User login
NLR useful for predicting 1-year mortality in PBC patients
An elevated baseline neutrophil-to-lymphocyte ratio (NLR) was associated with a poor 1-year mortality rate in hospitalized primary biliary cholangitis (PBC) patients, according to Lin Lin, MD, of Tianjin (China) Medical University General Hospital and the Tianjin Institute of Digestive Diseases and associates.
A retrospective analysis of 88 PBC patients hospitalized between June 2009 and January 2014 was performed for the study. NLR was a significant predictor of survival, with an odds ratio of 1.5, a sensitivity of 100%, and a specificity of 67.1%. A baseline NLR value of 2.18 was selected as the cutoff for 1-year mortality. Of the 33 patients above this value at initial hospitalization, 6 died, whereas none of the 55 patients below this value died.
The results of the retrospective study were confirmed in a prospective 1-year cohort that included 63 people with PBC. The patients with a baseline NLR of less than 2.18 had significantly longer survival times than those who had a baseline NLR of 2.18 or higher.
“NLR – an affordable, widely available and reproducible index – is closely related to short-term mortality in patients with PBC. Further studies are warranted to externally cross-validate our findings in other populations,” the investigators concluded.
Find the full study in BMJ Open (2017. doi: 10.1136/bmjopen-2016-015304).
An elevated baseline neutrophil-to-lymphocyte ratio (NLR) was associated with a poor 1-year mortality rate in hospitalized primary biliary cholangitis (PBC) patients, according to Lin Lin, MD, of Tianjin (China) Medical University General Hospital and the Tianjin Institute of Digestive Diseases and associates.
A retrospective analysis of 88 PBC patients hospitalized between June 2009 and January 2014 was performed for the study. NLR was a significant predictor of survival, with an odds ratio of 1.5, a sensitivity of 100%, and a specificity of 67.1%. A baseline NLR value of 2.18 was selected as the cutoff for 1-year mortality. Of the 33 patients above this value at initial hospitalization, 6 died, whereas none of the 55 patients below this value died.
The results of the retrospective study were confirmed in a prospective 1-year cohort that included 63 people with PBC. The patients with a baseline NLR of less than 2.18 had significantly longer survival times than those who had a baseline NLR of 2.18 or higher.
“NLR – an affordable, widely available and reproducible index – is closely related to short-term mortality in patients with PBC. Further studies are warranted to externally cross-validate our findings in other populations,” the investigators concluded.
Find the full study in BMJ Open (2017. doi: 10.1136/bmjopen-2016-015304).
An elevated baseline neutrophil-to-lymphocyte ratio (NLR) was associated with a poor 1-year mortality rate in hospitalized primary biliary cholangitis (PBC) patients, according to Lin Lin, MD, of Tianjin (China) Medical University General Hospital and the Tianjin Institute of Digestive Diseases and associates.
A retrospective analysis of 88 PBC patients hospitalized between June 2009 and January 2014 was performed for the study. NLR was a significant predictor of survival, with an odds ratio of 1.5, a sensitivity of 100%, and a specificity of 67.1%. A baseline NLR value of 2.18 was selected as the cutoff for 1-year mortality. Of the 33 patients above this value at initial hospitalization, 6 died, whereas none of the 55 patients below this value died.
The results of the retrospective study were confirmed in a prospective 1-year cohort that included 63 people with PBC. The patients with a baseline NLR of less than 2.18 had significantly longer survival times than those who had a baseline NLR of 2.18 or higher.
“NLR – an affordable, widely available and reproducible index – is closely related to short-term mortality in patients with PBC. Further studies are warranted to externally cross-validate our findings in other populations,” the investigators concluded.
Find the full study in BMJ Open (2017. doi: 10.1136/bmjopen-2016-015304).
FROM BMJ OPEN
VA cohort study: Individualize SSI prophylaxis based on patient factors
The combined use of vancomycin and a beta-lactam antibiotic for prophylaxis against surgical site infections is associated with both benefits and harms, according to findings from a national propensity-score–adjusted retrospective cohort study.
For example, the combination treatment reduced surgical site infections (SSIs) 30 days after cardiac surgical procedures but increased the risk of postoperative acute kidney injury (AKI) in some patients, Westyn Branch-Elliman, MD, of the VA Boston Healthcare System and her colleagues reported online July 10 in PLOS Medicine.
Among cardiac surgery patients, the incidence of surgical site infections was significantly lower for the 6,953 patients treated with both drugs vs. the 12,834 treated with a single agent (0.95% vs. 1.48%), the investigators found (PLOS Med. 2017 Jul 10. doi: 10.1371/journal.pmed.1002340).
SSI benefit with combination therapy
“After controlling for age, diabetes, ASA [American Society of Anesthesiologists] score, mupirocin administration, current smoking status, and preoperative MRSA [methicillin-resistant Staphylococcus aureus] colonization status, receipt of combination antimicrobial prophylaxis was associated with reduced SSI risk following cardiac surgical procedures (adjusted risk ratio, 0.61),” they wrote, noting that, when combination therapy was compared with either of the agents alone, the associations were similar and that no association between SSI reduction and the combination regimen was seen for the other types of surgical procedures assessed.
Secondary analyses showed that, among the cardiac patients, differences in the rates of SSIs were seen based on MRSA status in patients undergoing cardiac surgery. Among MRSA-colonized patients, SSIs occurred in 8 of 346 patients (2.3%) who received combination prophylaxis vs. 4 of 100 patients (4%) who received vancomycin alone (aRR, 0.53), and, among MRSA-negative and MRSA-unknown cardiac surgery patients, SSIs occurred in 58 of 6,607 patients (0.88%) receiving combination prophylaxis and 146 of 10,215 patients (1.4%) receiving a beta-lactam alone (aRR, 0.60).
“Among MRSA-colonized patients undergoing cardiac surgery, the associated absolute risk reduction for SSI was approximately triple that of the absolute risk reduction in MRSA-negative or -unknown patients, with a [number needed to treat] to prevent 1 SSI of 53 for the MRSA-colonized group, compared with 176 for the MRSA-negative or -unknown groups,” they wrote.
The incidence of Clostridium difficile infection was similar in both exposure groups (0.72% and 0.81% with combination and single agent prophylaxis, respectively).
Higher AKI risk with combination therapy
“In contrast, combination versus single prophylaxis was associated with higher relative risk of AKI in the 7-day postoperative period after adjusting for prophylaxis regimen duration, age, diabetes, ASA score, and smoking,” they said.
The rate of AKI was 23.75% among patients receiving combination prophylaxis, compared with 20.79% and 13.93% among those receiving vancomycin alone and a beta-lactam alone, respectively.
Significant associations between absolute risk of AKI and receipt of combination regimens were seen across all types of procedures, the investigators said.
“Overall, the NNH [number needed to harm] to cause one episode of AKI in cardiac surgery patients receiving combination therapy was 22, and, for stage 3 AKI, 167. The NNH associated with one additional episode of any postoperative AKI after receipt of combination therapy was 76 following orthopedic procedures and 25 following vascular surgical procedures,” they said.
The optimal approach for preventing SSIs is unclear. Although the multidisciplinary Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery recommend single agent prophylaxis most often, with a beta-lactam antibiotic, for most surgical procedures, the use of vancomycin alone is a consideration in MRSA-colonized patients and in centers with a high MRSA incidence, and combination prophylaxis with a beta-lactam plus vancomycin is increasing. However, the relative risks and benefit of this strategy have not been carefully studied, the investigators said.
Thus, the investigators used a propensity-adjusted, log-binomial regression model stratified by type of surgical procedure among the cases identified in the Veterans Affairs cohort to assess the association between SSIs and receipt of combination prophylaxis versus single agent prophylaxis.
Though limited by the observational study design and by factors such as a predominantly male and slightly older and more rural population, the findings suggest that “clinicians may need to individualize prophylaxis strategy based on patient-specific factors that influence the risk-versus-benefit equation,” they said, concluding that “future studies are needed to evaluate the utility of MRSA screening protocols for optimizing and individualizing surgical prophylaxis regimen.”
This study was funded by Veterans Affairs Health Services Research and Development. Dr. Branch-Elliman reported having no disclosures. One other author, Eli Perencevich, MD, received an investigator initiated Grant from Merck Pharmaceuticals in 2013.
The combined use of vancomycin and a beta-lactam antibiotic for prophylaxis against surgical site infections is associated with both benefits and harms, according to findings from a national propensity-score–adjusted retrospective cohort study.
For example, the combination treatment reduced surgical site infections (SSIs) 30 days after cardiac surgical procedures but increased the risk of postoperative acute kidney injury (AKI) in some patients, Westyn Branch-Elliman, MD, of the VA Boston Healthcare System and her colleagues reported online July 10 in PLOS Medicine.
Among cardiac surgery patients, the incidence of surgical site infections was significantly lower for the 6,953 patients treated with both drugs vs. the 12,834 treated with a single agent (0.95% vs. 1.48%), the investigators found (PLOS Med. 2017 Jul 10. doi: 10.1371/journal.pmed.1002340).
SSI benefit with combination therapy
“After controlling for age, diabetes, ASA [American Society of Anesthesiologists] score, mupirocin administration, current smoking status, and preoperative MRSA [methicillin-resistant Staphylococcus aureus] colonization status, receipt of combination antimicrobial prophylaxis was associated with reduced SSI risk following cardiac surgical procedures (adjusted risk ratio, 0.61),” they wrote, noting that, when combination therapy was compared with either of the agents alone, the associations were similar and that no association between SSI reduction and the combination regimen was seen for the other types of surgical procedures assessed.
Secondary analyses showed that, among the cardiac patients, differences in the rates of SSIs were seen based on MRSA status in patients undergoing cardiac surgery. Among MRSA-colonized patients, SSIs occurred in 8 of 346 patients (2.3%) who received combination prophylaxis vs. 4 of 100 patients (4%) who received vancomycin alone (aRR, 0.53), and, among MRSA-negative and MRSA-unknown cardiac surgery patients, SSIs occurred in 58 of 6,607 patients (0.88%) receiving combination prophylaxis and 146 of 10,215 patients (1.4%) receiving a beta-lactam alone (aRR, 0.60).
“Among MRSA-colonized patients undergoing cardiac surgery, the associated absolute risk reduction for SSI was approximately triple that of the absolute risk reduction in MRSA-negative or -unknown patients, with a [number needed to treat] to prevent 1 SSI of 53 for the MRSA-colonized group, compared with 176 for the MRSA-negative or -unknown groups,” they wrote.
The incidence of Clostridium difficile infection was similar in both exposure groups (0.72% and 0.81% with combination and single agent prophylaxis, respectively).
Higher AKI risk with combination therapy
“In contrast, combination versus single prophylaxis was associated with higher relative risk of AKI in the 7-day postoperative period after adjusting for prophylaxis regimen duration, age, diabetes, ASA score, and smoking,” they said.
The rate of AKI was 23.75% among patients receiving combination prophylaxis, compared with 20.79% and 13.93% among those receiving vancomycin alone and a beta-lactam alone, respectively.
Significant associations between absolute risk of AKI and receipt of combination regimens were seen across all types of procedures, the investigators said.
“Overall, the NNH [number needed to harm] to cause one episode of AKI in cardiac surgery patients receiving combination therapy was 22, and, for stage 3 AKI, 167. The NNH associated with one additional episode of any postoperative AKI after receipt of combination therapy was 76 following orthopedic procedures and 25 following vascular surgical procedures,” they said.
The optimal approach for preventing SSIs is unclear. Although the multidisciplinary Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery recommend single agent prophylaxis most often, with a beta-lactam antibiotic, for most surgical procedures, the use of vancomycin alone is a consideration in MRSA-colonized patients and in centers with a high MRSA incidence, and combination prophylaxis with a beta-lactam plus vancomycin is increasing. However, the relative risks and benefit of this strategy have not been carefully studied, the investigators said.
Thus, the investigators used a propensity-adjusted, log-binomial regression model stratified by type of surgical procedure among the cases identified in the Veterans Affairs cohort to assess the association between SSIs and receipt of combination prophylaxis versus single agent prophylaxis.
Though limited by the observational study design and by factors such as a predominantly male and slightly older and more rural population, the findings suggest that “clinicians may need to individualize prophylaxis strategy based on patient-specific factors that influence the risk-versus-benefit equation,” they said, concluding that “future studies are needed to evaluate the utility of MRSA screening protocols for optimizing and individualizing surgical prophylaxis regimen.”
This study was funded by Veterans Affairs Health Services Research and Development. Dr. Branch-Elliman reported having no disclosures. One other author, Eli Perencevich, MD, received an investigator initiated Grant from Merck Pharmaceuticals in 2013.
The combined use of vancomycin and a beta-lactam antibiotic for prophylaxis against surgical site infections is associated with both benefits and harms, according to findings from a national propensity-score–adjusted retrospective cohort study.
For example, the combination treatment reduced surgical site infections (SSIs) 30 days after cardiac surgical procedures but increased the risk of postoperative acute kidney injury (AKI) in some patients, Westyn Branch-Elliman, MD, of the VA Boston Healthcare System and her colleagues reported online July 10 in PLOS Medicine.
Among cardiac surgery patients, the incidence of surgical site infections was significantly lower for the 6,953 patients treated with both drugs vs. the 12,834 treated with a single agent (0.95% vs. 1.48%), the investigators found (PLOS Med. 2017 Jul 10. doi: 10.1371/journal.pmed.1002340).
SSI benefit with combination therapy
“After controlling for age, diabetes, ASA [American Society of Anesthesiologists] score, mupirocin administration, current smoking status, and preoperative MRSA [methicillin-resistant Staphylococcus aureus] colonization status, receipt of combination antimicrobial prophylaxis was associated with reduced SSI risk following cardiac surgical procedures (adjusted risk ratio, 0.61),” they wrote, noting that, when combination therapy was compared with either of the agents alone, the associations were similar and that no association between SSI reduction and the combination regimen was seen for the other types of surgical procedures assessed.
Secondary analyses showed that, among the cardiac patients, differences in the rates of SSIs were seen based on MRSA status in patients undergoing cardiac surgery. Among MRSA-colonized patients, SSIs occurred in 8 of 346 patients (2.3%) who received combination prophylaxis vs. 4 of 100 patients (4%) who received vancomycin alone (aRR, 0.53), and, among MRSA-negative and MRSA-unknown cardiac surgery patients, SSIs occurred in 58 of 6,607 patients (0.88%) receiving combination prophylaxis and 146 of 10,215 patients (1.4%) receiving a beta-lactam alone (aRR, 0.60).
“Among MRSA-colonized patients undergoing cardiac surgery, the associated absolute risk reduction for SSI was approximately triple that of the absolute risk reduction in MRSA-negative or -unknown patients, with a [number needed to treat] to prevent 1 SSI of 53 for the MRSA-colonized group, compared with 176 for the MRSA-negative or -unknown groups,” they wrote.
The incidence of Clostridium difficile infection was similar in both exposure groups (0.72% and 0.81% with combination and single agent prophylaxis, respectively).
Higher AKI risk with combination therapy
“In contrast, combination versus single prophylaxis was associated with higher relative risk of AKI in the 7-day postoperative period after adjusting for prophylaxis regimen duration, age, diabetes, ASA score, and smoking,” they said.
The rate of AKI was 23.75% among patients receiving combination prophylaxis, compared with 20.79% and 13.93% among those receiving vancomycin alone and a beta-lactam alone, respectively.
Significant associations between absolute risk of AKI and receipt of combination regimens were seen across all types of procedures, the investigators said.
“Overall, the NNH [number needed to harm] to cause one episode of AKI in cardiac surgery patients receiving combination therapy was 22, and, for stage 3 AKI, 167. The NNH associated with one additional episode of any postoperative AKI after receipt of combination therapy was 76 following orthopedic procedures and 25 following vascular surgical procedures,” they said.
The optimal approach for preventing SSIs is unclear. Although the multidisciplinary Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery recommend single agent prophylaxis most often, with a beta-lactam antibiotic, for most surgical procedures, the use of vancomycin alone is a consideration in MRSA-colonized patients and in centers with a high MRSA incidence, and combination prophylaxis with a beta-lactam plus vancomycin is increasing. However, the relative risks and benefit of this strategy have not been carefully studied, the investigators said.
Thus, the investigators used a propensity-adjusted, log-binomial regression model stratified by type of surgical procedure among the cases identified in the Veterans Affairs cohort to assess the association between SSIs and receipt of combination prophylaxis versus single agent prophylaxis.
Though limited by the observational study design and by factors such as a predominantly male and slightly older and more rural population, the findings suggest that “clinicians may need to individualize prophylaxis strategy based on patient-specific factors that influence the risk-versus-benefit equation,” they said, concluding that “future studies are needed to evaluate the utility of MRSA screening protocols for optimizing and individualizing surgical prophylaxis regimen.”
This study was funded by Veterans Affairs Health Services Research and Development. Dr. Branch-Elliman reported having no disclosures. One other author, Eli Perencevich, MD, received an investigator initiated Grant from Merck Pharmaceuticals in 2013.
FROM PLOS MEDICINE
Key clinical point:
Major finding: The SSI incidence was 0.95% vs. 1.48% with combination vs. single agent–therapy in cardiac surgery patients. Acute kidney injuries occurred in 23.75% of all surgery patients receiving combination prophylaxis, compared with 20.79% and 13.93% with vancomycin or a beta-lactam, respectively.
Data source: A retrospective cohort study of more than 70,000 surgical procedures.
Disclosures: This study was funded by Veterans Affairs Health Services Research and Development. Dr. Branch-Elliman reported having no disclosures. One other author, Eli Perencevich, MD, received an investigator initiated grant from Merck Pharmaceuticals in 2013.
Relamorelin for diabetic gastroparesis: Trial results
Gastroparesis is defined as delayed gastric emptying with associated symptoms in the absence of mechanical obstruction. The cardinal symptoms are upper abdominal pain, postprandial fullness, bloating, early satiety, nausea, and, with more severe disease, vomiting. Weight loss, malnutrition, dehydration, electrolyte imbalance, bezoar formation, and aspiration pneumonia may occur in advanced cases. Unfortunately, there are few approved or efficacious treatment options for diabetic gastroparesis. The 5-HT4 receptor agonist, cisapride, has been withdrawn from the prescription markets in most countries.

