve RRSs are thought to lie in the afferent limb.3 Our RRS‐CTP was not triggered in 1 of 2 instances in which criteria for mandatory initiation of the system were met. This is consistent with the findings of the Medical Early Response Intervention and Therapy (MERIT) trial, in which RRTs were called in only 41% of the patients meeting criteria and subsequently having adverse events,7 and with the ongoing monitoring of the use of the system at our hospital. Had the cross‐covering team seen the patient at the bedside initially, the PE might have been diagnosed while the patient was hemodynamically stable, giving the patient nearly a 3‐fold lower relative mortality.8 When the RRS‐CTP was activated, a prompt bedside evaluation occurred, allowing for lytic therapy to be administered before cardiopulmonary arrest (attendant mortality of 90%).9
While rapid response criteria were originally based upon published sensitivity analyses, more recent studies suggest that these criteria lack diagnostic accuracy. As demonstrated by Cretikos et al,10 to reach a sensitivity of 70%, the corresponding specificity would be only 86%. Given that the prevalence of adverse events in the MERIT trial was only 0.6%, the resulting positive predictive value (PPV) of rapid response call criteria is 3%. Accordingly, 33 calls would be needed to prevent 1 unplanned ICU transfer, cardiac arrest, or death. Nurses' attempts to minimize false‐positive calls may help explain the low call rates for patients meeting RRT criteria. The 2 avenues to increase the PPV of criteria are:
-
Increase the prevalence of disease in the population screened by risk factor stratification.
-
Increase the specificity of the call criteria, which has been limited by the associated decrease in sensitivity.10
Regarding the efferent response limb of RRS, our case demonstrates that the primary team (rather than a separate group of caregivers), when alerted appropriately, can effectively respond to critical changes in patient status. Accordingly, our data show that since the inception of the program, cardiopulmonary arrests have decreased from a mean of 4.1 per month to 2.3 per month (P = 0.03).
Many clinical trials of RRTs would not capture the success demonstrated in this case. For example, due to the low prevalence of events, the MERIT trial used a composite endpoint that included unplanned ICU transfers, cardiac arrests, and mortality. Because our patient still required an unplanned ICU transfer after being evaluated by the responding team, she would have been counted as a system failure.
Conclusion
While local needs should inform the type of RRS implemented, this case illustrates one of the major obstacles ubiquitous to RRS implementation: failure of system activation. With appropriate activation, an RRS‐CTP can meet RRS goals while maintaining continuity of care and maximizing existing resources. This case also illustrates the difficulty of achieving a statistically relevant outcome, while demonstrating the potential benefits of evolving RRSs.
Many in‐hospital cardiac arrests and other adverse events are heralded by warning signs that are evident in the preceding 6 to 8 hours.1 By promptly intervening before further deterioration occurs, rapid response teams (RRTs) are designed to decrease unexpected intensive care unit (ICU) transfers, cardiac arrests, and inpatient mortality. While implementing RRTs is 1 of the 6 initiatives recommended by the Institute for Healthcare Improvement,2 data supporting their effectiveness is equivocal.3, 4
In October 2006, at Denver Health Medical Center, an academic, safety net hospital, we initiated a rapid response systemclinical triggers program (RRS‐CTP).5 In our RRS‐CTP, an abrupt change in patient status (Figure 1) triggers a mandatory call by the patient's nurse to the primary team, which is then required to perform an immediate bedside evaluation. By incorporating the primary team into the RRT‐CTP, we sought to preserve as much continuity of care as possible. Also, since the same house staff compose our cardiopulmonary arrest or cor team, and staff the ICUs and non‐ICU hospital wards, we did not feel that creating a separate RRT was an efficient use of resources. Our nurses have undergone extensive education about the necessity of a prompt bedside evaluation and have been instructed and empowered to escalate concerns to senior physicians if needed. We present a case that illustrates challenges to both implementing an RRS and measuring its potential benefits.
Case
A 59‐year‐old woman with a history of bipolar mood disorder was admitted for altered mental status. At presentation, she had signs of acute mania with normal vital signs. After initial laboratory workup, her altered mental status was felt to be multifactorial due to urinary tract infection, hypernatremia (attributed to lithium‐induced nephrogenic diabetes insipidus), and acute mania (attributed to medication discontinuation). Because she was slow to recover from the acute mania, her hospital stay was prolonged. From admission, the patient was treated with heparin 5000 units subcutaneously twice daily for venous thromboembolism prophylaxis.
On hospital day 7, at 21:32, the patient was noted to have asymptomatic tachycardia at 149 beats per minute and a new oxygen requirement of 3 L/minute. The cross‐cover team was called; however, although criteria were met, the RRS‐CTP was not activated and a bedside evaluation was not performed. A chest X‐ray was found to be normal and, with the exception of the oxygen requirement, her vital signs normalized by 23:45. No further diagnostic testing was performed at the time.
The next morning, at 11:58, the patient was found to have a blood pressure of 60/40 mmHg and heart rate of 42 beats per minute. The RRS‐CTP was activated. The primary team arrived at the bedside at 12:00 and found the patient to be alert, oriented, and without complaints. Her respiratory rate was 30/minute, and her oxygen saturation was 86% on 3 L/minute. An arterial blood gas analysis demonstrated acute respiratory alkalosis with hypoxemia and an electrocardiogram showed sinus tachycardia with a new S1Q3T3 pattern. A computed tomography angiogram revealed a large, nearly occlusive pulmonary embolus (PE) filling an enlarged right pulmonary artery, as well as thrombus within the left main pulmonary artery. She was transferred to the medical ICU and alteplase was administered. The patient survived and was discharged in good clinical condition.
Discussion
Despite the strong theoretical benefit of the RRT concept, a recent review by Ranji et al.4 concluded that RRTs had not yet been shown to improve patient outcomes. In contrast to dedicated RRTs, this case illustrates a different type of RRS that was designed to address abrupt changes in patient status, while maintaining continuity of care and efficiently utilizing resources.
