User login
Therapy can produce durable CRs in NHL

When given after low-dose chemotherapy, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy can produce durable complete responses (CRs) in patients with relapsed/refractory non-Hodgkin lymphoma (NHL), according to research published in the Journal of Clinical Oncology.
In this phase 1 study, the overall response rate was 73%, and 50% of patients had an ongoing CR at last follow-up.
Fifty-five percent of patients experienced grade 3/4 neurologic toxicities, though these events eventually resolved.
This research was conducted under a cooperative research and development agreement between the National Cancer Institute and Kite Pharma, Inc.
Kite is developing the CAR T-cell therapy axicabtagene ciloleucel (formerly known as KTE-C19), and the therapy tested in this trial has the same CAR construct as axicabtagene ciloleucel.
Results from this study (NCT00924326) were previously published in the Journal of Clinical Oncology in 2014.
The current report included 22 patients with relapsed/refractory NHL. Seventeen patients had diffuse large B-cell lymphoma (DLBCL), 2 had primary mediastinal B-cell lymphoma (PMBCL), 2 had follicular lymphoma (FL), and 1 had mantle cell lymphoma (MCL).
Patients received a single dose of CAR T cells 2 days after a low-dose chemotherapy conditioning regimen consisting of cyclophosphamide and fludarabine.
Response
The overall response rate was 73% (16/22), with a CR rate of 55% (n=12) and a partial response (PR) rate of 18% (n=4).
Among patients with DLBCL, there were 9 CRs, 4 PRs, 1 patient with stable disease, and 3 patients with progressive disease.
Both FL patients achieved a CR, as did the patient with MCL. One patient with PMBCL had stable disease, and the other progressed.
Eleven of the 12 CRs are ongoing, with durations ranging from more than 7 months to more than 24 months. The median duration of CR is 12.5 months.
The researchers found that serum IL-15 levels and CAR T-cell expansion correlated with treatment response (CR or PR).
The median peak blood CAR+ cell level was 98/μL in patients who achieved a response and 15/μL in those who did not (P=0.027).
High serum IL-15 levels were significantly associated with high peak blood CAR+ cell levels (P=0.001) and response (P<0.001).
Toxicity
Fifty-five percent of patients had grade 3 or 4 neurologic toxicities, the most common of which were dysphasia (n=9) and confusion (n=8).
The researchers said all acute toxicities resolved completely, and none of the patients died as a result of toxicity.
One patient experienced vision loss 3 months after receiving CAR T-cell therapy. The researchers said they could not confirm the cause of the vision loss, but it is consistent with fludarabine toxicity.
One patient developed myelodysplastic syndrome, which was thought to be related to prior therapy.
The researchers noted that patients who experienced grade 3/4 neurologic toxicity had significantly higher levels of blood CAR+ cells than patients who had neurologic toxicities of a lower grade (P=0.003).
In addition, peak levels of serum IL-10 and IL-15 were higher in patients with grade 3/4 neurologic toxicities (P=0.006 and 0.014, respectively). ![]()
When given after low-dose chemotherapy, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy can produce durable complete responses (CRs) in patients with relapsed/refractory non-Hodgkin lymphoma (NHL), according to research published in the Journal of Clinical Oncology.
In this phase 1 study, the overall response rate was 73%, and 50% of patients had an ongoing CR at last follow-up.
Fifty-five percent of patients experienced grade 3/4 neurologic toxicities, though these events eventually resolved.
This research was conducted under a cooperative research and development agreement between the National Cancer Institute and Kite Pharma, Inc.
Kite is developing the CAR T-cell therapy axicabtagene ciloleucel (formerly known as KTE-C19), and the therapy tested in this trial has the same CAR construct as axicabtagene ciloleucel.
Results from this study (NCT00924326) were previously published in the Journal of Clinical Oncology in 2014.
The current report included 22 patients with relapsed/refractory NHL. Seventeen patients had diffuse large B-cell lymphoma (DLBCL), 2 had primary mediastinal B-cell lymphoma (PMBCL), 2 had follicular lymphoma (FL), and 1 had mantle cell lymphoma (MCL).
Patients received a single dose of CAR T cells 2 days after a low-dose chemotherapy conditioning regimen consisting of cyclophosphamide and fludarabine.
Response
The overall response rate was 73% (16/22), with a CR rate of 55% (n=12) and a partial response (PR) rate of 18% (n=4).
Among patients with DLBCL, there were 9 CRs, 4 PRs, 1 patient with stable disease, and 3 patients with progressive disease.
Both FL patients achieved a CR, as did the patient with MCL. One patient with PMBCL had stable disease, and the other progressed.
Eleven of the 12 CRs are ongoing, with durations ranging from more than 7 months to more than 24 months. The median duration of CR is 12.5 months.
The researchers found that serum IL-15 levels and CAR T-cell expansion correlated with treatment response (CR or PR).
The median peak blood CAR+ cell level was 98/μL in patients who achieved a response and 15/μL in those who did not (P=0.027).
High serum IL-15 levels were significantly associated with high peak blood CAR+ cell levels (P=0.001) and response (P<0.001).
Toxicity
Fifty-five percent of patients had grade 3 or 4 neurologic toxicities, the most common of which were dysphasia (n=9) and confusion (n=8).
The researchers said all acute toxicities resolved completely, and none of the patients died as a result of toxicity.
One patient experienced vision loss 3 months after receiving CAR T-cell therapy. The researchers said they could not confirm the cause of the vision loss, but it is consistent with fludarabine toxicity.
One patient developed myelodysplastic syndrome, which was thought to be related to prior therapy.
The researchers noted that patients who experienced grade 3/4 neurologic toxicity had significantly higher levels of blood CAR+ cells than patients who had neurologic toxicities of a lower grade (P=0.003).
In addition, peak levels of serum IL-10 and IL-15 were higher in patients with grade 3/4 neurologic toxicities (P=0.006 and 0.014, respectively). ![]()
When given after low-dose chemotherapy, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy can produce durable complete responses (CRs) in patients with relapsed/refractory non-Hodgkin lymphoma (NHL), according to research published in the Journal of Clinical Oncology.
In this phase 1 study, the overall response rate was 73%, and 50% of patients had an ongoing CR at last follow-up.
Fifty-five percent of patients experienced grade 3/4 neurologic toxicities, though these events eventually resolved.
This research was conducted under a cooperative research and development agreement between the National Cancer Institute and Kite Pharma, Inc.
Kite is developing the CAR T-cell therapy axicabtagene ciloleucel (formerly known as KTE-C19), and the therapy tested in this trial has the same CAR construct as axicabtagene ciloleucel.
Results from this study (NCT00924326) were previously published in the Journal of Clinical Oncology in 2014.
The current report included 22 patients with relapsed/refractory NHL. Seventeen patients had diffuse large B-cell lymphoma (DLBCL), 2 had primary mediastinal B-cell lymphoma (PMBCL), 2 had follicular lymphoma (FL), and 1 had mantle cell lymphoma (MCL).
Patients received a single dose of CAR T cells 2 days after a low-dose chemotherapy conditioning regimen consisting of cyclophosphamide and fludarabine.
Response
The overall response rate was 73% (16/22), with a CR rate of 55% (n=12) and a partial response (PR) rate of 18% (n=4).
Among patients with DLBCL, there were 9 CRs, 4 PRs, 1 patient with stable disease, and 3 patients with progressive disease.
Both FL patients achieved a CR, as did the patient with MCL. One patient with PMBCL had stable disease, and the other progressed.
Eleven of the 12 CRs are ongoing, with durations ranging from more than 7 months to more than 24 months. The median duration of CR is 12.5 months.
The researchers found that serum IL-15 levels and CAR T-cell expansion correlated with treatment response (CR or PR).
The median peak blood CAR+ cell level was 98/μL in patients who achieved a response and 15/μL in those who did not (P=0.027).
High serum IL-15 levels were significantly associated with high peak blood CAR+ cell levels (P=0.001) and response (P<0.001).
Toxicity
Fifty-five percent of patients had grade 3 or 4 neurologic toxicities, the most common of which were dysphasia (n=9) and confusion (n=8).
The researchers said all acute toxicities resolved completely, and none of the patients died as a result of toxicity.
One patient experienced vision loss 3 months after receiving CAR T-cell therapy. The researchers said they could not confirm the cause of the vision loss, but it is consistent with fludarabine toxicity.
One patient developed myelodysplastic syndrome, which was thought to be related to prior therapy.
The researchers noted that patients who experienced grade 3/4 neurologic toxicity had significantly higher levels of blood CAR+ cells than patients who had neurologic toxicities of a lower grade (P=0.003).
In addition, peak levels of serum IL-10 and IL-15 were higher in patients with grade 3/4 neurologic toxicities (P=0.006 and 0.014, respectively). ![]()
ADCs could treat myeloma, other malignancies
A class of antibody-drug conjugates (ADCs) have shown promise for treating hematologic and solid tumor malignancies, according to research published in Cell Chemical Biology.
The ADCs, known as selenomab-drug conjugates, demonstrated in vitro activity against breast cancer and multiple myeloma (MM).
The ADCs also inhibited tumor growth and prolonged survival in mouse models of both malignancies.
“We’ve been working on this technology for some time,” said study author Christoph Rader, PhD, of The Scripps Research Institute (TSRI) in Jupiter, Florida.
“It’s based on the rarely used natural amino acid selenocysteine, which we insert into our antibodies. We refer to these engineered antibodies as selenomabs.”
He then explained that selenomab-drug conjugates are ADCs that “utilize the unique reactivity of selenocysteine for drug attachment.”
For this study, Dr Rader and his colleagues generated selective selenomab-drug conjugates and tested them in vitro and in vivo.
The team found that CD138-targeting selenomab-drug conjugates were effective against MM cell lines (U266 and H929), and HER2-targeting selenomab-drug conjugates were effective against breast cancer cell lines.
Both types of ADCs demonstrated efficacy in mouse models as well.
One of the CD138-targeting selenomab-drug conjugates, known as CN29, was tested in a mouse model of MM.
One group of mice received CN29 at 3 mg/kg every 4 days for a total of 4 cycles, another group received unconjugated selenomab, and a third received vehicle control.
CN29 significantly inhibited tumor growth (P=0.000085) and extended survival time (P=0.0083) in the mice.
Based on these results, Dr Rader said selenomab-drug conjugates “promise broad utility for cancer therapy.” ![]()
A class of antibody-drug conjugates (ADCs) have shown promise for treating hematologic and solid tumor malignancies, according to research published in Cell Chemical Biology.
The ADCs, known as selenomab-drug conjugates, demonstrated in vitro activity against breast cancer and multiple myeloma (MM).
The ADCs also inhibited tumor growth and prolonged survival in mouse models of both malignancies.
“We’ve been working on this technology for some time,” said study author Christoph Rader, PhD, of The Scripps Research Institute (TSRI) in Jupiter, Florida.
“It’s based on the rarely used natural amino acid selenocysteine, which we insert into our antibodies. We refer to these engineered antibodies as selenomabs.”
He then explained that selenomab-drug conjugates are ADCs that “utilize the unique reactivity of selenocysteine for drug attachment.”
For this study, Dr Rader and his colleagues generated selective selenomab-drug conjugates and tested them in vitro and in vivo.
The team found that CD138-targeting selenomab-drug conjugates were effective against MM cell lines (U266 and H929), and HER2-targeting selenomab-drug conjugates were effective against breast cancer cell lines.
Both types of ADCs demonstrated efficacy in mouse models as well.
One of the CD138-targeting selenomab-drug conjugates, known as CN29, was tested in a mouse model of MM.
One group of mice received CN29 at 3 mg/kg every 4 days for a total of 4 cycles, another group received unconjugated selenomab, and a third received vehicle control.
CN29 significantly inhibited tumor growth (P=0.000085) and extended survival time (P=0.0083) in the mice.
Based on these results, Dr Rader said selenomab-drug conjugates “promise broad utility for cancer therapy.” ![]()
A class of antibody-drug conjugates (ADCs) have shown promise for treating hematologic and solid tumor malignancies, according to research published in Cell Chemical Biology.
The ADCs, known as selenomab-drug conjugates, demonstrated in vitro activity against breast cancer and multiple myeloma (MM).
The ADCs also inhibited tumor growth and prolonged survival in mouse models of both malignancies.
“We’ve been working on this technology for some time,” said study author Christoph Rader, PhD, of The Scripps Research Institute (TSRI) in Jupiter, Florida.
“It’s based on the rarely used natural amino acid selenocysteine, which we insert into our antibodies. We refer to these engineered antibodies as selenomabs.”
He then explained that selenomab-drug conjugates are ADCs that “utilize the unique reactivity of selenocysteine for drug attachment.”
For this study, Dr Rader and his colleagues generated selective selenomab-drug conjugates and tested them in vitro and in vivo.
The team found that CD138-targeting selenomab-drug conjugates were effective against MM cell lines (U266 and H929), and HER2-targeting selenomab-drug conjugates were effective against breast cancer cell lines.
Both types of ADCs demonstrated efficacy in mouse models as well.
One of the CD138-targeting selenomab-drug conjugates, known as CN29, was tested in a mouse model of MM.
One group of mice received CN29 at 3 mg/kg every 4 days for a total of 4 cycles, another group received unconjugated selenomab, and a third received vehicle control.
CN29 significantly inhibited tumor growth (P=0.000085) and extended survival time (P=0.0083) in the mice.
Based on these results, Dr Rader said selenomab-drug conjugates “promise broad utility for cancer therapy.” ![]()
Funders could do more to reduce research waste, team says

A study published in The Lancet suggests agencies that distribute public funds for research could do more to reduce waste.
Investigators evaluated 11 agencies from various countries and found the agencies aren’t always transparent about what they are doing to prevent waste in research.
