User login
Researchers compare world health authorities

A new study has revealed substantial differences between health authorities in different regions of the world.
A pair of researchers compared 12 different regulatory authorities responsible for approving drugs and medical products.
The researchers collected data* on annual budgets, new drug approvals per year, numbers of reviewers, standard and median review times, fees for new drug applications (NDAs), and other measurements.
The results were published in Nature Reviews Drug Discovery.
For the 2015 fiscal year, the US Food and Drug Administration (FDA) had the highest budget—$1.19 billion—and India’s Central Drugs Standard Control Organization (CDSCO) had the lowest—$26 million.
In 2016, the FDA again had the highest budget—$1.23 billion—while Health Canada and Switzerland’s SwissMedic had the lowest—$108 million.
In 2016, the European Medicines Agency (EMA) had the highest number of reviewers—4500—and SwissMedic had the lowest—60. (Data from 2015 were not included.)
In 2015, Japan’s Pharmaceuticals and Medical Devices Agency had the highest number of NDA submissions—127—and Health Canada had the lowest—27. Meanwhile, the Chinese FDA had the highest number of new drug approvals—72—and India’s CDSCO had the lowest—17.
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) technically had the most new drug approvals in 2015, at 146, but not all of these were unique, as the number included all decentralized applications, both with the UK as the reference member state and approvals from concerned member states.
In 2016, the EMA had the highest number of NDA submissions—68—and Health Canada had the lowest—25. Singapore’s Health Sciences Authority had the highest number of new drug approvals—72—while the US FDA and India’s CDSCO had the lowest—22.
The shortest standard review period was 210 days. This is the standard for the EMA, the UK’s MHRA, and Russia’s Roszdravnadzor. The regulatory agency with the longest standard review time—900 days—is the Chinese FDA.
The shortest median time to new drug approval in 2015 was 230 days, for the UK’s MHRA. The longest was 834 days, for the Brazilian Health Surveillance Agency.
The highest NDA review fees were those charged by the US FDA—$2.3 million. The lowest were those charged by India’s CDSCO—50,000 Indian rupees or about USD$1000.
The researchers noted that these data suggest products are being evaluated via different processes and according to different standards, which makes it challenging for pharmaceutical companies to develop drugs for simultaneous submission to all regulatory authorities.
Therefore, a harmonization of approval requirements and processes could significantly improve efficiency.
“Patients would profit especially since new drugs would be available faster and at lower prices,” said study author Thomas D. Szucs, MD, PhD, of the University of Basel in Switzerland.
“This suggests that companies and authorities should strengthen their international collaboration and communicate better with each other.” ![]()
*Some data were missing for most of the 12 agencies studied.
A new study has revealed substantial differences between health authorities in different regions of the world.
A pair of researchers compared 12 different regulatory authorities responsible for approving drugs and medical products.
The researchers collected data* on annual budgets, new drug approvals per year, numbers of reviewers, standard and median review times, fees for new drug applications (NDAs), and other measurements.
The results were published in Nature Reviews Drug Discovery.
For the 2015 fiscal year, the US Food and Drug Administration (FDA) had the highest budget—$1.19 billion—and India’s Central Drugs Standard Control Organization (CDSCO) had the lowest—$26 million.
In 2016, the FDA again had the highest budget—$1.23 billion—while Health Canada and Switzerland’s SwissMedic had the lowest—$108 million.
In 2016, the European Medicines Agency (EMA) had the highest number of reviewers—4500—and SwissMedic had the lowest—60. (Data from 2015 were not included.)
In 2015, Japan’s Pharmaceuticals and Medical Devices Agency had the highest number of NDA submissions—127—and Health Canada had the lowest—27. Meanwhile, the Chinese FDA had the highest number of new drug approvals—72—and India’s CDSCO had the lowest—17.
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) technically had the most new drug approvals in 2015, at 146, but not all of these were unique, as the number included all decentralized applications, both with the UK as the reference member state and approvals from concerned member states.
In 2016, the EMA had the highest number of NDA submissions—68—and Health Canada had the lowest—25. Singapore’s Health Sciences Authority had the highest number of new drug approvals—72—while the US FDA and India’s CDSCO had the lowest—22.
The shortest standard review period was 210 days. This is the standard for the EMA, the UK’s MHRA, and Russia’s Roszdravnadzor. The regulatory agency with the longest standard review time—900 days—is the Chinese FDA.
The shortest median time to new drug approval in 2015 was 230 days, for the UK’s MHRA. The longest was 834 days, for the Brazilian Health Surveillance Agency.
The highest NDA review fees were those charged by the US FDA—$2.3 million. The lowest were those charged by India’s CDSCO—50,000 Indian rupees or about USD$1000.
The researchers noted that these data suggest products are being evaluated via different processes and according to different standards, which makes it challenging for pharmaceutical companies to develop drugs for simultaneous submission to all regulatory authorities.
Therefore, a harmonization of approval requirements and processes could significantly improve efficiency.
“Patients would profit especially since new drugs would be available faster and at lower prices,” said study author Thomas D. Szucs, MD, PhD, of the University of Basel in Switzerland.
“This suggests that companies and authorities should strengthen their international collaboration and communicate better with each other.” ![]()
*Some data were missing for most of the 12 agencies studied.
A new study has revealed substantial differences between health authorities in different regions of the world.
A pair of researchers compared 12 different regulatory authorities responsible for approving drugs and medical products.
The researchers collected data* on annual budgets, new drug approvals per year, numbers of reviewers, standard and median review times, fees for new drug applications (NDAs), and other measurements.
The results were published in Nature Reviews Drug Discovery.
For the 2015 fiscal year, the US Food and Drug Administration (FDA) had the highest budget—$1.19 billion—and India’s Central Drugs Standard Control Organization (CDSCO) had the lowest—$26 million.
In 2016, the FDA again had the highest budget—$1.23 billion—while Health Canada and Switzerland’s SwissMedic had the lowest—$108 million.
In 2016, the European Medicines Agency (EMA) had the highest number of reviewers—4500—and SwissMedic had the lowest—60. (Data from 2015 were not included.)
In 2015, Japan’s Pharmaceuticals and Medical Devices Agency had the highest number of NDA submissions—127—and Health Canada had the lowest—27. Meanwhile, the Chinese FDA had the highest number of new drug approvals—72—and India’s CDSCO had the lowest—17.
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) technically had the most new drug approvals in 2015, at 146, but not all of these were unique, as the number included all decentralized applications, both with the UK as the reference member state and approvals from concerned member states.
In 2016, the EMA had the highest number of NDA submissions—68—and Health Canada had the lowest—25. Singapore’s Health Sciences Authority had the highest number of new drug approvals—72—while the US FDA and India’s CDSCO had the lowest—22.
The shortest standard review period was 210 days. This is the standard for the EMA, the UK’s MHRA, and Russia’s Roszdravnadzor. The regulatory agency with the longest standard review time—900 days—is the Chinese FDA.
The shortest median time to new drug approval in 2015 was 230 days, for the UK’s MHRA. The longest was 834 days, for the Brazilian Health Surveillance Agency.
The highest NDA review fees were those charged by the US FDA—$2.3 million. The lowest were those charged by India’s CDSCO—50,000 Indian rupees or about USD$1000.
The researchers noted that these data suggest products are being evaluated via different processes and according to different standards, which makes it challenging for pharmaceutical companies to develop drugs for simultaneous submission to all regulatory authorities.
Therefore, a harmonization of approval requirements and processes could significantly improve efficiency.
“Patients would profit especially since new drugs would be available faster and at lower prices,” said study author Thomas D. Szucs, MD, PhD, of the University of Basel in Switzerland.
“This suggests that companies and authorities should strengthen their international collaboration and communicate better with each other.” ![]()
*Some data were missing for most of the 12 agencies studied.
Test uses nanotechnology to diagnose Zika virus

Researchers say they have developed a point-of-care, paper-based test that quickly detects the presence of Zika virus in blood.
