User login
What is cell phone elbow, and what should we tell our patients?
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.
Small fiber neuropathy: A burning problem

In many of these patients, the findings on neurologic examination, nerve conduction studies, and electromyography are normal, although some may show signs of mild distal sensory loss on physical examination. The lack of objective findings on routine nerve conduction studies and electromyography may lead many physicians to attribute the symptoms to other disorders such as plantar fasciitis, vascular insufficiency, or degenerative lumbosacral spine disease.
The past 2 decades have seen the development of specialized tests that have greatly facilitated the diagnosis of small fiber neuropathy; these include skin biopsy to evaluate the density of nerve fibers in the epidermis and studies of autonomic nerve function. Common etiologies have been identified for small fiber neuropathy and can be specifically treated, which is critical for controlling progression of the disease. Pain management is becoming easier with more available options but is still quite challenging.
WHAT IS SMALL FIBER NEUROPATHY?
Peripheral nerve fibers can be classified according to size, which correlates with the degree of myelination.
- Large nerve fibers are heavily myelinated and include A-alpha fibers, which mediate motor strength, and A-beta fibers, which mediate vibratory and touch sensation.
- Medium-sized fibers, known as A-gamma fibers, are also myelinated and carry information to muscle spindles.
- Small fibers include myelinated A-delta fibers and unmyelinated C fibers, which innervate skin (somatic fibers) and involuntary muscles, including cardiac and smooth muscles (autonomic fibers). Together, they mediate pain, thermal sensation, and autonomic function.
Small fiber neuropathy results from selective impairment of small myelinated A-delta and unmyelinated C fibers.
Sensory symptoms: Pain, burning, tingling, numbness
Damage to or loss of small somatic nerve fibers results in pain, burning, tingling, or numbness that typically affects the limbs in a distal-to-proximal gradient. In rare cases, small fiber neuropathy follows a non-length-dependent distribution in which symptoms may be manifested predominantly in the arms, face, or trunk.
Symptoms may be mild initially, with some patients complaining of vague discomfort in one or both feet similar to the sensation of a sock gathering at the end of a shoe. Others report a wooden quality in their feet, numbness in their toes, or a feeling as if they are walking on pebbles, sand, or golf balls. The most bothersome and fairly typical symptom is burning pain in the feet that extends proximally in a stocking-glove distribution and is often accompanied by stabbing or aching pains, electric shock-like or pins-and-needles sensations, or cramping of the feet and calves.
Symptoms are usually worse at night and often affect sleep. Some patients say that their feet have become so exquisitely tender that they cannot bear having the bed sheets touch them, and so they sleep with their feet uncovered. A small number of patients do not have pain but report a feeling of tightness and swelling in their feet (even though the feet appear normal).
Examination often reveals allodynia (perception of nonpainful stimuli as being painful), hyperalgesia (perception of painful stimuli as being more painful than expected), or reduced pinprick and thermal sensation in the affected area. Vibratory sensation can be mildly reduced at the toes. Motor strength, tendon reflexes, and proprioception, however, are preserved because they are functions of large nerve fibers.
Autonomic symptoms
When autonomic fibers are affected, patients may experience dry eyes, dry mouth, orthostatic dizziness, constipation, bladder incontinence, sexual dysfunction, trouble sweating, or red or white skin discoloration.2 Examination may show orthostatic hypotension and skin changes. The skin over the affected area may appear atrophic, dry, shiny, discolored, or mildly edematous as the result of sudomotor and vasomotor abnormalities.
WHAT CAUSES SMALL FIBER NEUROPATHY?
Small fiber neuropathy has been associated with many medical conditions, including glucose dysmetabolism,3 connective tissue disease,4,5 dysthyroidism,6 vitamin B12 deficiency, paraproteinemia, human immunodeficiency virus (HIV) infection,7 hepatitis C virus infection, celiac disease,8 restless legs syndrome,9 neurotoxic drug exposure, hereditary diseases, and paraneoplastic syndrome. While most of these conditions cause a length-dependent small fiber neuropathy, others (Sjögren disease, celiac disease, and paraneoplastic syndrome) can cause a form of small fiber neuropathy that is not length-dependent.4,8,10
Diabetes and prediabetes
Glucose dysmetabolism, including diabetes and prediabetes with impaired oral glucose tolerance (a glucose level 140–199 mg/dL 2 hours after a 75-g oral dextrose load), is the most common identifiable associated condition, present in about one-third of patients with painful sensory neuropathy11 and in nearly half of those with otherwise idiopathic small fiber neuropathy.12–14
Research findings strongly suggest that even prediabetes is a risk factor for small fiber neuropathy, and that so-called “impaired glucose tolerance neuropathy” may represent the earliest stage of diabetic neuropathy. Several recent studies have found a high prevalence of impaired glucose tolerance in patients with sensory peripheral neuropathy,12–14 with a rate of up to 42% in cases initially thought to be idiopathic14 compared with 14% in the general population.15 Also, a dose-response relationship between the severity of hyperglycemia and the degree of neuropathy was demonstrated in one study, in which patients with impaired glucose tolerance more often had small fiber neuropathy, whereas those with diabetes more often had polyneuropathy involving both small and large fibers.14 And studies in animals and cell cultures have shown that intermittent hyperglycemia, which can be seen in patients with impaired glucose tolerance, caused sensory neuron and nerve fiber damage and increased spontaneous C-fiber firing, resulting in neuropathic pain.8,16,17
Metabolic syndrome
Insulin resistance with prediabetes and diabetes is a part of the metabolic syndrome, which also consists of hypertension, hyperlipidemia, and obesity. The individual components of the metabolic syndrome have been implicated as risk factors not only for cardiovascular and cerebrovascular disease but also for small fiber neuropathy.
One study in 548 patients with type 2 diabetes showed that those with the metabolic syndrome were twice as likely to have neuropathy as those without.18 Another study showed that in 1,200 patients with type 1 diabetes without neuropathy at baseline, hypertension, hyperlipidemia, and increased body mass index were each independently associated with a higher risk of developing neuropathy.19
A recent study of 219 patients with idiopathic distal symmetrical peripheral neuropathy and 175 diabetic patients without neuropathy found a higher prevalence of metabolic syndrome in patients with neuropathy than in normal populations. The prevalence of dyslipidemia (high levels of total and low-density lipoprotein cholesterol and triglycerides and low levels of high-density lipoprotein cholesterol), but not hypertension or obesity, was higher in patients with neuropathy than in patients with diabetes but no neuropathy.20 The findings linked dyslipidemia to neuropathy and showed the need for further studies of the potential pathogenic role of dyslipidemia in neuropathy.
Hereditary causes
Hereditary causes of small fiber neuropathy are rare and include Fabry disease, Tangier disease, hereditary sensory autonomic neuropathy, and hereditary amyloidosis.
HOW DO YOU EVALUATE PATIENTS WITH SUSPECTED SMALL FIBER NEUROPATHY?
A thorough history should be taken to obtain details regarding onset and features of neuropathy symptoms, exacerbating factors, and progression. It is also important to ascertain whether the patient has any associated conditions as mentioned above, a family history of neuropathy, risk factors for HIV or hepatitis C virus infection, or a history of neurotoxic drug exposure.
Clinical suspicion of small fiber neuropathy should be high if a patient presents with predominant small fiber symptoms and signs with preserved large fiber functions.
Nerve conduction studies and electromyography
For diagnostic testing, routine nerve conduction studies and electromyography assess the function of large nerve fibers only and are thus normal in small fiber neuropathy. These tests should still be ordered to rule out subclinical involvement of large fibers, which may affect the diagnostic evaluation, prognosis, and treatment plan. However, if the results of these tests are normal, specialized studies are needed to evaluate small fibers.
Although several tests are available to evaluate somatic and autonomic small fibers, the two that have the highest diagnostic efficiency for small fiber neuropathy and that are used most often are skin biopsy, to evaluate intraepidermal nerve fiber density, and quantitative sudomotor axon reflex testing (QSART), to assess sudomotor autonomic function.21–23
Skin biopsy
Skin biopsy is a minimally invasive procedure in which 3-mm-diameter punch biopsy specimens are taken from the distal leg, distal thigh, and proximal thigh of one lower limb. The procedure takes only 10 to 15 minutes.
Biopsy specimens are immunostained using an antibody against protein gene product 9.5, which is a panaxonal marker. Small nerve fibers in the epidermis are counted under a microscope, and intraepithelial nerve fiber densities are calculated and compared with established normative values. The diagnosis of small fiber neuropathy can be established if the intraepidermal nerve fiber density is lower than normal (Figure 1). Nerve fiber density may be normal in the early stage of small fiber neuropathy, but in this setting skin biopsy often shows abnormal morphologic changes in the small fibers, especially large swellings,24 and repeat biopsy in 6 to 12 months may be considered.
The diagnostic efficiency of skin biopsy is about 88%.21,23 For diagnosing small fiber neuropathy, it is more sensitive than quantitative sensory testing21,25 and more sensitive and less invasive than sural nerve biopsy.26 Intraepidermal nerve fiber density also correlates well with a variety of measures of severity of HIV distal sensory neuropathy and thus may be used to measure the severity and treatment response of small fiber neuropathy.27
Quantitative sudomotor axon reflex testing
QSART is an autonomic study that measures sweat output in response to acetylcholine, which reflects the function of postganglionic sympathetic unmyelinated sudomotor nerve fibers. Electrodes are placed on the arms and legs to record the volume of sweat produced by acetylcholine iontophoresis, in which a mild electrical stimulation on the skin allows acetylcholine to stimulate the sweat glands. The output is compared with normative values.
One prospective study showed that 67 (72.8%) of 92 patients with painful feet had abnormal results on QSART, ie, low sweat output.28 A retrospective study found that 77 (62%) of 125 patients with clinical features of distal small fiber neuropathy had a length-dependent pattern of QSART abnormalities.22 QSART abnormalities were detected in some patients without autonomic symptoms.
If these tests are not available
Skin biopsy and QSART are objective, reproducible, sensitive, and complementary in diagnosing small fiber neuropathy. One or both can be ordered, depending on whether the patient has somatic symptoms, autonomic symptoms, or both. However, these two tests are not widely available. Only a few laboratories in the country can process skin biopsy specimens to evaluate intraepidermal nerve fiber density. Nevertheless, it is easy to learn the skin punch biopsy procedure, and primary care physicians and neurologists can perform it after appropriate training. (A concern is avoiding damage to the epidermis.) They can then send specimens to one of the cutaneous nerve laboratories (but not to a routine reference laboratory).
A special technique, including unique fixative and cryoprotectant, is used to fix and process the biopsy specimens, because routine techniques for processing dermatologic punch biopsy specimens often result in lower intraepidermal nerve fiber densities. Therefore, it is very important to contact the laboratory regarding fixative and processing before performing a biopsy.
QSART requires specialized equipment and must be performed on site. In addition, the test is very sensitive to drugs that can affect sweating, such as antihistamines and antidepressants, and such drugs must be discontinued 48 hours before the study.
Basic laboratory tests to find the cause
Once the diagnosis of small fiber neuropathy is established, the next important step is to order a battery of laboratory tests to search for an underlying cause. The tests should include the following:
- Complete blood cell count
- Comprehensive metabolic panel
- Lipid panel
- Erythrocyte sedimentation rate
- Thyroid-stimulating hormone level
- Free thyroxine (T4) level
- Antinuclear antibody
- Extractable nuclear antigens
- Angiotensin-converting enzyme (ACE) level
- Serum and urine immunofixation tests
- Vitamin B12 level
- 2-hour oral glucose tolerance test.
Oral glucose tolerance testing is much more sensitive than measuring the hemoglobin A1c and fasting glucose levels in detecting diabetes and prediabetes. These two conditions were detected by oral glucose tolerance testing in more than 50% of patients with otherwise idiopathic sensory-predominant peripheral neuropathy and normal hemoglobin A1c and fasting glucose levels.13,14 Therefore, every patient with small fiber neuropathy without a known history of diabetes or prediabetes should have an oral glucose tolerance test.
Special laboratory tests in special cases
- If there is a history of gastrointestinal symptoms or herpetiform-like rash, then testing for gliadin antibody and tissue transglutaminase antibodies as well as small-bowel biopsy may be pursued to evaluate for celiac sprue.
- Serologic tests for HIV or hepatitis C should be ordered if the patient has risk factors.
- If there is a significant family history, further genetic testing should be considered.
- Lip biopsy or bone marrow biopsy should be considered if clinical suspicion is high for Sjögren disease, seronegative sicca syndrome, or amyloidosis.
- The serum ACE level has a low sensitivity and specificity; therefore, if sarcoid is suspected clinically, additional confirmatory testing, such as computed tomography of the chest, should be ordered despite a normal ACE value.
HOW DO YOU TREAT SMALL FIBER NEUROPATHY?
Treatment of small fiber neuropathy should target the underlying cause and neuropathic pain. Cause-specific treatment is a key in preventing small fiber neuropathy or slowing its progression.
Glucose control, weight control, and regular exercise
As glucose dysmetabolism is the condition most often associated with small fiber neuropathy (and since individual components of the metabolic syndrome are potential risk factors for it), tight glycemic control and lifestyle modification with diet control, weight control, and regular exercise are of paramount importance in patients with these conditions.
The Diabetic Prevention Program,29 a study in 3,234 people with prediabetes, found that diet and exercise were more effective than metformin (Glucophage) in preventing full-blown diabetes. At an average of 2.8 years of follow-up, the incidence of diabetes was 11.0 cases per 100 patient-years in a group assigned to receive placebo, compared with 7.8 in those assigned to receive metformin (31% lower), and 4.8 (58% lower) in those who were assigned to undergo a lifestyle intervention that included at least 150 minutes of physical activity per week with a weight-loss goal of 7%. Put another way, to prevent one case of diabetes over 3 years, 6.9 patients would have to undergo the lifestyle intervention program, or 13.9 would have to receive metformin. Since impaired glucose tolerance neuropathy may represent the earliest stage of diabetic neuropathy, the neuropathy at this stage may be reversible with lifestyle intervention and improvement of impaired glucose tolerance.
This concept is supported by a 3-year study in 31 people, which showed that lifestyle intervention significantly improved impaired glucose tolerance, reduced the body mass index, and lowered total serum cholesterol levels.30 Changes in these metabolic variables were accompanied by significant improvement of neuropathy as evidenced by significantly increased intraepidermal nerve fiber density, increased foot sweat volume, and decreased neuropathic pain.30
Treatment of other diseases
It has also been reported that treatment of sarcoidosis, autoimmune diseases, and celiac disease improved the symptoms of small fiber neuropathy resulting from these conditions.8,31 Therefore, it is important to identify the cause and treat it to prevent and slow the progression of small fiber neuropathy, and doing so may improve the disease in some mild cases.
Pain management
First-line choices of pain medications are the anticonvulsants gabapentin (Neurontin) and pregabalin (Lyrica), the tricyclic antidepressants amitriptyline (Elavil) and nortriptyline (Aventyl), a 5% lidocaine patch (Lidoderm), and the semisynthetic opioid analgesic tramadol (Ultram). These can be used alone or in combination.
Gabapentin is relatively well tolerated, but drowsiness can occur, especially with high starting doses. We usually start with 300 mg daily and increase it by 300 mg every week up to 1,200 mg three times a day as tolerated. Most patients need 600 to 900 mg three times a day.
Pregabalin is a newer antiepileptic drug, similar to gabapentin but less sedating. It can be started at 75 mg twice a day and gradually increased to 300 mg twice a day as needed. Weight gain and, rarely, swelling of the lower extremities may limit the use of both of these drugs.
Tricyclic antidepressants, such as amitriptyline, nortriptyline, and desipramine (Norpramin), are proven effective in controlling neuropathic pain, although no response with amitriptyline was seen in patients with painful HIV distal sensory neuropathy.34
Lidocaine patch is preferred if the painful area is small. Patients should be instructed to use the patch to cover the painful area 12 hours on and 12 hours off. If it does not provide relief within 1 week, it should be discontinued.
Tramadol is also helpful in treating neuropathic pain. It can be started at 50 mg two to four times a day as needed.
