User login
Three developmental screens differ in outcomes in comparative study
SAN FRANCISCO – The use of three different screening instruments to gauge behavioral development in children up to 5 years of age has yielded results that vary within a single practice and between different practices. This heterogeneity complicates the accurate and early identification of developmental disorders children in the primary care setting.
“The burden of diagnostic services that go along with developmental screening depends on the number of positive screens and the referral completion rate. These rates may vary markedly across practices that from the outside seem relatively homogeneous. This differential burden may help explain the variation between practices that has been observed,” said Radley Sheldrick, PhD, of Boston University School of Public Health.
The American Academy of Pediatrics has recommended the use of developmental screening instruments that have a track record in prior studies of a sensitivity and specificity of at least 70% each. Children who score positive can receive further services. The aim is laudable, Dr. Sheldrick said, but little is known of how different screens compare to one another in the results obtained, and the consistency of their performance in different practice settings.
A few years ago, Dr. Sheldrick and his colleagues at Tufts Medical Center, Boston, initiated the Screen Early, Screen Accurately for Child Well-Being (SESAW) head-to-head comparison of the effectiveness of three sets of developmental behavioral screening instruments used in the pediatric primary care setting: the Ages and Stages Questionnaire, 2nd edition (ASQ-2), Parent’s Evaluation of Developmental Status (PEDS), and the Survey of Well-Being of Young Children (SWYC).
The ASQ-2 and PEDS instruments have been in use for some time. Differences in their sensitivity and specificity of developmental concerns have been noted, although both can be used at the discretion of the physician. SWYC is a more recent instrument, which was developed at Tufts Medical Center. It was designed to be easy to read and quickly completed.
In the study, 1,000 parents of children aged 9 months to 5.5 years were enrolled at six pediatric practices in Massachusetts. About 50% of the children were boys, 10% were Hispanic, and 10% were African American. About one-quarter of the parents were receiving some form of public assistance. The parents completed the three screens. Children scoring positive on any screen were assessed further.
The researchers were especially interested in the agreement between the three screens and the variance across the six practices in the performance of the screens and the proportion of children who tested positive and actually received referral care.
Overall, about 44% of the children scored positive on at least one screen. Of these, 72% were assessed more comprehensively. A closer look at those who were assessed revealed agreement between all three screens in only 16% of the children.
The performance of the three screens was not consistent from practice to practice. Variations were evident with each screen in the different practices, and between the three screens in individual practices. The differences in the performance of the screens in the individual practices were not significantly different. However, considerable difference was noted between practices, the extreme being a 70% higher difference in one practice compared to another.
Referral completion rates also displayed variation between practices, although no significant difference was evident. Still, the extreme case was a 30% higher rate of completion of one of the practices, compared with another.
“As I’ve gotten further into this research, I’ve become struck by the number of things we don’t know about developmental screens [compared to] what we do know. Whether, for example, the sensitivity and specificity of a screen in one population carries over to other populations is an assumption we have made, but which we don’t really know,” said Dr. Sheldrick.
Another unknown is whether a developmental disorder identified by a screen at one age can be identified at a later age in someone who has not received specialized care.
Finally, the issue of false positive results is vexing. While a false positive might be suspected, not to do anything sends the wrong message.
“What to do when there is a problem between a clinical result and a screening result is one of the most important clinical questions we have right now. Clinicians have to make up their minds on this issue every day, and there is not a lot of research on it. The results need to be evaluated while recognizing that there are still some uncertainties with screening results, and recognizing other forms of information, such as parent reporting and observations of the child, that can be informative,” explained Dr. Sheldrick.
Tufts Medical Center sponsored the study, which was funded by the National Institutes of Health. Dr. Sheldrick reported having no relevant financial disclosures.
SAN FRANCISCO – The use of three different screening instruments to gauge behavioral development in children up to 5 years of age has yielded results that vary within a single practice and between different practices. This heterogeneity complicates the accurate and early identification of developmental disorders children in the primary care setting.
“The burden of diagnostic services that go along with developmental screening depends on the number of positive screens and the referral completion rate. These rates may vary markedly across practices that from the outside seem relatively homogeneous. This differential burden may help explain the variation between practices that has been observed,” said Radley Sheldrick, PhD, of Boston University School of Public Health.
The American Academy of Pediatrics has recommended the use of developmental screening instruments that have a track record in prior studies of a sensitivity and specificity of at least 70% each. Children who score positive can receive further services. The aim is laudable, Dr. Sheldrick said, but little is known of how different screens compare to one another in the results obtained, and the consistency of their performance in different practice settings.
A few years ago, Dr. Sheldrick and his colleagues at Tufts Medical Center, Boston, initiated the Screen Early, Screen Accurately for Child Well-Being (SESAW) head-to-head comparison of the effectiveness of three sets of developmental behavioral screening instruments used in the pediatric primary care setting: the Ages and Stages Questionnaire, 2nd edition (ASQ-2), Parent’s Evaluation of Developmental Status (PEDS), and the Survey of Well-Being of Young Children (SWYC).
The ASQ-2 and PEDS instruments have been in use for some time. Differences in their sensitivity and specificity of developmental concerns have been noted, although both can be used at the discretion of the physician. SWYC is a more recent instrument, which was developed at Tufts Medical Center. It was designed to be easy to read and quickly completed.
In the study, 1,000 parents of children aged 9 months to 5.5 years were enrolled at six pediatric practices in Massachusetts. About 50% of the children were boys, 10% were Hispanic, and 10% were African American. About one-quarter of the parents were receiving some form of public assistance. The parents completed the three screens. Children scoring positive on any screen were assessed further.
The researchers were especially interested in the agreement between the three screens and the variance across the six practices in the performance of the screens and the proportion of children who tested positive and actually received referral care.
Overall, about 44% of the children scored positive on at least one screen. Of these, 72% were assessed more comprehensively. A closer look at those who were assessed revealed agreement between all three screens in only 16% of the children.
The performance of the three screens was not consistent from practice to practice. Variations were evident with each screen in the different practices, and between the three screens in individual practices. The differences in the performance of the screens in the individual practices were not significantly different. However, considerable difference was noted between practices, the extreme being a 70% higher difference in one practice compared to another.
Referral completion rates also displayed variation between practices, although no significant difference was evident. Still, the extreme case was a 30% higher rate of completion of one of the practices, compared with another.
“As I’ve gotten further into this research, I’ve become struck by the number of things we don’t know about developmental screens [compared to] what we do know. Whether, for example, the sensitivity and specificity of a screen in one population carries over to other populations is an assumption we have made, but which we don’t really know,” said Dr. Sheldrick.
Another unknown is whether a developmental disorder identified by a screen at one age can be identified at a later age in someone who has not received specialized care.
Finally, the issue of false positive results is vexing. While a false positive might be suspected, not to do anything sends the wrong message.
“What to do when there is a problem between a clinical result and a screening result is one of the most important clinical questions we have right now. Clinicians have to make up their minds on this issue every day, and there is not a lot of research on it. The results need to be evaluated while recognizing that there are still some uncertainties with screening results, and recognizing other forms of information, such as parent reporting and observations of the child, that can be informative,” explained Dr. Sheldrick.
Tufts Medical Center sponsored the study, which was funded by the National Institutes of Health. Dr. Sheldrick reported having no relevant financial disclosures.
SAN FRANCISCO – The use of three different screening instruments to gauge behavioral development in children up to 5 years of age has yielded results that vary within a single practice and between different practices. This heterogeneity complicates the accurate and early identification of developmental disorders children in the primary care setting.
“The burden of diagnostic services that go along with developmental screening depends on the number of positive screens and the referral completion rate. These rates may vary markedly across practices that from the outside seem relatively homogeneous. This differential burden may help explain the variation between practices that has been observed,” said Radley Sheldrick, PhD, of Boston University School of Public Health.
The American Academy of Pediatrics has recommended the use of developmental screening instruments that have a track record in prior studies of a sensitivity and specificity of at least 70% each. Children who score positive can receive further services. The aim is laudable, Dr. Sheldrick said, but little is known of how different screens compare to one another in the results obtained, and the consistency of their performance in different practice settings.
A few years ago, Dr. Sheldrick and his colleagues at Tufts Medical Center, Boston, initiated the Screen Early, Screen Accurately for Child Well-Being (SESAW) head-to-head comparison of the effectiveness of three sets of developmental behavioral screening instruments used in the pediatric primary care setting: the Ages and Stages Questionnaire, 2nd edition (ASQ-2), Parent’s Evaluation of Developmental Status (PEDS), and the Survey of Well-Being of Young Children (SWYC).
The ASQ-2 and PEDS instruments have been in use for some time. Differences in their sensitivity and specificity of developmental concerns have been noted, although both can be used at the discretion of the physician. SWYC is a more recent instrument, which was developed at Tufts Medical Center. It was designed to be easy to read and quickly completed.
In the study, 1,000 parents of children aged 9 months to 5.5 years were enrolled at six pediatric practices in Massachusetts. About 50% of the children were boys, 10% were Hispanic, and 10% were African American. About one-quarter of the parents were receiving some form of public assistance. The parents completed the three screens. Children scoring positive on any screen were assessed further.
The researchers were especially interested in the agreement between the three screens and the variance across the six practices in the performance of the screens and the proportion of children who tested positive and actually received referral care.
Overall, about 44% of the children scored positive on at least one screen. Of these, 72% were assessed more comprehensively. A closer look at those who were assessed revealed agreement between all three screens in only 16% of the children.
The performance of the three screens was not consistent from practice to practice. Variations were evident with each screen in the different practices, and between the three screens in individual practices. The differences in the performance of the screens in the individual practices were not significantly different. However, considerable difference was noted between practices, the extreme being a 70% higher difference in one practice compared to another.
Referral completion rates also displayed variation between practices, although no significant difference was evident. Still, the extreme case was a 30% higher rate of completion of one of the practices, compared with another.
“As I’ve gotten further into this research, I’ve become struck by the number of things we don’t know about developmental screens [compared to] what we do know. Whether, for example, the sensitivity and specificity of a screen in one population carries over to other populations is an assumption we have made, but which we don’t really know,” said Dr. Sheldrick.