If one considers an RRS to have both afferent (criteria recognition) and efferent (RRT or primary team response) limbs, the afferent limb must be consistently activated in order to obtain the efferent limb's response.6 The greatest opportunities to improve RRSs are thought to lie in the afferent limb.3 Our RRS‐CTP was not triggered in 1 of 2 instances in which criteria for mandatory initiation of the system were met. This is consistent with the findings of the Medical Early Response Intervention and Therapy (MERIT) trial, in which RRTs were called in only 41% of the patients meeting criteria and subsequently having adverse events,7 and with the ongoing monitoring of the use of the system at our hospital. Had the cross‐covering team seen the patient at the bedside initially, the PE might have been diagnosed while the patient was hemodynamically stable, giving the patient nearly a 3‐fold lower relative mortality.8 When the RRS‐CTP was activated, a prompt bedside evaluation occurred, allowing for lytic therapy to be administered before cardiopulmonary arrest (attendant mortality of 90%).9
While rapid response criteria were originally based upon published sensitivity analyses, more recent studies suggest that these criteria lack diagnostic accuracy. As demonstrated by Cretikos et al,10 to reach a sensitivity of 70%, the corresponding specificity would be only 86%. Given that the prevalence of adverse events in the MERIT trial was only 0.6%, the resulting positive predictive value (PPV) of rapid response call criteria is 3%. Accordingly, 33 calls would be needed to prevent 1 unplanned ICU transfer, cardiac arrest, or death. Nurses' attempts to minimize false‐positive calls may help explain the low call rates for patients meeting RRT criteria. The 2 avenues to increase the PPV of criteria are:
-
Increase the prevalence of disease in the population screened by risk factor stratification.
-
Increase the specificity of the call criteria, which has been limited by the associated decrease in sensitivity.10
Regarding the efferent response limb of RRS, our case demonstrates that the primary team (rather than a separate group of caregivers), when alerted appropriately, can effectively respond to critical changes in patient status. Accordingly, our data show that since the inception of the program, cardiopulmonary arrests have decreased from a mean of 4.1 per month to 2.3 per month (P = 0.03).
Many clinical trials of RRTs would not capture the success demonstrated in this case. For example, due to the low prevalence of events, the MERIT trial used a composite endpoint that included unplanned ICU transfers, cardiac arrests, and mortality. Because our patient still required an unplanned ICU transfer after being evaluated by the responding team, she would have been counted as a system failure.
Conclusion
While local needs should inform the type of RRS implemented, this case illustrates one of the major obstacles ubiquitous to RRS implementation: failure of system activation. With appropriate activation, an RRS‐CTP can meet RRS goals while maintaining continuity of care and maximizing existing resources. This case also illustrates the difficulty of achieving a statistically relevant outcome, while demonstrating the potential benefits of evolving RRSs.
- ,,,,.Rapid response teams—do they make a difference.Dimens Crit Care Nurs.2007;26(6):253–260.
- Institute for Healthcare Improvement. 5 Million Lives Campaign. Available at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId=1IHI. Accessed February2009.
- .The rapid response team paradox: why doesn't anyone call for help?Crit Care Med.2008;36(2):634–636.
- ,,,,.Effects of rapid response systems on clinical outcomes: review and meta‐analyses.J Hosp Med.2007;2:422–432.
- ,,.Clinical triggers and rapid response escalation criteria.Patient Saf Qual Healthc.2007;4(2):12–13. Available at: http://www.psqh.com/archives.html. Accessed February 2009.
- ,,, et al.Use of medical emergency team responses to reduce hospital cardiopulmonary arrest.Qual Saf Health Care.2004;13:251–254.
- MERIT Study Investigators.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,.Acute pulmonary embolism: clinical outcomes in the international cooperative pulmonary embolism registry (ICOPER).Lancet.1999;353(9162):1386–1389.
- ,,,.Early predictors of mortality for hospitalized patients suffering cardiopulmonary arrest.Chest.1990;97(2):413–419.
- ,,,,,.The objective medical emergency team activation criteria: a case–control study.Resuscitation.2007;73:62–72.
- ,,,,.Rapid response teams—do they make a difference.Dimens Crit Care Nurs.2007;26(6):253–260.
- Institute for Healthcare Improvement. 5 Million Lives Campaign. Available at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId=1IHI. Accessed February2009.
- .The rapid response team paradox: why doesn't anyone call for help?Crit Care Med.2008;36(2):634–636.
- ,,,,.Effects of rapid response systems on clinical outcomes: review and meta‐analyses.J Hosp Med.2007;2:422–432.
- ,,.Clinical triggers and rapid response escalation criteria.Patient Saf Qual Healthc.2007;4(2):12–13. Available at: http://www.psqh.com/archives.html. Accessed February 2009.
- ,,, et al.Use of medical emergency team responses to reduce hospital cardiopulmonary arrest.Qual Saf Health Care.2004;13:251–254.
- MERIT Study Investigators.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,.Acute pulmonary embolism: clinical outcomes in the international cooperative pulmonary embolism registry (ICOPER).Lancet.1999;353(9162):1386–1389.
- ,,,.Early predictors of mortality for hospitalized patients suffering cardiopulmonary arrest.Chest.1990;97(2):413–419.
- ,,,,,.The objective medical emergency team activation criteria: a case–control study.Resuscitation.2007;73:62–72.
The Accidental Hospitalist
David Yu, MD, learned early on the value of being flexible. While attending Washington University in St. Louis, he found his calling when he changed his major from economics to biology. When the malpractice insurance crisis forced him to close his private practice, he embraced an opportunity to launch a program devoted to the “newfangled concept” of hospital medicine.
