User login
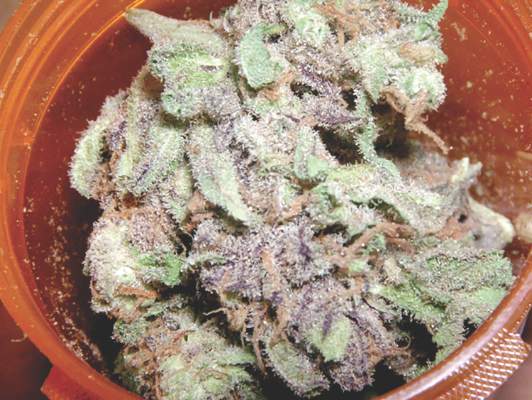
For Neuropathic Pain, Marijuana Yields Modest Benefits
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
EXPERT ANALYSIS FROM PAIN CARE FOR PRIMARY CARE
For neuropathic pain, marijuana yields modest benefits
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
LAKE BUENA VISTA, FLA. – As medical marijuana penetrates mainstream medical practice in the United States and elsewhere, awareness of the potential benefits, potential risks, and local laws governing its use for treatment of chronic pain gain importance, according to a specialist reviewing available data at Pain Care for Primary Care.
For many specific types of chronic pain, more data are needed to judge the benefit-to-risk ratio of marijuana relative to other options, but there are reasonable data suggesting both acceptable safety and meaningful efficacy of this analgesic in neuropathic pain, according to Mark A. Ware, MBBS, associate professor in the departments of anesthesia and family medicine, McGill University, Montreal.
In neuropathic pain, the evidence includes at least five randomized trials, according to Dr. Ware. In a recently published review article for which Dr. Ware served as senior author, the degree of neuropathic pain reductions were characterized as being on an order similar to those achieved with opioids and anticonvulsants (J Pain. 2016 Jun;17[6]:654-68). In one study, the number needed to treat (NNT) for a 50% pain reduction was just 2.
In Canada, marijuana is now available for at least some medical uses in every province. In the United States, 23 states have passed laws permitting clinical use of marijuana, according to Dr. Ware. He suggested that legalization of marijuana has fueled a growing acceptance of marijuana as a treatment option whether or not it is prescribed. For this reason, it’s necessary to examine the objective evidence to provide appropriate counseling.
“I think we are past the point where this option can simply be ignored,” Dr. Ware said. Even if they do not intend to prescribe marijuana for chronic pain, “clinicians should become familiar with the evidence regarding benefit and safety as well as the laws regarding its use.” In a study of long-term safety led by Dr. Ware, a standardized cannabis product containing 12.5% tetrahydrocannabinol was dispensed to 215 current or prior users of marijuana with a non-cancer chronic pain syndrome (J Pain. 2015 Dec;16[12]:1233-42). Followed for 1 year, adverse events in this group were compared with 216 control patients who also had chronic pain but were not using cannabis.
The odds ratio (OR) of non-serious adverse events in the categories of respiratory disorders (OR, 1.77) infectious disorders (OR, 1.51), nervous system disorders (OR, 1.77), and psychiatric disorders (OR, 2.74) were all significantly higher in the group treated with cannabis, but almost all were judged to be of mild to moderate severity. There was no significant difference in the risk of serious AEs. Dr. Ware also reported there was no difference between the cannabis group and controls for neurocognitive testing at baseline, 6 months, or the end of 1 year.
Pain control was also monitored over the course of the study. According to Dr. Ware, average pain scores in the cannabis group fell modestly but consistently over the course of the study. Over the same period, the pain scores rose slightly in the control group.
There is a long list of unanswered questions regarding effective use of marijuana in the control of chronic pain, he said. For example, Dr. Ware noted that the optimal composition of cannabinoids has yet to be determined. He noted that more than one of the complex constituents may contribute to pain control, and these constituents are not necessarily the same as those most favored by recreational users seeking a euphoric “high.”
There is also a long list of unanswered questions about safety. Dr. Ware reviewed some evidence that inhaled vaporized marijuana may be safer than traditional smoked marijuana due to a reduced exposure to toxins, but he suggested more rigorous studies are needed to generate objective data that can better quantify the benefit-to-risk of this and other methods of marijuana delivery.
Despite unanswered questions, marijuana is widely available and likely to be considered by patients for chronic pain whether or not it is recommended by physicians. It is for this reason that clinicians need to become familiar with both its potential risks and benefits.
“It will be helpful to patients if you can provide them practical and accurate information about what is and is not known about this treatment,” Dr. Ware suggested.
Dr. Ware reported a financial relationship with CanniMed. The meeting was held by the American Pain Society and Global Academy for Medical Education. Global Academy and this news organization are owned by the same company.
EXPERT ANALYSIS FROM PAIN CARE FOR PRIMARY CARE
HIV chemoprophylaxis in U.S. up 738% in recent 3-year period
DURBAN, SOUTH AFRICA – The number of Americans using oral emtricitabine/tenofovir (Truvada) to prevent HIV infection jumped by 738% during a recent 3-year period since the drug’s 2012 marketing approval. However, uptake in certain at-risk populations leaves much room for improvement, Scott McCallister, MD, said at the 21st International AIDS Conference.
“While there are encouraging signs in using Truvada for pre-exposure prophylaxis across the country as a whole, there are certainly barriers that must be addressed in women, those under age 25, and in certain regions of the U.S. where lifetime risk of HIV acquisition is high,” said Dr. McCallister, senior director for clinical research at Gilead Sciences in Foster City, Calif.

He presented key findings from a national survey of 80% of retail pharmacies that showed that more than three-quarters of the 79,684 individuals who started on emtricitabine/tenofovir for HIV chemoprophylaxis during the fourth quarter of 2012 through the end of 2015 were men. Just 11% of the men and 28% of women taking the drug for pre-exposure prophylaxis (PrEP) were under age 25, a particularly high-risk group.
Fifty-one percent of all patients on emtricitabine/tenofovir for PrEP resided in five states: Texas, New York, Florida, Illinois, and California. Yet that doesn’t reflect the distribution of the HIV epidemic. A 2016 Centers for Disease and Prevention report concluded that the highest lifetime risk of HIV infection occurs in eight southeastern states and the District of Columbia, as well as Texas and New York.
“Some of the states with the highest lifetime risks of HIV diagnosis are lagging behind and have low numbers for Truvada for PrEP,” Dr. McCallister observed.
The Centers for Disease Control and Prevention estimates that while the lifetime risk of HIV is 1 in 99 in the United States overall, it’s 1 in 48 among black or Hispanic men, 1 in 2 for black men who have sex with men, and 1 in 4 for Hispanic MSM. Moreover, the CDC has also reported that 44% of all new HIV diagnoses occur in African Americans. And while Dr. McCallister said it’s difficult to analyze race/ethnicity in the Gilead survey because the data were de-identified, it’s his impression from other studies and talking with clinicians that PrEP users are disproportionately white.
Asked why prescribing of emtricitabine/tenofovir to date for PrEP in men far outpaces that for women, Dr. McCallister offered a theory: “Based on conversations I’ve had with community-based physicians who are avid prescribers, I think it’s a matter of men having a greater comfort level in terms of using PrEP because their clinicians and the MSM communities are more knowledgeable about PrEP. Perhaps there are fewer touch points for women to see knowledgeable clinicians. They are probably most often going to an ob.gyn. or a primary care physician who may have slightly less knowledge of PrEP than the HIV specialists or sexual health clinics where many MSMs are going.”
He noted that in addition to the randomized trial evidence of safety and efficacy that won Food and Drug Administration approval of emtricitabine/tenofovir for HIV PrEP, the real-world experience accrued in 32 demonstration projects with a total of more than 7,000 person-years of follow-up showed an HIV seroconversion rate of 0.95% per year in patients on the daily oral medication.
Dr. McCallister is an employee of Gilead Sciences, which sponsored the national PrEP survey and markets emtricitabine/tenofovir.
DURBAN, SOUTH AFRICA – The number of Americans using oral emtricitabine/tenofovir (Truvada) to prevent HIV infection jumped by 738% during a recent 3-year period since the drug’s 2012 marketing approval. However, uptake in certain at-risk populations leaves much room for improvement, Scott McCallister, MD, said at the 21st International AIDS Conference.
“While there are encouraging signs in using Truvada for pre-exposure prophylaxis across the country as a whole, there are certainly barriers that must be addressed in women, those under age 25, and in certain regions of the U.S. where lifetime risk of HIV acquisition is high,” said Dr. McCallister, senior director for clinical research at Gilead Sciences in Foster City, Calif.
