NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Nonalcoholic fatty liver disease is the 21st century epidemic in liver disease, Zobair M. Younossi, MD, declared at the annual meeting of the American College of Physicians.
Bruce Jancin/MDedge News
Dr. Zobair M. Younossi
The massive growth in nonalcoholic fatty liver disease (NAFLD) is being fueled to a great extent by the related epidemics of obesity and type 2 diabetes mellitus. While the overall prevalence of NAFLD worldwide is 24%, almost three-quarters of patients with NAFLD are obese. And the prevalence of NAFLD in individuals with T2DM was 58% in a recent meta-analysis of studies from 20 countries conducted by Dr. Younossi and his coinvestigators.
“The prevalence of NAFLD in U.S. kids is about 10%. This is of course part of the coming tsunami because our kids are getting obese, diabetic, and they’re going to have problems with NASH [nonalcoholic steatohepatitis],” said Dr. Younossi, a gastroenterologist who is professor and chairman of the department of medicine at the Inova Fairfax (Va.) campus of Virginia Commonwealth University.
NASH is the form of NAFLD that has the strongest prognostic implications. It can progress to cirrhosis, liver failure, or hepatocellular carcinoma. As Dr. Younossi and his coworkers have shown (Hepat Commun. 2017 Jun 6;1[5]:421-8), it is associated with a significantly greater risk of both liver-related and all-cause mortality than that of non-NASH NAFLD, although NAFLD also carries an increased risk of cardiovascular disease, the leading cause of death in that population.
In addition to highlighting the enormous clinical, economic, and quality-of-life implications of the NAFLD epidemic, Dr. Younossi offered practical tips on how busy primary care physicians can identify patients in their practice who have high-risk NAFLD. They have not done a very good job of this to date. That’s possibly due to lack of incentive, since in 2018 there is no approved drug for the treatment of NASH. He cited one representative retrospective study in which only about 15% of patients identified as having NAFLD received a recommendation for lifestyle modification involving diet and exercise, which is the standard evidence-based treatment, albeit admittedly difficult to sustain. And only 3% of patients with advanced liver fibrosis were referred to a specialist for management.
“So NAFLD is common, but its recognition and doing something about it is quite a challenge,” Dr. Younossi observed.
He argued that patients who have NASH deserve to know it because of its prognostic implications and also so they can have the chance to participate in one of the roughly two dozen ongoing clinical trials of potential therapies, some of which look quite promising. All of the trials required a liver biopsy as a condition for enrollment. Plus, once a patient is known to have stage 3 fibrosis, it’s time to start screening for hepatocellular carcinoma and esophageal varices.
The scope of the epidemic
NASH is the most rapidly growing indication for liver transplantation in the United States, with most of the increase coming from the baby boomer population. NASH is now the second most common indication for placement on the wait list. Meanwhile, liver transplantation due to the consequences of hepatitis C, the No. 1 indication, is declining as a result of the spectacular advances in medical treatment introduced a few years ago. It’s likely that in coming years NASH will take over the top spot, according to Dr. Younossi.
He was coauthor of a recent study that modeled the estimated trends for the NAFLD epidemic in the United States through 2030. The forecast is that the prevalence of NAFLD among adults will climb to 33.5% and the proportion of NAFLD categorized as NASH will increase from 20% at present to 27%. Moreover, this will result in a 168% jump in the incidence of decompensated cirrhosis, a 137% increase in the incidence of hepatocellular carcinoma, and a 178% increase in liver-related mortality, which will account for an estimated 78,300 deaths in 2030 (Hepatology. 2018 Jan;67[1]:123-33).
Practical ways to identify high-risk patients
The best noninvasive means of detecting NAFLD is by ultrasound showing a fatty liver. Often the condition is detected as an incidental finding on abdominal ultrasound ordered for another reason. Elevated liver enzymes can be a tipoff as well. Of course, alcoholic liver disease and other causes must be excluded.
But what’s most important is to identify patients with NASH. It’s a diagnosis made by biopsy. However, it is unthinkable to perform liver biopsies in the entire vast population with NAFLD, so there is a great deal of interest in developing noninvasive diagnostic modalities that can help zero in on the subset of high-risk NAFLD patients who should be considered for referral for liver biopsy.
One useful clue is the presence of comorbid metabolic syndrome in patients with NAFLD. It confers a substantially higher mortality risk – especially cardiovascular mortality – than does NAFLD without metabolic syndrome. Dr. Younossi and his coinvestigators have shown in a study of 3,613 NAFLD patients followed long-term that those with one component of the metabolic syndrome – either hypertension, central obesity, increased fasting plasma glucose, or hyperlipidemia – had 8- and 16-year all-cause mortality rates of 4.7% and 11.9%, nearly double the 2.6% and 6% rates in NAFLD patients with no elements of the metabolic syndrome.
Moreover, the magnitude of risk increased with each additional metabolic syndrome condition: a 3.57-fold increased mortality risk in NAFLD patients with two components of metabolic syndrome, a 5.87-fold increase in those with three, and a 13.09-fold increase in NAFLD patients with all four elements of metabolic syndrome (Medicine [Baltimore]. 2018 Mar;97[13]:e0214. doi: 10.1097/MD.0000000000010214).
Dr. Younossi was a member of the American Association for the Study of Liver Disease expert panel that developed the latest practice guidance regarding the diagnosis and management of NAFLD (Hepatology. 2018 Jan;67[1]:328-57). He said that probably the best simple noninvasive scoring system for the detection of NASH with advanced fibrosis is the NAFLD fibrosis score, which is easily calculated using laboratory values and clinical parameters already in a patient’s chart.
A more sophisticated serum biomarker test known as ELF, or the Enhanced Liver Fibrosis test, combines serum levels of hyaluronic acid, tissue inhibitor of metalloproteinase I, and procollagen amino terminal peptide.
“ELF is a very, very good test. It’s approved in Europe and I suspect it will be in the U.S. within the next year or so,” said Dr. Younossi.
The most exciting noninvasive tests, however, involve imaging that measures liver stiffness, which provides a fairly accurate indication of the degree of scarring in the organ. There are two methods available: vibration wave transient elastography and magnetic resonance elastography.
Transient elastography using the FibroScan device is commercially available in the United States. “It’s a good test, very easy to do, noninvasive. I have a couple of these machines, and we use them all the time,” the gastroenterologist said.
MR elastography provides superior accuracy, but access is an issue.
“At our institution you sometimes have to wait for weeks to get an outpatient MRI, so if you have hundreds of patients with fatty liver disease it makes things difficult. So in our practice we use transient elastography,” he explained.
Both imaging modalities also measure the amount of fat in the liver.
Dr. Younossi uses transient elastography in patients who don’t have type 2 diabetes or frank insulin resistance. If the FibroScan score is 7 kiloPascals or more, he considers liver biopsy, since that’s the threshold for detection of earlier, potentially reversible stage 2 fibrosis. If, however, a patient has diabetes or insulin resistance along with a NAFLD fibrosis score suggesting a high possibility of fibrosis, he sends that patient for liver biopsy, since those endocrinologic disorders are known to be independent risk factors for mortality in the setting of NAFLD.
Dr. Younossi reported having no financial conflicts of interest regarding his presentation.
At birth, this child had a lesion on his shoulder that now—a year later—has doubled in size. His parents report no systemic symptoms or medication use for their son. They say that the child exhibits no distress; he does not attempt to scratch at the affected patch of skin. However, they observe that if the lesion is touched, it swells and then (within minutes) returns to normal.
There is no family history of similar problems. However, both the patient and his mother are highly atopic.
EXAMINATION The lesion—a low, orange, oval plaque—measures about 3.5 x 2 cm. Barely palpable, it urticates when stroked with a fingernail edge but does not appear to cause any discomfort.
No other lesions of note are found. The child appears quite healthy and is in no distress.
What is the diagnosis?
DISCUSSION Mastocytosis is caused by a localized accumulation of mast cells (a type of white blood cell) and CD34-positive mast cell precursors, which are normally present but widely scattered and sparse. This child has the most common form of cutaneous mastocytosis, which can manifest with solitary lesions or with dozens or hundreds of scattered lesions (the latter known as urticaria pigmentosa). Both types are typically benign and self-limited.
When stroked, mast cell lesions degranulate portions of the cell, releasing histamine precursors and leukotrienes (eg, IL 1 and IL 31). In most cases, stroking merely leads to short-lived urtication. But if the problem is more widespread (eg, urticaria pigmentosa) and the lesions are sufficiently traumatized, the release of these substances can lead to problems such as hypotension, malaise, fever, and abdominal pain.