Nonsteroidal anti-inflammatory drugs and selective serotonin reuptake inhibitors are typically less effective than the other drugs mentioned.
Opioids should be reserved for refractory cases, given the potential for addiction, but they are sometimes necessary in patients with disabling pain that does not respond to other drugs.
TENS may be of benefit. The patient controls a pocket-size device that sends electrical signals to leads placed on affected areas.
Alternative therapies for small fiber neuropathy, such as meditation, yoga, and acupuncture, have yet to be studied.
It is also important to explain to patients that the typical course of small fiber neuropathy is relatively benign, as many patients worry about developing weakness and eventually not being able to walk. These concerns and fears can aggravate pain and depression, which can make treatment difficult.
WHAT IS THE PROGNOSIS OF SMALL FIBER NEUROPATHY?
Most patients with small fiber neuropathy experience a slowly progressive course, with symptoms and signs spreading proximally over time.
In one study, only 13% of 124 patients with small fiber neuropathy showed evidence of large-fiber involvement over a 2-year period. 21 None went on to develop Charcot joints, foot ulcers, weakness, or sensory ataxia, as is often seen in patients with long-standing or severe large fiber neuropathy. Neuropathic pain worsened in 30% and resolved spontaneously in 11%.21
Most patients with small fiber neuropathy require chronic pain management. Again, treatment of the underlying cause is important and can improve the prognosis.
We believe that the overall progression of small fiber neuropathy is slow. A longitudinal study with a follow-up longer than 2 years would be useful to confirm this.
TAKE-HOME POINTS
As the population continues to age and as more patients develop diabetes and the metabolic syndrome, the prevalence of small fiber neuropathy will rise. Patients who present to their primary care physicians with painful, burning feet require a thorough diagnostic evaluation, which may include referral for specialized neurodiagnostic testing. Aggressive cause-specific treatment, lifestyle modification, and pain control are key elements of a team approach to managing small fiber neuropathy.
- Gregg EW, Gu Q, Williams D, et al. Prevalence of lower extremity diseases associated with normal glucose levels, impaired fasting glucose, and diabetes among U.S. adults aged 40 or older. Diabetes Res Clin Pract 2007; 77:485–488.
- Lacomis D. Small fiber neuropathy. Muscle Nerve 2002; 26:173–188.
- Smith AG, Singleton JR. Impaired glucose tolerance and neuropathy. Neurologist 2008; 14:23–29.
- Chai J, Herrmann DN, Stanton M, Barbano RL, Logigian EL. Painful small-fiber neuropathy in Sjogren syndrome. Neurology 2005; 65:925–927.
- Goransson LG, Tjensvoll AB, Herigstad A, Mellgren SI, Omdal R. Small-diameter nerve fiber neuropathy in systemic lupus erythematosus. Arch Neurol 2006; 63:401–404.
- Orstavik K, Norheim I, Jorum E. Pain and small-fiber neuropathy in patients with hypothyroidism. Neurology 2006; 67:786–791.
- McArthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. Lancet Neurol 2005; 4:543–555.
- Brannagan TH, Hays AP, Chin SS, et al. Small-fiber neuropathy/neuronopathy associated with celiac disease: skin biopsy findings. Arch Neurol 2005; 62:1574–1578.
- Polydefkis M, Allen RP, Hauer P, Earley CJ, Griffin JW, McArthur JC. Subclinical sensory neuropathy in late-onset restless legs syndrome. Neurology 2000; 55:1115–1121.
- Gorson KC, Herrmann DN, Thiagarajan R, et al. Non-length dependent small fibre neuropathy/ganglionopathy. J Neurol Neurosurg Psychiatry 2008; 79:163–169.
- Singleton JR, Smith AG, Bromberg MB. Increased prevalence of impaired glucose tolerance in patients with painful sensory neuropathy. Diabetes Care 2001; 24:1448–1453.
- Novella SP, Inzucchi SE, Goldstein JM. The frequency of undiagnosed diabetes and impaired glucose tolerance in patients with idiopathic sensory neuropathy. Muscle Nerve 2001; 24:1229–1231.
- Smith AG, Singleton JR. The diagnostic yield of a standardized approach to idiopathic sensory-predominant neuropathy. Arch Intern Med 2004; 164:1021–1025.
- Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003; 60:108–111.
- Gregg EW, Sorlie P, Paulose-Ram R, et al. Prevalence of lower-extremity disease in the US adult population >=40 years of age with and without diabetes: 1999–2000 National Health and Nutrition Examination Survey. Diabetes Care 2004; 27:1591–1597.
- Boulton A. What causes neuropathic pain? J Diabetes Complications 1992; 6:58–63.
- Russell JW, Sullivan KA, Windebank AJ, Herrmann DN, Feldman EL. Neurons undergo apoptosis in animal and cell culture models of diabetes. Neurobiol Dis 1999; 6:347–363.
- Costa LA, Canani LH, Lisboa HR, Tres GS, Gross JL. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in type 2 diabetes. Diabet Med 2004; 21:252–255.
- Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:341–350.
- Smith A, Rose K, Singleton J. Idiopathic neuropathy patients are at high risk for metabolic syndrome. J Neurol Sci 2008; 273:25–28.
- Devigili G, Tugnoli V, Penza P, et al. The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain 2008; 131:1912– 1925.
- Low VA, Sandroni P, Fealey RD, Low PA. Detection of small-fiber neuropathy by sudomotor testing. Muscle Nerve 2006; 34:57–61.
- McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW. Epidermal nerve fiber density: normative reference range and diagnostic efficiency. Arch Neurol 1998; 55:1513–1520.
- Gibbons CH, Griffin JW, Polydefkis M, et al. The utility of skin biopsy for prediction of progression in suspected small fiber neuropathy. Neurology 2006; 66:256–258.
- Polydefkis M, Yiannoutsos CT, Cohen BA, et al. Reduced intraepidermal nerve fiber density in HIV-associated sensory neuropathy. Neurology 2002; 58:115–119.
- Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC. Epidermal nerve fiber density and sural nerve morphometry in peripheral neuropathies. Neurology 1999; 53:1634–1640.
- Zhou L, Kitch DW, Evans SR, et al. Correlates of epidermal nerve fiber densities in HIV-associated distal sensory polyneuropathy. Neurology 2007; 68:2113–2119.
- Novak V, Freimer ML, Kissel JT, et al. Autonomic impairment in painful neuropathy. Neurology 2001; 56:861–868.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393–403.
- Smith AG, Russell J, Feldman EL, et al. Lifestyle intervention for prediabetic neuropathy. Diabetes Care 2006; 29:1294–1299.
- Hoitsma E, Faber CG, van Santen-Hoeufft M, De Vries J, Reulen JP, Drent M. Improvement of small fiber neuropathy in a sarcoidosis patient after treatment with infliximab. Sarcoidosis Vasc Diffuse Lung Dis 2006; 23:73–77.
- Chen H, Lamer TJ, Rho RH, et al. Contemporary management of neuropathic pain for the primary care physician. Mayo Clin Proc 2004; 79:1533–1545.
- Galluzzi KE. Managing neuropathic pain. J Am Osteopath Assoc 2007; 107( suppl 6):ES39–ES48.
- Kieburtz K, Simpson D, Yiannoutsos C, et al. A randomized trial of amitriptyline and mexiletine for painful neuropathy in HIV infection. AIDS Clinical Trial Group 242 Protocol Team. Neurology 1998; 51:1682–1688.
In many of these patients, the findings on neurologic examination, nerve conduction studies, and electromyography are normal, although some may show signs of mild distal sensory loss on physical examination. The lack of objective findings on routine nerve conduction studies and electromyography may lead many physicians to attribute the symptoms to other disorders such as plantar fasciitis, vascular insufficiency, or degenerative lumbosacral spine disease.
The past 2 decades have seen the development of specialized tests that have greatly facilitated the diagnosis of small fiber neuropathy; these include skin biopsy to evaluate the density of nerve fibers in the epidermis and studies of autonomic nerve function. Common etiologies have been identified for small fiber neuropathy and can be specifically treated, which is critical for controlling progression of the disease. Pain management is becoming easier with more available options but is still quite challenging.
WHAT IS SMALL FIBER NEUROPATHY?
Peripheral nerve fibers can be classified according to size, which correlates with the degree of myelination.
- Large nerve fibers are heavily myelinated and include A-alpha fibers, which mediate motor strength, and A-beta fibers, which mediate vibratory and touch sensation.
- Medium-sized fibers, known as A-gamma fibers, are also myelinated and carry information to muscle spindles.
- Small fibers include myelinated A-delta fibers and unmyelinated C fibers, which innervate skin (somatic fibers) and involuntary muscles, including cardiac and smooth muscles (autonomic fibers). Together, they mediate pain, thermal sensation, and autonomic function.
Small fiber neuropathy results from selective impairment of small myelinated A-delta and unmyelinated C fibers.
Sensory symptoms: Pain, burning, tingling, numbness
Damage to or loss of small somatic nerve fibers results in pain, burning, tingling, or numbness that typically affects the limbs in a distal-to-proximal gradient. In rare cases, small fiber neuropathy follows a non-length-dependent distribution in which symptoms may be manifested predominantly in the arms, face, or trunk.
Symptoms may be mild initially, with some patients complaining of vague discomfort in one or both feet similar to the sensation of a sock gathering at the end of a shoe. Others report a wooden quality in their feet, numbness in their toes, or a feeling as if they are walking on pebbles, sand, or golf balls. The most bothersome and fairly typical symptom is burning pain in the feet that extends proximally in a stocking-glove distribution and is often accompanied by stabbing or aching pains, electric shock-like or pins-and-needles sensations, or cramping of the feet and calves.
Symptoms are usually worse at night and often affect sleep. Some patients say that their feet have become so exquisitely tender that they cannot bear having the bed sheets touch them, and so they sleep with their feet uncovered. A small number of patients do not have pain but report a feeling of tightness and swelling in their feet (even though the feet appear normal).
Examination often reveals allodynia (perception of nonpainful stimuli as being painful), hyperalgesia (perception of painful stimuli as being more painful than expected), or reduced pinprick and thermal sensation in the affected area. Vibratory sensation can be mildly reduced at the toes. Motor strength, tendon reflexes, and proprioception, however, are preserved because they are functions of large nerve fibers.
Autonomic symptoms
When autonomic fibers are affected, patients may experience dry eyes, dry mouth, orthostatic dizziness, constipation, bladder incontinence, sexual dysfunction, trouble sweating, or red or white skin discoloration.2 Examination may show orthostatic hypotension and skin changes. The skin over the affected area may appear atrophic, dry, shiny, discolored, or mildly edematous as the result of sudomotor and vasomotor abnormalities.
WHAT CAUSES SMALL FIBER NEUROPATHY?
Small fiber neuropathy has been associated with many medical conditions, including glucose dysmetabolism,3 connective tissue disease,4,5 dysthyroidism,6 vitamin B12 deficiency, paraproteinemia, human immunodeficiency virus (HIV) infection,7 hepatitis C virus infection, celiac disease,8 restless legs syndrome,9 neurotoxic drug exposure, hereditary diseases, and paraneoplastic syndrome. While most of these conditions cause a length-dependent small fiber neuropathy, others (Sjögren disease, celiac disease, and paraneoplastic syndrome) can cause a form of small fiber neuropathy that is not length-dependent.4,8,10
Diabetes and prediabetes
Glucose dysmetabolism, including diabetes and prediabetes with impaired oral glucose tolerance (a glucose level 140–199 mg/dL 2 hours after a 75-g oral dextrose load), is the most common identifiable associated condition, present in about one-third of patients with painful sensory neuropathy11 and in nearly half of those with otherwise idiopathic small fiber neuropathy.12–14
Research findings strongly suggest that even prediabetes is a risk factor for small fiber neuropathy, and that so-called “impaired glucose tolerance neuropathy” may represent the earliest stage of diabetic neuropathy. Several recent studies have found a high prevalence of impaired glucose tolerance in patients with sensory peripheral neuropathy,12–14 with a rate of up to 42% in cases initially thought to be idiopathic14 compared with 14% in the general population.15 Also, a dose-response relationship between the severity of hyperglycemia and the degree of neuropathy was demonstrated in one study, in which patients with impaired glucose tolerance more often had small fiber neuropathy, whereas those with diabetes more often had polyneuropathy involving both small and large fibers.14 And studies in animals and cell cultures have shown that intermittent hyperglycemia, which can be seen in patients with impaired glucose tolerance, caused sensory neuron and nerve fiber damage and increased spontaneous C-fiber firing, resulting in neuropathic pain.8,16,17
Metabolic syndrome
Insulin resistance with prediabetes and diabetes is a part of the metabolic syndrome, which also consists of hypertension, hyperlipidemia, and obesity. The individual components of the metabolic syndrome have been implicated as risk factors not only for cardiovascular and cerebrovascular disease but also for small fiber neuropathy.
One study in 548 patients with type 2 diabetes showed that those with the metabolic syndrome were twice as likely to have neuropathy as those without.18 Another study showed that in 1,200 patients with type 1 diabetes without neuropathy at baseline, hypertension, hyperlipidemia, and increased body mass index were each independently associated with a higher risk of developing neuropathy.19
A recent study of 219 patients with idiopathic distal symmetrical peripheral neuropathy and 175 diabetic patients without neuropathy found a higher prevalence of metabolic syndrome in patients with neuropathy than in normal populations. The prevalence of dyslipidemia (high levels of total and low-density lipoprotein cholesterol and triglycerides and low levels of high-density lipoprotein cholesterol), but not hypertension or obesity, was higher in patients with neuropathy than in patients with diabetes but no neuropathy.20 The findings linked dyslipidemia to neuropathy and showed the need for further studies of the potential pathogenic role of dyslipidemia in neuropathy.
Hereditary causes
Hereditary causes of small fiber neuropathy are rare and include Fabry disease, Tangier disease, hereditary sensory autonomic neuropathy, and hereditary amyloidosis.
HOW DO YOU EVALUATE PATIENTS WITH SUSPECTED SMALL FIBER NEUROPATHY?
A thorough history should be taken to obtain details regarding onset and features of neuropathy symptoms, exacerbating factors, and progression. It is also important to ascertain whether the patient has any associated conditions as mentioned above, a family history of neuropathy, risk factors for HIV or hepatitis C virus infection, or a history of neurotoxic drug exposure.
Clinical suspicion of small fiber neuropathy should be high if a patient presents with predominant small fiber symptoms and signs with preserved large fiber functions.
Nerve conduction studies and electromyography
For diagnostic testing, routine nerve conduction studies and electromyography assess the function of large nerve fibers only and are thus normal in small fiber neuropathy. These tests should still be ordered to rule out subclinical involvement of large fibers, which may affect the diagnostic evaluation, prognosis, and treatment plan. However, if the results of these tests are normal, specialized studies are needed to evaluate small fibers.
Although several tests are available to evaluate somatic and autonomic small fibers, the two that have the highest diagnostic efficiency for small fiber neuropathy and that are used most often are skin biopsy, to evaluate intraepidermal nerve fiber density, and quantitative sudomotor axon reflex testing (QSART), to assess sudomotor autonomic function.21–23
Skin biopsy
Skin biopsy is a minimally invasive procedure in which 3-mm-diameter punch biopsy specimens are taken from the distal leg, distal thigh, and proximal thigh of one lower limb. The procedure takes only 10 to 15 minutes.
Biopsy specimens are immunostained using an antibody against protein gene product 9.5, which is a panaxonal marker. Small nerve fibers in the epidermis are counted under a microscope, and intraepithelial nerve fiber densities are calculated and compared with established normative values. The diagnosis of small fiber neuropathy can be established if the intraepidermal nerve fiber density is lower than normal (Figure 1). Nerve fiber density may be normal in the early stage of small fiber neuropathy, but in this setting skin biopsy often shows abnormal morphologic changes in the small fibers, especially large swellings,24 and repeat biopsy in 6 to 12 months may be considered.
