User login
Meningitis before age 3 months: Consider enterovirus and parechovirus
MADRID – Ninety-five percent of cases of enterovirus and parechovirus meningitis in infants younger than 90 days old in the United Kingdom and Ireland were diagnosed through lumbar puncture and identification of the virus in the CSF by PCR, Seilesh Kadambari, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“We recommend that routine testing of CSF for enterovirus and parechovirus in febrile infants should be promoted, even in the absence of pleocytosis,” said Dr. Kadambari of John Radcliffe Hospital in Oxford, England.

This active enhanced prospective surveillance study was undertaken because an earlier retrospective study concluded that the rate of viral meningitis across all pediatric and adult age groups had increased rapidly during a recent 10-year period in the United Kingdom and Ireland. Infants younger than 3 months of age were especially hard hit by enterovirus, which accounted in the earlier study for 92% of all viral meningitis cases in that age group. Dr. Kadambari and his coinvestigators decided to take a closer prospective look at the sub-3-month age group because it’s such an important time neurodevelopmentally.
During the 13-month period of June 2014 to June 2015, 710 patients younger than 90 days old were hospitalized for enterovirus or parechovirus meningitis across the United Kingdom and Republic of Ireland. Ninety-five percent were due to enterovirus. Only 6% of affected infants were born prematurely.
“One of the take-home messages for me from the study was that 12% of enterovirus cases and 23% of parechovirus meningitis cases required admission to an ICU setting,” the pediatrician observed.
Among the infants admitted to a pediatric ICU, half of those with enterovirus meningitis and all those with parechovirus meningitis required intubation and mechanical ventilation. One-fifth of the enterovirus meningitis patients in pediatric ICUs required inotropic support for cardiovascular stabilization, as did all young infants with parechovirus meningitis.
Among the 710 patients, the three most common clinical presenting features were fever, irritability, and reduced feeding, present in 85%, 66%, and 54%, respectively.
Upon physical examination, two noteworthy common findings were signs of shock, present in 27% of infants with enterovirus meningitis and 43% with parechovirus meningitis, and respiratory distress, seen in 12% and 26%, respectively.
None of the 710 infants had a secondary bacterial infection. “That has implications for antimicrobial stewardship programs,” according to Dr. Kadambari.
The majority of infants had a normal CSF WBC count and a normal-range C-reactive protein level.
“Raised inflammatory markers were not a common feature in our cohort,” he noted.
Two infants died: one of a massive pulmonary hemorrhage and the other as a result of septic shock. Of the remaining 708 patients, however, 699 (98.7%) were discharged without significant neurologic impairment. Seven infants with enterovirus meningitis and two with parechovirus meningitis were discharged with severe delay, including cases of fine motor and gross motor delay, visual abnormalities, and a single case of severe cardiac dysfunction requiring discharge on an ACE inhibitor.
This surveillance study was a collaboration between St. George’s University of London and Public Health England. Dr. Kadambari reported having no financial conflicts.
Future studies need to examine long-term neurodevelopmental outcomes in affected young infants out to age 24 months, he said.
MADRID – Ninety-five percent of cases of enterovirus and parechovirus meningitis in infants younger than 90 days old in the United Kingdom and Ireland were diagnosed through lumbar puncture and identification of the virus in the CSF by PCR, Seilesh Kadambari, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“We recommend that routine testing of CSF for enterovirus and parechovirus in febrile infants should be promoted, even in the absence of pleocytosis,” said Dr. Kadambari of John Radcliffe Hospital in Oxford, England.
This active enhanced prospective surveillance study was undertaken because an earlier retrospective study concluded that the rate of viral meningitis across all pediatric and adult age groups had increased rapidly during a recent 10-year period in the United Kingdom and Ireland. Infants younger than 3 months of age were especially hard hit by enterovirus, which accounted in the earlier study for 92% of all viral meningitis cases in that age group. Dr. Kadambari and his coinvestigators decided to take a closer prospective look at the sub-3-month age group because it’s such an important time neurodevelopmentally.
During the 13-month period of June 2014 to June 2015, 710 patients younger than 90 days old were hospitalized for enterovirus or parechovirus meningitis across the United Kingdom and Republic of Ireland. Ninety-five percent were due to enterovirus. Only 6% of affected infants were born prematurely.
“One of the take-home messages for me from the study was that 12% of enterovirus cases and 23% of parechovirus meningitis cases required admission to an ICU setting,” the pediatrician observed.
Among the infants admitted to a pediatric ICU, half of those with enterovirus meningitis and all those with parechovirus meningitis required intubation and mechanical ventilation. One-fifth of the enterovirus meningitis patients in pediatric ICUs required inotropic support for cardiovascular stabilization, as did all young infants with parechovirus meningitis.
Among the 710 patients, the three most common clinical presenting features were fever, irritability, and reduced feeding, present in 85%, 66%, and 54%, respectively.
Upon physical examination, two noteworthy common findings were signs of shock, present in 27% of infants with enterovirus meningitis and 43% with parechovirus meningitis, and respiratory distress, seen in 12% and 26%, respectively.
None of the 710 infants had a secondary bacterial infection. “That has implications for antimicrobial stewardship programs,” according to Dr. Kadambari.
The majority of infants had a normal CSF WBC count and a normal-range C-reactive protein level.
“Raised inflammatory markers were not a common feature in our cohort,” he noted.
Two infants died: one of a massive pulmonary hemorrhage and the other as a result of septic shock. Of the remaining 708 patients, however, 699 (98.7%) were discharged without significant neurologic impairment. Seven infants with enterovirus meningitis and two with parechovirus meningitis were discharged with severe delay, including cases of fine motor and gross motor delay, visual abnormalities, and a single case of severe cardiac dysfunction requiring discharge on an ACE inhibitor.
This surveillance study was a collaboration between St. George’s University of London and Public Health England. Dr. Kadambari reported having no financial conflicts.
Future studies need to examine long-term neurodevelopmental outcomes in affected young infants out to age 24 months, he said.
MADRID – Ninety-five percent of cases of enterovirus and parechovirus meningitis in infants younger than 90 days old in the United Kingdom and Ireland were diagnosed through lumbar puncture and identification of the virus in the CSF by PCR, Seilesh Kadambari, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“We recommend that routine testing of CSF for enterovirus and parechovirus in febrile infants should be promoted, even in the absence of pleocytosis,” said Dr. Kadambari of John Radcliffe Hospital in Oxford, England.
This active enhanced prospective surveillance study was undertaken because an earlier retrospective study concluded that the rate of viral meningitis across all pediatric and adult age groups had increased rapidly during a recent 10-year period in the United Kingdom and Ireland. Infants younger than 3 months of age were especially hard hit by enterovirus, which accounted in the earlier study for 92% of all viral meningitis cases in that age group. Dr. Kadambari and his coinvestigators decided to take a closer prospective look at the sub-3-month age group because it’s such an important time neurodevelopmentally.
During the 13-month period of June 2014 to June 2015, 710 patients younger than 90 days old were hospitalized for enterovirus or parechovirus meningitis across the United Kingdom and Republic of Ireland. Ninety-five percent were due to enterovirus. Only 6% of affected infants were born prematurely.
“One of the take-home messages for me from the study was that 12% of enterovirus cases and 23% of parechovirus meningitis cases required admission to an ICU setting,” the pediatrician observed.
Among the infants admitted to a pediatric ICU, half of those with enterovirus meningitis and all those with parechovirus meningitis required intubation and mechanical ventilation. One-fifth of the enterovirus meningitis patients in pediatric ICUs required inotropic support for cardiovascular stabilization, as did all young infants with parechovirus meningitis.
Among the 710 patients, the three most common clinical presenting features were fever, irritability, and reduced feeding, present in 85%, 66%, and 54%, respectively.
Upon physical examination, two noteworthy common findings were signs of shock, present in 27% of infants with enterovirus meningitis and 43% with parechovirus meningitis, and respiratory distress, seen in 12% and 26%, respectively.
None of the 710 infants had a secondary bacterial infection. “That has implications for antimicrobial stewardship programs,” according to Dr. Kadambari.
The majority of infants had a normal CSF WBC count and a normal-range C-reactive protein level.
“Raised inflammatory markers were not a common feature in our cohort,” he noted.
Two infants died: one of a massive pulmonary hemorrhage and the other as a result of septic shock. Of the remaining 708 patients, however, 699 (98.7%) were discharged without significant neurologic impairment. Seven infants with enterovirus meningitis and two with parechovirus meningitis were discharged with severe delay, including cases of fine motor and gross motor delay, visual abnormalities, and a single case of severe cardiac dysfunction requiring discharge on an ACE inhibitor.
This surveillance study was a collaboration between St. George’s University of London and Public Health England. Dr. Kadambari reported having no financial conflicts.
Future studies need to examine long-term neurodevelopmental outcomes in affected young infants out to age 24 months, he said.
AT ESPID 2017
Key clinical point:
Major finding: More than 98% of infants in the United Kingdom and Ireland younger than 90 days old with enterovirus or parechovirus meningitis were discharged without significant neurologic impairment.
Data source: A prospective active enhanced surveillance study including all 710 infants younger than 90 days old hospitalized for enterovirus or parechovirus meningitis in the United Kingdom and Ireland in a 13-month period.
Disclosures: The study was jointly sponsored by Public Health England and St. George’s University of London. The presenter reported having no financial conflicts.
New monotherapy approved for partial-onset seizures
The U.S. Food and Drug Administration has approved perampanel (Fycompa) for monotherapy treatment of partial-onset seizures (POS) in patients aged 12 years or older as of July 27. It was approved in 2012 for adjunctive use for POS and primary, generalized tonic-clonic seizures in patients aged 12 years or older.
Three clinical trials showed improvement in seizure control for the patients with POS taking perampanel, compared with placebo.
The drug is available in tablets from 2 mg to 12 mg and as an oral suspension formulation. It is taken once daily.
“Approximately one-third of people living with epilepsy have seizures that are not adequately controlled,” said Robert T. Wechsler, MD, PhD, medical director of the Idaho Comprehensive Epilepsy Center, in Eisai’s press release. “Having a new monotherapy option for partial-onset seizures that is once a day gives physicians and patients an effective treatment option that has the potential to make a difference in patients’ lives.”
The U.S. Food and Drug Administration has approved perampanel (Fycompa) for monotherapy treatment of partial-onset seizures (POS) in patients aged 12 years or older as of July 27. It was approved in 2012 for adjunctive use for POS and primary, generalized tonic-clonic seizures in patients aged 12 years or older.
Three clinical trials showed improvement in seizure control for the patients with POS taking perampanel, compared with placebo.
The drug is available in tablets from 2 mg to 12 mg and as an oral suspension formulation. It is taken once daily.
“Approximately one-third of people living with epilepsy have seizures that are not adequately controlled,” said Robert T. Wechsler, MD, PhD, medical director of the Idaho Comprehensive Epilepsy Center, in Eisai’s press release. “Having a new monotherapy option for partial-onset seizures that is once a day gives physicians and patients an effective treatment option that has the potential to make a difference in patients’ lives.”
The U.S. Food and Drug Administration has approved perampanel (Fycompa) for monotherapy treatment of partial-onset seizures (POS) in patients aged 12 years or older as of July 27. It was approved in 2012 for adjunctive use for POS and primary, generalized tonic-clonic seizures in patients aged 12 years or older.
Three clinical trials showed improvement in seizure control for the patients with POS taking perampanel, compared with placebo.
The drug is available in tablets from 2 mg to 12 mg and as an oral suspension formulation. It is taken once daily.
“Approximately one-third of people living with epilepsy have seizures that are not adequately controlled,” said Robert T. Wechsler, MD, PhD, medical director of the Idaho Comprehensive Epilepsy Center, in Eisai’s press release. “Having a new monotherapy option for partial-onset seizures that is once a day gives physicians and patients an effective treatment option that has the potential to make a difference in patients’ lives.”
Senate sinks GOP health care reform effort
After casting the deciding vote to begin debate in the Senate on the Republican effort to repeal and replace the Affordable Care Act, Sen. John McCain (R-Ariz.) brought the effort to an end when he voted against the so-called “skinny repeal” bill introduced by Senate Majority Leader Mitch McConnell (R-Ky.).
Sen. McCain crossed the aisle with Sen. Susan Collins (R-Maine) and Sen. Lisa Murkowski (R-Alaska) and voted with the 48 members of the chamber’s Democratic caucus to kill the bill. Republicans would have needed 50 votes to pass the measure, with Vice President Mike Pence on hand to cast a tie-breaking vote if necessary. With three senators voting against the measure, however, the 49 votes were not enough.
In the early evening on July 27, however, Sen. McCain made it clear during a press conference that he would not vote for a skinny repeal. Other senators expressed concern over the skinny repeal but said they would vote for it if there were assurances that the House would actually go to conference committee (a procedure used when the House and Senate pass different versions of the same bill to allow a bipartisan group to find consensus and create a unified bill) and work out a final bill and not simply move the skinny repeal straight to the president’s desk.
Speaker of the House Paul Ryan (R-Wisc.) had issued a statement to that effect, but the House was laying a path to simply move any bill passed by the Senate, leaving it up in the air as to whether a conference committee would actually be created.
Despite a reported phone call from Speaker Ryan and conversations directly with Vice President Pence on the Senate floor, Sen. McCain ultimately could not be convinced to vote with the majority of Republicans.
“From the beginning, I have believed that Obamacare should be repealed and replaced with a solution that increases competition, lowers costs, and improves care for the American people,” Sen. McCain said in a statement issued July 28, following the early-morning vote. “The so-called ‘skinny repeal’ amendment the Senate voted on today would not accomplish those goals. While the amendment would have repealed some of Obamacare’s most burdensome regulations, it offered no replacement to actually reform our health care system and deliver affordable, quality health care to our citizens. The Speaker’s statement that the House would be ‘willing’ to go to conference does not ease my concern that this shell of a bill could be taken up and passed at any time.”
The vote brought to an end a few days of minimal activity. Every attempt by the GOP to pass some form of amendment to move the process forward – from the tweaked version of the Better Care Replacement Act to a straight repeal of the ACA – failed. Sen. Steve Daines (R-Mont.) even introduced a single-payer amendment, but that failed to get a single yes vote, with all 52 GOP members and five Democrats voting against it and the remaining 43 Democrats voting “present.”

Very few amendments were proposed, though one did get passed in the process that would have permanently repealed the so-called “Cadillac tax,” which levies a 40% tax on plans that exceed a certain value. That amendment passed along party lines by a 52-48 vote.
The future of the ACA and future reform efforts remain unclear at the moment. Following the vote, a defeated Majority Leader McConnell asked the minority party what plan they have to offer. Senate Minority Leader Charles E. Schumer (D-N.Y.) echoed Sen. McCain’s speech earlier in the week after the vote was cast to start the debate to return to regular and hammer out a bipartisan solution though the committee process.
Meanwhile, President Donald Trump advocated via Twitter to simply let the ACA continue to crumble and when it failed, then to work on a deal.
The American Medical Association called on Congress to continue its work on fixing the health care system. “While we are relieved that the Senate did not adopt legislation that would have harmed patients and critical safety net programs, the status quo is not acceptable,” AMA President David Barbe said in a statement. “We urge Congress to initiate a bipartisan effort to address shortcomings in the Affordable Care Act. The first priority should be to stabilize the individual marketplace to achieve the goal of providing access to quality, affordable health coverage for more Americans.”
After casting the deciding vote to begin debate in the Senate on the Republican effort to repeal and replace the Affordable Care Act, Sen. John McCain (R-Ariz.) brought the effort to an end when he voted against the so-called “skinny repeal” bill introduced by Senate Majority Leader Mitch McConnell (R-Ky.).
Sen. McCain crossed the aisle with Sen. Susan Collins (R-Maine) and Sen. Lisa Murkowski (R-Alaska) and voted with the 48 members of the chamber’s Democratic caucus to kill the bill. Republicans would have needed 50 votes to pass the measure, with Vice President Mike Pence on hand to cast a tie-breaking vote if necessary. With three senators voting against the measure, however, the 49 votes were not enough.
In the early evening on July 27, however, Sen. McCain made it clear during a press conference that he would not vote for a skinny repeal. Other senators expressed concern over the skinny repeal but said they would vote for it if there were assurances that the House would actually go to conference committee (a procedure used when the House and Senate pass different versions of the same bill to allow a bipartisan group to find consensus and create a unified bill) and work out a final bill and not simply move the skinny repeal straight to the president’s desk.
Speaker of the House Paul Ryan (R-Wisc.) had issued a statement to that effect, but the House was laying a path to simply move any bill passed by the Senate, leaving it up in the air as to whether a conference committee would actually be created.
Despite a reported phone call from Speaker Ryan and conversations directly with Vice President Pence on the Senate floor, Sen. McCain ultimately could not be convinced to vote with the majority of Republicans.
“From the beginning, I have believed that Obamacare should be repealed and replaced with a solution that increases competition, lowers costs, and improves care for the American people,” Sen. McCain said in a statement issued July 28, following the early-morning vote. “The so-called ‘skinny repeal’ amendment the Senate voted on today would not accomplish those goals. While the amendment would have repealed some of Obamacare’s most burdensome regulations, it offered no replacement to actually reform our health care system and deliver affordable, quality health care to our citizens. The Speaker’s statement that the House would be ‘willing’ to go to conference does not ease my concern that this shell of a bill could be taken up and passed at any time.”
The vote brought to an end a few days of minimal activity. Every attempt by the GOP to pass some form of amendment to move the process forward – from the tweaked version of the Better Care Replacement Act to a straight repeal of the ACA – failed. Sen. Steve Daines (R-Mont.) even introduced a single-payer amendment, but that failed to get a single yes vote, with all 52 GOP members and five Democrats voting against it and the remaining 43 Democrats voting “present.”
Very few amendments were proposed, though one did get passed in the process that would have permanently repealed the so-called “Cadillac tax,” which levies a 40% tax on plans that exceed a certain value. That amendment passed along party lines by a 52-48 vote.
The future of the ACA and future reform efforts remain unclear at the moment. Following the vote, a defeated Majority Leader McConnell asked the minority party what plan they have to offer. Senate Minority Leader Charles E. Schumer (D-N.Y.) echoed Sen. McCain’s speech earlier in the week after the vote was cast to start the debate to return to regular and hammer out a bipartisan solution though the committee process.
Meanwhile, President Donald Trump advocated via Twitter to simply let the ACA continue to crumble and when it failed, then to work on a deal.