He presented key findings from a national survey of 80% of retail pharmacies that showed that more than three-quarters of the 79,684 individuals who started on emtricitabine/tenofovir for HIV chemoprophylaxis during the fourth quarter of 2012 through the end of 2015 were men. Just 11% of the men and 28% of women taking the drug for pre-exposure prophylaxis (PrEP) were under age 25, a particularly high-risk group.
Fifty-one percent of all patients on emtricitabine/tenofovir for PrEP resided in five states: Texas, New York, Florida, Illinois, and California. Yet that doesn’t reflect the distribution of the HIV epidemic. A 2016 Centers for Disease and Prevention report concluded that the highest lifetime risk of HIV infection occurs in eight southeastern states and the District of Columbia, as well as Texas and New York.
“Some of the states with the highest lifetime risks of HIV diagnosis are lagging behind and have low numbers for Truvada for PrEP,” Dr. McCallister observed.
The Centers for Disease Control and Prevention estimates that while the lifetime risk of HIV is 1 in 99 in the United States overall, it’s 1 in 48 among black or Hispanic men, 1 in 2 for black men who have sex with men, and 1 in 4 for Hispanic MSM. Moreover, the CDC has also reported that 44% of all new HIV diagnoses occur in African Americans. And while Dr. McCallister said it’s difficult to analyze race/ethnicity in the Gilead survey because the data were de-identified, it’s his impression from other studies and talking with clinicians that PrEP users are disproportionately white.
Asked why prescribing of emtricitabine/tenofovir to date for PrEP in men far outpaces that for women, Dr. McCallister offered a theory: “Based on conversations I’ve had with community-based physicians who are avid prescribers, I think it’s a matter of men having a greater comfort level in terms of using PrEP because their clinicians and the MSM communities are more knowledgeable about PrEP. Perhaps there are fewer touch points for women to see knowledgeable clinicians. They are probably most often going to an ob.gyn. or a primary care physician who may have slightly less knowledge of PrEP than the HIV specialists or sexual health clinics where many MSMs are going.”
He noted that in addition to the randomized trial evidence of safety and efficacy that won Food and Drug Administration approval of emtricitabine/tenofovir for HIV PrEP, the real-world experience accrued in 32 demonstration projects with a total of more than 7,000 person-years of follow-up showed an HIV seroconversion rate of 0.95% per year in patients on the daily oral medication.
Dr. McCallister is an employee of Gilead Sciences, which sponsored the national PrEP survey and markets emtricitabine/tenofovir.
DURBAN, SOUTH AFRICA – The number of Americans using oral emtricitabine/tenofovir (Truvada) to prevent HIV infection jumped by 738% during a recent 3-year period since the drug’s 2012 marketing approval. However, uptake in certain at-risk populations leaves much room for improvement, Scott McCallister, MD, said at the 21st International AIDS Conference.
“While there are encouraging signs in using Truvada for pre-exposure prophylaxis across the country as a whole, there are certainly barriers that must be addressed in women, those under age 25, and in certain regions of the U.S. where lifetime risk of HIV acquisition is high,” said Dr. McCallister, senior director for clinical research at Gilead Sciences in Foster City, Calif.
He presented key findings from a national survey of 80% of retail pharmacies that showed that more than three-quarters of the 79,684 individuals who started on emtricitabine/tenofovir for HIV chemoprophylaxis during the fourth quarter of 2012 through the end of 2015 were men. Just 11% of the men and 28% of women taking the drug for pre-exposure prophylaxis (PrEP) were under age 25, a particularly high-risk group.
Fifty-one percent of all patients on emtricitabine/tenofovir for PrEP resided in five states: Texas, New York, Florida, Illinois, and California. Yet that doesn’t reflect the distribution of the HIV epidemic. A 2016 Centers for Disease and Prevention report concluded that the highest lifetime risk of HIV infection occurs in eight southeastern states and the District of Columbia, as well as Texas and New York.
“Some of the states with the highest lifetime risks of HIV diagnosis are lagging behind and have low numbers for Truvada for PrEP,” Dr. McCallister observed.
The Centers for Disease Control and Prevention estimates that while the lifetime risk of HIV is 1 in 99 in the United States overall, it’s 1 in 48 among black or Hispanic men, 1 in 2 for black men who have sex with men, and 1 in 4 for Hispanic MSM. Moreover, the CDC has also reported that 44% of all new HIV diagnoses occur in African Americans. And while Dr. McCallister said it’s difficult to analyze race/ethnicity in the Gilead survey because the data were de-identified, it’s his impression from other studies and talking with clinicians that PrEP users are disproportionately white.
Asked why prescribing of emtricitabine/tenofovir to date for PrEP in men far outpaces that for women, Dr. McCallister offered a theory: “Based on conversations I’ve had with community-based physicians who are avid prescribers, I think it’s a matter of men having a greater comfort level in terms of using PrEP because their clinicians and the MSM communities are more knowledgeable about PrEP. Perhaps there are fewer touch points for women to see knowledgeable clinicians. They are probably most often going to an ob.gyn. or a primary care physician who may have slightly less knowledge of PrEP than the HIV specialists or sexual health clinics where many MSMs are going.”
He noted that in addition to the randomized trial evidence of safety and efficacy that won Food and Drug Administration approval of emtricitabine/tenofovir for HIV PrEP, the real-world experience accrued in 32 demonstration projects with a total of more than 7,000 person-years of follow-up showed an HIV seroconversion rate of 0.95% per year in patients on the daily oral medication.
Dr. McCallister is an employee of Gilead Sciences, which sponsored the national PrEP survey and markets emtricitabine/tenofovir.
AT AIDS 2016
Key clinical point: More than 79,000 Americans started taking emtricitabine/tenofovir for prevention of HIV infection in a recent 3-year period.
Major finding: Adoption of HIV chemoprophylaxis via daily oral emtricitabine/tenofovir has risen steeply of late in the United States, although not in close accord with the epidemiology of the HIV epidemic.
Data source: This national survey of patients starting on emtricitabine/tenofovir to prevent HIV infection was based upon de-identified data obtained from 80% of U.S. retail pharmacies for fourth quarter 2012 through 2015.
Disclosures: The national survey of HIV pre-exposure prophylaxis was sponsored by Gilead Sciences, which markets emtricitabine/tenofovir (Truvada). The presenter is a company employee.

Retinal nerve fiber layer thinning predicts cognitive decline
TORONTO – A thinner-than-normal layer of retinal nerve fibers in the eye is now linked with cognitive decline – another suggestion that extracranial physical findings could be leveraged into dementia screening tools.
The findings were seen in a cohort of 32,000 people enrolled in the U.K. Biobank– an ongoing prospective study following half a million people and collecting data on cancer, heart diseases, stroke, diabetes, arthritis, osteoporosis, eye disorders, depression, and dementia.
The correlation between retinal nerve fiber thickness and cognition was observed in the large cohort at baseline, Fang Sarah Ko, MD, said during a press briefing at the Alzheimer’s Association International Conference 2016. But after following 1,251 of these subjects for 3 years, she and her colleagues found that the correlation continued unabated.

“It’s amazing that we found this in such a healthy population,” Dr. Ko said during the briefing. “We wouldn’t have expected in just 3 years to see any cognitive decline in this cohort, much less measurable cognitive decline with a significant association with retinal nerve fiber layer thickness.”
Dr. Ko, an ophthalmologist in private practice in Tallahassee, Fla., said later during her main presentation of the study that the finding suggests a possible role for retinal imaging as a cognitive health screen.
“Thinner nerve fiber layer was associated with worse performance on memory, reasoning, and reaction time at baseline, and with a decline in each of these tests over time,” she said. “It may be that the nerve fiber layer could be used as a biomarker,” because it is easy to observe and measure with equipment available in most ophthalmology offices. “I would say the potential for clinical use is quite high.”
The U.K. Biobank recruits all of its subjects through the U.K. National Health Service patient registry. All undergo a standard battery of numerous tests; among them are tests of cognitive function and spectral-domain optical coherence tomography (S-DOCT) of the eye. S-DOCT is an increasingly common method of imaging the retina. It produces three-dimensional images of extremely fine resolution.
The 32,000 subjects included in the baseline cohort were all free of diabetes and ocular or neurological disease, and they had normal intraocular pressure. They undertook four tests of cognition: prospective memory, pairs matching, numeric and verbal reasoning, and reaction time. The relationship between these test results and retinal nerve fiber thickness was adjusted for age, sex, race, socioeconomic status, height, refraction, and intraocular pressure.
