User login
Sinus of Valsalva preserved in aortic valve replacement
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
With regard to the question, ‘‘Is it necessary to replace the sinuses of Valsalva in the setting of bicuspid aortic valve aortopathy?’’, the researchers “leverage their enormous institutional experience to find an answer. The results suggest that this answer is ‘no.’ At least not in all cases,” Thoralf M. Sundt, MD, wrote in his invited commentary on the paper (J Thorac Cardiovasc Surg. 2017;154:419-20).
“The findings of this study argue for us to take a step back and ask how much really needs be done,” he added. And although “it is hard to ask a surgeon to do less rather than more; however, the balance of judgment has to be between the operative risk of the more aggressive approach and the natural history of the disease. In other words, what does it ‘cost’ to be aggressive, and what do we gain?” he asked.
Bicuspid aortic valve aortopathy, it would appear, is not cancer after all. Regardless of theoretic arguments that are based on embryology and the migration of neural crest cells, it does not appear to require resection to ‘clean margins,’ even if we believe that the operative risk ‘in our hands’ is low,” concluded Dr. Sundt.
Thoralf M. Sundt, MD, is at Harvard Medical School, Boston. He reported having no disclosures.
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
The sinus of Valsalva segment can be preserved during aortic valve replacement irrespective of the type of valve pathology, according to a recent study by Rita Karianna Milewski, MD, and her colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Severe aortic root dilation coupled to aortic valve disease requires root replacement in patients with a tricuspid or bicuspid aortic valve. Commonly, an aortic valve replacement and supracoronary ascending aorta replacement (AVRSCAAR) procedure has been used for patients who have a mild to moderately dilated sinus segment. One advantage of the procedure is that it retains the sinus of Valsalva (SOV) and preserves the intact coronary ostia.
However, the long-term behavior and risk of aortic events for the retained SOV in both BAV and TAV patients remains unclear, according to Dr. Milewski and her colleagues.
Previous researchers have suggested that patients with BAV and TAV have different rates of complications of the remaining aorta and dilation of the proximal aorta and retained sinus segment. In addition, it has been suggested that the cause of aortic dilation is different in patients with aortic stenosis (AS) and aortic insufficiency (AI) and is based on TAV and BAV morphology, histology, and hemodynamic flow patterns.
However, in the August issue of the Journal of Thoracic and Cardiovascular Surgery, Dr. Milewski and her colleagues reported on their study showing that, in patients with nonaneurysmal SOV undergoing AVRSCAAR, the sinus of Valsalva segment can be preserved regardless of the type of valvular pathology (aortic stenosis vs. aortic insufficiency) or valvular morphology (BAV vs. TAV).
The researchers retrospectively reviewed a prospectively maintained institutional database to stratify all patients by BAV or TAV valvular pathology with concomitant ascending aortic aneurysm who underwent an elective AVRSCAAR from 2002 to 2015 (J Thorac Cardiovasc Surg. 2017;154:421-32).
The distribution of the 428 patients meeting inclusion criteria by subgroups was: BAV group (254 patients: BAV-AS = 178; BAV-AI = 76); TAV group (174 patients: TAV-AS = 61; TAV-AI =113). Preoperative sinus of Valsalva dimensions were divided into 3 subgroups (less than 40 mm, 40-45 mm, and greater than 45 mm).
The mean patient age for patients with BAV and TAV was 59 years and 72 years (P less than .001), respectively (with 78% with BAV being men and 57% with TAV being men). There was a significantly higher subpopulation of AS in the BAV cohort vs. TAV-AS (70% vs. 35%; P less than .001).
With regard to SOV sizing, there was no significant difference in mean preoperative aortic root diameters between BAV and TAV cohorts for the AS or AI subpopulations.
In-hospital/30-day mortality was significantly higher in patients with TAV (5.2%) than in patients with BAV (1.6%, P = .033). In addition, the incidence of transient ischemic attack/stroke was significantly higher in the TAV group (3.4%) vs. the BAV group (0.8%, P = .04).
Valvular morphology and pathology at baseline, preoperative SOV diameter, postoperative time course, and interaction effect of preoperative SOV diameters and postoperative time course were used as covariates to assess outcomes. Within-subject and within–stratified subgroup comparison failed to show main effects across the follow-up times on postoperative SOV size patterns (P = .935), implying that the SOV trends were stable and sustained (discharge to greater than or equal to 10 years) irrespective of valvular morphology and pathology (BAV-AI, BAV-AS, TAV-AI, and TAV-AS).
Preoperative SOV dimensions significantly affected the retained postoperative sinus dimensions (P less than .001), according to Dr. Milewski and her colleagues.
The data indicated that an initial and pronounced postoperative decrease in SOV dimensions occurs with AVRSCAAR independently of aortic valve morphology, aortic valve pathology, and age, they added.
The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively. The BAV group had significantly improved reoperation-free survival, compared with the TAV group (P less than .001), while the type of valvular pathology within each group did not show a significant survival difference.
“Irrespective of the aortic valve morphology or valve pathology, in patients with mild to moderate aortic root dilatation (less than 45 mm), preservation of the SOV segment in the context of an AVRSCAAR procedure is justified. Continued further follow-up will be important to understand the long-term outcomes of sinus preservation, especially in the younger population with BAVs,” the researchers concluded.
The authors reported having no financial conflicts to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point:
Major finding: The 10-year freedom from aortic reoperation rates were 97% and 95% in the BAV and TAV subgroups, respectively.
Data source: A retrospective review of 428 patients in a prospectively maintained database who met study inclusion criteria and were operated on between 2002 and 2015.
Disclosures: The authors reported having no financial conflicts to disclose.

Obinutuzumab-CHOP not superior to rituximab-CHOP in new DLBCL
Obinutuzumab with CHOP therapy did not improve progression-free survival, compared with rituximab plus CHOP, in patients with previously untreated diffuse large B-cell lymphoma (DLBCL), according to results from a phase 3 trial published in the Journal of Clinical Oncology. (2017 Aug 10. doi: 10.1200/JCO.2017.73.3402)
The findings suggest that obinutuzumab, a glycoengineered, type II, anti-CD20 monoclonal antibody, might not offer a benefit over standard treatment with rituximab, an anti-CD20 monoclonal antibody, when used with CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone).
A total of 1,418 patients were enrolled at 207 centers in 29 countries in the GOYA trial and were randomly assigned to one regimen or the other. The mean duration of exposure to the drugs was 25 weeks for both. The progression-free survival was 69.6% for obinutuzumab-CHOP – also known as G-CHOP – and 66.9% for rituximab-CHOP, not a statistically significant difference, wrote Umberto Vitolo, MD, of University-Hospital Città della Salute e della Scienza, Torino, Italy, and his fellow investigators.
The rate of adverse events was similar between the two groups. The lack of superiority of obinutuzumab comes after findings of its superiority in untreated follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL). The investigators suggested that this may be a sign that obinutuzumab’s efficacy is best seen in less aggressive disease types.
“Given the advantages of G-based therapy in patients with FL and CLL, the lack of benefit of G-CHOP in patients with DLBCL in the GOYA study was unexpected, and the reasons for it are unclear,” they wrote. “This lack of benefit might simply have resulted from the differences in biologic and clinical profiles between indolent lymphoproliferative diseases, such as FL and CLL, and aggressive ones, such as DLBCL.”
The study was sponsored by F. Hoffman-La Roche, the manufacturer of the two drugs, and had support from Fondazione Italiana Linfomi.
