User login
To Crush or Not to Crush
There are multiple reasons for crushing tablets or capsule contents before administering medications, but there are numerous medications that should not be crushed. These medications should not be chewed, either, usually due to their specific formulations and their pharmacokinetic properties.1 Most of the no-crush medications are sustained-release, oral-dosage formulas. The majority of extended-release products should not be crushed or chewed, although there are some newer slow-release tablet formulations available that are scored and can be divided or halved (e.g., Toprol XL).
A common reason for crushing a tablet or capsule is for use by a hospitalized patient with an enteral feeding tube. A recent review in the American Journal of Health-System Pharmacy provides more details about administering medications in patients with enteral feeding tubes.2 Oral solutions can be used when commercially available and medically appropriate. If an oral solution or suspension is not available, the hospital pharmacy should be consulted to determine if a liquid formulation of the product can be extemporaneously prepared. In some cases, after careful consideration of compatibility, stability, and drug absorption changes, an injectable formulation of a product may be used. You should always consult your hospital pharmacist for information on this modality of drug administration.
Some patients have difficulty swallowing tablets or capsules; some dislike the taste. In these cases, crushing of medication for powdered delivery (to be mixed with food or beverages) should be considered. But beware of certain caveats, as not all medications are suitable for crushing. Generally, meds that should not be crushed fall into one of these categories:
- Sustained-release tablets, which can be composed of multiple layers for different drug release times, as can beads within capsules. Some of the more common prefixes or suffixes for sustained-release, controlled-release, or controlled-delivery products include: 12-hour, 24-hour, CC, CD, CR, ER, LA, Retard, SA, Slo-, SR, XL, XR, or XT.
- Enteric-coated tablets, which are formulated because certain drugs can be irritating to the stomach or are degraded by stomach acid. By enteric-coating tablets or capsule beads, the drug’s release can be delayed until it reaches the small intestine. Prefixes include EN- and EC-.
Other medications have objectionable tastes and are sugar-coated to improve tolerability. If this type of medication is crushed, the patient would be subject to its unpleasant taste, which could significantly impair medication adherence. Additionally, both sublingual and effervescent medications should not be crushed because it will decrease the medication’s effectiveness.
Hospital Pharmacy publishes a wall chart that includes many of these types of formulations, along with their do’s and don’ts. If there is ever any doubt about the best way to administer a particular product or whether it can be halved or crushed, ask your pharmacist.3 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Mitchell J. Oral dosage forms that should not be crushed or chewed: facts and comparisons 4.0. Hospital Pharmacy Web site. Available at: online.factsandcomparisons.com/Viewer.aspx?book=atoz&monoID=fandc-atoz1040. Accessed March 5, 2009.
2. Williams NT. Medication administration through enteral feeding tubes. Am J Health Syst Pharm. 2008;65(24):2347-2357.
3. Mitchell JF. Oral dosage forms that should not be crushed: wall chart. Wolters Kluwer Health Web site. Available at: www.factsandcomparisons.com/Products/product.aspx?id=1111. Accessed Jan. 26, 2009.
4. Mylan's Matrix receives final FDA approval for the generic version of the antiretroviral Zerit capsules. Wolters Kluwer Health Web site. Available at: http://mylan.mediaroom.com/index.php?s=43&item=399. Accessed Jan. 23, 2009.
5. Product approval information. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/Cber/products/Cinryze.htm. Accessed Jan. 14, 2009.
6. FDA licenses for marketing new therapy for rare genetic disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/NEWS/2008/NEW01903.html. Accessed Jan. 14, 2009.
7. Sancuso patch approved for nausea and vomiting. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sancusopatchapprovedfornauseaandvomiting/article/122384/. Accessed Jan. 14, 2009.
8. TussiCaps now available for cough suppression. Monthly Prescribing Reference Web site. Available at: www.empr.com/TussiCapsnowavailableforcoughsuppression/article/122377/. Accessed Jan. 14, 2009.
9. UCB’s Vimpat approved by U.S. FDA as adjunctive therapy for partial onset seizures in adults. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/127354.php. Accessed Jan. 14, 2009.
10. Apriso granted FDA marketing approval for maintenance of remission of ulcerative colitis. Medical News Today Web site. Available at: http://www.medicalnewstoday.com/articles/127839.php. Accessed Jan. 14, 2009.
11. http://biz.yahoo.com/ap/081106/cv_therapeutics _ranexa.html?.v=1. Accessed February 2, 2009.
12. FDA approves Seroquel for bipolar maintenance. Monthly Prescribing Reference Web site. Available at: www.prescribingreference.com/news/showNews/which/SeroquelXRForBipolar10101. Accessed Jan. 14, 2009.
13. Seroquel XR Web site. Available at: www.pharmacistelink.com/news/2009/01/14_seroquel.pdf. Accessed Jan. 23, 2009.
14. Peck P. Smoking cessation drug linked to 1,001 new serious adverse events. Medpage Today Web site. Available at: www.medpagetoday.com/PrimaryCare/Smoking/11428. Accessed Jan. 14, 2009.
15. Public health advisory: important information on Chantix (varenicline). U.S. Food and Drug Administration Web site. Available at: www.fda.gov/CDER/Drug/advisory/varenicline.htm. Accessed Jan. 14, 2009.
There are multiple reasons for crushing tablets or capsule contents before administering medications, but there are numerous medications that should not be crushed. These medications should not be chewed, either, usually due to their specific formulations and their pharmacokinetic properties.1 Most of the no-crush medications are sustained-release, oral-dosage formulas. The majority of extended-release products should not be crushed or chewed, although there are some newer slow-release tablet formulations available that are scored and can be divided or halved (e.g., Toprol XL).
A common reason for crushing a tablet or capsule is for use by a hospitalized patient with an enteral feeding tube. A recent review in the American Journal of Health-System Pharmacy provides more details about administering medications in patients with enteral feeding tubes.2 Oral solutions can be used when commercially available and medically appropriate. If an oral solution or suspension is not available, the hospital pharmacy should be consulted to determine if a liquid formulation of the product can be extemporaneously prepared. In some cases, after careful consideration of compatibility, stability, and drug absorption changes, an injectable formulation of a product may be used. You should always consult your hospital pharmacist for information on this modality of drug administration.
Some patients have difficulty swallowing tablets or capsules; some dislike the taste. In these cases, crushing of medication for powdered delivery (to be mixed with food or beverages) should be considered. But beware of certain caveats, as not all medications are suitable for crushing. Generally, meds that should not be crushed fall into one of these categories:
- Sustained-release tablets, which can be composed of multiple layers for different drug release times, as can beads within capsules. Some of the more common prefixes or suffixes for sustained-release, controlled-release, or controlled-delivery products include: 12-hour, 24-hour, CC, CD, CR, ER, LA, Retard, SA, Slo-, SR, XL, XR, or XT.
- Enteric-coated tablets, which are formulated because certain drugs can be irritating to the stomach or are degraded by stomach acid. By enteric-coating tablets or capsule beads, the drug’s release can be delayed until it reaches the small intestine. Prefixes include EN- and EC-.
Other medications have objectionable tastes and are sugar-coated to improve tolerability. If this type of medication is crushed, the patient would be subject to its unpleasant taste, which could significantly impair medication adherence. Additionally, both sublingual and effervescent medications should not be crushed because it will decrease the medication’s effectiveness.
Hospital Pharmacy publishes a wall chart that includes many of these types of formulations, along with their do’s and don’ts. If there is ever any doubt about the best way to administer a particular product or whether it can be halved or crushed, ask your pharmacist.3 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Mitchell J. Oral dosage forms that should not be crushed or chewed: facts and comparisons 4.0. Hospital Pharmacy Web site. Available at: online.factsandcomparisons.com/Viewer.aspx?book=atoz&monoID=fandc-atoz1040. Accessed March 5, 2009.
2. Williams NT. Medication administration through enteral feeding tubes. Am J Health Syst Pharm. 2008;65(24):2347-2357.
3. Mitchell JF. Oral dosage forms that should not be crushed: wall chart. Wolters Kluwer Health Web site. Available at: www.factsandcomparisons.com/Products/product.aspx?id=1111. Accessed Jan. 26, 2009.
4. Mylan's Matrix receives final FDA approval for the generic version of the antiretroviral Zerit capsules. Wolters Kluwer Health Web site. Available at: http://mylan.mediaroom.com/index.php?s=43&item=399. Accessed Jan. 23, 2009.
5. Product approval information. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/Cber/products/Cinryze.htm. Accessed Jan. 14, 2009.
6. FDA licenses for marketing new therapy for rare genetic disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/NEWS/2008/NEW01903.html. Accessed Jan. 14, 2009.
7. Sancuso patch approved for nausea and vomiting. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sancusopatchapprovedfornauseaandvomiting/article/122384/. Accessed Jan. 14, 2009.
8. TussiCaps now available for cough suppression. Monthly Prescribing Reference Web site. Available at: www.empr.com/TussiCapsnowavailableforcoughsuppression/article/122377/. Accessed Jan. 14, 2009.
9. UCB’s Vimpat approved by U.S. FDA as adjunctive therapy for partial onset seizures in adults. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/127354.php. Accessed Jan. 14, 2009.
10. Apriso granted FDA marketing approval for maintenance of remission of ulcerative colitis. Medical News Today Web site. Available at: http://www.medicalnewstoday.com/articles/127839.php. Accessed Jan. 14, 2009.
11. http://biz.yahoo.com/ap/081106/cv_therapeutics _ranexa.html?.v=1. Accessed February 2, 2009.
12. FDA approves Seroquel for bipolar maintenance. Monthly Prescribing Reference Web site. Available at: www.prescribingreference.com/news/showNews/which/SeroquelXRForBipolar10101. Accessed Jan. 14, 2009.
13. Seroquel XR Web site. Available at: www.pharmacistelink.com/news/2009/01/14_seroquel.pdf. Accessed Jan. 23, 2009.
14. Peck P. Smoking cessation drug linked to 1,001 new serious adverse events. Medpage Today Web site. Available at: www.medpagetoday.com/PrimaryCare/Smoking/11428. Accessed Jan. 14, 2009.
15. Public health advisory: important information on Chantix (varenicline). U.S. Food and Drug Administration Web site. Available at: www.fda.gov/CDER/Drug/advisory/varenicline.htm. Accessed Jan. 14, 2009.
There are multiple reasons for crushing tablets or capsule contents before administering medications, but there are numerous medications that should not be crushed. These medications should not be chewed, either, usually due to their specific formulations and their pharmacokinetic properties.1 Most of the no-crush medications are sustained-release, oral-dosage formulas. The majority of extended-release products should not be crushed or chewed, although there are some newer slow-release tablet formulations available that are scored and can be divided or halved (e.g., Toprol XL).
A common reason for crushing a tablet or capsule is for use by a hospitalized patient with an enteral feeding tube. A recent review in the American Journal of Health-System Pharmacy provides more details about administering medications in patients with enteral feeding tubes.2 Oral solutions can be used when commercially available and medically appropriate. If an oral solution or suspension is not available, the hospital pharmacy should be consulted to determine if a liquid formulation of the product can be extemporaneously prepared. In some cases, after careful consideration of compatibility, stability, and drug absorption changes, an injectable formulation of a product may be used. You should always consult your hospital pharmacist for information on this modality of drug administration.
Some patients have difficulty swallowing tablets or capsules; some dislike the taste. In these cases, crushing of medication for powdered delivery (to be mixed with food or beverages) should be considered. But beware of certain caveats, as not all medications are suitable for crushing. Generally, meds that should not be crushed fall into one of these categories:
- Sustained-release tablets, which can be composed of multiple layers for different drug release times, as can beads within capsules. Some of the more common prefixes or suffixes for sustained-release, controlled-release, or controlled-delivery products include: 12-hour, 24-hour, CC, CD, CR, ER, LA, Retard, SA, Slo-, SR, XL, XR, or XT.
- Enteric-coated tablets, which are formulated because certain drugs can be irritating to the stomach or are degraded by stomach acid. By enteric-coating tablets or capsule beads, the drug’s release can be delayed until it reaches the small intestine. Prefixes include EN- and EC-.
Other medications have objectionable tastes and are sugar-coated to improve tolerability. If this type of medication is crushed, the patient would be subject to its unpleasant taste, which could significantly impair medication adherence. Additionally, both sublingual and effervescent medications should not be crushed because it will decrease the medication’s effectiveness.
Hospital Pharmacy publishes a wall chart that includes many of these types of formulations, along with their do’s and don’ts. If there is ever any doubt about the best way to administer a particular product or whether it can be halved or crushed, ask your pharmacist.3 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Mitchell J. Oral dosage forms that should not be crushed or chewed: facts and comparisons 4.0. Hospital Pharmacy Web site. Available at: online.factsandcomparisons.com/Viewer.aspx?book=atoz&monoID=fandc-atoz1040. Accessed March 5, 2009.
2. Williams NT. Medication administration through enteral feeding tubes. Am J Health Syst Pharm. 2008;65(24):2347-2357.
3. Mitchell JF. Oral dosage forms that should not be crushed: wall chart. Wolters Kluwer Health Web site. Available at: www.factsandcomparisons.com/Products/product.aspx?id=1111. Accessed Jan. 26, 2009.
4. Mylan's Matrix receives final FDA approval for the generic version of the antiretroviral Zerit capsules. Wolters Kluwer Health Web site. Available at: http://mylan.mediaroom.com/index.php?s=43&item=399. Accessed Jan. 23, 2009.
5. Product approval information. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/Cber/products/Cinryze.htm. Accessed Jan. 14, 2009.
6. FDA licenses for marketing new therapy for rare genetic disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/NEWS/2008/NEW01903.html. Accessed Jan. 14, 2009.
7. Sancuso patch approved for nausea and vomiting. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sancusopatchapprovedfornauseaandvomiting/article/122384/. Accessed Jan. 14, 2009.
8. TussiCaps now available for cough suppression. Monthly Prescribing Reference Web site. Available at: www.empr.com/TussiCapsnowavailableforcoughsuppression/article/122377/. Accessed Jan. 14, 2009.
9. UCB’s Vimpat approved by U.S. FDA as adjunctive therapy for partial onset seizures in adults. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/127354.php. Accessed Jan. 14, 2009.
10. Apriso granted FDA marketing approval for maintenance of remission of ulcerative colitis. Medical News Today Web site. Available at: http://www.medicalnewstoday.com/articles/127839.php. Accessed Jan. 14, 2009.
11. http://biz.yahoo.com/ap/081106/cv_therapeutics _ranexa.html?.v=1. Accessed February 2, 2009.
12. FDA approves Seroquel for bipolar maintenance. Monthly Prescribing Reference Web site. Available at: www.prescribingreference.com/news/showNews/which/SeroquelXRForBipolar10101. Accessed Jan. 14, 2009.
13. Seroquel XR Web site. Available at: www.pharmacistelink.com/news/2009/01/14_seroquel.pdf. Accessed Jan. 23, 2009.
14. Peck P. Smoking cessation drug linked to 1,001 new serious adverse events. Medpage Today Web site. Available at: www.medpagetoday.com/PrimaryCare/Smoking/11428. Accessed Jan. 14, 2009.
15. Public health advisory: important information on Chantix (varenicline). U.S. Food and Drug Administration Web site. Available at: www.fda.gov/CDER/Drug/advisory/varenicline.htm. Accessed Jan. 14, 2009.
Eliminate Inconsistency
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
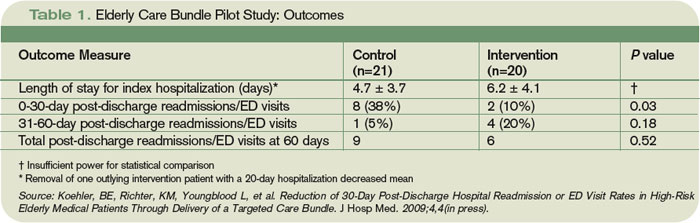
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.

—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.
—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
Three years ago, Andrew Masica, MD, MSCI, joined the MedProvider Inpatient Care Unit hospitalist group at Baylor University Medical Center (BUMC) in Dallas just as the national debate on Medicare recidivism rates was focusing on high-risk populations.
Dr. Masica’s master’s degree in clinical investigation, combined with the roughly 35 hospitalists operating at the 900-bed BUMC, suggested it made sense to see what Baylor’s doctors could add to the conversation. And a study was born: “Reduction of 30-Day Post-Discharge Hospital Readmission or ED Visit Rates in High-Risk Elderly Medical Patients Through Delivery of a Targeted Care Bundle.” The single-center study will be published in this month’s Journal of Hospital Medicine.
