User login
Common gut yeast may exacerbate IBD
A ubiquitous yeast strain may play a role in exacerbating inflammatory bowel disease (IBD), an animal study showed.
While research has shown that the composition of gut microbiota in people with IBD is different from that of healthy people, most of the attention has been focused on bacteria. The roles of other microorganisms, including yeasts, are still poorly understood.
In research published in Science Translational Medicine, Tyson Chiaro, of the University of Utah, Salt Lake City, and his colleagues inoculated sterile mice with either of two fungal species: Rhodotorula aurantiaca – an environmentally acquired yeast found in milk and fruit juices – or Saccharomyces cerevisiae – Baker’s yeast – for which some people with Crohn’s disease have been shown to have elevated antibodies. The mice were inoculated gradually over a period of a week to mimic consumption of food enriched with yeast products. The researchers then treated the mice with drugs to induce colitislike symptoms and analyzed colon tissues for damage. Mr. Chiaro and his colleagues found that colonization with S. cerevisiae, but not with R. aurantiaca, aggravated colitis and resulted in epithelial damage leading to greater gut permeability (Sci Transl Med. 2017;9[380] pii: eaaf9044]).
Mr. Chiaro and his colleagues then investigated whether heat-killed S. cerevisiae also induced aggravated colitis and found that it did not, suggesting that a metabolically active organism was required to aggravate disease. Mr. Chiaro and his colleagues performed screens of fecal metabolites in the mice and found that S. cerevisiae colonization enhanced purine metabolism, resulting in increased uric acid production.
To test whether this purine pathway was aggravating colitis, the researchers blocked it with allopurinol (10 mg/kg). The S. cerevisiae– inoculated mice that were treated with allopurinol had reduced uric acid–levels and ameliorated colitis–symptoms. The results suggest that allopurinol might be of more clinical value in treating IBD than previously thought. The drug has been used in patients with Crohn’s disease to increase the efficacy of other IBD medications, and “many patients who received adjunctive allopurinol therapy were reported to have major clinical improvement,” Mr. Chiaro and his colleagues noted. The results “suggest that some of the improvement might come from preventing yeast-induced–uric acid buildup in the intestine. Thus, allopurinol treatment in some IBD patients with adverse reactions to yeast and high uric acid might be of therapeutic benefit and should be explored.”
Mr. Chiaro’s coauthors reported a variety of individual grant and fellowship awards, including from the National Institute of Allergy and Infectious Disease and the National Institutes of Health. None declared commercial conflicts of interest.
A ubiquitous yeast strain may play a role in exacerbating inflammatory bowel disease (IBD), an animal study showed.
While research has shown that the composition of gut microbiota in people with IBD is different from that of healthy people, most of the attention has been focused on bacteria. The roles of other microorganisms, including yeasts, are still poorly understood.
In research published in Science Translational Medicine, Tyson Chiaro, of the University of Utah, Salt Lake City, and his colleagues inoculated sterile mice with either of two fungal species: Rhodotorula aurantiaca – an environmentally acquired yeast found in milk and fruit juices – or Saccharomyces cerevisiae – Baker’s yeast – for which some people with Crohn’s disease have been shown to have elevated antibodies. The mice were inoculated gradually over a period of a week to mimic consumption of food enriched with yeast products. The researchers then treated the mice with drugs to induce colitislike symptoms and analyzed colon tissues for damage. Mr. Chiaro and his colleagues found that colonization with S. cerevisiae, but not with R. aurantiaca, aggravated colitis and resulted in epithelial damage leading to greater gut permeability (Sci Transl Med. 2017;9[380] pii: eaaf9044]).
Mr. Chiaro and his colleagues then investigated whether heat-killed S. cerevisiae also induced aggravated colitis and found that it did not, suggesting that a metabolically active organism was required to aggravate disease. Mr. Chiaro and his colleagues performed screens of fecal metabolites in the mice and found that S. cerevisiae colonization enhanced purine metabolism, resulting in increased uric acid production.
To test whether this purine pathway was aggravating colitis, the researchers blocked it with allopurinol (10 mg/kg). The S. cerevisiae– inoculated mice that were treated with allopurinol had reduced uric acid–levels and ameliorated colitis–symptoms. The results suggest that allopurinol might be of more clinical value in treating IBD than previously thought. The drug has been used in patients with Crohn’s disease to increase the efficacy of other IBD medications, and “many patients who received adjunctive allopurinol therapy were reported to have major clinical improvement,” Mr. Chiaro and his colleagues noted. The results “suggest that some of the improvement might come from preventing yeast-induced–uric acid buildup in the intestine. Thus, allopurinol treatment in some IBD patients with adverse reactions to yeast and high uric acid might be of therapeutic benefit and should be explored.”
Mr. Chiaro’s coauthors reported a variety of individual grant and fellowship awards, including from the National Institute of Allergy and Infectious Disease and the National Institutes of Health. None declared commercial conflicts of interest.
A ubiquitous yeast strain may play a role in exacerbating inflammatory bowel disease (IBD), an animal study showed.
While research has shown that the composition of gut microbiota in people with IBD is different from that of healthy people, most of the attention has been focused on bacteria. The roles of other microorganisms, including yeasts, are still poorly understood.
In research published in Science Translational Medicine, Tyson Chiaro, of the University of Utah, Salt Lake City, and his colleagues inoculated sterile mice with either of two fungal species: Rhodotorula aurantiaca – an environmentally acquired yeast found in milk and fruit juices – or Saccharomyces cerevisiae – Baker’s yeast – for which some people with Crohn’s disease have been shown to have elevated antibodies. The mice were inoculated gradually over a period of a week to mimic consumption of food enriched with yeast products. The researchers then treated the mice with drugs to induce colitislike symptoms and analyzed colon tissues for damage. Mr. Chiaro and his colleagues found that colonization with S. cerevisiae, but not with R. aurantiaca, aggravated colitis and resulted in epithelial damage leading to greater gut permeability (Sci Transl Med. 2017;9[380] pii: eaaf9044]).
Mr. Chiaro and his colleagues then investigated whether heat-killed S. cerevisiae also induced aggravated colitis and found that it did not, suggesting that a metabolically active organism was required to aggravate disease. Mr. Chiaro and his colleagues performed screens of fecal metabolites in the mice and found that S. cerevisiae colonization enhanced purine metabolism, resulting in increased uric acid production.
To test whether this purine pathway was aggravating colitis, the researchers blocked it with allopurinol (10 mg/kg). The S. cerevisiae– inoculated mice that were treated with allopurinol had reduced uric acid–levels and ameliorated colitis–symptoms. The results suggest that allopurinol might be of more clinical value in treating IBD than previously thought. The drug has been used in patients with Crohn’s disease to increase the efficacy of other IBD medications, and “many patients who received adjunctive allopurinol therapy were reported to have major clinical improvement,” Mr. Chiaro and his colleagues noted. The results “suggest that some of the improvement might come from preventing yeast-induced–uric acid buildup in the intestine. Thus, allopurinol treatment in some IBD patients with adverse reactions to yeast and high uric acid might be of therapeutic benefit and should be explored.”
Mr. Chiaro’s coauthors reported a variety of individual grant and fellowship awards, including from the National Institute of Allergy and Infectious Disease and the National Institutes of Health. None declared commercial conflicts of interest.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: Sterile mice inoculated with S. cerevisiae and treated to induce colitis had more tissue damage than untreated mice or those treated with another type of yeast.
Data source: An experimental study on mice inoculated with one of two yeasts, then treated to induce colitislike symptoms.
Disclosures: Study authors had multiple sources of individual grant funding but no commercial conflicts of interest.
Can better operations improve CABG in women?
Worse outcomes after cardiovascular arterial bypass grafting (CABG) in women have been attributed to a number of clinical and nonclinical factors: older age, delayed diagnosis and treatment, more comorbidities, smaller body size, underuse of arterial grafts, and referral bias. However, a team of Cleveland Clinic researchers reported that women were less likely than men to have bilateral–internal thoracic artery (ITA) grafting and complete revascularization, both of which are linked to better long-term survival.
“Women had less favorable preoperative characteristics than men but received fewer bilateral-ITA grafts and less all-arterial grafting as part of their revascularization strategy,” Tamer Attia, MD, MSc, and his coauthors said in the study published in the Journal of Thoracic and Cardiovascular Surgery. They also found that women were more likely to die in the hospital after CABG and had lower risk-adjusted long-term survival than men (2017 March;153:571-9).
Survival was lowest in women who were not completely revascularized and had no ITA grafting, while survival was highest in men who were completely revascularized and had bilateral grafting, Dr. Attia and coauthors said.
The researchers’ goal was to use extensive risk adjustment to evaluate how differences in revascularization strategies influenced survival of men and women after CABG. They analyzed 57,943 primary, isolated CABG procedures performed at Cleveland Clinic from 1972 to 2011, including 11,009 procedures in women.
The researchers identified differences between sexes in three key areas: revascularization strategies, in-hospital outcomes, and time-related survival.
With regard to revascularization strategies, while men were significantly more likely to have incomplete revascularization than were women, women received significantly fewer arterial grafts (8.4% vs. 9.3% for men). This included fewer bilateral-ITA grafts and radial artery grafts, less use of total arterial revascularization, and greater use of saphenous vein grafts (SVGs) to the left anterior descending artery. Women were also significantly more likely to receive only SVGs for revascularization (32% vs. 30% for men; P less than .0001). Most operations for both women and men were done with cardiopulmonary bypass, but significantly more women had off-pump procedures (5.4% vs. 2.9%).
In the hospital after operations, women were significantly more prone to postoperative deep sternal–wound infections and septicemias, as well as strokes and renal failure, including dialysis-dependent renal failure. Women also had higher rates of new-onset atrial fibrillation (15% vs. 13% in men), and higher rates of mechanical ventilation for more than 24 hours (13% vs. 9.2%). Women spent more time in the ICU and hospital overall, and their in-hospital death rate was more than double that of men (2.7% vs. 1.1%).
Women also had shorter long-term survival, “and this has persisted since the beginning of CABG at Cleveland Clinic,” Dr. Attia and coauthors said. What’s more, the survival gap between women in the study and women in the general population post CABG was wider than that in men. “After we adjusted for patient and revascularization strategy differences, female sex remained an independent risk factor for death overall and both early and late after CABG.”
Incomplete revascularization had greater consequences for women than for men. At 10 years, 58% of women with incomplete revascularization survived, vs. 70% of men. At 20 years, the rates were 25% for women and 35% for men. “Use of ITA grafts was associated with better survival than use of SVGs alone and was best when bilateral-ITA grafting was performed,” Dr. Attia and coauthors said. However, the study determined that bilateral grafting seems less effective in women long-term. “Hence, a patient’s sex deserves special consideration in operative planning.”
Many questions about CABG in women remain: Identifying which female patients would benefit from more meticulous conduit harvesting, from better coronary artery selection, and from bilateral-ITA grafting and which are less susceptible to sternal would infections could increase appropriate use of bilateral-ITA grafting, the researchers noted. “The difference in effectiveness of bilateral-ITA grafting needs to be considered in women at elevated risk for bilateral-ITA harvesting complications.”
Coauthor Ellen Mayer Sabik, MD, is a principal investigator for Abbott Laboratories and is on the scientific advisory board of Medtronic. Dr. Attia and all other coauthors reported having no relevant financial relationships to disclose.
As with other long-term analyses, the answer in this study “is in the shadows as opposed to the spotlight,” George L. Hicks Jr., MD, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153[3]:580-1).
Dr. Hicks of the University of Rochester (N.Y.) noted key limitations of the study: use of all-cause mortality, substandard use of bilateral– or single–internal thoracic artery grafting, little data about postdischarge cholesterol levels, diabetes incidence, or blood pressure, among others. However, “the authors raise the banner for the continued need for increased use of arterial revascularization with the eventual hope that the Arterial Revascularization Trial will reinforce the survival benefits manifested by that strategy,” he said.
Reducing risks and not changing the type of operation will even out the differences in postoperative survival between genders, he indicated. “Furthermore, the extension of similar therapies – for example, [bilateral–internal thoracic artery] or all-arterial grafting and improved long-term risk modification in both men and women – may improve the inequality but not eliminate the differences until we know that both men and women come from the same planet,” he said.
Dr. Hicks reported having no relevant financial relationships to disclose.
As with other long-term analyses, the answer in this study “is in the shadows as opposed to the spotlight,” George L. Hicks Jr., MD, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153[3]:580-1).
Dr. Hicks of the University of Rochester (N.Y.) noted key limitations of the study: use of all-cause mortality, substandard use of bilateral– or single–internal thoracic artery grafting, little data about postdischarge cholesterol levels, diabetes incidence, or blood pressure, among others. However, “the authors raise the banner for the continued need for increased use of arterial revascularization with the eventual hope that the Arterial Revascularization Trial will reinforce the survival benefits manifested by that strategy,” he said.
Reducing risks and not changing the type of operation will even out the differences in postoperative survival between genders, he indicated. “Furthermore, the extension of similar therapies – for example, [bilateral–internal thoracic artery] or all-arterial grafting and improved long-term risk modification in both men and women – may improve the inequality but not eliminate the differences until we know that both men and women come from the same planet,” he said.
Dr. Hicks reported having no relevant financial relationships to disclose.
As with other long-term analyses, the answer in this study “is in the shadows as opposed to the spotlight,” George L. Hicks Jr., MD, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153[3]:580-1).
Dr. Hicks of the University of Rochester (N.Y.) noted key limitations of the study: use of all-cause mortality, substandard use of bilateral– or single–internal thoracic artery grafting, little data about postdischarge cholesterol levels, diabetes incidence, or blood pressure, among others. However, “the authors raise the banner for the continued need for increased use of arterial revascularization with the eventual hope that the Arterial Revascularization Trial will reinforce the survival benefits manifested by that strategy,” he said.
