User login
Odontogenic Sinusitis
A 55-year-old man who had experienced discolored nasal drainage and mucus plugs in the right side of his nose for 5 years was referred to the ear, nose, and throat clinic. A computerized tomography (CT) scan showed opacification of the right ethmoid and maxillary sinuses and periapical radiolucency in the first and second right maxillary molars (Figure 1). 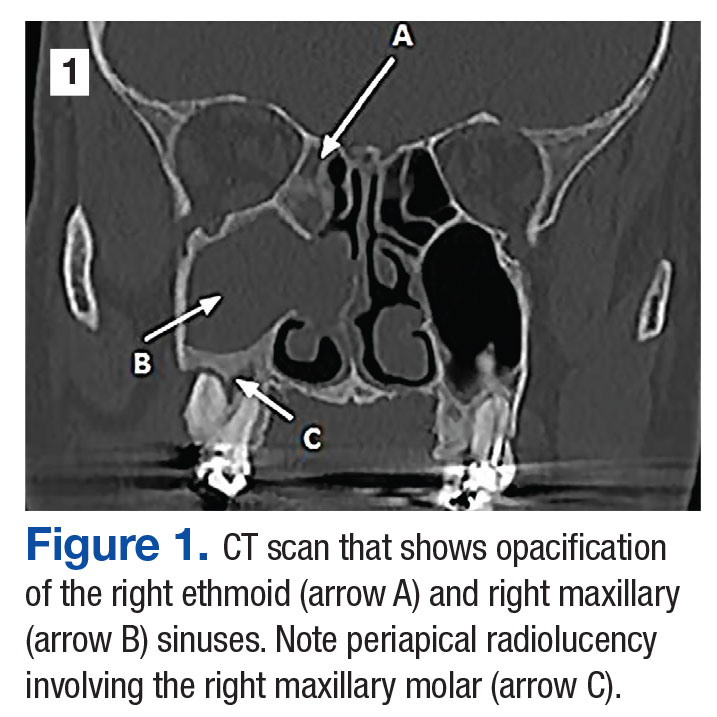
The patient was treated with antibiotics (amoxicillin and clavulanate; moxifloxacin) and nasal rinses but failed to improve. 
The maxillary molars were considered the source of the persistent sinus infection, and the patient was referred to oral surgery for extraction. Three months after oral surgery, the extraction sites were completely healed, and the right maxillary sinus appeared free of disease endoscopically (Figure 3). 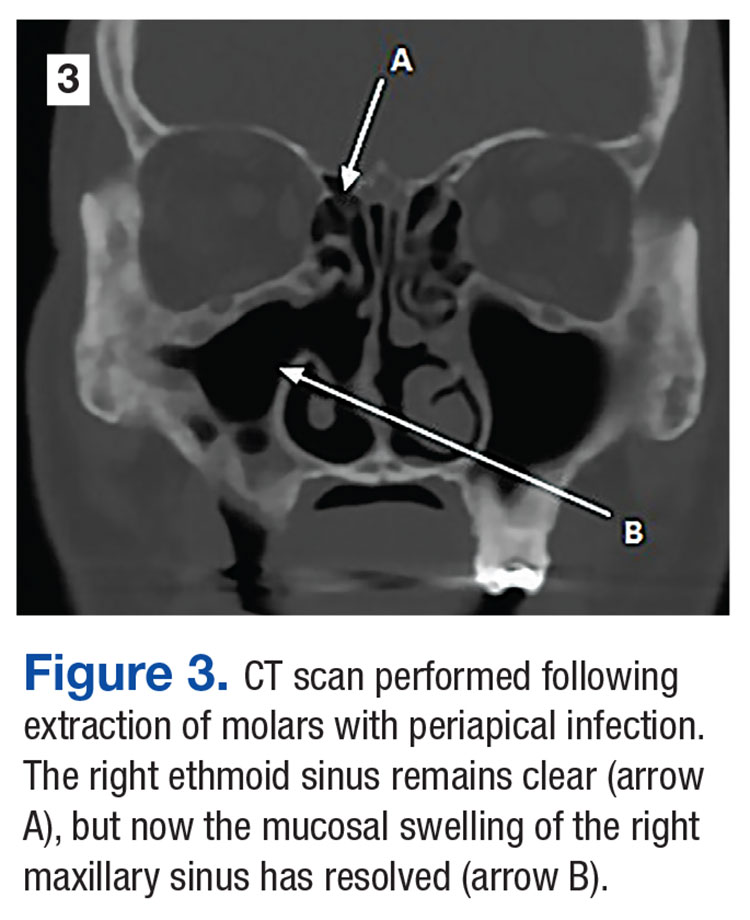
1 .
2. Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otolaryngol Head Neck Surg. 2012;20(1):24-28.
A 55-year-old man who had experienced discolored nasal drainage and mucus plugs in the right side of his nose for 5 years was referred to the ear, nose, and throat clinic. A computerized tomography (CT) scan showed opacification of the right ethmoid and maxillary sinuses and periapical radiolucency in the first and second right maxillary molars (Figure 1).
The patient was treated with antibiotics (amoxicillin and clavulanate; moxifloxacin) and nasal rinses but failed to improve.
The maxillary molars were considered the source of the persistent sinus infection, and the patient was referred to oral surgery for extraction. Three months after oral surgery, the extraction sites were completely healed, and the right maxillary sinus appeared free of disease endoscopically (Figure 3).
A 55-year-old man who had experienced discolored nasal drainage and mucus plugs in the right side of his nose for 5 years was referred to the ear, nose, and throat clinic. A computerized tomography (CT) scan showed opacification of the right ethmoid and maxillary sinuses and periapical radiolucency in the first and second right maxillary molars (Figure 1).
The patient was treated with antibiotics (amoxicillin and clavulanate; moxifloxacin) and nasal rinses but failed to improve.
The maxillary molars were considered the source of the persistent sinus infection, and the patient was referred to oral surgery for extraction. Three months after oral surgery, the extraction sites were completely healed, and the right maxillary sinus appeared free of disease endoscopically (Figure 3).
1 .
2. Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otolaryngol Head Neck Surg. 2012;20(1):24-28.
1 .
2. Patel NA, Ferguson BJ. Odontogenic sinusitis: an ancient but under-appreciated cause of maxillary sinusitis. Curr Opin Otolaryngol Head Neck Surg. 2012;20(1):24-28.
MRD predicts outcome of HSCT in ALL, study suggests
ORLANDO, FL—Minimal residual disease (MRD) measurements before and after hematopoietic stem cell transplant (HSCT) can help predict outcomes in patients with childhood acute lymphoblastic leukemia (ALL), according to researchers.
Their work also suggests several other factors can be used to predict event-free survival (EFS) in this patient population, and the team developed risk scores incorporating these factors.
Michael A. Pulsipher, MD, of Children’s Hospital Los Angeles in California, presented this work as one of the “Best Abstracts” at the 2017 BMT Tandem Meetings (abstract 4*).
“The new risk scores that we were able to develop very nicely predict outcomes post-transplant and can guide study planning,” Dr Pulsipher said.
“MRD pre-transplant was a very powerful predictor of outcome, and MRD post-transplant highlights individual patients at risk.”
For this study, Dr Pulsipher and his colleagues retrospectively analyzed 747 patients treated in Europe, North America, and Australia. The patients received transplants between September 1999 and May 2015.
Most patients had pre-B ALL (78%, n=586), 19% (n=145) had T-cell ALL, 2% had “other” ALLs (n=8) or no data on ALL type (n=8). Sixty-two percent (n=466) were male.