The study found readmission/ED visit rates were lower after 30 days for those given an individualized care bundle of educational information compared with those who received the center’s standard treatment (10% individualized care bundle compared with 38.1% for standard treatment, P=0.04). Analysis also showed that for those patients who had a readmission or post-discharge ED visit, the time interval to the second event was longer in the intervention group compared with the control group (36.2 days to 15.7 days, P=0.05). At 60 days, however, readmission/ED visit rates were not affected positively for the intervention group versus the control group (42.9% vs. 30%, P=0.52).
The study team emphasizes that its small sample size—20 in the intervention group, 21 in the control—make it nearly impossible to extrapolate the results to large population sets; however, the results fuel the debate. “We don’t want to overstate our conclusions,” says Dr. Masica, the principal study investigator. “Important questions need to be asked. Is it the specific characteristics of the care coordinators? Can you reproduce this at other facilities? Is it the care bundle or the personnel? …We view this as early-phase work that people can build upon.”
Expansion Opportunity
Still, Dr. Masica believes hospitalist-centric conclusions can be reached. Since the study used in-house personnel only, other HM groups could easily reproduce the bundle without added expense. Additionally, because the coordinated-care approach involves a checklist of patient interaction activities, not medical procedures, the barrier to replication is further reduced. However, hospitalists will need the cooperation of more than their own medical directors.
In BUMC’s case, that meant the assistance of patient-care support services and the pharmacy department. Liz Youngblood, RN, MBA, supervised the care coordination in her role as vice president of patient-care support services for the Baylor Health Care System. Brian Cohen, PharmD, MS, was the pharmacy lead. Dr. Masica notes the confluence between departments was one of the keys to the reduction in recidivism over the first 30 days post-discharge.
—Andrew Masica, MD, MSCI, hospitalist, MedProvider Inpatient Care Unit, Dallas
“If you pick the high-risk patients and deliver the care in a bundle, you would be able to improve outcomes,” Dr. Masica says. “When you deliver just pieces of the care—just the coordinated care or just the pharmacist—you get inconsistencies.”
The first struggle BUMC researchers encountered—once they secured funding from Baylor’s Institute for Health Care Research and Improvement—was enrolling enough patients who met the criteria set for the study. The high-risk patient thresholds were:
- At least 70 years old;
- Regular use of at least five medications;
- At least three chronic, comorbid conditions;
- Assistance with at least one activity of daily living; and
- Preadmission residence at home or at an assisted-living facility with a reasonable expectation of disposition back to that residence.
Researchers also wanted patients with common DRGs admitted, and set exclusion criteria as well: lack of fluency in English; admission primarily for a surgical procedure; terminal diagnosis with life expectancy of less than six months; and residency in a long-term care facility. Patients who could not be enrolled within 72 hours of admission were excluded.
Dr. Masica notes hospitalists interested in replicating the research should pay attention to the consent forms they used. When the Baylor team conducted its research from March to September 2007, they used a long-form consent waiver. Baylor’s consent form for similar studies has since been shortened, and Dr. Masica says a less complicated form would have helped encourage more patients to enroll. In the end, 60 patients declined to enroll in the Baylor study and 56 were unable to give their consent due to impairment.
Once enrolled, the patients were delivered the care bundle in stages (see Table 1). Care coordinators (CCs) saw patients daily, instructing them on specific health conditions with an eye toward teaching home care, should post-discharge problems arise. Clinical pharmacists (CPs) visited patients to focus on medication reconciliation and education. CCs and CPs would follow up with post-discharge phone calls to confirm receipt of medical equipment and medications, use and affects of those medications, home-health arrangements, and to schedule follow-up appointments. If patients indicated any issues, the coordinators recommended action plans.
“It would be surprising to find out how little patients really understand about why they’re in the hospital and what they’re being treated for,” Youngblood says. “To have the reinforcement is really valuable.”
Care Continuum
One topic the study skirts is the ever-contentious realm of post-discharge care and who takes over responsibility for patient care. While the Baylor study examined readmission/ED visit rates through 60 days, Dr. Masica says a transitional-care program is the best way to manage that care continuum.
“We did see a difference at 30 days,” Dr. Masica says. “At 60 days, that effectively washed out. That makes sense. You can only control things so much from the hospital side. After 30 days, you need transitional care, good primary care.”
Baylor’s research team is working on a follow-up study that would apply the coordinated-care bundle to specific disease management. Youngblood notes that directing specific services at a targeted population—for example, congestive heart failure patients—should show an even more concentrated reduction of 30-day recidivism. “The key is to identify the high-risk groups,” he says. “You can’t apply this to every single patient. That would be low-yield. Your yield is going to come in on the very high-risk folks.” TH
Richard Quinn is a freelance writer based in New Jersey.
The latest research you need to know
In This Edition
- Generic vs. brand-name drugs.
- Rapid-response teams and mortality.
- A new prediction rule for mortality in acute pancreatitis.
- Viral causes of community-acquired pneumonia.
- Intensive insulin therapy in the ICU.
- New preoperative and intraoperative risk factors.
- Timing of ICU feedings and mortality.
- Aspirin as primary prevention in diabetics.
Generic, Brand-Name Drugs Used for Cardiovascular Disease Are Clinically Equivalent
Clinical question: Is there a clinical risk when substituting generic drugs for brand-name drugs in the treatment of cardiovascular disease?
Background: Spending on healthcare in the U.S. has reached critical levels. Increasing prescription drug costs make up a large portion of healthcare expenditures. The high cost of medicines directly affect adherence to treatment regimens and contribute to poor health outcomes. Cardiovascular drugs make up the largest portion of outpatient prescription drug spending.
Study design: Systematic review of relevant articles with a meta-analysis performed to determine an aggregate effect size.
Setting: Multiple locations and varied patient populations.
Synopsis: A total of 47 articles were included in the review, of which 38 were randomized controlled trials (RCTs). The studies measured both clinical efficacy and safety end points. More than half the articles were published prior to 2000. Clinical equivalence was noted in all seven beta-blocker RCTs; 10 of 11 diuretic RCTs; five of seven calcium-channel-blocker RCTs; all three antiplatelet-agent RCTs (clopidogrel, enteric-coated aspirin); two statin RCTs; one ACE-inhibitor RCT; and one alpha-blocker RCT. For drugs with a narrow therapeutic index, clinical equivalence was noted in all five warfarin RCTs and a single Class 1 anti-arrhythmic-agent RCT.
The aggregate effect size was -0.03 (95% CI, -0.15 to 0.08), which indicates nearly complete overlap of the generic and brand-name distributions. The data show no evidence of superiority of brand-name to generic drugs in clinical outcomes measured in the various studies.
In a separate review of editorials addressing generic substitution for cardiovascular drugs, 53% expressed a negative view of generic-drug substitution.
Bottom line: There is clinical equivalency between generic and brand-name drugs used in the treatment of cardiovascular disease. Despite this conclusion, a substantial number of editorials advise against generic substitution, which affects both patient and physician drug preferences.
Citation: Kesselheim A, Misono A, Lee J, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008; 300(21):2514-2526.
PEDIATRIC LITERATURE

Oral Prednisolone Does Not Shorten Hospitalization in Preschool-Age Children with Acute Virus-Induced Wheezing
Clinical question: Does oral prednisolone shorten duration of hospitalization in preschool-age children with acute virus-induced wheezing?
Background: Wheezing illnesses in young children are commonly associated with viral infections and may resolve with age without further stigmata of atopic asthma. Although systemic corticosteroids are commonly recommended for this population, evidence of their effectiveness is limited.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Three hospitals in the United Kingdom.
Synopsis: Children between 10 and 60 months that presented to a hospital with a physician-diagnosed attack of wheezing preceded by a viral infection were randomized to receive oral prednisolone or a placebo. There was no significant difference between the groups in the time to hospital discharge. There also was no difference in the prespecified subgroup analysis of children at high risk for atopic asthma.
The median time between presentation and “fit for discharge” was relatively low in this sample—12 hours in the placebo group and 10.1 hours in the prednisolone group. Nearly half the patients were discharged within the first several hours after presentation, and not all patients were admitted to a pediatric ward. A short-stay observation ward within the ED was an option. Thus, the results may be most applicable to patients with mild to moderate disease, some of which may not be admitted to a traditional inpatient unit.
Bottom line: Systemic corticosteroids do not dramatically shorten hospital and ED stays in preschool-aged children with mild to moderate virus-induced wheezing.
Citation: Panickar J, Lakhanpaul M, Lambert P, et al. Oral prednisolone for preschool children with acute virus-induced wheezing. N Engl J Med. 2009;360(4):329-338.
Reviewed by pediatric editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
RRT Implement-ation Doesn’t Affect Hospitalwide Code Rates or Mortality
Clinical question: Does the use of a rapid-response team (RRT) affect hospitalwide code rates and mortality?
Background: In the 100,000 Lives campaign, the Institute for Healthcare Improvement recommended that hospitals implement RRTs to help reduce preventable, in-hospital deaths. Studies have demonstrated that rates of non-ICU codes decrease after RRT implementation. It is unclear if this translates to changes in mortality rates.
Study design: Prospective cohort study of adult inpatients.
Setting: Saint Luke’s Hospital, a 404-bed tertiary-care academic hospital in Kansas City, Mo.
Synopsis: The hospital documented a total of 376 RRT activations. After RRT implementation, mean hospitalwide code rates decreased to 7.5 per 1,000 admissions from 11.2 per 1,000 admissions. This was not associated with a statistically significant reduction in hospitalwide code rates (adjusted odds ratio 0.76; 95% CI; 0.57-1.01; P=0.06). Secondary analyses noted lower rates of non-ICU codes (0.59; 95% CI, 0.40-0.89) compared with ICU codes (0.95; 95% CI; 0.64-1.43; P=0.03 for interaction). Finally, the RRT implementation was not associated with lower hospital-wide mortality (0.95; 95% CI; 0.81-1.11; P=0.52).
Secondary analyses also revealed few instances of RRT undertreatment or underutilization that may have affected the mortality numbers.
A limitation of this study is that it was slightly underpowered (78%) to detect a significant mortality difference. The findings also represent a single institution experience, and may not be generalized to other adult hospital settings or RRT programs.
Bottom line: Implementation of an RRT does not confer lower rates of hospital-wide code arrests or mortality.
Citation: Chan P, Khalid A, Longmore L, et al. Hospital-wide code rates and mortality before and after implementation of a rapid response team. JAMA. 2008;300(21):2506-2513.
Simple Scoring System Provides Timely Prediction of Mortality in Acute Pancreatitis
Clinical question: How can physicians predict mortality in acute pancreatitis?
Background: Historical predictors of mortality in acute pancreatitis require up to 48 hours of data, such as with the Ranson Criteria, or extensive amounts of data, such as with the APACHE II score. An easier tool is needed to predict which patients are at higher risk of mortality.
Study design: Retrospective cohort.
Setting: Patients in the Cardinal Health clinical outcomes research database, which supports public reporting of hospital performance.
Synopsis: The authors identified patients with the principal diagnosis of pancreatitis from 2000-2001 and explored numerous diagnostic findings available within the first 24 hours. Ultimately, BUN >25, impaired mental status, presence of SIRS (systemic inflammatory response syndrome), age >60, and presence of a pleural effusion were found to be predictive of mortality. These diagnostic findings correspond to the mnemonic BISAP. The BISAP score was then validated in a second cohort that included patients from 2004-2005.
Each finding in the BISAP score was given one point. A score of less than 2 was present in approximately 60% of patients admitted with acute pancreatitis, and corresponded to a mortality of less than 1%. A score of 2 corresponded to a mortality of 2%. Higher scores were associated with steeply increasing mortality, with a score of 5 corresponding with greater than 20% mortality.
The BISAP score performed similarly to the APACHE II score, but the former is easier to calculate on the day of admission and has fewer parameters. A more challenging research step will be to demonstrate that using the BISAP score to determine treatment strategies can affect patient outcomes.
Bottom line: The easy-to-calculate BISAP score is a new method for predicting mortality in patients with acute pancreatitis. This tool should help hospitalists determine, on the day of admission, to what extent patients with acute pancreatitis need aggressive management, such as ICU admission and early involvement of specialists.
Citation: Wu B, Johannes R, Sun X, Tabak Y, Conwell D, Banks P. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008;57(12): 1698-1703.
Nasal Swabs Identify Viral Causes in CAP Patients
Clinical question: How often is viral infection associated with community-acquired pneumonia (CAP) in adults?
Background: CAP is a clinically important disease that is associated with significant hospitalization and mortality. CAP treatment guidelines acknowledge respiratory viruses as an etiology for pneumonia, but few recommendations are made regarding management of these viral infections.
Study design: Prospective study.
Setting: Five hospitals in Edmonton, Alberta, from 2004-2006.
Synopsis: The authors enrolled 193 hospitalized adults, median age 71. Nucleic amplification tests (NATs) from nasopharyngeal swab specimens were tested for human metapneumovirus, respiratory syncytial virus, rhinovirus, parainfluenza virus 1-4, coronaviruses, and adenovirus.
Fifteen percent of these patients had a nasal swab positive for a viral infection. Interestingly, 4% of patients had both a positive viral nasal swab and positive bacterial cultures. Compared with bacterial infection, patients with viral infection tended to be older (76 vs. 64 years, P=0.01), have limited ambulation (66% vs. 32%, P=0.006), and have a history of cardiac disease (66% vs. 32%, P=0.02). Patients with bacterial pneumonia showed a statistically significant trend toward having chest pain, an abnormal white blood count, and a lobar infiltrate on chest X-ray.
Further investigations might look at how nasal swab data could be used to improve infection control within the hospital for patients found to have easily transmissible viruses. Further research could explore the feasibility of avoiding antibiotic use in patients found to have viral pneumonia, assuming bacterial co-infection is reliably excluded.
Bottom line: Nasal swabs using NAT technology could play a significant role in identifying pathogens in CAP patients. How this technology should affect clinical decision-making and how it might improve outcomes remains unknown.
Citation: Johnstone J, Majumdar S, Fox J, Marrie T. Viral infection in adults hospitalized with community-acquired pneumonia: prevalence, pathogens, and presentation. Chest. 2008;134(6):1141-1148.
Intensive Insulin Therapy Doesn’t Reduce ICU Mortality
Clinical question: Does the use of intensive insulin therapy decrease mortality in the intensive-care unit (ICU)?
Background: In 2001, Van den Berghe et al (N Engl J Med. 2001;345(19):1359-67) reported a reduction in morbidity and mortality with intensive insulin therapy (IIT) in surgical ICU patients. This study led to the adoption of IIT protocols in many hospitals. Since 2001, further studies have failed to reproduce the same dramatic benefit of IIT.
Study design: Randomized, controlled trial.
Setting: National Guard King Abdulaziz Medical City, a tertiary-care teaching hospital in Saudi Arabia.
Synopsis: Patients were included in this study if they were 18 years or older with serum glucose levels greater than 110 mg/dL during the first 24 hours of ICU admission. There were multiple exclusion criteria, including patients with Type I diabetes, documented hypoglycemia on ICU admission (glucose <40), or diabetic ketoacidosis.
Enrolled patients were randomized to IIT or conventional insulin therapy (CIT). A multidisciplinary team designed the protocols to maintain glucose levels of 80 to 110 mg/dL and 180 to 200 mg/dL in the IIT and the CIT groups, respectively. The primary endpoint measured was ICU mortality.
The study did not produce a statistically significant difference in ICU mortality (13.5% for IIT vs. 17.1% for CIT; P=0.30). The adjusted hypoglycemia rate was 6.8 per 100 treatment days with IIT and 0.4 per 100 treatment days with CIT (P<0.0001). Patients with hypoglycemia had higher ICU mortality (23.8% vs. 13.7%, P=0.02).
In the measurement of secondary endpoints, there was a trend toward lower episodes of severe sepsis and septic shock in the IIT group (20.7% in IIT vs. 27.2% in CIT, P=0.08). However, this result was not statistically significant.
Bottom line: This well-designed study failed to show a survival benefit with IIT use in the critical-care setting. Given the findings of this and several other recent studies, one should question whether IIT should be prescribed as the standard of care in all critically-ill patients.
Citation: Arabi Y, Dabbagh O, Tamim H, et al. Intensive versus conventional insulin therapy: a randomized controlled trial in medical and surgical critically ill patients. Crit Care Med. 2008;36(12):3190-3197.
