User login
Photoparoxysmal Response Is High Among Teenagers With Autism and Epilepsy
A recent finding may indicate brain irritability or hypersensitivity in children with autism spectrum disorders.
BALTIMORE—The incidence of a photoparoxysmal response among children older than 15 with autism spectrum disorders (ASD) is 25%, which is much higher than that for younger children with ASD, according to a study presented at the 65th Annual Meeting of the American Epilepsy Society. When children in the sample population without epilepsy are excluded, the incidence of a photoparoxysmal response among children older than 15 with ASD is 29.4%.
Epilepsy and frequent interictal discharges are common among children with ASD. Photoparoxysmal responses are interictal EEG discharges correlated with generalized, photosensitive epilepsy. A flashing strobe light, for example, can trigger a photoparoxysmal response in a predisposed individual. “The brain picks up that stimulus through the eye, and for some children, it can cause an abnormal brainwave pattern,” explained Jill Miller-Horn, MD, an epilepsy fellow at Children’s Hospital Boston.
“We already know that abnormal brainwave responses to flashing light can be associated with epilepsy. You might be familiar with what happened in Japan with the Pokemon cartoon, where there was bright, flashing colored light on the screen and hundreds of children then had seizures,” she added. Dr. Miller-Horn and her colleagues decided to study photoparoxysmal responses to photic stimulation in children with ASD, a topic that she said no researchers had previously investigated.
Identifying a Cohort of Children With ASD
The team conducted a retrospective pilot study of children with ASD to determine the rate of the photoparoxysmal response caused by intermittent photic stimulation during EEG studies at Children’s Hospital Boston. The investigators searched medical records that identified 333 children with ASD who were treated at the hospital between December 2010 and May 2011.
Of these children, 206 had had EEGs. In the group of 206 children, 118 had comorbid ASD and epilepsy, and 88 had ASD without seizures. Intermittent photic stimulation was part of 177 children’s EEG studies. The group of 177 included 138 boys and 39 girls, and the children’s average age was 9.
Photoparoxysmal Response Increases in Adolescence
A photoparoxysmal response was elicited in 13 of the 177 children who received photic stimulation during their EEGs. The 7.3% incidence of a photoparoxysmal response in children with ASD was within the range previously reported in the normal population, according to Dr. Miller-Horn. “Our study found that in the ASD population, there is an association between the photoparoxysmal response and epilepsy, as has been previously reported in children with epilepsy without ASD,” she said.
“When we subdivided these children with autism by age, we found that there’s an increase in the photoparoxysmal response as they entered adolescence,” commented Dr. Miller-Horn. The meaning of the result is unclear, “but it’s a difference from the normal population, and it’s a difference from other children who have epilepsy,” she added.
“This is a new finding that may be a clue to the pathophysiology for the high rate of ASD and epilepsy comorbidity,” Dr. Miller-Horn continued. “There may be irritability or hypersensitivity in the brain for children with autism that’s being revealed with the clue that they are more photosensitive.”
Large-scale and prospective studies are needed to confirm the trend, according to the investigators. Further studies could reveal the findings’ significance in the pathophysiology of epilepsy in children with ASD.
—Erik Greb
Suggested Reading
Lo C, Shorvon S, Davis M, et al. Genetic linkage analysis of a large family with photoparoxysmal response. Epilepsy Res. 2011 Nov 7; [Epub ahead of print]
Lopes da Silva FH, Harding GF. Transition to seizure in photosensitive epilepsy. Epilepsy Res. 2011;97(3):278-282.
A recent finding may indicate brain irritability or hypersensitivity in children with autism spectrum disorders.
BALTIMORE—The incidence of a photoparoxysmal response among children older than 15 with autism spectrum disorders (ASD) is 25%, which is much higher than that for younger children with ASD, according to a study presented at the 65th Annual Meeting of the American Epilepsy Society. When children in the sample population without epilepsy are excluded, the incidence of a photoparoxysmal response among children older than 15 with ASD is 29.4%.
Epilepsy and frequent interictal discharges are common among children with ASD. Photoparoxysmal responses are interictal EEG discharges correlated with generalized, photosensitive epilepsy. A flashing strobe light, for example, can trigger a photoparoxysmal response in a predisposed individual. “The brain picks up that stimulus through the eye, and for some children, it can cause an abnormal brainwave pattern,” explained Jill Miller-Horn, MD, an epilepsy fellow at Children’s Hospital Boston.
“We already know that abnormal brainwave responses to flashing light can be associated with epilepsy. You might be familiar with what happened in Japan with the Pokemon cartoon, where there was bright, flashing colored light on the screen and hundreds of children then had seizures,” she added. Dr. Miller-Horn and her colleagues decided to study photoparoxysmal responses to photic stimulation in children with ASD, a topic that she said no researchers had previously investigated.
Identifying a Cohort of Children With ASD
The team conducted a retrospective pilot study of children with ASD to determine the rate of the photoparoxysmal response caused by intermittent photic stimulation during EEG studies at Children’s Hospital Boston. The investigators searched medical records that identified 333 children with ASD who were treated at the hospital between December 2010 and May 2011.
Of these children, 206 had had EEGs. In the group of 206 children, 118 had comorbid ASD and epilepsy, and 88 had ASD without seizures. Intermittent photic stimulation was part of 177 children’s EEG studies. The group of 177 included 138 boys and 39 girls, and the children’s average age was 9.
Photoparoxysmal Response Increases in Adolescence
A photoparoxysmal response was elicited in 13 of the 177 children who received photic stimulation during their EEGs. The 7.3% incidence of a photoparoxysmal response in children with ASD was within the range previously reported in the normal population, according to Dr. Miller-Horn. “Our study found that in the ASD population, there is an association between the photoparoxysmal response and epilepsy, as has been previously reported in children with epilepsy without ASD,” she said.
“When we subdivided these children with autism by age, we found that there’s an increase in the photoparoxysmal response as they entered adolescence,” commented Dr. Miller-Horn. The meaning of the result is unclear, “but it’s a difference from the normal population, and it’s a difference from other children who have epilepsy,” she added.
“This is a new finding that may be a clue to the pathophysiology for the high rate of ASD and epilepsy comorbidity,” Dr. Miller-Horn continued. “There may be irritability or hypersensitivity in the brain for children with autism that’s being revealed with the clue that they are more photosensitive.”
Large-scale and prospective studies are needed to confirm the trend, according to the investigators. Further studies could reveal the findings’ significance in the pathophysiology of epilepsy in children with ASD.
—Erik Greb
A recent finding may indicate brain irritability or hypersensitivity in children with autism spectrum disorders.
BALTIMORE—The incidence of a photoparoxysmal response among children older than 15 with autism spectrum disorders (ASD) is 25%, which is much higher than that for younger children with ASD, according to a study presented at the 65th Annual Meeting of the American Epilepsy Society. When children in the sample population without epilepsy are excluded, the incidence of a photoparoxysmal response among children older than 15 with ASD is 29.4%.
Epilepsy and frequent interictal discharges are common among children with ASD. Photoparoxysmal responses are interictal EEG discharges correlated with generalized, photosensitive epilepsy. A flashing strobe light, for example, can trigger a photoparoxysmal response in a predisposed individual. “The brain picks up that stimulus through the eye, and for some children, it can cause an abnormal brainwave pattern,” explained Jill Miller-Horn, MD, an epilepsy fellow at Children’s Hospital Boston.
“We already know that abnormal brainwave responses to flashing light can be associated with epilepsy. You might be familiar with what happened in Japan with the Pokemon cartoon, where there was bright, flashing colored light on the screen and hundreds of children then had seizures,” she added. Dr. Miller-Horn and her colleagues decided to study photoparoxysmal responses to photic stimulation in children with ASD, a topic that she said no researchers had previously investigated.
Identifying a Cohort of Children With ASD
The team conducted a retrospective pilot study of children with ASD to determine the rate of the photoparoxysmal response caused by intermittent photic stimulation during EEG studies at Children’s Hospital Boston. The investigators searched medical records that identified 333 children with ASD who were treated at the hospital between December 2010 and May 2011.
Of these children, 206 had had EEGs. In the group of 206 children, 118 had comorbid ASD and epilepsy, and 88 had ASD without seizures. Intermittent photic stimulation was part of 177 children’s EEG studies. The group of 177 included 138 boys and 39 girls, and the children’s average age was 9.
Photoparoxysmal Response Increases in Adolescence
A photoparoxysmal response was elicited in 13 of the 177 children who received photic stimulation during their EEGs. The 7.3% incidence of a photoparoxysmal response in children with ASD was within the range previously reported in the normal population, according to Dr. Miller-Horn. “Our study found that in the ASD population, there is an association between the photoparoxysmal response and epilepsy, as has been previously reported in children with epilepsy without ASD,” she said.
