User login
STD testing in youth hindered by confidentiality concerns
Adolescents and young adults on their parents’ health insurance plan are less likely to receive sexual preventive health care, such as sexual risk assessments and testing for sexually transmitted disease, a study found.
Further, teen girls (aged 15-17 years), were more than twice as likely to be tested for chlamydia if they met with their provider alone than if they did not, researchers found.
“Confidentiality issues, including concerns that parents might find out, might be barriers to the use of STD [sexually transmitted disease] services among some subpopulations,” Jami S. Leichliter, PhD, and colleagues at the Centers for Disease Control and Prevention wrote. “Public health efforts to reduce these confidentiality concerns might be useful,” such as providers meeting privately for at least part of an appointment with an adolescent (MMWR. 2017 Mar 10;66[9]:237-41).
The researchers examined data collected from the 2013-2015 National Survey of Family Growth regarding sexual and reproductive health care experiences and behaviors of youth with sexual experience, specifically teens aged 15-17 and young adults aged 18-25 who were on their parents’ health plan. Sexual experience refers to having ever had vaginal, anal, or oral sex with any partner.
Overall, 12.7% of these youth avoided seeking care for sexual and reproductive health because they worried their parents could find out. For those aged 15-17 years, the rate was even higher, at 22.6%.
These concerns were also reflected in the overall prevalence of chlamydia screenings: Just 17.1% of young women who worried about confidentiality had been screened for chlamydia, compared with 38.7% of young women who did not report that concern.
The researchers also compared teens aged 15-17 who had and had not received a sexual risk assessment, which includes being asked by a provider about their (or their partners’) sexual orientation, number of sexual partners, condom use, and types of sex. Among teens who met with a provider alone in the past year, 71.1% reported receiving a sexual risk assessment, compared with about 36.6% who did not meet privately with a provider.
Similarly, 34.0% of teen girls (aged 15-17 years) who saw their provider alone were tested for chlamydia, compared with 14.9% who never met with their provider alone. Slightly more teen boys (13.6%) received STD testing if they met with their provider alone than if they didn’t (9.5%), but this difference did not reach statistical significance.
The study was funded by the Centers for Disease Control and Prevention. The authors did not report any disclosures.
Adolescents and young adults on their parents’ health insurance plan are less likely to receive sexual preventive health care, such as sexual risk assessments and testing for sexually transmitted disease, a study found.
Further, teen girls (aged 15-17 years), were more than twice as likely to be tested for chlamydia if they met with their provider alone than if they did not, researchers found.
“Confidentiality issues, including concerns that parents might find out, might be barriers to the use of STD [sexually transmitted disease] services among some subpopulations,” Jami S. Leichliter, PhD, and colleagues at the Centers for Disease Control and Prevention wrote. “Public health efforts to reduce these confidentiality concerns might be useful,” such as providers meeting privately for at least part of an appointment with an adolescent (MMWR. 2017 Mar 10;66[9]:237-41).
The researchers examined data collected from the 2013-2015 National Survey of Family Growth regarding sexual and reproductive health care experiences and behaviors of youth with sexual experience, specifically teens aged 15-17 and young adults aged 18-25 who were on their parents’ health plan. Sexual experience refers to having ever had vaginal, anal, or oral sex with any partner.
Overall, 12.7% of these youth avoided seeking care for sexual and reproductive health because they worried their parents could find out. For those aged 15-17 years, the rate was even higher, at 22.6%.
These concerns were also reflected in the overall prevalence of chlamydia screenings: Just 17.1% of young women who worried about confidentiality had been screened for chlamydia, compared with 38.7% of young women who did not report that concern.
The researchers also compared teens aged 15-17 who had and had not received a sexual risk assessment, which includes being asked by a provider about their (or their partners’) sexual orientation, number of sexual partners, condom use, and types of sex. Among teens who met with a provider alone in the past year, 71.1% reported receiving a sexual risk assessment, compared with about 36.6% who did not meet privately with a provider.
Similarly, 34.0% of teen girls (aged 15-17 years) who saw their provider alone were tested for chlamydia, compared with 14.9% who never met with their provider alone. Slightly more teen boys (13.6%) received STD testing if they met with their provider alone than if they didn’t (9.5%), but this difference did not reach statistical significance.
The study was funded by the Centers for Disease Control and Prevention. The authors did not report any disclosures.
Adolescents and young adults on their parents’ health insurance plan are less likely to receive sexual preventive health care, such as sexual risk assessments and testing for sexually transmitted disease, a study found.
Further, teen girls (aged 15-17 years), were more than twice as likely to be tested for chlamydia if they met with their provider alone than if they did not, researchers found.
“Confidentiality issues, including concerns that parents might find out, might be barriers to the use of STD [sexually transmitted disease] services among some subpopulations,” Jami S. Leichliter, PhD, and colleagues at the Centers for Disease Control and Prevention wrote. “Public health efforts to reduce these confidentiality concerns might be useful,” such as providers meeting privately for at least part of an appointment with an adolescent (MMWR. 2017 Mar 10;66[9]:237-41).
The researchers examined data collected from the 2013-2015 National Survey of Family Growth regarding sexual and reproductive health care experiences and behaviors of youth with sexual experience, specifically teens aged 15-17 and young adults aged 18-25 who were on their parents’ health plan. Sexual experience refers to having ever had vaginal, anal, or oral sex with any partner.
Overall, 12.7% of these youth avoided seeking care for sexual and reproductive health because they worried their parents could find out. For those aged 15-17 years, the rate was even higher, at 22.6%.
These concerns were also reflected in the overall prevalence of chlamydia screenings: Just 17.1% of young women who worried about confidentiality had been screened for chlamydia, compared with 38.7% of young women who did not report that concern.
The researchers also compared teens aged 15-17 who had and had not received a sexual risk assessment, which includes being asked by a provider about their (or their partners’) sexual orientation, number of sexual partners, condom use, and types of sex. Among teens who met with a provider alone in the past year, 71.1% reported receiving a sexual risk assessment, compared with about 36.6% who did not meet privately with a provider.
Similarly, 34.0% of teen girls (aged 15-17 years) who saw their provider alone were tested for chlamydia, compared with 14.9% who never met with their provider alone. Slightly more teen boys (13.6%) received STD testing if they met with their provider alone than if they didn’t (9.5%), but this difference did not reach statistical significance.
The study was funded by the Centers for Disease Control and Prevention. The authors did not report any disclosures.
FROM MMWR
Key clinical point:
Major finding: Overall, 12.7% of sexually experienced youths (aged 15-25 years) who were on their parents’ health plan would not seek sexual and reproductive health care because of confidentiality concerns.
Data source: Responses from sexually experienced youth aged 15-25 years provided during the 2013-2015 U.S. National Survey of Family Growth.
Disclosures: The study was funded by the Centers for Disease Control and Prevention. The authors did not report any disclosures.
Senate confirms Verma as CMS administrator
The Senate confirmed Seema Verma as administrator of the Centers for Medicare & Medicaid Services on March 13 by a largely party line vote of 55-43.
Ms. Verma’s confirmation comes as Republicans begin their efforts to repeal and replace the Affordable Care Act. During the March 13 debate, Senate Finance Committee Chairman Orrin Hatch (R-Utah) reiterated his support for Ms. Verma, saying she will be a needed leader during the transition from the ACA.

Senate Finance Committee Ranking Member Ron Wyden (D-Ore.) continued to criticize Ms. Verma during the debate, stressing that she has presented no clear vision of her plans as the next CMS administrator.
“Ms. Verma gave the Finance Committee and the public virtually nothing to go by in terms of how she’d approach this job,” Sen. Wyden said during floor debate. “If confirmed, she’d be one of the top officials to implement Trumpcare, a bill that would raid Medicaid, slash Medicare, and kick millions of Americans off their health care... So I’m unable to support this nomination.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
During her confirmation hearing, senators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. But Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for Hewlett Packard. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
The Association for Community Affiliated Plans (ACAP) pledged to work with Ms. Verma as the Trump administration works toward changing how Medicaid is financed and administered. ACAP represents nonprofit safety net health plans in 28 states that serve patients enrolled in Medicaid, Medicare, the Children’s Health Insurance Program, marketplaces, and other publicly supported health programs.
“Flexibility is one of the great things about the Medicaid program today – this very flexibility is what has allowed the changes Ms. Verma helped to effect in Indiana,” ACAP CEO Margaret A. Murray said in a statement. “We look forward to working with Ms. Verma on pathways to refine the program while maintaining its guarantee of coverage for all eligible individuals, improving transparency and actuarial soundness in rate-setting, and assuring access to needed care and services.”
[email protected]
On Twitter @legal_med
The Senate confirmed Seema Verma as administrator of the Centers for Medicare & Medicaid Services on March 13 by a largely party line vote of 55-43.
Ms. Verma’s confirmation comes as Republicans begin their efforts to repeal and replace the Affordable Care Act. During the March 13 debate, Senate Finance Committee Chairman Orrin Hatch (R-Utah) reiterated his support for Ms. Verma, saying she will be a needed leader during the transition from the ACA.
Senate Finance Committee Ranking Member Ron Wyden (D-Ore.) continued to criticize Ms. Verma during the debate, stressing that she has presented no clear vision of her plans as the next CMS administrator.