Obinutuzumab with CHOP therapy did not improve progression-free survival, compared with rituximab plus CHOP, in patients with previously untreated diffuse large B-cell lymphoma (DLBCL), according to results from a phase 3 trial published in the Journal of Clinical Oncology. (2017 Aug 10. doi: 10.1200/JCO.2017.73.3402)
The findings suggest that obinutuzumab, a glycoengineered, type II, anti-CD20 monoclonal antibody, might not offer a benefit over standard treatment with rituximab, an anti-CD20 monoclonal antibody, when used with CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone).
A total of 1,418 patients were enrolled at 207 centers in 29 countries in the GOYA trial and were randomly assigned to one regimen or the other. The mean duration of exposure to the drugs was 25 weeks for both. The progression-free survival was 69.6% for obinutuzumab-CHOP – also known as G-CHOP – and 66.9% for rituximab-CHOP, not a statistically significant difference, wrote Umberto Vitolo, MD, of University-Hospital Città della Salute e della Scienza, Torino, Italy, and his fellow investigators.
The rate of adverse events was similar between the two groups. The lack of superiority of obinutuzumab comes after findings of its superiority in untreated follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL). The investigators suggested that this may be a sign that obinutuzumab’s efficacy is best seen in less aggressive disease types.
“Given the advantages of G-based therapy in patients with FL and CLL, the lack of benefit of G-CHOP in patients with DLBCL in the GOYA study was unexpected, and the reasons for it are unclear,” they wrote. “This lack of benefit might simply have resulted from the differences in biologic and clinical profiles between indolent lymphoproliferative diseases, such as FL and CLL, and aggressive ones, such as DLBCL.”
The study was sponsored by F. Hoffman-La Roche, the manufacturer of the two drugs, and had support from Fondazione Italiana Linfomi.
Obinutuzumab with CHOP therapy did not improve progression-free survival, compared with rituximab plus CHOP, in patients with previously untreated diffuse large B-cell lymphoma (DLBCL), according to results from a phase 3 trial published in the Journal of Clinical Oncology. (2017 Aug 10. doi: 10.1200/JCO.2017.73.3402)
The findings suggest that obinutuzumab, a glycoengineered, type II, anti-CD20 monoclonal antibody, might not offer a benefit over standard treatment with rituximab, an anti-CD20 monoclonal antibody, when used with CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone).
A total of 1,418 patients were enrolled at 207 centers in 29 countries in the GOYA trial and were randomly assigned to one regimen or the other. The mean duration of exposure to the drugs was 25 weeks for both. The progression-free survival was 69.6% for obinutuzumab-CHOP – also known as G-CHOP – and 66.9% for rituximab-CHOP, not a statistically significant difference, wrote Umberto Vitolo, MD, of University-Hospital Città della Salute e della Scienza, Torino, Italy, and his fellow investigators.
The rate of adverse events was similar between the two groups. The lack of superiority of obinutuzumab comes after findings of its superiority in untreated follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL). The investigators suggested that this may be a sign that obinutuzumab’s efficacy is best seen in less aggressive disease types.
“Given the advantages of G-based therapy in patients with FL and CLL, the lack of benefit of G-CHOP in patients with DLBCL in the GOYA study was unexpected, and the reasons for it are unclear,” they wrote. “This lack of benefit might simply have resulted from the differences in biologic and clinical profiles between indolent lymphoproliferative diseases, such as FL and CLL, and aggressive ones, such as DLBCL.”
The study was sponsored by F. Hoffman-La Roche, the manufacturer of the two drugs, and had support from Fondazione Italiana Linfomi.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Obinutuzumab with CHOP therapy did not improve progression-free survival for diffuse large B-cell lymphoma, compared with standard treatment with rituximab used with CHOP.
Major finding: The estimated PFS was 69.6% for obinutuzumab-CHOP and 66.9% for rituximab-CHOP, an insignificant difference.
Data source: A randomized phase 3 trial of 1,418 patients at 207 centers in 29 countries.
Disclosures: The study was sponsored by F. Hoffman-La Roche, the manufacturer of the two drugs, and had support from Fondazione Italiana Linfomi..
Inotuzumab ozogamicin approved for relapsed/refractory ALL
The Food and Drug Administration has approved the antibody drug conjugate inotuzumab ozogamicin for the treatment of adults with relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL).
The treatment, to be marketed by Pfizer as Besponsa, won approval based on the results of the INO-VATE ALL trial, which randomized 326 patients to receive either inotuzumab ozogamicin (164 patients) or a chemotherapy regimen of the investigator’s choice (162 patients). To be considered for inclusion in the trial, patients with Philadelphia chromosome–negative or –positive relapsed or refractory B-cell precursor ALL were required to have at least 5% bone marrow blasts and have received one or two induction chemotherapy regimens.
Adverse events that occurred in more than 20% of patients included thrombocytopenia, neutropenia, anemia, leukopenia, fatigue, hemorrhage, pyrexia, nausea, headache, febrile neutropenia, abdominal pain, and hyperbilirubinemia, as well as increases in gamma-glutamyltransferase and transaminases. Adverse events that led to discontinuation of treatment were infection, thrombocytopenia, hyperbilirubinemia, hemorrhage, and increases in transaminases.
Preliminary results were published in August 2016 (N Engl J Med. 2016;375:740-53).
Inotuzumab ozogamicin was granted orphan drug and breakthrough status, as well as priority review, by the FDA in February 2017.
[email protected]
On Twitter @denisefulton
The Food and Drug Administration has approved the antibody drug conjugate inotuzumab ozogamicin for the treatment of adults with relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL).
The treatment, to be marketed by Pfizer as Besponsa, won approval based on the results of the INO-VATE ALL trial, which randomized 326 patients to receive either inotuzumab ozogamicin (164 patients) or a chemotherapy regimen of the investigator’s choice (162 patients). To be considered for inclusion in the trial, patients with Philadelphia chromosome–negative or –positive relapsed or refractory B-cell precursor ALL were required to have at least 5% bone marrow blasts and have received one or two induction chemotherapy regimens.
Adverse events that occurred in more than 20% of patients included thrombocytopenia, neutropenia, anemia, leukopenia, fatigue, hemorrhage, pyrexia, nausea, headache, febrile neutropenia, abdominal pain, and hyperbilirubinemia, as well as increases in gamma-glutamyltransferase and transaminases. Adverse events that led to discontinuation of treatment were infection, thrombocytopenia, hyperbilirubinemia, hemorrhage, and increases in transaminases.
Preliminary results were published in August 2016 (N Engl J Med. 2016;375:740-53).
Inotuzumab ozogamicin was granted orphan drug and breakthrough status, as well as priority review, by the FDA in February 2017.
[email protected]
On Twitter @denisefulton
The Food and Drug Administration has approved the antibody drug conjugate inotuzumab ozogamicin for the treatment of adults with relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL).
The treatment, to be marketed by Pfizer as Besponsa, won approval based on the results of the INO-VATE ALL trial, which randomized 326 patients to receive either inotuzumab ozogamicin (164 patients) or a chemotherapy regimen of the investigator’s choice (162 patients). To be considered for inclusion in the trial, patients with Philadelphia chromosome–negative or –positive relapsed or refractory B-cell precursor ALL were required to have at least 5% bone marrow blasts and have received one or two induction chemotherapy regimens.
