User login
CHEST keynote to bridge the gap between generations
Scott Zimmer, a product of generation X, went through college with a passion for public speaking, as well as a deep interest in the generational divide. In 2013, he began working for a company called BridgeWorks and so began his career as one of three speakers at this firm of “generational junkies and trend spotters.”
Founded in 1998, Bridgeworks strives to bridge the generational gaps that are found in all workplaces through research, keynote speakers, workshops, blogs, training, trivia, and more. Bridgeworks is a team of 13 people coming from the baby boomer generation down to millennials on the cusp of being classified with generation Z (gen edgers, as Zimmer calls them). Each team member has their own interesting and diverse background with a passion for the topic of generations, and everyone engages this passion by conducting research with the BridgeWorks team.
There are generational clashes in every single industry, according to Zimmer. Just at BridgeWorks, he even notices when simply sending a text he perceives as “normal” to one of his millennial coworkers, that it is sometimes received as curt and leaves the recipient concerned that they have done something to offend him. This topic is not foreign to anyone— everyone has had a moment of saying “kids these days,” or “ugh, old people.” Because of this, Zimmer starts every session knowing that each person will leave with relevant insights and actionable takeaways.
Zimmer also loves to integrate nostalgia into his presentations, and working with generational theory at BridgeWorks allows him to do just that in a way that helps drive home points and makes ideas more relatable. “Some people like to say we are all just people and we grow out of certain things. But we develop specific traits and values at an impressionable age, and I love looking at what was happening in our lives during those formative years. What are these shared experiences that will form who we are?” This love of nostalgia set Zimmer up for a great opportunity to develop his own trivia gameshow at BridgeWorks. GenPOP! is an interactive trivia gameshow that pairs members of different generations up and quizzes them on all things pop culture from different decades, while also teaching audience members new things about the people they interact with every day.
“So much goes into who we are and who shows up to the workplace, what effects our behavior, and our motivation,” says Zimmer when asked where his passion for this topic stems. “It could be our gender, the region we grew up in, or birth order, and I personally like looking at it through the lens of these different generations.”
So, what will Zimmer bring to CHEST 2018? During his keynote presentation in San Antonio, Zimmer will examine the generational gaps that are existent in the medical community. “You don’t want your young medical professionals to feel like they are sitting at the ‘kids table’ or being talked down to when they have something to share because they do not have equal experience.”
Each generation and each member of a medical team communicates differently, and understanding those differences and feeling like an equal part of the team is very important. How information is conveyed to patients and medical team members of any age affects how they perceive given information and the level of comfort that is felt by each party. Finding ways to bridge the obvious gaps between the generations is a key component to making any team work efficiently.
Scott Zimmer, a product of generation X, went through college with a passion for public speaking, as well as a deep interest in the generational divide. In 2013, he began working for a company called BridgeWorks and so began his career as one of three speakers at this firm of “generational junkies and trend spotters.”
Founded in 1998, Bridgeworks strives to bridge the generational gaps that are found in all workplaces through research, keynote speakers, workshops, blogs, training, trivia, and more. Bridgeworks is a team of 13 people coming from the baby boomer generation down to millennials on the cusp of being classified with generation Z (gen edgers, as Zimmer calls them). Each team member has their own interesting and diverse background with a passion for the topic of generations, and everyone engages this passion by conducting research with the BridgeWorks team.
There are generational clashes in every single industry, according to Zimmer. Just at BridgeWorks, he even notices when simply sending a text he perceives as “normal” to one of his millennial coworkers, that it is sometimes received as curt and leaves the recipient concerned that they have done something to offend him. This topic is not foreign to anyone— everyone has had a moment of saying “kids these days,” or “ugh, old people.” Because of this, Zimmer starts every session knowing that each person will leave with relevant insights and actionable takeaways.
