User login
Clues to drug adulteration may lie skin deep
CHICAGO – Sometimes, the skin can provide the first clues that a patient has been exposed to a drug product that has been adulterated or an over-the-counter product illegally sold in this country that contains a prescription medication, according to pediatric dermatologist Scott Norton, MD.
Speaking at the World Congress of Pediatric Dermatology, he reviewed some of the reactions associated with exposure to counterfeit drugs, contraband drugs, as well as products, misrepresented as drugs that do not include any active pharmaceutical ingredients. The worldwide market for these products is a “hugely profitable industry,” and the scope of the problem should not be underestimated, said Dr. Norton, chief of dermatology at Children’s National Health System, Washington.

It’s particularly important to have a high index of suspicion for such products given an increasingly mobile worldwide population. Today, patients and their family members who travel out of the country – and even local shopkeepers – may bring in these sorts of products from outside the United States, many of which would require a prescription in the United States.
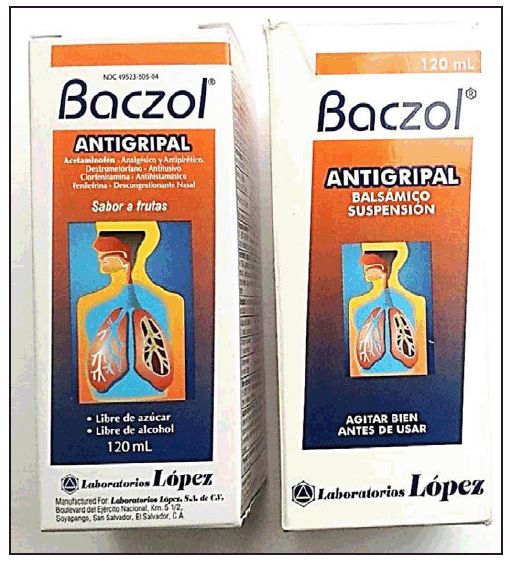
In the United States, there have been several reports of a mysterious fixed drug eruption in patients reported to have taken Baczol, a cold and flu remedy available over the counter in El Salvador for upper respiratory infections. Two of the ingredients listed on the Baczol label are sulfamethoxazole and trimethoprim, two prescription antibiotics. After determining that two Salvadoran American children with a suspected fixed drug eruption had taken a Baczol product, Dr. Norton, with the aid of medical students, was able to find Baczol containing trimethoprim-sulfamethoxazole for sale over the counter in more than one-third of the shops visited in the greater Washington area (MMWR Morb Mortal Wkly Rep. 2013 Nov 22;62[46]:914-6). Eventually, the Food and Drug Administration issued a consumer alert regarding certain Baczol products containing these ingredients, but Dr. Norton said he is still concerned about the possibility for more grave hypersensitivity reactions to these sulfa antibiotics in the Salvadoran product.
Sometimes, said Dr. Norton, the problem lies in the lack of an expected ingredient. He and his team at Children’s National Health System helped solve a medical mystery involving a skin ailment in very premature infants with cholestasis. An interdisciplinary team was convened after the neonatal intensive care unit at the hospital saw its third infant with severe blistering and erosions in an acral, perianal, and perioral pattern that did not respond to empiric treatment for herpes simplex virus and staphylococcal infection – a pattern reminiscent of zinc deficiency dermatitis. Dietitians reported that there was a nationwide shortage of sterile injectable zinc, so total parenteral nutrition was being formulated without zinc. All three of the premature infants were receiving total parenteral nutrition and were so premature that they had insufficient zinc stores. The problem was identified and corrected (MMWR 2014 Jan. 17;63[02];35-7).
A more pervasive issue, which has global significance, pertains to counterfeit vaccines prepared with absolutely no vaccine components, often made in China or Nigeria with high-quality and sophisticated packaging, said Dr. Norton.
Keeping a lid on counterfeit drugs is challenging since there are so many potential entry points into the supply chain, Dr. Norton pointed out. Weak points include mislabeled raw ingredients, packaging, storage, transportation, repackaging, and distribution. The proliferation of online pharmacies also makes regulation more difficult.
There is some international cooperation to detect and combat drug counterfeiting and adulteration: For example, Interpol, the International Coalition of Medicines Regulatory Authorities, the Pharmaceutical Security Institute, and even the United Nations are developing cooperative strategies to combat the problem.
In the meantime, he emphasized that physicians must maintain a high index of suspicion and keep in mind that the first signs of adulterated drugs or prescription drugs available OTC may appear on the skin.
Dr. Norton reported no conflicts of interest.
[email protected]
On Twitter @karioakes
CHICAGO – Sometimes, the skin can provide the first clues that a patient has been exposed to a drug product that has been adulterated or an over-the-counter product illegally sold in this country that contains a prescription medication, according to pediatric dermatologist Scott Norton, MD.
Speaking at the World Congress of Pediatric Dermatology, he reviewed some of the reactions associated with exposure to counterfeit drugs, contraband drugs, as well as products, misrepresented as drugs that do not include any active pharmaceutical ingredients. The worldwide market for these products is a “hugely profitable industry,” and the scope of the problem should not be underestimated, said Dr. Norton, chief of dermatology at Children’s National Health System, Washington.
It’s particularly important to have a high index of suspicion for such products given an increasingly mobile worldwide population. Today, patients and their family members who travel out of the country – and even local shopkeepers – may bring in these sorts of products from outside the United States, many of which would require a prescription in the United States.
In the United States, there have been several reports of a mysterious fixed drug eruption in patients reported to have taken Baczol, a cold and flu remedy available over the counter in El Salvador for upper respiratory infections. Two of the ingredients listed on the Baczol label are sulfamethoxazole and trimethoprim, two prescription antibiotics. After determining that two Salvadoran American children with a suspected fixed drug eruption had taken a Baczol product, Dr. Norton, with the aid of medical students, was able to find Baczol containing trimethoprim-sulfamethoxazole for sale over the counter in more than one-third of the shops visited in the greater Washington area (MMWR Morb Mortal Wkly Rep. 2013 Nov 22;62[46]:914-6). Eventually, the Food and Drug Administration issued a consumer alert regarding certain Baczol products containing these ingredients, but Dr. Norton said he is still concerned about the possibility for more grave hypersensitivity reactions to these sulfa antibiotics in the Salvadoran product.
Sometimes, said Dr. Norton, the problem lies in the lack of an expected ingredient. He and his team at Children’s National Health System helped solve a medical mystery involving a skin ailment in very premature infants with cholestasis. An interdisciplinary team was convened after the neonatal intensive care unit at the hospital saw its third infant with severe blistering and erosions in an acral, perianal, and perioral pattern that did not respond to empiric treatment for herpes simplex virus and staphylococcal infection – a pattern reminiscent of zinc deficiency dermatitis. Dietitians reported that there was a nationwide shortage of sterile injectable zinc, so total parenteral nutrition was being formulated without zinc. All three of the premature infants were receiving total parenteral nutrition and were so premature that they had insufficient zinc stores. The problem was identified and corrected (MMWR 2014 Jan. 17;63[02];35-7).
A more pervasive issue, which has global significance, pertains to counterfeit vaccines prepared with absolutely no vaccine components, often made in China or Nigeria with high-quality and sophisticated packaging, said Dr. Norton.
Keeping a lid on counterfeit drugs is challenging since there are so many potential entry points into the supply chain, Dr. Norton pointed out. Weak points include mislabeled raw ingredients, packaging, storage, transportation, repackaging, and distribution. The proliferation of online pharmacies also makes regulation more difficult.
There is some international cooperation to detect and combat drug counterfeiting and adulteration: For example, Interpol, the International Coalition of Medicines Regulatory Authorities, the Pharmaceutical Security Institute, and even the United Nations are developing cooperative strategies to combat the problem.
In the meantime, he emphasized that physicians must maintain a high index of suspicion and keep in mind that the first signs of adulterated drugs or prescription drugs available OTC may appear on the skin.
Dr. Norton reported no conflicts of interest.
[email protected]
On Twitter @karioakes
CHICAGO – Sometimes, the skin can provide the first clues that a patient has been exposed to a drug product that has been adulterated or an over-the-counter product illegally sold in this country that contains a prescription medication, according to pediatric dermatologist Scott Norton, MD.
Speaking at the World Congress of Pediatric Dermatology, he reviewed some of the reactions associated with exposure to counterfeit drugs, contraband drugs, as well as products, misrepresented as drugs that do not include any active pharmaceutical ingredients. The worldwide market for these products is a “hugely profitable industry,” and the scope of the problem should not be underestimated, said Dr. Norton, chief of dermatology at Children’s National Health System, Washington.
It’s particularly important to have a high index of suspicion for such products given an increasingly mobile worldwide population. Today, patients and their family members who travel out of the country – and even local shopkeepers – may bring in these sorts of products from outside the United States, many of which would require a prescription in the United States.
In the United States, there have been several reports of a mysterious fixed drug eruption in patients reported to have taken Baczol, a cold and flu remedy available over the counter in El Salvador for upper respiratory infections. Two of the ingredients listed on the Baczol label are sulfamethoxazole and trimethoprim, two prescription antibiotics. After determining that two Salvadoran American children with a suspected fixed drug eruption had taken a Baczol product, Dr. Norton, with the aid of medical students, was able to find Baczol containing trimethoprim-sulfamethoxazole for sale over the counter in more than one-third of the shops visited in the greater Washington area (MMWR Morb Mortal Wkly Rep. 2013 Nov 22;62[46]:914-6). Eventually, the Food and Drug Administration issued a consumer alert regarding certain Baczol products containing these ingredients, but Dr. Norton said he is still concerned about the possibility for more grave hypersensitivity reactions to these sulfa antibiotics in the Salvadoran product.
Sometimes, said Dr. Norton, the problem lies in the lack of an expected ingredient. He and his team at Children’s National Health System helped solve a medical mystery involving a skin ailment in very premature infants with cholestasis. An interdisciplinary team was convened after the neonatal intensive care unit at the hospital saw its third infant with severe blistering and erosions in an acral, perianal, and perioral pattern that did not respond to empiric treatment for herpes simplex virus and staphylococcal infection – a pattern reminiscent of zinc deficiency dermatitis. Dietitians reported that there was a nationwide shortage of sterile injectable zinc, so total parenteral nutrition was being formulated without zinc. All three of the premature infants were receiving total parenteral nutrition and were so premature that they had insufficient zinc stores. The problem was identified and corrected (MMWR 2014 Jan. 17;63[02];35-7).
A more pervasive issue, which has global significance, pertains to counterfeit vaccines prepared with absolutely no vaccine components, often made in China or Nigeria with high-quality and sophisticated packaging, said Dr. Norton.
Keeping a lid on counterfeit drugs is challenging since there are so many potential entry points into the supply chain, Dr. Norton pointed out. Weak points include mislabeled raw ingredients, packaging, storage, transportation, repackaging, and distribution. The proliferation of online pharmacies also makes regulation more difficult.
There is some international cooperation to detect and combat drug counterfeiting and adulteration: For example, Interpol, the International Coalition of Medicines Regulatory Authorities, the Pharmaceutical Security Institute, and even the United Nations are developing cooperative strategies to combat the problem.
In the meantime, he emphasized that physicians must maintain a high index of suspicion and keep in mind that the first signs of adulterated drugs or prescription drugs available OTC may appear on the skin.
Dr. Norton reported no conflicts of interest.
[email protected]
On Twitter @karioakes
EXPERT ANALYSIS FROM WCPD 2017
Small community hospitals need antibiotic stewardship programs
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Antibiotic use and misuse is driving drug resistance. Each year in the United States, at least 2 million people become infected with bacteria that are resistant to antibiotics, and at least 23,000 people die each year as a result of these infections, according to the Centers for Disease Control and Prevention.
Over 70% of U.S. hospitals are small community hospitals with 200 beds or fewer; however, our understanding of antibiotic use in these facilities is extremely limited. Most of the existing data on antibiotic use rates come from larger academic medical centers. Describing antibiotic usage patterns in small facilities is a high priority, given they constitute the majority of acute care hospitals and national antibiotic stewardship is forthcoming.
Intermountain has a long history of antibiotic use measurements and digital data support. All facilities use an electronic medical record system that transmits data to a centralized enterprise data warehouse. Since 2011, antibiotic use reports have been collected from the data system and submitted to the CDC’s National Healthcare and Safety Network Antimicrobial Use (NHSN AU) module.
Using data from the NHSN AU module from January 2011 through December 2013, we calculated monthly and 3-year antibiotic use rates for each facility, care unit type, and antibiotic category. Data included in the NHSN AU modules include:
• Patient care location.
• Facility-wide antibiotic use.
• Use of individual antibiotics.
• Classes of antibiotics.
• Days of therapy.
• Patient-day data.
Antibiotic agents were categorized into five groups based on antibiotic spectrum and ability to treat multidrug-resistant organisms (MDROs). Category one antibiotics are narrower-spectrum agents, and category five antibiotics are the broadest-spectrum antibiotics or associated with treating MDROs. Categories four and five were classified as broad-spectrum antibiotics. Hospital care units were categorized as intensive care, medical/surgical, pediatric, or miscellaneous.
Antibiotic use rates, expressed as days of therapy per 1,000 patient-days (DOT/1000PD), were calculated for each small community hospital and compared with rates in large community hospitals. Negative-binomial regression was used to relate antibiotic use.
The key findings of the study include:
• Total antibiotic use rates varied widely across the 15 small community hospitals and were similar to rates in four large community hospitals.
• The proportion of patient-days spent in the respective care unit types varied substantially within small community hospitals and had a large impact on facility-level antibiotic use rates.
• Broad-spectrum antibiotics accounted for 26% of use in small community hospitals, similar to the proportion in large community hospitals.
• Significant predictors of antibiotic use include case mix index, proportion of patient-days in specific care unit types, and season.
• Small community hospitals need to become a focus of antibiotic stewardship efforts.
All hospitals in 2017 are required to have an antibiotic stewardship program in place according to Joint Commission guidelines. Small community hospitals in the United States face significant challenges meeting the national antibiotic stewardship requirements. These challenges include: limited access to infectious diseases physician and/or pharmacist leadership, limited information technology support, and lack of antibiotic guidance.
In order to holistically address the growing problem of antibiotic-resistant bacteria, the infectious disease community must respond to antibiotic use in ALL hospitals, not just the large academic medical facilities. Small hospitals are least likely to have stewardship programs even though antibiotic usage patterns are similar to larger facilities. We need to bring stewardship support to ALL hospitals, but the challenges come in knowing how to do that.
To address the challenges, researchers at Intermountain Healthcare are currently conducting a study to identify recommendations that will help build antibiotic stewardship programs for these facilities.
Eddie Stenehjem, MD, is an infectious disease physician and researcher at Intermountain Medical Center, Salt Lake City, the flagship facility for the Intermountain Healthcare system.
Attitudes and beliefs affecting methotrexate adherence identified
MADRID – Negative beliefs and uncertainty regarding treatment with methotrexate, as well as dislike for the drug, contribute the most to rheumatoid arthritis patients’ nonadherence to the therapy, with one study finding that about one-third were nonadherent at the time they were eligible to start biologic therapy.
The French cross-sectional survey of 244 patients who were not responding to methotrexate found that 34% actually had poor adherence, including 54% who skipped doses and 38% who temporarily stopped treatment without their doctors’ recommendation. In comparison, patients who were deemed adherent had a lower rate of skipping doses (15%) or temporarily stopped treatment without their doctors’ recommendation (4%), both of which were statistically significant differences, Catherine Beauvais, MD, reported at the European Congress of Rheumatology. Nonadherence was defined as taking less than 80% of doses, according to the CQR19 (Compliance Questionnaire for Rheumatology).
“We have identified profiles of adherence,” Dr. Beauvais of Saint-Antoine Hospital in Paris commented in an interview.