“I’m kind of like the accidental tourist,” says Dr. Yu, medical director of hospitalist services at the 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale. “I didn’t really go to college with the mind-set of being a doctor, and when I became a doctor, there was no such thing as a hospitalist. … I went where the current took me and, fortunately, here I am.”
Question: What prompted the switch from economics to pre-med/biology?
Answer: When I got to the upper-level econ classes, I realized why the economy is the way it is: because nobody can understand how it works. My sister was in medical school. She really liked it and she talked me into it.
Q: You spent nine years in traditional practice. Why did you become a hospitalist?
A: In 2004, my malpractice insurance rate shot up 400% without any active lawsuits, so I had to close my practice. I had the choice of joining another traditional group, or Decatur (Memorial Hospital) was starting a new hospitalist program. To quote “The Godfather,” they made me an offer I couldn’t refuse.
Q: How did your experience in traditional practice prepare you for your role as a hospitalist?
A: I had been surrounded by incredible specialists. I saw how they interacted with me and how they treated my patients. As hospitalists, we are serving our patients, but really our clientele is the physicians we admit for. When I made the switch, I really had an idea of how a hospitalist should serve traditional practice.
Q: What is that service model?
A: It comes down to what I call the three A’s: You have to be available, you have to be able, and you have to be amicable. One of the problems in our field is a lot of hospitalists complain they’re treated like residents. They say they don’t get respect. They feel mistreated. That’s the wrong attitude. You can’t just ask for respect or demand it. You have to develop relationships.
Q: When Decatur’s hospitalist program started, you were on your own. Now there are seven physicians, two physician assistants, and a practice manager. How rewarding has it been to see it grow?
We have to find ways to help hospitalists take more ownership in their patients and their program. ... With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy.
—David Yu, MD, Decatur (Ill.)
Memorial Hospital
A: It’s been very rewarding. I’m honored to have been chosen as a member of Team Hospitalist, and I’m honored to be a committee member for SHM’s Non-Physician Provider Committee. Those are personal honors, but they are reflections on the success of the program. It’s an honor for the entire Decatur Memorial Hospital, and the administration, that a program started four and a half years ago, indirectly, has received national recognition.
Q: You implemented a one-week-on, one-week-off schedule for your hospitalists as a way to decrease signouts. How did that come about?
A: Signouts have been the bane of medical mistakes. Instead of having signouts twice a day, we have one physician on call for that entire week for his or her patients. It’s patient-centric versus schedule-centric. Physicians leave the hospital when their work is done, instead of looking at the clock and waiting to sign out at a certain time like a factory worker. It treats hospitalists not as shift workers but as attending physicians. It gives them due respect that they can manage their own patients responsibly.
Q: Do you think the schedule improves the quality of patient care?
A: The continuity of care is incredible. If you are admitted and discharged between Mondays, you have one hospitalist in charge of your entire case, instead of multiple physicians being on call for you. That increases patient satisfaction, reduces medical errors, and eliminates the need for unnecessary tests when new physicians take over. I’m also a huge believer that scheduling brings out the best and worst in hospitalists.
Q: How does it bring out the best in them?
A: As medical directors, we have to find ways to help hospitalists take more ownership in their patients and their program. If they’re thinking, “My shift is ending and I’m going to be off and I can hand this issue off to the next doctor,” that can have a tremendous effect on the quality of care and the way a hospitalist delivers medicine. With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy. … If something goes wrong or if the ball gets dropped, there’s no one else to blame it on.
Q: You developed a system at Decatur through which patient discharge summaries are sent electronically to primary-care physicians, often before the patient leaves the hospital. Have the primaries been receptive?
A: Absolutely. Communication is the mother’s milk of hospitalists. Some hospitalist programs are very large, they’re very busy, or there’s no incentive for them to do this because they’re the only game in town. But I practice in a mid-size community and I know all of these doctors. My reputation is my bond. I have to provide good service.
Q: What do you enjoy most about your role as a hospitalist?
A: I love solving problems for a patient. I also love how the relationship builds. You introduce yourself to a patient and their family as a hospitalist and they’re thinking, “Who the heck are you?” For a few seconds, it’s like meeting someone on a blind date. And when they’re discharged, they tell you they had a pleasant experience and they appreciate your help. It’s a courtship at a rapid pace.
Q: What do you consider to be your biggest challenge?
A: Recruitment; the administration asking us to take on more responsibilities; burnout. … We’re a typical hospitalist program; I think the problems are pretty universal.
Q: How do you address those challenges?
A: As medical director, you’re always navigating political and personal minefields. It comes back to developing relationships. The only way to earn goodwill is to give and provide service. That’s a problem some hospitalist programs run into. They want to instantly demand respect. You can’t demand it; you have to earn it. Sometimes hospitalists feel dumped on. Those are opportunities … to provide service in a willing and positive way instead of complaining. I’m not saying you have to be a whipping boy, but there are times when you have to give a little to get a little. That’s where the wisdom of the medical director comes in and sets the whole tone.
Q: What’s ahead for the academic side of your career?
A: We’re considering the possibility of starting a family practice fellowship program for attending residents who finish but want to go into the field of hospital medicine and want additional training. It’s not a done deal, but it’s an exciting possibility.
Q: How so?
A: Every medical director says they have a hard time recruiting. One way we can help solve the problem is by producing more hospitalists. We can’t just complain. We have to increase the pool of professionals interested in our model, train them, and get them integrated into our system.
Q: What advice would you give a student who is considering going that route?
A: You have to be a good communicator, you have to enjoy taking care of very sick people, and you have to enjoy solving very complex problems. You can’t just do it for the lifestyle. If you do, you won’t be happy in the long run. If I ask a medical student or resident why they want to be a hospitalist and they say, “I like the one-week-on, one-week-off schedule,” I tell them, “If that’s the reason you’re considering it, you really should reconsider.” TH
Mark Leiser is a freelance writer in New Jersey.
