User login
Discharge Before Noon
It is thought that late afternoon hospital discharges create admission bottlenecks in the emergency department (ED).[1] As hospital occupancy increases, so too does ED boarding time.[2] Increased ED boarding time can result in increased length of stay (LOS)[3] and reduced patient and staff satisfaction.[4] Early in the day discharge programs are intended to improve hospital throughput.[5, 6, 7, 8, 9] Yet, ED admission timing is, in part, determined by external fluctuations in ED volume and acuity that early discharges do not impact.[10] We previously reported that high levels of discharge before noon (DBN) from inpatient medicine units is achievable through a multidisciplinary intervention.[5] We now evaluate the effect of this intervention upon admission patterns and the sustainability of the DBN initiative.
The DBN intervention consisted of afternoon interdisciplinary rounds, a checklist of team members' responsibilities, a standardized electronic communication tool, and daily feedback on the DBN rate.[5] The intervention resulted in an increase in the DBN rate from 11% to 38% in the first 13 months. We previously reported effects upon the discharged patient as measured by the observed to expected length of stay (O:E LOS) and 30‐day readmission rate. We now assess the effect of our DBN initiative on the subsequent patient and hospital throughput. Our objectives for this study were: (1) to determine the effect of DBN on the admission arrival times and admissions per hour to the units, and (2) in a separate data collection and analysis, to determine if the increased DBN rate is sustainable. We hypothesize that DBN results in admissions arriving onto the units earlier in the day. We further hypothesize that because of this redistribution, DBN will level the load of admissions, reducing admissions per hour peaks that can occur late in the day.
METHODS
Study Design, Participants, and Setting
This is a pre‐/postretrospective analysis evaluating the effect of a previously described DBN intervention.[5] Two inpatient acute‐care medicine units at NYU Langone Medical Center's Tisch Hospital, a 725‐bed, urban, academic medical center, were included in the analysis. All patients admitted to the units underwent the intervention.
Intervention
The DBN intervention began with a multidisciplinary kickoff event in which all team members received education on the importance of DBN, a clear description of roles in the DBN process, and a corresponding checklist of responsibilities. The checklist was utilized at new afternoon interdisciplinary rounds intended to identify next‐day DBNs. Patients identified in afternoon interdisciplinary rounds were logged in a DBN website that generated twice‐daily automated emails to communicate the planned DBN list to frontline staff and key stakeholders. Daily, real‐time feedback on the DBN rate was provided to floor staff.
Measures
Admission Arrival Time
The arrival location and time to any hospital area (ED, radiology, inpatient medical unit) is recorded in the electronic medical record (Epic, Madison, WI) at the time the patient arrives by the patient unit assistant or unit clerk. We obtained the arrival time to each hospital unit throughout the patient's hospitalization for all patients arriving to the study units during their hospitalization between June 1, 2011 and March 4, 2012 (the baseline period) and March 5, 2012 and June 31, 2013 (the intervention period). Data from October 25, 2012 to the end of January 2013 were excluded due to hospital closure from Hurricane Sandy. These time periods and exclusions match those used in our previous DBN article.[5] To match that study's criteria, we excluded patients on the units in the patient class observation, inpatient hospice, and those patients whose discharge disposition was expired or hospice.
ED Admissions
All patients with a first inpatient unit location of ED and no other inpatient unit location prior to arrival on the study units were included in the ED admission analysis. Units that treat but do not provide long‐term boarding/housing of inpatientssuch as radiology, hemodialysis, and cardiac catheterizationwere not considered in determining ED admission status. Even if a patient had recorded arrival to those areas between ED and study unit arrival, these patients were considered ED admissions, as they were never admitted to another inpatient unit.
Transfers and Direct Admissions
All patients whose first inpatient unit location was the study units were included in the transfers and direct admissions analysis. Those patients who were recorded as coming from another inpatient unit (such as another medical, surgical, step‐down, intensive care, or other specialty unit) prior to study unit arrival were included as intrahospital transfers.
Level Load of Admissions
Level loading is a lean methodology term that describes reducing the unevenness in a production line to enhance efficiency.[11] We evaluated this by comparing the admissions per hour (density distribution) to the studied units in the pre‐ and postintervention periods.
Sustainability of the DBN Intervention
The DBN intervention, as described in our original article, continues uninterrupted. Using the same methodology, inclusion criteria, exclusion criteria, and data analysis previously described, we gathered the discharge date and time as recorded by the patient unit assistant for all patients discharged from the study units for the 18 months (July 1, 2013 to December 31, 2014) after our original article to evaluate the sustainability of our improvement in DBN rates.
Statistical Analysis
Median admission time to the floor was compared between the 2 time periods using the Wilcoxon rank sum test. This is a non parametric test of the null hypothesis that the two time periods have the same distributions of admission time to the floor. To evaluate statistical significance, each admission time is arranged in order of magnitude and assigned a rank. The sum of the ranks for each group is calculated and the smaller rank sum (the W statistic) is compared to an expected range of values based on the sample sizes. If this value is out of range then one can reject the null hypothesis. The density distributions of admissions during the 2 time periods were compared using the Kolmogorov‐Smirnov test. The 2‐sided Kolmogorov‐Smirnov test evaluates the maximum distance (D) between the distributions of 2 samples.[12] We chose this test because it evaluates differences between both the position and shape of the distributions of the samples.
RESULTS
Setting Characteristics
The units had an average occupancy rate of 86.8% for the duration of the study. The average number of total discharges per day was 9.8. The average absolute length of stay was 5.6 days.
Admission Arrival Time to the Unit
ED Admissions
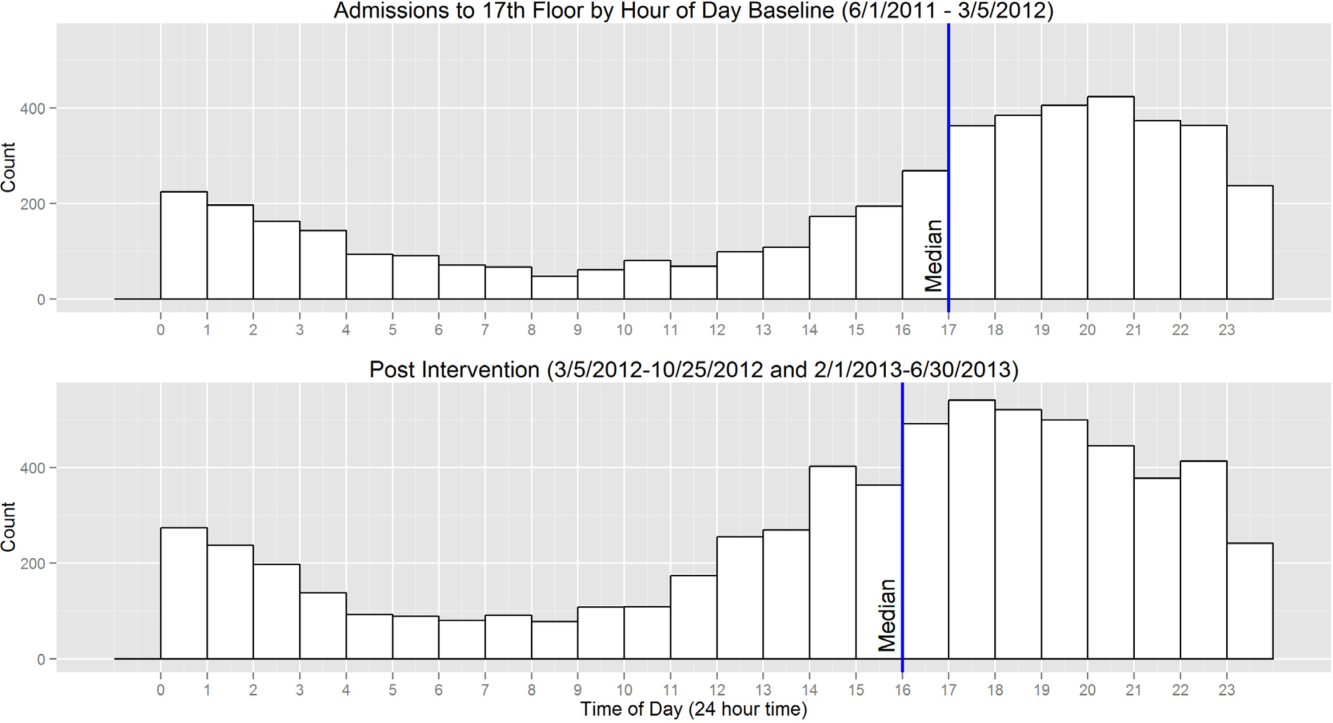
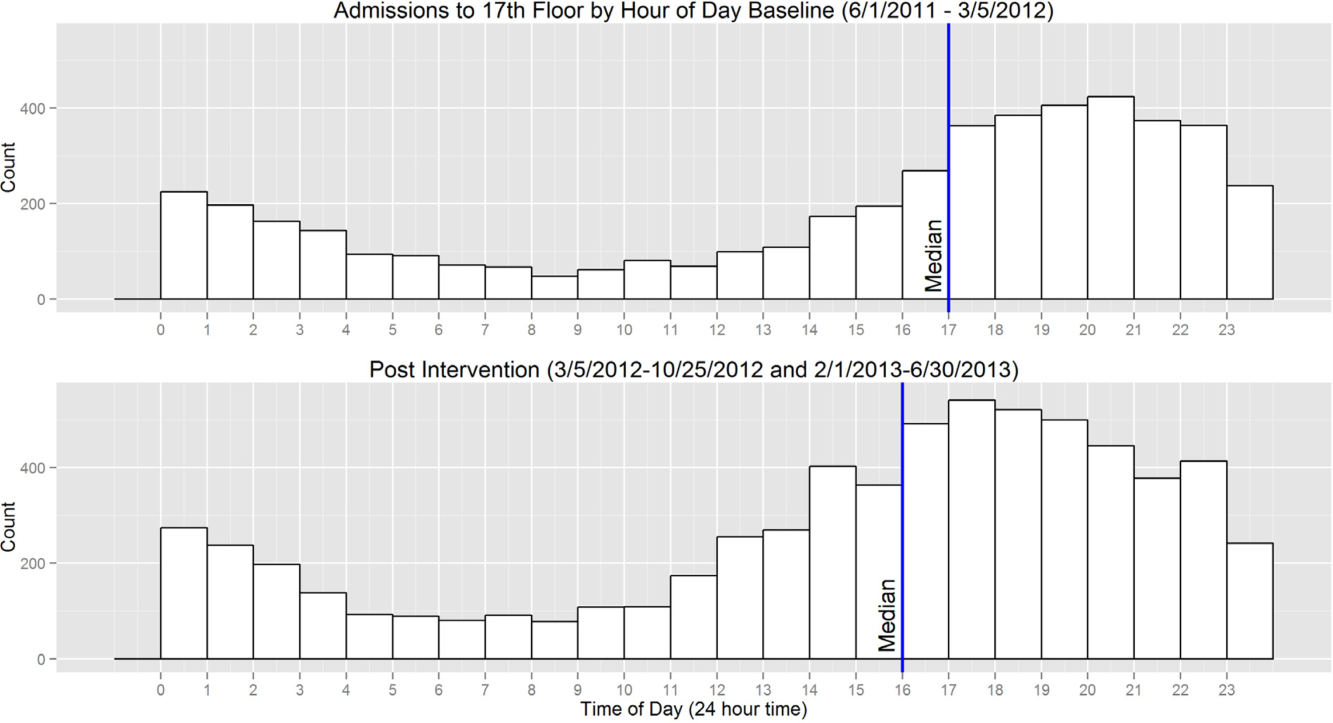
A total of 6566 patients were admitted from the ED to the units, 2756 in the baseline period and 3810 in the intervention period. The median arrival time to the units of ED admissions grouped by hour of the day moved by 1 hour, from 5 pm to 4 pm from the baseline to intervention period, and this change was statistically significant (W=16,211,778, P<0.01) (Figure 1).
Transfers and Direct Admissions
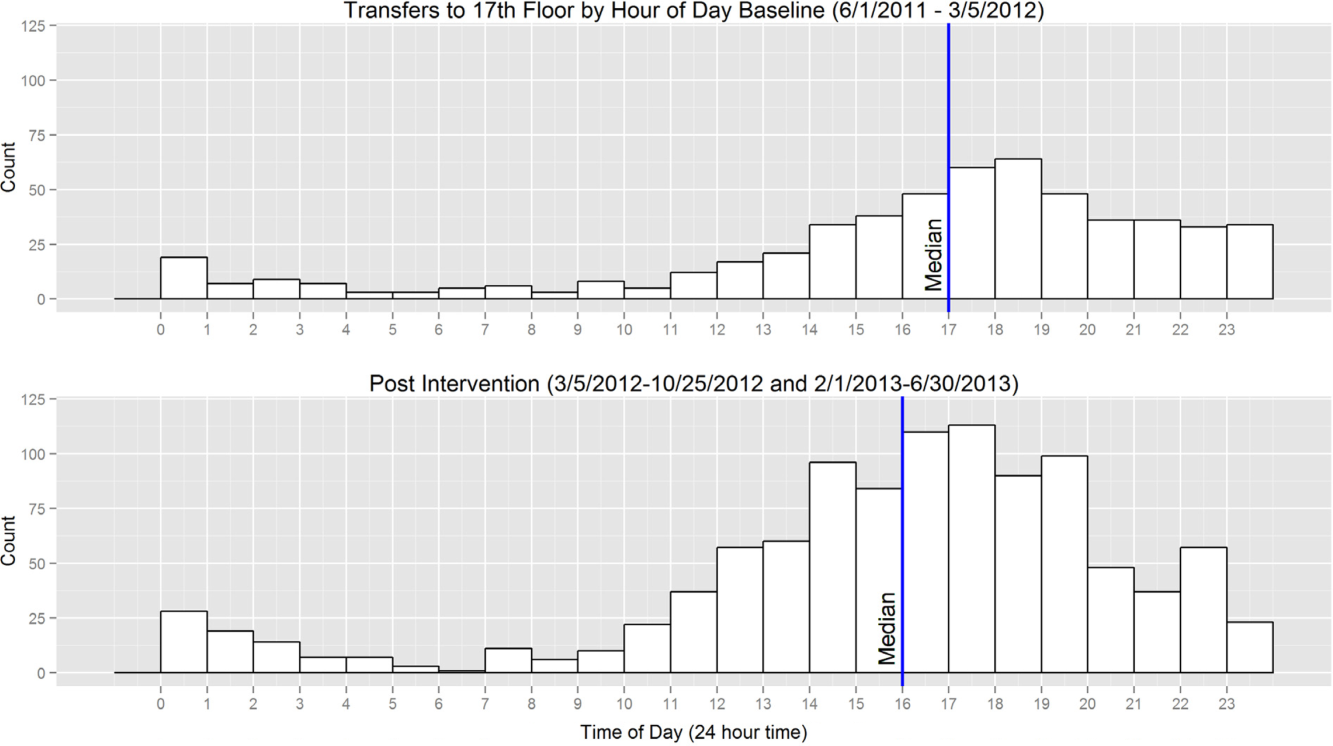
A total of 823 patients were transferred or directly admitted to the units, 310 in the baseline period and 513 in the intervention period. The median arrival time to the units grouped by hour of the day moved 1 hour from 5 pm to 4 pm, and this change was statistically significant (W=324,532, P<0.01) (Figure 2).
Level Load of Admissions
In the baseline period, the highest density of ED admissions occurred during the 5‐hour period from 5 pm to 10 pm, when 42.3% of daily admissions arrived (Figure 3). In the intervention period, the highest density of admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 40.0% of daily admissions arrived. The difference between the density distributions for the 2 time periods was found to be statistically significant using the Kolmogorov‐Smirnov test (D=0.03, P<0.01).
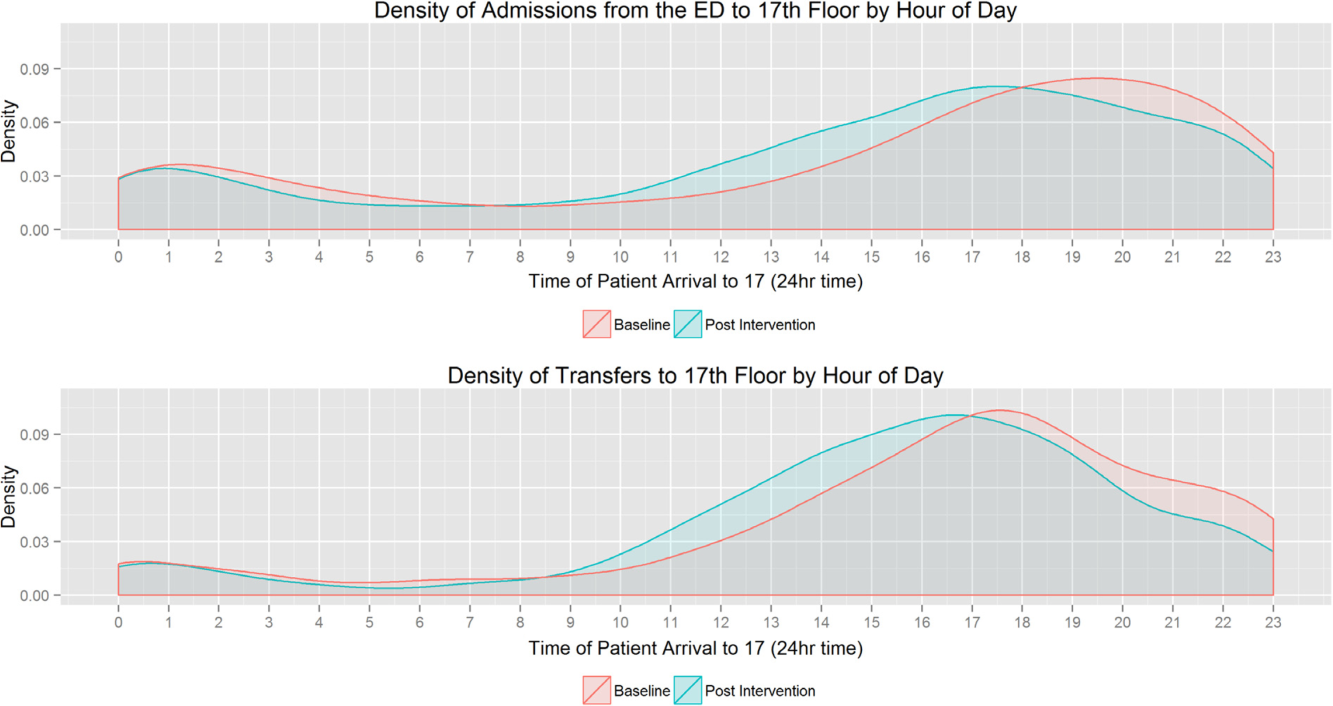
In the baseline period, the highest density of transfers and direct admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 51.7% of daily admissions arrived (Figure 3). In the intervention time period, the highest density of transfers and direct admissions occurred during the 5‐hour time period from 2 pm to 7 pm, when 50.3% of daily admissions arrived. The difference between the density distributions of transfers and direct admissions for the 2 time periods was not statistically significant using the Kolmogorov‐Smirnov test (D=0.04, P=0.3).
Sustainability of the DBN Intervention
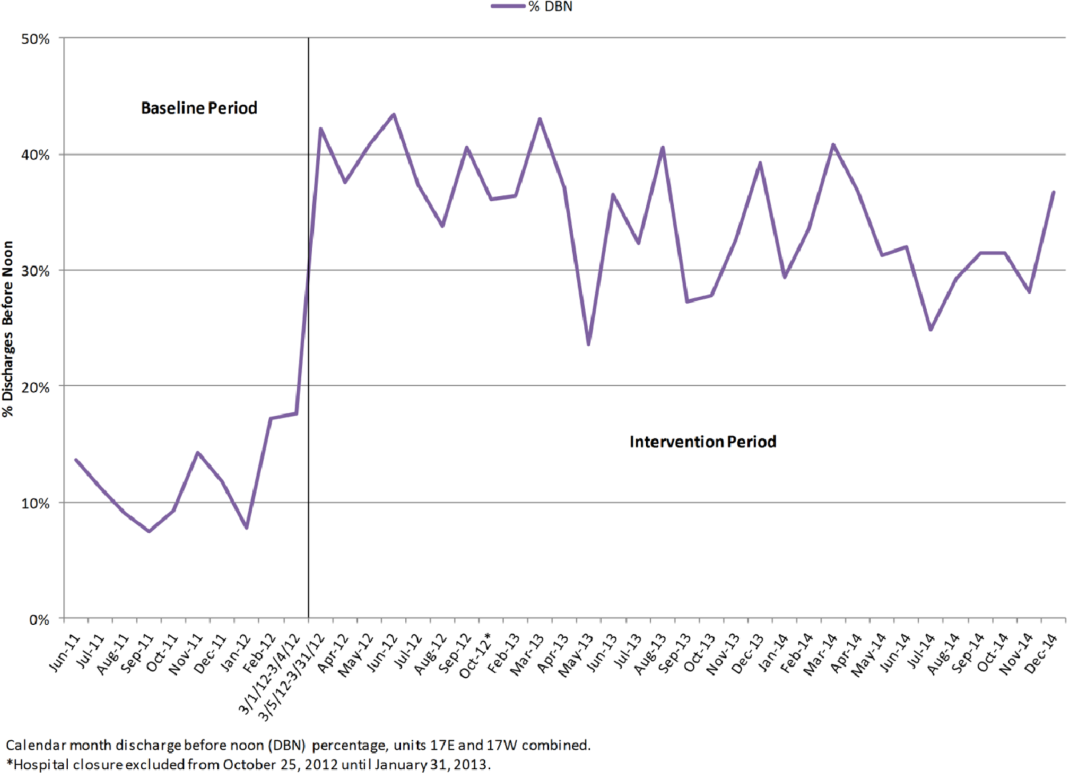
For the 18 months after the prior reported DBN intervention period, an additional 5505 total discharges were included for analysis. Of these, 1796 were DBN. The average DBN rate for the study units from March 5, 2012 until December 31, 2014 (the original intervention period plus the additional 18 months of new data) is 35% (Figure 4).
DISCUSSION
The potential effects of DBN are multiple. By reducing the O:E LOS and allowing patients the time to acquire their medications, make follow‐up appointments, and ask questions while providers are still in the hospital, our DBN initiative impacts the discharged patient's quality, safety, and efficiency of care.[5] We now report how the DBN initiative potentially impacts the subsequent patient's efficiency of care and hospital throughput. In addition, we show that the DBN initiative is sustainable over years.
Over the same time course as our initial DBN intervention, we found a statistically significant change in the time when admitted patients arrive on the floor. This was true of those patients admitted through the ED and those directly admitted to the floor. In a complex hospital system with many factors both internal (bed cleaning, patient transportation) and external (natural variations in ED volume and acuity) affecting the timing of admissions, it is important to note that increasing the DBN rate correlates with a change in median admission arrival time. From a patient safety standpoint, any initiative that moves admissions away from evening and night hours and takes advantage of (usually more robust) day staffing is a potentially favorable intervention.[13]
We observed a statistically significant reduction of highest frequency peaks of ED admissions. It appears that opening beds up earlier in the day through DBN may help level the load of admissions from the ED. There was no effect on highest frequency peaks of transfer admissions to the floor. This may be due to the timing of transfers being dependent on factors other than bed availability, such as timing of transportation to the hospital or the timing of planned treatment.
We also found that the DBN intervention has created sustainable increases in the DBN rate. Since our initial publication, we have received direct communication from physicians, administrators and managers in 6 different states and 2 foreign countries asking for additional information or reporting that their hospitals are pursuing similar goals. Some of the most common questions asked include: Are your results sustained? and What do you think is a reasonable DBN goal? We have attempted to answer both of these questions. We previously reported improvement to an average DBN rate of 38% over the first 13 intervention months. With more time, we now see an absolute DBN rate of 35%. In November 2014, we restructured our medicine service to become geographic, so that the same group of doctors, trainees, nurses, care managers, and social workers care for patients on a single ward. Since this initiative, our DBN rate has climbed to greater than 40%. We hope to report further on this new intervention in the future. Similar hospital centers can consider using our experience on an inpatient acute‐care medical unit in an urban environment as a benchmark for setting hospital metric goals for early‐in‐the‐day discharge.
Several studies have previously reported on early‐in‐the‐day discharge initiatives. These were smaller studies that focused on descriptions of the type of intervention, including a discharge brunch on an obstetrics floor,[8] scheduled discharges,[6] in‐room displays of expected day and time of discharge,[9] and a physician‐centered discharge process.[7] Our study is substantially larger, focused on inpatient medicine units, and reports the effect of significant changes in DBN on patient and hospital metrics.
Our study had several limitations. The study is based in a single site, potentially limiting the generalizability of our findings. The hospital underwent tremendous change during the course of the intervention, including its temporary closure due to Hurricane Sandy. We cannot exclude effects related to shifts in volume and possible differences in the pre‐ and post‐time period patient populations. The prior study evaluated the population of discharged patients, but the admission analysis in this study involves the population of admitted patients. There may be slight differences in the populations due to the inclusion of patients who were admitted but not discharged from the units (for instance due to transfer after admission). Though the findings on admission arrival time correlate well with the increasing DBN rates, as they occur during the same time and in the same direction (earlier in the day), we are unable to conclude if the effect is causative. There were many interventions ongoing throughout the hospital to improve throughput, and these programs could have created local trends that confound our data. We are also unable to evaluate the clinical significance of a 1‐hour shift in median admission arrival time. Each hospital system must determine for itself if the time and resource investment in DBN is worth the change in admission timing described. We completed this analysis with the perspective of the inpatient medical unit experience, including the timing and number of admissions arriving to the units. We cannot exclude the possibility that changes in arrival times or boarding trends in the ED contribute to our findings.
CONCLUSION
In our hospital, a successful DBN initiative correlates with movement of ED admissions and transfers onto the inpatient units earlier in the day. There was a leveling of the load for ED admissions over the same time period. DBN continues to be an achievable hospital goal, and we provide a potential benchmark for similar hospitals.
Disclosure
Nothing to report.
- , , , Impact of admission and discharge peak times on hospital overcrowding. Stud Health Technol Inform. 2011;168:82–88.
- , , , et al. Time series analysis of emergency department length of stay per 8‐hour shift. West J Emerg Med. 2012;13(2):163–168.
- , , , , , Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med. 2013;44(1):230–235.
- , Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–68.
- , , , et al. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210–214.
- , , All roads lead to scheduled discharges. Nursing. 2008;38(12):61–63.
- , , , Discharging patients earlier in the day: a concept worth evaluating. Health Care Manag (Frederick). 2007;26(2):142–146.
- , The discharge brunch: reducing chaos and increasing smiles on the OB unit. Nurs Womens Health. 2009;13(5):402–409.
- , , , et al. In‐room display of day and time patient is anticipated to leave hospital: a “discharge appointment”. J Hosp Med. 2007;2(1):13–16.
- , , , , , Emergency department crowding: factors influencing flow. West J Emerg Med. 2010;11(1):10–15.
- The Toyota Way: 14 Management Principles From the World's Greatest Manufacturer. New York, NY: McGraw‐Hill; 2004.
- Comparing Distributions. New York, NY: Springer; 2010.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299(7):785–792.
It is thought that late afternoon hospital discharges create admission bottlenecks in the emergency department (ED).[1] As hospital occupancy increases, so too does ED boarding time.[2] Increased ED boarding time can result in increased length of stay (LOS)[3] and reduced patient and staff satisfaction.[4] Early in the day discharge programs are intended to improve hospital throughput.[5, 6, 7, 8, 9] Yet, ED admission timing is, in part, determined by external fluctuations in ED volume and acuity that early discharges do not impact.[10] We previously reported that high levels of discharge before noon (DBN) from inpatient medicine units is achievable through a multidisciplinary intervention.[5] We now evaluate the effect of this intervention upon admission patterns and the sustainability of the DBN initiative.
The DBN intervention consisted of afternoon interdisciplinary rounds, a checklist of team members' responsibilities, a standardized electronic communication tool, and daily feedback on the DBN rate.[5] The intervention resulted in an increase in the DBN rate from 11% to 38% in the first 13 months. We previously reported effects upon the discharged patient as measured by the observed to expected length of stay (O:E LOS) and 30‐day readmission rate. We now assess the effect of our DBN initiative on the subsequent patient and hospital throughput. Our objectives for this study were: (1) to determine the effect of DBN on the admission arrival times and admissions per hour to the units, and (2) in a separate data collection and analysis, to determine if the increased DBN rate is sustainable. We hypothesize that DBN results in admissions arriving onto the units earlier in the day. We further hypothesize that because of this redistribution, DBN will level the load of admissions, reducing admissions per hour peaks that can occur late in the day.
METHODS
Study Design, Participants, and Setting
This is a pre‐/postretrospective analysis evaluating the effect of a previously described DBN intervention.[5] Two inpatient acute‐care medicine units at NYU Langone Medical Center's Tisch Hospital, a 725‐bed, urban, academic medical center, were included in the analysis. All patients admitted to the units underwent the intervention.
Intervention
The DBN intervention began with a multidisciplinary kickoff event in which all team members received education on the importance of DBN, a clear description of roles in the DBN process, and a corresponding checklist of responsibilities. The checklist was utilized at new afternoon interdisciplinary rounds intended to identify next‐day DBNs. Patients identified in afternoon interdisciplinary rounds were logged in a DBN website that generated twice‐daily automated emails to communicate the planned DBN list to frontline staff and key stakeholders. Daily, real‐time feedback on the DBN rate was provided to floor staff.
Measures
Admission Arrival Time
The arrival location and time to any hospital area (ED, radiology, inpatient medical unit) is recorded in the electronic medical record (Epic, Madison, WI) at the time the patient arrives by the patient unit assistant or unit clerk. We obtained the arrival time to each hospital unit throughout the patient's hospitalization for all patients arriving to the study units during their hospitalization between June 1, 2011 and March 4, 2012 (the baseline period) and March 5, 2012 and June 31, 2013 (the intervention period). Data from October 25, 2012 to the end of January 2013 were excluded due to hospital closure from Hurricane Sandy. These time periods and exclusions match those used in our previous DBN article.[5] To match that study's criteria, we excluded patients on the units in the patient class observation, inpatient hospice, and those patients whose discharge disposition was expired or hospice.
ED Admissions
All patients with a first inpatient unit location of ED and no other inpatient unit location prior to arrival on the study units were included in the ED admission analysis. Units that treat but do not provide long‐term boarding/housing of inpatientssuch as radiology, hemodialysis, and cardiac catheterizationwere not considered in determining ED admission status. Even if a patient had recorded arrival to those areas between ED and study unit arrival, these patients were considered ED admissions, as they were never admitted to another inpatient unit.
Transfers and Direct Admissions
All patients whose first inpatient unit location was the study units were included in the transfers and direct admissions analysis. Those patients who were recorded as coming from another inpatient unit (such as another medical, surgical, step‐down, intensive care, or other specialty unit) prior to study unit arrival were included as intrahospital transfers.
Level Load of Admissions
Level loading is a lean methodology term that describes reducing the unevenness in a production line to enhance efficiency.[11] We evaluated this by comparing the admissions per hour (density distribution) to the studied units in the pre‐ and postintervention periods.
Sustainability of the DBN Intervention
The DBN intervention, as described in our original article, continues uninterrupted. Using the same methodology, inclusion criteria, exclusion criteria, and data analysis previously described, we gathered the discharge date and time as recorded by the patient unit assistant for all patients discharged from the study units for the 18 months (July 1, 2013 to December 31, 2014) after our original article to evaluate the sustainability of our improvement in DBN rates.
Statistical Analysis
Median admission time to the floor was compared between the 2 time periods using the Wilcoxon rank sum test. This is a non parametric test of the null hypothesis that the two time periods have the same distributions of admission time to the floor. To evaluate statistical significance, each admission time is arranged in order of magnitude and assigned a rank. The sum of the ranks for each group is calculated and the smaller rank sum (the W statistic) is compared to an expected range of values based on the sample sizes. If this value is out of range then one can reject the null hypothesis. The density distributions of admissions during the 2 time periods were compared using the Kolmogorov‐Smirnov test. The 2‐sided Kolmogorov‐Smirnov test evaluates the maximum distance (D) between the distributions of 2 samples.[12] We chose this test because it evaluates differences between both the position and shape of the distributions of the samples.
RESULTS
Setting Characteristics
The units had an average occupancy rate of 86.8% for the duration of the study. The average number of total discharges per day was 9.8. The average absolute length of stay was 5.6 days.
Admission Arrival Time to the Unit
ED Admissions
A total of 6566 patients were admitted from the ED to the units, 2756 in the baseline period and 3810 in the intervention period. The median arrival time to the units of ED admissions grouped by hour of the day moved by 1 hour, from 5 pm to 4 pm from the baseline to intervention period, and this change was statistically significant (W=16,211,778, P<0.01) (Figure 1).
Transfers and Direct Admissions
A total of 823 patients were transferred or directly admitted to the units, 310 in the baseline period and 513 in the intervention period. The median arrival time to the units grouped by hour of the day moved 1 hour from 5 pm to 4 pm, and this change was statistically significant (W=324,532, P<0.01) (Figure 2).
Level Load of Admissions
In the baseline period, the highest density of ED admissions occurred during the 5‐hour period from 5 pm to 10 pm, when 42.3% of daily admissions arrived (Figure 3). In the intervention period, the highest density of admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 40.0% of daily admissions arrived. The difference between the density distributions for the 2 time periods was found to be statistically significant using the Kolmogorov‐Smirnov test (D=0.03, P<0.01).
In the baseline period, the highest density of transfers and direct admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 51.7% of daily admissions arrived (Figure 3). In the intervention time period, the highest density of transfers and direct admissions occurred during the 5‐hour time period from 2 pm to 7 pm, when 50.3% of daily admissions arrived. The difference between the density distributions of transfers and direct admissions for the 2 time periods was not statistically significant using the Kolmogorov‐Smirnov test (D=0.04, P=0.3).
Sustainability of the DBN Intervention
For the 18 months after the prior reported DBN intervention period, an additional 5505 total discharges were included for analysis. Of these, 1796 were DBN. The average DBN rate for the study units from March 5, 2012 until December 31, 2014 (the original intervention period plus the additional 18 months of new data) is 35% (Figure 4).
DISCUSSION
The potential effects of DBN are multiple. By reducing the O:E LOS and allowing patients the time to acquire their medications, make follow‐up appointments, and ask questions while providers are still in the hospital, our DBN initiative impacts the discharged patient's quality, safety, and efficiency of care.[5] We now report how the DBN initiative potentially impacts the subsequent patient's efficiency of care and hospital throughput. In addition, we show that the DBN initiative is sustainable over years.
Over the same time course as our initial DBN intervention, we found a statistically significant change in the time when admitted patients arrive on the floor. This was true of those patients admitted through the ED and those directly admitted to the floor. In a complex hospital system with many factors both internal (bed cleaning, patient transportation) and external (natural variations in ED volume and acuity) affecting the timing of admissions, it is important to note that increasing the DBN rate correlates with a change in median admission arrival time. From a patient safety standpoint, any initiative that moves admissions away from evening and night hours and takes advantage of (usually more robust) day staffing is a potentially favorable intervention.[13]
We observed a statistically significant reduction of highest frequency peaks of ED admissions. It appears that opening beds up earlier in the day through DBN may help level the load of admissions from the ED. There was no effect on highest frequency peaks of transfer admissions to the floor. This may be due to the timing of transfers being dependent on factors other than bed availability, such as timing of transportation to the hospital or the timing of planned treatment.
We also found that the DBN intervention has created sustainable increases in the DBN rate. Since our initial publication, we have received direct communication from physicians, administrators and managers in 6 different states and 2 foreign countries asking for additional information or reporting that their hospitals are pursuing similar goals. Some of the most common questions asked include: Are your results sustained? and What do you think is a reasonable DBN goal? We have attempted to answer both of these questions. We previously reported improvement to an average DBN rate of 38% over the first 13 intervention months. With more time, we now see an absolute DBN rate of 35%. In November 2014, we restructured our medicine service to become geographic, so that the same group of doctors, trainees, nurses, care managers, and social workers care for patients on a single ward. Since this initiative, our DBN rate has climbed to greater than 40%. We hope to report further on this new intervention in the future. Similar hospital centers can consider using our experience on an inpatient acute‐care medical unit in an urban environment as a benchmark for setting hospital metric goals for early‐in‐the‐day discharge.