Another unknown is whether a developmental disorder identified by a screen at one age can be identified at a later age in someone who has not received specialized care.
Finally, the issue of false positive results is vexing. While a false positive might be suspected, not to do anything sends the wrong message.
“What to do when there is a problem between a clinical result and a screening result is one of the most important clinical questions we have right now. Clinicians have to make up their minds on this issue every day, and there is not a lot of research on it. The results need to be evaluated while recognizing that there are still some uncertainties with screening results, and recognizing other forms of information, such as parent reporting and observations of the child, that can be informative,” explained Dr. Sheldrick.
Tufts Medical Center sponsored the study, which was funded by the National Institutes of Health. Dr. Sheldrick reported having no relevant financial disclosures.
AT PAS 17
Key clinical point: There were significant differences in the results of different developmental screening instruments within and between practices in a comparative study.
Major finding: The PEDS, ASQ-2, and SWYC developmental screens coidentified only 16% of 317 children aged 9 months to 5.5 years, with significant differences in the results of each developmental screen between practices.
Data source: The Screen Early, Screen Accurately for Child Well-Being (SESAW) head-to-head comparative effectiveness trial of three sets of developmental behavioral screening instruments used in pediatric primary care.
Disclosures: Tufts Medical Center sponsored the study, which was funded by the National Institutes of Health. Dr. Sheldrick reported having no relevant financial disclosures.
Endometrial cancer rates increased following WHI
SAN DIEGO – Endometrial cancer (EC) rates increased after 2002, coinciding with the release of results from the Women’s Health Initiative and including a 10% spike between 2006 and 2014, according to a large analysis of national data.
“Be aware of an increase of endometrial cancer and, whenever possible, look to minimize possible inciting causes,” Ginger Constantine, MD, lead study author, said in an interview prior to the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Be certain that the hormonal products that patients are taking are delivering adequate progesterone to the endometrium in those patients at an increased risk of endometrial cancer, such as those with unopposed estrogen.”

“We sought to look at possible causes for the increase of the known risk factors for EC,” she said. “What has changed in the years leading up to 2006?” To find out, she and her associates obtained EC incidence from the Surveillance, Epidemiology, and End Result Program database from 1975 through 2014. They evaluated the incidence of risk factors thought to be associated with EC, including age, obesity, race, number of menstrual cycles, gravidity and parity, metabolic syndromes, diet and exercise, and medications, including various types of hormone therapy, tamoxifen, and hormonal contraceptives.
Shelli Graham, PhD, vice president of medical affairs for Boca Raton, Florida–based TherapeuticsMD, presented the study findings on behalf of Dr. Constantine, who was unable to attend the meeting. The rates of EC were relatively constant from 1992 to 2002 (at about 76/100,000 cases per year) but have increased 2.5% annually, with a 10% increase from 2006 to 2014, especially in women aged 55-64 years.
Use of estrogen and progestin combinations have decreased while risk factors remained constant or decreased during the same time period. However, the researchers observed a “huge increase (of 1-2.5 million U.S. women) using non-FDA approved compounded estrogen and estrogen and progesterone, which may not provide adequate endometrial protection from estrogen, a known cause of EC,” Dr. Constantine said. “Additionally, there is less progestin use subsequent to the [Women’s Health Initiative] and it is known that progestin is protective on the endometrium.”
The researchers also examined the incidence of obesity – another known risk factor for EC – and found that, although obesity has continued to increase in incidence, “it does not appear to be increasing at the same rate as EC, so [it] does not appear to be enough to explain the increase in EC from 2006,” Dr. Constantine said. “I was surprised at the rate of increase of EC from 2006 to 2014 and have also been surprised by the amount of non-FDA compounded hormone use.”
Dr. Graham characterized the increase in EC incidence as “a public health concern that is most likely multifactorial in etiology.” Contributors, she said, include the combination of an increase in obesity with an inherent increase in endogenous estrogen, decreasing progesterone use from a decrease in the use of FDA-approved hormone therapy products, and an increase in compounded hormone therapy that may not deliver adequate endometrial protection.
Dr. Constantine acknowledged certain limitations of the study, including the fact that it is “an ecological analysis, not a randomized clinical trial. It is hypothesis-generating.”
Dr. Constantine reported that she is a consultant/advisory member for TherapeuticsMD and other pharmaceutical companies. She owns stock in TherapeuticsMD. Coauthor Steven R. Goldstein, MD, reported having numerous financial relationships with pharmaceutical companies including TherapeuticsMD. Dr. Graham is an employee of TherapeuticsMD.
SAN DIEGO – Endometrial cancer (EC) rates increased after 2002, coinciding with the release of results from the Women’s Health Initiative and including a 10% spike between 2006 and 2014, according to a large analysis of national data.
“Be aware of an increase of endometrial cancer and, whenever possible, look to minimize possible inciting causes,” Ginger Constantine, MD, lead study author, said in an interview prior to the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Be certain that the hormonal products that patients are taking are delivering adequate progesterone to the endometrium in those patients at an increased risk of endometrial cancer, such as those with unopposed estrogen.”
“We sought to look at possible causes for the increase of the known risk factors for EC,” she said. “What has changed in the years leading up to 2006?” To find out, she and her associates obtained EC incidence from the Surveillance, Epidemiology, and End Result Program database from 1975 through 2014. They evaluated the incidence of risk factors thought to be associated with EC, including age, obesity, race, number of menstrual cycles, gravidity and parity, metabolic syndromes, diet and exercise, and medications, including various types of hormone therapy, tamoxifen, and hormonal contraceptives.
Shelli Graham, PhD, vice president of medical affairs for Boca Raton, Florida–based TherapeuticsMD, presented the study findings on behalf of Dr. Constantine, who was unable to attend the meeting. The rates of EC were relatively constant from 1992 to 2002 (at about 76/100,000 cases per year) but have increased 2.5% annually, with a 10% increase from 2006 to 2014, especially in women aged 55-64 years.
Use of estrogen and progestin combinations have decreased while risk factors remained constant or decreased during the same time period. However, the researchers observed a “huge increase (of 1-2.5 million U.S. women) using non-FDA approved compounded estrogen and estrogen and progesterone, which may not provide adequate endometrial protection from estrogen, a known cause of EC,” Dr. Constantine said. “Additionally, there is less progestin use subsequent to the [Women’s Health Initiative] and it is known that progestin is protective on the endometrium.”
The researchers also examined the incidence of obesity – another known risk factor for EC – and found that, although obesity has continued to increase in incidence, “it does not appear to be increasing at the same rate as EC, so [it] does not appear to be enough to explain the increase in EC from 2006,” Dr. Constantine said. “I was surprised at the rate of increase of EC from 2006 to 2014 and have also been surprised by the amount of non-FDA compounded hormone use.”
Dr. Graham characterized the increase in EC incidence as “a public health concern that is most likely multifactorial in etiology.” Contributors, she said, include the combination of an increase in obesity with an inherent increase in endogenous estrogen, decreasing progesterone use from a decrease in the use of FDA-approved hormone therapy products, and an increase in compounded hormone therapy that may not deliver adequate endometrial protection.
Dr. Constantine acknowledged certain limitations of the study, including the fact that it is “an ecological analysis, not a randomized clinical trial. It is hypothesis-generating.”
Dr. Constantine reported that she is a consultant/advisory member for TherapeuticsMD and other pharmaceutical companies. She owns stock in TherapeuticsMD. Coauthor Steven R. Goldstein, MD, reported having numerous financial relationships with pharmaceutical companies including TherapeuticsMD. Dr. Graham is an employee of TherapeuticsMD.
SAN DIEGO – Endometrial cancer (EC) rates increased after 2002, coinciding with the release of results from the Women’s Health Initiative and including a 10% spike between 2006 and 2014, according to a large analysis of national data.
“Be aware of an increase of endometrial cancer and, whenever possible, look to minimize possible inciting causes,” Ginger Constantine, MD, lead study author, said in an interview prior to the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. “Be certain that the hormonal products that patients are taking are delivering adequate progesterone to the endometrium in those patients at an increased risk of endometrial cancer, such as those with unopposed estrogen.”
“We sought to look at possible causes for the increase of the known risk factors for EC,” she said. “What has changed in the years leading up to 2006?” To find out, she and her associates obtained EC incidence from the Surveillance, Epidemiology, and End Result Program database from 1975 through 2014. They evaluated the incidence of risk factors thought to be associated with EC, including age, obesity, race, number of menstrual cycles, gravidity and parity, metabolic syndromes, diet and exercise, and medications, including various types of hormone therapy, tamoxifen, and hormonal contraceptives.
Shelli Graham, PhD, vice president of medical affairs for Boca Raton, Florida–based TherapeuticsMD, presented the study findings on behalf of Dr. Constantine, who was unable to attend the meeting. The rates of EC were relatively constant from 1992 to 2002 (at about 76/100,000 cases per year) but have increased 2.5% annually, with a 10% increase from 2006 to 2014, especially in women aged 55-64 years.
Use of estrogen and progestin combinations have decreased while risk factors remained constant or decreased during the same time period. However, the researchers observed a “huge increase (of 1-2.5 million U.S. women) using non-FDA approved compounded estrogen and estrogen and progesterone, which may not provide adequate endometrial protection from estrogen, a known cause of EC,” Dr. Constantine said. “Additionally, there is less progestin use subsequent to the [Women’s Health Initiative] and it is known that progestin is protective on the endometrium.”
The researchers also examined the incidence of obesity – another known risk factor for EC – and found that, although obesity has continued to increase in incidence, “it does not appear to be increasing at the same rate as EC, so [it] does not appear to be enough to explain the increase in EC from 2006,” Dr. Constantine said. “I was surprised at the rate of increase of EC from 2006 to 2014 and have also been surprised by the amount of non-FDA compounded hormone use.”