The American Medical Association called on Congress to continue its work on fixing the health care system. “While we are relieved that the Senate did not adopt legislation that would have harmed patients and critical safety net programs, the status quo is not acceptable,” AMA President David Barbe said in a statement. “We urge Congress to initiate a bipartisan effort to address shortcomings in the Affordable Care Act. The first priority should be to stabilize the individual marketplace to achieve the goal of providing access to quality, affordable health coverage for more Americans.”
After casting the deciding vote to begin debate in the Senate on the Republican effort to repeal and replace the Affordable Care Act, Sen. John McCain (R-Ariz.) brought the effort to an end when he voted against the so-called “skinny repeal” bill introduced by Senate Majority Leader Mitch McConnell (R-Ky.).
Sen. McCain crossed the aisle with Sen. Susan Collins (R-Maine) and Sen. Lisa Murkowski (R-Alaska) and voted with the 48 members of the chamber’s Democratic caucus to kill the bill. Republicans would have needed 50 votes to pass the measure, with Vice President Mike Pence on hand to cast a tie-breaking vote if necessary. With three senators voting against the measure, however, the 49 votes were not enough.
In the early evening on July 27, however, Sen. McCain made it clear during a press conference that he would not vote for a skinny repeal. Other senators expressed concern over the skinny repeal but said they would vote for it if there were assurances that the House would actually go to conference committee (a procedure used when the House and Senate pass different versions of the same bill to allow a bipartisan group to find consensus and create a unified bill) and work out a final bill and not simply move the skinny repeal straight to the president’s desk.
Speaker of the House Paul Ryan (R-Wisc.) had issued a statement to that effect, but the House was laying a path to simply move any bill passed by the Senate, leaving it up in the air as to whether a conference committee would actually be created.
Despite a reported phone call from Speaker Ryan and conversations directly with Vice President Pence on the Senate floor, Sen. McCain ultimately could not be convinced to vote with the majority of Republicans.
“From the beginning, I have believed that Obamacare should be repealed and replaced with a solution that increases competition, lowers costs, and improves care for the American people,” Sen. McCain said in a statement issued July 28, following the early-morning vote. “The so-called ‘skinny repeal’ amendment the Senate voted on today would not accomplish those goals. While the amendment would have repealed some of Obamacare’s most burdensome regulations, it offered no replacement to actually reform our health care system and deliver affordable, quality health care to our citizens. The Speaker’s statement that the House would be ‘willing’ to go to conference does not ease my concern that this shell of a bill could be taken up and passed at any time.”
The vote brought to an end a few days of minimal activity. Every attempt by the GOP to pass some form of amendment to move the process forward – from the tweaked version of the Better Care Replacement Act to a straight repeal of the ACA – failed. Sen. Steve Daines (R-Mont.) even introduced a single-payer amendment, but that failed to get a single yes vote, with all 52 GOP members and five Democrats voting against it and the remaining 43 Democrats voting “present.”
Very few amendments were proposed, though one did get passed in the process that would have permanently repealed the so-called “Cadillac tax,” which levies a 40% tax on plans that exceed a certain value. That amendment passed along party lines by a 52-48 vote.
The future of the ACA and future reform efforts remain unclear at the moment. Following the vote, a defeated Majority Leader McConnell asked the minority party what plan they have to offer. Senate Minority Leader Charles E. Schumer (D-N.Y.) echoed Sen. McCain’s speech earlier in the week after the vote was cast to start the debate to return to regular and hammer out a bipartisan solution though the committee process.
Meanwhile, President Donald Trump advocated via Twitter to simply let the ACA continue to crumble and when it failed, then to work on a deal.
The American Medical Association called on Congress to continue its work on fixing the health care system. “While we are relieved that the Senate did not adopt legislation that would have harmed patients and critical safety net programs, the status quo is not acceptable,” AMA President David Barbe said in a statement. “We urge Congress to initiate a bipartisan effort to address shortcomings in the Affordable Care Act. The first priority should be to stabilize the individual marketplace to achieve the goal of providing access to quality, affordable health coverage for more Americans.”
Leonard Wood: Advocate of Military Preparedness
Unless you have been assigned to the post or the hospital, you have probably never heard of Leonard Wood. Leonard Wood arguably had the most distinguished military-government career of someone who did not become president. Wood was a Harvard-educated physician, pursued the Apache Chief Geronimo, received the Medal of Honor, was physician to 2 U.S. presidents, served as U.S. army chief of staff, was a successful military governor, ran for president, was a colleague of Walter Reed, and was commander-inarms for President Theodore Roosevelt.

Wood was born in 1860 to an established New England family; his father was a Union Army physician during the Civil War and was practicing on Cape Cod when he died unexpectedly in 1880. The family was left destitute, but Wood was able to continue his education when a wealthy family friend agreed to pay for him to attend Harvard Medical School, which at the time did not require any prior college. He graduated in 1883 and was selected for a prized internship at Boston City Hospital; however, he was dismissed for a rule violation that the program director later admitted was a mistake.
Unable to support himself in practice in Boston, Wood turned to the U.S. Army, a decision that would change his life. Assigned to Fort Huachuca in Arizona, Wood participated in the yearlong pursuit and final surrender of Geronimo; for his role he was awarded the Medal of Honor in 1898. His experiences in the wild and rugged terrain of the west triggered a legendary and lifelong pursuit of hard and stressful physical activity. Transferred to California, Wood met Louise Condit-Smith, ward of an associate justice of the U.S. Supreme Court. When they married in November 1890 in Washington, DC, the ceremony was attended by all of the Supreme Court justices.
In 1893 while assigned to Fort McPherson outside Atlanta, Wood, whose duties were not demanding, needed a physical outlet for his unbounded energies. He enrolled at Georgia Tech at age 33 to play football. He was eligible to play because he had not previously attended college. He scored 5 touchdowns, winning the game against rival University of Georgia.
Later, Wood was assigned to Washington, where he quickly became known and sought after as a physician. He served many of the political and military elite, including presidents Grover Cleveland and William McKinley. In 1897, he met Theodore Roosevelt, the 38-year-old assistant secretary of the U.S. Navy who shared his love of outdoor adventure and the military. They became fast friends/companions/competitors; Roosevelt wrote to a friend that he had found a “playmate.”
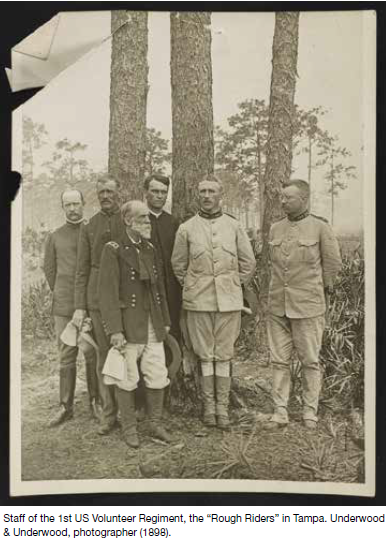
When the U.S.S. Maine was sunk in Havana Harbor in 1898 and war was declared on Spain, Wood and Roosevelt schemed on how to go to war together. Wood the career soldier and Roosevelt the career politician had excellent connections and became commander and deputy commander of the First Volunteer Calvary, later famously known as the Rough Riders. When a more senior general became ill, Wood was promoted to brigadier general, and Roosevelt became the regiment colonel.
After the war, Wood became military governor of Cuba and major general of volunteers. During the U.S. occupation, Walter Reed was sent to investigate infectious diseases, including yellow fever. Wood provided $10,000 to fund the second phase of Reed’s research and approved the use of human volunteers. When the U.S. occupation ended in 1902, Wood was to revert to captain, medical corps.
Wood’s success in Cuba was obvious and wel l known; President McKinley promoted him to U.S. Army brigadier general. At that time, as a brigadier general, Wood was essentially guaranteed a second star and a rotation through the chief of staff position. He served as chief of staff from 1910 to 1914, the only physician ever to do so. As chief of staff he eliminated the antiquated bureau system, developed the maneuver unit concept, and laid the groundwork for the Reserve Officers’ Training Corps.
Wood stayed on active duty and rotated through other senior-level positions. Because of Wood’s political activity promoting universal service and improving readiness, President Woodrow Wilson passed over him, instead selecting John J. Pershing to command the American Expeditionary Force in World War I. Wood stayed politically active and ran for the Republican presidential nomination in 1920, losing to Warren G. Harding at the convention. Wood was appointed governor general of the Philippines, a position he held until his death in 1927.
While in Cuba, Wood was severely injured by striking his head on a chandelier, most likely resulting in an undiagnosed skull fracture. Over time he developed neurologic symptoms and was seen by neurosurgeon Harvey Cushing, MD, at Johns Hopkins, who removed a meningioma in February 1910. Wood made a dramatic recovery. Over a decade later while in the Philippines, his symptoms returned, and after significant delay he went home to see Cushing who was then at Harvard Medical School. When Wood died after surgery, Cushing admitted that he should not have tackled such a difficult case so quickly after returning from a trip to Europe.
Fort Leonard Wood in Missouri and the on-base General Leonard Wood U.S. Army Community Hospital are named in Wood’s honor.
About this column
This column provides biographical sketches of the namesakes of military and VA health care facilities. To learn more about the individual
your facility was named for or to offer a topic suggestion, contact us at [email protected] or on Facebook.
Unless you have been assigned to the post or the hospital, you have probably never heard of Leonard Wood. Leonard Wood arguably had the most distinguished military-government career of someone who did not become president. Wood was a Harvard-educated physician, pursued the Apache Chief Geronimo, received the Medal of Honor, was physician to 2 U.S. presidents, served as U.S. army chief of staff, was a successful military governor, ran for president, was a colleague of Walter Reed, and was commander-inarms for President Theodore Roosevelt.
Wood was born in 1860 to an established New England family; his father was a Union Army physician during the Civil War and was practicing on Cape Cod when he died unexpectedly in 1880. The family was left destitute, but Wood was able to continue his education when a wealthy family friend agreed to pay for him to attend Harvard Medical School, which at the time did not require any prior college. He graduated in 1883 and was selected for a prized internship at Boston City Hospital; however, he was dismissed for a rule violation that the program director later admitted was a mistake.
Unable to support himself in practice in Boston, Wood turned to the U.S. Army, a decision that would change his life. Assigned to Fort Huachuca in Arizona, Wood participated in the yearlong pursuit and final surrender of Geronimo; for his role he was awarded the Medal of Honor in 1898. His experiences in the wild and rugged terrain of the west triggered a legendary and lifelong pursuit of hard and stressful physical activity. Transferred to California, Wood met Louise Condit-Smith, ward of an associate justice of the U.S. Supreme Court. When they married in November 1890 in Washington, DC, the ceremony was attended by all of the Supreme Court justices.
In 1893 while assigned to Fort McPherson outside Atlanta, Wood, whose duties were not demanding, needed a physical outlet for his unbounded energies. He enrolled at Georgia Tech at age 33 to play football. He was eligible to play because he had not previously attended college. He scored 5 touchdowns, winning the game against rival University of Georgia.
Later, Wood was assigned to Washington, where he quickly became known and sought after as a physician. He served many of the political and military elite, including presidents Grover Cleveland and William McKinley. In 1897, he met Theodore Roosevelt, the 38-year-old assistant secretary of the U.S. Navy who shared his love of outdoor adventure and the military. They became fast friends/companions/competitors; Roosevelt wrote to a friend that he had found a “playmate.”
When the U.S.S. Maine was sunk in Havana Harbor in 1898 and war was declared on Spain, Wood and Roosevelt schemed on how to go to war together. Wood the career soldier and Roosevelt the career politician had excellent connections and became commander and deputy commander of the First Volunteer Calvary, later famously known as the Rough Riders. When a more senior general became ill, Wood was promoted to brigadier general, and Roosevelt became the regiment colonel.
After the war, Wood became military governor of Cuba and major general of volunteers. During the U.S. occupation, Walter Reed was sent to investigate infectious diseases, including yellow fever. Wood provided $10,000 to fund the second phase of Reed’s research and approved the use of human volunteers. When the U.S. occupation ended in 1902, Wood was to revert to captain, medical corps.
Wood’s success in Cuba was obvious and wel l known; President McKinley promoted him to U.S. Army brigadier general. At that time, as a brigadier general, Wood was essentially guaranteed a second star and a rotation through the chief of staff position. He served as chief of staff from 1910 to 1914, the only physician ever to do so. As chief of staff he eliminated the antiquated bureau system, developed the maneuver unit concept, and laid the groundwork for the Reserve Officers’ Training Corps.
Wood stayed on active duty and rotated through other senior-level positions. Because of Wood’s political activity promoting universal service and improving readiness, President Woodrow Wilson passed over him, instead selecting John J. Pershing to command the American Expeditionary Force in World War I. Wood stayed politically active and ran for the Republican presidential nomination in 1920, losing to Warren G. Harding at the convention. Wood was appointed governor general of the Philippines, a position he held until his death in 1927.
While in Cuba, Wood was severely injured by striking his head on a chandelier, most likely resulting in an undiagnosed skull fracture. Over time he developed neurologic symptoms and was seen by neurosurgeon Harvey Cushing, MD, at Johns Hopkins, who removed a meningioma in February 1910. Wood made a dramatic recovery. Over a decade later while in the Philippines, his symptoms returned, and after significant delay he went home to see Cushing who was then at Harvard Medical School. When Wood died after surgery, Cushing admitted that he should not have tackled such a difficult case so quickly after returning from a trip to Europe.
Fort Leonard Wood in Missouri and the on-base General Leonard Wood U.S. Army Community Hospital are named in Wood’s honor.
About this column
This column provides biographical sketches of the namesakes of military and VA health care facilities. To learn more about the individual
your facility was named for or to offer a topic suggestion, contact us at [email protected] or on Facebook.
Unless you have been assigned to the post or the hospital, you have probably never heard of Leonard Wood. Leonard Wood arguably had the most distinguished military-government career of someone who did not become president. Wood was a Harvard-educated physician, pursued the Apache Chief Geronimo, received the Medal of Honor, was physician to 2 U.S. presidents, served as U.S. army chief of staff, was a successful military governor, ran for president, was a colleague of Walter Reed, and was commander-inarms for President Theodore Roosevelt.
Wood was born in 1860 to an established New England family; his father was a Union Army physician during the Civil War and was practicing on Cape Cod when he died unexpectedly in 1880. The family was left destitute, but Wood was able to continue his education when a wealthy family friend agreed to pay for him to attend Harvard Medical School, which at the time did not require any prior college. He graduated in 1883 and was selected for a prized internship at Boston City Hospital; however, he was dismissed for a rule violation that the program director later admitted was a mistake.
Unable to support himself in practice in Boston, Wood turned to the U.S. Army, a decision that would change his life. Assigned to Fort Huachuca in Arizona, Wood participated in the yearlong pursuit and final surrender of Geronimo; for his role he was awarded the Medal of Honor in 1898. His experiences in the wild and rugged terrain of the west triggered a legendary and lifelong pursuit of hard and stressful physical activity. Transferred to California, Wood met Louise Condit-Smith, ward of an associate justice of the U.S. Supreme Court. When they married in November 1890 in Washington, DC, the ceremony was attended by all of the Supreme Court justices.
In 1893 while assigned to Fort McPherson outside Atlanta, Wood, whose duties were not demanding, needed a physical outlet for his unbounded energies. He enrolled at Georgia Tech at age 33 to play football. He was eligible to play because he had not previously attended college. He scored 5 touchdowns, winning the game against rival University of Georgia.
Later, Wood was assigned to Washington, where he quickly became known and sought after as a physician. He served many of the political and military elite, including presidents Grover Cleveland and William McKinley. In 1897, he met Theodore Roosevelt, the 38-year-old assistant secretary of the U.S. Navy who shared his love of outdoor adventure and the military. They became fast friends/companions/competitors; Roosevelt wrote to a friend that he had found a “playmate.”
When the U.S.S. Maine was sunk in Havana Harbor in 1898 and war was declared on Spain, Wood and Roosevelt schemed on how to go to war together. Wood the career soldier and Roosevelt the career politician had excellent connections and became commander and deputy commander of the First Volunteer Calvary, later famously known as the Rough Riders. When a more senior general became ill, Wood was promoted to brigadier general, and Roosevelt became the regiment colonel.
After the war, Wood became military governor of Cuba and major general of volunteers. During the U.S. occupation, Walter Reed was sent to investigate infectious diseases, including yellow fever. Wood provided $10,000 to fund the second phase of Reed’s research and approved the use of human volunteers. When the U.S. occupation ended in 1902, Wood was to revert to captain, medical corps.
Wood’s success in Cuba was obvious and wel l known; President McKinley promoted him to U.S. Army brigadier general. At that time, as a brigadier general, Wood was essentially guaranteed a second star and a rotation through the chief of staff position. He served as chief of staff from 1910 to 1914, the only physician ever to do so. As chief of staff he eliminated the antiquated bureau system, developed the maneuver unit concept, and laid the groundwork for the Reserve Officers’ Training Corps.
Wood stayed on active duty and rotated through other senior-level positions. Because of Wood’s political activity promoting universal service and improving readiness, President Woodrow Wilson passed over him, instead selecting John J. Pershing to command the American Expeditionary Force in World War I. Wood stayed politically active and ran for the Republican presidential nomination in 1920, losing to Warren G. Harding at the convention. Wood was appointed governor general of the Philippines, a position he held until his death in 1927.
While in Cuba, Wood was severely injured by striking his head on a chandelier, most likely resulting in an undiagnosed skull fracture. Over time he developed neurologic symptoms and was seen by neurosurgeon Harvey Cushing, MD, at Johns Hopkins, who removed a meningioma in February 1910. Wood made a dramatic recovery. Over a decade later while in the Philippines, his symptoms returned, and after significant delay he went home to see Cushing who was then at Harvard Medical School. When Wood died after surgery, Cushing admitted that he should not have tackled such a difficult case so quickly after returning from a trip to Europe.
Fort Leonard Wood in Missouri and the on-base General Leonard Wood U.S. Army Community Hospital are named in Wood’s honor.
About this column
This column provides biographical sketches of the namesakes of military and VA health care facilities. To learn more about the individual
your facility was named for or to offer a topic suggestion, contact us at [email protected] or on Facebook.
CRISPR sheds light on dyskeratosis congenita
Gene editing has revealed how dyskeratosis congenita (DC) impairs the formation of blood cells, according to research published in Stem Cell Reports.