“Ms. Verma gave the Finance Committee and the public virtually nothing to go by in terms of how she’d approach this job,” Sen. Wyden said during floor debate. “If confirmed, she’d be one of the top officials to implement Trumpcare, a bill that would raid Medicaid, slash Medicare, and kick millions of Americans off their health care... So I’m unable to support this nomination.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
During her confirmation hearing, senators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. But Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for Hewlett Packard. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
The Association for Community Affiliated Plans (ACAP) pledged to work with Ms. Verma as the Trump administration works toward changing how Medicaid is financed and administered. ACAP represents nonprofit safety net health plans in 28 states that serve patients enrolled in Medicaid, Medicare, the Children’s Health Insurance Program, marketplaces, and other publicly supported health programs.
“Flexibility is one of the great things about the Medicaid program today – this very flexibility is what has allowed the changes Ms. Verma helped to effect in Indiana,” ACAP CEO Margaret A. Murray said in a statement. “We look forward to working with Ms. Verma on pathways to refine the program while maintaining its guarantee of coverage for all eligible individuals, improving transparency and actuarial soundness in rate-setting, and assuring access to needed care and services.”
[email protected]
On Twitter @legal_med
The Senate confirmed Seema Verma as administrator of the Centers for Medicare & Medicaid Services on March 13 by a largely party line vote of 55-43.
Ms. Verma’s confirmation comes as Republicans begin their efforts to repeal and replace the Affordable Care Act. During the March 13 debate, Senate Finance Committee Chairman Orrin Hatch (R-Utah) reiterated his support for Ms. Verma, saying she will be a needed leader during the transition from the ACA.
Senate Finance Committee Ranking Member Ron Wyden (D-Ore.) continued to criticize Ms. Verma during the debate, stressing that she has presented no clear vision of her plans as the next CMS administrator.
“Ms. Verma gave the Finance Committee and the public virtually nothing to go by in terms of how she’d approach this job,” Sen. Wyden said during floor debate. “If confirmed, she’d be one of the top officials to implement Trumpcare, a bill that would raid Medicaid, slash Medicare, and kick millions of Americans off their health care... So I’m unable to support this nomination.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
During her confirmation hearing, senators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. But Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for Hewlett Packard. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
The Association for Community Affiliated Plans (ACAP) pledged to work with Ms. Verma as the Trump administration works toward changing how Medicaid is financed and administered. ACAP represents nonprofit safety net health plans in 28 states that serve patients enrolled in Medicaid, Medicare, the Children’s Health Insurance Program, marketplaces, and other publicly supported health programs.
“Flexibility is one of the great things about the Medicaid program today – this very flexibility is what has allowed the changes Ms. Verma helped to effect in Indiana,” ACAP CEO Margaret A. Murray said in a statement. “We look forward to working with Ms. Verma on pathways to refine the program while maintaining its guarantee of coverage for all eligible individuals, improving transparency and actuarial soundness in rate-setting, and assuring access to needed care and services.”
[email protected]
On Twitter @legal_med
On vacation, my patients go with me
I’m in the process of planning our family vacations for the summer. I do something different from most when on the road: I take my patients with me.
Well, obviously not physically, but I do cover everything, no matter where I am.
Yes, it takes time. In a ritual my family is used to, two to three times a day I’ll call my staff and go over a list of calls that came in, refills needed, and test results. We go back and forth for a bit. For more complicated questions, I may have to wait until I have my laptop, with the charts on it. If there’s an emergency they’ll call me, and if I can’t be reached, they’ll dial up my call partners.

• I know my patients. I think we all feel that way. I’m more comfortable, and I hope they are too, with the doc who knows them making the decisions.
• My call partners don’t know them. We’re all in solo practice. They don’t have access to my charts any more than I do to theirs. That’s an okay arrangement for a weekend call, but not 2 weeks.
• No surprises. I know that I’m not going to be coming home to a pile of MRI and lab reports that I need to review and act on. If my patient was in the ER or admitted, I spoke to the physician handling it.
A long time ago, when I first started out, I asked another neurologist in my building to cover for me when I was leaving town. I didn’t know him very well, but I was still learning the ropes. He said fine.
When I came home, I found he’d actually “poached” several who’d called, having them come in and convincing them to switch doctors. He’d also changed medications on well-controlled epilepsy and migraine patients who’d needed refills, leaving me to deal with the complications of it when I returned.
Granted, I’ve since learned that he was unusual in that degree, but it really rattled me. I decided I’d rather handle things on my own from then on.
This isn’t an easy decision, but I’m glad I do it. I come home to an office with no surprises, no test results piled up to review, no medication changes that I look at and wonder about.
Does it ruin my vacation? Not at all. Yes, it’s 30-60 minutes out of each day that I have to spend with my office, but I think it’s worth it. It’s peace of mind for me, my staff, and my patients, at least as much as you can ever have in this field.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
[polldaddy:9696724]
I’m in the process of planning our family vacations for the summer. I do something different from most when on the road: I take my patients with me.
Well, obviously not physically, but I do cover everything, no matter where I am.
Yes, it takes time. In a ritual my family is used to, two to three times a day I’ll call my staff and go over a list of calls that came in, refills needed, and test results. We go back and forth for a bit. For more complicated questions, I may have to wait until I have my laptop, with the charts on it. If there’s an emergency they’ll call me, and if I can’t be reached, they’ll dial up my call partners.
• I know my patients. I think we all feel that way. I’m more comfortable, and I hope they are too, with the doc who knows them making the decisions.
• My call partners don’t know them. We’re all in solo practice. They don’t have access to my charts any more than I do to theirs. That’s an okay arrangement for a weekend call, but not 2 weeks.
• No surprises. I know that I’m not going to be coming home to a pile of MRI and lab reports that I need to review and act on. If my patient was in the ER or admitted, I spoke to the physician handling it.
A long time ago, when I first started out, I asked another neurologist in my building to cover for me when I was leaving town. I didn’t know him very well, but I was still learning the ropes. He said fine.
When I came home, I found he’d actually “poached” several who’d called, having them come in and convincing them to switch doctors. He’d also changed medications on well-controlled epilepsy and migraine patients who’d needed refills, leaving me to deal with the complications of it when I returned.
Granted, I’ve since learned that he was unusual in that degree, but it really rattled me. I decided I’d rather handle things on my own from then on.
This isn’t an easy decision, but I’m glad I do it. I come home to an office with no surprises, no test results piled up to review, no medication changes that I look at and wonder about.
Does it ruin my vacation? Not at all. Yes, it’s 30-60 minutes out of each day that I have to spend with my office, but I think it’s worth it. It’s peace of mind for me, my staff, and my patients, at least as much as you can ever have in this field.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
[polldaddy:9696724]
I’m in the process of planning our family vacations for the summer. I do something different from most when on the road: I take my patients with me.
Well, obviously not physically, but I do cover everything, no matter where I am.
Yes, it takes time. In a ritual my family is used to, two to three times a day I’ll call my staff and go over a list of calls that came in, refills needed, and test results. We go back and forth for a bit. For more complicated questions, I may have to wait until I have my laptop, with the charts on it. If there’s an emergency they’ll call me, and if I can’t be reached, they’ll dial up my call partners.
• I know my patients. I think we all feel that way. I’m more comfortable, and I hope they are too, with the doc who knows them making the decisions.
• My call partners don’t know them. We’re all in solo practice. They don’t have access to my charts any more than I do to theirs. That’s an okay arrangement for a weekend call, but not 2 weeks.
• No surprises. I know that I’m not going to be coming home to a pile of MRI and lab reports that I need to review and act on. If my patient was in the ER or admitted, I spoke to the physician handling it.
A long time ago, when I first started out, I asked another neurologist in my building to cover for me when I was leaving town. I didn’t know him very well, but I was still learning the ropes. He said fine.
When I came home, I found he’d actually “poached” several who’d called, having them come in and convincing them to switch doctors. He’d also changed medications on well-controlled epilepsy and migraine patients who’d needed refills, leaving me to deal with the complications of it when I returned.
Granted, I’ve since learned that he was unusual in that degree, but it really rattled me. I decided I’d rather handle things on my own from then on.
This isn’t an easy decision, but I’m glad I do it. I come home to an office with no surprises, no test results piled up to review, no medication changes that I look at and wonder about.
Does it ruin my vacation? Not at all. Yes, it’s 30-60 minutes out of each day that I have to spend with my office, but I think it’s worth it. It’s peace of mind for me, my staff, and my patients, at least as much as you can ever have in this field.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
[polldaddy:9696724]
Oral immunotherapy induced wheat allergy tolerance
ATLANTA – Oral immunotherapy with wheat gluten flour decreased wheat reactions in some allergic patients, according to a trial reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Wheat allergy is fairly common in young children; most people outgrow it. For some, though, it remains a dangerous problem, especially because wheat is almost impossible to avoid, said senior investigator Hugh Sampson, MD, the Kurt Hirschhorn Professor of Pediatrics at the Icahn School of Medicine at Mount Sinai and director of the Jaffe Food Allergy Institute at Mount Sinai Hospital, New York.
For example, one of the study subjects stopped for a bite on the way to the clinic. “He thought he ate a wheat-free breakfast but ended up arriving with anaphylaxis,” the physician said.