“When we subdivided these children with autism by age, we found that there’s an increase in the photoparoxysmal response as they entered adolescence,” commented Dr. Miller-Horn. The meaning of the result is unclear, “but it’s a difference from the normal population, and it’s a difference from other children who have epilepsy,” she added.
“This is a new finding that may be a clue to the pathophysiology for the high rate of ASD and epilepsy comorbidity,” Dr. Miller-Horn continued. “There may be irritability or hypersensitivity in the brain for children with autism that’s being revealed with the clue that they are more photosensitive.”
Large-scale and prospective studies are needed to confirm the trend, according to the investigators. Further studies could reveal the findings’ significance in the pathophysiology of epilepsy in children with ASD.
—Erik Greb
Suggested Reading
Lo C, Shorvon S, Davis M, et al. Genetic linkage analysis of a large family with photoparoxysmal response. Epilepsy Res. 2011 Nov 7; [Epub ahead of print]
Lopes da Silva FH, Harding GF. Transition to seizure in photosensitive epilepsy. Epilepsy Res. 2011;97(3):278-282.
Suggested Reading
Lo C, Shorvon S, Davis M, et al. Genetic linkage analysis of a large family with photoparoxysmal response. Epilepsy Res. 2011 Nov 7; [Epub ahead of print]
Lopes da Silva FH, Harding GF. Transition to seizure in photosensitive epilepsy. Epilepsy Res. 2011;97(3):278-282.
Grand Rounds: Man, 61, With Painful Oral Ulcerations
A 61-year-old man, who had recently emigrated from the Ukraine, presented to his primary care provider with a chief complaint of painful oral lesions and weight loss. The patient described the gradual onset of a severe sore throat and mouth pain three months earlier. Originally, he attributed his symptoms to an upper respiratory infection but became concerned when his symptoms did not resolve.
He reported that the pain had worsened over time and that he was now barely able to swallow solid food or tolerate acidic beverages due to considerable discomfort. His son, who accompanied him to the appointment, had also noted weight loss.
The patient denied any concomitant symptoms, including fever, cough, night sweats, fatigue, lymphadenopathy, abdominal pain, diarrhea, melena, or concomitant rash. His medical history was remarkable only for stage 1 hypertension, which had been well controlled on hydrochlorothiazide 12.5 mg/d for the previous three years. However, the patient had received only minimal preventive health care while living in the Ukraine. His family history was unknown.
One week earlier, the patient had seen a dentist complaining of mouth pain, and was referred to an oral medicine specialist; this specialist, in turn, referred the patient to a primary care nurse practitioner for lab work to confirm the suspected diagnosis of pemphigus vulgaris.
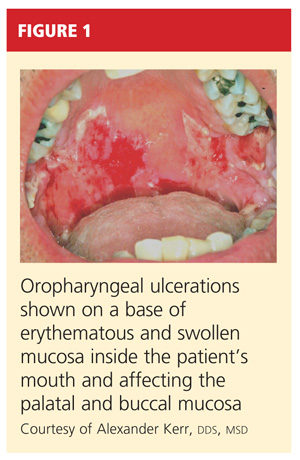
On physical examination, the patient appeared older than his stated age. He was a thin, mildly ill–appearing man, afebrile and normotensive, with heart rate and respirations within normal limits. However, intraoral examination revealed multiple oropharyngeal ulcerations of varying size on a base of erythematous and swollen mucosa on the inside of the man’s cheek and palatal and buccal mucosa (see Figure 1). On his upper back, two round, crusted blisters were noted in isolation (Figure 2). The remaining findings in the physical examination were unremarkable.

Based on the patient’s physical exam findings and clinical guideline recommendations regarding chronic oral ulcerations of unknown etiology,1,2 the patient was scheduled for a cytologic smear to be performed by oral medicine, followed by a gingival biopsy for a direct immunofluorescence test and routine histopathology.3 Unfortunately, due to extensive involvement and concern for possible mucosal shredding, an oral biopsy was not deemed possible.
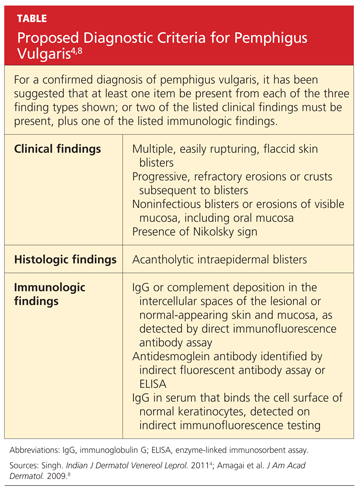
However, the oral medicine specialist, because he strongly suspected pemphigus vulgaris, recommended testing for circulating autoantibodies against the antigens desmogleins 1 and/or 3 in the epidermis, which are responsible for cellular adhesion. (A positive test result supports, but does not confirm, a diagnosis of pemphigus vulgaris.4)
Additionally, baseline labs were performed for signs of systemic illness, including infection, anemia, and liver and kidney disease. Frequent monitoring was conducted for steroid-induced symptoms of elevated blood sugars; the primary care provider was responsible for monitoring the patient for weight gain and steroid-induced psychosis. The patient was referred to gastroenterology for a colonoscopy to ensure that his weight loss and anorexia were not the result of gastrointestinal malignancy. However, the patient declined this test.
DISCUSSION
Painful oral lesions can have numerous etiologies of varying severity and complexity, including herpes simplex virus infection, aphthae, lichen planus, erythema multiforme, squamous cell and other oral carcinomas, primary HIV infection, lupus, and pemphigus. Differentiating among these conditions requires a careful medical history and complete physical exam.5
Pemphigus vulgaris (PV) is the most common variant of pemphigus, a group of chronic autoimmune diseases that cause blistering and ulceration of the mucous membranes and the skin.6 From the Greek pemphix (bubble), PV is more common in people of Ashkenazi Jewish or Mediterranean descent,6,7 usually occurs in middle-aged and older persons, and occurs about 1.5 times more commonly in women than men.5,7 Until the introduction of systemic steroids, pemphigus was often a fatal disease. Significant mortality still exists, mainly as a result of infection or adverse reactions to medication therapy.5
In patients with PV, flaccid bullae are formed on the skin in a process called acantholysis, in which epidermal cells lose their ability to adhere to one another. This results in rapidly expanding, thin-walled blisters on the oral mucosa, scalp, face, axillae, and groin. The blisters burst easily, leaving irregularly shaped, painful ulcerations.4 Painful oral mucosal membrane erosions are the first presenting sign of PV and often the only sign for an average of five months before other skin lesions develop.3 These lesions are noninfectious.
To make a definitive diagnosis of PV, clinical lesions must be present, with a confirmation of histologic findings, acantholysis on biopsy, and a confirmation of autoantibodies present in tissue and/or serum.4 (For proposed detailed diagnostic criteria, see table4,8.)
Initial misdiagnoses, which often lead to delayed or incorrect treatment, usually include aphthous stomatitis, gingivostomatitis, erythema multiforme, erosive lichen planus, herpes simplex virus, and/or oral candidiasis.3
Common Differentials
Herpes simplex virus. Affecting between 15% and 45% of the population, herpes simplex virus (HSV) infection, also known as cold sores, is the most common cause of recurrent oral ulcers.9 HSV is transmitted through direct contact with lesions or via viral shedding. Primary infection, which may occur with flu-like symptoms, causes the sudden onset of multiple clustered vesicles on an erythematous base that quickly ulcerate and crust. Recurrent infections tend to be less severe and are accompanied by minimal systemic symptoms.10
Diagnosis is usually made through history and physical exam. However, diagnostic tests, including Tzanck smears, biopsy, polymerase chain reaction (PCR) assay, and/or viral isolation in culture, are sometimes used to confirm a suspected case.10
Oral lichen planus (OLP). This is a common, chronic, mucocutaneous inflammatory disease of unknown etiology that affects skin and mucous membranes of the mouth, including the buccal mucosa, tongue, and/or gums. These lesions are noninfectious and are an immunologically mediated disease. Stress, anxiety, genetic predisposition, NSAID use, antihypertensive medications (eg, captopril, enalapril, propranolol; considered an oral lichenoid drug reaction), and altered cell-mediated immune response have been considered possible causative factors.11,12 Recent reports suggest an association between hepatitis C virus and OLP.13
Affecting about 4% of the general population, and more predominate in perimenopausal women, OLP lesions appear as white, lacey patches; red, swollen tissues; or open sores, most commonly on the inside of the mouth bilaterally. Patients will present with complaints of burning, roughness, or pain in the mouth, dry mouth, sensitivity to hot or spicy foods, and difficulty swallowing if the throat is involved. Diagnosis is based on history and physical examination and often a confirmatory biopsy. Topical high-potency corticosteroids are generally first-line therapy, with systemic medications such as oral prednisone used to treat severe cases.14,15
Oral candidiasis. Up to 80% of healthy individuals carry Candida albicans in their mouths16; this pathogen accounts for about half of all cases of oral candidiasis (oral thrush). Oral infections occur only with an underlying predisposing condition in the host. Oral thrush presents as creamy white lesions on the oral mucosa; a diagnostic feature is that the plaques can be removed to reveal an erythematous base.16,17
In the chronic form of candidiasis, the mucosal surface is bright red and smooth. When the tongue is involved, it may appear dry, fissured, or cracked. Patients may report a dry mouth, burning pain, and difficulty eating. Infection can be confirmed with periodic acid-Schiff staining of a smear to detect candidal hyphae.9
Use of antifungal creams and lozenges, as well as improved oral hygiene, will often lead to resolution of symptoms.9 Management of any associated underlying conditions, such as diabetes, asthma requiring long-term use of steroid inhalers, or infection with HIV/AIDS, is essential.18
Oral aphthae. Recurrent aphthous ulcers (commonly called canker sores; also referred to as recurrent aphthous stomatitis [RAS]) are a common oral condition. Etiology is unknown and most likely multifactorial, with a strong genetic tendency and multiple predisposing factors, including trauma, stress, food allergies, hormones, and smoking.19 Certain chronic illnesses, including celiac disease, inflammatory bowel disease (IBD), HIV, and neutropenia may also predispose patients to RAS or RAS-like syndromes.