The investigators also found evidence to suggest that some agencies are not taking certain steps that could reduce waste, and the governments responsible for the public money these agencies distribute are not holding them to account.
“Our investigation has shown that, on the whole, information about the policies and processes used by national funding agencies across the funding landscape are not transparent or readily available,” said Mona Nasser, DDS, of Plymouth University in the UK.
“It would appear that governments around the world often do not hold these agencies accountable for adding value to research and reducing research waste. This is not a call for governments to reduce spending on medical research, but, rather, as public funds become increasingly squeezed, there is no better time for funding agencies and governments to work together to ensure that we will all get the best ‘bang for the buck.’”
For this study, Dr Nasser and her colleagues investigated how research funders monitor and take steps to reduce waste in the research they support. The team also examined how funders support methodology research and the development of research infrastructures to reduce waste.
The investigators looked through the websites of 11 national research funders that distribute public funds in the US, UK, Australia, Canada, Germany, France, The Netherlands, Denmark, and Norway.
The team looked for information on how the agencies decide what to fund and how they ensure what they fund is not wasteful. The investigators also contacted these agencies to verify their findings.
The team found that approaches vary among the funders, but there are weaknesses that are applicable across all funding bodies.
One weakness is that grant committees tend to be dominated by academics and clinicians, which is a problem because patients’ interests may be overlooked.
The funders with the “most extensive” involvement of the general public are the National Institute of Health Research (NIHR) in the UK and ZonMW in The Netherlands.
Another weakness is the fact that practice and policy decisions are often made without the systematic assessment of existing research evidence.
The only funder to require reference to relevant systematic reviews in all funding applications is NIHR.
Yet another weakness is that only 6 of the 11 funding agencies require the publication of full reports of the research they have funded. And none of the funders have a comprehensive strategy to make data from all research projects freely available.
Based on these results, Dr Nasser and her colleagues concluded that more should be done to ensure transparency and accountability.
“In simple terms, there is a 2-pronged requirement for medical research funding bodies which distribute public funds,” Dr Nasser said. “The first is that they need to be fully responsible for how and why those funds are distributed because they are ultimately answerable to every tax payer in their home countries.”
“The second is that they need to ensure that public funds are not only invested wisely in research projects which represent both good value and waste-limited practice, but also to ensure that the results of these studies are made available in a usable format to the people who need them.” ![]()
A study published in The Lancet suggests agencies that distribute public funds for research could do more to reduce waste.
Investigators evaluated 11 agencies from various countries and found the agencies aren’t always transparent about what they are doing to prevent waste in research.
The investigators also found evidence to suggest that some agencies are not taking certain steps that could reduce waste, and the governments responsible for the public money these agencies distribute are not holding them to account.
“Our investigation has shown that, on the whole, information about the policies and processes used by national funding agencies across the funding landscape are not transparent or readily available,” said Mona Nasser, DDS, of Plymouth University in the UK.
“It would appear that governments around the world often do not hold these agencies accountable for adding value to research and reducing research waste. This is not a call for governments to reduce spending on medical research, but, rather, as public funds become increasingly squeezed, there is no better time for funding agencies and governments to work together to ensure that we will all get the best ‘bang for the buck.’”
For this study, Dr Nasser and her colleagues investigated how research funders monitor and take steps to reduce waste in the research they support. The team also examined how funders support methodology research and the development of research infrastructures to reduce waste.
The investigators looked through the websites of 11 national research funders that distribute public funds in the US, UK, Australia, Canada, Germany, France, The Netherlands, Denmark, and Norway.
The team looked for information on how the agencies decide what to fund and how they ensure what they fund is not wasteful. The investigators also contacted these agencies to verify their findings.
The team found that approaches vary among the funders, but there are weaknesses that are applicable across all funding bodies.
One weakness is that grant committees tend to be dominated by academics and clinicians, which is a problem because patients’ interests may be overlooked.
The funders with the “most extensive” involvement of the general public are the National Institute of Health Research (NIHR) in the UK and ZonMW in The Netherlands.
Another weakness is the fact that practice and policy decisions are often made without the systematic assessment of existing research evidence.
The only funder to require reference to relevant systematic reviews in all funding applications is NIHR.
Yet another weakness is that only 6 of the 11 funding agencies require the publication of full reports of the research they have funded. And none of the funders have a comprehensive strategy to make data from all research projects freely available.
Based on these results, Dr Nasser and her colleagues concluded that more should be done to ensure transparency and accountability.
“In simple terms, there is a 2-pronged requirement for medical research funding bodies which distribute public funds,” Dr Nasser said. “The first is that they need to be fully responsible for how and why those funds are distributed because they are ultimately answerable to every tax payer in their home countries.”
“The second is that they need to ensure that public funds are not only invested wisely in research projects which represent both good value and waste-limited practice, but also to ensure that the results of these studies are made available in a usable format to the people who need them.” ![]()
A study published in The Lancet suggests agencies that distribute public funds for research could do more to reduce waste.
Investigators evaluated 11 agencies from various countries and found the agencies aren’t always transparent about what they are doing to prevent waste in research.
The investigators also found evidence to suggest that some agencies are not taking certain steps that could reduce waste, and the governments responsible for the public money these agencies distribute are not holding them to account.
“Our investigation has shown that, on the whole, information about the policies and processes used by national funding agencies across the funding landscape are not transparent or readily available,” said Mona Nasser, DDS, of Plymouth University in the UK.
“It would appear that governments around the world often do not hold these agencies accountable for adding value to research and reducing research waste. This is not a call for governments to reduce spending on medical research, but, rather, as public funds become increasingly squeezed, there is no better time for funding agencies and governments to work together to ensure that we will all get the best ‘bang for the buck.’”
For this study, Dr Nasser and her colleagues investigated how research funders monitor and take steps to reduce waste in the research they support. The team also examined how funders support methodology research and the development of research infrastructures to reduce waste.
The investigators looked through the websites of 11 national research funders that distribute public funds in the US, UK, Australia, Canada, Germany, France, The Netherlands, Denmark, and Norway.
The team looked for information on how the agencies decide what to fund and how they ensure what they fund is not wasteful. The investigators also contacted these agencies to verify their findings.
The team found that approaches vary among the funders, but there are weaknesses that are applicable across all funding bodies.
One weakness is that grant committees tend to be dominated by academics and clinicians, which is a problem because patients’ interests may be overlooked.
The funders with the “most extensive” involvement of the general public are the National Institute of Health Research (NIHR) in the UK and ZonMW in The Netherlands.
Another weakness is the fact that practice and policy decisions are often made without the systematic assessment of existing research evidence.
The only funder to require reference to relevant systematic reviews in all funding applications is NIHR.
Yet another weakness is that only 6 of the 11 funding agencies require the publication of full reports of the research they have funded. And none of the funders have a comprehensive strategy to make data from all research projects freely available.
Based on these results, Dr Nasser and her colleagues concluded that more should be done to ensure transparency and accountability.
“In simple terms, there is a 2-pronged requirement for medical research funding bodies which distribute public funds,” Dr Nasser said. “The first is that they need to be fully responsible for how and why those funds are distributed because they are ultimately answerable to every tax payer in their home countries.”
“The second is that they need to ensure that public funds are not only invested wisely in research projects which represent both good value and waste-limited practice, but also to ensure that the results of these studies are made available in a usable format to the people who need them.” ![]()
What are indications, complications of acute blood transfusions in sickle cell anemia? Key Points Additional Reading
Case
A 19-year-old female with a history of sickle cell anemia and hemoglobin SS, presents with a 2-day history of worsening lower back pain and dyspnea. Physical exam reveals oxygen saturation of 87% on room air, a temperature of 39.2° C, respiratory rate of 24 breaths per minute, and right-sided rales. Her hemoglobin is 5.3 g/dL (baseline hemoglobin of 7.8 g/dL). Chest radiograph reveals a right upper lobe pneumonia, and she is diagnosed with acute chest syndrome.
What are indications and complications of acute transfusion in sickle cell anemia?
Background
Chronic hemolytic anemia is a trademark of sickle cell anemia (SCA) or hemoglobin (Hb) SS as is acute anemia during illness or vaso-occlusive crises. Blood transfusions were the first therapy used in sickle cell disease, long before the pathophysiology was understood. Transfusion of red blood cells (RBC) increases the percentage of circulating normal Hb A, thereby decreasing the percentage of abnormal, sickled cells. This increases the oxygen-carrying capacity of the patient’s RBCs, improves organ perfusion, prevents organ damage, and can be life saving. SCA patients are the largest users of the United States rare donor blood bank registry.1
Unfortunately, transfusion comes with many risks including infection, transfusion reactions, alloimmunization, iron overload, hyperviscosity, and volume overload.
As SCA is a low-prevalence disease in a minority population, very few studies have been performed. Currently, the guidance available regarding blood transfusion is primarily based on expert opinion.
What to transfuse

Leukoreduced and intensive phenotypically matched RBC are not possible in many medical centers. Previous studies have noted decreased incidence of febrile nonhemolytic anemia transfusion reactions, cytomegalovirus transmission, and human leukocyte antigen alloimmunization in leukoreduced blood transfusions, however, these studies did not include SCA patients.2
Complications from transfusion
Complications from blood transfusions include febrile nonhemolytic transfusion reaction, acute hemolytic transfusion reaction (ABO incompatibility), transfusion-associated lung injury (TRALI), transfusion-associated circulatory overload (TACO), infections, and anaphylaxis. The National Heart, Lung, and Blood Institute guidelines specifically highlight the complications of delayed hemolytic transfusion reaction, iron overload, and hyperviscosity in SCA.Approximately 30% of SCA patients have alloantibodies.2 SCA patients may also develop autoimmunization, an immune response to their own RBC, particularly if the patient has multiple autoantibodies.
Infection is a risk for all individuals receiving transfusion. Screening for hepatitis B, hepatitis C, HIV, human T-cell lymphotropic virus, syphilis, West Nile virus, Trympanosoma, and bacteria are routinely performed but not 100% conclusive. Other diseases not routinely screened for include Creutzfeldt-Jakob disease, Babesia, human herpesvirus-8, dengue fever, malaria, and newer concerns such as Zika virus. 2,3
Febrile nonhemolytic transfusion reactions present as an increase in body temperature of more than 1° C during or shortly after receiving a blood transfusion in the absence of other pyrexic stimulus. Febrile nonhemolytic transfusion reaction occurs more frequently in patients with a previous history of transfusions. The use of leukoreduced RBCs reduces the occurrence to less than 1%.2
TRALI presents with the acute onset of hypoxemia and noncardiogenic pulmonary edema within 6 hours of a blood transfusion in the absence of other etiologies. The mechanism of TRALI is caused by an inflammatory response causing injury to the alveolar capillary membrane and the development of pulmonary edema.1
TACO presents with cardiogenic pulmonary edema not from another etiology. This is usually seen after transfusion of excessive volumes of blood or after excessively rapid rates of transfusion.1
Delayed hemolytic transfusion reaction (DHTR) may be a life-threatening immune response to donor cell antigens. The reaction is identified by a drop in the patient’s hemoglobin below the pretransfusion level, reticulocytopenia, a positive direct Coombs test, and occasionally jaundice on physical exam.2 Patients may have an unexpectedly high hemoglobin S% after transfusion from the hemolysis of donor cells. The pathognomonic feature is development of a new alloantibody. DHTR occurs more often in individuals who have received recurrent transfusions and has been reported in 4%-11% of transfused SCA patients.3 Donor and native cells hemolyze intra- and extravascularly 5-20 days after receiving a transfusion.2 DHTR is likely underestimated in SCA as it may be confused for a vaso-occlusive crisis.
Iron overload from recurrent transfusions is a slow, chronic process resulting in end organ damage of the heart, liver, and pancreas. It is associated with more frequent hospitalizations and higher mortality in SCA.3 The average person has 4-5 g of iron with no process to remove the excess. One unit of packed red blood cells adds 250-300 mg of iron.2 Ferritin somewhat correlates to iron overload but is not a reliable method because it is an acute-phase reactant. Liver biopsy is the current diagnostic gold standard, however, noninvasive MRI is gaining diagnostic credibility.
