User login
Possible downside to cloth diapers: bullous diaper dermatitis
MINNEAPOLIS – A small study of cloth diaper–wearing toddlers with unusual vesiculobullous and erosive lesions found that the rashes fully resolved with aggressive barrier cream application and a switch to disposable diapers.
The four patients had previously received aggressive work-ups, including biopsy in some cases; all had received systemic antibiotics. Katya L. Harfmann, MD, a pediatric dermatologist at Nationwide Children’s Hospital in Columbus, Ohio, was the lead author in a poster presentation at the annual meeting of the Society for Pediatric Dermatology.
The toddlers, aged 17 months to 2 years, had diaper dermatitis of several weeks’ to several months’ duration, with a presentation of vesicles, bullae, and erosions. All of the children had been placed in cloth diapers since birth. The patients, three of them male, had undergone work-ups that included bacterial culture for three patients, herpes simplex virus (HSV) polymerase chain reaction (PCR) testing for three patients, and blood work for two patients. HSV cultures and viral cultures were each performed on one patient. With the exception of one bacterial culture returning methicillin-sensitive Staphylococcus aureus (MSSA), all results were negative.
Two patients underwent biopsies. One biopsy was reported as “spongiform dermatitis,” while the other was read as a “nonspecific ulcer.”
A variety of treatments had been tried for the children. All of the children had received systemic antibiotics; two received systemic antivirals as well. Two patients each received topical steroids and topical antibacterials, and one patient also received topical dapsone. Many treatments were given “in repetitive courses, without improvement in the lesions,” wrote Dr. Harfmann and her coauthor.
The families were advised to switch to exclusive use of disposable diapers and to begin frequent use of a zinc oxide–based thick diaper paste. For all patients, the diaper dermatitis completely resolved within as little as 2 weeks.
The medical literature documents an increased risk of diaper dermatitis with cloth diaper use. “Despite this knowledge in the medical community, nearly half of cloth diaper–using parents select cloth diapers with the assumption that diaper rash is less frequent with their usage,” the researchers noted.
They pointed out that bullae in the diaper region are often thought to be associated with such infectious conditions as impetigo and herpes simplex infection, and can also be associated with immunobullous disorders. Diaper changes are less frequent in older children, though, giving the opportunity for prolonged contact with the irritating chemicals in feces and urine. This prolonged contact, exacerbated by the moister environment of a cloth diaper, may account for the unusual, severe presentation seen in these cases.
Also, the three boys had vesicular lesions on their testicles and penis. “It is possible that the thinner skin in these areas has a lower irritation threshold or that the redundancy of skin often seen on the penile shaft leads to trapping of irritants with extended diaper use,” they wrote.
“An empiric trial of disposable diapers exclusively with aggressive barrier cream application for several weeks may eliminate the need for more invasive procedures and laboratory tests,” wrote Dr. Harfmann and her coauthor.
They reported no conflicts of interest.
On Twitter @karioakes
MINNEAPOLIS – A small study of cloth diaper–wearing toddlers with unusual vesiculobullous and erosive lesions found that the rashes fully resolved with aggressive barrier cream application and a switch to disposable diapers.
The four patients had previously received aggressive work-ups, including biopsy in some cases; all had received systemic antibiotics. Katya L. Harfmann, MD, a pediatric dermatologist at Nationwide Children’s Hospital in Columbus, Ohio, was the lead author in a poster presentation at the annual meeting of the Society for Pediatric Dermatology.
The toddlers, aged 17 months to 2 years, had diaper dermatitis of several weeks’ to several months’ duration, with a presentation of vesicles, bullae, and erosions. All of the children had been placed in cloth diapers since birth. The patients, three of them male, had undergone work-ups that included bacterial culture for three patients, herpes simplex virus (HSV) polymerase chain reaction (PCR) testing for three patients, and blood work for two patients. HSV cultures and viral cultures were each performed on one patient. With the exception of one bacterial culture returning methicillin-sensitive Staphylococcus aureus (MSSA), all results were negative.
Two patients underwent biopsies. One biopsy was reported as “spongiform dermatitis,” while the other was read as a “nonspecific ulcer.”
A variety of treatments had been tried for the children. All of the children had received systemic antibiotics; two received systemic antivirals as well. Two patients each received topical steroids and topical antibacterials, and one patient also received topical dapsone. Many treatments were given “in repetitive courses, without improvement in the lesions,” wrote Dr. Harfmann and her coauthor.
The families were advised to switch to exclusive use of disposable diapers and to begin frequent use of a zinc oxide–based thick diaper paste. For all patients, the diaper dermatitis completely resolved within as little as 2 weeks.