At baseline, the mean retinal nerve fiber layer was significantly thinner among subjects with abnormal scores on any of the cognitive tests. On the prospective memory test, the layer was an average of 53.3 micrometers for subjects who had correct first-time recall, 52.5 micrometers for those with correct second-time recall, and 51.9 micrometers for those who did not recall. The layer was also significantly thinner in subjects who had low scores on pairs matching, numeric and verbal reasoning, and reaction times.
And the relationship between test results and retinal nerve fiber thinning appeared additive, Dr. Ko said. For each test that a subject failed, the layer was about 1 micrometer thinner. In the multivariate analysis, thinner retinal nerve fiber layer was associated with worse performance on all of the tests: The layer was 0.13 micrometer thinner for each incorrect match on pairs matching; 0.14 micrometer thinner for every 2 points lower in score on numeric and verbal reasoning; and 0.14 micrometer thinner for every 100 millisecond slower reaction time.
The 3-year follow-up data confirmed that these baseline findings persisted, and predicted cognitive decline. “Again, this was true after controlling for all the variables,” Dr. Ko said. “We found that those with the thinnest layers at baseline got worse on more of the tests, compared to those who had the thickest nerve fiber layers at baseline.”
Although this is the first time retinal nerve fiber thickness has predicted cognitive decline, the association with cognition has been studied for a few years. A 2015 meta-analysis found 17 studies comparing the marker between patients with Alzheimer’s and healthy controls and 5 studies of patients with mild cognitive impairment MCI) and healthy controls (Alzheimers Dement (Amst). 2015 Apr 23;1[2]:136-43). All of these found significant retinal nerve fiber thinning in Alzheimer’s and MCI patients.
The lead author of that paper, Kelsey Thompson of the University of Edinburgh (United Kingdom), said the retinal ganglion cell axons can be seen as a sentinel marker for neurodegeneration in the brain.
“Retinal nerve fiber layer thinning in [Alzheimer’s disease] has been hypothesized to occur because of retrograde degeneration of the retinal ganglion cell axons, and these changes have been suggested to occur even before memory is affected. There is also a suggestion that neuroretinal atrophy may occur as a result of amyloid-beta plaque deposits within the retina, although this hypothesis remains more speculative.”
Dr. Ko had no financial declarations.
On Twitter @alz_gal
TORONTO – A thinner-than-normal layer of retinal nerve fibers in the eye is now linked with cognitive decline – another suggestion that extracranial physical findings could be leveraged into dementia screening tools.
The findings were seen in a cohort of 32,000 people enrolled in the U.K. Biobank– an ongoing prospective study following half a million people and collecting data on cancer, heart diseases, stroke, diabetes, arthritis, osteoporosis, eye disorders, depression, and dementia.
The correlation between retinal nerve fiber thickness and cognition was observed in the large cohort at baseline, Fang Sarah Ko, MD, said during a press briefing at the Alzheimer’s Association International Conference 2016. But after following 1,251 of these subjects for 3 years, she and her colleagues found that the correlation continued unabated.
“It’s amazing that we found this in such a healthy population,” Dr. Ko said during the briefing. “We wouldn’t have expected in just 3 years to see any cognitive decline in this cohort, much less measurable cognitive decline with a significant association with retinal nerve fiber layer thickness.”
Dr. Ko, an ophthalmologist in private practice in Tallahassee, Fla., said later during her main presentation of the study that the finding suggests a possible role for retinal imaging as a cognitive health screen.
“Thinner nerve fiber layer was associated with worse performance on memory, reasoning, and reaction time at baseline, and with a decline in each of these tests over time,” she said. “It may be that the nerve fiber layer could be used as a biomarker,” because it is easy to observe and measure with equipment available in most ophthalmology offices. “I would say the potential for clinical use is quite high.”
The U.K. Biobank recruits all of its subjects through the U.K. National Health Service patient registry. All undergo a standard battery of numerous tests; among them are tests of cognitive function and spectral-domain optical coherence tomography (S-DOCT) of the eye. S-DOCT is an increasingly common method of imaging the retina. It produces three-dimensional images of extremely fine resolution.
The 32,000 subjects included in the baseline cohort were all free of diabetes and ocular or neurological disease, and they had normal intraocular pressure. They undertook four tests of cognition: prospective memory, pairs matching, numeric and verbal reasoning, and reaction time. The relationship between these test results and retinal nerve fiber thickness was adjusted for age, sex, race, socioeconomic status, height, refraction, and intraocular pressure.
At baseline, the mean retinal nerve fiber layer was significantly thinner among subjects with abnormal scores on any of the cognitive tests. On the prospective memory test, the layer was an average of 53.3 micrometers for subjects who had correct first-time recall, 52.5 micrometers for those with correct second-time recall, and 51.9 micrometers for those who did not recall. The layer was also significantly thinner in subjects who had low scores on pairs matching, numeric and verbal reasoning, and reaction times.
And the relationship between test results and retinal nerve fiber thinning appeared additive, Dr. Ko said. For each test that a subject failed, the layer was about 1 micrometer thinner. In the multivariate analysis, thinner retinal nerve fiber layer was associated with worse performance on all of the tests: The layer was 0.13 micrometer thinner for each incorrect match on pairs matching; 0.14 micrometer thinner for every 2 points lower in score on numeric and verbal reasoning; and 0.14 micrometer thinner for every 100 millisecond slower reaction time.
The 3-year follow-up data confirmed that these baseline findings persisted, and predicted cognitive decline. “Again, this was true after controlling for all the variables,” Dr. Ko said. “We found that those with the thinnest layers at baseline got worse on more of the tests, compared to those who had the thickest nerve fiber layers at baseline.”
Although this is the first time retinal nerve fiber thickness has predicted cognitive decline, the association with cognition has been studied for a few years. A 2015 meta-analysis found 17 studies comparing the marker between patients with Alzheimer’s and healthy controls and 5 studies of patients with mild cognitive impairment MCI) and healthy controls (Alzheimers Dement (Amst). 2015 Apr 23;1[2]:136-43). All of these found significant retinal nerve fiber thinning in Alzheimer’s and MCI patients.
The lead author of that paper, Kelsey Thompson of the University of Edinburgh (United Kingdom), said the retinal ganglion cell axons can be seen as a sentinel marker for neurodegeneration in the brain.
“Retinal nerve fiber layer thinning in [Alzheimer’s disease] has been hypothesized to occur because of retrograde degeneration of the retinal ganglion cell axons, and these changes have been suggested to occur even before memory is affected. There is also a suggestion that neuroretinal atrophy may occur as a result of amyloid-beta plaque deposits within the retina, although this hypothesis remains more speculative.”
Dr. Ko had no financial declarations.
On Twitter @alz_gal
TORONTO – A thinner-than-normal layer of retinal nerve fibers in the eye is now linked with cognitive decline – another suggestion that extracranial physical findings could be leveraged into dementia screening tools.
The findings were seen in a cohort of 32,000 people enrolled in the U.K. Biobank– an ongoing prospective study following half a million people and collecting data on cancer, heart diseases, stroke, diabetes, arthritis, osteoporosis, eye disorders, depression, and dementia.
The correlation between retinal nerve fiber thickness and cognition was observed in the large cohort at baseline, Fang Sarah Ko, MD, said during a press briefing at the Alzheimer’s Association International Conference 2016. But after following 1,251 of these subjects for 3 years, she and her colleagues found that the correlation continued unabated.
“It’s amazing that we found this in such a healthy population,” Dr. Ko said during the briefing. “We wouldn’t have expected in just 3 years to see any cognitive decline in this cohort, much less measurable cognitive decline with a significant association with retinal nerve fiber layer thickness.”
Dr. Ko, an ophthalmologist in private practice in Tallahassee, Fla., said later during her main presentation of the study that the finding suggests a possible role for retinal imaging as a cognitive health screen.
“Thinner nerve fiber layer was associated with worse performance on memory, reasoning, and reaction time at baseline, and with a decline in each of these tests over time,” she said. “It may be that the nerve fiber layer could be used as a biomarker,” because it is easy to observe and measure with equipment available in most ophthalmology offices. “I would say the potential for clinical use is quite high.”
The U.K. Biobank recruits all of its subjects through the U.K. National Health Service patient registry. All undergo a standard battery of numerous tests; among them are tests of cognitive function and spectral-domain optical coherence tomography (S-DOCT) of the eye. S-DOCT is an increasingly common method of imaging the retina. It produces three-dimensional images of extremely fine resolution.