Hb SS blood has up to 10 times higher viscosity than does non–sickle cell blood at the same hemoglobin level. RBC transfusion increases the already hyperviscous state of SCA resulting in slow blood flow through vessels. The slow flow through small vessels from hyperviscosity may result in additional sickling and trigger or worsen a vaso-occlusive crisis. Avascular necrosis is theorized to be a result of hyperviscosity as it occurs more commonly in sickle cell patients with higher hemoglobin. It is important not to transfuse to baseline or above a hemoglobin of 10 g/dL to avoid worsening hyperviscosity.2
When to consider transfusion
Unfortunately, there are no strong randomized controlled trials to definitively dictate when simple transfusions or exchange transfusions are indicated. Acute simple transfusions should be considered in certain circumstances including acute chest syndrome, acute stroke, aplastic anemia, preoperative transfusion, splenic sequestration plus severe anemia, acute hepatic sequestration, and severe acute intrahepatic cholestasis.2
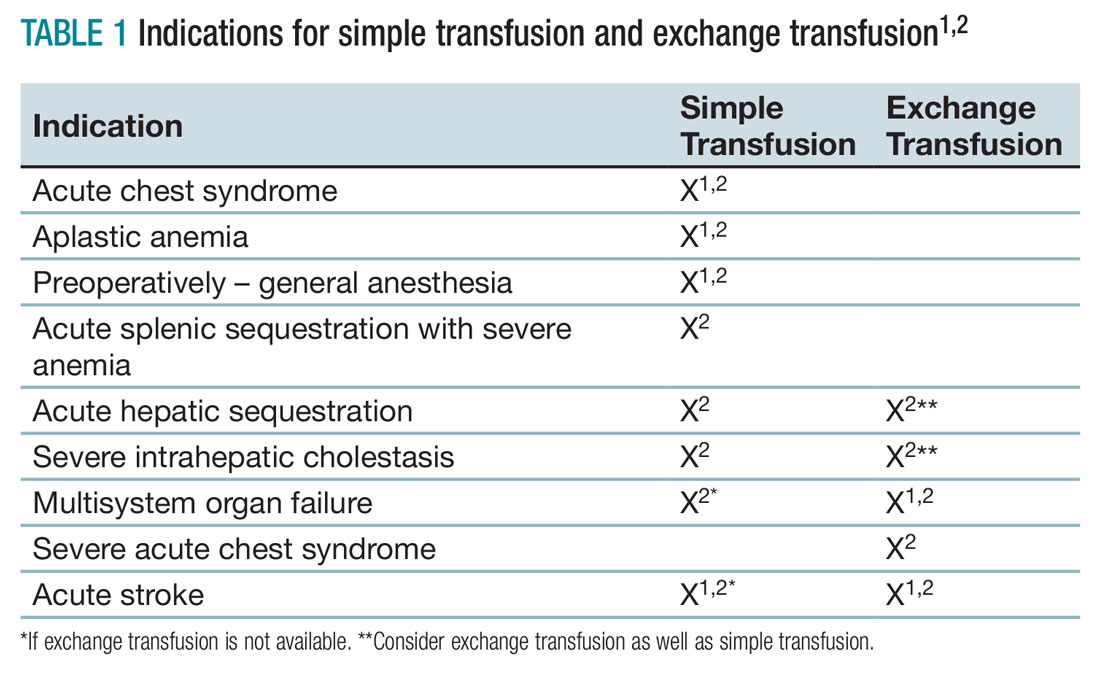
Few studies compare simple transfusion and exchange transfusion.2 The decision to use exchange transfusion over simple transfusion often is based on availability of exchange transfusion, ability of simple transfusion to decrease the percentage of hemoglobin S, and/or the patient’s current hemoglobin to avoid hyperviscosity from simple transfusion.3 Exchange transfusion should be considered for hemoglobin greater than 8-9 g/dL.2
Acute hepatic sequestration (AHS) occurs with the sequestration of RBCs in the liver and is marked by greater than 2 g/dL decrease in hemoglobin and hepatic enlargement, compared with baseline. The stretching of the hepatic capsule results in right upper quadrant pain. AHS often develops over a few hours to a few days with only mild elevation of liver function tests. AHS may be underestimated as two-thirds of SCA patients have hepatomegaly. Unless the hepatomegaly is radiographically monitored it may not be possible to determine an acute increase in liver size.2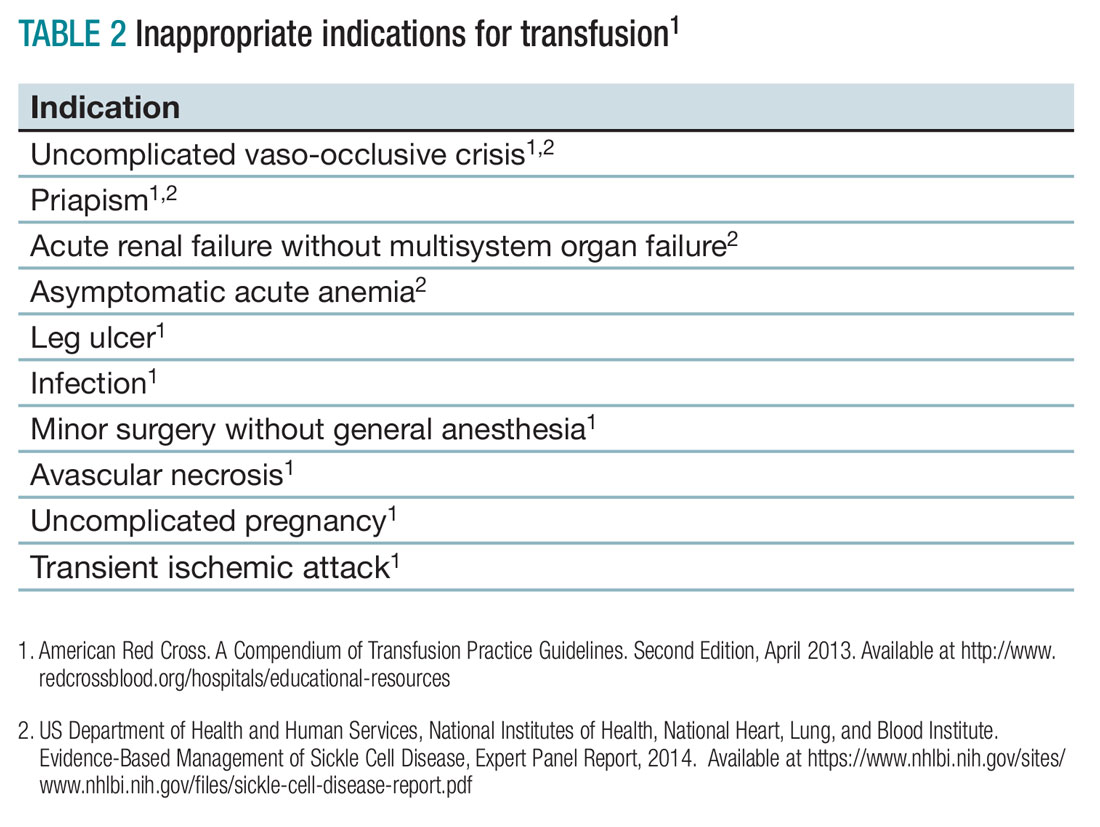
Aplastic crisis presents as a gradual onset of fatigue, shortness of breath, and sometimes syncope or fever. Physical examination may reveal tachycardia and occasionally frank heart failure. The hemoglobin is usually far below the patient’s baseline level with an inappropriate, severely low reticulocyte count. Aplastic crisis should be transfused immediately because of the markedly short life expectancy of hemoglobin S RBCs, but does not need to be transfused to baseline.2
Acute splenic sequestration presents as a decrease in hemoglobin by greater than 2 g/dL, elevated reticulocyte count and circulating nucleated red blood cells, thrombocytopenia, and sudden splenomegaly.2 The goal of transfusion is for partial correction because of the risk of hyperviscosity when the spleen releases the sequestered RBCs.
Acute chest syndrome (ACS) presents as a pneumonia radiographically consistent with a respiratory tract infection caused by cough, shortness of breath, retractions, and/or rales. ACS is the most common cause of death in SCA. ACS is usually from infection but may be because of fat embolism, intrapulmonary aggregates of sickled cells, atelectasis, or pulmonary edema.2 If ACS has a hemoglobin decrease of greater than 1g/dL, consider transfusion.1,2
Severe acute chest syndrome is distinguished by radiographic evidence of multilobe pneumonia, increased work of breathing, pleural effusions, and oxygen saturation below 95% with supplemental oxygen. Severe ACS may have a decrease in hemoglobin despite receiving transfusion. Exchange transfusion is recommended because of the high mortality in severe ACS.2
Preoperative transfusion is used to decrease the incidence of postoperative vaso-occlusive crisis, acute stroke, or ACS for patients receiving general anesthesia. The goal for transfusion hemoglobin is 10g/dL. In SCA patients with a hemoglobin greater than 9g/dL, exchange transfusion may be considered to avoid hyperviscosity.1,2
Multisystem organ failure (MSOF) is severe and life-threatening lung, liver, and/or kidney failure. MSOF may occur after several days of hospitalization. It is often unanticipated and swift, frequently presenting with fever, a rapid increase in anemia, thrombocytopenia, and altered mental status. Lung failure often presents as ACS. Liver failure is marked by hyperbilirubinemia, elevated transaminases, and coagulopathy. Kidney failure is marked by elevated creatinine, with or without change in urine output and hyperkalemia. Rapid treatment with transfusion or exchange transfusion reduces mortality.
The incidence of acute ischemic stroke in SCA decreases with prophylactic transfusion of patients with elevated transcranial Dopplers. Acute stroke is usually secondary to stenosis or an occlusion of the internal carotid or middle cerebral artery. Acute hemorrhagic stroke may present as severe headache and loss of consciousness. Acute stroke should be confirmed radiographically, then exchange transfusion instituted rapidly.2
When not to transfuse
- Do not transfuse for simple vaso-occlusive crisis in the absence of symptoms attributable to acute anemia.1-3
- Do not transfuse for priapism.2
- Do not transfuse for acute renal failure unless there is MSOF.2
Back to the case
The patient was admitted for vaso-occlusive crisis and was started on patient-controlled analgesia with hydromorphone and IV fluids. Azithromycin and ceftriaxone were initiated empirically for community-acquired pneumonia. She was given one unit of phenotypically matched, leukoreduced RBCs for acute chest syndrome. Her hemoglobin increased to 6.1 g/dL. Her fever resolved on day 2, and her dyspnea improved on day 3 of hospitalization. She was weaned off of her patient-controlled analgesia on day 4 and discharged home on day 5 with moxifloxacin to complete 7 days of antibiotics.
Bottom line
Acute simple transfusions and exchange transfusions are indicated for multiple serious and life-threatening complications in SCA. However, transfusion has many serious and life-threatening potential adverse effects. It is essential to conduct a thorough risk-benefit analysis for each individual SCA patient. Whenever possible, intensive phenotypically matched and leukoreduced RBCs should be used. TH
References
1. American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
2. US Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. Evidence-Based Management of Sickle Cell Disease, Expert Panel Report, 2014.
3. Smith-Whitely, K and Thompson, AA. Indications and complications of transfusions in sickle cell disease. Pediatr Blood Cancer. 2012;59(2):358-64.
- SCA patients are at risk for serious transfusion complications including iron overload, delayed hemolytic transfusion reaction, and hyperviscosity in addition to the usual transfusion risks.
- Do not transfuse an uncomplicated vaso-occlusive crisis without symptomatic anemia.1-3
- Repeated transfusions create alloimmunization in SCA patients increasing risk for life-threatening transfusion reactions and difficulty locating phenotypically matched RBCs.
- Transfusion should be considered in SCA patients experiencing acute chest syndrome, aplastic anemia, splenic sequestration with acute anemia, acute hepatic sequestration, and severe intrahepatic cholestasis.1,2
- If available, exchange transfusion should be considered for SCA patients experiencing multisystem organ failure, acute stroke, and severe acute chest syndrome.1,2
- American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
Case
A 19-year-old female with a history of sickle cell anemia and hemoglobin SS, presents with a 2-day history of worsening lower back pain and dyspnea. Physical exam reveals oxygen saturation of 87% on room air, a temperature of 39.2° C, respiratory rate of 24 breaths per minute, and right-sided rales. Her hemoglobin is 5.3 g/dL (baseline hemoglobin of 7.8 g/dL). Chest radiograph reveals a right upper lobe pneumonia, and she is diagnosed with acute chest syndrome.
What are indications and complications of acute transfusion in sickle cell anemia?
Background
Chronic hemolytic anemia is a trademark of sickle cell anemia (SCA) or hemoglobin (Hb) SS as is acute anemia during illness or vaso-occlusive crises. Blood transfusions were the first therapy used in sickle cell disease, long before the pathophysiology was understood. Transfusion of red blood cells (RBC) increases the percentage of circulating normal Hb A, thereby decreasing the percentage of abnormal, sickled cells. This increases the oxygen-carrying capacity of the patient’s RBCs, improves organ perfusion, prevents organ damage, and can be life saving. SCA patients are the largest users of the United States rare donor blood bank registry.1
Unfortunately, transfusion comes with many risks including infection, transfusion reactions, alloimmunization, iron overload, hyperviscosity, and volume overload.
As SCA is a low-prevalence disease in a minority population, very few studies have been performed. Currently, the guidance available regarding blood transfusion is primarily based on expert opinion.
What to transfuse
Leukoreduced and intensive phenotypically matched RBC are not possible in many medical centers. Previous studies have noted decreased incidence of febrile nonhemolytic anemia transfusion reactions, cytomegalovirus transmission, and human leukocyte antigen alloimmunization in leukoreduced blood transfusions, however, these studies did not include SCA patients.2
Complications from transfusion
Complications from blood transfusions include febrile nonhemolytic transfusion reaction, acute hemolytic transfusion reaction (ABO incompatibility), transfusion-associated lung injury (TRALI), transfusion-associated circulatory overload (TACO), infections, and anaphylaxis. The National Heart, Lung, and Blood Institute guidelines specifically highlight the complications of delayed hemolytic transfusion reaction, iron overload, and hyperviscosity in SCA.Approximately 30% of SCA patients have alloantibodies.2 SCA patients may also develop autoimmunization, an immune response to their own RBC, particularly if the patient has multiple autoantibodies.