Aphthous ulcers are classified as minor or major. Minor aphthae, which account for 90% of RAS cases, present as single or multiple, small, oval or round ulcers with an erythematous halo on the buccal or labial mucosa or tongue.19 The ulcers last 7 to 10 days and heal spontaneously without scarring.
Diagnosis, based on history and clinical presentation, may include evaluation for systemic causes of oral ulcers. Treatment for both minor and major apthae is palliative, with mainstays including topical corticosteroids, mouth rinses, and, in severe cases, thalidomide, although randomized controlled trials have not shown this agent to be of benefit.9
Treatment for Pemphigus Vulgaris
The outcome goal for management of pemphigus is to achieve and maintain remission. This includes the epithelialization of all skin and mucosal lesions, prevention of relapse, minimization of adverse treatment effects, and successful withdrawal of therapeutic medications.20
The response to treatment varies greatly among patients, as the optimal therapeutic regimen for pemphigus is unknown.20 Systemic glucocorticoids are considered the gold standard of treatment and management, but their use has been associated with several adverse effects, including weight gain and elevated blood sugar levels. Recently, the combination of IV immune globulin and biological therapies (eg, rituximab) that target specific molecules in the inflammatory process have been demonstrated as effective in cases of refractory pemphigus.21,22
PATIENT MANAGEMENT AND OUTCOME
Several referrals were made, including dermatology, for its familiarity with autoimmune diseases of the skin. There, the patient was fully examined and found to have a small truncal lesion compatible with PV. He was referred to an otolaryngologist for a nasal endoscopy to determine the extent of the lesions. They were found to extend far beyond his oral cavity into his esophagus.
Based on a positive enzyme-linked immunosorbent assay (ELISA) for PV antibodies, a cytologic smear with acantholytic cells, and a classic clinical presentation of PV, the patient was started on prednisone 80 mg/d with azathioprine 50 mg/d for the first 14 days.23,24 He responded quickly to these oral medications and underwent a confirmatory oral biopsy within a few weeks.
After several months, the patient was slowly titrated down to lower maintenance doses of prednisone and azathioprine. Now in remission, he continues to receive collaborative management from oral medicine, dermatology, and a nurse practitioner–managed primary care practice. Health care maintenance has included appropriate vaccination and discussion regarding prostate cancer screening, per 2010 guidelines from the US Preventive Services Task Force.25
CONCLUSION
Since the differential diagnosis for pemphigus vulgaris is extensive and the diagnostic criteria are exacting, many affected patients are undiagnosed or misdiagnosed, with a resulting delay in effective treatment. It is important for the primary care clinician to undertake a frequent review of common oral infections, particularly those with similar presentations.
The authors extend their thanks to Alexander Kerr, DDS, MSD, Clinical Associate Professor, Department of Oral and Maxillary Pathology, Radiology and Medicine, New York University College of Dentistry, for the images included in this article and for Dr. Kerr’s clinical expertise and partnership.
REFERENCES
1. Sciubba JJ. Oral mucosal diseases in the office setting. Part II. Oral lichen planus, pemphigus vulgaris, and mucosal pemphigoid. Gen Dent. 2007;55(5):464-476.
2. Muñoz-Corcuera M, Esparza-Gómez G, González-Moles MA, Bascones-Martínez A. Oral ulcers: clinical aspects. A tool for dermatologists. Part II. Chronic ulcers. Clin Exp Dermatol. 2009; 34(4):456-461.
3. Dagistan S, Goregen M, Miloglu O, Cakur B. Oral pemphigus vulgaris: a case report with review of the literature. J Oral Sci. 2008;50(3):359-362.
4. Singh S. Evidence-based treatments for pemphigus vulgaris, pemphigus foliaceus and bullous pemphigoid: a systematic review. Indian J Dermatol Venereol Leprol. 2011;77(4):456-469.
5. Ohta M, Osawa S, Endo H, et al. Pemphigus vulgaris confined to the gingiva: a case report. Int J Dent. 2011;2011:207153. Epub 2011 May 11.
6. Mignona MD, Fortuna G, Leuci S. Oral pemphigus. Minerva Stomatol. 2009;58(10):501-518.
7. Mimouni D, Bar H, Gdalevich M, et al. Pemphigus: analysis of epidemiological factors in 155 patients. J Eur Acad Dermatol Venereol. 2008; 22(10):1232-1235.
8. Amagai M, Ikeda S, Shimizu H, et al. A randomized double-blind trial of intravenous immunoglobulin for pemphigus. J Am Acad Dermatol. 2009;60(4):595-603.
9. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: Part I. Superficial mucosal lesions. Am Fam Physician. 2007;75(4):501-507.
10. Fatahzadeh M, Schwartz R. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57(5):737-763.
11. Sugerman PB, Savage NW. Oral lichen planus: causes, diagnosis and management. Aust Dent J. 2002;47(4):290-297.
12. Kaomongkolgit R. Oral lichenoid drug reaction associated with antihypertensive and hypoglycemic drugs. J Drugs Dermatol. 2010;9(1):73-75.
13. Petti S, Rabiei M, De Luca M, Scully C. The magnitude of the association between hepatitis C virus infection and oral lichen planus: meta-analysis and case control study. Odontology. 2011;99(2):168-178.
14. Usatine RP, Tinitigan M. Diagnosis and treatment of lichen planus. Am Fam Physician. 2011;84(1): 53-60.
15. Thongprasom K, Carrozzo M, Furness S, Lodi G. Interventions for treating oral lichen planus. Cochrane Database Syst Rev. 2011 Jul 6; (7):CD001168.
16. Giannini PJ, Shetty KV. Diagnosis and management of oral candidiasis. Otolaryngol Clin North Am. 2011;44(1):231-240, vii.
17. Lynch DP. Oral candidiasis. History, classification, and clinical presentation. Oral Surg Oral Med Oral Pathol. 1994;78(2):189-193.
18. Williams D, Lewis M. Pathogenesis and treatment of oral candidosis. J Oral Microbiol. 2011 Jan 28;3. doi: 10.3402/jom.v3i0.5771.
19. Scully C, Challacombe SJ. Pemphigus vulgaris: update on etiopathogenesis, oral manifestations, and management. Crit Rev Oral Biol Med. 2002;13(5):397-408.
20. Martin LK, Werth V, Villanueva E, Murrell DF. A systematic review of randomized controlled trials for pemphigus vulgaris and pemphigus foliaceus. J Am Acad Dermatol. 2011;64(5):903-908.
21. Joly P, Mouquet H, Roujeau JC, et al. A single cycle of rituximab for the treatment of severe pemphigus. N Engl J Med. 2007;357(6):545-552.
22. Diaz LA. Rituximab and pemphigus: a therapeutic advance. N Engl J Med. 2007;357(6):605-607.
23. Anstey AV, Wakelin S, Reynolds NJ. Guidelines for prescribing azathioprine in dermatology. Br J Dermatol. 2004;151(6):1123-1132.
24. Chams-Davatchi C, Daneshpazhooh M. Prednisolone dosage in pemphigus vulgaris. J Am Acad Dermatol. 2005;53(3):547.
25. Agency for Healthcare Research and Quality. Guide to Clinical Preventive Services, 2010-2011: recommendations of the US Preventive Services Task Force. AHRQ Publication No. 10-05145, September 2010. www.ahrq.gov/clinic/pocketgd1011/pocketgd1011.pdf. Accessed January 23, 2012.
A 61-year-old man, who had recently emigrated from the Ukraine, presented to his primary care provider with a chief complaint of painful oral lesions and weight loss. The patient described the gradual onset of a severe sore throat and mouth pain three months earlier. Originally, he attributed his symptoms to an upper respiratory infection but became concerned when his symptoms did not resolve.
