User login
Study compares sterile vs. nonsterile gloves for outpatient derm procedures
The use of sterile or nonsterile gloves during outpatient dermatologic and dental procedures resulted in similar rates of postoperative surgical site infections (SSIs), results from a large systematic review and meta-analysis demonstrated.
“During the past few decades, the use of surgical gloves has become standard practice to prevent postoperative wound infections or surgical site infection,” researchers led by Dr. Jerry Brewer wrote in a study published online Aug. 3, 2016 in JAMA Dermatology. “However, whether the use of sterile vs. non-sterile gloves makes a difference in the development of postoperative SSIs in the setting of cutaneous and minor outpatient surgical procedures remains unclear.”

In an effort to examine that question, Dr. Brewer of the division of dermatologic surgery at Mayo Clinic, Rochester, Minn., and his associates conducted a systematic review and meta-analysis of randomized clinical trials and comparative studies with information on sterile vs. non-sterile gloves in outpatient surgical procedures (JAMA Dermatol. 2016 Aug. 3. doi: 10.1001/jamadermatol.2016.1965). Patients in the studies underwent outpatient cutaneous or mucosal surgical procedures, including Mohs micrographic surgery, repair of a laceration, standard excisions, and tooth extractions.
The final meta-analysis included 11,071 patients from 13 studies. Of these, 6,040 underwent procedures with sterile gloves and 5,031 underwent procedures with nonsterile gloves. The researchers reported that a total of 228 patients (2.1%) had a postoperative SSI, including 107 in the nonsterile glove group (2.1%), and 121 in the sterile glove group (2%). The overall relative risk for an SSI with nonsterile glove use was 1.06.
In an interview, Dr. Brewer estimated that sterile gloves cost anywhere from $0.27 to $1.29 per pair, compared with about 8 cents per pair for clean nonsterile gloves. “This cost difference may not seem like much, but if you think about all the surgeries that are done on a regular basis across the country, that’s a huge difference in cost,” he said.
The authors acknowledged certain limitations of the study, including the potential for selection bias, since many of the studies included in the meta-analysis were observational. They also noted that findings from some previous studies on the topic run counter to theirs (see Dermatol. Surg. 2010; 36[10]:1529-36 and J. Hosp. Infect. 2007;65[3]:258-63 ). “Although the broad use of nonsterile clean gloves may be justified, caution is advised in generalizing this justification to more advanced outpatient surgical procedures that may not pertain to the information summarized in this review and meta-analysis,” they concluded. “Future study could include whether duration of surgery and complexity of the repair influence postoperative SSI development in the setting of sterile vs. nonsterile gloves.”
The researchers reported having no financial disclosures.
The use of sterile or nonsterile gloves during outpatient dermatologic and dental procedures resulted in similar rates of postoperative surgical site infections (SSIs), results from a large systematic review and meta-analysis demonstrated.
“During the past few decades, the use of surgical gloves has become standard practice to prevent postoperative wound infections or surgical site infection,” researchers led by Dr. Jerry Brewer wrote in a study published online Aug. 3, 2016 in JAMA Dermatology. “However, whether the use of sterile vs. non-sterile gloves makes a difference in the development of postoperative SSIs in the setting of cutaneous and minor outpatient surgical procedures remains unclear.”
In an effort to examine that question, Dr. Brewer of the division of dermatologic surgery at Mayo Clinic, Rochester, Minn., and his associates conducted a systematic review and meta-analysis of randomized clinical trials and comparative studies with information on sterile vs. non-sterile gloves in outpatient surgical procedures (JAMA Dermatol. 2016 Aug. 3. doi: 10.1001/jamadermatol.2016.1965). Patients in the studies underwent outpatient cutaneous or mucosal surgical procedures, including Mohs micrographic surgery, repair of a laceration, standard excisions, and tooth extractions.
The final meta-analysis included 11,071 patients from 13 studies. Of these, 6,040 underwent procedures with sterile gloves and 5,031 underwent procedures with nonsterile gloves. The researchers reported that a total of 228 patients (2.1%) had a postoperative SSI, including 107 in the nonsterile glove group (2.1%), and 121 in the sterile glove group (2%). The overall relative risk for an SSI with nonsterile glove use was 1.06.
In an interview, Dr. Brewer estimated that sterile gloves cost anywhere from $0.27 to $1.29 per pair, compared with about 8 cents per pair for clean nonsterile gloves. “This cost difference may not seem like much, but if you think about all the surgeries that are done on a regular basis across the country, that’s a huge difference in cost,” he said.
The authors acknowledged certain limitations of the study, including the potential for selection bias, since many of the studies included in the meta-analysis were observational. They also noted that findings from some previous studies on the topic run counter to theirs (see Dermatol. Surg. 2010; 36[10]:1529-36 and J. Hosp. Infect. 2007;65[3]:258-63 ). “Although the broad use of nonsterile clean gloves may be justified, caution is advised in generalizing this justification to more advanced outpatient surgical procedures that may not pertain to the information summarized in this review and meta-analysis,” they concluded. “Future study could include whether duration of surgery and complexity of the repair influence postoperative SSI development in the setting of sterile vs. nonsterile gloves.”
The researchers reported having no financial disclosures.
The use of sterile or nonsterile gloves during outpatient dermatologic and dental procedures resulted in similar rates of postoperative surgical site infections (SSIs), results from a large systematic review and meta-analysis demonstrated.
“During the past few decades, the use of surgical gloves has become standard practice to prevent postoperative wound infections or surgical site infection,” researchers led by Dr. Jerry Brewer wrote in a study published online Aug. 3, 2016 in JAMA Dermatology. “However, whether the use of sterile vs. non-sterile gloves makes a difference in the development of postoperative SSIs in the setting of cutaneous and minor outpatient surgical procedures remains unclear.”
In an effort to examine that question, Dr. Brewer of the division of dermatologic surgery at Mayo Clinic, Rochester, Minn., and his associates conducted a systematic review and meta-analysis of randomized clinical trials and comparative studies with information on sterile vs. non-sterile gloves in outpatient surgical procedures (JAMA Dermatol. 2016 Aug. 3. doi: 10.1001/jamadermatol.2016.1965). Patients in the studies underwent outpatient cutaneous or mucosal surgical procedures, including Mohs micrographic surgery, repair of a laceration, standard excisions, and tooth extractions.
The final meta-analysis included 11,071 patients from 13 studies. Of these, 6,040 underwent procedures with sterile gloves and 5,031 underwent procedures with nonsterile gloves. The researchers reported that a total of 228 patients (2.1%) had a postoperative SSI, including 107 in the nonsterile glove group (2.1%), and 121 in the sterile glove group (2%). The overall relative risk for an SSI with nonsterile glove use was 1.06.
In an interview, Dr. Brewer estimated that sterile gloves cost anywhere from $0.27 to $1.29 per pair, compared with about 8 cents per pair for clean nonsterile gloves. “This cost difference may not seem like much, but if you think about all the surgeries that are done on a regular basis across the country, that’s a huge difference in cost,” he said.
The authors acknowledged certain limitations of the study, including the potential for selection bias, since many of the studies included in the meta-analysis were observational. They also noted that findings from some previous studies on the topic run counter to theirs (see Dermatol. Surg. 2010; 36[10]:1529-36 and J. Hosp. Infect. 2007;65[3]:258-63 ). “Although the broad use of nonsterile clean gloves may be justified, caution is advised in generalizing this justification to more advanced outpatient surgical procedures that may not pertain to the information summarized in this review and meta-analysis,” they concluded. “Future study could include whether duration of surgery and complexity of the repair influence postoperative SSI development in the setting of sterile vs. nonsterile gloves.”
The researchers reported having no financial disclosures.
FROM JAMA DERMATOLOGY
Key clinical point: No difference was observed in the rate of postoperative SSIs between outpatient surgical procedures performed with sterile versus nonsterile gloves.
Major finding: Overall, 2.1% of patients had a postoperative SSI, including 2.1% in the nonsterile glove group and 2% in the sterile glove group.
Data source: A meta-analysis that included 11,071 patients from 13 studies with information on sterile vs. nonsterile gloves in outpatient surgical procedures.
Disclosures: The researchers reported having no financial disclosures.

Extended-release naltrexone helps alcohol-dependent HIV-positive prisoners transition to community
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Extended-release naltrexone provides clinically meaningful benefits in HIV-infected prisoners with alcohol use disorder and multiple comorbid conditions as they transition back into the community, according to the findings of a double-blind randomized clinical trial.
“I think it’s important to know that a very effective medication, which has not previously been given to this population, was accepted by this group. It may be a feasible conduit to care as they transition to the community, even among those with severe psychosocial disparities like homelessness and mental illness,” Sandra A. Springer, MD, said in presenting the study findings at the 21st International AIDS Conference.
Extended-release naltrexone (Vivitrol) is a mu-opioid receptor antagonist approved for the treatment of alcohol use disorder, where it has been shown to decrease consumption. But prior to her study, the once-monthly injectable drug hadn’t been studied in alcohol-dependent prisoners living with HIV who are transitioning from jail or prison into the community, noted Dr. Springer, an infectious disease specialist at Yale University in New Haven, Conn.
This is a large, important, and seriously neglected patient population, she observed. The United States has the highest incarceration rate in the world. The prevalence of HIV infection is at least three times greater in U.S. criminal justice settings than in the general population. Alcohol use disorders are eightfold more common. Release from prison or jail in affected individuals often is complicated by relapse to alcohol use, which in turn is associated with poor HIV treatment outcomes.
Dr. Springer reported on 100 HIV-positive adult prisoners with alcohol use disorder diagnosed by DSM-IV criteria who were randomized double-blind two-to-one to 6 monthly 380-mg intramuscular injections of extended-release naltrexone or placebo, with the first dose given 3-7 days prior to release. Participants were required to have no baseline clinical evidence of cirrhosis or very high liver enzyme levels.
Half of participants had chronic hepatitis C. Eighty-seven percent of subjects scored 20 or higher on the Alcohol Use Disorders Identification test, indicating alcohol dependence. On the Mini International Neuropsychiatric Interview, 15% of participants met criteria for major depressive disorder, 16% for bipolar disorder, 59% for cocaine use disorder, 16% for narcotic use disorder, and 16% for cannabis use disorder. Most of the subjects were homeless or had an unstable housing situation.
Alcohol outcomes were assessed monthly during the 6-month trial. Not surprisingly, the better the treatment adherence, the better the outcomes. During the 90 days before incarceration, patients self-reported that 70% of those days were heavy drinking days, defined in men as having five or more drinks per day and in women as four or more. Their average consumption on those heavy drinking days was 28 drinks per day. In contrast, patients who accepted four or more extended-release naltrexone injections during 180 days of follow-up after release from custody drank heavily on just 7.6% of days, with an average of 8.6 drinks per day on those heavy drinking days. Subjects who received four or more placebo injections drank heavily on 11.6% of days, consuming an average of 12 drinks per heavy drinking day.
The time to first heavy drinking day was longer in patients who accepted 4-6 monthly injections of extended-release naltrexone than in those with 4-6 placebo injections. However, the difference achieved statistical significance only in the younger subgroup of participants aged 21-29 years. In that subgroup, the average time to the first heavy drinking day was 24.1 days, compared with 9.5 days with placebo.
On a composite alcohol consumption index comprised of time to first heavy drinking day after release, mean number of drinks per drinking day, change from before to after incarceration in average number of drinks per drinking day, alcohol craving score, and total number of drinking days, subjects who received four or more extended-release naltrexone injections had a significantly more favorable result, with a mean score of 3.15, compared with 2.93 in patients who took four or more placebo injections.
Moreover, consistent use of extended-release naltrexone was associated with significantly lower HIV viral load counts, compared with placebo-treated controls.
Treatment with extended-release naltrexone was safe. No serious side effects occurred, even in patients with comorbid hepatitis C who were on antiretroviral therapy. The most common side effects were the same as in seen in studies of the drug in other populations: mild to moderate nausea, headache, decreased appetite, fatigue, and dizziness.
Elsewhere at AIDS 2016, Chris Beyrer, MD, president of the International AIDS Society, included prisoners on his list of the populations most vulnerable to HIV because of discriminatory laws and policies in many parts of the world. Others on the list were transgender people, sex workers, men who have sex with men, and injection drug users.
“We’ll never be able to end AIDS without addressing the needs of these most vulnerable individuals and communities, and yet we know in 2016 far too many are being left behind,” said Dr. Beyrer, professor of epidemiology at Johns Hopkins University, Baltimore.
Transgender individuals, for example, are 49 times more likely to have HIV infection than other adults. Injection drug users and men who have sex with men are each 24-fold more likely to become HIV infected than the general population. Sex workers are 10 times more likely to acquire HIV infection than others in their reproductive years. And prisoners have a fivefold greater prevalence of HIV.
“In 2014 these vulnerable groups accounted for more than one-third of all new HIV infections. That’s an extraordinary proportion of HIV,” he observed. “This truly is the undone work of the HIV response. If there’s any silver lining in this cloud, it’s this: We’re talking about a relatively small number of people who are at high risk of infection relative to the world’s population. And that means that turning this around doesn’t require massive new commitments to very large populations. What it does require is an honest acknowledgment of where the epidemic is hitting hardest and directing resources to that need.”
Unfortunately, screening and treatment programs are rarely tailored to reach these highly vulnerable groups effectively, he added.
Dr. Beyrer was a contributor to a special issue of the Lancet devoted to HIV infection among prisoners published with the AIDS 2016 conference.
Dr. Springer’s study was funded by the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Drug Abuse. She reported having no financial conflicts of interest.
AT AIDS 2016
Key clinical point: Extended-release naltrexone helps HIV-infected prisoners with alcohol use disorder in transitioning to the community.
Major finding: The mean time to the first heavy drinking day among 21- to 29-year-old HIV-infected prisoners with an alcohol use disorder was 24.1 days following release from prison or jail in those on extended-release naltrexone versus 9.5 days with placebo.
Data source: This randomized, double-blind clinical trial included 100 HIV-positive prisoners with alcohol use disorder who were released into the community. Two-thirds received six monthly injections of extended-release naltrexone, the rest placebo.
Disclosures: The study was funded by the National Institute on Alcohol Abuse and Alcoholism and the National Institute on Drug Abuse. The presenter reported having no financial conflicts of interest.
FDA grants fast track status to volixibat
The Food and Drug Administration has granted fast track status to volixibat, an investigational treatment manufactured by Shire.
“The FDA’s fast track is a process designed to facilitate the development, and expedite the review, of drugs to treat serious conditions and fill an unmet medical need,” the Dublin-based pharmaceutical company explained in a statement. “However, it does not guarantee that the FDA will ultimately approve [volixibat] for NASH [nonalcoholic steatohepatitis] or the timing of any such approval.”

Volixibat, also known as SHP626, is meant to treat NASH with liver fibrosis in adult patients via an apical sodium-dependent bile acid transporter inhibitor, which is a protein that recycles bile acids from the intestine and into the liver. This orally administered, once-daily treatment would be the first ever treatment available for NASH.
“This fast track designation is further recognition of the critical need to develop new, effective therapeutic options for patients with this serious condition,” said Philip J. Vickers, PhD, head of research and development for Shire, in a statement.
Preclinical and phase I studies have already been completed, the results of which contributed to the FDA granting volixibat fast track status. A randomized, placebo-controlled, double-blind phase II trial is set to get underway shortly at centers in the United States, Canada, and the United Kingdom, which will examine safety, tolerability, and efficacy of a three-dose volixibat regimen administered over the course of 48 weeks.
The Food and Drug Administration has granted fast track status to volixibat, an investigational treatment manufactured by Shire.
“The FDA’s fast track is a process designed to facilitate the development, and expedite the review, of drugs to treat serious conditions and fill an unmet medical need,” the Dublin-based pharmaceutical company explained in a statement. “However, it does not guarantee that the FDA will ultimately approve [volixibat] for NASH [nonalcoholic steatohepatitis] or the timing of any such approval.”
Volixibat, also known as SHP626, is meant to treat NASH with liver fibrosis in adult patients via an apical sodium-dependent bile acid transporter inhibitor, which is a protein that recycles bile acids from the intestine and into the liver. This orally administered, once-daily treatment would be the first ever treatment available for NASH.
“This fast track designation is further recognition of the critical need to develop new, effective therapeutic options for patients with this serious condition,” said Philip J. Vickers, PhD, head of research and development for Shire, in a statement.
Preclinical and phase I studies have already been completed, the results of which contributed to the FDA granting volixibat fast track status. A randomized, placebo-controlled, double-blind phase II trial is set to get underway shortly at centers in the United States, Canada, and the United Kingdom, which will examine safety, tolerability, and efficacy of a three-dose volixibat regimen administered over the course of 48 weeks.
The Food and Drug Administration has granted fast track status to volixibat, an investigational treatment manufactured by Shire.
“The FDA’s fast track is a process designed to facilitate the development, and expedite the review, of drugs to treat serious conditions and fill an unmet medical need,” the Dublin-based pharmaceutical company explained in a statement. “However, it does not guarantee that the FDA will ultimately approve [volixibat] for NASH [nonalcoholic steatohepatitis] or the timing of any such approval.”
Volixibat, also known as SHP626, is meant to treat NASH with liver fibrosis in adult patients via an apical sodium-dependent bile acid transporter inhibitor, which is a protein that recycles bile acids from the intestine and into the liver. This orally administered, once-daily treatment would be the first ever treatment available for NASH.
“This fast track designation is further recognition of the critical need to develop new, effective therapeutic options for patients with this serious condition,” said Philip J. Vickers, PhD, head of research and development for Shire, in a statement.
Preclinical and phase I studies have already been completed, the results of which contributed to the FDA granting volixibat fast track status. A randomized, placebo-controlled, double-blind phase II trial is set to get underway shortly at centers in the United States, Canada, and the United Kingdom, which will examine safety, tolerability, and efficacy of a three-dose volixibat regimen administered over the course of 48 weeks.

Studies highlight diagnostic and treatment challenges in hidradenitis suppurativa
SCOTTSDALE, ARIZ. – Patients with hidradenitis suppurativa (HS) may be misdiagnosed when they see providers who are not dermatologists – as is usually the case during the initial years of their disease, according to a large analysis of medical claims data.
The findings highlight the need for visual diagnostic aids and specific guidelines for treating HS that target nondermatologists, Melissa Butt, MPH, of Penn State Hershey (Pa.) Medical Center, said during an interview at the annual meeting of the Society for Investigative Dermatology. She presented the findings during a poster session at the meeting.
HS is a chronic inflammatory disease of the hair follicles that affects 0.5%-4% of people in the United States. In past studies, up to 12 years elapsed between disease onset and diagnosis, in part because patients often cannot readily access dermatologists, Ms. Butt said. To better understand patterns of health care use during the years leading up to HS diagnosis, she and her colleagues used MarketScan data to identify 1,733 patients with HS-specific medical care claims filed in 2012 and 2013. Then they looked back at medical claims for these patients during 2008 through 2011, before the patients were diagnosed with HS. The cohort averaged 37 years of age (standard deviation, 15 years), and 73% were female.
Among 239,892 claims filed before patients were diagnosed with HS, 11,381 (4.7%) included codes for other diseases of the skin and subcutaneous tissues, Ms. Butt said. Dermatologists filed only 31% of these skin-specific claims, while 69% were filed by other providers, such as family practitioners, internists, emergency department physicians, and acute care hospitalists.
Notably, about two-thirds of the skin-specific diagnostic codes could have represented a misdiagnosis of HS. These codes included conditions such as abscesses, carbuncles, local infections, ulcers, and diseases of the sebaceous glands.
The fact that 78% of visits occurred in offices and other outpatient settings further underscores the need to improve the detection and care of HS in these environments, Ms. Butt said. Given current national shortages of dermatologists, visual HS diagnostic aids and “detailed, multistep clinical practice guidelines” for nondermatologists could help improve care of HS while patients wait to see the specialists, she added.
A second poster presented at the meeting provided results of a study on the use and impact of antibiotics in the treatment of HS. Alexander Fischer of Johns Hopkins University, Baltimore, and his associates studied antibiotic prescriptions and bacterial cultures from the lesions of 239 patients with HS who were treated at Johns Hopkins medical facilities between 2010 and 2015. Not only were 51% of HS patients on antibiotics at the time of culture, but these patients’ lesions were significantly more likely to contain antibiotic-resistant bacteria than were those of patients not on antibiotics.
Strikingly, Proteus species were isolated from nearly half of patients on trimethoprim-sulfamethoxazole (TMP/SMX), and 88% of colonies were resistant to TMP/SMX, while only 13% of cultures from untreated patients grew Proteus (P less than .001) and all were TMP/SMX-susceptible (P less than .001). Likewise, 100% of methicillin-resistant Staphylococcus aureus (MRSA) strains from patients prescribed ciprofloxacin were resistant to it, compared with a 10% background rate of ciprofloxacin resistance among MRSA from patients not taking antibiotics (P = .04). In addition, the proportion of other S. aureus strains that were clindamycin-resistant was higher when patients were taking this antibiotic than when they were not (63% versus 17%; P = .03).