The 32,000 subjects included in the baseline cohort were all free of diabetes and ocular or neurological disease, and they had normal intraocular pressure. They undertook four tests of cognition: prospective memory, pairs matching, numeric and verbal reasoning, and reaction time. The relationship between these test results and retinal nerve fiber thickness was adjusted for age, sex, race, socioeconomic status, height, refraction, and intraocular pressure.
At baseline, the mean retinal nerve fiber layer was significantly thinner among subjects with abnormal scores on any of the cognitive tests. On the prospective memory test, the layer was an average of 53.3 micrometers for subjects who had correct first-time recall, 52.5 micrometers for those with correct second-time recall, and 51.9 micrometers for those who did not recall. The layer was also significantly thinner in subjects who had low scores on pairs matching, numeric and verbal reasoning, and reaction times.
And the relationship between test results and retinal nerve fiber thinning appeared additive, Dr. Ko said. For each test that a subject failed, the layer was about 1 micrometer thinner. In the multivariate analysis, thinner retinal nerve fiber layer was associated with worse performance on all of the tests: The layer was 0.13 micrometer thinner for each incorrect match on pairs matching; 0.14 micrometer thinner for every 2 points lower in score on numeric and verbal reasoning; and 0.14 micrometer thinner for every 100 millisecond slower reaction time.
The 3-year follow-up data confirmed that these baseline findings persisted, and predicted cognitive decline. “Again, this was true after controlling for all the variables,” Dr. Ko said. “We found that those with the thinnest layers at baseline got worse on more of the tests, compared to those who had the thickest nerve fiber layers at baseline.”
Although this is the first time retinal nerve fiber thickness has predicted cognitive decline, the association with cognition has been studied for a few years. A 2015 meta-analysis found 17 studies comparing the marker between patients with Alzheimer’s and healthy controls and 5 studies of patients with mild cognitive impairment MCI) and healthy controls (Alzheimers Dement (Amst). 2015 Apr 23;1[2]:136-43). All of these found significant retinal nerve fiber thinning in Alzheimer’s and MCI patients.
The lead author of that paper, Kelsey Thompson of the University of Edinburgh (United Kingdom), said the retinal ganglion cell axons can be seen as a sentinel marker for neurodegeneration in the brain.
“Retinal nerve fiber layer thinning in [Alzheimer’s disease] has been hypothesized to occur because of retrograde degeneration of the retinal ganglion cell axons, and these changes have been suggested to occur even before memory is affected. There is also a suggestion that neuroretinal atrophy may occur as a result of amyloid-beta plaque deposits within the retina, although this hypothesis remains more speculative.”
Dr. Ko had no financial declarations.
On Twitter @alz_gal
AT AAIC 2016
Key clinical point: Thinning of the retinal nerve fiber layer was associated with poorer cognitive performance and predicted cognitive decline as well.
Major finding: On a prospective memory test, the layer was an average of 53.3 micrometers for subjects who had correct first-time recall, vs. 51.9 micrometers for those who did not recall.
Data source: The study comprised 32,000 patients at baseline, of whom 1,251 were followed for 3 years.
Disclosures: Dr. Ko had no financial disclosures.

Starting antiretroviral therapy on same day as HIV testing improves outcomes
DURBAN, SOUTH AFRICA – Same-day HIV testing and initiation of antiretroviral therapy results in significantly better outcomes at 12 months than does the common practice of delaying ART for days to weeks in order to provide counseling and conduct further tests, Serena Koenig, MD, reported at the 21st International AIDS Conference.
“With standard testing protocols, patients are given the terrible news that they are HIV-positive and then discharged home without treatment. We believe that if we roll out the red carpet on that very challenging first day and provide extra attention and same-day ART, we increase a sense of hope, optimism, and connectedness to health care providers,” explained Dr. Koenig of Brigham and Women’s Hospital, Boston.

She presented a randomized, prospective clinical trial involving 577 patients at the GHESKIO Clinic in Port-au-Prince, Haiti, the world’s oldest HIV/AIDS treatment clinic and the largest provider of HIV/AIDS care in the Caribbean. Participants, all of whom had a positive HIV test, were randomized to same-day initiation of ART or to standard care, which was discharge home with instructions to return once per week for three counseling and clinical evaluation visits, with ART to begin on day 21.
Both groups received identical services and the same number of contacts with physicians and social workers in the first month following their HIV diagnosis. The only difference was the timing of ART initiation.
Study eligibility was restricted to patients with World Health Organization stage 1 or 2 HIV disease and a same-day chest x-ray showing no indication of tuberculosis or pneumonia.
The primary study endpoint was the rate of retention in care with a plasma HIV RNA viral load of less than 50 copies/mL at 12 months follow-up. This target was achieved in 54% of the same-day ART group, compared with 42% of controls.
Same-day ART also proved significantly better than the standard protocol in terms of the secondary study endpoints. It was associated with 3% mortality at 12 months, compared with 7% in the control arm. Also, 61% of patients in the same-day ART group were retained in care with a viral load of less than 1,000 copies/mL at 12 months, compared with 50% of controls.
In a multivariate regression analysis adjusted for patient demographics and clinical factors, same-day ART was independently associated with a 76% greater likelihood of retention in care with a viral load below 50 copies/mL at 12 months, a 65% reduction in the risk of mortality, and a 67% greater likelihood of retention in care with a viral load of less than 1,000 copies/mL.
The usual rationale for scheduling multiple pre-ART clinic visits is that patients may need time to come to grips with the reality that they require lifelong treatment, coupled with a feeling among many clinicians that there is no real urgency regarding ART initiation. But Dr. Koenig characterized the standard practice of requiring several clinic visits before starting ART as “a missed opportunity.”
“Delays in treatment are associated with increased mortality, diminished recovery of CD4+ cells, higher cost of treatment for opportunistic infections, and ongoing HIV transmission,” she said. “In addition to making things logistically easy, a big part of our study of same-day ART was the foundation of hope.”
Dr. Koenig reported having no financial conflicts with regard to this study, which was funded by the National Institute of Allergy and Infectious Diseases.
DURBAN, SOUTH AFRICA – Same-day HIV testing and initiation of antiretroviral therapy results in significantly better outcomes at 12 months than does the common practice of delaying ART for days to weeks in order to provide counseling and conduct further tests, Serena Koenig, MD, reported at the 21st International AIDS Conference.
“With standard testing protocols, patients are given the terrible news that they are HIV-positive and then discharged home without treatment. We believe that if we roll out the red carpet on that very challenging first day and provide extra attention and same-day ART, we increase a sense of hope, optimism, and connectedness to health care providers,” explained Dr. Koenig of Brigham and Women’s Hospital, Boston.
She presented a randomized, prospective clinical trial involving 577 patients at the GHESKIO Clinic in Port-au-Prince, Haiti, the world’s oldest HIV/AIDS treatment clinic and the largest provider of HIV/AIDS care in the Caribbean. Participants, all of whom had a positive HIV test, were randomized to same-day initiation of ART or to standard care, which was discharge home with instructions to return once per week for three counseling and clinical evaluation visits, with ART to begin on day 21.
Both groups received identical services and the same number of contacts with physicians and social workers in the first month following their HIV diagnosis. The only difference was the timing of ART initiation.
Study eligibility was restricted to patients with World Health Organization stage 1 or 2 HIV disease and a same-day chest x-ray showing no indication of tuberculosis or pneumonia.
The primary study endpoint was the rate of retention in care with a plasma HIV RNA viral load of less than 50 copies/mL at 12 months follow-up. This target was achieved in 54% of the same-day ART group, compared with 42% of controls.
Same-day ART also proved significantly better than the standard protocol in terms of the secondary study endpoints. It was associated with 3% mortality at 12 months, compared with 7% in the control arm. Also, 61% of patients in the same-day ART group were retained in care with a viral load of less than 1,000 copies/mL at 12 months, compared with 50% of controls.
In a multivariate regression analysis adjusted for patient demographics and clinical factors, same-day ART was independently associated with a 76% greater likelihood of retention in care with a viral load below 50 copies/mL at 12 months, a 65% reduction in the risk of mortality, and a 67% greater likelihood of retention in care with a viral load of less than 1,000 copies/mL.
The usual rationale for scheduling multiple pre-ART clinic visits is that patients may need time to come to grips with the reality that they require lifelong treatment, coupled with a feeling among many clinicians that there is no real urgency regarding ART initiation. But Dr. Koenig characterized the standard practice of requiring several clinic visits before starting ART as “a missed opportunity.”
“Delays in treatment are associated with increased mortality, diminished recovery of CD4+ cells, higher cost of treatment for opportunistic infections, and ongoing HIV transmission,” she said. “In addition to making things logistically easy, a big part of our study of same-day ART was the foundation of hope.”