Infection is a risk for all individuals receiving transfusion. Screening for hepatitis B, hepatitis C, HIV, human T-cell lymphotropic virus, syphilis, West Nile virus, Trympanosoma, and bacteria are routinely performed but not 100% conclusive. Other diseases not routinely screened for include Creutzfeldt-Jakob disease, Babesia, human herpesvirus-8, dengue fever, malaria, and newer concerns such as Zika virus. 2,3
Febrile nonhemolytic transfusion reactions present as an increase in body temperature of more than 1° C during or shortly after receiving a blood transfusion in the absence of other pyrexic stimulus. Febrile nonhemolytic transfusion reaction occurs more frequently in patients with a previous history of transfusions. The use of leukoreduced RBCs reduces the occurrence to less than 1%.2
TRALI presents with the acute onset of hypoxemia and noncardiogenic pulmonary edema within 6 hours of a blood transfusion in the absence of other etiologies. The mechanism of TRALI is caused by an inflammatory response causing injury to the alveolar capillary membrane and the development of pulmonary edema.1
TACO presents with cardiogenic pulmonary edema not from another etiology. This is usually seen after transfusion of excessive volumes of blood or after excessively rapid rates of transfusion.1
Delayed hemolytic transfusion reaction (DHTR) may be a life-threatening immune response to donor cell antigens. The reaction is identified by a drop in the patient’s hemoglobin below the pretransfusion level, reticulocytopenia, a positive direct Coombs test, and occasionally jaundice on physical exam.2 Patients may have an unexpectedly high hemoglobin S% after transfusion from the hemolysis of donor cells. The pathognomonic feature is development of a new alloantibody. DHTR occurs more often in individuals who have received recurrent transfusions and has been reported in 4%-11% of transfused SCA patients.3 Donor and native cells hemolyze intra- and extravascularly 5-20 days after receiving a transfusion.2 DHTR is likely underestimated in SCA as it may be confused for a vaso-occlusive crisis.
Iron overload from recurrent transfusions is a slow, chronic process resulting in end organ damage of the heart, liver, and pancreas. It is associated with more frequent hospitalizations and higher mortality in SCA.3 The average person has 4-5 g of iron with no process to remove the excess. One unit of packed red blood cells adds 250-300 mg of iron.2 Ferritin somewhat correlates to iron overload but is not a reliable method because it is an acute-phase reactant. Liver biopsy is the current diagnostic gold standard, however, noninvasive MRI is gaining diagnostic credibility.
Hb SS blood has up to 10 times higher viscosity than does non–sickle cell blood at the same hemoglobin level. RBC transfusion increases the already hyperviscous state of SCA resulting in slow blood flow through vessels. The slow flow through small vessels from hyperviscosity may result in additional sickling and trigger or worsen a vaso-occlusive crisis. Avascular necrosis is theorized to be a result of hyperviscosity as it occurs more commonly in sickle cell patients with higher hemoglobin. It is important not to transfuse to baseline or above a hemoglobin of 10 g/dL to avoid worsening hyperviscosity.2
When to consider transfusion
Unfortunately, there are no strong randomized controlled trials to definitively dictate when simple transfusions or exchange transfusions are indicated. Acute simple transfusions should be considered in certain circumstances including acute chest syndrome, acute stroke, aplastic anemia, preoperative transfusion, splenic sequestration plus severe anemia, acute hepatic sequestration, and severe acute intrahepatic cholestasis.2
Few studies compare simple transfusion and exchange transfusion.2 The decision to use exchange transfusion over simple transfusion often is based on availability of exchange transfusion, ability of simple transfusion to decrease the percentage of hemoglobin S, and/or the patient’s current hemoglobin to avoid hyperviscosity from simple transfusion.3 Exchange transfusion should be considered for hemoglobin greater than 8-9 g/dL.2
Acute hepatic sequestration (AHS) occurs with the sequestration of RBCs in the liver and is marked by greater than 2 g/dL decrease in hemoglobin and hepatic enlargement, compared with baseline. The stretching of the hepatic capsule results in right upper quadrant pain. AHS often develops over a few hours to a few days with only mild elevation of liver function tests. AHS may be underestimated as two-thirds of SCA patients have hepatomegaly. Unless the hepatomegaly is radiographically monitored it may not be possible to determine an acute increase in liver size.2
Aplastic crisis presents as a gradual onset of fatigue, shortness of breath, and sometimes syncope or fever. Physical examination may reveal tachycardia and occasionally frank heart failure. The hemoglobin is usually far below the patient’s baseline level with an inappropriate, severely low reticulocyte count. Aplastic crisis should be transfused immediately because of the markedly short life expectancy of hemoglobin S RBCs, but does not need to be transfused to baseline.2
Acute splenic sequestration presents as a decrease in hemoglobin by greater than 2 g/dL, elevated reticulocyte count and circulating nucleated red blood cells, thrombocytopenia, and sudden splenomegaly.2 The goal of transfusion is for partial correction because of the risk of hyperviscosity when the spleen releases the sequestered RBCs.
Acute chest syndrome (ACS) presents as a pneumonia radiographically consistent with a respiratory tract infection caused by cough, shortness of breath, retractions, and/or rales. ACS is the most common cause of death in SCA. ACS is usually from infection but may be because of fat embolism, intrapulmonary aggregates of sickled cells, atelectasis, or pulmonary edema.2 If ACS has a hemoglobin decrease of greater than 1g/dL, consider transfusion.1,2
Severe acute chest syndrome is distinguished by radiographic evidence of multilobe pneumonia, increased work of breathing, pleural effusions, and oxygen saturation below 95% with supplemental oxygen. Severe ACS may have a decrease in hemoglobin despite receiving transfusion. Exchange transfusion is recommended because of the high mortality in severe ACS.2
Preoperative transfusion is used to decrease the incidence of postoperative vaso-occlusive crisis, acute stroke, or ACS for patients receiving general anesthesia. The goal for transfusion hemoglobin is 10g/dL. In SCA patients with a hemoglobin greater than 9g/dL, exchange transfusion may be considered to avoid hyperviscosity.1,2
Multisystem organ failure (MSOF) is severe and life-threatening lung, liver, and/or kidney failure. MSOF may occur after several days of hospitalization. It is often unanticipated and swift, frequently presenting with fever, a rapid increase in anemia, thrombocytopenia, and altered mental status. Lung failure often presents as ACS. Liver failure is marked by hyperbilirubinemia, elevated transaminases, and coagulopathy. Kidney failure is marked by elevated creatinine, with or without change in urine output and hyperkalemia. Rapid treatment with transfusion or exchange transfusion reduces mortality.
The incidence of acute ischemic stroke in SCA decreases with prophylactic transfusion of patients with elevated transcranial Dopplers. Acute stroke is usually secondary to stenosis or an occlusion of the internal carotid or middle cerebral artery. Acute hemorrhagic stroke may present as severe headache and loss of consciousness. Acute stroke should be confirmed radiographically, then exchange transfusion instituted rapidly.2
When not to transfuse
- Do not transfuse for simple vaso-occlusive crisis in the absence of symptoms attributable to acute anemia.1-3
- Do not transfuse for priapism.2
- Do not transfuse for acute renal failure unless there is MSOF.2
Back to the case
The patient was admitted for vaso-occlusive crisis and was started on patient-controlled analgesia with hydromorphone and IV fluids. Azithromycin and ceftriaxone were initiated empirically for community-acquired pneumonia. She was given one unit of phenotypically matched, leukoreduced RBCs for acute chest syndrome. Her hemoglobin increased to 6.1 g/dL. Her fever resolved on day 2, and her dyspnea improved on day 3 of hospitalization. She was weaned off of her patient-controlled analgesia on day 4 and discharged home on day 5 with moxifloxacin to complete 7 days of antibiotics.
Bottom line
Acute simple transfusions and exchange transfusions are indicated for multiple serious and life-threatening complications in SCA. However, transfusion has many serious and life-threatening potential adverse effects. It is essential to conduct a thorough risk-benefit analysis for each individual SCA patient. Whenever possible, intensive phenotypically matched and leukoreduced RBCs should be used. TH
References
1. American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
2. US Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. Evidence-Based Management of Sickle Cell Disease, Expert Panel Report, 2014.
3. Smith-Whitely, K and Thompson, AA. Indications and complications of transfusions in sickle cell disease. Pediatr Blood Cancer. 2012;59(2):358-64.
- SCA patients are at risk for serious transfusion complications including iron overload, delayed hemolytic transfusion reaction, and hyperviscosity in addition to the usual transfusion risks.
- Do not transfuse an uncomplicated vaso-occlusive crisis without symptomatic anemia.1-3
- Repeated transfusions create alloimmunization in SCA patients increasing risk for life-threatening transfusion reactions and difficulty locating phenotypically matched RBCs.
- Transfusion should be considered in SCA patients experiencing acute chest syndrome, aplastic anemia, splenic sequestration with acute anemia, acute hepatic sequestration, and severe intrahepatic cholestasis.1,2
- If available, exchange transfusion should be considered for SCA patients experiencing multisystem organ failure, acute stroke, and severe acute chest syndrome.1,2
- American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
Case
A 19-year-old female with a history of sickle cell anemia and hemoglobin SS, presents with a 2-day history of worsening lower back pain and dyspnea. Physical exam reveals oxygen saturation of 87% on room air, a temperature of 39.2° C, respiratory rate of 24 breaths per minute, and right-sided rales. Her hemoglobin is 5.3 g/dL (baseline hemoglobin of 7.8 g/dL). Chest radiograph reveals a right upper lobe pneumonia, and she is diagnosed with acute chest syndrome.
What are indications and complications of acute transfusion in sickle cell anemia?
Background
Chronic hemolytic anemia is a trademark of sickle cell anemia (SCA) or hemoglobin (Hb) SS as is acute anemia during illness or vaso-occlusive crises. Blood transfusions were the first therapy used in sickle cell disease, long before the pathophysiology was understood. Transfusion of red blood cells (RBC) increases the percentage of circulating normal Hb A, thereby decreasing the percentage of abnormal, sickled cells. This increases the oxygen-carrying capacity of the patient’s RBCs, improves organ perfusion, prevents organ damage, and can be life saving. SCA patients are the largest users of the United States rare donor blood bank registry.1
Unfortunately, transfusion comes with many risks including infection, transfusion reactions, alloimmunization, iron overload, hyperviscosity, and volume overload.
As SCA is a low-prevalence disease in a minority population, very few studies have been performed. Currently, the guidance available regarding blood transfusion is primarily based on expert opinion.
What to transfuse
Leukoreduced and intensive phenotypically matched RBC are not possible in many medical centers. Previous studies have noted decreased incidence of febrile nonhemolytic anemia transfusion reactions, cytomegalovirus transmission, and human leukocyte antigen alloimmunization in leukoreduced blood transfusions, however, these studies did not include SCA patients.2
Complications from transfusion
Complications from blood transfusions include febrile nonhemolytic transfusion reaction, acute hemolytic transfusion reaction (ABO incompatibility), transfusion-associated lung injury (TRALI), transfusion-associated circulatory overload (TACO), infections, and anaphylaxis. The National Heart, Lung, and Blood Institute guidelines specifically highlight the complications of delayed hemolytic transfusion reaction, iron overload, and hyperviscosity in SCA.Approximately 30% of SCA patients have alloantibodies.2 SCA patients may also develop autoimmunization, an immune response to their own RBC, particularly if the patient has multiple autoantibodies.
Infection is a risk for all individuals receiving transfusion. Screening for hepatitis B, hepatitis C, HIV, human T-cell lymphotropic virus, syphilis, West Nile virus, Trympanosoma, and bacteria are routinely performed but not 100% conclusive. Other diseases not routinely screened for include Creutzfeldt-Jakob disease, Babesia, human herpesvirus-8, dengue fever, malaria, and newer concerns such as Zika virus. 2,3
Febrile nonhemolytic transfusion reactions present as an increase in body temperature of more than 1° C during or shortly after receiving a blood transfusion in the absence of other pyrexic stimulus. Febrile nonhemolytic transfusion reaction occurs more frequently in patients with a previous history of transfusions. The use of leukoreduced RBCs reduces the occurrence to less than 1%.2
TRALI presents with the acute onset of hypoxemia and noncardiogenic pulmonary edema within 6 hours of a blood transfusion in the absence of other etiologies. The mechanism of TRALI is caused by an inflammatory response causing injury to the alveolar capillary membrane and the development of pulmonary edema.1
TACO presents with cardiogenic pulmonary edema not from another etiology. This is usually seen after transfusion of excessive volumes of blood or after excessively rapid rates of transfusion.1
Delayed hemolytic transfusion reaction (DHTR) may be a life-threatening immune response to donor cell antigens. The reaction is identified by a drop in the patient’s hemoglobin below the pretransfusion level, reticulocytopenia, a positive direct Coombs test, and occasionally jaundice on physical exam.2 Patients may have an unexpectedly high hemoglobin S% after transfusion from the hemolysis of donor cells. The pathognomonic feature is development of a new alloantibody. DHTR occurs more often in individuals who have received recurrent transfusions and has been reported in 4%-11% of transfused SCA patients.3 Donor and native cells hemolyze intra- and extravascularly 5-20 days after receiving a transfusion.2 DHTR is likely underestimated in SCA as it may be confused for a vaso-occlusive crisis.
Iron overload from recurrent transfusions is a slow, chronic process resulting in end organ damage of the heart, liver, and pancreas. It is associated with more frequent hospitalizations and higher mortality in SCA.3 The average person has 4-5 g of iron with no process to remove the excess. One unit of packed red blood cells adds 250-300 mg of iron.2 Ferritin somewhat correlates to iron overload but is not a reliable method because it is an acute-phase reactant. Liver biopsy is the current diagnostic gold standard, however, noninvasive MRI is gaining diagnostic credibility.