He reported that the pain had worsened over time and that he was now barely able to swallow solid food or tolerate acidic beverages due to considerable discomfort. His son, who accompanied him to the appointment, had also noted weight loss.
The patient denied any concomitant symptoms, including fever, cough, night sweats, fatigue, lymphadenopathy, abdominal pain, diarrhea, melena, or concomitant rash. His medical history was remarkable only for stage 1 hypertension, which had been well controlled on hydrochlorothiazide 12.5 mg/d for the previous three years. However, the patient had received only minimal preventive health care while living in the Ukraine. His family history was unknown.
One week earlier, the patient had seen a dentist complaining of mouth pain, and was referred to an oral medicine specialist; this specialist, in turn, referred the patient to a primary care nurse practitioner for lab work to confirm the suspected diagnosis of pemphigus vulgaris.
On physical examination, the patient appeared older than his stated age. He was a thin, mildly ill–appearing man, afebrile and normotensive, with heart rate and respirations within normal limits. However, intraoral examination revealed multiple oropharyngeal ulcerations of varying size on a base of erythematous and swollen mucosa on the inside of the man’s cheek and palatal and buccal mucosa (see Figure 1). On his upper back, two round, crusted blisters were noted in isolation (Figure 2). The remaining findings in the physical examination were unremarkable.
Based on the patient’s physical exam findings and clinical guideline recommendations regarding chronic oral ulcerations of unknown etiology,1,2 the patient was scheduled for a cytologic smear to be performed by oral medicine, followed by a gingival biopsy for a direct immunofluorescence test and routine histopathology.3 Unfortunately, due to extensive involvement and concern for possible mucosal shredding, an oral biopsy was not deemed possible.
However, the oral medicine specialist, because he strongly suspected pemphigus vulgaris, recommended testing for circulating autoantibodies against the antigens desmogleins 1 and/or 3 in the epidermis, which are responsible for cellular adhesion. (A positive test result supports, but does not confirm, a diagnosis of pemphigus vulgaris.4)
Additionally, baseline labs were performed for signs of systemic illness, including infection, anemia, and liver and kidney disease. Frequent monitoring was conducted for steroid-induced symptoms of elevated blood sugars; the primary care provider was responsible for monitoring the patient for weight gain and steroid-induced psychosis. The patient was referred to gastroenterology for a colonoscopy to ensure that his weight loss and anorexia were not the result of gastrointestinal malignancy. However, the patient declined this test.
DISCUSSION
Painful oral lesions can have numerous etiologies of varying severity and complexity, including herpes simplex virus infection, aphthae, lichen planus, erythema multiforme, squamous cell and other oral carcinomas, primary HIV infection, lupus, and pemphigus. Differentiating among these conditions requires a careful medical history and complete physical exam.5
Pemphigus vulgaris (PV) is the most common variant of pemphigus, a group of chronic autoimmune diseases that cause blistering and ulceration of the mucous membranes and the skin.6 From the Greek pemphix (bubble), PV is more common in people of Ashkenazi Jewish or Mediterranean descent,6,7 usually occurs in middle-aged and older persons, and occurs about 1.5 times more commonly in women than men.5,7 Until the introduction of systemic steroids, pemphigus was often a fatal disease. Significant mortality still exists, mainly as a result of infection or adverse reactions to medication therapy.5
In patients with PV, flaccid bullae are formed on the skin in a process called acantholysis, in which epidermal cells lose their ability to adhere to one another. This results in rapidly expanding, thin-walled blisters on the oral mucosa, scalp, face, axillae, and groin. The blisters burst easily, leaving irregularly shaped, painful ulcerations.4 Painful oral mucosal membrane erosions are the first presenting sign of PV and often the only sign for an average of five months before other skin lesions develop.3 These lesions are noninfectious.
To make a definitive diagnosis of PV, clinical lesions must be present, with a confirmation of histologic findings, acantholysis on biopsy, and a confirmation of autoantibodies present in tissue and/or serum.4 (For proposed detailed diagnostic criteria, see table4,8.)
Initial misdiagnoses, which often lead to delayed or incorrect treatment, usually include aphthous stomatitis, gingivostomatitis, erythema multiforme, erosive lichen planus, herpes simplex virus, and/or oral candidiasis.3
Common Differentials
Herpes simplex virus. Affecting between 15% and 45% of the population, herpes simplex virus (HSV) infection, also known as cold sores, is the most common cause of recurrent oral ulcers.9 HSV is transmitted through direct contact with lesions or via viral shedding. Primary infection, which may occur with flu-like symptoms, causes the sudden onset of multiple clustered vesicles on an erythematous base that quickly ulcerate and crust. Recurrent infections tend to be less severe and are accompanied by minimal systemic symptoms.10
Diagnosis is usually made through history and physical exam. However, diagnostic tests, including Tzanck smears, biopsy, polymerase chain reaction (PCR) assay, and/or viral isolation in culture, are sometimes used to confirm a suspected case.10
Oral lichen planus (OLP). This is a common, chronic, mucocutaneous inflammatory disease of unknown etiology that affects skin and mucous membranes of the mouth, including the buccal mucosa, tongue, and/or gums. These lesions are noninfectious and are an immunologically mediated disease. Stress, anxiety, genetic predisposition, NSAID use, antihypertensive medications (eg, captopril, enalapril, propranolol; considered an oral lichenoid drug reaction), and altered cell-mediated immune response have been considered possible causative factors.11,12 Recent reports suggest an association between hepatitis C virus and OLP.13
Affecting about 4% of the general population, and more predominate in perimenopausal women, OLP lesions appear as white, lacey patches; red, swollen tissues; or open sores, most commonly on the inside of the mouth bilaterally. Patients will present with complaints of burning, roughness, or pain in the mouth, dry mouth, sensitivity to hot or spicy foods, and difficulty swallowing if the throat is involved. Diagnosis is based on history and physical examination and often a confirmatory biopsy. Topical high-potency corticosteroids are generally first-line therapy, with systemic medications such as oral prednisone used to treat severe cases.14,15
Oral candidiasis. Up to 80% of healthy individuals carry Candida albicans in their mouths16; this pathogen accounts for about half of all cases of oral candidiasis (oral thrush). Oral infections occur only with an underlying predisposing condition in the host. Oral thrush presents as creamy white lesions on the oral mucosa; a diagnostic feature is that the plaques can be removed to reveal an erythematous base.16,17
In the chronic form of candidiasis, the mucosal surface is bright red and smooth. When the tongue is involved, it may appear dry, fissured, or cracked. Patients may report a dry mouth, burning pain, and difficulty eating. Infection can be confirmed with periodic acid-Schiff staining of a smear to detect candidal hyphae.9
Use of antifungal creams and lozenges, as well as improved oral hygiene, will often lead to resolution of symptoms.9 Management of any associated underlying conditions, such as diabetes, asthma requiring long-term use of steroid inhalers, or infection with HIV/AIDS, is essential.18
Oral aphthae. Recurrent aphthous ulcers (commonly called canker sores; also referred to as recurrent aphthous stomatitis [RAS]) are a common oral condition. Etiology is unknown and most likely multifactorial, with a strong genetic tendency and multiple predisposing factors, including trauma, stress, food allergies, hormones, and smoking.19 Certain chronic illnesses, including celiac disease, inflammatory bowel disease (IBD), HIV, and neutropenia may also predispose patients to RAS or RAS-like syndromes.
Aphthous ulcers are classified as minor or major. Minor aphthae, which account for 90% of RAS cases, present as single or multiple, small, oval or round ulcers with an erythematous halo on the buccal or labial mucosa or tongue.19 The ulcers last 7 to 10 days and heal spontaneously without scarring.
Diagnosis, based on history and clinical presentation, may include evaluation for systemic causes of oral ulcers. Treatment for both minor and major apthae is palliative, with mainstays including topical corticosteroids, mouth rinses, and, in severe cases, thalidomide, although randomized controlled trials have not shown this agent to be of benefit.9
Treatment for Pemphigus Vulgaris
The outcome goal for management of pemphigus is to achieve and maintain remission. This includes the epithelialization of all skin and mucosal lesions, prevention of relapse, minimization of adverse treatment effects, and successful withdrawal of therapeutic medications.20
The response to treatment varies greatly among patients, as the optimal therapeutic regimen for pemphigus is unknown.20 Systemic glucocorticoids are considered the gold standard of treatment and management, but their use has been associated with several adverse effects, including weight gain and elevated blood sugar levels. Recently, the combination of IV immune globulin and biological therapies (eg, rituximab) that target specific molecules in the inflammatory process have been demonstrated as effective in cases of refractory pemphigus.21,22
PATIENT MANAGEMENT AND OUTCOME
Several referrals were made, including dermatology, for its familiarity with autoimmune diseases of the skin. There, the patient was fully examined and found to have a small truncal lesion compatible with PV. He was referred to an otolaryngologist for a nasal endoscopy to determine the extent of the lesions. They were found to extend far beyond his oral cavity into his esophagus.
