User login
Reducing the Risk of Overt Hepatic Encephalopathy (HE) Recurrence and HE-Related Hospitalizations

In this supplement to The Hospitalist, Dr. Hameed Ali discusses HE and the importance of identifying and properly managing this common complication of cirrhosis.
Topics include:
- The various stages of HE
- The burden of HE and hospital readmission rates
- A medication for overt HE management
About the Author:
Hameed Q. Ali, DO, FHM
Clinical Assistant Professor
Department of Internal Medicine
Texas A&M Health Science Center
Temple, TX
XIF.0097.USA.18
In this supplement to The Hospitalist, Dr. Hameed Ali discusses HE and the importance of identifying and properly managing this common complication of cirrhosis.
Topics include:
- The various stages of HE
- The burden of HE and hospital readmission rates
- A medication for overt HE management
About the Author:
Hameed Q. Ali, DO, FHM
Clinical Assistant Professor
Department of Internal Medicine
Texas A&M Health Science Center
Temple, TX
XIF.0097.USA.18
In this supplement to The Hospitalist, Dr. Hameed Ali discusses HE and the importance of identifying and properly managing this common complication of cirrhosis.
Topics include:
- The various stages of HE
- The burden of HE and hospital readmission rates
- A medication for overt HE management
About the Author:
Hameed Q. Ali, DO, FHM
Clinical Assistant Professor
Department of Internal Medicine
Texas A&M Health Science Center
Temple, TX
XIF.0097.USA.18

Venetoclax plus ibrutinib yields encouraging MRD results in first-line CLL
CHICAGO – The combination of ibrutinib plus venetoclax yielded a high rate of undetectable minimal residual disease (MRD) when used as first-line treatment for chronic lymphocytic leukemia (CLL), according to preliminary results of the CAPTIVATE trial.
Of the first 30 patients in the trial, 23 (77%) had undetectable blood MRD after just six cycles of combined treatment, said investigator William G. Wierda, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.

“These early results show a highly active and safe treatment with 12 cycles of combined treatment with ibrutinib and venetoclax,” Dr. Wierda said in a presentation of the CAPTIVATE results at the annual meeting of the American Society of Clinical Oncology.
Those MRD results are “at least as good as we can achieve with chemoimmunotherapy,” Bruce D. Cheson, MD, head of hematology at Georgetown University, Washington, said during a discussion of the CAPTIVATE study results.
Dr. Cheson referenced MRD results from a 2016 analysis of the CLL8 and CLL10 trials, which included patients treated with fludarabine, cyclophosphamide, and rituximab (FCR) and bendamustine plus rituximab (BR). In that analysis, 33.6% of patients achieved MRD-negative complete response and 29.1% achieved MRD-negative partial response.
In CAPTIVATE, by contrast, all of the complete remissions were MRD negative, as were a majority of the partial responders, Dr. Cheson noted.
Venetoclax and ibrutinib have “clinically complimentary activity” that provided a rationale for combining the two, Dr. Wierda said at ASCO. Ibrutinib is a BTK inhibitor that has a high rate of response and durable disease control, though continuous treatment is indicated, he said, because most patients achieve partial remissions as best response and continue to have residual disease in blood or bone marrow. Venetoclax, he added, is a BCL-2 inhibitor that produces durable partial remissions, though “residual disease is typically present in the form of persistently enlarged lymph nodes,” he said. “Venetoclax is highly effective at clearing disease from blood and bone marrow.”
The phase 2 CAPTIVATE trial includes a total of 164 patients younger than 70 years of age who receive a 3-cycle ibrutinib lead-in, followed by ibrutinib plus venetoclax for 12 cycles. At that point, patients are randomized according to MRD status. Patients with confirmed undetectable MRD are randomized to further treatment with ibrutinib or placebo, and those with undetectable MRD not confirmed are randomized to ibrutinib versus ibrutinib plus venetoclax.
In addition to early efficacy data, Dr. Wierda also reported some safety data. Compared with the single-agent ibrutinib lead-in period, combined ibrutinib plus venetoclax treatment had more gastrointestinal-associated events and neutropenia. Almost half of patients (45%) have had a treatment-related grade 3-4 adverse event, though just 18 (11%) have had treatment-related adverse events classified as serious, and there have been no adverse event-related deaths on study.
The high activity of ibrutinib plus venetoclax in CAPTIVATE supports further study of the combination, Dr. Wierda said. A randomized, open-label phase 3 trial of ibrutinib plus venetoclax versus chlorambucil plus obinutuzumab as first-line treatment for CLL is currently recruiting.
The study was sponsored by Pharmacyclics, an AbbVie company. Dr. Wierda reported consulting and research funding from Pharmacyclics, AbbVie, and several other companies.
SOURCE: Wierda WG et al. ASCO 2018, Abstract 7502.
CHICAGO – The combination of ibrutinib plus venetoclax yielded a high rate of undetectable minimal residual disease (MRD) when used as first-line treatment for chronic lymphocytic leukemia (CLL), according to preliminary results of the CAPTIVATE trial.
Of the first 30 patients in the trial, 23 (77%) had undetectable blood MRD after just six cycles of combined treatment, said investigator William G. Wierda, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.
“These early results show a highly active and safe treatment with 12 cycles of combined treatment with ibrutinib and venetoclax,” Dr. Wierda said in a presentation of the CAPTIVATE results at the annual meeting of the American Society of Clinical Oncology.
Those MRD results are “at least as good as we can achieve with chemoimmunotherapy,” Bruce D. Cheson, MD, head of hematology at Georgetown University, Washington, said during a discussion of the CAPTIVATE study results.
Dr. Cheson referenced MRD results from a 2016 analysis of the CLL8 and CLL10 trials, which included patients treated with fludarabine, cyclophosphamide, and rituximab (FCR) and bendamustine plus rituximab (BR). In that analysis, 33.6% of patients achieved MRD-negative complete response and 29.1% achieved MRD-negative partial response.
In CAPTIVATE, by contrast, all of the complete remissions were MRD negative, as were a majority of the partial responders, Dr. Cheson noted.
Venetoclax and ibrutinib have “clinically complimentary activity” that provided a rationale for combining the two, Dr. Wierda said at ASCO. Ibrutinib is a BTK inhibitor that has a high rate of response and durable disease control, though continuous treatment is indicated, he said, because most patients achieve partial remissions as best response and continue to have residual disease in blood or bone marrow. Venetoclax, he added, is a BCL-2 inhibitor that produces durable partial remissions, though “residual disease is typically present in the form of persistently enlarged lymph nodes,” he said. “Venetoclax is highly effective at clearing disease from blood and bone marrow.”
The phase 2 CAPTIVATE trial includes a total of 164 patients younger than 70 years of age who receive a 3-cycle ibrutinib lead-in, followed by ibrutinib plus venetoclax for 12 cycles. At that point, patients are randomized according to MRD status. Patients with confirmed undetectable MRD are randomized to further treatment with ibrutinib or placebo, and those with undetectable MRD not confirmed are randomized to ibrutinib versus ibrutinib plus venetoclax.
In addition to early efficacy data, Dr. Wierda also reported some safety data. Compared with the single-agent ibrutinib lead-in period, combined ibrutinib plus venetoclax treatment had more gastrointestinal-associated events and neutropenia. Almost half of patients (45%) have had a treatment-related grade 3-4 adverse event, though just 18 (11%) have had treatment-related adverse events classified as serious, and there have been no adverse event-related deaths on study.
The high activity of ibrutinib plus venetoclax in CAPTIVATE supports further study of the combination, Dr. Wierda said. A randomized, open-label phase 3 trial of ibrutinib plus venetoclax versus chlorambucil plus obinutuzumab as first-line treatment for CLL is currently recruiting.
The study was sponsored by Pharmacyclics, an AbbVie company. Dr. Wierda reported consulting and research funding from Pharmacyclics, AbbVie, and several other companies.
SOURCE: Wierda WG et al. ASCO 2018, Abstract 7502.
CHICAGO – The combination of ibrutinib plus venetoclax yielded a high rate of undetectable minimal residual disease (MRD) when used as first-line treatment for chronic lymphocytic leukemia (CLL), according to preliminary results of the CAPTIVATE trial.
Of the first 30 patients in the trial, 23 (77%) had undetectable blood MRD after just six cycles of combined treatment, said investigator William G. Wierda, MD, PhD, of the University of Texas MD Anderson Cancer Center, Houston.
“These early results show a highly active and safe treatment with 12 cycles of combined treatment with ibrutinib and venetoclax,” Dr. Wierda said in a presentation of the CAPTIVATE results at the annual meeting of the American Society of Clinical Oncology.
Those MRD results are “at least as good as we can achieve with chemoimmunotherapy,” Bruce D. Cheson, MD, head of hematology at Georgetown University, Washington, said during a discussion of the CAPTIVATE study results.
Dr. Cheson referenced MRD results from a 2016 analysis of the CLL8 and CLL10 trials, which included patients treated with fludarabine, cyclophosphamide, and rituximab (FCR) and bendamustine plus rituximab (BR). In that analysis, 33.6% of patients achieved MRD-negative complete response and 29.1% achieved MRD-negative partial response.
In CAPTIVATE, by contrast, all of the complete remissions were MRD negative, as were a majority of the partial responders, Dr. Cheson noted.
Venetoclax and ibrutinib have “clinically complimentary activity” that provided a rationale for combining the two, Dr. Wierda said at ASCO. Ibrutinib is a BTK inhibitor that has a high rate of response and durable disease control, though continuous treatment is indicated, he said, because most patients achieve partial remissions as best response and continue to have residual disease in blood or bone marrow. Venetoclax, he added, is a BCL-2 inhibitor that produces durable partial remissions, though “residual disease is typically present in the form of persistently enlarged lymph nodes,” he said. “Venetoclax is highly effective at clearing disease from blood and bone marrow.”
The phase 2 CAPTIVATE trial includes a total of 164 patients younger than 70 years of age who receive a 3-cycle ibrutinib lead-in, followed by ibrutinib plus venetoclax for 12 cycles. At that point, patients are randomized according to MRD status. Patients with confirmed undetectable MRD are randomized to further treatment with ibrutinib or placebo, and those with undetectable MRD not confirmed are randomized to ibrutinib versus ibrutinib plus venetoclax.