Zimmer also loves to integrate nostalgia into his presentations, and working with generational theory at BridgeWorks allows him to do just that in a way that helps drive home points and makes ideas more relatable. “Some people like to say we are all just people and we grow out of certain things. But we develop specific traits and values at an impressionable age, and I love looking at what was happening in our lives during those formative years. What are these shared experiences that will form who we are?” This love of nostalgia set Zimmer up for a great opportunity to develop his own trivia gameshow at BridgeWorks. GenPOP! is an interactive trivia gameshow that pairs members of different generations up and quizzes them on all things pop culture from different decades, while also teaching audience members new things about the people they interact with every day.
“So much goes into who we are and who shows up to the workplace, what effects our behavior, and our motivation,” says Zimmer when asked where his passion for this topic stems. “It could be our gender, the region we grew up in, or birth order, and I personally like looking at it through the lens of these different generations.”
So, what will Zimmer bring to CHEST 2018? During his keynote presentation in San Antonio, Zimmer will examine the generational gaps that are existent in the medical community. “You don’t want your young medical professionals to feel like they are sitting at the ‘kids table’ or being talked down to when they have something to share because they do not have equal experience.”
Each generation and each member of a medical team communicates differently, and understanding those differences and feeling like an equal part of the team is very important. How information is conveyed to patients and medical team members of any age affects how they perceive given information and the level of comfort that is felt by each party. Finding ways to bridge the obvious gaps between the generations is a key component to making any team work efficiently.
Scott Zimmer, a product of generation X, went through college with a passion for public speaking, as well as a deep interest in the generational divide. In 2013, he began working for a company called BridgeWorks and so began his career as one of three speakers at this firm of “generational junkies and trend spotters.”
Founded in 1998, Bridgeworks strives to bridge the generational gaps that are found in all workplaces through research, keynote speakers, workshops, blogs, training, trivia, and more. Bridgeworks is a team of 13 people coming from the baby boomer generation down to millennials on the cusp of being classified with generation Z (gen edgers, as Zimmer calls them). Each team member has their own interesting and diverse background with a passion for the topic of generations, and everyone engages this passion by conducting research with the BridgeWorks team.
There are generational clashes in every single industry, according to Zimmer. Just at BridgeWorks, he even notices when simply sending a text he perceives as “normal” to one of his millennial coworkers, that it is sometimes received as curt and leaves the recipient concerned that they have done something to offend him. This topic is not foreign to anyone— everyone has had a moment of saying “kids these days,” or “ugh, old people.” Because of this, Zimmer starts every session knowing that each person will leave with relevant insights and actionable takeaways.
Zimmer also loves to integrate nostalgia into his presentations, and working with generational theory at BridgeWorks allows him to do just that in a way that helps drive home points and makes ideas more relatable. “Some people like to say we are all just people and we grow out of certain things. But we develop specific traits and values at an impressionable age, and I love looking at what was happening in our lives during those formative years. What are these shared experiences that will form who we are?” This love of nostalgia set Zimmer up for a great opportunity to develop his own trivia gameshow at BridgeWorks. GenPOP! is an interactive trivia gameshow that pairs members of different generations up and quizzes them on all things pop culture from different decades, while also teaching audience members new things about the people they interact with every day.
“So much goes into who we are and who shows up to the workplace, what effects our behavior, and our motivation,” says Zimmer when asked where his passion for this topic stems. “It could be our gender, the region we grew up in, or birth order, and I personally like looking at it through the lens of these different generations.”
So, what will Zimmer bring to CHEST 2018? During his keynote presentation in San Antonio, Zimmer will examine the generational gaps that are existent in the medical community. “You don’t want your young medical professionals to feel like they are sitting at the ‘kids table’ or being talked down to when they have something to share because they do not have equal experience.”
Each generation and each member of a medical team communicates differently, and understanding those differences and feeling like an equal part of the team is very important. How information is conveyed to patients and medical team members of any age affects how they perceive given information and the level of comfort that is felt by each party. Finding ways to bridge the obvious gaps between the generations is a key component to making any team work efficiently.