Currently, testing for Zika requires that a blood sample be refrigerated and shipped to a medical center or laboratory, delaying diagnosis and possible treatment.
The new test, on the other hand, does not require refrigeration and can produce results in minutes.
“If an assay requires electricity and refrigeration, it defeats the purpose of developing something to use in a resource-limited setting, especially in tropical areas of the world,” said Srikanth Singamaneni, PhD, of Washington University in St. Louis, Missouri.
“We wanted to make the test immune from variations in temperature and humidity.”
Dr Singamaneni and his colleagues described this test in Advanced Biosystems.
The researchers used the test on blood samples from 4 subjects known to be infected with Zika virus and samples from 5 subjects who did not have the virus.
The test showed positive results for the Zika-infected patients and negative results for controls. There were no false-positives.
How the test works
The test uses gold nanorods mounted on paper to detect Zika infection in the blood.
The test relies on a protein made by Zika virus that causes an immune response in infected individuals— ZIKV-nonstructural protein 1 (NS1). The ZIKV-NS1 protein is attached to gold nanorods mounted on a piece of paper.
The paper is then covered with protective nanocrystals. The nanocrystals allow the diagnostic nanorods to be shipped and stored without refrigeration prior to use.
To use the test, a technician rinses the paper with slightly acidic water, removing the protective crystals and exposing the protein mounted on the nanorods.
Then, a drop of the patient’s blood is applied. If the patient has come into contact with the virus, the blood will contain immunoglobulins that react with the ZIKV-NS1 protein.
“We’re taking advantage of the fact that patients mount an immune attack against this viral protein,” said study author Jeremiah J. Morrissey, PhD, of Washington University.
“The immunoglobulins persist in the blood for a few months, and when they come into contact with the gold nanorods, the nanorods undergo a slight color change that can be detected with a hand-held spectrophotometer. With this test, results will be clear before the patient leaves the clinic, allowing immediate counseling and access to treatment.”
The color change cannot be seen with the naked eye, but the researchers are working to change that. They’re also working on developing ways to use saliva rather than blood.
Although the test uses gold, the nanorods are very small. The researchers estimate the cost of the gold used in one of the assays would be 10 to 15 cents. ![]()
Researchers say they have developed a point-of-care, paper-based test that quickly detects the presence of Zika virus in blood.
Currently, testing for Zika requires that a blood sample be refrigerated and shipped to a medical center or laboratory, delaying diagnosis and possible treatment.
The new test, on the other hand, does not require refrigeration and can produce results in minutes.
“If an assay requires electricity and refrigeration, it defeats the purpose of developing something to use in a resource-limited setting, especially in tropical areas of the world,” said Srikanth Singamaneni, PhD, of Washington University in St. Louis, Missouri.
“We wanted to make the test immune from variations in temperature and humidity.”
Dr Singamaneni and his colleagues described this test in Advanced Biosystems.
The researchers used the test on blood samples from 4 subjects known to be infected with Zika virus and samples from 5 subjects who did not have the virus.
The test showed positive results for the Zika-infected patients and negative results for controls. There were no false-positives.
How the test works
The test uses gold nanorods mounted on paper to detect Zika infection in the blood.
The test relies on a protein made by Zika virus that causes an immune response in infected individuals— ZIKV-nonstructural protein 1 (NS1). The ZIKV-NS1 protein is attached to gold nanorods mounted on a piece of paper.
The paper is then covered with protective nanocrystals. The nanocrystals allow the diagnostic nanorods to be shipped and stored without refrigeration prior to use.
To use the test, a technician rinses the paper with slightly acidic water, removing the protective crystals and exposing the protein mounted on the nanorods.
Then, a drop of the patient’s blood is applied. If the patient has come into contact with the virus, the blood will contain immunoglobulins that react with the ZIKV-NS1 protein.
“We’re taking advantage of the fact that patients mount an immune attack against this viral protein,” said study author Jeremiah J. Morrissey, PhD, of Washington University.
“The immunoglobulins persist in the blood for a few months, and when they come into contact with the gold nanorods, the nanorods undergo a slight color change that can be detected with a hand-held spectrophotometer. With this test, results will be clear before the patient leaves the clinic, allowing immediate counseling and access to treatment.”
The color change cannot be seen with the naked eye, but the researchers are working to change that. They’re also working on developing ways to use saliva rather than blood.
Although the test uses gold, the nanorods are very small. The researchers estimate the cost of the gold used in one of the assays would be 10 to 15 cents. ![]()
Researchers say they have developed a point-of-care, paper-based test that quickly detects the presence of Zika virus in blood.
Currently, testing for Zika requires that a blood sample be refrigerated and shipped to a medical center or laboratory, delaying diagnosis and possible treatment.
The new test, on the other hand, does not require refrigeration and can produce results in minutes.
“If an assay requires electricity and refrigeration, it defeats the purpose of developing something to use in a resource-limited setting, especially in tropical areas of the world,” said Srikanth Singamaneni, PhD, of Washington University in St. Louis, Missouri.
“We wanted to make the test immune from variations in temperature and humidity.”
Dr Singamaneni and his colleagues described this test in Advanced Biosystems.
The researchers used the test on blood samples from 4 subjects known to be infected with Zika virus and samples from 5 subjects who did not have the virus.
The test showed positive results for the Zika-infected patients and negative results for controls. There were no false-positives.
How the test works
The test uses gold nanorods mounted on paper to detect Zika infection in the blood.
The test relies on a protein made by Zika virus that causes an immune response in infected individuals— ZIKV-nonstructural protein 1 (NS1). The ZIKV-NS1 protein is attached to gold nanorods mounted on a piece of paper.
The paper is then covered with protective nanocrystals. The nanocrystals allow the diagnostic nanorods to be shipped and stored without refrigeration prior to use.
To use the test, a technician rinses the paper with slightly acidic water, removing the protective crystals and exposing the protein mounted on the nanorods.
Then, a drop of the patient’s blood is applied. If the patient has come into contact with the virus, the blood will contain immunoglobulins that react with the ZIKV-NS1 protein.
“We’re taking advantage of the fact that patients mount an immune attack against this viral protein,” said study author Jeremiah J. Morrissey, PhD, of Washington University.
“The immunoglobulins persist in the blood for a few months, and when they come into contact with the gold nanorods, the nanorods undergo a slight color change that can be detected with a hand-held spectrophotometer. With this test, results will be clear before the patient leaves the clinic, allowing immediate counseling and access to treatment.”
The color change cannot be seen with the naked eye, but the researchers are working to change that. They’re also working on developing ways to use saliva rather than blood.
Although the test uses gold, the nanorods are very small. The researchers estimate the cost of the gold used in one of the assays would be 10 to 15 cents. ![]()
Exelixis seeks expanded indication for cabozantinib in RCC
Exelixis has submitted a supplemental New Drug Application to the Food and Drug Administration for cabozantinib (Cabometyx) for the treatment of previously untreated advanced renal cell carcinoma (RCC).
The application, announced on Aug. 16, seeks to allow the manufacturer to modify the label. Cabozantinib was approved in April 2016 for treatment of patients with advanced RCC who had previously received antiangiogenic therapy.![]()
The results of the trial were published in the Journal of Clinical Oncology (2017 Feb 20;35[6]:591-7). An independent review committee confirmed the primary efficacy endpoint results in June 2017.
Exelixis has submitted a supplemental New Drug Application to the Food and Drug Administration for cabozantinib (Cabometyx) for the treatment of previously untreated advanced renal cell carcinoma (RCC).
The application, announced on Aug. 16, seeks to allow the manufacturer to modify the label. Cabozantinib was approved in April 2016 for treatment of patients with advanced RCC who had previously received antiangiogenic therapy.![]()
The results of the trial were published in the Journal of Clinical Oncology (2017 Feb 20;35[6]:591-7). An independent review committee confirmed the primary efficacy endpoint results in June 2017.