Several studies have previously reported on early‐in‐the‐day discharge initiatives. These were smaller studies that focused on descriptions of the type of intervention, including a discharge brunch on an obstetrics floor,[8] scheduled discharges,[6] in‐room displays of expected day and time of discharge,[9] and a physician‐centered discharge process.[7] Our study is substantially larger, focused on inpatient medicine units, and reports the effect of significant changes in DBN on patient and hospital metrics.
Our study had several limitations. The study is based in a single site, potentially limiting the generalizability of our findings. The hospital underwent tremendous change during the course of the intervention, including its temporary closure due to Hurricane Sandy. We cannot exclude effects related to shifts in volume and possible differences in the pre‐ and post‐time period patient populations. The prior study evaluated the population of discharged patients, but the admission analysis in this study involves the population of admitted patients. There may be slight differences in the populations due to the inclusion of patients who were admitted but not discharged from the units (for instance due to transfer after admission). Though the findings on admission arrival time correlate well with the increasing DBN rates, as they occur during the same time and in the same direction (earlier in the day), we are unable to conclude if the effect is causative. There were many interventions ongoing throughout the hospital to improve throughput, and these programs could have created local trends that confound our data. We are also unable to evaluate the clinical significance of a 1‐hour shift in median admission arrival time. Each hospital system must determine for itself if the time and resource investment in DBN is worth the change in admission timing described. We completed this analysis with the perspective of the inpatient medical unit experience, including the timing and number of admissions arriving to the units. We cannot exclude the possibility that changes in arrival times or boarding trends in the ED contribute to our findings.
CONCLUSION
In our hospital, a successful DBN initiative correlates with movement of ED admissions and transfers onto the inpatient units earlier in the day. There was a leveling of the load for ED admissions over the same time period. DBN continues to be an achievable hospital goal, and we provide a potential benchmark for similar hospitals.
Disclosure
Nothing to report.
It is thought that late afternoon hospital discharges create admission bottlenecks in the emergency department (ED).[1] As hospital occupancy increases, so too does ED boarding time.[2] Increased ED boarding time can result in increased length of stay (LOS)[3] and reduced patient and staff satisfaction.[4] Early in the day discharge programs are intended to improve hospital throughput.[5, 6, 7, 8, 9] Yet, ED admission timing is, in part, determined by external fluctuations in ED volume and acuity that early discharges do not impact.[10] We previously reported that high levels of discharge before noon (DBN) from inpatient medicine units is achievable through a multidisciplinary intervention.[5] We now evaluate the effect of this intervention upon admission patterns and the sustainability of the DBN initiative.
The DBN intervention consisted of afternoon interdisciplinary rounds, a checklist of team members' responsibilities, a standardized electronic communication tool, and daily feedback on the DBN rate.[5] The intervention resulted in an increase in the DBN rate from 11% to 38% in the first 13 months. We previously reported effects upon the discharged patient as measured by the observed to expected length of stay (O:E LOS) and 30‐day readmission rate. We now assess the effect of our DBN initiative on the subsequent patient and hospital throughput. Our objectives for this study were: (1) to determine the effect of DBN on the admission arrival times and admissions per hour to the units, and (2) in a separate data collection and analysis, to determine if the increased DBN rate is sustainable. We hypothesize that DBN results in admissions arriving onto the units earlier in the day. We further hypothesize that because of this redistribution, DBN will level the load of admissions, reducing admissions per hour peaks that can occur late in the day.
METHODS
Study Design, Participants, and Setting
This is a pre‐/postretrospective analysis evaluating the effect of a previously described DBN intervention.[5] Two inpatient acute‐care medicine units at NYU Langone Medical Center's Tisch Hospital, a 725‐bed, urban, academic medical center, were included in the analysis. All patients admitted to the units underwent the intervention.
Intervention
The DBN intervention began with a multidisciplinary kickoff event in which all team members received education on the importance of DBN, a clear description of roles in the DBN process, and a corresponding checklist of responsibilities. The checklist was utilized at new afternoon interdisciplinary rounds intended to identify next‐day DBNs. Patients identified in afternoon interdisciplinary rounds were logged in a DBN website that generated twice‐daily automated emails to communicate the planned DBN list to frontline staff and key stakeholders. Daily, real‐time feedback on the DBN rate was provided to floor staff.
Measures
Admission Arrival Time
The arrival location and time to any hospital area (ED, radiology, inpatient medical unit) is recorded in the electronic medical record (Epic, Madison, WI) at the time the patient arrives by the patient unit assistant or unit clerk. We obtained the arrival time to each hospital unit throughout the patient's hospitalization for all patients arriving to the study units during their hospitalization between June 1, 2011 and March 4, 2012 (the baseline period) and March 5, 2012 and June 31, 2013 (the intervention period). Data from October 25, 2012 to the end of January 2013 were excluded due to hospital closure from Hurricane Sandy. These time periods and exclusions match those used in our previous DBN article.[5] To match that study's criteria, we excluded patients on the units in the patient class observation, inpatient hospice, and those patients whose discharge disposition was expired or hospice.
ED Admissions
All patients with a first inpatient unit location of ED and no other inpatient unit location prior to arrival on the study units were included in the ED admission analysis. Units that treat but do not provide long‐term boarding/housing of inpatientssuch as radiology, hemodialysis, and cardiac catheterizationwere not considered in determining ED admission status. Even if a patient had recorded arrival to those areas between ED and study unit arrival, these patients were considered ED admissions, as they were never admitted to another inpatient unit.
Transfers and Direct Admissions
All patients whose first inpatient unit location was the study units were included in the transfers and direct admissions analysis. Those patients who were recorded as coming from another inpatient unit (such as another medical, surgical, step‐down, intensive care, or other specialty unit) prior to study unit arrival were included as intrahospital transfers.
Level Load of Admissions
Level loading is a lean methodology term that describes reducing the unevenness in a production line to enhance efficiency.[11] We evaluated this by comparing the admissions per hour (density distribution) to the studied units in the pre‐ and postintervention periods.
Sustainability of the DBN Intervention
The DBN intervention, as described in our original article, continues uninterrupted. Using the same methodology, inclusion criteria, exclusion criteria, and data analysis previously described, we gathered the discharge date and time as recorded by the patient unit assistant for all patients discharged from the study units for the 18 months (July 1, 2013 to December 31, 2014) after our original article to evaluate the sustainability of our improvement in DBN rates.
Statistical Analysis
Median admission time to the floor was compared between the 2 time periods using the Wilcoxon rank sum test. This is a non parametric test of the null hypothesis that the two time periods have the same distributions of admission time to the floor. To evaluate statistical significance, each admission time is arranged in order of magnitude and assigned a rank. The sum of the ranks for each group is calculated and the smaller rank sum (the W statistic) is compared to an expected range of values based on the sample sizes. If this value is out of range then one can reject the null hypothesis. The density distributions of admissions during the 2 time periods were compared using the Kolmogorov‐Smirnov test. The 2‐sided Kolmogorov‐Smirnov test evaluates the maximum distance (D) between the distributions of 2 samples.[12] We chose this test because it evaluates differences between both the position and shape of the distributions of the samples.
RESULTS
Setting Characteristics
The units had an average occupancy rate of 86.8% for the duration of the study. The average number of total discharges per day was 9.8. The average absolute length of stay was 5.6 days.
Admission Arrival Time to the Unit
ED Admissions
A total of 6566 patients were admitted from the ED to the units, 2756 in the baseline period and 3810 in the intervention period. The median arrival time to the units of ED admissions grouped by hour of the day moved by 1 hour, from 5 pm to 4 pm from the baseline to intervention period, and this change was statistically significant (W=16,211,778, P<0.01) (Figure 1).
Transfers and Direct Admissions
A total of 823 patients were transferred or directly admitted to the units, 310 in the baseline period and 513 in the intervention period. The median arrival time to the units grouped by hour of the day moved 1 hour from 5 pm to 4 pm, and this change was statistically significant (W=324,532, P<0.01) (Figure 2).
Level Load of Admissions
In the baseline period, the highest density of ED admissions occurred during the 5‐hour period from 5 pm to 10 pm, when 42.3% of daily admissions arrived (Figure 3). In the intervention period, the highest density of admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 40.0% of daily admissions arrived. The difference between the density distributions for the 2 time periods was found to be statistically significant using the Kolmogorov‐Smirnov test (D=0.03, P<0.01).
In the baseline period, the highest density of transfers and direct admissions occurred during the 5‐hour period from 3 pm to 8 pm, when 51.7% of daily admissions arrived (Figure 3). In the intervention time period, the highest density of transfers and direct admissions occurred during the 5‐hour time period from 2 pm to 7 pm, when 50.3% of daily admissions arrived. The difference between the density distributions of transfers and direct admissions for the 2 time periods was not statistically significant using the Kolmogorov‐Smirnov test (D=0.04, P=0.3).
Sustainability of the DBN Intervention
For the 18 months after the prior reported DBN intervention period, an additional 5505 total discharges were included for analysis. Of these, 1796 were DBN. The average DBN rate for the study units from March 5, 2012 until December 31, 2014 (the original intervention period plus the additional 18 months of new data) is 35% (Figure 4).
DISCUSSION
The potential effects of DBN are multiple. By reducing the O:E LOS and allowing patients the time to acquire their medications, make follow‐up appointments, and ask questions while providers are still in the hospital, our DBN initiative impacts the discharged patient's quality, safety, and efficiency of care.[5] We now report how the DBN initiative potentially impacts the subsequent patient's efficiency of care and hospital throughput. In addition, we show that the DBN initiative is sustainable over years.
Over the same time course as our initial DBN intervention, we found a statistically significant change in the time when admitted patients arrive on the floor. This was true of those patients admitted through the ED and those directly admitted to the floor. In a complex hospital system with many factors both internal (bed cleaning, patient transportation) and external (natural variations in ED volume and acuity) affecting the timing of admissions, it is important to note that increasing the DBN rate correlates with a change in median admission arrival time. From a patient safety standpoint, any initiative that moves admissions away from evening and night hours and takes advantage of (usually more robust) day staffing is a potentially favorable intervention.[13]
We observed a statistically significant reduction of highest frequency peaks of ED admissions. It appears that opening beds up earlier in the day through DBN may help level the load of admissions from the ED. There was no effect on highest frequency peaks of transfer admissions to the floor. This may be due to the timing of transfers being dependent on factors other than bed availability, such as timing of transportation to the hospital or the timing of planned treatment.
We also found that the DBN intervention has created sustainable increases in the DBN rate. Since our initial publication, we have received direct communication from physicians, administrators and managers in 6 different states and 2 foreign countries asking for additional information or reporting that their hospitals are pursuing similar goals. Some of the most common questions asked include: Are your results sustained? and What do you think is a reasonable DBN goal? We have attempted to answer both of these questions. We previously reported improvement to an average DBN rate of 38% over the first 13 intervention months. With more time, we now see an absolute DBN rate of 35%. In November 2014, we restructured our medicine service to become geographic, so that the same group of doctors, trainees, nurses, care managers, and social workers care for patients on a single ward. Since this initiative, our DBN rate has climbed to greater than 40%. We hope to report further on this new intervention in the future. Similar hospital centers can consider using our experience on an inpatient acute‐care medical unit in an urban environment as a benchmark for setting hospital metric goals for early‐in‐the‐day discharge.
Several studies have previously reported on early‐in‐the‐day discharge initiatives. These were smaller studies that focused on descriptions of the type of intervention, including a discharge brunch on an obstetrics floor,[8] scheduled discharges,[6] in‐room displays of expected day and time of discharge,[9] and a physician‐centered discharge process.[7] Our study is substantially larger, focused on inpatient medicine units, and reports the effect of significant changes in DBN on patient and hospital metrics.
Our study had several limitations. The study is based in a single site, potentially limiting the generalizability of our findings. The hospital underwent tremendous change during the course of the intervention, including its temporary closure due to Hurricane Sandy. We cannot exclude effects related to shifts in volume and possible differences in the pre‐ and post‐time period patient populations. The prior study evaluated the population of discharged patients, but the admission analysis in this study involves the population of admitted patients. There may be slight differences in the populations due to the inclusion of patients who were admitted but not discharged from the units (for instance due to transfer after admission). Though the findings on admission arrival time correlate well with the increasing DBN rates, as they occur during the same time and in the same direction (earlier in the day), we are unable to conclude if the effect is causative. There were many interventions ongoing throughout the hospital to improve throughput, and these programs could have created local trends that confound our data. We are also unable to evaluate the clinical significance of a 1‐hour shift in median admission arrival time. Each hospital system must determine for itself if the time and resource investment in DBN is worth the change in admission timing described. We completed this analysis with the perspective of the inpatient medical unit experience, including the timing and number of admissions arriving to the units. We cannot exclude the possibility that changes in arrival times or boarding trends in the ED contribute to our findings.
CONCLUSION
In our hospital, a successful DBN initiative correlates with movement of ED admissions and transfers onto the inpatient units earlier in the day. There was a leveling of the load for ED admissions over the same time period. DBN continues to be an achievable hospital goal, and we provide a potential benchmark for similar hospitals.
Disclosure
Nothing to report.
- , , , Impact of admission and discharge peak times on hospital overcrowding. Stud Health Technol Inform. 2011;168:82–88.
- , , , et al. Time series analysis of emergency department length of stay per 8‐hour shift. West J Emerg Med. 2012;13(2):163–168.
- , , , , , Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med. 2013;44(1):230–235.
- , Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–68.
- , , , et al. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210–214.
- , , All roads lead to scheduled discharges. Nursing. 2008;38(12):61–63.
- , , , Discharging patients earlier in the day: a concept worth evaluating. Health Care Manag (Frederick). 2007;26(2):142–146.
- , The discharge brunch: reducing chaos and increasing smiles on the OB unit. Nurs Womens Health. 2009;13(5):402–409.
- , , , et al. In‐room display of day and time patient is anticipated to leave hospital: a “discharge appointment”. J Hosp Med. 2007;2(1):13–16.
- , , , , , Emergency department crowding: factors influencing flow. West J Emerg Med. 2010;11(1):10–15.
- The Toyota Way: 14 Management Principles From the World's Greatest Manufacturer. New York, NY: McGraw‐Hill; 2004.
- Comparing Distributions. New York, NY: Springer; 2010.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299(7):785–792.
- , , , Impact of admission and discharge peak times on hospital overcrowding. Stud Health Technol Inform. 2011;168:82–88.
- , , , et al. Time series analysis of emergency department length of stay per 8‐hour shift. West J Emerg Med. 2012;13(2):163–168.
- , , , , , Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med. 2013;44(1):230–235.
- , Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–68.
- , , , et al. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210–214.
- , , All roads lead to scheduled discharges. Nursing. 2008;38(12):61–63.
- , , , Discharging patients earlier in the day: a concept worth evaluating. Health Care Manag (Frederick). 2007;26(2):142–146.
- , The discharge brunch: reducing chaos and increasing smiles on the OB unit. Nurs Womens Health. 2009;13(5):402–409.
- , , , et al. In‐room display of day and time patient is anticipated to leave hospital: a “discharge appointment”. J Hosp Med. 2007;2(1):13–16.
- , , , , , Emergency department crowding: factors influencing flow. West J Emerg Med. 2010;11(1):10–15.
- The Toyota Way: 14 Management Principles From the World's Greatest Manufacturer. New York, NY: McGraw‐Hill; 2004.
- Comparing Distributions. New York, NY: Springer; 2010.
- , , , et al. Survival from in‐hospital cardiac arrest during nights and weekends. JAMA. 2008;299(7):785–792.
© 2015 Society of Hospital Medicine
Nebulized Bronchodilator Instead of MDI
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CASE PRESENTATION
A 54‐year‐old woman presented to the emergency department (ED) with shortness of breath. She reported that her primary care physician diagnosed her with chronic obstructive pulmonary disease (COPD). Her physician had prescribed her an albuterol inhaler to use as needed for shortness of breath. Over the past few weeks she had been trying to use the inhaler, but she noted that it did not seem to help her increasing wheezing, coughing, and sputum production. In the ED, she received continuous albuterol treatments via nebulizer, Solu‐Medrol 125 mg intravenously, antibiotics, and a chest x‐ray. She was admitted to the hospital medicine service for COPD exacerbation and started on nebulized bronchodilator treatments every 4 hours. By the fourth day of her hospital stay, she was discharged to home with an albuterol inhaler, oral prednisone, oral doxycycline, and a follow‐up appointment. Dedicated patient education regarding proper inhaler administration did not occur during hospitalization.
WHY YOU MIGHT THINK NEBULIZED TREATMENTS IN INPATIENTS ARE HELPFUL
Inhaled bronchodilators are a mainstay of therapy for acute obstructive pulmonary diseases, including COPD and asthma exacerbations.[1, 2] Inhaled bronchodilators may be delivered by metered‐dose inhalers (MDIs) or via wet nebulizers powered by compressed air or oxygen. Current practice patterns in EDs and hospital wards tend to favor the use of nebulizers due to many apparent advantages of these devices.[3] For instance, nebulizers do not require any special inhalation technique and can be effectively used by patients at any age.[3, 4] There is also a common perception that nebulizers are more effective, possibly stemming from the assumption that hospitalized patients have already failed their outpatient MDI therapy and an almost mystical belief in the healing power of mist. Moreover, many clinicians have been trained to routinely use nebulizer therapies and may lack sufficient knowledge or comfort about the relative efficacy and equivalence dosing of MDI therapies.
WHY NEBULIZERS ARE NOT BETTER THAN MDIs FOR PATIENTS HOSPITALIZED WITH OBSTRUCTIVE PULMONARY SYMPTOMS
Decades of research support that MDIs are effective, efficient, and less costly (depending on circumstances) than nebulizers for the routine treatment of obstructive pulmonary exacerbations.[3, 4, 5, 6, 7, 8, 9, 10, 11] The clinical effectiveness of MDIs has been shown in studies across populations of adults with acute COPD symptoms,[3, 4, 7, 8] as well as children and adults with asthma exacerbations.[3, 4, 5, 6, 9, 10] A 2005 joint report by the American College of Chest Physicians (ACCP) and the American College of Asthma, Allergy and Immunology (ACAAI), concluded none of the pooled meta‐analyses showed a significant difference between devices in any efficacy outcome in any patient group for each of the clinical settings.[4] Many different outcomes have been investigated, including forced expiratory volumes (FEV), peak flows, symptoms and specific symptom scores, and physical findings.[4]
Compared to MDIs, there are a number of drawbacks to the use of nebulizers: nebulizers are more expensive to buy and maintain, are less portable, and take longer to set up, use, and clean following each use.[12] In addition, nebulizers have been associated with greater increases in heart rate and tremors compared to MDIs, suggesting nebulizers lead to higher systemically absorbed ‐agonist doses.[4]
Of note, nearly all of the clinical effectiveness studies administered MDIs with a valved holding chamber or spacer, facilitating the delivery of drug to the airways.[3, 4] Although valved holding chambers are commonly referred to as a spacer, a true spacer does not have a valve and is rarely used today.[12]
THE EVIDENCE EXAMINING NEBULIZERS VERSUS MDIs IN PATIENTS WITH ASTHMA OR COPD EXACERBATIONS
A 2013 Cochrane review sought to establish the relative efficacy of MDIs with holding chambers versus nebulizers for children and adults who presented to a community setting or emergency department with acute asthma.[6] The review included a total of 1897 children and 729 adults in 39 randomized controlled trials. The authors judged the overall evidence to be of moderate quality. Children with acute asthma treated with MDIs in the ED had shorter lengths of stay in the ED (70 minutes vs 103 minutes), similar peak flow and FEV measurements, lower heart rates, and less tremor compared to children treated with nebulizers.[5, 6] There were no significant differences found between devices for the treatment of adult patients with asthma.[6]
In a separate double‐blind, randomized, placebo‐controlled study evaluating albuterol administered by nebulizer versus MDI with spacer for children <2 years old presenting to an ED with wheezing, the use of MDIs with a spacer and facemask was equally efficacious and may have led to fewer hospital admissions.[10]
Mandelberg et al. performed a double‐blind, randomized, placebo‐controlled trial for unselected adult patients presenting to an ED with obstructive pulmonary symptoms.[8] Patients received either 2 puffs of a placebo MDI with a spacer along with nebulized salbutamol 0.5 mL in 1.5 mL saline solution (n=25), or a salbutamol MDI along with a nebulized placebo saline solution (n=25). Treatments were repeated every 15 minutes up to 3 times, unless side effects occurred. Spirometric measurements were performed following each treatment. No differences were seen between the groups at any point during the study period. The authors concluded, Even in the setting of the unselected group of patient referrals to the [Department of Emergency Medicine] for episodes of severe airflow limitation, the clinical and objective bronchodilator responses to the administration of salbutamol are independent of the method of delivery: MDI with large spacer or aerosol nebulization.[8]
There are surprisingly few studies examining the use of nebulizers versus MDIs in the inpatient setting for both children and adults. Dolovich et al. reviewed 6 studies that included 253 total patients and reported no significant differences in pulmonary function between devices.[4] Based on these findings, the ACCP/ACAAI group recommended both nebulizers and MDIs with spacers/holding chambers are appropriate for use in the inpatient setting. Quality of evidence: good.[4]
WHY USE MDIs FOR INPATIENTS
If MDI and nebulizer treatments are equally effective, why change current practice? The use of MDIs, rather than nebulizers, in hospitals could lead to fewer side effects such as tachycardia, arrhythmias, and tremors. MDIs are also more portable and do not require specialized set‐up. Furthermore, MDI administrations during hospitalization may provide a golden opportunity to have respiratory therapists, pharmacists, or other health professionals spend time teaching patients proper inhaler usage, rather than providing time‐consuming nebulizer treatments.[13] In a recent study, approximately 86% of hospitalized patients with asthma or COPD could not demonstrate appropriate use of an MDI. However, 100% of patients were able to achieve mastery following a short teach‐back session.[14] It is conceivable that transitioning patients to MDIs earlier during hospitalization and providing them with education regarding proper MDI administration could instill confidence in their use of inhalers and result in downstream effects such as shorter lengths of stay, less frequent hospital readmissions, or improved quality of life.
MDI use may result in cost savings in certain settings, although the relative costs of nebulizer versus MDI treatments depends on many institution‐specific factors. Such factors include the institutional policies on who delivers the nebulizer or the MDI and how they are compensated and staffed. For example in the Nebs No More After 24 program initiated at the University of California, San Francisco, the vast majority of the realized cost savings are due to the reduction in respiratory therapist time spent delivering MDIs, which reflects the local policies and compensation structure.[13] Previous inpatient interventions to convert from nebulizers to MDIs also showed cost savings resulting from decreased labor needs.[15] In some hospitals, nurses deliver nebulizer treatments, whereas in others only respiratory therapists are allowed to provide nebulizers. Moreover, whether the MDI can go home with the patient upon discharge depends on whether the hospital has a dispensing pharmacy or not. Formal economic evaluations specific to the local institution are necessary.
WHAT WE SHOULD DO INSTEAD: ENCOURAGE THE USE OF MDIs FOR INPATIENTS
For effective inpatient MDI treatments, MDI technique must be good. Thus, it is vital to enlist the right people to provide proper MDI teaching and supervision. Respiratory therapists are generally trained for this task, and may be complemented by appropriately trained physicians, nurses, or pharmacists. Many institutions have successfully implemented respiratory therapist‐driven protocols for the administration of MDIs, which has led to measurable improvements in the utilization of appropriate respiratory care resources.[15, 16] At University of California, San Francisco, this was accomplished by recruiting respiratory therapists and nurses to help support the transition of patients from nebulizers to MDIs and to provide bedside teaching on proper MDI usage. The institution then launched a Nebs No More After 24 campaign that sought to transition patients from nebulizers to MDIs within 24 hours of hospitalization. This campaign included an educational program for physicians, prepared facilitator guides to assist attending physicians with teaching about the new initiative, publicity efforts including pens and strategically placed posters, and regular feedback regarding nebulizer utilization on the pilot ward. Although the evidence suggests that patients can be started on MDIs immediately upon presentation to the ED, the UCSF campaign focused on transitioning patients within 24 hours so to alleviate concerns about transitions in care between the ED and the medical ward, as well as between overnight and day teams. MDIs are only as or more effective than nebulizers if the correct administration technique is employed. The 24‐hour transition period allows for MDI teaching and transition during regular daytime hours.
Inpatient use of nebulizers may be more appropriate than MDIs for patients with dementia or altered mental status, as well as those in extreme distress resulting in an inability to coordinate inhaler usage. Very low health literacy may be an additional barrier to appropriate MDI teaching and usage.
RECOMMENDATIONS
In patients with obstructive pulmonary symptoms, transition patients from nebulizers to MDIs early in their hospital course, unless the patient is unable to use an inhaler due to altered mental status, dementia, or other circumstances. Ensure that patients are instructed and supervised on proper MDI technique. Enlisting respiratory therapists and appropriately trained staff (pharmacists, nurses, physicians) is key to the successful use of MDIs. Frequency and dosage of MDIs used should be comparable to that of nebulized treatments. Although studies have used a relatively wide range of albuterol MDI dosing, prior programs have determined a dose of albuterol 4 puffs via MDI as being equivalent to the standard albuterol 2.5 mg nebulizer dosage.[17, 18] Some studies have advocated for using a range of 2 to 10 puffs albuterol MDI, with the actual dose based on clinical response.[17] One study in children with mild acute asthma found that 2 puffs of albuterol by MDI was just as effective as higher doses delivered by MDI (610 puffs) or by nebulizer.[19]
CONCLUSION
MDIs with holding chambers are clinically equivalent to nebulizer therapy for the treatment of both children and adults with obstructive pulmonary symptoms, as long as MDI technique and MDI dosing is adequate. This is based on good data in the ED setting but fewer studies in adult inpatients. There are a number of advantages to the use of inpatient MDIs over nebulizers; MDIs are more portable, often less expensive to use, may result in fewer side effects, and will hopefully improve outpatient MDI technique. The delivery of MDIs during hospitalization should be accompanied with patient education regarding proper administration technique.
Disclosure
Nothing to report.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of COPD. Available at: http://www.goldcopd.org/guidelines‐global‐strategy‐for‐diagnosis‐management.html. Updated January 2015. Accessed September 25, 2014.
- National Heart Lung and Blood Institute. National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Published 2007. Updated April 2012. Accessed September 25, 2014.
- , , , Bronchodilator delivery in acute airflow obstruction. A meta‐analysis. Arch Intern Med. 1997;157(15):1736–1744.
- , , , et al. Device selection and outcomes of aerosol therapy: Evidence‐based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335–371.
- , Beta‐agonists through metered‐dose inhaler with valved holding chamber versus nebulizer for acute exacerbation of wheezing or asthma in children under 5 years of age: a systematic review with meta‐analysis. J Pediatr. 2004;145(2):172–177.
- , , Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , , Nebulizer vs spacer for bronchodilator delivery in patients hospitalized for acute exacerbations of COPD. Chest. 1989;96(6):1241–1246.
- , , , Nebulized wet aerosol treatment in emergency department—is it essential? Comparison with large spacer device for metered‐dose inhaler. Chest. 1997;112(6):1501–1505.
- , , , , , Randomized controlled trial of salbutamol aerosol therapy via metered dose inhaler‐spacer vs. jet nebulizer in young children with wheezing. Pediatr Pulmonol. 2005;39(5):466–472.
- , , , Nebulizers vs metered‐dose inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med. 2003;157(1):76–80.
- , , , A review and economic evaluation of bronchodilator delivery methods in hospitalized patients. Arch Intern Med. 1996;156(18):2113–2118.
- , Asthma medication delivery: mists and myths. Paediatr Respir Rev. 2013;14(2):112–118.
- , , , , “Nebs no more after 24”: a pilot program to improve the use of appropriate respiratory therapies. JAMA Intern Med. 2013;173(17):1647–1648.
- , , , et al. Misuse of respiratory inhalers in hospitalized patients with asthma or COPD. J Gen Intern Med. 2011;26(6):635–642.
- , , A model for conversion from small volume nebulizer to metered dose inhaler aerosol therapy. Chest. 1992;101(3):634–637.
- , , Physician‐ordered aerosol therapy versus respiratory therapist‐driven aerosol protocol: the effect on resource utilization. Respir Care. 2013;58(3):431–437.
- , , , Automatic replacement of albuterol nebulizer therapy by metered‐dose inhaler and valved holding chamber. Am J Health Syst Pharm. 2005;62(10):1053–1061.
- , , , , The conversion to metered‐dose inhaler with valved holding chamber to administer inhaled albuterol: a pediatric hospital experience. Respir Care. 2008;53(3):338–345.
- , , , , , Comparison of albuterol delivered by a metered dose inhaler with spacer versus a nebulizer in children with mild acute asthma. J Pediatr. 1999;135(1):22–27.
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CASE PRESENTATION
A 54‐year‐old woman presented to the emergency department (ED) with shortness of breath. She reported that her primary care physician diagnosed her with chronic obstructive pulmonary disease (COPD). Her physician had prescribed her an albuterol inhaler to use as needed for shortness of breath. Over the past few weeks she had been trying to use the inhaler, but she noted that it did not seem to help her increasing wheezing, coughing, and sputum production. In the ED, she received continuous albuterol treatments via nebulizer, Solu‐Medrol 125 mg intravenously, antibiotics, and a chest x‐ray. She was admitted to the hospital medicine service for COPD exacerbation and started on nebulized bronchodilator treatments every 4 hours. By the fourth day of her hospital stay, she was discharged to home with an albuterol inhaler, oral prednisone, oral doxycycline, and a follow‐up appointment. Dedicated patient education regarding proper inhaler administration did not occur during hospitalization.
WHY YOU MIGHT THINK NEBULIZED TREATMENTS IN INPATIENTS ARE HELPFUL
Inhaled bronchodilators are a mainstay of therapy for acute obstructive pulmonary diseases, including COPD and asthma exacerbations.[1, 2] Inhaled bronchodilators may be delivered by metered‐dose inhalers (MDIs) or via wet nebulizers powered by compressed air or oxygen. Current practice patterns in EDs and hospital wards tend to favor the use of nebulizers due to many apparent advantages of these devices.[3] For instance, nebulizers do not require any special inhalation technique and can be effectively used by patients at any age.[3, 4] There is also a common perception that nebulizers are more effective, possibly stemming from the assumption that hospitalized patients have already failed their outpatient MDI therapy and an almost mystical belief in the healing power of mist. Moreover, many clinicians have been trained to routinely use nebulizer therapies and may lack sufficient knowledge or comfort about the relative efficacy and equivalence dosing of MDI therapies.
WHY NEBULIZERS ARE NOT BETTER THAN MDIs FOR PATIENTS HOSPITALIZED WITH OBSTRUCTIVE PULMONARY SYMPTOMS
Decades of research support that MDIs are effective, efficient, and less costly (depending on circumstances) than nebulizers for the routine treatment of obstructive pulmonary exacerbations.[3, 4, 5, 6, 7, 8, 9, 10, 11] The clinical effectiveness of MDIs has been shown in studies across populations of adults with acute COPD symptoms,[3, 4, 7, 8] as well as children and adults with asthma exacerbations.[3, 4, 5, 6, 9, 10] A 2005 joint report by the American College of Chest Physicians (ACCP) and the American College of Asthma, Allergy and Immunology (ACAAI), concluded none of the pooled meta‐analyses showed a significant difference between devices in any efficacy outcome in any patient group for each of the clinical settings.[4] Many different outcomes have been investigated, including forced expiratory volumes (FEV), peak flows, symptoms and specific symptom scores, and physical findings.[4]
Compared to MDIs, there are a number of drawbacks to the use of nebulizers: nebulizers are more expensive to buy and maintain, are less portable, and take longer to set up, use, and clean following each use.[12] In addition, nebulizers have been associated with greater increases in heart rate and tremors compared to MDIs, suggesting nebulizers lead to higher systemically absorbed ‐agonist doses.[4]
Of note, nearly all of the clinical effectiveness studies administered MDIs with a valved holding chamber or spacer, facilitating the delivery of drug to the airways.[3, 4] Although valved holding chambers are commonly referred to as a spacer, a true spacer does not have a valve and is rarely used today.[12]
THE EVIDENCE EXAMINING NEBULIZERS VERSUS MDIs IN PATIENTS WITH ASTHMA OR COPD EXACERBATIONS
A 2013 Cochrane review sought to establish the relative efficacy of MDIs with holding chambers versus nebulizers for children and adults who presented to a community setting or emergency department with acute asthma.[6] The review included a total of 1897 children and 729 adults in 39 randomized controlled trials. The authors judged the overall evidence to be of moderate quality. Children with acute asthma treated with MDIs in the ED had shorter lengths of stay in the ED (70 minutes vs 103 minutes), similar peak flow and FEV measurements, lower heart rates, and less tremor compared to children treated with nebulizers.[5, 6] There were no significant differences found between devices for the treatment of adult patients with asthma.[6]
In a separate double‐blind, randomized, placebo‐controlled study evaluating albuterol administered by nebulizer versus MDI with spacer for children <2 years old presenting to an ED with wheezing, the use of MDIs with a spacer and facemask was equally efficacious and may have led to fewer hospital admissions.[10]
Mandelberg et al. performed a double‐blind, randomized, placebo‐controlled trial for unselected adult patients presenting to an ED with obstructive pulmonary symptoms.[8] Patients received either 2 puffs of a placebo MDI with a spacer along with nebulized salbutamol 0.5 mL in 1.5 mL saline solution (n=25), or a salbutamol MDI along with a nebulized placebo saline solution (n=25). Treatments were repeated every 15 minutes up to 3 times, unless side effects occurred. Spirometric measurements were performed following each treatment. No differences were seen between the groups at any point during the study period. The authors concluded, Even in the setting of the unselected group of patient referrals to the [Department of Emergency Medicine] for episodes of severe airflow limitation, the clinical and objective bronchodilator responses to the administration of salbutamol are independent of the method of delivery: MDI with large spacer or aerosol nebulization.[8]
There are surprisingly few studies examining the use of nebulizers versus MDIs in the inpatient setting for both children and adults. Dolovich et al. reviewed 6 studies that included 253 total patients and reported no significant differences in pulmonary function between devices.[4] Based on these findings, the ACCP/ACAAI group recommended both nebulizers and MDIs with spacers/holding chambers are appropriate for use in the inpatient setting. Quality of evidence: good.[4]
WHY USE MDIs FOR INPATIENTS
If MDI and nebulizer treatments are equally effective, why change current practice? The use of MDIs, rather than nebulizers, in hospitals could lead to fewer side effects such as tachycardia, arrhythmias, and tremors. MDIs are also more portable and do not require specialized set‐up. Furthermore, MDI administrations during hospitalization may provide a golden opportunity to have respiratory therapists, pharmacists, or other health professionals spend time teaching patients proper inhaler usage, rather than providing time‐consuming nebulizer treatments.[13] In a recent study, approximately 86% of hospitalized patients with asthma or COPD could not demonstrate appropriate use of an MDI. However, 100% of patients were able to achieve mastery following a short teach‐back session.[14] It is conceivable that transitioning patients to MDIs earlier during hospitalization and providing them with education regarding proper MDI administration could instill confidence in their use of inhalers and result in downstream effects such as shorter lengths of stay, less frequent hospital readmissions, or improved quality of life.
MDI use may result in cost savings in certain settings, although the relative costs of nebulizer versus MDI treatments depends on many institution‐specific factors. Such factors include the institutional policies on who delivers the nebulizer or the MDI and how they are compensated and staffed. For example in the Nebs No More After 24 program initiated at the University of California, San Francisco, the vast majority of the realized cost savings are due to the reduction in respiratory therapist time spent delivering MDIs, which reflects the local policies and compensation structure.[13] Previous inpatient interventions to convert from nebulizers to MDIs also showed cost savings resulting from decreased labor needs.[15] In some hospitals, nurses deliver nebulizer treatments, whereas in others only respiratory therapists are allowed to provide nebulizers. Moreover, whether the MDI can go home with the patient upon discharge depends on whether the hospital has a dispensing pharmacy or not. Formal economic evaluations specific to the local institution are necessary.