In addition to early efficacy data, Dr. Wierda also reported some safety data. Compared with the single-agent ibrutinib lead-in period, combined ibrutinib plus venetoclax treatment had more gastrointestinal-associated events and neutropenia. Almost half of patients (45%) have had a treatment-related grade 3-4 adverse event, though just 18 (11%) have had treatment-related adverse events classified as serious, and there have been no adverse event-related deaths on study.
The high activity of ibrutinib plus venetoclax in CAPTIVATE supports further study of the combination, Dr. Wierda said. A randomized, open-label phase 3 trial of ibrutinib plus venetoclax versus chlorambucil plus obinutuzumab as first-line treatment for CLL is currently recruiting.
The study was sponsored by Pharmacyclics, an AbbVie company. Dr. Wierda reported consulting and research funding from Pharmacyclics, AbbVie, and several other companies.
SOURCE: Wierda WG et al. ASCO 2018, Abstract 7502.
REPORTING FROM ASCO 2018
Key clinical point:
Major finding: Of 14 patients, 12 (86%) who completed 12 cycles of treatment had undetectable bone marrow MRD.
Study details: Early results of the phase 2 CAPTIVATE trial including 164 patients younger than 70 years of age with previously untreated CLL.
Disclosures: The study was sponsored by Pharmacyclics, an Abbvie company. Dr. Wierda reported consulting and research funding from Pharmacyclics, AbbVie, and several other companies.
Source: Wierda WG et al. ASCO 2018, Abstract 7502.

Sleep apnea treatment may not prevent sleepiness
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.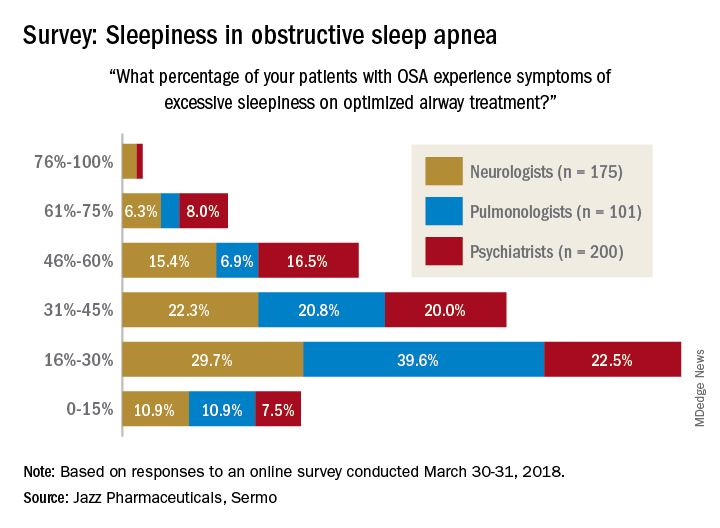
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Physicians who treat obstructive sleep apnea reported that patients with OSA can experience excessive sleepiness despite being on optimized airway treatment, findings from an online surgery of clinicians show.
Jazz Pharmaceuticals and the social media network Sermo conducted an online questionnaire on topics in excessive sleepiness and obstructive sleep apnea. The study was conducted March 30-31, 2018.
When asked how often they assess their OSA patients’ sleepiness, 46% of respondents said every 3 months, 28% said every 6 months, 19% said once a month, 6% said once a year, and 0.4% (one neurologist and one pulmonologist) said never. The method of evaluation varied by specialty: 82% of pulmonologists most often use the Epworth Sleepiness Scale and 76% of psychiatrists primarily use an informal set of questions, with neurologists in between but leaning toward informal questions, Jazz reported.
“As more scientific evidence emerges around the neuronal injury occurring due to OSA and the potential neurocognitive effects of excessive sleepiness, it’s imperative that pulmonologists, neurologists and psychiatrists understand the impact ES [excessive sleepiness] can have on patients’ lives,” Richard K. Bogan, MD, of the University of South Carolina, Columbia, a paid consultant to Jazz, said in a written statement.
Customized airway stents show promise in feasibility trial
SAN DIEGO – for whom conventional stents were not suitable or failed, results from a small study demonstrated.
“Anatomically complex airway stenosis remains a challenging situation,” lead study author Nicolas Guibert, MD, said at an international conference of the American Thoracic Society. “Conventional devices are either not suited or may result in a significant complication rate, including poor clinical tolerance, migration, or granulation tissue reaction due to lack of congruence.”

Dr. Guibert reported results from eight patients. Of these, three had posttransplant complex airway stenoses involving the bronchus intermedius. Each improved after placement of the customized stents. For example, one patient with vanishing bronchus intermedius syndrome experienced improvements in NYHA dyspnea score from 3 to 1, the VQ11 score from 22 to 11/55, and forced expiratory volume in 1 second (FEV1) from 70% to 107%. The stent was removed after 3 months. Meanwhile, a patient with localized malacia and stenosis of the right main bronchus experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 score from 27 to 15/55, and FEV1 from 70% to 102%. That person’s stent is still in place with no complications. Another patient with localized malacia and stenosis of the bronchus intermedius experienced improvements in FEV1 from 84% to 100%. That person’s device was removed after 3 months, with no residual stenosis.
A fourth patient underwent stent placement for localized malacia (cartilage ring rupture). That person experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 from 23 to 15/55, and FEV1 from 66% to 92%, and peak flow from 49% to 82%. The device is still in place with no complications. A fifth patient received stent placement for extensive tracheobronchomalacia, but it had imperfect congruence and was removed after 3 months because it caused intense cough.
One patient with post-tracheotomy stenosis experienced improvements in NYHA dyspnea score from 3 to 0, VQ11 from 29 to 12/55, and peak flow from 45% to 81%. That person’s device is still in place, Dr. Guibert said. Two other patients treated for post-tracheotomy experienced stent migration (conventional stents also migrated in these two cases), despite good bronchoscopic congruence after placement.
“Tracheal diseases result in suboptimal congruence, probably due to higher respiratory variation,” Dr. Guibert said. “These devices need to be studied in less selected populations and the technology has to be improved.” He reported having no financial disclosures.
SOURCE: Guibert N et al. ATS 2018, Abstract 4433.
SAN DIEGO – for whom conventional stents were not suitable or failed, results from a small study demonstrated.
“Anatomically complex airway stenosis remains a challenging situation,” lead study author Nicolas Guibert, MD, said at an international conference of the American Thoracic Society. “Conventional devices are either not suited or may result in a significant complication rate, including poor clinical tolerance, migration, or granulation tissue reaction due to lack of congruence.”
Dr. Guibert reported results from eight patients. Of these, three had posttransplant complex airway stenoses involving the bronchus intermedius. Each improved after placement of the customized stents. For example, one patient with vanishing bronchus intermedius syndrome experienced improvements in NYHA dyspnea score from 3 to 1, the VQ11 score from 22 to 11/55, and forced expiratory volume in 1 second (FEV1) from 70% to 107%. The stent was removed after 3 months. Meanwhile, a patient with localized malacia and stenosis of the right main bronchus experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 score from 27 to 15/55, and FEV1 from 70% to 102%. That person’s stent is still in place with no complications. Another patient with localized malacia and stenosis of the bronchus intermedius experienced improvements in FEV1 from 84% to 100%. That person’s device was removed after 3 months, with no residual stenosis.
A fourth patient underwent stent placement for localized malacia (cartilage ring rupture). That person experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 from 23 to 15/55, and FEV1 from 66% to 92%, and peak flow from 49% to 82%. The device is still in place with no complications. A fifth patient received stent placement for extensive tracheobronchomalacia, but it had imperfect congruence and was removed after 3 months because it caused intense cough.
One patient with post-tracheotomy stenosis experienced improvements in NYHA dyspnea score from 3 to 0, VQ11 from 29 to 12/55, and peak flow from 45% to 81%. That person’s device is still in place, Dr. Guibert said. Two other patients treated for post-tracheotomy experienced stent migration (conventional stents also migrated in these two cases), despite good bronchoscopic congruence after placement.
“Tracheal diseases result in suboptimal congruence, probably due to higher respiratory variation,” Dr. Guibert said. “These devices need to be studied in less selected populations and the technology has to be improved.” He reported having no financial disclosures.
SOURCE: Guibert N et al. ATS 2018, Abstract 4433.
SAN DIEGO – for whom conventional stents were not suitable or failed, results from a small study demonstrated.
“Anatomically complex airway stenosis remains a challenging situation,” lead study author Nicolas Guibert, MD, said at an international conference of the American Thoracic Society. “Conventional devices are either not suited or may result in a significant complication rate, including poor clinical tolerance, migration, or granulation tissue reaction due to lack of congruence.”
Dr. Guibert reported results from eight patients. Of these, three had posttransplant complex airway stenoses involving the bronchus intermedius. Each improved after placement of the customized stents. For example, one patient with vanishing bronchus intermedius syndrome experienced improvements in NYHA dyspnea score from 3 to 1, the VQ11 score from 22 to 11/55, and forced expiratory volume in 1 second (FEV1) from 70% to 107%. The stent was removed after 3 months. Meanwhile, a patient with localized malacia and stenosis of the right main bronchus experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 score from 27 to 15/55, and FEV1 from 70% to 102%. That person’s stent is still in place with no complications. Another patient with localized malacia and stenosis of the bronchus intermedius experienced improvements in FEV1 from 84% to 100%. That person’s device was removed after 3 months, with no residual stenosis.
A fourth patient underwent stent placement for localized malacia (cartilage ring rupture). That person experienced improvements in NYHA dyspnea score from 3 to 1, VQ11 from 23 to 15/55, and FEV1 from 66% to 92%, and peak flow from 49% to 82%. The device is still in place with no complications. A fifth patient received stent placement for extensive tracheobronchomalacia, but it had imperfect congruence and was removed after 3 months because it caused intense cough.
One patient with post-tracheotomy stenosis experienced improvements in NYHA dyspnea score from 3 to 0, VQ11 from 29 to 12/55, and peak flow from 45% to 81%. That person’s device is still in place, Dr. Guibert said. Two other patients treated for post-tracheotomy experienced stent migration (conventional stents also migrated in these two cases), despite good bronchoscopic congruence after placement.