Nearly half of patients were between the ages of 2 and 10 (49%, n=365), 47% (n=351) were older than 10, and 4% (n=31) were younger than 2.
Transplant details
Patients received grafts from matched unrelated donors (42%, n=314), matched sibling donors (30%, n=227), mismatched donors (10%, n=75), and cord blood from unrelated donors (17%, n=128). There was no data on donor type for 3 patients.
Most patients received bone marrow transplants (61%, n=458), 20% (n=147) received cord blood, and 18% (n=131) received peripheral blood stem cells. Eight patients received “other” types of transplants, and 3 patients had no data on stem cell source.
More than half of the patients (55%, n=410) were in their second complete remission (CR) at transplant. Thirty-seven percent were in their first CR (n=275), 7% were in their third or greater CR (n=53), and 1% were not in remission (n=7). Two patients had no data on remission status.
MRD
MRD was assessed before HSCT as well as after—on or near days 30, 60, 90, 180, 365, and beyond.
There were 4 MRD categories:
- MRD negative: No signal
- MRD low: >0 to <10-4 (<0.01%)
- MRD high: ≥10-4 to <10-3 (0.01 to 0.1%)
- MRD very high: ≥10-3 to <10-2 (>0.1%).
Dr Pulsipher noted that, when analyzing MRD pre-HSCT or at 30 days after HSCT, the estimated 5-year EFS was similar for patients in the MRD-negative and MRD-low groups. However, as time went on (at days 90, 180, and 365), any detectable level of MRD was associated with a poor prognosis.
“And patients arriving at day 365 with no detectable MRD had an exceptional prognosis, with survival approaching 90%,” Dr Pulsipher said.
He also pointed out an interaction between acute graft-vs-host disease (aGVHD) and MRD post-HSCT. He and his colleagues observed better survival for MRD-positive patients with aGVHD (grade 1-2) than for MRD-positive patients without aGVHD.
Pre-HSCT risk score
Via an adjusted Cox regression analysis, the researchers identified several pre-transplant factors that predicted EFS at 18 months.
These included remission status, donor type, immunophenotype, and MRD. The researchers assigned points to each of these factors to create a risk score.
Compared to patients in first CR, the hazard ratio (HR) for patients in early second CR was 2.53, and the score was 3. For patients in third CR or greater, the HR was 1.95, and the score was 2.
Compared to patients with a matched sibling donor, the HR for patients with a mismatched donor was 1.41, and the score was 1. For patients who received cord blood from an unrelated donor, the HR was 1.48, and the score was 1.
Compared to patients with T-cell ALL, the HR for patients with pre-B ALL was 1.35, and the score was 1.
Compared to patients with MRD <10-4, the HR for patients with MRD ≥10-4 was 2.32, and the score was 2.
The probability of EFS at 18 months was 78% ± 2% for patients with 0 to 1 points, 54% ± 3% for those with 2 to 3 points, and 46% ± 5% for patients with 4 or more points.
Day 30 post-HSCT risk score
When considering patients at day 30 post-HSCT, factors that predicted 18-month EFS included remission status, donor type, immunophenotype, aGVHD status, and MRD.
The HR for patients in early second CR was 2.51, and the score was 3. For patients in third CR or greater, the HR was 2.09, and the score was 2.
The HR for patients with a mismatched donor was 1.75, and the score was 2. The HR for patients with pre-B ALL was 1.40, and the score was 1.
Compared to patients with grade 1-2 aGVHD, the HR was 2.02 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 3 aGVHD, the HR was 1.44, and the score was 1. For patients with grade 4 aGVHD, the HR was 7.12, and the score was 7.
The researchers evaluated MRD prior to HSCT and MRD at day 30, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 30, the HR was 2.29, and the score was 2.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 30, the HR was 3.17, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 30, the HR was 3.63, and the score was 4.
The probability of EFS at 18 months was 80% ± 2% for patients with 0 to 3 points, 54% ± 4% for those with 4 to 6 points, and 25% ± 6% for those with 7 or more points.
Day 90 post-HSCT risk score
When considering patients at day 90 post-HSCT, factors that predicted 18-month EFS included remission status, aGVHD status, and MRD.
For patients in early second CR, the HR was 2.81, and the score was 3. For those in third CR or greater, the HR was 1.85, and the score was 2.
Compared to patients with grade 1-2 aGVHD, the HR was 1.60 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 4 aGVHD, the HR was 2.49, and the score was 2.
The researchers assessed MRD prior to HSCT and MRD at day 90, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 90, the HR was 6.03, and the score was 6.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 90, the HR was 3.11, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 90, the HR was 4.59, and the score was 5.
The probability of EFS at 18 months was 83% ± 2% for patients with 0 to 2 points, 60% ± 4% for those with 3 to 5 points, and 17% ± 11 for those with 6 or more points. ![]()
*Information in the abstract differs from the presentation.
ORLANDO, FL—Minimal residual disease (MRD) measurements before and after hematopoietic stem cell transplant (HSCT) can help predict outcomes in patients with childhood acute lymphoblastic leukemia (ALL), according to researchers.
Their work also suggests several other factors can be used to predict event-free survival (EFS) in this patient population, and the team developed risk scores incorporating these factors.
Michael A. Pulsipher, MD, of Children’s Hospital Los Angeles in California, presented this work as one of the “Best Abstracts” at the 2017 BMT Tandem Meetings (abstract 4*).
“The new risk scores that we were able to develop very nicely predict outcomes post-transplant and can guide study planning,” Dr Pulsipher said.
“MRD pre-transplant was a very powerful predictor of outcome, and MRD post-transplant highlights individual patients at risk.”
For this study, Dr Pulsipher and his colleagues retrospectively analyzed 747 patients treated in Europe, North America, and Australia. The patients received transplants between September 1999 and May 2015.
Most patients had pre-B ALL (78%, n=586), 19% (n=145) had T-cell ALL, 2% had “other” ALLs (n=8) or no data on ALL type (n=8). Sixty-two percent (n=466) were male.
Nearly half of patients were between the ages of 2 and 10 (49%, n=365), 47% (n=351) were older than 10, and 4% (n=31) were younger than 2.
Transplant details
Patients received grafts from matched unrelated donors (42%, n=314), matched sibling donors (30%, n=227), mismatched donors (10%, n=75), and cord blood from unrelated donors (17%, n=128). There was no data on donor type for 3 patients.
Most patients received bone marrow transplants (61%, n=458), 20% (n=147) received cord blood, and 18% (n=131) received peripheral blood stem cells. Eight patients received “other” types of transplants, and 3 patients had no data on stem cell source.
More than half of the patients (55%, n=410) were in their second complete remission (CR) at transplant. Thirty-seven percent were in their first CR (n=275), 7% were in their third or greater CR (n=53), and 1% were not in remission (n=7). Two patients had no data on remission status.
MRD
MRD was assessed before HSCT as well as after—on or near days 30, 60, 90, 180, 365, and beyond.
There were 4 MRD categories:
- MRD negative: No signal
- MRD low: >0 to <10-4 (<0.01%)
- MRD high: ≥10-4 to <10-3 (0.01 to 0.1%)
- MRD very high: ≥10-3 to <10-2 (>0.1%).
Dr Pulsipher noted that, when analyzing MRD pre-HSCT or at 30 days after HSCT, the estimated 5-year EFS was similar for patients in the MRD-negative and MRD-low groups. However, as time went on (at days 90, 180, and 365), any detectable level of MRD was associated with a poor prognosis.