Preoperative and Intraoperative Predictors of Cardiac Adverse Events
Clinical question: What are the incidence and risk factors for perioperative cardiac adverse events after noncardiac surgery?
Background: In the past few decades, the incidence of cardiac adverse events (CAEs) for a general surgery population has remained largely unchanged (approximately 1%). This is in spite of multiple studies evaluating predictive models and attempts at preventive treatment, including preoperative coronary revascularization and perioperative beta blockers.
Study design: Prospective observational study.
Setting: Single, large, tertiary-care university hospital.
Synopsis: A total of 7,740 cases were reviewed in this study, which consisted of general surgery (4,937), vascular surgery (1,846), and urological surgery (957). A trained nurse followed up for perioperative CAEs as many as 30 days after the operation via medical chart review, phone calls, and letters. CAEs were defined as: Q-wave myocardial infarction (MI), non-ST elevation MI, cardiac arrest, or new cardiac dysrhythmia. A total of 83 CAEs (1.1% of patients) had cardiac arrest, with cardiac dysrhythmia being most common.
A total of seven preoperative risk factors were identified as independent predictors for CAEs: age 68, BMI 30, emergent surgery, prior coronary intervention or cardiac surgery, active congestive heart failure, cerebrovascular disease, and hypertension. In addition, two intraoperative risk factors were identified: intraoperative transfusion of packed red blood cells and operative duration of 3.8 hours. (The P value was 0.05 for all independent predictors.)
A further evaluation of intraoperative parameters of high-risk patients experiencing a CAE showed that these patients were more likely to have an episode of mean arterial pressure (MAP) <50 mmHg, an episode of 40% decrease in MAP, and an episode of tachycardia (heart rate >100).
Bottom line: A combination of preoperative predictors and intraoperative elements can help improve risk assessment for perioperative CAEs after noncardiac surgery.
Citation: Kheterpal S, O’Reilly M, Englesbe M, et al. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110(1):58-66.
Early Feeding in the ICU Does Not Affect Hospital Mortality
Clinical question: Will implementing evidence-based feeding guidelines improve feeding practices and reduce mortality in ICU patients?
Background: There is evidence suggesting that providing nutritional support to ICU patients within 24 hours of admission may decrease mortality. It is widely understood that patient care varies between ICUs, and there exist no uniform, evidence-based guidelines for nutritional support. Many patients remain unfed after 48 hours.
Study design: Cluster, randomized-controlled trial.
Setting: ICUs in 27 community and tertiary-care hospitals in Australia and New Zealand.
Synopsis: Hospitals were randomized to intervention or control groups. Dietitian and intensivist co-investigators from intervention ICUs developed guidelines using the Clinical Practice Guideline Development Cycle. Control ICUs were requested to make no new ICU nutritional management changes. The study enrolled 1,118 eligible patients and included adults expected to stay longer than two days. Excluded were patients taking oral diets, patients receiving palliative care or with suspected brain death, and patients sent from other facilities.
Guidelines were implemented using several methods—educational outreach visits, one-on-one conversations, active reminders, passive reminders, and educational in-services. The guidelines were successful in evoking significant practice changes in all of the intervention ICUs. Significantly more patients received nutritional support during their ICU stays in guideline ICUs, and patients in these ICUs were fed significantly earlier. There were, however, no significant differences between guideline and control ICUs with regard to hospital discharge mortality (28.9% vs. 27.4%; 95% CI; -6.3% to 12.0%; P=0.75). The groups also showed no statistical difference in hospital or ICU length of stay.
Bottom line: Significantly more patients in the guideline ICUs were fed within 24 hours, but this did not translate into improvements in mortality or other clinical outcomes.
Citation: Doig G, Simpson F, Finfer S, et al. Effect of evidence-based feeding guidelines on mortality of critically ill adults: a cluster randomized controlled trial. JAMA. 2008;300(23):2731-2741.
Low-Dose Aspirin Doesn’t Reduce Cardiovascular Events in Type 2 Diabetes Patients
Clinical question: Is low-dose aspirin effective for the primary prevention of atherosclerotic events in patients with Type 2 diabetes?
Background: Diabetes is a significant risk factor for cardiovascular events. Several prior studies have shown that aspirin therapy is effective as a secondary prevention strategy for cardiovascular events. The American Diabetes Association also recommends use of aspirin as a primary prevention strategy. Clinical trial data is currently insufficient in this area.
Study design: Prospective, randomized, open-label, controlled trial with blinded endpoint assessment.
Setting: 163 institutions in Japan.
Synopsis: The study enrolled 2,539 diabetic patients between 30 and 85 years old—mean age was 65—and included patients without EKG changes or a significant history or ongoing treatment of atherosclerotic disease. Patients were randomly assigned into an aspirin group (81 mg or 100 mg once daily) or a nonaspirin group. Patients had a median follow up of 4.37 years.
The primary endpoint was any atherosclerotic event, ranging from sudden death to ischemic heart disease or stroke. The incidence of atherosclerotic events was not statistically different in the aspirin group (68 events, 5.4%) than in the nonaspirin group (86 events, 6.7%) (HR, 0.80; 95% CI; 0.58-1.10; log-rank test, P=0.16). However, there was a suggested benefit of primary prevention in the subgroup aged 65 years or older. In addition, the combined endpoint of fatal coronary and cerebrovascular events occurred in one patient in the aspirin group and 10 patients in the nonaspirin group (HR, 0.10; 95 % CI, 0.01-0.79; P=.0037). This study is limited by the low incidence of atherosclerotic disease in Japan.
Bottom line: Low-dose aspirin used in patients with Type 2 diabetes does not significantly demonstrate primary prevention of cardiovascular events.
Citation: Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA. 2008;300(18):2134-2141. TH
In This Edition
- Generic vs. brand-name drugs.
- Rapid-response teams and mortality.
- A new prediction rule for mortality in acute pancreatitis.
- Viral causes of community-acquired pneumonia.
- Intensive insulin therapy in the ICU.
- New preoperative and intraoperative risk factors.
- Timing of ICU feedings and mortality.
- Aspirin as primary prevention in diabetics.
Generic, Brand-Name Drugs Used for Cardiovascular Disease Are Clinically Equivalent
Clinical question: Is there a clinical risk when substituting generic drugs for brand-name drugs in the treatment of cardiovascular disease?
Background: Spending on healthcare in the U.S. has reached critical levels. Increasing prescription drug costs make up a large portion of healthcare expenditures. The high cost of medicines directly affect adherence to treatment regimens and contribute to poor health outcomes. Cardiovascular drugs make up the largest portion of outpatient prescription drug spending.
Study design: Systematic review of relevant articles with a meta-analysis performed to determine an aggregate effect size.
Setting: Multiple locations and varied patient populations.
Synopsis: A total of 47 articles were included in the review, of which 38 were randomized controlled trials (RCTs). The studies measured both clinical efficacy and safety end points. More than half the articles were published prior to 2000. Clinical equivalence was noted in all seven beta-blocker RCTs; 10 of 11 diuretic RCTs; five of seven calcium-channel-blocker RCTs; all three antiplatelet-agent RCTs (clopidogrel, enteric-coated aspirin); two statin RCTs; one ACE-inhibitor RCT; and one alpha-blocker RCT. For drugs with a narrow therapeutic index, clinical equivalence was noted in all five warfarin RCTs and a single Class 1 anti-arrhythmic-agent RCT.
The aggregate effect size was -0.03 (95% CI, -0.15 to 0.08), which indicates nearly complete overlap of the generic and brand-name distributions. The data show no evidence of superiority of brand-name to generic drugs in clinical outcomes measured in the various studies.
In a separate review of editorials addressing generic substitution for cardiovascular drugs, 53% expressed a negative view of generic-drug substitution.
Bottom line: There is clinical equivalency between generic and brand-name drugs used in the treatment of cardiovascular disease. Despite this conclusion, a substantial number of editorials advise against generic substitution, which affects both patient and physician drug preferences.
Citation: Kesselheim A, Misono A, Lee J, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008; 300(21):2514-2526.
PEDIATRIC LITERATURE
Oral Prednisolone Does Not Shorten Hospitalization in Preschool-Age Children with Acute Virus-Induced Wheezing
Clinical question: Does oral prednisolone shorten duration of hospitalization in preschool-age children with acute virus-induced wheezing?
Background: Wheezing illnesses in young children are commonly associated with viral infections and may resolve with age without further stigmata of atopic asthma. Although systemic corticosteroids are commonly recommended for this population, evidence of their effectiveness is limited.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Three hospitals in the United Kingdom.
Synopsis: Children between 10 and 60 months that presented to a hospital with a physician-diagnosed attack of wheezing preceded by a viral infection were randomized to receive oral prednisolone or a placebo. There was no significant difference between the groups in the time to hospital discharge. There also was no difference in the prespecified subgroup analysis of children at high risk for atopic asthma.
The median time between presentation and “fit for discharge” was relatively low in this sample—12 hours in the placebo group and 10.1 hours in the prednisolone group. Nearly half the patients were discharged within the first several hours after presentation, and not all patients were admitted to a pediatric ward. A short-stay observation ward within the ED was an option. Thus, the results may be most applicable to patients with mild to moderate disease, some of which may not be admitted to a traditional inpatient unit.
Bottom line: Systemic corticosteroids do not dramatically shorten hospital and ED stays in preschool-aged children with mild to moderate virus-induced wheezing.
Citation: Panickar J, Lakhanpaul M, Lambert P, et al. Oral prednisolone for preschool children with acute virus-induced wheezing. N Engl J Med. 2009;360(4):329-338.
Reviewed by pediatric editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
RRT Implement-ation Doesn’t Affect Hospitalwide Code Rates or Mortality
Clinical question: Does the use of a rapid-response team (RRT) affect hospitalwide code rates and mortality?
Background: In the 100,000 Lives campaign, the Institute for Healthcare Improvement recommended that hospitals implement RRTs to help reduce preventable, in-hospital deaths. Studies have demonstrated that rates of non-ICU codes decrease after RRT implementation. It is unclear if this translates to changes in mortality rates.
Study design: Prospective cohort study of adult inpatients.
Setting: Saint Luke’s Hospital, a 404-bed tertiary-care academic hospital in Kansas City, Mo.
Synopsis: The hospital documented a total of 376 RRT activations. After RRT implementation, mean hospitalwide code rates decreased to 7.5 per 1,000 admissions from 11.2 per 1,000 admissions. This was not associated with a statistically significant reduction in hospitalwide code rates (adjusted odds ratio 0.76; 95% CI; 0.57-1.01; P=0.06). Secondary analyses noted lower rates of non-ICU codes (0.59; 95% CI, 0.40-0.89) compared with ICU codes (0.95; 95% CI; 0.64-1.43; P=0.03 for interaction). Finally, the RRT implementation was not associated with lower hospital-wide mortality (0.95; 95% CI; 0.81-1.11; P=0.52).
Secondary analyses also revealed few instances of RRT undertreatment or underutilization that may have affected the mortality numbers.
A limitation of this study is that it was slightly underpowered (78%) to detect a significant mortality difference. The findings also represent a single institution experience, and may not be generalized to other adult hospital settings or RRT programs.
Bottom line: Implementation of an RRT does not confer lower rates of hospital-wide code arrests or mortality.
Citation: Chan P, Khalid A, Longmore L, et al. Hospital-wide code rates and mortality before and after implementation of a rapid response team. JAMA. 2008;300(21):2506-2513.
Simple Scoring System Provides Timely Prediction of Mortality in Acute Pancreatitis
Clinical question: How can physicians predict mortality in acute pancreatitis?
Background: Historical predictors of mortality in acute pancreatitis require up to 48 hours of data, such as with the Ranson Criteria, or extensive amounts of data, such as with the APACHE II score. An easier tool is needed to predict which patients are at higher risk of mortality.
Study design: Retrospective cohort.
Setting: Patients in the Cardinal Health clinical outcomes research database, which supports public reporting of hospital performance.
Synopsis: The authors identified patients with the principal diagnosis of pancreatitis from 2000-2001 and explored numerous diagnostic findings available within the first 24 hours. Ultimately, BUN >25, impaired mental status, presence of SIRS (systemic inflammatory response syndrome), age >60, and presence of a pleural effusion were found to be predictive of mortality. These diagnostic findings correspond to the mnemonic BISAP. The BISAP score was then validated in a second cohort that included patients from 2004-2005.
Each finding in the BISAP score was given one point. A score of less than 2 was present in approximately 60% of patients admitted with acute pancreatitis, and corresponded to a mortality of less than 1%. A score of 2 corresponded to a mortality of 2%. Higher scores were associated with steeply increasing mortality, with a score of 5 corresponding with greater than 20% mortality.
The BISAP score performed similarly to the APACHE II score, but the former is easier to calculate on the day of admission and has fewer parameters. A more challenging research step will be to demonstrate that using the BISAP score to determine treatment strategies can affect patient outcomes.
Bottom line: The easy-to-calculate BISAP score is a new method for predicting mortality in patients with acute pancreatitis. This tool should help hospitalists determine, on the day of admission, to what extent patients with acute pancreatitis need aggressive management, such as ICU admission and early involvement of specialists.
Citation: Wu B, Johannes R, Sun X, Tabak Y, Conwell D, Banks P. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008;57(12): 1698-1703.
Nasal Swabs Identify Viral Causes in CAP Patients
Clinical question: How often is viral infection associated with community-acquired pneumonia (CAP) in adults?
Background: CAP is a clinically important disease that is associated with significant hospitalization and mortality. CAP treatment guidelines acknowledge respiratory viruses as an etiology for pneumonia, but few recommendations are made regarding management of these viral infections.
Study design: Prospective study.
Setting: Five hospitals in Edmonton, Alberta, from 2004-2006.
Synopsis: The authors enrolled 193 hospitalized adults, median age 71. Nucleic amplification tests (NATs) from nasopharyngeal swab specimens were tested for human metapneumovirus, respiratory syncytial virus, rhinovirus, parainfluenza virus 1-4, coronaviruses, and adenovirus.
Fifteen percent of these patients had a nasal swab positive for a viral infection. Interestingly, 4% of patients had both a positive viral nasal swab and positive bacterial cultures. Compared with bacterial infection, patients with viral infection tended to be older (76 vs. 64 years, P=0.01), have limited ambulation (66% vs. 32%, P=0.006), and have a history of cardiac disease (66% vs. 32%, P=0.02). Patients with bacterial pneumonia showed a statistically significant trend toward having chest pain, an abnormal white blood count, and a lobar infiltrate on chest X-ray.
Further investigations might look at how nasal swab data could be used to improve infection control within the hospital for patients found to have easily transmissible viruses. Further research could explore the feasibility of avoiding antibiotic use in patients found to have viral pneumonia, assuming bacterial co-infection is reliably excluded.
Bottom line: Nasal swabs using NAT technology could play a significant role in identifying pathogens in CAP patients. How this technology should affect clinical decision-making and how it might improve outcomes remains unknown.
Citation: Johnstone J, Majumdar S, Fox J, Marrie T. Viral infection in adults hospitalized with community-acquired pneumonia: prevalence, pathogens, and presentation. Chest. 2008;134(6):1141-1148.
Intensive Insulin Therapy Doesn’t Reduce ICU Mortality
Clinical question: Does the use of intensive insulin therapy decrease mortality in the intensive-care unit (ICU)?
Background: In 2001, Van den Berghe et al (N Engl J Med. 2001;345(19):1359-67) reported a reduction in morbidity and mortality with intensive insulin therapy (IIT) in surgical ICU patients. This study led to the adoption of IIT protocols in many hospitals. Since 2001, further studies have failed to reproduce the same dramatic benefit of IIT.
Study design: Randomized, controlled trial.
Setting: National Guard King Abdulaziz Medical City, a tertiary-care teaching hospital in Saudi Arabia.
Synopsis: Patients were included in this study if they were 18 years or older with serum glucose levels greater than 110 mg/dL during the first 24 hours of ICU admission. There were multiple exclusion criteria, including patients with Type I diabetes, documented hypoglycemia on ICU admission (glucose <40), or diabetic ketoacidosis.
Enrolled patients were randomized to IIT or conventional insulin therapy (CIT). A multidisciplinary team designed the protocols to maintain glucose levels of 80 to 110 mg/dL and 180 to 200 mg/dL in the IIT and the CIT groups, respectively. The primary endpoint measured was ICU mortality.