Gluten is the protein-rich allergenic part of wheat; using gluten flour instead of regular flour allowed for smaller, more convenient doses. It was sprinkled over applesauce and other foods. Twelve of the 23 gluten flour subjects (52%), but no one in the placebo group, tolerated a challenge of 4,443 mg at 1 year.
Next, placebo subjects were started on their own gluten flour regimen, but they shot for a higher maximum dose of 3,870 mg/day. The original gluten group stayed on their dose, a maximum of 1,445 mg/day.
The higher dose was more effective at 2-year follow-up; 7 of 23 patients (30%) in the 1,445-mg group tolerated a challenge of 7,443 mg at 2 years, versus 12 of 21 patients (57%) in the 3,870-mg group.
Just over 10% of the doses triggered adverse reactions. Most of the reactions were mild – itching in the throat or mouth, nausea, and the like – but epinephrine was needed after 0.05% of the doses. The adverse reaction rate was similar to that with other forms of oral immunotherapy, and there were no statistically significant differences in the number of reactions between the low- and high-dose gluten groups.
For anyone who reads the study and thinks about running to the grocery store for gluten flour, Dr. Sampson cautioned against it. There’s no Food and Drug Administration–approved product, and, more importantly, “you can run into [serious medical] problems” if, for instance, immunotherapy triggers anaphylaxis with too much exercise afterward.
The study “has nothing to do with” the kind of gluten intolerance that’s led to an explosion in gluten-free products in recent years, he said. “Our study was directed at IgE-mediated reactions. Celiac disease has a very different mechanism.”
Also, only a few people remained tolerant after being backed off wheat immunotherapy for a couple of months. There’s no such thing as a cure for food allergies at this point.
“We are trying to get people into remission. Nobody yet has demonstrated that you can make a permanent change in somebody [who] is hypersensitive, even to a bee sting,” Dr. Sampson said.
The study results are big enough to protect wheat-allergic people from accidental exposure. In the case of the study subject who reacted to wheat in his breakfast, he probably reacted to far less than 7,443 mg of wheat protein – about the amount in a plate of pasta – before immunotherapy. No one with a wheat allergy is intentionally going to order something like that, Dr. Sampson said.
The next step is industry funding for a larger trial. “These studies are expensive, and we hope somebody will take up the torch. We have to get industry involved,” he said.
Private philanthropies funded the work. Dr. Sampson is chief scientific officer for DBV Technologies, a company developing a patch for peanut allergies.
ATLANTA – Oral immunotherapy with wheat gluten flour decreased wheat reactions in some allergic patients, according to a trial reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Wheat allergy is fairly common in young children; most people outgrow it. For some, though, it remains a dangerous problem, especially because wheat is almost impossible to avoid, said senior investigator Hugh Sampson, MD, the Kurt Hirschhorn Professor of Pediatrics at the Icahn School of Medicine at Mount Sinai and director of the Jaffe Food Allergy Institute at Mount Sinai Hospital, New York.
For example, one of the study subjects stopped for a bite on the way to the clinic. “He thought he ate a wheat-free breakfast but ended up arriving with anaphylaxis,” the physician said.
Gluten is the protein-rich allergenic part of wheat; using gluten flour instead of regular flour allowed for smaller, more convenient doses. It was sprinkled over applesauce and other foods. Twelve of the 23 gluten flour subjects (52%), but no one in the placebo group, tolerated a challenge of 4,443 mg at 1 year.
Next, placebo subjects were started on their own gluten flour regimen, but they shot for a higher maximum dose of 3,870 mg/day. The original gluten group stayed on their dose, a maximum of 1,445 mg/day.
The higher dose was more effective at 2-year follow-up; 7 of 23 patients (30%) in the 1,445-mg group tolerated a challenge of 7,443 mg at 2 years, versus 12 of 21 patients (57%) in the 3,870-mg group.
Just over 10% of the doses triggered adverse reactions. Most of the reactions were mild – itching in the throat or mouth, nausea, and the like – but epinephrine was needed after 0.05% of the doses. The adverse reaction rate was similar to that with other forms of oral immunotherapy, and there were no statistically significant differences in the number of reactions between the low- and high-dose gluten groups.
For anyone who reads the study and thinks about running to the grocery store for gluten flour, Dr. Sampson cautioned against it. There’s no Food and Drug Administration–approved product, and, more importantly, “you can run into [serious medical] problems” if, for instance, immunotherapy triggers anaphylaxis with too much exercise afterward.
The study “has nothing to do with” the kind of gluten intolerance that’s led to an explosion in gluten-free products in recent years, he said. “Our study was directed at IgE-mediated reactions. Celiac disease has a very different mechanism.”
Also, only a few people remained tolerant after being backed off wheat immunotherapy for a couple of months. There’s no such thing as a cure for food allergies at this point.
“We are trying to get people into remission. Nobody yet has demonstrated that you can make a permanent change in somebody [who] is hypersensitive, even to a bee sting,” Dr. Sampson said.
The study results are big enough to protect wheat-allergic people from accidental exposure. In the case of the study subject who reacted to wheat in his breakfast, he probably reacted to far less than 7,443 mg of wheat protein – about the amount in a plate of pasta – before immunotherapy. No one with a wheat allergy is intentionally going to order something like that, Dr. Sampson said.
The next step is industry funding for a larger trial. “These studies are expensive, and we hope somebody will take up the torch. We have to get industry involved,” he said.
Private philanthropies funded the work. Dr. Sampson is chief scientific officer for DBV Technologies, a company developing a patch for peanut allergies.
ATLANTA – Oral immunotherapy with wheat gluten flour decreased wheat reactions in some allergic patients, according to a trial reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Wheat allergy is fairly common in young children; most people outgrow it. For some, though, it remains a dangerous problem, especially because wheat is almost impossible to avoid, said senior investigator Hugh Sampson, MD, the Kurt Hirschhorn Professor of Pediatrics at the Icahn School of Medicine at Mount Sinai and director of the Jaffe Food Allergy Institute at Mount Sinai Hospital, New York.
For example, one of the study subjects stopped for a bite on the way to the clinic. “He thought he ate a wheat-free breakfast but ended up arriving with anaphylaxis,” the physician said.
Gluten is the protein-rich allergenic part of wheat; using gluten flour instead of regular flour allowed for smaller, more convenient doses. It was sprinkled over applesauce and other foods. Twelve of the 23 gluten flour subjects (52%), but no one in the placebo group, tolerated a challenge of 4,443 mg at 1 year.
Next, placebo subjects were started on their own gluten flour regimen, but they shot for a higher maximum dose of 3,870 mg/day. The original gluten group stayed on their dose, a maximum of 1,445 mg/day.
The higher dose was more effective at 2-year follow-up; 7 of 23 patients (30%) in the 1,445-mg group tolerated a challenge of 7,443 mg at 2 years, versus 12 of 21 patients (57%) in the 3,870-mg group.
Just over 10% of the doses triggered adverse reactions. Most of the reactions were mild – itching in the throat or mouth, nausea, and the like – but epinephrine was needed after 0.05% of the doses. The adverse reaction rate was similar to that with other forms of oral immunotherapy, and there were no statistically significant differences in the number of reactions between the low- and high-dose gluten groups.
For anyone who reads the study and thinks about running to the grocery store for gluten flour, Dr. Sampson cautioned against it. There’s no Food and Drug Administration–approved product, and, more importantly, “you can run into [serious medical] problems” if, for instance, immunotherapy triggers anaphylaxis with too much exercise afterward.
The study “has nothing to do with” the kind of gluten intolerance that’s led to an explosion in gluten-free products in recent years, he said. “Our study was directed at IgE-mediated reactions. Celiac disease has a very different mechanism.”
Also, only a few people remained tolerant after being backed off wheat immunotherapy for a couple of months. There’s no such thing as a cure for food allergies at this point.
“We are trying to get people into remission. Nobody yet has demonstrated that you can make a permanent change in somebody [who] is hypersensitive, even to a bee sting,” Dr. Sampson said.
The study results are big enough to protect wheat-allergic people from accidental exposure. In the case of the study subject who reacted to wheat in his breakfast, he probably reacted to far less than 7,443 mg of wheat protein – about the amount in a plate of pasta – before immunotherapy. No one with a wheat allergy is intentionally going to order something like that, Dr. Sampson said.
The next step is industry funding for a larger trial. “These studies are expensive, and we hope somebody will take up the torch. We have to get industry involved,” he said.
Private philanthropies funded the work. Dr. Sampson is chief scientific officer for DBV Technologies, a company developing a patch for peanut allergies.
AT 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: Twelve of the 23 gluten flour subjects (52%), but no one in the placebo group, tolerated a challenge dose of 4,443 mg at 1 year.
Data source: A randomized trial of 46 wheat-allergic patients.
Disclosures: Private philanthropies funded the work. The senior investigator is chief scientific officer for DBV Technologies, a company developing a patch for peanut allergies.
FDA approves ribociclib for HR+, HER2– advanced breast cancer
The Food and Drug Administration has approved ribociclib, a cyclin-dependent kinase (CDK) 4/6 inhibitor, in combination with an aromatase inhibitor as initial endocrine-based therapy for the treatment of postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer.