Dr. Graham characterized the increase in EC incidence as “a public health concern that is most likely multifactorial in etiology.” Contributors, she said, include the combination of an increase in obesity with an inherent increase in endogenous estrogen, decreasing progesterone use from a decrease in the use of FDA-approved hormone therapy products, and an increase in compounded hormone therapy that may not deliver adequate endometrial protection.
Dr. Constantine acknowledged certain limitations of the study, including the fact that it is “an ecological analysis, not a randomized clinical trial. It is hypothesis-generating.”
Dr. Constantine reported that she is a consultant/advisory member for TherapeuticsMD and other pharmaceutical companies. She owns stock in TherapeuticsMD. Coauthor Steven R. Goldstein, MD, reported having numerous financial relationships with pharmaceutical companies including TherapeuticsMD. Dr. Graham is an employee of TherapeuticsMD.
Key clinical point:
Major finding: Rates of endometrial cancer increased 10% between 2006 and 2014.
Data source: An analysis of the Surveillance, Epidemiology, and End Result Program database.
Disclosures: Dr. Constantine reported that she is a consultant/advisory board member for TherapeuticsMD as well as other pharmaceutical companies. She also owns stock in TherapeuticsMD. Coauthor Steven R. Goldstein, MD, reported having numerous financial relationships with pharmaceutical companies including TherapeuticsMD. Dr. Graham is an employee of TherapeuticsMD.
Hospitalists share strategies to secure, excel at jobs
LAS VEGAS – In the view of academic hospitalist Alfred Burger, MD, SFHM, portability was long a dirty word in HM circles. But not anymore.
“My good friends in law and business do this all the time,” said Dr. Burger, associate program director of the internal medicine residency program at Mount Sinai Beth Israel in New York. “You’re not going to make partner in city X, but they’ve got an opening to be partner in city Y if you go there and perform for a year. People up and leave coasts, people up and leave states, people have up and left the country. ... Doctors are starting to view it the same way.”
The lessons of career development were a focal point of HM17, particularly for younger physicians who could take advantage of the Early-Career Hospitalists mini-track. But Dr. Burger said that those strategies of upward mobility can apply whether someone is chasing their first job or their fifth.
First, identify one’s strengths and play to those. Then identify the skills you don’t have or don’t excel at, and address those deficiencies.
“How can you acquire the skills to put yourself in the best position to move up, if you wish to develop your career as a leader?” Dr. Burger said. “If you wish to be the best clinician, you still need to stay on top of the game. Things like coming to SHM, staying on top of the content. That’s important.”
Another skill set is self-advocacy.
“Be your own champion,” said Brian Markoff, MD, SFHM, chief of hospital medicine at Mount Sinai St. Luke’s in New York. “Many of us are very good at this and many of us are terrible at this. You may fall somewhere in between, but you do have to be your own champion.”
Dr. Burger said that he understands that there is a fine line between too much self-promotion and too little. But he urged hospitalists at all career points to take responsibility for marketing themselves.
“Nobody is going to invest in your career unless you yourself invest in it,” he added. “You have to put it as a priority, and not in a selfish way, but in a way [that,] if you wish to move forward and move up, you’ve got to put the time in. It’s not a natural assumption anymore that, if you are the best and brightest of a group of doctors, you will just be chosen to lead.”
In a similar vein, networking is a major boon to career development that can be a double-edged scalpel.
“Having a great ‘social game’ is important, but if all you bring to the table is a social game, you’ll find yourself out of a job just as quickly as you found that job,” Dr. Burger said. “Meaning, you might be able to get it based on that, but you’re not going to be able to sustain it. At the same time, being highly accomplished and having no social graces is also a killer. So, you need to be sort of strong in both areas.”
Many of the meeting’s opportunities for tips on professional development are personal, but HM group leaders have to consider developing the careers of their employees. One of the main planks of that is physician engagement, said Flora Kisuule, MD, MPH, SFHM, of Johns Hopkins University, Baltimore.
“I don’t believe your institution or your organization can go anywhere if your employees are not engaged or if the people you work with are not engaged,” she said, adding that disengaged employees “are actively working against you. You don’t want that. You can’t go in any direction when there are people rowing in the opposite direction. At best, you stay in one place. At worst, you can end up losing ground.”
Hospitalist Christie Masters, MD, MBA, MHA, who practices at UCLA, disclosed during a session that she also runs a wellness coaching firm. She added that a focus on personal wellness and well-being is its own form of career development. It works in tandem with engagement, morale, and professional growth.
“If you’re only focusing on wellness and you don’t have hospitalists or a group that’s engaged or with high morale, they’re going to burnout or they’re going to leave,” Dr. Masters said. “And nobody wants that for their group. So, if we surround ourselves with people who feel well and feel whole, that’s going to have intangible benefits ... that affect the bottom line.”
LAS VEGAS – In the view of academic hospitalist Alfred Burger, MD, SFHM, portability was long a dirty word in HM circles. But not anymore.
“My good friends in law and business do this all the time,” said Dr. Burger, associate program director of the internal medicine residency program at Mount Sinai Beth Israel in New York. “You’re not going to make partner in city X, but they’ve got an opening to be partner in city Y if you go there and perform for a year. People up and leave coasts, people up and leave states, people have up and left the country. ... Doctors are starting to view it the same way.”
The lessons of career development were a focal point of HM17, particularly for younger physicians who could take advantage of the Early-Career Hospitalists mini-track. But Dr. Burger said that those strategies of upward mobility can apply whether someone is chasing their first job or their fifth.
First, identify one’s strengths and play to those. Then identify the skills you don’t have or don’t excel at, and address those deficiencies.
“How can you acquire the skills to put yourself in the best position to move up, if you wish to develop your career as a leader?” Dr. Burger said. “If you wish to be the best clinician, you still need to stay on top of the game. Things like coming to SHM, staying on top of the content. That’s important.”
Another skill set is self-advocacy.
“Be your own champion,” said Brian Markoff, MD, SFHM, chief of hospital medicine at Mount Sinai St. Luke’s in New York. “Many of us are very good at this and many of us are terrible at this. You may fall somewhere in between, but you do have to be your own champion.”
Dr. Burger said that he understands that there is a fine line between too much self-promotion and too little. But he urged hospitalists at all career points to take responsibility for marketing themselves.
“Nobody is going to invest in your career unless you yourself invest in it,” he added. “You have to put it as a priority, and not in a selfish way, but in a way [that,] if you wish to move forward and move up, you’ve got to put the time in. It’s not a natural assumption anymore that, if you are the best and brightest of a group of doctors, you will just be chosen to lead.”
In a similar vein, networking is a major boon to career development that can be a double-edged scalpel.
“Having a great ‘social game’ is important, but if all you bring to the table is a social game, you’ll find yourself out of a job just as quickly as you found that job,” Dr. Burger said. “Meaning, you might be able to get it based on that, but you’re not going to be able to sustain it. At the same time, being highly accomplished and having no social graces is also a killer. So, you need to be sort of strong in both areas.”
Many of the meeting’s opportunities for tips on professional development are personal, but HM group leaders have to consider developing the careers of their employees. One of the main planks of that is physician engagement, said Flora Kisuule, MD, MPH, SFHM, of Johns Hopkins University, Baltimore.
“I don’t believe your institution or your organization can go anywhere if your employees are not engaged or if the people you work with are not engaged,” she said, adding that disengaged employees “are actively working against you. You don’t want that. You can’t go in any direction when there are people rowing in the opposite direction. At best, you stay in one place. At worst, you can end up losing ground.”
Hospitalist Christie Masters, MD, MBA, MHA, who practices at UCLA, disclosed during a session that she also runs a wellness coaching firm. She added that a focus on personal wellness and well-being is its own form of career development. It works in tandem with engagement, morale, and professional growth.
“If you’re only focusing on wellness and you don’t have hospitalists or a group that’s engaged or with high morale, they’re going to burnout or they’re going to leave,” Dr. Masters said. “And nobody wants that for their group. So, if we surround ourselves with people who feel well and feel whole, that’s going to have intangible benefits ... that affect the bottom line.”
LAS VEGAS – In the view of academic hospitalist Alfred Burger, MD, SFHM, portability was long a dirty word in HM circles. But not anymore.
“My good friends in law and business do this all the time,” said Dr. Burger, associate program director of the internal medicine residency program at Mount Sinai Beth Israel in New York. “You’re not going to make partner in city X, but they’ve got an opening to be partner in city Y if you go there and perform for a year. People up and leave coasts, people up and leave states, people have up and left the country. ... Doctors are starting to view it the same way.”
The lessons of career development were a focal point of HM17, particularly for younger physicians who could take advantage of the Early-Career Hospitalists mini-track. But Dr. Burger said that those strategies of upward mobility can apply whether someone is chasing their first job or their fifth.
First, identify one’s strengths and play to those. Then identify the skills you don’t have or don’t excel at, and address those deficiencies.
“How can you acquire the skills to put yourself in the best position to move up, if you wish to develop your career as a leader?” Dr. Burger said. “If you wish to be the best clinician, you still need to stay on top of the game. Things like coming to SHM, staying on top of the content. That’s important.”
Another skill set is self-advocacy.
“Be your own champion,” said Brian Markoff, MD, SFHM, chief of hospital medicine at Mount Sinai St. Luke’s in New York. “Many of us are very good at this and many of us are terrible at this. You may fall somewhere in between, but you do have to be your own champion.”
Dr. Burger said that he understands that there is a fine line between too much self-promotion and too little. But he urged hospitalists at all career points to take responsibility for marketing themselves.
“Nobody is going to invest in your career unless you yourself invest in it,” he added. “You have to put it as a priority, and not in a selfish way, but in a way [that,] if you wish to move forward and move up, you’ve got to put the time in. It’s not a natural assumption anymore that, if you are the best and brightest of a group of doctors, you will just be chosen to lead.”
In a similar vein, networking is a major boon to career development that can be a double-edged scalpel.
“Having a great ‘social game’ is important, but if all you bring to the table is a social game, you’ll find yourself out of a job just as quickly as you found that job,” Dr. Burger said. “Meaning, you might be able to get it based on that, but you’re not going to be able to sustain it. At the same time, being highly accomplished and having no social graces is also a killer. So, you need to be sort of strong in both areas.”