The study did not produce a statistically significant difference in ICU mortality (13.5% for IIT vs. 17.1% for CIT; P=0.30). The adjusted hypoglycemia rate was 6.8 per 100 treatment days with IIT and 0.4 per 100 treatment days with CIT (P<0.0001). Patients with hypoglycemia had higher ICU mortality (23.8% vs. 13.7%, P=0.02).
In the measurement of secondary endpoints, there was a trend toward lower episodes of severe sepsis and septic shock in the IIT group (20.7% in IIT vs. 27.2% in CIT, P=0.08). However, this result was not statistically significant.
Bottom line: This well-designed study failed to show a survival benefit with IIT use in the critical-care setting. Given the findings of this and several other recent studies, one should question whether IIT should be prescribed as the standard of care in all critically-ill patients.
Citation: Arabi Y, Dabbagh O, Tamim H, et al. Intensive versus conventional insulin therapy: a randomized controlled trial in medical and surgical critically ill patients. Crit Care Med. 2008;36(12):3190-3197.
Preoperative and Intraoperative Predictors of Cardiac Adverse Events
Clinical question: What are the incidence and risk factors for perioperative cardiac adverse events after noncardiac surgery?
Background: In the past few decades, the incidence of cardiac adverse events (CAEs) for a general surgery population has remained largely unchanged (approximately 1%). This is in spite of multiple studies evaluating predictive models and attempts at preventive treatment, including preoperative coronary revascularization and perioperative beta blockers.
Study design: Prospective observational study.
Setting: Single, large, tertiary-care university hospital.
Synopsis: A total of 7,740 cases were reviewed in this study, which consisted of general surgery (4,937), vascular surgery (1,846), and urological surgery (957). A trained nurse followed up for perioperative CAEs as many as 30 days after the operation via medical chart review, phone calls, and letters. CAEs were defined as: Q-wave myocardial infarction (MI), non-ST elevation MI, cardiac arrest, or new cardiac dysrhythmia. A total of 83 CAEs (1.1% of patients) had cardiac arrest, with cardiac dysrhythmia being most common.
A total of seven preoperative risk factors were identified as independent predictors for CAEs: age 68, BMI 30, emergent surgery, prior coronary intervention or cardiac surgery, active congestive heart failure, cerebrovascular disease, and hypertension. In addition, two intraoperative risk factors were identified: intraoperative transfusion of packed red blood cells and operative duration of 3.8 hours. (The P value was 0.05 for all independent predictors.)
A further evaluation of intraoperative parameters of high-risk patients experiencing a CAE showed that these patients were more likely to have an episode of mean arterial pressure (MAP) <50 mmHg, an episode of 40% decrease in MAP, and an episode of tachycardia (heart rate >100).
Bottom line: A combination of preoperative predictors and intraoperative elements can help improve risk assessment for perioperative CAEs after noncardiac surgery.
Citation: Kheterpal S, O’Reilly M, Englesbe M, et al. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110(1):58-66.
Early Feeding in the ICU Does Not Affect Hospital Mortality
Clinical question: Will implementing evidence-based feeding guidelines improve feeding practices and reduce mortality in ICU patients?
Background: There is evidence suggesting that providing nutritional support to ICU patients within 24 hours of admission may decrease mortality. It is widely understood that patient care varies between ICUs, and there exist no uniform, evidence-based guidelines for nutritional support. Many patients remain unfed after 48 hours.
Study design: Cluster, randomized-controlled trial.
Setting: ICUs in 27 community and tertiary-care hospitals in Australia and New Zealand.
Synopsis: Hospitals were randomized to intervention or control groups. Dietitian and intensivist co-investigators from intervention ICUs developed guidelines using the Clinical Practice Guideline Development Cycle. Control ICUs were requested to make no new ICU nutritional management changes. The study enrolled 1,118 eligible patients and included adults expected to stay longer than two days. Excluded were patients taking oral diets, patients receiving palliative care or with suspected brain death, and patients sent from other facilities.
Guidelines were implemented using several methods—educational outreach visits, one-on-one conversations, active reminders, passive reminders, and educational in-services. The guidelines were successful in evoking significant practice changes in all of the intervention ICUs. Significantly more patients received nutritional support during their ICU stays in guideline ICUs, and patients in these ICUs were fed significantly earlier. There were, however, no significant differences between guideline and control ICUs with regard to hospital discharge mortality (28.9% vs. 27.4%; 95% CI; -6.3% to 12.0%; P=0.75). The groups also showed no statistical difference in hospital or ICU length of stay.
Bottom line: Significantly more patients in the guideline ICUs were fed within 24 hours, but this did not translate into improvements in mortality or other clinical outcomes.
Citation: Doig G, Simpson F, Finfer S, et al. Effect of evidence-based feeding guidelines on mortality of critically ill adults: a cluster randomized controlled trial. JAMA. 2008;300(23):2731-2741.
Low-Dose Aspirin Doesn’t Reduce Cardiovascular Events in Type 2 Diabetes Patients
Clinical question: Is low-dose aspirin effective for the primary prevention of atherosclerotic events in patients with Type 2 diabetes?
Background: Diabetes is a significant risk factor for cardiovascular events. Several prior studies have shown that aspirin therapy is effective as a secondary prevention strategy for cardiovascular events. The American Diabetes Association also recommends use of aspirin as a primary prevention strategy. Clinical trial data is currently insufficient in this area.
Study design: Prospective, randomized, open-label, controlled trial with blinded endpoint assessment.
Setting: 163 institutions in Japan.
Synopsis: The study enrolled 2,539 diabetic patients between 30 and 85 years old—mean age was 65—and included patients without EKG changes or a significant history or ongoing treatment of atherosclerotic disease. Patients were randomly assigned into an aspirin group (81 mg or 100 mg once daily) or a nonaspirin group. Patients had a median follow up of 4.37 years.
The primary endpoint was any atherosclerotic event, ranging from sudden death to ischemic heart disease or stroke. The incidence of atherosclerotic events was not statistically different in the aspirin group (68 events, 5.4%) than in the nonaspirin group (86 events, 6.7%) (HR, 0.80; 95% CI; 0.58-1.10; log-rank test, P=0.16). However, there was a suggested benefit of primary prevention in the subgroup aged 65 years or older. In addition, the combined endpoint of fatal coronary and cerebrovascular events occurred in one patient in the aspirin group and 10 patients in the nonaspirin group (HR, 0.10; 95 % CI, 0.01-0.79; P=.0037). This study is limited by the low incidence of atherosclerotic disease in Japan.
Bottom line: Low-dose aspirin used in patients with Type 2 diabetes does not significantly demonstrate primary prevention of cardiovascular events.
Citation: Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA. 2008;300(18):2134-2141. TH
In This Edition
- Generic vs. brand-name drugs.
- Rapid-response teams and mortality.
- A new prediction rule for mortality in acute pancreatitis.
- Viral causes of community-acquired pneumonia.
- Intensive insulin therapy in the ICU.
- New preoperative and intraoperative risk factors.
- Timing of ICU feedings and mortality.
- Aspirin as primary prevention in diabetics.
Generic, Brand-Name Drugs Used for Cardiovascular Disease Are Clinically Equivalent
Clinical question: Is there a clinical risk when substituting generic drugs for brand-name drugs in the treatment of cardiovascular disease?
Background: Spending on healthcare in the U.S. has reached critical levels. Increasing prescription drug costs make up a large portion of healthcare expenditures. The high cost of medicines directly affect adherence to treatment regimens and contribute to poor health outcomes. Cardiovascular drugs make up the largest portion of outpatient prescription drug spending.
Study design: Systematic review of relevant articles with a meta-analysis performed to determine an aggregate effect size.
Setting: Multiple locations and varied patient populations.
Synopsis: A total of 47 articles were included in the review, of which 38 were randomized controlled trials (RCTs). The studies measured both clinical efficacy and safety end points. More than half the articles were published prior to 2000. Clinical equivalence was noted in all seven beta-blocker RCTs; 10 of 11 diuretic RCTs; five of seven calcium-channel-blocker RCTs; all three antiplatelet-agent RCTs (clopidogrel, enteric-coated aspirin); two statin RCTs; one ACE-inhibitor RCT; and one alpha-blocker RCT. For drugs with a narrow therapeutic index, clinical equivalence was noted in all five warfarin RCTs and a single Class 1 anti-arrhythmic-agent RCT.
The aggregate effect size was -0.03 (95% CI, -0.15 to 0.08), which indicates nearly complete overlap of the generic and brand-name distributions. The data show no evidence of superiority of brand-name to generic drugs in clinical outcomes measured in the various studies.
In a separate review of editorials addressing generic substitution for cardiovascular drugs, 53% expressed a negative view of generic-drug substitution.
Bottom line: There is clinical equivalency between generic and brand-name drugs used in the treatment of cardiovascular disease. Despite this conclusion, a substantial number of editorials advise against generic substitution, which affects both patient and physician drug preferences.
Citation: Kesselheim A, Misono A, Lee J, et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis. JAMA. 2008; 300(21):2514-2526.
PEDIATRIC LITERATURE
Oral Prednisolone Does Not Shorten Hospitalization in Preschool-Age Children with Acute Virus-Induced Wheezing
Clinical question: Does oral prednisolone shorten duration of hospitalization in preschool-age children with acute virus-induced wheezing?
Background: Wheezing illnesses in young children are commonly associated with viral infections and may resolve with age without further stigmata of atopic asthma. Although systemic corticosteroids are commonly recommended for this population, evidence of their effectiveness is limited.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Three hospitals in the United Kingdom.
Synopsis: Children between 10 and 60 months that presented to a hospital with a physician-diagnosed attack of wheezing preceded by a viral infection were randomized to receive oral prednisolone or a placebo. There was no significant difference between the groups in the time to hospital discharge. There also was no difference in the prespecified subgroup analysis of children at high risk for atopic asthma.
The median time between presentation and “fit for discharge” was relatively low in this sample—12 hours in the placebo group and 10.1 hours in the prednisolone group. Nearly half the patients were discharged within the first several hours after presentation, and not all patients were admitted to a pediatric ward. A short-stay observation ward within the ED was an option. Thus, the results may be most applicable to patients with mild to moderate disease, some of which may not be admitted to a traditional inpatient unit.
Bottom line: Systemic corticosteroids do not dramatically shorten hospital and ED stays in preschool-aged children with mild to moderate virus-induced wheezing.
Citation: Panickar J, Lakhanpaul M, Lambert P, et al. Oral prednisolone for preschool children with acute virus-induced wheezing. N Engl J Med. 2009;360(4):329-338.
Reviewed by pediatric editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
RRT Implement-ation Doesn’t Affect Hospitalwide Code Rates or Mortality
Clinical question: Does the use of a rapid-response team (RRT) affect hospitalwide code rates and mortality?
Background: In the 100,000 Lives campaign, the Institute for Healthcare Improvement recommended that hospitals implement RRTs to help reduce preventable, in-hospital deaths. Studies have demonstrated that rates of non-ICU codes decrease after RRT implementation. It is unclear if this translates to changes in mortality rates.
Study design: Prospective cohort study of adult inpatients.
Setting: Saint Luke’s Hospital, a 404-bed tertiary-care academic hospital in Kansas City, Mo.
Synopsis: The hospital documented a total of 376 RRT activations. After RRT implementation, mean hospitalwide code rates decreased to 7.5 per 1,000 admissions from 11.2 per 1,000 admissions. This was not associated with a statistically significant reduction in hospitalwide code rates (adjusted odds ratio 0.76; 95% CI; 0.57-1.01; P=0.06). Secondary analyses noted lower rates of non-ICU codes (0.59; 95% CI, 0.40-0.89) compared with ICU codes (0.95; 95% CI; 0.64-1.43; P=0.03 for interaction). Finally, the RRT implementation was not associated with lower hospital-wide mortality (0.95; 95% CI; 0.81-1.11; P=0.52).
Secondary analyses also revealed few instances of RRT undertreatment or underutilization that may have affected the mortality numbers.
A limitation of this study is that it was slightly underpowered (78%) to detect a significant mortality difference. The findings also represent a single institution experience, and may not be generalized to other adult hospital settings or RRT programs.
Bottom line: Implementation of an RRT does not confer lower rates of hospital-wide code arrests or mortality.
Citation: Chan P, Khalid A, Longmore L, et al. Hospital-wide code rates and mortality before and after implementation of a rapid response team. JAMA. 2008;300(21):2506-2513.
Simple Scoring System Provides Timely Prediction of Mortality in Acute Pancreatitis
Clinical question: How can physicians predict mortality in acute pancreatitis?
Background: Historical predictors of mortality in acute pancreatitis require up to 48 hours of data, such as with the Ranson Criteria, or extensive amounts of data, such as with the APACHE II score. An easier tool is needed to predict which patients are at higher risk of mortality.
Study design: Retrospective cohort.
Setting: Patients in the Cardinal Health clinical outcomes research database, which supports public reporting of hospital performance.
Synopsis: The authors identified patients with the principal diagnosis of pancreatitis from 2000-2001 and explored numerous diagnostic findings available within the first 24 hours. Ultimately, BUN >25, impaired mental status, presence of SIRS (systemic inflammatory response syndrome), age >60, and presence of a pleural effusion were found to be predictive of mortality. These diagnostic findings correspond to the mnemonic BISAP. The BISAP score was then validated in a second cohort that included patients from 2004-2005.
Each finding in the BISAP score was given one point. A score of less than 2 was present in approximately 60% of patients admitted with acute pancreatitis, and corresponded to a mortality of less than 1%. A score of 2 corresponded to a mortality of 2%. Higher scores were associated with steeply increasing mortality, with a score of 5 corresponding with greater than 20% mortality.
The BISAP score performed similarly to the APACHE II score, but the former is easier to calculate on the day of admission and has fewer parameters. A more challenging research step will be to demonstrate that using the BISAP score to determine treatment strategies can affect patient outcomes.
Bottom line: The easy-to-calculate BISAP score is a new method for predicting mortality in patients with acute pancreatitis. This tool should help hospitalists determine, on the day of admission, to what extent patients with acute pancreatitis need aggressive management, such as ICU admission and early involvement of specialists.
Citation: Wu B, Johannes R, Sun X, Tabak Y, Conwell D, Banks P. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008;57(12): 1698-1703.
Nasal Swabs Identify Viral Causes in CAP Patients
Clinical question: How often is viral infection associated with community-acquired pneumonia (CAP) in adults?
Background: CAP is a clinically important disease that is associated with significant hospitalization and mortality. CAP treatment guidelines acknowledge respiratory viruses as an etiology for pneumonia, but few recommendations are made regarding management of these viral infections.
Study design: Prospective study.
Setting: Five hospitals in Edmonton, Alberta, from 2004-2006.
Synopsis: The authors enrolled 193 hospitalized adults, median age 71. Nucleic amplification tests (NATs) from nasopharyngeal swab specimens were tested for human metapneumovirus, respiratory syncytial virus, rhinovirus, parainfluenza virus 1-4, coronaviruses, and adenovirus.
Fifteen percent of these patients had a nasal swab positive for a viral infection. Interestingly, 4% of patients had both a positive viral nasal swab and positive bacterial cultures. Compared with bacterial infection, patients with viral infection tended to be older (76 vs. 64 years, P=0.01), have limited ambulation (66% vs. 32%, P=0.006), and have a history of cardiac disease (66% vs. 32%, P=0.02). Patients with bacterial pneumonia showed a statistically significant trend toward having chest pain, an abnormal white blood count, and a lobar infiltrate on chest X-ray.
Further investigations might look at how nasal swab data could be used to improve infection control within the hospital for patients found to have easily transmissible viruses. Further research could explore the feasibility of avoiding antibiotic use in patients found to have viral pneumonia, assuming bacterial co-infection is reliably excluded.
Bottom line: Nasal swabs using NAT technology could play a significant role in identifying pathogens in CAP patients. How this technology should affect clinical decision-making and how it might improve outcomes remains unknown.
Citation: Johnstone J, Majumdar S, Fox J, Marrie T. Viral infection in adults hospitalized with community-acquired pneumonia: prevalence, pathogens, and presentation. Chest. 2008;134(6):1141-1148.
Intensive Insulin Therapy Doesn’t Reduce ICU Mortality
Clinical question: Does the use of intensive insulin therapy decrease mortality in the intensive-care unit (ICU)?
Background: In 2001, Van den Berghe et al (N Engl J Med. 2001;345(19):1359-67) reported a reduction in morbidity and mortality with intensive insulin therapy (IIT) in surgical ICU patients. This study led to the adoption of IIT protocols in many hospitals. Since 2001, further studies have failed to reproduce the same dramatic benefit of IIT.