Overall survival data is immature but approval was based on improvement in progression-free survival (PFS) among 334 women randomized to receive ribociclib plus letrozole compared to 334 women randomized to receive placebo plus letrozole in phase III MONALEESA-2 (hazard ratio, 0.556; 95% CI: 0.429, 0.720; P less than .0001).

Ribociclib 600 mg or placebo was administered orally once daily for 21 consecutive days, followed by 7 days off, with letrozole 2.5 mg administered orally once daily for 28 days. All patients were postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer who received no prior therapy for advanced disease. Treatment continued until disease progression or unacceptable toxicity,
The most common adverse reactions in patients taking ribociclib were neutropenia, nausea, fatigue, diarrhea, leukopenia, alopecia, vomiting, constipation, headache, and back pain. The most common grade 3 or 4 adverse reactions were neutropenia, leukopenia, abnormal liver function tests, lymphopenia, and vomiting. Ribociclib has been shown to prolong the QT interval in a concentration-dependent manner, the FDA warns.
Ribociclib is the second CDK4/6 inhibitor to receive approval for advanced breast cancer, following the accelerated approval of palbociclib (Ibrance) plus letrozole (Femara) as a first-line treatment for postmenopausal women with ER-postive, HER2-negative metastatic breast cancer in 2015. The FDA expanded the indication for fulvestrant to include use in combination with palbociclib in 2016.
Phase II trial data indicating activity of a third CDK 4/6 inhibitor, abemaciclib, in this patient population was presented at the 2016 ASCO Annual Meeting.
The recommended starting dose of ribociclib is 600 mg orally (three 200-mg tablets) taken once daily with or without food for 21 consecutive days followed by 7 days off treatment.
Full prescribing information for ribociclib is available here.
Ribociclib is being marketed as Kisqali by Novartis Pharmaceuticals Corp.
[email protected]
On Twitter @NikolaidesLaura
The Food and Drug Administration has approved ribociclib, a cyclin-dependent kinase (CDK) 4/6 inhibitor, in combination with an aromatase inhibitor as initial endocrine-based therapy for the treatment of postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer.
Overall survival data is immature but approval was based on improvement in progression-free survival (PFS) among 334 women randomized to receive ribociclib plus letrozole compared to 334 women randomized to receive placebo plus letrozole in phase III MONALEESA-2 (hazard ratio, 0.556; 95% CI: 0.429, 0.720; P less than .0001).
Ribociclib 600 mg or placebo was administered orally once daily for 21 consecutive days, followed by 7 days off, with letrozole 2.5 mg administered orally once daily for 28 days. All patients were postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer who received no prior therapy for advanced disease. Treatment continued until disease progression or unacceptable toxicity,
The most common adverse reactions in patients taking ribociclib were neutropenia, nausea, fatigue, diarrhea, leukopenia, alopecia, vomiting, constipation, headache, and back pain. The most common grade 3 or 4 adverse reactions were neutropenia, leukopenia, abnormal liver function tests, lymphopenia, and vomiting. Ribociclib has been shown to prolong the QT interval in a concentration-dependent manner, the FDA warns.
Ribociclib is the second CDK4/6 inhibitor to receive approval for advanced breast cancer, following the accelerated approval of palbociclib (Ibrance) plus letrozole (Femara) as a first-line treatment for postmenopausal women with ER-postive, HER2-negative metastatic breast cancer in 2015. The FDA expanded the indication for fulvestrant to include use in combination with palbociclib in 2016.
Phase II trial data indicating activity of a third CDK 4/6 inhibitor, abemaciclib, in this patient population was presented at the 2016 ASCO Annual Meeting.
The recommended starting dose of ribociclib is 600 mg orally (three 200-mg tablets) taken once daily with or without food for 21 consecutive days followed by 7 days off treatment.
Full prescribing information for ribociclib is available here.
Ribociclib is being marketed as Kisqali by Novartis Pharmaceuticals Corp.
[email protected]
On Twitter @NikolaidesLaura
The Food and Drug Administration has approved ribociclib, a cyclin-dependent kinase (CDK) 4/6 inhibitor, in combination with an aromatase inhibitor as initial endocrine-based therapy for the treatment of postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer.
Overall survival data is immature but approval was based on improvement in progression-free survival (PFS) among 334 women randomized to receive ribociclib plus letrozole compared to 334 women randomized to receive placebo plus letrozole in phase III MONALEESA-2 (hazard ratio, 0.556; 95% CI: 0.429, 0.720; P less than .0001).
Ribociclib 600 mg or placebo was administered orally once daily for 21 consecutive days, followed by 7 days off, with letrozole 2.5 mg administered orally once daily for 28 days. All patients were postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer who received no prior therapy for advanced disease. Treatment continued until disease progression or unacceptable toxicity,
The most common adverse reactions in patients taking ribociclib were neutropenia, nausea, fatigue, diarrhea, leukopenia, alopecia, vomiting, constipation, headache, and back pain. The most common grade 3 or 4 adverse reactions were neutropenia, leukopenia, abnormal liver function tests, lymphopenia, and vomiting. Ribociclib has been shown to prolong the QT interval in a concentration-dependent manner, the FDA warns.
Ribociclib is the second CDK4/6 inhibitor to receive approval for advanced breast cancer, following the accelerated approval of palbociclib (Ibrance) plus letrozole (Femara) as a first-line treatment for postmenopausal women with ER-postive, HER2-negative metastatic breast cancer in 2015. The FDA expanded the indication for fulvestrant to include use in combination with palbociclib in 2016.
Phase II trial data indicating activity of a third CDK 4/6 inhibitor, abemaciclib, in this patient population was presented at the 2016 ASCO Annual Meeting.
The recommended starting dose of ribociclib is 600 mg orally (three 200-mg tablets) taken once daily with or without food for 21 consecutive days followed by 7 days off treatment.
Full prescribing information for ribociclib is available here.
Ribociclib is being marketed as Kisqali by Novartis Pharmaceuticals Corp.
[email protected]
On Twitter @NikolaidesLaura
Isolated tumor cells did not predict progression in endometrial cancer
NATIONAL HARBOR, MD. – Patients with endometrial cancer should not receive adjuvant chemotherapy or radiotherapy solely because they have isolated tumor cells in their sentinel lymph nodes, Marie Plante, MD, said during an oral presentation at the annual meeting of the Society of Gynecologic Oncology.
In a single-center prospective cohort study, about 96% of patients with endometrial cancer were alive and progression free at 3 years, a rate which resembles those reported for node-negative patients, said Dr. Plante of Laval University, Quebec City. Moreover, all 10 patients who did not receive adjuvant therapy remained alive and progression free during follow-up, she said. “Patients with isolated tumor cells carry an excellent prognosis,” she added. “Adjuvant treatment should be tailored based on uterine factors and histology and not solely on the presence of isolated tumor cells in sentinel lymph nodes.”
Pathologic ultrastaging has boosted the detection of low-volume metastases, which comprise anywhere from 35% to 63% of nodal metastases in patients with endometrial cancer. Clinicians continue to debate management when this low-volume disease consists of isolated tumor cells (ITC), defined as fewer than 200 carcinoma cells found singly or in small clusters. Finding ITC in endometrial cancer is uncommon, and few studies have examined this subgroup, Dr. Plante noted.
She and her associates evaluated 519 patients who underwent hysterectomy, salpingo-oophorectomy, lymphadenectomy, or sentinel lymph node mapping for endometrial cancer at their center between 2010 and 2015. Pathologic ultrastaging identified 31 patients with ITC (6%), of whom 11 patients received adjuvant chemotherapy, 14 received pelvic radiation therapy, and 10 underwent only brachytherapy or observation, with some patients receiving more than one treatment. Another 54 patients in the cohort had metastatic disease, including 43 patients with macrometastasis and 11 with micrometastasis.
Stage, not treatment, predicted progression-free survival (PFS), Dr. Plante emphasized. After a median follow-up period of 29 months, the estimated 3-year rate of PFS was significantly better among patients with ITC (96%), node-negative disease (88%), or micrometastasis (86%) than among those with macrometastasis (59%; P = .001), even though macrometastasis patients received significantly more chemotherapy (P = .0001).
Rates of PFS did not statistically differ between the ITC and node-negative groups, Dr. Plante noted. The single recurrence in an ITC patient involved a 7 cm carcinosarcoma that recurred despite adjuvant chemotherapy and radiation therapy. There were no recurrences among patients with endometrioid histology.
Among ITC patients who received no adjuvant treatment, half had stage IA endometrial cancer and half were stage IB, half were grade 1 and half were grade 2, all had endometrioid histology, and seven (70%) had evidence of lymphovascular space invasion, Dr. Plante said. All remained alive and progression free at follow-up.
Ultrastaging should only be performed if a sentinel lymph node is negative on initial hematoxylin and eosin stain and if there is myoinvasion, commented Nadeem R. Abu-Rustum, MD, chief of the gynecology service at Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study. “Ultrastaging increases positive-node detection by about 8%,” he said during the scientific plenary session at the conference. “Finding positive nodes can change management, and we have to be careful not to overtreat.”
Ongoing research is examining the topography and anatomic location of ITC in sentinel lymph nodes, Dr. Abu-Rustum said. In the meantime, he advised clinicians to consider any ultrastaging result of ITC in context. “When modeling the risk of ITCs, don’t look at them in isolation. Don’t be ‘node-centric,’ ” he advised. “Look at the uterine factors and the overall bigger picture.”