Hb SS blood has up to 10 times higher viscosity than does non–sickle cell blood at the same hemoglobin level. RBC transfusion increases the already hyperviscous state of SCA resulting in slow blood flow through vessels. The slow flow through small vessels from hyperviscosity may result in additional sickling and trigger or worsen a vaso-occlusive crisis. Avascular necrosis is theorized to be a result of hyperviscosity as it occurs more commonly in sickle cell patients with higher hemoglobin. It is important not to transfuse to baseline or above a hemoglobin of 10 g/dL to avoid worsening hyperviscosity.2
When to consider transfusion
Unfortunately, there are no strong randomized controlled trials to definitively dictate when simple transfusions or exchange transfusions are indicated. Acute simple transfusions should be considered in certain circumstances including acute chest syndrome, acute stroke, aplastic anemia, preoperative transfusion, splenic sequestration plus severe anemia, acute hepatic sequestration, and severe acute intrahepatic cholestasis.2
Few studies compare simple transfusion and exchange transfusion.2 The decision to use exchange transfusion over simple transfusion often is based on availability of exchange transfusion, ability of simple transfusion to decrease the percentage of hemoglobin S, and/or the patient’s current hemoglobin to avoid hyperviscosity from simple transfusion.3 Exchange transfusion should be considered for hemoglobin greater than 8-9 g/dL.2
Acute hepatic sequestration (AHS) occurs with the sequestration of RBCs in the liver and is marked by greater than 2 g/dL decrease in hemoglobin and hepatic enlargement, compared with baseline. The stretching of the hepatic capsule results in right upper quadrant pain. AHS often develops over a few hours to a few days with only mild elevation of liver function tests. AHS may be underestimated as two-thirds of SCA patients have hepatomegaly. Unless the hepatomegaly is radiographically monitored it may not be possible to determine an acute increase in liver size.2
Aplastic crisis presents as a gradual onset of fatigue, shortness of breath, and sometimes syncope or fever. Physical examination may reveal tachycardia and occasionally frank heart failure. The hemoglobin is usually far below the patient’s baseline level with an inappropriate, severely low reticulocyte count. Aplastic crisis should be transfused immediately because of the markedly short life expectancy of hemoglobin S RBCs, but does not need to be transfused to baseline.2
Acute splenic sequestration presents as a decrease in hemoglobin by greater than 2 g/dL, elevated reticulocyte count and circulating nucleated red blood cells, thrombocytopenia, and sudden splenomegaly.2 The goal of transfusion is for partial correction because of the risk of hyperviscosity when the spleen releases the sequestered RBCs.
Acute chest syndrome (ACS) presents as a pneumonia radiographically consistent with a respiratory tract infection caused by cough, shortness of breath, retractions, and/or rales. ACS is the most common cause of death in SCA. ACS is usually from infection but may be because of fat embolism, intrapulmonary aggregates of sickled cells, atelectasis, or pulmonary edema.2 If ACS has a hemoglobin decrease of greater than 1g/dL, consider transfusion.1,2
Severe acute chest syndrome is distinguished by radiographic evidence of multilobe pneumonia, increased work of breathing, pleural effusions, and oxygen saturation below 95% with supplemental oxygen. Severe ACS may have a decrease in hemoglobin despite receiving transfusion. Exchange transfusion is recommended because of the high mortality in severe ACS.2
Preoperative transfusion is used to decrease the incidence of postoperative vaso-occlusive crisis, acute stroke, or ACS for patients receiving general anesthesia. The goal for transfusion hemoglobin is 10g/dL. In SCA patients with a hemoglobin greater than 9g/dL, exchange transfusion may be considered to avoid hyperviscosity.1,2
Multisystem organ failure (MSOF) is severe and life-threatening lung, liver, and/or kidney failure. MSOF may occur after several days of hospitalization. It is often unanticipated and swift, frequently presenting with fever, a rapid increase in anemia, thrombocytopenia, and altered mental status. Lung failure often presents as ACS. Liver failure is marked by hyperbilirubinemia, elevated transaminases, and coagulopathy. Kidney failure is marked by elevated creatinine, with or without change in urine output and hyperkalemia. Rapid treatment with transfusion or exchange transfusion reduces mortality.
The incidence of acute ischemic stroke in SCA decreases with prophylactic transfusion of patients with elevated transcranial Dopplers. Acute stroke is usually secondary to stenosis or an occlusion of the internal carotid or middle cerebral artery. Acute hemorrhagic stroke may present as severe headache and loss of consciousness. Acute stroke should be confirmed radiographically, then exchange transfusion instituted rapidly.2
When not to transfuse
- Do not transfuse for simple vaso-occlusive crisis in the absence of symptoms attributable to acute anemia.1-3
- Do not transfuse for priapism.2
- Do not transfuse for acute renal failure unless there is MSOF.2
Back to the case
The patient was admitted for vaso-occlusive crisis and was started on patient-controlled analgesia with hydromorphone and IV fluids. Azithromycin and ceftriaxone were initiated empirically for community-acquired pneumonia. She was given one unit of phenotypically matched, leukoreduced RBCs for acute chest syndrome. Her hemoglobin increased to 6.1 g/dL. Her fever resolved on day 2, and her dyspnea improved on day 3 of hospitalization. She was weaned off of her patient-controlled analgesia on day 4 and discharged home on day 5 with moxifloxacin to complete 7 days of antibiotics.
Bottom line
Acute simple transfusions and exchange transfusions are indicated for multiple serious and life-threatening complications in SCA. However, transfusion has many serious and life-threatening potential adverse effects. It is essential to conduct a thorough risk-benefit analysis for each individual SCA patient. Whenever possible, intensive phenotypically matched and leukoreduced RBCs should be used. TH
References
1. American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
2. US Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. Evidence-Based Management of Sickle Cell Disease, Expert Panel Report, 2014.
3. Smith-Whitely, K and Thompson, AA. Indications and complications of transfusions in sickle cell disease. Pediatr Blood Cancer. 2012;59(2):358-64.
- SCA patients are at risk for serious transfusion complications including iron overload, delayed hemolytic transfusion reaction, and hyperviscosity in addition to the usual transfusion risks.
- Do not transfuse an uncomplicated vaso-occlusive crisis without symptomatic anemia.1-3
- Repeated transfusions create alloimmunization in SCA patients increasing risk for life-threatening transfusion reactions and difficulty locating phenotypically matched RBCs.
- Transfusion should be considered in SCA patients experiencing acute chest syndrome, aplastic anemia, splenic sequestration with acute anemia, acute hepatic sequestration, and severe intrahepatic cholestasis.1,2
- If available, exchange transfusion should be considered for SCA patients experiencing multisystem organ failure, acute stroke, and severe acute chest syndrome.1,2
- American Red Cross. A Compendium of Transfusion Practice Guidelines. Second Edition, April 2013.
EBUS scope, EUS-FNA similarly effective
When assessing a patient for lung cancer, a procedure involving the insertion of an EBUS scope in the esophagus – EUS-B-FNA – can achieve similarly accurate results as endoscopic ultrasound guided–fine-needle aspiration (EUS-FNA), according to a new study.
This finding could lead patients to choose EUS-B-FNA over EUS-FNA – the standard of care for analyzing potential metastasis of the left adrenal glands (LAGs) – resulting in both time and cost savings for patients.

“A recent report showed that LAG visualization using the EBUS scope was possible in 85% of patients,” according to the authors of this study, including Prof. Jouke T. Annema, MD of the University of Amsterdam. Prior to this new research, it was unknown to what extent a single EBUS scope adequately assess and sample the LAGs and how its performance related to the use of a conventional endoscopic ultrasound–guided scope (Lung Cancer. 2017. doi: org/10.1016/j.lungcan.2017.02.011).
Dr. Annema and his coauthors recruited patients from four centers – three in the Netherlands, one in Poland – and followed them prospectively. Patients with “(suspected) lung cancer [who] had an indication for both mediastinal lymph node and LAG sampling” were recruited for the study. The researchers followed 44 patients through final diagnosis to determine if they ultimately had lung cancer.
Subjects first received complete mediastinal and hilar staging of lung cancer and any present tumors via an EBUS and EUS-B procedure. Following an EBUS examination of the mediastinum, the EBUS scope was retracted from the trachea and positioned into the esophagus for an examination of the mediastinal nodes. Then, the EBUS scope was advanced into the stomach for identification of the LAG. Afterward, the routine EUS-FNA was performed. LAG analysis across both methods involved visualizing the LAG and collecting an adequate tissue sample for testing.
“In short, in order to locate the LAG, a structured three step approach was used according to the EUS assessment tool (EUS-AT): identification of the liver, abdominal aorta, coeliac trunk, left kidney, and LAG,” the authors noted. “By turning the EBUS scope clockwise from the liver, the abdominal aorta and coeliac trun[k] are identified. By subsequently turning the EBUS scope gently in caudal direction, the left kidney and LAG are identified.”
Endoscopists then evaluated both procedures in each subject according to feasibility and practicability to determine if the findings of the experimental procedure were usable. Finally, a cytologic exam was conducted, using Giemsa or Papanicolaou staining to determine if any present cancer had metastasized, and a final diagnosis was made.
LAG analysis had a success rate of 89% (39/44; 95% confidence interval, 76-95%) for EUS-B-FNA, compared with 93% (41/44; 95% CI, 82-98%) for EUS-FNA. Similarly, when looking at the rate of sensitivity for LAG metastases, EUS-B had a rate of sensitivity for LAG metastases of at least 87% (95% CI, 65-97%), while EUS-FNA was found to be at least 83% (95% CI, 62-95%. Endoscopists were equally satisfied with both procedures in the “majority” of cases in this study.
“In [five] cases (11%), the EUS-B-FNA procedure was unsuccessful, due to the inability to make good contact of the ultrasound transducer and the stomach wall,” the authors explained. “The conventional EUS scope is more stable as a result of the increased tube diameter. Another advantage of the conventional echo-endoscope is its wider scanning angle. ... The conventional EUS scope is also longer than the EBUS scope, [but that] does not seem to be the limiting factor.”
No funding source was disclosed for this study. The authors reported no relevant financial disclosures.
When assessing a patient for lung cancer, a procedure involving the insertion of an EBUS scope in the esophagus – EUS-B-FNA – can achieve similarly accurate results as endoscopic ultrasound guided–fine-needle aspiration (EUS-FNA), according to a new study.
This finding could lead patients to choose EUS-B-FNA over EUS-FNA – the standard of care for analyzing potential metastasis of the left adrenal glands (LAGs) – resulting in both time and cost savings for patients.
“A recent report showed that LAG visualization using the EBUS scope was possible in 85% of patients,” according to the authors of this study, including Prof. Jouke T. Annema, MD of the University of Amsterdam. Prior to this new research, it was unknown to what extent a single EBUS scope adequately assess and sample the LAGs and how its performance related to the use of a conventional endoscopic ultrasound–guided scope (Lung Cancer. 2017. doi: org/10.1016/j.lungcan.2017.02.011).
Dr. Annema and his coauthors recruited patients from four centers – three in the Netherlands, one in Poland – and followed them prospectively. Patients with “(suspected) lung cancer [who] had an indication for both mediastinal lymph node and LAG sampling” were recruited for the study. The researchers followed 44 patients through final diagnosis to determine if they ultimately had lung cancer.
Subjects first received complete mediastinal and hilar staging of lung cancer and any present tumors via an EBUS and EUS-B procedure. Following an EBUS examination of the mediastinum, the EBUS scope was retracted from the trachea and positioned into the esophagus for an examination of the mediastinal nodes. Then, the EBUS scope was advanced into the stomach for identification of the LAG. Afterward, the routine EUS-FNA was performed. LAG analysis across both methods involved visualizing the LAG and collecting an adequate tissue sample for testing.
“In short, in order to locate the LAG, a structured three step approach was used according to the EUS assessment tool (EUS-AT): identification of the liver, abdominal aorta, coeliac trunk, left kidney, and LAG,” the authors noted. “By turning the EBUS scope clockwise from the liver, the abdominal aorta and coeliac trun[k] are identified. By subsequently turning the EBUS scope gently in caudal direction, the left kidney and LAG are identified.”
Endoscopists then evaluated both procedures in each subject according to feasibility and practicability to determine if the findings of the experimental procedure were usable. Finally, a cytologic exam was conducted, using Giemsa or Papanicolaou staining to determine if any present cancer had metastasized, and a final diagnosis was made.
LAG analysis had a success rate of 89% (39/44; 95% confidence interval, 76-95%) for EUS-B-FNA, compared with 93% (41/44; 95% CI, 82-98%) for EUS-FNA. Similarly, when looking at the rate of sensitivity for LAG metastases, EUS-B had a rate of sensitivity for LAG metastases of at least 87% (95% CI, 65-97%), while EUS-FNA was found to be at least 83% (95% CI, 62-95%. Endoscopists were equally satisfied with both procedures in the “majority” of cases in this study.
“In [five] cases (11%), the EUS-B-FNA procedure was unsuccessful, due to the inability to make good contact of the ultrasound transducer and the stomach wall,” the authors explained. “The conventional EUS scope is more stable as a result of the increased tube diameter. Another advantage of the conventional echo-endoscope is its wider scanning angle. ... The conventional EUS scope is also longer than the EBUS scope, [but that] does not seem to be the limiting factor.”
No funding source was disclosed for this study. The authors reported no relevant financial disclosures.
When assessing a patient for lung cancer, a procedure involving the insertion of an EBUS scope in the esophagus – EUS-B-FNA – can achieve similarly accurate results as endoscopic ultrasound guided–fine-needle aspiration (EUS-FNA), according to a new study.
This finding could lead patients to choose EUS-B-FNA over EUS-FNA – the standard of care for analyzing potential metastasis of the left adrenal glands (LAGs) – resulting in both time and cost savings for patients.
“A recent report showed that LAG visualization using the EBUS scope was possible in 85% of patients,” according to the authors of this study, including Prof. Jouke T. Annema, MD of the University of Amsterdam. Prior to this new research, it was unknown to what extent a single EBUS scope adequately assess and sample the LAGs and how its performance related to the use of a conventional endoscopic ultrasound–guided scope (Lung Cancer. 2017. doi: org/10.1016/j.lungcan.2017.02.011).
Dr. Annema and his coauthors recruited patients from four centers – three in the Netherlands, one in Poland – and followed them prospectively. Patients with “(suspected) lung cancer [who] had an indication for both mediastinal lymph node and LAG sampling” were recruited for the study. The researchers followed 44 patients through final diagnosis to determine if they ultimately had lung cancer.