Exelixis has submitted a supplemental New Drug Application to the Food and Drug Administration for cabozantinib (Cabometyx) for the treatment of previously untreated advanced renal cell carcinoma (RCC).
The application, announced on Aug. 16, seeks to allow the manufacturer to modify the label. Cabozantinib was approved in April 2016 for treatment of patients with advanced RCC who had previously received antiangiogenic therapy.![]()
The results of the trial were published in the Journal of Clinical Oncology (2017 Feb 20;35[6]:591-7). An independent review committee confirmed the primary efficacy endpoint results in June 2017.
NASH did not increase risk of poor liver transplantation outcomes
Adults with nonalcoholic steatohepatitis (NASH) fared as well on key outcome measures as other liver transplant recipients, despite having significantly more comorbidities, according to the results of a single-center retrospective cohort study.
Major morbidity, mortality, and rates of graft survival after 90 days were similar between patients who underwent transplantation for NASH and those who underwent it for another cirrhotic liver condition, wrote Eline H. van den Berg, MD, of University Medical Center Groningen (the Netherlands) with her associates. “These results are comforting, considering the expected increase of patients with NASH cirrhosis in the near future,” the researchers concluded. “Future analysis regarding the recurrence of nonalcoholic fatty liver disease, development of long-term complications, long-term graft patency, and occurrence of comorbid diseases after LT [liver transplantation] is mandatory to better understand the natural history and risk profile of NASH patients and to prevent and treat its complications.” The findings were published online in Digestive and Liver Disease (Dig Liver Dis. 2017 Aug 11. doi: 10.1016/j.dld.2017.08.022).
Nonalcoholic fatty liver disease begins as steatosis and can progress to NASH, fibrosis, and cirrhosis. The global obesity epidemic is amplifying its incidence, and about 26% of patients who develop NASH ultimately develop cirrhosis. Cirrhosis itself increases the risk of in-hospital death or prolonged length of postoperative stay, but patients with NASH also have obesity and cardiovascular disease, which might “tremendously increase” the risk of poor postoperative outcomes, the researchers said. Because prior research had focused mainly on mortality and had reported conflicting results, they used the Clavien-Dindo classification system to retrospectively study rates of complications among 169 adults who underwent liver transplantation at their center from 2009 through 2015, including 34 (20%) patients with NASH cirrhosis.
Patients with NASH were significantly older than other transplant recipients (59 versus 55 years, P = .01) and had markedly higher rates of obesity (62% versus 8%; P less than .01), diabetes mellitus (74% versus 20%; P less than .01), metabolic syndrome (83% versus 38%; P less than .01), hypertension (61% versus 30%; P less than .01), and cardiovascular disease (29% versus 11%; P less than .01). Despite these differences, the groups had statistically similar rates of postoperative mortality (3% in both groups), 90-day graft survival posttransplantation (94% and 90%, respectively), and major postoperative complications, including biopsy-proven acute cellular rejection (3% and 7%), hepatic artery thrombosis (0% and 7%), relaparotomy (15% and 24%), primary nonfunction (0% and 1.6%), retransplantation (6% and 7%), sepsis (12% and 13%), gastrointestinal infection (24% and 36%), fever of unknown origin (18% and 14%), and renal replacement therapy (15% and 24%).
After accounting for age, sex, transplant year, and donor characteristics, NASH patients were at significantly increased risk of grade 2 urogenital infections, compared with other patients (odds ratio, 3.4; 95% confidence interval, 1.1 to 10.6; P = .03). Grade 1 complications also were more common with NASH than otherwise (77% versus 59%), and the difference remained statistically significant in the multivariable analysis (OR, 1.6; 95% CI, 1.03 to 2.63; P = .04).
The study used a strict, internationally accepted definition of NASH – all patients either had cases confirmed by biopsy, had metabolic syndrome, or had obesity and type 2 diabetes mellitus, and, further, none had hepatitis or alcoholic liver disease. None of the patients in the study received transplants for acute liver failure or noncirrhotic liver disease, and none were 70 years or older, which is the cutoff age for liver transplantation in the Netherlands.
The investigators received no funding for the study and reported having no conflicts of interest.
Adults with nonalcoholic steatohepatitis (NASH) fared as well on key outcome measures as other liver transplant recipients, despite having significantly more comorbidities, according to the results of a single-center retrospective cohort study.
Major morbidity, mortality, and rates of graft survival after 90 days were similar between patients who underwent transplantation for NASH and those who underwent it for another cirrhotic liver condition, wrote Eline H. van den Berg, MD, of University Medical Center Groningen (the Netherlands) with her associates. “These results are comforting, considering the expected increase of patients with NASH cirrhosis in the near future,” the researchers concluded. “Future analysis regarding the recurrence of nonalcoholic fatty liver disease, development of long-term complications, long-term graft patency, and occurrence of comorbid diseases after LT [liver transplantation] is mandatory to better understand the natural history and risk profile of NASH patients and to prevent and treat its complications.” The findings were published online in Digestive and Liver Disease (Dig Liver Dis. 2017 Aug 11. doi: 10.1016/j.dld.2017.08.022).
Nonalcoholic fatty liver disease begins as steatosis and can progress to NASH, fibrosis, and cirrhosis. The global obesity epidemic is amplifying its incidence, and about 26% of patients who develop NASH ultimately develop cirrhosis. Cirrhosis itself increases the risk of in-hospital death or prolonged length of postoperative stay, but patients with NASH also have obesity and cardiovascular disease, which might “tremendously increase” the risk of poor postoperative outcomes, the researchers said. Because prior research had focused mainly on mortality and had reported conflicting results, they used the Clavien-Dindo classification system to retrospectively study rates of complications among 169 adults who underwent liver transplantation at their center from 2009 through 2015, including 34 (20%) patients with NASH cirrhosis.
Patients with NASH were significantly older than other transplant recipients (59 versus 55 years, P = .01) and had markedly higher rates of obesity (62% versus 8%; P less than .01), diabetes mellitus (74% versus 20%; P less than .01), metabolic syndrome (83% versus 38%; P less than .01), hypertension (61% versus 30%; P less than .01), and cardiovascular disease (29% versus 11%; P less than .01). Despite these differences, the groups had statistically similar rates of postoperative mortality (3% in both groups), 90-day graft survival posttransplantation (94% and 90%, respectively), and major postoperative complications, including biopsy-proven acute cellular rejection (3% and 7%), hepatic artery thrombosis (0% and 7%), relaparotomy (15% and 24%), primary nonfunction (0% and 1.6%), retransplantation (6% and 7%), sepsis (12% and 13%), gastrointestinal infection (24% and 36%), fever of unknown origin (18% and 14%), and renal replacement therapy (15% and 24%).
After accounting for age, sex, transplant year, and donor characteristics, NASH patients were at significantly increased risk of grade 2 urogenital infections, compared with other patients (odds ratio, 3.4; 95% confidence interval, 1.1 to 10.6; P = .03). Grade 1 complications also were more common with NASH than otherwise (77% versus 59%), and the difference remained statistically significant in the multivariable analysis (OR, 1.6; 95% CI, 1.03 to 2.63; P = .04).
The study used a strict, internationally accepted definition of NASH – all patients either had cases confirmed by biopsy, had metabolic syndrome, or had obesity and type 2 diabetes mellitus, and, further, none had hepatitis or alcoholic liver disease. None of the patients in the study received transplants for acute liver failure or noncirrhotic liver disease, and none were 70 years or older, which is the cutoff age for liver transplantation in the Netherlands.
The investigators received no funding for the study and reported having no conflicts of interest.
Adults with nonalcoholic steatohepatitis (NASH) fared as well on key outcome measures as other liver transplant recipients, despite having significantly more comorbidities, according to the results of a single-center retrospective cohort study.