The results “raise questions” about whether antibiotics should be used in HS patients who are not clearly benefiting from them, according to the researchers.
The authors of both studies reported no funding sources and had no disclosures.
SCOTTSDALE, ARIZ. – Patients with hidradenitis suppurativa (HS) may be misdiagnosed when they see providers who are not dermatologists – as is usually the case during the initial years of their disease, according to a large analysis of medical claims data.
The findings highlight the need for visual diagnostic aids and specific guidelines for treating HS that target nondermatologists, Melissa Butt, MPH, of Penn State Hershey (Pa.) Medical Center, said during an interview at the annual meeting of the Society for Investigative Dermatology. She presented the findings during a poster session at the meeting.
HS is a chronic inflammatory disease of the hair follicles that affects 0.5%-4% of people in the United States. In past studies, up to 12 years elapsed between disease onset and diagnosis, in part because patients often cannot readily access dermatologists, Ms. Butt said. To better understand patterns of health care use during the years leading up to HS diagnosis, she and her colleagues used MarketScan data to identify 1,733 patients with HS-specific medical care claims filed in 2012 and 2013. Then they looked back at medical claims for these patients during 2008 through 2011, before the patients were diagnosed with HS. The cohort averaged 37 years of age (standard deviation, 15 years), and 73% were female.
Among 239,892 claims filed before patients were diagnosed with HS, 11,381 (4.7%) included codes for other diseases of the skin and subcutaneous tissues, Ms. Butt said. Dermatologists filed only 31% of these skin-specific claims, while 69% were filed by other providers, such as family practitioners, internists, emergency department physicians, and acute care hospitalists.
Notably, about two-thirds of the skin-specific diagnostic codes could have represented a misdiagnosis of HS. These codes included conditions such as abscesses, carbuncles, local infections, ulcers, and diseases of the sebaceous glands.
The fact that 78% of visits occurred in offices and other outpatient settings further underscores the need to improve the detection and care of HS in these environments, Ms. Butt said. Given current national shortages of dermatologists, visual HS diagnostic aids and “detailed, multistep clinical practice guidelines” for nondermatologists could help improve care of HS while patients wait to see the specialists, she added.
A second poster presented at the meeting provided results of a study on the use and impact of antibiotics in the treatment of HS. Alexander Fischer of Johns Hopkins University, Baltimore, and his associates studied antibiotic prescriptions and bacterial cultures from the lesions of 239 patients with HS who were treated at Johns Hopkins medical facilities between 2010 and 2015. Not only were 51% of HS patients on antibiotics at the time of culture, but these patients’ lesions were significantly more likely to contain antibiotic-resistant bacteria than were those of patients not on antibiotics.
Strikingly, Proteus species were isolated from nearly half of patients on trimethoprim-sulfamethoxazole (TMP/SMX), and 88% of colonies were resistant to TMP/SMX, while only 13% of cultures from untreated patients grew Proteus (P less than .001) and all were TMP/SMX-susceptible (P less than .001). Likewise, 100% of methicillin-resistant Staphylococcus aureus (MRSA) strains from patients prescribed ciprofloxacin were resistant to it, compared with a 10% background rate of ciprofloxacin resistance among MRSA from patients not taking antibiotics (P = .04). In addition, the proportion of other S. aureus strains that were clindamycin-resistant was higher when patients were taking this antibiotic than when they were not (63% versus 17%; P = .03).
The results “raise questions” about whether antibiotics should be used in HS patients who are not clearly benefiting from them, according to the researchers.
The authors of both studies reported no funding sources and had no disclosures.
SCOTTSDALE, ARIZ. – Patients with hidradenitis suppurativa (HS) may be misdiagnosed when they see providers who are not dermatologists – as is usually the case during the initial years of their disease, according to a large analysis of medical claims data.
The findings highlight the need for visual diagnostic aids and specific guidelines for treating HS that target nondermatologists, Melissa Butt, MPH, of Penn State Hershey (Pa.) Medical Center, said during an interview at the annual meeting of the Society for Investigative Dermatology. She presented the findings during a poster session at the meeting.
HS is a chronic inflammatory disease of the hair follicles that affects 0.5%-4% of people in the United States. In past studies, up to 12 years elapsed between disease onset and diagnosis, in part because patients often cannot readily access dermatologists, Ms. Butt said. To better understand patterns of health care use during the years leading up to HS diagnosis, she and her colleagues used MarketScan data to identify 1,733 patients with HS-specific medical care claims filed in 2012 and 2013. Then they looked back at medical claims for these patients during 2008 through 2011, before the patients were diagnosed with HS. The cohort averaged 37 years of age (standard deviation, 15 years), and 73% were female.
Among 239,892 claims filed before patients were diagnosed with HS, 11,381 (4.7%) included codes for other diseases of the skin and subcutaneous tissues, Ms. Butt said. Dermatologists filed only 31% of these skin-specific claims, while 69% were filed by other providers, such as family practitioners, internists, emergency department physicians, and acute care hospitalists.
Notably, about two-thirds of the skin-specific diagnostic codes could have represented a misdiagnosis of HS. These codes included conditions such as abscesses, carbuncles, local infections, ulcers, and diseases of the sebaceous glands.
The fact that 78% of visits occurred in offices and other outpatient settings further underscores the need to improve the detection and care of HS in these environments, Ms. Butt said. Given current national shortages of dermatologists, visual HS diagnostic aids and “detailed, multistep clinical practice guidelines” for nondermatologists could help improve care of HS while patients wait to see the specialists, she added.
A second poster presented at the meeting provided results of a study on the use and impact of antibiotics in the treatment of HS. Alexander Fischer of Johns Hopkins University, Baltimore, and his associates studied antibiotic prescriptions and bacterial cultures from the lesions of 239 patients with HS who were treated at Johns Hopkins medical facilities between 2010 and 2015. Not only were 51% of HS patients on antibiotics at the time of culture, but these patients’ lesions were significantly more likely to contain antibiotic-resistant bacteria than were those of patients not on antibiotics.
Strikingly, Proteus species were isolated from nearly half of patients on trimethoprim-sulfamethoxazole (TMP/SMX), and 88% of colonies were resistant to TMP/SMX, while only 13% of cultures from untreated patients grew Proteus (P less than .001) and all were TMP/SMX-susceptible (P less than .001). Likewise, 100% of methicillin-resistant Staphylococcus aureus (MRSA) strains from patients prescribed ciprofloxacin were resistant to it, compared with a 10% background rate of ciprofloxacin resistance among MRSA from patients not taking antibiotics (P = .04). In addition, the proportion of other S. aureus strains that were clindamycin-resistant was higher when patients were taking this antibiotic than when they were not (63% versus 17%; P = .03).
The results “raise questions” about whether antibiotics should be used in HS patients who are not clearly benefiting from them, according to the researchers.
The authors of both studies reported no funding sources and had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: Two studies underscored current challenges in diagnosing and treating hidradenitis suppurativa (HS).
Major finding: HS was usually diagnosed in outpatient settings by nondermatologists who often initially filed claims for carbuncles, ulcers, and other conditions that are confused with HS. In a separate study, antibiotic-resistant bacteria were significantly more prevalent in the lesions of HS patients who were receiving antibiotics than in patients who were not taking antibiotics.
Data source: A medical claims analysis of 1,733 patients with HS, and a study of antibiotic prescriptions and bacterial cultures from 239 patients with HS.
Disclosures: The authors of both studies reported no funding sources and had no disclosures.
Are Periodic Endoscopies Useful for Patients Under 40?
Endoscopies do not necessarily help catch early gastric cancer in young people, say researchers from Severance Hospital, Seoul, and Hanyang University, Guri, both in Korea.
In countries such as Korea and Japan, where the researchers say Helicobacter pylori is endemic and gastric cancer is prevalent, screening for gastric cancer is recommended for people aged ≥ 40 years. In a previous study, they found that biennial endoscopies increased the diagnosis of gastric neoplasms, including gastric cancer and adenoma, at an early stage in people aged ≥ 40 years. Noting that disease-free status and overall survival of younger patients with gastric cancer are dependent on the cancer’s stage at diagnosis, as is the case with middle-aged patients, they wanted to find out whether earlier periodic endoscopies would be useful.
Related:Clarifying the Links Between Gallbladder Disease and Cancer
In their study, 101 patients underwent screening endoscopy within 24 months after receiving their gastric cancer diagnosis. Another 463 had not had an endoscopy within 2 years. Overall, 65% to 68% had early gastric cancer, but the researchers found no significant difference between the 2 groups. However, the proportion of lesions that were treated with endoscopic submucosal dissection (ESD) differed according to the interval: 9.8% for ≤ 24 and 4.5% for ≥ 24 months.
The only factor associated with early gastric cancer was gastrointestinal symptoms at the time of diagnosis.
Related: How Much Is Too Much Cancer Screening?
Performing an earlier endoscopy detected gastric cancer at a smaller size (23.8 mm in the ≤ 24-month group vs 30.5 mm in the ≥ 24-month group), which could facilitate treatment with ESD, the researchers say. They suggest that although not necessarily influencing early diagnosis, periodic endoscopies may help increase the proportion of lesions treated with ESD.
Source:
Park CH, Kim EH, Chung H, et al. PLoS One. 2016;11(7):e0159759.
doi: 10.1371/journal.pone.0159759.
Endoscopies do not necessarily help catch early gastric cancer in young people, say researchers from Severance Hospital, Seoul, and Hanyang University, Guri, both in Korea.
In countries such as Korea and Japan, where the researchers say Helicobacter pylori is endemic and gastric cancer is prevalent, screening for gastric cancer is recommended for people aged ≥ 40 years. In a previous study, they found that biennial endoscopies increased the diagnosis of gastric neoplasms, including gastric cancer and adenoma, at an early stage in people aged ≥ 40 years. Noting that disease-free status and overall survival of younger patients with gastric cancer are dependent on the cancer’s stage at diagnosis, as is the case with middle-aged patients, they wanted to find out whether earlier periodic endoscopies would be useful.
Related:Clarifying the Links Between Gallbladder Disease and Cancer
In their study, 101 patients underwent screening endoscopy within 24 months after receiving their gastric cancer diagnosis. Another 463 had not had an endoscopy within 2 years. Overall, 65% to 68% had early gastric cancer, but the researchers found no significant difference between the 2 groups. However, the proportion of lesions that were treated with endoscopic submucosal dissection (ESD) differed according to the interval: 9.8% for ≤ 24 and 4.5% for ≥ 24 months.
The only factor associated with early gastric cancer was gastrointestinal symptoms at the time of diagnosis.
Related: How Much Is Too Much Cancer Screening?
Performing an earlier endoscopy detected gastric cancer at a smaller size (23.8 mm in the ≤ 24-month group vs 30.5 mm in the ≥ 24-month group), which could facilitate treatment with ESD, the researchers say. They suggest that although not necessarily influencing early diagnosis, periodic endoscopies may help increase the proportion of lesions treated with ESD.
Source:
Park CH, Kim EH, Chung H, et al. PLoS One. 2016;11(7):e0159759.
doi: 10.1371/journal.pone.0159759.
Endoscopies do not necessarily help catch early gastric cancer in young people, say researchers from Severance Hospital, Seoul, and Hanyang University, Guri, both in Korea.
In countries such as Korea and Japan, where the researchers say Helicobacter pylori is endemic and gastric cancer is prevalent, screening for gastric cancer is recommended for people aged ≥ 40 years. In a previous study, they found that biennial endoscopies increased the diagnosis of gastric neoplasms, including gastric cancer and adenoma, at an early stage in people aged ≥ 40 years. Noting that disease-free status and overall survival of younger patients with gastric cancer are dependent on the cancer’s stage at diagnosis, as is the case with middle-aged patients, they wanted to find out whether earlier periodic endoscopies would be useful.
Related:Clarifying the Links Between Gallbladder Disease and Cancer
In their study, 101 patients underwent screening endoscopy within 24 months after receiving their gastric cancer diagnosis. Another 463 had not had an endoscopy within 2 years. Overall, 65% to 68% had early gastric cancer, but the researchers found no significant difference between the 2 groups. However, the proportion of lesions that were treated with endoscopic submucosal dissection (ESD) differed according to the interval: 9.8% for ≤ 24 and 4.5% for ≥ 24 months.
The only factor associated with early gastric cancer was gastrointestinal symptoms at the time of diagnosis.
Related: How Much Is Too Much Cancer Screening?
Performing an earlier endoscopy detected gastric cancer at a smaller size (23.8 mm in the ≤ 24-month group vs 30.5 mm in the ≥ 24-month group), which could facilitate treatment with ESD, the researchers say. They suggest that although not necessarily influencing early diagnosis, periodic endoscopies may help increase the proportion of lesions treated with ESD.
Source:
Park CH, Kim EH, Chung H, et al. PLoS One. 2016;11(7):e0159759.
doi: 10.1371/journal.pone.0159759.
Emergency Imaging: Shortness of breath
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
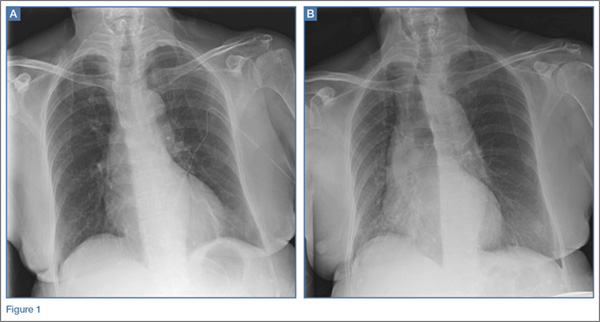
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
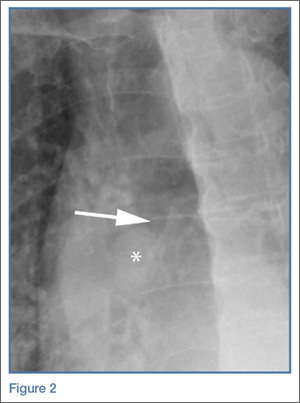
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
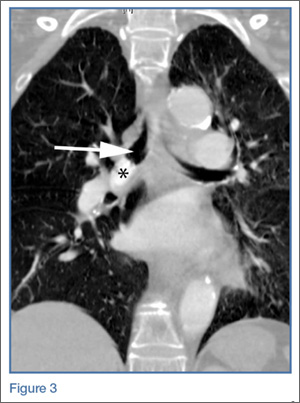
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
2. McGuirt WF, Holmes KD, Feehs R, Browne JD. Tracheobronchial foreign bodies. Laryngoscope. 1988;98(6 Pt 1):615-618.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
2. McGuirt WF, Holmes KD, Feehs R, Browne JD. Tracheobronchial foreign bodies. Laryngoscope. 1988;98(6 Pt 1):615-618.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
2. McGuirt WF, Holmes KD, Feehs R, Browne JD. Tracheobronchial foreign bodies. Laryngoscope. 1988;98(6 Pt 1):615-618.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.

An Unusual Cause of Syncope With T-Wave Abnormalities
Case
A 34-year-old man presented to our ED via emergency medical services (EMS) following a syncopal episode. The patient stated that as he was getting ready for work earlier that morning, he experienced sudden lightheadedness and passed out, whereupon his wife immediately called EMS. The patient denied any previous history of syncope, but said he had been experiencing frequent episodes of nausea and vomiting over the past week. He also complained of a mild occipital headache that acetaminophen had failed to relieve.
The patient had been seen at a different ED 3 days earlier for nausea and vomiting. After evaluating the patient, the emergency physician (EP) at this facility felt the most likely cause of the patient’s gastrointestinal issues was related to hydralazine, his antihypertensive medication, and advised the patient to discontinue its use.
During evaluation at our ED, the patient denied fever, chills, neck stiffness, numbness, weakness, tingling of the extremities, or difficulty walking. He also denied chest pain, shortness of breath, or urinary symptoms. The patient’s medical history was significant only for hypertension; he had not taken any antihypertensive or other medications for the past 3 days, as previously instructed by the EP at the other ED. The patient denied alcohol or drug abuse.
On physical examination, the patient’s vital signs were: temperature, 98.6°F; heart rate, 58 beats/minute; blood pressure, 130/90 mm Hg; and respiratory rate, 16 breaths/minute. Oxygen saturation was 100% on room air. Examination of the head was normal and without evidence of trauma. Both pupils measured 4 mm and were equally round and reactive to light; the patient’s extraocular movements were intact. The remainder of the head, eyes, ears, nose, and throat examination was normal. The neck was supple, without masses or meningeal signs. The cardiopulmonary and abdominal examinations were all normal. On neurological examination, the patient was awake, alert, and oriented to person, place, and time. Cranial nerves II through XII were intact, and the patient had 5/5 motor strength in all four extremities and a normal gait.
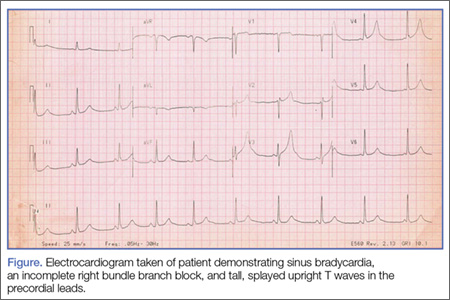
Because we were concerned about the patient’s unexplained syncopal episode, we ordered laboratory tests, including a complete blood count (CBC), evaluation of electrolytes and glucose levels, and kidney function. In addition, we also ordered an electrocardiogram (ECG) and a noncontrast computed tomography (CT) scan of the head. All laboratory test results were within normal range. The ECG, however, demonstrated sinus bradycardia (approximately 58 beats/minute), a normal PR and QRS interval, a normal axis, and an incomplete right bundle branch block with tall, large, splayed upright T waves in the precordial leads (Figure). Based on the abnormal ECG results, we ordered serum cardiac marker studies, the values of which were all within normal range. The noncontrast CT scan of the head revealed a low-density posterior fossa mass compressing the fourth ventricle with secondary hydrocephalus.
The patient was placed with his head in an upright position and given 1 g/kg mannitol and 10 mg dexamethasone intravenously (IV). Neurosurgery services were consulted, and the patient underwent surgery the following morning. Surgery confirmed the presence of a hemangioblastoma. The hemangioblastoma was successfully excised, and the patient had an uneventful recovery. Interestingly, the significant T-wave changes in the precordial leads were no longer present postoperatively.
Discussion
Syncope and near-syncope are common reasons for ED visits. Syncope is a syndrome characterized by a transient, self-limited episode of loss of consciousness occurring as a result of a brief interruption of the oxygen supply to the brain.1 This interruption is almost always due to a transient cessation of blood flow.1 In true syncope (as opposed to seizures or hypoglycemia), the episode is characterized by a rapid onset of loss of consciousness—with or without warning symptoms.1 It is important to determine the cause of syncope, because 7% to 23% of such patients will suffer serious outcomes within 7 to 30 days of their ED visit—either within a hospital setting or at home.2
Etiology
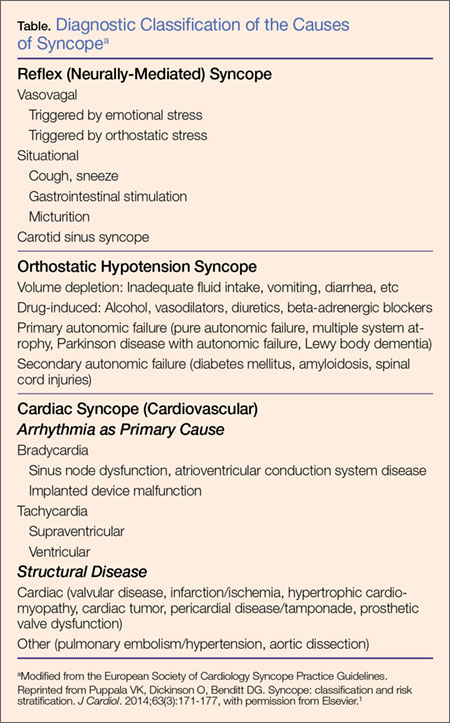
There are many causes of syncope. In most cases, the etiology falls under one of three broad categories: neurally mediated (or reflex mediated), orthostatic hypotensive-mediated, or cardiovascular (CV)-mediated. Less common causes of syncope include cerebrovascular injury.1 The Table outlines both common and uncommon causes of syncope.
On presentation, our patient had several possible causes for his syncopal episode: an abnormal ECG (CV); multiple episodes of emesis (volume depletion); and headache (cerebrovascular). The EP worked up all three of these signs and symptoms simultaneously as is the appropriate protocol when evaluating an ED patient presenting with undifferentiated syncope.
Signs and Symptoms
Patients with undiagnosed brain tumors normally present with headache, seizures, nausea, vomiting, focal neurological deficits, or an altered mental status.3 Syncope is a very rare manifestation of a brain tumor3; however, our patient did complain of headache, nausea, and vomiting.