Subjects first received complete mediastinal and hilar staging of lung cancer and any present tumors via an EBUS and EUS-B procedure. Following an EBUS examination of the mediastinum, the EBUS scope was retracted from the trachea and positioned into the esophagus for an examination of the mediastinal nodes. Then, the EBUS scope was advanced into the stomach for identification of the LAG. Afterward, the routine EUS-FNA was performed. LAG analysis across both methods involved visualizing the LAG and collecting an adequate tissue sample for testing.
“In short, in order to locate the LAG, a structured three step approach was used according to the EUS assessment tool (EUS-AT): identification of the liver, abdominal aorta, coeliac trunk, left kidney, and LAG,” the authors noted. “By turning the EBUS scope clockwise from the liver, the abdominal aorta and coeliac trun[k] are identified. By subsequently turning the EBUS scope gently in caudal direction, the left kidney and LAG are identified.”
Endoscopists then evaluated both procedures in each subject according to feasibility and practicability to determine if the findings of the experimental procedure were usable. Finally, a cytologic exam was conducted, using Giemsa or Papanicolaou staining to determine if any present cancer had metastasized, and a final diagnosis was made.
LAG analysis had a success rate of 89% (39/44; 95% confidence interval, 76-95%) for EUS-B-FNA, compared with 93% (41/44; 95% CI, 82-98%) for EUS-FNA. Similarly, when looking at the rate of sensitivity for LAG metastases, EUS-B had a rate of sensitivity for LAG metastases of at least 87% (95% CI, 65-97%), while EUS-FNA was found to be at least 83% (95% CI, 62-95%. Endoscopists were equally satisfied with both procedures in the “majority” of cases in this study.
“In [five] cases (11%), the EUS-B-FNA procedure was unsuccessful, due to the inability to make good contact of the ultrasound transducer and the stomach wall,” the authors explained. “The conventional EUS scope is more stable as a result of the increased tube diameter. Another advantage of the conventional echo-endoscope is its wider scanning angle. ... The conventional EUS scope is also longer than the EBUS scope, [but that] does not seem to be the limiting factor.”
No funding source was disclosed for this study. The authors reported no relevant financial disclosures.
FROM LUNG CANCER
Key clinical point:
Major finding: EUS-B-FNA had a success rate of 89%, versus 93% for EUS-FNA, while sensitivity for LAG metastases were 87% and 83%, respectively.
Data source: Multicenter, prospective study of 44 consecutive suspected lung cancer patients.
Disclosures: No funding source disclosed. Authors reported no relevant financial disclosures.
Antiviral medication successful for treating HCV in hepatocellular carcinoma
Direct-acting antiviral (DAA) medication was successful in treating hepatitis C in 74.5% of patients with hepatocellular carcinoma, and 93.4% of patients with HCC who underwent liver transplants, according to a study funded by Veterans Affairs.
In order to study the effectiveness of DAAs in this setting, Lauren A. Beste, MD, and her colleagues studied a cohort of 17,487 veterans; 624 patients reported having HCC, including 142 with HCC and liver transplantation (J Hepatol. 2017. doi. org/10.1016/j.jhep.2017.02.027).
Effects of the DAAs were also studied based on the genotype of patients’ HCV. According to analysis, patients with the genotype 1 HCV virus were most susceptible to the medication, with sustained virologic response (SVR) rates calculated at 79.1% for patients with HCC, 96.4% for HCC and transplant, and 93.1% for non-HCC.
For patients with genotype 2 virus, the SVR rate was 68.9% for those with HCC, and 86.5% for patients without HCC; for genotype 3, the rate of SVR was 68.9% and 86.5% for patients with and without HCC, respectively; and for genotype 4, the SVR rate was 50% and 90.2% for patients with and without HCC, respectively.
Unlike the genotype 1 population, which had 111 patients with HCC and liver transplantation, genotypes 2, 3, and 4 had only 4, 18, and 0 patients, respectively.
Dr. Beste and her colleagues attribute this to how common genotype 1 is, which made up 11,761 of 11,871 patients (99%) with known genotypes treated with either of the two medications.
An LDV/SOF-based regimen was given to more of those with genotype 1 who had HCC (88.1%) or HCC and liver transplantation (99.1%) than to those without HCC.
When comparing fibrosis and cirrhosis (FIB-4) scores among patients with an LDV/SOF-based and PrOD p/m ribavirin regimens, patients given PrOD regimens were less likely to have a higher FIB-4 score (47.7% vs. 73.1%), thrombocytopenia (23.1% vs. 40.2%), or elevated bilirubin (21.6% vs. 35.9%).
Patients with genotype 4 showed similar results in favor of PrOD treatment and genotype 2 patients only received LDV/SOF-based treatment; however genotype 3 showed the most positive results with LDV/SOF-based regimens, reporting a 100% success rate for the seven patients treated in the specific sample.
Overall, treatment was less successful for patients with HCC, compared with those without or who underwent transplantation. While Dr. Beste and her colleagues could not definitively explain this, the researchers suggested that it might be from the HCC itself. “The association between HCC and treatment failure persisted after adjustment for cirrhosis, markers of liver dysfunction, and genotype,” said Dr. Beste. “Therefore, these factors cannot explain the lower SVR in patients with HCC, and lead us to suspect that HCC itself could be causally linked to antiviral treatment failure.”
The researcher’s presented the hypothesis that “altered hepatic immune processes may predispose both to HCC and to poorer antiviral treatment outcomes.”
While the study was strengthened by the size and scope of the cohort, researchers were limited by a lack of data, including SVR data for 11.6% of HCC patients and 6.3% of HCC patients with transplantations. Researchers were also unable to attain HCC treatment data for nearly 24% of nontransplanted cases. Finally, the sample size was “overwhelmingly” male, which may give the study “limited generalizability to women.”
[email protected]
On Twitter @EAZweets
Direct-acting antiviral (DAA) medication was successful in treating hepatitis C in 74.5% of patients with hepatocellular carcinoma, and 93.4% of patients with HCC who underwent liver transplants, according to a study funded by Veterans Affairs.
In order to study the effectiveness of DAAs in this setting, Lauren A. Beste, MD, and her colleagues studied a cohort of 17,487 veterans; 624 patients reported having HCC, including 142 with HCC and liver transplantation (J Hepatol. 2017. doi. org/10.1016/j.jhep.2017.02.027).
Effects of the DAAs were also studied based on the genotype of patients’ HCV. According to analysis, patients with the genotype 1 HCV virus were most susceptible to the medication, with sustained virologic response (SVR) rates calculated at 79.1% for patients with HCC, 96.4% for HCC and transplant, and 93.1% for non-HCC.
For patients with genotype 2 virus, the SVR rate was 68.9% for those with HCC, and 86.5% for patients without HCC; for genotype 3, the rate of SVR was 68.9% and 86.5% for patients with and without HCC, respectively; and for genotype 4, the SVR rate was 50% and 90.2% for patients with and without HCC, respectively.
Unlike the genotype 1 population, which had 111 patients with HCC and liver transplantation, genotypes 2, 3, and 4 had only 4, 18, and 0 patients, respectively.
Dr. Beste and her colleagues attribute this to how common genotype 1 is, which made up 11,761 of 11,871 patients (99%) with known genotypes treated with either of the two medications.
An LDV/SOF-based regimen was given to more of those with genotype 1 who had HCC (88.1%) or HCC and liver transplantation (99.1%) than to those without HCC.
When comparing fibrosis and cirrhosis (FIB-4) scores among patients with an LDV/SOF-based and PrOD p/m ribavirin regimens, patients given PrOD regimens were less likely to have a higher FIB-4 score (47.7% vs. 73.1%), thrombocytopenia (23.1% vs. 40.2%), or elevated bilirubin (21.6% vs. 35.9%).
Patients with genotype 4 showed similar results in favor of PrOD treatment and genotype 2 patients only received LDV/SOF-based treatment; however genotype 3 showed the most positive results with LDV/SOF-based regimens, reporting a 100% success rate for the seven patients treated in the specific sample.
Overall, treatment was less successful for patients with HCC, compared with those without or who underwent transplantation. While Dr. Beste and her colleagues could not definitively explain this, the researchers suggested that it might be from the HCC itself. “The association between HCC and treatment failure persisted after adjustment for cirrhosis, markers of liver dysfunction, and genotype,” said Dr. Beste. “Therefore, these factors cannot explain the lower SVR in patients with HCC, and lead us to suspect that HCC itself could be causally linked to antiviral treatment failure.”
The researcher’s presented the hypothesis that “altered hepatic immune processes may predispose both to HCC and to poorer antiviral treatment outcomes.”
While the study was strengthened by the size and scope of the cohort, researchers were limited by a lack of data, including SVR data for 11.6% of HCC patients and 6.3% of HCC patients with transplantations. Researchers were also unable to attain HCC treatment data for nearly 24% of nontransplanted cases. Finally, the sample size was “overwhelmingly” male, which may give the study “limited generalizability to women.”
[email protected]
On Twitter @EAZweets
Direct-acting antiviral (DAA) medication was successful in treating hepatitis C in 74.5% of patients with hepatocellular carcinoma, and 93.4% of patients with HCC who underwent liver transplants, according to a study funded by Veterans Affairs.
In order to study the effectiveness of DAAs in this setting, Lauren A. Beste, MD, and her colleagues studied a cohort of 17,487 veterans; 624 patients reported having HCC, including 142 with HCC and liver transplantation (J Hepatol. 2017. doi. org/10.1016/j.jhep.2017.02.027).
Effects of the DAAs were also studied based on the genotype of patients’ HCV. According to analysis, patients with the genotype 1 HCV virus were most susceptible to the medication, with sustained virologic response (SVR) rates calculated at 79.1% for patients with HCC, 96.4% for HCC and transplant, and 93.1% for non-HCC.
For patients with genotype 2 virus, the SVR rate was 68.9% for those with HCC, and 86.5% for patients without HCC; for genotype 3, the rate of SVR was 68.9% and 86.5% for patients with and without HCC, respectively; and for genotype 4, the SVR rate was 50% and 90.2% for patients with and without HCC, respectively.
Unlike the genotype 1 population, which had 111 patients with HCC and liver transplantation, genotypes 2, 3, and 4 had only 4, 18, and 0 patients, respectively.
Dr. Beste and her colleagues attribute this to how common genotype 1 is, which made up 11,761 of 11,871 patients (99%) with known genotypes treated with either of the two medications.
An LDV/SOF-based regimen was given to more of those with genotype 1 who had HCC (88.1%) or HCC and liver transplantation (99.1%) than to those without HCC.
When comparing fibrosis and cirrhosis (FIB-4) scores among patients with an LDV/SOF-based and PrOD p/m ribavirin regimens, patients given PrOD regimens were less likely to have a higher FIB-4 score (47.7% vs. 73.1%), thrombocytopenia (23.1% vs. 40.2%), or elevated bilirubin (21.6% vs. 35.9%).
Patients with genotype 4 showed similar results in favor of PrOD treatment and genotype 2 patients only received LDV/SOF-based treatment; however genotype 3 showed the most positive results with LDV/SOF-based regimens, reporting a 100% success rate for the seven patients treated in the specific sample.
Overall, treatment was less successful for patients with HCC, compared with those without or who underwent transplantation. While Dr. Beste and her colleagues could not definitively explain this, the researchers suggested that it might be from the HCC itself. “The association between HCC and treatment failure persisted after adjustment for cirrhosis, markers of liver dysfunction, and genotype,” said Dr. Beste. “Therefore, these factors cannot explain the lower SVR in patients with HCC, and lead us to suspect that HCC itself could be causally linked to antiviral treatment failure.”
The researcher’s presented the hypothesis that “altered hepatic immune processes may predispose both to HCC and to poorer antiviral treatment outcomes.”
While the study was strengthened by the size and scope of the cohort, researchers were limited by a lack of data, including SVR data for 11.6% of HCC patients and 6.3% of HCC patients with transplantations. Researchers were also unable to attain HCC treatment data for nearly 24% of nontransplanted cases. Finally, the sample size was “overwhelmingly” male, which may give the study “limited generalizability to women.”
[email protected]
On Twitter @EAZweets
FROM JOURNAL OF HEPATOLOGY
Key clinical point:
Major finding: Of the 17,487 patients given HCV treatment, sustained virologic response was found in 91.9% of patients without HCC, 74.5% with HCC, and 93.4% of patients with HCC and liver transplantation.
Data source: 17,487 patient records from 2014-2015 obtained through the Veterans Affairs Corporate Data Warehouse. Tests were approved by the VA Puget Sound Institutional Review Board.
Disclosures: The study was funded in part by Clinical Science Research and Development, Office of Research and Development, Veterans Affairs. Researchers reported no conflicts of interest.
Robert Hauser, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Jonathan Eskenazi, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Wouter Schievink, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Bluish Gray Hyperpigmentation on the Face and Neck
The Diagnosis: Erythema Dyschromicum Perstans
Erythema dyschromicum perstans (EDP), also referred to as ashy dermatosis, was first described by Ramirez1 in 1957 who labeled the patients los cenicientos (the ashen ones). It preferentially affects women in the second decade of life; however, patients of all ages can be affected, with reported cases occurring in children as young as 2 years of age.2 Most patients have Fitzpatrick skin type IV, mainly Amerindian, Hispanic South Asian, and Southwest Asian; however, there are cases reported worldwide.3 A genetic predisposition is proposed, as major histocompatibility complex genes associated with HLA-DR4⁎0407 are frequent in Mexican patients with ashy dermatosis and in the Amerindian population.4
The etiology of EDP is unknown. Various contributing factors have been reported including alimentary, occupational, and climatic factors,5,6 yet none have been conclusively demonstrated. High expression of CD36 (thrombospondin receptor not found in normal skin) in spinous and granular layers, CD94 (cytotoxic cell marker) in the basal cell layer and in the inflammatory dermal infiltrate,7 and focal keratinocytic expression of intercellular adhesion molecule I (CD54) in the active lesions of EDP, as well as the absence of these findings in normal skin, suggests an immunologic role in the development of the disease.8
Erythema dyschromicum perstans presents clinically with blue-gray hyperpigmented macules varying in size and shape and developing symmetrically in both sun-exposed and sun-protected areas of the face, neck, trunk, arms, and sometimes the dorsal hands (Figures 1 and 2). Notable sparing of the palms, soles, scalp, and mucous membranes occurs.