“Tracheal diseases result in suboptimal congruence, probably due to higher respiratory variation,” Dr. Guibert said. “These devices need to be studied in less selected populations and the technology has to be improved.” He reported having no financial disclosures.
SOURCE: Guibert N et al. ATS 2018, Abstract 4433.
REPORTING FROM ATS 2018
Key clinical point: Customized, 3-D airway stents have the potential for improving tolerance and decreasing the complication rate.
Major finding: Congruence and outcomes tended to be better in stenoses involving the bronchial level (three of three, no complications).
Study details: A feasibility study of eight patients with nonmalignant, anatomically complex, and symptomatic stenosis for which conventional stents were not suitable.
Disclosures: Dr. Guibert reported having no financial disclosures.
Source: Guibert N et al. ATS 2018, Abstract 4433.
New cell-free DNA assays hold promise for lung cancer screening
CHICAGO – according to the first interim report from a substudy of the large, ongoing Circulating Cell-free Genome Atlas (CCGA).
“Lung cancer screening with low-dose CT is known to improve outcomes. And yet, CT-based lung cancer screening is not widely adopted,” said lead study author Geoffrey R. Oxnard, MD, associate professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the study was reported. “Criticisms of low-dose CT include the risk of false positives and overdiagnosis. We proposed to investigate an untapped opportunity for cancer detection, which is using cell-free DNA.”

Main substudy results among 164 patients with lung cancer and 923 comparable individuals without known cancer showed that at a specificity of 98%, the three assays evaluated detected up to 51% of early-stage (stage I-IIIA) lung cancers and up to 91% of late-stage (stage IIIB-IV) lung cancers. And among the healthy participants with false-positive results for lung cancer, several were ultimately found to have cancers of other types.
“This first interim analysis of the CCGA study demonstrates that comprehensive sequencing of the plasma cell-free DNA can generate high-quality data across the entire genome, and it permits noninvasive cancer detection. The assays can detect lung cancer across stages, across histologies, across populations,” Dr. Oxnard said.
“Together, these results support the promise of using cell-free, DNA-based assays to develop an early cancer detection test with high specificity. Further assay and clinical development is ongoing: There is a separate prospective trial enrolling, the STRIVE study, and there remain thousands of patients still on this CCGA study to be analyzed for further optimization and focusing of this assay towards an eventual cancer diagnostic.”
The cohort studied was not a screening population, so the assays’ performance cannot be compared with that of low-dose CT at this point, he said. But the hypothesis going forward is that the assays will have comparatively higher specificity, sparing some patients an unnecessary diagnostic work-up.
The population in which the final blood test might be used will depend on its diagnostic performance once the assays are fully refined and clinic ready, which will take some time, according to Dr. Oxnard. However, “2 years ago, this was a pipe dream. Two years ago, it was completely just a brainstorm that had no data to support it, and I didn’t believe that this could be done. Today, we actually have data to show that this is really feasible to find early-stage cancer in the blood. So this is a huge step forward and actually means that this is going to be a reality.”

“This is an important first step towards an easier way to detect lung cancer at earlier and hopefully more curable stages,” agreed ASCO Expert David Graham, MD, who is also medical director at the Levine Cancer Institute in Charlotte, N.C. “If the promise of this report holds, we could easily see a day when a person could be screened for lung cancer and possibly other cancers simply by going into their regular doctor’s office for a blood draw.”
Study details
The CCGA study has enrolled more than 12,000 of its planned 15,000 participants (70% with cancer, 30% without) across 142 U.S. and Canadian sites.
The substudy reported had a development cohort (118 patients with lung cancer, 561 individuals without cancer) and a validation cohort (46 patients with lung cancer, 362 individuals without cancer), with the lung cancer and noncancer groups matched on age, race, and body mass index. “Having a comparable control cohort is very important in developing such a diagnostic for accurate analysis of the potential false-positive rate,” Dr. Oxnard noted.
Three prototype assays were tested: A targeted sequencing assay entailing very deep sequencing across 507 genes for somatic mutations such as single-nucleotide variants and small insertions and/or deletions; a novel, whole-genome sequencing assay to detect somatic gene copy number changes; and a novel, whole-genome methylation sequencing assay to detect abnormal epigenetic changes.
Sequencing was also performed on DNA from white blood cells. “That’s very important. The white blood cells are rich with mutations that can pollute the DNA and make you think that there is cancer present in the cell-free DNA,” Dr. Oxnard explained. “You screen out this interference from the white blood cells and other biologic noise, and you are left with the final features: mutations, copy number variations, and methylation signatures that then go into the final assays being studied.”
Results showed that when assay specificity was 98%, sensitivity for early-stage (stage I-IIIA) lung cancer ranged from 38% to 51%, and sensitivity for late-stage (stage IIIB-IV) lung cancer ranged from 87% to 91%.
Among five presumed cancer-free individuals having positive results on all three assays, two subsequently received a cancer diagnosis (one with stage III ovarian cancer, one with stage II endometrial cancer).
An additional 19 cancer types across all stages were tested in the CCGA substudy. Early results for breast, gastrointestinal, gynecologic, blood, and other cancers were also reported at the meeting (abstracts 536, 12021, and 12003).
Dr. Oxnard disclosed that he has a consulting or advisory role with AstraZeneca, Inivata, Boehringer Ingelheim, Takeda, Genentech/Roche, Novartis, Loxo Oncology, Ignyta, DropWorks, and GRAIL, and that he has patents, royalties, and/or other intellectual property with Chugai Pharmaceutical, Bio-Rad, Sysmex, and Guardant Health. The study was funded by GRAIL.
SOURCE: Oxnard GR et al. ASCO 2018. Abstract LBA8501.
CHICAGO – according to the first interim report from a substudy of the large, ongoing Circulating Cell-free Genome Atlas (CCGA).
“Lung cancer screening with low-dose CT is known to improve outcomes. And yet, CT-based lung cancer screening is not widely adopted,” said lead study author Geoffrey R. Oxnard, MD, associate professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the study was reported. “Criticisms of low-dose CT include the risk of false positives and overdiagnosis. We proposed to investigate an untapped opportunity for cancer detection, which is using cell-free DNA.”
Main substudy results among 164 patients with lung cancer and 923 comparable individuals without known cancer showed that at a specificity of 98%, the three assays evaluated detected up to 51% of early-stage (stage I-IIIA) lung cancers and up to 91% of late-stage (stage IIIB-IV) lung cancers. And among the healthy participants with false-positive results for lung cancer, several were ultimately found to have cancers of other types.
“This first interim analysis of the CCGA study demonstrates that comprehensive sequencing of the plasma cell-free DNA can generate high-quality data across the entire genome, and it permits noninvasive cancer detection. The assays can detect lung cancer across stages, across histologies, across populations,” Dr. Oxnard said.
“Together, these results support the promise of using cell-free, DNA-based assays to develop an early cancer detection test with high specificity. Further assay and clinical development is ongoing: There is a separate prospective trial enrolling, the STRIVE study, and there remain thousands of patients still on this CCGA study to be analyzed for further optimization and focusing of this assay towards an eventual cancer diagnostic.”
The cohort studied was not a screening population, so the assays’ performance cannot be compared with that of low-dose CT at this point, he said. But the hypothesis going forward is that the assays will have comparatively higher specificity, sparing some patients an unnecessary diagnostic work-up.
The population in which the final blood test might be used will depend on its diagnostic performance once the assays are fully refined and clinic ready, which will take some time, according to Dr. Oxnard. However, “2 years ago, this was a pipe dream. Two years ago, it was completely just a brainstorm that had no data to support it, and I didn’t believe that this could be done. Today, we actually have data to show that this is really feasible to find early-stage cancer in the blood. So this is a huge step forward and actually means that this is going to be a reality.”
“This is an important first step towards an easier way to detect lung cancer at earlier and hopefully more curable stages,” agreed ASCO Expert David Graham, MD, who is also medical director at the Levine Cancer Institute in Charlotte, N.C. “If the promise of this report holds, we could easily see a day when a person could be screened for lung cancer and possibly other cancers simply by going into their regular doctor’s office for a blood draw.”
Study details
The CCGA study has enrolled more than 12,000 of its planned 15,000 participants (70% with cancer, 30% without) across 142 U.S. and Canadian sites.
The substudy reported had a development cohort (118 patients with lung cancer, 561 individuals without cancer) and a validation cohort (46 patients with lung cancer, 362 individuals without cancer), with the lung cancer and noncancer groups matched on age, race, and body mass index. “Having a comparable control cohort is very important in developing such a diagnostic for accurate analysis of the potential false-positive rate,” Dr. Oxnard noted.
Three prototype assays were tested: A targeted sequencing assay entailing very deep sequencing across 507 genes for somatic mutations such as single-nucleotide variants and small insertions and/or deletions; a novel, whole-genome sequencing assay to detect somatic gene copy number changes; and a novel, whole-genome methylation sequencing assay to detect abnormal epigenetic changes.
Sequencing was also performed on DNA from white blood cells. “That’s very important. The white blood cells are rich with mutations that can pollute the DNA and make you think that there is cancer present in the cell-free DNA,” Dr. Oxnard explained. “You screen out this interference from the white blood cells and other biologic noise, and you are left with the final features: mutations, copy number variations, and methylation signatures that then go into the final assays being studied.”
Results showed that when assay specificity was 98%, sensitivity for early-stage (stage I-IIIA) lung cancer ranged from 38% to 51%, and sensitivity for late-stage (stage IIIB-IV) lung cancer ranged from 87% to 91%.
Among five presumed cancer-free individuals having positive results on all three assays, two subsequently received a cancer diagnosis (one with stage III ovarian cancer, one with stage II endometrial cancer).
An additional 19 cancer types across all stages were tested in the CCGA substudy. Early results for breast, gastrointestinal, gynecologic, blood, and other cancers were also reported at the meeting (abstracts 536, 12021, and 12003).