The diagnostic efficiency of skin biopsy is about 88%.21,23 For diagnosing small fiber neuropathy, it is more sensitive than quantitative sensory testing21,25 and more sensitive and less invasive than sural nerve biopsy.26 Intraepidermal nerve fiber density also correlates well with a variety of measures of severity of HIV distal sensory neuropathy and thus may be used to measure the severity and treatment response of small fiber neuropathy.27
Quantitative sudomotor axon reflex testing
QSART is an autonomic study that measures sweat output in response to acetylcholine, which reflects the function of postganglionic sympathetic unmyelinated sudomotor nerve fibers. Electrodes are placed on the arms and legs to record the volume of sweat produced by acetylcholine iontophoresis, in which a mild electrical stimulation on the skin allows acetylcholine to stimulate the sweat glands. The output is compared with normative values.
One prospective study showed that 67 (72.8%) of 92 patients with painful feet had abnormal results on QSART, ie, low sweat output.28 A retrospective study found that 77 (62%) of 125 patients with clinical features of distal small fiber neuropathy had a length-dependent pattern of QSART abnormalities.22 QSART abnormalities were detected in some patients without autonomic symptoms.
If these tests are not available
Skin biopsy and QSART are objective, reproducible, sensitive, and complementary in diagnosing small fiber neuropathy. One or both can be ordered, depending on whether the patient has somatic symptoms, autonomic symptoms, or both. However, these two tests are not widely available. Only a few laboratories in the country can process skin biopsy specimens to evaluate intraepidermal nerve fiber density. Nevertheless, it is easy to learn the skin punch biopsy procedure, and primary care physicians and neurologists can perform it after appropriate training. (A concern is avoiding damage to the epidermis.) They can then send specimens to one of the cutaneous nerve laboratories (but not to a routine reference laboratory).
A special technique, including unique fixative and cryoprotectant, is used to fix and process the biopsy specimens, because routine techniques for processing dermatologic punch biopsy specimens often result in lower intraepidermal nerve fiber densities. Therefore, it is very important to contact the laboratory regarding fixative and processing before performing a biopsy.
QSART requires specialized equipment and must be performed on site. In addition, the test is very sensitive to drugs that can affect sweating, such as antihistamines and antidepressants, and such drugs must be discontinued 48 hours before the study.
Basic laboratory tests to find the cause
Once the diagnosis of small fiber neuropathy is established, the next important step is to order a battery of laboratory tests to search for an underlying cause. The tests should include the following:
- Complete blood cell count
- Comprehensive metabolic panel
- Lipid panel
- Erythrocyte sedimentation rate
- Thyroid-stimulating hormone level
- Free thyroxine (T4) level
- Antinuclear antibody
- Extractable nuclear antigens
- Angiotensin-converting enzyme (ACE) level
- Serum and urine immunofixation tests
- Vitamin B12 level
- 2-hour oral glucose tolerance test.
Oral glucose tolerance testing is much more sensitive than measuring the hemoglobin A1c and fasting glucose levels in detecting diabetes and prediabetes. These two conditions were detected by oral glucose tolerance testing in more than 50% of patients with otherwise idiopathic sensory-predominant peripheral neuropathy and normal hemoglobin A1c and fasting glucose levels.13,14 Therefore, every patient with small fiber neuropathy without a known history of diabetes or prediabetes should have an oral glucose tolerance test.
Special laboratory tests in special cases
- If there is a history of gastrointestinal symptoms or herpetiform-like rash, then testing for gliadin antibody and tissue transglutaminase antibodies as well as small-bowel biopsy may be pursued to evaluate for celiac sprue.
- Serologic tests for HIV or hepatitis C should be ordered if the patient has risk factors.
- If there is a significant family history, further genetic testing should be considered.
- Lip biopsy or bone marrow biopsy should be considered if clinical suspicion is high for Sjögren disease, seronegative sicca syndrome, or amyloidosis.
- The serum ACE level has a low sensitivity and specificity; therefore, if sarcoid is suspected clinically, additional confirmatory testing, such as computed tomography of the chest, should be ordered despite a normal ACE value.
HOW DO YOU TREAT SMALL FIBER NEUROPATHY?
Treatment of small fiber neuropathy should target the underlying cause and neuropathic pain. Cause-specific treatment is a key in preventing small fiber neuropathy or slowing its progression.
Glucose control, weight control, and regular exercise
As glucose dysmetabolism is the condition most often associated with small fiber neuropathy (and since individual components of the metabolic syndrome are potential risk factors for it), tight glycemic control and lifestyle modification with diet control, weight control, and regular exercise are of paramount importance in patients with these conditions.
The Diabetic Prevention Program,29 a study in 3,234 people with prediabetes, found that diet and exercise were more effective than metformin (Glucophage) in preventing full-blown diabetes. At an average of 2.8 years of follow-up, the incidence of diabetes was 11.0 cases per 100 patient-years in a group assigned to receive placebo, compared with 7.8 in those assigned to receive metformin (31% lower), and 4.8 (58% lower) in those who were assigned to undergo a lifestyle intervention that included at least 150 minutes of physical activity per week with a weight-loss goal of 7%. Put another way, to prevent one case of diabetes over 3 years, 6.9 patients would have to undergo the lifestyle intervention program, or 13.9 would have to receive metformin. Since impaired glucose tolerance neuropathy may represent the earliest stage of diabetic neuropathy, the neuropathy at this stage may be reversible with lifestyle intervention and improvement of impaired glucose tolerance.
This concept is supported by a 3-year study in 31 people, which showed that lifestyle intervention significantly improved impaired glucose tolerance, reduced the body mass index, and lowered total serum cholesterol levels.30 Changes in these metabolic variables were accompanied by significant improvement of neuropathy as evidenced by significantly increased intraepidermal nerve fiber density, increased foot sweat volume, and decreased neuropathic pain.30
Treatment of other diseases
It has also been reported that treatment of sarcoidosis, autoimmune diseases, and celiac disease improved the symptoms of small fiber neuropathy resulting from these conditions.8,31 Therefore, it is important to identify the cause and treat it to prevent and slow the progression of small fiber neuropathy, and doing so may improve the disease in some mild cases.
Pain management
First-line choices of pain medications are the anticonvulsants gabapentin (Neurontin) and pregabalin (Lyrica), the tricyclic antidepressants amitriptyline (Elavil) and nortriptyline (Aventyl), a 5% lidocaine patch (Lidoderm), and the semisynthetic opioid analgesic tramadol (Ultram). These can be used alone or in combination.
Gabapentin is relatively well tolerated, but drowsiness can occur, especially with high starting doses. We usually start with 300 mg daily and increase it by 300 mg every week up to 1,200 mg three times a day as tolerated. Most patients need 600 to 900 mg three times a day.
Pregabalin is a newer antiepileptic drug, similar to gabapentin but less sedating. It can be started at 75 mg twice a day and gradually increased to 300 mg twice a day as needed. Weight gain and, rarely, swelling of the lower extremities may limit the use of both of these drugs.
Tricyclic antidepressants, such as amitriptyline, nortriptyline, and desipramine (Norpramin), are proven effective in controlling neuropathic pain, although no response with amitriptyline was seen in patients with painful HIV distal sensory neuropathy.34
Lidocaine patch is preferred if the painful area is small. Patients should be instructed to use the patch to cover the painful area 12 hours on and 12 hours off. If it does not provide relief within 1 week, it should be discontinued.
Tramadol is also helpful in treating neuropathic pain. It can be started at 50 mg two to four times a day as needed.
Nonsteroidal anti-inflammatory drugs and selective serotonin reuptake inhibitors are typically less effective than the other drugs mentioned.
Opioids should be reserved for refractory cases, given the potential for addiction, but they are sometimes necessary in patients with disabling pain that does not respond to other drugs.
TENS may be of benefit. The patient controls a pocket-size device that sends electrical signals to leads placed on affected areas.
Alternative therapies for small fiber neuropathy, such as meditation, yoga, and acupuncture, have yet to be studied.
It is also important to explain to patients that the typical course of small fiber neuropathy is relatively benign, as many patients worry about developing weakness and eventually not being able to walk. These concerns and fears can aggravate pain and depression, which can make treatment difficult.
WHAT IS THE PROGNOSIS OF SMALL FIBER NEUROPATHY?
Most patients with small fiber neuropathy experience a slowly progressive course, with symptoms and signs spreading proximally over time.
In one study, only 13% of 124 patients with small fiber neuropathy showed evidence of large-fiber involvement over a 2-year period. 21 None went on to develop Charcot joints, foot ulcers, weakness, or sensory ataxia, as is often seen in patients with long-standing or severe large fiber neuropathy. Neuropathic pain worsened in 30% and resolved spontaneously in 11%.21
Most patients with small fiber neuropathy require chronic pain management. Again, treatment of the underlying cause is important and can improve the prognosis.
We believe that the overall progression of small fiber neuropathy is slow. A longitudinal study with a follow-up longer than 2 years would be useful to confirm this.
TAKE-HOME POINTS
As the population continues to age and as more patients develop diabetes and the metabolic syndrome, the prevalence of small fiber neuropathy will rise. Patients who present to their primary care physicians with painful, burning feet require a thorough diagnostic evaluation, which may include referral for specialized neurodiagnostic testing. Aggressive cause-specific treatment, lifestyle modification, and pain control are key elements of a team approach to managing small fiber neuropathy.
In many of these patients, the findings on neurologic examination, nerve conduction studies, and electromyography are normal, although some may show signs of mild distal sensory loss on physical examination. The lack of objective findings on routine nerve conduction studies and electromyography may lead many physicians to attribute the symptoms to other disorders such as plantar fasciitis, vascular insufficiency, or degenerative lumbosacral spine disease.
The past 2 decades have seen the development of specialized tests that have greatly facilitated the diagnosis of small fiber neuropathy; these include skin biopsy to evaluate the density of nerve fibers in the epidermis and studies of autonomic nerve function. Common etiologies have been identified for small fiber neuropathy and can be specifically treated, which is critical for controlling progression of the disease. Pain management is becoming easier with more available options but is still quite challenging.
WHAT IS SMALL FIBER NEUROPATHY?
Peripheral nerve fibers can be classified according to size, which correlates with the degree of myelination.
- Large nerve fibers are heavily myelinated and include A-alpha fibers, which mediate motor strength, and A-beta fibers, which mediate vibratory and touch sensation.
- Medium-sized fibers, known as A-gamma fibers, are also myelinated and carry information to muscle spindles.
- Small fibers include myelinated A-delta fibers and unmyelinated C fibers, which innervate skin (somatic fibers) and involuntary muscles, including cardiac and smooth muscles (autonomic fibers). Together, they mediate pain, thermal sensation, and autonomic function.
Small fiber neuropathy results from selective impairment of small myelinated A-delta and unmyelinated C fibers.
Sensory symptoms: Pain, burning, tingling, numbness
Damage to or loss of small somatic nerve fibers results in pain, burning, tingling, or numbness that typically affects the limbs in a distal-to-proximal gradient. In rare cases, small fiber neuropathy follows a non-length-dependent distribution in which symptoms may be manifested predominantly in the arms, face, or trunk.
Symptoms may be mild initially, with some patients complaining of vague discomfort in one or both feet similar to the sensation of a sock gathering at the end of a shoe. Others report a wooden quality in their feet, numbness in their toes, or a feeling as if they are walking on pebbles, sand, or golf balls. The most bothersome and fairly typical symptom is burning pain in the feet that extends proximally in a stocking-glove distribution and is often accompanied by stabbing or aching pains, electric shock-like or pins-and-needles sensations, or cramping of the feet and calves.
Symptoms are usually worse at night and often affect sleep. Some patients say that their feet have become so exquisitely tender that they cannot bear having the bed sheets touch them, and so they sleep with their feet uncovered. A small number of patients do not have pain but report a feeling of tightness and swelling in their feet (even though the feet appear normal).
Examination often reveals allodynia (perception of nonpainful stimuli as being painful), hyperalgesia (perception of painful stimuli as being more painful than expected), or reduced pinprick and thermal sensation in the affected area. Vibratory sensation can be mildly reduced at the toes. Motor strength, tendon reflexes, and proprioception, however, are preserved because they are functions of large nerve fibers.
Autonomic symptoms
When autonomic fibers are affected, patients may experience dry eyes, dry mouth, orthostatic dizziness, constipation, bladder incontinence, sexual dysfunction, trouble sweating, or red or white skin discoloration.2 Examination may show orthostatic hypotension and skin changes. The skin over the affected area may appear atrophic, dry, shiny, discolored, or mildly edematous as the result of sudomotor and vasomotor abnormalities.
WHAT CAUSES SMALL FIBER NEUROPATHY?
Small fiber neuropathy has been associated with many medical conditions, including glucose dysmetabolism,3 connective tissue disease,4,5 dysthyroidism,6 vitamin B12 deficiency, paraproteinemia, human immunodeficiency virus (HIV) infection,7 hepatitis C virus infection, celiac disease,8 restless legs syndrome,9 neurotoxic drug exposure, hereditary diseases, and paraneoplastic syndrome. While most of these conditions cause a length-dependent small fiber neuropathy, others (Sjögren disease, celiac disease, and paraneoplastic syndrome) can cause a form of small fiber neuropathy that is not length-dependent.4,8,10
Diabetes and prediabetes
Glucose dysmetabolism, including diabetes and prediabetes with impaired oral glucose tolerance (a glucose level 140–199 mg/dL 2 hours after a 75-g oral dextrose load), is the most common identifiable associated condition, present in about one-third of patients with painful sensory neuropathy11 and in nearly half of those with otherwise idiopathic small fiber neuropathy.12–14
Research findings strongly suggest that even prediabetes is a risk factor for small fiber neuropathy, and that so-called “impaired glucose tolerance neuropathy” may represent the earliest stage of diabetic neuropathy. Several recent studies have found a high prevalence of impaired glucose tolerance in patients with sensory peripheral neuropathy,12–14 with a rate of up to 42% in cases initially thought to be idiopathic14 compared with 14% in the general population.15 Also, a dose-response relationship between the severity of hyperglycemia and the degree of neuropathy was demonstrated in one study, in which patients with impaired glucose tolerance more often had small fiber neuropathy, whereas those with diabetes more often had polyneuropathy involving both small and large fibers.14 And studies in animals and cell cultures have shown that intermittent hyperglycemia, which can be seen in patients with impaired glucose tolerance, caused sensory neuron and nerve fiber damage and increased spontaneous C-fiber firing, resulting in neuropathic pain.8,16,17
Metabolic syndrome
Insulin resistance with prediabetes and diabetes is a part of the metabolic syndrome, which also consists of hypertension, hyperlipidemia, and obesity. The individual components of the metabolic syndrome have been implicated as risk factors not only for cardiovascular and cerebrovascular disease but also for small fiber neuropathy.
One study in 548 patients with type 2 diabetes showed that those with the metabolic syndrome were twice as likely to have neuropathy as those without.18 Another study showed that in 1,200 patients with type 1 diabetes without neuropathy at baseline, hypertension, hyperlipidemia, and increased body mass index were each independently associated with a higher risk of developing neuropathy.19
A recent study of 219 patients with idiopathic distal symmetrical peripheral neuropathy and 175 diabetic patients without neuropathy found a higher prevalence of metabolic syndrome in patients with neuropathy than in normal populations. The prevalence of dyslipidemia (high levels of total and low-density lipoprotein cholesterol and triglycerides and low levels of high-density lipoprotein cholesterol), but not hypertension or obesity, was higher in patients with neuropathy than in patients with diabetes but no neuropathy.20 The findings linked dyslipidemia to neuropathy and showed the need for further studies of the potential pathogenic role of dyslipidemia in neuropathy.
Hereditary causes
Hereditary causes of small fiber neuropathy are rare and include Fabry disease, Tangier disease, hereditary sensory autonomic neuropathy, and hereditary amyloidosis.
HOW DO YOU EVALUATE PATIENTS WITH SUSPECTED SMALL FIBER NEUROPATHY?
A thorough history should be taken to obtain details regarding onset and features of neuropathy symptoms, exacerbating factors, and progression. It is also important to ascertain whether the patient has any associated conditions as mentioned above, a family history of neuropathy, risk factors for HIV or hepatitis C virus infection, or a history of neurotoxic drug exposure.
Clinical suspicion of small fiber neuropathy should be high if a patient presents with predominant small fiber symptoms and signs with preserved large fiber functions.