“Among nonadherent patients, there are two profiles,” she added. “We have patients who are not responding to methotrexate but they also have negative beliefs, low levels of support, and they have professional impairment. [Then,] there are patients who do not like their treatment [although it is being well tolerated].”
The other profiles identified were of patients with good adherence to methotrexate with a higher or lower impact on patient outcomes.
In a poster presentation, Dr. Beauvais and her coauthors suggested that the “detection of patients’ profiles may allow targeted strategies to improve or maintain adherence.”
The FORGET survey was conducted over a 3-month period starting in July 2016. A total of 78 rheumatologists recruited patients who were inadequately responding to methotrexate and, thus, eligible to start biologic treatment for rheumatoid arthritis. Both the rheumatologists and the patients completed questionnaires, with 200 questionnaires being completed by patients and their rheumatologist.
As might be suspected for an RA population, 72% of respondents were women, with a mean age of 54 years. Over half (58%) had at least one comorbidity, and the mean disease activity score in 28 joints at the time of the survey was 4.07.
Significant factors for nonadherence were feeling constrained about taking treatment, cited by 29% of respondents; feeling “less good” with a change in dosage (31%); and feeling that treatment was “doing me more harm than good” (19% of respondents).
Surprisingly, most rheumatologists seemed to be unaware of their patients’ lack of adherence to their medication, despite saying that they asked about adherence in more than 80% of their patients.
Rheumatologists proposed the addition of a biologic to methotrexate more often if patients were nonadherent than if patients showed good compliance (91% vs. 68%; P less than .01).
Effect of patient attitudes on compliance
A team of U.K. researchers evaluated how attitudes toward treatment with methotrexate affected patients’ compliance in a separate poster presentation at the meeting.

RAMS is a 1-year observational study of patients with RA who are starting treatment with methotrexate. Patients recruited into the study completed weekly diaries, noting whether they took methotrexate (adherence) and, if not, their reasons for not doing so. Patients were deemed nonadherent if they did not take methotrexate correctly for 90% of the time over a period of 6 months.
Lower adherence was significantly associated with negative or uncertain views about treatment, with an odds ratio of 2.7. Conversely, being positive or certain about treatment lowered patients’ odds of being nonadherent (OR, 0.32).
“People who are uncertain about how to attribute illness events are less likely to adhere within the first 6 months of starting methotrexate therapy,” Ms. Hope and her coauthors observed.
“Encouraging patients to actively monitor their progress with therapy and providing them with support to understand likely effects of methotrexate may help optimize disease-modifying antirheumatic drug use,” they concluded.
Ms. Hope and Dr. Beauvais had no conflicts of interest to disclose. The FORGET survey was funded by Chugai Pharma France.
MADRID – Negative beliefs and uncertainty regarding treatment with methotrexate, as well as dislike for the drug, contribute the most to rheumatoid arthritis patients’ nonadherence to the therapy, with one study finding that about one-third were nonadherent at the time they were eligible to start biologic therapy.
The French cross-sectional survey of 244 patients who were not responding to methotrexate found that 34% actually had poor adherence, including 54% who skipped doses and 38% who temporarily stopped treatment without their doctors’ recommendation. In comparison, patients who were deemed adherent had a lower rate of skipping doses (15%) or temporarily stopped treatment without their doctors’ recommendation (4%), both of which were statistically significant differences, Catherine Beauvais, MD, reported at the European Congress of Rheumatology. Nonadherence was defined as taking less than 80% of doses, according to the CQR19 (Compliance Questionnaire for Rheumatology).
“We have identified profiles of adherence,” Dr. Beauvais of Saint-Antoine Hospital in Paris commented in an interview.
“Among nonadherent patients, there are two profiles,” she added. “We have patients who are not responding to methotrexate but they also have negative beliefs, low levels of support, and they have professional impairment. [Then,] there are patients who do not like their treatment [although it is being well tolerated].”
The other profiles identified were of patients with good adherence to methotrexate with a higher or lower impact on patient outcomes.
In a poster presentation, Dr. Beauvais and her coauthors suggested that the “detection of patients’ profiles may allow targeted strategies to improve or maintain adherence.”
The FORGET survey was conducted over a 3-month period starting in July 2016. A total of 78 rheumatologists recruited patients who were inadequately responding to methotrexate and, thus, eligible to start biologic treatment for rheumatoid arthritis. Both the rheumatologists and the patients completed questionnaires, with 200 questionnaires being completed by patients and their rheumatologist.
As might be suspected for an RA population, 72% of respondents were women, with a mean age of 54 years. Over half (58%) had at least one comorbidity, and the mean disease activity score in 28 joints at the time of the survey was 4.07.
Significant factors for nonadherence were feeling constrained about taking treatment, cited by 29% of respondents; feeling “less good” with a change in dosage (31%); and feeling that treatment was “doing me more harm than good” (19% of respondents).
Surprisingly, most rheumatologists seemed to be unaware of their patients’ lack of adherence to their medication, despite saying that they asked about adherence in more than 80% of their patients.
Rheumatologists proposed the addition of a biologic to methotrexate more often if patients were nonadherent than if patients showed good compliance (91% vs. 68%; P less than .01).
Effect of patient attitudes on compliance
A team of U.K. researchers evaluated how attitudes toward treatment with methotrexate affected patients’ compliance in a separate poster presentation at the meeting.
RAMS is a 1-year observational study of patients with RA who are starting treatment with methotrexate. Patients recruited into the study completed weekly diaries, noting whether they took methotrexate (adherence) and, if not, their reasons for not doing so. Patients were deemed nonadherent if they did not take methotrexate correctly for 90% of the time over a period of 6 months.
Lower adherence was significantly associated with negative or uncertain views about treatment, with an odds ratio of 2.7. Conversely, being positive or certain about treatment lowered patients’ odds of being nonadherent (OR, 0.32).
“People who are uncertain about how to attribute illness events are less likely to adhere within the first 6 months of starting methotrexate therapy,” Ms. Hope and her coauthors observed.
“Encouraging patients to actively monitor their progress with therapy and providing them with support to understand likely effects of methotrexate may help optimize disease-modifying antirheumatic drug use,” they concluded.
Ms. Hope and Dr. Beauvais had no conflicts of interest to disclose. The FORGET survey was funded by Chugai Pharma France.
MADRID – Negative beliefs and uncertainty regarding treatment with methotrexate, as well as dislike for the drug, contribute the most to rheumatoid arthritis patients’ nonadherence to the therapy, with one study finding that about one-third were nonadherent at the time they were eligible to start biologic therapy.
The French cross-sectional survey of 244 patients who were not responding to methotrexate found that 34% actually had poor adherence, including 54% who skipped doses and 38% who temporarily stopped treatment without their doctors’ recommendation. In comparison, patients who were deemed adherent had a lower rate of skipping doses (15%) or temporarily stopped treatment without their doctors’ recommendation (4%), both of which were statistically significant differences, Catherine Beauvais, MD, reported at the European Congress of Rheumatology. Nonadherence was defined as taking less than 80% of doses, according to the CQR19 (Compliance Questionnaire for Rheumatology).
“We have identified profiles of adherence,” Dr. Beauvais of Saint-Antoine Hospital in Paris commented in an interview.
“Among nonadherent patients, there are two profiles,” she added. “We have patients who are not responding to methotrexate but they also have negative beliefs, low levels of support, and they have professional impairment. [Then,] there are patients who do not like their treatment [although it is being well tolerated].”
The other profiles identified were of patients with good adherence to methotrexate with a higher or lower impact on patient outcomes.
In a poster presentation, Dr. Beauvais and her coauthors suggested that the “detection of patients’ profiles may allow targeted strategies to improve or maintain adherence.”
The FORGET survey was conducted over a 3-month period starting in July 2016. A total of 78 rheumatologists recruited patients who were inadequately responding to methotrexate and, thus, eligible to start biologic treatment for rheumatoid arthritis. Both the rheumatologists and the patients completed questionnaires, with 200 questionnaires being completed by patients and their rheumatologist.
As might be suspected for an RA population, 72% of respondents were women, with a mean age of 54 years. Over half (58%) had at least one comorbidity, and the mean disease activity score in 28 joints at the time of the survey was 4.07.
Significant factors for nonadherence were feeling constrained about taking treatment, cited by 29% of respondents; feeling “less good” with a change in dosage (31%); and feeling that treatment was “doing me more harm than good” (19% of respondents).
Surprisingly, most rheumatologists seemed to be unaware of their patients’ lack of adherence to their medication, despite saying that they asked about adherence in more than 80% of their patients.
Rheumatologists proposed the addition of a biologic to methotrexate more often if patients were nonadherent than if patients showed good compliance (91% vs. 68%; P less than .01).
Effect of patient attitudes on compliance
A team of U.K. researchers evaluated how attitudes toward treatment with methotrexate affected patients’ compliance in a separate poster presentation at the meeting.
RAMS is a 1-year observational study of patients with RA who are starting treatment with methotrexate. Patients recruited into the study completed weekly diaries, noting whether they took methotrexate (adherence) and, if not, their reasons for not doing so. Patients were deemed nonadherent if they did not take methotrexate correctly for 90% of the time over a period of 6 months.
Lower adherence was significantly associated with negative or uncertain views about treatment, with an odds ratio of 2.7. Conversely, being positive or certain about treatment lowered patients’ odds of being nonadherent (OR, 0.32).
“People who are uncertain about how to attribute illness events are less likely to adhere within the first 6 months of starting methotrexate therapy,” Ms. Hope and her coauthors observed.
“Encouraging patients to actively monitor their progress with therapy and providing them with support to understand likely effects of methotrexate may help optimize disease-modifying antirheumatic drug use,” they concluded.
Ms. Hope and Dr. Beauvais had no conflicts of interest to disclose. The FORGET survey was funded by Chugai Pharma France.
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: One-third (34%) of RA patients were nonadherent to methotrexate at the initiation of biologic therapy; having negative and uncertain beliefs about the effects of treatment increased the odds of nonadherence.
Data source: The cross-sectional FORGET survey of 78 rheumatologists and 269 patients with rheumatoid arthritis conducted in France and the Rheumatoid Arthritis Medications Study (RAMS) of 200 adherent and nonadherent patients.
Disclosures: The authors had no conflicts of interest to disclose. The FORGET survey was funded by Chugai Pharma France.
Acute liver failure in the ED
Acute liver failure (ALF), is a life-threatening deterioration of liver function in people without preexisting cirrhosis. It can be caused by acetaminophen toxicity, pregnancy, ischemia, hepatitis A infection, and Wilson disease, among other things.
In emergency medicine, ALF can pose serious dilemmas. While transplantation has drastically improved survival rates in recent decades, it is not always required, and no firm criteria for transplantation exist.
But delays in the decision to go ahead with a liver transplant can lead to death.
A new literature review aims to distill the decision-making process for emergency medicine practitioners. Knowing which candidates will benefit and when to perform transplantation “is crucial in improving the likelihood of survival,” its authors say, because of the many factors involved.
In a paper published online in May in The American Journal of Emergency Medicine (2017 May. doi. 10.1016/j.ajem.2017.05.028), Hamid Shokoohi, MD, and his colleagues at George Washington University Medical Center in Washington say that establishing the cause of acute liver failure is essential to making treatment decisions, as some causes are associated with poorer prognosis without transplantation.
“We wanted to improve awareness among emergency medicine physicians, who are the first in the chain of command for transferring patients to a transplant site,” said Ali Pourmand, MD, of George Washington University, Washington, and the corresponding author of the study. “The high risk of early death among these cases makes it necessary for emergency physicians to consider coexisting etiology, be aware of indications and criteria available to determine the need for emergent transplantation, and be able to expedite patient transfer to a transplant center, when indicated.”
As patients presenting with ALF are likely too impaired be able to provide a history, and physical exam findings may be nonspecific, laboratory findings are key in establishing both severity and likely cause. ALF patients in general will have a prolonged prothrombin time, markedly elevated aminotransferase levels, elevated bilirubin, and low platelet count.
Patients with ALF caused by acetaminophen toxicity (the most common cause of ALF in the United States) are likely to present with very high aminotransferase levels, low bilirubin, and high international normalized ratio (INR). Those with viral causes of ALF, meanwhile, tend to have aminotransferase levels of 1,000-2,000 IU/L, and alanine transaminase higher than aspartate transaminase.
Prognosis without transplantation is considerably poorer in patients with severe ALF caused by Wilson disease, Budd-Chiari syndrome, or idiosyncratic drug reactions, compared with those who experience viral hepatitis or acetaminophen toxicity.
Dr. Shokoohi and his colleagues noted that two validated scoring systems can be used to assess prognosis for severe ALF. The King’s College Criteria can be used to establish prognosis for ALF caused by acetaminophen, and ALF from other causes, while the MELD score, recommended by the American Association for the Study of Liver Diseases, incorporates bilirubin, INR, sodium, and creatinine levels to predict prognosis. Both of these scoring systems can be used to inform decisions about transplantation.
Finally, the authors advised that patients with alcoholic liver disease be considered under the same criteria for transplantation as those with other causes of ALF. “Recent research has shown that only a minority of patients ... will have poor follow-up and noncompliance to therapy and/or will revert to heavy alcohol use or abuse after transplant,” they wrote in their analysis. The researchers disclosed no outside funding of conflicts of interest related to their article.
Acute liver failure (ALF), is a life-threatening deterioration of liver function in people without preexisting cirrhosis. It can be caused by acetaminophen toxicity, pregnancy, ischemia, hepatitis A infection, and Wilson disease, among other things.
In emergency medicine, ALF can pose serious dilemmas. While transplantation has drastically improved survival rates in recent decades, it is not always required, and no firm criteria for transplantation exist.
But delays in the decision to go ahead with a liver transplant can lead to death.
A new literature review aims to distill the decision-making process for emergency medicine practitioners. Knowing which candidates will benefit and when to perform transplantation “is crucial in improving the likelihood of survival,” its authors say, because of the many factors involved.
In a paper published online in May in The American Journal of Emergency Medicine (2017 May. doi. 10.1016/j.ajem.2017.05.028), Hamid Shokoohi, MD, and his colleagues at George Washington University Medical Center in Washington say that establishing the cause of acute liver failure is essential to making treatment decisions, as some causes are associated with poorer prognosis without transplantation.
“We wanted to improve awareness among emergency medicine physicians, who are the first in the chain of command for transferring patients to a transplant site,” said Ali Pourmand, MD, of George Washington University, Washington, and the corresponding author of the study. “The high risk of early death among these cases makes it necessary for emergency physicians to consider coexisting etiology, be aware of indications and criteria available to determine the need for emergent transplantation, and be able to expedite patient transfer to a transplant center, when indicated.”
As patients presenting with ALF are likely too impaired be able to provide a history, and physical exam findings may be nonspecific, laboratory findings are key in establishing both severity and likely cause. ALF patients in general will have a prolonged prothrombin time, markedly elevated aminotransferase levels, elevated bilirubin, and low platelet count.
Patients with ALF caused by acetaminophen toxicity (the most common cause of ALF in the United States) are likely to present with very high aminotransferase levels, low bilirubin, and high international normalized ratio (INR). Those with viral causes of ALF, meanwhile, tend to have aminotransferase levels of 1,000-2,000 IU/L, and alanine transaminase higher than aspartate transaminase.
Prognosis without transplantation is considerably poorer in patients with severe ALF caused by Wilson disease, Budd-Chiari syndrome, or idiosyncratic drug reactions, compared with those who experience viral hepatitis or acetaminophen toxicity.
Dr. Shokoohi and his colleagues noted that two validated scoring systems can be used to assess prognosis for severe ALF. The King’s College Criteria can be used to establish prognosis for ALF caused by acetaminophen, and ALF from other causes, while the MELD score, recommended by the American Association for the Study of Liver Diseases, incorporates bilirubin, INR, sodium, and creatinine levels to predict prognosis. Both of these scoring systems can be used to inform decisions about transplantation.
