User login
Trump administration floats 18% budget cut to HHS
The Department of Health & Human Services would see an 18% funding cut under the first budget proposal from the Trump administration.
The proposal, submitted to Congress March 16, would cut $15.1 billion from fiscal 2017 levels, funding the agency at $69 billion for fiscal year 2018. More than a third of the cuts come from the National Institutes of Health.
The NIH’s overall budget would drop to $25.9 billion in FY 2018, down $5.8 billion from this year (fiscal 2017). The proposal includes “a major reorganization of NIH’s institutes and centers to help focus resources on the highest priority research and training activities, including: eliminating the Fogarty International Center, consolidating the Agency for Healthcare Research and Quality within the NIH, and other consolidations and structural changes across NIH organizations and activities,” according to summary documents from the Office of Management and Budget.
The proposed cuts also account for the funds that are to be appropriated for the 21st Century Cures Act, which was supposed to add $4.8 billion in new appropriated funding, including funds dedicated to the Cancer Moonshot and the BRAIN Initiative.
The Centers for Disease Control and Prevention also would be reformed, getting a new $500 million block grant “to increase state flexibility and focus on the leading public health challenges specific to each state.” It also creates a new Federal Emergency Response Fund to respond to public health outbreaks such as the Zika virus.
Another area receiving a boost under the proposal is the funding for the Health Care Fraud and Abuse Control program at the CMS, which would receive $751 million in fiscal 2018, about 10% more than it did in fiscal 2017. The budget document notes that the “return on investment for the HCFAC account was $5 returned for every $1 expended from 2014-2016.”
Other cuts highlighted by the proposal include elimination of $403 million in health professions and nursing training programs, “which lack evidence that they significantly improve the nation’s health workforce,” and a $4.2 billion cut from the elimination of discretionary programs within the Office of Community Services.
The Department of Health & Human Services would see an 18% funding cut under the first budget proposal from the Trump administration.
The proposal, submitted to Congress March 16, would cut $15.1 billion from fiscal 2017 levels, funding the agency at $69 billion for fiscal year 2018. More than a third of the cuts come from the National Institutes of Health.
The NIH’s overall budget would drop to $25.9 billion in FY 2018, down $5.8 billion from this year (fiscal 2017). The proposal includes “a major reorganization of NIH’s institutes and centers to help focus resources on the highest priority research and training activities, including: eliminating the Fogarty International Center, consolidating the Agency for Healthcare Research and Quality within the NIH, and other consolidations and structural changes across NIH organizations and activities,” according to summary documents from the Office of Management and Budget.
The proposed cuts also account for the funds that are to be appropriated for the 21st Century Cures Act, which was supposed to add $4.8 billion in new appropriated funding, including funds dedicated to the Cancer Moonshot and the BRAIN Initiative.
The Centers for Disease Control and Prevention also would be reformed, getting a new $500 million block grant “to increase state flexibility and focus on the leading public health challenges specific to each state.” It also creates a new Federal Emergency Response Fund to respond to public health outbreaks such as the Zika virus.
Another area receiving a boost under the proposal is the funding for the Health Care Fraud and Abuse Control program at the CMS, which would receive $751 million in fiscal 2018, about 10% more than it did in fiscal 2017. The budget document notes that the “return on investment for the HCFAC account was $5 returned for every $1 expended from 2014-2016.”
Other cuts highlighted by the proposal include elimination of $403 million in health professions and nursing training programs, “which lack evidence that they significantly improve the nation’s health workforce,” and a $4.2 billion cut from the elimination of discretionary programs within the Office of Community Services.
The Department of Health & Human Services would see an 18% funding cut under the first budget proposal from the Trump administration.
The proposal, submitted to Congress March 16, would cut $15.1 billion from fiscal 2017 levels, funding the agency at $69 billion for fiscal year 2018. More than a third of the cuts come from the National Institutes of Health.
The NIH’s overall budget would drop to $25.9 billion in FY 2018, down $5.8 billion from this year (fiscal 2017). The proposal includes “a major reorganization of NIH’s institutes and centers to help focus resources on the highest priority research and training activities, including: eliminating the Fogarty International Center, consolidating the Agency for Healthcare Research and Quality within the NIH, and other consolidations and structural changes across NIH organizations and activities,” according to summary documents from the Office of Management and Budget.
The proposed cuts also account for the funds that are to be appropriated for the 21st Century Cures Act, which was supposed to add $4.8 billion in new appropriated funding, including funds dedicated to the Cancer Moonshot and the BRAIN Initiative.
The Centers for Disease Control and Prevention also would be reformed, getting a new $500 million block grant “to increase state flexibility and focus on the leading public health challenges specific to each state.” It also creates a new Federal Emergency Response Fund to respond to public health outbreaks such as the Zika virus.
Another area receiving a boost under the proposal is the funding for the Health Care Fraud and Abuse Control program at the CMS, which would receive $751 million in fiscal 2018, about 10% more than it did in fiscal 2017. The budget document notes that the “return on investment for the HCFAC account was $5 returned for every $1 expended from 2014-2016.”
Other cuts highlighted by the proposal include elimination of $403 million in health professions and nursing training programs, “which lack evidence that they significantly improve the nation’s health workforce,” and a $4.2 billion cut from the elimination of discretionary programs within the Office of Community Services.
HCV ‘cure’ within the VA appears likely
The number of Veterans Affairs patients with hepatitis C who have achieved a sustained virologic response to antiviral therapy has escalated so rapidly and reached such a height that the disease may well be eradicated in that health care system within a few years, according to a report in Alimentary Pharmacology and Therapeutics.
The potential public health benefits are substantial, “considering that HCV infection is the most common cause of cirrhosis and liver cancer in the VA and the United States, that the benefits of SVR are long-lasting, and that HCV clearance reduces the risk of liver cancer by 76% and all-cause mortality by 50%,” said Andrew M. Moon, MD, of the division of general internal medicine, University of Washington, Seattle, and his associates.
An estimated 124,662 VA patients currently are infected, and curing them “would substantially reduce the burden of HCV within the entire country and prevent tens of thousands of deaths,” they noted.
The VA dramatically increased the number of patients who were offered treatment in recent years, because it was able to allocate nearly $700 million to offset the high costs of highly effective direct antiviral agents, which in turn made these better-tolerated drugs more widely available at clinics across the country. The VA also removed all treatment prioritization criteria, allowing all patients, not just those with severe disease, to receive highly effective direct antiviral agents. This is “in stark contrast to most health care systems, state Medicaid programs, and insurance carriers in the U.S., which still restrict access ... based on severity of liver disease,” the investigators said (Aliment Pharmacol Ther. 2017 March 8. doi: 10.1111/apt.14021).
To examine the impact of these changes, Dr. Moon and his associates performed a retrospective cohort study, analyzing the electronic medical records of all 105,369 HCV treatment regimens given to 78,947 VA patients (mean age, 56 years) during a 17-year period. They found that annual treatment rates more than doubled from 2,726 to 6,679 patients when pegylated interferon was introduced, declined for a while and then rose modestly to 4,900 patients when boceprevir and telaprevir were introduced, declined again to an all-time low of 2,609 and then rebounded to 9,180 patients when sofosbuvir and simeprevir were introduced, and finally skyrocketed to 31,028 patients when ledipasvir/sofosbuvir and paritaprevir/ritonavir/ombitasvir/dasabuvir were introduced.
Correspondingly, SVR rates rose from less than 25% at the beginning of the study period to a “remarkable” 90.5% at the end. The improvement in SVR rates was even more pronounced among traditionally “hard to treat” cases, such as patients with concomitant cirrhosis (from 11.0% to 87.0%), decompensated cirrhosis (from 14.6% to 85.2%), highly refractory infection (from 16.4% to 89.3%), and genotype-1 infection (from 1.3% to 91.7%). “The number of patients achieving SVR increased 21-fold from 1,313 in 2010 to an estimated 28,084 in 2015,” Dr. Moon and his associates said.
“We believe that our findings based on the VA health care system might be relevant and informative for other comprehensive health care systems,” providing proof-of-concept that similar results can be achieved if aggressive screening; affordable, tolerable treatment; and open access to all patients are implemented.
The number of Veterans Affairs patients with hepatitis C who have achieved a sustained virologic response to antiviral therapy has escalated so rapidly and reached such a height that the disease may well be eradicated in that health care system within a few years, according to a report in Alimentary Pharmacology and Therapeutics.
The potential public health benefits are substantial, “considering that HCV infection is the most common cause of cirrhosis and liver cancer in the VA and the United States, that the benefits of SVR are long-lasting, and that HCV clearance reduces the risk of liver cancer by 76% and all-cause mortality by 50%,” said Andrew M. Moon, MD, of the division of general internal medicine, University of Washington, Seattle, and his associates.
An estimated 124,662 VA patients currently are infected, and curing them “would substantially reduce the burden of HCV within the entire country and prevent tens of thousands of deaths,” they noted.
The VA dramatically increased the number of patients who were offered treatment in recent years, because it was able to allocate nearly $700 million to offset the high costs of highly effective direct antiviral agents, which in turn made these better-tolerated drugs more widely available at clinics across the country. The VA also removed all treatment prioritization criteria, allowing all patients, not just those with severe disease, to receive highly effective direct antiviral agents. This is “in stark contrast to most health care systems, state Medicaid programs, and insurance carriers in the U.S., which still restrict access ... based on severity of liver disease,” the investigators said (Aliment Pharmacol Ther. 2017 March 8. doi: 10.1111/apt.14021).
To examine the impact of these changes, Dr. Moon and his associates performed a retrospective cohort study, analyzing the electronic medical records of all 105,369 HCV treatment regimens given to 78,947 VA patients (mean age, 56 years) during a 17-year period. They found that annual treatment rates more than doubled from 2,726 to 6,679 patients when pegylated interferon was introduced, declined for a while and then rose modestly to 4,900 patients when boceprevir and telaprevir were introduced, declined again to an all-time low of 2,609 and then rebounded to 9,180 patients when sofosbuvir and simeprevir were introduced, and finally skyrocketed to 31,028 patients when ledipasvir/sofosbuvir and paritaprevir/ritonavir/ombitasvir/dasabuvir were introduced.
Correspondingly, SVR rates rose from less than 25% at the beginning of the study period to a “remarkable” 90.5% at the end. The improvement in SVR rates was even more pronounced among traditionally “hard to treat” cases, such as patients with concomitant cirrhosis (from 11.0% to 87.0%), decompensated cirrhosis (from 14.6% to 85.2%), highly refractory infection (from 16.4% to 89.3%), and genotype-1 infection (from 1.3% to 91.7%). “The number of patients achieving SVR increased 21-fold from 1,313 in 2010 to an estimated 28,084 in 2015,” Dr. Moon and his associates said.
“We believe that our findings based on the VA health care system might be relevant and informative for other comprehensive health care systems,” providing proof-of-concept that similar results can be achieved if aggressive screening; affordable, tolerable treatment; and open access to all patients are implemented.
The number of Veterans Affairs patients with hepatitis C who have achieved a sustained virologic response to antiviral therapy has escalated so rapidly and reached such a height that the disease may well be eradicated in that health care system within a few years, according to a report in Alimentary Pharmacology and Therapeutics.
The potential public health benefits are substantial, “considering that HCV infection is the most common cause of cirrhosis and liver cancer in the VA and the United States, that the benefits of SVR are long-lasting, and that HCV clearance reduces the risk of liver cancer by 76% and all-cause mortality by 50%,” said Andrew M. Moon, MD, of the division of general internal medicine, University of Washington, Seattle, and his associates.
An estimated 124,662 VA patients currently are infected, and curing them “would substantially reduce the burden of HCV within the entire country and prevent tens of thousands of deaths,” they noted.
The VA dramatically increased the number of patients who were offered treatment in recent years, because it was able to allocate nearly $700 million to offset the high costs of highly effective direct antiviral agents, which in turn made these better-tolerated drugs more widely available at clinics across the country. The VA also removed all treatment prioritization criteria, allowing all patients, not just those with severe disease, to receive highly effective direct antiviral agents. This is “in stark contrast to most health care systems, state Medicaid programs, and insurance carriers in the U.S., which still restrict access ... based on severity of liver disease,” the investigators said (Aliment Pharmacol Ther. 2017 March 8. doi: 10.1111/apt.14021).
To examine the impact of these changes, Dr. Moon and his associates performed a retrospective cohort study, analyzing the electronic medical records of all 105,369 HCV treatment regimens given to 78,947 VA patients (mean age, 56 years) during a 17-year period. They found that annual treatment rates more than doubled from 2,726 to 6,679 patients when pegylated interferon was introduced, declined for a while and then rose modestly to 4,900 patients when boceprevir and telaprevir were introduced, declined again to an all-time low of 2,609 and then rebounded to 9,180 patients when sofosbuvir and simeprevir were introduced, and finally skyrocketed to 31,028 patients when ledipasvir/sofosbuvir and paritaprevir/ritonavir/ombitasvir/dasabuvir were introduced.