Adverse events that occurred in more than 20% of patients included thrombocytopenia, neutropenia, anemia, leukopenia, fatigue, hemorrhage, pyrexia, nausea, headache, febrile neutropenia, abdominal pain, and hyperbilirubinemia, as well as increases in gamma-glutamyltransferase and transaminases. Adverse events that led to discontinuation of treatment were infection, thrombocytopenia, hyperbilirubinemia, hemorrhage, and increases in transaminases.
Preliminary results were published in August 2016 (N Engl J Med. 2016;375:740-53).
Inotuzumab ozogamicin was granted orphan drug and breakthrough status, as well as priority review, by the FDA in February 2017.
[email protected]
On Twitter @denisefulton
How to make the move away from opioids for chronic noncancer pain
Standard care of chronic noncancer pain should start moving away from chronic opioid treatment, which can put patients in greater danger of developing a substance use disorder, according to evidence presented at a meeting held by the American Pain Society and Global Academy for Medical Education.
As the effects of the U.S. opioid epidemic continue to gain public attention – recently spurring a declaration of a state of emergency –
Use of opioid therapy for pain conditions such as osteoarthritis, fibromyalgia, and migraine – once a common treatment approach – has been shown to be a dangerous breeding ground for opioid substance use disorders, and physicians would do well to re-evaluate their treatment methods, according to Edwin Salsitz, MD, assistant clinical professor at Mount Sinai Beth Israel Hospital, New York.
“Each prescriber is going to have to review this, digest it, reflect on it, and decide what they are going to do,” said Dr. Salsitz in an interview. “Base it on the Centers for Disease Control and Prevention’s guideline as a good starting point, and then individualize it for yourself and your patients.”
One of the major steps toward lowering the rate of opioid addiction through prescription is avoiding opioids as a treatment for acute pain.
“The first recommendation [of the CDC guideline] is nonpharmaceutical therapy, including physical therapy, massage therapy, acupuncture, and cognitive-behavioral therapy – and there’s a whole lot of evidence for these types of therapy,” said Dr. Salsitz. “The second option is that if you’re going to use medications, use those that aren’t opioids, like Tylenol, Motrin, and antidepressants.”
If opioids are necessary, said Dr. Salsitz, immediate-release opioids in limited prescriptions are a good way to lower the risk of addiction.
“The extended-release opioids have many more milligrams than the immediate-release opioids,” according to Dr. Salsitz. “For example, in New York state, we have a law now that says for acute pain, you cannot prescribe for more than a 7-day amount.”
That 7-day limit helps keep excess opioids out of households, he noted, making it harder for patients to share their medication with friends and family, which has proven to be the most common source for opioids during the onset of substance use disorders. In the first 12 months of use, friends and family members accounted for 55% of reported sources of opioids, according to the U.S. 2010 National Survey on Drug Use and Health.
Providers may also want to consider screening pain patients for psychological disorders, Dr. Salsitz said, as many psychological conditions are associated with a high risk of developing a substance use disorder. Patients with major depression, dysthymia, or panic disorder were 3.43, 6.51, and 5.37 times more likely, respectively, than those without to initiate a prescription for and regularly use opioids, according to a study cited by Dr. Salsitz (Arch Intern Med. 2006 Oct 23;166[19]:2087-93).
One of the largest barriers preventing providers from implementing these methods, however, is a lack of resources, particularly in rural areas with increasing rates of opioid substance use disorders and limited provider options.
While these limitations do pose a problem, physicians should not feel they can’t provide proper care, according to Dr. Salsitz. “I think that each individual provider, wherever they are located, can do a reasonable job.”
Global Academy and this news organization are owned by the same company.
[email protected]
On Twitter @eaztweets
Standard care of chronic noncancer pain should start moving away from chronic opioid treatment, which can put patients in greater danger of developing a substance use disorder, according to evidence presented at a meeting held by the American Pain Society and Global Academy for Medical Education.
As the effects of the U.S. opioid epidemic continue to gain public attention – recently spurring a declaration of a state of emergency –
Use of opioid therapy for pain conditions such as osteoarthritis, fibromyalgia, and migraine – once a common treatment approach – has been shown to be a dangerous breeding ground for opioid substance use disorders, and physicians would do well to re-evaluate their treatment methods, according to Edwin Salsitz, MD, assistant clinical professor at Mount Sinai Beth Israel Hospital, New York.
“Each prescriber is going to have to review this, digest it, reflect on it, and decide what they are going to do,” said Dr. Salsitz in an interview. “Base it on the Centers for Disease Control and Prevention’s guideline as a good starting point, and then individualize it for yourself and your patients.”
One of the major steps toward lowering the rate of opioid addiction through prescription is avoiding opioids as a treatment for acute pain.
“The first recommendation [of the CDC guideline] is nonpharmaceutical therapy, including physical therapy, massage therapy, acupuncture, and cognitive-behavioral therapy – and there’s a whole lot of evidence for these types of therapy,” said Dr. Salsitz. “The second option is that if you’re going to use medications, use those that aren’t opioids, like Tylenol, Motrin, and antidepressants.”
If opioids are necessary, said Dr. Salsitz, immediate-release opioids in limited prescriptions are a good way to lower the risk of addiction.
“The extended-release opioids have many more milligrams than the immediate-release opioids,” according to Dr. Salsitz. “For example, in New York state, we have a law now that says for acute pain, you cannot prescribe for more than a 7-day amount.”
That 7-day limit helps keep excess opioids out of households, he noted, making it harder for patients to share their medication with friends and family, which has proven to be the most common source for opioids during the onset of substance use disorders. In the first 12 months of use, friends and family members accounted for 55% of reported sources of opioids, according to the U.S. 2010 National Survey on Drug Use and Health.
Providers may also want to consider screening pain patients for psychological disorders, Dr. Salsitz said, as many psychological conditions are associated with a high risk of developing a substance use disorder. Patients with major depression, dysthymia, or panic disorder were 3.43, 6.51, and 5.37 times more likely, respectively, than those without to initiate a prescription for and regularly use opioids, according to a study cited by Dr. Salsitz (Arch Intern Med. 2006 Oct 23;166[19]:2087-93).
One of the largest barriers preventing providers from implementing these methods, however, is a lack of resources, particularly in rural areas with increasing rates of opioid substance use disorders and limited provider options.
While these limitations do pose a problem, physicians should not feel they can’t provide proper care, according to Dr. Salsitz. “I think that each individual provider, wherever they are located, can do a reasonable job.”
Global Academy and this news organization are owned by the same company.
[email protected]
On Twitter @eaztweets
Standard care of chronic noncancer pain should start moving away from chronic opioid treatment, which can put patients in greater danger of developing a substance use disorder, according to evidence presented at a meeting held by the American Pain Society and Global Academy for Medical Education.
As the effects of the U.S. opioid epidemic continue to gain public attention – recently spurring a declaration of a state of emergency –
Use of opioid therapy for pain conditions such as osteoarthritis, fibromyalgia, and migraine – once a common treatment approach – has been shown to be a dangerous breeding ground for opioid substance use disorders, and physicians would do well to re-evaluate their treatment methods, according to Edwin Salsitz, MD, assistant clinical professor at Mount Sinai Beth Israel Hospital, New York.
“Each prescriber is going to have to review this, digest it, reflect on it, and decide what they are going to do,” said Dr. Salsitz in an interview. “Base it on the Centers for Disease Control and Prevention’s guideline as a good starting point, and then individualize it for yourself and your patients.”
One of the major steps toward lowering the rate of opioid addiction through prescription is avoiding opioids as a treatment for acute pain.