The medical literature documents an increased risk of diaper dermatitis with cloth diaper use. “Despite this knowledge in the medical community, nearly half of cloth diaper–using parents select cloth diapers with the assumption that diaper rash is less frequent with their usage,” the researchers noted.
They pointed out that bullae in the diaper region are often thought to be associated with such infectious conditions as impetigo and herpes simplex infection, and can also be associated with immunobullous disorders. Diaper changes are less frequent in older children, though, giving the opportunity for prolonged contact with the irritating chemicals in feces and urine. This prolonged contact, exacerbated by the moister environment of a cloth diaper, may account for the unusual, severe presentation seen in these cases.
Also, the three boys had vesicular lesions on their testicles and penis. “It is possible that the thinner skin in these areas has a lower irritation threshold or that the redundancy of skin often seen on the penile shaft leads to trapping of irritants with extended diaper use,” they wrote.
“An empiric trial of disposable diapers exclusively with aggressive barrier cream application for several weeks may eliminate the need for more invasive procedures and laboratory tests,” wrote Dr. Harfmann and her coauthor.
They reported no conflicts of interest.
On Twitter @karioakes
MINNEAPOLIS – A small study of cloth diaper–wearing toddlers with unusual vesiculobullous and erosive lesions found that the rashes fully resolved with aggressive barrier cream application and a switch to disposable diapers.
The four patients had previously received aggressive work-ups, including biopsy in some cases; all had received systemic antibiotics. Katya L. Harfmann, MD, a pediatric dermatologist at Nationwide Children’s Hospital in Columbus, Ohio, was the lead author in a poster presentation at the annual meeting of the Society for Pediatric Dermatology.
The toddlers, aged 17 months to 2 years, had diaper dermatitis of several weeks’ to several months’ duration, with a presentation of vesicles, bullae, and erosions. All of the children had been placed in cloth diapers since birth. The patients, three of them male, had undergone work-ups that included bacterial culture for three patients, herpes simplex virus (HSV) polymerase chain reaction (PCR) testing for three patients, and blood work for two patients. HSV cultures and viral cultures were each performed on one patient. With the exception of one bacterial culture returning methicillin-sensitive Staphylococcus aureus (MSSA), all results were negative.
Two patients underwent biopsies. One biopsy was reported as “spongiform dermatitis,” while the other was read as a “nonspecific ulcer.”
A variety of treatments had been tried for the children. All of the children had received systemic antibiotics; two received systemic antivirals as well. Two patients each received topical steroids and topical antibacterials, and one patient also received topical dapsone. Many treatments were given “in repetitive courses, without improvement in the lesions,” wrote Dr. Harfmann and her coauthor.
The families were advised to switch to exclusive use of disposable diapers and to begin frequent use of a zinc oxide–based thick diaper paste. For all patients, the diaper dermatitis completely resolved within as little as 2 weeks.
The medical literature documents an increased risk of diaper dermatitis with cloth diaper use. “Despite this knowledge in the medical community, nearly half of cloth diaper–using parents select cloth diapers with the assumption that diaper rash is less frequent with their usage,” the researchers noted.
They pointed out that bullae in the diaper region are often thought to be associated with such infectious conditions as impetigo and herpes simplex infection, and can also be associated with immunobullous disorders. Diaper changes are less frequent in older children, though, giving the opportunity for prolonged contact with the irritating chemicals in feces and urine. This prolonged contact, exacerbated by the moister environment of a cloth diaper, may account for the unusual, severe presentation seen in these cases.
Also, the three boys had vesicular lesions on their testicles and penis. “It is possible that the thinner skin in these areas has a lower irritation threshold or that the redundancy of skin often seen on the penile shaft leads to trapping of irritants with extended diaper use,” they wrote.
“An empiric trial of disposable diapers exclusively with aggressive barrier cream application for several weeks may eliminate the need for more invasive procedures and laboratory tests,” wrote Dr. Harfmann and her coauthor.
They reported no conflicts of interest.
On Twitter @karioakes
AT THE SPD ANNUAL MEETING
Key clinical point: A distinct, vesiculobullous form of diaper dermatitis may be associated with cloth diaper use in toddlers.
Major finding: Disposable diapers and barrier protection resolved vesiculobullous lesions in cloth diaper–wearing toddlers.
Data source: A case series of four children with extensive negative work-ups for erosive and vesiculobullous eruptions.
Disclosures: The study investigators reported no disclosures.
Small Study: Placebo Bests Chondroitin, Glucosamine Combo for Knee Osteoarthritis
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).

Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).
Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).
Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
FROM ARTHRITIS & RHEUMATOLOGY

Small study: Placebo bests chondroitin, glucosamine combo for knee osteoarthritis
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).

Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).
Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
Combination therapy involving chondroitin sulfate and glucosamine sulfate proved no better than placebo for the management of pain and functional impairment brought on by knee osteoarthritis, in a double-blind, randomized trial.