Many of the meeting’s opportunities for tips on professional development are personal, but HM group leaders have to consider developing the careers of their employees. One of the main planks of that is physician engagement, said Flora Kisuule, MD, MPH, SFHM, of Johns Hopkins University, Baltimore.
“I don’t believe your institution or your organization can go anywhere if your employees are not engaged or if the people you work with are not engaged,” she said, adding that disengaged employees “are actively working against you. You don’t want that. You can’t go in any direction when there are people rowing in the opposite direction. At best, you stay in one place. At worst, you can end up losing ground.”
Hospitalist Christie Masters, MD, MBA, MHA, who practices at UCLA, disclosed during a session that she also runs a wellness coaching firm. She added that a focus on personal wellness and well-being is its own form of career development. It works in tandem with engagement, morale, and professional growth.
“If you’re only focusing on wellness and you don’t have hospitalists or a group that’s engaged or with high morale, they’re going to burnout or they’re going to leave,” Dr. Masters said. “And nobody wants that for their group. So, if we surround ourselves with people who feel well and feel whole, that’s going to have intangible benefits ... that affect the bottom line.”
Hospitalists’ EMR frustrations continue: SHM report
LAS VEGAS – Ronald Schaefer, MD, a hospitalist with Hawaii Pacific Health who also works on creating digital templates for his hospital, can’t input hemoglobin A1c levels from three different labs into his electronic medical records (EMR) system the same way.
Hospitalist George Dimitriou, MD, FHM, who splits his time at Allegheny Health Network in Pittsburgh between clinical work and medical informatics, worries there are so many fields in his EMR that physicians can get distracted.
Yevgeniy “Eugene” Gitelman, MD, a clinical informatics manager at the Perelman School of Medicine at University of Pennsylvania Health in Philadelphia, wonders how good any systems can be with the privacy concerns related to HIPAA.
This was the nexus of IT and HM17, a time when hospitalists said they are stymied and frustrated by continuing issues of interoperability, functionality, and access. The meeting highlighted new smartphone and tablet applications, as well as medical devices available to hospitalists, but tech-focused physicians say the biggest issue remains the day-to-day workings of EMR.
“If you build something really good, people will use it. If you build something that makes their documentation process a lot easier and a lot faster and a lot better, they’ll use it,” said Dr. Schaefer. “The tools aren’t there yet. I don’t think the technology is mature enough.”
If the tech hasn’t yet come of full age, the concerns surely have. SHM unveiled a white paper at HM17 that codified hospitalists’ worries about the current state of IT. The report, “Hospitalist Perspectives on Electronic Medical Records,” found that “a staggering” 85% of providers said they spend more time interacting with their inpatient EMR than their actual inpatients.
Rupesh Prasad, MD, MPH, SFHM, chair of SHM’s Health IT Committee, says the report is meant to foster discussion about the issues surrounding EMRs. The data points, generated from 462 respondents, are stark. Just 40% said they were happy with their EMR. Some 52% would change vendors if they could. One-quarter of respondents would revert to using paper if given the option.
“By sharing these results, we hope to raise awareness of the unacceptable performance of existing systems,” the report states. “This continues to contribute to our slower than desired improvement in quality and safety, as well as increasing provider frustration. We strongly believe that we need a renewed focus on initial goals of technology adoption in health care.”
Dr. Prasad said that he hopes hospitalists heed that call to action and use the report in discussions with various stakeholders, including vendors, public policy officials, and their own bosses.
“We want to give hospitalists ammunition to go back to their systems and talk to their administrators to see if they can influence [it],” he said.
Dr. Prasad is pleased that the society is sensitive to the issues surrounding technology. He encourages hospitalists to actively participate in HMX, SHM’s online portal to discuss health IT issues and crowd-source potential solutions. Patrick Vulgamore, MPH, SHM’s director of governance and practice management, said the society is formulating a potential special-interest working group to further seek to solve problems.
Hospitalists were also urged to apply for American Board of Medical Specialties (ABMS) certification in clinical informatics. Physicians can grandfather into eligibility via the “practice pathway” through the end of the year, if they’ve been working in informatics professionally for at least 25% of their time during any three of the previous five years. Next year, only graduates of two-year Accreditation Council for Graduate Medical Education–accredited fellowships will be board eligible.
“As end users of technology, we understand the problems better than anybody else,” Dr. Prasad said. “Obviously, the next step would be try to solve the problems. And what better way then to get involved and become experts in what you do?”
While much of the meeting’s tech talk was frustration, both former National Coordinator for Health IT Karen DeSalvo, MD, MPH, MSc, and HM Dean Robert Wachter, MD, MHM, forecast a future when artificial intelligence and intuitive computers work alongside physicians. Imagine the user-friendliness of Apple’s Siri or Google’s Alexa married to the existing functionalities provided by firms such as Epic or Cerner.
But that’s years away, and hospitalists like Dr. Dimitriou want help now.
“The speed of medicine, the speed of what’s happening in real time, is still faster than what our electronic tools seem to be able to keep up with,” he said. “There are encouraging signs that we’ve definitely moved in the right direction. We’ve come a long way ... but again, the speed at which things are moving? We aren’t keeping up. We’ve got to do more.”
LAS VEGAS – Ronald Schaefer, MD, a hospitalist with Hawaii Pacific Health who also works on creating digital templates for his hospital, can’t input hemoglobin A1c levels from three different labs into his electronic medical records (EMR) system the same way.
Hospitalist George Dimitriou, MD, FHM, who splits his time at Allegheny Health Network in Pittsburgh between clinical work and medical informatics, worries there are so many fields in his EMR that physicians can get distracted.
Yevgeniy “Eugene” Gitelman, MD, a clinical informatics manager at the Perelman School of Medicine at University of Pennsylvania Health in Philadelphia, wonders how good any systems can be with the privacy concerns related to HIPAA.
This was the nexus of IT and HM17, a time when hospitalists said they are stymied and frustrated by continuing issues of interoperability, functionality, and access. The meeting highlighted new smartphone and tablet applications, as well as medical devices available to hospitalists, but tech-focused physicians say the biggest issue remains the day-to-day workings of EMR.
“If you build something really good, people will use it. If you build something that makes their documentation process a lot easier and a lot faster and a lot better, they’ll use it,” said Dr. Schaefer. “The tools aren’t there yet. I don’t think the technology is mature enough.”
If the tech hasn’t yet come of full age, the concerns surely have. SHM unveiled a white paper at HM17 that codified hospitalists’ worries about the current state of IT. The report, “Hospitalist Perspectives on Electronic Medical Records,” found that “a staggering” 85% of providers said they spend more time interacting with their inpatient EMR than their actual inpatients.
Rupesh Prasad, MD, MPH, SFHM, chair of SHM’s Health IT Committee, says the report is meant to foster discussion about the issues surrounding EMRs. The data points, generated from 462 respondents, are stark. Just 40% said they were happy with their EMR. Some 52% would change vendors if they could. One-quarter of respondents would revert to using paper if given the option.
“By sharing these results, we hope to raise awareness of the unacceptable performance of existing systems,” the report states. “This continues to contribute to our slower than desired improvement in quality and safety, as well as increasing provider frustration. We strongly believe that we need a renewed focus on initial goals of technology adoption in health care.”
Dr. Prasad said that he hopes hospitalists heed that call to action and use the report in discussions with various stakeholders, including vendors, public policy officials, and their own bosses.
“We want to give hospitalists ammunition to go back to their systems and talk to their administrators to see if they can influence [it],” he said.
Dr. Prasad is pleased that the society is sensitive to the issues surrounding technology. He encourages hospitalists to actively participate in HMX, SHM’s online portal to discuss health IT issues and crowd-source potential solutions. Patrick Vulgamore, MPH, SHM’s director of governance and practice management, said the society is formulating a potential special-interest working group to further seek to solve problems.
Hospitalists were also urged to apply for American Board of Medical Specialties (ABMS) certification in clinical informatics. Physicians can grandfather into eligibility via the “practice pathway” through the end of the year, if they’ve been working in informatics professionally for at least 25% of their time during any three of the previous five years. Next year, only graduates of two-year Accreditation Council for Graduate Medical Education–accredited fellowships will be board eligible.
“As end users of technology, we understand the problems better than anybody else,” Dr. Prasad said. “Obviously, the next step would be try to solve the problems. And what better way then to get involved and become experts in what you do?”
While much of the meeting’s tech talk was frustration, both former National Coordinator for Health IT Karen DeSalvo, MD, MPH, MSc, and HM Dean Robert Wachter, MD, MHM, forecast a future when artificial intelligence and intuitive computers work alongside physicians. Imagine the user-friendliness of Apple’s Siri or Google’s Alexa married to the existing functionalities provided by firms such as Epic or Cerner.
But that’s years away, and hospitalists like Dr. Dimitriou want help now.
“The speed of medicine, the speed of what’s happening in real time, is still faster than what our electronic tools seem to be able to keep up with,” he said. “There are encouraging signs that we’ve definitely moved in the right direction. We’ve come a long way ... but again, the speed at which things are moving? We aren’t keeping up. We’ve got to do more.”
LAS VEGAS – Ronald Schaefer, MD, a hospitalist with Hawaii Pacific Health who also works on creating digital templates for his hospital, can’t input hemoglobin A1c levels from three different labs into his electronic medical records (EMR) system the same way.
Hospitalist George Dimitriou, MD, FHM, who splits his time at Allegheny Health Network in Pittsburgh between clinical work and medical informatics, worries there are so many fields in his EMR that physicians can get distracted.
Yevgeniy “Eugene” Gitelman, MD, a clinical informatics manager at the Perelman School of Medicine at University of Pennsylvania Health in Philadelphia, wonders how good any systems can be with the privacy concerns related to HIPAA.
