User login
Prolonged antimalarial therapy linked to elevated cardiac biomarkers, cardiomyopathy
People with systemic lupus erythematosus (SLE) taking antimalarials, particularly for prolonged periods, could be at risk for cardiomyopathy, and measuring specific myocardial biomarkers could help identify patients at particularly high risk, researchers have suggested.
Writing in the Journal of Rheumatology, the research team led by Konstantinos Tselios, MD, PhD, of the University of Toronto Lupus Clinic at the Centre for Prognosis Studies in the Rheumatic Diseases, noted that antimalarial-induced cardiomyopathy (AMIC) had been reported in 47 patients to date, 19 of whom had SLE, with duration and cumulative use of antimalarials thought to be the cause.
The authors suggested that AMIC could be underrecognized because antimalarials were currently recommended for all patients with SLE (without known contraindications) for prolonged periods. It was speculated that the mechanism by which AMIC occurred involved the deposition of antimalarials in the myocardial fibers and that this could lead to chronic, subclinical tissue necrosis, a process which, if not reversed, could lead to heart failure.
“Heart-specific biomarkers, such as cardiac troponin (for the assessment of myocardial necrosis) and brain natriuretic peptide (BNP; for the assessment of volume and/or pressure overload), may be of value in identifying subclinical heart damage,” the research team suggested.
The current study involved 151 consecutive patients with SLE who had no prior cardiac disease and were attending the University of Toronto Lupus Clinic from March to May 2016.
During the course of the disease, 28 of the patients had been taking chloroquine, and 137 had been taking hydroxychloroquine (14 patients had been treated with both drugs at different time periods). In the study, normal range was less than 26 ng/mL for high-sensitivity cardiac troponin I (cTnI) and less than 100 pg/mL for BNP.
Overall, 16 patients (10.6%) had abnormal BNP, of whom 9 (6%) also had abnormal cTnI. Prolonged antimalarial use (greater than 5.6 yrs) was associated with increased risk for these elevated biomarkers, regardless of age and SLE disease duration.
“Because duration of AM [antimalarial] treatment is the critical predictor of AMIC, the majority of patients with SLE should be considered at risk because most of them receive long-term maintenance therapy,” the researchers wrote.
They said that elevations of the biomarkers implicated possible active myocardial necrosis (elevated cTnI) and/or increased intracardiac ventricular pressure (elevated BNP).
“In this context, AM deposition in the myocardium, leading over time to overt cardiomyopathy, may be an important contributing factor. Indeed, 6 out of 16 of these patients were ultimately diagnosed with definite or possible AMIC, while 3 of them were completely asymptomatic, and their investigation was initiated because of the abnormal biomarkers,” they wrote.
The researchers also found that persistent creatine phosphokinase (CPK) elevation was also an important predictor for elevated cardiac biomarkers.
“We showed that chronic AM use is associated with a more than threefold increased risk for elevated CPK (after excluding patients with active myositis and statin therapy). ... It is not known whether elevated CPK may predict patients at risk for development of AMIC or whether certain patients are predisposed to AM-related muscle damage,” they said.
“Prolonged AM therapy and persistent CPK elevation conferred an increased risk for abnormal BNP and cTnI, which might predict AMIC,” they concluded.
Nevertheless, the authors acknowledged that expensive and invasive investigation was unjustified in asymptomatic individuals. They therefore suggested that identifying heart-specific biomarkers for the detection of subclinical heart damage could allow patients to be stratified according to their risk.
“Cardiac biomarkers could become a screening test for patients with SLE using AM for longer than 5.6 years and/or who have persistently elevated CPK levels. Further research is needed to delineate the differential toxicity of CQ [chloroquine] and HCQ [hydroxychloroquine],” they suggested.
The University of Toronto Lupus Research Program is supported by the University Health Network, Lou and Marissa Rocca, and the Lupus Foundation of Ontario. Dr. Tselios is financially supported by Lupus Ontario.
SOURCE: Tselios K et al. J Rheumatol. 2018. doi: 10.3899/jrheum.171436.
People with systemic lupus erythematosus (SLE) taking antimalarials, particularly for prolonged periods, could be at risk for cardiomyopathy, and measuring specific myocardial biomarkers could help identify patients at particularly high risk, researchers have suggested.
Writing in the Journal of Rheumatology, the research team led by Konstantinos Tselios, MD, PhD, of the University of Toronto Lupus Clinic at the Centre for Prognosis Studies in the Rheumatic Diseases, noted that antimalarial-induced cardiomyopathy (AMIC) had been reported in 47 patients to date, 19 of whom had SLE, with duration and cumulative use of antimalarials thought to be the cause.
The authors suggested that AMIC could be underrecognized because antimalarials were currently recommended for all patients with SLE (without known contraindications) for prolonged periods. It was speculated that the mechanism by which AMIC occurred involved the deposition of antimalarials in the myocardial fibers and that this could lead to chronic, subclinical tissue necrosis, a process which, if not reversed, could lead to heart failure.
“Heart-specific biomarkers, such as cardiac troponin (for the assessment of myocardial necrosis) and brain natriuretic peptide (BNP; for the assessment of volume and/or pressure overload), may be of value in identifying subclinical heart damage,” the research team suggested.
The current study involved 151 consecutive patients with SLE who had no prior cardiac disease and were attending the University of Toronto Lupus Clinic from March to May 2016.
During the course of the disease, 28 of the patients had been taking chloroquine, and 137 had been taking hydroxychloroquine (14 patients had been treated with both drugs at different time periods). In the study, normal range was less than 26 ng/mL for high-sensitivity cardiac troponin I (cTnI) and less than 100 pg/mL for BNP.
Overall, 16 patients (10.6%) had abnormal BNP, of whom 9 (6%) also had abnormal cTnI. Prolonged antimalarial use (greater than 5.6 yrs) was associated with increased risk for these elevated biomarkers, regardless of age and SLE disease duration.
“Because duration of AM [antimalarial] treatment is the critical predictor of AMIC, the majority of patients with SLE should be considered at risk because most of them receive long-term maintenance therapy,” the researchers wrote.
They said that elevations of the biomarkers implicated possible active myocardial necrosis (elevated cTnI) and/or increased intracardiac ventricular pressure (elevated BNP).
“In this context, AM deposition in the myocardium, leading over time to overt cardiomyopathy, may be an important contributing factor. Indeed, 6 out of 16 of these patients were ultimately diagnosed with definite or possible AMIC, while 3 of them were completely asymptomatic, and their investigation was initiated because of the abnormal biomarkers,” they wrote.
The researchers also found that persistent creatine phosphokinase (CPK) elevation was also an important predictor for elevated cardiac biomarkers.
“We showed that chronic AM use is associated with a more than threefold increased risk for elevated CPK (after excluding patients with active myositis and statin therapy). ... It is not known whether elevated CPK may predict patients at risk for development of AMIC or whether certain patients are predisposed to AM-related muscle damage,” they said.
“Prolonged AM therapy and persistent CPK elevation conferred an increased risk for abnormal BNP and cTnI, which might predict AMIC,” they concluded.
Nevertheless, the authors acknowledged that expensive and invasive investigation was unjustified in asymptomatic individuals. They therefore suggested that identifying heart-specific biomarkers for the detection of subclinical heart damage could allow patients to be stratified according to their risk.
“Cardiac biomarkers could become a screening test for patients with SLE using AM for longer than 5.6 years and/or who have persistently elevated CPK levels. Further research is needed to delineate the differential toxicity of CQ [chloroquine] and HCQ [hydroxychloroquine],” they suggested.
The University of Toronto Lupus Research Program is supported by the University Health Network, Lou and Marissa Rocca, and the Lupus Foundation of Ontario. Dr. Tselios is financially supported by Lupus Ontario.
SOURCE: Tselios K et al. J Rheumatol. 2018. doi: 10.3899/jrheum.171436.
People with systemic lupus erythematosus (SLE) taking antimalarials, particularly for prolonged periods, could be at risk for cardiomyopathy, and measuring specific myocardial biomarkers could help identify patients at particularly high risk, researchers have suggested.
Writing in the Journal of Rheumatology, the research team led by Konstantinos Tselios, MD, PhD, of the University of Toronto Lupus Clinic at the Centre for Prognosis Studies in the Rheumatic Diseases, noted that antimalarial-induced cardiomyopathy (AMIC) had been reported in 47 patients to date, 19 of whom had SLE, with duration and cumulative use of antimalarials thought to be the cause.
The authors suggested that AMIC could be underrecognized because antimalarials were currently recommended for all patients with SLE (without known contraindications) for prolonged periods. It was speculated that the mechanism by which AMIC occurred involved the deposition of antimalarials in the myocardial fibers and that this could lead to chronic, subclinical tissue necrosis, a process which, if not reversed, could lead to heart failure.
“Heart-specific biomarkers, such as cardiac troponin (for the assessment of myocardial necrosis) and brain natriuretic peptide (BNP; for the assessment of volume and/or pressure overload), may be of value in identifying subclinical heart damage,” the research team suggested.
The current study involved 151 consecutive patients with SLE who had no prior cardiac disease and were attending the University of Toronto Lupus Clinic from March to May 2016.
During the course of the disease, 28 of the patients had been taking chloroquine, and 137 had been taking hydroxychloroquine (14 patients had been treated with both drugs at different time periods). In the study, normal range was less than 26 ng/mL for high-sensitivity cardiac troponin I (cTnI) and less than 100 pg/mL for BNP.
Overall, 16 patients (10.6%) had abnormal BNP, of whom 9 (6%) also had abnormal cTnI. Prolonged antimalarial use (greater than 5.6 yrs) was associated with increased risk for these elevated biomarkers, regardless of age and SLE disease duration.
“Because duration of AM [antimalarial] treatment is the critical predictor of AMIC, the majority of patients with SLE should be considered at risk because most of them receive long-term maintenance therapy,” the researchers wrote.
They said that elevations of the biomarkers implicated possible active myocardial necrosis (elevated cTnI) and/or increased intracardiac ventricular pressure (elevated BNP).
“In this context, AM deposition in the myocardium, leading over time to overt cardiomyopathy, may be an important contributing factor. Indeed, 6 out of 16 of these patients were ultimately diagnosed with definite or possible AMIC, while 3 of them were completely asymptomatic, and their investigation was initiated because of the abnormal biomarkers,” they wrote.
The researchers also found that persistent creatine phosphokinase (CPK) elevation was also an important predictor for elevated cardiac biomarkers.
“We showed that chronic AM use is associated with a more than threefold increased risk for elevated CPK (after excluding patients with active myositis and statin therapy). ... It is not known whether elevated CPK may predict patients at risk for development of AMIC or whether certain patients are predisposed to AM-related muscle damage,” they said.
“Prolonged AM therapy and persistent CPK elevation conferred an increased risk for abnormal BNP and cTnI, which might predict AMIC,” they concluded.
Nevertheless, the authors acknowledged that expensive and invasive investigation was unjustified in asymptomatic individuals. They therefore suggested that identifying heart-specific biomarkers for the detection of subclinical heart damage could allow patients to be stratified according to their risk.
“Cardiac biomarkers could become a screening test for patients with SLE using AM for longer than 5.6 years and/or who have persistently elevated CPK levels. Further research is needed to delineate the differential toxicity of CQ [chloroquine] and HCQ [hydroxychloroquine],” they suggested.
The University of Toronto Lupus Research Program is supported by the University Health Network, Lou and Marissa Rocca, and the Lupus Foundation of Ontario. Dr. Tselios is financially supported by Lupus Ontario.
SOURCE: Tselios K et al. J Rheumatol. 2018. doi: 10.3899/jrheum.171436.
FROM JOURNAL OF RHEUMATOLOGY
Key clinical point: Patients with SLE who receive prolonged antimalarial treatment (greater than 5.6 years) are at increased risk for elevated cardiac biomarkers (BNP/cTnI), particularly when persistently elevated creatine phosphokinase is present. These biomarkers could be used to predict antimalarial-induced cardiomyopathy.
Major finding: Of a cohort of 151 patients with SLE, 10% had elevated myocardial biomarkers in the absence of prior cardiac disease or pulmonary arterial hypertension. One-third of the patients were diagnosed with antimalarial-induced cardiomyopathy.
Study details: The study enrolled 151 consecutive patients attending the University of Toronto Lupus Clinic from March to May 2016.
Disclosures: The University of Toronto Lupus Research Program is supported by the University Health Network, Lou and Marissa Rocca, and the Lupus Foundation of Ontario. Dr. Tselios is financially supported by Lupus Ontario.
Source: Tselios K et al. J Rheumatol. 2018. doi: 10.3899/jrheum.171436.
The second victim: More ob.gyn. organizations recognize need for support
When Patrice Weiss, MD, was a resident, a healthy, low-risk patient underwent what should have been an uncomplicated vaginal hysterectomy. But the patient developed a series of postoperative complications leading to multisystem organ failure and a lengthy stay in intensive care.
“None of us could really figure out how this happened. I still can’t figure out how this person who was relatively young developed all these complications,” said Dr. Weiss, now chief medical officer of Carilion Clinic and professor of obstetrics and gynecology at Virginia Tech Carilion School of Medicine and Research Institute, both in Roanoke, Va. “There are times when you don’t know why something happened or what you could have done differently – and the answer may be nothing – but that dramatic, potentially very complicated outcome can really weigh on people. You still harbor those feelings of a second victim.”
It’s the health care professional who is that “second victim,” a term coined in 2000 by Albert W. Wu, MD, professor of public health at Johns Hopkins University, Baltimore, to describe an increasingly recognized phenomenon following unexpected adverse patient events, medical errors, or patient injuries (BMJ. 2000 Mar 18;320[7237]:726-7). The patients and their loved ones are the first victims, but a health care professional’s feelings of guilt, shame, inadequacy, and other powerful, complicated emotions can have long-lasting effects on his or her psyche, clinical practice, and career, particularly if he or she does not receive validation, support, and access to resources to work through the experience.
“Second victims ... become victimized in the sense that the provider is traumatized by the event,” Susan D. Scott, PhD, of the University of Missouri Health System, Columbia, and her colleagues wrote in a 2009 paper about the phenomenon (Qual Saf Health Care. 2009;18[5]:325-30). “Frequently, these individuals feel personally responsible for the patient outcome. Many feel as though they have failed the patient, second-guessing their clinical skills and knowledge base,” they said.
It’s that latter part that can fester and potentially poison a health care professional’s ability to function, according to Charlie Jaynes, MD, senior director of medical operations for Ob Hospitalist Group in Greenville, S.C.
“ and therefore can have a direct effect on patient care and lead to poor outcomes,” Dr. Jaynes said. “It’s a very dangerous phenomenon because it can degrade the quality of medical care provided.”
Most physicians are trained to internalize and compartmentalize these experiences, to “suck it up and get on with it,” he said, but it’s now become clear that such a strategy can have disastrous professional and personal consequences.
“In the worst case scenario, people burn out, drop out or commit suicide, their marriage ends up in shambles, or they turn to drugs and alcohol,” Dr. Jaynes said. “What Dr. Wu did was open the box to allow some empathy and compassion to be introduced to the situation.”
Dangers of unaddressed second victim impact
Estimates vary widely on the prevalence of second victim phenomenon among physicians and nurses who have been involved in a medical error or unexpected serious outcome. Across the medical field, estimates range from 10% in a study among otolaryngologists (Laryngoscope. 2006 Jul;116[7]:1114-20) to up to 30% and 50% more broadly, although some fields may be more susceptible than others (Jt Comm J Qual Patient Saf. 2010;36[5]:233-40; BMJ Qual Saf. 2012;21[4]:267-70).