In addition to the unusual cause of the syncope, the abnormally large upright T waves make this case even more notable. T-wave changes are the most common ECG abnormality, seen in about 50% of abnormal tracings reviewed in a hospital population and in 2.4% of all ECGs.4
In general, T-wave changes are a result of local changes in the duration of repolarization. T-wave inversion is the most common T-wave abnormality and is typically observed in the setting of ischemia, post-ingestion of food, following an episode of tachycardia or anxiety, and autonomic dysfunction.5 However, in patients who have a cerebral etiology (usually hemorrhage), the T-wave changes may be either upright (as in our case) or inverted.5 Historically, subarachnoid hemorrhage (SAH) has been associated with ST-segment elevation and T-wave inversion. Hypothalamic stimulation and autonomic dysfunction have been linked to abnormal T-waves, but this has not been conclusively proven to be the cause of the abnormality.6 For all of the aforementioned reasons, the specificity for a given cause of T-wave changes is exceedingly low.5
Hyperacute T-wave amplitude, with prominent symmetrical T waves in at least two continuous leads, may be the earliest sign of acute transmural myocardial infarction (MI).7 It usually persists for only a brief time before other ECG findings of acute MI are observed. Other common causes of hyperacute T waves include hyperkalemia (usually narrow-based, and peaked), early repolarization, left ventricular hypertrophy, and acute myocarditis.8 Less common causes of prominent T waves include pre-excitation syndromes, pericarditis, and scorpion stings.9,10
Summary
It is unclear why our patient, who had a hemangioblastoma, demonstrated hyperacute T-wave abnormality on ECG. The abnormal upright T waves may have occurred secondary to the same theories regarding SAH, hypothalamic stimulation, or autonomic dysfunction. Regardless of the underlying etiology, this case serves as a reminder to the EP that not all T-wave changes on ECG are cardiac in origin.
1. Puppala VK, Dickinson O, Benditt DG. Syncope: classification and risk stratification. J Cardiol. 2014;63(3):171-177.
2. Thiruganasambandamoorthy V, Stiell IG, Sivilotti ML, et al. Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study. BMC Emerg Med. 2014;14(1):8.
3. van der Sluijs BM, Renier WO, Kappelle AC. Brain tumor as a rare cause of cardiac syncope. J Neurooncol. 2004;67(1-2):241-244.
4. Friedberg CK, Zagar A. Nonspecific ST and T-wave changes. Circulation. 1961;23:665-661.
5. Fisch C. T wave abnormalities due to extracardiac “functional” causes. ACC Curr J Rev. 1997;6(2):101-104.
6. Chatterjee S. ECG changes in subarachnoid hemorrhage: a synopsis. Neth Heart J. 2011;19(1):31-47.
7. Vojáčeka, J, Janskýb P, Janotac T. Third universal definition of myocardial infarction. Cor Vasa. 2013;55:e228-e235.
8. Levis JT. ECG diagnosis: hyperacute T waves. Perm J. 2015;19(3):79.
9. Somers MP, Brady WJ, Perron AD, Mattu A. The prominent T wave: electrocardiographic differential diagnosis. Am J Emerg Med. 2002;20(3):243-251.
10. Kumar MR, Bharath RV, Subrahmanyam BV, Rammohan P, Agrawal A. Scorpion envenomation and its management in adults. Sahel Med J. 2013;16(2):60-63.
Case
A 34-year-old man presented to our ED via emergency medical services (EMS) following a syncopal episode. The patient stated that as he was getting ready for work earlier that morning, he experienced sudden lightheadedness and passed out, whereupon his wife immediately called EMS. The patient denied any previous history of syncope, but said he had been experiencing frequent episodes of nausea and vomiting over the past week. He also complained of a mild occipital headache that acetaminophen had failed to relieve.
The patient had been seen at a different ED 3 days earlier for nausea and vomiting. After evaluating the patient, the emergency physician (EP) at this facility felt the most likely cause of the patient’s gastrointestinal issues was related to hydralazine, his antihypertensive medication, and advised the patient to discontinue its use.
During evaluation at our ED, the patient denied fever, chills, neck stiffness, numbness, weakness, tingling of the extremities, or difficulty walking. He also denied chest pain, shortness of breath, or urinary symptoms. The patient’s medical history was significant only for hypertension; he had not taken any antihypertensive or other medications for the past 3 days, as previously instructed by the EP at the other ED. The patient denied alcohol or drug abuse.
On physical examination, the patient’s vital signs were: temperature, 98.6°F; heart rate, 58 beats/minute; blood pressure, 130/90 mm Hg; and respiratory rate, 16 breaths/minute. Oxygen saturation was 100% on room air. Examination of the head was normal and without evidence of trauma. Both pupils measured 4 mm and were equally round and reactive to light; the patient’s extraocular movements were intact. The remainder of the head, eyes, ears, nose, and throat examination was normal. The neck was supple, without masses or meningeal signs. The cardiopulmonary and abdominal examinations were all normal. On neurological examination, the patient was awake, alert, and oriented to person, place, and time. Cranial nerves II through XII were intact, and the patient had 5/5 motor strength in all four extremities and a normal gait.
Because we were concerned about the patient’s unexplained syncopal episode, we ordered laboratory tests, including a complete blood count (CBC), evaluation of electrolytes and glucose levels, and kidney function. In addition, we also ordered an electrocardiogram (ECG) and a noncontrast computed tomography (CT) scan of the head. All laboratory test results were within normal range. The ECG, however, demonstrated sinus bradycardia (approximately 58 beats/minute), a normal PR and QRS interval, a normal axis, and an incomplete right bundle branch block with tall, large, splayed upright T waves in the precordial leads (Figure). Based on the abnormal ECG results, we ordered serum cardiac marker studies, the values of which were all within normal range. The noncontrast CT scan of the head revealed a low-density posterior fossa mass compressing the fourth ventricle with secondary hydrocephalus.
The patient was placed with his head in an upright position and given 1 g/kg mannitol and 10 mg dexamethasone intravenously (IV). Neurosurgery services were consulted, and the patient underwent surgery the following morning. Surgery confirmed the presence of a hemangioblastoma. The hemangioblastoma was successfully excised, and the patient had an uneventful recovery. Interestingly, the significant T-wave changes in the precordial leads were no longer present postoperatively.
Discussion
Syncope and near-syncope are common reasons for ED visits. Syncope is a syndrome characterized by a transient, self-limited episode of loss of consciousness occurring as a result of a brief interruption of the oxygen supply to the brain.1 This interruption is almost always due to a transient cessation of blood flow.1 In true syncope (as opposed to seizures or hypoglycemia), the episode is characterized by a rapid onset of loss of consciousness—with or without warning symptoms.1 It is important to determine the cause of syncope, because 7% to 23% of such patients will suffer serious outcomes within 7 to 30 days of their ED visit—either within a hospital setting or at home.2
Etiology
There are many causes of syncope. In most cases, the etiology falls under one of three broad categories: neurally mediated (or reflex mediated), orthostatic hypotensive-mediated, or cardiovascular (CV)-mediated. Less common causes of syncope include cerebrovascular injury.1 The Table outlines both common and uncommon causes of syncope.
On presentation, our patient had several possible causes for his syncopal episode: an abnormal ECG (CV); multiple episodes of emesis (volume depletion); and headache (cerebrovascular). The EP worked up all three of these signs and symptoms simultaneously as is the appropriate protocol when evaluating an ED patient presenting with undifferentiated syncope.
Signs and Symptoms
Patients with undiagnosed brain tumors normally present with headache, seizures, nausea, vomiting, focal neurological deficits, or an altered mental status.3 Syncope is a very rare manifestation of a brain tumor3; however, our patient did complain of headache, nausea, and vomiting.
In addition to the unusual cause of the syncope, the abnormally large upright T waves make this case even more notable. T-wave changes are the most common ECG abnormality, seen in about 50% of abnormal tracings reviewed in a hospital population and in 2.4% of all ECGs.4
In general, T-wave changes are a result of local changes in the duration of repolarization. T-wave inversion is the most common T-wave abnormality and is typically observed in the setting of ischemia, post-ingestion of food, following an episode of tachycardia or anxiety, and autonomic dysfunction.5 However, in patients who have a cerebral etiology (usually hemorrhage), the T-wave changes may be either upright (as in our case) or inverted.5 Historically, subarachnoid hemorrhage (SAH) has been associated with ST-segment elevation and T-wave inversion. Hypothalamic stimulation and autonomic dysfunction have been linked to abnormal T-waves, but this has not been conclusively proven to be the cause of the abnormality.6 For all of the aforementioned reasons, the specificity for a given cause of T-wave changes is exceedingly low.5
Hyperacute T-wave amplitude, with prominent symmetrical T waves in at least two continuous leads, may be the earliest sign of acute transmural myocardial infarction (MI).7 It usually persists for only a brief time before other ECG findings of acute MI are observed. Other common causes of hyperacute T waves include hyperkalemia (usually narrow-based, and peaked), early repolarization, left ventricular hypertrophy, and acute myocarditis.8 Less common causes of prominent T waves include pre-excitation syndromes, pericarditis, and scorpion stings.9,10
Summary
It is unclear why our patient, who had a hemangioblastoma, demonstrated hyperacute T-wave abnormality on ECG. The abnormal upright T waves may have occurred secondary to the same theories regarding SAH, hypothalamic stimulation, or autonomic dysfunction. Regardless of the underlying etiology, this case serves as a reminder to the EP that not all T-wave changes on ECG are cardiac in origin.
Case
A 34-year-old man presented to our ED via emergency medical services (EMS) following a syncopal episode. The patient stated that as he was getting ready for work earlier that morning, he experienced sudden lightheadedness and passed out, whereupon his wife immediately called EMS. The patient denied any previous history of syncope, but said he had been experiencing frequent episodes of nausea and vomiting over the past week. He also complained of a mild occipital headache that acetaminophen had failed to relieve.
The patient had been seen at a different ED 3 days earlier for nausea and vomiting. After evaluating the patient, the emergency physician (EP) at this facility felt the most likely cause of the patient’s gastrointestinal issues was related to hydralazine, his antihypertensive medication, and advised the patient to discontinue its use.
During evaluation at our ED, the patient denied fever, chills, neck stiffness, numbness, weakness, tingling of the extremities, or difficulty walking. He also denied chest pain, shortness of breath, or urinary symptoms. The patient’s medical history was significant only for hypertension; he had not taken any antihypertensive or other medications for the past 3 days, as previously instructed by the EP at the other ED. The patient denied alcohol or drug abuse.
On physical examination, the patient’s vital signs were: temperature, 98.6°F; heart rate, 58 beats/minute; blood pressure, 130/90 mm Hg; and respiratory rate, 16 breaths/minute. Oxygen saturation was 100% on room air. Examination of the head was normal and without evidence of trauma. Both pupils measured 4 mm and were equally round and reactive to light; the patient’s extraocular movements were intact. The remainder of the head, eyes, ears, nose, and throat examination was normal. The neck was supple, without masses or meningeal signs. The cardiopulmonary and abdominal examinations were all normal. On neurological examination, the patient was awake, alert, and oriented to person, place, and time. Cranial nerves II through XII were intact, and the patient had 5/5 motor strength in all four extremities and a normal gait.
Because we were concerned about the patient’s unexplained syncopal episode, we ordered laboratory tests, including a complete blood count (CBC), evaluation of electrolytes and glucose levels, and kidney function. In addition, we also ordered an electrocardiogram (ECG) and a noncontrast computed tomography (CT) scan of the head. All laboratory test results were within normal range. The ECG, however, demonstrated sinus bradycardia (approximately 58 beats/minute), a normal PR and QRS interval, a normal axis, and an incomplete right bundle branch block with tall, large, splayed upright T waves in the precordial leads (Figure). Based on the abnormal ECG results, we ordered serum cardiac marker studies, the values of which were all within normal range. The noncontrast CT scan of the head revealed a low-density posterior fossa mass compressing the fourth ventricle with secondary hydrocephalus.
The patient was placed with his head in an upright position and given 1 g/kg mannitol and 10 mg dexamethasone intravenously (IV). Neurosurgery services were consulted, and the patient underwent surgery the following morning. Surgery confirmed the presence of a hemangioblastoma. The hemangioblastoma was successfully excised, and the patient had an uneventful recovery. Interestingly, the significant T-wave changes in the precordial leads were no longer present postoperatively.
Discussion
Syncope and near-syncope are common reasons for ED visits. Syncope is a syndrome characterized by a transient, self-limited episode of loss of consciousness occurring as a result of a brief interruption of the oxygen supply to the brain.1 This interruption is almost always due to a transient cessation of blood flow.1 In true syncope (as opposed to seizures or hypoglycemia), the episode is characterized by a rapid onset of loss of consciousness—with or without warning symptoms.1 It is important to determine the cause of syncope, because 7% to 23% of such patients will suffer serious outcomes within 7 to 30 days of their ED visit—either within a hospital setting or at home.2
Etiology
There are many causes of syncope. In most cases, the etiology falls under one of three broad categories: neurally mediated (or reflex mediated), orthostatic hypotensive-mediated, or cardiovascular (CV)-mediated. Less common causes of syncope include cerebrovascular injury.1 The Table outlines both common and uncommon causes of syncope.
On presentation, our patient had several possible causes for his syncopal episode: an abnormal ECG (CV); multiple episodes of emesis (volume depletion); and headache (cerebrovascular). The EP worked up all three of these signs and symptoms simultaneously as is the appropriate protocol when evaluating an ED patient presenting with undifferentiated syncope.
Signs and Symptoms
Patients with undiagnosed brain tumors normally present with headache, seizures, nausea, vomiting, focal neurological deficits, or an altered mental status.3 Syncope is a very rare manifestation of a brain tumor3; however, our patient did complain of headache, nausea, and vomiting.
In addition to the unusual cause of the syncope, the abnormally large upright T waves make this case even more notable. T-wave changes are the most common ECG abnormality, seen in about 50% of abnormal tracings reviewed in a hospital population and in 2.4% of all ECGs.4
In general, T-wave changes are a result of local changes in the duration of repolarization. T-wave inversion is the most common T-wave abnormality and is typically observed in the setting of ischemia, post-ingestion of food, following an episode of tachycardia or anxiety, and autonomic dysfunction.5 However, in patients who have a cerebral etiology (usually hemorrhage), the T-wave changes may be either upright (as in our case) or inverted.5 Historically, subarachnoid hemorrhage (SAH) has been associated with ST-segment elevation and T-wave inversion. Hypothalamic stimulation and autonomic dysfunction have been linked to abnormal T-waves, but this has not been conclusively proven to be the cause of the abnormality.6 For all of the aforementioned reasons, the specificity for a given cause of T-wave changes is exceedingly low.5
Hyperacute T-wave amplitude, with prominent symmetrical T waves in at least two continuous leads, may be the earliest sign of acute transmural myocardial infarction (MI).7 It usually persists for only a brief time before other ECG findings of acute MI are observed. Other common causes of hyperacute T waves include hyperkalemia (usually narrow-based, and peaked), early repolarization, left ventricular hypertrophy, and acute myocarditis.8 Less common causes of prominent T waves include pre-excitation syndromes, pericarditis, and scorpion stings.9,10
Summary
It is unclear why our patient, who had a hemangioblastoma, demonstrated hyperacute T-wave abnormality on ECG. The abnormal upright T waves may have occurred secondary to the same theories regarding SAH, hypothalamic stimulation, or autonomic dysfunction. Regardless of the underlying etiology, this case serves as a reminder to the EP that not all T-wave changes on ECG are cardiac in origin.
1. Puppala VK, Dickinson O, Benditt DG. Syncope: classification and risk stratification. J Cardiol. 2014;63(3):171-177.
2. Thiruganasambandamoorthy V, Stiell IG, Sivilotti ML, et al. Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study. BMC Emerg Med. 2014;14(1):8.
3. van der Sluijs BM, Renier WO, Kappelle AC. Brain tumor as a rare cause of cardiac syncope. J Neurooncol. 2004;67(1-2):241-244.
4. Friedberg CK, Zagar A. Nonspecific ST and T-wave changes. Circulation. 1961;23:665-661.
5. Fisch C. T wave abnormalities due to extracardiac “functional” causes. ACC Curr J Rev. 1997;6(2):101-104.
6. Chatterjee S. ECG changes in subarachnoid hemorrhage: a synopsis. Neth Heart J. 2011;19(1):31-47.
7. Vojáčeka, J, Janskýb P, Janotac T. Third universal definition of myocardial infarction. Cor Vasa. 2013;55:e228-e235.
8. Levis JT. ECG diagnosis: hyperacute T waves. Perm J. 2015;19(3):79.
9. Somers MP, Brady WJ, Perron AD, Mattu A. The prominent T wave: electrocardiographic differential diagnosis. Am J Emerg Med. 2002;20(3):243-251.
10. Kumar MR, Bharath RV, Subrahmanyam BV, Rammohan P, Agrawal A. Scorpion envenomation and its management in adults. Sahel Med J. 2013;16(2):60-63.
1. Puppala VK, Dickinson O, Benditt DG. Syncope: classification and risk stratification. J Cardiol. 2014;63(3):171-177.
2. Thiruganasambandamoorthy V, Stiell IG, Sivilotti ML, et al. Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study. BMC Emerg Med. 2014;14(1):8.
3. van der Sluijs BM, Renier WO, Kappelle AC. Brain tumor as a rare cause of cardiac syncope. J Neurooncol. 2004;67(1-2):241-244.
4. Friedberg CK, Zagar A. Nonspecific ST and T-wave changes. Circulation. 1961;23:665-661.
5. Fisch C. T wave abnormalities due to extracardiac “functional” causes. ACC Curr J Rev. 1997;6(2):101-104.
6. Chatterjee S. ECG changes in subarachnoid hemorrhage: a synopsis. Neth Heart J. 2011;19(1):31-47.
7. Vojáčeka, J, Janskýb P, Janotac T. Third universal definition of myocardial infarction. Cor Vasa. 2013;55:e228-e235.
8. Levis JT. ECG diagnosis: hyperacute T waves. Perm J. 2015;19(3):79.
9. Somers MP, Brady WJ, Perron AD, Mattu A. The prominent T wave: electrocardiographic differential diagnosis. Am J Emerg Med. 2002;20(3):243-251.
10. Kumar MR, Bharath RV, Subrahmanyam BV, Rammohan P, Agrawal A. Scorpion envenomation and its management in adults. Sahel Med J. 2013;16(2):60-63.
A Rare Case of Traumatic Tension Pneumo-orbitum
Traumatic eye injuries ranging from mild corneal abrasions to penetrating globe injuries are commonly seen in the ED, and ocular trauma accounts for nearly 1% of all complaints in the ED.1 Up to 29% of facial fractures have associated eye injuries.2 Emergency physicians (EPs) must be aware of possible eye injuries, including traumatic vision loss, and the indicators for emergent interventions.
Tension pneumo-orbitum following facial trauma is rarely reported. We present a case of orbital compartment syndrome (OCS) in an elderly woman who sustained an orbital floor fracture and required emergent lateral canthotomy to preserve vision.
Case
A 76-year-old woman presented to the ED for evaluation of pain, swelling, and loss of vision in the right eye. She said she had been sitting in a chair tying her shoes when she lost her balance and fell forward, striking her head and the right side of her face against the floor. She experienced no loss of consciousness and denied any neck pain, jaw pain, or dizziness. She also denied any chest pain, shortness of breath, weakness, or loss of function in either her arms or legs. She did, however, note a small nosebleed that had stopped before she arrived at the ED. The patient’s primary complaint was a possible nasal bone fracture.
Her medical history was significant for hypertension and coronary artery disease. Her medications include amitriptyline, an antihistamine, aspirin, clopidogrel, diltiazem, folic acid, furosemide, hydralazine, levothyroxine, prednisone, and zolpidem. She stated that she was allergic to amoxicillin and sulfa drugs.
The patient’s vital signs at presentation were: blood pressure (BP), 193/82 mm Hg; heart rate, 71 beats/minute; respiratory rate, 16 breaths/minute; and temperature, 97°F. She was alert, oriented, and in no distress. Her head and neck examination showed no scalp lacerations or swelling. There was, however, significant swelling and ecchymosis around the right eye and swelling and ecchymosis around the nose, with dried blood in both nares. No septal hematoma was present. The patient had tenderness to palpation over the infraorbital area and nose. No gross facial instability was present, and Battle sign was not appreciated. No jaw or dental abnormalities were noted.
The patient’s right pupil was fixed and dilated, and she could not perceive light. She did have upward and lateral movement of the eye, but was unable to look down. A minimal amount of proptosis was noted. Her intraocular pressure (IOP) was elevated at 54 mm Hg (normal range, 10-20 mm Hg). The remainder of the examination, including the neurological examination, was unremarkable.
The patient received emergent head and facial computed tomography (CT) scans. The head CT showed no acute intracranial hemorrhage, mass, or infarct. The facial CT was read as a right orbital floor fracture with intraorbital air, and a right maxillary sinus hematoma. Laboratory evaluation revealed a hematocrit of 38% and a platelet count of 544,000/mcL (normal range, 150,000-450,000/mcL). The prothrombin time was 10.9 seconds (normal range, 11-13.5 seconds); the international normalized ratio was 0.8 (normal range, 0.8-1.1); and the partial thromboplastin time was 22.5 seconds (normal range, 25-35 seconds).