This was the nexus of IT and HM17, a time when hospitalists said they are stymied and frustrated by continuing issues of interoperability, functionality, and access. The meeting highlighted new smartphone and tablet applications, as well as medical devices available to hospitalists, but tech-focused physicians say the biggest issue remains the day-to-day workings of EMR.
“If you build something really good, people will use it. If you build something that makes their documentation process a lot easier and a lot faster and a lot better, they’ll use it,” said Dr. Schaefer. “The tools aren’t there yet. I don’t think the technology is mature enough.”
If the tech hasn’t yet come of full age, the concerns surely have. SHM unveiled a white paper at HM17 that codified hospitalists’ worries about the current state of IT. The report, “Hospitalist Perspectives on Electronic Medical Records,” found that “a staggering” 85% of providers said they spend more time interacting with their inpatient EMR than their actual inpatients.
Rupesh Prasad, MD, MPH, SFHM, chair of SHM’s Health IT Committee, says the report is meant to foster discussion about the issues surrounding EMRs. The data points, generated from 462 respondents, are stark. Just 40% said they were happy with their EMR. Some 52% would change vendors if they could. One-quarter of respondents would revert to using paper if given the option.
“By sharing these results, we hope to raise awareness of the unacceptable performance of existing systems,” the report states. “This continues to contribute to our slower than desired improvement in quality and safety, as well as increasing provider frustration. We strongly believe that we need a renewed focus on initial goals of technology adoption in health care.”
Dr. Prasad said that he hopes hospitalists heed that call to action and use the report in discussions with various stakeholders, including vendors, public policy officials, and their own bosses.
“We want to give hospitalists ammunition to go back to their systems and talk to their administrators to see if they can influence [it],” he said.
Dr. Prasad is pleased that the society is sensitive to the issues surrounding technology. He encourages hospitalists to actively participate in HMX, SHM’s online portal to discuss health IT issues and crowd-source potential solutions. Patrick Vulgamore, MPH, SHM’s director of governance and practice management, said the society is formulating a potential special-interest working group to further seek to solve problems.
Hospitalists were also urged to apply for American Board of Medical Specialties (ABMS) certification in clinical informatics. Physicians can grandfather into eligibility via the “practice pathway” through the end of the year, if they’ve been working in informatics professionally for at least 25% of their time during any three of the previous five years. Next year, only graduates of two-year Accreditation Council for Graduate Medical Education–accredited fellowships will be board eligible.
“As end users of technology, we understand the problems better than anybody else,” Dr. Prasad said. “Obviously, the next step would be try to solve the problems. And what better way then to get involved and become experts in what you do?”
While much of the meeting’s tech talk was frustration, both former National Coordinator for Health IT Karen DeSalvo, MD, MPH, MSc, and HM Dean Robert Wachter, MD, MHM, forecast a future when artificial intelligence and intuitive computers work alongside physicians. Imagine the user-friendliness of Apple’s Siri or Google’s Alexa married to the existing functionalities provided by firms such as Epic or Cerner.
But that’s years away, and hospitalists like Dr. Dimitriou want help now.
“The speed of medicine, the speed of what’s happening in real time, is still faster than what our electronic tools seem to be able to keep up with,” he said. “There are encouraging signs that we’ve definitely moved in the right direction. We’ve come a long way ... but again, the speed at which things are moving? We aren’t keeping up. We’ve got to do more.”
UTI predictors identified in infants under 3 months of age
SAN FRANCISCO – Serum leukocytosis, pyuria, and urine leukocyte esterase have been identified as predictors of urinary tract infection (UTI) in infants younger than 90 days of age, with males being more likely to develop UTI than females.
The chance of the infection declined in older infants.
“Really young infants have a less well developed immune system, which may increase their susceptibility to UTIs,” said Sarah Berman, DO, a pediatric resident at Winthrop-University Hospital, Mineola, N.Y.
In 2011, the American Academy of Pediatrics issued “Urinary Tract Infection: Clinical Practice Guidelines for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months” (Pediatrics. 2011. doi: 10.1542/peds.2011-1330) concerning the diagnosis and management of the presence of bacteria in urine – a possible warning sign of UTI, but the AAP guidelines did not consider infants in the first 2 months of life.
To address this gap, the Winthrop-University Hospital researchers reviewed the medical records for all infants younger than 90 days of age diagnosed with UTI, fever, or viral illness from the beginning of 2009 to September 2015. Residence in neonatal intensive care, known congenital abnormalities, and prior antibiotic use were grounds for exclusion. Standard growth-based definitions of UTI and bacteriuria were used.
Of the 315 mainly white or Hispanic patients, 73 had a diagnosis of UTI and 261 did not. Both groups had the same mean age of 45 days. Fever within 24 hours of admission was more prevalent in those without UTI than those with (57% vs. 41%; P = .035). Those with UTI were significantly more likely (all P lesser than .001) to display serum leukocytosis (35% vs. 12%), pyuria (71% vs. 12%), and urine detection of leukocyte esterase (87% vs. 14%) and nitrite (19% vs. 0%).
In a univariate analysis, factors that were associated with UTI included serum leukocytosis, white blood cells in the urine, and urine leukocyte esterase, with fever within 24 hours of admission associated with reduced chance of UTI. A multivariate analysis that accounted for age, gender, and gestational age identified serum leukocytosis, pyruria, urine leukocyte esterase, and male sex as predictors of UTI, with increased odds ratio of 6.25, 3.19, 28, and 3.88, respectively.
The reduced likelihood of UTI in those who developed a fever within 24 hours of admission held up in the multivariate analysis (odds ratio 0.34).
Validation of the findings will require a prospective study, which is in the planning stage. If the findings bear out, the result could be improved diagnosis of UTI from birth onward, according to Dr. Berman.
Dr. Berman reported having no relevant financial disclosures.
SAN FRANCISCO – Serum leukocytosis, pyuria, and urine leukocyte esterase have been identified as predictors of urinary tract infection (UTI) in infants younger than 90 days of age, with males being more likely to develop UTI than females.
The chance of the infection declined in older infants.
“Really young infants have a less well developed immune system, which may increase their susceptibility to UTIs,” said Sarah Berman, DO, a pediatric resident at Winthrop-University Hospital, Mineola, N.Y.
In 2011, the American Academy of Pediatrics issued “Urinary Tract Infection: Clinical Practice Guidelines for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months” (Pediatrics. 2011. doi: 10.1542/peds.2011-1330) concerning the diagnosis and management of the presence of bacteria in urine – a possible warning sign of UTI, but the AAP guidelines did not consider infants in the first 2 months of life.
To address this gap, the Winthrop-University Hospital researchers reviewed the medical records for all infants younger than 90 days of age diagnosed with UTI, fever, or viral illness from the beginning of 2009 to September 2015. Residence in neonatal intensive care, known congenital abnormalities, and prior antibiotic use were grounds for exclusion. Standard growth-based definitions of UTI and bacteriuria were used.
Of the 315 mainly white or Hispanic patients, 73 had a diagnosis of UTI and 261 did not. Both groups had the same mean age of 45 days. Fever within 24 hours of admission was more prevalent in those without UTI than those with (57% vs. 41%; P = .035). Those with UTI were significantly more likely (all P lesser than .001) to display serum leukocytosis (35% vs. 12%), pyuria (71% vs. 12%), and urine detection of leukocyte esterase (87% vs. 14%) and nitrite (19% vs. 0%).
In a univariate analysis, factors that were associated with UTI included serum leukocytosis, white blood cells in the urine, and urine leukocyte esterase, with fever within 24 hours of admission associated with reduced chance of UTI. A multivariate analysis that accounted for age, gender, and gestational age identified serum leukocytosis, pyruria, urine leukocyte esterase, and male sex as predictors of UTI, with increased odds ratio of 6.25, 3.19, 28, and 3.88, respectively.
The reduced likelihood of UTI in those who developed a fever within 24 hours of admission held up in the multivariate analysis (odds ratio 0.34).
Validation of the findings will require a prospective study, which is in the planning stage. If the findings bear out, the result could be improved diagnosis of UTI from birth onward, according to Dr. Berman.
Dr. Berman reported having no relevant financial disclosures.
SAN FRANCISCO – Serum leukocytosis, pyuria, and urine leukocyte esterase have been identified as predictors of urinary tract infection (UTI) in infants younger than 90 days of age, with males being more likely to develop UTI than females.
The chance of the infection declined in older infants.
“Really young infants have a less well developed immune system, which may increase their susceptibility to UTIs,” said Sarah Berman, DO, a pediatric resident at Winthrop-University Hospital, Mineola, N.Y.
In 2011, the American Academy of Pediatrics issued “Urinary Tract Infection: Clinical Practice Guidelines for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months” (Pediatrics. 2011. doi: 10.1542/peds.2011-1330) concerning the diagnosis and management of the presence of bacteria in urine – a possible warning sign of UTI, but the AAP guidelines did not consider infants in the first 2 months of life.
To address this gap, the Winthrop-University Hospital researchers reviewed the medical records for all infants younger than 90 days of age diagnosed with UTI, fever, or viral illness from the beginning of 2009 to September 2015. Residence in neonatal intensive care, known congenital abnormalities, and prior antibiotic use were grounds for exclusion. Standard growth-based definitions of UTI and bacteriuria were used.
Of the 315 mainly white or Hispanic patients, 73 had a diagnosis of UTI and 261 did not. Both groups had the same mean age of 45 days. Fever within 24 hours of admission was more prevalent in those without UTI than those with (57% vs. 41%; P = .035). Those with UTI were significantly more likely (all P lesser than .001) to display serum leukocytosis (35% vs. 12%), pyuria (71% vs. 12%), and urine detection of leukocyte esterase (87% vs. 14%) and nitrite (19% vs. 0%).
In a univariate analysis, factors that were associated with UTI included serum leukocytosis, white blood cells in the urine, and urine leukocyte esterase, with fever within 24 hours of admission associated with reduced chance of UTI. A multivariate analysis that accounted for age, gender, and gestational age identified serum leukocytosis, pyruria, urine leukocyte esterase, and male sex as predictors of UTI, with increased odds ratio of 6.25, 3.19, 28, and 3.88, respectively.