“In the world of obstetrics, we spend 99.9% of our time in a happy field of medicine filled with joy and new life,” Dr. Weiss said. “Whether consciously or unconsciously, those become the expectations of the patients and the providers, so when there is an outcome that is less than optimal, that’s when you’re even more affected because of what your expectations are going into it.”
Dr. Scott and her colleagues noted that the stages of being a second victim are similar to the Kübler-Ross stages:
- Stage 1: Chaos and event repair.
- Stage 2: Intrusive thoughts, “what if.”
- Stage 3: Restoring personal identity.
- Stage 4: Enduring the inquisition.
- Stage 5: Obtaining emotional first aid.
- Stage 6: Moving on or dropping out; surviving and/or thriving.”
“This can go on for years. Someone can spend years just surviving and not thriving,” Dr. Weiss said. “It can really happen along a continuum.”
Although studies have not looked specifically at second victims and patient care, research has shown that second victims have a higher risk of burnout, and that physicians with high burnout tend to order more tests, spend less time with patients, and have greater risk of making medical errors, Dr. Weiss said.
A study looking at the emotional impact of medical errors on physicians found that 61% had greater anxiety about making future medical errors, 44% had a loss of confidence, 42% had trouble sleeping, and 42% were less satisfied in their job (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
“You have the risk of the provider leaving medicine altogether or significantly changing their practice patterns, or giving up obstetric care because of the emotional toll it takes on providers,” she said. “We already know that one of the crises facing medicine right now is burnout, so you have the risk of additional or worsening burnout.”
Recognizing the need for formal support programs
Research does clearly show a need for programs formally addressing these experiences. A 2007 survey found that only 10% of 3,171 of internal medicine doctors, pediatricians, family physicians, and surgeons felt their health care organizations provided adequate support in managing stress following a medical error, yet about 8 in 10 wanted support (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
Organizations are responding. One of the first second-victim programs is the “forYOU” program implemented at the University of Missouri Health Care’s Office of Clinical Effectiveness in 2007. The free, 24-7 program provides a “safe zone” for expressing emotions and reactions confidentially.
Ob Hospitalist Group just launched the CARE (Clinician Assistance, Recovery & Encouragement) Program, the first national peer-support program for second victims. The first 25 volunteers who underwent training in September will serve the organization’s more than 700 health care professionals across 32 states.
Instead of psychological counseling or intervention, the program emphasizes active listening, nonjudgment, and compassion during confidential calls; peers don’t take notes or record the conversations.
“We will be quiet and listen and speak at the appropriate times to be compassionate and not make judgments,” Dr. Jaynes said. “I think its critical to realize that in order to do that you have to be one of us. If you haven’t been there yourself when a baby dies in utero or you have a mother almost die by hemorrhage or a complication of surgery ... it creates emotional turmoil. Everybody who’s worth their salt questions, ‘What did I do wrong?’ and we’re really harsh on ourselves. If I can say I realize it’s a horrible place to be because I’ve been there myself, I can be a useful peer.”
At Dr. Weiss’s institution, Carilion Clinic spent 5 years developing and implementing the TRUST second-victim program, emphasizing Treatment, Respect, Understanding/compassion, Supportive care, and Transparency. Dr. Weiss said the first step in developing such a program is talking about the problem.
“You need hospital leadership addressing the phenomenon of the second victim, recognizing it is real, that it’s not a sign of weakness for providers to have any of these signs,” she said. “It has to be done at an organizational level. There has to be a place where providers can talk freely about the emotional impact of the outcome, not just the clinical outcomes.”
Johns Hopkins Hospital in Baltimore published findings in September 2017 about its program RISE (Resilience In Stressful Events) (Jt Comm J Qual Patient Saf. 2017 Sep;43[9]:471-83 that was featured by the Joint Commission as a program that employs some of the tools the commission describes in its toolkit for health care organizations to develop second-victim support programs (Jt Comm J Qual Patient Saf. 2012 May;38[5]:235-40, 193).
It’s important that health care professionals are not expected or required to seek counseling or similar interventions, Dr. Weiss said, but they know of available resources.
“People need to be able to talk about it when they’re ready. It doesn’t necessarily matter how your peers judge your actions because these are feelings that come from within,” Dr. Weiss said, although colleagues can validate a second victim’s experience or feelings by sharing their own.
“It’s helpful when someone in a leadership role can acknowledge that this is real and say to a provider, ‘I’ve been there, and this is what helped me,’ or ‘I’ve been there, and there was no resource and I went without help for years,’ ” she said.
In fact, it’s her own past experiences that have made Dr. Weiss so passionate about raising awareness about second victims.
“I’ve been involved in cases of unanticipated outcomes and personally witnessed medical errors, and I’ve seen how very close colleagues can be affected,” she said. “This is a topic that really, really hits home for me.”
Signs and symptoms: How to recognize a possible second victim
Anyone can become a second victim, regardless of their training, experience, or years of practice, Dr. Weiss said. A health care professional may practice for years and witness many unanticipated poor outcomes before one suddenly drums up feelings they don’t expect.
“It’s almost inevitable that providers are going to have unanticipated outcomes or unexpected outcomes,” Dr. Weiss said. “The challenge with the second victim is no one can ever predict how someone is going to respond to an outcome, including ourselves. This may be the first time they have a response to something they never saw coming.”
Two aspects correlated with a higher risk of second victim are the severity of the morbidity or mortality of the patient and the degree of personal responsibility the health care professional feels. The signs and symptoms of being a second victim can be indistinguishable from those of depression, anxiety, or posttraumatic stress syndrome, but the biggest indicator is a change in a person’s normal behavior, Dr. Weiss said.
“The person who is never late to work is late to work. The person who is always mild-mannered is on edge,” she said. “A lot of it is subtle personality or behavior changes, or you begin to notice practice pattern differences, such as ordering a bunch of labs.”
Perhaps the providers are snapping at people when they’ve never snapped before, or they express more cynicism or sarcasm, she added. “A change in their sleeping or eating patterns or in their personal hygiene are all things that one could look for.”
According to Dr. Jaynes, emotional signs may include irritability, fear, anger, grief, remorse, frustration, desperation, numbness, guilt, loneliness, shock and feeling disconnected, feeling hopeless or out of control. Physical symptoms include headaches, muscle tension, chest pain, extreme fatigue, sleeping problems, appetite changes or gastrointestinal symptoms, dizziness, frequent illnesses, being easily startled, or increased heart rate, blood pressure, or breathing rate. Other possible signs include flashbacks, nightmares, social avoidance, difficulties concentrating, poor memory, avoiding patient care areas, fearing repercussions to their reputations, and decreased job satisfaction. Second victims also may experience a loss in confidence or spiritual connection, or loss of interest in work, usual activities, and connections with others.
Dr. Weiss and Dr. Jaynes said they had no relevant financial disclosures.
When Patrice Weiss, MD, was a resident, a healthy, low-risk patient underwent what should have been an uncomplicated vaginal hysterectomy. But the patient developed a series of postoperative complications leading to multisystem organ failure and a lengthy stay in intensive care.
“None of us could really figure out how this happened. I still can’t figure out how this person who was relatively young developed all these complications,” said Dr. Weiss, now chief medical officer of Carilion Clinic and professor of obstetrics and gynecology at Virginia Tech Carilion School of Medicine and Research Institute, both in Roanoke, Va. “There are times when you don’t know why something happened or what you could have done differently – and the answer may be nothing – but that dramatic, potentially very complicated outcome can really weigh on people. You still harbor those feelings of a second victim.”
It’s the health care professional who is that “second victim,” a term coined in 2000 by Albert W. Wu, MD, professor of public health at Johns Hopkins University, Baltimore, to describe an increasingly recognized phenomenon following unexpected adverse patient events, medical errors, or patient injuries (BMJ. 2000 Mar 18;320[7237]:726-7). The patients and their loved ones are the first victims, but a health care professional’s feelings of guilt, shame, inadequacy, and other powerful, complicated emotions can have long-lasting effects on his or her psyche, clinical practice, and career, particularly if he or she does not receive validation, support, and access to resources to work through the experience.
“Second victims ... become victimized in the sense that the provider is traumatized by the event,” Susan D. Scott, PhD, of the University of Missouri Health System, Columbia, and her colleagues wrote in a 2009 paper about the phenomenon (Qual Saf Health Care. 2009;18[5]:325-30). “Frequently, these individuals feel personally responsible for the patient outcome. Many feel as though they have failed the patient, second-guessing their clinical skills and knowledge base,” they said.
It’s that latter part that can fester and potentially poison a health care professional’s ability to function, according to Charlie Jaynes, MD, senior director of medical operations for Ob Hospitalist Group in Greenville, S.C.
“ and therefore can have a direct effect on patient care and lead to poor outcomes,” Dr. Jaynes said. “It’s a very dangerous phenomenon because it can degrade the quality of medical care provided.”
Most physicians are trained to internalize and compartmentalize these experiences, to “suck it up and get on with it,” he said, but it’s now become clear that such a strategy can have disastrous professional and personal consequences.
“In the worst case scenario, people burn out, drop out or commit suicide, their marriage ends up in shambles, or they turn to drugs and alcohol,” Dr. Jaynes said. “What Dr. Wu did was open the box to allow some empathy and compassion to be introduced to the situation.”
Dangers of unaddressed second victim impact
Estimates vary widely on the prevalence of second victim phenomenon among physicians and nurses who have been involved in a medical error or unexpected serious outcome. Across the medical field, estimates range from 10% in a study among otolaryngologists (Laryngoscope. 2006 Jul;116[7]:1114-20) to up to 30% and 50% more broadly, although some fields may be more susceptible than others (Jt Comm J Qual Patient Saf. 2010;36[5]:233-40; BMJ Qual Saf. 2012;21[4]:267-70).
“In the world of obstetrics, we spend 99.9% of our time in a happy field of medicine filled with joy and new life,” Dr. Weiss said. “Whether consciously or unconsciously, those become the expectations of the patients and the providers, so when there is an outcome that is less than optimal, that’s when you’re even more affected because of what your expectations are going into it.”
Dr. Scott and her colleagues noted that the stages of being a second victim are similar to the Kübler-Ross stages:
- Stage 1: Chaos and event repair.
- Stage 2: Intrusive thoughts, “what if.”
- Stage 3: Restoring personal identity.
- Stage 4: Enduring the inquisition.
- Stage 5: Obtaining emotional first aid.
- Stage 6: Moving on or dropping out; surviving and/or thriving.”
“This can go on for years. Someone can spend years just surviving and not thriving,” Dr. Weiss said. “It can really happen along a continuum.”
Although studies have not looked specifically at second victims and patient care, research has shown that second victims have a higher risk of burnout, and that physicians with high burnout tend to order more tests, spend less time with patients, and have greater risk of making medical errors, Dr. Weiss said.
A study looking at the emotional impact of medical errors on physicians found that 61% had greater anxiety about making future medical errors, 44% had a loss of confidence, 42% had trouble sleeping, and 42% were less satisfied in their job (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
“You have the risk of the provider leaving medicine altogether or significantly changing their practice patterns, or giving up obstetric care because of the emotional toll it takes on providers,” she said. “We already know that one of the crises facing medicine right now is burnout, so you have the risk of additional or worsening burnout.”
Recognizing the need for formal support programs
Research does clearly show a need for programs formally addressing these experiences. A 2007 survey found that only 10% of 3,171 of internal medicine doctors, pediatricians, family physicians, and surgeons felt their health care organizations provided adequate support in managing stress following a medical error, yet about 8 in 10 wanted support (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
Organizations are responding. One of the first second-victim programs is the “forYOU” program implemented at the University of Missouri Health Care’s Office of Clinical Effectiveness in 2007. The free, 24-7 program provides a “safe zone” for expressing emotions and reactions confidentially.
Ob Hospitalist Group just launched the CARE (Clinician Assistance, Recovery & Encouragement) Program, the first national peer-support program for second victims. The first 25 volunteers who underwent training in September will serve the organization’s more than 700 health care professionals across 32 states.
Instead of psychological counseling or intervention, the program emphasizes active listening, nonjudgment, and compassion during confidential calls; peers don’t take notes or record the conversations.
“We will be quiet and listen and speak at the appropriate times to be compassionate and not make judgments,” Dr. Jaynes said. “I think its critical to realize that in order to do that you have to be one of us. If you haven’t been there yourself when a baby dies in utero or you have a mother almost die by hemorrhage or a complication of surgery ... it creates emotional turmoil. Everybody who’s worth their salt questions, ‘What did I do wrong?’ and we’re really harsh on ourselves. If I can say I realize it’s a horrible place to be because I’ve been there myself, I can be a useful peer.”
At Dr. Weiss’s institution, Carilion Clinic spent 5 years developing and implementing the TRUST second-victim program, emphasizing Treatment, Respect, Understanding/compassion, Supportive care, and Transparency. Dr. Weiss said the first step in developing such a program is talking about the problem.
“You need hospital leadership addressing the phenomenon of the second victim, recognizing it is real, that it’s not a sign of weakness for providers to have any of these signs,” she said. “It has to be done at an organizational level. There has to be a place where providers can talk freely about the emotional impact of the outcome, not just the clinical outcomes.”
Johns Hopkins Hospital in Baltimore published findings in September 2017 about its program RISE (Resilience In Stressful Events) (Jt Comm J Qual Patient Saf. 2017 Sep;43[9]:471-83 that was featured by the Joint Commission as a program that employs some of the tools the commission describes in its toolkit for health care organizations to develop second-victim support programs (Jt Comm J Qual Patient Saf. 2012 May;38[5]:235-40, 193).
It’s important that health care professionals are not expected or required to seek counseling or similar interventions, Dr. Weiss said, but they know of available resources.
“People need to be able to talk about it when they’re ready. It doesn’t necessarily matter how your peers judge your actions because these are feelings that come from within,” Dr. Weiss said, although colleagues can validate a second victim’s experience or feelings by sharing their own.
“It’s helpful when someone in a leadership role can acknowledge that this is real and say to a provider, ‘I’ve been there, and this is what helped me,’ or ‘I’ve been there, and there was no resource and I went without help for years,’ ” she said.
In fact, it’s her own past experiences that have made Dr. Weiss so passionate about raising awareness about second victims.
“I’ve been involved in cases of unanticipated outcomes and personally witnessed medical errors, and I’ve seen how very close colleagues can be affected,” she said. “This is a topic that really, really hits home for me.”
Signs and symptoms: How to recognize a possible second victim
Anyone can become a second victim, regardless of their training, experience, or years of practice, Dr. Weiss said. A health care professional may practice for years and witness many unanticipated poor outcomes before one suddenly drums up feelings they don’t expect.
“It’s almost inevitable that providers are going to have unanticipated outcomes or unexpected outcomes,” Dr. Weiss said. “The challenge with the second victim is no one can ever predict how someone is going to respond to an outcome, including ourselves. This may be the first time they have a response to something they never saw coming.”
Two aspects correlated with a higher risk of second victim are the severity of the morbidity or mortality of the patient and the degree of personal responsibility the health care professional feels. The signs and symptoms of being a second victim can be indistinguishable from those of depression, anxiety, or posttraumatic stress syndrome, but the biggest indicator is a change in a person’s normal behavior, Dr. Weiss said.
