User login
Up Close and Personal
There has been a lot of talk recently about pharmacogenomics and personalized medicine. Pharmaco-genomics—the way an individual responds to a medication—includes both positive and negative reactions, and how individual genetic differences affect drug response. It also examines the inherited variations in genes that dictate drug response and explores how these variations can be used to predict what type of response a patient will have to a particular drug, whether that is a good response, a bad response, or no response at all.1
In the race to catalog all the different gene variations, variations known as single nucleotide polymorphisms (SNPs, or “snips”) are used diagnostically to predict a patient’s response to a drug. In the future, pharmaceutical companies could use pharmacogenomics to predict which patients will have a negative response to a particular drug in clinical trials and, therefore, not study the medication in those patients.2 In essence, it would be a way to “streamline” therapy to those in most need of it or for those who likely will have a positive response with minimal adverse events.
By pre-screening patients, clinical trials could be smaller, faster, and less costly. The capability to pre-assess whether a patient will benefit from a particular medication before it is prescribed is a major advantage when it comes to medication use. It also might increase a prescriber’s confidence before starting a patient on a medication, and it might improve a patient’s confidence in taking the medication, which could increase medication adherence and lead to better patient outcomes.
Researchers have found that when patients with certain SNP variants of cytochrome P450 (CYP) take warfarin, metabolism and patient sensitivity are affected. Once this was discovered, the Food and Drug Administration (FDA) subsequently approved prescribing label changes for warfarin that incorporated pharmacogenomics information.3 This change included information on increased bleeding risk for patients carrying either the CYP2C9*2 or CYP2C9*3 alleles.4
More recently, Eckman et al published a cost-effectiveness analysis evaluating pharmacogenetic information related to warfarin dosing in patients with nonvalvular atrial fibrillation.5 In the study, the authors concluded that currently limited data exist utilizing pharmacogenomics for dosing of warfarin and its effects on major bleeding. They did note, however, that genotyping may be beneficial and cost-effective in patients who are at high risk of hemorrhage.
Additionally, there has been recent media coverage of the genetic variations of CYP2C19 affecting clopidogrel metabolism and efficacy.6,7 Both Mega et al and Collet et al noted that patients carrying at least one genetic variation of CYP2C19 had diminished platelet inhibition. Published earlier this year, both studies noted that patients carrying the genetic variation of CYP2C19 exhibited a higher rate of major cardiovascular events—including death, stent thrombosis, myocardial infarction, or stroke—than did noncarriers.
The FDA warned healthcare providers in November 2008 about using phenytoin or fosphenytoin in patients with the HLA-B*1502 allele due to a potentially increased risk of Stevens-Johnson syndrome and toxic epidermal necrolysis. A similar warning exists for carbamazepine in the same patient population. This is another example of pharmacogenomics information at work.8
Patient-specific variables have been identified that can help determine how an individual will respond to certain medications. Ultimately, this could decrease healthcare costs. It is a slow process and might be the wave of the future, but we are not there yet. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Just the facts: a basic introduction to the science underlying NCBI resources. National Center for Biotechnology Information Web site. Available at: www.ncbi.nlm.nih.gov/About/primer/pharm.html. Accessed Jan. 31, 2009.
- Gulseth MP, Grice GR, Dager WE. Pharmacogenomics of warfarin: uncovering a piece of the warfarin mystery. Am J Health Syst Pharm. 2009;66:123-133.
- FDA letter on approval of pharmacogenomics information for Coumadin label. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/appletter/2007/009218s105ltr.pdf. Accessed Feb. 4, 2009.
- Coumadin label updated. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2007/009218s105lblv2.pdf. Accessed Feb. 4, 2009.
- Eckman MH, Rosand J, Greenberg SM, Gage BF. Cost-effectiveness of using pharmacogenetic information in warfarin dosing for patients with nonvalvular atrial fibrillation. Ann Intern Med. 2009;150:73-83.
- Mega JL, Close SL, Wiviott SD, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009;360:354-362.
- Collet JP, Hulot JS, Pena A, et al. Cytochrome P450) 2C19 polymorphism in young patients treated with clopidogrel after myocardial infarction: a cohort study. Lancet. 2009;373:309-317.
- Phenytoin and fosphenytoin information. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/infopage/phenytoin_fosphenytoin/default.htm. Accessed Feb. 4, 2009.
- Mylan receives final approval for first-to-file generic version of antiepileptic Keppra and launches immediately. Mylan Web site. Available at: investor.mylan.com/phoenix.zhtml?c=66563&p=irol-newsArticle&ID=1221778. Accessed Feb. 4, 2009.
- Prism pharmaceuticals receives FDA approval of Nexterone for life-threatening ventricular fibrillation and ventricular tachycardia. Prism Pharmaceuticals Web site. Available at: www.prismpharma.com/news.html. Accessed Feb. 4, 2009.
- Now in double concentration. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025CFED437DC0261D862. Accessed Feb. 4, 2009.
- Meeting of the Cardiovascular and Renal Drugs Advisory Committee. Food and Drug Administration Web site. Available at: www.fda.gov/cder/audiences/acspage/meetings/crdac_meeting_20090203.htm. Accessed Feb. 4, 2009.
- Bratulic, A. FDA panel recommends Eli Lilly’s, Daiichi Sankyo’s Effient. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=F4B502BDC684486986AE56DED7B532F3&logRowId=281890. Accessed Feb. 4, 2009.
- Now available 12-mg tablets. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025C1D5D3BD762CE3ECB. Accessed Feb. 4, 2009.
- Tom WC. New venlafaxine extended-release formulation. Pharmacist’s Letter/Prescriber’s Letter. 2009;25(1)250108.
There has been a lot of talk recently about pharmacogenomics and personalized medicine. Pharmaco-genomics—the way an individual responds to a medication—includes both positive and negative reactions, and how individual genetic differences affect drug response. It also examines the inherited variations in genes that dictate drug response and explores how these variations can be used to predict what type of response a patient will have to a particular drug, whether that is a good response, a bad response, or no response at all.1
In the race to catalog all the different gene variations, variations known as single nucleotide polymorphisms (SNPs, or “snips”) are used diagnostically to predict a patient’s response to a drug. In the future, pharmaceutical companies could use pharmacogenomics to predict which patients will have a negative response to a particular drug in clinical trials and, therefore, not study the medication in those patients.2 In essence, it would be a way to “streamline” therapy to those in most need of it or for those who likely will have a positive response with minimal adverse events.
By pre-screening patients, clinical trials could be smaller, faster, and less costly. The capability to pre-assess whether a patient will benefit from a particular medication before it is prescribed is a major advantage when it comes to medication use. It also might increase a prescriber’s confidence before starting a patient on a medication, and it might improve a patient’s confidence in taking the medication, which could increase medication adherence and lead to better patient outcomes.
Researchers have found that when patients with certain SNP variants of cytochrome P450 (CYP) take warfarin, metabolism and patient sensitivity are affected. Once this was discovered, the Food and Drug Administration (FDA) subsequently approved prescribing label changes for warfarin that incorporated pharmacogenomics information.3 This change included information on increased bleeding risk for patients carrying either the CYP2C9*2 or CYP2C9*3 alleles.4
More recently, Eckman et al published a cost-effectiveness analysis evaluating pharmacogenetic information related to warfarin dosing in patients with nonvalvular atrial fibrillation.5 In the study, the authors concluded that currently limited data exist utilizing pharmacogenomics for dosing of warfarin and its effects on major bleeding. They did note, however, that genotyping may be beneficial and cost-effective in patients who are at high risk of hemorrhage.
Additionally, there has been recent media coverage of the genetic variations of CYP2C19 affecting clopidogrel metabolism and efficacy.6,7 Both Mega et al and Collet et al noted that patients carrying at least one genetic variation of CYP2C19 had diminished platelet inhibition. Published earlier this year, both studies noted that patients carrying the genetic variation of CYP2C19 exhibited a higher rate of major cardiovascular events—including death, stent thrombosis, myocardial infarction, or stroke—than did noncarriers.
The FDA warned healthcare providers in November 2008 about using phenytoin or fosphenytoin in patients with the HLA-B*1502 allele due to a potentially increased risk of Stevens-Johnson syndrome and toxic epidermal necrolysis. A similar warning exists for carbamazepine in the same patient population. This is another example of pharmacogenomics information at work.8
Patient-specific variables have been identified that can help determine how an individual will respond to certain medications. Ultimately, this could decrease healthcare costs. It is a slow process and might be the wave of the future, but we are not there yet. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Just the facts: a basic introduction to the science underlying NCBI resources. National Center for Biotechnology Information Web site. Available at: www.ncbi.nlm.nih.gov/About/primer/pharm.html. Accessed Jan. 31, 2009.
- Gulseth MP, Grice GR, Dager WE. Pharmacogenomics of warfarin: uncovering a piece of the warfarin mystery. Am J Health Syst Pharm. 2009;66:123-133.
- FDA letter on approval of pharmacogenomics information for Coumadin label. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/appletter/2007/009218s105ltr.pdf. Accessed Feb. 4, 2009.
- Coumadin label updated. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2007/009218s105lblv2.pdf. Accessed Feb. 4, 2009.
- Eckman MH, Rosand J, Greenberg SM, Gage BF. Cost-effectiveness of using pharmacogenetic information in warfarin dosing for patients with nonvalvular atrial fibrillation. Ann Intern Med. 2009;150:73-83.
- Mega JL, Close SL, Wiviott SD, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009;360:354-362.
- Collet JP, Hulot JS, Pena A, et al. Cytochrome P450) 2C19 polymorphism in young patients treated with clopidogrel after myocardial infarction: a cohort study. Lancet. 2009;373:309-317.
- Phenytoin and fosphenytoin information. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/infopage/phenytoin_fosphenytoin/default.htm. Accessed Feb. 4, 2009.
- Mylan receives final approval for first-to-file generic version of antiepileptic Keppra and launches immediately. Mylan Web site. Available at: investor.mylan.com/phoenix.zhtml?c=66563&p=irol-newsArticle&ID=1221778. Accessed Feb. 4, 2009.
- Prism pharmaceuticals receives FDA approval of Nexterone for life-threatening ventricular fibrillation and ventricular tachycardia. Prism Pharmaceuticals Web site. Available at: www.prismpharma.com/news.html. Accessed Feb. 4, 2009.
- Now in double concentration. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025CFED437DC0261D862. Accessed Feb. 4, 2009.
- Meeting of the Cardiovascular and Renal Drugs Advisory Committee. Food and Drug Administration Web site. Available at: www.fda.gov/cder/audiences/acspage/meetings/crdac_meeting_20090203.htm. Accessed Feb. 4, 2009.
- Bratulic, A. FDA panel recommends Eli Lilly’s, Daiichi Sankyo’s Effient. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=F4B502BDC684486986AE56DED7B532F3&logRowId=281890. Accessed Feb. 4, 2009.
- Now available 12-mg tablets. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025C1D5D3BD762CE3ECB. Accessed Feb. 4, 2009.
- Tom WC. New venlafaxine extended-release formulation. Pharmacist’s Letter/Prescriber’s Letter. 2009;25(1)250108.
There has been a lot of talk recently about pharmacogenomics and personalized medicine. Pharmaco-genomics—the way an individual responds to a medication—includes both positive and negative reactions, and how individual genetic differences affect drug response. It also examines the inherited variations in genes that dictate drug response and explores how these variations can be used to predict what type of response a patient will have to a particular drug, whether that is a good response, a bad response, or no response at all.1
In the race to catalog all the different gene variations, variations known as single nucleotide polymorphisms (SNPs, or “snips”) are used diagnostically to predict a patient’s response to a drug. In the future, pharmaceutical companies could use pharmacogenomics to predict which patients will have a negative response to a particular drug in clinical trials and, therefore, not study the medication in those patients.2 In essence, it would be a way to “streamline” therapy to those in most need of it or for those who likely will have a positive response with minimal adverse events.
By pre-screening patients, clinical trials could be smaller, faster, and less costly. The capability to pre-assess whether a patient will benefit from a particular medication before it is prescribed is a major advantage when it comes to medication use. It also might increase a prescriber’s confidence before starting a patient on a medication, and it might improve a patient’s confidence in taking the medication, which could increase medication adherence and lead to better patient outcomes.
Researchers have found that when patients with certain SNP variants of cytochrome P450 (CYP) take warfarin, metabolism and patient sensitivity are affected. Once this was discovered, the Food and Drug Administration (FDA) subsequently approved prescribing label changes for warfarin that incorporated pharmacogenomics information.3 This change included information on increased bleeding risk for patients carrying either the CYP2C9*2 or CYP2C9*3 alleles.4
More recently, Eckman et al published a cost-effectiveness analysis evaluating pharmacogenetic information related to warfarin dosing in patients with nonvalvular atrial fibrillation.5 In the study, the authors concluded that currently limited data exist utilizing pharmacogenomics for dosing of warfarin and its effects on major bleeding. They did note, however, that genotyping may be beneficial and cost-effective in patients who are at high risk of hemorrhage.
Additionally, there has been recent media coverage of the genetic variations of CYP2C19 affecting clopidogrel metabolism and efficacy.6,7 Both Mega et al and Collet et al noted that patients carrying at least one genetic variation of CYP2C19 had diminished platelet inhibition. Published earlier this year, both studies noted that patients carrying the genetic variation of CYP2C19 exhibited a higher rate of major cardiovascular events—including death, stent thrombosis, myocardial infarction, or stroke—than did noncarriers.
The FDA warned healthcare providers in November 2008 about using phenytoin or fosphenytoin in patients with the HLA-B*1502 allele due to a potentially increased risk of Stevens-Johnson syndrome and toxic epidermal necrolysis. A similar warning exists for carbamazepine in the same patient population. This is another example of pharmacogenomics information at work.8
Patient-specific variables have been identified that can help determine how an individual will respond to certain medications. Ultimately, this could decrease healthcare costs. It is a slow process and might be the wave of the future, but we are not there yet. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Just the facts: a basic introduction to the science underlying NCBI resources. National Center for Biotechnology Information Web site. Available at: www.ncbi.nlm.nih.gov/About/primer/pharm.html. Accessed Jan. 31, 2009.
- Gulseth MP, Grice GR, Dager WE. Pharmacogenomics of warfarin: uncovering a piece of the warfarin mystery. Am J Health Syst Pharm. 2009;66:123-133.
- FDA letter on approval of pharmacogenomics information for Coumadin label. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/appletter/2007/009218s105ltr.pdf. Accessed Feb. 4, 2009.
- Coumadin label updated. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2007/009218s105lblv2.pdf. Accessed Feb. 4, 2009.
- Eckman MH, Rosand J, Greenberg SM, Gage BF. Cost-effectiveness of using pharmacogenetic information in warfarin dosing for patients with nonvalvular atrial fibrillation. Ann Intern Med. 2009;150:73-83.
- Mega JL, Close SL, Wiviott SD, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009;360:354-362.
- Collet JP, Hulot JS, Pena A, et al. Cytochrome P450) 2C19 polymorphism in young patients treated with clopidogrel after myocardial infarction: a cohort study. Lancet. 2009;373:309-317.
- Phenytoin and fosphenytoin information. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/infopage/phenytoin_fosphenytoin/default.htm. Accessed Feb. 4, 2009.
- Mylan receives final approval for first-to-file generic version of antiepileptic Keppra and launches immediately. Mylan Web site. Available at: investor.mylan.com/phoenix.zhtml?c=66563&p=irol-newsArticle&ID=1221778. Accessed Feb. 4, 2009.
- Prism pharmaceuticals receives FDA approval of Nexterone for life-threatening ventricular fibrillation and ventricular tachycardia. Prism Pharmaceuticals Web site. Available at: www.prismpharma.com/news.html. Accessed Feb. 4, 2009.
- Now in double concentration. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025CFED437DC0261D862. Accessed Feb. 4, 2009.
- Meeting of the Cardiovascular and Renal Drugs Advisory Committee. Food and Drug Administration Web site. Available at: www.fda.gov/cder/audiences/acspage/meetings/crdac_meeting_20090203.htm. Accessed Feb. 4, 2009.
- Bratulic, A. FDA panel recommends Eli Lilly’s, Daiichi Sankyo’s Effient. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=F4B502BDC684486986AE56DED7B532F3&logRowId=281890. Accessed Feb. 4, 2009.
- Now available 12-mg tablets. E-Pharm/alert Web site. Available at: whatcounts.jobson.com/dm?id=0CCEED6291EC025C1D5D3BD762CE3ECB. Accessed Feb. 4, 2009.
- Tom WC. New venlafaxine extended-release formulation. Pharmacist’s Letter/Prescriber’s Letter. 2009;25(1)250108.
The latest research you need to know
Literature at a Glance
- Discharge innovation and readmission rates.
- Electronic medical records and outcomes.
- CXR findings predict outcomes.
- NSAIDs and congestive heart failure morbidity.
- Outcomes of interpreter use.
- Predictors and outcomes of postoperative delirium.
- Perioperative beta-blockers.
- Perioperative stroke risk.
Standardized Discharge Intervention Decreases Readmission Rates
Clinical question: Does a standardized discharge intervention lead to a decrease in ED visits and readmission rates following hospital discharge?
Background: Hospital discharge is a complex process that is not standardized at many institutions. Deficiencies in the process can lead to poor outcomes, unnecessary rehospitalizations, and increased costs. Previous studies of peridischarge interventions have yielded mixed results and typically focus on specific patient populations.
Study design: Randomized trial.
Setting: Boston Medical Center, a large, urban, academic medical center.
Synopsis: In this single-institution study, 749 English-speaking hospitalized adults were randomly assigned one of two discharge plans: a multidisciplinary package of discharge services or the usual discharge process. Patients in the intervention group were assigned a nurse discharge advocate who performed patient education, medication reconciliation, discharge coordination, and scheduled follow-up appointments. A pharmacist also telephoned participants two to four days after discharge to reinforce the discharge plan and review medications.
Participants in the intervention group had a 30% relative reduction in hospital utilization (defined as ED visit or hospital readmission) at 30 days. Overall, 21.6% of intervention patients and 26.9% of usual-discharge patients had at least one hospital utilization within 30 days of discharge.
This study was limited to a single center, and 27% of the patients did not meet eligibility criteria. The applicability also is limited by the resource utilization required for the intervention. The authors estimated that 0.5 full-time-equivalent (FTE) nursing time and 0.15 FTE pharmacist time was required to maintain 14 patients per week.
Bottom line: A systematic, intensive approach to discharges can reduce ED return visits and readmission rates.
Citation: Jack B, Chetty V, Anthony D, et al. A re-engineered hospital discharge program to decrease re-hospitalization. Ann Intern Med. 2009:150(3):178-187.
EMR Equals Lower Mortality, Fewer Complications, Lower Costs
Clinical question: Is improved automation of hospital information associated with reduced rates of inpatient mortality, complications, cost, and length of stay (LOS)?
Background: Clinical information technologies, including electronic medical records (EMR), are touted as an antidote for the fragmented, unsafe, and expensive American healthcare system. Most studies on the effect of such technologies are limited to a single site, and few involve commercially available information systems.
Study design: Cross-sectional study.
Setting: Urban hospitals in Texas.
Synopsis: Researchers used the previously validated Clinical Information Technology Assessment Tool to survey physicians providing inpatient care in 72 Texas hospitals. This tool measures the degree to which clinical information processes are computerized. Automation is divided into four subdomains: test results, notes and records, order entry, and decision support. To achieve a high score, a process must be fully computerized, the physician must know how to activate it, and the physician must choose the computerized process over alternatives. The authors examined the association between a hospital’s degree of automation and mortality, costs, and LOS among patients with myocardial infarction, congestive heart failure, coronary artery bypass grafting, and pneumonia.
Overall, greater automation was associated with lower mortality, fewer complications, and lower costs. No clear impact on LOS was found. Higher scores in the notes and records subdomains were most associated with lower mortality. Higher decision-support scores were most associated with lower complication rates and costs.
This study is one of the first to demonstrate the benefits of clinical information technologies across a variety of institutions using different information systems.
Bottom line: Hospitals with EMR, order entry, and clinical decision support have lower mortality rates, fewer complications, and lower costs.
Citation: Amarasingham R, Plantinga L, Diener-West M, et al. Clinical information technologies and inpatient outcomes. Arch Intern Med. 2009;169(2):108-114.
Radiologic Progression of Pulmonary Infiltrates Portends Worse Prognosis in Severe CAP Patients
Clinical question: In patients admitted to the ICU with severe community-acquired pneumonia (CAP), do bacteremia and rapid radiologic progression of pulmonary infiltrates increase the risk of shock and mortality?
Background: Severe CAP is associated with considerable morbidity and mortality; however, data focusing on short-term outcomes is limited. The role of the chest radiograph is established in diagnosis but is unclear as a prognostic tool. Bacteremia is associated with higher mortality risk but also is more common in patients with comorbid illnesses.
Study design: Retrospective cohort.
Setting: 33 hospitals in Spain.
Synopsis: This study retrospectively analyzed 457 patients with severe CAP admitted to the ICU between Dec. 1, 2000, and Feb. 28, 2002. Patients were classified into four groups according to the presence or absence of rapid radiographic spread of pulmonary infiltrates and CAP-associated bacteremia. Patients demonstrating significant worsening by chest radiography within the first 48 hours after admission had a threefold increase in the risk of death. Bacteremia was not associated with increased mortality.
The retrospective nature of this study is its major limitation. Other limitations are the probable inclusion of unrecognized bacteremia in the nonbacteremic groups, the fact that repeat chest radiographs were obtained only once (at 48 hours), and that the cause of radiographic deterioration was not examined.
This study contributes to the literature by identifying a subset of patients (those with worsening chest radiographs at 48 hours) who may benefit from further study and targeted interventions.
Bottom line: In severe CAP patients, radiographic worsening at 48 hours is a negative prognostic factor, while bacteremia is not associated with worse outcomes.
Citation: Lisboa T, Blot S, Waterer G, et al. Radiologic progression of pulmonary infiltrates predicts a worse prognosis in severe community-acquired pneumonia than bacteremia. Chest. 2009;135(1):165-172.
NSAIDs Increase Risk of Death and Cardiovascular Morbidity in CHF Patients
Clinical question: Is NSAID use by patients with congestive heart failure (CHF) associated with a higher risk of death or hospitalization due to acute myocardial infarction (MI) or heart failure?
Background: NSAID use is widespread and generally perceived to be low-risk given their over-the-counter availability. However, clinical guidelines discourage the use of NSAIDs in patients with chronic heart failure due to the risk of fluid retention and worsening heart failure.
Study design: Retrospective cohort.
Setting: All hospitals in Denmark.
Synopsis: This study identified 107,092 patients who survived their first hospitalizations due to heart failure between 1995 and 2004. Subsequent use of NSAIDs was determined from a national prescription registry. Patient records were retrospectively analyzed to assess mortality and hospitalization due to MI or heart failure.
At least one NSAID prescription was claimed by 33.9% of the patients after discharge. All NSAIDs were associated with higher death rates, and there was a dose-dependent increase in the risk of death. Ibuprofen and naproxen demonstrated increased mortality only at high doses. All NSAIDs that were studied increased the risk of hospitalization for MI or heart failure.
The observational design is the study’s major limitation. Other important limitations include lack of detailed information about heart failure diagnoses and indication for starting NSAID therapy.
This study intensifies the debate regarding the increased risk of cardiovascular events in NSAID patients, which has been ongoing since the publication of the VIGOR Study in 2000.
Bottom line: In patients with a history of heart failure, NSAIDs are associated with an increased risk of death and cardiovascular morbidity.
Citation: Gislason G, Rasmussen J, Abildstrom S, et al. Increased mortality and cardiovascular morbidity associated with use of non-steroidal anti-inflammatory drugs in chronic heart failure. Arch Intern Med. 2009;169(2):141-149.
Language Barriers Present Obstacle during ICU Family Meetings
Clinical question: Do family meetings that require the use of an interpreter have different characteristics than those in which an interpreter is not needed?
Background: Communication about end-of-life care is essential in the ICU, yet limited English proficiency (LEP) can be a barrier to effective discussions. Overall, outcomes and satisfaction are improved when interpreters are used, but specific effects on ICU family conferences are unknown.