Dr. Koenig reported having no financial conflicts with regard to this study, which was funded by the National Institute of Allergy and Infectious Diseases.
DURBAN, SOUTH AFRICA – Same-day HIV testing and initiation of antiretroviral therapy results in significantly better outcomes at 12 months than does the common practice of delaying ART for days to weeks in order to provide counseling and conduct further tests, Serena Koenig, MD, reported at the 21st International AIDS Conference.
“With standard testing protocols, patients are given the terrible news that they are HIV-positive and then discharged home without treatment. We believe that if we roll out the red carpet on that very challenging first day and provide extra attention and same-day ART, we increase a sense of hope, optimism, and connectedness to health care providers,” explained Dr. Koenig of Brigham and Women’s Hospital, Boston.
She presented a randomized, prospective clinical trial involving 577 patients at the GHESKIO Clinic in Port-au-Prince, Haiti, the world’s oldest HIV/AIDS treatment clinic and the largest provider of HIV/AIDS care in the Caribbean. Participants, all of whom had a positive HIV test, were randomized to same-day initiation of ART or to standard care, which was discharge home with instructions to return once per week for three counseling and clinical evaluation visits, with ART to begin on day 21.
Both groups received identical services and the same number of contacts with physicians and social workers in the first month following their HIV diagnosis. The only difference was the timing of ART initiation.
Study eligibility was restricted to patients with World Health Organization stage 1 or 2 HIV disease and a same-day chest x-ray showing no indication of tuberculosis or pneumonia.
The primary study endpoint was the rate of retention in care with a plasma HIV RNA viral load of less than 50 copies/mL at 12 months follow-up. This target was achieved in 54% of the same-day ART group, compared with 42% of controls.
Same-day ART also proved significantly better than the standard protocol in terms of the secondary study endpoints. It was associated with 3% mortality at 12 months, compared with 7% in the control arm. Also, 61% of patients in the same-day ART group were retained in care with a viral load of less than 1,000 copies/mL at 12 months, compared with 50% of controls.
In a multivariate regression analysis adjusted for patient demographics and clinical factors, same-day ART was independently associated with a 76% greater likelihood of retention in care with a viral load below 50 copies/mL at 12 months, a 65% reduction in the risk of mortality, and a 67% greater likelihood of retention in care with a viral load of less than 1,000 copies/mL.
The usual rationale for scheduling multiple pre-ART clinic visits is that patients may need time to come to grips with the reality that they require lifelong treatment, coupled with a feeling among many clinicians that there is no real urgency regarding ART initiation. But Dr. Koenig characterized the standard practice of requiring several clinic visits before starting ART as “a missed opportunity.”
“Delays in treatment are associated with increased mortality, diminished recovery of CD4+ cells, higher cost of treatment for opportunistic infections, and ongoing HIV transmission,” she said. “In addition to making things logistically easy, a big part of our study of same-day ART was the foundation of hope.”
Dr. Koenig reported having no financial conflicts with regard to this study, which was funded by the National Institute of Allergy and Infectious Diseases.
AT AIDS 2016
Key clinical point: Starting antiretroviral therapy on the same day a patient undergoes HIV testing is clinically advantageous.
Major finding: Patients who started antiretroviral therapy the same day they tested positive for HIV were 76% more likely to remain in care with a plasma HIV RNA viral load of less than 50 copies/mL at 12 months follow-up than were those whose treatment start was delayed 3 weeks for pre-treatment counseling sessions and further testing.
Data source: This prospective, randomized trial included 577 HIV-positive patients who were randomized to initiation of antiretroviral therapy on the same day they underwent HIV testing or to initiation of therapy 21 days later, after three additional clinic visits.
Disclosures: The presenter reported having no financial conflicts with regard to this study, which was funded by the National Institute of Allergy and Infectious Diseases.

Deals likely the way forward for Medicaid coverage of hepatitis C drugs
As state governments struggle to find a balance between access to hepatitis C drugs and being able to afford them, it appears that individual deals with drug manufacturers will be the way to get these drugs to a wider portion of the population.
Most recently, MassHealth, Massachusetts’ state Medicaid agency, negotiated with Gilead Sciences on new rebates that the agency said will “significantly” lower the cost on the hepatitis C drug Harvoni.
“I think it probably is the direction we are going in hepatitis C coverage,” Matt Salo, executive director of the National Association of Medicaid Directors (NAMD), said in an interivew. “Pricing has been a real challenge nationwide, certainly for Medicaid itself. Medicaid’s got an obligation to … like state budgets, balance a budget every single year. When we’ve got massive cost spikes in any one particular area, it generally tends to come with trade-offs you have to make elsewhere that aren’t necessarily in the best interest of everybody involved.”
According to the deal, Harvoni will be the exclusive drug used to treat hepatitis C for about 80% of patients in need. MassHealth also negotiated rebates for Gilead’s Sovaldi and Bristol-Myers Squibb’s Daklinza, which are indicated for about 20% of hepatitis C patients. The state expects to be able to cover most people in the state with hepatitis C.
Given the cost of hepatitis C drugs, which can reach into the $90,000 range for a course of treatment, state Medicaid agencies were putting access restrictions on the drug. However, as lawsuits were limiting states’ abilities to apply utilization management, negotiations with the drug companies became another avenue.
“When those lawsuits hit and were decided, most recently in Washington state and Delaware, it basically said and basically confirmed that Medicaid has to cover everybody,” Mr. Salo said. “That put the pricing issue right back in the forefront, because states like Massachusetts, Florida, and New York are going down this road of trying to figure out if we are going to open up coverage to everybody. How do we manage this?”
He noted that competition has helped make the price more manageable, but challenges still remain because of the cost of these drugs and prices still need to come down.
“Now that you’ve got three manufacturers – Gilead, AbbVie, and Merck – there is a little bit more of a competitive market at play,” Mr. Salo noted. “When the Merck product came on, they intentionally priced it lower than the other stuff in the market, which is good. These are all good things, but I still think the challenge we are going to face now is it’s still not gotten down to a price that’s low enough to really make it affordable to cover a million people in the Medicaid program.”
However, Mr. Salo said he does not see prices themselves coming down much further, unless perhaps a new competitor can come in and shake the market up further. As such, NAMD is looking toward legislative solutions to address the hepatitis C drug market.
He narrowed it down to three areas: price, cost, and access control.
Mr. Salo was quick to note that Congress doing something about price would look very much like price controls and would probably be a tough sell politically.
However, the federal government could help in other ways, such as creating a fund similar to the one the government uses to help pay for HIV/AIDS drugs.
“These are a bunch of things that wouldn’t touch on the manufacturers’ profit margin but might be things like an increased federal match for the drugs or perhaps creating a separate standalone federal program to provide hepatitis C treatments for patients much in the same way that Congress created the Ryan White program when it was clear that the cost of HIV/AIDS treatments were too much for the market to bear,” he said.
He also suggested that perhaps Medicare could help pay for the Medicaid coverage of hepatitis C drugs.
“If you think about cost savings to the system, the savings will be reaped by Medicare because it won’t be until those folks are 65 and older that the liver fibrosis and other types of things will really start to take effect,” he said. “Is there a way to bring Medicare in to offset some of the cost?”
Finally, he suggested Congress give state Medicaid agencies explicit authority to apply utilization management to help prioritize patients in need of these treatments.
As state governments struggle to find a balance between access to hepatitis C drugs and being able to afford them, it appears that individual deals with drug manufacturers will be the way to get these drugs to a wider portion of the population.
Most recently, MassHealth, Massachusetts’ state Medicaid agency, negotiated with Gilead Sciences on new rebates that the agency said will “significantly” lower the cost on the hepatitis C drug Harvoni.
“I think it probably is the direction we are going in hepatitis C coverage,” Matt Salo, executive director of the National Association of Medicaid Directors (NAMD), said in an interivew. “Pricing has been a real challenge nationwide, certainly for Medicaid itself. Medicaid’s got an obligation to … like state budgets, balance a budget every single year. When we’ve got massive cost spikes in any one particular area, it generally tends to come with trade-offs you have to make elsewhere that aren’t necessarily in the best interest of everybody involved.”
According to the deal, Harvoni will be the exclusive drug used to treat hepatitis C for about 80% of patients in need. MassHealth also negotiated rebates for Gilead’s Sovaldi and Bristol-Myers Squibb’s Daklinza, which are indicated for about 20% of hepatitis C patients. The state expects to be able to cover most people in the state with hepatitis C.
