User login
Who was responsible for excessive oxytocin doses? $18.2M verdict

Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Who was responsible for excessive oxytocin doses? $18.2M verdict
Early in the morning, a woman at 40 weeks’ gestation presented to the hospital for induction of labor managed by her ObGyn. Labor was lengthy, and the mother was given increasing doses of 22, 24, and 26 mIU/min of oxytocin to stimulate labor. The baby was delivered in the evening. The child suffered a hypoxic birth injury and has cerebral palsy.
Parents’ claim Excessive oxytocin was administered, causing uterine hyperstimulation and excessive contractions. Nurses failed to inform the ObGyn of an abnormal fetal heart rate during the afternoon.
Defendants’ defense The parties disputed the oxytocin orders. The ObGyn claimed she has a standing order against oxytocin doses over 20 mIU/min. The nurses claimed that the dosage was based on the ObGyn’s verbal orders, which the ObGyn denied. The ObGyn denied negligence and maintained that if she’d known of the oxytocin administration greater than 20 mIU/min and the abnormal fetal heart rate, she immediately would have called for cesarean delivery. The hospital denied negligence and maintained that the oxytocin was administered 10 hours before delivery and played no role in fetal distress.
Verdict At trial, the ObGyn did not call expert witnesses and, in closing arguments, the physician’s attorney asked for exoneration of the ObGyn and a finding of fault solely against the hospital. An $18.2 million Washington verdict was returned against the hospital.
What caused the child’s Erb’s palsy?
A mother presented to the hospital for induction of labor. Oxytocin was administered and the first stage of labor progressed normally. When the mother began pushing, the ObGyn noted a turtle sign at crowning and called for assistance. The ObGyn attempted to deliver the fetus with downward guidance of the fetal head but encountered shoulder dystocia and a nuchal cord. He unwrapped the cord and instructed the nursing staff to place the mother in the McRobert’s position to help dislodge the right shoulder. When that did not work, the ObGyn performed a first-degree episiotomy and completed delivery. The child was found to have Erb’s palsy of the right arm. She underwent decompression and neurolysis of the brachial plexus using sural nerve grafts but still has reduced use of her right arm.
Parents’ claim Shoulder dystocia was improperly managed, causing the brachial plexus injury.
Defendants’ defense The ObGyn and hospital system denied negligence. The child’s injury occurred in utero due to natural forces of the mother’s uterine contractions.
Verdict An Ohio defense verdict was returned.
Woman claims lack of proper consent
A 47-year-old woman underwent endometrial ablation performed by her ObGyn. During the procedure, the uterus was perforated and the ObGyn performed a hysterectomy. Six days later, the patient was found to have peritonitis and underwent bowel repair surgery. The patient developed untreatable bowel adhesions that cause chronic pain.
Patient’s claim There were less expensive and invasive alternatives to the ablation that the ObGyn did not offer. The patient claimed lack of informed consent for the ablation and hysterectomy and negligence in perforating the bowel. The ObGyn was also negligent in failing to recognize the perforation and to diagnose peritonitis in a timely manner.
Texas state law requires consent for hysterectomies without documented evidence of immediate danger to life. Her husband did not have the authority to consent on her behalf.
Physician’s defense The husband gave informed consent. Failure to recognize the perforation was not negligent; it is a known risk of the surgery. The patient’s care was transferred to another physician after the second postoperative day.
Verdict A $200,000 Texas settlement was reached.
Bowel obstruction in pregnant woman
A 29-year-old woman at 27 weeks’ gestation had abdominal pain. She went to a community hospital where a hospitalist was assigned to her care. After a day, the patient was found to have a small bowel obstruction and necrosis of the bowel. The baby was delivered preterm. The mother underwent 12 operations; half of her intestines were resected. The mother is being treated for posttraumatic stress syndrome. The child is autistic.
Parents’ claim The hospitalist did not diagnose the mother’s intestinal blockage in a timely manner and did not obtain an obstetric consult or notify the patient’s ObGyn. The hospital staff did not follow protocol to notify the mother’s ObGyn. The child’s autism is a result of preterm delivery.
Defendants’ defense The hospital denied any duty to notify the ObGyn if the patient was admitted to the hospital for nonobstetric reasons. The case was settled during trial.
Verdict A $4.2 million Washington settlement was reached including $3 million from the hospital.
Fourth-degree perineal tear and continuing pain after delivery
A woman in her 30s went to the hospital for induction of labor. After many hours, the ObGyn used vacuum extraction due to maternal fatigue. The baby emerged in compound presentation, with her hand at the side of her head. She weighed 9 lb 12 oz at birth. A fourth-degree perineal tear occurred at birth. Postpartum, a rectovaginal fistula developed that required several repair operations. The mother is unable to have intercourse due to continuing vaginal pain and discomfort.
Patient’s Claim Knowing that the father’s head was overly large, the ObGyn should have better estimated the fetus’ size, and should have performed cesarean delivery.
Physician’s defense The ObGyn admitted that he knew the baby was large but maintained that a large fetus does not mandate a cesarean delivery. There were no indications that the baby’s head or body was too large to fit through the mother’s pelvis, so a vaginal delivery was appropriate. A perineal tear is a known complication of childbirth and could not be prevented. The patient’s current pain is unrelated to the perineal tear.
Verdict A Pennsylvania defense verdict was returned.
Breast cancer missed in woman with dense breasts
In 2003, a 44-year-old woman was told she had dense fibrocystic breasts. From 2003 through 2009 she regularly saw a breast surgeon due to concern that breast cancer might be difficult to detect.
In August 2009, her ObGyn identified a questionable mass in her left breast after ultrasonography and mammography. The patient saw the surgeon in late September 2009; no further imaging was ordered and she was told to return in a year.
The patient, concerned about the mass, returned to the surgeon in May 2010. Testing revealed cancer, and she underwent radical mastectomy and other treatment.
Patient’s claim Because the mass had not been treated in a timely manner, her 5-year survival rate in May 2010 was less than 50%. The surgeon was negligent in failing to order additional testing in September 2009. Magnetic resonance imaging (MRI) would have detected the cancer at a time when her survival rate could have been 80%.
Physician’s defense The cancer was diagnosed in a timely manner. An earlier diagnosis would not have changed the outcome.
Verdict A Tennessee defense verdict was returned.
Child stillborn, mother injured after vacuum extraction
When the mother’s labor slowed at a birthing center, she received several medications including castor oil, blue cohosh, and black cohosh to induce labor. The mother was later transferred by ambulance to a hospital. Ninety minutes after admission, the ObGyn used vacuum extraction to deliver a stillborn child. The mother sustained damage to her rectum, uterus, and vagina, had repair surgery, and has been unable to get pregnant again.
Parents’ claim While in labor at the birthing center, the castor oil, blue cohosh, and black cohosh caused the patient’s uterus to contract excessively and contributed to fetal death. The patient should have been transferred to the hospital earlier. Cesarean delivery should have been performed immediately upon her arrival at the hospital but the ObGyn did not arrive at the hospital for an hour after the patient’s admission.
Defendants’ defense The head midwife at the birthing center conceded negligence. The hospital claimed that the fetus was already dead before the mother arrived. The ObGyn denied negligence, arguing that he had no supervisory role or ownership in the birthing center and was not present during the mother’s labor. He also claimed that the fetus was dead in utero 12 or more hours before delivery and that an infectious process had developed in the mother during the 17 hours that she was at the birthing center.
Verdict A $4,095,000 Florida verdict was returned against the ObGyn. A directed verdict was granted for the hospital.
Patient still in pain after labia reduction
A 44-year-old woman underwent surgical reduction of her labia minora performed by a gynecologist. The procedure was intended to relieve discomfort during sexual activity. The patient continues to have pain.
Patient’s claim An excessive amount of the right labia minora was removed because proper presurgical demarcation of the operative area was not performed. Her pain during intercourse has worsened and she cannot properly urinate.
Physician’s defense Presurgical demarcation was correctly completed using clamps. Surgery was properly performed. The asymmetry is due to poor healing of the surgical wound. The patient’s clitoris was not scarred. The patient never reported complications related to urination to her gynecologist. Her ongoing pain is due to an estrogen deficiency.
Verdict A New York defense verdict was returned.
Uterine rupture after version for breech presentation: $7M
A woman went to the hospital for delivery of her baby. The fetus was in breech position, but the mother requested vaginal delivery. When the ObGyn attempted an external cephalic version to turn the baby, the uterus ruptured and the placenta was damaged. The baby sustained hypoxic-ischemic encephalopathy resulting in cerebral palsy (CP). He requires constant nursing care.
Parents’ claim The ObGyn failed to recognize fetal distress during the breech version. The ObGyn improperly performed the version, causing the uterine rupture. There was lack of informed consent for the version.
Defendants’ defense The case was settled during trial.
Verdict A $7 million New Jersey settlement was reached.
Sepsis following hysterectomy
An ObGyn performed total abdominal hysterectomy to treat uterine fibroids in a 26-year-old woman. Despite reporting abdominal pain, the patient was discharged on postsurgical day 4.
Three days later, she went to a different hospital with moderate diffuse abdominal pain, constipation, nausea, emesis, tachycardia, and low-grade fever. An abdominal radiograph was taken, the patient was given morphine and ketorolac, and she was sent home.
She returned to the first hospital 3 days later reporting fever, nausea, emesis, diarrhea, and severe abdominal pain. After an abdominal computed tomography (CT) scan revealed numerous fluid- and gas-filled collections, indicative of abscess, intravenous antibiotics were ordered and administered.
Six days later, an infectious disease physician was consulted. He made a diagnosis of sepsis secondary to abdominal infection.
The next day, an abdominal CT scan revealed enlargement of multiple abdominal and pelvic fluid collections.
At exploratory laparotomy, purulent fluid was found in the anterior fascial compartment, with gross pus in the abdomen. The entire bowel was dilated, inflamed, and matted. Necrotic rind and infection were noted on multiple surfaces of the colon and small intestine and the transverse colon was gangrenous and sealed to the right lower quadrant. The patient’s intestines were resected and an ileostomy was placed, which was reversed several months later.
Patient’s claim The ObGyn did not offer an alternative to hysterectomy. The ObGyn was negligent in injuring the small intestine during surgery and failing to recognize and treat it intraoperatively. The patient should not have been discharged based on her reported symptoms. Failure to recognize and treat the injury led to sepsis with severe complications and months of recuperation.
Physician’s defense There was no negligence; small bowel injury is a known risk of hysterectomy. Other caregivers at both hospitals were at fault for not properly diagnosing and treating the infection.
Verdict A $901,420 Nevada verdict was returned; the ObGyn was found 85% at fault and other parties 15% at fault. The court granted the physician’s motion to reduce the verdict to $436,954, which included $371,411 from the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements, & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In this article
- What caused the child’s Erb’s palsy?
- Woman claims lack of proper consent
- Bowel obstruction in pregnant woman
- Fourth-degree perineal tear and continuing pain after delivery
- Breast cancer missed in woman with dense breasts
- Child stillborn, mother injured after vacuum extraction
- Patient still in pain after labia reduction
- Uterine rupture after version for breech presentation: $7M
- Sepsis following hysterectomy

Anticoagulant antidote effective in healthy volunteers

TORONTO—An antidote to factor Xa inhibitors can safely reverse the anticoagulant effect of apixaban in healthy volunteers, results of the ANNEXA-A study suggest.
The first part of this study showed that a bolus of the antidote, andexanet alfa, was effective. And none of the volunteers had serious adverse events, thrombotic events, or antibodies to factor X or Xa.
In the second part of the study, researchers tested a bolus and a 2-hour infusion of andexanet alfa.
The drug normalized coagulation parameters immediately post-bolus, and this effect was sustained during the infusion. The reversal of anti-factor Xa activity lasted 1 to 2 hours post-infusion.
As in part 1, there were no serious adverse events or thrombotic events, and none of the subjects developed antibodies to factor X or Xa.
Mark Crowther, MD, of McMaster University in Hamilton, Ontario, Canada, presented details on part 2 of ANNEXA-A at the ISTH 2015 Congress (abstract LB004). The trial was sponsored by Portola Pharmaceuticals, Inc., the company developing andexanet alfa.
The goal of the randomized, double-blind ANNEXA-A study was to evaluate the safety and efficacy of andexanet alfa in reversing apixaban-induced anticoagulation in healthy volunteers ages 50 to 75.
In part 1, 33 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus (n=24) or to placebo (n=9). Results from this part of the study were presented at the American Heart Association 2014 Scientific Sessions.
In the second part of the study, 32 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus followed by a continuous infusion of 4 mg/min for 120 minutes (n=24) or to placebo (n=8).
Safety
One subject in the andexanet alfa arm discontinued treatment during the infusion due to mild hives. The subject did not have any other allergic
manifestations or cardiorespiratory effects.
Six subjects had mild infusion-related reactions, 4 (16.7%) in the andexanet alfa arm and 2 (25%) in the placebo arm.
None of the subjects had an increase in D-dimer (more than 2 times the upper limit of normal) on more than 1 day.
The majority of andexanet-alfa-treated subjects had transient elevation of F1 and F2, but, in all cases, levels returned to less than or equal to 2 times the upper limit of normal by the fourth day.
Efficacy
Twenty-three subjects in the andexanet alfa arm and all 8 subjects in the placebo arm were evaluable for efficacy.
All evaluable subjects in the andexanet alfa arm had an 80% or greater reduction in anti-factor Xa activity post-infusion nadir, compared to none of the subjects on placebo (P<0.0001).
The mean percent change in anti-factor Xa activity from baseline to post-infusion nadir was 92% in the andexanet alfa arm (P<0.0001 vs placebo). And the mean percent change from baseline to post-bolus nadir was 93% (P<0.0001 vs placebo).
The mean change in free apixaban concentration from baseline to post-infusion nadir was 1.39 ng/mL in the andexanet alfa arm (P=0.0002 vs placebo).
Thrombin generation was restored to the day 1, pre-apixaban baseline range in all 23 subjects on andexanet alfa (P<0.0001). And there was no long-term effect on thrombin generation.
The researchers said andexanet alfa demonstrated rapid onset and offset of action. Furthermore, it seems that either a bolus dose alone or a bolus plus infusion can reverse apixaban’s anticoagulant activity, which could provide flexibility for bleeding patients.
Andexanet alfa is also under investigation as an antidote to rivaroxaban, edoxaban, enoxaparin, and betrixaban. ![]()
TORONTO—An antidote to factor Xa inhibitors can safely reverse the anticoagulant effect of apixaban in healthy volunteers, results of the ANNEXA-A study suggest.
The first part of this study showed that a bolus of the antidote, andexanet alfa, was effective. And none of the volunteers had serious adverse events, thrombotic events, or antibodies to factor X or Xa.
In the second part of the study, researchers tested a bolus and a 2-hour infusion of andexanet alfa.
The drug normalized coagulation parameters immediately post-bolus, and this effect was sustained during the infusion. The reversal of anti-factor Xa activity lasted 1 to 2 hours post-infusion.
As in part 1, there were no serious adverse events or thrombotic events, and none of the subjects developed antibodies to factor X or Xa.
Mark Crowther, MD, of McMaster University in Hamilton, Ontario, Canada, presented details on part 2 of ANNEXA-A at the ISTH 2015 Congress (abstract LB004). The trial was sponsored by Portola Pharmaceuticals, Inc., the company developing andexanet alfa.
The goal of the randomized, double-blind ANNEXA-A study was to evaluate the safety and efficacy of andexanet alfa in reversing apixaban-induced anticoagulation in healthy volunteers ages 50 to 75.
In part 1, 33 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus (n=24) or to placebo (n=9). Results from this part of the study were presented at the American Heart Association 2014 Scientific Sessions.
In the second part of the study, 32 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus followed by a continuous infusion of 4 mg/min for 120 minutes (n=24) or to placebo (n=8).
Safety
One subject in the andexanet alfa arm discontinued treatment during the infusion due to mild hives. The subject did not have any other allergic
manifestations or cardiorespiratory effects.
Six subjects had mild infusion-related reactions, 4 (16.7%) in the andexanet alfa arm and 2 (25%) in the placebo arm.
None of the subjects had an increase in D-dimer (more than 2 times the upper limit of normal) on more than 1 day.
The majority of andexanet-alfa-treated subjects had transient elevation of F1 and F2, but, in all cases, levels returned to less than or equal to 2 times the upper limit of normal by the fourth day.
Efficacy
Twenty-three subjects in the andexanet alfa arm and all 8 subjects in the placebo arm were evaluable for efficacy.
All evaluable subjects in the andexanet alfa arm had an 80% or greater reduction in anti-factor Xa activity post-infusion nadir, compared to none of the subjects on placebo (P<0.0001).
The mean percent change in anti-factor Xa activity from baseline to post-infusion nadir was 92% in the andexanet alfa arm (P<0.0001 vs placebo). And the mean percent change from baseline to post-bolus nadir was 93% (P<0.0001 vs placebo).
The mean change in free apixaban concentration from baseline to post-infusion nadir was 1.39 ng/mL in the andexanet alfa arm (P=0.0002 vs placebo).
Thrombin generation was restored to the day 1, pre-apixaban baseline range in all 23 subjects on andexanet alfa (P<0.0001). And there was no long-term effect on thrombin generation.
The researchers said andexanet alfa demonstrated rapid onset and offset of action. Furthermore, it seems that either a bolus dose alone or a bolus plus infusion can reverse apixaban’s anticoagulant activity, which could provide flexibility for bleeding patients.
Andexanet alfa is also under investigation as an antidote to rivaroxaban, edoxaban, enoxaparin, and betrixaban. ![]()
TORONTO—An antidote to factor Xa inhibitors can safely reverse the anticoagulant effect of apixaban in healthy volunteers, results of the ANNEXA-A study suggest.
The first part of this study showed that a bolus of the antidote, andexanet alfa, was effective. And none of the volunteers had serious adverse events, thrombotic events, or antibodies to factor X or Xa.
In the second part of the study, researchers tested a bolus and a 2-hour infusion of andexanet alfa.
The drug normalized coagulation parameters immediately post-bolus, and this effect was sustained during the infusion. The reversal of anti-factor Xa activity lasted 1 to 2 hours post-infusion.
As in part 1, there were no serious adverse events or thrombotic events, and none of the subjects developed antibodies to factor X or Xa.
Mark Crowther, MD, of McMaster University in Hamilton, Ontario, Canada, presented details on part 2 of ANNEXA-A at the ISTH 2015 Congress (abstract LB004). The trial was sponsored by Portola Pharmaceuticals, Inc., the company developing andexanet alfa.
The goal of the randomized, double-blind ANNEXA-A study was to evaluate the safety and efficacy of andexanet alfa in reversing apixaban-induced anticoagulation in healthy volunteers ages 50 to 75.
In part 1, 33 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus (n=24) or to placebo (n=9). Results from this part of the study were presented at the American Heart Association 2014 Scientific Sessions.
In the second part of the study, 32 healthy volunteers received apixaban at 5 mg twice daily for 4 days and were then randomized in a 3:1 ratio to andexanet alfa administered as a 400 mg intravenous bolus followed by a continuous infusion of 4 mg/min for 120 minutes (n=24) or to placebo (n=8).
Safety
One subject in the andexanet alfa arm discontinued treatment during the infusion due to mild hives. The subject did not have any other allergic
manifestations or cardiorespiratory effects.
Six subjects had mild infusion-related reactions, 4 (16.7%) in the andexanet alfa arm and 2 (25%) in the placebo arm.
None of the subjects had an increase in D-dimer (more than 2 times the upper limit of normal) on more than 1 day.
The majority of andexanet-alfa-treated subjects had transient elevation of F1 and F2, but, in all cases, levels returned to less than or equal to 2 times the upper limit of normal by the fourth day.
Efficacy
Twenty-three subjects in the andexanet alfa arm and all 8 subjects in the placebo arm were evaluable for efficacy.
All evaluable subjects in the andexanet alfa arm had an 80% or greater reduction in anti-factor Xa activity post-infusion nadir, compared to none of the subjects on placebo (P<0.0001).
The mean percent change in anti-factor Xa activity from baseline to post-infusion nadir was 92% in the andexanet alfa arm (P<0.0001 vs placebo). And the mean percent change from baseline to post-bolus nadir was 93% (P<0.0001 vs placebo).
The mean change in free apixaban concentration from baseline to post-infusion nadir was 1.39 ng/mL in the andexanet alfa arm (P=0.0002 vs placebo).
Thrombin generation was restored to the day 1, pre-apixaban baseline range in all 23 subjects on andexanet alfa (P<0.0001). And there was no long-term effect on thrombin generation.
The researchers said andexanet alfa demonstrated rapid onset and offset of action. Furthermore, it seems that either a bolus dose alone or a bolus plus infusion can reverse apixaban’s anticoagulant activity, which could provide flexibility for bleeding patients.
Andexanet alfa is also under investigation as an antidote to rivaroxaban, edoxaban, enoxaparin, and betrixaban. ![]()
‘Radically different’ PI3Kδ inhibitor lacks hepatotoxicity

Photo by Larry Young
LUGANO—Updated phase 1 results with TGR-1202 suggest this next-generation PI3kδ inhibitor lacks the hepatotoxicity associated with other PI3Kδ inhibitors.
Investigators also confirmed that no case of colitis has been reported to date with TGR-1202, and only 2% of evaluable patients on this trial have experienced grade 3-4 diarrhea.
The study is an ongoing, first-in-human trial in patients with relapsed or refractory hematologic malignancies.
Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York, shared results from this trial at the 13th International Congress on Malignant Lymphoma (abstract 038*). The trial is sponsored by TG Therapeutics, Inc., the company developing TGR-1202.
“TGR-1202 is a radically different sort of PI3kδ inhibitor,” Dr O’Connor said. “[I]t’s really a unique chemical entity that is different from the previous 2 structures [idelalisib and duvelisib] that you’ve probably heard something about.”
Study design
This ongoing trial of TGR-1202 is open to patients with hematologic malignancies who relapsed after or were refractory to at least 1 prior treatment regimen. Patients are eligible if they have an ECOG performance status of 2 or less with adequate organ system function, including absolute neutrophil count of 750/μL or greater and platelets of 50,000/μL or greater.
TGR-1202 is dosed orally, once a day in continuous, 28-day cycles. The original dose-escalation portion of the study was a classic 3+3 design, starting at 50 mg and increasing to 1800 mg. Patients who received prior therapy with a PI3K and/or mTOR inhibitor were excluded from the dose-escalation cohorts but were allowed in the expansion cohorts.
Dr O’Connor pointed out that, through cohort 5, TGR-1202 was taken in the fasting state. However, pharmacokinetic studies performed in the fed state revealed that the area under the curve (AUC) and Cmax could be doubled by taking the drug with food. So the expansions in the ongoing 800 mg and 1200 mg cohorts are being conducted in the fed state.
Dr O’Connor also noted that a subsequent, micronized version of TGR-1202 was developed. The micronization “essentially increases the surface area of the formulation, allowing for better bioavailability and markedly increases the AUC and Cmax exposure,” he said.
So the investigators conducted a second escalation with the micronized formulation, starting at 200 mg and increasing to 800 mg. At present, they are enrolling patients to the 800 mg and 1200 mg cohorts conducted in the fed state with the micronized formulation.
Demographics
Dr O’Connor presented data on 66 patients who were evaluable for safety and 51 for efficacy. The patients’ median age was 66 (range, 22–85), and 46 were male.
In all, there were 20 patients with chronic lymphocytic leukemia (CLL), 17 with follicular lymphoma, 10 with diffuse large B-cell lymphoma, 9 with Hodgkin lymphoma, 5 with mantle cell lymphoma, 3 with marginal zone lymphoma, 1 with Waldenström’s macroglobulinemia, and 1 with hairy cell leukemia.
Patients had received a median of 3 prior therapies (range, 1–14), and 36 (55%) had 3 or more prior therapies. Thirty-four patients (52%) were refractory to their prior therapy.
Efficacy
Dr O’Connor reported that higher doses of TGR-1202—1200 mg of the initial formulation and 600 mg or more of the micronized version—demonstrated rapid and profound responses in CLL, follicular lymphoma, and marginal zone lymphoma.
Responses have been limited in diffuse large B-cell lymphoma, Hodgkin lymphoma, and mantle cell lymphoma.
Eighty-eight percent of CLL patients achieved a nodal partial remission, and 63% achieved a response according to iwCLL criteria (Hallek 2008).
Safety and tolerability
Adverse events occurring in more than 10% of patients included nausea (41%), diarrhea (32%), fatigue (32%), headache (23%), vomiting (23%), cough (21%), decreased appetite (17%), rash (17%), constipation (14%), hypokalemia (14%), anemia, dizziness, dyspnea, neutropenia, and pyrexia (12% each), and abdominal pain (11%).
The most common grade 3-4 toxicity was neutropenia, occurring in 11% of patients.
“But other than that, the bulk of the toxicities in terms of grade 3-4 events were relatively modest,” Dr O’Connor said. “[I]t’s worth pointing out that diarrhea grade 3-4 only occurred in about 2% of patients in the population.”
Approximately 50% of patients (n=31) have been on study for more than 6 months, and approximately 30% taking a higher dose level have been on study for 6 months or more. Twenty-five of 37 patients exposed to 800 mg or more of the micronized formulation currently remain on study.
“So this gives you a sense that it is a very well-tolerated drug, with patients staying on for extended periods of time,” Dr O’Connor said.
He added that time on study becomes relevant in assessing some of the gastrointestinal toxicities seen with other PI3Kδ inhibitors, where it seems the median time to gastrointestinal toxicity is beyond 6 months.
“So far, and I’m willing to concede it’s early, but with half the patients being treated for over 6 months, [diarrhea/colitis] seems to be much lower than the experience with the other PI3 kinase inhibitors,” Dr O’Connor said.
“I think one of the more important features of [TGR-1202], and one that allows me to think we might be able to integrate this drug a little more readily into various combination regimens, are the discontinuations due to other adverse events.”
“Only 4% treated with [TGR-1202] had discontinuations secondary to adverse events. [A]nd it looks like the efficacy is in line with what we’d expect with some of the other drugs, but this [study] is actively accruing still.” ![]()
*Information in the abstract differs from that presented at the meeting.
Photo by Larry Young
LUGANO—Updated phase 1 results with TGR-1202 suggest this next-generation PI3kδ inhibitor lacks the hepatotoxicity associated with other PI3Kδ inhibitors.
Investigators also confirmed that no case of colitis has been reported to date with TGR-1202, and only 2% of evaluable patients on this trial have experienced grade 3-4 diarrhea.
The study is an ongoing, first-in-human trial in patients with relapsed or refractory hematologic malignancies.
Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York, shared results from this trial at the 13th International Congress on Malignant Lymphoma (abstract 038*). The trial is sponsored by TG Therapeutics, Inc., the company developing TGR-1202.
“TGR-1202 is a radically different sort of PI3kδ inhibitor,” Dr O’Connor said. “[I]t’s really a unique chemical entity that is different from the previous 2 structures [idelalisib and duvelisib] that you’ve probably heard something about.”
Study design
This ongoing trial of TGR-1202 is open to patients with hematologic malignancies who relapsed after or were refractory to at least 1 prior treatment regimen. Patients are eligible if they have an ECOG performance status of 2 or less with adequate organ system function, including absolute neutrophil count of 750/μL or greater and platelets of 50,000/μL or greater.
TGR-1202 is dosed orally, once a day in continuous, 28-day cycles. The original dose-escalation portion of the study was a classic 3+3 design, starting at 50 mg and increasing to 1800 mg. Patients who received prior therapy with a PI3K and/or mTOR inhibitor were excluded from the dose-escalation cohorts but were allowed in the expansion cohorts.
Dr O’Connor pointed out that, through cohort 5, TGR-1202 was taken in the fasting state. However, pharmacokinetic studies performed in the fed state revealed that the area under the curve (AUC) and Cmax could be doubled by taking the drug with food. So the expansions in the ongoing 800 mg and 1200 mg cohorts are being conducted in the fed state.
Dr O’Connor also noted that a subsequent, micronized version of TGR-1202 was developed. The micronization “essentially increases the surface area of the formulation, allowing for better bioavailability and markedly increases the AUC and Cmax exposure,” he said.
So the investigators conducted a second escalation with the micronized formulation, starting at 200 mg and increasing to 800 mg. At present, they are enrolling patients to the 800 mg and 1200 mg cohorts conducted in the fed state with the micronized formulation.
Demographics
Dr O’Connor presented data on 66 patients who were evaluable for safety and 51 for efficacy. The patients’ median age was 66 (range, 22–85), and 46 were male.
In all, there were 20 patients with chronic lymphocytic leukemia (CLL), 17 with follicular lymphoma, 10 with diffuse large B-cell lymphoma, 9 with Hodgkin lymphoma, 5 with mantle cell lymphoma, 3 with marginal zone lymphoma, 1 with Waldenström’s macroglobulinemia, and 1 with hairy cell leukemia.
Patients had received a median of 3 prior therapies (range, 1–14), and 36 (55%) had 3 or more prior therapies. Thirty-four patients (52%) were refractory to their prior therapy.
Efficacy
Dr O’Connor reported that higher doses of TGR-1202—1200 mg of the initial formulation and 600 mg or more of the micronized version—demonstrated rapid and profound responses in CLL, follicular lymphoma, and marginal zone lymphoma.
Responses have been limited in diffuse large B-cell lymphoma, Hodgkin lymphoma, and mantle cell lymphoma.
Eighty-eight percent of CLL patients achieved a nodal partial remission, and 63% achieved a response according to iwCLL criteria (Hallek 2008).
Safety and tolerability
Adverse events occurring in more than 10% of patients included nausea (41%), diarrhea (32%), fatigue (32%), headache (23%), vomiting (23%), cough (21%), decreased appetite (17%), rash (17%), constipation (14%), hypokalemia (14%), anemia, dizziness, dyspnea, neutropenia, and pyrexia (12% each), and abdominal pain (11%).
The most common grade 3-4 toxicity was neutropenia, occurring in 11% of patients.
“But other than that, the bulk of the toxicities in terms of grade 3-4 events were relatively modest,” Dr O’Connor said. “[I]t’s worth pointing out that diarrhea grade 3-4 only occurred in about 2% of patients in the population.”
Approximately 50% of patients (n=31) have been on study for more than 6 months, and approximately 30% taking a higher dose level have been on study for 6 months or more. Twenty-five of 37 patients exposed to 800 mg or more of the micronized formulation currently remain on study.
“So this gives you a sense that it is a very well-tolerated drug, with patients staying on for extended periods of time,” Dr O’Connor said.
He added that time on study becomes relevant in assessing some of the gastrointestinal toxicities seen with other PI3Kδ inhibitors, where it seems the median time to gastrointestinal toxicity is beyond 6 months.
“So far, and I’m willing to concede it’s early, but with half the patients being treated for over 6 months, [diarrhea/colitis] seems to be much lower than the experience with the other PI3 kinase inhibitors,” Dr O’Connor said.
“I think one of the more important features of [TGR-1202], and one that allows me to think we might be able to integrate this drug a little more readily into various combination regimens, are the discontinuations due to other adverse events.”
“Only 4% treated with [TGR-1202] had discontinuations secondary to adverse events. [A]nd it looks like the efficacy is in line with what we’d expect with some of the other drugs, but this [study] is actively accruing still.” ![]()
*Information in the abstract differs from that presented at the meeting.
Photo by Larry Young
LUGANO—Updated phase 1 results with TGR-1202 suggest this next-generation PI3kδ inhibitor lacks the hepatotoxicity associated with other PI3Kδ inhibitors.
Investigators also confirmed that no case of colitis has been reported to date with TGR-1202, and only 2% of evaluable patients on this trial have experienced grade 3-4 diarrhea.
The study is an ongoing, first-in-human trial in patients with relapsed or refractory hematologic malignancies.
Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York, shared results from this trial at the 13th International Congress on Malignant Lymphoma (abstract 038*). The trial is sponsored by TG Therapeutics, Inc., the company developing TGR-1202.
“TGR-1202 is a radically different sort of PI3kδ inhibitor,” Dr O’Connor said. “[I]t’s really a unique chemical entity that is different from the previous 2 structures [idelalisib and duvelisib] that you’ve probably heard something about.”
Study design
This ongoing trial of TGR-1202 is open to patients with hematologic malignancies who relapsed after or were refractory to at least 1 prior treatment regimen. Patients are eligible if they have an ECOG performance status of 2 or less with adequate organ system function, including absolute neutrophil count of 750/μL or greater and platelets of 50,000/μL or greater.
TGR-1202 is dosed orally, once a day in continuous, 28-day cycles. The original dose-escalation portion of the study was a classic 3+3 design, starting at 50 mg and increasing to 1800 mg. Patients who received prior therapy with a PI3K and/or mTOR inhibitor were excluded from the dose-escalation cohorts but were allowed in the expansion cohorts.
Dr O’Connor pointed out that, through cohort 5, TGR-1202 was taken in the fasting state. However, pharmacokinetic studies performed in the fed state revealed that the area under the curve (AUC) and Cmax could be doubled by taking the drug with food. So the expansions in the ongoing 800 mg and 1200 mg cohorts are being conducted in the fed state.
Dr O’Connor also noted that a subsequent, micronized version of TGR-1202 was developed. The micronization “essentially increases the surface area of the formulation, allowing for better bioavailability and markedly increases the AUC and Cmax exposure,” he said.
So the investigators conducted a second escalation with the micronized formulation, starting at 200 mg and increasing to 800 mg. At present, they are enrolling patients to the 800 mg and 1200 mg cohorts conducted in the fed state with the micronized formulation.
Demographics
Dr O’Connor presented data on 66 patients who were evaluable for safety and 51 for efficacy. The patients’ median age was 66 (range, 22–85), and 46 were male.
In all, there were 20 patients with chronic lymphocytic leukemia (CLL), 17 with follicular lymphoma, 10 with diffuse large B-cell lymphoma, 9 with Hodgkin lymphoma, 5 with mantle cell lymphoma, 3 with marginal zone lymphoma, 1 with Waldenström’s macroglobulinemia, and 1 with hairy cell leukemia.
Patients had received a median of 3 prior therapies (range, 1–14), and 36 (55%) had 3 or more prior therapies. Thirty-four patients (52%) were refractory to their prior therapy.
Efficacy
Dr O’Connor reported that higher doses of TGR-1202—1200 mg of the initial formulation and 600 mg or more of the micronized version—demonstrated rapid and profound responses in CLL, follicular lymphoma, and marginal zone lymphoma.
Responses have been limited in diffuse large B-cell lymphoma, Hodgkin lymphoma, and mantle cell lymphoma.
Eighty-eight percent of CLL patients achieved a nodal partial remission, and 63% achieved a response according to iwCLL criteria (Hallek 2008).
Safety and tolerability
Adverse events occurring in more than 10% of patients included nausea (41%), diarrhea (32%), fatigue (32%), headache (23%), vomiting (23%), cough (21%), decreased appetite (17%), rash (17%), constipation (14%), hypokalemia (14%), anemia, dizziness, dyspnea, neutropenia, and pyrexia (12% each), and abdominal pain (11%).
The most common grade 3-4 toxicity was neutropenia, occurring in 11% of patients.