Nerve conduction studies and electromyography
For diagnostic testing, routine nerve conduction studies and electromyography assess the function of large nerve fibers only and are thus normal in small fiber neuropathy. These tests should still be ordered to rule out subclinical involvement of large fibers, which may affect the diagnostic evaluation, prognosis, and treatment plan. However, if the results of these tests are normal, specialized studies are needed to evaluate small fibers.
Although several tests are available to evaluate somatic and autonomic small fibers, the two that have the highest diagnostic efficiency for small fiber neuropathy and that are used most often are skin biopsy, to evaluate intraepidermal nerve fiber density, and quantitative sudomotor axon reflex testing (QSART), to assess sudomotor autonomic function.21–23
Skin biopsy
Skin biopsy is a minimally invasive procedure in which 3-mm-diameter punch biopsy specimens are taken from the distal leg, distal thigh, and proximal thigh of one lower limb. The procedure takes only 10 to 15 minutes.
Biopsy specimens are immunostained using an antibody against protein gene product 9.5, which is a panaxonal marker. Small nerve fibers in the epidermis are counted under a microscope, and intraepithelial nerve fiber densities are calculated and compared with established normative values. The diagnosis of small fiber neuropathy can be established if the intraepidermal nerve fiber density is lower than normal (Figure 1). Nerve fiber density may be normal in the early stage of small fiber neuropathy, but in this setting skin biopsy often shows abnormal morphologic changes in the small fibers, especially large swellings,24 and repeat biopsy in 6 to 12 months may be considered.
The diagnostic efficiency of skin biopsy is about 88%.21,23 For diagnosing small fiber neuropathy, it is more sensitive than quantitative sensory testing21,25 and more sensitive and less invasive than sural nerve biopsy.26 Intraepidermal nerve fiber density also correlates well with a variety of measures of severity of HIV distal sensory neuropathy and thus may be used to measure the severity and treatment response of small fiber neuropathy.27
Quantitative sudomotor axon reflex testing
QSART is an autonomic study that measures sweat output in response to acetylcholine, which reflects the function of postganglionic sympathetic unmyelinated sudomotor nerve fibers. Electrodes are placed on the arms and legs to record the volume of sweat produced by acetylcholine iontophoresis, in which a mild electrical stimulation on the skin allows acetylcholine to stimulate the sweat glands. The output is compared with normative values.
One prospective study showed that 67 (72.8%) of 92 patients with painful feet had abnormal results on QSART, ie, low sweat output.28 A retrospective study found that 77 (62%) of 125 patients with clinical features of distal small fiber neuropathy had a length-dependent pattern of QSART abnormalities.22 QSART abnormalities were detected in some patients without autonomic symptoms.
If these tests are not available
Skin biopsy and QSART are objective, reproducible, sensitive, and complementary in diagnosing small fiber neuropathy. One or both can be ordered, depending on whether the patient has somatic symptoms, autonomic symptoms, or both. However, these two tests are not widely available. Only a few laboratories in the country can process skin biopsy specimens to evaluate intraepidermal nerve fiber density. Nevertheless, it is easy to learn the skin punch biopsy procedure, and primary care physicians and neurologists can perform it after appropriate training. (A concern is avoiding damage to the epidermis.) They can then send specimens to one of the cutaneous nerve laboratories (but not to a routine reference laboratory).
A special technique, including unique fixative and cryoprotectant, is used to fix and process the biopsy specimens, because routine techniques for processing dermatologic punch biopsy specimens often result in lower intraepidermal nerve fiber densities. Therefore, it is very important to contact the laboratory regarding fixative and processing before performing a biopsy.
QSART requires specialized equipment and must be performed on site. In addition, the test is very sensitive to drugs that can affect sweating, such as antihistamines and antidepressants, and such drugs must be discontinued 48 hours before the study.
Basic laboratory tests to find the cause
Once the diagnosis of small fiber neuropathy is established, the next important step is to order a battery of laboratory tests to search for an underlying cause. The tests should include the following:
- Complete blood cell count
- Comprehensive metabolic panel
- Lipid panel
- Erythrocyte sedimentation rate
- Thyroid-stimulating hormone level
- Free thyroxine (T4) level
- Antinuclear antibody
- Extractable nuclear antigens
- Angiotensin-converting enzyme (ACE) level
- Serum and urine immunofixation tests
- Vitamin B12 level
- 2-hour oral glucose tolerance test.
Oral glucose tolerance testing is much more sensitive than measuring the hemoglobin A1c and fasting glucose levels in detecting diabetes and prediabetes. These two conditions were detected by oral glucose tolerance testing in more than 50% of patients with otherwise idiopathic sensory-predominant peripheral neuropathy and normal hemoglobin A1c and fasting glucose levels.13,14 Therefore, every patient with small fiber neuropathy without a known history of diabetes or prediabetes should have an oral glucose tolerance test.
Special laboratory tests in special cases
- If there is a history of gastrointestinal symptoms or herpetiform-like rash, then testing for gliadin antibody and tissue transglutaminase antibodies as well as small-bowel biopsy may be pursued to evaluate for celiac sprue.
- Serologic tests for HIV or hepatitis C should be ordered if the patient has risk factors.
- If there is a significant family history, further genetic testing should be considered.
- Lip biopsy or bone marrow biopsy should be considered if clinical suspicion is high for Sjögren disease, seronegative sicca syndrome, or amyloidosis.
- The serum ACE level has a low sensitivity and specificity; therefore, if sarcoid is suspected clinically, additional confirmatory testing, such as computed tomography of the chest, should be ordered despite a normal ACE value.
HOW DO YOU TREAT SMALL FIBER NEUROPATHY?
Treatment of small fiber neuropathy should target the underlying cause and neuropathic pain. Cause-specific treatment is a key in preventing small fiber neuropathy or slowing its progression.
Glucose control, weight control, and regular exercise
As glucose dysmetabolism is the condition most often associated with small fiber neuropathy (and since individual components of the metabolic syndrome are potential risk factors for it), tight glycemic control and lifestyle modification with diet control, weight control, and regular exercise are of paramount importance in patients with these conditions.
The Diabetic Prevention Program,29 a study in 3,234 people with prediabetes, found that diet and exercise were more effective than metformin (Glucophage) in preventing full-blown diabetes. At an average of 2.8 years of follow-up, the incidence of diabetes was 11.0 cases per 100 patient-years in a group assigned to receive placebo, compared with 7.8 in those assigned to receive metformin (31% lower), and 4.8 (58% lower) in those who were assigned to undergo a lifestyle intervention that included at least 150 minutes of physical activity per week with a weight-loss goal of 7%. Put another way, to prevent one case of diabetes over 3 years, 6.9 patients would have to undergo the lifestyle intervention program, or 13.9 would have to receive metformin. Since impaired glucose tolerance neuropathy may represent the earliest stage of diabetic neuropathy, the neuropathy at this stage may be reversible with lifestyle intervention and improvement of impaired glucose tolerance.
This concept is supported by a 3-year study in 31 people, which showed that lifestyle intervention significantly improved impaired glucose tolerance, reduced the body mass index, and lowered total serum cholesterol levels.30 Changes in these metabolic variables were accompanied by significant improvement of neuropathy as evidenced by significantly increased intraepidermal nerve fiber density, increased foot sweat volume, and decreased neuropathic pain.30
Treatment of other diseases
It has also been reported that treatment of sarcoidosis, autoimmune diseases, and celiac disease improved the symptoms of small fiber neuropathy resulting from these conditions.8,31 Therefore, it is important to identify the cause and treat it to prevent and slow the progression of small fiber neuropathy, and doing so may improve the disease in some mild cases.
Pain management
First-line choices of pain medications are the anticonvulsants gabapentin (Neurontin) and pregabalin (Lyrica), the tricyclic antidepressants amitriptyline (Elavil) and nortriptyline (Aventyl), a 5% lidocaine patch (Lidoderm), and the semisynthetic opioid analgesic tramadol (Ultram). These can be used alone or in combination.
Gabapentin is relatively well tolerated, but drowsiness can occur, especially with high starting doses. We usually start with 300 mg daily and increase it by 300 mg every week up to 1,200 mg three times a day as tolerated. Most patients need 600 to 900 mg three times a day.
Pregabalin is a newer antiepileptic drug, similar to gabapentin but less sedating. It can be started at 75 mg twice a day and gradually increased to 300 mg twice a day as needed. Weight gain and, rarely, swelling of the lower extremities may limit the use of both of these drugs.
Tricyclic antidepressants, such as amitriptyline, nortriptyline, and desipramine (Norpramin), are proven effective in controlling neuropathic pain, although no response with amitriptyline was seen in patients with painful HIV distal sensory neuropathy.34
Lidocaine patch is preferred if the painful area is small. Patients should be instructed to use the patch to cover the painful area 12 hours on and 12 hours off. If it does not provide relief within 1 week, it should be discontinued.
Tramadol is also helpful in treating neuropathic pain. It can be started at 50 mg two to four times a day as needed.
Nonsteroidal anti-inflammatory drugs and selective serotonin reuptake inhibitors are typically less effective than the other drugs mentioned.
Opioids should be reserved for refractory cases, given the potential for addiction, but they are sometimes necessary in patients with disabling pain that does not respond to other drugs.
TENS may be of benefit. The patient controls a pocket-size device that sends electrical signals to leads placed on affected areas.
Alternative therapies for small fiber neuropathy, such as meditation, yoga, and acupuncture, have yet to be studied.
It is also important to explain to patients that the typical course of small fiber neuropathy is relatively benign, as many patients worry about developing weakness and eventually not being able to walk. These concerns and fears can aggravate pain and depression, which can make treatment difficult.
WHAT IS THE PROGNOSIS OF SMALL FIBER NEUROPATHY?
Most patients with small fiber neuropathy experience a slowly progressive course, with symptoms and signs spreading proximally over time.
In one study, only 13% of 124 patients with small fiber neuropathy showed evidence of large-fiber involvement over a 2-year period. 21 None went on to develop Charcot joints, foot ulcers, weakness, or sensory ataxia, as is often seen in patients with long-standing or severe large fiber neuropathy. Neuropathic pain worsened in 30% and resolved spontaneously in 11%.21
Most patients with small fiber neuropathy require chronic pain management. Again, treatment of the underlying cause is important and can improve the prognosis.
We believe that the overall progression of small fiber neuropathy is slow. A longitudinal study with a follow-up longer than 2 years would be useful to confirm this.
TAKE-HOME POINTS
As the population continues to age and as more patients develop diabetes and the metabolic syndrome, the prevalence of small fiber neuropathy will rise. Patients who present to their primary care physicians with painful, burning feet require a thorough diagnostic evaluation, which may include referral for specialized neurodiagnostic testing. Aggressive cause-specific treatment, lifestyle modification, and pain control are key elements of a team approach to managing small fiber neuropathy.
- Gregg EW, Gu Q, Williams D, et al. Prevalence of lower extremity diseases associated with normal glucose levels, impaired fasting glucose, and diabetes among U.S. adults aged 40 or older. Diabetes Res Clin Pract 2007; 77:485–488.
- Lacomis D. Small fiber neuropathy. Muscle Nerve 2002; 26:173–188.
- Smith AG, Singleton JR. Impaired glucose tolerance and neuropathy. Neurologist 2008; 14:23–29.
- Chai J, Herrmann DN, Stanton M, Barbano RL, Logigian EL. Painful small-fiber neuropathy in Sjogren syndrome. Neurology 2005; 65:925–927.
- Goransson LG, Tjensvoll AB, Herigstad A, Mellgren SI, Omdal R. Small-diameter nerve fiber neuropathy in systemic lupus erythematosus. Arch Neurol 2006; 63:401–404.
- Orstavik K, Norheim I, Jorum E. Pain and small-fiber neuropathy in patients with hypothyroidism. Neurology 2006; 67:786–791.
- McArthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. Lancet Neurol 2005; 4:543–555.
- Brannagan TH, Hays AP, Chin SS, et al. Small-fiber neuropathy/neuronopathy associated with celiac disease: skin biopsy findings. Arch Neurol 2005; 62:1574–1578.
- Polydefkis M, Allen RP, Hauer P, Earley CJ, Griffin JW, McArthur JC. Subclinical sensory neuropathy in late-onset restless legs syndrome. Neurology 2000; 55:1115–1121.
- Gorson KC, Herrmann DN, Thiagarajan R, et al. Non-length dependent small fibre neuropathy/ganglionopathy. J Neurol Neurosurg Psychiatry 2008; 79:163–169.
- Singleton JR, Smith AG, Bromberg MB. Increased prevalence of impaired glucose tolerance in patients with painful sensory neuropathy. Diabetes Care 2001; 24:1448–1453.
- Novella SP, Inzucchi SE, Goldstein JM. The frequency of undiagnosed diabetes and impaired glucose tolerance in patients with idiopathic sensory neuropathy. Muscle Nerve 2001; 24:1229–1231.
- Smith AG, Singleton JR. The diagnostic yield of a standardized approach to idiopathic sensory-predominant neuropathy. Arch Intern Med 2004; 164:1021–1025.
- Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003; 60:108–111.
- Gregg EW, Sorlie P, Paulose-Ram R, et al. Prevalence of lower-extremity disease in the US adult population >=40 years of age with and without diabetes: 1999–2000 National Health and Nutrition Examination Survey. Diabetes Care 2004; 27:1591–1597.
- Boulton A. What causes neuropathic pain? J Diabetes Complications 1992; 6:58–63.
- Russell JW, Sullivan KA, Windebank AJ, Herrmann DN, Feldman EL. Neurons undergo apoptosis in animal and cell culture models of diabetes. Neurobiol Dis 1999; 6:347–363.
- Costa LA, Canani LH, Lisboa HR, Tres GS, Gross JL. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in type 2 diabetes. Diabet Med 2004; 21:252–255.
- Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:341–350.
- Smith A, Rose K, Singleton J. Idiopathic neuropathy patients are at high risk for metabolic syndrome. J Neurol Sci 2008; 273:25–28.
- Devigili G, Tugnoli V, Penza P, et al. The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain 2008; 131:1912– 1925.
- Low VA, Sandroni P, Fealey RD, Low PA. Detection of small-fiber neuropathy by sudomotor testing. Muscle Nerve 2006; 34:57–61.
- McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW. Epidermal nerve fiber density: normative reference range and diagnostic efficiency. Arch Neurol 1998; 55:1513–1520.
- Gibbons CH, Griffin JW, Polydefkis M, et al. The utility of skin biopsy for prediction of progression in suspected small fiber neuropathy. Neurology 2006; 66:256–258.
- Polydefkis M, Yiannoutsos CT, Cohen BA, et al. Reduced intraepidermal nerve fiber density in HIV-associated sensory neuropathy. Neurology 2002; 58:115–119.
- Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC. Epidermal nerve fiber density and sural nerve morphometry in peripheral neuropathies. Neurology 1999; 53:1634–1640.
- Zhou L, Kitch DW, Evans SR, et al. Correlates of epidermal nerve fiber densities in HIV-associated distal sensory polyneuropathy. Neurology 2007; 68:2113–2119.
- Novak V, Freimer ML, Kissel JT, et al. Autonomic impairment in painful neuropathy. Neurology 2001; 56:861–868.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393–403.
- Smith AG, Russell J, Feldman EL, et al. Lifestyle intervention for prediabetic neuropathy. Diabetes Care 2006; 29:1294–1299.
- Hoitsma E, Faber CG, van Santen-Hoeufft M, De Vries J, Reulen JP, Drent M. Improvement of small fiber neuropathy in a sarcoidosis patient after treatment with infliximab. Sarcoidosis Vasc Diffuse Lung Dis 2006; 23:73–77.
- Chen H, Lamer TJ, Rho RH, et al. Contemporary management of neuropathic pain for the primary care physician. Mayo Clin Proc 2004; 79:1533–1545.
- Galluzzi KE. Managing neuropathic pain. J Am Osteopath Assoc 2007; 107( suppl 6):ES39–ES48.
- Kieburtz K, Simpson D, Yiannoutsos C, et al. A randomized trial of amitriptyline and mexiletine for painful neuropathy in HIV infection. AIDS Clinical Trial Group 242 Protocol Team. Neurology 1998; 51:1682–1688.