Given the cost of hepatitis C drugs, which can reach into the $90,000 range for a course of treatment, state Medicaid agencies were putting access restrictions on the drug. However, as lawsuits were limiting states’ abilities to apply utilization management, negotiations with the drug companies became another avenue.
“When those lawsuits hit and were decided, most recently in Washington state and Delaware, it basically said and basically confirmed that Medicaid has to cover everybody,” Mr. Salo said. “That put the pricing issue right back in the forefront, because states like Massachusetts, Florida, and New York are going down this road of trying to figure out if we are going to open up coverage to everybody. How do we manage this?”
He noted that competition has helped make the price more manageable, but challenges still remain because of the cost of these drugs and prices still need to come down.
“Now that you’ve got three manufacturers – Gilead, AbbVie, and Merck – there is a little bit more of a competitive market at play,” Mr. Salo noted. “When the Merck product came on, they intentionally priced it lower than the other stuff in the market, which is good. These are all good things, but I still think the challenge we are going to face now is it’s still not gotten down to a price that’s low enough to really make it affordable to cover a million people in the Medicaid program.”
However, Mr. Salo said he does not see prices themselves coming down much further, unless perhaps a new competitor can come in and shake the market up further. As such, NAMD is looking toward legislative solutions to address the hepatitis C drug market.
He narrowed it down to three areas: price, cost, and access control.
Mr. Salo was quick to note that Congress doing something about price would look very much like price controls and would probably be a tough sell politically.
However, the federal government could help in other ways, such as creating a fund similar to the one the government uses to help pay for HIV/AIDS drugs.
“These are a bunch of things that wouldn’t touch on the manufacturers’ profit margin but might be things like an increased federal match for the drugs or perhaps creating a separate standalone federal program to provide hepatitis C treatments for patients much in the same way that Congress created the Ryan White program when it was clear that the cost of HIV/AIDS treatments were too much for the market to bear,” he said.
He also suggested that perhaps Medicare could help pay for the Medicaid coverage of hepatitis C drugs.
“If you think about cost savings to the system, the savings will be reaped by Medicare because it won’t be until those folks are 65 and older that the liver fibrosis and other types of things will really start to take effect,” he said. “Is there a way to bring Medicare in to offset some of the cost?”
Finally, he suggested Congress give state Medicaid agencies explicit authority to apply utilization management to help prioritize patients in need of these treatments.
As state governments struggle to find a balance between access to hepatitis C drugs and being able to afford them, it appears that individual deals with drug manufacturers will be the way to get these drugs to a wider portion of the population.
Most recently, MassHealth, Massachusetts’ state Medicaid agency, negotiated with Gilead Sciences on new rebates that the agency said will “significantly” lower the cost on the hepatitis C drug Harvoni.
“I think it probably is the direction we are going in hepatitis C coverage,” Matt Salo, executive director of the National Association of Medicaid Directors (NAMD), said in an interivew. “Pricing has been a real challenge nationwide, certainly for Medicaid itself. Medicaid’s got an obligation to … like state budgets, balance a budget every single year. When we’ve got massive cost spikes in any one particular area, it generally tends to come with trade-offs you have to make elsewhere that aren’t necessarily in the best interest of everybody involved.”
According to the deal, Harvoni will be the exclusive drug used to treat hepatitis C for about 80% of patients in need. MassHealth also negotiated rebates for Gilead’s Sovaldi and Bristol-Myers Squibb’s Daklinza, which are indicated for about 20% of hepatitis C patients. The state expects to be able to cover most people in the state with hepatitis C.
Given the cost of hepatitis C drugs, which can reach into the $90,000 range for a course of treatment, state Medicaid agencies were putting access restrictions on the drug. However, as lawsuits were limiting states’ abilities to apply utilization management, negotiations with the drug companies became another avenue.
“When those lawsuits hit and were decided, most recently in Washington state and Delaware, it basically said and basically confirmed that Medicaid has to cover everybody,” Mr. Salo said. “That put the pricing issue right back in the forefront, because states like Massachusetts, Florida, and New York are going down this road of trying to figure out if we are going to open up coverage to everybody. How do we manage this?”
He noted that competition has helped make the price more manageable, but challenges still remain because of the cost of these drugs and prices still need to come down.
“Now that you’ve got three manufacturers – Gilead, AbbVie, and Merck – there is a little bit more of a competitive market at play,” Mr. Salo noted. “When the Merck product came on, they intentionally priced it lower than the other stuff in the market, which is good. These are all good things, but I still think the challenge we are going to face now is it’s still not gotten down to a price that’s low enough to really make it affordable to cover a million people in the Medicaid program.”
However, Mr. Salo said he does not see prices themselves coming down much further, unless perhaps a new competitor can come in and shake the market up further. As such, NAMD is looking toward legislative solutions to address the hepatitis C drug market.
He narrowed it down to three areas: price, cost, and access control.
Mr. Salo was quick to note that Congress doing something about price would look very much like price controls and would probably be a tough sell politically.
However, the federal government could help in other ways, such as creating a fund similar to the one the government uses to help pay for HIV/AIDS drugs.
“These are a bunch of things that wouldn’t touch on the manufacturers’ profit margin but might be things like an increased federal match for the drugs or perhaps creating a separate standalone federal program to provide hepatitis C treatments for patients much in the same way that Congress created the Ryan White program when it was clear that the cost of HIV/AIDS treatments were too much for the market to bear,” he said.
He also suggested that perhaps Medicare could help pay for the Medicaid coverage of hepatitis C drugs.
“If you think about cost savings to the system, the savings will be reaped by Medicare because it won’t be until those folks are 65 and older that the liver fibrosis and other types of things will really start to take effect,” he said. “Is there a way to bring Medicare in to offset some of the cost?”
Finally, he suggested Congress give state Medicaid agencies explicit authority to apply utilization management to help prioritize patients in need of these treatments.
COMFORT mnemonic can help guide malignant wound care
BOSTON – Malignancy in a chronic leg wound can be very aggressive, and multidisciplinary care is a must – particularly in those who oppose amputation, according to Tania J. Phillips, MD.
“When you get a more advanced, malignant, ulcerated wound, this is really a complex situation that requires multidisciplinary care,” she said at the American Academy of Dermatology summer meeting.
In addition to dermatologic care, patients may need medical oncology, surgery, radiation, and good nursing care, she explained.
For patients with malignancy who oppose amputation, a palliative care team may also be a necessity, said Dr. Phillips, professor of dermatology at Boston University. She described one patient she cared for who had an ulcerated wound with squamous cell carcinoma. The patient was treated daily 5 days per week for 2 months. The wound did not heal.
“In these kinds of patients you may not heal the wound; you may just have to try to keep the wound clean, free of pain, and free of infection, she said.
COMFORT is a valuable mnemonic device for caring for such patients, she said: Care for pain and itching, use Odor control, Manage exudate and bleeding, Fight infection, Optimize peri-wound skin integrity, use Reparative and aesthetic wound dressings, Treat the cancer.
Pain is a major issue in patients with such wounds. It is important assess the wound etiology and treat the underlying disease, but it is also important to assess the pain and try to manage it, Dr. Phillips said. Often, addressing local wound management will help with the pain. Appropriate dressing selection is particularly important, as dressing changes can be very painful, she said, recommending the use of non-stick dressings that keep the wound moist. Local and systemic treatment may also be necessary to control pain and itching, she said.
Odor control is another concern. Necrotic tissue has a lot of odor, so debridement can help.
“Use a 19-guage needle to cleanse the wound,” she suggested, noting that this provides higher pressure that can be effective for cleansing.
Dressings that contain nanocrystalline silver or activated charcoal can also help.
As for managing exudate and bleeding, dressing choice is again an important consideration. More absorbent dressings like alginates are useful and have hemostatic properties that can also help with bleeding. Frequent dressing changes are also important.
“And obviously, you want to treat infection,” Dr. Phillips added. Metronidazole gel or powder can help with both infection and odor, she noted.
Peri-wound skin can be very fragile, so it is important to provide protection. In some cases, this can be addressed simply with zinc oxide or petrolatum. Various skin sealants are also available, and can be used to form a barrier to dressings that can be damaging to the skin.
Silicone dressings are very powerful because they don’t stick to the skin, and are not painful or damaging when removed, she said.
The use of a window with hydrocolloid dressing, which allows for changing only the inside of the dressing, is another useful approach, and using mesh rather than tape to hold the dressing in place can help to protect peri-wound skin.
Dr. Phillips reported a financial relationship with Hygeia.