“The first recommendation [of the CDC guideline] is nonpharmaceutical therapy, including physical therapy, massage therapy, acupuncture, and cognitive-behavioral therapy – and there’s a whole lot of evidence for these types of therapy,” said Dr. Salsitz. “The second option is that if you’re going to use medications, use those that aren’t opioids, like Tylenol, Motrin, and antidepressants.”
If opioids are necessary, said Dr. Salsitz, immediate-release opioids in limited prescriptions are a good way to lower the risk of addiction.
“The extended-release opioids have many more milligrams than the immediate-release opioids,” according to Dr. Salsitz. “For example, in New York state, we have a law now that says for acute pain, you cannot prescribe for more than a 7-day amount.”
That 7-day limit helps keep excess opioids out of households, he noted, making it harder for patients to share their medication with friends and family, which has proven to be the most common source for opioids during the onset of substance use disorders. In the first 12 months of use, friends and family members accounted for 55% of reported sources of opioids, according to the U.S. 2010 National Survey on Drug Use and Health.
Providers may also want to consider screening pain patients for psychological disorders, Dr. Salsitz said, as many psychological conditions are associated with a high risk of developing a substance use disorder. Patients with major depression, dysthymia, or panic disorder were 3.43, 6.51, and 5.37 times more likely, respectively, than those without to initiate a prescription for and regularly use opioids, according to a study cited by Dr. Salsitz (Arch Intern Med. 2006 Oct 23;166[19]:2087-93).
One of the largest barriers preventing providers from implementing these methods, however, is a lack of resources, particularly in rural areas with increasing rates of opioid substance use disorders and limited provider options.
While these limitations do pose a problem, physicians should not feel they can’t provide proper care, according to Dr. Salsitz. “I think that each individual provider, wherever they are located, can do a reasonable job.”
Global Academy and this news organization are owned by the same company.
[email protected]
On Twitter @eaztweets
FROM PAIN CARE FOR PRIMARY CARE
Study shows more changes, less stopping of PsA systemic drugs
Among psoriatic arthritis (PsA) patients who started a systemic disease-modifying antirheumatic drug (DMARD) in the United States during 2004-2015, treatment modification rates went up and discontinuation rates decreased over the 11-year period, according to results from a large study of national claims data.
The increased rate of treatment modification may not be surprising given the “significant advancement in PsA treatment and expanding pharmacotherapy options in the past decade,” wrote researchers led by Moa P. Lee, PharmD, of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital and Harvard Medical School, Boston (Arthritis Care Res. 2017 Aug 13. doi: 10.1002/acr.23337).
The researchers reviewed records between July 1, 2004, and Sept. 30, 2015, from the Clinformatics Datamart data set, which contains demographic and longitudinal claims information for all United Healthcare beneficiaries. They observed an increasing trend in treatment modifications over the 11-year study period (P = .03) and found that 5% of all patients discontinued treatment, with the discontinuation rates decreasing over time (P less than .001).
Of the 9,222 PsA patients who initiated DMARDs, 43% received a biologic agent (bDMARD) and 57% received a conventional synthetic agent (csDMARD). Patients who were initiated on bDMARDs had an average age of 48 years, compared with 52 years in csDMARD initiators. Biologic DMARD initiators also had generally fewer comorbidities.
The most frequently used DMARD overall was methotrexate, which constituted 81% of csDMARD initiations. The most commonly prescribed bDMARDs were etanercept and adalimumab (49% vs. 34%, respectively).
When the researchers evaluated 12-month follow-up data after the first DMARD initiation, they found that 20% of bDMARD initiators had their initial DMARD regimen modified, compared with 31% of csDMARD initiators. Treatment modifications occurred more quickly after starting a csDMARD (median of 102 days) when compared against bDMARD initiators (148 days), and the rate of modification was also higher for patients who first started a csDMARD (adjusted incidence rate of 39.3 cases per 100 patient-years vs. 21.1 cases per 100 person-years for bDMARDs).
The most common modification made by csDMARD initiators was the addition of a bDMARD to methotrexate, particularly etanercept or adalimumab, in 16%. For bDMARD initiators, the most common modification was adding methotrexate in 7%, followed by switches between etanercept and adalimumab in 6%.
“In a rapidly evolving field of PsA treatment, further studies that elucidate more comprehensive real-world trends in the use of available treatment, including more recent novel therapies for PsA, may be needed,” the researchers concluded.
There was no specific funding source for the study. The researchers reported having no financial disclosures relevant to the study.
Among psoriatic arthritis (PsA) patients who started a systemic disease-modifying antirheumatic drug (DMARD) in the United States during 2004-2015, treatment modification rates went up and discontinuation rates decreased over the 11-year period, according to results from a large study of national claims data.
The increased rate of treatment modification may not be surprising given the “significant advancement in PsA treatment and expanding pharmacotherapy options in the past decade,” wrote researchers led by Moa P. Lee, PharmD, of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital and Harvard Medical School, Boston (Arthritis Care Res. 2017 Aug 13. doi: 10.1002/acr.23337).
The researchers reviewed records between July 1, 2004, and Sept. 30, 2015, from the Clinformatics Datamart data set, which contains demographic and longitudinal claims information for all United Healthcare beneficiaries. They observed an increasing trend in treatment modifications over the 11-year study period (P = .03) and found that 5% of all patients discontinued treatment, with the discontinuation rates decreasing over time (P less than .001).
Of the 9,222 PsA patients who initiated DMARDs, 43% received a biologic agent (bDMARD) and 57% received a conventional synthetic agent (csDMARD). Patients who were initiated on bDMARDs had an average age of 48 years, compared with 52 years in csDMARD initiators. Biologic DMARD initiators also had generally fewer comorbidities.
The most frequently used DMARD overall was methotrexate, which constituted 81% of csDMARD initiations. The most commonly prescribed bDMARDs were etanercept and adalimumab (49% vs. 34%, respectively).
When the researchers evaluated 12-month follow-up data after the first DMARD initiation, they found that 20% of bDMARD initiators had their initial DMARD regimen modified, compared with 31% of csDMARD initiators. Treatment modifications occurred more quickly after starting a csDMARD (median of 102 days) when compared against bDMARD initiators (148 days), and the rate of modification was also higher for patients who first started a csDMARD (adjusted incidence rate of 39.3 cases per 100 patient-years vs. 21.1 cases per 100 person-years for bDMARDs).
The most common modification made by csDMARD initiators was the addition of a bDMARD to methotrexate, particularly etanercept or adalimumab, in 16%. For bDMARD initiators, the most common modification was adding methotrexate in 7%, followed by switches between etanercept and adalimumab in 6%.
“In a rapidly evolving field of PsA treatment, further studies that elucidate more comprehensive real-world trends in the use of available treatment, including more recent novel therapies for PsA, may be needed,” the researchers concluded.
There was no specific funding source for the study. The researchers reported having no financial disclosures relevant to the study.
Among psoriatic arthritis (PsA) patients who started a systemic disease-modifying antirheumatic drug (DMARD) in the United States during 2004-2015, treatment modification rates went up and discontinuation rates decreased over the 11-year period, according to results from a large study of national claims data.
The increased rate of treatment modification may not be surprising given the “significant advancement in PsA treatment and expanding pharmacotherapy options in the past decade,” wrote researchers led by Moa P. Lee, PharmD, of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital and Harvard Medical School, Boston (Arthritis Care Res. 2017 Aug 13. doi: 10.1002/acr.23337).