“The person who is never late to work is late to work. The person who is always mild-mannered is on edge,” she said. “A lot of it is subtle personality or behavior changes, or you begin to notice practice pattern differences, such as ordering a bunch of labs.”
Perhaps the providers are snapping at people when they’ve never snapped before, or they express more cynicism or sarcasm, she added. “A change in their sleeping or eating patterns or in their personal hygiene are all things that one could look for.”
According to Dr. Jaynes, emotional signs may include irritability, fear, anger, grief, remorse, frustration, desperation, numbness, guilt, loneliness, shock and feeling disconnected, feeling hopeless or out of control. Physical symptoms include headaches, muscle tension, chest pain, extreme fatigue, sleeping problems, appetite changes or gastrointestinal symptoms, dizziness, frequent illnesses, being easily startled, or increased heart rate, blood pressure, or breathing rate. Other possible signs include flashbacks, nightmares, social avoidance, difficulties concentrating, poor memory, avoiding patient care areas, fearing repercussions to their reputations, and decreased job satisfaction. Second victims also may experience a loss in confidence or spiritual connection, or loss of interest in work, usual activities, and connections with others.
Dr. Weiss and Dr. Jaynes said they had no relevant financial disclosures.
When Patrice Weiss, MD, was a resident, a healthy, low-risk patient underwent what should have been an uncomplicated vaginal hysterectomy. But the patient developed a series of postoperative complications leading to multisystem organ failure and a lengthy stay in intensive care.
“None of us could really figure out how this happened. I still can’t figure out how this person who was relatively young developed all these complications,” said Dr. Weiss, now chief medical officer of Carilion Clinic and professor of obstetrics and gynecology at Virginia Tech Carilion School of Medicine and Research Institute, both in Roanoke, Va. “There are times when you don’t know why something happened or what you could have done differently – and the answer may be nothing – but that dramatic, potentially very complicated outcome can really weigh on people. You still harbor those feelings of a second victim.”
It’s the health care professional who is that “second victim,” a term coined in 2000 by Albert W. Wu, MD, professor of public health at Johns Hopkins University, Baltimore, to describe an increasingly recognized phenomenon following unexpected adverse patient events, medical errors, or patient injuries (BMJ. 2000 Mar 18;320[7237]:726-7). The patients and their loved ones are the first victims, but a health care professional’s feelings of guilt, shame, inadequacy, and other powerful, complicated emotions can have long-lasting effects on his or her psyche, clinical practice, and career, particularly if he or she does not receive validation, support, and access to resources to work through the experience.
“Second victims ... become victimized in the sense that the provider is traumatized by the event,” Susan D. Scott, PhD, of the University of Missouri Health System, Columbia, and her colleagues wrote in a 2009 paper about the phenomenon (Qual Saf Health Care. 2009;18[5]:325-30). “Frequently, these individuals feel personally responsible for the patient outcome. Many feel as though they have failed the patient, second-guessing their clinical skills and knowledge base,” they said.
It’s that latter part that can fester and potentially poison a health care professional’s ability to function, according to Charlie Jaynes, MD, senior director of medical operations for Ob Hospitalist Group in Greenville, S.C.
“ and therefore can have a direct effect on patient care and lead to poor outcomes,” Dr. Jaynes said. “It’s a very dangerous phenomenon because it can degrade the quality of medical care provided.”
Most physicians are trained to internalize and compartmentalize these experiences, to “suck it up and get on with it,” he said, but it’s now become clear that such a strategy can have disastrous professional and personal consequences.
“In the worst case scenario, people burn out, drop out or commit suicide, their marriage ends up in shambles, or they turn to drugs and alcohol,” Dr. Jaynes said. “What Dr. Wu did was open the box to allow some empathy and compassion to be introduced to the situation.”
Dangers of unaddressed second victim impact
Estimates vary widely on the prevalence of second victim phenomenon among physicians and nurses who have been involved in a medical error or unexpected serious outcome. Across the medical field, estimates range from 10% in a study among otolaryngologists (Laryngoscope. 2006 Jul;116[7]:1114-20) to up to 30% and 50% more broadly, although some fields may be more susceptible than others (Jt Comm J Qual Patient Saf. 2010;36[5]:233-40; BMJ Qual Saf. 2012;21[4]:267-70).
“In the world of obstetrics, we spend 99.9% of our time in a happy field of medicine filled with joy and new life,” Dr. Weiss said. “Whether consciously or unconsciously, those become the expectations of the patients and the providers, so when there is an outcome that is less than optimal, that’s when you’re even more affected because of what your expectations are going into it.”
Dr. Scott and her colleagues noted that the stages of being a second victim are similar to the Kübler-Ross stages:
- Stage 1: Chaos and event repair.
- Stage 2: Intrusive thoughts, “what if.”
- Stage 3: Restoring personal identity.
- Stage 4: Enduring the inquisition.
- Stage 5: Obtaining emotional first aid.
- Stage 6: Moving on or dropping out; surviving and/or thriving.”
“This can go on for years. Someone can spend years just surviving and not thriving,” Dr. Weiss said. “It can really happen along a continuum.”
Although studies have not looked specifically at second victims and patient care, research has shown that second victims have a higher risk of burnout, and that physicians with high burnout tend to order more tests, spend less time with patients, and have greater risk of making medical errors, Dr. Weiss said.
A study looking at the emotional impact of medical errors on physicians found that 61% had greater anxiety about making future medical errors, 44% had a loss of confidence, 42% had trouble sleeping, and 42% were less satisfied in their job (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
“You have the risk of the provider leaving medicine altogether or significantly changing their practice patterns, or giving up obstetric care because of the emotional toll it takes on providers,” she said. “We already know that one of the crises facing medicine right now is burnout, so you have the risk of additional or worsening burnout.”
Recognizing the need for formal support programs
Research does clearly show a need for programs formally addressing these experiences. A 2007 survey found that only 10% of 3,171 of internal medicine doctors, pediatricians, family physicians, and surgeons felt their health care organizations provided adequate support in managing stress following a medical error, yet about 8 in 10 wanted support (Jt Comm J Qual Patient Saf. 2007;33[8]:467-76).
Organizations are responding. One of the first second-victim programs is the “forYOU” program implemented at the University of Missouri Health Care’s Office of Clinical Effectiveness in 2007. The free, 24-7 program provides a “safe zone” for expressing emotions and reactions confidentially.
Ob Hospitalist Group just launched the CARE (Clinician Assistance, Recovery & Encouragement) Program, the first national peer-support program for second victims. The first 25 volunteers who underwent training in September will serve the organization’s more than 700 health care professionals across 32 states.
Instead of psychological counseling or intervention, the program emphasizes active listening, nonjudgment, and compassion during confidential calls; peers don’t take notes or record the conversations.
“We will be quiet and listen and speak at the appropriate times to be compassionate and not make judgments,” Dr. Jaynes said. “I think its critical to realize that in order to do that you have to be one of us. If you haven’t been there yourself when a baby dies in utero or you have a mother almost die by hemorrhage or a complication of surgery ... it creates emotional turmoil. Everybody who’s worth their salt questions, ‘What did I do wrong?’ and we’re really harsh on ourselves. If I can say I realize it’s a horrible place to be because I’ve been there myself, I can be a useful peer.”
At Dr. Weiss’s institution, Carilion Clinic spent 5 years developing and implementing the TRUST second-victim program, emphasizing Treatment, Respect, Understanding/compassion, Supportive care, and Transparency. Dr. Weiss said the first step in developing such a program is talking about the problem.
“You need hospital leadership addressing the phenomenon of the second victim, recognizing it is real, that it’s not a sign of weakness for providers to have any of these signs,” she said. “It has to be done at an organizational level. There has to be a place where providers can talk freely about the emotional impact of the outcome, not just the clinical outcomes.”
Johns Hopkins Hospital in Baltimore published findings in September 2017 about its program RISE (Resilience In Stressful Events) (Jt Comm J Qual Patient Saf. 2017 Sep;43[9]:471-83 that was featured by the Joint Commission as a program that employs some of the tools the commission describes in its toolkit for health care organizations to develop second-victim support programs (Jt Comm J Qual Patient Saf. 2012 May;38[5]:235-40, 193).
It’s important that health care professionals are not expected or required to seek counseling or similar interventions, Dr. Weiss said, but they know of available resources.
“People need to be able to talk about it when they’re ready. It doesn’t necessarily matter how your peers judge your actions because these are feelings that come from within,” Dr. Weiss said, although colleagues can validate a second victim’s experience or feelings by sharing their own.
“It’s helpful when someone in a leadership role can acknowledge that this is real and say to a provider, ‘I’ve been there, and this is what helped me,’ or ‘I’ve been there, and there was no resource and I went without help for years,’ ” she said.
In fact, it’s her own past experiences that have made Dr. Weiss so passionate about raising awareness about second victims.
“I’ve been involved in cases of unanticipated outcomes and personally witnessed medical errors, and I’ve seen how very close colleagues can be affected,” she said. “This is a topic that really, really hits home for me.”
Signs and symptoms: How to recognize a possible second victim
Anyone can become a second victim, regardless of their training, experience, or years of practice, Dr. Weiss said. A health care professional may practice for years and witness many unanticipated poor outcomes before one suddenly drums up feelings they don’t expect.
“It’s almost inevitable that providers are going to have unanticipated outcomes or unexpected outcomes,” Dr. Weiss said. “The challenge with the second victim is no one can ever predict how someone is going to respond to an outcome, including ourselves. This may be the first time they have a response to something they never saw coming.”
Two aspects correlated with a higher risk of second victim are the severity of the morbidity or mortality of the patient and the degree of personal responsibility the health care professional feels. The signs and symptoms of being a second victim can be indistinguishable from those of depression, anxiety, or posttraumatic stress syndrome, but the biggest indicator is a change in a person’s normal behavior, Dr. Weiss said.
“The person who is never late to work is late to work. The person who is always mild-mannered is on edge,” she said. “A lot of it is subtle personality or behavior changes, or you begin to notice practice pattern differences, such as ordering a bunch of labs.”
Perhaps the providers are snapping at people when they’ve never snapped before, or they express more cynicism or sarcasm, she added. “A change in their sleeping or eating patterns or in their personal hygiene are all things that one could look for.”
According to Dr. Jaynes, emotional signs may include irritability, fear, anger, grief, remorse, frustration, desperation, numbness, guilt, loneliness, shock and feeling disconnected, feeling hopeless or out of control. Physical symptoms include headaches, muscle tension, chest pain, extreme fatigue, sleeping problems, appetite changes or gastrointestinal symptoms, dizziness, frequent illnesses, being easily startled, or increased heart rate, blood pressure, or breathing rate. Other possible signs include flashbacks, nightmares, social avoidance, difficulties concentrating, poor memory, avoiding patient care areas, fearing repercussions to their reputations, and decreased job satisfaction. Second victims also may experience a loss in confidence or spiritual connection, or loss of interest in work, usual activities, and connections with others.
Dr. Weiss and Dr. Jaynes said they had no relevant financial disclosures.

Hot Topics in Primary Care 2018
Click here to read the full supplement.

This supplement includes 1.0 CME credits (scroll down for more information).
Articles include:
- Approach to the Identification and Differentiation of Migraine
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- Individualizing Treatment with Statin Therapy
- Advances in Type 2 Diabetes: Focus on Basal Insulin/Glucagon-Like Peptide-1 Receptor Agonist Combination Therapy
- From Randomized Controlled Trials to the Real World: Putting Evidence into Context
- Approaches to Increase Colorectal Cancer Screening Rates: Key Information for the Family Physician
This supplement offers the opportunity to earn a total of 1.0 CME credits.
Credit is awarded for successful completion of the online evaluations at the link below. This link may also be found within the supplement on the first page of the article.
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- To complete the online evaluation and receive 1 CME credit for this article: please click on the link at the end of the article or go to www.pceconsortium.org/gout.
Click here to read the full supplement.
This supplement includes 1.0 CME credits (scroll down for more information).
Articles include:
- Approach to the Identification and Differentiation of Migraine
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- Individualizing Treatment with Statin Therapy
- Advances in Type 2 Diabetes: Focus on Basal Insulin/Glucagon-Like Peptide-1 Receptor Agonist Combination Therapy
- From Randomized Controlled Trials to the Real World: Putting Evidence into Context
- Approaches to Increase Colorectal Cancer Screening Rates: Key Information for the Family Physician
This supplement offers the opportunity to earn a total of 1.0 CME credits.
Credit is awarded for successful completion of the online evaluations at the link below. This link may also be found within the supplement on the first page of the article.
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- To complete the online evaluation and receive 1 CME credit for this article: please click on the link at the end of the article or go to www.pceconsortium.org/gout.
Click here to read the full supplement.
This supplement includes 1.0 CME credits (scroll down for more information).
Articles include:
- Approach to the Identification and Differentiation of Migraine
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- Individualizing Treatment with Statin Therapy
- Advances in Type 2 Diabetes: Focus on Basal Insulin/Glucagon-Like Peptide-1 Receptor Agonist Combination Therapy
- From Randomized Controlled Trials to the Real World: Putting Evidence into Context
- Approaches to Increase Colorectal Cancer Screening Rates: Key Information for the Family Physician
This supplement offers the opportunity to earn a total of 1.0 CME credits.
Credit is awarded for successful completion of the online evaluations at the link below. This link may also be found within the supplement on the first page of the article.
- Long-term Treatment of Gout: New Opportunities for Improved Outcomes
- To complete the online evaluation and receive 1 CME credit for this article: please click on the link at the end of the article or go to www.pceconsortium.org/gout.

Address physical health risks of people with SMI
ROCKVILLE, MD. – The problem of medical comorbidities in people with serious mental illness (SMI) persists and must be addressed, researchers said at a National Institute on Mental Health conference on mental health services research. Part of that effort, they said, is a more careful consideration of risks tied to the off-label use of second-generation antipsychotics.

The researchers discussed strategies aimed at combating obesity and diabetes, as well as behaviors such as smoking and sedentary lifestyle.
“One of the things that jumps out is the tremendous need for evidence-based strategies to address these physical health problems that are common in general population but even more of a burden for people with serious mental illness,” said Susan T. Azrin, PhD, of the NIMH, in an interview.
A study published in 2015, estimated that people with schizophrenia, for example, might lose almost 30 years of life because of premature death. Individuals with serious mental illness also experience elevated morbidity from cardiovascular disease and cancer. The NIMH and other federal agencies have in recent years looked for ways to help people with SMI quit smoking, and better control their weight and cholesterol.
But approaches that sound promising for boosting physical fitness in this group of patients have not always proven successful. Joshua Breslau, PhD, ScD, of the Rand Corp. discussed findings from a 2014 paper where he and his colleagues reported somewhat disappointing results from a study of federal Primary and Behavioral Health Care Integration grants.
The researchers matched clinics receiving this funding with similar ones that did not. They found that people with mental illness treated at the clinics receiving the grants showed improvements in some indicators of physical health (diastolic blood pressure, total cholesterol, LDL cholesterol, and fasting plasma glucose) but not in others (systolic blood pressure, body mass index, HDL cholesterol, hemoglobin A1c, triglycerides, self-reported smoking). Dr. Breslau said he and his colleagues also found only limited benefits in quality of care for physical health conditions associated with the grant program. Still, he remains hopeful.