Fortunately, this is rare, as is systemic mastocytosis—a condition in which mast cells infiltrate internal organs and bone marrow, interrupting normal function and, in the extreme, leading to mast cell leukemia. Our patient is not at risk for these complications; his lesion should resolve completely by age 3.
The differential for this patient’s lesion includes congenital nevus, lichen aureus, and café au lait spot.
TAKE-HOME LEARNING POINTS
Cutaneous mastocytosis manifests as a reddish orange maculopapular patch, which urticates upon forceful stroking.
Stroking the lesion degranulates the mast cells comprising it, leading to the release of histamine precursors.
Mast cells can infiltrate internal organs and bone marrow, leading, in the extreme, to mast cell leukemia.
Urticaria pigmentosa is a variation of mastocytosis in which hundreds of such lesions develop all over the body.
At birth, this child had a lesion on his shoulder that now—a year later—has doubled in size. His parents report no systemic symptoms or medication use for their son. They say that the child exhibits no distress; he does not attempt to scratch at the affected patch of skin. However, they observe that if the lesion is touched, it swells and then (within minutes) returns to normal.
There is no family history of similar problems. However, both the patient and his mother are highly atopic.
EXAMINATION The lesion—a low, orange, oval plaque—measures about 3.5 x 2 cm. Barely palpable, it urticates when stroked with a fingernail edge but does not appear to cause any discomfort.
No other lesions of note are found. The child appears quite healthy and is in no distress.
What is the diagnosis?
DISCUSSION Mastocytosis is caused by a localized accumulation of mast cells (a type of white blood cell) and CD34-positive mast cell precursors, which are normally present but widely scattered and sparse. This child has the most common form of cutaneous mastocytosis, which can manifest with solitary lesions or with dozens or hundreds of scattered lesions (the latter known as urticaria pigmentosa). Both types are typically benign and self-limited.
When stroked, mast cell lesions degranulate portions of the cell, releasing histamine precursors and leukotrienes (eg, IL 1 and IL 31). In most cases, stroking merely leads to short-lived urtication. But if the problem is more widespread (eg, urticaria pigmentosa) and the lesions are sufficiently traumatized, the release of these substances can lead to problems such as hypotension, malaise, fever, and abdominal pain.
Fortunately, this is rare, as is systemic mastocytosis—a condition in which mast cells infiltrate internal organs and bone marrow, interrupting normal function and, in the extreme, leading to mast cell leukemia. Our patient is not at risk for these complications; his lesion should resolve completely by age 3.
The differential for this patient’s lesion includes congenital nevus, lichen aureus, and café au lait spot.
TAKE-HOME LEARNING POINTS
Cutaneous mastocytosis manifests as a reddish orange maculopapular patch, which urticates upon forceful stroking.
Stroking the lesion degranulates the mast cells comprising it, leading to the release of histamine precursors.
Mast cells can infiltrate internal organs and bone marrow, leading, in the extreme, to mast cell leukemia.
Urticaria pigmentosa is a variation of mastocytosis in which hundreds of such lesions develop all over the body.
At birth, this child had a lesion on his shoulder that now—a year later—has doubled in size. His parents report no systemic symptoms or medication use for their son. They say that the child exhibits no distress; he does not attempt to scratch at the affected patch of skin. However, they observe that if the lesion is touched, it swells and then (within minutes) returns to normal.
There is no family history of similar problems. However, both the patient and his mother are highly atopic.
EXAMINATION The lesion—a low, orange, oval plaque—measures about 3.5 x 2 cm. Barely palpable, it urticates when stroked with a fingernail edge but does not appear to cause any discomfort.
No other lesions of note are found. The child appears quite healthy and is in no distress.
What is the diagnosis?
DISCUSSION Mastocytosis is caused by a localized accumulation of mast cells (a type of white blood cell) and CD34-positive mast cell precursors, which are normally present but widely scattered and sparse. This child has the most common form of cutaneous mastocytosis, which can manifest with solitary lesions or with dozens or hundreds of scattered lesions (the latter known as urticaria pigmentosa). Both types are typically benign and self-limited.
When stroked, mast cell lesions degranulate portions of the cell, releasing histamine precursors and leukotrienes (eg, IL 1 and IL 31). In most cases, stroking merely leads to short-lived urtication. But if the problem is more widespread (eg, urticaria pigmentosa) and the lesions are sufficiently traumatized, the release of these substances can lead to problems such as hypotension, malaise, fever, and abdominal pain.
Fortunately, this is rare, as is systemic mastocytosis—a condition in which mast cells infiltrate internal organs and bone marrow, interrupting normal function and, in the extreme, leading to mast cell leukemia. Our patient is not at risk for these complications; his lesion should resolve completely by age 3.
The differential for this patient’s lesion includes congenital nevus, lichen aureus, and café au lait spot.
TAKE-HOME LEARNING POINTS
Cutaneous mastocytosis manifests as a reddish orange maculopapular patch, which urticates upon forceful stroking.
Stroking the lesion degranulates the mast cells comprising it, leading to the release of histamine precursors.
Mast cells can infiltrate internal organs and bone marrow, leading, in the extreme, to mast cell leukemia.
Urticaria pigmentosa is a variation of mastocytosis in which hundreds of such lesions develop all over the body.
Medicare beneficiaries with myeloma who have prescription drug coverage have shown both decreased used of classic cytotoxic chemotherapy and better survival, according to new research.
vitanovski/Thinkstock.com
The findings suggested that prescription drug coverage brings better access to all existing treatment options.
“In this analysis of Medicare beneficiaries with myeloma, the receipt of therapy and survival differed according to prescription drug coverage status,” Adam Olszewski, MD, of the Lifespan Cancer Institute at Rhode Island Hospital in Providence, R.I., and his colleagues noted in the study. “Patients with PDP [prescription drug plan coverage through Medicare Part D] or OCC [other credible prescription drug coverage] more often received active myeloma care, compared to those without coverage,” they wrote in Journal of Clinical Oncology.
The researchers looked at 9,755 patients diagnosed with myeloma during 2006-2011 and examined what was used to treat the myeloma as a first line treatment. The cohort included 1,460 patients with no prescription drug coverage, 3,283 with PDP coverage, 3,607 with OCC, and 1,405 dual eligibility for Medicare and Medicaid coverage.
The study found that, compared with beneficiaries with no coverage, Medicare beneficiaries with PDP coverage “were 14% less likely to be treated with parenteral chemotherapy and 38% less likely to receive classic cytotoxic agents.” Additionally, among the cohort of beneficiaries that were without drug coverage prior to the diagnosis of myeloma, 41% actively obtained coverage, but even then, their survival was “significantly worse, compared with the beneficiaries who had coverage at diagnosis.”
Beneficiaries classified as having other credible coverage were 3% more likely to receive active myeloma care than were those without coverage, but the use of parenteral regimens did not differ between those groups.
Researchers noted that overall survival was 10% higher at 1 year and 6% higher at 3 years for beneficiaries with PDP coverage or OCC than it was for those without coverage, but they added that the analysis required cautious interpretation “as it is confounded by multiple baseline factors and mediated by the quality of cancer treatment. ... We could not discern whether worse survival in the group without coverage was a result of not receiving therapy at all, an inability to access IMiDs [immunomodulatory drugs], or poor control of other medical issues.”
However, a comparison with the control group “strongly suggest[s] that patients with myeloma without prescription drug coverage may not have received the most effective first-line therapy,” Dr. Olszewski and his colleagues added. “Survival for PDP and OCC groups remained identical, which supports the notion that having any prescription drug coverage contributed to optimal treatment and outcomes.”
The study was limited by the fact that unobserved clinical differences between beneficiaries with or without prescription drug coverage could have accounted for differences in mortality and that the comparison of treatments was restricted to parenteral regimens because IMiDs were observed to have been administered only for PDP enrollees.
Dr. Olszewski and study coauthor Amy Davidoff, PhD, of Yale University, New Haven, Conn., disclosed acting in consulting or advisory roles and receiving research funding from several pharmaceutical companies that develop cancer treatments.
Medicare beneficiaries with myeloma who have prescription drug coverage have shown both decreased used of classic cytotoxic chemotherapy and better survival, according to new research.
vitanovski/Thinkstock.com
The findings suggested that prescription drug coverage brings better access to all existing treatment options.
“In this analysis of Medicare beneficiaries with myeloma, the receipt of therapy and survival differed according to prescription drug coverage status,” Adam Olszewski, MD, of the Lifespan Cancer Institute at Rhode Island Hospital in Providence, R.I., and his colleagues noted in the study. “Patients with PDP [prescription drug plan coverage through Medicare Part D] or OCC [other credible prescription drug coverage] more often received active myeloma care, compared to those without coverage,” they wrote in Journal of Clinical Oncology.