Reducing risks and not changing the type of operation will even out the differences in postoperative survival between genders, he indicated. “Furthermore, the extension of similar therapies – for example, [bilateral–internal thoracic artery] or all-arterial grafting and improved long-term risk modification in both men and women – may improve the inequality but not eliminate the differences until we know that both men and women come from the same planet,” he said.
Dr. Hicks reported having no relevant financial relationships to disclose.
Worse outcomes after cardiovascular arterial bypass grafting (CABG) in women have been attributed to a number of clinical and nonclinical factors: older age, delayed diagnosis and treatment, more comorbidities, smaller body size, underuse of arterial grafts, and referral bias. However, a team of Cleveland Clinic researchers reported that women were less likely than men to have bilateral–internal thoracic artery (ITA) grafting and complete revascularization, both of which are linked to better long-term survival.
“Women had less favorable preoperative characteristics than men but received fewer bilateral-ITA grafts and less all-arterial grafting as part of their revascularization strategy,” Tamer Attia, MD, MSc, and his coauthors said in the study published in the Journal of Thoracic and Cardiovascular Surgery. They also found that women were more likely to die in the hospital after CABG and had lower risk-adjusted long-term survival than men (2017 March;153:571-9).
Survival was lowest in women who were not completely revascularized and had no ITA grafting, while survival was highest in men who were completely revascularized and had bilateral grafting, Dr. Attia and coauthors said.
The researchers’ goal was to use extensive risk adjustment to evaluate how differences in revascularization strategies influenced survival of men and women after CABG. They analyzed 57,943 primary, isolated CABG procedures performed at Cleveland Clinic from 1972 to 2011, including 11,009 procedures in women.
The researchers identified differences between sexes in three key areas: revascularization strategies, in-hospital outcomes, and time-related survival.
With regard to revascularization strategies, while men were significantly more likely to have incomplete revascularization than were women, women received significantly fewer arterial grafts (8.4% vs. 9.3% for men). This included fewer bilateral-ITA grafts and radial artery grafts, less use of total arterial revascularization, and greater use of saphenous vein grafts (SVGs) to the left anterior descending artery. Women were also significantly more likely to receive only SVGs for revascularization (32% vs. 30% for men; P less than .0001). Most operations for both women and men were done with cardiopulmonary bypass, but significantly more women had off-pump procedures (5.4% vs. 2.9%).
In the hospital after operations, women were significantly more prone to postoperative deep sternal–wound infections and septicemias, as well as strokes and renal failure, including dialysis-dependent renal failure. Women also had higher rates of new-onset atrial fibrillation (15% vs. 13% in men), and higher rates of mechanical ventilation for more than 24 hours (13% vs. 9.2%). Women spent more time in the ICU and hospital overall, and their in-hospital death rate was more than double that of men (2.7% vs. 1.1%).
Women also had shorter long-term survival, “and this has persisted since the beginning of CABG at Cleveland Clinic,” Dr. Attia and coauthors said. What’s more, the survival gap between women in the study and women in the general population post CABG was wider than that in men. “After we adjusted for patient and revascularization strategy differences, female sex remained an independent risk factor for death overall and both early and late after CABG.”
Incomplete revascularization had greater consequences for women than for men. At 10 years, 58% of women with incomplete revascularization survived, vs. 70% of men. At 20 years, the rates were 25% for women and 35% for men. “Use of ITA grafts was associated with better survival than use of SVGs alone and was best when bilateral-ITA grafting was performed,” Dr. Attia and coauthors said. However, the study determined that bilateral grafting seems less effective in women long-term. “Hence, a patient’s sex deserves special consideration in operative planning.”
Many questions about CABG in women remain: Identifying which female patients would benefit from more meticulous conduit harvesting, from better coronary artery selection, and from bilateral-ITA grafting and which are less susceptible to sternal would infections could increase appropriate use of bilateral-ITA grafting, the researchers noted. “The difference in effectiveness of bilateral-ITA grafting needs to be considered in women at elevated risk for bilateral-ITA harvesting complications.”
Coauthor Ellen Mayer Sabik, MD, is a principal investigator for Abbott Laboratories and is on the scientific advisory board of Medtronic. Dr. Attia and all other coauthors reported having no relevant financial relationships to disclose.
Worse outcomes after cardiovascular arterial bypass grafting (CABG) in women have been attributed to a number of clinical and nonclinical factors: older age, delayed diagnosis and treatment, more comorbidities, smaller body size, underuse of arterial grafts, and referral bias. However, a team of Cleveland Clinic researchers reported that women were less likely than men to have bilateral–internal thoracic artery (ITA) grafting and complete revascularization, both of which are linked to better long-term survival.
“Women had less favorable preoperative characteristics than men but received fewer bilateral-ITA grafts and less all-arterial grafting as part of their revascularization strategy,” Tamer Attia, MD, MSc, and his coauthors said in the study published in the Journal of Thoracic and Cardiovascular Surgery. They also found that women were more likely to die in the hospital after CABG and had lower risk-adjusted long-term survival than men (2017 March;153:571-9).
Survival was lowest in women who were not completely revascularized and had no ITA grafting, while survival was highest in men who were completely revascularized and had bilateral grafting, Dr. Attia and coauthors said.
The researchers’ goal was to use extensive risk adjustment to evaluate how differences in revascularization strategies influenced survival of men and women after CABG. They analyzed 57,943 primary, isolated CABG procedures performed at Cleveland Clinic from 1972 to 2011, including 11,009 procedures in women.
The researchers identified differences between sexes in three key areas: revascularization strategies, in-hospital outcomes, and time-related survival.
With regard to revascularization strategies, while men were significantly more likely to have incomplete revascularization than were women, women received significantly fewer arterial grafts (8.4% vs. 9.3% for men). This included fewer bilateral-ITA grafts and radial artery grafts, less use of total arterial revascularization, and greater use of saphenous vein grafts (SVGs) to the left anterior descending artery. Women were also significantly more likely to receive only SVGs for revascularization (32% vs. 30% for men; P less than .0001). Most operations for both women and men were done with cardiopulmonary bypass, but significantly more women had off-pump procedures (5.4% vs. 2.9%).
In the hospital after operations, women were significantly more prone to postoperative deep sternal–wound infections and septicemias, as well as strokes and renal failure, including dialysis-dependent renal failure. Women also had higher rates of new-onset atrial fibrillation (15% vs. 13% in men), and higher rates of mechanical ventilation for more than 24 hours (13% vs. 9.2%). Women spent more time in the ICU and hospital overall, and their in-hospital death rate was more than double that of men (2.7% vs. 1.1%).
Women also had shorter long-term survival, “and this has persisted since the beginning of CABG at Cleveland Clinic,” Dr. Attia and coauthors said. What’s more, the survival gap between women in the study and women in the general population post CABG was wider than that in men. “After we adjusted for patient and revascularization strategy differences, female sex remained an independent risk factor for death overall and both early and late after CABG.”
Incomplete revascularization had greater consequences for women than for men. At 10 years, 58% of women with incomplete revascularization survived, vs. 70% of men. At 20 years, the rates were 25% for women and 35% for men. “Use of ITA grafts was associated with better survival than use of SVGs alone and was best when bilateral-ITA grafting was performed,” Dr. Attia and coauthors said. However, the study determined that bilateral grafting seems less effective in women long-term. “Hence, a patient’s sex deserves special consideration in operative planning.”
Many questions about CABG in women remain: Identifying which female patients would benefit from more meticulous conduit harvesting, from better coronary artery selection, and from bilateral-ITA grafting and which are less susceptible to sternal would infections could increase appropriate use of bilateral-ITA grafting, the researchers noted. “The difference in effectiveness of bilateral-ITA grafting needs to be considered in women at elevated risk for bilateral-ITA harvesting complications.”
Coauthor Ellen Mayer Sabik, MD, is a principal investigator for Abbott Laboratories and is on the scientific advisory board of Medtronic. Dr. Attia and all other coauthors reported having no relevant financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Survival rates after CABG are worse for women than for men.
Major finding: In both men and women, complete revascularization and use of bilateral-ITA grafting achieve better long-term survival than incomplete revascularization and single-ITA grafting.
Data source: Analysis of 57,943 adults who had primary isolated CABG from 1972 to 2011 at Cleveland Clinic.
Disclosure: Coauthor Ellen Mayer Sabik, MD, is a principal investigator for Abbott Laboratories and is on the scientific advisory board of Medtronic. Dr. Attia and all other coauthors reported having no relevant financial disclosures.
By The Numbers: Trump’s choice for FDA chief is versatile, entrenched in Pharma
President Donald Trump’s pick to lead the Food and Drug Administration has deep ties to the pharmaceutical industry as a consultant, investor, and board member. Scott Gottlieb, MD, 44, also has worn many hats in a career that included two previous stints at the FDA, practicing as a physician, and writer/editor roles at prestigious medical journals.
“It seems like the main question is, ‘Which Gottlieb are we going to get?’” said Dr. Robert Califf, who stepped down from his position as the commissioner of the Food and Drug Administration in January.
Here’s a look at Dr. Gottlieb’s career, by the numbers:
188 companies
New Enterprise Associates, the venture capital firm in which Dr. Gottlieb is a partner, is currently or has been invested in 188 health care companies.
8 boards of directors
Dr. Gottlieb serves or has served on eight boards of directors, according to his LinkedIn profile. The firms include pharmaceutical companies Gradalis and Tolero Pharmaceuticals, which are developing cancer treatments, among other things; and Glytec, which offers glycemic management tools for patients with diabetes.
8 drug and device companies
Eight pharmaceutical companies disclosed payments to Dr. Gottlieb in 2015, according to the open payments database: Vertex Pharmaceuticals, GlaxoSmithKline, Daiichi, Valeant, Pfizer, Millennium, SI-BONE, and E.R. Squibb & Sons. Payments included travel to Philadelphia, San Francisco, and London.
9 recusals
In a memo, Dr. Gottlieb wrote that he had a consulting relationship with nine health care companies before his stint as the FDA’s deputy commissioner for medical and scientific affairs during the George W. Bush administration. Those ties disqualified him from dealing with matters concerning those companies for at least a year. The firms included Eli Lilly, Roche, and Sanofi-Aventis.
The recusals generated some headlines during the avian flu scare because Dr. Gottlieb had to recuse himself from some of the planning efforts around vaccines.
7 years
Starting in 1997, Dr. Gottlieb spent 7 years as a staff writer for BMJ, one of the top medical journals in the world. And he was an editor at the Pulse section of JAMA, the Journal of the American Medical Association, from 1996 to 2001.
Dr. Gottlieb also spent the past 7 years as an adviser to drug maker GlaxoSmithKline’s product investment board, according to his LinkedIn page.
33 years old
Dr. Gottlieb was 33 when he got the No. 2 job at the FDA in 2005. He had done a short stint at the agency a few years earlier but was considered a controversial pick because of his ties to Wall Street. He stayed until 2007.
“He has done a lot of thinking about how FDA should be managed – his operational sophistication is going to be a great asset,” said former FDA attorney Coleen Klasmeier, who worked with Dr. Gottlieb and coauthored articles with him. “He also has very strong relationships among career FDA personnel and will be able to hit the ground running on a range of important initiatives.”
18 times before Congress
Dr. Gottlieb testified before Congress as an expert witness 18 times. He has spoken about drug prices, revamping the FDA approval process and the vaccine supply.
“Most people watching at the FDA would breathe a sigh of relief,” Joshua Sharfstein, MD, who served as the FDA’s principal deputy commissioner until 2011, said of Dr. Gottlieb’s impending nomination. He added that Dr. Gottlieb is “not someone who has expressed antagonism to the core principles of the agency.”
36,000 Twitter followers
More than 36,000 people follow Dr. Gottlieb on Twitter, although he follows only 845 people, as of Tuesday. He has tweeted at least 10,400 times, lately about different strains of the flu.
72 percent
Almost three-fourths of the 53 drug companies surveyed by Mizuho said they’d prefer Dr. Gottlieb to head the FDA.
$414,000
Pharmaceutical companies paid Dr. Gottlieb nearly $414,000 from 2013 through 2015, according to federal open payments data, for speeches, consulting, travel, and meals.
That included $65,780 from a pharmaceutical company to promote a controversial cystic fibrosis drug called Kalydeco (ivacaftor). Only one other doctor received more money toward promoting the drug.
The drug’s price tag was controversial because the nonprofit Cystic Fibrosis Foundation kicked in $150 million toward finding a cure for the fatal disease and got a rich $3.3 billion payday for selling its rights to royalties for the drug. Vertex Pharmaceuticals priced Kalydeco at more than $300,000 a year.
Nearly $30,000
Dr. Gottlieb has contributed nearly $30,000 toward Republican political campaigns and joint fundraising committees from 2005 to 2014. He has donated toward the presidential runs of Mitt Romney and Sen. John McCain. He also donated more than once to Speaker Paul Ryan.
Dr. Gottlieb contributed the most money toward Sen. Ben Sasse (R-Neb.), spending $2,600 in the primary and $2,600 again in the general election in 2013. Sen. Sasse was a vocal anti-Trump supporter, penning an open letter in February 2016 about how he could not support Trump, who was “dividing” the nation, in his view.
“But have you noticed how Mr. Trump uses the word ‘Reign’ – like he thinks he’s running for King?” Sen. Sasse asked in the post.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump’s pick to lead the Food and Drug Administration has deep ties to the pharmaceutical industry as a consultant, investor, and board member. Scott Gottlieb, MD, 44, also has worn many hats in a career that included two previous stints at the FDA, practicing as a physician, and writer/editor roles at prestigious medical journals.
“It seems like the main question is, ‘Which Gottlieb are we going to get?’” said Dr. Robert Califf, who stepped down from his position as the commissioner of the Food and Drug Administration in January.