The study aim was to evaluate the efficacy of relamorelin on disease symptoms and gastric emptying in moderate to severe diabetic gastroparesis. In a 12-week, double-blind, placebo-controlled, parallel-group, randomized, controlled trial, with a 2-week, single-blind placebo run-in, patients were randomized to 10 microg b.i.d., 30 microg b.i.d., 100 microg b.i.d., or placebo b.i.d. Patients completed a daily e-diary of symptoms (Diabetic Gastroparesis Symptom Severity Diary [DGSSD]: nausea, abdominal pain, postprandial fullness, and bloating on a 0–10 scale) and vomiting episodes, which were summarized by treatment week. The primary endpoint was a change from baseline in vomiting frequency; a key secondary endpoint was change from baseline in a four-symptom composite of DGSSD symptoms.
A longitudinal analysis over the 12-week trial showed there were reductions in nausea, postprandial fullness, abdominal pain, and bloating individually and as a composite score. Relamorelin accelerated gastric emptying T1/2 at all three doses compared with placebo. However, there were no effects on vomiting frequency, which showed a high placebo response. More hyperglycemia events and diarrhea events were observed with relamorelin treatment compared with placebo. The diarrhea reflects the previously demonstrated stimulation of colonic transit and motility and reduction of symptoms of constipation in patients with chronic constipation. The hyperglycemia likely resulted from accelerated gastric emptying rather than potential inhibition of insulin production, which has been reported with high levels of ghrelin in animal studies or with high levels of ghrelin associated with starvation.
Thus, relamorelin demonstrated substantially improved core symptoms of diabetic gastroparesis, was generally safe and well tolerated, and should be further assessed in pivotal phase 3 trials. The results in this trial suggest that there is no dose-response relationship between the three doses of relamorelin tested and that future trials of relamorelin might not need to include the 100-microg b.i.d. dose. Importantly, this study also suggests the importance to prospectively manage the hyperglycemia in future trials.
Dr. Camilleri is a faculty member in the department of gastroenterology and hepatology at the Mayo Clinic in Rochester, Minn. His comments were made during the AGA Institute Presidential Plenary at the Annual Digestive Disease Week.
Gastroparesis is defined as delayed gastric emptying with associated symptoms in the absence of mechanical obstruction. The cardinal symptoms are upper abdominal pain, postprandial fullness, bloating, early satiety, nausea, and, with more severe disease, vomiting. Weight loss, malnutrition, dehydration, electrolyte imbalance, bezoar formation, and aspiration pneumonia may occur in advanced cases. Unfortunately, there are few approved or efficacious treatment options for diabetic gastroparesis. The 5-HT4 receptor agonist, cisapride, has been withdrawn from the prescription markets in most countries.
The study aim was to evaluate the efficacy of relamorelin on disease symptoms and gastric emptying in moderate to severe diabetic gastroparesis. In a 12-week, double-blind, placebo-controlled, parallel-group, randomized, controlled trial, with a 2-week, single-blind placebo run-in, patients were randomized to 10 microg b.i.d., 30 microg b.i.d., 100 microg b.i.d., or placebo b.i.d. Patients completed a daily e-diary of symptoms (Diabetic Gastroparesis Symptom Severity Diary [DGSSD]: nausea, abdominal pain, postprandial fullness, and bloating on a 0–10 scale) and vomiting episodes, which were summarized by treatment week. The primary endpoint was a change from baseline in vomiting frequency; a key secondary endpoint was change from baseline in a four-symptom composite of DGSSD symptoms.
A longitudinal analysis over the 12-week trial showed there were reductions in nausea, postprandial fullness, abdominal pain, and bloating individually and as a composite score. Relamorelin accelerated gastric emptying T1/2 at all three doses compared with placebo. However, there were no effects on vomiting frequency, which showed a high placebo response. More hyperglycemia events and diarrhea events were observed with relamorelin treatment compared with placebo. The diarrhea reflects the previously demonstrated stimulation of colonic transit and motility and reduction of symptoms of constipation in patients with chronic constipation. The hyperglycemia likely resulted from accelerated gastric emptying rather than potential inhibition of insulin production, which has been reported with high levels of ghrelin in animal studies or with high levels of ghrelin associated with starvation.
Thus, relamorelin demonstrated substantially improved core symptoms of diabetic gastroparesis, was generally safe and well tolerated, and should be further assessed in pivotal phase 3 trials. The results in this trial suggest that there is no dose-response relationship between the three doses of relamorelin tested and that future trials of relamorelin might not need to include the 100-microg b.i.d. dose. Importantly, this study also suggests the importance to prospectively manage the hyperglycemia in future trials.
Dr. Camilleri is a faculty member in the department of gastroenterology and hepatology at the Mayo Clinic in Rochester, Minn. His comments were made during the AGA Institute Presidential Plenary at the Annual Digestive Disease Week.
Gastroparesis is defined as delayed gastric emptying with associated symptoms in the absence of mechanical obstruction. The cardinal symptoms are upper abdominal pain, postprandial fullness, bloating, early satiety, nausea, and, with more severe disease, vomiting. Weight loss, malnutrition, dehydration, electrolyte imbalance, bezoar formation, and aspiration pneumonia may occur in advanced cases. Unfortunately, there are few approved or efficacious treatment options for diabetic gastroparesis. The 5-HT4 receptor agonist, cisapride, has been withdrawn from the prescription markets in most countries.
The study aim was to evaluate the efficacy of relamorelin on disease symptoms and gastric emptying in moderate to severe diabetic gastroparesis. In a 12-week, double-blind, placebo-controlled, parallel-group, randomized, controlled trial, with a 2-week, single-blind placebo run-in, patients were randomized to 10 microg b.i.d., 30 microg b.i.d., 100 microg b.i.d., or placebo b.i.d. Patients completed a daily e-diary of symptoms (Diabetic Gastroparesis Symptom Severity Diary [DGSSD]: nausea, abdominal pain, postprandial fullness, and bloating on a 0–10 scale) and vomiting episodes, which were summarized by treatment week. The primary endpoint was a change from baseline in vomiting frequency; a key secondary endpoint was change from baseline in a four-symptom composite of DGSSD symptoms.
A longitudinal analysis over the 12-week trial showed there were reductions in nausea, postprandial fullness, abdominal pain, and bloating individually and as a composite score. Relamorelin accelerated gastric emptying T1/2 at all three doses compared with placebo. However, there were no effects on vomiting frequency, which showed a high placebo response. More hyperglycemia events and diarrhea events were observed with relamorelin treatment compared with placebo. The diarrhea reflects the previously demonstrated stimulation of colonic transit and motility and reduction of symptoms of constipation in patients with chronic constipation. The hyperglycemia likely resulted from accelerated gastric emptying rather than potential inhibition of insulin production, which has been reported with high levels of ghrelin in animal studies or with high levels of ghrelin associated with starvation.
Thus, relamorelin demonstrated substantially improved core symptoms of diabetic gastroparesis, was generally safe and well tolerated, and should be further assessed in pivotal phase 3 trials. The results in this trial suggest that there is no dose-response relationship between the three doses of relamorelin tested and that future trials of relamorelin might not need to include the 100-microg b.i.d. dose. Importantly, this study also suggests the importance to prospectively manage the hyperglycemia in future trials.
Dr. Camilleri is a faculty member in the department of gastroenterology and hepatology at the Mayo Clinic in Rochester, Minn. His comments were made during the AGA Institute Presidential Plenary at the Annual Digestive Disease Week.
Co-occurrence of Steatocystoma Multiplex, Eruptive Vellus Hair Cysts, and Trichofolliculomas
An association between steatocystoma multiplex (SCM) and eruptive vellus hair cysts (EVHCs) has been recognized. They are related conditions representing nevoid malformations of the pilosebaceous junctions1-10 that have similar clinical features but distinctive histologic features. Both conditions most commonly involve the anterior aspect of the chest. Six cases of a rare facial variant of SCM have been reported,11-16 3 involving lesions limited to the forehead.13-15 Two patients with a rare facial variant of EVHC also have been reported.17 The development of separate lesions of SCM and EVHC on the trunk can uncommonly occur.5,6,10 One case of SCM and EVHC on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. The simultaneous occurrence of multiple trichoblastomas, trichoepitheliomas, and SCM on the face and trunk has been reported in 1 case.18 Milia, SCM, and EVHC on the face and trunk have been reported in 1 family.4 A report of facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus also has occurred in 1 patient.19 Here, we report the simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead.
Case Report
A 37-year-old man had an increasing number of flesh-colored to yellow papules on the forehead that had been present since puberty. Although the lesions were asymptomatic, some had recently become tender, which led him to seek medical care. There was no history of trauma, burns, irradiation, or application of topical agents to the area or use of eyeglasses or goggles. The patient’s father had similar lesions limited to the forehead, which developed during adolescence.
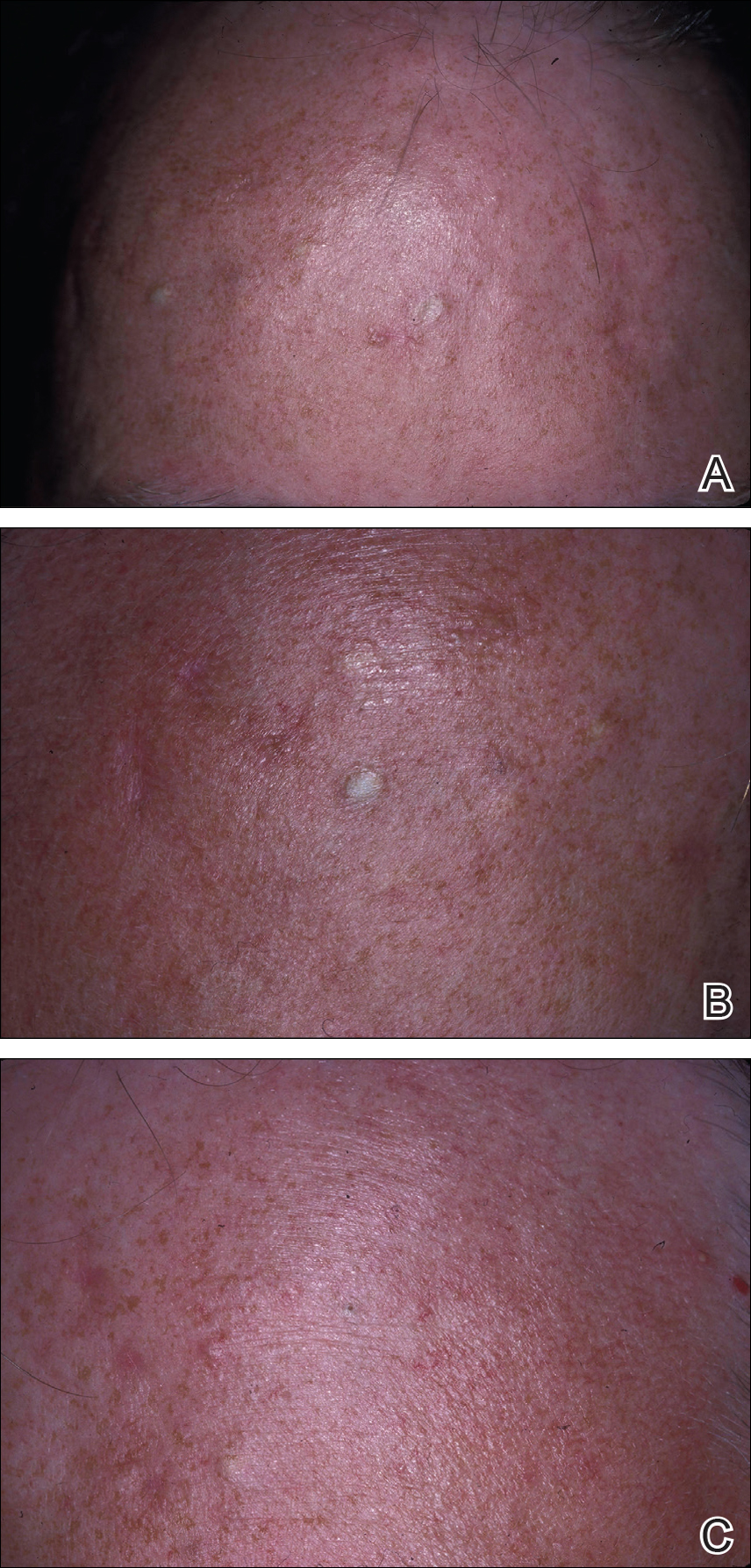
On evaluation at our clinic, skin examination revealed 16 discrete, 0.3- to 1-cm, flesh-colored, yellow to blue, mobile, smooth papules, as well as flesh-colored papules with a central black punctum, on the forehead (Figure 1). Similar lesions were not present on the rest of the face; around the ears; or on the scalp, neck, chest, back, abdomen, genitalia, buttocks, palms, soles, axillae, arms, or legs. There were no nail abnormalities.
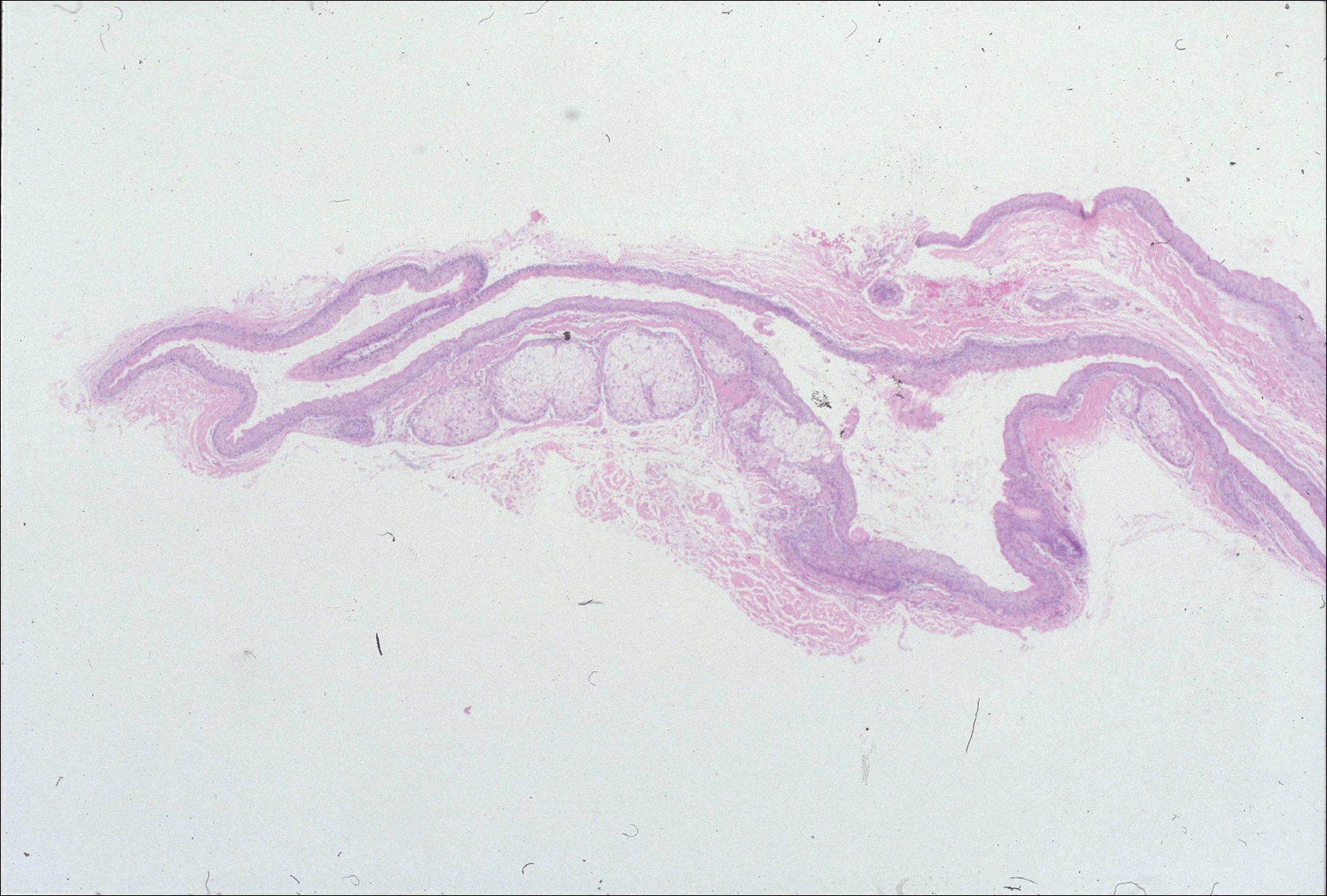
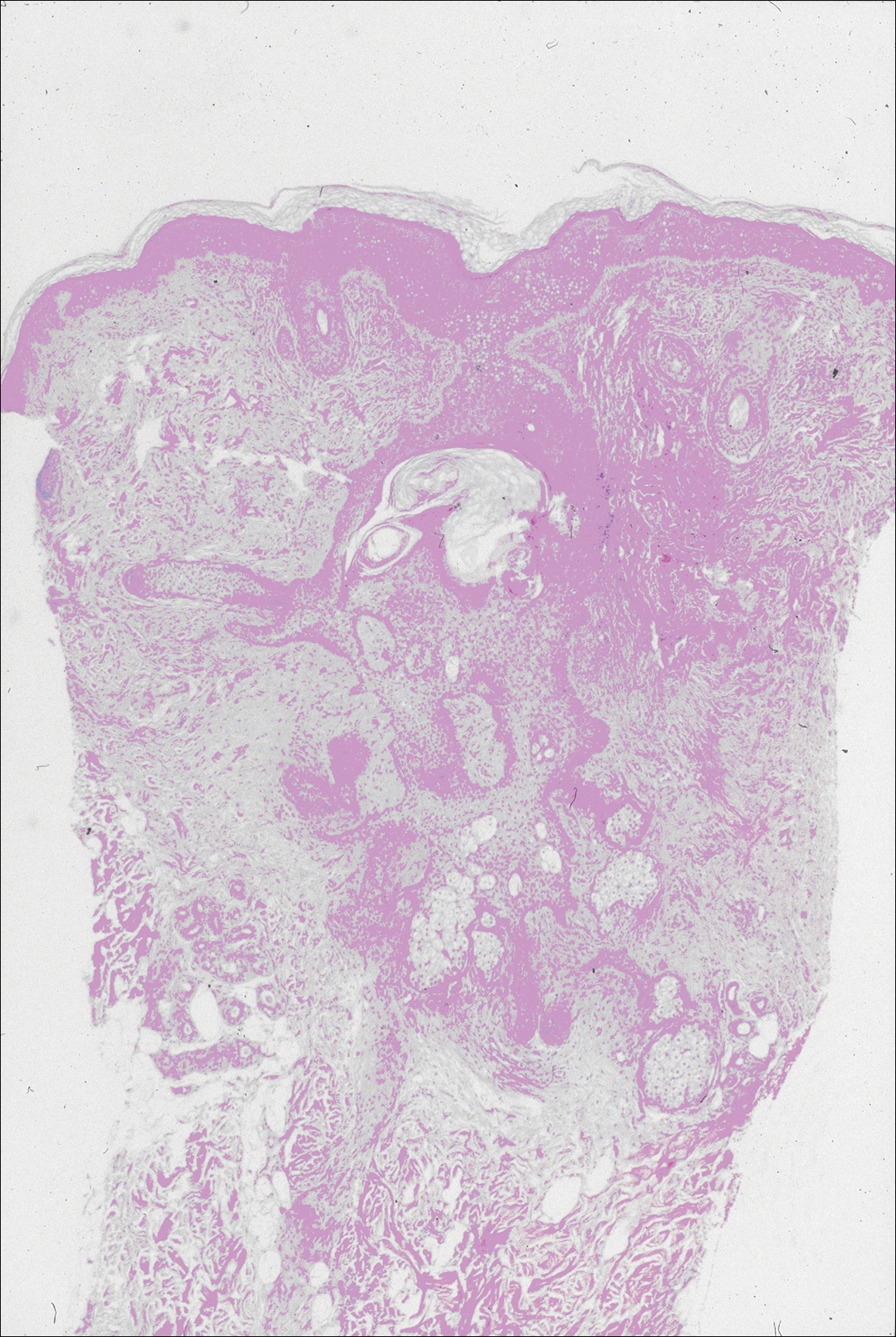
Multiple 3-, 4-, and 6-mm punch and excisional biopsies were performed to remove all 16 lesions on the forehead. Histologic examination revealed a collapsed cystic structure in the mid dermis in 10 lesions. The cysts were lined with a squamous epithelium without a granular layer but with an eosinophilic corrugated lining, and the cyst cavity contained scant homogeneous eosinophilic secretion. Mature sebaceous glands were adjacent to the outer portion of the cyst wall. These histologic findings were consistent with SCM (Figure 2).