Dr. Plante did not acknowledge external funding sources. Dr. Plante and Dr. Abu-Rustum reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Patients with endometrial cancer should not receive adjuvant chemotherapy or radiotherapy solely because they have isolated tumor cells in their sentinel lymph nodes, Marie Plante, MD, said during an oral presentation at the annual meeting of the Society of Gynecologic Oncology.
In a single-center prospective cohort study, about 96% of patients with endometrial cancer were alive and progression free at 3 years, a rate which resembles those reported for node-negative patients, said Dr. Plante of Laval University, Quebec City. Moreover, all 10 patients who did not receive adjuvant therapy remained alive and progression free during follow-up, she said. “Patients with isolated tumor cells carry an excellent prognosis,” she added. “Adjuvant treatment should be tailored based on uterine factors and histology and not solely on the presence of isolated tumor cells in sentinel lymph nodes.”
Pathologic ultrastaging has boosted the detection of low-volume metastases, which comprise anywhere from 35% to 63% of nodal metastases in patients with endometrial cancer. Clinicians continue to debate management when this low-volume disease consists of isolated tumor cells (ITC), defined as fewer than 200 carcinoma cells found singly or in small clusters. Finding ITC in endometrial cancer is uncommon, and few studies have examined this subgroup, Dr. Plante noted.
She and her associates evaluated 519 patients who underwent hysterectomy, salpingo-oophorectomy, lymphadenectomy, or sentinel lymph node mapping for endometrial cancer at their center between 2010 and 2015. Pathologic ultrastaging identified 31 patients with ITC (6%), of whom 11 patients received adjuvant chemotherapy, 14 received pelvic radiation therapy, and 10 underwent only brachytherapy or observation, with some patients receiving more than one treatment. Another 54 patients in the cohort had metastatic disease, including 43 patients with macrometastasis and 11 with micrometastasis.
Stage, not treatment, predicted progression-free survival (PFS), Dr. Plante emphasized. After a median follow-up period of 29 months, the estimated 3-year rate of PFS was significantly better among patients with ITC (96%), node-negative disease (88%), or micrometastasis (86%) than among those with macrometastasis (59%; P = .001), even though macrometastasis patients received significantly more chemotherapy (P = .0001).
Rates of PFS did not statistically differ between the ITC and node-negative groups, Dr. Plante noted. The single recurrence in an ITC patient involved a 7 cm carcinosarcoma that recurred despite adjuvant chemotherapy and radiation therapy. There were no recurrences among patients with endometrioid histology.
Among ITC patients who received no adjuvant treatment, half had stage IA endometrial cancer and half were stage IB, half were grade 1 and half were grade 2, all had endometrioid histology, and seven (70%) had evidence of lymphovascular space invasion, Dr. Plante said. All remained alive and progression free at follow-up.
Ultrastaging should only be performed if a sentinel lymph node is negative on initial hematoxylin and eosin stain and if there is myoinvasion, commented Nadeem R. Abu-Rustum, MD, chief of the gynecology service at Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study. “Ultrastaging increases positive-node detection by about 8%,” he said during the scientific plenary session at the conference. “Finding positive nodes can change management, and we have to be careful not to overtreat.”
Ongoing research is examining the topography and anatomic location of ITC in sentinel lymph nodes, Dr. Abu-Rustum said. In the meantime, he advised clinicians to consider any ultrastaging result of ITC in context. “When modeling the risk of ITCs, don’t look at them in isolation. Don’t be ‘node-centric,’ ” he advised. “Look at the uterine factors and the overall bigger picture.”
Dr. Plante did not acknowledge external funding sources. Dr. Plante and Dr. Abu-Rustum reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Patients with endometrial cancer should not receive adjuvant chemotherapy or radiotherapy solely because they have isolated tumor cells in their sentinel lymph nodes, Marie Plante, MD, said during an oral presentation at the annual meeting of the Society of Gynecologic Oncology.
In a single-center prospective cohort study, about 96% of patients with endometrial cancer were alive and progression free at 3 years, a rate which resembles those reported for node-negative patients, said Dr. Plante of Laval University, Quebec City. Moreover, all 10 patients who did not receive adjuvant therapy remained alive and progression free during follow-up, she said. “Patients with isolated tumor cells carry an excellent prognosis,” she added. “Adjuvant treatment should be tailored based on uterine factors and histology and not solely on the presence of isolated tumor cells in sentinel lymph nodes.”
Pathologic ultrastaging has boosted the detection of low-volume metastases, which comprise anywhere from 35% to 63% of nodal metastases in patients with endometrial cancer. Clinicians continue to debate management when this low-volume disease consists of isolated tumor cells (ITC), defined as fewer than 200 carcinoma cells found singly or in small clusters. Finding ITC in endometrial cancer is uncommon, and few studies have examined this subgroup, Dr. Plante noted.
She and her associates evaluated 519 patients who underwent hysterectomy, salpingo-oophorectomy, lymphadenectomy, or sentinel lymph node mapping for endometrial cancer at their center between 2010 and 2015. Pathologic ultrastaging identified 31 patients with ITC (6%), of whom 11 patients received adjuvant chemotherapy, 14 received pelvic radiation therapy, and 10 underwent only brachytherapy or observation, with some patients receiving more than one treatment. Another 54 patients in the cohort had metastatic disease, including 43 patients with macrometastasis and 11 with micrometastasis.
Stage, not treatment, predicted progression-free survival (PFS), Dr. Plante emphasized. After a median follow-up period of 29 months, the estimated 3-year rate of PFS was significantly better among patients with ITC (96%), node-negative disease (88%), or micrometastasis (86%) than among those with macrometastasis (59%; P = .001), even though macrometastasis patients received significantly more chemotherapy (P = .0001).
Rates of PFS did not statistically differ between the ITC and node-negative groups, Dr. Plante noted. The single recurrence in an ITC patient involved a 7 cm carcinosarcoma that recurred despite adjuvant chemotherapy and radiation therapy. There were no recurrences among patients with endometrioid histology.
Among ITC patients who received no adjuvant treatment, half had stage IA endometrial cancer and half were stage IB, half were grade 1 and half were grade 2, all had endometrioid histology, and seven (70%) had evidence of lymphovascular space invasion, Dr. Plante said. All remained alive and progression free at follow-up.
Ultrastaging should only be performed if a sentinel lymph node is negative on initial hematoxylin and eosin stain and if there is myoinvasion, commented Nadeem R. Abu-Rustum, MD, chief of the gynecology service at Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study. “Ultrastaging increases positive-node detection by about 8%,” he said during the scientific plenary session at the conference. “Finding positive nodes can change management, and we have to be careful not to overtreat.”
Ongoing research is examining the topography and anatomic location of ITC in sentinel lymph nodes, Dr. Abu-Rustum said. In the meantime, he advised clinicians to consider any ultrastaging result of ITC in context. “When modeling the risk of ITCs, don’t look at them in isolation. Don’t be ‘node-centric,’ ” he advised. “Look at the uterine factors and the overall bigger picture.”
Dr. Plante did not acknowledge external funding sources. Dr. Plante and Dr. Abu-Rustum reported having no conflicts of interest.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: For patients with endometrial cancer, isolated tumor cells in sentinel lymph nodes did not lead to disease progression and were not an indication for adjuvant treatments.
Major finding: At 3 years, the estimated rate of progression-free survival was 100% among patients who underwent only pelvic brachytherapy or observation.
Data source: A single-center prospective study of 519 patients undergoing hysterectomy, salpingo-oophorectomy, lymphadenectomy, and sentinel lymph node mapping for endometrial cancer, including 31 patients with isolated tumor cells identified in sentinel lymph nodes.
Disclosures: Dr. Plante did not report having external funding sources. Dr. Plante and Dr. Abu-Rustum had no disclosures.
More pushback from docs after CBO scores GOP health care plan
Physician groups continue to push back against a Republican plan to repeal and replace the Affordable Care Act following a Congressional Budget Office analysis that showed up to 24 million patients would not be insured under the plan.
According to the CBO analysis, 14 million more patients would become uninsured in the first year of the American Health Care Act than under current law, with most dropping coverage because of the repeal of the ACA’s individual health insurance mandate.
By 2020, an additional 7 million patients would lose coverage largely because of the bill’s rollback of expansion in favor of a per capita allotment to states to cover their Medicaid population.
“In 2026, an estimated 52 million would be uninsured, compared with 28 million who would lack insurance that year under current law,” according to the CBO analysis.
American Medical Association President Andrew Gurman, MD, called the uptick in uninsured “unacceptable.”
“While the Affordable Care Act was an imperfect law, it was a significant improvement on the status quo at the time, and the AMA believes we need continued progress to expand coverage for the uninsured. Unfortunately, the current proposal – as the CBO analysis shows – would result in the most vulnerable population losing their coverage,” Dr. Gurman said in a statement.
Likewise, the American Osteopathic Association voiced its objections to the GOP proposal.
“The AOA urges Congress to halt any further progression of the American Health Care Act as written and take a more comprehensive approach that addresses such systemic issues while providing stability for the insurance marketplace and the millions of Americans who rely on it for coverage,” President Boyd Buser, DO, said in a statement.