BOSTON – Malignancy in a chronic leg wound can be very aggressive, and multidisciplinary care is a must – particularly in those who oppose amputation, according to Tania J. Phillips, MD.
“When you get a more advanced, malignant, ulcerated wound, this is really a complex situation that requires multidisciplinary care,” she said at the American Academy of Dermatology summer meeting.
In addition to dermatologic care, patients may need medical oncology, surgery, radiation, and good nursing care, she explained.
For patients with malignancy who oppose amputation, a palliative care team may also be a necessity, said Dr. Phillips, professor of dermatology at Boston University. She described one patient she cared for who had an ulcerated wound with squamous cell carcinoma. The patient was treated daily 5 days per week for 2 months. The wound did not heal.
“In these kinds of patients you may not heal the wound; you may just have to try to keep the wound clean, free of pain, and free of infection, she said.
COMFORT is a valuable mnemonic device for caring for such patients, she said: Care for pain and itching, use Odor control, Manage exudate and bleeding, Fight infection, Optimize peri-wound skin integrity, use Reparative and aesthetic wound dressings, Treat the cancer.
Pain is a major issue in patients with such wounds. It is important assess the wound etiology and treat the underlying disease, but it is also important to assess the pain and try to manage it, Dr. Phillips said. Often, addressing local wound management will help with the pain. Appropriate dressing selection is particularly important, as dressing changes can be very painful, she said, recommending the use of non-stick dressings that keep the wound moist. Local and systemic treatment may also be necessary to control pain and itching, she said.
Odor control is another concern. Necrotic tissue has a lot of odor, so debridement can help.
“Use a 19-guage needle to cleanse the wound,” she suggested, noting that this provides higher pressure that can be effective for cleansing.
Dressings that contain nanocrystalline silver or activated charcoal can also help.
As for managing exudate and bleeding, dressing choice is again an important consideration. More absorbent dressings like alginates are useful and have hemostatic properties that can also help with bleeding. Frequent dressing changes are also important.
“And obviously, you want to treat infection,” Dr. Phillips added. Metronidazole gel or powder can help with both infection and odor, she noted.
Peri-wound skin can be very fragile, so it is important to provide protection. In some cases, this can be addressed simply with zinc oxide or petrolatum. Various skin sealants are also available, and can be used to form a barrier to dressings that can be damaging to the skin.
Silicone dressings are very powerful because they don’t stick to the skin, and are not painful or damaging when removed, she said.
The use of a window with hydrocolloid dressing, which allows for changing only the inside of the dressing, is another useful approach, and using mesh rather than tape to hold the dressing in place can help to protect peri-wound skin.
Dr. Phillips reported a financial relationship with Hygeia.
BOSTON – Malignancy in a chronic leg wound can be very aggressive, and multidisciplinary care is a must – particularly in those who oppose amputation, according to Tania J. Phillips, MD.
“When you get a more advanced, malignant, ulcerated wound, this is really a complex situation that requires multidisciplinary care,” she said at the American Academy of Dermatology summer meeting.
In addition to dermatologic care, patients may need medical oncology, surgery, radiation, and good nursing care, she explained.
For patients with malignancy who oppose amputation, a palliative care team may also be a necessity, said Dr. Phillips, professor of dermatology at Boston University. She described one patient she cared for who had an ulcerated wound with squamous cell carcinoma. The patient was treated daily 5 days per week for 2 months. The wound did not heal.
“In these kinds of patients you may not heal the wound; you may just have to try to keep the wound clean, free of pain, and free of infection, she said.
COMFORT is a valuable mnemonic device for caring for such patients, she said: Care for pain and itching, use Odor control, Manage exudate and bleeding, Fight infection, Optimize peri-wound skin integrity, use Reparative and aesthetic wound dressings, Treat the cancer.
Pain is a major issue in patients with such wounds. It is important assess the wound etiology and treat the underlying disease, but it is also important to assess the pain and try to manage it, Dr. Phillips said. Often, addressing local wound management will help with the pain. Appropriate dressing selection is particularly important, as dressing changes can be very painful, she said, recommending the use of non-stick dressings that keep the wound moist. Local and systemic treatment may also be necessary to control pain and itching, she said.
Odor control is another concern. Necrotic tissue has a lot of odor, so debridement can help.
“Use a 19-guage needle to cleanse the wound,” she suggested, noting that this provides higher pressure that can be effective for cleansing.
Dressings that contain nanocrystalline silver or activated charcoal can also help.
As for managing exudate and bleeding, dressing choice is again an important consideration. More absorbent dressings like alginates are useful and have hemostatic properties that can also help with bleeding. Frequent dressing changes are also important.
“And obviously, you want to treat infection,” Dr. Phillips added. Metronidazole gel or powder can help with both infection and odor, she noted.
Peri-wound skin can be very fragile, so it is important to provide protection. In some cases, this can be addressed simply with zinc oxide or petrolatum. Various skin sealants are also available, and can be used to form a barrier to dressings that can be damaging to the skin.
Silicone dressings are very powerful because they don’t stick to the skin, and are not painful or damaging when removed, she said.
The use of a window with hydrocolloid dressing, which allows for changing only the inside of the dressing, is another useful approach, and using mesh rather than tape to hold the dressing in place can help to protect peri-wound skin.
Dr. Phillips reported a financial relationship with Hygeia.
EXPERT ANALYSIS FROM AAD SUMMER ACADEMY 2016
Early Alzheimer’s Treatment Decreases Both Costs and Mortality
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.

It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.
It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.
It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
AT AAIC 2016

Early Alzheimer’s treatment decreases both costs and mortality
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.

It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
On Twitter @alz_gal
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.
It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
On Twitter @alz_gal
TORONTO – For patients with Alzheimer’s disease, early treatment may translate into lower health care costs and better survival, based on study results reported at the Alzheimer’s Association International Conference 2016.
A review of Medicare claims data from more than 1,300 patients who received a diagnosis of Alzheimer’s disease during 2010-2013 found that patients who got standard anti-dementia therapy within a month of an Alzheimer’s diagnosis had a 28% lower risk of dying by 6 months than did patients who weren’t treated. And while their health care costs spiked at the time of diagnosis, monthly costs were consistently lower, yielding an overall savings of about $1,700 by the end of the study.
It’s not that the drugs themselves exerted any lifesaving effects, said study co-author Christopher Black, associate director of outcomes research at Merck Research Laboratories, Rahway, N.J. Rather, the observed benefit is probably because the patients who got treated also then got consistent medical attention for health-threatening comorbidities.
“This is an important caveat,” Mr. Black said in an interview at the meeting. “We are not saying that anti-dementia treatment is causing longer survival. It’s a proxy for better care. Typically, dementia patients die of complications from comorbidities that are exacerbated by Alzheimer’s symptoms.”
Mr. Black and his colleagues examined healthcare costs and utilization during the 12 months before diagnosis and in the 6 months after diagnosis. They also looked at mortality incidence. He and his colleagues identified 6,553 incident Alzheimer’s patients. Just 35% received a prescription for an anti-dementia medication within the month after diagnosis. Most patients (67%) got donepezil. Other prescribed medications were memantine (19%), rivastigmine (12%) and galantamine (2%).
There were several significant differences between the treated and untreated groups. Untreated patients were older (84 vs. 81 years) and had a significantly higher Charlson comorbidity index (3.5 vs. 3.2). To account for these differences, the researchers used propensity score matching on the basis of medical comorbidities, age, and other demographics to compare 694 patients from each group.
At the end of 6 months, treated patients had a 28% lower risk of dying (hazard ratio, 0.72) than did non-treated patients. Health care costs and utilization showed significant differences as well. Before diagnosis, monthly medical costs were similar (average $665). During the month of diagnosis, costs surged for both groups, although more so in the group that was untreated (mean $6,711 vs. $5,535). This probably reflected the general health differences between the two groups, as well as the cost of transitioning into a hospital, or from a hospital to a long-term care facility, Mr. Black said.
“This spike at the time of diagnosis is important,” he said in an interview. “The major cost driver was inpatient hospitalization and skilled nursing home placement, and this was driven by 10% of the patients.”
After the first month, costs declined and stabilized in each group. However, the between-group differences remained. There were half as many hospice visits per month among the treated patients (0.04 vs. 0.09; P = .0001). Monthly costs overall were lower, but not to a statistically significant extent ($2,207 vs. $2,349; P = .3037). Total health care costs by the end of the follow-up period averaged about $1,700 less in treated patients.