- Gregg EW, Gu Q, Williams D, et al. Prevalence of lower extremity diseases associated with normal glucose levels, impaired fasting glucose, and diabetes among U.S. adults aged 40 or older. Diabetes Res Clin Pract 2007; 77:485–488.
- Lacomis D. Small fiber neuropathy. Muscle Nerve 2002; 26:173–188.
- Smith AG, Singleton JR. Impaired glucose tolerance and neuropathy. Neurologist 2008; 14:23–29.
- Chai J, Herrmann DN, Stanton M, Barbano RL, Logigian EL. Painful small-fiber neuropathy in Sjogren syndrome. Neurology 2005; 65:925–927.
- Goransson LG, Tjensvoll AB, Herigstad A, Mellgren SI, Omdal R. Small-diameter nerve fiber neuropathy in systemic lupus erythematosus. Arch Neurol 2006; 63:401–404.
- Orstavik K, Norheim I, Jorum E. Pain and small-fiber neuropathy in patients with hypothyroidism. Neurology 2006; 67:786–791.
- McArthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. Lancet Neurol 2005; 4:543–555.
- Brannagan TH, Hays AP, Chin SS, et al. Small-fiber neuropathy/neuronopathy associated with celiac disease: skin biopsy findings. Arch Neurol 2005; 62:1574–1578.
- Polydefkis M, Allen RP, Hauer P, Earley CJ, Griffin JW, McArthur JC. Subclinical sensory neuropathy in late-onset restless legs syndrome. Neurology 2000; 55:1115–1121.
- Gorson KC, Herrmann DN, Thiagarajan R, et al. Non-length dependent small fibre neuropathy/ganglionopathy. J Neurol Neurosurg Psychiatry 2008; 79:163–169.
- Singleton JR, Smith AG, Bromberg MB. Increased prevalence of impaired glucose tolerance in patients with painful sensory neuropathy. Diabetes Care 2001; 24:1448–1453.
- Novella SP, Inzucchi SE, Goldstein JM. The frequency of undiagnosed diabetes and impaired glucose tolerance in patients with idiopathic sensory neuropathy. Muscle Nerve 2001; 24:1229–1231.
- Smith AG, Singleton JR. The diagnostic yield of a standardized approach to idiopathic sensory-predominant neuropathy. Arch Intern Med 2004; 164:1021–1025.
- Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003; 60:108–111.
- Gregg EW, Sorlie P, Paulose-Ram R, et al. Prevalence of lower-extremity disease in the US adult population >=40 years of age with and without diabetes: 1999–2000 National Health and Nutrition Examination Survey. Diabetes Care 2004; 27:1591–1597.
- Boulton A. What causes neuropathic pain? J Diabetes Complications 1992; 6:58–63.
- Russell JW, Sullivan KA, Windebank AJ, Herrmann DN, Feldman EL. Neurons undergo apoptosis in animal and cell culture models of diabetes. Neurobiol Dis 1999; 6:347–363.
- Costa LA, Canani LH, Lisboa HR, Tres GS, Gross JL. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in type 2 diabetes. Diabet Med 2004; 21:252–255.
- Tesfaye S, Chaturvedi N, Eaton SE, et al. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352:341–350.
- Smith A, Rose K, Singleton J. Idiopathic neuropathy patients are at high risk for metabolic syndrome. J Neurol Sci 2008; 273:25–28.
- Devigili G, Tugnoli V, Penza P, et al. The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain 2008; 131:1912– 1925.
- Low VA, Sandroni P, Fealey RD, Low PA. Detection of small-fiber neuropathy by sudomotor testing. Muscle Nerve 2006; 34:57–61.
- McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW. Epidermal nerve fiber density: normative reference range and diagnostic efficiency. Arch Neurol 1998; 55:1513–1520.
- Gibbons CH, Griffin JW, Polydefkis M, et al. The utility of skin biopsy for prediction of progression in suspected small fiber neuropathy. Neurology 2006; 66:256–258.
- Polydefkis M, Yiannoutsos CT, Cohen BA, et al. Reduced intraepidermal nerve fiber density in HIV-associated sensory neuropathy. Neurology 2002; 58:115–119.
- Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC. Epidermal nerve fiber density and sural nerve morphometry in peripheral neuropathies. Neurology 1999; 53:1634–1640.
- Zhou L, Kitch DW, Evans SR, et al. Correlates of epidermal nerve fiber densities in HIV-associated distal sensory polyneuropathy. Neurology 2007; 68:2113–2119.
- Novak V, Freimer ML, Kissel JT, et al. Autonomic impairment in painful neuropathy. Neurology 2001; 56:861–868.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393–403.
- Smith AG, Russell J, Feldman EL, et al. Lifestyle intervention for prediabetic neuropathy. Diabetes Care 2006; 29:1294–1299.
- Hoitsma E, Faber CG, van Santen-Hoeufft M, De Vries J, Reulen JP, Drent M. Improvement of small fiber neuropathy in a sarcoidosis patient after treatment with infliximab. Sarcoidosis Vasc Diffuse Lung Dis 2006; 23:73–77.
- Chen H, Lamer TJ, Rho RH, et al. Contemporary management of neuropathic pain for the primary care physician. Mayo Clin Proc 2004; 79:1533–1545.
- Galluzzi KE. Managing neuropathic pain. J Am Osteopath Assoc 2007; 107( suppl 6):ES39–ES48.
- Kieburtz K, Simpson D, Yiannoutsos C, et al. A randomized trial of amitriptyline and mexiletine for painful neuropathy in HIV infection. AIDS Clinical Trial Group 242 Protocol Team. Neurology 1998; 51:1682–1688.
KEY POINTS
- Symptoms of small fiber neuropathy typically start with burning feet and numb toes.
- Causes and associated conditions can be found in over 50% of cases. These include glucose dysmetabolism, connective tissue diseases, sarcoidosis, dysthyroidism, vitamin B12 deficiency, paraproteinemia, human immunodeficiency virus infection, celiac disease, neurotoxic drug exposure, and paraneoplastic syndrome.
- Findings on routine nerve conduction studies and electromyography are typically normal in this disease.
- Management includes aggressively identifying and treating the underlying cause, advising lifestyle modifications, and alleviating pain.
Advance care planning: Beyond the living will
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
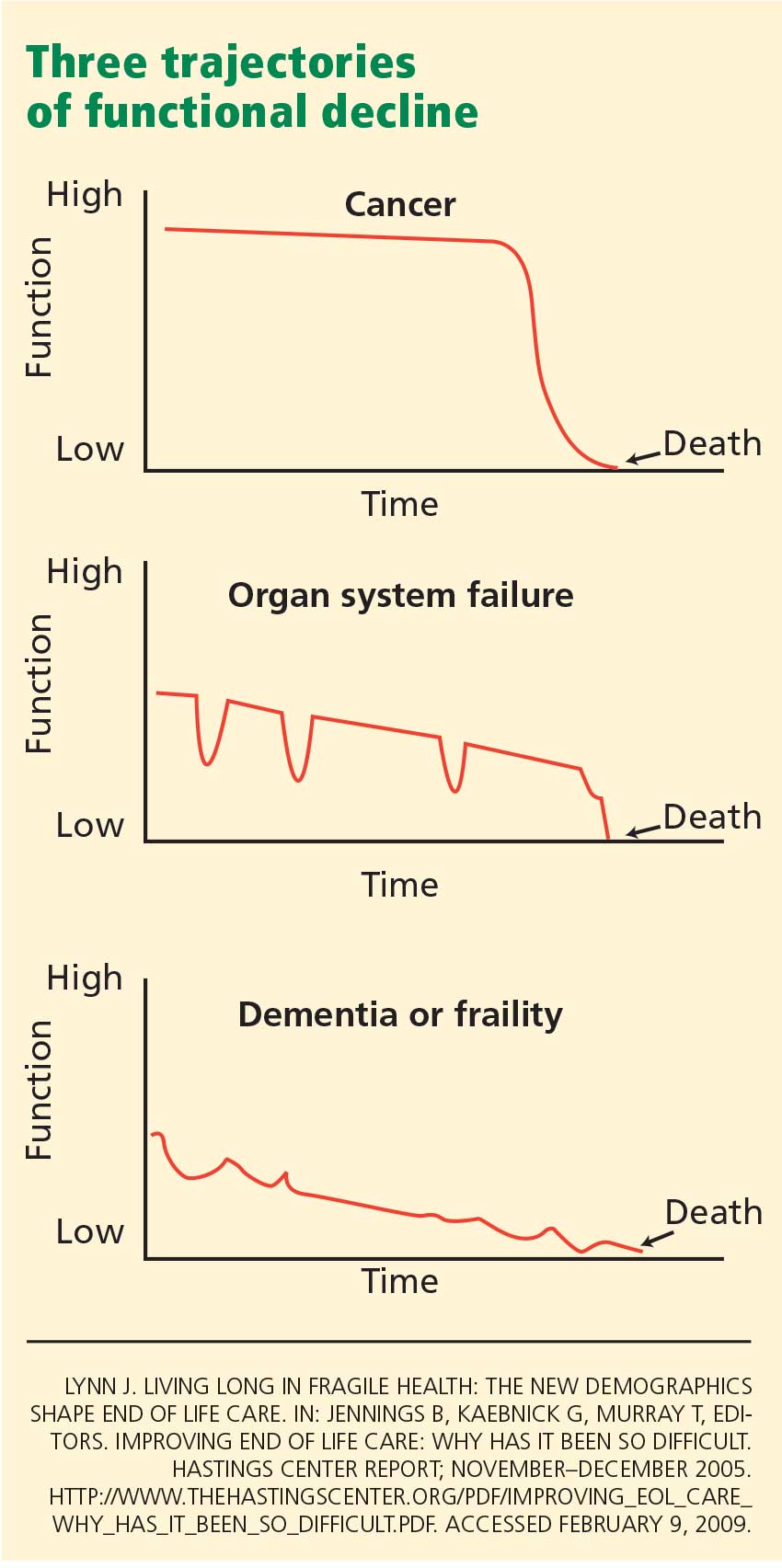
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
KEY POINTS
- In the ambulatory setting, start by assessing the patient’s prognosis and his or her receptiveness to advance care planning.
- For a patient in declining health who is willing to participate in the care planning process, it may be useful to take a full values history and to review the goals of care.
- For a patient with advanced disease who is unable or unwilling to participate in advance care planning, a limited approach may be appropriate, ie, identifying a surrogate decision-maker and ascertaining how much flexibility the surrogate should have with health care decisions.
- Whatever the patient’s life expectancy and level of receptivity, brief, episodic discussions are more useful than a one-time description of available written advance directives.
Advance care planning is an art, not an algorithm
The article by Drs. Messinger-Rapport et al in this issue of the Cleveland Clinic Journal of Medicine makes several assertions about advance care planning with which I disagree. As a practicing oncologist and hospice medical director in a community setting for almost 20 years, I believe the authors’ attempt to reduce a complex physician-patient interaction to a practice algorithm oversimplifies the issues.
INTUITION, EXPERIENCE, AND TRAINING PLAY A VITAL ROLE
I agree with the authors that advance care planning is an oft-mentioned but underperformed function of being a physician in current American society. Our nation has become a people who deny physical vulnerability, frailty, and death. This area is not well taught in our medical schools and residency training programs.
However, the algorithms in the paper do not effectively address the timing and process of advance care planning. It is clearly not effective to have an end-of-life discussion at the bedside of a critically ill patient about to be intubated. It also seems futile to have a superficial discussion with patients about advance care planning at a time when they are healthy and in the setting of a routine and brief office visit. In this healthy population, the episodic discussions recommended by the authors could become background noise and could seem irrelevant to a patient. Physicians are already overburdened with responsibilities. Re-educating society that lives are not infinite is a social issue that needs to begin early in our lives.
In any setting, a social history, properly taken, should identify family structure, responsible next of kin, and family issues of discord that could affect treatment decisions and patient care. This is all that is needed as a minimal discussion about advance care planning.
Once patients develop significant illness, speaking to them about advance care planning becomes more relevant to their lives. As patients struggle with their illnesses and physical decline, the opportunity for further discussion grows and the impact of these interventions becomes greater. The energy and time it takes to have such discussions are better spent in these settings.
Discussing long-term planning with a patient is where intuition, experience, and training play a vital role. The balance between the pragmatic need for advance care planning and the need for allowing the patient to have hope of wellness is difficult to achieve and different for every patient, every family, and every care situation. It is for this reason that I find the flowcharts outlined in the paper difficult to follow and not very useful for the care of patients. Given the diversity of patients for whom we care, it seems impossible to me to condense the subject down to a care-flow matrix. This is an area in which the art of patient care and the art of being a physician come fully into play and cannot be replaced by an algorithm. Individual and small-group training with mentors, at all levels of medical education, would allow a physician to grow in comfort and skill in dealing with advance care planning.
LIVING WILLS CAN BE USEFUL
Another point on which I disagree with Dr. Messinger-Rapport et al is their assessment of the utility of the living will. They state that a living will applies only to patients who are terminally ill or in a persistent vegetative state. However, I find that it can also supply important information at all stages of illness. While it may lie “dormant” in a legal sense, it can give important information for a family by providing a window into the patient’s state of mind as it relates to the patient’s willingness to limit care in certain settings. Once a patient is able to articulate situations that warrant limiting care, a surrogate decision-maker (or the patient) can try to broaden those limits. It is up to the physician to articulate prognosis so the patient and family can decide how much they are willing to do to maintain that limited level of function. Any treatment can be declined at any time during a patient’s life or illness.
The living will also provides a framework in which to discuss end-of-life issues with a patient. It can open the discussion about current quality of life as perceived by the patient and what level of medical treatment the patient is willing to pursue. As the authors note in their article, those desires are fluid and can change over time. This does not render the living will useless. It shows that the living will needs to be adapted over time to suit the patient’s current situation.
The authors describe a patient with Alzheimer disease for whom a percutaneous endoscopic gastrostomy tube was recommended by a physician but declined by his wife. They assert that a living will does not offer guidance in this situation, since the patient was not, strictly speaking, terminally ill. I disagree. Medical care can delay death for years. If the patient’s quality of life is poor, that delay may violate the implied wishes of the patient and should be discussed. Before he became severely demented, the patient may not have wanted to have his life prolonged if the end result was a continued decline in his already compromised quality of life. The family should have been given that option to consider.
RE-EDUCATING PEOPLE ABOUT LIFE, ILLNESS, AND DEATH
Advance care planning is an essential component of being a physician and taking care of patients. A broad movement needs to be undertaken to re-educate people about the realities of life, illness, and death. The training of our physicians about advance care planning should begin early and should be continued throughout their medical education and careers. One-on-one or small-group mentoring would be an ideal method of training. The attempt to develop an algorithm to guide those discussions tries to simplify a process that is extraordinarily complex. Each situation is different and requires well-developed skills and practiced and mentored intuition. Experience and the art of being a physician cannot be reduced to a “model approach” or a flowchart.
The article by Drs. Messinger-Rapport et al in this issue of the Cleveland Clinic Journal of Medicine makes several assertions about advance care planning with which I disagree. As a practicing oncologist and hospice medical director in a community setting for almost 20 years, I believe the authors’ attempt to reduce a complex physician-patient interaction to a practice algorithm oversimplifies the issues.
INTUITION, EXPERIENCE, AND TRAINING PLAY A VITAL ROLE
I agree with the authors that advance care planning is an oft-mentioned but underperformed function of being a physician in current American society. Our nation has become a people who deny physical vulnerability, frailty, and death. This area is not well taught in our medical schools and residency training programs.
However, the algorithms in the paper do not effectively address the timing and process of advance care planning. It is clearly not effective to have an end-of-life discussion at the bedside of a critically ill patient about to be intubated. It also seems futile to have a superficial discussion with patients about advance care planning at a time when they are healthy and in the setting of a routine and brief office visit. In this healthy population, the episodic discussions recommended by the authors could become background noise and could seem irrelevant to a patient. Physicians are already overburdened with responsibilities. Re-educating society that lives are not infinite is a social issue that needs to begin early in our lives.