The reduced likelihood of UTI in those who developed a fever within 24 hours of admission held up in the multivariate analysis (odds ratio 0.34).
Validation of the findings will require a prospective study, which is in the planning stage. If the findings bear out, the result could be improved diagnosis of UTI from birth onward, according to Dr. Berman.
Dr. Berman reported having no relevant financial disclosures.
AT PAS 17
Key clinical point: Pyuria, urine leukocyte esterase, and serum leukocytosis appear to be predictors of urinary tract infection in infants younger than 90 days of age.
Major finding: A multivariate analysis identified serum leukocytosis, pyruria, and urine leukocyte esterase as predictors of UTI, with increased odds ratio of 6.25, 3.19, and 28, respectively.
Data source: Retrospective analysis of medical records from one hospital.
Disclosures: Dr. Berman reported having no relevant financial disclosures.
Unilateral Verrucous Porokeratosis of the Gluteal Cleft
To the Editor:
Verrucous porokeratosis of the gluteal cleft is a rare skin condition that has distinct clinical and histologic features. A review of 5 cases described a characteristic clinical presentation of a butterfly-shaped bilateral gluteal cleft lesion on most patients.1 We present an unusual case of verrucous porokeratosis presenting as a unilateral single lesion in the gluteal area that emulated seborrheic keratosis with histology consistent with verrucous porokeratosis. This case adds to the variable presentation of this unusual disease.
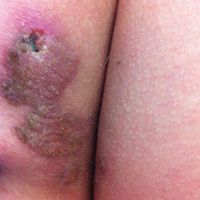
A 40-year-old man who presented to the dermatology clinic for a follow-up on a basal cell carcinoma of the temple region was concerned about a lesion on the left buttock of 1 year’s duration. Physical examination revealed a unilateral hyperkeratotic plaque that clinically resembled seborrheic keratosis (Figure 1). Biopsy revealed hyperkeratosis with numerous columns of parakeratosis, psoriasiform epidermal hyperplasia (Figures 2A and 2B), dyskeratotic keratinocytes (Figure 2C), pigment incontinence, and mild superficial chronic inflammation consistent with verrucous porokeratosis. The patient was treated with urea lotion but ultimately was lost to follow-up.

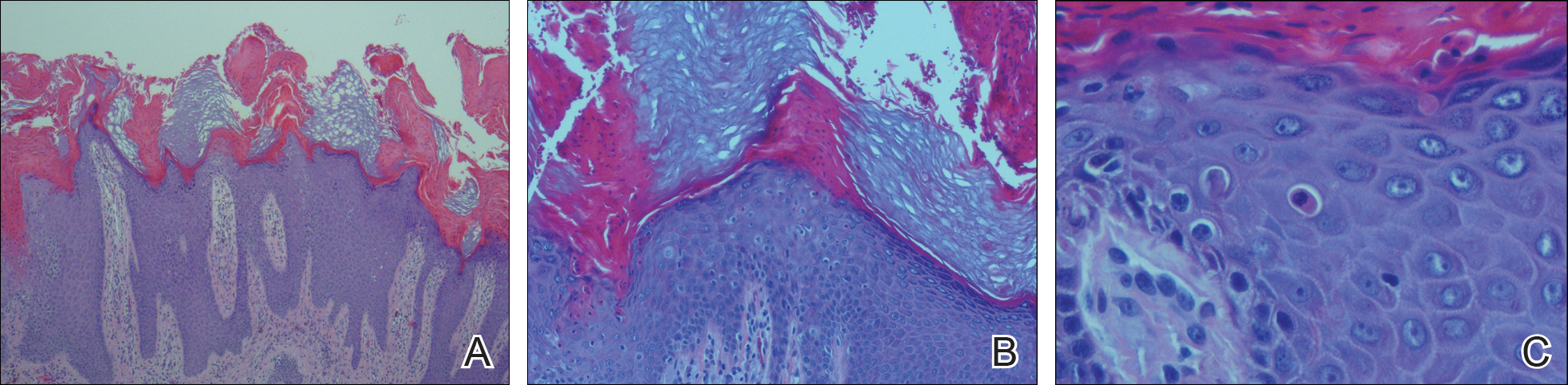
We present a unique case of unilateral verrucous porokeratosis of the gluteal cleft. The clinical differential diagnosis included seborrheic keratosis, condyloma acuminata, and inflammatory linear verrucous epidermal nevus. Histopathology was consistent with verrucous porokeratosis. Porokeratosis is a heterogeneous group of keratinization disorders containing several described variants such as classici porokeratosis of Mibelli, disseminated superficial porokeratosis, porokeratosis palmaris et plantaris disseminata, linear porokeratosis, and punctuate porokeratosis.1,2 Most patients present clinically with plaquelike bilateral (butterfly) lesions with threadlike (ridge) borders, though some patients initially have a unilateral lesion that subsequently develops into a bilateral lesion.1 The clinical course is slow growing, but it can potentially give rise to malignancies such as squamous cell carcinoma.3 Histologically, numerous columns of parakeratosis overlying epidermal cells with attenuated granular layer are observed with the concentric cornoid lamellae considered unique to the verrucous variant.1 Although our patient had only a single unilateral lesion on the gluteal cleft, the histology was consistent with verrucous porokeratosis. Our case adds to the growing clinical presentations of this unusual disease.
- Takiguchi R, White K, Clifton W, et al. Verrucous porokeratosis of the gluteal cleft (porokeratosis stychotropica): a rare disorder easily misdiagnosed. J Cutan Pathol. 2010;37:802-807.
- McGuigan K, Shurman D, Campanelli C, et al. Porokeratosis ptychotropica: a clinically distinct variant of porokeratosis. J Am Acad Dermatol. 2009;60:501-503.
- Malek J, Chedraoui A, Kibbi AG, et al. Genitogluteal porokeratosis: 10 years to make the diagnosis! Am J Dermatopathol. 2009;31:604-606.
To the Editor:
Verrucous porokeratosis of the gluteal cleft is a rare skin condition that has distinct clinical and histologic features. A review of 5 cases described a characteristic clinical presentation of a butterfly-shaped bilateral gluteal cleft lesion on most patients.1 We present an unusual case of verrucous porokeratosis presenting as a unilateral single lesion in the gluteal area that emulated seborrheic keratosis with histology consistent with verrucous porokeratosis. This case adds to the variable presentation of this unusual disease.
A 40-year-old man who presented to the dermatology clinic for a follow-up on a basal cell carcinoma of the temple region was concerned about a lesion on the left buttock of 1 year’s duration. Physical examination revealed a unilateral hyperkeratotic plaque that clinically resembled seborrheic keratosis (Figure 1). Biopsy revealed hyperkeratosis with numerous columns of parakeratosis, psoriasiform epidermal hyperplasia (Figures 2A and 2B), dyskeratotic keratinocytes (Figure 2C), pigment incontinence, and mild superficial chronic inflammation consistent with verrucous porokeratosis. The patient was treated with urea lotion but ultimately was lost to follow-up.
We present a unique case of unilateral verrucous porokeratosis of the gluteal cleft. The clinical differential diagnosis included seborrheic keratosis, condyloma acuminata, and inflammatory linear verrucous epidermal nevus. Histopathology was consistent with verrucous porokeratosis. Porokeratosis is a heterogeneous group of keratinization disorders containing several described variants such as classici porokeratosis of Mibelli, disseminated superficial porokeratosis, porokeratosis palmaris et plantaris disseminata, linear porokeratosis, and punctuate porokeratosis.1,2 Most patients present clinically with plaquelike bilateral (butterfly) lesions with threadlike (ridge) borders, though some patients initially have a unilateral lesion that subsequently develops into a bilateral lesion.1 The clinical course is slow growing, but it can potentially give rise to malignancies such as squamous cell carcinoma.3 Histologically, numerous columns of parakeratosis overlying epidermal cells with attenuated granular layer are observed with the concentric cornoid lamellae considered unique to the verrucous variant.1 Although our patient had only a single unilateral lesion on the gluteal cleft, the histology was consistent with verrucous porokeratosis. Our case adds to the growing clinical presentations of this unusual disease.
To the Editor:
Verrucous porokeratosis of the gluteal cleft is a rare skin condition that has distinct clinical and histologic features. A review of 5 cases described a characteristic clinical presentation of a butterfly-shaped bilateral gluteal cleft lesion on most patients.1 We present an unusual case of verrucous porokeratosis presenting as a unilateral single lesion in the gluteal area that emulated seborrheic keratosis with histology consistent with verrucous porokeratosis. This case adds to the variable presentation of this unusual disease.
A 40-year-old man who presented to the dermatology clinic for a follow-up on a basal cell carcinoma of the temple region was concerned about a lesion on the left buttock of 1 year’s duration. Physical examination revealed a unilateral hyperkeratotic plaque that clinically resembled seborrheic keratosis (Figure 1). Biopsy revealed hyperkeratosis with numerous columns of parakeratosis, psoriasiform epidermal hyperplasia (Figures 2A and 2B), dyskeratotic keratinocytes (Figure 2C), pigment incontinence, and mild superficial chronic inflammation consistent with verrucous porokeratosis. The patient was treated with urea lotion but ultimately was lost to follow-up.
We present a unique case of unilateral verrucous porokeratosis of the gluteal cleft. The clinical differential diagnosis included seborrheic keratosis, condyloma acuminata, and inflammatory linear verrucous epidermal nevus. Histopathology was consistent with verrucous porokeratosis. Porokeratosis is a heterogeneous group of keratinization disorders containing several described variants such as classici porokeratosis of Mibelli, disseminated superficial porokeratosis, porokeratosis palmaris et plantaris disseminata, linear porokeratosis, and punctuate porokeratosis.1,2 Most patients present clinically with plaquelike bilateral (butterfly) lesions with threadlike (ridge) borders, though some patients initially have a unilateral lesion that subsequently develops into a bilateral lesion.1 The clinical course is slow growing, but it can potentially give rise to malignancies such as squamous cell carcinoma.3 Histologically, numerous columns of parakeratosis overlying epidermal cells with attenuated granular layer are observed with the concentric cornoid lamellae considered unique to the verrucous variant.1 Although our patient had only a single unilateral lesion on the gluteal cleft, the histology was consistent with verrucous porokeratosis. Our case adds to the growing clinical presentations of this unusual disease.