Major morbidity, mortality, and rates of graft survival after 90 days were similar between patients who underwent transplantation for NASH and those who underwent it for another cirrhotic liver condition, wrote Eline H. van den Berg, MD, of University Medical Center Groningen (the Netherlands) with her associates. “These results are comforting, considering the expected increase of patients with NASH cirrhosis in the near future,” the researchers concluded. “Future analysis regarding the recurrence of nonalcoholic fatty liver disease, development of long-term complications, long-term graft patency, and occurrence of comorbid diseases after LT [liver transplantation] is mandatory to better understand the natural history and risk profile of NASH patients and to prevent and treat its complications.” The findings were published online in Digestive and Liver Disease (Dig Liver Dis. 2017 Aug 11. doi: 10.1016/j.dld.2017.08.022).
Nonalcoholic fatty liver disease begins as steatosis and can progress to NASH, fibrosis, and cirrhosis. The global obesity epidemic is amplifying its incidence, and about 26% of patients who develop NASH ultimately develop cirrhosis. Cirrhosis itself increases the risk of in-hospital death or prolonged length of postoperative stay, but patients with NASH also have obesity and cardiovascular disease, which might “tremendously increase” the risk of poor postoperative outcomes, the researchers said. Because prior research had focused mainly on mortality and had reported conflicting results, they used the Clavien-Dindo classification system to retrospectively study rates of complications among 169 adults who underwent liver transplantation at their center from 2009 through 2015, including 34 (20%) patients with NASH cirrhosis.
Patients with NASH were significantly older than other transplant recipients (59 versus 55 years, P = .01) and had markedly higher rates of obesity (62% versus 8%; P less than .01), diabetes mellitus (74% versus 20%; P less than .01), metabolic syndrome (83% versus 38%; P less than .01), hypertension (61% versus 30%; P less than .01), and cardiovascular disease (29% versus 11%; P less than .01). Despite these differences, the groups had statistically similar rates of postoperative mortality (3% in both groups), 90-day graft survival posttransplantation (94% and 90%, respectively), and major postoperative complications, including biopsy-proven acute cellular rejection (3% and 7%), hepatic artery thrombosis (0% and 7%), relaparotomy (15% and 24%), primary nonfunction (0% and 1.6%), retransplantation (6% and 7%), sepsis (12% and 13%), gastrointestinal infection (24% and 36%), fever of unknown origin (18% and 14%), and renal replacement therapy (15% and 24%).
After accounting for age, sex, transplant year, and donor characteristics, NASH patients were at significantly increased risk of grade 2 urogenital infections, compared with other patients (odds ratio, 3.4; 95% confidence interval, 1.1 to 10.6; P = .03). Grade 1 complications also were more common with NASH than otherwise (77% versus 59%), and the difference remained statistically significant in the multivariable analysis (OR, 1.6; 95% CI, 1.03 to 2.63; P = .04).
The study used a strict, internationally accepted definition of NASH – all patients either had cases confirmed by biopsy, had metabolic syndrome, or had obesity and type 2 diabetes mellitus, and, further, none had hepatitis or alcoholic liver disease. None of the patients in the study received transplants for acute liver failure or noncirrhotic liver disease, and none were 70 years or older, which is the cutoff age for liver transplantation in the Netherlands.
The investigators received no funding for the study and reported having no conflicts of interest.
FROM DIGESTIVE AND LIVER DISEASES
Key clinical point: Adults with nonalcoholic steatohepatitis (NASH) fared as well as on key outcome measures as other liver transplant recipients, despite having significantly more comorbidities.
Major finding: Patients with and without NASH had statistically similar rates of postoperative mortality (3% in both groups), 90-day graft survival (94% and 90%, respectively), and major postoperative complications.
Data source: A single-center retrospective cohort study of 169 adult liver transplant recipients, of whom 20% were transplanted for NASH cirrhosis.
Disclosures: The investigators received no funding for the study and reported having no conflicts of interest.
Brain scan study suggests serotonin drives early cognitive decline
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
FROM NEUROBIOLOGY OF DISEASE
Key clinical point: Levels of serotonin transporters were significantly lower in the cortical, striatal, thalamic, and limbic regions of the brain of adults with mild cognitive impairment, compared with healthy controls.
Major finding: The decrease in serotonin transporters (SERT) ranged from 10% to 38% in MCI adults, compared with healthy controls.
Data source: The data come from a comparison study of 28 adults with MCI and 28 healthy controls.
Disclosures: Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. The study was supported by the NIH.
Breaking bad news
As psychiatrists, we do not often encounter situations in which we need to inform patients and their families that they have a life-threatening diagnosis. Nonetheless, on the rare occasions when we work with such patients, new psychiatrists may find their clinical skills challenged. Breaking bad news remains an aspect of clinical training that is often overlooked by medical schools.
Here I present a case that illustrates the challenges residents and medical students face when they need to deliver bad news and review the current literature on how to present patients with this type of information.
Case
Bizarre behavior, difficult diagnosis
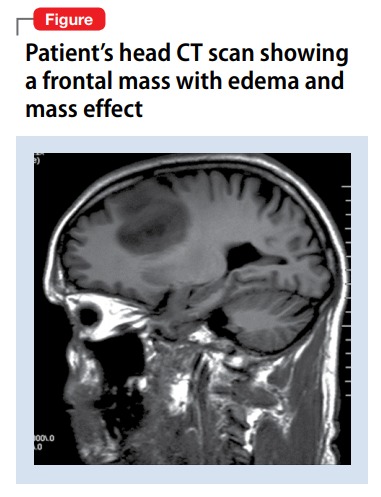
Mr. C, age 59, with a 1-year history of major depressive disorder, was brought to the emergency department by his wife for worsening depression and disorganized behavior over the course of 3 weeks. Mr. C had obsessive thoughts about arranging things in symmetrical patterns, difficulty sleeping, loss of appetite, and anhedonia. His wife reported that his bizarre, disorganized behavior further intensified in the previous week; he was urinating on the rug, rubbing his genitals against the bathroom counter, staring into space without moving for prolonged periods of time, and arranging his food in symmetrical patterns. Mr. C has no reported substance use or suicidal or homicidal ideation.
Strategies for delivering bad news
Initially, I struggled when I realized I would have to deliver the news of this potentially life-threatening diagnosis to the patient and his wife because I had not received any training on how to do so. However, I took time to look into the literature and used the skills that we as psychiatrists have, including empathy, listening, and validation. My experience with Mr. C and his family made me realize that delivering bad news with empathy and being involved in the struggle that follows can make a significant difference to their suffering.
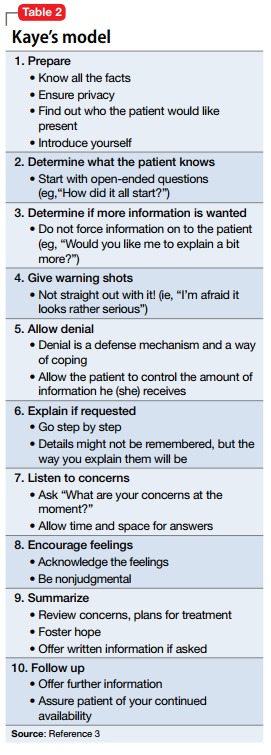
There are various models and techniques for breaking bad news to patients. Two of the most commonly used models in the oncology setting are the SPIKES (Set up, Perception, Interview, Knowledge, Emotions, Strategize and Summarize) model (Table 12) and Kaye’s model (Table 23).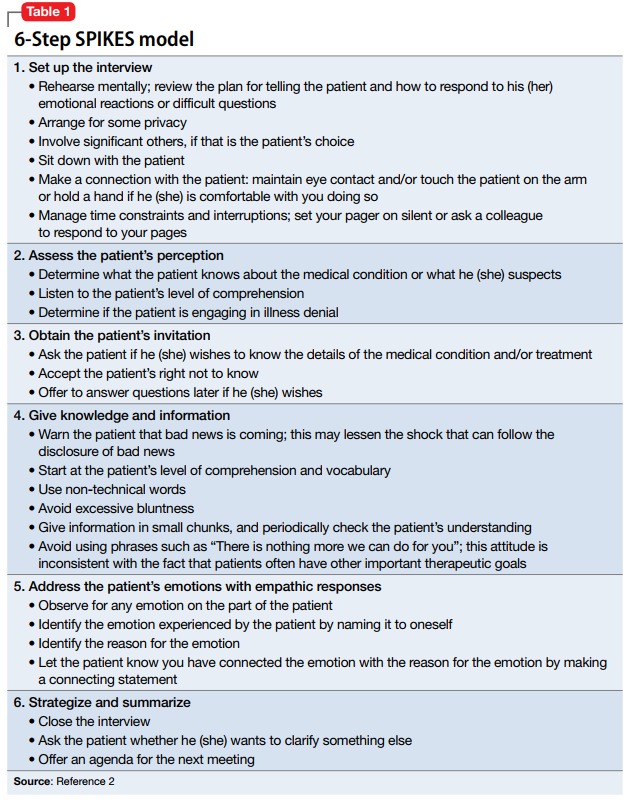
A clinician’s attitude and communication skills play a crucial role in how well patients and family members cope when they receive bad news. When delivering bad news:
- Choose a setting with adequate privacy, use simple language that distills medical facts into appreciable pieces of information, and give the recipients ample space and time to process the implications. Doing so will foster better understanding and facilitate their acceptance of the bad news.