The researchers looked at 9,755 patients diagnosed with myeloma during 2006-2011 and examined what was used to treat the myeloma as a first line treatment. The cohort included 1,460 patients with no prescription drug coverage, 3,283 with PDP coverage, 3,607 with OCC, and 1,405 dual eligibility for Medicare and Medicaid coverage.
The study found that, compared with beneficiaries with no coverage, Medicare beneficiaries with PDP coverage “were 14% less likely to be treated with parenteral chemotherapy and 38% less likely to receive classic cytotoxic agents.” Additionally, among the cohort of beneficiaries that were without drug coverage prior to the diagnosis of myeloma, 41% actively obtained coverage, but even then, their survival was “significantly worse, compared with the beneficiaries who had coverage at diagnosis.”
Beneficiaries classified as having other credible coverage were 3% more likely to receive active myeloma care than were those without coverage, but the use of parenteral regimens did not differ between those groups.
Researchers noted that overall survival was 10% higher at 1 year and 6% higher at 3 years for beneficiaries with PDP coverage or OCC than it was for those without coverage, but they added that the analysis required cautious interpretation “as it is confounded by multiple baseline factors and mediated by the quality of cancer treatment. ... We could not discern whether worse survival in the group without coverage was a result of not receiving therapy at all, an inability to access IMiDs [immunomodulatory drugs], or poor control of other medical issues.”
However, a comparison with the control group “strongly suggest[s] that patients with myeloma without prescription drug coverage may not have received the most effective first-line therapy,” Dr. Olszewski and his colleagues added. “Survival for PDP and OCC groups remained identical, which supports the notion that having any prescription drug coverage contributed to optimal treatment and outcomes.”
The study was limited by the fact that unobserved clinical differences between beneficiaries with or without prescription drug coverage could have accounted for differences in mortality and that the comparison of treatments was restricted to parenteral regimens because IMiDs were observed to have been administered only for PDP enrollees.
Dr. Olszewski and study coauthor Amy Davidoff, PhD, of Yale University, New Haven, Conn., disclosed acting in consulting or advisory roles and receiving research funding from several pharmaceutical companies that develop cancer treatments.
Medicare beneficiaries with myeloma who have prescription drug coverage have shown both decreased used of classic cytotoxic chemotherapy and better survival, according to new research.
vitanovski/Thinkstock.com
The findings suggested that prescription drug coverage brings better access to all existing treatment options.
“In this analysis of Medicare beneficiaries with myeloma, the receipt of therapy and survival differed according to prescription drug coverage status,” Adam Olszewski, MD, of the Lifespan Cancer Institute at Rhode Island Hospital in Providence, R.I., and his colleagues noted in the study. “Patients with PDP [prescription drug plan coverage through Medicare Part D] or OCC [other credible prescription drug coverage] more often received active myeloma care, compared to those without coverage,” they wrote in Journal of Clinical Oncology.
The researchers looked at 9,755 patients diagnosed with myeloma during 2006-2011 and examined what was used to treat the myeloma as a first line treatment. The cohort included 1,460 patients with no prescription drug coverage, 3,283 with PDP coverage, 3,607 with OCC, and 1,405 dual eligibility for Medicare and Medicaid coverage.
The study found that, compared with beneficiaries with no coverage, Medicare beneficiaries with PDP coverage “were 14% less likely to be treated with parenteral chemotherapy and 38% less likely to receive classic cytotoxic agents.” Additionally, among the cohort of beneficiaries that were without drug coverage prior to the diagnosis of myeloma, 41% actively obtained coverage, but even then, their survival was “significantly worse, compared with the beneficiaries who had coverage at diagnosis.”
Beneficiaries classified as having other credible coverage were 3% more likely to receive active myeloma care than were those without coverage, but the use of parenteral regimens did not differ between those groups.
Researchers noted that overall survival was 10% higher at 1 year and 6% higher at 3 years for beneficiaries with PDP coverage or OCC than it was for those without coverage, but they added that the analysis required cautious interpretation “as it is confounded by multiple baseline factors and mediated by the quality of cancer treatment. ... We could not discern whether worse survival in the group without coverage was a result of not receiving therapy at all, an inability to access IMiDs [immunomodulatory drugs], or poor control of other medical issues.”
However, a comparison with the control group “strongly suggest[s] that patients with myeloma without prescription drug coverage may not have received the most effective first-line therapy,” Dr. Olszewski and his colleagues added. “Survival for PDP and OCC groups remained identical, which supports the notion that having any prescription drug coverage contributed to optimal treatment and outcomes.”
The study was limited by the fact that unobserved clinical differences between beneficiaries with or without prescription drug coverage could have accounted for differences in mortality and that the comparison of treatments was restricted to parenteral regimens because IMiDs were observed to have been administered only for PDP enrollees.
Dr. Olszewski and study coauthor Amy Davidoff, PhD, of Yale University, New Haven, Conn., disclosed acting in consulting or advisory roles and receiving research funding from several pharmaceutical companies that develop cancer treatments.
Key clinical point: Prescription drug coverage is related to better outcomes for Medicare patients with myeloma.
Major finding: Compared with patients without coverage, patients with prescription drug plan coverage through Medicare Part D were 14% less likely to receive parenteral chemotherapy and 38% less likely to receive classic cytotoxic agents.
Study details: Observational study using SEER-Medicare data for 9,755 beneficiaries diagnosed with myeloma during 2006-2011.
Disclosures: The study was supported by scholar awards from the American Cancer Society and the American Society of Hematology and by a grant from the National Institute of General Medical Sciences. Report authors Dr. Olszewski and one coauthor disclosed receiving research funding and other financial compensation from several pharmaceutical companies that develop cancer treatments.
Source: Olszewski A et al. J Clin Oncol. 2018 Aug 16. doi: 10.1200/JCO.2018.77.8894
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
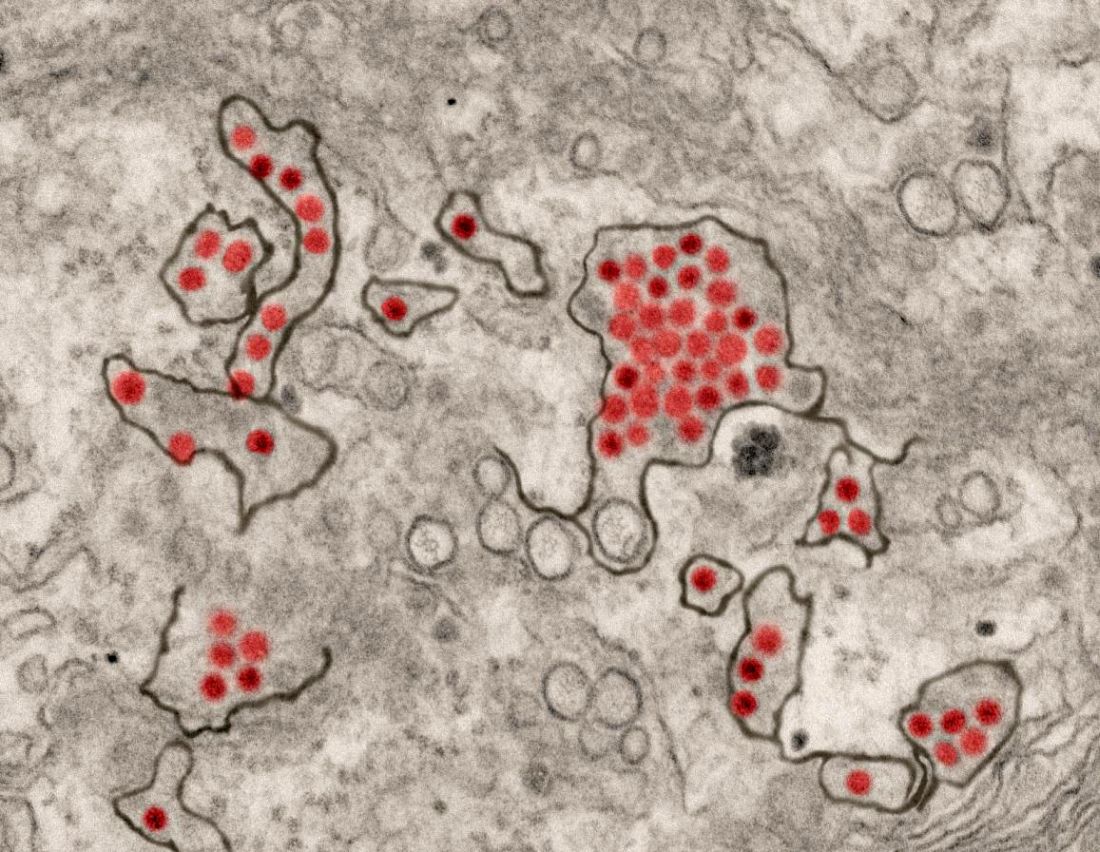
A first-in-human trial of a live, attenuated Zika virus vaccine has begun, according to an announcement by the National Institutes of Health.