“But other than that, the bulk of the toxicities in terms of grade 3-4 events were relatively modest,” Dr O’Connor said. “[I]t’s worth pointing out that diarrhea grade 3-4 only occurred in about 2% of patients in the population.”
Approximately 50% of patients (n=31) have been on study for more than 6 months, and approximately 30% taking a higher dose level have been on study for 6 months or more. Twenty-five of 37 patients exposed to 800 mg or more of the micronized formulation currently remain on study.
“So this gives you a sense that it is a very well-tolerated drug, with patients staying on for extended periods of time,” Dr O’Connor said.
He added that time on study becomes relevant in assessing some of the gastrointestinal toxicities seen with other PI3Kδ inhibitors, where it seems the median time to gastrointestinal toxicity is beyond 6 months.
“So far, and I’m willing to concede it’s early, but with half the patients being treated for over 6 months, [diarrhea/colitis] seems to be much lower than the experience with the other PI3 kinase inhibitors,” Dr O’Connor said.
“I think one of the more important features of [TGR-1202], and one that allows me to think we might be able to integrate this drug a little more readily into various combination regimens, are the discontinuations due to other adverse events.”
“Only 4% treated with [TGR-1202] had discontinuations secondary to adverse events. [A]nd it looks like the efficacy is in line with what we’d expect with some of the other drugs, but this [study] is actively accruing still.” ![]()
*Information in the abstract differs from that presented at the meeting.
Cord milking better than delayed clamping for some preterm infants

Photo courtesy of Meutia
Chaerani & Indradi Soemardjan
Umbilical cord milking may be more beneficial than delayed cord clamping for preterm infants delivered by Cesarean section, according to new research.
The study showed that cord milking produced greater blood circulation, higher hemoglobin levels, and higher blood pressure, but only in preterm infants delivered by Cesarean.
For preterm infants delivered vaginally, there was no significant difference between the milking and delayed clamping groups.
Anup C. Katheria, MD, of the Neonatal Research Institute at the Sharp Mary Birch Hospital in San Diego, California, and his colleagues reported these findings in Pediatrics.
The researchers noted that, in 2012, the American College of Obstetricians and Gynecologists recommended a 30- to 60-second delay before clamping the umbilical cord in all preterm deliveries.
This is thought to allow sufficient time for blood from the umbilical cord to fill the blood vessels in the infant’s lungs and to protect infants from intraventricular hemorrhage. However, some previous studies failed to find a reduction in intraventricular hemorrhage from delayed cord clamping among preterm infants delivered by Cesarean.
Dr Katheria and his colleagues theorized that the use of an anesthetic in Cesarean delivery reduces uterine contractions and therefore hinders the exodus of blood from the umbilical cord.
They reasoned that cord milking—encircling the cord with thumb and forefingers, gently squeezing, and slowly pushing the blood through the cord to the infant’s abdomen—might compensate for diminished blood flow through the umbilical cord and increase the amount of blood available to the infant.
To test this theory, the researchers enrolled 197 infants in a prospective study. Mothers went into labor at or before the 32nd week of pregnancy.
Of the 154 infants delivered by Cesarean, 75 were randomized to the umbilical cord milking (UCM) group and 79 to the delayed cord clamping (DCC) group.
Infants in the UCM group had significantly higher blood flow in the superior vena cava than those in the DCC group—93 ± 24 mL/kg per min vs 81 ± 29 mL/kg per min (P<0.05)—and a significantly higher output of blood from the right ventricle—261 ± 80 mL/kg per min vs 216 ±73 mL/kg per min (P<0.001).
These measures, taken together, are an indication of blood circulation in the brain and body.
Infants in the UCM group had significantly higher hemoglobin levels at birth than infants in the DCC group—16.3 ± 2.4 g/dL vs 15.6 ± 2.2 g/dL (P<0.05). And mean arterial pressure in the first 15 hours of life was significantly higher in the UCM group than the DCC group (P=0.02).
Among the 43 infants who were delivered vaginally, the researchers found no significant differences in outcomes between infants randomized to UCM or DCC. ![]()
Photo courtesy of Meutia
Chaerani & Indradi Soemardjan
Umbilical cord milking may be more beneficial than delayed cord clamping for preterm infants delivered by Cesarean section, according to new research.
The study showed that cord milking produced greater blood circulation, higher hemoglobin levels, and higher blood pressure, but only in preterm infants delivered by Cesarean.
For preterm infants delivered vaginally, there was no significant difference between the milking and delayed clamping groups.
Anup C. Katheria, MD, of the Neonatal Research Institute at the Sharp Mary Birch Hospital in San Diego, California, and his colleagues reported these findings in Pediatrics.
The researchers noted that, in 2012, the American College of Obstetricians and Gynecologists recommended a 30- to 60-second delay before clamping the umbilical cord in all preterm deliveries.
This is thought to allow sufficient time for blood from the umbilical cord to fill the blood vessels in the infant’s lungs and to protect infants from intraventricular hemorrhage. However, some previous studies failed to find a reduction in intraventricular hemorrhage from delayed cord clamping among preterm infants delivered by Cesarean.
Dr Katheria and his colleagues theorized that the use of an anesthetic in Cesarean delivery reduces uterine contractions and therefore hinders the exodus of blood from the umbilical cord.
They reasoned that cord milking—encircling the cord with thumb and forefingers, gently squeezing, and slowly pushing the blood through the cord to the infant’s abdomen—might compensate for diminished blood flow through the umbilical cord and increase the amount of blood available to the infant.
To test this theory, the researchers enrolled 197 infants in a prospective study. Mothers went into labor at or before the 32nd week of pregnancy.
Of the 154 infants delivered by Cesarean, 75 were randomized to the umbilical cord milking (UCM) group and 79 to the delayed cord clamping (DCC) group.
Infants in the UCM group had significantly higher blood flow in the superior vena cava than those in the DCC group—93 ± 24 mL/kg per min vs 81 ± 29 mL/kg per min (P<0.05)—and a significantly higher output of blood from the right ventricle—261 ± 80 mL/kg per min vs 216 ±73 mL/kg per min (P<0.001).
These measures, taken together, are an indication of blood circulation in the brain and body.
Infants in the UCM group had significantly higher hemoglobin levels at birth than infants in the DCC group—16.3 ± 2.4 g/dL vs 15.6 ± 2.2 g/dL (P<0.05). And mean arterial pressure in the first 15 hours of life was significantly higher in the UCM group than the DCC group (P=0.02).
Among the 43 infants who were delivered vaginally, the researchers found no significant differences in outcomes between infants randomized to UCM or DCC. ![]()
Photo courtesy of Meutia
Chaerani & Indradi Soemardjan
Umbilical cord milking may be more beneficial than delayed cord clamping for preterm infants delivered by Cesarean section, according to new research.
The study showed that cord milking produced greater blood circulation, higher hemoglobin levels, and higher blood pressure, but only in preterm infants delivered by Cesarean.
For preterm infants delivered vaginally, there was no significant difference between the milking and delayed clamping groups.
Anup C. Katheria, MD, of the Neonatal Research Institute at the Sharp Mary Birch Hospital in San Diego, California, and his colleagues reported these findings in Pediatrics.
The researchers noted that, in 2012, the American College of Obstetricians and Gynecologists recommended a 30- to 60-second delay before clamping the umbilical cord in all preterm deliveries.
This is thought to allow sufficient time for blood from the umbilical cord to fill the blood vessels in the infant’s lungs and to protect infants from intraventricular hemorrhage. However, some previous studies failed to find a reduction in intraventricular hemorrhage from delayed cord clamping among preterm infants delivered by Cesarean.
Dr Katheria and his colleagues theorized that the use of an anesthetic in Cesarean delivery reduces uterine contractions and therefore hinders the exodus of blood from the umbilical cord.
They reasoned that cord milking—encircling the cord with thumb and forefingers, gently squeezing, and slowly pushing the blood through the cord to the infant’s abdomen—might compensate for diminished blood flow through the umbilical cord and increase the amount of blood available to the infant.
To test this theory, the researchers enrolled 197 infants in a prospective study. Mothers went into labor at or before the 32nd week of pregnancy.
Of the 154 infants delivered by Cesarean, 75 were randomized to the umbilical cord milking (UCM) group and 79 to the delayed cord clamping (DCC) group.
Infants in the UCM group had significantly higher blood flow in the superior vena cava than those in the DCC group—93 ± 24 mL/kg per min vs 81 ± 29 mL/kg per min (P<0.05)—and a significantly higher output of blood from the right ventricle—261 ± 80 mL/kg per min vs 216 ±73 mL/kg per min (P<0.001).
These measures, taken together, are an indication of blood circulation in the brain and body.
Infants in the UCM group had significantly higher hemoglobin levels at birth than infants in the DCC group—16.3 ± 2.4 g/dL vs 15.6 ± 2.2 g/dL (P<0.05). And mean arterial pressure in the first 15 hours of life was significantly higher in the UCM group than the DCC group (P=0.02).
Among the 43 infants who were delivered vaginally, the researchers found no significant differences in outcomes between infants randomized to UCM or DCC. ![]()
SCAMP Tool for an Old Problem
The traditional tools of observation, retrospective studies, registries, clinical practice guidelines (CPGs), prospective studies, and randomized control trials have all contributed to much of the progress of modern medicine to date. However, each of these tools has inherent tensions, strengths, and weaknesses: prospective versus retrospective, standardization versus personalization, and the art versus the science of medicine. As the field of medicine continually evolves, so too should our tools and methods. We review the Standardized Clinical Assessment and Management Plan (SCAMP) as a complementary tool to facilitate learning and discovery.
WHAT IS A SCAMP?
The methodology and major components of a SCAMP have been described in detail.[1, 2, 3] The goals of SCAMPs are to (1) reduce practice variation, (2) improve patient outcomes, and to (3) identify unnecessary resource utilization. SCAMPs leverage concepts from CPGs and prospective trials and infuse the iterative Plan, Do, Study, Act Cycle quality‐improvement techniques. Like most novel initiatives, SCAMPs methodology itself has matured over time and with experience. Briefly, creating a SCAMP has the following steps. Step 1 is to summarize the available data and expert opinions on a topic of interest. This is a critical first step, as it identifies gaps in our knowledge base and can help focus areas for the SCAMP to explore. Occasionally, retrospective studies are needed to provide data regarding local practices, procedures, and outcome metrics. These data can be used as a historical benchmark to compare SCAMP data with. Step 2 is to convene a group of clinicians who are engaged by the topic to define the patients to be included and to create a standardized care algorithm. Decision points and recommendations made within these algorithms should be precise and concrete, knowing that they can be changed or improved after data analysis and review. Figure 1 is a partial snapshot of the algorithm from the Hypertrophic Cardiomyopathy SCAMP describing the follow‐up in adults with known hypertrophic cardiomyopathy. Creation of the algorithm is often done in parallel with step 3, which is the generation of a set of targeted data statements (TDSs). TDSs are driven by the main objectives of the SCAMP, focus on areas of high uncertainty and variation in care, and frame the SCAMP to keep the amount of data collected in scope. A good TDS is concrete, measurable, and clearly relates to the recommendations in the algorithm. Here is an example of a TDS from the adult Congestive Heart Failure SCAMP: Greater than 75% of patients will be discharged on at least their admission doses of ‐blockers, angiotensin‐converting enzyme inhibitors, and angiotensin receptor blockers.
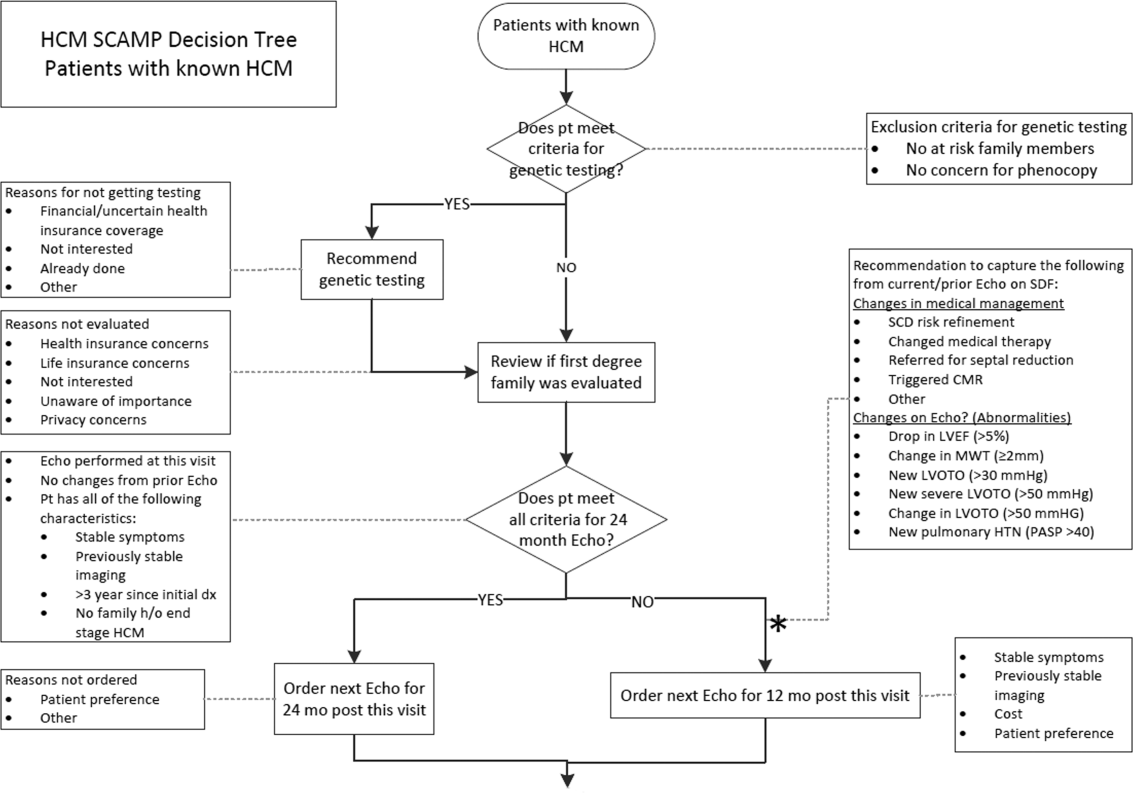
The last step for SCAMP creation involves developing online or paper data forms that allow for efficient data capture at the point of care. The key to these data forms is limiting the data capture to only what is needed to answer the TDS and documenting the reasons why clinicians chose not to follow SCAMP recommendations. Figure 2 is a partial data form from the adult Distal Radius Fracture SCAMP. Implementation of a SCAMP is a key component to a SCAMP's success but is outside the scope of this review.
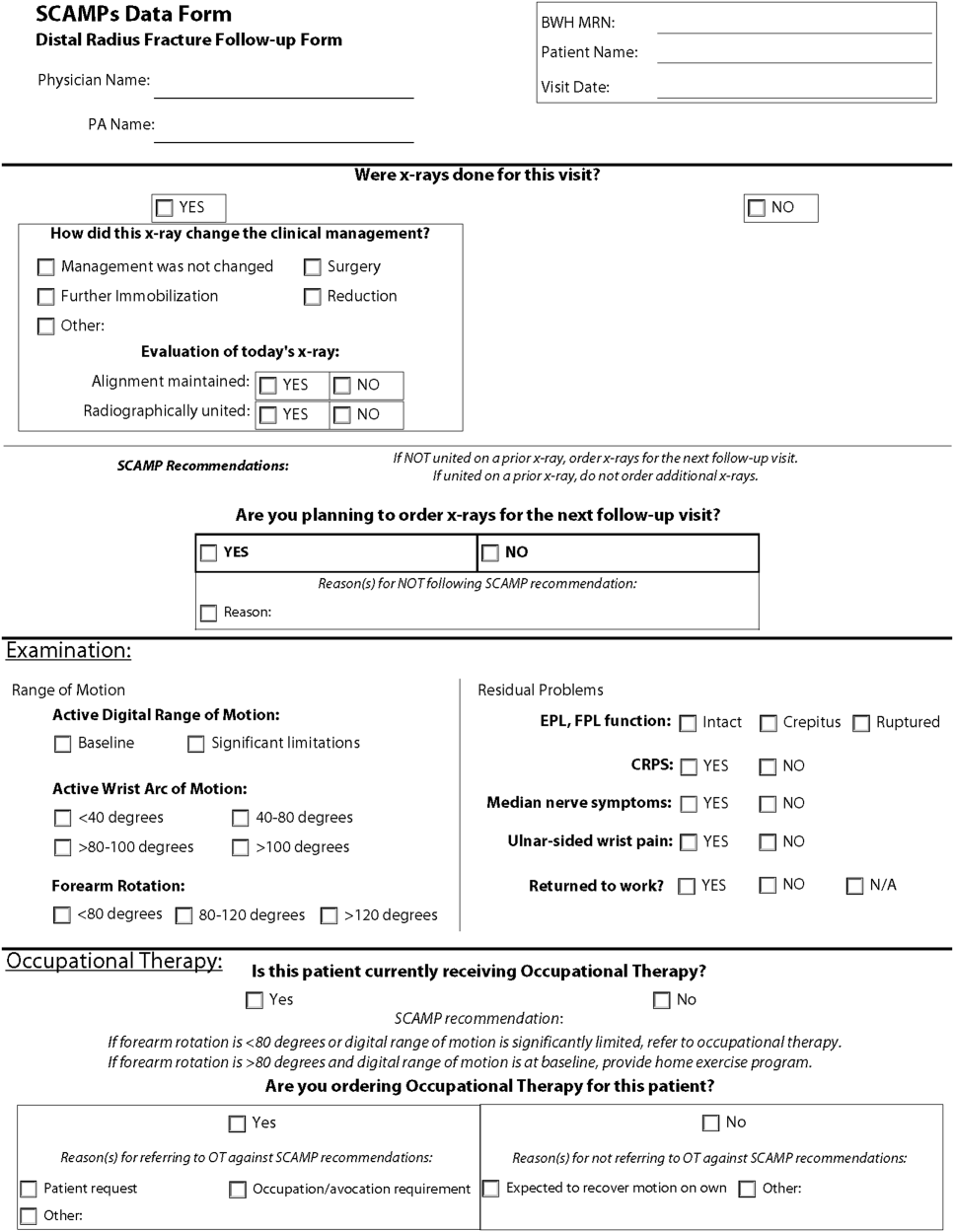
One of the hallmark features of SCAMPs is iterative, rapid data analysis, which is meant to inform and help change the SCAMP algorithm. For example, the Congestive Heart Failure TDS example above was based on the assumption that patients should be discharged home on equal or higher doses of their home medications. However, analysis of SCAMP patients showed that, in fact, clinicians were discharging a large number of patients on lower doses despite algorithm recommendations. The SCAMP algorithm was changed to explore and better understand the associations between neurohormonal medication dose changes and patients' renal function, blood pressures, and overall hemodynamic stability. This type of data capture, analysis, and algorithm change to improve the SCAMP itself can occur in relatively rapid fashion (typically in 6‐ to 12‐month cycles).
WHAT MAKES A GOOD SCAMP TOPIC?
A good SCAMP topic typically involves high stakes. The subject matter or the anticipated impact must be substantial enough to warrant the time and resource investments. These interests often parallel the overall goals of the SCAMP. The best SCAMPs target areas where the stakes are high in terms of the costs of practice variation, the importance of patient outcomes, and the waste of unnecessary resource utilization. We have shown that SCAMPs can apply to the spectrum of clinical care (inpatient, outpatient, procedures, adult, pediatric, long‐ or short‐range episodes of care) and to both common and rare diagnoses in medicine. To date, there have been 47 SCAMPs created and implemented across a network of 11 centers and societies. A full list of available adult and pediatric SCAMPs can be found at
WHAT MAKES A SCAMP DIFFERENT?
More Than a Clinical Practice Guideline
The initial process of developing a SCAMP is very similar to developing a CPG. There is reliance on available published data and expert opinion to create the TDS and algorithms. However, in contrast to CPGs, there is a fundamental tenet to the SCAMPs methodology that, within a given knowledge base on a particular subject, there are considerable holes where definitive truth is not known. There are errors in our data and understanding, but we do not know exactly which assumptions are correct or misguided. Acknowledging the limitations of our knowledge base gives the freedom to make recommendations in the algorithm that are, essentially, educated guesses. Within a short time period, the authors will get informed data and the opportunity to make adjustments, as necessary, to the algorithm. This type of prospective data collection and rapid analyses are generally not part of CPGs.
The Role of Diversions
No CPG, prospective study, randomized trial, or SCAMP algorithm will perfectly fit every patient, every time. The bedside clinician will occasionally have insights into that particular patient's care that justify not following an algorithm, regardless if it comes from a CPG, trial, or SCAMP. SCAMPs encourage these diversions, as they are a rich set of data that can be used to highlight deficiencies in the algorithms, especially when numerous providers identify similar concerns. In a CPG, these diversions are typically chalked up to noncompliance, whereas in a SCAMP, the decision, as well as the rationale behind the decision making, is captured. The key to diversions is capturing the logic and rationale of the decision making for that patient. These critical clinical decision‐making data are often lost or buried within an electronic medical record, in a form (e.g. free text) that cannot easily be identified or analyzed. During the analysis, the data regarding diversions are reviewed, looking for similar patterns of why clinicians did not follow the SCAMP algorithm. For example, in the adult Inpatient Chest Pain SCAMP, there was a high rate of diversions regarding the amount of inpatient testing being done for the evaluation of patients at low or intermediate risk for acute coronary syndrome. In analysis of the diversions, it seems that many of these patients did not have a primary cardiologist or lived far away. The SCAMP algorithm was modified to have different recommendations based on where the patient lived and if they had a cardiologist. In the next analysis, this subgroup can be compared against patients who live closer and had a primary cardiologist to see if additional inpatient testing did or did not affect outcomes.
Little Data Instead of Big Data
There has been a lot of focus across hospital systems on the analysis of big data. Over the last several years, there has been an explosion in the availability of large, often unstructured, datasets. In many ways, big data analytics look to find meaning across very large datasets because the critical data (e.g. clinical decision making) is not captured in a discrete analyzable fashion. In electronic health records, much of the decision making as to why the clinician chose the red pill instead of the blue pill is lost in the free text abyss of clinic and inpatient notes. Through the use of TDSs, the SCAMP authors are asked to identify the critical data elements needed to say which patient should get what pill. By doing this, the clinical decision making is codified in a way that will facilitate future analysis and SCAMP modifications. Decisions made by clinicians and how they got to those decisions (either via the SCAMP algorithm or by diversion) are captured in an easily analyzable form. This approach, choosing only critical and targeted little data, also reduces the data collection burden and increases clinician compliance.
A Grassroots Effort
Many CPGs are created by panels of international experts in the field/subject matter. The origins of most SCAMPs tend to start more locally, often by frustrated clinicians who struggle with the data and knowledge gaps. They are often motivated to improve their care delivery, not necessarily on a national level, but in their clinic or inpatient setting. The data they get back in the interim analyses are about their patientstheir data. This empowers them to expand and grow the SCAMP. The flexibility of allowing diversions increases this engagement. SCAMPs are created and authored by clinicians on the front lines. This more grassroots approach feels more palatable compared to the top down verdicts that come from CPGs.
SCAMPs are a novel, complementary, but alternative tool to help deliver better care. By focusing on targeted little data collection, allowing diversions, and performing rapid analysis to iteratively improve the algorithm, SCAMPs blend the strengths of many of our traditional tools of good change to affect better change. By choosing topics with high stakes, they allow the frontline clinicians to shape and improve how they delivery care.
Disclosure: Nothing to report.
- , , , et al. A novel approach to gathering and acting on relevant clinical information: SCAMPs. Congenit Heart Dis. 2010;5:343–353.
- , , , et al. Standardized clinical assessment and management plans (SCAMPs) provide a better alternative to clinical practice guidelines. Health Aff (Millwood). 2013;32:911–920.
- , , , Gathering and learning from relevant clinical data: a new framework. Acad Med. 2015;90(2):143–148.
The traditional tools of observation, retrospective studies, registries, clinical practice guidelines (CPGs), prospective studies, and randomized control trials have all contributed to much of the progress of modern medicine to date. However, each of these tools has inherent tensions, strengths, and weaknesses: prospective versus retrospective, standardization versus personalization, and the art versus the science of medicine. As the field of medicine continually evolves, so too should our tools and methods. We review the Standardized Clinical Assessment and Management Plan (SCAMP) as a complementary tool to facilitate learning and discovery.
WHAT IS A SCAMP?
The methodology and major components of a SCAMP have been described in detail.[1, 2, 3] The goals of SCAMPs are to (1) reduce practice variation, (2) improve patient outcomes, and to (3) identify unnecessary resource utilization. SCAMPs leverage concepts from CPGs and prospective trials and infuse the iterative Plan, Do, Study, Act Cycle quality‐improvement techniques. Like most novel initiatives, SCAMPs methodology itself has matured over time and with experience. Briefly, creating a SCAMP has the following steps. Step 1 is to summarize the available data and expert opinions on a topic of interest. This is a critical first step, as it identifies gaps in our knowledge base and can help focus areas for the SCAMP to explore. Occasionally, retrospective studies are needed to provide data regarding local practices, procedures, and outcome metrics. These data can be used as a historical benchmark to compare SCAMP data with. Step 2 is to convene a group of clinicians who are engaged by the topic to define the patients to be included and to create a standardized care algorithm. Decision points and recommendations made within these algorithms should be precise and concrete, knowing that they can be changed or improved after data analysis and review. Figure 1 is a partial snapshot of the algorithm from the Hypertrophic Cardiomyopathy SCAMP describing the follow‐up in adults with known hypertrophic cardiomyopathy. Creation of the algorithm is often done in parallel with step 3, which is the generation of a set of targeted data statements (TDSs). TDSs are driven by the main objectives of the SCAMP, focus on areas of high uncertainty and variation in care, and frame the SCAMP to keep the amount of data collected in scope. A good TDS is concrete, measurable, and clearly relates to the recommendations in the algorithm. Here is an example of a TDS from the adult Congestive Heart Failure SCAMP: Greater than 75% of patients will be discharged on at least their admission doses of ‐blockers, angiotensin‐converting enzyme inhibitors, and angiotensin receptor blockers.
The last step for SCAMP creation involves developing online or paper data forms that allow for efficient data capture at the point of care. The key to these data forms is limiting the data capture to only what is needed to answer the TDS and documenting the reasons why clinicians chose not to follow SCAMP recommendations. Figure 2 is a partial data form from the adult Distal Radius Fracture SCAMP. Implementation of a SCAMP is a key component to a SCAMP's success but is outside the scope of this review.
One of the hallmark features of SCAMPs is iterative, rapid data analysis, which is meant to inform and help change the SCAMP algorithm. For example, the Congestive Heart Failure TDS example above was based on the assumption that patients should be discharged home on equal or higher doses of their home medications. However, analysis of SCAMP patients showed that, in fact, clinicians were discharging a large number of patients on lower doses despite algorithm recommendations. The SCAMP algorithm was changed to explore and better understand the associations between neurohormonal medication dose changes and patients' renal function, blood pressures, and overall hemodynamic stability. This type of data capture, analysis, and algorithm change to improve the SCAMP itself can occur in relatively rapid fashion (typically in 6‐ to 12‐month cycles).
WHAT MAKES A GOOD SCAMP TOPIC?
A good SCAMP topic typically involves high stakes. The subject matter or the anticipated impact must be substantial enough to warrant the time and resource investments. These interests often parallel the overall goals of the SCAMP. The best SCAMPs target areas where the stakes are high in terms of the costs of practice variation, the importance of patient outcomes, and the waste of unnecessary resource utilization. We have shown that SCAMPs can apply to the spectrum of clinical care (inpatient, outpatient, procedures, adult, pediatric, long‐ or short‐range episodes of care) and to both common and rare diagnoses in medicine. To date, there have been 47 SCAMPs created and implemented across a network of 11 centers and societies. A full list of available adult and pediatric SCAMPs can be found at
WHAT MAKES A SCAMP DIFFERENT?
More Than a Clinical Practice Guideline
The initial process of developing a SCAMP is very similar to developing a CPG. There is reliance on available published data and expert opinion to create the TDS and algorithms. However, in contrast to CPGs, there is a fundamental tenet to the SCAMPs methodology that, within a given knowledge base on a particular subject, there are considerable holes where definitive truth is not known. There are errors in our data and understanding, but we do not know exactly which assumptions are correct or misguided. Acknowledging the limitations of our knowledge base gives the freedom to make recommendations in the algorithm that are, essentially, educated guesses. Within a short time period, the authors will get informed data and the opportunity to make adjustments, as necessary, to the algorithm. This type of prospective data collection and rapid analyses are generally not part of CPGs.
The Role of Diversions
No CPG, prospective study, randomized trial, or SCAMP algorithm will perfectly fit every patient, every time. The bedside clinician will occasionally have insights into that particular patient's care that justify not following an algorithm, regardless if it comes from a CPG, trial, or SCAMP. SCAMPs encourage these diversions, as they are a rich set of data that can be used to highlight deficiencies in the algorithms, especially when numerous providers identify similar concerns. In a CPG, these diversions are typically chalked up to noncompliance, whereas in a SCAMP, the decision, as well as the rationale behind the decision making, is captured. The key to diversions is capturing the logic and rationale of the decision making for that patient. These critical clinical decision‐making data are often lost or buried within an electronic medical record, in a form (e.g. free text) that cannot easily be identified or analyzed. During the analysis, the data regarding diversions are reviewed, looking for similar patterns of why clinicians did not follow the SCAMP algorithm. For example, in the adult Inpatient Chest Pain SCAMP, there was a high rate of diversions regarding the amount of inpatient testing being done for the evaluation of patients at low or intermediate risk for acute coronary syndrome. In analysis of the diversions, it seems that many of these patients did not have a primary cardiologist or lived far away. The SCAMP algorithm was modified to have different recommendations based on where the patient lived and if they had a cardiologist. In the next analysis, this subgroup can be compared against patients who live closer and had a primary cardiologist to see if additional inpatient testing did or did not affect outcomes.
Little Data Instead of Big Data
There has been a lot of focus across hospital systems on the analysis of big data. Over the last several years, there has been an explosion in the availability of large, often unstructured, datasets. In many ways, big data analytics look to find meaning across very large datasets because the critical data (e.g. clinical decision making) is not captured in a discrete analyzable fashion. In electronic health records, much of the decision making as to why the clinician chose the red pill instead of the blue pill is lost in the free text abyss of clinic and inpatient notes. Through the use of TDSs, the SCAMP authors are asked to identify the critical data elements needed to say which patient should get what pill. By doing this, the clinical decision making is codified in a way that will facilitate future analysis and SCAMP modifications. Decisions made by clinicians and how they got to those decisions (either via the SCAMP algorithm or by diversion) are captured in an easily analyzable form. This approach, choosing only critical and targeted little data, also reduces the data collection burden and increases clinician compliance.
A Grassroots Effort
Many CPGs are created by panels of international experts in the field/subject matter. The origins of most SCAMPs tend to start more locally, often by frustrated clinicians who struggle with the data and knowledge gaps. They are often motivated to improve their care delivery, not necessarily on a national level, but in their clinic or inpatient setting. The data they get back in the interim analyses are about their patientstheir data. This empowers them to expand and grow the SCAMP. The flexibility of allowing diversions increases this engagement. SCAMPs are created and authored by clinicians on the front lines. This more grassroots approach feels more palatable compared to the top down verdicts that come from CPGs.
SCAMPs are a novel, complementary, but alternative tool to help deliver better care. By focusing on targeted little data collection, allowing diversions, and performing rapid analysis to iteratively improve the algorithm, SCAMPs blend the strengths of many of our traditional tools of good change to affect better change. By choosing topics with high stakes, they allow the frontline clinicians to shape and improve how they delivery care.
Disclosure: Nothing to report.
The traditional tools of observation, retrospective studies, registries, clinical practice guidelines (CPGs), prospective studies, and randomized control trials have all contributed to much of the progress of modern medicine to date. However, each of these tools has inherent tensions, strengths, and weaknesses: prospective versus retrospective, standardization versus personalization, and the art versus the science of medicine. As the field of medicine continually evolves, so too should our tools and methods. We review the Standardized Clinical Assessment and Management Plan (SCAMP) as a complementary tool to facilitate learning and discovery.
WHAT IS A SCAMP?
The methodology and major components of a SCAMP have been described in detail.[1, 2, 3] The goals of SCAMPs are to (1) reduce practice variation, (2) improve patient outcomes, and to (3) identify unnecessary resource utilization. SCAMPs leverage concepts from CPGs and prospective trials and infuse the iterative Plan, Do, Study, Act Cycle quality‐improvement techniques. Like most novel initiatives, SCAMPs methodology itself has matured over time and with experience. Briefly, creating a SCAMP has the following steps. Step 1 is to summarize the available data and expert opinions on a topic of interest. This is a critical first step, as it identifies gaps in our knowledge base and can help focus areas for the SCAMP to explore. Occasionally, retrospective studies are needed to provide data regarding local practices, procedures, and outcome metrics. These data can be used as a historical benchmark to compare SCAMP data with. Step 2 is to convene a group of clinicians who are engaged by the topic to define the patients to be included and to create a standardized care algorithm. Decision points and recommendations made within these algorithms should be precise and concrete, knowing that they can be changed or improved after data analysis and review. Figure 1 is a partial snapshot of the algorithm from the Hypertrophic Cardiomyopathy SCAMP describing the follow‐up in adults with known hypertrophic cardiomyopathy. Creation of the algorithm is often done in parallel with step 3, which is the generation of a set of targeted data statements (TDSs). TDSs are driven by the main objectives of the SCAMP, focus on areas of high uncertainty and variation in care, and frame the SCAMP to keep the amount of data collected in scope. A good TDS is concrete, measurable, and clearly relates to the recommendations in the algorithm. Here is an example of a TDS from the adult Congestive Heart Failure SCAMP: Greater than 75% of patients will be discharged on at least their admission doses of ‐blockers, angiotensin‐converting enzyme inhibitors, and angiotensin receptor blockers.
The last step for SCAMP creation involves developing online or paper data forms that allow for efficient data capture at the point of care. The key to these data forms is limiting the data capture to only what is needed to answer the TDS and documenting the reasons why clinicians chose not to follow SCAMP recommendations. Figure 2 is a partial data form from the adult Distal Radius Fracture SCAMP. Implementation of a SCAMP is a key component to a SCAMP's success but is outside the scope of this review.
One of the hallmark features of SCAMPs is iterative, rapid data analysis, which is meant to inform and help change the SCAMP algorithm. For example, the Congestive Heart Failure TDS example above was based on the assumption that patients should be discharged home on equal or higher doses of their home medications. However, analysis of SCAMP patients showed that, in fact, clinicians were discharging a large number of patients on lower doses despite algorithm recommendations. The SCAMP algorithm was changed to explore and better understand the associations between neurohormonal medication dose changes and patients' renal function, blood pressures, and overall hemodynamic stability. This type of data capture, analysis, and algorithm change to improve the SCAMP itself can occur in relatively rapid fashion (typically in 6‐ to 12‐month cycles).