The discovery has opened up new lines of investigation into how to treat DC, which is characterized by shortened telomeres.
“Lengthening telomeres seems like a logical way to help these patients, but it could possibly come with its own set of problems,” said study author Luis F.Z. Batista, PhD, of the Washington University School of Medicine in St. Louis, Missouri.
“We would worry about encouraging cancer formation, for example, as high levels of the protein that lengthens telomeres—telomerase—are commonly found with cancer. But if we could find a way to block the signaling pathways that short telomeres activate—that specifically lead to the problems in blood cell formation—it could allow these patients to continue making blood cells.”
With this in mind, Dr Batista and his colleagues used CRISPR to edit into human embryonic stem cells a pair of mutations associated with DC— DKC1_A353V and TERT_P704S. These cells reproduced the telomere-shortening defect seen in patients with DC.
With this model, the researchers showed how the telomere defect leads to the gradual loss of blood cell formation and how blocking the downstream effects of the defect can reverse this loss, leading to normal production of blood cells.
Blocking this signaling pathway did not lengthen telomeres or stop their shortening, but it allowed the manufacturing of different types of blood cells to continue.
The researchers also made a discovery that provides a distinction regarding the detrimental effect of short telomeres during early development. The team found the defect did not hinder primitive hematopoiesis, but it did impair definitive hematopoiesis.
“This was tremendously interesting from a developmental biology perspective as well as from a disease modeling perspective,” said study author Christopher M. Sturgeon, PhD, of the Washington University School of Medicine. “We now have a platform to really dig deeper into understanding the mechanisms behind some forms of bone marrow failure.”
The researchers implicated high levels of the protein p53 as one of the signals that leads to the drop in definitive hematopoiesis.
“P53 is thought of as a guardian of the genome,” Dr Batista noted. “Mutations that disable p53 are associated with different types of cancer. Because of this, we would not consider directly trying to block p53 in these patients.”
“But what this study provides is proof-of-concept that this pathway is involved in this response. So we now are looking for ways to block the pathway further downstream without necessarily blocking p53 directly.”
Drs Batista and Sturgeon recently received a grant from the Department of Defense to investigate the pathway. The pair believes the strategy used in this study could be relevant for other bone marrow failure syndromes as well, such as Fanconi anemia and aplastic anemia. ![]()
Gene editing has revealed how dyskeratosis congenita (DC) impairs the formation of blood cells, according to research published in Stem Cell Reports.
The discovery has opened up new lines of investigation into how to treat DC, which is characterized by shortened telomeres.
“Lengthening telomeres seems like a logical way to help these patients, but it could possibly come with its own set of problems,” said study author Luis F.Z. Batista, PhD, of the Washington University School of Medicine in St. Louis, Missouri.
“We would worry about encouraging cancer formation, for example, as high levels of the protein that lengthens telomeres—telomerase—are commonly found with cancer. But if we could find a way to block the signaling pathways that short telomeres activate—that specifically lead to the problems in blood cell formation—it could allow these patients to continue making blood cells.”
With this in mind, Dr Batista and his colleagues used CRISPR to edit into human embryonic stem cells a pair of mutations associated with DC— DKC1_A353V and TERT_P704S. These cells reproduced the telomere-shortening defect seen in patients with DC.
With this model, the researchers showed how the telomere defect leads to the gradual loss of blood cell formation and how blocking the downstream effects of the defect can reverse this loss, leading to normal production of blood cells.
Blocking this signaling pathway did not lengthen telomeres or stop their shortening, but it allowed the manufacturing of different types of blood cells to continue.
The researchers also made a discovery that provides a distinction regarding the detrimental effect of short telomeres during early development. The team found the defect did not hinder primitive hematopoiesis, but it did impair definitive hematopoiesis.
“This was tremendously interesting from a developmental biology perspective as well as from a disease modeling perspective,” said study author Christopher M. Sturgeon, PhD, of the Washington University School of Medicine. “We now have a platform to really dig deeper into understanding the mechanisms behind some forms of bone marrow failure.”
The researchers implicated high levels of the protein p53 as one of the signals that leads to the drop in definitive hematopoiesis.
“P53 is thought of as a guardian of the genome,” Dr Batista noted. “Mutations that disable p53 are associated with different types of cancer. Because of this, we would not consider directly trying to block p53 in these patients.”
“But what this study provides is proof-of-concept that this pathway is involved in this response. So we now are looking for ways to block the pathway further downstream without necessarily blocking p53 directly.”
Drs Batista and Sturgeon recently received a grant from the Department of Defense to investigate the pathway. The pair believes the strategy used in this study could be relevant for other bone marrow failure syndromes as well, such as Fanconi anemia and aplastic anemia. ![]()
Gene editing has revealed how dyskeratosis congenita (DC) impairs the formation of blood cells, according to research published in Stem Cell Reports.
The discovery has opened up new lines of investigation into how to treat DC, which is characterized by shortened telomeres.
“Lengthening telomeres seems like a logical way to help these patients, but it could possibly come with its own set of problems,” said study author Luis F.Z. Batista, PhD, of the Washington University School of Medicine in St. Louis, Missouri.
“We would worry about encouraging cancer formation, for example, as high levels of the protein that lengthens telomeres—telomerase—are commonly found with cancer. But if we could find a way to block the signaling pathways that short telomeres activate—that specifically lead to the problems in blood cell formation—it could allow these patients to continue making blood cells.”
With this in mind, Dr Batista and his colleagues used CRISPR to edit into human embryonic stem cells a pair of mutations associated with DC— DKC1_A353V and TERT_P704S. These cells reproduced the telomere-shortening defect seen in patients with DC.
With this model, the researchers showed how the telomere defect leads to the gradual loss of blood cell formation and how blocking the downstream effects of the defect can reverse this loss, leading to normal production of blood cells.
Blocking this signaling pathway did not lengthen telomeres or stop their shortening, but it allowed the manufacturing of different types of blood cells to continue.
The researchers also made a discovery that provides a distinction regarding the detrimental effect of short telomeres during early development. The team found the defect did not hinder primitive hematopoiesis, but it did impair definitive hematopoiesis.
“This was tremendously interesting from a developmental biology perspective as well as from a disease modeling perspective,” said study author Christopher M. Sturgeon, PhD, of the Washington University School of Medicine. “We now have a platform to really dig deeper into understanding the mechanisms behind some forms of bone marrow failure.”
The researchers implicated high levels of the protein p53 as one of the signals that leads to the drop in definitive hematopoiesis.
“P53 is thought of as a guardian of the genome,” Dr Batista noted. “Mutations that disable p53 are associated with different types of cancer. Because of this, we would not consider directly trying to block p53 in these patients.”
“But what this study provides is proof-of-concept that this pathway is involved in this response. So we now are looking for ways to block the pathway further downstream without necessarily blocking p53 directly.”
Drs Batista and Sturgeon recently received a grant from the Department of Defense to investigate the pathway. The pair believes the strategy used in this study could be relevant for other bone marrow failure syndromes as well, such as Fanconi anemia and aplastic anemia. ![]()
Developing better mouse models

Researchers say they have developed a new approach to model human immune variation that overcomes the limitations of traditional mouse models.
With this approach, the team identified genetic markers that directly correlate with the outcome of inflammatory and malignant diseases in humans, including chronic lymphocytic leukemia and Burkitt lymphoma.
The findings suggest that accounting for immune diversity is critical to the success of predicting disease outcomes based on immune cell measurements.
The team reported these findings in Nature Communications.
Traditionally, researchers have relied on inbred mouse strains to gain insight into human diseases while reducing experimental noise.
“If you take a black, a brown, or a white mouse, each one will give you a different answer in the same assay,” said Klaus Ley, MD, of La Jolla Institute for Allergy and Immunology in California.
“For example, if you vaccinate them, their responses will be different, which creates a lot of experimental noise. However, when you think about patients, or even healthy people, we are all different.”
To mine those differences for information, the researchers embraced the experimental noise. Instead of analyzing a single inbred mouse strain, they turned to the hybrid mouse diversity panel (HDMP).
The HDMP is a panel of about 100 different inbred mouse strains that mirror the breadth of genetic and immunological diversity found in the human population.
The researchers studied the natural variation in the activation pattern of abdominal macrophages. Macrophages isolated from 83 different mouse strains from the HDMP were exposed to lipopolysaccharide (LPS), a major component of the outer wall of gram-negative bacteria.
“Fundamentally, when the immune system is confronted with gram-negative bacteria, it can deal with the situation in 2 ways—either it gets very angry and tries to kill the bacteria or it can wall them off in an attempt to live with it,” explained Dr Ley. “Both strategies carry a certain risk, but a long evolutionary history has ensured that mice and people can survive with either strategy.”
The LPS-induced reactions of the macrophages covered the whole spectrum—from very aggressive (LPS+) to very tolerant (LPS-), depending on the mouse strain.
Next, the researchers asked which genes were active during each type of response to identify gene signatures that correlated with LPS responsiveness.
The team then ran these gene signatures across various human gene expression data sets and discovered they strongly correlated with human disease outcomes.
For example, macrophages isolated from healthy joints were enriched in LPS-tolerant genes, whereas macrophages from rheumatoid arthritis patients were strongly skewed toward LPS-aggressive.
Since it was known that mice and people with the aggressive phenotype are better at fighting cancer, the researchers specifically asked whether the level of LPS responsiveness could predict tumor survival.
After analyzing data from 18,000 biopsies across 39 different tumor types, the team found the LPS+ gene signature strongly correlated with survival, while the LPS- signature correlated with cancer death.
The pattern was significant across many types of cancer, including chronic lymphocytic leukemia, Burkitt lymphoma, osteosarcoma, melanoma, and large-cell lung carcinoma. ![]()
Researchers say they have developed a new approach to model human immune variation that overcomes the limitations of traditional mouse models.
With this approach, the team identified genetic markers that directly correlate with the outcome of inflammatory and malignant diseases in humans, including chronic lymphocytic leukemia and Burkitt lymphoma.
The findings suggest that accounting for immune diversity is critical to the success of predicting disease outcomes based on immune cell measurements.
The team reported these findings in Nature Communications.
Traditionally, researchers have relied on inbred mouse strains to gain insight into human diseases while reducing experimental noise.
“If you take a black, a brown, or a white mouse, each one will give you a different answer in the same assay,” said Klaus Ley, MD, of La Jolla Institute for Allergy and Immunology in California.
“For example, if you vaccinate them, their responses will be different, which creates a lot of experimental noise. However, when you think about patients, or even healthy people, we are all different.”
To mine those differences for information, the researchers embraced the experimental noise. Instead of analyzing a single inbred mouse strain, they turned to the hybrid mouse diversity panel (HDMP).
The HDMP is a panel of about 100 different inbred mouse strains that mirror the breadth of genetic and immunological diversity found in the human population.
The researchers studied the natural variation in the activation pattern of abdominal macrophages. Macrophages isolated from 83 different mouse strains from the HDMP were exposed to lipopolysaccharide (LPS), a major component of the outer wall of gram-negative bacteria.
“Fundamentally, when the immune system is confronted with gram-negative bacteria, it can deal with the situation in 2 ways—either it gets very angry and tries to kill the bacteria or it can wall them off in an attempt to live with it,” explained Dr Ley. “Both strategies carry a certain risk, but a long evolutionary history has ensured that mice and people can survive with either strategy.”
The LPS-induced reactions of the macrophages covered the whole spectrum—from very aggressive (LPS+) to very tolerant (LPS-), depending on the mouse strain.
Next, the researchers asked which genes were active during each type of response to identify gene signatures that correlated with LPS responsiveness.
The team then ran these gene signatures across various human gene expression data sets and discovered they strongly correlated with human disease outcomes.
For example, macrophages isolated from healthy joints were enriched in LPS-tolerant genes, whereas macrophages from rheumatoid arthritis patients were strongly skewed toward LPS-aggressive.
Since it was known that mice and people with the aggressive phenotype are better at fighting cancer, the researchers specifically asked whether the level of LPS responsiveness could predict tumor survival.
After analyzing data from 18,000 biopsies across 39 different tumor types, the team found the LPS+ gene signature strongly correlated with survival, while the LPS- signature correlated with cancer death.
The pattern was significant across many types of cancer, including chronic lymphocytic leukemia, Burkitt lymphoma, osteosarcoma, melanoma, and large-cell lung carcinoma. ![]()
Researchers say they have developed a new approach to model human immune variation that overcomes the limitations of traditional mouse models.
With this approach, the team identified genetic markers that directly correlate with the outcome of inflammatory and malignant diseases in humans, including chronic lymphocytic leukemia and Burkitt lymphoma.
The findings suggest that accounting for immune diversity is critical to the success of predicting disease outcomes based on immune cell measurements.
The team reported these findings in Nature Communications.
Traditionally, researchers have relied on inbred mouse strains to gain insight into human diseases while reducing experimental noise.
“If you take a black, a brown, or a white mouse, each one will give you a different answer in the same assay,” said Klaus Ley, MD, of La Jolla Institute for Allergy and Immunology in California.
“For example, if you vaccinate them, their responses will be different, which creates a lot of experimental noise. However, when you think about patients, or even healthy people, we are all different.”
To mine those differences for information, the researchers embraced the experimental noise. Instead of analyzing a single inbred mouse strain, they turned to the hybrid mouse diversity panel (HDMP).
The HDMP is a panel of about 100 different inbred mouse strains that mirror the breadth of genetic and immunological diversity found in the human population.
The researchers studied the natural variation in the activation pattern of abdominal macrophages. Macrophages isolated from 83 different mouse strains from the HDMP were exposed to lipopolysaccharide (LPS), a major component of the outer wall of gram-negative bacteria.
“Fundamentally, when the immune system is confronted with gram-negative bacteria, it can deal with the situation in 2 ways—either it gets very angry and tries to kill the bacteria or it can wall them off in an attempt to live with it,” explained Dr Ley. “Both strategies carry a certain risk, but a long evolutionary history has ensured that mice and people can survive with either strategy.”
The LPS-induced reactions of the macrophages covered the whole spectrum—from very aggressive (LPS+) to very tolerant (LPS-), depending on the mouse strain.
Next, the researchers asked which genes were active during each type of response to identify gene signatures that correlated with LPS responsiveness.
The team then ran these gene signatures across various human gene expression data sets and discovered they strongly correlated with human disease outcomes.
For example, macrophages isolated from healthy joints were enriched in LPS-tolerant genes, whereas macrophages from rheumatoid arthritis patients were strongly skewed toward LPS-aggressive.
Since it was known that mice and people with the aggressive phenotype are better at fighting cancer, the researchers specifically asked whether the level of LPS responsiveness could predict tumor survival.
After analyzing data from 18,000 biopsies across 39 different tumor types, the team found the LPS+ gene signature strongly correlated with survival, while the LPS- signature correlated with cancer death.
The pattern was significant across many types of cancer, including chronic lymphocytic leukemia, Burkitt lymphoma, osteosarcoma, melanoma, and large-cell lung carcinoma. ![]()
Team makes ‘fundamental’ AML discovery

A newly identified pathway plays a “fundamental” role in acute myeloid leukemia (AML), according to researchers.
The team discovered that AML cells have a secretory pathway that leads to the production and release of the immune receptor Tim-3 and its ligand galectin-9, both of which prevent natural killer (NK) and other cytotoxic cells from killing the AML cells.
Vadim Sumbayev, PhD, of the University of Kent in the UK, and his colleagues recounted these findings in EBioMedicine.
The researchers found that AML cells—but not healthy blood cells—express a receptor called latrophilin 1 (LPHN1). LPHN1 induces activation of PKCα, which triggers the translation and secretion of Tim-3 and galectin-9.
Soluble Tim-3 prevents the secretion of interleukin 2, which is required for the activation of NK cells and cytotoxic T cells. Galectin-9 impairs the AML-cell-killing ability of NK cells and other cytotoxic lymphocytes.
The researchers said their work revealed both biomarkers for AML diagnostics and potential targets for AML treatment.
“Targeting this pathway will crucially enhance patients’ own immune defenses, helping them to eliminate leukemia cells,” Dr Sumbayev said.
He added that his group’s discovery might be applied to the treatment of other cancers as well. ![]()
A newly identified pathway plays a “fundamental” role in acute myeloid leukemia (AML), according to researchers.
The team discovered that AML cells have a secretory pathway that leads to the production and release of the immune receptor Tim-3 and its ligand galectin-9, both of which prevent natural killer (NK) and other cytotoxic cells from killing the AML cells.
Vadim Sumbayev, PhD, of the University of Kent in the UK, and his colleagues recounted these findings in EBioMedicine.
The researchers found that AML cells—but not healthy blood cells—express a receptor called latrophilin 1 (LPHN1). LPHN1 induces activation of PKCα, which triggers the translation and secretion of Tim-3 and galectin-9.
Soluble Tim-3 prevents the secretion of interleukin 2, which is required for the activation of NK cells and cytotoxic T cells. Galectin-9 impairs the AML-cell-killing ability of NK cells and other cytotoxic lymphocytes.
The researchers said their work revealed both biomarkers for AML diagnostics and potential targets for AML treatment.
“Targeting this pathway will crucially enhance patients’ own immune defenses, helping them to eliminate leukemia cells,” Dr Sumbayev said.
He added that his group’s discovery might be applied to the treatment of other cancers as well. ![]()
A newly identified pathway plays a “fundamental” role in acute myeloid leukemia (AML), according to researchers.
The team discovered that AML cells have a secretory pathway that leads to the production and release of the immune receptor Tim-3 and its ligand galectin-9, both of which prevent natural killer (NK) and other cytotoxic cells from killing the AML cells.
Vadim Sumbayev, PhD, of the University of Kent in the UK, and his colleagues recounted these findings in EBioMedicine.
The researchers found that AML cells—but not healthy blood cells—express a receptor called latrophilin 1 (LPHN1). LPHN1 induces activation of PKCα, which triggers the translation and secretion of Tim-3 and galectin-9.
Soluble Tim-3 prevents the secretion of interleukin 2, which is required for the activation of NK cells and cytotoxic T cells. Galectin-9 impairs the AML-cell-killing ability of NK cells and other cytotoxic lymphocytes.
The researchers said their work revealed both biomarkers for AML diagnostics and potential targets for AML treatment.
“Targeting this pathway will crucially enhance patients’ own immune defenses, helping them to eliminate leukemia cells,” Dr Sumbayev said.