Study design: Cross-sectional evaluation of family meetings.
Setting: Four hospitals in Seattle.
Synopsis: Fifty-one noninterpreted (English-speaking members only) and 10 interpreted (non-English-speaking members present) ICU family meetings were recorded and analyzed for the amount of speaking time and content. The total duration was similar for interpreted versus noninterpreted conferences (26.3 minutes vs. 32.0 minutes, P=0.25), but clinician speech was significantly less in the interpreted group (10.9 minutes vs. 19.6 minutes, P=0.001). Family speaking time was similar in both interpreted and noninterpreted conversations (7.1 minutes vs. 8.2 minutes, P=0.66). Clinicians used more emotional support for families in noninterpreted meetings, including active listening and pausing for questions.
This study is limited by the use of an audio recorder; a video recorder would have provided researchers with participants’ physical interaction and expressions. Additionally, the study does not differentiate between cultural and linguistic difficulties, or provide a reference for the degree of complexity of each conference.
Bottom line: Family meetings in the ICU that require the use of an interpreter provide less information and emotional support to family members than those in which an interpreter is not required.
Citation: Thornton J, Pham K, Engelberg R, et al. Families with limited English proficiency receive less information and support in interpreted intensive care unit family conferences. Crit Care Med. 2009;37(1):89-95.
Postoperative Delirium and Poor Outcomes
Clinical question: In patients 50 and older, what are the risk factors for the development of postoperative delirium, and how are outcomes affected by delirium?
Background: Delirium in the elderly postoperative patient is common. It results in increased costs, morbidity, and mortality. As the population ages, more elderly patients will undergo surgical procedures, so identification of delirium risk factors is essential.
Study design: Prospective, observational, cohort study.
Setting: Veterans Affairs Medical Center, Denver.
Synopsis: Researchers assessed 144 patients 50 and older who were scheduled to undergo surgical procedures with a planned, postoperative ICU stay for cognitive function, overall functional status, and comorbidities. Postoperatively, patients were assessed daily for the development of dementia using the cognitive assessment method-ICU instrument (CAM-ICU). Additionally, a validated chart review method for diagnosing delirium was used. The overall delirium incidence was 44%, and only 12% of cases had an identifiable etiology. The mean onset of delirium was 2.4 days; duration was 4.5 days. The incidence of delirium increased with age, reaching 92% in the 80- to 89-year-old group. In multivariate analysis, preoperative cognitive dysfunction was the strongest predictor of delirium.
Delirium development in patients 50 and older was associated with marked increases in costs ($50,000 vs. $32,000), length of stay (16 days vs. eight days), discharge to a facility (33% vs. 1%), and mortality (9% vs. 1%).
Limitations of this study included the patient population studied (97% men) and lack of data regarding medication use during hospitalization.
Bottom line: In older patients undergoing surgery requiring postoperative ICU care, delirium is common, is associated with prior cognitive dysfunction, and results in significant increases in LOS and mortality.
Citation: Robinson T, Raeburn C, Tran Z, et al. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249(1):173-178.
Meta-Analysis of Perioperative Beta-Blockers Doesn’t Support Routine Use
Clinical question: Are perioperative beta-blockers effective in preventing cardiac events in noncardiac surgery?
Background: The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines for noncardiac surgery recommend beta-blockers for high-risk patients undergoing intermediate or high-risk surgery. The results of previous randomized controlled trials have been inconsistent.
Study design: Meta-analysis.
Setting: Literature search of PubMed, Embase, and the Cochrane Library.
Synopsis: Thirty-three randomized, controlled trials—which included 12,306 patients—were selected for statistical analysis. In these trials, beta-blockers were initiated in the perioperative period with 30-day followup for outcomes of interest. Overall, perioperative beta-blocker use was associated with a 35% risk reduction in nonfatal MI, a 116% increased risk of nonfatal stroke, and no significant difference in all-cause mortality. Trials with higher levels of bias showed greater statistical benefit of beta-blockers. Of note, the POISE trial carried the largest amount of weight, accounting for nearly two-thirds of the total number of patients included in treatment arms.
The application of this data is challenging, as studies differ in several important variables, such as timing of beta-blocker initiation, dosing regimen, and duration of treatment. The POISE trial, in particular, employed a very large dose of metoprolol, compared with doses of beta-blockers used in other studies. There is less data regarding the perioperative efficacy of beta-blockers when therapy is started well before surgery.
Bottom line: Current evidence does not support the routine use of beta-blockers started immediately prior to noncardiac surgery to prevent perioperative cardiac events.
Citation: Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta-blockers in patients having non-cardiac surgery: a meta-analysis. Lancet. 2008;372:1962-1976.
Perioperative Ischemic Stroke an Important Cause of Morbidity and Mortality in Noncardiac Surgery
Clinical question: What are the incidence, risk factors, and outcomes of acute ischemic stroke in nonvascular surgery?
Background: Ischemic stroke is a well-understood complication of cardiovascular surgery. However, little data exist in medical literature regarding the frequency, associations, and outcomes of perioperative ischemic stroke in noncardiac surgery.
Study design: Observational chart review using administrative data.
Setting: The Nationwide Inpatient Sample, a public-use database, in which approximately 1,000 hospitals submit data from nonfederal acute-care hospitals.
Synopsis: Three common surgeries were sampled from an administrative database to characterize the epidemiology of perioperative ischemic stroke in noncardiac surgery. This outcome occurred in 0.7% of hemicolectomy patients; 0.2% of total hip replacement patients; and 0.6% of lobectomy/segmental lung resection patients. Studying the rate of perioperative ischemic stroke in coronary artery bypass graft (CABG) patients validated the authors’ method of data extraction. This rate was consistent with prior studies of this outcome in cardiovascular surgery patients.
Multivariate analysis showed that renal disease (odds ratio 3.0), atrial fibrillation (OR 2.0), prior stroke (OR 1.6), and valvular disease (OR 1.5) are statistically associated with an increased risk of perioperative ischemic stroke. The primary outcome was associated with a marked increase in the odds of in-hospital mortality or need for chronic care upon hospital discharge.
This study is limited by its use of administrative coding data, as well as potential bias introduced by the use of only three major types of surgery.
Bottom line: Ischemic stroke is a serious complication of intermediate and major noncardiovascular surgery. It is associated with poor patient outcomes; more evidence is needed to confirm associations with this outcome and to discover strategies to reduce risk.
Citation: Bateman B, Schum-acher H, Wang S, et al. Perioperative acute ischemic stroke in non-cardiac and nonvascular surgery. Anesthesiology. 2009;110:231-238.
Literature at a Glance
- Discharge innovation and readmission rates.
- Electronic medical records and outcomes.
- CXR findings predict outcomes.
- NSAIDs and congestive heart failure morbidity.
- Outcomes of interpreter use.
- Predictors and outcomes of postoperative delirium.
- Perioperative beta-blockers.
- Perioperative stroke risk.
Standardized Discharge Intervention Decreases Readmission Rates
Clinical question: Does a standardized discharge intervention lead to a decrease in ED visits and readmission rates following hospital discharge?
Background: Hospital discharge is a complex process that is not standardized at many institutions. Deficiencies in the process can lead to poor outcomes, unnecessary rehospitalizations, and increased costs. Previous studies of peridischarge interventions have yielded mixed results and typically focus on specific patient populations.
Study design: Randomized trial.
Setting: Boston Medical Center, a large, urban, academic medical center.
Synopsis: In this single-institution study, 749 English-speaking hospitalized adults were randomly assigned one of two discharge plans: a multidisciplinary package of discharge services or the usual discharge process. Patients in the intervention group were assigned a nurse discharge advocate who performed patient education, medication reconciliation, discharge coordination, and scheduled follow-up appointments. A pharmacist also telephoned participants two to four days after discharge to reinforce the discharge plan and review medications.
Participants in the intervention group had a 30% relative reduction in hospital utilization (defined as ED visit or hospital readmission) at 30 days. Overall, 21.6% of intervention patients and 26.9% of usual-discharge patients had at least one hospital utilization within 30 days of discharge.
This study was limited to a single center, and 27% of the patients did not meet eligibility criteria. The applicability also is limited by the resource utilization required for the intervention. The authors estimated that 0.5 full-time-equivalent (FTE) nursing time and 0.15 FTE pharmacist time was required to maintain 14 patients per week.
Bottom line: A systematic, intensive approach to discharges can reduce ED return visits and readmission rates.
Citation: Jack B, Chetty V, Anthony D, et al. A re-engineered hospital discharge program to decrease re-hospitalization. Ann Intern Med. 2009:150(3):178-187.
EMR Equals Lower Mortality, Fewer Complications, Lower Costs
Clinical question: Is improved automation of hospital information associated with reduced rates of inpatient mortality, complications, cost, and length of stay (LOS)?
Background: Clinical information technologies, including electronic medical records (EMR), are touted as an antidote for the fragmented, unsafe, and expensive American healthcare system. Most studies on the effect of such technologies are limited to a single site, and few involve commercially available information systems.
Study design: Cross-sectional study.
Setting: Urban hospitals in Texas.
Synopsis: Researchers used the previously validated Clinical Information Technology Assessment Tool to survey physicians providing inpatient care in 72 Texas hospitals. This tool measures the degree to which clinical information processes are computerized. Automation is divided into four subdomains: test results, notes and records, order entry, and decision support. To achieve a high score, a process must be fully computerized, the physician must know how to activate it, and the physician must choose the computerized process over alternatives. The authors examined the association between a hospital’s degree of automation and mortality, costs, and LOS among patients with myocardial infarction, congestive heart failure, coronary artery bypass grafting, and pneumonia.
Overall, greater automation was associated with lower mortality, fewer complications, and lower costs. No clear impact on LOS was found. Higher scores in the notes and records subdomains were most associated with lower mortality. Higher decision-support scores were most associated with lower complication rates and costs.
This study is one of the first to demonstrate the benefits of clinical information technologies across a variety of institutions using different information systems.
Bottom line: Hospitals with EMR, order entry, and clinical decision support have lower mortality rates, fewer complications, and lower costs.
Citation: Amarasingham R, Plantinga L, Diener-West M, et al. Clinical information technologies and inpatient outcomes. Arch Intern Med. 2009;169(2):108-114.
Radiologic Progression of Pulmonary Infiltrates Portends Worse Prognosis in Severe CAP Patients
Clinical question: In patients admitted to the ICU with severe community-acquired pneumonia (CAP), do bacteremia and rapid radiologic progression of pulmonary infiltrates increase the risk of shock and mortality?
Background: Severe CAP is associated with considerable morbidity and mortality; however, data focusing on short-term outcomes is limited. The role of the chest radiograph is established in diagnosis but is unclear as a prognostic tool. Bacteremia is associated with higher mortality risk but also is more common in patients with comorbid illnesses.
Study design: Retrospective cohort.
Setting: 33 hospitals in Spain.
Synopsis: This study retrospectively analyzed 457 patients with severe CAP admitted to the ICU between Dec. 1, 2000, and Feb. 28, 2002. Patients were classified into four groups according to the presence or absence of rapid radiographic spread of pulmonary infiltrates and CAP-associated bacteremia. Patients demonstrating significant worsening by chest radiography within the first 48 hours after admission had a threefold increase in the risk of death. Bacteremia was not associated with increased mortality.
The retrospective nature of this study is its major limitation. Other limitations are the probable inclusion of unrecognized bacteremia in the nonbacteremic groups, the fact that repeat chest radiographs were obtained only once (at 48 hours), and that the cause of radiographic deterioration was not examined.
This study contributes to the literature by identifying a subset of patients (those with worsening chest radiographs at 48 hours) who may benefit from further study and targeted interventions.
Bottom line: In severe CAP patients, radiographic worsening at 48 hours is a negative prognostic factor, while bacteremia is not associated with worse outcomes.
Citation: Lisboa T, Blot S, Waterer G, et al. Radiologic progression of pulmonary infiltrates predicts a worse prognosis in severe community-acquired pneumonia than bacteremia. Chest. 2009;135(1):165-172.
NSAIDs Increase Risk of Death and Cardiovascular Morbidity in CHF Patients
Clinical question: Is NSAID use by patients with congestive heart failure (CHF) associated with a higher risk of death or hospitalization due to acute myocardial infarction (MI) or heart failure?
Background: NSAID use is widespread and generally perceived to be low-risk given their over-the-counter availability. However, clinical guidelines discourage the use of NSAIDs in patients with chronic heart failure due to the risk of fluid retention and worsening heart failure.
Study design: Retrospective cohort.
Setting: All hospitals in Denmark.
Synopsis: This study identified 107,092 patients who survived their first hospitalizations due to heart failure between 1995 and 2004. Subsequent use of NSAIDs was determined from a national prescription registry. Patient records were retrospectively analyzed to assess mortality and hospitalization due to MI or heart failure.
At least one NSAID prescription was claimed by 33.9% of the patients after discharge. All NSAIDs were associated with higher death rates, and there was a dose-dependent increase in the risk of death. Ibuprofen and naproxen demonstrated increased mortality only at high doses. All NSAIDs that were studied increased the risk of hospitalization for MI or heart failure.
The observational design is the study’s major limitation. Other important limitations include lack of detailed information about heart failure diagnoses and indication for starting NSAID therapy.
This study intensifies the debate regarding the increased risk of cardiovascular events in NSAID patients, which has been ongoing since the publication of the VIGOR Study in 2000.
Bottom line: In patients with a history of heart failure, NSAIDs are associated with an increased risk of death and cardiovascular morbidity.
Citation: Gislason G, Rasmussen J, Abildstrom S, et al. Increased mortality and cardiovascular morbidity associated with use of non-steroidal anti-inflammatory drugs in chronic heart failure. Arch Intern Med. 2009;169(2):141-149.
Language Barriers Present Obstacle during ICU Family Meetings
Clinical question: Do family meetings that require the use of an interpreter have different characteristics than those in which an interpreter is not needed?
Background: Communication about end-of-life care is essential in the ICU, yet limited English proficiency (LEP) can be a barrier to effective discussions. Overall, outcomes and satisfaction are improved when interpreters are used, but specific effects on ICU family conferences are unknown.
Study design: Cross-sectional evaluation of family meetings.
Setting: Four hospitals in Seattle.
Synopsis: Fifty-one noninterpreted (English-speaking members only) and 10 interpreted (non-English-speaking members present) ICU family meetings were recorded and analyzed for the amount of speaking time and content. The total duration was similar for interpreted versus noninterpreted conferences (26.3 minutes vs. 32.0 minutes, P=0.25), but clinician speech was significantly less in the interpreted group (10.9 minutes vs. 19.6 minutes, P=0.001). Family speaking time was similar in both interpreted and noninterpreted conversations (7.1 minutes vs. 8.2 minutes, P=0.66). Clinicians used more emotional support for families in noninterpreted meetings, including active listening and pausing for questions.
This study is limited by the use of an audio recorder; a video recorder would have provided researchers with participants’ physical interaction and expressions. Additionally, the study does not differentiate between cultural and linguistic difficulties, or provide a reference for the degree of complexity of each conference.
Bottom line: Family meetings in the ICU that require the use of an interpreter provide less information and emotional support to family members than those in which an interpreter is not required.
Citation: Thornton J, Pham K, Engelberg R, et al. Families with limited English proficiency receive less information and support in interpreted intensive care unit family conferences. Crit Care Med. 2009;37(1):89-95.
Postoperative Delirium and Poor Outcomes
Clinical question: In patients 50 and older, what are the risk factors for the development of postoperative delirium, and how are outcomes affected by delirium?
Background: Delirium in the elderly postoperative patient is common. It results in increased costs, morbidity, and mortality. As the population ages, more elderly patients will undergo surgical procedures, so identification of delirium risk factors is essential.
Study design: Prospective, observational, cohort study.
Setting: Veterans Affairs Medical Center, Denver.
Synopsis: Researchers assessed 144 patients 50 and older who were scheduled to undergo surgical procedures with a planned, postoperative ICU stay for cognitive function, overall functional status, and comorbidities. Postoperatively, patients were assessed daily for the development of dementia using the cognitive assessment method-ICU instrument (CAM-ICU). Additionally, a validated chart review method for diagnosing delirium was used. The overall delirium incidence was 44%, and only 12% of cases had an identifiable etiology. The mean onset of delirium was 2.4 days; duration was 4.5 days. The incidence of delirium increased with age, reaching 92% in the 80- to 89-year-old group. In multivariate analysis, preoperative cognitive dysfunction was the strongest predictor of delirium.
Delirium development in patients 50 and older was associated with marked increases in costs ($50,000 vs. $32,000), length of stay (16 days vs. eight days), discharge to a facility (33% vs. 1%), and mortality (9% vs. 1%).
Limitations of this study included the patient population studied (97% men) and lack of data regarding medication use during hospitalization.
Bottom line: In older patients undergoing surgery requiring postoperative ICU care, delirium is common, is associated with prior cognitive dysfunction, and results in significant increases in LOS and mortality.
Citation: Robinson T, Raeburn C, Tran Z, et al. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249(1):173-178.
Meta-Analysis of Perioperative Beta-Blockers Doesn’t Support Routine Use
Clinical question: Are perioperative beta-blockers effective in preventing cardiac events in noncardiac surgery?
Background: The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines for noncardiac surgery recommend beta-blockers for high-risk patients undergoing intermediate or high-risk surgery. The results of previous randomized controlled trials have been inconsistent.
Study design: Meta-analysis.
Setting: Literature search of PubMed, Embase, and the Cochrane Library.
Synopsis: Thirty-three randomized, controlled trials—which included 12,306 patients—were selected for statistical analysis. In these trials, beta-blockers were initiated in the perioperative period with 30-day followup for outcomes of interest. Overall, perioperative beta-blocker use was associated with a 35% risk reduction in nonfatal MI, a 116% increased risk of nonfatal stroke, and no significant difference in all-cause mortality. Trials with higher levels of bias showed greater statistical benefit of beta-blockers. Of note, the POISE trial carried the largest amount of weight, accounting for nearly two-thirds of the total number of patients included in treatment arms.
The application of this data is challenging, as studies differ in several important variables, such as timing of beta-blocker initiation, dosing regimen, and duration of treatment. The POISE trial, in particular, employed a very large dose of metoprolol, compared with doses of beta-blockers used in other studies. There is less data regarding the perioperative efficacy of beta-blockers when therapy is started well before surgery.
Bottom line: Current evidence does not support the routine use of beta-blockers started immediately prior to noncardiac surgery to prevent perioperative cardiac events.
Citation: Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta-blockers in patients having non-cardiac surgery: a meta-analysis. Lancet. 2008;372:1962-1976.
Perioperative Ischemic Stroke an Important Cause of Morbidity and Mortality in Noncardiac Surgery
Clinical question: What are the incidence, risk factors, and outcomes of acute ischemic stroke in nonvascular surgery?
Background: Ischemic stroke is a well-understood complication of cardiovascular surgery. However, little data exist in medical literature regarding the frequency, associations, and outcomes of perioperative ischemic stroke in noncardiac surgery.
Study design: Observational chart review using administrative data.
Setting: The Nationwide Inpatient Sample, a public-use database, in which approximately 1,000 hospitals submit data from nonfederal acute-care hospitals.
Synopsis: Three common surgeries were sampled from an administrative database to characterize the epidemiology of perioperative ischemic stroke in noncardiac surgery. This outcome occurred in 0.7% of hemicolectomy patients; 0.2% of total hip replacement patients; and 0.6% of lobectomy/segmental lung resection patients. Studying the rate of perioperative ischemic stroke in coronary artery bypass graft (CABG) patients validated the authors’ method of data extraction. This rate was consistent with prior studies of this outcome in cardiovascular surgery patients.
Multivariate analysis showed that renal disease (odds ratio 3.0), atrial fibrillation (OR 2.0), prior stroke (OR 1.6), and valvular disease (OR 1.5) are statistically associated with an increased risk of perioperative ischemic stroke. The primary outcome was associated with a marked increase in the odds of in-hospital mortality or need for chronic care upon hospital discharge.
This study is limited by its use of administrative coding data, as well as potential bias introduced by the use of only three major types of surgery.
Bottom line: Ischemic stroke is a serious complication of intermediate and major noncardiovascular surgery. It is associated with poor patient outcomes; more evidence is needed to confirm associations with this outcome and to discover strategies to reduce risk.
Citation: Bateman B, Schum-acher H, Wang S, et al. Perioperative acute ischemic stroke in non-cardiac and nonvascular surgery. Anesthesiology. 2009;110:231-238.
Literature at a Glance
- Discharge innovation and readmission rates.
- Electronic medical records and outcomes.
- CXR findings predict outcomes.
- NSAIDs and congestive heart failure morbidity.
- Outcomes of interpreter use.
- Predictors and outcomes of postoperative delirium.
- Perioperative beta-blockers.
- Perioperative stroke risk.
Standardized Discharge Intervention Decreases Readmission Rates
Clinical question: Does a standardized discharge intervention lead to a decrease in ED visits and readmission rates following hospital discharge?
Background: Hospital discharge is a complex process that is not standardized at many institutions. Deficiencies in the process can lead to poor outcomes, unnecessary rehospitalizations, and increased costs. Previous studies of peridischarge interventions have yielded mixed results and typically focus on specific patient populations.
Study design: Randomized trial.
Setting: Boston Medical Center, a large, urban, academic medical center.
Synopsis: In this single-institution study, 749 English-speaking hospitalized adults were randomly assigned one of two discharge plans: a multidisciplinary package of discharge services or the usual discharge process. Patients in the intervention group were assigned a nurse discharge advocate who performed patient education, medication reconciliation, discharge coordination, and scheduled follow-up appointments. A pharmacist also telephoned participants two to four days after discharge to reinforce the discharge plan and review medications.
Participants in the intervention group had a 30% relative reduction in hospital utilization (defined as ED visit or hospital readmission) at 30 days. Overall, 21.6% of intervention patients and 26.9% of usual-discharge patients had at least one hospital utilization within 30 days of discharge.
This study was limited to a single center, and 27% of the patients did not meet eligibility criteria. The applicability also is limited by the resource utilization required for the intervention. The authors estimated that 0.5 full-time-equivalent (FTE) nursing time and 0.15 FTE pharmacist time was required to maintain 14 patients per week.
Bottom line: A systematic, intensive approach to discharges can reduce ED return visits and readmission rates.
Citation: Jack B, Chetty V, Anthony D, et al. A re-engineered hospital discharge program to decrease re-hospitalization. Ann Intern Med. 2009:150(3):178-187.
EMR Equals Lower Mortality, Fewer Complications, Lower Costs
Clinical question: Is improved automation of hospital information associated with reduced rates of inpatient mortality, complications, cost, and length of stay (LOS)?
Background: Clinical information technologies, including electronic medical records (EMR), are touted as an antidote for the fragmented, unsafe, and expensive American healthcare system. Most studies on the effect of such technologies are limited to a single site, and few involve commercially available information systems.
Study design: Cross-sectional study.
Setting: Urban hospitals in Texas.
Synopsis: Researchers used the previously validated Clinical Information Technology Assessment Tool to survey physicians providing inpatient care in 72 Texas hospitals. This tool measures the degree to which clinical information processes are computerized. Automation is divided into four subdomains: test results, notes and records, order entry, and decision support. To achieve a high score, a process must be fully computerized, the physician must know how to activate it, and the physician must choose the computerized process over alternatives. The authors examined the association between a hospital’s degree of automation and mortality, costs, and LOS among patients with myocardial infarction, congestive heart failure, coronary artery bypass grafting, and pneumonia.
Overall, greater automation was associated with lower mortality, fewer complications, and lower costs. No clear impact on LOS was found. Higher scores in the notes and records subdomains were most associated with lower mortality. Higher decision-support scores were most associated with lower complication rates and costs.
This study is one of the first to demonstrate the benefits of clinical information technologies across a variety of institutions using different information systems.
Bottom line: Hospitals with EMR, order entry, and clinical decision support have lower mortality rates, fewer complications, and lower costs.
Citation: Amarasingham R, Plantinga L, Diener-West M, et al. Clinical information technologies and inpatient outcomes. Arch Intern Med. 2009;169(2):108-114.