“There is some potential here,” Dr. Breslau said. “Sometimes, we are seeing positive effects, but it’s certainly not a slam-dunk.”
He noted that opening a new setting for primary care services could strain a workforce that’s already in short supply. In addition, he said, attempts to fold primary care services into mental health programs could, in some cases, result in replication of care of chronic conditions for certain patients with SMI.
We “may still not reach that portion of the target population that has the greatest need,” Dr. Breslau said in an interview. “The new services may turn out to be duplicative rather than filling a gap.”
In another session, Gail L. Daumit, MD, MHS, of Johns Hopkins University, Baltimore, discussed her plan to build on a past success in helping people with SMI lose weight.
In the ACHIEVE (Achieving Healthy Lifestyles In Psych Rehabilitation) trial, Dr. Daumit and her colleagues found that people enrolled in an intervention group lost an average of 3.2 kg more than did a control group after 18 months (N Engl J Med. 2013;368:1594-602). The intervention steps included alternating group and individual weight management sessions, on-site group physical activity three times weekly, and weigh-ins. The study had 291 patients who were randomized between the control and intervention groups.
that can be used more broadly. She’s seeking to scale up effective interventions to address cardiovascular risk factors in people with SMI.
“Our goal is not just to get process-of-care measures like ‘counseling was delivered,’ ‘a medicine was started,’ but to actually show impact on health outcomes,” Dr. Daumit said.
Risks tied to antipsychotics
People with SMI face cardiovascular risks not only from unhealthy behaviors but also from the medications used to treat their psychiatric conditions. The American Diabetes Association and American Psychiatric Association in 2004 released a consensus statement on the impact of antipsychotics such as clozapine, olanzapine, and risperidone on obesity and diabetes. It included guidelines for monitoring the metabolic status of patients both at baseline and after initiating treatment, including checking body mass index, waist circumference, blood pressure, fasting glucose, and fasting lipids.
Yet, substantial evidence suggests that the medical community still has not paid enough attention to the health risks of those medications, said Alisa Busch, MD, of Harvard Medical School, Boston.
“A slew of research has shown since then that we have done a very poor job in adhering to those monitoring guidelines,” Dr. Busch said.
A fellow panelist, Marcela Horvitz-Lennon, MD, MPH, of the Rand Corp., presented results from her study showing continued common use of second-generation antipsychotics for off-label use for treatment of anxiety, posttraumatic stress disorder, and dementia in people of all ages.
Consistent with previous research, Dr. Horvitz-Lennon and her colleagues found that off-label use of second-generation antipsychotics was common during 2008-2012 in the four states they studied. They looked at available data from fee-for-service Medicare, Medicaid, and dually (Medicaid-Medicare) covered adult beneficiaries in California, Georgia, Mississippi, and Oklahoma.
Throughout the study period, California had the highest rate of fee-for-service beneficiaries whose SGA use was consistently off label (44.6%). Georgia had the lowest rate of always off-label use (35.1%), while Mississippi (42%) and Oklahoma (36.3%) fell somewhere in the middle.
When second-generation antipsychotics have approved uses such as schizophrenia, the known profile of a medication gives some assurance that the benefit of the medications will exceed the risk for that patient, she said. “When the medication is used off label, the implication is that there is no good evidence that the benefits are there,” Dr. Horvitz-Lennon said. “Hence, the potential for harm is most likely exceeding that likely or unlikely benefit.”
Dr. Daumit, Dr. Breslau, and Dr. Horvitz-Lennon said they had no financial disclosures.
ROCKVILLE, MD. – The problem of medical comorbidities in people with serious mental illness (SMI) persists and must be addressed, researchers said at a National Institute on Mental Health conference on mental health services research. Part of that effort, they said, is a more careful consideration of risks tied to the off-label use of second-generation antipsychotics.
The researchers discussed strategies aimed at combating obesity and diabetes, as well as behaviors such as smoking and sedentary lifestyle.
“One of the things that jumps out is the tremendous need for evidence-based strategies to address these physical health problems that are common in general population but even more of a burden for people with serious mental illness,” said Susan T. Azrin, PhD, of the NIMH, in an interview.
A study published in 2015, estimated that people with schizophrenia, for example, might lose almost 30 years of life because of premature death. Individuals with serious mental illness also experience elevated morbidity from cardiovascular disease and cancer. The NIMH and other federal agencies have in recent years looked for ways to help people with SMI quit smoking, and better control their weight and cholesterol.
But approaches that sound promising for boosting physical fitness in this group of patients have not always proven successful. Joshua Breslau, PhD, ScD, of the Rand Corp. discussed findings from a 2014 paper where he and his colleagues reported somewhat disappointing results from a study of federal Primary and Behavioral Health Care Integration grants.
The researchers matched clinics receiving this funding with similar ones that did not. They found that people with mental illness treated at the clinics receiving the grants showed improvements in some indicators of physical health (diastolic blood pressure, total cholesterol, LDL cholesterol, and fasting plasma glucose) but not in others (systolic blood pressure, body mass index, HDL cholesterol, hemoglobin A1c, triglycerides, self-reported smoking). Dr. Breslau said he and his colleagues also found only limited benefits in quality of care for physical health conditions associated with the grant program. Still, he remains hopeful.
“There is some potential here,” Dr. Breslau said. “Sometimes, we are seeing positive effects, but it’s certainly not a slam-dunk.”
He noted that opening a new setting for primary care services could strain a workforce that’s already in short supply. In addition, he said, attempts to fold primary care services into mental health programs could, in some cases, result in replication of care of chronic conditions for certain patients with SMI.
We “may still not reach that portion of the target population that has the greatest need,” Dr. Breslau said in an interview. “The new services may turn out to be duplicative rather than filling a gap.”
In another session, Gail L. Daumit, MD, MHS, of Johns Hopkins University, Baltimore, discussed her plan to build on a past success in helping people with SMI lose weight.
In the ACHIEVE (Achieving Healthy Lifestyles In Psych Rehabilitation) trial, Dr. Daumit and her colleagues found that people enrolled in an intervention group lost an average of 3.2 kg more than did a control group after 18 months (N Engl J Med. 2013;368:1594-602). The intervention steps included alternating group and individual weight management sessions, on-site group physical activity three times weekly, and weigh-ins. The study had 291 patients who were randomized between the control and intervention groups.
that can be used more broadly. She’s seeking to scale up effective interventions to address cardiovascular risk factors in people with SMI.
“Our goal is not just to get process-of-care measures like ‘counseling was delivered,’ ‘a medicine was started,’ but to actually show impact on health outcomes,” Dr. Daumit said.
Risks tied to antipsychotics
People with SMI face cardiovascular risks not only from unhealthy behaviors but also from the medications used to treat their psychiatric conditions. The American Diabetes Association and American Psychiatric Association in 2004 released a consensus statement on the impact of antipsychotics such as clozapine, olanzapine, and risperidone on obesity and diabetes. It included guidelines for monitoring the metabolic status of patients both at baseline and after initiating treatment, including checking body mass index, waist circumference, blood pressure, fasting glucose, and fasting lipids.
Yet, substantial evidence suggests that the medical community still has not paid enough attention to the health risks of those medications, said Alisa Busch, MD, of Harvard Medical School, Boston.
“A slew of research has shown since then that we have done a very poor job in adhering to those monitoring guidelines,” Dr. Busch said.
A fellow panelist, Marcela Horvitz-Lennon, MD, MPH, of the Rand Corp., presented results from her study showing continued common use of second-generation antipsychotics for off-label use for treatment of anxiety, posttraumatic stress disorder, and dementia in people of all ages.
Consistent with previous research, Dr. Horvitz-Lennon and her colleagues found that off-label use of second-generation antipsychotics was common during 2008-2012 in the four states they studied. They looked at available data from fee-for-service Medicare, Medicaid, and dually (Medicaid-Medicare) covered adult beneficiaries in California, Georgia, Mississippi, and Oklahoma.
Throughout the study period, California had the highest rate of fee-for-service beneficiaries whose SGA use was consistently off label (44.6%). Georgia had the lowest rate of always off-label use (35.1%), while Mississippi (42%) and Oklahoma (36.3%) fell somewhere in the middle.
When second-generation antipsychotics have approved uses such as schizophrenia, the known profile of a medication gives some assurance that the benefit of the medications will exceed the risk for that patient, she said. “When the medication is used off label, the implication is that there is no good evidence that the benefits are there,” Dr. Horvitz-Lennon said. “Hence, the potential for harm is most likely exceeding that likely or unlikely benefit.”
Dr. Daumit, Dr. Breslau, and Dr. Horvitz-Lennon said they had no financial disclosures.
ROCKVILLE, MD. – The problem of medical comorbidities in people with serious mental illness (SMI) persists and must be addressed, researchers said at a National Institute on Mental Health conference on mental health services research. Part of that effort, they said, is a more careful consideration of risks tied to the off-label use of second-generation antipsychotics.
The researchers discussed strategies aimed at combating obesity and diabetes, as well as behaviors such as smoking and sedentary lifestyle.
“One of the things that jumps out is the tremendous need for evidence-based strategies to address these physical health problems that are common in general population but even more of a burden for people with serious mental illness,” said Susan T. Azrin, PhD, of the NIMH, in an interview.
A study published in 2015, estimated that people with schizophrenia, for example, might lose almost 30 years of life because of premature death. Individuals with serious mental illness also experience elevated morbidity from cardiovascular disease and cancer. The NIMH and other federal agencies have in recent years looked for ways to help people with SMI quit smoking, and better control their weight and cholesterol.
But approaches that sound promising for boosting physical fitness in this group of patients have not always proven successful. Joshua Breslau, PhD, ScD, of the Rand Corp. discussed findings from a 2014 paper where he and his colleagues reported somewhat disappointing results from a study of federal Primary and Behavioral Health Care Integration grants.
The researchers matched clinics receiving this funding with similar ones that did not. They found that people with mental illness treated at the clinics receiving the grants showed improvements in some indicators of physical health (diastolic blood pressure, total cholesterol, LDL cholesterol, and fasting plasma glucose) but not in others (systolic blood pressure, body mass index, HDL cholesterol, hemoglobin A1c, triglycerides, self-reported smoking). Dr. Breslau said he and his colleagues also found only limited benefits in quality of care for physical health conditions associated with the grant program. Still, he remains hopeful.
“There is some potential here,” Dr. Breslau said. “Sometimes, we are seeing positive effects, but it’s certainly not a slam-dunk.”
He noted that opening a new setting for primary care services could strain a workforce that’s already in short supply. In addition, he said, attempts to fold primary care services into mental health programs could, in some cases, result in replication of care of chronic conditions for certain patients with SMI.
We “may still not reach that portion of the target population that has the greatest need,” Dr. Breslau said in an interview. “The new services may turn out to be duplicative rather than filling a gap.”
In another session, Gail L. Daumit, MD, MHS, of Johns Hopkins University, Baltimore, discussed her plan to build on a past success in helping people with SMI lose weight.
In the ACHIEVE (Achieving Healthy Lifestyles In Psych Rehabilitation) trial, Dr. Daumit and her colleagues found that people enrolled in an intervention group lost an average of 3.2 kg more than did a control group after 18 months (N Engl J Med. 2013;368:1594-602). The intervention steps included alternating group and individual weight management sessions, on-site group physical activity three times weekly, and weigh-ins. The study had 291 patients who were randomized between the control and intervention groups.
that can be used more broadly. She’s seeking to scale up effective interventions to address cardiovascular risk factors in people with SMI.
“Our goal is not just to get process-of-care measures like ‘counseling was delivered,’ ‘a medicine was started,’ but to actually show impact on health outcomes,” Dr. Daumit said.
Risks tied to antipsychotics
People with SMI face cardiovascular risks not only from unhealthy behaviors but also from the medications used to treat their psychiatric conditions. The American Diabetes Association and American Psychiatric Association in 2004 released a consensus statement on the impact of antipsychotics such as clozapine, olanzapine, and risperidone on obesity and diabetes. It included guidelines for monitoring the metabolic status of patients both at baseline and after initiating treatment, including checking body mass index, waist circumference, blood pressure, fasting glucose, and fasting lipids.
Yet, substantial evidence suggests that the medical community still has not paid enough attention to the health risks of those medications, said Alisa Busch, MD, of Harvard Medical School, Boston.
“A slew of research has shown since then that we have done a very poor job in adhering to those monitoring guidelines,” Dr. Busch said.
A fellow panelist, Marcela Horvitz-Lennon, MD, MPH, of the Rand Corp., presented results from her study showing continued common use of second-generation antipsychotics for off-label use for treatment of anxiety, posttraumatic stress disorder, and dementia in people of all ages.
Consistent with previous research, Dr. Horvitz-Lennon and her colleagues found that off-label use of second-generation antipsychotics was common during 2008-2012 in the four states they studied. They looked at available data from fee-for-service Medicare, Medicaid, and dually (Medicaid-Medicare) covered adult beneficiaries in California, Georgia, Mississippi, and Oklahoma.
Throughout the study period, California had the highest rate of fee-for-service beneficiaries whose SGA use was consistently off label (44.6%). Georgia had the lowest rate of always off-label use (35.1%), while Mississippi (42%) and Oklahoma (36.3%) fell somewhere in the middle.
When second-generation antipsychotics have approved uses such as schizophrenia, the known profile of a medication gives some assurance that the benefit of the medications will exceed the risk for that patient, she said. “When the medication is used off label, the implication is that there is no good evidence that the benefits are there,” Dr. Horvitz-Lennon said. “Hence, the potential for harm is most likely exceeding that likely or unlikely benefit.”
Dr. Daumit, Dr. Breslau, and Dr. Horvitz-Lennon said they had no financial disclosures.
REPORTING FROM AN NIMH CONFERENCE
Breast arterial calcification, low bone mass predict CAD in women
Breast arterial calcification and low bone mass (LBM) were strongly linked to risk of coronary artery disease in asymptomatic women, according to a cross-sectional registry study. 
The results suggest that breast arterial calcification – easily visible on every mammogram – “provides an independent and incremental predictive value over conventional risk factors,” wrote Yeonyee E. Yoon, MD, and colleagues from Seoul National University Bundang Hospital in Seongnam, South Korea.
In addition, they show that “atherosclerosis imaging allows a more direct visualization of the cumulative effects of all risk determinants in an individual patient,” they noted. The report is in JACC: Cardiovascular Imaging.
The researchers evaluated 2,100 asymptomatic women aged at least 40 years in the Women Health Registry Study for Bone, Breast, and Coronary Artery Disease (BBC study). All underwent a self-referred health evaluation that included simultaneous dual-energy x-ray absorptiometry (DXA), coronary computed tomography angiography (CCTA), and digital mammography. They predicted the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) with the Korean Risk Prediction Model (KRPM) and Pooled Cohort Equation (PCE).
Overall, Dr. Yoon and colleagues found that 199 patients (9.5%) had BAC and 716 patients (34.1%) had LBM, with 235 patients (11.2%) having coronary artery calcification (CAC) and 328 with coronary artery plaque (CAP, 15.6%). BAC presence was associated with CAC (unadjusted odds ratio, 3.54), with mild (OR, 2.84) and severe BAC scores (OR, 5.50) having a greater association with CAC. All associations were statistically significant at P less than .001.