- Although physicians can rarely appreciate the patient’s feelings at a personal level, make every effort to validate their thoughts and offer emotional support. In such situations, it is often appropriate to move closer to the recipient and make brief physical gestures, such as laying a hand on the shoulder, which might comfort them.
- In the aftermath of such encounters, it is important to remain active in the patient’s emotional journey and available for further clarification, which can mitigate uncertainties and facilitate the difficult process of coming to terms with new realities.4,5
1. Munjal S, Pahlajani S, Baxi A, et al. Delayed diagnosis of glioblastoma multiforme presenting with atypical psychiatric symptoms. Prim Care Companion CNS Disord. 2016;18(6). doi: 10.4088/PCC.16l01972.
2. Baile WF, Buckman R, Lenzi R, et al. SPIKES-a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311.
3. Kaye P. Breaking bad news: a 10 step approach. Northampton, MA: EPL Publications; 1995.
4. Chaturvedi SK, Chandra PS. Breaking bad news-issues important for psychiatrists. Asian J Psychiatr. 2010;3(2):87-89.
5. VandeKieft GK. Breaking bad news. Am Fam Physician. 2001;64(12):1975-1978.
As psychiatrists, we do not often encounter situations in which we need to inform patients and their families that they have a life-threatening diagnosis. Nonetheless, on the rare occasions when we work with such patients, new psychiatrists may find their clinical skills challenged. Breaking bad news remains an aspect of clinical training that is often overlooked by medical schools.
Here I present a case that illustrates the challenges residents and medical students face when they need to deliver bad news and review the current literature on how to present patients with this type of information.
Case
Bizarre behavior, difficult diagnosis
Mr. C, age 59, with a 1-year history of major depressive disorder, was brought to the emergency department by his wife for worsening depression and disorganized behavior over the course of 3 weeks. Mr. C had obsessive thoughts about arranging things in symmetrical patterns, difficulty sleeping, loss of appetite, and anhedonia. His wife reported that his bizarre, disorganized behavior further intensified in the previous week; he was urinating on the rug, rubbing his genitals against the bathroom counter, staring into space without moving for prolonged periods of time, and arranging his food in symmetrical patterns. Mr. C has no reported substance use or suicidal or homicidal ideation.
Strategies for delivering bad news
Initially, I struggled when I realized I would have to deliver the news of this potentially life-threatening diagnosis to the patient and his wife because I had not received any training on how to do so. However, I took time to look into the literature and used the skills that we as psychiatrists have, including empathy, listening, and validation. My experience with Mr. C and his family made me realize that delivering bad news with empathy and being involved in the struggle that follows can make a significant difference to their suffering.
There are various models and techniques for breaking bad news to patients. Two of the most commonly used models in the oncology setting are the SPIKES (Set up, Perception, Interview, Knowledge, Emotions, Strategize and Summarize) model (Table 12) and Kaye’s model (Table 23).
A clinician’s attitude and communication skills play a crucial role in how well patients and family members cope when they receive bad news. When delivering bad news:
- Choose a setting with adequate privacy, use simple language that distills medical facts into appreciable pieces of information, and give the recipients ample space and time to process the implications. Doing so will foster better understanding and facilitate their acceptance of the bad news.
- Although physicians can rarely appreciate the patient’s feelings at a personal level, make every effort to validate their thoughts and offer emotional support. In such situations, it is often appropriate to move closer to the recipient and make brief physical gestures, such as laying a hand on the shoulder, which might comfort them.
- In the aftermath of such encounters, it is important to remain active in the patient’s emotional journey and available for further clarification, which can mitigate uncertainties and facilitate the difficult process of coming to terms with new realities.4,5
As psychiatrists, we do not often encounter situations in which we need to inform patients and their families that they have a life-threatening diagnosis. Nonetheless, on the rare occasions when we work with such patients, new psychiatrists may find their clinical skills challenged. Breaking bad news remains an aspect of clinical training that is often overlooked by medical schools.
Here I present a case that illustrates the challenges residents and medical students face when they need to deliver bad news and review the current literature on how to present patients with this type of information.
Case
Bizarre behavior, difficult diagnosis
Mr. C, age 59, with a 1-year history of major depressive disorder, was brought to the emergency department by his wife for worsening depression and disorganized behavior over the course of 3 weeks. Mr. C had obsessive thoughts about arranging things in symmetrical patterns, difficulty sleeping, loss of appetite, and anhedonia. His wife reported that his bizarre, disorganized behavior further intensified in the previous week; he was urinating on the rug, rubbing his genitals against the bathroom counter, staring into space without moving for prolonged periods of time, and arranging his food in symmetrical patterns. Mr. C has no reported substance use or suicidal or homicidal ideation.
Strategies for delivering bad news
Initially, I struggled when I realized I would have to deliver the news of this potentially life-threatening diagnosis to the patient and his wife because I had not received any training on how to do so. However, I took time to look into the literature and used the skills that we as psychiatrists have, including empathy, listening, and validation. My experience with Mr. C and his family made me realize that delivering bad news with empathy and being involved in the struggle that follows can make a significant difference to their suffering.
There are various models and techniques for breaking bad news to patients. Two of the most commonly used models in the oncology setting are the SPIKES (Set up, Perception, Interview, Knowledge, Emotions, Strategize and Summarize) model (Table 12) and Kaye’s model (Table 23).
A clinician’s attitude and communication skills play a crucial role in how well patients and family members cope when they receive bad news. When delivering bad news:
- Choose a setting with adequate privacy, use simple language that distills medical facts into appreciable pieces of information, and give the recipients ample space and time to process the implications. Doing so will foster better understanding and facilitate their acceptance of the bad news.
- Although physicians can rarely appreciate the patient’s feelings at a personal level, make every effort to validate their thoughts and offer emotional support. In such situations, it is often appropriate to move closer to the recipient and make brief physical gestures, such as laying a hand on the shoulder, which might comfort them.
- In the aftermath of such encounters, it is important to remain active in the patient’s emotional journey and available for further clarification, which can mitigate uncertainties and facilitate the difficult process of coming to terms with new realities.4,5
1. Munjal S, Pahlajani S, Baxi A, et al. Delayed diagnosis of glioblastoma multiforme presenting with atypical psychiatric symptoms. Prim Care Companion CNS Disord. 2016;18(6). doi: 10.4088/PCC.16l01972.