Radiologic Progression of Pulmonary Infiltrates Portends Worse Prognosis in Severe CAP Patients
Clinical question: In patients admitted to the ICU with severe community-acquired pneumonia (CAP), do bacteremia and rapid radiologic progression of pulmonary infiltrates increase the risk of shock and mortality?
Background: Severe CAP is associated with considerable morbidity and mortality; however, data focusing on short-term outcomes is limited. The role of the chest radiograph is established in diagnosis but is unclear as a prognostic tool. Bacteremia is associated with higher mortality risk but also is more common in patients with comorbid illnesses.
Study design: Retrospective cohort.
Setting: 33 hospitals in Spain.
Synopsis: This study retrospectively analyzed 457 patients with severe CAP admitted to the ICU between Dec. 1, 2000, and Feb. 28, 2002. Patients were classified into four groups according to the presence or absence of rapid radiographic spread of pulmonary infiltrates and CAP-associated bacteremia. Patients demonstrating significant worsening by chest radiography within the first 48 hours after admission had a threefold increase in the risk of death. Bacteremia was not associated with increased mortality.
The retrospective nature of this study is its major limitation. Other limitations are the probable inclusion of unrecognized bacteremia in the nonbacteremic groups, the fact that repeat chest radiographs were obtained only once (at 48 hours), and that the cause of radiographic deterioration was not examined.
This study contributes to the literature by identifying a subset of patients (those with worsening chest radiographs at 48 hours) who may benefit from further study and targeted interventions.
Bottom line: In severe CAP patients, radiographic worsening at 48 hours is a negative prognostic factor, while bacteremia is not associated with worse outcomes.
Citation: Lisboa T, Blot S, Waterer G, et al. Radiologic progression of pulmonary infiltrates predicts a worse prognosis in severe community-acquired pneumonia than bacteremia. Chest. 2009;135(1):165-172.
NSAIDs Increase Risk of Death and Cardiovascular Morbidity in CHF Patients
Clinical question: Is NSAID use by patients with congestive heart failure (CHF) associated with a higher risk of death or hospitalization due to acute myocardial infarction (MI) or heart failure?
Background: NSAID use is widespread and generally perceived to be low-risk given their over-the-counter availability. However, clinical guidelines discourage the use of NSAIDs in patients with chronic heart failure due to the risk of fluid retention and worsening heart failure.
Study design: Retrospective cohort.
Setting: All hospitals in Denmark.
Synopsis: This study identified 107,092 patients who survived their first hospitalizations due to heart failure between 1995 and 2004. Subsequent use of NSAIDs was determined from a national prescription registry. Patient records were retrospectively analyzed to assess mortality and hospitalization due to MI or heart failure.
At least one NSAID prescription was claimed by 33.9% of the patients after discharge. All NSAIDs were associated with higher death rates, and there was a dose-dependent increase in the risk of death. Ibuprofen and naproxen demonstrated increased mortality only at high doses. All NSAIDs that were studied increased the risk of hospitalization for MI or heart failure.
The observational design is the study’s major limitation. Other important limitations include lack of detailed information about heart failure diagnoses and indication for starting NSAID therapy.
This study intensifies the debate regarding the increased risk of cardiovascular events in NSAID patients, which has been ongoing since the publication of the VIGOR Study in 2000.
Bottom line: In patients with a history of heart failure, NSAIDs are associated with an increased risk of death and cardiovascular morbidity.
Citation: Gislason G, Rasmussen J, Abildstrom S, et al. Increased mortality and cardiovascular morbidity associated with use of non-steroidal anti-inflammatory drugs in chronic heart failure. Arch Intern Med. 2009;169(2):141-149.
Language Barriers Present Obstacle during ICU Family Meetings
Clinical question: Do family meetings that require the use of an interpreter have different characteristics than those in which an interpreter is not needed?
Background: Communication about end-of-life care is essential in the ICU, yet limited English proficiency (LEP) can be a barrier to effective discussions. Overall, outcomes and satisfaction are improved when interpreters are used, but specific effects on ICU family conferences are unknown.
Study design: Cross-sectional evaluation of family meetings.
Setting: Four hospitals in Seattle.
Synopsis: Fifty-one noninterpreted (English-speaking members only) and 10 interpreted (non-English-speaking members present) ICU family meetings were recorded and analyzed for the amount of speaking time and content. The total duration was similar for interpreted versus noninterpreted conferences (26.3 minutes vs. 32.0 minutes, P=0.25), but clinician speech was significantly less in the interpreted group (10.9 minutes vs. 19.6 minutes, P=0.001). Family speaking time was similar in both interpreted and noninterpreted conversations (7.1 minutes vs. 8.2 minutes, P=0.66). Clinicians used more emotional support for families in noninterpreted meetings, including active listening and pausing for questions.
This study is limited by the use of an audio recorder; a video recorder would have provided researchers with participants’ physical interaction and expressions. Additionally, the study does not differentiate between cultural and linguistic difficulties, or provide a reference for the degree of complexity of each conference.
Bottom line: Family meetings in the ICU that require the use of an interpreter provide less information and emotional support to family members than those in which an interpreter is not required.
Citation: Thornton J, Pham K, Engelberg R, et al. Families with limited English proficiency receive less information and support in interpreted intensive care unit family conferences. Crit Care Med. 2009;37(1):89-95.
Postoperative Delirium and Poor Outcomes
Clinical question: In patients 50 and older, what are the risk factors for the development of postoperative delirium, and how are outcomes affected by delirium?
Background: Delirium in the elderly postoperative patient is common. It results in increased costs, morbidity, and mortality. As the population ages, more elderly patients will undergo surgical procedures, so identification of delirium risk factors is essential.
Study design: Prospective, observational, cohort study.
Setting: Veterans Affairs Medical Center, Denver.
Synopsis: Researchers assessed 144 patients 50 and older who were scheduled to undergo surgical procedures with a planned, postoperative ICU stay for cognitive function, overall functional status, and comorbidities. Postoperatively, patients were assessed daily for the development of dementia using the cognitive assessment method-ICU instrument (CAM-ICU). Additionally, a validated chart review method for diagnosing delirium was used. The overall delirium incidence was 44%, and only 12% of cases had an identifiable etiology. The mean onset of delirium was 2.4 days; duration was 4.5 days. The incidence of delirium increased with age, reaching 92% in the 80- to 89-year-old group. In multivariate analysis, preoperative cognitive dysfunction was the strongest predictor of delirium.
Delirium development in patients 50 and older was associated with marked increases in costs ($50,000 vs. $32,000), length of stay (16 days vs. eight days), discharge to a facility (33% vs. 1%), and mortality (9% vs. 1%).
Limitations of this study included the patient population studied (97% men) and lack of data regarding medication use during hospitalization.
Bottom line: In older patients undergoing surgery requiring postoperative ICU care, delirium is common, is associated with prior cognitive dysfunction, and results in significant increases in LOS and mortality.
Citation: Robinson T, Raeburn C, Tran Z, et al. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249(1):173-178.
Meta-Analysis of Perioperative Beta-Blockers Doesn’t Support Routine Use
Clinical question: Are perioperative beta-blockers effective in preventing cardiac events in noncardiac surgery?
Background: The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines for noncardiac surgery recommend beta-blockers for high-risk patients undergoing intermediate or high-risk surgery. The results of previous randomized controlled trials have been inconsistent.
Study design: Meta-analysis.
Setting: Literature search of PubMed, Embase, and the Cochrane Library.
Synopsis: Thirty-three randomized, controlled trials—which included 12,306 patients—were selected for statistical analysis. In these trials, beta-blockers were initiated in the perioperative period with 30-day followup for outcomes of interest. Overall, perioperative beta-blocker use was associated with a 35% risk reduction in nonfatal MI, a 116% increased risk of nonfatal stroke, and no significant difference in all-cause mortality. Trials with higher levels of bias showed greater statistical benefit of beta-blockers. Of note, the POISE trial carried the largest amount of weight, accounting for nearly two-thirds of the total number of patients included in treatment arms.
The application of this data is challenging, as studies differ in several important variables, such as timing of beta-blocker initiation, dosing regimen, and duration of treatment. The POISE trial, in particular, employed a very large dose of metoprolol, compared with doses of beta-blockers used in other studies. There is less data regarding the perioperative efficacy of beta-blockers when therapy is started well before surgery.
Bottom line: Current evidence does not support the routine use of beta-blockers started immediately prior to noncardiac surgery to prevent perioperative cardiac events.
Citation: Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta-blockers in patients having non-cardiac surgery: a meta-analysis. Lancet. 2008;372:1962-1976.
Perioperative Ischemic Stroke an Important Cause of Morbidity and Mortality in Noncardiac Surgery
Clinical question: What are the incidence, risk factors, and outcomes of acute ischemic stroke in nonvascular surgery?
Background: Ischemic stroke is a well-understood complication of cardiovascular surgery. However, little data exist in medical literature regarding the frequency, associations, and outcomes of perioperative ischemic stroke in noncardiac surgery.
Study design: Observational chart review using administrative data.
Setting: The Nationwide Inpatient Sample, a public-use database, in which approximately 1,000 hospitals submit data from nonfederal acute-care hospitals.
Synopsis: Three common surgeries were sampled from an administrative database to characterize the epidemiology of perioperative ischemic stroke in noncardiac surgery. This outcome occurred in 0.7% of hemicolectomy patients; 0.2% of total hip replacement patients; and 0.6% of lobectomy/segmental lung resection patients. Studying the rate of perioperative ischemic stroke in coronary artery bypass graft (CABG) patients validated the authors’ method of data extraction. This rate was consistent with prior studies of this outcome in cardiovascular surgery patients.
Multivariate analysis showed that renal disease (odds ratio 3.0), atrial fibrillation (OR 2.0), prior stroke (OR 1.6), and valvular disease (OR 1.5) are statistically associated with an increased risk of perioperative ischemic stroke. The primary outcome was associated with a marked increase in the odds of in-hospital mortality or need for chronic care upon hospital discharge.
This study is limited by its use of administrative coding data, as well as potential bias introduced by the use of only three major types of surgery.
Bottom line: Ischemic stroke is a serious complication of intermediate and major noncardiovascular surgery. It is associated with poor patient outcomes; more evidence is needed to confirm associations with this outcome and to discover strategies to reduce risk.
Citation: Bateman B, Schum-acher H, Wang S, et al. Perioperative acute ischemic stroke in non-cardiac and nonvascular surgery. Anesthesiology. 2009;110:231-238.
2010: HM Goes to Washington
Enter text here
Enter text here
Enter text here
SHM’s Down with Digital
When hospitalist Robert Wachter, MD, FHM, started his HM blog almost two years ago, he didn’t anticipate that one of his blog entries would be about pop-music icon Britney Spears. Or that it would become his most popular, attracting nearly double the number of readers as his next-most-popular post.
Dr. Wachter—professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World” (www.wachtersworld.com)—attributes the popularity of that post partly to Spears, but also to the fact it touched on a topic that always sparks interest among hospitalists, other healthcare providers, and hospital executives: the relationship between doctors and nurses in a hospital setting. Dr. Wachter’s most-popular post used Spears’ hospitalization in early 2008 and the controversy surrounding care providers who sneaked a peek at her medical records to make a point about how physicians and nurses often are treated differently in a hospital setting.
—Robert Chang, MD, hospitalist, University of Michigan Medical Center, Ann Arbor
But that was just one story. In the first year alone, Dr. Wachter wrote 76 blog posts, each of which easily exceeded 1,000 words. During the first year of blogging, the average post was read more than 1,800 times and the Web site attracted nearly 140,000 views.
“This has been one of the most gratifying things I’ve done in my career,” Dr. Wachter says. “I’ve published hundreds of articles in journals, but something about this form has an immediacy and connection to the audience that feels very important.”
And he isn’t alone. Blogs and HM have experienced similar growth trajectories in recent years. Now they are coming together to help hospitalists understand the most pressing issues in the specialty and provide the best care to hospitalized patients.
A Blog Primer
Blogs are Web sites that feature regular articles, or “posts.” The topic, length, and regularity of the posts are entirely at the discretion of the author, also known as the blogger. Some blogs are updated dozens of times a day; others, such as Wachter’s World, only feature new posts every week or so, but often with more depth and insight.
Although initially dismissed by many as outlets for trivial information, blogs are now recognized by experts in nearly every field as an important and cost-effective way to spark conversation and take positions on issues of the day.
Compared with more traditional media outlets, the ability to create dialogue is perhaps the most distinctive blog characteristic. Bloggers often invite readers to post or e-mail comments, creating interactivity between author and reader. In addition, many blogs automatically e-mail and distribute new blog posts to subscribers.
The “viral” aspect of blogs is a major contributor to their success. For instance, say Dr. Wachter writes a new blog post at 8:30 in the morning. Shortly thereafter, his readers will receive an automatically generated e-mail from the blog informing readers that Dr. Wachter has posted a new blog entry. When the reader visits the blog and reads the new post, they might think it could be of interest to a colleague, so they forward it to a colleague via e-mail. The colleague not only reads the article, but they also are impressed and post a comment for the rest of the blog’s readers to view.
SHM Blogs Advance the Specialty
The feedback loop of blogs isn’t limited to the on-screen world. That’s the lesson learned by clinical hospitalist Danielle Scheurer, MD, MSCR, SHM’s Web editor and director of General Medical Services at Brigham and Women’s Hospital in Boston.
As the author of SHM’s new clinical practice blog, “Hospital Medicine Quick Hits,” Dr. Scheurer knew the fledgling blog provided a valuable resource to busy clinicians, but she didn’t expect it to get back to her. She recalls that one day, “my blog was quoted to me by one of my house staff, who said, ‘I found this great hospital medicine blog today,’ and he didn’t realize I was the author.”
For the blog, Scheurer scours through 50 of the top medical journals for articles that are relevant to practicing clinical hospitalists. She posts concise overviews of the articles, along with links to the original research.
For hospitalists who have an interest in practice management, SHM offers another new blog, “The Hospitalist Leader.” It shares perspectives and ideas on the day-to-day interactions that hospitalists encounter and how best to administer a hospital practice. Four hospitalist co-authors—Robert Chang, MD, FHM, a hospitalist at the University of Michigan Medical Center in Ann Arbor; Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare; John Nelson, MD, FHM, principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm; and Robert Bessler, MD, FHM, a hospitalist with Sound Inpatient Physicians in Tacoma, Wash.—use many of their own experiences in the hospital as raw material for the blog.
Dr. Chang views the blog as another way to move HM forward: “I trust and hope that we can use the blog to help the professional status of our profession, as this ultimately will determine the choices we make, large and small,” he says.
What’s Next
If you’re attending HM09 this year, don’t be surprised if you see someone else in the crowd excitedly typing into an iPhone or BlackBerry. You just might find a new blog post on the session you just attended.
Gone are the old images of a blogger in slippers and pajamas stealthily typing on the computer in the basement. These days, posting at or during an event, on site and in real time, is standard practice for many bloggers. In fact, SHM made a concerted effort to invite the most influential bloggers in the industry to HM09.
And if the person typing away isn’t “live blogging,” he may be “tweeting,” or adding super-short updates to the popular Web site Twitter. For many bloggers, it’s a way of communicating instantaneously with their audiences; once they post a blog article, they “tweet”—or send out—the link to thousands of readers.
SHM has its own Twitter account—@SHMLive—and uses the account to keep interested hospitalists updated on new blog posts, society news, and other HM developments.
“Hospital medicine is constantly evolving,” says Heather Abdel-Salam, SHM’s public relations and marketing coordinator, “and so do our efforts t.o communicate the best practices in the specialty. Blogs, Twitter feeds, and other online outreach are a big part of how we promote hospital medicine and help it grow within the healthcare arena.” TH
Brendon Shank is a freelance writer based in Philadelphia.
When hospitalist Robert Wachter, MD, FHM, started his HM blog almost two years ago, he didn’t anticipate that one of his blog entries would be about pop-music icon Britney Spears. Or that it would become his most popular, attracting nearly double the number of readers as his next-most-popular post.
Dr. Wachter—professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World” (www.wachtersworld.com)—attributes the popularity of that post partly to Spears, but also to the fact it touched on a topic that always sparks interest among hospitalists, other healthcare providers, and hospital executives: the relationship between doctors and nurses in a hospital setting. Dr. Wachter’s most-popular post used Spears’ hospitalization in early 2008 and the controversy surrounding care providers who sneaked a peek at her medical records to make a point about how physicians and nurses often are treated differently in a hospital setting.
—Robert Chang, MD, hospitalist, University of Michigan Medical Center, Ann Arbor
But that was just one story. In the first year alone, Dr. Wachter wrote 76 blog posts, each of which easily exceeded 1,000 words. During the first year of blogging, the average post was read more than 1,800 times and the Web site attracted nearly 140,000 views.
“This has been one of the most gratifying things I’ve done in my career,” Dr. Wachter says. “I’ve published hundreds of articles in journals, but something about this form has an immediacy and connection to the audience that feels very important.”
And he isn’t alone. Blogs and HM have experienced similar growth trajectories in recent years. Now they are coming together to help hospitalists understand the most pressing issues in the specialty and provide the best care to hospitalized patients.
A Blog Primer
Blogs are Web sites that feature regular articles, or “posts.” The topic, length, and regularity of the posts are entirely at the discretion of the author, also known as the blogger. Some blogs are updated dozens of times a day; others, such as Wachter’s World, only feature new posts every week or so, but often with more depth and insight.
Although initially dismissed by many as outlets for trivial information, blogs are now recognized by experts in nearly every field as an important and cost-effective way to spark conversation and take positions on issues of the day.
Compared with more traditional media outlets, the ability to create dialogue is perhaps the most distinctive blog characteristic. Bloggers often invite readers to post or e-mail comments, creating interactivity between author and reader. In addition, many blogs automatically e-mail and distribute new blog posts to subscribers.
The “viral” aspect of blogs is a major contributor to their success. For instance, say Dr. Wachter writes a new blog post at 8:30 in the morning. Shortly thereafter, his readers will receive an automatically generated e-mail from the blog informing readers that Dr. Wachter has posted a new blog entry. When the reader visits the blog and reads the new post, they might think it could be of interest to a colleague, so they forward it to a colleague via e-mail. The colleague not only reads the article, but they also are impressed and post a comment for the rest of the blog’s readers to view.
SHM Blogs Advance the Specialty
The feedback loop of blogs isn’t limited to the on-screen world. That’s the lesson learned by clinical hospitalist Danielle Scheurer, MD, MSCR, SHM’s Web editor and director of General Medical Services at Brigham and Women’s Hospital in Boston.
As the author of SHM’s new clinical practice blog, “Hospital Medicine Quick Hits,” Dr. Scheurer knew the fledgling blog provided a valuable resource to busy clinicians, but she didn’t expect it to get back to her. She recalls that one day, “my blog was quoted to me by one of my house staff, who said, ‘I found this great hospital medicine blog today,’ and he didn’t realize I was the author.”
For the blog, Scheurer scours through 50 of the top medical journals for articles that are relevant to practicing clinical hospitalists. She posts concise overviews of the articles, along with links to the original research.
For hospitalists who have an interest in practice management, SHM offers another new blog, “The Hospitalist Leader.” It shares perspectives and ideas on the day-to-day interactions that hospitalists encounter and how best to administer a hospital practice. Four hospitalist co-authors—Robert Chang, MD, FHM, a hospitalist at the University of Michigan Medical Center in Ann Arbor; Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare; John Nelson, MD, FHM, principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm; and Robert Bessler, MD, FHM, a hospitalist with Sound Inpatient Physicians in Tacoma, Wash.—use many of their own experiences in the hospital as raw material for the blog.
Dr. Chang views the blog as another way to move HM forward: “I trust and hope that we can use the blog to help the professional status of our profession, as this ultimately will determine the choices we make, large and small,” he says.
What’s Next
If you’re attending HM09 this year, don’t be surprised if you see someone else in the crowd excitedly typing into an iPhone or BlackBerry. You just might find a new blog post on the session you just attended.
Gone are the old images of a blogger in slippers and pajamas stealthily typing on the computer in the basement. These days, posting at or during an event, on site and in real time, is standard practice for many bloggers. In fact, SHM made a concerted effort to invite the most influential bloggers in the industry to HM09.
And if the person typing away isn’t “live blogging,” he may be “tweeting,” or adding super-short updates to the popular Web site Twitter. For many bloggers, it’s a way of communicating instantaneously with their audiences; once they post a blog article, they “tweet”—or send out—the link to thousands of readers.
SHM has its own Twitter account—@SHMLive—and uses the account to keep interested hospitalists updated on new blog posts, society news, and other HM developments.
“Hospital medicine is constantly evolving,” says Heather Abdel-Salam, SHM’s public relations and marketing coordinator, “and so do our efforts t.o communicate the best practices in the specialty. Blogs, Twitter feeds, and other online outreach are a big part of how we promote hospital medicine and help it grow within the healthcare arena.” TH
Brendon Shank is a freelance writer based in Philadelphia.
When hospitalist Robert Wachter, MD, FHM, started his HM blog almost two years ago, he didn’t anticipate that one of his blog entries would be about pop-music icon Britney Spears. Or that it would become his most popular, attracting nearly double the number of readers as his next-most-popular post.
Dr. Wachter—professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World” (www.wachtersworld.com)—attributes the popularity of that post partly to Spears, but also to the fact it touched on a topic that always sparks interest among hospitalists, other healthcare providers, and hospital executives: the relationship between doctors and nurses in a hospital setting. Dr. Wachter’s most-popular post used Spears’ hospitalization in early 2008 and the controversy surrounding care providers who sneaked a peek at her medical records to make a point about how physicians and nurses often are treated differently in a hospital setting.
—Robert Chang, MD, hospitalist, University of Michigan Medical Center, Ann Arbor
But that was just one story. In the first year alone, Dr. Wachter wrote 76 blog posts, each of which easily exceeded 1,000 words. During the first year of blogging, the average post was read more than 1,800 times and the Web site attracted nearly 140,000 views.
“This has been one of the most gratifying things I’ve done in my career,” Dr. Wachter says. “I’ve published hundreds of articles in journals, but something about this form has an immediacy and connection to the audience that feels very important.”
And he isn’t alone. Blogs and HM have experienced similar growth trajectories in recent years. Now they are coming together to help hospitalists understand the most pressing issues in the specialty and provide the best care to hospitalized patients.
A Blog Primer
Blogs are Web sites that feature regular articles, or “posts.” The topic, length, and regularity of the posts are entirely at the discretion of the author, also known as the blogger. Some blogs are updated dozens of times a day; others, such as Wachter’s World, only feature new posts every week or so, but often with more depth and insight.
Although initially dismissed by many as outlets for trivial information, blogs are now recognized by experts in nearly every field as an important and cost-effective way to spark conversation and take positions on issues of the day.
Compared with more traditional media outlets, the ability to create dialogue is perhaps the most distinctive blog characteristic. Bloggers often invite readers to post or e-mail comments, creating interactivity between author and reader. In addition, many blogs automatically e-mail and distribute new blog posts to subscribers.
The “viral” aspect of blogs is a major contributor to their success. For instance, say Dr. Wachter writes a new blog post at 8:30 in the morning. Shortly thereafter, his readers will receive an automatically generated e-mail from the blog informing readers that Dr. Wachter has posted a new blog entry. When the reader visits the blog and reads the new post, they might think it could be of interest to a colleague, so they forward it to a colleague via e-mail. The colleague not only reads the article, but they also are impressed and post a comment for the rest of the blog’s readers to view.
SHM Blogs Advance the Specialty
The feedback loop of blogs isn’t limited to the on-screen world. That’s the lesson learned by clinical hospitalist Danielle Scheurer, MD, MSCR, SHM’s Web editor and director of General Medical Services at Brigham and Women’s Hospital in Boston.
As the author of SHM’s new clinical practice blog, “Hospital Medicine Quick Hits,” Dr. Scheurer knew the fledgling blog provided a valuable resource to busy clinicians, but she didn’t expect it to get back to her. She recalls that one day, “my blog was quoted to me by one of my house staff, who said, ‘I found this great hospital medicine blog today,’ and he didn’t realize I was the author.”