David Yu, MD, learned early on the value of being flexible. While attending Washington University in St. Louis, he found his calling when he changed his major from economics to biology. When the malpractice insurance crisis forced him to close his private practice, he embraced an opportunity to launch a program devoted to the “newfangled concept” of hospital medicine.
“I’m kind of like the accidental tourist,” says Dr. Yu, medical director of hospitalist services at the 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale. “I didn’t really go to college with the mind-set of being a doctor, and when I became a doctor, there was no such thing as a hospitalist. … I went where the current took me and, fortunately, here I am.”
Question: What prompted the switch from economics to pre-med/biology?
Answer: When I got to the upper-level econ classes, I realized why the economy is the way it is: because nobody can understand how it works. My sister was in medical school. She really liked it and she talked me into it.
Q: You spent nine years in traditional practice. Why did you become a hospitalist?
A: In 2004, my malpractice insurance rate shot up 400% without any active lawsuits, so I had to close my practice. I had the choice of joining another traditional group, or Decatur (Memorial Hospital) was starting a new hospitalist program. To quote “The Godfather,” they made me an offer I couldn’t refuse.
Q: How did your experience in traditional practice prepare you for your role as a hospitalist?
A: I had been surrounded by incredible specialists. I saw how they interacted with me and how they treated my patients. As hospitalists, we are serving our patients, but really our clientele is the physicians we admit for. When I made the switch, I really had an idea of how a hospitalist should serve traditional practice.
Q: What is that service model?
A: It comes down to what I call the three A’s: You have to be available, you have to be able, and you have to be amicable. One of the problems in our field is a lot of hospitalists complain they’re treated like residents. They say they don’t get respect. They feel mistreated. That’s the wrong attitude. You can’t just ask for respect or demand it. You have to develop relationships.
Q: When Decatur’s hospitalist program started, you were on your own. Now there are seven physicians, two physician assistants, and a practice manager. How rewarding has it been to see it grow?
We have to find ways to help hospitalists take more ownership in their patients and their program. ... With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy.
—David Yu, MD, Decatur (Ill.)
Memorial Hospital
A: It’s been very rewarding. I’m honored to have been chosen as a member of Team Hospitalist, and I’m honored to be a committee member for SHM’s Non-Physician Provider Committee. Those are personal honors, but they are reflections on the success of the program. It’s an honor for the entire Decatur Memorial Hospital, and the administration, that a program started four and a half years ago, indirectly, has received national recognition.
Q: You implemented a one-week-on, one-week-off schedule for your hospitalists as a way to decrease signouts. How did that come about?
A: Signouts have been the bane of medical mistakes. Instead of having signouts twice a day, we have one physician on call for that entire week for his or her patients. It’s patient-centric versus schedule-centric. Physicians leave the hospital when their work is done, instead of looking at the clock and waiting to sign out at a certain time like a factory worker. It treats hospitalists not as shift workers but as attending physicians. It gives them due respect that they can manage their own patients responsibly.
Q: Do you think the schedule improves the quality of patient care?
A: The continuity of care is incredible. If you are admitted and discharged between Mondays, you have one hospitalist in charge of your entire case, instead of multiple physicians being on call for you. That increases patient satisfaction, reduces medical errors, and eliminates the need for unnecessary tests when new physicians take over. I’m also a huge believer that scheduling brings out the best and worst in hospitalists.
Q: How does it bring out the best in them?
A: As medical directors, we have to find ways to help hospitalists take more ownership in their patients and their program. If they’re thinking, “My shift is ending and I’m going to be off and I can hand this issue off to the next doctor,” that can have a tremendous effect on the quality of care and the way a hospitalist delivers medicine. With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy. … If something goes wrong or if the ball gets dropped, there’s no one else to blame it on.
Q: You developed a system at Decatur through which patient discharge summaries are sent electronically to primary-care physicians, often before the patient leaves the hospital. Have the primaries been receptive?
A: Absolutely. Communication is the mother’s milk of hospitalists. Some hospitalist programs are very large, they’re very busy, or there’s no incentive for them to do this because they’re the only game in town. But I practice in a mid-size community and I know all of these doctors. My reputation is my bond. I have to provide good service.
Q: What do you enjoy most about your role as a hospitalist?
A: I love solving problems for a patient. I also love how the relationship builds. You introduce yourself to a patient and their family as a hospitalist and they’re thinking, “Who the heck are you?” For a few seconds, it’s like meeting someone on a blind date. And when they’re discharged, they tell you they had a pleasant experience and they appreciate your help. It’s a courtship at a rapid pace.
Q: What do you consider to be your biggest challenge?
A: Recruitment; the administration asking us to take on more responsibilities; burnout. … We’re a typical hospitalist program; I think the problems are pretty universal.
Q: How do you address those challenges?
A: As medical director, you’re always navigating political and personal minefields. It comes back to developing relationships. The only way to earn goodwill is to give and provide service. That’s a problem some hospitalist programs run into. They want to instantly demand respect. You can’t demand it; you have to earn it. Sometimes hospitalists feel dumped on. Those are opportunities … to provide service in a willing and positive way instead of complaining. I’m not saying you have to be a whipping boy, but there are times when you have to give a little to get a little. That’s where the wisdom of the medical director comes in and sets the whole tone.
Q: What’s ahead for the academic side of your career?
A: We’re considering the possibility of starting a family practice fellowship program for attending residents who finish but want to go into the field of hospital medicine and want additional training. It’s not a done deal, but it’s an exciting possibility.
Q: How so?
A: Every medical director says they have a hard time recruiting. One way we can help solve the problem is by producing more hospitalists. We can’t just complain. We have to increase the pool of professionals interested in our model, train them, and get them integrated into our system.
Q: What advice would you give a student who is considering going that route?