Finally, the authors advised that patients with alcoholic liver disease be considered under the same criteria for transplantation as those with other causes of ALF. “Recent research has shown that only a minority of patients ... will have poor follow-up and noncompliance to therapy and/or will revert to heavy alcohol use or abuse after transplant,” they wrote in their analysis. The researchers disclosed no outside funding of conflicts of interest related to their article.
Acute liver failure (ALF), is a life-threatening deterioration of liver function in people without preexisting cirrhosis. It can be caused by acetaminophen toxicity, pregnancy, ischemia, hepatitis A infection, and Wilson disease, among other things.
In emergency medicine, ALF can pose serious dilemmas. While transplantation has drastically improved survival rates in recent decades, it is not always required, and no firm criteria for transplantation exist.
But delays in the decision to go ahead with a liver transplant can lead to death.
A new literature review aims to distill the decision-making process for emergency medicine practitioners. Knowing which candidates will benefit and when to perform transplantation “is crucial in improving the likelihood of survival,” its authors say, because of the many factors involved.
In a paper published online in May in The American Journal of Emergency Medicine (2017 May. doi. 10.1016/j.ajem.2017.05.028), Hamid Shokoohi, MD, and his colleagues at George Washington University Medical Center in Washington say that establishing the cause of acute liver failure is essential to making treatment decisions, as some causes are associated with poorer prognosis without transplantation.
“We wanted to improve awareness among emergency medicine physicians, who are the first in the chain of command for transferring patients to a transplant site,” said Ali Pourmand, MD, of George Washington University, Washington, and the corresponding author of the study. “The high risk of early death among these cases makes it necessary for emergency physicians to consider coexisting etiology, be aware of indications and criteria available to determine the need for emergent transplantation, and be able to expedite patient transfer to a transplant center, when indicated.”
As patients presenting with ALF are likely too impaired be able to provide a history, and physical exam findings may be nonspecific, laboratory findings are key in establishing both severity and likely cause. ALF patients in general will have a prolonged prothrombin time, markedly elevated aminotransferase levels, elevated bilirubin, and low platelet count.
Patients with ALF caused by acetaminophen toxicity (the most common cause of ALF in the United States) are likely to present with very high aminotransferase levels, low bilirubin, and high international normalized ratio (INR). Those with viral causes of ALF, meanwhile, tend to have aminotransferase levels of 1,000-2,000 IU/L, and alanine transaminase higher than aspartate transaminase.
Prognosis without transplantation is considerably poorer in patients with severe ALF caused by Wilson disease, Budd-Chiari syndrome, or idiosyncratic drug reactions, compared with those who experience viral hepatitis or acetaminophen toxicity.
Dr. Shokoohi and his colleagues noted that two validated scoring systems can be used to assess prognosis for severe ALF. The King’s College Criteria can be used to establish prognosis for ALF caused by acetaminophen, and ALF from other causes, while the MELD score, recommended by the American Association for the Study of Liver Diseases, incorporates bilirubin, INR, sodium, and creatinine levels to predict prognosis. Both of these scoring systems can be used to inform decisions about transplantation.
Finally, the authors advised that patients with alcoholic liver disease be considered under the same criteria for transplantation as those with other causes of ALF. “Recent research has shown that only a minority of patients ... will have poor follow-up and noncompliance to therapy and/or will revert to heavy alcohol use or abuse after transplant,” they wrote in their analysis. The researchers disclosed no outside funding of conflicts of interest related to their article.
FROM THE AMERICAN JOURNAL OF EMERGENCY MEDICINE
Vaginal salpingo-oophorectomy: Tips and tricks

Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
This video is brought to you by![]()
Four drugs better than three for myeloma induction
MADRID – A four-drug induction regimen induced quicker and deeper remissions than sequential triplet regimens in patients with newly diagnosed multiple myeloma.
In addition, fast, deep remissions may lead to improved progression-free survival (PFS) following autologous stem cell transplantation (ASCT), said investigators from a U.K. Medical Research Council study.
In the phase 3 randomized, parallel group Myeloma XI study, very good partial responses (VGPR) or better were seen following induction in 79.5% of patients assigned to the quadruplet (KCRD) of carfilzomib (Kyprolis), cyclophosphamide, lenalidomide (Revlimid), and dexamethasone, compared with 60.8% for those assigned to cyclophosphamide, lenalidomide, and dexamethasone (CRD) and 52.8% for those assigned to cyclophosphamide, thalidomide, and dexamethasone (CTD), said Charlotte Pawlyn, MD, PhD, at the annual congress of the European Hematology Association.
“In our study, we see a very much deeper response after initial induction with the quadruplet regimen, compared with triplet regimens,” Dr. Pawlyn of the Institute of Cancer Research, London, said in an interview.
Medical Research Council investigators showed in the Myeloma IX study that among patients who had a less than VGPR to an immunomodulator-based triplet regimen such as CRD, a triplet regimen including the proteasome inhibitor bortezomib (Velcade) could improve both pre- and post-transplant response rates, and that the improved responses translated into improved PFS.
For the Myeloma XI study, the investigators employed the same response-adapted approach to compare outcomes following induction with the proteasome inhibitor–containing KCRD regimen and the lenalidomide- or thalidomide-based regimens.

They chose carfilzomib as the proteasome-inhibitor backbone of the quadruplet because of its selective, irreversible target binding, lower incidence of peripheral neuropathy (compared with bortezomib), and efficacy in both the frontline and relapsed/refractory setting, she said.
Asked why the comparator regimens did not contain a proteasome inhibitor, Dr. Pawlyn said that while the current standard for induction therapy in the United Kingdom is bortezomib, thalidomide, and dexamethasone, CTD was the standard of care at the time of study planning and initial enrollment.
The trial was open to all patients in the United Kingdom of all ages with newly diagnosed symptomatic multiple myeloma, with pathways for both transplant-eligible and transplant-ineligible patients. The only main exclusion criteria were for patients with dialysis-dependent renal failure and for those who had a prior or concurrent malignancy.
A total of 1,021 patients were assigned to each of the CTD and CRD cohorts, and 526 patients were assigned to the KCRD cohort. The cohorts were well balanced by sex, age, World Health Organization performance score, and other parameters.
Patients randomized to either CTD or CRD were assessed for response after a minimum of four induction cycles, with treatment continued until best response. Those with a VGPR or better went on to ASCT, while those with a partial response were randomized to either a second induction with cyclophosphamide, bortezomib, and dexamethasone (CVD) or no CVD, and then proceeded to transplant. Patients with stable disease or disease progression in either of these arms went on to CVD prior to ASCT.
In the KCRD arm, all patients went from induction to transplant. Following ASCT, patients were randomized to either observation or lenalidomide maintenance.
A higher proportion of patients assigned to KCRD completed the minimum of four induction cycles, and few patients in any trial arm had to stop induction therapy because of adverse events. Dose modifications were required in 63.9% of patients on KCRD, 56.3% of patients on CRD, and 82.2% of patients on CTD.
There was no significant cardiac signal seen in the study, and no difference in the incidence of venous thromboembolic events among the treatment arms.
As noted before, rates of VGPR or better after initial induction were highest in the KCRD arm, at 79.5%, compared with 60% for CRD, and 52.8% for CTD.
“The KCRD quadruplet achieved the highest speed and depth of response,” Dr. Pawlyn said.
The pattern of responses was similar across all cytogenetic risk groups, she added.
A higher proportion of patients treated with KCRD went on to ASCT, and the pattern of deeper responses among patients who underwent induction with KCRD persisted, with 92.1% of patients having a post-transplant VGPR or better, compared with 81.8% for CRD and 77.0% for CTD (statistical significance not shown).
Again, the pattern of responses post-transplant was similar across cytogenetic risk groups.
The investigators anticipate receiving PFS results from the Myeloma XI study in the third or fourth quarter of 2017.
The study was sponsored by the University of Leeds (England), with support from the U.K. National Cancer Research Institute, Cancer Research UK, and Myeloma UK, and collaboration with Celgene, Merck Sharp & Dohme, and Amgen. Dr. Pawlyn disclosed travel support from Celgene and Janssen, and honoraria from Celgene and Takeda.
MADRID – A four-drug induction regimen induced quicker and deeper remissions than sequential triplet regimens in patients with newly diagnosed multiple myeloma.
In addition, fast, deep remissions may lead to improved progression-free survival (PFS) following autologous stem cell transplantation (ASCT), said investigators from a U.K. Medical Research Council study.
In the phase 3 randomized, parallel group Myeloma XI study, very good partial responses (VGPR) or better were seen following induction in 79.5% of patients assigned to the quadruplet (KCRD) of carfilzomib (Kyprolis), cyclophosphamide, lenalidomide (Revlimid), and dexamethasone, compared with 60.8% for those assigned to cyclophosphamide, lenalidomide, and dexamethasone (CRD) and 52.8% for those assigned to cyclophosphamide, thalidomide, and dexamethasone (CTD), said Charlotte Pawlyn, MD, PhD, at the annual congress of the European Hematology Association.
“In our study, we see a very much deeper response after initial induction with the quadruplet regimen, compared with triplet regimens,” Dr. Pawlyn of the Institute of Cancer Research, London, said in an interview.
Medical Research Council investigators showed in the Myeloma IX study that among patients who had a less than VGPR to an immunomodulator-based triplet regimen such as CRD, a triplet regimen including the proteasome inhibitor bortezomib (Velcade) could improve both pre- and post-transplant response rates, and that the improved responses translated into improved PFS.
For the Myeloma XI study, the investigators employed the same response-adapted approach to compare outcomes following induction with the proteasome inhibitor–containing KCRD regimen and the lenalidomide- or thalidomide-based regimens.
They chose carfilzomib as the proteasome-inhibitor backbone of the quadruplet because of its selective, irreversible target binding, lower incidence of peripheral neuropathy (compared with bortezomib), and efficacy in both the frontline and relapsed/refractory setting, she said.
Asked why the comparator regimens did not contain a proteasome inhibitor, Dr. Pawlyn said that while the current standard for induction therapy in the United Kingdom is bortezomib, thalidomide, and dexamethasone, CTD was the standard of care at the time of study planning and initial enrollment.
The trial was open to all patients in the United Kingdom of all ages with newly diagnosed symptomatic multiple myeloma, with pathways for both transplant-eligible and transplant-ineligible patients. The only main exclusion criteria were for patients with dialysis-dependent renal failure and for those who had a prior or concurrent malignancy.
A total of 1,021 patients were assigned to each of the CTD and CRD cohorts, and 526 patients were assigned to the KCRD cohort. The cohorts were well balanced by sex, age, World Health Organization performance score, and other parameters.
Patients randomized to either CTD or CRD were assessed for response after a minimum of four induction cycles, with treatment continued until best response. Those with a VGPR or better went on to ASCT, while those with a partial response were randomized to either a second induction with cyclophosphamide, bortezomib, and dexamethasone (CVD) or no CVD, and then proceeded to transplant. Patients with stable disease or disease progression in either of these arms went on to CVD prior to ASCT.
In the KCRD arm, all patients went from induction to transplant. Following ASCT, patients were randomized to either observation or lenalidomide maintenance.
A higher proportion of patients assigned to KCRD completed the minimum of four induction cycles, and few patients in any trial arm had to stop induction therapy because of adverse events. Dose modifications were required in 63.9% of patients on KCRD, 56.3% of patients on CRD, and 82.2% of patients on CTD.
There was no significant cardiac signal seen in the study, and no difference in the incidence of venous thromboembolic events among the treatment arms.
As noted before, rates of VGPR or better after initial induction were highest in the KCRD arm, at 79.5%, compared with 60% for CRD, and 52.8% for CTD.
“The KCRD quadruplet achieved the highest speed and depth of response,” Dr. Pawlyn said.
The pattern of responses was similar across all cytogenetic risk groups, she added.
A higher proportion of patients treated with KCRD went on to ASCT, and the pattern of deeper responses among patients who underwent induction with KCRD persisted, with 92.1% of patients having a post-transplant VGPR or better, compared with 81.8% for CRD and 77.0% for CTD (statistical significance not shown).
Again, the pattern of responses post-transplant was similar across cytogenetic risk groups.
The investigators anticipate receiving PFS results from the Myeloma XI study in the third or fourth quarter of 2017.
The study was sponsored by the University of Leeds (England), with support from the U.K. National Cancer Research Institute, Cancer Research UK, and Myeloma UK, and collaboration with Celgene, Merck Sharp & Dohme, and Amgen. Dr. Pawlyn disclosed travel support from Celgene and Janssen, and honoraria from Celgene and Takeda.
MADRID – A four-drug induction regimen induced quicker and deeper remissions than sequential triplet regimens in patients with newly diagnosed multiple myeloma.
In addition, fast, deep remissions may lead to improved progression-free survival (PFS) following autologous stem cell transplantation (ASCT), said investigators from a U.K. Medical Research Council study.
In the phase 3 randomized, parallel group Myeloma XI study, very good partial responses (VGPR) or better were seen following induction in 79.5% of patients assigned to the quadruplet (KCRD) of carfilzomib (Kyprolis), cyclophosphamide, lenalidomide (Revlimid), and dexamethasone, compared with 60.8% for those assigned to cyclophosphamide, lenalidomide, and dexamethasone (CRD) and 52.8% for those assigned to cyclophosphamide, thalidomide, and dexamethasone (CTD), said Charlotte Pawlyn, MD, PhD, at the annual congress of the European Hematology Association.
“In our study, we see a very much deeper response after initial induction with the quadruplet regimen, compared with triplet regimens,” Dr. Pawlyn of the Institute of Cancer Research, London, said in an interview.
Medical Research Council investigators showed in the Myeloma IX study that among patients who had a less than VGPR to an immunomodulator-based triplet regimen such as CRD, a triplet regimen including the proteasome inhibitor bortezomib (Velcade) could improve both pre- and post-transplant response rates, and that the improved responses translated into improved PFS.
For the Myeloma XI study, the investigators employed the same response-adapted approach to compare outcomes following induction with the proteasome inhibitor–containing KCRD regimen and the lenalidomide- or thalidomide-based regimens.
They chose carfilzomib as the proteasome-inhibitor backbone of the quadruplet because of its selective, irreversible target binding, lower incidence of peripheral neuropathy (compared with bortezomib), and efficacy in both the frontline and relapsed/refractory setting, she said.
Asked why the comparator regimens did not contain a proteasome inhibitor, Dr. Pawlyn said that while the current standard for induction therapy in the United Kingdom is bortezomib, thalidomide, and dexamethasone, CTD was the standard of care at the time of study planning and initial enrollment.
The trial was open to all patients in the United Kingdom of all ages with newly diagnosed symptomatic multiple myeloma, with pathways for both transplant-eligible and transplant-ineligible patients. The only main exclusion criteria were for patients with dialysis-dependent renal failure and for those who had a prior or concurrent malignancy.
A total of 1,021 patients were assigned to each of the CTD and CRD cohorts, and 526 patients were assigned to the KCRD cohort. The cohorts were well balanced by sex, age, World Health Organization performance score, and other parameters.
Patients randomized to either CTD or CRD were assessed for response after a minimum of four induction cycles, with treatment continued until best response. Those with a VGPR or better went on to ASCT, while those with a partial response were randomized to either a second induction with cyclophosphamide, bortezomib, and dexamethasone (CVD) or no CVD, and then proceeded to transplant. Patients with stable disease or disease progression in either of these arms went on to CVD prior to ASCT.
In the KCRD arm, all patients went from induction to transplant. Following ASCT, patients were randomized to either observation or lenalidomide maintenance.
A higher proportion of patients assigned to KCRD completed the minimum of four induction cycles, and few patients in any trial arm had to stop induction therapy because of adverse events. Dose modifications were required in 63.9% of patients on KCRD, 56.3% of patients on CRD, and 82.2% of patients on CTD.