WHAT MAKES A GOOD SCAMP TOPIC?
A good SCAMP topic typically involves high stakes. The subject matter or the anticipated impact must be substantial enough to warrant the time and resource investments. These interests often parallel the overall goals of the SCAMP. The best SCAMPs target areas where the stakes are high in terms of the costs of practice variation, the importance of patient outcomes, and the waste of unnecessary resource utilization. We have shown that SCAMPs can apply to the spectrum of clinical care (inpatient, outpatient, procedures, adult, pediatric, long‐ or short‐range episodes of care) and to both common and rare diagnoses in medicine. To date, there have been 47 SCAMPs created and implemented across a network of 11 centers and societies. A full list of available adult and pediatric SCAMPs can be found at
WHAT MAKES A SCAMP DIFFERENT?
More Than a Clinical Practice Guideline
The initial process of developing a SCAMP is very similar to developing a CPG. There is reliance on available published data and expert opinion to create the TDS and algorithms. However, in contrast to CPGs, there is a fundamental tenet to the SCAMPs methodology that, within a given knowledge base on a particular subject, there are considerable holes where definitive truth is not known. There are errors in our data and understanding, but we do not know exactly which assumptions are correct or misguided. Acknowledging the limitations of our knowledge base gives the freedom to make recommendations in the algorithm that are, essentially, educated guesses. Within a short time period, the authors will get informed data and the opportunity to make adjustments, as necessary, to the algorithm. This type of prospective data collection and rapid analyses are generally not part of CPGs.
The Role of Diversions
No CPG, prospective study, randomized trial, or SCAMP algorithm will perfectly fit every patient, every time. The bedside clinician will occasionally have insights into that particular patient's care that justify not following an algorithm, regardless if it comes from a CPG, trial, or SCAMP. SCAMPs encourage these diversions, as they are a rich set of data that can be used to highlight deficiencies in the algorithms, especially when numerous providers identify similar concerns. In a CPG, these diversions are typically chalked up to noncompliance, whereas in a SCAMP, the decision, as well as the rationale behind the decision making, is captured. The key to diversions is capturing the logic and rationale of the decision making for that patient. These critical clinical decision‐making data are often lost or buried within an electronic medical record, in a form (e.g. free text) that cannot easily be identified or analyzed. During the analysis, the data regarding diversions are reviewed, looking for similar patterns of why clinicians did not follow the SCAMP algorithm. For example, in the adult Inpatient Chest Pain SCAMP, there was a high rate of diversions regarding the amount of inpatient testing being done for the evaluation of patients at low or intermediate risk for acute coronary syndrome. In analysis of the diversions, it seems that many of these patients did not have a primary cardiologist or lived far away. The SCAMP algorithm was modified to have different recommendations based on where the patient lived and if they had a cardiologist. In the next analysis, this subgroup can be compared against patients who live closer and had a primary cardiologist to see if additional inpatient testing did or did not affect outcomes.
Little Data Instead of Big Data
There has been a lot of focus across hospital systems on the analysis of big data. Over the last several years, there has been an explosion in the availability of large, often unstructured, datasets. In many ways, big data analytics look to find meaning across very large datasets because the critical data (e.g. clinical decision making) is not captured in a discrete analyzable fashion. In electronic health records, much of the decision making as to why the clinician chose the red pill instead of the blue pill is lost in the free text abyss of clinic and inpatient notes. Through the use of TDSs, the SCAMP authors are asked to identify the critical data elements needed to say which patient should get what pill. By doing this, the clinical decision making is codified in a way that will facilitate future analysis and SCAMP modifications. Decisions made by clinicians and how they got to those decisions (either via the SCAMP algorithm or by diversion) are captured in an easily analyzable form. This approach, choosing only critical and targeted little data, also reduces the data collection burden and increases clinician compliance.
A Grassroots Effort
Many CPGs are created by panels of international experts in the field/subject matter. The origins of most SCAMPs tend to start more locally, often by frustrated clinicians who struggle with the data and knowledge gaps. They are often motivated to improve their care delivery, not necessarily on a national level, but in their clinic or inpatient setting. The data they get back in the interim analyses are about their patientstheir data. This empowers them to expand and grow the SCAMP. The flexibility of allowing diversions increases this engagement. SCAMPs are created and authored by clinicians on the front lines. This more grassroots approach feels more palatable compared to the top down verdicts that come from CPGs.
SCAMPs are a novel, complementary, but alternative tool to help deliver better care. By focusing on targeted little data collection, allowing diversions, and performing rapid analysis to iteratively improve the algorithm, SCAMPs blend the strengths of many of our traditional tools of good change to affect better change. By choosing topics with high stakes, they allow the frontline clinicians to shape and improve how they delivery care.
Disclosure: Nothing to report.
- , , , et al. A novel approach to gathering and acting on relevant clinical information: SCAMPs. Congenit Heart Dis. 2010;5:343–353.
- , , , et al. Standardized clinical assessment and management plans (SCAMPs) provide a better alternative to clinical practice guidelines. Health Aff (Millwood). 2013;32:911–920.
- , , , Gathering and learning from relevant clinical data: a new framework. Acad Med. 2015;90(2):143–148.
- , , , et al. A novel approach to gathering and acting on relevant clinical information: SCAMPs. Congenit Heart Dis. 2010;5:343–353.
- , , , et al. Standardized clinical assessment and management plans (SCAMPs) provide a better alternative to clinical practice guidelines. Health Aff (Millwood). 2013;32:911–920.
- , , , Gathering and learning from relevant clinical data: a new framework. Acad Med. 2015;90(2):143–148.
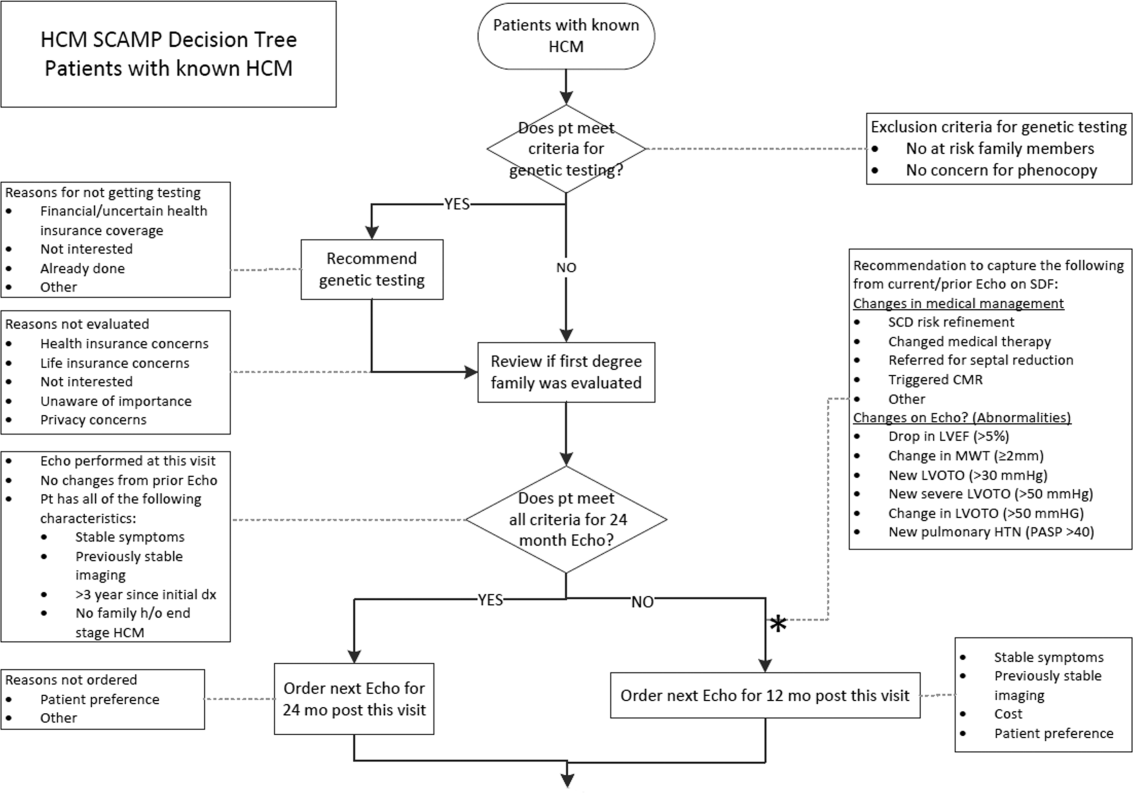
Hospital Deaths Among HIV Patients
Successfully treated human immunodeficiency virus (HIV)‐infected individuals in the United States currently have life expectancy and mortality rates that are similar to the general population.[1, 2, 3, 4] A large multinational study found that the excess mortality rate among HIV‐positive individuals decreased from 40.8 to 6.1 per 1000 person‐years from pre‐1995 to 2006.1 This is largely due to improved access to comprehensive HIV care, in particular widespread antiretroviral (ART) use. However, the proportion of deaths that are not classically considered acquired immunodeficiency syndrome (AIDS)‐related such as liver disease, cardiovascular disease, and non‐AIDS malignancy has increased,[1, 5, 6, 7] particularly among patients with higher CD4 T‐cell counts.[5, 8] Additionally, despite overall decline in mortality, there is evidence of racial and gender differences, with increased mortality risk associated with female gender and black race.[9, 10]
In the current ART era, HIV care has shifted focus from inpatient to outpatient care, with more emphasis on chronic disease management. However, hospitalization rates among HIV‐positive persons remain higher than that of the general population.[11, 12] A cross‐sectional study of HIV‐infected persons in the United States estimated a hospitalization rate of 26.6 per 100 persons in 2009,[13] compared to a rate of 11.9 for the general population during the same year.[14] Possible reasons for higher hospitalization rates include complications of aging or other chronic comorbidities, and consequences of behavioral risk factors such tobacco use and substance abuse.
Characterizing deaths among inpatient HIV‐infected individuals in the ART era is important to developing targeted interventions to further reduce mortality. Prior studies examining in‐hospital deaths of HIV‐positive patients evaluated more limited time periods,[15, 16, 17, 18] and thus did not necessarily assess the full spectrum of changes in mortality that have occurred with the introduction of ART. Furthermore, these studies described causes of death, but did not consistently identify factors associated with non‐AIDS deaths. We examined the trends in in‐hospital deaths among HIV‐infected patients from 1995 to 2011 and identified contributing factors to mortality. As the HIV population is aging, we hypothesized that HIV‐infected patients are more likely to die from nonAIDS‐related death in the late ART era due to factors related to cardiovascular and liver disease, compared to the early ART era.
METHODS
The study was performed at YaleNew Haven Hospital, an urban tertiary care academic teaching hospital with 1008 beds and the state of Connecticut's largest ambulatory HIV clinic. Connecticut ranks seventh nationally (10/100,000) in HIV prevalence; New Haven is second among Connecticut cities in the number of people living with HIV/AIDS.[19] We reviewed all patients with an International Classification of Diseases, Ninth Revision (ICD‐9) code of HIV or AIDS (ICD‐9 codes V08 and 042) who died during hospitalization between January 1, 1995 to December 31, 2011. The Yale Human Investigation Committee granted ethical approval to conduct the study.
A standardized data collection tool was used to abstract demographic characteristics (ie, age, gender, and race), medical comorbidities (ie, diabetes, chronic kidney disease, chronic hepatitis B or C, liver cirrhosis, hypertension, coronary artery disease, congestive heart failure, chronic obstructive lung disease, alcohol and substance abuse), ART use (yes or no), HIV viral load (VL), CD4 cell count, and causes of death. Comorbidities were defined using the Coding of Death in HIV Project protocol, a multinational endeavor to standardize data collection in studies of HIV‐positive patients.[20] Chronic kidney disease included individuals with National Kidney Foundation stage I to V disease. Chronic hepatitis B or C infection was identified in patients who had serologic testing indicative of prior infection. Alcohol and substance abuse were identified when source documents mentioned any history of current alcohol or illicit drug abuse or dependence. ART use was defined as documentation of ART on admission or prescription during hospitalization. This included individuals who were on 2 or more ART agents. The last HIV VL and CD4 cell count available within 1 year and closest to death were recorded. HIV VL suppression was defined as <400 copies/mL.
Two clinicians independently classified the cause of death as AIDS related or non‐AIDS related in accordance with published definitions.[21, 22] Cause of death was determined by review of the medical record, discharge diagnosis, and autopsy report when available. Official death certificates were not available for review. There was discordance in assigning 23 of the 400 causes of death. In these cases, the medical record was reviewed and determined by consensus between the 2 clinicians.
AIDS‐related deaths were categorized as nonspecified AIDS, AIDS infection, and AIDS malignancy. AIDS‐related deaths were defined as those caused by conditions meeting the Centers for Disease Control and Prevention AIDS case definition.[22] Non‐specified AIDS deaths were those occurring in patients with a CD4 count 50 cells/mm3 or with an AIDS‐defining illness, who died from a condition that was not clearly AIDS related. This included septic shock of unclear etiology, first known episode of pneumonia, a gastrointestinal bleed of unclear etiology, and altered mental status of unclear etiology when cerebrospinal fluid analysis or imaging of the brain was not available.
Non‐AIDS deaths included non‐AIDS infection in patients with a CD4 count >50 cells/mm3, cardiovascular disease, liver disease, non‐AIDS malignancy, and renal disease (Table 1). Deaths classified as other incorporated the deaths that did not fall into these categories. Chronic obstructive pulmonary disease (COPD) exacerbation and status asthmaticus were included in this category, because there was only 1 death from each of these causes.
| |
| Non‐AIDS infection | Infectious etiology not on the list of AIDS‐defining conditions, such as Clostridium difficile colitis, endocarditis, bacteremia, nonrecurrent bacterial pneumonia, or septic shock of unclear cause without a CD4 count of less than 50 cells/mm3 or a documented opportunistic infection |
| Cardiovascular disease | Cardiac arrest without clear cause, ischemic or hemorrhagic stroke, congestive heart failure (respiratory failure most likely due to pulmonary edema in the setting of known systolic or diastolic heart failure), myocardial infarction, and cardiac arrhythmia |
| Liver disease | Complications of cirrhosis such as variceal bleed, hepatic encephalopathy, hepatorenal syndrome, and acute liver failure |
| Renal disease | Complications of acute renal failure such as hyperkalemia leading to cardiac arrest. Complications of end‐stage renal disease such as stopping hemodialysis or calciphylaxis |
| Non‐AIDS malignancy | Malignancies not on the AIDS indicator diagnostic list |
| Other causes | Drug overdose, trauma, suicide, Stevens‐Johnson syndrome, macrophage activation syndrome, hemorrhagic pancreatitis, status asthmaticus, COPD exacerbation, status epilepticus of unclear cause, complications of idiopathic thrombocytopenic purpura, and diabetic ketoacidosis |
The early ART era was defined as 1995 to 2001 and the late ART era from 2002 to 2011. During the early period, combination ART was introduced and significantly impacted overall mortality.[23, 24] The late ART era better reflected current in‐hospital deaths and was compared to the early era to evaluate trends over time.[15, 25]
2 analysis and parametric (t test and analysis of variance) methods compared categorical and continuous variables, respectively. Bivariate analysis was used to determine associations with AIDS versus non‐AIDS deaths in the entire study cohort. Multivariable logistic regression was used to identify correlates of non‐AIDS deaths in the (1) complete 17‐year period and (2) late ART era. For all analyses, a P value <0.05 was considered statistically significant. All statistical analysis was performed using SAS 9.3 (SAS Institute, Cary, NC).
RESULTS
Among 12,183 hospital discharges of HIV‐infected patients from 1995 to 2011, 406 (3.3%) died. Six medical records were missing or incomplete; 400 were available for review. The proportion of hospitalized HIV‐infected patients who died declined from 6.2% in 1995 to 1.5% in 2011 (P<0.0001).
Table 2 summarizes all 400 patients' demographic and clinical characteristics, and cause of death. The majority were male (65.5%), nonwhite (73.3%), and taking ART (65.9%), though only one‐third achieved a VL <400 copies/mL on the most recent measurement available in the year prior to death. The majority (56.3%) died due to nonAIDS‐related causes.
| Total, n=400 | Early Era, n=207 | Late Era, n=193 | P Value | |
|---|---|---|---|---|
| ||||
| Median age, y (IQR) | 45 (3852) | 41 (3547) | 49 (4357) | <0.0001 |
| Male gender, no. (%) | 262 (65.5) | 141 (68.1) | 121 (62.7) | 0.25 |
| Race, no. (%) | ||||
| Black | 238 (59.5) | 124 (59.9) | 114 (59.1) | 0.87 |
| White | 105 (26.3) | 55 (26.6) | 50 (25.9) | 0.88 |
| Hispanic | 55 (13.8) | 27 (13.0) | 28 (14.5) | 0.67 |
| Median CD4 cells/mm3 (IQR)a | 90 (12248) | 50 (10150) | 153 (22399) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 77 (31.3) | 12 (13.3) | 65 (41.7) | <0.0001 |
| On ART, no. (%) | 257 (65.9) | 120 (58.3) | 137 (74.5) | 0.0008 |
| Cause of death, no. (%) | ||||
| AIDS‐related, no. (%) | 175 (43.8) | 118 (57.0) | 57 (29.5) | <0.0001 |
| AIDS infection | 85 (21.3) | 58 (28.0) | 27 (14.0) | 0.82 |
| Nonspecified AIDS | 73 (18.3) | 46 (22.2) | 27 (14.0) | 0.99 |
| AIDS malignancy | 17 (4.3) | 14 (6.8) | 3 (1.6) | 0.17 |
| Non‐AIDS‐related, no. (%) | 225 (56.3) | 89 (43.0) | 136 (70.5) | <0.0001 |
| Non‐AIDS infection | 81 (20.3) | 32 (15.5) | 49 (25.4) | 0.99 |
| Cardiovascular | 45 (11.3) | 16 (7.7) | 29 (15.0) | 0.54 |
| Liver related | 34 (8.5) | 18 (8.7) | 16 (8.3) | 0.08 |
| Malignancy | 31 (7.8) | 6 (2.9) | 25 (13.0) | 0.01 |
| Renal failure | 18 (4.5) | 8 (3.9) | 10 (5.2) | 0.66 |
| Other, no. (%) | 16 (4.1) | 9 (4.5) | 7 (3.6) | 0.16 |
Among all AIDS‐related deaths from 1995 to 2011 (Table 2), AIDS‐defining infection was the most common cause (21.3%), followed by nonspecified AIDS (18.3%), and AIDS malignancy (4.3%). The proportion of nonAIDS‐related deaths increased significantly over time (Figure 1). The most common cause of nonAIDS‐related deaths was non‐AIDS infection (20.3%), followed by cardiovascular disease (11.3%), liver disease (8.5%), malignancy (7.8%), and renal failure (4.5%). The most common non‐AIDS infection was sepsis in 43 patients (60.6%), followed by nonrecurrent bacterial pneumonia in 24 patients (33.8%) and Clostridium difficile infection in 4 patients (5.6%). NonAIDS‐related malignancy was the only category to significantly increase from the early ART to late ART era (P=0.01).

Compared to those dying of AIDS‐related causes over the 17‐year period (Table 3), patients dying of nonAIDS‐related causes were older (P<0.0001), less likely to have a CD4 count 200 cells/mm3 (P<0.0001), and more likely to be on ART and virologically suppressed (P<0.0001). Patients who died from nonAIDS‐related causes were also more likely to have diabetes mellitus (P=0.01), chronic kidney disease (P<0.0001), hepatitis C (P<0.0001), liver cirrhosis (P<0.0001), hypertension (P=0.0002), coronary artery disease (P=0.004), and COPD (P=0.04). Of note, there was no statistically significant difference in gender, race, or substance abuse between AIDS‐related and nonAIDS‐related deaths.
| AIDS, n=175 | Non‐AIDS, n=225 | P Value | |
|---|---|---|---|
| |||
| Median age, y (IQR) | 40 (3548) | 48 (4255) | <0.0001 |
| Male gender, no. (%) | 115 (43.9) | 147 (56.1) | 0.94 |
| Race, no. (%) | |||
| Black | 105 (60.3) | 133 (59.4) | 0.84 |
| White | 41 (23.6) | 64 (28.6) | 0.26 |
| Hispanic | 28 (16.1) | 27 (12.1) | 0.25 |
| On ART, no. (%) | 97 (55.8) | 160 (74.1) | 0.0001 |
| CD4 <200 cells/mm3, no. (%)a | 167 (97.1) | 95 (47.2) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 2 (4.1) | 75 (38.1) | <0.0001 |
| Comorbidities, no. (%) | |||
| Diabetes | 13 (7.4) | 35 (15.6) | 0.01 |
| Renal disease | |||
| CKD | 21 (12) | 73 (32.4) | <0.0001 |
| On dialysis | 9 (5.1) | 47 (20.9) | <0.0001 |
| Liver disease | |||
| Hepatitis C | 38 (21.7) | 130 (57.8) | <0.0001 |
| Cirrhosis | 14 (8) | 67 (29.8) | <0.0001 |
| Cardiovascular disease | |||
| Hypertension | 18 (10.3) | 56 (24.9) | 0.0002 |
| CAD | 2 (1.1) | 16 (7.1) | 0.004 |
| CHF | 13 (7.4) | 29 (12.9) | 0.08 |
| COPD | 5 (2.9) | 17 (7.6) | 0.04 |
| Alcohol abuse | 9 (5.1) | 18 (8.0) | 0.26 |
| Polysubstance abuse | 10 (5.7) | 22 (9.8) | 0.14 |
Associations With Non‐AIDS Deaths
Among all clinical factors associated with non‐AIDS deaths (Table 4), only the last CD4 within the year prior to death >200 cells/mm3, VL 400 copies/mL in the year prior to death, and liver and cardiovascular comorbidities were independently associated with non‐AIDS deaths. The last CD4 count >200 cells/mm3 in the year prior to death was the strongest correlate (odds ratio [OR]: 16.5; 95% CI: 5.351.4) of non‐AIDS deaths, whereas gender and race were not significant.
| Overall (19952011) | Early Era (19952001) | Late Era (20022011) | ||||
|---|---|---|---|---|---|---|
| Deaths | 400 | 207 | 193 | |||
| Non‐AIDS | 225 | 89 | 136 | |||
| AIDS | 175 | 118 | 57 | |||
| Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | Odds Ratio (95% CI)a | Adjusted Odds Ratiob (95% CI) | Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | |
| ||||||
| Clinical factors | ||||||
| Age (per year) | 1.06 (1.04‐1.08) | c | 1.03 (1.01‐1.06) | c | 1.07 (1.03‐1.1) | c |
| Male gender | 0.98 (0.6‐1.5) | c | 1.04 (0.6‐1.9) | c | 1.1 (0.6‐2.0) | c |
| White race (vs nonwhite) | 0.8 (0.5‐1.2) | c | 1.2 (0.6‐2.2) | c | 0.4 (0.2‐0.8) | c |
| CD4 >200 cells/mm3d | 37.6 (14.895.5) | 16.5 (5.351.4) | 24.4 (7.183.2) | 17.4 (3.488.3) | 45.4 (10.5195.5) | 25.9 (5.0134.5) |
| HIV VL 400 copies/mL‖ | 13.6 (5.235.3) | 7.5 (2.324.4) | 9.4 (1.276.6) | c | 15.6 (5.246.4) | 10.9 (2.448.8) |
| On ART | 2.3 (1.5‐3.5) | c | 1.6 (0.9‐2.8) | c | 2.7 (1.35.3) | c |
| Comorbidities | ||||||
| Lung diseasee | 1.9 (1.013.5) | c | 2.4 (1.025.5) | c | 1.5 (0.6‐3.9) | c |
| Kidney diseasee | 3.5 (2.16.0) | c | 3.5 (1.7‐7.3) | 4.9 (1.417.8) | 3.1 (1.47.2) | c |
| Depression | 1.6 (0.8‐ 3.2) | c | 2.5 (0.9‐6.6) | c | 0.95 (0.4‐2.5) | c |
| Substance abusee | 1.9 (1.13.6) | c | 3.7 (1.59.5) | c | 0.9 (0.4‐2.1) | c |
| Diabetes | 2.3 (1.24.5) | c | 2.0 (0.7‐5.5) | c | 1.9 (0.7‐5.0) | c |
| Liver diseasee | 3.6 (2.45.4) | 4.5 (2.29.3) | 2.4 (1.4‐4.3) | 4.4 (1.512.7) | 4.3 (2.28.3) | 7.5 (2.423.4) |
| Cardiovascular diseasee | 2.9 (1.8‐4.6) | 4.2 (1.89.9) | 1.8 (0.9‐3.5) | 4.6 (2.010.3) | 6.8 (1.924.0) | |
In the early ART era (19952001), only CD4 count, renal disease, and cardiovascular disease were independently associated with non‐AIDS deaths; the last CD4 count <200 cells/mm3 in the year prior to death was associated most strongly (OR: 17.4; 95% CI: 3.488.3) with non‐AIDS death, whereas again, gender and race were not significant correlates of non‐AIDS death.
In the late ART era (20022011), similar to those for the entire 17‐year time period, independent correlates of non‐AIDS deaths included last CD4 <200 cells/mm3 in the year prior to death, VL 400 copies/mL in the last year prior to death, and liver and cardiovascular disease. Last CD4 count >200 cells/mm3 in the year prior to death (OR: 25.9; 95% CI: 5134.5) was most strongly correlated with non‐AIDS deaths in the late ART era. Nonwhite patients had a lower likelihood of nonAIDS‐related death (OR: 0.4; 95% CI: 0.2‐0.8), but this was not significant on multivariable regression analysis. Gender difference was not statistically significant.
DISCUSSION
Our study demonstrated changes in the causes of death among HIV‐infected hospitalized patients from 1995 to 2011. To our knowledge, this is the longest duration retrospective analysis of in‐hospital deaths among HIV‐infected patients during the ART era. Knowledge of the changes in comorbidities and causes of death among hospitalized HIV‐infected patients during the ART era could help inpatient providers focus diagnostic and therapeutic efforts and improve overall care. Our findings emphasize that HIV‐infected patients remain at high risk for complications from non‐AIDS infections, even when their immune system has been restored as measured by the CD4 cell count, and at increased risk of cardiovascular and liver disease, which highlights the need to carefully monitor HIV‐positive patients admitted with these conditions.
Comparison of AIDS‐related and nonAIDS‐related deaths in 2 time periods has revealed important findings. First, inpatient deaths of HIV‐infected patients have decreased dramatically (from 6.2% to 1.5%, P<0.0001), and the mortality due to nonAIDS‐related causes has increased significantly over time. Second, we defined demographic and clinical characteristics independently associated with HIV‐infected inpatient mortality. Third, a substantial proportion of in‐hospital deaths were caused by potentially preventable non‐AIDS as well as AIDS‐related diseases.
The striking decline in hospital deaths over time is likely the result of expanded ART use resulting in improved immunologic profiles. NonAIDS‐related causes were responsible for almost three‐quarters of deaths in this large inpatient HIV‐positive population during the late ART era. Similar findings have been reported from other settings in industrialized countries.[5, 7, 16, 17, 18, 26, 27] In our urban population, although cardiovascular disease, liver disease, renal failure, and malignancy were frequent causes of non‐AIDS death, the most common cause was non‐AIDS infection. Further, the proportion of deaths due to non‐AIDS infections did not decrease significantly over time.
A similar study of HIV‐positive inpatients in New York City also found that the majority of non‐AIDS deaths were due to non‐AIDS infections in the ART era.[17] The most common causes of non‐AIDS infection identified in the study were identical to ours: unspecified sepsis followed by nonrecurrent bacterial pneumonia and Clostridium difficile infection. Evidence suggests that individuals with HIV infection have multiple immunological defects that not only lead to increased susceptibility to bacterial infection but also to an unregulated inflammatory response, even in patients who are on ART and virologically suppressed.[28, 29] This highlights the need for hospital physicians to evaluate an HIV‐infected patient's risk for more routine infections that are not commonly considered AIDS related in addition to traditional opportunistic infections. It also implies that inpatient providers should carefully monitor HIV‐positive patients admitted for bacterial infections, as they remain at higher risk for the development of septic shock.
Cardiovascular and liver disease represented the next most common causes of death, which is similar to the New York City study and is consistent with other studies from the ART era.[15, 16, 17, 18] Although deaths due directly to cardiovascular and liver disease did not significantly change over time, these represented the major comorbidities associated with non‐AIDS mortality and, along with renal disease, increased significantly over the study period. There are accumulating studies indicating that HIV infection is associated with accelerated coronary artery disease due to the immune and inflammatory response to the viral replication.[30] Additionally, ART side effects such as hyperlipidemia, metabolic syndrome, and insulin resistance contribute to an increased cardiovascular risk profile.[31] Our findings emphasize the importance of assessing comorbidities not classically considered HIV related. For example, acute coronary syndrome should be in the differential diagnosis for HIV‐infected patients admitted with chest pain regardless of age. Furthermore, HIV‐infected patients are at increased risk for hepatitis B and C coinfection due to related behavioral risk, and coinfection is associated with rapid progression to liver cirrhosis[32, 33, 34] and increased risk for oncogenesis over time rapidly expanding therapeutic options will benefit patients with chronic liver disease.[35, 36, 37]
Although the numbers are relatively small, non‐AIDS malignancy deaths more than quadrupled from the early to the late ART eras. This finding likely underestimates the proportion of overall hospital deaths due to non‐AIDS malignancies given the increased use of hospice facilities and community‐based care,[38] though it is consistent with increasing trends noted in other studies.[39] Doubling of malignancy as a cause of death among AIDS patients from 2000 to 2010 was reported in a French study, as well as in a large multicohort study from 1999 to 2011, consistent with our findings.[16, 40] Developing and implementing screening guidelines for non‐AIDS malignancy among those with HIV at the primary care level may potentially reduce this upward trend.[41] Inpatient providers need to be aware of this trend and consider undiagnosed non‐AIDS malignancy as part of their differential diagnosis when evaluating HIV‐positive patients.
Although emphasis has been placed on non‐AIDS causes, nearly one‐half of all deaths for the entire period, and almost one‐third of deaths in the late ART era were still due to AIDS‐related causes. This is similar to a study of 40,000 patients in Europe and North America from 1996 to 2006, where AIDS deaths comprised almost half of all deaths,[7] as well as a French national study,[16] and remains characteristic of resource‐limited settings.[42] This indicates the need for continued vigilance toward earlier HIV case detection and retention in care to prevent disease progression and AIDS‐related mortality. Primary care and hospital physicians should assess risk for HIV infection in all patients and institute universal HIV testing in both the inpatient and outpatient settings.
Although the majority of our sample was nonwhite and male, there was sufficient demographic diversity to determine that race and gender differences were not statistically significant contributors to mortality. In contrast, hospital‐based and population‐based studies reporting racial and gender disparities in HIV‐associated mortality have attributed this to poor access to health care.[9, 17, 43, 44, 45, 46] Compared to the New York City study, patients in our study had comparable median age and CD4 cell count, but also had greater ART use and better virologic control.[17] We speculate that in our smaller urban area, characterized by strong community and clinical HIV programs, patients may have had improved access to care without regard to race and gender.
Our study strengths include a large sample size, a diverse population with a relatively high proportion of women, and varied age and race, as well as data acquired in a standardized fashion over a prolonged period of ART availability. Further, 2 clinicians classified causes of death independently, utilizing validated definitions to minimize bias. Our late ART era evaluation is consistent with other HIV cohort studies,[25] though we utilized multivariate analysis to uncover independent correlates of mortality, a feature not employed in other studies.[16, 17]
We also recognize several limitations in our study. Our study design was associated with the recognized limitations of retrospective research, including missing data. We examined in‐hospital deaths at a single urban hospital in the Northeastern United States only, affecting the generalizability of our findings. The study did not include a control group of hospitalized HIV‐infected patients who survived or hospitalized HIV‐negative patients who died, which might have further strengthened our findings. Despite these limitations, this study provides important observations that can inform strategies to impact HIV‐associated mortality in the inpatient setting.
In conclusion, the mortality profile of hospitalized HIV‐infected patients has evolved with the epidemic. Caring for the hospitalized HIV‐infected patient has become increasingly complex because patients are more likely to suffer from multiple comorbidities, especially cardiovascular and liver diseases, and to die from non‐AIDS causes. Inpatient providers need to understand the changing trends in chronic HIV disease management as patients are living longer with antiretroviral therapy and are increasingly likely to succumb to nonAIDS‐related causes of death. Clinicians can no longer remain focused on AIDS‐defining opportunistic infections and need to recognize the emerging importance of chronic comorbidities when developing a differential diagnosis, and the higher risk of death due to non‐AIDS infectious causes. Physicians caring for hospitalized patients should appreciate the current trends in the HIV epidemic to provide comprehensive and appropriate interventions that can reduce mortality for HIV‐infected inpatients.
Disclosures: This research was supported by the National Institute of Allergy and Infectious Diseases (S.S.; 1K23AI089260). The authors report no conflicts of interest.
- , , , et al. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA. 2008;300:51–59.
- , , . Improvement in the health of HIV‐infected persons in care: reducing disparities. Clin Infect Dis. 2012;55:1242–1251.
- , , , et al. Mortality in well controlled HIV in the continuous antiretroviral therapy arms of the SMART and ESPRIT trials compared with the general population. AIDS. 2013;27:973–979.
- , , , et al. Mortality of HIV‐infected patients starting potent antiretroviral therapy: comparison with the general population in nine industrialized countries. Int J Epidemiol. 2009;38:1624–1633.
- , , , et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34.
- , , , et al. Risk, predictors, and mortality associated with non‐AIDS events in newly diagnosed HIV‐infected patients: role of antiretroviral therapy. AIDS. 2013;27:181–189.
- Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV‐1‐infected patients treated with antiretroviral therapy, 1996–2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis. 2010;50:1387–1396.
- , , , et al. Risk of all‐cause mortality associated with nonfatal AIDS and serious non‐AIDS events among adults infected with HIV. AIDS. 2010;24:697–706.
- , , , et al. Race and sex differences in antiretroviral therapy use and mortality among HIV‐infected persons in care. J Infect Dis. 2009;199:991–998.
- , , , . The influence of sex, race/ethnicity, and educational attainment on human immunodeficiency virus death rates among adults, 1993–2007. Arch Intern Med. 2012;172:1591–1598.
- , , , et al. Rates of hospitalizations and associated diagnoses in a large multisite cohort of HIV patients in the United States, 1994–2005. AIDS. 2008;22:1345–1354.
- , , , et al. Trends and causes of hospitalizations among HIV‐infected persons during the late HAART era: what is the impact of CD4 counts and HAART use? J Acquir Immune Defic Syndr. 2010;54:248–257.
- , . Hospitalization rates of people living with HIV in the United States, 2009. Public Health Rep. 2014;129:178–186.
- Agency for Healthcare Research and Quality. 2009 National Healthcare Quality Report. Available at: http://archive.ahrq.gov/research/findings/nhqrdr/nhqr09. Accessed May 8, 2015.