Impact factor news for the journal CHEST®
The journal CHEST® was recently awarded a 2-year impact factor of 7.652, the highest in its history, which equates to a 24% increase over last year’s score. In addition, our 5-year impact factor is 7.854, a 7% increase over last year. With respect to the 2-year factor, CHEST® is ranked 4th out of 33 journals in the Critical Care category and 7th out of 59 journals in the Respiratory System category.
Our recent Eigenfactor places us as the second-highest ranked journal in both respiratory and critical care categories. The Eigenfactor metric adjusts the impact factor by eliminating self-citations and factoring in citations in the top-tier journals.
Congratulations to our journal CHEST® !
The journal CHEST® was recently awarded a 2-year impact factor of 7.652, the highest in its history, which equates to a 24% increase over last year’s score. In addition, our 5-year impact factor is 7.854, a 7% increase over last year. With respect to the 2-year factor, CHEST® is ranked 4th out of 33 journals in the Critical Care category and 7th out of 59 journals in the Respiratory System category.
Our recent Eigenfactor places us as the second-highest ranked journal in both respiratory and critical care categories. The Eigenfactor metric adjusts the impact factor by eliminating self-citations and factoring in citations in the top-tier journals.
Congratulations to our journal CHEST® !
The journal CHEST® was recently awarded a 2-year impact factor of 7.652, the highest in its history, which equates to a 24% increase over last year’s score. In addition, our 5-year impact factor is 7.854, a 7% increase over last year. With respect to the 2-year factor, CHEST® is ranked 4th out of 33 journals in the Critical Care category and 7th out of 59 journals in the Respiratory System category.
Our recent Eigenfactor places us as the second-highest ranked journal in both respiratory and critical care categories. The Eigenfactor metric adjusts the impact factor by eliminating self-citations and factoring in citations in the top-tier journals.
Congratulations to our journal CHEST® !
CHEST NetWorks
Palliative and End-of-Life Care
Patient-tailored goals-of-care discussions: Is this the new standard?
Goals-of-care discussions can be challenging conversations for even the most seasoned physicians. The challenge often is not just the timing but also knowing how to stitch together the content of the discussion. In most cases, physicians have minimal prior knowledge of patient and family preferences, and this adds to the complexity. In addition, the majority of these discussions happen in the inpatient setting (Mack et al. Ann Intern Med. 2012;156[3]:204) where the acuity of the illness adds to the barriers of effective communication (Fulmer et al. J Am Geriatr Soc. 2018;May 23. doi: 10.1111/jgs.15374. [Epub ahead of print]). Can these discussions be tailored to suit individual patient needs and can such attempts better goals-of-care communication? A recent publication by Curtis et al in JAMA Internal Medicine (2018;178[7]:930) attempts to shed light on these unanswered questions and provide physician guidance to better engage in these critical discussions. The cluster-randomized trial included both clinicians and patients. Patients were sent a survey assessing their individual preferences, and physicians were given a summary and communication tips based on these preferences (Jumpstart-Tips). This simple, cost-effective yet scalable intervention was able to improve the frequency, documentation, and patient-assessed quality of goals-of-care discussions in an outpatient setting. In addition, the delivery of goal-concordant care was increased at 3 months in the subgroup of patients with stable goals. A notable limitation of this study was the low participation among physicians. Further studies will be needed to further dissect the characteristics of participating and nonparticipating physicians. Research will also be needed to ascertain how to seamlessly integrate this into health-care delivery. But one irrefutable point is that interventions to improve communication hold the key to better end-of-life care delivery for our patients with serious illnesses. Drs. Paladino and Bernacki have aptly noted in their commentary (JAMA Intern Med. 2018;178[7]:940): “In the age of precision medicine, one can imagine a future of precision communication, where we….provide customized direction for clinicians to begin these discussions based on patient-specific needs.” One question remains. Will this be the new standard? The answer lies with us, the clinicians. My answer to this is a resounding “Yes,” and I hope early adopters will lead the way and prove me right.