LBM also had a positive link with CAC that grew with its severity. Specifically, the odds ratio of CAC with osteopenia, defined as a T-score between –1.0 and –2.5, was 2.06, and that for osteoporosis, defined as a T-score at or below –2.5, was 3.21. All links were significant at P less than .001.
Similarly, BAC and LBM were also significantly tied to coronary artery plaque, with mild (OR, 2.61) and moderate (OR, 4.15) BAC severity as well as osteopenia (OR, 1.76) and osteoporosis (OR 2.82) being significantly associated with CAP (all P less than .001).
In a multivariable analysis, BAC presence and BAC score were significantly associated with CAC and CAP after adjustment for 10-year ASCVD risk. Predictions for CAC and CAP under the KRPM and PCE curve analyses showed a significant increase of areas under the curve (0.71 vs. 0.64), while adding BAC presence significantly increased the AUCs for the KRPM curve analysis (0.61 vs 0.64).
“Being able to predict CAC or CAP presence in an individual patient based on the presence and severity of BAC in addition to the use of conventional risk stratification algorithms may help clinicians decide when to recommend further cardiac tests and how aggressive interventions to prescribe in order to prevent the onset of clinical CAD,” the researchers noted.
They added that patients were all self-referred women, and results may not be generalizable to a larger population. The study’s retrospective nature also is a limitation, the researchers wrote. However, they said they are planning a future trial that will attempt to determine whether there is a long-term clinical benefit to identifying BAC and LBM in women without symptoms of CAD.
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea; the Ministry of Science, ICT, and Future Planning; and the Seoul National University Bundang Hospital Research Fund. The authors report no relevant financial disclosures.
SOURCE: Yoon YE et al. JACC: Cardiovasc Imaging. 2018 Aug 15. doi: 10.1016/j.jcmg.2018.07.004.
Breast arterial calcification and low bone mass (LBM) were strongly linked to risk of coronary artery disease in asymptomatic women, according to a cross-sectional registry study.
The results suggest that breast arterial calcification – easily visible on every mammogram – “provides an independent and incremental predictive value over conventional risk factors,” wrote Yeonyee E. Yoon, MD, and colleagues from Seoul National University Bundang Hospital in Seongnam, South Korea.
In addition, they show that “atherosclerosis imaging allows a more direct visualization of the cumulative effects of all risk determinants in an individual patient,” they noted. The report is in JACC: Cardiovascular Imaging.
The researchers evaluated 2,100 asymptomatic women aged at least 40 years in the Women Health Registry Study for Bone, Breast, and Coronary Artery Disease (BBC study). All underwent a self-referred health evaluation that included simultaneous dual-energy x-ray absorptiometry (DXA), coronary computed tomography angiography (CCTA), and digital mammography. They predicted the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) with the Korean Risk Prediction Model (KRPM) and Pooled Cohort Equation (PCE).
Overall, Dr. Yoon and colleagues found that 199 patients (9.5%) had BAC and 716 patients (34.1%) had LBM, with 235 patients (11.2%) having coronary artery calcification (CAC) and 328 with coronary artery plaque (CAP, 15.6%). BAC presence was associated with CAC (unadjusted odds ratio, 3.54), with mild (OR, 2.84) and severe BAC scores (OR, 5.50) having a greater association with CAC. All associations were statistically significant at P less than .001.
LBM also had a positive link with CAC that grew with its severity. Specifically, the odds ratio of CAC with osteopenia, defined as a T-score between –1.0 and –2.5, was 2.06, and that for osteoporosis, defined as a T-score at or below –2.5, was 3.21. All links were significant at P less than .001.
Similarly, BAC and LBM were also significantly tied to coronary artery plaque, with mild (OR, 2.61) and moderate (OR, 4.15) BAC severity as well as osteopenia (OR, 1.76) and osteoporosis (OR 2.82) being significantly associated with CAP (all P less than .001).
In a multivariable analysis, BAC presence and BAC score were significantly associated with CAC and CAP after adjustment for 10-year ASCVD risk. Predictions for CAC and CAP under the KRPM and PCE curve analyses showed a significant increase of areas under the curve (0.71 vs. 0.64), while adding BAC presence significantly increased the AUCs for the KRPM curve analysis (0.61 vs 0.64).
“Being able to predict CAC or CAP presence in an individual patient based on the presence and severity of BAC in addition to the use of conventional risk stratification algorithms may help clinicians decide when to recommend further cardiac tests and how aggressive interventions to prescribe in order to prevent the onset of clinical CAD,” the researchers noted.
They added that patients were all self-referred women, and results may not be generalizable to a larger population. The study’s retrospective nature also is a limitation, the researchers wrote. However, they said they are planning a future trial that will attempt to determine whether there is a long-term clinical benefit to identifying BAC and LBM in women without symptoms of CAD.
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea; the Ministry of Science, ICT, and Future Planning; and the Seoul National University Bundang Hospital Research Fund. The authors report no relevant financial disclosures.
SOURCE: Yoon YE et al. JACC: Cardiovasc Imaging. 2018 Aug 15. doi: 10.1016/j.jcmg.2018.07.004.
Breast arterial calcification and low bone mass (LBM) were strongly linked to risk of coronary artery disease in asymptomatic women, according to a cross-sectional registry study.
The results suggest that breast arterial calcification – easily visible on every mammogram – “provides an independent and incremental predictive value over conventional risk factors,” wrote Yeonyee E. Yoon, MD, and colleagues from Seoul National University Bundang Hospital in Seongnam, South Korea.
In addition, they show that “atherosclerosis imaging allows a more direct visualization of the cumulative effects of all risk determinants in an individual patient,” they noted. The report is in JACC: Cardiovascular Imaging.
The researchers evaluated 2,100 asymptomatic women aged at least 40 years in the Women Health Registry Study for Bone, Breast, and Coronary Artery Disease (BBC study). All underwent a self-referred health evaluation that included simultaneous dual-energy x-ray absorptiometry (DXA), coronary computed tomography angiography (CCTA), and digital mammography. They predicted the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) with the Korean Risk Prediction Model (KRPM) and Pooled Cohort Equation (PCE).
Overall, Dr. Yoon and colleagues found that 199 patients (9.5%) had BAC and 716 patients (34.1%) had LBM, with 235 patients (11.2%) having coronary artery calcification (CAC) and 328 with coronary artery plaque (CAP, 15.6%). BAC presence was associated with CAC (unadjusted odds ratio, 3.54), with mild (OR, 2.84) and severe BAC scores (OR, 5.50) having a greater association with CAC. All associations were statistically significant at P less than .001.
LBM also had a positive link with CAC that grew with its severity. Specifically, the odds ratio of CAC with osteopenia, defined as a T-score between –1.0 and –2.5, was 2.06, and that for osteoporosis, defined as a T-score at or below –2.5, was 3.21. All links were significant at P less than .001.
Similarly, BAC and LBM were also significantly tied to coronary artery plaque, with mild (OR, 2.61) and moderate (OR, 4.15) BAC severity as well as osteopenia (OR, 1.76) and osteoporosis (OR 2.82) being significantly associated with CAP (all P less than .001).
In a multivariable analysis, BAC presence and BAC score were significantly associated with CAC and CAP after adjustment for 10-year ASCVD risk. Predictions for CAC and CAP under the KRPM and PCE curve analyses showed a significant increase of areas under the curve (0.71 vs. 0.64), while adding BAC presence significantly increased the AUCs for the KRPM curve analysis (0.61 vs 0.64).
“Being able to predict CAC or CAP presence in an individual patient based on the presence and severity of BAC in addition to the use of conventional risk stratification algorithms may help clinicians decide when to recommend further cardiac tests and how aggressive interventions to prescribe in order to prevent the onset of clinical CAD,” the researchers noted.
They added that patients were all self-referred women, and results may not be generalizable to a larger population. The study’s retrospective nature also is a limitation, the researchers wrote. However, they said they are planning a future trial that will attempt to determine whether there is a long-term clinical benefit to identifying BAC and LBM in women without symptoms of CAD.
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea; the Ministry of Science, ICT, and Future Planning; and the Seoul National University Bundang Hospital Research Fund. The authors report no relevant financial disclosures.
SOURCE: Yoon YE et al. JACC: Cardiovasc Imaging. 2018 Aug 15. doi: 10.1016/j.jcmg.2018.07.004.
FROM JACC: CARDIOVASCULAR IMAGING
Key clinical point:
Major finding: Breast arterial calcification (BAC) carried an odds ratio of 3.54 and low bone mass (LBM) carried an OR of 2.22 for the associated presence of coronary artery calcification, while BAC had an OR of 3.02 and LBM had an OR of 1.92 for associated presence of coronary atherosclerotic plaque.
Study details: A cross-sectional study of 2,100 women analyzed for subclinical coronary artery disease in the Bone, Breast, and CAD health registry study.
Disclosures: This study was supported by the Basic Science Research Program through the National Research Foundation of Korea; the Ministry of Science, ICT, and Future Planning; and the Seoul National University Bundang Hospital Research Fund. The authors report no relevant financial disclosures.
Source: Yoon YE et al. JACC: Cardiovasc Imaging. 2018 Aug 15; doi: 10.1016/j.jcmg.2018.07.004.
First-ever gestational trophoblastic neoplasia guidelines published
The National Comprehensive Cancer Network (NCCN) has issued its first-ever clinical practice guidelines for the treatment of gestational trophoblastic neoplasia (GTN), a rare, serious complication of pregnancy that can often be cured, but can have devastating consequences if mismanaged or if treatment is needlessly delayed.
David Mutch, MD, of the Siteman Cancer Center at Barnes-Jewish Hospital and Washington University in St. Louis, who heads the NCCN Clinical Practice Guidelines in Oncology Committee for GTN, explained the critical importance of the GTN guidelines.
“It’s a rare disease, people weren’t that familiar with it, and they often are patients treated with single-agent therapy when they should be treated with multi-agent therapy,” he said in an interview.
“There wasn’t a clear understanding of what to do except by those people who treated these patients regularly. The only thing most people knew was that it was very chemosensitive and should be curable, but it’s only curable if you follow the appropriate algorithms,” he continued.
The algorithms he referred to were established by a handful of centers with expertise and experience in diagnosing and treating these rare conditions, including noninvasive hydatidiform mole, invasive mole, and choriocarcinoma, the most aggressive form of GTN.
Neil Horowitz, MD, director of clinical research in gynecologic oncology at the Dana-Farber Cancer Institute in Boston, works with colleagues in one of those referral centers, the New England Trophoblastic Disease Center, and is familiar with the new guidelines. As with other rare malignancies, there are data to suggest that patients with GTN who are treated in centers of excellence with higher patient volumes have better outcomes than do similar patients treated in a community setting, he said in an interview.
Placental origins
GTNs arise from placental rather than maternal tissue. They most commonly present with vaginal bleeding and a rapidly enlarging uterus, and may be accompanied by pelvic pain or pressure, anemia, severe nausea/vomiting (hyperemesis gravidarum), hyperthyroidism, or early-pregnancy preeclampsia.
The overall reported incidence of GTN in the United States, including hydatidiform mole, is approximately 110 to 120 per 100,000 pregnancies, and the reported incidence of choriocarcinoma is about 2 to 7 per 100,000, according to the National Cancer Institute.
The GTN guidelines provide evidence-based recommendations about optimal approaches to GTN in all of its known forms. For example, the section on noninvasive hydatidiform mole recommends the tests that should be routinely performed during workup, followed by surgery with either suction, dilation and curettage – preferably under ultrasound guidance – or hysterectomy for women who are older or who do not wish to preserve fertility.
The guidelines also specify steps that should be taken for diagnosis and staging of GTN as well as risk-based therapeutic approaches.
For example, the guidelines recommend therapy with either methotrexate alone or alternating with leucovorin, or dactinomycin alone for patients with confirmed low risk GTN, defined as a prognostic score less than 7.
The prognostic scoring index, also included in the guidelines, considers risk factors such as age, prior pregnancies, interval from an index pregnancy, pretreatment human chorionic gonadotropin (hCG) levels, site and number of metastases, largest tumor size, and previous chemotherapy failure.
For patients with high-risk GTN, defined as FIGO (Fédération Internationale de Gynécologie et d’Obstétrique) stages II-III with a prognostic score of 7 or greater, or FIGO stage IV, chemotherapy with the EMA/CO regimen is recommended. This aggressive regimen consists of etoposide, methotrexate, dactinomycin (the “EMA “component) plus cyclophosphamide and vincristine (the “CO” component).
“In my mind, the most important part of the guidelines is reiterating how the diagnosis of GTN should be made, and importantly, how the score should be calculated so that women are put in the appropriate low-risk or high-risk category, so they get the right treatment,” Dr. Horowitz said.
Reassuring insurers
Dr. Mutch said that he and his colleagues in GTN centers sometimes treat patients with intermediate or high-risk disease who were started on single-agent therapy or suboptimal therapies and present with advanced, drug-resistant disease.
“These guidelines were established so that people could see exactly what needs to be done when,” he said.
The guidelines also are critical for convincing third-party payers about the need for specific treatments, he added.
“I had a high-risk patient who needed EMA/CO, and the insurance company said ‘well, there’s no NCCN guidelines – we won’t approve it.’ So then I had to wait 3 days while it went through peer review. Meanwhile, the tumor doubled in size, and then the nurse who was reviewing it declined the ‘CO’ part, so that was delayed a week, and it really jeopardized this patient’s survival,” Dr. Mutch said.
The guidelines also include recommendations for patients with special clinical situations, such as women with clinical responses to EMA/CO who continue to have plateauing low levels of hCG or have a re-elevation of hCG levels after having a complete response to EMA/CO.
There are also specific recommendations for treatment of two even rarer intermediate trophoblastic tumor types: placental-site trophoblastic tumor and epithelioid trophoblastic tumor.
The guidelines are supported by the NCCN. Dr. Mutch reported consulting/advisory board participation for Clovis. Dr. Horowitz reported having no relationships to disclose.
SOURCE: Gestational Trophoblastic Neoplasia. NCCN.org, Version 1.2019, published Aug. 9, 2018.
The National Comprehensive Cancer Network (NCCN) has issued its first-ever clinical practice guidelines for the treatment of gestational trophoblastic neoplasia (GTN), a rare, serious complication of pregnancy that can often be cured, but can have devastating consequences if mismanaged or if treatment is needlessly delayed.
David Mutch, MD, of the Siteman Cancer Center at Barnes-Jewish Hospital and Washington University in St. Louis, who heads the NCCN Clinical Practice Guidelines in Oncology Committee for GTN, explained the critical importance of the GTN guidelines.
“It’s a rare disease, people weren’t that familiar with it, and they often are patients treated with single-agent therapy when they should be treated with multi-agent therapy,” he said in an interview.
“There wasn’t a clear understanding of what to do except by those people who treated these patients regularly. The only thing most people knew was that it was very chemosensitive and should be curable, but it’s only curable if you follow the appropriate algorithms,” he continued.
The algorithms he referred to were established by a handful of centers with expertise and experience in diagnosing and treating these rare conditions, including noninvasive hydatidiform mole, invasive mole, and choriocarcinoma, the most aggressive form of GTN.
Neil Horowitz, MD, director of clinical research in gynecologic oncology at the Dana-Farber Cancer Institute in Boston, works with colleagues in one of those referral centers, the New England Trophoblastic Disease Center, and is familiar with the new guidelines. As with other rare malignancies, there are data to suggest that patients with GTN who are treated in centers of excellence with higher patient volumes have better outcomes than do similar patients treated in a community setting, he said in an interview.