2. Baile WF, Buckman R, Lenzi R, et al. SPIKES-a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311.
3. Kaye P. Breaking bad news: a 10 step approach. Northampton, MA: EPL Publications; 1995.
4. Chaturvedi SK, Chandra PS. Breaking bad news-issues important for psychiatrists. Asian J Psychiatr. 2010;3(2):87-89.
5. VandeKieft GK. Breaking bad news. Am Fam Physician. 2001;64(12):1975-1978.
1. Munjal S, Pahlajani S, Baxi A, et al. Delayed diagnosis of glioblastoma multiforme presenting with atypical psychiatric symptoms. Prim Care Companion CNS Disord. 2016;18(6). doi: 10.4088/PCC.16l01972.
2. Baile WF, Buckman R, Lenzi R, et al. SPIKES-a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311.
3. Kaye P. Breaking bad news: a 10 step approach. Northampton, MA: EPL Publications; 1995.
4. Chaturvedi SK, Chandra PS. Breaking bad news-issues important for psychiatrists. Asian J Psychiatr. 2010;3(2):87-89.
5. VandeKieft GK. Breaking bad news. Am Fam Physician. 2001;64(12):1975-1978.

Big changes coming for thyroid cancer staging
BOSTON – When the American Joint Committee on Cancer’s Eighth Edition Cancer Staging Manual becomes effective for U.S. practice on Jan. 1, 2018, substantially more patients with thyroid cancer will meet the definition for stage I disease, but their survival prognosis will remain as good as it was for the smaller slice of patients defined with stage I thyroid cancer by the seventh edition, Bryan R. Haugen, MD, predicted during a talk at the World Congress on Thyroid Cancer.
Under current stage definitions in the seventh edition, roughly 60% of thyroid cancer patients have stage I disease, but this will kick up to about 80% under the eighth edition, said Dr. Haugen, professor of medicine and head of the division of endocrinology, metabolism, and diabetes at the University of Colorado in Aurora. Despite this influx of more patients, “survival rates in stage I patients haven’t changed,” with a disease-specific survival (DSS) of 98%-100% for stage I patients in the eighth edition compared with 97%-100% in the seventh edition, he noted.
Dr. Haugen credited this apparent paradox to the revised staging system’s superior discrimination among various grades of disease progression. “The eighth edition better separates patients based on their projected survival.” As more patients fit stage I classification with its highest level of projected survival, fewer patients will classify with more advanced disease and its worse projected survival.
For example, in the seventh edition patients with stage IV disease had a projected DSS rate of 50%-75%; in the eighth edition that rate is now less than 50%. The projected DSS rate for patients with stage II disease has down shifted from 97%-100% in the seventh edition to 85%-95% in the eighth. For patients with stage III thyroid cancer the DSS rate of 88%-95% in the seventh edition became 60%-70% in the eighth edition.
‘The new system will take some getting used to,” Dr. Haugen admitted, and it involves even more “big” changes, he warned. These include:
• Changing the cutpoint separating younger from older patients to 55 years of age in the eighth edition, a rise from the 45-year-old cutpoint in the seventh edition.
• Allowing tumors classified as stage I to be as large as 4 cm, up from the 2 cm or less defining stage I in the seventh edition.
• Reserving stage II designation for patients with tumors larger than 4 cm. In the seventh edition tumors had to be 2-4 cm in size.
• Expanding stage II disease to include not only patients with disease confined to their thyroid, but also patients with N1 lymph node spread or gross extrathyroidal extension. In the seventh edition tumor spread like this put patients into stage III.
• Specifying in the eighth edition that stage III disease must feature gross extrathyroidal extension into the larynx, trachea, esophagus, or recurrent laryngial nerve. To qualify for stage IV in the eighth edition, spread must extend into prevertebral fascia or encase major vessels, for stage IVA, or involve distant metastases for stage IVB.
• Paring down three stage IV subgroups, A, B, and C, in the seventh edition to just an A or B subgroup in the eighth edition.
Dr. Haugen coauthored a recent editorial that laid out an assessment of the eighth edition in greater detail (Thyroid. 2017 Jun;27[6]:751-6).
[email protected]
On Twitter @mitchelzoler
BOSTON – When the American Joint Committee on Cancer’s Eighth Edition Cancer Staging Manual becomes effective for U.S. practice on Jan. 1, 2018, substantially more patients with thyroid cancer will meet the definition for stage I disease, but their survival prognosis will remain as good as it was for the smaller slice of patients defined with stage I thyroid cancer by the seventh edition, Bryan R. Haugen, MD, predicted during a talk at the World Congress on Thyroid Cancer.
Under current stage definitions in the seventh edition, roughly 60% of thyroid cancer patients have stage I disease, but this will kick up to about 80% under the eighth edition, said Dr. Haugen, professor of medicine and head of the division of endocrinology, metabolism, and diabetes at the University of Colorado in Aurora. Despite this influx of more patients, “survival rates in stage I patients haven’t changed,” with a disease-specific survival (DSS) of 98%-100% for stage I patients in the eighth edition compared with 97%-100% in the seventh edition, he noted.
Dr. Haugen credited this apparent paradox to the revised staging system’s superior discrimination among various grades of disease progression. “The eighth edition better separates patients based on their projected survival.” As more patients fit stage I classification with its highest level of projected survival, fewer patients will classify with more advanced disease and its worse projected survival.
For example, in the seventh edition patients with stage IV disease had a projected DSS rate of 50%-75%; in the eighth edition that rate is now less than 50%. The projected DSS rate for patients with stage II disease has down shifted from 97%-100% in the seventh edition to 85%-95% in the eighth. For patients with stage III thyroid cancer the DSS rate of 88%-95% in the seventh edition became 60%-70% in the eighth edition.
‘The new system will take some getting used to,” Dr. Haugen admitted, and it involves even more “big” changes, he warned. These include:
• Changing the cutpoint separating younger from older patients to 55 years of age in the eighth edition, a rise from the 45-year-old cutpoint in the seventh edition.
• Allowing tumors classified as stage I to be as large as 4 cm, up from the 2 cm or less defining stage I in the seventh edition.
• Reserving stage II designation for patients with tumors larger than 4 cm. In the seventh edition tumors had to be 2-4 cm in size.
• Expanding stage II disease to include not only patients with disease confined to their thyroid, but also patients with N1 lymph node spread or gross extrathyroidal extension. In the seventh edition tumor spread like this put patients into stage III.
• Specifying in the eighth edition that stage III disease must feature gross extrathyroidal extension into the larynx, trachea, esophagus, or recurrent laryngial nerve. To qualify for stage IV in the eighth edition, spread must extend into prevertebral fascia or encase major vessels, for stage IVA, or involve distant metastases for stage IVB.
• Paring down three stage IV subgroups, A, B, and C, in the seventh edition to just an A or B subgroup in the eighth edition.
Dr. Haugen coauthored a recent editorial that laid out an assessment of the eighth edition in greater detail (Thyroid. 2017 Jun;27[6]:751-6).
[email protected]
On Twitter @mitchelzoler
BOSTON – When the American Joint Committee on Cancer’s Eighth Edition Cancer Staging Manual becomes effective for U.S. practice on Jan. 1, 2018, substantially more patients with thyroid cancer will meet the definition for stage I disease, but their survival prognosis will remain as good as it was for the smaller slice of patients defined with stage I thyroid cancer by the seventh edition, Bryan R. Haugen, MD, predicted during a talk at the World Congress on Thyroid Cancer.
Under current stage definitions in the seventh edition, roughly 60% of thyroid cancer patients have stage I disease, but this will kick up to about 80% under the eighth edition, said Dr. Haugen, professor of medicine and head of the division of endocrinology, metabolism, and diabetes at the University of Colorado in Aurora. Despite this influx of more patients, “survival rates in stage I patients haven’t changed,” with a disease-specific survival (DSS) of 98%-100% for stage I patients in the eighth edition compared with 97%-100% in the seventh edition, he noted.
Dr. Haugen credited this apparent paradox to the revised staging system’s superior discrimination among various grades of disease progression. “The eighth edition better separates patients based on their projected survival.” As more patients fit stage I classification with its highest level of projected survival, fewer patients will classify with more advanced disease and its worse projected survival.