According to the CBO analysis, the individual health insurance market “would probably be stable in most areas under either current law or the legislation.” However, there could be large premium increases for some patients, based on age group.
Tom Price, MD, secretary of the Department of Health & Human Services, criticized the CBO projections.
“The CBO report’s coverage numbers defy logic,” he said in a statement. “They project that zeroing out the individual mandate – allowing Americans to choose whether to have insurance – will result in 14 million Americans opting out of coverage in 1 year. For there to be the reductions in coverage they project in just the first year, they assume 5 million Americans on Medicaid will drop off of health insurance for which they pay very little, and another 9 million will stop participating in the individual and employer markets. These types of assumptions do not translate to the real world, and they do not accurately estimate the effects of this bill.”
Rep. Kevin Brady (R-Texas), chairman of the House Ways & Means Committee, also disputed the increase in the uninsured population.
“The American Health Care Act is a dramatic departure from Obamacare, which forced Americans to buy expensive, one-size-fits-all health insurance,” Chairman Brady said in a statement. “Our legislation gives individuals and families the freedom to access health care options that are tailored to the needs, not Washington’s.”
Rep. Brady and Dr. Price also pointed out that the AHCA is just the first step of a three-step process, which will include a review of ACA regulations as well as passage of further legislation aimed at providing high quality care at lower costs. However, those cannot be scored by CBO as those details have yet to be released, the GOP leaders pointed out.
The CBO analysis predicts that premiums for those buying insurance in the individual marketplace would increase of 15%-20% from 2018 to 2019, but starting in 2020, average premiums are expected to decrease from states using federal government funds to help offset costs from high users of health care and more younger people coming into the health insurance market.
“By 2026, average premiums for single policyholders in the nongroup market under the legislation would be roughly 10% lower than under current law,” according to the analysis, although since the law allows for higher premiums for older individuals, the congressional budget watchdog sees the provisions of the AHCA as “substantially reducing premiums for young adults and substantially raising premiums for older people.”
The CBO estimates that enacting this legislation would reduce federal deficits by $337 billion over the 2017-2026 period, mainly from reductions in Medicaid spending and the elimination of the current premium subsidies, though the deficit reduction is somewhat offset by the refundable premium tax credits that replace the ACA’s subsidies.
Physician groups continue to push back against a Republican plan to repeal and replace the Affordable Care Act following a Congressional Budget Office analysis that showed up to 24 million patients would not be insured under the plan.
According to the CBO analysis, 14 million more patients would become uninsured in the first year of the American Health Care Act than under current law, with most dropping coverage because of the repeal of the ACA’s individual health insurance mandate.
By 2020, an additional 7 million patients would lose coverage largely because of the bill’s rollback of expansion in favor of a per capita allotment to states to cover their Medicaid population.
“In 2026, an estimated 52 million would be uninsured, compared with 28 million who would lack insurance that year under current law,” according to the CBO analysis.
American Medical Association President Andrew Gurman, MD, called the uptick in uninsured “unacceptable.”
“While the Affordable Care Act was an imperfect law, it was a significant improvement on the status quo at the time, and the AMA believes we need continued progress to expand coverage for the uninsured. Unfortunately, the current proposal – as the CBO analysis shows – would result in the most vulnerable population losing their coverage,” Dr. Gurman said in a statement.
Likewise, the American Osteopathic Association voiced its objections to the GOP proposal.
“The AOA urges Congress to halt any further progression of the American Health Care Act as written and take a more comprehensive approach that addresses such systemic issues while providing stability for the insurance marketplace and the millions of Americans who rely on it for coverage,” President Boyd Buser, DO, said in a statement.
According to the CBO analysis, the individual health insurance market “would probably be stable in most areas under either current law or the legislation.” However, there could be large premium increases for some patients, based on age group.
Tom Price, MD, secretary of the Department of Health & Human Services, criticized the CBO projections.
“The CBO report’s coverage numbers defy logic,” he said in a statement. “They project that zeroing out the individual mandate – allowing Americans to choose whether to have insurance – will result in 14 million Americans opting out of coverage in 1 year. For there to be the reductions in coverage they project in just the first year, they assume 5 million Americans on Medicaid will drop off of health insurance for which they pay very little, and another 9 million will stop participating in the individual and employer markets. These types of assumptions do not translate to the real world, and they do not accurately estimate the effects of this bill.”
Rep. Kevin Brady (R-Texas), chairman of the House Ways & Means Committee, also disputed the increase in the uninsured population.
“The American Health Care Act is a dramatic departure from Obamacare, which forced Americans to buy expensive, one-size-fits-all health insurance,” Chairman Brady said in a statement. “Our legislation gives individuals and families the freedom to access health care options that are tailored to the needs, not Washington’s.”
Rep. Brady and Dr. Price also pointed out that the AHCA is just the first step of a three-step process, which will include a review of ACA regulations as well as passage of further legislation aimed at providing high quality care at lower costs. However, those cannot be scored by CBO as those details have yet to be released, the GOP leaders pointed out.
The CBO analysis predicts that premiums for those buying insurance in the individual marketplace would increase of 15%-20% from 2018 to 2019, but starting in 2020, average premiums are expected to decrease from states using federal government funds to help offset costs from high users of health care and more younger people coming into the health insurance market.
“By 2026, average premiums for single policyholders in the nongroup market under the legislation would be roughly 10% lower than under current law,” according to the analysis, although since the law allows for higher premiums for older individuals, the congressional budget watchdog sees the provisions of the AHCA as “substantially reducing premiums for young adults and substantially raising premiums for older people.”
The CBO estimates that enacting this legislation would reduce federal deficits by $337 billion over the 2017-2026 period, mainly from reductions in Medicaid spending and the elimination of the current premium subsidies, though the deficit reduction is somewhat offset by the refundable premium tax credits that replace the ACA’s subsidies.
Physician groups continue to push back against a Republican plan to repeal and replace the Affordable Care Act following a Congressional Budget Office analysis that showed up to 24 million patients would not be insured under the plan.
According to the CBO analysis, 14 million more patients would become uninsured in the first year of the American Health Care Act than under current law, with most dropping coverage because of the repeal of the ACA’s individual health insurance mandate.
By 2020, an additional 7 million patients would lose coverage largely because of the bill’s rollback of expansion in favor of a per capita allotment to states to cover their Medicaid population.
“In 2026, an estimated 52 million would be uninsured, compared with 28 million who would lack insurance that year under current law,” according to the CBO analysis.
American Medical Association President Andrew Gurman, MD, called the uptick in uninsured “unacceptable.”
“While the Affordable Care Act was an imperfect law, it was a significant improvement on the status quo at the time, and the AMA believes we need continued progress to expand coverage for the uninsured. Unfortunately, the current proposal – as the CBO analysis shows – would result in the most vulnerable population losing their coverage,” Dr. Gurman said in a statement.
Likewise, the American Osteopathic Association voiced its objections to the GOP proposal.
“The AOA urges Congress to halt any further progression of the American Health Care Act as written and take a more comprehensive approach that addresses such systemic issues while providing stability for the insurance marketplace and the millions of Americans who rely on it for coverage,” President Boyd Buser, DO, said in a statement.
According to the CBO analysis, the individual health insurance market “would probably be stable in most areas under either current law or the legislation.” However, there could be large premium increases for some patients, based on age group.
Tom Price, MD, secretary of the Department of Health & Human Services, criticized the CBO projections.
“The CBO report’s coverage numbers defy logic,” he said in a statement. “They project that zeroing out the individual mandate – allowing Americans to choose whether to have insurance – will result in 14 million Americans opting out of coverage in 1 year. For there to be the reductions in coverage they project in just the first year, they assume 5 million Americans on Medicaid will drop off of health insurance for which they pay very little, and another 9 million will stop participating in the individual and employer markets. These types of assumptions do not translate to the real world, and they do not accurately estimate the effects of this bill.”
Rep. Kevin Brady (R-Texas), chairman of the House Ways & Means Committee, also disputed the increase in the uninsured population.
“The American Health Care Act is a dramatic departure from Obamacare, which forced Americans to buy expensive, one-size-fits-all health insurance,” Chairman Brady said in a statement. “Our legislation gives individuals and families the freedom to access health care options that are tailored to the needs, not Washington’s.”
Rep. Brady and Dr. Price also pointed out that the AHCA is just the first step of a three-step process, which will include a review of ACA regulations as well as passage of further legislation aimed at providing high quality care at lower costs. However, those cannot be scored by CBO as those details have yet to be released, the GOP leaders pointed out.
The CBO analysis predicts that premiums for those buying insurance in the individual marketplace would increase of 15%-20% from 2018 to 2019, but starting in 2020, average premiums are expected to decrease from states using federal government funds to help offset costs from high users of health care and more younger people coming into the health insurance market.
“By 2026, average premiums for single policyholders in the nongroup market under the legislation would be roughly 10% lower than under current law,” according to the analysis, although since the law allows for higher premiums for older individuals, the congressional budget watchdog sees the provisions of the AHCA as “substantially reducing premiums for young adults and substantially raising premiums for older people.”