Occasionally, in the early active stage of the disease, elevated erythematous borders are noted surrounding the hyperpigmented macules. Eventually a hypopigmented halo develops after a prolonged duration of disease.9 The eruption typically is chronic and asymptomatic, though some cases may be pruritic.10
Histopathologically, the early lesions of EDP with an erythematous active border reveal lichenoid dermatitis with basal vacuolar change and occasional Civatte bodies. A mild to moderate perivascular lymphohistiocytic infiltrate admixed with melanophages can be seen in the papillary dermis (Figure 3). In older lesions, the inflammatory infiltrate is sparse, and pigment incontinence consistent with postinflammatory pigmentation is prominent, though melanophages extending deep into the reticular dermis may aid in distinguishing EDP from other causes of postinflammatory pigment alteration.7,11
Erythema dyschromicum perstans and lichen planus pigmentosus (LPP) may be indistinguishable histopathologically and may both be variants of lichen planus actinicus. Lichen planus pigmentosus often differs from EDP in that it presents with brown-black macules and patches often on the face and flexural areas. A subset of cases of LPP also may have mucous membrane involvement. The erythematous border that characterizes the active lesion of EDP is characteristically absent in LPP. In addition, pruritus often is reported with LPP. Direct immunofluorescence is not a beneficial tool in distinguishing the entities.12
Other differential diagnoses of predominantly facial hyperpigmentation include a lichenoid drug eruption; drug-induced hyperpigmentation (deposition disorder); postinflammatory hyperpigmentation following atopic dermatitis; contact dermatitis or photosensitivity reaction; early pinta; and cutaneous findings of systemic diseases manifesting with diffuse hyperpigmentation such as lupus erythematosus, dermatomyositis, hemochromatosis, and Addison disease. A detailed history including medication use, thorough clinical examination, and careful histopathologic evaluation will help distinguish these conditions.
Chrysiasis is a rare bluish to slate gray discoloration of the skin that predominantly occurs in sun-exposed areas. It is caused by chronic use of gold salts, which have been used to treat rheumatoid arthritis. UV light may contribute to induce the uptake of gold and subsequently stimulate tyrosinase activity.13 Histologic features of chrysiasis include dermal and perivascular gold deposition within the macrophages and endothelial cells as well as extracellular granules. It demonstrates an orange-red birefringence on fluorescent microscopy.14,15
Minocycline-induced hyperpigmentation is a well-recognized side effect of this drug. It is dose dependent and appears as a blue-black pigmentation that most frequently affects the shins, ankles, and arms.16 Three distinct types were documented: abnormal discoloration of the skin that has been linked to deposition of pigmented metabolites of minocycline producing blue-black pigmentation at the site of scarring or prior inflammation (type 1); blue-gray pigmentation affecting normal skin, mainly the legs (type 2); and elevated levels of melanin on the sun-exposed areas producing dirty skin syndrome (type 3).17,18
Topical and systemic corticosteroids, UV light therapy, oral dapsone, griseofulvin, retinoids, and clofazimine are reported as treatment options for ashy dermatosis, though results typically are disappointing.7
- Ramirez CO. Los cenicientos: problema clinica. In: Memoria del Primer Congresso Centroamericano de Dermatologica, December 5-8, 1957. San Salvador, El Salvador; 1957:122-130.
- Lee SJ, Chung KY. Erythema dyschromicum perstans in early childhood. J Dermatol. 1999;26:119-121.
- Homez-Chacin, Barroso C. On the etiopathogenic of the erythema dyschromicum perstans: possibility of a melanosis neurocutaneous. Dermatol Venez. 1996;4:149-151.
- Correa MC, Memije EV, Vargas-Alarcon G, et al. HLA-DR association with the genetic susceptibility to develop ashy dermatosis in Mexican Mestizo patients [published online November 20, 2006]. J Am Acad Dermatol. 2007;56:617-620.
- Jablonska S. Ingestion of ammonium nitrate as a possible cause of erythema dyschromicum perstans (ashy dermatosis). Dermatologica. 1975;150:287-291.
- Stevenson JR, Miura M. Erythema dyschromicum perstans (ashy dermatosis). Arch Dermatol. 1966;94:196-199.
- Baranda L, Torres-Alvarez B, Cortes-Franco R, et al. Involvement of cell adhesion and activation molecules in the pathogenesis of erythema dyschromicum perstans (ashy dermatitis). the effect of clofazimine therapy. Arch Dermatol. 1997;133:325-329.
- Vasquez-Ochoa LA, Isaza-Guzman DM, Orozco-Mora B, et al. Immunopathologic study of erythema dyschromicum perstans (ashy dermatosis). Int J Dermatol. 2006;45:937-941.
- Convit J, Kerdel-Vegas F, Roderiguez G. Erythema dyschromicum perstans: a hiltherto undescribed skin disease. J Invest Dermatol. 1961;36:457-462.
- Ono S, Miyachi Y, Kabashima K. Ashy dermatosis with prior pruritic and scaling skin lesions. J Dermatol. 2012;39:1103-1104.
- Sanchez NP, Pathak MA, Sato SS, et al. Circumscribed dermal melaninoses: classification, light, histochemical, and electron microscopic studies on three patients with the erythema dyschromicum perstans type. Int J Dermatol. 1982;21:25-32.
- Vega ME, Waxtein L, Arenas R, et al. Ashy dermatosis and lichen planus pigmentosus: a clinicopathologic study of 31 cases. Int J Dermatol. 1992;31:90-94.
- Ahmed SV, Sajjan R. Chrysiasis: a gold "curse!" [published online May 21, 2009]. BMJ Case Rep. 2009;2009.
- Fiscus V, Hankinson A, Alweis R. Minocycline-induced hyperpigmentation. J Community Hosp Intern Med Perspect. 2014;4. doi:10.3402/jchimp.v4.24063.
- Cox AJ, Marich KW. Gold in the dermis following gold therapy for rheumatoid arthritis. Arch Dermatol. 1973;108:655-657.
- al-Talib RK, Wright DH, Theaker JM. Orange-red birefringence of gold particles in paraffin wax embedded sections: an aid to the diagnosis of chrysiasis. Histopathology. 1994;24:176-178.
- Meyer AJ, Nahass GT. Hyperpigmented patches on the dorsa of the feet. minocycline pigmentation. Arch Dermatol. 1995;131:1447-1450.
- Bayne-Poorman M, Shubrook J. Bluish pigmentation of face and sclera. J Fam Pract. 2010;59:519-522.
The Diagnosis: Erythema Dyschromicum Perstans
Erythema dyschromicum perstans (EDP), also referred to as ashy dermatosis, was first described by Ramirez1 in 1957 who labeled the patients los cenicientos (the ashen ones). It preferentially affects women in the second decade of life; however, patients of all ages can be affected, with reported cases occurring in children as young as 2 years of age.2 Most patients have Fitzpatrick skin type IV, mainly Amerindian, Hispanic South Asian, and Southwest Asian; however, there are cases reported worldwide.3 A genetic predisposition is proposed, as major histocompatibility complex genes associated with HLA-DR4⁎0407 are frequent in Mexican patients with ashy dermatosis and in the Amerindian population.4
The etiology of EDP is unknown. Various contributing factors have been reported including alimentary, occupational, and climatic factors,5,6 yet none have been conclusively demonstrated. High expression of CD36 (thrombospondin receptor not found in normal skin) in spinous and granular layers, CD94 (cytotoxic cell marker) in the basal cell layer and in the inflammatory dermal infiltrate,7 and focal keratinocytic expression of intercellular adhesion molecule I (CD54) in the active lesions of EDP, as well as the absence of these findings in normal skin, suggests an immunologic role in the development of the disease.8
Erythema dyschromicum perstans presents clinically with blue-gray hyperpigmented macules varying in size and shape and developing symmetrically in both sun-exposed and sun-protected areas of the face, neck, trunk, arms, and sometimes the dorsal hands (Figures 1 and 2). Notable sparing of the palms, soles, scalp, and mucous membranes occurs.
Occasionally, in the early active stage of the disease, elevated erythematous borders are noted surrounding the hyperpigmented macules. Eventually a hypopigmented halo develops after a prolonged duration of disease.9 The eruption typically is chronic and asymptomatic, though some cases may be pruritic.10
Histopathologically, the early lesions of EDP with an erythematous active border reveal lichenoid dermatitis with basal vacuolar change and occasional Civatte bodies. A mild to moderate perivascular lymphohistiocytic infiltrate admixed with melanophages can be seen in the papillary dermis (Figure 3). In older lesions, the inflammatory infiltrate is sparse, and pigment incontinence consistent with postinflammatory pigmentation is prominent, though melanophages extending deep into the reticular dermis may aid in distinguishing EDP from other causes of postinflammatory pigment alteration.7,11
Erythema dyschromicum perstans and lichen planus pigmentosus (LPP) may be indistinguishable histopathologically and may both be variants of lichen planus actinicus. Lichen planus pigmentosus often differs from EDP in that it presents with brown-black macules and patches often on the face and flexural areas. A subset of cases of LPP also may have mucous membrane involvement. The erythematous border that characterizes the active lesion of EDP is characteristically absent in LPP. In addition, pruritus often is reported with LPP. Direct immunofluorescence is not a beneficial tool in distinguishing the entities.12
Other differential diagnoses of predominantly facial hyperpigmentation include a lichenoid drug eruption; drug-induced hyperpigmentation (deposition disorder); postinflammatory hyperpigmentation following atopic dermatitis; contact dermatitis or photosensitivity reaction; early pinta; and cutaneous findings of systemic diseases manifesting with diffuse hyperpigmentation such as lupus erythematosus, dermatomyositis, hemochromatosis, and Addison disease. A detailed history including medication use, thorough clinical examination, and careful histopathologic evaluation will help distinguish these conditions.
Chrysiasis is a rare bluish to slate gray discoloration of the skin that predominantly occurs in sun-exposed areas. It is caused by chronic use of gold salts, which have been used to treat rheumatoid arthritis. UV light may contribute to induce the uptake of gold and subsequently stimulate tyrosinase activity.13 Histologic features of chrysiasis include dermal and perivascular gold deposition within the macrophages and endothelial cells as well as extracellular granules. It demonstrates an orange-red birefringence on fluorescent microscopy.14,15
Minocycline-induced hyperpigmentation is a well-recognized side effect of this drug. It is dose dependent and appears as a blue-black pigmentation that most frequently affects the shins, ankles, and arms.16 Three distinct types were documented: abnormal discoloration of the skin that has been linked to deposition of pigmented metabolites of minocycline producing blue-black pigmentation at the site of scarring or prior inflammation (type 1); blue-gray pigmentation affecting normal skin, mainly the legs (type 2); and elevated levels of melanin on the sun-exposed areas producing dirty skin syndrome (type 3).17,18
Topical and systemic corticosteroids, UV light therapy, oral dapsone, griseofulvin, retinoids, and clofazimine are reported as treatment options for ashy dermatosis, though results typically are disappointing.7
The Diagnosis: Erythema Dyschromicum Perstans
Erythema dyschromicum perstans (EDP), also referred to as ashy dermatosis, was first described by Ramirez1 in 1957 who labeled the patients los cenicientos (the ashen ones). It preferentially affects women in the second decade of life; however, patients of all ages can be affected, with reported cases occurring in children as young as 2 years of age.2 Most patients have Fitzpatrick skin type IV, mainly Amerindian, Hispanic South Asian, and Southwest Asian; however, there are cases reported worldwide.3 A genetic predisposition is proposed, as major histocompatibility complex genes associated with HLA-DR4⁎0407 are frequent in Mexican patients with ashy dermatosis and in the Amerindian population.4
The etiology of EDP is unknown. Various contributing factors have been reported including alimentary, occupational, and climatic factors,5,6 yet none have been conclusively demonstrated. High expression of CD36 (thrombospondin receptor not found in normal skin) in spinous and granular layers, CD94 (cytotoxic cell marker) in the basal cell layer and in the inflammatory dermal infiltrate,7 and focal keratinocytic expression of intercellular adhesion molecule I (CD54) in the active lesions of EDP, as well as the absence of these findings in normal skin, suggests an immunologic role in the development of the disease.8
Erythema dyschromicum perstans presents clinically with blue-gray hyperpigmented macules varying in size and shape and developing symmetrically in both sun-exposed and sun-protected areas of the face, neck, trunk, arms, and sometimes the dorsal hands (Figures 1 and 2). Notable sparing of the palms, soles, scalp, and mucous membranes occurs.