Based on a positive enzyme-linked immunosorbent assay (ELISA) for PV antibodies, a cytologic smear with acantholytic cells, and a classic clinical presentation of PV, the patient was started on prednisone 80 mg/d with azathioprine 50 mg/d for the first 14 days.23,24 He responded quickly to these oral medications and underwent a confirmatory oral biopsy within a few weeks.
After several months, the patient was slowly titrated down to lower maintenance doses of prednisone and azathioprine. Now in remission, he continues to receive collaborative management from oral medicine, dermatology, and a nurse practitioner–managed primary care practice. Health care maintenance has included appropriate vaccination and discussion regarding prostate cancer screening, per 2010 guidelines from the US Preventive Services Task Force.25
CONCLUSION
Since the differential diagnosis for pemphigus vulgaris is extensive and the diagnostic criteria are exacting, many affected patients are undiagnosed or misdiagnosed, with a resulting delay in effective treatment. It is important for the primary care clinician to undertake a frequent review of common oral infections, particularly those with similar presentations.
The authors extend their thanks to Alexander Kerr, DDS, MSD, Clinical Associate Professor, Department of Oral and Maxillary Pathology, Radiology and Medicine, New York University College of Dentistry, for the images included in this article and for Dr. Kerr’s clinical expertise and partnership.
REFERENCES
1. Sciubba JJ. Oral mucosal diseases in the office setting. Part II. Oral lichen planus, pemphigus vulgaris, and mucosal pemphigoid. Gen Dent. 2007;55(5):464-476.
2. Muñoz-Corcuera M, Esparza-Gómez G, González-Moles MA, Bascones-Martínez A. Oral ulcers: clinical aspects. A tool for dermatologists. Part II. Chronic ulcers. Clin Exp Dermatol. 2009; 34(4):456-461.
3. Dagistan S, Goregen M, Miloglu O, Cakur B. Oral pemphigus vulgaris: a case report with review of the literature. J Oral Sci. 2008;50(3):359-362.
4. Singh S. Evidence-based treatments for pemphigus vulgaris, pemphigus foliaceus and bullous pemphigoid: a systematic review. Indian J Dermatol Venereol Leprol. 2011;77(4):456-469.
5. Ohta M, Osawa S, Endo H, et al. Pemphigus vulgaris confined to the gingiva: a case report. Int J Dent. 2011;2011:207153. Epub 2011 May 11.
6. Mignona MD, Fortuna G, Leuci S. Oral pemphigus. Minerva Stomatol. 2009;58(10):501-518.
7. Mimouni D, Bar H, Gdalevich M, et al. Pemphigus: analysis of epidemiological factors in 155 patients. J Eur Acad Dermatol Venereol. 2008; 22(10):1232-1235.
8. Amagai M, Ikeda S, Shimizu H, et al. A randomized double-blind trial of intravenous immunoglobulin for pemphigus. J Am Acad Dermatol. 2009;60(4):595-603.
9. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: Part I. Superficial mucosal lesions. Am Fam Physician. 2007;75(4):501-507.
10. Fatahzadeh M, Schwartz R. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57(5):737-763.
11. Sugerman PB, Savage NW. Oral lichen planus: causes, diagnosis and management. Aust Dent J. 2002;47(4):290-297.
12. Kaomongkolgit R. Oral lichenoid drug reaction associated with antihypertensive and hypoglycemic drugs. J Drugs Dermatol. 2010;9(1):73-75.
13. Petti S, Rabiei M, De Luca M, Scully C. The magnitude of the association between hepatitis C virus infection and oral lichen planus: meta-analysis and case control study. Odontology. 2011;99(2):168-178.
14. Usatine RP, Tinitigan M. Diagnosis and treatment of lichen planus. Am Fam Physician. 2011;84(1): 53-60.
15. Thongprasom K, Carrozzo M, Furness S, Lodi G. Interventions for treating oral lichen planus. Cochrane Database Syst Rev. 2011 Jul 6; (7):CD001168.
16. Giannini PJ, Shetty KV. Diagnosis and management of oral candidiasis. Otolaryngol Clin North Am. 2011;44(1):231-240, vii.
17. Lynch DP. Oral candidiasis. History, classification, and clinical presentation. Oral Surg Oral Med Oral Pathol. 1994;78(2):189-193.
18. Williams D, Lewis M. Pathogenesis and treatment of oral candidosis. J Oral Microbiol. 2011 Jan 28;3. doi: 10.3402/jom.v3i0.5771.
19. Scully C, Challacombe SJ. Pemphigus vulgaris: update on etiopathogenesis, oral manifestations, and management. Crit Rev Oral Biol Med. 2002;13(5):397-408.
20. Martin LK, Werth V, Villanueva E, Murrell DF. A systematic review of randomized controlled trials for pemphigus vulgaris and pemphigus foliaceus. J Am Acad Dermatol. 2011;64(5):903-908.
21. Joly P, Mouquet H, Roujeau JC, et al. A single cycle of rituximab for the treatment of severe pemphigus. N Engl J Med. 2007;357(6):545-552.
22. Diaz LA. Rituximab and pemphigus: a therapeutic advance. N Engl J Med. 2007;357(6):605-607.
23. Anstey AV, Wakelin S, Reynolds NJ. Guidelines for prescribing azathioprine in dermatology. Br J Dermatol. 2004;151(6):1123-1132.
24. Chams-Davatchi C, Daneshpazhooh M. Prednisolone dosage in pemphigus vulgaris. J Am Acad Dermatol. 2005;53(3):547.
25. Agency for Healthcare Research and Quality. Guide to Clinical Preventive Services, 2010-2011: recommendations of the US Preventive Services Task Force. AHRQ Publication No. 10-05145, September 2010. www.ahrq.gov/clinic/pocketgd1011/pocketgd1011.pdf. Accessed January 23, 2012.
A 61-year-old man, who had recently emigrated from the Ukraine, presented to his primary care provider with a chief complaint of painful oral lesions and weight loss. The patient described the gradual onset of a severe sore throat and mouth pain three months earlier. Originally, he attributed his symptoms to an upper respiratory infection but became concerned when his symptoms did not resolve.
He reported that the pain had worsened over time and that he was now barely able to swallow solid food or tolerate acidic beverages due to considerable discomfort. His son, who accompanied him to the appointment, had also noted weight loss.
The patient denied any concomitant symptoms, including fever, cough, night sweats, fatigue, lymphadenopathy, abdominal pain, diarrhea, melena, or concomitant rash. His medical history was remarkable only for stage 1 hypertension, which had been well controlled on hydrochlorothiazide 12.5 mg/d for the previous three years. However, the patient had received only minimal preventive health care while living in the Ukraine. His family history was unknown.
One week earlier, the patient had seen a dentist complaining of mouth pain, and was referred to an oral medicine specialist; this specialist, in turn, referred the patient to a primary care nurse practitioner for lab work to confirm the suspected diagnosis of pemphigus vulgaris.
On physical examination, the patient appeared older than his stated age. He was a thin, mildly ill–appearing man, afebrile and normotensive, with heart rate and respirations within normal limits. However, intraoral examination revealed multiple oropharyngeal ulcerations of varying size on a base of erythematous and swollen mucosa on the inside of the man’s cheek and palatal and buccal mucosa (see Figure 1). On his upper back, two round, crusted blisters were noted in isolation (Figure 2). The remaining findings in the physical examination were unremarkable.
Based on the patient’s physical exam findings and clinical guideline recommendations regarding chronic oral ulcerations of unknown etiology,1,2 the patient was scheduled for a cytologic smear to be performed by oral medicine, followed by a gingival biopsy for a direct immunofluorescence test and routine histopathology.3 Unfortunately, due to extensive involvement and concern for possible mucosal shredding, an oral biopsy was not deemed possible.
However, the oral medicine specialist, because he strongly suspected pemphigus vulgaris, recommended testing for circulating autoantibodies against the antigens desmogleins 1 and/or 3 in the epidermis, which are responsible for cellular adhesion. (A positive test result supports, but does not confirm, a diagnosis of pemphigus vulgaris.4)
Additionally, baseline labs were performed for signs of systemic illness, including infection, anemia, and liver and kidney disease. Frequent monitoring was conducted for steroid-induced symptoms of elevated blood sugars; the primary care provider was responsible for monitoring the patient for weight gain and steroid-induced psychosis. The patient was referred to gastroenterology for a colonoscopy to ensure that his weight loss and anorexia were not the result of gastrointestinal malignancy. However, the patient declined this test.