Study design: Randomized, controlled trial.
Setting: National Guard King Abdulaziz Medical City, a tertiary-care teaching hospital in Saudi Arabia.
Synopsis: Patients were included in this study if they were 18 years or older with serum glucose levels greater than 110 mg/dL during the first 24 hours of ICU admission. There were multiple exclusion criteria, including patients with Type I diabetes, documented hypoglycemia on ICU admission (glucose <40), or diabetic ketoacidosis.
Enrolled patients were randomized to IIT or conventional insulin therapy (CIT). A multidisciplinary team designed the protocols to maintain glucose levels of 80 to 110 mg/dL and 180 to 200 mg/dL in the IIT and the CIT groups, respectively. The primary endpoint measured was ICU mortality.
The study did not produce a statistically significant difference in ICU mortality (13.5% for IIT vs. 17.1% for CIT; P=0.30). The adjusted hypoglycemia rate was 6.8 per 100 treatment days with IIT and 0.4 per 100 treatment days with CIT (P<0.0001). Patients with hypoglycemia had higher ICU mortality (23.8% vs. 13.7%, P=0.02).
In the measurement of secondary endpoints, there was a trend toward lower episodes of severe sepsis and septic shock in the IIT group (20.7% in IIT vs. 27.2% in CIT, P=0.08). However, this result was not statistically significant.
Bottom line: This well-designed study failed to show a survival benefit with IIT use in the critical-care setting. Given the findings of this and several other recent studies, one should question whether IIT should be prescribed as the standard of care in all critically-ill patients.
Citation: Arabi Y, Dabbagh O, Tamim H, et al. Intensive versus conventional insulin therapy: a randomized controlled trial in medical and surgical critically ill patients. Crit Care Med. 2008;36(12):3190-3197.
Preoperative and Intraoperative Predictors of Cardiac Adverse Events
Clinical question: What are the incidence and risk factors for perioperative cardiac adverse events after noncardiac surgery?
Background: In the past few decades, the incidence of cardiac adverse events (CAEs) for a general surgery population has remained largely unchanged (approximately 1%). This is in spite of multiple studies evaluating predictive models and attempts at preventive treatment, including preoperative coronary revascularization and perioperative beta blockers.
Study design: Prospective observational study.
Setting: Single, large, tertiary-care university hospital.
Synopsis: A total of 7,740 cases were reviewed in this study, which consisted of general surgery (4,937), vascular surgery (1,846), and urological surgery (957). A trained nurse followed up for perioperative CAEs as many as 30 days after the operation via medical chart review, phone calls, and letters. CAEs were defined as: Q-wave myocardial infarction (MI), non-ST elevation MI, cardiac arrest, or new cardiac dysrhythmia. A total of 83 CAEs (1.1% of patients) had cardiac arrest, with cardiac dysrhythmia being most common.
A total of seven preoperative risk factors were identified as independent predictors for CAEs: age 68, BMI 30, emergent surgery, prior coronary intervention or cardiac surgery, active congestive heart failure, cerebrovascular disease, and hypertension. In addition, two intraoperative risk factors were identified: intraoperative transfusion of packed red blood cells and operative duration of 3.8 hours. (The P value was 0.05 for all independent predictors.)
A further evaluation of intraoperative parameters of high-risk patients experiencing a CAE showed that these patients were more likely to have an episode of mean arterial pressure (MAP) <50 mmHg, an episode of 40% decrease in MAP, and an episode of tachycardia (heart rate >100).
Bottom line: A combination of preoperative predictors and intraoperative elements can help improve risk assessment for perioperative CAEs after noncardiac surgery.
Citation: Kheterpal S, O’Reilly M, Englesbe M, et al. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110(1):58-66.
Early Feeding in the ICU Does Not Affect Hospital Mortality
Clinical question: Will implementing evidence-based feeding guidelines improve feeding practices and reduce mortality in ICU patients?
Background: There is evidence suggesting that providing nutritional support to ICU patients within 24 hours of admission may decrease mortality. It is widely understood that patient care varies between ICUs, and there exist no uniform, evidence-based guidelines for nutritional support. Many patients remain unfed after 48 hours.
Study design: Cluster, randomized-controlled trial.
Setting: ICUs in 27 community and tertiary-care hospitals in Australia and New Zealand.
Synopsis: Hospitals were randomized to intervention or control groups. Dietitian and intensivist co-investigators from intervention ICUs developed guidelines using the Clinical Practice Guideline Development Cycle. Control ICUs were requested to make no new ICU nutritional management changes. The study enrolled 1,118 eligible patients and included adults expected to stay longer than two days. Excluded were patients taking oral diets, patients receiving palliative care or with suspected brain death, and patients sent from other facilities.
Guidelines were implemented using several methods—educational outreach visits, one-on-one conversations, active reminders, passive reminders, and educational in-services. The guidelines were successful in evoking significant practice changes in all of the intervention ICUs. Significantly more patients received nutritional support during their ICU stays in guideline ICUs, and patients in these ICUs were fed significantly earlier. There were, however, no significant differences between guideline and control ICUs with regard to hospital discharge mortality (28.9% vs. 27.4%; 95% CI; -6.3% to 12.0%; P=0.75). The groups also showed no statistical difference in hospital or ICU length of stay.
Bottom line: Significantly more patients in the guideline ICUs were fed within 24 hours, but this did not translate into improvements in mortality or other clinical outcomes.
Citation: Doig G, Simpson F, Finfer S, et al. Effect of evidence-based feeding guidelines on mortality of critically ill adults: a cluster randomized controlled trial. JAMA. 2008;300(23):2731-2741.
Low-Dose Aspirin Doesn’t Reduce Cardiovascular Events in Type 2 Diabetes Patients
Clinical question: Is low-dose aspirin effective for the primary prevention of atherosclerotic events in patients with Type 2 diabetes?
Background: Diabetes is a significant risk factor for cardiovascular events. Several prior studies have shown that aspirin therapy is effective as a secondary prevention strategy for cardiovascular events. The American Diabetes Association also recommends use of aspirin as a primary prevention strategy. Clinical trial data is currently insufficient in this area.
Study design: Prospective, randomized, open-label, controlled trial with blinded endpoint assessment.
Setting: 163 institutions in Japan.
Synopsis: The study enrolled 2,539 diabetic patients between 30 and 85 years old—mean age was 65—and included patients without EKG changes or a significant history or ongoing treatment of atherosclerotic disease. Patients were randomly assigned into an aspirin group (81 mg or 100 mg once daily) or a nonaspirin group. Patients had a median follow up of 4.37 years.
The primary endpoint was any atherosclerotic event, ranging from sudden death to ischemic heart disease or stroke. The incidence of atherosclerotic events was not statistically different in the aspirin group (68 events, 5.4%) than in the nonaspirin group (86 events, 6.7%) (HR, 0.80; 95% CI; 0.58-1.10; log-rank test, P=0.16). However, there was a suggested benefit of primary prevention in the subgroup aged 65 years or older. In addition, the combined endpoint of fatal coronary and cerebrovascular events occurred in one patient in the aspirin group and 10 patients in the nonaspirin group (HR, 0.10; 95 % CI, 0.01-0.79; P=.0037). This study is limited by the low incidence of atherosclerotic disease in Japan.
Bottom line: Low-dose aspirin used in patients with Type 2 diabetes does not significantly demonstrate primary prevention of cardiovascular events.
Citation: Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA. 2008;300(18):2134-2141. TH
See You in Chicago
Having grown up in the shadows of the Windy City, I always wanted to work in the Sears Tower, jog along Lake Shore Drive, catch a comedy show at the Chicago Theater, and—just like every other 11-year-old boy—hop the subway to Wrigley Field for Chicago Cubs’ day games. It’s been nearly two decades since I left Chicago’s suburbs, yet I still refer to the Windy City as my home.
It’s safe to say I’m a little excited about attending my first annual meeting in my favorite U.S. city. An expanded HM09 runs May 14-17 at the Hyatt Regency in downtown Chicago. The 2,000-room base hotel is the perfect location for learning and leisure. It’s just a stone’s throw from Lake Michigan, Navy Pier, museums, great restaurants, and shopping. If you weren’t able to make it to HM05 in Chicago—or aren’t familiar with the stretch of Michigan Avenue known as the Magnificent Mile—it has something for everyone, and it’s easily accessible on foot or by taxi, subway, or horse-drawn carriage.
I know times are tough, but if you can, plan to spend an extra day or two and soak up all that Chicago has to offer. May is a great time to visit Chicago: The temperature should be in the 70s, and thousands of tulips will be in full bloom. The Art Institute of Chicago is opening a new wing and admission will be free May 16-22; the 11th annual Great Chicago Places & Spaces festival is May 16 and offers hundreds of free architectural tours; and Lincoln Park Zoo (a 15-minute cab ride from downtown) is celebrating Bear Awareness Week. For you green thumbs, the Chicago Farmers Market, which offers fresh fruit, vegetables, and flowers, is right around the corner from the Hyatt at Daley Plaza. Feeling ambitious? You can embark on a tour of President Obama’s Chicago; just follow the user-friendly map at www.chicagotribune.com/travel/chi-obama-chicago-htmlstory,0,506256.htmlstory.
Chicago’s nightlife offers something for every taste—beer gardens, IMAX theaters, comedy shows, and live music of all genres. If you’re a sports fan, the Cubs will be in town, and the resurgent Blackhawks could be in the NHL playoffs. If you are looking for a sports bar to watch your favorite team, look no further than Houlihan’s (right next door to the hotel) and Mother Hubbard’s (two blocks north of the hotel).
Dare I forget to mention the main reason HM09 attracts thousands of the nation’s top hospitalists—a world-class continuing medical education lineup, first-rate faculty, and endless networking opportunities? The addition of a fourth meeting day dedicated solely to clinical and practice management precourses not only allows for a less-hectic meeting schedule, but it also cements HM09 as a forward-thinking, education-focused annual conference.
In addition to a pair of powerhouse keynote speakers and the annual Awards of Excellence, SHM will induct its first class of Fellows in Hospital Medicine at HM09. Built using SHM’s Core Competencies, the FHM designation recognizes individuals who have chosen HM as a career and have the credentials to represent the emerging specialty. SHM received more than 600 applications for the FHM designation, and more than 400 hospitalists will be inducted in the first class.
It hardly seems possible, but HM09 is right around the corner. The editorial team here at The Hospitalist has a few aces up our sleeves, too. More on those in the May issue! Also, don’t forget to stop by The Hospitalist booth (listed in the program as the Wiley-Blackwell booth) to introduce yourself, exchange business cards, sign up for a cool prize, and share your ideas on the future of HM. TH
Jason Carris is editor of The Hospitalist.
Having grown up in the shadows of the Windy City, I always wanted to work in the Sears Tower, jog along Lake Shore Drive, catch a comedy show at the Chicago Theater, and—just like every other 11-year-old boy—hop the subway to Wrigley Field for Chicago Cubs’ day games. It’s been nearly two decades since I left Chicago’s suburbs, yet I still refer to the Windy City as my home.
It’s safe to say I’m a little excited about attending my first annual meeting in my favorite U.S. city. An expanded HM09 runs May 14-17 at the Hyatt Regency in downtown Chicago. The 2,000-room base hotel is the perfect location for learning and leisure. It’s just a stone’s throw from Lake Michigan, Navy Pier, museums, great restaurants, and shopping. If you weren’t able to make it to HM05 in Chicago—or aren’t familiar with the stretch of Michigan Avenue known as the Magnificent Mile—it has something for everyone, and it’s easily accessible on foot or by taxi, subway, or horse-drawn carriage.
I know times are tough, but if you can, plan to spend an extra day or two and soak up all that Chicago has to offer. May is a great time to visit Chicago: The temperature should be in the 70s, and thousands of tulips will be in full bloom. The Art Institute of Chicago is opening a new wing and admission will be free May 16-22; the 11th annual Great Chicago Places & Spaces festival is May 16 and offers hundreds of free architectural tours; and Lincoln Park Zoo (a 15-minute cab ride from downtown) is celebrating Bear Awareness Week. For you green thumbs, the Chicago Farmers Market, which offers fresh fruit, vegetables, and flowers, is right around the corner from the Hyatt at Daley Plaza. Feeling ambitious? You can embark on a tour of President Obama’s Chicago; just follow the user-friendly map at www.chicagotribune.com/travel/chi-obama-chicago-htmlstory,0,506256.htmlstory.
Chicago’s nightlife offers something for every taste—beer gardens, IMAX theaters, comedy shows, and live music of all genres. If you’re a sports fan, the Cubs will be in town, and the resurgent Blackhawks could be in the NHL playoffs. If you are looking for a sports bar to watch your favorite team, look no further than Houlihan’s (right next door to the hotel) and Mother Hubbard’s (two blocks north of the hotel).
Dare I forget to mention the main reason HM09 attracts thousands of the nation’s top hospitalists—a world-class continuing medical education lineup, first-rate faculty, and endless networking opportunities? The addition of a fourth meeting day dedicated solely to clinical and practice management precourses not only allows for a less-hectic meeting schedule, but it also cements HM09 as a forward-thinking, education-focused annual conference.
In addition to a pair of powerhouse keynote speakers and the annual Awards of Excellence, SHM will induct its first class of Fellows in Hospital Medicine at HM09. Built using SHM’s Core Competencies, the FHM designation recognizes individuals who have chosen HM as a career and have the credentials to represent the emerging specialty. SHM received more than 600 applications for the FHM designation, and more than 400 hospitalists will be inducted in the first class.
It hardly seems possible, but HM09 is right around the corner. The editorial team here at The Hospitalist has a few aces up our sleeves, too. More on those in the May issue! Also, don’t forget to stop by The Hospitalist booth (listed in the program as the Wiley-Blackwell booth) to introduce yourself, exchange business cards, sign up for a cool prize, and share your ideas on the future of HM. TH
Jason Carris is editor of The Hospitalist.
Having grown up in the shadows of the Windy City, I always wanted to work in the Sears Tower, jog along Lake Shore Drive, catch a comedy show at the Chicago Theater, and—just like every other 11-year-old boy—hop the subway to Wrigley Field for Chicago Cubs’ day games. It’s been nearly two decades since I left Chicago’s suburbs, yet I still refer to the Windy City as my home.
It’s safe to say I’m a little excited about attending my first annual meeting in my favorite U.S. city. An expanded HM09 runs May 14-17 at the Hyatt Regency in downtown Chicago. The 2,000-room base hotel is the perfect location for learning and leisure. It’s just a stone’s throw from Lake Michigan, Navy Pier, museums, great restaurants, and shopping. If you weren’t able to make it to HM05 in Chicago—or aren’t familiar with the stretch of Michigan Avenue known as the Magnificent Mile—it has something for everyone, and it’s easily accessible on foot or by taxi, subway, or horse-drawn carriage.
I know times are tough, but if you can, plan to spend an extra day or two and soak up all that Chicago has to offer. May is a great time to visit Chicago: The temperature should be in the 70s, and thousands of tulips will be in full bloom. The Art Institute of Chicago is opening a new wing and admission will be free May 16-22; the 11th annual Great Chicago Places & Spaces festival is May 16 and offers hundreds of free architectural tours; and Lincoln Park Zoo (a 15-minute cab ride from downtown) is celebrating Bear Awareness Week. For you green thumbs, the Chicago Farmers Market, which offers fresh fruit, vegetables, and flowers, is right around the corner from the Hyatt at Daley Plaza. Feeling ambitious? You can embark on a tour of President Obama’s Chicago; just follow the user-friendly map at www.chicagotribune.com/travel/chi-obama-chicago-htmlstory,0,506256.htmlstory.
Chicago’s nightlife offers something for every taste—beer gardens, IMAX theaters, comedy shows, and live music of all genres. If you’re a sports fan, the Cubs will be in town, and the resurgent Blackhawks could be in the NHL playoffs. If you are looking for a sports bar to watch your favorite team, look no further than Houlihan’s (right next door to the hotel) and Mother Hubbard’s (two blocks north of the hotel).
Dare I forget to mention the main reason HM09 attracts thousands of the nation’s top hospitalists—a world-class continuing medical education lineup, first-rate faculty, and endless networking opportunities? The addition of a fourth meeting day dedicated solely to clinical and practice management precourses not only allows for a less-hectic meeting schedule, but it also cements HM09 as a forward-thinking, education-focused annual conference.