Dr. Oxnard disclosed that he has a consulting or advisory role with AstraZeneca, Inivata, Boehringer Ingelheim, Takeda, Genentech/Roche, Novartis, Loxo Oncology, Ignyta, DropWorks, and GRAIL, and that he has patents, royalties, and/or other intellectual property with Chugai Pharmaceutical, Bio-Rad, Sysmex, and Guardant Health. The study was funded by GRAIL.
SOURCE: Oxnard GR et al. ASCO 2018. Abstract LBA8501.
CHICAGO – according to the first interim report from a substudy of the large, ongoing Circulating Cell-free Genome Atlas (CCGA).
“Lung cancer screening with low-dose CT is known to improve outcomes. And yet, CT-based lung cancer screening is not widely adopted,” said lead study author Geoffrey R. Oxnard, MD, associate professor of medicine at Dana-Farber Cancer Institute and Harvard Medical School, Boston, in a press briefing at the annual meeting of the American Society of Clinical Oncology, where the study was reported. “Criticisms of low-dose CT include the risk of false positives and overdiagnosis. We proposed to investigate an untapped opportunity for cancer detection, which is using cell-free DNA.”
Main substudy results among 164 patients with lung cancer and 923 comparable individuals without known cancer showed that at a specificity of 98%, the three assays evaluated detected up to 51% of early-stage (stage I-IIIA) lung cancers and up to 91% of late-stage (stage IIIB-IV) lung cancers. And among the healthy participants with false-positive results for lung cancer, several were ultimately found to have cancers of other types.
“This first interim analysis of the CCGA study demonstrates that comprehensive sequencing of the plasma cell-free DNA can generate high-quality data across the entire genome, and it permits noninvasive cancer detection. The assays can detect lung cancer across stages, across histologies, across populations,” Dr. Oxnard said.
“Together, these results support the promise of using cell-free, DNA-based assays to develop an early cancer detection test with high specificity. Further assay and clinical development is ongoing: There is a separate prospective trial enrolling, the STRIVE study, and there remain thousands of patients still on this CCGA study to be analyzed for further optimization and focusing of this assay towards an eventual cancer diagnostic.”
The cohort studied was not a screening population, so the assays’ performance cannot be compared with that of low-dose CT at this point, he said. But the hypothesis going forward is that the assays will have comparatively higher specificity, sparing some patients an unnecessary diagnostic work-up.
The population in which the final blood test might be used will depend on its diagnostic performance once the assays are fully refined and clinic ready, which will take some time, according to Dr. Oxnard. However, “2 years ago, this was a pipe dream. Two years ago, it was completely just a brainstorm that had no data to support it, and I didn’t believe that this could be done. Today, we actually have data to show that this is really feasible to find early-stage cancer in the blood. So this is a huge step forward and actually means that this is going to be a reality.”
“This is an important first step towards an easier way to detect lung cancer at earlier and hopefully more curable stages,” agreed ASCO Expert David Graham, MD, who is also medical director at the Levine Cancer Institute in Charlotte, N.C. “If the promise of this report holds, we could easily see a day when a person could be screened for lung cancer and possibly other cancers simply by going into their regular doctor’s office for a blood draw.”
Study details
The CCGA study has enrolled more than 12,000 of its planned 15,000 participants (70% with cancer, 30% without) across 142 U.S. and Canadian sites.
The substudy reported had a development cohort (118 patients with lung cancer, 561 individuals without cancer) and a validation cohort (46 patients with lung cancer, 362 individuals without cancer), with the lung cancer and noncancer groups matched on age, race, and body mass index. “Having a comparable control cohort is very important in developing such a diagnostic for accurate analysis of the potential false-positive rate,” Dr. Oxnard noted.
Three prototype assays were tested: A targeted sequencing assay entailing very deep sequencing across 507 genes for somatic mutations such as single-nucleotide variants and small insertions and/or deletions; a novel, whole-genome sequencing assay to detect somatic gene copy number changes; and a novel, whole-genome methylation sequencing assay to detect abnormal epigenetic changes.
Sequencing was also performed on DNA from white blood cells. “That’s very important. The white blood cells are rich with mutations that can pollute the DNA and make you think that there is cancer present in the cell-free DNA,” Dr. Oxnard explained. “You screen out this interference from the white blood cells and other biologic noise, and you are left with the final features: mutations, copy number variations, and methylation signatures that then go into the final assays being studied.”
Results showed that when assay specificity was 98%, sensitivity for early-stage (stage I-IIIA) lung cancer ranged from 38% to 51%, and sensitivity for late-stage (stage IIIB-IV) lung cancer ranged from 87% to 91%.
Among five presumed cancer-free individuals having positive results on all three assays, two subsequently received a cancer diagnosis (one with stage III ovarian cancer, one with stage II endometrial cancer).
An additional 19 cancer types across all stages were tested in the CCGA substudy. Early results for breast, gastrointestinal, gynecologic, blood, and other cancers were also reported at the meeting (abstracts 536, 12021, and 12003).
Dr. Oxnard disclosed that he has a consulting or advisory role with AstraZeneca, Inivata, Boehringer Ingelheim, Takeda, Genentech/Roche, Novartis, Loxo Oncology, Ignyta, DropWorks, and GRAIL, and that he has patents, royalties, and/or other intellectual property with Chugai Pharmaceutical, Bio-Rad, Sysmex, and Guardant Health. The study was funded by GRAIL.
SOURCE: Oxnard GR et al. ASCO 2018. Abstract LBA8501.
REPORTING FROM ASCO 2018
Key clinical point: Three blood-based assays performed moderately well for identifying lung cancer in early, potentially curable stages.
Major finding: At 98% specificity, the assays had sensitivities of 38%-51% for detecting lung cancers of stage I-IIIA.
Study details: A case-control study of circulating cell-free DNA assays among 164 patients with lung cancer and 923 comparable individuals without cancer.
Disclosures: Dr. Oxnard disclosed that he has a consulting or advisory role with AstraZeneca, Inivata, Boehringer Ingelheim, Takeda, Genentech/Roche, Novartis, Loxo Oncology, Ignyta, DropWorks, and GRAIL, and that he has patents, royalties, and/or other intellectual property with Chugai Pharmaceutical, Bio-Rad, Sysmex, and Guardant Health. The study was funded by GRAIL.
Source: Oxnard GR et al. ASCO 2018. Abstract LBA8501.
What Are Predictors of Mortality in Veterans With MS?
A retrospective study finds that 39% of patients who died during follow-up were never on a disease-modifying therapy, compared with 22% of those who were still alive.
NASHVILLE—Among veterans with multiple sclerosis (MS), excess MS-related mortality is mainly influenced by initial presentation with progressive MS, sensory and cerebellar complaints, and higher levels of disability. Excess mortality also may be influenced by motor complaints and low BMI, according to research presented at the 2018 CMSC Annual Meeting. Main causes of death include MS itself, infection, respiratory disease, and cancer.
These findings suggest a need to pay more attention “to preventive strategies such as yearly influenza immunization, aggressively treating MS-related complications, and comorbidities, especially vascular risk factors,” said the researchers.
Studying mortality in chronic neurologic diseases may help identify treatable risk factors, and population-based studies of English death records have found that about 64% of patients with MS have a neurologic cause of death.
To identify the predictors of mortality in veterans with MS attending outpatient clinics, Meheroz H. Rabadi, MD, Clinical Professor of Neurology at the University of Oklahoma College of Medicine and Medical Director of the Oklahoma City Veterans Affairs Medical Center MS Program, and Christopher E. Aston, PhD, Associate Research Professor of Pediatrics and a biostatistician at the University of Oklahoma Sciences Center, conducted a retrospective study.
Data From a Veterans Affairs Medical Center
The researchers conducted a retrospective electronic chart review of data from 229 veterans with MS diagnosed based on the McDonald criteria who were registered in the MS program at the Oklahoma City Veterans Affairs Medical Center between January 1, 2000, and December 31, 2014. Participants were followed up every four months in the clinic.
Data included age at initial clinic visit, gender, ethnicity and race, age at MS diagnosis, clinical MS subtype (ie, relapsing-remitting, secondary progressive, primary progressive, clinically isolated syndrome, or radiologically isolated syndrome), and initial presenting features (eg, visual complaints, motor weakness, balance disorder, and sensory complaints).
Drs. Rabadi and Aston determined an impairment index based on the presence or absence of motor and nonmotor signs on initial examination. MS severity was measured by initial Expanded Disability Status Scale and total Functional Independence Measure scores.
The researchers recorded the presence of pre-existing and new-onset comorbidities that are commonly encountered in veterans and are the most common causes of disability and death in the United States, such as hypertension, hyperlipidemia, diabetes mellitus, BMI, and history of smoking. They also recorded the presence of MS-related complications such as pressure ulcers, neurogenic bowel, and neurogenic bladder.
Main Causes of Death
A total of 226 participants were included in the analysis; 17% were female. Most participants were white (81%), 13% were black, 1% were Hispanic, and 2% were Native American.
The mortality rate at the end of the 15-year study period was 14%. Among the 33 patients who died, the main causes of death documented were MS disease itself (57% of cases), infection (43%), cancer (18%), and respiratory failure (18%). Cox regression analysis using the whole cohort found that significant predictors of mortality were progressive MS type; older age at entry into the study; the presence of sensory, cerebellar, or motor complaints on presentation; more disability on presentation; lower BMI; diabetes; not having been on disease-modifying therapy; and the presence of pressure ulcers or neurogenic bladder.
Among patients who died during follow up, 36% had primary progressive MS, compared with 17% of patients who were alive; 42% of patients who died had secondary progressive MS, compared with 21% of those who were alive.
In addition, patients who died had an average age of 56 at study entry, compared with an average age of 48 among those who were alive. BMI among those who died was 23.7, compared with 28 among patients who were alive. Thirty-nine percent of patients who died were never on a disease-modifying therapy, compared with 22% of patients who were alive. Thirty-three percent of patients who died had diabetes mellitus, compared with 16% of those who were alive. Finally, 12% of patients who died had pressure ulcers, compared with 2% of patients who were alive, and 82% of patients who died had neurogenic bladder, compared with 53% of patients who were alive.
—Erica Tricarico
A retrospective study finds that 39% of patients who died during follow-up were never on a disease-modifying therapy, compared with 22% of those who were still alive.