The CBO estimates that enacting this legislation would reduce federal deficits by $337 billion over the 2017-2026 period, mainly from reductions in Medicaid spending and the elimination of the current premium subsidies, though the deficit reduction is somewhat offset by the refundable premium tax credits that replace the ACA’s subsidies.
VIDEO: Cell-free DNA mutations linked with recurrence of ovarian cancer
NATIONAL HARBOR, MD. – Next-generation sequencing of high-grade serous ovarian tumor specimens taken during interval debulking identified several mutations that matched those in cell-free DNA (cfDNA), Rebecca C. Arend, MD, said at the annual meeting of the Society of Gynecologic Oncology.
Furthermore, three of four patients whose ovarian cancer recurred had mutations in cfDNA that were previously detected in tumors, said Dr. Arend of the University of Alabama at Birmingham.
Researchers continue to search for ways to spare patients with ovarian cancer from serial biopsies, Dr. Arend noted during a video interview. As part of that work, she and her associates performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens from 14 patients with high-grade serous ovarian cancer.
Mutations found only in tumors were relatively consistent before and after neoadjuvant chemotherapy, while mutations found only in cell-free DNA varied substantially.
The researchers also sequenced plasma samples from four patients at cancer recurrence. Three patients had at least one mutation that was previously detected in their tumor sample. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Many studies have sought circulating tumor markers that reliably predict tumor recurrence. When it comes to cfDNA, “we are not there yet,” but the work is worthwhile, Dr. Arend stressed. Sequencing tumor and cfDNA specimens from patients at multiple points during their journey might one day help pinpoint mutations that reliably predict cancer recurrence, sparing patients from repeated biopsies and helping them efficiently enter clinical trials that target their specific mutation, she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – Next-generation sequencing of high-grade serous ovarian tumor specimens taken during interval debulking identified several mutations that matched those in cell-free DNA (cfDNA), Rebecca C. Arend, MD, said at the annual meeting of the Society of Gynecologic Oncology.
Furthermore, three of four patients whose ovarian cancer recurred had mutations in cfDNA that were previously detected in tumors, said Dr. Arend of the University of Alabama at Birmingham.
Researchers continue to search for ways to spare patients with ovarian cancer from serial biopsies, Dr. Arend noted during a video interview. As part of that work, she and her associates performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens from 14 patients with high-grade serous ovarian cancer.
Mutations found only in tumors were relatively consistent before and after neoadjuvant chemotherapy, while mutations found only in cell-free DNA varied substantially.
The researchers also sequenced plasma samples from four patients at cancer recurrence. Three patients had at least one mutation that was previously detected in their tumor sample. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Many studies have sought circulating tumor markers that reliably predict tumor recurrence. When it comes to cfDNA, “we are not there yet,” but the work is worthwhile, Dr. Arend stressed. Sequencing tumor and cfDNA specimens from patients at multiple points during their journey might one day help pinpoint mutations that reliably predict cancer recurrence, sparing patients from repeated biopsies and helping them efficiently enter clinical trials that target their specific mutation, she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – Next-generation sequencing of high-grade serous ovarian tumor specimens taken during interval debulking identified several mutations that matched those in cell-free DNA (cfDNA), Rebecca C. Arend, MD, said at the annual meeting of the Society of Gynecologic Oncology.
Furthermore, three of four patients whose ovarian cancer recurred had mutations in cfDNA that were previously detected in tumors, said Dr. Arend of the University of Alabama at Birmingham.
Researchers continue to search for ways to spare patients with ovarian cancer from serial biopsies, Dr. Arend noted during a video interview. As part of that work, she and her associates performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens from 14 patients with high-grade serous ovarian cancer.
Mutations found only in tumors were relatively consistent before and after neoadjuvant chemotherapy, while mutations found only in cell-free DNA varied substantially.
The researchers also sequenced plasma samples from four patients at cancer recurrence. Three patients had at least one mutation that was previously detected in their tumor sample. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Many studies have sought circulating tumor markers that reliably predict tumor recurrence. When it comes to cfDNA, “we are not there yet,” but the work is worthwhile, Dr. Arend stressed. Sequencing tumor and cfDNA specimens from patients at multiple points during their journey might one day help pinpoint mutations that reliably predict cancer recurrence, sparing patients from repeated biopsies and helping them efficiently enter clinical trials that target their specific mutation, she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Next-generation sequencing of cell-free DNA specimens (liquid biopsies) might one day help identify tumor recurrence in patients with high-grade serous ovarian cancer.
Major finding: Three of four patients whose cancer recurred had mutations in cell-free DNA that were previously detected in tumor specimens collected during interval debulking.
Data source: Next-generation sequencing of tumor and cell-free (plasma) DNA from 14 patients with high-grade serous ovarian cancer before and after platinum-based neoadjuvant chemotherapy.
Disclosures: Dr. Arend cited no funding sources and reported having no conflicts of interest.

U.S. flu activity continues to decline
The 2016-2017 U.S. influenza season appears to have peaked, as activity measures dropped for the third consecutive week, the Centers for Disease Control and Prevention reported.
For the week ending March 4, there were 11 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity, with another three in the “high” range at levels 8 and 9. The previous week (Feb. 25), there were 22 states at level 10, with a total of 27 in the high range of ILI activity. At the peak of activity during the week of Feb. 11, there were 25 states at level 10, data from the CDC’s Outpatient ILI Surveillance Network show.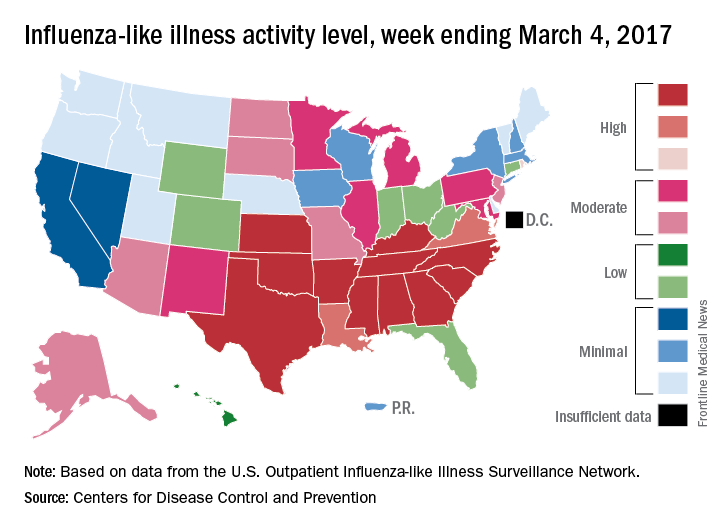
There were eight ILI-related pediatric deaths reported during the week ending March 4, although all occurred in earlier weeks. For the 2016-2017 season so far, 48 ILI-related pediatric deaths have been reported, the CDC said.
For the 70 counties in 13 states that report to the Influenza Hospitalization Surveillance Network, the flu-related hospitalization rate for the season is 43.5 per 100,000 population. The highest rate by age group is for those 65 years and over at 198.8 per 100,000, followed by 50- to 64-year-olds at 42.2 per 100,000 and children aged 0-4 years at 28.8 per 100,000, according to the CDC.
The 2016-2017 U.S. influenza season appears to have peaked, as activity measures dropped for the third consecutive week, the Centers for Disease Control and Prevention reported.
For the week ending March 4, there were 11 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity, with another three in the “high” range at levels 8 and 9. The previous week (Feb. 25), there were 22 states at level 10, with a total of 27 in the high range of ILI activity. At the peak of activity during the week of Feb. 11, there were 25 states at level 10, data from the CDC’s Outpatient ILI Surveillance Network show.
There were eight ILI-related pediatric deaths reported during the week ending March 4, although all occurred in earlier weeks. For the 2016-2017 season so far, 48 ILI-related pediatric deaths have been reported, the CDC said.
For the 70 counties in 13 states that report to the Influenza Hospitalization Surveillance Network, the flu-related hospitalization rate for the season is 43.5 per 100,000 population. The highest rate by age group is for those 65 years and over at 198.8 per 100,000, followed by 50- to 64-year-olds at 42.2 per 100,000 and children aged 0-4 years at 28.8 per 100,000, according to the CDC.
The 2016-2017 U.S. influenza season appears to have peaked, as activity measures dropped for the third consecutive week, the Centers for Disease Control and Prevention reported.
For the week ending March 4, there were 11 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity, with another three in the “high” range at levels 8 and 9. The previous week (Feb. 25), there were 22 states at level 10, with a total of 27 in the high range of ILI activity. At the peak of activity during the week of Feb. 11, there were 25 states at level 10, data from the CDC’s Outpatient ILI Surveillance Network show.
There were eight ILI-related pediatric deaths reported during the week ending March 4, although all occurred in earlier weeks. For the 2016-2017 season so far, 48 ILI-related pediatric deaths have been reported, the CDC said.
For the 70 counties in 13 states that report to the Influenza Hospitalization Surveillance Network, the flu-related hospitalization rate for the season is 43.5 per 100,000 population. The highest rate by age group is for those 65 years and over at 198.8 per 100,000, followed by 50- to 64-year-olds at 42.2 per 100,000 and children aged 0-4 years at 28.8 per 100,000, according to the CDC.
No benefit found for routine inpatient rehab after knee replacement
A new randomized study from Australia suggests that for many patients, brief inpatient rehabilitation after knee replacement provides no benefits in several measures, compared with rehab at home.