Here’s a look at Dr. Gottlieb’s career, by the numbers:
188 companies
New Enterprise Associates, the venture capital firm in which Dr. Gottlieb is a partner, is currently or has been invested in 188 health care companies.
8 boards of directors
Dr. Gottlieb serves or has served on eight boards of directors, according to his LinkedIn profile. The firms include pharmaceutical companies Gradalis and Tolero Pharmaceuticals, which are developing cancer treatments, among other things; and Glytec, which offers glycemic management tools for patients with diabetes.
8 drug and device companies
Eight pharmaceutical companies disclosed payments to Dr. Gottlieb in 2015, according to the open payments database: Vertex Pharmaceuticals, GlaxoSmithKline, Daiichi, Valeant, Pfizer, Millennium, SI-BONE, and E.R. Squibb & Sons. Payments included travel to Philadelphia, San Francisco, and London.
9 recusals
In a memo, Dr. Gottlieb wrote that he had a consulting relationship with nine health care companies before his stint as the FDA’s deputy commissioner for medical and scientific affairs during the George W. Bush administration. Those ties disqualified him from dealing with matters concerning those companies for at least a year. The firms included Eli Lilly, Roche, and Sanofi-Aventis.
The recusals generated some headlines during the avian flu scare because Dr. Gottlieb had to recuse himself from some of the planning efforts around vaccines.
7 years
Starting in 1997, Dr. Gottlieb spent 7 years as a staff writer for BMJ, one of the top medical journals in the world. And he was an editor at the Pulse section of JAMA, the Journal of the American Medical Association, from 1996 to 2001.
Dr. Gottlieb also spent the past 7 years as an adviser to drug maker GlaxoSmithKline’s product investment board, according to his LinkedIn page.
33 years old
Dr. Gottlieb was 33 when he got the No. 2 job at the FDA in 2005. He had done a short stint at the agency a few years earlier but was considered a controversial pick because of his ties to Wall Street. He stayed until 2007.
“He has done a lot of thinking about how FDA should be managed – his operational sophistication is going to be a great asset,” said former FDA attorney Coleen Klasmeier, who worked with Dr. Gottlieb and coauthored articles with him. “He also has very strong relationships among career FDA personnel and will be able to hit the ground running on a range of important initiatives.”
18 times before Congress
Dr. Gottlieb testified before Congress as an expert witness 18 times. He has spoken about drug prices, revamping the FDA approval process and the vaccine supply.
“Most people watching at the FDA would breathe a sigh of relief,” Joshua Sharfstein, MD, who served as the FDA’s principal deputy commissioner until 2011, said of Dr. Gottlieb’s impending nomination. He added that Dr. Gottlieb is “not someone who has expressed antagonism to the core principles of the agency.”
36,000 Twitter followers
More than 36,000 people follow Dr. Gottlieb on Twitter, although he follows only 845 people, as of Tuesday. He has tweeted at least 10,400 times, lately about different strains of the flu.
72 percent
Almost three-fourths of the 53 drug companies surveyed by Mizuho said they’d prefer Dr. Gottlieb to head the FDA.
$414,000
Pharmaceutical companies paid Dr. Gottlieb nearly $414,000 from 2013 through 2015, according to federal open payments data, for speeches, consulting, travel, and meals.
That included $65,780 from a pharmaceutical company to promote a controversial cystic fibrosis drug called Kalydeco (ivacaftor). Only one other doctor received more money toward promoting the drug.
The drug’s price tag was controversial because the nonprofit Cystic Fibrosis Foundation kicked in $150 million toward finding a cure for the fatal disease and got a rich $3.3 billion payday for selling its rights to royalties for the drug. Vertex Pharmaceuticals priced Kalydeco at more than $300,000 a year.
Nearly $30,000
Dr. Gottlieb has contributed nearly $30,000 toward Republican political campaigns and joint fundraising committees from 2005 to 2014. He has donated toward the presidential runs of Mitt Romney and Sen. John McCain. He also donated more than once to Speaker Paul Ryan.
Dr. Gottlieb contributed the most money toward Sen. Ben Sasse (R-Neb.), spending $2,600 in the primary and $2,600 again in the general election in 2013. Sen. Sasse was a vocal anti-Trump supporter, penning an open letter in February 2016 about how he could not support Trump, who was “dividing” the nation, in his view.
“But have you noticed how Mr. Trump uses the word ‘Reign’ – like he thinks he’s running for King?” Sen. Sasse asked in the post.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump’s pick to lead the Food and Drug Administration has deep ties to the pharmaceutical industry as a consultant, investor, and board member. Scott Gottlieb, MD, 44, also has worn many hats in a career that included two previous stints at the FDA, practicing as a physician, and writer/editor roles at prestigious medical journals.
“It seems like the main question is, ‘Which Gottlieb are we going to get?’” said Dr. Robert Califf, who stepped down from his position as the commissioner of the Food and Drug Administration in January.
Here’s a look at Dr. Gottlieb’s career, by the numbers:
188 companies
New Enterprise Associates, the venture capital firm in which Dr. Gottlieb is a partner, is currently or has been invested in 188 health care companies.
8 boards of directors
Dr. Gottlieb serves or has served on eight boards of directors, according to his LinkedIn profile. The firms include pharmaceutical companies Gradalis and Tolero Pharmaceuticals, which are developing cancer treatments, among other things; and Glytec, which offers glycemic management tools for patients with diabetes.
8 drug and device companies
Eight pharmaceutical companies disclosed payments to Dr. Gottlieb in 2015, according to the open payments database: Vertex Pharmaceuticals, GlaxoSmithKline, Daiichi, Valeant, Pfizer, Millennium, SI-BONE, and E.R. Squibb & Sons. Payments included travel to Philadelphia, San Francisco, and London.
9 recusals
In a memo, Dr. Gottlieb wrote that he had a consulting relationship with nine health care companies before his stint as the FDA’s deputy commissioner for medical and scientific affairs during the George W. Bush administration. Those ties disqualified him from dealing with matters concerning those companies for at least a year. The firms included Eli Lilly, Roche, and Sanofi-Aventis.
The recusals generated some headlines during the avian flu scare because Dr. Gottlieb had to recuse himself from some of the planning efforts around vaccines.
7 years
Starting in 1997, Dr. Gottlieb spent 7 years as a staff writer for BMJ, one of the top medical journals in the world. And he was an editor at the Pulse section of JAMA, the Journal of the American Medical Association, from 1996 to 2001.
Dr. Gottlieb also spent the past 7 years as an adviser to drug maker GlaxoSmithKline’s product investment board, according to his LinkedIn page.
33 years old
Dr. Gottlieb was 33 when he got the No. 2 job at the FDA in 2005. He had done a short stint at the agency a few years earlier but was considered a controversial pick because of his ties to Wall Street. He stayed until 2007.
“He has done a lot of thinking about how FDA should be managed – his operational sophistication is going to be a great asset,” said former FDA attorney Coleen Klasmeier, who worked with Dr. Gottlieb and coauthored articles with him. “He also has very strong relationships among career FDA personnel and will be able to hit the ground running on a range of important initiatives.”
18 times before Congress
Dr. Gottlieb testified before Congress as an expert witness 18 times. He has spoken about drug prices, revamping the FDA approval process and the vaccine supply.
“Most people watching at the FDA would breathe a sigh of relief,” Joshua Sharfstein, MD, who served as the FDA’s principal deputy commissioner until 2011, said of Dr. Gottlieb’s impending nomination. He added that Dr. Gottlieb is “not someone who has expressed antagonism to the core principles of the agency.”
36,000 Twitter followers
More than 36,000 people follow Dr. Gottlieb on Twitter, although he follows only 845 people, as of Tuesday. He has tweeted at least 10,400 times, lately about different strains of the flu.
72 percent
Almost three-fourths of the 53 drug companies surveyed by Mizuho said they’d prefer Dr. Gottlieb to head the FDA.
$414,000
Pharmaceutical companies paid Dr. Gottlieb nearly $414,000 from 2013 through 2015, according to federal open payments data, for speeches, consulting, travel, and meals.
That included $65,780 from a pharmaceutical company to promote a controversial cystic fibrosis drug called Kalydeco (ivacaftor). Only one other doctor received more money toward promoting the drug.
The drug’s price tag was controversial because the nonprofit Cystic Fibrosis Foundation kicked in $150 million toward finding a cure for the fatal disease and got a rich $3.3 billion payday for selling its rights to royalties for the drug. Vertex Pharmaceuticals priced Kalydeco at more than $300,000 a year.
Nearly $30,000
Dr. Gottlieb has contributed nearly $30,000 toward Republican political campaigns and joint fundraising committees from 2005 to 2014. He has donated toward the presidential runs of Mitt Romney and Sen. John McCain. He also donated more than once to Speaker Paul Ryan.
Dr. Gottlieb contributed the most money toward Sen. Ben Sasse (R-Neb.), spending $2,600 in the primary and $2,600 again in the general election in 2013. Sen. Sasse was a vocal anti-Trump supporter, penning an open letter in February 2016 about how he could not support Trump, who was “dividing” the nation, in his view.
“But have you noticed how Mr. Trump uses the word ‘Reign’ – like he thinks he’s running for King?” Sen. Sasse asked in the post.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Set a goal, or two, or three
In today’s health care space, tracking progress and achieving specified metrics are all part of the job. Most fast-paced physician groups incentivize clinicians for efficiency, consistency, quality, and loyalty. Setting and achieving goals, although it might sound somewhat cliche, can play an important role in daily performance, as well as have an impact on long-term satisfaction with an HM career, according to experts in the field.
“Health care insurers and individuals choosing where to obtain health care want evidence that hospitalists are delivering the best care possible,” says Judith S. Treharne, consulting executive at Halley Consulting Group in Westerville, Ohio. “This requires goal setting, measuring performance related to those goals, and continually developing processes that enhance performance in order to achieve goals.”
Hospitalists are at the forefront of healthcare transformations taking place both inside the hospital and when patients are discharged to different settings. The opportunities for setting goals – personal and group-wide – are endless.

For employed hospitalists, goal setting – and achievement – can counter career stagnation, says Sanjay Bhatia, MD, FHM, CDIP.
“They show up, do a job, and go home. Many are not encouraged to develop their careers,” says Dr. Bhatia, chief medical officer, Prime Healthcare–Lower Bucks Hospital, Bristol, Pa.; founding partner, First Docs/Mercer Bucks Medical, Levittown, Pa.; and CEO/president, Prime Clinical Solutions, Freehold, N.J.

Setting goals will help hospitalists establish skill sets and achieve accomplishments that will keep their career growth on track, adds Surinder Yadav, MD, SFHM, vice president of hospital medicine at Emeryville, Calif.–based CEP America, a national organization specializing in acute-care staffing, including hospitalist, intensivist, and emergency medicine programs.
when someone consistently reaches their goals (that is, improving outcomes) and feels accomplished, it enhances engagement of their work, says Treharne, who advises hospitalist groups.
Determine, pursue goals
There are many reasons why goal setting is important. So what guidelines can a hospitalist use to set goals? In order to establish goals for your current role, Treharne advises reviewing your job description – which should be updated as your role evolves.
“Determine what you need to do in order to progress toward meeting these requirements,” she says. “Find out what resources are available to support your efforts.”
Regarding setting career goals, Dr. Jaffer says hospitalists should consider things that really move them.
“For hospitalists in the early stages of their careers, it may take some time to determine them,” he says. “But when a passion develops, hospitalists can identify opportunities which will allow them to create a niche for themselves or an area of expertise.”
Then, hospitalists can work with individuals within their organization and beyond to increase their expertise.
“Find one or more mentors, take educational courses or even pursue an advanced degree, and write about your area of expertise either by publishing articles or abstracts, giving poster presentations, or lecturing,” Dr. Jaffer advises. “That will establish you as an expert and lead to promotions.”
Dr. Bhatia believes it’s natural and important for hospitalists to pursue administrative roles and become experts on how hospitals and post–acute care facilities work, because they transition patients to these institutions and they employ hospitalists. He has also seen hospitalists pursue entrepreneurial goals, such as becoming involved in information technology by developing apps or becoming C-suite executives, and starting other medical-based businesses such as home-based physician visits and telemedicine ventures and even nonmedical-based businesses such as real estate investing. Another avenue is teaching residency programs and developing an academic career.
“The key is to have good teammates, partners, and ancillary staff in each endeavor,” Dr. Bhatia says. “You can learn a lot from them as well. My experiences beyond being a hospitalist make me very valuable as a hospitalist. I’ve found that varied experiences create a synergistic and value-added service to a hospital.”
Stay on target
In order to reach your goals, Dr. Bhatia recommends creating daily task lists as well as setting goals quarterly and annually and evaluating them at those intervals. Determine action steps to reach long-term goals. “I keep these lists on my smartphone, so they’re always in my mind’s eye,” he says. “I look at the big picture on a daily basis and work toward my goals.”
In an effort to help faculty members reach their goals, Dr. Jaffer, when he was a division director at Rush University Medical Center in Chicago, scheduled biannual professional reviews with each team member. It was a formal process adapted from the annual professional review that he learned while at the Cleveland Clinic. Members were asked to complete a faculty self-reflection assessment and answer questions such as:
- Since our last meeting, what committees and educational opportunities have you participated in?
- What types of quality improvement projects and presentations have you done?
- What achievements are you most proud of?
- Regarding the goals you listed at your last review, where have you had the most growth? What would you define as opportunities for growth?
At Rush, Dr. Jaffer asked members of his division to set one or two professional goals each year. “I suggested they set goals that will make them feel fulfilled professionally, so their careers remain gratifying,” he says.
Group goals
Hospitalists should play an integral role in developing a hospital’s strategic and operational plan. “By having hospitalists provide feedback in the planning process, prior to annual finalization of the plan, the hospital’s and hospitalist program’s objectives can be aligned,” Treharne says. “It’s important that their goals align, in order for both to be successful.”