Placental origins
GTNs arise from placental rather than maternal tissue. They most commonly present with vaginal bleeding and a rapidly enlarging uterus, and may be accompanied by pelvic pain or pressure, anemia, severe nausea/vomiting (hyperemesis gravidarum), hyperthyroidism, or early-pregnancy preeclampsia.
The overall reported incidence of GTN in the United States, including hydatidiform mole, is approximately 110 to 120 per 100,000 pregnancies, and the reported incidence of choriocarcinoma is about 2 to 7 per 100,000, according to the National Cancer Institute.
The GTN guidelines provide evidence-based recommendations about optimal approaches to GTN in all of its known forms. For example, the section on noninvasive hydatidiform mole recommends the tests that should be routinely performed during workup, followed by surgery with either suction, dilation and curettage – preferably under ultrasound guidance – or hysterectomy for women who are older or who do not wish to preserve fertility.
The guidelines also specify steps that should be taken for diagnosis and staging of GTN as well as risk-based therapeutic approaches.
For example, the guidelines recommend therapy with either methotrexate alone or alternating with leucovorin, or dactinomycin alone for patients with confirmed low risk GTN, defined as a prognostic score less than 7.
The prognostic scoring index, also included in the guidelines, considers risk factors such as age, prior pregnancies, interval from an index pregnancy, pretreatment human chorionic gonadotropin (hCG) levels, site and number of metastases, largest tumor size, and previous chemotherapy failure.
For patients with high-risk GTN, defined as FIGO (Fédération Internationale de Gynécologie et d’Obstétrique) stages II-III with a prognostic score of 7 or greater, or FIGO stage IV, chemotherapy with the EMA/CO regimen is recommended. This aggressive regimen consists of etoposide, methotrexate, dactinomycin (the “EMA “component) plus cyclophosphamide and vincristine (the “CO” component).
“In my mind, the most important part of the guidelines is reiterating how the diagnosis of GTN should be made, and importantly, how the score should be calculated so that women are put in the appropriate low-risk or high-risk category, so they get the right treatment,” Dr. Horowitz said.
Reassuring insurers
Dr. Mutch said that he and his colleagues in GTN centers sometimes treat patients with intermediate or high-risk disease who were started on single-agent therapy or suboptimal therapies and present with advanced, drug-resistant disease.
“These guidelines were established so that people could see exactly what needs to be done when,” he said.
The guidelines also are critical for convincing third-party payers about the need for specific treatments, he added.
“I had a high-risk patient who needed EMA/CO, and the insurance company said ‘well, there’s no NCCN guidelines – we won’t approve it.’ So then I had to wait 3 days while it went through peer review. Meanwhile, the tumor doubled in size, and then the nurse who was reviewing it declined the ‘CO’ part, so that was delayed a week, and it really jeopardized this patient’s survival,” Dr. Mutch said.
The guidelines also include recommendations for patients with special clinical situations, such as women with clinical responses to EMA/CO who continue to have plateauing low levels of hCG or have a re-elevation of hCG levels after having a complete response to EMA/CO.
There are also specific recommendations for treatment of two even rarer intermediate trophoblastic tumor types: placental-site trophoblastic tumor and epithelioid trophoblastic tumor.
The guidelines are supported by the NCCN. Dr. Mutch reported consulting/advisory board participation for Clovis. Dr. Horowitz reported having no relationships to disclose.
SOURCE: Gestational Trophoblastic Neoplasia. NCCN.org, Version 1.2019, published Aug. 9, 2018.
The National Comprehensive Cancer Network (NCCN) has issued its first-ever clinical practice guidelines for the treatment of gestational trophoblastic neoplasia (GTN), a rare, serious complication of pregnancy that can often be cured, but can have devastating consequences if mismanaged or if treatment is needlessly delayed.
David Mutch, MD, of the Siteman Cancer Center at Barnes-Jewish Hospital and Washington University in St. Louis, who heads the NCCN Clinical Practice Guidelines in Oncology Committee for GTN, explained the critical importance of the GTN guidelines.
“It’s a rare disease, people weren’t that familiar with it, and they often are patients treated with single-agent therapy when they should be treated with multi-agent therapy,” he said in an interview.
“There wasn’t a clear understanding of what to do except by those people who treated these patients regularly. The only thing most people knew was that it was very chemosensitive and should be curable, but it’s only curable if you follow the appropriate algorithms,” he continued.
The algorithms he referred to were established by a handful of centers with expertise and experience in diagnosing and treating these rare conditions, including noninvasive hydatidiform mole, invasive mole, and choriocarcinoma, the most aggressive form of GTN.
Neil Horowitz, MD, director of clinical research in gynecologic oncology at the Dana-Farber Cancer Institute in Boston, works with colleagues in one of those referral centers, the New England Trophoblastic Disease Center, and is familiar with the new guidelines. As with other rare malignancies, there are data to suggest that patients with GTN who are treated in centers of excellence with higher patient volumes have better outcomes than do similar patients treated in a community setting, he said in an interview.
Placental origins
GTNs arise from placental rather than maternal tissue. They most commonly present with vaginal bleeding and a rapidly enlarging uterus, and may be accompanied by pelvic pain or pressure, anemia, severe nausea/vomiting (hyperemesis gravidarum), hyperthyroidism, or early-pregnancy preeclampsia.
The overall reported incidence of GTN in the United States, including hydatidiform mole, is approximately 110 to 120 per 100,000 pregnancies, and the reported incidence of choriocarcinoma is about 2 to 7 per 100,000, according to the National Cancer Institute.
The GTN guidelines provide evidence-based recommendations about optimal approaches to GTN in all of its known forms. For example, the section on noninvasive hydatidiform mole recommends the tests that should be routinely performed during workup, followed by surgery with either suction, dilation and curettage – preferably under ultrasound guidance – or hysterectomy for women who are older or who do not wish to preserve fertility.
The guidelines also specify steps that should be taken for diagnosis and staging of GTN as well as risk-based therapeutic approaches.
For example, the guidelines recommend therapy with either methotrexate alone or alternating with leucovorin, or dactinomycin alone for patients with confirmed low risk GTN, defined as a prognostic score less than 7.
The prognostic scoring index, also included in the guidelines, considers risk factors such as age, prior pregnancies, interval from an index pregnancy, pretreatment human chorionic gonadotropin (hCG) levels, site and number of metastases, largest tumor size, and previous chemotherapy failure.
For patients with high-risk GTN, defined as FIGO (Fédération Internationale de Gynécologie et d’Obstétrique) stages II-III with a prognostic score of 7 or greater, or FIGO stage IV, chemotherapy with the EMA/CO regimen is recommended. This aggressive regimen consists of etoposide, methotrexate, dactinomycin (the “EMA “component) plus cyclophosphamide and vincristine (the “CO” component).
“In my mind, the most important part of the guidelines is reiterating how the diagnosis of GTN should be made, and importantly, how the score should be calculated so that women are put in the appropriate low-risk or high-risk category, so they get the right treatment,” Dr. Horowitz said.
Reassuring insurers
Dr. Mutch said that he and his colleagues in GTN centers sometimes treat patients with intermediate or high-risk disease who were started on single-agent therapy or suboptimal therapies and present with advanced, drug-resistant disease.
“These guidelines were established so that people could see exactly what needs to be done when,” he said.
The guidelines also are critical for convincing third-party payers about the need for specific treatments, he added.
“I had a high-risk patient who needed EMA/CO, and the insurance company said ‘well, there’s no NCCN guidelines – we won’t approve it.’ So then I had to wait 3 days while it went through peer review. Meanwhile, the tumor doubled in size, and then the nurse who was reviewing it declined the ‘CO’ part, so that was delayed a week, and it really jeopardized this patient’s survival,” Dr. Mutch said.
The guidelines also include recommendations for patients with special clinical situations, such as women with clinical responses to EMA/CO who continue to have plateauing low levels of hCG or have a re-elevation of hCG levels after having a complete response to EMA/CO.
There are also specific recommendations for treatment of two even rarer intermediate trophoblastic tumor types: placental-site trophoblastic tumor and epithelioid trophoblastic tumor.
The guidelines are supported by the NCCN. Dr. Mutch reported consulting/advisory board participation for Clovis. Dr. Horowitz reported having no relationships to disclose.
SOURCE: Gestational Trophoblastic Neoplasia. NCCN.org, Version 1.2019, published Aug. 9, 2018.
Key clinical point: Gestational trophoblastic neoplasia (GTN) is a complication of pregnancy involving rare placental derived tumors that are generally curable with appropriate therapy, best delivered at a center of excellence.
Major finding: National Comprehensive Cancer Network Guidelines specify risk-based therapy for GTN based on staging and prognostic indicators.
Study details: Evidence-based guidelines issued by the National Comprehensive Cancer Network.
Disclosures: The guidelines are supported by the NCCN. Dr. Mutch reported consulting/advisory board participation for Clovis. Dr. Horowitz reported having no disclosures to report.
Source: Gestational Trophoblastic Neoplasia. NCCN.org, Version 1.2019, published Aug. 9, 2018.
Phase 1 CAR T trial for NHL launches in Cleveland
University Hospitals Seidman Cancer Center in Cleveland has launched a phase 1 clinical trial to study the safety of CAR T therapy for non-Hodgkin lymphoma.
The trial will enroll 12-15 adult patients with non-Hodgkin lymphoma who have not responded to standard therapies, according to a statement from University Hospitals Seidman Cancer Center.
The principal investigator for the trial will be Paolo Caimi, MD, of UH Seidman and Case Western Reserve University.
UH Seidman, affiliated with Case Western Reserve University, is one of a handful of centers that has the ability to manufacture the CAR T cells from the patient’s own genetically modified T cells on site in the shared Case Western Reserve University National Center for Regenerative Medicine and the UH Seidman Cellular Therapy Laboratory, saving time for patients.
“Having the ability to make cells on-site means there will be a shorter turnaround time in having the cells available for the patient, compared to shipping them off-site,” said Dr. Caimi in the press statement.
University Hospitals Seidman Cancer Center in Cleveland has launched a phase 1 clinical trial to study the safety of CAR T therapy for non-Hodgkin lymphoma.
The trial will enroll 12-15 adult patients with non-Hodgkin lymphoma who have not responded to standard therapies, according to a statement from University Hospitals Seidman Cancer Center.
The principal investigator for the trial will be Paolo Caimi, MD, of UH Seidman and Case Western Reserve University.
UH Seidman, affiliated with Case Western Reserve University, is one of a handful of centers that has the ability to manufacture the CAR T cells from the patient’s own genetically modified T cells on site in the shared Case Western Reserve University National Center for Regenerative Medicine and the UH Seidman Cellular Therapy Laboratory, saving time for patients.
“Having the ability to make cells on-site means there will be a shorter turnaround time in having the cells available for the patient, compared to shipping them off-site,” said Dr. Caimi in the press statement.
University Hospitals Seidman Cancer Center in Cleveland has launched a phase 1 clinical trial to study the safety of CAR T therapy for non-Hodgkin lymphoma.
The trial will enroll 12-15 adult patients with non-Hodgkin lymphoma who have not responded to standard therapies, according to a statement from University Hospitals Seidman Cancer Center.
The principal investigator for the trial will be Paolo Caimi, MD, of UH Seidman and Case Western Reserve University.
UH Seidman, affiliated with Case Western Reserve University, is one of a handful of centers that has the ability to manufacture the CAR T cells from the patient’s own genetically modified T cells on site in the shared Case Western Reserve University National Center for Regenerative Medicine and the UH Seidman Cellular Therapy Laboratory, saving time for patients.
“Having the ability to make cells on-site means there will be a shorter turnaround time in having the cells available for the patient, compared to shipping them off-site,” said Dr. Caimi in the press statement.
Key clinical point: A phase 1 trial of CAR T therapy is enrolling adult patients with NHL who have not responded to standard therapies.
Major finding: The trial site has the ability to manufacture the cells on site, saving patients time.
Study details: A phase 1 trial to evaluate safety.
Disclosures: The study will be funded by University Hospitals Seidman Cancer Center.
Dr David Henry's top ASCO selections in hematology and bone health
David Henry, MD, the Editor-in-Chief of The Journal of Community and Supportive Oncology, shares his top selections in hematology and bone health from this year's line-up of abstracts at the annual meeting of the American Society of Clinical Oncology in Chicago.
8004 Phase 2 study of venetoclax plus carfilzomib and dexamethasone in patients with relapsed refractory myeloma (Luciano J Costa et al). Of 17 patients evaluated after completing at least two cycles of therapy, 3 had complete responses, 2 had very good partial response, 3 had partial response, 3 experienced stable disease, and 2 had progressive disease (response data for 4 patients still to come). The study drug combination was well tolerated, and phase 3 trial is planned.
8008 FDA analysis of pembrolizumab trials in multiple myeloma: immune-related adverse events and response (Aviva C Krauss et al). An evaluation of the KEYNOTE-183 and KEYNOTE-185 trials of nearly 250 patients showed no significant myeloma response with pembrolizumab compared with the control arm of pomalidomide+dexamethasone.
10113 Prospsective phase II pilot study to evaluate the use of intravenous iron in the treatment of anemia in cancer patients (Youjin Kim et al). IV iron supplementation alone showed encouraging results in improving anemia, with hepcidin level possibly predicting response to IV iron and may be superior to the TSAT test.
500 Adjuvant denosumab in early breast cancer: disease free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
David Henry, MD, the Editor-in-Chief of The Journal of Community and Supportive Oncology, shares his top selections in hematology and bone health from this year's line-up of abstracts at the annual meeting of the American Society of Clinical Oncology in Chicago.
8004 Phase 2 study of venetoclax plus carfilzomib and dexamethasone in patients with relapsed refractory myeloma (Luciano J Costa et al). Of 17 patients evaluated after completing at least two cycles of therapy, 3 had complete responses, 2 had very good partial response, 3 had partial response, 3 experienced stable disease, and 2 had progressive disease (response data for 4 patients still to come). The study drug combination was well tolerated, and phase 3 trial is planned.
8008 FDA analysis of pembrolizumab trials in multiple myeloma: immune-related adverse events and response (Aviva C Krauss et al). An evaluation of the KEYNOTE-183 and KEYNOTE-185 trials of nearly 250 patients showed no significant myeloma response with pembrolizumab compared with the control arm of pomalidomide+dexamethasone.
10113 Prospsective phase II pilot study to evaluate the use of intravenous iron in the treatment of anemia in cancer patients (Youjin Kim et al). IV iron supplementation alone showed encouraging results in improving anemia, with hepcidin level possibly predicting response to IV iron and may be superior to the TSAT test.
500 Adjuvant denosumab in early breast cancer: disease free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
David Henry, MD, the Editor-in-Chief of The Journal of Community and Supportive Oncology, shares his top selections in hematology and bone health from this year's line-up of abstracts at the annual meeting of the American Society of Clinical Oncology in Chicago.
8004 Phase 2 study of venetoclax plus carfilzomib and dexamethasone in patients with relapsed refractory myeloma (Luciano J Costa et al). Of 17 patients evaluated after completing at least two cycles of therapy, 3 had complete responses, 2 had very good partial response, 3 had partial response, 3 experienced stable disease, and 2 had progressive disease (response data for 4 patients still to come). The study drug combination was well tolerated, and phase 3 trial is planned.