In 3 lesions, histologic examination revealed a cystic structure lined by a few layers of stratified squamous epithelium in the mid dermis. The cyst cavity contained numerous small vellus hairs and laminated keratin. These histologic findings were consistent with EVHC (Figure 3).
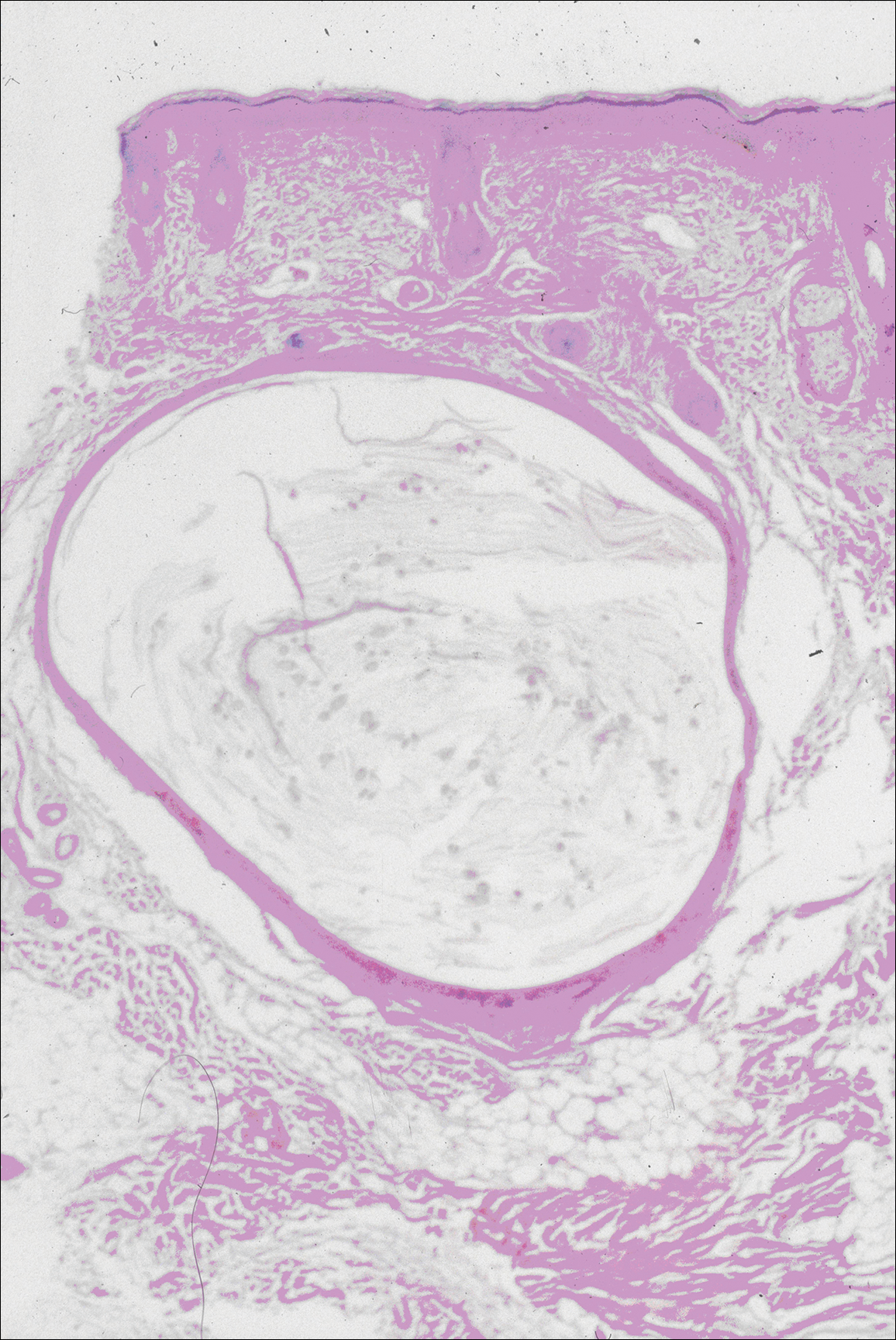
In the other 3 lesions, histologic examination revealed a dilated central cystic cavity filled with laminated keratin in the mid dermis. Multiple small follicles arose from the cysts and showed differentiation toward germinative epithelium. The surrounding stroma was fibrotic and contained a patchy lymphocytic infiltrate. These histologic findings were consistent with trichofolliculomas (Figure 4).
Comment
Characteristics of SCM
Steatocystoma multiplex is an uncommon condition characterized by the formation of asymptomatic, 0.2- to 2-cm, yellow to flesh-colored, soft, mobile papules or nodules on the trunk, extremities, axillae, genitalia, and/or chest. The lesions contain a clear or opaque, oily, milky or yellow, odorless fluid and most commonly are located on the anterior aspect of the chest. The face is not a commonly involved site in this condition. Six cases of a rare facial variant of SCM have been reported,11-16 with lesions limited to the forehead in 3 cases.13-15
In 1937, Mount20 credited Bozellini for describing the first case, though 3 cases reported in the late 1800s probably were SCM.21 In 1899, Pringle22 coined the term steatocystoma multiplex for this condition. It can be sporadic or have an autosomal-dominant inheritance pattern. Steatocystoma multiplex can occur at any age, though lesions develop most frequently in adolescence or young adulthood. There is no sex predilection.
Steatocystoma multiplex with pachyonychia congenita has been reported in a familial case.23 Other findings reported in patients with SCM include ichthyosis, koilonychia, acrokeratosis verruciformis of Hopf and hypertrophic lichen planus, hidradenitis suppurativa, hypotrichosis, multiple keratoacanthomas, and rheumatoid arthritis.12,24-26
Steatocystoma multiplex is a cyst lined by stratified squamous epithelium without a granular layer but with a thick eosinophilic cuticle. Mature sebaceous lobules are closely associated with the cyst wall. Steatocystoma multiplex arises from the sebaceous duct because the lining of the lumen is composed of undulating eosinophilic cuticle.
Characteristics of EVHCs
Eruptive vellus hair cysts, which were first described by Esterly et al,27 can occur at any age but develop most frequently in adolescents or young adults. Sometimes the lesions are congenital or appear in childhood. There is no sex predilection. They can be sporadic or have an autosomal-dominant inheritance pattern.
Eruptive vellus hair cysts are asymptomatic, 1- to 2-mm, smooth, crusted, or umbilicated papules on the chest or arms and legs. Eruptive vellus hair cysts most commonly involve the anterior aspect of the chest. The lesions are flesh-colored to yellow, though they have a slate gray color in darker-skinned individuals. A rare facial variant has been reported in 2 patients of Asian descent.17
Eruptive vellus hair cysts are small cystic structures lined by a stratified squamous epithelium with a granular layer. The cyst cavity contains numerous small vellus hair shafts and laminated keratin. Eruptive vellus hair cysts originate from the infundibulum or less frequently the isthmus or infundibular-isthmic junction of the hair follicle.
Characteristics of Trichofolliculomas
Trichofolliculomas are solitary, 3- to 5-mm, flesh-colored papules that occur on the face. They are highly differentiated, benign, neoplastic proliferations of an actively trichogenic epithelium, with structural components reflecting all portions of the pilosebaceous unit. Trichofolliculomas consist of a central dilated primary follicle contiguous with the surface epidermis embedded in a fibrous stroma. Multiple small secondary follicles with varying degrees of follicular differentiation arise from the primary follicle.
Co-occurrence of Lesions
An association between SCM and EVHC has been recognized.5-10 Steatocystoma multiplex and EVHC have similar clinical features but distinctive histologic features. They also have a similar age of onset, location/appearance of lesions, and mode of inheritance. Steatocystoma multiplex and EVHC can be distinguished by immunohistochemical techniques: SCM shows expression of keratin 10 and keratin 17, whereas EVHCs express only keratin 17.28
Steatocystoma multiplex and EVHC have only rarely been reported to occur together on the trunk. One case of SCM and EVHC occurring on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. Milia, SCM, and EVHC on the face and trunk have been reported in 1 family,4 and facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus was reported in 1 patient.19 Although trichofolliculomas have not been reported to occur with SCM or EVHC, 2 related follicular neoplasms—trichoepitheliomas and trichoblastomas—have been reported to occur in association with SCM on the face and chest and around the ears in 1 case.18
Differential Diagnosis
The clinical differential diagnosis includes multiple epidermoid cysts, dermoid cysts, Gardner syndrome, sebaceous adenomas, Muir-Torre syndrome, syringomas, milia, leiomyomas, lipomas, acneiform folliculitis, multiple familial and nonfamilial trichoepitheliomas, cylindromas, and angiofibromas.3,29
Conclusion
Our patient represents a rare case of simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead. The patient had multiple neoplasms involving differentiation toward various regions of the pilosebaceous unit. This case gives further support to the hypothesis that these benign follicular neoplasms are closely related but are distinct conditions within the spectrum of the same disease process. They represent nevoid malformations of the pilosebaceous unit that can be sporadic or inherited in an autosomal-dominant pattern. Pure types of these lesions may represent one end of the spectrum, but in some patients, there are overlapping features or hybrids of each condition. Several biopsies from patients with multiple lesions should be performed to establish an accurate diagnosis.
- Cho S, Chang SE, Choi JH, et al. Clinical and histologic features of 64 cases of steatocystoma multiplex. J Dermatol. 2002;29:152-156.
- Ogawa Y, Nogita T, Kawashima M. The coexistence of eruptive vellus hair cysts and steatocystoma multiplex. J Dermatol. 1992;19:570-571.
- Sanchez Yus E, Requena L. Eruptive vellus hair cyst and steatocystoma multiplex. Am J Dermatopathol. 1990;12:536-537.
- Patrizi A, Neri I, Guerrini V, et al. Persistent milia, steatocystoma multiplex and eruptive vellus hair cysts: variable expression of multiple pilosebaceous cysts within an affected family. Dermatology. 1998;196:392-396.
- Ohtake N, Kubota Y, Takayama O, et al. Relationship between steatocystoma multiplex and eruptive vellus hair cysts. J Am Acad Dermatol. 1992;26(5, pt 2):876-878.
- Kiene P, Hauschild A, Christophers E. Eruptive vellus hair cysts and steatocystoma multiplex: variants of one entity? Br J Dermatol. 1996;134:365-367.
- Hurlimann AF, Panizzon RG, Burg G. Eruptive vellus hair cyst and steatocystoma multiplex: hybrid cysts. Dermatology. 1996;192:64-66.
- Sexton M, Murdock DK. Eruptive vellus hair cysts: a follicular cyst of the sebaceous duct (sometimes). Am J Dermatopathol. 1989;11:364-368.
- Sanchez-Yus E, Aguilar-Martinez A, Cristobal-Gil MC, et al. Eruptive vellus hair cyst and steatocystoma multiplex: two related conditions? J Cutan Pathol. 1988;15:40-42.
- Ahn SK, Chung J, Lee WS, et al. Hybrid cysts showing alternate combination of eruptive vellus hair cyst, steatocystoma multiplex, and epidermoid cyst, and an association among the three conditions. Am J Dermatopathol. 1996;18:645-649.
- Ahn SK, Hwang SM, Lee SH, et al. Steatocystoma multiplex localized only in the face. Int J Dermatol. 1997;36:372-373.
- Cole LA. Steatocystoma multiplex. Arch Dermatol. 1976;112:1437-1439.
- Hansen KK, Troy JL, Fairley JA. Multiple papules of the scalp and forehead. steatocystoma multiplex (facial papular variant). Arch Dermatol. 1995;131:835-838.
- Nishimura M, Kohda H, Urabe A. Steatocystoma multiplex: a facial popular variant. Arch Dermatol. 1986;122:205-207.
- Requena L, Martin L, Renedo G, et al. A facial variant of steatocystoma multiplex. Cutis. 1993;51:449-452.
- Holmes R, Black MM. Steatocystoma multiplex with unusually prominent cysts on the face. Br J Dermatol. 1980;102:711-713.
- Kumakiri M, Takashima I, Iju M, et al. Eruptive vellus hair cysts: a facial variant. J Am Acad Dermatol. 1982;7:461-467.
- Gianotti R, Cavicchini S, Alessi E. Simultaneous occurrence of multiple trichoblastomas and steatocystoma multiplex. Am J Dermatopathol. 1997;19:294-298.
- Sardana K, Sharma RC, Jain A, et al. Facial steatocystoma multiplex associated with pilar cyst and bilateral preauricular sinus. J Dermatol. 2002;29:157-159.
- Mount LB. Steatocystoma multiplex. Arch Dermatol Syphilol. 1937;36:31-39.
- Dubreuilh W, Auche B. Kystes grassieux sudoripares. Arch Clin de Bordeaux. 1896;5:387-391.
- Pringle JJ. A case of peculiar multiple sebaceous cysts (steatocystoma multiplex). Br J Dermatol. 1899;11:381-88.
- Vineyard WR, Scott RA. Steatocystoma multiplex with pachyonychia congenital: eight cases in four generations. Arch Dermatol. 1961;84:824-827.
- Contreras MA, Costello MJ. Steatocystoma multiplex with embryonal hair formation: case presentation and consideration of pathogenesis. AMA Arch Derm. 1957;76:720-725.
- Sohn D, Chin TC, Fellner MJ. Multiple keratoacanthomas associated with steatocystoma multiplex and rheumatoid arthritis: a case report. Arch Dermatol. 1980;116:913-915.
- Verbov J. Acrokeratosis verruciformis of Hopf with steatocystoma multiplex and hypertrophic lichen planus. Br J Dermatol. 1972;86:91-94.
- Esterly NB, Fretzin DF, Pinkus H. Eruptive vellus hair cysts. Arch Dermatol. 1977;113:500-503.
- Tomkova H, Fujimoto W, Arata J. Expression of keratins (K10 and K17) in steatocystoma multiplex, eruptive vellus hair cysts, and epidermoid and trichilemmal cysts. Am J Dermatopathol. 1997;19:250-253.
- Feinstein A, Trau H, Movshovitz M, et al. Steatocystoma multiplex. Cutis. 1983;31:425-427.
An association between steatocystoma multiplex (SCM) and eruptive vellus hair cysts (EVHCs) has been recognized. They are related conditions representing nevoid malformations of the pilosebaceous junctions1-10 that have similar clinical features but distinctive histologic features. Both conditions most commonly involve the anterior aspect of the chest. Six cases of a rare facial variant of SCM have been reported,11-16 3 involving lesions limited to the forehead.13-15 Two patients with a rare facial variant of EVHC also have been reported.17 The development of separate lesions of SCM and EVHC on the trunk can uncommonly occur.5,6,10 One case of SCM and EVHC on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. The simultaneous occurrence of multiple trichoblastomas, trichoepitheliomas, and SCM on the face and trunk has been reported in 1 case.18 Milia, SCM, and EVHC on the face and trunk have been reported in 1 family.4 A report of facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus also has occurred in 1 patient.19 Here, we report the simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead.
Case Report
A 37-year-old man had an increasing number of flesh-colored to yellow papules on the forehead that had been present since puberty. Although the lesions were asymptomatic, some had recently become tender, which led him to seek medical care. There was no history of trauma, burns, irradiation, or application of topical agents to the area or use of eyeglasses or goggles. The patient’s father had similar lesions limited to the forehead, which developed during adolescence.