- , , , et al. Comparisons of causes of death and mortality rates among HIV‐infected persons: analysis of the pre‐, early, and late HAART (Highly Active Antiretroviral Therapy) Eras. J Acquir Immune Defic Syndr. 2006;41:194–200.
- , , , et al. Causes of death among HIV‐infected patients in France in 2010 (national survey): trends since 2000. AIDS. 2014;28:1181–1191.
- , , , , , . All‐cause mortality in hospitalized HIV‐infected patients at an acute tertiary care hospital with a comprehensive outpatient HIV care program in New York City in the era of highly active antiretroviral therapy (HAART). Infection. 2013;41:545–551.
- , , , . Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann Intern Med. 2006;145:397–406.
- Connecticut Department of Public Health. TB, HIV, STD 12:109–117.
- , , , et al. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992;41:1–19.
- , , , et al. Patterns of the hazard of death after AIDS through the evolution of antiretroviral therapy: 1984–2004. AIDS. 2005;19:2009–2018.
- , , , et al. Continued improvement in survival among HIV‐infected individuals with newer forms of highly active antiretroviral therapy. AIDS. 2007;21:685–692.
- , , , et al. Predictive accuracy of the Veterans Aging Cohort Study index for mortality with HIV infection: a North American cross cohort analysis. J Acquir Immune Defic Syndr. 2013;62:149–163.
- , , , et al. Non‐AIDS‐defining deaths and immunodeficiency in the era of combination antiretroviral therapy. AIDS. 2009;23:1743–1753.
- , , , et al. Causes of death in HIV‐infected patients from the Cologne‐Bonn cohort. Infection. 2014;42:135–140.
- , , , et al. Invasive pneumococcal disease in patients infected with HIV: still a threat in the era of highly active antiretroviral therapy. Clin Infect Dis. 2004;38:1623–1628.
- , , . The effect of HIV infection on the host response to bacterial sepsis. Lancet Infect Dis. 2015;15:95–108.
- , , , et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173:614–622.
- . Epidemiology of coronary heart disease in patients with human immunodeficiency virus. Rev Cardiovasc Med. 2014;15(suppl 1):S1–S8.
- , . Impact of human immunodeficiency virus infection on the prevalence and severity of steatosis in patients with chronic hepatitis C virus infection. J Hepatol. 2006;44:1026–1032.
- , , , et al. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta‐analysis. Clin Infect Dis. 2001;33:562–569.
- , . Coinfection with HIV‐1 and HCV–a one‐two punch. Gastroenterology. 2009;137:795–814.
- , , , et al. Hepatocellular carcinoma in HIV‐infected patients: epidemiological features, clinical presentation and outcome. AIDS. 2004;18:2285–2293.
- , , , et al. Presentation and outcome of hepatocellular carcinoma in HIV‐infected patients: a U.S.‐Canadian multicenter study. J Hepatol. 2007;47:527–537.
- , , , et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370:1879–1888.
- , , , et al. HIV as a chronic disease: implications for long‐term care at an AIDS‐dedicated skilled nursing facility. J Urban Health. 2000;77:187–203.
- , , , , , . Causes of death in HIV patients and the evolution of an AIDS hospice: 1988–2008. AIDS Res Treat. 2012;2012:390406.
- , , , et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384:241–248.
- , . Screening guidelines for non‐AIDS defining cancers in HIV‐infected individuals. Curr Opin Oncol. 2013;25:518–525.
- , , , et al. Disease patterns and causes of death of hospitalized HIV‐positive adults in West Africa: a multicountry survey in the antiretroviral treatment era. J Int AIDS Soc. 2014;17:18797.
- , , , . Recent trends in hospital utilization and mortality for HIV infection: 2000–2005. J Natl Med Assoc. 2010;102:1131–1138.
- , . Differences in HIV‐related hospitalization among white, black, and Hispanic men and women of Florida. Women Health. 2008;47:1–18.
- , , , . Effect of race and/or ethnicity in use of antiretrovirals and prophylaxis for opportunistic infection: a review of the literature. Public Health Rep. 2002;117:233–251; discussion 1–2.
- . HIV/AIDS in women and racial/ethnic minorities in the U.S. Curr Infect Dis Rep. 2012;14:53–60.
- , , , . Management of human immunodeficiency virus infection in advanced age. JAMA. 2013;309:1397–1405.
Successfully treated human immunodeficiency virus (HIV)‐infected individuals in the United States currently have life expectancy and mortality rates that are similar to the general population.[1, 2, 3, 4] A large multinational study found that the excess mortality rate among HIV‐positive individuals decreased from 40.8 to 6.1 per 1000 person‐years from pre‐1995 to 2006.1 This is largely due to improved access to comprehensive HIV care, in particular widespread antiretroviral (ART) use. However, the proportion of deaths that are not classically considered acquired immunodeficiency syndrome (AIDS)‐related such as liver disease, cardiovascular disease, and non‐AIDS malignancy has increased,[1, 5, 6, 7] particularly among patients with higher CD4 T‐cell counts.[5, 8] Additionally, despite overall decline in mortality, there is evidence of racial and gender differences, with increased mortality risk associated with female gender and black race.[9, 10]
In the current ART era, HIV care has shifted focus from inpatient to outpatient care, with more emphasis on chronic disease management. However, hospitalization rates among HIV‐positive persons remain higher than that of the general population.[11, 12] A cross‐sectional study of HIV‐infected persons in the United States estimated a hospitalization rate of 26.6 per 100 persons in 2009,[13] compared to a rate of 11.9 for the general population during the same year.[14] Possible reasons for higher hospitalization rates include complications of aging or other chronic comorbidities, and consequences of behavioral risk factors such tobacco use and substance abuse.
Characterizing deaths among inpatient HIV‐infected individuals in the ART era is important to developing targeted interventions to further reduce mortality. Prior studies examining in‐hospital deaths of HIV‐positive patients evaluated more limited time periods,[15, 16, 17, 18] and thus did not necessarily assess the full spectrum of changes in mortality that have occurred with the introduction of ART. Furthermore, these studies described causes of death, but did not consistently identify factors associated with non‐AIDS deaths. We examined the trends in in‐hospital deaths among HIV‐infected patients from 1995 to 2011 and identified contributing factors to mortality. As the HIV population is aging, we hypothesized that HIV‐infected patients are more likely to die from nonAIDS‐related death in the late ART era due to factors related to cardiovascular and liver disease, compared to the early ART era.
METHODS
The study was performed at YaleNew Haven Hospital, an urban tertiary care academic teaching hospital with 1008 beds and the state of Connecticut's largest ambulatory HIV clinic. Connecticut ranks seventh nationally (10/100,000) in HIV prevalence; New Haven is second among Connecticut cities in the number of people living with HIV/AIDS.[19] We reviewed all patients with an International Classification of Diseases, Ninth Revision (ICD‐9) code of HIV or AIDS (ICD‐9 codes V08 and 042) who died during hospitalization between January 1, 1995 to December 31, 2011. The Yale Human Investigation Committee granted ethical approval to conduct the study.
A standardized data collection tool was used to abstract demographic characteristics (ie, age, gender, and race), medical comorbidities (ie, diabetes, chronic kidney disease, chronic hepatitis B or C, liver cirrhosis, hypertension, coronary artery disease, congestive heart failure, chronic obstructive lung disease, alcohol and substance abuse), ART use (yes or no), HIV viral load (VL), CD4 cell count, and causes of death. Comorbidities were defined using the Coding of Death in HIV Project protocol, a multinational endeavor to standardize data collection in studies of HIV‐positive patients.[20] Chronic kidney disease included individuals with National Kidney Foundation stage I to V disease. Chronic hepatitis B or C infection was identified in patients who had serologic testing indicative of prior infection. Alcohol and substance abuse were identified when source documents mentioned any history of current alcohol or illicit drug abuse or dependence. ART use was defined as documentation of ART on admission or prescription during hospitalization. This included individuals who were on 2 or more ART agents. The last HIV VL and CD4 cell count available within 1 year and closest to death were recorded. HIV VL suppression was defined as <400 copies/mL.
Two clinicians independently classified the cause of death as AIDS related or non‐AIDS related in accordance with published definitions.[21, 22] Cause of death was determined by review of the medical record, discharge diagnosis, and autopsy report when available. Official death certificates were not available for review. There was discordance in assigning 23 of the 400 causes of death. In these cases, the medical record was reviewed and determined by consensus between the 2 clinicians.
AIDS‐related deaths were categorized as nonspecified AIDS, AIDS infection, and AIDS malignancy. AIDS‐related deaths were defined as those caused by conditions meeting the Centers for Disease Control and Prevention AIDS case definition.[22] Non‐specified AIDS deaths were those occurring in patients with a CD4 count 50 cells/mm3 or with an AIDS‐defining illness, who died from a condition that was not clearly AIDS related. This included septic shock of unclear etiology, first known episode of pneumonia, a gastrointestinal bleed of unclear etiology, and altered mental status of unclear etiology when cerebrospinal fluid analysis or imaging of the brain was not available.
Non‐AIDS deaths included non‐AIDS infection in patients with a CD4 count >50 cells/mm3, cardiovascular disease, liver disease, non‐AIDS malignancy, and renal disease (Table 1). Deaths classified as other incorporated the deaths that did not fall into these categories. Chronic obstructive pulmonary disease (COPD) exacerbation and status asthmaticus were included in this category, because there was only 1 death from each of these causes.
| |
| Non‐AIDS infection | Infectious etiology not on the list of AIDS‐defining conditions, such as Clostridium difficile colitis, endocarditis, bacteremia, nonrecurrent bacterial pneumonia, or septic shock of unclear cause without a CD4 count of less than 50 cells/mm3 or a documented opportunistic infection |
| Cardiovascular disease | Cardiac arrest without clear cause, ischemic or hemorrhagic stroke, congestive heart failure (respiratory failure most likely due to pulmonary edema in the setting of known systolic or diastolic heart failure), myocardial infarction, and cardiac arrhythmia |
| Liver disease | Complications of cirrhosis such as variceal bleed, hepatic encephalopathy, hepatorenal syndrome, and acute liver failure |
| Renal disease | Complications of acute renal failure such as hyperkalemia leading to cardiac arrest. Complications of end‐stage renal disease such as stopping hemodialysis or calciphylaxis |
| Non‐AIDS malignancy | Malignancies not on the AIDS indicator diagnostic list |
| Other causes | Drug overdose, trauma, suicide, Stevens‐Johnson syndrome, macrophage activation syndrome, hemorrhagic pancreatitis, status asthmaticus, COPD exacerbation, status epilepticus of unclear cause, complications of idiopathic thrombocytopenic purpura, and diabetic ketoacidosis |
The early ART era was defined as 1995 to 2001 and the late ART era from 2002 to 2011. During the early period, combination ART was introduced and significantly impacted overall mortality.[23, 24] The late ART era better reflected current in‐hospital deaths and was compared to the early era to evaluate trends over time.[15, 25]
2 analysis and parametric (t test and analysis of variance) methods compared categorical and continuous variables, respectively. Bivariate analysis was used to determine associations with AIDS versus non‐AIDS deaths in the entire study cohort. Multivariable logistic regression was used to identify correlates of non‐AIDS deaths in the (1) complete 17‐year period and (2) late ART era. For all analyses, a P value <0.05 was considered statistically significant. All statistical analysis was performed using SAS 9.3 (SAS Institute, Cary, NC).
RESULTS
Among 12,183 hospital discharges of HIV‐infected patients from 1995 to 2011, 406 (3.3%) died. Six medical records were missing or incomplete; 400 were available for review. The proportion of hospitalized HIV‐infected patients who died declined from 6.2% in 1995 to 1.5% in 2011 (P<0.0001).
Table 2 summarizes all 400 patients' demographic and clinical characteristics, and cause of death. The majority were male (65.5%), nonwhite (73.3%), and taking ART (65.9%), though only one‐third achieved a VL <400 copies/mL on the most recent measurement available in the year prior to death. The majority (56.3%) died due to nonAIDS‐related causes.
| Total, n=400 | Early Era, n=207 | Late Era, n=193 | P Value | |
|---|---|---|---|---|
| ||||
| Median age, y (IQR) | 45 (3852) | 41 (3547) | 49 (4357) | <0.0001 |
| Male gender, no. (%) | 262 (65.5) | 141 (68.1) | 121 (62.7) | 0.25 |
| Race, no. (%) | ||||
| Black | 238 (59.5) | 124 (59.9) | 114 (59.1) | 0.87 |
| White | 105 (26.3) | 55 (26.6) | 50 (25.9) | 0.88 |
| Hispanic | 55 (13.8) | 27 (13.0) | 28 (14.5) | 0.67 |
| Median CD4 cells/mm3 (IQR)a | 90 (12248) | 50 (10150) | 153 (22399) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 77 (31.3) | 12 (13.3) | 65 (41.7) | <0.0001 |
| On ART, no. (%) | 257 (65.9) | 120 (58.3) | 137 (74.5) | 0.0008 |
| Cause of death, no. (%) | ||||
| AIDS‐related, no. (%) | 175 (43.8) | 118 (57.0) | 57 (29.5) | <0.0001 |
| AIDS infection | 85 (21.3) | 58 (28.0) | 27 (14.0) | 0.82 |
| Nonspecified AIDS | 73 (18.3) | 46 (22.2) | 27 (14.0) | 0.99 |
| AIDS malignancy | 17 (4.3) | 14 (6.8) | 3 (1.6) | 0.17 |
| Non‐AIDS‐related, no. (%) | 225 (56.3) | 89 (43.0) | 136 (70.5) | <0.0001 |
| Non‐AIDS infection | 81 (20.3) | 32 (15.5) | 49 (25.4) | 0.99 |
| Cardiovascular | 45 (11.3) | 16 (7.7) | 29 (15.0) | 0.54 |
| Liver related | 34 (8.5) | 18 (8.7) | 16 (8.3) | 0.08 |
| Malignancy | 31 (7.8) | 6 (2.9) | 25 (13.0) | 0.01 |
| Renal failure | 18 (4.5) | 8 (3.9) | 10 (5.2) | 0.66 |
| Other, no. (%) | 16 (4.1) | 9 (4.5) | 7 (3.6) | 0.16 |
Among all AIDS‐related deaths from 1995 to 2011 (Table 2), AIDS‐defining infection was the most common cause (21.3%), followed by nonspecified AIDS (18.3%), and AIDS malignancy (4.3%). The proportion of nonAIDS‐related deaths increased significantly over time (Figure 1). The most common cause of nonAIDS‐related deaths was non‐AIDS infection (20.3%), followed by cardiovascular disease (11.3%), liver disease (8.5%), malignancy (7.8%), and renal failure (4.5%). The most common non‐AIDS infection was sepsis in 43 patients (60.6%), followed by nonrecurrent bacterial pneumonia in 24 patients (33.8%) and Clostridium difficile infection in 4 patients (5.6%). NonAIDS‐related malignancy was the only category to significantly increase from the early ART to late ART era (P=0.01).
Compared to those dying of AIDS‐related causes over the 17‐year period (Table 3), patients dying of nonAIDS‐related causes were older (P<0.0001), less likely to have a CD4 count 200 cells/mm3 (P<0.0001), and more likely to be on ART and virologically suppressed (P<0.0001). Patients who died from nonAIDS‐related causes were also more likely to have diabetes mellitus (P=0.01), chronic kidney disease (P<0.0001), hepatitis C (P<0.0001), liver cirrhosis (P<0.0001), hypertension (P=0.0002), coronary artery disease (P=0.004), and COPD (P=0.04). Of note, there was no statistically significant difference in gender, race, or substance abuse between AIDS‐related and nonAIDS‐related deaths.
| AIDS, n=175 | Non‐AIDS, n=225 | P Value | |
|---|---|---|---|
| |||
| Median age, y (IQR) | 40 (3548) | 48 (4255) | <0.0001 |
| Male gender, no. (%) | 115 (43.9) | 147 (56.1) | 0.94 |
| Race, no. (%) | |||
| Black | 105 (60.3) | 133 (59.4) | 0.84 |
| White | 41 (23.6) | 64 (28.6) | 0.26 |
| Hispanic | 28 (16.1) | 27 (12.1) | 0.25 |
| On ART, no. (%) | 97 (55.8) | 160 (74.1) | 0.0001 |
| CD4 <200 cells/mm3, no. (%)a | 167 (97.1) | 95 (47.2) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 2 (4.1) | 75 (38.1) | <0.0001 |
| Comorbidities, no. (%) | |||
| Diabetes | 13 (7.4) | 35 (15.6) | 0.01 |
| Renal disease | |||
| CKD | 21 (12) | 73 (32.4) | <0.0001 |
| On dialysis | 9 (5.1) | 47 (20.9) | <0.0001 |
| Liver disease | |||
| Hepatitis C | 38 (21.7) | 130 (57.8) | <0.0001 |
| Cirrhosis | 14 (8) | 67 (29.8) | <0.0001 |
| Cardiovascular disease | |||
| Hypertension | 18 (10.3) | 56 (24.9) | 0.0002 |
| CAD | 2 (1.1) | 16 (7.1) | 0.004 |
| CHF | 13 (7.4) | 29 (12.9) | 0.08 |
| COPD | 5 (2.9) | 17 (7.6) | 0.04 |
| Alcohol abuse | 9 (5.1) | 18 (8.0) | 0.26 |
| Polysubstance abuse | 10 (5.7) | 22 (9.8) | 0.14 |
Associations With Non‐AIDS Deaths
Among all clinical factors associated with non‐AIDS deaths (Table 4), only the last CD4 within the year prior to death >200 cells/mm3, VL 400 copies/mL in the year prior to death, and liver and cardiovascular comorbidities were independently associated with non‐AIDS deaths. The last CD4 count >200 cells/mm3 in the year prior to death was the strongest correlate (odds ratio [OR]: 16.5; 95% CI: 5.351.4) of non‐AIDS deaths, whereas gender and race were not significant.
| Overall (19952011) | Early Era (19952001) | Late Era (20022011) | ||||
|---|---|---|---|---|---|---|
| Deaths | 400 | 207 | 193 | |||
| Non‐AIDS | 225 | 89 | 136 | |||
| AIDS | 175 | 118 | 57 | |||
| Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | Odds Ratio (95% CI)a | Adjusted Odds Ratiob (95% CI) | Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | |
| ||||||
| Clinical factors | ||||||
| Age (per year) | 1.06 (1.04‐1.08) | c | 1.03 (1.01‐1.06) | c | 1.07 (1.03‐1.1) | c |
| Male gender | 0.98 (0.6‐1.5) | c | 1.04 (0.6‐1.9) | c | 1.1 (0.6‐2.0) | c |
| White race (vs nonwhite) | 0.8 (0.5‐1.2) | c | 1.2 (0.6‐2.2) | c | 0.4 (0.2‐0.8) | c |
| CD4 >200 cells/mm3d | 37.6 (14.895.5) | 16.5 (5.351.4) | 24.4 (7.183.2) | 17.4 (3.488.3) | 45.4 (10.5195.5) | 25.9 (5.0134.5) |
| HIV VL 400 copies/mL‖ | 13.6 (5.235.3) | 7.5 (2.324.4) | 9.4 (1.276.6) | c | 15.6 (5.246.4) | 10.9 (2.448.8) |
| On ART | 2.3 (1.5‐3.5) | c | 1.6 (0.9‐2.8) | c | 2.7 (1.35.3) | c |
| Comorbidities | ||||||
| Lung diseasee | 1.9 (1.013.5) | c | 2.4 (1.025.5) | c | 1.5 (0.6‐3.9) | c |
| Kidney diseasee | 3.5 (2.16.0) | c | 3.5 (1.7‐7.3) | 4.9 (1.417.8) | 3.1 (1.47.2) | c |
| Depression | 1.6 (0.8‐ 3.2) | c | 2.5 (0.9‐6.6) | c | 0.95 (0.4‐2.5) | c |
| Substance abusee | 1.9 (1.13.6) | c | 3.7 (1.59.5) | c | 0.9 (0.4‐2.1) | c |
| Diabetes | 2.3 (1.24.5) | c | 2.0 (0.7‐5.5) | c | 1.9 (0.7‐5.0) | c |
| Liver diseasee | 3.6 (2.45.4) | 4.5 (2.29.3) | 2.4 (1.4‐4.3) | 4.4 (1.512.7) | 4.3 (2.28.3) | 7.5 (2.423.4) |
| Cardiovascular diseasee | 2.9 (1.8‐4.6) | 4.2 (1.89.9) | 1.8 (0.9‐3.5) | 4.6 (2.010.3) | 6.8 (1.924.0) | |
In the early ART era (19952001), only CD4 count, renal disease, and cardiovascular disease were independently associated with non‐AIDS deaths; the last CD4 count <200 cells/mm3 in the year prior to death was associated most strongly (OR: 17.4; 95% CI: 3.488.3) with non‐AIDS death, whereas again, gender and race were not significant correlates of non‐AIDS death.
In the late ART era (20022011), similar to those for the entire 17‐year time period, independent correlates of non‐AIDS deaths included last CD4 <200 cells/mm3 in the year prior to death, VL 400 copies/mL in the last year prior to death, and liver and cardiovascular disease. Last CD4 count >200 cells/mm3 in the year prior to death (OR: 25.9; 95% CI: 5134.5) was most strongly correlated with non‐AIDS deaths in the late ART era. Nonwhite patients had a lower likelihood of nonAIDS‐related death (OR: 0.4; 95% CI: 0.2‐0.8), but this was not significant on multivariable regression analysis. Gender difference was not statistically significant.
DISCUSSION
Our study demonstrated changes in the causes of death among HIV‐infected hospitalized patients from 1995 to 2011. To our knowledge, this is the longest duration retrospective analysis of in‐hospital deaths among HIV‐infected patients during the ART era. Knowledge of the changes in comorbidities and causes of death among hospitalized HIV‐infected patients during the ART era could help inpatient providers focus diagnostic and therapeutic efforts and improve overall care. Our findings emphasize that HIV‐infected patients remain at high risk for complications from non‐AIDS infections, even when their immune system has been restored as measured by the CD4 cell count, and at increased risk of cardiovascular and liver disease, which highlights the need to carefully monitor HIV‐positive patients admitted with these conditions.
Comparison of AIDS‐related and nonAIDS‐related deaths in 2 time periods has revealed important findings. First, inpatient deaths of HIV‐infected patients have decreased dramatically (from 6.2% to 1.5%, P<0.0001), and the mortality due to nonAIDS‐related causes has increased significantly over time. Second, we defined demographic and clinical characteristics independently associated with HIV‐infected inpatient mortality. Third, a substantial proportion of in‐hospital deaths were caused by potentially preventable non‐AIDS as well as AIDS‐related diseases.
The striking decline in hospital deaths over time is likely the result of expanded ART use resulting in improved immunologic profiles. NonAIDS‐related causes were responsible for almost three‐quarters of deaths in this large inpatient HIV‐positive population during the late ART era. Similar findings have been reported from other settings in industrialized countries.[5, 7, 16, 17, 18, 26, 27] In our urban population, although cardiovascular disease, liver disease, renal failure, and malignancy were frequent causes of non‐AIDS death, the most common cause was non‐AIDS infection. Further, the proportion of deaths due to non‐AIDS infections did not decrease significantly over time.
A similar study of HIV‐positive inpatients in New York City also found that the majority of non‐AIDS deaths were due to non‐AIDS infections in the ART era.[17] The most common causes of non‐AIDS infection identified in the study were identical to ours: unspecified sepsis followed by nonrecurrent bacterial pneumonia and Clostridium difficile infection. Evidence suggests that individuals with HIV infection have multiple immunological defects that not only lead to increased susceptibility to bacterial infection but also to an unregulated inflammatory response, even in patients who are on ART and virologically suppressed.[28, 29] This highlights the need for hospital physicians to evaluate an HIV‐infected patient's risk for more routine infections that are not commonly considered AIDS related in addition to traditional opportunistic infections. It also implies that inpatient providers should carefully monitor HIV‐positive patients admitted for bacterial infections, as they remain at higher risk for the development of septic shock.
Cardiovascular and liver disease represented the next most common causes of death, which is similar to the New York City study and is consistent with other studies from the ART era.[15, 16, 17, 18] Although deaths due directly to cardiovascular and liver disease did not significantly change over time, these represented the major comorbidities associated with non‐AIDS mortality and, along with renal disease, increased significantly over the study period. There are accumulating studies indicating that HIV infection is associated with accelerated coronary artery disease due to the immune and inflammatory response to the viral replication.[30] Additionally, ART side effects such as hyperlipidemia, metabolic syndrome, and insulin resistance contribute to an increased cardiovascular risk profile.[31] Our findings emphasize the importance of assessing comorbidities not classically considered HIV related. For example, acute coronary syndrome should be in the differential diagnosis for HIV‐infected patients admitted with chest pain regardless of age. Furthermore, HIV‐infected patients are at increased risk for hepatitis B and C coinfection due to related behavioral risk, and coinfection is associated with rapid progression to liver cirrhosis[32, 33, 34] and increased risk for oncogenesis over time rapidly expanding therapeutic options will benefit patients with chronic liver disease.[35, 36, 37]
Although the numbers are relatively small, non‐AIDS malignancy deaths more than quadrupled from the early to the late ART eras. This finding likely underestimates the proportion of overall hospital deaths due to non‐AIDS malignancies given the increased use of hospice facilities and community‐based care,[38] though it is consistent with increasing trends noted in other studies.[39] Doubling of malignancy as a cause of death among AIDS patients from 2000 to 2010 was reported in a French study, as well as in a large multicohort study from 1999 to 2011, consistent with our findings.[16, 40] Developing and implementing screening guidelines for non‐AIDS malignancy among those with HIV at the primary care level may potentially reduce this upward trend.[41] Inpatient providers need to be aware of this trend and consider undiagnosed non‐AIDS malignancy as part of their differential diagnosis when evaluating HIV‐positive patients.
Although emphasis has been placed on non‐AIDS causes, nearly one‐half of all deaths for the entire period, and almost one‐third of deaths in the late ART era were still due to AIDS‐related causes. This is similar to a study of 40,000 patients in Europe and North America from 1996 to 2006, where AIDS deaths comprised almost half of all deaths,[7] as well as a French national study,[16] and remains characteristic of resource‐limited settings.[42] This indicates the need for continued vigilance toward earlier HIV case detection and retention in care to prevent disease progression and AIDS‐related mortality. Primary care and hospital physicians should assess risk for HIV infection in all patients and institute universal HIV testing in both the inpatient and outpatient settings.
Although the majority of our sample was nonwhite and male, there was sufficient demographic diversity to determine that race and gender differences were not statistically significant contributors to mortality. In contrast, hospital‐based and population‐based studies reporting racial and gender disparities in HIV‐associated mortality have attributed this to poor access to health care.[9, 17, 43, 44, 45, 46] Compared to the New York City study, patients in our study had comparable median age and CD4 cell count, but also had greater ART use and better virologic control.[17] We speculate that in our smaller urban area, characterized by strong community and clinical HIV programs, patients may have had improved access to care without regard to race and gender.
Our study strengths include a large sample size, a diverse population with a relatively high proportion of women, and varied age and race, as well as data acquired in a standardized fashion over a prolonged period of ART availability. Further, 2 clinicians classified causes of death independently, utilizing validated definitions to minimize bias. Our late ART era evaluation is consistent with other HIV cohort studies,[25] though we utilized multivariate analysis to uncover independent correlates of mortality, a feature not employed in other studies.[16, 17]
We also recognize several limitations in our study. Our study design was associated with the recognized limitations of retrospective research, including missing data. We examined in‐hospital deaths at a single urban hospital in the Northeastern United States only, affecting the generalizability of our findings. The study did not include a control group of hospitalized HIV‐infected patients who survived or hospitalized HIV‐negative patients who died, which might have further strengthened our findings. Despite these limitations, this study provides important observations that can inform strategies to impact HIV‐associated mortality in the inpatient setting.
In conclusion, the mortality profile of hospitalized HIV‐infected patients has evolved with the epidemic. Caring for the hospitalized HIV‐infected patient has become increasingly complex because patients are more likely to suffer from multiple comorbidities, especially cardiovascular and liver diseases, and to die from non‐AIDS causes. Inpatient providers need to understand the changing trends in chronic HIV disease management as patients are living longer with antiretroviral therapy and are increasingly likely to succumb to nonAIDS‐related causes of death. Clinicians can no longer remain focused on AIDS‐defining opportunistic infections and need to recognize the emerging importance of chronic comorbidities when developing a differential diagnosis, and the higher risk of death due to non‐AIDS infectious causes. Physicians caring for hospitalized patients should appreciate the current trends in the HIV epidemic to provide comprehensive and appropriate interventions that can reduce mortality for HIV‐infected inpatients.
Disclosures: This research was supported by the National Institute of Allergy and Infectious Diseases (S.S.; 1K23AI089260). The authors report no conflicts of interest.
Successfully treated human immunodeficiency virus (HIV)‐infected individuals in the United States currently have life expectancy and mortality rates that are similar to the general population.[1, 2, 3, 4] A large multinational study found that the excess mortality rate among HIV‐positive individuals decreased from 40.8 to 6.1 per 1000 person‐years from pre‐1995 to 2006.1 This is largely due to improved access to comprehensive HIV care, in particular widespread antiretroviral (ART) use. However, the proportion of deaths that are not classically considered acquired immunodeficiency syndrome (AIDS)‐related such as liver disease, cardiovascular disease, and non‐AIDS malignancy has increased,[1, 5, 6, 7] particularly among patients with higher CD4 T‐cell counts.[5, 8] Additionally, despite overall decline in mortality, there is evidence of racial and gender differences, with increased mortality risk associated with female gender and black race.[9, 10]
In the current ART era, HIV care has shifted focus from inpatient to outpatient care, with more emphasis on chronic disease management. However, hospitalization rates among HIV‐positive persons remain higher than that of the general population.[11, 12] A cross‐sectional study of HIV‐infected persons in the United States estimated a hospitalization rate of 26.6 per 100 persons in 2009,[13] compared to a rate of 11.9 for the general population during the same year.[14] Possible reasons for higher hospitalization rates include complications of aging or other chronic comorbidities, and consequences of behavioral risk factors such tobacco use and substance abuse.
Characterizing deaths among inpatient HIV‐infected individuals in the ART era is important to developing targeted interventions to further reduce mortality. Prior studies examining in‐hospital deaths of HIV‐positive patients evaluated more limited time periods,[15, 16, 17, 18] and thus did not necessarily assess the full spectrum of changes in mortality that have occurred with the introduction of ART. Furthermore, these studies described causes of death, but did not consistently identify factors associated with non‐AIDS deaths. We examined the trends in in‐hospital deaths among HIV‐infected patients from 1995 to 2011 and identified contributing factors to mortality. As the HIV population is aging, we hypothesized that HIV‐infected patients are more likely to die from nonAIDS‐related death in the late ART era due to factors related to cardiovascular and liver disease, compared to the early ART era.
METHODS
The study was performed at YaleNew Haven Hospital, an urban tertiary care academic teaching hospital with 1008 beds and the state of Connecticut's largest ambulatory HIV clinic. Connecticut ranks seventh nationally (10/100,000) in HIV prevalence; New Haven is second among Connecticut cities in the number of people living with HIV/AIDS.[19] We reviewed all patients with an International Classification of Diseases, Ninth Revision (ICD‐9) code of HIV or AIDS (ICD‐9 codes V08 and 042) who died during hospitalization between January 1, 1995 to December 31, 2011. The Yale Human Investigation Committee granted ethical approval to conduct the study.
A standardized data collection tool was used to abstract demographic characteristics (ie, age, gender, and race), medical comorbidities (ie, diabetes, chronic kidney disease, chronic hepatitis B or C, liver cirrhosis, hypertension, coronary artery disease, congestive heart failure, chronic obstructive lung disease, alcohol and substance abuse), ART use (yes or no), HIV viral load (VL), CD4 cell count, and causes of death. Comorbidities were defined using the Coding of Death in HIV Project protocol, a multinational endeavor to standardize data collection in studies of HIV‐positive patients.[20] Chronic kidney disease included individuals with National Kidney Foundation stage I to V disease. Chronic hepatitis B or C infection was identified in patients who had serologic testing indicative of prior infection. Alcohol and substance abuse were identified when source documents mentioned any history of current alcohol or illicit drug abuse or dependence. ART use was defined as documentation of ART on admission or prescription during hospitalization. This included individuals who were on 2 or more ART agents. The last HIV VL and CD4 cell count available within 1 year and closest to death were recorded. HIV VL suppression was defined as <400 copies/mL.
Two clinicians independently classified the cause of death as AIDS related or non‐AIDS related in accordance with published definitions.[21, 22] Cause of death was determined by review of the medical record, discharge diagnosis, and autopsy report when available. Official death certificates were not available for review. There was discordance in assigning 23 of the 400 causes of death. In these cases, the medical record was reviewed and determined by consensus between the 2 clinicians.
AIDS‐related deaths were categorized as nonspecified AIDS, AIDS infection, and AIDS malignancy. AIDS‐related deaths were defined as those caused by conditions meeting the Centers for Disease Control and Prevention AIDS case definition.[22] Non‐specified AIDS deaths were those occurring in patients with a CD4 count 50 cells/mm3 or with an AIDS‐defining illness, who died from a condition that was not clearly AIDS related. This included septic shock of unclear etiology, first known episode of pneumonia, a gastrointestinal bleed of unclear etiology, and altered mental status of unclear etiology when cerebrospinal fluid analysis or imaging of the brain was not available.
Non‐AIDS deaths included non‐AIDS infection in patients with a CD4 count >50 cells/mm3, cardiovascular disease, liver disease, non‐AIDS malignancy, and renal disease (Table 1). Deaths classified as other incorporated the deaths that did not fall into these categories. Chronic obstructive pulmonary disease (COPD) exacerbation and status asthmaticus were included in this category, because there was only 1 death from each of these causes.
| |
| Non‐AIDS infection | Infectious etiology not on the list of AIDS‐defining conditions, such as Clostridium difficile colitis, endocarditis, bacteremia, nonrecurrent bacterial pneumonia, or septic shock of unclear cause without a CD4 count of less than 50 cells/mm3 or a documented opportunistic infection |
| Cardiovascular disease | Cardiac arrest without clear cause, ischemic or hemorrhagic stroke, congestive heart failure (respiratory failure most likely due to pulmonary edema in the setting of known systolic or diastolic heart failure), myocardial infarction, and cardiac arrhythmia |
| Liver disease | Complications of cirrhosis such as variceal bleed, hepatic encephalopathy, hepatorenal syndrome, and acute liver failure |
| Renal disease | Complications of acute renal failure such as hyperkalemia leading to cardiac arrest. Complications of end‐stage renal disease such as stopping hemodialysis or calciphylaxis |
| Non‐AIDS malignancy | Malignancies not on the AIDS indicator diagnostic list |
| Other causes | Drug overdose, trauma, suicide, Stevens‐Johnson syndrome, macrophage activation syndrome, hemorrhagic pancreatitis, status asthmaticus, COPD exacerbation, status epilepticus of unclear cause, complications of idiopathic thrombocytopenic purpura, and diabetic ketoacidosis |
The early ART era was defined as 1995 to 2001 and the late ART era from 2002 to 2011. During the early period, combination ART was introduced and significantly impacted overall mortality.[23, 24] The late ART era better reflected current in‐hospital deaths and was compared to the early era to evaluate trends over time.[15, 25]
2 analysis and parametric (t test and analysis of variance) methods compared categorical and continuous variables, respectively. Bivariate analysis was used to determine associations with AIDS versus non‐AIDS deaths in the entire study cohort. Multivariable logistic regression was used to identify correlates of non‐AIDS deaths in the (1) complete 17‐year period and (2) late ART era. For all analyses, a P value <0.05 was considered statistically significant. All statistical analysis was performed using SAS 9.3 (SAS Institute, Cary, NC).