Correspondingly, SVR rates rose from less than 25% at the beginning of the study period to a “remarkable” 90.5% at the end. The improvement in SVR rates was even more pronounced among traditionally “hard to treat” cases, such as patients with concomitant cirrhosis (from 11.0% to 87.0%), decompensated cirrhosis (from 14.6% to 85.2%), highly refractory infection (from 16.4% to 89.3%), and genotype-1 infection (from 1.3% to 91.7%). “The number of patients achieving SVR increased 21-fold from 1,313 in 2010 to an estimated 28,084 in 2015,” Dr. Moon and his associates said.
“We believe that our findings based on the VA health care system might be relevant and informative for other comprehensive health care systems,” providing proof-of-concept that similar results can be achieved if aggressive screening; affordable, tolerable treatment; and open access to all patients are implemented.
FROM ALIMENTARY PHARMACOLOGY AND THERAPEUTICS
Key clinical point: The number of VA patients with hepatitis C virus who have achieved a sustained virologic response has escalated so rapidly and so high that the disease may be eradicated in that health care system within a few years.
Major finding: SVR rates rose from less than 25% at the beginning of the study period to a “remarkable” 90.5% at the end; the number of patients achieving SVR increased 21-fold from 1,313 in 2010 to an estimated 28,084 in 2015.
Data source: A retrospective cohort study examining all 105,369 antiviral regimens administered within the VA in 1999-2016.
Disclosures: The VA Office of Research and Development funded the study. Dr. Moon and his associates reported having no relevant financial disclosures.
Alan Finkel, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Lars Edvinsson, MD, PhD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Parental reasons for HPV nonvaccination are shifting
NATIONAL HARBOR, MD. – Parents are now less concerned about whether their daughters are sexually active when weighing whether to vaccinate against human papillomavirus (HPV), compared with just a few years ago.
This shift in parental attitudes can inform physician guidance and shift the HPV vaccination discussion, Anna Beavis, MD, a clinical fellow in gynecologic oncology at Johns Hopkins Medicine, Baltimore, said at the annual meeting of the Society of Gynecologic Oncology.
About 90% of cervical cancer is preventable with the HPV vaccine, but “U.S. vaccination rates are still suboptimal,” putting the United States far behind many other developed countries, Dr. Beavis said.
It’s been shown that the physician recommendation is one of the strongest predictors of whether an adolescent will be immunized against HPV, yet many providers remain reluctant to raise the issue, she said. Discomfort about discussing adolescent sexuality with the teen and with parents has been cited by physicians as a primary barrier.
To evaluate why parents of adolescent girls would opt out of HPV vaccination and to identify whether the reasons had changed over time, Dr. Beavis and her colleagues formulated a study that compared parent responses to a nationwide survey about HPV vaccination given in 2014 to those in 2010.
The study drew from the National Immunization Survey–Teen, a random digit-dialing survey administered by the Centers for Disease Control and Prevention. Only data pertaining to girls aged 13-17 years was included in the analysis, and for the sake of accuracy, only provider-verified responses were used.
Of the 49,345 responses that could be provider verified during the period from 2010 to 2014, 54% had received at least one HPV vaccination. Of the remaining responses, 55% of the parents said they had no intention of vaccinating their daughters.
During this period, vaccination rates have climbed slowly, from a little less than half in 2010 to about 60% in 2014 (test of trend, P less than .001), according to Dr. Beavis.
However, the reasons parents gave for declining vaccination has shifted over time, she said. The primary reason given in 2010 was concern about safety or side effects, followed by the sense that the vaccine was not necessary. These remained the top two reasons in 2014, though they had swapped places.
In 2010, the third most common reason parents gave for declining the HPV vaccination was that their daughters were not sexually active. By 2014, this reason had slid to the bottom of the top five reasons, and now was given by fewer than 10% of parents (test of trend, P less than .01).
This is important information for physicians, Dr. Beavis said in a video interview. If a physician has been reluctant to start the HPV discussion for fear of stepping into awkward territory with parents of teen girls, they should know that it’s significantly less likely that issues of sexuality will be on the parental radar when talking about HPV vaccination.
Looking deeper into the data, the investigators found that white race, younger patient age, and living above the poverty level were risk factors for nonvaccination. This means, Dr. Beavis said, that physicians should consider “developing a targeted HPV message” for families at higher risk of nonvaccination.
“This vaccine message should focus on cancer prevention, necessity, and the safety of the HPV vaccine,” Dr. Beavis said.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @karioakes
NATIONAL HARBOR, MD. – Parents are now less concerned about whether their daughters are sexually active when weighing whether to vaccinate against human papillomavirus (HPV), compared with just a few years ago.
This shift in parental attitudes can inform physician guidance and shift the HPV vaccination discussion, Anna Beavis, MD, a clinical fellow in gynecologic oncology at Johns Hopkins Medicine, Baltimore, said at the annual meeting of the Society of Gynecologic Oncology.
About 90% of cervical cancer is preventable with the HPV vaccine, but “U.S. vaccination rates are still suboptimal,” putting the United States far behind many other developed countries, Dr. Beavis said.
It’s been shown that the physician recommendation is one of the strongest predictors of whether an adolescent will be immunized against HPV, yet many providers remain reluctant to raise the issue, she said. Discomfort about discussing adolescent sexuality with the teen and with parents has been cited by physicians as a primary barrier.
To evaluate why parents of adolescent girls would opt out of HPV vaccination and to identify whether the reasons had changed over time, Dr. Beavis and her colleagues formulated a study that compared parent responses to a nationwide survey about HPV vaccination given in 2014 to those in 2010.
The study drew from the National Immunization Survey–Teen, a random digit-dialing survey administered by the Centers for Disease Control and Prevention. Only data pertaining to girls aged 13-17 years was included in the analysis, and for the sake of accuracy, only provider-verified responses were used.
Of the 49,345 responses that could be provider verified during the period from 2010 to 2014, 54% had received at least one HPV vaccination. Of the remaining responses, 55% of the parents said they had no intention of vaccinating their daughters.
During this period, vaccination rates have climbed slowly, from a little less than half in 2010 to about 60% in 2014 (test of trend, P less than .001), according to Dr. Beavis.
However, the reasons parents gave for declining vaccination has shifted over time, she said. The primary reason given in 2010 was concern about safety or side effects, followed by the sense that the vaccine was not necessary. These remained the top two reasons in 2014, though they had swapped places.
In 2010, the third most common reason parents gave for declining the HPV vaccination was that their daughters were not sexually active. By 2014, this reason had slid to the bottom of the top five reasons, and now was given by fewer than 10% of parents (test of trend, P less than .01).
This is important information for physicians, Dr. Beavis said in a video interview. If a physician has been reluctant to start the HPV discussion for fear of stepping into awkward territory with parents of teen girls, they should know that it’s significantly less likely that issues of sexuality will be on the parental radar when talking about HPV vaccination.
Looking deeper into the data, the investigators found that white race, younger patient age, and living above the poverty level were risk factors for nonvaccination. This means, Dr. Beavis said, that physicians should consider “developing a targeted HPV message” for families at higher risk of nonvaccination.
“This vaccine message should focus on cancer prevention, necessity, and the safety of the HPV vaccine,” Dr. Beavis said.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @karioakes
NATIONAL HARBOR, MD. – Parents are now less concerned about whether their daughters are sexually active when weighing whether to vaccinate against human papillomavirus (HPV), compared with just a few years ago.
This shift in parental attitudes can inform physician guidance and shift the HPV vaccination discussion, Anna Beavis, MD, a clinical fellow in gynecologic oncology at Johns Hopkins Medicine, Baltimore, said at the annual meeting of the Society of Gynecologic Oncology.
About 90% of cervical cancer is preventable with the HPV vaccine, but “U.S. vaccination rates are still suboptimal,” putting the United States far behind many other developed countries, Dr. Beavis said.
It’s been shown that the physician recommendation is one of the strongest predictors of whether an adolescent will be immunized against HPV, yet many providers remain reluctant to raise the issue, she said. Discomfort about discussing adolescent sexuality with the teen and with parents has been cited by physicians as a primary barrier.
To evaluate why parents of adolescent girls would opt out of HPV vaccination and to identify whether the reasons had changed over time, Dr. Beavis and her colleagues formulated a study that compared parent responses to a nationwide survey about HPV vaccination given in 2014 to those in 2010.
The study drew from the National Immunization Survey–Teen, a random digit-dialing survey administered by the Centers for Disease Control and Prevention. Only data pertaining to girls aged 13-17 years was included in the analysis, and for the sake of accuracy, only provider-verified responses were used.
Of the 49,345 responses that could be provider verified during the period from 2010 to 2014, 54% had received at least one HPV vaccination. Of the remaining responses, 55% of the parents said they had no intention of vaccinating their daughters.
During this period, vaccination rates have climbed slowly, from a little less than half in 2010 to about 60% in 2014 (test of trend, P less than .001), according to Dr. Beavis.
However, the reasons parents gave for declining vaccination has shifted over time, she said. The primary reason given in 2010 was concern about safety or side effects, followed by the sense that the vaccine was not necessary. These remained the top two reasons in 2014, though they had swapped places.
In 2010, the third most common reason parents gave for declining the HPV vaccination was that their daughters were not sexually active. By 2014, this reason had slid to the bottom of the top five reasons, and now was given by fewer than 10% of parents (test of trend, P less than .01).
This is important information for physicians, Dr. Beavis said in a video interview. If a physician has been reluctant to start the HPV discussion for fear of stepping into awkward territory with parents of teen girls, they should know that it’s significantly less likely that issues of sexuality will be on the parental radar when talking about HPV vaccination.
Looking deeper into the data, the investigators found that white race, younger patient age, and living above the poverty level were risk factors for nonvaccination. This means, Dr. Beavis said, that physicians should consider “developing a targeted HPV message” for families at higher risk of nonvaccination.
“This vaccine message should focus on cancer prevention, necessity, and the safety of the HPV vaccine,” Dr. Beavis said.
She reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @karioakes
AT THE ANNUAL MEETING ON WOMEN’S CANCER

Postoperative Henoch-Schönlein Purpura
To the Editor:
A 57-year-old man with a history of type 2 diabetes mellitus and hypertension was hospitalized for heart disease resulting in an aortic valve replacement and multiple-vessel bypass grafting. He experienced a stormy septic postoperative course during which he developed numerous palpable purplish plaques (Figure 1). The lesions were bilateral and more heavily involved the lower legs and buttocks. The head and neck remained free of skin lesions. Additionally, the patient reported a bilateral burning sensation from the knees to the feet.

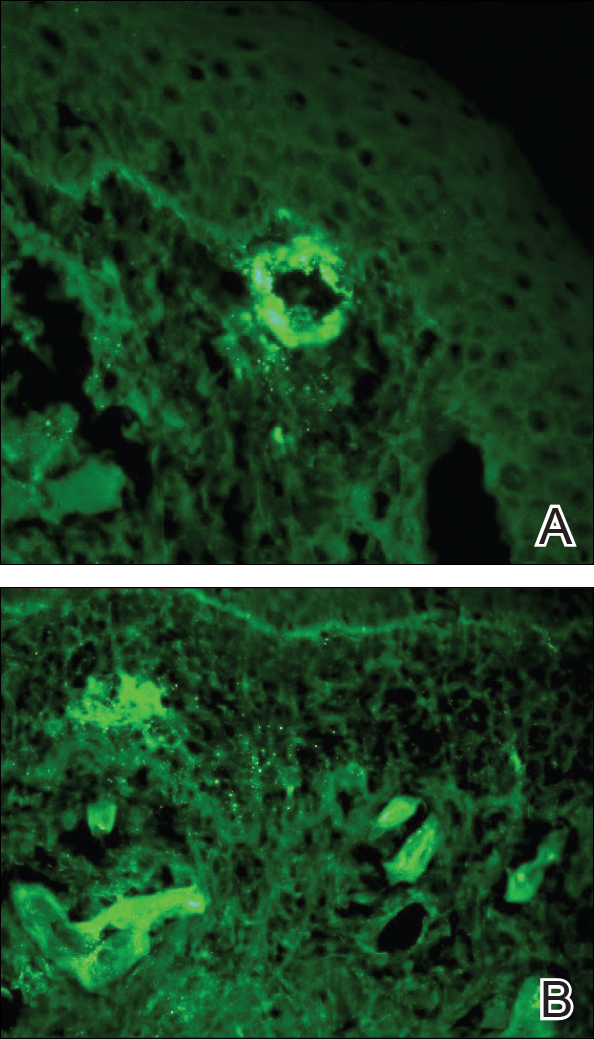
Punch biopsies of lesions from the right upper arm were obtained. Hematoxylin and eosin staining revealed neutrophilic-predominant small vessel vasculitis (Figure 2A) with the upper dermal location more heavily involved, as demonstrated by involvement of a superficial vascular plexus (Figures 2B and 2C) that was consistent with Henoch-Schönlein purpura (HSP). The diagnosis later was confirmed with immunofluorescence. Direct immunofluorescence revealed granular IgA deposition around the superficial vascular plexus (Figure 3). No IgG, IgM, C3, C5b-9 complement complex, or fibrinogen deposition was seen. Additionally, periodic acid-Schiff staining failed to show microorganisms, thrombi, or intravascular hyaline material.