Courtesy National Institute of Allergy and Infectious Diseases
Zika virus particles (red) shown in African green monkey kidney cells.
The vaccine, developed by scientists at the National Institute of Allergy and Infectious Diseases will be tested in 28 healthy, nonpregnant adults aged 18-50 years at two centers, the Johns Hopkins Bloomberg School of Public Health Center for Immunization Research in Baltimore, and the Vaccine Testing Center at the University of Vermont in Burlington.
The challenge virus in the vaccine is an attenuated genetic chimera consisting of a dengue virus 4 backbone that expresses Zika virus surface proteins designed to elicit an immune response. The virus was previously tested in rhesus macaque monkeys.
Study participants for the phase 1 trial, Evaluation of the Safety and Immunogenicity of the Live Attenuated Zika Vaccine rZIKV/D4Δ30-713 in Flavivirus-Naive Adults, (NCT03611946) will be assessed based on local and general adverse events to the vaccine and peak neutralizing antibody titer to Zika virus as measured up to 90 days after vaccination. The trial is expected to be reach primary completion by Dec. 31, 2018.
If the phase 1 trial is successful, the goal is to integrate the vaccine with a live, attenuated dengue vaccine candidate called TV003, which is designed to elicit antibodies against all four dengue virus serotypes. The TV003 experimental vaccine is currently under evaluation in a phase 3 clinical trial (NCT02406729) underway in Brazil. Both Zika and dengue viruses frequently are endemic in the same regions and a single vaccine against both diseases would be valued. Stephen Whitehead, PhD of NIAID’s Laboratory of Viral Diseases led the efforts to develop both experimental vaccines.
A first-in-human trial of a live, attenuated Zika virus vaccine has begun, according to an announcement by the National Institutes of Health.
Courtesy National Institute of Allergy and Infectious Diseases
Zika virus particles (red) shown in African green monkey kidney cells.
The vaccine, developed by scientists at the National Institute of Allergy and Infectious Diseases will be tested in 28 healthy, nonpregnant adults aged 18-50 years at two centers, the Johns Hopkins Bloomberg School of Public Health Center for Immunization Research in Baltimore, and the Vaccine Testing Center at the University of Vermont in Burlington.
The challenge virus in the vaccine is an attenuated genetic chimera consisting of a dengue virus 4 backbone that expresses Zika virus surface proteins designed to elicit an immune response. The virus was previously tested in rhesus macaque monkeys.
Study participants for the phase 1 trial, Evaluation of the Safety and Immunogenicity of the Live Attenuated Zika Vaccine rZIKV/D4Δ30-713 in Flavivirus-Naive Adults, (NCT03611946) will be assessed based on local and general adverse events to the vaccine and peak neutralizing antibody titer to Zika virus as measured up to 90 days after vaccination. The trial is expected to be reach primary completion by Dec. 31, 2018.
If the phase 1 trial is successful, the goal is to integrate the vaccine with a live, attenuated dengue vaccine candidate called TV003, which is designed to elicit antibodies against all four dengue virus serotypes. The TV003 experimental vaccine is currently under evaluation in a phase 3 clinical trial (NCT02406729) underway in Brazil. Both Zika and dengue viruses frequently are endemic in the same regions and a single vaccine against both diseases would be valued. Stephen Whitehead, PhD of NIAID’s Laboratory of Viral Diseases led the efforts to develop both experimental vaccines.
A first-in-human trial of a live, attenuated Zika virus vaccine has begun, according to an announcement by the National Institutes of Health.
Courtesy National Institute of Allergy and Infectious Diseases
Zika virus particles (red) shown in African green monkey kidney cells.
The vaccine, developed by scientists at the National Institute of Allergy and Infectious Diseases will be tested in 28 healthy, nonpregnant adults aged 18-50 years at two centers, the Johns Hopkins Bloomberg School of Public Health Center for Immunization Research in Baltimore, and the Vaccine Testing Center at the University of Vermont in Burlington.
The challenge virus in the vaccine is an attenuated genetic chimera consisting of a dengue virus 4 backbone that expresses Zika virus surface proteins designed to elicit an immune response. The virus was previously tested in rhesus macaque monkeys.
Study participants for the phase 1 trial, Evaluation of the Safety and Immunogenicity of the Live Attenuated Zika Vaccine rZIKV/D4Δ30-713 in Flavivirus-Naive Adults, (NCT03611946) will be assessed based on local and general adverse events to the vaccine and peak neutralizing antibody titer to Zika virus as measured up to 90 days after vaccination. The trial is expected to be reach primary completion by Dec. 31, 2018.
If the phase 1 trial is successful, the goal is to integrate the vaccine with a live, attenuated dengue vaccine candidate called TV003, which is designed to elicit antibodies against all four dengue virus serotypes. The TV003 experimental vaccine is currently under evaluation in a phase 3 clinical trial (NCT02406729) underway in Brazil. Both Zika and dengue viruses frequently are endemic in the same regions and a single vaccine against both diseases would be valued. Stephen Whitehead, PhD of NIAID’s Laboratory of Viral Diseases led the efforts to develop both experimental vaccines.
Prominent in the news has been the plight of thousands of immigrant families who are separated from one another at the Mexico-United States border. Now, as reunification is occurring for some, what is the aftermath of the forced separations?
A recent report by the PBS News Hour focused on 3-year-old “Sofi” (last name withheld). She and her grandmother and guardian, Angelina, were among those separated when they made their way legally from Mexico to a U.S. immigration checkpoint in Texas, seeking to escape reprisals from a Mexican drug cartel. For 47 days, infant Sofi was on her own without her family, first in a migrant shelter in El Paso, Texas, and then in a facility in Pennsylvania. For Ana, whose mother was in California already, the time apart from Sofi was one of mind-numbing worry over the fate of her daughter and mother.
Now, life is better. Through an interpreter, Ana said: “I feel good, very good to see her with my mom, and to know that she will now be with us, and she won’t be apart from me.”
The separation was hard on Sofi.
“She cried all the time, told me she didn’t want to be there,” said Ana of Sofi’s ordeal. “One time, she didn’t sound OK. She couldn’t speak clearly, and they were giving her a bad look. They would scold her. And she wanted to tell me something, but couldn’t, because they would scold her. So that had me very worried.”
The early days of reunification have gone fairly well. But unease remains. Sofi mentioned medicine she was given and of being punished for crying or refusing to eat. Whether those incidents are real or embellished, and whether emotional scars remain, is the stuff of the unknown.
“We haven’t asked her many questions because she says that it was a bad place. We want to eventually ask her little by little how she was treated. I think that, with time, we need to let her know that they separated her from us for some time,” Angelina said. “We want to take her to see a therapist, for her to be examined to see how she is, how her health is, because she looks good now – but who knows how she will react later on.” Sofi is home. But hundreds of other children reportedly remain separated from their families.
Prominent in the news has been the plight of thousands of immigrant families who are separated from one another at the Mexico-United States border. Now, as reunification is occurring for some, what is the aftermath of the forced separations?
A recent report by the PBS News Hour focused on 3-year-old “Sofi” (last name withheld). She and her grandmother and guardian, Angelina, were among those separated when they made their way legally from Mexico to a U.S. immigration checkpoint in Texas, seeking to escape reprisals from a Mexican drug cartel. For 47 days, infant Sofi was on her own without her family, first in a migrant shelter in El Paso, Texas, and then in a facility in Pennsylvania. For Ana, whose mother was in California already, the time apart from Sofi was one of mind-numbing worry over the fate of her daughter and mother.
Now, life is better. Through an interpreter, Ana said: “I feel good, very good to see her with my mom, and to know that she will now be with us, and she won’t be apart from me.”
The separation was hard on Sofi.
“She cried all the time, told me she didn’t want to be there,” said Ana of Sofi’s ordeal. “One time, she didn’t sound OK. She couldn’t speak clearly, and they were giving her a bad look. They would scold her. And she wanted to tell me something, but couldn’t, because they would scold her. So that had me very worried.”
The early days of reunification have gone fairly well. But unease remains. Sofi mentioned medicine she was given and of being punished for crying or refusing to eat. Whether those incidents are real or embellished, and whether emotional scars remain, is the stuff of the unknown.