He added that his group’s discovery might be applied to the treatment of other cancers as well. ![]()
PANS and PANDAS – A step forward?
In the Journal of Child and Adolescent Psychopharmacology’s July 2017 issue, a group of respected individuals representing diverse expertise published “guidelines” to support clinical management of pediatric acute-onset neuropsychiatric syndrome (PANS) and its subclass PANDAS (those associated with streptococcal infection). PANS represents an enigmatic clinical syndrome that includes abrupt onset of obsessive-compulsive disorder (OCD) or eating restriction in combination with anxiety, attention deficit, hyperkinesia, emotional lability, irritability, aggressive or oppositional behavior, or academic decline. Neurologic findings also may be present; these are most often motor or vocal tics, but choreiform movements of the finger (repetitive motions that are rapid, jerky, and involuntary), deteriorating penmanship, sleep disruptions, or urinary frequency also may be present. The clinical course most often is relapsing and remitting with overall improvement over months or years.
(J Child Adolesc Psychopharmacol. 2017 Apr 7. doi: 10.1089/cap.2016.0151).
Specific recommendations include:
1. Searching for a coexisting infectious etiology with history, exam, and appropriate laboratory testing (including ASO and ADB antibodies), and, when present, treating accordingly. Even in the absence of definitive evidence of GAS infection, they recommend an initial course of antimicrobial therapy such as that given to patients with rheumatic fever.
2. For children with PANDAS (PANS with either culture or serologic evidence of GAS), consider instituting long-term streptococcal prophylaxis. The data on its value is mixed; however, most studies find more than 40% (and as many as 75%) of exacerbations are associated with GAS, and at least one study reports a reduction in neuropsychiatric exacerbations in children on penicillin or azithromycin prophylaxis for a 1-year period. Such decisions should be individualized: In children with strong evidence of exacerbations linked to GAS, there was thought to be greater likelihood of benefit, while, in those with no evidence for prior GAS infection, the potential for benefit was thought to be insufficient to justify prophylaxis. Furthermore, the optimal duration of prophylaxis is unknown. The guidelines recommend up to 2 years, but individualization is appropriate since severe cases may warrant prolonged prophylaxis.
3. In children who present with PANDAS and a positive throat culture for GAS, follow-up should be the same as that given for rheumatic fever, with reculture at 2-7 days and retreatment if there is persistence of GAS.
4. Vigilance for GAS infection in family members is appropriate, including obtaining throat cultures from persons with pharyngitis and treating them promptly when results are positive.
5. When GAS infection is not identified, the clinician should search for alternative infectious agents, such as Mycoplasma pneumoniae (using polymerase chain reaction on throat or nasopharyngeal swab), influenza virus, or alternative infections such as sinusitis, and treat accordingly.
6. Children with PANS and PANDAS should be immunized according to Advisory Committee of Immunization Practices recommendations, which includes annual influenza immunization. The committee reported that symptom flares after immunization were uncommon, brief, and manageable with NSAIDs.
7. The committee suggested that optimization of serum vitamin D levels among children with PANS and PANDAS could be of benefit, despite limited evidence. The committee members recommended treating children with PANS/PANDAS with vitamin D3 as needed to maintain serum 25-hydroxy vitamin D levels above 30 ng/mL. No benefit for adenotonsillectomy was identified. The committee recommended that tonsillectomy and/or adenoidectomy should limited to those with traditional indications (sleep apnea, failure to thrive, and abnormally large tonsils, etc.). The committee also found no evidence to suggest that probiotics modulate this condition.
These guidelines come with an important caveat. They represent a practical clinical approach for the management of infection in the context of PANS or PANDAS and rely heavily on the clinical experience of the members of the PANS/PANDAS Consortium. They provide criteria for the retrospective diagnosis of GAS infection and recommend treatment of GAS in all patients with newly diagnosed PANS. The suggested guidelines are supported by limited data and recognize that further prospective study of the mechanistic link between infection and PANS, clarification of the risk factors for development of PANS, and definitive study of the risks and benefits of antimicrobial prophylaxis are needed.
The consortium also has published two accompanying guidelines that address psychiatric (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0145) and immunomodulatory management (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0148) in the same issue of the Journal of Child and Adolescent Psychopharmacology.
Proposed criteria for documenting GAS infection in PANS pediatric patients
- A rise in serial antibody level, regardless of rapid test or culture result. This definition does not require clinical pharyngitis.
- Acute pharyngitis with a positive GAS throat culture, with or without a rising antibody level.
- Pharyngitis with characteristic palatal petechiae.
- Pharyngitis with a characteristic scarlatiniform rash.
- Pharyngitis without a throat swab or serology, but intimate (usually household) exposure to a proven GAS case.
- Asymptomatic pharyngeal colonization documented after an intimate exposure.
- Asymptomatic pharyngeal colonization after a negative throat swab documented within the prior 3-4 months.
- Single ASO or ADB antibody level within 6 months after the initial onset of neuropsychiatric symptoms may be accepted as positive if it is more than 95th percentile, using the laboratory’s normal standard for children of comparable age, or provisionally ASO greater than or equal to 1:480 or ADB greater than or equal to 1:1280.
- Both ASO and ADB are elevated at more than 80% percentile for age in the same serum sample within 6 months after the initial onset of neuropsychiatric symptoms.
- Culture-documented streptococcal dermatitis.
Source: J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0151.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at [email protected].
In the Journal of Child and Adolescent Psychopharmacology’s July 2017 issue, a group of respected individuals representing diverse expertise published “guidelines” to support clinical management of pediatric acute-onset neuropsychiatric syndrome (PANS) and its subclass PANDAS (those associated with streptococcal infection). PANS represents an enigmatic clinical syndrome that includes abrupt onset of obsessive-compulsive disorder (OCD) or eating restriction in combination with anxiety, attention deficit, hyperkinesia, emotional lability, irritability, aggressive or oppositional behavior, or academic decline. Neurologic findings also may be present; these are most often motor or vocal tics, but choreiform movements of the finger (repetitive motions that are rapid, jerky, and involuntary), deteriorating penmanship, sleep disruptions, or urinary frequency also may be present. The clinical course most often is relapsing and remitting with overall improvement over months or years.
(J Child Adolesc Psychopharmacol. 2017 Apr 7. doi: 10.1089/cap.2016.0151).
Specific recommendations include:
1. Searching for a coexisting infectious etiology with history, exam, and appropriate laboratory testing (including ASO and ADB antibodies), and, when present, treating accordingly. Even in the absence of definitive evidence of GAS infection, they recommend an initial course of antimicrobial therapy such as that given to patients with rheumatic fever.
2. For children with PANDAS (PANS with either culture or serologic evidence of GAS), consider instituting long-term streptococcal prophylaxis. The data on its value is mixed; however, most studies find more than 40% (and as many as 75%) of exacerbations are associated with GAS, and at least one study reports a reduction in neuropsychiatric exacerbations in children on penicillin or azithromycin prophylaxis for a 1-year period. Such decisions should be individualized: In children with strong evidence of exacerbations linked to GAS, there was thought to be greater likelihood of benefit, while, in those with no evidence for prior GAS infection, the potential for benefit was thought to be insufficient to justify prophylaxis. Furthermore, the optimal duration of prophylaxis is unknown. The guidelines recommend up to 2 years, but individualization is appropriate since severe cases may warrant prolonged prophylaxis.
3. In children who present with PANDAS and a positive throat culture for GAS, follow-up should be the same as that given for rheumatic fever, with reculture at 2-7 days and retreatment if there is persistence of GAS.
4. Vigilance for GAS infection in family members is appropriate, including obtaining throat cultures from persons with pharyngitis and treating them promptly when results are positive.
5. When GAS infection is not identified, the clinician should search for alternative infectious agents, such as Mycoplasma pneumoniae (using polymerase chain reaction on throat or nasopharyngeal swab), influenza virus, or alternative infections such as sinusitis, and treat accordingly.
6. Children with PANS and PANDAS should be immunized according to Advisory Committee of Immunization Practices recommendations, which includes annual influenza immunization. The committee reported that symptom flares after immunization were uncommon, brief, and manageable with NSAIDs.
7. The committee suggested that optimization of serum vitamin D levels among children with PANS and PANDAS could be of benefit, despite limited evidence. The committee members recommended treating children with PANS/PANDAS with vitamin D3 as needed to maintain serum 25-hydroxy vitamin D levels above 30 ng/mL. No benefit for adenotonsillectomy was identified. The committee recommended that tonsillectomy and/or adenoidectomy should limited to those with traditional indications (sleep apnea, failure to thrive, and abnormally large tonsils, etc.). The committee also found no evidence to suggest that probiotics modulate this condition.
These guidelines come with an important caveat. They represent a practical clinical approach for the management of infection in the context of PANS or PANDAS and rely heavily on the clinical experience of the members of the PANS/PANDAS Consortium. They provide criteria for the retrospective diagnosis of GAS infection and recommend treatment of GAS in all patients with newly diagnosed PANS. The suggested guidelines are supported by limited data and recognize that further prospective study of the mechanistic link between infection and PANS, clarification of the risk factors for development of PANS, and definitive study of the risks and benefits of antimicrobial prophylaxis are needed.
The consortium also has published two accompanying guidelines that address psychiatric (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0145) and immunomodulatory management (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0148) in the same issue of the Journal of Child and Adolescent Psychopharmacology.
Proposed criteria for documenting GAS infection in PANS pediatric patients
- A rise in serial antibody level, regardless of rapid test or culture result. This definition does not require clinical pharyngitis.
- Acute pharyngitis with a positive GAS throat culture, with or without a rising antibody level.
- Pharyngitis with characteristic palatal petechiae.
- Pharyngitis with a characteristic scarlatiniform rash.
- Pharyngitis without a throat swab or serology, but intimate (usually household) exposure to a proven GAS case.
- Asymptomatic pharyngeal colonization documented after an intimate exposure.
- Asymptomatic pharyngeal colonization after a negative throat swab documented within the prior 3-4 months.
- Single ASO or ADB antibody level within 6 months after the initial onset of neuropsychiatric symptoms may be accepted as positive if it is more than 95th percentile, using the laboratory’s normal standard for children of comparable age, or provisionally ASO greater than or equal to 1:480 or ADB greater than or equal to 1:1280.
- Both ASO and ADB are elevated at more than 80% percentile for age in the same serum sample within 6 months after the initial onset of neuropsychiatric symptoms.
- Culture-documented streptococcal dermatitis.
Source: J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0151.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at [email protected].
In the Journal of Child and Adolescent Psychopharmacology’s July 2017 issue, a group of respected individuals representing diverse expertise published “guidelines” to support clinical management of pediatric acute-onset neuropsychiatric syndrome (PANS) and its subclass PANDAS (those associated with streptococcal infection). PANS represents an enigmatic clinical syndrome that includes abrupt onset of obsessive-compulsive disorder (OCD) or eating restriction in combination with anxiety, attention deficit, hyperkinesia, emotional lability, irritability, aggressive or oppositional behavior, or academic decline. Neurologic findings also may be present; these are most often motor or vocal tics, but choreiform movements of the finger (repetitive motions that are rapid, jerky, and involuntary), deteriorating penmanship, sleep disruptions, or urinary frequency also may be present. The clinical course most often is relapsing and remitting with overall improvement over months or years.
(J Child Adolesc Psychopharmacol. 2017 Apr 7. doi: 10.1089/cap.2016.0151).
Specific recommendations include:
1. Searching for a coexisting infectious etiology with history, exam, and appropriate laboratory testing (including ASO and ADB antibodies), and, when present, treating accordingly. Even in the absence of definitive evidence of GAS infection, they recommend an initial course of antimicrobial therapy such as that given to patients with rheumatic fever.
2. For children with PANDAS (PANS with either culture or serologic evidence of GAS), consider instituting long-term streptococcal prophylaxis. The data on its value is mixed; however, most studies find more than 40% (and as many as 75%) of exacerbations are associated with GAS, and at least one study reports a reduction in neuropsychiatric exacerbations in children on penicillin or azithromycin prophylaxis for a 1-year period. Such decisions should be individualized: In children with strong evidence of exacerbations linked to GAS, there was thought to be greater likelihood of benefit, while, in those with no evidence for prior GAS infection, the potential for benefit was thought to be insufficient to justify prophylaxis. Furthermore, the optimal duration of prophylaxis is unknown. The guidelines recommend up to 2 years, but individualization is appropriate since severe cases may warrant prolonged prophylaxis.
3. In children who present with PANDAS and a positive throat culture for GAS, follow-up should be the same as that given for rheumatic fever, with reculture at 2-7 days and retreatment if there is persistence of GAS.
4. Vigilance for GAS infection in family members is appropriate, including obtaining throat cultures from persons with pharyngitis and treating them promptly when results are positive.
5. When GAS infection is not identified, the clinician should search for alternative infectious agents, such as Mycoplasma pneumoniae (using polymerase chain reaction on throat or nasopharyngeal swab), influenza virus, or alternative infections such as sinusitis, and treat accordingly.
6. Children with PANS and PANDAS should be immunized according to Advisory Committee of Immunization Practices recommendations, which includes annual influenza immunization. The committee reported that symptom flares after immunization were uncommon, brief, and manageable with NSAIDs.
7. The committee suggested that optimization of serum vitamin D levels among children with PANS and PANDAS could be of benefit, despite limited evidence. The committee members recommended treating children with PANS/PANDAS with vitamin D3 as needed to maintain serum 25-hydroxy vitamin D levels above 30 ng/mL. No benefit for adenotonsillectomy was identified. The committee recommended that tonsillectomy and/or adenoidectomy should limited to those with traditional indications (sleep apnea, failure to thrive, and abnormally large tonsils, etc.). The committee also found no evidence to suggest that probiotics modulate this condition.
These guidelines come with an important caveat. They represent a practical clinical approach for the management of infection in the context of PANS or PANDAS and rely heavily on the clinical experience of the members of the PANS/PANDAS Consortium. They provide criteria for the retrospective diagnosis of GAS infection and recommend treatment of GAS in all patients with newly diagnosed PANS. The suggested guidelines are supported by limited data and recognize that further prospective study of the mechanistic link between infection and PANS, clarification of the risk factors for development of PANS, and definitive study of the risks and benefits of antimicrobial prophylaxis are needed.
The consortium also has published two accompanying guidelines that address psychiatric (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0145) and immunomodulatory management (J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0148) in the same issue of the Journal of Child and Adolescent Psychopharmacology.
Proposed criteria for documenting GAS infection in PANS pediatric patients
- A rise in serial antibody level, regardless of rapid test or culture result. This definition does not require clinical pharyngitis.
- Acute pharyngitis with a positive GAS throat culture, with or without a rising antibody level.
- Pharyngitis with characteristic palatal petechiae.
- Pharyngitis with a characteristic scarlatiniform rash.
- Pharyngitis without a throat swab or serology, but intimate (usually household) exposure to a proven GAS case.
- Asymptomatic pharyngeal colonization documented after an intimate exposure.
- Asymptomatic pharyngeal colonization after a negative throat swab documented within the prior 3-4 months.
- Single ASO or ADB antibody level within 6 months after the initial onset of neuropsychiatric symptoms may be accepted as positive if it is more than 95th percentile, using the laboratory’s normal standard for children of comparable age, or provisionally ASO greater than or equal to 1:480 or ADB greater than or equal to 1:1280.
- Both ASO and ADB are elevated at more than 80% percentile for age in the same serum sample within 6 months after the initial onset of neuropsychiatric symptoms.
- Culture-documented streptococcal dermatitis.
Source: J Child Adolesc Psychopharmacol. 2017. doi: 10.1089/cap.2016.0151.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. Dr. Pelton said he had no relevant financial disclosures. Email him at [email protected].
Disease-Modifying Drug Treatment Before, During, and After Pregnancy in Women With MS
NEW ORLEANS—In a population of women with multiple sclerosis (MS) and a live birth, the rate of disease-modifying drug treatment decreased before and during pregnancy and increased steadily post partum, according to a report presented at the 31st Annual Meeting of the Consortium of MS Centers. In a separate analysis by the same researchers, they reported that less than one-third of women with MS and a live birth initiated a disease-modifying treatment within one year after delivery. “The rate of disease-modifying drug initiation increased with the number of relapses the patient experienced prior to pregnancy,” said Maria K. Houtchens, MD, on behalf of her research collaborators. Dr. Houtchens is an Assistant Professor in the Department of Neurology at Harvard Medical School and Director of the Women’s Health Program at the Partners MS Center at Brigham and Women’s Hospital in Boston.

Treatment Before, During, and After Pregnancy
To evaluate treatment patterns before, during, and after pregnancy in women with MS and a live birth, Dr. Houtchens and colleagues used a US administrative claims database to conduct a retrospective analysis of women ages 18 to 65 with MS, a claim indicative of a live birth, and one-year continuous eligibility before and after pregnancy in the IMS Health Real World Data Adjudicated Claims US database from January 1, 2006, to June 30, 2015. Disease-modifying drug treatment was evaluated during the year prior to pregnancy (at three-month intervals), the three trimesters of pregnancy, puerperium (six weeks post pregnancy), and one year post pregnancy (seven to 12 weeks post pregnancy and three to six, six to nine, and nine to 12 months post pregnancy). The researchers evaluated the proportion of women exposed to disease-modifying drug treatment during the 12 time periods. Results were also stratified by the number of relapses women experienced in the year prior to pregnancy.
Of 190,475 women with MS, 2,158 met eligibility criteria. Mean age was 30.26. Most women had commercial health insurance (98%) and were from the Midwest (32%), South (30%), or Northeast (29%) regions of the US.
The proportion of women with MS and a live birth treated with any disease-modifying drug was 20.48% at nine to 12 months pre-pregnancy, 21.46% at six to nine months pre-pregnancy, 20.62% at three to six months pre-pregnancy, and 17.75% at three months pre-pregnancy. During pregnancy, the proportion of women treated with a disease-modifying drug decreased to 12.05% during the first trimester and 1.90% during the second trimester, and then increased slightly to 2.97% during the third trimester. The proportion of women treated with disease-modifying drugs increased to 8.34% during puerperium, 12.93% during seven to 12 weeks post partum, 21.97% during three to six months post partum, 24.47% during six to nine months post partum, and 25.49% during nine to 12 months post partum. The majority of women (81.9%) had received disease-modifying drug treatment by six to nine months post partum. The proportion of women with disease-modifying drug treatment before and after pregnancy increased numerically with the number of relapses experienced before pregnancy.