In addition to a pair of powerhouse keynote speakers and the annual Awards of Excellence, SHM will induct its first class of Fellows in Hospital Medicine at HM09. Built using SHM’s Core Competencies, the FHM designation recognizes individuals who have chosen HM as a career and have the credentials to represent the emerging specialty. SHM received more than 600 applications for the FHM designation, and more than 400 hospitalists will be inducted in the first class.
It hardly seems possible, but HM09 is right around the corner. The editorial team here at The Hospitalist has a few aces up our sleeves, too. More on those in the May issue! Also, don’t forget to stop by The Hospitalist booth (listed in the program as the Wiley-Blackwell booth) to introduce yourself, exchange business cards, sign up for a cool prize, and share your ideas on the future of HM. TH
Jason Carris is editor of The Hospitalist.
Telemedicine Can Help Solve Intensivist Shortage
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
Non-Physician Providers: Vital HM Resources
Enter text here
Enter text here
Enter text here
Project BOOST Expands
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) is an initiative to improve practices in transition care and reduce readmission rates for hospitals across the country. The project’s toolkit, mentoring program, and national advocacy efforts have proven so successful that the program is expanding this year.
In 2008, SHM began the first round of the Project BOOST mentoring program in six pilot hospitals. The first full cycle of Project BOOST mentoring sites began in March at 24 sites. The Hospitalist will feature updates on the full cycle of Project BOOST later this year. For more information about Project BOOST, visit www.hospitalmedicine.org/BOOST or e-mail [email protected].
As a pilot site, Southwestern Vermont Medical Center in Bennington has worked with mentors for the past six months. We caught up with project leader Jennifer Fells, RN, MS, to discuss the institution’s participation.
—Jennifer Fells, RN, MS, Southwestern Vermont Medical Center, Bennington
Question: Why did your group choose to participate in the mentoring program?
Answer: We wanted to reduce our readmission rate, and we knew we weren’t doing a service to patients. This was also a goal of our organization overall; it’s not only a benefit to the hospital, but a larger value when the patient goes back to the community.
Q: How has the BOOST mentoring program benefited your program?
A: It helped us get organized by beginning the process and affirmed our belief that there were ways to address readmissions. The toolkit has proved to be invaluable. The mentors helped us keep on track and offered us guidance. They share the experiences of the other Project BOOST teams, and we benefit from that information.
Chapter Updates

Georgia Coastal
The chapter’s second meeting was well attended by both of the large hospitalist groups in Atlanta; two hospitalists from a rural institution also were in attendance. Leena Dutta, MD, of North Fulton Regional Hospital in Roswell, spoke about her experience as a hospitalist and the uses of Tygacil.

Los Angeles
The chapter met Feb. 3 for dinner at Valentino’s Restaurant in Santa Monica. Twenty-five hospitalists and residents from academic and private institutions attended the meeting, which featured two presentations. The night started off with a discussion about the management of bloodstream infections, led by Anjay Rastogi, MD, of UCLA Medical Center. Robert Schultz and Craig Steinhauer of financial planning services firm NWF discussed “Navigating Through Rocky Times: A Guide to Investment and Retirement Strategies.”
Miami/South Florida
The chapter met Jan. 22, and the keynote speaker was treasurer Efren Manjarrez, MD, who gave a presentation on “Transition of Care.” He revealed data from a soon-to-be-released SHM task force paper. The presentation was well received, and the local HM programs agreed to collaborate to collect more data for future studies.
The changes in the approach to the discharge process were a surprise to us. After we developed our team, we discovered how fragmented the discharge process was throughout the entire organization. Discharges were handled over multiple disciplines, and it was fragmented by design.
For example, our documentation, discharge plans, discharge recommendations, and patient-education materials are in different parts of our documentation system.
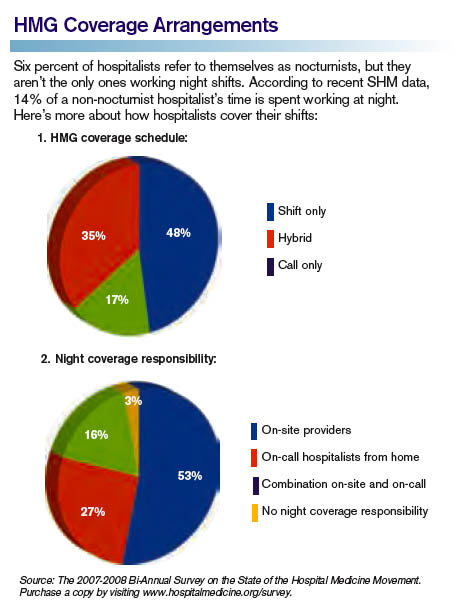
Q: What did you learn about your program through the initial Project BOOST step: analyze care delivery?
A: We realized that disciplines were not coordinated with one another and there was not enough time for the physician to complete the discharge plan. The process was cumbersome, awkward, and very time-consuming. We were looking to create efficiency in the information that needs to be coordinated to do those discharge orders.
Q: What additional changes do you hope to see in the remaining time with BOOST mentors?
A: We definitely hope to improve our process. We want to have implemented the tools and have a coordinated discharge process, and a centralized way to communicate the discharge plan. We found a lack of communication creates a barrier among disciplines, and we hope to correct that and become more customer-friendly to patients.
Q: How did your site’s BOOST mentor assist in the implementation process? What was the outcome?
A: Our site mentor helped with the clarification of data to be collected for measurement, keeping us on track with the toolkit, and served as another set of eyes. When you are in an organization, and even when you have the appropriate team, you always need somebody to say, “What do you think about this?” or “Did you think about this item?”
It’s another perspective, sharing gained knowledge from other organizations. That’s very critical.
SHM marketing coordinator Nadia Clenending contributed to this report.
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) is an initiative to improve practices in transition care and reduce readmission rates for hospitals across the country. The project’s toolkit, mentoring program, and national advocacy efforts have proven so successful that the program is expanding this year.
In 2008, SHM began the first round of the Project BOOST mentoring program in six pilot hospitals. The first full cycle of Project BOOST mentoring sites began in March at 24 sites. The Hospitalist will feature updates on the full cycle of Project BOOST later this year. For more information about Project BOOST, visit www.hospitalmedicine.org/BOOST or e-mail [email protected].
As a pilot site, Southwestern Vermont Medical Center in Bennington has worked with mentors for the past six months. We caught up with project leader Jennifer Fells, RN, MS, to discuss the institution’s participation.
—Jennifer Fells, RN, MS, Southwestern Vermont Medical Center, Bennington
Question: Why did your group choose to participate in the mentoring program?
Answer: We wanted to reduce our readmission rate, and we knew we weren’t doing a service to patients. This was also a goal of our organization overall; it’s not only a benefit to the hospital, but a larger value when the patient goes back to the community.
Q: How has the BOOST mentoring program benefited your program?
A: It helped us get organized by beginning the process and affirmed our belief that there were ways to address readmissions. The toolkit has proved to be invaluable. The mentors helped us keep on track and offered us guidance. They share the experiences of the other Project BOOST teams, and we benefit from that information.
Chapter Updates
Georgia Coastal
The chapter’s second meeting was well attended by both of the large hospitalist groups in Atlanta; two hospitalists from a rural institution also were in attendance. Leena Dutta, MD, of North Fulton Regional Hospital in Roswell, spoke about her experience as a hospitalist and the uses of Tygacil.
Los Angeles
The chapter met Feb. 3 for dinner at Valentino’s Restaurant in Santa Monica. Twenty-five hospitalists and residents from academic and private institutions attended the meeting, which featured two presentations. The night started off with a discussion about the management of bloodstream infections, led by Anjay Rastogi, MD, of UCLA Medical Center. Robert Schultz and Craig Steinhauer of financial planning services firm NWF discussed “Navigating Through Rocky Times: A Guide to Investment and Retirement Strategies.”
Miami/South Florida
The chapter met Jan. 22, and the keynote speaker was treasurer Efren Manjarrez, MD, who gave a presentation on “Transition of Care.” He revealed data from a soon-to-be-released SHM task force paper. The presentation was well received, and the local HM programs agreed to collaborate to collect more data for future studies.
The changes in the approach to the discharge process were a surprise to us. After we developed our team, we discovered how fragmented the discharge process was throughout the entire organization. Discharges were handled over multiple disciplines, and it was fragmented by design.
For example, our documentation, discharge plans, discharge recommendations, and patient-education materials are in different parts of our documentation system.
Q: What did you learn about your program through the initial Project BOOST step: analyze care delivery?
A: We realized that disciplines were not coordinated with one another and there was not enough time for the physician to complete the discharge plan. The process was cumbersome, awkward, and very time-consuming. We were looking to create efficiency in the information that needs to be coordinated to do those discharge orders.
Q: What additional changes do you hope to see in the remaining time with BOOST mentors?
A: We definitely hope to improve our process. We want to have implemented the tools and have a coordinated discharge process, and a centralized way to communicate the discharge plan. We found a lack of communication creates a barrier among disciplines, and we hope to correct that and become more customer-friendly to patients.
Q: How did your site’s BOOST mentor assist in the implementation process? What was the outcome?
A: Our site mentor helped with the clarification of data to be collected for measurement, keeping us on track with the toolkit, and served as another set of eyes. When you are in an organization, and even when you have the appropriate team, you always need somebody to say, “What do you think about this?” or “Did you think about this item?”
It’s another perspective, sharing gained knowledge from other organizations. That’s very critical.
SHM marketing coordinator Nadia Clenending contributed to this report.
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) is an initiative to improve practices in transition care and reduce readmission rates for hospitals across the country. The project’s toolkit, mentoring program, and national advocacy efforts have proven so successful that the program is expanding this year.
In 2008, SHM began the first round of the Project BOOST mentoring program in six pilot hospitals. The first full cycle of Project BOOST mentoring sites began in March at 24 sites. The Hospitalist will feature updates on the full cycle of Project BOOST later this year. For more information about Project BOOST, visit www.hospitalmedicine.org/BOOST or e-mail [email protected].
As a pilot site, Southwestern Vermont Medical Center in Bennington has worked with mentors for the past six months. We caught up with project leader Jennifer Fells, RN, MS, to discuss the institution’s participation.
—Jennifer Fells, RN, MS, Southwestern Vermont Medical Center, Bennington
Question: Why did your group choose to participate in the mentoring program?
Answer: We wanted to reduce our readmission rate, and we knew we weren’t doing a service to patients. This was also a goal of our organization overall; it’s not only a benefit to the hospital, but a larger value when the patient goes back to the community.
Q: How has the BOOST mentoring program benefited your program?
A: It helped us get organized by beginning the process and affirmed our belief that there were ways to address readmissions. The toolkit has proved to be invaluable. The mentors helped us keep on track and offered us guidance. They share the experiences of the other Project BOOST teams, and we benefit from that information.
Chapter Updates
Georgia Coastal
The chapter’s second meeting was well attended by both of the large hospitalist groups in Atlanta; two hospitalists from a rural institution also were in attendance. Leena Dutta, MD, of North Fulton Regional Hospital in Roswell, spoke about her experience as a hospitalist and the uses of Tygacil.
Los Angeles
The chapter met Feb. 3 for dinner at Valentino’s Restaurant in Santa Monica. Twenty-five hospitalists and residents from academic and private institutions attended the meeting, which featured two presentations. The night started off with a discussion about the management of bloodstream infections, led by Anjay Rastogi, MD, of UCLA Medical Center. Robert Schultz and Craig Steinhauer of financial planning services firm NWF discussed “Navigating Through Rocky Times: A Guide to Investment and Retirement Strategies.”
Miami/South Florida
The chapter met Jan. 22, and the keynote speaker was treasurer Efren Manjarrez, MD, who gave a presentation on “Transition of Care.” He revealed data from a soon-to-be-released SHM task force paper. The presentation was well received, and the local HM programs agreed to collaborate to collect more data for future studies.
The changes in the approach to the discharge process were a surprise to us. After we developed our team, we discovered how fragmented the discharge process was throughout the entire organization. Discharges were handled over multiple disciplines, and it was fragmented by design.
For example, our documentation, discharge plans, discharge recommendations, and patient-education materials are in different parts of our documentation system.
Q: What did you learn about your program through the initial Project BOOST step: analyze care delivery?
A: We realized that disciplines were not coordinated with one another and there was not enough time for the physician to complete the discharge plan. The process was cumbersome, awkward, and very time-consuming. We were looking to create efficiency in the information that needs to be coordinated to do those discharge orders.
Q: What additional changes do you hope to see in the remaining time with BOOST mentors?
A: We definitely hope to improve our process. We want to have implemented the tools and have a coordinated discharge process, and a centralized way to communicate the discharge plan. We found a lack of communication creates a barrier among disciplines, and we hope to correct that and become more customer-friendly to patients.
Q: How did your site’s BOOST mentor assist in the implementation process? What was the outcome?
A: Our site mentor helped with the clarification of data to be collected for measurement, keeping us on track with the toolkit, and served as another set of eyes. When you are in an organization, and even when you have the appropriate team, you always need somebody to say, “What do you think about this?” or “Did you think about this item?”
It’s another perspective, sharing gained knowledge from other organizations. That’s very critical.
SHM marketing coordinator Nadia Clenending contributed to this report.
Consumer-Driven Healthcare
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition

According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition
According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
Joseph Forrester, DO, a critical-care hospitalist and pulmonologist in Denver, discovered firsthand how scoping out and paying for healthcare now resembles shopping for other big-ticket items. Unlike purchasing and paying down a diamond ring or a 60-inch flat-screen TV, for which the final price and payment is duly noted and balances promptly adjusted, hospital billing attempted to overcharge Dr. Forrester by 500%. He already had paid $4,000 toward his 2008 out-of-pocket deductible for medical expenses and was surprised when the hospital said he would have to pay the full $5,000 deductible before he could receive care. The savvy doc went to a real-time claims adjudication tool that he uses in his own practice to show the hospital he’d already satisfied the first 80% of the $5,000 deductible.
The hospital’s billing department listened and responded.
Dr. Forrester paid the remaining $1,000 to fulfill his deductible, and his insurer covered the rest of the treatment cost. “Having access to this information allowed him to receive care immediately, without having to wait weeks for the hospital to correct its mistaken information,” says Chris Stanley, MD, a medical director with United Healthcare.
High-deductible health plans (HDHPs) like Dr. Forrester’s have been growing in popularity since the establishment of health savings accounts (HSAs). Designed to help individuals save for future medical and retiree health expenses on a tax-free basis, HSAs were signed into law by President Bush in December 2003. These products are just beginning to influence how hospitals collect fees and how patients negotiate with their physicians—including hospitalists—about which medications, tests, and procedures they’re willing to pay for.
Break from Tradition
According to the U.S. Treasury Department Web site, HSAs allow individuals to “own and control the money in your HSA. Decisions on how to spend the money are made by the consumer without relying on a third party or a health insurer. Consumers will also decide what types of investments to make with the money in the account in order to make it grow.”
HSAs only are available to individuals covered solely through an HDHP. Individuals receiving veterans benefits or already on Medicare are not eligible; however, if they establish an HSA before enrolling in Medicare, they can keep it—but not add to it.
HDHPs offer consumers—especially young, healthy individuals—low premiums and high deductibles (between $1,150 and $2,900 for individuals and $2,300 to $5,800 for family plans). In addition to paying a low premium, consumers can put money into an HSA to pay for out-of-pocket expenses, including deductibles, co-pays, and co-insurance. The maximum amount of tax-free money a consumer can stash in an HSA this year is $5,800 for individuals and $11,600 for families. (Those 55 and older can contribute an additional $1,000 annually to their HSAs to accelerate their savings rates.)
Consumers can access HSA funds through a debit card, or they can pay for a service, then file for reimbursement.
An HSA should not be confused with a flexible spending account (FSA). Both are paid for by employees with pre-tax dollars; however, FSAs:
- Carry no insurance requirements;
- Are capped at $5,000 in annual contributions;
- Do not pay interest on the account balance; and
- Must be used—or forfeited—by the end of the plan year.
In contrast, an HSA:
- Is funded by the employee or jointly by employer and employee (known as a health reimbursement account, or HRA);
- Has insurance requirements on deductibles and out-of-pocket contributions;
- Pays the provider directly and submits receipts to the account administrator;
- Accumulates interest through a financial institution; and
- Allows unused funds to be carried forward.