“We haven’t asked her many questions because she says that it was a bad place. We want to eventually ask her little by little how she was treated. I think that, with time, we need to let her know that they separated her from us for some time,” Angelina said. “We want to take her to see a therapist, for her to be examined to see how she is, how her health is, because she looks good now – but who knows how she will react later on.” Sofi is home. But hundreds of other children reportedly remain separated from their families.
Prominent in the news has been the plight of thousands of immigrant families who are separated from one another at the Mexico-United States border. Now, as reunification is occurring for some, what is the aftermath of the forced separations?
A recent report by the PBS News Hour focused on 3-year-old “Sofi” (last name withheld). She and her grandmother and guardian, Angelina, were among those separated when they made their way legally from Mexico to a U.S. immigration checkpoint in Texas, seeking to escape reprisals from a Mexican drug cartel. For 47 days, infant Sofi was on her own without her family, first in a migrant shelter in El Paso, Texas, and then in a facility in Pennsylvania. For Ana, whose mother was in California already, the time apart from Sofi was one of mind-numbing worry over the fate of her daughter and mother.
Now, life is better. Through an interpreter, Ana said: “I feel good, very good to see her with my mom, and to know that she will now be with us, and she won’t be apart from me.”
The separation was hard on Sofi.
“She cried all the time, told me she didn’t want to be there,” said Ana of Sofi’s ordeal. “One time, she didn’t sound OK. She couldn’t speak clearly, and they were giving her a bad look. They would scold her. And she wanted to tell me something, but couldn’t, because they would scold her. So that had me very worried.”
The early days of reunification have gone fairly well. But unease remains. Sofi mentioned medicine she was given and of being punished for crying or refusing to eat. Whether those incidents are real or embellished, and whether emotional scars remain, is the stuff of the unknown.
“We haven’t asked her many questions because she says that it was a bad place. We want to eventually ask her little by little how she was treated. I think that, with time, we need to let her know that they separated her from us for some time,” Angelina said. “We want to take her to see a therapist, for her to be examined to see how she is, how her health is, because she looks good now – but who knows how she will react later on.” Sofi is home. But hundreds of other children reportedly remain separated from their families.
Many men (yours truly included) are not the smoothest creatures on the dance floor. But what is embarrassing dorky in public works like magic at home, with the clunky moves drawing howls of laughter from family.
But there’s the rub ... behavior that is fun in private can become something to be avoided in public. The drumbeat of generations past about men who are strong and capable can surface, curbing those tapping feet and sending dads to the edge of the dance floor.
That’s why the latest Internet rage is welcome. Videos of dads putting on their best moves are providing an example of how love can overcome less-than-stellar footwork. Check out https://www.youtube.com/watch?v=SGSSHSJPhv4 for an example.
According to Sarah L. Kaufman, dance critic at the Washington Post, “therein lies the coolness of the real-life dancing dad. He’s the opposite of embarrassing! He’s uplifting by way of a profound, unspoken understanding of the situation and of his child.”
Motivated by love and unafraid to show the world their moves, the dorky dancing dad can become heroic dancing dad, especially to a son or daughter who is on shaky ground and in need of support. The behavior of these dads also runs counter to the toxic masculinity that seems to pervade much of American culture.
“Within his body, stereotypes are vanquished. The distant dad is overshadowed by the physically present dad. The clueless dad yields to the one who knows exactly what his kid needs,” Ms. Kaufman wrote.
Many men (yours truly included) are not the smoothest creatures on the dance floor. But what is embarrassing dorky in public works like magic at home, with the clunky moves drawing howls of laughter from family.
But there’s the rub ... behavior that is fun in private can become something to be avoided in public. The drumbeat of generations past about men who are strong and capable can surface, curbing those tapping feet and sending dads to the edge of the dance floor.
That’s why the latest Internet rage is welcome. Videos of dads putting on their best moves are providing an example of how love can overcome less-than-stellar footwork. Check out https://www.youtube.com/watch?v=SGSSHSJPhv4 for an example.
According to Sarah L. Kaufman, dance critic at the Washington Post, “therein lies the coolness of the real-life dancing dad. He’s the opposite of embarrassing! He’s uplifting by way of a profound, unspoken understanding of the situation and of his child.”
Motivated by love and unafraid to show the world their moves, the dorky dancing dad can become heroic dancing dad, especially to a son or daughter who is on shaky ground and in need of support. The behavior of these dads also runs counter to the toxic masculinity that seems to pervade much of American culture.
“Within his body, stereotypes are vanquished. The distant dad is overshadowed by the physically present dad. The clueless dad yields to the one who knows exactly what his kid needs,” Ms. Kaufman wrote.
Many men (yours truly included) are not the smoothest creatures on the dance floor. But what is embarrassing dorky in public works like magic at home, with the clunky moves drawing howls of laughter from family.
But there’s the rub ... behavior that is fun in private can become something to be avoided in public. The drumbeat of generations past about men who are strong and capable can surface, curbing those tapping feet and sending dads to the edge of the dance floor.
That’s why the latest Internet rage is welcome. Videos of dads putting on their best moves are providing an example of how love can overcome less-than-stellar footwork. Check out https://www.youtube.com/watch?v=SGSSHSJPhv4 for an example.
According to Sarah L. Kaufman, dance critic at the Washington Post, “therein lies the coolness of the real-life dancing dad. He’s the opposite of embarrassing! He’s uplifting by way of a profound, unspoken understanding of the situation and of his child.”
Motivated by love and unafraid to show the world their moves, the dorky dancing dad can become heroic dancing dad, especially to a son or daughter who is on shaky ground and in need of support. The behavior of these dads also runs counter to the toxic masculinity that seems to pervade much of American culture.
“Within his body, stereotypes are vanquished. The distant dad is overshadowed by the physically present dad. The clueless dad yields to the one who knows exactly what his kid needs,” Ms. Kaufman wrote.
Among psoriasis patients, treatment with infliximab was associated with an increased risk of serious infections that led to hospitalization, the use of intravenous antimicrobial therapy, or death, according to a prospective cohort study of cases in the United Kingdom and the Republic of Ireland.
The new data suggest a risk associated with infliximab treatment that previous clinical trials and observational studies were insufficiently powered to detect, according to the investigators, led by Zenas Yiu, of the University of Manchester (England). They found no associations between infection risk and treatment with etanercept, adalimumab, or ustekinumab, and they noted that there are no such data yet on more recently approved biologic therapies for psoriasis, such as secukinumab or ixekizumab.
The British Association of Dermatologists (BAD) recommends infliximab, a tumor necrosis factor (TNF)–blocker, only for severe cases of psoriasis (Psoriasis Area and Severity Index greater than or equal to 20 and a Dermatology Life Quality Index greater than 18), or when other biologics fail or cannot be used.
To address the insufficient power of earlier studies, the researchers used data from the BAD Biologic Interventions Register (BADBIR), a large, prospective psoriasis registry in the United Kingdom and Ireland established in 2007. The analysis included 3,421 subjects in the nonbiologic systemic therapy cohort, and 422 subjects in the all-lines infliximab cohort. The median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.*
Treatment with infliximab was associated with a statistically significant increased risk of serious infection (defined as an infection associated with prolonged hospitalization or use of IV antimicrobial therapy; or an infection that resulted in death), with an adjusted hazard ratio of 1.95 (95% confidence interval, 1.01-3.75), compared with nonbiologic systemic treatments. The risk was higher in the first 6 months (adjusted HR, 3.49; 95% CI, 1.14-10.70), and from 6 months to 1 year (aHR, 2.99; 95% CI, 1.10-8.14,) but did not reach statistical significance at 1 year to 2 years (aHR, 2.03; 95% CI, 0.61-6.79).
There was also an increased risk of serious infection with infliximab compared with methotrexate (aHR, 2.96; 95% CI, 1.58-5.57).
“Given our findings of a higher risk of serious infection associated with infliximab, we provide real-world evidence to reinforce the position of infliximab in the psoriasis treatment hierarchy,” the authors wrote, adding that “patients with severe psoriasis who fulfill the criteria for the prescription of infliximab should be counseled” about the risk of serious infection.
Dr. Yiu disclosed having received nonfinancial support form Novartis, two authors had no disclosures, and the remainder had various disclosures related to pharmaceutical companies. BADBIR is funded by BAD, which receives funding from Pfizer, Janssen Cilag, AbbVie, Novartis, Samsung Bioepis and Eli Lilly for providing pharmacovigilance services.
*This article was updated to correctly indicate that the median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.
Among psoriasis patients, treatment with infliximab was associated with an increased risk of serious infections that led to hospitalization, the use of intravenous antimicrobial therapy, or death, according to a prospective cohort study of cases in the United Kingdom and the Republic of Ireland.