Treatment After a Live Birth
In a separate analysis using the same cohort, Dr. Houtchens and colleagues looked closer at the time to initiation of disease-modifying drug treatment after a live birth in women with MS. Of the 2,094 women included in this analysis, the proportion with a live birth initiating a disease-modifying drug treatment within one year was 28.46%, and the proportion with no disease-modifying treatment within one year was 71.54%.
For those initiating a disease-modifying treatment within one year, mean time from live birth to first treatment was 118.98 days, and median time to first treatment was 93.50 days. A total of 16.11% received a disease-modifying drug less than 30 days after live birth, approximately half initiated a treatment within 90 days (47.82%), and three-quarters initiated a disease-modifying drug within six months (75.5%). The proportion of patients initiating treatment within one year after live birth increased with higher numbers of pre-pregnancy relapses (zero relapses, n = 441, 24.53%; one relapse, n = 108, 50.94%; two relapses, n = 33, 54.10%; three or more relapses, n = 14, 60.87%). The mean number of days until disease-modifying drug initiation for those receiving
This study was supported by EMD Serono.
NEW ORLEANS—In a population of women with multiple sclerosis (MS) and a live birth, the rate of disease-modifying drug treatment decreased before and during pregnancy and increased steadily post partum, according to a report presented at the 31st Annual Meeting of the Consortium of MS Centers. In a separate analysis by the same researchers, they reported that less than one-third of women with MS and a live birth initiated a disease-modifying treatment within one year after delivery. “The rate of disease-modifying drug initiation increased with the number of relapses the patient experienced prior to pregnancy,” said Maria K. Houtchens, MD, on behalf of her research collaborators. Dr. Houtchens is an Assistant Professor in the Department of Neurology at Harvard Medical School and Director of the Women’s Health Program at the Partners MS Center at Brigham and Women’s Hospital in Boston.
Treatment Before, During, and After Pregnancy
To evaluate treatment patterns before, during, and after pregnancy in women with MS and a live birth, Dr. Houtchens and colleagues used a US administrative claims database to conduct a retrospective analysis of women ages 18 to 65 with MS, a claim indicative of a live birth, and one-year continuous eligibility before and after pregnancy in the IMS Health Real World Data Adjudicated Claims US database from January 1, 2006, to June 30, 2015. Disease-modifying drug treatment was evaluated during the year prior to pregnancy (at three-month intervals), the three trimesters of pregnancy, puerperium (six weeks post pregnancy), and one year post pregnancy (seven to 12 weeks post pregnancy and three to six, six to nine, and nine to 12 months post pregnancy). The researchers evaluated the proportion of women exposed to disease-modifying drug treatment during the 12 time periods. Results were also stratified by the number of relapses women experienced in the year prior to pregnancy.
Of 190,475 women with MS, 2,158 met eligibility criteria. Mean age was 30.26. Most women had commercial health insurance (98%) and were from the Midwest (32%), South (30%), or Northeast (29%) regions of the US.
The proportion of women with MS and a live birth treated with any disease-modifying drug was 20.48% at nine to 12 months pre-pregnancy, 21.46% at six to nine months pre-pregnancy, 20.62% at three to six months pre-pregnancy, and 17.75% at three months pre-pregnancy. During pregnancy, the proportion of women treated with a disease-modifying drug decreased to 12.05% during the first trimester and 1.90% during the second trimester, and then increased slightly to 2.97% during the third trimester. The proportion of women treated with disease-modifying drugs increased to 8.34% during puerperium, 12.93% during seven to 12 weeks post partum, 21.97% during three to six months post partum, 24.47% during six to nine months post partum, and 25.49% during nine to 12 months post partum. The majority of women (81.9%) had received disease-modifying drug treatment by six to nine months post partum. The proportion of women with disease-modifying drug treatment before and after pregnancy increased numerically with the number of relapses experienced before pregnancy.
Treatment After a Live Birth
In a separate analysis using the same cohort, Dr. Houtchens and colleagues looked closer at the time to initiation of disease-modifying drug treatment after a live birth in women with MS. Of the 2,094 women included in this analysis, the proportion with a live birth initiating a disease-modifying drug treatment within one year was 28.46%, and the proportion with no disease-modifying treatment within one year was 71.54%.
For those initiating a disease-modifying treatment within one year, mean time from live birth to first treatment was 118.98 days, and median time to first treatment was 93.50 days. A total of 16.11% received a disease-modifying drug less than 30 days after live birth, approximately half initiated a treatment within 90 days (47.82%), and three-quarters initiated a disease-modifying drug within six months (75.5%). The proportion of patients initiating treatment within one year after live birth increased with higher numbers of pre-pregnancy relapses (zero relapses, n = 441, 24.53%; one relapse, n = 108, 50.94%; two relapses, n = 33, 54.10%; three or more relapses, n = 14, 60.87%). The mean number of days until disease-modifying drug initiation for those receiving
This study was supported by EMD Serono.
NEW ORLEANS—In a population of women with multiple sclerosis (MS) and a live birth, the rate of disease-modifying drug treatment decreased before and during pregnancy and increased steadily post partum, according to a report presented at the 31st Annual Meeting of the Consortium of MS Centers. In a separate analysis by the same researchers, they reported that less than one-third of women with MS and a live birth initiated a disease-modifying treatment within one year after delivery. “The rate of disease-modifying drug initiation increased with the number of relapses the patient experienced prior to pregnancy,” said Maria K. Houtchens, MD, on behalf of her research collaborators. Dr. Houtchens is an Assistant Professor in the Department of Neurology at Harvard Medical School and Director of the Women’s Health Program at the Partners MS Center at Brigham and Women’s Hospital in Boston.
Treatment Before, During, and After Pregnancy
To evaluate treatment patterns before, during, and after pregnancy in women with MS and a live birth, Dr. Houtchens and colleagues used a US administrative claims database to conduct a retrospective analysis of women ages 18 to 65 with MS, a claim indicative of a live birth, and one-year continuous eligibility before and after pregnancy in the IMS Health Real World Data Adjudicated Claims US database from January 1, 2006, to June 30, 2015. Disease-modifying drug treatment was evaluated during the year prior to pregnancy (at three-month intervals), the three trimesters of pregnancy, puerperium (six weeks post pregnancy), and one year post pregnancy (seven to 12 weeks post pregnancy and three to six, six to nine, and nine to 12 months post pregnancy). The researchers evaluated the proportion of women exposed to disease-modifying drug treatment during the 12 time periods. Results were also stratified by the number of relapses women experienced in the year prior to pregnancy.
Of 190,475 women with MS, 2,158 met eligibility criteria. Mean age was 30.26. Most women had commercial health insurance (98%) and were from the Midwest (32%), South (30%), or Northeast (29%) regions of the US.
The proportion of women with MS and a live birth treated with any disease-modifying drug was 20.48% at nine to 12 months pre-pregnancy, 21.46% at six to nine months pre-pregnancy, 20.62% at three to six months pre-pregnancy, and 17.75% at three months pre-pregnancy. During pregnancy, the proportion of women treated with a disease-modifying drug decreased to 12.05% during the first trimester and 1.90% during the second trimester, and then increased slightly to 2.97% during the third trimester. The proportion of women treated with disease-modifying drugs increased to 8.34% during puerperium, 12.93% during seven to 12 weeks post partum, 21.97% during three to six months post partum, 24.47% during six to nine months post partum, and 25.49% during nine to 12 months post partum. The majority of women (81.9%) had received disease-modifying drug treatment by six to nine months post partum. The proportion of women with disease-modifying drug treatment before and after pregnancy increased numerically with the number of relapses experienced before pregnancy.
Treatment After a Live Birth
In a separate analysis using the same cohort, Dr. Houtchens and colleagues looked closer at the time to initiation of disease-modifying drug treatment after a live birth in women with MS. Of the 2,094 women included in this analysis, the proportion with a live birth initiating a disease-modifying drug treatment within one year was 28.46%, and the proportion with no disease-modifying treatment within one year was 71.54%.
For those initiating a disease-modifying treatment within one year, mean time from live birth to first treatment was 118.98 days, and median time to first treatment was 93.50 days. A total of 16.11% received a disease-modifying drug less than 30 days after live birth, approximately half initiated a treatment within 90 days (47.82%), and three-quarters initiated a disease-modifying drug within six months (75.5%). The proportion of patients initiating treatment within one year after live birth increased with higher numbers of pre-pregnancy relapses (zero relapses, n = 441, 24.53%; one relapse, n = 108, 50.94%; two relapses, n = 33, 54.10%; three or more relapses, n = 14, 60.87%). The mean number of days until disease-modifying drug initiation for those receiving
This study was supported by EMD Serono.
A shot in the arm: Boost your knowledge about immunizations for psychiatric patients
Patients with chronic, severe mental illness live much shorter lives than the general population. The 25-year loss in life expectancy for people with chronic mental illness has been attributed to higher rates of cardiovascular disease driven by increased smoking, obesity, poverty, and poor nutrition.1 These individuals also face the added burden of struggling with a psychiatric condition that often interferes with their ability to make optimal preventative health decisions, including staying up to date on vaccinations.2 A recent review from Toronto, Canada, found that the influenza vaccination rates among homeless adults with mental illness—a population at high risk of respiratory illness—was only 6.7% compared with 31.1% for the general population of Ontario.3
Mental health professionals may serve as the only contacts to offer medical care to this vulnerable population, leading some psychiatric leaders to advocate that psychiatrists be considered primary care providers within accountable care organizations. Because most vaccines are easily available, mental health professionals should know about key immunizations to guide their patients accordingly.
In the United States, approximately 45,000 adults die annually from vaccine-preventable diseases, the majority from influenza.4 When combined with the most recent Adult Immunization Schedule and general recommendations adapted from the CDC,5,6 the mnemonic ARM SHOT allows for a quick assessment of risk factors to guide administration and education about most vaccinations (Table 1). ARM SHOT involves assessing the following components of an individual’s health status and living arrangements to determine one’s risk of contracting communicable diseases:
- Age
- Risk of exposure
- Medical conditions (comorbidities)
- Substance use history
- HIV status or other immunocompromised states
- Occupancy, or living arrangements
- Tobacco use.

We recommend keeping a copy of the Adult Immunization Schedule (age ≥19) and/or the immunization schedule for children and adolescents (age ≤18) close for quick reference. Here, we provide a case and then explore how each component of the ARM SHOT mnemonic applies in decision-making.
Case Evaluating risk, assess needs
Ms. W, age 24, has bipolar I disorder, most recently manic with psychotic features. She presents for follow-up in clinic after a 5-day hospitalization for mania and comorbid alcohol use disorder. Her medical comorbidities include asthma and active tobacco use. She is taking lurasidone, 20 mg/d, and lithium, 900 mg/d. Her case manager is working to place Ms. W in a residential substance use disorder treatment program. Ms. W is on a waiting list to establish care with a primary care physician and has a history of poor engagement with medical services in general; prior attempts to place her with a primary care physician failed.
In advance of Ms. W’s transfer to a residential treatment facility, you have been asked to place a Mantoux screening test for tuberculosis (purified protein derivative), which raises the important question about her susceptibility to infectious diseases in general. To protect Ms. W from preventable diseases for which vaccines are available, you review the ARM SHOT mnemonic to broadly assess her candidacy for vaccinations.
Age
Age may be the most important determinant of a patient’s need for vaccination (Table 2). The CDC immunization schedules account for age-specific risks for diseases, complications, and responses to vaccination (Figure 1).6
Influenza vaccination. Adults can have an intramuscular or intradermal inactivated influenza vaccination yearly in the fall or winter, unless they have an allergy to a vaccine component such as egg protein. Those with such an allergy can receive a recombinant influenza vaccine. Until the 2016 to 2017 flu season, an intranasal mist of live, attenuated influenza vaccine was available to healthy, non-pregnant women, ages 2 to 49, without high-risk medical conditions. However, the CDC dropped its recommendation for this vaccine because data showed it did not effectively prevent the flu.7 Individuals age ≥65 can receive either the standard- or high-dose inactivated influenza vaccination. The latter contains 4 times the amount of antigen with the intention of triggering a stronger immune response in older adults.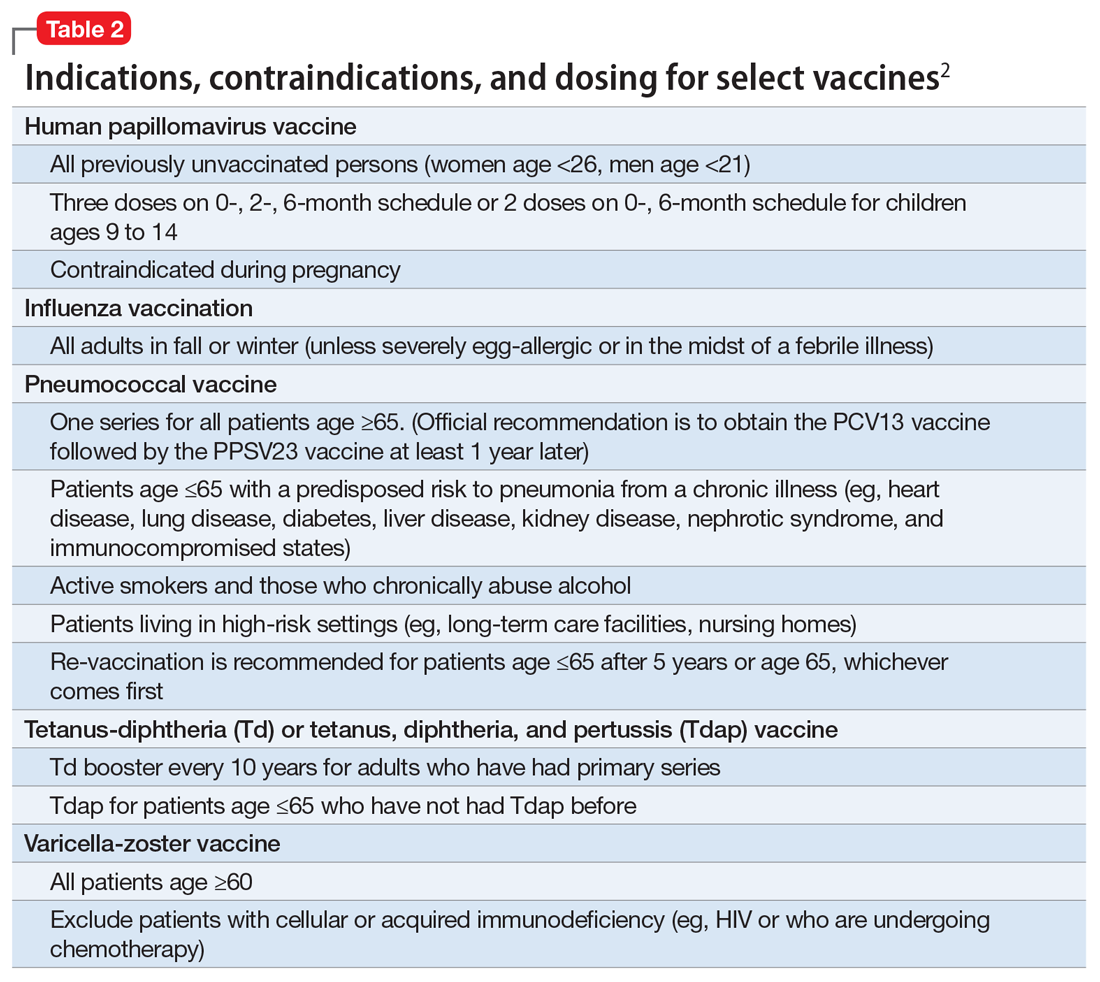
Pneumonia immunization. All patients age ≥65 should receive vaccinations for Streptococcus pneumoniae and its variants in the form of one 13-valent pneumococcal conjugate vaccine and, at least 1 year later, one 23-valent pneumococcal polysaccharide vaccine (PPSV23). Immunization reduces the morbidity and mortality from pneumococcal illness by decreasing the burden of a pneumonia, bacteremia, or meningitis infection. Adults, ages 19 to 64, with a chronic disease (referred to as “special populations” in CDC tables), such as diabetes, heart or lung disease, alcoholism, or cirrhosis, or those who smoke cigarettes, should receive PPSV23 with a second dose administered at least 5 years after the first. The CDC recommends a 1-time re-vaccination at age 65 for patients if >5 years have passed since the last PPSV23 and if the patient was younger than age 65 at the time of primary vaccine for S. pneumoniae. This can be a rather tricky clinical situation; the health care provider should verify a patient’s immunization history to ensure that she (he) is receiving only necessary vaccines. However, when the history cannot be verified, err on the side of inclusion, because risks are minimal.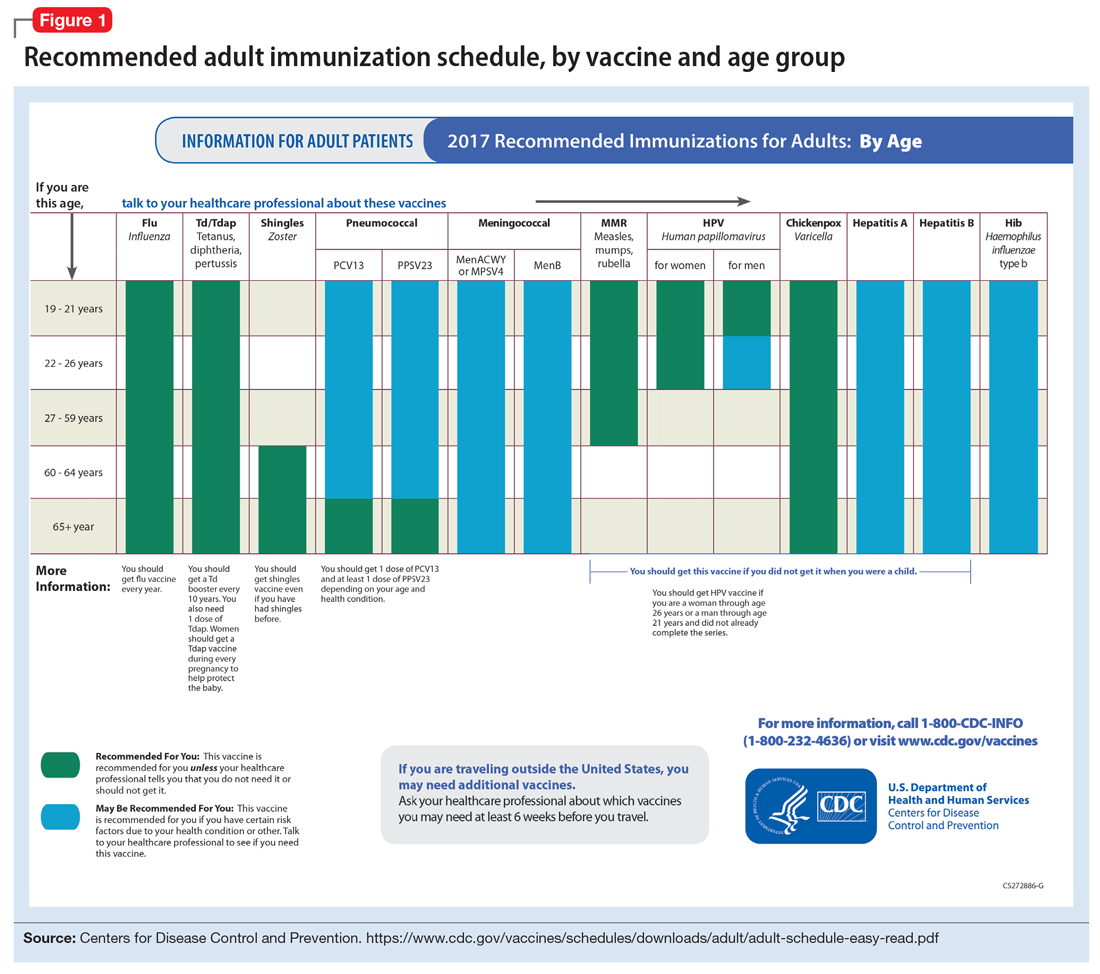
Shingles vaccination. Adults age ≥60 who are not immunocompromised should receive a single dose of live attenuated vaccine from varicella-zoster virus (VZV) to limit the risk of shingles from a prior chickenpox infection. The vaccine is approximately 66.5% effective at preventing postherpetic neuralgia for up to 4.9 years. Individuals as young as age 50 may have the vaccine because the risk of herpes zoster radically increases from then on,8 although most insurers only cover VZV vaccination after age 60.