RESULTS
Among 12,183 hospital discharges of HIV‐infected patients from 1995 to 2011, 406 (3.3%) died. Six medical records were missing or incomplete; 400 were available for review. The proportion of hospitalized HIV‐infected patients who died declined from 6.2% in 1995 to 1.5% in 2011 (P<0.0001).
Table 2 summarizes all 400 patients' demographic and clinical characteristics, and cause of death. The majority were male (65.5%), nonwhite (73.3%), and taking ART (65.9%), though only one‐third achieved a VL <400 copies/mL on the most recent measurement available in the year prior to death. The majority (56.3%) died due to nonAIDS‐related causes.
| Total, n=400 | Early Era, n=207 | Late Era, n=193 | P Value | |
|---|---|---|---|---|
| ||||
| Median age, y (IQR) | 45 (3852) | 41 (3547) | 49 (4357) | <0.0001 |
| Male gender, no. (%) | 262 (65.5) | 141 (68.1) | 121 (62.7) | 0.25 |
| Race, no. (%) | ||||
| Black | 238 (59.5) | 124 (59.9) | 114 (59.1) | 0.87 |
| White | 105 (26.3) | 55 (26.6) | 50 (25.9) | 0.88 |
| Hispanic | 55 (13.8) | 27 (13.0) | 28 (14.5) | 0.67 |
| Median CD4 cells/mm3 (IQR)a | 90 (12248) | 50 (10150) | 153 (22399) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 77 (31.3) | 12 (13.3) | 65 (41.7) | <0.0001 |
| On ART, no. (%) | 257 (65.9) | 120 (58.3) | 137 (74.5) | 0.0008 |
| Cause of death, no. (%) | ||||
| AIDS‐related, no. (%) | 175 (43.8) | 118 (57.0) | 57 (29.5) | <0.0001 |
| AIDS infection | 85 (21.3) | 58 (28.0) | 27 (14.0) | 0.82 |
| Nonspecified AIDS | 73 (18.3) | 46 (22.2) | 27 (14.0) | 0.99 |
| AIDS malignancy | 17 (4.3) | 14 (6.8) | 3 (1.6) | 0.17 |
| Non‐AIDS‐related, no. (%) | 225 (56.3) | 89 (43.0) | 136 (70.5) | <0.0001 |
| Non‐AIDS infection | 81 (20.3) | 32 (15.5) | 49 (25.4) | 0.99 |
| Cardiovascular | 45 (11.3) | 16 (7.7) | 29 (15.0) | 0.54 |
| Liver related | 34 (8.5) | 18 (8.7) | 16 (8.3) | 0.08 |
| Malignancy | 31 (7.8) | 6 (2.9) | 25 (13.0) | 0.01 |
| Renal failure | 18 (4.5) | 8 (3.9) | 10 (5.2) | 0.66 |
| Other, no. (%) | 16 (4.1) | 9 (4.5) | 7 (3.6) | 0.16 |
Among all AIDS‐related deaths from 1995 to 2011 (Table 2), AIDS‐defining infection was the most common cause (21.3%), followed by nonspecified AIDS (18.3%), and AIDS malignancy (4.3%). The proportion of nonAIDS‐related deaths increased significantly over time (Figure 1). The most common cause of nonAIDS‐related deaths was non‐AIDS infection (20.3%), followed by cardiovascular disease (11.3%), liver disease (8.5%), malignancy (7.8%), and renal failure (4.5%). The most common non‐AIDS infection was sepsis in 43 patients (60.6%), followed by nonrecurrent bacterial pneumonia in 24 patients (33.8%) and Clostridium difficile infection in 4 patients (5.6%). NonAIDS‐related malignancy was the only category to significantly increase from the early ART to late ART era (P=0.01).
Compared to those dying of AIDS‐related causes over the 17‐year period (Table 3), patients dying of nonAIDS‐related causes were older (P<0.0001), less likely to have a CD4 count 200 cells/mm3 (P<0.0001), and more likely to be on ART and virologically suppressed (P<0.0001). Patients who died from nonAIDS‐related causes were also more likely to have diabetes mellitus (P=0.01), chronic kidney disease (P<0.0001), hepatitis C (P<0.0001), liver cirrhosis (P<0.0001), hypertension (P=0.0002), coronary artery disease (P=0.004), and COPD (P=0.04). Of note, there was no statistically significant difference in gender, race, or substance abuse between AIDS‐related and nonAIDS‐related deaths.
| AIDS, n=175 | Non‐AIDS, n=225 | P Value | |
|---|---|---|---|
| |||
| Median age, y (IQR) | 40 (3548) | 48 (4255) | <0.0001 |
| Male gender, no. (%) | 115 (43.9) | 147 (56.1) | 0.94 |
| Race, no. (%) | |||
| Black | 105 (60.3) | 133 (59.4) | 0.84 |
| White | 41 (23.6) | 64 (28.6) | 0.26 |
| Hispanic | 28 (16.1) | 27 (12.1) | 0.25 |
| On ART, no. (%) | 97 (55.8) | 160 (74.1) | 0.0001 |
| CD4 <200 cells/mm3, no. (%)a | 167 (97.1) | 95 (47.2) | <0.0001 |
| HIV VL 400 copies/mL, no. (%)b | 2 (4.1) | 75 (38.1) | <0.0001 |
| Comorbidities, no. (%) | |||
| Diabetes | 13 (7.4) | 35 (15.6) | 0.01 |
| Renal disease | |||
| CKD | 21 (12) | 73 (32.4) | <0.0001 |
| On dialysis | 9 (5.1) | 47 (20.9) | <0.0001 |
| Liver disease | |||
| Hepatitis C | 38 (21.7) | 130 (57.8) | <0.0001 |
| Cirrhosis | 14 (8) | 67 (29.8) | <0.0001 |
| Cardiovascular disease | |||
| Hypertension | 18 (10.3) | 56 (24.9) | 0.0002 |
| CAD | 2 (1.1) | 16 (7.1) | 0.004 |
| CHF | 13 (7.4) | 29 (12.9) | 0.08 |
| COPD | 5 (2.9) | 17 (7.6) | 0.04 |
| Alcohol abuse | 9 (5.1) | 18 (8.0) | 0.26 |
| Polysubstance abuse | 10 (5.7) | 22 (9.8) | 0.14 |
Associations With Non‐AIDS Deaths
Among all clinical factors associated with non‐AIDS deaths (Table 4), only the last CD4 within the year prior to death >200 cells/mm3, VL 400 copies/mL in the year prior to death, and liver and cardiovascular comorbidities were independently associated with non‐AIDS deaths. The last CD4 count >200 cells/mm3 in the year prior to death was the strongest correlate (odds ratio [OR]: 16.5; 95% CI: 5.351.4) of non‐AIDS deaths, whereas gender and race were not significant.
| Overall (19952011) | Early Era (19952001) | Late Era (20022011) | ||||
|---|---|---|---|---|---|---|
| Deaths | 400 | 207 | 193 | |||
| Non‐AIDS | 225 | 89 | 136 | |||
| AIDS | 175 | 118 | 57 | |||
| Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | Odds Ratio (95% CI)a | Adjusted Odds Ratiob (95% CI) | Odds Ratio (95% CI)a | Adjusted Odds Ratio (95% CI)b | |
| ||||||
| Clinical factors | ||||||
| Age (per year) | 1.06 (1.04‐1.08) | c | 1.03 (1.01‐1.06) | c | 1.07 (1.03‐1.1) | c |
| Male gender | 0.98 (0.6‐1.5) | c | 1.04 (0.6‐1.9) | c | 1.1 (0.6‐2.0) | c |
| White race (vs nonwhite) | 0.8 (0.5‐1.2) | c | 1.2 (0.6‐2.2) | c | 0.4 (0.2‐0.8) | c |
| CD4 >200 cells/mm3d | 37.6 (14.895.5) | 16.5 (5.351.4) | 24.4 (7.183.2) | 17.4 (3.488.3) | 45.4 (10.5195.5) | 25.9 (5.0134.5) |
| HIV VL 400 copies/mL‖ | 13.6 (5.235.3) | 7.5 (2.324.4) | 9.4 (1.276.6) | c | 15.6 (5.246.4) | 10.9 (2.448.8) |
| On ART | 2.3 (1.5‐3.5) | c | 1.6 (0.9‐2.8) | c | 2.7 (1.35.3) | c |
| Comorbidities | ||||||
| Lung diseasee | 1.9 (1.013.5) | c | 2.4 (1.025.5) | c | 1.5 (0.6‐3.9) | c |
| Kidney diseasee | 3.5 (2.16.0) | c | 3.5 (1.7‐7.3) | 4.9 (1.417.8) | 3.1 (1.47.2) | c |
| Depression | 1.6 (0.8‐ 3.2) | c | 2.5 (0.9‐6.6) | c | 0.95 (0.4‐2.5) | c |
| Substance abusee | 1.9 (1.13.6) | c | 3.7 (1.59.5) | c | 0.9 (0.4‐2.1) | c |
| Diabetes | 2.3 (1.24.5) | c | 2.0 (0.7‐5.5) | c | 1.9 (0.7‐5.0) | c |
| Liver diseasee | 3.6 (2.45.4) | 4.5 (2.29.3) | 2.4 (1.4‐4.3) | 4.4 (1.512.7) | 4.3 (2.28.3) | 7.5 (2.423.4) |
| Cardiovascular diseasee | 2.9 (1.8‐4.6) | 4.2 (1.89.9) | 1.8 (0.9‐3.5) | 4.6 (2.010.3) | 6.8 (1.924.0) | |
In the early ART era (19952001), only CD4 count, renal disease, and cardiovascular disease were independently associated with non‐AIDS deaths; the last CD4 count <200 cells/mm3 in the year prior to death was associated most strongly (OR: 17.4; 95% CI: 3.488.3) with non‐AIDS death, whereas again, gender and race were not significant correlates of non‐AIDS death.
In the late ART era (20022011), similar to those for the entire 17‐year time period, independent correlates of non‐AIDS deaths included last CD4 <200 cells/mm3 in the year prior to death, VL 400 copies/mL in the last year prior to death, and liver and cardiovascular disease. Last CD4 count >200 cells/mm3 in the year prior to death (OR: 25.9; 95% CI: 5134.5) was most strongly correlated with non‐AIDS deaths in the late ART era. Nonwhite patients had a lower likelihood of nonAIDS‐related death (OR: 0.4; 95% CI: 0.2‐0.8), but this was not significant on multivariable regression analysis. Gender difference was not statistically significant.
DISCUSSION
Our study demonstrated changes in the causes of death among HIV‐infected hospitalized patients from 1995 to 2011. To our knowledge, this is the longest duration retrospective analysis of in‐hospital deaths among HIV‐infected patients during the ART era. Knowledge of the changes in comorbidities and causes of death among hospitalized HIV‐infected patients during the ART era could help inpatient providers focus diagnostic and therapeutic efforts and improve overall care. Our findings emphasize that HIV‐infected patients remain at high risk for complications from non‐AIDS infections, even when their immune system has been restored as measured by the CD4 cell count, and at increased risk of cardiovascular and liver disease, which highlights the need to carefully monitor HIV‐positive patients admitted with these conditions.
Comparison of AIDS‐related and nonAIDS‐related deaths in 2 time periods has revealed important findings. First, inpatient deaths of HIV‐infected patients have decreased dramatically (from 6.2% to 1.5%, P<0.0001), and the mortality due to nonAIDS‐related causes has increased significantly over time. Second, we defined demographic and clinical characteristics independently associated with HIV‐infected inpatient mortality. Third, a substantial proportion of in‐hospital deaths were caused by potentially preventable non‐AIDS as well as AIDS‐related diseases.
The striking decline in hospital deaths over time is likely the result of expanded ART use resulting in improved immunologic profiles. NonAIDS‐related causes were responsible for almost three‐quarters of deaths in this large inpatient HIV‐positive population during the late ART era. Similar findings have been reported from other settings in industrialized countries.[5, 7, 16, 17, 18, 26, 27] In our urban population, although cardiovascular disease, liver disease, renal failure, and malignancy were frequent causes of non‐AIDS death, the most common cause was non‐AIDS infection. Further, the proportion of deaths due to non‐AIDS infections did not decrease significantly over time.
A similar study of HIV‐positive inpatients in New York City also found that the majority of non‐AIDS deaths were due to non‐AIDS infections in the ART era.[17] The most common causes of non‐AIDS infection identified in the study were identical to ours: unspecified sepsis followed by nonrecurrent bacterial pneumonia and Clostridium difficile infection. Evidence suggests that individuals with HIV infection have multiple immunological defects that not only lead to increased susceptibility to bacterial infection but also to an unregulated inflammatory response, even in patients who are on ART and virologically suppressed.[28, 29] This highlights the need for hospital physicians to evaluate an HIV‐infected patient's risk for more routine infections that are not commonly considered AIDS related in addition to traditional opportunistic infections. It also implies that inpatient providers should carefully monitor HIV‐positive patients admitted for bacterial infections, as they remain at higher risk for the development of septic shock.
Cardiovascular and liver disease represented the next most common causes of death, which is similar to the New York City study and is consistent with other studies from the ART era.[15, 16, 17, 18] Although deaths due directly to cardiovascular and liver disease did not significantly change over time, these represented the major comorbidities associated with non‐AIDS mortality and, along with renal disease, increased significantly over the study period. There are accumulating studies indicating that HIV infection is associated with accelerated coronary artery disease due to the immune and inflammatory response to the viral replication.[30] Additionally, ART side effects such as hyperlipidemia, metabolic syndrome, and insulin resistance contribute to an increased cardiovascular risk profile.[31] Our findings emphasize the importance of assessing comorbidities not classically considered HIV related. For example, acute coronary syndrome should be in the differential diagnosis for HIV‐infected patients admitted with chest pain regardless of age. Furthermore, HIV‐infected patients are at increased risk for hepatitis B and C coinfection due to related behavioral risk, and coinfection is associated with rapid progression to liver cirrhosis[32, 33, 34] and increased risk for oncogenesis over time rapidly expanding therapeutic options will benefit patients with chronic liver disease.[35, 36, 37]
Although the numbers are relatively small, non‐AIDS malignancy deaths more than quadrupled from the early to the late ART eras. This finding likely underestimates the proportion of overall hospital deaths due to non‐AIDS malignancies given the increased use of hospice facilities and community‐based care,[38] though it is consistent with increasing trends noted in other studies.[39] Doubling of malignancy as a cause of death among AIDS patients from 2000 to 2010 was reported in a French study, as well as in a large multicohort study from 1999 to 2011, consistent with our findings.[16, 40] Developing and implementing screening guidelines for non‐AIDS malignancy among those with HIV at the primary care level may potentially reduce this upward trend.[41] Inpatient providers need to be aware of this trend and consider undiagnosed non‐AIDS malignancy as part of their differential diagnosis when evaluating HIV‐positive patients.
Although emphasis has been placed on non‐AIDS causes, nearly one‐half of all deaths for the entire period, and almost one‐third of deaths in the late ART era were still due to AIDS‐related causes. This is similar to a study of 40,000 patients in Europe and North America from 1996 to 2006, where AIDS deaths comprised almost half of all deaths,[7] as well as a French national study,[16] and remains characteristic of resource‐limited settings.[42] This indicates the need for continued vigilance toward earlier HIV case detection and retention in care to prevent disease progression and AIDS‐related mortality. Primary care and hospital physicians should assess risk for HIV infection in all patients and institute universal HIV testing in both the inpatient and outpatient settings.
Although the majority of our sample was nonwhite and male, there was sufficient demographic diversity to determine that race and gender differences were not statistically significant contributors to mortality. In contrast, hospital‐based and population‐based studies reporting racial and gender disparities in HIV‐associated mortality have attributed this to poor access to health care.[9, 17, 43, 44, 45, 46] Compared to the New York City study, patients in our study had comparable median age and CD4 cell count, but also had greater ART use and better virologic control.[17] We speculate that in our smaller urban area, characterized by strong community and clinical HIV programs, patients may have had improved access to care without regard to race and gender.
Our study strengths include a large sample size, a diverse population with a relatively high proportion of women, and varied age and race, as well as data acquired in a standardized fashion over a prolonged period of ART availability. Further, 2 clinicians classified causes of death independently, utilizing validated definitions to minimize bias. Our late ART era evaluation is consistent with other HIV cohort studies,[25] though we utilized multivariate analysis to uncover independent correlates of mortality, a feature not employed in other studies.[16, 17]
We also recognize several limitations in our study. Our study design was associated with the recognized limitations of retrospective research, including missing data. We examined in‐hospital deaths at a single urban hospital in the Northeastern United States only, affecting the generalizability of our findings. The study did not include a control group of hospitalized HIV‐infected patients who survived or hospitalized HIV‐negative patients who died, which might have further strengthened our findings. Despite these limitations, this study provides important observations that can inform strategies to impact HIV‐associated mortality in the inpatient setting.
In conclusion, the mortality profile of hospitalized HIV‐infected patients has evolved with the epidemic. Caring for the hospitalized HIV‐infected patient has become increasingly complex because patients are more likely to suffer from multiple comorbidities, especially cardiovascular and liver diseases, and to die from non‐AIDS causes. Inpatient providers need to understand the changing trends in chronic HIV disease management as patients are living longer with antiretroviral therapy and are increasingly likely to succumb to nonAIDS‐related causes of death. Clinicians can no longer remain focused on AIDS‐defining opportunistic infections and need to recognize the emerging importance of chronic comorbidities when developing a differential diagnosis, and the higher risk of death due to non‐AIDS infectious causes. Physicians caring for hospitalized patients should appreciate the current trends in the HIV epidemic to provide comprehensive and appropriate interventions that can reduce mortality for HIV‐infected inpatients.
Disclosures: This research was supported by the National Institute of Allergy and Infectious Diseases (S.S.; 1K23AI089260). The authors report no conflicts of interest.
- , , , et al. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA. 2008;300:51–59.
- , , . Improvement in the health of HIV‐infected persons in care: reducing disparities. Clin Infect Dis. 2012;55:1242–1251.
- , , , et al. Mortality in well controlled HIV in the continuous antiretroviral therapy arms of the SMART and ESPRIT trials compared with the general population. AIDS. 2013;27:973–979.
- , , , et al. Mortality of HIV‐infected patients starting potent antiretroviral therapy: comparison with the general population in nine industrialized countries. Int J Epidemiol. 2009;38:1624–1633.
- , , , et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34.
- , , , et al. Risk, predictors, and mortality associated with non‐AIDS events in newly diagnosed HIV‐infected patients: role of antiretroviral therapy. AIDS. 2013;27:181–189.
- Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV‐1‐infected patients treated with antiretroviral therapy, 1996–2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis. 2010;50:1387–1396.
- , , , et al. Risk of all‐cause mortality associated with nonfatal AIDS and serious non‐AIDS events among adults infected with HIV. AIDS. 2010;24:697–706.
- , , , et al. Race and sex differences in antiretroviral therapy use and mortality among HIV‐infected persons in care. J Infect Dis. 2009;199:991–998.
- , , , . The influence of sex, race/ethnicity, and educational attainment on human immunodeficiency virus death rates among adults, 1993–2007. Arch Intern Med. 2012;172:1591–1598.
- , , , et al. Rates of hospitalizations and associated diagnoses in a large multisite cohort of HIV patients in the United States, 1994–2005. AIDS. 2008;22:1345–1354.
- , , , et al. Trends and causes of hospitalizations among HIV‐infected persons during the late HAART era: what is the impact of CD4 counts and HAART use? J Acquir Immune Defic Syndr. 2010;54:248–257.
- , . Hospitalization rates of people living with HIV in the United States, 2009. Public Health Rep. 2014;129:178–186.
- Agency for Healthcare Research and Quality. 2009 National Healthcare Quality Report. Available at: http://archive.ahrq.gov/research/findings/nhqrdr/nhqr09. Accessed May 8, 2015.
- , , , et al. Comparisons of causes of death and mortality rates among HIV‐infected persons: analysis of the pre‐, early, and late HAART (Highly Active Antiretroviral Therapy) Eras. J Acquir Immune Defic Syndr. 2006;41:194–200.
- , , , et al. Causes of death among HIV‐infected patients in France in 2010 (national survey): trends since 2000. AIDS. 2014;28:1181–1191.
- , , , , , . All‐cause mortality in hospitalized HIV‐infected patients at an acute tertiary care hospital with a comprehensive outpatient HIV care program in New York City in the era of highly active antiretroviral therapy (HAART). Infection. 2013;41:545–551.
- , , , . Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann Intern Med. 2006;145:397–406.
- Connecticut Department of Public Health. TB, HIV, STD 12:109–117.
- , , , et al. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992;41:1–19.
- , , , et al. Patterns of the hazard of death after AIDS through the evolution of antiretroviral therapy: 1984–2004. AIDS. 2005;19:2009–2018.
- , , , et al. Continued improvement in survival among HIV‐infected individuals with newer forms of highly active antiretroviral therapy. AIDS. 2007;21:685–692.
- , , , et al. Predictive accuracy of the Veterans Aging Cohort Study index for mortality with HIV infection: a North American cross cohort analysis. J Acquir Immune Defic Syndr. 2013;62:149–163.
- , , , et al. Non‐AIDS‐defining deaths and immunodeficiency in the era of combination antiretroviral therapy. AIDS. 2009;23:1743–1753.
- , , , et al. Causes of death in HIV‐infected patients from the Cologne‐Bonn cohort. Infection. 2014;42:135–140.
- , , , et al. Invasive pneumococcal disease in patients infected with HIV: still a threat in the era of highly active antiretroviral therapy. Clin Infect Dis. 2004;38:1623–1628.
- , , . The effect of HIV infection on the host response to bacterial sepsis. Lancet Infect Dis. 2015;15:95–108.
- , , , et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173:614–622.
- . Epidemiology of coronary heart disease in patients with human immunodeficiency virus. Rev Cardiovasc Med. 2014;15(suppl 1):S1–S8.
- , . Impact of human immunodeficiency virus infection on the prevalence and severity of steatosis in patients with chronic hepatitis C virus infection. J Hepatol. 2006;44:1026–1032.
- , , , et al. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta‐analysis. Clin Infect Dis. 2001;33:562–569.
- , . Coinfection with HIV‐1 and HCV–a one‐two punch. Gastroenterology. 2009;137:795–814.
- , , , et al. Hepatocellular carcinoma in HIV‐infected patients: epidemiological features, clinical presentation and outcome. AIDS. 2004;18:2285–2293.
- , , , et al. Presentation and outcome of hepatocellular carcinoma in HIV‐infected patients: a U.S.‐Canadian multicenter study. J Hepatol. 2007;47:527–537.
- , , , et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370:1879–1888.
- , , , et al. HIV as a chronic disease: implications for long‐term care at an AIDS‐dedicated skilled nursing facility. J Urban Health. 2000;77:187–203.
- , , , , , . Causes of death in HIV patients and the evolution of an AIDS hospice: 1988–2008. AIDS Res Treat. 2012;2012:390406.
- , , , et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384:241–248.
- , . Screening guidelines for non‐AIDS defining cancers in HIV‐infected individuals. Curr Opin Oncol. 2013;25:518–525.
- , , , et al. Disease patterns and causes of death of hospitalized HIV‐positive adults in West Africa: a multicountry survey in the antiretroviral treatment era. J Int AIDS Soc. 2014;17:18797.
- , , , . Recent trends in hospital utilization and mortality for HIV infection: 2000–2005. J Natl Med Assoc. 2010;102:1131–1138.
- , . Differences in HIV‐related hospitalization among white, black, and Hispanic men and women of Florida. Women Health. 2008;47:1–18.
- , , , . Effect of race and/or ethnicity in use of antiretrovirals and prophylaxis for opportunistic infection: a review of the literature. Public Health Rep. 2002;117:233–251; discussion 1–2.
- . HIV/AIDS in women and racial/ethnic minorities in the U.S. Curr Infect Dis Rep. 2012;14:53–60.
- , , , . Management of human immunodeficiency virus infection in advanced age. JAMA. 2013;309:1397–1405.
- , , , et al. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA. 2008;300:51–59.
- , , . Improvement in the health of HIV‐infected persons in care: reducing disparities. Clin Infect Dis. 2012;55:1242–1251.
- , , , et al. Mortality in well controlled HIV in the continuous antiretroviral therapy arms of the SMART and ESPRIT trials compared with the general population. AIDS. 2013;27:973–979.
- , , , et al. Mortality of HIV‐infected patients starting potent antiretroviral therapy: comparison with the general population in nine industrialized countries. Int J Epidemiol. 2009;38:1624–1633.
- , , , et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34.
- , , , et al. Risk, predictors, and mortality associated with non‐AIDS events in newly diagnosed HIV‐infected patients: role of antiretroviral therapy. AIDS. 2013;27:181–189.
- Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV‐1‐infected patients treated with antiretroviral therapy, 1996–2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis. 2010;50:1387–1396.
- , , , et al. Risk of all‐cause mortality associated with nonfatal AIDS and serious non‐AIDS events among adults infected with HIV. AIDS. 2010;24:697–706.
- , , , et al. Race and sex differences in antiretroviral therapy use and mortality among HIV‐infected persons in care. J Infect Dis. 2009;199:991–998.
- , , , . The influence of sex, race/ethnicity, and educational attainment on human immunodeficiency virus death rates among adults, 1993–2007. Arch Intern Med. 2012;172:1591–1598.
- , , , et al. Rates of hospitalizations and associated diagnoses in a large multisite cohort of HIV patients in the United States, 1994–2005. AIDS. 2008;22:1345–1354.
- , , , et al. Trends and causes of hospitalizations among HIV‐infected persons during the late HAART era: what is the impact of CD4 counts and HAART use? J Acquir Immune Defic Syndr. 2010;54:248–257.
- , . Hospitalization rates of people living with HIV in the United States, 2009. Public Health Rep. 2014;129:178–186.
- Agency for Healthcare Research and Quality. 2009 National Healthcare Quality Report. Available at: http://archive.ahrq.gov/research/findings/nhqrdr/nhqr09. Accessed May 8, 2015.
- , , , et al. Comparisons of causes of death and mortality rates among HIV‐infected persons: analysis of the pre‐, early, and late HAART (Highly Active Antiretroviral Therapy) Eras. J Acquir Immune Defic Syndr. 2006;41:194–200.
- , , , et al. Causes of death among HIV‐infected patients in France in 2010 (national survey): trends since 2000. AIDS. 2014;28:1181–1191.
- , , , , , . All‐cause mortality in hospitalized HIV‐infected patients at an acute tertiary care hospital with a comprehensive outpatient HIV care program in New York City in the era of highly active antiretroviral therapy (HAART). Infection. 2013;41:545–551.
- , , , . Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York City. Ann Intern Med. 2006;145:397–406.
- Connecticut Department of Public Health. TB, HIV, STD 12:109–117.
- , , , et al. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992;41:1–19.
- , , , et al. Patterns of the hazard of death after AIDS through the evolution of antiretroviral therapy: 1984–2004. AIDS. 2005;19:2009–2018.
- , , , et al. Continued improvement in survival among HIV‐infected individuals with newer forms of highly active antiretroviral therapy. AIDS. 2007;21:685–692.
- , , , et al. Predictive accuracy of the Veterans Aging Cohort Study index for mortality with HIV infection: a North American cross cohort analysis. J Acquir Immune Defic Syndr. 2013;62:149–163.
- , , , et al. Non‐AIDS‐defining deaths and immunodeficiency in the era of combination antiretroviral therapy. AIDS. 2009;23:1743–1753.
- , , , et al. Causes of death in HIV‐infected patients from the Cologne‐Bonn cohort. Infection. 2014;42:135–140.
- , , , et al. Invasive pneumococcal disease in patients infected with HIV: still a threat in the era of highly active antiretroviral therapy. Clin Infect Dis. 2004;38:1623–1628.
- , , . The effect of HIV infection on the host response to bacterial sepsis. Lancet Infect Dis. 2015;15:95–108.
- , , , et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173:614–622.
- . Epidemiology of coronary heart disease in patients with human immunodeficiency virus. Rev Cardiovasc Med. 2014;15(suppl 1):S1–S8.
- , . Impact of human immunodeficiency virus infection on the prevalence and severity of steatosis in patients with chronic hepatitis C virus infection. J Hepatol. 2006;44:1026–1032.
- , , , et al. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta‐analysis. Clin Infect Dis. 2001;33:562–569.
- , . Coinfection with HIV‐1 and HCV–a one‐two punch. Gastroenterology. 2009;137:795–814.
- , , , et al. Hepatocellular carcinoma in HIV‐infected patients: epidemiological features, clinical presentation and outcome. AIDS. 2004;18:2285–2293.
- , , , et al. Presentation and outcome of hepatocellular carcinoma in HIV‐infected patients: a U.S.‐Canadian multicenter study. J Hepatol. 2007;47:527–537.
- , , , et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370:1879–1888.
- , , , et al. HIV as a chronic disease: implications for long‐term care at an AIDS‐dedicated skilled nursing facility. J Urban Health. 2000;77:187–203.
- , , , , , . Causes of death in HIV patients and the evolution of an AIDS hospice: 1988–2008. AIDS Res Treat. 2012;2012:390406.
- , , , et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384:241–248.
- , . Screening guidelines for non‐AIDS defining cancers in HIV‐infected individuals. Curr Opin Oncol. 2013;25:518–525.
- , , , et al. Disease patterns and causes of death of hospitalized HIV‐positive adults in West Africa: a multicountry survey in the antiretroviral treatment era. J Int AIDS Soc. 2014;17:18797.
- , , , . Recent trends in hospital utilization and mortality for HIV infection: 2000–2005. J Natl Med Assoc. 2010;102:1131–1138.
- , . Differences in HIV‐related hospitalization among white, black, and Hispanic men and women of Florida. Women Health. 2008;47:1–18.
- , , , . Effect of race and/or ethnicity in use of antiretrovirals and prophylaxis for opportunistic infection: a review of the literature. Public Health Rep. 2002;117:233–251; discussion 1–2.
- . HIV/AIDS in women and racial/ethnic minorities in the U.S. Curr Infect Dis Rep. 2012;14:53–60.
- , , , . Management of human immunodeficiency virus infection in advanced age. JAMA. 2013;309:1397–1405.
© 2015 Society of Hospital Medicine

Predictors of Prolonged Hospitalizations
Hospitalizations frequently last longer than warranted by medical necessity alone, due to inefficiencies within the US healthcare system.[1, 2] Discharge delays place patients at risk for hospital‐acquired complications and increase costs. With the growing emphasis on high‐value care, hospital length of stay (LOS) has emerged as a key metric for inpatient care and will remain a central focus of hospital‐based improvement initiatives for the foreseeable future.
Hospitals may find it difficult to identify the primary drivers of inpatient LOS in a dynamic and increasingly complex healthcare system. Multiple recent policy changes have affected inpatient care. The Health Information Technology for Economic and Clinical Health Act of 2009 has led to widespread adoption of electronic health records (EHRs) that have markedly impacted provider workflows.[3] In October 2013, the Centers for Medicare & Medicaid Services implemented the 2‐midnight rule, which reclassified lower acuity inpatients with an expected stay 48 hours to observation status.[4] In January 2014, expansion of insurance coverage under the Affordable Care Act (ACA) altered payer mix for hospitals nationwide.[5] At a local level, hospitals that are rapidly adjusting resource allocation, capital investments, and marketing efforts and making complex operational decisions (eg, to open new units or change admission or referral algorithms) may simultaneously experience shifts in patient volumes, case‐mix index, and staffing ratios with downstream effects on LOS.
Given the myriad factors influencing inpatient LOS, hospital leaders may encounter real challenges in designing effective LOS reduction strategies. For example, they may expend significant resources on real‐time demand‐capacity management systems to improve hospital‐wide patient flow, but the resultant emphasis on bed placement and early discharges may shave only hours off average LOS.[6, 7] An alternative approach may be to target the small percentage of patients with prolonged hospitalizations who contribute disproportionately to the average LOS, as other initiatives focused on high utilizers have done.[8, 9, 10]
Our institution noted an increase in the average inpatient LOS for general medicine patients from 2012 to 2014, prompting a call to action by hospital leaders. We sought to characterize the predictors of prolonged hospitalizations among medicine patients to guide future efforts aimed at mitigating the contribution of prolonged LOS to overall LOS.
METHODS
Study Design
We performed a retrospective analysis of medicine patients discharged between January 1, 2012 and December 31, 2014, from the University of Colorado Hospital, a 551‐bed urban, quaternary‐care academic medical center in Aurora, Colorado. Patients were included if they were admitted under inpatient status, 18 years of age, and discharged from 1 of our 10 medicine services: 7 services with residents, staffed by hospitalists, general internists, or subspecialists; and 3 services with advanced practice providers, staffed by hospitalists.
Data Collection
We obtained LOS, calendar year of discharge, demographic data, insurance type, discharge disposition, number of medications, consults, intensive care unit (ICU) stays, surgeries (ie, procedures requiring anesthesia), and primary diagnosis by International Classification of Diseases, Ninth Revision codes from an administrative database that had been developed, validated, and maintained by our hospital medicine group. This database was populated with variables from our EHR, which was implemented in September 2011; to minimize variability in data input during the EHR rollout, we excluded data from September 2011 through December 2011. The Colorado Multiple Institutional Review Board reviewed and exempted this database (protocol 13‐2953) as a program evaluation.
Outcomes
We defined a prolonged hospitalization or LOS as >21 days in duration. This represented approximately 2 standard deviations above the mean LOS in our cohort. This cutoff also helped to remove provider‐level variability, as each medicine service was staffed by 2 attendings per month, each working approximately 7 days on and 7 days off. We examined LOS >14 and >30 days in sensitivity analyses to ensure that the selection of >21 days did not impose an arbitrary and invalid limitation on our statistical analysis.
Statistical Analysis
Demographic and clinical data were compared in the group with LOS 21 days versus the group with LOS >21 days with a 2 test for dichotomous variables and Student t test for continuous variables. We then built a multivariable logistic regression model to predict LOS >21 days using the variables that were significantly different between groups in bivariate analyses. A two‐sided P value of 0.05 was considered statistically significant. All data analyses were performed using Stata 12.0 (StataCorp, College Station, TX).
RESULTS
We identified 18,363 inpatient discharges among 12,511 medicine patients between January 1, 2012 and December 31, 2014. Of these discharges, 416 (2.3%) demonstrated prolonged LOS. Prolonged hospitalizations accounted for 18.6% of total inpatient days. The average LOS during the study period was 4.8 days including patients with prolonged LOS and 4.0 days excluding patients with prolonged LOS, a contribution of 0.8 days.