“And patients arriving at day 365 with no detectable MRD had an exceptional prognosis, with survival approaching 90%,” Dr Pulsipher said.
He also pointed out an interaction between acute graft-vs-host disease (aGVHD) and MRD post-HSCT. He and his colleagues observed better survival for MRD-positive patients with aGVHD (grade 1-2) than for MRD-positive patients without aGVHD.
Pre-HSCT risk score
Via an adjusted Cox regression analysis, the researchers identified several pre-transplant factors that predicted EFS at 18 months.
These included remission status, donor type, immunophenotype, and MRD. The researchers assigned points to each of these factors to create a risk score.
Compared to patients in first CR, the hazard ratio (HR) for patients in early second CR was 2.53, and the score was 3. For patients in third CR or greater, the HR was 1.95, and the score was 2.
Compared to patients with a matched sibling donor, the HR for patients with a mismatched donor was 1.41, and the score was 1. For patients who received cord blood from an unrelated donor, the HR was 1.48, and the score was 1.
Compared to patients with T-cell ALL, the HR for patients with pre-B ALL was 1.35, and the score was 1.
Compared to patients with MRD <10-4, the HR for patients with MRD ≥10-4 was 2.32, and the score was 2.
The probability of EFS at 18 months was 78% ± 2% for patients with 0 to 1 points, 54% ± 3% for those with 2 to 3 points, and 46% ± 5% for patients with 4 or more points.
Day 30 post-HSCT risk score
When considering patients at day 30 post-HSCT, factors that predicted 18-month EFS included remission status, donor type, immunophenotype, aGVHD status, and MRD.
The HR for patients in early second CR was 2.51, and the score was 3. For patients in third CR or greater, the HR was 2.09, and the score was 2.
The HR for patients with a mismatched donor was 1.75, and the score was 2. The HR for patients with pre-B ALL was 1.40, and the score was 1.
Compared to patients with grade 1-2 aGVHD, the HR was 2.02 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 3 aGVHD, the HR was 1.44, and the score was 1. For patients with grade 4 aGVHD, the HR was 7.12, and the score was 7.
The researchers evaluated MRD prior to HSCT and MRD at day 30, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 30, the HR was 2.29, and the score was 2.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 30, the HR was 3.17, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 30, the HR was 3.63, and the score was 4.
The probability of EFS at 18 months was 80% ± 2% for patients with 0 to 3 points, 54% ± 4% for those with 4 to 6 points, and 25% ± 6% for those with 7 or more points.
Day 90 post-HSCT risk score
When considering patients at day 90 post-HSCT, factors that predicted 18-month EFS included remission status, aGVHD status, and MRD.
For patients in early second CR, the HR was 2.81, and the score was 3. For those in third CR or greater, the HR was 1.85, and the score was 2.
Compared to patients with grade 1-2 aGVHD, the HR was 1.60 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 4 aGVHD, the HR was 2.49, and the score was 2.
The researchers assessed MRD prior to HSCT and MRD at day 90, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 90, the HR was 6.03, and the score was 6.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 90, the HR was 3.11, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 90, the HR was 4.59, and the score was 5.
The probability of EFS at 18 months was 83% ± 2% for patients with 0 to 2 points, 60% ± 4% for those with 3 to 5 points, and 17% ± 11 for those with 6 or more points. ![]()
*Information in the abstract differs from the presentation.
ORLANDO, FL—Minimal residual disease (MRD) measurements before and after hematopoietic stem cell transplant (HSCT) can help predict outcomes in patients with childhood acute lymphoblastic leukemia (ALL), according to researchers.
Their work also suggests several other factors can be used to predict event-free survival (EFS) in this patient population, and the team developed risk scores incorporating these factors.
Michael A. Pulsipher, MD, of Children’s Hospital Los Angeles in California, presented this work as one of the “Best Abstracts” at the 2017 BMT Tandem Meetings (abstract 4*).
“The new risk scores that we were able to develop very nicely predict outcomes post-transplant and can guide study planning,” Dr Pulsipher said.
“MRD pre-transplant was a very powerful predictor of outcome, and MRD post-transplant highlights individual patients at risk.”
For this study, Dr Pulsipher and his colleagues retrospectively analyzed 747 patients treated in Europe, North America, and Australia. The patients received transplants between September 1999 and May 2015.
Most patients had pre-B ALL (78%, n=586), 19% (n=145) had T-cell ALL, 2% had “other” ALLs (n=8) or no data on ALL type (n=8). Sixty-two percent (n=466) were male.
Nearly half of patients were between the ages of 2 and 10 (49%, n=365), 47% (n=351) were older than 10, and 4% (n=31) were younger than 2.
Transplant details
Patients received grafts from matched unrelated donors (42%, n=314), matched sibling donors (30%, n=227), mismatched donors (10%, n=75), and cord blood from unrelated donors (17%, n=128). There was no data on donor type for 3 patients.
Most patients received bone marrow transplants (61%, n=458), 20% (n=147) received cord blood, and 18% (n=131) received peripheral blood stem cells. Eight patients received “other” types of transplants, and 3 patients had no data on stem cell source.
More than half of the patients (55%, n=410) were in their second complete remission (CR) at transplant. Thirty-seven percent were in their first CR (n=275), 7% were in their third or greater CR (n=53), and 1% were not in remission (n=7). Two patients had no data on remission status.
MRD
MRD was assessed before HSCT as well as after—on or near days 30, 60, 90, 180, 365, and beyond.
There were 4 MRD categories:
- MRD negative: No signal
- MRD low: >0 to <10-4 (<0.01%)
- MRD high: ≥10-4 to <10-3 (0.01 to 0.1%)
- MRD very high: ≥10-3 to <10-2 (>0.1%).
Dr Pulsipher noted that, when analyzing MRD pre-HSCT or at 30 days after HSCT, the estimated 5-year EFS was similar for patients in the MRD-negative and MRD-low groups. However, as time went on (at days 90, 180, and 365), any detectable level of MRD was associated with a poor prognosis.
“And patients arriving at day 365 with no detectable MRD had an exceptional prognosis, with survival approaching 90%,” Dr Pulsipher said.
He also pointed out an interaction between acute graft-vs-host disease (aGVHD) and MRD post-HSCT. He and his colleagues observed better survival for MRD-positive patients with aGVHD (grade 1-2) than for MRD-positive patients without aGVHD.
Pre-HSCT risk score
Via an adjusted Cox regression analysis, the researchers identified several pre-transplant factors that predicted EFS at 18 months.
These included remission status, donor type, immunophenotype, and MRD. The researchers assigned points to each of these factors to create a risk score.
Compared to patients in first CR, the hazard ratio (HR) for patients in early second CR was 2.53, and the score was 3. For patients in third CR or greater, the HR was 1.95, and the score was 2.
Compared to patients with a matched sibling donor, the HR for patients with a mismatched donor was 1.41, and the score was 1. For patients who received cord blood from an unrelated donor, the HR was 1.48, and the score was 1.
Compared to patients with T-cell ALL, the HR for patients with pre-B ALL was 1.35, and the score was 1.
Compared to patients with MRD <10-4, the HR for patients with MRD ≥10-4 was 2.32, and the score was 2.
The probability of EFS at 18 months was 78% ± 2% for patients with 0 to 1 points, 54% ± 3% for those with 2 to 3 points, and 46% ± 5% for patients with 4 or more points.