WHAT WE SHOULD DO INSTEAD: ENCOURAGE THE USE OF MDIs FOR INPATIENTS
For effective inpatient MDI treatments, MDI technique must be good. Thus, it is vital to enlist the right people to provide proper MDI teaching and supervision. Respiratory therapists are generally trained for this task, and may be complemented by appropriately trained physicians, nurses, or pharmacists. Many institutions have successfully implemented respiratory therapist‐driven protocols for the administration of MDIs, which has led to measurable improvements in the utilization of appropriate respiratory care resources.[15, 16] At University of California, San Francisco, this was accomplished by recruiting respiratory therapists and nurses to help support the transition of patients from nebulizers to MDIs and to provide bedside teaching on proper MDI usage. The institution then launched a Nebs No More After 24 campaign that sought to transition patients from nebulizers to MDIs within 24 hours of hospitalization. This campaign included an educational program for physicians, prepared facilitator guides to assist attending physicians with teaching about the new initiative, publicity efforts including pens and strategically placed posters, and regular feedback regarding nebulizer utilization on the pilot ward. Although the evidence suggests that patients can be started on MDIs immediately upon presentation to the ED, the UCSF campaign focused on transitioning patients within 24 hours so to alleviate concerns about transitions in care between the ED and the medical ward, as well as between overnight and day teams. MDIs are only as or more effective than nebulizers if the correct administration technique is employed. The 24‐hour transition period allows for MDI teaching and transition during regular daytime hours.
Inpatient use of nebulizers may be more appropriate than MDIs for patients with dementia or altered mental status, as well as those in extreme distress resulting in an inability to coordinate inhaler usage. Very low health literacy may be an additional barrier to appropriate MDI teaching and usage.
RECOMMENDATIONS
In patients with obstructive pulmonary symptoms, transition patients from nebulizers to MDIs early in their hospital course, unless the patient is unable to use an inhaler due to altered mental status, dementia, or other circumstances. Ensure that patients are instructed and supervised on proper MDI technique. Enlisting respiratory therapists and appropriately trained staff (pharmacists, nurses, physicians) is key to the successful use of MDIs. Frequency and dosage of MDIs used should be comparable to that of nebulized treatments. Although studies have used a relatively wide range of albuterol MDI dosing, prior programs have determined a dose of albuterol 4 puffs via MDI as being equivalent to the standard albuterol 2.5 mg nebulizer dosage.[17, 18] Some studies have advocated for using a range of 2 to 10 puffs albuterol MDI, with the actual dose based on clinical response.[17] One study in children with mild acute asthma found that 2 puffs of albuterol by MDI was just as effective as higher doses delivered by MDI (610 puffs) or by nebulizer.[19]
CONCLUSION
MDIs with holding chambers are clinically equivalent to nebulizer therapy for the treatment of both children and adults with obstructive pulmonary symptoms, as long as MDI technique and MDI dosing is adequate. This is based on good data in the ED setting but fewer studies in adult inpatients. There are a number of advantages to the use of inpatient MDIs over nebulizers; MDIs are more portable, often less expensive to use, may result in fewer side effects, and will hopefully improve outpatient MDI technique. The delivery of MDIs during hospitalization should be accompanied with patient education regarding proper administration technique.
Disclosure
Nothing to report.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected]
The Things We Do for No Reason (TWDFNR) series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent black and white conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CASE PRESENTATION
A 54‐year‐old woman presented to the emergency department (ED) with shortness of breath. She reported that her primary care physician diagnosed her with chronic obstructive pulmonary disease (COPD). Her physician had prescribed her an albuterol inhaler to use as needed for shortness of breath. Over the past few weeks she had been trying to use the inhaler, but she noted that it did not seem to help her increasing wheezing, coughing, and sputum production. In the ED, she received continuous albuterol treatments via nebulizer, Solu‐Medrol 125 mg intravenously, antibiotics, and a chest x‐ray. She was admitted to the hospital medicine service for COPD exacerbation and started on nebulized bronchodilator treatments every 4 hours. By the fourth day of her hospital stay, she was discharged to home with an albuterol inhaler, oral prednisone, oral doxycycline, and a follow‐up appointment. Dedicated patient education regarding proper inhaler administration did not occur during hospitalization.
WHY YOU MIGHT THINK NEBULIZED TREATMENTS IN INPATIENTS ARE HELPFUL
Inhaled bronchodilators are a mainstay of therapy for acute obstructive pulmonary diseases, including COPD and asthma exacerbations.[1, 2] Inhaled bronchodilators may be delivered by metered‐dose inhalers (MDIs) or via wet nebulizers powered by compressed air or oxygen. Current practice patterns in EDs and hospital wards tend to favor the use of nebulizers due to many apparent advantages of these devices.[3] For instance, nebulizers do not require any special inhalation technique and can be effectively used by patients at any age.[3, 4] There is also a common perception that nebulizers are more effective, possibly stemming from the assumption that hospitalized patients have already failed their outpatient MDI therapy and an almost mystical belief in the healing power of mist. Moreover, many clinicians have been trained to routinely use nebulizer therapies and may lack sufficient knowledge or comfort about the relative efficacy and equivalence dosing of MDI therapies.
WHY NEBULIZERS ARE NOT BETTER THAN MDIs FOR PATIENTS HOSPITALIZED WITH OBSTRUCTIVE PULMONARY SYMPTOMS
Decades of research support that MDIs are effective, efficient, and less costly (depending on circumstances) than nebulizers for the routine treatment of obstructive pulmonary exacerbations.[3, 4, 5, 6, 7, 8, 9, 10, 11] The clinical effectiveness of MDIs has been shown in studies across populations of adults with acute COPD symptoms,[3, 4, 7, 8] as well as children and adults with asthma exacerbations.[3, 4, 5, 6, 9, 10] A 2005 joint report by the American College of Chest Physicians (ACCP) and the American College of Asthma, Allergy and Immunology (ACAAI), concluded none of the pooled meta‐analyses showed a significant difference between devices in any efficacy outcome in any patient group for each of the clinical settings.[4] Many different outcomes have been investigated, including forced expiratory volumes (FEV), peak flows, symptoms and specific symptom scores, and physical findings.[4]
Compared to MDIs, there are a number of drawbacks to the use of nebulizers: nebulizers are more expensive to buy and maintain, are less portable, and take longer to set up, use, and clean following each use.[12] In addition, nebulizers have been associated with greater increases in heart rate and tremors compared to MDIs, suggesting nebulizers lead to higher systemically absorbed ‐agonist doses.[4]
Of note, nearly all of the clinical effectiveness studies administered MDIs with a valved holding chamber or spacer, facilitating the delivery of drug to the airways.[3, 4] Although valved holding chambers are commonly referred to as a spacer, a true spacer does not have a valve and is rarely used today.[12]
THE EVIDENCE EXAMINING NEBULIZERS VERSUS MDIs IN PATIENTS WITH ASTHMA OR COPD EXACERBATIONS
A 2013 Cochrane review sought to establish the relative efficacy of MDIs with holding chambers versus nebulizers for children and adults who presented to a community setting or emergency department with acute asthma.[6] The review included a total of 1897 children and 729 adults in 39 randomized controlled trials. The authors judged the overall evidence to be of moderate quality. Children with acute asthma treated with MDIs in the ED had shorter lengths of stay in the ED (70 minutes vs 103 minutes), similar peak flow and FEV measurements, lower heart rates, and less tremor compared to children treated with nebulizers.[5, 6] There were no significant differences found between devices for the treatment of adult patients with asthma.[6]
In a separate double‐blind, randomized, placebo‐controlled study evaluating albuterol administered by nebulizer versus MDI with spacer for children <2 years old presenting to an ED with wheezing, the use of MDIs with a spacer and facemask was equally efficacious and may have led to fewer hospital admissions.[10]
Mandelberg et al. performed a double‐blind, randomized, placebo‐controlled trial for unselected adult patients presenting to an ED with obstructive pulmonary symptoms.[8] Patients received either 2 puffs of a placebo MDI with a spacer along with nebulized salbutamol 0.5 mL in 1.5 mL saline solution (n=25), or a salbutamol MDI along with a nebulized placebo saline solution (n=25). Treatments were repeated every 15 minutes up to 3 times, unless side effects occurred. Spirometric measurements were performed following each treatment. No differences were seen between the groups at any point during the study period. The authors concluded, Even in the setting of the unselected group of patient referrals to the [Department of Emergency Medicine] for episodes of severe airflow limitation, the clinical and objective bronchodilator responses to the administration of salbutamol are independent of the method of delivery: MDI with large spacer or aerosol nebulization.[8]
There are surprisingly few studies examining the use of nebulizers versus MDIs in the inpatient setting for both children and adults. Dolovich et al. reviewed 6 studies that included 253 total patients and reported no significant differences in pulmonary function between devices.[4] Based on these findings, the ACCP/ACAAI group recommended both nebulizers and MDIs with spacers/holding chambers are appropriate for use in the inpatient setting. Quality of evidence: good.[4]
WHY USE MDIs FOR INPATIENTS
If MDI and nebulizer treatments are equally effective, why change current practice? The use of MDIs, rather than nebulizers, in hospitals could lead to fewer side effects such as tachycardia, arrhythmias, and tremors. MDIs are also more portable and do not require specialized set‐up. Furthermore, MDI administrations during hospitalization may provide a golden opportunity to have respiratory therapists, pharmacists, or other health professionals spend time teaching patients proper inhaler usage, rather than providing time‐consuming nebulizer treatments.[13] In a recent study, approximately 86% of hospitalized patients with asthma or COPD could not demonstrate appropriate use of an MDI. However, 100% of patients were able to achieve mastery following a short teach‐back session.[14] It is conceivable that transitioning patients to MDIs earlier during hospitalization and providing them with education regarding proper MDI administration could instill confidence in their use of inhalers and result in downstream effects such as shorter lengths of stay, less frequent hospital readmissions, or improved quality of life.
MDI use may result in cost savings in certain settings, although the relative costs of nebulizer versus MDI treatments depends on many institution‐specific factors. Such factors include the institutional policies on who delivers the nebulizer or the MDI and how they are compensated and staffed. For example in the Nebs No More After 24 program initiated at the University of California, San Francisco, the vast majority of the realized cost savings are due to the reduction in respiratory therapist time spent delivering MDIs, which reflects the local policies and compensation structure.[13] Previous inpatient interventions to convert from nebulizers to MDIs also showed cost savings resulting from decreased labor needs.[15] In some hospitals, nurses deliver nebulizer treatments, whereas in others only respiratory therapists are allowed to provide nebulizers. Moreover, whether the MDI can go home with the patient upon discharge depends on whether the hospital has a dispensing pharmacy or not. Formal economic evaluations specific to the local institution are necessary.
WHAT WE SHOULD DO INSTEAD: ENCOURAGE THE USE OF MDIs FOR INPATIENTS
For effective inpatient MDI treatments, MDI technique must be good. Thus, it is vital to enlist the right people to provide proper MDI teaching and supervision. Respiratory therapists are generally trained for this task, and may be complemented by appropriately trained physicians, nurses, or pharmacists. Many institutions have successfully implemented respiratory therapist‐driven protocols for the administration of MDIs, which has led to measurable improvements in the utilization of appropriate respiratory care resources.[15, 16] At University of California, San Francisco, this was accomplished by recruiting respiratory therapists and nurses to help support the transition of patients from nebulizers to MDIs and to provide bedside teaching on proper MDI usage. The institution then launched a Nebs No More After 24 campaign that sought to transition patients from nebulizers to MDIs within 24 hours of hospitalization. This campaign included an educational program for physicians, prepared facilitator guides to assist attending physicians with teaching about the new initiative, publicity efforts including pens and strategically placed posters, and regular feedback regarding nebulizer utilization on the pilot ward. Although the evidence suggests that patients can be started on MDIs immediately upon presentation to the ED, the UCSF campaign focused on transitioning patients within 24 hours so to alleviate concerns about transitions in care between the ED and the medical ward, as well as between overnight and day teams. MDIs are only as or more effective than nebulizers if the correct administration technique is employed. The 24‐hour transition period allows for MDI teaching and transition during regular daytime hours.
Inpatient use of nebulizers may be more appropriate than MDIs for patients with dementia or altered mental status, as well as those in extreme distress resulting in an inability to coordinate inhaler usage. Very low health literacy may be an additional barrier to appropriate MDI teaching and usage.
RECOMMENDATIONS
In patients with obstructive pulmonary symptoms, transition patients from nebulizers to MDIs early in their hospital course, unless the patient is unable to use an inhaler due to altered mental status, dementia, or other circumstances. Ensure that patients are instructed and supervised on proper MDI technique. Enlisting respiratory therapists and appropriately trained staff (pharmacists, nurses, physicians) is key to the successful use of MDIs. Frequency and dosage of MDIs used should be comparable to that of nebulized treatments. Although studies have used a relatively wide range of albuterol MDI dosing, prior programs have determined a dose of albuterol 4 puffs via MDI as being equivalent to the standard albuterol 2.5 mg nebulizer dosage.[17, 18] Some studies have advocated for using a range of 2 to 10 puffs albuterol MDI, with the actual dose based on clinical response.[17] One study in children with mild acute asthma found that 2 puffs of albuterol by MDI was just as effective as higher doses delivered by MDI (610 puffs) or by nebulizer.[19]
CONCLUSION
MDIs with holding chambers are clinically equivalent to nebulizer therapy for the treatment of both children and adults with obstructive pulmonary symptoms, as long as MDI technique and MDI dosing is adequate. This is based on good data in the ED setting but fewer studies in adult inpatients. There are a number of advantages to the use of inpatient MDIs over nebulizers; MDIs are more portable, often less expensive to use, may result in fewer side effects, and will hopefully improve outpatient MDI technique. The delivery of MDIs during hospitalization should be accompanied with patient education regarding proper administration technique.
Disclosure
Nothing to report.
Do you think this is a low‐value practice? Is this truly a Thing We Do for No Reason? Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and Liking It on Facebook. We invite you to propose ideas for other Things We Do for No Reason topics by emailing [email protected]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of COPD. Available at: http://www.goldcopd.org/guidelines‐global‐strategy‐for‐diagnosis‐management.html. Updated January 2015. Accessed September 25, 2014.
- National Heart Lung and Blood Institute. National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Published 2007. Updated April 2012. Accessed September 25, 2014.
- , , , Bronchodilator delivery in acute airflow obstruction. A meta‐analysis. Arch Intern Med. 1997;157(15):1736–1744.
- , , , et al. Device selection and outcomes of aerosol therapy: Evidence‐based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335–371.
- , Beta‐agonists through metered‐dose inhaler with valved holding chamber versus nebulizer for acute exacerbation of wheezing or asthma in children under 5 years of age: a systematic review with meta‐analysis. J Pediatr. 2004;145(2):172–177.
- , , Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , , Nebulizer vs spacer for bronchodilator delivery in patients hospitalized for acute exacerbations of COPD. Chest. 1989;96(6):1241–1246.
- , , , Nebulized wet aerosol treatment in emergency department—is it essential? Comparison with large spacer device for metered‐dose inhaler. Chest. 1997;112(6):1501–1505.
- , , , , , Randomized controlled trial of salbutamol aerosol therapy via metered dose inhaler‐spacer vs. jet nebulizer in young children with wheezing. Pediatr Pulmonol. 2005;39(5):466–472.
- , , , Nebulizers vs metered‐dose inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med. 2003;157(1):76–80.
- , , , A review and economic evaluation of bronchodilator delivery methods in hospitalized patients. Arch Intern Med. 1996;156(18):2113–2118.
- , Asthma medication delivery: mists and myths. Paediatr Respir Rev. 2013;14(2):112–118.
- , , , , “Nebs no more after 24”: a pilot program to improve the use of appropriate respiratory therapies. JAMA Intern Med. 2013;173(17):1647–1648.
- , , , et al. Misuse of respiratory inhalers in hospitalized patients with asthma or COPD. J Gen Intern Med. 2011;26(6):635–642.
- , , A model for conversion from small volume nebulizer to metered dose inhaler aerosol therapy. Chest. 1992;101(3):634–637.
- , , Physician‐ordered aerosol therapy versus respiratory therapist‐driven aerosol protocol: the effect on resource utilization. Respir Care. 2013;58(3):431–437.
- , , , Automatic replacement of albuterol nebulizer therapy by metered‐dose inhaler and valved holding chamber. Am J Health Syst Pharm. 2005;62(10):1053–1061.
- , , , , The conversion to metered‐dose inhaler with valved holding chamber to administer inhaled albuterol: a pediatric hospital experience. Respir Care. 2008;53(3):338–345.
- , , , , , Comparison of albuterol delivered by a metered dose inhaler with spacer versus a nebulizer in children with mild acute asthma. J Pediatr. 1999;135(1):22–27.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of COPD. Available at: http://www.goldcopd.org/guidelines‐global‐strategy‐for‐diagnosis‐management.html. Updated January 2015. Accessed September 25, 2014.
- National Heart Lung and Blood Institute. National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Published 2007. Updated April 2012. Accessed September 25, 2014.
- , , , Bronchodilator delivery in acute airflow obstruction. A meta‐analysis. Arch Intern Med. 1997;157(15):1736–1744.
- , , , et al. Device selection and outcomes of aerosol therapy: Evidence‐based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335–371.
- , Beta‐agonists through metered‐dose inhaler with valved holding chamber versus nebulizer for acute exacerbation of wheezing or asthma in children under 5 years of age: a systematic review with meta‐analysis. J Pediatr. 2004;145(2):172–177.
- , , Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , , Nebulizer vs spacer for bronchodilator delivery in patients hospitalized for acute exacerbations of COPD. Chest. 1989;96(6):1241–1246.
- , , , Nebulized wet aerosol treatment in emergency department—is it essential? Comparison with large spacer device for metered‐dose inhaler. Chest. 1997;112(6):1501–1505.
- , , , , , Randomized controlled trial of salbutamol aerosol therapy via metered dose inhaler‐spacer vs. jet nebulizer in young children with wheezing. Pediatr Pulmonol. 2005;39(5):466–472.
- , , , Nebulizers vs metered‐dose inhalers with spacers for bronchodilator therapy to treat wheezing in children aged 2 to 24 months in a pediatric emergency department. Arch Pediatr Adolesc Med. 2003;157(1):76–80.
- , , , A review and economic evaluation of bronchodilator delivery methods in hospitalized patients. Arch Intern Med. 1996;156(18):2113–2118.
- , Asthma medication delivery: mists and myths. Paediatr Respir Rev. 2013;14(2):112–118.
- , , , , “Nebs no more after 24”: a pilot program to improve the use of appropriate respiratory therapies. JAMA Intern Med. 2013;173(17):1647–1648.
- , , , et al. Misuse of respiratory inhalers in hospitalized patients with asthma or COPD. J Gen Intern Med. 2011;26(6):635–642.
- , , A model for conversion from small volume nebulizer to metered dose inhaler aerosol therapy. Chest. 1992;101(3):634–637.
- , , Physician‐ordered aerosol therapy versus respiratory therapist‐driven aerosol protocol: the effect on resource utilization. Respir Care. 2013;58(3):431–437.
- , , , Automatic replacement of albuterol nebulizer therapy by metered‐dose inhaler and valved holding chamber. Am J Health Syst Pharm. 2005;62(10):1053–1061.
- , , , , The conversion to metered‐dose inhaler with valved holding chamber to administer inhaled albuterol: a pediatric hospital experience. Respir Care. 2008;53(3):338–345.
- , , , , , Comparison of albuterol delivered by a metered dose inhaler with spacer versus a nebulizer in children with mild acute asthma. J Pediatr. 1999;135(1):22–27.
© 2015 Society of Hospital Medicine
Variation in Readmission Rates by EDs
Readmissions of Medicare beneficiaries within 30 days of discharge are frequent and costly.[1] Concern about readmissions has prompted the Centers for Medicare & Medicaid Services (CMS) to reduce payments to hospitals with excess readmissions.[2] Research has identified a number of patient clinical and socio‐demographic factors associated with readmissions.[3] However, interventions designed to reduce readmissions have met with limited success. In a systematic review, no single intervention was regularly effective in reducing readmissions, despite the fact that interventions have targeted both predischarge, transition of care, and postdischarge processes of care.[4]
The different trajectories of care experienced by patients after hospital discharge, and their effect on risk of readmission, have been incompletely studied. Although early outpatient follow‐up after discharge is associated with lower readmission rates,[5, 6] a factor that has been minimally studied is the role of the emergency department (ED) and the ED provider in readmissions. The ED and ED providers feature prominently in the care received by patients shortly after discharge from a hospital. About a quarter of all hospitalized Medicare patients are evaluated in an ED within 30 days of discharge,[7, 8] and a majority of readmissions within 30 days of discharge are precipitated by an ED visit.[9] Hence, we asked whether when a recently discharged patient is seen in an ED, does the rate of readmission vary by ED provider and by ED facility?
We used Texas Medicare claims data to examine patients visiting the ED within 30 days of discharge from an initial hospitalization to determine if their risk of readmission varies by the ED provider caring for them and by the ED facility they visit.
METHODS
Sources of Data
We used claims from the years 2007 to 2011 for 100% of Texas Medicare beneficiaries, including Medicare beneficiary summary files, Medicare Provider Analysis and Review (MedPAR) files, Outpatient Standard Analytical Files (OutSAF), and Medicare Carrier files. We obtained diagnosis‐related group associated information, including weights, and Major Diagnostic Category from CMS, and used Provider of Services files to determine facility characteristics.
Establishment of the Study Cohort
From 2008 through 2011 MedPAR files, we initially selected all hospital discharges from acute‐care hospitals in Texas. From these 3,191,160 admissions, we excluded those discharged dead or transferred to other acute‐care hospitals (N=230,343), those who were younger than 66 years at admission (N=736,685) and those without complete Parts A and B enrollment or with any health maintenance organization enrollment in the 12 months prior to and 2 months after the admission of interest (N=596,427). From the remaining 1,627,705 discharges, we identified 302,949 discharges that were followed by at least 1 ED visit within 30 days.
We applied the algorithm developed by Kaskie et al. to identify ED visits.[10] We identified claims for ED services with Current Procedural Terminology (CPT) codes 99281‐99285 from Carrier files and bundled claims with overlapping dates or those that were within 1 day of each other. Then we identified claims for ED services using the same CPT codes from OutSAF and bundled those with overlapping dates or those that were within 3 days of each other. Finally, we bundled Carrier and OutSAF claims with overlapping dates and defined them as the same ED visit. From these, we retained only the first ED visit. We excluded those receiving care from multiple ED providers during the ED visit (N=38,565), and those who had a readmission before the first ED visit (N=1436), leaving 262,948 ED visits. For patients who had more than 1 hospitalization followed by an ED visit in a given year, we selected the first hospitalization, resulting in 199,143 ED visits. We then selected ED providers associated with at least 30 ED visits in this cohort, resulting in 1922 ED providers and 174,209 ED visits. For analyses where we examined both ED provider and facility variation in admission rates, we eliminated ED providers that generated charges from more than 1 ED facility, resulting in 525 providers and 48,883 ED visits at 143 ED facilities.
Measures
Patient Characteristics
We categorized beneficiaries by age, gender, and ethnicity using Medicare beneficiary summary files. We used the Medicaid indicator as a proxy of low socioeconomic status. We obtained information on weekend admission, emergent admission, discharge destination, and diagnosis‐related groupt (DRG) from MedPAR files. We identified comorbidities using the claims from MedPAR, Carrier, and OutSAF files in the year prior to the admission.[11] We identified total hospitalizations and outpatient visits in the prior year from MedPAR files and Carrier files, respectively. We obtained education status at the level of zip code of residence from the 2011 American Community Survey estimates from the United States Census Bureau. We determined urban or rural residence using the 2013 Rural‐Urban Continuum Codes developed by the United States Department of Agriculture.
ED Facility Characteristics
We used the provider number of the ED facility to link to the Provider of Services files and obtained information on medical school affiliation, facility size, and for profit status.
Study Outcomes
The outcome of this study was readmission after an ED visit within 30 days of discharge from an initial hospitalization. We defined readmission after an ED visit as a hospitalization starting the day of or the day following the ED visit
Statistical Analyses
We performed 2‐level analyses where patients were clustered with ED providers to examine variation among ED providers. The effect of ED providers was modeled as a random effect to account for the correlation among the patients cared for by the same ED provider. We derived ED provider‐specific estimates from models adjusted for patient age, gender, race/ethnicity, rural or urban residence, Medicaid eligibility, education at the zip code level of residence, and characteristics of the initial admission (emergency admission, weekend admission, discharge destination, its major diagnostic category and DRG weight). We also adjusted for comorbidities, number of hospitalizations, and number of physician visits in the year before the initial admission.
We also conducted 2‐level analyses where patients were nested in ED facilities and 3‐level analyses where patients were nested in ED providers and ED providers were nested in ED facilities. We adjusted for all factors described above. We computed the change in the variance between 2‐level and 2‐level analyses to determine the variation in readmission rates that was explained by the ED provider and the ED facility. All analyses were performed with SAS version 9.2 (SAS Institute Inc., Cary, NC).
RESULTS
We identified 174,209 patients who visited an ED within 30 days of discharge from an initial hospitalization. Table 1 describes the characteristics of these patients as well as the readmission rates associated with these characteristics. The rate of readmission of our cohort of 1,627,705 discharges with or without a following ED visit was 16.2%, whereas the rate of readmission following an ED visit in our final cohort of 174,209 patients was 52.67%. This readmission rate increased with age, from 49.31% for patients between 66 and 70 years of age to 55.33% for patients older than 85 years. There were minor variations by gender and ethnicity. Patients residing in metropolitan areas or in zip codes with low education levels had higher readmission rates, as did those whose original admission was classified as emergency or those who were not discharged home.
| Patient Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| MeanSD, Median (Q1Q3) | Odds Ratio (95% CI)a | ||
| |||
| Overall | 174,209 (100) | 52.67 | |
| Age, y | |||
| 6670 | 32,962 (18.92) | 49.31 | 1.00 |
| 7175 | 34,979 (20.08) | 51.48 | 1.10 (1.06‐1.13)b |
| 7680 | 36,728 (21.08) | 53.01 | 1.15 (1.12‐1.19)b |
| 8185 | 34,784 (19.97) | 54.05 | 1.19 (1.15‐1.23)b |
| >85 | 34,756 (19.95) | 55.33 | 1.25 (1.21‐1.29)b |
| Gender | |||
| Male | 71,049 (40.78) | 52.95 | 1.02 (1.00‐1.04) |
| Female | 103,160 (59.22) | 52.48 | 1.00 |
| Race | |||
| Non‐Hispanic white | 124,312 (71.36) | 52.77 | 1.00 |
| Black | 16,809 (9.65) | 51.45 | 0.84 (0.81‐0.87)b |
| Hispanic | 30,618 (17.58) | 52.70 | 0.88 (0.85‐0.91)b |
| Other | 2,470 (1.42) | 55.71 | 1.06 (0.97‐1.15) |
| Rural/urban residence | |||
| Metropolitan | 136,739 (78.49) | 53.88 | 1.00 |
| Nonmetropolitan | 35,000 (20.09) | 48.16 | 0.96 (0.93‐0.99)b |
| Rural | 2,448 (1.41) | 50.04 | 1.04 (0.95‐1.13) |
| Medicaid eligible | |||
| No | 128,909 (74.00) | 52.65 | 1.00 |
| Yes | 45,300 (26.00) | 52.72 | 0.97 (0.94‐0.99)b |
| Education levelc | |||
| 1st quartile (lowest) | 43,863 (25.18) | 54.61 | 1.00 |
| 2nd quartile | 43,316 (24.86) | 53.92 | 1.00 (0.97‐1.03) |
| 3rd quartile | 43,571 (25.01) | 50.72 | 0.99 (0.96‐1.02) |
| 4th quartile (highest) | 43,318 (24.87) | 51.98 | 1.01 (0.97‐1.04) |
| Emergency admission | |||
| No | 99,101 (56.89) | 51.15 | 1.00 |
| Yes | 75,108 (43.11) | 54.68 | 1.07 (1.05‐1.09)b |
| Weekend admission | |||
| No | 131,266 (75.35) | 52.45 | 1.00 |
| Yes | 42,943 (24.65) | 53.35 | 1.01 (0.99‐1.04) |
| Discharge destination | |||
| Home | 122,542 (70.34) | 50.90 | 1.00 |
| Inpatient rehabilitation facility | 9,512 (5.46) | 55.48 | 1.31 (1.25‐1.37)b |
| Skilled nursing facility | 37,248 (21.38) | 57.25 | 1.29 (1.26‐1.33)b |
| Other | 4,907 (2.82) | 56.88 | 1.14 (1.07‐1.21)b |
| DRG weight (per unit) | 1.561.27, 0.82 (1.16‐1.83) | 1.06 (1.05‐1.07)b | |
| Hospitalization in the prior year (per hospitalization) | 1.031.49, 0.00 (1.00‐2.00) | 1.04 (1.03‐1.04)b | |
| Physician visits in the prior year (per 10 visits) | 11.759.80, 5.00 (10.00‐17.00) | 0.97 (0.96‐0.98)b | |
Table 1 also presents the odds of readmission adjusted for all other factors in the table and also adjusted for clustering within ED providers in a 2‐level model. Increasing age, white race, metropolitan residence, nonhome discharge, higher severity of illness, more hospitalizations in the prior year, fewer physician visits in the prior year, and an emergency initial admission were each associated with a higher readmission rate.
We next generated estimates of readmission rates for each ED provider from the adjusted 2‐level models. Figure 1 shows the adjusted cumulative readmission rates for the 1922 ED providers. This figure shows the mean value and 95% confidence intervals of the readmission rates for each provider. Dark vertical lines indicate providers whose readmission rate differed significantly from the mean adjusted readmission rate of 52.1% for all providers. Of the ED providers, 14.2% had significantly higher readmission rates. The mean readmission rate for these 272 providers was 67.2%. Of the ED providers, 14.7% had significantly lower readmission rates. The mean readmission rate for these 283 providers was 36.8%.
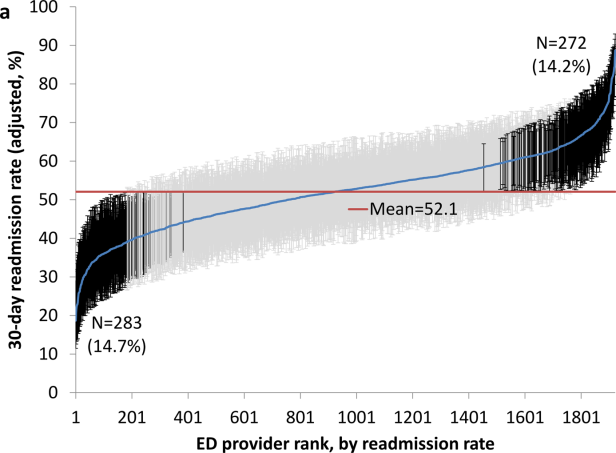
To determine the contribution of the ED facility to the variation in readmission rates, we restricted our analysis to 48,883 patients (28.06% of our cohort) seen by 525 ED providers who were associated with only 1 facility (total of 143 facilities). Table 2 describes the unadjusted readmission rates stratified by specific characteristics of those facilities. The unadjusted readmission rate increased with the size of the associated hospital, from 47.61% for hospitals with less than 100 beds to 57.06% for hospitals with more than 400 beds. The readmission rate for nonprofit facilities was 53.81% and for for‐profit facilities was 57.39%. Facilities with no medical school affiliation had a readmission rate of 54.51%, whereas those with a major affiliation had a readmission rate of 58.72%.
| ED Facility Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| |||
| Overall | 48,883 | ||
| Total beds | |||
| 100 | 3,936 (8.05) | 47.61 | 1.00 |
| 101200 | 6,251 (12.79) | 52.07 | 1.38 (1.06‐1.81)b |
| 201400 | 13,000 (26.59) | 56.26 | 1.69 (1.32‐2.17)b |
| >400 | 25,696 (52.57) | 57.06 | 1.77 (1.35‐2.33)b |
| Type of control | |||
| Nonprofit | 24,999 (51.14) | 53.81 | 1.00 |
| Proprietary | 17,108 (35.00) | 57.39 | 1.32 (1.09‐1.61)b |
| Government | 6,776 (13.86) | 56.60 | 1.11 (0.88‐1.41) |
| Medical school affiliation | |||
| Major | 6,487 (13.27) | 58.72 | 1.00 |
| Limited | 7,066 (14.45) | 56.37 | 0.85 (0.58‐1.25) |
| Graduate | 3,164 (6.47) | 56.19 | 0.71 (0.44‐1.15) |
| No affiliation | 32,166 (65.80) | 54.51 | 0.78 (0.57‐1.05) |
| If the same hospital patient was discharged from | |||
| Yes | 38,532 (78.82) | 55.64 | 0.96 (0.91‐1.00) |
| No | 10,351 (21.18) | 54.73 | 1.00 |
With this smaller cohort, we performed 2 types of 2‐level models, where patients clustered within ED facilities and ER providers, respectively, and a 3‐level model accounting for clustering of patients within providers and of providers within facilities. From the facility‐patient 2‐level model, the variance of the ED facility was 0.2718 (95% confidence interval [CI]: 0.2083‐0.3696). From the provider‐patient 2‐level model, the variance of ED provider was 0.2532 (95% CI: 0.2166‐0.3002). However, when the 3‐level model was performed, the variance of ED provider decreased to 0.0893 (95% CI: 0.0723‐0.1132) and the variance of ED facility dropped to 0.2316 (95% CI: 0.1704‐0.3331) . This indicates 65% of the variation among ED providers was explained by the ED facility, and in contrast, 15% of the variation among ED facilities was explained by ED providers.
Table 2 also shows the adjusted odds of readmission generated from the 3‐level model. Patients receiving care in ED facilities in hospitals with more beds and in for‐profit hospitals were at higher risk for readmission. It is possible that patients seen at the ED associated with the discharging hospital had a lower risk of readmission. This finding was close to being statistically significant (P=0.051).
We repeated all the above analyses using an outcome of readmission anytime between the ED visit and 30 days after discharge from the initial hospitalization (rather than readmission on the day of or after the ED visit). All analyses produced results similar to the results presented above. For example, Figure 2 shows the adjusted cumulative readmission rates for the 1922 ED providers using this outcome. Of the ED providers, 12.8% had higher and 12.5% had lower readmission rates as compared to the mean readmission rate for all ED providers. The Spearman correlation coefficient between the rank of ED providers in immediate readmission rate (Figure 1) and readmission rate within 30 days of hospital discharge (Figure 2) was 0.94 (P<0.001).
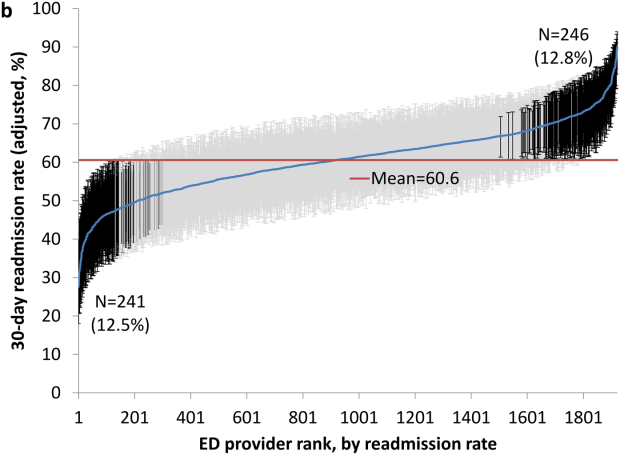
DISCUSSION
This study found substantial variation in readmission rates by ED provider, despite controlling for patient clinical and sociodemographic factors. In 3‐level models, the ED facility explained a substantial part of the variation by ED provider, with patients seen at larger facilities and for‐profit facilities having higher readmission rates.