Table 1 compares the characteristics of patients with and without prolonged LOS. Age, insurance, discharge disposition, palliative care consults, ICU stays, and surgeries were among the variables that differed significantly between the 2 groups. Among patients undergoing surgery, those with prolonged LOS were more likely to have surgery >24 hours after admission than those without prolonged LOS (85.7% vs 51.4%, P0.001).
| Variable | LOS 21 Days, N=17,947 | LOS >21 Days, N=416 | P Value |
|---|---|---|---|
| |||
| Age, y, mean (SD) | 56.4 (18.7) | 54.4 (17.1) | 0.030 |
| Female | 9,256 (52%) | 199 (48%) | 0.132 |
| Year of discharge | 0.001 | ||
| 2012 | 5,486 (31%) | 69 (17%) | |
| 2013 | 6,193 (35%) | 162 (39%) | |
| 2014 | 6,268 (35%) | 185 (44%) | |
| Race/ethnicity | 0.003 | ||
| White non‐Hispanic | 9,702 (54%) | 242 (58%) | |
| Black non‐Hispanic | 4,000 (22%) | 68 (16%) | |
| Hispanic | 2,872(16%) | 67 (16%) | |
| Asian | 578 (3%) | 9 (2%) | |
| Other or unknown | 795 (4%) | 30 (7%) | |
| Language preference | 0.795 | ||
| English | 16,049 (89%) | 376 (90%) | |
| Spanish | 1,052 (6%) | 23 (6%) | |
| Other | 846 (5%) | 17 (4%) | |
| Insurance | 0.001 | ||
| Medicare | 5,462 (30%) | 109 (26%) | |
| Medicaid | 3,406 (19%) | 126 (30%) | |
| Dual | 2,815 (16%) | 64 (15%) | |
| Private | 2,714 (15%) | 60 (14%) | |
| Indigent/self‐pay | 2,829 (16%) | 42 (10%) | |
| Other | 721 (4%) | 15 (4%) | |
| Length of stay, d (SD) | 4.0 (3.5) | 39.5 (37.3) | 0.001 |
| Discharge disposition | 0.001 | ||
| Home with self‐care | 13,276 (74%) | 115 (28%) | |
| Home with home health | 1,584 (9%) | 79 (19%) | |
| Hospicehome or inpatient | 369 (2%) | 19 (5%) | |
| Postacute‐care facility or LTAC | 1,761 (10%) | 141 (34%) | |
| Expired | 113 (1%) | 18 (4%) | |
| Other | 844 (5%) | 44 (11%) | |
| No. of admission medications (SD) | 9.7 (7.4) | 10.9 (7.8) | 0.002 |
| Primary diagnosis by ICD‐9 code* | |||
| Sepsis, unspecified | 1,548 (9%) | 55 (13%) | 0.001 |
| Acute respiratory failure | 293 (2%) | 9 (2%) | 0.400 |
| MSSA septicemia | 36 (0.2%) | 8 (2%) | 0.001 |
| MRSA septicemia | 13 (0.1%) | 7 (2%) | 0.001 |
| Alcoholic cirrhosis of the liver | 111 (1%) | 7 (2%) | 0.007 |
| Palliative care consult | 398 (2%) | 64 (15%) | 0.001 |
| ICU stay | 2,030 (11%) | 246 (59%) | 0.001 |
| Surgical procedure | 1,800 (10%) | 182 (44%) | 0.001 |
Unspecified sepsis was the most frequent primary diagnosis, regardless of LOS category (Table 2). However, the second through fifth most frequent diagnoses differed for patients with and without prolonged LOS.
| N | % | |
|---|---|---|
| ||
| LOS 21 days | ||
| 1. Sepsis, unspecified | 1,548 | 8.6% |
| 2. Acute pancreatitis | 435 | 2.4% |
| 3. Pneumonia | 431 | 2.4% |
| 4. Acute kidney failure | 363 | 2.0% |
| 5. COPD exacerbation | 320 | 1.8% |
| LOS >21 days | ||
| 1. Sepsis, unspecified | 55 | 13.0% |
| 2. Acute respiratory failure | 9 | 2.2% |
| 3. Methicillin‐sensitive Staphylococcus aureus septicemia | 8 | 1.9% |
| 4. Methicillin‐resistant Staphylococcus aureus septicemia | 7 | 1.7% |
| 5. Alcoholic cirrhosis of the liver | 7 | 1.7% |
In an adjusted logistic regression model (Table 3), we found lower odds of prolonged LOS for each 10‐year increase in age and higher odds of prolonged LOS for Medicaid insurance, discharge to home with home health, discharge to a postacute‐care or long‐term acute‐care facility, and in‐hospital death. Methicillin‐resistant Staphylococcus aureus (MRSA) septicemia, palliative care consults, ICU stays, and surgeries were all also associated with increased odds of prolonged LOS. We identified a statistically significant interaction between ICU stay and surgical procedure (odds ratio: 2.53, 95% confidence interval: 1.51‐4.26, P0.001).
| Outcome: LOS >21 Days | Odds Ratio | 95% CI | P Value |
|---|---|---|---|
| |||
| Age, per 10 years increase in age | 0.80 | 0.73‐0.87 | 0.001 |
| Year of discharge | |||
| 2012 | 0.47 | 0.34‐0.67 | 0.001 |
| 2013 | 1.10 | 0.84‐1.43 | 0.493 |
| 2014 | Ref | ||
| Race/ethnicity | |||
| White non‐Hispanic | Ref | ||
| Black non‐Hispanic | 0.89 | 0.64‐1.22 | 0.454 |
| Hispanic | 1.01 | 0.70‐1.46 | 0.952 |
| Asian | 0.85 | 0.40‐1.83 | 0.679 |
| Other or unknown | 1.29 | 0.73‐2.26 | 0.378 |
| Insurance | |||
| Medicare | Ref | ||
| Medicaid | 1.99 | 1.29‐3.05 | 0.002 |
| Dual | 1.06 | 0.72‐1.57 | 0.765 |
| Private | 1.13 | 0.70‐1.82 | 0.620 |
| Indigent/self‐pay | 1.66 | 0.95‐2.88 | 0.073 |
| Other | 0.96 | 0.47‐1.96 | 0.908 |
| Discharge disposition | |||
| Home with self‐care | Ref | ||
| Home with home health | 4.48 | 3.10‐6.48 | 0.001 |
| Hospicehome or inpatient | 2.11 | 0.98‐4.55 | 0.057 |
| Postacute‐care facility or LTAC | 10.37 | 6.92‐15.56 | 0.001 |
| Expired | 5.38 | 2.27‐12.75 | 0.001 |
| Other | 4.04 | 2.64‐6.18 | 0.001 |
| No. of admission medications | 1.00 | 0.99‐1.02 | 0.775 |
| Primary diagnosis by ICD‐9 code | |||
| Sepsis, unspecified | 1.11 | 0.78‐1.58 | 0.575 |
| MSSA septicemia | 2.44 | 0.68‐8.67 | 0.074 |
| MRSA septicemia | 8.83 | 1.72‐45.36 | 0.009 |
| Alcoholic cirrhosis of the liver | 1.25 | 0.43‐3.65 | 0.687 |
| Palliative care consult | 4.63 | 2.86‐7.49 | 0.001 |
| ICU stay | 6.66 | 5.22‐8.50 | 0.001 |
| Surgical procedure | 5.04 | 3.90‐6.52 | 0.001 |
Sensitivity analyses using LOS >14 and >30 days yielded similar results to LOS >21 days (see Supporting Appendix Table 1 in the online version of this article).
DISCUSSION
We found that a small proportion of medicine patients with prolonged hospitalizations contributed substantially to both total inpatient days and average inpatient LOS. Such disproportionate healthcare utilization is concerning in light of the Institute of Medicine's charge for health systems to deliver timely, efficient, and equitable care.[11]
Few studies in the United States have analyzed patient characteristics that predict prolonged LOS, and to our knowledge, none have evaluated prolonged LOS specifically in general medicine patients.[12, 13, 14] Among selected surgical populations, prolonged hospitalizations are most often related to placement difficulties, operational delays, and payer‐related issues, rather than severity of illness, baseline comorbidities, or in‐hospital complications.[12, 13] In our study, we found that patients with prolonged LOS were more likely to require a palliative care consult, ICU stay, or surgery, all proxies for disease severity. Patients with prolonged LOS were also more likely to undergo surgery >24 hours after admission than those without prolonged LOS, suggesting that the former were either too unstable to proceed directly to surgery or developed complications later during their hospitalization. Even after controlling for palliative care consults, ICU stays, and surgeries, placement at a postacute‐care facility was strongly associated with prolonged LOS. Patients with prolonged LOS were also more likely to have Medicaid compared to other insurance types.
Our findings have several potential implications for efforts aimed at decreasing the number of and length of prolonged hospitalizations. Although demographic and clinical factors such as Medicaid insurance, ICU stays, and surgeries are generally not modifiable, they could, particularly in combination, be used to trigger earlier and more intensive case management involvement. A streamlined insurance approval process for Medicaid pending inpatients could be beneficial, given the recent expansion of Medicaid eligibility under the ACA. Hospital partnerships with postacute‐care facilities could also relieve bottlenecks in placement.[8] Chart review of the patients with MRSA septicemia and prolonged LOS indicated that development of an intensive outpatient parenteral antimicrobial therapy pathway with substance abuse counseling could provide an alternative to extended inpatient treatment for intravenous drug users with complicated infections.[15]
This study has several limitations. First, given the lack of consensus in the literature regarding the definition of a prolonged hospitalization, it is difficult to directly compare our results with existing studies.[8, 12, 13, 14] However, we believe LOS >21 days to be a meaningful cutoff for our cohort. Most demographic and clinical variables that were predictive at >21 days were also predictive at >14 and >30 days, which reassured us that the relationship between variables and prolonged LOS was stable at different thresholds. Second, our database did not allow us to fully adjust for baseline comorbidities or categorize the reasons for discharge delays. Finally, this was a single‐center program evaluation. Although this limits generalization to other institutions, we believe our approach may serve as a guide for others interested in reducing prolonged hospitalizations.
In summary, prolonged hospitalizations represent a potentially high‐yield target for LOS reduction efforts. Prolonged hospitalizations among medicine patients at our institution particularly affected Medicaid enrollees with complex hospital stays who were not discharged home. Further studies are needed to determine the specific reasons for unnecessary hospital days in this population.
Acknowledgements
The authors thank Essey Yirdaw for her contributions to the building and management of the database that informed this work.
Disclosure: M.E.A. conceived of the study concept and design and drafted the manuscript. J.J.G. assisted with the study design and made critical revisions to the final manuscript. D.A., R.P., and R.C. assisted with the study design and made critical revisions to the manuscript. C.D.J. assisted with the study design, performed data analyses, and made critical revisions to the manuscript. RC has disclosed that her time is funded by a National Institutes of Health grant unrelated to this study. A modified abstract was presented in poster format at the Society of Hospital Medicine Research, Innovations, and Vignettes Competition 2015 Annual Meeting, held March 29 April 1, 2015, in National Harbor, Maryland. The authors have no conflicts of interest to disclose.
- , , , et al. Excess hospitalization days in an academic medical center: perceptions of hospitalists and discharge planners. Am J Manag Care. 2011;17(2):e34–e42.
- , , A prospective study of reasons for prolonged hospitalizations on a general medicine teaching service. J Gen Intern Med. 2005;20(2):108–115.
- , , , et al. Adoption of electronic health records grows rapidly, but fewer than half of U.S. hospitals had at least a basic system in 2012. Health Aff (Millwood). 2013;32(8):1478–1485.
- , , , et al. Observation and inpatient status: clinical impact of the 2‐midnight rule. J Hosp Med. 2014;9(4):203–209.
- , , Impact of insurance expansion on hospital uncompensated care costs in 2014. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. Available at: http://aspe.hhs.gov/health/reports/2014/uncompensatedcare/ib_uncompensatedcare.pdf. Accessed March 28, 2015.
- , , , Using real‐time demand capacity management to improve hospital‐wide patient flow. Jt Comm J Qual Patient Saf. 2011;37(5):217–227.
- , , , , , Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226–233.
- , , , Addressing hospital length of stay outlier patients: a community‐wide approach. Adv Biosci Biotechol. 2014;5:188–196.
- , American medical home runs. Health Aff (Millwood). 2009;28(5):1317–1326.
- The hot spotters: can we lower medical costs by giving the neediest patients better care? New Yorker. January 2011:40–51.
- Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
- , , , et al. Excessively long hospital stays after trauma are not related to the severity of illness: let's aim to the right target! JAMA Surg. 2013;148(1):956–961.
- , , Extended length of stay after surgery: complications, inefficient practice, or sick patients? JAMA Surg. 2014;149(8):815–820.
- , , , , Nonmedical factors associated with prolonged hospital length of stay in an urban homebound population. J Hosp Med. 2012;7(2):73–78.
- , , , Safe and successful treatment of intravenous drug users with a peripherally inserted central catheter in an outpatient parenteral antibiotic treatment service. J Antimicrob Chemother. 2010;65(12):2641–2644.
Hospitalizations frequently last longer than warranted by medical necessity alone, due to inefficiencies within the US healthcare system.[1, 2] Discharge delays place patients at risk for hospital‐acquired complications and increase costs. With the growing emphasis on high‐value care, hospital length of stay (LOS) has emerged as a key metric for inpatient care and will remain a central focus of hospital‐based improvement initiatives for the foreseeable future.
Hospitals may find it difficult to identify the primary drivers of inpatient LOS in a dynamic and increasingly complex healthcare system. Multiple recent policy changes have affected inpatient care. The Health Information Technology for Economic and Clinical Health Act of 2009 has led to widespread adoption of electronic health records (EHRs) that have markedly impacted provider workflows.[3] In October 2013, the Centers for Medicare & Medicaid Services implemented the 2‐midnight rule, which reclassified lower acuity inpatients with an expected stay 48 hours to observation status.[4] In January 2014, expansion of insurance coverage under the Affordable Care Act (ACA) altered payer mix for hospitals nationwide.[5] At a local level, hospitals that are rapidly adjusting resource allocation, capital investments, and marketing efforts and making complex operational decisions (eg, to open new units or change admission or referral algorithms) may simultaneously experience shifts in patient volumes, case‐mix index, and staffing ratios with downstream effects on LOS.
Given the myriad factors influencing inpatient LOS, hospital leaders may encounter real challenges in designing effective LOS reduction strategies. For example, they may expend significant resources on real‐time demand‐capacity management systems to improve hospital‐wide patient flow, but the resultant emphasis on bed placement and early discharges may shave only hours off average LOS.[6, 7] An alternative approach may be to target the small percentage of patients with prolonged hospitalizations who contribute disproportionately to the average LOS, as other initiatives focused on high utilizers have done.[8, 9, 10]
Our institution noted an increase in the average inpatient LOS for general medicine patients from 2012 to 2014, prompting a call to action by hospital leaders. We sought to characterize the predictors of prolonged hospitalizations among medicine patients to guide future efforts aimed at mitigating the contribution of prolonged LOS to overall LOS.
METHODS
Study Design
We performed a retrospective analysis of medicine patients discharged between January 1, 2012 and December 31, 2014, from the University of Colorado Hospital, a 551‐bed urban, quaternary‐care academic medical center in Aurora, Colorado. Patients were included if they were admitted under inpatient status, 18 years of age, and discharged from 1 of our 10 medicine services: 7 services with residents, staffed by hospitalists, general internists, or subspecialists; and 3 services with advanced practice providers, staffed by hospitalists.
Data Collection
We obtained LOS, calendar year of discharge, demographic data, insurance type, discharge disposition, number of medications, consults, intensive care unit (ICU) stays, surgeries (ie, procedures requiring anesthesia), and primary diagnosis by International Classification of Diseases, Ninth Revision codes from an administrative database that had been developed, validated, and maintained by our hospital medicine group. This database was populated with variables from our EHR, which was implemented in September 2011; to minimize variability in data input during the EHR rollout, we excluded data from September 2011 through December 2011. The Colorado Multiple Institutional Review Board reviewed and exempted this database (protocol 13‐2953) as a program evaluation.
Outcomes
We defined a prolonged hospitalization or LOS as >21 days in duration. This represented approximately 2 standard deviations above the mean LOS in our cohort. This cutoff also helped to remove provider‐level variability, as each medicine service was staffed by 2 attendings per month, each working approximately 7 days on and 7 days off. We examined LOS >14 and >30 days in sensitivity analyses to ensure that the selection of >21 days did not impose an arbitrary and invalid limitation on our statistical analysis.
Statistical Analysis
Demographic and clinical data were compared in the group with LOS 21 days versus the group with LOS >21 days with a 2 test for dichotomous variables and Student t test for continuous variables. We then built a multivariable logistic regression model to predict LOS >21 days using the variables that were significantly different between groups in bivariate analyses. A two‐sided P value of 0.05 was considered statistically significant. All data analyses were performed using Stata 12.0 (StataCorp, College Station, TX).
RESULTS
We identified 18,363 inpatient discharges among 12,511 medicine patients between January 1, 2012 and December 31, 2014. Of these discharges, 416 (2.3%) demonstrated prolonged LOS. Prolonged hospitalizations accounted for 18.6% of total inpatient days. The average LOS during the study period was 4.8 days including patients with prolonged LOS and 4.0 days excluding patients with prolonged LOS, a contribution of 0.8 days.
Table 1 compares the characteristics of patients with and without prolonged LOS. Age, insurance, discharge disposition, palliative care consults, ICU stays, and surgeries were among the variables that differed significantly between the 2 groups. Among patients undergoing surgery, those with prolonged LOS were more likely to have surgery >24 hours after admission than those without prolonged LOS (85.7% vs 51.4%, P0.001).
| Variable | LOS 21 Days, N=17,947 | LOS >21 Days, N=416 | P Value |
|---|---|---|---|
| |||
| Age, y, mean (SD) | 56.4 (18.7) | 54.4 (17.1) | 0.030 |
| Female | 9,256 (52%) | 199 (48%) | 0.132 |
| Year of discharge | 0.001 | ||
| 2012 | 5,486 (31%) | 69 (17%) | |
| 2013 | 6,193 (35%) | 162 (39%) | |
| 2014 | 6,268 (35%) | 185 (44%) | |
| Race/ethnicity | 0.003 | ||
| White non‐Hispanic | 9,702 (54%) | 242 (58%) | |
| Black non‐Hispanic | 4,000 (22%) | 68 (16%) | |
| Hispanic | 2,872(16%) | 67 (16%) | |
| Asian | 578 (3%) | 9 (2%) | |
| Other or unknown | 795 (4%) | 30 (7%) | |
| Language preference | 0.795 | ||
| English | 16,049 (89%) | 376 (90%) | |
| Spanish | 1,052 (6%) | 23 (6%) | |
| Other | 846 (5%) | 17 (4%) | |
| Insurance | 0.001 | ||
| Medicare | 5,462 (30%) | 109 (26%) | |
| Medicaid | 3,406 (19%) | 126 (30%) | |
| Dual | 2,815 (16%) | 64 (15%) | |
| Private | 2,714 (15%) | 60 (14%) | |
| Indigent/self‐pay | 2,829 (16%) | 42 (10%) | |
| Other | 721 (4%) | 15 (4%) | |
| Length of stay, d (SD) | 4.0 (3.5) | 39.5 (37.3) | 0.001 |
| Discharge disposition | 0.001 | ||
| Home with self‐care | 13,276 (74%) | 115 (28%) | |
| Home with home health | 1,584 (9%) | 79 (19%) | |
| Hospicehome or inpatient | 369 (2%) | 19 (5%) | |
| Postacute‐care facility or LTAC | 1,761 (10%) | 141 (34%) | |
| Expired | 113 (1%) | 18 (4%) | |
| Other | 844 (5%) | 44 (11%) | |
| No. of admission medications (SD) | 9.7 (7.4) | 10.9 (7.8) | 0.002 |
| Primary diagnosis by ICD‐9 code* | |||
| Sepsis, unspecified | 1,548 (9%) | 55 (13%) | 0.001 |
| Acute respiratory failure | 293 (2%) | 9 (2%) | 0.400 |
| MSSA septicemia | 36 (0.2%) | 8 (2%) | 0.001 |
| MRSA septicemia | 13 (0.1%) | 7 (2%) | 0.001 |
| Alcoholic cirrhosis of the liver | 111 (1%) | 7 (2%) | 0.007 |
| Palliative care consult | 398 (2%) | 64 (15%) | 0.001 |
| ICU stay | 2,030 (11%) | 246 (59%) | 0.001 |
| Surgical procedure | 1,800 (10%) | 182 (44%) | 0.001 |
Unspecified sepsis was the most frequent primary diagnosis, regardless of LOS category (Table 2). However, the second through fifth most frequent diagnoses differed for patients with and without prolonged LOS.
| N | % | |
|---|---|---|
| ||
| LOS 21 days | ||
| 1. Sepsis, unspecified | 1,548 | 8.6% |
| 2. Acute pancreatitis | 435 | 2.4% |
| 3. Pneumonia | 431 | 2.4% |
| 4. Acute kidney failure | 363 | 2.0% |
| 5. COPD exacerbation | 320 | 1.8% |
| LOS >21 days | ||
| 1. Sepsis, unspecified | 55 | 13.0% |
| 2. Acute respiratory failure | 9 | 2.2% |
| 3. Methicillin‐sensitive Staphylococcus aureus septicemia | 8 | 1.9% |
| 4. Methicillin‐resistant Staphylococcus aureus septicemia | 7 | 1.7% |
| 5. Alcoholic cirrhosis of the liver | 7 | 1.7% |
In an adjusted logistic regression model (Table 3), we found lower odds of prolonged LOS for each 10‐year increase in age and higher odds of prolonged LOS for Medicaid insurance, discharge to home with home health, discharge to a postacute‐care or long‐term acute‐care facility, and in‐hospital death. Methicillin‐resistant Staphylococcus aureus (MRSA) septicemia, palliative care consults, ICU stays, and surgeries were all also associated with increased odds of prolonged LOS. We identified a statistically significant interaction between ICU stay and surgical procedure (odds ratio: 2.53, 95% confidence interval: 1.51‐4.26, P0.001).
| Outcome: LOS >21 Days | Odds Ratio | 95% CI | P Value |
|---|---|---|---|
| |||
| Age, per 10 years increase in age | 0.80 | 0.73‐0.87 | 0.001 |
| Year of discharge | |||
| 2012 | 0.47 | 0.34‐0.67 | 0.001 |
| 2013 | 1.10 | 0.84‐1.43 | 0.493 |
| 2014 | Ref | ||
| Race/ethnicity | |||
| White non‐Hispanic | Ref | ||
| Black non‐Hispanic | 0.89 | 0.64‐1.22 | 0.454 |
| Hispanic | 1.01 | 0.70‐1.46 | 0.952 |
| Asian | 0.85 | 0.40‐1.83 | 0.679 |
| Other or unknown | 1.29 | 0.73‐2.26 | 0.378 |
| Insurance | |||
| Medicare | Ref | ||
| Medicaid | 1.99 | 1.29‐3.05 | 0.002 |
| Dual | 1.06 | 0.72‐1.57 | 0.765 |
| Private | 1.13 | 0.70‐1.82 | 0.620 |
| Indigent/self‐pay | 1.66 | 0.95‐2.88 | 0.073 |
| Other | 0.96 | 0.47‐1.96 | 0.908 |
| Discharge disposition | |||
| Home with self‐care | Ref | ||
| Home with home health | 4.48 | 3.10‐6.48 | 0.001 |
| Hospicehome or inpatient | 2.11 | 0.98‐4.55 | 0.057 |
| Postacute‐care facility or LTAC | 10.37 | 6.92‐15.56 | 0.001 |
| Expired | 5.38 | 2.27‐12.75 | 0.001 |
| Other | 4.04 | 2.64‐6.18 | 0.001 |
| No. of admission medications | 1.00 | 0.99‐1.02 | 0.775 |
| Primary diagnosis by ICD‐9 code | |||
| Sepsis, unspecified | 1.11 | 0.78‐1.58 | 0.575 |
| MSSA septicemia | 2.44 | 0.68‐8.67 | 0.074 |
| MRSA septicemia | 8.83 | 1.72‐45.36 | 0.009 |
| Alcoholic cirrhosis of the liver | 1.25 | 0.43‐3.65 | 0.687 |
| Palliative care consult | 4.63 | 2.86‐7.49 | 0.001 |
| ICU stay | 6.66 | 5.22‐8.50 | 0.001 |
| Surgical procedure | 5.04 | 3.90‐6.52 | 0.001 |
Sensitivity analyses using LOS >14 and >30 days yielded similar results to LOS >21 days (see Supporting Appendix Table 1 in the online version of this article).
DISCUSSION
We found that a small proportion of medicine patients with prolonged hospitalizations contributed substantially to both total inpatient days and average inpatient LOS. Such disproportionate healthcare utilization is concerning in light of the Institute of Medicine's charge for health systems to deliver timely, efficient, and equitable care.[11]
Few studies in the United States have analyzed patient characteristics that predict prolonged LOS, and to our knowledge, none have evaluated prolonged LOS specifically in general medicine patients.[12, 13, 14] Among selected surgical populations, prolonged hospitalizations are most often related to placement difficulties, operational delays, and payer‐related issues, rather than severity of illness, baseline comorbidities, or in‐hospital complications.[12, 13] In our study, we found that patients with prolonged LOS were more likely to require a palliative care consult, ICU stay, or surgery, all proxies for disease severity. Patients with prolonged LOS were also more likely to undergo surgery >24 hours after admission than those without prolonged LOS, suggesting that the former were either too unstable to proceed directly to surgery or developed complications later during their hospitalization. Even after controlling for palliative care consults, ICU stays, and surgeries, placement at a postacute‐care facility was strongly associated with prolonged LOS. Patients with prolonged LOS were also more likely to have Medicaid compared to other insurance types.
Our findings have several potential implications for efforts aimed at decreasing the number of and length of prolonged hospitalizations. Although demographic and clinical factors such as Medicaid insurance, ICU stays, and surgeries are generally not modifiable, they could, particularly in combination, be used to trigger earlier and more intensive case management involvement. A streamlined insurance approval process for Medicaid pending inpatients could be beneficial, given the recent expansion of Medicaid eligibility under the ACA. Hospital partnerships with postacute‐care facilities could also relieve bottlenecks in placement.[8] Chart review of the patients with MRSA septicemia and prolonged LOS indicated that development of an intensive outpatient parenteral antimicrobial therapy pathway with substance abuse counseling could provide an alternative to extended inpatient treatment for intravenous drug users with complicated infections.[15]
This study has several limitations. First, given the lack of consensus in the literature regarding the definition of a prolonged hospitalization, it is difficult to directly compare our results with existing studies.[8, 12, 13, 14] However, we believe LOS >21 days to be a meaningful cutoff for our cohort. Most demographic and clinical variables that were predictive at >21 days were also predictive at >14 and >30 days, which reassured us that the relationship between variables and prolonged LOS was stable at different thresholds. Second, our database did not allow us to fully adjust for baseline comorbidities or categorize the reasons for discharge delays. Finally, this was a single‐center program evaluation. Although this limits generalization to other institutions, we believe our approach may serve as a guide for others interested in reducing prolonged hospitalizations.
In summary, prolonged hospitalizations represent a potentially high‐yield target for LOS reduction efforts. Prolonged hospitalizations among medicine patients at our institution particularly affected Medicaid enrollees with complex hospital stays who were not discharged home. Further studies are needed to determine the specific reasons for unnecessary hospital days in this population.
Acknowledgements
The authors thank Essey Yirdaw for her contributions to the building and management of the database that informed this work.
Disclosure: M.E.A. conceived of the study concept and design and drafted the manuscript. J.J.G. assisted with the study design and made critical revisions to the final manuscript. D.A., R.P., and R.C. assisted with the study design and made critical revisions to the manuscript. C.D.J. assisted with the study design, performed data analyses, and made critical revisions to the manuscript. RC has disclosed that her time is funded by a National Institutes of Health grant unrelated to this study. A modified abstract was presented in poster format at the Society of Hospital Medicine Research, Innovations, and Vignettes Competition 2015 Annual Meeting, held March 29 April 1, 2015, in National Harbor, Maryland. The authors have no conflicts of interest to disclose.
Hospitalizations frequently last longer than warranted by medical necessity alone, due to inefficiencies within the US healthcare system.[1, 2] Discharge delays place patients at risk for hospital‐acquired complications and increase costs. With the growing emphasis on high‐value care, hospital length of stay (LOS) has emerged as a key metric for inpatient care and will remain a central focus of hospital‐based improvement initiatives for the foreseeable future.
Hospitals may find it difficult to identify the primary drivers of inpatient LOS in a dynamic and increasingly complex healthcare system. Multiple recent policy changes have affected inpatient care. The Health Information Technology for Economic and Clinical Health Act of 2009 has led to widespread adoption of electronic health records (EHRs) that have markedly impacted provider workflows.[3] In October 2013, the Centers for Medicare & Medicaid Services implemented the 2‐midnight rule, which reclassified lower acuity inpatients with an expected stay 48 hours to observation status.[4] In January 2014, expansion of insurance coverage under the Affordable Care Act (ACA) altered payer mix for hospitals nationwide.[5] At a local level, hospitals that are rapidly adjusting resource allocation, capital investments, and marketing efforts and making complex operational decisions (eg, to open new units or change admission or referral algorithms) may simultaneously experience shifts in patient volumes, case‐mix index, and staffing ratios with downstream effects on LOS.
Given the myriad factors influencing inpatient LOS, hospital leaders may encounter real challenges in designing effective LOS reduction strategies. For example, they may expend significant resources on real‐time demand‐capacity management systems to improve hospital‐wide patient flow, but the resultant emphasis on bed placement and early discharges may shave only hours off average LOS.[6, 7] An alternative approach may be to target the small percentage of patients with prolonged hospitalizations who contribute disproportionately to the average LOS, as other initiatives focused on high utilizers have done.[8, 9, 10]
Our institution noted an increase in the average inpatient LOS for general medicine patients from 2012 to 2014, prompting a call to action by hospital leaders. We sought to characterize the predictors of prolonged hospitalizations among medicine patients to guide future efforts aimed at mitigating the contribution of prolonged LOS to overall LOS.
METHODS
Study Design
We performed a retrospective analysis of medicine patients discharged between January 1, 2012 and December 31, 2014, from the University of Colorado Hospital, a 551‐bed urban, quaternary‐care academic medical center in Aurora, Colorado. Patients were included if they were admitted under inpatient status, 18 years of age, and discharged from 1 of our 10 medicine services: 7 services with residents, staffed by hospitalists, general internists, or subspecialists; and 3 services with advanced practice providers, staffed by hospitalists.
Data Collection
We obtained LOS, calendar year of discharge, demographic data, insurance type, discharge disposition, number of medications, consults, intensive care unit (ICU) stays, surgeries (ie, procedures requiring anesthesia), and primary diagnosis by International Classification of Diseases, Ninth Revision codes from an administrative database that had been developed, validated, and maintained by our hospital medicine group. This database was populated with variables from our EHR, which was implemented in September 2011; to minimize variability in data input during the EHR rollout, we excluded data from September 2011 through December 2011. The Colorado Multiple Institutional Review Board reviewed and exempted this database (protocol 13‐2953) as a program evaluation.
Outcomes
We defined a prolonged hospitalization or LOS as >21 days in duration. This represented approximately 2 standard deviations above the mean LOS in our cohort. This cutoff also helped to remove provider‐level variability, as each medicine service was staffed by 2 attendings per month, each working approximately 7 days on and 7 days off. We examined LOS >14 and >30 days in sensitivity analyses to ensure that the selection of >21 days did not impose an arbitrary and invalid limitation on our statistical analysis.
Statistical Analysis
Demographic and clinical data were compared in the group with LOS 21 days versus the group with LOS >21 days with a 2 test for dichotomous variables and Student t test for continuous variables. We then built a multivariable logistic regression model to predict LOS >21 days using the variables that were significantly different between groups in bivariate analyses. A two‐sided P value of 0.05 was considered statistically significant. All data analyses were performed using Stata 12.0 (StataCorp, College Station, TX).
RESULTS
We identified 18,363 inpatient discharges among 12,511 medicine patients between January 1, 2012 and December 31, 2014. Of these discharges, 416 (2.3%) demonstrated prolonged LOS. Prolonged hospitalizations accounted for 18.6% of total inpatient days. The average LOS during the study period was 4.8 days including patients with prolonged LOS and 4.0 days excluding patients with prolonged LOS, a contribution of 0.8 days.