On evaluation at our clinic, skin examination revealed 16 discrete, 0.3- to 1-cm, flesh-colored, yellow to blue, mobile, smooth papules, as well as flesh-colored papules with a central black punctum, on the forehead (Figure 1). Similar lesions were not present on the rest of the face; around the ears; or on the scalp, neck, chest, back, abdomen, genitalia, buttocks, palms, soles, axillae, arms, or legs. There were no nail abnormalities.
Multiple 3-, 4-, and 6-mm punch and excisional biopsies were performed to remove all 16 lesions on the forehead. Histologic examination revealed a collapsed cystic structure in the mid dermis in 10 lesions. The cysts were lined with a squamous epithelium without a granular layer but with an eosinophilic corrugated lining, and the cyst cavity contained scant homogeneous eosinophilic secretion. Mature sebaceous glands were adjacent to the outer portion of the cyst wall. These histologic findings were consistent with SCM (Figure 2).
In 3 lesions, histologic examination revealed a cystic structure lined by a few layers of stratified squamous epithelium in the mid dermis. The cyst cavity contained numerous small vellus hairs and laminated keratin. These histologic findings were consistent with EVHC (Figure 3).
In the other 3 lesions, histologic examination revealed a dilated central cystic cavity filled with laminated keratin in the mid dermis. Multiple small follicles arose from the cysts and showed differentiation toward germinative epithelium. The surrounding stroma was fibrotic and contained a patchy lymphocytic infiltrate. These histologic findings were consistent with trichofolliculomas (Figure 4).
Comment
Characteristics of SCM
Steatocystoma multiplex is an uncommon condition characterized by the formation of asymptomatic, 0.2- to 2-cm, yellow to flesh-colored, soft, mobile papules or nodules on the trunk, extremities, axillae, genitalia, and/or chest. The lesions contain a clear or opaque, oily, milky or yellow, odorless fluid and most commonly are located on the anterior aspect of the chest. The face is not a commonly involved site in this condition. Six cases of a rare facial variant of SCM have been reported,11-16 with lesions limited to the forehead in 3 cases.13-15
In 1937, Mount20 credited Bozellini for describing the first case, though 3 cases reported in the late 1800s probably were SCM.21 In 1899, Pringle22 coined the term steatocystoma multiplex for this condition. It can be sporadic or have an autosomal-dominant inheritance pattern. Steatocystoma multiplex can occur at any age, though lesions develop most frequently in adolescence or young adulthood. There is no sex predilection.
Steatocystoma multiplex with pachyonychia congenita has been reported in a familial case.23 Other findings reported in patients with SCM include ichthyosis, koilonychia, acrokeratosis verruciformis of Hopf and hypertrophic lichen planus, hidradenitis suppurativa, hypotrichosis, multiple keratoacanthomas, and rheumatoid arthritis.12,24-26
Steatocystoma multiplex is a cyst lined by stratified squamous epithelium without a granular layer but with a thick eosinophilic cuticle. Mature sebaceous lobules are closely associated with the cyst wall. Steatocystoma multiplex arises from the sebaceous duct because the lining of the lumen is composed of undulating eosinophilic cuticle.
Characteristics of EVHCs
Eruptive vellus hair cysts, which were first described by Esterly et al,27 can occur at any age but develop most frequently in adolescents or young adults. Sometimes the lesions are congenital or appear in childhood. There is no sex predilection. They can be sporadic or have an autosomal-dominant inheritance pattern.
Eruptive vellus hair cysts are asymptomatic, 1- to 2-mm, smooth, crusted, or umbilicated papules on the chest or arms and legs. Eruptive vellus hair cysts most commonly involve the anterior aspect of the chest. The lesions are flesh-colored to yellow, though they have a slate gray color in darker-skinned individuals. A rare facial variant has been reported in 2 patients of Asian descent.17
Eruptive vellus hair cysts are small cystic structures lined by a stratified squamous epithelium with a granular layer. The cyst cavity contains numerous small vellus hair shafts and laminated keratin. Eruptive vellus hair cysts originate from the infundibulum or less frequently the isthmus or infundibular-isthmic junction of the hair follicle.
Characteristics of Trichofolliculomas
Trichofolliculomas are solitary, 3- to 5-mm, flesh-colored papules that occur on the face. They are highly differentiated, benign, neoplastic proliferations of an actively trichogenic epithelium, with structural components reflecting all portions of the pilosebaceous unit. Trichofolliculomas consist of a central dilated primary follicle contiguous with the surface epidermis embedded in a fibrous stroma. Multiple small secondary follicles with varying degrees of follicular differentiation arise from the primary follicle.
Co-occurrence of Lesions
An association between SCM and EVHC has been recognized.5-10 Steatocystoma multiplex and EVHC have similar clinical features but distinctive histologic features. They also have a similar age of onset, location/appearance of lesions, and mode of inheritance. Steatocystoma multiplex and EVHC can be distinguished by immunohistochemical techniques: SCM shows expression of keratin 10 and keratin 17, whereas EVHCs express only keratin 17.28
Steatocystoma multiplex and EVHC have only rarely been reported to occur together on the trunk. One case of SCM and EVHC occurring on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. Milia, SCM, and EVHC on the face and trunk have been reported in 1 family,4 and facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus was reported in 1 patient.19 Although trichofolliculomas have not been reported to occur with SCM or EVHC, 2 related follicular neoplasms—trichoepitheliomas and trichoblastomas—have been reported to occur in association with SCM on the face and chest and around the ears in 1 case.18
Differential Diagnosis
The clinical differential diagnosis includes multiple epidermoid cysts, dermoid cysts, Gardner syndrome, sebaceous adenomas, Muir-Torre syndrome, syringomas, milia, leiomyomas, lipomas, acneiform folliculitis, multiple familial and nonfamilial trichoepitheliomas, cylindromas, and angiofibromas.3,29
Conclusion
Our patient represents a rare case of simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead. The patient had multiple neoplasms involving differentiation toward various regions of the pilosebaceous unit. This case gives further support to the hypothesis that these benign follicular neoplasms are closely related but are distinct conditions within the spectrum of the same disease process. They represent nevoid malformations of the pilosebaceous unit that can be sporadic or inherited in an autosomal-dominant pattern. Pure types of these lesions may represent one end of the spectrum, but in some patients, there are overlapping features or hybrids of each condition. Several biopsies from patients with multiple lesions should be performed to establish an accurate diagnosis.
An association between steatocystoma multiplex (SCM) and eruptive vellus hair cysts (EVHCs) has been recognized. They are related conditions representing nevoid malformations of the pilosebaceous junctions1-10 that have similar clinical features but distinctive histologic features. Both conditions most commonly involve the anterior aspect of the chest. Six cases of a rare facial variant of SCM have been reported,11-16 3 involving lesions limited to the forehead.13-15 Two patients with a rare facial variant of EVHC also have been reported.17 The development of separate lesions of SCM and EVHC on the trunk can uncommonly occur.5,6,10 One case of SCM and EVHC on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. The simultaneous occurrence of multiple trichoblastomas, trichoepitheliomas, and SCM on the face and trunk has been reported in 1 case.18 Milia, SCM, and EVHC on the face and trunk have been reported in 1 family.4 A report of facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus also has occurred in 1 patient.19 Here, we report the simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead.
Case Report
A 37-year-old man had an increasing number of flesh-colored to yellow papules on the forehead that had been present since puberty. Although the lesions were asymptomatic, some had recently become tender, which led him to seek medical care. There was no history of trauma, burns, irradiation, or application of topical agents to the area or use of eyeglasses or goggles. The patient’s father had similar lesions limited to the forehead, which developed during adolescence.
On evaluation at our clinic, skin examination revealed 16 discrete, 0.3- to 1-cm, flesh-colored, yellow to blue, mobile, smooth papules, as well as flesh-colored papules with a central black punctum, on the forehead (Figure 1). Similar lesions were not present on the rest of the face; around the ears; or on the scalp, neck, chest, back, abdomen, genitalia, buttocks, palms, soles, axillae, arms, or legs. There were no nail abnormalities.
Multiple 3-, 4-, and 6-mm punch and excisional biopsies were performed to remove all 16 lesions on the forehead. Histologic examination revealed a collapsed cystic structure in the mid dermis in 10 lesions. The cysts were lined with a squamous epithelium without a granular layer but with an eosinophilic corrugated lining, and the cyst cavity contained scant homogeneous eosinophilic secretion. Mature sebaceous glands were adjacent to the outer portion of the cyst wall. These histologic findings were consistent with SCM (Figure 2).
In 3 lesions, histologic examination revealed a cystic structure lined by a few layers of stratified squamous epithelium in the mid dermis. The cyst cavity contained numerous small vellus hairs and laminated keratin. These histologic findings were consistent with EVHC (Figure 3).
In the other 3 lesions, histologic examination revealed a dilated central cystic cavity filled with laminated keratin in the mid dermis. Multiple small follicles arose from the cysts and showed differentiation toward germinative epithelium. The surrounding stroma was fibrotic and contained a patchy lymphocytic infiltrate. These histologic findings were consistent with trichofolliculomas (Figure 4).
Comment
Characteristics of SCM
Steatocystoma multiplex is an uncommon condition characterized by the formation of asymptomatic, 0.2- to 2-cm, yellow to flesh-colored, soft, mobile papules or nodules on the trunk, extremities, axillae, genitalia, and/or chest. The lesions contain a clear or opaque, oily, milky or yellow, odorless fluid and most commonly are located on the anterior aspect of the chest. The face is not a commonly involved site in this condition. Six cases of a rare facial variant of SCM have been reported,11-16 with lesions limited to the forehead in 3 cases.13-15
In 1937, Mount20 credited Bozellini for describing the first case, though 3 cases reported in the late 1800s probably were SCM.21 In 1899, Pringle22 coined the term steatocystoma multiplex for this condition. It can be sporadic or have an autosomal-dominant inheritance pattern. Steatocystoma multiplex can occur at any age, though lesions develop most frequently in adolescence or young adulthood. There is no sex predilection.
Steatocystoma multiplex with pachyonychia congenita has been reported in a familial case.23 Other findings reported in patients with SCM include ichthyosis, koilonychia, acrokeratosis verruciformis of Hopf and hypertrophic lichen planus, hidradenitis suppurativa, hypotrichosis, multiple keratoacanthomas, and rheumatoid arthritis.12,24-26
Steatocystoma multiplex is a cyst lined by stratified squamous epithelium without a granular layer but with a thick eosinophilic cuticle. Mature sebaceous lobules are closely associated with the cyst wall. Steatocystoma multiplex arises from the sebaceous duct because the lining of the lumen is composed of undulating eosinophilic cuticle.
Characteristics of EVHCs
Eruptive vellus hair cysts, which were first described by Esterly et al,27 can occur at any age but develop most frequently in adolescents or young adults. Sometimes the lesions are congenital or appear in childhood. There is no sex predilection. They can be sporadic or have an autosomal-dominant inheritance pattern.
Eruptive vellus hair cysts are asymptomatic, 1- to 2-mm, smooth, crusted, or umbilicated papules on the chest or arms and legs. Eruptive vellus hair cysts most commonly involve the anterior aspect of the chest. The lesions are flesh-colored to yellow, though they have a slate gray color in darker-skinned individuals. A rare facial variant has been reported in 2 patients of Asian descent.17
Eruptive vellus hair cysts are small cystic structures lined by a stratified squamous epithelium with a granular layer. The cyst cavity contains numerous small vellus hair shafts and laminated keratin. Eruptive vellus hair cysts originate from the infundibulum or less frequently the isthmus or infundibular-isthmic junction of the hair follicle.
Characteristics of Trichofolliculomas
Trichofolliculomas are solitary, 3- to 5-mm, flesh-colored papules that occur on the face. They are highly differentiated, benign, neoplastic proliferations of an actively trichogenic epithelium, with structural components reflecting all portions of the pilosebaceous unit. Trichofolliculomas consist of a central dilated primary follicle contiguous with the surface epidermis embedded in a fibrous stroma. Multiple small secondary follicles with varying degrees of follicular differentiation arise from the primary follicle.
Co-occurrence of Lesions
An association between SCM and EVHC has been recognized.5-10 Steatocystoma multiplex and EVHC have similar clinical features but distinctive histologic features. They also have a similar age of onset, location/appearance of lesions, and mode of inheritance. Steatocystoma multiplex and EVHC can be distinguished by immunohistochemical techniques: SCM shows expression of keratin 10 and keratin 17, whereas EVHCs express only keratin 17.28
Steatocystoma multiplex and EVHC have only rarely been reported to occur together on the trunk. One case of SCM and EVHC occurring on the forehead has been described.3 Other types of benign follicular neoplasms simultaneously developing in association with SCM or EVHC also are rare. Milia, SCM, and EVHC on the face and trunk have been reported in 1 family,4 and facial steatocystoma associated with a pilar cyst and bilateral preauricular sinus was reported in 1 patient.19 Although trichofolliculomas have not been reported to occur with SCM or EVHC, 2 related follicular neoplasms—trichoepitheliomas and trichoblastomas—have been reported to occur in association with SCM on the face and chest and around the ears in 1 case.18
Differential Diagnosis
The clinical differential diagnosis includes multiple epidermoid cysts, dermoid cysts, Gardner syndrome, sebaceous adenomas, Muir-Torre syndrome, syringomas, milia, leiomyomas, lipomas, acneiform folliculitis, multiple familial and nonfamilial trichoepitheliomas, cylindromas, and angiofibromas.3,29
Conclusion
Our patient represents a rare case of simultaneous occurrence of SCM, EVHC, and trichofolliculomas localized to the forehead. The patient had multiple neoplasms involving differentiation toward various regions of the pilosebaceous unit. This case gives further support to the hypothesis that these benign follicular neoplasms are closely related but are distinct conditions within the spectrum of the same disease process. They represent nevoid malformations of the pilosebaceous unit that can be sporadic or inherited in an autosomal-dominant pattern. Pure types of these lesions may represent one end of the spectrum, but in some patients, there are overlapping features or hybrids of each condition. Several biopsies from patients with multiple lesions should be performed to establish an accurate diagnosis.
- Cho S, Chang SE, Choi JH, et al. Clinical and histologic features of 64 cases of steatocystoma multiplex. J Dermatol. 2002;29:152-156.
- Ogawa Y, Nogita T, Kawashima M. The coexistence of eruptive vellus hair cysts and steatocystoma multiplex. J Dermatol. 1992;19:570-571.
- Sanchez Yus E, Requena L. Eruptive vellus hair cyst and steatocystoma multiplex. Am J Dermatopathol. 1990;12:536-537.
- Patrizi A, Neri I, Guerrini V, et al. Persistent milia, steatocystoma multiplex and eruptive vellus hair cysts: variable expression of multiple pilosebaceous cysts within an affected family. Dermatology. 1998;196:392-396.
- Ohtake N, Kubota Y, Takayama O, et al. Relationship between steatocystoma multiplex and eruptive vellus hair cysts. J Am Acad Dermatol. 1992;26(5, pt 2):876-878.
- Kiene P, Hauschild A, Christophers E. Eruptive vellus hair cysts and steatocystoma multiplex: variants of one entity? Br J Dermatol. 1996;134:365-367.
- Hurlimann AF, Panizzon RG, Burg G. Eruptive vellus hair cyst and steatocystoma multiplex: hybrid cysts. Dermatology. 1996;192:64-66.
- Sexton M, Murdock DK. Eruptive vellus hair cysts: a follicular cyst of the sebaceous duct (sometimes). Am J Dermatopathol. 1989;11:364-368.
- Sanchez-Yus E, Aguilar-Martinez A, Cristobal-Gil MC, et al. Eruptive vellus hair cyst and steatocystoma multiplex: two related conditions? J Cutan Pathol. 1988;15:40-42.
- Ahn SK, Chung J, Lee WS, et al. Hybrid cysts showing alternate combination of eruptive vellus hair cyst, steatocystoma multiplex, and epidermoid cyst, and an association among the three conditions. Am J Dermatopathol. 1996;18:645-649.
- Ahn SK, Hwang SM, Lee SH, et al. Steatocystoma multiplex localized only in the face. Int J Dermatol. 1997;36:372-373.
- Cole LA. Steatocystoma multiplex. Arch Dermatol. 1976;112:1437-1439.
- Hansen KK, Troy JL, Fairley JA. Multiple papules of the scalp and forehead. steatocystoma multiplex (facial papular variant). Arch Dermatol. 1995;131:835-838.
- Nishimura M, Kohda H, Urabe A. Steatocystoma multiplex: a facial popular variant. Arch Dermatol. 1986;122:205-207.
- Requena L, Martin L, Renedo G, et al. A facial variant of steatocystoma multiplex. Cutis. 1993;51:449-452.
- Holmes R, Black MM. Steatocystoma multiplex with unusually prominent cysts on the face. Br J Dermatol. 1980;102:711-713.
- Kumakiri M, Takashima I, Iju M, et al. Eruptive vellus hair cysts: a facial variant. J Am Acad Dermatol. 1982;7:461-467.
- Gianotti R, Cavicchini S, Alessi E. Simultaneous occurrence of multiple trichoblastomas and steatocystoma multiplex. Am J Dermatopathol. 1997;19:294-298.
- Sardana K, Sharma RC, Jain A, et al. Facial steatocystoma multiplex associated with pilar cyst and bilateral preauricular sinus. J Dermatol. 2002;29:157-159.
- Mount LB. Steatocystoma multiplex. Arch Dermatol Syphilol. 1937;36:31-39.
- Dubreuilh W, Auche B. Kystes grassieux sudoripares. Arch Clin de Bordeaux. 1896;5:387-391.
- Pringle JJ. A case of peculiar multiple sebaceous cysts (steatocystoma multiplex). Br J Dermatol. 1899;11:381-88.
- Vineyard WR, Scott RA. Steatocystoma multiplex with pachyonychia congenital: eight cases in four generations. Arch Dermatol. 1961;84:824-827.
- Contreras MA, Costello MJ. Steatocystoma multiplex with embryonal hair formation: case presentation and consideration of pathogenesis. AMA Arch Derm. 1957;76:720-725.
- Sohn D, Chin TC, Fellner MJ. Multiple keratoacanthomas associated with steatocystoma multiplex and rheumatoid arthritis: a case report. Arch Dermatol. 1980;116:913-915.