“This is the first RCT sponsored by a pharmaceutical company to evaluate the efficacy of a combination of CS [chondroitin sulfate] plus GS [glucosamine sulfate] and including a [Data and Safety Monitoring Board] composed of independent experts charged with ensuring participant safety and accurate, bias-free data,” wrote the authors, led by Jorge A. Roman-Blas, MD, of Fundación Jiménez Díaz in Madrid (Arthritis Rheumatol. 2016 Jul 31. doi: 10.1002/art.39819).
Dr. Roman-Blas and his coinvestigators recruited patients with Kellgren-Lawrence stages II-III knee osteoarthritis from one orthopedic surgery and nine rheumatology centers across Spain. The study was split into two parts; the first part would have half of the patients complete the study in 6 months, followed by an interim analysis and evaluation of the data. If deemed okay by the Data and Safety Monitoring Board, the second part of the study would proceed, in which half of the patients would again complete the study in 6 months.
Ultimately, the study comprised 164 patients. They were randomized in a 1:1 ratio into cohorts receiving either a placebo or a regimen of 1,200 mg CS derived from bovine tracheal cartilage plus 1,500 mg of crystalline GS derived from crustaceans. The primary endpoint was reduction in pain from baseline evaluation, which was based on the visual analog scale (VAS) of 1-100 mm.
Patients in the combination therapy cohort had a lower average reduction in pain at 6 months than did those taking the placebo. In the modified intention-to-treat population, those taking CS+GS therapy had an average reduction of 11.8 ± 2.4 mm, or 19%, compared with baseline. On the other hand, those in the placebo cohort recorded a 20.5 ± 2.4 mm, or 33%, reduction in pain (P = .029). Based on this analysis, the trial was stopped early at 6 months to prevent “overexposure of additional patients to placebo treatment,” the investigators said.
However, pain measured by VAS did not differ between the groups in a per-protocol analysis. Furthermore, when taking Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores into account, there was no significant difference in improvement between CS+GS therapy and placebo in pain and function, for both intention-to-treat and per-protocol subjects.
Although placebo was more effective in pain reduction in the modified intent-to-treat analysis than was CS plus GS combination treatment, the effect size of placebo was small and the effect size of CS plus GS in this study was smaller than in previous studies, the investigators noted. “These findings may be related to the fact that GS may interfere with the absorption of CS and therefore reduce its local effect. Eventually, our patients may have had less severe pain than those in other studies, which would justify a lesser effect after the pharmacological intervention,” the authors wrote. “Furthermore, when the main outcome studied is particularly subjective, the placebo effect can overcome the effect of the active drug.”
Tedec Meiji Farma SA of Madrid funded the study. Dr. Roman-Blas and his coauthors did not report any relevant financial disclosures.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Chondroitin sulfate plus glucosamine sulfate is ineffective at reducing pain and functional impairment in patients with knee osteoarthritis.
Major finding: CS plus GS treatment registered a 19% reduction in joint pain in the modified intention-to-treat population, versus the 33% reduction brought on by the placebo (P = .029).
Data source: A multicenter, randomized, double-blind, placebo-controlled study of 164 patients with Kellgren-Lawrence stages II-III knee osteoarthritis.
Disclosures: Tedec Meiji Farma SA of Madrid funded the study. The authors reported no relevant financial disclosures.

Ali Rezai, MD

Psychotropic drug use more likely with ASD diagnosis at older age
Older age at the time of autism spectrum disorder diagnosis was associated with a higher likelihood of psychotropic medication in children aged 6-11, according to Katharine Zuckerman, MD, and her associates.
The mean age at diagnosis for the 722 children included in the study was 4.4 years, with a mean diagnostic delay of 2.2 years. The adjusted odds ratio for psychotropic drug use in children who were diagnosed with autism spectrum disorder (ASD) after the age of 4 was 3.09, compared with children diagnosed before the age of 4. Children diagnosed at a later age were less likely to receive behavioral intervention (BI) therapy (adjusted odds ratio = 0.44), complementary and alternative medicine (aOR = 0.63), and school-based therapy (aOR = 0.38).

Children who experienced at least 2 years of delay before diagnosis were also significantly more likely to use psychotropic drugs (aOR = 1.77), and less likely to receive BI therapy (aOR = 0.54) and school-based therapy (aOR = 0.59). However, a delay of at least 2 years was associated with a greater chance of receiving complementary and alternative medicine (aOR = 2.81).
“Results suggest that if long-term ASD therapy use is a priority, payers and policymakers may need to proactively accelerate diagnosis by incentivizing screening or enhancing case management of children at high risk of diagnostic delays. From a population standpoint, as children receive earlier ASD diagnoses, payers may expect changes in service use patterns toward more therapy use and less pharmacology,” the investigators wrote.