Tetanus, diphtheria, and acellular pertussis (Tdap) vaccine. All adults should complete the 3-dose primary vaccination series for tetanus, diphtheria, and pertussis (also known as whooping cough) and this should include 1 dose of Tdap. Administration of the primary series is staged so that the second dose is given 4 weeks after the initial dose and the final dose 6 to 12 months after the first dose. After receiving the primary series, adults should receive a tetanus-diphtheria booster dose every 10 years. For adults ages 19 to 64, the Advisory Committee on Immunization Practices (ACIP) recommends 1 dose of Tdap in place of a booster vaccination to decrease the transmission risk of pertussis to vulnerable persons, especially children.
Human papillomavirus (HPV) immunization. The ACIP recommendation9 has been for children to receive routine vaccination for the 4 major strains of HPV—strains 6, 11, 16, and 18—starting at ages 11 to 12 to confer protection from HPV-associated diseases, such as genital warts, oropharyngeal cancer, and anal cancer; cancers of the cervix, vulva, and vagina in women; and penile cancer in men. Ideally, the vaccines are administered prior to HPV exposure from sexual contact. The quadrivalent HPV vaccine is safe and is administered as a 3-dose series, with the second and third doses given 2 and 6 months, respectively, after the initial dose. Adolescent girls also have the option of a bivalent HPV vaccine.
In 2016, the FDA approved a 9-valent HPV vaccine, a simpler 2-dose schedule for children ages 9 to 14 (2 doses at least 6 months apart). Leading cancer centers have endorsed this vaccine based on strong comparative data with the 3-dose regimen.10 For those not previously vaccinated, the HPV vaccine is available for women ages 13 to 26 and for men ages 13 to 21 (although men ages 22 to 26 can receive the vaccine, and it is recommended for men who have sex with men [MSM]). Women do not require Papanicolaou, serum pregnancy, HPV DNA, or HPV antibody tests prior to vaccination. If a woman becomes pregnant, remaining doses of the vaccine should be postponed until after delivery. Women still need to follow recommendations for cervical cancer screening because the HPV vaccine does not cover all genital strains of the virus. For sexually active individuals who might have HPV or genital warts, immunization has no clinical effect except to prevent other HPV strains.
Measles, mumps, and rubella (MMR) vaccine. All adults should receive, at minimum, 1 dose of MMR vaccination unless serological immunity can be verified or if contraindicated. Two doses of the vaccine are recommended for students attending post-high school institutions, health care personnel, and international travelers because they are at higher risk for exposure and transmission of measles and mumps. Individuals born before 1957 are considered immune to measles and mumps. A measles outbreak from December 2014 to February 201511 highlighted the importance of maintaining one’s immunity status for MMR.
Case continued
Based on Ms. W’s age, she should be offered vaccinations for influenza and opportunities to receive vaccinations for HPV, Tdap (the primary series, a Tdap or Td booster), and MMR, if appropriate and not completed previously.
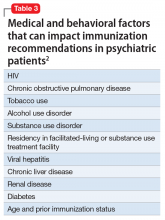
Risk of exposure
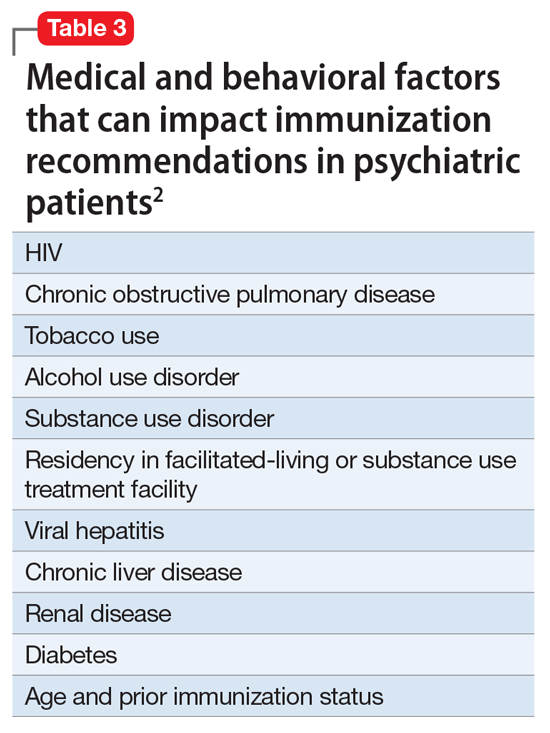
Certain behaviors will increase the risk of exposure to and transmission of diseases communicable by blood and other bodily fluids (Table 3). These behaviors include needle injections (eg, during use of illicit drugs) and sexual activity with multiple partners, including MSM or promiscuity/impulsivity during a manic episode. A common consequence of risky behaviors is comorbid infection of HIV and viral hepatitis for those with substance use disorder or those who engage in high-risk sexual practices.12,13
Hepatitis B virus (HBV) immunization. Vaccination is one of the most effective ways to prevent HBV infection, which is why it is offered to all health care workers. HBV immunization is a 3-dose series in which the second and third doses are given 1 and 6 months after the initial doses, respectively. In addition to certain medical risk factors or conditions that indicate HBV vaccination, people should be offered the vaccine if they are in a higher risk occupation, travel, are of Asian or Pacific Islander ethnicity from an endemic area, or have any present or suspected sexually transmitted diseases.
Hepatitis A virus (HAV) vaccination. HAV is transmitted via fecal–oral routes, often from contaminated water or food, or through household or sexual contact with an infected person. Individuals should receive the HAV vaccine if they use illicit drugs by any route of administration, work with primates infected with HAV, travel to countries with unknown or high rates of HAV, or have chronic liver disease (ie, hepatitis, alcohol use disorder, or non-alcoholic fatty liver disease) or clotting deficiencies. The CDC Health Information for International Travel, commonly called the “Yellow Book,” publishes vaccination recommendations for those who plan travel to specific countries.14
Case continued
Ms. W’s history of mania (if such episodes included increased sexual activity) and substance use would make her a candidate for the HBV and HAV vaccinations and could also strengthen our previous recommendation that she receive the HPV vaccination.
Medical conditions
Patients with certain medical conditions may have difficulty fighting infections or become more susceptible to morbidity and mortality from coinfection with vaccine-preventable illnesses. Secondary effects of psychotropic medications that may carry implications for vaccine recommendations (eg, risk of agranulocytosis and impaired cell-medicated immunity with mirtazapine and clozapine or renal impairment from lithium use) are of particular concern in psychiatric patients.2
To help care for these patients, the CDC has developed a “medical conditions” schedule (Figure 2). This schedule makes vaccination recommendations for those with a weakened immune system, including patients with HIV, chronic obstructive pulmonary disease (COPD), diabetes, hepatitis, asplenia, end-stage renal disease, cardiac disease, and pregnancy.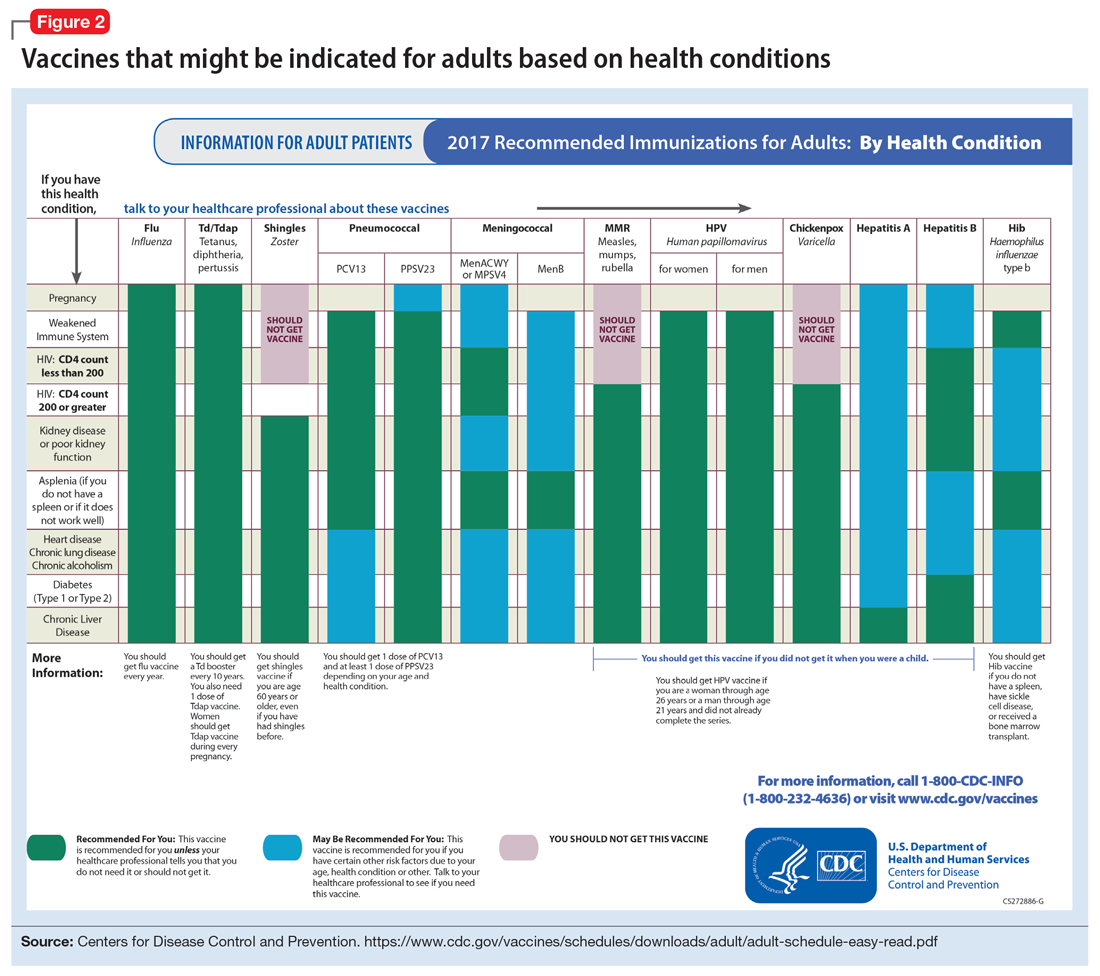
Because patients with psychiatric illness face a greater risk of heart disease and diabetes, these conditions may warrant special reference on the schedule. The increased cardiometabolic risk factors in these patients may be due in part to genetics, socioeconomic status, lifestyle behaviors, and medications to treat their mental illness (eg, antipsychotics). Patients with bipolar disorder or schizophrenia in particular tend to have higher rates of COPD (mainly from chronic bronchitis) and asthma than the general population.12 Pay special attention to the indications schedule for those with chronic lung disease, especially patients who continue to smoke cigarettes.
Case continued
Because of Ms. W’s asthma, the CDC schedule recommends ensuring she is up to date on her influenza, pneumococcal, and Tdap vaccinations.
Substance use
Patients with combined psychiatric and substance use disorders (“dual diagnosis”) have lower rates of receiving preventive care than patients with either condition alone.15 Substance use can be behaviorally disinhibiting, leading to increased risk of exposures from sexual contact or other risky activities. The use of illicit substances can provide a nidus for infection depending on the route of administration and can result in negative effects on organ systems, compromising one’s ability to ward off infection.
Patients who use any illicit drugs, regardless of the method of delivery, should be recommended for HAV vaccination. For those with alcohol use disorder and/or chronic liver disease, and/or seeking treatment for substance use, hepatitis B screening and vaccination is recommended.
Case continued
From a substance use perspective, discussion of vaccination status for both hepatitis A and B would be important for Ms. W.
HIV or immunocompromised
Persons with severe mental illness have high rates of HIV, with almost 8 times the risk of exposure, compared with the general population due to myriad reasons, including greater rates of substance abuse, higher risk sexual behavior, and lack of awareness of HIV transmission.12,13 Patients with mental illness are also at risk of leukopenia and agranulocytosis from certain drugs used to treat their conditions, such as clozapine.
Pregnancy is a challenge for women with mental illness because of the pharmacologic risk and immune-system compromise to the mother and baby. A pregnant woman who has HIV with a CD4 count <200, or has a weakened immune system from an organ transplant or a similar condition, is a candidate for certain vaccines based on the Adult Immunization Schedule (Figure 2). However, these patients should avoid live vaccines, such as the intranasal mist of live influenza, MMR, VZV, and varicella, to avoid illness from these inoculations.
Case continued
Ms. W should undergo testing for pregnancy and HIV (and preferably other sexually transmitted infections per general preventive health guidelines) before receiving any live vaccinations.
Occupancy
Aside from direct transmission of bodily fluids, infectious diseases also can spread through droplets/secretions from the throat and respiratory tract. Close quarters or lengthy contact enhances communicability by droplets, and therefore people who reside in a communal living space (eg, individuals in substance use treatment facilities or those who reside in a nursing home) are most susceptible.
The bacterial disease Neisseria meningitidis (meningococcus) can spread through droplets and can cause pneumonia, bacteremia, and meningitis. Vaccination is indicated, and in some states is mandated, for college students who live in residence halls and missed routine vaccination by age 16. Meningococcus conjugate vaccine is administered in 2 doses; each dose may be given at least 2 months apart for those with HIV, asplenia, or persistent complement-related disorders. A single dose may be recommended for travelers to areas where meningococcal disease is hyperendemic or epidemic, military recruits, or microbiologists. For those age ≥55 and older, meningococcal polysaccharide vaccine is recommended over meningococcal conjugate vaccine.
Influenza, MMR, diphtheria, pertussis, and pneumococcus also spread through droplet contact.
Case continued
If Ms. W had not previously received the meningococcus vaccine as part of adolescent immunizations, she could benefit from this vaccine because she plans to enter a residential substance use disorder treatment program.
Tobacco use
Patients with psychiatric illness are twice as likely to smoke compared with the general population.16 Adult smokers, especially those with chronic lung disease, are at higher risk for influenza and pneumococcal-related illness; they should be vaccinated against these illnesses regardless of age (as discussed in the “Age” section).
Case continued
Because she smokes, Ms. W should receive counseling on vaccinations, such as influenza and pneumonia, to lessen her risk of respiratory illnesses and downstream sepsis.
Conclusion
Ms. W’s case represents an unfortunately all-too-common scenario where her multifaceted biopsychosocial circumstances place her at high risk for vaccine-preventable conditions. Her weight is recorded and laboratory work ordered to evaluate her pregnancy status, blood counts, lipids, complete metabolic panel, lithium level, and HIV status. Fortunately, she had received her series of MMR, meningococcal, and Tdap vaccinations when she was younger. Influenza, HPV, HAV, HBV, and pneumococcal vaccinations were all recommended to her, all of which can be given on the same day (HAV and HBV often are available as a combined vaccine). Ms. W receives a renewal of her psychiatric medications and counseling on healthy living habits (eg, diet and exercise, quitting tobacco and alcohol use, and safe sex practices) and the importance of immunizations.
Vaccination is 1 of the 10 great public health achievements of the 20th century when one considers how immunization of vaccine-preventable diseases has reduced morbidity, mortality, and health-associated costs.17 As mental health professionals, we can help pass on the direct and indirect benefits of immunizations to an often underserved and undertreated population to help improve their health outcomes and quality of life.
1. Newcomer JW, Hennekens CH. Severe mental illness and risk of cardiovascular disease. JAMA. 2007;298(15):1794-1796.
2. Raj YP, Lloyd L. Adult immunizations. In: McCarron RM, Xiong GL, Keenan GR, et al, eds. Preventive medical care in psychiatry. Arlington, VA: American Psychiatric Publishing. 2015;215-227.
3. Young S, Dosani N, Whisler A, et al. Influenza vaccination rates among homeless adults with mental illness in Toronto. J Prim Care Community Health. 2015;6(3):211-214.
4. Kroger AT, Atkinson WL, Marcues EK, et al; Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC). General recommendations on immunization: recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55(RR-15):1-48.
5. Centers for Disease Control and Prevention. Recommended Adult Immunization by Vaccine and Age Group. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated February 27, 2017. Accessed February 1, 2017.
6. National Center for Immunization and Respiratory Diseases. General recommendations on immunization—recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(2):1-64.
7. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. https://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Updated June 22, 2016. Accessed February 1, 2017.