8008 FDA analysis of pembrolizumab trials in multiple myeloma: immune-related adverse events and response (Aviva C Krauss et al). An evaluation of the KEYNOTE-183 and KEYNOTE-185 trials of nearly 250 patients showed no significant myeloma response with pembrolizumab compared with the control arm of pomalidomide+dexamethasone.
10113 Prospsective phase II pilot study to evaluate the use of intravenous iron in the treatment of anemia in cancer patients (Youjin Kim et al). IV iron supplementation alone showed encouraging results in improving anemia, with hepcidin level possibly predicting response to IV iron and may be superior to the TSAT test.
500 Adjuvant denosumab in early breast cancer: disease free survival analysis of postmenopausal patients in the ABCSG-18 trial (Michael Gnant et al). In this double-blind placebo controlled trial, disease-free survival in the denosumab group was 89% at 5 years and 80% at 8 years, compared with 87% and 77%, respectively, for placebo.
New myeloma drugs improve response and extend survival
In this interview, Dr David Henry, the Editor-in-Chief of The Journal of Community and Supportive Oncology, and Dr Ken Anderson, the Kraft Family Professor of Medicine at Harvard Medical School and an international thought leader and investigator in myeloma, discuss three cases of patients with myeloma that are indicative of the remarkable therapeutic advances in oncology in general, and in myeloma in particular.
Listen to the podcast below
In this interview, Dr David Henry, the Editor-in-Chief of The Journal of Community and Supportive Oncology, and Dr Ken Anderson, the Kraft Family Professor of Medicine at Harvard Medical School and an international thought leader and investigator in myeloma, discuss three cases of patients with myeloma that are indicative of the remarkable therapeutic advances in oncology in general, and in myeloma in particular.
Listen to the podcast below
In this interview, Dr David Henry, the Editor-in-Chief of The Journal of Community and Supportive Oncology, and Dr Ken Anderson, the Kraft Family Professor of Medicine at Harvard Medical School and an international thought leader and investigator in myeloma, discuss three cases of patients with myeloma that are indicative of the remarkable therapeutic advances in oncology in general, and in myeloma in particular.
Listen to the podcast below
First CAR T-cell therapy approvals bolster booming immunotherapy market
There were a number of landmark approvals by the US Food and Drug Administration (FDA) in 2017 for cancer therapies, among them, the approval of the first two chimeric antigen receptor (CAR) T-cell therapies for cancer: tisagenlecleucel (in August) and axicabtagene ciloluecel (in October).1 CAR T-cells are a type of adoptive cell therapy or immunotherapy, in which the patient’s own immune cells are genetically engineered to target a tumor-associated antigen, in this case CD19. In tisagenlecleucel, CD19 proteins on B cells are targeted in the treatment of B-cell precursor acute lymphoblastic leukemia. Axicabtagene ciloluecel, the second anti-CD19 CAR T-cell therapy, was approved for the treatment of refractory, aggressive B-cell non-Hodgkin lymphoma.
Tisagenlecleucel
Tisagenlecleucel was approved for the treatment of pediatric patients up to 25 years of age with B-cell precursor acute lymphoblastic leukemia (ALL) whose disease is refractory to treatment or who have relapsed after second-line therapy or beyond.2 Approval was based on the pivotal ELIANA trial, a single-arm, global phase 2 trial conducted at 25 centers worldwide during April 2015 through April 2017. Patients were eligible for enrollment if they had relapsed or refractory B-cell ALL and were at least 3 years of age at screening and no older than 21 years of age at diagnosis, had at least 5% lymphoblasts in the bone marrow at screening, had tumor expression of CD19, had adequate organ function, and a Karnofsky (adult) or Lansky (child) Performance Status of ≥50 (with the worst allowable score, 50, indicating a patient who requires considerable assistance and frequent medical care [Karnofsky] and lying around much of the day, but gets dressed; no active playing but participates in all quiet play and activities [Lansky]). Exclusion criteria included previous receipt of anti-CD19 therapy, concomitant genetic syndromes associated with bone marrow failure, previous malignancy, and/or active or latent hepatitis B or C virus (HBV/HCV) infection.
The overall remission rate (ORR) was evaluated in 75 patients who were given a single dose of tisagenlecleucel (a median weight-adjusted dose of 3.1 x 106 transduced viable T cells per kg of body weight) within 14 days of completing a lymphodepleting chemotherapy regimen. The confirmed ORR after at least 3 months of follow-up, as assessed by independent central review, was 81%, which included 60% of patients in complete remission (CR) and 21% in complete remission with incomplete hematologic recovery, all of whom were negative for minimal residual disease.
The most common adverse events (AEs) associated with tisagenlecleucel treatment were cytokine release syndrome (CRS), hypogammaglobulinemia, infection, pyrexia, decreased appetite, headache, encephalopathy, hypotension, bleeding episodes, tachycardia, nausea, diarrhea, vomiting, viral infectious disorders, hypoxia, fatigue, acute kidney injury, and delirium. AEs were of grade 3/4 severity in 84% of patients.3
To combat serious safety issues, including CRS and neurologic toxicities, the FDA approved tisagenlecleucel with a Risk Evaluation and Mitigation Strategy (REMS) that, in part, requires health care providers who administer the drug to be trained in their management. It also requires the facility where treatment is administered to have immediate, onsite access to the drug tocilizumab, which was approved in conjunction with tisagenlecleucel for the treatment of patients who experience CRS.
In addition to information about the REMS, the prescribing information details warnings and precautions relating to several other common toxicities. These include hypersensitivity reactions, serious infections, prolonged cytopenias, and hypogammaglobulinemia.
Patients should be monitored for signs and symptoms of infection and treated appropriately. Viral reactivation can occur after tisagenlecleucel treatment, so patients should be screened for HBV, HCV, and human immunodeficiency virus before collection of cells.
The administration of myeloid growth factors is not recommended during the first 3 weeks after infusion or until CRS has resolved. Immunoglobulin levels should be monitored after treatment and hypogammaglobulinemia managed using infection precautions, antibiotic prophylaxis, and immunoglobulin replacement according to standard guidelines.
Patients treated with tisagenlecleucel should also be monitored for life for secondary malignancies, should not be treated with live vaccines from 2 weeks before the start of lymphodepleting chemotherapy until immune recovery after tisagenlecleucel infusion, and should be aware of the potential for neurological events to impact their ability to drive and use dangerous machinery.4
Tisagenlecleucel is marketed as Kymriah by Novartis Pharmaceuticals. The recommended dose is 1 infusion of 0.2-5 x 106 CAR-positive viable T cells per kilogram of body weight intravenously (for patients ≤50kg) and 0.1-2.5 x 108 cells/kg (for patients >50kg), administered 2-14 days after lymphodepleting chemotherapy.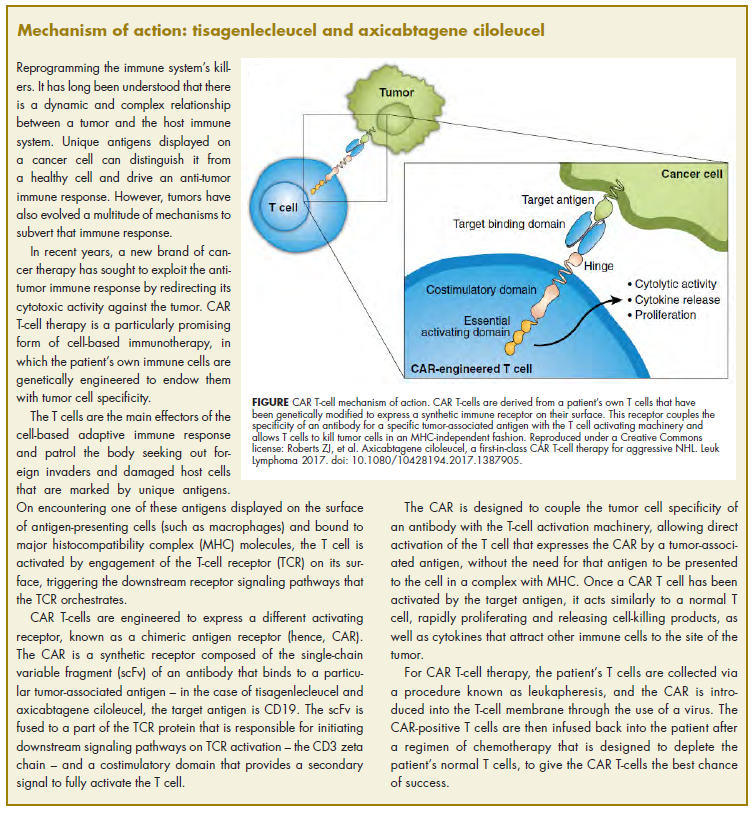
Axicabtagene ciloleucel
Axicabtagene ciloleucel was approved for the treatment of adult patients with certain types of relapsed or refractory large B-cell lymphoma, including diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma (PMBCL), high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma.5 It is not indicated for the treatment of patients with primary central nervous system lymphoma.
Approval followed positive results from the phase 2 single-arm, multicenter ZUMA-1 trial.6 Patients were included if they were aged 18 years of age and older, had histologically confirmed aggressive B-cell non-Hodgkin lymphoma that was chemotherapy refractory, had received adequate previous therapy, had at least 1 measurable lesion, had completed radiation or systemic therapy at least 2 weeks before, had resolved toxicities related to previous therapy, and had an Eastern Cooperative Oncology Group Performance Status of 0 (asymptomatic) or 1 (symptomatic), an absolute neutrophil count of ≥1000/µL, a platelet count of ≥50,000/µL, and adequate hepatic, renal and cardiac function. They were treated with a single infusion of axicabtagene ciloleucel after lymphodepleting chemotherapy.
Patients who had received previous CD19-targeted therapy, who had concomitant genetic syndromes associated with bone marrow failure, who had previous malignancy, and who had active or latent HBV/HCV infection were among those excluded from the study.
Patients were enrolled in 2 cohorts; those with DLBCL (n = 77) and those with PMBCL or transformed follicular lymphoma (n = 24). The primary endpoint was objective response rate, and after a primary analysis at a minimum of 6 months follow-up, the objective response rate was 82%, with a CR rate of 52%. Among patients who achieved CR, the median duration of response was not reached after a median follow-up of 7.9 months.
A subsequent updated analysis was performed when 108 patients had been followed for a minimum of 1 year. The objective response rate was 82%, and the CR rate was 58%, with some patients having CR in the absence of additional therapies as late as 15 months after treatment. At this updated analysis, 42% of patients continued to have a response, 40% of whom remained in CR.
The most common grade 3 or higher AEs included febrile neutropenia, fever, CRS, encephalopathy, infections, hypotension, and hypoxia. Serious AEs occurred in 52% of patients and included CRS, neurologic toxicity, prolonged cytopenias, and serious infections. Grade 3 or higher CRS or neurologic toxicities occurred in 13% and 28% of patients, respectively. Three patients died during treatment.
To mitigate the risk of CRS and neurologic toxicity, axicabtagene ciloleucel is approved with an REMS that requires appropriate certification and training before hospitals are cleared to administer the therapy.
Other warnings and precautions in the prescribing information relate to serious infections (monitor for signs and symptoms and treat appropriately), prolonged cytopenias (monitor blood counts), hypogammaglobulinemia (monitor immunoglobulin levels and manage appropriately), secondary malignancies (life-long monitoring), and the potential effects of neurologic events on a patient’s ability to drive and operate dangerous machinery (avoid for at least 8 weeks after infusion).7
Axicabtagene ciloleucel is marketed as Yescarta by Kite Pharma Inc. The recommended dose is a single intravenous infusion with a target of 2 x 106 CAR-positive viable T cells per kilogram of body weight, preceded by fludarabine and cyclophosphamide lymphodepleting chemotherapy.
1. Bosserman LD. Cancer care in 2017: the promise of more cures with the challenges of an unstable health care system. JCSO 2017;15(6):e283-e290.
2. FDA approves tisagenlecleucel for B-cell ALL and tocilizumab for cytokine release syndrome. FDA News Release. August 30, 2017. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/
ucm574154.htm. Accessed March 31, 2018.
3. Maude S.L, Laetsch T.W, Buechner S, et al. Tisagenlecleucel in children and young adults with B-Cell lymphoblastic leukemia. N Engl J Med. 2018;378:439-48.
4. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Novartis Pharmaceuticals Corporation, August, 2017. https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.
com/files/kymriah.pdf. Accessed March 31, 2018.
5. FDA approves axicabtagene ciloleucel for large B-cell lymphoma. FDA News Release. October 18, 2017. https://www.fda.gov/Drugs/
InformationOnDrugs/ApprovedDrugs/ucm581296.htm. Accessed March 31, 2018.
6. Neelapu, S.S, Locke F.L, Bartlett, L.J, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med. 2017;377:2531-44.
7. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Kite Pharma Inc. October 2017. https://www.yescarta.com/wp-content/uploads/yescarta-pi.pdf. Accessed March 31, 2018.
There were a number of landmark approvals by the US Food and Drug Administration (FDA) in 2017 for cancer therapies, among them, the approval of the first two chimeric antigen receptor (CAR) T-cell therapies for cancer: tisagenlecleucel (in August) and axicabtagene ciloluecel (in October).1 CAR T-cells are a type of adoptive cell therapy or immunotherapy, in which the patient’s own immune cells are genetically engineered to target a tumor-associated antigen, in this case CD19. In tisagenlecleucel, CD19 proteins on B cells are targeted in the treatment of B-cell precursor acute lymphoblastic leukemia. Axicabtagene ciloluecel, the second anti-CD19 CAR T-cell therapy, was approved for the treatment of refractory, aggressive B-cell non-Hodgkin lymphoma.
Tisagenlecleucel
Tisagenlecleucel was approved for the treatment of pediatric patients up to 25 years of age with B-cell precursor acute lymphoblastic leukemia (ALL) whose disease is refractory to treatment or who have relapsed after second-line therapy or beyond.2 Approval was based on the pivotal ELIANA trial, a single-arm, global phase 2 trial conducted at 25 centers worldwide during April 2015 through April 2017. Patients were eligible for enrollment if they had relapsed or refractory B-cell ALL and were at least 3 years of age at screening and no older than 21 years of age at diagnosis, had at least 5% lymphoblasts in the bone marrow at screening, had tumor expression of CD19, had adequate organ function, and a Karnofsky (adult) or Lansky (child) Performance Status of ≥50 (with the worst allowable score, 50, indicating a patient who requires considerable assistance and frequent medical care [Karnofsky] and lying around much of the day, but gets dressed; no active playing but participates in all quiet play and activities [Lansky]). Exclusion criteria included previous receipt of anti-CD19 therapy, concomitant genetic syndromes associated with bone marrow failure, previous malignancy, and/or active or latent hepatitis B or C virus (HBV/HCV) infection.
The overall remission rate (ORR) was evaluated in 75 patients who were given a single dose of tisagenlecleucel (a median weight-adjusted dose of 3.1 x 106 transduced viable T cells per kg of body weight) within 14 days of completing a lymphodepleting chemotherapy regimen. The confirmed ORR after at least 3 months of follow-up, as assessed by independent central review, was 81%, which included 60% of patients in complete remission (CR) and 21% in complete remission with incomplete hematologic recovery, all of whom were negative for minimal residual disease.