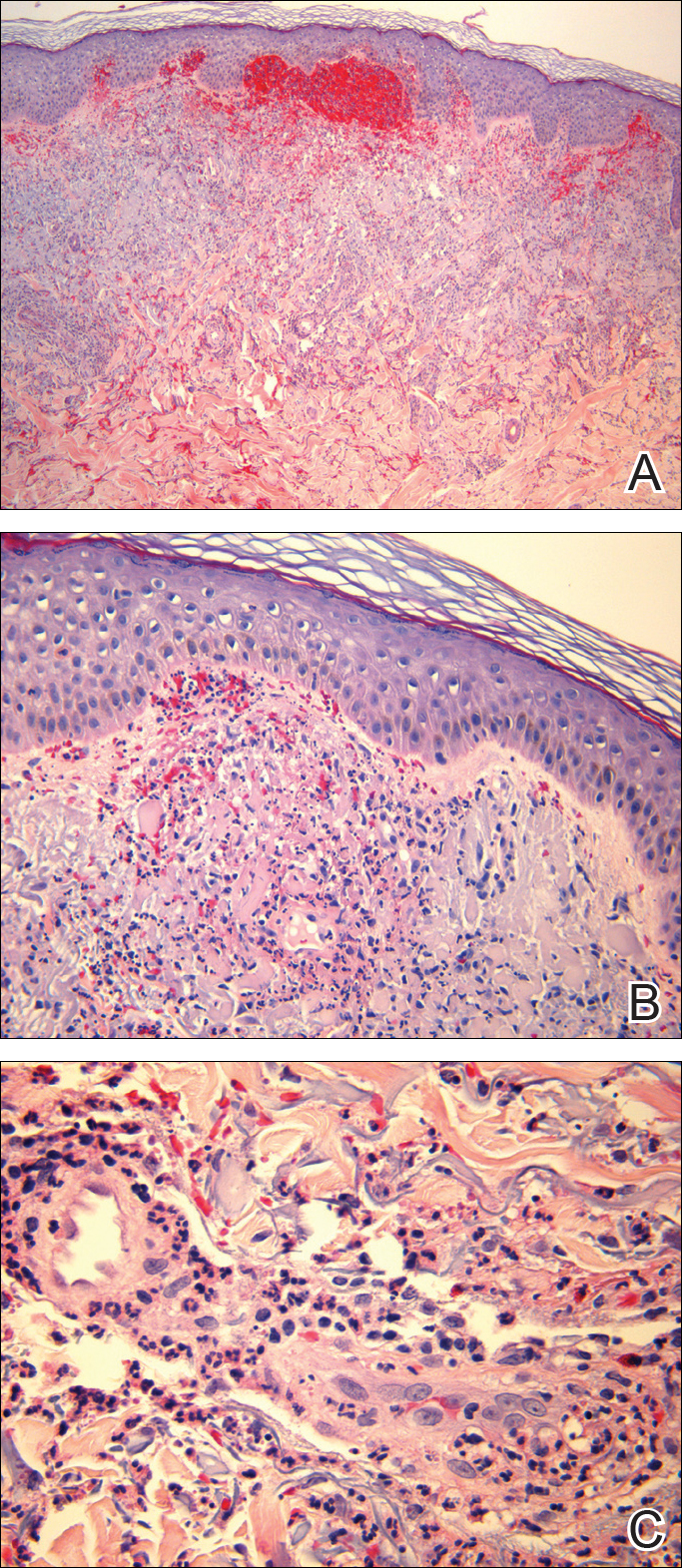
At our initial consultation, we observed an ill-appearing afebrile man with purplish plaques. Our impression was that he had vasculitis and not warfarin necrosis, which had been suspected by the cardiovascular team. The burning sensation noted by the patient lent credence to our vasculitic diagnosis. Proteinuria and hematuria were present; however, the values for blood urea nitrogen, creatinine, and glomerular filtration rate all remained within reference range. His signs and symptoms responded dramatically to prednisone. He remains on 1 mg of prednisone daily and a nephrologist continues to monitor renal function as an outpatient.
Henoch-Schönlein purpura is a systemic leukocytoclastic vasculitis involving small vessels. The small vessel vasculitis is associated with IgA antigen-antibody complex deposition in areas throughout the body. Palpable purpura typically is seen on the skin, which characteristically involves dependent areas such as the legs and the buttocks. Lesions normally are present bilaterally in a symmetric distribution. Initially, the lesions develop as erythematous macules that progress to purple, nonblanching, palpable, and purpuric plaques.1 Henoch-Schönlein purpura most commonly involves the skin; however, other locations for the immune complexes include the gastrointestinal tract, joints, and kidneys.2 The cause for the body's immunogenic deposition response is unknown in a majority of cases.
Henoch-Schönlein purpura most commonly is seen in the pediatric population with a predilection for males.3 The incidence in the pediatric population is 13.5 to 20 per 100,000 children per year; HSP is more rare in adults.4-6 Henoch-Schönlein purpura most often is a self-limiting disease that requires only supportive treatment. The signs and symptoms last 4 to 6 weeks in most patients and resolve completely in 94% of children and 89% of adults.7 Renal involvement carries a worse prognosis. Adult patients have a higher incidence of renal involvement, renal insufficiency, and subsequent progression to end-stage renal disease.3,8-10 In a study by Hung et al8 of 65 children and 22 adult HSP patients, 12 adults presented with renal involvement in which hematuria or proteinuria were present. Of them, 6 progressed to renal insufficiency (defined as having a plasma creatinine concentration>1.2 mg/dL).8 Fogazzi et al11 reported similar findings; 8 of 16 patients affected with HSP progressed to renal insufficiency with creatinine clearances ranging from 31 to 60 mL/min, and 3 patients required chronic dialysis. Pillebout et al9 evaluated 250 adults with HSP and 32% reached renal insufficiency with creatinine clearances of less than 50 mL/min, with 11% of patients developing end-stage renal disease. The degree of hematuria and/or proteinuria has been shown to be an effective prognostic indicator.9,10 Coppo et al10 found a similar prognosis among children and adults with HSP-related nephritis.
Our patient described the burning sensation as occurring bilaterally from the knees down to the feet, which provided an additional clue that small vessel vasculitis was involved, as occluded blood vessels can cause ischemia to nerves and perivascular involvement can affect nearby neural structures. Sais et al12 demonstrated that paresthesia in the setting of HSP was a risk factor for systemic involvement. Of note, our patient's paresthesia lasted only several days.
The cause of HSP is not always as evident in the adult population as in the pediatric population. Early diagnosis of HSP in adults may allow for the proper instatement of treatment to deter long-term renal complications. Follow-up with urinalysis is recommended because a small percentage of patients have a late progression to renal failure.13,14
Because the dermatologists involved in this case knew where and what types of biopsies to perform, a correct diagnosis was obtained quickly, allowing for the correct therapeutic intervention. After the diagnosis of HSP is made in an adult, nephrology should be consulted early in the treatment course.
- Rai A, Nast C, Adler S. Henoch-Schönlein purpura nephritis. J Am Soc Nephrol. 1999;10:2637-2644.
- Helander SD, De Castro FR, Gibson LE. Henoch-Schönlein purpura: clinicopathologic correlation of cutaneous vascular IgA deposits and the relationship to leukocytoclastic vasculitis. Acta Derm Venereol. 1995;75:125-129.
- Garcia-Porrua C, Calvino MC, Llorca J, et al. Henoch-Schönlein purpura in children and adults: clinical differences in a defined population. Semin Arthritis Rheum. 2002;32:149-156.
- Stewart M, Savage JM, Bell B, et al. Long term renal prognosis of Henoch-Schönlein purpura in an unselected childhood population. Eur J Pediatr. 1988;147:113-115.
- Watts RA, Scott DG. Epidemiology of the vasculitides. Semin Respir Crit Care. 2004;25:455-464.
- Gardner-Medwin JM, Dolezalova P, Cummins C, et al. Incidence of Henoch-Schönlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet. 2002;360:1197-1202.
- Blanco R, Martínez-Taboada VM, Rodríguez-Valverde V, et al. Henoch-Schönlein purpura in adulthood and childhood: two different expressions of the same syndrome. Arthritis Rheum. 1997;40:859-864.
- Hung SP, Yang YH, Lin YT, et al. Clinical manifestations and outcomes of Henoch-Schönlein purpura: comparison between adults and children. Pediatr Neonatol. 2009;50:162-168.
- Pillebout E, Thervet E, Hill G, et al. Henoch-Schönlein purpura in adults: outcomes and prognostic factors. J Am Soc Nephrol. 2002;13:1271-1278.
- Coppo R, Mazzucco G, Cagnoli L, et al. Long-term prognosis of Henoch-Schönlein nephritis in adults and children. Italian Group of Renal Immunopathology collaborative study on Henoch-Schönlein purpura. Nephrol Dial Transplant. 1997;12:2277-2283.
- Fogazzi GB, Pasquali S, Moriggi M, et al. Long-term outcome of Schönlein-Henoch nephritis in the adult. Clin Nephrol. 1989;31:60-66.
- Sais G, Vidaller A, Jucgla A. Prognostic factors in leukocytoclastic vasculitis. a clinicopathologic study of 160 patients. Arch Dermatol. 1998;134:309-315.
- Kraft DM, McKee D, Scott C. Henoch-Schönlein purpura: a review. Am Fam Physician. 1998;58:405-408.
- Narchi H. Risk of long-term renal impairment and duration of follow up recommended for Henoch-Schönlein purpura with normal or minimal urinary findings: a systematic review. Arch Dis Child. 2005;90:916-920.
To the Editor:
A 57-year-old man with a history of type 2 diabetes mellitus and hypertension was hospitalized for heart disease resulting in an aortic valve replacement and multiple-vessel bypass grafting. He experienced a stormy septic postoperative course during which he developed numerous palpable purplish plaques (Figure 1). The lesions were bilateral and more heavily involved the lower legs and buttocks. The head and neck remained free of skin lesions. Additionally, the patient reported a bilateral burning sensation from the knees to the feet.
Punch biopsies of lesions from the right upper arm were obtained. Hematoxylin and eosin staining revealed neutrophilic-predominant small vessel vasculitis (Figure 2A) with the upper dermal location more heavily involved, as demonstrated by involvement of a superficial vascular plexus (Figures 2B and 2C) that was consistent with Henoch-Schönlein purpura (HSP). The diagnosis later was confirmed with immunofluorescence. Direct immunofluorescence revealed granular IgA deposition around the superficial vascular plexus (Figure 3). No IgG, IgM, C3, C5b-9 complement complex, or fibrinogen deposition was seen. Additionally, periodic acid-Schiff staining failed to show microorganisms, thrombi, or intravascular hyaline material.
At our initial consultation, we observed an ill-appearing afebrile man with purplish plaques. Our impression was that he had vasculitis and not warfarin necrosis, which had been suspected by the cardiovascular team. The burning sensation noted by the patient lent credence to our vasculitic diagnosis. Proteinuria and hematuria were present; however, the values for blood urea nitrogen, creatinine, and glomerular filtration rate all remained within reference range. His signs and symptoms responded dramatically to prednisone. He remains on 1 mg of prednisone daily and a nephrologist continues to monitor renal function as an outpatient.
Henoch-Schönlein purpura is a systemic leukocytoclastic vasculitis involving small vessels. The small vessel vasculitis is associated with IgA antigen-antibody complex deposition in areas throughout the body. Palpable purpura typically is seen on the skin, which characteristically involves dependent areas such as the legs and the buttocks. Lesions normally are present bilaterally in a symmetric distribution. Initially, the lesions develop as erythematous macules that progress to purple, nonblanching, palpable, and purpuric plaques.1 Henoch-Schönlein purpura most commonly involves the skin; however, other locations for the immune complexes include the gastrointestinal tract, joints, and kidneys.2 The cause for the body's immunogenic deposition response is unknown in a majority of cases.
Henoch-Schönlein purpura most commonly is seen in the pediatric population with a predilection for males.3 The incidence in the pediatric population is 13.5 to 20 per 100,000 children per year; HSP is more rare in adults.4-6 Henoch-Schönlein purpura most often is a self-limiting disease that requires only supportive treatment. The signs and symptoms last 4 to 6 weeks in most patients and resolve completely in 94% of children and 89% of adults.7 Renal involvement carries a worse prognosis. Adult patients have a higher incidence of renal involvement, renal insufficiency, and subsequent progression to end-stage renal disease.3,8-10 In a study by Hung et al8 of 65 children and 22 adult HSP patients, 12 adults presented with renal involvement in which hematuria or proteinuria were present. Of them, 6 progressed to renal insufficiency (defined as having a plasma creatinine concentration>1.2 mg/dL).8 Fogazzi et al11 reported similar findings; 8 of 16 patients affected with HSP progressed to renal insufficiency with creatinine clearances ranging from 31 to 60 mL/min, and 3 patients required chronic dialysis. Pillebout et al9 evaluated 250 adults with HSP and 32% reached renal insufficiency with creatinine clearances of less than 50 mL/min, with 11% of patients developing end-stage renal disease. The degree of hematuria and/or proteinuria has been shown to be an effective prognostic indicator.9,10 Coppo et al10 found a similar prognosis among children and adults with HSP-related nephritis.