A: You have to be a good communicator, you have to enjoy taking care of very sick people, and you have to enjoy solving very complex problems. You can’t just do it for the lifestyle. If you do, you won’t be happy in the long run. If I ask a medical student or resident why they want to be a hospitalist and they say, “I like the one-week-on, one-week-off schedule,” I tell them, “If that’s the reason you’re considering it, you really should reconsider.” TH
Mark Leiser is a freelance writer in New Jersey.
David Yu, MD, learned early on the value of being flexible. While attending Washington University in St. Louis, he found his calling when he changed his major from economics to biology. When the malpractice insurance crisis forced him to close his private practice, he embraced an opportunity to launch a program devoted to the “newfangled concept” of hospital medicine.
“I’m kind of like the accidental tourist,” says Dr. Yu, medical director of hospitalist services at the 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale. “I didn’t really go to college with the mind-set of being a doctor, and when I became a doctor, there was no such thing as a hospitalist. … I went where the current took me and, fortunately, here I am.”
Question: What prompted the switch from economics to pre-med/biology?
Answer: When I got to the upper-level econ classes, I realized why the economy is the way it is: because nobody can understand how it works. My sister was in medical school. She really liked it and she talked me into it.
Q: You spent nine years in traditional practice. Why did you become a hospitalist?
A: In 2004, my malpractice insurance rate shot up 400% without any active lawsuits, so I had to close my practice. I had the choice of joining another traditional group, or Decatur (Memorial Hospital) was starting a new hospitalist program. To quote “The Godfather,” they made me an offer I couldn’t refuse.
Q: How did your experience in traditional practice prepare you for your role as a hospitalist?
A: I had been surrounded by incredible specialists. I saw how they interacted with me and how they treated my patients. As hospitalists, we are serving our patients, but really our clientele is the physicians we admit for. When I made the switch, I really had an idea of how a hospitalist should serve traditional practice.
Q: What is that service model?
A: It comes down to what I call the three A’s: You have to be available, you have to be able, and you have to be amicable. One of the problems in our field is a lot of hospitalists complain they’re treated like residents. They say they don’t get respect. They feel mistreated. That’s the wrong attitude. You can’t just ask for respect or demand it. You have to develop relationships.
Q: When Decatur’s hospitalist program started, you were on your own. Now there are seven physicians, two physician assistants, and a practice manager. How rewarding has it been to see it grow?
We have to find ways to help hospitalists take more ownership in their patients and their program. ... With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy.
—David Yu, MD, Decatur (Ill.)
Memorial Hospital
A: It’s been very rewarding. I’m honored to have been chosen as a member of Team Hospitalist, and I’m honored to be a committee member for SHM’s Non-Physician Provider Committee. Those are personal honors, but they are reflections on the success of the program. It’s an honor for the entire Decatur Memorial Hospital, and the administration, that a program started four and a half years ago, indirectly, has received national recognition.
Q: You implemented a one-week-on, one-week-off schedule for your hospitalists as a way to decrease signouts. How did that come about?
A: Signouts have been the bane of medical mistakes. Instead of having signouts twice a day, we have one physician on call for that entire week for his or her patients. It’s patient-centric versus schedule-centric. Physicians leave the hospital when their work is done, instead of looking at the clock and waiting to sign out at a certain time like a factory worker. It treats hospitalists not as shift workers but as attending physicians. It gives them due respect that they can manage their own patients responsibly.
Q: Do you think the schedule improves the quality of patient care?
A: The continuity of care is incredible. If you are admitted and discharged between Mondays, you have one hospitalist in charge of your entire case, instead of multiple physicians being on call for you. That increases patient satisfaction, reduces medical errors, and eliminates the need for unnecessary tests when new physicians take over. I’m also a huge believer that scheduling brings out the best and worst in hospitalists.
Q: How does it bring out the best in them?
A: As medical directors, we have to find ways to help hospitalists take more ownership in their patients and their program. If they’re thinking, “My shift is ending and I’m going to be off and I can hand this issue off to the next doctor,” that can have a tremendous effect on the quality of care and the way a hospitalist delivers medicine. With our schedule, you can’t pawn off your responsibility to the nocturnist or the weekend guy. … If something goes wrong or if the ball gets dropped, there’s no one else to blame it on.
Q: You developed a system at Decatur through which patient discharge summaries are sent electronically to primary-care physicians, often before the patient leaves the hospital. Have the primaries been receptive?
A: Absolutely. Communication is the mother’s milk of hospitalists. Some hospitalist programs are very large, they’re very busy, or there’s no incentive for them to do this because they’re the only game in town. But I practice in a mid-size community and I know all of these doctors. My reputation is my bond. I have to provide good service.
Q: What do you enjoy most about your role as a hospitalist?
A: I love solving problems for a patient. I also love how the relationship builds. You introduce yourself to a patient and their family as a hospitalist and they’re thinking, “Who the heck are you?” For a few seconds, it’s like meeting someone on a blind date. And when they’re discharged, they tell you they had a pleasant experience and they appreciate your help. It’s a courtship at a rapid pace.
Q: What do you consider to be your biggest challenge?
A: Recruitment; the administration asking us to take on more responsibilities; burnout. … We’re a typical hospitalist program; I think the problems are pretty universal.
Q: How do you address those challenges?
A: As medical director, you’re always navigating political and personal minefields. It comes back to developing relationships. The only way to earn goodwill is to give and provide service. That’s a problem some hospitalist programs run into. They want to instantly demand respect. You can’t demand it; you have to earn it. Sometimes hospitalists feel dumped on. Those are opportunities … to provide service in a willing and positive way instead of complaining. I’m not saying you have to be a whipping boy, but there are times when you have to give a little to get a little. That’s where the wisdom of the medical director comes in and sets the whole tone.
Q: What’s ahead for the academic side of your career?