A retrospective study finds that 39% of patients who died during follow-up were never on a disease-modifying therapy, compared with 22% of those who were still alive.
NASHVILLE—Among veterans with multiple sclerosis (MS), excess MS-related mortality is mainly influenced by initial presentation with progressive MS, sensory and cerebellar complaints, and higher levels of disability. Excess mortality also may be influenced by motor complaints and low BMI, according to research presented at the 2018 CMSC Annual Meeting. Main causes of death include MS itself, infection, respiratory disease, and cancer.
These findings suggest a need to pay more attention “to preventive strategies such as yearly influenza immunization, aggressively treating MS-related complications, and comorbidities, especially vascular risk factors,” said the researchers.
Studying mortality in chronic neurologic diseases may help identify treatable risk factors, and population-based studies of English death records have found that about 64% of patients with MS have a neurologic cause of death.
To identify the predictors of mortality in veterans with MS attending outpatient clinics, Meheroz H. Rabadi, MD, Clinical Professor of Neurology at the University of Oklahoma College of Medicine and Medical Director of the Oklahoma City Veterans Affairs Medical Center MS Program, and Christopher E. Aston, PhD, Associate Research Professor of Pediatrics and a biostatistician at the University of Oklahoma Sciences Center, conducted a retrospective study.
Data From a Veterans Affairs Medical Center
The researchers conducted a retrospective electronic chart review of data from 229 veterans with MS diagnosed based on the McDonald criteria who were registered in the MS program at the Oklahoma City Veterans Affairs Medical Center between January 1, 2000, and December 31, 2014. Participants were followed up every four months in the clinic.
Data included age at initial clinic visit, gender, ethnicity and race, age at MS diagnosis, clinical MS subtype (ie, relapsing-remitting, secondary progressive, primary progressive, clinically isolated syndrome, or radiologically isolated syndrome), and initial presenting features (eg, visual complaints, motor weakness, balance disorder, and sensory complaints).
Drs. Rabadi and Aston determined an impairment index based on the presence or absence of motor and nonmotor signs on initial examination. MS severity was measured by initial Expanded Disability Status Scale and total Functional Independence Measure scores.
The researchers recorded the presence of pre-existing and new-onset comorbidities that are commonly encountered in veterans and are the most common causes of disability and death in the United States, such as hypertension, hyperlipidemia, diabetes mellitus, BMI, and history of smoking. They also recorded the presence of MS-related complications such as pressure ulcers, neurogenic bowel, and neurogenic bladder.
Main Causes of Death
A total of 226 participants were included in the analysis; 17% were female. Most participants were white (81%), 13% were black, 1% were Hispanic, and 2% were Native American.
The mortality rate at the end of the 15-year study period was 14%. Among the 33 patients who died, the main causes of death documented were MS disease itself (57% of cases), infection (43%), cancer (18%), and respiratory failure (18%). Cox regression analysis using the whole cohort found that significant predictors of mortality were progressive MS type; older age at entry into the study; the presence of sensory, cerebellar, or motor complaints on presentation; more disability on presentation; lower BMI; diabetes; not having been on disease-modifying therapy; and the presence of pressure ulcers or neurogenic bladder.
Among patients who died during follow up, 36% had primary progressive MS, compared with 17% of patients who were alive; 42% of patients who died had secondary progressive MS, compared with 21% of those who were alive.
In addition, patients who died had an average age of 56 at study entry, compared with an average age of 48 among those who were alive. BMI among those who died was 23.7, compared with 28 among patients who were alive. Thirty-nine percent of patients who died were never on a disease-modifying therapy, compared with 22% of patients who were alive. Thirty-three percent of patients who died had diabetes mellitus, compared with 16% of those who were alive. Finally, 12% of patients who died had pressure ulcers, compared with 2% of patients who were alive, and 82% of patients who died had neurogenic bladder, compared with 53% of patients who were alive.
—Erica Tricarico
NASHVILLE—Among veterans with multiple sclerosis (MS), excess MS-related mortality is mainly influenced by initial presentation with progressive MS, sensory and cerebellar complaints, and higher levels of disability. Excess mortality also may be influenced by motor complaints and low BMI, according to research presented at the 2018 CMSC Annual Meeting. Main causes of death include MS itself, infection, respiratory disease, and cancer.
These findings suggest a need to pay more attention “to preventive strategies such as yearly influenza immunization, aggressively treating MS-related complications, and comorbidities, especially vascular risk factors,” said the researchers.
Studying mortality in chronic neurologic diseases may help identify treatable risk factors, and population-based studies of English death records have found that about 64% of patients with MS have a neurologic cause of death.
To identify the predictors of mortality in veterans with MS attending outpatient clinics, Meheroz H. Rabadi, MD, Clinical Professor of Neurology at the University of Oklahoma College of Medicine and Medical Director of the Oklahoma City Veterans Affairs Medical Center MS Program, and Christopher E. Aston, PhD, Associate Research Professor of Pediatrics and a biostatistician at the University of Oklahoma Sciences Center, conducted a retrospective study.
Data From a Veterans Affairs Medical Center
The researchers conducted a retrospective electronic chart review of data from 229 veterans with MS diagnosed based on the McDonald criteria who were registered in the MS program at the Oklahoma City Veterans Affairs Medical Center between January 1, 2000, and December 31, 2014. Participants were followed up every four months in the clinic.
Data included age at initial clinic visit, gender, ethnicity and race, age at MS diagnosis, clinical MS subtype (ie, relapsing-remitting, secondary progressive, primary progressive, clinically isolated syndrome, or radiologically isolated syndrome), and initial presenting features (eg, visual complaints, motor weakness, balance disorder, and sensory complaints).
Drs. Rabadi and Aston determined an impairment index based on the presence or absence of motor and nonmotor signs on initial examination. MS severity was measured by initial Expanded Disability Status Scale and total Functional Independence Measure scores.
The researchers recorded the presence of pre-existing and new-onset comorbidities that are commonly encountered in veterans and are the most common causes of disability and death in the United States, such as hypertension, hyperlipidemia, diabetes mellitus, BMI, and history of smoking. They also recorded the presence of MS-related complications such as pressure ulcers, neurogenic bowel, and neurogenic bladder.
Main Causes of Death
A total of 226 participants were included in the analysis; 17% were female. Most participants were white (81%), 13% were black, 1% were Hispanic, and 2% were Native American.
The mortality rate at the end of the 15-year study period was 14%. Among the 33 patients who died, the main causes of death documented were MS disease itself (57% of cases), infection (43%), cancer (18%), and respiratory failure (18%). Cox regression analysis using the whole cohort found that significant predictors of mortality were progressive MS type; older age at entry into the study; the presence of sensory, cerebellar, or motor complaints on presentation; more disability on presentation; lower BMI; diabetes; not having been on disease-modifying therapy; and the presence of pressure ulcers or neurogenic bladder.
Among patients who died during follow up, 36% had primary progressive MS, compared with 17% of patients who were alive; 42% of patients who died had secondary progressive MS, compared with 21% of those who were alive.
In addition, patients who died had an average age of 56 at study entry, compared with an average age of 48 among those who were alive. BMI among those who died was 23.7, compared with 28 among patients who were alive. Thirty-nine percent of patients who died were never on a disease-modifying therapy, compared with 22% of patients who were alive. Thirty-three percent of patients who died had diabetes mellitus, compared with 16% of those who were alive. Finally, 12% of patients who died had pressure ulcers, compared with 2% of patients who were alive, and 82% of patients who died had neurogenic bladder, compared with 53% of patients who were alive.
—Erica Tricarico
Allergies linked to autism spectrum disorder in children
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).

Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).
Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The results of this study add to a “growing body of literature supporting an immune-mediated subtype of autism spectrum disorder (ASD),” Christopher J. McDougle, MD, wrote in an editorial published with the study.
Although prior studies have identified an association between ASD and respiratory and skin allergy, this study is “the first to document the association of food allergy with ASD with confidence, in part based on the large sample size they accessed,” he said (JAMA Network Open. 2018;1[2]:e180280. doi: 10.1001/jamanetworkopen.2018.0280).
Dr. McDougle is affiliated with the Lurie Center for Autism at Massachusetts General Hospital.
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
The prevalence of food, respiratory, and skin allergy is greater in U.S. children with autism spectrum disorder (ASD) than in U.S. children without the disorder, according to findings published June 8 in JAMA Network Open.
An analysis of data from the National Health Interview Survey found that the weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Survey data were collected between 1997 and 2016, and included patients aged 3-17 years. Allergic conditions were defined by the respondent, usually a parent, answering in the affirmative that the child had any kind of food, digestive, respiratory, or skin allergy in the past 12 months. ASD was defined based on an affirmative response to a question asking whether the child received an ASD diagnosis from a health professional. The question was asked as part of a 10-condition checklist from 1997 to 2013, and as a standalone item from 2014 onward, with revised wording to distinguish autism, Asperger’s disorder, pervasive developmental disorder, and ASD, wrote Guifeng Xu, MD, of the department of epidemiology at the University of Iowa, Iowa City, and her coauthors.
Of the 199,520 children included in the study, 8,734 had food allergy, 24,555 had respiratory allergy, and 19,399 had skin allergy. An ASD diagnosis was reported in 1,868 children. The weighted prevalence was 4.31% for food allergy (95% confidence interval, 4.20%-4.43%), 12.15% for respiratory allergy (95% CI, 11.92%-12.38%), and 9.91% for skin allergy (95% CI, 9.72%-10.10%), the authors said.
Children with ASD were more likely than were children without ASD to have food allergy, respiratory allergy, and skin allergy (P less than .001). After adjustment for factors including age, sex, ethnicity, and family education level, the odds ratio of ASD was more than double among children with food allergy, compared with those without food allergy (odds ratio, 2.72; 95% CI, 2.26-3.28; P less than .001).
Respiratory allergy and skin allergy also were significantly associated with ASD, but to a lesser degree, with an OR of 1.53 (95% CI, 1.32-1.78; P less than .001) for respiratory allergy and 1.80 (95% CI, 1.55-2.09; P less than .001) for skin allergy, Dr. Xu and her colleagues reported.