Our patient described the burning sensation as occurring bilaterally from the knees down to the feet, which provided an additional clue that small vessel vasculitis was involved, as occluded blood vessels can cause ischemia to nerves and perivascular involvement can affect nearby neural structures. Sais et al12 demonstrated that paresthesia in the setting of HSP was a risk factor for systemic involvement. Of note, our patient's paresthesia lasted only several days.
The cause of HSP is not always as evident in the adult population as in the pediatric population. Early diagnosis of HSP in adults may allow for the proper instatement of treatment to deter long-term renal complications. Follow-up with urinalysis is recommended because a small percentage of patients have a late progression to renal failure.13,14
Because the dermatologists involved in this case knew where and what types of biopsies to perform, a correct diagnosis was obtained quickly, allowing for the correct therapeutic intervention. After the diagnosis of HSP is made in an adult, nephrology should be consulted early in the treatment course.
To the Editor:
A 57-year-old man with a history of type 2 diabetes mellitus and hypertension was hospitalized for heart disease resulting in an aortic valve replacement and multiple-vessel bypass grafting. He experienced a stormy septic postoperative course during which he developed numerous palpable purplish plaques (Figure 1). The lesions were bilateral and more heavily involved the lower legs and buttocks. The head and neck remained free of skin lesions. Additionally, the patient reported a bilateral burning sensation from the knees to the feet.
Punch biopsies of lesions from the right upper arm were obtained. Hematoxylin and eosin staining revealed neutrophilic-predominant small vessel vasculitis (Figure 2A) with the upper dermal location more heavily involved, as demonstrated by involvement of a superficial vascular plexus (Figures 2B and 2C) that was consistent with Henoch-Schönlein purpura (HSP). The diagnosis later was confirmed with immunofluorescence. Direct immunofluorescence revealed granular IgA deposition around the superficial vascular plexus (Figure 3). No IgG, IgM, C3, C5b-9 complement complex, or fibrinogen deposition was seen. Additionally, periodic acid-Schiff staining failed to show microorganisms, thrombi, or intravascular hyaline material.
At our initial consultation, we observed an ill-appearing afebrile man with purplish plaques. Our impression was that he had vasculitis and not warfarin necrosis, which had been suspected by the cardiovascular team. The burning sensation noted by the patient lent credence to our vasculitic diagnosis. Proteinuria and hematuria were present; however, the values for blood urea nitrogen, creatinine, and glomerular filtration rate all remained within reference range. His signs and symptoms responded dramatically to prednisone. He remains on 1 mg of prednisone daily and a nephrologist continues to monitor renal function as an outpatient.
Henoch-Schönlein purpura is a systemic leukocytoclastic vasculitis involving small vessels. The small vessel vasculitis is associated with IgA antigen-antibody complex deposition in areas throughout the body. Palpable purpura typically is seen on the skin, which characteristically involves dependent areas such as the legs and the buttocks. Lesions normally are present bilaterally in a symmetric distribution. Initially, the lesions develop as erythematous macules that progress to purple, nonblanching, palpable, and purpuric plaques.1 Henoch-Schönlein purpura most commonly involves the skin; however, other locations for the immune complexes include the gastrointestinal tract, joints, and kidneys.2 The cause for the body's immunogenic deposition response is unknown in a majority of cases.
Henoch-Schönlein purpura most commonly is seen in the pediatric population with a predilection for males.3 The incidence in the pediatric population is 13.5 to 20 per 100,000 children per year; HSP is more rare in adults.4-6 Henoch-Schönlein purpura most often is a self-limiting disease that requires only supportive treatment. The signs and symptoms last 4 to 6 weeks in most patients and resolve completely in 94% of children and 89% of adults.7 Renal involvement carries a worse prognosis. Adult patients have a higher incidence of renal involvement, renal insufficiency, and subsequent progression to end-stage renal disease.3,8-10 In a study by Hung et al8 of 65 children and 22 adult HSP patients, 12 adults presented with renal involvement in which hematuria or proteinuria were present. Of them, 6 progressed to renal insufficiency (defined as having a plasma creatinine concentration>1.2 mg/dL).8 Fogazzi et al11 reported similar findings; 8 of 16 patients affected with HSP progressed to renal insufficiency with creatinine clearances ranging from 31 to 60 mL/min, and 3 patients required chronic dialysis. Pillebout et al9 evaluated 250 adults with HSP and 32% reached renal insufficiency with creatinine clearances of less than 50 mL/min, with 11% of patients developing end-stage renal disease. The degree of hematuria and/or proteinuria has been shown to be an effective prognostic indicator.9,10 Coppo et al10 found a similar prognosis among children and adults with HSP-related nephritis.
Our patient described the burning sensation as occurring bilaterally from the knees down to the feet, which provided an additional clue that small vessel vasculitis was involved, as occluded blood vessels can cause ischemia to nerves and perivascular involvement can affect nearby neural structures. Sais et al12 demonstrated that paresthesia in the setting of HSP was a risk factor for systemic involvement. Of note, our patient's paresthesia lasted only several days.
The cause of HSP is not always as evident in the adult population as in the pediatric population. Early diagnosis of HSP in adults may allow for the proper instatement of treatment to deter long-term renal complications. Follow-up with urinalysis is recommended because a small percentage of patients have a late progression to renal failure.13,14
Because the dermatologists involved in this case knew where and what types of biopsies to perform, a correct diagnosis was obtained quickly, allowing for the correct therapeutic intervention. After the diagnosis of HSP is made in an adult, nephrology should be consulted early in the treatment course.
- Rai A, Nast C, Adler S. Henoch-Schönlein purpura nephritis. J Am Soc Nephrol. 1999;10:2637-2644.
- Helander SD, De Castro FR, Gibson LE. Henoch-Schönlein purpura: clinicopathologic correlation of cutaneous vascular IgA deposits and the relationship to leukocytoclastic vasculitis. Acta Derm Venereol. 1995;75:125-129.
- Garcia-Porrua C, Calvino MC, Llorca J, et al. Henoch-Schönlein purpura in children and adults: clinical differences in a defined population. Semin Arthritis Rheum. 2002;32:149-156.
- Stewart M, Savage JM, Bell B, et al. Long term renal prognosis of Henoch-Schönlein purpura in an unselected childhood population. Eur J Pediatr. 1988;147:113-115.
- Watts RA, Scott DG. Epidemiology of the vasculitides. Semin Respir Crit Care. 2004;25:455-464.
- Gardner-Medwin JM, Dolezalova P, Cummins C, et al. Incidence of Henoch-Schönlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet. 2002;360:1197-1202.
- Blanco R, Martínez-Taboada VM, Rodríguez-Valverde V, et al. Henoch-Schönlein purpura in adulthood and childhood: two different expressions of the same syndrome. Arthritis Rheum. 1997;40:859-864.
- Hung SP, Yang YH, Lin YT, et al. Clinical manifestations and outcomes of Henoch-Schönlein purpura: comparison between adults and children. Pediatr Neonatol. 2009;50:162-168.
- Pillebout E, Thervet E, Hill G, et al. Henoch-Schönlein purpura in adults: outcomes and prognostic factors. J Am Soc Nephrol. 2002;13:1271-1278.
- Coppo R, Mazzucco G, Cagnoli L, et al. Long-term prognosis of Henoch-Schönlein nephritis in adults and children. Italian Group of Renal Immunopathology collaborative study on Henoch-Schönlein purpura. Nephrol Dial Transplant. 1997;12:2277-2283.
- Fogazzi GB, Pasquali S, Moriggi M, et al. Long-term outcome of Schönlein-Henoch nephritis in the adult. Clin Nephrol. 1989;31:60-66.
- Sais G, Vidaller A, Jucgla A. Prognostic factors in leukocytoclastic vasculitis. a clinicopathologic study of 160 patients. Arch Dermatol. 1998;134:309-315.
- Kraft DM, McKee D, Scott C. Henoch-Schönlein purpura: a review. Am Fam Physician. 1998;58:405-408.
- Narchi H. Risk of long-term renal impairment and duration of follow up recommended for Henoch-Schönlein purpura with normal or minimal urinary findings: a systematic review. Arch Dis Child. 2005;90:916-920.
- Rai A, Nast C, Adler S. Henoch-Schönlein purpura nephritis. J Am Soc Nephrol. 1999;10:2637-2644.
- Helander SD, De Castro FR, Gibson LE. Henoch-Schönlein purpura: clinicopathologic correlation of cutaneous vascular IgA deposits and the relationship to leukocytoclastic vasculitis. Acta Derm Venereol. 1995;75:125-129.
- Garcia-Porrua C, Calvino MC, Llorca J, et al. Henoch-Schönlein purpura in children and adults: clinical differences in a defined population. Semin Arthritis Rheum. 2002;32:149-156.
- Stewart M, Savage JM, Bell B, et al. Long term renal prognosis of Henoch-Schönlein purpura in an unselected childhood population. Eur J Pediatr. 1988;147:113-115.
- Watts RA, Scott DG. Epidemiology of the vasculitides. Semin Respir Crit Care. 2004;25:455-464.
- Gardner-Medwin JM, Dolezalova P, Cummins C, et al. Incidence of Henoch-Schönlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet. 2002;360:1197-1202.
- Blanco R, Martínez-Taboada VM, Rodríguez-Valverde V, et al. Henoch-Schönlein purpura in adulthood and childhood: two different expressions of the same syndrome. Arthritis Rheum. 1997;40:859-864.
- Hung SP, Yang YH, Lin YT, et al. Clinical manifestations and outcomes of Henoch-Schönlein purpura: comparison between adults and children. Pediatr Neonatol. 2009;50:162-168.
- Pillebout E, Thervet E, Hill G, et al. Henoch-Schönlein purpura in adults: outcomes and prognostic factors. J Am Soc Nephrol. 2002;13:1271-1278.
- Coppo R, Mazzucco G, Cagnoli L, et al. Long-term prognosis of Henoch-Schönlein nephritis in adults and children. Italian Group of Renal Immunopathology collaborative study on Henoch-Schönlein purpura. Nephrol Dial Transplant. 1997;12:2277-2283.
- Fogazzi GB, Pasquali S, Moriggi M, et al. Long-term outcome of Schönlein-Henoch nephritis in the adult. Clin Nephrol. 1989;31:60-66.
- Sais G, Vidaller A, Jucgla A. Prognostic factors in leukocytoclastic vasculitis. a clinicopathologic study of 160 patients. Arch Dermatol. 1998;134:309-315.
- Kraft DM, McKee D, Scott C. Henoch-Schönlein purpura: a review. Am Fam Physician. 1998;58:405-408.
- Narchi H. Risk of long-term renal impairment and duration of follow up recommended for Henoch-Schönlein purpura with normal or minimal urinary findings: a systematic review. Arch Dis Child. 2005;90:916-920.
Practice Points
- Henoch-Schönlein purpura is a multidisciplinary problem.
- Henoch-Schönlein purpura is an IgA-mediated disorder that is more common in children and has a more severe course in adults.

Maintenance taxane therapy of no benefit in advanced ovarian cancer
NATIONAL HARBOR, MD. – Using either a polymerized formulation of paclitaxel or paclitaxel alone as maintenance therapy conferred no survival benefit for women with advanced ovarian, fallopian tube, or peritoneal cancer.
In a phase III randomized trial, patients survived a median 54.8 months with surveillance alone, 51.3 months with maintenance paclitaxel, and 60.0 months with maintenance paclitaxel poliglumex; these differences were not statistically significant.
In a presentation at the annual meeting of the Society of Gynecologic Oncology, Larry Copeland, MD, a professor of gynecologic oncology at Ohio State University, Columbus, said that treatment with surgery and chemotherapy yields a clinical complete response in many patients with these cancers. However, he said, recurrent progressive disease is still very common; the rationale behind maintenance chemotherapy is that it may “reduce the risk of recurrence and extend survival.”
There had been promising earlier data supporting this approach from a previous phase III comparison trial that evaluated the difference in clinical complete response between 3 or 12 cycles of paclitaxel, said Dr. Copeland. The results of a predefined interim analysis prompted the data monitoring committee to close that study (J Clin Oncol. 2003;21[13]:2460-5) since the 12-cycle, 7-month arm of the study had better progression-free survival. However, the 12-cycle protocol did not confer a benefit in overall survival, the investigators later reported (Gynecol Oncol 2009;114[2]:195-8).
The current stage III randomized trial enrolled women with stage III or IV ovarian, fallopian tube, or peritoneal cancer who had had five to eight cycles of chemotherapy and achieved clinical complete response. If patients had neuropathy, it could not exceed grade 1, and their cancer performance status scores could not exceed 2, Dr. Copeland said.
Patients were randomized 1:1:1 to a surveillance arm, to receive paclitaxel as a 3-hour infusion, or to receive paclitaxel poliglumex as a 10- to 20-minute infusion. Both study drugs were dosed at 35 mg/m2 every 28 days for 12 cycles.
The study ran from March 2005 to January 2014, enrolling 1,157 patients who were followed for a median of 71 months. Over 80% of patients in each study arm had ovarian cancer, and a similar number had stage III cancer and serous histology. Over 90% of patients in each arm had grade 2 or higher histology.