Variation among ED facilities and ED providers in readmission rates has not previously been studied. There is literature on the variation in ED facility and ED provider admission rates. As readmissions are a subset of all admissions, this literature provides context to our findings. Abualenain et al. examined admission rates for 89 ED physicians for adult patients presenting with an acute medical or surgical complaint at 3 EDs in a health system.[12] After adjusting for patient and clinical characteristics, admission rates varied from 21% to 49% among physicians and from 27% to 41% among 3 facilities. Two other studies from single hospitals have found similar variation among providers.[13, 14] The reasons for the variation among ED providers presumably relate to subjective aspects of clinical assessment and the reluctance of providers to rely solely on objective scales, even when they are available.[14, 15] Variation in admission rates among different facilities may relate to clustering of providers with similar practice styles within facilities, lack of clinical guidelines for certain conditions, as well as differences among facilities in the socioeconomic status and access to primary care of their clientele.[12, 16, 17] For example, Pines et al. have shown that ED facility admission rates are higher in communities with fewer primary care physicians per capita and are influenced by the prevailing county level admission rates.[16] Capp et al. showed persistent variation in admission rates across hospitals, despite adjusting for clinical criteria such as vital signs, chief complaints, and severity of illness.[18]
Structural differences in ED facilities may also influence the decision to admit. We found that patients visiting ED facilities in hospitals with more beds had a higher readmission rate. ED facility systems of care such as observation units or protocols are associated with lower admission rates.[19, 20] Finally, certain hospitals may actively influence the admission practice patterns of their ED providers. We noted that patients seen at for‐profit ED facilities had a greater risk of readmission. A similar finding has been described by Pines et al., who noted higher admission rates at for‐profit facilities.[16] In an extreme example, a recent Justice Department lawsuit alleged that a for‐profit hospital chain used software systems and financial incentives to ED providers to increase admissions.[21]
It is possible that the providers with low readmission rates may have inappropriately released patients who truly should have been admitted. A signal that this occurred would be if these patients were readmitted in the days after the ED visits. We examined this possibility by additionally examining readmissions occurring anytime between the ED visit until 30 days after discharge from the initial hospitalization. The results were similar to when we only included readmissions that occurred immediately following the ED visit, with a very high correlation (r=0.94) between the ranking of the ED providers by readmission rates in both circumstances. This suggests that the decisions of the ED providers with low readmission rates to admit or release from the ED were likely appropriate.
Our research has limitations. We studied patients with fee‐for‐service Medicare in a single large state in the United States over a 4‐year period. Our findings may not be generalizable to younger patient populations, other regions with different sociodemographic patterns and healthcare systems, or other time periods. We could not control for many factors that may impact the risk of readmission but are not measured in Medicare databases (eg, clinical data such as vital signs, measures of quality of transition from discharging hospital, ED provider workload). To attribute care to a single ED provider, we excluded patients who were taken care of by multiple ED providers. These patients may have different needs from our study population (eg, more complex issues and longer stays in the ED) and may bias our results.
This study provides a new direction for research and quality improvement targeting readmissions. Research should extend beyond the discharge transition and examine the entire trajectory of posthospitalization care to better understand readmissions. Based directly on this study, research could investigate the practice patterns of ED providers and systems of care at ED facilities that affect readmissions rates. Such investigation could inform quality improvement efforts to standardize care for patients in the ED.
CMS policies hold hospitals accountable for readmissions of the patients they discharge, but do not address the admission process in the ED that leads to readmissions of recently discharged patients. Given the present study, and the fact that the proportion of all hospital admissions that occur through the ED has grown to 44%,[22] consideration of the role of the ED in public policy efforts to discourage unnecessary inpatient care may be appropriate.
In summary, this study shows that a recently discharged patient's chances of being readmitted depends partly on the ED provider who evaluates them and on the ED facility at which they seek care. ED provider practice patterns and ED facility systems of care may be a target for interventions aimed at decreasing readmission rates.
Disclosures
This research was supported by grants from the National Institutes of Health (AG033134 and K05CA134923) and from the Agency for Healthcare Research and Quality (R24H5022134). The authors report no conflicts of interest.
- , , Rehospitalizations among patients in the Medicare Fee‐for‐Service Program. N Engl J Med. 2009;360:1418–1428.
- Centers for Medicare 306:1688–1698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155:520–528.
- , , , , Outpatient follow‐up visit and 30‐day emergency department visit and readmission in patients hospitalized for chronic obstructive pulmonary disease. Arch Intern Med. 2010;170:1664–1670.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303:1716–1722.
- , , After hospitalization: a Dartmouth Atlas report on post‐acute care for Medicare beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed August 8, 2013.
- , , , Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013;62:145–150.
- , , , Emergency department visits after surgery are common for Medicare patients, suggesting opportunities to improve care. Health Aff (Millwood). 2013;32:1600–1607.
- , , , et al. Defining emergency department episodes by severity and intensity: a 15‐year study of Medicare beneficiaries. BMC Health Serv Res. 2010;10:1–13.
- , , , Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- , , , , , Emergency department physician‐level and hospital‐level variation in admission rates. Ann Emerg Med. 2013;61:638–643.
- , , , et al. Hospital admission decision for patients with community‐acquired pneumonia: variability among physicians in an emergency department. Ann Emerg Med. 2012;59:35–41.
- , , Individual emergency physician admission rates: predictably unpredictable. CJEM. 2009;11(2):149–155.
- , , , , , Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis. 2009;49:e100–e108.
- , , Variation in emergency department admission rates across the United States. Med Care Res Rev. 2013;70:218–231.
- , , , , , Variation in US hospital emergency department admission rates by clinical condition. Med Care. 2015;53:237–244.
- , , , et al. Hospital variation in risk‐standardized hospital admission rates from US EDs among adults. Am J Emerg Med. 2014;32:837–843.
- , , The effect of an observation unit on the rate of ED admission and discharge for pyelonephritis. Am J Emerg Med. 2010;28:682–688.
- , , , , , Protocol‐driven emergency department observation units offer savings, shorter stays, and reduced admissions. Health Aff (Millwood). 2013;32:2149–2156.
- , Hospital chain said to scheme to inflate bills. New York Times. January 23, 2014. Available at: http://www.nytimes.com/2014/01/24/business/hospital‐chain‐said‐to‐scheme‐to‐inflate‐bills.html?emc=eta1367:391–393.
Readmissions of Medicare beneficiaries within 30 days of discharge are frequent and costly.[1] Concern about readmissions has prompted the Centers for Medicare & Medicaid Services (CMS) to reduce payments to hospitals with excess readmissions.[2] Research has identified a number of patient clinical and socio‐demographic factors associated with readmissions.[3] However, interventions designed to reduce readmissions have met with limited success. In a systematic review, no single intervention was regularly effective in reducing readmissions, despite the fact that interventions have targeted both predischarge, transition of care, and postdischarge processes of care.[4]
The different trajectories of care experienced by patients after hospital discharge, and their effect on risk of readmission, have been incompletely studied. Although early outpatient follow‐up after discharge is associated with lower readmission rates,[5, 6] a factor that has been minimally studied is the role of the emergency department (ED) and the ED provider in readmissions. The ED and ED providers feature prominently in the care received by patients shortly after discharge from a hospital. About a quarter of all hospitalized Medicare patients are evaluated in an ED within 30 days of discharge,[7, 8] and a majority of readmissions within 30 days of discharge are precipitated by an ED visit.[9] Hence, we asked whether when a recently discharged patient is seen in an ED, does the rate of readmission vary by ED provider and by ED facility?
We used Texas Medicare claims data to examine patients visiting the ED within 30 days of discharge from an initial hospitalization to determine if their risk of readmission varies by the ED provider caring for them and by the ED facility they visit.
METHODS
Sources of Data
We used claims from the years 2007 to 2011 for 100% of Texas Medicare beneficiaries, including Medicare beneficiary summary files, Medicare Provider Analysis and Review (MedPAR) files, Outpatient Standard Analytical Files (OutSAF), and Medicare Carrier files. We obtained diagnosis‐related group associated information, including weights, and Major Diagnostic Category from CMS, and used Provider of Services files to determine facility characteristics.
Establishment of the Study Cohort
From 2008 through 2011 MedPAR files, we initially selected all hospital discharges from acute‐care hospitals in Texas. From these 3,191,160 admissions, we excluded those discharged dead or transferred to other acute‐care hospitals (N=230,343), those who were younger than 66 years at admission (N=736,685) and those without complete Parts A and B enrollment or with any health maintenance organization enrollment in the 12 months prior to and 2 months after the admission of interest (N=596,427). From the remaining 1,627,705 discharges, we identified 302,949 discharges that were followed by at least 1 ED visit within 30 days.
We applied the algorithm developed by Kaskie et al. to identify ED visits.[10] We identified claims for ED services with Current Procedural Terminology (CPT) codes 99281‐99285 from Carrier files and bundled claims with overlapping dates or those that were within 1 day of each other. Then we identified claims for ED services using the same CPT codes from OutSAF and bundled those with overlapping dates or those that were within 3 days of each other. Finally, we bundled Carrier and OutSAF claims with overlapping dates and defined them as the same ED visit. From these, we retained only the first ED visit. We excluded those receiving care from multiple ED providers during the ED visit (N=38,565), and those who had a readmission before the first ED visit (N=1436), leaving 262,948 ED visits. For patients who had more than 1 hospitalization followed by an ED visit in a given year, we selected the first hospitalization, resulting in 199,143 ED visits. We then selected ED providers associated with at least 30 ED visits in this cohort, resulting in 1922 ED providers and 174,209 ED visits. For analyses where we examined both ED provider and facility variation in admission rates, we eliminated ED providers that generated charges from more than 1 ED facility, resulting in 525 providers and 48,883 ED visits at 143 ED facilities.
Measures
Patient Characteristics
We categorized beneficiaries by age, gender, and ethnicity using Medicare beneficiary summary files. We used the Medicaid indicator as a proxy of low socioeconomic status. We obtained information on weekend admission, emergent admission, discharge destination, and diagnosis‐related groupt (DRG) from MedPAR files. We identified comorbidities using the claims from MedPAR, Carrier, and OutSAF files in the year prior to the admission.[11] We identified total hospitalizations and outpatient visits in the prior year from MedPAR files and Carrier files, respectively. We obtained education status at the level of zip code of residence from the 2011 American Community Survey estimates from the United States Census Bureau. We determined urban or rural residence using the 2013 Rural‐Urban Continuum Codes developed by the United States Department of Agriculture.
ED Facility Characteristics
We used the provider number of the ED facility to link to the Provider of Services files and obtained information on medical school affiliation, facility size, and for profit status.
Study Outcomes
The outcome of this study was readmission after an ED visit within 30 days of discharge from an initial hospitalization. We defined readmission after an ED visit as a hospitalization starting the day of or the day following the ED visit
Statistical Analyses
We performed 2‐level analyses where patients were clustered with ED providers to examine variation among ED providers. The effect of ED providers was modeled as a random effect to account for the correlation among the patients cared for by the same ED provider. We derived ED provider‐specific estimates from models adjusted for patient age, gender, race/ethnicity, rural or urban residence, Medicaid eligibility, education at the zip code level of residence, and characteristics of the initial admission (emergency admission, weekend admission, discharge destination, its major diagnostic category and DRG weight). We also adjusted for comorbidities, number of hospitalizations, and number of physician visits in the year before the initial admission.
We also conducted 2‐level analyses where patients were nested in ED facilities and 3‐level analyses where patients were nested in ED providers and ED providers were nested in ED facilities. We adjusted for all factors described above. We computed the change in the variance between 2‐level and 2‐level analyses to determine the variation in readmission rates that was explained by the ED provider and the ED facility. All analyses were performed with SAS version 9.2 (SAS Institute Inc., Cary, NC).
RESULTS
We identified 174,209 patients who visited an ED within 30 days of discharge from an initial hospitalization. Table 1 describes the characteristics of these patients as well as the readmission rates associated with these characteristics. The rate of readmission of our cohort of 1,627,705 discharges with or without a following ED visit was 16.2%, whereas the rate of readmission following an ED visit in our final cohort of 174,209 patients was 52.67%. This readmission rate increased with age, from 49.31% for patients between 66 and 70 years of age to 55.33% for patients older than 85 years. There were minor variations by gender and ethnicity. Patients residing in metropolitan areas or in zip codes with low education levels had higher readmission rates, as did those whose original admission was classified as emergency or those who were not discharged home.
| Patient Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| MeanSD, Median (Q1Q3) | Odds Ratio (95% CI)a | ||
| |||
| Overall | 174,209 (100) | 52.67 | |
| Age, y | |||
| 6670 | 32,962 (18.92) | 49.31 | 1.00 |
| 7175 | 34,979 (20.08) | 51.48 | 1.10 (1.06‐1.13)b |
| 7680 | 36,728 (21.08) | 53.01 | 1.15 (1.12‐1.19)b |
| 8185 | 34,784 (19.97) | 54.05 | 1.19 (1.15‐1.23)b |
| >85 | 34,756 (19.95) | 55.33 | 1.25 (1.21‐1.29)b |
| Gender | |||
| Male | 71,049 (40.78) | 52.95 | 1.02 (1.00‐1.04) |
| Female | 103,160 (59.22) | 52.48 | 1.00 |
| Race | |||
| Non‐Hispanic white | 124,312 (71.36) | 52.77 | 1.00 |
| Black | 16,809 (9.65) | 51.45 | 0.84 (0.81‐0.87)b |
| Hispanic | 30,618 (17.58) | 52.70 | 0.88 (0.85‐0.91)b |
| Other | 2,470 (1.42) | 55.71 | 1.06 (0.97‐1.15) |
| Rural/urban residence | |||
| Metropolitan | 136,739 (78.49) | 53.88 | 1.00 |
| Nonmetropolitan | 35,000 (20.09) | 48.16 | 0.96 (0.93‐0.99)b |
| Rural | 2,448 (1.41) | 50.04 | 1.04 (0.95‐1.13) |
| Medicaid eligible | |||
| No | 128,909 (74.00) | 52.65 | 1.00 |
| Yes | 45,300 (26.00) | 52.72 | 0.97 (0.94‐0.99)b |
| Education levelc | |||
| 1st quartile (lowest) | 43,863 (25.18) | 54.61 | 1.00 |
| 2nd quartile | 43,316 (24.86) | 53.92 | 1.00 (0.97‐1.03) |
| 3rd quartile | 43,571 (25.01) | 50.72 | 0.99 (0.96‐1.02) |
| 4th quartile (highest) | 43,318 (24.87) | 51.98 | 1.01 (0.97‐1.04) |
| Emergency admission | |||
| No | 99,101 (56.89) | 51.15 | 1.00 |
| Yes | 75,108 (43.11) | 54.68 | 1.07 (1.05‐1.09)b |
| Weekend admission | |||
| No | 131,266 (75.35) | 52.45 | 1.00 |
| Yes | 42,943 (24.65) | 53.35 | 1.01 (0.99‐1.04) |
| Discharge destination | |||
| Home | 122,542 (70.34) | 50.90 | 1.00 |
| Inpatient rehabilitation facility | 9,512 (5.46) | 55.48 | 1.31 (1.25‐1.37)b |
| Skilled nursing facility | 37,248 (21.38) | 57.25 | 1.29 (1.26‐1.33)b |
| Other | 4,907 (2.82) | 56.88 | 1.14 (1.07‐1.21)b |
| DRG weight (per unit) | 1.561.27, 0.82 (1.16‐1.83) | 1.06 (1.05‐1.07)b | |
| Hospitalization in the prior year (per hospitalization) | 1.031.49, 0.00 (1.00‐2.00) | 1.04 (1.03‐1.04)b | |
| Physician visits in the prior year (per 10 visits) | 11.759.80, 5.00 (10.00‐17.00) | 0.97 (0.96‐0.98)b | |
Table 1 also presents the odds of readmission adjusted for all other factors in the table and also adjusted for clustering within ED providers in a 2‐level model. Increasing age, white race, metropolitan residence, nonhome discharge, higher severity of illness, more hospitalizations in the prior year, fewer physician visits in the prior year, and an emergency initial admission were each associated with a higher readmission rate.
We next generated estimates of readmission rates for each ED provider from the adjusted 2‐level models. Figure 1 shows the adjusted cumulative readmission rates for the 1922 ED providers. This figure shows the mean value and 95% confidence intervals of the readmission rates for each provider. Dark vertical lines indicate providers whose readmission rate differed significantly from the mean adjusted readmission rate of 52.1% for all providers. Of the ED providers, 14.2% had significantly higher readmission rates. The mean readmission rate for these 272 providers was 67.2%. Of the ED providers, 14.7% had significantly lower readmission rates. The mean readmission rate for these 283 providers was 36.8%.
To determine the contribution of the ED facility to the variation in readmission rates, we restricted our analysis to 48,883 patients (28.06% of our cohort) seen by 525 ED providers who were associated with only 1 facility (total of 143 facilities). Table 2 describes the unadjusted readmission rates stratified by specific characteristics of those facilities. The unadjusted readmission rate increased with the size of the associated hospital, from 47.61% for hospitals with less than 100 beds to 57.06% for hospitals with more than 400 beds. The readmission rate for nonprofit facilities was 53.81% and for for‐profit facilities was 57.39%. Facilities with no medical school affiliation had a readmission rate of 54.51%, whereas those with a major affiliation had a readmission rate of 58.72%.
| ED Facility Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| |||
| Overall | 48,883 | ||
| Total beds | |||
| 100 | 3,936 (8.05) | 47.61 | 1.00 |
| 101200 | 6,251 (12.79) | 52.07 | 1.38 (1.06‐1.81)b |
| 201400 | 13,000 (26.59) | 56.26 | 1.69 (1.32‐2.17)b |
| >400 | 25,696 (52.57) | 57.06 | 1.77 (1.35‐2.33)b |
| Type of control | |||
| Nonprofit | 24,999 (51.14) | 53.81 | 1.00 |
| Proprietary | 17,108 (35.00) | 57.39 | 1.32 (1.09‐1.61)b |
| Government | 6,776 (13.86) | 56.60 | 1.11 (0.88‐1.41) |
| Medical school affiliation | |||
| Major | 6,487 (13.27) | 58.72 | 1.00 |
| Limited | 7,066 (14.45) | 56.37 | 0.85 (0.58‐1.25) |
| Graduate | 3,164 (6.47) | 56.19 | 0.71 (0.44‐1.15) |
| No affiliation | 32,166 (65.80) | 54.51 | 0.78 (0.57‐1.05) |
| If the same hospital patient was discharged from | |||
| Yes | 38,532 (78.82) | 55.64 | 0.96 (0.91‐1.00) |
| No | 10,351 (21.18) | 54.73 | 1.00 |
With this smaller cohort, we performed 2 types of 2‐level models, where patients clustered within ED facilities and ER providers, respectively, and a 3‐level model accounting for clustering of patients within providers and of providers within facilities. From the facility‐patient 2‐level model, the variance of the ED facility was 0.2718 (95% confidence interval [CI]: 0.2083‐0.3696). From the provider‐patient 2‐level model, the variance of ED provider was 0.2532 (95% CI: 0.2166‐0.3002). However, when the 3‐level model was performed, the variance of ED provider decreased to 0.0893 (95% CI: 0.0723‐0.1132) and the variance of ED facility dropped to 0.2316 (95% CI: 0.1704‐0.3331) . This indicates 65% of the variation among ED providers was explained by the ED facility, and in contrast, 15% of the variation among ED facilities was explained by ED providers.
Table 2 also shows the adjusted odds of readmission generated from the 3‐level model. Patients receiving care in ED facilities in hospitals with more beds and in for‐profit hospitals were at higher risk for readmission. It is possible that patients seen at the ED associated with the discharging hospital had a lower risk of readmission. This finding was close to being statistically significant (P=0.051).
We repeated all the above analyses using an outcome of readmission anytime between the ED visit and 30 days after discharge from the initial hospitalization (rather than readmission on the day of or after the ED visit). All analyses produced results similar to the results presented above. For example, Figure 2 shows the adjusted cumulative readmission rates for the 1922 ED providers using this outcome. Of the ED providers, 12.8% had higher and 12.5% had lower readmission rates as compared to the mean readmission rate for all ED providers. The Spearman correlation coefficient between the rank of ED providers in immediate readmission rate (Figure 1) and readmission rate within 30 days of hospital discharge (Figure 2) was 0.94 (P<0.001).
DISCUSSION
This study found substantial variation in readmission rates by ED provider, despite controlling for patient clinical and sociodemographic factors. In 3‐level models, the ED facility explained a substantial part of the variation by ED provider, with patients seen at larger facilities and for‐profit facilities having higher readmission rates.
Variation among ED facilities and ED providers in readmission rates has not previously been studied. There is literature on the variation in ED facility and ED provider admission rates. As readmissions are a subset of all admissions, this literature provides context to our findings. Abualenain et al. examined admission rates for 89 ED physicians for adult patients presenting with an acute medical or surgical complaint at 3 EDs in a health system.[12] After adjusting for patient and clinical characteristics, admission rates varied from 21% to 49% among physicians and from 27% to 41% among 3 facilities. Two other studies from single hospitals have found similar variation among providers.[13, 14] The reasons for the variation among ED providers presumably relate to subjective aspects of clinical assessment and the reluctance of providers to rely solely on objective scales, even when they are available.[14, 15] Variation in admission rates among different facilities may relate to clustering of providers with similar practice styles within facilities, lack of clinical guidelines for certain conditions, as well as differences among facilities in the socioeconomic status and access to primary care of their clientele.[12, 16, 17] For example, Pines et al. have shown that ED facility admission rates are higher in communities with fewer primary care physicians per capita and are influenced by the prevailing county level admission rates.[16] Capp et al. showed persistent variation in admission rates across hospitals, despite adjusting for clinical criteria such as vital signs, chief complaints, and severity of illness.[18]
Structural differences in ED facilities may also influence the decision to admit. We found that patients visiting ED facilities in hospitals with more beds had a higher readmission rate. ED facility systems of care such as observation units or protocols are associated with lower admission rates.[19, 20] Finally, certain hospitals may actively influence the admission practice patterns of their ED providers. We noted that patients seen at for‐profit ED facilities had a greater risk of readmission. A similar finding has been described by Pines et al., who noted higher admission rates at for‐profit facilities.[16] In an extreme example, a recent Justice Department lawsuit alleged that a for‐profit hospital chain used software systems and financial incentives to ED providers to increase admissions.[21]
It is possible that the providers with low readmission rates may have inappropriately released patients who truly should have been admitted. A signal that this occurred would be if these patients were readmitted in the days after the ED visits. We examined this possibility by additionally examining readmissions occurring anytime between the ED visit until 30 days after discharge from the initial hospitalization. The results were similar to when we only included readmissions that occurred immediately following the ED visit, with a very high correlation (r=0.94) between the ranking of the ED providers by readmission rates in both circumstances. This suggests that the decisions of the ED providers with low readmission rates to admit or release from the ED were likely appropriate.
Our research has limitations. We studied patients with fee‐for‐service Medicare in a single large state in the United States over a 4‐year period. Our findings may not be generalizable to younger patient populations, other regions with different sociodemographic patterns and healthcare systems, or other time periods. We could not control for many factors that may impact the risk of readmission but are not measured in Medicare databases (eg, clinical data such as vital signs, measures of quality of transition from discharging hospital, ED provider workload). To attribute care to a single ED provider, we excluded patients who were taken care of by multiple ED providers. These patients may have different needs from our study population (eg, more complex issues and longer stays in the ED) and may bias our results.
This study provides a new direction for research and quality improvement targeting readmissions. Research should extend beyond the discharge transition and examine the entire trajectory of posthospitalization care to better understand readmissions. Based directly on this study, research could investigate the practice patterns of ED providers and systems of care at ED facilities that affect readmissions rates. Such investigation could inform quality improvement efforts to standardize care for patients in the ED.
CMS policies hold hospitals accountable for readmissions of the patients they discharge, but do not address the admission process in the ED that leads to readmissions of recently discharged patients. Given the present study, and the fact that the proportion of all hospital admissions that occur through the ED has grown to 44%,[22] consideration of the role of the ED in public policy efforts to discourage unnecessary inpatient care may be appropriate.
In summary, this study shows that a recently discharged patient's chances of being readmitted depends partly on the ED provider who evaluates them and on the ED facility at which they seek care. ED provider practice patterns and ED facility systems of care may be a target for interventions aimed at decreasing readmission rates.
Disclosures
This research was supported by grants from the National Institutes of Health (AG033134 and K05CA134923) and from the Agency for Healthcare Research and Quality (R24H5022134). The authors report no conflicts of interest.
Readmissions of Medicare beneficiaries within 30 days of discharge are frequent and costly.[1] Concern about readmissions has prompted the Centers for Medicare & Medicaid Services (CMS) to reduce payments to hospitals with excess readmissions.[2] Research has identified a number of patient clinical and socio‐demographic factors associated with readmissions.[3] However, interventions designed to reduce readmissions have met with limited success. In a systematic review, no single intervention was regularly effective in reducing readmissions, despite the fact that interventions have targeted both predischarge, transition of care, and postdischarge processes of care.[4]
The different trajectories of care experienced by patients after hospital discharge, and their effect on risk of readmission, have been incompletely studied. Although early outpatient follow‐up after discharge is associated with lower readmission rates,[5, 6] a factor that has been minimally studied is the role of the emergency department (ED) and the ED provider in readmissions. The ED and ED providers feature prominently in the care received by patients shortly after discharge from a hospital. About a quarter of all hospitalized Medicare patients are evaluated in an ED within 30 days of discharge,[7, 8] and a majority of readmissions within 30 days of discharge are precipitated by an ED visit.[9] Hence, we asked whether when a recently discharged patient is seen in an ED, does the rate of readmission vary by ED provider and by ED facility?
We used Texas Medicare claims data to examine patients visiting the ED within 30 days of discharge from an initial hospitalization to determine if their risk of readmission varies by the ED provider caring for them and by the ED facility they visit.
METHODS
Sources of Data
We used claims from the years 2007 to 2011 for 100% of Texas Medicare beneficiaries, including Medicare beneficiary summary files, Medicare Provider Analysis and Review (MedPAR) files, Outpatient Standard Analytical Files (OutSAF), and Medicare Carrier files. We obtained diagnosis‐related group associated information, including weights, and Major Diagnostic Category from CMS, and used Provider of Services files to determine facility characteristics.
Establishment of the Study Cohort
From 2008 through 2011 MedPAR files, we initially selected all hospital discharges from acute‐care hospitals in Texas. From these 3,191,160 admissions, we excluded those discharged dead or transferred to other acute‐care hospitals (N=230,343), those who were younger than 66 years at admission (N=736,685) and those without complete Parts A and B enrollment or with any health maintenance organization enrollment in the 12 months prior to and 2 months after the admission of interest (N=596,427). From the remaining 1,627,705 discharges, we identified 302,949 discharges that were followed by at least 1 ED visit within 30 days.
We applied the algorithm developed by Kaskie et al. to identify ED visits.[10] We identified claims for ED services with Current Procedural Terminology (CPT) codes 99281‐99285 from Carrier files and bundled claims with overlapping dates or those that were within 1 day of each other. Then we identified claims for ED services using the same CPT codes from OutSAF and bundled those with overlapping dates or those that were within 3 days of each other. Finally, we bundled Carrier and OutSAF claims with overlapping dates and defined them as the same ED visit. From these, we retained only the first ED visit. We excluded those receiving care from multiple ED providers during the ED visit (N=38,565), and those who had a readmission before the first ED visit (N=1436), leaving 262,948 ED visits. For patients who had more than 1 hospitalization followed by an ED visit in a given year, we selected the first hospitalization, resulting in 199,143 ED visits. We then selected ED providers associated with at least 30 ED visits in this cohort, resulting in 1922 ED providers and 174,209 ED visits. For analyses where we examined both ED provider and facility variation in admission rates, we eliminated ED providers that generated charges from more than 1 ED facility, resulting in 525 providers and 48,883 ED visits at 143 ED facilities.
Measures
Patient Characteristics
We categorized beneficiaries by age, gender, and ethnicity using Medicare beneficiary summary files. We used the Medicaid indicator as a proxy of low socioeconomic status. We obtained information on weekend admission, emergent admission, discharge destination, and diagnosis‐related groupt (DRG) from MedPAR files. We identified comorbidities using the claims from MedPAR, Carrier, and OutSAF files in the year prior to the admission.[11] We identified total hospitalizations and outpatient visits in the prior year from MedPAR files and Carrier files, respectively. We obtained education status at the level of zip code of residence from the 2011 American Community Survey estimates from the United States Census Bureau. We determined urban or rural residence using the 2013 Rural‐Urban Continuum Codes developed by the United States Department of Agriculture.
ED Facility Characteristics
We used the provider number of the ED facility to link to the Provider of Services files and obtained information on medical school affiliation, facility size, and for profit status.
Study Outcomes
The outcome of this study was readmission after an ED visit within 30 days of discharge from an initial hospitalization. We defined readmission after an ED visit as a hospitalization starting the day of or the day following the ED visit
Statistical Analyses
We performed 2‐level analyses where patients were clustered with ED providers to examine variation among ED providers. The effect of ED providers was modeled as a random effect to account for the correlation among the patients cared for by the same ED provider. We derived ED provider‐specific estimates from models adjusted for patient age, gender, race/ethnicity, rural or urban residence, Medicaid eligibility, education at the zip code level of residence, and characteristics of the initial admission (emergency admission, weekend admission, discharge destination, its major diagnostic category and DRG weight). We also adjusted for comorbidities, number of hospitalizations, and number of physician visits in the year before the initial admission.
We also conducted 2‐level analyses where patients were nested in ED facilities and 3‐level analyses where patients were nested in ED providers and ED providers were nested in ED facilities. We adjusted for all factors described above. We computed the change in the variance between 2‐level and 2‐level analyses to determine the variation in readmission rates that was explained by the ED provider and the ED facility. All analyses were performed with SAS version 9.2 (SAS Institute Inc., Cary, NC).
RESULTS
We identified 174,209 patients who visited an ED within 30 days of discharge from an initial hospitalization. Table 1 describes the characteristics of these patients as well as the readmission rates associated with these characteristics. The rate of readmission of our cohort of 1,627,705 discharges with or without a following ED visit was 16.2%, whereas the rate of readmission following an ED visit in our final cohort of 174,209 patients was 52.67%. This readmission rate increased with age, from 49.31% for patients between 66 and 70 years of age to 55.33% for patients older than 85 years. There were minor variations by gender and ethnicity. Patients residing in metropolitan areas or in zip codes with low education levels had higher readmission rates, as did those whose original admission was classified as emergency or those who were not discharged home.
| Patient Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| MeanSD, Median (Q1Q3) | Odds Ratio (95% CI)a | ||
| |||
| Overall | 174,209 (100) | 52.67 | |
| Age, y | |||
| 6670 | 32,962 (18.92) | 49.31 | 1.00 |
| 7175 | 34,979 (20.08) | 51.48 | 1.10 (1.06‐1.13)b |
| 7680 | 36,728 (21.08) | 53.01 | 1.15 (1.12‐1.19)b |
| 8185 | 34,784 (19.97) | 54.05 | 1.19 (1.15‐1.23)b |
| >85 | 34,756 (19.95) | 55.33 | 1.25 (1.21‐1.29)b |
| Gender | |||
| Male | 71,049 (40.78) | 52.95 | 1.02 (1.00‐1.04) |
| Female | 103,160 (59.22) | 52.48 | 1.00 |
| Race | |||
| Non‐Hispanic white | 124,312 (71.36) | 52.77 | 1.00 |
| Black | 16,809 (9.65) | 51.45 | 0.84 (0.81‐0.87)b |
| Hispanic | 30,618 (17.58) | 52.70 | 0.88 (0.85‐0.91)b |
| Other | 2,470 (1.42) | 55.71 | 1.06 (0.97‐1.15) |
| Rural/urban residence | |||
| Metropolitan | 136,739 (78.49) | 53.88 | 1.00 |
| Nonmetropolitan | 35,000 (20.09) | 48.16 | 0.96 (0.93‐0.99)b |
| Rural | 2,448 (1.41) | 50.04 | 1.04 (0.95‐1.13) |
| Medicaid eligible | |||
| No | 128,909 (74.00) | 52.65 | 1.00 |
| Yes | 45,300 (26.00) | 52.72 | 0.97 (0.94‐0.99)b |
| Education levelc | |||
| 1st quartile (lowest) | 43,863 (25.18) | 54.61 | 1.00 |
| 2nd quartile | 43,316 (24.86) | 53.92 | 1.00 (0.97‐1.03) |
| 3rd quartile | 43,571 (25.01) | 50.72 | 0.99 (0.96‐1.02) |
| 4th quartile (highest) | 43,318 (24.87) | 51.98 | 1.01 (0.97‐1.04) |
| Emergency admission | |||
| No | 99,101 (56.89) | 51.15 | 1.00 |
| Yes | 75,108 (43.11) | 54.68 | 1.07 (1.05‐1.09)b |
| Weekend admission | |||
| No | 131,266 (75.35) | 52.45 | 1.00 |
| Yes | 42,943 (24.65) | 53.35 | 1.01 (0.99‐1.04) |
| Discharge destination | |||
| Home | 122,542 (70.34) | 50.90 | 1.00 |
| Inpatient rehabilitation facility | 9,512 (5.46) | 55.48 | 1.31 (1.25‐1.37)b |
| Skilled nursing facility | 37,248 (21.38) | 57.25 | 1.29 (1.26‐1.33)b |
| Other | 4,907 (2.82) | 56.88 | 1.14 (1.07‐1.21)b |
| DRG weight (per unit) | 1.561.27, 0.82 (1.16‐1.83) | 1.06 (1.05‐1.07)b | |
| Hospitalization in the prior year (per hospitalization) | 1.031.49, 0.00 (1.00‐2.00) | 1.04 (1.03‐1.04)b | |
| Physician visits in the prior year (per 10 visits) | 11.759.80, 5.00 (10.00‐17.00) | 0.97 (0.96‐0.98)b | |
Table 1 also presents the odds of readmission adjusted for all other factors in the table and also adjusted for clustering within ED providers in a 2‐level model. Increasing age, white race, metropolitan residence, nonhome discharge, higher severity of illness, more hospitalizations in the prior year, fewer physician visits in the prior year, and an emergency initial admission were each associated with a higher readmission rate.
We next generated estimates of readmission rates for each ED provider from the adjusted 2‐level models. Figure 1 shows the adjusted cumulative readmission rates for the 1922 ED providers. This figure shows the mean value and 95% confidence intervals of the readmission rates for each provider. Dark vertical lines indicate providers whose readmission rate differed significantly from the mean adjusted readmission rate of 52.1% for all providers. Of the ED providers, 14.2% had significantly higher readmission rates. The mean readmission rate for these 272 providers was 67.2%. Of the ED providers, 14.7% had significantly lower readmission rates. The mean readmission rate for these 283 providers was 36.8%.
To determine the contribution of the ED facility to the variation in readmission rates, we restricted our analysis to 48,883 patients (28.06% of our cohort) seen by 525 ED providers who were associated with only 1 facility (total of 143 facilities). Table 2 describes the unadjusted readmission rates stratified by specific characteristics of those facilities. The unadjusted readmission rate increased with the size of the associated hospital, from 47.61% for hospitals with less than 100 beds to 57.06% for hospitals with more than 400 beds. The readmission rate for nonprofit facilities was 53.81% and for for‐profit facilities was 57.39%. Facilities with no medical school affiliation had a readmission rate of 54.51%, whereas those with a major affiliation had a readmission rate of 58.72%.
| ED Facility Characteristic | No. of ED Visits (%) | % Readmitted | Odds Ratio (95% CI)a |
|---|---|---|---|
| |||
| Overall | 48,883 | ||
| Total beds | |||
| 100 | 3,936 (8.05) | 47.61 | 1.00 |
| 101200 | 6,251 (12.79) | 52.07 | 1.38 (1.06‐1.81)b |
| 201400 | 13,000 (26.59) | 56.26 | 1.69 (1.32‐2.17)b |
| >400 | 25,696 (52.57) | 57.06 | 1.77 (1.35‐2.33)b |
| Type of control | |||
| Nonprofit | 24,999 (51.14) | 53.81 | 1.00 |
| Proprietary | 17,108 (35.00) | 57.39 | 1.32 (1.09‐1.61)b |
| Government | 6,776 (13.86) | 56.60 | 1.11 (0.88‐1.41) |
| Medical school affiliation | |||
| Major | 6,487 (13.27) | 58.72 | 1.00 |
| Limited | 7,066 (14.45) | 56.37 | 0.85 (0.58‐1.25) |
| Graduate | 3,164 (6.47) | 56.19 | 0.71 (0.44‐1.15) |
| No affiliation | 32,166 (65.80) | 54.51 | 0.78 (0.57‐1.05) |
| If the same hospital patient was discharged from | |||
| Yes | 38,532 (78.82) | 55.64 | 0.96 (0.91‐1.00) |
| No | 10,351 (21.18) | 54.73 | 1.00 |
With this smaller cohort, we performed 2 types of 2‐level models, where patients clustered within ED facilities and ER providers, respectively, and a 3‐level model accounting for clustering of patients within providers and of providers within facilities. From the facility‐patient 2‐level model, the variance of the ED facility was 0.2718 (95% confidence interval [CI]: 0.2083‐0.3696). From the provider‐patient 2‐level model, the variance of ED provider was 0.2532 (95% CI: 0.2166‐0.3002). However, when the 3‐level model was performed, the variance of ED provider decreased to 0.0893 (95% CI: 0.0723‐0.1132) and the variance of ED facility dropped to 0.2316 (95% CI: 0.1704‐0.3331) . This indicates 65% of the variation among ED providers was explained by the ED facility, and in contrast, 15% of the variation among ED facilities was explained by ED providers.