Find the full study online in Psychiatric Services (doi:10.1176/appi.ps.201500549).
Older age at the time of autism spectrum disorder diagnosis was associated with a higher likelihood of psychotropic medication in children aged 6-11, according to Katharine Zuckerman, MD, and her associates.
The mean age at diagnosis for the 722 children included in the study was 4.4 years, with a mean diagnostic delay of 2.2 years. The adjusted odds ratio for psychotropic drug use in children who were diagnosed with autism spectrum disorder (ASD) after the age of 4 was 3.09, compared with children diagnosed before the age of 4. Children diagnosed at a later age were less likely to receive behavioral intervention (BI) therapy (adjusted odds ratio = 0.44), complementary and alternative medicine (aOR = 0.63), and school-based therapy (aOR = 0.38).
Children who experienced at least 2 years of delay before diagnosis were also significantly more likely to use psychotropic drugs (aOR = 1.77), and less likely to receive BI therapy (aOR = 0.54) and school-based therapy (aOR = 0.59). However, a delay of at least 2 years was associated with a greater chance of receiving complementary and alternative medicine (aOR = 2.81).
“Results suggest that if long-term ASD therapy use is a priority, payers and policymakers may need to proactively accelerate diagnosis by incentivizing screening or enhancing case management of children at high risk of diagnostic delays. From a population standpoint, as children receive earlier ASD diagnoses, payers may expect changes in service use patterns toward more therapy use and less pharmacology,” the investigators wrote.
Find the full study online in Psychiatric Services (doi:10.1176/appi.ps.201500549).
Older age at the time of autism spectrum disorder diagnosis was associated with a higher likelihood of psychotropic medication in children aged 6-11, according to Katharine Zuckerman, MD, and her associates.
The mean age at diagnosis for the 722 children included in the study was 4.4 years, with a mean diagnostic delay of 2.2 years. The adjusted odds ratio for psychotropic drug use in children who were diagnosed with autism spectrum disorder (ASD) after the age of 4 was 3.09, compared with children diagnosed before the age of 4. Children diagnosed at a later age were less likely to receive behavioral intervention (BI) therapy (adjusted odds ratio = 0.44), complementary and alternative medicine (aOR = 0.63), and school-based therapy (aOR = 0.38).
Children who experienced at least 2 years of delay before diagnosis were also significantly more likely to use psychotropic drugs (aOR = 1.77), and less likely to receive BI therapy (aOR = 0.54) and school-based therapy (aOR = 0.59). However, a delay of at least 2 years was associated with a greater chance of receiving complementary and alternative medicine (aOR = 2.81).
“Results suggest that if long-term ASD therapy use is a priority, payers and policymakers may need to proactively accelerate diagnosis by incentivizing screening or enhancing case management of children at high risk of diagnostic delays. From a population standpoint, as children receive earlier ASD diagnoses, payers may expect changes in service use patterns toward more therapy use and less pharmacology,” the investigators wrote.
Find the full study online in Psychiatric Services (doi:10.1176/appi.ps.201500549).
FROM PSYCHIATRIC SERVICES

Malpractice cases serve to warn about careful use of EHRs
Buy our EHR. Come to a dinner and see our EHR. Our EHR is the best.
I hear that a lot, but am not rushing out to get one. Yes, I have an EHR, but it’s one I designed myself. It works very well for my dinky little practice, and I’m happy with it.
I get notes from practices that use commercial EHRs all the time. They’re usually a pile of gobbledygook, mixing labs, vital signs, medication lists, and ICD-10 codes that tell you absolutely nothing about the patient or the physician’s thought process.

Recently, while reviewing malpractice cases, I saw some where I thought that the EHR was contributing to the problem. Medication lists that showed everything a patient had ever taken, without showing when some were discontinued. Prescribing lists that allowed you to enter only certain doses or schedules, therefore blocking the physician from tailoring them to a specific person’s needs. Physical exam forms that allowed only positive or negative answers, with nowhere to comment on unusual findings.
Of course, I’m just one person, so I thought “maybe it’s just me.” After all, a lot of practices out there use EHRs.
But apparently I’m not the only one. A recent report by one of the nation’s largest doctor-owned malpractice companies found that EHRs may increase the risks of liability and medical errors. In 2013, The Doctor’s Company found 28 closed claims where the EHR contributed, and 26 in just the first half of 2014.
These include both technological problems with the systems and human error in their use. Troubles included erroneous medication dose and schedules, diagnosis-related errors, and the sadly common pitfall of cutting and pasting previous notes without modification.
Medicine has always been, and will always be, a thinking profession, and trying to have computers take part of this job off of us is never good. EHRs, while they have advantages in convenience and space savings, are as imperfect as those who write them.