The study was designed as a superiority design, and patients were not to receive other cancer treatments until they had disease progression. Primary clinical endpoints for the study included overall survival, quality of life as measured by the Ovarian Specific Questionnaire Quality of Life–Cancer, and patient-reported neurotoxicity as reported on the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group/Neurotoxicity questionnaire.
The third scheduled interim analysis, in May 2016, examined the primary endpoint of overall survival, triggered when at least 200 deaths occurred in the surveillance group. The overall final analysis had been scheduled for the point at which at least 301 deaths happened in the surveillance group. In the abstract accompanying the presentation, Dr. Copeland wrote that the data at the point of this interim analysis indicated that “the relative death hazards passed the futility boundaries for both taxane regimens.”
“The log-rank statistic for each taxane regimen was below the interval specific in the study design, making it unlikely either of the taxane regimens has superior overall survival compared to surveillance,” said Dr. Copeland.
The hazard ratio for overall survival of the paclitaxel group compared to surveillance was 1.104, with a 97.5% confidence interval (CI) of 0.884-1.38. For the paclitaxel poliglumex group, the hazard ratio compared to surveillance alone was 0.979 (97.5% CI, 0.781-1.23).
Dr. Copeland and his colleagues also looked at progression-free survival, not a primary endpoint of the study. For the paclitaxel patients compared to surveillance, the HR for progression-free survival was 0.783 (95% CI, 0.666-0.921). For paclitaxel poliglumex, the HR was 0.847 (95% CI, 0.666-0.921).
Not unexpectedly, more patients who received taxane treatment than those in the surveillance arm experienced adverse events, said Dr. Copeland. The most common adverse events were hypersensitivity or allergic reactions, fatigue, alopecia, nausea, constipation, and sensory neuropathies. Grade 2 alopecia was experienced by about a quarter of the paclitaxel poliglumex cohort, and by a little less than half of the paclitaxel cohort. Neurologic adverse events were very common, reported by three quarters of the paclitaxel poliglumex cohort, four in five of the paclitaxel group, and by a little over half of the surveillance cohort.
Overall quality of life scores did not differ significantly among the treatment arms.
In an exploratory analysis, Dr. Copeland and his colleagues determined that patients with no residual disease (R0 patients) after initial cytoreductive surgery fared better, with a median 70 months of survival compared to a median 43.6 months for individuals with gross residual disease. When those patients were sorted out by treatment arm, there was no significant difference in OS for R0 patients who received any intervention or surveillance.
“Overall survival was not improved with taxane maintenance, though progression-free survival is slightly delayed,” Dr. Copeland concluded.
In discussion after the presentation, he said that he is not sure that further investigations will be pursued for paclitaxel poliglumex in the treatment of ovarian cancers.
Paclitaxel poliglumex (CT-2103; Opaxio) is paclitaxel conjugated to a polyglutamate polymer, a formulation that may enhance tumor penetration and retention, and that allows shorter infusion at a peripheral site. Previous work had shown that CT-2103’s structure enhanced pharmacokinetics and potentially decreased toxicity (Expert Opin Investig Drugs. 2004 Nov;13[11]:1501-8).
Dr. Copeland reported receiving consulting or honoraria fees from Clovis, Advaxis, Janssen, and Tesaro, and is a stockholder or shareholder in Merck, Eli Lilly, and Cardinal Health. The study was sponsored by the Cancer Therapy Evaluation Program of the National Cancer Institute and by Cell Therapeutics, which plans to market paclitaxel poliglumex.
[email protected]
On Twitter @karioakes
NATIONAL HARBOR, MD. – Using either a polymerized formulation of paclitaxel or paclitaxel alone as maintenance therapy conferred no survival benefit for women with advanced ovarian, fallopian tube, or peritoneal cancer.
In a phase III randomized trial, patients survived a median 54.8 months with surveillance alone, 51.3 months with maintenance paclitaxel, and 60.0 months with maintenance paclitaxel poliglumex; these differences were not statistically significant.
In a presentation at the annual meeting of the Society of Gynecologic Oncology, Larry Copeland, MD, a professor of gynecologic oncology at Ohio State University, Columbus, said that treatment with surgery and chemotherapy yields a clinical complete response in many patients with these cancers. However, he said, recurrent progressive disease is still very common; the rationale behind maintenance chemotherapy is that it may “reduce the risk of recurrence and extend survival.”
There had been promising earlier data supporting this approach from a previous phase III comparison trial that evaluated the difference in clinical complete response between 3 or 12 cycles of paclitaxel, said Dr. Copeland. The results of a predefined interim analysis prompted the data monitoring committee to close that study (J Clin Oncol. 2003;21[13]:2460-5) since the 12-cycle, 7-month arm of the study had better progression-free survival. However, the 12-cycle protocol did not confer a benefit in overall survival, the investigators later reported (Gynecol Oncol 2009;114[2]:195-8).
The current stage III randomized trial enrolled women with stage III or IV ovarian, fallopian tube, or peritoneal cancer who had had five to eight cycles of chemotherapy and achieved clinical complete response. If patients had neuropathy, it could not exceed grade 1, and their cancer performance status scores could not exceed 2, Dr. Copeland said.
Patients were randomized 1:1:1 to a surveillance arm, to receive paclitaxel as a 3-hour infusion, or to receive paclitaxel poliglumex as a 10- to 20-minute infusion. Both study drugs were dosed at 35 mg/m2 every 28 days for 12 cycles.
The study ran from March 2005 to January 2014, enrolling 1,157 patients who were followed for a median of 71 months. Over 80% of patients in each study arm had ovarian cancer, and a similar number had stage III cancer and serous histology. Over 90% of patients in each arm had grade 2 or higher histology.
The study was designed as a superiority design, and patients were not to receive other cancer treatments until they had disease progression. Primary clinical endpoints for the study included overall survival, quality of life as measured by the Ovarian Specific Questionnaire Quality of Life–Cancer, and patient-reported neurotoxicity as reported on the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group/Neurotoxicity questionnaire.
The third scheduled interim analysis, in May 2016, examined the primary endpoint of overall survival, triggered when at least 200 deaths occurred in the surveillance group. The overall final analysis had been scheduled for the point at which at least 301 deaths happened in the surveillance group. In the abstract accompanying the presentation, Dr. Copeland wrote that the data at the point of this interim analysis indicated that “the relative death hazards passed the futility boundaries for both taxane regimens.”
“The log-rank statistic for each taxane regimen was below the interval specific in the study design, making it unlikely either of the taxane regimens has superior overall survival compared to surveillance,” said Dr. Copeland.
The hazard ratio for overall survival of the paclitaxel group compared to surveillance was 1.104, with a 97.5% confidence interval (CI) of 0.884-1.38. For the paclitaxel poliglumex group, the hazard ratio compared to surveillance alone was 0.979 (97.5% CI, 0.781-1.23).
Dr. Copeland and his colleagues also looked at progression-free survival, not a primary endpoint of the study. For the paclitaxel patients compared to surveillance, the HR for progression-free survival was 0.783 (95% CI, 0.666-0.921). For paclitaxel poliglumex, the HR was 0.847 (95% CI, 0.666-0.921).
Not unexpectedly, more patients who received taxane treatment than those in the surveillance arm experienced adverse events, said Dr. Copeland. The most common adverse events were hypersensitivity or allergic reactions, fatigue, alopecia, nausea, constipation, and sensory neuropathies. Grade 2 alopecia was experienced by about a quarter of the paclitaxel poliglumex cohort, and by a little less than half of the paclitaxel cohort. Neurologic adverse events were very common, reported by three quarters of the paclitaxel poliglumex cohort, four in five of the paclitaxel group, and by a little over half of the surveillance cohort.
Overall quality of life scores did not differ significantly among the treatment arms.
In an exploratory analysis, Dr. Copeland and his colleagues determined that patients with no residual disease (R0 patients) after initial cytoreductive surgery fared better, with a median 70 months of survival compared to a median 43.6 months for individuals with gross residual disease. When those patients were sorted out by treatment arm, there was no significant difference in OS for R0 patients who received any intervention or surveillance.
“Overall survival was not improved with taxane maintenance, though progression-free survival is slightly delayed,” Dr. Copeland concluded.
In discussion after the presentation, he said that he is not sure that further investigations will be pursued for paclitaxel poliglumex in the treatment of ovarian cancers.
Paclitaxel poliglumex (CT-2103; Opaxio) is paclitaxel conjugated to a polyglutamate polymer, a formulation that may enhance tumor penetration and retention, and that allows shorter infusion at a peripheral site. Previous work had shown that CT-2103’s structure enhanced pharmacokinetics and potentially decreased toxicity (Expert Opin Investig Drugs. 2004 Nov;13[11]:1501-8).
Dr. Copeland reported receiving consulting or honoraria fees from Clovis, Advaxis, Janssen, and Tesaro, and is a stockholder or shareholder in Merck, Eli Lilly, and Cardinal Health. The study was sponsored by the Cancer Therapy Evaluation Program of the National Cancer Institute and by Cell Therapeutics, which plans to market paclitaxel poliglumex.
[email protected]
On Twitter @karioakes
NATIONAL HARBOR, MD. – Using either a polymerized formulation of paclitaxel or paclitaxel alone as maintenance therapy conferred no survival benefit for women with advanced ovarian, fallopian tube, or peritoneal cancer.
In a phase III randomized trial, patients survived a median 54.8 months with surveillance alone, 51.3 months with maintenance paclitaxel, and 60.0 months with maintenance paclitaxel poliglumex; these differences were not statistically significant.
In a presentation at the annual meeting of the Society of Gynecologic Oncology, Larry Copeland, MD, a professor of gynecologic oncology at Ohio State University, Columbus, said that treatment with surgery and chemotherapy yields a clinical complete response in many patients with these cancers. However, he said, recurrent progressive disease is still very common; the rationale behind maintenance chemotherapy is that it may “reduce the risk of recurrence and extend survival.”
There had been promising earlier data supporting this approach from a previous phase III comparison trial that evaluated the difference in clinical complete response between 3 or 12 cycles of paclitaxel, said Dr. Copeland. The results of a predefined interim analysis prompted the data monitoring committee to close that study (J Clin Oncol. 2003;21[13]:2460-5) since the 12-cycle, 7-month arm of the study had better progression-free survival. However, the 12-cycle protocol did not confer a benefit in overall survival, the investigators later reported (Gynecol Oncol 2009;114[2]:195-8).
The current stage III randomized trial enrolled women with stage III or IV ovarian, fallopian tube, or peritoneal cancer who had had five to eight cycles of chemotherapy and achieved clinical complete response. If patients had neuropathy, it could not exceed grade 1, and their cancer performance status scores could not exceed 2, Dr. Copeland said.
Patients were randomized 1:1:1 to a surveillance arm, to receive paclitaxel as a 3-hour infusion, or to receive paclitaxel poliglumex as a 10- to 20-minute infusion. Both study drugs were dosed at 35 mg/m2 every 28 days for 12 cycles.
The study ran from March 2005 to January 2014, enrolling 1,157 patients who were followed for a median of 71 months. Over 80% of patients in each study arm had ovarian cancer, and a similar number had stage III cancer and serous histology. Over 90% of patients in each arm had grade 2 or higher histology.
The study was designed as a superiority design, and patients were not to receive other cancer treatments until they had disease progression. Primary clinical endpoints for the study included overall survival, quality of life as measured by the Ovarian Specific Questionnaire Quality of Life–Cancer, and patient-reported neurotoxicity as reported on the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group/Neurotoxicity questionnaire.
The third scheduled interim analysis, in May 2016, examined the primary endpoint of overall survival, triggered when at least 200 deaths occurred in the surveillance group. The overall final analysis had been scheduled for the point at which at least 301 deaths happened in the surveillance group. In the abstract accompanying the presentation, Dr. Copeland wrote that the data at the point of this interim analysis indicated that “the relative death hazards passed the futility boundaries for both taxane regimens.”
“The log-rank statistic for each taxane regimen was below the interval specific in the study design, making it unlikely either of the taxane regimens has superior overall survival compared to surveillance,” said Dr. Copeland.
The hazard ratio for overall survival of the paclitaxel group compared to surveillance was 1.104, with a 97.5% confidence interval (CI) of 0.884-1.38. For the paclitaxel poliglumex group, the hazard ratio compared to surveillance alone was 0.979 (97.5% CI, 0.781-1.23).
Dr. Copeland and his colleagues also looked at progression-free survival, not a primary endpoint of the study. For the paclitaxel patients compared to surveillance, the HR for progression-free survival was 0.783 (95% CI, 0.666-0.921). For paclitaxel poliglumex, the HR was 0.847 (95% CI, 0.666-0.921).
Not unexpectedly, more patients who received taxane treatment than those in the surveillance arm experienced adverse events, said Dr. Copeland. The most common adverse events were hypersensitivity or allergic reactions, fatigue, alopecia, nausea, constipation, and sensory neuropathies. Grade 2 alopecia was experienced by about a quarter of the paclitaxel poliglumex cohort, and by a little less than half of the paclitaxel cohort. Neurologic adverse events were very common, reported by three quarters of the paclitaxel poliglumex cohort, four in five of the paclitaxel group, and by a little over half of the surveillance cohort.