Table 2 also shows the adjusted odds of readmission generated from the 3‐level model. Patients receiving care in ED facilities in hospitals with more beds and in for‐profit hospitals were at higher risk for readmission. It is possible that patients seen at the ED associated with the discharging hospital had a lower risk of readmission. This finding was close to being statistically significant (P=0.051).
We repeated all the above analyses using an outcome of readmission anytime between the ED visit and 30 days after discharge from the initial hospitalization (rather than readmission on the day of or after the ED visit). All analyses produced results similar to the results presented above. For example, Figure 2 shows the adjusted cumulative readmission rates for the 1922 ED providers using this outcome. Of the ED providers, 12.8% had higher and 12.5% had lower readmission rates as compared to the mean readmission rate for all ED providers. The Spearman correlation coefficient between the rank of ED providers in immediate readmission rate (Figure 1) and readmission rate within 30 days of hospital discharge (Figure 2) was 0.94 (P<0.001).
DISCUSSION
This study found substantial variation in readmission rates by ED provider, despite controlling for patient clinical and sociodemographic factors. In 3‐level models, the ED facility explained a substantial part of the variation by ED provider, with patients seen at larger facilities and for‐profit facilities having higher readmission rates.
Variation among ED facilities and ED providers in readmission rates has not previously been studied. There is literature on the variation in ED facility and ED provider admission rates. As readmissions are a subset of all admissions, this literature provides context to our findings. Abualenain et al. examined admission rates for 89 ED physicians for adult patients presenting with an acute medical or surgical complaint at 3 EDs in a health system.[12] After adjusting for patient and clinical characteristics, admission rates varied from 21% to 49% among physicians and from 27% to 41% among 3 facilities. Two other studies from single hospitals have found similar variation among providers.[13, 14] The reasons for the variation among ED providers presumably relate to subjective aspects of clinical assessment and the reluctance of providers to rely solely on objective scales, even when they are available.[14, 15] Variation in admission rates among different facilities may relate to clustering of providers with similar practice styles within facilities, lack of clinical guidelines for certain conditions, as well as differences among facilities in the socioeconomic status and access to primary care of their clientele.[12, 16, 17] For example, Pines et al. have shown that ED facility admission rates are higher in communities with fewer primary care physicians per capita and are influenced by the prevailing county level admission rates.[16] Capp et al. showed persistent variation in admission rates across hospitals, despite adjusting for clinical criteria such as vital signs, chief complaints, and severity of illness.[18]
Structural differences in ED facilities may also influence the decision to admit. We found that patients visiting ED facilities in hospitals with more beds had a higher readmission rate. ED facility systems of care such as observation units or protocols are associated with lower admission rates.[19, 20] Finally, certain hospitals may actively influence the admission practice patterns of their ED providers. We noted that patients seen at for‐profit ED facilities had a greater risk of readmission. A similar finding has been described by Pines et al., who noted higher admission rates at for‐profit facilities.[16] In an extreme example, a recent Justice Department lawsuit alleged that a for‐profit hospital chain used software systems and financial incentives to ED providers to increase admissions.[21]
It is possible that the providers with low readmission rates may have inappropriately released patients who truly should have been admitted. A signal that this occurred would be if these patients were readmitted in the days after the ED visits. We examined this possibility by additionally examining readmissions occurring anytime between the ED visit until 30 days after discharge from the initial hospitalization. The results were similar to when we only included readmissions that occurred immediately following the ED visit, with a very high correlation (r=0.94) between the ranking of the ED providers by readmission rates in both circumstances. This suggests that the decisions of the ED providers with low readmission rates to admit or release from the ED were likely appropriate.
Our research has limitations. We studied patients with fee‐for‐service Medicare in a single large state in the United States over a 4‐year period. Our findings may not be generalizable to younger patient populations, other regions with different sociodemographic patterns and healthcare systems, or other time periods. We could not control for many factors that may impact the risk of readmission but are not measured in Medicare databases (eg, clinical data such as vital signs, measures of quality of transition from discharging hospital, ED provider workload). To attribute care to a single ED provider, we excluded patients who were taken care of by multiple ED providers. These patients may have different needs from our study population (eg, more complex issues and longer stays in the ED) and may bias our results.
This study provides a new direction for research and quality improvement targeting readmissions. Research should extend beyond the discharge transition and examine the entire trajectory of posthospitalization care to better understand readmissions. Based directly on this study, research could investigate the practice patterns of ED providers and systems of care at ED facilities that affect readmissions rates. Such investigation could inform quality improvement efforts to standardize care for patients in the ED.
CMS policies hold hospitals accountable for readmissions of the patients they discharge, but do not address the admission process in the ED that leads to readmissions of recently discharged patients. Given the present study, and the fact that the proportion of all hospital admissions that occur through the ED has grown to 44%,[22] consideration of the role of the ED in public policy efforts to discourage unnecessary inpatient care may be appropriate.
In summary, this study shows that a recently discharged patient's chances of being readmitted depends partly on the ED provider who evaluates them and on the ED facility at which they seek care. ED provider practice patterns and ED facility systems of care may be a target for interventions aimed at decreasing readmission rates.
Disclosures
This research was supported by grants from the National Institutes of Health (AG033134 and K05CA134923) and from the Agency for Healthcare Research and Quality (R24H5022134). The authors report no conflicts of interest.
- , , Rehospitalizations among patients in the Medicare Fee‐for‐Service Program. N Engl J Med. 2009;360:1418–1428.
- Centers for Medicare 306:1688–1698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155:520–528.
- , , , , Outpatient follow‐up visit and 30‐day emergency department visit and readmission in patients hospitalized for chronic obstructive pulmonary disease. Arch Intern Med. 2010;170:1664–1670.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303:1716–1722.
- , , After hospitalization: a Dartmouth Atlas report on post‐acute care for Medicare beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed August 8, 2013.
- , , , Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013;62:145–150.
- , , , Emergency department visits after surgery are common for Medicare patients, suggesting opportunities to improve care. Health Aff (Millwood). 2013;32:1600–1607.
- , , , et al. Defining emergency department episodes by severity and intensity: a 15‐year study of Medicare beneficiaries. BMC Health Serv Res. 2010;10:1–13.
- , , , Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- , , , , , Emergency department physician‐level and hospital‐level variation in admission rates. Ann Emerg Med. 2013;61:638–643.
- , , , et al. Hospital admission decision for patients with community‐acquired pneumonia: variability among physicians in an emergency department. Ann Emerg Med. 2012;59:35–41.
- , , Individual emergency physician admission rates: predictably unpredictable. CJEM. 2009;11(2):149–155.
- , , , , , Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis. 2009;49:e100–e108.
- , , Variation in emergency department admission rates across the United States. Med Care Res Rev. 2013;70:218–231.
- , , , , , Variation in US hospital emergency department admission rates by clinical condition. Med Care. 2015;53:237–244.
- , , , et al. Hospital variation in risk‐standardized hospital admission rates from US EDs among adults. Am J Emerg Med. 2014;32:837–843.
- , , The effect of an observation unit on the rate of ED admission and discharge for pyelonephritis. Am J Emerg Med. 2010;28:682–688.
- , , , , , Protocol‐driven emergency department observation units offer savings, shorter stays, and reduced admissions. Health Aff (Millwood). 2013;32:2149–2156.
- , Hospital chain said to scheme to inflate bills. New York Times. January 23, 2014. Available at: http://www.nytimes.com/2014/01/24/business/hospital‐chain‐said‐to‐scheme‐to‐inflate‐bills.html?emc=eta1367:391–393.
- , , Rehospitalizations among patients in the Medicare Fee‐for‐Service Program. N Engl J Med. 2009;360:1418–1428.
- Centers for Medicare 306:1688–1698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155:520–528.
- , , , , Outpatient follow‐up visit and 30‐day emergency department visit and readmission in patients hospitalized for chronic obstructive pulmonary disease. Arch Intern Med. 2010;170:1664–1670.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303:1716–1722.
- , , After hospitalization: a Dartmouth Atlas report on post‐acute care for Medicare beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed August 8, 2013.
- , , , Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013;62:145–150.
- , , , Emergency department visits after surgery are common for Medicare patients, suggesting opportunities to improve care. Health Aff (Millwood). 2013;32:1600–1607.
- , , , et al. Defining emergency department episodes by severity and intensity: a 15‐year study of Medicare beneficiaries. BMC Health Serv Res. 2010;10:1–13.
- , , , Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
- , , , , , Emergency department physician‐level and hospital‐level variation in admission rates. Ann Emerg Med. 2013;61:638–643.
- , , , et al. Hospital admission decision for patients with community‐acquired pneumonia: variability among physicians in an emergency department. Ann Emerg Med. 2012;59:35–41.
- , , Individual emergency physician admission rates: predictably unpredictable. CJEM. 2009;11(2):149–155.
- , , , , , Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis. 2009;49:e100–e108.
- , , Variation in emergency department admission rates across the United States. Med Care Res Rev. 2013;70:218–231.
- , , , , , Variation in US hospital emergency department admission rates by clinical condition. Med Care. 2015;53:237–244.
- , , , et al. Hospital variation in risk‐standardized hospital admission rates from US EDs among adults. Am J Emerg Med. 2014;32:837–843.
- , , The effect of an observation unit on the rate of ED admission and discharge for pyelonephritis. Am J Emerg Med. 2010;28:682–688.
- , , , , , Protocol‐driven emergency department observation units offer savings, shorter stays, and reduced admissions. Health Aff (Millwood). 2013;32:2149–2156.
- , Hospital chain said to scheme to inflate bills. New York Times. January 23, 2014. Available at: http://www.nytimes.com/2014/01/24/business/hospital‐chain‐said‐to‐scheme‐to‐inflate‐bills.html?emc=eta1367:391–393.
© 2015 Society of Hospital Medicine
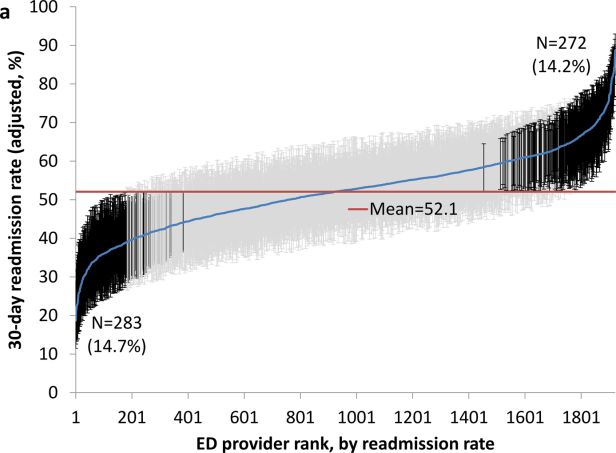
Weekend Discharge and Readmission
Hospital readmission, defined as an admission to a hospital within 30 days of discharge from an acute‐care hospitalization, is associated with short‐term morbidity, mortality, and medical costs.[1] In 2013, the Patient Protection and Affordable Care Act began assigning financial penalties to hospitals based on performance against benchmarks on readmission for acute myocardial infarction (AMI), pneumonia (PNA), and congestive heart failure (CHF) through its Hospital Readmission Reduction Program (HRRP).[2] In its third year, the program recently announced penalties for 2,610 hospitals that will total over $428 million.[3] Despite increased attention to this issue, few interventions have been identified that effectively reduce hospital readmissions.[4, 5]
Hospital discharge is a complex process that aims to achieve the safe transfer of care of a hospitalized patient to another setting (eg, home, skilled nursing facility [SNF]). Success depends on adequate staffing of physicians, nurses, case managers, social workers, and pharmacists; clear communication among patients and providers; and integrated coordination of care. Although much focus has been placed on the association between weekend hospital admission and increased mortality,[6, 7, 8] very little is known about the impact of weekend hospital discharge on outcomes, specifically hospital readmission rates. Furthermore, previous studies on this topic, based on Canadian data, have produced conflicting results.[9, 10, 11]
Staffing of physicians, physician extenders (eg, physician assistants or nurse practitioners), nurses, case managers, social workers, and ancillary staff (eg, physical and occupational therapists) are all typically reduced on the weekend. Patients may be cared for by covering healthcare providers. These factors may have important implications on the timeliness of discharge, accuracy of discharge instructions, safety of discharge (eg, clearance by physical therapy), and medication reconciliation, among others. Clinic offices are more likely to be closed, and therefore, some follow‐up appointments may inadvertently not be scheduled, and lack of timely postdischarge follow‐up may be associated with higher rates of readmission.[12] Reduced outpatient pharmacy availability may also cause delays in patients receiving their medications,[13] which may exacerbate failed transition to the outpatient setting due to medication noncompliance.[14]
Based on this rationale, the current study was designed to investigate the association between weekend discharge and 30‐ and 90‐ day readmissions in patients hospitalized for medical diagnoses included in Centers for Medicare and Medicaid Services' HRRP.[15] To do so, a large‐state, all‐payer discharge database with individual patient record linkage numbers (RLN) was selected to capture all readmissions, even those to a different hospital. We hypothesized that patients who are discharged on a weekend would have higher hospital readmission rates compared to those discharged on a weekday.
METHODS
Approval was obtained from both the California Committee for the Protection of Human Subjects and the Stanford University Institutional Review Board. The California Office of State Health Planning and Development (OSHPD) 2012 Patient Discharge Data (PDD) was utilized for this study. The OSHPD‐PDD contains records for all patients admitted and eventually discharged from every general, acute, nonfederal hospital within the state. Demographic variables contained in the dataset include age, gender, race, and a unique RLN (an individually assigned number based on the patient's social security number and other demographics) to associate discharged patients with subsequent hospitalizations. Clinical information collected included principal diagnosis (indication for admission), 24 additional diagnoses with an indicator as to whether or not the condition was present on admission (POA) to differentiate comorbidities from complications, and principle procedure codes. Details about the admission included date of admission and discharge, admission type (scheduled or unscheduled), expected payer/emnsurance and disposition (home, acute rehabilitation, skilled nursing facility, residential facility, other). Details about the hospital included a unique identification number to indicate the location of care for both index/discharge and subsequent readmission.
International Classification of Disease, Ninth Edition, Clinical Modification (ICD‐9‐CM) coding schema were used to identify all patients admitted with the principal diagnosis of AMI (ICD‐9‐CM code 410.xx), CHF (428.xx), or PNA (480.xx‐486.xx). We excluded patients who were coded as having in‐hospital mortality, as these patients would not be eligible for readmission, those who were transferred to a different inpatient acute‐care facility, and those with invalid RLNs. Patients were separated into 2 groups based on the day of discharge. Weekday was defined as Monday through Friday, whereas weekend was defined as Saturday and Sunday. The Charlson Comorbidity Index was calculated based on POA comorbidities.
Demographic data, hospital variables, and readmission rates were directly compared for patients discharged on a weekend compared to weekday after admission for AMI, CHF, or PNA. Hospital readmission was defined as the first inpatient hospitalization for any reason at either 30 or 90 days following discharge from an index acute‐care hospitalization. Hospital identification codes were used to determine whether the readmission occurred at the index (discharging) hospital or to a different facility. The principal diagnosis for the subsequent admission was assessed to identify the most common reasons for readmission.
The [2] test and Student t test were used to compare mean values between the 2 groups when appropriate, with statistical significance set as P<0.05. Univariate and multivariable logistic regression models were built to estimate the odds of hospital readmission based on weekend versus weekday discharge after controlling for age, gender, race, Charlson Comorbidity Index, discharge disposition, payer status, length of stay, presence of complication, and admission type. All statistical analyses were 2‐tailed and performed using SAS 9.3 for windows (SAS Institute Inc., Cary, NC). The odds ratio (OR) was considered significant when it was not equal to 1, the 95% confidence interval (CI) did not include 1, and the P value was less than 0.05.
RESULTS
Patient Characteristics
There were 266,519 patients hospitalized with a principal diagnosis of AMI, CHF, or PNA in California during 2012 and met all inclusion criteria. The cohort consisted of 77,853 (29.2%) with AMI, 91,327 (34.3%) with CHF, and 97,339 (36.5%) with PNA. A total of 60,097 (22.5%) patients were discharged on the weekend compared to 206,422 (77.5%) on a weekday, which was similar across diagnosis groups. Differences in gender, age, race, Charlson comorbidity score, insurance status, type of admission, or occurrence of complications between patients who were discharged on the weekend versus weekday are listed in Table 1. Patients discharged on a weekend had a shorter average length of stay (LOS) (AMI: 4.05.6 days vs 4.67.7 days; CHF: 5.19.3 vs 6.034.1; PNA: 5.011.7 vs 5.710.7). A higher proportion of these patients were discharged to home (AMI: 67.1% vs 63.8%; CHF: 53.3% vs 49.4%; PNA: 57.0% vs 52.9%), whereas a smaller proportion were discharged to an SNF (AMI: 7.0% vs 9.6%; CHF: 11.2% vs 15.9%; PNA: 12.8% vs 17.8%).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Weekend | Weekday | Weekend | Weekday | Weekend | Weekday | |
| ||||||
| No. (%) | 18,061 (23.2) | 59,792 (76.8) | 20,487 (22.4) | 70,840 (77.6) | 21,549 (22.1) | 75,790 (77.9) |
| Age, y | ||||||
| 044 | 4.7 | 4.5 | 4.5 | 4.1 | 9.4 | 8.6 |
| 4554 | 13.1 | 13.0 | 8.5 | 8.3 | 9.8 | 9.9 |
| 5564 | 22.6 | 22.4 | 14.3 | 14.6 | 14.9 | 14.9 |
| 6574 | 22.5 | 22.7 | 19.2 | 18.7 | 18.3 | 18.0 |
| 7584 | 21.4 | 21.4 | 26.4 | 26.3 | 24.1 | 24.0 |
| 85+ | 15.6 | 16.0 | 27.2 | 28.0 | 23.5 | 24.5 |
| Mean (SD) | 68.5 (14.3) | 68.7 (14.3) | 73.3 (15.1) | 3.6 (15.0) | 70.0 (17.6) | 70.5 (17.4) |
| Sex | ||||||
| Male | 62.0 | 61.7 | 51.7 | 51.4 | 47.9 | 47.0 |
| Female | 38.0 | 38.3 | 48.3 | 48.6 | 52.1 | 52.1 |
| Race | ||||||
| White | 63.5 | 62.9 | 58.7 | 58.5 | 63.0 | 62.4 |
| Black | 6.9 | 7.3 | 12.0 | 12.1 | 7.7 | 8.0 |
| Hispanic | 19.5 | 20.0 | 20.3 | 20.6 | 20.4 | 20.7 |
| API | 10.0 | 9.7 | 9.0 | 8.8 | 8.8 | 8.9 |
| Charlson Comorbidity Index | ||||||
| 0 | 30.7 | 30.1 | 9.4 | 9.5 | 23.0 | 22.2 |
| 1 | 25.1 | 24.9 | 19.5 | 19.8 | 25.7 | 26.4 |
| 2 | 14.9 | 15.2 | 20.4 | 20.3 | 17.3 | 17.4 |
| 3 | 29.2 | 29.8 | 50.8 | 50.4 | 34.0 | 34.1 |
| Mean (SD) | 2.1 (2.2) | 2.1 (2.2) | 3.0 (2.3) | 3.0 (2.3) | 2.4 (2.6) | 2.4 (2.5) |
| Payer status | ||||||
| Private | 25.4 | 25.1 | 11.3 | 10.7 | 15.7 | 14.4 |
| Medicare | 57.6 | 57.9 | 72.7 | 73.1 | 67.1 | 68.1 |
| Medicaid | 8.0 | 8.0 | 10.0 | 10.6 | 11.5 | 11.8 |
| No insurance | 4.2 | 4.0 | 2.7 | 2.3 | 2.6 | 2.5 |
| Unknown | 4.8 | 4.9 | 3.3 | 3.3 | 3.2 | 3.2 |
| Complication | ||||||
| Urinary tract infection | 6.0 | 6.8 | 10.3 | 10.8 | 10.2 | 11.0 |
| Acute MI | 6.7 | 6.9 | 2.7 | 2.6 | 1.2 | 1.2 |
| DVT/PE | 0.02 | 0.02 | 0.01 | 0.01 | 0.03 | 0.03 |
| Pneumonia | 0.06 | 0.05 | 0.09 | 0.08 | 0.1 | 0.1 |
| Hemorrhage | 1.7 | 1.7 | 1.5 | 1.5 | 1.2 | 1.1 |
| Sepsis | 3.5 | 3.6 | 6.2 | 6.0 | 7.4 | 7.6 |
| Mean length of stay (SD) | 4.0 (5.6) | 4.6 (7.7) | 5.1 (9.3) | 6.0 (34.1) | 5.0 (11.7) | 5.7 (10.7) |
| Disposition | ||||||
| Home | 67.1 | 63.8 | 53.3 | 49.4 | 57.0 | 52.9 |
| Acute rehabilitation | 1.9 | 3.2 | 0.7 | 0.9 | 0.5 | 0.7 |
| Skilled nursing facility | 7.0 | 9.6 | 11.2 | 15.9 | 12.8 | 17.8 |
| Residential facility | 0.4 | 0.5 | 0.9 | 1.0 | 1.1 | 1.4 |
| Other | 23.6 | 23.0 | 33.9 | 32.8 | 28.6 | 27.2 |
| Admission type | ||||||
| Elective | 8.9 | 10.1 | 7.9 | 9.1 | 7.1 | 7.6 |
| Unplanned | 91.0 | 89.9 | 92.1 | 90.9 | 92.9 | 92.3 |
Rate, Reason, and Location of Readmission
Table 2 shows overall rates of readmission. Among all patients, there were no significant differences in the unadjusted readmission rates for patients being discharged on a weekend versus weekday at either 30 days (16.7% vs 17.0%, P=0.14) or 90 days (26.9% vs 27.5%, P=0.05) (Table 2). Unadjusted 30‐day readmission rates were similar between the 2 groups for AMI (21.9% vs 21.9%, P=0.94) and PNA (12.1% vs 12.4%, P=0.28), whereas they were higher for weekday discharges in CHF (15.4% vs 16.0%, P=0.04). Similar results were seen for 90‐day readmission rates. To elucidate the impact of discharge disposition, a subset analysis was performed based on day of discharge and disposition (Figure 1). There was no difference in rates of readmission among patients discharged home on a weekend versus weekday (AMI: 21.3% vs 21.1%, P=0.78; CHF: 12.2% vs 12.6%, P=0.29; PNA: 8.3% vs 8.6%, P=0.29).
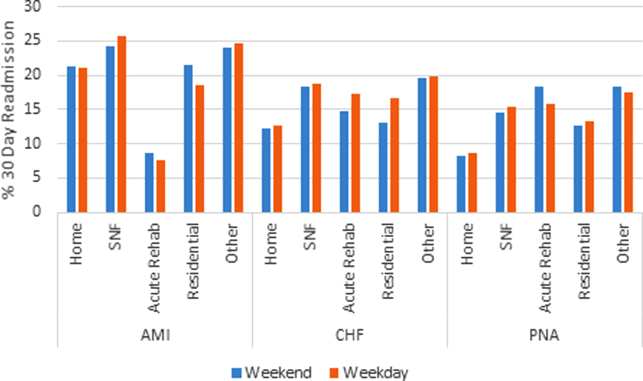
Abbreviations: AMI, acute myocardial infarction; CHF, congestive heart failure; PNA, pneumonia; SNF, skilled nursing facility.
| AMI | CHF | PNA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Weekend | Weekday | P Value | Weekend | Weekday | P Value | Weekend | Weekday | P Value | |
| |||||||||
| 30‐day readmission (%) | 3,954 (21.9) | 13,106 (21.9) | 0.94 | 3,162 (15.4) | 11,366 (16.0) | 0.04 | 2,608 (12.1) | 9,380 (12.4) | 0.28 |
| 90‐day readmission (%) | 5,253 (29.1) | 17,344 (29.0) | 0.84 | 5,994 (29.3) | 21,355 (30.2) | 0.008 | 4,698 (21.8) | 16,910 (22.3) | 0.11 |
The reason for hospital readmission was most frequently related to the principal diagnosis. Among patients discharged after hospitalization for AMI, 45.3% of readmissions had a principal diagnosis of AMI, whereas 13.9% listed readmission for angina or coronary artery disease. Of CHF discharges, at least 26.7% of readmissions were for CHF. PNA was the principal diagnosis in 19.8% of readmissions after admission for PNA. A significant proportion of patients (AMI: 64.8%, CHF: 35.0%, PNA: 32.9%) were readmitted to a different hospital than the discharging hospital.
Predictors of Readmission
On univariate logistic regression, discharge on a weekend was not associated with hospital readmission for patients admitted with AMI (OR: 1.0, 95% CI: 0.96‐1.04) or PNA (OR: 0.97, 95% CI: 0.93‐1.02) but was inversely associated for CHF (OR: 0.96, 95% CI: 0.91‐1.0). In multivariable models, weekend discharge was not associated with increased risk of readmission for any diagnosis (AMI [OR: 1.02, 95% CI: 0.98‐1.07], CHF [OR: 0.99, 95% CI: 0.95‐1.03], or PNA [OR: 1.02, 95% CI: 0.98‐1.07]; Table 3).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Univariate OR (95% CI) | Multivariable OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | |
| ||||||
| Weekend discharge | 1 (0.96‐1.04) | 1.02 (0.98‐1.06) | 0.96 (0.91‐1) | 0.99 (0.94‐1.03) | 0.97 (0.93‐1.02) | 1.02 (0.98‐1.07) |
| Age, y | ||||||
| 044 | ||||||
| 4554 | 1.02 (0.92‐1.12) | 0.96 (0.87‐1.07) | 1.04 (0.93‐1.16) | 1.00 (0.89‐1.11) | 1.08 (0.98‐1.19) | 0.93 (0.84‐1.03) |
| 5564 | 1.11 (1.02‐1.22) | 1.00 (0.91‐1.10) | 1.11 (1.01‐1.23) | 0.97 (0.88‐1.08) | 1.23 (1.13‐1.34) | 0.94 (0.86‐1.03) |
| 6574 | 1.31 (1.19‐1.43) | 1.04 (0.94‐1.15) | 1.1 (1‐1.22) | 0.90 (0.81‐1.01) | 1.29 (1.19‐1.41) | 0.87 (0.79‐0.96) |
| 7584 | 1.29 (1.18‐1.41) | 0.94 (0.85‐1.05) | 1.06 (0.97‐1.17) | 0.84 (0.75‐0.93) | 1.37 (1.27‐1.49) | 0.87 (0.79‐0.95) |
| 85+ | 1.03 (0.94‐1.13) | 0.72 (0.64‐0.81) | 0.98 (0.89‐1.08) | 0.76 (0.68‐0.84) | 1.31 (1.2‐1.41) | 0.78 (0.71‐0.86) |
| Gender | ||||||
| Female | ||||||
| Male | 1 (0.97‐1.04) | 1.1 (1.05‐1.14) | 1.06 (1.02‐1.1) | 1.08 (1.04‐1.12) | 1.13 (1.09‐1.18) | 1.15 (1.10‐1.19) |
| Race | ||||||
| White | ||||||
| Black | 1.17 (1.1‐1.25) | 1.12 (1.05‐1.20) | 1.06 (1‐1.12) | 1.03 (0.97‐1.09) | 1.11 (1.04‐1.19) | 1.07 (0.99‐1.15) |
| Hispanic | 1.11 (1.06‐1.16) | 1.12 (1.06‐1.17) | 1.05 (1‐1.1) | 1.04 (1.00‐1.10) | 0.93 (0.89‐0.98) | 0.95 (0.90‐1.00) |
| API | 1.14 (1.07‐1.2) | 1.09 (1.03‐1.16) | 1.01 (0.95‐1.08) | 1.00 (0.94‐1.07) | 0.97 (0.91‐1.04) | 0.93 (0.86‐0.99) |
| Charlson Comorbidity Index | ||||||
| 0 | ||||||
| 1 | 1.54 (1.46‐1.62) | 1.40 (1.32‐1.48) | 1.02 (0.95‐1.1) | 1.0 (0.92‐1.08) | 1.19 (1.12‐1.26) | 1.11 (1.04‐1.19) |
| 2 | 1.78 (1.69‐1.89) | 1.60 (1.51‐1.70) | 1.16 (1.08‐1.25) | 1.11 (1.03‐1.20) | 1.43 (1.34‐1.53) | 1.22 (1.14‐1.31) |
| 3 | 2.07 (1.97‐2.17) | 1.83 (1.73‐1.93) | 1.41 (1.32‐1.51) | 1.24 (1.15‐1.32) | 1.79 (1.69‐1.89) | 1.40 (1.31‐1.48) |
| Payer status | ||||||
| Private | ||||||
| Medicare | 1.02 (0.98‐1.06) | 0.89 (0.84‐0.95) | 1.04 (0.98‐1.11) | 1.04 (0.98‐1.12) | 1.29 (1.22‐1.37) | 1.06 (0.98‐1.13) |
| Medicaid | 0.89 (0.83‐0.96) | 0.83 (0.77‐0.89) | 1.2 (1.12‐1.3) | 1.23 (1.13‐1.33) | 1.28 (1.18‐1.38) | 1.18 (1.09‐1.28) |
| No insurance | 0.52 (0.46‐0.58) | 0.60 (0.53‐0.67) | 0.66 (0.57‐0.76) | 0.79 (0.68‐0.91) | 0.64 (0.54‐0.75) | 0.73 (0.61‐0.87) |
| Unknown | 0.71 (0.65‐0.78) | 0.77 (0.70‐0.84) | 0.91 (0.81‐1.03) | 1.02 (0.9‐1.15) | 0.9 (0.79‐1.03) | 0.93 (0.81‐1.06) |
| Disposition | ||||||
| Home | ||||||
| Acute care | 0.32 (0.27‐0.37) | 0.35 (0.29‐0.41) | 1.42 (1.18‐1.71) | 1.2 (1.05‐1.55) | 2.08 (1.69‐2.56) | 1.64 (1.32‐2.03) |
| SNF | 1.27 (1.2‐1.34) | 1.18 (1.10‐1.26) | 1.61 (1.53‐1.7) | 1.54 (1.46‐1.63) | 1.9 (1.81‐2.01) | 1.61 (1.52‐1.71) |
| Residential facility | 0.89 (0.68‐1.15) | 0.94 (0.72‐1.24) | 1.31 (1.1‐1.58) | 1.40 (1.16‐1.69) | 1.61 (1.37‐1.89) | 1.52 (1.29‐1.80) |
| Other | 1.21 (1.16‐1.26) | 1.10 (1.05‐1.15) | 1.72 (1.66‐1.79) | 1.59 (1.52‐1.66) | 2.31 (2.21‐2.41) | 1.88 (1.79‐1.98) |
| Length of stay* | 1.04 (1.02‐1.05) | 0.89 (0.87‐0.90) | 1.20 (1.19‐1.22) | 1.09 (1.08‐1.11) | 1.31 (1.29‐1.32) | 1.13 (1.1‐1.14) |
| Any complication | 3.14 (3.02‐3.26) | 2.61 (2.50‐2.73) | 1.52 (1.46‐1.59) | 1.35 (1.29‐1.41) | 1.70 (1.62‐1.78) | 1.39 (1.32‐1.45) |
| Admission type | ||||||
| Elective | ||||||
| Unplanned | 0.28 (0.27‐0.29) | 0.33 (0.31‐0.34) | 0.56 (0.54‐0.59) | 0.57 (0.53‐0.6) | 0.39 (0.37‐0.42) | 0.45 (0.42‐0.48) |
Increasing age, male gender, black race, greater Charlson Comorbidity Index, occurrence of any complication, and increased LOS were all associated with need for readmission on univariate analysis, though many of these associations weakened on multivariable analysis (Table 3). The effect of payer status on readmission was complex. Compared to private insurance, Medicare was associated with readmissions for patients with PNA (OR: 1.29, 95% CI: 1.22‐1.37) but not AMI (OR: 1.02, 95% CI: 0.98‐1.06) or CHF (OR: 1.04, 95% CI: 0.98‐1.11). Medicaid insurance was associated with readmission for CHF (OR: 1.20, 95% CI: 1.12‐1.30) and PNA (OR: 1.28, 95% CI: 1.18‐1.38) but appeared to be protective from readmission for AMI (OR: 0.89, 95% CI: 0.83‐0.96). Lack of insurance was associated with decreased odds of readmission for all diagnoses (P<0.05 for all models).
Models predicting 90‐day readmission rates showed similar results in all categories; therefore, the data are not shown.
DISCUSSION
We used a California statewide discharge database that linked individual patient records from all nonfederal hospitals to examine 30‐ and 90‐day hospital readmissions for CHF, AMI, and PNA. We hypothesized, but did not find, that weekend hospital discharge would be associated with higher hospital readmission rates. We did find other factors that were associated with hospital readmissions, including race, age, greater comorbidities, male gender, and discharge to an SNF. Nearly half of patients were readmitted for the same diagnosis as the initial discharge diagnosis, and nearly two‐thirds of the patients were readmitted to a hospital different from the discharging hospital.
Our study found some findings similar to prior investigations. First, the factors that predicted hospital readmission were complex and included age, race, gender, comorbidities, payer status, length of hospital stay, and the occurrence of a complication; most of these factors persisted after multivariable analysis but were not necessarily consistent across all admission diagnoses.[16, 17, 18] One finding of particular interest was the impact of insurance status. Specifically, lack of insurance was inversely associated with hospital readmission; this finding warrants further investigation. Our study is also similar to others in that we found that the most common reasons for readmission are typically related to the reason for the principal admission. Dharmarajan et al. previously studied the reason for readmission among hospitalized Medicare patients with AMI, CHF, and PNA, and found similarly high rates of identical admission diagnoses.[19] Furthermore, in our study, between 32% and 65% of 30‐day readmissions were to a hospital different than the discharging facility. Although few prior studies have had the ability to assess readmission to alternative hospitals, those who have done so in the past have found similar rates of divergence from the index facility.[20, 21]
Despite the apparent similarities to other studies, the current research question was specifically designed to investigate the weekend effect of hospital discharge. The term weekend effect refers to a phenomenon of worse clinical outcomes (eg, morbidity,[22] mortality,[6, 7] intensive care unit [ICU] readmission,[23] delays in appropriate diagnostic imaging[24, 25] and intervention,[26, 27] LOS,[28] and hospital costs[29]) for care delivered on a weekend. In a landmark study, Bell and Redelmeier demonstrated increased in‐house mortality for patients with ruptured abdominal aortic aneurysm, pulmonary embolism, or acute epiglottitis admitted through the emergency department on a weekend compared to weekday.[6] After controlling for patient variables, the association persisted, suggesting system‐related factors were contributory. Similarly, Kostis et al. showed that patients admitted to the hospital on a weekend with AMI had higher 30‐day mortality rates compared to those with weekday admission.[7] Finally, Aylin et al. demonstrated that mortality was 44% higher for patients undergoing elective surgery on a Friday and 82% higher for surgery on a weekend compared to a Monday.[30]
Despite this robust literature, fewer studies have evaluated the relationship between timing of discharge and outcomes. Much of the initial research has been focused on timing of discharge from the ICU. For example, transfer out of the ICU at night has been associated with higher in‐hospital mortality[31, 32, 33, 34, 35] as well as ICU readmission.[36, 37] Discharge from the ICU on a weekend has been associated with increased mortality in some studies[23] but not in others.[35, 38] Van Walraven and Bell were the first to investigate the impact of weekend hospital discharge on outcomes. In their analysis of all discharges from Ontario hospitals between 1990 and 2000, patients discharged on a Friday were at increased risk of death and 30‐day readmission compared to discharge on a Wednesday.[9] Beck et al. performed a similar study in pediatric patients but did not find a statistically significant effect of Friday discharge on readmission rates.[39] McAlister et al. specifically studied the effect of weekend (Saturday or Sunday) discharge on patients with CHF by analyzing discharges from Alberta, Canada hospitals between 1999 and 2009. Despite being comprised of lower‐risk patients, weekend discharge was associated with greater rates of 30‐ and 90‐day death and hospital readmission.[10] Conversely, McAlister et al. evaluated general medicine discharges from teaching hospitals in Alberta, Canada between 2009 and 2011 and found no difference in hospital readmission rates among those discharged on a weekend versus weekday.[11] The current investigation is the first to study hospitals in the United States to address this topic, an important consideration given differences in American and Canadian healthcare systems. Nevertheless, our results are similar to those of McAlister et al.,[11] who found no difference in hospital readmission rates based on day of discharge among patients with AMI, CHF, or PNA.