Day 30 post-HSCT risk score
When considering patients at day 30 post-HSCT, factors that predicted 18-month EFS included remission status, donor type, immunophenotype, aGVHD status, and MRD.
The HR for patients in early second CR was 2.51, and the score was 3. For patients in third CR or greater, the HR was 2.09, and the score was 2.
The HR for patients with a mismatched donor was 1.75, and the score was 2. The HR for patients with pre-B ALL was 1.40, and the score was 1.
Compared to patients with grade 1-2 aGVHD, the HR was 2.02 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 3 aGVHD, the HR was 1.44, and the score was 1. For patients with grade 4 aGVHD, the HR was 7.12, and the score was 7.
The researchers evaluated MRD prior to HSCT and MRD at day 30, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 30, the HR was 2.29, and the score was 2.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 30, the HR was 3.17, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 30, the HR was 3.63, and the score was 4.
The probability of EFS at 18 months was 80% ± 2% for patients with 0 to 3 points, 54% ± 4% for those with 4 to 6 points, and 25% ± 6% for those with 7 or more points.
Day 90 post-HSCT risk score
When considering patients at day 90 post-HSCT, factors that predicted 18-month EFS included remission status, aGVHD status, and MRD.
For patients in early second CR, the HR was 2.81, and the score was 3. For those in third CR or greater, the HR was 1.85, and the score was 2.
Compared to patients with grade 1-2 aGVHD, the HR was 1.60 for patients with grade 0 aGVHD, and the score was 2. For patients with grade 4 aGVHD, the HR was 2.49, and the score was 2.
The researchers assessed MRD prior to HSCT and MRD at day 90, using a reference of MRD <10-4 at both time points. For patients with MRD <10-4 pre-HSCT and ≥10-4 at day 90, the HR was 6.03, and the score was 6.
For patients with MRD ≥10-4 pre-HSCT and <10-4 at day 90, the HR was 3.11, and the score was 3. For patients with MRD ≥10-4 pre-HSCT and at day 90, the HR was 4.59, and the score was 5.
The probability of EFS at 18 months was 83% ± 2% for patients with 0 to 2 points, 60% ± 4% for those with 3 to 5 points, and 17% ± 11 for those with 6 or more points. ![]()
*Information in the abstract differs from the presentation.
Drug receives orphan designation for DLBCL

The US Food and Drug Administration (FDA) has granted orphan drug designation for eFT508 to treat diffuse large B-cell lymphoma (DLBCL).
eFT508 is a highly selective inhibitor of MNK1 and MNK2, enzymes that integrate signals from several oncogenic and immune signaling pathways.
The FDA grants orphan designation to drugs or biologics intended to treat a disease or condition affecting fewer than 200,000 patients in the US.
The orphan designation for eFT508 provides several incentives for eFFECTOR Therapeutics, the company developing eFT508.
These incentives include increased access to FDA reviewers to discuss clinical trial designs, the ability to qualify for tax credits for certain clinical research costs, the ability to apply for annual grant funding, a waiver of Prescription Drug User Fee Act filing fees, and the potential for 7 years of US marketing exclusivity if eFT508 is approved.
eFFECTOR has dosed the first subject in a phase 1/2 trial of eFT508 in patients with B-cell hematologic malignancies. The study is designed to evaluate the safety, pharmacokinetics, pharmacodynamics, and antitumor activity of eFT508.
eFFECTOR presented preclinical research of eFT508 in DLBCL at the 2015 ASH Annual Meeting. The poster is available for download from the eFFECTOR website.
The researchers reported that eFT508 demonstrated anti-proliferative activity against multiple DLBCL cell lines, including the TMD8, OCI-Ly3, and HBL1 cell lines.
eFT508 also exhibited “significant anti-tumor activity” in mouse models of TMD8 and HBL-1 ABC-DLBCL.
Finally, the researchers found that eFT508 synergized with everolimus, ibrutinib, and venetoclax both in vitro and in vivo. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation for eFT508 to treat diffuse large B-cell lymphoma (DLBCL).
eFT508 is a highly selective inhibitor of MNK1 and MNK2, enzymes that integrate signals from several oncogenic and immune signaling pathways.
The FDA grants orphan designation to drugs or biologics intended to treat a disease or condition affecting fewer than 200,000 patients in the US.
The orphan designation for eFT508 provides several incentives for eFFECTOR Therapeutics, the company developing eFT508.
These incentives include increased access to FDA reviewers to discuss clinical trial designs, the ability to qualify for tax credits for certain clinical research costs, the ability to apply for annual grant funding, a waiver of Prescription Drug User Fee Act filing fees, and the potential for 7 years of US marketing exclusivity if eFT508 is approved.
eFFECTOR has dosed the first subject in a phase 1/2 trial of eFT508 in patients with B-cell hematologic malignancies. The study is designed to evaluate the safety, pharmacokinetics, pharmacodynamics, and antitumor activity of eFT508.
eFFECTOR presented preclinical research of eFT508 in DLBCL at the 2015 ASH Annual Meeting. The poster is available for download from the eFFECTOR website.
The researchers reported that eFT508 demonstrated anti-proliferative activity against multiple DLBCL cell lines, including the TMD8, OCI-Ly3, and HBL1 cell lines.
eFT508 also exhibited “significant anti-tumor activity” in mouse models of TMD8 and HBL-1 ABC-DLBCL.
Finally, the researchers found that eFT508 synergized with everolimus, ibrutinib, and venetoclax both in vitro and in vivo. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation for eFT508 to treat diffuse large B-cell lymphoma (DLBCL).
eFT508 is a highly selective inhibitor of MNK1 and MNK2, enzymes that integrate signals from several oncogenic and immune signaling pathways.
The FDA grants orphan designation to drugs or biologics intended to treat a disease or condition affecting fewer than 200,000 patients in the US.
The orphan designation for eFT508 provides several incentives for eFFECTOR Therapeutics, the company developing eFT508.
These incentives include increased access to FDA reviewers to discuss clinical trial designs, the ability to qualify for tax credits for certain clinical research costs, the ability to apply for annual grant funding, a waiver of Prescription Drug User Fee Act filing fees, and the potential for 7 years of US marketing exclusivity if eFT508 is approved.
eFFECTOR has dosed the first subject in a phase 1/2 trial of eFT508 in patients with B-cell hematologic malignancies. The study is designed to evaluate the safety, pharmacokinetics, pharmacodynamics, and antitumor activity of eFT508.
eFFECTOR presented preclinical research of eFT508 in DLBCL at the 2015 ASH Annual Meeting. The poster is available for download from the eFFECTOR website.
The researchers reported that eFT508 demonstrated anti-proliferative activity against multiple DLBCL cell lines, including the TMD8, OCI-Ly3, and HBL1 cell lines.
eFT508 also exhibited “significant anti-tumor activity” in mouse models of TMD8 and HBL-1 ABC-DLBCL.
Finally, the researchers found that eFT508 synergized with everolimus, ibrutinib, and venetoclax both in vitro and in vivo. ![]()
Infectious Penile Lesions
1. A 63-year-old man complains of a mildly painful and tender rash on his penis that has been there for almost two years. The patient is uncircumcised; when the foreskin is retracted, a bright red, erythematous, nonscaly, circumferential plaque is visible on the glans penis, spreading to the foreskin. He denies pain on urination, discharge, fever, malaise, arthralgias, and sexual contact outside of his marriage.