For the blog, Scheurer scours through 50 of the top medical journals for articles that are relevant to practicing clinical hospitalists. She posts concise overviews of the articles, along with links to the original research.
For hospitalists who have an interest in practice management, SHM offers another new blog, “The Hospitalist Leader.” It shares perspectives and ideas on the day-to-day interactions that hospitalists encounter and how best to administer a hospital practice. Four hospitalist co-authors—Robert Chang, MD, FHM, a hospitalist at the University of Michigan Medical Center in Ann Arbor; Rusty Holman, MD, FHM, chief operating officer of Brentwood, Tenn.-based Cogent Healthcare; John Nelson, MD, FHM, principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm; and Robert Bessler, MD, FHM, a hospitalist with Sound Inpatient Physicians in Tacoma, Wash.—use many of their own experiences in the hospital as raw material for the blog.
Dr. Chang views the blog as another way to move HM forward: “I trust and hope that we can use the blog to help the professional status of our profession, as this ultimately will determine the choices we make, large and small,” he says.
What’s Next
If you’re attending HM09 this year, don’t be surprised if you see someone else in the crowd excitedly typing into an iPhone or BlackBerry. You just might find a new blog post on the session you just attended.
Gone are the old images of a blogger in slippers and pajamas stealthily typing on the computer in the basement. These days, posting at or during an event, on site and in real time, is standard practice for many bloggers. In fact, SHM made a concerted effort to invite the most influential bloggers in the industry to HM09.
And if the person typing away isn’t “live blogging,” he may be “tweeting,” or adding super-short updates to the popular Web site Twitter. For many bloggers, it’s a way of communicating instantaneously with their audiences; once they post a blog article, they “tweet”—or send out—the link to thousands of readers.
SHM has its own Twitter account—@SHMLive—and uses the account to keep interested hospitalists updated on new blog posts, society news, and other HM developments.
“Hospital medicine is constantly evolving,” says Heather Abdel-Salam, SHM’s public relations and marketing coordinator, “and so do our efforts t.o communicate the best practices in the specialty. Blogs, Twitter feeds, and other online outreach are a big part of how we promote hospital medicine and help it grow within the healthcare arena.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Clinical tips for managing safety in patients with borderline personality disorder
Issues in Hepatitis B Virus Infection
Supplement Editor:
William D. Carey, MD
Contents
The prevalence and natural history of hepatitis B in the 21st century
William D. Carey, MD
Risk of hepatocellular carcinoma in hepatitis B and prevention through treatment
Morris Sherman, MD, PhD
Understanding cultural barriers in hepatitis B virus infection
Tram T. Tran, MD
Hepatitis B treatment: Current best practices, avoiding resistance
Robert G. Gish, MD
Monotherapy vs multiple-drug therapy: The experts debate
Robert G. Gish, MD, and Pierre M. Gholam,MD
Management of hepatitis B in pregnancy: Weighing the options
Tram T. Tran, MD
Strategies for managing coinfection with hepatitis B virus and HIV
Morris Sherman, MD, PhD
Supplement Editor:
William D. Carey, MD
Contents
The prevalence and natural history of hepatitis B in the 21st century
William D. Carey, MD
Risk of hepatocellular carcinoma in hepatitis B and prevention through treatment
Morris Sherman, MD, PhD
Understanding cultural barriers in hepatitis B virus infection
Tram T. Tran, MD
Hepatitis B treatment: Current best practices, avoiding resistance
Robert G. Gish, MD
Monotherapy vs multiple-drug therapy: The experts debate
Robert G. Gish, MD, and Pierre M. Gholam,MD
Management of hepatitis B in pregnancy: Weighing the options
Tram T. Tran, MD
Strategies for managing coinfection with hepatitis B virus and HIV
Morris Sherman, MD, PhD
Supplement Editor:
William D. Carey, MD
Contents
The prevalence and natural history of hepatitis B in the 21st century
William D. Carey, MD
Risk of hepatocellular carcinoma in hepatitis B and prevention through treatment
Morris Sherman, MD, PhD
Understanding cultural barriers in hepatitis B virus infection
Tram T. Tran, MD
Hepatitis B treatment: Current best practices, avoiding resistance
Robert G. Gish, MD
Monotherapy vs multiple-drug therapy: The experts debate
Robert G. Gish, MD, and Pierre M. Gholam,MD
Management of hepatitis B in pregnancy: Weighing the options
Tram T. Tran, MD
Strategies for managing coinfection with hepatitis B virus and HIV
Morris Sherman, MD, PhD
The prevalence and natural history of hepatitis B in the 21st century
Hepatitis B virus (HBV) infection is highly prevalent worldwide and is a major cause of morbidity and death. Two billion people globally have been infected with HBV, 350 to 400 million are chronic carriers, and tens of millions of new cases occur annually. Of those infected, 15% to 40% develop HBV complications, namely cirrhosis or hepatocellular carcinoma (HCC).1–3
The high prevalence of HBV infection represents an enormous failure of public health, considering that HBV immunization has been available for an entire generation, and where it has been employed it has been highly effective at reducing the incidence of HBV infection. Immunization, however, has been underused.
This supplement to the Cleveland Clinic Journal of Medicine, derived from a live symposium, aims to enhance awareness of the natural history of HBV infection and clarify its management recommendations with illustrative case histories. The supplement starts with a brief review of HBV terminology, natural history, and epidemiology.
CHRONIC HBV INFECTION TERMINOLOGY
Familiarity with the terms commonly used to describe chronic HBV infection will help clinicians in the management of the disease4:
- Chronic HBV infection is defined as presence of hepatitis B surface antigen (HBsAg) for more than 6 months. Those with infection may also express another antigen, HB e antigen (HBeAg), a marker of heightened infectivity. At the same time, those who are HBeAg positive are better responders to antiviral therapy compared with those who are HBeAg negative.
- An inactive HBsAg carrier is an individual who is HBsAg positive with a very low level of circulating virus, liver enzyme levels within normal limits, and a low likelihood of having chronic progressive disease.
- Resolved HBV infection is defined as previous HBV infection with no remaining evidence of active disease. Such individuals test negative for HBsAg and positive for antibody to HBsAg (anti-HBs) and to HB core antigen (anti-HBc). They also have no detectable viral load, or HBV DNA, in their blood. In most instances, they are protected from reinfection.
- Reactivation is the reappearance of HBV infection in someone who is known to be an inactive HBsAg carrier or whose previous HBV infection had resolved (see “Case: Recurrence despite anti-HBs and HBsAg negativity”).
- HBeAg seroconversion is the transition from HBeAg-positive to HBeAg-negative status and development of antibody to HBeAg (anti-HBe), usually accompanied by less active liver disease and lower viral loads.
- HBeAg clearance is disappearance of HBeAg without the development of anti-HBe; reactivation or reversion to HBeAg-positive status can occur.
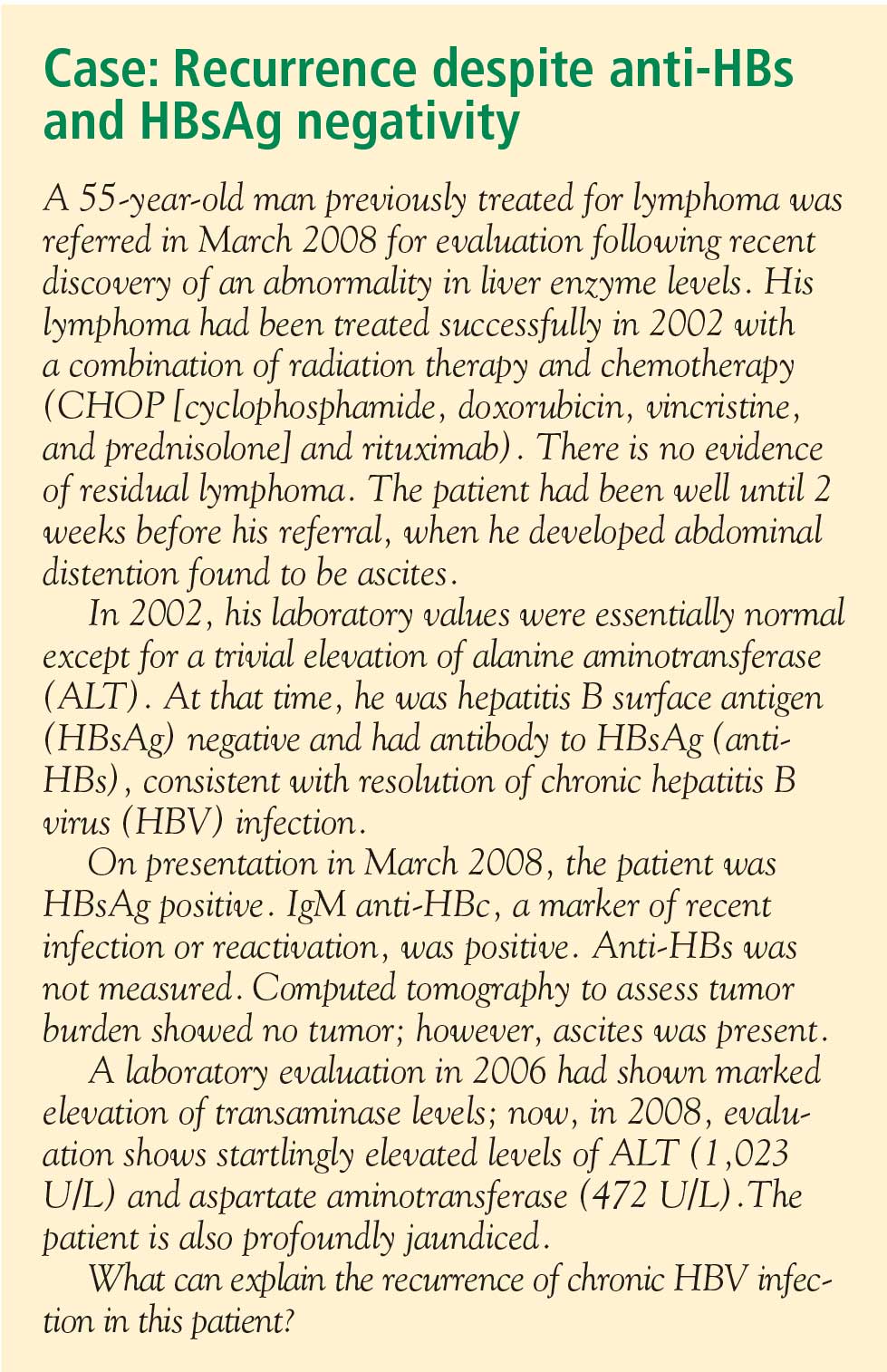
GEOGRAPHIC DISTRIBUTION OF CHRONIC HBV INFECTION
The global prevalence of HBV varies widely. Regions are divided into areas of low, intermediate, and high prevalence, defined as follows4:
- High prevalence implies that at least 8% of the population is currently infected, with a lifetime likelihood of active or resolved infection greater than 60%. About 45% of the world’s population lives in regions of high prevalence. Among this group, early childhood infections are common, with the virus usually transmitted from mother to infant during the perinatal period.
- Intermediate prevalence is defined as 2% to 7%, with a lifetime risk of infection of 20% to 60%. These regions represent about 43% of the global population. In intermediate-prevalence areas, infections occur in all age groups.
- Low prevalence is defined as less than 2% and represents only 12% of the global population. In these regions, the lifetime risk of infection is less than 20%.
North America is a low-prevalence area except for the northern rim, where Inuit and Yupik Eskimos have a high prevalence, and communities that have a substantial immigrant population from high-prevalence areas, such as sub-Saharan Africa and many parts of Asia.
Chronic HBV infection in the United States
Approximately 1.25 million individuals in the United States are HBsAg carriers.2,4 In Asian Americans and Alaskan natives, the prevalence of HBsAg positivity, or chronic disease, is 5% to 15%.5,6 Similarly, US health statistics sources estimate that among those who are chronically infected, approximately half are Asian American.7 As the Asian American population continues to increase (1.5 million to 7 million from 1970 to 19905,8; 11.9 million in the 2000 US Census8), the total prevalence of chronic HBV infection will increase as well.
NATURAL HISTORY OF CHRONIC HBV INFECTION
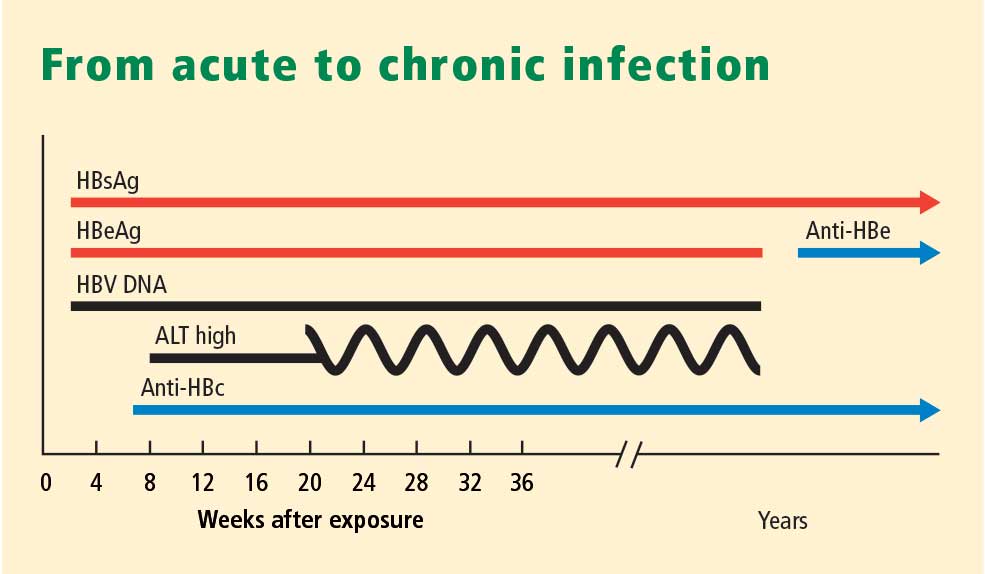
Chronic HBV usually causes microinflammatory changes that evoke a fibrotic response in the liver, and many infected individuals will eventually develop cirrhosis and are at risk for the development of HCC. Inactive HBsAg carriers often bypass the development of cirrhosis but remain at risk for HCC if their viral load is very high. This is particularly true when infection is acquired in infancy.
The age at acquisition of HBV has a large impact on the likelihood of the disease becoming chronic. The chance of chronic infection is 90% or greater among neonates who become infected with HBV through perinatal transmission. Exposure during adolescence or young adulthood is associated with a 95% or greater likelihood that the disease will be self-limiting.
The typical North American patient with HBV acquires the infection as an adolescent or young adult and is not at risk of HCC unless cirrhosis develops. In most patients who acquire the disease in adolescence or adulthood, the infection resolves after weeks or a few months and they are not at risk of either cirrhosis or HCC. However, an individual such as the one described in the accompanying case, who becomes immunocompromised, is at risk of reactivation of HBV infection (see “Case revisited”).
HBV MODES OF TRANSMISSION
In low-prevalence areas, such as most of North America, most cases of HBV infection are acquired during adolescence to midadulthood, a period during which behaviors that increase the risk of HBV infection (ie, intravenous drug abuse or unprotected sexual activity) are most likely.9,10 Sex workers and homosexuals are at particular risk of sexual transmission of HBV. Intravenous drug abusers and health workers are at risk of parenteral transmission.
In high-prevalence areas, HBV is mostly transmitted during the perinatal period from mother to infant, conferring a high likelihood of chronicity.9,10 Mothers who are HBsAg positive, particularly those who are also HBeAg positive, are much more likely than others to transmit HBV to their offspring.
FACTORS THAT INFLUENCE THE COURSE OF HBV INFECTION
Viral load has emerged as the most significant factor implicated in the development of cirrhosis or HCC. Iloeje et al11 found that viral load predicted progression to cirrhosis among a cohort of nearly 4,000 Taiwanese. Other factors that can influence the course of HBV infection include age at onset, male sex, and comorbidities (ie, alcohol use, human immunodeficiency virus infection, hepatitis C virus infection). Core promoter and precore mutants may affect the likelihood of developing HCC. A genetic signature that predisposes liver cells to proliferate, termed field effects, may also lead to the development of HCC. The influence of smoking and diabetes on the development of HCC in HBV-infected individuals is not well documented.
Reduction or elimination of measurable virus is the current holy grail of treatment; available antiviral therapies are potent tools that lower viral load with the hope of reducing the likelihood of either cirrhosis or HCC.
HBV genotypes may be implicated in the progression of liver disease or the risk of development of HCC. HBV genotypes differ by region and may correlate with ethnicity and disease progression. In a study of 694 US patients with chronic HBV, Chu et al12 found that genotypes A and C were associated with a higher prevalence of HBsAg positivity than other genotypes. Genotypes B and C were the most common among Asian American patients, while genotype A was the most common among Caucasian and African American patients. The authors suggested that HBV genotypes may explain the heterogeneity in the manifestation of the disease.
- Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004; 11:97–107.
- Hepatitis B Foundation. Statistics. Hepatitis B Foundation Web site. http://www.hepb.org/hepb/statistics.htm. Published 2003–2008. Accessed January 9, 2009.
- Hepatitis Foundation International. The ABC’s of hepatitis. Hepatitis Foundation International Web site. http://www.hepfi.org/living/liv_abc.html. Published 2003. Accessed January 9, 2009.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Tong MJ, Hwang S-J. Hepatitis B virus infection in Asian Americans. Gastroenterol Clin North Am 1994; 23:523–536.
- McMahon BJ, Schoenberg S, Bulkow L, et al. Seroprevalence of hepatitis B viral markers in 52,000 Alaska natives. Am J Epidemiol 1993; 138:544–549.
- US Department of Health and Human Services. Hepatitis and Asian Americans. The Office of Minority Health Web site. http://www.omhrc.gov/templates/content.aspx?lvl=3&lvlid=541&ID=6495. Updated May 5, 2008. Accessed January 12, 2009.
- Barnes JS, Bennett CE. The Asian population: 2000. Census 2000 brief. United States Census 2000 Web site. http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed January 12, 2009.
- Lok AS, McMahon BJ; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Chronic hepatitis B. Hepatology 2001; 34:1225–1241.
- Lok AS, Heathcote EJ, Hoofnagle JH. Management of hepatitis B: 2000—summary of a workshop. Gastroenterology 2001; 120:1828–1853.
- Iloeje UH, Yang H-I, Su J, Jen C-L, You S-L, Chen C-J, and The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-in HBV (the REVEAL-HBV) Study Group. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006; 130:678–686.
- Chu CJ, Keeffe EB, Han SH, et al. Hepatitis B virus genotypes in the United States: results of a nationwide study. Gastroenterology 2003; 125:444–451.
Hepatitis B virus (HBV) infection is highly prevalent worldwide and is a major cause of morbidity and death. Two billion people globally have been infected with HBV, 350 to 400 million are chronic carriers, and tens of millions of new cases occur annually. Of those infected, 15% to 40% develop HBV complications, namely cirrhosis or hepatocellular carcinoma (HCC).1–3
The high prevalence of HBV infection represents an enormous failure of public health, considering that HBV immunization has been available for an entire generation, and where it has been employed it has been highly effective at reducing the incidence of HBV infection. Immunization, however, has been underused.
This supplement to the Cleveland Clinic Journal of Medicine, derived from a live symposium, aims to enhance awareness of the natural history of HBV infection and clarify its management recommendations with illustrative case histories. The supplement starts with a brief review of HBV terminology, natural history, and epidemiology.
CHRONIC HBV INFECTION TERMINOLOGY
Familiarity with the terms commonly used to describe chronic HBV infection will help clinicians in the management of the disease4:
- Chronic HBV infection is defined as presence of hepatitis B surface antigen (HBsAg) for more than 6 months. Those with infection may also express another antigen, HB e antigen (HBeAg), a marker of heightened infectivity. At the same time, those who are HBeAg positive are better responders to antiviral therapy compared with those who are HBeAg negative.
- An inactive HBsAg carrier is an individual who is HBsAg positive with a very low level of circulating virus, liver enzyme levels within normal limits, and a low likelihood of having chronic progressive disease.
- Resolved HBV infection is defined as previous HBV infection with no remaining evidence of active disease. Such individuals test negative for HBsAg and positive for antibody to HBsAg (anti-HBs) and to HB core antigen (anti-HBc). They also have no detectable viral load, or HBV DNA, in their blood. In most instances, they are protected from reinfection.
- Reactivation is the reappearance of HBV infection in someone who is known to be an inactive HBsAg carrier or whose previous HBV infection had resolved (see “Case: Recurrence despite anti-HBs and HBsAg negativity”).
- HBeAg seroconversion is the transition from HBeAg-positive to HBeAg-negative status and development of antibody to HBeAg (anti-HBe), usually accompanied by less active liver disease and lower viral loads.
- HBeAg clearance is disappearance of HBeAg without the development of anti-HBe; reactivation or reversion to HBeAg-positive status can occur.
GEOGRAPHIC DISTRIBUTION OF CHRONIC HBV INFECTION
The global prevalence of HBV varies widely. Regions are divided into areas of low, intermediate, and high prevalence, defined as follows4:
- High prevalence implies that at least 8% of the population is currently infected, with a lifetime likelihood of active or resolved infection greater than 60%. About 45% of the world’s population lives in regions of high prevalence. Among this group, early childhood infections are common, with the virus usually transmitted from mother to infant during the perinatal period.
- Intermediate prevalence is defined as 2% to 7%, with a lifetime risk of infection of 20% to 60%. These regions represent about 43% of the global population. In intermediate-prevalence areas, infections occur in all age groups.
- Low prevalence is defined as less than 2% and represents only 12% of the global population. In these regions, the lifetime risk of infection is less than 20%.
North America is a low-prevalence area except for the northern rim, where Inuit and Yupik Eskimos have a high prevalence, and communities that have a substantial immigrant population from high-prevalence areas, such as sub-Saharan Africa and many parts of Asia.
Chronic HBV infection in the United States
Approximately 1.25 million individuals in the United States are HBsAg carriers.2,4 In Asian Americans and Alaskan natives, the prevalence of HBsAg positivity, or chronic disease, is 5% to 15%.5,6 Similarly, US health statistics sources estimate that among those who are chronically infected, approximately half are Asian American.7 As the Asian American population continues to increase (1.5 million to 7 million from 1970 to 19905,8; 11.9 million in the 2000 US Census8), the total prevalence of chronic HBV infection will increase as well.
NATURAL HISTORY OF CHRONIC HBV INFECTION
Chronic HBV usually causes microinflammatory changes that evoke a fibrotic response in the liver, and many infected individuals will eventually develop cirrhosis and are at risk for the development of HCC. Inactive HBsAg carriers often bypass the development of cirrhosis but remain at risk for HCC if their viral load is very high. This is particularly true when infection is acquired in infancy.
The age at acquisition of HBV has a large impact on the likelihood of the disease becoming chronic. The chance of chronic infection is 90% or greater among neonates who become infected with HBV through perinatal transmission. Exposure during adolescence or young adulthood is associated with a 95% or greater likelihood that the disease will be self-limiting.
The typical North American patient with HBV acquires the infection as an adolescent or young adult and is not at risk of HCC unless cirrhosis develops. In most patients who acquire the disease in adolescence or adulthood, the infection resolves after weeks or a few months and they are not at risk of either cirrhosis or HCC. However, an individual such as the one described in the accompanying case, who becomes immunocompromised, is at risk of reactivation of HBV infection (see “Case revisited”).
HBV MODES OF TRANSMISSION
In low-prevalence areas, such as most of North America, most cases of HBV infection are acquired during adolescence to midadulthood, a period during which behaviors that increase the risk of HBV infection (ie, intravenous drug abuse or unprotected sexual activity) are most likely.9,10 Sex workers and homosexuals are at particular risk of sexual transmission of HBV. Intravenous drug abusers and health workers are at risk of parenteral transmission.
In high-prevalence areas, HBV is mostly transmitted during the perinatal period from mother to infant, conferring a high likelihood of chronicity.9,10 Mothers who are HBsAg positive, particularly those who are also HBeAg positive, are much more likely than others to transmit HBV to their offspring.