There was no significant cardiac signal seen in the study, and no difference in the incidence of venous thromboembolic events among the treatment arms.
As noted before, rates of VGPR or better after initial induction were highest in the KCRD arm, at 79.5%, compared with 60% for CRD, and 52.8% for CTD.
“The KCRD quadruplet achieved the highest speed and depth of response,” Dr. Pawlyn said.
The pattern of responses was similar across all cytogenetic risk groups, she added.
A higher proportion of patients treated with KCRD went on to ASCT, and the pattern of deeper responses among patients who underwent induction with KCRD persisted, with 92.1% of patients having a post-transplant VGPR or better, compared with 81.8% for CRD and 77.0% for CTD (statistical significance not shown).
Again, the pattern of responses post-transplant was similar across cytogenetic risk groups.
The investigators anticipate receiving PFS results from the Myeloma XI study in the third or fourth quarter of 2017.
The study was sponsored by the University of Leeds (England), with support from the U.K. National Cancer Research Institute, Cancer Research UK, and Myeloma UK, and collaboration with Celgene, Merck Sharp & Dohme, and Amgen. Dr. Pawlyn disclosed travel support from Celgene and Janssen, and honoraria from Celgene and Takeda.
AT THE EHA CONGRESS
Key clinical point:
Major finding: An induction quadruplet containing carfilzomib induced a higher rate of very good partial responses or better vs. regimens without a proteasome inhibitor.
Data source: A randomized, open-label, parallel group study of 2,568 patients with newly diagnosed multiple myeloma.
Disclosures: The study was sponsored by the University of Leeds (England), with support from the U.K. National Cancer Research Institute, Cancer Research UK, and Myeloma UK, and collaboration with Celgene, Merck Sharp & Dohme, and Amgen. Dr. Pawlyn disclosed travel support from Celgene and Janssen, and honoraria from Celgene and Takeda.
Surgeons can take steps to reduce excess opioids
NEW YORK – Surgeons prescribe approximately 10% of the 280 million schedule II prescriptions written every year. Because patients report taking on average 20%-30% of their opioid pills, a large amount of these drugs end up being diverted to nonpatients and contributing to the opioid epidemic in the United States, said Jonah J. Stulberg, MD.
”You can’t turn on the television, pick up the newspaper, do anything on social media without seeing a lot of headlines about the tragedies occurring because of opioid abuse,” said Dr. Stulberg, assistant professor of surgery at Northwestern University in Chicago.
The majority of opioid abusers are obtaining the drugs through diversion, he said. “So the prescriptions we’re writing and the excess pills we have available, they do make a difference. They’re making it down the pipeline.”
Some practical steps
There are practical actions surgeons can take to try to reduce the sheer volume of prescription opioids that end up in the hands of people for whom they are not intended, Dr. Stulberg said at the American College of Surgeons Quality and Safety Conference.
Sign up for a prescription monitoring program, he suggested. These programs are now available in 49 states (Missouri is the exception). “It’s really easy to create an account as a provider.” Just search online for your state’s prescription monitoring program and enter your contact information, he said. The state will then ask you for some basic information.
Take it one step further and integrate your prescription monitoring program into your electronic medical records, Dr. Stulberg said. “We’re starting to integrate it in all hospitals in Illinois. That means when the surgeon or the nurse providers look up the patient, they will know if the patient got two other prescriptions in the last 2 weeks.” He added, “You can ask if they need more pills before adding to the surplus.”
Another practical strategy is to give patients better access to opioid disposal. Find out where the nearest drug return receptacle or kiosk is located – a pharmacy, police station, or elsewhere – and inform your patients. “We put opioid retrieval boxes in our clinic. When patients are educated about this, they bring [excess pills] back.”
Minimizing opioid prescribing in surgery
“This is not a problem of one individual specialty,” Dr. Stulberg said. “We have a problem of culture, a problem of mindset. So we need to approach solving this problem, in my opinion, from that perspective.”
Start with setting patient expectations in the preoperative period. Explain what the surgery entails and the amount of pain they should expect. “Patients have to understand what we’re doing hurts but we can manage that pain. It can make a big difference in their satisfaction … and also in how much medication they end up taking.”
In addition, perform preoperative risk screening for opioid abuse. “There is very good evidence that patients with addictions to other drugs, alcohol, or who have previous drug use, are much more likely to continue using prescription pain medications after a surgical encounter – 6 months to 12 months later.”
In addition, a paradigm shift in thinking is needed. “When we’re talking about pain control in the clinic and minimizing opioids during a surgical episode, we should be focusing on function,” he said. Orthopedic surgery is a prime example, where physicians encourage patients to start mobility exercises the same day of surgery because evidence shows it helps restore function faster.
Surgeons should tell patients that “the goal of how we are treating your pain is getting you to your optimal function.” Then check on function recovery postoperatively, he added. “We don’t follow-up – that is not part of our standard postoperative pathway in any way.”
Consider prescribing fewer pills postoperatively
If surgeons have a prescription feedback mechanism in place, they might know how many opioid pills patients are actually taking. “If I gave 20 pills to the last 10 patients but they only took 8 on average – can I go lower?” Dr. Stulberg said.
Researchers conducted a study to determine opioid needs for 80% of the patients at their institution after certain types of surgery (Ann Surg. 2017;265:709-14).
The study determined the number of pills that 80% of patients found controlled their pain: after partial mastectomy, 5; after partial mastectomy with sentinel lymph node biopsy, 10; after laparoscopic cholecystectomy, 15; after laparoscopic inguinal hernia repair, 15; and after open inguinal hernia repair, 15. These numbers represent about 43% of the actual number prescribed overall, so many patients are getting more medications than they require.
Dr. Stulberg suggested that surgeons could use the data from this study to counter any pushback from others at their institution reluctant to prescribe fewer opioids for their patients.
Dr. Stulberg did not have any relevant disclosures.
NEW YORK – Surgeons prescribe approximately 10% of the 280 million schedule II prescriptions written every year. Because patients report taking on average 20%-30% of their opioid pills, a large amount of these drugs end up being diverted to nonpatients and contributing to the opioid epidemic in the United States, said Jonah J. Stulberg, MD.
”You can’t turn on the television, pick up the newspaper, do anything on social media without seeing a lot of headlines about the tragedies occurring because of opioid abuse,” said Dr. Stulberg, assistant professor of surgery at Northwestern University in Chicago.
The majority of opioid abusers are obtaining the drugs through diversion, he said. “So the prescriptions we’re writing and the excess pills we have available, they do make a difference. They’re making it down the pipeline.”
Some practical steps
There are practical actions surgeons can take to try to reduce the sheer volume of prescription opioids that end up in the hands of people for whom they are not intended, Dr. Stulberg said at the American College of Surgeons Quality and Safety Conference.
Sign up for a prescription monitoring program, he suggested. These programs are now available in 49 states (Missouri is the exception). “It’s really easy to create an account as a provider.” Just search online for your state’s prescription monitoring program and enter your contact information, he said. The state will then ask you for some basic information.
Take it one step further and integrate your prescription monitoring program into your electronic medical records, Dr. Stulberg said. “We’re starting to integrate it in all hospitals in Illinois. That means when the surgeon or the nurse providers look up the patient, they will know if the patient got two other prescriptions in the last 2 weeks.” He added, “You can ask if they need more pills before adding to the surplus.”
Another practical strategy is to give patients better access to opioid disposal. Find out where the nearest drug return receptacle or kiosk is located – a pharmacy, police station, or elsewhere – and inform your patients. “We put opioid retrieval boxes in our clinic. When patients are educated about this, they bring [excess pills] back.”
Minimizing opioid prescribing in surgery
“This is not a problem of one individual specialty,” Dr. Stulberg said. “We have a problem of culture, a problem of mindset. So we need to approach solving this problem, in my opinion, from that perspective.”
Start with setting patient expectations in the preoperative period. Explain what the surgery entails and the amount of pain they should expect. “Patients have to understand what we’re doing hurts but we can manage that pain. It can make a big difference in their satisfaction … and also in how much medication they end up taking.”
In addition, perform preoperative risk screening for opioid abuse. “There is very good evidence that patients with addictions to other drugs, alcohol, or who have previous drug use, are much more likely to continue using prescription pain medications after a surgical encounter – 6 months to 12 months later.”
In addition, a paradigm shift in thinking is needed. “When we’re talking about pain control in the clinic and minimizing opioids during a surgical episode, we should be focusing on function,” he said. Orthopedic surgery is a prime example, where physicians encourage patients to start mobility exercises the same day of surgery because evidence shows it helps restore function faster.
Surgeons should tell patients that “the goal of how we are treating your pain is getting you to your optimal function.” Then check on function recovery postoperatively, he added. “We don’t follow-up – that is not part of our standard postoperative pathway in any way.”
Consider prescribing fewer pills postoperatively
If surgeons have a prescription feedback mechanism in place, they might know how many opioid pills patients are actually taking. “If I gave 20 pills to the last 10 patients but they only took 8 on average – can I go lower?” Dr. Stulberg said.
Researchers conducted a study to determine opioid needs for 80% of the patients at their institution after certain types of surgery (Ann Surg. 2017;265:709-14).
The study determined the number of pills that 80% of patients found controlled their pain: after partial mastectomy, 5; after partial mastectomy with sentinel lymph node biopsy, 10; after laparoscopic cholecystectomy, 15; after laparoscopic inguinal hernia repair, 15; and after open inguinal hernia repair, 15. These numbers represent about 43% of the actual number prescribed overall, so many patients are getting more medications than they require.
Dr. Stulberg suggested that surgeons could use the data from this study to counter any pushback from others at their institution reluctant to prescribe fewer opioids for their patients.
Dr. Stulberg did not have any relevant disclosures.
NEW YORK – Surgeons prescribe approximately 10% of the 280 million schedule II prescriptions written every year. Because patients report taking on average 20%-30% of their opioid pills, a large amount of these drugs end up being diverted to nonpatients and contributing to the opioid epidemic in the United States, said Jonah J. Stulberg, MD.
”You can’t turn on the television, pick up the newspaper, do anything on social media without seeing a lot of headlines about the tragedies occurring because of opioid abuse,” said Dr. Stulberg, assistant professor of surgery at Northwestern University in Chicago.
The majority of opioid abusers are obtaining the drugs through diversion, he said. “So the prescriptions we’re writing and the excess pills we have available, they do make a difference. They’re making it down the pipeline.”
Some practical steps
There are practical actions surgeons can take to try to reduce the sheer volume of prescription opioids that end up in the hands of people for whom they are not intended, Dr. Stulberg said at the American College of Surgeons Quality and Safety Conference.
Sign up for a prescription monitoring program, he suggested. These programs are now available in 49 states (Missouri is the exception). “It’s really easy to create an account as a provider.” Just search online for your state’s prescription monitoring program and enter your contact information, he said. The state will then ask you for some basic information.
Take it one step further and integrate your prescription monitoring program into your electronic medical records, Dr. Stulberg said. “We’re starting to integrate it in all hospitals in Illinois. That means when the surgeon or the nurse providers look up the patient, they will know if the patient got two other prescriptions in the last 2 weeks.” He added, “You can ask if they need more pills before adding to the surplus.”
Another practical strategy is to give patients better access to opioid disposal. Find out where the nearest drug return receptacle or kiosk is located – a pharmacy, police station, or elsewhere – and inform your patients. “We put opioid retrieval boxes in our clinic. When patients are educated about this, they bring [excess pills] back.”
Minimizing opioid prescribing in surgery
“This is not a problem of one individual specialty,” Dr. Stulberg said. “We have a problem of culture, a problem of mindset. So we need to approach solving this problem, in my opinion, from that perspective.”
Start with setting patient expectations in the preoperative period. Explain what the surgery entails and the amount of pain they should expect. “Patients have to understand what we’re doing hurts but we can manage that pain. It can make a big difference in their satisfaction … and also in how much medication they end up taking.”
In addition, perform preoperative risk screening for opioid abuse. “There is very good evidence that patients with addictions to other drugs, alcohol, or who have previous drug use, are much more likely to continue using prescription pain medications after a surgical encounter – 6 months to 12 months later.”
In addition, a paradigm shift in thinking is needed. “When we’re talking about pain control in the clinic and minimizing opioids during a surgical episode, we should be focusing on function,” he said. Orthopedic surgery is a prime example, where physicians encourage patients to start mobility exercises the same day of surgery because evidence shows it helps restore function faster.
Surgeons should tell patients that “the goal of how we are treating your pain is getting you to your optimal function.” Then check on function recovery postoperatively, he added. “We don’t follow-up – that is not part of our standard postoperative pathway in any way.”
Consider prescribing fewer pills postoperatively
If surgeons have a prescription feedback mechanism in place, they might know how many opioid pills patients are actually taking. “If I gave 20 pills to the last 10 patients but they only took 8 on average – can I go lower?” Dr. Stulberg said.
Researchers conducted a study to determine opioid needs for 80% of the patients at their institution after certain types of surgery (Ann Surg. 2017;265:709-14).
The study determined the number of pills that 80% of patients found controlled their pain: after partial mastectomy, 5; after partial mastectomy with sentinel lymph node biopsy, 10; after laparoscopic cholecystectomy, 15; after laparoscopic inguinal hernia repair, 15; and after open inguinal hernia repair, 15. These numbers represent about 43% of the actual number prescribed overall, so many patients are getting more medications than they require.
Dr. Stulberg suggested that surgeons could use the data from this study to counter any pushback from others at their institution reluctant to prescribe fewer opioids for their patients.
Dr. Stulberg did not have any relevant disclosures.
EXPERT ANALYSIS AT THE ACS QUALITY & SAFETY CONFERENCE
Outcomes improved with ERAS pathway tailored to colorectal surgery
NEW YORK – A protocol that standardizes care before, during, and after colorectal surgery cut average hospital stays from almost 6 days to less than 3, reduced complications, and slashed costs an estimated $11,227 per procedure.
“We decided to take a look at our own data, and we saw that a couple of variables were higher than we wanted them to be,” said Deepa Bhat, MD, a second year surgery resident at Advocate Illinois Masonic Medical Center in Chicago. Length of stay was one. Colorectal surgery patients were staying in the hospital an average 5.65 days, for example.
Their surgical site infection rate also warranted attention, Dr. Bhat said during a poster session at the American College of Surgeons Quality and Safety Conference. The overall complication rate was 6.45%.
“So, we decided to implement this enhanced recovery pathway in the hope that it would, one, get patients out of the hospital faster and allow them to recover at home and, two, decrease the rate of complications, including surgical site infections.”
Prior to the protocol, individual surgeons chose when to initiate fluids, when to discharge a patient, and many other preoperative factors. “Now, care is standardized so that every patient experiences the same pre-, intra-, and postoperative protocol, which leads to better outcomes,” Dr. Bhat said.
The multidisciplinary Enhanced Recovery After Colorectal Surgery (ERACS) pathway also now emphasizes more patient education prior to surgery. “The patients go into surgery having a very clear idea of what they can expect, such as how their pain will be controlled, when they can start liquids, and what their expectations are for ambulation,” she said. “By making patients active participants in their own care, they tend to do better.”
The investigators studied 246 elective colorectal surgery patients at their large, urban, community teaching hospital. They compared outcomes in 2014, versus 2015, to gauge the effectiveness of the ERACS. “The change in length of stay was really rather remarkable,” Dr. Bhat said. In fact, the typical number of days in the hospital decreased by about half from 5.65 to 2.89 days, a statistically significant difference (P less than .0001).
Historically, “the whole reason we don’t send patients home sooner is we’re worried they’re going to bounce right back, and that’s an issue for the 30-day readmission rate,” Dr. Bhat said. However, the enhanced recovery protocol was designed to minimize that risk, and the study verified that it works. “We wanted to show that you can send patients home safely and also not worry that they would come back more often.”
Patient satisfaction seems higher too. Dr. Bhat added, “Who doesn’t feel better at home?”