Patients are not one-size-fits-all, and individual treatments have to be customized in ways that current systems often don’t recognize, sometimes with sad consequences for all involved.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Buy our EHR. Come to a dinner and see our EHR. Our EHR is the best.
I hear that a lot, but am not rushing out to get one. Yes, I have an EHR, but it’s one I designed myself. It works very well for my dinky little practice, and I’m happy with it.
I get notes from practices that use commercial EHRs all the time. They’re usually a pile of gobbledygook, mixing labs, vital signs, medication lists, and ICD-10 codes that tell you absolutely nothing about the patient or the physician’s thought process.
Recently, while reviewing malpractice cases, I saw some where I thought that the EHR was contributing to the problem. Medication lists that showed everything a patient had ever taken, without showing when some were discontinued. Prescribing lists that allowed you to enter only certain doses or schedules, therefore blocking the physician from tailoring them to a specific person’s needs. Physical exam forms that allowed only positive or negative answers, with nowhere to comment on unusual findings.
Of course, I’m just one person, so I thought “maybe it’s just me.” After all, a lot of practices out there use EHRs.
But apparently I’m not the only one. A recent report by one of the nation’s largest doctor-owned malpractice companies found that EHRs may increase the risks of liability and medical errors. In 2013, The Doctor’s Company found 28 closed claims where the EHR contributed, and 26 in just the first half of 2014.
These include both technological problems with the systems and human error in their use. Troubles included erroneous medication dose and schedules, diagnosis-related errors, and the sadly common pitfall of cutting and pasting previous notes without modification.
Medicine has always been, and will always be, a thinking profession, and trying to have computers take part of this job off of us is never good. EHRs, while they have advantages in convenience and space savings, are as imperfect as those who write them.
Patients are not one-size-fits-all, and individual treatments have to be customized in ways that current systems often don’t recognize, sometimes with sad consequences for all involved.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Buy our EHR. Come to a dinner and see our EHR. Our EHR is the best.
I hear that a lot, but am not rushing out to get one. Yes, I have an EHR, but it’s one I designed myself. It works very well for my dinky little practice, and I’m happy with it.
I get notes from practices that use commercial EHRs all the time. They’re usually a pile of gobbledygook, mixing labs, vital signs, medication lists, and ICD-10 codes that tell you absolutely nothing about the patient or the physician’s thought process.
Recently, while reviewing malpractice cases, I saw some where I thought that the EHR was contributing to the problem. Medication lists that showed everything a patient had ever taken, without showing when some were discontinued. Prescribing lists that allowed you to enter only certain doses or schedules, therefore blocking the physician from tailoring them to a specific person’s needs. Physical exam forms that allowed only positive or negative answers, with nowhere to comment on unusual findings.
Of course, I’m just one person, so I thought “maybe it’s just me.” After all, a lot of practices out there use EHRs.
But apparently I’m not the only one. A recent report by one of the nation’s largest doctor-owned malpractice companies found that EHRs may increase the risks of liability and medical errors. In 2013, The Doctor’s Company found 28 closed claims where the EHR contributed, and 26 in just the first half of 2014.
These include both technological problems with the systems and human error in their use. Troubles included erroneous medication dose and schedules, diagnosis-related errors, and the sadly common pitfall of cutting and pasting previous notes without modification.
Medicine has always been, and will always be, a thinking profession, and trying to have computers take part of this job off of us is never good. EHRs, while they have advantages in convenience and space savings, are as imperfect as those who write them.
Patients are not one-size-fits-all, and individual treatments have to be customized in ways that current systems often don’t recognize, sometimes with sad consequences for all involved.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Using transcatheter aortic valves for severe mitral annular calcification
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.

She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
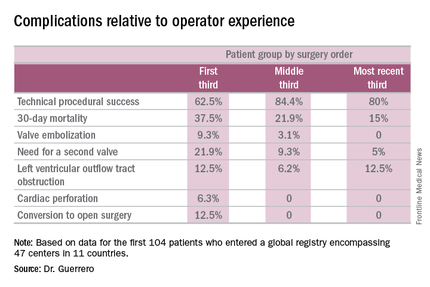
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.

Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.
She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.
Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
PARIS – Transcatheter mitral valve replacement using a repurposed transcatheter aortic valve in patients with severe symptomatic native mitral valve disease and severe mitral annular calcification is feasible and may be an option in carefully selected patients who aren’t candidates for surgery, Mayra Guerrero, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
However, at this early point in development, the procedure is associated with an exceptionally steep learning curve, said Dr. Guerrero, director of cardiac structural interventions at the NorthShore University Health System in Evanston, Ill.