Because the patient was at risk for permanent visual impairment due to increased IOP from the injury, a lateral canthotomy was immediately performed. A small amount of air was released, and the proptosis was notably reduced.
At this point, the ophthalmologist arrived and used an 18-gauge needle to explore the retrobulbar space. Two pockets of air were released, which markedly reduced the tactile pressure of the globe. Repeat tonography of the globe was 28 mm Hg. The wound was left open to drain, and the patient was started on azithromycin. She was discharged home to follow up with ophthalmology.
The patient presented to the ED 2 months later for an unrelated condition. At that time, she reported a complete return of her vision with no deficits and no noticeable scarring around the eye.
Discussion
The orbit is an enclosed space, bordered by bone laterally and posteriorly—the orbital septa superiorly and inferiorly, and the globe anteriorly.3 The lateral canthus is a combined tendon-ligament that helps attach the tarsal plates of the lids and the orbicularis oculi muscles to the lateral orbital wall and zygoma, which forms the posterior orbital wall.3,4 The lateral canthal tendon is located beneath the lateral canthus and is comprised of the inferior and superior crus, which attaches to the inner aspect of the lateral orbital wall, forming a structure called Whitnall’s tubercle.3,4
Other than globe injuries, the most common findings in patients with orbital trauma are periocular lacerations (96%), orbital fractures (16%), and retrobulbar hemorrhage (8%).5 The most common cause of retrobulbar hemorrhage is ocular trauma, but it is also observed in facial fractures, orbital surgery, retrobulbar injections, venous anomalies, atherosclerosis, intraorbital aneurysm of the ophthalmic artery, lacerated ophthalmic artery, hypertension, hemophilia, leukemia, von Willebrand disease, and straining.3,6,7
In retrobulbar hemorrhage, an increased pressure in the orbital space can lead to optic nerve compression and vascular compromise.6 Important alternative diagnoses to consider include orbital cellulitis, orbital fracture, and globe rupture.3 Retrobulbar hemorrhage should be suspected in the clinical setting of exophthalmos, proptosis, diffuse subconjunctival hemorrhage, pain, visual loss or diplopia, periorbital edema, partial or complete ophthalmoplegia, resistance to retropulsion, increased IOP, a blanched ophthalmic artery on funduscopic examination, and an afferent pupillary defect.3,4,8,9 Less commonly, periorbital crepitus and infraorbital hypoesthesia can be appreciated.3
If a patient with a retrobulbar hemorrhage is experiencing diminished vision, an emergent lateral canthotomy should be attempted. Retrobulbar hemorrhage can be difficult to diagnose in the setting of trauma. There can be damage to the optic nerve with associated edema and vision loss that is not associated with a retrobulbar hemorrhage and does not require a lateral canthotomy.3,7 A dedicated CT scan of the orbits can aid in the diagnosis, but treatment should not be delayed.8
Patients with retrobulbar hemorrhage may initially present to the ED with intact visual acuity, but as the pressure behind the globe increases, vision will diminish.3 Although the medical literature has not established a definitive timeframe, it is believed that permanent visual compromise develops between 1 to 3 hours after ischemia develops.6 Animal studies show that visual loss due to central retinal artery ischemia may be reversible up to 100 minutes.3
Not all cases of retrobulbar hemorrhage are associated with vision loss. In patients without diminished vision, conservative treatments such as bed rest, elevation of the head of the bed, ice packs, analgesia, lowering BP, and sedatives should be attempted first.5 Acetazolamide and mannitol can also be considered in consultation with an ophthalmologist.
Pneumo-orbitum
The presence of pneumo-orbitum should alert the clinician to either a communication with a paranasal sinus, a gas-forming organism, or (rarely) Munchausen syndrome.10 Unlike most case presentations, most causes of pneumo-orbitum do not involve OCS and are self-limited.11 Traumatic pneumo-orbitum without OCS has been reported in the literature.12-15 However, traumatic tension pneumo-orbitum is rare.12-16 One case report involved an elderly man with an orbital floor fracture who developed recurrent tension pneumo-orbitum after blowing his nose while intoxicated.12 Another case involved a boy with tension pneumo-orbitum that required surgical decompression.16
In a patient who has experienced trauma, the combination of proptosis, elevated IOP, and vision loss likely represent a retrobulbar hematoma or OCS. A lateral canthotomy can help relieve IOP from either condition.17,18 Orbital compartment syndrome can be caused by edema, emphysema, and caroticocavernous fistula, leading to increased orbital pressure and decreased perfusion.17,18
In a review of 10 trauma patients with OCS, all cases were intubated due to the severity of the head trauma, and all had OCS due to edema.17 In a review of eight trauma patients with OCS, all had eye pain, reduced visual acuity, and proptosis.18 Most of the patients had periorbital edema, ophthalmoparesis, a relative afferent pupillary defect (as compared to a fixed and dilated pupil), and chemosis.18,19 All of the patients with OCS required cantholysis or a lateral canthotomy.18
Lateral Canthotomy
Although EPs rarely perform lateral canthotomy, knowledge of this procedure is important, because it can prevent vision loss in the appropriate clinical setting. To perform a lateral canthotomy, the area around the affected eye is cleaned with saline irrigation.4 One percent or 2% lidocaine with epinephrine is then injected into the lateral canthus of the affected eye.4,10 A straight hemostat is applied between the upper and lower lids, producing a crush injury along the site of local anesthesia for 1 to 2 minutes.3,4,10 This is done to reduce the risk of bleeding by devitalizing the tissue.4 Straight scissors are then used to make a 1-cm horizontal incision from the lateral canthal tendon to the lateral orbital rim.4 This initial incision exposes the orbicularis muscle, orbital septum, palpebral conjunctiva, and an area called Eisler’s pocket that sits anterior to the lateral canthal tendon.3
Cantholysis can then be performed by blunt dissection.10 The inferior crus of the lateral canthus is identified either visually or by palpation, and a 1- to 2-cm inferior-posterior cut of the inferior crus accomplishes the lateral canthotomy.3-4 After cutting the inferior crus, the lower lid should be pulled away easily, and if this does not occur, repeated attempts at cutting the inferior crus should be made.3 Pulling the lower eyelid down and away from the lateral orbital rim separates the skin and conjunctiva, aiding in visualization.4
After cutting the inferior crus, only a small amount of blood or air typically is expressed, but this is usually enough to prevent vision loss.3 When the procedure is performed correctly, the practitioner should be able to palpate a difference in the pressure of the globe, and tonography will show a reduced IOP. If the ocular pressure is still significantly elevated, the physician can proceed to cut the superior canthus of the lateral canthal tendon in a manner similar to cutting the inferior crus of the tendon.4 After the procedure is performed, urgent ophthalmologic consultation is required.
The risks of performing a lateral canthotomy include mechanical injury, hemorrhage, and infection.4 The incision from a lateral canthotomy generally does not need suturing and will heal without significant scarring.4 If the scissors are aimed superiorly instead of inferiorly for the inferior crus of the lateral canthal tendon, there is risk of injuring the levator aponeurosis leading to ptosis, as well as a small risk of injury to the lacrimal gland and lacrimal artery.3
Conclusion
Our patient demonstrates a case of traumatic OCS, a vision-threatening medical condition that requires rapid diagnosis and lateral canthotomy to lower IOP and reduce the risk of permanent vision loss. While an orbital CT scan may assist in confirming the diagnosis, treatment of IOP should not be delayed.
1. McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2001 Emergency Department Summary. Advance Data from Vital Health and Statistics; No. 335. https://www.cdc.gov/nchs/data/ad/ad335.pdf. Accessed July 22, 2016.
2. Knoop KJ, Dennis WR. Eye trauma. In: Wolfson AB, Hendy GW, Hendy PL, et al (eds). Harwood-Nuss’ Clinical Practice of Emergency Medicine. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
3. Vassallo S, Hartstein M, Howard D, Stetz J. Traumatic retrobulbar hemorrhage: emergent decompression by lateral canthotomy and cantholysis. J Emerg Med. 2002;22(3):251-256.
4. Roberts JR, Hedges JR (eds). Clinical Procedures in Emergency Medicine, 4th ed. Philadelphia, PA: Saunders; 2004.
5. Hatton MP, Thakker MM, Ray S. Orbital and adnexal trauma associated with open-globe injuries. Ophthal Plast Reconstr Surg. 2002;18(6):458-461.
6. Suner S, Simmons W, Savitt DL. A porcine model for instruction of lateral canthotomy. Acad Emerg Med. 2000;7(7):837-838.
7. Goodall KL, Brahma A, Bates A, Leatherbarrow B. Lateral canthotomy and inferior cantholysis: an effective method of urgent orbital decompression for sight threatening acute retrobulbar hemorrhage. Injury. 1999;30(7):485-490.
8. Gerbino G, Ramieri GA, Nasi A. Diagnosis and treatment of retrobulbar haematomas following blunt orbital trauma: a description of eight cases. Int J Oral Maxillofac Surg. 2005;34(2):127-131.
9. Machado RA, Silveira RL, Borges HO, Filho AM, de Oliveira GM. Retrobulbar hemorrhage: A case report. J Contemp Dent Pract. 2006;7(2):130-136.
10. Winans JM, House LR, Robinson HE. Self-induced orbital emphysema as a presenting sign of Munchausen’s syndrome. Laryngoscope. 1983;93(9):1209-1211.
11. Zimmer-Galler IE, Bartley GB. Orbital emphysema: case reports and review of the literature. Mayo Clin Proc. 1994;69(2):115-121.
12. Ahnood D, Toft PB. Recurrent orbital compartment syndrome caused by a blow-out fracture and accumulation of air; management by orbital punctures. Acta Ophthalmol. 2012;90(12):199-200.
13. Martin PW, Williams AC. Supraorbital emphysema: report of a case. J Oral Surg. 1972;30(12):901-902.
14. Per BL, Sanders BB. Post-traumatic intraorbital pneumatocele--a rare case of unilateral exophthalmos. Br J Radio. 1971;44(519):214-215.
15. Haller ML, Brackup AH, Shiffman F. Intraorbital aerocele. Arch Ophthalmol. 1980;98(9):1612-1613.
16. Chaudhry IA, Al-Amri A, Shamsi FA, Al-Rashed W. Visual recovery after evacuation of orbital emphysema. Orbit. 2007;26(4):283-285.
17. Perry M. Acute proptosis in trauma: retrobulbar hemorrhage or orbital compartment syndrome—does it really matter? J Oral Maxillofac Surg. 2008;66(9):1913-1920.
18. Sun MT, Chan WO, Selva D. Traumatic orbital compartment syndrome: importance of the lateral canthotomy and cantholysis. Emerg Med Australas. 2014;26(3):274-278.
19. Belliveau MJ, Johnson D. Orbital compartment syndrome after head trauma. Lancet Neurol. 2015;14(2):136-137.
Traumatic eye injuries ranging from mild corneal abrasions to penetrating globe injuries are commonly seen in the ED, and ocular trauma accounts for nearly 1% of all complaints in the ED.1 Up to 29% of facial fractures have associated eye injuries.2 Emergency physicians (EPs) must be aware of possible eye injuries, including traumatic vision loss, and the indicators for emergent interventions.
Tension pneumo-orbitum following facial trauma is rarely reported. We present a case of orbital compartment syndrome (OCS) in an elderly woman who sustained an orbital floor fracture and required emergent lateral canthotomy to preserve vision.
Case
A 76-year-old woman presented to the ED for evaluation of pain, swelling, and loss of vision in the right eye. She said she had been sitting in a chair tying her shoes when she lost her balance and fell forward, striking her head and the right side of her face against the floor. She experienced no loss of consciousness and denied any neck pain, jaw pain, or dizziness. She also denied any chest pain, shortness of breath, weakness, or loss of function in either her arms or legs. She did, however, note a small nosebleed that had stopped before she arrived at the ED. The patient’s primary complaint was a possible nasal bone fracture.
Her medical history was significant for hypertension and coronary artery disease. Her medications include amitriptyline, an antihistamine, aspirin, clopidogrel, diltiazem, folic acid, furosemide, hydralazine, levothyroxine, prednisone, and zolpidem. She stated that she was allergic to amoxicillin and sulfa drugs.
The patient’s vital signs at presentation were: blood pressure (BP), 193/82 mm Hg; heart rate, 71 beats/minute; respiratory rate, 16 breaths/minute; and temperature, 97°F. She was alert, oriented, and in no distress. Her head and neck examination showed no scalp lacerations or swelling. There was, however, significant swelling and ecchymosis around the right eye and swelling and ecchymosis around the nose, with dried blood in both nares. No septal hematoma was present. The patient had tenderness to palpation over the infraorbital area and nose. No gross facial instability was present, and Battle sign was not appreciated. No jaw or dental abnormalities were noted.
The patient’s right pupil was fixed and dilated, and she could not perceive light. She did have upward and lateral movement of the eye, but was unable to look down. A minimal amount of proptosis was noted. Her intraocular pressure (IOP) was elevated at 54 mm Hg (normal range, 10-20 mm Hg). The remainder of the examination, including the neurological examination, was unremarkable.
The patient received emergent head and facial computed tomography (CT) scans. The head CT showed no acute intracranial hemorrhage, mass, or infarct. The facial CT was read as a right orbital floor fracture with intraorbital air, and a right maxillary sinus hematoma. Laboratory evaluation revealed a hematocrit of 38% and a platelet count of 544,000/mcL (normal range, 150,000-450,000/mcL). The prothrombin time was 10.9 seconds (normal range, 11-13.5 seconds); the international normalized ratio was 0.8 (normal range, 0.8-1.1); and the partial thromboplastin time was 22.5 seconds (normal range, 25-35 seconds).
Because the patient was at risk for permanent visual impairment due to increased IOP from the injury, a lateral canthotomy was immediately performed. A small amount of air was released, and the proptosis was notably reduced.
At this point, the ophthalmologist arrived and used an 18-gauge needle to explore the retrobulbar space. Two pockets of air were released, which markedly reduced the tactile pressure of the globe. Repeat tonography of the globe was 28 mm Hg. The wound was left open to drain, and the patient was started on azithromycin. She was discharged home to follow up with ophthalmology.
The patient presented to the ED 2 months later for an unrelated condition. At that time, she reported a complete return of her vision with no deficits and no noticeable scarring around the eye.
Discussion
The orbit is an enclosed space, bordered by bone laterally and posteriorly—the orbital septa superiorly and inferiorly, and the globe anteriorly.3 The lateral canthus is a combined tendon-ligament that helps attach the tarsal plates of the lids and the orbicularis oculi muscles to the lateral orbital wall and zygoma, which forms the posterior orbital wall.3,4 The lateral canthal tendon is located beneath the lateral canthus and is comprised of the inferior and superior crus, which attaches to the inner aspect of the lateral orbital wall, forming a structure called Whitnall’s tubercle.3,4
Other than globe injuries, the most common findings in patients with orbital trauma are periocular lacerations (96%), orbital fractures (16%), and retrobulbar hemorrhage (8%).5 The most common cause of retrobulbar hemorrhage is ocular trauma, but it is also observed in facial fractures, orbital surgery, retrobulbar injections, venous anomalies, atherosclerosis, intraorbital aneurysm of the ophthalmic artery, lacerated ophthalmic artery, hypertension, hemophilia, leukemia, von Willebrand disease, and straining.3,6,7
In retrobulbar hemorrhage, an increased pressure in the orbital space can lead to optic nerve compression and vascular compromise.6 Important alternative diagnoses to consider include orbital cellulitis, orbital fracture, and globe rupture.3 Retrobulbar hemorrhage should be suspected in the clinical setting of exophthalmos, proptosis, diffuse subconjunctival hemorrhage, pain, visual loss or diplopia, periorbital edema, partial or complete ophthalmoplegia, resistance to retropulsion, increased IOP, a blanched ophthalmic artery on funduscopic examination, and an afferent pupillary defect.3,4,8,9 Less commonly, periorbital crepitus and infraorbital hypoesthesia can be appreciated.3
If a patient with a retrobulbar hemorrhage is experiencing diminished vision, an emergent lateral canthotomy should be attempted. Retrobulbar hemorrhage can be difficult to diagnose in the setting of trauma. There can be damage to the optic nerve with associated edema and vision loss that is not associated with a retrobulbar hemorrhage and does not require a lateral canthotomy.3,7 A dedicated CT scan of the orbits can aid in the diagnosis, but treatment should not be delayed.8
Patients with retrobulbar hemorrhage may initially present to the ED with intact visual acuity, but as the pressure behind the globe increases, vision will diminish.3 Although the medical literature has not established a definitive timeframe, it is believed that permanent visual compromise develops between 1 to 3 hours after ischemia develops.6 Animal studies show that visual loss due to central retinal artery ischemia may be reversible up to 100 minutes.3
Not all cases of retrobulbar hemorrhage are associated with vision loss. In patients without diminished vision, conservative treatments such as bed rest, elevation of the head of the bed, ice packs, analgesia, lowering BP, and sedatives should be attempted first.5 Acetazolamide and mannitol can also be considered in consultation with an ophthalmologist.
Pneumo-orbitum
The presence of pneumo-orbitum should alert the clinician to either a communication with a paranasal sinus, a gas-forming organism, or (rarely) Munchausen syndrome.10 Unlike most case presentations, most causes of pneumo-orbitum do not involve OCS and are self-limited.11 Traumatic pneumo-orbitum without OCS has been reported in the literature.12-15 However, traumatic tension pneumo-orbitum is rare.12-16 One case report involved an elderly man with an orbital floor fracture who developed recurrent tension pneumo-orbitum after blowing his nose while intoxicated.12 Another case involved a boy with tension pneumo-orbitum that required surgical decompression.16
In a patient who has experienced trauma, the combination of proptosis, elevated IOP, and vision loss likely represent a retrobulbar hematoma or OCS. A lateral canthotomy can help relieve IOP from either condition.17,18 Orbital compartment syndrome can be caused by edema, emphysema, and caroticocavernous fistula, leading to increased orbital pressure and decreased perfusion.17,18
In a review of 10 trauma patients with OCS, all cases were intubated due to the severity of the head trauma, and all had OCS due to edema.17 In a review of eight trauma patients with OCS, all had eye pain, reduced visual acuity, and proptosis.18 Most of the patients had periorbital edema, ophthalmoparesis, a relative afferent pupillary defect (as compared to a fixed and dilated pupil), and chemosis.18,19 All of the patients with OCS required cantholysis or a lateral canthotomy.18
Lateral Canthotomy
Although EPs rarely perform lateral canthotomy, knowledge of this procedure is important, because it can prevent vision loss in the appropriate clinical setting. To perform a lateral canthotomy, the area around the affected eye is cleaned with saline irrigation.4 One percent or 2% lidocaine with epinephrine is then injected into the lateral canthus of the affected eye.4,10 A straight hemostat is applied between the upper and lower lids, producing a crush injury along the site of local anesthesia for 1 to 2 minutes.3,4,10 This is done to reduce the risk of bleeding by devitalizing the tissue.4 Straight scissors are then used to make a 1-cm horizontal incision from the lateral canthal tendon to the lateral orbital rim.4 This initial incision exposes the orbicularis muscle, orbital septum, palpebral conjunctiva, and an area called Eisler’s pocket that sits anterior to the lateral canthal tendon.3
Cantholysis can then be performed by blunt dissection.10 The inferior crus of the lateral canthus is identified either visually or by palpation, and a 1- to 2-cm inferior-posterior cut of the inferior crus accomplishes the lateral canthotomy.3-4 After cutting the inferior crus, the lower lid should be pulled away easily, and if this does not occur, repeated attempts at cutting the inferior crus should be made.3 Pulling the lower eyelid down and away from the lateral orbital rim separates the skin and conjunctiva, aiding in visualization.4
After cutting the inferior crus, only a small amount of blood or air typically is expressed, but this is usually enough to prevent vision loss.3 When the procedure is performed correctly, the practitioner should be able to palpate a difference in the pressure of the globe, and tonography will show a reduced IOP. If the ocular pressure is still significantly elevated, the physician can proceed to cut the superior canthus of the lateral canthal tendon in a manner similar to cutting the inferior crus of the tendon.4 After the procedure is performed, urgent ophthalmologic consultation is required.
The risks of performing a lateral canthotomy include mechanical injury, hemorrhage, and infection.4 The incision from a lateral canthotomy generally does not need suturing and will heal without significant scarring.4 If the scissors are aimed superiorly instead of inferiorly for the inferior crus of the lateral canthal tendon, there is risk of injuring the levator aponeurosis leading to ptosis, as well as a small risk of injury to the lacrimal gland and lacrimal artery.3
Conclusion
Our patient demonstrates a case of traumatic OCS, a vision-threatening medical condition that requires rapid diagnosis and lateral canthotomy to lower IOP and reduce the risk of permanent vision loss. While an orbital CT scan may assist in confirming the diagnosis, treatment of IOP should not be delayed.