Overall quality of life scores did not differ significantly among the treatment arms.
In an exploratory analysis, Dr. Copeland and his colleagues determined that patients with no residual disease (R0 patients) after initial cytoreductive surgery fared better, with a median 70 months of survival compared to a median 43.6 months for individuals with gross residual disease. When those patients were sorted out by treatment arm, there was no significant difference in OS for R0 patients who received any intervention or surveillance.
“Overall survival was not improved with taxane maintenance, though progression-free survival is slightly delayed,” Dr. Copeland concluded.
In discussion after the presentation, he said that he is not sure that further investigations will be pursued for paclitaxel poliglumex in the treatment of ovarian cancers.
Paclitaxel poliglumex (CT-2103; Opaxio) is paclitaxel conjugated to a polyglutamate polymer, a formulation that may enhance tumor penetration and retention, and that allows shorter infusion at a peripheral site. Previous work had shown that CT-2103’s structure enhanced pharmacokinetics and potentially decreased toxicity (Expert Opin Investig Drugs. 2004 Nov;13[11]:1501-8).
Dr. Copeland reported receiving consulting or honoraria fees from Clovis, Advaxis, Janssen, and Tesaro, and is a stockholder or shareholder in Merck, Eli Lilly, and Cardinal Health. The study was sponsored by the Cancer Therapy Evaluation Program of the National Cancer Institute and by Cell Therapeutics, which plans to market paclitaxel poliglumex.
[email protected]
On Twitter @karioakes
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point:
Major finding: There was no statistically significant overall survival benefit of maintenance taxane therapy for advanced ovarian, fallopian tube, or peritoneal cancer, compared with surveillance.
Data source: Phase III randomized trial of 1,157 patients with advanced ovarian, fallopian tube, or peritoneal cancer.
Disclosures: Dr. Copeland reported receiving consulting or honoraria fees from Clovis, Advaxis, Janssen, and Tesaro, and is a stockholder or shareholder in Merck, Eli Lilly, and Cardinal Health. The study was sponsored by the Cancer Therapy Evaluation Program of the National Cancer Institute and by Cell Therapeutics, which plans to market paclitaxel poliglumex.
Are new medications on horizon for patients with depression, inflammation?
SCOTTSDALE, ARIZ. – Inflammation is inextricably linked to depression in a subset of patients who differ from other depressed patients in their responses to certain interventions, according to Charles L. Raison, MD.
“The brains of people who are depressed and who have inflammation look very different from those of people who are depressed without inflammation,” Dr. Raison said in an interview at the annual meeting of the American College of Psychiatrists. “They have different connectivity patterns, different glutaminergic patterns, different signaling. It seems that inflammatory processes change the way different parts of the brain talk to each other and seem to do so in consistent ways.”
Dr. Raison, the Mary Sue and Mike Shannon Chair for Healthy Minds, Children & Families at the University of Wisconsin–Madison, told a plenary audience at the meeting: “We [psychiatrists] are so brain centric, it’s easy to forget how much the immune system drives us. It’s either like a second brain, or it is at least part of the brain.”

Over the years, Dr. Raison and his colleagues have observed how inflammation can interfere with mood, leading to depression in people who previously did not report or describe depressive symptoms.
In the early 2000s, Dr. Raison and others such as Andrew H. Miller, MD, a psychiatric oncologist, investigated the inflammatory response and levels of depression in people treated with interferon-alpha for hepatitis C infection (J Clin Psychiatry. 2005 Jan;66[1]:41-8). They found that more than half of people who had not reported or described depressive symptoms at baseline subsequently reported depressive symptoms. “In a nutshell, we found that interferon-alpha induces every single brain-body function associated with regular old major depression,” said Dr. Raison, also a professor of psychiatry at the university.
In another study, this one led by neuropsychosomatic specialist Dominique L. Musselman, MD, a similar cohort of hepatitis C patients assessed for baseline depression was randomly assigned to either placebo or paroxetine during the course of interferon-alpha treatment. Patients treated with placebo had a 0.24 relative risk (95% confidence interval, 0.08-0.93) of developing depression, compared with the paroxetine group (N Eng J Med. 2001;344:961-6).
The real “breakthrough” in understanding the role of inflammation in depression, Dr. Raison said, came from studies that made the association between early-life adversity, depression, and inflammation. In one particular study, Dr. Raison and colleagues found that stress-induced spikes in interleukin-6 and NF-kappaB DNA-binding were greater in patients with higher baseline levels of depression and higher levels of early life stress (Am J Psychiatry. 2006 Sep;163[9]:1630-3).
Spikes in the inflammatory response independently correlated with depression severity but not with early life stress, which Dr. Raison said suggests that adversity likely can cause inflammation – and thus predisposes people to depression, and not necessarily vice versa.
“Something about early adversity in life programs the brain-body complex to run inflammatory systems hot, probably because it’s an effective way to be ready for [a stream of] unpredictable miseries,” Dr. Raison said during the session. “Chronic, elevated inflammation [early on] seems to predict increased depression later.”
Now that the link has been established between some depression and inflammation, the next step for science is to tease out who is most likely to respond to anti-inflammatory interventions for depression, Dr. Raison said.
“Something that is just starting to emerge is that maybe the relationship between inflammation and depression is not a straight line but a U-shaped curve, such that if you have too much inflammation, you’re in trouble, and if you have too little, you’re also in trouble,” he said in the interview, citing a study he and others conducted into blocking the inflammatory response. In that study, people with major depression who were otherwise medically healthy received either three infusions of the anti-inflammatory tumor necrosis factor–alpha antagonist infliximab (5 mg/kg), or of salt water. The investigators found that placebo worked just as well as infliximab. But patients with lower levels of inflammation at baseline had the greatest improvements in their Hamilton Rating Scale for Depression scores with placebo when compared with treatment (JAMA Psychiatry. 2013 Jan;70[1]:31-41).
Data are not yet conclusive, but Dr. Raison said the field soon could use biomarkers such as levels of C-reactive protein to determine whether patients will respond to anti-inflammatories such as omega-3 essential fatty acids. “Everyone in psychiatry is desperate to find clear, unambiguous answers. We’re right on the edge, but we’re not there yet.”
Until then, Dr. Raison cautioned against the “indiscriminate” use of anti-inflammatories, lest they exacerbate patients’ depressive symptoms. “For instance, omega-3 fatty acids might actually be counterproductive in a lot of depressed people,” he said. Still, he believes that “developing and studying anti-inflammatory strategies is probably going to lead to a novel way of treating depression in some people. What is beautiful is that if these studies continue, we might actually be able – for the first time – to target a subgroup of patients for a specific treatment.”
Dr. Raison is on the scientific advisory board of the Usona Institute, a nonprofit medical research firm.
[email protected]
On Twitter @whitneymcknight
SCOTTSDALE, ARIZ. – Inflammation is inextricably linked to depression in a subset of patients who differ from other depressed patients in their responses to certain interventions, according to Charles L. Raison, MD.
“The brains of people who are depressed and who have inflammation look very different from those of people who are depressed without inflammation,” Dr. Raison said in an interview at the annual meeting of the American College of Psychiatrists. “They have different connectivity patterns, different glutaminergic patterns, different signaling. It seems that inflammatory processes change the way different parts of the brain talk to each other and seem to do so in consistent ways.”
Dr. Raison, the Mary Sue and Mike Shannon Chair for Healthy Minds, Children & Families at the University of Wisconsin–Madison, told a plenary audience at the meeting: “We [psychiatrists] are so brain centric, it’s easy to forget how much the immune system drives us. It’s either like a second brain, or it is at least part of the brain.”
Over the years, Dr. Raison and his colleagues have observed how inflammation can interfere with mood, leading to depression in people who previously did not report or describe depressive symptoms.
In the early 2000s, Dr. Raison and others such as Andrew H. Miller, MD, a psychiatric oncologist, investigated the inflammatory response and levels of depression in people treated with interferon-alpha for hepatitis C infection (J Clin Psychiatry. 2005 Jan;66[1]:41-8). They found that more than half of people who had not reported or described depressive symptoms at baseline subsequently reported depressive symptoms. “In a nutshell, we found that interferon-alpha induces every single brain-body function associated with regular old major depression,” said Dr. Raison, also a professor of psychiatry at the university.
In another study, this one led by neuropsychosomatic specialist Dominique L. Musselman, MD, a similar cohort of hepatitis C patients assessed for baseline depression was randomly assigned to either placebo or paroxetine during the course of interferon-alpha treatment. Patients treated with placebo had a 0.24 relative risk (95% confidence interval, 0.08-0.93) of developing depression, compared with the paroxetine group (N Eng J Med. 2001;344:961-6).
The real “breakthrough” in understanding the role of inflammation in depression, Dr. Raison said, came from studies that made the association between early-life adversity, depression, and inflammation. In one particular study, Dr. Raison and colleagues found that stress-induced spikes in interleukin-6 and NF-kappaB DNA-binding were greater in patients with higher baseline levels of depression and higher levels of early life stress (Am J Psychiatry. 2006 Sep;163[9]:1630-3).
Spikes in the inflammatory response independently correlated with depression severity but not with early life stress, which Dr. Raison said suggests that adversity likely can cause inflammation – and thus predisposes people to depression, and not necessarily vice versa.
“Something about early adversity in life programs the brain-body complex to run inflammatory systems hot, probably because it’s an effective way to be ready for [a stream of] unpredictable miseries,” Dr. Raison said during the session. “Chronic, elevated inflammation [early on] seems to predict increased depression later.”
Now that the link has been established between some depression and inflammation, the next step for science is to tease out who is most likely to respond to anti-inflammatory interventions for depression, Dr. Raison said.
“Something that is just starting to emerge is that maybe the relationship between inflammation and depression is not a straight line but a U-shaped curve, such that if you have too much inflammation, you’re in trouble, and if you have too little, you’re also in trouble,” he said in the interview, citing a study he and others conducted into blocking the inflammatory response. In that study, people with major depression who were otherwise medically healthy received either three infusions of the anti-inflammatory tumor necrosis factor–alpha antagonist infliximab (5 mg/kg), or of salt water. The investigators found that placebo worked just as well as infliximab. But patients with lower levels of inflammation at baseline had the greatest improvements in their Hamilton Rating Scale for Depression scores with placebo when compared with treatment (JAMA Psychiatry. 2013 Jan;70[1]:31-41).
Data are not yet conclusive, but Dr. Raison said the field soon could use biomarkers such as levels of C-reactive protein to determine whether patients will respond to anti-inflammatories such as omega-3 essential fatty acids. “Everyone in psychiatry is desperate to find clear, unambiguous answers. We’re right on the edge, but we’re not there yet.”
Until then, Dr. Raison cautioned against the “indiscriminate” use of anti-inflammatories, lest they exacerbate patients’ depressive symptoms. “For instance, omega-3 fatty acids might actually be counterproductive in a lot of depressed people,” he said. Still, he believes that “developing and studying anti-inflammatory strategies is probably going to lead to a novel way of treating depression in some people. What is beautiful is that if these studies continue, we might actually be able – for the first time – to target a subgroup of patients for a specific treatment.”
Dr. Raison is on the scientific advisory board of the Usona Institute, a nonprofit medical research firm.
[email protected]
On Twitter @whitneymcknight
SCOTTSDALE, ARIZ. – Inflammation is inextricably linked to depression in a subset of patients who differ from other depressed patients in their responses to certain interventions, according to Charles L. Raison, MD.
“The brains of people who are depressed and who have inflammation look very different from those of people who are depressed without inflammation,” Dr. Raison said in an interview at the annual meeting of the American College of Psychiatrists. “They have different connectivity patterns, different glutaminergic patterns, different signaling. It seems that inflammatory processes change the way different parts of the brain talk to each other and seem to do so in consistent ways.”
Dr. Raison, the Mary Sue and Mike Shannon Chair for Healthy Minds, Children & Families at the University of Wisconsin–Madison, told a plenary audience at the meeting: “We [psychiatrists] are so brain centric, it’s easy to forget how much the immune system drives us. It’s either like a second brain, or it is at least part of the brain.”
Over the years, Dr. Raison and his colleagues have observed how inflammation can interfere with mood, leading to depression in people who previously did not report or describe depressive symptoms.
In the early 2000s, Dr. Raison and others such as Andrew H. Miller, MD, a psychiatric oncologist, investigated the inflammatory response and levels of depression in people treated with interferon-alpha for hepatitis C infection (J Clin Psychiatry. 2005 Jan;66[1]:41-8). They found that more than half of people who had not reported or described depressive symptoms at baseline subsequently reported depressive symptoms. “In a nutshell, we found that interferon-alpha induces every single brain-body function associated with regular old major depression,” said Dr. Raison, also a professor of psychiatry at the university.
In another study, this one led by neuropsychosomatic specialist Dominique L. Musselman, MD, a similar cohort of hepatitis C patients assessed for baseline depression was randomly assigned to either placebo or paroxetine during the course of interferon-alpha treatment. Patients treated with placebo had a 0.24 relative risk (95% confidence interval, 0.08-0.93) of developing depression, compared with the paroxetine group (N Eng J Med. 2001;344:961-6).