Dr. Jaffer suggests starting at the beginning of each fiscal year. HM groups should, as a team, create quality, operational, and efficiency goals, which align closely with the hospital’s goals. Some examples: clinical productivity work relative value units (wRVUs), doctor-patient communication scores, observed-to-expected length of stay, readmission rates, and percentage of patients discharged by 1 p.m.
“We set goals both as individuals and as a group,” Dr. Jaffer says. “Then, we create a scorecard for each hospitalist on a quarterly basis and share each hospitalist’s data with them, as well as create a group dashboard. As a group, hospitalists can view both individual data and the group’s data. This feedback helps them identify where they need to improve their performance.”
Dr. Bhatia has found that setting group goals on a quarterly basis works well. Goals involve recruitment needs, patient satisfaction, case mix index, Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), utilization, and length of stay.
“Metrics should be recorded and shared monthly by either the hospital’s information technology department or the hospitalist group’s software,” he says.
Data: top of mind
Each provider needs to understand that success for the team also means individual success.
“Focus on helping each other to achieve high performance and high quality care,” Dr. Yadav says. “Engage with each other and with the hospital at large. Aim to be involved in projects and to help find solutions to problems or barriers within the system.”
When you implement a change in a process and expect to see improvement regarding a particular measure, be sure to give the new process adequate time to shift the outcome.
“Many good ideas have been cast aside because they were deemed unsuccessful before there was sufficient time for the process to stabilize and the improvement to be seen,” Treharne says.
When setting targets and measures, set expectations regarding how long the new process will need to be in place prior to evaluating the change.
“Pilot programs are often a good way to try something out before completely changing a process with potential unwanted outcomes,” she says.
If a clinical operational or efficiency goal that involves the whole group and performance is below target, look to best practices to help you achieve success, Dr. Jaffer says. Create a work group and appoint a champion.
Hopefully, reaching your goals will translate into success.
“Success for me is about having a positive impact on people and processes, and being content with my personal life and having time and resources to pursue my passions,” Dr. Jaffer concludes.
Setting Goals for Now and Then
When looking to set goals, Treharne recommends starting with long-term goal setting.
“Set goals for the next year, or five years and beyond, by establishing a vision – dream to be more than you are today,” she says. “Envision a future that gets you excited to participate in change and come to work every day.”

- I could become more valued in my job by doing _____.
- I could make more income by _____.
- I’d like to increase my knowledge of _____.
Then, develop short-term goals that will help you work toward achieving your long-term goals.
“Map out a path from today using the metrics available and applicable to the future state,” Treharne says. “Creating that path allows you to determine the short-term goals. How far can you get in what period of time? Be realistic, but stretch yourself so you’re not complacent.”
Document this path in a quarterly action plan with a complementary monthly tactical plan. Plans should identify accountable parties, resources needed, data requirements, and timelines, Treharne says. Review your progress monthly.
Check in and articulate your goals with those in your inner circle – seek their advice on a regular basis, Uy says. Measure results and be willing to adapt if you’re not progressing as you’ve envisioned.
Karen Appold is a freelance writer in Pennsylvania.
In today’s health care space, tracking progress and achieving specified metrics are all part of the job. Most fast-paced physician groups incentivize clinicians for efficiency, consistency, quality, and loyalty. Setting and achieving goals, although it might sound somewhat cliche, can play an important role in daily performance, as well as have an impact on long-term satisfaction with an HM career, according to experts in the field.
“Health care insurers and individuals choosing where to obtain health care want evidence that hospitalists are delivering the best care possible,” says Judith S. Treharne, consulting executive at Halley Consulting Group in Westerville, Ohio. “This requires goal setting, measuring performance related to those goals, and continually developing processes that enhance performance in order to achieve goals.”
Hospitalists are at the forefront of healthcare transformations taking place both inside the hospital and when patients are discharged to different settings. The opportunities for setting goals – personal and group-wide – are endless.
For employed hospitalists, goal setting – and achievement – can counter career stagnation, says Sanjay Bhatia, MD, FHM, CDIP.
“They show up, do a job, and go home. Many are not encouraged to develop their careers,” says Dr. Bhatia, chief medical officer, Prime Healthcare–Lower Bucks Hospital, Bristol, Pa.; founding partner, First Docs/Mercer Bucks Medical, Levittown, Pa.; and CEO/president, Prime Clinical Solutions, Freehold, N.J.
Setting goals will help hospitalists establish skill sets and achieve accomplishments that will keep their career growth on track, adds Surinder Yadav, MD, SFHM, vice president of hospital medicine at Emeryville, Calif.–based CEP America, a national organization specializing in acute-care staffing, including hospitalist, intensivist, and emergency medicine programs.
when someone consistently reaches their goals (that is, improving outcomes) and feels accomplished, it enhances engagement of their work, says Treharne, who advises hospitalist groups.
Determine, pursue goals
There are many reasons why goal setting is important. So what guidelines can a hospitalist use to set goals? In order to establish goals for your current role, Treharne advises reviewing your job description – which should be updated as your role evolves.
“Determine what you need to do in order to progress toward meeting these requirements,” she says. “Find out what resources are available to support your efforts.”
Regarding setting career goals, Dr. Jaffer says hospitalists should consider things that really move them.
“For hospitalists in the early stages of their careers, it may take some time to determine them,” he says. “But when a passion develops, hospitalists can identify opportunities which will allow them to create a niche for themselves or an area of expertise.”
Then, hospitalists can work with individuals within their organization and beyond to increase their expertise.
“Find one or more mentors, take educational courses or even pursue an advanced degree, and write about your area of expertise either by publishing articles or abstracts, giving poster presentations, or lecturing,” Dr. Jaffer advises. “That will establish you as an expert and lead to promotions.”
Dr. Bhatia believes it’s natural and important for hospitalists to pursue administrative roles and become experts on how hospitals and post–acute care facilities work, because they transition patients to these institutions and they employ hospitalists. He has also seen hospitalists pursue entrepreneurial goals, such as becoming involved in information technology by developing apps or becoming C-suite executives, and starting other medical-based businesses such as home-based physician visits and telemedicine ventures and even nonmedical-based businesses such as real estate investing. Another avenue is teaching residency programs and developing an academic career.
“The key is to have good teammates, partners, and ancillary staff in each endeavor,” Dr. Bhatia says. “You can learn a lot from them as well. My experiences beyond being a hospitalist make me very valuable as a hospitalist. I’ve found that varied experiences create a synergistic and value-added service to a hospital.”
Stay on target
In order to reach your goals, Dr. Bhatia recommends creating daily task lists as well as setting goals quarterly and annually and evaluating them at those intervals. Determine action steps to reach long-term goals. “I keep these lists on my smartphone, so they’re always in my mind’s eye,” he says. “I look at the big picture on a daily basis and work toward my goals.”
In an effort to help faculty members reach their goals, Dr. Jaffer, when he was a division director at Rush University Medical Center in Chicago, scheduled biannual professional reviews with each team member. It was a formal process adapted from the annual professional review that he learned while at the Cleveland Clinic. Members were asked to complete a faculty self-reflection assessment and answer questions such as:
- Since our last meeting, what committees and educational opportunities have you participated in?
- What types of quality improvement projects and presentations have you done?
- What achievements are you most proud of?
- Regarding the goals you listed at your last review, where have you had the most growth? What would you define as opportunities for growth?
At Rush, Dr. Jaffer asked members of his division to set one or two professional goals each year. “I suggested they set goals that will make them feel fulfilled professionally, so their careers remain gratifying,” he says.
Group goals
Hospitalists should play an integral role in developing a hospital’s strategic and operational plan. “By having hospitalists provide feedback in the planning process, prior to annual finalization of the plan, the hospital’s and hospitalist program’s objectives can be aligned,” Treharne says. “It’s important that their goals align, in order for both to be successful.”
Dr. Jaffer suggests starting at the beginning of each fiscal year. HM groups should, as a team, create quality, operational, and efficiency goals, which align closely with the hospital’s goals. Some examples: clinical productivity work relative value units (wRVUs), doctor-patient communication scores, observed-to-expected length of stay, readmission rates, and percentage of patients discharged by 1 p.m.
“We set goals both as individuals and as a group,” Dr. Jaffer says. “Then, we create a scorecard for each hospitalist on a quarterly basis and share each hospitalist’s data with them, as well as create a group dashboard. As a group, hospitalists can view both individual data and the group’s data. This feedback helps them identify where they need to improve their performance.”
Dr. Bhatia has found that setting group goals on a quarterly basis works well. Goals involve recruitment needs, patient satisfaction, case mix index, Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), utilization, and length of stay.
“Metrics should be recorded and shared monthly by either the hospital’s information technology department or the hospitalist group’s software,” he says.
Data: top of mind
Each provider needs to understand that success for the team also means individual success.
“Focus on helping each other to achieve high performance and high quality care,” Dr. Yadav says. “Engage with each other and with the hospital at large. Aim to be involved in projects and to help find solutions to problems or barriers within the system.”
When you implement a change in a process and expect to see improvement regarding a particular measure, be sure to give the new process adequate time to shift the outcome.
“Many good ideas have been cast aside because they were deemed unsuccessful before there was sufficient time for the process to stabilize and the improvement to be seen,” Treharne says.
When setting targets and measures, set expectations regarding how long the new process will need to be in place prior to evaluating the change.
“Pilot programs are often a good way to try something out before completely changing a process with potential unwanted outcomes,” she says.
If a clinical operational or efficiency goal that involves the whole group and performance is below target, look to best practices to help you achieve success, Dr. Jaffer says. Create a work group and appoint a champion.
Hopefully, reaching your goals will translate into success.
“Success for me is about having a positive impact on people and processes, and being content with my personal life and having time and resources to pursue my passions,” Dr. Jaffer concludes.
Setting Goals for Now and Then
When looking to set goals, Treharne recommends starting with long-term goal setting.
“Set goals for the next year, or five years and beyond, by establishing a vision – dream to be more than you are today,” she says. “Envision a future that gets you excited to participate in change and come to work every day.”
- I could become more valued in my job by doing _____.
- I could make more income by _____.
- I’d like to increase my knowledge of _____.
Then, develop short-term goals that will help you work toward achieving your long-term goals.
“Map out a path from today using the metrics available and applicable to the future state,” Treharne says. “Creating that path allows you to determine the short-term goals. How far can you get in what period of time? Be realistic, but stretch yourself so you’re not complacent.”
Document this path in a quarterly action plan with a complementary monthly tactical plan. Plans should identify accountable parties, resources needed, data requirements, and timelines, Treharne says. Review your progress monthly.
Check in and articulate your goals with those in your inner circle – seek their advice on a regular basis, Uy says. Measure results and be willing to adapt if you’re not progressing as you’ve envisioned.
Karen Appold is a freelance writer in Pennsylvania.
In today’s health care space, tracking progress and achieving specified metrics are all part of the job. Most fast-paced physician groups incentivize clinicians for efficiency, consistency, quality, and loyalty. Setting and achieving goals, although it might sound somewhat cliche, can play an important role in daily performance, as well as have an impact on long-term satisfaction with an HM career, according to experts in the field.
“Health care insurers and individuals choosing where to obtain health care want evidence that hospitalists are delivering the best care possible,” says Judith S. Treharne, consulting executive at Halley Consulting Group in Westerville, Ohio. “This requires goal setting, measuring performance related to those goals, and continually developing processes that enhance performance in order to achieve goals.”
Hospitalists are at the forefront of healthcare transformations taking place both inside the hospital and when patients are discharged to different settings. The opportunities for setting goals – personal and group-wide – are endless.
For employed hospitalists, goal setting – and achievement – can counter career stagnation, says Sanjay Bhatia, MD, FHM, CDIP.
“They show up, do a job, and go home. Many are not encouraged to develop their careers,” says Dr. Bhatia, chief medical officer, Prime Healthcare–Lower Bucks Hospital, Bristol, Pa.; founding partner, First Docs/Mercer Bucks Medical, Levittown, Pa.; and CEO/president, Prime Clinical Solutions, Freehold, N.J.
Setting goals will help hospitalists establish skill sets and achieve accomplishments that will keep their career growth on track, adds Surinder Yadav, MD, SFHM, vice president of hospital medicine at Emeryville, Calif.–based CEP America, a national organization specializing in acute-care staffing, including hospitalist, intensivist, and emergency medicine programs.
when someone consistently reaches their goals (that is, improving outcomes) and feels accomplished, it enhances engagement of their work, says Treharne, who advises hospitalist groups.
Determine, pursue goals
There are many reasons why goal setting is important. So what guidelines can a hospitalist use to set goals? In order to establish goals for your current role, Treharne advises reviewing your job description – which should be updated as your role evolves.
“Determine what you need to do in order to progress toward meeting these requirements,” she says. “Find out what resources are available to support your efforts.”
Regarding setting career goals, Dr. Jaffer says hospitalists should consider things that really move them.
“For hospitalists in the early stages of their careers, it may take some time to determine them,” he says. “But when a passion develops, hospitalists can identify opportunities which will allow them to create a niche for themselves or an area of expertise.”
Then, hospitalists can work with individuals within their organization and beyond to increase their expertise.
“Find one or more mentors, take educational courses or even pursue an advanced degree, and write about your area of expertise either by publishing articles or abstracts, giving poster presentations, or lecturing,” Dr. Jaffer advises. “That will establish you as an expert and lead to promotions.”
Dr. Bhatia believes it’s natural and important for hospitalists to pursue administrative roles and become experts on how hospitals and post–acute care facilities work, because they transition patients to these institutions and they employ hospitalists. He has also seen hospitalists pursue entrepreneurial goals, such as becoming involved in information technology by developing apps or becoming C-suite executives, and starting other medical-based businesses such as home-based physician visits and telemedicine ventures and even nonmedical-based businesses such as real estate investing. Another avenue is teaching residency programs and developing an academic career.