Table 1 compares the characteristics of patients with and without prolonged LOS. Age, insurance, discharge disposition, palliative care consults, ICU stays, and surgeries were among the variables that differed significantly between the 2 groups. Among patients undergoing surgery, those with prolonged LOS were more likely to have surgery >24 hours after admission than those without prolonged LOS (85.7% vs 51.4%, P0.001).
| Variable | LOS 21 Days, N=17,947 | LOS >21 Days, N=416 | P Value |
|---|---|---|---|
| |||
| Age, y, mean (SD) | 56.4 (18.7) | 54.4 (17.1) | 0.030 |
| Female | 9,256 (52%) | 199 (48%) | 0.132 |
| Year of discharge | 0.001 | ||
| 2012 | 5,486 (31%) | 69 (17%) | |
| 2013 | 6,193 (35%) | 162 (39%) | |
| 2014 | 6,268 (35%) | 185 (44%) | |
| Race/ethnicity | 0.003 | ||
| White non‐Hispanic | 9,702 (54%) | 242 (58%) | |
| Black non‐Hispanic | 4,000 (22%) | 68 (16%) | |
| Hispanic | 2,872(16%) | 67 (16%) | |
| Asian | 578 (3%) | 9 (2%) | |
| Other or unknown | 795 (4%) | 30 (7%) | |
| Language preference | 0.795 | ||
| English | 16,049 (89%) | 376 (90%) | |
| Spanish | 1,052 (6%) | 23 (6%) | |
| Other | 846 (5%) | 17 (4%) | |
| Insurance | 0.001 | ||
| Medicare | 5,462 (30%) | 109 (26%) | |
| Medicaid | 3,406 (19%) | 126 (30%) | |
| Dual | 2,815 (16%) | 64 (15%) | |
| Private | 2,714 (15%) | 60 (14%) | |
| Indigent/self‐pay | 2,829 (16%) | 42 (10%) | |
| Other | 721 (4%) | 15 (4%) | |
| Length of stay, d (SD) | 4.0 (3.5) | 39.5 (37.3) | 0.001 |
| Discharge disposition | 0.001 | ||
| Home with self‐care | 13,276 (74%) | 115 (28%) | |
| Home with home health | 1,584 (9%) | 79 (19%) | |
| Hospicehome or inpatient | 369 (2%) | 19 (5%) | |
| Postacute‐care facility or LTAC | 1,761 (10%) | 141 (34%) | |
| Expired | 113 (1%) | 18 (4%) | |
| Other | 844 (5%) | 44 (11%) | |
| No. of admission medications (SD) | 9.7 (7.4) | 10.9 (7.8) | 0.002 |
| Primary diagnosis by ICD‐9 code* | |||
| Sepsis, unspecified | 1,548 (9%) | 55 (13%) | 0.001 |
| Acute respiratory failure | 293 (2%) | 9 (2%) | 0.400 |
| MSSA septicemia | 36 (0.2%) | 8 (2%) | 0.001 |
| MRSA septicemia | 13 (0.1%) | 7 (2%) | 0.001 |
| Alcoholic cirrhosis of the liver | 111 (1%) | 7 (2%) | 0.007 |
| Palliative care consult | 398 (2%) | 64 (15%) | 0.001 |
| ICU stay | 2,030 (11%) | 246 (59%) | 0.001 |
| Surgical procedure | 1,800 (10%) | 182 (44%) | 0.001 |
Unspecified sepsis was the most frequent primary diagnosis, regardless of LOS category (Table 2). However, the second through fifth most frequent diagnoses differed for patients with and without prolonged LOS.
| N | % | |
|---|---|---|
| ||
| LOS 21 days | ||
| 1. Sepsis, unspecified | 1,548 | 8.6% |
| 2. Acute pancreatitis | 435 | 2.4% |
| 3. Pneumonia | 431 | 2.4% |
| 4. Acute kidney failure | 363 | 2.0% |
| 5. COPD exacerbation | 320 | 1.8% |
| LOS >21 days | ||
| 1. Sepsis, unspecified | 55 | 13.0% |
| 2. Acute respiratory failure | 9 | 2.2% |
| 3. Methicillin‐sensitive Staphylococcus aureus septicemia | 8 | 1.9% |
| 4. Methicillin‐resistant Staphylococcus aureus septicemia | 7 | 1.7% |
| 5. Alcoholic cirrhosis of the liver | 7 | 1.7% |
In an adjusted logistic regression model (Table 3), we found lower odds of prolonged LOS for each 10‐year increase in age and higher odds of prolonged LOS for Medicaid insurance, discharge to home with home health, discharge to a postacute‐care or long‐term acute‐care facility, and in‐hospital death. Methicillin‐resistant Staphylococcus aureus (MRSA) septicemia, palliative care consults, ICU stays, and surgeries were all also associated with increased odds of prolonged LOS. We identified a statistically significant interaction between ICU stay and surgical procedure (odds ratio: 2.53, 95% confidence interval: 1.51‐4.26, P0.001).
| Outcome: LOS >21 Days | Odds Ratio | 95% CI | P Value |
|---|---|---|---|
| |||
| Age, per 10 years increase in age | 0.80 | 0.73‐0.87 | 0.001 |
| Year of discharge | |||
| 2012 | 0.47 | 0.34‐0.67 | 0.001 |
| 2013 | 1.10 | 0.84‐1.43 | 0.493 |
| 2014 | Ref | ||
| Race/ethnicity | |||
| White non‐Hispanic | Ref | ||
| Black non‐Hispanic | 0.89 | 0.64‐1.22 | 0.454 |
| Hispanic | 1.01 | 0.70‐1.46 | 0.952 |
| Asian | 0.85 | 0.40‐1.83 | 0.679 |
| Other or unknown | 1.29 | 0.73‐2.26 | 0.378 |
| Insurance | |||
| Medicare | Ref | ||
| Medicaid | 1.99 | 1.29‐3.05 | 0.002 |
| Dual | 1.06 | 0.72‐1.57 | 0.765 |
| Private | 1.13 | 0.70‐1.82 | 0.620 |
| Indigent/self‐pay | 1.66 | 0.95‐2.88 | 0.073 |
| Other | 0.96 | 0.47‐1.96 | 0.908 |
| Discharge disposition | |||
| Home with self‐care | Ref | ||
| Home with home health | 4.48 | 3.10‐6.48 | 0.001 |
| Hospicehome or inpatient | 2.11 | 0.98‐4.55 | 0.057 |
| Postacute‐care facility or LTAC | 10.37 | 6.92‐15.56 | 0.001 |
| Expired | 5.38 | 2.27‐12.75 | 0.001 |
| Other | 4.04 | 2.64‐6.18 | 0.001 |
| No. of admission medications | 1.00 | 0.99‐1.02 | 0.775 |
| Primary diagnosis by ICD‐9 code | |||
| Sepsis, unspecified | 1.11 | 0.78‐1.58 | 0.575 |
| MSSA septicemia | 2.44 | 0.68‐8.67 | 0.074 |
| MRSA septicemia | 8.83 | 1.72‐45.36 | 0.009 |
| Alcoholic cirrhosis of the liver | 1.25 | 0.43‐3.65 | 0.687 |
| Palliative care consult | 4.63 | 2.86‐7.49 | 0.001 |
| ICU stay | 6.66 | 5.22‐8.50 | 0.001 |
| Surgical procedure | 5.04 | 3.90‐6.52 | 0.001 |
Sensitivity analyses using LOS >14 and >30 days yielded similar results to LOS >21 days (see Supporting Appendix Table 1 in the online version of this article).
DISCUSSION
We found that a small proportion of medicine patients with prolonged hospitalizations contributed substantially to both total inpatient days and average inpatient LOS. Such disproportionate healthcare utilization is concerning in light of the Institute of Medicine's charge for health systems to deliver timely, efficient, and equitable care.[11]
Few studies in the United States have analyzed patient characteristics that predict prolonged LOS, and to our knowledge, none have evaluated prolonged LOS specifically in general medicine patients.[12, 13, 14] Among selected surgical populations, prolonged hospitalizations are most often related to placement difficulties, operational delays, and payer‐related issues, rather than severity of illness, baseline comorbidities, or in‐hospital complications.[12, 13] In our study, we found that patients with prolonged LOS were more likely to require a palliative care consult, ICU stay, or surgery, all proxies for disease severity. Patients with prolonged LOS were also more likely to undergo surgery >24 hours after admission than those without prolonged LOS, suggesting that the former were either too unstable to proceed directly to surgery or developed complications later during their hospitalization. Even after controlling for palliative care consults, ICU stays, and surgeries, placement at a postacute‐care facility was strongly associated with prolonged LOS. Patients with prolonged LOS were also more likely to have Medicaid compared to other insurance types.
Our findings have several potential implications for efforts aimed at decreasing the number of and length of prolonged hospitalizations. Although demographic and clinical factors such as Medicaid insurance, ICU stays, and surgeries are generally not modifiable, they could, particularly in combination, be used to trigger earlier and more intensive case management involvement. A streamlined insurance approval process for Medicaid pending inpatients could be beneficial, given the recent expansion of Medicaid eligibility under the ACA. Hospital partnerships with postacute‐care facilities could also relieve bottlenecks in placement.[8] Chart review of the patients with MRSA septicemia and prolonged LOS indicated that development of an intensive outpatient parenteral antimicrobial therapy pathway with substance abuse counseling could provide an alternative to extended inpatient treatment for intravenous drug users with complicated infections.[15]
This study has several limitations. First, given the lack of consensus in the literature regarding the definition of a prolonged hospitalization, it is difficult to directly compare our results with existing studies.[8, 12, 13, 14] However, we believe LOS >21 days to be a meaningful cutoff for our cohort. Most demographic and clinical variables that were predictive at >21 days were also predictive at >14 and >30 days, which reassured us that the relationship between variables and prolonged LOS was stable at different thresholds. Second, our database did not allow us to fully adjust for baseline comorbidities or categorize the reasons for discharge delays. Finally, this was a single‐center program evaluation. Although this limits generalization to other institutions, we believe our approach may serve as a guide for others interested in reducing prolonged hospitalizations.
In summary, prolonged hospitalizations represent a potentially high‐yield target for LOS reduction efforts. Prolonged hospitalizations among medicine patients at our institution particularly affected Medicaid enrollees with complex hospital stays who were not discharged home. Further studies are needed to determine the specific reasons for unnecessary hospital days in this population.
Acknowledgements
The authors thank Essey Yirdaw for her contributions to the building and management of the database that informed this work.
Disclosure: M.E.A. conceived of the study concept and design and drafted the manuscript. J.J.G. assisted with the study design and made critical revisions to the final manuscript. D.A., R.P., and R.C. assisted with the study design and made critical revisions to the manuscript. C.D.J. assisted with the study design, performed data analyses, and made critical revisions to the manuscript. RC has disclosed that her time is funded by a National Institutes of Health grant unrelated to this study. A modified abstract was presented in poster format at the Society of Hospital Medicine Research, Innovations, and Vignettes Competition 2015 Annual Meeting, held March 29 April 1, 2015, in National Harbor, Maryland. The authors have no conflicts of interest to disclose.
- , , , et al. Excess hospitalization days in an academic medical center: perceptions of hospitalists and discharge planners. Am J Manag Care. 2011;17(2):e34–e42.
- , , A prospective study of reasons for prolonged hospitalizations on a general medicine teaching service. J Gen Intern Med. 2005;20(2):108–115.
- , , , et al. Adoption of electronic health records grows rapidly, but fewer than half of U.S. hospitals had at least a basic system in 2012. Health Aff (Millwood). 2013;32(8):1478–1485.
- , , , et al. Observation and inpatient status: clinical impact of the 2‐midnight rule. J Hosp Med. 2014;9(4):203–209.
- , , Impact of insurance expansion on hospital uncompensated care costs in 2014. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. Available at: http://aspe.hhs.gov/health/reports/2014/uncompensatedcare/ib_uncompensatedcare.pdf. Accessed March 28, 2015.
- , , , Using real‐time demand capacity management to improve hospital‐wide patient flow. Jt Comm J Qual Patient Saf. 2011;37(5):217–227.
- , , , , , Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226–233.
- , , , Addressing hospital length of stay outlier patients: a community‐wide approach. Adv Biosci Biotechol. 2014;5:188–196.
- , American medical home runs. Health Aff (Millwood). 2009;28(5):1317–1326.
- The hot spotters: can we lower medical costs by giving the neediest patients better care? New Yorker. January 2011:40–51.
- Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
- , , , et al. Excessively long hospital stays after trauma are not related to the severity of illness: let's aim to the right target! JAMA Surg. 2013;148(1):956–961.
- , , Extended length of stay after surgery: complications, inefficient practice, or sick patients? JAMA Surg. 2014;149(8):815–820.
- , , , , Nonmedical factors associated with prolonged hospital length of stay in an urban homebound population. J Hosp Med. 2012;7(2):73–78.
- , , , Safe and successful treatment of intravenous drug users with a peripherally inserted central catheter in an outpatient parenteral antibiotic treatment service. J Antimicrob Chemother. 2010;65(12):2641–2644.
- , , , et al. Excess hospitalization days in an academic medical center: perceptions of hospitalists and discharge planners. Am J Manag Care. 2011;17(2):e34–e42.
- , , A prospective study of reasons for prolonged hospitalizations on a general medicine teaching service. J Gen Intern Med. 2005;20(2):108–115.
- , , , et al. Adoption of electronic health records grows rapidly, but fewer than half of U.S. hospitals had at least a basic system in 2012. Health Aff (Millwood). 2013;32(8):1478–1485.
- , , , et al. Observation and inpatient status: clinical impact of the 2‐midnight rule. J Hosp Med. 2014;9(4):203–209.
- , , Impact of insurance expansion on hospital uncompensated care costs in 2014. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. Available at: http://aspe.hhs.gov/health/reports/2014/uncompensatedcare/ib_uncompensatedcare.pdf. Accessed March 28, 2015.
- , , , Using real‐time demand capacity management to improve hospital‐wide patient flow. Jt Comm J Qual Patient Saf. 2011;37(5):217–227.
- , , , , , Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226–233.
- , , , Addressing hospital length of stay outlier patients: a community‐wide approach. Adv Biosci Biotechol. 2014;5:188–196.
- , American medical home runs. Health Aff (Millwood). 2009;28(5):1317–1326.
- The hot spotters: can we lower medical costs by giving the neediest patients better care? New Yorker. January 2011:40–51.
- Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
- , , , et al. Excessively long hospital stays after trauma are not related to the severity of illness: let's aim to the right target! JAMA Surg. 2013;148(1):956–961.
- , , Extended length of stay after surgery: complications, inefficient practice, or sick patients? JAMA Surg. 2014;149(8):815–820.
- , , , , Nonmedical factors associated with prolonged hospital length of stay in an urban homebound population. J Hosp Med. 2012;7(2):73–78.
- , , , Safe and successful treatment of intravenous drug users with a peripherally inserted central catheter in an outpatient parenteral antibiotic treatment service. J Antimicrob Chemother. 2010;65(12):2641–2644.
Hospital Medicine Management Dictums
In the spring of 1998 at the Society of Hospital Medicine's (SHM) (then known as the National Association of Inpatient Physicians) first annual meeting, Dr. John Eisenberg asked, If the hospitalist model of practice were a drug, do we have enough evidence about its risks and benefits to support its use? His question is only one of many often‐repeated dictums and phrases regarding how the hospitalist model of practice is organized and performs. These can serve as useful lenses to assess the past and future of the field.
Data and opinions used to answer Dr. Eisenberg's question continue to evolve. Many studies and opinions of its effects on costs and quality have appeared in the peer‐reviewed literature, including the Journal of Hospital Medicine, which has become a principal home for studies of the hospitalist model of care. In 1998, hospital medicine's impact on outcomes and costs was only beginning, and descriptions of the hospitalist's role in implementation of new programs, such as team‐based rounding models, geographic assignment of hospitalists, or the costs of interruptions, were not even on our radar. Effective management of these and other operational concerns will help ensure we are able to answer Dr. Eisenberg's question with an increasingly confident yes.
Early in the history of hospital medicine, it became common to speak of the voltage drop of information loss as a patient's care transitions to and from hospitalists and other caregivers. This term remains in common use today and encourages a focus on handoff communication. As of April 2015, the Journal of Hospital Medicine has published 15 articles that mention handoffs in the title, and many more that address the topic more peripherally.[1] Collectively, these provide thoughtful strategies to mitigate a voltage drop and its risks,[2] even though it persists and more work is needed to overcome it.
Referring to work as a hospitalist, many have said that this is a young doctor's game; one cannot do it for a whole career. The field is young enough that one cannot convincingly prove or disprove this idea, and evidence can be found on either side. Hospitalist burnout is distressingly common, though potentially similar to many other physician specialties.[3, 4, 5] Through both peer‐reviewed literature and more informal channels, primarily SHM activities, there is a substantial and growing set of data and opinions regarding factors related to burnout and potential mitigation strategies.
Donald Redelmeier observed that a hospitalist's time is to a large degree governed by a pager, in contrast to an office‐based physician whose time is governed by a clock.[6] Frequent interruptions delivered by a pager, many of which are of low importance and not urgent, are a significant issue for hospitalists, and to some extent all healthcare providers, and one begging for solutions.[7] Technology that replaces pagers will be helpful and will need to be paired with new methods around what is communicated, how urgently, and by what method.
Perhaps the most common dictum used by those who think about sharing best practices across our field is: If you have seen one hospitalist practice, you have seen one hospitalist practice. This has been invoked countless times as shorthand for the myriad ways hospitalist practices are organized, differing significantly in scheduling, workloads, compensation, leadership, cost structure, and other operational details. Here, the SHM serves as a valuable forum for exchange of ideas and information about the relative merits of different operational structures, and in 2014 published expert opinion regarding valuable characteristics of hospital medicine groups associated with success.[8]
In the 1990s, the principal mission of a hospitalist group was to replace primary care physicians who were leaving hospital practice and to increase efficiency of care. Many activities have since been added to this still‐important original mission, including improving performance on patient safety, quality, and satisfaction, and ensuring good hospital performance during the transition to dramatically different forms of reimbursement for services. Moreover, hospitals are increasingly organized into networks, most of which are now seeking to reduce variation in hospitalist organizational models and performance across all of their hospitals.[9]
This final dictum is a foundational one for our field, and will help us solve the challenges posed by the others: A hospitalist's job is to provide care for the sick person occupying a room in the hospital, and to care for and improve the performance of the hospital itself. Laurence Wellikson, Chief Executive Officer of the SHM, may have said this first. By embracing both of these goals, hospitalists have the opportunity to achieve much on behalf of individual patients and the healthcare system as a whole.
New dictums and sayings are sure to arise, and there is ample room for optimism that they will increasingly highlight the successes and vital role of hospital medicine.
Disclosure
Nothing to report.
- Journal of Hospital Medicine website. Available at: http://onlinelibrary.wiley.com/journal/10.1002/%28ISSN%291553‐5606. Accessed April 8, 2015.
- , Handoffs: a story in evolution. J Hosp Med. 2015;10(3):202–203.
- , , , A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
- , , , , Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- A Canadian perspective on the American hospitalist movement. Arch Intern Med. 1999;159(15):1665–1668.
- , , , , Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353–359.
- , , , et al. The key principles and characteristics of an effective hospital medicine group: an assessment guide for hospitals and hospitalists. J Hosp Med. 2014;9(2):123–128.
- Multi‐site hospital medicine group leaders face similar challenges. The Hospitalist. November 1, 2013. Available at: http://www.the‐hospitalist.org/article/multi‐site‐hospital‐medicine‐group‐leaders‐face‐similar‐challenges. Accessed April 8, 2015.
In the spring of 1998 at the Society of Hospital Medicine's (SHM) (then known as the National Association of Inpatient Physicians) first annual meeting, Dr. John Eisenberg asked, If the hospitalist model of practice were a drug, do we have enough evidence about its risks and benefits to support its use? His question is only one of many often‐repeated dictums and phrases regarding how the hospitalist model of practice is organized and performs. These can serve as useful lenses to assess the past and future of the field.
Data and opinions used to answer Dr. Eisenberg's question continue to evolve. Many studies and opinions of its effects on costs and quality have appeared in the peer‐reviewed literature, including the Journal of Hospital Medicine, which has become a principal home for studies of the hospitalist model of care. In 1998, hospital medicine's impact on outcomes and costs was only beginning, and descriptions of the hospitalist's role in implementation of new programs, such as team‐based rounding models, geographic assignment of hospitalists, or the costs of interruptions, were not even on our radar. Effective management of these and other operational concerns will help ensure we are able to answer Dr. Eisenberg's question with an increasingly confident yes.
Early in the history of hospital medicine, it became common to speak of the voltage drop of information loss as a patient's care transitions to and from hospitalists and other caregivers. This term remains in common use today and encourages a focus on handoff communication. As of April 2015, the Journal of Hospital Medicine has published 15 articles that mention handoffs in the title, and many more that address the topic more peripherally.[1] Collectively, these provide thoughtful strategies to mitigate a voltage drop and its risks,[2] even though it persists and more work is needed to overcome it.
Referring to work as a hospitalist, many have said that this is a young doctor's game; one cannot do it for a whole career. The field is young enough that one cannot convincingly prove or disprove this idea, and evidence can be found on either side. Hospitalist burnout is distressingly common, though potentially similar to many other physician specialties.[3, 4, 5] Through both peer‐reviewed literature and more informal channels, primarily SHM activities, there is a substantial and growing set of data and opinions regarding factors related to burnout and potential mitigation strategies.
Donald Redelmeier observed that a hospitalist's time is to a large degree governed by a pager, in contrast to an office‐based physician whose time is governed by a clock.[6] Frequent interruptions delivered by a pager, many of which are of low importance and not urgent, are a significant issue for hospitalists, and to some extent all healthcare providers, and one begging for solutions.[7] Technology that replaces pagers will be helpful and will need to be paired with new methods around what is communicated, how urgently, and by what method.
Perhaps the most common dictum used by those who think about sharing best practices across our field is: If you have seen one hospitalist practice, you have seen one hospitalist practice. This has been invoked countless times as shorthand for the myriad ways hospitalist practices are organized, differing significantly in scheduling, workloads, compensation, leadership, cost structure, and other operational details. Here, the SHM serves as a valuable forum for exchange of ideas and information about the relative merits of different operational structures, and in 2014 published expert opinion regarding valuable characteristics of hospital medicine groups associated with success.[8]
In the 1990s, the principal mission of a hospitalist group was to replace primary care physicians who were leaving hospital practice and to increase efficiency of care. Many activities have since been added to this still‐important original mission, including improving performance on patient safety, quality, and satisfaction, and ensuring good hospital performance during the transition to dramatically different forms of reimbursement for services. Moreover, hospitals are increasingly organized into networks, most of which are now seeking to reduce variation in hospitalist organizational models and performance across all of their hospitals.[9]
This final dictum is a foundational one for our field, and will help us solve the challenges posed by the others: A hospitalist's job is to provide care for the sick person occupying a room in the hospital, and to care for and improve the performance of the hospital itself. Laurence Wellikson, Chief Executive Officer of the SHM, may have said this first. By embracing both of these goals, hospitalists have the opportunity to achieve much on behalf of individual patients and the healthcare system as a whole.
New dictums and sayings are sure to arise, and there is ample room for optimism that they will increasingly highlight the successes and vital role of hospital medicine.
Disclosure
Nothing to report.
In the spring of 1998 at the Society of Hospital Medicine's (SHM) (then known as the National Association of Inpatient Physicians) first annual meeting, Dr. John Eisenberg asked, If the hospitalist model of practice were a drug, do we have enough evidence about its risks and benefits to support its use? His question is only one of many often‐repeated dictums and phrases regarding how the hospitalist model of practice is organized and performs. These can serve as useful lenses to assess the past and future of the field.
Data and opinions used to answer Dr. Eisenberg's question continue to evolve. Many studies and opinions of its effects on costs and quality have appeared in the peer‐reviewed literature, including the Journal of Hospital Medicine, which has become a principal home for studies of the hospitalist model of care. In 1998, hospital medicine's impact on outcomes and costs was only beginning, and descriptions of the hospitalist's role in implementation of new programs, such as team‐based rounding models, geographic assignment of hospitalists, or the costs of interruptions, were not even on our radar. Effective management of these and other operational concerns will help ensure we are able to answer Dr. Eisenberg's question with an increasingly confident yes.
Early in the history of hospital medicine, it became common to speak of the voltage drop of information loss as a patient's care transitions to and from hospitalists and other caregivers. This term remains in common use today and encourages a focus on handoff communication. As of April 2015, the Journal of Hospital Medicine has published 15 articles that mention handoffs in the title, and many more that address the topic more peripherally.[1] Collectively, these provide thoughtful strategies to mitigate a voltage drop and its risks,[2] even though it persists and more work is needed to overcome it.
Referring to work as a hospitalist, many have said that this is a young doctor's game; one cannot do it for a whole career. The field is young enough that one cannot convincingly prove or disprove this idea, and evidence can be found on either side. Hospitalist burnout is distressingly common, though potentially similar to many other physician specialties.[3, 4, 5] Through both peer‐reviewed literature and more informal channels, primarily SHM activities, there is a substantial and growing set of data and opinions regarding factors related to burnout and potential mitigation strategies.
Donald Redelmeier observed that a hospitalist's time is to a large degree governed by a pager, in contrast to an office‐based physician whose time is governed by a clock.[6] Frequent interruptions delivered by a pager, many of which are of low importance and not urgent, are a significant issue for hospitalists, and to some extent all healthcare providers, and one begging for solutions.[7] Technology that replaces pagers will be helpful and will need to be paired with new methods around what is communicated, how urgently, and by what method.
Perhaps the most common dictum used by those who think about sharing best practices across our field is: If you have seen one hospitalist practice, you have seen one hospitalist practice. This has been invoked countless times as shorthand for the myriad ways hospitalist practices are organized, differing significantly in scheduling, workloads, compensation, leadership, cost structure, and other operational details. Here, the SHM serves as a valuable forum for exchange of ideas and information about the relative merits of different operational structures, and in 2014 published expert opinion regarding valuable characteristics of hospital medicine groups associated with success.[8]
In the 1990s, the principal mission of a hospitalist group was to replace primary care physicians who were leaving hospital practice and to increase efficiency of care. Many activities have since been added to this still‐important original mission, including improving performance on patient safety, quality, and satisfaction, and ensuring good hospital performance during the transition to dramatically different forms of reimbursement for services. Moreover, hospitals are increasingly organized into networks, most of which are now seeking to reduce variation in hospitalist organizational models and performance across all of their hospitals.[9]
This final dictum is a foundational one for our field, and will help us solve the challenges posed by the others: A hospitalist's job is to provide care for the sick person occupying a room in the hospital, and to care for and improve the performance of the hospital itself. Laurence Wellikson, Chief Executive Officer of the SHM, may have said this first. By embracing both of these goals, hospitalists have the opportunity to achieve much on behalf of individual patients and the healthcare system as a whole.
New dictums and sayings are sure to arise, and there is ample room for optimism that they will increasingly highlight the successes and vital role of hospital medicine.
Disclosure
Nothing to report.
- Journal of Hospital Medicine website. Available at: http://onlinelibrary.wiley.com/journal/10.1002/%28ISSN%291553‐5606. Accessed April 8, 2015.
- , Handoffs: a story in evolution. J Hosp Med. 2015;10(3):202–203.
- , , , A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
- , , , , Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- A Canadian perspective on the American hospitalist movement. Arch Intern Med. 1999;159(15):1665–1668.
- , , , , Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353–359.
- , , , et al. The key principles and characteristics of an effective hospital medicine group: an assessment guide for hospitals and hospitalists. J Hosp Med. 2014;9(2):123–128.
- Multi‐site hospital medicine group leaders face similar challenges. The Hospitalist. November 1, 2013. Available at: http://www.the‐hospitalist.org/article/multi‐site‐hospital‐medicine‐group‐leaders‐face‐similar‐challenges. Accessed April 8, 2015.
- Journal of Hospital Medicine website. Available at: http://onlinelibrary.wiley.com/journal/10.1002/%28ISSN%291553‐5606. Accessed April 8, 2015.
- , Handoffs: a story in evolution. J Hosp Med. 2015;10(3):202–203.
- , , , A national comparison of burnout and work‐life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176–181.
- , , , , Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- A Canadian perspective on the American hospitalist movement. Arch Intern Med. 1999;159(15):1665–1668.
- , , , , Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353–359.
- , , , et al. The key principles and characteristics of an effective hospital medicine group: an assessment guide for hospitals and hospitalists. J Hosp Med. 2014;9(2):123–128.
- Multi‐site hospital medicine group leaders face similar challenges. The Hospitalist. November 1, 2013. Available at: http://www.the‐hospitalist.org/article/multi‐site‐hospital‐medicine‐group‐leaders‐face‐similar‐challenges. Accessed April 8, 2015.
Priorities and Gender Pay Gap
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
Hospitalists are a growing workforce numbering over 40,000 physicians, one‐third of whom are women.[1] Flexibility of work schedules and control over personal time have been the traditional selling points of the specialty.[2] Multiple studies of physician work life reveal growing physician dissatisfaction and a high prevalence of burnout.[3] To mitigate burnout risk, leaders in hospital medicine recognize the importance of creating a sustainable profession that offers both job and career satisfaction as well as work‐life balance and, importantly, fairness within the work environment.[4] Although success in some of these endeavors has been realized sporadically, sustaining work‐life balance and fairness in the specialty remains a work in progress, whereas evidence of high job attrition and pay inequities remain.[5, 6]
Pay inequity for women relative to men continues to be pervasive in medicine, including among early‐career physicians, researchers, and various specialists.[6, 7, 8, 9, 10, 11, 12, 13] The earnings gap seems to persist for physicians, even as federal efforts such as the Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aim to end wage discrimination.[11, 14] Differences in specialty, part‐time status, and practice type do not mitigate the disparity.[8, 10, 15] Additional explanations have been proposed to explain the variability, including gender differences in negotiating skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.[12, 16, 17, 18, 19, 20]
The earnings gap is also a consequence of what is commonly called the glass ceiling.[18, 19] Most agree that obstacles to fair advancement of women include absence of collaborative environments and role models who have successfully achieved work‐life balance.[17, 20, 21, 22] Somewhat surprisingly, women leaders in medicine seem to suffer greater income disparity than nonleaders; this income gap is prevalent among leaders in other elite professions as well.[7, 23] It is unknown whether women physicians' emphasis on work‐life balance, seen repeatedly in surveys, explains any of the pay disparity.[24] Little research to date has examined whether work‐life priorities of women in hospital medicine differ from men.
In this study, we sought to examine differences in job priorities between men and women hospitalists. In particular, we examine the relative prioritization of substantial pay to job satisfaction. We also examined gender differences in work patterns and earnings to explore potential sources of the persistent gender earnings gap.
METHODS
We analyzed data from the 20092010 Hospital Medicine Physician Worklife Survey, the design of which is detailed elsewhere.[4] Briefly, a 118‐item survey was administered by mail to a stratified sample of hospitalists from the Society of Hospital Medicine database and 3 large multisite hospitalist groups. A single survey item asked respondents to identify up to 4 out of 12 most important domains to their satisfaction with a hospitalist job. The domains were distilled from focus groups of nationally representative hospitalists as described previously,[4] and the survey item allowed up to one‐third of these domains to be identified as respondents' personal priorities. The list included: optimal variety of tasks, optimal workload, substantial pay, collegiality with other physicians, recognition by leaders, rewarding relationships with patients, satisfaction with nurses, optimal autonomy, control over personal time, fairness within organization, ample availability of resources to do job, and organizational climate of trust and belonging. We tabulated and ranked the frequency with which respondents selected each satisfaction domain by gender. Due to the nonstandard format of the survey item, we a priori decided to analyze only responses that were completed as instructed.
We also used demographic data including detailed work characteristics, clinical and nonclinical workload, total pretax earnings in 2009 as a hospitalist, and self‐identification as leader of their hospital medicine group. Respondent characteristics were tabulated and gender differences were tested using the t test, rank sum test, and the Fischer exact test as appropriate. We also listed the number of nonrespondents for each item. In estimating gender differences in earnings, we opted to use multiple‐imputation techniques to more conservatively account for greater variance inherent in the presence of missing data. Consistent with existing guidelines,[25] we demonstrated that item responses were not missing monotonically by visually inspecting patterns of nonresponse. We further demonstrated that data were missing at random by showing that response patterns of completed survey items did not predict whether or not a given variable response was missing using logistic regression models. We found no significant differences between respondents with complete and missing data. We verified that appropriate regression models for each variable on every other variable converged. We used Stata 13.1 (StataCorp, College Station, TX) to perform multiple imputations using chain equations (mi impute chain) to create 10 imputed tables for 7 normally distributed continuous variables using the ordinary least squares method, 3 non‐normally distributed variables using the predictive mean matching method, 2 nonordinal categorical variables using the multinomial logit method, and 1 binary variable using the logit method.[26, 27] Gender, pediatric specialty status, region of practice, and whether or not respondents prioritized substantial pay for job satisfaction were used as regular variables without missing data points.
Differences in earnings were assessed using a multivariate ordinary linear regression model applied to the imputed datasets fitted by forward selection of explanatory variables using P < 0.20 in bivariate analysis for inclusion and manual backward elimination of all statistically nonsignificant variables. We tested the significance of the women leader interaction term in the final parsimonious model. We used the usual significance threshold of P < 0.05 for inferences. Our analysis of publicly available anonymous data was exempt from IRB review.
RESULTS
Of the 816 survey respondents (response rate 25.6%), 40 either omitted the item soliciting work priorities or completed it incorrectly. Data from the remaining 776 respondents were used for the present analysis. Respondent characteristics are tabulated in Table 1. The characteristics of hospitalists by age, gender, specialty, practice model, and practice region were representative of US hospitalists from other surveys.[28]
| Women | Men | P Value | No. of Missing Responses | |
|---|---|---|---|---|
| ||||
| No. | 263 | 513 | 0 | |
| Role, n (%) | <0.01 | 0 | ||
| Frontline hospitalist | 201 (76) | 337 (66) | ||
| Hospitalist leader | 53 (24) | 176 (34) | ||
| Age, y, mean (SD) | 42 (8) | 45 (9) | <0.01 | 67 |
| Years in current job, mean (SD) | 5 (4) | 6 (5) | 0.07 | 14 |
| Specialty, n (%) | <0.01 | 0 | ||
| Internal medicine | 160 (61) | 369 (72) | ||
| Pediatrics | 56 (21) | 57 (11) | ||
| Other | 39 (15) | 47 (9) | ||
| Family medicine | 8 (3) | 40 (8) | ||
| Practice model, n (%) | 0.02 | 19 | ||
| Hospital employed | 110 (43) | 227 (46) | ||
| Multispecialty group | 44 (17) | 68 (14) | ||
| University/medical school | 47 (18) | 58 (12) | ||
| Multistate group | 27 (11) | 73 (15) | ||
| Local hospitalist group | 22 (8) | 65 (13) | ||
| Other | 7 (3) | 9 (2) | ||
| Practice region, n (%) | 0.14 | 0 | ||
| Southeast | 56 (21) | 151 (29) | ||
| Midwest | 58 (22) | 106 (21) | ||
| Northeast | 54 (21) | 96 (19) | ||
| Southwest | 44 (17) | 83 (16) | ||
| West | 51 (19) | 77 (15) | ||
| Full‐time equivalents, n (%) | <0.01 | 42 | ||
| <100% | 46 (18) | 60 (12) | ||
| 100% | 202 (81) | 402 (83) | ||
| >100% | 2 (1) | 22 (5) | ||
| Days per month doing clinical work if FTE 100%, median (IQR) | 15 (1418) | 16 (1420) | 0.12 | 11 |
| Hours per day doing clinical work, median (IQR) | 11 (912) | 11 (912) | 0.67 | 30 |
| Consecutive days doing clinical work, median (IQR) | 7 (57) | 7 (57) | 0.94 | 17 |
| Percentage of work at night, median (IQR) | 15 (530) | 15 (525) | 0.45 | 16 |
| Percentage of night work in hospital if working nights, median (IQR) | 100 (5100) | 100 (10100) | 0.12 | 8 |
| Hours per month doing nonclinical work, median (IQR) | 12 (540) | 15 (540) | 0.77 | 26 |
| Estimated daily billable encounters, mean (IQR) | 14 (1116) | 15 (1218) | 0.01 | 54 |
| Total earnings in fiscal year 2009, median US$1,000 (IQR) | 185 (150210) | 202 (180240) | <0.01 | 56 |
| Marriage/domestic partnership status, n (%) | 0.15 | 43 | ||
| Married/currently in DP | 197 (80) | 421 (86) | ||
| Never married/never in DP | 26 (11) | 42 (9) | ||
| Divorced or separated | 18 (7) | 20 (4) | ||
| Other | 4 (2) | 5 (1) | ||
| Dependent children under 7 years old living in home, n (%) | 0.22 | 42 | ||
| 0 | 136 (55) | 265 (54) | ||
| 1 | 47 (19) | 92 (19) | ||
| 2 | 52 (21) | 87 (18) | ||
| 3 | 12 (5) | 43 (9) | ||
Several gender differences were seen in the characteristics of hospitalists and their work (Table 1). Women compared to men hospitalists were less likely to be leaders, more likely to be pediatricians, work in university settings, and practice in Western states. Women compared to men, on average, were younger by 3 years, worked fewer full‐time equivalents (FTEs), worked a greater percentage of nights, and reported fewer billable encounters per shift. They were also more likely to be divorced or separated.