- Verbov J. Acrokeratosis verruciformis of Hopf with steatocystoma multiplex and hypertrophic lichen planus. Br J Dermatol. 1972;86:91-94.
- Esterly NB, Fretzin DF, Pinkus H. Eruptive vellus hair cysts. Arch Dermatol. 1977;113:500-503.
- Tomkova H, Fujimoto W, Arata J. Expression of keratins (K10 and K17) in steatocystoma multiplex, eruptive vellus hair cysts, and epidermoid and trichilemmal cysts. Am J Dermatopathol. 1997;19:250-253.
- Feinstein A, Trau H, Movshovitz M, et al. Steatocystoma multiplex. Cutis. 1983;31:425-427.
- Cho S, Chang SE, Choi JH, et al. Clinical and histologic features of 64 cases of steatocystoma multiplex. J Dermatol. 2002;29:152-156.
- Ogawa Y, Nogita T, Kawashima M. The coexistence of eruptive vellus hair cysts and steatocystoma multiplex. J Dermatol. 1992;19:570-571.
- Sanchez Yus E, Requena L. Eruptive vellus hair cyst and steatocystoma multiplex. Am J Dermatopathol. 1990;12:536-537.
- Patrizi A, Neri I, Guerrini V, et al. Persistent milia, steatocystoma multiplex and eruptive vellus hair cysts: variable expression of multiple pilosebaceous cysts within an affected family. Dermatology. 1998;196:392-396.
- Ohtake N, Kubota Y, Takayama O, et al. Relationship between steatocystoma multiplex and eruptive vellus hair cysts. J Am Acad Dermatol. 1992;26(5, pt 2):876-878.
- Kiene P, Hauschild A, Christophers E. Eruptive vellus hair cysts and steatocystoma multiplex: variants of one entity? Br J Dermatol. 1996;134:365-367.
- Hurlimann AF, Panizzon RG, Burg G. Eruptive vellus hair cyst and steatocystoma multiplex: hybrid cysts. Dermatology. 1996;192:64-66.
- Sexton M, Murdock DK. Eruptive vellus hair cysts: a follicular cyst of the sebaceous duct (sometimes). Am J Dermatopathol. 1989;11:364-368.
- Sanchez-Yus E, Aguilar-Martinez A, Cristobal-Gil MC, et al. Eruptive vellus hair cyst and steatocystoma multiplex: two related conditions? J Cutan Pathol. 1988;15:40-42.
- Ahn SK, Chung J, Lee WS, et al. Hybrid cysts showing alternate combination of eruptive vellus hair cyst, steatocystoma multiplex, and epidermoid cyst, and an association among the three conditions. Am J Dermatopathol. 1996;18:645-649.
- Ahn SK, Hwang SM, Lee SH, et al. Steatocystoma multiplex localized only in the face. Int J Dermatol. 1997;36:372-373.
- Cole LA. Steatocystoma multiplex. Arch Dermatol. 1976;112:1437-1439.
- Hansen KK, Troy JL, Fairley JA. Multiple papules of the scalp and forehead. steatocystoma multiplex (facial papular variant). Arch Dermatol. 1995;131:835-838.
- Nishimura M, Kohda H, Urabe A. Steatocystoma multiplex: a facial popular variant. Arch Dermatol. 1986;122:205-207.
- Requena L, Martin L, Renedo G, et al. A facial variant of steatocystoma multiplex. Cutis. 1993;51:449-452.
- Holmes R, Black MM. Steatocystoma multiplex with unusually prominent cysts on the face. Br J Dermatol. 1980;102:711-713.
- Kumakiri M, Takashima I, Iju M, et al. Eruptive vellus hair cysts: a facial variant. J Am Acad Dermatol. 1982;7:461-467.
- Gianotti R, Cavicchini S, Alessi E. Simultaneous occurrence of multiple trichoblastomas and steatocystoma multiplex. Am J Dermatopathol. 1997;19:294-298.
- Sardana K, Sharma RC, Jain A, et al. Facial steatocystoma multiplex associated with pilar cyst and bilateral preauricular sinus. J Dermatol. 2002;29:157-159.
- Mount LB. Steatocystoma multiplex. Arch Dermatol Syphilol. 1937;36:31-39.
- Dubreuilh W, Auche B. Kystes grassieux sudoripares. Arch Clin de Bordeaux. 1896;5:387-391.
- Pringle JJ. A case of peculiar multiple sebaceous cysts (steatocystoma multiplex). Br J Dermatol. 1899;11:381-88.
- Vineyard WR, Scott RA. Steatocystoma multiplex with pachyonychia congenital: eight cases in four generations. Arch Dermatol. 1961;84:824-827.
- Contreras MA, Costello MJ. Steatocystoma multiplex with embryonal hair formation: case presentation and consideration of pathogenesis. AMA Arch Derm. 1957;76:720-725.
- Sohn D, Chin TC, Fellner MJ. Multiple keratoacanthomas associated with steatocystoma multiplex and rheumatoid arthritis: a case report. Arch Dermatol. 1980;116:913-915.
- Verbov J. Acrokeratosis verruciformis of Hopf with steatocystoma multiplex and hypertrophic lichen planus. Br J Dermatol. 1972;86:91-94.
- Esterly NB, Fretzin DF, Pinkus H. Eruptive vellus hair cysts. Arch Dermatol. 1977;113:500-503.
- Tomkova H, Fujimoto W, Arata J. Expression of keratins (K10 and K17) in steatocystoma multiplex, eruptive vellus hair cysts, and epidermoid and trichilemmal cysts. Am J Dermatopathol. 1997;19:250-253.
- Feinstein A, Trau H, Movshovitz M, et al. Steatocystoma multiplex. Cutis. 1983;31:425-427.
Practice Points
- Steatocystoma multiplex (SCM) and eruptive vellus hair cysts (EVHCs) have similar clinical features but distinctive histologic features.
- Milia, pilar cyst, trichoepitheliomas, and trichoblastomas simultaneously developing in association with SCM or EVHC on the face are rare.
- This case supports the hypothesis that these benign follicular neoplasms are related but distinct nevoid malformations of the pilosebaceous unit within the same disease spectrum.

No, you still can’t diagnose Trump
On the morning of July 25, I scrolled through my Twitter account to see tweets flying: Psychiatrists can now defy the Goldwater Rule! Oops, wrong organization; no ,they can’t. Over the course of the day, articles appeared in Scientific American, the Los Angeles Times, Newsweek, International Business Times; and statements were issued by both the American Psychiatric Association and the American Psychoanalytic Association.
So what happened?

On July 6, 2017, the ApsaA had sent an email to all its members informing them of this decision. The email also stated: “However, it is important to note that members of APsaA are free to comment about political figures as individuals. The American Psychiatric Association’s ethical stance on the Goldwater Rule applies to its members only. The APsaA does not consider political commentary by its individual members an ethical matter.” (Bolding per the email). This was not considered to be a change in its policy.
Citing that email, on July 25, STAT reporter Sharon Begley wrote an article titled, “Psychiatry group tells members they can ignore ‘Goldwater rule’ and comment on Trump’s mental health.” The article was linked to on Twitter, and the retweets and comments started to fly. As a single example, Josh Marshall, editor and publisher of Talking Points Memo, tweeted out to his 215,000 followers: “Truly amazing am psych assoc says Trump so f’ing nuts they’re lifting Goldwater Rule.” The APA issued several statements over the course of the day, notably: “We are the largest psychiatric organization in the world with more than 37,000 members. The Goldwater Rules applies to our members.” Commenters expressed frustration with the Goldwater Rule, and suggested that the APA had a duty to warn.
Shortly after noon that day, the APsaA put a statement on its website to clarify information in the STAT article: “In an email to association members, our leadership did not encourage members to defy the “Goldwater Rule” which is a part of the ethics code of a different mental health organization, the American Psychiatric Association (APA). Rather, it articulated a distinct ethics position that represents the viewpoint of psychoanalysts. The field of psychoanalysis addresses the full spectrum of human behavior, and we feel that our concepts and understanding are applicable and valuable to understanding a wide range of human behaviors and cultural phenomenon.”
Later in the afternoon, I spoke with Wylie Tene, director of pubic affairs for the APsaA. He noted: “The article in StatNews had a misleading and sensational headline. It didn’t represent what our email was about.”
I found it interesting that a sensational headline on STAT’s website could lead to so much comment and so many articles in major news outlets. July 25, 2017, was not a slow news day: John McCain (R-Ariz) returned to the Senate that day and voted to proceed with the debate to repeal Obamacare. A single vote cast by Vice President Mike Pence broke the tie, allowing the debate to go forward.
Like many, I feel conflicted about the Goldwater Rule but for a single reason: I am a strong believer in free speech, and the rule squelches psychiatrists. But as I noted in a column in August 2016, I don’t believe that our opinions should, would, or could change our political environment. Psychiatric treatment is about compassion and healing, and diagnoses are based on symptoms that patients often tell us about in a setting of intimacy and trust. Diagnosing celebrities, on the other hand, is often about name calling; it risks insulting our patients and perpetuating stigma.
Regarding Mr. Trump, I’m going to finish with the same words I wrote back in August, prior to his election as president. You’ll note that my insights in Clinical Psychiatry News and circulated on the Internet – devoid of a diagnosis – did not influence the outcome of the general election. Psychiatric diagnoses are made by observing a constellation of symptoms that occur together.
Mr. Trump has given the whole world years of data – he’s lived his life in a very public way. As a real estate developer, he has had countless employees who all know how they’ve been treated. We’ve seen him through three marriages and watched how he interacts with his children. We’ve seen him take out full-page ads calling for the death penalty for a group of young men who were wrongly convicted in the rape and assault of the Central Park jogger in 1989. If that’s not enough, he has hosted his own reality television show, and we’ve now seen him countless times in debates and rallies. We know how he treats his running mates, journalist Megyn Kelly, a news reporter with a disability, and the parents of a fallen soldier. We’ve watched him allude to the size of his genitals during a primary debate. Every individual is free to decide if Mr. Trump’s widely viewed patterns of behavior represent much-needed spunk and change with political beliefs that align with their own, or if his words and behaviors represent cruelty, impulsivity, poor judgment, and a pattern of actions that some might not feel is dignified enough for our country’s leader. No degree is required to observe and draw conclusions.
Dr. Miller, who practices in Baltimore, is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
On the morning of July 25, I scrolled through my Twitter account to see tweets flying: Psychiatrists can now defy the Goldwater Rule! Oops, wrong organization; no ,they can’t. Over the course of the day, articles appeared in Scientific American, the Los Angeles Times, Newsweek, International Business Times; and statements were issued by both the American Psychiatric Association and the American Psychoanalytic Association.
So what happened?
On July 6, 2017, the ApsaA had sent an email to all its members informing them of this decision. The email also stated: “However, it is important to note that members of APsaA are free to comment about political figures as individuals. The American Psychiatric Association’s ethical stance on the Goldwater Rule applies to its members only. The APsaA does not consider political commentary by its individual members an ethical matter.” (Bolding per the email). This was not considered to be a change in its policy.
Citing that email, on July 25, STAT reporter Sharon Begley wrote an article titled, “Psychiatry group tells members they can ignore ‘Goldwater rule’ and comment on Trump’s mental health.” The article was linked to on Twitter, and the retweets and comments started to fly. As a single example, Josh Marshall, editor and publisher of Talking Points Memo, tweeted out to his 215,000 followers: “Truly amazing am psych assoc says Trump so f’ing nuts they’re lifting Goldwater Rule.” The APA issued several statements over the course of the day, notably: “We are the largest psychiatric organization in the world with more than 37,000 members. The Goldwater Rules applies to our members.” Commenters expressed frustration with the Goldwater Rule, and suggested that the APA had a duty to warn.
Shortly after noon that day, the APsaA put a statement on its website to clarify information in the STAT article: “In an email to association members, our leadership did not encourage members to defy the “Goldwater Rule” which is a part of the ethics code of a different mental health organization, the American Psychiatric Association (APA). Rather, it articulated a distinct ethics position that represents the viewpoint of psychoanalysts. The field of psychoanalysis addresses the full spectrum of human behavior, and we feel that our concepts and understanding are applicable and valuable to understanding a wide range of human behaviors and cultural phenomenon.”
Later in the afternoon, I spoke with Wylie Tene, director of pubic affairs for the APsaA. He noted: “The article in StatNews had a misleading and sensational headline. It didn’t represent what our email was about.”
I found it interesting that a sensational headline on STAT’s website could lead to so much comment and so many articles in major news outlets. July 25, 2017, was not a slow news day: John McCain (R-Ariz) returned to the Senate that day and voted to proceed with the debate to repeal Obamacare. A single vote cast by Vice President Mike Pence broke the tie, allowing the debate to go forward.
Like many, I feel conflicted about the Goldwater Rule but for a single reason: I am a strong believer in free speech, and the rule squelches psychiatrists. But as I noted in a column in August 2016, I don’t believe that our opinions should, would, or could change our political environment. Psychiatric treatment is about compassion and healing, and diagnoses are based on symptoms that patients often tell us about in a setting of intimacy and trust. Diagnosing celebrities, on the other hand, is often about name calling; it risks insulting our patients and perpetuating stigma.
Regarding Mr. Trump, I’m going to finish with the same words I wrote back in August, prior to his election as president. You’ll note that my insights in Clinical Psychiatry News and circulated on the Internet – devoid of a diagnosis – did not influence the outcome of the general election. Psychiatric diagnoses are made by observing a constellation of symptoms that occur together.
Mr. Trump has given the whole world years of data – he’s lived his life in a very public way. As a real estate developer, he has had countless employees who all know how they’ve been treated. We’ve seen him through three marriages and watched how he interacts with his children. We’ve seen him take out full-page ads calling for the death penalty for a group of young men who were wrongly convicted in the rape and assault of the Central Park jogger in 1989. If that’s not enough, he has hosted his own reality television show, and we’ve now seen him countless times in debates and rallies. We know how he treats his running mates, journalist Megyn Kelly, a news reporter with a disability, and the parents of a fallen soldier. We’ve watched him allude to the size of his genitals during a primary debate. Every individual is free to decide if Mr. Trump’s widely viewed patterns of behavior represent much-needed spunk and change with political beliefs that align with their own, or if his words and behaviors represent cruelty, impulsivity, poor judgment, and a pattern of actions that some might not feel is dignified enough for our country’s leader. No degree is required to observe and draw conclusions.
Dr. Miller, who practices in Baltimore, is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
On the morning of July 25, I scrolled through my Twitter account to see tweets flying: Psychiatrists can now defy the Goldwater Rule! Oops, wrong organization; no ,they can’t. Over the course of the day, articles appeared in Scientific American, the Los Angeles Times, Newsweek, International Business Times; and statements were issued by both the American Psychiatric Association and the American Psychoanalytic Association.
So what happened?
On July 6, 2017, the ApsaA had sent an email to all its members informing them of this decision. The email also stated: “However, it is important to note that members of APsaA are free to comment about political figures as individuals. The American Psychiatric Association’s ethical stance on the Goldwater Rule applies to its members only. The APsaA does not consider political commentary by its individual members an ethical matter.” (Bolding per the email). This was not considered to be a change in its policy.
Citing that email, on July 25, STAT reporter Sharon Begley wrote an article titled, “Psychiatry group tells members they can ignore ‘Goldwater rule’ and comment on Trump’s mental health.” The article was linked to on Twitter, and the retweets and comments started to fly. As a single example, Josh Marshall, editor and publisher of Talking Points Memo, tweeted out to his 215,000 followers: “Truly amazing am psych assoc says Trump so f’ing nuts they’re lifting Goldwater Rule.” The APA issued several statements over the course of the day, notably: “We are the largest psychiatric organization in the world with more than 37,000 members. The Goldwater Rules applies to our members.” Commenters expressed frustration with the Goldwater Rule, and suggested that the APA had a duty to warn.
Shortly after noon that day, the APsaA put a statement on its website to clarify information in the STAT article: “In an email to association members, our leadership did not encourage members to defy the “Goldwater Rule” which is a part of the ethics code of a different mental health organization, the American Psychiatric Association (APA). Rather, it articulated a distinct ethics position that represents the viewpoint of psychoanalysts. The field of psychoanalysis addresses the full spectrum of human behavior, and we feel that our concepts and understanding are applicable and valuable to understanding a wide range of human behaviors and cultural phenomenon.”
Later in the afternoon, I spoke with Wylie Tene, director of pubic affairs for the APsaA. He noted: “The article in StatNews had a misleading and sensational headline. It didn’t represent what our email was about.”
I found it interesting that a sensational headline on STAT’s website could lead to so much comment and so many articles in major news outlets. July 25, 2017, was not a slow news day: John McCain (R-Ariz) returned to the Senate that day and voted to proceed with the debate to repeal Obamacare. A single vote cast by Vice President Mike Pence broke the tie, allowing the debate to go forward.
Like many, I feel conflicted about the Goldwater Rule but for a single reason: I am a strong believer in free speech, and the rule squelches psychiatrists. But as I noted in a column in August 2016, I don’t believe that our opinions should, would, or could change our political environment. Psychiatric treatment is about compassion and healing, and diagnoses are based on symptoms that patients often tell us about in a setting of intimacy and trust. Diagnosing celebrities, on the other hand, is often about name calling; it risks insulting our patients and perpetuating stigma.
Regarding Mr. Trump, I’m going to finish with the same words I wrote back in August, prior to his election as president. You’ll note that my insights in Clinical Psychiatry News and circulated on the Internet – devoid of a diagnosis – did not influence the outcome of the general election. Psychiatric diagnoses are made by observing a constellation of symptoms that occur together.
Mr. Trump has given the whole world years of data – he’s lived his life in a very public way. As a real estate developer, he has had countless employees who all know how they’ve been treated. We’ve seen him through three marriages and watched how he interacts with his children. We’ve seen him take out full-page ads calling for the death penalty for a group of young men who were wrongly convicted in the rape and assault of the Central Park jogger in 1989. If that’s not enough, he has hosted his own reality television show, and we’ve now seen him countless times in debates and rallies. We know how he treats his running mates, journalist Megyn Kelly, a news reporter with a disability, and the parents of a fallen soldier. We’ve watched him allude to the size of his genitals during a primary debate. Every individual is free to decide if Mr. Trump’s widely viewed patterns of behavior represent much-needed spunk and change with political beliefs that align with their own, or if his words and behaviors represent cruelty, impulsivity, poor judgment, and a pattern of actions that some might not feel is dignified enough for our country’s leader. No degree is required to observe and draw conclusions.