In any setting, a social history, properly taken, should identify family structure, responsible next of kin, and family issues of discord that could affect treatment decisions and patient care. This is all that is needed as a minimal discussion about advance care planning.
Once patients develop significant illness, speaking to them about advance care planning becomes more relevant to their lives. As patients struggle with their illnesses and physical decline, the opportunity for further discussion grows and the impact of these interventions becomes greater. The energy and time it takes to have such discussions are better spent in these settings.
Discussing long-term planning with a patient is where intuition, experience, and training play a vital role. The balance between the pragmatic need for advance care planning and the need for allowing the patient to have hope of wellness is difficult to achieve and different for every patient, every family, and every care situation. It is for this reason that I find the flowcharts outlined in the paper difficult to follow and not very useful for the care of patients. Given the diversity of patients for whom we care, it seems impossible to me to condense the subject down to a care-flow matrix. This is an area in which the art of patient care and the art of being a physician come fully into play and cannot be replaced by an algorithm. Individual and small-group training with mentors, at all levels of medical education, would allow a physician to grow in comfort and skill in dealing with advance care planning.
LIVING WILLS CAN BE USEFUL
Another point on which I disagree with Dr. Messinger-Rapport et al is their assessment of the utility of the living will. They state that a living will applies only to patients who are terminally ill or in a persistent vegetative state. However, I find that it can also supply important information at all stages of illness. While it may lie “dormant” in a legal sense, it can give important information for a family by providing a window into the patient’s state of mind as it relates to the patient’s willingness to limit care in certain settings. Once a patient is able to articulate situations that warrant limiting care, a surrogate decision-maker (or the patient) can try to broaden those limits. It is up to the physician to articulate prognosis so the patient and family can decide how much they are willing to do to maintain that limited level of function. Any treatment can be declined at any time during a patient’s life or illness.
The living will also provides a framework in which to discuss end-of-life issues with a patient. It can open the discussion about current quality of life as perceived by the patient and what level of medical treatment the patient is willing to pursue. As the authors note in their article, those desires are fluid and can change over time. This does not render the living will useless. It shows that the living will needs to be adapted over time to suit the patient’s current situation.
The authors describe a patient with Alzheimer disease for whom a percutaneous endoscopic gastrostomy tube was recommended by a physician but declined by his wife. They assert that a living will does not offer guidance in this situation, since the patient was not, strictly speaking, terminally ill. I disagree. Medical care can delay death for years. If the patient’s quality of life is poor, that delay may violate the implied wishes of the patient and should be discussed. Before he became severely demented, the patient may not have wanted to have his life prolonged if the end result was a continued decline in his already compromised quality of life. The family should have been given that option to consider.
RE-EDUCATING PEOPLE ABOUT LIFE, ILLNESS, AND DEATH
Advance care planning is an essential component of being a physician and taking care of patients. A broad movement needs to be undertaken to re-educate people about the realities of life, illness, and death. The training of our physicians about advance care planning should begin early and should be continued throughout their medical education and careers. One-on-one or small-group mentoring would be an ideal method of training. The attempt to develop an algorithm to guide those discussions tries to simplify a process that is extraordinarily complex. Each situation is different and requires well-developed skills and practiced and mentored intuition. Experience and the art of being a physician cannot be reduced to a “model approach” or a flowchart.
The article by Drs. Messinger-Rapport et al in this issue of the Cleveland Clinic Journal of Medicine makes several assertions about advance care planning with which I disagree. As a practicing oncologist and hospice medical director in a community setting for almost 20 years, I believe the authors’ attempt to reduce a complex physician-patient interaction to a practice algorithm oversimplifies the issues.
INTUITION, EXPERIENCE, AND TRAINING PLAY A VITAL ROLE
I agree with the authors that advance care planning is an oft-mentioned but underperformed function of being a physician in current American society. Our nation has become a people who deny physical vulnerability, frailty, and death. This area is not well taught in our medical schools and residency training programs.
However, the algorithms in the paper do not effectively address the timing and process of advance care planning. It is clearly not effective to have an end-of-life discussion at the bedside of a critically ill patient about to be intubated. It also seems futile to have a superficial discussion with patients about advance care planning at a time when they are healthy and in the setting of a routine and brief office visit. In this healthy population, the episodic discussions recommended by the authors could become background noise and could seem irrelevant to a patient. Physicians are already overburdened with responsibilities. Re-educating society that lives are not infinite is a social issue that needs to begin early in our lives.
In any setting, a social history, properly taken, should identify family structure, responsible next of kin, and family issues of discord that could affect treatment decisions and patient care. This is all that is needed as a minimal discussion about advance care planning.
Once patients develop significant illness, speaking to them about advance care planning becomes more relevant to their lives. As patients struggle with their illnesses and physical decline, the opportunity for further discussion grows and the impact of these interventions becomes greater. The energy and time it takes to have such discussions are better spent in these settings.
Discussing long-term planning with a patient is where intuition, experience, and training play a vital role. The balance between the pragmatic need for advance care planning and the need for allowing the patient to have hope of wellness is difficult to achieve and different for every patient, every family, and every care situation. It is for this reason that I find the flowcharts outlined in the paper difficult to follow and not very useful for the care of patients. Given the diversity of patients for whom we care, it seems impossible to me to condense the subject down to a care-flow matrix. This is an area in which the art of patient care and the art of being a physician come fully into play and cannot be replaced by an algorithm. Individual and small-group training with mentors, at all levels of medical education, would allow a physician to grow in comfort and skill in dealing with advance care planning.
LIVING WILLS CAN BE USEFUL
Another point on which I disagree with Dr. Messinger-Rapport et al is their assessment of the utility of the living will. They state that a living will applies only to patients who are terminally ill or in a persistent vegetative state. However, I find that it can also supply important information at all stages of illness. While it may lie “dormant” in a legal sense, it can give important information for a family by providing a window into the patient’s state of mind as it relates to the patient’s willingness to limit care in certain settings. Once a patient is able to articulate situations that warrant limiting care, a surrogate decision-maker (or the patient) can try to broaden those limits. It is up to the physician to articulate prognosis so the patient and family can decide how much they are willing to do to maintain that limited level of function. Any treatment can be declined at any time during a patient’s life or illness.
The living will also provides a framework in which to discuss end-of-life issues with a patient. It can open the discussion about current quality of life as perceived by the patient and what level of medical treatment the patient is willing to pursue. As the authors note in their article, those desires are fluid and can change over time. This does not render the living will useless. It shows that the living will needs to be adapted over time to suit the patient’s current situation.
The authors describe a patient with Alzheimer disease for whom a percutaneous endoscopic gastrostomy tube was recommended by a physician but declined by his wife. They assert that a living will does not offer guidance in this situation, since the patient was not, strictly speaking, terminally ill. I disagree. Medical care can delay death for years. If the patient’s quality of life is poor, that delay may violate the implied wishes of the patient and should be discussed. Before he became severely demented, the patient may not have wanted to have his life prolonged if the end result was a continued decline in his already compromised quality of life. The family should have been given that option to consider.
RE-EDUCATING PEOPLE ABOUT LIFE, ILLNESS, AND DEATH
Advance care planning is an essential component of being a physician and taking care of patients. A broad movement needs to be undertaken to re-educate people about the realities of life, illness, and death. The training of our physicians about advance care planning should begin early and should be continued throughout their medical education and careers. One-on-one or small-group mentoring would be an ideal method of training. The attempt to develop an algorithm to guide those discussions tries to simplify a process that is extraordinarily complex. Each situation is different and requires well-developed skills and practiced and mentored intuition. Experience and the art of being a physician cannot be reduced to a “model approach” or a flowchart.
VA Reports More Infections With Possible Links to Endoscopic Errors
Aquatic Antagonists: Indirect Nematocyst Envenomation and Acute Allergic Contact Dermatitis Due to Nudibranchs
Vesiculopustular Eruption Associated With Transient Myeloproliferative Disorder
Smoking allowed: Is hospital policy a liability risk?
Dear Dr. Mossman:
I work at a state mental hospital where all patients are adults who are court-committed, and at least 75% of them smoke. The hospital allows smoking in part of the only outdoor area where patients—smokers and nonsmokers—may go while in our most restrictive treatment phase. Patients come to us after spending at least 2 weeks in nonsmoking facilities where smokers receive nicotine replacement therapy. If patients want to smoke but have no money, in the past our hospital provided “unit cigarettes.”
In my state, a court commitment means the patient lacks the capacity to make decisions about psychiatric care. Of course nicotine is a psychoactive drug. If a patient starts smoking while in our care, would the hospital be liable for health-related expenses the patient may later incur?—Submitted by “Dr. A”
Speaking as one colleague to another about malpractice liability, letting psychiatric patients smoke is not breaching the standard of care toward smoking patients. But you care for nonsmoking patients as well, and other types of liability besides malpractice exist.
Doctors have moral duties for lots of things we can’t be sued for. Dr. A is right to be concerned. To explain, we’ll look at:
- changes in attitudes about smoking
- the link between smoking and mental illness
- smoking bans in psychiatric facilities
- malpractice potential
- other issues Dr. A’s hospital should consider, such as offering patients assistance with smoking cessation.
Changing attitudes about smoking
Thirty years ago, doctors smoked during medical meetings, and smoking on airplanes and in public was commonplace. I worked at an adolescent inpatient unit, and line staff carried lighters. We thought lighting kids’ cigarettes was a legitimate way to establish rapport. Times and attitudes have changed. No hospital condones smoking these days, let alone smoking by minor patients. Since the Surgeon General first declared in 1964 that smoking was hazardous, U.S. adult smoking rates have dropped from 42% to under 20%.1
In the early 1990s, California issued the first statewide ban on smoking in work-places, including bars and restaurants.2 Nearly 3,000 state or local jurisdictions require workplaces and/or commercial establishments to be smoke-free.3 Recently, the legislature in Virginia—a major tobacco-producing state—voted to prohibit smoking in restaurants,4 and many other state governments are considering smoking bans. Smoking bans are intended to protect nonsmokers—especially children—from risks of secondhand smoke,5 but they also discourage individuals from taking up the habit6 and encourage smokers to quit.7
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Smoking and mental illness
Persons with serious psychiatric disorders have smoking rates 2 to 3 times higher than those of the general population.8,9 As Dr. A notes, nicotine is a psychoactive drug. Smoking may be a genuine—although ultimately unhealthy—form of self-medication and may have positive psychological effects, such as antidepressant activity for many mentally ill persons.10,11 The Joint Commission on Accreditation of Healthcare Organizations banned smoking in hospitals in 1992 but made an exception for psychiatric units. Out of sympathy for patients and concern about what could happen when they are deprived of a substance they intensely crave, many psychiatric wards continue to accommodate smokers.12
What some institutions have done
An increasing number of psychiatric facilities have instituted or are considering bans on smoking.13 The first psychiatric smoking bans were implemented despite fears that patient violence would increase and opposition from hospital employees—a group that often includes smokers. Experience shows that although not all smoking bans are successful or problem-free,14 they usually cause fewer problems than anticipated. We also know what factors help make smoke-free programs successful (Table).15
Table
Smoke-free plans that work: How to clear the air
| • Take time—more than 6 months—to plan smoke-free initiatives |
| • Supply patient and staff smokers with nicotine replacement therapy |
| • Present clear, consistent, visible leadership |
| • Encourage cohesive teamwork |
| • Provide extensive education and training for staff |
| • Reduce staff smoking rates |
| • Offer programs and education to promote smoking cessation among staff members |
| • Enforce nonsmoking policies |
| Source: Adapted from reference 15 |
Aggression, seclusion, discharges against medical advice, and “prn” medication use do not increase after smoking bans,5,16,17 and many patients experience health benefits.18 After discharge, however, most patients resume tobacco use.11,19,20
Smoking bans have been opposed on grounds that they abridge psychiatric patients’ rights and are unduly coercive.21,22 In the United States and United Kingdom, however, legal actions to block smoking bans have not succeeded, and courts have not recognized a fundamental “right to smoke.”23-25
Is allowing smoking malpractice?
Now that many psychiatric facilities have ended smoking, clinicians may worry—as does Dr. A—that we could incur malpractice liability if we let inpatients smoke. One of my University of Cincinnati law students, Amanda Smith, and I researched this topic and found no case report that said letting psychiatric inpatients smoke violated the standard of care.
This makes sense, because in the malpractice context, a practitioner is judged by what prudent, similarly situated physicians with similar training would do in similar circumstances. Many psychiatric facilities still permit smoking, so letting patients smoke does not breach the standard of care, even if it seems negligent.26
The ill effects of smoking accrue over years, not weeks or months. Almost all patients who smoke in hospitals also have smoked before hospitalization, and most smokers who are barred from smoking while inpatients resume soon after discharge. To succeed, a malpractice lawsuit must show that the defendant’s actions caused damages. A jury might find it hard to conclude that a permissive hospital smoking policy was the primary cause of a long-term smoker’s health problems.
4 other concerns
Nonsmokers’ rights. Arrangements at Dr. A’s hospital expose nonsmokers to secondhand cigarette smoke, which raises the possibility of legal action by nonsmokers. In 1993, the U.S. Supreme Court held that a prison inmate’s heavy exposure to secondhand smoke violated the Eighth Amendment ban on cruel and unusual punishment.27 Involuntary hospitalization is not punishment, but suits such as this might be brought on other grounds, such as violation of patients’ civil rights.28
Competence. In some states, civil commitment requires a finding that the respondent is not competent to make treatment decisions. Can persons who are not competent to make treatment decisions make good decisions about whether to smoke? Shouldn’t the hospital deal with patients’ nicotine dependence more therapeutically—and paternalistically—by providing nicotine replacement and encouraging smoking cessation? Shouldn’t the hospital also discourage patients who don’t smoke from starting?
Protecting patients. Dr. A’s hospital provides cigarettes to patients. Though compassion may be the motive, is the hospital failing to protect its incompetent patients and abetting their self-injurious behavior?
Helping smokers quit. Does the hospital offer treatment to help smokers quit? Although the problems that lead to civil commitment are immediate and serious, addressing long-term health issues is consistent with treating acute psychiatric crises. Many hospitals that permit smoking also encourage participation in smoking-cessation programs. Having these available to patients might make claims that the hospital failed in its duties to care for patients less plausible.
Related resources
- Maryland Hospital Association. Smoke-free hospital campus tool-kit. www.mdhospitals.org/mha/Community_Health_Resources/Smoke_Free_Hospital_Campuses.shtml.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
1. Centers for Disease Control and Prevention. Cigarette smoking among adults—United States, 2007. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a2.htm. Accessed April 10, 2009.
2. Calif. Labor Code § 6404.5.
3. American Nonsmokers’ Rights Foundation. Overview list–how many smokefree laws? Available at: http://www.no-smoke.org/pdf/mediaordlist.pdf. Accessed February 11, 2009.
4. Kumar A. Va. House approves ban on smoking: most restaurants would be affected. Washington Post. February 10, 2009: Page A01.
5. U.S. Department of Health and Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services; 2006.
6. Siegel M, Albers AB, Cheng DM, et al. Local restaurant smoking regulations and the adolescent smoking initiation process: results of a multilevel contextual analysis among Massachusetts youth. Arch Pediatr Adolesc Med. 2008;162(5):477-483.
7. Longo DR, Feldman MM, Kruse RL, et al. Implementing smoking bans in American hospitals: results of a national survey. Tob Control. 1998;7(1):47-55.
8. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
9. Morris CD, Giese AA, Turnbull JJ, et al. Predictors of tobacco use among persons with mental illnesses in a statewide population. Psychiatr Serv. 2006;57(7):1035-1038.
10. Cattapan-Ludewig K, Ludewig S, Jaquenoud Sirot E, et al. Why do schizophrenic patients smoke? Nervenarzt. 2005;76(3):287-294.
11. El-Guebaly N, Cathcart J, Currie S, et al. Public health and therapeutic aspects of smoking bans in mental health and addiction settings. Psychiatr Serv. 2002;53(12):1617-1622.
12. Williams JM. Eliminating tobacco use in mental health facilities: patients’ rights, public health, and policy issues. JAMA. 2008;299(5):571-573.