“It is pretty remarkable that you can send somebody home in less than 3 days and they don’t come back to the hospital with complications, versus having them stay double that amount of time,” Dr. Bhat said. The direct variable cost was approximately $3,705 lower with the ERACS, and total hospitalization costs decreased by up to $11,227 per patient. For the institution overall, that outcome translated into savings of approximately $1 million for the year.
Dr. Bhat continues to see increasing gains from the protocol ERACS since the study period ended. “Our enhanced recovery pathway is getting better and better and more efficient.” The institution is now looking to expand enhanced recovery protocols to other types of surgery.
Dr. Deepa Bhat had no relevant financial disclosures.
NEW YORK – A protocol that standardizes care before, during, and after colorectal surgery cut average hospital stays from almost 6 days to less than 3, reduced complications, and slashed costs an estimated $11,227 per procedure.
“We decided to take a look at our own data, and we saw that a couple of variables were higher than we wanted them to be,” said Deepa Bhat, MD, a second year surgery resident at Advocate Illinois Masonic Medical Center in Chicago. Length of stay was one. Colorectal surgery patients were staying in the hospital an average 5.65 days, for example.
Their surgical site infection rate also warranted attention, Dr. Bhat said during a poster session at the American College of Surgeons Quality and Safety Conference. The overall complication rate was 6.45%.
“So, we decided to implement this enhanced recovery pathway in the hope that it would, one, get patients out of the hospital faster and allow them to recover at home and, two, decrease the rate of complications, including surgical site infections.”
Prior to the protocol, individual surgeons chose when to initiate fluids, when to discharge a patient, and many other preoperative factors. “Now, care is standardized so that every patient experiences the same pre-, intra-, and postoperative protocol, which leads to better outcomes,” Dr. Bhat said.
The multidisciplinary Enhanced Recovery After Colorectal Surgery (ERACS) pathway also now emphasizes more patient education prior to surgery. “The patients go into surgery having a very clear idea of what they can expect, such as how their pain will be controlled, when they can start liquids, and what their expectations are for ambulation,” she said. “By making patients active participants in their own care, they tend to do better.”
The investigators studied 246 elective colorectal surgery patients at their large, urban, community teaching hospital. They compared outcomes in 2014, versus 2015, to gauge the effectiveness of the ERACS. “The change in length of stay was really rather remarkable,” Dr. Bhat said. In fact, the typical number of days in the hospital decreased by about half from 5.65 to 2.89 days, a statistically significant difference (P less than .0001).
Historically, “the whole reason we don’t send patients home sooner is we’re worried they’re going to bounce right back, and that’s an issue for the 30-day readmission rate,” Dr. Bhat said. However, the enhanced recovery protocol was designed to minimize that risk, and the study verified that it works. “We wanted to show that you can send patients home safely and also not worry that they would come back more often.”
Patient satisfaction seems higher too. Dr. Bhat added, “Who doesn’t feel better at home?”
“It is pretty remarkable that you can send somebody home in less than 3 days and they don’t come back to the hospital with complications, versus having them stay double that amount of time,” Dr. Bhat said. The direct variable cost was approximately $3,705 lower with the ERACS, and total hospitalization costs decreased by up to $11,227 per patient. For the institution overall, that outcome translated into savings of approximately $1 million for the year.
Dr. Bhat continues to see increasing gains from the protocol ERACS since the study period ended. “Our enhanced recovery pathway is getting better and better and more efficient.” The institution is now looking to expand enhanced recovery protocols to other types of surgery.
Dr. Deepa Bhat had no relevant financial disclosures.
NEW YORK – A protocol that standardizes care before, during, and after colorectal surgery cut average hospital stays from almost 6 days to less than 3, reduced complications, and slashed costs an estimated $11,227 per procedure.
“We decided to take a look at our own data, and we saw that a couple of variables were higher than we wanted them to be,” said Deepa Bhat, MD, a second year surgery resident at Advocate Illinois Masonic Medical Center in Chicago. Length of stay was one. Colorectal surgery patients were staying in the hospital an average 5.65 days, for example.
Their surgical site infection rate also warranted attention, Dr. Bhat said during a poster session at the American College of Surgeons Quality and Safety Conference. The overall complication rate was 6.45%.
“So, we decided to implement this enhanced recovery pathway in the hope that it would, one, get patients out of the hospital faster and allow them to recover at home and, two, decrease the rate of complications, including surgical site infections.”
Prior to the protocol, individual surgeons chose when to initiate fluids, when to discharge a patient, and many other preoperative factors. “Now, care is standardized so that every patient experiences the same pre-, intra-, and postoperative protocol, which leads to better outcomes,” Dr. Bhat said.
The multidisciplinary Enhanced Recovery After Colorectal Surgery (ERACS) pathway also now emphasizes more patient education prior to surgery. “The patients go into surgery having a very clear idea of what they can expect, such as how their pain will be controlled, when they can start liquids, and what their expectations are for ambulation,” she said. “By making patients active participants in their own care, they tend to do better.”
The investigators studied 246 elective colorectal surgery patients at their large, urban, community teaching hospital. They compared outcomes in 2014, versus 2015, to gauge the effectiveness of the ERACS. “The change in length of stay was really rather remarkable,” Dr. Bhat said. In fact, the typical number of days in the hospital decreased by about half from 5.65 to 2.89 days, a statistically significant difference (P less than .0001).
Historically, “the whole reason we don’t send patients home sooner is we’re worried they’re going to bounce right back, and that’s an issue for the 30-day readmission rate,” Dr. Bhat said. However, the enhanced recovery protocol was designed to minimize that risk, and the study verified that it works. “We wanted to show that you can send patients home safely and also not worry that they would come back more often.”
Patient satisfaction seems higher too. Dr. Bhat added, “Who doesn’t feel better at home?”
“It is pretty remarkable that you can send somebody home in less than 3 days and they don’t come back to the hospital with complications, versus having them stay double that amount of time,” Dr. Bhat said. The direct variable cost was approximately $3,705 lower with the ERACS, and total hospitalization costs decreased by up to $11,227 per patient. For the institution overall, that outcome translated into savings of approximately $1 million for the year.
Dr. Bhat continues to see increasing gains from the protocol ERACS since the study period ended. “Our enhanced recovery pathway is getting better and better and more efficient.” The institution is now looking to expand enhanced recovery protocols to other types of surgery.
Dr. Deepa Bhat had no relevant financial disclosures.
AT THE ACS QUALITY AND SAFETY CONFERENCE
Key clinical point: An Enhanced Recovery After Colorectal Surgery (ERACS) protocol cut colorectal surgical site infections and reduced length of stay.
Major finding: The intervention decreased the hospital stays from an average of 6 days to 3 days and saved an estimated $11,227 per surgery.
Data source: A retrospective study of 246 patients undergoing elective colorectal surgery at a large, urban, community teaching hospital.
Disclosures: Dr. Deepa Bhat had no relevant financial disclosures.
From Obamacare to Trumpcare – implications for gastroenterologists
The June issue of CGH was the final column under my management. I have enjoyed the opportunity to provide you with information about practice management and health care reform. I also have enjoyed working with the Clinical Gastroenterology and Hepatology board of editors, and Erin Landis and Brook Simpson from AGA headquarters. Beginning in July 2017, this section will become the responsibility of Ziad Gellad, MD, MPH, AGAF, from Duke University. I have worked with Ziad for many years, and he serves on my board of editors for GI & Hepatology News. I have great confidence in his knowledge and ability.
During the last 5 years, we have published 58 columns beginning with an article where I made several broad predictions. I have tried to present important concepts and management tools related to private and academic clinical practice, health care reform, and health economics. This article was written in early January 2017 just before the inauguration of Donald Trump. As I wrote, we did not know the full extent or the pace of “Repeal and Replace,” as Obamacare becomes Trumpcare (www.healthaffairs.org/obamacare-to-trumpcare).
The extent of current Republican control of federal and state governments is unprecedented in modern political history. Per Newt Gingrich (The Economist, Jan. 7, 2017, p. 25), this will be the third attempt, after Ronald Reagan’s election in 1980 and Gingrich’s “Contract with America” in 1994, to break free from a “Big Government” mindset initiated by Franklin Roosevelt’s New Deal. In this article, I will speculate how a right-leaning shift in American health care policy might impact the business model of gastroenterology. No matter how government regulations or funds flow change, we (physicians) will ultimately be responsible for digestive care provided to our patients. In the words of Martin Luther King Jr. (as he paraphrased Theodore Parker), “The arc of the moral universe is long, but it bends toward justice.” What is remembered by fewer people, however, are words he then added during his speeches: “but only if we march.”
John I. Allen, MD, MBA, AGAF
Editor in Chief
The first column was published in July 2012.1 I wrote about five dominant themes that would alter our gastroenterology practices in the ensuing years. They were 1) an increasing requirement for us to demonstrate value, 2) the need to think about population management in addition to individual patient care, 3) consolidation that would occur at all levels of health care delivery, 4) increasing cost pressure, and 5) how medical decisions would be linked to reimbursement (now called value-based payment). I fully expected the Patient Protection and Affordable Care Act (ACA) would shape the health care landscape for the rest of our careers. After the article’s publication, I was invited to speak about health care reform at many academic centers and private practices. My last talk before the election was in Pasadena, Calif. (Oct. 28, 2016) where I confidently spoke about the implications of President Clinton’s cementing ACA into the fabric of U.S. medicine.

Donald Trump is now the 45th President of the United States. Republicans hold a 52-48 majority in the Senate and a 241-194 majority in the House. As of January 2017, one Supreme Court seat was available, and three more may open because of retirements (Justice Ginsburg is 83 years old, Justice Kennedy is 80, and Justice Breyer is 78). Republicans control all three branches of government in 25 states and dominate in 8 others. Conservative politicians control a large majority of county and city boards.
Until this year, Republicans have controlled all three branches of government only twice since 1945 (modern political history), and only once (George Bush in 2005) did the president have a Senate majority.2 With his win, Mr. Trump can lead a conservative revolution to reverse key initiatives begun when the Democratic Party held majority power. Repeal of the ACA, signed into legislation on March 23, 2010, is the Republican Party’s top priority.
Equally important, Congress can alter previously implemented federal regulations. Each year about 3,000 regulations are written by federal agencies that act with authority delegated by Congress (albeit Congress retains power to overturn them). Regulations are published in the Federal Register as preliminary rules during each year, and Final Rules are published after a public comment period and implemented shortly thereafter. Regulations carry the force of law and are codified in the Code of Federal Regulations. The Code of Federal Regulations is divided into 50 sections (Titles), with Title 42 (Public Health) and Title 45 (Public Welfare) most pertinent to us.
Other policies are created through executive orders, issued by the president (federal) or governors (states), without involvement of legislative or judicial branches (they were not mentioned in the Constitution, by the way). Executive orders issued by President Obama could, theoretically, be overturned by new executive orders.
Repeal and replace
Destruction of the ACA is a top priority of President Trump and Republican leaders of both houses of Congress. The ACA was a Democratic bill (passed with no Republican support), although it had many similarities to previous Republican legislative ideas dating from 1993.3
Although outright repeal could be blocked by a Democratic filibuster, the law could be drastically modified through budget reconciliation whose passage takes only a simple Senate majority. Thus, a simple budget-related bill could serve as a vehicle to defund many parts of ACA, including money for Medicaid expansion, insurance risk corridors, money to offset out-of-pocket expenses and individual premium subsidies, for example.4,5
There would be substantial problems if ACA were repealed even with a 2- or 3-year delay, a scenario proposed to provide time for a replacement bill. On Jan. 4, 2017, the House Republican Study Committee introduced the American Health Care Reform Act (AHCRA) as a replacement proposal, with the stipulation that ACA would be repealed as of Jan. 1, 2018. This initial bill hinted at Republican intent and was detailed in a Health Affairs blog.6 Importantly, there were distinct similarities between this and prior Republican proposals put forward by Representative Tom Price (nominated to head the Department of Health & Human Services under President Trump) and Speaker of the House Paul Ryan.7,8
Consistently, Republicans have advocated for expansion of health savings accounts, altering the tax code to allow individuals to deduct health insurance premiums, establishment of association risk pools, imposition of malpractice limits, protections for people with preexisting conditions, and further restrictions on abortion coverage. The AHCRA changes financial subsidies for purchasing insurance from a tax credit (which can be paid to people even if they do not pay taxes) to a tax deduction (only applicable to people who pay taxes). Analysis of a similar proposal made by President Trump during the campaign found that this plan would increase the number of uninsured people by more than 15 million.
If ACA is repealed, effects would be broader than just factors related to insurance coverage.9 ACA provides for preventive care (including colonoscopy) without copays, education of additional medical personnel, closing the donut hole for Medicare Part D (medications), approval of generic biologics, and Medicaid expansions, among other initiatives. If ACA were defunded without restoring pre-ACA support for Disproportion Share Hospital charity care, research, and graduate medical education, then safety-net hospitals and many academic medical centers (AMCs) could face enormous funding cuts.10 Defunding Medicaid expansion would adversely affect states in many ways, as pointed out by Ayanian et al.11 Medicaid expansion had broad economic impact in states that accepted federal money to expand. In Michigan for example, 30,900 jobs were added to the state in 2016 because of Medicaid expansion, with two-thirds outside of the health care industry. President Obama defined his view about the effects of ACA repeal in the New England Journal of Medicine.12
Lessons learned
Economic principles and unique characteristics of United States health care help explain why solutions to its high cost and uneven coverage are so difficult to achieve. These include higher prices for goods in the United States compared with other countries, variation in price (unrelated to quality), restraints on government price negotiations, inefficiencies due to variation in size of delivery systems, and “moral hazard” related to rich insurance coverage, which are some of the factors that doom any simple solutions. These are reviewed by Victor Fuchs13 in an excellent article in Annals of Internal Medicine. Payment methods for health care services also distort resource use and efficiencies. Understanding the eight basic payment methodologies in health care and current predictions about future health care spending will be important in shaping reimbursement policies.14,15
Disruptions in health care are unpopular and, as Uve Reinardt stated: “Our health care financing system will always remain a horrendous mess and a fountain for such dismay among the providers of health care as well as among patients.”4 Lessons to inform the next iteration of health care policy, learned from the 2009-2010 experience, might be as follows:
1. If a bill is to be passed, the president must personally lead in explaining the bill to the public in simple terms.
2. Even the threat of repeal may disrupt the current market and force insurance companies to exit quickly.
3. Coverage must be affordable to individuals, state budgets, and health care providers. Because expansion states saw positive impacts to state budgets8 and mental health and substance abuse services became part of Medicaid benefits, how will a replacement bill maintain coverage and compensate for new state moneys used now for other imperatives such as education and infrastructure?
4. Health care is like a massive cargo ship, not a sports car, so a bill to replace the ACA may take a long time (and might never be passed).
5. Health care is intensely personal, so it will always be politically charged.
Ultimately, physicians will need to make strategic guesses and rapid adjustments to sustain financial viability and provide high-value care. Strategies differ depending on your practice situation. Keep in mind the five principles listed in the opening paragraph of this article. It is likely that the most important principle to factor into your practice strategy is continuing reduction in reimbursements. No matter what model is adopted to reform the ACA, the financial pot (Medicare, Medicaid, commercial insurance, bundled payments, fee-for-service payments) will be reduced, and the number of uninsured patients will increase. How would you change your practice if Medicare was your best payer (“manage to Medicare”)?