However, “we are not concluding that there is no role for inpatient rehabilitation after knee arthroplasty,” said study coauthor Justine Naylor, PhD, of the University of New South Wales, Liverpool, Australia. “We are simply saying that for people who are otherwise well enough to be discharged directly home, inpatient rehabilitation does not provide more superior recovery across a range of outcomes.”
For the new study, conducted at two Australian hospitals during 2012-2015, researchers recruited patients aged 40 years or older with a primary diagnosis of osteoarthritis who were undergoing a primary unilateral knee arthroplasty and did not have complications such as a need for inpatient care in recovery beyond an initial 5 days after surgery.
The researchers randomly assigned 165 knee arthroplasty patients with uncomplicated cases to undergo either inpatient rehabilitation for 10 days and then recover at home for 6 weeks or a monitored 6-week home rehab program that began 2 weeks after surgery (JAMA. 2017;317[10]:1037-46).
A third group of 112 patients, 87 of whom were included in the primary analysis, were observed as they entered the home rehab protocol. They were in an initial group of 215 who declined to be randomized, mostly because they wanted to get home quickly after surgery.
The average age of all participants was 67 years, and just over two-thirds were women.
At 26 weeks, the researchers found that there was no significant difference in how the patients in the three groups fared on a 6-minute walk test (mean difference, −1.01 meters; 95% confidence interval, −25.56 to 23.55). They also found no significant difference in measurements of patient-reported pain and function (knee score mean difference, 2.06; 95% CI, −0.59 to 4.71), and quality of life (EQ-5D visual analog scale mean difference, 1.41; 95% CI, −6.42 to 3.60).
However, the patients did seem to have a preference. “Satisfaction with rehabilitation was significantly higher with inpatient rehab, average 92% vs. 83%, though both modes were well received overall,” Dr. Naylor said in an interview.
“Many patients who went to inpatient rehabilitation really enjoyed it,” she added. “We have observed that patients and carers like the convenience of inpatient rehab – a one-stop shop where patients get access to multiple clinicians, gyms, and other patients and do not have to prepare meals.”
However, she said, while “we have no doubt the inpatient rehabilitation environment is nurturing, there must also be advantages to being discharged directly home, otherwise we would have seen differences between the groups. It is possible that monitored home programs like the one provided in this study help people gain independence quickly and empower patients in their recovery.”
Dr. Naylor cautioned that inpatient rehabilitation does have potential benefits for certain patients, such as those who are the most impaired and those without someone available to care for them at home. “Future research could focus on what is best in those situations or, at least, design community-based programs [that] offer some of the perceived benefits of inpatient therapy,” she said. “In addition, we also need to know what the best rehabilitation approach is after hip arthroplasty.”
The study was funded by various sources, including a foundation grant. The study authors reported no relevant disclosures.
A new randomized study from Australia suggests that for many patients, brief inpatient rehabilitation after knee replacement provides no benefits in several measures, compared with rehab at home.
However, “we are not concluding that there is no role for inpatient rehabilitation after knee arthroplasty,” said study coauthor Justine Naylor, PhD, of the University of New South Wales, Liverpool, Australia. “We are simply saying that for people who are otherwise well enough to be discharged directly home, inpatient rehabilitation does not provide more superior recovery across a range of outcomes.”
For the new study, conducted at two Australian hospitals during 2012-2015, researchers recruited patients aged 40 years or older with a primary diagnosis of osteoarthritis who were undergoing a primary unilateral knee arthroplasty and did not have complications such as a need for inpatient care in recovery beyond an initial 5 days after surgery.
The researchers randomly assigned 165 knee arthroplasty patients with uncomplicated cases to undergo either inpatient rehabilitation for 10 days and then recover at home for 6 weeks or a monitored 6-week home rehab program that began 2 weeks after surgery (JAMA. 2017;317[10]:1037-46).
A third group of 112 patients, 87 of whom were included in the primary analysis, were observed as they entered the home rehab protocol. They were in an initial group of 215 who declined to be randomized, mostly because they wanted to get home quickly after surgery.
The average age of all participants was 67 years, and just over two-thirds were women.
At 26 weeks, the researchers found that there was no significant difference in how the patients in the three groups fared on a 6-minute walk test (mean difference, −1.01 meters; 95% confidence interval, −25.56 to 23.55). They also found no significant difference in measurements of patient-reported pain and function (knee score mean difference, 2.06; 95% CI, −0.59 to 4.71), and quality of life (EQ-5D visual analog scale mean difference, 1.41; 95% CI, −6.42 to 3.60).
However, the patients did seem to have a preference. “Satisfaction with rehabilitation was significantly higher with inpatient rehab, average 92% vs. 83%, though both modes were well received overall,” Dr. Naylor said in an interview.
“Many patients who went to inpatient rehabilitation really enjoyed it,” she added. “We have observed that patients and carers like the convenience of inpatient rehab – a one-stop shop where patients get access to multiple clinicians, gyms, and other patients and do not have to prepare meals.”
However, she said, while “we have no doubt the inpatient rehabilitation environment is nurturing, there must also be advantages to being discharged directly home, otherwise we would have seen differences between the groups. It is possible that monitored home programs like the one provided in this study help people gain independence quickly and empower patients in their recovery.”
Dr. Naylor cautioned that inpatient rehabilitation does have potential benefits for certain patients, such as those who are the most impaired and those without someone available to care for them at home. “Future research could focus on what is best in those situations or, at least, design community-based programs [that] offer some of the perceived benefits of inpatient therapy,” she said. “In addition, we also need to know what the best rehabilitation approach is after hip arthroplasty.”
The study was funded by various sources, including a foundation grant. The study authors reported no relevant disclosures.
A new randomized study from Australia suggests that for many patients, brief inpatient rehabilitation after knee replacement provides no benefits in several measures, compared with rehab at home.
However, “we are not concluding that there is no role for inpatient rehabilitation after knee arthroplasty,” said study coauthor Justine Naylor, PhD, of the University of New South Wales, Liverpool, Australia. “We are simply saying that for people who are otherwise well enough to be discharged directly home, inpatient rehabilitation does not provide more superior recovery across a range of outcomes.”
For the new study, conducted at two Australian hospitals during 2012-2015, researchers recruited patients aged 40 years or older with a primary diagnosis of osteoarthritis who were undergoing a primary unilateral knee arthroplasty and did not have complications such as a need for inpatient care in recovery beyond an initial 5 days after surgery.
The researchers randomly assigned 165 knee arthroplasty patients with uncomplicated cases to undergo either inpatient rehabilitation for 10 days and then recover at home for 6 weeks or a monitored 6-week home rehab program that began 2 weeks after surgery (JAMA. 2017;317[10]:1037-46).
A third group of 112 patients, 87 of whom were included in the primary analysis, were observed as they entered the home rehab protocol. They were in an initial group of 215 who declined to be randomized, mostly because they wanted to get home quickly after surgery.
The average age of all participants was 67 years, and just over two-thirds were women.
At 26 weeks, the researchers found that there was no significant difference in how the patients in the three groups fared on a 6-minute walk test (mean difference, −1.01 meters; 95% confidence interval, −25.56 to 23.55). They also found no significant difference in measurements of patient-reported pain and function (knee score mean difference, 2.06; 95% CI, −0.59 to 4.71), and quality of life (EQ-5D visual analog scale mean difference, 1.41; 95% CI, −6.42 to 3.60).
However, the patients did seem to have a preference. “Satisfaction with rehabilitation was significantly higher with inpatient rehab, average 92% vs. 83%, though both modes were well received overall,” Dr. Naylor said in an interview.
“Many patients who went to inpatient rehabilitation really enjoyed it,” she added. “We have observed that patients and carers like the convenience of inpatient rehab – a one-stop shop where patients get access to multiple clinicians, gyms, and other patients and do not have to prepare meals.”
However, she said, while “we have no doubt the inpatient rehabilitation environment is nurturing, there must also be advantages to being discharged directly home, otherwise we would have seen differences between the groups. It is possible that monitored home programs like the one provided in this study help people gain independence quickly and empower patients in their recovery.”
Dr. Naylor cautioned that inpatient rehabilitation does have potential benefits for certain patients, such as those who are the most impaired and those without someone available to care for them at home. “Future research could focus on what is best in those situations or, at least, design community-based programs [that] offer some of the perceived benefits of inpatient therapy,” she said. “In addition, we also need to know what the best rehabilitation approach is after hip arthroplasty.”
The study was funded by various sources, including a foundation grant. The study authors reported no relevant disclosures.
FROM JAMA
Key clinical point:
Major finding: There were no significant differences in the primary outcome of a 6-minute walk test at 26 weeks or in pain, function, and quality of life measures between patients randomized to inpatient or at-home rehab protocols.
Data source: A parallel, randomized controlled trial of 165 uncomplicated knee arthroplasty patients assigned to undergo either inpatient rehab for 10 days then in-home monitored rehab for 6 weeks or to a monitored 6-week home rehab 2 weeks after surgery. The study also included a third observational group of 112 patients (87 included in analysis) who underwent at-home rehab.
Disclosures: The study was funded by various sources, including a foundation grant. The study authors reported no relevant disclosures.