FACTORS THAT INFLUENCE THE COURSE OF HBV INFECTION
Viral load has emerged as the most significant factor implicated in the development of cirrhosis or HCC. Iloeje et al11 found that viral load predicted progression to cirrhosis among a cohort of nearly 4,000 Taiwanese. Other factors that can influence the course of HBV infection include age at onset, male sex, and comorbidities (ie, alcohol use, human immunodeficiency virus infection, hepatitis C virus infection). Core promoter and precore mutants may affect the likelihood of developing HCC. A genetic signature that predisposes liver cells to proliferate, termed field effects, may also lead to the development of HCC. The influence of smoking and diabetes on the development of HCC in HBV-infected individuals is not well documented.
Reduction or elimination of measurable virus is the current holy grail of treatment; available antiviral therapies are potent tools that lower viral load with the hope of reducing the likelihood of either cirrhosis or HCC.
HBV genotypes may be implicated in the progression of liver disease or the risk of development of HCC. HBV genotypes differ by region and may correlate with ethnicity and disease progression. In a study of 694 US patients with chronic HBV, Chu et al12 found that genotypes A and C were associated with a higher prevalence of HBsAg positivity than other genotypes. Genotypes B and C were the most common among Asian American patients, while genotype A was the most common among Caucasian and African American patients. The authors suggested that HBV genotypes may explain the heterogeneity in the manifestation of the disease.
Hepatitis B virus (HBV) infection is highly prevalent worldwide and is a major cause of morbidity and death. Two billion people globally have been infected with HBV, 350 to 400 million are chronic carriers, and tens of millions of new cases occur annually. Of those infected, 15% to 40% develop HBV complications, namely cirrhosis or hepatocellular carcinoma (HCC).1–3
The high prevalence of HBV infection represents an enormous failure of public health, considering that HBV immunization has been available for an entire generation, and where it has been employed it has been highly effective at reducing the incidence of HBV infection. Immunization, however, has been underused.
This supplement to the Cleveland Clinic Journal of Medicine, derived from a live symposium, aims to enhance awareness of the natural history of HBV infection and clarify its management recommendations with illustrative case histories. The supplement starts with a brief review of HBV terminology, natural history, and epidemiology.
CHRONIC HBV INFECTION TERMINOLOGY
Familiarity with the terms commonly used to describe chronic HBV infection will help clinicians in the management of the disease4:
- Chronic HBV infection is defined as presence of hepatitis B surface antigen (HBsAg) for more than 6 months. Those with infection may also express another antigen, HB e antigen (HBeAg), a marker of heightened infectivity. At the same time, those who are HBeAg positive are better responders to antiviral therapy compared with those who are HBeAg negative.
- An inactive HBsAg carrier is an individual who is HBsAg positive with a very low level of circulating virus, liver enzyme levels within normal limits, and a low likelihood of having chronic progressive disease.
- Resolved HBV infection is defined as previous HBV infection with no remaining evidence of active disease. Such individuals test negative for HBsAg and positive for antibody to HBsAg (anti-HBs) and to HB core antigen (anti-HBc). They also have no detectable viral load, or HBV DNA, in their blood. In most instances, they are protected from reinfection.
- Reactivation is the reappearance of HBV infection in someone who is known to be an inactive HBsAg carrier or whose previous HBV infection had resolved (see “Case: Recurrence despite anti-HBs and HBsAg negativity”).
- HBeAg seroconversion is the transition from HBeAg-positive to HBeAg-negative status and development of antibody to HBeAg (anti-HBe), usually accompanied by less active liver disease and lower viral loads.
- HBeAg clearance is disappearance of HBeAg without the development of anti-HBe; reactivation or reversion to HBeAg-positive status can occur.
GEOGRAPHIC DISTRIBUTION OF CHRONIC HBV INFECTION
The global prevalence of HBV varies widely. Regions are divided into areas of low, intermediate, and high prevalence, defined as follows4:
- High prevalence implies that at least 8% of the population is currently infected, with a lifetime likelihood of active or resolved infection greater than 60%. About 45% of the world’s population lives in regions of high prevalence. Among this group, early childhood infections are common, with the virus usually transmitted from mother to infant during the perinatal period.
- Intermediate prevalence is defined as 2% to 7%, with a lifetime risk of infection of 20% to 60%. These regions represent about 43% of the global population. In intermediate-prevalence areas, infections occur in all age groups.
- Low prevalence is defined as less than 2% and represents only 12% of the global population. In these regions, the lifetime risk of infection is less than 20%.
North America is a low-prevalence area except for the northern rim, where Inuit and Yupik Eskimos have a high prevalence, and communities that have a substantial immigrant population from high-prevalence areas, such as sub-Saharan Africa and many parts of Asia.
Chronic HBV infection in the United States
Approximately 1.25 million individuals in the United States are HBsAg carriers.2,4 In Asian Americans and Alaskan natives, the prevalence of HBsAg positivity, or chronic disease, is 5% to 15%.5,6 Similarly, US health statistics sources estimate that among those who are chronically infected, approximately half are Asian American.7 As the Asian American population continues to increase (1.5 million to 7 million from 1970 to 19905,8; 11.9 million in the 2000 US Census8), the total prevalence of chronic HBV infection will increase as well.
NATURAL HISTORY OF CHRONIC HBV INFECTION
Chronic HBV usually causes microinflammatory changes that evoke a fibrotic response in the liver, and many infected individuals will eventually develop cirrhosis and are at risk for the development of HCC. Inactive HBsAg carriers often bypass the development of cirrhosis but remain at risk for HCC if their viral load is very high. This is particularly true when infection is acquired in infancy.
The age at acquisition of HBV has a large impact on the likelihood of the disease becoming chronic. The chance of chronic infection is 90% or greater among neonates who become infected with HBV through perinatal transmission. Exposure during adolescence or young adulthood is associated with a 95% or greater likelihood that the disease will be self-limiting.
The typical North American patient with HBV acquires the infection as an adolescent or young adult and is not at risk of HCC unless cirrhosis develops. In most patients who acquire the disease in adolescence or adulthood, the infection resolves after weeks or a few months and they are not at risk of either cirrhosis or HCC. However, an individual such as the one described in the accompanying case, who becomes immunocompromised, is at risk of reactivation of HBV infection (see “Case revisited”).
HBV MODES OF TRANSMISSION
In low-prevalence areas, such as most of North America, most cases of HBV infection are acquired during adolescence to midadulthood, a period during which behaviors that increase the risk of HBV infection (ie, intravenous drug abuse or unprotected sexual activity) are most likely.9,10 Sex workers and homosexuals are at particular risk of sexual transmission of HBV. Intravenous drug abusers and health workers are at risk of parenteral transmission.
In high-prevalence areas, HBV is mostly transmitted during the perinatal period from mother to infant, conferring a high likelihood of chronicity.9,10 Mothers who are HBsAg positive, particularly those who are also HBeAg positive, are much more likely than others to transmit HBV to their offspring.
FACTORS THAT INFLUENCE THE COURSE OF HBV INFECTION
Viral load has emerged as the most significant factor implicated in the development of cirrhosis or HCC. Iloeje et al11 found that viral load predicted progression to cirrhosis among a cohort of nearly 4,000 Taiwanese. Other factors that can influence the course of HBV infection include age at onset, male sex, and comorbidities (ie, alcohol use, human immunodeficiency virus infection, hepatitis C virus infection). Core promoter and precore mutants may affect the likelihood of developing HCC. A genetic signature that predisposes liver cells to proliferate, termed field effects, may also lead to the development of HCC. The influence of smoking and diabetes on the development of HCC in HBV-infected individuals is not well documented.
Reduction or elimination of measurable virus is the current holy grail of treatment; available antiviral therapies are potent tools that lower viral load with the hope of reducing the likelihood of either cirrhosis or HCC.
HBV genotypes may be implicated in the progression of liver disease or the risk of development of HCC. HBV genotypes differ by region and may correlate with ethnicity and disease progression. In a study of 694 US patients with chronic HBV, Chu et al12 found that genotypes A and C were associated with a higher prevalence of HBsAg positivity than other genotypes. Genotypes B and C were the most common among Asian American patients, while genotype A was the most common among Caucasian and African American patients. The authors suggested that HBV genotypes may explain the heterogeneity in the manifestation of the disease.
- Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004; 11:97–107.
- Hepatitis B Foundation. Statistics. Hepatitis B Foundation Web site. http://www.hepb.org/hepb/statistics.htm. Published 2003–2008. Accessed January 9, 2009.
- Hepatitis Foundation International. The ABC’s of hepatitis. Hepatitis Foundation International Web site. http://www.hepfi.org/living/liv_abc.html. Published 2003. Accessed January 9, 2009.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Tong MJ, Hwang S-J. Hepatitis B virus infection in Asian Americans. Gastroenterol Clin North Am 1994; 23:523–536.
- McMahon BJ, Schoenberg S, Bulkow L, et al. Seroprevalence of hepatitis B viral markers in 52,000 Alaska natives. Am J Epidemiol 1993; 138:544–549.
- US Department of Health and Human Services. Hepatitis and Asian Americans. The Office of Minority Health Web site. http://www.omhrc.gov/templates/content.aspx?lvl=3&lvlid=541&ID=6495. Updated May 5, 2008. Accessed January 12, 2009.
- Barnes JS, Bennett CE. The Asian population: 2000. Census 2000 brief. United States Census 2000 Web site. http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed January 12, 2009.
- Lok AS, McMahon BJ; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Chronic hepatitis B. Hepatology 2001; 34:1225–1241.
- Lok AS, Heathcote EJ, Hoofnagle JH. Management of hepatitis B: 2000—summary of a workshop. Gastroenterology 2001; 120:1828–1853.
- Iloeje UH, Yang H-I, Su J, Jen C-L, You S-L, Chen C-J, and The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-in HBV (the REVEAL-HBV) Study Group. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006; 130:678–686.
- Chu CJ, Keeffe EB, Han SH, et al. Hepatitis B virus genotypes in the United States: results of a nationwide study. Gastroenterology 2003; 125:444–451.
- Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004; 11:97–107.
- Hepatitis B Foundation. Statistics. Hepatitis B Foundation Web site. http://www.hepb.org/hepb/statistics.htm. Published 2003–2008. Accessed January 9, 2009.
- Hepatitis Foundation International. The ABC’s of hepatitis. Hepatitis Foundation International Web site. http://www.hepfi.org/living/liv_abc.html. Published 2003. Accessed January 9, 2009.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Tong MJ, Hwang S-J. Hepatitis B virus infection in Asian Americans. Gastroenterol Clin North Am 1994; 23:523–536.
- McMahon BJ, Schoenberg S, Bulkow L, et al. Seroprevalence of hepatitis B viral markers in 52,000 Alaska natives. Am J Epidemiol 1993; 138:544–549.
- US Department of Health and Human Services. Hepatitis and Asian Americans. The Office of Minority Health Web site. http://www.omhrc.gov/templates/content.aspx?lvl=3&lvlid=541&ID=6495. Updated May 5, 2008. Accessed January 12, 2009.
- Barnes JS, Bennett CE. The Asian population: 2000. Census 2000 brief. United States Census 2000 Web site. http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed January 12, 2009.
- Lok AS, McMahon BJ; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Chronic hepatitis B. Hepatology 2001; 34:1225–1241.
- Lok AS, Heathcote EJ, Hoofnagle JH. Management of hepatitis B: 2000—summary of a workshop. Gastroenterology 2001; 120:1828–1853.
- Iloeje UH, Yang H-I, Su J, Jen C-L, You S-L, Chen C-J, and The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-in HBV (the REVEAL-HBV) Study Group. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006; 130:678–686.
- Chu CJ, Keeffe EB, Han SH, et al. Hepatitis B virus genotypes in the United States: results of a nationwide study. Gastroenterology 2003; 125:444–451.
KEY POINTS
- The prevalence of chronic HBV infection in the United States is expected to increase as Asian immigrants constitute a larger proportion of the US population.
- The chance of chronic infection is 90% or greater with perinatal transmission; conversely, the risk of chronic disease is less than 10% with adult-acquired infection.
- In addition to viral load, predictors of disease progression include age at onset, male sex, and comorbidities.
Risk of hepatocellular carcinoma in hepatitis B and prevention through treatment
The role of hepatitis B virus (HBV) as a risk factor for the development of hepatocellular carcinoma (HCC) is well established. Not every patient with HBV infection develops HCC; yet, the current guidelines issued by the American Association for the Study of Liver Diseases1 recommend screening all patients who have HBV infection when they reach certain ages associated with increased risk. Improved identification of risk factors specifically associated with the likelihood of developing HCC may spare some patients the burden of unnecessary testing. This article reviews up-to-date information that will help identify patients who are at risk of HCC based on factors with more specificity than age, and considers whether treatment can alter their risk.
ASSESSING RISK
Several factors are associated with increased risk of developing HCC (see “Case: Hepatocellular carcinoma in a young woman”):
- An elevated serum alanine aminotransferase (ALT) level signifies the presence of active disease and increases risk, particularly if the ALT is persistently or intermittently elevated over years.
- Persistently elevated alpha-fetoprotein level is a reflection of enhanced regenerative state in the liver; the increased rate of cell division increases the risk of mutation, leading to increased risk of HCC.
- A low platelet count suggests the presence of cirrhosis, which itself increases the risk of HCC.
- Histologic risk factors revealed at biopsy include dysplasia, geographic morphologic changes that suggest clonal populations of cells, and a positive stain for proliferating cell nuclear antigen.
- Viral load (HBV DNA) is a significant predictor of HCC; two recent large, prospective studies—the Haimen City study2,3 and the REVEAL-HBV (Risk Evaluation of Viral Load Evaluation and Associated Liver Disease/Cancer-Hepatitis B Virus) study4—support the importance of this risk factor.
Haimen City study
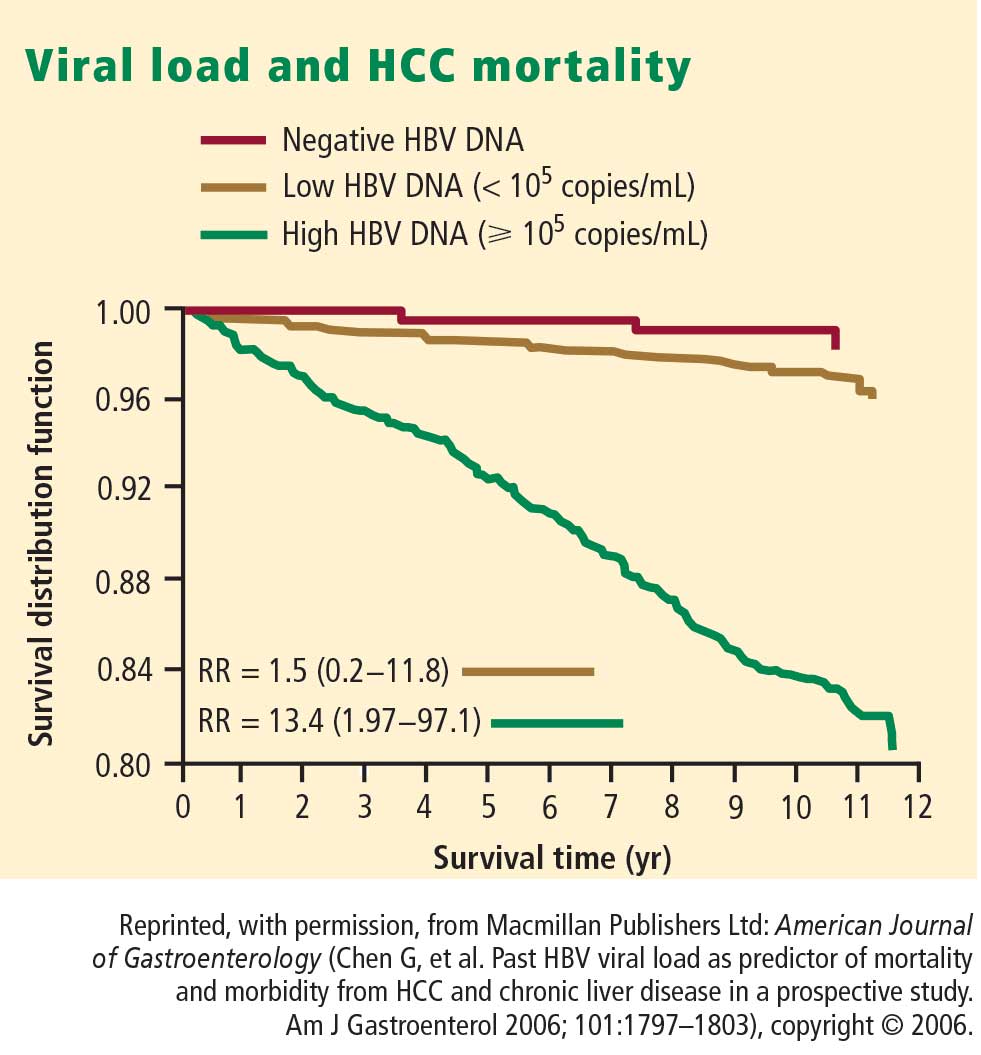
The REVEAL-HBV study
The REVEAL-HBV study was a multicenter observational cohort study of 23,820 Taiwanese individuals aged 30 to 65 years old who were free of HCC at baseline.4 Of these, 3,653 were seropositive for HBsAg and seronegative for antibodies to hepatitis C virus.
Some 1,619 men and women had serum HBV DNA levels greater than or equal to 104 copies/mL at study entry.4 A direct correlation was observed between baseline HBV DNA levels and the incidence of HCC.During a mean follow-up period of 11.4 years, there were 164 new cases of HCC. In a model that integrated baseline and follow-up HBV DNA levels, the cumulative incidence of HCC ranged from 1.3% of those with undetectable levels of HBV DNA to 14.9% of those with HBV DNA levels of 106 copies/mL or greater. The same association between viral load and incidence of HCC was evident in patients who upon study entry had normal ALT levels and were hepatitis B e antigen (HBeAg) negative, a group previously considered to be inactive carriers of HBV.
The incidence of HCC was higher in the subjects with persistent viremia than in those whose viral load decreased over time, representing a biologic gradient of risk. Compared with the reference group (baseline HBV DNA < 104 copies/mL), the adjusted relative risk was nine times greater in those who maintained HBV DNA levels of 105 copies/mL or greater.
Genotype further defines risk
In addition to viral load, genotype may further define the risk of HCC in HBV carriers aged 30 years or older. In a nested case-control study, genotype C was associated with fivefold increased risk of HCC compared with other genotypes.5 Consistent with other studies, the risk of HCC increased with increasing viral load.
Caveats to the viral load–HCC link
The association between viral load and the development of HCC applies to patients aged 30 years or older, the subjects of the aforementioned studies. Younger patients who present with a high viral load and are HBeAg positive are likely to be in an immune-tolerant phase of HBV infection. Among patients aged 30 years or older, the association between viral load and HCC applies to HBeAg-positive as well as HBeAg-negative status. The longer the HBeAg-positive state is maintained, the greater the risk of developing cirrhosis and HCC, which is a reflection of active disease over a prolonged period. The association applies equally to patients with normal or elevated ALT levels. A risk nomogram is being developed that will help identify patients at highest risk of HCC.6
ALT AS PROGNOSTIC DETERMINANT
The risk of developing liver complications from chronic HBV infection increases with increasing concentrations of ALT. Yuen et al7 followed 3,233 Chinese patients with chronic HBV infection for approximately 4 years. The risk of developing complications from liver disease increased as ALT concentration increased from less than 0.5 times the upper limit of normal (ULN) to two to six times the ULN; ALT levels one to two times the ULN were associated with the highest risk of development of complications.
Interestingly, an ALT level greater than six times the ULN was associated with a significantly lower risk of liver complications. The speculation is that this phenomenon represents inactivation of disease following HBeAg seroconversion.
VIRAL LOAD SUPPRESSION LIMITS DISEASE PROGRESSION
Disease activity may flare during the natural course of chronic HBV infection, and repeated episodes may lead to progressive fibrosis, cirrhosis, and end-stage liver disease, as well as HCC. Patients whose cirrhosis has progressed to end-stage liver disease are candidates for transplant.
Continuous antiviral therapy with lamivudine has been shown to dramatically reduce the risk of complications and disease progression in patients with chronic HBV infection. In a placebo-controlled trial of 651 patients with chronic HBV infection and advanced fibrosis or cirrhosis, those randomized to lamivudine who remained sensitive to the drug had a 7.8% risk of complications over approximately 3 years, compared with a 17.7% risk in the patients randomized to placebo.8 The difference was significant and sizeable enough that the study was terminated after a mean duration of 32.4 months. Patients who developed resistance to lamivudine, caused by a mutation in HBV (YMDD mutation, a sign of lamivudine resistance), lost the protection provided by viral suppression.
The risk of disease progression to cirrhosis or HCC was also significantly lower among HBeAg-positive patients without cirrhosis who were treated with lamivudine for a median of 89.9 months compared with placebo, Yuen et al found.9 As in other studies, patients in whom the YMDD mutation developed lost the protection of viral suppression.
In a retrospective study, Di Marco et al10 also found that a loss of response to lamivudine was associated with higher risk of development of HCC, whereas patients who maintained a response to lamivudine were much less likely to develop progressive disease. The authors found that cirrhosis and loss of antiviral response were independently related to mortality and development of HCC.
SUMMARY
Patients with HBV are at risk for cancer, and the risk factors can be identified. Although not yet fully evaluated, awareness of these factors will make the screening process more efficient and less burdensome than current guidelines recommend. The publication and eventual validation of a risk nomogram will facilitate the determination of risk. An especially strong predictor of adverse outcomes, including HCC, is HBV DNA concentration higher than 104 copies/mL, as shown by two recent large studies; further, investigators observed a correlation between HBV DNA level and incidence of HCC.
Antiviral therapy has dramatically reduced the risk of complications and progression of HBV infection. Those who develop resistance to therapy lose the protection provided by viral suppression.
DISCUSSION
William D. Carey, MD: Does biopsy of nontumorous portions of the liver have value, either by showing dysplasia or perhaps through a staining technique, in predicting the development of liver cancer?
Morris Sherman, MD, PhD: I believe that you’re referring to a recent study in which microarray technology was used to identify patients at risk for the development of a de novo tumor after a resection of the first tumor.11 Liver tissue surrounding the tumor was analyzed by microarray technology, and gene expression profiling accurately predicted the development of a new tumor in another part of the liver more than 2 years later. This discovery suggests the presence of a field defect, or a propensity for the development of new tumors in a damaged organ. Patients who have a field defect identified by the microarray technique are at much higher risk of developing a subsequent cancer. These patients might be candidates for liver transplant despite apparent surgical cure of their HCC. However, because the subsequent liver malignancy occurs some time later and is a new primary tumor, the need for transplant is less urgent than it is for a patient with a progressive hepatoma, for example.
Pierre M. Gholam, MD: Do you consider ethnicity in addition to age, viral load, and other factors in your decision to screen patients for HCC?
Dr. Sherman: We traditionally think of ethnicity as a major factor because HBV is concentrated in Asian and African populations. I’m not entirely sure whether ethnicity or the viral genotypes are more important, because the viral genotypes are distributed along ethnic lines. We know that genotypes B and C, which are common in the Far East, are associated with a high rate of progressive liver disease. Genotype D, observed mainly in Middle Eastern and Greek populations, is associated with a much higher rate of progressive liver disease than genotypes common in Western Europe and most of North America. I believe that genotype should be a factor in decisions to screen.
Robert G. Gish, MD: In your case presentation you described the aspartate aminotransferase (AST) and ALT as being normal. New criteria define an AST/ALT of 20 as being “healthy” for a woman. I like the word “healthy” better than “normal.” How would you have described those test results to the patient?
Dr. Sherman: I would have told her that although her AST and ALT levels were within the laboratory reference range, ideally for a young woman the ALT should be closer to 20 U/L. Her actual levels were at least twice the upper range of ideal, and therefore, I believe a biopsy to determine the extent of injury in the liver would be important.
Tram T. Tran, MD: Are there any new serum markers for liver cancer that have promise?