,” though the underlying mechanisms still need to be identified, the authors wrote.
Particularly striking were the connections found between ASD and food allergy. “Although the underlying mechanisms for the observed association between food allergy and ASD remain to be elucidated, the gut-brain-behavior axis could be one of the potential mechanisms,” Dr. Xu and her coauthors wrote. “Previous studies found higher prevalence of gastrointestinal symptoms among children with ASD.”
Limitations to the study include possible recall bias and misreporting, as well as an absence of information about onset of allergy and ASD diagnosis.
“Large prospective cohort studies starting from birth or early life are needed to confirm our findings,” the authors concluded.
No conflicts of interest were reported.
SOURCE: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
FROM JAMA NETWORK OPEN
Key clinical point: The prevalence of food, respiratory, and skin allergy was greater in children with autism spectrum disorder (ASD).
Major finding: The weighted prevalence of food, respiratory, and skin allergies was 11.25%, 18.73%, and 16.81%, respectively, in children with ASD, compared with 4.25%, 12.08%, and 9.84%, respectively, in children without ASD (P less than .001).
Study details: A population-based study of 199,520 children aged 3-17 years in the National Health Interview Survey.
Disclosures: No conflicts of interest were reported.
Source: Guifeng X et al. JAMA Network Open. 2018 Jun 8. doi: 10.1001/jamanetworkopen.2018.0279.
Cladribine Tablets Improve MRI Outcomes in Patients With Highly Active Relapsing-Remitting MS
The relative risk ratio for cumulative new T1 gadolinium-enhancing lesions was significantly lower in the cladribine 3.5 mg/kg group, compared with placebo.
NASHVILLE—Treatment with cladribine tablets 3.5 mg/kg reduces MRI markers of disease activity in patients with highly active relapsing-remitting multiple sclerosis (MS), according to research described at the 2018 CMSC Annual Meeting. Results of a post hoc analysis of the CLARITY study indicated that in patients with relapsing MS who were selected for further study based on high disease activity, treatment with cladribine tablets 3.5 mg/kg showed efficacy in reducing MRI markers of disease activity comparable with the overall CLARITY study population.
In the CLARITY study, treatment with cladribine tablets versus placebo showed strong efficacy in a large cohort of patients with relapsing MS over two years. Because patients with high disease activity have a high risk of relapses and disability, Gavin Giovannoni, MBBCh, PhD, and his CLARITY collaborators conducted a post hoc analysis to compare the effects of cladribine tablets 3.5 mg/kg versus placebo on outcomes assessed by MRI in subgroups of CLARITY patients with evidence of high disease activity at study entry. Professor Giovannoni is Chair of Neurology at the Blizard Institute of Cell and Molecular Science, Barts and the London School of Medicine and Dentistry at Queen Mary University of London.

The researchers retrospectively analyzed CLARITY participants randomized to cladribine tablets 3.5 mg/kg or placebo using the following two sets of high disease activity criteria based on relapse history, prior treatment, and MRI characteristics: 1) high relapse activity, which was defined as two or more relapses during the year before study entry whether on disease-modifying therapy or not; 2) high relapse activity plus treatment nonresponse, in which treatment nonresponse was defined as one or more relapses and one or more T1 gadolinium-enhancing lesions or nine or more T2 lesions during the year before study entry and while on therapy with other disease-modifying therapy.
For cumulative new T1 gadolinium-enhancing lesions, the relative risk ratio in the high relapse activity subgroup (0.087) was significantly lower in favor of cladribine tablets 3.5 mg/kg (n = 130) over placebo (n = 131). In the high relapse activity plus treatment nonresponse subgroup, the relative risk ratio (0.077) also significantly favored cladribine tablets 3.5 mg/kg (n = 140) versus placebo (n = 149). The risk reductions (91% and 92%, respectively) were similar to the 90% reduction in the overall CLARITY population (0.097), said the researchers.
For cumulative active T2 lesions, the relative risk ratio also significantly favored cladribine tablets 3.5 mg/kg versus placebo for the high relapse activity (0.263) and the high relapse activity plus treatment nonresponse subgroups (0.254), with risk reductions of 74% and 75%, reflecting the 73% reduction in the overall population (0.272).
The relative risk ratio for cumulative combined unique active lesions significantly favored cladribine tablets 3.5 mg/kg versus placebo for high relapse activity (0.212) and high relapse activity plus treatment nonresponse (0.203) with risk reductions of 79% and 80%, reflecting the 77% overall population reduction (0.234). Comparable results were observed in the non-high-disease activity counterparts, with no significant treatment-subgroup interactions.
—Erica Tricarico
Suggested Reading
Giovannoni G, Soelberg Sorensen P, Cook S, et al. Efficacy of cladribine tablets in high disease activity subgroups of patients with relapsing multiple sclerosis: A post hoc analysis of the CLARITY Study. Mult Scler. 2018 April 1 [Epub ahead of print].
The relative risk ratio for cumulative new T1 gadolinium-enhancing lesions was significantly lower in the cladribine 3.5 mg/kg group, compared with placebo.
The relative risk ratio for cumulative new T1 gadolinium-enhancing lesions was significantly lower in the cladribine 3.5 mg/kg group, compared with placebo.
NASHVILLE—Treatment with cladribine tablets 3.5 mg/kg reduces MRI markers of disease activity in patients with highly active relapsing-remitting multiple sclerosis (MS), according to research described at the 2018 CMSC Annual Meeting. Results of a post hoc analysis of the CLARITY study indicated that in patients with relapsing MS who were selected for further study based on high disease activity, treatment with cladribine tablets 3.5 mg/kg showed efficacy in reducing MRI markers of disease activity comparable with the overall CLARITY study population.
In the CLARITY study, treatment with cladribine tablets versus placebo showed strong efficacy in a large cohort of patients with relapsing MS over two years. Because patients with high disease activity have a high risk of relapses and disability, Gavin Giovannoni, MBBCh, PhD, and his CLARITY collaborators conducted a post hoc analysis to compare the effects of cladribine tablets 3.5 mg/kg versus placebo on outcomes assessed by MRI in subgroups of CLARITY patients with evidence of high disease activity at study entry. Professor Giovannoni is Chair of Neurology at the Blizard Institute of Cell and Molecular Science, Barts and the London School of Medicine and Dentistry at Queen Mary University of London.
The researchers retrospectively analyzed CLARITY participants randomized to cladribine tablets 3.5 mg/kg or placebo using the following two sets of high disease activity criteria based on relapse history, prior treatment, and MRI characteristics: 1) high relapse activity, which was defined as two or more relapses during the year before study entry whether on disease-modifying therapy or not; 2) high relapse activity plus treatment nonresponse, in which treatment nonresponse was defined as one or more relapses and one or more T1 gadolinium-enhancing lesions or nine or more T2 lesions during the year before study entry and while on therapy with other disease-modifying therapy.
For cumulative new T1 gadolinium-enhancing lesions, the relative risk ratio in the high relapse activity subgroup (0.087) was significantly lower in favor of cladribine tablets 3.5 mg/kg (n = 130) over placebo (n = 131). In the high relapse activity plus treatment nonresponse subgroup, the relative risk ratio (0.077) also significantly favored cladribine tablets 3.5 mg/kg (n = 140) versus placebo (n = 149). The risk reductions (91% and 92%, respectively) were similar to the 90% reduction in the overall CLARITY population (0.097), said the researchers.
For cumulative active T2 lesions, the relative risk ratio also significantly favored cladribine tablets 3.5 mg/kg versus placebo for the high relapse activity (0.263) and the high relapse activity plus treatment nonresponse subgroups (0.254), with risk reductions of 74% and 75%, reflecting the 73% reduction in the overall population (0.272).
The relative risk ratio for cumulative combined unique active lesions significantly favored cladribine tablets 3.5 mg/kg versus placebo for high relapse activity (0.212) and high relapse activity plus treatment nonresponse (0.203) with risk reductions of 79% and 80%, reflecting the 77% overall population reduction (0.234). Comparable results were observed in the non-high-disease activity counterparts, with no significant treatment-subgroup interactions.
—Erica Tricarico
Suggested Reading
Giovannoni G, Soelberg Sorensen P, Cook S, et al. Efficacy of cladribine tablets in high disease activity subgroups of patients with relapsing multiple sclerosis: A post hoc analysis of the CLARITY Study. Mult Scler. 2018 April 1 [Epub ahead of print].
NASHVILLE—Treatment with cladribine tablets 3.5 mg/kg reduces MRI markers of disease activity in patients with highly active relapsing-remitting multiple sclerosis (MS), according to research described at the 2018 CMSC Annual Meeting. Results of a post hoc analysis of the CLARITY study indicated that in patients with relapsing MS who were selected for further study based on high disease activity, treatment with cladribine tablets 3.5 mg/kg showed efficacy in reducing MRI markers of disease activity comparable with the overall CLARITY study population.
In the CLARITY study, treatment with cladribine tablets versus placebo showed strong efficacy in a large cohort of patients with relapsing MS over two years. Because patients with high disease activity have a high risk of relapses and disability, Gavin Giovannoni, MBBCh, PhD, and his CLARITY collaborators conducted a post hoc analysis to compare the effects of cladribine tablets 3.5 mg/kg versus placebo on outcomes assessed by MRI in subgroups of CLARITY patients with evidence of high disease activity at study entry. Professor Giovannoni is Chair of Neurology at the Blizard Institute of Cell and Molecular Science, Barts and the London School of Medicine and Dentistry at Queen Mary University of London.
The researchers retrospectively analyzed CLARITY participants randomized to cladribine tablets 3.5 mg/kg or placebo using the following two sets of high disease activity criteria based on relapse history, prior treatment, and MRI characteristics: 1) high relapse activity, which was defined as two or more relapses during the year before study entry whether on disease-modifying therapy or not; 2) high relapse activity plus treatment nonresponse, in which treatment nonresponse was defined as one or more relapses and one or more T1 gadolinium-enhancing lesions or nine or more T2 lesions during the year before study entry and while on therapy with other disease-modifying therapy.