Easy Business Decision
Employers are jumping on the HDHP bandwagon, largely to shift more health insurance costs to employees. HDHPs allow consumers to save on upfront costs (e.g., premiums and routine medical expenses) while allowing them to partner with their physicians when deciding how and when they will spend their HSA dollars.
Allowing patients to be involved in the testing, medication, and length-of-stay decisions relative to their care is a reversal from the status quo. Physicians working with hospitalized patients aren’t used to patients questioning treatment or asking for a cost analysis of medications. Another way to think about working with patients who have nontraditional plans: If you were eating at a soup kitchen, you probably wouldn’t complain about having to eat off of paper plates. But if you were dining at a five-star restaurant, you’d freely complain to the maître d’ if your soup was cold or the salad limp.
The 2008 National Study of Employer-Sponsored Health Plans, conducted by international human resources consulting firm Mercer, reported consumer-directed health plans, coupled with either an HSA or an HRA, are offered by 45% of companies with 25,000 or more employees (up from 22% in 2005). Nine percent of companies with 10 to 499 employees offer consumer-directed health plans, up from 2% in 2005.
Mercer partner Blaine Bos notes that raising deductibles is the fallback for employers faced with medical cost increases they can’t—or won’t—absorb. “The introduction of HSAs may have changed employers’ thinking on just how high a deductible can go without causing employees to revolt,” Bos says in the survey analysis. He predicts bad economic times will accelerate consumer-directed health plan uptake in small and large firms because they deliver substantially lower costs than PPOs and HMOs. In 2008, CDHP costs averaged $6,207 per employee, compared with $7,815 for PPOs and $7,768 for HMOs.
Data from ehealthinsurance.com indicate consumers are taking full advantage of HDHPs: Fifteen percent choose the highest deductibles, 48% the mid-range, and 37% the lowest deductible.
Still on HM’s Horizon
Consumer-driven healthcare has yet to significantly affect hospitals and—by extension—HM groups, although hospital admissions were down 2% nationally in 2008 and hospital debts are climbing. Adam Singer, MD, CEO of IPC: The Hospitalist Company, says the impact of HSAs on HM isn’t noticeable yet because patients haven’t adapted to the new model. “Consumers usually aren’t price-shopping the facility, because they’re committed to their physicians and will go to the hospital where their physician has privileges,” Dr. Singer says. “Additionally, the patients hospitalists see are very sick. Many came in through the ED and had no choice about how they got there. They certainly don’t pick their hospitalists.”
By extension, the ED isn’t immune to market forces driving consumer-directed care. Karen McConnell, PhD, director of the Oregon Health and Science University’s Center for Policy and Research in Emergency Medicine, posits that rapid adoption of high-deductible plans could change ED utilization (Ann Emerg Med. 2005;46(6):536-40). Although the ED may be insulated from extensive shopping and price negotiation because visits generally are for urgent conditions, Dr. McConnell says, ED utilization patterns may change if cost-conscious HSA holders forego other necessary medical care or seek substitutes for less-urgent problems.
The reality of consumer-directed healthcare and patients footing more of their own medical bills could eventually have a significant impact on HM programs. “Hospitals are under attack,” Dr. Singer says. “The 20% to 50% of hospital medicine program revenues received as support payments from their hospitals may drop as high-deductible plans with HSAs drive down hospital revenues. So as hospital revenues fall, the subsidies—particularly some of the more absurd, seven-figure subsidies that hospitalists enjoy—are vulnerable.”
Patients Take Charge
With their own money at stake, HSA consumers are engaged in the decision to spend—or save—their healthcare dollars. Although the shift in the doctor-patient decision-making process has slowly found its way into the hospital, it is playing out in doctor’s offices—one of several pipelines for hospital admissions. As a consumer, Linda Waldmann, manager of MyCost, a real-time claims-adjudication tool offered by Alegent Health, introduced cost when making treatment decisions after she was diagnosed with carpal tunnel syndrome. She asked her orthopedic surgeon lots of questions, absorbed what he said, then made her own treatment choices.
“My orthopedist wanted me to have three tests, but I elected to postpone one test until my HSA replenished the following year,” Waldmann says. “Doctors are still hesitant about negotiating with patients, but this one understood my concern.”
Blue Cross/Blue Shield of Tennessee’s (BCBST) Maggie Fox, director of application systems, saw a large jump (to 33% in 2009 from 8% in 2008) among BCBST’s 5,000 employees opting for HSAs. The Tennessee company emphasizes prevention, education, and wellness as critical components of consumer-directed care, and the company’s HSA consumers are offered a variety of discounts for adhering to healthy lifestyles.
At BCBST, HSAs have opened dialogue between patients, physicians, and hospitals. Through a Web-based portal called “Blue Access,” providers receive information on a patient’s financial liability in as little as 10 seconds. “HSAs and HRAs have created a patient liability that never existed before,” Fox says. “Higher out-of-pocket costs change everything. Providers need to collect payment at the point of care, whether that’s the office or hospital. There’s more work at checkout, but at least patients and providers know the exact amount the care costs and how much the patient has to pay.”
Davis Liu, MD, a Wharton School of Business graduate and family physician with Northern California Permanente Medical Group, advises hospitalists to be ready for patients with HSAs to challenge treatment decisions because of the cost. He says hospitalists must prepare to communicate clearly and effectively with HSA patients, especially when it comes to necessary testing and medications. The task might be difficult because information about testing costs and procedures is limited, and prices vary dramatically by hospital and region. “While it is extremely unlikely that patients will refuse testing when hospitalized, hospitalists must be acutely aware that these patients may skip follow-up appointments, testing, and surgeries,” Dr. Liu says.
United Healthcare’s Dr. Stanley sees physician decision-making evolving as HSA patients become more aware of the economics of treatment options. “Patients are already questioning doctors who order four tests when they’re only willing to pay for three, wanting to postpone procedures, and asking about costs for additional tests and procedures,” he says. “Eventually, cost consciousness will impact group practices. They will have to decrease overhead, revamp collection processes, and strive for administrative simplicity.” Woe to the physician who believes cost isn’t their responsibility, Dr. Stanley says, as they “must realize they’re small-business owners and act accordingly.”
The Future
Consumer-driven healthcare might have little effect on hospitals right now, but change is on the horizon, according to Greg Scandlen, president and CEO of Consumers for Health Care Choice in Hagerstown, Md. He cites the 2008 National Health Interview Survey conducted by the Centers for Disease Control and Prevention, which shows 20% of Americans have an HDHP, as proof positive these new plans are increasing market penetration.
“We’re at a tipping point where every provider will have to deal with cash-paying clients,” he says. “Hospitals with Chargemaster pricing [the list price for services and procedures charged to self-pay and other uninsured clients, usually three to three and a half times the normal Medicare reimbursement] won’t get away with that much longer. They’ll have to charge reasonable, negotiated rates rather than slamming self-pay patients.”
It looks as though the days when patients entered the hospital worried about getting well and dealing with the bills later will soon be in the rearview mirror. Not far into the future, individuals with self-pay components to their health insurance might demand and receive full financial disclosure of all their expected hospital costs (see “Patients Can Shop Around,” p. 29) at the time of admission, with necessary adjustments at discharge.
“Hospitals can’t have secret pricing in a transparent, consumer-driven world,” says Scandlen. “The HDHP model hasn’t fully hit hospitals yet, but they’ll get clobbered in about two years if they don’t adapt.” TH
Marlene Piturro is a freelance writer based in Hastings-on-Hudson, NY.
Proceedings of the 2008 Heart-Brain Summit

Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Preface
Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Introduction: Heart-brain medicine: Update 2008
Marc S. Penn, MD, PhD, and Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Bakken Lecture: The brain, the heart, and therapeutic hypothermia
Patrick M. Kochanek, MD
Session 1: Pathways Involved in Neuromodulation of Risks in Coronary Artery Disease
Depression and heart rate variability in patients with coronary heart disease
Robert M. Carney, PhD, and Kenneth E. Freedland, PhD
Autonomic function and prognosis
Michael S. Lauer, MD
Vagal tone and the inflammatory reflex
Julian F. Thayer, PhD
Inflammation, atherosclerosis, and arterial thrombosis: Role of the scavenger receptors CD36
Roy L. Silverstein, MD
Pioneer Award Address: Ignorance isn't biased: Comments on receiving the Pioneer Award
David S. Goldstein, MD, PhD
Session II: Measures and Strategies for Modulation of Heart-Brain Interactions
Heart rate variability with deep breathing as a clinical test of cardiovagal function
Robert W. Shields, Jr, MD
Basic research models for the study of underlying mechanisms of electrical neuromodulation and ischemi heart-brain interactions
Mike J.L. DeJongste, MD, PhD, FESC; Gert J. TerHorst, PhD; and Robert D. Foreman, PhD
Session III: Annual Review of Key Papers in Heart-Brain Medicine
Key papers in the field published during the year prior to the Summit were discussed; two of those papers are reported here.
Cardiac sympathetic denervation preceding motor signs in Parkinson disease
David S. Goldstein, MD, PhD; Yehonatan Sharabi, MD; Barbara I. Karp, MD; Oladi Bentho; Ahmed Saleem, MD; Karel Pacak, MD, PhD; and Graeme Eisenhofer, PhD
Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation
Jeffrey P. Moak, MD; David S. Goldstein, MD, PhD; Basil A. Eldadah, MD, PhD; Ahmed Saleem, MD; Courtney Holmes, CMT; Sandra Pechnik, RN; and Yehonatan Sharabi, MD
Session IV: Code Lavender—Strategies for Implementing Heart-Brain Medicine
Is posttraumatic stress disorder related to development of heart disease? An update
Laura D. Kubzansky, PhD, and Karestan C. Koenen, PhD
Creating a healing environment: Rationale and research overview
Jone Geimer-Flanders, DO
Redesigning the neurocritical care unit to enhance family participation and improve outcomes
Owen Samuels, MD
Session V: Insights into Neuromodulation of Cardiovascular Function
Neuromodulation of cardiac pain and cerebral vasculature: Neural mechanisms
Robert D. Foreman, PhD, and Chao Qin, MD, PhD
Pinacidil induces vascular dilation and hyperemia in vivo and does not impact biophysical properties of neurons and astrocytes in vitro
Rosa Cao; Bryan T. Higashikubo; Jessica Cardin; Ulf Knoblich; Raddy Ramos, PhD; Mark T. Nelson, PhD; Christopher I. Moore, PhD; and Joshua C. Brumberg, PhD
The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system
Stephen W. Porges, PhD
Poster Abstracts
Abstract 1: Insulin use does not protect against restenosis in diabetic patients presenting with acute coronary syndrome or symptomatic angina
Matthew C. Becker, MD; John M. Galla, MD; Saif Anwaruddin, MD; Samir Kapadia, MD; and Richard A. Krasuski, MD
Abstract 2: Postoperative statin use and lower LDL cholesterol concentration are associated with reduced incidence of stroke
Matthew C. Becker, John M. Galla, Ryan P. Daly, Femi Philip, Peter Zimbwa, Stephen O. Chen, Chen H. Chow, Tingfei Hu, Richard A. Krasuski, and Arman T. Askari
Abstract 3: Brain edema and blood-brain barrier leakage influence antiepileptic drug levels
Giulia Betto, Vincent Fazio, Damir Janigro, and Chaitali Ghosh
Abstract 4: CPAP treatment vs conservative treatment in mild obstructive sleep apnea: Implications on cardiovascular morbidity
Kumar Budur, MD, and Nattapong Jaimchariyatam, MD
Abstract 5: New bioinformatics program identifies behavioral medicine interventions for epidemic cardiovascular disease in the developing world: Analysis of multidisciplinary findings for launching a new global public health initiative in heart-brain medicine
William C. Bushell, PhD
Abstract 6: Do systemic inflammation and blood-brain barrier failure play a role in pediatric psychosis?
Erin Carlton, Tatiana Falcone, Ayush Batra, Vince Fazio, Kathleen Franco, and Damir Janigro
Abstract 7: Brain, heart, and education
Linda Bryant Caviness, PhD
Abstract 8: Tobacco smoke mediates a monocytic and endothelial proinflammatory activation that synergistically affects BBB integrity
L. Cucullo, T. Sathe, M. Hossain, and D. Janigro
Abstract 9: Dynamic changes in ECG predict poor outcome after aneurysmal subarachnoid hemorrhage (aSAH)
H.A. Elsharkawy, MD; S.M. El Hadi, MD, PhD; J.E. Tetzlaff, MD; and J.J. Provencio, MD, FCCM
Abstract 10: Mechanism studies of malformation of cortical development by prenatal exposure of combined methylazoxymethanol and thalidomide
Q. Fan, S. Ramakrishna, N. Marchi, V. Fazio, K. Hallene, and D. Janigro
Abstract 11: Proapolipoprotein A1 demonstrates improved potential as a serum marker for brain metastases without vascular disease interference
Vince Fazio, Peter Mazzone, Nicola Marchi, Thomas Masaryk, and Damir Janigro
Abstract 12: Biofeedback-assisted stress management training to reverse myocardial remodeling in patients with end-stage heart failure
Dana L. Frank, BS; Mary E. Klecka, BA; Jerry Kiffer, MA; Heather Henrickson, PhD; Michael G. McKee, PhD; and Christine S. Moravec, PhD
Abstract 13: Nitric oxide and arginine metabolism in depression: Effect of a serotonin-norepinephrine reuptake inhibitor
Angelos Halaris, John Piletz, Omer Iqbal, Debra Hoppensteadt, Jawed Fareed, He Zhu, James Sinacore, and C. Lindsay DeVane
Abstract 14: Association between excessive daytime sleepiness and oxygen desaturation in obstructive sleep apnea syndrome: Nadir oxygen saturation vs mean oxygen saturation vs time spent below 90% oxygen saturation—which is important?
Nattapong Jaimchariyatam, MD, and Kumar Budur, MD
Abstract 15: Endotoxin preconditioning of the CNS: Microglia activation and neuroprotection
Walid Jalabi, Ranjan Dutta, Yongming Jin, Gerson Criste, Xinghua Yin, Grahame J. Kidd, and Bruce D. Trapp
Abstract 16: Pilot of stress reduction strategies for patients after a coronary event
R. Lindquist, D. Windenburg, K. Savik, and U. Bronas
Abstract 17: Cerebrovascular substrates of seizures after cardiopulmonary bypass
Rebecca O’Dwyer, Tim Wehner, Dileep Nair, Giulia Betto, Nicola Marchi, and Damir Janigro
Abstract 18: Depression and whole blood serotonin in patients with coronary heart disease from the heart and soul study
Lawson Wulsin, Dominique Musselman, Christian Otte, Erica Bruce, Sadia Ali, and Mary Whooley
Abstract 19: Gender differences prominent in linking anxiety to long-term mortality among the elderly
Jianping Zhang, MD, PhD; Boaz Kahana, PhD; Eva Kahana, PhD; Bo Hu, PhD; and Leo Pozuelo, MD
Abstract 20: Temporal lobe and sinus node: A case report provides evidence for bidirectional effects
Rebecca O’Dwyer, MD; Andreas Alexopoulos, MD, MPH; Walid Saliba, MD; Imad Najm, MD; and Richard Burgess, MD, PhD
Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Preface
Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Introduction: Heart-brain medicine: Update 2008
Marc S. Penn, MD, PhD, and Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Bakken Lecture: The brain, the heart, and therapeutic hypothermia
Patrick M. Kochanek, MD
Session 1: Pathways Involved in Neuromodulation of Risks in Coronary Artery Disease
Depression and heart rate variability in patients with coronary heart disease
Robert M. Carney, PhD, and Kenneth E. Freedland, PhD
Autonomic function and prognosis
Michael S. Lauer, MD
Vagal tone and the inflammatory reflex
Julian F. Thayer, PhD
Inflammation, atherosclerosis, and arterial thrombosis: Role of the scavenger receptors CD36
Roy L. Silverstein, MD
Pioneer Award Address: Ignorance isn't biased: Comments on receiving the Pioneer Award
David S. Goldstein, MD, PhD
Session II: Measures and Strategies for Modulation of Heart-Brain Interactions
Heart rate variability with deep breathing as a clinical test of cardiovagal function
Robert W. Shields, Jr, MD
Basic research models for the study of underlying mechanisms of electrical neuromodulation and ischemi heart-brain interactions
Mike J.L. DeJongste, MD, PhD, FESC; Gert J. TerHorst, PhD; and Robert D. Foreman, PhD
Session III: Annual Review of Key Papers in Heart-Brain Medicine
Key papers in the field published during the year prior to the Summit were discussed; two of those papers are reported here.