Dr. Miller, who practices in Baltimore, is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
Pediatric News welcomes Dr. Kelly Curran
Pediatric News welcomes Kelly Curran, MD, MA, to its Editorial Advisory Board.
Dr. Curran is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, practicing adolescent medicine. Dr. Curran is member of the Society for Adolescent Health and Medicine and the American Academy of Pediatrics, where she serves as an editorial board member for the AAP’s Adolescent Medicine PREP series. Her areas of interest include bioethics, reproductive health care, and adolescent mental health care.

Pediatric News welcomes Kelly Curran, MD, MA, to its Editorial Advisory Board.
Dr. Curran is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, practicing adolescent medicine. Dr. Curran is member of the Society for Adolescent Health and Medicine and the American Academy of Pediatrics, where she serves as an editorial board member for the AAP’s Adolescent Medicine PREP series. Her areas of interest include bioethics, reproductive health care, and adolescent mental health care.
Pediatric News welcomes Kelly Curran, MD, MA, to its Editorial Advisory Board.
Dr. Curran is an assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, practicing adolescent medicine. Dr. Curran is member of the Society for Adolescent Health and Medicine and the American Academy of Pediatrics, where she serves as an editorial board member for the AAP’s Adolescent Medicine PREP series. Her areas of interest include bioethics, reproductive health care, and adolescent mental health care.
50 years of pediatrics: What has changed for female pediatricians?
In the last 50 years, the field of pediatrics has vastly changed, particularly for female physicians.
For starters, the number of female pediatricians has rapidly grown over the last few decades. In 1970, 21% of pediatricians were women, compared with 59% in 2013, according to the American Medical Association physician characteristics and distribution data 2015 edition. The overall pediatric workforce also has increased: A total of 18,332 pediatricians were practicing in 1970, and 84,559 pediatricians were in practice in 2013.
Along with numbers, the field of pediatrics has seen significant changes in practice size, technology, clinical responsibilities, and record keeping, to name a few. However, longtime pediatricians say there are also many ways that the specialty has stayed the same.
Dr. Bennett’s story
When Jean L. Bennett, MD, opened her solo pediatric practice in 1963, she initially had no nurses or team of assistants to help carry out clinical duties. With one receptionist answering phones and Dr. Bennett in the exam room, the Clearwater, Fla., practice opened for business. There was no shortage of patients, Dr. Bennett recalls.
“There was no such thing as neonatology. As a pediatrician, one took care of well and sick newborns and of course, saw a variety of infectious diseases in the office,” Dr. Bennett said in an interview. “We started our own IVs, we did our own lumbar punctures, we did subdural taps, we did exchange transfusions. We did all of those ourselves.”

Dr. Bennett was no stranger to being the lone woman on the job. She was the first woman to graduate from the University of Florida College of Medicine in Gainesville, the first woman to serve as chief of staff at Morton F. Plant Hospital in Clearwater, and the first woman to chair the hospital’s department of pediatrics. Despite being the first in many cases, Dr. Bennett does not remember facing discrimination from colleagues or community members, nor experiencing prejudice against her gender as a medical student or young resident
“My experience was different, of course, than other people graduating at that time, but I can truly say that I always felt the playing field was level,” Dr. Bennett said. “Nobody gave me anything for being a woman, and nobody took anything away.”
Compared with concerns that physicians have today, such as electronic medical records and increasing regulations, Dr. Bennett remembers a relatively worry-free career. She recalls some concern over the medical malpractice crisis in the 1970s and 1980s, but said the majority of her tenure was spent with a clear mind and positive attitude.
“In the 60s, I was naive enough not to worry a whole lot,” she said. “I was in the process of getting my practice started, and I was raising in a family at the same time. I would struggle to tell you the things I spent time worrying about. I went to work every day with a joyful attitude, grateful that I was in a community where I could serve.”
Two of the most significant changes Dr. Bennett witnessed during her career were the development of pediatric subspecialists and the establishment of children’s hospitals. Both markedly altered the field of pediatrics and the way in which children were cared for, she said.
“Early in medicine, children were thought of as the stepchildren of medicine, if you will,” she said. “All the attention research-wise and provision-wise was for adults. During my tenure, I saw that attitude change. The attitude that children were just little adults certainly changed, and the development of specialty hospitals for children, that was a real plus.”
Dr. Bennett spent 27 years in solo practice before hiring additional doctors at what is now Myrtle Avenue Pediatrics, a group practice in Clearwater. She retired in 2003 after a career spanning 40 years. The best advice she would offer young pediatricians is to treat their staff well, especially the front office staff who answer phones and make appointments. Pay them well, train them, and treat them right in order to retain loyal employees and reduce turnover.
In addition, Dr. Bennett stresses that young women who want to be pediatricians should not focus on their gender. “I would remind them that they are physicians who happen to be women,” and they should not think of themselves as female physicians, she said. “Personally I believe becoming a physician is a calling, and I don’t think it is gender oriented. I think males and females can have that calling. I see no difference.”
Dr. Eaton’s story
In the 1960s, when most young pediatricians were opening practices or joining small groups, Antoinette P. Eaton, MD, chose an different path. A passion for serving undeserved families led her to back to what is now Nationwide Children’s Hospital in Columbus, Ohio, where she had completed her residency. In the early 60s, Dr. Eaton served as assistant medical director at the hospital, and in 1965 she become director of the hospital’s birth defect center.
Back then, insurers operated much differently, Dr. Eaton recalled. Insurance companies would not pay for outpatient care, and so children with developmental or congenital disorders would have to be admitted to the hospital for treatment. “It was a complete reversal of what it is like now,” she said.

“We all saw each patient, and then we would get together and conference on the patient and decide on the best approach,” Dr. Eaton said in an interview. “I would definitely say it was unique. It certainly ingrained in me how valuable the team approach to medicine was then and is now. It’s become a very popular approach, and I’m happy to see that, but that was my approach way back in the mid-60s and mid-70s.”
Like female pediatricians of today, Dr. Eaton worked to juggle her career and her role as a mother to four children. She found balance by working part time when necessary and getting off early when her children were school-aged. “Being a mother and being a physician, especially in leadership, there’s always going to be pressure for allocating your time appropriately between all of those demands, but I can tell you I always made being a mother my top priority, and I don’t think I sacrificed my professional duties as a result,” she said. “I think it was possible to combine them, although it’s certainly challenging at times.”
Dr. Eaton went on to become director for maternal health at the Ohio Department of Health and later served as president for the AAP Ohio Chapter and as AAP president from 1990 to 1991.
Her most important achievement however, was being a strong voice for children, she said. “My biggest accomplishment, I hope, was standing up for children and speaking out for children and assuming leadership roles in organizations like AAP to underscore that important role as an advocate.”
[email protected]
On Twitter @legal_med
In the last 50 years, the field of pediatrics has vastly changed, particularly for female physicians.
For starters, the number of female pediatricians has rapidly grown over the last few decades. In 1970, 21% of pediatricians were women, compared with 59% in 2013, according to the American Medical Association physician characteristics and distribution data 2015 edition. The overall pediatric workforce also has increased: A total of 18,332 pediatricians were practicing in 1970, and 84,559 pediatricians were in practice in 2013.
Along with numbers, the field of pediatrics has seen significant changes in practice size, technology, clinical responsibilities, and record keeping, to name a few. However, longtime pediatricians say there are also many ways that the specialty has stayed the same.
Dr. Bennett’s story
When Jean L. Bennett, MD, opened her solo pediatric practice in 1963, she initially had no nurses or team of assistants to help carry out clinical duties. With one receptionist answering phones and Dr. Bennett in the exam room, the Clearwater, Fla., practice opened for business. There was no shortage of patients, Dr. Bennett recalls.
“There was no such thing as neonatology. As a pediatrician, one took care of well and sick newborns and of course, saw a variety of infectious diseases in the office,” Dr. Bennett said in an interview. “We started our own IVs, we did our own lumbar punctures, we did subdural taps, we did exchange transfusions. We did all of those ourselves.”
Dr. Bennett was no stranger to being the lone woman on the job. She was the first woman to graduate from the University of Florida College of Medicine in Gainesville, the first woman to serve as chief of staff at Morton F. Plant Hospital in Clearwater, and the first woman to chair the hospital’s department of pediatrics. Despite being the first in many cases, Dr. Bennett does not remember facing discrimination from colleagues or community members, nor experiencing prejudice against her gender as a medical student or young resident
“My experience was different, of course, than other people graduating at that time, but I can truly say that I always felt the playing field was level,” Dr. Bennett said. “Nobody gave me anything for being a woman, and nobody took anything away.”
Compared with concerns that physicians have today, such as electronic medical records and increasing regulations, Dr. Bennett remembers a relatively worry-free career. She recalls some concern over the medical malpractice crisis in the 1970s and 1980s, but said the majority of her tenure was spent with a clear mind and positive attitude.
“In the 60s, I was naive enough not to worry a whole lot,” she said. “I was in the process of getting my practice started, and I was raising in a family at the same time. I would struggle to tell you the things I spent time worrying about. I went to work every day with a joyful attitude, grateful that I was in a community where I could serve.”
Two of the most significant changes Dr. Bennett witnessed during her career were the development of pediatric subspecialists and the establishment of children’s hospitals. Both markedly altered the field of pediatrics and the way in which children were cared for, she said.
“Early in medicine, children were thought of as the stepchildren of medicine, if you will,” she said. “All the attention research-wise and provision-wise was for adults. During my tenure, I saw that attitude change. The attitude that children were just little adults certainly changed, and the development of specialty hospitals for children, that was a real plus.”
Dr. Bennett spent 27 years in solo practice before hiring additional doctors at what is now Myrtle Avenue Pediatrics, a group practice in Clearwater. She retired in 2003 after a career spanning 40 years. The best advice she would offer young pediatricians is to treat their staff well, especially the front office staff who answer phones and make appointments. Pay them well, train them, and treat them right in order to retain loyal employees and reduce turnover.
In addition, Dr. Bennett stresses that young women who want to be pediatricians should not focus on their gender. “I would remind them that they are physicians who happen to be women,” and they should not think of themselves as female physicians, she said. “Personally I believe becoming a physician is a calling, and I don’t think it is gender oriented. I think males and females can have that calling. I see no difference.”
Dr. Eaton’s story
In the 1960s, when most young pediatricians were opening practices or joining small groups, Antoinette P. Eaton, MD, chose an different path. A passion for serving undeserved families led her to back to what is now Nationwide Children’s Hospital in Columbus, Ohio, where she had completed her residency. In the early 60s, Dr. Eaton served as assistant medical director at the hospital, and in 1965 she become director of the hospital’s birth defect center.
Back then, insurers operated much differently, Dr. Eaton recalled. Insurance companies would not pay for outpatient care, and so children with developmental or congenital disorders would have to be admitted to the hospital for treatment. “It was a complete reversal of what it is like now,” she said.
“We all saw each patient, and then we would get together and conference on the patient and decide on the best approach,” Dr. Eaton said in an interview. “I would definitely say it was unique. It certainly ingrained in me how valuable the team approach to medicine was then and is now. It’s become a very popular approach, and I’m happy to see that, but that was my approach way back in the mid-60s and mid-70s.”
Like female pediatricians of today, Dr. Eaton worked to juggle her career and her role as a mother to four children. She found balance by working part time when necessary and getting off early when her children were school-aged. “Being a mother and being a physician, especially in leadership, there’s always going to be pressure for allocating your time appropriately between all of those demands, but I can tell you I always made being a mother my top priority, and I don’t think I sacrificed my professional duties as a result,” she said. “I think it was possible to combine them, although it’s certainly challenging at times.”
Dr. Eaton went on to become director for maternal health at the Ohio Department of Health and later served as president for the AAP Ohio Chapter and as AAP president from 1990 to 1991.
Her most important achievement however, was being a strong voice for children, she said. “My biggest accomplishment, I hope, was standing up for children and speaking out for children and assuming leadership roles in organizations like AAP to underscore that important role as an advocate.”
[email protected]
On Twitter @legal_med
In the last 50 years, the field of pediatrics has vastly changed, particularly for female physicians.
For starters, the number of female pediatricians has rapidly grown over the last few decades. In 1970, 21% of pediatricians were women, compared with 59% in 2013, according to the American Medical Association physician characteristics and distribution data 2015 edition. The overall pediatric workforce also has increased: A total of 18,332 pediatricians were practicing in 1970, and 84,559 pediatricians were in practice in 2013.
Along with numbers, the field of pediatrics has seen significant changes in practice size, technology, clinical responsibilities, and record keeping, to name a few. However, longtime pediatricians say there are also many ways that the specialty has stayed the same.
Dr. Bennett’s story
When Jean L. Bennett, MD, opened her solo pediatric practice in 1963, she initially had no nurses or team of assistants to help carry out clinical duties. With one receptionist answering phones and Dr. Bennett in the exam room, the Clearwater, Fla., practice opened for business. There was no shortage of patients, Dr. Bennett recalls.
“There was no such thing as neonatology. As a pediatrician, one took care of well and sick newborns and of course, saw a variety of infectious diseases in the office,” Dr. Bennett said in an interview. “We started our own IVs, we did our own lumbar punctures, we did subdural taps, we did exchange transfusions. We did all of those ourselves.”
Dr. Bennett was no stranger to being the lone woman on the job. She was the first woman to graduate from the University of Florida College of Medicine in Gainesville, the first woman to serve as chief of staff at Morton F. Plant Hospital in Clearwater, and the first woman to chair the hospital’s department of pediatrics. Despite being the first in many cases, Dr. Bennett does not remember facing discrimination from colleagues or community members, nor experiencing prejudice against her gender as a medical student or young resident
“My experience was different, of course, than other people graduating at that time, but I can truly say that I always felt the playing field was level,” Dr. Bennett said. “Nobody gave me anything for being a woman, and nobody took anything away.”
Compared with concerns that physicians have today, such as electronic medical records and increasing regulations, Dr. Bennett remembers a relatively worry-free career. She recalls some concern over the medical malpractice crisis in the 1970s and 1980s, but said the majority of her tenure was spent with a clear mind and positive attitude.
“In the 60s, I was naive enough not to worry a whole lot,” she said. “I was in the process of getting my practice started, and I was raising in a family at the same time. I would struggle to tell you the things I spent time worrying about. I went to work every day with a joyful attitude, grateful that I was in a community where I could serve.”
Two of the most significant changes Dr. Bennett witnessed during her career were the development of pediatric subspecialists and the establishment of children’s hospitals. Both markedly altered the field of pediatrics and the way in which children were cared for, she said.
“Early in medicine, children were thought of as the stepchildren of medicine, if you will,” she said. “All the attention research-wise and provision-wise was for adults. During my tenure, I saw that attitude change. The attitude that children were just little adults certainly changed, and the development of specialty hospitals for children, that was a real plus.”
Dr. Bennett spent 27 years in solo practice before hiring additional doctors at what is now Myrtle Avenue Pediatrics, a group practice in Clearwater. She retired in 2003 after a career spanning 40 years. The best advice she would offer young pediatricians is to treat their staff well, especially the front office staff who answer phones and make appointments. Pay them well, train them, and treat them right in order to retain loyal employees and reduce turnover.
In addition, Dr. Bennett stresses that young women who want to be pediatricians should not focus on their gender. “I would remind them that they are physicians who happen to be women,” and they should not think of themselves as female physicians, she said. “Personally I believe becoming a physician is a calling, and I don’t think it is gender oriented. I think males and females can have that calling. I see no difference.”
Dr. Eaton’s story
In the 1960s, when most young pediatricians were opening practices or joining small groups, Antoinette P. Eaton, MD, chose an different path. A passion for serving undeserved families led her to back to what is now Nationwide Children’s Hospital in Columbus, Ohio, where she had completed her residency. In the early 60s, Dr. Eaton served as assistant medical director at the hospital, and in 1965 she become director of the hospital’s birth defect center.
Back then, insurers operated much differently, Dr. Eaton recalled. Insurance companies would not pay for outpatient care, and so children with developmental or congenital disorders would have to be admitted to the hospital for treatment. “It was a complete reversal of what it is like now,” she said.
“We all saw each patient, and then we would get together and conference on the patient and decide on the best approach,” Dr. Eaton said in an interview. “I would definitely say it was unique. It certainly ingrained in me how valuable the team approach to medicine was then and is now. It’s become a very popular approach, and I’m happy to see that, but that was my approach way back in the mid-60s and mid-70s.”
Like female pediatricians of today, Dr. Eaton worked to juggle her career and her role as a mother to four children. She found balance by working part time when necessary and getting off early when her children were school-aged. “Being a mother and being a physician, especially in leadership, there’s always going to be pressure for allocating your time appropriately between all of those demands, but I can tell you I always made being a mother my top priority, and I don’t think I sacrificed my professional duties as a result,” she said. “I think it was possible to combine them, although it’s certainly challenging at times.”
Dr. Eaton went on to become director for maternal health at the Ohio Department of Health and later served as president for the AAP Ohio Chapter and as AAP president from 1990 to 1991.
Her most important achievement however, was being a strong voice for children, she said. “My biggest accomplishment, I hope, was standing up for children and speaking out for children and assuming leadership roles in organizations like AAP to underscore that important role as an advocate.”
[email protected]
On Twitter @legal_med
M13-982 trial in del(17p) CLL: High, durable response rates to venetoclax
New York – Venetoclax monotherapy is associated with high and durable objective response rates in patients with del(17p) chronic lymphocytic leukemia (CLL), according to efficacy findings from the open-label M13-982 trial.
Additionally, a safety expansion of the pivotal phase 2 study showed that treatment was well tolerated, and assessment of minimal residual disease (MRD) status in the peripheral blood and bone marrow of study participants correlated with the 24-month progression-free survival estimate of 100% for patients with complete remission/complete remission with incomplete blood count recovery (CR/CRi), Stephan Stilgenbauer, MD, of the University of Ulm, Germany, and his colleagues reported in a poster at the annual meeting of the International Workshop on Chronic Lymphocytic Leukemia.