She presented the procedural and 30-day outcomes for the first 104 patients entered into a global registry encompassing 47 centers in 11 countries. Nearly 90% of patients received an Edwards SAPIEN XT or SAPIEN 3 valve. The EuroPCR results update an earlier report on the first 64 patients in the registry (JACC Cardiovasc Interv. 2016 Jul 11;9[13]:1361-71).
The results, she said, are reminiscent of the early days in transcatheter aortic valve replacement, which were marked by an initial very high early mortality rate that fell dramatically as technology and techniques improved.
“We know that there are important things we need to improve. Left ventricular outflow tract obstruction is the Achilles heel of this procedure; we need to work on its prevention and management. We need better annulus sizing methods. We need to find the best delivery method and improve our patient selection in order to avoid taking on patients who are too sick. Still, even during this early experience, the technical success rate has improved, and 30-day mortality continues to drop,” Dr. Guerrero said.
Indeed, the 30-day all-cause mortality rate of 25% in the first 104 patients doesn’t tell the whole story. The rate was 37.5% in the first third of patients, fell to 21.9% in the second tertile, and then to 15% in the most recent tertile.
Similarly, the technical success rate of the procedure according to Mitral Valve Academic Research Consortium criteria improved from 62.5% in the first tertile of patients to 84.4% and 80% in the second and third, respectively, she continued.
The rates of almost all complications went down with greater operator experience, too. The notable exception was left ventricular outflow tract obstruction (LVOTO). It occurred in 12.5% of patients in the first tertile and remained unchanged in the third.
It’s noteworthy that the majority of deaths were noncardiac in nature. Patients with mitral annular calcification are a high-risk group even before they develop valvular dysfunction. They are typically older and have multiple comorbidities. Participants in the global registry had a mean Society of Thoracic Surgeons score of 14.4; 38% had diabetes, 45% had chronic obstructive pulmonary disease, 35% had heart failure, 34% had previously undergone coronary artery bypass surgery, and roughly half of patients had a prior aortic valve replacement.
Causes of noncardiac mortality within 30 days included multiorgan failure in 8.6% of subjects, pneumonia in 2.9%, infection in 1.9%, and one fatal thoracentesis-related bleeding complication.
Cardiovascular deaths included two cases due to left ventricular perforation, two fatal strokes, an MI due to air emboli, a lethal complete atrioventricular block, and three deaths owing to LVOTO.
Alcohol ablation met with some success as a bailout treatment in cases of LVOTO with hemodynamic compromise after transmitral valve replacement in the global registry. All six treated patients had significant improvement initially, although the LVOTO recurred the next day in one instance. Four of the six patients were discharged from the hospital. One patient died because of atrioventricular block, and another from multiorgan failure 3 weeks after alcohol ablation of the LVOTO.
Dr. Guerrero has been a leader in this new field. She reported the first percutaneous implantation of a balloon expandable transcatheter valve in a native mitral valve without a surgical incision (Catheter Cardiovasc Interv. 2014 Jun 1;83[7]:E287-91), and more recently, together with coworkers developed a percutaneous alcohol ablation technique for acute reduction of LVOTO due to transcatheter mitral valve replacement (Catheter Cardiovasc Interv. 2016 Jul 5. doi:10.1002/ccd.26649).
She is now the principal investigator in the ongoing Mitral Implantation of Transcatheter Valves (MITRAL) trial, a physician-sponsored, 90-patient pilot study underway at six U.S. sites. MITRAL is recruiting three patient populations for transcatheter mitral valve replacement: patients like those in the global registry, with native mitral valve disease and severe mitral annular calcification; those with a symptomatic failing surgical ring with severe mitral regurgitation or stenosis; and patients with a symptomatic failing surgical bioprosthesis with severe mitral regurgitation or stenosis.
Discussant Nicolo Piazza, MD, of McGill University, Montreal, said transcatheter mitral valve replacement in mitral valve disease with severe mitral annular calcification in patients unsuitable for surgery “definitely represents an unmet clinical need in our practice today.” But he urged caution in interpreting the global registry data.
“This is a real world registry study with inherent selection bias and physician reporting bias,” the cardiologist said.
“We are leveraging a therapy from the aortic field into the mitral field. Of course, we do not have dedicated devices yet to treat these patients. The main finding of this study is that the procedure is actually feasible,” Dr. Piazza said.
Still, it’s sobering that at least 1 in 10 treated patients experiences LVOTO, 1 in 10 requires a second valve, and technical success is achieved in 3 out of 4 patients, he added.
Dr. Piazza predicted that multislice CT scans will be “extremely important” in refining patient selection criteria for the procedure, and echocardiography will be helpful in understanding the optimal procedural techniques and viewing angles. Work also needs to be done on developing optimal anticoagulation protocols in order to avoid valve thrombosis.