“The key is to have good teammates, partners, and ancillary staff in each endeavor,” Dr. Bhatia says. “You can learn a lot from them as well. My experiences beyond being a hospitalist make me very valuable as a hospitalist. I’ve found that varied experiences create a synergistic and value-added service to a hospital.”
Stay on target
In order to reach your goals, Dr. Bhatia recommends creating daily task lists as well as setting goals quarterly and annually and evaluating them at those intervals. Determine action steps to reach long-term goals. “I keep these lists on my smartphone, so they’re always in my mind’s eye,” he says. “I look at the big picture on a daily basis and work toward my goals.”
In an effort to help faculty members reach their goals, Dr. Jaffer, when he was a division director at Rush University Medical Center in Chicago, scheduled biannual professional reviews with each team member. It was a formal process adapted from the annual professional review that he learned while at the Cleveland Clinic. Members were asked to complete a faculty self-reflection assessment and answer questions such as:
- Since our last meeting, what committees and educational opportunities have you participated in?
- What types of quality improvement projects and presentations have you done?
- What achievements are you most proud of?
- Regarding the goals you listed at your last review, where have you had the most growth? What would you define as opportunities for growth?
At Rush, Dr. Jaffer asked members of his division to set one or two professional goals each year. “I suggested they set goals that will make them feel fulfilled professionally, so their careers remain gratifying,” he says.
Group goals
Hospitalists should play an integral role in developing a hospital’s strategic and operational plan. “By having hospitalists provide feedback in the planning process, prior to annual finalization of the plan, the hospital’s and hospitalist program’s objectives can be aligned,” Treharne says. “It’s important that their goals align, in order for both to be successful.”
Dr. Jaffer suggests starting at the beginning of each fiscal year. HM groups should, as a team, create quality, operational, and efficiency goals, which align closely with the hospital’s goals. Some examples: clinical productivity work relative value units (wRVUs), doctor-patient communication scores, observed-to-expected length of stay, readmission rates, and percentage of patients discharged by 1 p.m.
“We set goals both as individuals and as a group,” Dr. Jaffer says. “Then, we create a scorecard for each hospitalist on a quarterly basis and share each hospitalist’s data with them, as well as create a group dashboard. As a group, hospitalists can view both individual data and the group’s data. This feedback helps them identify where they need to improve their performance.”
Dr. Bhatia has found that setting group goals on a quarterly basis works well. Goals involve recruitment needs, patient satisfaction, case mix index, Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS), utilization, and length of stay.
“Metrics should be recorded and shared monthly by either the hospital’s information technology department or the hospitalist group’s software,” he says.
Data: top of mind
Each provider needs to understand that success for the team also means individual success.
“Focus on helping each other to achieve high performance and high quality care,” Dr. Yadav says. “Engage with each other and with the hospital at large. Aim to be involved in projects and to help find solutions to problems or barriers within the system.”
When you implement a change in a process and expect to see improvement regarding a particular measure, be sure to give the new process adequate time to shift the outcome.
“Many good ideas have been cast aside because they were deemed unsuccessful before there was sufficient time for the process to stabilize and the improvement to be seen,” Treharne says.
When setting targets and measures, set expectations regarding how long the new process will need to be in place prior to evaluating the change.
“Pilot programs are often a good way to try something out before completely changing a process with potential unwanted outcomes,” she says.
If a clinical operational or efficiency goal that involves the whole group and performance is below target, look to best practices to help you achieve success, Dr. Jaffer says. Create a work group and appoint a champion.
Hopefully, reaching your goals will translate into success.
“Success for me is about having a positive impact on people and processes, and being content with my personal life and having time and resources to pursue my passions,” Dr. Jaffer concludes.
Setting Goals for Now and Then
When looking to set goals, Treharne recommends starting with long-term goal setting.
“Set goals for the next year, or five years and beyond, by establishing a vision – dream to be more than you are today,” she says. “Envision a future that gets you excited to participate in change and come to work every day.”
- I could become more valued in my job by doing _____.
- I could make more income by _____.
- I’d like to increase my knowledge of _____.
Then, develop short-term goals that will help you work toward achieving your long-term goals.
“Map out a path from today using the metrics available and applicable to the future state,” Treharne says. “Creating that path allows you to determine the short-term goals. How far can you get in what period of time? Be realistic, but stretch yourself so you’re not complacent.”
Document this path in a quarterly action plan with a complementary monthly tactical plan. Plans should identify accountable parties, resources needed, data requirements, and timelines, Treharne says. Review your progress monthly.
Check in and articulate your goals with those in your inner circle – seek their advice on a regular basis, Uy says. Measure results and be willing to adapt if you’re not progressing as you’ve envisioned.
Karen Appold is a freelance writer in Pennsylvania.
The dermatologic tourist
I’m not much of a traveler. I like to see the world through the adventures of my patients.
This is especially nice in the winter, such as during school vacation week. Within the past 24 hours, I’ve gotten messages from patients in Hawaii, Arizona, and Orlando.
Writing from Hawaii, Melvin showed me a photo of a small white spot that appeared on the outer aspect of his arm. I couldn’t make much of it except to tell him that it doesn’t look like anything that warrants a 9-hour flight to show it to me, at least not until he gets back to town.

Finally, Svetlana forwarded a photograph of a rash on her foot that she said had “just come yesterday.” This was the nicest case of cutaneous larva migrans that I’ve seen in quite some time, although I am fairly sure it has been there for more than a day. I tried not to sound too excited about her diagnosis, of course (“You’ve got the coolest parasite!”), and just suggested that she come in to see me on her return next week.
North, South, West. I’ve been all over, without leaving the chair facing my computer screen. (Nobody seems to have gotten a volcanic eruption in Iceland this year.) All this with no packing, no waiting in airports, no TSA lines. Who says traveling can’t be a pleasure?
Practice dermatology – see the world!
* * * * * * * * * * * * * * * * * * * * * * *
Brian was delighted. The fungal infection on his calf, treated for weeks with a topical steroid that had produced only intolerable itch, was subsiding nicely with oral terbinafine and topical ketoconazole.
“Can I drink when I take this medicine?” he asked. “The Internet says I shouldn’t.”
“It’s only another week, Brian,” I said. “Best to hold off ‘till then.”
“Because I really needed a drink last week,” he said.
“Why was that?”
“I was on a vacation with my father.”
“I see.”
“It was my father and his 70-year-old girlfriend.”
“Oh.”
“We were at a nudist colony.”
“You know, Brian,” I said. “Just hearing about that makes me want a drink myself.”
Practice can take you places you never went, places you’ll never get to, places you never want to get to.
* * * * * * * * * * * * * * * * * * * * * * *
Although I have patients fill out the usual consent form on oral isotretinoin, on which they promise to contact me if they become depressed, I rarely find anyone who does. Instead, people tend to become rather happy once their acne improves.
Since I’m not a psychiatrist, I try to do an amateur job of assessing mood when patients come in for their monthly follow-up. I pass on my technique for any of you might find it useful.
“Hello, Peter, are you having any problems?”
“No.”
“Do you get headaches?”
“No.”
“Nosebleeds?”
“No.”
“Any aches and pains in your muscles?”
“No.”
“Are you depressed?”
“No.”
“Are you always this negative?”
If the patient smiles while saying, “No,” you’re in good shape. If not, consider suggesting a therapist.
Better still, send the patient to the Caribbean. Then propose that you go come along yourself as a consultant, just to keep an eye on things.
And bring sunscreen. For the two of you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
I’m not much of a traveler. I like to see the world through the adventures of my patients.
This is especially nice in the winter, such as during school vacation week. Within the past 24 hours, I’ve gotten messages from patients in Hawaii, Arizona, and Orlando.
Writing from Hawaii, Melvin showed me a photo of a small white spot that appeared on the outer aspect of his arm. I couldn’t make much of it except to tell him that it doesn’t look like anything that warrants a 9-hour flight to show it to me, at least not until he gets back to town.
Finally, Svetlana forwarded a photograph of a rash on her foot that she said had “just come yesterday.” This was the nicest case of cutaneous larva migrans that I’ve seen in quite some time, although I am fairly sure it has been there for more than a day. I tried not to sound too excited about her diagnosis, of course (“You’ve got the coolest parasite!”), and just suggested that she come in to see me on her return next week.
North, South, West. I’ve been all over, without leaving the chair facing my computer screen. (Nobody seems to have gotten a volcanic eruption in Iceland this year.) All this with no packing, no waiting in airports, no TSA lines. Who says traveling can’t be a pleasure?
Practice dermatology – see the world!
* * * * * * * * * * * * * * * * * * * * * * *
Brian was delighted. The fungal infection on his calf, treated for weeks with a topical steroid that had produced only intolerable itch, was subsiding nicely with oral terbinafine and topical ketoconazole.
“Can I drink when I take this medicine?” he asked. “The Internet says I shouldn’t.”
“It’s only another week, Brian,” I said. “Best to hold off ‘till then.”
“Because I really needed a drink last week,” he said.
“Why was that?”
“I was on a vacation with my father.”
“I see.”
“It was my father and his 70-year-old girlfriend.”
“Oh.”
“We were at a nudist colony.”
“You know, Brian,” I said. “Just hearing about that makes me want a drink myself.”
Practice can take you places you never went, places you’ll never get to, places you never want to get to.
* * * * * * * * * * * * * * * * * * * * * * *
Although I have patients fill out the usual consent form on oral isotretinoin, on which they promise to contact me if they become depressed, I rarely find anyone who does. Instead, people tend to become rather happy once their acne improves.
Since I’m not a psychiatrist, I try to do an amateur job of assessing mood when patients come in for their monthly follow-up. I pass on my technique for any of you might find it useful.
“Hello, Peter, are you having any problems?”
“No.”
“Do you get headaches?”
“No.”
“Nosebleeds?”
“No.”
“Any aches and pains in your muscles?”
“No.”
“Are you depressed?”
“No.”
“Are you always this negative?”
If the patient smiles while saying, “No,” you’re in good shape. If not, consider suggesting a therapist.
Better still, send the patient to the Caribbean. Then propose that you go come along yourself as a consultant, just to keep an eye on things.
And bring sunscreen. For the two of you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
I’m not much of a traveler. I like to see the world through the adventures of my patients.
This is especially nice in the winter, such as during school vacation week. Within the past 24 hours, I’ve gotten messages from patients in Hawaii, Arizona, and Orlando.
Writing from Hawaii, Melvin showed me a photo of a small white spot that appeared on the outer aspect of his arm. I couldn’t make much of it except to tell him that it doesn’t look like anything that warrants a 9-hour flight to show it to me, at least not until he gets back to town.
Finally, Svetlana forwarded a photograph of a rash on her foot that she said had “just come yesterday.” This was the nicest case of cutaneous larva migrans that I’ve seen in quite some time, although I am fairly sure it has been there for more than a day. I tried not to sound too excited about her diagnosis, of course (“You’ve got the coolest parasite!”), and just suggested that she come in to see me on her return next week.
North, South, West. I’ve been all over, without leaving the chair facing my computer screen. (Nobody seems to have gotten a volcanic eruption in Iceland this year.) All this with no packing, no waiting in airports, no TSA lines. Who says traveling can’t be a pleasure?
Practice dermatology – see the world!
* * * * * * * * * * * * * * * * * * * * * * *
Brian was delighted. The fungal infection on his calf, treated for weeks with a topical steroid that had produced only intolerable itch, was subsiding nicely with oral terbinafine and topical ketoconazole.
“Can I drink when I take this medicine?” he asked. “The Internet says I shouldn’t.”
“It’s only another week, Brian,” I said. “Best to hold off ‘till then.”
“Because I really needed a drink last week,” he said.
“Why was that?”
“I was on a vacation with my father.”
“I see.”
“It was my father and his 70-year-old girlfriend.”
“Oh.”
“We were at a nudist colony.”
“You know, Brian,” I said. “Just hearing about that makes me want a drink myself.”
Practice can take you places you never went, places you’ll never get to, places you never want to get to.
* * * * * * * * * * * * * * * * * * * * * * *
Although I have patients fill out the usual consent form on oral isotretinoin, on which they promise to contact me if they become depressed, I rarely find anyone who does. Instead, people tend to become rather happy once their acne improves.
Since I’m not a psychiatrist, I try to do an amateur job of assessing mood when patients come in for their monthly follow-up. I pass on my technique for any of you might find it useful.
“Hello, Peter, are you having any problems?”
“No.”
“Do you get headaches?”
“No.”
“Nosebleeds?”
“No.”
“Any aches and pains in your muscles?”
“No.”
“Are you depressed?”
“No.”
“Are you always this negative?”
If the patient smiles while saying, “No,” you’re in good shape. If not, consider suggesting a therapist.
Better still, send the patient to the Caribbean. Then propose that you go come along yourself as a consultant, just to keep an eye on things.
And bring sunscreen. For the two of you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Children with poor lung function develop ACOS
Children with poor lung function will be more likely to develop asthma-chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS), suggesting that prevention of this disease should be attempted in early life, a study shows.
While other research has found that patients with poor lung function in early life have poor lung function as adults, this was the first study to investigate the relationship between childhood lung function and ACOS in adult life, according to Dinh S. Bui of the University of Melbourne, and his colleagues.
The study, published in the American Journal of Respiratory and Critical Care Medicine, used multinomial regression models to investigate associations between childhood lung parameters at age 7 years and asthma, COPD, and ACOS at age 45 years (Am J Respir Crit Care Med. 2017 Feb 1. doi: 10.1164/rccm.201606-1272OC).