A: We’re considering the possibility of starting a family practice fellowship program for attending residents who finish but want to go into the field of hospital medicine and want additional training. It’s not a done deal, but it’s an exciting possibility.
Q: How so?
A: Every medical director says they have a hard time recruiting. One way we can help solve the problem is by producing more hospitalists. We can’t just complain. We have to increase the pool of professionals interested in our model, train them, and get them integrated into our system.
Q: What advice would you give a student who is considering going that route?
A: You have to be a good communicator, you have to enjoy taking care of very sick people, and you have to enjoy solving very complex problems. You can’t just do it for the lifestyle. If you do, you won’t be happy in the long run. If I ask a medical student or resident why they want to be a hospitalist and they say, “I like the one-week-on, one-week-off schedule,” I tell them, “If that’s the reason you’re considering it, you really should reconsider.” TH
Mark Leiser is a freelance writer in New Jersey.
Palliative-Care Payment
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
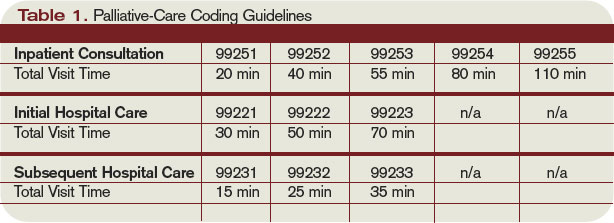
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
A Pivotal Year for Policy
Change is in the air. With a new ad-ministration promising to be a change agent, an overhauled Congress, and a seemingly unanimous national interest in tackling healthcare reform, what changes can hospital medicine expect in 2009?
“I think there’s certainly the political will and interest now,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “We haven’t had enough political will to ‘go big’ until recently. Now that we have it, the trillion-dollar question is where the money will come from.”
With that in mind, let’s explore three of the hottest healthcare issues:
Comprehensive Healthcare Reform
Providing healthcare coverage to all or most Americans was a centerpiece of President Obama’s campaign and a significant part of a proposal published by Senate Finance Committee Chairman Max Baucus (D-Mont.). Any actual reform will come through legislation, which will have to spell out who is covered and how, and where the money will come from. Any legislation will have to pass both the House and the Senate before Obama can sign it into law.
“The Democrats have certainly said [healthcare reform] is going to happen. Obama has talked about it … but how bipartisan will the effort be?” Dr. Siegal says. “This is too big and important for unilateral action; any durable healthcare reform must have bipartisan support. I do think that everyone can agree that the healthcare system is going to bankrupt itself if we don’t make changes.”
Dr. Siegal is skeptical that a major reform bill of any stripe will be passed anytime soon. “Given the depth of the recession and the projected cost of the stimulus package, my guess is that we will not see significant healthcare reform legislation passed in 2009,” he predicts. “However, I think that 2009 is still going to be an important year in that Congress will lay much of the foundation for new legislation. My guess is that 2010 is the year to look for major healthcare reform. And we want to make sure that the reform that happens is in the best interests of healthcare and of hospitalists.”
Less encompassing aspects of healthcare reform, the “easy stuff,” should have enough votes to pass in 2009, Dr. Siegal says. A good example is the State Children’s Health Insurance Program (SCHIP), which was passed the first week of February and increases the number of children eligible for free medical coverage from 7 million to 11 million. “SCHIP was as close to a slam dunk as possible.”
Major overhauls to the system, such as the healthcare exchange outlined in Sen. Baucus’ proposal or a major reworking of Medicare, may come about further down the road. “Those are going to take a lot of time, energy, and money,” Dr. Siegal says, “and I think that Congress has bigger fish to fry right now.”
Physician Fee Schedule
Last summer, physician fees paid by Medicare were slashed by 10.6% and then restored—with a 1.1% increase—when Congress overrode a presidential veto. SHM members were among the many physicians who fought the fee cut with letters and e-mails to Congress. However, the current fee schedule is short-lived: A 20% fee cut is scheduled for 2010. Will hospitalists and others have to go through the same battle all over again to maintain their Medicare payments?
Bradley Flansbaum, DO, MPH, chief of the hospitalist section at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, points out “there are some proposals to modify the SGR [sustainable growth rate] formula, so this may not be the hot issue it was in 2008.” The SGR is used to set reimbursement rates for specific services and have been targeted by numerous stakeholders as flawed.
Regardless of the reimbursement formula, the Centers for Medicare and Medicaid Services (CMS) physician fee schedule might become less crucial to hospitalists’ income. “In the context of healthcare reform, you have to wonder if fee-for-service is even going to be relevant,” Dr. Flansbaum explains. “I think that Congress and MedPAC will think things through and admit that we can’t keep Band-Aiding a broken system.”
A major system overhaul might be looming. “This may not happen this year,” he says, “but I think that if Congress needs to avert the pay cut, then they will say they’re doing this one more time, with the caveat that payment will be drastically different” in the near future.
Delivery System Reform
A third hot topic for 2009 is legislation and consideration of changes in the healthcare delivery system, including payment reform, healthcare information technology, and improving care coordination.
“We think that payment reform is central to reshaping the healthcare system,” Dr. Siegal says.
As for moving toward a fee-for-quality system: “Well, there’s politics and there’s policy,” Dr. Flansbaum says. “Politics says we need to reward quality. However, the policy is that the methods of measuring quality haven’t evolved to the point where we can go forward. Everything is in beta-testing right now; we’re not ready to make any sweeping decisions. The delivery system has to be well-thought-out. It’s complicated.”
For example, in 2008, the CMS published a proposed inpatient prospective payment system rule, which included additional categories of hospital-acquired conditions that would no longer carry higher Medicare payments. The list caused industry alarm because some of the conditions—including Clostridium difficile-associated disease (see “Clostridium Difficile Infection: Are We Doing Enough,” p. 12)—were seen as only partially preventable in hospitalized patients or not entirely hospital-acquired.