Dr. Sherman: The problem with serum markers, or biomarkers in general, is the confusion over their intended use, such as for screening, risk stratification, or diagnosis.
I assume that your question refers to their potential use in screening, and so far none of the existing biomarkers is adequate to find small tumors. For screening purposes, you ideally want to find tumors that are 2 cm or smaller, and none of the biomarkers is efficient with those small tumors. A biomarker is not needed to identify tumors that are 5 or 6 cm.
- Bruix J, Sherman M. Management of hepatocellular carcinoma. AASLD Practice Guideline. Hepatology 2005; 42:1208–1235.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol 2006; 101:1797–1803.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Chronic hepatitis B virus infection and mortality from nonliver causes: results from the Haimen City cohort study [published online ahead of print January 19, 2005]. Int J Epidemiol 2005; 34:132–137.
- Chen C-J, Yang H-I, Su J, et al; for the REVEAL-HBV Study Group. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006; 295:65–73.
- Yu M-W, Yeh S-H, Chen P-J, et al. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl Cancer Inst 2005; 97:265–272.
- Chen C-J, Yang H-I, Iloeje UH, et al. A risk function nomogram for predicting HCC in patients with chronic hepatitis B: the REVEAL-HBV study [AASLD abstract S1766]. Gastroenterology 2007; 132(suppl 2):A761.
- Yuen M-F, Yuan H-J, Wong DK-H, et al. Prognostic determinants for chronic hepatitis B in Asians: therapeutic implications. Gut 2005; 54:1610–1614.
- Liaw Y-F, Sung JJY, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004; 351:1521–1531.
- Yuen MF, Seto WK, Chow DHF, et al. Long-term beneficial outcome of Chinese asymptomatic patients with HBeAg-positive chronic hepatitis B on continuous lamivudine therapy: 7-year experience [AASLD abstract 985]. Hepatology 2005; 42(suppl 1):583A.
- Di Marco V, Marzano A, Lampertico P, et al. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology 2004; 40:883–891.
- Hoshida Y, Villaneuva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med 2008; 359:1995–2004.
The role of hepatitis B virus (HBV) as a risk factor for the development of hepatocellular carcinoma (HCC) is well established. Not every patient with HBV infection develops HCC; yet, the current guidelines issued by the American Association for the Study of Liver Diseases1 recommend screening all patients who have HBV infection when they reach certain ages associated with increased risk. Improved identification of risk factors specifically associated with the likelihood of developing HCC may spare some patients the burden of unnecessary testing. This article reviews up-to-date information that will help identify patients who are at risk of HCC based on factors with more specificity than age, and considers whether treatment can alter their risk.
ASSESSING RISK
Several factors are associated with increased risk of developing HCC (see “Case: Hepatocellular carcinoma in a young woman”):
- An elevated serum alanine aminotransferase (ALT) level signifies the presence of active disease and increases risk, particularly if the ALT is persistently or intermittently elevated over years.
- Persistently elevated alpha-fetoprotein level is a reflection of enhanced regenerative state in the liver; the increased rate of cell division increases the risk of mutation, leading to increased risk of HCC.
- A low platelet count suggests the presence of cirrhosis, which itself increases the risk of HCC.
- Histologic risk factors revealed at biopsy include dysplasia, geographic morphologic changes that suggest clonal populations of cells, and a positive stain for proliferating cell nuclear antigen.
- Viral load (HBV DNA) is a significant predictor of HCC; two recent large, prospective studies—the Haimen City study2,3 and the REVEAL-HBV (Risk Evaluation of Viral Load Evaluation and Associated Liver Disease/Cancer-Hepatitis B Virus) study4—support the importance of this risk factor.
Haimen City study
The REVEAL-HBV study
The REVEAL-HBV study was a multicenter observational cohort study of 23,820 Taiwanese individuals aged 30 to 65 years old who were free of HCC at baseline.4 Of these, 3,653 were seropositive for HBsAg and seronegative for antibodies to hepatitis C virus.
Some 1,619 men and women had serum HBV DNA levels greater than or equal to 104 copies/mL at study entry.4 A direct correlation was observed between baseline HBV DNA levels and the incidence of HCC.During a mean follow-up period of 11.4 years, there were 164 new cases of HCC. In a model that integrated baseline and follow-up HBV DNA levels, the cumulative incidence of HCC ranged from 1.3% of those with undetectable levels of HBV DNA to 14.9% of those with HBV DNA levels of 106 copies/mL or greater. The same association between viral load and incidence of HCC was evident in patients who upon study entry had normal ALT levels and were hepatitis B e antigen (HBeAg) negative, a group previously considered to be inactive carriers of HBV.
The incidence of HCC was higher in the subjects with persistent viremia than in those whose viral load decreased over time, representing a biologic gradient of risk. Compared with the reference group (baseline HBV DNA < 104 copies/mL), the adjusted relative risk was nine times greater in those who maintained HBV DNA levels of 105 copies/mL or greater.
Genotype further defines risk
In addition to viral load, genotype may further define the risk of HCC in HBV carriers aged 30 years or older. In a nested case-control study, genotype C was associated with fivefold increased risk of HCC compared with other genotypes.5 Consistent with other studies, the risk of HCC increased with increasing viral load.
Caveats to the viral load–HCC link
The association between viral load and the development of HCC applies to patients aged 30 years or older, the subjects of the aforementioned studies. Younger patients who present with a high viral load and are HBeAg positive are likely to be in an immune-tolerant phase of HBV infection. Among patients aged 30 years or older, the association between viral load and HCC applies to HBeAg-positive as well as HBeAg-negative status. The longer the HBeAg-positive state is maintained, the greater the risk of developing cirrhosis and HCC, which is a reflection of active disease over a prolonged period. The association applies equally to patients with normal or elevated ALT levels. A risk nomogram is being developed that will help identify patients at highest risk of HCC.6
ALT AS PROGNOSTIC DETERMINANT
The risk of developing liver complications from chronic HBV infection increases with increasing concentrations of ALT. Yuen et al7 followed 3,233 Chinese patients with chronic HBV infection for approximately 4 years. The risk of developing complications from liver disease increased as ALT concentration increased from less than 0.5 times the upper limit of normal (ULN) to two to six times the ULN; ALT levels one to two times the ULN were associated with the highest risk of development of complications.
Interestingly, an ALT level greater than six times the ULN was associated with a significantly lower risk of liver complications. The speculation is that this phenomenon represents inactivation of disease following HBeAg seroconversion.
VIRAL LOAD SUPPRESSION LIMITS DISEASE PROGRESSION
Disease activity may flare during the natural course of chronic HBV infection, and repeated episodes may lead to progressive fibrosis, cirrhosis, and end-stage liver disease, as well as HCC. Patients whose cirrhosis has progressed to end-stage liver disease are candidates for transplant.
Continuous antiviral therapy with lamivudine has been shown to dramatically reduce the risk of complications and disease progression in patients with chronic HBV infection. In a placebo-controlled trial of 651 patients with chronic HBV infection and advanced fibrosis or cirrhosis, those randomized to lamivudine who remained sensitive to the drug had a 7.8% risk of complications over approximately 3 years, compared with a 17.7% risk in the patients randomized to placebo.8 The difference was significant and sizeable enough that the study was terminated after a mean duration of 32.4 months. Patients who developed resistance to lamivudine, caused by a mutation in HBV (YMDD mutation, a sign of lamivudine resistance), lost the protection provided by viral suppression.
The risk of disease progression to cirrhosis or HCC was also significantly lower among HBeAg-positive patients without cirrhosis who were treated with lamivudine for a median of 89.9 months compared with placebo, Yuen et al found.9 As in other studies, patients in whom the YMDD mutation developed lost the protection of viral suppression.
In a retrospective study, Di Marco et al10 also found that a loss of response to lamivudine was associated with higher risk of development of HCC, whereas patients who maintained a response to lamivudine were much less likely to develop progressive disease. The authors found that cirrhosis and loss of antiviral response were independently related to mortality and development of HCC.
SUMMARY
Patients with HBV are at risk for cancer, and the risk factors can be identified. Although not yet fully evaluated, awareness of these factors will make the screening process more efficient and less burdensome than current guidelines recommend. The publication and eventual validation of a risk nomogram will facilitate the determination of risk. An especially strong predictor of adverse outcomes, including HCC, is HBV DNA concentration higher than 104 copies/mL, as shown by two recent large studies; further, investigators observed a correlation between HBV DNA level and incidence of HCC.
Antiviral therapy has dramatically reduced the risk of complications and progression of HBV infection. Those who develop resistance to therapy lose the protection provided by viral suppression.
DISCUSSION
William D. Carey, MD: Does biopsy of nontumorous portions of the liver have value, either by showing dysplasia or perhaps through a staining technique, in predicting the development of liver cancer?
Morris Sherman, MD, PhD: I believe that you’re referring to a recent study in which microarray technology was used to identify patients at risk for the development of a de novo tumor after a resection of the first tumor.11 Liver tissue surrounding the tumor was analyzed by microarray technology, and gene expression profiling accurately predicted the development of a new tumor in another part of the liver more than 2 years later. This discovery suggests the presence of a field defect, or a propensity for the development of new tumors in a damaged organ. Patients who have a field defect identified by the microarray technique are at much higher risk of developing a subsequent cancer. These patients might be candidates for liver transplant despite apparent surgical cure of their HCC. However, because the subsequent liver malignancy occurs some time later and is a new primary tumor, the need for transplant is less urgent than it is for a patient with a progressive hepatoma, for example.
Pierre M. Gholam, MD: Do you consider ethnicity in addition to age, viral load, and other factors in your decision to screen patients for HCC?
Dr. Sherman: We traditionally think of ethnicity as a major factor because HBV is concentrated in Asian and African populations. I’m not entirely sure whether ethnicity or the viral genotypes are more important, because the viral genotypes are distributed along ethnic lines. We know that genotypes B and C, which are common in the Far East, are associated with a high rate of progressive liver disease. Genotype D, observed mainly in Middle Eastern and Greek populations, is associated with a much higher rate of progressive liver disease than genotypes common in Western Europe and most of North America. I believe that genotype should be a factor in decisions to screen.
Robert G. Gish, MD: In your case presentation you described the aspartate aminotransferase (AST) and ALT as being normal. New criteria define an AST/ALT of 20 as being “healthy” for a woman. I like the word “healthy” better than “normal.” How would you have described those test results to the patient?
Dr. Sherman: I would have told her that although her AST and ALT levels were within the laboratory reference range, ideally for a young woman the ALT should be closer to 20 U/L. Her actual levels were at least twice the upper range of ideal, and therefore, I believe a biopsy to determine the extent of injury in the liver would be important.
Tram T. Tran, MD: Are there any new serum markers for liver cancer that have promise?
Dr. Sherman: The problem with serum markers, or biomarkers in general, is the confusion over their intended use, such as for screening, risk stratification, or diagnosis.
I assume that your question refers to their potential use in screening, and so far none of the existing biomarkers is adequate to find small tumors. For screening purposes, you ideally want to find tumors that are 2 cm or smaller, and none of the biomarkers is efficient with those small tumors. A biomarker is not needed to identify tumors that are 5 or 6 cm.
The role of hepatitis B virus (HBV) as a risk factor for the development of hepatocellular carcinoma (HCC) is well established. Not every patient with HBV infection develops HCC; yet, the current guidelines issued by the American Association for the Study of Liver Diseases1 recommend screening all patients who have HBV infection when they reach certain ages associated with increased risk. Improved identification of risk factors specifically associated with the likelihood of developing HCC may spare some patients the burden of unnecessary testing. This article reviews up-to-date information that will help identify patients who are at risk of HCC based on factors with more specificity than age, and considers whether treatment can alter their risk.
ASSESSING RISK
Several factors are associated with increased risk of developing HCC (see “Case: Hepatocellular carcinoma in a young woman”):
- An elevated serum alanine aminotransferase (ALT) level signifies the presence of active disease and increases risk, particularly if the ALT is persistently or intermittently elevated over years.
- Persistently elevated alpha-fetoprotein level is a reflection of enhanced regenerative state in the liver; the increased rate of cell division increases the risk of mutation, leading to increased risk of HCC.
- A low platelet count suggests the presence of cirrhosis, which itself increases the risk of HCC.
- Histologic risk factors revealed at biopsy include dysplasia, geographic morphologic changes that suggest clonal populations of cells, and a positive stain for proliferating cell nuclear antigen.
- Viral load (HBV DNA) is a significant predictor of HCC; two recent large, prospective studies—the Haimen City study2,3 and the REVEAL-HBV (Risk Evaluation of Viral Load Evaluation and Associated Liver Disease/Cancer-Hepatitis B Virus) study4—support the importance of this risk factor.
Haimen City study
The REVEAL-HBV study
The REVEAL-HBV study was a multicenter observational cohort study of 23,820 Taiwanese individuals aged 30 to 65 years old who were free of HCC at baseline.4 Of these, 3,653 were seropositive for HBsAg and seronegative for antibodies to hepatitis C virus.
Some 1,619 men and women had serum HBV DNA levels greater than or equal to 104 copies/mL at study entry.4 A direct correlation was observed between baseline HBV DNA levels and the incidence of HCC.During a mean follow-up period of 11.4 years, there were 164 new cases of HCC. In a model that integrated baseline and follow-up HBV DNA levels, the cumulative incidence of HCC ranged from 1.3% of those with undetectable levels of HBV DNA to 14.9% of those with HBV DNA levels of 106 copies/mL or greater. The same association between viral load and incidence of HCC was evident in patients who upon study entry had normal ALT levels and were hepatitis B e antigen (HBeAg) negative, a group previously considered to be inactive carriers of HBV.
The incidence of HCC was higher in the subjects with persistent viremia than in those whose viral load decreased over time, representing a biologic gradient of risk. Compared with the reference group (baseline HBV DNA < 104 copies/mL), the adjusted relative risk was nine times greater in those who maintained HBV DNA levels of 105 copies/mL or greater.
Genotype further defines risk
In addition to viral load, genotype may further define the risk of HCC in HBV carriers aged 30 years or older. In a nested case-control study, genotype C was associated with fivefold increased risk of HCC compared with other genotypes.5 Consistent with other studies, the risk of HCC increased with increasing viral load.
Caveats to the viral load–HCC link
The association between viral load and the development of HCC applies to patients aged 30 years or older, the subjects of the aforementioned studies. Younger patients who present with a high viral load and are HBeAg positive are likely to be in an immune-tolerant phase of HBV infection. Among patients aged 30 years or older, the association between viral load and HCC applies to HBeAg-positive as well as HBeAg-negative status. The longer the HBeAg-positive state is maintained, the greater the risk of developing cirrhosis and HCC, which is a reflection of active disease over a prolonged period. The association applies equally to patients with normal or elevated ALT levels. A risk nomogram is being developed that will help identify patients at highest risk of HCC.6
ALT AS PROGNOSTIC DETERMINANT
The risk of developing liver complications from chronic HBV infection increases with increasing concentrations of ALT. Yuen et al7 followed 3,233 Chinese patients with chronic HBV infection for approximately 4 years. The risk of developing complications from liver disease increased as ALT concentration increased from less than 0.5 times the upper limit of normal (ULN) to two to six times the ULN; ALT levels one to two times the ULN were associated with the highest risk of development of complications.
Interestingly, an ALT level greater than six times the ULN was associated with a significantly lower risk of liver complications. The speculation is that this phenomenon represents inactivation of disease following HBeAg seroconversion.
VIRAL LOAD SUPPRESSION LIMITS DISEASE PROGRESSION
Disease activity may flare during the natural course of chronic HBV infection, and repeated episodes may lead to progressive fibrosis, cirrhosis, and end-stage liver disease, as well as HCC. Patients whose cirrhosis has progressed to end-stage liver disease are candidates for transplant.
Continuous antiviral therapy with lamivudine has been shown to dramatically reduce the risk of complications and disease progression in patients with chronic HBV infection. In a placebo-controlled trial of 651 patients with chronic HBV infection and advanced fibrosis or cirrhosis, those randomized to lamivudine who remained sensitive to the drug had a 7.8% risk of complications over approximately 3 years, compared with a 17.7% risk in the patients randomized to placebo.8 The difference was significant and sizeable enough that the study was terminated after a mean duration of 32.4 months. Patients who developed resistance to lamivudine, caused by a mutation in HBV (YMDD mutation, a sign of lamivudine resistance), lost the protection provided by viral suppression.
The risk of disease progression to cirrhosis or HCC was also significantly lower among HBeAg-positive patients without cirrhosis who were treated with lamivudine for a median of 89.9 months compared with placebo, Yuen et al found.9 As in other studies, patients in whom the YMDD mutation developed lost the protection of viral suppression.
In a retrospective study, Di Marco et al10 also found that a loss of response to lamivudine was associated with higher risk of development of HCC, whereas patients who maintained a response to lamivudine were much less likely to develop progressive disease. The authors found that cirrhosis and loss of antiviral response were independently related to mortality and development of HCC.
SUMMARY
Patients with HBV are at risk for cancer, and the risk factors can be identified. Although not yet fully evaluated, awareness of these factors will make the screening process more efficient and less burdensome than current guidelines recommend. The publication and eventual validation of a risk nomogram will facilitate the determination of risk. An especially strong predictor of adverse outcomes, including HCC, is HBV DNA concentration higher than 104 copies/mL, as shown by two recent large studies; further, investigators observed a correlation between HBV DNA level and incidence of HCC.
Antiviral therapy has dramatically reduced the risk of complications and progression of HBV infection. Those who develop resistance to therapy lose the protection provided by viral suppression.
DISCUSSION
William D. Carey, MD: Does biopsy of nontumorous portions of the liver have value, either by showing dysplasia or perhaps through a staining technique, in predicting the development of liver cancer?
Morris Sherman, MD, PhD: I believe that you’re referring to a recent study in which microarray technology was used to identify patients at risk for the development of a de novo tumor after a resection of the first tumor.11 Liver tissue surrounding the tumor was analyzed by microarray technology, and gene expression profiling accurately predicted the development of a new tumor in another part of the liver more than 2 years later. This discovery suggests the presence of a field defect, or a propensity for the development of new tumors in a damaged organ. Patients who have a field defect identified by the microarray technique are at much higher risk of developing a subsequent cancer. These patients might be candidates for liver transplant despite apparent surgical cure of their HCC. However, because the subsequent liver malignancy occurs some time later and is a new primary tumor, the need for transplant is less urgent than it is for a patient with a progressive hepatoma, for example.
Pierre M. Gholam, MD: Do you consider ethnicity in addition to age, viral load, and other factors in your decision to screen patients for HCC?
Dr. Sherman: We traditionally think of ethnicity as a major factor because HBV is concentrated in Asian and African populations. I’m not entirely sure whether ethnicity or the viral genotypes are more important, because the viral genotypes are distributed along ethnic lines. We know that genotypes B and C, which are common in the Far East, are associated with a high rate of progressive liver disease. Genotype D, observed mainly in Middle Eastern and Greek populations, is associated with a much higher rate of progressive liver disease than genotypes common in Western Europe and most of North America. I believe that genotype should be a factor in decisions to screen.
Robert G. Gish, MD: In your case presentation you described the aspartate aminotransferase (AST) and ALT as being normal. New criteria define an AST/ALT of 20 as being “healthy” for a woman. I like the word “healthy” better than “normal.” How would you have described those test results to the patient?
Dr. Sherman: I would have told her that although her AST and ALT levels were within the laboratory reference range, ideally for a young woman the ALT should be closer to 20 U/L. Her actual levels were at least twice the upper range of ideal, and therefore, I believe a biopsy to determine the extent of injury in the liver would be important.
Tram T. Tran, MD: Are there any new serum markers for liver cancer that have promise?
Dr. Sherman: The problem with serum markers, or biomarkers in general, is the confusion over their intended use, such as for screening, risk stratification, or diagnosis.
I assume that your question refers to their potential use in screening, and so far none of the existing biomarkers is adequate to find small tumors. For screening purposes, you ideally want to find tumors that are 2 cm or smaller, and none of the biomarkers is efficient with those small tumors. A biomarker is not needed to identify tumors that are 5 or 6 cm.
- Bruix J, Sherman M. Management of hepatocellular carcinoma. AASLD Practice Guideline. Hepatology 2005; 42:1208–1235.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol 2006; 101:1797–1803.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Chronic hepatitis B virus infection and mortality from nonliver causes: results from the Haimen City cohort study [published online ahead of print January 19, 2005]. Int J Epidemiol 2005; 34:132–137.
- Chen C-J, Yang H-I, Su J, et al; for the REVEAL-HBV Study Group. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006; 295:65–73.
- Yu M-W, Yeh S-H, Chen P-J, et al. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl Cancer Inst 2005; 97:265–272.
- Chen C-J, Yang H-I, Iloeje UH, et al. A risk function nomogram for predicting HCC in patients with chronic hepatitis B: the REVEAL-HBV study [AASLD abstract S1766]. Gastroenterology 2007; 132(suppl 2):A761.
- Yuen M-F, Yuan H-J, Wong DK-H, et al. Prognostic determinants for chronic hepatitis B in Asians: therapeutic implications. Gut 2005; 54:1610–1614.
- Liaw Y-F, Sung JJY, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004; 351:1521–1531.
- Yuen MF, Seto WK, Chow DHF, et al. Long-term beneficial outcome of Chinese asymptomatic patients with HBeAg-positive chronic hepatitis B on continuous lamivudine therapy: 7-year experience [AASLD abstract 985]. Hepatology 2005; 42(suppl 1):583A.
- Di Marco V, Marzano A, Lampertico P, et al. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology 2004; 40:883–891.
- Hoshida Y, Villaneuva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med 2008; 359:1995–2004.
- Bruix J, Sherman M. Management of hepatocellular carcinoma. AASLD Practice Guideline. Hepatology 2005; 42:1208–1235.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol 2006; 101:1797–1803.
- Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Chronic hepatitis B virus infection and mortality from nonliver causes: results from the Haimen City cohort study [published online ahead of print January 19, 2005]. Int J Epidemiol 2005; 34:132–137.
- Chen C-J, Yang H-I, Su J, et al; for the REVEAL-HBV Study Group. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006; 295:65–73.
- Yu M-W, Yeh S-H, Chen P-J, et al. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl Cancer Inst 2005; 97:265–272.
- Chen C-J, Yang H-I, Iloeje UH, et al. A risk function nomogram for predicting HCC in patients with chronic hepatitis B: the REVEAL-HBV study [AASLD abstract S1766]. Gastroenterology 2007; 132(suppl 2):A761.
- Yuen M-F, Yuan H-J, Wong DK-H, et al. Prognostic determinants for chronic hepatitis B in Asians: therapeutic implications. Gut 2005; 54:1610–1614.
- Liaw Y-F, Sung JJY, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004; 351:1521–1531.
- Yuen MF, Seto WK, Chow DHF, et al. Long-term beneficial outcome of Chinese asymptomatic patients with HBeAg-positive chronic hepatitis B on continuous lamivudine therapy: 7-year experience [AASLD abstract 985]. Hepatology 2005; 42(suppl 1):583A.
- Di Marco V, Marzano A, Lampertico P, et al. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology 2004; 40:883–891.
- Hoshida Y, Villaneuva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med 2008; 359:1995–2004.
KEY POINTS
- A high viral load is a significant predictor of the development of hepatocellular carcinoma in patients aged 30 years or older with chronic HBV infection.
- The risk of developing liver complications from chronic HBV infection increases with increasing concentrations of alanine aminotransferase.
- Continuous antiviral therapy to suppress viral load dramatically reduces the risk of complications from HBV infection and reduces the rate of disease progression, as long as patients maintain a therapeutic response.