8. Hales CM, Harpaz, R, Ortega-Sanchez I, et al; Centers for Disease Control and Prevention. Update on recommendations for use of herpes zoster vaccine. MMWR Morb Mortal Wkly Rep. 2014;63(33):729-731.
9. Petrosky E, Bocchini Jr JA, Hariri S, et al; Centers for Disease Control and Prevention (CDC). Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccine recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2015;64(11)300-304.
10. Iversen OE, Miranda MJ, Ulied A, et al. Immunogenicity of the 9-valent HPV vaccine using 2-dose regimens in girls and boys vs a 3-dose regimen in women. JAMA. 2016;316(22):2411-2421.
11. Zipprich J, Winter K, Hacker J, et al; Centers for Disease Control and Prevention (CDC). Measles outbreak—California, December 2014-February 2015. MMWR Morb Mortal Wkly Rep. 2015;64(6):153-154.
12. De Hert M, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52-77.
13. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Public Health. 2001;91(1):31-37.
14. Centers for Disease for Control and Prevention. CDC yellow book 2018: health information for international travel. New York, NY: Oxford University Press; 2017.
15. Druss BG, Rosenheck RA, Desai MM, et al. Quality of preventive medical care for patients with mental disorders. Med Care. 2002;40(2):129-136.
16. Lasser K, Boyd J, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
17. Centers for Disease Control and Prevention (CDC). Ten great public health achievements—United States, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011;60(19);619-623.
Patients with chronic, severe mental illness live much shorter lives than the general population. The 25-year loss in life expectancy for people with chronic mental illness has been attributed to higher rates of cardiovascular disease driven by increased smoking, obesity, poverty, and poor nutrition.1 These individuals also face the added burden of struggling with a psychiatric condition that often interferes with their ability to make optimal preventative health decisions, including staying up to date on vaccinations.2 A recent review from Toronto, Canada, found that the influenza vaccination rates among homeless adults with mental illness—a population at high risk of respiratory illness—was only 6.7% compared with 31.1% for the general population of Ontario.3
Mental health professionals may serve as the only contacts to offer medical care to this vulnerable population, leading some psychiatric leaders to advocate that psychiatrists be considered primary care providers within accountable care organizations. Because most vaccines are easily available, mental health professionals should know about key immunizations to guide their patients accordingly.
In the United States, approximately 45,000 adults die annually from vaccine-preventable diseases, the majority from influenza.4 When combined with the most recent Adult Immunization Schedule and general recommendations adapted from the CDC,5,6 the mnemonic ARM SHOT allows for a quick assessment of risk factors to guide administration and education about most vaccinations (Table 1). ARM SHOT involves assessing the following components of an individual’s health status and living arrangements to determine one’s risk of contracting communicable diseases:
- Age
- Risk of exposure
- Medical conditions (comorbidities)
- Substance use history
- HIV status or other immunocompromised states
- Occupancy, or living arrangements
- Tobacco use.
We recommend keeping a copy of the Adult Immunization Schedule (age ≥19) and/or the immunization schedule for children and adolescents (age ≤18) close for quick reference. Here, we provide a case and then explore how each component of the ARM SHOT mnemonic applies in decision-making.
Case Evaluating risk, assess needs
Ms. W, age 24, has bipolar I disorder, most recently manic with psychotic features. She presents for follow-up in clinic after a 5-day hospitalization for mania and comorbid alcohol use disorder. Her medical comorbidities include asthma and active tobacco use. She is taking lurasidone, 20 mg/d, and lithium, 900 mg/d. Her case manager is working to place Ms. W in a residential substance use disorder treatment program. Ms. W is on a waiting list to establish care with a primary care physician and has a history of poor engagement with medical services in general; prior attempts to place her with a primary care physician failed.
In advance of Ms. W’s transfer to a residential treatment facility, you have been asked to place a Mantoux screening test for tuberculosis (purified protein derivative), which raises the important question about her susceptibility to infectious diseases in general. To protect Ms. W from preventable diseases for which vaccines are available, you review the ARM SHOT mnemonic to broadly assess her candidacy for vaccinations.
Age
Age may be the most important determinant of a patient’s need for vaccination (Table 2). The CDC immunization schedules account for age-specific risks for diseases, complications, and responses to vaccination (Figure 1).6
Influenza vaccination. Adults can have an intramuscular or intradermal inactivated influenza vaccination yearly in the fall or winter, unless they have an allergy to a vaccine component such as egg protein. Those with such an allergy can receive a recombinant influenza vaccine. Until the 2016 to 2017 flu season, an intranasal mist of live, attenuated influenza vaccine was available to healthy, non-pregnant women, ages 2 to 49, without high-risk medical conditions. However, the CDC dropped its recommendation for this vaccine because data showed it did not effectively prevent the flu.7 Individuals age ≥65 can receive either the standard- or high-dose inactivated influenza vaccination. The latter contains 4 times the amount of antigen with the intention of triggering a stronger immune response in older adults.
Pneumonia immunization. All patients age ≥65 should receive vaccinations for Streptococcus pneumoniae and its variants in the form of one 13-valent pneumococcal conjugate vaccine and, at least 1 year later, one 23-valent pneumococcal polysaccharide vaccine (PPSV23). Immunization reduces the morbidity and mortality from pneumococcal illness by decreasing the burden of a pneumonia, bacteremia, or meningitis infection. Adults, ages 19 to 64, with a chronic disease (referred to as “special populations” in CDC tables), such as diabetes, heart or lung disease, alcoholism, or cirrhosis, or those who smoke cigarettes, should receive PPSV23 with a second dose administered at least 5 years after the first. The CDC recommends a 1-time re-vaccination at age 65 for patients if >5 years have passed since the last PPSV23 and if the patient was younger than age 65 at the time of primary vaccine for S. pneumoniae. This can be a rather tricky clinical situation; the health care provider should verify a patient’s immunization history to ensure that she (he) is receiving only necessary vaccines. However, when the history cannot be verified, err on the side of inclusion, because risks are minimal.
Shingles vaccination. Adults age ≥60 who are not immunocompromised should receive a single dose of live attenuated vaccine from varicella-zoster virus (VZV) to limit the risk of shingles from a prior chickenpox infection. The vaccine is approximately 66.5% effective at preventing postherpetic neuralgia for up to 4.9 years. Individuals as young as age 50 may have the vaccine because the risk of herpes zoster radically increases from then on,8 although most insurers only cover VZV vaccination after age 60.
Tetanus, diphtheria, and acellular pertussis (Tdap) vaccine. All adults should complete the 3-dose primary vaccination series for tetanus, diphtheria, and pertussis (also known as whooping cough) and this should include 1 dose of Tdap. Administration of the primary series is staged so that the second dose is given 4 weeks after the initial dose and the final dose 6 to 12 months after the first dose. After receiving the primary series, adults should receive a tetanus-diphtheria booster dose every 10 years. For adults ages 19 to 64, the Advisory Committee on Immunization Practices (ACIP) recommends 1 dose of Tdap in place of a booster vaccination to decrease the transmission risk of pertussis to vulnerable persons, especially children.
Human papillomavirus (HPV) immunization. The ACIP recommendation9 has been for children to receive routine vaccination for the 4 major strains of HPV—strains 6, 11, 16, and 18—starting at ages 11 to 12 to confer protection from HPV-associated diseases, such as genital warts, oropharyngeal cancer, and anal cancer; cancers of the cervix, vulva, and vagina in women; and penile cancer in men. Ideally, the vaccines are administered prior to HPV exposure from sexual contact. The quadrivalent HPV vaccine is safe and is administered as a 3-dose series, with the second and third doses given 2 and 6 months, respectively, after the initial dose. Adolescent girls also have the option of a bivalent HPV vaccine.
In 2016, the FDA approved a 9-valent HPV vaccine, a simpler 2-dose schedule for children ages 9 to 14 (2 doses at least 6 months apart). Leading cancer centers have endorsed this vaccine based on strong comparative data with the 3-dose regimen.10 For those not previously vaccinated, the HPV vaccine is available for women ages 13 to 26 and for men ages 13 to 21 (although men ages 22 to 26 can receive the vaccine, and it is recommended for men who have sex with men [MSM]). Women do not require Papanicolaou, serum pregnancy, HPV DNA, or HPV antibody tests prior to vaccination. If a woman becomes pregnant, remaining doses of the vaccine should be postponed until after delivery. Women still need to follow recommendations for cervical cancer screening because the HPV vaccine does not cover all genital strains of the virus. For sexually active individuals who might have HPV or genital warts, immunization has no clinical effect except to prevent other HPV strains.
Measles, mumps, and rubella (MMR) vaccine. All adults should receive, at minimum, 1 dose of MMR vaccination unless serological immunity can be verified or if contraindicated. Two doses of the vaccine are recommended for students attending post-high school institutions, health care personnel, and international travelers because they are at higher risk for exposure and transmission of measles and mumps. Individuals born before 1957 are considered immune to measles and mumps. A measles outbreak from December 2014 to February 201511 highlighted the importance of maintaining one’s immunity status for MMR.
Case continued
Based on Ms. W’s age, she should be offered vaccinations for influenza and opportunities to receive vaccinations for HPV, Tdap (the primary series, a Tdap or Td booster), and MMR, if appropriate and not completed previously.
Risk of exposure
Certain behaviors will increase the risk of exposure to and transmission of diseases communicable by blood and other bodily fluids (Table 3). These behaviors include needle injections (eg, during use of illicit drugs) and sexual activity with multiple partners, including MSM or promiscuity/impulsivity during a manic episode. A common consequence of risky behaviors is comorbid infection of HIV and viral hepatitis for those with substance use disorder or those who engage in high-risk sexual practices.12,13
Hepatitis B virus (HBV) immunization. Vaccination is one of the most effective ways to prevent HBV infection, which is why it is offered to all health care workers. HBV immunization is a 3-dose series in which the second and third doses are given 1 and 6 months after the initial doses, respectively. In addition to certain medical risk factors or conditions that indicate HBV vaccination, people should be offered the vaccine if they are in a higher risk occupation, travel, are of Asian or Pacific Islander ethnicity from an endemic area, or have any present or suspected sexually transmitted diseases.
Hepatitis A virus (HAV) vaccination. HAV is transmitted via fecal–oral routes, often from contaminated water or food, or through household or sexual contact with an infected person. Individuals should receive the HAV vaccine if they use illicit drugs by any route of administration, work with primates infected with HAV, travel to countries with unknown or high rates of HAV, or have chronic liver disease (ie, hepatitis, alcohol use disorder, or non-alcoholic fatty liver disease) or clotting deficiencies. The CDC Health Information for International Travel, commonly called the “Yellow Book,” publishes vaccination recommendations for those who plan travel to specific countries.14
Case continued
Ms. W’s history of mania (if such episodes included increased sexual activity) and substance use would make her a candidate for the HBV and HAV vaccinations and could also strengthen our previous recommendation that she receive the HPV vaccination.
Medical conditions
Patients with certain medical conditions may have difficulty fighting infections or become more susceptible to morbidity and mortality from coinfection with vaccine-preventable illnesses. Secondary effects of psychotropic medications that may carry implications for vaccine recommendations (eg, risk of agranulocytosis and impaired cell-medicated immunity with mirtazapine and clozapine or renal impairment from lithium use) are of particular concern in psychiatric patients.2
To help care for these patients, the CDC has developed a “medical conditions” schedule (Figure 2). This schedule makes vaccination recommendations for those with a weakened immune system, including patients with HIV, chronic obstructive pulmonary disease (COPD), diabetes, hepatitis, asplenia, end-stage renal disease, cardiac disease, and pregnancy.
Because patients with psychiatric illness face a greater risk of heart disease and diabetes, these conditions may warrant special reference on the schedule. The increased cardiometabolic risk factors in these patients may be due in part to genetics, socioeconomic status, lifestyle behaviors, and medications to treat their mental illness (eg, antipsychotics). Patients with bipolar disorder or schizophrenia in particular tend to have higher rates of COPD (mainly from chronic bronchitis) and asthma than the general population.12 Pay special attention to the indications schedule for those with chronic lung disease, especially patients who continue to smoke cigarettes.
Case continued
Because of Ms. W’s asthma, the CDC schedule recommends ensuring she is up to date on her influenza, pneumococcal, and Tdap vaccinations.
Substance use
Patients with combined psychiatric and substance use disorders (“dual diagnosis”) have lower rates of receiving preventive care than patients with either condition alone.15 Substance use can be behaviorally disinhibiting, leading to increased risk of exposures from sexual contact or other risky activities. The use of illicit substances can provide a nidus for infection depending on the route of administration and can result in negative effects on organ systems, compromising one’s ability to ward off infection.
Patients who use any illicit drugs, regardless of the method of delivery, should be recommended for HAV vaccination. For those with alcohol use disorder and/or chronic liver disease, and/or seeking treatment for substance use, hepatitis B screening and vaccination is recommended.
Case continued
From a substance use perspective, discussion of vaccination status for both hepatitis A and B would be important for Ms. W.
HIV or immunocompromised
Persons with severe mental illness have high rates of HIV, with almost 8 times the risk of exposure, compared with the general population due to myriad reasons, including greater rates of substance abuse, higher risk sexual behavior, and lack of awareness of HIV transmission.12,13 Patients with mental illness are also at risk of leukopenia and agranulocytosis from certain drugs used to treat their conditions, such as clozapine.
Pregnancy is a challenge for women with mental illness because of the pharmacologic risk and immune-system compromise to the mother and baby. A pregnant woman who has HIV with a CD4 count <200, or has a weakened immune system from an organ transplant or a similar condition, is a candidate for certain vaccines based on the Adult Immunization Schedule (Figure 2). However, these patients should avoid live vaccines, such as the intranasal mist of live influenza, MMR, VZV, and varicella, to avoid illness from these inoculations.
Case continued
Ms. W should undergo testing for pregnancy and HIV (and preferably other sexually transmitted infections per general preventive health guidelines) before receiving any live vaccinations.
Occupancy
Aside from direct transmission of bodily fluids, infectious diseases also can spread through droplets/secretions from the throat and respiratory tract. Close quarters or lengthy contact enhances communicability by droplets, and therefore people who reside in a communal living space (eg, individuals in substance use treatment facilities or those who reside in a nursing home) are most susceptible.
The bacterial disease Neisseria meningitidis (meningococcus) can spread through droplets and can cause pneumonia, bacteremia, and meningitis. Vaccination is indicated, and in some states is mandated, for college students who live in residence halls and missed routine vaccination by age 16. Meningococcus conjugate vaccine is administered in 2 doses; each dose may be given at least 2 months apart for those with HIV, asplenia, or persistent complement-related disorders. A single dose may be recommended for travelers to areas where meningococcal disease is hyperendemic or epidemic, military recruits, or microbiologists. For those age ≥55 and older, meningococcal polysaccharide vaccine is recommended over meningococcal conjugate vaccine.
Influenza, MMR, diphtheria, pertussis, and pneumococcus also spread through droplet contact.
Case continued
If Ms. W had not previously received the meningococcus vaccine as part of adolescent immunizations, she could benefit from this vaccine because she plans to enter a residential substance use disorder treatment program.
Tobacco use
Patients with psychiatric illness are twice as likely to smoke compared with the general population.16 Adult smokers, especially those with chronic lung disease, are at higher risk for influenza and pneumococcal-related illness; they should be vaccinated against these illnesses regardless of age (as discussed in the “Age” section).
Case continued
Because she smokes, Ms. W should receive counseling on vaccinations, such as influenza and pneumonia, to lessen her risk of respiratory illnesses and downstream sepsis.
Conclusion
Ms. W’s case represents an unfortunately all-too-common scenario where her multifaceted biopsychosocial circumstances place her at high risk for vaccine-preventable conditions. Her weight is recorded and laboratory work ordered to evaluate her pregnancy status, blood counts, lipids, complete metabolic panel, lithium level, and HIV status. Fortunately, she had received her series of MMR, meningococcal, and Tdap vaccinations when she was younger. Influenza, HPV, HAV, HBV, and pneumococcal vaccinations were all recommended to her, all of which can be given on the same day (HAV and HBV often are available as a combined vaccine). Ms. W receives a renewal of her psychiatric medications and counseling on healthy living habits (eg, diet and exercise, quitting tobacco and alcohol use, and safe sex practices) and the importance of immunizations.
Vaccination is 1 of the 10 great public health achievements of the 20th century when one considers how immunization of vaccine-preventable diseases has reduced morbidity, mortality, and health-associated costs.17 As mental health professionals, we can help pass on the direct and indirect benefits of immunizations to an often underserved and undertreated population to help improve their health outcomes and quality of life.
Patients with chronic, severe mental illness live much shorter lives than the general population. The 25-year loss in life expectancy for people with chronic mental illness has been attributed to higher rates of cardiovascular disease driven by increased smoking, obesity, poverty, and poor nutrition.1 These individuals also face the added burden of struggling with a psychiatric condition that often interferes with their ability to make optimal preventative health decisions, including staying up to date on vaccinations.2 A recent review from Toronto, Canada, found that the influenza vaccination rates among homeless adults with mental illness—a population at high risk of respiratory illness—was only 6.7% compared with 31.1% for the general population of Ontario.3
Mental health professionals may serve as the only contacts to offer medical care to this vulnerable population, leading some psychiatric leaders to advocate that psychiatrists be considered primary care providers within accountable care organizations. Because most vaccines are easily available, mental health professionals should know about key immunizations to guide their patients accordingly.
In the United States, approximately 45,000 adults die annually from vaccine-preventable diseases, the majority from influenza.4 When combined with the most recent Adult Immunization Schedule and general recommendations adapted from the CDC,5,6 the mnemonic ARM SHOT allows for a quick assessment of risk factors to guide administration and education about most vaccinations (Table 1). ARM SHOT involves assessing the following components of an individual’s health status and living arrangements to determine one’s risk of contracting communicable diseases:
- Age
- Risk of exposure
- Medical conditions (comorbidities)
- Substance use history
- HIV status or other immunocompromised states
- Occupancy, or living arrangements
- Tobacco use.
We recommend keeping a copy of the Adult Immunization Schedule (age ≥19) and/or the immunization schedule for children and adolescents (age ≤18) close for quick reference. Here, we provide a case and then explore how each component of the ARM SHOT mnemonic applies in decision-making.