One potential explanation for finding a lack of correlation between weekend discharge and readmissions is that patients at higher risk for readmission are already selected toward weekday discharge. Our study found that patients discharged to an SNF, a group with higher odds of readmission, were less often discharged on a weekend. There may be other unmeasurable factors that differ between patients discharged on weekends versus weekdays. Also, factors that bias healthcare providers' decision making on timing of discharge are difficult to quantify and may differ between the 2 groups. Although our study hypothesis was driven by the perception that weekend discharges may fare poorly because of inadequate resources on the weekend, an alternative explanation for finding no association may be that current systems in place already do an effective job of discharge coordination on the weekend. Despite fears that staffing and equipment are significantly reduced during the weekend, perhaps weekend discharge resources are not the limiting factor in efforts to reduce readmissions.
Our results challenge the idea that weekend discharges predict hospital readmissions in California and argue for the relative safety of weekend discharges. Based on these findings, the routine delay in discharge of the complex medical patient until Monday for fear of discharge on a weekend does not seem warranted. Avoiding unnecessary delays in discharge should have positive effects on healthcare costs by reducing LOS. Two additional implications of our work are that single institution studies may underestimate readmission rates,[40] and that discharge to an SNF should receive special consideration in calculation of hospital‐level penalties for subsequent readmissions, as this group is associated with particularly higher risk.
There are some limitations to our study that should be acknowledged. The use of administrative data has well known limitations and the possibility of coding inaccuracy cannot be excluded.[41] Certain factors that could potentially differ between groups, such as illness severity, as well as details on the discharge process, were not available in this administrative database. In addition, elective readmissions were not excluded from the study. Also, because of the way the data were coded, a significant percentage of discharge dispositions were unknown. Finally, although morbidity and mortality have been studied in previous reports,[9, 10, 39] these data were not available for the current study, limiting the applicability of its conclusions.
CONCLUSIONS
In conclusion, among patients admitted with AMI, CHF, or PNA in California, discharge on a weekend is not associated with hospital readmission. Future studies on hospital readmissions should use a population‐based approach to accurately capture all readmissions following discharge.
Acknowledgments
Disclosure: Nothing to report.
- , Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160(8):1074–1081.
- , Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306(16):1794–1795.
- Medicare fines 2,610 hospitals in third round of readmission penalties. Kaiser Health News. Available at: http://www.kaiserhealthnews.org/Stories/2014/October/02/Medicare‐readmissions‐penalties‐2015.aspx. Published October 2, 2014. Accessed October 2, 2014.
- , Interventions to decrease hospital readmissions: keys for cost‐effectiveness. JAMA Intern Med. 2013;173(8):695–698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001;345(9):663–668.
- , , , et al. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med. 2007;356(11):1099–1109.
- , , , , , Mortality rate after nonelective hospital admission. Arch Surg 2011;146(5):545–551.
- , Risk of death or readmission among people discharged from hospital on Fridays. CMAJ. 2002;166(13):1672–1673.
- , , , , Postdischarge outcomes in heart failure are better for teaching hospitals and weekday discharges. Circ Heart Fail. 2013;6(5):922–929.
- , , , Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
- , , Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , , , The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429.
- Readmissions Reduction Program. August 2014. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html. Accessed October 2, 2014.
- , , Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25(3):211–219.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- , , , et al. Diagnoses and timing of 30‐day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355–363.
- , , , et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: a population‐based appraisal. Ann Surg Oncol. 2009;16(3):554–561.
- , , , et al. Is same‐hospital readmission rate a good surrogate for all‐hospital readmission rate? Med Care. 2010;48(5):477–481.
- , , , et al. Worse outcomes in patients undergoing urgent surgery for left‐sided diverticulitis admitted on weekends vs weekdays: a population‐based study of 31 832 patients. Arch Surg. 2012;147(7):649–655.
- , , , et al. Mortality after discharge from the intensive care unit during the early weekend period: a population‐based cohort study in Denmark. Acta Anaesthesiol Scand. 2007;51(9):1225–1230.
- , , , Something for the weekend? JAMA Neurol. 2013;70(1):130.
- , , , , Dying for the weekend: a retrospective cohort study on the association between day of hospital presentation and the quality and safety of stroke care. Arch Neurol. 2012;69(10):1296–1302.
- , , , Effects of weekend admission on the outcomes and management of ruptured aortic aneurysms. J Vasc Surg. 2014;60(2):318–324
- , , , et al. Treatment delay in patients undergoing primary percutaneous coronary intervention for ST‐elevation myocardial infarction: a key process analysis of patient and program factors. Am Heart J. 2008;155(2):290–297.
- , , , et al. Weekend hospital admission and discharge for heart failure: association with quality of care and clinical outcomes. Am Heart J. 2009;158(3):451–458.
- , , , , Comparison of perioperative outcomes and cost of spinal fusion for cervical trauma: weekday versus weekend admissions. Spine. 2013;38(25):2178–2183.
- , , , , Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
- , Consequences of discharges from intensive care at night. Lancet. 2000;355(9210):1138–1142.
- , , Waiting for the break of dawn? The effects of discharge time, discharge TISS scores and discharge facility on hospital mortality after intensive care. Intensive Care Med. 2002;28(9):1287–1293.
- , After‐hours discharges from intensive care are associated with increased mortality. Med J Aust. 2006;184(7):334–337.
- , Impact of intensive care unit discharge time on patient outcome. Crit Care Med. 2006;34(12):2946–2951.
- , , , Hospital mortality among adults admitted to and discharged from intensive care on weekends and evenings. J Crit Care. 2008;23(3):317–324.
- , , , et al. Factors associated with increased risk of readmission to intensive care in Australia. Intensive Care Med. 2011;37(11):1800–1808.
- , , , , After‐hours discharge from intensive care increases the risk of readmission and death. Anaesth Intensive Care. 2007;35(4):477–485.
- , , The effects of ICU admission and discharge times on mortality in Finland. Intensive Care Med. 2003;29(12):2144–2148.
- , , , , Day of discharge and hospital readmission rates within 30 days in children: a population‐based study. Paediatr Child Health. 2006;11(7):409–412.
- , , , Using same‐hospital readmission rates to estimate all‐hospital readmission rates. J Am Coll Surg. 2014;219(4):656–663.
- , , , et al. Evaluation of hospital readmissions in surgical patients: do administrative data tell the real story? JAMA Surg. 2014;149(8):759–764.
Hospital readmission, defined as an admission to a hospital within 30 days of discharge from an acute‐care hospitalization, is associated with short‐term morbidity, mortality, and medical costs.[1] In 2013, the Patient Protection and Affordable Care Act began assigning financial penalties to hospitals based on performance against benchmarks on readmission for acute myocardial infarction (AMI), pneumonia (PNA), and congestive heart failure (CHF) through its Hospital Readmission Reduction Program (HRRP).[2] In its third year, the program recently announced penalties for 2,610 hospitals that will total over $428 million.[3] Despite increased attention to this issue, few interventions have been identified that effectively reduce hospital readmissions.[4, 5]
Hospital discharge is a complex process that aims to achieve the safe transfer of care of a hospitalized patient to another setting (eg, home, skilled nursing facility [SNF]). Success depends on adequate staffing of physicians, nurses, case managers, social workers, and pharmacists; clear communication among patients and providers; and integrated coordination of care. Although much focus has been placed on the association between weekend hospital admission and increased mortality,[6, 7, 8] very little is known about the impact of weekend hospital discharge on outcomes, specifically hospital readmission rates. Furthermore, previous studies on this topic, based on Canadian data, have produced conflicting results.[9, 10, 11]
Staffing of physicians, physician extenders (eg, physician assistants or nurse practitioners), nurses, case managers, social workers, and ancillary staff (eg, physical and occupational therapists) are all typically reduced on the weekend. Patients may be cared for by covering healthcare providers. These factors may have important implications on the timeliness of discharge, accuracy of discharge instructions, safety of discharge (eg, clearance by physical therapy), and medication reconciliation, among others. Clinic offices are more likely to be closed, and therefore, some follow‐up appointments may inadvertently not be scheduled, and lack of timely postdischarge follow‐up may be associated with higher rates of readmission.[12] Reduced outpatient pharmacy availability may also cause delays in patients receiving their medications,[13] which may exacerbate failed transition to the outpatient setting due to medication noncompliance.[14]
Based on this rationale, the current study was designed to investigate the association between weekend discharge and 30‐ and 90‐ day readmissions in patients hospitalized for medical diagnoses included in Centers for Medicare and Medicaid Services' HRRP.[15] To do so, a large‐state, all‐payer discharge database with individual patient record linkage numbers (RLN) was selected to capture all readmissions, even those to a different hospital. We hypothesized that patients who are discharged on a weekend would have higher hospital readmission rates compared to those discharged on a weekday.
METHODS
Approval was obtained from both the California Committee for the Protection of Human Subjects and the Stanford University Institutional Review Board. The California Office of State Health Planning and Development (OSHPD) 2012 Patient Discharge Data (PDD) was utilized for this study. The OSHPD‐PDD contains records for all patients admitted and eventually discharged from every general, acute, nonfederal hospital within the state. Demographic variables contained in the dataset include age, gender, race, and a unique RLN (an individually assigned number based on the patient's social security number and other demographics) to associate discharged patients with subsequent hospitalizations. Clinical information collected included principal diagnosis (indication for admission), 24 additional diagnoses with an indicator as to whether or not the condition was present on admission (POA) to differentiate comorbidities from complications, and principle procedure codes. Details about the admission included date of admission and discharge, admission type (scheduled or unscheduled), expected payer/emnsurance and disposition (home, acute rehabilitation, skilled nursing facility, residential facility, other). Details about the hospital included a unique identification number to indicate the location of care for both index/discharge and subsequent readmission.
International Classification of Disease, Ninth Edition, Clinical Modification (ICD‐9‐CM) coding schema were used to identify all patients admitted with the principal diagnosis of AMI (ICD‐9‐CM code 410.xx), CHF (428.xx), or PNA (480.xx‐486.xx). We excluded patients who were coded as having in‐hospital mortality, as these patients would not be eligible for readmission, those who were transferred to a different inpatient acute‐care facility, and those with invalid RLNs. Patients were separated into 2 groups based on the day of discharge. Weekday was defined as Monday through Friday, whereas weekend was defined as Saturday and Sunday. The Charlson Comorbidity Index was calculated based on POA comorbidities.
Demographic data, hospital variables, and readmission rates were directly compared for patients discharged on a weekend compared to weekday after admission for AMI, CHF, or PNA. Hospital readmission was defined as the first inpatient hospitalization for any reason at either 30 or 90 days following discharge from an index acute‐care hospitalization. Hospital identification codes were used to determine whether the readmission occurred at the index (discharging) hospital or to a different facility. The principal diagnosis for the subsequent admission was assessed to identify the most common reasons for readmission.
The [2] test and Student t test were used to compare mean values between the 2 groups when appropriate, with statistical significance set as P<0.05. Univariate and multivariable logistic regression models were built to estimate the odds of hospital readmission based on weekend versus weekday discharge after controlling for age, gender, race, Charlson Comorbidity Index, discharge disposition, payer status, length of stay, presence of complication, and admission type. All statistical analyses were 2‐tailed and performed using SAS 9.3 for windows (SAS Institute Inc., Cary, NC). The odds ratio (OR) was considered significant when it was not equal to 1, the 95% confidence interval (CI) did not include 1, and the P value was less than 0.05.
RESULTS
Patient Characteristics
There were 266,519 patients hospitalized with a principal diagnosis of AMI, CHF, or PNA in California during 2012 and met all inclusion criteria. The cohort consisted of 77,853 (29.2%) with AMI, 91,327 (34.3%) with CHF, and 97,339 (36.5%) with PNA. A total of 60,097 (22.5%) patients were discharged on the weekend compared to 206,422 (77.5%) on a weekday, which was similar across diagnosis groups. Differences in gender, age, race, Charlson comorbidity score, insurance status, type of admission, or occurrence of complications between patients who were discharged on the weekend versus weekday are listed in Table 1. Patients discharged on a weekend had a shorter average length of stay (LOS) (AMI: 4.05.6 days vs 4.67.7 days; CHF: 5.19.3 vs 6.034.1; PNA: 5.011.7 vs 5.710.7). A higher proportion of these patients were discharged to home (AMI: 67.1% vs 63.8%; CHF: 53.3% vs 49.4%; PNA: 57.0% vs 52.9%), whereas a smaller proportion were discharged to an SNF (AMI: 7.0% vs 9.6%; CHF: 11.2% vs 15.9%; PNA: 12.8% vs 17.8%).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Weekend | Weekday | Weekend | Weekday | Weekend | Weekday | |
| ||||||
| No. (%) | 18,061 (23.2) | 59,792 (76.8) | 20,487 (22.4) | 70,840 (77.6) | 21,549 (22.1) | 75,790 (77.9) |
| Age, y | ||||||
| 044 | 4.7 | 4.5 | 4.5 | 4.1 | 9.4 | 8.6 |
| 4554 | 13.1 | 13.0 | 8.5 | 8.3 | 9.8 | 9.9 |
| 5564 | 22.6 | 22.4 | 14.3 | 14.6 | 14.9 | 14.9 |
| 6574 | 22.5 | 22.7 | 19.2 | 18.7 | 18.3 | 18.0 |
| 7584 | 21.4 | 21.4 | 26.4 | 26.3 | 24.1 | 24.0 |
| 85+ | 15.6 | 16.0 | 27.2 | 28.0 | 23.5 | 24.5 |
| Mean (SD) | 68.5 (14.3) | 68.7 (14.3) | 73.3 (15.1) | 3.6 (15.0) | 70.0 (17.6) | 70.5 (17.4) |
| Sex | ||||||
| Male | 62.0 | 61.7 | 51.7 | 51.4 | 47.9 | 47.0 |
| Female | 38.0 | 38.3 | 48.3 | 48.6 | 52.1 | 52.1 |
| Race | ||||||
| White | 63.5 | 62.9 | 58.7 | 58.5 | 63.0 | 62.4 |
| Black | 6.9 | 7.3 | 12.0 | 12.1 | 7.7 | 8.0 |
| Hispanic | 19.5 | 20.0 | 20.3 | 20.6 | 20.4 | 20.7 |
| API | 10.0 | 9.7 | 9.0 | 8.8 | 8.8 | 8.9 |
| Charlson Comorbidity Index | ||||||
| 0 | 30.7 | 30.1 | 9.4 | 9.5 | 23.0 | 22.2 |
| 1 | 25.1 | 24.9 | 19.5 | 19.8 | 25.7 | 26.4 |
| 2 | 14.9 | 15.2 | 20.4 | 20.3 | 17.3 | 17.4 |
| 3 | 29.2 | 29.8 | 50.8 | 50.4 | 34.0 | 34.1 |
| Mean (SD) | 2.1 (2.2) | 2.1 (2.2) | 3.0 (2.3) | 3.0 (2.3) | 2.4 (2.6) | 2.4 (2.5) |
| Payer status | ||||||
| Private | 25.4 | 25.1 | 11.3 | 10.7 | 15.7 | 14.4 |
| Medicare | 57.6 | 57.9 | 72.7 | 73.1 | 67.1 | 68.1 |
| Medicaid | 8.0 | 8.0 | 10.0 | 10.6 | 11.5 | 11.8 |
| No insurance | 4.2 | 4.0 | 2.7 | 2.3 | 2.6 | 2.5 |
| Unknown | 4.8 | 4.9 | 3.3 | 3.3 | 3.2 | 3.2 |
| Complication | ||||||
| Urinary tract infection | 6.0 | 6.8 | 10.3 | 10.8 | 10.2 | 11.0 |
| Acute MI | 6.7 | 6.9 | 2.7 | 2.6 | 1.2 | 1.2 |
| DVT/PE | 0.02 | 0.02 | 0.01 | 0.01 | 0.03 | 0.03 |
| Pneumonia | 0.06 | 0.05 | 0.09 | 0.08 | 0.1 | 0.1 |
| Hemorrhage | 1.7 | 1.7 | 1.5 | 1.5 | 1.2 | 1.1 |
| Sepsis | 3.5 | 3.6 | 6.2 | 6.0 | 7.4 | 7.6 |
| Mean length of stay (SD) | 4.0 (5.6) | 4.6 (7.7) | 5.1 (9.3) | 6.0 (34.1) | 5.0 (11.7) | 5.7 (10.7) |
| Disposition | ||||||
| Home | 67.1 | 63.8 | 53.3 | 49.4 | 57.0 | 52.9 |
| Acute rehabilitation | 1.9 | 3.2 | 0.7 | 0.9 | 0.5 | 0.7 |
| Skilled nursing facility | 7.0 | 9.6 | 11.2 | 15.9 | 12.8 | 17.8 |
| Residential facility | 0.4 | 0.5 | 0.9 | 1.0 | 1.1 | 1.4 |
| Other | 23.6 | 23.0 | 33.9 | 32.8 | 28.6 | 27.2 |
| Admission type | ||||||
| Elective | 8.9 | 10.1 | 7.9 | 9.1 | 7.1 | 7.6 |
| Unplanned | 91.0 | 89.9 | 92.1 | 90.9 | 92.9 | 92.3 |
Rate, Reason, and Location of Readmission
Table 2 shows overall rates of readmission. Among all patients, there were no significant differences in the unadjusted readmission rates for patients being discharged on a weekend versus weekday at either 30 days (16.7% vs 17.0%, P=0.14) or 90 days (26.9% vs 27.5%, P=0.05) (Table 2). Unadjusted 30‐day readmission rates were similar between the 2 groups for AMI (21.9% vs 21.9%, P=0.94) and PNA (12.1% vs 12.4%, P=0.28), whereas they were higher for weekday discharges in CHF (15.4% vs 16.0%, P=0.04). Similar results were seen for 90‐day readmission rates. To elucidate the impact of discharge disposition, a subset analysis was performed based on day of discharge and disposition (Figure 1). There was no difference in rates of readmission among patients discharged home on a weekend versus weekday (AMI: 21.3% vs 21.1%, P=0.78; CHF: 12.2% vs 12.6%, P=0.29; PNA: 8.3% vs 8.6%, P=0.29).
Abbreviations: AMI, acute myocardial infarction; CHF, congestive heart failure; PNA, pneumonia; SNF, skilled nursing facility.
| AMI | CHF | PNA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Weekend | Weekday | P Value | Weekend | Weekday | P Value | Weekend | Weekday | P Value | |
| |||||||||
| 30‐day readmission (%) | 3,954 (21.9) | 13,106 (21.9) | 0.94 | 3,162 (15.4) | 11,366 (16.0) | 0.04 | 2,608 (12.1) | 9,380 (12.4) | 0.28 |
| 90‐day readmission (%) | 5,253 (29.1) | 17,344 (29.0) | 0.84 | 5,994 (29.3) | 21,355 (30.2) | 0.008 | 4,698 (21.8) | 16,910 (22.3) | 0.11 |
The reason for hospital readmission was most frequently related to the principal diagnosis. Among patients discharged after hospitalization for AMI, 45.3% of readmissions had a principal diagnosis of AMI, whereas 13.9% listed readmission for angina or coronary artery disease. Of CHF discharges, at least 26.7% of readmissions were for CHF. PNA was the principal diagnosis in 19.8% of readmissions after admission for PNA. A significant proportion of patients (AMI: 64.8%, CHF: 35.0%, PNA: 32.9%) were readmitted to a different hospital than the discharging hospital.
Predictors of Readmission
On univariate logistic regression, discharge on a weekend was not associated with hospital readmission for patients admitted with AMI (OR: 1.0, 95% CI: 0.96‐1.04) or PNA (OR: 0.97, 95% CI: 0.93‐1.02) but was inversely associated for CHF (OR: 0.96, 95% CI: 0.91‐1.0). In multivariable models, weekend discharge was not associated with increased risk of readmission for any diagnosis (AMI [OR: 1.02, 95% CI: 0.98‐1.07], CHF [OR: 0.99, 95% CI: 0.95‐1.03], or PNA [OR: 1.02, 95% CI: 0.98‐1.07]; Table 3).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Univariate OR (95% CI) | Multivariable OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | |
| ||||||
| Weekend discharge | 1 (0.96‐1.04) | 1.02 (0.98‐1.06) | 0.96 (0.91‐1) | 0.99 (0.94‐1.03) | 0.97 (0.93‐1.02) | 1.02 (0.98‐1.07) |
| Age, y | ||||||
| 044 | ||||||
| 4554 | 1.02 (0.92‐1.12) | 0.96 (0.87‐1.07) | 1.04 (0.93‐1.16) | 1.00 (0.89‐1.11) | 1.08 (0.98‐1.19) | 0.93 (0.84‐1.03) |
| 5564 | 1.11 (1.02‐1.22) | 1.00 (0.91‐1.10) | 1.11 (1.01‐1.23) | 0.97 (0.88‐1.08) | 1.23 (1.13‐1.34) | 0.94 (0.86‐1.03) |
| 6574 | 1.31 (1.19‐1.43) | 1.04 (0.94‐1.15) | 1.1 (1‐1.22) | 0.90 (0.81‐1.01) | 1.29 (1.19‐1.41) | 0.87 (0.79‐0.96) |
| 7584 | 1.29 (1.18‐1.41) | 0.94 (0.85‐1.05) | 1.06 (0.97‐1.17) | 0.84 (0.75‐0.93) | 1.37 (1.27‐1.49) | 0.87 (0.79‐0.95) |
| 85+ | 1.03 (0.94‐1.13) | 0.72 (0.64‐0.81) | 0.98 (0.89‐1.08) | 0.76 (0.68‐0.84) | 1.31 (1.2‐1.41) | 0.78 (0.71‐0.86) |
| Gender | ||||||
| Female | ||||||
| Male | 1 (0.97‐1.04) | 1.1 (1.05‐1.14) | 1.06 (1.02‐1.1) | 1.08 (1.04‐1.12) | 1.13 (1.09‐1.18) | 1.15 (1.10‐1.19) |
| Race | ||||||
| White | ||||||
| Black | 1.17 (1.1‐1.25) | 1.12 (1.05‐1.20) | 1.06 (1‐1.12) | 1.03 (0.97‐1.09) | 1.11 (1.04‐1.19) | 1.07 (0.99‐1.15) |
| Hispanic | 1.11 (1.06‐1.16) | 1.12 (1.06‐1.17) | 1.05 (1‐1.1) | 1.04 (1.00‐1.10) | 0.93 (0.89‐0.98) | 0.95 (0.90‐1.00) |
| API | 1.14 (1.07‐1.2) | 1.09 (1.03‐1.16) | 1.01 (0.95‐1.08) | 1.00 (0.94‐1.07) | 0.97 (0.91‐1.04) | 0.93 (0.86‐0.99) |
| Charlson Comorbidity Index | ||||||
| 0 | ||||||
| 1 | 1.54 (1.46‐1.62) | 1.40 (1.32‐1.48) | 1.02 (0.95‐1.1) | 1.0 (0.92‐1.08) | 1.19 (1.12‐1.26) | 1.11 (1.04‐1.19) |
| 2 | 1.78 (1.69‐1.89) | 1.60 (1.51‐1.70) | 1.16 (1.08‐1.25) | 1.11 (1.03‐1.20) | 1.43 (1.34‐1.53) | 1.22 (1.14‐1.31) |
| 3 | 2.07 (1.97‐2.17) | 1.83 (1.73‐1.93) | 1.41 (1.32‐1.51) | 1.24 (1.15‐1.32) | 1.79 (1.69‐1.89) | 1.40 (1.31‐1.48) |
| Payer status | ||||||
| Private | ||||||
| Medicare | 1.02 (0.98‐1.06) | 0.89 (0.84‐0.95) | 1.04 (0.98‐1.11) | 1.04 (0.98‐1.12) | 1.29 (1.22‐1.37) | 1.06 (0.98‐1.13) |
| Medicaid | 0.89 (0.83‐0.96) | 0.83 (0.77‐0.89) | 1.2 (1.12‐1.3) | 1.23 (1.13‐1.33) | 1.28 (1.18‐1.38) | 1.18 (1.09‐1.28) |
| No insurance | 0.52 (0.46‐0.58) | 0.60 (0.53‐0.67) | 0.66 (0.57‐0.76) | 0.79 (0.68‐0.91) | 0.64 (0.54‐0.75) | 0.73 (0.61‐0.87) |
| Unknown | 0.71 (0.65‐0.78) | 0.77 (0.70‐0.84) | 0.91 (0.81‐1.03) | 1.02 (0.9‐1.15) | 0.9 (0.79‐1.03) | 0.93 (0.81‐1.06) |
| Disposition | ||||||
| Home | ||||||
| Acute care | 0.32 (0.27‐0.37) | 0.35 (0.29‐0.41) | 1.42 (1.18‐1.71) | 1.2 (1.05‐1.55) | 2.08 (1.69‐2.56) | 1.64 (1.32‐2.03) |
| SNF | 1.27 (1.2‐1.34) | 1.18 (1.10‐1.26) | 1.61 (1.53‐1.7) | 1.54 (1.46‐1.63) | 1.9 (1.81‐2.01) | 1.61 (1.52‐1.71) |
| Residential facility | 0.89 (0.68‐1.15) | 0.94 (0.72‐1.24) | 1.31 (1.1‐1.58) | 1.40 (1.16‐1.69) | 1.61 (1.37‐1.89) | 1.52 (1.29‐1.80) |
| Other | 1.21 (1.16‐1.26) | 1.10 (1.05‐1.15) | 1.72 (1.66‐1.79) | 1.59 (1.52‐1.66) | 2.31 (2.21‐2.41) | 1.88 (1.79‐1.98) |
| Length of stay* | 1.04 (1.02‐1.05) | 0.89 (0.87‐0.90) | 1.20 (1.19‐1.22) | 1.09 (1.08‐1.11) | 1.31 (1.29‐1.32) | 1.13 (1.1‐1.14) |
| Any complication | 3.14 (3.02‐3.26) | 2.61 (2.50‐2.73) | 1.52 (1.46‐1.59) | 1.35 (1.29‐1.41) | 1.70 (1.62‐1.78) | 1.39 (1.32‐1.45) |
| Admission type | ||||||
| Elective | ||||||
| Unplanned | 0.28 (0.27‐0.29) | 0.33 (0.31‐0.34) | 0.56 (0.54‐0.59) | 0.57 (0.53‐0.6) | 0.39 (0.37‐0.42) | 0.45 (0.42‐0.48) |
Increasing age, male gender, black race, greater Charlson Comorbidity Index, occurrence of any complication, and increased LOS were all associated with need for readmission on univariate analysis, though many of these associations weakened on multivariable analysis (Table 3). The effect of payer status on readmission was complex. Compared to private insurance, Medicare was associated with readmissions for patients with PNA (OR: 1.29, 95% CI: 1.22‐1.37) but not AMI (OR: 1.02, 95% CI: 0.98‐1.06) or CHF (OR: 1.04, 95% CI: 0.98‐1.11). Medicaid insurance was associated with readmission for CHF (OR: 1.20, 95% CI: 1.12‐1.30) and PNA (OR: 1.28, 95% CI: 1.18‐1.38) but appeared to be protective from readmission for AMI (OR: 0.89, 95% CI: 0.83‐0.96). Lack of insurance was associated with decreased odds of readmission for all diagnoses (P<0.05 for all models).
Models predicting 90‐day readmission rates showed similar results in all categories; therefore, the data are not shown.
DISCUSSION
We used a California statewide discharge database that linked individual patient records from all nonfederal hospitals to examine 30‐ and 90‐day hospital readmissions for CHF, AMI, and PNA. We hypothesized, but did not find, that weekend hospital discharge would be associated with higher hospital readmission rates. We did find other factors that were associated with hospital readmissions, including race, age, greater comorbidities, male gender, and discharge to an SNF. Nearly half of patients were readmitted for the same diagnosis as the initial discharge diagnosis, and nearly two‐thirds of the patients were readmitted to a hospital different from the discharging hospital.
Our study found some findings similar to prior investigations. First, the factors that predicted hospital readmission were complex and included age, race, gender, comorbidities, payer status, length of hospital stay, and the occurrence of a complication; most of these factors persisted after multivariable analysis but were not necessarily consistent across all admission diagnoses.[16, 17, 18] One finding of particular interest was the impact of insurance status. Specifically, lack of insurance was inversely associated with hospital readmission; this finding warrants further investigation. Our study is also similar to others in that we found that the most common reasons for readmission are typically related to the reason for the principal admission. Dharmarajan et al. previously studied the reason for readmission among hospitalized Medicare patients with AMI, CHF, and PNA, and found similarly high rates of identical admission diagnoses.[19] Furthermore, in our study, between 32% and 65% of 30‐day readmissions were to a hospital different than the discharging facility. Although few prior studies have had the ability to assess readmission to alternative hospitals, those who have done so in the past have found similar rates of divergence from the index facility.[20, 21]
Despite the apparent similarities to other studies, the current research question was specifically designed to investigate the weekend effect of hospital discharge. The term weekend effect refers to a phenomenon of worse clinical outcomes (eg, morbidity,[22] mortality,[6, 7] intensive care unit [ICU] readmission,[23] delays in appropriate diagnostic imaging[24, 25] and intervention,[26, 27] LOS,[28] and hospital costs[29]) for care delivered on a weekend. In a landmark study, Bell and Redelmeier demonstrated increased in‐house mortality for patients with ruptured abdominal aortic aneurysm, pulmonary embolism, or acute epiglottitis admitted through the emergency department on a weekend compared to weekday.[6] After controlling for patient variables, the association persisted, suggesting system‐related factors were contributory. Similarly, Kostis et al. showed that patients admitted to the hospital on a weekend with AMI had higher 30‐day mortality rates compared to those with weekday admission.[7] Finally, Aylin et al. demonstrated that mortality was 44% higher for patients undergoing elective surgery on a Friday and 82% higher for surgery on a weekend compared to a Monday.[30]
Despite this robust literature, fewer studies have evaluated the relationship between timing of discharge and outcomes. Much of the initial research has been focused on timing of discharge from the ICU. For example, transfer out of the ICU at night has been associated with higher in‐hospital mortality[31, 32, 33, 34, 35] as well as ICU readmission.[36, 37] Discharge from the ICU on a weekend has been associated with increased mortality in some studies[23] but not in others.[35, 38] Van Walraven and Bell were the first to investigate the impact of weekend hospital discharge on outcomes. In their analysis of all discharges from Ontario hospitals between 1990 and 2000, patients discharged on a Friday were at increased risk of death and 30‐day readmission compared to discharge on a Wednesday.[9] Beck et al. performed a similar study in pediatric patients but did not find a statistically significant effect of Friday discharge on readmission rates.[39] McAlister et al. specifically studied the effect of weekend (Saturday or Sunday) discharge on patients with CHF by analyzing discharges from Alberta, Canada hospitals between 1999 and 2009. Despite being comprised of lower‐risk patients, weekend discharge was associated with greater rates of 30‐ and 90‐day death and hospital readmission.[10] Conversely, McAlister et al. evaluated general medicine discharges from teaching hospitals in Alberta, Canada between 2009 and 2011 and found no difference in hospital readmission rates among those discharged on a weekend versus weekday.[11] The current investigation is the first to study hospitals in the United States to address this topic, an important consideration given differences in American and Canadian healthcare systems. Nevertheless, our results are similar to those of McAlister et al.,[11] who found no difference in hospital readmission rates based on day of discharge among patients with AMI, CHF, or PNA.
One potential explanation for finding a lack of correlation between weekend discharge and readmissions is that patients at higher risk for readmission are already selected toward weekday discharge. Our study found that patients discharged to an SNF, a group with higher odds of readmission, were less often discharged on a weekend. There may be other unmeasurable factors that differ between patients discharged on weekends versus weekdays. Also, factors that bias healthcare providers' decision making on timing of discharge are difficult to quantify and may differ between the 2 groups. Although our study hypothesis was driven by the perception that weekend discharges may fare poorly because of inadequate resources on the weekend, an alternative explanation for finding no association may be that current systems in place already do an effective job of discharge coordination on the weekend. Despite fears that staffing and equipment are significantly reduced during the weekend, perhaps weekend discharge resources are not the limiting factor in efforts to reduce readmissions.
Our results challenge the idea that weekend discharges predict hospital readmissions in California and argue for the relative safety of weekend discharges. Based on these findings, the routine delay in discharge of the complex medical patient until Monday for fear of discharge on a weekend does not seem warranted. Avoiding unnecessary delays in discharge should have positive effects on healthcare costs by reducing LOS. Two additional implications of our work are that single institution studies may underestimate readmission rates,[40] and that discharge to an SNF should receive special consideration in calculation of hospital‐level penalties for subsequent readmissions, as this group is associated with particularly higher risk.
There are some limitations to our study that should be acknowledged. The use of administrative data has well known limitations and the possibility of coding inaccuracy cannot be excluded.[41] Certain factors that could potentially differ between groups, such as illness severity, as well as details on the discharge process, were not available in this administrative database. In addition, elective readmissions were not excluded from the study. Also, because of the way the data were coded, a significant percentage of discharge dispositions were unknown. Finally, although morbidity and mortality have been studied in previous reports,[9, 10, 39] these data were not available for the current study, limiting the applicability of its conclusions.
CONCLUSIONS
In conclusion, among patients admitted with AMI, CHF, or PNA in California, discharge on a weekend is not associated with hospital readmission. Future studies on hospital readmissions should use a population‐based approach to accurately capture all readmissions following discharge.
Acknowledgments
Disclosure: Nothing to report.
Hospital readmission, defined as an admission to a hospital within 30 days of discharge from an acute‐care hospitalization, is associated with short‐term morbidity, mortality, and medical costs.[1] In 2013, the Patient Protection and Affordable Care Act began assigning financial penalties to hospitals based on performance against benchmarks on readmission for acute myocardial infarction (AMI), pneumonia (PNA), and congestive heart failure (CHF) through its Hospital Readmission Reduction Program (HRRP).[2] In its third year, the program recently announced penalties for 2,610 hospitals that will total over $428 million.[3] Despite increased attention to this issue, few interventions have been identified that effectively reduce hospital readmissions.[4, 5]
Hospital discharge is a complex process that aims to achieve the safe transfer of care of a hospitalized patient to another setting (eg, home, skilled nursing facility [SNF]). Success depends on adequate staffing of physicians, nurses, case managers, social workers, and pharmacists; clear communication among patients and providers; and integrated coordination of care. Although much focus has been placed on the association between weekend hospital admission and increased mortality,[6, 7, 8] very little is known about the impact of weekend hospital discharge on outcomes, specifically hospital readmission rates. Furthermore, previous studies on this topic, based on Canadian data, have produced conflicting results.[9, 10, 11]
Staffing of physicians, physician extenders (eg, physician assistants or nurse practitioners), nurses, case managers, social workers, and ancillary staff (eg, physical and occupational therapists) are all typically reduced on the weekend. Patients may be cared for by covering healthcare providers. These factors may have important implications on the timeliness of discharge, accuracy of discharge instructions, safety of discharge (eg, clearance by physical therapy), and medication reconciliation, among others. Clinic offices are more likely to be closed, and therefore, some follow‐up appointments may inadvertently not be scheduled, and lack of timely postdischarge follow‐up may be associated with higher rates of readmission.[12] Reduced outpatient pharmacy availability may also cause delays in patients receiving their medications,[13] which may exacerbate failed transition to the outpatient setting due to medication noncompliance.[14]
Based on this rationale, the current study was designed to investigate the association between weekend discharge and 30‐ and 90‐ day readmissions in patients hospitalized for medical diagnoses included in Centers for Medicare and Medicaid Services' HRRP.[15] To do so, a large‐state, all‐payer discharge database with individual patient record linkage numbers (RLN) was selected to capture all readmissions, even those to a different hospital. We hypothesized that patients who are discharged on a weekend would have higher hospital readmission rates compared to those discharged on a weekday.