The researchers reviewed records between July 1, 2004, and Sept. 30, 2015, from the Clinformatics Datamart data set, which contains demographic and longitudinal claims information for all United Healthcare beneficiaries. They observed an increasing trend in treatment modifications over the 11-year study period (P = .03) and found that 5% of all patients discontinued treatment, with the discontinuation rates decreasing over time (P less than .001).
Of the 9,222 PsA patients who initiated DMARDs, 43% received a biologic agent (bDMARD) and 57% received a conventional synthetic agent (csDMARD). Patients who were initiated on bDMARDs had an average age of 48 years, compared with 52 years in csDMARD initiators. Biologic DMARD initiators also had generally fewer comorbidities.
The most frequently used DMARD overall was methotrexate, which constituted 81% of csDMARD initiations. The most commonly prescribed bDMARDs were etanercept and adalimumab (49% vs. 34%, respectively).
When the researchers evaluated 12-month follow-up data after the first DMARD initiation, they found that 20% of bDMARD initiators had their initial DMARD regimen modified, compared with 31% of csDMARD initiators. Treatment modifications occurred more quickly after starting a csDMARD (median of 102 days) when compared against bDMARD initiators (148 days), and the rate of modification was also higher for patients who first started a csDMARD (adjusted incidence rate of 39.3 cases per 100 patient-years vs. 21.1 cases per 100 person-years for bDMARDs).
The most common modification made by csDMARD initiators was the addition of a bDMARD to methotrexate, particularly etanercept or adalimumab, in 16%. For bDMARD initiators, the most common modification was adding methotrexate in 7%, followed by switches between etanercept and adalimumab in 6%.
“In a rapidly evolving field of PsA treatment, further studies that elucidate more comprehensive real-world trends in the use of available treatment, including more recent novel therapies for PsA, may be needed,” the researchers concluded.
There was no specific funding source for the study. The researchers reported having no financial disclosures relevant to the study.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point:
Major finding: 20% of bDMARD initiators had their initial DMARD regimen modified, compared with 31% of csDMARD initiators.
Data source: Data from a national claims database on 9,222 psoriatic arthritis patients who initiated DMARDs.
Disclosures: There was no specific funding source for the study. The researchers reported having no financial disclosures relevant to the study.
Why you should use sunscreens indoors
It may be surprising that there are dermatologic risks of UV exposure from lamps and other indoor light sources that we use daily. Is long-term daily exposure to presumably low-irradiance lights of clinical significance to photodermatoses? Recent findings suggest that skin protection must be practiced indoors to adequately protect the skin against UV rays.
Photodermatoses, such as lupus, actinic prurigo, and xeroderma pigmentosum, are only a few of the skin diseases that are triggered by UV exposure; however, chronic low-dose exposures to UV light, such as those associated with indoor lighting, may also be triggers of such conditions. Melasma, for example, can be triggered by heat or UV light. Chronic exposure to ambient light may darken the skin, necessitating daily UV protection in both indoor and outdoor settings.
A study examining light sources in the environment of a child with xeroderma pigmentosum suggested that indoor lights emit unexpected amounts of UV light as measured by a spectral radiometer. This finding illustrated that cumulative, chronic doses of indoor lighting may be of clinical significance.
Interior lighting is also implicated in worsening of melasma and other photosensitive dermatoses. Incandescent bulbs have little to no UV irradiance. However, fluorescent lighting has been shown to increase lifetime UV exposure by 3% based on the distance the lamp is from the skin. If the lamp is close – particularly desk lamps, bed lamps, and overhead lamps – the light and heat emitted can worsen photoexacerbated dermatitidis. Avoiding close contact with the light or adding acrylic or plastic diffusers to the light can help reduce exposure.
Halogen bulbs are filled with an inert gas and a halogen, such as iodine. These bulbs are usually made of quartz because quartz is more resistant to the high heat emitted by these bulbs. But the quartz, however, does not block UV radiation, which is why manufacturers add UV-blocking agents and heat-resistant glass to block the UV; however, the amount blocked is usually unknown. As with fluorescent bulbs, the distance from the bulb is essential to protect against both the UV and heat emitted. Light-emitting diodes (LEDs) generate a light from a semiconductor material that converts blue light into white light with the use of phosphorus; LEDs do not emit UV rays and, therefore, are a safer light source for the skin.

In addition to the use of lamps, the light that passes through glass is easy to underestimate. Unlike UVB rays, UVA rays pass through glass and affect the skin. The percentage of UVA rays that pass through glass depends on the type of glass and the coating on the glass. There are three types of window glass: clear, reflective, and tinted. Clear glass allows 75% of UVA through,while reflective and tinted glass allow only 25%-50% of UVA rays to pass through. Low-emissivity glass (Low-E) is made to reduce heat transfer and is similar to clear glass. The most protective glass is laminated or UV-coated glass that filters out 95%-99% of all UVA rays. Unfortunately, most residential and commercial buildings do not have UVA protection. The use of blinds, shades, and tinted glass, and increasing the distance from windows and doors are the best methods of protection from chronic daily UVA exposures.
In most cars, windshield is made of laminated glass (two layers of glass with a layer of plastic in between), which blocks all UVB and approximately 50% of UVA rays. However, side and rear windows are often clear glass, which does not prevent UVA rays from penetrating through. Patients with photosensitive dermatoses and all melasma patients are encouraged to tint the side windows of their vehicles to reduce UVA exposures to 15%-30%. Tinting, however, must be in compliance with federally mandated standard of 70% minimum visible light transmittance. In my practice, daily UV protection is recommended for all patients, even within an automobile or in an office. Daily cumulative exposure can cause chronic skin damage and early signs of photoaging.
Other sources of indoor exposures include TV monitors, computers, tablets, and UV sterilization devices in the workplace. Older cathode ray tube screens emit UV radiation; however, newer liquid crystal display (LCD) or flat panel monitors most commonly on laptops, desktops, and mobile devices do not emit UV radiation. They do emit blue light – although a small fraction compared to that emitted by the sun. The amount of time spent in front of these screens and their proximity can pose a problem as blue light can increase reactive oxygen species, which is the most common contributor to premature aging. These devices also emit heat, which can exacerbate erythema ab igne and other heat-sensitive skin conditions.

The risks of indoor UV and blue light exposures are commonly overlooked. Skin protection with broad-spectrum sunscreen both inside and outside should be used daily for maximum protection. Care should also be taken to limit exposure times and increase distance of these objects from the skin and eyes.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
It may be surprising that there are dermatologic risks of UV exposure from lamps and other indoor light sources that we use daily. Is long-term daily exposure to presumably low-irradiance lights of clinical significance to photodermatoses? Recent findings suggest that skin protection must be practiced indoors to adequately protect the skin against UV rays.
Photodermatoses, such as lupus, actinic prurigo, and xeroderma pigmentosum, are only a few of the skin diseases that are triggered by UV exposure; however, chronic low-dose exposures to UV light, such as those associated with indoor lighting, may also be triggers of such conditions. Melasma, for example, can be triggered by heat or UV light. Chronic exposure to ambient light may darken the skin, necessitating daily UV protection in both indoor and outdoor settings.
A study examining light sources in the environment of a child with xeroderma pigmentosum suggested that indoor lights emit unexpected amounts of UV light as measured by a spectral radiometer. This finding illustrated that cumulative, chronic doses of indoor lighting may be of clinical significance.