For example, in the seventh edition patients with stage IV disease had a projected DSS rate of 50%-75%; in the eighth edition that rate is now less than 50%. The projected DSS rate for patients with stage II disease has down shifted from 97%-100% in the seventh edition to 85%-95% in the eighth. For patients with stage III thyroid cancer the DSS rate of 88%-95% in the seventh edition became 60%-70% in the eighth edition.
‘The new system will take some getting used to,” Dr. Haugen admitted, and it involves even more “big” changes, he warned. These include:
• Changing the cutpoint separating younger from older patients to 55 years of age in the eighth edition, a rise from the 45-year-old cutpoint in the seventh edition.
• Allowing tumors classified as stage I to be as large as 4 cm, up from the 2 cm or less defining stage I in the seventh edition.
• Reserving stage II designation for patients with tumors larger than 4 cm. In the seventh edition tumors had to be 2-4 cm in size.
• Expanding stage II disease to include not only patients with disease confined to their thyroid, but also patients with N1 lymph node spread or gross extrathyroidal extension. In the seventh edition tumor spread like this put patients into stage III.
• Specifying in the eighth edition that stage III disease must feature gross extrathyroidal extension into the larynx, trachea, esophagus, or recurrent laryngial nerve. To qualify for stage IV in the eighth edition, spread must extend into prevertebral fascia or encase major vessels, for stage IVA, or involve distant metastases for stage IVB.
• Paring down three stage IV subgroups, A, B, and C, in the seventh edition to just an A or B subgroup in the eighth edition.
Dr. Haugen coauthored a recent editorial that laid out an assessment of the eighth edition in greater detail (Thyroid. 2017 Jun;27[6]:751-6).
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM WCTC 2017
Cancer screening in elderly: When to just say no
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – A simple walking speed measurement over a 20-foot distance is an invaluable guide to physiologic age as part of individualized decision making about when to stop cancer screening in elderly patients, according to Jeff Wallace, MD, professor of geriatric medicine at the University of Colorado at Denver.
“If you have one measurement to assess ‘am I aging well?’ it’s your gait speed. A lot of us in geriatrics are advocating evaluation of gait speed in all patients as a fifth vital sign. It’s probably more useful than blood pressure in some of the older adults coming into our clinics,” he said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wallace also gave a shout-out to the ePrognosis cancer-screening decision tool, available free at www.eprognosis.org, as an aid in shared decision-making conversations regarding when to stop cancer screening. This tool, developed by researchers at the University of California, San Francisco, allows physicians to plug key individual patient characteristics into its model, including comorbid conditions, functional status, and body mass index, and then spits out data-driven estimated benefits and harms a patient can expect from advanced-age screening for colon or breast cancer.
Of course, guidelines as to when to stop screening for various cancers are available from the U.S. Preventive Services Task Force, the American Cancer Society, and specialty societies. However, it’s important that nongeriatricians understand the serious limitations of those guidelines.
“We’re not guidelines followers in the geriatrics world because the guidelines don’t apply to most of our patients,” he explained. “We hate guidelines in geriatrics because few studies – and no lung cancer or breast cancer trials – enroll patients over age 75 with comorbid conditions. Also, most of these guidelines do not incorporate patient preferences, which probably should be a primary goal. So we’re left extrapolating.“
Regrettably, though, “it turns out most Americans are drinking the Kool-Aid when it comes to patient preferences. It’s amazing how much cancer screening is going on in this country. We’re doing a lot more than we should,” said Dr. Wallace.
All of that is clearly overscreening. Experts unanimously agree that if someone is not going to live for 10 years, that person is not likely to benefit from cancer screening. The one exception is lung cancer screening of high-risk patients, where there are data to show that annual low-dose CT screening is beneficial in those with even a 5-year life expectancy.
As part of the Choosing Wisely program, the American Geriatric Society has advocated that physicians “don’t recommend screening for breast, colorectal, prostate, or lung cancer without considering life expectancy and the risks of testing, overdiagnosis, and overtreatment.”
That’s where gait speed and ePrognosis come in handy in discussions with patients regarding what they can realistically expect from cancer screening at an advanced age.
The importance of gait speed was highlighted in a pooled analysis of nine cohort studies totaling more than 34,000 community-dwelling adults aged 65 years and older with 6-21 years of follow-up. Investigators at the University of Pittsburgh identified a strong relationship between gait speed and survival. Every 0.1-m/sec made a significant difference (JAMA. 2011 Jan 5;305[1]:50-8).
A gait speed evaluation is simple: The patient is asked to walk 20 feet at a normal speed, not racing. For men age 75, the Pittsburgh investigators found, gait speed predicted 10-year survival across a range of 19%-87%. The median speed was 0.8 m/sec, or about 1.8 mph, so a middle-of-the-pack walker ought to stop all cancer screening by age 75. A fast-walking older man won’t reach a 10-year remaining life expectancy until he’s in his early to mid-80s; a slow walker reaches that life expectancy as early as his late 60s, depending upon just how slow he walks. A woman at age 80 with an average gait speed has roughly 10 years of remaining life, factoring in plus or minus 5 years from that landmark depending upon whether she is a faster- or slower-than-average walker, Dr. Wallace explained.
The U.S. Preventive Services Task Force currently recommends colon cancer screening routinely for 50- to 75-year-olds, declaring in accord with other groups that this strategy has a high certainty of substantial net benefit. But the USPSTF also recommends selective screening for those aged 76-85, with a weaker C recommendation (JAMA. 2016 Jun 21;315[23]:2564-75).
What are the practical implications of that recommendation for selective screening after age 75?
Investigators at Harvard Medical School and the University of Oslo recently took a closer look. Their population-based, prospective, observational study included 1,355,692 Medicare beneficiaries aged 70-79 years at average risk for colorectal cancer who had not had a colonoscopy within the previous 5 years.
The investigators demonstrated that the benefit of screening colonoscopy decreased with age. For patients aged 70-74, the 8-year risk of colorectal cancer was 2.19% in those who were screened, compared with 2.62% in those who weren’t, for an absolute 0.43% difference. The number needed to be screened to detect one additional case of colorectal cancer was 283. Among those aged 75-79, the number needed to be screened climbed to 714 (Ann Intern Med. 2017 Jan 3;166[1]18-26).
Moreover, the risk of colonoscopy-related adverse events also climbed with age. These included perforations, falls while racing to the bathroom during the preprocedural bowel prep, and the humiliation of fecal incontinence. The excess 30-day risk for any adverse event in the colonoscopy group was 5.6 events per 1,000 patients aged 70-74 and 10.3 per 1,000 in 75- to 79-year-olds.
In a similar vein, Mara A. Schonberg, MD, of Harvard Medical School, Boston, has shed light on the risks and benefits of biannual mammographic screening for breast cancer in 70- to 79-year-olds, a practice recommended in American Cancer Society guidelines for women who are in overall good health and have at least a 10-year life expectancy.
She estimated that 2 women per 1,000 screened would avoid death due to breast cancer, for a number needed to screen of 500. But roughly 200 of those 1,000 women would experience a false-positive mammogram, and 20-40 of those false-positive imaging studies would result in a breast biopsy. Also, roughly 30% of the screen-detected cancers would not otherwise become apparent in an older woman’s lifetime, yet nearly all of the malignancies would undergo breast cancer therapy (J Am Geriatr Soc. 2016 Dec;64[12]:2413-8).
Dr. Schonberg’s research speaks to Dr. Wallace.
“It’s breast cancer therapy: It’s procedures; it’s medicalizing the patient’s whole life and creating a high degree of angst when she’s 75 or 80,” he said.
As to when to ‘just say no’ to cancer screening, Dr. Wallace said his answer is after age 65 for cervical cancer screening in women with at least two normal screens in the past 10 years or a prior total hysterectomy for a benign indication. All of the guidelines agree on that, although the American Congress of Obstetricians and Gynecologists recommends in addition that women with cervical intraepithelial neoplasia 2 be screened for the next 20 years.