Shine Raju, MD, MBBS
Steering Committee Member
Respiratory Care
Prevention of health-care professional errors in use of inhalers
Asthma affects approximately 300 million people worldwide. The 2018 Global Initiative for Asthma (GINA) guidelines recommend assessing the patient’s inhaler technique on a regular basis (www.ginasthma.org. Updated 2018. Accessed August 1, 2018).
The pressurized metered-dose inhaler (pMDI) and dry powder inhaler (DPI) are the most common aerosolized medication delivery devices.
Proper inhaler technique optimizes delivery of medication, and patients rely on a variety of their health-care providers (HCP) to teach them to use the devices. Unfortunately, evidence demonstrates patients are unable to use their inhalers properly (Sanchis et al. Chest. 2016;150[2]:394). Improper and inadequate inhaler technique is commonly associated with poor disease control, exacerbations, hospitalization stays, and need for systemic corticosteroids and antibiotic therapy (Capanoglu et al. J Asthma. 2015;52[8]:838; Levy et al. Prim Care Respir J. 2013;22:406; Westerik et al. J Asthma. 2015;53[3]:1).
Incorrect inhaler use is attributed to the design of the device, poor patient understanding, and HCPs having insufficient knowledge of the inhalers and performed the correct inhaled technique 15.5% of the time (Plaza et al. J Allergy Clin Immunol Prac. 2018;6[3]:987).
Health-care providers who are directly responsible for managing patients with pulmonary disease must have knowledge of correct inhaler techniques to effectively teach patients and properly assess their use of these devices. The quality of the HCP instruction to the patient is key to reducing poor inhaler technique (Klijn et al. NPJ Prim Care Respir Med. 2017;;27[1]:24. doi: 10.1038/s41533-017-0022-1). Targeted inhaler technique educational programs for HCPs have been shown to improve clinical outcomes of patients with asthma (Myers. Respir Care. 2015;60[8]:1190). The Respiratory Care NetWork is developing HCP and patient handouts for each aerosol delivery device which may be available in early 2019.
De De Gardner, DrPH, RRT-NPS, FCCP
Steering Committee Member
Sleep Medicine
Pediatric Sleep Disorders
The Sleep Medicine Network has worked hard to contribute to the CHEST 2018 exciting program of events by highlighting hot topics, discussing clinical controversies, and presenting challenging cases in sleep medicine. The goal of the Sleep Medicine Network has been to design content relevant to the diverse audience attending CHEST in San Antonio this year.
This goal includes topics relevant to pediatric sleep medicine. Why is this important to the larger audience at CHEST? Demand for pediatric sleep physicians significantly out paces access in many areas of this country (Phillips et al. Am J Respir Crit Care Med. 2015;192[8]:915). Adult sleep physicians may treat older children or adolescents in their practice, they may care for medically complex children when they transition to adulthood, and they may be asked for advice regarding the sleep concerns of children of their friends and colleagues. Sleep problems in children are common and may affect up to a quarter of children at some point during their lifetime (Owens. Prim Care. 2008;35[3]:533). The entire household is affected when children are not receiving adequate sleep; the sleep of their caregivers and family members is impacted. While many similarities exist between adult and pediatric sleep medicine, physicians who regularly care for children need to be aware of the important differences in the evaluation and treatment of pediatric sleep disorders.
How else can we connect with your practice? If you have an important topic you would like considered for CHEST 2019 please seek out the Sleep Medicine Network meeting in San Antonio, so we can continue to generate relevant content for your practice.
Julie Baughn, MD
Steering Committee Member
Palliative and End-of-Life Care
Patient-tailored goals-of-care discussions: Is this the new standard?