Dr. Guerrero reported serving as a consultant to Edwards Lifesciences. Dr. Piazza is a consultant to Medtronic and MicroPort.
AT EUROPCR 2016
Key clinical point: A report from a global registry of transcatheter aortic valve implantation in the mitral position shows the procedure is feasible.
Major finding: Thirty-day mortality fell from 37.5% in the first third of treated patients to 15% in the most recent tertile.
Data source: A real world registry that includes 104 patients at 47 centers in 11 countries to date.
Disclosures: The study presenter reported serving as a consultant to Edwards Lifesciences.

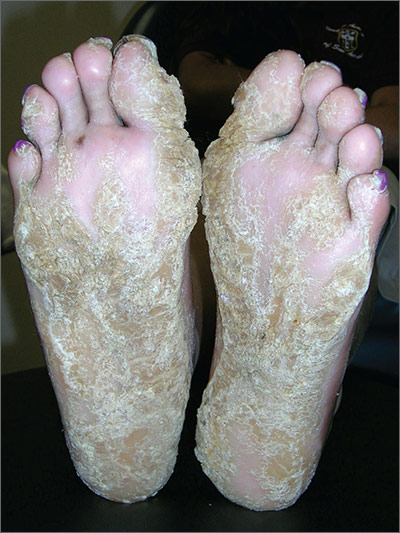
Thickening of skin on feet
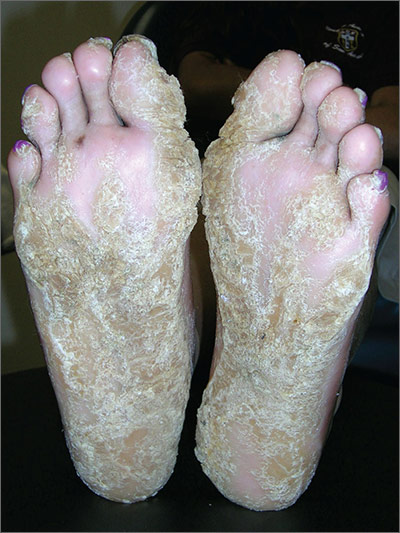
The FP recognized this as diffuse palmoplantar keratoderma of the palms and soles. This is an inherited genodermatosis that may be autosomal dominant or sporadic. Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had diffuse hyperkeratosis, which can be distributed over most of the plantar surface.
This condition can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief. The family hoped that there would be some genetic treatment for this in the future.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP recognized this as diffuse palmoplantar keratoderma of the palms and soles. This is an inherited genodermatosis that may be autosomal dominant or sporadic. Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had diffuse hyperkeratosis, which can be distributed over most of the plantar surface.
This condition can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief. The family hoped that there would be some genetic treatment for this in the future.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP recognized this as diffuse palmoplantar keratoderma of the palms and soles. This is an inherited genodermatosis that may be autosomal dominant or sporadic. Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had diffuse hyperkeratosis, which can be distributed over most of the plantar surface.
This condition can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief. The family hoped that there would be some genetic treatment for this in the future.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
Scaly palms and soles

The FP recognized this as focal palmoplantar keratoderma of the palms and soles, which is an inherited genodermatosis that is autosomal dominant. The lesions are located mainly on high pressure areas and spare the arches of the feet.
Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had focal hyperkeratosis, which is located mainly on pressure points and sites of recurrent friction.
Palmoplantar keratoderma can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP recognized this as focal palmoplantar keratoderma of the palms and soles, which is an inherited genodermatosis that is autosomal dominant. The lesions are located mainly on high pressure areas and spare the arches of the feet.
Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had focal hyperkeratosis, which is located mainly on pressure points and sites of recurrent friction.
Palmoplantar keratoderma can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP recognized this as focal palmoplantar keratoderma of the palms and soles, which is an inherited genodermatosis that is autosomal dominant. The lesions are located mainly on high pressure areas and spare the arches of the feet.
Palmoplantar keratoderma includes a rare heterogeneous group of disorders that are characterized by thickening of the palms and the soles that can also be an associated feature of some very rare syndromes. The patient in this case had focal hyperkeratosis, which is located mainly on pressure points and sites of recurrent friction.
Palmoplantar keratoderma can be differentiated from plantar warts as it is present on more diffuse locations on the palmoplantar surfaces (including palms and soles) and it lacks the black dots of thrombosed capillaries that are seen in plantar warts.
There is no cure for this genetic condition and the goals of treatment are functional and cosmetic improvement. The FP prescribed 12% ammonium lactate as an emollient and keratolytic. The patient applied this twice daily with some symptomatic relief.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Growths on palms

The FP diagnosed this patient with palmar warts, which are similar in morphology to plantar warts. Plantar (or palmar) warts are lesions caused by human papillomavirus (HPV) that occur on the soles of the feet and palms of the hands. Plantar warts occur mostly in adolescents and young adults and affect up to 10% of people in these age groups.