DISCUSSION
Painful oral lesions can have numerous etiologies of varying severity and complexity, including herpes simplex virus infection, aphthae, lichen planus, erythema multiforme, squamous cell and other oral carcinomas, primary HIV infection, lupus, and pemphigus. Differentiating among these conditions requires a careful medical history and complete physical exam.5
Pemphigus vulgaris (PV) is the most common variant of pemphigus, a group of chronic autoimmune diseases that cause blistering and ulceration of the mucous membranes and the skin.6 From the Greek pemphix (bubble), PV is more common in people of Ashkenazi Jewish or Mediterranean descent,6,7 usually occurs in middle-aged and older persons, and occurs about 1.5 times more commonly in women than men.5,7 Until the introduction of systemic steroids, pemphigus was often a fatal disease. Significant mortality still exists, mainly as a result of infection or adverse reactions to medication therapy.5
In patients with PV, flaccid bullae are formed on the skin in a process called acantholysis, in which epidermal cells lose their ability to adhere to one another. This results in rapidly expanding, thin-walled blisters on the oral mucosa, scalp, face, axillae, and groin. The blisters burst easily, leaving irregularly shaped, painful ulcerations.4 Painful oral mucosal membrane erosions are the first presenting sign of PV and often the only sign for an average of five months before other skin lesions develop.3 These lesions are noninfectious.
To make a definitive diagnosis of PV, clinical lesions must be present, with a confirmation of histologic findings, acantholysis on biopsy, and a confirmation of autoantibodies present in tissue and/or serum.4 (For proposed detailed diagnostic criteria, see table4,8.)
Initial misdiagnoses, which often lead to delayed or incorrect treatment, usually include aphthous stomatitis, gingivostomatitis, erythema multiforme, erosive lichen planus, herpes simplex virus, and/or oral candidiasis.3
Common Differentials
Herpes simplex virus. Affecting between 15% and 45% of the population, herpes simplex virus (HSV) infection, also known as cold sores, is the most common cause of recurrent oral ulcers.9 HSV is transmitted through direct contact with lesions or via viral shedding. Primary infection, which may occur with flu-like symptoms, causes the sudden onset of multiple clustered vesicles on an erythematous base that quickly ulcerate and crust. Recurrent infections tend to be less severe and are accompanied by minimal systemic symptoms.10
Diagnosis is usually made through history and physical exam. However, diagnostic tests, including Tzanck smears, biopsy, polymerase chain reaction (PCR) assay, and/or viral isolation in culture, are sometimes used to confirm a suspected case.10
Oral lichen planus (OLP). This is a common, chronic, mucocutaneous inflammatory disease of unknown etiology that affects skin and mucous membranes of the mouth, including the buccal mucosa, tongue, and/or gums. These lesions are noninfectious and are an immunologically mediated disease. Stress, anxiety, genetic predisposition, NSAID use, antihypertensive medications (eg, captopril, enalapril, propranolol; considered an oral lichenoid drug reaction), and altered cell-mediated immune response have been considered possible causative factors.11,12 Recent reports suggest an association between hepatitis C virus and OLP.13
Affecting about 4% of the general population, and more predominate in perimenopausal women, OLP lesions appear as white, lacey patches; red, swollen tissues; or open sores, most commonly on the inside of the mouth bilaterally. Patients will present with complaints of burning, roughness, or pain in the mouth, dry mouth, sensitivity to hot or spicy foods, and difficulty swallowing if the throat is involved. Diagnosis is based on history and physical examination and often a confirmatory biopsy. Topical high-potency corticosteroids are generally first-line therapy, with systemic medications such as oral prednisone used to treat severe cases.14,15
Oral candidiasis. Up to 80% of healthy individuals carry Candida albicans in their mouths16; this pathogen accounts for about half of all cases of oral candidiasis (oral thrush). Oral infections occur only with an underlying predisposing condition in the host. Oral thrush presents as creamy white lesions on the oral mucosa; a diagnostic feature is that the plaques can be removed to reveal an erythematous base.16,17
In the chronic form of candidiasis, the mucosal surface is bright red and smooth. When the tongue is involved, it may appear dry, fissured, or cracked. Patients may report a dry mouth, burning pain, and difficulty eating. Infection can be confirmed with periodic acid-Schiff staining of a smear to detect candidal hyphae.9
Use of antifungal creams and lozenges, as well as improved oral hygiene, will often lead to resolution of symptoms.9 Management of any associated underlying conditions, such as diabetes, asthma requiring long-term use of steroid inhalers, or infection with HIV/AIDS, is essential.18
Oral aphthae. Recurrent aphthous ulcers (commonly called canker sores; also referred to as recurrent aphthous stomatitis [RAS]) are a common oral condition. Etiology is unknown and most likely multifactorial, with a strong genetic tendency and multiple predisposing factors, including trauma, stress, food allergies, hormones, and smoking.19 Certain chronic illnesses, including celiac disease, inflammatory bowel disease (IBD), HIV, and neutropenia may also predispose patients to RAS or RAS-like syndromes.
Aphthous ulcers are classified as minor or major. Minor aphthae, which account for 90% of RAS cases, present as single or multiple, small, oval or round ulcers with an erythematous halo on the buccal or labial mucosa or tongue.19 The ulcers last 7 to 10 days and heal spontaneously without scarring.
Diagnosis, based on history and clinical presentation, may include evaluation for systemic causes of oral ulcers. Treatment for both minor and major apthae is palliative, with mainstays including topical corticosteroids, mouth rinses, and, in severe cases, thalidomide, although randomized controlled trials have not shown this agent to be of benefit.9
Treatment for Pemphigus Vulgaris
The outcome goal for management of pemphigus is to achieve and maintain remission. This includes the epithelialization of all skin and mucosal lesions, prevention of relapse, minimization of adverse treatment effects, and successful withdrawal of therapeutic medications.20
The response to treatment varies greatly among patients, as the optimal therapeutic regimen for pemphigus is unknown.20 Systemic glucocorticoids are considered the gold standard of treatment and management, but their use has been associated with several adverse effects, including weight gain and elevated blood sugar levels. Recently, the combination of IV immune globulin and biological therapies (eg, rituximab) that target specific molecules in the inflammatory process have been demonstrated as effective in cases of refractory pemphigus.21,22
PATIENT MANAGEMENT AND OUTCOME
Several referrals were made, including dermatology, for its familiarity with autoimmune diseases of the skin. There, the patient was fully examined and found to have a small truncal lesion compatible with PV. He was referred to an otolaryngologist for a nasal endoscopy to determine the extent of the lesions. They were found to extend far beyond his oral cavity into his esophagus.
Based on a positive enzyme-linked immunosorbent assay (ELISA) for PV antibodies, a cytologic smear with acantholytic cells, and a classic clinical presentation of PV, the patient was started on prednisone 80 mg/d with azathioprine 50 mg/d for the first 14 days.23,24 He responded quickly to these oral medications and underwent a confirmatory oral biopsy within a few weeks.
After several months, the patient was slowly titrated down to lower maintenance doses of prednisone and azathioprine. Now in remission, he continues to receive collaborative management from oral medicine, dermatology, and a nurse practitioner–managed primary care practice. Health care maintenance has included appropriate vaccination and discussion regarding prostate cancer screening, per 2010 guidelines from the US Preventive Services Task Force.25
CONCLUSION
Since the differential diagnosis for pemphigus vulgaris is extensive and the diagnostic criteria are exacting, many affected patients are undiagnosed or misdiagnosed, with a resulting delay in effective treatment. It is important for the primary care clinician to undertake a frequent review of common oral infections, particularly those with similar presentations.
The authors extend their thanks to Alexander Kerr, DDS, MSD, Clinical Associate Professor, Department of Oral and Maxillary Pathology, Radiology and Medicine, New York University College of Dentistry, for the images included in this article and for Dr. Kerr’s clinical expertise and partnership.
REFERENCES
1. Sciubba JJ. Oral mucosal diseases in the office setting. Part II. Oral lichen planus, pemphigus vulgaris, and mucosal pemphigoid. Gen Dent. 2007;55(5):464-476.
2. Muñoz-Corcuera M, Esparza-Gómez G, González-Moles MA, Bascones-Martínez A. Oral ulcers: clinical aspects. A tool for dermatologists. Part II. Chronic ulcers. Clin Exp Dermatol. 2009; 34(4):456-461.
3. Dagistan S, Goregen M, Miloglu O, Cakur B. Oral pemphigus vulgaris: a case report with review of the literature. J Oral Sci. 2008;50(3):359-362.
4. Singh S. Evidence-based treatments for pemphigus vulgaris, pemphigus foliaceus and bullous pemphigoid: a systematic review. Indian J Dermatol Venereol Leprol. 2011;77(4):456-469.
5. Ohta M, Osawa S, Endo H, et al. Pemphigus vulgaris confined to the gingiva: a case report. Int J Dent. 2011;2011:207153. Epub 2011 May 11.
6. Mignona MD, Fortuna G, Leuci S. Oral pemphigus. Minerva Stomatol. 2009;58(10):501-518.
7. Mimouni D, Bar H, Gdalevich M, et al. Pemphigus: analysis of epidemiological factors in 155 patients. J Eur Acad Dermatol Venereol. 2008; 22(10):1232-1235.