“Even after adjusting for demographic and clinical differences, results suggested that treated Alzheimer’s patients had lower all-cause health care costs and lower mortality rates compared to untreated patients,” Mr. Black said. “The arguments for early treatment are myriad, but this study shows greater survival and less all-cause health care costs among those receiving treatment for dementia. These results indicate that choosing not to treat, or even a delay in starting treatment, may lead to less favorable results. Early diagnosis and time to treatment should be a priority for policymakers, physicians and the public.”
On Twitter @alz_gal
AT AAIC 2016
Key clinical point: Alzheimer’s patients who get early medical treatment have less risk of dying and incur lower health care costs.
Major finding: By 6 months after diagnosis, treated patients had a 28% lower risk of dying, and had incurred about $1,700 less in health care expenditures.
Data source: The Medicare claims database study comprised about 1,300 patients.
Disclosures: Christopher Black is an associate director of outcomes research at Merck Research Laboratories, Rahway, N.J.

Color correcting – for skin blemishes
One of the most frustrating problems we encounter is helping patients with skin issues that we cannot immediately fix or cure. Teaching them the art of concealing skin blemishes gives patients a sense of relief. Color correction is an art and requires an understanding of basic color theory and Fitzpatrick skin type.
On the color wheel, each color sits directly across from another color, making them complementary colors.
If we look at red, the color opposing it is green. When red and green are combined, they neutralize each other. One of the greatest dermatologists of all time and my mentor, Timothy Berger, MD, taught me that in dermatology color “hue” is a clue to understanding morphology. Everything that is red cannot just be called “erythematous.” There is orange/red (pityriasis rosea, tinea versicolor, seborrheic dermatitis), deep red (cellulitis, Sweet’s syndrome, acne scars, rosacea, psoriasis), purple/red (vasculitis, lichen planus (LP), veins, under-eye circles), brown/red (pigmented purpura, pigmented acne scars, sarcoid).
The combination of the underlying pathology, morphology, and Fitzpatrick type is both a clue to diagnosis and a pallet for skin concealers. We can use the following techniques to help patients color correct skin imperfections:

Red: rosacea, acne scars, acne
Green-based concealers and primers are the best option to significantly reduce the redness. While green primers and correctors tend to be great for Fitzpatrick skin types I-III, a yellow-based concealer/corrector can help to cover redness on those with skin types IV-VI.
Blue: periorbital veins
If you are dealing with blue-toned skin lesions, such as periorbital veins, the ideal corrector is one with a peach or orange undertones. For skin types I-III, a peach/salmon corrector works best, whereas skin types IV-VI requires an orange-toned corrector.
Purple: under-eye circles, LP, postprocedure bruising
If under-eye circles tend to have a more purple hue to them, a yellow-based corrector works best for skin types I-III. For skin types IV-VI skin types, you will need a corrector with a red undertone.
Yellow: bruising
Purple/lavender correctors are best suited for eliminating yellow tones from the face. Purple also combats sallow undertones of the skin.
Brown: lentigines, melasma, seborrheic keratosis, post-inflammatory hyperpigmentation, nevi, café au lait spots

Brown is actually the hardest of all colors to correct. The deeper the pigment (ashy dermatitis, melasma) the more gray the areas appear with skin concealers. The more superficial the pigment (ephelides, lentigines), the easier it is to correct. Generally speaking, peach toned concealers work best, not beige or brown. The corrector, however, should be lighter than the skin tone or the lesion itself will appear darker.
Helping patients conceal imperfections with these simple guidelines is a great way to help relieve some anxiety and help our patients fell more confident in their skin.
Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].
One of the most frustrating problems we encounter is helping patients with skin issues that we cannot immediately fix or cure. Teaching them the art of concealing skin blemishes gives patients a sense of relief. Color correction is an art and requires an understanding of basic color theory and Fitzpatrick skin type.
On the color wheel, each color sits directly across from another color, making them complementary colors.
If we look at red, the color opposing it is green. When red and green are combined, they neutralize each other. One of the greatest dermatologists of all time and my mentor, Timothy Berger, MD, taught me that in dermatology color “hue” is a clue to understanding morphology. Everything that is red cannot just be called “erythematous.” There is orange/red (pityriasis rosea, tinea versicolor, seborrheic dermatitis), deep red (cellulitis, Sweet’s syndrome, acne scars, rosacea, psoriasis), purple/red (vasculitis, lichen planus (LP), veins, under-eye circles), brown/red (pigmented purpura, pigmented acne scars, sarcoid).
The combination of the underlying pathology, morphology, and Fitzpatrick type is both a clue to diagnosis and a pallet for skin concealers. We can use the following techniques to help patients color correct skin imperfections:
Red: rosacea, acne scars, acne
Green-based concealers and primers are the best option to significantly reduce the redness. While green primers and correctors tend to be great for Fitzpatrick skin types I-III, a yellow-based concealer/corrector can help to cover redness on those with skin types IV-VI.
Blue: periorbital veins
If you are dealing with blue-toned skin lesions, such as periorbital veins, the ideal corrector is one with a peach or orange undertones. For skin types I-III, a peach/salmon corrector works best, whereas skin types IV-VI requires an orange-toned corrector.
Purple: under-eye circles, LP, postprocedure bruising
If under-eye circles tend to have a more purple hue to them, a yellow-based corrector works best for skin types I-III. For skin types IV-VI skin types, you will need a corrector with a red undertone.
Yellow: bruising
Purple/lavender correctors are best suited for eliminating yellow tones from the face. Purple also combats sallow undertones of the skin.
Brown: lentigines, melasma, seborrheic keratosis, post-inflammatory hyperpigmentation, nevi, café au lait spots
Brown is actually the hardest of all colors to correct. The deeper the pigment (ashy dermatitis, melasma) the more gray the areas appear with skin concealers. The more superficial the pigment (ephelides, lentigines), the easier it is to correct. Generally speaking, peach toned concealers work best, not beige or brown. The corrector, however, should be lighter than the skin tone or the lesion itself will appear darker.
Helping patients conceal imperfections with these simple guidelines is a great way to help relieve some anxiety and help our patients fell more confident in their skin.
Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].
One of the most frustrating problems we encounter is helping patients with skin issues that we cannot immediately fix or cure. Teaching them the art of concealing skin blemishes gives patients a sense of relief. Color correction is an art and requires an understanding of basic color theory and Fitzpatrick skin type.
On the color wheel, each color sits directly across from another color, making them complementary colors.
If we look at red, the color opposing it is green. When red and green are combined, they neutralize each other. One of the greatest dermatologists of all time and my mentor, Timothy Berger, MD, taught me that in dermatology color “hue” is a clue to understanding morphology. Everything that is red cannot just be called “erythematous.” There is orange/red (pityriasis rosea, tinea versicolor, seborrheic dermatitis), deep red (cellulitis, Sweet’s syndrome, acne scars, rosacea, psoriasis), purple/red (vasculitis, lichen planus (LP), veins, under-eye circles), brown/red (pigmented purpura, pigmented acne scars, sarcoid).
The combination of the underlying pathology, morphology, and Fitzpatrick type is both a clue to diagnosis and a pallet for skin concealers. We can use the following techniques to help patients color correct skin imperfections:
Red: rosacea, acne scars, acne
Green-based concealers and primers are the best option to significantly reduce the redness. While green primers and correctors tend to be great for Fitzpatrick skin types I-III, a yellow-based concealer/corrector can help to cover redness on those with skin types IV-VI.
Blue: periorbital veins
If you are dealing with blue-toned skin lesions, such as periorbital veins, the ideal corrector is one with a peach or orange undertones. For skin types I-III, a peach/salmon corrector works best, whereas skin types IV-VI requires an orange-toned corrector.
Purple: under-eye circles, LP, postprocedure bruising
If under-eye circles tend to have a more purple hue to them, a yellow-based corrector works best for skin types I-III. For skin types IV-VI skin types, you will need a corrector with a red undertone.
Yellow: bruising
Purple/lavender correctors are best suited for eliminating yellow tones from the face. Purple also combats sallow undertones of the skin.
Brown: lentigines, melasma, seborrheic keratosis, post-inflammatory hyperpigmentation, nevi, café au lait spots
Brown is actually the hardest of all colors to correct. The deeper the pigment (ashy dermatitis, melasma) the more gray the areas appear with skin concealers. The more superficial the pigment (ephelides, lentigines), the easier it is to correct. Generally speaking, peach toned concealers work best, not beige or brown. The corrector, however, should be lighter than the skin tone or the lesion itself will appear darker.
Helping patients conceal imperfections with these simple guidelines is a great way to help relieve some anxiety and help our patients fell more confident in their skin.
Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].