The real “breakthrough” in understanding the role of inflammation in depression, Dr. Raison said, came from studies that made the association between early-life adversity, depression, and inflammation. In one particular study, Dr. Raison and colleagues found that stress-induced spikes in interleukin-6 and NF-kappaB DNA-binding were greater in patients with higher baseline levels of depression and higher levels of early life stress (Am J Psychiatry. 2006 Sep;163[9]:1630-3).
Spikes in the inflammatory response independently correlated with depression severity but not with early life stress, which Dr. Raison said suggests that adversity likely can cause inflammation – and thus predisposes people to depression, and not necessarily vice versa.
“Something about early adversity in life programs the brain-body complex to run inflammatory systems hot, probably because it’s an effective way to be ready for [a stream of] unpredictable miseries,” Dr. Raison said during the session. “Chronic, elevated inflammation [early on] seems to predict increased depression later.”
Now that the link has been established between some depression and inflammation, the next step for science is to tease out who is most likely to respond to anti-inflammatory interventions for depression, Dr. Raison said.
“Something that is just starting to emerge is that maybe the relationship between inflammation and depression is not a straight line but a U-shaped curve, such that if you have too much inflammation, you’re in trouble, and if you have too little, you’re also in trouble,” he said in the interview, citing a study he and others conducted into blocking the inflammatory response. In that study, people with major depression who were otherwise medically healthy received either three infusions of the anti-inflammatory tumor necrosis factor–alpha antagonist infliximab (5 mg/kg), or of salt water. The investigators found that placebo worked just as well as infliximab. But patients with lower levels of inflammation at baseline had the greatest improvements in their Hamilton Rating Scale for Depression scores with placebo when compared with treatment (JAMA Psychiatry. 2013 Jan;70[1]:31-41).
Data are not yet conclusive, but Dr. Raison said the field soon could use biomarkers such as levels of C-reactive protein to determine whether patients will respond to anti-inflammatories such as omega-3 essential fatty acids. “Everyone in psychiatry is desperate to find clear, unambiguous answers. We’re right on the edge, but we’re not there yet.”
Until then, Dr. Raison cautioned against the “indiscriminate” use of anti-inflammatories, lest they exacerbate patients’ depressive symptoms. “For instance, omega-3 fatty acids might actually be counterproductive in a lot of depressed people,” he said. Still, he believes that “developing and studying anti-inflammatory strategies is probably going to lead to a novel way of treating depression in some people. What is beautiful is that if these studies continue, we might actually be able – for the first time – to target a subgroup of patients for a specific treatment.”
Dr. Raison is on the scientific advisory board of the Usona Institute, a nonprofit medical research firm.
[email protected]
On Twitter @whitneymcknight
EXPERT OPINION FROM THE AMERICAN COLLEGE OF PSYCHIATRISTS MEETING
Portfolio of physician-led measures nets better quality of care
ORLANDO – A multifaceted portfolio of physician-led measures with feedback and financial incentives can dramatically improve the quality of care provided at cancer centers, suggests the experience of Stanford (Calif.) Health Care.
Physician leaders of 13 disease-specific cancer care programs (CCPs) identified measures of care that were meaningful to their team and patients, spanning the spectrum from new diagnosis through end of life and survivorship care. Quality and analytics teams developed 16 corresponding metrics and performance reports used for feedback. Programs were also given a financial incentive to meet jointly set targets.
After a year, the CCPs had improved on 12 of the metrics and maintained high baseline levels of performance on the other 4 metrics, investigators reported at a symposium on quality care sponsored by the American Society of Clinical Oncology. For example, they got better at entering staging information in a dedicated field in the electronic health record (+50% absolute increase), recording hand and foot pain (+34%), performing hepatitis B testing before rituximab use (+17%), and referring patients with ovarian cancer for genetic counseling (+43%).

“The main drivers, I would argue, besides the Hawthorne effect, were a high level of physician engagement in the selection, management, and improvement of the metrics, and these metrics excited the care teams, which also provided some motivation,” she said. “We provided real-time, high-quality feedback of performance. And last but probably not least was a financial incentive for the CCP as a team, not part of any individual compensation.”
The investigators plan to continue measuring the metrics, to expand them to other sites in their network, and to add new metrics that are common across the programs to minimize measurement burden, according to Ms. Porter. “We also plan to build cohorts for value-based care and unplanned care like ED visits and unplanned admissions. Finally, we want to keep momentum going and capitalize upon a provider engagement in value measurement and improvement,” she said.
“Based on this work and prior abstracts, … there are many validated metrics to be used. So, to choose those metrics and to choose them through local leadership support, most importantly, engaging frontline staff and having their buy-in of the measures that you are collecting are important,” commented invited discussant Jessica A. Zerillo, MD, MPH, of the Beth Israel Deaconess Medical Center in Boston. “And this can include using incentives that drive such stakeholders, whether they be financial or simply pride with public reporting.”

Study details
“In the summer of 2015, we were starting to feel a lot of pressure to prepare for evolving reimbursement models,” Ms. Porter said, explaining the initiative’s genesis. “Mainly, how do we define our value, and how can we measure and improve on that value of the care we deliver? One answer, of course, is to measure and reduce unnecessary variation. And we knew, to be successful, we had to increase our physician engagement and leadership in the selection and improvement of our metrics.”
Physician leaders of the CCPs were asked to choose quality measures that met three criteria: they were meaningful and important to both the care team and patients, they had pertinent data elements already available in existing databases (to reduce documentation burden), and they were multidisciplinary in nature, reflecting the care provided by the whole program. The measures ultimately selected included a variety of those put forth by American Society of Clinical Oncology’s Quality Oncology Practice Initiative and the American Society for Radiation Oncology. CCPs were offered a financial incentive for meeting targets ranging from $75,000 to $125,000 that was based on number of providers and patient volume, rather than on the impact of improved metric. “This was really meant for reinvestment back into their quality programs,” Ms. Porter said. “I would argue this was really a culture-building year for us, and we hope that next year there might be a little bit more tangible value with the metrics.”
The quality team gave CCPs monthly or quarterly performance reports with unblinded physician- and patient-level details that were ultimately disseminated to all the other CCPs. They also investigated any missing data for individual metrics.
Study results showed that half of the 16 measures the physician leaders chose pertained to the diagnosis and treatment planning phase of care, according to Ms. Porter. “It was important to many of our CCPs to ensure that specific testing was done, which would then, in turn, drive treatment planning decisions,” she commented.
At the end of the year, each metric was assessed among 13 to 2,406 patients. “All CCPs met their predetermined target and earned their financial incentive award for the year,” Ms. Porter reported.
Improvement was most marked, with a 50% absolute increase, for the metric of completing a staging module, which required conversion of staging information (historically embedded in progress notes) into a structured format in a dedicated field in the electronic health record within 45 days of a patient’s first cancer treatment. This practice enables ready identification of stage cohorts in which value of care can be assessed, she noted.
There were also sizable absolute increases in relevant CCPs in the proportion of blood and marrow transplant recipients referred to survivorship care by day 100 (+20%) and visiting that service by day 180 (+13%), recording of hand and foot pain (+34%) and radiation dermatitis (+21%), mismatch repair testing in patients with newly diagnosed colorectal cancer (+10%), referral of patients with newly diagnosed ovarian cancer for genetic counseling (+43%), cytogenetic testing in patients with newly diagnosed hematologic malignancies (+17%), hepatitis B testing before rituximab administration (+17%), and allowance of at least 2 nights for treatment plan physics–quality assurance before the start of a nonemergent radiation oncology treatment (+14%).
Meanwhile, there were decreases, considered favorable changes, in chemotherapy use in the last 2 weeks of life among neuro-oncology patients (–9%) and in patients’ receipt of more than 10 fractions of radiation therapy for palliation of bone metastases (–9%).
Finally, there was no change in several metrics of quality that were already at very high or low levels, as appropriate, at baseline: molecular testing in patients with newly diagnosed acute myeloid leukemia (stable at 95%), hospice enrollment at the time of death for neuro-oncology patients (stable at 100%), chemotherapy in the last 2 weeks of life for patients with sarcoma (stable at 0%), and epidermal growth factor receptor testing in patients with newly diagnosed lung adenocarcinoma (stable at 98%).
ORLANDO – A multifaceted portfolio of physician-led measures with feedback and financial incentives can dramatically improve the quality of care provided at cancer centers, suggests the experience of Stanford (Calif.) Health Care.
Physician leaders of 13 disease-specific cancer care programs (CCPs) identified measures of care that were meaningful to their team and patients, spanning the spectrum from new diagnosis through end of life and survivorship care. Quality and analytics teams developed 16 corresponding metrics and performance reports used for feedback. Programs were also given a financial incentive to meet jointly set targets.
After a year, the CCPs had improved on 12 of the metrics and maintained high baseline levels of performance on the other 4 metrics, investigators reported at a symposium on quality care sponsored by the American Society of Clinical Oncology. For example, they got better at entering staging information in a dedicated field in the electronic health record (+50% absolute increase), recording hand and foot pain (+34%), performing hepatitis B testing before rituximab use (+17%), and referring patients with ovarian cancer for genetic counseling (+43%).
“The main drivers, I would argue, besides the Hawthorne effect, were a high level of physician engagement in the selection, management, and improvement of the metrics, and these metrics excited the care teams, which also provided some motivation,” she said. “We provided real-time, high-quality feedback of performance. And last but probably not least was a financial incentive for the CCP as a team, not part of any individual compensation.”
The investigators plan to continue measuring the metrics, to expand them to other sites in their network, and to add new metrics that are common across the programs to minimize measurement burden, according to Ms. Porter. “We also plan to build cohorts for value-based care and unplanned care like ED visits and unplanned admissions. Finally, we want to keep momentum going and capitalize upon a provider engagement in value measurement and improvement,” she said.
“Based on this work and prior abstracts, … there are many validated metrics to be used. So, to choose those metrics and to choose them through local leadership support, most importantly, engaging frontline staff and having their buy-in of the measures that you are collecting are important,” commented invited discussant Jessica A. Zerillo, MD, MPH, of the Beth Israel Deaconess Medical Center in Boston. “And this can include using incentives that drive such stakeholders, whether they be financial or simply pride with public reporting.”
Study details
“In the summer of 2015, we were starting to feel a lot of pressure to prepare for evolving reimbursement models,” Ms. Porter said, explaining the initiative’s genesis. “Mainly, how do we define our value, and how can we measure and improve on that value of the care we deliver? One answer, of course, is to measure and reduce unnecessary variation. And we knew, to be successful, we had to increase our physician engagement and leadership in the selection and improvement of our metrics.”
Physician leaders of the CCPs were asked to choose quality measures that met three criteria: they were meaningful and important to both the care team and patients, they had pertinent data elements already available in existing databases (to reduce documentation burden), and they were multidisciplinary in nature, reflecting the care provided by the whole program. The measures ultimately selected included a variety of those put forth by American Society of Clinical Oncology’s Quality Oncology Practice Initiative and the American Society for Radiation Oncology. CCPs were offered a financial incentive for meeting targets ranging from $75,000 to $125,000 that was based on number of providers and patient volume, rather than on the impact of improved metric. “This was really meant for reinvestment back into their quality programs,” Ms. Porter said. “I would argue this was really a culture-building year for us, and we hope that next year there might be a little bit more tangible value with the metrics.”
The quality team gave CCPs monthly or quarterly performance reports with unblinded physician- and patient-level details that were ultimately disseminated to all the other CCPs. They also investigated any missing data for individual metrics.
Study results showed that half of the 16 measures the physician leaders chose pertained to the diagnosis and treatment planning phase of care, according to Ms. Porter. “It was important to many of our CCPs to ensure that specific testing was done, which would then, in turn, drive treatment planning decisions,” she commented.
At the end of the year, each metric was assessed among 13 to 2,406 patients. “All CCPs met their predetermined target and earned their financial incentive award for the year,” Ms. Porter reported.
Improvement was most marked, with a 50% absolute increase, for the metric of completing a staging module, which required conversion of staging information (historically embedded in progress notes) into a structured format in a dedicated field in the electronic health record within 45 days of a patient’s first cancer treatment. This practice enables ready identification of stage cohorts in which value of care can be assessed, she noted.
There were also sizable absolute increases in relevant CCPs in the proportion of blood and marrow transplant recipients referred to survivorship care by day 100 (+20%) and visiting that service by day 180 (+13%), recording of hand and foot pain (+34%) and radiation dermatitis (+21%), mismatch repair testing in patients with newly diagnosed colorectal cancer (+10%), referral of patients with newly diagnosed ovarian cancer for genetic counseling (+43%), cytogenetic testing in patients with newly diagnosed hematologic malignancies (+17%), hepatitis B testing before rituximab administration (+17%), and allowance of at least 2 nights for treatment plan physics–quality assurance before the start of a nonemergent radiation oncology treatment (+14%).