13. Parks J, Jewell P, eds,, Burke M. Technical report on smoking policy and treatment in state operated psychiatric facilities. Alexandria, VA: National Association of State Mental Health Program Directors Medical Directors Council; 2006. Technical Report 12.
14. Campion J, Lawn S, Brownlie A, et al. Implementing smoke-free policies in mental health inpatient units: learning from unsuccessful experience. Australas Psychiatry. 2008;16(2):92-97.
15. Lawn S, Campion J. Smoke-free initiatives in psychiatric inpatient units: a national survey of Australian sites. Adelaide, Australia: Flinders University; 2008.
16. Lawn S, Pols R. Smoking bans in psychiatric inpatient settings? A review of the research. Aust N Z J Psychiatry. 2005;39(10):866-885.
17. Hempel AG, Kownacki R, Malin DH, et al. Effect of a total smoking ban in a maximum security psychiatric hospital. Behav Sci Law. 2002;20(5):507-522.
18. Harris GT, Parle D, Gagné J. Effects of a tobacco ban on long-term psychiatric patients. J Behav Health Serv Res. 2007;34(1):43-55.
19. Shmueli D, Fletcher L, Hall SE, et al. Changes in psychiatric patients’ thoughts about quitting smoking during a smoke-free hospitalization. Nicotine Tob Res. 2008;10(5):875-881.
20. Prochaska JJ, Fletcher L, Hall SE, et al. Return to smoking following a smoke-free psychiatric hospitalization. Am J Addict. 2006;15(1):15-22.
21. Marcus K. Smoking bans in long-term inpatient settings: a dilemma. Psychiatr Serv. 2008;59(3):330.-
22. Remal G. Hospital preparing to kick habit; A lawyer for smokers at Riverview Psychiatric Center sees little chance of reversing a smoking ban. Portland (Maine) Press Herald. December 29, 2006.
23. Arbogast v Peterson, 631 N.E.2d 673 (Ohio App 1993).
24. R (G) v Nottinghamshire Healthcare NHS Trust and others (2008).
25. Thiel v Nelson, 422 F.Supp. 2d 1024 (WD Wis 2006).
26. New Jersey Department of Health Services. Testimony of Kevin Martone, Assistant Commissioner, Department of Human Services, Division of Mental Health Services, New Jersey Assembly Human Services Committee, A-2308 Smoking Cessation, March 6, 2008. Trenton, NJ: New Jersey Department of Health Services. Available at: http://www.state.nj.us/humanservices/dmhs/Assembly_smoking_testimony_03_2008.pdf. Accessed February 14, 2009.
27. Helling v McKinney, 509 U.S. 25 (1993).
28. Appelbaum PS. Do hospitalized patients have a right to smoke? Psychiatr Serv. 1995;46(7):653-654, 660.

Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine.
Dear Dr. Mossman:
I work at a state mental hospital where all patients are adults who are court-committed, and at least 75% of them smoke. The hospital allows smoking in part of the only outdoor area where patients—smokers and nonsmokers—may go while in our most restrictive treatment phase. Patients come to us after spending at least 2 weeks in nonsmoking facilities where smokers receive nicotine replacement therapy. If patients want to smoke but have no money, in the past our hospital provided “unit cigarettes.”
In my state, a court commitment means the patient lacks the capacity to make decisions about psychiatric care. Of course nicotine is a psychoactive drug. If a patient starts smoking while in our care, would the hospital be liable for health-related expenses the patient may later incur?—Submitted by “Dr. A”
Speaking as one colleague to another about malpractice liability, letting psychiatric patients smoke is not breaching the standard of care toward smoking patients. But you care for nonsmoking patients as well, and other types of liability besides malpractice exist.
Doctors have moral duties for lots of things we can’t be sued for. Dr. A is right to be concerned. To explain, we’ll look at:
- changes in attitudes about smoking
- the link between smoking and mental illness
- smoking bans in psychiatric facilities
- malpractice potential
- other issues Dr. A’s hospital should consider, such as offering patients assistance with smoking cessation.
Changing attitudes about smoking
Thirty years ago, doctors smoked during medical meetings, and smoking on airplanes and in public was commonplace. I worked at an adolescent inpatient unit, and line staff carried lighters. We thought lighting kids’ cigarettes was a legitimate way to establish rapport. Times and attitudes have changed. No hospital condones smoking these days, let alone smoking by minor patients. Since the Surgeon General first declared in 1964 that smoking was hazardous, U.S. adult smoking rates have dropped from 42% to under 20%.1
In the early 1990s, California issued the first statewide ban on smoking in work-places, including bars and restaurants.2 Nearly 3,000 state or local jurisdictions require workplaces and/or commercial establishments to be smoke-free.3 Recently, the legislature in Virginia—a major tobacco-producing state—voted to prohibit smoking in restaurants,4 and many other state governments are considering smoking bans. Smoking bans are intended to protect nonsmokers—especially children—from risks of secondhand smoke,5 but they also discourage individuals from taking up the habit6 and encourage smokers to quit.7
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Smoking and mental illness
Persons with serious psychiatric disorders have smoking rates 2 to 3 times higher than those of the general population.8,9 As Dr. A notes, nicotine is a psychoactive drug. Smoking may be a genuine—although ultimately unhealthy—form of self-medication and may have positive psychological effects, such as antidepressant activity for many mentally ill persons.10,11 The Joint Commission on Accreditation of Healthcare Organizations banned smoking in hospitals in 1992 but made an exception for psychiatric units. Out of sympathy for patients and concern about what could happen when they are deprived of a substance they intensely crave, many psychiatric wards continue to accommodate smokers.12
What some institutions have done
An increasing number of psychiatric facilities have instituted or are considering bans on smoking.13 The first psychiatric smoking bans were implemented despite fears that patient violence would increase and opposition from hospital employees—a group that often includes smokers. Experience shows that although not all smoking bans are successful or problem-free,14 they usually cause fewer problems than anticipated. We also know what factors help make smoke-free programs successful (Table).15
Table
Smoke-free plans that work: How to clear the air
| • Take time—more than 6 months—to plan smoke-free initiatives |
| • Supply patient and staff smokers with nicotine replacement therapy |
| • Present clear, consistent, visible leadership |
| • Encourage cohesive teamwork |
| • Provide extensive education and training for staff |
| • Reduce staff smoking rates |
| • Offer programs and education to promote smoking cessation among staff members |
| • Enforce nonsmoking policies |
| Source: Adapted from reference 15 |
Aggression, seclusion, discharges against medical advice, and “prn” medication use do not increase after smoking bans,5,16,17 and many patients experience health benefits.18 After discharge, however, most patients resume tobacco use.11,19,20
Smoking bans have been opposed on grounds that they abridge psychiatric patients’ rights and are unduly coercive.21,22 In the United States and United Kingdom, however, legal actions to block smoking bans have not succeeded, and courts have not recognized a fundamental “right to smoke.”23-25
Is allowing smoking malpractice?
Now that many psychiatric facilities have ended smoking, clinicians may worry—as does Dr. A—that we could incur malpractice liability if we let inpatients smoke. One of my University of Cincinnati law students, Amanda Smith, and I researched this topic and found no case report that said letting psychiatric inpatients smoke violated the standard of care.
This makes sense, because in the malpractice context, a practitioner is judged by what prudent, similarly situated physicians with similar training would do in similar circumstances. Many psychiatric facilities still permit smoking, so letting patients smoke does not breach the standard of care, even if it seems negligent.26
The ill effects of smoking accrue over years, not weeks or months. Almost all patients who smoke in hospitals also have smoked before hospitalization, and most smokers who are barred from smoking while inpatients resume soon after discharge. To succeed, a malpractice lawsuit must show that the defendant’s actions caused damages. A jury might find it hard to conclude that a permissive hospital smoking policy was the primary cause of a long-term smoker’s health problems.
4 other concerns
Nonsmokers’ rights. Arrangements at Dr. A’s hospital expose nonsmokers to secondhand cigarette smoke, which raises the possibility of legal action by nonsmokers. In 1993, the U.S. Supreme Court held that a prison inmate’s heavy exposure to secondhand smoke violated the Eighth Amendment ban on cruel and unusual punishment.27 Involuntary hospitalization is not punishment, but suits such as this might be brought on other grounds, such as violation of patients’ civil rights.28
Competence. In some states, civil commitment requires a finding that the respondent is not competent to make treatment decisions. Can persons who are not competent to make treatment decisions make good decisions about whether to smoke? Shouldn’t the hospital deal with patients’ nicotine dependence more therapeutically—and paternalistically—by providing nicotine replacement and encouraging smoking cessation? Shouldn’t the hospital also discourage patients who don’t smoke from starting?
Protecting patients. Dr. A’s hospital provides cigarettes to patients. Though compassion may be the motive, is the hospital failing to protect its incompetent patients and abetting their self-injurious behavior?
Helping smokers quit. Does the hospital offer treatment to help smokers quit? Although the problems that lead to civil commitment are immediate and serious, addressing long-term health issues is consistent with treating acute psychiatric crises. Many hospitals that permit smoking also encourage participation in smoking-cessation programs. Having these available to patients might make claims that the hospital failed in its duties to care for patients less plausible.
Related resources
- Maryland Hospital Association. Smoke-free hospital campus tool-kit. www.mdhospitals.org/mha/Community_Health_Resources/Smoke_Free_Hospital_Campuses.shtml.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Dear Dr. Mossman:
I work at a state mental hospital where all patients are adults who are court-committed, and at least 75% of them smoke. The hospital allows smoking in part of the only outdoor area where patients—smokers and nonsmokers—may go while in our most restrictive treatment phase. Patients come to us after spending at least 2 weeks in nonsmoking facilities where smokers receive nicotine replacement therapy. If patients want to smoke but have no money, in the past our hospital provided “unit cigarettes.”
In my state, a court commitment means the patient lacks the capacity to make decisions about psychiatric care. Of course nicotine is a psychoactive drug. If a patient starts smoking while in our care, would the hospital be liable for health-related expenses the patient may later incur?—Submitted by “Dr. A”
Speaking as one colleague to another about malpractice liability, letting psychiatric patients smoke is not breaching the standard of care toward smoking patients. But you care for nonsmoking patients as well, and other types of liability besides malpractice exist.
Doctors have moral duties for lots of things we can’t be sued for. Dr. A is right to be concerned. To explain, we’ll look at:
- changes in attitudes about smoking
- the link between smoking and mental illness
- smoking bans in psychiatric facilities
- malpractice potential
- other issues Dr. A’s hospital should consider, such as offering patients assistance with smoking cessation.
Changing attitudes about smoking
Thirty years ago, doctors smoked during medical meetings, and smoking on airplanes and in public was commonplace. I worked at an adolescent inpatient unit, and line staff carried lighters. We thought lighting kids’ cigarettes was a legitimate way to establish rapport. Times and attitudes have changed. No hospital condones smoking these days, let alone smoking by minor patients. Since the Surgeon General first declared in 1964 that smoking was hazardous, U.S. adult smoking rates have dropped from 42% to under 20%.1
In the early 1990s, California issued the first statewide ban on smoking in work-places, including bars and restaurants.2 Nearly 3,000 state or local jurisdictions require workplaces and/or commercial establishments to be smoke-free.3 Recently, the legislature in Virginia—a major tobacco-producing state—voted to prohibit smoking in restaurants,4 and many other state governments are considering smoking bans. Smoking bans are intended to protect nonsmokers—especially children—from risks of secondhand smoke,5 but they also discourage individuals from taking up the habit6 and encourage smokers to quit.7
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Smoking and mental illness
Persons with serious psychiatric disorders have smoking rates 2 to 3 times higher than those of the general population.8,9 As Dr. A notes, nicotine is a psychoactive drug. Smoking may be a genuine—although ultimately unhealthy—form of self-medication and may have positive psychological effects, such as antidepressant activity for many mentally ill persons.10,11 The Joint Commission on Accreditation of Healthcare Organizations banned smoking in hospitals in 1992 but made an exception for psychiatric units. Out of sympathy for patients and concern about what could happen when they are deprived of a substance they intensely crave, many psychiatric wards continue to accommodate smokers.12
What some institutions have done
An increasing number of psychiatric facilities have instituted or are considering bans on smoking.13 The first psychiatric smoking bans were implemented despite fears that patient violence would increase and opposition from hospital employees—a group that often includes smokers. Experience shows that although not all smoking bans are successful or problem-free,14 they usually cause fewer problems than anticipated. We also know what factors help make smoke-free programs successful (Table).15
Table
Smoke-free plans that work: How to clear the air
| • Take time—more than 6 months—to plan smoke-free initiatives |
| • Supply patient and staff smokers with nicotine replacement therapy |
| • Present clear, consistent, visible leadership |
| • Encourage cohesive teamwork |
| • Provide extensive education and training for staff |
| • Reduce staff smoking rates |
| • Offer programs and education to promote smoking cessation among staff members |
| • Enforce nonsmoking policies |
| Source: Adapted from reference 15 |
Aggression, seclusion, discharges against medical advice, and “prn” medication use do not increase after smoking bans,5,16,17 and many patients experience health benefits.18 After discharge, however, most patients resume tobacco use.11,19,20
Smoking bans have been opposed on grounds that they abridge psychiatric patients’ rights and are unduly coercive.21,22 In the United States and United Kingdom, however, legal actions to block smoking bans have not succeeded, and courts have not recognized a fundamental “right to smoke.”23-25
Is allowing smoking malpractice?
Now that many psychiatric facilities have ended smoking, clinicians may worry—as does Dr. A—that we could incur malpractice liability if we let inpatients smoke. One of my University of Cincinnati law students, Amanda Smith, and I researched this topic and found no case report that said letting psychiatric inpatients smoke violated the standard of care.
This makes sense, because in the malpractice context, a practitioner is judged by what prudent, similarly situated physicians with similar training would do in similar circumstances. Many psychiatric facilities still permit smoking, so letting patients smoke does not breach the standard of care, even if it seems negligent.26
The ill effects of smoking accrue over years, not weeks or months. Almost all patients who smoke in hospitals also have smoked before hospitalization, and most smokers who are barred from smoking while inpatients resume soon after discharge. To succeed, a malpractice lawsuit must show that the defendant’s actions caused damages. A jury might find it hard to conclude that a permissive hospital smoking policy was the primary cause of a long-term smoker’s health problems.
4 other concerns
Nonsmokers’ rights. Arrangements at Dr. A’s hospital expose nonsmokers to secondhand cigarette smoke, which raises the possibility of legal action by nonsmokers. In 1993, the U.S. Supreme Court held that a prison inmate’s heavy exposure to secondhand smoke violated the Eighth Amendment ban on cruel and unusual punishment.27 Involuntary hospitalization is not punishment, but suits such as this might be brought on other grounds, such as violation of patients’ civil rights.28
Competence. In some states, civil commitment requires a finding that the respondent is not competent to make treatment decisions. Can persons who are not competent to make treatment decisions make good decisions about whether to smoke? Shouldn’t the hospital deal with patients’ nicotine dependence more therapeutically—and paternalistically—by providing nicotine replacement and encouraging smoking cessation? Shouldn’t the hospital also discourage patients who don’t smoke from starting?
Protecting patients. Dr. A’s hospital provides cigarettes to patients. Though compassion may be the motive, is the hospital failing to protect its incompetent patients and abetting their self-injurious behavior?
Helping smokers quit. Does the hospital offer treatment to help smokers quit? Although the problems that lead to civil commitment are immediate and serious, addressing long-term health issues is consistent with treating acute psychiatric crises. Many hospitals that permit smoking also encourage participation in smoking-cessation programs. Having these available to patients might make claims that the hospital failed in its duties to care for patients less plausible.
Related resources
- Maryland Hospital Association. Smoke-free hospital campus tool-kit. www.mdhospitals.org/mha/Community_Health_Resources/Smoke_Free_Hospital_Campuses.shtml.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
1. Centers for Disease Control and Prevention. Cigarette smoking among adults—United States, 2007. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a2.htm. Accessed April 10, 2009.
2. Calif. Labor Code § 6404.5.
3. American Nonsmokers’ Rights Foundation. Overview list–how many smokefree laws? Available at: http://www.no-smoke.org/pdf/mediaordlist.pdf. Accessed February 11, 2009.