Independent practices
Physicians in small- to medium-size independent practices continue to struggle with reducing reimbursements, reporting burdens, increasing overhead expenses, crushing regulatory requirements, and provider burnout. Trumpcare will favor small practices more than Obamacare from a policy (not necessarily a financial) perspective. Regulations on small business and reporting burdens may ease, but the move toward value-based reimbursement as outlined in the MACRA (passed with overwhelming bipartisan support) will not end.16 Practices in small communities continue to thrive because they give excellent care with limited competition and low overhead. Some practices in suburban and urban centers struggle because payers tend to favor (with enhanced managed care rates) larger practices and health systems. Large, horizontally integrated, efficient gastroenterology practices will continue to thrive because they can develop a “must-have” position with payers. Building remote patient monitoring, teleconsulting, and capabilities around value demonstration will be strategically advantageous.
Options for independent physicians include 1) maintaining status quo, 2) retiring, or 3) exiting the independent business model through a practice sale. Traditionally, physicians who wanted to sell their practices turned to hospitals or health systems. Recently, a physician-run model funded by venture capital has emerged where reduced overhead (through centralization of services) is combined with enhanced power during payer negotiations (because of scale). This model has allowed practices to merge into a physician organization and remain free from health system employment.17
Large health systems
Physicians employed by large health systems, whether they are nonprofit, for-profit, or AMCs, will see their future tied directly to health system success. If bundled payment, alternative payment, and capitation models of health care financing continue to grow in popularity, then success will be determined by a health system’s market share and its ability to form true clinical integration. In a capitated environment, expansion of market share (especially of relatively healthy patients) will help support margins. However, financial success will come from a system’s ability to manage high-cost patients, those 5% of patients who consume 50% of health care resources.18
Hospitals with a financially challenged patient base (safety-net hospitals) will have enormous financial pressures going forward. Repeal of ACA without restoration of pre-ACA funding will affect directly the financial health of systems including AMCs. AMCs and other health systems will be forced to reduce fixed overhead, enhance productivity of faculty, and restrict nonfunded activities (teaching for example). Although most AMCs are now in an active acquisition mode, this strategy is naturally limited by the number of remaining acquisition targets. Traditional high managed care rates enjoyed by AMCs will shrink, as will federal research funding (which typically comes with high indirect financial support). Health systems and GI societies will need to dedicate much more attention to state policy makers as Trumpcare progresses.
Finally, all providers will need to manage the business implications of retail health. As people assume higher deductibles and copays and health savings accounts grow, patients will change their patterns of purchasing services. Reputation counts for less when people are facing large price differences, so attention to patient-centric amenities, price, patient engagement, and patient satisfaction will become even more important.
Conclusion
The United States has undergone a massive and rapid political transformation. The mandate felt by conservative politicians, perhaps not supported by numbers, will carry a conservative platform forward. In areas where progressive Democrats emphasized federal power and socialized regulation (religion, education, civil rights, income security, and health policy), conservatives will transfer decision power as much as possible to states, local communities, and individuals. Maintaining the concept of “health as a right” will test the conscience of all of us.
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Gill KE. Visual guide: the balance of power between Congress and the Presidency (1901-2016). Wired Pen. November 2016. Available from http://wiredpen.com/resources/political-commentary-and-analysis/a-visual-guide-balance-of-power-congress-presidency/. Accessed Dec. 30, 2016.
3. Mertens M. Chart: comparing health reform bills – Democrats and Republicans 2009, Republics 1993. Kaiser Health News. Feb. 24, 2010. Available from http://khn.org/022310-bill-comparison/. Accessed Jan. 8, 2017.
4. Hotchkiss M. Q&A: what a Trump presidency means for the Affordable Care Act. Nov. 16, 2016 News at Princeton. Princeton University. Available from https://www.princeton.edu/main/news/archive/S47/93/09C11/index.xml?section=topstories. Accessed Dec. 30, 2016.
5. Jost T. Taking stock of health reform: where we’ve been, where we’re going. Health Affairs Blog. Available from http://healthaffairs.org/blog/2016/12/06/taking-stock-of-health-reform-where-weve-been-where-were-going/. Accessed Dec. 30, 2016.
6. Jost T. The Republican Study Committee’s ACA replacement proposal (updated). Health Affairs Blog. Available from http://healthaffairs.org/blog/2017/01/05/the-republican-study-committees-aca-replacement-proposal/. Accessed Jan. 10, 2017.
7. Price T. Empowering patients first. Available from http://tomprice.house.gov/sites/tomprice.house.gov/files/HR%202300%20Empowering%20Patients%20First%20Act%202015.pdf. Accessed Dec. 30, 2016.
8. Ryan P. A better way. Available from https://abetterway.speaker.gov/_assets/pdf/ABetterWay-HealthCare-PolicyPaper.pdf. Accessed Dec. 30, 2016.
9. Oberlander, J. The end of Obamacare. N Engl J Med. 2017;376:1-3.
10. Goodnough A. Hospitals in safety net brace for health care law’s repeal. New York Times. Dec. 28, 2016. Available from http://www.nytimes.com/2016/12/28/health/hospitals-medicaid-obamacare-trump.html?smprod=nytcore-iphone&smid=nytcore-iphone-share&_r=0. Accessed Jan. 10, 2017.
11. Ayanian, J.Z., Ehrlich, G.M., Grimes, D.R., et al. Economic effects of Medicaid expansion in Michigan. N Engl J Med. 2017;376:407-10.
12. Obama, B.H. Repealing the ACA without a replacement: the risks to American health care. N Engl J Med. 2017;376:297-9.
13. Fuchs, V.R. Major concepts of health economics. Ann Intern Med. 2015;162:380-3.
14. Quinn, K. The 8 basic payment methods in health care. Ann Intern Med. 2015;163:300-6.
15. Schoenman JA. A detailed look at US health care spending: a presentation from the National Institute for Health Care Management (NIHCM). Oct. 25, 2012. Available from http://www.nihcm.org/images/stories/Health_care_spending_slides_-_MILI_-_Schoenman.pdf. Accessed Dec. 30, 2016.
16. Allen, J.I., Allen, C.C., Brill, J.V. Gastroenterology 2020: no time for WIMPs. Gastroenterology. 2016;150:295-9.
17. Sciacca R. Weekly Byte: GI roundtable and navigating uncharted waters in health care. The PMD Blog. Available from https://www.pmd.com/blog/post/weekly-byte-gi-roundtable-and-navigating-uncharted-waters-in-health-care. Accessed Jan. 10, 2017.
18. Powers, B.W., Chaguturu, S.K. ACOs and high-cost patients. N Engl J Med. 2016;374:203-5.
Dr. Allen is professor of medicine, University of Michigan School of Medicine, Institute for Health Care Policy and Innovations, and associate medical director of Network Strategy and Business Development – Michigan Medicine, Ann Arbor. He discloses no conflicts.
The June issue of CGH was the final column under my management. I have enjoyed the opportunity to provide you with information about practice management and health care reform. I also have enjoyed working with the Clinical Gastroenterology and Hepatology board of editors, and Erin Landis and Brook Simpson from AGA headquarters. Beginning in July 2017, this section will become the responsibility of Ziad Gellad, MD, MPH, AGAF, from Duke University. I have worked with Ziad for many years, and he serves on my board of editors for GI & Hepatology News. I have great confidence in his knowledge and ability.
During the last 5 years, we have published 58 columns beginning with an article where I made several broad predictions. I have tried to present important concepts and management tools related to private and academic clinical practice, health care reform, and health economics. This article was written in early January 2017 just before the inauguration of Donald Trump. As I wrote, we did not know the full extent or the pace of “Repeal and Replace,” as Obamacare becomes Trumpcare (www.healthaffairs.org/obamacare-to-trumpcare).
The extent of current Republican control of federal and state governments is unprecedented in modern political history. Per Newt Gingrich (The Economist, Jan. 7, 2017, p. 25), this will be the third attempt, after Ronald Reagan’s election in 1980 and Gingrich’s “Contract with America” in 1994, to break free from a “Big Government” mindset initiated by Franklin Roosevelt’s New Deal. In this article, I will speculate how a right-leaning shift in American health care policy might impact the business model of gastroenterology. No matter how government regulations or funds flow change, we (physicians) will ultimately be responsible for digestive care provided to our patients. In the words of Martin Luther King Jr. (as he paraphrased Theodore Parker), “The arc of the moral universe is long, but it bends toward justice.” What is remembered by fewer people, however, are words he then added during his speeches: “but only if we march.”
John I. Allen, MD, MBA, AGAF
Editor in Chief
The first column was published in July 2012.1 I wrote about five dominant themes that would alter our gastroenterology practices in the ensuing years. They were 1) an increasing requirement for us to demonstrate value, 2) the need to think about population management in addition to individual patient care, 3) consolidation that would occur at all levels of health care delivery, 4) increasing cost pressure, and 5) how medical decisions would be linked to reimbursement (now called value-based payment). I fully expected the Patient Protection and Affordable Care Act (ACA) would shape the health care landscape for the rest of our careers. After the article’s publication, I was invited to speak about health care reform at many academic centers and private practices. My last talk before the election was in Pasadena, Calif. (Oct. 28, 2016) where I confidently spoke about the implications of President Clinton’s cementing ACA into the fabric of U.S. medicine.
Donald Trump is now the 45th President of the United States. Republicans hold a 52-48 majority in the Senate and a 241-194 majority in the House. As of January 2017, one Supreme Court seat was available, and three more may open because of retirements (Justice Ginsburg is 83 years old, Justice Kennedy is 80, and Justice Breyer is 78). Republicans control all three branches of government in 25 states and dominate in 8 others. Conservative politicians control a large majority of county and city boards.
Until this year, Republicans have controlled all three branches of government only twice since 1945 (modern political history), and only once (George Bush in 2005) did the president have a Senate majority.2 With his win, Mr. Trump can lead a conservative revolution to reverse key initiatives begun when the Democratic Party held majority power. Repeal of the ACA, signed into legislation on March 23, 2010, is the Republican Party’s top priority.
Equally important, Congress can alter previously implemented federal regulations. Each year about 3,000 regulations are written by federal agencies that act with authority delegated by Congress (albeit Congress retains power to overturn them). Regulations are published in the Federal Register as preliminary rules during each year, and Final Rules are published after a public comment period and implemented shortly thereafter. Regulations carry the force of law and are codified in the Code of Federal Regulations. The Code of Federal Regulations is divided into 50 sections (Titles), with Title 42 (Public Health) and Title 45 (Public Welfare) most pertinent to us.
Other policies are created through executive orders, issued by the president (federal) or governors (states), without involvement of legislative or judicial branches (they were not mentioned in the Constitution, by the way). Executive orders issued by President Obama could, theoretically, be overturned by new executive orders.
Repeal and replace
Destruction of the ACA is a top priority of President Trump and Republican leaders of both houses of Congress. The ACA was a Democratic bill (passed with no Republican support), although it had many similarities to previous Republican legislative ideas dating from 1993.3
Although outright repeal could be blocked by a Democratic filibuster, the law could be drastically modified through budget reconciliation whose passage takes only a simple Senate majority. Thus, a simple budget-related bill could serve as a vehicle to defund many parts of ACA, including money for Medicaid expansion, insurance risk corridors, money to offset out-of-pocket expenses and individual premium subsidies, for example.4,5
There would be substantial problems if ACA were repealed even with a 2- or 3-year delay, a scenario proposed to provide time for a replacement bill. On Jan. 4, 2017, the House Republican Study Committee introduced the American Health Care Reform Act (AHCRA) as a replacement proposal, with the stipulation that ACA would be repealed as of Jan. 1, 2018. This initial bill hinted at Republican intent and was detailed in a Health Affairs blog.6 Importantly, there were distinct similarities between this and prior Republican proposals put forward by Representative Tom Price (nominated to head the Department of Health & Human Services under President Trump) and Speaker of the House Paul Ryan.7,8
Consistently, Republicans have advocated for expansion of health savings accounts, altering the tax code to allow individuals to deduct health insurance premiums, establishment of association risk pools, imposition of malpractice limits, protections for people with preexisting conditions, and further restrictions on abortion coverage. The AHCRA changes financial subsidies for purchasing insurance from a tax credit (which can be paid to people even if they do not pay taxes) to a tax deduction (only applicable to people who pay taxes). Analysis of a similar proposal made by President Trump during the campaign found that this plan would increase the number of uninsured people by more than 15 million.
If ACA is repealed, effects would be broader than just factors related to insurance coverage.9 ACA provides for preventive care (including colonoscopy) without copays, education of additional medical personnel, closing the donut hole for Medicare Part D (medications), approval of generic biologics, and Medicaid expansions, among other initiatives. If ACA were defunded without restoring pre-ACA support for Disproportion Share Hospital charity care, research, and graduate medical education, then safety-net hospitals and many academic medical centers (AMCs) could face enormous funding cuts.10 Defunding Medicaid expansion would adversely affect states in many ways, as pointed out by Ayanian et al.11 Medicaid expansion had broad economic impact in states that accepted federal money to expand. In Michigan for example, 30,900 jobs were added to the state in 2016 because of Medicaid expansion, with two-thirds outside of the health care industry. President Obama defined his view about the effects of ACA repeal in the New England Journal of Medicine.12
Lessons learned
Economic principles and unique characteristics of United States health care help explain why solutions to its high cost and uneven coverage are so difficult to achieve. These include higher prices for goods in the United States compared with other countries, variation in price (unrelated to quality), restraints on government price negotiations, inefficiencies due to variation in size of delivery systems, and “moral hazard” related to rich insurance coverage, which are some of the factors that doom any simple solutions. These are reviewed by Victor Fuchs13 in an excellent article in Annals of Internal Medicine. Payment methods for health care services also distort resource use and efficiencies. Understanding the eight basic payment methodologies in health care and current predictions about future health care spending will be important in shaping reimbursement policies.14,15
Disruptions in health care are unpopular and, as Uve Reinardt stated: “Our health care financing system will always remain a horrendous mess and a fountain for such dismay among the providers of health care as well as among patients.”4 Lessons to inform the next iteration of health care policy, learned from the 2009-2010 experience, might be as follows:
1. If a bill is to be passed, the president must personally lead in explaining the bill to the public in simple terms.
2. Even the threat of repeal may disrupt the current market and force insurance companies to exit quickly.
3. Coverage must be affordable to individuals, state budgets, and health care providers. Because expansion states saw positive impacts to state budgets8 and mental health and substance abuse services became part of Medicaid benefits, how will a replacement bill maintain coverage and compensate for new state moneys used now for other imperatives such as education and infrastructure?
4. Health care is like a massive cargo ship, not a sports car, so a bill to replace the ACA may take a long time (and might never be passed).
5. Health care is intensely personal, so it will always be politically charged.
Ultimately, physicians will need to make strategic guesses and rapid adjustments to sustain financial viability and provide high-value care. Strategies differ depending on your practice situation. Keep in mind the five principles listed in the opening paragraph of this article. It is likely that the most important principle to factor into your practice strategy is continuing reduction in reimbursements. No matter what model is adopted to reform the ACA, the financial pot (Medicare, Medicaid, commercial insurance, bundled payments, fee-for-service payments) will be reduced, and the number of uninsured patients will increase. How would you change your practice if Medicare was your best payer (“manage to Medicare”)?
Independent practices
Physicians in small- to medium-size independent practices continue to struggle with reducing reimbursements, reporting burdens, increasing overhead expenses, crushing regulatory requirements, and provider burnout. Trumpcare will favor small practices more than Obamacare from a policy (not necessarily a financial) perspective. Regulations on small business and reporting burdens may ease, but the move toward value-based reimbursement as outlined in the MACRA (passed with overwhelming bipartisan support) will not end.16 Practices in small communities continue to thrive because they give excellent care with limited competition and low overhead. Some practices in suburban and urban centers struggle because payers tend to favor (with enhanced managed care rates) larger practices and health systems. Large, horizontally integrated, efficient gastroenterology practices will continue to thrive because they can develop a “must-have” position with payers. Building remote patient monitoring, teleconsulting, and capabilities around value demonstration will be strategically advantageous.