The new data suggest a risk associated with infliximab treatment that previous clinical trials and observational studies were insufficiently powered to detect, according to the investigators, led by Zenas Yiu, of the University of Manchester (England). They found no associations between infection risk and treatment with etanercept, adalimumab, or ustekinumab, and they noted that there are no such data yet on more recently approved biologic therapies for psoriasis, such as secukinumab or ixekizumab.
The British Association of Dermatologists (BAD) recommends infliximab, a tumor necrosis factor (TNF)–blocker, only for severe cases of psoriasis (Psoriasis Area and Severity Index greater than or equal to 20 and a Dermatology Life Quality Index greater than 18), or when other biologics fail or cannot be used.
To address the insufficient power of earlier studies, the researchers used data from the BAD Biologic Interventions Register (BADBIR), a large, prospective psoriasis registry in the United Kingdom and Ireland established in 2007. The analysis included 3,421 subjects in the nonbiologic systemic therapy cohort, and 422 subjects in the all-lines infliximab cohort. The median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.*
Treatment with infliximab was associated with a statistically significant increased risk of serious infection (defined as an infection associated with prolonged hospitalization or use of IV antimicrobial therapy; or an infection that resulted in death), with an adjusted hazard ratio of 1.95 (95% confidence interval, 1.01-3.75), compared with nonbiologic systemic treatments. The risk was higher in the first 6 months (adjusted HR, 3.49; 95% CI, 1.14-10.70), and from 6 months to 1 year (aHR, 2.99; 95% CI, 1.10-8.14,) but did not reach statistical significance at 1 year to 2 years (aHR, 2.03; 95% CI, 0.61-6.79).
There was also an increased risk of serious infection with infliximab compared with methotrexate (aHR, 2.96; 95% CI, 1.58-5.57).
“Given our findings of a higher risk of serious infection associated with infliximab, we provide real-world evidence to reinforce the position of infliximab in the psoriasis treatment hierarchy,” the authors wrote, adding that “patients with severe psoriasis who fulfill the criteria for the prescription of infliximab should be counseled” about the risk of serious infection.
Dr. Yiu disclosed having received nonfinancial support form Novartis, two authors had no disclosures, and the remainder had various disclosures related to pharmaceutical companies. BADBIR is funded by BAD, which receives funding from Pfizer, Janssen Cilag, AbbVie, Novartis, Samsung Bioepis and Eli Lilly for providing pharmacovigilance services.
*This article was updated to correctly indicate that the median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.
Among psoriasis patients, treatment with infliximab was associated with an increased risk of serious infections that led to hospitalization, the use of intravenous antimicrobial therapy, or death, according to a prospective cohort study of cases in the United Kingdom and the Republic of Ireland.
The new data suggest a risk associated with infliximab treatment that previous clinical trials and observational studies were insufficiently powered to detect, according to the investigators, led by Zenas Yiu, of the University of Manchester (England). They found no associations between infection risk and treatment with etanercept, adalimumab, or ustekinumab, and they noted that there are no such data yet on more recently approved biologic therapies for psoriasis, such as secukinumab or ixekizumab.
The British Association of Dermatologists (BAD) recommends infliximab, a tumor necrosis factor (TNF)–blocker, only for severe cases of psoriasis (Psoriasis Area and Severity Index greater than or equal to 20 and a Dermatology Life Quality Index greater than 18), or when other biologics fail or cannot be used.
To address the insufficient power of earlier studies, the researchers used data from the BAD Biologic Interventions Register (BADBIR), a large, prospective psoriasis registry in the United Kingdom and Ireland established in 2007. The analysis included 3,421 subjects in the nonbiologic systemic therapy cohort, and 422 subjects in the all-lines infliximab cohort. The median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.*
Treatment with infliximab was associated with a statistically significant increased risk of serious infection (defined as an infection associated with prolonged hospitalization or use of IV antimicrobial therapy; or an infection that resulted in death), with an adjusted hazard ratio of 1.95 (95% confidence interval, 1.01-3.75), compared with nonbiologic systemic treatments. The risk was higher in the first 6 months (adjusted HR, 3.49; 95% CI, 1.14-10.70), and from 6 months to 1 year (aHR, 2.99; 95% CI, 1.10-8.14,) but did not reach statistical significance at 1 year to 2 years (aHR, 2.03; 95% CI, 0.61-6.79).
There was also an increased risk of serious infection with infliximab compared with methotrexate (aHR, 2.96; 95% CI, 1.58-5.57).
“Given our findings of a higher risk of serious infection associated with infliximab, we provide real-world evidence to reinforce the position of infliximab in the psoriasis treatment hierarchy,” the authors wrote, adding that “patients with severe psoriasis who fulfill the criteria for the prescription of infliximab should be counseled” about the risk of serious infection.
Dr. Yiu disclosed having received nonfinancial support form Novartis, two authors had no disclosures, and the remainder had various disclosures related to pharmaceutical companies. BADBIR is funded by BAD, which receives funding from Pfizer, Janssen Cilag, AbbVie, Novartis, Samsung Bioepis and Eli Lilly for providing pharmacovigilance services.
*This article was updated to correctly indicate that the median follow-up period was 1.49 person-years (interquartile range, 2.50 person-years) for the all-lines (not just first-line) infliximab group, and 1.51 person-years (1.84 person-years) for the nonbiologics group.
Key clinical point: The study reinforces British guidelines that infliximab should be restricted to most severe cases.
Major finding: Infliximab was associated with a hazard ratio of 1.95 for severe infections, compared with non-biologic systemic therapies.
Study details: Prospective cohort analysis of a psoriasis treatment database of 3,843 individuals.
Disclosures: Dr. Yiu disclosed having received non-financial support form Novartis, two authors had no disclosures, and the remainder had various disclosures related to pharmaceutical companies. BADBIR is funded by BAD, which receives funding from Pfizer, Janssen Cilag, AbbVie, Novartis, Samsung Bioepis and Eli Lilly for providing pharmacovigilance services.
Source: Yiu ZZN et al. Br J Dermatol. 2018 Aug 2. doi: 10.1111/bjd.17036.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
Black women who smoke cigarettes are at increased risk of systemic lupus erythematosus (SLE), while those who drink alcohol in moderation have a decreased risk, data from the prospective Black Women’s Health Study suggests.
The current findings among black women, who are the demographic group at the highest risk of SLE in the U.S. population, are consistent with the previously reported positive association of cigarette smoking with risk of SLE and inverse association of alcohol consumption with SLE,” lead researchers Yvette Cozier, DSc, and Medha Barbhaiya, MD, and their colleagues wrote in a study published in Arthritis Care & Research.
“The role of environmental factors in the pathogenesis of SLE is of great interest, as genetic factors do not explain a major portion of the incidence. Cigarette smoking has been associated with SLE risk in several, but not all, past studies,” wrote Dr. Cozier of the Slone Epidemiology Center at Boston University and Dr. Barbhaiya of the Hospital for Special Surgery, New York, and their coauthors.
Their analysis of data from the Black Women’s Health Study, a prospective study following 59,000 black women in the United States since 1995, identified 127 new cases of SLE between 1995 and 2015 that were confirmed by medical records.
At baseline, 8,851 women (16%) were current smokers, and 10,447 (18%) were past smokers. A total of 14,001 (25%) were current drinkers, and 10,255 (18%) were past drinkers.
The researchers reported that, compared with never smokers, women who had ever smoked had a 45% higher risk for SLE than did never smokers (hazard ratio, 1.45; 95% confidence interval, 0.97-2.18), but the finding was not statistically significant.
The risk of SLE was greater among current smokers (52% higher risk) than among past smokers (41% higher risk), and greater for 20 or more pack-years of smoking (60% higher risk) than for less than 20 pack-years of smoking (37% higher risk), although the authors noted that none of these differences were statistically significant.
Current and past alcohol consumption were associated with nonsignificant reductions in risk for SLE, 29% and 21%, respectively. However, “moderate” current alcohol consumption, measured as four or more drinks per week, was associated with a 57% reduction in risk for SLE (HR, 0.43; 95% CI, 0.19-0.96).
The researchers said that the associations between cigarette smoking and alcohol intake with SLE risk were biologically plausible and may lead to insights into SLE pathogenesis. For example, exposure to toxic components from cigarette smoke was associated with increased oxidative stress and stimulation of autoantibody production, and such exposure can directly damage endogenous proteins and DNA. Alcohol suppresses the synthesis of proinflammatory cytokines and may inhibit DNA synthesis.
The small number of lupus cases in the Black Women’s Health Study cohort limited the statistical power of the analysis. Smoking and alcohol use were also relatively uncommon among women in the Black Women’s Health Study cohort, the investigators said.