4. Kumar A. Va. House approves ban on smoking: most restaurants would be affected. Washington Post. February 10, 2009: Page A01.
5. U.S. Department of Health and Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services; 2006.
6. Siegel M, Albers AB, Cheng DM, et al. Local restaurant smoking regulations and the adolescent smoking initiation process: results of a multilevel contextual analysis among Massachusetts youth. Arch Pediatr Adolesc Med. 2008;162(5):477-483.
7. Longo DR, Feldman MM, Kruse RL, et al. Implementing smoking bans in American hospitals: results of a national survey. Tob Control. 1998;7(1):47-55.
8. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
9. Morris CD, Giese AA, Turnbull JJ, et al. Predictors of tobacco use among persons with mental illnesses in a statewide population. Psychiatr Serv. 2006;57(7):1035-1038.
10. Cattapan-Ludewig K, Ludewig S, Jaquenoud Sirot E, et al. Why do schizophrenic patients smoke? Nervenarzt. 2005;76(3):287-294.
11. El-Guebaly N, Cathcart J, Currie S, et al. Public health and therapeutic aspects of smoking bans in mental health and addiction settings. Psychiatr Serv. 2002;53(12):1617-1622.
12. Williams JM. Eliminating tobacco use in mental health facilities: patients’ rights, public health, and policy issues. JAMA. 2008;299(5):571-573.
13. Parks J, Jewell P, eds,, Burke M. Technical report on smoking policy and treatment in state operated psychiatric facilities. Alexandria, VA: National Association of State Mental Health Program Directors Medical Directors Council; 2006. Technical Report 12.
14. Campion J, Lawn S, Brownlie A, et al. Implementing smoke-free policies in mental health inpatient units: learning from unsuccessful experience. Australas Psychiatry. 2008;16(2):92-97.
15. Lawn S, Campion J. Smoke-free initiatives in psychiatric inpatient units: a national survey of Australian sites. Adelaide, Australia: Flinders University; 2008.
16. Lawn S, Pols R. Smoking bans in psychiatric inpatient settings? A review of the research. Aust N Z J Psychiatry. 2005;39(10):866-885.
17. Hempel AG, Kownacki R, Malin DH, et al. Effect of a total smoking ban in a maximum security psychiatric hospital. Behav Sci Law. 2002;20(5):507-522.
18. Harris GT, Parle D, Gagné J. Effects of a tobacco ban on long-term psychiatric patients. J Behav Health Serv Res. 2007;34(1):43-55.
19. Shmueli D, Fletcher L, Hall SE, et al. Changes in psychiatric patients’ thoughts about quitting smoking during a smoke-free hospitalization. Nicotine Tob Res. 2008;10(5):875-881.
20. Prochaska JJ, Fletcher L, Hall SE, et al. Return to smoking following a smoke-free psychiatric hospitalization. Am J Addict. 2006;15(1):15-22.
21. Marcus K. Smoking bans in long-term inpatient settings: a dilemma. Psychiatr Serv. 2008;59(3):330.-
22. Remal G. Hospital preparing to kick habit; A lawyer for smokers at Riverview Psychiatric Center sees little chance of reversing a smoking ban. Portland (Maine) Press Herald. December 29, 2006.
23. Arbogast v Peterson, 631 N.E.2d 673 (Ohio App 1993).
24. R (G) v Nottinghamshire Healthcare NHS Trust and others (2008).
25. Thiel v Nelson, 422 F.Supp. 2d 1024 (WD Wis 2006).
26. New Jersey Department of Health Services. Testimony of Kevin Martone, Assistant Commissioner, Department of Human Services, Division of Mental Health Services, New Jersey Assembly Human Services Committee, A-2308 Smoking Cessation, March 6, 2008. Trenton, NJ: New Jersey Department of Health Services. Available at: http://www.state.nj.us/humanservices/dmhs/Assembly_smoking_testimony_03_2008.pdf. Accessed February 14, 2009.
27. Helling v McKinney, 509 U.S. 25 (1993).
28. Appelbaum PS. Do hospitalized patients have a right to smoke? Psychiatr Serv. 1995;46(7):653-654, 660.
1. Centers for Disease Control and Prevention. Cigarette smoking among adults—United States, 2007. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a2.htm. Accessed April 10, 2009.
2. Calif. Labor Code § 6404.5.
3. American Nonsmokers’ Rights Foundation. Overview list–how many smokefree laws? Available at: http://www.no-smoke.org/pdf/mediaordlist.pdf. Accessed February 11, 2009.
4. Kumar A. Va. House approves ban on smoking: most restaurants would be affected. Washington Post. February 10, 2009: Page A01.
5. U.S. Department of Health and Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services; 2006.
6. Siegel M, Albers AB, Cheng DM, et al. Local restaurant smoking regulations and the adolescent smoking initiation process: results of a multilevel contextual analysis among Massachusetts youth. Arch Pediatr Adolesc Med. 2008;162(5):477-483.
7. Longo DR, Feldman MM, Kruse RL, et al. Implementing smoking bans in American hospitals: results of a national survey. Tob Control. 1998;7(1):47-55.
8. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
9. Morris CD, Giese AA, Turnbull JJ, et al. Predictors of tobacco use among persons with mental illnesses in a statewide population. Psychiatr Serv. 2006;57(7):1035-1038.
10. Cattapan-Ludewig K, Ludewig S, Jaquenoud Sirot E, et al. Why do schizophrenic patients smoke? Nervenarzt. 2005;76(3):287-294.
11. El-Guebaly N, Cathcart J, Currie S, et al. Public health and therapeutic aspects of smoking bans in mental health and addiction settings. Psychiatr Serv. 2002;53(12):1617-1622.
12. Williams JM. Eliminating tobacco use in mental health facilities: patients’ rights, public health, and policy issues. JAMA. 2008;299(5):571-573.
13. Parks J, Jewell P, eds,, Burke M. Technical report on smoking policy and treatment in state operated psychiatric facilities. Alexandria, VA: National Association of State Mental Health Program Directors Medical Directors Council; 2006. Technical Report 12.
14. Campion J, Lawn S, Brownlie A, et al. Implementing smoke-free policies in mental health inpatient units: learning from unsuccessful experience. Australas Psychiatry. 2008;16(2):92-97.
15. Lawn S, Campion J. Smoke-free initiatives in psychiatric inpatient units: a national survey of Australian sites. Adelaide, Australia: Flinders University; 2008.
16. Lawn S, Pols R. Smoking bans in psychiatric inpatient settings? A review of the research. Aust N Z J Psychiatry. 2005;39(10):866-885.
17. Hempel AG, Kownacki R, Malin DH, et al. Effect of a total smoking ban in a maximum security psychiatric hospital. Behav Sci Law. 2002;20(5):507-522.
18. Harris GT, Parle D, Gagné J. Effects of a tobacco ban on long-term psychiatric patients. J Behav Health Serv Res. 2007;34(1):43-55.
19. Shmueli D, Fletcher L, Hall SE, et al. Changes in psychiatric patients’ thoughts about quitting smoking during a smoke-free hospitalization. Nicotine Tob Res. 2008;10(5):875-881.
20. Prochaska JJ, Fletcher L, Hall SE, et al. Return to smoking following a smoke-free psychiatric hospitalization. Am J Addict. 2006;15(1):15-22.
21. Marcus K. Smoking bans in long-term inpatient settings: a dilemma. Psychiatr Serv. 2008;59(3):330.-
22. Remal G. Hospital preparing to kick habit; A lawyer for smokers at Riverview Psychiatric Center sees little chance of reversing a smoking ban. Portland (Maine) Press Herald. December 29, 2006.
23. Arbogast v Peterson, 631 N.E.2d 673 (Ohio App 1993).
24. R (G) v Nottinghamshire Healthcare NHS Trust and others (2008).
25. Thiel v Nelson, 422 F.Supp. 2d 1024 (WD Wis 2006).
26. New Jersey Department of Health Services. Testimony of Kevin Martone, Assistant Commissioner, Department of Human Services, Division of Mental Health Services, New Jersey Assembly Human Services Committee, A-2308 Smoking Cessation, March 6, 2008. Trenton, NJ: New Jersey Department of Health Services. Available at: http://www.state.nj.us/humanservices/dmhs/Assembly_smoking_testimony_03_2008.pdf. Accessed February 14, 2009.
27. Helling v McKinney, 509 U.S. 25 (1993).
28. Appelbaum PS. Do hospitalized patients have a right to smoke? Psychiatr Serv. 1995;46(7):653-654, 660.
New Medicare Rule Reduces Retroactive Billing Period
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
Medicare enrollment rules for retroactive billing implemented this month may catch some hospital medicine leaders by surprise—and cost them billing revenue.
The new rules from the Centers for Medicare and Medicaid Services (CMS), effective April 1, cut from 27 months to 30 days the window in which physicians can back-bill for services after successful enrollment or re-enrollment in Medicare. Most HM groups routinely allow new hospitalists to work prior to payor credentialing, then retroactively bill for those services once credentialing is completed, says Leslie Flores, MHA, a principal in Nelson/Flores Associates, an HM consulting firm in La Quinta, Calif., and director of SHM's Practice Management Institute.
Another provision of the rules states that practices must alert contractors of any changes in practice locations within 30 days, or risk expulsion from Medicare for as much as two years.
“This is likely to impact hospital medicine more than other specialties because of our rapid growth, the proportion of new graduates we hire, and the frequency with which hospitalists move around,” Flores says.
Marshall Maglothin, chief operating officer of Inpatient Specialists, which staffs 70 hospitalists at three Washington, D.C.-area hospitalists, suggests HM leaders read the new Medicare Provider Enrollment Toolkit, recently issued by the American Medical Association (AMA) and the Medical Group Management Association (MGMA). The resource includes an introduction to CMS’ Web-based version of the Provider Enrollment, Chain and Ownership System (PECOS), which became available this month for both HM groups and individual hospitalists. To download the toolkit, visit www.mgma.com.
“Until this gets worked over the next couple of months, there’s going to be a lot of missed revenue,” says Maglothin, who also runs HM advisory firm Blue Oak Consulting. “This is the ideal timeline, but it’s totally unrealistic when you’re dealing with over 600,000 physicians in the United States. There should have been an ease-in process.”
To help smooth the transition, CMS will hold a conference call to discuss provider issues at 2 p.m. (EST) Thursday. Capacity is limited, but to participate, call (800) 837-1935 and reference conference No. 94109369.
Pandemic Preparation
Now that more swine flu cases have been reported in New York City than in any other part of the U.S., local hospitalists are preparing to handle a potential influx of ill patients.
Dahlia Rizk, DO, FHM, director of the hospitalist program at Beth Israel Medical Center (BIMC) in New York City, says her 20-member team is receiving daily briefings from the hospital’s infection control expert. Hospitalists are learning about the latest confirmed cases and guidelines from the Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO), and the NYC Department of Health and Mental Hygiene. Dr. Rizk is sharing the information with the rest of the hospital staff.
"This is our home; this is where we spend 90% of our day, if not 100%," Dr. Rizk says. “The staff know us, they rely on us, recognize us, and expect information and help from us when it comes to these kinds of situations."
John Novotny, MD, associate director of the hospitalist program at BIMC, says the hospital's strategy focuses on containing the virus and protecting other patients and staff from becoming infected by placing suspected swine flu patients in an isolation room that prevents the illness from being transmitted through droplets in the air. In addition, staff members will be expected to wear an N95 respirator facemask when entering the rooms of swine flu patients. Patients who are placed in the isolation room will be administered a PCR nasal swab test to confirm whether they are infected with influenza.
Dr. Rizk says patients showing mild to moderate symptoms will be asked to go home and remain there for seven days to reduce the chances of infecting others. “During this emergency, it is especially important to limit admissions of suspected influenza to those patients with more serious clinical conditions or significant comorbidities," she explains. "We need to focus on the priority of avoiding exposing other vulnerable inpatients to influenza, such as the elderly, the immune-compromised, or those with chronic heart and lung conditions.”
Drs. Novotny and Rizk suggest hospitalists follow these swine flu preparation tips:
- Communicate. Keep nurses and other staff up to date about the latest treatment and containment guidelines.
- Establish expectations. Be aware that staffers are looking to hospitalists for guidance during this emergency situation.
- Monitor for updates. Stay informed through your infectious disease division, the CDC, the WHO, and your local public health department.
For more information, visit the CDC website.
Now that more swine flu cases have been reported in New York City than in any other part of the U.S., local hospitalists are preparing to handle a potential influx of ill patients.
Dahlia Rizk, DO, FHM, director of the hospitalist program at Beth Israel Medical Center (BIMC) in New York City, says her 20-member team is receiving daily briefings from the hospital’s infection control expert. Hospitalists are learning about the latest confirmed cases and guidelines from the Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO), and the NYC Department of Health and Mental Hygiene. Dr. Rizk is sharing the information with the rest of the hospital staff.
"This is our home; this is where we spend 90% of our day, if not 100%," Dr. Rizk says. “The staff know us, they rely on us, recognize us, and expect information and help from us when it comes to these kinds of situations."
John Novotny, MD, associate director of the hospitalist program at BIMC, says the hospital's strategy focuses on containing the virus and protecting other patients and staff from becoming infected by placing suspected swine flu patients in an isolation room that prevents the illness from being transmitted through droplets in the air. In addition, staff members will be expected to wear an N95 respirator facemask when entering the rooms of swine flu patients. Patients who are placed in the isolation room will be administered a PCR nasal swab test to confirm whether they are infected with influenza.
Dr. Rizk says patients showing mild to moderate symptoms will be asked to go home and remain there for seven days to reduce the chances of infecting others. “During this emergency, it is especially important to limit admissions of suspected influenza to those patients with more serious clinical conditions or significant comorbidities," she explains. "We need to focus on the priority of avoiding exposing other vulnerable inpatients to influenza, such as the elderly, the immune-compromised, or those with chronic heart and lung conditions.”
Drs. Novotny and Rizk suggest hospitalists follow these swine flu preparation tips:
- Communicate. Keep nurses and other staff up to date about the latest treatment and containment guidelines.
- Establish expectations. Be aware that staffers are looking to hospitalists for guidance during this emergency situation.
- Monitor for updates. Stay informed through your infectious disease division, the CDC, the WHO, and your local public health department.
For more information, visit the CDC website.
Now that more swine flu cases have been reported in New York City than in any other part of the U.S., local hospitalists are preparing to handle a potential influx of ill patients.
Dahlia Rizk, DO, FHM, director of the hospitalist program at Beth Israel Medical Center (BIMC) in New York City, says her 20-member team is receiving daily briefings from the hospital’s infection control expert. Hospitalists are learning about the latest confirmed cases and guidelines from the Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO), and the NYC Department of Health and Mental Hygiene. Dr. Rizk is sharing the information with the rest of the hospital staff.
"This is our home; this is where we spend 90% of our day, if not 100%," Dr. Rizk says. “The staff know us, they rely on us, recognize us, and expect information and help from us when it comes to these kinds of situations."
John Novotny, MD, associate director of the hospitalist program at BIMC, says the hospital's strategy focuses on containing the virus and protecting other patients and staff from becoming infected by placing suspected swine flu patients in an isolation room that prevents the illness from being transmitted through droplets in the air. In addition, staff members will be expected to wear an N95 respirator facemask when entering the rooms of swine flu patients. Patients who are placed in the isolation room will be administered a PCR nasal swab test to confirm whether they are infected with influenza.
Dr. Rizk says patients showing mild to moderate symptoms will be asked to go home and remain there for seven days to reduce the chances of infecting others. “During this emergency, it is especially important to limit admissions of suspected influenza to those patients with more serious clinical conditions or significant comorbidities," she explains. "We need to focus on the priority of avoiding exposing other vulnerable inpatients to influenza, such as the elderly, the immune-compromised, or those with chronic heart and lung conditions.”
Drs. Novotny and Rizk suggest hospitalists follow these swine flu preparation tips:
- Communicate. Keep nurses and other staff up to date about the latest treatment and containment guidelines.
- Establish expectations. Be aware that staffers are looking to hospitalists for guidance during this emergency situation.
- Monitor for updates. Stay informed through your infectious disease division, the CDC, the WHO, and your local public health department.
For more information, visit the CDC website.