For cumulative new T1 gadolinium-enhancing lesions, the relative risk ratio in the high relapse activity subgroup (0.087) was significantly lower in favor of cladribine tablets 3.5 mg/kg (n = 130) over placebo (n = 131). In the high relapse activity plus treatment nonresponse subgroup, the relative risk ratio (0.077) also significantly favored cladribine tablets 3.5 mg/kg (n = 140) versus placebo (n = 149). The risk reductions (91% and 92%, respectively) were similar to the 90% reduction in the overall CLARITY population (0.097), said the researchers.
For cumulative active T2 lesions, the relative risk ratio also significantly favored cladribine tablets 3.5 mg/kg versus placebo for the high relapse activity (0.263) and the high relapse activity plus treatment nonresponse subgroups (0.254), with risk reductions of 74% and 75%, reflecting the 73% reduction in the overall population (0.272).
The relative risk ratio for cumulative combined unique active lesions significantly favored cladribine tablets 3.5 mg/kg versus placebo for high relapse activity (0.212) and high relapse activity plus treatment nonresponse (0.203) with risk reductions of 79% and 80%, reflecting the 77% overall population reduction (0.234). Comparable results were observed in the non-high-disease activity counterparts, with no significant treatment-subgroup interactions.
—Erica Tricarico
Suggested Reading
Giovannoni G, Soelberg Sorensen P, Cook S, et al. Efficacy of cladribine tablets in high disease activity subgroups of patients with relapsing multiple sclerosis: A post hoc analysis of the CLARITY Study. Mult Scler. 2018 April 1 [Epub ahead of print].
Caring for the offensive patient
“I only see Jewish doctors.”
The middle-aged lady across my desk repeated that several times during her visit, apparently hoping to get some response from me. I just ignored it each time.

Imagine if she’d said, “I only see white doctors,” or “I only see black doctors.” To say you came to a doctor solely because of his or her ethnicity is, to me, ignorant at best and blatant discrimination at worst.
Of course, I continued the appointment. While I found her comment offensive, I’m a doctor. Unlike a restaurant owner, I can’t refuse to serve someone because of their personal beliefs, no matter how much I disagree. I took an oath to provide equal care to all, regardless of personal differences. I try hard to measure up to that.
We live in a world that seems to be increasingly divided along tribal lines. Us against them. Me against you. Everyone for themselves.
I’m not going to play that game. For better or worse, I’ll take the high road and continue treating all people as equal. If you want to believe that religion, or color, or any other difference makes someone a better or worse physician (or person, for that matter), you’re entitled to your opinion.
I may not be able to change your mind, but that’s not going to stop me from trying to be the best doctor I can to everyone who comes to me, regardless of who they are.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“I only see Jewish doctors.”
The middle-aged lady across my desk repeated that several times during her visit, apparently hoping to get some response from me. I just ignored it each time.
Imagine if she’d said, “I only see white doctors,” or “I only see black doctors.” To say you came to a doctor solely because of his or her ethnicity is, to me, ignorant at best and blatant discrimination at worst.
Of course, I continued the appointment. While I found her comment offensive, I’m a doctor. Unlike a restaurant owner, I can’t refuse to serve someone because of their personal beliefs, no matter how much I disagree. I took an oath to provide equal care to all, regardless of personal differences. I try hard to measure up to that.
We live in a world that seems to be increasingly divided along tribal lines. Us against them. Me against you. Everyone for themselves.
I’m not going to play that game. For better or worse, I’ll take the high road and continue treating all people as equal. If you want to believe that religion, or color, or any other difference makes someone a better or worse physician (or person, for that matter), you’re entitled to your opinion.
I may not be able to change your mind, but that’s not going to stop me from trying to be the best doctor I can to everyone who comes to me, regardless of who they are.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
“I only see Jewish doctors.”
The middle-aged lady across my desk repeated that several times during her visit, apparently hoping to get some response from me. I just ignored it each time.
Imagine if she’d said, “I only see white doctors,” or “I only see black doctors.” To say you came to a doctor solely because of his or her ethnicity is, to me, ignorant at best and blatant discrimination at worst.
Of course, I continued the appointment. While I found her comment offensive, I’m a doctor. Unlike a restaurant owner, I can’t refuse to serve someone because of their personal beliefs, no matter how much I disagree. I took an oath to provide equal care to all, regardless of personal differences. I try hard to measure up to that.
We live in a world that seems to be increasingly divided along tribal lines. Us against them. Me against you. Everyone for themselves.
I’m not going to play that game. For better or worse, I’ll take the high road and continue treating all people as equal. If you want to believe that religion, or color, or any other difference makes someone a better or worse physician (or person, for that matter), you’re entitled to your opinion.
I may not be able to change your mind, but that’s not going to stop me from trying to be the best doctor I can to everyone who comes to me, regardless of who they are.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Everolimus/exemestane improves PFS of ER+/HER2– breast cancer vs. everolimus alone
CHICAGO – For women with estrogen receptor–positive breast cancer resistant to endocrine therapy, the combination of everolimus and exemestane had better efficacy than did everolimus alone, but single-agent capecitabine appeared to offer benefit comparable to that of the combination therapy, results of the BOLERO-6 trial suggest.
Among 309 postmenopausal women with ER-positive, HER2-negative advanced breast cancer, the combination of everolimus (Afinitor) and exemestane (Aromasin and generics) was associated with a 26% improvement in progression-free survival (PFS) compared with everolimus alone, reported Guy Jerusalem, MD, PhD, of Liege University, Belgium.
There was also, however, a numerical but not statistically significant difference in PFS favoring capecitabine (Xeloda and generics) “which may be attributed to various baseline characteristics favoring capecitabine, and potential informative censoring,” he said at the annual meeting of the American Society of Clinical Oncology.
“We have noted in BOLERO-6 a better-than-expected outcome in median progression-free survival of capecitabine compared with the previously reported 4.1 to 7.9 months median progression-free survival,” he said.
BOLERO-6, results of which were published online June 3 in JAMA Oncology, was a postmarketing study by the sponsors to fulfill commitments to both the Food and Drug Administration and the European Medicines Agency to estimate the treatment benefit with combined everolimus and exemestane vs. monotherapy with everolimus or capecitabine in patients with ER-positive, HER2-negative breast cancer that progressed during nonsteroidal aromatase inhibitor therapy.
Patients from 83 centers in 18 countries were enrolled in the open label, phase 2 study and randomly assigned to receive oral everolimus 10 mg daily with oral exemestane 25 mg daily, everolimus at the same dose alone, or oral capecitabine 1,250 mg/m2 twice daily for 2 weeks on, 1 week off.
The trial was not powered for statistical comparisons between arms, but was instead designed with the primary objective of estimated investigator-assessed PFS for the combination vs. everolimus alone.
At baseline, more patients assigned to capecitabine vs. everolimus-containing regimens were younger than 65, white, had an Eastern Cooperative Oncology Group status of 0 (fully active), and had bone-only metastases. In addition, fewer patients in the capecitabine arm had three or more metastatic sites, Dr. Jerusalem noted,
For the primary analysis, the median PFS with everolimus/exemestane was 8.4 months, compared with 6.8 months for everolimus alone. The estimated hazard ratio (HR) for PFS with everolimus/exemestane vs. everolimus alone was 0.74 (90% confidence interval [CI], 0.57-0.97)
In contrast, median PFS with capecitabine was 9.6 months, with a nonsignificant hazard ratio of 1.26 for the combination (90% CI, 0.96-1.66).
A stratified multivariate Cox regression model controlling for baseline difference and known prognostic factor yielded an HR for PFS of 1.15 (90% CI, 0.86-1.52) for the combination.
Censoring of patients was more frequent in the capecitabine arm (33% vs. 23% in the combination arm), which included 20% of patients on capecitabine who were censored for starting on a new antineoplastic therapy vs. 9% of patients on everolimus/exemestane.
The median time to treatment failure was 5.8 months with the combination, vs. 4.2 months with everolimus alone (HR, 0.66, 90% CI, 0.52-0.4), and 6.2 months with capecitabine alone (HR, 1.03, 90% CI, 0.81-1.31).
Median overall survival was 23.1 months in the combination arm, 29.3 months in the everolimus arm, and 25.6 months in the capecitabine arm. There were no statistically significant differences in overall survival among the groups.
Grade 3 or greater adverse events were more frequent in the combination vs. everolimus arms, and comparable between the combination and capecitabine arms, Dr. Jerusalem said.
Serious adverse events of any grade were more frequent in the combination arm than in the other two arms, but there were no significant differences in discontinuations due to adverse events
“The results of the present study suggest that mTOR inhibitor and endocrine therapy combinations remain important for aromatase inhibitor–refractory disease. Safety and PFS with everolimus plus exemestane in this study were consistent with BOLERO-2 and are now supported by real-world evidence,” the investigators wrote.
“The take home from the BOLERO-6 trial is that the progression-free survival for the combination of everolimus and exemestane is superior to everolimus alone, and is in line with data from the BOLERO-2 trial, and also the PrE0102 study, demonstrating the consistent activity of mTOR inhibition in combination with endocrine therapy in the aromatase inhibitor resistance setting, and this supports our use of the combination in the endocrine resistant patients,” said Cynthia X. Ma, MD, PhD, of Washington University, St. Louis, the invited discussant.
Novartis funded the study. Dr Jerusalem received research funding from Novartis and Roche; honoraria from Novartis, Roche, Pfizer, Lilly, Celgene, Amgen, BMS, and Puma Technology; and nonfinancial support from Novartis, Roche, Pfizer, Lilly, Amgen, and BMS. Dr. Ma reported consulting/advising, travel expenses, and institutional research funding from Novartis and others.
SOURCE: Jerusalem G et al. ASCO 2018 Abstract 1005
CHICAGO – For women with estrogen receptor–positive breast cancer resistant to endocrine therapy, the combination of everolimus and exemestane had better efficacy than did everolimus alone, but single-agent capecitabine appeared to offer benefit comparable to that of the combination therapy, results of the BOLERO-6 trial suggest.
Among 309 postmenopausal women with ER-positive, HER2-negative advanced breast cancer, the combination of everolimus (Afinitor) and exemestane (Aromasin and generics) was associated with a 26% improvement in progression-free survival (PFS) compared with everolimus alone, reported Guy Jerusalem, MD, PhD, of Liege University, Belgium.