Traumatic eye injuries ranging from mild corneal abrasions to penetrating globe injuries are commonly seen in the ED, and ocular trauma accounts for nearly 1% of all complaints in the ED.1 Up to 29% of facial fractures have associated eye injuries.2 Emergency physicians (EPs) must be aware of possible eye injuries, including traumatic vision loss, and the indicators for emergent interventions.
Tension pneumo-orbitum following facial trauma is rarely reported. We present a case of orbital compartment syndrome (OCS) in an elderly woman who sustained an orbital floor fracture and required emergent lateral canthotomy to preserve vision.
Case
A 76-year-old woman presented to the ED for evaluation of pain, swelling, and loss of vision in the right eye. She said she had been sitting in a chair tying her shoes when she lost her balance and fell forward, striking her head and the right side of her face against the floor. She experienced no loss of consciousness and denied any neck pain, jaw pain, or dizziness. She also denied any chest pain, shortness of breath, weakness, or loss of function in either her arms or legs. She did, however, note a small nosebleed that had stopped before she arrived at the ED. The patient’s primary complaint was a possible nasal bone fracture.
Her medical history was significant for hypertension and coronary artery disease. Her medications include amitriptyline, an antihistamine, aspirin, clopidogrel, diltiazem, folic acid, furosemide, hydralazine, levothyroxine, prednisone, and zolpidem. She stated that she was allergic to amoxicillin and sulfa drugs.
The patient’s vital signs at presentation were: blood pressure (BP), 193/82 mm Hg; heart rate, 71 beats/minute; respiratory rate, 16 breaths/minute; and temperature, 97°F. She was alert, oriented, and in no distress. Her head and neck examination showed no scalp lacerations or swelling. There was, however, significant swelling and ecchymosis around the right eye and swelling and ecchymosis around the nose, with dried blood in both nares. No septal hematoma was present. The patient had tenderness to palpation over the infraorbital area and nose. No gross facial instability was present, and Battle sign was not appreciated. No jaw or dental abnormalities were noted.
The patient’s right pupil was fixed and dilated, and she could not perceive light. She did have upward and lateral movement of the eye, but was unable to look down. A minimal amount of proptosis was noted. Her intraocular pressure (IOP) was elevated at 54 mm Hg (normal range, 10-20 mm Hg). The remainder of the examination, including the neurological examination, was unremarkable.
The patient received emergent head and facial computed tomography (CT) scans. The head CT showed no acute intracranial hemorrhage, mass, or infarct. The facial CT was read as a right orbital floor fracture with intraorbital air, and a right maxillary sinus hematoma. Laboratory evaluation revealed a hematocrit of 38% and a platelet count of 544,000/mcL (normal range, 150,000-450,000/mcL). The prothrombin time was 10.9 seconds (normal range, 11-13.5 seconds); the international normalized ratio was 0.8 (normal range, 0.8-1.1); and the partial thromboplastin time was 22.5 seconds (normal range, 25-35 seconds).
Because the patient was at risk for permanent visual impairment due to increased IOP from the injury, a lateral canthotomy was immediately performed. A small amount of air was released, and the proptosis was notably reduced.
At this point, the ophthalmologist arrived and used an 18-gauge needle to explore the retrobulbar space. Two pockets of air were released, which markedly reduced the tactile pressure of the globe. Repeat tonography of the globe was 28 mm Hg. The wound was left open to drain, and the patient was started on azithromycin. She was discharged home to follow up with ophthalmology.
The patient presented to the ED 2 months later for an unrelated condition. At that time, she reported a complete return of her vision with no deficits and no noticeable scarring around the eye.
Discussion
The orbit is an enclosed space, bordered by bone laterally and posteriorly—the orbital septa superiorly and inferiorly, and the globe anteriorly.3 The lateral canthus is a combined tendon-ligament that helps attach the tarsal plates of the lids and the orbicularis oculi muscles to the lateral orbital wall and zygoma, which forms the posterior orbital wall.3,4 The lateral canthal tendon is located beneath the lateral canthus and is comprised of the inferior and superior crus, which attaches to the inner aspect of the lateral orbital wall, forming a structure called Whitnall’s tubercle.3,4
Other than globe injuries, the most common findings in patients with orbital trauma are periocular lacerations (96%), orbital fractures (16%), and retrobulbar hemorrhage (8%).5 The most common cause of retrobulbar hemorrhage is ocular trauma, but it is also observed in facial fractures, orbital surgery, retrobulbar injections, venous anomalies, atherosclerosis, intraorbital aneurysm of the ophthalmic artery, lacerated ophthalmic artery, hypertension, hemophilia, leukemia, von Willebrand disease, and straining.3,6,7
In retrobulbar hemorrhage, an increased pressure in the orbital space can lead to optic nerve compression and vascular compromise.6 Important alternative diagnoses to consider include orbital cellulitis, orbital fracture, and globe rupture.3 Retrobulbar hemorrhage should be suspected in the clinical setting of exophthalmos, proptosis, diffuse subconjunctival hemorrhage, pain, visual loss or diplopia, periorbital edema, partial or complete ophthalmoplegia, resistance to retropulsion, increased IOP, a blanched ophthalmic artery on funduscopic examination, and an afferent pupillary defect.3,4,8,9 Less commonly, periorbital crepitus and infraorbital hypoesthesia can be appreciated.3
If a patient with a retrobulbar hemorrhage is experiencing diminished vision, an emergent lateral canthotomy should be attempted. Retrobulbar hemorrhage can be difficult to diagnose in the setting of trauma. There can be damage to the optic nerve with associated edema and vision loss that is not associated with a retrobulbar hemorrhage and does not require a lateral canthotomy.3,7 A dedicated CT scan of the orbits can aid in the diagnosis, but treatment should not be delayed.8
Patients with retrobulbar hemorrhage may initially present to the ED with intact visual acuity, but as the pressure behind the globe increases, vision will diminish.3 Although the medical literature has not established a definitive timeframe, it is believed that permanent visual compromise develops between 1 to 3 hours after ischemia develops.6 Animal studies show that visual loss due to central retinal artery ischemia may be reversible up to 100 minutes.3
Not all cases of retrobulbar hemorrhage are associated with vision loss. In patients without diminished vision, conservative treatments such as bed rest, elevation of the head of the bed, ice packs, analgesia, lowering BP, and sedatives should be attempted first.5 Acetazolamide and mannitol can also be considered in consultation with an ophthalmologist.
Pneumo-orbitum
The presence of pneumo-orbitum should alert the clinician to either a communication with a paranasal sinus, a gas-forming organism, or (rarely) Munchausen syndrome.10 Unlike most case presentations, most causes of pneumo-orbitum do not involve OCS and are self-limited.11 Traumatic pneumo-orbitum without OCS has been reported in the literature.12-15 However, traumatic tension pneumo-orbitum is rare.12-16 One case report involved an elderly man with an orbital floor fracture who developed recurrent tension pneumo-orbitum after blowing his nose while intoxicated.12 Another case involved a boy with tension pneumo-orbitum that required surgical decompression.16
In a patient who has experienced trauma, the combination of proptosis, elevated IOP, and vision loss likely represent a retrobulbar hematoma or OCS. A lateral canthotomy can help relieve IOP from either condition.17,18 Orbital compartment syndrome can be caused by edema, emphysema, and caroticocavernous fistula, leading to increased orbital pressure and decreased perfusion.17,18
In a review of 10 trauma patients with OCS, all cases were intubated due to the severity of the head trauma, and all had OCS due to edema.17 In a review of eight trauma patients with OCS, all had eye pain, reduced visual acuity, and proptosis.18 Most of the patients had periorbital edema, ophthalmoparesis, a relative afferent pupillary defect (as compared to a fixed and dilated pupil), and chemosis.18,19 All of the patients with OCS required cantholysis or a lateral canthotomy.18
Lateral Canthotomy
Although EPs rarely perform lateral canthotomy, knowledge of this procedure is important, because it can prevent vision loss in the appropriate clinical setting. To perform a lateral canthotomy, the area around the affected eye is cleaned with saline irrigation.4 One percent or 2% lidocaine with epinephrine is then injected into the lateral canthus of the affected eye.4,10 A straight hemostat is applied between the upper and lower lids, producing a crush injury along the site of local anesthesia for 1 to 2 minutes.3,4,10 This is done to reduce the risk of bleeding by devitalizing the tissue.4 Straight scissors are then used to make a 1-cm horizontal incision from the lateral canthal tendon to the lateral orbital rim.4 This initial incision exposes the orbicularis muscle, orbital septum, palpebral conjunctiva, and an area called Eisler’s pocket that sits anterior to the lateral canthal tendon.3
Cantholysis can then be performed by blunt dissection.10 The inferior crus of the lateral canthus is identified either visually or by palpation, and a 1- to 2-cm inferior-posterior cut of the inferior crus accomplishes the lateral canthotomy.3-4 After cutting the inferior crus, the lower lid should be pulled away easily, and if this does not occur, repeated attempts at cutting the inferior crus should be made.3 Pulling the lower eyelid down and away from the lateral orbital rim separates the skin and conjunctiva, aiding in visualization.4
After cutting the inferior crus, only a small amount of blood or air typically is expressed, but this is usually enough to prevent vision loss.3 When the procedure is performed correctly, the practitioner should be able to palpate a difference in the pressure of the globe, and tonography will show a reduced IOP. If the ocular pressure is still significantly elevated, the physician can proceed to cut the superior canthus of the lateral canthal tendon in a manner similar to cutting the inferior crus of the tendon.4 After the procedure is performed, urgent ophthalmologic consultation is required.
The risks of performing a lateral canthotomy include mechanical injury, hemorrhage, and infection.4 The incision from a lateral canthotomy generally does not need suturing and will heal without significant scarring.4 If the scissors are aimed superiorly instead of inferiorly for the inferior crus of the lateral canthal tendon, there is risk of injuring the levator aponeurosis leading to ptosis, as well as a small risk of injury to the lacrimal gland and lacrimal artery.3
Conclusion
Our patient demonstrates a case of traumatic OCS, a vision-threatening medical condition that requires rapid diagnosis and lateral canthotomy to lower IOP and reduce the risk of permanent vision loss. While an orbital CT scan may assist in confirming the diagnosis, treatment of IOP should not be delayed.
1. McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2001 Emergency Department Summary. Advance Data from Vital Health and Statistics; No. 335. https://www.cdc.gov/nchs/data/ad/ad335.pdf. Accessed July 22, 2016.
2. Knoop KJ, Dennis WR. Eye trauma. In: Wolfson AB, Hendy GW, Hendy PL, et al (eds). Harwood-Nuss’ Clinical Practice of Emergency Medicine. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
3. Vassallo S, Hartstein M, Howard D, Stetz J. Traumatic retrobulbar hemorrhage: emergent decompression by lateral canthotomy and cantholysis. J Emerg Med. 2002;22(3):251-256.
4. Roberts JR, Hedges JR (eds). Clinical Procedures in Emergency Medicine, 4th ed. Philadelphia, PA: Saunders; 2004.
5. Hatton MP, Thakker MM, Ray S. Orbital and adnexal trauma associated with open-globe injuries. Ophthal Plast Reconstr Surg. 2002;18(6):458-461.
6. Suner S, Simmons W, Savitt DL. A porcine model for instruction of lateral canthotomy. Acad Emerg Med. 2000;7(7):837-838.
7. Goodall KL, Brahma A, Bates A, Leatherbarrow B. Lateral canthotomy and inferior cantholysis: an effective method of urgent orbital decompression for sight threatening acute retrobulbar hemorrhage. Injury. 1999;30(7):485-490.
8. Gerbino G, Ramieri GA, Nasi A. Diagnosis and treatment of retrobulbar haematomas following blunt orbital trauma: a description of eight cases. Int J Oral Maxillofac Surg. 2005;34(2):127-131.
9. Machado RA, Silveira RL, Borges HO, Filho AM, de Oliveira GM. Retrobulbar hemorrhage: A case report. J Contemp Dent Pract. 2006;7(2):130-136.
10. Winans JM, House LR, Robinson HE. Self-induced orbital emphysema as a presenting sign of Munchausen’s syndrome. Laryngoscope. 1983;93(9):1209-1211.
11. Zimmer-Galler IE, Bartley GB. Orbital emphysema: case reports and review of the literature. Mayo Clin Proc. 1994;69(2):115-121.
12. Ahnood D, Toft PB. Recurrent orbital compartment syndrome caused by a blow-out fracture and accumulation of air; management by orbital punctures. Acta Ophthalmol. 2012;90(12):199-200.
13. Martin PW, Williams AC. Supraorbital emphysema: report of a case. J Oral Surg. 1972;30(12):901-902.
14. Per BL, Sanders BB. Post-traumatic intraorbital pneumatocele--a rare case of unilateral exophthalmos. Br J Radio. 1971;44(519):214-215.
15. Haller ML, Brackup AH, Shiffman F. Intraorbital aerocele. Arch Ophthalmol. 1980;98(9):1612-1613.
16. Chaudhry IA, Al-Amri A, Shamsi FA, Al-Rashed W. Visual recovery after evacuation of orbital emphysema. Orbit. 2007;26(4):283-285.
17. Perry M. Acute proptosis in trauma: retrobulbar hemorrhage or orbital compartment syndrome—does it really matter? J Oral Maxillofac Surg. 2008;66(9):1913-1920.
18. Sun MT, Chan WO, Selva D. Traumatic orbital compartment syndrome: importance of the lateral canthotomy and cantholysis. Emerg Med Australas. 2014;26(3):274-278.
19. Belliveau MJ, Johnson D. Orbital compartment syndrome after head trauma. Lancet Neurol. 2015;14(2):136-137.
1. McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2001 Emergency Department Summary. Advance Data from Vital Health and Statistics; No. 335. https://www.cdc.gov/nchs/data/ad/ad335.pdf. Accessed July 22, 2016.
2. Knoop KJ, Dennis WR. Eye trauma. In: Wolfson AB, Hendy GW, Hendy PL, et al (eds). Harwood-Nuss’ Clinical Practice of Emergency Medicine. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
3. Vassallo S, Hartstein M, Howard D, Stetz J. Traumatic retrobulbar hemorrhage: emergent decompression by lateral canthotomy and cantholysis. J Emerg Med. 2002;22(3):251-256.
4. Roberts JR, Hedges JR (eds). Clinical Procedures in Emergency Medicine, 4th ed. Philadelphia, PA: Saunders; 2004.
5. Hatton MP, Thakker MM, Ray S. Orbital and adnexal trauma associated with open-globe injuries. Ophthal Plast Reconstr Surg. 2002;18(6):458-461.
6. Suner S, Simmons W, Savitt DL. A porcine model for instruction of lateral canthotomy. Acad Emerg Med. 2000;7(7):837-838.
7. Goodall KL, Brahma A, Bates A, Leatherbarrow B. Lateral canthotomy and inferior cantholysis: an effective method of urgent orbital decompression for sight threatening acute retrobulbar hemorrhage. Injury. 1999;30(7):485-490.
8. Gerbino G, Ramieri GA, Nasi A. Diagnosis and treatment of retrobulbar haematomas following blunt orbital trauma: a description of eight cases. Int J Oral Maxillofac Surg. 2005;34(2):127-131.
9. Machado RA, Silveira RL, Borges HO, Filho AM, de Oliveira GM. Retrobulbar hemorrhage: A case report. J Contemp Dent Pract. 2006;7(2):130-136.
10. Winans JM, House LR, Robinson HE. Self-induced orbital emphysema as a presenting sign of Munchausen’s syndrome. Laryngoscope. 1983;93(9):1209-1211.
11. Zimmer-Galler IE, Bartley GB. Orbital emphysema: case reports and review of the literature. Mayo Clin Proc. 1994;69(2):115-121.
12. Ahnood D, Toft PB. Recurrent orbital compartment syndrome caused by a blow-out fracture and accumulation of air; management by orbital punctures. Acta Ophthalmol. 2012;90(12):199-200.
13. Martin PW, Williams AC. Supraorbital emphysema: report of a case. J Oral Surg. 1972;30(12):901-902.
14. Per BL, Sanders BB. Post-traumatic intraorbital pneumatocele--a rare case of unilateral exophthalmos. Br J Radio. 1971;44(519):214-215.
15. Haller ML, Brackup AH, Shiffman F. Intraorbital aerocele. Arch Ophthalmol. 1980;98(9):1612-1613.
16. Chaudhry IA, Al-Amri A, Shamsi FA, Al-Rashed W. Visual recovery after evacuation of orbital emphysema. Orbit. 2007;26(4):283-285.
17. Perry M. Acute proptosis in trauma: retrobulbar hemorrhage or orbital compartment syndrome—does it really matter? J Oral Maxillofac Surg. 2008;66(9):1913-1920.
18. Sun MT, Chan WO, Selva D. Traumatic orbital compartment syndrome: importance of the lateral canthotomy and cantholysis. Emerg Med Australas. 2014;26(3):274-278.
19. Belliveau MJ, Johnson D. Orbital compartment syndrome after head trauma. Lancet Neurol. 2015;14(2):136-137.

The Orlando Nightclub Shooting: Firsthand Accounts and Lessons Learned
Orlando Regional Medical Center (ORMC) is an urban, academic, Level 1 trauma center with an ED that treats in excess of 85,000 patients each year. There are more than 4,500 annual trauma admissions, including penetrating and blunt mechanism injuries. We have a 3-year emergency medicine (EM) residency program, originally established in 1986, that now has 14 residents per year. The events that we experienced on the early morning of June 12, 2016 were tragic and unexpected and tested our community, our teams, and our organization. The following is a description of activity perspectives, personal reflections and feelings, and important lessons learned from which other EDs may benefit.

Prehospital/Rescue Period
The prehospital approach to a mass-casualty incident (MCI) caused by gunfire has changed significantly over the last decade, with lessons gleaned from the experience of military and domestic attacks. The Orange County (Florida) Emergency Medical Services (EMS) System, including the agencies involved in the response to the June 12, 2016 Pulse nightclub shooting incident (Orlando Fire Department, Rural Metro Ambulance, and Orange County Fire Rescue), have trained specifically on the evolving priorities during an active shooter incident. This includes targeted hemorrhage control, swift extrication, minimal interventions, and immediate transport to the appropriate receiving center. In June 2015, 1 year prior to the Pulse nightclub shooting, a protocol variance was written by medical directors, explaining that “EMS providers may engage in initial patient care with only the supplies deemed absolutely necessary for rapid evaluation and removal into a safe triage zone.” This variance applies when there is an active shooter scenario. In addition, in 2014, 2015, and 2016, we conducted large scale, multiagency community exercises, encompassing shooting/active shooter scenarios and drills.
On June 12, 2016, EMS units were on scene of the Pulse nightclub in downtown Orlando less than 5 minutes after shooting began. It became immediately obvious that additional resources would be necessary. Soon after the incident, an MCI alert was activated from the Orlando Fire Department Communications Center, utilizing a software system to notify area hospitals and the medical directors that up to 20 patients had been shot, and requesting status on bed availability. Christopher L. Hunter, MD, PhD, one of our associate EMS medical directors, was working in the ED at a hospital several miles away from the incident and began coordinating efforts to distribute patients to the appropriate destination via radio and phone communication between the scene, the communications center, and the trauma center.
On scene, a group of law enforcement officers were engaging the shooter while others assisted in extracting victims from the club and surrounding area. Injured victims were brought to a casualty collection point, under cover, across the street and were transported as units became available. Initially, law enforcement vehicles and ambulances would make the two-block drive from the scene to ORMC carrying as many patients as they safely could, and return immediately after offload. Per previous training, minimal interventions were performed, and unlike standard procedure, EMS could offer no prearrival report to the hospital. The decision was made to triage only patients meeting Florida’s state trauma alert criteria to ORMC, and funnel other patients to nearby nontrauma centers. Dr Hunter attempted to notify the hospitals of patients as they were transported off the scene; however, the extremely short transport times made this process difficult.
Over the course of the incident, on-scene commands designated a casualty collection point, a transport unit staging area, and a hospital liaison. Emergency medical service responders cooperated with law enforcement to transport injured patients throughout the response. By the end of the event, nearly 100 EMS providers utilizing dozens of vehicles had responded to the scene.
The ED Period
The overnight shift of Saturday, June 11 was slower than usual in the ORMC ED, and triage housed the typical Saturday-night complaints. One of our mid-level providers, Brian Clayton, ARNP, worked in the fast track pod treating lower acuity illnesses, while the four senior residents discussed who might receive the honor of leaving early. Even the senior attending, Gary A. Parrish, MD, wrapped up his patients and was ready to leave right on time. The 11:00 pm to 7:00 am attending, Kathryn J. Bondani, MD, was looking forward to an easy shift with four graduating senior residents. We had just called in an order from a popular nearby sandwich shop when suddenly, a slew of police cars flew past the hospital—not unusual given our proximity to downtown. The radio squawked “Multiple gunshots wounds en route.” Someone said “a club downtown got shot up.” In anticipation of multiple patient arrivals, resident Amanda M. Stone, MD, and the attending hurried to the trauma/ressuscitation bay. Another resident, Amanda F. Tarkowski, MD, called the trauma attending to rally his team downstairs, informing him that “A club downtown has a shooter and we have multiple patients with a 2-minute ETA.” Multiple gunshot wounds (GSWs) at once is not unusual for our Level 1 trauma center.