Meanwhile, there were decreases, considered favorable changes, in chemotherapy use in the last 2 weeks of life among neuro-oncology patients (–9%) and in patients’ receipt of more than 10 fractions of radiation therapy for palliation of bone metastases (–9%).
Finally, there was no change in several metrics of quality that were already at very high or low levels, as appropriate, at baseline: molecular testing in patients with newly diagnosed acute myeloid leukemia (stable at 95%), hospice enrollment at the time of death for neuro-oncology patients (stable at 100%), chemotherapy in the last 2 weeks of life for patients with sarcoma (stable at 0%), and epidermal growth factor receptor testing in patients with newly diagnosed lung adenocarcinoma (stable at 98%).
ORLANDO – A multifaceted portfolio of physician-led measures with feedback and financial incentives can dramatically improve the quality of care provided at cancer centers, suggests the experience of Stanford (Calif.) Health Care.
Physician leaders of 13 disease-specific cancer care programs (CCPs) identified measures of care that were meaningful to their team and patients, spanning the spectrum from new diagnosis through end of life and survivorship care. Quality and analytics teams developed 16 corresponding metrics and performance reports used for feedback. Programs were also given a financial incentive to meet jointly set targets.
After a year, the CCPs had improved on 12 of the metrics and maintained high baseline levels of performance on the other 4 metrics, investigators reported at a symposium on quality care sponsored by the American Society of Clinical Oncology. For example, they got better at entering staging information in a dedicated field in the electronic health record (+50% absolute increase), recording hand and foot pain (+34%), performing hepatitis B testing before rituximab use (+17%), and referring patients with ovarian cancer for genetic counseling (+43%).
“The main drivers, I would argue, besides the Hawthorne effect, were a high level of physician engagement in the selection, management, and improvement of the metrics, and these metrics excited the care teams, which also provided some motivation,” she said. “We provided real-time, high-quality feedback of performance. And last but probably not least was a financial incentive for the CCP as a team, not part of any individual compensation.”
The investigators plan to continue measuring the metrics, to expand them to other sites in their network, and to add new metrics that are common across the programs to minimize measurement burden, according to Ms. Porter. “We also plan to build cohorts for value-based care and unplanned care like ED visits and unplanned admissions. Finally, we want to keep momentum going and capitalize upon a provider engagement in value measurement and improvement,” she said.
“Based on this work and prior abstracts, … there are many validated metrics to be used. So, to choose those metrics and to choose them through local leadership support, most importantly, engaging frontline staff and having their buy-in of the measures that you are collecting are important,” commented invited discussant Jessica A. Zerillo, MD, MPH, of the Beth Israel Deaconess Medical Center in Boston. “And this can include using incentives that drive such stakeholders, whether they be financial or simply pride with public reporting.”
Study details
“In the summer of 2015, we were starting to feel a lot of pressure to prepare for evolving reimbursement models,” Ms. Porter said, explaining the initiative’s genesis. “Mainly, how do we define our value, and how can we measure and improve on that value of the care we deliver? One answer, of course, is to measure and reduce unnecessary variation. And we knew, to be successful, we had to increase our physician engagement and leadership in the selection and improvement of our metrics.”
Physician leaders of the CCPs were asked to choose quality measures that met three criteria: they were meaningful and important to both the care team and patients, they had pertinent data elements already available in existing databases (to reduce documentation burden), and they were multidisciplinary in nature, reflecting the care provided by the whole program. The measures ultimately selected included a variety of those put forth by American Society of Clinical Oncology’s Quality Oncology Practice Initiative and the American Society for Radiation Oncology. CCPs were offered a financial incentive for meeting targets ranging from $75,000 to $125,000 that was based on number of providers and patient volume, rather than on the impact of improved metric. “This was really meant for reinvestment back into their quality programs,” Ms. Porter said. “I would argue this was really a culture-building year for us, and we hope that next year there might be a little bit more tangible value with the metrics.”
The quality team gave CCPs monthly or quarterly performance reports with unblinded physician- and patient-level details that were ultimately disseminated to all the other CCPs. They also investigated any missing data for individual metrics.
Study results showed that half of the 16 measures the physician leaders chose pertained to the diagnosis and treatment planning phase of care, according to Ms. Porter. “It was important to many of our CCPs to ensure that specific testing was done, which would then, in turn, drive treatment planning decisions,” she commented.
At the end of the year, each metric was assessed among 13 to 2,406 patients. “All CCPs met their predetermined target and earned their financial incentive award for the year,” Ms. Porter reported.
Improvement was most marked, with a 50% absolute increase, for the metric of completing a staging module, which required conversion of staging information (historically embedded in progress notes) into a structured format in a dedicated field in the electronic health record within 45 days of a patient’s first cancer treatment. This practice enables ready identification of stage cohorts in which value of care can be assessed, she noted.
There were also sizable absolute increases in relevant CCPs in the proportion of blood and marrow transplant recipients referred to survivorship care by day 100 (+20%) and visiting that service by day 180 (+13%), recording of hand and foot pain (+34%) and radiation dermatitis (+21%), mismatch repair testing in patients with newly diagnosed colorectal cancer (+10%), referral of patients with newly diagnosed ovarian cancer for genetic counseling (+43%), cytogenetic testing in patients with newly diagnosed hematologic malignancies (+17%), hepatitis B testing before rituximab administration (+17%), and allowance of at least 2 nights for treatment plan physics–quality assurance before the start of a nonemergent radiation oncology treatment (+14%).
Meanwhile, there were decreases, considered favorable changes, in chemotherapy use in the last 2 weeks of life among neuro-oncology patients (–9%) and in patients’ receipt of more than 10 fractions of radiation therapy for palliation of bone metastases (–9%).
Finally, there was no change in several metrics of quality that were already at very high or low levels, as appropriate, at baseline: molecular testing in patients with newly diagnosed acute myeloid leukemia (stable at 95%), hospice enrollment at the time of death for neuro-oncology patients (stable at 100%), chemotherapy in the last 2 weeks of life for patients with sarcoma (stable at 0%), and epidermal growth factor receptor testing in patients with newly diagnosed lung adenocarcinoma (stable at 98%).
AT THE QUALITY CARE SYMPOSIUM
Key clinical point:
Major finding: Over a 1-year period, the center saw improvements in practices such as completion of staging modules (+50%), recording of hand and foot pain (+34%), hepatitis B testing before rituximab use (+17%), and referral of patients with ovarian cancer for genetic counseling (+43%).
Data source: An initiative targeting 16 quality metrics undertaken by 13 cancer care programs at Stanford Health Care.
Disclosures: Ms. Porter disclosed that she had no relevant conflicts of interest.
Machine learning melanoma
What if an app could diagnose melanoma from a photo? That was my idea. In December 2009, Google introduced Google Goggles, an application that recognized images. At the time, I thought, “Wouldn’t it be neat if we could use this with telederm?” I even pitched it to a friend at the search giant. “Great idea!” he wrote back, placating me. For those uninitiated in innovation, “Great idea!” is a euphemism for “Yeah, we thought of that.”
Yes, it isn’t only mine; no doubt, many of you had this same idea: Let’s use amazing image interpretation capabilities from companies like Google or Apple to help us make diagnoses. Sounds simple. It isn’t. This is why most melanoma-finding apps are for entertainment purposes only – they don’t work.

So can melanoma be diagnosed from an app? A Stanford University team believes so. They trained a machine learning system to make dermatologic diagnoses from photos of skin lesions. To overcome previous barriers, they used open-sourced software from Google and awesome processors. For a start, they pretrained the program on over 1.28 million images. Then they fed it 128,450 images of known diagnoses.
Then, just as when Google’s AlphaGo algorithm challenged Lee Sedol, the world Go champion, the Stanford research team challenged 21 dermatologists. They had to choose if they would biopsy/treat or reassure patients based on photos of benign lesions, keratinocyte carcinomas, clinical melanomas, and dermoscopic melanomas. Guess who won?
In a stunning victory (or defeat, if you’re rooting for our team), the trained algorithm matched or outperformed all the dermatologists when scored on sensitivity-specificity curves. While we dermatologists, of course, use more than just a photo to diagnose skin cancer, many around the globe don’t have access to us. Based on these findings, they might need access only to a smartphone to get potentially life-saving advice.
But, what does this mean? Will we someday be outsourced to AI? Will a future POTUS promise to “bring back the doctor industry?” Not if we adapt. The future is bright – if we learn to apply machine learning in ways that can have an impact. (Brain + Computer > Brain.) Consider the following: An optimized ophthalmologist who reads retinal scans prediagnosed by a computer. A teledermatologist who uses AI to perform perfectly in diagnosing melanoma.
Patients have always wanted high quality and high touch care. In the history of medicine, we’ve never been better at both than we are today. Until tomorrow, when we’ll be better still.
Jeff Benabio, MD, MBA, is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]. He has no disclosures related to this column.
What if an app could diagnose melanoma from a photo? That was my idea. In December 2009, Google introduced Google Goggles, an application that recognized images. At the time, I thought, “Wouldn’t it be neat if we could use this with telederm?” I even pitched it to a friend at the search giant. “Great idea!” he wrote back, placating me. For those uninitiated in innovation, “Great idea!” is a euphemism for “Yeah, we thought of that.”
Yes, it isn’t only mine; no doubt, many of you had this same idea: Let’s use amazing image interpretation capabilities from companies like Google or Apple to help us make diagnoses. Sounds simple. It isn’t. This is why most melanoma-finding apps are for entertainment purposes only – they don’t work.
So can melanoma be diagnosed from an app? A Stanford University team believes so. They trained a machine learning system to make dermatologic diagnoses from photos of skin lesions. To overcome previous barriers, they used open-sourced software from Google and awesome processors. For a start, they pretrained the program on over 1.28 million images. Then they fed it 128,450 images of known diagnoses.
Then, just as when Google’s AlphaGo algorithm challenged Lee Sedol, the world Go champion, the Stanford research team challenged 21 dermatologists. They had to choose if they would biopsy/treat or reassure patients based on photos of benign lesions, keratinocyte carcinomas, clinical melanomas, and dermoscopic melanomas. Guess who won?
In a stunning victory (or defeat, if you’re rooting for our team), the trained algorithm matched or outperformed all the dermatologists when scored on sensitivity-specificity curves. While we dermatologists, of course, use more than just a photo to diagnose skin cancer, many around the globe don’t have access to us. Based on these findings, they might need access only to a smartphone to get potentially life-saving advice.
But, what does this mean? Will we someday be outsourced to AI? Will a future POTUS promise to “bring back the doctor industry?” Not if we adapt. The future is bright – if we learn to apply machine learning in ways that can have an impact. (Brain + Computer > Brain.) Consider the following: An optimized ophthalmologist who reads retinal scans prediagnosed by a computer. A teledermatologist who uses AI to perform perfectly in diagnosing melanoma.
Patients have always wanted high quality and high touch care. In the history of medicine, we’ve never been better at both than we are today. Until tomorrow, when we’ll be better still.
Jeff Benabio, MD, MBA, is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]. He has no disclosures related to this column.
What if an app could diagnose melanoma from a photo? That was my idea. In December 2009, Google introduced Google Goggles, an application that recognized images. At the time, I thought, “Wouldn’t it be neat if we could use this with telederm?” I even pitched it to a friend at the search giant. “Great idea!” he wrote back, placating me. For those uninitiated in innovation, “Great idea!” is a euphemism for “Yeah, we thought of that.”
Yes, it isn’t only mine; no doubt, many of you had this same idea: Let’s use amazing image interpretation capabilities from companies like Google or Apple to help us make diagnoses. Sounds simple. It isn’t. This is why most melanoma-finding apps are for entertainment purposes only – they don’t work.
So can melanoma be diagnosed from an app? A Stanford University team believes so. They trained a machine learning system to make dermatologic diagnoses from photos of skin lesions. To overcome previous barriers, they used open-sourced software from Google and awesome processors. For a start, they pretrained the program on over 1.28 million images. Then they fed it 128,450 images of known diagnoses.
Then, just as when Google’s AlphaGo algorithm challenged Lee Sedol, the world Go champion, the Stanford research team challenged 21 dermatologists. They had to choose if they would biopsy/treat or reassure patients based on photos of benign lesions, keratinocyte carcinomas, clinical melanomas, and dermoscopic melanomas. Guess who won?
In a stunning victory (or defeat, if you’re rooting for our team), the trained algorithm matched or outperformed all the dermatologists when scored on sensitivity-specificity curves. While we dermatologists, of course, use more than just a photo to diagnose skin cancer, many around the globe don’t have access to us. Based on these findings, they might need access only to a smartphone to get potentially life-saving advice.
But, what does this mean? Will we someday be outsourced to AI? Will a future POTUS promise to “bring back the doctor industry?” Not if we adapt. The future is bright – if we learn to apply machine learning in ways that can have an impact. (Brain + Computer > Brain.) Consider the following: An optimized ophthalmologist who reads retinal scans prediagnosed by a computer. A teledermatologist who uses AI to perform perfectly in diagnosing melanoma.
Patients have always wanted high quality and high touch care. In the history of medicine, we’ve never been better at both than we are today. Until tomorrow, when we’ll be better still.
Jeff Benabio, MD, MBA, is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]. He has no disclosures related to this column.