Job satisfaction priorities differed for women and men hospitalists. Table 2 lists job satisfaction domains in descending order of the frequency prioritized by men. The largest proportion of women and men prioritized optimal workload. However, although substantial pay was prioritized next most frequently by men, more women prioritized collegiality and control over personal time than substantial pay.
| Women, % | Rank | Men, % | Rank | |
|---|---|---|---|---|
| Optimal workload | 59 | 1 | 59 | 1 |
| Substantial pay | 41 | 4 | 50 | 2 |
| Control over personal time | 44 | 3 | 41 | 3 |
| Collegiality with physicians | 47 | 2 | 38 | 4 |
| Rewarding relationships with patients | 35 | 5 | 34 | 5 |
| Organizational climate of trust and belonging | 27 | 7 | 33 | 6 |
| Ample availability of resources to do job | 24 | 9 | 27 | 7 |
| Optimal autonomy | 26 | 8 | 24 | 8 |
| Fairness within organization | 15 | 10 | 23 | 9 |
| Optimal variety of tasks | 29 | 6 | 22 | 10 |
| Recognition by leaders | 11 | 12 | 10 | 11 |
| Satisfaction with nurses | 12 | 11 | 7 | 12 |
Key differences in individual characteristics, work patterns, and indicating substantial pay as a priority were associated with self‐reported total earnings in 2009 from respondents' work as a hospitalist. As shown in Table 3, the inclusion of detailed productivity measures such as FTE, days of monthly clinical work, and estimated number of daily billable encounters yielded a model that explained 33% of variance in earnings. After adjusting for significant covariates including pediatric specialty, practice model, geography, and amount and type of clinical work, the estimated underpayment of women compared to men was $14,581. Hospitalists who prioritized substantial pay earned $10,771 more than those who did not. The female x leader interaction term testing the hypothesis that gender disparity is greater among leaders than frontline hospitalists was not statistically significant ($16,720, P = 0.087) and excluded from the final model.
| Differences in Salary, 2009 US$ (95% CI) | P Value | |
|---|---|---|
| ||
| Women | 14,581 (23,074 to 6,089) | <0.01 |
| Leader | 21,997 (13,313 to 30,682) | <0.01 |
| Prioritized substantial pay | 10,771 (2,651 to 18,891) | <0.01 |
| Pediatric specialty | 31,126 (43,007 to 19,244) | <0.01 |
| Practice model | ||
| Hospital employed | REF | |
| Multispecialty group | 1,922 (13,891 to 10,047) | 0.75 |
| University/medical school | 33,503 (46,336 to 20,671) | <0.01 |
| Multistate group | 6,505 (72,69 to 20,279) | 0.35 |
| Local hospitalist group | 9,330 (4,352 to 23,012) | 0.18 |
| Other | 17,364 (45,741 to 11,012) | 0.23 |
| Practice region | ||
| Southeast | REF | |
| Midwest | 1,225 (10,595 to 13,044) | 0.84 |
| Northeast | 15,712 (28,182 to 3,242) | 0.01 |
| Southwest | 722 (13,545 to 12,101) | 0.91 |
| West | 5,251 (7,383 to 17,885) | 0.41 |
| FTE | 1,021 (762 to 1,279) | <0.01 |
| Days per month doing clinical work | 1,209 (443 to 1,975) | <0.01 |
| Estimated daily billable encounters | 608 (20 to 1,196) | 0.04 |
DISCUSSION
In a national stratified sample of US hospitalists, we found gender differences in job satisfaction priorities and hospitalist work characteristics. We also confirmed the persistence of a substantial gender earnings disparity. Lower earnings among women compared to men hospitalists were present in our data after controlling for age, pediatric specialty, practice model, geography, type of clinical work, and productivity measures. The gender earnings disparity noted in 1999[6] persists, although it appears to have decreased, possibly indicating progress toward equity. We showed that women hospitalists' relative tendency not to prioritize pay explains a significant portion of the residual income gap.
Hoff examined hospitalist earnings in a large national survey of hospitalists in 1999. Our cohorts differed in age and experience (both lower in the Hoff study). An estimated $24,000 ($124,266 vs. $148,132) earnings gap between women and men was greater than our estimate of $14,581 following an interval of 10 years. Although survey items differed, both studies found that women were less interested in pay than men when considering a hospitalist job. Hoff also found that work setting and attitudes about pay and lifestyle were significantly related to earnings. We extended the previous analyses of gender differences in job satisfaction priorities, work, and demographic characteristics to explain the earnings gap and understand how it may be remedied.
When considering job satisfaction, we found that more men than women prioritized substantial pay and that prioritization of substantial pay was directly related to higher earnings. Therefore, fewer women prioritizing pay partly explains women's lower earnings. Reasons for why fewer women prioritize pay were not assessed in this study but may include factors like being part of 2‐income households and competing commitments.[29] Priorities may even be influenced by empirically observed gender differences in discussions of financial matters, governed by cultural norms. Such norms may implicitly sanction employers to offer women less pay than men for the same or similar work. Women may disadvantage themselves by negotiating less or less well than men for higher starting and promotion salaries. They may be perceived more negatively than men when they do negotiate pay, leading to unintended negative consequences such as loss of social networks, decreased likability, and even loss of job offers.[29, 30, 31, 32]
More women prioritized optimal variety of tasks (6th most prevalent among women and 10th among men). Women who highly rate optimal variety of tasks as a job satisfier may choose positions in which they teach, perform research, and participate in hospital committees and quality‐improvement work, but offer lower pay. Yet hours per month doing nonclinical work was not significantly different between men and women, nor associated with earnings differences in our earnings models. Understanding whether women self‐select into hospitalist jobs with like‐minded colleagues to achieve complementary fit or end up supplementing their skills with hospitalists with different priorities may inform strategies to reduce the gender income disparity.[5] Unlike disparities between various hospital medicine groups, systematic disparities within practices risk generating low levels of organizational fairness and burnout among employees.
Not surprisingly, productivity was positively associated with earnings but did not fully account for the gender earnings gap. Our data demonstrated that women, on average, were associated with work characteristics that expectedly generate less compensation. For example, women were younger, more often part time, academic, pediatric, less often leaders, and reported fewer billable encounters compared to men. These differences account for some of the earnings gap between men and women, but these factors were controlled for in the earnings model. In addition, our analysis may have underestimated the gap by not incorporating loss of fringe benefits from part‐time status and not comprehensively counting incentive pay associated with high productivity. Other work patterns more commonly associated with women suggest an imbalance in reimbursement. More women than men work nights that are often compensated at higher rates than daytime work, yet their average pay was less, suggesting that compensation for night work may need to be adjusted to reflect its unique burdens and responsibilities.[33]
Although the gender pay gap was not more extreme among leaders compared to frontline hospitalists in our data, the trend, nonetheless, underscores an important consideration. Whereas clinical work is paid for in mostly measurable ways, pay for leadership may be influenced by intangible factors such as reputation, negotiation, and confidence that may disadvantage women relative to men.[7, 19, 23, 34, 35, 36] Efforts to overcome implicit gender bias should be most effective when we consciously couple fair promotion of women to leadership with fair compensation commensurate with their male peers.[21]
Our data are vulnerable to nonresponse bias.[1, 4, 5] Post hoc analyses demonstrated that distributions of age, gender, practice model and region of our respondents were similar to other nationally representative cohorts of hospitalists. Consequently, we believe our data can make valid estimates about a nationally representative sample of hospitalists. However, we acknowledge several additional weaknesses of self‐reported data, including recall bias and accuracy of productivity figures, which were rounded to variable significant digits by respondents. Earnings analysis using this data was intended to be exploratory, but the findings echoed analyses using more authoritative data sources.[11] Still, we made inferences conservatively by adopting multiple imputation techniques for dealing with nonresponse surveys in adherence to established reporting guidelines.[25] We also note several limitations relevant to multiple imputations. The greater prevalence of missing data for survey items soliciting earnings and the number of billable encounters suggest they were not truly missing at random as assumed. However, we showed that missingness is unrelated to the variables under study, justifying use of the technique. The wider measures of variance derived from multiple imputations make us vulnerable to not detecting associations that may exist.
The gender earnings gap found in hospital medicine echoes the gap found in multiple medical specialties, including but not limited to pediatrics, academic medicine, gastroenterology, and plastic surgery.[7, 8, 9, 11, 12, 13, 37] Hospital medicine employment models and practice patterns have important structural differences compared to previously studied populations that could mitigate factors contributing to women physicians' lower earnings. However, despite well‐defined working hours, lack of control over the number of patient encounters per day and high prevalence of hospital‐employed practice models, the gender earnings gap persists. We showed that lower prioritization for pay may reflect the self‐selection of women into lower paying jobs. Unmeasured factors, including implicit bias and differences in negotiations, social networks and mentoring opportunities[38, 39] may also contribute to pay differences between men and women hospitalists. As hospital medicine tackles gender inequities and other disparities, strategies to assess and address fair physician compensation must be on the table.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task F. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- , . The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335(7):514–517.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO study. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation. Vol. 1. Research Findings. Rockville, MD; Agency for Healthcare Research and Quality; 2005.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , . Person‐job fit: an exploratory cross‐sectional analysis of hospitalists. J Hosp Med. 2013;8(2):96–101.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- , , , . Compensation and advancement of women in academic medicine: Is there equity? Ann Intern Med. 2004;141(3):205–212.
- . Differences in earnings between male and female physicians. N Engl J Med. 1996;334(15):960–964.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , , , . The work lives of women physicians results from the physician work life study. The SGIM Career Satisfaction Study Group. J Gen Intern Med. 2000;15(6):372–380.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30(2):193–201.
- , , , . Assessing gender equity in a large academic department of pediatrics. Acad Med. 2012;87(1):98–104.
- , , , , , . Gender disparity in the practice of gastroenterology: the first 5 years of a career. Am J Gastroenterol. 2005;100(2):259–264.
- H.R. 438, Fair Pay Act of 2013. 113th Congress (2013‐2014).
- , , , , . Topics to ponder: part‐time practice and pay parity. Gend Med. 2010;7(4):350–356.
- , . Understanding and finding mentorship: a review for junior faculty. J Palliat Med. 2010;13(11):1373–1379.
- , , , et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA. 1996;276(11):898–905.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335(17):1282–1289.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–1025.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86(6):752–758.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , . Why aren't there more women leaders in academic medicine? tHe views of clinical department chairs. Acad Med. 2001;76(5):453–465.
- . The gender gap in executive compensation: the role of female directors and chief executive officers. Ann Am Acad Pol Soc Sci. 2012(639):258–278.
- , , . Keys to career satisfaction: insights from a survey of women pediatric surgeons. J Pediatr Surg. 2004;39(6):984–990.
- , , , et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393.
- Imputation and Variance Estimation Software [computer program]. Ann Arbor, MI: Universtiy of Michigan; 2007.
- , , . Multiple Imputation using chained equations: issues and guidance for practice. Stat Med. 2010;30(4):377–399.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2010.
- , . The Changing Face of Medicine: Women Doctors and the Evolution Of Health Care in America. Ithaca, NY: ILR Press/Cornell University Press; 2008.
- , . Women Don't Ask: Negotiation and the Gender Divide. Princeton, NJ: Princeton University Press; 2003.
- , , , et al. Negotiation in academic medicine: a necessary career skill. J Womens Health (Larchmt). 2007;16(2):235–244.
- . Women and salary negotiation: the costs of self‐advocacy. Psychol Women Q. 2001;25:65–76.
- State of Hospital Medicine: 2014 Report Based on 2013 Data. Englewood, CO and Philadelphia, PA: Medical Group Management Association and Society of Hospital Medicine; 2014.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , . Sociology. The gender gap in NIH grant applications. Science. 2008;322(5907):1472–1474.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , . Gender differences in the professional and private lives of plastic surgeons. Ann Plast Surg. 2010;64(6):775–779.
- . Gender and supportive co‐worker relations in the medical profession. Gend Work Organ. 2014;21(1):1–17.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
© 2015 Society of Hospital Medicine
Gender and Hospital Medicine
From a new concept to 44,000 practitioners in just 18 years,[1] there is no doubt that the word hospitalist is synonymous with innovation, leadership, growth, and change. Yet 2 articles in this month's Journal of Hospital Medicine prove that even our new field faces age‐old problems. Although women comprise half of all academic hospitalist and general internal medicine faculty, Burden et al.[2] showed that female hospitalists are less likely than male hospitalists to be division or section heads of hospital medicine, speakers at national meetings, and first or last authors on both research publications and editorials. This is made more concerning given that women are more likely to choose academic hospital medicine careers,[3] as they represent one‐third of all hospitalists but half of the academic hospitalist workforce.[2, 3] Findings in general internal medicine were similar, except that equal numbers of women and men were national meeting speakers and first authors on research publications (but not editorials). Weaver et al.[4] shed even more light on this disparity, and found that female hospitalists made $14,581 less per year than their male counterparts, even after adjusting for relevant differences. Weaver and colleagues also found other gender‐specific differences: women worked more nights and had fewer billable encounters per hospitalist shift than men.
Unfortunately, these trends are not new or limited to hospital medicine. For decades, almost equal numbers of women and men have entered medical school,[5] yet women are under‐represented in high status specialties,[6] less likely to be first or senior authors on original research studies compared to men,[7] less likely to be promoted,[8] and women physicians are consistently paid less than men across specialties.[9, 10] Simple analyses have not yet explained these disparities. Compared with men, women have similar leadership aspirations[11, 12] and are at least as effective as leaders.[13, 14, 15] Yet equity has not been attained.
Implicit bias research suggests that gender stereotypes influence women at all career stages.[16, 17, 18] For example, an elegant study conducted by Correll et al. identified a motherhood penalty, where indicating membership in the elementary school parent‐teacher organization on one's curriculum vitae hurt women's chances of employment and pay, but actually helped men.[19] Gender stereotypes exist, even among those who do not support their content. The universal reinforcement of such stereotypes over time leads to implicit but prescriptive rules about how women and men should act.[20] In particular, communal behaviors, including being cooperative, kind, and understanding, are typically associated with women, and agentic behaviors, including being ambitious and acting as a leader, are considered appropriate for men.[21] This leads to the think leader, think male phenomena, where we automatically associate men with leadership and higher status tasks (like first authorship or speaker invitations).[22, 23] Furthermore, acting against the stereotype (eg, a woman showing anger[24] or negotiating for more pay[25] or a man showing sadness[26]) can negatively impact wage and employment. Expecting social censure for violating gender norms, women develop a fear of the backlash that alone may shape behavior such that women may not express interest in having a high salary or negotiate for a raise.[27, 28, 29]
The specific system and institutional barriers that prevent female hospitalists from receiving equal pay and opportunities for leadership are not known, but one can surmise they are similar to those found in other specialties.[10, 30, 31] The findings of the studies of Burden et al.[2] and Weaver et al.[4] invite investigation of new questions specific to hospital medicine. Why are women in hospital medicine working more night shifts? Does this impact leadership or scholarship opportunities? Why are women documenting less productivity? Are they spending more time with patients, as they do in other settings?[32] What influences their practice choice? We would like to believe that there is something about hospital medicine that can explain the gender differences identified in these 2 studies. However, these data should prompt a serious and thorough examination of our specialty. We must accept that despite being a new specialty and a change leader, hospital medicine may not have escaped systematic gender bias that constrains the full participation and advancement of women.
But we believe that hospitalistsinnovators and change leaders in medicinewill be spurred to action to address the possibility of gender inequities. We do not need to know all of the causes to begin to address disparities, of every type, on an individual, institutional, and national level. As individuals, we can acknowledge that there are implicit assumptions that influence our decision making. No matter how unintentional, and even conflicting with evidence, these assumptions can lead us to judge women as less capable leaders than men or to automatically envision a high salary for a woman and man as different amounts. However, these automatic gender biases function as habits of mind, so they can be broken like any other unwanted habit.[33] Institutionally, we can also hold ourselves accountable for transparency in mentorship, leadership, scholarship, promotions, and wages to ensure diverse representation. We should routinely examine our practices to ensure the equitable hiring, pay, and promotion of our workforce.[18] National organizations and their respective journals should actively pursue diverse representation in leadership and membership on boards and committees, award nominees and recipients, and opportunities for invited editorials. Hospital medicinebeing young, innovative, and committed to changeis uniquely well suited to lead the charge for workforce equity. We can, and will, show the rest of medicine how it is done.
Disclosure
Nothing to report.
- Society of Hospital Medicine. Milestones in the hospital medicine movement. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Industry/shm_History.aspx. Accessed March 23, 2015.
- , , , et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(X):000–000.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7:402–410.
- , , , . A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486–490.
- Association of American Medical Colleges. Table 1: medical students, selected years, 1965–2013. Available at: https://www.aamc.org/download/411782/data/2014_table1.pdf. Accessed March 23, 2015.
- , , , . Sex, role models, and specialty choices among graduates of US medical schools in 2006‐2008. J Am Coll Surg. 2014;218(3):345–352.
- , , , et al. The “Gender Gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355(3):281–287.
- . Women physicians in academic medicine. N Engl J Med. 2000;342(6):399–405.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Affairs. 2011;30(2):193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500–508.
- . Faculty and staff members perceptions of effective leadership: are there differences between men and women leaders? Equity Excell Educ. 2003;36(1):71–81.
- , , . Transformational, transactional, and lasissez‐faire leadership styles: a meta‐analysis comparing women and men. Psychol Bull. 2003;129(4):569–591.
- , , . A qualitative study of faculty members' views of women chairs. J Womens Health (Larchmt). 2010;19(3):533–546.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
- , . Women and the labyrinth of leadership. Harv Bus Rev. 2007;85(9):62–71.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , , . Getting a job: is there a motherhood penalty? Am J Sociol. 2017;112(5):1297–1339.
- , , , , . Afraid of being “witchy with a ‘b’”: a qualitative study of how gender influences residents' experiences leading cardiopulmonary resuscitation. Acad Med. 2014;89(9):1276–1281.
- . The measurement of psychological androgyny. J Consult Clin Psychol. 1974;42:155–162.
- , , , . Think manager—think male: A global phenomenon? J Organ Behav. 1996;17(1):33–41.
- , , , . Are leader stereotypes masculine? A meta‐analysis of three research paradigms. Psychol Bull. 2011;137(4):616–642.
- , . Can an angry woman get ahead? Status conferral, gender, and expression of emotion in the workplace. Psychol Sci. 2008;19(3):268–275.
- , , . Social incentives for gender differences in the propensity to initiate negations: sometimes it does hurt to ask. Organ Behav Hum Decis Process 2007;103:84–103.
- . Anger and advancement versus sadness and subjugation: the effect of negative emotion expressions on social status conferral. J Pers Soc Psychol. 2001;80(1):86–94.
- , , . Battle of the sexes: gender stereotype confirmation and reactance in negotiations. J Pers Soc Psychol. 2001;80(6):942–958.
- , . Prejudice toward female leaders: Backlash effects and women's impression management dilemma. Soc Personal Psychol Compass. 2010;4(10):807–820.
- . Commentary: deconstructing gender difference. Acad Med. 2010;85(4):575–577.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , , , , . Survey results: a decade of change in professional life in cardiology: a 2008 report of the ACC women in cardiology council. J Am Coll Cardiol. 2008;52(25):2215–2226.
- , , , , . Effect of physicians' gender on communication and consultation length: a systematic review and meta‐analysis. J Health Serv Res Policy. 2013;18:242–248.
- , , , et al. The effect of an intervention to break the gender bias habit for faculty at one institution: a cluster randomized, controlled trial. Acad Med. 2015;90(2):221–230.
From a new concept to 44,000 practitioners in just 18 years,[1] there is no doubt that the word hospitalist is synonymous with innovation, leadership, growth, and change. Yet 2 articles in this month's Journal of Hospital Medicine prove that even our new field faces age‐old problems. Although women comprise half of all academic hospitalist and general internal medicine faculty, Burden et al.[2] showed that female hospitalists are less likely than male hospitalists to be division or section heads of hospital medicine, speakers at national meetings, and first or last authors on both research publications and editorials. This is made more concerning given that women are more likely to choose academic hospital medicine careers,[3] as they represent one‐third of all hospitalists but half of the academic hospitalist workforce.[2, 3] Findings in general internal medicine were similar, except that equal numbers of women and men were national meeting speakers and first authors on research publications (but not editorials). Weaver et al.[4] shed even more light on this disparity, and found that female hospitalists made $14,581 less per year than their male counterparts, even after adjusting for relevant differences. Weaver and colleagues also found other gender‐specific differences: women worked more nights and had fewer billable encounters per hospitalist shift than men.
Unfortunately, these trends are not new or limited to hospital medicine. For decades, almost equal numbers of women and men have entered medical school,[5] yet women are under‐represented in high status specialties,[6] less likely to be first or senior authors on original research studies compared to men,[7] less likely to be promoted,[8] and women physicians are consistently paid less than men across specialties.[9, 10] Simple analyses have not yet explained these disparities. Compared with men, women have similar leadership aspirations[11, 12] and are at least as effective as leaders.[13, 14, 15] Yet equity has not been attained.
Implicit bias research suggests that gender stereotypes influence women at all career stages.[16, 17, 18] For example, an elegant study conducted by Correll et al. identified a motherhood penalty, where indicating membership in the elementary school parent‐teacher organization on one's curriculum vitae hurt women's chances of employment and pay, but actually helped men.[19] Gender stereotypes exist, even among those who do not support their content. The universal reinforcement of such stereotypes over time leads to implicit but prescriptive rules about how women and men should act.[20] In particular, communal behaviors, including being cooperative, kind, and understanding, are typically associated with women, and agentic behaviors, including being ambitious and acting as a leader, are considered appropriate for men.[21] This leads to the think leader, think male phenomena, where we automatically associate men with leadership and higher status tasks (like first authorship or speaker invitations).[22, 23] Furthermore, acting against the stereotype (eg, a woman showing anger[24] or negotiating for more pay[25] or a man showing sadness[26]) can negatively impact wage and employment. Expecting social censure for violating gender norms, women develop a fear of the backlash that alone may shape behavior such that women may not express interest in having a high salary or negotiate for a raise.[27, 28, 29]
The specific system and institutional barriers that prevent female hospitalists from receiving equal pay and opportunities for leadership are not known, but one can surmise they are similar to those found in other specialties.[10, 30, 31] The findings of the studies of Burden et al.[2] and Weaver et al.[4] invite investigation of new questions specific to hospital medicine. Why are women in hospital medicine working more night shifts? Does this impact leadership or scholarship opportunities? Why are women documenting less productivity? Are they spending more time with patients, as they do in other settings?[32] What influences their practice choice? We would like to believe that there is something about hospital medicine that can explain the gender differences identified in these 2 studies. However, these data should prompt a serious and thorough examination of our specialty. We must accept that despite being a new specialty and a change leader, hospital medicine may not have escaped systematic gender bias that constrains the full participation and advancement of women.
But we believe that hospitalistsinnovators and change leaders in medicinewill be spurred to action to address the possibility of gender inequities. We do not need to know all of the causes to begin to address disparities, of every type, on an individual, institutional, and national level. As individuals, we can acknowledge that there are implicit assumptions that influence our decision making. No matter how unintentional, and even conflicting with evidence, these assumptions can lead us to judge women as less capable leaders than men or to automatically envision a high salary for a woman and man as different amounts. However, these automatic gender biases function as habits of mind, so they can be broken like any other unwanted habit.[33] Institutionally, we can also hold ourselves accountable for transparency in mentorship, leadership, scholarship, promotions, and wages to ensure diverse representation. We should routinely examine our practices to ensure the equitable hiring, pay, and promotion of our workforce.[18] National organizations and their respective journals should actively pursue diverse representation in leadership and membership on boards and committees, award nominees and recipients, and opportunities for invited editorials. Hospital medicinebeing young, innovative, and committed to changeis uniquely well suited to lead the charge for workforce equity. We can, and will, show the rest of medicine how it is done.
Disclosure
Nothing to report.
From a new concept to 44,000 practitioners in just 18 years,[1] there is no doubt that the word hospitalist is synonymous with innovation, leadership, growth, and change. Yet 2 articles in this month's Journal of Hospital Medicine prove that even our new field faces age‐old problems. Although women comprise half of all academic hospitalist and general internal medicine faculty, Burden et al.[2] showed that female hospitalists are less likely than male hospitalists to be division or section heads of hospital medicine, speakers at national meetings, and first or last authors on both research publications and editorials. This is made more concerning given that women are more likely to choose academic hospital medicine careers,[3] as they represent one‐third of all hospitalists but half of the academic hospitalist workforce.[2, 3] Findings in general internal medicine were similar, except that equal numbers of women and men were national meeting speakers and first authors on research publications (but not editorials). Weaver et al.[4] shed even more light on this disparity, and found that female hospitalists made $14,581 less per year than their male counterparts, even after adjusting for relevant differences. Weaver and colleagues also found other gender‐specific differences: women worked more nights and had fewer billable encounters per hospitalist shift than men.
Unfortunately, these trends are not new or limited to hospital medicine. For decades, almost equal numbers of women and men have entered medical school,[5] yet women are under‐represented in high status specialties,[6] less likely to be first or senior authors on original research studies compared to men,[7] less likely to be promoted,[8] and women physicians are consistently paid less than men across specialties.[9, 10] Simple analyses have not yet explained these disparities. Compared with men, women have similar leadership aspirations[11, 12] and are at least as effective as leaders.[13, 14, 15] Yet equity has not been attained.
Implicit bias research suggests that gender stereotypes influence women at all career stages.[16, 17, 18] For example, an elegant study conducted by Correll et al. identified a motherhood penalty, where indicating membership in the elementary school parent‐teacher organization on one's curriculum vitae hurt women's chances of employment and pay, but actually helped men.[19] Gender stereotypes exist, even among those who do not support their content. The universal reinforcement of such stereotypes over time leads to implicit but prescriptive rules about how women and men should act.[20] In particular, communal behaviors, including being cooperative, kind, and understanding, are typically associated with women, and agentic behaviors, including being ambitious and acting as a leader, are considered appropriate for men.[21] This leads to the think leader, think male phenomena, where we automatically associate men with leadership and higher status tasks (like first authorship or speaker invitations).[22, 23] Furthermore, acting against the stereotype (eg, a woman showing anger[24] or negotiating for more pay[25] or a man showing sadness[26]) can negatively impact wage and employment. Expecting social censure for violating gender norms, women develop a fear of the backlash that alone may shape behavior such that women may not express interest in having a high salary or negotiate for a raise.[27, 28, 29]
The specific system and institutional barriers that prevent female hospitalists from receiving equal pay and opportunities for leadership are not known, but one can surmise they are similar to those found in other specialties.[10, 30, 31] The findings of the studies of Burden et al.[2] and Weaver et al.[4] invite investigation of new questions specific to hospital medicine. Why are women in hospital medicine working more night shifts? Does this impact leadership or scholarship opportunities? Why are women documenting less productivity? Are they spending more time with patients, as they do in other settings?[32] What influences their practice choice? We would like to believe that there is something about hospital medicine that can explain the gender differences identified in these 2 studies. However, these data should prompt a serious and thorough examination of our specialty. We must accept that despite being a new specialty and a change leader, hospital medicine may not have escaped systematic gender bias that constrains the full participation and advancement of women.
But we believe that hospitalistsinnovators and change leaders in medicinewill be spurred to action to address the possibility of gender inequities. We do not need to know all of the causes to begin to address disparities, of every type, on an individual, institutional, and national level. As individuals, we can acknowledge that there are implicit assumptions that influence our decision making. No matter how unintentional, and even conflicting with evidence, these assumptions can lead us to judge women as less capable leaders than men or to automatically envision a high salary for a woman and man as different amounts. However, these automatic gender biases function as habits of mind, so they can be broken like any other unwanted habit.[33] Institutionally, we can also hold ourselves accountable for transparency in mentorship, leadership, scholarship, promotions, and wages to ensure diverse representation. We should routinely examine our practices to ensure the equitable hiring, pay, and promotion of our workforce.[18] National organizations and their respective journals should actively pursue diverse representation in leadership and membership on boards and committees, award nominees and recipients, and opportunities for invited editorials. Hospital medicinebeing young, innovative, and committed to changeis uniquely well suited to lead the charge for workforce equity. We can, and will, show the rest of medicine how it is done.
Disclosure
Nothing to report.
- Society of Hospital Medicine. Milestones in the hospital medicine movement. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Industry/shm_History.aspx. Accessed March 23, 2015.
- , , , et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(X):000–000.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7:402–410.
- , , , . A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486–490.
- Association of American Medical Colleges. Table 1: medical students, selected years, 1965–2013. Available at: https://www.aamc.org/download/411782/data/2014_table1.pdf. Accessed March 23, 2015.
- , , , . Sex, role models, and specialty choices among graduates of US medical schools in 2006‐2008. J Am Coll Surg. 2014;218(3):345–352.
- , , , et al. The “Gender Gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355(3):281–287.
- . Women physicians in academic medicine. N Engl J Med. 2000;342(6):399–405.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Affairs. 2011;30(2):193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500–508.
- . Faculty and staff members perceptions of effective leadership: are there differences between men and women leaders? Equity Excell Educ. 2003;36(1):71–81.
- , , . Transformational, transactional, and lasissez‐faire leadership styles: a meta‐analysis comparing women and men. Psychol Bull. 2003;129(4):569–591.
- , , . A qualitative study of faculty members' views of women chairs. J Womens Health (Larchmt). 2010;19(3):533–546.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
- , . Women and the labyrinth of leadership. Harv Bus Rev. 2007;85(9):62–71.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , , . Getting a job: is there a motherhood penalty? Am J Sociol. 2017;112(5):1297–1339.
- , , , , . Afraid of being “witchy with a ‘b’”: a qualitative study of how gender influences residents' experiences leading cardiopulmonary resuscitation. Acad Med. 2014;89(9):1276–1281.
- . The measurement of psychological androgyny. J Consult Clin Psychol. 1974;42:155–162.
- , , , . Think manager—think male: A global phenomenon? J Organ Behav. 1996;17(1):33–41.
- , , , . Are leader stereotypes masculine? A meta‐analysis of three research paradigms. Psychol Bull. 2011;137(4):616–642.
- , . Can an angry woman get ahead? Status conferral, gender, and expression of emotion in the workplace. Psychol Sci. 2008;19(3):268–275.
- , , . Social incentives for gender differences in the propensity to initiate negations: sometimes it does hurt to ask. Organ Behav Hum Decis Process 2007;103:84–103.
- . Anger and advancement versus sadness and subjugation: the effect of negative emotion expressions on social status conferral. J Pers Soc Psychol. 2001;80(1):86–94.
- , , . Battle of the sexes: gender stereotype confirmation and reactance in negotiations. J Pers Soc Psychol. 2001;80(6):942–958.
- , . Prejudice toward female leaders: Backlash effects and women's impression management dilemma. Soc Personal Psychol Compass. 2010;4(10):807–820.
- . Commentary: deconstructing gender difference. Acad Med. 2010;85(4):575–577.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , , , , . Survey results: a decade of change in professional life in cardiology: a 2008 report of the ACC women in cardiology council. J Am Coll Cardiol. 2008;52(25):2215–2226.
- , , , , . Effect of physicians' gender on communication and consultation length: a systematic review and meta‐analysis. J Health Serv Res Policy. 2013;18:242–248.
- , , , et al. The effect of an intervention to break the gender bias habit for faculty at one institution: a cluster randomized, controlled trial. Acad Med. 2015;90(2):221–230.
- Society of Hospital Medicine. Milestones in the hospital medicine movement. Available at: http://www.hospitalmedicine.org/Web/About_SHM/Industry/shm_History.aspx. Accessed March 23, 2015.
- , , , et al. Gender disparities in leadership and scholarly productivity of academic hospitalists. J Hosp Med. 2015;10(X):000–000.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7:402–410.
- , , , . A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486–490.
- Association of American Medical Colleges. Table 1: medical students, selected years, 1965–2013. Available at: https://www.aamc.org/download/411782/data/2014_table1.pdf. Accessed March 23, 2015.
- , , , . Sex, role models, and specialty choices among graduates of US medical schools in 2006‐2008. J Am Coll Surg. 2014;218(3):345–352.
- , , , et al. The “Gender Gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355(3):281–287.
- . Women physicians in academic medicine. N Engl J Med. 2000;342(6):399–405.
- , , , , , . Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Affairs. 2011;30(2):193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28(2):201–207.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500–508.
- . Faculty and staff members perceptions of effective leadership: are there differences between men and women leaders? Equity Excell Educ. 2003;36(1):71–81.
- , , . Transformational, transactional, and lasissez‐faire leadership styles: a meta‐analysis comparing women and men. Psychol Bull. 2003;129(4):569–591.
- , , . A qualitative study of faculty members' views of women chairs. J Womens Health (Larchmt). 2010;19(3):533–546.
- , . Stuck in the out‐group: Jennifer can't grow up, Jane's invisible, and Janet's over the hill. J Womens Health (Larchmt). 2014;23(6):481–484.
- , . Women and the labyrinth of leadership. Harv Bus Rev. 2007;85(9):62–71.
- , , . Interventions that affect gender bias in hiring: a systematic review. Acad Med. 2009;84(10):1440–1446.
- , , . Getting a job: is there a motherhood penalty? Am J Sociol. 2017;112(5):1297–1339.
- , , , , . Afraid of being “witchy with a ‘b’”: a qualitative study of how gender influences residents' experiences leading cardiopulmonary resuscitation. Acad Med. 2014;89(9):1276–1281.
- . The measurement of psychological androgyny. J Consult Clin Psychol. 1974;42:155–162.
- , , , . Think manager—think male: A global phenomenon? J Organ Behav. 1996;17(1):33–41.
- , , , . Are leader stereotypes masculine? A meta‐analysis of three research paradigms. Psychol Bull. 2011;137(4):616–642.
- , . Can an angry woman get ahead? Status conferral, gender, and expression of emotion in the workplace. Psychol Sci. 2008;19(3):268–275.
- , , . Social incentives for gender differences in the propensity to initiate negations: sometimes it does hurt to ask. Organ Behav Hum Decis Process 2007;103:84–103.
- . Anger and advancement versus sadness and subjugation: the effect of negative emotion expressions on social status conferral. J Pers Soc Psychol. 2001;80(1):86–94.
- , , . Battle of the sexes: gender stereotype confirmation and reactance in negotiations. J Pers Soc Psychol. 2001;80(6):942–958.
- , . Prejudice toward female leaders: Backlash effects and women's impression management dilemma. Soc Personal Psychol Compass. 2010;4(10):807–820.
- . Commentary: deconstructing gender difference. Acad Med. 2010;85(4):575–577.
- , , , . Organizational climate and family life: how these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
- , , , , , . Survey results: a decade of change in professional life in cardiology: a 2008 report of the ACC women in cardiology council. J Am Coll Cardiol. 2008;52(25):2215–2226.
- , , , , . Effect of physicians' gender on communication and consultation length: a systematic review and meta‐analysis. J Health Serv Res Policy. 2013;18:242–248.
- , , , et al. The effect of an intervention to break the gender bias habit for faculty at one institution: a cluster randomized, controlled trial. Acad Med. 2015;90(2):221–230.