8. Amagai M, Ikeda S, Shimizu H, et al. A randomized double-blind trial of intravenous immunoglobulin for pemphigus. J Am Acad Dermatol. 2009;60(4):595-603.
9. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: Part I. Superficial mucosal lesions. Am Fam Physician. 2007;75(4):501-507.
10. Fatahzadeh M, Schwartz R. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57(5):737-763.
11. Sugerman PB, Savage NW. Oral lichen planus: causes, diagnosis and management. Aust Dent J. 2002;47(4):290-297.
12. Kaomongkolgit R. Oral lichenoid drug reaction associated with antihypertensive and hypoglycemic drugs. J Drugs Dermatol. 2010;9(1):73-75.
13. Petti S, Rabiei M, De Luca M, Scully C. The magnitude of the association between hepatitis C virus infection and oral lichen planus: meta-analysis and case control study. Odontology. 2011;99(2):168-178.
14. Usatine RP, Tinitigan M. Diagnosis and treatment of lichen planus. Am Fam Physician. 2011;84(1): 53-60.
15. Thongprasom K, Carrozzo M, Furness S, Lodi G. Interventions for treating oral lichen planus. Cochrane Database Syst Rev. 2011 Jul 6; (7):CD001168.
16. Giannini PJ, Shetty KV. Diagnosis and management of oral candidiasis. Otolaryngol Clin North Am. 2011;44(1):231-240, vii.
17. Lynch DP. Oral candidiasis. History, classification, and clinical presentation. Oral Surg Oral Med Oral Pathol. 1994;78(2):189-193.
18. Williams D, Lewis M. Pathogenesis and treatment of oral candidosis. J Oral Microbiol. 2011 Jan 28;3. doi: 10.3402/jom.v3i0.5771.
19. Scully C, Challacombe SJ. Pemphigus vulgaris: update on etiopathogenesis, oral manifestations, and management. Crit Rev Oral Biol Med. 2002;13(5):397-408.
20. Martin LK, Werth V, Villanueva E, Murrell DF. A systematic review of randomized controlled trials for pemphigus vulgaris and pemphigus foliaceus. J Am Acad Dermatol. 2011;64(5):903-908.
21. Joly P, Mouquet H, Roujeau JC, et al. A single cycle of rituximab for the treatment of severe pemphigus. N Engl J Med. 2007;357(6):545-552.
22. Diaz LA. Rituximab and pemphigus: a therapeutic advance. N Engl J Med. 2007;357(6):605-607.
23. Anstey AV, Wakelin S, Reynolds NJ. Guidelines for prescribing azathioprine in dermatology. Br J Dermatol. 2004;151(6):1123-1132.
24. Chams-Davatchi C, Daneshpazhooh M. Prednisolone dosage in pemphigus vulgaris. J Am Acad Dermatol. 2005;53(3):547.
25. Agency for Healthcare Research and Quality. Guide to Clinical Preventive Services, 2010-2011: recommendations of the US Preventive Services Task Force. AHRQ Publication No. 10-05145, September 2010. www.ahrq.gov/clinic/pocketgd1011/pocketgd1011.pdf. Accessed January 23, 2012.
An Unusual Presentation of Subacute Osteomyelitis: A Talus Brodie Abscess With Tendon Involvement
An Analysis of Suboptimal Outcomes of Medial Malleolus Fractures in Skeletally Immature Children
A Survey on Management of Chronic Achilles Tendon Ruptures
Burkitt Lymphoma in a Child With Atopic Dermatitis and a 7-Year History of Regular Topical Tacrolimus Use
Obsessive and inattentive
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Perfect breath
Mr. C, a 20-year-old college student, is diagnosed with obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD), and tic disorder (TD). His obsessions consist of a persistent sense that he is not breathing “correctly” or “perfectly.” He compulsively holds his breath to “rush blood to my head” until “the pressure feels just right.” Mr. C says that his OCD has had longstanding, significant negative impact on his academic performance and capacity to engage in other activities. Tics have been present for years and manifest as coughing and throat-clearing. After multiple syncopal epi-sodes from breath-holding with Valsalva maneuver—some of which caused falls and head injury—Mr. C is admitted to a residential psychiatric unit specializing in treating OCD. At the time of his admission, his Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores1,2 are 23 total, 12 on the obsessions subscale, and 11 on the compulsions subscale, indicating moderate to severe illness. Cognitive-behavioral therapy (CBT) is offered, along with a combination of escitalopram, 60 mg/d, and quetiapine, 50 mg/d. Quetiapine is over-sedating at subtherapeutic doses and Mr. C’s compulsions worsen. He reports that “[it] took longer and longer to get the ‘just right’ feeling.’” Quetiapine is discontinued and risperidone, 0.5 mg/d, is started, which decreases the frequency of his tics. When he is discharged after a 36-day stay, Mr. C’s Y-BOCS scores are greatly improved at 13 total, 7 on the obsessions subscale, and 3 on the compulsions subscale.
Mr. C’s psychologist refers him to our outpatient clinic for continued psychiatric evaluation and treatment of his OCD, ADHD, and TD. At this time, he is prescribed escitalopram, 60 mg/d, and risperidone, 0.5 mg/d, along with CBT with his psychologist. We do not readminister the Y-BOCS at this time, but Mr. C reports that his OCD is “60% improved.” However, he describes prominent obsessive thoughts regarding his breathing similar to those he experienced before residential treatment. These obsessive thoughts arise in the context of specific environmental “triggers,” such as other people coughing or his own tics. The obsessions lead to compulsive urges to engage in breath-holding rituals. Mr. C experiences the thoughts and compulsions as deeply troubling and they consume 5 to 6 hours each day. Mr. C reports impaired concentration in class and during studying: “I can focus for 5 minutes, then not for 2 minutes, then for 3 minutes… I can never stay focused for more than a couple minutes,” before becoming distracted “by my OCD” or other environmental stimuli. We note on exam prominent breath-holding occurring several times per minute. Mr. C says his OCD has not impaired his ability to socialize.
Mr. C notes that he has been exposed to an array of CBT techniques, but he has difficulty using these techniques because his “mind wanders” or he lacks “motivation.” He admits he occasionally has taken a classmate’s ADHD medication (mixed amphetamine salts [MAS], dose unspecified) and found it improved his ability to focus on his academic work.
The authors’ observations
Researchers have established a relationship among OCD, ADHD, and TD across all combinations of comorbidity (OCD and ADHD,3 ADHD and TD,4 OCD and TD,5,6 and all 3 entities7). Data suggests a poorer prognosis for OCD when comorbid with either or both of these conditions.8 Researchers have raised concerns that psychostimulants could exacerbate or potentiate tic behaviors in patients with ADHD,9,10 although safe and effective use of these medications has been documented in controlled trials of patients with comorbid ADHD and tics.11-13 Furthermore, tic suppression has been reported with psychostimulants,14 as well as a differential effect of stimulants on motor vs vocal tics.15 Despite these data (Table 1),9-15 the FDA regards using psychostimulants in patients with TD as a contraindication,16 although clinicians often recognize that this practice may be unavoidable in some circumstances because of high comorbidity rates. Psychostimulants could exacerbate obsessions or compulsions in some patients because of their dopaminergic properties or through mitigation of the purported anti-obsessional properties of dopamine antagonists.17
Although there is evidence that the prevalence of prescribed psychostimulant abuse is low among ADHD patients,18 diversion of prescribed medication is a risk inherent in the use of these agents, particularly among college-age patients.19,20
Table 1
Evidence of effect of psychostimulants on tics
| Study/disorder(s) | Medication and study design | Relevant findings |
|---|---|---|
| Lipkin et al, 19949; ADHD without TD | Chart review (N = 122) to determine the incidence of tics or dyskinesias in children treated with stimulants | Approximately 9% of children developed tics or dyskinesias, which predominantly were transient, with <1% developing chronic tics or Tourette’s syndrome. Personal or family tic history and medication selection or dosage were not related to onset of tics or dyskinesias |
| Gadow et al, 199515; ADHD with TD | Methylphenidate variable dose, placebo-controlled, 2-week trials (N = 24) | All children’s ADHD symptoms improved. At a 0.1 mg/kg dose, motor tics observed in the classroom increased, but there were fewer vocal tics observed in the lunchroom |
| Castellanos et al, 199710; ADHD with Tourette’s syndrome | Methylphenidate, dextroamphetamine, variable-dose, double-blind, placebo-controlled, 9-week crossover (N = 20) | 3 patients had consistent worsening of tics while taking stimulants. Stimulants reduced hyperactivity rates compared with placebo (P = .03). Stimulants improved ADHD symptoms and had acceptable effects on tics. Methylphenidate was better tolerated than dextroamphetamine |
| Gadow et al, 199911; ADHD with TD | 34 methylphenidate-treated children, followed at 6-month intervals for 2 years | No evidence that frequency or severity of motor or vocal tics changed during maintenance therapy |
| Tourette Syndrome Study Group, 200213; ADHD with TD | Clonidine alone, methylphenidate alone, clonidine plus methylphenidate, or placebo | Worsening of tics was not reported in any group at a rate significantly higher than placebo. Tic severity was more reduced in the 2 clonidine groups than in the methylphenidate group |
| Lyon et al, 201014; ADHD with Tourette’s syndrome | Dexmethylphenidate, single-dose challenge. Ten patients with or without TSP | Acute dexmethylphenidate administration resulted in tic suppression but did not augment TSP |
| Gadow et al, 200712; ADHD with TD | Double-blind, placebo-controlled, 2-week trials each of 3 doses of methylphenidate and placebo (N = 71) | MPH-IR did not alter the overall severity of TD or OCD behaviors. Teacher ratings indicated that MPH-IR therapy decreased tic frequency and severity |
| ADHD: attention-deficit/hyperactivity disorder; MPH-IR: methylphenidate immediate release; OCD: obsessive-compulsive disorder; TD: tic disorder; TSP: tic suppression protocol | ||
TREATMENT: Weighing options
To manage impaired attention and executive function difficulties secondary to ADHD, we offer Mr. C several options, including bupropion, modafinil, and memantine augmentation. Mr. C asks for a psychostimulant because exam week is approaching and he wants a treatment with quick therapeutic effect. We discuss with Mr. C the potential for dopaminergic agents, such as psychostimulants, to exacerbate tics or OCD symptoms. Ultimately, we prescribe immediate-release MAS, 20 mg/d.