- Takiguchi R, White K, Clifton W, et al. Verrucous porokeratosis of the gluteal cleft (porokeratosis stychotropica): a rare disorder easily misdiagnosed. J Cutan Pathol. 2010;37:802-807.
- McGuigan K, Shurman D, Campanelli C, et al. Porokeratosis ptychotropica: a clinically distinct variant of porokeratosis. J Am Acad Dermatol. 2009;60:501-503.
- Malek J, Chedraoui A, Kibbi AG, et al. Genitogluteal porokeratosis: 10 years to make the diagnosis! Am J Dermatopathol. 2009;31:604-606.
- Takiguchi R, White K, Clifton W, et al. Verrucous porokeratosis of the gluteal cleft (porokeratosis stychotropica): a rare disorder easily misdiagnosed. J Cutan Pathol. 2010;37:802-807.
- McGuigan K, Shurman D, Campanelli C, et al. Porokeratosis ptychotropica: a clinically distinct variant of porokeratosis. J Am Acad Dermatol. 2009;60:501-503.
- Malek J, Chedraoui A, Kibbi AG, et al. Genitogluteal porokeratosis: 10 years to make the diagnosis! Am J Dermatopathol. 2009;31:604-606.
Practice Point
- Porokeratosis of the gluteal cleft typically is bilateral but may be unilateral.
Is Your Practice Biosimilar Ready?
Click Here to Read the Full Supplement.

Topics include:
- The Pathway for Biosimilar Approval
- The Difference between Biosimilars and Generics
- Draft Interchangeablity Guidelines
- ACR Position Statement on Biosimilars
- Effect of the Reimbursement Model on Biosimilars
Click Here to Read the Full Supplement.
Topics include:
- The Pathway for Biosimilar Approval
- The Difference between Biosimilars and Generics
- Draft Interchangeablity Guidelines
- ACR Position Statement on Biosimilars
- Effect of the Reimbursement Model on Biosimilars
Click Here to Read the Full Supplement.
Topics include:
- The Pathway for Biosimilar Approval
- The Difference between Biosimilars and Generics
- Draft Interchangeablity Guidelines
- ACR Position Statement on Biosimilars
- Effect of the Reimbursement Model on Biosimilars
Decision to remove breast cancer metastases depends on location of lesions
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain

Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain
Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
LAS VEGAS – Determination of whether excision of persistent breast cancer metastases can benefit the patient and even prolong survival depends on the location of the metastatic lesions, an investigator said at the annual meeting of the American Society of Breast Surgeons.
Before making the decision, it’s important to restage the patient’s disease and to recheck the receptor status if a biopsy is accessible, said Roshni Rao, MD, of the University of Texas Southwestern Medical Center.
Brain
Survival is worse when there are concurrent extracranial metastases or when brain metastases are greater than 5 cm, in patients with triple negative tumors, and in patients with a Karnofsky score of 70 or less, Dr. Rao said.
Surgery has the greatest benefit in patients with a single metastasis, with no extracranial disease, and who are able to undergo adjuvant whole brain radiation. In these cases, surgery improves survival, lowers recurrence rates, and reduces the risk of death neurological causes, she said.
Long-term survival is most common with continuous adjuvant therapy, either trastuzumab or hormonal, and in patients with a longer time interval to development of metastases. One series showed a 20-month survival increase.
Liver
Approximately 15% of patients with synchronous metastases will have liver metastases, and about half of stage IV patients will experience liver metastases at some point during treatment.
There is evidence from colorectal cancer that removing liver metastases is beneficial, and that has prompted interest in a similar approach in breast cancer. Liver resection has also become safer with new advances.
Dr. Rao discussed a single-institution study which took an aggressive approach to liver resection in 85 patients (Ann Surg. 2006;244:897-907). The researchers found that increased survival was associated with a good response to adjuvant chemotherapy, an r0 or r1 resection, and in patients who had a previous liver resection and were healthy enough to undergo another resection.
Overall, existing studies support liver resection if there are one to three lesions, if negative margins can be achieved, if the tumors are hormone receptor positive, and if the cancer is hormone positive and has good response to chemotherapy.
Dr. Rao emphasized that liver resections should be performed with a multidisciplinary team and should only be attempted at centers with low morbidity and where the doctors are experienced with liver resection.
When it’s possible, liver resection is beneficial. “There have been multiple reports of long-term survivors with no evidence of disease. There is likely a survival benefit with careful selection of these patients,” Dr. Rao said.
Lung
Lung surgeries are becoming safer, especially with the availability of video-assisted techniques, and pulmonary metastases are increasingly being spotted using more sensitive techniques such as higher resolution computed tomography.
A lung metastasis registry analysis showed three factors improved survival: prolonged disease-free survival, especially longer than 36 months; a complete resection; and a small number of metastases and success in resecting them all (Eur J Cardiothorac Surg. 2002;22:335-44). A more recent meta-analysis showed the same results (J Thorac Dis. 2015;7:1441-51).
Bone
Bone metastases remain rare choices for surgical treatment. Most of the time, morbidity will be too high, and there are good options for systemic treatment. That leaves surgery reserved mostly for stabilization or the treatment of fractures.
However, there are a couple of exceptions, according to Dr. Rao. One multi-institutional randomized trial looked at metastatic epidural spinal cord compression. Subjects either underwent decompressive surgery with stabilization and radiation or radiation alone. Patients in the surgical group had a longer ambulatory period and had a lower usage rate of steroids and opioids. Morbidity outcomes were similar in both groups. Patients whose primary tumor was in the breast seemed to benefit the most with respect to ambulatory time (Lancet. 2005;9486:643-8; J Neurosurg Spine. 2008;8:271-8).
Sternal metastases represent another special case. 70% of the time, patients with sternal metastases have it as their only metastatic site. A French series of 33 patients who underwent aggressive chest wall and rib resection reported a 36% complication rate, while another study of 28 patients showed a 21% complication rate. Those complications are a problem, “but if you’re able to perform this in a resected tumor, there are long term survivors. As usual, triple negative breast cancers predicted a worse prognosis,” said Dr. Rao.
Dr. Rao concluded that resection of metastatic sites has a role. “I think it’s our responsibility as breast surgeons who are many times continuously following these patients to consider appropriate operations,” said Dr. Rao.
However, she did sound one note of caution. Surgery can interrupt therapy that is helping a patient. “Let’s say you have someone get a big liver resection, and then they have a tough time with recovery. There could be a long period of time they can’t get the therapy that was keeping them alive. That’s the real concern,” she said.
EXPERT ANALYSIS FROM ASBS 2017
Black Linear Streaks on the Face With Pruritic Plaques on the Trunk and Arms
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.

A 68-year-old man presented to the emergency department with pruritic, edematous, pink plaques on the trunk and arms, as well as black linear streaks on the face, prompting dermatology consultation for possible tissue necrosis. The patient reported working outdoors in his garden 3 days prior to presentation.

Breastfeeding among factors that modify neonatal abstinence syndrome
SAN FRANCISCO – The good news of a prospective, multicenter study presented at the Pediatric Academic Societies meeting was that neonates who were breastfed were less likely to require neonatal abstinence syndrome (NAS) treatment and displayed milder symptoms.
The study also identified other risk factors associated with the need for NAS treatment and the severity of NAS.
“These findings are important because many of these risk factors are modifiable. Prenatal care providers strive to provide the best treatments for both the mother and the fetus. Our findings regarding the association of NAS with some maternal drug exposures can be shared with opiate-dependent mothers during general counseling about tobacco and illicit use in pregnancy and in counseling about NAS,” explained Megan Stover, MD, a fellow in maternal-fetal medicine and genetics at Tufts Medical Center in Boston.
The current standard of care for opioid-dependent pregnant women is medication-assisted treatment with either methadone or buprenorphine. The intervention can be effective in curbing continued opioid abuse and preventing relapse. However, for many of their unborn children, the damage has already been done.
The scope of the problem in the United States is staggering. Between 2004 and 2013, there was a fourfold to fivefold increase in the rate of admissions to neonatal intensive care units (NICUs) for NAS. “It has been estimated that, every minute in the United States, one neonate will require treatment for NAS,” said Dr. Stover. The glum reality for the Tufts researchers is that 50%-80% of opiate-exposed infants will require treatment for NAS. The aim is to reduce this rate.
Dr. Stover was part of a study conducted at hospitals on the U.S. East Coast that aimed to clarify factors before and after birth that were associated with NAS. The enrolled mothers had been treated during their third trimester or following admission for birth for opioid dependence or had received an opioid for relief of chronic pain. They had given birth to their child at term.
Neonates who were born prematurely or who had comorbidities judged to be significant were not part of the analyses. Of the 306 neonates included, 52% required treatment for NAS and 48% did not. The two groups were similar in age of the mother and for neonatal characteristics of gestational age, sex, ethnicity, and body measurements at birth. The severity of NAS was gauged in two ways. One was the number of days of treatment required to free the neonates from the opioid-induced symptoms, with less than 10 days indicating mild NAS, greater than 30 days indicating severe NAS, and the intervening days indicating moderate NAS. Severe NAS also was indicated by the use of two or more medications.
There was good news. Neonates were significantly less likely to require NAS treatment if they were breastfed exclusively, compared with formula fed babies (15% vs 67%; P less than .0001). NAS was usually mild in breastfed babies and often severe in formula-fed babies (P less than .002).
“Our findings regarding the favorable outcomes seen with breastfeeding support recent research regarding the influence of nonpharmacologic approaches to the prevention and management of NAS, namely that more soothing environments, like those outside the NICU, may be more optimal settings for infants undergoing surveillance for NAS,” said Dr. Stover.