Interior lighting is also implicated in worsening of melasma and other photosensitive dermatoses. Incandescent bulbs have little to no UV irradiance. However, fluorescent lighting has been shown to increase lifetime UV exposure by 3% based on the distance the lamp is from the skin. If the lamp is close – particularly desk lamps, bed lamps, and overhead lamps – the light and heat emitted can worsen photoexacerbated dermatitidis. Avoiding close contact with the light or adding acrylic or plastic diffusers to the light can help reduce exposure.
Halogen bulbs are filled with an inert gas and a halogen, such as iodine. These bulbs are usually made of quartz because quartz is more resistant to the high heat emitted by these bulbs. But the quartz, however, does not block UV radiation, which is why manufacturers add UV-blocking agents and heat-resistant glass to block the UV; however, the amount blocked is usually unknown. As with fluorescent bulbs, the distance from the bulb is essential to protect against both the UV and heat emitted. Light-emitting diodes (LEDs) generate a light from a semiconductor material that converts blue light into white light with the use of phosphorus; LEDs do not emit UV rays and, therefore, are a safer light source for the skin.
In addition to the use of lamps, the light that passes through glass is easy to underestimate. Unlike UVB rays, UVA rays pass through glass and affect the skin. The percentage of UVA rays that pass through glass depends on the type of glass and the coating on the glass. There are three types of window glass: clear, reflective, and tinted. Clear glass allows 75% of UVA through,while reflective and tinted glass allow only 25%-50% of UVA rays to pass through. Low-emissivity glass (Low-E) is made to reduce heat transfer and is similar to clear glass. The most protective glass is laminated or UV-coated glass that filters out 95%-99% of all UVA rays. Unfortunately, most residential and commercial buildings do not have UVA protection. The use of blinds, shades, and tinted glass, and increasing the distance from windows and doors are the best methods of protection from chronic daily UVA exposures.
In most cars, windshield is made of laminated glass (two layers of glass with a layer of plastic in between), which blocks all UVB and approximately 50% of UVA rays. However, side and rear windows are often clear glass, which does not prevent UVA rays from penetrating through. Patients with photosensitive dermatoses and all melasma patients are encouraged to tint the side windows of their vehicles to reduce UVA exposures to 15%-30%. Tinting, however, must be in compliance with federally mandated standard of 70% minimum visible light transmittance. In my practice, daily UV protection is recommended for all patients, even within an automobile or in an office. Daily cumulative exposure can cause chronic skin damage and early signs of photoaging.
Other sources of indoor exposures include TV monitors, computers, tablets, and UV sterilization devices in the workplace. Older cathode ray tube screens emit UV radiation; however, newer liquid crystal display (LCD) or flat panel monitors most commonly on laptops, desktops, and mobile devices do not emit UV radiation. They do emit blue light – although a small fraction compared to that emitted by the sun. The amount of time spent in front of these screens and their proximity can pose a problem as blue light can increase reactive oxygen species, which is the most common contributor to premature aging. These devices also emit heat, which can exacerbate erythema ab igne and other heat-sensitive skin conditions.
The risks of indoor UV and blue light exposures are commonly overlooked. Skin protection with broad-spectrum sunscreen both inside and outside should be used daily for maximum protection. Care should also be taken to limit exposure times and increase distance of these objects from the skin and eyes.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
It may be surprising that there are dermatologic risks of UV exposure from lamps and other indoor light sources that we use daily. Is long-term daily exposure to presumably low-irradiance lights of clinical significance to photodermatoses? Recent findings suggest that skin protection must be practiced indoors to adequately protect the skin against UV rays.
Photodermatoses, such as lupus, actinic prurigo, and xeroderma pigmentosum, are only a few of the skin diseases that are triggered by UV exposure; however, chronic low-dose exposures to UV light, such as those associated with indoor lighting, may also be triggers of such conditions. Melasma, for example, can be triggered by heat or UV light. Chronic exposure to ambient light may darken the skin, necessitating daily UV protection in both indoor and outdoor settings.
A study examining light sources in the environment of a child with xeroderma pigmentosum suggested that indoor lights emit unexpected amounts of UV light as measured by a spectral radiometer. This finding illustrated that cumulative, chronic doses of indoor lighting may be of clinical significance.
Interior lighting is also implicated in worsening of melasma and other photosensitive dermatoses. Incandescent bulbs have little to no UV irradiance. However, fluorescent lighting has been shown to increase lifetime UV exposure by 3% based on the distance the lamp is from the skin. If the lamp is close – particularly desk lamps, bed lamps, and overhead lamps – the light and heat emitted can worsen photoexacerbated dermatitidis. Avoiding close contact with the light or adding acrylic or plastic diffusers to the light can help reduce exposure.
Halogen bulbs are filled with an inert gas and a halogen, such as iodine. These bulbs are usually made of quartz because quartz is more resistant to the high heat emitted by these bulbs. But the quartz, however, does not block UV radiation, which is why manufacturers add UV-blocking agents and heat-resistant glass to block the UV; however, the amount blocked is usually unknown. As with fluorescent bulbs, the distance from the bulb is essential to protect against both the UV and heat emitted. Light-emitting diodes (LEDs) generate a light from a semiconductor material that converts blue light into white light with the use of phosphorus; LEDs do not emit UV rays and, therefore, are a safer light source for the skin.
In addition to the use of lamps, the light that passes through glass is easy to underestimate. Unlike UVB rays, UVA rays pass through glass and affect the skin. The percentage of UVA rays that pass through glass depends on the type of glass and the coating on the glass. There are three types of window glass: clear, reflective, and tinted. Clear glass allows 75% of UVA through,while reflective and tinted glass allow only 25%-50% of UVA rays to pass through. Low-emissivity glass (Low-E) is made to reduce heat transfer and is similar to clear glass. The most protective glass is laminated or UV-coated glass that filters out 95%-99% of all UVA rays. Unfortunately, most residential and commercial buildings do not have UVA protection. The use of blinds, shades, and tinted glass, and increasing the distance from windows and doors are the best methods of protection from chronic daily UVA exposures.
In most cars, windshield is made of laminated glass (two layers of glass with a layer of plastic in between), which blocks all UVB and approximately 50% of UVA rays. However, side and rear windows are often clear glass, which does not prevent UVA rays from penetrating through. Patients with photosensitive dermatoses and all melasma patients are encouraged to tint the side windows of their vehicles to reduce UVA exposures to 15%-30%. Tinting, however, must be in compliance with federally mandated standard of 70% minimum visible light transmittance. In my practice, daily UV protection is recommended for all patients, even within an automobile or in an office. Daily cumulative exposure can cause chronic skin damage and early signs of photoaging.
Other sources of indoor exposures include TV monitors, computers, tablets, and UV sterilization devices in the workplace. Older cathode ray tube screens emit UV radiation; however, newer liquid crystal display (LCD) or flat panel monitors most commonly on laptops, desktops, and mobile devices do not emit UV radiation. They do emit blue light – although a small fraction compared to that emitted by the sun. The amount of time spent in front of these screens and their proximity can pose a problem as blue light can increase reactive oxygen species, which is the most common contributor to premature aging. These devices also emit heat, which can exacerbate erythema ab igne and other heat-sensitive skin conditions.
The risks of indoor UV and blue light exposures are commonly overlooked. Skin protection with broad-spectrum sunscreen both inside and outside should be used daily for maximum protection. Care should also be taken to limit exposure times and increase distance of these objects from the skin and eyes.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
Potential pitfalls of social media
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?

Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Mindfulness and child health
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.

Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.

Physicians shift on support of single-payer system
, according to a recent survey by physician recruiting firm Merritt Hawkins.
A single-payer system was “strongly supported” by 42% and “somewhat supported” by 14% of the 1,033 physicians who responded to the email survey, which was sent out on Aug. 3. Compared with the 41% who expressed opposition to a single payer – 35% “strongly opposed” and 6% “somewhat opposed” – the total of 56% supporting it was more than enough to cover the margin of error of ±3.1%. The remaining 3% of physicians said that they neither support nor oppose a single-payer system, Merritt Hawkins reported.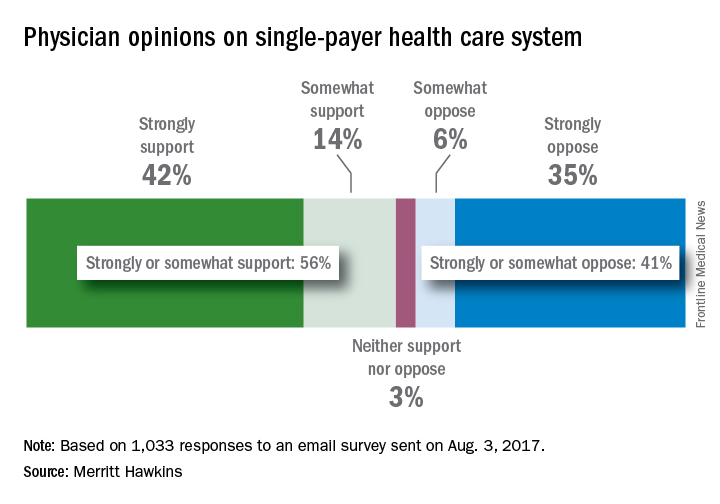
In a survey the company conducted in 2008, just 42% of physicians supported a single-payer system and 58% opposed it. “Physicians appear to have evolved on single payer,” Travis Singleton, senior vice president of Merritt Hawkins, said in a statement. “Whether they are enthusiastic about it, are merely resigned to it, or are just seeking clarity, single payer is a concept many physicians appear to be embracing.”
, according to a recent survey by physician recruiting firm Merritt Hawkins.
A single-payer system was “strongly supported” by 42% and “somewhat supported” by 14% of the 1,033 physicians who responded to the email survey, which was sent out on Aug. 3. Compared with the 41% who expressed opposition to a single payer – 35% “strongly opposed” and 6% “somewhat opposed” – the total of 56% supporting it was more than enough to cover the margin of error of ±3.1%. The remaining 3% of physicians said that they neither support nor oppose a single-payer system, Merritt Hawkins reported.
In a survey the company conducted in 2008, just 42% of physicians supported a single-payer system and 58% opposed it. “Physicians appear to have evolved on single payer,” Travis Singleton, senior vice president of Merritt Hawkins, said in a statement. “Whether they are enthusiastic about it, are merely resigned to it, or are just seeking clarity, single payer is a concept many physicians appear to be embracing.”
, according to a recent survey by physician recruiting firm Merritt Hawkins.
A single-payer system was “strongly supported” by 42% and “somewhat supported” by 14% of the 1,033 physicians who responded to the email survey, which was sent out on Aug. 3. Compared with the 41% who expressed opposition to a single payer – 35% “strongly opposed” and 6% “somewhat opposed” – the total of 56% supporting it was more than enough to cover the margin of error of ±3.1%. The remaining 3% of physicians said that they neither support nor oppose a single-payer system, Merritt Hawkins reported.
In a survey the company conducted in 2008, just 42% of physicians supported a single-payer system and 58% opposed it. “Physicians appear to have evolved on single payer,” Travis Singleton, senior vice president of Merritt Hawkins, said in a statement. “Whether they are enthusiastic about it, are merely resigned to it, or are just seeking clarity, single payer is a concept many physicians appear to be embracing.”
QI enthusiast to QI leader: Luci Leykum, MD
Editor’s Note: This ongoing series highlights the professional pathways of quality improvement leaders. This month features the story of Luci Leykum, MD, division chief, general and hospital medicine at the University of Texas Health Science Center, San Antonio.
Luci Leykum, MD, MBA, MSc, FACP, SFHM, became familiar with inpatient medicine at age 9 years, when her grandfather contracted non-AB hepatitis from a postoperative blood transfusion. In the ensuing years, Dr. Leykum visited her grandfather during his frequent hospitalizations, keeping a close watch on the physicians charged with his care.
“It was when HIV and what we now think is hep C were just emerging, and there was a lot to figure out,” Dr. Leykum recalled of these formative experiences. Her interests in problem-solving, human relationships, and physiology led to enrollment years later as a medical student at Columbia University’s College of Physicians and Surgeons, where her keen observation skills led to a life-changing, “how did we get here?” moment.

Shortly before Dr. Leykum entered residency in 1999, New York Hospital and Columbia Presbyterian Hospital announced that they were merging. The timing was ideal for someone with Dr. Leykum’s acumen in business and medicine, and, as a resident, she began working with the chief medical officer for quality at the new, combined health system to identify quality improvement opportunities.
From there, the projects began pouring in: tracking phone hold times for residents; updating policies to reduce staff exposure to blood-borne pathogens and other infectious diseases; and monitoring flow through the hospitalization process. “In the progression of a few years, I was able to see important aspects of how the system came together,” said Dr. Leykum, “and how decisions were made around standards and metrics for the system as a whole and for its multiple individual hospital facilities.”
In 2004, two years out of residency, Dr. Leykum relocated to San Antonio to accept a clinician investigator position with the South Texas Veterans Health Care System/University of Texas Health Science Center San Antonio (UTHSCSA). Research, she said, has allowed her to delve deeper into the underlying mechanisms that impact systems of health care. She sees the complementary sides of quality improvement and research.
“Through our quality improvement initiatives, we can evaluate and improve specific aspects of care, in specific contexts or systems,” Dr. Leykum explained. “In our research projects, we look for new insights that can be more broadly applied across contexts. With funding, you are able to look at things with a scope, depth, or time horizon beyond what you typically have with a QI project.”
Since joining the UTHSCSA/VA system, Dr. Leykum has participated in more than 15 externally funded studies, 6 as principal investigator. She joined SHM’s research committee in 2009, serving as chair for 6 years, and is currently working with the committee to implement the Improving Hospital Outcomes through Patient Engagement (i-HOPE) Study.
I-HOPE, funded through the Patient-Centered Outcomes Research Institute, is a project to develop a patient- and stakeholder-partnered research agenda to improve the care of hospitalized patients. Dr. Leykum is also involved in implementing a collaborative care model at University Health System, a patient-partnered, interprofessional model that “focuses on improving interconnections, relationships, and sense making,” in the hospital system, she explained. “It was motivated strongly by our desire to improve our partnerships with patients and other providers in the hospital as a strategy to improve care.”
In addition to the many professional responsibilities she manages as division chief of general and hospital medicine at UTHSCSA – a position she has held for hospital medicine since 2006 and for the combined division since 2016 – Dr. Leykum continues to play an integral role in multiple academic and research initiatives for SHM.
She encourages anyone considering a concentration in QI and research to seek opportunities to actively learn these skills and, more importantly, let other people know their interests.