“Future studies are needed to confirm these findings and establish the biologic mechanisms by which cigarette smoking and alcohol consumption influence the risk of SLE in this population and others,“ they wrote.
The study was supported by individual investigators’ grant awards from the National Cancer Institute, the National Institute of Arthritis and Musculoskeletal and Skin Diseases, the Rheumatology Research Foundation, and the Lupus Foundation of America. The authors declared no relevant conflicts of interest.
Black women who smoke cigarettes are at increased risk of systemic lupus erythematosus (SLE), while those who drink alcohol in moderation have a decreased risk, data from the prospective Black Women’s Health Study suggests.
The current findings among black women, who are the demographic group at the highest risk of SLE in the U.S. population, are consistent with the previously reported positive association of cigarette smoking with risk of SLE and inverse association of alcohol consumption with SLE,” lead researchers Yvette Cozier, DSc, and Medha Barbhaiya, MD, and their colleagues wrote in a study published in Arthritis Care & Research.
“The role of environmental factors in the pathogenesis of SLE is of great interest, as genetic factors do not explain a major portion of the incidence. Cigarette smoking has been associated with SLE risk in several, but not all, past studies,” wrote Dr. Cozier of the Slone Epidemiology Center at Boston University and Dr. Barbhaiya of the Hospital for Special Surgery, New York, and their coauthors.
Their analysis of data from the Black Women’s Health Study, a prospective study following 59,000 black women in the United States since 1995, identified 127 new cases of SLE between 1995 and 2015 that were confirmed by medical records.
At baseline, 8,851 women (16%) were current smokers, and 10,447 (18%) were past smokers. A total of 14,001 (25%) were current drinkers, and 10,255 (18%) were past drinkers.
The researchers reported that, compared with never smokers, women who had ever smoked had a 45% higher risk for SLE than did never smokers (hazard ratio, 1.45; 95% confidence interval, 0.97-2.18), but the finding was not statistically significant.
The risk of SLE was greater among current smokers (52% higher risk) than among past smokers (41% higher risk), and greater for 20 or more pack-years of smoking (60% higher risk) than for less than 20 pack-years of smoking (37% higher risk), although the authors noted that none of these differences were statistically significant.
Current and past alcohol consumption were associated with nonsignificant reductions in risk for SLE, 29% and 21%, respectively. However, “moderate” current alcohol consumption, measured as four or more drinks per week, was associated with a 57% reduction in risk for SLE (HR, 0.43; 95% CI, 0.19-0.96).
The researchers said that the associations between cigarette smoking and alcohol intake with SLE risk were biologically plausible and may lead to insights into SLE pathogenesis. For example, exposure to toxic components from cigarette smoke was associated with increased oxidative stress and stimulation of autoantibody production, and such exposure can directly damage endogenous proteins and DNA. Alcohol suppresses the synthesis of proinflammatory cytokines and may inhibit DNA synthesis.
The small number of lupus cases in the Black Women’s Health Study cohort limited the statistical power of the analysis. Smoking and alcohol use were also relatively uncommon among women in the Black Women’s Health Study cohort, the investigators said.
“Future studies are needed to confirm these findings and establish the biologic mechanisms by which cigarette smoking and alcohol consumption influence the risk of SLE in this population and others,“ they wrote.
The study was supported by individual investigators’ grant awards from the National Cancer Institute, the National Institute of Arthritis and Musculoskeletal and Skin Diseases, the Rheumatology Research Foundation, and the Lupus Foundation of America. The authors declared no relevant conflicts of interest.
Black women who smoke cigarettes are at increased risk of systemic lupus erythematosus (SLE), while those who drink alcohol in moderation have a decreased risk, data from the prospective Black Women’s Health Study suggests.
The current findings among black women, who are the demographic group at the highest risk of SLE in the U.S. population, are consistent with the previously reported positive association of cigarette smoking with risk of SLE and inverse association of alcohol consumption with SLE,” lead researchers Yvette Cozier, DSc, and Medha Barbhaiya, MD, and their colleagues wrote in a study published in Arthritis Care & Research.
“The role of environmental factors in the pathogenesis of SLE is of great interest, as genetic factors do not explain a major portion of the incidence. Cigarette smoking has been associated with SLE risk in several, but not all, past studies,” wrote Dr. Cozier of the Slone Epidemiology Center at Boston University and Dr. Barbhaiya of the Hospital for Special Surgery, New York, and their coauthors.
Their analysis of data from the Black Women’s Health Study, a prospective study following 59,000 black women in the United States since 1995, identified 127 new cases of SLE between 1995 and 2015 that were confirmed by medical records.
At baseline, 8,851 women (16%) were current smokers, and 10,447 (18%) were past smokers. A total of 14,001 (25%) were current drinkers, and 10,255 (18%) were past drinkers.
The researchers reported that, compared with never smokers, women who had ever smoked had a 45% higher risk for SLE than did never smokers (hazard ratio, 1.45; 95% confidence interval, 0.97-2.18), but the finding was not statistically significant.
The risk of SLE was greater among current smokers (52% higher risk) than among past smokers (41% higher risk), and greater for 20 or more pack-years of smoking (60% higher risk) than for less than 20 pack-years of smoking (37% higher risk), although the authors noted that none of these differences were statistically significant.
Current and past alcohol consumption were associated with nonsignificant reductions in risk for SLE, 29% and 21%, respectively. However, “moderate” current alcohol consumption, measured as four or more drinks per week, was associated with a 57% reduction in risk for SLE (HR, 0.43; 95% CI, 0.19-0.96).
The researchers said that the associations between cigarette smoking and alcohol intake with SLE risk were biologically plausible and may lead to insights into SLE pathogenesis. For example, exposure to toxic components from cigarette smoke was associated with increased oxidative stress and stimulation of autoantibody production, and such exposure can directly damage endogenous proteins and DNA. Alcohol suppresses the synthesis of proinflammatory cytokines and may inhibit DNA synthesis.
The small number of lupus cases in the Black Women’s Health Study cohort limited the statistical power of the analysis. Smoking and alcohol use were also relatively uncommon among women in the Black Women’s Health Study cohort, the investigators said.
“Future studies are needed to confirm these findings and establish the biologic mechanisms by which cigarette smoking and alcohol consumption influence the risk of SLE in this population and others,“ they wrote.
The study was supported by individual investigators’ grant awards from the National Cancer Institute, the National Institute of Arthritis and Musculoskeletal and Skin Diseases, the Rheumatology Research Foundation, and the Lupus Foundation of America. The authors declared no relevant conflicts of interest.
Key clinical point:Like Asian and white women, black women are at an increased risk of SLE if they smoke and at a decreased risk with moderate alcohol consumption.
Major finding: There was an estimated 45% increase in risk of SLE for ever smoking relative to never smoking, but the finding was of borderline statistical significance. Moderate current alcohol consumption, measured as four or more drinks per week, was associated with a 57% reduction in SLE risk.
Study details: Analysis of data from 59,000 women enrolled in the prospective Black Women’s Health Study between 1995 and 2015.
Disclosures: The study was supported by individual investigators’ grant awards from the National Cancer Institute, the National Institute of Arthritis and Musculoskeletal and Skin Diseases, the Rheumatology Research Foundation, and the Lupus Foundation of America. The authors declared no relevant conflicts of interest.
Source: Cozier Y et al. Arthritis Care Res. 2018 Aug 9. doi: 10.1002/acr.23703.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
An update to the first-ever guideline on adult congenital heart disease, released today, provides new recommendations and a more nuanced classification system based on data and expertise accrued in the field over the past decade.
Dr. Curt J Daniels
Recommendations for more than two dozen specific lesion types are included in the 2018 American Heart Association/American College of Cardiology Guideline for the Management of Adults With Congenital Heart Disease.
The 172-page document, published online in the Journal of the American College of Cardiology and Circulation, also includes recommendations on general principles ranging from evaluation of suspected disease to palliative care and end-of-life issues.
“The original guidelines, I think everyone would agree, were just a lot more best practice and expert consensus, whereas now we have at least some data to support our recommendations,” said guideline-writing committee vice chair Curt J. Daniels, MD.
Better road map
The document is intended to provide a “better road map” for all providers who will see such patients in their practice, said Dr. Daniels, director of the adult congenital heart disease and pulmonary hypertension program at Ohio State University Heart Center and Nationwide Children’s Hospital, Columbus.
“There are not enough adult congenital heart disease cardiologists and programs in the country to care for the almost 1.5 million adults with congenital heart disease in the United States, so we know these patients are cared for by general cardiologists,” Dr. Daniels said in an interview. “Having some guidelines about when to refer to those patients was a huge part of the purpose of these updated guidelines.”