The first patient arrived shortly after 2:00 am and had multiple GSWs to the abdomen, but was awake and talking. He was mildly tachycardic, but his blood pressure (BP) was stable. We all gaped at the fist-sized wound on his back—some of us had never seen a GSW like this before. It was apparent that he needed to go to the operating room, but before preparations could be made, three more patients rolled into the ED. Instead of our usual organized, methodical EMS report, these patients were dropped off by a police pickup truck and rolled in on our own stretchers by nurses and technicians. Soon, all six of our trauma bays were filled with critical patients. Christopher H. Ponder, MD, recalled, “I heard an overhead page for ‘all available trauma nurses to the trauma bay’ shortly followed by a more concerned-sounding ‘all available staff to the trauma bay.’” All four senior EM residents, both EM attendings, the trauma attending, four trauma residents, multiple ED nurses, technicians, and various ancillary staff quickly descended on the patients. Chest tubes were placed, and multiple patients were intubated. Several thoracotomies were performed at the initial point when the team was unaware of the exact number of patients who would ultimately follow. Blood bags were hung and tranexamic acid was administered liberally. Unfortunately, some of these initial attempts were unsuccessful, as the first wave contained the most critically injured patients.
We barely had time to reflect on the dead as more patients filled the hallways. In the midst of all of this, triage decisions came quickly—awake and talking patients with an acceptable BP were moved out of the trauma bay in favor of less stable patients. Intubation and chest-tube placement decisions were made instantly. There was no time for routine X-rays or laboratory evaluation. Nurses, technicians, and doctors crowded the trauma bay desperately trying to stabilize the critically injured. Vital signs were taken manually. Dr Ponder called his colleague Thomas N. Smith, MD, who was also a graduating senior EM resident, and who happened to be staffing the children’s ED across the street that night. “Is there any way you can make it over here right now?” he shouted into the phone. Dr Smith quickly grabbed several trauma supplies and hitched a ride with security to the ORMC ED to assist. He was confronted with the scene of the previously mentioned “first wave” and grabbed an ultrasound machine to help triage these unfortunate patients. In addition to Dr Smith, unit clerks continued making calls to additional off-duty medical, nursing, and support staff. Critical care attendings and fellows responded from upstairs to assist in the ED. The Hospital Incident Command System (HICS) was initiated to provide hospital and corporate coordination of services. Timothy B. Bullard, MD, another EM attending physician and medical staff director of HICS, was en route to the ED to assist in the response.
Amidst the overwhelming mass of mortally and critically wounded patients, we were told stories of terror from just down the road. The sense of horror was almost contagious, and we all wondered if the violence would spread to the hospital.
About an hour into the ordeal, we heard another page overhead “Code Silver, ED Triage. Code Silver, ED Triage.” Everyone in the trauma bay froze. We heard someone shout from the hallway “Shots fired in triage!” After a few seconds, those nearest the trauma bay doors pushed them shut. One of the trauma surgeons shouted, “Keep caring for your patients, push the portable X-ray machines in front of the doors.” That is exactly what happened, and we worked in the barricaded trauma room for the longest few minutes of the night. We would later learn that this report was false, but fearing for our own lives as well as the lives of our patients is an experience that few, if any, of us had previously been through. The fact that we continued to work in such a situation illustrates everyone’s dedication to their patients and mission.
After the first wave of patients, it was clear that reassessing patients was now our greatest challenge. There were multiple patients with stable vital signs but who had GSWs to the abdomen, pelvis, and thorax and required surgery. Having realized that the ultrasound machine and focused assessment with sonography for trauma (FAST) examinations were the most practical rapid imaging modality, Drs Tarkowski, Ponder, and Smith grabbed the machine and went from room to room repeating the FAST examinations, vital signs, and assessments for missed wounds. A portable computer allowed us to order X-ray orders for patients with extremity wounds. Several patients who initially had negative FASTs had a repeat examination that was positive for free fluid. The operating room triage list shuffled based on these examinations.
At this point, there seemed to be a never-ending list of “Doe” names on the electronic medical record (EMR) tracking board. Tracking the location of patients was a dynamic process, and updating the tracking board was difficult. Patients were continually cycled in and out of the trauma bay, shuffled in and out of treatment rooms, lined up in the hallways, and transported up to the intensive care unit (ICU). Some of those “Doe” names belonged to patients who had succumbed to their injuries. Some patients had empty, bloody charts next to them on their stretcher. Every patient had a wristband. Dr Tarkowski improvised a rapid documentation system using quarter sheets of scrap paper that were taped either to the stretcher or door with a patient name, brief list of injuries, FAST examination result, pending tests, and medications given. This system was an efficient way of identifying which patients had been evaluated, what had been done, and what was pending.
While we were “rounding” on our patients, down the street, law enforcement had broken down the club’s wall, and a second wave of patients began to arrive. Two residents completed the secondary evaluations while the other three resuscitated new patients. The second wave seemed like a repeat of the first. Several extremity-only injuries were triaged directly to the hallways to be seen by the two residents outside of the trauma bay. By this time, the orthopedic surgery service had come down to the ED and was washing out wounds, splinting, and making plans for surgery. The internal medicine service and the medical critical care team were helping reassess patients as well.
There were many emotional moments. Dr Ponder remembered, “One of the first few patients I saw was pulseless, and as I went to start chest compressions, I was stopped by a trauma surgeon who said, ‘He’s gone, focus on the ones we can help.’ That’s when I realized the gravity of our situation. For almost 2 hours, each resident cycled through patients.” Dr Stone recounted, “I just went down the line of patients, from head of the bed to head of the bed, some patients still on EMS stretchers, intubating many of them. It was surreal to see that many severely injured in one place.” Tory L. Weatherford, MD, recalled, “It was controlled chaos. My training kicked in, and it became about just trying to do anything possible to help.”
Dr Bondani, the overnight attending, said she does not remember many specifics from the event. “Faces and injuries blurred together. I remember looking in one young man’s eyes and telling him, ‘We are going to help you, just hang in there,’ and telling another panicking woman, ‘You’re talking, you can feel pain, you’re alive. Calm down.’ It was organized chaos as we swept from patient to patient moving as quickly as possible. Your training kicks in and you do what needs to be done in the moment.”
We were fortunate to have the EM team we did, and to be in the place that we were. On duty, we had five senior graduating residents, essentially with attending-level skills and training, who had been together since day one. “We gave everything we had; there was no time to stop. We went where our hands could be helpful—it didn’t matter if it was your traditional role or not,” said Dr Weatherford.
Dr Tarkowski remembered what it was like leaving the walls of the ED later that morning. “Leaving the hospital didn’t feel like a success. We knew the work we did was good, that we did everything we could, but it didn’t feel like it. It felt heavy. It felt empty.” Afterward, the emotional toll set in. We gathered up the names of the deceased and looked at a status board littered with “Doe” names, and we tried hard not to break down at the violence and the pain we witnessed.
Immediate Recovery Period (Prehospital Setting)
In the aftermath of the initial rescue operation, stabilization of injured victims, and demobilization of resources, a second “event” unfolded—hundreds of family members flooded to ORMC looking for unaccounted loved ones. At this point, there were dozens of deceased and critically injured patients who remained unidentified, and addressing the needs of both the victims and the families was becoming overwhelming. With the cooperation of federal, state, county, city, and private resources, a family reunification center (FRC; a family staging area/family reception center) was created and managed initially within the hospital. At this site, grief counselors, victim advocates, law enforcement and medical examiner’s officials, hospital chaplains, and translators gathered with the loved ones of those missing to synchronize efforts to identify and reunite them. The Emergency Operations Center quickly created a telephone hotline and Web site to guide those in need to this resource. Food and housing for those in need were provided by the generosity of our community—which cannot be overstated in the wake of this tragedy. As days passed, the FRC transitioned to a new location as the Orlando United Assistance Center, and will continue to serve as a navigation point for those who are and will be affected by the event for months to come.
Hospital Incident Command System
The HICS was activated shortly past 3:00 am, just after the initial wave of victims flooded our ED and the gravity of the situation became apparent. The ED and trauma services were already near full staff due to timing, rapid response, and communication between the traumatologists, as well as a bit of luck. Because of the time of the disaster, our normal notification process for incident command and all personnel was severely limited. In retrospect, this turned out to be a blessing. While everyone who normally would respond to HICS was not available, individuals serving in key positions were reached by personal phone calls and were on-site quickly. One of the main functions of HICS is to control the internal chaos that arises when a disaster occurs and all personnel want to assist in some manner. We have spent hours during drills crafting communications that target key personnel necessary to meet the mission, while controlling well-intentioned but unnecessary personnel. In our drills, this is not an issue because everyone knows the exercise is not reality; however, in a real disaster, everyone wants to help. This was confirmed by the guilt that so many of our team members expressed at not being involved that Sunday.
With an initial skeleton crew in incident command, it was easy to focus on the immediate needs of patient care. The strong leadership and cool heads of our incident command leadership led to rapid role definition and responsibility, and set forth an easy path for execution. Hospital command personnel adapted their usual roles and performed functions and assignments as needed. Many HICS staff had direct face-to-face contact with frontline providers in the ED and other vital areas. This was possible because of the close proximity of the hospital command headquarters to the ED. The need for additional resources was rapidly identified, and the hospital command leaders assumed direct responsibility for procuring them instead of delegating. A great example of this was when Orlando Health’s chief executive officer and chief operating officer went to our nearby hospitals to gather additional chest tubes after learning that we were running in short supply. Their main responsibilities lay ahead of them, and they were willing to help in any manner they could at the time. Some of the medical personnel were able to switch roles and pitch in to treat the second wave of victims that arrived at around 5:00 am.
As the flow of victims to the ED subsided and order began to be restored, HICS shifted gears and took on a much broader role: coordinating activities with multiple agencies, including local law enforcement, the Federal Bureau of Investigation, news media, and an array of patient and family services. Again, the timing of this tragic event allowed the needs and functions of our hospital command to concentrate the focus in a more structured manner than might have been possible during regular operational hours.
Lessons Learned and Recommendations
As with any MCI, it is important to perform after-incident debriefings to reflect upon the prehospital, ED, and hospital care to assess for areas in need of improvement. Obviously, depending on the number and type of patients who are received and the resources available at the institution, such events can stress EDs that are already at or above their capacity. At the time of this writing (less than 2 months after the incident), although we are still in the early stages of our post-incident debriefing process, we offer the following suggestions and recommendations that we believe will be a benefit to other institutions faced with similar challenges.
Dedicated Disaster Preparedness Program
Depending on the size of the institution and whether or not it is a trauma-receiving center, it is vitally important to have a team of individuals dedicated to the development and maintenance of a disaster readiness program. Eric Alberts, manager of Emergency Preparedness at Orlando Heath, emphasized the need to harness and leverage preparedness efforts and relationships with community partners, law enforcement, and EMS. In addition, he noted that these trained individuals can provide education and coordination for mass-casualty drills, assist in developing and maintaining policies and protocols, and coordinate with hospital incident command during actual events.
Practice, Practice, Practice
In order for medical staff, nursing staff, and support personnel to understand their roles and responsibilities if an MCI occurs, they must practice simulated drills. Tabletop and full-scale emergency intake drills, with a range of scenarios occurring at different times of the day and night, will improve teamwork and coordination. At least once a year, a large, full-scale community exercise that involves scene casualty collection points, law enforcement and EMS involvement, multiple EDs, and hospital-wide integration will educate staff members on their duties. There should be enough patients in these drills to stress the entire system—both ED and in-hospital. Physician involvement in these exercises is crucial. In March 2016, a full-scale community exercise was performed in the Central Florida area in which more than 500 volunteers, 50 agencies, and 15 hospitals participated. A segment of that exercise involved an active shooter impersonating a patient brought to the ED. We feel this recent exercise, and others like it, were helpful in managing our actual mass casualty event.
Notification
When the shootings at the Pulse nightclub started, we were advised that there might be as many as 20 victims, but over the next few hours, we received more than twice as many injured patients. In any scenario where it is felt additional ED resources and personnel are needed, it is advantageous to begin the notification process as early as possible. Ideally, there are redundant methods in place to notify in-house and off-duty personnel, preferably in a multilayered system of electronic and voice communications that provides feedback as to staff availability. During daytime hours, it is easier for off-duty staff to learn of an event through news and social media. However, during early morning hours, such as when these shootings occurred, it may be difficult to notify sleeping staff that they are needed. With the trend of using mobile devices instead of landline phones, and with the ability to silence those devices during nighttime sleep hours, it has become increasingly difficult to “break through” the silence. In our event, group e-mail notifications were activated, but individual phone calls were also required. Initially, some calls to staff went to voice mail rather than being
answered directly.
Communication
Communication is an area of opportunity for improvement in almost any mass-casualty event. Redundant methods of electronic, voice, telephone, and radio communications are crucial for personnel to coordinate efforts. It is imperative that HICS and ED personnel receive updates about events on the scene and the status of potential incoming patients. An infrastructure of communications is paramount for the coordination that is needed between prehospital, ED, and in-house resources.
Throughput
Facilitating ED and hospital throughput and improving operational efficiencies are regular topics of discussion in most busy EDs. However, when it becomes necessary to intake large numbers of patients in an ED within a short period of time, the need to move patients out of the department intensifies. In many cases, to continue intake of patients, it will be necessary to quickly find areas outside of the ED—such as operating rooms, ICUs, and general floors—to transport patients to. At our facility, we normally have two operating rooms staffed throughout the night for traumas. On the night of the shootings, a total of six operating rooms were activated quickly to manage the penetrating injuries of these patients. Previously admitted medical patients were retrieved by in-house nursing staff to free up ED beds.
Media
It is important to recognize the intense social, print, online, and television media exposure that will occur with such tragedies, and have personnel and systems in place to manage it. The Pulse nightclub is located only a few short blocks south of ORMC, and the majority of all injured patients, including those with the most severe injuries, presented to our facility. As a result, the intense media coverage at our hospital physically overlapped the intense media coverage at the scene. Nearby businesses were shut down, access to several main thoroughfare roads were blocked, and some individuals mistakenly thought the hospital was closed. Our media relations department felt the most efficient way to manage information dissemination was to hold a “presser”—a press conference with a few of the health professionals involved in the care of the patients. The press conference helped to relieve some of the media presence and pressure, and provided welcomed transparency to the community.
Expect the Unexpected
Even when physicians and staff conduct regular training exercises and are familiar with policies and procedures, the controlled chaos that is typical of a true mass-casualty event will likely result in some unexpected occurrences. After injured patients began arriving at our ED, during a period when patient influx and medical care was intense, there was a brief time when we were concerned an active shooter was also in our ED. Since the mass shootings were only a few blocks from the ED, and we did not know the scope or number of shooters, it was a reasonable assumption that a perpetrator could present to the ED as a patient or active shooter. During an event such as this, it is the practice at ORMC to have security officers place the facility on lockdown; however; the added concern that an active shooter was physically present in the ED required additional law enforcement officers to methodically search the entire facility until the threat of a shooter was eliminated. Although this did not directly impact patient care, it did create another level of complexity and stress to the already challenging situation.

Emotional Impact
One should not underestimate the emotional impact of a mass-casualty event. Emergency physicians and personnel are well equipped to manage illness, injury, and death. However, an event of this magnitude, with the number and manner of injuries and deaths that presented to our ED, along with the closeness to a scene of bloodshed where many young lives were taken in a senseless act of violence, will likely have a lasting impression on many staff members. Any institution encountering such an event should have behavioral health and support counselors readily available as soon as possible.
Conclusion
When patients present in truckloads, as they did in our ambulance bay in the early hours of June 12, an ED may be inundated with injured patients without notice or preparation. Teams need to trust their instincts, their training, and one another. It is unlikely that your normal ED practice patterns will be sufficient to take care of a large surge of patients, and you will need to turn to your ingenuity, creativity, and resourcefulness to do what you think is best to save the lives of as many patients as possible. As Sarah Duran, BSN, the trauma nurse who was working as the ED charge nurse the night of the shootings, stated, “I don’t think anyone can fully prepare for anything on the scale of what happened in Orlando, but with a good foundation of protocols in place, strong set of staff, constant vigilance, and great teamwork, any hospital can be successful in handling a mass casualty incident.”
Orlando Regional Medical Center (ORMC) is an urban, academic, Level 1 trauma center with an ED that treats in excess of 85,000 patients each year. There are more than 4,500 annual trauma admissions, including penetrating and blunt mechanism injuries. We have a 3-year emergency medicine (EM) residency program, originally established in 1986, that now has 14 residents per year. The events that we experienced on the early morning of June 12, 2016 were tragic and unexpected and tested our community, our teams, and our organization. The following is a description of activity perspectives, personal reflections and feelings, and important lessons learned from which other EDs may benefit.
Prehospital/Rescue Period
The prehospital approach to a mass-casualty incident (MCI) caused by gunfire has changed significantly over the last decade, with lessons gleaned from the experience of military and domestic attacks. The Orange County (Florida) Emergency Medical Services (EMS) System, including the agencies involved in the response to the June 12, 2016 Pulse nightclub shooting incident (Orlando Fire Department, Rural Metro Ambulance, and Orange County Fire Rescue), have trained specifically on the evolving priorities during an active shooter incident. This includes targeted hemorrhage control, swift extrication, minimal interventions, and immediate transport to the appropriate receiving center. In June 2015, 1 year prior to the Pulse nightclub shooting, a protocol variance was written by medical directors, explaining that “EMS providers may engage in initial patient care with only the supplies deemed absolutely necessary for rapid evaluation and removal into a safe triage zone.” This variance applies when there is an active shooter scenario. In addition, in 2014, 2015, and 2016, we conducted large scale, multiagency community exercises, encompassing shooting/active shooter scenarios and drills.
On June 12, 2016, EMS units were on scene of the Pulse nightclub in downtown Orlando less than 5 minutes after shooting began. It became immediately obvious that additional resources would be necessary. Soon after the incident, an MCI alert was activated from the Orlando Fire Department Communications Center, utilizing a software system to notify area hospitals and the medical directors that up to 20 patients had been shot, and requesting status on bed availability. Christopher L. Hunter, MD, PhD, one of our associate EMS medical directors, was working in the ED at a hospital several miles away from the incident and began coordinating efforts to distribute patients to the appropriate destination via radio and phone communication between the scene, the communications center, and the trauma center.
On scene, a group of law enforcement officers were engaging the shooter while others assisted in extracting victims from the club and surrounding area. Injured victims were brought to a casualty collection point, under cover, across the street and were transported as units became available. Initially, law enforcement vehicles and ambulances would make the two-block drive from the scene to ORMC carrying as many patients as they safely could, and return immediately after offload. Per previous training, minimal interventions were performed, and unlike standard procedure, EMS could offer no prearrival report to the hospital. The decision was made to triage only patients meeting Florida’s state trauma alert criteria to ORMC, and funnel other patients to nearby nontrauma centers. Dr Hunter attempted to notify the hospitals of patients as they were transported off the scene; however, the extremely short transport times made this process difficult.
Over the course of the incident, on-scene commands designated a casualty collection point, a transport unit staging area, and a hospital liaison. Emergency medical service responders cooperated with law enforcement to transport injured patients throughout the response. By the end of the event, nearly 100 EMS providers utilizing dozens of vehicles had responded to the scene.
The ED Period
The overnight shift of Saturday, June 11 was slower than usual in the ORMC ED, and triage housed the typical Saturday-night complaints. One of our mid-level providers, Brian Clayton, ARNP, worked in the fast track pod treating lower acuity illnesses, while the four senior residents discussed who might receive the honor of leaving early. Even the senior attending, Gary A. Parrish, MD, wrapped up his patients and was ready to leave right on time. The 11:00 pm to 7:00 am attending, Kathryn J. Bondani, MD, was looking forward to an easy shift with four graduating senior residents. We had just called in an order from a popular nearby sandwich shop when suddenly, a slew of police cars flew past the hospital—not unusual given our proximity to downtown. The radio squawked “Multiple gunshots wounds en route.” Someone said “a club downtown got shot up.” In anticipation of multiple patient arrivals, resident Amanda M. Stone, MD, and the attending hurried to the trauma/ressuscitation bay. Another resident, Amanda F. Tarkowski, MD, called the trauma attending to rally his team downstairs, informing him that “A club downtown has a shooter and we have multiple patients with a 2-minute ETA.” Multiple gunshot wounds (GSWs) at once is not unusual for our Level 1 trauma center.