“We found that ACOS participants showed evidence of persistently lower FEV1 [forced expiratory volume in 1 second] and FEV1/FVC [forced vital capacity] from childhood. This suggests that poorer childhood lung function tracked to early adult life, leading to impaired maximally attained lung function,” the researchers said.
“The study highlights that low childhood lung function is a risk factor for COPD (and ACOS) independent of smoking,” they noted.
The 1,355 study participants who had postbronchodilator (post-BD) lung function available were categorized into the following four mutually exclusive groups at age 45 years based on their asthma and COPD status: having neither asthma nor COPD (unaffected) (n = 959); having asthma alone (n = 269); having COPD alone (n = 59); having ACOS (n = 68).
Once adjusted for the sampling weights, the prevalence of current asthma alone was 13.5%, COPD alone was 4.1%, and ACOS was 2.9%. The researchers defined COPD at age 45 years as post-BD FEV1/FVC less than the Global Lung Initiative lower limit of normal. Because the associations between childhood lung function and both ACOS and COPD alone were nonlinear, the patients were grouped into quartiles based on their characteristics, such as their percent predicted FEV1 and percent predicted FEV1/FVC at 7 years, the investigators said.
Patients in the lowest quartile for FEV1 percent predicted at 7 years were 2.93 times more likely to have ACOS, compared with patients in the other quartiles for FEV1 percent predicted. Patients in the lowest quartile for FEV1/FVC percent predicted at 7 years were 16.3 times more likely to have ACOS and 5.76 times more likely to have COPD alone, compared with patients in the higher quartiles.
The researchers found large variation in childhood lung function among patients in the lowest quartiles for FEV1 and FEV1/FVC. To account for this, they conducted a sensitivity analysis, which excluded those with less than 80% predicted FEV1 and FEV1/FVC (n = 76 and 13, respectively).The associations between lung function measures and diseases in adulthood for patients in the lowest quartiles differed slightly following this adjustment. The sensitivity analysis showed that patients in the lowest quartile for FEV1 had an odds ratio of 2.4 for ACOS and that those patients in the lowest quartile for FEV1/FVC had an odds ratio of 5.2 for COPD alone and 15.1 for ACOS.
A sensitivity analysis that excluded patients with remitted asthma from the unaffected group showed childhood FEV1 was more strongly associated with ACOS for patients in the lowest quartile, compared with patients in the highest quartile (OR: 7.0, 95% CI: 2.7-18.3). This same analysis found that patients from the lowest quartile and second quartile for childhood FEV1/FVC were 6.8 and 3.9 times more likely to have COPD, respectively, compared with patients in the other quartiles. This sensitivity analysis also found that patients in the first quartile for FEV1/FVC were 19.1 times more likely to have ACOS, and patients in the second quartile for FEV1/FVC were 5.3 times more likely to have ACOS.
The researchers analyzed data from the Tasmanian Longitudinal Health Study, which began in 1968 when Tasmanian children born in 1961 and attending school in Tasmania were studied with respiratory health surveys and prebronchodilator (pre-BD) spirometry measurements. The most recent survey started in 2002. Survey respondents who had participated in past follow-up studies and/or reported symptoms of asthma or cough were invited to participate in a more detailed laboratory study from 2006 to 2008. That study included completing a questionnaire, pre-BD and post-BD spirometry, and skin prick testing. The predicted and percent predicted values for spirometry were derived from the Global Lung Initiative reference equations.
The final multinomial model was adjusted for various factors including childhood asthma, maternal smoking, and paternal smoking during childhood.
History of active smoking was significantly more frequent in patients with ACOS (73.5%) and COPD alone (73%) than in the unaffected (57%) groups. Childhood asthma, maternal asthma and atopy were more prevalent in the ACOS and asthma alone groups. ACOS and COPD participants had a higher prevalence of maternal smoking during childhood.
Individuals with ACOS had the lowest pre-BD FEV1 (percent predicted values) over time. Those with COPD alone or ACOS had significantly lower pre-BD FEV1/FVC (percent predicted values) at all time points, when patients were assessed, compared with unaffected participants. “Participants with COPD alone had significantly higher FVC at 7 and 13 years, while ACOS participants had significantly lower FVC at 45 years,” the researchers said.
“There was no evidence of effect modification by childhood lung infections, childhood asthma, maternal asthma, maternal smoking, or paternal smoking during childhood on the associations between childhood lung and the disease groups,” they noted.
The study was limited by its “relatively small sample sizes for the ACOS and COPD alone groups” and the absence of post-BD spirometry at 7 years, they added.
The researchers concluded that “screening of lung function in school-aged children may provide an opportunity to detect children likely to have ongoing poorer lung health, such as those with lung function below the lower limit of normal,” and that “[multifaceted] intervention strategies could then be implemented to reduce the burden of COPD and ACOS in adulthood.”

“I suspect that genetics may play a big role in the results, and there is increasing interest in learning how genetics are involved in COPD. A better understanding of the risk factors for lower lung function in children may also provide targets of intervention. The groups with ACOS and COPD have higher rates of maternal smoking, and while this study determined that the association between childhood low lung function and development of COPD and ACOS is independent of maternal smoking, maternal smoking still seems like a good area to target,” she said in an interview.
It would also be interesting to further study the first quartile of patients, she added. “The clinical disease for this quartile of patients covers a wide range of severities. I would be interested in dividing this group up further and learning the outcomes of their lung function and development of COPD and ACOS.”

Using inhaled corticosteroids and other medications for maintenance control, reducing and monitoring impairment, educating patients and patients’ guardians on triggers, avoiding triggers, and having an action plan for changing therapy based on symptoms or measured flows are ways to aggressively treat such conditions, said Dr. Gartman, assistant professor of medicine at Brown University, Providence, R.I*. He cited avoiding exposure to smoke, environmental pollutants, and living near highways, for those with low childhood function, as interventions that might prevent people with low lung function from later developing COPD.
Dr. Gartman added that differences between the availability of medication for children with asthma today and at the time of the study may mean there are differences between the children with low lung function in the study and those children who have low function today. A population of children with low lung function now may be experiencing relatively less asthma and more chronic lung disorders brought on by prematurity or cystic fibrosis, he noted. “As such, identification of poor function in today’s young children may carry with it a significantly different set of interventions and challenges,” Dr. Gartman said.
While asthma in children is better controlled now than it was at the time of the study, because the researchers did not provide any information about the asthma control of the study participants, “it [is] hard for me to say if better asthma drugs in those children would have made a difference in long-term outcomes of COPD and ACOS as an adult,” Dr. Swaminathan noted.
“The best thing we currently can do for children with low lung function is try and determine the underlying cause and treat any active diseases [such as asthma] that we can. This study reminds us of the need to keep searching for causes of low lung function that may be reversible,” she said.
The investigators recommended future research to understand the risk factors for lower lung function in children. They called for studies that address “the risk factors over adulthood that interact with lower lung function to increase the risk of rapid lung function decline.”
The study was supported by a National Health and Medical Research Council of Australia research grant, the University of Melbourne, Clifford Craig Medical Research Trust of Tasmania, the Victorian, Queensland & Tasmanian Asthma Foundations, The Royal Hobart Hospital, Helen MacPherson Smith Trust, GlaxoSmithKline, and John L Hopper. Five authors were supported by the research grant; the others reported no conflicts. Dr. Swaminathan and Dr. Gartman had no disclosures.
*This story was updated March 16, 2017, with Dr. Gartman's full affiliation.
Children with poor lung function will be more likely to develop asthma-chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS), suggesting that prevention of this disease should be attempted in early life, a study shows.
While other research has found that patients with poor lung function in early life have poor lung function as adults, this was the first study to investigate the relationship between childhood lung function and ACOS in adult life, according to Dinh S. Bui of the University of Melbourne, and his colleagues.
The study, published in the American Journal of Respiratory and Critical Care Medicine, used multinomial regression models to investigate associations between childhood lung parameters at age 7 years and asthma, COPD, and ACOS at age 45 years (Am J Respir Crit Care Med. 2017 Feb 1. doi: 10.1164/rccm.201606-1272OC).
“We found that ACOS participants showed evidence of persistently lower FEV1 [forced expiratory volume in 1 second] and FEV1/FVC [forced vital capacity] from childhood. This suggests that poorer childhood lung function tracked to early adult life, leading to impaired maximally attained lung function,” the researchers said.
“The study highlights that low childhood lung function is a risk factor for COPD (and ACOS) independent of smoking,” they noted.
The 1,355 study participants who had postbronchodilator (post-BD) lung function available were categorized into the following four mutually exclusive groups at age 45 years based on their asthma and COPD status: having neither asthma nor COPD (unaffected) (n = 959); having asthma alone (n = 269); having COPD alone (n = 59); having ACOS (n = 68).
Once adjusted for the sampling weights, the prevalence of current asthma alone was 13.5%, COPD alone was 4.1%, and ACOS was 2.9%. The researchers defined COPD at age 45 years as post-BD FEV1/FVC less than the Global Lung Initiative lower limit of normal. Because the associations between childhood lung function and both ACOS and COPD alone were nonlinear, the patients were grouped into quartiles based on their characteristics, such as their percent predicted FEV1 and percent predicted FEV1/FVC at 7 years, the investigators said.
Patients in the lowest quartile for FEV1 percent predicted at 7 years were 2.93 times more likely to have ACOS, compared with patients in the other quartiles for FEV1 percent predicted. Patients in the lowest quartile for FEV1/FVC percent predicted at 7 years were 16.3 times more likely to have ACOS and 5.76 times more likely to have COPD alone, compared with patients in the higher quartiles.
The researchers found large variation in childhood lung function among patients in the lowest quartiles for FEV1 and FEV1/FVC. To account for this, they conducted a sensitivity analysis, which excluded those with less than 80% predicted FEV1 and FEV1/FVC (n = 76 and 13, respectively).The associations between lung function measures and diseases in adulthood for patients in the lowest quartiles differed slightly following this adjustment. The sensitivity analysis showed that patients in the lowest quartile for FEV1 had an odds ratio of 2.4 for ACOS and that those patients in the lowest quartile for FEV1/FVC had an odds ratio of 5.2 for COPD alone and 15.1 for ACOS.
A sensitivity analysis that excluded patients with remitted asthma from the unaffected group showed childhood FEV1 was more strongly associated with ACOS for patients in the lowest quartile, compared with patients in the highest quartile (OR: 7.0, 95% CI: 2.7-18.3). This same analysis found that patients from the lowest quartile and second quartile for childhood FEV1/FVC were 6.8 and 3.9 times more likely to have COPD, respectively, compared with patients in the other quartiles. This sensitivity analysis also found that patients in the first quartile for FEV1/FVC were 19.1 times more likely to have ACOS, and patients in the second quartile for FEV1/FVC were 5.3 times more likely to have ACOS.
The researchers analyzed data from the Tasmanian Longitudinal Health Study, which began in 1968 when Tasmanian children born in 1961 and attending school in Tasmania were studied with respiratory health surveys and prebronchodilator (pre-BD) spirometry measurements. The most recent survey started in 2002. Survey respondents who had participated in past follow-up studies and/or reported symptoms of asthma or cough were invited to participate in a more detailed laboratory study from 2006 to 2008. That study included completing a questionnaire, pre-BD and post-BD spirometry, and skin prick testing. The predicted and percent predicted values for spirometry were derived from the Global Lung Initiative reference equations.
The final multinomial model was adjusted for various factors including childhood asthma, maternal smoking, and paternal smoking during childhood.
History of active smoking was significantly more frequent in patients with ACOS (73.5%) and COPD alone (73%) than in the unaffected (57%) groups. Childhood asthma, maternal asthma and atopy were more prevalent in the ACOS and asthma alone groups. ACOS and COPD participants had a higher prevalence of maternal smoking during childhood.
Individuals with ACOS had the lowest pre-BD FEV1 (percent predicted values) over time. Those with COPD alone or ACOS had significantly lower pre-BD FEV1/FVC (percent predicted values) at all time points, when patients were assessed, compared with unaffected participants. “Participants with COPD alone had significantly higher FVC at 7 and 13 years, while ACOS participants had significantly lower FVC at 45 years,” the researchers said.
“There was no evidence of effect modification by childhood lung infections, childhood asthma, maternal asthma, maternal smoking, or paternal smoking during childhood on the associations between childhood lung and the disease groups,” they noted.
The study was limited by its “relatively small sample sizes for the ACOS and COPD alone groups” and the absence of post-BD spirometry at 7 years, they added.
The researchers concluded that “screening of lung function in school-aged children may provide an opportunity to detect children likely to have ongoing poorer lung health, such as those with lung function below the lower limit of normal,” and that “[multifaceted] intervention strategies could then be implemented to reduce the burden of COPD and ACOS in adulthood.”
“I suspect that genetics may play a big role in the results, and there is increasing interest in learning how genetics are involved in COPD. A better understanding of the risk factors for lower lung function in children may also provide targets of intervention. The groups with ACOS and COPD have higher rates of maternal smoking, and while this study determined that the association between childhood low lung function and development of COPD and ACOS is independent of maternal smoking, maternal smoking still seems like a good area to target,” she said in an interview.
It would also be interesting to further study the first quartile of patients, she added. “The clinical disease for this quartile of patients covers a wide range of severities. I would be interested in dividing this group up further and learning the outcomes of their lung function and development of COPD and ACOS.”
Using inhaled corticosteroids and other medications for maintenance control, reducing and monitoring impairment, educating patients and patients’ guardians on triggers, avoiding triggers, and having an action plan for changing therapy based on symptoms or measured flows are ways to aggressively treat such conditions, said Dr. Gartman, assistant professor of medicine at Brown University, Providence, R.I*. He cited avoiding exposure to smoke, environmental pollutants, and living near highways, for those with low childhood function, as interventions that might prevent people with low lung function from later developing COPD.