Options for independent physicians include 1) maintaining status quo, 2) retiring, or 3) exiting the independent business model through a practice sale. Traditionally, physicians who wanted to sell their practices turned to hospitals or health systems. Recently, a physician-run model funded by venture capital has emerged where reduced overhead (through centralization of services) is combined with enhanced power during payer negotiations (because of scale). This model has allowed practices to merge into a physician organization and remain free from health system employment.17
Large health systems
Physicians employed by large health systems, whether they are nonprofit, for-profit, or AMCs, will see their future tied directly to health system success. If bundled payment, alternative payment, and capitation models of health care financing continue to grow in popularity, then success will be determined by a health system’s market share and its ability to form true clinical integration. In a capitated environment, expansion of market share (especially of relatively healthy patients) will help support margins. However, financial success will come from a system’s ability to manage high-cost patients, those 5% of patients who consume 50% of health care resources.18
Hospitals with a financially challenged patient base (safety-net hospitals) will have enormous financial pressures going forward. Repeal of ACA without restoration of pre-ACA funding will affect directly the financial health of systems including AMCs. AMCs and other health systems will be forced to reduce fixed overhead, enhance productivity of faculty, and restrict nonfunded activities (teaching for example). Although most AMCs are now in an active acquisition mode, this strategy is naturally limited by the number of remaining acquisition targets. Traditional high managed care rates enjoyed by AMCs will shrink, as will federal research funding (which typically comes with high indirect financial support). Health systems and GI societies will need to dedicate much more attention to state policy makers as Trumpcare progresses.
Finally, all providers will need to manage the business implications of retail health. As people assume higher deductibles and copays and health savings accounts grow, patients will change their patterns of purchasing services. Reputation counts for less when people are facing large price differences, so attention to patient-centric amenities, price, patient engagement, and patient satisfaction will become even more important.
Conclusion
The United States has undergone a massive and rapid political transformation. The mandate felt by conservative politicians, perhaps not supported by numbers, will carry a conservative platform forward. In areas where progressive Democrats emphasized federal power and socialized regulation (religion, education, civil rights, income security, and health policy), conservatives will transfer decision power as much as possible to states, local communities, and individuals. Maintaining the concept of “health as a right” will test the conscience of all of us.
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Gill KE. Visual guide: the balance of power between Congress and the Presidency (1901-2016). Wired Pen. November 2016. Available from http://wiredpen.com/resources/political-commentary-and-analysis/a-visual-guide-balance-of-power-congress-presidency/. Accessed Dec. 30, 2016.
3. Mertens M. Chart: comparing health reform bills – Democrats and Republicans 2009, Republics 1993. Kaiser Health News. Feb. 24, 2010. Available from http://khn.org/022310-bill-comparison/. Accessed Jan. 8, 2017.
4. Hotchkiss M. Q&A: what a Trump presidency means for the Affordable Care Act. Nov. 16, 2016 News at Princeton. Princeton University. Available from https://www.princeton.edu/main/news/archive/S47/93/09C11/index.xml?section=topstories. Accessed Dec. 30, 2016.
5. Jost T. Taking stock of health reform: where we’ve been, where we’re going. Health Affairs Blog. Available from http://healthaffairs.org/blog/2016/12/06/taking-stock-of-health-reform-where-weve-been-where-were-going/. Accessed Dec. 30, 2016.
6. Jost T. The Republican Study Committee’s ACA replacement proposal (updated). Health Affairs Blog. Available from http://healthaffairs.org/blog/2017/01/05/the-republican-study-committees-aca-replacement-proposal/. Accessed Jan. 10, 2017.
7. Price T. Empowering patients first. Available from http://tomprice.house.gov/sites/tomprice.house.gov/files/HR%202300%20Empowering%20Patients%20First%20Act%202015.pdf. Accessed Dec. 30, 2016.
8. Ryan P. A better way. Available from https://abetterway.speaker.gov/_assets/pdf/ABetterWay-HealthCare-PolicyPaper.pdf. Accessed Dec. 30, 2016.
9. Oberlander, J. The end of Obamacare. N Engl J Med. 2017;376:1-3.
10. Goodnough A. Hospitals in safety net brace for health care law’s repeal. New York Times. Dec. 28, 2016. Available from http://www.nytimes.com/2016/12/28/health/hospitals-medicaid-obamacare-trump.html?smprod=nytcore-iphone&smid=nytcore-iphone-share&_r=0. Accessed Jan. 10, 2017.
11. Ayanian, J.Z., Ehrlich, G.M., Grimes, D.R., et al. Economic effects of Medicaid expansion in Michigan. N Engl J Med. 2017;376:407-10.
12. Obama, B.H. Repealing the ACA without a replacement: the risks to American health care. N Engl J Med. 2017;376:297-9.
13. Fuchs, V.R. Major concepts of health economics. Ann Intern Med. 2015;162:380-3.
14. Quinn, K. The 8 basic payment methods in health care. Ann Intern Med. 2015;163:300-6.
15. Schoenman JA. A detailed look at US health care spending: a presentation from the National Institute for Health Care Management (NIHCM). Oct. 25, 2012. Available from http://www.nihcm.org/images/stories/Health_care_spending_slides_-_MILI_-_Schoenman.pdf. Accessed Dec. 30, 2016.
16. Allen, J.I., Allen, C.C., Brill, J.V. Gastroenterology 2020: no time for WIMPs. Gastroenterology. 2016;150:295-9.
17. Sciacca R. Weekly Byte: GI roundtable and navigating uncharted waters in health care. The PMD Blog. Available from https://www.pmd.com/blog/post/weekly-byte-gi-roundtable-and-navigating-uncharted-waters-in-health-care. Accessed Jan. 10, 2017.
18. Powers, B.W., Chaguturu, S.K. ACOs and high-cost patients. N Engl J Med. 2016;374:203-5.
Dr. Allen is professor of medicine, University of Michigan School of Medicine, Institute for Health Care Policy and Innovations, and associate medical director of Network Strategy and Business Development – Michigan Medicine, Ann Arbor. He discloses no conflicts.
The June issue of CGH was the final column under my management. I have enjoyed the opportunity to provide you with information about practice management and health care reform. I also have enjoyed working with the Clinical Gastroenterology and Hepatology board of editors, and Erin Landis and Brook Simpson from AGA headquarters. Beginning in July 2017, this section will become the responsibility of Ziad Gellad, MD, MPH, AGAF, from Duke University. I have worked with Ziad for many years, and he serves on my board of editors for GI & Hepatology News. I have great confidence in his knowledge and ability.
During the last 5 years, we have published 58 columns beginning with an article where I made several broad predictions. I have tried to present important concepts and management tools related to private and academic clinical practice, health care reform, and health economics. This article was written in early January 2017 just before the inauguration of Donald Trump. As I wrote, we did not know the full extent or the pace of “Repeal and Replace,” as Obamacare becomes Trumpcare (www.healthaffairs.org/obamacare-to-trumpcare).
The extent of current Republican control of federal and state governments is unprecedented in modern political history. Per Newt Gingrich (The Economist, Jan. 7, 2017, p. 25), this will be the third attempt, after Ronald Reagan’s election in 1980 and Gingrich’s “Contract with America” in 1994, to break free from a “Big Government” mindset initiated by Franklin Roosevelt’s New Deal. In this article, I will speculate how a right-leaning shift in American health care policy might impact the business model of gastroenterology. No matter how government regulations or funds flow change, we (physicians) will ultimately be responsible for digestive care provided to our patients. In the words of Martin Luther King Jr. (as he paraphrased Theodore Parker), “The arc of the moral universe is long, but it bends toward justice.” What is remembered by fewer people, however, are words he then added during his speeches: “but only if we march.”
John I. Allen, MD, MBA, AGAF
Editor in Chief
The first column was published in July 2012.1 I wrote about five dominant themes that would alter our gastroenterology practices in the ensuing years. They were 1) an increasing requirement for us to demonstrate value, 2) the need to think about population management in addition to individual patient care, 3) consolidation that would occur at all levels of health care delivery, 4) increasing cost pressure, and 5) how medical decisions would be linked to reimbursement (now called value-based payment). I fully expected the Patient Protection and Affordable Care Act (ACA) would shape the health care landscape for the rest of our careers. After the article’s publication, I was invited to speak about health care reform at many academic centers and private practices. My last talk before the election was in Pasadena, Calif. (Oct. 28, 2016) where I confidently spoke about the implications of President Clinton’s cementing ACA into the fabric of U.S. medicine.
Donald Trump is now the 45th President of the United States. Republicans hold a 52-48 majority in the Senate and a 241-194 majority in the House. As of January 2017, one Supreme Court seat was available, and three more may open because of retirements (Justice Ginsburg is 83 years old, Justice Kennedy is 80, and Justice Breyer is 78). Republicans control all three branches of government in 25 states and dominate in 8 others. Conservative politicians control a large majority of county and city boards.
Until this year, Republicans have controlled all three branches of government only twice since 1945 (modern political history), and only once (George Bush in 2005) did the president have a Senate majority.2 With his win, Mr. Trump can lead a conservative revolution to reverse key initiatives begun when the Democratic Party held majority power. Repeal of the ACA, signed into legislation on March 23, 2010, is the Republican Party’s top priority.
Equally important, Congress can alter previously implemented federal regulations. Each year about 3,000 regulations are written by federal agencies that act with authority delegated by Congress (albeit Congress retains power to overturn them). Regulations are published in the Federal Register as preliminary rules during each year, and Final Rules are published after a public comment period and implemented shortly thereafter. Regulations carry the force of law and are codified in the Code of Federal Regulations. The Code of Federal Regulations is divided into 50 sections (Titles), with Title 42 (Public Health) and Title 45 (Public Welfare) most pertinent to us.
Other policies are created through executive orders, issued by the president (federal) or governors (states), without involvement of legislative or judicial branches (they were not mentioned in the Constitution, by the way). Executive orders issued by President Obama could, theoretically, be overturned by new executive orders.
Repeal and replace
Destruction of the ACA is a top priority of President Trump and Republican leaders of both houses of Congress. The ACA was a Democratic bill (passed with no Republican support), although it had many similarities to previous Republican legislative ideas dating from 1993.3
Although outright repeal could be blocked by a Democratic filibuster, the law could be drastically modified through budget reconciliation whose passage takes only a simple Senate majority. Thus, a simple budget-related bill could serve as a vehicle to defund many parts of ACA, including money for Medicaid expansion, insurance risk corridors, money to offset out-of-pocket expenses and individual premium subsidies, for example.4,5
There would be substantial problems if ACA were repealed even with a 2- or 3-year delay, a scenario proposed to provide time for a replacement bill. On Jan. 4, 2017, the House Republican Study Committee introduced the American Health Care Reform Act (AHCRA) as a replacement proposal, with the stipulation that ACA would be repealed as of Jan. 1, 2018. This initial bill hinted at Republican intent and was detailed in a Health Affairs blog.6 Importantly, there were distinct similarities between this and prior Republican proposals put forward by Representative Tom Price (nominated to head the Department of Health & Human Services under President Trump) and Speaker of the House Paul Ryan.7,8
Consistently, Republicans have advocated for expansion of health savings accounts, altering the tax code to allow individuals to deduct health insurance premiums, establishment of association risk pools, imposition of malpractice limits, protections for people with preexisting conditions, and further restrictions on abortion coverage. The AHCRA changes financial subsidies for purchasing insurance from a tax credit (which can be paid to people even if they do not pay taxes) to a tax deduction (only applicable to people who pay taxes). Analysis of a similar proposal made by President Trump during the campaign found that this plan would increase the number of uninsured people by more than 15 million.
If ACA is repealed, effects would be broader than just factors related to insurance coverage.9 ACA provides for preventive care (including colonoscopy) without copays, education of additional medical personnel, closing the donut hole for Medicare Part D (medications), approval of generic biologics, and Medicaid expansions, among other initiatives. If ACA were defunded without restoring pre-ACA support for Disproportion Share Hospital charity care, research, and graduate medical education, then safety-net hospitals and many academic medical centers (AMCs) could face enormous funding cuts.10 Defunding Medicaid expansion would adversely affect states in many ways, as pointed out by Ayanian et al.11 Medicaid expansion had broad economic impact in states that accepted federal money to expand. In Michigan for example, 30,900 jobs were added to the state in 2016 because of Medicaid expansion, with two-thirds outside of the health care industry. President Obama defined his view about the effects of ACA repeal in the New England Journal of Medicine.12
Lessons learned
Economic principles and unique characteristics of United States health care help explain why solutions to its high cost and uneven coverage are so difficult to achieve. These include higher prices for goods in the United States compared with other countries, variation in price (unrelated to quality), restraints on government price negotiations, inefficiencies due to variation in size of delivery systems, and “moral hazard” related to rich insurance coverage, which are some of the factors that doom any simple solutions. These are reviewed by Victor Fuchs13 in an excellent article in Annals of Internal Medicine. Payment methods for health care services also distort resource use and efficiencies. Understanding the eight basic payment methodologies in health care and current predictions about future health care spending will be important in shaping reimbursement policies.14,15
Disruptions in health care are unpopular and, as Uve Reinardt stated: “Our health care financing system will always remain a horrendous mess and a fountain for such dismay among the providers of health care as well as among patients.”4 Lessons to inform the next iteration of health care policy, learned from the 2009-2010 experience, might be as follows:
1. If a bill is to be passed, the president must personally lead in explaining the bill to the public in simple terms.
2. Even the threat of repeal may disrupt the current market and force insurance companies to exit quickly.
3. Coverage must be affordable to individuals, state budgets, and health care providers. Because expansion states saw positive impacts to state budgets8 and mental health and substance abuse services became part of Medicaid benefits, how will a replacement bill maintain coverage and compensate for new state moneys used now for other imperatives such as education and infrastructure?
4. Health care is like a massive cargo ship, not a sports car, so a bill to replace the ACA may take a long time (and might never be passed).
5. Health care is intensely personal, so it will always be politically charged.
Ultimately, physicians will need to make strategic guesses and rapid adjustments to sustain financial viability and provide high-value care. Strategies differ depending on your practice situation. Keep in mind the five principles listed in the opening paragraph of this article. It is likely that the most important principle to factor into your practice strategy is continuing reduction in reimbursements. No matter what model is adopted to reform the ACA, the financial pot (Medicare, Medicaid, commercial insurance, bundled payments, fee-for-service payments) will be reduced, and the number of uninsured patients will increase. How would you change your practice if Medicare was your best payer (“manage to Medicare”)?
Independent practices
Physicians in small- to medium-size independent practices continue to struggle with reducing reimbursements, reporting burdens, increasing overhead expenses, crushing regulatory requirements, and provider burnout. Trumpcare will favor small practices more than Obamacare from a policy (not necessarily a financial) perspective. Regulations on small business and reporting burdens may ease, but the move toward value-based reimbursement as outlined in the MACRA (passed with overwhelming bipartisan support) will not end.16 Practices in small communities continue to thrive because they give excellent care with limited competition and low overhead. Some practices in suburban and urban centers struggle because payers tend to favor (with enhanced managed care rates) larger practices and health systems. Large, horizontally integrated, efficient gastroenterology practices will continue to thrive because they can develop a “must-have” position with payers. Building remote patient monitoring, teleconsulting, and capabilities around value demonstration will be strategically advantageous.