That response was maintained at 1 year in 85% of participants.
The current findings, which represent data through April 2017 for those 107 patients from the main cohort, as well as for 51 patients in the safety expansion study, show an overall response rate of 77%, with 20% CR/CRi.
The median time to first response was 1 month, and time to CR/CRi was 9.8 months, they said.
Estimates at 24 months for duration of response, progression-free survival, and overall survival were 66%, 54%, and 73%, respectively.
Additionally, objective responses were seen in four of five previously untreated patients who were enrolled in the safety expansion, and two of them had complete remissions. One patient with best response of stable disease decided to discontinue treatment but remained in follow-up with stable disease.
“All patients were alive at the time of analysis and remain progression free,” the investigators wrote.
In 18 patients who received prior B-cell receptor pathway inhibitor (BCRi) therapy, the objective response rate was 61% and the complete remission rate was 11%, with 12-month, progression-free and overall survival estimates of 50% and 54%, respectively.
Treatment-emergent adverse events of any grade occurred in 98% of patients, and led to dosing interruption in 40% and dosing adjustment in 17%. The most common adverse event was neutropenia; grade 3/4 neutropenia occurred in 40% of patients.
Neutropenia lead to a dose reduction in 8% of patients and to treatment interruption in 6% of patients; no discontinuations were reported.
Infections occurred in 81% of 158 patients, and grade 3/4 infections occurred in 23%; these infections were consistent with the underlying disease, the investigators said.
Laboratory tumor lysis syndrome (TLS) occurred in 5% of patients, but there were no episodes of clinical TLS, they said, noting that five TLS patients required dose interruptions. TLS occurred in four patients with medium risk at screening and in four with high risk. All episodes of TLS occurred during initial dosing or ramp-up, and all resolved. Affected patients were able to resume venetoclax with dose escalation to 400 mg/day.
The rate of minimal residual disease negativity was 30% in the intention-to-treat population as demonstrated by flow cytometry and confirmed by next generation sequencing (NGS) in 21 of 29 patients with an evaluable matched time point specimen. Bone marrow MRD negativity was observed in 20 patients by flow cytometry, and in 9 patients by NGS.
When looking at flow cytometry and NGS data combined, the MRD negativity rate in peripheral blood was 25% overall and 40% in evaluable patients, and the MRD negativity rate in bone marrow was 11% overall and 24% in evaluable patients.
Of those who achieved CR/CRi, 69% were MRD negative in peripheral blood by flow cytometry, with a 24-month, progression-free survival estimate of 100%, and 13 of those had confirmed MRD-negative blood by NGS, 2 had MRD-positive blood by NGS at a matched flow cytometry assessment, and 7 were not evaluated by NGS. For the remaining CR/CRi patients, who were MRD-positive by flow cytometry, the 24-month progression-free survival estimate was 86%.
Study participants in the main cohort were adults with a median age of 67 years who had relapsed/refractory CLL with an indication for treatment by iwCLL criteria, del(17p), good performance status, adequate bone marrow function, and creatinine clearance of at least 50 mg/min. They received a single test dose of 20 mg on day 1, with gradual ramp up to 400 mg over 4-5 weeks based on laboratory assessments. All were hospitalized for the first 20 mg and 50 mg venetoclax doses during ramp up.
Those in the safety expansion were treated with once-daily oral venetoclax starting at a dose of 20 mg/day for 1 week and ramped up to 400 mg by week 5. To mitigate TLS risk, uric acid–lowering agents and hydration were started at least 72 hours prior to administering the first dose. Those with high TLS risk – and some with medium risk – were hospitalized for the first 20-mg and 50-mg doses. Those with low TLS risk – and most with medium risk – received initial venetoclax dosing in an outpatient setting.
“Continued follow-up of patients in this trial will provide additional data on the durability of response with venetoclax in patients with del(17p) CLL,” the investigators wrote.
This study was supported by AbbVie and Genentech. Dr. Stilgenbauer received research funding, honoraria, and travel support from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Genentech, Genzyme, Gilead, GSK, Janssen, Mundipharma, Novartis, Pharmacyclics, Hoffmann La-Roche, and Sanofi.
New York – Venetoclax monotherapy is associated with high and durable objective response rates in patients with del(17p) chronic lymphocytic leukemia (CLL), according to efficacy findings from the open-label M13-982 trial.
Additionally, a safety expansion of the pivotal phase 2 study showed that treatment was well tolerated, and assessment of minimal residual disease (MRD) status in the peripheral blood and bone marrow of study participants correlated with the 24-month progression-free survival estimate of 100% for patients with complete remission/complete remission with incomplete blood count recovery (CR/CRi), Stephan Stilgenbauer, MD, of the University of Ulm, Germany, and his colleagues reported in a poster at the annual meeting of the International Workshop on Chronic Lymphocytic Leukemia.
That response was maintained at 1 year in 85% of participants.
The current findings, which represent data through April 2017 for those 107 patients from the main cohort, as well as for 51 patients in the safety expansion study, show an overall response rate of 77%, with 20% CR/CRi.
The median time to first response was 1 month, and time to CR/CRi was 9.8 months, they said.
Estimates at 24 months for duration of response, progression-free survival, and overall survival were 66%, 54%, and 73%, respectively.
Additionally, objective responses were seen in four of five previously untreated patients who were enrolled in the safety expansion, and two of them had complete remissions. One patient with best response of stable disease decided to discontinue treatment but remained in follow-up with stable disease.
“All patients were alive at the time of analysis and remain progression free,” the investigators wrote.
In 18 patients who received prior B-cell receptor pathway inhibitor (BCRi) therapy, the objective response rate was 61% and the complete remission rate was 11%, with 12-month, progression-free and overall survival estimates of 50% and 54%, respectively.
Treatment-emergent adverse events of any grade occurred in 98% of patients, and led to dosing interruption in 40% and dosing adjustment in 17%. The most common adverse event was neutropenia; grade 3/4 neutropenia occurred in 40% of patients.
Neutropenia lead to a dose reduction in 8% of patients and to treatment interruption in 6% of patients; no discontinuations were reported.
Infections occurred in 81% of 158 patients, and grade 3/4 infections occurred in 23%; these infections were consistent with the underlying disease, the investigators said.
Laboratory tumor lysis syndrome (TLS) occurred in 5% of patients, but there were no episodes of clinical TLS, they said, noting that five TLS patients required dose interruptions. TLS occurred in four patients with medium risk at screening and in four with high risk. All episodes of TLS occurred during initial dosing or ramp-up, and all resolved. Affected patients were able to resume venetoclax with dose escalation to 400 mg/day.
The rate of minimal residual disease negativity was 30% in the intention-to-treat population as demonstrated by flow cytometry and confirmed by next generation sequencing (NGS) in 21 of 29 patients with an evaluable matched time point specimen. Bone marrow MRD negativity was observed in 20 patients by flow cytometry, and in 9 patients by NGS.
When looking at flow cytometry and NGS data combined, the MRD negativity rate in peripheral blood was 25% overall and 40% in evaluable patients, and the MRD negativity rate in bone marrow was 11% overall and 24% in evaluable patients.
Of those who achieved CR/CRi, 69% were MRD negative in peripheral blood by flow cytometry, with a 24-month, progression-free survival estimate of 100%, and 13 of those had confirmed MRD-negative blood by NGS, 2 had MRD-positive blood by NGS at a matched flow cytometry assessment, and 7 were not evaluated by NGS. For the remaining CR/CRi patients, who were MRD-positive by flow cytometry, the 24-month progression-free survival estimate was 86%.
Study participants in the main cohort were adults with a median age of 67 years who had relapsed/refractory CLL with an indication for treatment by iwCLL criteria, del(17p), good performance status, adequate bone marrow function, and creatinine clearance of at least 50 mg/min. They received a single test dose of 20 mg on day 1, with gradual ramp up to 400 mg over 4-5 weeks based on laboratory assessments. All were hospitalized for the first 20 mg and 50 mg venetoclax doses during ramp up.
Those in the safety expansion were treated with once-daily oral venetoclax starting at a dose of 20 mg/day for 1 week and ramped up to 400 mg by week 5. To mitigate TLS risk, uric acid–lowering agents and hydration were started at least 72 hours prior to administering the first dose. Those with high TLS risk – and some with medium risk – were hospitalized for the first 20-mg and 50-mg doses. Those with low TLS risk – and most with medium risk – received initial venetoclax dosing in an outpatient setting.
“Continued follow-up of patients in this trial will provide additional data on the durability of response with venetoclax in patients with del(17p) CLL,” the investigators wrote.
This study was supported by AbbVie and Genentech. Dr. Stilgenbauer received research funding, honoraria, and travel support from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Genentech, Genzyme, Gilead, GSK, Janssen, Mundipharma, Novartis, Pharmacyclics, Hoffmann La-Roche, and Sanofi.
New York – Venetoclax monotherapy is associated with high and durable objective response rates in patients with del(17p) chronic lymphocytic leukemia (CLL), according to efficacy findings from the open-label M13-982 trial.
Additionally, a safety expansion of the pivotal phase 2 study showed that treatment was well tolerated, and assessment of minimal residual disease (MRD) status in the peripheral blood and bone marrow of study participants correlated with the 24-month progression-free survival estimate of 100% for patients with complete remission/complete remission with incomplete blood count recovery (CR/CRi), Stephan Stilgenbauer, MD, of the University of Ulm, Germany, and his colleagues reported in a poster at the annual meeting of the International Workshop on Chronic Lymphocytic Leukemia.
That response was maintained at 1 year in 85% of participants.
The current findings, which represent data through April 2017 for those 107 patients from the main cohort, as well as for 51 patients in the safety expansion study, show an overall response rate of 77%, with 20% CR/CRi.
The median time to first response was 1 month, and time to CR/CRi was 9.8 months, they said.
Estimates at 24 months for duration of response, progression-free survival, and overall survival were 66%, 54%, and 73%, respectively.
Additionally, objective responses were seen in four of five previously untreated patients who were enrolled in the safety expansion, and two of them had complete remissions. One patient with best response of stable disease decided to discontinue treatment but remained in follow-up with stable disease.
“All patients were alive at the time of analysis and remain progression free,” the investigators wrote.
In 18 patients who received prior B-cell receptor pathway inhibitor (BCRi) therapy, the objective response rate was 61% and the complete remission rate was 11%, with 12-month, progression-free and overall survival estimates of 50% and 54%, respectively.
Treatment-emergent adverse events of any grade occurred in 98% of patients, and led to dosing interruption in 40% and dosing adjustment in 17%. The most common adverse event was neutropenia; grade 3/4 neutropenia occurred in 40% of patients.
Neutropenia lead to a dose reduction in 8% of patients and to treatment interruption in 6% of patients; no discontinuations were reported.
Infections occurred in 81% of 158 patients, and grade 3/4 infections occurred in 23%; these infections were consistent with the underlying disease, the investigators said.
Laboratory tumor lysis syndrome (TLS) occurred in 5% of patients, but there were no episodes of clinical TLS, they said, noting that five TLS patients required dose interruptions. TLS occurred in four patients with medium risk at screening and in four with high risk. All episodes of TLS occurred during initial dosing or ramp-up, and all resolved. Affected patients were able to resume venetoclax with dose escalation to 400 mg/day.
The rate of minimal residual disease negativity was 30% in the intention-to-treat population as demonstrated by flow cytometry and confirmed by next generation sequencing (NGS) in 21 of 29 patients with an evaluable matched time point specimen. Bone marrow MRD negativity was observed in 20 patients by flow cytometry, and in 9 patients by NGS.
When looking at flow cytometry and NGS data combined, the MRD negativity rate in peripheral blood was 25% overall and 40% in evaluable patients, and the MRD negativity rate in bone marrow was 11% overall and 24% in evaluable patients.
Of those who achieved CR/CRi, 69% were MRD negative in peripheral blood by flow cytometry, with a 24-month, progression-free survival estimate of 100%, and 13 of those had confirmed MRD-negative blood by NGS, 2 had MRD-positive blood by NGS at a matched flow cytometry assessment, and 7 were not evaluated by NGS. For the remaining CR/CRi patients, who were MRD-positive by flow cytometry, the 24-month progression-free survival estimate was 86%.
Study participants in the main cohort were adults with a median age of 67 years who had relapsed/refractory CLL with an indication for treatment by iwCLL criteria, del(17p), good performance status, adequate bone marrow function, and creatinine clearance of at least 50 mg/min. They received a single test dose of 20 mg on day 1, with gradual ramp up to 400 mg over 4-5 weeks based on laboratory assessments. All were hospitalized for the first 20 mg and 50 mg venetoclax doses during ramp up.
Those in the safety expansion were treated with once-daily oral venetoclax starting at a dose of 20 mg/day for 1 week and ramped up to 400 mg by week 5. To mitigate TLS risk, uric acid–lowering agents and hydration were started at least 72 hours prior to administering the first dose. Those with high TLS risk – and some with medium risk – were hospitalized for the first 20-mg and 50-mg doses. Those with low TLS risk – and most with medium risk – received initial venetoclax dosing in an outpatient setting.
“Continued follow-up of patients in this trial will provide additional data on the durability of response with venetoclax in patients with del(17p) CLL,” the investigators wrote.
This study was supported by AbbVie and Genentech. Dr. Stilgenbauer received research funding, honoraria, and travel support from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Genentech, Genzyme, Gilead, GSK, Janssen, Mundipharma, Novartis, Pharmacyclics, Hoffmann La-Roche, and Sanofi.
AT THE iwCLL MEETING
Key clinical point:
Major finding: At April 2017 data analysis, the overall response rate was 77% with 20% CR/CRi.
Data source: The phase 2 open-label M13-982 Trial and safety expansion cohort of 158 total patients.
Disclosures: This study was supported by AbbVie and Genentech. Dr. Stilgenbauer received research funding, honoraria, and travel support from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Genentech, Genzyme, Gilead, GSK, Janssen, Mundipharma, Novartis, Pharmacyclics, Hoffmann La-Roche, and Sanofi.
Multiple factors predict surgical site infection risk after lower extremity revascularization
Patient, operative, and hospital factors were found to be significant predictors of the risk of surgical site infection in patients who underwent open lower extremity bypass procedures, according to the results of a retrospective data analysis.
The study assessed the outcomes of 3,033 patients who underwent elective or urgent open LEB procedures between January 2012 and June 2015 using data from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 VIC), a statewide cardiovascular consortium of 35 hospitals, according to Frank M. Davis, MD, and his colleagues at the University of Michigan, Ann Arbor.
Demographic information, medical history, laboratory test results before and after the procedure, procedural indication, procedural urgency, technical details of procedures, and associated complications were assessed for each patient. Women comprised 31% of patients, the average patient age was 66 years, and 83% of the population was white (J Vasc Surg. 2017 Jun;65[6]:1769-78).
Among all of the patients treated, 320 developed SSIs and 2,713 did not. The procedural indications included one or more of the following: claudication (72%), rest pain (50.5%), ulcer/gangrene (32.4%), or acute limb ischemia (15.1%). Antibiotics were appropriately administered to 97% of the patients, according to the researchers, “demonstrating high compliance across the BMC2 VIC.”
- Patient factors: As indicated by previous studies, obesity (odds ratio, 1.78), dialysis dependence (OR, 4.33), and hypertension (OR, 4.29) conferred a significant increased risk of SSI after LEB, according to Dr. Davis and his colleagues. In addition, however, they found that previous vascular surgery (OR, 1.57), previous percutaneous coronary intervention (OR, 1.47), use of antiplatelet medication (OR, 4.29), and low Peripheral Artery Questionnaire symptom severity (OR, 1.48) were significant independent predictors of SSI.
- Operative factors: Prolonged procedural length (OR, 2.95), iodine-only antiseptic skin preparation (OR, 1.73), and high peak intraoperative glucose (defined as a peak glucose greater than 180 mg/dL; OR, 1.99) were significant independent predictors of SSI. However, concomitant stent placement was found to be significantly predictive (OR, .38), “perhaps due to improvement in regional and subcutaneous vascular flow after the intervention,” the researchers suggested.
- Hospital factors: Larger overall hospital size (OR, 2.22) and major teaching center (OR, 1.66) were associated with increased risk of SSI. “Interestingly, we did not find an association with SSI and the hospital annual volume or the hospital urgent/emergent procedure rate,” the researchers added.
SSIs were not found to be significantly associated with a difference in 30-day mortality. However, they were significantly associated with an increased rate of several postoperative morbidities, including transfusion, lymph leak, major amputation, and open surgical bypass revision at or within 30 days of the index operation, according to Dr. Davis and his colleagues.
“Although some factors, such as patients comorbidities, are not modifiable, others represent areas for quality improvement in at-risk patients,” the researchers indicated. “Diligence should be devoted to decreasing operative length, controlling intraoperative glucose levels, and avoiding iodine-only skin preparation to decrease the rate of SSIs and its numerous associate morbidities in vascular surgery patients.”
In discussing the issue of antiplatelet medication being an indicator of increased risk, the authors pointed out that it was a hitherto unreported factor in the vascular literature, and of concern because, “as expected, a high percentage of patients (78.7%) were taking antiplatelet medication at the time of their LEB.”
Because the association of antiplatelet medication with SSIs was independent of the need for operative transfusion or the need for repeat intervention, the researchers speculated that “all antiplatelet agents have the theoretical potential to diminish activation-dependent platelet immune functions.” They referred to previous studies showing that clopidogrel was associated with significantly higher clinical rates of infection, particularly pneumonia.
Limitations cited for the study were the retrospective nature of the database analysis, the possibility of confounders not assessed in the data, and the fact that outcomes were limited to 30-day events, which would not take into account longer-term graft failure or mortality.
The authors reported having no conflicts of interest with regard to the study.
Patient, operative, and hospital factors were found to be significant predictors of the risk of surgical site infection in patients who underwent open lower extremity bypass procedures, according to the results of a retrospective data analysis.
The study assessed the outcomes of 3,033 patients who underwent elective or urgent open LEB procedures between January 2012 and June 2015 using data from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 VIC), a statewide cardiovascular consortium of 35 hospitals, according to Frank M. Davis, MD, and his colleagues at the University of Michigan, Ann Arbor.