Understanding cultural barriers in hepatitis B virus infection
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
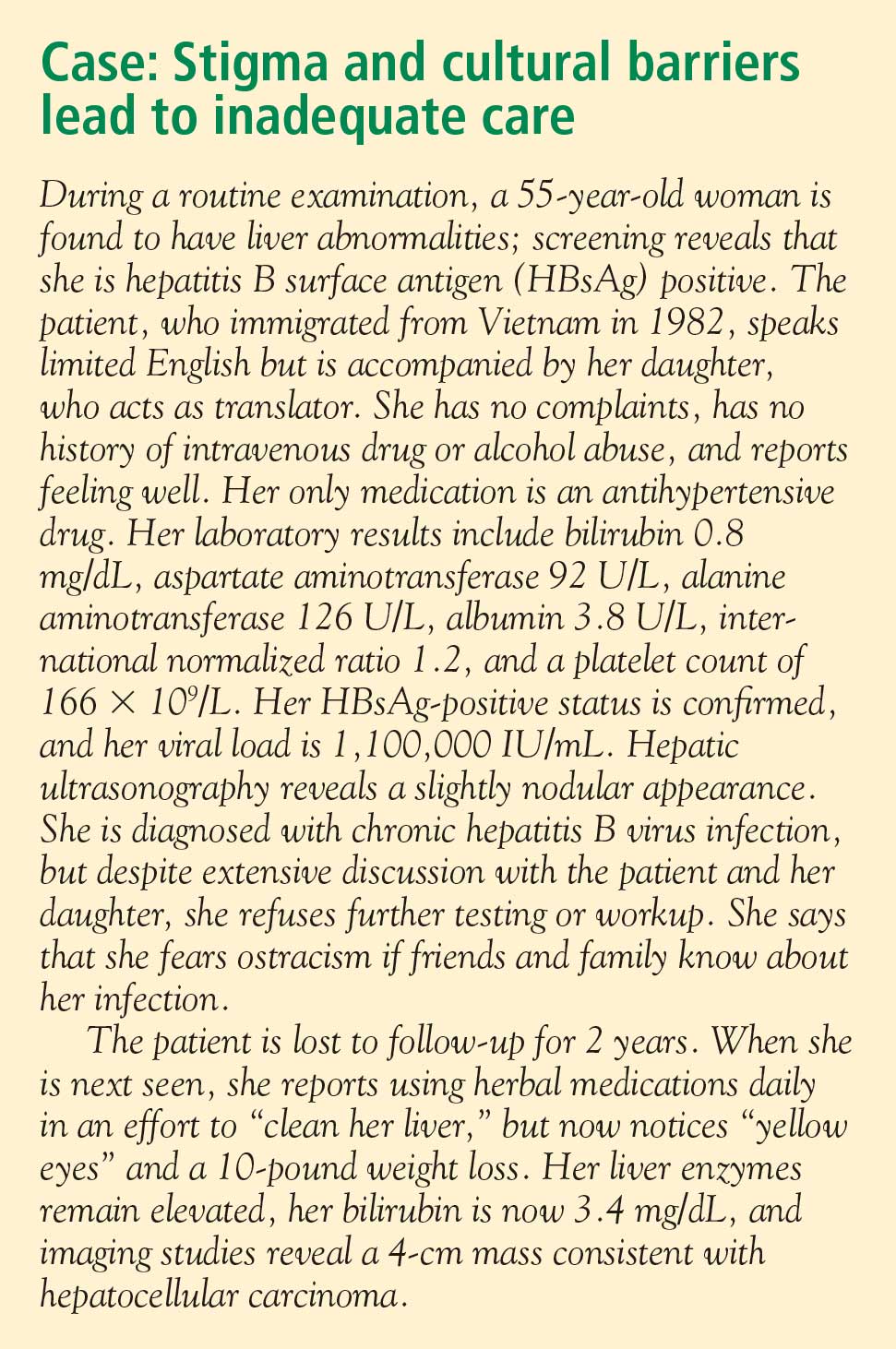
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
Asian Americans represent 4% of the population in the United States, and their share of the US population is projected to grow to 9% by 2050.1 These numbers are significant because of the high prevalence of hepatitis B virus (HBV) infection in this community and the cultural barriers to its effective management.
Appreciating the impact of cultural barriers on health care among Asian Americans requires an understanding of the diversity of the Asian continent, which is composed of 52 countries where 100 languages and dialects are spoken. Within each region are religious, cultural, and societal differences. Asians have immigrated to the United States over the course of several generations, and the era in which they immigrated may affect their ability to understand English, integrate into American culture, and navigate the US health care system. Successful integration into American life favors those whose families immigrated several generations earlier.
The overall prevalence of HBV infection in the United States is 0.4%2; however, estimates of prevalence range from 5% to 15% in Asian American populations, and are as high as 20% in some Pacific Rim populations.3,4 The prevalence of HBV infection in Asian Americans differs by subpopulation, with the highest prevalence among immigrants from Vietnam, Laos, and China, and the lowest among those from Japan.
Of the approximately 1 million Americans estimated to be infected with HBV as of 2005, more than 750,000 had access to health care; of these, 205,000 were diagnosed with HBV infection,5 suggesting substantial underdiagnosis. Referrals to specialists were even fewer (175,000), and only about 31,000 patients chronically infected with HBV received antiviral treatment, a figure that has likely increased with greater awareness of HBV and the availability of new antiviral medications.
BARRIERS TO DIAGNOSIS AND TREATMENT
The barriers to effective management of HBV infection in Asian Americans include cultural, socioeconomic, and accessibility issues (see “Case: Stigma and cultural barriers lead to inadequate care”).
Language and linguistic isolation
Limited proficiency in English is a large, if not the largest, barrier to effective management of chronic HBV infection. According to the US Census Bureau, a person with limited English proficiency is one who does not speak English “very well.”6 This terminology has implications for allocation of federal government resources; ie, the percentage of a community’s residents with limited English proficiency is a criterion for receipt of governmental grants and other forms of assistance, including translation services.6
Linguistic isolation, another barrier to medical care, is lack of an English-speaking household member who is older than 14 years.7 By this definition, more than one-third of Korean, Taiwanese, Chinese, Hmong, and Bangladeshi households, and almost half of Vietnamese households, are linguistically isolated, with limited ability to communicate with health care providers.8
Lack of health insurance and its correlates
The high percentage of Asian immigrants without health insurance is a challenge to providing adequate health care. Health insurance coverage is lacking for about one-third of Korean immigrants, about one in five immigrants from Southeast Asia and South Asia, and about 15% of Filipino and Chinese immigrants.9
One reason for the large proportion of uninsured among these groups is the high rate of small business ownership among Asian Americans and the difficulty that small business owners have in obtaining affordable health insurance coverage. In addition, although Asian Americans are as likely as other US residents to be employed full time, their employment options may be less likely to include health insurance benefits.
Poverty affects the ability to acquire health insurance. Although the popular image of the Asian immigrant is an educated person with high earning potential, the reality is that poverty strikes immigrants from Southeast Asia at a high rate. Almost 40% of the Hmong population, for example, lives below the poverty level, and poverty rates among the Cambodian, Bangladeshi, Malaysian, and several other Asian subpopulations are nearly as high.8
Citizenship correlates with the ability to obtain health insurance; it is estimated that 42% to 57% of noncitizens lack health insurance, compared with 15% of citizens.8 Only half of Asian immigrants become naturalized citizens, with wide variability among subgroups. Two-thirds of Filipinos who immigrate to the United States eventually become naturalized compared with less than one-third of Malaysian, Japanese, Indonesian, and Hmong immigrants.8
Educational achievement is associated with attainment of financial security and health insurance. The vast majority of Taiwanese, Japanese, Filipino, and Korean Americans obtain a high school education or higher, with correspondingly higher rates of health insurance coverage. Among those from Southeast Asia (Hmong, Cambodians, Laotians, and Vietnamese), whose immigration to this country is relatively recent, fewer than half complete a high school education.8
Health care workforce representation
Certain Asian subgroups are underrepresented in the racial composition of the US health care workforce; this imbalance may affect accessibility to the health care system and adherence to medical prescriptions and instructions among underrepresented groups. Racial concordance between patient and health care provider is associated with greater patient participation in care, according to the Institute of Medicine.10 In addition to racial similarity, linguistic similarity enhances communication and adherence to instructions.
Belief systems and attitudes toward health care
An immigrant patient’s religious beliefs and cultural attitudes toward Western medicine may pose difficulties in successfully managing disease. Many Asian Americans are Buddhists, who may believe that suffering is an integral part of life; proactively seeking medical care may not be imperative for them. Confucianism, the worship of ancestors and the subjugation of the self to the well-being of the family, is a common belief system among Asians that may inhibit the desire to seek needed medical care. For example, a family elder may instruct a young man not to seek medical care for his HBV infection because this would jeopardize his siblings’ marriage prospects. Taoism involves the belief that perfection is achieved when events are allowed to take the more natural course. Intervention is therefore frowned upon.
Some belief systems may impede care because they incorporate indifference toward suffering. Many Hmong believe that the length of life is predetermined, so lifesaving care is pointless. Cultural value may be placed on stoicism, discouraging visits to health care providers. A belief that disease is caused by supernatural events rather than organic etiologies is another perception that serves as a barrier to seeking medical care.
Distrust of, or unfamiliarity with, Western medicine may delay care, and the resulting poor outcomes may be falsely attributed to Western medicine itself. In some cultures, there is a pervasive belief that a physician can touch the pulse and identify the problem. Some Laotians believe that immunizations are dangerous for a baby’s spirit, and therefore forgo immunization against HBV when it is indicated.
The patient’s relationship with his or her health care provider is an important determinant of quality of care and willingness to continue to receive care. The best possible scenario is concordance in language and culture. Asian cultures emphasize politeness, respect for authority, filial piety, and avoidance of shame. Because Asian patients often view physicians as authority figures, they may not ask questions or voice reservations or fears about their treatment regimens; instead, they may express their agreement with physicians’ advice, but with no intent to return or follow instructions.
Infection with HBV carries a stigma about the mode of transmission that can interfere with patients’ daily lives. A study of attitudes about HBV found that HBV-infected patients feel less welcome to stay overnight or share the same bathroom at friends’ or relatives’ houses, that noninfected persons fear that the disease may be passed to them by HBV-positive friends, and that HBV-infected patients are concerned about whether their choices may have led to the infection.11
OVERCOMING BARRIERS
Sensitivity to cultural attitudes may enhance communication and the likelihood that patients will accept physicians’ recommendations. Several office visits may be necessary to confirm that a patient is receptive to the health care provider’s instructions and is adhering to them. Referral to access programs can aid communication. For example, most cities have community centers where patients can seek medical advice from physicians who speak the patients’ language; these centers also may provide native-language materials and interpreters.
Offering reassurance to patients in their own language and in a culturally sensitive setting will help break down barriers and improve care. Patients who are educated about HBV transmission and the availability of an effective vaccine may be instrumental in preventing transmission of the disease to household members.
Cultural sensitivity training will benefit health care providers and staffs whose patients include Asian Americans. Educational programs should be specific to the needs of the community, as different subpopulations have different needs. Resource materials are available for such training; for example, the federal government’s Office of Minority Health Web site (http://www.omhrc.gov/) offers links to resources for cultural training. In addition to educating themselves and their staffs, health care providers have a responsibility to advocate for funding and equal access to care, and for the creation of more cultural and community health centers that can serve as resources to overcome cultural barriers.
DISCUSSION
Robert G. Gish, MD: How often are herbal remedies tried for chronic HBV infection in the patients you see, especially in the Vietnamese population?
Tram T. Tran, MD: Once patients are diagnosed with chronic HBV infection, the use of herbal remedies is very high; it approaches 80% in my practice. Patients may not admit to it unless you ask them specifically, because they know herbal remedies may be somewhat frowned upon by Western physicians. If you are careful and ask very gently about their use of herbals, they will tell you that they do believe in herbal medicines pretty strongly.
Morris Sherman, MD, PhD: I’d like to emphasize the need to be able to communicate with patients in their own language. In Toronto, 50% of the population was born outside of Canada. We have a huge immigrant population; given the nature of hepatology, we have many patients from Southeast and South Asia, and from all over the world, who don’t speak English. My hospital has a multilingual interpreter service, which we use freely. Scarcely a day goes by without two or three interpreters coming to the clinic to talk to patients, and as a result it’s rare that I can’t make myself understood. Maybe what I’ve said hasn’t been accepted, but patients can at least understand what I’m saying.
William D. Carey, MD: I interview many applicants for our medical school, and many of them are Asians, including Hmong and Vietnamese. With the high value that most of these groups put on education and their success with educational attainment, is their access to care improving? Are we doing a better job of training nurses, allied health personnel, and physicians to deal with this problem?
Dr. Tran: I think so, yes. For instance, the Southeast Asian immigrant population arrived in two different eras. The Vietnamese who immigrated in 1975 have been in the United States longer and in general have been able to attain a higher level of education than those who came later. The group that arrived earlier is therefore more likely to have health insurance, and it has been easier to get them into the health care system. More recent immigrants have had more difficulty navigating the system. In general, their socioeconomic status and therefore access to care is directly related to how long they’ve been in the country.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
- President’s Advisory Commission on Asian Americans and Pacific Islanders. Asian Americans and Pacific Islanders: a people looking forward. Action for access and partnerships in the 21st century. Interim report to the president and the nation. http://permanent.access.gpo.gov/lps17931/www.aapi.gov/intreport.htm. Published January 2001. Accessed December 21, 2008.
- National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Hepatitis B index. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm. Updated July 8, 2008. Accessed January 21, 2009.
- Do S. The natural history of hepatitis B in Asian Americans. Asian Am Pac Isl J Health 2001; 9:141–153.
- Stanford University School of Medicine. FAQ about hepatitis B. Asian Liver Center Web site. http://liver.stanford.edu/Education/faq.html. Updated July 10, 2008. Accessed January 21, 2009.
- Di Bisceglie AM, Keeffe E, Atillasoy E, Varshneya R, Bergstein G. Management of chronic hepatitis B—an analysis of physician practices [DDW abstract M918]. Gastroenterology 2005; 128(suppl 2):A739.
- US Census Bureau. American community survey. US Census Bureau Web site. http://www.census.gov/acs/www/SBasics/SQuest/fact_pdf/P%2013%20factsheetlanguageathome2.pdf. Published January 29, 2004. Accessed January 21, 2009.
- Lestina FA. Analysis of the linguistically isolated population in Census 2000. http://www.census.gov/pred/www/rpts/A.5a.pdf. Published September 30, 2003. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Diverse communities, diverse experiences: the status of Asian Americans and Pacific Islanders in the U.S. http://www.apiahf.org/resources/pdf/Diverse%20Communities%20Diverse%20Experiences.pdf. Accessed January 21, 2009.
- Asian & Pacific Islander American Health Forum. Race, ethnicity and health care fact sheet. Henry J. Kaiser Family Foundation Web site. http://www.kff.org/minorityhealth/upload/7745.pdf. Published April 2008. Accessed January 21, 2009.
- Smedley BD, Stith AY, Nelson AR, eds; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. http://www.nap.edu/openbook.php?isbn=030908265X. Published 2003. Accessed January 21, 2009.
- Speigel BMR, Bollus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology 2007; 46:113–121.
KEY POINTS
- Some Asian Americans have limited proficiency in English and are isolated linguistically, limiting their ability to communicate with health care providers.
- Asian Americans may view Western medicine with suspicion, causing delays in seeking care and making it difficult to successfully manage chronic HBV infection.
- Sensitivity to cultural attitudes may enhance communication and the likelihood that immigrant patients will accept health care providers’ recommendations; cultural sensitivity training may be helpful.
Hepatitis B treatment: Current best practices, avoiding resistance
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
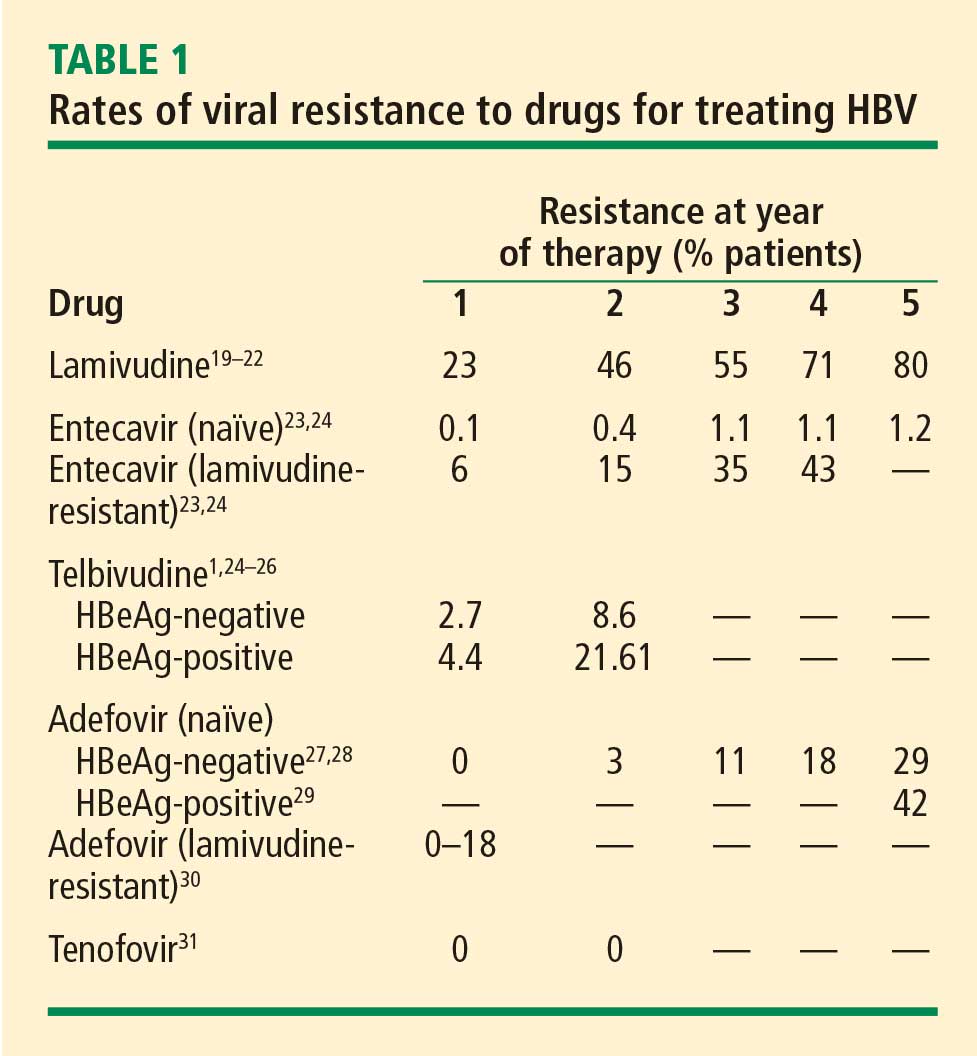
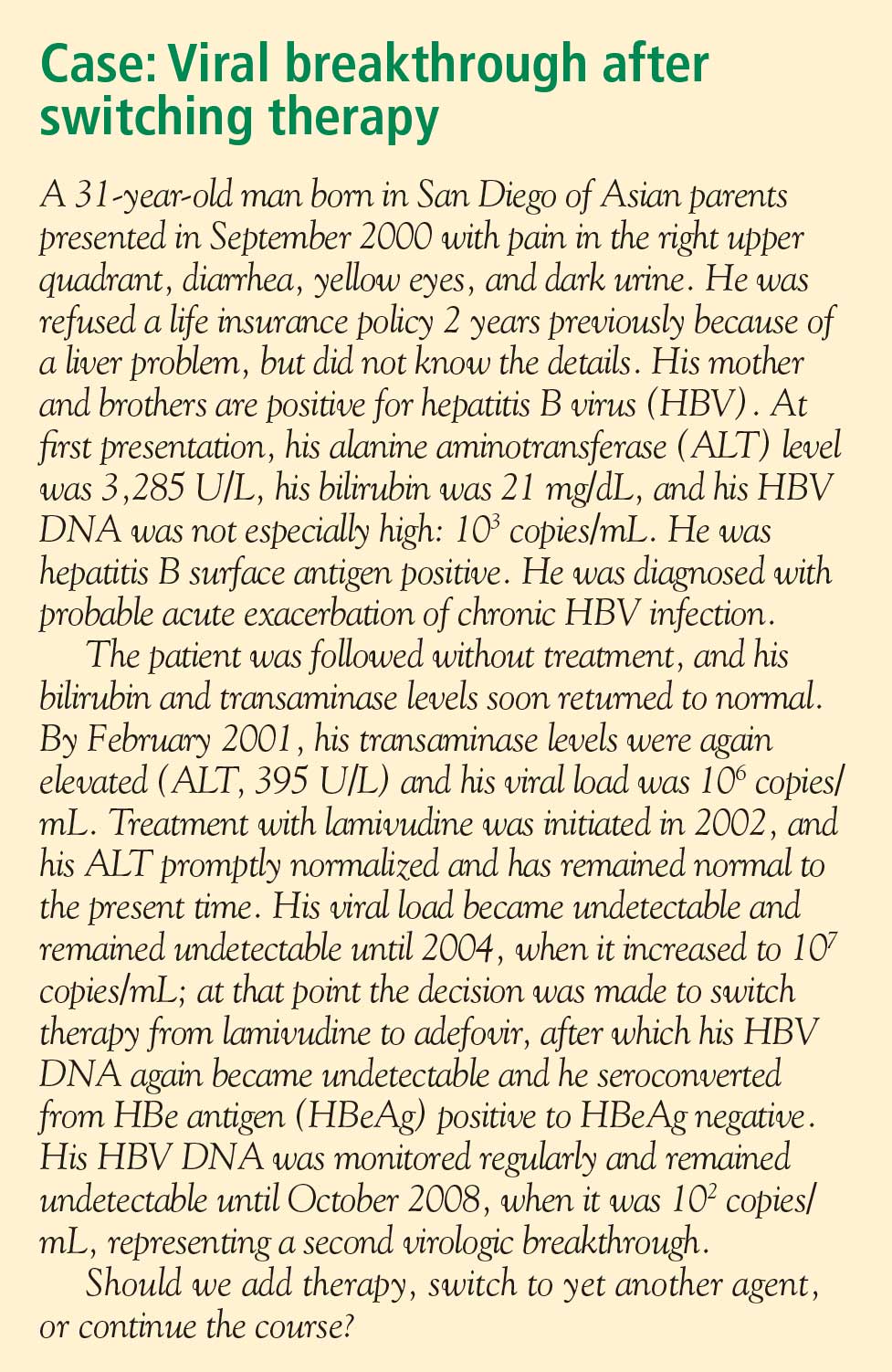
Nucleoside analogues
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
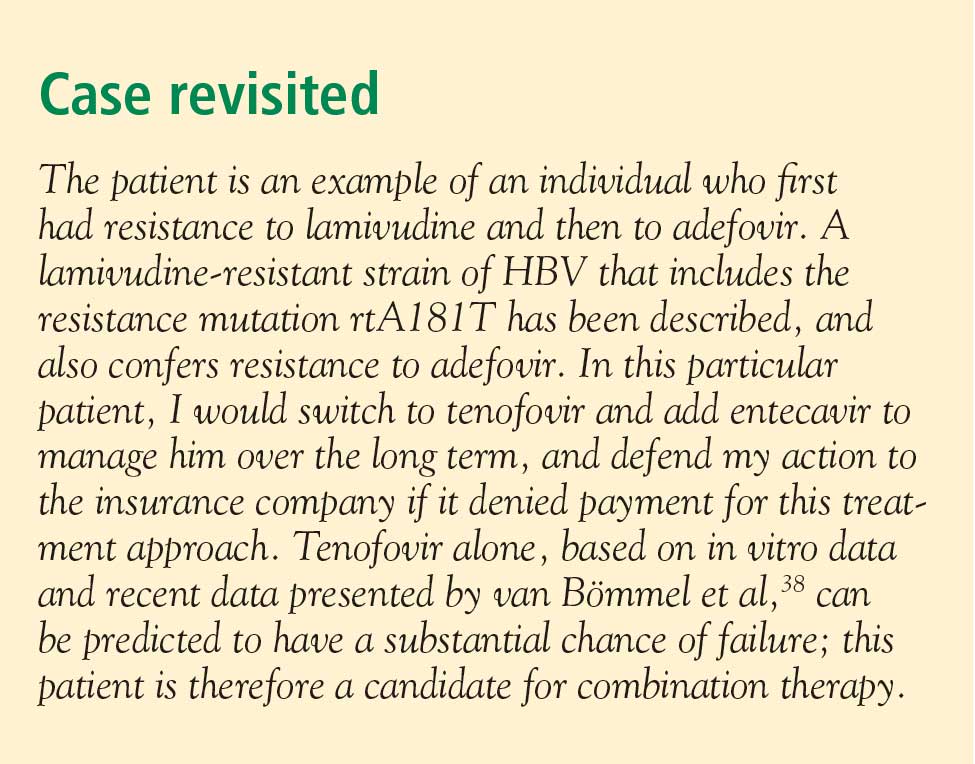
Managing resistance
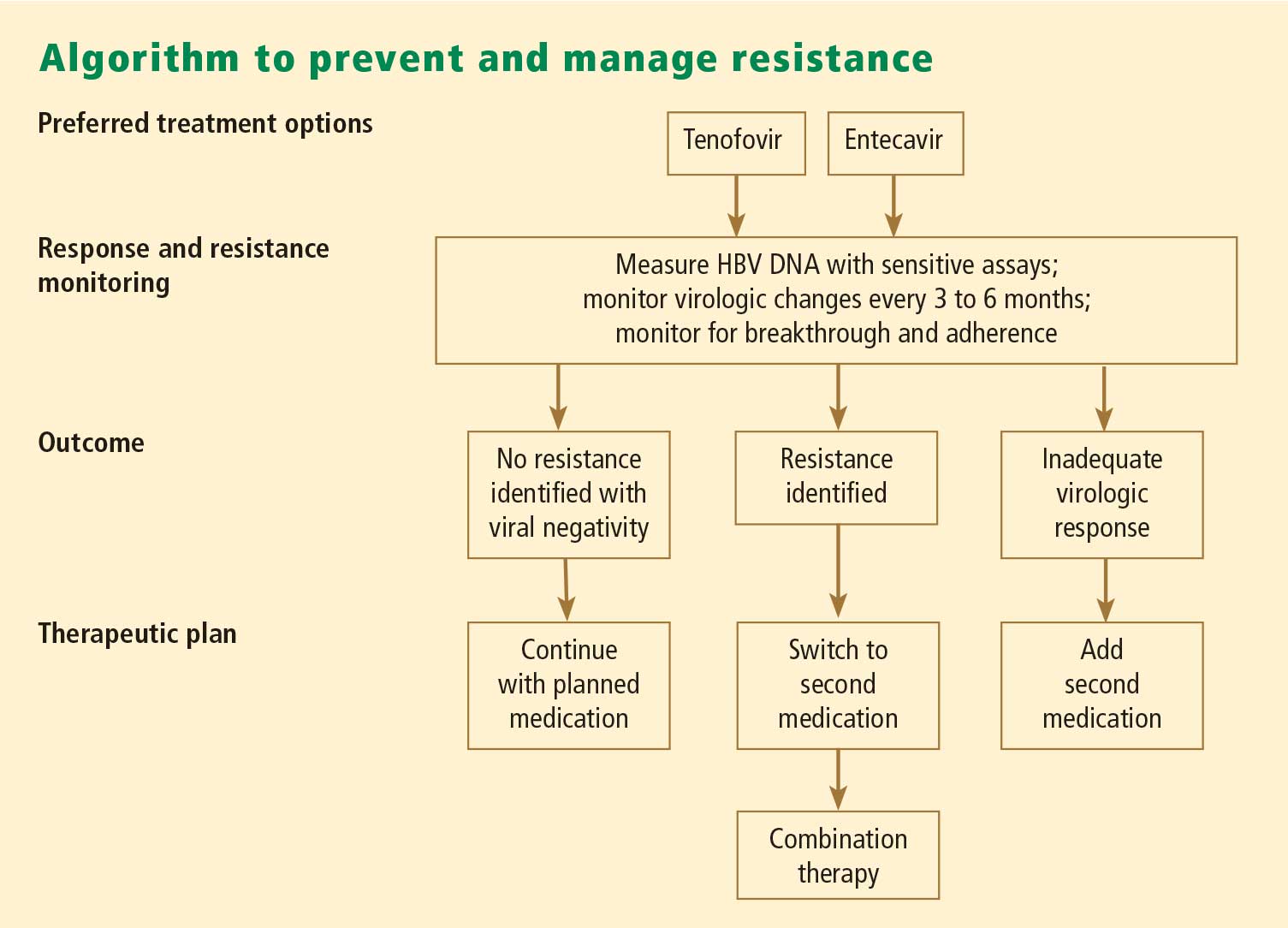
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
Nucleoside analogues
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
Managing resistance
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
Guidelines for the management of hepatitis B virus (HBV) infection can be daunting to clinicians. Further, although established practice guidelines can provide direction, treatment of chronic HBV infection is characterized by uncertainties that can hinder optimal patient care. Reservations about when to initiate and terminate therapy, cost issues, and the development of resistance to therapy are among the factors that impede adequate treatment. This article offers a straightforward roadmap for the management of chronic HBV infection, based on interpretation of recently released guidelines,1–3 and strategies for preventing and managing resistance to antiviral therapy.