METHODS
Approval was obtained from both the California Committee for the Protection of Human Subjects and the Stanford University Institutional Review Board. The California Office of State Health Planning and Development (OSHPD) 2012 Patient Discharge Data (PDD) was utilized for this study. The OSHPD‐PDD contains records for all patients admitted and eventually discharged from every general, acute, nonfederal hospital within the state. Demographic variables contained in the dataset include age, gender, race, and a unique RLN (an individually assigned number based on the patient's social security number and other demographics) to associate discharged patients with subsequent hospitalizations. Clinical information collected included principal diagnosis (indication for admission), 24 additional diagnoses with an indicator as to whether or not the condition was present on admission (POA) to differentiate comorbidities from complications, and principle procedure codes. Details about the admission included date of admission and discharge, admission type (scheduled or unscheduled), expected payer/emnsurance and disposition (home, acute rehabilitation, skilled nursing facility, residential facility, other). Details about the hospital included a unique identification number to indicate the location of care for both index/discharge and subsequent readmission.
International Classification of Disease, Ninth Edition, Clinical Modification (ICD‐9‐CM) coding schema were used to identify all patients admitted with the principal diagnosis of AMI (ICD‐9‐CM code 410.xx), CHF (428.xx), or PNA (480.xx‐486.xx). We excluded patients who were coded as having in‐hospital mortality, as these patients would not be eligible for readmission, those who were transferred to a different inpatient acute‐care facility, and those with invalid RLNs. Patients were separated into 2 groups based on the day of discharge. Weekday was defined as Monday through Friday, whereas weekend was defined as Saturday and Sunday. The Charlson Comorbidity Index was calculated based on POA comorbidities.
Demographic data, hospital variables, and readmission rates were directly compared for patients discharged on a weekend compared to weekday after admission for AMI, CHF, or PNA. Hospital readmission was defined as the first inpatient hospitalization for any reason at either 30 or 90 days following discharge from an index acute‐care hospitalization. Hospital identification codes were used to determine whether the readmission occurred at the index (discharging) hospital or to a different facility. The principal diagnosis for the subsequent admission was assessed to identify the most common reasons for readmission.
The [2] test and Student t test were used to compare mean values between the 2 groups when appropriate, with statistical significance set as P<0.05. Univariate and multivariable logistic regression models were built to estimate the odds of hospital readmission based on weekend versus weekday discharge after controlling for age, gender, race, Charlson Comorbidity Index, discharge disposition, payer status, length of stay, presence of complication, and admission type. All statistical analyses were 2‐tailed and performed using SAS 9.3 for windows (SAS Institute Inc., Cary, NC). The odds ratio (OR) was considered significant when it was not equal to 1, the 95% confidence interval (CI) did not include 1, and the P value was less than 0.05.
RESULTS
Patient Characteristics
There were 266,519 patients hospitalized with a principal diagnosis of AMI, CHF, or PNA in California during 2012 and met all inclusion criteria. The cohort consisted of 77,853 (29.2%) with AMI, 91,327 (34.3%) with CHF, and 97,339 (36.5%) with PNA. A total of 60,097 (22.5%) patients were discharged on the weekend compared to 206,422 (77.5%) on a weekday, which was similar across diagnosis groups. Differences in gender, age, race, Charlson comorbidity score, insurance status, type of admission, or occurrence of complications between patients who were discharged on the weekend versus weekday are listed in Table 1. Patients discharged on a weekend had a shorter average length of stay (LOS) (AMI: 4.05.6 days vs 4.67.7 days; CHF: 5.19.3 vs 6.034.1; PNA: 5.011.7 vs 5.710.7). A higher proportion of these patients were discharged to home (AMI: 67.1% vs 63.8%; CHF: 53.3% vs 49.4%; PNA: 57.0% vs 52.9%), whereas a smaller proportion were discharged to an SNF (AMI: 7.0% vs 9.6%; CHF: 11.2% vs 15.9%; PNA: 12.8% vs 17.8%).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Weekend | Weekday | Weekend | Weekday | Weekend | Weekday | |
| ||||||
| No. (%) | 18,061 (23.2) | 59,792 (76.8) | 20,487 (22.4) | 70,840 (77.6) | 21,549 (22.1) | 75,790 (77.9) |
| Age, y | ||||||
| 044 | 4.7 | 4.5 | 4.5 | 4.1 | 9.4 | 8.6 |
| 4554 | 13.1 | 13.0 | 8.5 | 8.3 | 9.8 | 9.9 |
| 5564 | 22.6 | 22.4 | 14.3 | 14.6 | 14.9 | 14.9 |
| 6574 | 22.5 | 22.7 | 19.2 | 18.7 | 18.3 | 18.0 |
| 7584 | 21.4 | 21.4 | 26.4 | 26.3 | 24.1 | 24.0 |
| 85+ | 15.6 | 16.0 | 27.2 | 28.0 | 23.5 | 24.5 |
| Mean (SD) | 68.5 (14.3) | 68.7 (14.3) | 73.3 (15.1) | 3.6 (15.0) | 70.0 (17.6) | 70.5 (17.4) |
| Sex | ||||||
| Male | 62.0 | 61.7 | 51.7 | 51.4 | 47.9 | 47.0 |
| Female | 38.0 | 38.3 | 48.3 | 48.6 | 52.1 | 52.1 |
| Race | ||||||
| White | 63.5 | 62.9 | 58.7 | 58.5 | 63.0 | 62.4 |
| Black | 6.9 | 7.3 | 12.0 | 12.1 | 7.7 | 8.0 |
| Hispanic | 19.5 | 20.0 | 20.3 | 20.6 | 20.4 | 20.7 |
| API | 10.0 | 9.7 | 9.0 | 8.8 | 8.8 | 8.9 |
| Charlson Comorbidity Index | ||||||
| 0 | 30.7 | 30.1 | 9.4 | 9.5 | 23.0 | 22.2 |
| 1 | 25.1 | 24.9 | 19.5 | 19.8 | 25.7 | 26.4 |
| 2 | 14.9 | 15.2 | 20.4 | 20.3 | 17.3 | 17.4 |
| 3 | 29.2 | 29.8 | 50.8 | 50.4 | 34.0 | 34.1 |
| Mean (SD) | 2.1 (2.2) | 2.1 (2.2) | 3.0 (2.3) | 3.0 (2.3) | 2.4 (2.6) | 2.4 (2.5) |
| Payer status | ||||||
| Private | 25.4 | 25.1 | 11.3 | 10.7 | 15.7 | 14.4 |
| Medicare | 57.6 | 57.9 | 72.7 | 73.1 | 67.1 | 68.1 |
| Medicaid | 8.0 | 8.0 | 10.0 | 10.6 | 11.5 | 11.8 |
| No insurance | 4.2 | 4.0 | 2.7 | 2.3 | 2.6 | 2.5 |
| Unknown | 4.8 | 4.9 | 3.3 | 3.3 | 3.2 | 3.2 |
| Complication | ||||||
| Urinary tract infection | 6.0 | 6.8 | 10.3 | 10.8 | 10.2 | 11.0 |
| Acute MI | 6.7 | 6.9 | 2.7 | 2.6 | 1.2 | 1.2 |
| DVT/PE | 0.02 | 0.02 | 0.01 | 0.01 | 0.03 | 0.03 |
| Pneumonia | 0.06 | 0.05 | 0.09 | 0.08 | 0.1 | 0.1 |
| Hemorrhage | 1.7 | 1.7 | 1.5 | 1.5 | 1.2 | 1.1 |
| Sepsis | 3.5 | 3.6 | 6.2 | 6.0 | 7.4 | 7.6 |
| Mean length of stay (SD) | 4.0 (5.6) | 4.6 (7.7) | 5.1 (9.3) | 6.0 (34.1) | 5.0 (11.7) | 5.7 (10.7) |
| Disposition | ||||||
| Home | 67.1 | 63.8 | 53.3 | 49.4 | 57.0 | 52.9 |
| Acute rehabilitation | 1.9 | 3.2 | 0.7 | 0.9 | 0.5 | 0.7 |
| Skilled nursing facility | 7.0 | 9.6 | 11.2 | 15.9 | 12.8 | 17.8 |
| Residential facility | 0.4 | 0.5 | 0.9 | 1.0 | 1.1 | 1.4 |
| Other | 23.6 | 23.0 | 33.9 | 32.8 | 28.6 | 27.2 |
| Admission type | ||||||
| Elective | 8.9 | 10.1 | 7.9 | 9.1 | 7.1 | 7.6 |
| Unplanned | 91.0 | 89.9 | 92.1 | 90.9 | 92.9 | 92.3 |
Rate, Reason, and Location of Readmission
Table 2 shows overall rates of readmission. Among all patients, there were no significant differences in the unadjusted readmission rates for patients being discharged on a weekend versus weekday at either 30 days (16.7% vs 17.0%, P=0.14) or 90 days (26.9% vs 27.5%, P=0.05) (Table 2). Unadjusted 30‐day readmission rates were similar between the 2 groups for AMI (21.9% vs 21.9%, P=0.94) and PNA (12.1% vs 12.4%, P=0.28), whereas they were higher for weekday discharges in CHF (15.4% vs 16.0%, P=0.04). Similar results were seen for 90‐day readmission rates. To elucidate the impact of discharge disposition, a subset analysis was performed based on day of discharge and disposition (Figure 1). There was no difference in rates of readmission among patients discharged home on a weekend versus weekday (AMI: 21.3% vs 21.1%, P=0.78; CHF: 12.2% vs 12.6%, P=0.29; PNA: 8.3% vs 8.6%, P=0.29).
Abbreviations: AMI, acute myocardial infarction; CHF, congestive heart failure; PNA, pneumonia; SNF, skilled nursing facility.
| AMI | CHF | PNA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Weekend | Weekday | P Value | Weekend | Weekday | P Value | Weekend | Weekday | P Value | |
| |||||||||
| 30‐day readmission (%) | 3,954 (21.9) | 13,106 (21.9) | 0.94 | 3,162 (15.4) | 11,366 (16.0) | 0.04 | 2,608 (12.1) | 9,380 (12.4) | 0.28 |
| 90‐day readmission (%) | 5,253 (29.1) | 17,344 (29.0) | 0.84 | 5,994 (29.3) | 21,355 (30.2) | 0.008 | 4,698 (21.8) | 16,910 (22.3) | 0.11 |
The reason for hospital readmission was most frequently related to the principal diagnosis. Among patients discharged after hospitalization for AMI, 45.3% of readmissions had a principal diagnosis of AMI, whereas 13.9% listed readmission for angina or coronary artery disease. Of CHF discharges, at least 26.7% of readmissions were for CHF. PNA was the principal diagnosis in 19.8% of readmissions after admission for PNA. A significant proportion of patients (AMI: 64.8%, CHF: 35.0%, PNA: 32.9%) were readmitted to a different hospital than the discharging hospital.
Predictors of Readmission
On univariate logistic regression, discharge on a weekend was not associated with hospital readmission for patients admitted with AMI (OR: 1.0, 95% CI: 0.96‐1.04) or PNA (OR: 0.97, 95% CI: 0.93‐1.02) but was inversely associated for CHF (OR: 0.96, 95% CI: 0.91‐1.0). In multivariable models, weekend discharge was not associated with increased risk of readmission for any diagnosis (AMI [OR: 1.02, 95% CI: 0.98‐1.07], CHF [OR: 0.99, 95% CI: 0.95‐1.03], or PNA [OR: 1.02, 95% CI: 0.98‐1.07]; Table 3).
| AMI | CHF | PNA | ||||
|---|---|---|---|---|---|---|
| Univariate OR (95% CI) | Multivariable OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | Univariate OR (95% CI) | Multivariate OR (95% CI) | |
| ||||||
| Weekend discharge | 1 (0.96‐1.04) | 1.02 (0.98‐1.06) | 0.96 (0.91‐1) | 0.99 (0.94‐1.03) | 0.97 (0.93‐1.02) | 1.02 (0.98‐1.07) |
| Age, y | ||||||
| 044 | ||||||
| 4554 | 1.02 (0.92‐1.12) | 0.96 (0.87‐1.07) | 1.04 (0.93‐1.16) | 1.00 (0.89‐1.11) | 1.08 (0.98‐1.19) | 0.93 (0.84‐1.03) |
| 5564 | 1.11 (1.02‐1.22) | 1.00 (0.91‐1.10) | 1.11 (1.01‐1.23) | 0.97 (0.88‐1.08) | 1.23 (1.13‐1.34) | 0.94 (0.86‐1.03) |
| 6574 | 1.31 (1.19‐1.43) | 1.04 (0.94‐1.15) | 1.1 (1‐1.22) | 0.90 (0.81‐1.01) | 1.29 (1.19‐1.41) | 0.87 (0.79‐0.96) |
| 7584 | 1.29 (1.18‐1.41) | 0.94 (0.85‐1.05) | 1.06 (0.97‐1.17) | 0.84 (0.75‐0.93) | 1.37 (1.27‐1.49) | 0.87 (0.79‐0.95) |
| 85+ | 1.03 (0.94‐1.13) | 0.72 (0.64‐0.81) | 0.98 (0.89‐1.08) | 0.76 (0.68‐0.84) | 1.31 (1.2‐1.41) | 0.78 (0.71‐0.86) |
| Gender | ||||||
| Female | ||||||
| Male | 1 (0.97‐1.04) | 1.1 (1.05‐1.14) | 1.06 (1.02‐1.1) | 1.08 (1.04‐1.12) | 1.13 (1.09‐1.18) | 1.15 (1.10‐1.19) |
| Race | ||||||
| White | ||||||
| Black | 1.17 (1.1‐1.25) | 1.12 (1.05‐1.20) | 1.06 (1‐1.12) | 1.03 (0.97‐1.09) | 1.11 (1.04‐1.19) | 1.07 (0.99‐1.15) |
| Hispanic | 1.11 (1.06‐1.16) | 1.12 (1.06‐1.17) | 1.05 (1‐1.1) | 1.04 (1.00‐1.10) | 0.93 (0.89‐0.98) | 0.95 (0.90‐1.00) |
| API | 1.14 (1.07‐1.2) | 1.09 (1.03‐1.16) | 1.01 (0.95‐1.08) | 1.00 (0.94‐1.07) | 0.97 (0.91‐1.04) | 0.93 (0.86‐0.99) |
| Charlson Comorbidity Index | ||||||
| 0 | ||||||
| 1 | 1.54 (1.46‐1.62) | 1.40 (1.32‐1.48) | 1.02 (0.95‐1.1) | 1.0 (0.92‐1.08) | 1.19 (1.12‐1.26) | 1.11 (1.04‐1.19) |
| 2 | 1.78 (1.69‐1.89) | 1.60 (1.51‐1.70) | 1.16 (1.08‐1.25) | 1.11 (1.03‐1.20) | 1.43 (1.34‐1.53) | 1.22 (1.14‐1.31) |
| 3 | 2.07 (1.97‐2.17) | 1.83 (1.73‐1.93) | 1.41 (1.32‐1.51) | 1.24 (1.15‐1.32) | 1.79 (1.69‐1.89) | 1.40 (1.31‐1.48) |
| Payer status | ||||||
| Private | ||||||
| Medicare | 1.02 (0.98‐1.06) | 0.89 (0.84‐0.95) | 1.04 (0.98‐1.11) | 1.04 (0.98‐1.12) | 1.29 (1.22‐1.37) | 1.06 (0.98‐1.13) |
| Medicaid | 0.89 (0.83‐0.96) | 0.83 (0.77‐0.89) | 1.2 (1.12‐1.3) | 1.23 (1.13‐1.33) | 1.28 (1.18‐1.38) | 1.18 (1.09‐1.28) |
| No insurance | 0.52 (0.46‐0.58) | 0.60 (0.53‐0.67) | 0.66 (0.57‐0.76) | 0.79 (0.68‐0.91) | 0.64 (0.54‐0.75) | 0.73 (0.61‐0.87) |
| Unknown | 0.71 (0.65‐0.78) | 0.77 (0.70‐0.84) | 0.91 (0.81‐1.03) | 1.02 (0.9‐1.15) | 0.9 (0.79‐1.03) | 0.93 (0.81‐1.06) |
| Disposition | ||||||
| Home | ||||||
| Acute care | 0.32 (0.27‐0.37) | 0.35 (0.29‐0.41) | 1.42 (1.18‐1.71) | 1.2 (1.05‐1.55) | 2.08 (1.69‐2.56) | 1.64 (1.32‐2.03) |
| SNF | 1.27 (1.2‐1.34) | 1.18 (1.10‐1.26) | 1.61 (1.53‐1.7) | 1.54 (1.46‐1.63) | 1.9 (1.81‐2.01) | 1.61 (1.52‐1.71) |
| Residential facility | 0.89 (0.68‐1.15) | 0.94 (0.72‐1.24) | 1.31 (1.1‐1.58) | 1.40 (1.16‐1.69) | 1.61 (1.37‐1.89) | 1.52 (1.29‐1.80) |
| Other | 1.21 (1.16‐1.26) | 1.10 (1.05‐1.15) | 1.72 (1.66‐1.79) | 1.59 (1.52‐1.66) | 2.31 (2.21‐2.41) | 1.88 (1.79‐1.98) |
| Length of stay* | 1.04 (1.02‐1.05) | 0.89 (0.87‐0.90) | 1.20 (1.19‐1.22) | 1.09 (1.08‐1.11) | 1.31 (1.29‐1.32) | 1.13 (1.1‐1.14) |
| Any complication | 3.14 (3.02‐3.26) | 2.61 (2.50‐2.73) | 1.52 (1.46‐1.59) | 1.35 (1.29‐1.41) | 1.70 (1.62‐1.78) | 1.39 (1.32‐1.45) |
| Admission type | ||||||
| Elective | ||||||
| Unplanned | 0.28 (0.27‐0.29) | 0.33 (0.31‐0.34) | 0.56 (0.54‐0.59) | 0.57 (0.53‐0.6) | 0.39 (0.37‐0.42) | 0.45 (0.42‐0.48) |
Increasing age, male gender, black race, greater Charlson Comorbidity Index, occurrence of any complication, and increased LOS were all associated with need for readmission on univariate analysis, though many of these associations weakened on multivariable analysis (Table 3). The effect of payer status on readmission was complex. Compared to private insurance, Medicare was associated with readmissions for patients with PNA (OR: 1.29, 95% CI: 1.22‐1.37) but not AMI (OR: 1.02, 95% CI: 0.98‐1.06) or CHF (OR: 1.04, 95% CI: 0.98‐1.11). Medicaid insurance was associated with readmission for CHF (OR: 1.20, 95% CI: 1.12‐1.30) and PNA (OR: 1.28, 95% CI: 1.18‐1.38) but appeared to be protective from readmission for AMI (OR: 0.89, 95% CI: 0.83‐0.96). Lack of insurance was associated with decreased odds of readmission for all diagnoses (P<0.05 for all models).
Models predicting 90‐day readmission rates showed similar results in all categories; therefore, the data are not shown.
DISCUSSION
We used a California statewide discharge database that linked individual patient records from all nonfederal hospitals to examine 30‐ and 90‐day hospital readmissions for CHF, AMI, and PNA. We hypothesized, but did not find, that weekend hospital discharge would be associated with higher hospital readmission rates. We did find other factors that were associated with hospital readmissions, including race, age, greater comorbidities, male gender, and discharge to an SNF. Nearly half of patients were readmitted for the same diagnosis as the initial discharge diagnosis, and nearly two‐thirds of the patients were readmitted to a hospital different from the discharging hospital.
Our study found some findings similar to prior investigations. First, the factors that predicted hospital readmission were complex and included age, race, gender, comorbidities, payer status, length of hospital stay, and the occurrence of a complication; most of these factors persisted after multivariable analysis but were not necessarily consistent across all admission diagnoses.[16, 17, 18] One finding of particular interest was the impact of insurance status. Specifically, lack of insurance was inversely associated with hospital readmission; this finding warrants further investigation. Our study is also similar to others in that we found that the most common reasons for readmission are typically related to the reason for the principal admission. Dharmarajan et al. previously studied the reason for readmission among hospitalized Medicare patients with AMI, CHF, and PNA, and found similarly high rates of identical admission diagnoses.[19] Furthermore, in our study, between 32% and 65% of 30‐day readmissions were to a hospital different than the discharging facility. Although few prior studies have had the ability to assess readmission to alternative hospitals, those who have done so in the past have found similar rates of divergence from the index facility.[20, 21]
Despite the apparent similarities to other studies, the current research question was specifically designed to investigate the weekend effect of hospital discharge. The term weekend effect refers to a phenomenon of worse clinical outcomes (eg, morbidity,[22] mortality,[6, 7] intensive care unit [ICU] readmission,[23] delays in appropriate diagnostic imaging[24, 25] and intervention,[26, 27] LOS,[28] and hospital costs[29]) for care delivered on a weekend. In a landmark study, Bell and Redelmeier demonstrated increased in‐house mortality for patients with ruptured abdominal aortic aneurysm, pulmonary embolism, or acute epiglottitis admitted through the emergency department on a weekend compared to weekday.[6] After controlling for patient variables, the association persisted, suggesting system‐related factors were contributory. Similarly, Kostis et al. showed that patients admitted to the hospital on a weekend with AMI had higher 30‐day mortality rates compared to those with weekday admission.[7] Finally, Aylin et al. demonstrated that mortality was 44% higher for patients undergoing elective surgery on a Friday and 82% higher for surgery on a weekend compared to a Monday.[30]
Despite this robust literature, fewer studies have evaluated the relationship between timing of discharge and outcomes. Much of the initial research has been focused on timing of discharge from the ICU. For example, transfer out of the ICU at night has been associated with higher in‐hospital mortality[31, 32, 33, 34, 35] as well as ICU readmission.[36, 37] Discharge from the ICU on a weekend has been associated with increased mortality in some studies[23] but not in others.[35, 38] Van Walraven and Bell were the first to investigate the impact of weekend hospital discharge on outcomes. In their analysis of all discharges from Ontario hospitals between 1990 and 2000, patients discharged on a Friday were at increased risk of death and 30‐day readmission compared to discharge on a Wednesday.[9] Beck et al. performed a similar study in pediatric patients but did not find a statistically significant effect of Friday discharge on readmission rates.[39] McAlister et al. specifically studied the effect of weekend (Saturday or Sunday) discharge on patients with CHF by analyzing discharges from Alberta, Canada hospitals between 1999 and 2009. Despite being comprised of lower‐risk patients, weekend discharge was associated with greater rates of 30‐ and 90‐day death and hospital readmission.[10] Conversely, McAlister et al. evaluated general medicine discharges from teaching hospitals in Alberta, Canada between 2009 and 2011 and found no difference in hospital readmission rates among those discharged on a weekend versus weekday.[11] The current investigation is the first to study hospitals in the United States to address this topic, an important consideration given differences in American and Canadian healthcare systems. Nevertheless, our results are similar to those of McAlister et al.,[11] who found no difference in hospital readmission rates based on day of discharge among patients with AMI, CHF, or PNA.
One potential explanation for finding a lack of correlation between weekend discharge and readmissions is that patients at higher risk for readmission are already selected toward weekday discharge. Our study found that patients discharged to an SNF, a group with higher odds of readmission, were less often discharged on a weekend. There may be other unmeasurable factors that differ between patients discharged on weekends versus weekdays. Also, factors that bias healthcare providers' decision making on timing of discharge are difficult to quantify and may differ between the 2 groups. Although our study hypothesis was driven by the perception that weekend discharges may fare poorly because of inadequate resources on the weekend, an alternative explanation for finding no association may be that current systems in place already do an effective job of discharge coordination on the weekend. Despite fears that staffing and equipment are significantly reduced during the weekend, perhaps weekend discharge resources are not the limiting factor in efforts to reduce readmissions.
Our results challenge the idea that weekend discharges predict hospital readmissions in California and argue for the relative safety of weekend discharges. Based on these findings, the routine delay in discharge of the complex medical patient until Monday for fear of discharge on a weekend does not seem warranted. Avoiding unnecessary delays in discharge should have positive effects on healthcare costs by reducing LOS. Two additional implications of our work are that single institution studies may underestimate readmission rates,[40] and that discharge to an SNF should receive special consideration in calculation of hospital‐level penalties for subsequent readmissions, as this group is associated with particularly higher risk.
There are some limitations to our study that should be acknowledged. The use of administrative data has well known limitations and the possibility of coding inaccuracy cannot be excluded.[41] Certain factors that could potentially differ between groups, such as illness severity, as well as details on the discharge process, were not available in this administrative database. In addition, elective readmissions were not excluded from the study. Also, because of the way the data were coded, a significant percentage of discharge dispositions were unknown. Finally, although morbidity and mortality have been studied in previous reports,[9, 10, 39] these data were not available for the current study, limiting the applicability of its conclusions.
CONCLUSIONS
In conclusion, among patients admitted with AMI, CHF, or PNA in California, discharge on a weekend is not associated with hospital readmission. Future studies on hospital readmissions should use a population‐based approach to accurately capture all readmissions following discharge.
Acknowledgments
Disclosure: Nothing to report.
- , Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160(8):1074–1081.
- , Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306(16):1794–1795.
- Medicare fines 2,610 hospitals in third round of readmission penalties. Kaiser Health News. Available at: http://www.kaiserhealthnews.org/Stories/2014/October/02/Medicare‐readmissions‐penalties‐2015.aspx. Published October 2, 2014. Accessed October 2, 2014.
- , Interventions to decrease hospital readmissions: keys for cost‐effectiveness. JAMA Intern Med. 2013;173(8):695–698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001;345(9):663–668.
- , , , et al. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med. 2007;356(11):1099–1109.
- , , , , , Mortality rate after nonelective hospital admission. Arch Surg 2011;146(5):545–551.
- , Risk of death or readmission among people discharged from hospital on Fridays. CMAJ. 2002;166(13):1672–1673.
- , , , , Postdischarge outcomes in heart failure are better for teaching hospitals and weekday discharges. Circ Heart Fail. 2013;6(5):922–929.
- , , , Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
- , , Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , , , The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429.
- Readmissions Reduction Program. August 2014. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html. Accessed October 2, 2014.
- , , Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25(3):211–219.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- , , , et al. Diagnoses and timing of 30‐day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355–363.
- , , , et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: a population‐based appraisal. Ann Surg Oncol. 2009;16(3):554–561.
- , , , et al. Is same‐hospital readmission rate a good surrogate for all‐hospital readmission rate? Med Care. 2010;48(5):477–481.
- , , , et al. Worse outcomes in patients undergoing urgent surgery for left‐sided diverticulitis admitted on weekends vs weekdays: a population‐based study of 31 832 patients. Arch Surg. 2012;147(7):649–655.
- , , , et al. Mortality after discharge from the intensive care unit during the early weekend period: a population‐based cohort study in Denmark. Acta Anaesthesiol Scand. 2007;51(9):1225–1230.
- , , , Something for the weekend? JAMA Neurol. 2013;70(1):130.
- , , , , Dying for the weekend: a retrospective cohort study on the association between day of hospital presentation and the quality and safety of stroke care. Arch Neurol. 2012;69(10):1296–1302.
- , , , Effects of weekend admission on the outcomes and management of ruptured aortic aneurysms. J Vasc Surg. 2014;60(2):318–324
- , , , et al. Treatment delay in patients undergoing primary percutaneous coronary intervention for ST‐elevation myocardial infarction: a key process analysis of patient and program factors. Am Heart J. 2008;155(2):290–297.
- , , , et al. Weekend hospital admission and discharge for heart failure: association with quality of care and clinical outcomes. Am Heart J. 2009;158(3):451–458.
- , , , , Comparison of perioperative outcomes and cost of spinal fusion for cervical trauma: weekday versus weekend admissions. Spine. 2013;38(25):2178–2183.
- , , , , Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
- , Consequences of discharges from intensive care at night. Lancet. 2000;355(9210):1138–1142.
- , , Waiting for the break of dawn? The effects of discharge time, discharge TISS scores and discharge facility on hospital mortality after intensive care. Intensive Care Med. 2002;28(9):1287–1293.
- , After‐hours discharges from intensive care are associated with increased mortality. Med J Aust. 2006;184(7):334–337.
- , Impact of intensive care unit discharge time on patient outcome. Crit Care Med. 2006;34(12):2946–2951.
- , , , Hospital mortality among adults admitted to and discharged from intensive care on weekends and evenings. J Crit Care. 2008;23(3):317–324.
- , , , et al. Factors associated with increased risk of readmission to intensive care in Australia. Intensive Care Med. 2011;37(11):1800–1808.
- , , , , After‐hours discharge from intensive care increases the risk of readmission and death. Anaesth Intensive Care. 2007;35(4):477–485.
- , , The effects of ICU admission and discharge times on mortality in Finland. Intensive Care Med. 2003;29(12):2144–2148.
- , , , , Day of discharge and hospital readmission rates within 30 days in children: a population‐based study. Paediatr Child Health. 2006;11(7):409–412.
- , , , Using same‐hospital readmission rates to estimate all‐hospital readmission rates. J Am Coll Surg. 2014;219(4):656–663.
- , , , et al. Evaluation of hospital readmissions in surgical patients: do administrative data tell the real story? JAMA Surg. 2014;149(8):759–764.
- , Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160(8):1074–1081.
- , Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306(16):1794–1795.
- Medicare fines 2,610 hospitals in third round of readmission penalties. Kaiser Health News. Available at: http://www.kaiserhealthnews.org/Stories/2014/October/02/Medicare‐readmissions‐penalties‐2015.aspx. Published October 2, 2014. Accessed October 2, 2014.
- , Interventions to decrease hospital readmissions: keys for cost‐effectiveness. JAMA Intern Med. 2013;173(8):695–698.
- , , , , Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- , Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001;345(9):663–668.
- , , , et al. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med. 2007;356(11):1099–1109.
- , , , , , Mortality rate after nonelective hospital admission. Arch Surg 2011;146(5):545–551.
- , Risk of death or readmission among people discharged from hospital on Fridays. CMAJ. 2002;166(13):1672–1673.
- , , , , Postdischarge outcomes in heart failure are better for teaching hospitals and weekday discharges. Circ Heart Fail. 2013;6(5):922–929.
- , , , Similar outcomes among general medicine patients discharged on weekends. J Hosp Med. 2015;10(2):69–74.
- , , Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , , , The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429.
- Readmissions Reduction Program. August 2014. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html. Accessed October 2, 2014.
- , , Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25(3):211–219.
- , , Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- , , , et al. Diagnoses and timing of 30‐day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355–363.
- , , , et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: a population‐based appraisal. Ann Surg Oncol. 2009;16(3):554–561.
- , , , et al. Is same‐hospital readmission rate a good surrogate for all‐hospital readmission rate? Med Care. 2010;48(5):477–481.
- , , , et al. Worse outcomes in patients undergoing urgent surgery for left‐sided diverticulitis admitted on weekends vs weekdays: a population‐based study of 31 832 patients. Arch Surg. 2012;147(7):649–655.
- , , , et al. Mortality after discharge from the intensive care unit during the early weekend period: a population‐based cohort study in Denmark. Acta Anaesthesiol Scand. 2007;51(9):1225–1230.
- , , , Something for the weekend? JAMA Neurol. 2013;70(1):130.
- , , , , Dying for the weekend: a retrospective cohort study on the association between day of hospital presentation and the quality and safety of stroke care. Arch Neurol. 2012;69(10):1296–1302.
- , , , Effects of weekend admission on the outcomes and management of ruptured aortic aneurysms. J Vasc Surg. 2014;60(2):318–324
- , , , et al. Treatment delay in patients undergoing primary percutaneous coronary intervention for ST‐elevation myocardial infarction: a key process analysis of patient and program factors. Am Heart J. 2008;155(2):290–297.
- , , , et al. Weekend hospital admission and discharge for heart failure: association with quality of care and clinical outcomes. Am Heart J. 2009;158(3):451–458.
- , , , , Comparison of perioperative outcomes and cost of spinal fusion for cervical trauma: weekday versus weekend admissions. Spine. 2013;38(25):2178–2183.
- , , , , Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
- , Consequences of discharges from intensive care at night. Lancet. 2000;355(9210):1138–1142.
- , , Waiting for the break of dawn? The effects of discharge time, discharge TISS scores and discharge facility on hospital mortality after intensive care. Intensive Care Med. 2002;28(9):1287–1293.
- , After‐hours discharges from intensive care are associated with increased mortality. Med J Aust. 2006;184(7):334–337.
- , Impact of intensive care unit discharge time on patient outcome. Crit Care Med. 2006;34(12):2946–2951.
- , , , Hospital mortality among adults admitted to and discharged from intensive care on weekends and evenings. J Crit Care. 2008;23(3):317–324.
- , , , et al. Factors associated with increased risk of readmission to intensive care in Australia. Intensive Care Med. 2011;37(11):1800–1808.
- , , , , After‐hours discharge from intensive care increases the risk of readmission and death. Anaesth Intensive Care. 2007;35(4):477–485.
- , , The effects of ICU admission and discharge times on mortality in Finland. Intensive Care Med. 2003;29(12):2144–2148.
- , , , , Day of discharge and hospital readmission rates within 30 days in children: a population‐based study. Paediatr Child Health. 2006;11(7):409–412.
- , , , Using same‐hospital readmission rates to estimate all‐hospital readmission rates. J Am Coll Surg. 2014;219(4):656–663.
- , , , et al. Evaluation of hospital readmissions in surgical patients: do administrative data tell the real story? JAMA Surg. 2014;149(8):759–764.
© 2015 Society of Hospital Medicine
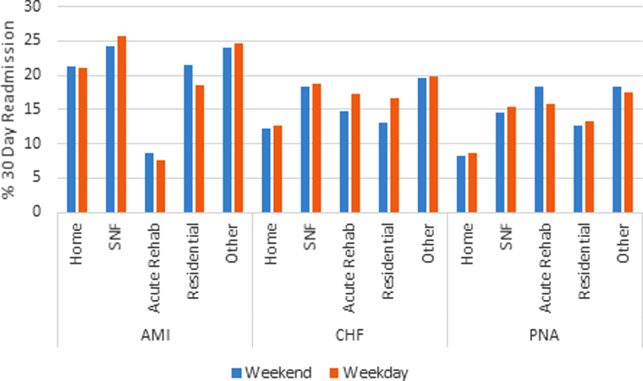
David Henry's JCSO podcast, June 2015
This month, Dr David Henry of The Journal of Community and Supportive Oncology examines the use olaparib, which was recently approved for the treatment of BRCA-mutated advanced ovarian cancer, as well as four Original Research articles that focus on patient care, support, and quality of life. There’s a comparison of the antiemetic efficacy and safety of palonosetron and ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children; a study that looks at the rationale, dosimetric parameters, and preliminary clinical outcomes in patients who undergo postoperative stereotactic radiosurgery with simultaneous integrated boost for brain metastases; an examination of the impact of nurse navigation on the timeliness of diagnostic medical services in patients with newly diagnosed lung cancer; and a study that draws on a novel approach to improving end-of-life care by measuring patterns of care among recently deceased patients. The podcast concludes with a round-up of some recent studies on cardiovascular disease in oncology, including the toxicity of cancer therapy and treatment guidelines from the American Society of Clinical Oncology.
This month, Dr David Henry of The Journal of Community and Supportive Oncology examines the use olaparib, which was recently approved for the treatment of BRCA-mutated advanced ovarian cancer, as well as four Original Research articles that focus on patient care, support, and quality of life. There’s a comparison of the antiemetic efficacy and safety of palonosetron and ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children; a study that looks at the rationale, dosimetric parameters, and preliminary clinical outcomes in patients who undergo postoperative stereotactic radiosurgery with simultaneous integrated boost for brain metastases; an examination of the impact of nurse navigation on the timeliness of diagnostic medical services in patients with newly diagnosed lung cancer; and a study that draws on a novel approach to improving end-of-life care by measuring patterns of care among recently deceased patients. The podcast concludes with a round-up of some recent studies on cardiovascular disease in oncology, including the toxicity of cancer therapy and treatment guidelines from the American Society of Clinical Oncology.