There was also, however, a numerical but not statistically significant difference in PFS favoring capecitabine (Xeloda and generics) “which may be attributed to various baseline characteristics favoring capecitabine, and potential informative censoring,” he said at the annual meeting of the American Society of Clinical Oncology.
“We have noted in BOLERO-6 a better-than-expected outcome in median progression-free survival of capecitabine compared with the previously reported 4.1 to 7.9 months median progression-free survival,” he said.
BOLERO-6, results of which were published online June 3 in JAMA Oncology, was a postmarketing study by the sponsors to fulfill commitments to both the Food and Drug Administration and the European Medicines Agency to estimate the treatment benefit with combined everolimus and exemestane vs. monotherapy with everolimus or capecitabine in patients with ER-positive, HER2-negative breast cancer that progressed during nonsteroidal aromatase inhibitor therapy.
Patients from 83 centers in 18 countries were enrolled in the open label, phase 2 study and randomly assigned to receive oral everolimus 10 mg daily with oral exemestane 25 mg daily, everolimus at the same dose alone, or oral capecitabine 1,250 mg/m2 twice daily for 2 weeks on, 1 week off.
The trial was not powered for statistical comparisons between arms, but was instead designed with the primary objective of estimated investigator-assessed PFS for the combination vs. everolimus alone.
At baseline, more patients assigned to capecitabine vs. everolimus-containing regimens were younger than 65, white, had an Eastern Cooperative Oncology Group status of 0 (fully active), and had bone-only metastases. In addition, fewer patients in the capecitabine arm had three or more metastatic sites, Dr. Jerusalem noted,
For the primary analysis, the median PFS with everolimus/exemestane was 8.4 months, compared with 6.8 months for everolimus alone. The estimated hazard ratio (HR) for PFS with everolimus/exemestane vs. everolimus alone was 0.74 (90% confidence interval [CI], 0.57-0.97)
In contrast, median PFS with capecitabine was 9.6 months, with a nonsignificant hazard ratio of 1.26 for the combination (90% CI, 0.96-1.66).
A stratified multivariate Cox regression model controlling for baseline difference and known prognostic factor yielded an HR for PFS of 1.15 (90% CI, 0.86-1.52) for the combination.
Censoring of patients was more frequent in the capecitabine arm (33% vs. 23% in the combination arm), which included 20% of patients on capecitabine who were censored for starting on a new antineoplastic therapy vs. 9% of patients on everolimus/exemestane.
The median time to treatment failure was 5.8 months with the combination, vs. 4.2 months with everolimus alone (HR, 0.66, 90% CI, 0.52-0.4), and 6.2 months with capecitabine alone (HR, 1.03, 90% CI, 0.81-1.31).
Median overall survival was 23.1 months in the combination arm, 29.3 months in the everolimus arm, and 25.6 months in the capecitabine arm. There were no statistically significant differences in overall survival among the groups.
Grade 3 or greater adverse events were more frequent in the combination vs. everolimus arms, and comparable between the combination and capecitabine arms, Dr. Jerusalem said.
Serious adverse events of any grade were more frequent in the combination arm than in the other two arms, but there were no significant differences in discontinuations due to adverse events
“The results of the present study suggest that mTOR inhibitor and endocrine therapy combinations remain important for aromatase inhibitor–refractory disease. Safety and PFS with everolimus plus exemestane in this study were consistent with BOLERO-2 and are now supported by real-world evidence,” the investigators wrote.
“The take home from the BOLERO-6 trial is that the progression-free survival for the combination of everolimus and exemestane is superior to everolimus alone, and is in line with data from the BOLERO-2 trial, and also the PrE0102 study, demonstrating the consistent activity of mTOR inhibition in combination with endocrine therapy in the aromatase inhibitor resistance setting, and this supports our use of the combination in the endocrine resistant patients,” said Cynthia X. Ma, MD, PhD, of Washington University, St. Louis, the invited discussant.
Novartis funded the study. Dr Jerusalem received research funding from Novartis and Roche; honoraria from Novartis, Roche, Pfizer, Lilly, Celgene, Amgen, BMS, and Puma Technology; and nonfinancial support from Novartis, Roche, Pfizer, Lilly, Amgen, and BMS. Dr. Ma reported consulting/advising, travel expenses, and institutional research funding from Novartis and others.
SOURCE: Jerusalem G et al. ASCO 2018 Abstract 1005
CHICAGO – For women with estrogen receptor–positive breast cancer resistant to endocrine therapy, the combination of everolimus and exemestane had better efficacy than did everolimus alone, but single-agent capecitabine appeared to offer benefit comparable to that of the combination therapy, results of the BOLERO-6 trial suggest.
Among 309 postmenopausal women with ER-positive, HER2-negative advanced breast cancer, the combination of everolimus (Afinitor) and exemestane (Aromasin and generics) was associated with a 26% improvement in progression-free survival (PFS) compared with everolimus alone, reported Guy Jerusalem, MD, PhD, of Liege University, Belgium.
There was also, however, a numerical but not statistically significant difference in PFS favoring capecitabine (Xeloda and generics) “which may be attributed to various baseline characteristics favoring capecitabine, and potential informative censoring,” he said at the annual meeting of the American Society of Clinical Oncology.
“We have noted in BOLERO-6 a better-than-expected outcome in median progression-free survival of capecitabine compared with the previously reported 4.1 to 7.9 months median progression-free survival,” he said.
BOLERO-6, results of which were published online June 3 in JAMA Oncology, was a postmarketing study by the sponsors to fulfill commitments to both the Food and Drug Administration and the European Medicines Agency to estimate the treatment benefit with combined everolimus and exemestane vs. monotherapy with everolimus or capecitabine in patients with ER-positive, HER2-negative breast cancer that progressed during nonsteroidal aromatase inhibitor therapy.
Patients from 83 centers in 18 countries were enrolled in the open label, phase 2 study and randomly assigned to receive oral everolimus 10 mg daily with oral exemestane 25 mg daily, everolimus at the same dose alone, or oral capecitabine 1,250 mg/m2 twice daily for 2 weeks on, 1 week off.
The trial was not powered for statistical comparisons between arms, but was instead designed with the primary objective of estimated investigator-assessed PFS for the combination vs. everolimus alone.
At baseline, more patients assigned to capecitabine vs. everolimus-containing regimens were younger than 65, white, had an Eastern Cooperative Oncology Group status of 0 (fully active), and had bone-only metastases. In addition, fewer patients in the capecitabine arm had three or more metastatic sites, Dr. Jerusalem noted,
For the primary analysis, the median PFS with everolimus/exemestane was 8.4 months, compared with 6.8 months for everolimus alone. The estimated hazard ratio (HR) for PFS with everolimus/exemestane vs. everolimus alone was 0.74 (90% confidence interval [CI], 0.57-0.97)
In contrast, median PFS with capecitabine was 9.6 months, with a nonsignificant hazard ratio of 1.26 for the combination (90% CI, 0.96-1.66).
A stratified multivariate Cox regression model controlling for baseline difference and known prognostic factor yielded an HR for PFS of 1.15 (90% CI, 0.86-1.52) for the combination.
Censoring of patients was more frequent in the capecitabine arm (33% vs. 23% in the combination arm), which included 20% of patients on capecitabine who were censored for starting on a new antineoplastic therapy vs. 9% of patients on everolimus/exemestane.
The median time to treatment failure was 5.8 months with the combination, vs. 4.2 months with everolimus alone (HR, 0.66, 90% CI, 0.52-0.4), and 6.2 months with capecitabine alone (HR, 1.03, 90% CI, 0.81-1.31).
Median overall survival was 23.1 months in the combination arm, 29.3 months in the everolimus arm, and 25.6 months in the capecitabine arm. There were no statistically significant differences in overall survival among the groups.
Grade 3 or greater adverse events were more frequent in the combination vs. everolimus arms, and comparable between the combination and capecitabine arms, Dr. Jerusalem said.
Serious adverse events of any grade were more frequent in the combination arm than in the other two arms, but there were no significant differences in discontinuations due to adverse events
“The results of the present study suggest that mTOR inhibitor and endocrine therapy combinations remain important for aromatase inhibitor–refractory disease. Safety and PFS with everolimus plus exemestane in this study were consistent with BOLERO-2 and are now supported by real-world evidence,” the investigators wrote.
“The take home from the BOLERO-6 trial is that the progression-free survival for the combination of everolimus and exemestane is superior to everolimus alone, and is in line with data from the BOLERO-2 trial, and also the PrE0102 study, demonstrating the consistent activity of mTOR inhibition in combination with endocrine therapy in the aromatase inhibitor resistance setting, and this supports our use of the combination in the endocrine resistant patients,” said Cynthia X. Ma, MD, PhD, of Washington University, St. Louis, the invited discussant.
Novartis funded the study. Dr Jerusalem received research funding from Novartis and Roche; honoraria from Novartis, Roche, Pfizer, Lilly, Celgene, Amgen, BMS, and Puma Technology; and nonfinancial support from Novartis, Roche, Pfizer, Lilly, Amgen, and BMS. Dr. Ma reported consulting/advising, travel expenses, and institutional research funding from Novartis and others.
SOURCE: Jerusalem G et al. ASCO 2018 Abstract 1005
REPORTING FROM ASCO 2018
Key clinical point: The combination of everolimus and exemestane had better efficacy than did everolimus alone in women with ER+/HER2– breast cancer resistant to endocrine therapy.
Major finding: Median PFS with everolimus/exemestane was 8.4 months vs 6.8 months for everolimus.
Study details: Randomized, open label, phase 2 trial of 309 women with ER-positive, HER2-negative breast cancer that progressed during nonsteroidal aromatase inhibitor therapy.
Disclosures: Novartis funded the study. Dr Jerusalem received research funding from Novartis and Roche; honoraria from Novartis, Roche, Pfizer, Lilly, Celgene, Amgen, BMS, and Puma Technology; and nonfinancial support from Novartis, Roche, Pfizer, Lilly, Amgen, and BMS. Dr. Ma reported consulting/advising, travel expenses, and institutional research funding from Novartis and others.
Source: Jerusalem G et al. ASCO 2018, Abstract 1005.