Dr. Gartman added that differences between the availability of medication for children with asthma today and at the time of the study may mean there are differences between the children with low lung function in the study and those children who have low function today. A population of children with low lung function now may be experiencing relatively less asthma and more chronic lung disorders brought on by prematurity or cystic fibrosis, he noted. “As such, identification of poor function in today’s young children may carry with it a significantly different set of interventions and challenges,” Dr. Gartman said.
While asthma in children is better controlled now than it was at the time of the study, because the researchers did not provide any information about the asthma control of the study participants, “it [is] hard for me to say if better asthma drugs in those children would have made a difference in long-term outcomes of COPD and ACOS as an adult,” Dr. Swaminathan noted.
“The best thing we currently can do for children with low lung function is try and determine the underlying cause and treat any active diseases [such as asthma] that we can. This study reminds us of the need to keep searching for causes of low lung function that may be reversible,” she said.
The investigators recommended future research to understand the risk factors for lower lung function in children. They called for studies that address “the risk factors over adulthood that interact with lower lung function to increase the risk of rapid lung function decline.”
The study was supported by a National Health and Medical Research Council of Australia research grant, the University of Melbourne, Clifford Craig Medical Research Trust of Tasmania, the Victorian, Queensland & Tasmanian Asthma Foundations, The Royal Hobart Hospital, Helen MacPherson Smith Trust, GlaxoSmithKline, and John L Hopper. Five authors were supported by the research grant; the others reported no conflicts. Dr. Swaminathan and Dr. Gartman had no disclosures.
*This story was updated March 16, 2017, with Dr. Gartman's full affiliation.
Children with poor lung function will be more likely to develop asthma-chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS), suggesting that prevention of this disease should be attempted in early life, a study shows.
While other research has found that patients with poor lung function in early life have poor lung function as adults, this was the first study to investigate the relationship between childhood lung function and ACOS in adult life, according to Dinh S. Bui of the University of Melbourne, and his colleagues.
The study, published in the American Journal of Respiratory and Critical Care Medicine, used multinomial regression models to investigate associations between childhood lung parameters at age 7 years and asthma, COPD, and ACOS at age 45 years (Am J Respir Crit Care Med. 2017 Feb 1. doi: 10.1164/rccm.201606-1272OC).
“We found that ACOS participants showed evidence of persistently lower FEV1 [forced expiratory volume in 1 second] and FEV1/FVC [forced vital capacity] from childhood. This suggests that poorer childhood lung function tracked to early adult life, leading to impaired maximally attained lung function,” the researchers said.
“The study highlights that low childhood lung function is a risk factor for COPD (and ACOS) independent of smoking,” they noted.
The 1,355 study participants who had postbronchodilator (post-BD) lung function available were categorized into the following four mutually exclusive groups at age 45 years based on their asthma and COPD status: having neither asthma nor COPD (unaffected) (n = 959); having asthma alone (n = 269); having COPD alone (n = 59); having ACOS (n = 68).
Once adjusted for the sampling weights, the prevalence of current asthma alone was 13.5%, COPD alone was 4.1%, and ACOS was 2.9%. The researchers defined COPD at age 45 years as post-BD FEV1/FVC less than the Global Lung Initiative lower limit of normal. Because the associations between childhood lung function and both ACOS and COPD alone were nonlinear, the patients were grouped into quartiles based on their characteristics, such as their percent predicted FEV1 and percent predicted FEV1/FVC at 7 years, the investigators said.
Patients in the lowest quartile for FEV1 percent predicted at 7 years were 2.93 times more likely to have ACOS, compared with patients in the other quartiles for FEV1 percent predicted. Patients in the lowest quartile for FEV1/FVC percent predicted at 7 years were 16.3 times more likely to have ACOS and 5.76 times more likely to have COPD alone, compared with patients in the higher quartiles.
The researchers found large variation in childhood lung function among patients in the lowest quartiles for FEV1 and FEV1/FVC. To account for this, they conducted a sensitivity analysis, which excluded those with less than 80% predicted FEV1 and FEV1/FVC (n = 76 and 13, respectively).The associations between lung function measures and diseases in adulthood for patients in the lowest quartiles differed slightly following this adjustment. The sensitivity analysis showed that patients in the lowest quartile for FEV1 had an odds ratio of 2.4 for ACOS and that those patients in the lowest quartile for FEV1/FVC had an odds ratio of 5.2 for COPD alone and 15.1 for ACOS.
A sensitivity analysis that excluded patients with remitted asthma from the unaffected group showed childhood FEV1 was more strongly associated with ACOS for patients in the lowest quartile, compared with patients in the highest quartile (OR: 7.0, 95% CI: 2.7-18.3). This same analysis found that patients from the lowest quartile and second quartile for childhood FEV1/FVC were 6.8 and 3.9 times more likely to have COPD, respectively, compared with patients in the other quartiles. This sensitivity analysis also found that patients in the first quartile for FEV1/FVC were 19.1 times more likely to have ACOS, and patients in the second quartile for FEV1/FVC were 5.3 times more likely to have ACOS.
The researchers analyzed data from the Tasmanian Longitudinal Health Study, which began in 1968 when Tasmanian children born in 1961 and attending school in Tasmania were studied with respiratory health surveys and prebronchodilator (pre-BD) spirometry measurements. The most recent survey started in 2002. Survey respondents who had participated in past follow-up studies and/or reported symptoms of asthma or cough were invited to participate in a more detailed laboratory study from 2006 to 2008. That study included completing a questionnaire, pre-BD and post-BD spirometry, and skin prick testing. The predicted and percent predicted values for spirometry were derived from the Global Lung Initiative reference equations.
The final multinomial model was adjusted for various factors including childhood asthma, maternal smoking, and paternal smoking during childhood.
History of active smoking was significantly more frequent in patients with ACOS (73.5%) and COPD alone (73%) than in the unaffected (57%) groups. Childhood asthma, maternal asthma and atopy were more prevalent in the ACOS and asthma alone groups. ACOS and COPD participants had a higher prevalence of maternal smoking during childhood.
Individuals with ACOS had the lowest pre-BD FEV1 (percent predicted values) over time. Those with COPD alone or ACOS had significantly lower pre-BD FEV1/FVC (percent predicted values) at all time points, when patients were assessed, compared with unaffected participants. “Participants with COPD alone had significantly higher FVC at 7 and 13 years, while ACOS participants had significantly lower FVC at 45 years,” the researchers said.
“There was no evidence of effect modification by childhood lung infections, childhood asthma, maternal asthma, maternal smoking, or paternal smoking during childhood on the associations between childhood lung and the disease groups,” they noted.
The study was limited by its “relatively small sample sizes for the ACOS and COPD alone groups” and the absence of post-BD spirometry at 7 years, they added.
The researchers concluded that “screening of lung function in school-aged children may provide an opportunity to detect children likely to have ongoing poorer lung health, such as those with lung function below the lower limit of normal,” and that “[multifaceted] intervention strategies could then be implemented to reduce the burden of COPD and ACOS in adulthood.”
“I suspect that genetics may play a big role in the results, and there is increasing interest in learning how genetics are involved in COPD. A better understanding of the risk factors for lower lung function in children may also provide targets of intervention. The groups with ACOS and COPD have higher rates of maternal smoking, and while this study determined that the association between childhood low lung function and development of COPD and ACOS is independent of maternal smoking, maternal smoking still seems like a good area to target,” she said in an interview.
It would also be interesting to further study the first quartile of patients, she added. “The clinical disease for this quartile of patients covers a wide range of severities. I would be interested in dividing this group up further and learning the outcomes of their lung function and development of COPD and ACOS.”
Using inhaled corticosteroids and other medications for maintenance control, reducing and monitoring impairment, educating patients and patients’ guardians on triggers, avoiding triggers, and having an action plan for changing therapy based on symptoms or measured flows are ways to aggressively treat such conditions, said Dr. Gartman, assistant professor of medicine at Brown University, Providence, R.I*. He cited avoiding exposure to smoke, environmental pollutants, and living near highways, for those with low childhood function, as interventions that might prevent people with low lung function from later developing COPD.
Dr. Gartman added that differences between the availability of medication for children with asthma today and at the time of the study may mean there are differences between the children with low lung function in the study and those children who have low function today. A population of children with low lung function now may be experiencing relatively less asthma and more chronic lung disorders brought on by prematurity or cystic fibrosis, he noted. “As such, identification of poor function in today’s young children may carry with it a significantly different set of interventions and challenges,” Dr. Gartman said.
While asthma in children is better controlled now than it was at the time of the study, because the researchers did not provide any information about the asthma control of the study participants, “it [is] hard for me to say if better asthma drugs in those children would have made a difference in long-term outcomes of COPD and ACOS as an adult,” Dr. Swaminathan noted.
“The best thing we currently can do for children with low lung function is try and determine the underlying cause and treat any active diseases [such as asthma] that we can. This study reminds us of the need to keep searching for causes of low lung function that may be reversible,” she said.
The investigators recommended future research to understand the risk factors for lower lung function in children. They called for studies that address “the risk factors over adulthood that interact with lower lung function to increase the risk of rapid lung function decline.”
The study was supported by a National Health and Medical Research Council of Australia research grant, the University of Melbourne, Clifford Craig Medical Research Trust of Tasmania, the Victorian, Queensland & Tasmanian Asthma Foundations, The Royal Hobart Hospital, Helen MacPherson Smith Trust, GlaxoSmithKline, and John L Hopper. Five authors were supported by the research grant; the others reported no conflicts. Dr. Swaminathan and Dr. Gartman had no disclosures.
*This story was updated March 16, 2017, with Dr. Gartman's full affiliation.
FROM AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
David Henry's JCSO podcast, March-April 2017
For the March-April issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses two informative “how-to” articles, one on the implementation of a distress management program at an oncology hospital in Puerto Rico, the other on the prevention and treatment options for mTOR inhibitor-associated stomatitis. Dr Henry also shares his preferences for addressing health care reform, and he highlights a letter to the journal in response to the January-February issue Commentary on physician-assisted dying. Immunotherapies are at the fore again, this time with an insightful essay by Jane de Lartigue who writes that combination therapy is likely to be key in expanding the scope of immunotherapy into currently unresponsive patient populations, which raises questions about the optimal combinations and the timing and sequencing of combination immunotherapy. Three Original Reports span the clinical, supportive, and quality- and value-based care components of cancer care, with their respective foci on APF530 for nausea and vomiting prevention after cisplatin; patterns of care in whole-brain radiotherapy technique and delivery; and emergency department use by newly diagnosed cancer patients. As usual, there is a line-up of rare and challenging presentations in Case Reports on pulmonary sarcomatoid carcinoma presenting as a necrotizing cavitary lung lesions, palmoplantar exacerbation of psoriasis after nivolumab for lung cancer, primary cardiac prosthetic valve-associated lymphoma; and atraumatic splenic rupture as an initial presentation of chronic myelogenous leukemia.
Listen to the podcast below.
For the March-April issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses two informative “how-to” articles, one on the implementation of a distress management program at an oncology hospital in Puerto Rico, the other on the prevention and treatment options for mTOR inhibitor-associated stomatitis. Dr Henry also shares his preferences for addressing health care reform, and he highlights a letter to the journal in response to the January-February issue Commentary on physician-assisted dying. Immunotherapies are at the fore again, this time with an insightful essay by Jane de Lartigue who writes that combination therapy is likely to be key in expanding the scope of immunotherapy into currently unresponsive patient populations, which raises questions about the optimal combinations and the timing and sequencing of combination immunotherapy. Three Original Reports span the clinical, supportive, and quality- and value-based care components of cancer care, with their respective foci on APF530 for nausea and vomiting prevention after cisplatin; patterns of care in whole-brain radiotherapy technique and delivery; and emergency department use by newly diagnosed cancer patients. As usual, there is a line-up of rare and challenging presentations in Case Reports on pulmonary sarcomatoid carcinoma presenting as a necrotizing cavitary lung lesions, palmoplantar exacerbation of psoriasis after nivolumab for lung cancer, primary cardiac prosthetic valve-associated lymphoma; and atraumatic splenic rupture as an initial presentation of chronic myelogenous leukemia.
Listen to the podcast below.
For the March-April issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses two informative “how-to” articles, one on the implementation of a distress management program at an oncology hospital in Puerto Rico, the other on the prevention and treatment options for mTOR inhibitor-associated stomatitis. Dr Henry also shares his preferences for addressing health care reform, and he highlights a letter to the journal in response to the January-February issue Commentary on physician-assisted dying. Immunotherapies are at the fore again, this time with an insightful essay by Jane de Lartigue who writes that combination therapy is likely to be key in expanding the scope of immunotherapy into currently unresponsive patient populations, which raises questions about the optimal combinations and the timing and sequencing of combination immunotherapy. Three Original Reports span the clinical, supportive, and quality- and value-based care components of cancer care, with their respective foci on APF530 for nausea and vomiting prevention after cisplatin; patterns of care in whole-brain radiotherapy technique and delivery; and emergency department use by newly diagnosed cancer patients. As usual, there is a line-up of rare and challenging presentations in Case Reports on pulmonary sarcomatoid carcinoma presenting as a necrotizing cavitary lung lesions, palmoplantar exacerbation of psoriasis after nivolumab for lung cancer, primary cardiac prosthetic valve-associated lymphoma; and atraumatic splenic rupture as an initial presentation of chronic myelogenous leukemia.
Listen to the podcast below.
Increased IUD use suggests ‘Trump effect’
Patient visits for IUD prescriptions and insertions were up 21% between October 2016 and January 2017, compared with those in the same period a year earlier, according to athenahealth, a provider of EHR systems and point-of-care mobile applications.