The first patient arrived shortly after 2:00 am and had multiple GSWs to the abdomen, but was awake and talking. He was mildly tachycardic, but his blood pressure (BP) was stable. We all gaped at the fist-sized wound on his back—some of us had never seen a GSW like this before. It was apparent that he needed to go to the operating room, but before preparations could be made, three more patients rolled into the ED. Instead of our usual organized, methodical EMS report, these patients were dropped off by a police pickup truck and rolled in on our own stretchers by nurses and technicians. Soon, all six of our trauma bays were filled with critical patients. Christopher H. Ponder, MD, recalled, “I heard an overhead page for ‘all available trauma nurses to the trauma bay’ shortly followed by a more concerned-sounding ‘all available staff to the trauma bay.’” All four senior EM residents, both EM attendings, the trauma attending, four trauma residents, multiple ED nurses, technicians, and various ancillary staff quickly descended on the patients. Chest tubes were placed, and multiple patients were intubated. Several thoracotomies were performed at the initial point when the team was unaware of the exact number of patients who would ultimately follow. Blood bags were hung and tranexamic acid was administered liberally. Unfortunately, some of these initial attempts were unsuccessful, as the first wave contained the most critically injured patients.
We barely had time to reflect on the dead as more patients filled the hallways. In the midst of all of this, triage decisions came quickly—awake and talking patients with an acceptable BP were moved out of the trauma bay in favor of less stable patients. Intubation and chest-tube placement decisions were made instantly. There was no time for routine X-rays or laboratory evaluation. Nurses, technicians, and doctors crowded the trauma bay desperately trying to stabilize the critically injured. Vital signs were taken manually. Dr Ponder called his colleague Thomas N. Smith, MD, who was also a graduating senior EM resident, and who happened to be staffing the children’s ED across the street that night. “Is there any way you can make it over here right now?” he shouted into the phone. Dr Smith quickly grabbed several trauma supplies and hitched a ride with security to the ORMC ED to assist. He was confronted with the scene of the previously mentioned “first wave” and grabbed an ultrasound machine to help triage these unfortunate patients. In addition to Dr Smith, unit clerks continued making calls to additional off-duty medical, nursing, and support staff. Critical care attendings and fellows responded from upstairs to assist in the ED. The Hospital Incident Command System (HICS) was initiated to provide hospital and corporate coordination of services. Timothy B. Bullard, MD, another EM attending physician and medical staff director of HICS, was en route to the ED to assist in the response.
Amidst the overwhelming mass of mortally and critically wounded patients, we were told stories of terror from just down the road. The sense of horror was almost contagious, and we all wondered if the violence would spread to the hospital.
About an hour into the ordeal, we heard another page overhead “Code Silver, ED Triage. Code Silver, ED Triage.” Everyone in the trauma bay froze. We heard someone shout from the hallway “Shots fired in triage!” After a few seconds, those nearest the trauma bay doors pushed them shut. One of the trauma surgeons shouted, “Keep caring for your patients, push the portable X-ray machines in front of the doors.” That is exactly what happened, and we worked in the barricaded trauma room for the longest few minutes of the night. We would later learn that this report was false, but fearing for our own lives as well as the lives of our patients is an experience that few, if any, of us had previously been through. The fact that we continued to work in such a situation illustrates everyone’s dedication to their patients and mission.
After the first wave of patients, it was clear that reassessing patients was now our greatest challenge. There were multiple patients with stable vital signs but who had GSWs to the abdomen, pelvis, and thorax and required surgery. Having realized that the ultrasound machine and focused assessment with sonography for trauma (FAST) examinations were the most practical rapid imaging modality, Drs Tarkowski, Ponder, and Smith grabbed the machine and went from room to room repeating the FAST examinations, vital signs, and assessments for missed wounds. A portable computer allowed us to order X-ray orders for patients with extremity wounds. Several patients who initially had negative FASTs had a repeat examination that was positive for free fluid. The operating room triage list shuffled based on these examinations.
At this point, there seemed to be a never-ending list of “Doe” names on the electronic medical record (EMR) tracking board. Tracking the location of patients was a dynamic process, and updating the tracking board was difficult. Patients were continually cycled in and out of the trauma bay, shuffled in and out of treatment rooms, lined up in the hallways, and transported up to the intensive care unit (ICU). Some of those “Doe” names belonged to patients who had succumbed to their injuries. Some patients had empty, bloody charts next to them on their stretcher. Every patient had a wristband. Dr Tarkowski improvised a rapid documentation system using quarter sheets of scrap paper that were taped either to the stretcher or door with a patient name, brief list of injuries, FAST examination result, pending tests, and medications given. This system was an efficient way of identifying which patients had been evaluated, what had been done, and what was pending.
While we were “rounding” on our patients, down the street, law enforcement had broken down the club’s wall, and a second wave of patients began to arrive. Two residents completed the secondary evaluations while the other three resuscitated new patients. The second wave seemed like a repeat of the first. Several extremity-only injuries were triaged directly to the hallways to be seen by the two residents outside of the trauma bay. By this time, the orthopedic surgery service had come down to the ED and was washing out wounds, splinting, and making plans for surgery. The internal medicine service and the medical critical care team were helping reassess patients as well.
There were many emotional moments. Dr Ponder remembered, “One of the first few patients I saw was pulseless, and as I went to start chest compressions, I was stopped by a trauma surgeon who said, ‘He’s gone, focus on the ones we can help.’ That’s when I realized the gravity of our situation. For almost 2 hours, each resident cycled through patients.” Dr Stone recounted, “I just went down the line of patients, from head of the bed to head of the bed, some patients still on EMS stretchers, intubating many of them. It was surreal to see that many severely injured in one place.” Tory L. Weatherford, MD, recalled, “It was controlled chaos. My training kicked in, and it became about just trying to do anything possible to help.”
Dr Bondani, the overnight attending, said she does not remember many specifics from the event. “Faces and injuries blurred together. I remember looking in one young man’s eyes and telling him, ‘We are going to help you, just hang in there,’ and telling another panicking woman, ‘You’re talking, you can feel pain, you’re alive. Calm down.’ It was organized chaos as we swept from patient to patient moving as quickly as possible. Your training kicks in and you do what needs to be done in the moment.”
We were fortunate to have the EM team we did, and to be in the place that we were. On duty, we had five senior graduating residents, essentially with attending-level skills and training, who had been together since day one. “We gave everything we had; there was no time to stop. We went where our hands could be helpful—it didn’t matter if it was your traditional role or not,” said Dr Weatherford.
Dr Tarkowski remembered what it was like leaving the walls of the ED later that morning. “Leaving the hospital didn’t feel like a success. We knew the work we did was good, that we did everything we could, but it didn’t feel like it. It felt heavy. It felt empty.” Afterward, the emotional toll set in. We gathered up the names of the deceased and looked at a status board littered with “Doe” names, and we tried hard not to break down at the violence and the pain we witnessed.
Immediate Recovery Period (Prehospital Setting)
In the aftermath of the initial rescue operation, stabilization of injured victims, and demobilization of resources, a second “event” unfolded—hundreds of family members flooded to ORMC looking for unaccounted loved ones. At this point, there were dozens of deceased and critically injured patients who remained unidentified, and addressing the needs of both the victims and the families was becoming overwhelming. With the cooperation of federal, state, county, city, and private resources, a family reunification center (FRC; a family staging area/family reception center) was created and managed initially within the hospital. At this site, grief counselors, victim advocates, law enforcement and medical examiner’s officials, hospital chaplains, and translators gathered with the loved ones of those missing to synchronize efforts to identify and reunite them. The Emergency Operations Center quickly created a telephone hotline and Web site to guide those in need to this resource. Food and housing for those in need were provided by the generosity of our community—which cannot be overstated in the wake of this tragedy. As days passed, the FRC transitioned to a new location as the Orlando United Assistance Center, and will continue to serve as a navigation point for those who are and will be affected by the event for months to come.
Hospital Incident Command System
The HICS was activated shortly past 3:00 am, just after the initial wave of victims flooded our ED and the gravity of the situation became apparent. The ED and trauma services were already near full staff due to timing, rapid response, and communication between the traumatologists, as well as a bit of luck. Because of the time of the disaster, our normal notification process for incident command and all personnel was severely limited. In retrospect, this turned out to be a blessing. While everyone who normally would respond to HICS was not available, individuals serving in key positions were reached by personal phone calls and were on-site quickly. One of the main functions of HICS is to control the internal chaos that arises when a disaster occurs and all personnel want to assist in some manner. We have spent hours during drills crafting communications that target key personnel necessary to meet the mission, while controlling well-intentioned but unnecessary personnel. In our drills, this is not an issue because everyone knows the exercise is not reality; however, in a real disaster, everyone wants to help. This was confirmed by the guilt that so many of our team members expressed at not being involved that Sunday.
With an initial skeleton crew in incident command, it was easy to focus on the immediate needs of patient care. The strong leadership and cool heads of our incident command leadership led to rapid role definition and responsibility, and set forth an easy path for execution. Hospital command personnel adapted their usual roles and performed functions and assignments as needed. Many HICS staff had direct face-to-face contact with frontline providers in the ED and other vital areas. This was possible because of the close proximity of the hospital command headquarters to the ED. The need for additional resources was rapidly identified, and the hospital command leaders assumed direct responsibility for procuring them instead of delegating. A great example of this was when Orlando Health’s chief executive officer and chief operating officer went to our nearby hospitals to gather additional chest tubes after learning that we were running in short supply. Their main responsibilities lay ahead of them, and they were willing to help in any manner they could at the time. Some of the medical personnel were able to switch roles and pitch in to treat the second wave of victims that arrived at around 5:00 am.
As the flow of victims to the ED subsided and order began to be restored, HICS shifted gears and took on a much broader role: coordinating activities with multiple agencies, including local law enforcement, the Federal Bureau of Investigation, news media, and an array of patient and family services. Again, the timing of this tragic event allowed the needs and functions of our hospital command to concentrate the focus in a more structured manner than might have been possible during regular operational hours.
Lessons Learned and Recommendations
As with any MCI, it is important to perform after-incident debriefings to reflect upon the prehospital, ED, and hospital care to assess for areas in need of improvement. Obviously, depending on the number and type of patients who are received and the resources available at the institution, such events can stress EDs that are already at or above their capacity. At the time of this writing (less than 2 months after the incident), although we are still in the early stages of our post-incident debriefing process, we offer the following suggestions and recommendations that we believe will be a benefit to other institutions faced with similar challenges.
Dedicated Disaster Preparedness Program
Depending on the size of the institution and whether or not it is a trauma-receiving center, it is vitally important to have a team of individuals dedicated to the development and maintenance of a disaster readiness program. Eric Alberts, manager of Emergency Preparedness at Orlando Heath, emphasized the need to harness and leverage preparedness efforts and relationships with community partners, law enforcement, and EMS. In addition, he noted that these trained individuals can provide education and coordination for mass-casualty drills, assist in developing and maintaining policies and protocols, and coordinate with hospital incident command during actual events.
Practice, Practice, Practice
In order for medical staff, nursing staff, and support personnel to understand their roles and responsibilities if an MCI occurs, they must practice simulated drills. Tabletop and full-scale emergency intake drills, with a range of scenarios occurring at different times of the day and night, will improve teamwork and coordination. At least once a year, a large, full-scale community exercise that involves scene casualty collection points, law enforcement and EMS involvement, multiple EDs, and hospital-wide integration will educate staff members on their duties. There should be enough patients in these drills to stress the entire system—both ED and in-hospital. Physician involvement in these exercises is crucial. In March 2016, a full-scale community exercise was performed in the Central Florida area in which more than 500 volunteers, 50 agencies, and 15 hospitals participated. A segment of that exercise involved an active shooter impersonating a patient brought to the ED. We feel this recent exercise, and others like it, were helpful in managing our actual mass casualty event.
Notification
When the shootings at the Pulse nightclub started, we were advised that there might be as many as 20 victims, but over the next few hours, we received more than twice as many injured patients. In any scenario where it is felt additional ED resources and personnel are needed, it is advantageous to begin the notification process as early as possible. Ideally, there are redundant methods in place to notify in-house and off-duty personnel, preferably in a multilayered system of electronic and voice communications that provides feedback as to staff availability. During daytime hours, it is easier for off-duty staff to learn of an event through news and social media. However, during early morning hours, such as when these shootings occurred, it may be difficult to notify sleeping staff that they are needed. With the trend of using mobile devices instead of landline phones, and with the ability to silence those devices during nighttime sleep hours, it has become increasingly difficult to “break through” the silence. In our event, group e-mail notifications were activated, but individual phone calls were also required. Initially, some calls to staff went to voice mail rather than being
answered directly.
Communication
Communication is an area of opportunity for improvement in almost any mass-casualty event. Redundant methods of electronic, voice, telephone, and radio communications are crucial for personnel to coordinate efforts. It is imperative that HICS and ED personnel receive updates about events on the scene and the status of potential incoming patients. An infrastructure of communications is paramount for the coordination that is needed between prehospital, ED, and in-house resources.
Throughput
Facilitating ED and hospital throughput and improving operational efficiencies are regular topics of discussion in most busy EDs. However, when it becomes necessary to intake large numbers of patients in an ED within a short period of time, the need to move patients out of the department intensifies. In many cases, to continue intake of patients, it will be necessary to quickly find areas outside of the ED—such as operating rooms, ICUs, and general floors—to transport patients to. At our facility, we normally have two operating rooms staffed throughout the night for traumas. On the night of the shootings, a total of six operating rooms were activated quickly to manage the penetrating injuries of these patients. Previously admitted medical patients were retrieved by in-house nursing staff to free up ED beds.
Media
It is important to recognize the intense social, print, online, and television media exposure that will occur with such tragedies, and have personnel and systems in place to manage it. The Pulse nightclub is located only a few short blocks south of ORMC, and the majority of all injured patients, including those with the most severe injuries, presented to our facility. As a result, the intense media coverage at our hospital physically overlapped the intense media coverage at the scene. Nearby businesses were shut down, access to several main thoroughfare roads were blocked, and some individuals mistakenly thought the hospital was closed. Our media relations department felt the most efficient way to manage information dissemination was to hold a “presser”—a press conference with a few of the health professionals involved in the care of the patients. The press conference helped to relieve some of the media presence and pressure, and provided welcomed transparency to the community.
Expect the Unexpected
Even when physicians and staff conduct regular training exercises and are familiar with policies and procedures, the controlled chaos that is typical of a true mass-casualty event will likely result in some unexpected occurrences. After injured patients began arriving at our ED, during a period when patient influx and medical care was intense, there was a brief time when we were concerned an active shooter was also in our ED. Since the mass shootings were only a few blocks from the ED, and we did not know the scope or number of shooters, it was a reasonable assumption that a perpetrator could present to the ED as a patient or active shooter. During an event such as this, it is the practice at ORMC to have security officers place the facility on lockdown; however; the added concern that an active shooter was physically present in the ED required additional law enforcement officers to methodically search the entire facility until the threat of a shooter was eliminated. Although this did not directly impact patient care, it did create another level of complexity and stress to the already challenging situation.
Emotional Impact
One should not underestimate the emotional impact of a mass-casualty event. Emergency physicians and personnel are well equipped to manage illness, injury, and death. However, an event of this magnitude, with the number and manner of injuries and deaths that presented to our ED, along with the closeness to a scene of bloodshed where many young lives were taken in a senseless act of violence, will likely have a lasting impression on many staff members. Any institution encountering such an event should have behavioral health and support counselors readily available as soon as possible.
Conclusion
When patients present in truckloads, as they did in our ambulance bay in the early hours of June 12, an ED may be inundated with injured patients without notice or preparation. Teams need to trust their instincts, their training, and one another. It is unlikely that your normal ED practice patterns will be sufficient to take care of a large surge of patients, and you will need to turn to your ingenuity, creativity, and resourcefulness to do what you think is best to save the lives of as many patients as possible. As Sarah Duran, BSN, the trauma nurse who was working as the ED charge nurse the night of the shootings, stated, “I don’t think anyone can fully prepare for anything on the scale of what happened in Orlando, but with a good foundation of protocols in place, strong set of staff, constant vigilance, and great teamwork, any hospital can be successful in handling a mass casualty incident.”
Orlando Regional Medical Center (ORMC) is an urban, academic, Level 1 trauma center with an ED that treats in excess of 85,000 patients each year. There are more than 4,500 annual trauma admissions, including penetrating and blunt mechanism injuries. We have a 3-year emergency medicine (EM) residency program, originally established in 1986, that now has 14 residents per year. The events that we experienced on the early morning of June 12, 2016 were tragic and unexpected and tested our community, our teams, and our organization. The following is a description of activity perspectives, personal reflections and feelings, and important lessons learned from which other EDs may benefit.
Prehospital/Rescue Period
The prehospital approach to a mass-casualty incident (MCI) caused by gunfire has changed significantly over the last decade, with lessons gleaned from the experience of military and domestic attacks. The Orange County (Florida) Emergency Medical Services (EMS) System, including the agencies involved in the response to the June 12, 2016 Pulse nightclub shooting incident (Orlando Fire Department, Rural Metro Ambulance, and Orange County Fire Rescue), have trained specifically on the evolving priorities during an active shooter incident. This includes targeted hemorrhage control, swift extrication, minimal interventions, and immediate transport to the appropriate receiving center. In June 2015, 1 year prior to the Pulse nightclub shooting, a protocol variance was written by medical directors, explaining that “EMS providers may engage in initial patient care with only the supplies deemed absolutely necessary for rapid evaluation and removal into a safe triage zone.” This variance applies when there is an active shooter scenario. In addition, in 2014, 2015, and 2016, we conducted large scale, multiagency community exercises, encompassing shooting/active shooter scenarios and drills.
On June 12, 2016, EMS units were on scene of the Pulse nightclub in downtown Orlando less than 5 minutes after shooting began. It became immediately obvious that additional resources would be necessary. Soon after the incident, an MCI alert was activated from the Orlando Fire Department Communications Center, utilizing a software system to notify area hospitals and the medical directors that up to 20 patients had been shot, and requesting status on bed availability. Christopher L. Hunter, MD, PhD, one of our associate EMS medical directors, was working in the ED at a hospital several miles away from the incident and began coordinating efforts to distribute patients to the appropriate destination via radio and phone communication between the scene, the communications center, and the trauma center.
On scene, a group of law enforcement officers were engaging the shooter while others assisted in extracting victims from the club and surrounding area. Injured victims were brought to a casualty collection point, under cover, across the street and were transported as units became available. Initially, law enforcement vehicles and ambulances would make the two-block drive from the scene to ORMC carrying as many patients as they safely could, and return immediately after offload. Per previous training, minimal interventions were performed, and unlike standard procedure, EMS could offer no prearrival report to the hospital. The decision was made to triage only patients meeting Florida’s state trauma alert criteria to ORMC, and funnel other patients to nearby nontrauma centers. Dr Hunter attempted to notify the hospitals of patients as they were transported off the scene; however, the extremely short transport times made this process difficult.
Over the course of the incident, on-scene commands designated a casualty collection point, a transport unit staging area, and a hospital liaison. Emergency medical service responders cooperated with law enforcement to transport injured patients throughout the response. By the end of the event, nearly 100 EMS providers utilizing dozens of vehicles had responded to the scene.
The ED Period
The overnight shift of Saturday, June 11 was slower than usual in the ORMC ED, and triage housed the typical Saturday-night complaints. One of our mid-level providers, Brian Clayton, ARNP, worked in the fast track pod treating lower acuity illnesses, while the four senior residents discussed who might receive the honor of leaving early. Even the senior attending, Gary A. Parrish, MD, wrapped up his patients and was ready to leave right on time. The 11:00 pm to 7:00 am attending, Kathryn J. Bondani, MD, was looking forward to an easy shift with four graduating senior residents. We had just called in an order from a popular nearby sandwich shop when suddenly, a slew of police cars flew past the hospital—not unusual given our proximity to downtown. The radio squawked “Multiple gunshots wounds en route.” Someone said “a club downtown got shot up.” In anticipation of multiple patient arrivals, resident Amanda M. Stone, MD, and the attending hurried to the trauma/ressuscitation bay. Another resident, Amanda F. Tarkowski, MD, called the trauma attending to rally his team downstairs, informing him that “A club downtown has a shooter and we have multiple patients with a 2-minute ETA.” Multiple gunshot wounds (GSWs) at once is not unusual for our Level 1 trauma center.
The first patient arrived shortly after 2:00 am and had multiple GSWs to the abdomen, but was awake and talking. He was mildly tachycardic, but his blood pressure (BP) was stable. We all gaped at the fist-sized wound on his back—some of us had never seen a GSW like this before. It was apparent that he needed to go to the operating room, but before preparations could be made, three more patients rolled into the ED. Instead of our usual organized, methodical EMS report, these patients were dropped off by a police pickup truck and rolled in on our own stretchers by nurses and technicians. Soon, all six of our trauma bays were filled with critical patients. Christopher H. Ponder, MD, recalled, “I heard an overhead page for ‘all available trauma nurses to the trauma bay’ shortly followed by a more concerned-sounding ‘all available staff to the trauma bay.’” All four senior EM residents, both EM attendings, the trauma attending, four trauma residents, multiple ED nurses, technicians, and various ancillary staff quickly descended on the patients. Chest tubes were placed, and multiple patients were intubated. Several thoracotomies were performed at the initial point when the team was unaware of the exact number of patients who would ultimately follow. Blood bags were hung and tranexamic acid was administered liberally. Unfortunately, some of these initial attempts were unsuccessful, as the first wave contained the most critically injured patients.