This month, Dr David Henry of The Journal of Community and Supportive Oncology examines the use olaparib, which was recently approved for the treatment of BRCA-mutated advanced ovarian cancer, as well as four Original Research articles that focus on patient care, support, and quality of life. There’s a comparison of the antiemetic efficacy and safety of palonosetron and ondansetron in the prevention of chemotherapy-induced nausea and vomiting in children; a study that looks at the rationale, dosimetric parameters, and preliminary clinical outcomes in patients who undergo postoperative stereotactic radiosurgery with simultaneous integrated boost for brain metastases; an examination of the impact of nurse navigation on the timeliness of diagnostic medical services in patients with newly diagnosed lung cancer; and a study that draws on a novel approach to improving end-of-life care by measuring patterns of care among recently deceased patients. The podcast concludes with a round-up of some recent studies on cardiovascular disease in oncology, including the toxicity of cancer therapy and treatment guidelines from the American Society of Clinical Oncology.
VIDEO: Anticipatory guidance can reduce chronic postconcussion syndrome
WASHINGTON – Regardless of the number of tests and tools for helping to diagnose pediatric sports concussions, Dr. Christopher Giza, professor of pediatric neurology and neurosurgery at the University of California, Los Angeles, says it’s important for clinicians to remember that “concussion is a clinical diagnosis.”
In this video interview recorded at Summit in Neurology & Psychiatry, Dr. Giza offers pearls and insights into the latest in sports concussion management. He describes the four “Rs” of treating sports concussions and urges primary care personnel to offer anticipatory guidance to patients and their families. Such guidance can lead to a 20% decrease in chronic postconcussion syndrome in children and adolescents, he said at the meeting held by Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
WASHINGTON – Regardless of the number of tests and tools for helping to diagnose pediatric sports concussions, Dr. Christopher Giza, professor of pediatric neurology and neurosurgery at the University of California, Los Angeles, says it’s important for clinicians to remember that “concussion is a clinical diagnosis.”
In this video interview recorded at Summit in Neurology & Psychiatry, Dr. Giza offers pearls and insights into the latest in sports concussion management. He describes the four “Rs” of treating sports concussions and urges primary care personnel to offer anticipatory guidance to patients and their families. Such guidance can lead to a 20% decrease in chronic postconcussion syndrome in children and adolescents, he said at the meeting held by Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
WASHINGTON – Regardless of the number of tests and tools for helping to diagnose pediatric sports concussions, Dr. Christopher Giza, professor of pediatric neurology and neurosurgery at the University of California, Los Angeles, says it’s important for clinicians to remember that “concussion is a clinical diagnosis.”
In this video interview recorded at Summit in Neurology & Psychiatry, Dr. Giza offers pearls and insights into the latest in sports concussion management. He describes the four “Rs” of treating sports concussions and urges primary care personnel to offer anticipatory guidance to patients and their families. Such guidance can lead to a 20% decrease in chronic postconcussion syndrome in children and adolescents, he said at the meeting held by Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
AT SUMMIT IN NEUROLOGY & PSYCHIATRY

DDW: Antibiotic rifaximin eases functional dyspepsia
WASHINGTON – Two weeks of antibiotic therapy with rifaximin provided relief from functional dyspepsia symptoms in a phase III double-blind, randomized trial.
“This is the first study that demonstrates that rifaximin is efficacious in the treatment of functional dyspepsia, particularly for global dyspeptic symptoms, bloating, and possibly belching. Our finding may suggest a role for the gut microbiota in the pathogenesis of functional dyspepsia,” Dr. Victoria Tan said at the annual Digestive Disease Week.

Rifaximin (Xifaxan) works by reducing or altering bacteria in the gut and has been shown to be efficacious in the treatment of diarrhea-predominant irritable bowel syndrome. It is approved to treat traveler’s diarrhea caused by Escherichia coli and to prevent hepatic encephalopathy.
The study randomly assigned 95 consecutive adults with functional dyspepsia as per ROME III criteria who had a normal gastroscopy within the last 2 years, had active symptoms in the month prior to enrollment, and were Helicobacter pylori negative, to rifaximin 400 mg or placebo three times a day for 2 weeks. In all, 33 rifaximin and 39 placebo patients were evaluable for the primary efficacy outcome of adequate relief of global dyspeptic symptoms (either no or mild dyspeptic symptoms) at any of the follow-up time points.
At baseline, 77% of patients had moderate to severe global dyspepsia symptoms, 74% of the placebo group and 55%% of the rifaximin group had moderate to severe belching, and roughly half of all patients were not on any GI medications. Mean age of the patients was 52 years.
Global dyspepsia symptoms improved with rifaximin beginning at week 2 and significantly favored rifaximin by week 8, with 23.5% of rifaximin patients reporting moderate to severe symptoms compared with 47.4% given placebo (P value = .04), said Dr. Tan of the University of Hong Kong.
Rates of moderate to severe belching were significantly improved with rifaximin at week 4 compared with placebo (14.3% vs. 35.7%; P = .03), but this difference was no longer significant at week 8 (26.5% vs. 29%).
The story was similar for moderate to severe bloating: Rates declined significantly with rifaximin at week 4 (20% vs. 43%; P = .03), but were no longer significant at week 8 (26.5% vs. 34.2%), she said.
A subgroup analysis of female patients showed significant improvements in moderate to severe global dyspeptic symptoms with rifaximin compared with placebo at week 4 (20.8% vs. 59.4%; P = .006) and week 8 (20% vs. 48.4%; P = .048).
Treatment response was not reflected in change in hydrogen breath response, Dr. Tan said. Results of a 3-hour hydrogen breath test performed after a 12-hour overnight fast showed no differences between the rifaximin and placebo groups for H2 peak above baseline (2.94 ppm vs. 0.11 ppm; P = .29), H2 area under the curve (+43.64 ppm vs. –49.71 ppm; P = .76), and oro-cecal transit time (24.23 minutes vs. 16.5 minutes; P = .68).
Adverse events were very similar between the two groups at both 4 and 8 weeks, Dr. Tan said. Only one major event occurred, a severe case of acute hepatitis in a woman in the placebo arm who also took traditional Chinese herbs.
On Twitter @pwendl
WASHINGTON – Two weeks of antibiotic therapy with rifaximin provided relief from functional dyspepsia symptoms in a phase III double-blind, randomized trial.
“This is the first study that demonstrates that rifaximin is efficacious in the treatment of functional dyspepsia, particularly for global dyspeptic symptoms, bloating, and possibly belching. Our finding may suggest a role for the gut microbiota in the pathogenesis of functional dyspepsia,” Dr. Victoria Tan said at the annual Digestive Disease Week.
Rifaximin (Xifaxan) works by reducing or altering bacteria in the gut and has been shown to be efficacious in the treatment of diarrhea-predominant irritable bowel syndrome. It is approved to treat traveler’s diarrhea caused by Escherichia coli and to prevent hepatic encephalopathy.
The study randomly assigned 95 consecutive adults with functional dyspepsia as per ROME III criteria who had a normal gastroscopy within the last 2 years, had active symptoms in the month prior to enrollment, and were Helicobacter pylori negative, to rifaximin 400 mg or placebo three times a day for 2 weeks. In all, 33 rifaximin and 39 placebo patients were evaluable for the primary efficacy outcome of adequate relief of global dyspeptic symptoms (either no or mild dyspeptic symptoms) at any of the follow-up time points.
At baseline, 77% of patients had moderate to severe global dyspepsia symptoms, 74% of the placebo group and 55%% of the rifaximin group had moderate to severe belching, and roughly half of all patients were not on any GI medications. Mean age of the patients was 52 years.
Global dyspepsia symptoms improved with rifaximin beginning at week 2 and significantly favored rifaximin by week 8, with 23.5% of rifaximin patients reporting moderate to severe symptoms compared with 47.4% given placebo (P value = .04), said Dr. Tan of the University of Hong Kong.
Rates of moderate to severe belching were significantly improved with rifaximin at week 4 compared with placebo (14.3% vs. 35.7%; P = .03), but this difference was no longer significant at week 8 (26.5% vs. 29%).
The story was similar for moderate to severe bloating: Rates declined significantly with rifaximin at week 4 (20% vs. 43%; P = .03), but were no longer significant at week 8 (26.5% vs. 34.2%), she said.
A subgroup analysis of female patients showed significant improvements in moderate to severe global dyspeptic symptoms with rifaximin compared with placebo at week 4 (20.8% vs. 59.4%; P = .006) and week 8 (20% vs. 48.4%; P = .048).
Treatment response was not reflected in change in hydrogen breath response, Dr. Tan said. Results of a 3-hour hydrogen breath test performed after a 12-hour overnight fast showed no differences between the rifaximin and placebo groups for H2 peak above baseline (2.94 ppm vs. 0.11 ppm; P = .29), H2 area under the curve (+43.64 ppm vs. –49.71 ppm; P = .76), and oro-cecal transit time (24.23 minutes vs. 16.5 minutes; P = .68).
Adverse events were very similar between the two groups at both 4 and 8 weeks, Dr. Tan said. Only one major event occurred, a severe case of acute hepatitis in a woman in the placebo arm who also took traditional Chinese herbs.
On Twitter @pwendl
WASHINGTON – Two weeks of antibiotic therapy with rifaximin provided relief from functional dyspepsia symptoms in a phase III double-blind, randomized trial.
“This is the first study that demonstrates that rifaximin is efficacious in the treatment of functional dyspepsia, particularly for global dyspeptic symptoms, bloating, and possibly belching. Our finding may suggest a role for the gut microbiota in the pathogenesis of functional dyspepsia,” Dr. Victoria Tan said at the annual Digestive Disease Week.
Rifaximin (Xifaxan) works by reducing or altering bacteria in the gut and has been shown to be efficacious in the treatment of diarrhea-predominant irritable bowel syndrome. It is approved to treat traveler’s diarrhea caused by Escherichia coli and to prevent hepatic encephalopathy.
The study randomly assigned 95 consecutive adults with functional dyspepsia as per ROME III criteria who had a normal gastroscopy within the last 2 years, had active symptoms in the month prior to enrollment, and were Helicobacter pylori negative, to rifaximin 400 mg or placebo three times a day for 2 weeks. In all, 33 rifaximin and 39 placebo patients were evaluable for the primary efficacy outcome of adequate relief of global dyspeptic symptoms (either no or mild dyspeptic symptoms) at any of the follow-up time points.
At baseline, 77% of patients had moderate to severe global dyspepsia symptoms, 74% of the placebo group and 55%% of the rifaximin group had moderate to severe belching, and roughly half of all patients were not on any GI medications. Mean age of the patients was 52 years.
Global dyspepsia symptoms improved with rifaximin beginning at week 2 and significantly favored rifaximin by week 8, with 23.5% of rifaximin patients reporting moderate to severe symptoms compared with 47.4% given placebo (P value = .04), said Dr. Tan of the University of Hong Kong.
Rates of moderate to severe belching were significantly improved with rifaximin at week 4 compared with placebo (14.3% vs. 35.7%; P = .03), but this difference was no longer significant at week 8 (26.5% vs. 29%).
The story was similar for moderate to severe bloating: Rates declined significantly with rifaximin at week 4 (20% vs. 43%; P = .03), but were no longer significant at week 8 (26.5% vs. 34.2%), she said.
A subgroup analysis of female patients showed significant improvements in moderate to severe global dyspeptic symptoms with rifaximin compared with placebo at week 4 (20.8% vs. 59.4%; P = .006) and week 8 (20% vs. 48.4%; P = .048).
Treatment response was not reflected in change in hydrogen breath response, Dr. Tan said. Results of a 3-hour hydrogen breath test performed after a 12-hour overnight fast showed no differences between the rifaximin and placebo groups for H2 peak above baseline (2.94 ppm vs. 0.11 ppm; P = .29), H2 area under the curve (+43.64 ppm vs. –49.71 ppm; P = .76), and oro-cecal transit time (24.23 minutes vs. 16.5 minutes; P = .68).
Adverse events were very similar between the two groups at both 4 and 8 weeks, Dr. Tan said. Only one major event occurred, a severe case of acute hepatitis in a woman in the placebo arm who also took traditional Chinese herbs.
On Twitter @pwendl
AT DDW® 2015

Updated acute stroke guideline boosts thrombectomy
Pivotal new high-quality evidence from randomized clinical trials and other sources published since 2013 has prompted the American Heart Association and the American Stroke Association to update their joint clinical practice guideline on endovascular treatment of acute ischemic stroke.
The revisions were published online June 29 in Stroke.
Unchanged is the key recommendation that intravenous recombinant tissue-type plasminogen activator (r-tPA) remain the mainstay of initial therapy, even if endovascular treatment is being considered. But a new recommendation adds that a period of observation to assess patients’ clinical response to r-tPA before proceeding with endovascular therapy is not necessary and is not advisable, said Dr. William J. Powers, chair of the guideline writing committee and professor and chairman of the department of neurology, University of North Carolina, Durham, and his associates.
Most of the updates pertain to the use of a stent retriever, which is now recommended for all patients with acute ischemic stroke who meet these seven criteria:
1. A prestroke modified Rankin scale (mRS) score of 0-1.
2. Receipt of r-tPA within 4.5 hours of symptom onset.
3. Causative occlusion of the internal carotid artery or proximal middle cerebral artery.
4. Age of 18 years or older.
5. A National Institutes of Health Stroke Scale (NIHSS) score of 6 or greater.
6. An Alberta Stroke Program Early CT Score (ASPECTS) of 6 or greater.
7. Initiation of the procedure within 6 hours of symptom onset.
Use of stent retrievers also is now considered “reasonable” in carefully selected patients with occlusion of the anterior circulation who have contraindications to r-tPA, such as current use of anticoagulants, prior stroke, serious head trauma, or hemorrhagic coagulopathy. It also may be reasonable in selected patients who have causative occlusion of the M2 or M3 portion of the middle cerebral arteries, anterior cerebral arteries, vertebral arteries, basilar artery, or posterior cerebral arteries, although the benefits are “uncertain” in this patient population.
Similarly, endovascular therapy using stent retrievers may be reasonable for some patients younger than age 18 who otherwise meet the seven criteria, even though the benefits of treatment haven’t been established in this age group. And it likewise may be reasonable in patients with prestroke mRS scores greater than 1, an ASPECTS of less than 6, or NIHSS scores of less than 6 if there is causative occlusion of the internal carotid artery or the proximal middle cerebral artery.
The updated guideline also says that stent retrievers are preferable to the Merci device, but that other mechanical thrombectomy devices may be reasonable to use in some circumstances. And adjunctive use of a proximal balloon guide catheter or a large-bore distal access catheter rather than a cervical guide catheter along with stent retrievers also may be beneficial.
In addition, “the technical goal of the thrombectomy procedure should be a TICI [Thrombolysis in Cerebral Infarction] 2b/3 angiographic result to maximize the probability of a good functional outcome. Use of salvage technical adjuncts including intra-arterial fibrinolysis may be reasonable to achieve these angiographic results, if completed within 6 hours of symptom onset,” the guideline states (Stroke 2015 June 29 [doi:10.1161/STR.0000000000000074]).
Also with regard to intra-arterial rather than intravenous fibrinolysis, stent retrievers are now preferable to intra-arterial fibrinolysis as first-line therapy.
The updated guideline also has added the recommendation that conscious sedation may be preferable to general anesthesia during endovascular therapy, depending on patient risk factors, tolerance of the procedure, and other clinical characteristics. It also revised recommendations addressing imaging studies and systems of stroke care.
Five prospective, randomized controlled trials have come out in the past few months, and triggered a revolution in acute stroke therapy. All five studies – MR CLEAN, ESCAPE, EXTENT IA, SWIFT PRIME, and REVASCAT – were halted early because of the significant advantage mechanical endovascular therapy with stents or thrombus retrieval devices demonstrated over standard therapy featuring clot thrombolysis with r-tPA.
Collectively, the five trials showed a 60% greater chance for good functional recovery from stroke with endovascular interventions. The rate of a favorable neurologic outcome as reflected in a modified Rankin score of 0-2 was 48% with the use of stent/retriever devices, compared with 30% with thrombolysis alone, said Dr. Petr Widimsky, professor and chair of the cardiology department at Charles University in Prague, at the annual congress of the European Association of Percutaneous Cardiovascular Interventions (EuroPCR) held in Paris in May.
The American Academy of Neurology “affirms the value of this guideline as an educational tool for neurologists.” The revised guideline is endorsed by the American Association of Neurological Surgeons, the Congress of Neurological Surgeons, the American Society of Neuroradiology, and the Society of Vascular and Interventional Neurology. A copy of the document is available at http://myamericanheart.org/statements.
Pivotal new high-quality evidence from randomized clinical trials and other sources published since 2013 has prompted the American Heart Association and the American Stroke Association to update their joint clinical practice guideline on endovascular treatment of acute ischemic stroke.
The revisions were published online June 29 in Stroke.
Unchanged is the key recommendation that intravenous recombinant tissue-type plasminogen activator (r-tPA) remain the mainstay of initial therapy, even if endovascular treatment is being considered. But a new recommendation adds that a period of observation to assess patients’ clinical response to r-tPA before proceeding with endovascular therapy is not necessary and is not advisable, said Dr. William J. Powers, chair of the guideline writing committee and professor and chairman of the department of neurology, University of North Carolina, Durham, and his associates.
Most of the updates pertain to the use of a stent retriever, which is now recommended for all patients with acute ischemic stroke who meet these seven criteria:
1. A prestroke modified Rankin scale (mRS) score of 0-1.
2. Receipt of r-tPA within 4.5 hours of symptom onset.
3. Causative occlusion of the internal carotid artery or proximal middle cerebral artery.
4. Age of 18 years or older.
5. A National Institutes of Health Stroke Scale (NIHSS) score of 6 or greater.
6. An Alberta Stroke Program Early CT Score (ASPECTS) of 6 or greater.
7. Initiation of the procedure within 6 hours of symptom onset.
Use of stent retrievers also is now considered “reasonable” in carefully selected patients with occlusion of the anterior circulation who have contraindications to r-tPA, such as current use of anticoagulants, prior stroke, serious head trauma, or hemorrhagic coagulopathy. It also may be reasonable in selected patients who have causative occlusion of the M2 or M3 portion of the middle cerebral arteries, anterior cerebral arteries, vertebral arteries, basilar artery, or posterior cerebral arteries, although the benefits are “uncertain” in this patient population.
Similarly, endovascular therapy using stent retrievers may be reasonable for some patients younger than age 18 who otherwise meet the seven criteria, even though the benefits of treatment haven’t been established in this age group. And it likewise may be reasonable in patients with prestroke mRS scores greater than 1, an ASPECTS of less than 6, or NIHSS scores of less than 6 if there is causative occlusion of the internal carotid artery or the proximal middle cerebral artery.
The updated guideline also says that stent retrievers are preferable to the Merci device, but that other mechanical thrombectomy devices may be reasonable to use in some circumstances. And adjunctive use of a proximal balloon guide catheter or a large-bore distal access catheter rather than a cervical guide catheter along with stent retrievers also may be beneficial.
In addition, “the technical goal of the thrombectomy procedure should be a TICI [Thrombolysis in Cerebral Infarction] 2b/3 angiographic result to maximize the probability of a good functional outcome. Use of salvage technical adjuncts including intra-arterial fibrinolysis may be reasonable to achieve these angiographic results, if completed within 6 hours of symptom onset,” the guideline states (Stroke 2015 June 29 [doi:10.1161/STR.0000000000000074]).
Also with regard to intra-arterial rather than intravenous fibrinolysis, stent retrievers are now preferable to intra-arterial fibrinolysis as first-line therapy.
The updated guideline also has added the recommendation that conscious sedation may be preferable to general anesthesia during endovascular therapy, depending on patient risk factors, tolerance of the procedure, and other clinical characteristics. It also revised recommendations addressing imaging studies and systems of stroke care.
Five prospective, randomized controlled trials have come out in the past few months, and triggered a revolution in acute stroke therapy. All five studies – MR CLEAN, ESCAPE, EXTENT IA, SWIFT PRIME, and REVASCAT – were halted early because of the significant advantage mechanical endovascular therapy with stents or thrombus retrieval devices demonstrated over standard therapy featuring clot thrombolysis with r-tPA.
Collectively, the five trials showed a 60% greater chance for good functional recovery from stroke with endovascular interventions. The rate of a favorable neurologic outcome as reflected in a modified Rankin score of 0-2 was 48% with the use of stent/retriever devices, compared with 30% with thrombolysis alone, said Dr. Petr Widimsky, professor and chair of the cardiology department at Charles University in Prague, at the annual congress of the European Association of Percutaneous Cardiovascular Interventions (EuroPCR) held in Paris in May.
The American Academy of Neurology “affirms the value of this guideline as an educational tool for neurologists.” The revised guideline is endorsed by the American Association of Neurological Surgeons, the Congress of Neurological Surgeons, the American Society of Neuroradiology, and the Society of Vascular and Interventional Neurology. A copy of the document is available at http://myamericanheart.org/statements.
Pivotal new high-quality evidence from randomized clinical trials and other sources published since 2013 has prompted the American Heart Association and the American Stroke Association to update their joint clinical practice guideline on endovascular treatment of acute ischemic stroke.
The revisions were published online June 29 in Stroke.
Unchanged is the key recommendation that intravenous recombinant tissue-type plasminogen activator (r-tPA) remain the mainstay of initial therapy, even if endovascular treatment is being considered. But a new recommendation adds that a period of observation to assess patients’ clinical response to r-tPA before proceeding with endovascular therapy is not necessary and is not advisable, said Dr. William J. Powers, chair of the guideline writing committee and professor and chairman of the department of neurology, University of North Carolina, Durham, and his associates.
Most of the updates pertain to the use of a stent retriever, which is now recommended for all patients with acute ischemic stroke who meet these seven criteria:
1. A prestroke modified Rankin scale (mRS) score of 0-1.
2. Receipt of r-tPA within 4.5 hours of symptom onset.
3. Causative occlusion of the internal carotid artery or proximal middle cerebral artery.
4. Age of 18 years or older.
5. A National Institutes of Health Stroke Scale (NIHSS) score of 6 or greater.
6. An Alberta Stroke Program Early CT Score (ASPECTS) of 6 or greater.
7. Initiation of the procedure within 6 hours of symptom onset.
Use of stent retrievers also is now considered “reasonable” in carefully selected patients with occlusion of the anterior circulation who have contraindications to r-tPA, such as current use of anticoagulants, prior stroke, serious head trauma, or hemorrhagic coagulopathy. It also may be reasonable in selected patients who have causative occlusion of the M2 or M3 portion of the middle cerebral arteries, anterior cerebral arteries, vertebral arteries, basilar artery, or posterior cerebral arteries, although the benefits are “uncertain” in this patient population.
Similarly, endovascular therapy using stent retrievers may be reasonable for some patients younger than age 18 who otherwise meet the seven criteria, even though the benefits of treatment haven’t been established in this age group. And it likewise may be reasonable in patients with prestroke mRS scores greater than 1, an ASPECTS of less than 6, or NIHSS scores of less than 6 if there is causative occlusion of the internal carotid artery or the proximal middle cerebral artery.
The updated guideline also says that stent retrievers are preferable to the Merci device, but that other mechanical thrombectomy devices may be reasonable to use in some circumstances. And adjunctive use of a proximal balloon guide catheter or a large-bore distal access catheter rather than a cervical guide catheter along with stent retrievers also may be beneficial.
In addition, “the technical goal of the thrombectomy procedure should be a TICI [Thrombolysis in Cerebral Infarction] 2b/3 angiographic result to maximize the probability of a good functional outcome. Use of salvage technical adjuncts including intra-arterial fibrinolysis may be reasonable to achieve these angiographic results, if completed within 6 hours of symptom onset,” the guideline states (Stroke 2015 June 29 [doi:10.1161/STR.0000000000000074]).
Also with regard to intra-arterial rather than intravenous fibrinolysis, stent retrievers are now preferable to intra-arterial fibrinolysis as first-line therapy.
The updated guideline also has added the recommendation that conscious sedation may be preferable to general anesthesia during endovascular therapy, depending on patient risk factors, tolerance of the procedure, and other clinical characteristics. It also revised recommendations addressing imaging studies and systems of stroke care.
Five prospective, randomized controlled trials have come out in the past few months, and triggered a revolution in acute stroke therapy. All five studies – MR CLEAN, ESCAPE, EXTENT IA, SWIFT PRIME, and REVASCAT – were halted early because of the significant advantage mechanical endovascular therapy with stents or thrombus retrieval devices demonstrated over standard therapy featuring clot thrombolysis with r-tPA.
Collectively, the five trials showed a 60% greater chance for good functional recovery from stroke with endovascular interventions. The rate of a favorable neurologic outcome as reflected in a modified Rankin score of 0-2 was 48% with the use of stent/retriever devices, compared with 30% with thrombolysis alone, said Dr. Petr Widimsky, professor and chair of the cardiology department at Charles University in Prague, at the annual congress of the European Association of Percutaneous Cardiovascular Interventions (EuroPCR) held in Paris in May.
The American Academy of Neurology “affirms the value of this guideline as an educational tool for neurologists.” The revised guideline is endorsed by the American Association of Neurological Surgeons, the Congress of Neurological Surgeons, the American Society of Neuroradiology, and the Society of Vascular and Interventional Neurology. A copy of the document is available at http://myamericanheart.org/statements.
FROM STROKE
Key clinical point: Pivotal new evidence prompted several changes in the 2013 AHA/ASA clinical practice guideline for early endovascular treatment of acute ischemic stroke.
Major finding: Most of the updates pertain to use of stent retrievers, which is now recommended for all patients with acute ischemic stroke who meet seven criteria.
Data source: A detailed review of eight randomized clinical trials and other relevant data published since 2013.
Disclosures: This work was supported by the American Heart Association and the American Stroke Association; Medtronic/Covidien, maker of the stent retriever newly recommended in this guideline, is a corporate sponsor of both the AHA and the ASA. Dr. Powers reported having no relevant financial disclosures; his associates on the writing committee reported ties to Microvention, Penumbra, Silk Road, Pulse Therapeutics, Covidien, Genentech, Stryker, Roche, Sequent, Lazarus, Codman, and Aldagn/Cytomedix.
VIDEO: Sometimes, comfort care is best for ruptured AAAs
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE 2015 VASCULAR ANNUAL MEETING

DDW: Novel acid blocker holds its own against PPIs
WASHINGTON – An experimental acid suppressant was effective for prevention of peptic ulcer recurrence during NSAID therapy, with a safety profile similar to that of a currently marketed proton pump inhibitor, investigators reported.
At 2 years of follow-up, rates of recurrent peptic ulcers or hemorrhagic lesions in the stomach or duodenum among patients who took vonoprazan (marketed in Japan as Takecab) at a 10-mg or 20-mg daily oral dose were numerically but not statistically significantly lower than those for patients who took a 15-mg once daily dose of lansoprazole (Prevacid), said Dr. Yuji Mizokami of University of Tsukuba Hospital in Ibaraki, Japan.

“The long-term safety profile of vonoprazan was similar to lansoprazole, and no safety issues were identified,” he said at the annual Digestive Disease Week.
Proton pump inhibitors (PPIs) such as lansoprazole are frequently prescribed as concomitant gastroprotective agents in patients on long-term therapy with a nonsteroidal anti-inflammatory drug (NSAID) such as aspirin or ibuprofen.
PIs have relatively short half-lives, however, which may limit their effectiveness as gastroprotectives. In addition, polymorphisms in the gene encoding for cytochrome P2C19 (CYP2C19) can affect PPI metabolism, Dr. Mizokami said.
Vonoprazan belongs to a new class of acid-suppressing drugs called potassium-competitive acid blockers (PCABs), which, unlike PPIs, do not need to be activated by acid to become effective and are not affected by genetic variations. Vonoprazan migrates from blood into the secretory canaliculus of acid-secreting parietal cells, and because of its longer elimination half-life and stability in acidic environments, provides a strong acid-inhibiting effect from the first dose, and remains effective for 24 hours, Dr. Mizokami explained.
He presented data from a 2-year extension of a phase III, 24-week noninferiority study comparing vonoprazan with lansoprazole for prevention of peptic ulcer recurrence. In that study, 5.5% of patients on lansoprazole had recurrent gastric or duodenal ulcers by week 24, compared with 3.3% of patients on 10 mg vonoprazan, and 3.4% of those on 20 mg vonoprazan.
A total of 357 patients completed the extension study: 108 initially assigned to lansoprazole, 131 to vonoprazan 10 mg, and 118 to vonoprazan 20 mg.
At 1 year, the rates of recurrent ulcers were 7% for patients on lansoprazole, 3.6% for those on vonoprazan 10 mg, and 5.4% for those on vonoprazan 20 mg. The respective rates at 2 years were 7.5%. 3.8%, and 5.9%. In a safety analysis (intention-to-treat), treatment-emergent adverse events were mild, did not appear to be dose dependent with vonoprazan, and did not increase over time.
Serious treatment-emergent events occurred in 8.6% among the patients on lansoprazole, 8.3% among patients on 10 mg vonoprazan, and 14.2% among those on 20 mg. Events leading to drug discontinuation occurred in 7.6%, 4.1%, and 12.2% of patients, respectively.
In all three study arms, but especially in the vonoprazan arms, there was an increase in serum gastrin seen at week 4, which increased moderately until week 52. After that, it began to decline among patients on vonoprazan, while plateauing among patients on lansoprazole.
There were also increases in pepsinogen I and II at week 4 in all three treatment groups; the levels remained stable thereafter, as did the ratio of pepsinogen I to pepsinogen II.
Vonoprazan is currently approved only in Japan. The manufacturer, Takeda, has not said if or when it intends to file for a New Drug Application in the United States. The study was supported by Takeda Pharmaceuticals. Dr. Mizokami disclosed serving as a consultant on the study. Four of the coauthors are company employees.
WASHINGTON – An experimental acid suppressant was effective for prevention of peptic ulcer recurrence during NSAID therapy, with a safety profile similar to that of a currently marketed proton pump inhibitor, investigators reported.
At 2 years of follow-up, rates of recurrent peptic ulcers or hemorrhagic lesions in the stomach or duodenum among patients who took vonoprazan (marketed in Japan as Takecab) at a 10-mg or 20-mg daily oral dose were numerically but not statistically significantly lower than those for patients who took a 15-mg once daily dose of lansoprazole (Prevacid), said Dr. Yuji Mizokami of University of Tsukuba Hospital in Ibaraki, Japan.
“The long-term safety profile of vonoprazan was similar to lansoprazole, and no safety issues were identified,” he said at the annual Digestive Disease Week.
Proton pump inhibitors (PPIs) such as lansoprazole are frequently prescribed as concomitant gastroprotective agents in patients on long-term therapy with a nonsteroidal anti-inflammatory drug (NSAID) such as aspirin or ibuprofen.
PIs have relatively short half-lives, however, which may limit their effectiveness as gastroprotectives. In addition, polymorphisms in the gene encoding for cytochrome P2C19 (CYP2C19) can affect PPI metabolism, Dr. Mizokami said.
Vonoprazan belongs to a new class of acid-suppressing drugs called potassium-competitive acid blockers (PCABs), which, unlike PPIs, do not need to be activated by acid to become effective and are not affected by genetic variations. Vonoprazan migrates from blood into the secretory canaliculus of acid-secreting parietal cells, and because of its longer elimination half-life and stability in acidic environments, provides a strong acid-inhibiting effect from the first dose, and remains effective for 24 hours, Dr. Mizokami explained.
He presented data from a 2-year extension of a phase III, 24-week noninferiority study comparing vonoprazan with lansoprazole for prevention of peptic ulcer recurrence. In that study, 5.5% of patients on lansoprazole had recurrent gastric or duodenal ulcers by week 24, compared with 3.3% of patients on 10 mg vonoprazan, and 3.4% of those on 20 mg vonoprazan.
A total of 357 patients completed the extension study: 108 initially assigned to lansoprazole, 131 to vonoprazan 10 mg, and 118 to vonoprazan 20 mg.
At 1 year, the rates of recurrent ulcers were 7% for patients on lansoprazole, 3.6% for those on vonoprazan 10 mg, and 5.4% for those on vonoprazan 20 mg. The respective rates at 2 years were 7.5%. 3.8%, and 5.9%. In a safety analysis (intention-to-treat), treatment-emergent adverse events were mild, did not appear to be dose dependent with vonoprazan, and did not increase over time.
Serious treatment-emergent events occurred in 8.6% among the patients on lansoprazole, 8.3% among patients on 10 mg vonoprazan, and 14.2% among those on 20 mg. Events leading to drug discontinuation occurred in 7.6%, 4.1%, and 12.2% of patients, respectively.
In all three study arms, but especially in the vonoprazan arms, there was an increase in serum gastrin seen at week 4, which increased moderately until week 52. After that, it began to decline among patients on vonoprazan, while plateauing among patients on lansoprazole.
There were also increases in pepsinogen I and II at week 4 in all three treatment groups; the levels remained stable thereafter, as did the ratio of pepsinogen I to pepsinogen II.
Vonoprazan is currently approved only in Japan. The manufacturer, Takeda, has not said if or when it intends to file for a New Drug Application in the United States. The study was supported by Takeda Pharmaceuticals. Dr. Mizokami disclosed serving as a consultant on the study. Four of the coauthors are company employees.
WASHINGTON – An experimental acid suppressant was effective for prevention of peptic ulcer recurrence during NSAID therapy, with a safety profile similar to that of a currently marketed proton pump inhibitor, investigators reported.
At 2 years of follow-up, rates of recurrent peptic ulcers or hemorrhagic lesions in the stomach or duodenum among patients who took vonoprazan (marketed in Japan as Takecab) at a 10-mg or 20-mg daily oral dose were numerically but not statistically significantly lower than those for patients who took a 15-mg once daily dose of lansoprazole (Prevacid), said Dr. Yuji Mizokami of University of Tsukuba Hospital in Ibaraki, Japan.
“The long-term safety profile of vonoprazan was similar to lansoprazole, and no safety issues were identified,” he said at the annual Digestive Disease Week.
Proton pump inhibitors (PPIs) such as lansoprazole are frequently prescribed as concomitant gastroprotective agents in patients on long-term therapy with a nonsteroidal anti-inflammatory drug (NSAID) such as aspirin or ibuprofen.
PIs have relatively short half-lives, however, which may limit their effectiveness as gastroprotectives. In addition, polymorphisms in the gene encoding for cytochrome P2C19 (CYP2C19) can affect PPI metabolism, Dr. Mizokami said.
Vonoprazan belongs to a new class of acid-suppressing drugs called potassium-competitive acid blockers (PCABs), which, unlike PPIs, do not need to be activated by acid to become effective and are not affected by genetic variations. Vonoprazan migrates from blood into the secretory canaliculus of acid-secreting parietal cells, and because of its longer elimination half-life and stability in acidic environments, provides a strong acid-inhibiting effect from the first dose, and remains effective for 24 hours, Dr. Mizokami explained.
He presented data from a 2-year extension of a phase III, 24-week noninferiority study comparing vonoprazan with lansoprazole for prevention of peptic ulcer recurrence. In that study, 5.5% of patients on lansoprazole had recurrent gastric or duodenal ulcers by week 24, compared with 3.3% of patients on 10 mg vonoprazan, and 3.4% of those on 20 mg vonoprazan.
A total of 357 patients completed the extension study: 108 initially assigned to lansoprazole, 131 to vonoprazan 10 mg, and 118 to vonoprazan 20 mg.
At 1 year, the rates of recurrent ulcers were 7% for patients on lansoprazole, 3.6% for those on vonoprazan 10 mg, and 5.4% for those on vonoprazan 20 mg. The respective rates at 2 years were 7.5%. 3.8%, and 5.9%. In a safety analysis (intention-to-treat), treatment-emergent adverse events were mild, did not appear to be dose dependent with vonoprazan, and did not increase over time.
Serious treatment-emergent events occurred in 8.6% among the patients on lansoprazole, 8.3% among patients on 10 mg vonoprazan, and 14.2% among those on 20 mg. Events leading to drug discontinuation occurred in 7.6%, 4.1%, and 12.2% of patients, respectively.
In all three study arms, but especially in the vonoprazan arms, there was an increase in serum gastrin seen at week 4, which increased moderately until week 52. After that, it began to decline among patients on vonoprazan, while plateauing among patients on lansoprazole.
There were also increases in pepsinogen I and II at week 4 in all three treatment groups; the levels remained stable thereafter, as did the ratio of pepsinogen I to pepsinogen II.
Vonoprazan is currently approved only in Japan. The manufacturer, Takeda, has not said if or when it intends to file for a New Drug Application in the United States. The study was supported by Takeda Pharmaceuticals. Dr. Mizokami disclosed serving as a consultant on the study. Four of the coauthors are company employees.
AT DDW® 2015