Plantar warts usually occur at points of maximum pressure, such as on the heels or over the heads of the metatarsal bones, but may appear anywhere on the plantar surface, including the tips of the toes. A cluster of multiple warts that appear to fuse together is referred to as a mosaic wart. HIV is a risk factor for any type of HPV infection.
Distinguish warts from calluses by noting the skin lines; warts lack skin lines crossing their surface, whereas normal skin lines cross through a callus without any disturbance. Additionally, plantar/palmar warts may have a highly organized mosaic pattern on the surface when examined with a hand lens and have prominent black dots (thrombosed capillaries).
The most common treatments for warts include topical salicylic acid and cryotherapy. Topical salicylic acid preparations are nonscarring, minimally painful, and relatively effective, but require persistent application of medication once a day for weeks to months. Cryotherapy with liquid nitrogen therapy is commonly used, but plantar warts are more resistant than other HPV lesions. The liquid nitrogen is applied to form a freeze ball that covers the lesion and 2 mm of surrounding normal tissue for usually 10 to 20 seconds per treatment. This can be performed as a single long freeze or divided into 2 freezing episodes with thawing in between. This allows for more freeze time in a way that is less painful to the patient.
In this case, the patient chose cryotherapy and arranged for a follow-up appointment in 3 to 4 weeks for a second round.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed this patient with palmar warts, which are similar in morphology to plantar warts. Plantar (or palmar) warts are lesions caused by human papillomavirus (HPV) that occur on the soles of the feet and palms of the hands. Plantar warts occur mostly in adolescents and young adults and affect up to 10% of people in these age groups.
Plantar warts usually occur at points of maximum pressure, such as on the heels or over the heads of the metatarsal bones, but may appear anywhere on the plantar surface, including the tips of the toes. A cluster of multiple warts that appear to fuse together is referred to as a mosaic wart. HIV is a risk factor for any type of HPV infection.
Distinguish warts from calluses by noting the skin lines; warts lack skin lines crossing their surface, whereas normal skin lines cross through a callus without any disturbance. Additionally, plantar/palmar warts may have a highly organized mosaic pattern on the surface when examined with a hand lens and have prominent black dots (thrombosed capillaries).
The most common treatments for warts include topical salicylic acid and cryotherapy. Topical salicylic acid preparations are nonscarring, minimally painful, and relatively effective, but require persistent application of medication once a day for weeks to months. Cryotherapy with liquid nitrogen therapy is commonly used, but plantar warts are more resistant than other HPV lesions. The liquid nitrogen is applied to form a freeze ball that covers the lesion and 2 mm of surrounding normal tissue for usually 10 to 20 seconds per treatment. This can be performed as a single long freeze or divided into 2 freezing episodes with thawing in between. This allows for more freeze time in a way that is less painful to the patient.
In this case, the patient chose cryotherapy and arranged for a follow-up appointment in 3 to 4 weeks for a second round.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed this patient with palmar warts, which are similar in morphology to plantar warts. Plantar (or palmar) warts are lesions caused by human papillomavirus (HPV) that occur on the soles of the feet and palms of the hands. Plantar warts occur mostly in adolescents and young adults and affect up to 10% of people in these age groups.
Plantar warts usually occur at points of maximum pressure, such as on the heels or over the heads of the metatarsal bones, but may appear anywhere on the plantar surface, including the tips of the toes. A cluster of multiple warts that appear to fuse together is referred to as a mosaic wart. HIV is a risk factor for any type of HPV infection.
Distinguish warts from calluses by noting the skin lines; warts lack skin lines crossing their surface, whereas normal skin lines cross through a callus without any disturbance. Additionally, plantar/palmar warts may have a highly organized mosaic pattern on the surface when examined with a hand lens and have prominent black dots (thrombosed capillaries).
The most common treatments for warts include topical salicylic acid and cryotherapy. Topical salicylic acid preparations are nonscarring, minimally painful, and relatively effective, but require persistent application of medication once a day for weeks to months. Cryotherapy with liquid nitrogen therapy is commonly used, but plantar warts are more resistant than other HPV lesions. The liquid nitrogen is applied to form a freeze ball that covers the lesion and 2 mm of surrounding normal tissue for usually 10 to 20 seconds per treatment. This can be performed as a single long freeze or divided into 2 freezing episodes with thawing in between. This allows for more freeze time in a way that is less painful to the patient.
In this case, the patient chose cryotherapy and arranged for a follow-up appointment in 3 to 4 weeks for a second round.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ. Plantar warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:766-770.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