Cardiac sympathetic denervation preceding motor signs in Parkinson disease
David S. Goldstein, MD, PhD; Yehonatan Sharabi, MD; Barbara I. Karp, MD; Oladi Bentho; Ahmed Saleem, MD; Karel Pacak, MD, PhD; and Graeme Eisenhofer, PhD
Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation
Jeffrey P. Moak, MD; David S. Goldstein, MD, PhD; Basil A. Eldadah, MD, PhD; Ahmed Saleem, MD; Courtney Holmes, CMT; Sandra Pechnik, RN; and Yehonatan Sharabi, MD
Session IV: Code Lavender—Strategies for Implementing Heart-Brain Medicine
Is posttraumatic stress disorder related to development of heart disease? An update
Laura D. Kubzansky, PhD, and Karestan C. Koenen, PhD
Creating a healing environment: Rationale and research overview
Jone Geimer-Flanders, DO
Redesigning the neurocritical care unit to enhance family participation and improve outcomes
Owen Samuels, MD
Session V: Insights into Neuromodulation of Cardiovascular Function
Neuromodulation of cardiac pain and cerebral vasculature: Neural mechanisms
Robert D. Foreman, PhD, and Chao Qin, MD, PhD
Pinacidil induces vascular dilation and hyperemia in vivo and does not impact biophysical properties of neurons and astrocytes in vitro
Rosa Cao; Bryan T. Higashikubo; Jessica Cardin; Ulf Knoblich; Raddy Ramos, PhD; Mark T. Nelson, PhD; Christopher I. Moore, PhD; and Joshua C. Brumberg, PhD
The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system
Stephen W. Porges, PhD
Poster Abstracts
Abstract 1: Insulin use does not protect against restenosis in diabetic patients presenting with acute coronary syndrome or symptomatic angina
Matthew C. Becker, MD; John M. Galla, MD; Saif Anwaruddin, MD; Samir Kapadia, MD; and Richard A. Krasuski, MD
Abstract 2: Postoperative statin use and lower LDL cholesterol concentration are associated with reduced incidence of stroke
Matthew C. Becker, John M. Galla, Ryan P. Daly, Femi Philip, Peter Zimbwa, Stephen O. Chen, Chen H. Chow, Tingfei Hu, Richard A. Krasuski, and Arman T. Askari
Abstract 3: Brain edema and blood-brain barrier leakage influence antiepileptic drug levels
Giulia Betto, Vincent Fazio, Damir Janigro, and Chaitali Ghosh
Abstract 4: CPAP treatment vs conservative treatment in mild obstructive sleep apnea: Implications on cardiovascular morbidity
Kumar Budur, MD, and Nattapong Jaimchariyatam, MD
Abstract 5: New bioinformatics program identifies behavioral medicine interventions for epidemic cardiovascular disease in the developing world: Analysis of multidisciplinary findings for launching a new global public health initiative in heart-brain medicine
William C. Bushell, PhD
Abstract 6: Do systemic inflammation and blood-brain barrier failure play a role in pediatric psychosis?
Erin Carlton, Tatiana Falcone, Ayush Batra, Vince Fazio, Kathleen Franco, and Damir Janigro
Abstract 7: Brain, heart, and education
Linda Bryant Caviness, PhD
Abstract 8: Tobacco smoke mediates a monocytic and endothelial proinflammatory activation that synergistically affects BBB integrity
L. Cucullo, T. Sathe, M. Hossain, and D. Janigro
Abstract 9: Dynamic changes in ECG predict poor outcome after aneurysmal subarachnoid hemorrhage (aSAH)
H.A. Elsharkawy, MD; S.M. El Hadi, MD, PhD; J.E. Tetzlaff, MD; and J.J. Provencio, MD, FCCM
Abstract 10: Mechanism studies of malformation of cortical development by prenatal exposure of combined methylazoxymethanol and thalidomide
Q. Fan, S. Ramakrishna, N. Marchi, V. Fazio, K. Hallene, and D. Janigro
Abstract 11: Proapolipoprotein A1 demonstrates improved potential as a serum marker for brain metastases without vascular disease interference
Vince Fazio, Peter Mazzone, Nicola Marchi, Thomas Masaryk, and Damir Janigro
Abstract 12: Biofeedback-assisted stress management training to reverse myocardial remodeling in patients with end-stage heart failure
Dana L. Frank, BS; Mary E. Klecka, BA; Jerry Kiffer, MA; Heather Henrickson, PhD; Michael G. McKee, PhD; and Christine S. Moravec, PhD
Abstract 13: Nitric oxide and arginine metabolism in depression: Effect of a serotonin-norepinephrine reuptake inhibitor
Angelos Halaris, John Piletz, Omer Iqbal, Debra Hoppensteadt, Jawed Fareed, He Zhu, James Sinacore, and C. Lindsay DeVane
Abstract 14: Association between excessive daytime sleepiness and oxygen desaturation in obstructive sleep apnea syndrome: Nadir oxygen saturation vs mean oxygen saturation vs time spent below 90% oxygen saturation—which is important?
Nattapong Jaimchariyatam, MD, and Kumar Budur, MD
Abstract 15: Endotoxin preconditioning of the CNS: Microglia activation and neuroprotection
Walid Jalabi, Ranjan Dutta, Yongming Jin, Gerson Criste, Xinghua Yin, Grahame J. Kidd, and Bruce D. Trapp
Abstract 16: Pilot of stress reduction strategies for patients after a coronary event
R. Lindquist, D. Windenburg, K. Savik, and U. Bronas
Abstract 17: Cerebrovascular substrates of seizures after cardiopulmonary bypass
Rebecca O’Dwyer, Tim Wehner, Dileep Nair, Giulia Betto, Nicola Marchi, and Damir Janigro
Abstract 18: Depression and whole blood serotonin in patients with coronary heart disease from the heart and soul study
Lawson Wulsin, Dominique Musselman, Christian Otte, Erica Bruce, Sadia Ali, and Mary Whooley
Abstract 19: Gender differences prominent in linking anxiety to long-term mortality among the elderly
Jianping Zhang, MD, PhD; Boaz Kahana, PhD; Eva Kahana, PhD; Bo Hu, PhD; and Leo Pozuelo, MD
Abstract 20: Temporal lobe and sinus node: A case report provides evidence for bidirectional effects
Rebecca O’Dwyer, MD; Andreas Alexopoulos, MD, MPH; Walid Saliba, MD; Imad Najm, MD; and Richard Burgess, MD, PhD
Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Preface
Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Introduction: Heart-brain medicine: Update 2008
Marc S. Penn, MD, PhD, and Earl E. Bakken, MD, HonC, Hon DSc (3), Hon DHL (2)
Bakken Lecture: The brain, the heart, and therapeutic hypothermia
Patrick M. Kochanek, MD
Session 1: Pathways Involved in Neuromodulation of Risks in Coronary Artery Disease
Depression and heart rate variability in patients with coronary heart disease
Robert M. Carney, PhD, and Kenneth E. Freedland, PhD
Autonomic function and prognosis
Michael S. Lauer, MD
Vagal tone and the inflammatory reflex
Julian F. Thayer, PhD
Inflammation, atherosclerosis, and arterial thrombosis: Role of the scavenger receptors CD36
Roy L. Silverstein, MD
Pioneer Award Address: Ignorance isn't biased: Comments on receiving the Pioneer Award
David S. Goldstein, MD, PhD
Session II: Measures and Strategies for Modulation of Heart-Brain Interactions
Heart rate variability with deep breathing as a clinical test of cardiovagal function
Robert W. Shields, Jr, MD
Basic research models for the study of underlying mechanisms of electrical neuromodulation and ischemi heart-brain interactions
Mike J.L. DeJongste, MD, PhD, FESC; Gert J. TerHorst, PhD; and Robert D. Foreman, PhD
Session III: Annual Review of Key Papers in Heart-Brain Medicine
Key papers in the field published during the year prior to the Summit were discussed; two of those papers are reported here.
Cardiac sympathetic denervation preceding motor signs in Parkinson disease
David S. Goldstein, MD, PhD; Yehonatan Sharabi, MD; Barbara I. Karp, MD; Oladi Bentho; Ahmed Saleem, MD; Karel Pacak, MD, PhD; and Graeme Eisenhofer, PhD
Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation
Jeffrey P. Moak, MD; David S. Goldstein, MD, PhD; Basil A. Eldadah, MD, PhD; Ahmed Saleem, MD; Courtney Holmes, CMT; Sandra Pechnik, RN; and Yehonatan Sharabi, MD
Session IV: Code Lavender—Strategies for Implementing Heart-Brain Medicine
Is posttraumatic stress disorder related to development of heart disease? An update
Laura D. Kubzansky, PhD, and Karestan C. Koenen, PhD
Creating a healing environment: Rationale and research overview
Jone Geimer-Flanders, DO
Redesigning the neurocritical care unit to enhance family participation and improve outcomes
Owen Samuels, MD
Session V: Insights into Neuromodulation of Cardiovascular Function
Neuromodulation of cardiac pain and cerebral vasculature: Neural mechanisms
Robert D. Foreman, PhD, and Chao Qin, MD, PhD
Pinacidil induces vascular dilation and hyperemia in vivo and does not impact biophysical properties of neurons and astrocytes in vitro
Rosa Cao; Bryan T. Higashikubo; Jessica Cardin; Ulf Knoblich; Raddy Ramos, PhD; Mark T. Nelson, PhD; Christopher I. Moore, PhD; and Joshua C. Brumberg, PhD
The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system
Stephen W. Porges, PhD
Poster Abstracts
Abstract 1: Insulin use does not protect against restenosis in diabetic patients presenting with acute coronary syndrome or symptomatic angina
Matthew C. Becker, MD; John M. Galla, MD; Saif Anwaruddin, MD; Samir Kapadia, MD; and Richard A. Krasuski, MD
Abstract 2: Postoperative statin use and lower LDL cholesterol concentration are associated with reduced incidence of stroke
Matthew C. Becker, John M. Galla, Ryan P. Daly, Femi Philip, Peter Zimbwa, Stephen O. Chen, Chen H. Chow, Tingfei Hu, Richard A. Krasuski, and Arman T. Askari
Abstract 3: Brain edema and blood-brain barrier leakage influence antiepileptic drug levels
Giulia Betto, Vincent Fazio, Damir Janigro, and Chaitali Ghosh
Abstract 4: CPAP treatment vs conservative treatment in mild obstructive sleep apnea: Implications on cardiovascular morbidity
Kumar Budur, MD, and Nattapong Jaimchariyatam, MD
Abstract 5: New bioinformatics program identifies behavioral medicine interventions for epidemic cardiovascular disease in the developing world: Analysis of multidisciplinary findings for launching a new global public health initiative in heart-brain medicine
William C. Bushell, PhD
Abstract 6: Do systemic inflammation and blood-brain barrier failure play a role in pediatric psychosis?
Erin Carlton, Tatiana Falcone, Ayush Batra, Vince Fazio, Kathleen Franco, and Damir Janigro
Abstract 7: Brain, heart, and education
Linda Bryant Caviness, PhD
Abstract 8: Tobacco smoke mediates a monocytic and endothelial proinflammatory activation that synergistically affects BBB integrity
L. Cucullo, T. Sathe, M. Hossain, and D. Janigro
Abstract 9: Dynamic changes in ECG predict poor outcome after aneurysmal subarachnoid hemorrhage (aSAH)
H.A. Elsharkawy, MD; S.M. El Hadi, MD, PhD; J.E. Tetzlaff, MD; and J.J. Provencio, MD, FCCM
Abstract 10: Mechanism studies of malformation of cortical development by prenatal exposure of combined methylazoxymethanol and thalidomide
Q. Fan, S. Ramakrishna, N. Marchi, V. Fazio, K. Hallene, and D. Janigro
Abstract 11: Proapolipoprotein A1 demonstrates improved potential as a serum marker for brain metastases without vascular disease interference
Vince Fazio, Peter Mazzone, Nicola Marchi, Thomas Masaryk, and Damir Janigro
Abstract 12: Biofeedback-assisted stress management training to reverse myocardial remodeling in patients with end-stage heart failure
Dana L. Frank, BS; Mary E. Klecka, BA; Jerry Kiffer, MA; Heather Henrickson, PhD; Michael G. McKee, PhD; and Christine S. Moravec, PhD
Abstract 13: Nitric oxide and arginine metabolism in depression: Effect of a serotonin-norepinephrine reuptake inhibitor
Angelos Halaris, John Piletz, Omer Iqbal, Debra Hoppensteadt, Jawed Fareed, He Zhu, James Sinacore, and C. Lindsay DeVane
Abstract 14: Association between excessive daytime sleepiness and oxygen desaturation in obstructive sleep apnea syndrome: Nadir oxygen saturation vs mean oxygen saturation vs time spent below 90% oxygen saturation—which is important?
Nattapong Jaimchariyatam, MD, and Kumar Budur, MD
Abstract 15: Endotoxin preconditioning of the CNS: Microglia activation and neuroprotection
Walid Jalabi, Ranjan Dutta, Yongming Jin, Gerson Criste, Xinghua Yin, Grahame J. Kidd, and Bruce D. Trapp
Abstract 16: Pilot of stress reduction strategies for patients after a coronary event
R. Lindquist, D. Windenburg, K. Savik, and U. Bronas
Abstract 17: Cerebrovascular substrates of seizures after cardiopulmonary bypass
Rebecca O’Dwyer, Tim Wehner, Dileep Nair, Giulia Betto, Nicola Marchi, and Damir Janigro
Abstract 18: Depression and whole blood serotonin in patients with coronary heart disease from the heart and soul study
Lawson Wulsin, Dominique Musselman, Christian Otte, Erica Bruce, Sadia Ali, and Mary Whooley
Abstract 19: Gender differences prominent in linking anxiety to long-term mortality among the elderly
Jianping Zhang, MD, PhD; Boaz Kahana, PhD; Eva Kahana, PhD; Bo Hu, PhD; and Leo Pozuelo, MD
Abstract 20: Temporal lobe and sinus node: A case report provides evidence for bidirectional effects
Rebecca O’Dwyer, MD; Andreas Alexopoulos, MD, MPH; Walid Saliba, MD; Imad Najm, MD; and Richard Burgess, MD, PhD
Platelet Response in Acute Coronary Syndromes
Supplement Editors:
Deepak L. Bhatt, MD, MPH, and W. Frank Peacock, MD
Contents
Importance of platelets and platelet response in acute coronary syndromes
Kandice Kottke-Marchant, MD, PhD
Novel antiplatelet strategies in acute coronary syndromes
Marc S. Sabatine, MD, MPH
The current state of antiplatelet therapy in acute coronary syndromes: The data and the real word
John H. Alexander, MD, MHSc
Platelet response in practice: Applying new insights and tools for testing and treatment
Deepak L. Bhatt, MD, MPH; Kandice Kottke-Marchant, MD, PhD; John H. Alexander, MD, MHSc; W. Frank Peacock, MD; and Marc S. Sabatine, MD, MPH
Supplement Editors:
Deepak L. Bhatt, MD, MPH, and W. Frank Peacock, MD
Contents
Importance of platelets and platelet response in acute coronary syndromes
Kandice Kottke-Marchant, MD, PhD
Novel antiplatelet strategies in acute coronary syndromes
Marc S. Sabatine, MD, MPH
The current state of antiplatelet therapy in acute coronary syndromes: The data and the real word
John H. Alexander, MD, MHSc
Platelet response in practice: Applying new insights and tools for testing and treatment
Deepak L. Bhatt, MD, MPH; Kandice Kottke-Marchant, MD, PhD; John H. Alexander, MD, MHSc; W. Frank Peacock, MD; and Marc S. Sabatine, MD, MPH
Supplement Editors:
Deepak L. Bhatt, MD, MPH, and W. Frank Peacock, MD
Contents
Importance of platelets and platelet response in acute coronary syndromes
Kandice Kottke-Marchant, MD, PhD
Novel antiplatelet strategies in acute coronary syndromes
Marc S. Sabatine, MD, MPH
The current state of antiplatelet therapy in acute coronary syndromes: The data and the real word
John H. Alexander, MD, MHSc
Platelet response in practice: Applying new insights and tools for testing and treatment
Deepak L. Bhatt, MD, MPH; Kandice Kottke-Marchant, MD, PhD; John H. Alexander, MD, MHSc; W. Frank Peacock, MD; and Marc S. Sabatine, MD, MPH