Occasionally, in the early active stage of the disease, elevated erythematous borders are noted surrounding the hyperpigmented macules. Eventually a hypopigmented halo develops after a prolonged duration of disease.9 The eruption typically is chronic and asymptomatic, though some cases may be pruritic.10
Histopathologically, the early lesions of EDP with an erythematous active border reveal lichenoid dermatitis with basal vacuolar change and occasional Civatte bodies. A mild to moderate perivascular lymphohistiocytic infiltrate admixed with melanophages can be seen in the papillary dermis (Figure 3). In older lesions, the inflammatory infiltrate is sparse, and pigment incontinence consistent with postinflammatory pigmentation is prominent, though melanophages extending deep into the reticular dermis may aid in distinguishing EDP from other causes of postinflammatory pigment alteration.7,11
Erythema dyschromicum perstans and lichen planus pigmentosus (LPP) may be indistinguishable histopathologically and may both be variants of lichen planus actinicus. Lichen planus pigmentosus often differs from EDP in that it presents with brown-black macules and patches often on the face and flexural areas. A subset of cases of LPP also may have mucous membrane involvement. The erythematous border that characterizes the active lesion of EDP is characteristically absent in LPP. In addition, pruritus often is reported with LPP. Direct immunofluorescence is not a beneficial tool in distinguishing the entities.12
Other differential diagnoses of predominantly facial hyperpigmentation include a lichenoid drug eruption; drug-induced hyperpigmentation (deposition disorder); postinflammatory hyperpigmentation following atopic dermatitis; contact dermatitis or photosensitivity reaction; early pinta; and cutaneous findings of systemic diseases manifesting with diffuse hyperpigmentation such as lupus erythematosus, dermatomyositis, hemochromatosis, and Addison disease. A detailed history including medication use, thorough clinical examination, and careful histopathologic evaluation will help distinguish these conditions.
Chrysiasis is a rare bluish to slate gray discoloration of the skin that predominantly occurs in sun-exposed areas. It is caused by chronic use of gold salts, which have been used to treat rheumatoid arthritis. UV light may contribute to induce the uptake of gold and subsequently stimulate tyrosinase activity.13 Histologic features of chrysiasis include dermal and perivascular gold deposition within the macrophages and endothelial cells as well as extracellular granules. It demonstrates an orange-red birefringence on fluorescent microscopy.14,15
Minocycline-induced hyperpigmentation is a well-recognized side effect of this drug. It is dose dependent and appears as a blue-black pigmentation that most frequently affects the shins, ankles, and arms.16 Three distinct types were documented: abnormal discoloration of the skin that has been linked to deposition of pigmented metabolites of minocycline producing blue-black pigmentation at the site of scarring or prior inflammation (type 1); blue-gray pigmentation affecting normal skin, mainly the legs (type 2); and elevated levels of melanin on the sun-exposed areas producing dirty skin syndrome (type 3).17,18
Topical and systemic corticosteroids, UV light therapy, oral dapsone, griseofulvin, retinoids, and clofazimine are reported as treatment options for ashy dermatosis, though results typically are disappointing.7
- Ramirez CO. Los cenicientos: problema clinica. In: Memoria del Primer Congresso Centroamericano de Dermatologica, December 5-8, 1957. San Salvador, El Salvador; 1957:122-130.
- Lee SJ, Chung KY. Erythema dyschromicum perstans in early childhood. J Dermatol. 1999;26:119-121.
- Homez-Chacin, Barroso C. On the etiopathogenic of the erythema dyschromicum perstans: possibility of a melanosis neurocutaneous. Dermatol Venez. 1996;4:149-151.
- Correa MC, Memije EV, Vargas-Alarcon G, et al. HLA-DR association with the genetic susceptibility to develop ashy dermatosis in Mexican Mestizo patients [published online November 20, 2006]. J Am Acad Dermatol. 2007;56:617-620.
- Jablonska S. Ingestion of ammonium nitrate as a possible cause of erythema dyschromicum perstans (ashy dermatosis). Dermatologica. 1975;150:287-291.
- Stevenson JR, Miura M. Erythema dyschromicum perstans (ashy dermatosis). Arch Dermatol. 1966;94:196-199.
- Baranda L, Torres-Alvarez B, Cortes-Franco R, et al. Involvement of cell adhesion and activation molecules in the pathogenesis of erythema dyschromicum perstans (ashy dermatitis). the effect of clofazimine therapy. Arch Dermatol. 1997;133:325-329.
- Vasquez-Ochoa LA, Isaza-Guzman DM, Orozco-Mora B, et al. Immunopathologic study of erythema dyschromicum perstans (ashy dermatosis). Int J Dermatol. 2006;45:937-941.
- Convit J, Kerdel-Vegas F, Roderiguez G. Erythema dyschromicum perstans: a hiltherto undescribed skin disease. J Invest Dermatol. 1961;36:457-462.
- Ono S, Miyachi Y, Kabashima K. Ashy dermatosis with prior pruritic and scaling skin lesions. J Dermatol. 2012;39:1103-1104.
- Sanchez NP, Pathak MA, Sato SS, et al. Circumscribed dermal melaninoses: classification, light, histochemical, and electron microscopic studies on three patients with the erythema dyschromicum perstans type. Int J Dermatol. 1982;21:25-32.
- Vega ME, Waxtein L, Arenas R, et al. Ashy dermatosis and lichen planus pigmentosus: a clinicopathologic study of 31 cases. Int J Dermatol. 1992;31:90-94.
- Ahmed SV, Sajjan R. Chrysiasis: a gold "curse!" [published online May 21, 2009]. BMJ Case Rep. 2009;2009.
- Fiscus V, Hankinson A, Alweis R. Minocycline-induced hyperpigmentation. J Community Hosp Intern Med Perspect. 2014;4. doi:10.3402/jchimp.v4.24063.
- Cox AJ, Marich KW. Gold in the dermis following gold therapy for rheumatoid arthritis. Arch Dermatol. 1973;108:655-657.
- al-Talib RK, Wright DH, Theaker JM. Orange-red birefringence of gold particles in paraffin wax embedded sections: an aid to the diagnosis of chrysiasis. Histopathology. 1994;24:176-178.
- Meyer AJ, Nahass GT. Hyperpigmented patches on the dorsa of the feet. minocycline pigmentation. Arch Dermatol. 1995;131:1447-1450.
- Bayne-Poorman M, Shubrook J. Bluish pigmentation of face and sclera. J Fam Pract. 2010;59:519-522.
- Ramirez CO. Los cenicientos: problema clinica. In: Memoria del Primer Congresso Centroamericano de Dermatologica, December 5-8, 1957. San Salvador, El Salvador; 1957:122-130.
- Lee SJ, Chung KY. Erythema dyschromicum perstans in early childhood. J Dermatol. 1999;26:119-121.
- Homez-Chacin, Barroso C. On the etiopathogenic of the erythema dyschromicum perstans: possibility of a melanosis neurocutaneous. Dermatol Venez. 1996;4:149-151.
- Correa MC, Memije EV, Vargas-Alarcon G, et al. HLA-DR association with the genetic susceptibility to develop ashy dermatosis in Mexican Mestizo patients [published online November 20, 2006]. J Am Acad Dermatol. 2007;56:617-620.
- Jablonska S. Ingestion of ammonium nitrate as a possible cause of erythema dyschromicum perstans (ashy dermatosis). Dermatologica. 1975;150:287-291.
- Stevenson JR, Miura M. Erythema dyschromicum perstans (ashy dermatosis). Arch Dermatol. 1966;94:196-199.
- Baranda L, Torres-Alvarez B, Cortes-Franco R, et al. Involvement of cell adhesion and activation molecules in the pathogenesis of erythema dyschromicum perstans (ashy dermatitis). the effect of clofazimine therapy. Arch Dermatol. 1997;133:325-329.
- Vasquez-Ochoa LA, Isaza-Guzman DM, Orozco-Mora B, et al. Immunopathologic study of erythema dyschromicum perstans (ashy dermatosis). Int J Dermatol. 2006;45:937-941.
- Convit J, Kerdel-Vegas F, Roderiguez G. Erythema dyschromicum perstans: a hiltherto undescribed skin disease. J Invest Dermatol. 1961;36:457-462.
- Ono S, Miyachi Y, Kabashima K. Ashy dermatosis with prior pruritic and scaling skin lesions. J Dermatol. 2012;39:1103-1104.
- Sanchez NP, Pathak MA, Sato SS, et al. Circumscribed dermal melaninoses: classification, light, histochemical, and electron microscopic studies on three patients with the erythema dyschromicum perstans type. Int J Dermatol. 1982;21:25-32.
- Vega ME, Waxtein L, Arenas R, et al. Ashy dermatosis and lichen planus pigmentosus: a clinicopathologic study of 31 cases. Int J Dermatol. 1992;31:90-94.
- Ahmed SV, Sajjan R. Chrysiasis: a gold "curse!" [published online May 21, 2009]. BMJ Case Rep. 2009;2009.
- Fiscus V, Hankinson A, Alweis R. Minocycline-induced hyperpigmentation. J Community Hosp Intern Med Perspect. 2014;4. doi:10.3402/jchimp.v4.24063.
- Cox AJ, Marich KW. Gold in the dermis following gold therapy for rheumatoid arthritis. Arch Dermatol. 1973;108:655-657.
- al-Talib RK, Wright DH, Theaker JM. Orange-red birefringence of gold particles in paraffin wax embedded sections: an aid to the diagnosis of chrysiasis. Histopathology. 1994;24:176-178.
- Meyer AJ, Nahass GT. Hyperpigmented patches on the dorsa of the feet. minocycline pigmentation. Arch Dermatol. 1995;131:1447-1450.
- Bayne-Poorman M, Shubrook J. Bluish pigmentation of face and sclera. J Fam Pract. 2010;59:519-522.
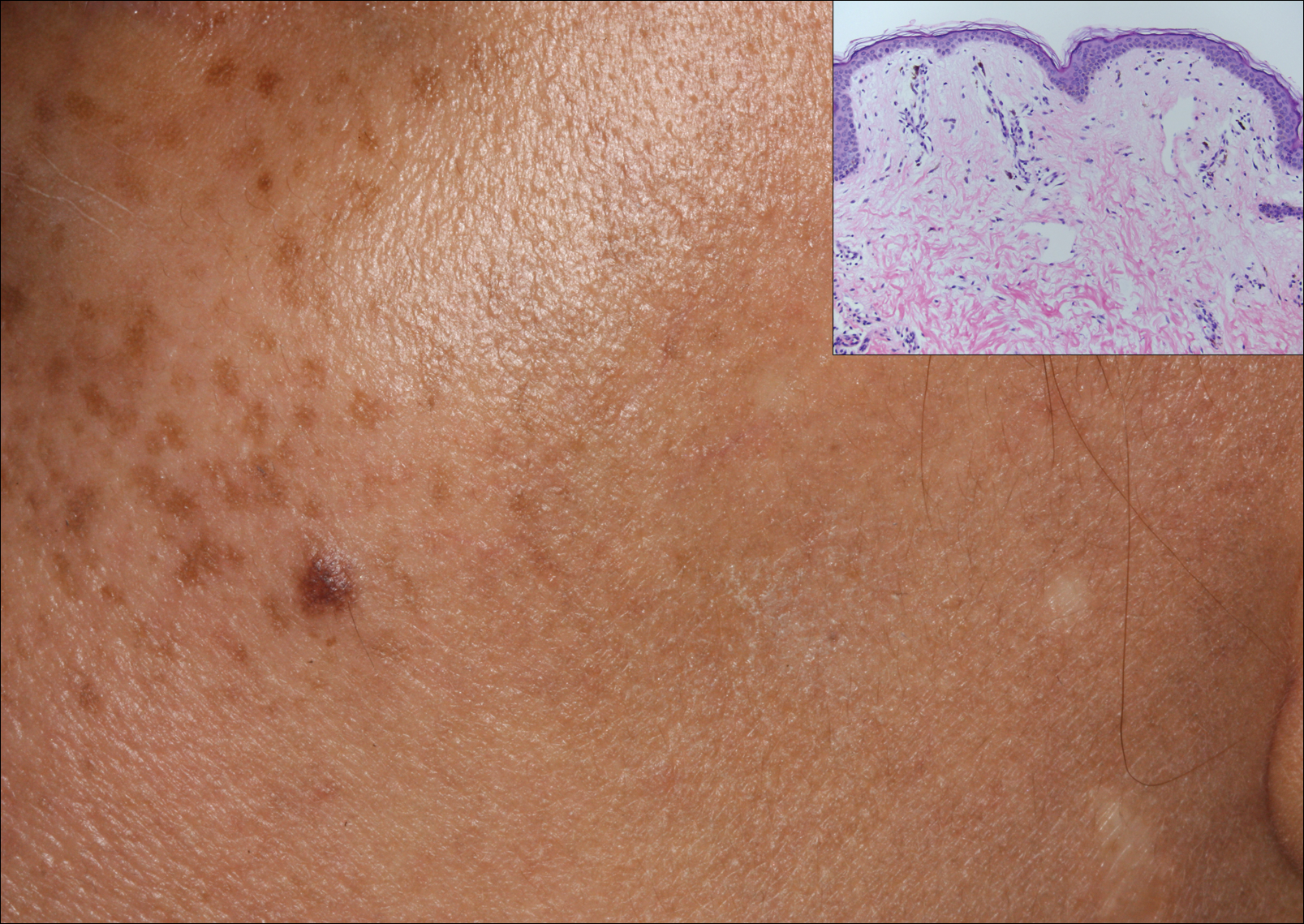
A middle-aged woman with Fitzpatrick skin type IV was evaluated for progressive hyperpigmentation of several months' duration involving the neck, jawline, both sides of the face, and forehead. The lesions were mildly pruritic. She denied contact with any new substance and there was no history of an eruption preceding the hyperpigmentation. Medical history included chronic anemia that was managed with iron supplementation. On physical examination, blue-gray nonscaly macules and patches were observed distributed symmetrically on the neck, jawline, sides of the face, and forehead. Microscopic examination of 2 shave biopsies revealed subtle vacuolar interface dermatitis with mild perivascular lymphocytic infiltrate and dermal melanophages (inset).