For prostate cancer, Dr. Wallace recommends his colleagues just say no to screening at age 70 and above because harm is more likely than benefit to ensue.
“I don’t know about you, but I have a ton of patients over age 70 asking me for PSAs. That’s one place I won’t do any screening. I tell them I know you’re in great shape for 76 and you think it’s a good idea, but I think it’s bad medicine and I won’t do it. Even the American Urological Association says don’t do it after age 70,” he said.
For prostate cancer screening at age 55-69, however, patient preference rules the day, he added.
He draws the line at any cancer screening in patients aged 90 or over. Mean survival at age 90 is another 4-5 years. Only 11% of 90-year-old women will reach 100.
“Everybody has to die eventually,” he mused.
Dr. Wallace reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
New acellular pertussis vaccine may solve waning immunogenicity problem
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.

Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.
Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.
Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
AT ESPID 2017
Key clinical point:
Major finding: One year after teens received a single dose of a novel acellular pertussis vaccine, they had a geometric mean titer of PT neutralizing antibody of 77 IU/mL, compared with just 12 IU/mL in adolescents who received a conventional Tdap vaccine.
Data source: This randomized, triple-arm, pivotal phase 3 clinical trial included 450 Thai 12- to 17-year-olds followed for 1 year after receiving a single dose of a novel monovalent pertussis vaccine or a novel Tdap vaccine, both of which contain genetically inactivated pertussis toxin, or, instead of those, a widely utilized conventional Tdap vaccine.
Disclosures: The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
Cerebral NIRS may be flawed for assessing infant brains after stage 1 palliation of HLHS
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).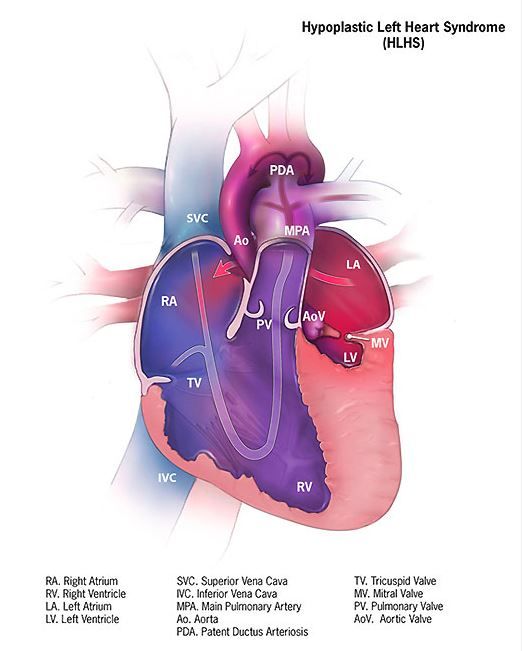
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The use of postoperative cerebral venous oxygen saturation monitoring (ScvO2) through an internal jugular vein catheter allows better monitoring of circulation, which may lead to better outcomes, but it is invasive and challenging. NIRS, being noninvasive, has proved attractive, but clinical interpretation in terms of both absolute values and trends is difficult, Edward Buratto, MBBS, and his colleagues noted in their invited commentary (doi: 10.1016/j.jtcvs.2017.04.061).
Dr. Rescoe and her colleagues have analyzed the correlation of NIRS-derived data with ScvO2 measured by co-oximetry from the internal jugular vein in 73 neonates after stage 1 palliation for hypoplastic left heart syndrome. They demonstrated that cerebral rSO2 correlated poorly with low ScvO2, and they suggest that cerebral rSO2 not be used in isolation. This problem was somewhat ameliorated by correction of the signal for arterial contamination. NIRS appears to be too valuable a tool to be simply discarded, they said, suggesting that a perioperative risk assessment that would include multisite NIRS and hemodynamic monitoring might still allow early determination of low-cardiac output.
“Two numbers are better than one,” wrote Dr. Buratto and his colleagues. “Whether the NIRS technology will add any useful information to a simple bedside assessment by an astute clinician is yet to be seen.”
Edward Buratto, MBBS, Steve Horton, PhD, and Igor E. Konstantinov, MD, are from the Department of Cardiothoracic Surgery, The Royal Children’s Hospital; the Department of Pediatrics, University of Melbourne; and Murdoch Children’s Research Institute, Melbourne. They reported having no financial conflicts of interest.
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
The regional oxygenation index (rSO2) based on near infrared spectroscopy (NIRS) measurement is frequently used to assess the adequacy of oxygen delivery after stage 1 palliation of hypoplastic left heart syndrome (HLHS). However, a recent study showed that cerebral rSO2 has low sensitivity and should not be considered reassuring even at rSO2 of 50 or greater. In addition, values below 30 were not found to be sensitive for detecting compromised oxygen delivery, according to a report published online in the Journal of Thoracic and Cardiovascular Surgery.
Erin Rescoe, MD, of Boston Children’s Hospital, and her colleagues at Harvard Medical School, Boston, performed a retrospective study of 73 neonates assessed with cerebral venous oxyhemoglobin saturation (ScvO2) measured by co-oximetry from the internal jugular vein, which is considered the preferred method for assessing the adequacy of tissue oxygen delivery, compared with cerebral rSO2 after stage 1 palliation of HLHS (doi: 10.1016/j.jtcvs.2017.03.154).
To determine the suggested benefit of NIRS as an effective trend monitor, the researchers used their interpolated data to examine changes in rSO2 and changes in ScvO2 at hourly intervals and compared these values.Of particular concern is the result showing that, in all instances where ScvO2 was less than 30%, rSO2 was greater than 30%. In terms of the sensitivity (the true positive rate) and specificity (the true negative rate) of using NIRS, time-matched pairs of rSO2 and ScvO2 showed that the receiver operating characteristic curves for rSO2 as a diagnostic test to detect ScvO2 less than 30%, less than 40%, and less than 50% were 0.82, 0.84, and 0.87, respectively, showing good specificity, with a value of rSO2 less than 30% indicating that ScvO2 will be less than 30% 99% of the time.
“However, the sensitivity of rSO2 in the range of clinical interest in detecting ScvO2 less than 30% is extremely low,” according to the researchers. Thus, NIRS is likely to produce false negatives, missing patients with clinically low postoperative oxygen saturation.
In fact, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%. Similar results were seen in comparing values at the less than 40% mark (equivalent less than 1% of the time). Better results showed at the less than 50% mark, with equivalence seen 46% of the time.
NIRS measures a composite of arterial and venous blood, according to Dr. Rescoe and her colleagues. Therefore, to do a more direct comparison, they adjusted their NIRS results by calculating an rSO2-based ScvO2 designed to remove arterial contamination from the rSO2 signal: rSO2-based ScvO2 = (rSO2 arterial oxygen saturation x 0.3)/0.7.
This significantly improved the sensitivity of rSO2 to detect ScvO2 at less than 30% to 6.5%, to 29% for rSO2 at less than 40%, and 77.4% for rSO2 less than 50%.
The researchers “were surprised by the extremely low sensitivity of cerebral NIRS to detect even the most severe aberrations in DO2” (i.e., ScvO2 less than 30%, which has been found to be associated with poor outcomes).
“Cerebral rSO2 in isolation should not be used to detect low ScvO2, because its sensitivity is low, although correction of rSO2 for arterial contamination significantly improves sensitivity. Cerebral rSO2 of 50 or greater should not be considered reassuring with regard to ScvO2, although values less than 30 are specific for low ScvO2,” the researchers concluded.
The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:
Major finding: In terms of sensitivity, rSO2 was less than 30% less than 1% of the time that ScvO2 was less than 30%.
Data source: A retrospective single institution study of 73 neonates assessed after stage 1 palliation
Disclosures: The study was sponsored by the Gerber Foundation, the Hess Family Philanthropic Fund, and Boston Children’s Hospital Heart Center Strategic Investment Fund. The authors disclosed that they had no financial conflicts.