Diagnosis: Zoon balanitis is a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The lesion associated with Zoon balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
For more information on this case, see “Erythematous penile lesion.” J Fam Pract. 2012;61(12):753-755.
2. A 21-year-old man presents with bumps on his penis. He admits to having unprotected sexual intercourse with more than six women in the past year. He is otherwise healthy.

Diagnosis: Genital warts are caused by human papillomavirus infection. The incubation period after exposure ranges from three weeks to eight months. Anogenital warts represent the most common viral sexually transmitted infection in the United States; there are approximately 1 million new cases of genital warts per year. Most infections are transient and clear up within two years, but some infections persist and recur.
The diagnosis is usually clinical; genital warts are typically asymptomatic and present as flesh-colored, exophytic lesions on the genitalia, including the penis, vulva, vagina, scrotum, perineum, and perianal skin. External warts can appear as small bumps, or they may be flat, verrucous, or pedunculated. Treatment options include cryotherapy and prescription imiquimod cream.
For more information on this case, see “Genital bumps.”
3. A 27-year-old man is worried that he may have contracted chlamydia. About five days ago, he experienced pain and a burning feeling with urination. Three days ago, a painful, growing lump near the head of his penis developed. The patient has a purulent urethral discharge and fluctuant, yellowish white, tender swelling on the left side of the frenulum. There are no ulcers, but there is a single 2-cm lymph node in the right inguinal area that is of normal consistency, mobile, nontender, and nonfluctuant.

Diagnosis: The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.
For more information on this case, see “Returning traveler with painful penile mass.” J Fam Pract. 2011 May;60(5):285-287.
4. A 32-year-old man presents with a week-long history of painful vesicles on the shaft of his penis associated with tender groin adenopathy. Two days ago, the vesicles broke and the pain worsened. The patient had similar lesions a year ago but did not seek medical care. He has had three different female sexual partners over the past two years but has no knowledge of them having any sores or diseases.

Diagnosis: Genital herpes presents with multiple transient, painful vesicles that appear on the penis, vulva, buttocks, perineum, vagina, or cervix. The vesicles break down and become ulcers that develop crusts while healing. Recurrences typically occur 2 to 3 times a year. The duration is shorter and less painful than in primary infections. The lesions often heal completely by 8 to 10 days.
Antiviral therapy is recommended for an initial genital herpes outbreak. Although systemic antiviral drugs can partially control the signs and symptoms of herpes episodes, they do not eradicate the latent virus.
For more information on this case, see “Painful vesicles on penis.”
1. A 63-year-old man complains of a mildly painful and tender rash on his penis that has been there for almost two years. The patient is uncircumcised; when the foreskin is retracted, a bright red, erythematous, nonscaly, circumferential plaque is visible on the glans penis, spreading to the foreskin. He denies pain on urination, discharge, fever, malaise, arthralgias, and sexual contact outside of his marriage.
Diagnosis: Zoon balanitis is a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The lesion associated with Zoon balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
For more information on this case, see “Erythematous penile lesion.” J Fam Pract. 2012;61(12):753-755.
2. A 21-year-old man presents with bumps on his penis. He admits to having unprotected sexual intercourse with more than six women in the past year. He is otherwise healthy.
Diagnosis: Genital warts are caused by human papillomavirus infection. The incubation period after exposure ranges from three weeks to eight months. Anogenital warts represent the most common viral sexually transmitted infection in the United States; there are approximately 1 million new cases of genital warts per year. Most infections are transient and clear up within two years, but some infections persist and recur.
The diagnosis is usually clinical; genital warts are typically asymptomatic and present as flesh-colored, exophytic lesions on the genitalia, including the penis, vulva, vagina, scrotum, perineum, and perianal skin. External warts can appear as small bumps, or they may be flat, verrucous, or pedunculated. Treatment options include cryotherapy and prescription imiquimod cream.
For more information on this case, see “Genital bumps.”
3. A 27-year-old man is worried that he may have contracted chlamydia. About five days ago, he experienced pain and a burning feeling with urination. Three days ago, a painful, growing lump near the head of his penis developed. The patient has a purulent urethral discharge and fluctuant, yellowish white, tender swelling on the left side of the frenulum. There are no ulcers, but there is a single 2-cm lymph node in the right inguinal area that is of normal consistency, mobile, nontender, and nonfluctuant.
Diagnosis: The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.
For more information on this case, see “Returning traveler with painful penile mass.” J Fam Pract. 2011 May;60(5):285-287.
4. A 32-year-old man presents with a week-long history of painful vesicles on the shaft of his penis associated with tender groin adenopathy. Two days ago, the vesicles broke and the pain worsened. The patient had similar lesions a year ago but did not seek medical care. He has had three different female sexual partners over the past two years but has no knowledge of them having any sores or diseases.
Diagnosis: Genital herpes presents with multiple transient, painful vesicles that appear on the penis, vulva, buttocks, perineum, vagina, or cervix. The vesicles break down and become ulcers that develop crusts while healing. Recurrences typically occur 2 to 3 times a year. The duration is shorter and less painful than in primary infections. The lesions often heal completely by 8 to 10 days.
Antiviral therapy is recommended for an initial genital herpes outbreak. Although systemic antiviral drugs can partially control the signs and symptoms of herpes episodes, they do not eradicate the latent virus.
For more information on this case, see “Painful vesicles on penis.”
1. A 63-year-old man complains of a mildly painful and tender rash on his penis that has been there for almost two years. The patient is uncircumcised; when the foreskin is retracted, a bright red, erythematous, nonscaly, circumferential plaque is visible on the glans penis, spreading to the foreskin. He denies pain on urination, discharge, fever, malaise, arthralgias, and sexual contact outside of his marriage.
Diagnosis: Zoon balanitis is a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The lesion associated with Zoon balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
For more information on this case, see “Erythematous penile lesion.” J Fam Pract. 2012;61(12):753-755.
2. A 21-year-old man presents with bumps on his penis. He admits to having unprotected sexual intercourse with more than six women in the past year. He is otherwise healthy.
Diagnosis: Genital warts are caused by human papillomavirus infection. The incubation period after exposure ranges from three weeks to eight months. Anogenital warts represent the most common viral sexually transmitted infection in the United States; there are approximately 1 million new cases of genital warts per year. Most infections are transient and clear up within two years, but some infections persist and recur.
The diagnosis is usually clinical; genital warts are typically asymptomatic and present as flesh-colored, exophytic lesions on the genitalia, including the penis, vulva, vagina, scrotum, perineum, and perianal skin. External warts can appear as small bumps, or they may be flat, verrucous, or pedunculated. Treatment options include cryotherapy and prescription imiquimod cream.
For more information on this case, see “Genital bumps.”
3. A 27-year-old man is worried that he may have contracted chlamydia. About five days ago, he experienced pain and a burning feeling with urination. Three days ago, a painful, growing lump near the head of his penis developed. The patient has a purulent urethral discharge and fluctuant, yellowish white, tender swelling on the left side of the frenulum. There are no ulcers, but there is a single 2-cm lymph node in the right inguinal area that is of normal consistency, mobile, nontender, and nonfluctuant.
Diagnosis: The clinical history was consistent with a diagnosis of gonococcal urethritis complicated by a periurethral gland abscess. The location of the swelling was most consistent with an abscess in the Tyson’s gland (also known as tysonitis). The Tyson’s (or preputial) glands of the penis are sebaceous-type glands on either side of the frenulum at the balanopreputial sulcus.1 In women, an abscess of the periurethral Skene’s gland is an analogous gonorrheal complication.