The most common adverse events (AEs) associated with tisagenlecleucel treatment were cytokine release syndrome (CRS), hypogammaglobulinemia, infection, pyrexia, decreased appetite, headache, encephalopathy, hypotension, bleeding episodes, tachycardia, nausea, diarrhea, vomiting, viral infectious disorders, hypoxia, fatigue, acute kidney injury, and delirium. AEs were of grade 3/4 severity in 84% of patients.3
To combat serious safety issues, including CRS and neurologic toxicities, the FDA approved tisagenlecleucel with a Risk Evaluation and Mitigation Strategy (REMS) that, in part, requires health care providers who administer the drug to be trained in their management. It also requires the facility where treatment is administered to have immediate, onsite access to the drug tocilizumab, which was approved in conjunction with tisagenlecleucel for the treatment of patients who experience CRS.
In addition to information about the REMS, the prescribing information details warnings and precautions relating to several other common toxicities. These include hypersensitivity reactions, serious infections, prolonged cytopenias, and hypogammaglobulinemia.
Patients should be monitored for signs and symptoms of infection and treated appropriately. Viral reactivation can occur after tisagenlecleucel treatment, so patients should be screened for HBV, HCV, and human immunodeficiency virus before collection of cells.
The administration of myeloid growth factors is not recommended during the first 3 weeks after infusion or until CRS has resolved. Immunoglobulin levels should be monitored after treatment and hypogammaglobulinemia managed using infection precautions, antibiotic prophylaxis, and immunoglobulin replacement according to standard guidelines.
Patients treated with tisagenlecleucel should also be monitored for life for secondary malignancies, should not be treated with live vaccines from 2 weeks before the start of lymphodepleting chemotherapy until immune recovery after tisagenlecleucel infusion, and should be aware of the potential for neurological events to impact their ability to drive and use dangerous machinery.4
Tisagenlecleucel is marketed as Kymriah by Novartis Pharmaceuticals. The recommended dose is 1 infusion of 0.2-5 x 106 CAR-positive viable T cells per kilogram of body weight intravenously (for patients ≤50kg) and 0.1-2.5 x 108 cells/kg (for patients >50kg), administered 2-14 days after lymphodepleting chemotherapy.
Axicabtagene ciloleucel
Axicabtagene ciloleucel was approved for the treatment of adult patients with certain types of relapsed or refractory large B-cell lymphoma, including diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma (PMBCL), high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma.5 It is not indicated for the treatment of patients with primary central nervous system lymphoma.
Approval followed positive results from the phase 2 single-arm, multicenter ZUMA-1 trial.6 Patients were included if they were aged 18 years of age and older, had histologically confirmed aggressive B-cell non-Hodgkin lymphoma that was chemotherapy refractory, had received adequate previous therapy, had at least 1 measurable lesion, had completed radiation or systemic therapy at least 2 weeks before, had resolved toxicities related to previous therapy, and had an Eastern Cooperative Oncology Group Performance Status of 0 (asymptomatic) or 1 (symptomatic), an absolute neutrophil count of ≥1000/µL, a platelet count of ≥50,000/µL, and adequate hepatic, renal and cardiac function. They were treated with a single infusion of axicabtagene ciloleucel after lymphodepleting chemotherapy.
Patients who had received previous CD19-targeted therapy, who had concomitant genetic syndromes associated with bone marrow failure, who had previous malignancy, and who had active or latent HBV/HCV infection were among those excluded from the study.
Patients were enrolled in 2 cohorts; those with DLBCL (n = 77) and those with PMBCL or transformed follicular lymphoma (n = 24). The primary endpoint was objective response rate, and after a primary analysis at a minimum of 6 months follow-up, the objective response rate was 82%, with a CR rate of 52%. Among patients who achieved CR, the median duration of response was not reached after a median follow-up of 7.9 months.
A subsequent updated analysis was performed when 108 patients had been followed for a minimum of 1 year. The objective response rate was 82%, and the CR rate was 58%, with some patients having CR in the absence of additional therapies as late as 15 months after treatment. At this updated analysis, 42% of patients continued to have a response, 40% of whom remained in CR.
The most common grade 3 or higher AEs included febrile neutropenia, fever, CRS, encephalopathy, infections, hypotension, and hypoxia. Serious AEs occurred in 52% of patients and included CRS, neurologic toxicity, prolonged cytopenias, and serious infections. Grade 3 or higher CRS or neurologic toxicities occurred in 13% and 28% of patients, respectively. Three patients died during treatment.
To mitigate the risk of CRS and neurologic toxicity, axicabtagene ciloleucel is approved with an REMS that requires appropriate certification and training before hospitals are cleared to administer the therapy.
Other warnings and precautions in the prescribing information relate to serious infections (monitor for signs and symptoms and treat appropriately), prolonged cytopenias (monitor blood counts), hypogammaglobulinemia (monitor immunoglobulin levels and manage appropriately), secondary malignancies (life-long monitoring), and the potential effects of neurologic events on a patient’s ability to drive and operate dangerous machinery (avoid for at least 8 weeks after infusion).7
Axicabtagene ciloleucel is marketed as Yescarta by Kite Pharma Inc. The recommended dose is a single intravenous infusion with a target of 2 x 106 CAR-positive viable T cells per kilogram of body weight, preceded by fludarabine and cyclophosphamide lymphodepleting chemotherapy.
There were a number of landmark approvals by the US Food and Drug Administration (FDA) in 2017 for cancer therapies, among them, the approval of the first two chimeric antigen receptor (CAR) T-cell therapies for cancer: tisagenlecleucel (in August) and axicabtagene ciloluecel (in October).1 CAR T-cells are a type of adoptive cell therapy or immunotherapy, in which the patient’s own immune cells are genetically engineered to target a tumor-associated antigen, in this case CD19. In tisagenlecleucel, CD19 proteins on B cells are targeted in the treatment of B-cell precursor acute lymphoblastic leukemia. Axicabtagene ciloluecel, the second anti-CD19 CAR T-cell therapy, was approved for the treatment of refractory, aggressive B-cell non-Hodgkin lymphoma.
Tisagenlecleucel
Tisagenlecleucel was approved for the treatment of pediatric patients up to 25 years of age with B-cell precursor acute lymphoblastic leukemia (ALL) whose disease is refractory to treatment or who have relapsed after second-line therapy or beyond.2 Approval was based on the pivotal ELIANA trial, a single-arm, global phase 2 trial conducted at 25 centers worldwide during April 2015 through April 2017. Patients were eligible for enrollment if they had relapsed or refractory B-cell ALL and were at least 3 years of age at screening and no older than 21 years of age at diagnosis, had at least 5% lymphoblasts in the bone marrow at screening, had tumor expression of CD19, had adequate organ function, and a Karnofsky (adult) or Lansky (child) Performance Status of ≥50 (with the worst allowable score, 50, indicating a patient who requires considerable assistance and frequent medical care [Karnofsky] and lying around much of the day, but gets dressed; no active playing but participates in all quiet play and activities [Lansky]). Exclusion criteria included previous receipt of anti-CD19 therapy, concomitant genetic syndromes associated with bone marrow failure, previous malignancy, and/or active or latent hepatitis B or C virus (HBV/HCV) infection.
The overall remission rate (ORR) was evaluated in 75 patients who were given a single dose of tisagenlecleucel (a median weight-adjusted dose of 3.1 x 106 transduced viable T cells per kg of body weight) within 14 days of completing a lymphodepleting chemotherapy regimen. The confirmed ORR after at least 3 months of follow-up, as assessed by independent central review, was 81%, which included 60% of patients in complete remission (CR) and 21% in complete remission with incomplete hematologic recovery, all of whom were negative for minimal residual disease.
The most common adverse events (AEs) associated with tisagenlecleucel treatment were cytokine release syndrome (CRS), hypogammaglobulinemia, infection, pyrexia, decreased appetite, headache, encephalopathy, hypotension, bleeding episodes, tachycardia, nausea, diarrhea, vomiting, viral infectious disorders, hypoxia, fatigue, acute kidney injury, and delirium. AEs were of grade 3/4 severity in 84% of patients.3
To combat serious safety issues, including CRS and neurologic toxicities, the FDA approved tisagenlecleucel with a Risk Evaluation and Mitigation Strategy (REMS) that, in part, requires health care providers who administer the drug to be trained in their management. It also requires the facility where treatment is administered to have immediate, onsite access to the drug tocilizumab, which was approved in conjunction with tisagenlecleucel for the treatment of patients who experience CRS.
In addition to information about the REMS, the prescribing information details warnings and precautions relating to several other common toxicities. These include hypersensitivity reactions, serious infections, prolonged cytopenias, and hypogammaglobulinemia.
Patients should be monitored for signs and symptoms of infection and treated appropriately. Viral reactivation can occur after tisagenlecleucel treatment, so patients should be screened for HBV, HCV, and human immunodeficiency virus before collection of cells.
The administration of myeloid growth factors is not recommended during the first 3 weeks after infusion or until CRS has resolved. Immunoglobulin levels should be monitored after treatment and hypogammaglobulinemia managed using infection precautions, antibiotic prophylaxis, and immunoglobulin replacement according to standard guidelines.
Patients treated with tisagenlecleucel should also be monitored for life for secondary malignancies, should not be treated with live vaccines from 2 weeks before the start of lymphodepleting chemotherapy until immune recovery after tisagenlecleucel infusion, and should be aware of the potential for neurological events to impact their ability to drive and use dangerous machinery.4
Tisagenlecleucel is marketed as Kymriah by Novartis Pharmaceuticals. The recommended dose is 1 infusion of 0.2-5 x 106 CAR-positive viable T cells per kilogram of body weight intravenously (for patients ≤50kg) and 0.1-2.5 x 108 cells/kg (for patients >50kg), administered 2-14 days after lymphodepleting chemotherapy.
Axicabtagene ciloleucel
Axicabtagene ciloleucel was approved for the treatment of adult patients with certain types of relapsed or refractory large B-cell lymphoma, including diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma (PMBCL), high-grade B-cell lymphoma, and DLBCL arising from follicular lymphoma.5 It is not indicated for the treatment of patients with primary central nervous system lymphoma.
Approval followed positive results from the phase 2 single-arm, multicenter ZUMA-1 trial.6 Patients were included if they were aged 18 years of age and older, had histologically confirmed aggressive B-cell non-Hodgkin lymphoma that was chemotherapy refractory, had received adequate previous therapy, had at least 1 measurable lesion, had completed radiation or systemic therapy at least 2 weeks before, had resolved toxicities related to previous therapy, and had an Eastern Cooperative Oncology Group Performance Status of 0 (asymptomatic) or 1 (symptomatic), an absolute neutrophil count of ≥1000/µL, a platelet count of ≥50,000/µL, and adequate hepatic, renal and cardiac function. They were treated with a single infusion of axicabtagene ciloleucel after lymphodepleting chemotherapy.
Patients who had received previous CD19-targeted therapy, who had concomitant genetic syndromes associated with bone marrow failure, who had previous malignancy, and who had active or latent HBV/HCV infection were among those excluded from the study.
Patients were enrolled in 2 cohorts; those with DLBCL (n = 77) and those with PMBCL or transformed follicular lymphoma (n = 24). The primary endpoint was objective response rate, and after a primary analysis at a minimum of 6 months follow-up, the objective response rate was 82%, with a CR rate of 52%. Among patients who achieved CR, the median duration of response was not reached after a median follow-up of 7.9 months.
A subsequent updated analysis was performed when 108 patients had been followed for a minimum of 1 year. The objective response rate was 82%, and the CR rate was 58%, with some patients having CR in the absence of additional therapies as late as 15 months after treatment. At this updated analysis, 42% of patients continued to have a response, 40% of whom remained in CR.
The most common grade 3 or higher AEs included febrile neutropenia, fever, CRS, encephalopathy, infections, hypotension, and hypoxia. Serious AEs occurred in 52% of patients and included CRS, neurologic toxicity, prolonged cytopenias, and serious infections. Grade 3 or higher CRS or neurologic toxicities occurred in 13% and 28% of patients, respectively. Three patients died during treatment.
To mitigate the risk of CRS and neurologic toxicity, axicabtagene ciloleucel is approved with an REMS that requires appropriate certification and training before hospitals are cleared to administer the therapy.
Other warnings and precautions in the prescribing information relate to serious infections (monitor for signs and symptoms and treat appropriately), prolonged cytopenias (monitor blood counts), hypogammaglobulinemia (monitor immunoglobulin levels and manage appropriately), secondary malignancies (life-long monitoring), and the potential effects of neurologic events on a patient’s ability to drive and operate dangerous machinery (avoid for at least 8 weeks after infusion).7
Axicabtagene ciloleucel is marketed as Yescarta by Kite Pharma Inc. The recommended dose is a single intravenous infusion with a target of 2 x 106 CAR-positive viable T cells per kilogram of body weight, preceded by fludarabine and cyclophosphamide lymphodepleting chemotherapy.
1. Bosserman LD. Cancer care in 2017: the promise of more cures with the challenges of an unstable health care system. JCSO 2017;15(6):e283-e290.
2. FDA approves tisagenlecleucel for B-cell ALL and tocilizumab for cytokine release syndrome. FDA News Release. August 30, 2017. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/
ucm574154.htm. Accessed March 31, 2018.
3. Maude S.L, Laetsch T.W, Buechner S, et al. Tisagenlecleucel in children and young adults with B-Cell lymphoblastic leukemia. N Engl J Med. 2018;378:439-48.
4. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Novartis Pharmaceuticals Corporation, August, 2017. https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.
com/files/kymriah.pdf. Accessed March 31, 2018.
5. FDA approves axicabtagene ciloleucel for large B-cell lymphoma. FDA News Release. October 18, 2017. https://www.fda.gov/Drugs/
InformationOnDrugs/ApprovedDrugs/ucm581296.htm. Accessed March 31, 2018.
6. Neelapu, S.S, Locke F.L, Bartlett, L.J, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med. 2017;377:2531-44.
7. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Kite Pharma Inc. October 2017. https://www.yescarta.com/wp-content/uploads/yescarta-pi.pdf. Accessed March 31, 2018.
1. Bosserman LD. Cancer care in 2017: the promise of more cures with the challenges of an unstable health care system. JCSO 2017;15(6):e283-e290.
2. FDA approves tisagenlecleucel for B-cell ALL and tocilizumab for cytokine release syndrome. FDA News Release. August 30, 2017. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/
ucm574154.htm. Accessed March 31, 2018.
3. Maude S.L, Laetsch T.W, Buechner S, et al. Tisagenlecleucel in children and young adults with B-Cell lymphoblastic leukemia. N Engl J Med. 2018;378:439-48.
4. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Novartis Pharmaceuticals Corporation, August, 2017. https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.
com/files/kymriah.pdf. Accessed March 31, 2018.
5. FDA approves axicabtagene ciloleucel for large B-cell lymphoma. FDA News Release. October 18, 2017. https://www.fda.gov/Drugs/
InformationOnDrugs/ApprovedDrugs/ucm581296.htm. Accessed March 31, 2018.
6. Neelapu, S.S, Locke F.L, Bartlett, L.J, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med. 2017;377:2531-44.
7. Kymriah (tisagenlecleucel) suspension for intravenous use. Prescribing information. Kite Pharma Inc. October 2017. https://www.yescarta.com/wp-content/uploads/yescarta-pi.pdf. Accessed March 31, 2018.