Neonatal treatment was more prevalent for women whose opioid substitution therapy involved methadone (54% vs 28% of untreated neonates; P less than .0001). When therapy used buprenorphine, 62% of the neonates did not display NAS. The drug used for substitution therapy had no effect on the length of treatment of the neonates.
“Our data regarding methadone exposure [versus buprenorphine] adds to a growing literature surrounding more favorable neonatal effects seen with this opiate maintenance agent over methadone,” commented Dr. Stover.
NAS treatment was more prevalent for mothers who smoked during pregnancy, compared with those who did not (76% vs 42%; P equal to .02), and for maternal use of illicit drugs (50% vs 34%; P equal to .002), with no effect on length of neonatal treatment.
Maternal psychiatric diagnosis was associated with neonatal NAS (P equal to .03), as was prescription benzodiazepine use in the third trimester of pregnancy (P equal to .02). Benzodiazepine use did not influence the length of treatment. However, maternal alprazolam use did, as it was associated with more severe NAS (P less than .001). Use of selective serotonin reuptake inhibitor during pregnancy was also associated with more severe NAS (P equal to 0.01).
The researchers are currently sifting through the genetic data gathered in the study. The goal is to combine the clinical and genetic data to create a risk score that will be used to tailor care before birth and in the early weeks following birth.
The study was sponsored by Tufts Medical Center and was funded by National Institute on Drug Abuse. Dr. Stover reported having no relevant financial disclosures.
SAN FRANCISCO – The good news of a prospective, multicenter study presented at the Pediatric Academic Societies meeting was that neonates who were breastfed were less likely to require neonatal abstinence syndrome (NAS) treatment and displayed milder symptoms.
The study also identified other risk factors associated with the need for NAS treatment and the severity of NAS.
“These findings are important because many of these risk factors are modifiable. Prenatal care providers strive to provide the best treatments for both the mother and the fetus. Our findings regarding the association of NAS with some maternal drug exposures can be shared with opiate-dependent mothers during general counseling about tobacco and illicit use in pregnancy and in counseling about NAS,” explained Megan Stover, MD, a fellow in maternal-fetal medicine and genetics at Tufts Medical Center in Boston.
The current standard of care for opioid-dependent pregnant women is medication-assisted treatment with either methadone or buprenorphine. The intervention can be effective in curbing continued opioid abuse and preventing relapse. However, for many of their unborn children, the damage has already been done.
The scope of the problem in the United States is staggering. Between 2004 and 2013, there was a fourfold to fivefold increase in the rate of admissions to neonatal intensive care units (NICUs) for NAS. “It has been estimated that, every minute in the United States, one neonate will require treatment for NAS,” said Dr. Stover. The glum reality for the Tufts researchers is that 50%-80% of opiate-exposed infants will require treatment for NAS. The aim is to reduce this rate.
Dr. Stover was part of a study conducted at hospitals on the U.S. East Coast that aimed to clarify factors before and after birth that were associated with NAS. The enrolled mothers had been treated during their third trimester or following admission for birth for opioid dependence or had received an opioid for relief of chronic pain. They had given birth to their child at term.
Neonates who were born prematurely or who had comorbidities judged to be significant were not part of the analyses. Of the 306 neonates included, 52% required treatment for NAS and 48% did not. The two groups were similar in age of the mother and for neonatal characteristics of gestational age, sex, ethnicity, and body measurements at birth. The severity of NAS was gauged in two ways. One was the number of days of treatment required to free the neonates from the opioid-induced symptoms, with less than 10 days indicating mild NAS, greater than 30 days indicating severe NAS, and the intervening days indicating moderate NAS. Severe NAS also was indicated by the use of two or more medications.
There was good news. Neonates were significantly less likely to require NAS treatment if they were breastfed exclusively, compared with formula fed babies (15% vs 67%; P less than .0001). NAS was usually mild in breastfed babies and often severe in formula-fed babies (P less than .002).
“Our findings regarding the favorable outcomes seen with breastfeeding support recent research regarding the influence of nonpharmacologic approaches to the prevention and management of NAS, namely that more soothing environments, like those outside the NICU, may be more optimal settings for infants undergoing surveillance for NAS,” said Dr. Stover.
Neonatal treatment was more prevalent for women whose opioid substitution therapy involved methadone (54% vs 28% of untreated neonates; P less than .0001). When therapy used buprenorphine, 62% of the neonates did not display NAS. The drug used for substitution therapy had no effect on the length of treatment of the neonates.
“Our data regarding methadone exposure [versus buprenorphine] adds to a growing literature surrounding more favorable neonatal effects seen with this opiate maintenance agent over methadone,” commented Dr. Stover.
NAS treatment was more prevalent for mothers who smoked during pregnancy, compared with those who did not (76% vs 42%; P equal to .02), and for maternal use of illicit drugs (50% vs 34%; P equal to .002), with no effect on length of neonatal treatment.
Maternal psychiatric diagnosis was associated with neonatal NAS (P equal to .03), as was prescription benzodiazepine use in the third trimester of pregnancy (P equal to .02). Benzodiazepine use did not influence the length of treatment. However, maternal alprazolam use did, as it was associated with more severe NAS (P less than .001). Use of selective serotonin reuptake inhibitor during pregnancy was also associated with more severe NAS (P equal to 0.01).
The researchers are currently sifting through the genetic data gathered in the study. The goal is to combine the clinical and genetic data to create a risk score that will be used to tailor care before birth and in the early weeks following birth.
The study was sponsored by Tufts Medical Center and was funded by National Institute on Drug Abuse. Dr. Stover reported having no relevant financial disclosures.
SAN FRANCISCO – The good news of a prospective, multicenter study presented at the Pediatric Academic Societies meeting was that neonates who were breastfed were less likely to require neonatal abstinence syndrome (NAS) treatment and displayed milder symptoms.
The study also identified other risk factors associated with the need for NAS treatment and the severity of NAS.
“These findings are important because many of these risk factors are modifiable. Prenatal care providers strive to provide the best treatments for both the mother and the fetus. Our findings regarding the association of NAS with some maternal drug exposures can be shared with opiate-dependent mothers during general counseling about tobacco and illicit use in pregnancy and in counseling about NAS,” explained Megan Stover, MD, a fellow in maternal-fetal medicine and genetics at Tufts Medical Center in Boston.
The current standard of care for opioid-dependent pregnant women is medication-assisted treatment with either methadone or buprenorphine. The intervention can be effective in curbing continued opioid abuse and preventing relapse. However, for many of their unborn children, the damage has already been done.
The scope of the problem in the United States is staggering. Between 2004 and 2013, there was a fourfold to fivefold increase in the rate of admissions to neonatal intensive care units (NICUs) for NAS. “It has been estimated that, every minute in the United States, one neonate will require treatment for NAS,” said Dr. Stover. The glum reality for the Tufts researchers is that 50%-80% of opiate-exposed infants will require treatment for NAS. The aim is to reduce this rate.
Dr. Stover was part of a study conducted at hospitals on the U.S. East Coast that aimed to clarify factors before and after birth that were associated with NAS. The enrolled mothers had been treated during their third trimester or following admission for birth for opioid dependence or had received an opioid for relief of chronic pain. They had given birth to their child at term.
Neonates who were born prematurely or who had comorbidities judged to be significant were not part of the analyses. Of the 306 neonates included, 52% required treatment for NAS and 48% did not. The two groups were similar in age of the mother and for neonatal characteristics of gestational age, sex, ethnicity, and body measurements at birth. The severity of NAS was gauged in two ways. One was the number of days of treatment required to free the neonates from the opioid-induced symptoms, with less than 10 days indicating mild NAS, greater than 30 days indicating severe NAS, and the intervening days indicating moderate NAS. Severe NAS also was indicated by the use of two or more medications.
There was good news. Neonates were significantly less likely to require NAS treatment if they were breastfed exclusively, compared with formula fed babies (15% vs 67%; P less than .0001). NAS was usually mild in breastfed babies and often severe in formula-fed babies (P less than .002).
“Our findings regarding the favorable outcomes seen with breastfeeding support recent research regarding the influence of nonpharmacologic approaches to the prevention and management of NAS, namely that more soothing environments, like those outside the NICU, may be more optimal settings for infants undergoing surveillance for NAS,” said Dr. Stover.
Neonatal treatment was more prevalent for women whose opioid substitution therapy involved methadone (54% vs 28% of untreated neonates; P less than .0001). When therapy used buprenorphine, 62% of the neonates did not display NAS. The drug used for substitution therapy had no effect on the length of treatment of the neonates.
“Our data regarding methadone exposure [versus buprenorphine] adds to a growing literature surrounding more favorable neonatal effects seen with this opiate maintenance agent over methadone,” commented Dr. Stover.
NAS treatment was more prevalent for mothers who smoked during pregnancy, compared with those who did not (76% vs 42%; P equal to .02), and for maternal use of illicit drugs (50% vs 34%; P equal to .002), with no effect on length of neonatal treatment.
Maternal psychiatric diagnosis was associated with neonatal NAS (P equal to .03), as was prescription benzodiazepine use in the third trimester of pregnancy (P equal to .02). Benzodiazepine use did not influence the length of treatment. However, maternal alprazolam use did, as it was associated with more severe NAS (P less than .001). Use of selective serotonin reuptake inhibitor during pregnancy was also associated with more severe NAS (P equal to 0.01).
The researchers are currently sifting through the genetic data gathered in the study. The goal is to combine the clinical and genetic data to create a risk score that will be used to tailor care before birth and in the early weeks following birth.
The study was sponsored by Tufts Medical Center and was funded by National Institute on Drug Abuse. Dr. Stover reported having no relevant financial disclosures.
AT PAS 2017
Key clinical point: Clinical factors associated with the need for treatment of neonatal abstinence syndrome and for its severity were identified.
Major finding: Breastfeeding was also associated with less severe NAS (P equal to .0003).
Data source: Prospective cohort analysis as part of a multisite trial.
Disclosures: The study was sponsored by Tufts Medical Center and was funded by the National Institute on Drug Abuse. Dr. Stover reported having no relevant financial disclosures.