Options for independent physicians include 1) maintaining status quo, 2) retiring, or 3) exiting the independent business model through a practice sale. Traditionally, physicians who wanted to sell their practices turned to hospitals or health systems. Recently, a physician-run model funded by venture capital has emerged where reduced overhead (through centralization of services) is combined with enhanced power during payer negotiations (because of scale). This model has allowed practices to merge into a physician organization and remain free from health system employment.17
Large health systems
Physicians employed by large health systems, whether they are nonprofit, for-profit, or AMCs, will see their future tied directly to health system success. If bundled payment, alternative payment, and capitation models of health care financing continue to grow in popularity, then success will be determined by a health system’s market share and its ability to form true clinical integration. In a capitated environment, expansion of market share (especially of relatively healthy patients) will help support margins. However, financial success will come from a system’s ability to manage high-cost patients, those 5% of patients who consume 50% of health care resources.18
Hospitals with a financially challenged patient base (safety-net hospitals) will have enormous financial pressures going forward. Repeal of ACA without restoration of pre-ACA funding will affect directly the financial health of systems including AMCs. AMCs and other health systems will be forced to reduce fixed overhead, enhance productivity of faculty, and restrict nonfunded activities (teaching for example). Although most AMCs are now in an active acquisition mode, this strategy is naturally limited by the number of remaining acquisition targets. Traditional high managed care rates enjoyed by AMCs will shrink, as will federal research funding (which typically comes with high indirect financial support). Health systems and GI societies will need to dedicate much more attention to state policy makers as Trumpcare progresses.
Finally, all providers will need to manage the business implications of retail health. As people assume higher deductibles and copays and health savings accounts grow, patients will change their patterns of purchasing services. Reputation counts for less when people are facing large price differences, so attention to patient-centric amenities, price, patient engagement, and patient satisfaction will become even more important.
Conclusion
The United States has undergone a massive and rapid political transformation. The mandate felt by conservative politicians, perhaps not supported by numbers, will carry a conservative platform forward. In areas where progressive Democrats emphasized federal power and socialized regulation (religion, education, civil rights, income security, and health policy), conservatives will transfer decision power as much as possible to states, local communities, and individuals. Maintaining the concept of “health as a right” will test the conscience of all of us.
References
1. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692-6.
2. Gill KE. Visual guide: the balance of power between Congress and the Presidency (1901-2016). Wired Pen. November 2016. Available from http://wiredpen.com/resources/political-commentary-and-analysis/a-visual-guide-balance-of-power-congress-presidency/. Accessed Dec. 30, 2016.
3. Mertens M. Chart: comparing health reform bills – Democrats and Republicans 2009, Republics 1993. Kaiser Health News. Feb. 24, 2010. Available from http://khn.org/022310-bill-comparison/. Accessed Jan. 8, 2017.
4. Hotchkiss M. Q&A: what a Trump presidency means for the Affordable Care Act. Nov. 16, 2016 News at Princeton. Princeton University. Available from https://www.princeton.edu/main/news/archive/S47/93/09C11/index.xml?section=topstories. Accessed Dec. 30, 2016.
5. Jost T. Taking stock of health reform: where we’ve been, where we’re going. Health Affairs Blog. Available from http://healthaffairs.org/blog/2016/12/06/taking-stock-of-health-reform-where-weve-been-where-were-going/. Accessed Dec. 30, 2016.
6. Jost T. The Republican Study Committee’s ACA replacement proposal (updated). Health Affairs Blog. Available from http://healthaffairs.org/blog/2017/01/05/the-republican-study-committees-aca-replacement-proposal/. Accessed Jan. 10, 2017.
7. Price T. Empowering patients first. Available from http://tomprice.house.gov/sites/tomprice.house.gov/files/HR%202300%20Empowering%20Patients%20First%20Act%202015.pdf. Accessed Dec. 30, 2016.
8. Ryan P. A better way. Available from https://abetterway.speaker.gov/_assets/pdf/ABetterWay-HealthCare-PolicyPaper.pdf. Accessed Dec. 30, 2016.
9. Oberlander, J. The end of Obamacare. N Engl J Med. 2017;376:1-3.
10. Goodnough A. Hospitals in safety net brace for health care law’s repeal. New York Times. Dec. 28, 2016. Available from http://www.nytimes.com/2016/12/28/health/hospitals-medicaid-obamacare-trump.html?smprod=nytcore-iphone&smid=nytcore-iphone-share&_r=0. Accessed Jan. 10, 2017.
11. Ayanian, J.Z., Ehrlich, G.M., Grimes, D.R., et al. Economic effects of Medicaid expansion in Michigan. N Engl J Med. 2017;376:407-10.
12. Obama, B.H. Repealing the ACA without a replacement: the risks to American health care. N Engl J Med. 2017;376:297-9.
13. Fuchs, V.R. Major concepts of health economics. Ann Intern Med. 2015;162:380-3.
14. Quinn, K. The 8 basic payment methods in health care. Ann Intern Med. 2015;163:300-6.
15. Schoenman JA. A detailed look at US health care spending: a presentation from the National Institute for Health Care Management (NIHCM). Oct. 25, 2012. Available from http://www.nihcm.org/images/stories/Health_care_spending_slides_-_MILI_-_Schoenman.pdf. Accessed Dec. 30, 2016.
16. Allen, J.I., Allen, C.C., Brill, J.V. Gastroenterology 2020: no time for WIMPs. Gastroenterology. 2016;150:295-9.
17. Sciacca R. Weekly Byte: GI roundtable and navigating uncharted waters in health care. The PMD Blog. Available from https://www.pmd.com/blog/post/weekly-byte-gi-roundtable-and-navigating-uncharted-waters-in-health-care. Accessed Jan. 10, 2017.
18. Powers, B.W., Chaguturu, S.K. ACOs and high-cost patients. N Engl J Med. 2016;374:203-5.
Dr. Allen is professor of medicine, University of Michigan School of Medicine, Institute for Health Care Policy and Innovations, and associate medical director of Network Strategy and Business Development – Michigan Medicine, Ann Arbor. He discloses no conflicts.

New cryoballoon treatment eradicated esophageal squamous cell neoplasias
For the first time, endoscopists have used focal cryoballoon ablation to eradicate early esophageal squamous cell neoplasias, including high-grade lesions in treatment-experienced patients.
A single session of treatment with the novel, portable nitrous oxide system (C2 Therapeutics, Redwood City, Calif.) produced complete pathologic and endoscopic responses at 3 months in 8 of 10 patients, reported Marcia Irene Canto, MD, of Johns Hopkins University in Baltimore, with her associates. Two to five sessions produced complete responses in the other two patients, and all patients were disease-free at their last visit (median follow-up, 10.7 months; interquartile range, 4-14 months). The study was published online July 15 in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.07.013).
Standard treatments for esophageal squamous cell neoplasia have drawbacks. Submucosal dissection can cause bleeding, perforation, and stenosis, and radiofrequency ablation (RFA) is associated with stricture. To test an alternative, the researchers used a portable, hand-held, battery-powered cryoballoon ablation system that successfully eradicated Barrett’s esophagus lesions in two prior studies. The machine contains liquid nitrous oxide, which turns to gas when released into a balloon catheter in the endoscope. The gas inflates the balloon, enabling the endoscopist to see through it to the neoplastic mucosa, which is pretreated with Lugol chromoendoscopy. The endoscopist then cryoablates the target lesion across the balloon wall. Unlike cryospray, the entire dose of cryogen hits the lesion, the investigators noted. Also, the gas is automatically evacuated without the need for suctioning or decompression, and the treatment process does not require heavy gas tanks or repeated freeze-thaw cycles.
In this study, all 10 patients achieved complete endoscopic and pathologic responses at 3 months. Seven patients were followed for 1 year, and none showed biopsy evidence of neoplastic progression. In contrast, a prospective trial of circumferential radiofrequency ablation without endoscopic mucosal resection or endoscopic submucosal dissection reported a 12-month rate of complete response of 84%, the researchers noted (Endoscopy. 2015;47:398-408). There were no serious treatment-related adverse events. Pain was usually self-limited, although one patient required 2 days of narcotics. Two patients developed symptomatic strictures 6-8 weeks after treatment that resolved with balloon dilation. Both of these patients had undergone extensive multifocal ablation. “Circumferential treatment of ESCN [esophageal squamous cell neoplasia] remains problematic for all endoscopic ablative therapies, with a high stricture rate of 20% in our small pilot study of cryoablation and 20%-23% with RFA,” the investigators wrote. “The risk for postablation stricture appears to be related to a long length of ESCN. Optimizing the cryogen dose, technique, and decrease in Lugol’s solution concentration might alter the incidence of postablation strictures for ablative treatments.”
Study participants were 55-90 years old, and six were female. Four were treatment naive, and six had progressed despite endoscopic mucosal resection, RFA, spray cryotherapy, argon plasma coagulation, or multiple therapies. Seven patients had high-grade lesions, two had low-grade lesions, and one had early esophageal squamous cell carcinoma. Most lesions were distally located, but two were in the middle esophagus and one was proximal. The largest lesion measured 4 cm and the maximum length of all lesions in a single patient was 10 cm. Patients did not have visible esophageal masses or evidence of advanced or metastatic disease.
“Comparative effectiveness trials might eventually determine the role of cryoablation in the treatment of early ESCN,” the researchers concluded. An open-label, nonrandomized clinical trial of the balloon cryotherapy device is underway in China (NCT02605759). The article did not list funding sources or disclosures.
For the first time, endoscopists have used focal cryoballoon ablation to eradicate early esophageal squamous cell neoplasias, including high-grade lesions in treatment-experienced patients.
A single session of treatment with the novel, portable nitrous oxide system (C2 Therapeutics, Redwood City, Calif.) produced complete pathologic and endoscopic responses at 3 months in 8 of 10 patients, reported Marcia Irene Canto, MD, of Johns Hopkins University in Baltimore, with her associates. Two to five sessions produced complete responses in the other two patients, and all patients were disease-free at their last visit (median follow-up, 10.7 months; interquartile range, 4-14 months). The study was published online July 15 in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.07.013).
Standard treatments for esophageal squamous cell neoplasia have drawbacks. Submucosal dissection can cause bleeding, perforation, and stenosis, and radiofrequency ablation (RFA) is associated with stricture. To test an alternative, the researchers used a portable, hand-held, battery-powered cryoballoon ablation system that successfully eradicated Barrett’s esophagus lesions in two prior studies. The machine contains liquid nitrous oxide, which turns to gas when released into a balloon catheter in the endoscope. The gas inflates the balloon, enabling the endoscopist to see through it to the neoplastic mucosa, which is pretreated with Lugol chromoendoscopy. The endoscopist then cryoablates the target lesion across the balloon wall. Unlike cryospray, the entire dose of cryogen hits the lesion, the investigators noted. Also, the gas is automatically evacuated without the need for suctioning or decompression, and the treatment process does not require heavy gas tanks or repeated freeze-thaw cycles.
In this study, all 10 patients achieved complete endoscopic and pathologic responses at 3 months. Seven patients were followed for 1 year, and none showed biopsy evidence of neoplastic progression. In contrast, a prospective trial of circumferential radiofrequency ablation without endoscopic mucosal resection or endoscopic submucosal dissection reported a 12-month rate of complete response of 84%, the researchers noted (Endoscopy. 2015;47:398-408). There were no serious treatment-related adverse events. Pain was usually self-limited, although one patient required 2 days of narcotics. Two patients developed symptomatic strictures 6-8 weeks after treatment that resolved with balloon dilation. Both of these patients had undergone extensive multifocal ablation. “Circumferential treatment of ESCN [esophageal squamous cell neoplasia] remains problematic for all endoscopic ablative therapies, with a high stricture rate of 20% in our small pilot study of cryoablation and 20%-23% with RFA,” the investigators wrote. “The risk for postablation stricture appears to be related to a long length of ESCN. Optimizing the cryogen dose, technique, and decrease in Lugol’s solution concentration might alter the incidence of postablation strictures for ablative treatments.”
Study participants were 55-90 years old, and six were female. Four were treatment naive, and six had progressed despite endoscopic mucosal resection, RFA, spray cryotherapy, argon plasma coagulation, or multiple therapies. Seven patients had high-grade lesions, two had low-grade lesions, and one had early esophageal squamous cell carcinoma. Most lesions were distally located, but two were in the middle esophagus and one was proximal. The largest lesion measured 4 cm and the maximum length of all lesions in a single patient was 10 cm. Patients did not have visible esophageal masses or evidence of advanced or metastatic disease.
“Comparative effectiveness trials might eventually determine the role of cryoablation in the treatment of early ESCN,” the researchers concluded. An open-label, nonrandomized clinical trial of the balloon cryotherapy device is underway in China (NCT02605759). The article did not list funding sources or disclosures.
For the first time, endoscopists have used focal cryoballoon ablation to eradicate early esophageal squamous cell neoplasias, including high-grade lesions in treatment-experienced patients.
A single session of treatment with the novel, portable nitrous oxide system (C2 Therapeutics, Redwood City, Calif.) produced complete pathologic and endoscopic responses at 3 months in 8 of 10 patients, reported Marcia Irene Canto, MD, of Johns Hopkins University in Baltimore, with her associates. Two to five sessions produced complete responses in the other two patients, and all patients were disease-free at their last visit (median follow-up, 10.7 months; interquartile range, 4-14 months). The study was published online July 15 in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.07.013).
Standard treatments for esophageal squamous cell neoplasia have drawbacks. Submucosal dissection can cause bleeding, perforation, and stenosis, and radiofrequency ablation (RFA) is associated with stricture. To test an alternative, the researchers used a portable, hand-held, battery-powered cryoballoon ablation system that successfully eradicated Barrett’s esophagus lesions in two prior studies. The machine contains liquid nitrous oxide, which turns to gas when released into a balloon catheter in the endoscope. The gas inflates the balloon, enabling the endoscopist to see through it to the neoplastic mucosa, which is pretreated with Lugol chromoendoscopy. The endoscopist then cryoablates the target lesion across the balloon wall. Unlike cryospray, the entire dose of cryogen hits the lesion, the investigators noted. Also, the gas is automatically evacuated without the need for suctioning or decompression, and the treatment process does not require heavy gas tanks or repeated freeze-thaw cycles.
In this study, all 10 patients achieved complete endoscopic and pathologic responses at 3 months. Seven patients were followed for 1 year, and none showed biopsy evidence of neoplastic progression. In contrast, a prospective trial of circumferential radiofrequency ablation without endoscopic mucosal resection or endoscopic submucosal dissection reported a 12-month rate of complete response of 84%, the researchers noted (Endoscopy. 2015;47:398-408). There were no serious treatment-related adverse events. Pain was usually self-limited, although one patient required 2 days of narcotics. Two patients developed symptomatic strictures 6-8 weeks after treatment that resolved with balloon dilation. Both of these patients had undergone extensive multifocal ablation. “Circumferential treatment of ESCN [esophageal squamous cell neoplasia] remains problematic for all endoscopic ablative therapies, with a high stricture rate of 20% in our small pilot study of cryoablation and 20%-23% with RFA,” the investigators wrote. “The risk for postablation stricture appears to be related to a long length of ESCN. Optimizing the cryogen dose, technique, and decrease in Lugol’s solution concentration might alter the incidence of postablation strictures for ablative treatments.”
Study participants were 55-90 years old, and six were female. Four were treatment naive, and six had progressed despite endoscopic mucosal resection, RFA, spray cryotherapy, argon plasma coagulation, or multiple therapies. Seven patients had high-grade lesions, two had low-grade lesions, and one had early esophageal squamous cell carcinoma. Most lesions were distally located, but two were in the middle esophagus and one was proximal. The largest lesion measured 4 cm and the maximum length of all lesions in a single patient was 10 cm. Patients did not have visible esophageal masses or evidence of advanced or metastatic disease.
“Comparative effectiveness trials might eventually determine the role of cryoablation in the treatment of early ESCN,” the researchers concluded. An open-label, nonrandomized clinical trial of the balloon cryotherapy device is underway in China (NCT02605759). The article did not list funding sources or disclosures.
FROM GIE
Key clinical point: In a first-in-kind study, endoscopists used focal cryoballoon ablation to eradicate early esophageal squamous cell neoplasias.
Major finding: All 10 patients had a complete response at 3 months. All remained disease free at last follow-up (median, 10.7 months).
Data source: A multicenter study of 10 patients with early high-grade or low-grade esophageal squamous cell neoplasias or early squamous cell carcinomas.
Disclosures: The article did not list funding sources or disclosures.