The lesson learned? Any reform to healthcare delivery must be carefully considered, along with input from the medical community. “Healthcare is 16% of the gross domestic product. You don’t take that and spin it around in one day,” Dr. Flansbaum says. “It’s best to approach reform slowly and really think it through.”
Even so, there is no guarantee that reform legislation will make it through Congress.
“Another aspect to consider is that there are ideological differences between Democrats and Republicans,” Dr. Flansbaum adds. “ … Many Republicans are miles away from [Democrats] ideologically. Further still, with Daschle’s exit, it is unclear how his replacement will approach any overhaul.”
Of course, nobody has a crystal ball. This year may bring forth less drastic changes than hospital medicine is predicting. Then again, considering the economic and political climate, reform could take place faster than seems possible.
Only time will tell. TH
Jane Jerrard is a medical writer based in Chicago.
Change is in the air. With a new ad-ministration promising to be a change agent, an overhauled Congress, and a seemingly unanimous national interest in tackling healthcare reform, what changes can hospital medicine expect in 2009?
“I think there’s certainly the political will and interest now,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “We haven’t had enough political will to ‘go big’ until recently. Now that we have it, the trillion-dollar question is where the money will come from.”
With that in mind, let’s explore three of the hottest healthcare issues:
Comprehensive Healthcare Reform
Providing healthcare coverage to all or most Americans was a centerpiece of President Obama’s campaign and a significant part of a proposal published by Senate Finance Committee Chairman Max Baucus (D-Mont.). Any actual reform will come through legislation, which will have to spell out who is covered and how, and where the money will come from. Any legislation will have to pass both the House and the Senate before Obama can sign it into law.
“The Democrats have certainly said [healthcare reform] is going to happen. Obama has talked about it … but how bipartisan will the effort be?” Dr. Siegal says. “This is too big and important for unilateral action; any durable healthcare reform must have bipartisan support. I do think that everyone can agree that the healthcare system is going to bankrupt itself if we don’t make changes.”
Dr. Siegal is skeptical that a major reform bill of any stripe will be passed anytime soon. “Given the depth of the recession and the projected cost of the stimulus package, my guess is that we will not see significant healthcare reform legislation passed in 2009,” he predicts. “However, I think that 2009 is still going to be an important year in that Congress will lay much of the foundation for new legislation. My guess is that 2010 is the year to look for major healthcare reform. And we want to make sure that the reform that happens is in the best interests of healthcare and of hospitalists.”
Less encompassing aspects of healthcare reform, the “easy stuff,” should have enough votes to pass in 2009, Dr. Siegal says. A good example is the State Children’s Health Insurance Program (SCHIP), which was passed the first week of February and increases the number of children eligible for free medical coverage from 7 million to 11 million. “SCHIP was as close to a slam dunk as possible.”
Major overhauls to the system, such as the healthcare exchange outlined in Sen. Baucus’ proposal or a major reworking of Medicare, may come about further down the road. “Those are going to take a lot of time, energy, and money,” Dr. Siegal says, “and I think that Congress has bigger fish to fry right now.”
Physician Fee Schedule
Last summer, physician fees paid by Medicare were slashed by 10.6% and then restored—with a 1.1% increase—when Congress overrode a presidential veto. SHM members were among the many physicians who fought the fee cut with letters and e-mails to Congress. However, the current fee schedule is short-lived: A 20% fee cut is scheduled for 2010. Will hospitalists and others have to go through the same battle all over again to maintain their Medicare payments?
Bradley Flansbaum, DO, MPH, chief of the hospitalist section at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, points out “there are some proposals to modify the SGR [sustainable growth rate] formula, so this may not be the hot issue it was in 2008.” The SGR is used to set reimbursement rates for specific services and have been targeted by numerous stakeholders as flawed.
Regardless of the reimbursement formula, the Centers for Medicare and Medicaid Services (CMS) physician fee schedule might become less crucial to hospitalists’ income. “In the context of healthcare reform, you have to wonder if fee-for-service is even going to be relevant,” Dr. Flansbaum explains. “I think that Congress and MedPAC will think things through and admit that we can’t keep Band-Aiding a broken system.”
A major system overhaul might be looming. “This may not happen this year,” he says, “but I think that if Congress needs to avert the pay cut, then they will say they’re doing this one more time, with the caveat that payment will be drastically different” in the near future.
Delivery System Reform
A third hot topic for 2009 is legislation and consideration of changes in the healthcare delivery system, including payment reform, healthcare information technology, and improving care coordination.
“We think that payment reform is central to reshaping the healthcare system,” Dr. Siegal says.
As for moving toward a fee-for-quality system: “Well, there’s politics and there’s policy,” Dr. Flansbaum says. “Politics says we need to reward quality. However, the policy is that the methods of measuring quality haven’t evolved to the point where we can go forward. Everything is in beta-testing right now; we’re not ready to make any sweeping decisions. The delivery system has to be well-thought-out. It’s complicated.”
For example, in 2008, the CMS published a proposed inpatient prospective payment system rule, which included additional categories of hospital-acquired conditions that would no longer carry higher Medicare payments. The list caused industry alarm because some of the conditions—including Clostridium difficile-associated disease (see “Clostridium Difficile Infection: Are We Doing Enough,” p. 12)—were seen as only partially preventable in hospitalized patients or not entirely hospital-acquired.
The lesson learned? Any reform to healthcare delivery must be carefully considered, along with input from the medical community. “Healthcare is 16% of the gross domestic product. You don’t take that and spin it around in one day,” Dr. Flansbaum says. “It’s best to approach reform slowly and really think it through.”
Even so, there is no guarantee that reform legislation will make it through Congress.