The rise in IUD-related visits since the presidential election – the first time in 5 years that the volume of visits for IUD procedures and follow-ups has increased in both November and December – suggests a “Trump effect.” As the replacement of the Affordable Care Act is debated, “uncertainly swirls over whether any new law would mandate free insurance coverage without copays for birth control and contraception devices,” athenahealth said.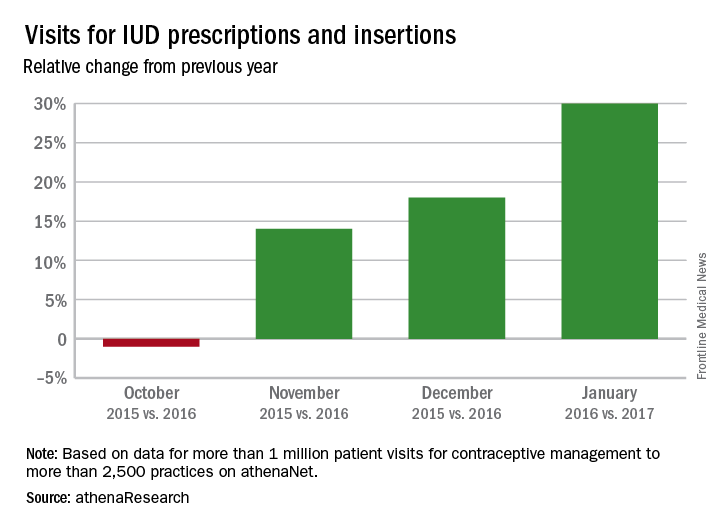
The athenahealth data include more than 1 million visits for IUD management to more than 2,500 practices using the company’s EHRs.
Patient visits for IUD prescriptions and insertions were up 21% between October 2016 and January 2017, compared with those in the same period a year earlier, according to athenahealth, a provider of EHR systems and point-of-care mobile applications.
The rise in IUD-related visits since the presidential election – the first time in 5 years that the volume of visits for IUD procedures and follow-ups has increased in both November and December – suggests a “Trump effect.” As the replacement of the Affordable Care Act is debated, “uncertainly swirls over whether any new law would mandate free insurance coverage without copays for birth control and contraception devices,” athenahealth said.
The athenahealth data include more than 1 million visits for IUD management to more than 2,500 practices using the company’s EHRs.
Patient visits for IUD prescriptions and insertions were up 21% between October 2016 and January 2017, compared with those in the same period a year earlier, according to athenahealth, a provider of EHR systems and point-of-care mobile applications.
The rise in IUD-related visits since the presidential election – the first time in 5 years that the volume of visits for IUD procedures and follow-ups has increased in both November and December – suggests a “Trump effect.” As the replacement of the Affordable Care Act is debated, “uncertainly swirls over whether any new law would mandate free insurance coverage without copays for birth control and contraception devices,” athenahealth said.
The athenahealth data include more than 1 million visits for IUD management to more than 2,500 practices using the company’s EHRs.
VIDEO: Striking improvement in PFS with olaparib for ovarian cancer
NATIONAL HARBOR, MD. – Maintenance therapy with the first-in-class PARP inhibitor olaparib was associated with a striking improvement in progression-free survival in patients with platinum-sensitive relapsed ovarian cancer and BRCA 1/2 mutation in the randomized, placebo-controlled phase III SOLO2 trial.
Compared with placebo, the tablet formulation of olaparib was associated with investigator-assessed PFS of 19.1 months in 196 patients, compared with 5.5 months in 99 patients who received placebo (hazard ratio, 0.30), Dr. Eric Pujade-Lauraine reported at the annual meeting of the Society of Gynecologic Oncology.
The SOLO2 results were both clinically meaningful and highly statistically significant, said Dr. Pujade-Lauraine of Hopital Hotel-Dieu, Paris.
Active treatment, which involved a twice-daily 300-mg oral dose of olaparib, was well tolerated; 75% of patients completed the study without dose reduction, he noted.
In this video interview, Dr. Pujade-Lauraine discussed the SOLO2 study and findings, which confirmed those of the phase II Study 19. Study 19 looked at olaparib in all-comers with platinum-sensitive relapsed ovarian cancer and involved a different formulation of the drug, which required that patients take 16 capsules each day to achieve a twice-daily dose of 400 mg. Patients with BRCA mutations were found in that study to derive the most benefit from olaparib.
The current findings are practice changing, Dr. Pujade-Lauraine said, concluding that “it is important to test BRCA, and if this test is positive, to offer olaparib in patients who are platinum sensitive.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – Maintenance therapy with the first-in-class PARP inhibitor olaparib was associated with a striking improvement in progression-free survival in patients with platinum-sensitive relapsed ovarian cancer and BRCA 1/2 mutation in the randomized, placebo-controlled phase III SOLO2 trial.
Compared with placebo, the tablet formulation of olaparib was associated with investigator-assessed PFS of 19.1 months in 196 patients, compared with 5.5 months in 99 patients who received placebo (hazard ratio, 0.30), Dr. Eric Pujade-Lauraine reported at the annual meeting of the Society of Gynecologic Oncology.
The SOLO2 results were both clinically meaningful and highly statistically significant, said Dr. Pujade-Lauraine of Hopital Hotel-Dieu, Paris.
Active treatment, which involved a twice-daily 300-mg oral dose of olaparib, was well tolerated; 75% of patients completed the study without dose reduction, he noted.
In this video interview, Dr. Pujade-Lauraine discussed the SOLO2 study and findings, which confirmed those of the phase II Study 19. Study 19 looked at olaparib in all-comers with platinum-sensitive relapsed ovarian cancer and involved a different formulation of the drug, which required that patients take 16 capsules each day to achieve a twice-daily dose of 400 mg. Patients with BRCA mutations were found in that study to derive the most benefit from olaparib.
The current findings are practice changing, Dr. Pujade-Lauraine said, concluding that “it is important to test BRCA, and if this test is positive, to offer olaparib in patients who are platinum sensitive.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – Maintenance therapy with the first-in-class PARP inhibitor olaparib was associated with a striking improvement in progression-free survival in patients with platinum-sensitive relapsed ovarian cancer and BRCA 1/2 mutation in the randomized, placebo-controlled phase III SOLO2 trial.
Compared with placebo, the tablet formulation of olaparib was associated with investigator-assessed PFS of 19.1 months in 196 patients, compared with 5.5 months in 99 patients who received placebo (hazard ratio, 0.30), Dr. Eric Pujade-Lauraine reported at the annual meeting of the Society of Gynecologic Oncology.
The SOLO2 results were both clinically meaningful and highly statistically significant, said Dr. Pujade-Lauraine of Hopital Hotel-Dieu, Paris.
Active treatment, which involved a twice-daily 300-mg oral dose of olaparib, was well tolerated; 75% of patients completed the study without dose reduction, he noted.
In this video interview, Dr. Pujade-Lauraine discussed the SOLO2 study and findings, which confirmed those of the phase II Study 19. Study 19 looked at olaparib in all-comers with platinum-sensitive relapsed ovarian cancer and involved a different formulation of the drug, which required that patients take 16 capsules each day to achieve a twice-daily dose of 400 mg. Patients with BRCA mutations were found in that study to derive the most benefit from olaparib.
The current findings are practice changing, Dr. Pujade-Lauraine said, concluding that “it is important to test BRCA, and if this test is positive, to offer olaparib in patients who are platinum sensitive.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ANNUAL MEETING ON WOMEN'S CANCER

VIDEO: Vaginal brachytherapy linked with better survival in rare uterine cancer
NATIONAL HARBOR, MD. – A large retrospective database study linked the use of vaginal brachytherapy and chemotherapy with improved survival among patients with early-stage uterine papillary serous carcinoma.
The findings offer a degree of clinical guidance on the adjuvant treatment of this relatively rare, aggressive histologic cancer subtype, Stephanie Cham, MD, said during a video interview at the annual meeting of the Society of Gynecologic Oncology.
Large dataset analyses can be especially helpful for exploring the treatment of rare diseases for which clinical trials can be infeasible, said Dr. Cham of Columbia University College of Physicians and Surgeons in New York. To evaluate chemotherapy, vaginal brachytherapy, and whole beam pelvic radiation therapy in stage I and stage II uterine papillary serous carcinoma, she and her associates analyzed the National Cancer Database.
Among 7,325 patients treated between 1998 and 2012, 38% of patients had received chemotherapy, 18% had received external beam radiation, and 20% received brachytherapy, Dr. Cham said. The use of chemotherapy rose significantly over time, regardless of stage (P less than .0001), as did the use of brachytherapy, while the use of external beam radiation decreased.
After the researchers controlled for numerous demographic and clinical variables, chemotherapy was associated with a statistically significant decrease in the risk of death overall (hazard ratio, 0.78; 95% confidence interval, 0.69 to 0.88) and in patients with stage IB (HR, 0.58; 95% CI, 0.44-0.77) or stage II cancer (HR, 0.74; 95% CI, 0.60-0.90). The use of brachytherapy also was associated with significantly improved survival overall (HR, 0.67), in stage IA cancer (HR, 0.67), and in stage II cancer (HR, 0.64).
The survival effect of brachytherapy held up in additional subgroup analyses, Dr. Cham explained. In contrast, external beam radiation therapy was not associated with improved survival overall or in any subgroup, she said. The results highlight the potential use of vaginal brachytherapy in early-stage uterine papillary serous carcinoma, she emphasized.
Dr. Cham cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – A large retrospective database study linked the use of vaginal brachytherapy and chemotherapy with improved survival among patients with early-stage uterine papillary serous carcinoma.
The findings offer a degree of clinical guidance on the adjuvant treatment of this relatively rare, aggressive histologic cancer subtype, Stephanie Cham, MD, said during a video interview at the annual meeting of the Society of Gynecologic Oncology.
Large dataset analyses can be especially helpful for exploring the treatment of rare diseases for which clinical trials can be infeasible, said Dr. Cham of Columbia University College of Physicians and Surgeons in New York. To evaluate chemotherapy, vaginal brachytherapy, and whole beam pelvic radiation therapy in stage I and stage II uterine papillary serous carcinoma, she and her associates analyzed the National Cancer Database.
Among 7,325 patients treated between 1998 and 2012, 38% of patients had received chemotherapy, 18% had received external beam radiation, and 20% received brachytherapy, Dr. Cham said. The use of chemotherapy rose significantly over time, regardless of stage (P less than .0001), as did the use of brachytherapy, while the use of external beam radiation decreased.
After the researchers controlled for numerous demographic and clinical variables, chemotherapy was associated with a statistically significant decrease in the risk of death overall (hazard ratio, 0.78; 95% confidence interval, 0.69 to 0.88) and in patients with stage IB (HR, 0.58; 95% CI, 0.44-0.77) or stage II cancer (HR, 0.74; 95% CI, 0.60-0.90). The use of brachytherapy also was associated with significantly improved survival overall (HR, 0.67), in stage IA cancer (HR, 0.67), and in stage II cancer (HR, 0.64).
The survival effect of brachytherapy held up in additional subgroup analyses, Dr. Cham explained. In contrast, external beam radiation therapy was not associated with improved survival overall or in any subgroup, she said. The results highlight the potential use of vaginal brachytherapy in early-stage uterine papillary serous carcinoma, she emphasized.
Dr. Cham cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NATIONAL HARBOR, MD. – A large retrospective database study linked the use of vaginal brachytherapy and chemotherapy with improved survival among patients with early-stage uterine papillary serous carcinoma.
The findings offer a degree of clinical guidance on the adjuvant treatment of this relatively rare, aggressive histologic cancer subtype, Stephanie Cham, MD, said during a video interview at the annual meeting of the Society of Gynecologic Oncology.
Large dataset analyses can be especially helpful for exploring the treatment of rare diseases for which clinical trials can be infeasible, said Dr. Cham of Columbia University College of Physicians and Surgeons in New York. To evaluate chemotherapy, vaginal brachytherapy, and whole beam pelvic radiation therapy in stage I and stage II uterine papillary serous carcinoma, she and her associates analyzed the National Cancer Database.
Among 7,325 patients treated between 1998 and 2012, 38% of patients had received chemotherapy, 18% had received external beam radiation, and 20% received brachytherapy, Dr. Cham said. The use of chemotherapy rose significantly over time, regardless of stage (P less than .0001), as did the use of brachytherapy, while the use of external beam radiation decreased.
After the researchers controlled for numerous demographic and clinical variables, chemotherapy was associated with a statistically significant decrease in the risk of death overall (hazard ratio, 0.78; 95% confidence interval, 0.69 to 0.88) and in patients with stage IB (HR, 0.58; 95% CI, 0.44-0.77) or stage II cancer (HR, 0.74; 95% CI, 0.60-0.90). The use of brachytherapy also was associated with significantly improved survival overall (HR, 0.67), in stage IA cancer (HR, 0.67), and in stage II cancer (HR, 0.64).
The survival effect of brachytherapy held up in additional subgroup analyses, Dr. Cham explained. In contrast, external beam radiation therapy was not associated with improved survival overall or in any subgroup, she said. The results highlight the potential use of vaginal brachytherapy in early-stage uterine papillary serous carcinoma, she emphasized.
Dr. Cham cited no funding sources and reported having no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Chemotherapy and brachytherapy were independently associated with survival in early-stage uterine papillary serous carcinoma.
Major finding: Multivariable analyses linked chemotherapy with a statistically significant decrease in the risk of death overall (hazard ratio, 0.78) and in stage IB (HR, 0.58; 95% CI, 0.44 to 0.77) and stage II cancer (HR, 0.74; 95% CI, 0.60 to 0.90). The use of brachytherapy also was associated with significantly improved survival in the entire cohort (HR, 0.67), in stage IA cancer (HR, 0.67), and in stage II cancer (HR, 0.64).
Data source: A retrospective analysis of patients with stage I or II uterine papillary serous carcinoma from the National Cancer Database.
Disclosures: Dr. Cham cited no funding sources and reported having no conflicts of interest.