We barely had time to reflect on the dead as more patients filled the hallways. In the midst of all of this, triage decisions came quickly—awake and talking patients with an acceptable BP were moved out of the trauma bay in favor of less stable patients. Intubation and chest-tube placement decisions were made instantly. There was no time for routine X-rays or laboratory evaluation. Nurses, technicians, and doctors crowded the trauma bay desperately trying to stabilize the critically injured. Vital signs were taken manually. Dr Ponder called his colleague Thomas N. Smith, MD, who was also a graduating senior EM resident, and who happened to be staffing the children’s ED across the street that night. “Is there any way you can make it over here right now?” he shouted into the phone. Dr Smith quickly grabbed several trauma supplies and hitched a ride with security to the ORMC ED to assist. He was confronted with the scene of the previously mentioned “first wave” and grabbed an ultrasound machine to help triage these unfortunate patients. In addition to Dr Smith, unit clerks continued making calls to additional off-duty medical, nursing, and support staff. Critical care attendings and fellows responded from upstairs to assist in the ED. The Hospital Incident Command System (HICS) was initiated to provide hospital and corporate coordination of services. Timothy B. Bullard, MD, another EM attending physician and medical staff director of HICS, was en route to the ED to assist in the response.
Amidst the overwhelming mass of mortally and critically wounded patients, we were told stories of terror from just down the road. The sense of horror was almost contagious, and we all wondered if the violence would spread to the hospital.
About an hour into the ordeal, we heard another page overhead “Code Silver, ED Triage. Code Silver, ED Triage.” Everyone in the trauma bay froze. We heard someone shout from the hallway “Shots fired in triage!” After a few seconds, those nearest the trauma bay doors pushed them shut. One of the trauma surgeons shouted, “Keep caring for your patients, push the portable X-ray machines in front of the doors.” That is exactly what happened, and we worked in the barricaded trauma room for the longest few minutes of the night. We would later learn that this report was false, but fearing for our own lives as well as the lives of our patients is an experience that few, if any, of us had previously been through. The fact that we continued to work in such a situation illustrates everyone’s dedication to their patients and mission.
After the first wave of patients, it was clear that reassessing patients was now our greatest challenge. There were multiple patients with stable vital signs but who had GSWs to the abdomen, pelvis, and thorax and required surgery. Having realized that the ultrasound machine and focused assessment with sonography for trauma (FAST) examinations were the most practical rapid imaging modality, Drs Tarkowski, Ponder, and Smith grabbed the machine and went from room to room repeating the FAST examinations, vital signs, and assessments for missed wounds. A portable computer allowed us to order X-ray orders for patients with extremity wounds. Several patients who initially had negative FASTs had a repeat examination that was positive for free fluid. The operating room triage list shuffled based on these examinations.
At this point, there seemed to be a never-ending list of “Doe” names on the electronic medical record (EMR) tracking board. Tracking the location of patients was a dynamic process, and updating the tracking board was difficult. Patients were continually cycled in and out of the trauma bay, shuffled in and out of treatment rooms, lined up in the hallways, and transported up to the intensive care unit (ICU). Some of those “Doe” names belonged to patients who had succumbed to their injuries. Some patients had empty, bloody charts next to them on their stretcher. Every patient had a wristband. Dr Tarkowski improvised a rapid documentation system using quarter sheets of scrap paper that were taped either to the stretcher or door with a patient name, brief list of injuries, FAST examination result, pending tests, and medications given. This system was an efficient way of identifying which patients had been evaluated, what had been done, and what was pending.
While we were “rounding” on our patients, down the street, law enforcement had broken down the club’s wall, and a second wave of patients began to arrive. Two residents completed the secondary evaluations while the other three resuscitated new patients. The second wave seemed like a repeat of the first. Several extremity-only injuries were triaged directly to the hallways to be seen by the two residents outside of the trauma bay. By this time, the orthopedic surgery service had come down to the ED and was washing out wounds, splinting, and making plans for surgery. The internal medicine service and the medical critical care team were helping reassess patients as well.
There were many emotional moments. Dr Ponder remembered, “One of the first few patients I saw was pulseless, and as I went to start chest compressions, I was stopped by a trauma surgeon who said, ‘He’s gone, focus on the ones we can help.’ That’s when I realized the gravity of our situation. For almost 2 hours, each resident cycled through patients.” Dr Stone recounted, “I just went down the line of patients, from head of the bed to head of the bed, some patients still on EMS stretchers, intubating many of them. It was surreal to see that many severely injured in one place.” Tory L. Weatherford, MD, recalled, “It was controlled chaos. My training kicked in, and it became about just trying to do anything possible to help.”
Dr Bondani, the overnight attending, said she does not remember many specifics from the event. “Faces and injuries blurred together. I remember looking in one young man’s eyes and telling him, ‘We are going to help you, just hang in there,’ and telling another panicking woman, ‘You’re talking, you can feel pain, you’re alive. Calm down.’ It was organized chaos as we swept from patient to patient moving as quickly as possible. Your training kicks in and you do what needs to be done in the moment.”
We were fortunate to have the EM team we did, and to be in the place that we were. On duty, we had five senior graduating residents, essentially with attending-level skills and training, who had been together since day one. “We gave everything we had; there was no time to stop. We went where our hands could be helpful—it didn’t matter if it was your traditional role or not,” said Dr Weatherford.
Dr Tarkowski remembered what it was like leaving the walls of the ED later that morning. “Leaving the hospital didn’t feel like a success. We knew the work we did was good, that we did everything we could, but it didn’t feel like it. It felt heavy. It felt empty.” Afterward, the emotional toll set in. We gathered up the names of the deceased and looked at a status board littered with “Doe” names, and we tried hard not to break down at the violence and the pain we witnessed.
Immediate Recovery Period (Prehospital Setting)
In the aftermath of the initial rescue operation, stabilization of injured victims, and demobilization of resources, a second “event” unfolded—hundreds of family members flooded to ORMC looking for unaccounted loved ones. At this point, there were dozens of deceased and critically injured patients who remained unidentified, and addressing the needs of both the victims and the families was becoming overwhelming. With the cooperation of federal, state, county, city, and private resources, a family reunification center (FRC; a family staging area/family reception center) was created and managed initially within the hospital. At this site, grief counselors, victim advocates, law enforcement and medical examiner’s officials, hospital chaplains, and translators gathered with the loved ones of those missing to synchronize efforts to identify and reunite them. The Emergency Operations Center quickly created a telephone hotline and Web site to guide those in need to this resource. Food and housing for those in need were provided by the generosity of our community—which cannot be overstated in the wake of this tragedy. As days passed, the FRC transitioned to a new location as the Orlando United Assistance Center, and will continue to serve as a navigation point for those who are and will be affected by the event for months to come.
Hospital Incident Command System
The HICS was activated shortly past 3:00 am, just after the initial wave of victims flooded our ED and the gravity of the situation became apparent. The ED and trauma services were already near full staff due to timing, rapid response, and communication between the traumatologists, as well as a bit of luck. Because of the time of the disaster, our normal notification process for incident command and all personnel was severely limited. In retrospect, this turned out to be a blessing. While everyone who normally would respond to HICS was not available, individuals serving in key positions were reached by personal phone calls and were on-site quickly. One of the main functions of HICS is to control the internal chaos that arises when a disaster occurs and all personnel want to assist in some manner. We have spent hours during drills crafting communications that target key personnel necessary to meet the mission, while controlling well-intentioned but unnecessary personnel. In our drills, this is not an issue because everyone knows the exercise is not reality; however, in a real disaster, everyone wants to help. This was confirmed by the guilt that so many of our team members expressed at not being involved that Sunday.
With an initial skeleton crew in incident command, it was easy to focus on the immediate needs of patient care. The strong leadership and cool heads of our incident command leadership led to rapid role definition and responsibility, and set forth an easy path for execution. Hospital command personnel adapted their usual roles and performed functions and assignments as needed. Many HICS staff had direct face-to-face contact with frontline providers in the ED and other vital areas. This was possible because of the close proximity of the hospital command headquarters to the ED. The need for additional resources was rapidly identified, and the hospital command leaders assumed direct responsibility for procuring them instead of delegating. A great example of this was when Orlando Health’s chief executive officer and chief operating officer went to our nearby hospitals to gather additional chest tubes after learning that we were running in short supply. Their main responsibilities lay ahead of them, and they were willing to help in any manner they could at the time. Some of the medical personnel were able to switch roles and pitch in to treat the second wave of victims that arrived at around 5:00 am.
As the flow of victims to the ED subsided and order began to be restored, HICS shifted gears and took on a much broader role: coordinating activities with multiple agencies, including local law enforcement, the Federal Bureau of Investigation, news media, and an array of patient and family services. Again, the timing of this tragic event allowed the needs and functions of our hospital command to concentrate the focus in a more structured manner than might have been possible during regular operational hours.
Lessons Learned and Recommendations
As with any MCI, it is important to perform after-incident debriefings to reflect upon the prehospital, ED, and hospital care to assess for areas in need of improvement. Obviously, depending on the number and type of patients who are received and the resources available at the institution, such events can stress EDs that are already at or above their capacity. At the time of this writing (less than 2 months after the incident), although we are still in the early stages of our post-incident debriefing process, we offer the following suggestions and recommendations that we believe will be a benefit to other institutions faced with similar challenges.
Dedicated Disaster Preparedness Program
Depending on the size of the institution and whether or not it is a trauma-receiving center, it is vitally important to have a team of individuals dedicated to the development and maintenance of a disaster readiness program. Eric Alberts, manager of Emergency Preparedness at Orlando Heath, emphasized the need to harness and leverage preparedness efforts and relationships with community partners, law enforcement, and EMS. In addition, he noted that these trained individuals can provide education and coordination for mass-casualty drills, assist in developing and maintaining policies and protocols, and coordinate with hospital incident command during actual events.
Practice, Practice, Practice
In order for medical staff, nursing staff, and support personnel to understand their roles and responsibilities if an MCI occurs, they must practice simulated drills. Tabletop and full-scale emergency intake drills, with a range of scenarios occurring at different times of the day and night, will improve teamwork and coordination. At least once a year, a large, full-scale community exercise that involves scene casualty collection points, law enforcement and EMS involvement, multiple EDs, and hospital-wide integration will educate staff members on their duties. There should be enough patients in these drills to stress the entire system—both ED and in-hospital. Physician involvement in these exercises is crucial. In March 2016, a full-scale community exercise was performed in the Central Florida area in which more than 500 volunteers, 50 agencies, and 15 hospitals participated. A segment of that exercise involved an active shooter impersonating a patient brought to the ED. We feel this recent exercise, and others like it, were helpful in managing our actual mass casualty event.
Notification
When the shootings at the Pulse nightclub started, we were advised that there might be as many as 20 victims, but over the next few hours, we received more than twice as many injured patients. In any scenario where it is felt additional ED resources and personnel are needed, it is advantageous to begin the notification process as early as possible. Ideally, there are redundant methods in place to notify in-house and off-duty personnel, preferably in a multilayered system of electronic and voice communications that provides feedback as to staff availability. During daytime hours, it is easier for off-duty staff to learn of an event through news and social media. However, during early morning hours, such as when these shootings occurred, it may be difficult to notify sleeping staff that they are needed. With the trend of using mobile devices instead of landline phones, and with the ability to silence those devices during nighttime sleep hours, it has become increasingly difficult to “break through” the silence. In our event, group e-mail notifications were activated, but individual phone calls were also required. Initially, some calls to staff went to voice mail rather than being
answered directly.
Communication
Communication is an area of opportunity for improvement in almost any mass-casualty event. Redundant methods of electronic, voice, telephone, and radio communications are crucial for personnel to coordinate efforts. It is imperative that HICS and ED personnel receive updates about events on the scene and the status of potential incoming patients. An infrastructure of communications is paramount for the coordination that is needed between prehospital, ED, and in-house resources.
Throughput
Facilitating ED and hospital throughput and improving operational efficiencies are regular topics of discussion in most busy EDs. However, when it becomes necessary to intake large numbers of patients in an ED within a short period of time, the need to move patients out of the department intensifies. In many cases, to continue intake of patients, it will be necessary to quickly find areas outside of the ED—such as operating rooms, ICUs, and general floors—to transport patients to. At our facility, we normally have two operating rooms staffed throughout the night for traumas. On the night of the shootings, a total of six operating rooms were activated quickly to manage the penetrating injuries of these patients. Previously admitted medical patients were retrieved by in-house nursing staff to free up ED beds.
Media
It is important to recognize the intense social, print, online, and television media exposure that will occur with such tragedies, and have personnel and systems in place to manage it. The Pulse nightclub is located only a few short blocks south of ORMC, and the majority of all injured patients, including those with the most severe injuries, presented to our facility. As a result, the intense media coverage at our hospital physically overlapped the intense media coverage at the scene. Nearby businesses were shut down, access to several main thoroughfare roads were blocked, and some individuals mistakenly thought the hospital was closed. Our media relations department felt the most efficient way to manage information dissemination was to hold a “presser”—a press conference with a few of the health professionals involved in the care of the patients. The press conference helped to relieve some of the media presence and pressure, and provided welcomed transparency to the community.
Expect the Unexpected
Even when physicians and staff conduct regular training exercises and are familiar with policies and procedures, the controlled chaos that is typical of a true mass-casualty event will likely result in some unexpected occurrences. After injured patients began arriving at our ED, during a period when patient influx and medical care was intense, there was a brief time when we were concerned an active shooter was also in our ED. Since the mass shootings were only a few blocks from the ED, and we did not know the scope or number of shooters, it was a reasonable assumption that a perpetrator could present to the ED as a patient or active shooter. During an event such as this, it is the practice at ORMC to have security officers place the facility on lockdown; however; the added concern that an active shooter was physically present in the ED required additional law enforcement officers to methodically search the entire facility until the threat of a shooter was eliminated. Although this did not directly impact patient care, it did create another level of complexity and stress to the already challenging situation.
Emotional Impact
One should not underestimate the emotional impact of a mass-casualty event. Emergency physicians and personnel are well equipped to manage illness, injury, and death. However, an event of this magnitude, with the number and manner of injuries and deaths that presented to our ED, along with the closeness to a scene of bloodshed where many young lives were taken in a senseless act of violence, will likely have a lasting impression on many staff members. Any institution encountering such an event should have behavioral health and support counselors readily available as soon as possible.
Conclusion
When patients present in truckloads, as they did in our ambulance bay in the early hours of June 12, an ED may be inundated with injured patients without notice or preparation. Teams need to trust their instincts, their training, and one another. It is unlikely that your normal ED practice patterns will be sufficient to take care of a large surge of patients, and you will need to turn to your ingenuity, creativity, and resourcefulness to do what you think is best to save the lives of as many patients as possible. As Sarah Duran, BSN, the trauma nurse who was working as the ED charge nurse the night of the shootings, stated, “I don’t think anyone can fully prepare for anything on the scale of what happened in Orlando, but with a good foundation of protocols in place, strong set of staff, constant vigilance, and great teamwork, any hospital can be successful in handling a mass casualty incident.”

Experts assess soft filler procedures for hand rejuvenation
Cosmetic dermatology patients are increasingly seeking hand rejuvenation procedures to eliminate appearance discrepancies between the face and hands, reported Ramin Fathi, MD, and Joel L. Cohen, MD, FAAD, who reviewed the benefits and complications of soft filler methods.
Pre-procedure evaluation includes assessing volume of lost fat from the skin via the Merz hand grading scale. Prior to augmentation, a detailed patient history, including medications, medical problems, and bleeding abnormalities, is typically taken, as well as assessment of patient lifestyle issues involving extensive hand activity, such as typing on a keyboard or playing piano. The authors reviewed three hand rejuvenation methods: autologous fat grafting, hyaluronic acid (HA), and poly-L-lactic acid (PLLA).
Although autologous fat grafting is still done in some practices, it is more invasive compared with soft tissue fillers, and can result in complications such as infection, cyst formation, temporary dysesthesia, and significant edema, the authors noted. PLLA is not approved for dorsal hand augmentation, and is used off label.
Hyaluronic acid (HA) fillers such as Restylane, Belotero, and Juvederm are approved only in the United States for facial soft tissue augmentation, and are also used off label for hand rejuvenation. The authors cited a small study of 16 patients evaluating small gel particle HA in the dorsal hand, in which vascular, tendon, bony prominence, and skin turgor were improved by 60.9%, 65.2%, 73.7%, and 26.3%, respectively, 2 weeks after treatment. “A distinct advantage of HA is that imperfections or undesired product can usually be reversed in the short term using hyaluronidase enzyme,” they added.
Despite the common adverse effects of erythema, pruritus, ecchymosis, and edema, “hand augmentation with soft tissue filler, alone or in conjunction with other rejuvenation modalities, can have a significant impact on improving appearance of the dorsal hands,” satisfying patient cosmetic objectives, the authors concluded.
Read the full article in the Journal of Drugs in Dermatology (J Drugs Dermatol. 2016;15[7]:809-15).
Cosmetic dermatology patients are increasingly seeking hand rejuvenation procedures to eliminate appearance discrepancies between the face and hands, reported Ramin Fathi, MD, and Joel L. Cohen, MD, FAAD, who reviewed the benefits and complications of soft filler methods.
Pre-procedure evaluation includes assessing volume of lost fat from the skin via the Merz hand grading scale. Prior to augmentation, a detailed patient history, including medications, medical problems, and bleeding abnormalities, is typically taken, as well as assessment of patient lifestyle issues involving extensive hand activity, such as typing on a keyboard or playing piano. The authors reviewed three hand rejuvenation methods: autologous fat grafting, hyaluronic acid (HA), and poly-L-lactic acid (PLLA).
Although autologous fat grafting is still done in some practices, it is more invasive compared with soft tissue fillers, and can result in complications such as infection, cyst formation, temporary dysesthesia, and significant edema, the authors noted. PLLA is not approved for dorsal hand augmentation, and is used off label.
Hyaluronic acid (HA) fillers such as Restylane, Belotero, and Juvederm are approved only in the United States for facial soft tissue augmentation, and are also used off label for hand rejuvenation. The authors cited a small study of 16 patients evaluating small gel particle HA in the dorsal hand, in which vascular, tendon, bony prominence, and skin turgor were improved by 60.9%, 65.2%, 73.7%, and 26.3%, respectively, 2 weeks after treatment. “A distinct advantage of HA is that imperfections or undesired product can usually be reversed in the short term using hyaluronidase enzyme,” they added.
Despite the common adverse effects of erythema, pruritus, ecchymosis, and edema, “hand augmentation with soft tissue filler, alone or in conjunction with other rejuvenation modalities, can have a significant impact on improving appearance of the dorsal hands,” satisfying patient cosmetic objectives, the authors concluded.
Read the full article in the Journal of Drugs in Dermatology (J Drugs Dermatol. 2016;15[7]:809-15).
Cosmetic dermatology patients are increasingly seeking hand rejuvenation procedures to eliminate appearance discrepancies between the face and hands, reported Ramin Fathi, MD, and Joel L. Cohen, MD, FAAD, who reviewed the benefits and complications of soft filler methods.
Pre-procedure evaluation includes assessing volume of lost fat from the skin via the Merz hand grading scale. Prior to augmentation, a detailed patient history, including medications, medical problems, and bleeding abnormalities, is typically taken, as well as assessment of patient lifestyle issues involving extensive hand activity, such as typing on a keyboard or playing piano. The authors reviewed three hand rejuvenation methods: autologous fat grafting, hyaluronic acid (HA), and poly-L-lactic acid (PLLA).
Although autologous fat grafting is still done in some practices, it is more invasive compared with soft tissue fillers, and can result in complications such as infection, cyst formation, temporary dysesthesia, and significant edema, the authors noted. PLLA is not approved for dorsal hand augmentation, and is used off label.
Hyaluronic acid (HA) fillers such as Restylane, Belotero, and Juvederm are approved only in the United States for facial soft tissue augmentation, and are also used off label for hand rejuvenation. The authors cited a small study of 16 patients evaluating small gel particle HA in the dorsal hand, in which vascular, tendon, bony prominence, and skin turgor were improved by 60.9%, 65.2%, 73.7%, and 26.3%, respectively, 2 weeks after treatment. “A distinct advantage of HA is that imperfections or undesired product can usually be reversed in the short term using hyaluronidase enzyme,” they added.
Despite the common adverse effects of erythema, pruritus, ecchymosis, and edema, “hand augmentation with soft tissue filler, alone or in conjunction with other rejuvenation modalities, can have a significant impact on improving appearance of the dorsal hands,” satisfying patient cosmetic objectives, the authors concluded.
Read the full article in the Journal of Drugs in Dermatology (J Drugs Dermatol. 2016;15[7]:809-15).
FROM THE JOURNAL OF DRUGS IN DERMATOLOGY