The differential diagnosis of acute swelling on the penile shaft includes syphilis, chancroid, lymphogranuloma venereum, herpes simplex virus, Behçet’s syndrome, a drug reaction, erythema multiforme, Crohn’s disease, lichen planus, amebiasis, scabies, trauma, and cancer.
For more information on this case, see “Returning traveler with painful penile mass.” J Fam Pract. 2011 May;60(5):285-287.
4. A 32-year-old man presents with a week-long history of painful vesicles on the shaft of his penis associated with tender groin adenopathy. Two days ago, the vesicles broke and the pain worsened. The patient had similar lesions a year ago but did not seek medical care. He has had three different female sexual partners over the past two years but has no knowledge of them having any sores or diseases.
Diagnosis: Genital herpes presents with multiple transient, painful vesicles that appear on the penis, vulva, buttocks, perineum, vagina, or cervix. The vesicles break down and become ulcers that develop crusts while healing. Recurrences typically occur 2 to 3 times a year. The duration is shorter and less painful than in primary infections. The lesions often heal completely by 8 to 10 days.
Antiviral therapy is recommended for an initial genital herpes outbreak. Although systemic antiviral drugs can partially control the signs and symptoms of herpes episodes, they do not eradicate the latent virus.
For more information on this case, see “Painful vesicles on penis.”
VIDEO: Residual cancer burden may be better outcome measure than pCR
MIAMI BEACH – The Food and Drug Administration has accepted pathological complete response rate (pCR) as a surrogate endpoint for disease-free and overall survival in clinical trials for neoadjuvant therapy of breast cancer.
Yet the specimen collection and histopathologic methods used to measure pCR have differed considerably across major neoadjuvant trials for breast cancer, said Michael F. Press, MD, PhD, of the USC/Norris Comprehensive Cancer Center at the University of California, Los Angeles.
In a video interview conducted at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource, Dr. Press outlined the problems associated with a lack of standardization of outcomes measures, and described how residual cancer burden may be a more effective, validated measures for comparing outcomes across clinical trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Press disclosed grant/research support from Cepheid, and consulting with Cepheid, Karyopharm Therapeutics, Eli Lilly, Puma Biotechnology, Halozyme Therapeutics, Biocartis SA, and ADC Therapeutics.
MIAMI BEACH – The Food and Drug Administration has accepted pathological complete response rate (pCR) as a surrogate endpoint for disease-free and overall survival in clinical trials for neoadjuvant therapy of breast cancer.
Yet the specimen collection and histopathologic methods used to measure pCR have differed considerably across major neoadjuvant trials for breast cancer, said Michael F. Press, MD, PhD, of the USC/Norris Comprehensive Cancer Center at the University of California, Los Angeles.
In a video interview conducted at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource, Dr. Press outlined the problems associated with a lack of standardization of outcomes measures, and described how residual cancer burden may be a more effective, validated measures for comparing outcomes across clinical trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Press disclosed grant/research support from Cepheid, and consulting with Cepheid, Karyopharm Therapeutics, Eli Lilly, Puma Biotechnology, Halozyme Therapeutics, Biocartis SA, and ADC Therapeutics.
MIAMI BEACH – The Food and Drug Administration has accepted pathological complete response rate (pCR) as a surrogate endpoint for disease-free and overall survival in clinical trials for neoadjuvant therapy of breast cancer.
Yet the specimen collection and histopathologic methods used to measure pCR have differed considerably across major neoadjuvant trials for breast cancer, said Michael F. Press, MD, PhD, of the USC/Norris Comprehensive Cancer Center at the University of California, Los Angeles.
In a video interview conducted at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource, Dr. Press outlined the problems associated with a lack of standardization of outcomes measures, and described how residual cancer burden may be a more effective, validated measures for comparing outcomes across clinical trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Press disclosed grant/research support from Cepheid, and consulting with Cepheid, Karyopharm Therapeutics, Eli Lilly, Puma Biotechnology, Halozyme Therapeutics, Biocartis SA, and ADC Therapeutics.
AT MBCC

Gender impacts risk of atopic diseases
ATLANTA – Obese females who live in urban settings are significantly more likely to develop atopic diseases, compared with their male counterparts, results from a single-center study showed.
“Some research has shown that obese girls are much more likely to be atopic, but many of them only look at one disease alone, such as atopic dermatitis or food allergies,” lead study author Sairaman Nagarajan, MD, MPH, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “Most of the studies are in asthma.”

The mean age of patients was 9 years, 23% were obese, and 55% were male. The researchers observed no differences in laboratory biomarkers nor in the prevalence of individual/or cumulative atopic disease in obese children, compared with controls. When stratified by gender, obese females had a significantly higher mean atopic disease score, compared with controls (4.00 vs. 2.62, respectively; P less than .001), while males had a significantly lower mean atopic disease score, compared with controls (3 vs. 3.42; P less than .001). Regression models yielded similar results; obese females had a significantly higher mean atopic disease score, compared with controls (by a mean elevation of 1.37 points; P less than .005), while males had a significantly lower mean atopic disease score (by a mean decline of -0.42 points; P less than .006). “From this we can say that female gender is a positive risk factor for atopy, and urban obese females may be particularly likely to benefit from lifestyle modification therapy like exercise and diet in controlling weight, and thereby allergies,” Dr. Nagarajan said.
He noted that it remains unclear whether the findings would apply to children who live in nonurban settings. “It’s difficult to say because there are some variables which are unique to urban minority populations like the housing that they live in and the kind of stores they buy food from,” he said.
Dr. Nagarajan reported having no financial disclosures.
ATLANTA – Obese females who live in urban settings are significantly more likely to develop atopic diseases, compared with their male counterparts, results from a single-center study showed.
“Some research has shown that obese girls are much more likely to be atopic, but many of them only look at one disease alone, such as atopic dermatitis or food allergies,” lead study author Sairaman Nagarajan, MD, MPH, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “Most of the studies are in asthma.”
The mean age of patients was 9 years, 23% were obese, and 55% were male. The researchers observed no differences in laboratory biomarkers nor in the prevalence of individual/or cumulative atopic disease in obese children, compared with controls. When stratified by gender, obese females had a significantly higher mean atopic disease score, compared with controls (4.00 vs. 2.62, respectively; P less than .001), while males had a significantly lower mean atopic disease score, compared with controls (3 vs. 3.42; P less than .001). Regression models yielded similar results; obese females had a significantly higher mean atopic disease score, compared with controls (by a mean elevation of 1.37 points; P less than .005), while males had a significantly lower mean atopic disease score (by a mean decline of -0.42 points; P less than .006). “From this we can say that female gender is a positive risk factor for atopy, and urban obese females may be particularly likely to benefit from lifestyle modification therapy like exercise and diet in controlling weight, and thereby allergies,” Dr. Nagarajan said.
He noted that it remains unclear whether the findings would apply to children who live in nonurban settings. “It’s difficult to say because there are some variables which are unique to urban minority populations like the housing that they live in and the kind of stores they buy food from,” he said.
Dr. Nagarajan reported having no financial disclosures.
ATLANTA – Obese females who live in urban settings are significantly more likely to develop atopic diseases, compared with their male counterparts, results from a single-center study showed.
“Some research has shown that obese girls are much more likely to be atopic, but many of them only look at one disease alone, such as atopic dermatitis or food allergies,” lead study author Sairaman Nagarajan, MD, MPH, said in an interview at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “Most of the studies are in asthma.”