Two days later, Mr. C says he has taken 3 MAS doses and describes a marked reduction in obsessions, significant decrease in frequency of “triggers,” and greater capacity to use CBT saying, “when I am [triggered], I am able to move past the urges without doing any compulsions.” Daily time spent “stuck on” obsessions or compulsions decreases from 5 to 6 hours per day to “about 2 and a half minutes.”
Mr. C reports a modest increase in the prevalence of tics, experienced as “little throat clears and quick stuttering of breath.” He notes that, although in the past such tics would be followed by urges for “perfecting the tic and making it feel just right,” he presently “had no desire to do so.”
OUTCOME: Sharper focus
Increasing MAS immediate release from 20 mg/d to 30 mg/d suppresses Mr. C’s obsessions and compulsions for 8 hours. On the 19th day of treatment, MAS immediate release was replaced with an extended release formulation, 30 mg/d, which preserves therapeutic effect and tolerability for 16 weeks. Repeat Y-BOCS yields 9 total, 3 on obsessions subscale, and 6 on compulsions subscale scores.
One month later, Mr. C reports that his symptoms have been “improving ever since” the previous appointment. He continues to be able to access skills for managing his OCD and is doing well in his 2 accelerated summer courses, saying “I focus really well” in 3-hour class sessions. On exam, tic behaviors are nearly absent. Mr. C describes occasional bouts of anxiety associated with urges to engage in tic behaviors, in turn arising from fear of symptomatic recurrence as he worked toward stopping smoking as advised by his primary care physician and psychiatrist.
The authors’ observations
The results of the repeat Y-BOCS are consistent with improvement in obsessions but possible worsening of compulsions since Mr. C was discharged from residential treatment. Alternatively, compulsions may have worsened immediately after discharge and declined again with introduction of MAS.
A substantial body of literature describes the challenges associated with treating ADHD with comorbid tics, including the relative degree of risk of tic exacerbation associated with treating ADHD with psychostimulants. The range of FDA-approved pharmacologic options for treatment of this comorbidity is limited (Table 2),21 particularly given the risk for tardive dyskinesia associated with the typical antipsychotics haloperidol and chlorpromazine. Data support using the α-2 agonist clonidine to treat hyperactivity associated with ADHD22 and TD23 and an extended-release preparation of this medication is FDA-approved for the former but not the latter indication (an α-2A receptor subtype agonist, guanfacine, also is FDA-approved for ADHD in pediatric patients). Mr. C’s experience of robust, sustained reduction in obsessions, if not compulsions, after treatment with MAS is consistent with the few studies of stimulant use in ADHD with comorbid OCD.24,25
Effective treatment of ADHD may help Mr. C better access CBT strategies and thereby potentiate treatment of comorbid OCD.
Table 2
FDA-approved medications for ADHD, OCD, and TD
| Disorder | Medications |
|---|---|
| ADHD | Amphetamine (racemic), atomoxetine, chlorpromazine (hyperactivity), clonidine extended release, dexmethylphenidate, dextroamphetamine, guanfacine extended release, haloperidol (hyperactivity, second-line), lisdexamfetamine, methylphenidate (racemic) |
| OCD | Clomipramine, fluoxetine, fluvoxamine, paroxetine, sertraline |
| TD/Tourette’s syndrome | Haloperidol (Tourette’s), pimozide (Tourette’s) |
| ADHD: attention-deficit/hyperactivity disorder; OCD: obsessive-compulsive disorder; TD: tic disorder Source: Reference 21 | |
Related Resources
- Pliszka SR. Treating ADHD and comorbid disorders: psychosocial and psychopharmacological interventions. New York, NY: The Guilford Press; 2011.
- Pollak Y, Benarroch F, Kanengisser L, et al. Tourette syndrome-associated psychopathology: roles of comorbid attention-deficit hyperactivity disorder and obsessive-compulsive disorder. J Dev Behav Pediatr. 2009;30(5):413-419.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Clonidine extended release • Kapvay
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Guanfacine • Intuniv, Tenex
- Haloperidol • Haldol
- Lisdexamfetamine • Vyvanse
- Memantine • Namenda
- Methylphenidate • Methylin, Ritalin
- Modafinil • Provigil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
1. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use and reliability. Arch Gen Psych. 1989;46(11):1006-1011.
2. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: II. Validity. Arch Gen Psych. 1989;46(11):1012-1016.
3. Geller DA, Biederman J, Faraone S, et al. Re-examining comorbidity of obsessive compulsive and attention-deficit hyperactivity disorder using an empirically derived taxonomy. Eur Child Adolesc Psychiatry. 2004;13(2):83-91.
4. Freeman RD. Attention deficit hyperactivity disorder in the presence of Tourette syndrome. Neurol Clin. 1997;15(2):411-420.
5. Geller DA. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr Clin North Am. 2006;29(2):353-370.
6. Eapen V, Fox-Hiley P, Banerjee S, et al. Clinical features and associated psychopathology in a Tourette syndrome cohort. Acta Neurol Scand. 2004;109(4):255-260.
7. Kano Y, Ohta M, Nagai Y, et al. Association between Tourette syndrome and comorbidities in Japan. Brain Dev. 2010;32(3):201-207.
8. Grados M, Riddle M. Do all obsessive-compulsive disorder subtypes respond to medication? Int Rev Psychiatry. 2008;20(2):189-193.
9. Lipkin PH, Goldstein IH, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med. 1994;148(8):859-861.
10. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry. 1997;36(5):589-596.
11. Gadow K, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry. 1999;56(4):330-333.
12. Gadow KD, Sverd J, Nolan EE, et al. Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):840-848.
13. Tourette’s Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology. 2002;58(4):527-536.
14. Lyon GJ, Samar SM, Conelea C, et al. Testing tic suppression: comparing the effects of dexmethylphenidate to no mediation in children and adolescents with attention-deficit/hyperactivity disorder and Tourette’s disorder. J Child Adolesc Psychopharmacol. 2010;20(4):283-289.
15. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry. 1995;52(6):444-455.
16. Bloch MH, Panza KE, Landerso-Weisenberger A, et al. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J Am Acad Child Adolesc Psychiatry. 2009;48(9):884-893.
17. McDougle CJ, Goodman WK, Price LH. Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry. 1994;55(suppl):24-31.
18. Wilens TE, Morrison NR. The intersection of attention-deficit/hyperactivity disorder and substance abuse. Curr Opin Psychiatry. 2011;24(4):280-285.
19. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
20. Schubiner H. Substance abuse in patients with attention-deficit hyperactivity disorder: therapeutic implications. CNS Drugs. 2005;19(8):643-655.
21. Stahl SM. The prescriber’s guide. Stahl’s essential psychopharmacology. 3rd ed. New York NY: Cambridge University Press; 2009.
22. Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(2):171-179.
23. Hedderick EF, Morris CM, Singer HS. Double-blind crossover study of clonidine and levetiracetam in Tourette syndrome. Pediatr Neurol. 2009;40(6):420-425.
24. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11(4):237-241.
25. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80(3):231-235.
Counseling is a must with this smoking cessation aid
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
Copyright © 2012 The Family Physicians Inquiries Network.
All rights reserved.
Fatty liver disease in type 2 diabetes: Common and often unmanaged
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
ACIP immunization update
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.