“Another aspect to consider is that there are ideological differences between Democrats and Republicans,” Dr. Flansbaum adds. “ … Many Republicans are miles away from [Democrats] ideologically. Further still, with Daschle’s exit, it is unclear how his replacement will approach any overhaul.”
Of course, nobody has a crystal ball. This year may bring forth less drastic changes than hospital medicine is predicting. Then again, considering the economic and political climate, reform could take place faster than seems possible.
Only time will tell. TH
Jane Jerrard is a medical writer based in Chicago.
Change is in the air. With a new ad-ministration promising to be a change agent, an overhauled Congress, and a seemingly unanimous national interest in tackling healthcare reform, what changes can hospital medicine expect in 2009?
“I think there’s certainly the political will and interest now,” says Eric Siegal, MD, chair of SHM’s Public Policy Committee. “We haven’t had enough political will to ‘go big’ until recently. Now that we have it, the trillion-dollar question is where the money will come from.”
With that in mind, let’s explore three of the hottest healthcare issues:
Comprehensive Healthcare Reform
Providing healthcare coverage to all or most Americans was a centerpiece of President Obama’s campaign and a significant part of a proposal published by Senate Finance Committee Chairman Max Baucus (D-Mont.). Any actual reform will come through legislation, which will have to spell out who is covered and how, and where the money will come from. Any legislation will have to pass both the House and the Senate before Obama can sign it into law.
“The Democrats have certainly said [healthcare reform] is going to happen. Obama has talked about it … but how bipartisan will the effort be?” Dr. Siegal says. “This is too big and important for unilateral action; any durable healthcare reform must have bipartisan support. I do think that everyone can agree that the healthcare system is going to bankrupt itself if we don’t make changes.”
Dr. Siegal is skeptical that a major reform bill of any stripe will be passed anytime soon. “Given the depth of the recession and the projected cost of the stimulus package, my guess is that we will not see significant healthcare reform legislation passed in 2009,” he predicts. “However, I think that 2009 is still going to be an important year in that Congress will lay much of the foundation for new legislation. My guess is that 2010 is the year to look for major healthcare reform. And we want to make sure that the reform that happens is in the best interests of healthcare and of hospitalists.”
Less encompassing aspects of healthcare reform, the “easy stuff,” should have enough votes to pass in 2009, Dr. Siegal says. A good example is the State Children’s Health Insurance Program (SCHIP), which was passed the first week of February and increases the number of children eligible for free medical coverage from 7 million to 11 million. “SCHIP was as close to a slam dunk as possible.”
Major overhauls to the system, such as the healthcare exchange outlined in Sen. Baucus’ proposal or a major reworking of Medicare, may come about further down the road. “Those are going to take a lot of time, energy, and money,” Dr. Siegal says, “and I think that Congress has bigger fish to fry right now.”
Physician Fee Schedule
Last summer, physician fees paid by Medicare were slashed by 10.6% and then restored—with a 1.1% increase—when Congress overrode a presidential veto. SHM members were among the many physicians who fought the fee cut with letters and e-mails to Congress. However, the current fee schedule is short-lived: A 20% fee cut is scheduled for 2010. Will hospitalists and others have to go through the same battle all over again to maintain their Medicare payments?
Bradley Flansbaum, DO, MPH, chief of the hospitalist section at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, points out “there are some proposals to modify the SGR [sustainable growth rate] formula, so this may not be the hot issue it was in 2008.” The SGR is used to set reimbursement rates for specific services and have been targeted by numerous stakeholders as flawed.
Regardless of the reimbursement formula, the Centers for Medicare and Medicaid Services (CMS) physician fee schedule might become less crucial to hospitalists’ income. “In the context of healthcare reform, you have to wonder if fee-for-service is even going to be relevant,” Dr. Flansbaum explains. “I think that Congress and MedPAC will think things through and admit that we can’t keep Band-Aiding a broken system.”
A major system overhaul might be looming. “This may not happen this year,” he says, “but I think that if Congress needs to avert the pay cut, then they will say they’re doing this one more time, with the caveat that payment will be drastically different” in the near future.
Delivery System Reform
A third hot topic for 2009 is legislation and consideration of changes in the healthcare delivery system, including payment reform, healthcare information technology, and improving care coordination.
“We think that payment reform is central to reshaping the healthcare system,” Dr. Siegal says.
As for moving toward a fee-for-quality system: “Well, there’s politics and there’s policy,” Dr. Flansbaum says. “Politics says we need to reward quality. However, the policy is that the methods of measuring quality haven’t evolved to the point where we can go forward. Everything is in beta-testing right now; we’re not ready to make any sweeping decisions. The delivery system has to be well-thought-out. It’s complicated.”
For example, in 2008, the CMS published a proposed inpatient prospective payment system rule, which included additional categories of hospital-acquired conditions that would no longer carry higher Medicare payments. The list caused industry alarm because some of the conditions—including Clostridium difficile-associated disease (see “Clostridium Difficile Infection: Are We Doing Enough,” p. 12)—were seen as only partially preventable in hospitalized patients or not entirely hospital-acquired.
The lesson learned? Any reform to healthcare delivery must be carefully considered, along with input from the medical community. “Healthcare is 16% of the gross domestic product. You don’t take that and spin it around in one day,” Dr. Flansbaum says. “It’s best to approach reform slowly and really think it through.”
Even so, there is no guarantee that reform legislation will make it through Congress.
“Another aspect to consider is that there are ideological differences between Democrats and Republicans,” Dr. Flansbaum adds. “ … Many Republicans are miles away from [Democrats] ideologically. Further still, with Daschle’s exit, it is unclear how his replacement will approach any overhaul.”
Of course, nobody has a crystal ball. This year may bring forth less drastic changes than hospital medicine is predicting. Then again, considering the economic and political climate, reform could take place faster than seems possible.
Only time will tell. TH
Jane Jerrard is a medical writer based in Chicago.