The mean age of patients was 9 years, 23% were obese, and 55% were male. The researchers observed no differences in laboratory biomarkers nor in the prevalence of individual/or cumulative atopic disease in obese children, compared with controls. When stratified by gender, obese females had a significantly higher mean atopic disease score, compared with controls (4.00 vs. 2.62, respectively; P less than .001), while males had a significantly lower mean atopic disease score, compared with controls (3 vs. 3.42; P less than .001). Regression models yielded similar results; obese females had a significantly higher mean atopic disease score, compared with controls (by a mean elevation of 1.37 points; P less than .005), while males had a significantly lower mean atopic disease score (by a mean decline of -0.42 points; P less than .006). “From this we can say that female gender is a positive risk factor for atopy, and urban obese females may be particularly likely to benefit from lifestyle modification therapy like exercise and diet in controlling weight, and thereby allergies,” Dr. Nagarajan said.
He noted that it remains unclear whether the findings would apply to children who live in nonurban settings. “It’s difficult to say because there are some variables which are unique to urban minority populations like the housing that they live in and the kind of stores they buy food from,” he said.
Dr. Nagarajan reported having no financial disclosures.
AT 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: When stratified by gender, obese females had a significantly higher mean atopic disease score, compared with controls (4 vs. 2.62, respectively; P less than .001), while males had a significantly lower mean atopic disease score, compared with controls (3 vs. 3.42; P less than .001).
Data source: A retrospective review of 113 children who were evaluated for a history of allergic rhinitis, eczema, asthma, food allergies, and IgE, the percentage of eosinophils, and absolute eosinophil counts.
Disclosures: Dr. Nagarajan reported having no financial disclosures.
In children, peanut IgE levels increase over time
ATLANTA – Within a cohort of children diagnosed with peanut allergy who were followed since 2001, peanut IgE levels increased significantly over time in all races, according to a preliminary analysis of data.
In an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology, lead study author Yasmin Hamzavi, MD, said that recent publications have implicated race as a factor in food sensitization, but how this may impact the management of food allergy has not been elucidated. “The novel aspect of this study is that we are not just looking at the baseline peanut IgE levels between the races, but at the rate of change in peanut IgE over time between the different races,” said Dr. Hamzavi, a fellow in the division of allergy and immunology at Northwell Health, Great Neck, N.Y. “My question was, does the level of peanut IgE decrease or increase faster in one race versus another?”

A significant increase in peanut IgE over time was observed among all races (P less than .0002). In addition, white and Asian children showed an increasing trend in peanut IgE, while black children demonstrated a decreasing trend over time (P less than .099), a finding that Dr. Hamzavi described as “surprising and unusual.” She called for larger studies exploring factors for the noted increase among all races, such as changes in testing methods, food avoidance, and increasing sensitization. “Understanding the changes in peanut sensitization over time is a crucial step in determining the likelihood of clinical reactivity,” she said.
Dr. Hamzavi is reviewing data for a similar analysis of children with milk and egg allergy. She reported having no financial disclosures.
ATLANTA – Within a cohort of children diagnosed with peanut allergy who were followed since 2001, peanut IgE levels increased significantly over time in all races, according to a preliminary analysis of data.
In an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology, lead study author Yasmin Hamzavi, MD, said that recent publications have implicated race as a factor in food sensitization, but how this may impact the management of food allergy has not been elucidated. “The novel aspect of this study is that we are not just looking at the baseline peanut IgE levels between the races, but at the rate of change in peanut IgE over time between the different races,” said Dr. Hamzavi, a fellow in the division of allergy and immunology at Northwell Health, Great Neck, N.Y. “My question was, does the level of peanut IgE decrease or increase faster in one race versus another?”
A significant increase in peanut IgE over time was observed among all races (P less than .0002). In addition, white and Asian children showed an increasing trend in peanut IgE, while black children demonstrated a decreasing trend over time (P less than .099), a finding that Dr. Hamzavi described as “surprising and unusual.” She called for larger studies exploring factors for the noted increase among all races, such as changes in testing methods, food avoidance, and increasing sensitization. “Understanding the changes in peanut sensitization over time is a crucial step in determining the likelihood of clinical reactivity,” she said.
Dr. Hamzavi is reviewing data for a similar analysis of children with milk and egg allergy. She reported having no financial disclosures.
ATLANTA – Within a cohort of children diagnosed with peanut allergy who were followed since 2001, peanut IgE levels increased significantly over time in all races, according to a preliminary analysis of data.
In an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology, lead study author Yasmin Hamzavi, MD, said that recent publications have implicated race as a factor in food sensitization, but how this may impact the management of food allergy has not been elucidated. “The novel aspect of this study is that we are not just looking at the baseline peanut IgE levels between the races, but at the rate of change in peanut IgE over time between the different races,” said Dr. Hamzavi, a fellow in the division of allergy and immunology at Northwell Health, Great Neck, N.Y. “My question was, does the level of peanut IgE decrease or increase faster in one race versus another?”
A significant increase in peanut IgE over time was observed among all races (P less than .0002). In addition, white and Asian children showed an increasing trend in peanut IgE, while black children demonstrated a decreasing trend over time (P less than .099), a finding that Dr. Hamzavi described as “surprising and unusual.” She called for larger studies exploring factors for the noted increase among all races, such as changes in testing methods, food avoidance, and increasing sensitization. “Understanding the changes in peanut sensitization over time is a crucial step in determining the likelihood of clinical reactivity,” she said.
Dr. Hamzavi is reviewing data for a similar analysis of children with milk and egg allergy. She reported having no financial disclosures.
AT 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: A significant increase in peanut IgE over time was observed among white, black, and Asian children (P less than .0002).
Data source: A retrospective review of 193 children diagnosed with peanut allergy .
Disclosures: Dr. Hamzavi reported having no financial disclosures.
VIDEO: Genomics, other advances further highlight how breast cancer differs in men
MIAMI BEACH – Growing evidence continues to point to a widening separation between female and male breast cancers, particularly with discoveries suggesting different pathways to disease and important genetic distinctions.
Therefore, the traditional practice of extrapolating findings from female breast cancer research to men with breast cancer no longer makes sense, Patrick I. Borgen, MD, said at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The incidence of male breast cancer is increasing. At the same time, fewer men with breast cancer get referred for and undergo genetic testing for their disease, said Dr. Borgen, chair of the department of surgery at Maimonides Medical Center in Brooklyn, N.Y.
Dr. Borgen explained in a video interview that both maternal and paternal inheritance of breast cancer are important, and they tie the lineage into a hypothesis for why BRCA mutations – which can predispose people to worse survival – have persisted through generations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Borgen is a member of the speakers bureau for Genomic Health Inc., NanoString Technologies, Genentech, and Pacira Inc.
MIAMI BEACH – Growing evidence continues to point to a widening separation between female and male breast cancers, particularly with discoveries suggesting different pathways to disease and important genetic distinctions.
Therefore, the traditional practice of extrapolating findings from female breast cancer research to men with breast cancer no longer makes sense, Patrick I. Borgen, MD, said at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The incidence of male breast cancer is increasing. At the same time, fewer men with breast cancer get referred for and undergo genetic testing for their disease, said Dr. Borgen, chair of the department of surgery at Maimonides Medical Center in Brooklyn, N.Y.