The revamped classification system underlying the new guidelines seeks to better characterize disease severity based on the complexity of its anatomy and physiology, according to Dr. Daniels.
Previous documents, including the original 2008 AHA/ACC guideline (Circulation. 2008 Nov 7;118:e714-833), focused mainly on anatomic classifications to rank severity, he said.
“Traditionally, we’ve based the severity of congenital heart disease based on the complexity of anatomy they were born with, but that goes only so far,” Dr. Daniels said in an interview.
More than just anatomy
Dr. Robert Jaquiss
In the new system, anatomy is classified as simple (I, e.g., isolated small atrial septal defect), moderately complex (II, e.g., coarctation of the aorta), or greatly complex (III, e.g., cyanotic congenital heart defect), while physiologic stages range from A to D, increasing along with the severity of physiologic variables such as New York Heart Association functional class; exercise capacity; aortic enlargement; arrhythmias; renal, hepatic, or pulmonary function; and venal or arterial stenosis.
A normotensive patient with repaired coarctation of the aorta would be classified as IIA if she had normal end-organ function and exercise capacity, whereas a similar patient with an ascending aortic diameter of 4.0 cm would be classified as IIB, and with the addition of moderate aortic stenosis, would be classified as IIIC, according to an example provided in the guidelines.
Congenital heart disease specialist Robert “Jake” Jaquiss, MD, said in an interview that consideration of physiology alongside anatomy is one of the most important features of the new guidelines.
“This is a way of thinking about patients that involves not just their anatomy, but also considering a variety of domains in which there may be physiologic dysfunction that can modify the underlying anatomy,” said Dr. Jaquiss, chief of pediatric and congenital heart surgery at Children’s Medical Center/University of Texas Southwestern Medical Center, Dallas. “I think that is a more clinically relevant way to think about patients and patient evaluation management, and I commend the authors for that focus.”
For example, one patient who has undergone a Fontan procedure may be fully functional, whereas another with nearly identical anatomy may be burdened by arrhythmias, fluid retention, and impaired exercise function. “If we don’t grasp the physiologic difference, we treat the two patients the same way, which is obviously inappropriate,” Dr. Jaquiss said.
Research directions
Much more research needs to be done, according to guideline authors, who list 60 unresolved research questions that represent evidence gaps and future directions for study.
For example, outstanding questions related to tetralogy of Fallot focus on the optimal timing for pulmonary valve replacement, the role of pulmonary valve replacement and ventricular tachycardia ablation in decreasing sudden cardiac death risk, and whether implantable cardioverter-defibrillators reduce mortality.
“These are the kinds of evolutionary sort of understandings and alterations in the intervention, both at the original operation and for assessment of care, and what we think about it and how we think about it in 2018 is quite different than how we thought in 2008, and I dare say it’ll be even more different in 2028,” Dr. Jaquiss said.
The AHA/ACC guideline was developed in association with the American Association for Thoracic Surgery, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons.
Dr. Daniels reported a relevant relationship with Actelion. Guideline coauthors reported relevant relationships in that same category with Actelion, Boehringer Ingelheim, Cormatrix, Edward Lifesciences, Gilead, Medtronic, Novartis, Sorin (LivaNova), St. Jude Medical, and United Therapeutics. No other disclosures were reported.
Even as summer continues on, the long, hot, sunny days and backyard barbecues can be tinged with the realization that the new school year looms ahead. For those in traditional school systems, September is the return to the classroom. This has long been a source of angst for many children who may face a new school or a return to the challenging, even overwhelming, business of learning.
“The end of summer and the beginning of a new school year can be a stressful time for parents and children,” says psychologist Lynn Bufka, PhD, assistant execute director for practice, research, and policy for the American Psychological Association. “While trying to manage work and the household, parents can sometimes overlook their children’s feelings of nervousness or anxiety as school begins. Working with your children to build resilience and manage their emotions can be beneficial for the psychological health of the whole family.”
According to the association, parents can help ease their child’s worries by offering support and encouragement and by listening to their child’s concerns, which can help foster their resilience. A dry run about a week before the big day can help reset the summer sleep schedule. Getting school supplies together and ready for action is another bit of preparation that helps get the mind ready for the reality of school. Visiting a new school, if permitted, can remove some sense of the unknown and lay the path for that first day through the front door. Empathy can be a powerful aid; understanding that a child might be apprehensive can prevent the potentially misguided advice to just tough it out.
But children aren’t the only ones with back-to-school anxiety. Increasingly, this time of year is generating stress for parents. When budgets are stretched tight, the additional school expenses can be a strain. The horrors of school shooting incidents can be on parents’ minds, especially when their child is enrolled in a new and unfamiliar school. An era of heightened competitiveness for postsecondary education and scholarship money comes with the baggage of worry that a son or daughter is lagging and already might be behind the eight ball in the game of life.
Parental stress can be tough to deal with. Budget planning, participating in safe-school activities, fostering relationships with teachers and staff, having a heightened awareness of signs of school-related stress in their children, and maintaining faith in their children’s ability to learn and succeed can go a long way toward easing the parental burden.
Even as summer continues on, the long, hot, sunny days and backyard barbecues can be tinged with the realization that the new school year looms ahead. For those in traditional school systems, September is the return to the classroom. This has long been a source of angst for many children who may face a new school or a return to the challenging, even overwhelming, business of learning.
“The end of summer and the beginning of a new school year can be a stressful time for parents and children,” says psychologist Lynn Bufka, PhD, assistant execute director for practice, research, and policy for the American Psychological Association. “While trying to manage work and the household, parents can sometimes overlook their children’s feelings of nervousness or anxiety as school begins. Working with your children to build resilience and manage their emotions can be beneficial for the psychological health of the whole family.”
According to the association, parents can help ease their child’s worries by offering support and encouragement and by listening to their child’s concerns, which can help foster their resilience. A dry run about a week before the big day can help reset the summer sleep schedule. Getting school supplies together and ready for action is another bit of preparation that helps get the mind ready for the reality of school. Visiting a new school, if permitted, can remove some sense of the unknown and lay the path for that first day through the front door. Empathy can be a powerful aid; understanding that a child might be apprehensive can prevent the potentially misguided advice to just tough it out.
But children aren’t the only ones with back-to-school anxiety. Increasingly, this time of year is generating stress for parents. When budgets are stretched tight, the additional school expenses can be a strain. The horrors of school shooting incidents can be on parents’ minds, especially when their child is enrolled in a new and unfamiliar school. An era of heightened competitiveness for postsecondary education and scholarship money comes with the baggage of worry that a son or daughter is lagging and already might be behind the eight ball in the game of life.
Parental stress can be tough to deal with. Budget planning, participating in safe-school activities, fostering relationships with teachers and staff, having a heightened awareness of signs of school-related stress in their children, and maintaining faith in their children’s ability to learn and succeed can go a long way toward easing the parental burden.
Even as summer continues on, the long, hot, sunny days and backyard barbecues can be tinged with the realization that the new school year looms ahead. For those in traditional school systems, September is the return to the classroom. This has long been a source of angst for many children who may face a new school or a return to the challenging, even overwhelming, business of learning.
“The end of summer and the beginning of a new school year can be a stressful time for parents and children,” says psychologist Lynn Bufka, PhD, assistant execute director for practice, research, and policy for the American Psychological Association. “While trying to manage work and the household, parents can sometimes overlook their children’s feelings of nervousness or anxiety as school begins. Working with your children to build resilience and manage their emotions can be beneficial for the psychological health of the whole family.”
According to the association, parents can help ease their child’s worries by offering support and encouragement and by listening to their child’s concerns, which can help foster their resilience. A dry run about a week before the big day can help reset the summer sleep schedule. Getting school supplies together and ready for action is another bit of preparation that helps get the mind ready for the reality of school. Visiting a new school, if permitted, can remove some sense of the unknown and lay the path for that first day through the front door. Empathy can be a powerful aid; understanding that a child might be apprehensive can prevent the potentially misguided advice to just tough it out.
But children aren’t the only ones with back-to-school anxiety. Increasingly, this time of year is generating stress for parents. When budgets are stretched tight, the additional school expenses can be a strain. The horrors of school shooting incidents can be on parents’ minds, especially when their child is enrolled in a new and unfamiliar school. An era of heightened competitiveness for postsecondary education and scholarship money comes with the baggage of worry that a son or daughter is lagging and already might be behind the eight ball in the game of life.
Parental stress can be tough to deal with. Budget planning, participating in safe-school activities, fostering relationships with teachers and staff, having a heightened awareness of signs of school-related stress in their children, and maintaining faith in their children’s ability to learn and succeed can go a long way toward easing the parental burden.