Case Evaluating risk, assess needs
Ms. W, age 24, has bipolar I disorder, most recently manic with psychotic features. She presents for follow-up in clinic after a 5-day hospitalization for mania and comorbid alcohol use disorder. Her medical comorbidities include asthma and active tobacco use. She is taking lurasidone, 20 mg/d, and lithium, 900 mg/d. Her case manager is working to place Ms. W in a residential substance use disorder treatment program. Ms. W is on a waiting list to establish care with a primary care physician and has a history of poor engagement with medical services in general; prior attempts to place her with a primary care physician failed.
In advance of Ms. W’s transfer to a residential treatment facility, you have been asked to place a Mantoux screening test for tuberculosis (purified protein derivative), which raises the important question about her susceptibility to infectious diseases in general. To protect Ms. W from preventable diseases for which vaccines are available, you review the ARM SHOT mnemonic to broadly assess her candidacy for vaccinations.
Age
Age may be the most important determinant of a patient’s need for vaccination (Table 2). The CDC immunization schedules account for age-specific risks for diseases, complications, and responses to vaccination (Figure 1).6
Influenza vaccination. Adults can have an intramuscular or intradermal inactivated influenza vaccination yearly in the fall or winter, unless they have an allergy to a vaccine component such as egg protein. Those with such an allergy can receive a recombinant influenza vaccine. Until the 2016 to 2017 flu season, an intranasal mist of live, attenuated influenza vaccine was available to healthy, non-pregnant women, ages 2 to 49, without high-risk medical conditions. However, the CDC dropped its recommendation for this vaccine because data showed it did not effectively prevent the flu.7 Individuals age ≥65 can receive either the standard- or high-dose inactivated influenza vaccination. The latter contains 4 times the amount of antigen with the intention of triggering a stronger immune response in older adults.
Pneumonia immunization. All patients age ≥65 should receive vaccinations for Streptococcus pneumoniae and its variants in the form of one 13-valent pneumococcal conjugate vaccine and, at least 1 year later, one 23-valent pneumococcal polysaccharide vaccine (PPSV23). Immunization reduces the morbidity and mortality from pneumococcal illness by decreasing the burden of a pneumonia, bacteremia, or meningitis infection. Adults, ages 19 to 64, with a chronic disease (referred to as “special populations” in CDC tables), such as diabetes, heart or lung disease, alcoholism, or cirrhosis, or those who smoke cigarettes, should receive PPSV23 with a second dose administered at least 5 years after the first. The CDC recommends a 1-time re-vaccination at age 65 for patients if >5 years have passed since the last PPSV23 and if the patient was younger than age 65 at the time of primary vaccine for S. pneumoniae. This can be a rather tricky clinical situation; the health care provider should verify a patient’s immunization history to ensure that she (he) is receiving only necessary vaccines. However, when the history cannot be verified, err on the side of inclusion, because risks are minimal.
Shingles vaccination. Adults age ≥60 who are not immunocompromised should receive a single dose of live attenuated vaccine from varicella-zoster virus (VZV) to limit the risk of shingles from a prior chickenpox infection. The vaccine is approximately 66.5% effective at preventing postherpetic neuralgia for up to 4.9 years. Individuals as young as age 50 may have the vaccine because the risk of herpes zoster radically increases from then on,8 although most insurers only cover VZV vaccination after age 60.
Tetanus, diphtheria, and acellular pertussis (Tdap) vaccine. All adults should complete the 3-dose primary vaccination series for tetanus, diphtheria, and pertussis (also known as whooping cough) and this should include 1 dose of Tdap. Administration of the primary series is staged so that the second dose is given 4 weeks after the initial dose and the final dose 6 to 12 months after the first dose. After receiving the primary series, adults should receive a tetanus-diphtheria booster dose every 10 years. For adults ages 19 to 64, the Advisory Committee on Immunization Practices (ACIP) recommends 1 dose of Tdap in place of a booster vaccination to decrease the transmission risk of pertussis to vulnerable persons, especially children.
Human papillomavirus (HPV) immunization. The ACIP recommendation9 has been for children to receive routine vaccination for the 4 major strains of HPV—strains 6, 11, 16, and 18—starting at ages 11 to 12 to confer protection from HPV-associated diseases, such as genital warts, oropharyngeal cancer, and anal cancer; cancers of the cervix, vulva, and vagina in women; and penile cancer in men. Ideally, the vaccines are administered prior to HPV exposure from sexual contact. The quadrivalent HPV vaccine is safe and is administered as a 3-dose series, with the second and third doses given 2 and 6 months, respectively, after the initial dose. Adolescent girls also have the option of a bivalent HPV vaccine.
In 2016, the FDA approved a 9-valent HPV vaccine, a simpler 2-dose schedule for children ages 9 to 14 (2 doses at least 6 months apart). Leading cancer centers have endorsed this vaccine based on strong comparative data with the 3-dose regimen.10 For those not previously vaccinated, the HPV vaccine is available for women ages 13 to 26 and for men ages 13 to 21 (although men ages 22 to 26 can receive the vaccine, and it is recommended for men who have sex with men [MSM]). Women do not require Papanicolaou, serum pregnancy, HPV DNA, or HPV antibody tests prior to vaccination. If a woman becomes pregnant, remaining doses of the vaccine should be postponed until after delivery. Women still need to follow recommendations for cervical cancer screening because the HPV vaccine does not cover all genital strains of the virus. For sexually active individuals who might have HPV or genital warts, immunization has no clinical effect except to prevent other HPV strains.
Measles, mumps, and rubella (MMR) vaccine. All adults should receive, at minimum, 1 dose of MMR vaccination unless serological immunity can be verified or if contraindicated. Two doses of the vaccine are recommended for students attending post-high school institutions, health care personnel, and international travelers because they are at higher risk for exposure and transmission of measles and mumps. Individuals born before 1957 are considered immune to measles and mumps. A measles outbreak from December 2014 to February 201511 highlighted the importance of maintaining one’s immunity status for MMR.
Case continued
Based on Ms. W’s age, she should be offered vaccinations for influenza and opportunities to receive vaccinations for HPV, Tdap (the primary series, a Tdap or Td booster), and MMR, if appropriate and not completed previously.
Risk of exposure
Certain behaviors will increase the risk of exposure to and transmission of diseases communicable by blood and other bodily fluids (Table 3). These behaviors include needle injections (eg, during use of illicit drugs) and sexual activity with multiple partners, including MSM or promiscuity/impulsivity during a manic episode. A common consequence of risky behaviors is comorbid infection of HIV and viral hepatitis for those with substance use disorder or those who engage in high-risk sexual practices.12,13
Hepatitis B virus (HBV) immunization. Vaccination is one of the most effective ways to prevent HBV infection, which is why it is offered to all health care workers. HBV immunization is a 3-dose series in which the second and third doses are given 1 and 6 months after the initial doses, respectively. In addition to certain medical risk factors or conditions that indicate HBV vaccination, people should be offered the vaccine if they are in a higher risk occupation, travel, are of Asian or Pacific Islander ethnicity from an endemic area, or have any present or suspected sexually transmitted diseases.
Hepatitis A virus (HAV) vaccination. HAV is transmitted via fecal–oral routes, often from contaminated water or food, or through household or sexual contact with an infected person. Individuals should receive the HAV vaccine if they use illicit drugs by any route of administration, work with primates infected with HAV, travel to countries with unknown or high rates of HAV, or have chronic liver disease (ie, hepatitis, alcohol use disorder, or non-alcoholic fatty liver disease) or clotting deficiencies. The CDC Health Information for International Travel, commonly called the “Yellow Book,” publishes vaccination recommendations for those who plan travel to specific countries.14
Case continued
Ms. W’s history of mania (if such episodes included increased sexual activity) and substance use would make her a candidate for the HBV and HAV vaccinations and could also strengthen our previous recommendation that she receive the HPV vaccination.
Medical conditions
Patients with certain medical conditions may have difficulty fighting infections or become more susceptible to morbidity and mortality from coinfection with vaccine-preventable illnesses. Secondary effects of psychotropic medications that may carry implications for vaccine recommendations (eg, risk of agranulocytosis and impaired cell-medicated immunity with mirtazapine and clozapine or renal impairment from lithium use) are of particular concern in psychiatric patients.2
To help care for these patients, the CDC has developed a “medical conditions” schedule (Figure 2). This schedule makes vaccination recommendations for those with a weakened immune system, including patients with HIV, chronic obstructive pulmonary disease (COPD), diabetes, hepatitis, asplenia, end-stage renal disease, cardiac disease, and pregnancy.
Because patients with psychiatric illness face a greater risk of heart disease and diabetes, these conditions may warrant special reference on the schedule. The increased cardiometabolic risk factors in these patients may be due in part to genetics, socioeconomic status, lifestyle behaviors, and medications to treat their mental illness (eg, antipsychotics). Patients with bipolar disorder or schizophrenia in particular tend to have higher rates of COPD (mainly from chronic bronchitis) and asthma than the general population.12 Pay special attention to the indications schedule for those with chronic lung disease, especially patients who continue to smoke cigarettes.
Case continued
Because of Ms. W’s asthma, the CDC schedule recommends ensuring she is up to date on her influenza, pneumococcal, and Tdap vaccinations.
Substance use
Patients with combined psychiatric and substance use disorders (“dual diagnosis”) have lower rates of receiving preventive care than patients with either condition alone.15 Substance use can be behaviorally disinhibiting, leading to increased risk of exposures from sexual contact or other risky activities. The use of illicit substances can provide a nidus for infection depending on the route of administration and can result in negative effects on organ systems, compromising one’s ability to ward off infection.
Patients who use any illicit drugs, regardless of the method of delivery, should be recommended for HAV vaccination. For those with alcohol use disorder and/or chronic liver disease, and/or seeking treatment for substance use, hepatitis B screening and vaccination is recommended.
Case continued
From a substance use perspective, discussion of vaccination status for both hepatitis A and B would be important for Ms. W.
HIV or immunocompromised
Persons with severe mental illness have high rates of HIV, with almost 8 times the risk of exposure, compared with the general population due to myriad reasons, including greater rates of substance abuse, higher risk sexual behavior, and lack of awareness of HIV transmission.12,13 Patients with mental illness are also at risk of leukopenia and agranulocytosis from certain drugs used to treat their conditions, such as clozapine.
Pregnancy is a challenge for women with mental illness because of the pharmacologic risk and immune-system compromise to the mother and baby. A pregnant woman who has HIV with a CD4 count <200, or has a weakened immune system from an organ transplant or a similar condition, is a candidate for certain vaccines based on the Adult Immunization Schedule (Figure 2). However, these patients should avoid live vaccines, such as the intranasal mist of live influenza, MMR, VZV, and varicella, to avoid illness from these inoculations.
Case continued
Ms. W should undergo testing for pregnancy and HIV (and preferably other sexually transmitted infections per general preventive health guidelines) before receiving any live vaccinations.
Occupancy
Aside from direct transmission of bodily fluids, infectious diseases also can spread through droplets/secretions from the throat and respiratory tract. Close quarters or lengthy contact enhances communicability by droplets, and therefore people who reside in a communal living space (eg, individuals in substance use treatment facilities or those who reside in a nursing home) are most susceptible.
The bacterial disease Neisseria meningitidis (meningococcus) can spread through droplets and can cause pneumonia, bacteremia, and meningitis. Vaccination is indicated, and in some states is mandated, for college students who live in residence halls and missed routine vaccination by age 16. Meningococcus conjugate vaccine is administered in 2 doses; each dose may be given at least 2 months apart for those with HIV, asplenia, or persistent complement-related disorders. A single dose may be recommended for travelers to areas where meningococcal disease is hyperendemic or epidemic, military recruits, or microbiologists. For those age ≥55 and older, meningococcal polysaccharide vaccine is recommended over meningococcal conjugate vaccine.
Influenza, MMR, diphtheria, pertussis, and pneumococcus also spread through droplet contact.
Case continued
If Ms. W had not previously received the meningococcus vaccine as part of adolescent immunizations, she could benefit from this vaccine because she plans to enter a residential substance use disorder treatment program.
Tobacco use
Patients with psychiatric illness are twice as likely to smoke compared with the general population.16 Adult smokers, especially those with chronic lung disease, are at higher risk for influenza and pneumococcal-related illness; they should be vaccinated against these illnesses regardless of age (as discussed in the “Age” section).
Case continued
Because she smokes, Ms. W should receive counseling on vaccinations, such as influenza and pneumonia, to lessen her risk of respiratory illnesses and downstream sepsis.
Conclusion
Ms. W’s case represents an unfortunately all-too-common scenario where her multifaceted biopsychosocial circumstances place her at high risk for vaccine-preventable conditions. Her weight is recorded and laboratory work ordered to evaluate her pregnancy status, blood counts, lipids, complete metabolic panel, lithium level, and HIV status. Fortunately, she had received her series of MMR, meningococcal, and Tdap vaccinations when she was younger. Influenza, HPV, HAV, HBV, and pneumococcal vaccinations were all recommended to her, all of which can be given on the same day (HAV and HBV often are available as a combined vaccine). Ms. W receives a renewal of her psychiatric medications and counseling on healthy living habits (eg, diet and exercise, quitting tobacco and alcohol use, and safe sex practices) and the importance of immunizations.
Vaccination is 1 of the 10 great public health achievements of the 20th century when one considers how immunization of vaccine-preventable diseases has reduced morbidity, mortality, and health-associated costs.17 As mental health professionals, we can help pass on the direct and indirect benefits of immunizations to an often underserved and undertreated population to help improve their health outcomes and quality of life.
1. Newcomer JW, Hennekens CH. Severe mental illness and risk of cardiovascular disease. JAMA. 2007;298(15):1794-1796.
2. Raj YP, Lloyd L. Adult immunizations. In: McCarron RM, Xiong GL, Keenan GR, et al, eds. Preventive medical care in psychiatry. Arlington, VA: American Psychiatric Publishing. 2015;215-227.
3. Young S, Dosani N, Whisler A, et al. Influenza vaccination rates among homeless adults with mental illness in Toronto. J Prim Care Community Health. 2015;6(3):211-214.
4. Kroger AT, Atkinson WL, Marcues EK, et al; Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC). General recommendations on immunization: recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55(RR-15):1-48.
5. Centers for Disease Control and Prevention. Recommended Adult Immunization by Vaccine and Age Group. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated February 27, 2017. Accessed February 1, 2017.
6. National Center for Immunization and Respiratory Diseases. General recommendations on immunization—recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(2):1-64.
7. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. https://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Updated June 22, 2016. Accessed February 1, 2017.
8. Hales CM, Harpaz, R, Ortega-Sanchez I, et al; Centers for Disease Control and Prevention. Update on recommendations for use of herpes zoster vaccine. MMWR Morb Mortal Wkly Rep. 2014;63(33):729-731.
9. Petrosky E, Bocchini Jr JA, Hariri S, et al; Centers for Disease Control and Prevention (CDC). Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccine recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2015;64(11)300-304.
10. Iversen OE, Miranda MJ, Ulied A, et al. Immunogenicity of the 9-valent HPV vaccine using 2-dose regimens in girls and boys vs a 3-dose regimen in women. JAMA. 2016;316(22):2411-2421.
11. Zipprich J, Winter K, Hacker J, et al; Centers for Disease Control and Prevention (CDC). Measles outbreak—California, December 2014-February 2015. MMWR Morb Mortal Wkly Rep. 2015;64(6):153-154.
12. De Hert M, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52-77.
13. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Public Health. 2001;91(1):31-37.
14. Centers for Disease for Control and Prevention. CDC yellow book 2018: health information for international travel. New York, NY: Oxford University Press; 2017.
15. Druss BG, Rosenheck RA, Desai MM, et al. Quality of preventive medical care for patients with mental disorders. Med Care. 2002;40(2):129-136.
16. Lasser K, Boyd J, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
17. Centers for Disease Control and Prevention (CDC). Ten great public health achievements—United States, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011;60(19);619-623.
1. Newcomer JW, Hennekens CH. Severe mental illness and risk of cardiovascular disease. JAMA. 2007;298(15):1794-1796.
2. Raj YP, Lloyd L. Adult immunizations. In: McCarron RM, Xiong GL, Keenan GR, et al, eds. Preventive medical care in psychiatry. Arlington, VA: American Psychiatric Publishing. 2015;215-227.
3. Young S, Dosani N, Whisler A, et al. Influenza vaccination rates among homeless adults with mental illness in Toronto. J Prim Care Community Health. 2015;6(3):211-214.
4. Kroger AT, Atkinson WL, Marcues EK, et al; Advisory Committee on Immunization Practices (ACIP) Centers for Disease Control and Prevention (CDC). General recommendations on immunization: recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55(RR-15):1-48.
5. Centers for Disease Control and Prevention. Recommended Adult Immunization by Vaccine and Age Group. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated February 27, 2017. Accessed February 1, 2017.
6. National Center for Immunization and Respiratory Diseases. General recommendations on immunization—recommendations on the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(2):1-64.
7. Centers for Disease Control and Prevention. ACIP votes down use of LAIV for 2016-2017 flu season. https://www.cdc.gov/media/releases/2016/s0622-laiv-flu.html. Updated June 22, 2016. Accessed February 1, 2017.
8. Hales CM, Harpaz, R, Ortega-Sanchez I, et al; Centers for Disease Control and Prevention. Update on recommendations for use of herpes zoster vaccine. MMWR Morb Mortal Wkly Rep. 2014;63(33):729-731.
9. Petrosky E, Bocchini Jr JA, Hariri S, et al; Centers for Disease Control and Prevention (CDC). Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccine recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2015;64(11)300-304.
10. Iversen OE, Miranda MJ, Ulied A, et al. Immunogenicity of the 9-valent HPV vaccine using 2-dose regimens in girls and boys vs a 3-dose regimen in women. JAMA. 2016;316(22):2411-2421.
11. Zipprich J, Winter K, Hacker J, et al; Centers for Disease Control and Prevention (CDC). Measles outbreak—California, December 2014-February 2015. MMWR Morb Mortal Wkly Rep. 2015;64(6):153-154.
12. De Hert M, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52-77.
13. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Public Health. 2001;91(1):31-37.
14. Centers for Disease for Control and Prevention. CDC yellow book 2018: health information for international travel. New York, NY: Oxford University Press; 2017.
15. Druss BG, Rosenheck RA, Desai MM, et al. Quality of preventive medical care for patients with mental disorders. Med Care. 2002;40(2):129-136.
16. Lasser K, Boyd J, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA. 2000;284(20):2606-2610.
17. Centers for Disease Control and Prevention (CDC). Ten great public health achievements—United States, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011;60(19);619-623.