Demographic information, medical history, laboratory test results before and after the procedure, procedural indication, procedural urgency, technical details of procedures, and associated complications were assessed for each patient. Women comprised 31% of patients, the average patient age was 66 years, and 83% of the population was white (J Vasc Surg. 2017 Jun;65[6]:1769-78).
Among all of the patients treated, 320 developed SSIs and 2,713 did not. The procedural indications included one or more of the following: claudication (72%), rest pain (50.5%), ulcer/gangrene (32.4%), or acute limb ischemia (15.1%). Antibiotics were appropriately administered to 97% of the patients, according to the researchers, “demonstrating high compliance across the BMC2 VIC.”
- Patient factors: As indicated by previous studies, obesity (odds ratio, 1.78), dialysis dependence (OR, 4.33), and hypertension (OR, 4.29) conferred a significant increased risk of SSI after LEB, according to Dr. Davis and his colleagues. In addition, however, they found that previous vascular surgery (OR, 1.57), previous percutaneous coronary intervention (OR, 1.47), use of antiplatelet medication (OR, 4.29), and low Peripheral Artery Questionnaire symptom severity (OR, 1.48) were significant independent predictors of SSI.
- Operative factors: Prolonged procedural length (OR, 2.95), iodine-only antiseptic skin preparation (OR, 1.73), and high peak intraoperative glucose (defined as a peak glucose greater than 180 mg/dL; OR, 1.99) were significant independent predictors of SSI. However, concomitant stent placement was found to be significantly predictive (OR, .38), “perhaps due to improvement in regional and subcutaneous vascular flow after the intervention,” the researchers suggested.
- Hospital factors: Larger overall hospital size (OR, 2.22) and major teaching center (OR, 1.66) were associated with increased risk of SSI. “Interestingly, we did not find an association with SSI and the hospital annual volume or the hospital urgent/emergent procedure rate,” the researchers added.
SSIs were not found to be significantly associated with a difference in 30-day mortality. However, they were significantly associated with an increased rate of several postoperative morbidities, including transfusion, lymph leak, major amputation, and open surgical bypass revision at or within 30 days of the index operation, according to Dr. Davis and his colleagues.
“Although some factors, such as patients comorbidities, are not modifiable, others represent areas for quality improvement in at-risk patients,” the researchers indicated. “Diligence should be devoted to decreasing operative length, controlling intraoperative glucose levels, and avoiding iodine-only skin preparation to decrease the rate of SSIs and its numerous associate morbidities in vascular surgery patients.”
In discussing the issue of antiplatelet medication being an indicator of increased risk, the authors pointed out that it was a hitherto unreported factor in the vascular literature, and of concern because, “as expected, a high percentage of patients (78.7%) were taking antiplatelet medication at the time of their LEB.”
Because the association of antiplatelet medication with SSIs was independent of the need for operative transfusion or the need for repeat intervention, the researchers speculated that “all antiplatelet agents have the theoretical potential to diminish activation-dependent platelet immune functions.” They referred to previous studies showing that clopidogrel was associated with significantly higher clinical rates of infection, particularly pneumonia.
Limitations cited for the study were the retrospective nature of the database analysis, the possibility of confounders not assessed in the data, and the fact that outcomes were limited to 30-day events, which would not take into account longer-term graft failure or mortality.
The authors reported having no conflicts of interest with regard to the study.
Patient, operative, and hospital factors were found to be significant predictors of the risk of surgical site infection in patients who underwent open lower extremity bypass procedures, according to the results of a retrospective data analysis.
The study assessed the outcomes of 3,033 patients who underwent elective or urgent open LEB procedures between January 2012 and June 2015 using data from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Vascular Intervention Collaborative (BMC2 VIC), a statewide cardiovascular consortium of 35 hospitals, according to Frank M. Davis, MD, and his colleagues at the University of Michigan, Ann Arbor.
Demographic information, medical history, laboratory test results before and after the procedure, procedural indication, procedural urgency, technical details of procedures, and associated complications were assessed for each patient. Women comprised 31% of patients, the average patient age was 66 years, and 83% of the population was white (J Vasc Surg. 2017 Jun;65[6]:1769-78).
Among all of the patients treated, 320 developed SSIs and 2,713 did not. The procedural indications included one or more of the following: claudication (72%), rest pain (50.5%), ulcer/gangrene (32.4%), or acute limb ischemia (15.1%). Antibiotics were appropriately administered to 97% of the patients, according to the researchers, “demonstrating high compliance across the BMC2 VIC.”
- Patient factors: As indicated by previous studies, obesity (odds ratio, 1.78), dialysis dependence (OR, 4.33), and hypertension (OR, 4.29) conferred a significant increased risk of SSI after LEB, according to Dr. Davis and his colleagues. In addition, however, they found that previous vascular surgery (OR, 1.57), previous percutaneous coronary intervention (OR, 1.47), use of antiplatelet medication (OR, 4.29), and low Peripheral Artery Questionnaire symptom severity (OR, 1.48) were significant independent predictors of SSI.
- Operative factors: Prolonged procedural length (OR, 2.95), iodine-only antiseptic skin preparation (OR, 1.73), and high peak intraoperative glucose (defined as a peak glucose greater than 180 mg/dL; OR, 1.99) were significant independent predictors of SSI. However, concomitant stent placement was found to be significantly predictive (OR, .38), “perhaps due to improvement in regional and subcutaneous vascular flow after the intervention,” the researchers suggested.
- Hospital factors: Larger overall hospital size (OR, 2.22) and major teaching center (OR, 1.66) were associated with increased risk of SSI. “Interestingly, we did not find an association with SSI and the hospital annual volume or the hospital urgent/emergent procedure rate,” the researchers added.
SSIs were not found to be significantly associated with a difference in 30-day mortality. However, they were significantly associated with an increased rate of several postoperative morbidities, including transfusion, lymph leak, major amputation, and open surgical bypass revision at or within 30 days of the index operation, according to Dr. Davis and his colleagues.
“Although some factors, such as patients comorbidities, are not modifiable, others represent areas for quality improvement in at-risk patients,” the researchers indicated. “Diligence should be devoted to decreasing operative length, controlling intraoperative glucose levels, and avoiding iodine-only skin preparation to decrease the rate of SSIs and its numerous associate morbidities in vascular surgery patients.”
In discussing the issue of antiplatelet medication being an indicator of increased risk, the authors pointed out that it was a hitherto unreported factor in the vascular literature, and of concern because, “as expected, a high percentage of patients (78.7%) were taking antiplatelet medication at the time of their LEB.”
Because the association of antiplatelet medication with SSIs was independent of the need for operative transfusion or the need for repeat intervention, the researchers speculated that “all antiplatelet agents have the theoretical potential to diminish activation-dependent platelet immune functions.” They referred to previous studies showing that clopidogrel was associated with significantly higher clinical rates of infection, particularly pneumonia.
Limitations cited for the study were the retrospective nature of the database analysis, the possibility of confounders not assessed in the data, and the fact that outcomes were limited to 30-day events, which would not take into account longer-term graft failure or mortality.
The authors reported having no conflicts of interest with regard to the study.
FROM THE JOURNAL OF VASCULAR SURGERY
Key clinical point:
Major finding: SSIs occurred in 10.6% of lower extremity bypasses.
Data source: A retrospective analysis of 3,033 elective or urgent open LEB procedures performed over a 3.5-year period in a statewide cardiovascular consortium of 35 hospitals.
Disclosures: The authors reported having no conflicts of interest with regard to the study.
Better bariatric surgery outcomes with lower preoperative BMI
Delaying bariatric surgery until body mass index is highly elevated may reduce the likelihood of achieving a BMI of less than 30 within a year, according to a paper published online July 26 in JAMA Surgery.
A retrospective study using prospectively gathered clinical data of 27,320 adults who underwent bariatric surgery in Michigan showed around one in three (36%) achieved a BMI below 30 within a year after surgery (JAMA Surgery 2017, July 26. doi: 10.1001/jamasurg.2017.2348). But obese patients with a body mass index of less than 40 kg/m2 before undergoing bariatric surgery are significantly more likely to achieve a postoperative BMI of under 30.
Individuals who had a preoperative BMI of less than 40 had a 12-fold higher chance of getting their BMI below 30, compared to those whose preoperative BMI was 40 or above (95% confidence interval 1.71-14.16, P less than .001). Only 8.5% of individuals with a BMI at or above 50 achieved a postoperative BMI below 30.

The likelihood of getting below 30 within a year was eightfold higher in patients who had a sleeve gastrectomy, 21 times greater in those who underwent Roux-en-Y bypass, and 82 times higher in those who had a duodenal switch, compared with patients who had adjustable gastric banding (P less than .001).
The researchers also compared other outcomes in individuals whose BMI dropped below 30 and in those who did not achieve this degree of weight loss. The analysis showed that those with a BMI below 30 after 1 year had at least a twofold greater chance of discontinuing cholesterol-lowering medications, insulin, diabetes medications, antihypertensives, and CPAP for sleep apnea, compared with those whose BMI remained at 30 or above. They were also more than three times more likely to report being ‘very satisfied’ with the outcomes of surgery.
The authors noted that the cohort’s mean BMI was 48, which was above the established threshold for bariatric surgery, namely a BMI of 40, or 35 with weight-related comorbidities.
“Our results suggest that patients with morbid obesity should be targeted for surgery when their BMI is still less than 40, as these patients are more likely to achieve a target BMI that results in substantial reduction in weight-related comorbidities,” the authors wrote.
However, they stressed that their findings should not be taken as a reason to exclude patients with a BMI above 40 from surgery, pointing out that even for patients with higher preoperative BMIs, bariatric surgery offered substantial health and quality of life benefits.
They also acknowledged that 1-year weight data was available for around 50% of patients in the registry, which may have led to selection bias.
“Policies and practice patterns that delay or incentivize patients to pursue bariatric surgery only once the BMI is highly elevated can result in inferior outcomes,” the investigators concluded.
Blue Cross Blue Shield of Michigan/Blue Care Network funded the study. Three authors had received salary support from Blue Cross Blue Shield. No other conflicts of interest were declared.
The authors’ conclusion that bariatric surgery should be more liberally applied to patients with less severe obesity is consistent with multiple reports of improved control of type 2 diabetes, if not remission, among lower-BMI patient populations following MBS [metabolic and bariatric surgery]. However, these reports generally do not refute the importance of weight loss in achieving important clinical benefit among patients with obesity-related comorbid disease.
One strength of the present study is that it is a clinical database. However, 50% attrition of the follow-up weight loss data at 1 year is potentially problematic.
Bruce M. Wolfe, MD, FACS, and Elizaveta Walker, MPH, are in the division of bariatric surgery, department of surgery, at Oregon Health & Science University, Portland. These comments are taken from an accompanying editorial (JAMA Surgery 2017 Jul 26. doi: 10.1001/jamasurg.2017.2349). No conflicts of interest were declared.
The authors’ conclusion that bariatric surgery should be more liberally applied to patients with less severe obesity is consistent with multiple reports of improved control of type 2 diabetes, if not remission, among lower-BMI patient populations following MBS [metabolic and bariatric surgery]. However, these reports generally do not refute the importance of weight loss in achieving important clinical benefit among patients with obesity-related comorbid disease.
One strength of the present study is that it is a clinical database. However, 50% attrition of the follow-up weight loss data at 1 year is potentially problematic.
Bruce M. Wolfe, MD, FACS, and Elizaveta Walker, MPH, are in the division of bariatric surgery, department of surgery, at Oregon Health & Science University, Portland. These comments are taken from an accompanying editorial (JAMA Surgery 2017 Jul 26. doi: 10.1001/jamasurg.2017.2349). No conflicts of interest were declared.
The authors’ conclusion that bariatric surgery should be more liberally applied to patients with less severe obesity is consistent with multiple reports of improved control of type 2 diabetes, if not remission, among lower-BMI patient populations following MBS [metabolic and bariatric surgery]. However, these reports generally do not refute the importance of weight loss in achieving important clinical benefit among patients with obesity-related comorbid disease.
One strength of the present study is that it is a clinical database. However, 50% attrition of the follow-up weight loss data at 1 year is potentially problematic.
Bruce M. Wolfe, MD, FACS, and Elizaveta Walker, MPH, are in the division of bariatric surgery, department of surgery, at Oregon Health & Science University, Portland. These comments are taken from an accompanying editorial (JAMA Surgery 2017 Jul 26. doi: 10.1001/jamasurg.2017.2349). No conflicts of interest were declared.
Delaying bariatric surgery until body mass index is highly elevated may reduce the likelihood of achieving a BMI of less than 30 within a year, according to a paper published online July 26 in JAMA Surgery.
A retrospective study using prospectively gathered clinical data of 27,320 adults who underwent bariatric surgery in Michigan showed around one in three (36%) achieved a BMI below 30 within a year after surgery (JAMA Surgery 2017, July 26. doi: 10.1001/jamasurg.2017.2348). But obese patients with a body mass index of less than 40 kg/m2 before undergoing bariatric surgery are significantly more likely to achieve a postoperative BMI of under 30.
Individuals who had a preoperative BMI of less than 40 had a 12-fold higher chance of getting their BMI below 30, compared to those whose preoperative BMI was 40 or above (95% confidence interval 1.71-14.16, P less than .001). Only 8.5% of individuals with a BMI at or above 50 achieved a postoperative BMI below 30.
The likelihood of getting below 30 within a year was eightfold higher in patients who had a sleeve gastrectomy, 21 times greater in those who underwent Roux-en-Y bypass, and 82 times higher in those who had a duodenal switch, compared with patients who had adjustable gastric banding (P less than .001).
The researchers also compared other outcomes in individuals whose BMI dropped below 30 and in those who did not achieve this degree of weight loss. The analysis showed that those with a BMI below 30 after 1 year had at least a twofold greater chance of discontinuing cholesterol-lowering medications, insulin, diabetes medications, antihypertensives, and CPAP for sleep apnea, compared with those whose BMI remained at 30 or above. They were also more than three times more likely to report being ‘very satisfied’ with the outcomes of surgery.
The authors noted that the cohort’s mean BMI was 48, which was above the established threshold for bariatric surgery, namely a BMI of 40, or 35 with weight-related comorbidities.
“Our results suggest that patients with morbid obesity should be targeted for surgery when their BMI is still less than 40, as these patients are more likely to achieve a target BMI that results in substantial reduction in weight-related comorbidities,” the authors wrote.
However, they stressed that their findings should not be taken as a reason to exclude patients with a BMI above 40 from surgery, pointing out that even for patients with higher preoperative BMIs, bariatric surgery offered substantial health and quality of life benefits.
They also acknowledged that 1-year weight data was available for around 50% of patients in the registry, which may have led to selection bias.
“Policies and practice patterns that delay or incentivize patients to pursue bariatric surgery only once the BMI is highly elevated can result in inferior outcomes,” the investigators concluded.
Blue Cross Blue Shield of Michigan/Blue Care Network funded the study. Three authors had received salary support from Blue Cross Blue Shield. No other conflicts of interest were declared.
Delaying bariatric surgery until body mass index is highly elevated may reduce the likelihood of achieving a BMI of less than 30 within a year, according to a paper published online July 26 in JAMA Surgery.
A retrospective study using prospectively gathered clinical data of 27,320 adults who underwent bariatric surgery in Michigan showed around one in three (36%) achieved a BMI below 30 within a year after surgery (JAMA Surgery 2017, July 26. doi: 10.1001/jamasurg.2017.2348). But obese patients with a body mass index of less than 40 kg/m2 before undergoing bariatric surgery are significantly more likely to achieve a postoperative BMI of under 30.
Individuals who had a preoperative BMI of less than 40 had a 12-fold higher chance of getting their BMI below 30, compared to those whose preoperative BMI was 40 or above (95% confidence interval 1.71-14.16, P less than .001). Only 8.5% of individuals with a BMI at or above 50 achieved a postoperative BMI below 30.
The likelihood of getting below 30 within a year was eightfold higher in patients who had a sleeve gastrectomy, 21 times greater in those who underwent Roux-en-Y bypass, and 82 times higher in those who had a duodenal switch, compared with patients who had adjustable gastric banding (P less than .001).
The researchers also compared other outcomes in individuals whose BMI dropped below 30 and in those who did not achieve this degree of weight loss. The analysis showed that those with a BMI below 30 after 1 year had at least a twofold greater chance of discontinuing cholesterol-lowering medications, insulin, diabetes medications, antihypertensives, and CPAP for sleep apnea, compared with those whose BMI remained at 30 or above. They were also more than three times more likely to report being ‘very satisfied’ with the outcomes of surgery.
The authors noted that the cohort’s mean BMI was 48, which was above the established threshold for bariatric surgery, namely a BMI of 40, or 35 with weight-related comorbidities.
“Our results suggest that patients with morbid obesity should be targeted for surgery when their BMI is still less than 40, as these patients are more likely to achieve a target BMI that results in substantial reduction in weight-related comorbidities,” the authors wrote.
However, they stressed that their findings should not be taken as a reason to exclude patients with a BMI above 40 from surgery, pointing out that even for patients with higher preoperative BMIs, bariatric surgery offered substantial health and quality of life benefits.
They also acknowledged that 1-year weight data was available for around 50% of patients in the registry, which may have led to selection bias.
“Policies and practice patterns that delay or incentivize patients to pursue bariatric surgery only once the BMI is highly elevated can result in inferior outcomes,” the investigators concluded.
Blue Cross Blue Shield of Michigan/Blue Care Network funded the study. Three authors had received salary support from Blue Cross Blue Shield. No other conflicts of interest were declared.
FROM JAMA SURGERY
Key clinical point: A BMI below 40 prior to undergoing bariatric surgery gives patients a significantly better chance of achieving a 1-year postoperative BMI under 30.
Major finding: Obese patients with a BMI less than 40 before undergoing bariatric surgery are more than 12 times more likely to achieve a postoperative BMI of under 30.
Data source: A retrospective study using prospectively gathered clinical data of 27, 320 adults who underwent bariatric surgery.
Disclosures: Blue Cross Blue Shield of Michigan/Blue Care Network funded the study. Three authors had received salary support from Blue Cross Blue Shield. No other conflicts of interest were declared.