Dr. Borgen explained in a video interview that both maternal and paternal inheritance of breast cancer are important, and they tie the lineage into a hypothesis for why BRCA mutations – which can predispose people to worse survival – have persisted through generations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Borgen is a member of the speakers bureau for Genomic Health Inc., NanoString Technologies, Genentech, and Pacira Inc.
MIAMI BEACH – Growing evidence continues to point to a widening separation between female and male breast cancers, particularly with discoveries suggesting different pathways to disease and important genetic distinctions.
Therefore, the traditional practice of extrapolating findings from female breast cancer research to men with breast cancer no longer makes sense, Patrick I. Borgen, MD, said at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The incidence of male breast cancer is increasing. At the same time, fewer men with breast cancer get referred for and undergo genetic testing for their disease, said Dr. Borgen, chair of the department of surgery at Maimonides Medical Center in Brooklyn, N.Y.
Dr. Borgen explained in a video interview that both maternal and paternal inheritance of breast cancer are important, and they tie the lineage into a hypothesis for why BRCA mutations – which can predispose people to worse survival – have persisted through generations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Borgen is a member of the speakers bureau for Genomic Health Inc., NanoString Technologies, Genentech, and Pacira Inc.
AT MBCC

VIDEO: It’s too early to give up on immunotherapy for breast cancer
MIAMI BEACH – The remarkable progress seen with immune checkpoint inhibitors in metastatic melanoma, non–small-cell lung cancer, and other tumors has yet to be replicated in breast cancer, but it’s early days yet, and breast cancer researchers need more time before the ultimate clinical benefits of immunotherapy in breast cancer can be ascertained, said Adam M. Brufsky, MD, PhD, of the University of Pittsburgh.
Early studies with inhibitors of programmed death-1 (PD-1) and its ligand PD-L1 in patients with advanced triple-negative breast cancer have yielded only minimal response rates to date, but it it’s far too early to give up on the concept, Dr. Brufsky cautioned at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
In a video interview, he discussed the challenges of treating breast cancers, which may be less immunogenic and have a lower tumor mutational burden than other malignancies that respond more readily to PD-1 inhibition. Several large, phase III clinical trials of checkpoint inhibitors combined with cytotoxic chemotherapy are underway, he said, and those eventual findings may shed light on the optimal approach to using immunotherapy to treat patients with refractory metastatic breast cancers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brufsky disclosed consulting with Novartis, Eisai, Celgene, Lilly, Pfizer, Agendia, Genomic Health, NanoString Technologies and Biotheranostics.
MIAMI BEACH – The remarkable progress seen with immune checkpoint inhibitors in metastatic melanoma, non–small-cell lung cancer, and other tumors has yet to be replicated in breast cancer, but it’s early days yet, and breast cancer researchers need more time before the ultimate clinical benefits of immunotherapy in breast cancer can be ascertained, said Adam M. Brufsky, MD, PhD, of the University of Pittsburgh.
Early studies with inhibitors of programmed death-1 (PD-1) and its ligand PD-L1 in patients with advanced triple-negative breast cancer have yielded only minimal response rates to date, but it it’s far too early to give up on the concept, Dr. Brufsky cautioned at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
In a video interview, he discussed the challenges of treating breast cancers, which may be less immunogenic and have a lower tumor mutational burden than other malignancies that respond more readily to PD-1 inhibition. Several large, phase III clinical trials of checkpoint inhibitors combined with cytotoxic chemotherapy are underway, he said, and those eventual findings may shed light on the optimal approach to using immunotherapy to treat patients with refractory metastatic breast cancers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brufsky disclosed consulting with Novartis, Eisai, Celgene, Lilly, Pfizer, Agendia, Genomic Health, NanoString Technologies and Biotheranostics.
MIAMI BEACH – The remarkable progress seen with immune checkpoint inhibitors in metastatic melanoma, non–small-cell lung cancer, and other tumors has yet to be replicated in breast cancer, but it’s early days yet, and breast cancer researchers need more time before the ultimate clinical benefits of immunotherapy in breast cancer can be ascertained, said Adam M. Brufsky, MD, PhD, of the University of Pittsburgh.
Early studies with inhibitors of programmed death-1 (PD-1) and its ligand PD-L1 in patients with advanced triple-negative breast cancer have yielded only minimal response rates to date, but it it’s far too early to give up on the concept, Dr. Brufsky cautioned at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
In a video interview, he discussed the challenges of treating breast cancers, which may be less immunogenic and have a lower tumor mutational burden than other malignancies that respond more readily to PD-1 inhibition. Several large, phase III clinical trials of checkpoint inhibitors combined with cytotoxic chemotherapy are underway, he said, and those eventual findings may shed light on the optimal approach to using immunotherapy to treat patients with refractory metastatic breast cancers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Brufsky disclosed consulting with Novartis, Eisai, Celgene, Lilly, Pfizer, Agendia, Genomic Health, NanoString Technologies and Biotheranostics.
AT MBCC
VIDEO: Multiple PARP inhibitors show promise in breast cancer treatment
MIAMI BEACH – Driven by efficacy demonstrated in ovarian cancer, a number of PARP inhibitors are in development and hold promise for treatment of breast cancer as well, including patients positive for the BRCA mutation.
Interestingly, early evidence suggests these agents could also treat BRCA-negative women, potentially expanding their future clinical utility, Kimberly L. Blackwell, MD, said in a video interview at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Although it’s early, PARP inhibitors potentially could also be combined with standard platinum-based chemotherapy agents, although toxicity and the optimal timing of the regimens need further evaluation, said Dr. Blackwell, professor of medicine and assistant professor of radiation oncology at Duke University Medical Center, Durham, N.C.
Approval of the first PARP inhibitor indicated for breast cancer is expected in 2017, she said.
Dr. Blackwell received institutional grant support from AstraZeneca and Pfizer.
MIAMI BEACH – Driven by efficacy demonstrated in ovarian cancer, a number of PARP inhibitors are in development and hold promise for treatment of breast cancer as well, including patients positive for the BRCA mutation.
Interestingly, early evidence suggests these agents could also treat BRCA-negative women, potentially expanding their future clinical utility, Kimberly L. Blackwell, MD, said in a video interview at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Although it’s early, PARP inhibitors potentially could also be combined with standard platinum-based chemotherapy agents, although toxicity and the optimal timing of the regimens need further evaluation, said Dr. Blackwell, professor of medicine and assistant professor of radiation oncology at Duke University Medical Center, Durham, N.C.
Approval of the first PARP inhibitor indicated for breast cancer is expected in 2017, she said.
Dr. Blackwell received institutional grant support from AstraZeneca and Pfizer.
MIAMI BEACH – Driven by efficacy demonstrated in ovarian cancer, a number of PARP inhibitors are in development and hold promise for treatment of breast cancer as well, including patients positive for the BRCA mutation.
Interestingly, early evidence suggests these agents could also treat BRCA-negative women, potentially expanding their future clinical utility, Kimberly L. Blackwell, MD, said in a video interview at the annual Miami Breast Cancer Conference, held by Physicians’ Education Resource.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Although it’s early, PARP inhibitors potentially could also be combined with standard platinum-based chemotherapy agents, although toxicity and the optimal timing of the regimens need further evaluation, said Dr. Blackwell, professor of medicine and assistant professor of radiation oncology at Duke University Medical Center, Durham, N.C.
Approval of the first PARP inhibitor indicated for breast cancer is expected in 2017, she said.
Dr. Blackwell received institutional grant support from AstraZeneca and Pfizer.
AT MBCC