“The value of talking with colleagues at other places is so high,” she said. “When you actively reach out, you find that most people are happy to share their knowledge. Networking is one of the best parts of the SHM annual meeting – there’s an energy and excitement in learning about what others are doing. Wander into the poster and special interest sessions and see what people are working on, get email addresses, and participate on committees.”
Editor’s Note: This ongoing series highlights the professional pathways of quality improvement leaders. This month features the story of Luci Leykum, MD, division chief, general and hospital medicine at the University of Texas Health Science Center, San Antonio.
Luci Leykum, MD, MBA, MSc, FACP, SFHM, became familiar with inpatient medicine at age 9 years, when her grandfather contracted non-AB hepatitis from a postoperative blood transfusion. In the ensuing years, Dr. Leykum visited her grandfather during his frequent hospitalizations, keeping a close watch on the physicians charged with his care.
“It was when HIV and what we now think is hep C were just emerging, and there was a lot to figure out,” Dr. Leykum recalled of these formative experiences. Her interests in problem-solving, human relationships, and physiology led to enrollment years later as a medical student at Columbia University’s College of Physicians and Surgeons, where her keen observation skills led to a life-changing, “how did we get here?” moment.
Shortly before Dr. Leykum entered residency in 1999, New York Hospital and Columbia Presbyterian Hospital announced that they were merging. The timing was ideal for someone with Dr. Leykum’s acumen in business and medicine, and, as a resident, she began working with the chief medical officer for quality at the new, combined health system to identify quality improvement opportunities.
From there, the projects began pouring in: tracking phone hold times for residents; updating policies to reduce staff exposure to blood-borne pathogens and other infectious diseases; and monitoring flow through the hospitalization process. “In the progression of a few years, I was able to see important aspects of how the system came together,” said Dr. Leykum, “and how decisions were made around standards and metrics for the system as a whole and for its multiple individual hospital facilities.”
In 2004, two years out of residency, Dr. Leykum relocated to San Antonio to accept a clinician investigator position with the South Texas Veterans Health Care System/University of Texas Health Science Center San Antonio (UTHSCSA). Research, she said, has allowed her to delve deeper into the underlying mechanisms that impact systems of health care. She sees the complementary sides of quality improvement and research.
“Through our quality improvement initiatives, we can evaluate and improve specific aspects of care, in specific contexts or systems,” Dr. Leykum explained. “In our research projects, we look for new insights that can be more broadly applied across contexts. With funding, you are able to look at things with a scope, depth, or time horizon beyond what you typically have with a QI project.”
Since joining the UTHSCSA/VA system, Dr. Leykum has participated in more than 15 externally funded studies, 6 as principal investigator. She joined SHM’s research committee in 2009, serving as chair for 6 years, and is currently working with the committee to implement the Improving Hospital Outcomes through Patient Engagement (i-HOPE) Study.
I-HOPE, funded through the Patient-Centered Outcomes Research Institute, is a project to develop a patient- and stakeholder-partnered research agenda to improve the care of hospitalized patients. Dr. Leykum is also involved in implementing a collaborative care model at University Health System, a patient-partnered, interprofessional model that “focuses on improving interconnections, relationships, and sense making,” in the hospital system, she explained. “It was motivated strongly by our desire to improve our partnerships with patients and other providers in the hospital as a strategy to improve care.”
In addition to the many professional responsibilities she manages as division chief of general and hospital medicine at UTHSCSA – a position she has held for hospital medicine since 2006 and for the combined division since 2016 – Dr. Leykum continues to play an integral role in multiple academic and research initiatives for SHM.
She encourages anyone considering a concentration in QI and research to seek opportunities to actively learn these skills and, more importantly, let other people know their interests.
“The value of talking with colleagues at other places is so high,” she said. “When you actively reach out, you find that most people are happy to share their knowledge. Networking is one of the best parts of the SHM annual meeting – there’s an energy and excitement in learning about what others are doing. Wander into the poster and special interest sessions and see what people are working on, get email addresses, and participate on committees.”
Editor’s Note: This ongoing series highlights the professional pathways of quality improvement leaders. This month features the story of Luci Leykum, MD, division chief, general and hospital medicine at the University of Texas Health Science Center, San Antonio.
Luci Leykum, MD, MBA, MSc, FACP, SFHM, became familiar with inpatient medicine at age 9 years, when her grandfather contracted non-AB hepatitis from a postoperative blood transfusion. In the ensuing years, Dr. Leykum visited her grandfather during his frequent hospitalizations, keeping a close watch on the physicians charged with his care.
“It was when HIV and what we now think is hep C were just emerging, and there was a lot to figure out,” Dr. Leykum recalled of these formative experiences. Her interests in problem-solving, human relationships, and physiology led to enrollment years later as a medical student at Columbia University’s College of Physicians and Surgeons, where her keen observation skills led to a life-changing, “how did we get here?” moment.
Shortly before Dr. Leykum entered residency in 1999, New York Hospital and Columbia Presbyterian Hospital announced that they were merging. The timing was ideal for someone with Dr. Leykum’s acumen in business and medicine, and, as a resident, she began working with the chief medical officer for quality at the new, combined health system to identify quality improvement opportunities.
From there, the projects began pouring in: tracking phone hold times for residents; updating policies to reduce staff exposure to blood-borne pathogens and other infectious diseases; and monitoring flow through the hospitalization process. “In the progression of a few years, I was able to see important aspects of how the system came together,” said Dr. Leykum, “and how decisions were made around standards and metrics for the system as a whole and for its multiple individual hospital facilities.”
In 2004, two years out of residency, Dr. Leykum relocated to San Antonio to accept a clinician investigator position with the South Texas Veterans Health Care System/University of Texas Health Science Center San Antonio (UTHSCSA). Research, she said, has allowed her to delve deeper into the underlying mechanisms that impact systems of health care. She sees the complementary sides of quality improvement and research.
“Through our quality improvement initiatives, we can evaluate and improve specific aspects of care, in specific contexts or systems,” Dr. Leykum explained. “In our research projects, we look for new insights that can be more broadly applied across contexts. With funding, you are able to look at things with a scope, depth, or time horizon beyond what you typically have with a QI project.”
Since joining the UTHSCSA/VA system, Dr. Leykum has participated in more than 15 externally funded studies, 6 as principal investigator. She joined SHM’s research committee in 2009, serving as chair for 6 years, and is currently working with the committee to implement the Improving Hospital Outcomes through Patient Engagement (i-HOPE) Study.
I-HOPE, funded through the Patient-Centered Outcomes Research Institute, is a project to develop a patient- and stakeholder-partnered research agenda to improve the care of hospitalized patients. Dr. Leykum is also involved in implementing a collaborative care model at University Health System, a patient-partnered, interprofessional model that “focuses on improving interconnections, relationships, and sense making,” in the hospital system, she explained. “It was motivated strongly by our desire to improve our partnerships with patients and other providers in the hospital as a strategy to improve care.”
In addition to the many professional responsibilities she manages as division chief of general and hospital medicine at UTHSCSA – a position she has held for hospital medicine since 2006 and for the combined division since 2016 – Dr. Leykum continues to play an integral role in multiple academic and research initiatives for SHM.
She encourages anyone considering a concentration in QI and research to seek opportunities to actively learn these skills and, more importantly, let other people know their interests.
“The value of talking with colleagues at other places is so high,” she said. “When you actively reach out, you find that most people are happy to share their knowledge. Networking is one of the best parts of the SHM annual meeting – there’s an energy and excitement in learning about what others are doing. Wander into the poster and special interest sessions and see what people are working on, get email addresses, and participate on committees.”