DECIDING TO TREAT
Key factors: Viral load and ALT
Two important factors influencing the decision to treat are viral load (HBV DNA) and alanine aminotransferase (ALT) level; although these are relatively straightforward measures, other factors can cause clinicians to avoid or delay treatment.
A simple guideline is to discuss treatment with any patient who is positive for HBV DNA. The most recent guidelines for the treatment of HBV infection, published by the European Association for the Study of the Liver (EASL), recommend an HBV DNA level of 2,000 copies/mL as a threshold for initiating therapy; this recommendation applies to patients who are either positive or negative for hepatitis B e antigen (HBeAg).3
The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study investigators used ultrasensitive polymerase chain reaction (PCR) to quantify HBV DNA levels and conducted a time-dependent multiple Cox regression analysis of HBV DNA level and the risk of hepatocellular carcinoma (HCC).4,5 The length of time at a given DNA level was weighted in determining the adjusted hazard ratio. With an HBV DNA level less than 300 copies/mL defined as the reference group, risk of HCC increased commensurate with increasing HBV DNA level; even at levels ranging from 300 to 10,000 copies/mL, longer duration of HBV DNA positivity increased risk. This group also found HBV DNA level to be an independent risk factor for cirrhosis.
Patients who are HBV DNA negative are at much lower risk of cirrhosis and HCC than HBV DNA–positive patients; HBV DNA–negative patients being treated with antiviral drugs are much less likely to develop resistance to treatment, provided that first-line medications such as tenofovir or entecavir are used.
The definition of a “healthy” ALT level is controversial. In my opinion, an abnormal ALT is greater than 19 IU/mL for women and greater than 25 IU/mL for men; in either setting, treatment should be instituted if the patient is HBV DNA positive. This position is supported by a recently published algorithm,6 a recent National Institutes of Health conference on management of HBV,7 and other sources.8–12
Barriers to optimal treatment
Patient reluctance to undergo invasive tests, concerns about resistance, confusion about when to initiate therapy, cost, and other issues can impede timely and effective treatment of HBV infection.
Invasive studies. Liver histology is a key driver for initiating treatment, but many patients resist undergoing a liver biopsy. Ultrasonography has enabled noninvasive determination of spleen size, portal vein size, and liver tissue and surface heterogeneity; noninvasive assessments such as measurement of aspartate aminotransferase, varices, serum markers of fibrosis, and platelet count may provide clues to advanced liver fibrosis. Eventually, ultrasonographic elastography to measure liver stiffness and magnetic resonance scans may be common in clinical practice for noninvasive evaluation of liver damage. Ultimately, however, liver biopsy remains a valuable tool to motivate patients with chronic HBV infection to initiate and continue antiviral therapy.
Rationales for avoiding or delaying treatment. Concern about the development of resistance to treatment, as with antiviral therapy directed against human immunodeficiency virus (HIV), is one reason not to treat. The absence of clear guidelines regarding the appropriate time to terminate therapy has also led to avoidance or delay of treatment. The lack of risk calculators similar to the Framingham risk score, which estimates the risk of coronary heart disease, has limited the treatment of chronic HBV infection.
Cost. Cost must be examined in relation to the cost of resistance developing and the cost of treating complications. Lamivudine, considered a third-line treatment for chronic HBV infection, is an inexpensive drug. However, up to 70% of patients will develop resistance to lamivudine over 5 years3,6; most will require combination therapy, with its attendant costs, and may eventually require transplants or experience poor clinical outcomes. Although the initial costs of potent first-line therapies (tenofovir, entecavir, and pegylated interferon) are high, cost modeling shows that they are less expensive over the long term when the overall cost of care is considered.13,14
GOALS OF THERAPY: VIRAL LOAD SUPPRESSION, SEROCONVERSION
Profound suppression of viral load reduces the risk of resistance and is the ultimate goal of therapy for HBV infection. We can infer from recent data15 that achieving HBV DNA negativity has led to improved outcomes in patients with chronic HBV infection; ie, with the increased use of antiviral drugs in the United States over the past 2 decades, the number of liver transplants for end-stage liver disease has fallen dramatically,15 suggesting that profound suppression of viral loads has translated into fewer cases of liver failure and less need for transplants.
Over the same period, the number of patients diagnosed annually with HCC has increased by 146%.15 One interpretation of these data is that patients with chronic HBV infection are living longer, allowing time for HCC to develop. In addition, aggressive surveillance guidelines may account for the increased number of HCC cases since 1990. If detected early, HCC is curable by liver transplant at a rate exceeding 80%.16–18
In discussing treatment duration with patients, I present the ultimate goal of therapy as loss of HB surface antigen (HBsAg), or seroconversion to anti-HBs. At our clinic, we monitor HBsAg at least annually when patients are on long-term therapy.
The cost-effectiveness of treating all patients until they are HBsAg negative needs to be assessed. Incremental cost-effectiveness ratios per quality-adjusted life-year are key to identifying the best course of action.
TREATMENT OPTIONS
Nucleoside analogues
Lamivudine. The incidence of lamivudine resistance increases with increased treatment duration, reaching a peak of 80% after 5 years of treatment19–22; use of this agent eventually requires combination therapy. For this reason, lamivudine is considered a third-line drug and is not recommended as a first-line therapy.
Entecavir. Entecavir induces profound suppression of HBV DNA (to undetectable levels by weeks 24 to 36) in patients who are HBeAg positive or negative, regardless of baseline HBV DNA levels; resistance rates are very low in treatment-naïve patients,23 and entecavir is therefore considered first-line therapy. More than 90% of HBeAg-positive or -negative patients who are adherent to entecavir are HBV DNA negative at 5 years.24 Loss of HBsAg is 5% in entecavir-treated patients at follow-up of approximately 80 weeks, which is roughly double the rate of HBsAg loss with lamivudine.32
Telbivudine. Telbivudine has a secondary role in treatment of HBV infection. In a study by Lai et al,25,26 the cumulative incidence of telbivudine resistance and virologic breakthrough in HBeAg-positive patients rose from nearly 5% after 1 year to 22% after 2 years of treatment. Although the incidence was lower in HBeAg-negative patients, rates of genotypic resistance with virologic breakthrough rose to 9% in this population.
Since these results report genotypic resistance and virologic breakthrough, the rates of genotypic resistance in these patients may actually be higher than reported. Indeed, genotypic resistance was detected in 6.8% of the entire study population after 1 year of treatment. In this study, it must be remembered that patients with HBV DNA levels that were detectable by PCR (≥ 300 copies/mL) but were less than 1,000 copies/mL were not assessed for resistance.
Because of high rates of resistance associated with telbivudine, its role in the treatment of chronic HBV is secondary. I may use it in pregnant patients because most other nucleoside analogues are category C drugs and telbivudine is a category B agent (see “Management of hepatitis B in pregnancy: Weighing the options”). There are risks of myositis and neuropathy with telbivudine; although these risks are low, I mention them to patients when discussing a treatment plan.
Nucleotide analogues
Adefovir. Adefovir is considered second-line or add-on therapy when resistance to lamivudine develops because of its low potency in suppressing viral load. At 48 weeks, only 12% of HBeAg-positive patients are HBV DNA negative when treated with adefovir monotherapy.33,34
In a phase 3 clinical trial, genotypic resistance to adefovir was detected in 29% of HBeAg-negative patients treated for up to 5 years.27 The probability of resistance with virologic breakthrough was 3%, 8%, 14%, and 20% after 2, 3, 4, and 5 years of treatment, respectively.
In patients infected with lamivudine-resistant HBV, the probability of adefovir resistance is reduced by adding adefovir to ongoing lamivudine therapy, according to data from a large retrospective comparative study.35 In patients treated with adefovir monotherapy, the probability of virologic breakthrough (defined as > 1 log10 rebound in HBV DNA compared with on-treatment nadir) reached 30% over 36 months. In patients treated with add-on adefovir, the probability of virologic breakthrough was reduced to 6%. Similarly, the probability of adefovir resistance over 36 months of treatment was greater in the adefovir monotherapy group (16%) than in the add-on adefovir group (0%).
Although adefovir resistance is observed infrequently when adefovir is added to lamivudine, the effectiveness of adding adefovir is still limited by its low potency.
Tenofovir. More than 90% of HBeAg-negative patients and nearly 80% of HBeAg-positive patients treated with tenofovir have persistent virologic responses and HBV DNA levels less than 400 copies/mL by 72 weeks, with minimal side effects.33,34 Marcellin et al reported no development of resistance to tenofovir after 48 weeks of treatment.31 Although the nucleotide analogues have been associated with renal toxicity,36 the risk of renal toxicity associated with tenofovir is 1% or less per year; it can be reduced even further by calculating renal function through the use of the Cockroft-Gault equation or the Modification of Diet in Renal Disease equation prior to therapy and adjusting the dosage accordingly.37
With profound HBV DNA suppression, HBsAg loss occurs in about 5% of tenofovir-treated patients at 64 weeks.33
Treatment with tenofovir in treatment-experienced patients leads to potent suppression of HBV DNA independent of HBV genotype, HBV mutations (YMDD mutations) that signal lamivudine resistance, or HBeAg status at baseline.38 Patients with genotypic resistance to adefovir at baseline had a lower probability of achieving HBV DNA suppression during treatment with tenofovir.
Pegylated interferon
Pegylated interferon has proven useful in subsets of HBV DNA–positive patients. These include patients with genotype A or B who are young, those with high ALT levels (≥ 2 or 3 times the upper limit of normal) and low viral load (< 107 copies/mL), and patients without significant comorbidities.6 Pegylated interferon is also an option for patients who require a defined treatment period (eg, a woman wishing to become pregnant in 1 to 2 years). The patients who would benefit from pegylated interferon as first-line therapy must be better defined, and early markers of virologic response need to be identified.
PREVENTING AND MANAGING RESISTANCE
Antiviral drug resistance has a negative impact on the treatment of patients with chronic HBV infection. The development of resistance can result in virologic breakthrough (a confirmed 1 log10 increase in plasma HBV DNA levels)1; increased ALT levels1,39; and the progression of liver disease,40 including hepatic decompensation, development of HCC, and need for liver transplant. In addition, resistance mutations may re-emerge, with covalently closed circular DNA representing a genetic archive for development of resistance; this can significantly limit future treatment options.41 Early detection and regular monitoring are critical to prevention and management of resistance.
Detection
Detecting virologic breakthrough as early as possible increases the likelihood of achieving virologic response. In a study by Rapti and colleagues,42 patients with lamivudine-resistant chronic HBV were treated with a combination of lamivudine and adefovir. The 3-year cumulative probability of virologic response (< 103 copies/mL) was 99% with the addition of adefovir when baseline viral load levels were less than 5 log10 copies/mL, but only 71% when baseline viral loads were greater than 6 log10 copies/mL.
Monitoring
Patient response must be defined correctly. In adherent patients who show an early favorable response to therapy, I advise HBV DNA testing every 3 to 6 months. For those whose response flattens and whose viral load remains high, switching therapy or adding on should be considered. We continue therapy and monitor regularly after HBV DNA reaches an undetectable level. If the response is suboptimal, the treatment regimen is adapted by adding a new agent or switching to an alternative therapy (see “Case revisited”).
For patients who are being treated with tenofovir or entecavir, I typically extend the interval of measuring DNA levels to every 6 months because rates of resistance with these agents are low. If response is suboptimal but resistance is absent, I consider switching to the opposite drug. In those patients with a resistance mutation, I add the other agent.
Managing resistance
Combination therapy has a role in individuals in whom medication has failed to suppress viral load, in the setting of drug resistance, after liver transplant, and in individuals coinfected with HIV (see “Strategies for managing coinfection with hepatitis B virus and HIV”). If patients demonstrate resistance to their current therapy, we examine viral factors, adherence to therapy, and medication availability (eg, cost and insurance coverage). Switching to entecavir in adefovir-resistant patients produces profound suppression of HBV DNA. Patients in whom entecavir or lamivudine have failed may respond to tenofovir, depending on the resistance mutations.
A POTENTIAL FUTURE OPTION
Clevudine is a nucleoside analogue in phase 3 clinical studies in the United States. Its potential role in therapy is not yet clear. To be determined is whether it will induce a long-term, off-treatment viral response, in which case treatment may be able to be terminated earlier, and whether it will show clinically important cross-resistance with other nucleoside analogues. The availability of more sensitive assays to demonstrate the emergence of early viral resistance would enable earlier changes in treatment for more successful outcomes.
SUMMARY
Preventing resistance is crucial to the success of antiviral drug therapy for treatment of chronic HBV; a persistently high viral load increases the risk of cirrhosis and HCC, and resistance is associated with increased HBV DNA levels. The best chance for long-term success depends on initiating therapy before cirrhosis develops, when viral load is still low; profound suppression of viral load using the most potent agents as first-line therapy; and long-term monitoring of HBV DNA. The development of resistance can result in virologic breakthrough and liver complications. Entecavir and tenofovir represent the most effective first-line options to suppress HBV DNA. Because cross-resistance can occur, adding another agent is preferred to switching agents if resistance to initial therapy develops.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
- Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007; 45:507–539.
- Liaw Y-F, Leung N, Kao J-H, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int 2008; 2:263–283.
- European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol 2009; 50:227–242.
- Chen CJ, Yang HI, Su J, et al. Serial monitoring of viral load and serum alanine aminotransferase level and the risk of hepatocellular carcinoma (HCC): R.E.V.E.A.L.-HBV study update [abstract 141]. J Hepatol 2008; 48(suppl 2):S61.
- Chen JD, Yang HI, Iloeje UH, et al. Liver disease progression in chronic hepatitis B infected persons with normal serum alanine amino transferase level: update from the R.E.V.E.A.L.-HBV study [abstract 644]. J Hepatol 2008; 48(suppl 2):S240.
- Keeffe EG, Dieterich DT, Han S-H B, et al. Special report. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008; 6:1315–1341.
- Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference statement: management of hepatitis B. Ann Intern Med 2009; 150:104–112.
- Piton A, Poynard T, Imbert-Bismut F, et al. Factors associated with serum alanine aminotransaminase activity in healthy subjects: consequences for the definition of normal values, for selection of blood donors, and for patients with chronic hepatitis C. MULTIVIRC group. Hepatology 1998; 27:1213–1219.
- Kim CH, Nam CM, Jee SH, Khan KH, Oh DK, Suh I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study. BMJ 2004; 328:983–986.
- Ioannou GN, Weiss NS, Boyko EJ, Mozaffarian D, Lee SP. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006; 43:1145–1151.
- Puoti C, Magrini A, Stati TN, et al. Clinical, histological, and virological features of hepatitis C virus carriers with persistently normal or abnormal alanine transaminase levels. Hepatology 1997; 26:1393–1398.
- Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002; 137:1–9.
- Deniz B, Buti M, Brosa M, et al. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate, lamivudine, adefovir dipivoxil, and entecavir of HbeAg negative patients with chronic hepatitis B in Spain [EASL abstract 558]. J Hepatol 2008; 48(suppl 2):S209.
- Deniz B, Everhard R. Cost-effectiveness simulation analysis of tenofovir disoproxil fumarate in HBeAg negative patients with chronic hepatitis B in Italy and France [EASL abstract 559]. J Hepatol 2008; 48(suppl 2):S210.
- Kim W, Benson JT, Hindman A, Brosgart C, Fortner-Burton C. Decline in the need for liver transplantation for end stage liver disease secondary to hepatitis B in the US. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 12.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334:693–700.
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 1999; 30:1434–1440.
- Yao FY, Bass NM, Nikolai B, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl 2003; 9:684–692.
- Lai CL, Ratziu V, Yuen M-F, Poynard T. Viral hepatitis B. Lancet 2003; 362:2089–2094.
- Leung NW, Lai C-L, Chang T-T, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology 2001; 33:1527–1532.
- Benhamou Y, Bochet M, Thibault V, et al. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999; 30:1302–1306.
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003; 125:1714–1722.
- Colonno RJ, Rose R, Baldick CJ, et al. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology 2006; 44:1656–1665.
- Perrillo RP. Current treatment of chronic hepatitis B: benefits and limitations. Semin Liver Dis 2005; 25(suppl 1):20–28.
- Lai C-L, Gane E, Liaw Y-F, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007; 357:2576–2588.
- Lai C-L, Gane E, Hsu C-W, et al. Two-year results from the GLOBE trial in patients with hepatitis B: greater clinical and antiviral efficacy for telbivudine (LDT) vs. lamivudine [AASLD abstract 91]. Hepatology 2006; 44(suppl 1):222A.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B [EASL abstract 36]. J Hepatol 2005; 42(suppl 2):17.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al; Adefovir Dipivoxil 438 Study Group. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005; 352:2673–2681.
- Hepsera [package insert]. Foster City, CA: Gilead Sciences, Inc; 2008.
- Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology 2006; 43:1385–1391.
- Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008; 359:2442–2455.
- Gish R, Chang T-T, Lai C-L, et al. Hepatitis B surface antigen loss in antiviral-treated patients with HBeAg(+) chronic hepatitis B infection: observations from antiviral-naïve patients treated with entecavir or lamivudine. Paper presented at: 58th Annual Meeting of the American Association for the Study of Liver Diseases; November 2–6, 2007; Boston, MA. Abstract 992.
- Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [EASL abstract 71]. J Hepatol 2008; 48(suppl 2):S32.
- Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [EASL abstract 57]. J Hepatol 2008; 48(suppl 2):S26.
- Lampertico P, Marzano A, Levrero M, et al. Adefovir and lamivudine combination therapy is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-negative chronic hepatitis B [EASL abstract 502]. J Hepatol 2007; 46(suppl 1):S191.
- Ha NB, Ha NB, Trinh HN. Changes in creatinine clearance (CRCL) in chronic hepatitis B (CHB) patients treated with adefovir dipivoxil (ADV) [AASLD abstract 901]. Hepatology 2008; 48:709A–710A.
- Gallant J, Staszewski S, Pozniak AL, et al; for the 903 Study Team. Similar renal safety profile between tenofovir DF (TDF) and stavudine (d4T) using modification of diet in renal disease (MDRD) and Cockcroft-Gault (CG) estimations of glomerular filtration rate (GFR) in antiretroviral-naïve patients through 144 weeks. In: Program and Abstracts of the 45th Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16–19, 2005; Washington, DC. Abstract H-350.
- van Bömmel F, de Man RA, Stein K, et al. A multicenter analysis of antiviral response after one year of tenofovir monotherapy in HBV-monoinfected patients with prior nucleos(t)ide analog experience [EASL abstract 73]. J Hepatol 2008; 48(suppl 2):S32.
- Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004; 9:1013–1026.
- Gish RG. Chronic hepatitis B virus: treating patients to prevent and manage resistance. US Gastroenterology Review 2007; March:51–54.
- Zoulim F. Mechanism of viral persistence and resistance to nucleoside and nucleotide analogs in chronic hepatitis B virus infection. Antiviral Res 2004; 64:1–15.
- Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007; 45:307–313.
KEY POINTS
- Consider treatment for chronic HBV infection for all patients who are positive for HBV DNA, as viral load levels as low as 300 copies/mL confer a risk for hepatocellular carcinoma.
- The goal of therapy is an undetectable level of HBV DNA; initiate therapy with the most potent agent to limit the possibility of resistance.
- Preventing resistance to therapy is crucial for successful treatment of chronic HBV infection.