Goals-of-care discussions can be challenging conversations for even the most seasoned physicians. The challenge often is not just the timing but also knowing how to stitch together the content of the discussion. In most cases, physicians have minimal prior knowledge of patient and family preferences, and this adds to the complexity. In addition, the majority of these discussions happen in the inpatient setting (Mack et al. Ann Intern Med. 2012;156[3]:204) where the acuity of the illness adds to the barriers of effective communication (Fulmer et al. J Am Geriatr Soc. 2018;May 23. doi: 10.1111/jgs.15374. [Epub ahead of print]). Can these discussions be tailored to suit individual patient needs and can such attempts better goals-of-care communication? A recent publication by Curtis et al in JAMA Internal Medicine (2018;178[7]:930) attempts to shed light on these unanswered questions and provide physician guidance to better engage in these critical discussions. The cluster-randomized trial included both clinicians and patients. Patients were sent a survey assessing their individual preferences, and physicians were given a summary and communication tips based on these preferences (Jumpstart-Tips). This simple, cost-effective yet scalable intervention was able to improve the frequency, documentation, and patient-assessed quality of goals-of-care discussions in an outpatient setting. In addition, the delivery of goal-concordant care was increased at 3 months in the subgroup of patients with stable goals. A notable limitation of this study was the low participation among physicians. Further studies will be needed to further dissect the characteristics of participating and nonparticipating physicians. Research will also be needed to ascertain how to seamlessly integrate this into health-care delivery. But one irrefutable point is that interventions to improve communication hold the key to better end-of-life care delivery for our patients with serious illnesses. Drs. Paladino and Bernacki have aptly noted in their commentary (JAMA Intern Med. 2018;178[7]:940): “In the age of precision medicine, one can imagine a future of precision communication, where we….provide customized direction for clinicians to begin these discussions based on patient-specific needs.” One question remains. Will this be the new standard? The answer lies with us, the clinicians. My answer to this is a resounding “Yes,” and I hope early adopters will lead the way and prove me right.
Shine Raju, MD, MBBS
Steering Committee Member
Respiratory Care
Prevention of health-care professional errors in use of inhalers
Asthma affects approximately 300 million people worldwide. The 2018 Global Initiative for Asthma (GINA) guidelines recommend assessing the patient’s inhaler technique on a regular basis (www.ginasthma.org. Updated 2018. Accessed August 1, 2018).
The pressurized metered-dose inhaler (pMDI) and dry powder inhaler (DPI) are the most common aerosolized medication delivery devices.
Proper inhaler technique optimizes delivery of medication, and patients rely on a variety of their health-care providers (HCP) to teach them to use the devices. Unfortunately, evidence demonstrates patients are unable to use their inhalers properly (Sanchis et al. Chest. 2016;150[2]:394). Improper and inadequate inhaler technique is commonly associated with poor disease control, exacerbations, hospitalization stays, and need for systemic corticosteroids and antibiotic therapy (Capanoglu et al. J Asthma. 2015;52[8]:838; Levy et al. Prim Care Respir J. 2013;22:406; Westerik et al. J Asthma. 2015;53[3]:1).
Incorrect inhaler use is attributed to the design of the device, poor patient understanding, and HCPs having insufficient knowledge of the inhalers and performed the correct inhaled technique 15.5% of the time (Plaza et al. J Allergy Clin Immunol Prac. 2018;6[3]:987).
Health-care providers who are directly responsible for managing patients with pulmonary disease must have knowledge of correct inhaler techniques to effectively teach patients and properly assess their use of these devices. The quality of the HCP instruction to the patient is key to reducing poor inhaler technique (Klijn et al. NPJ Prim Care Respir Med. 2017;;27[1]:24. doi: 10.1038/s41533-017-0022-1). Targeted inhaler technique educational programs for HCPs have been shown to improve clinical outcomes of patients with asthma (Myers. Respir Care. 2015;60[8]:1190). The Respiratory Care NetWork is developing HCP and patient handouts for each aerosol delivery device which may be available in early 2019.
De De Gardner, DrPH, RRT-NPS, FCCP
Steering Committee Member
Sleep Medicine
Pediatric Sleep Disorders
The Sleep Medicine Network has worked hard to contribute to the CHEST 2018 exciting program of events by highlighting hot topics, discussing clinical controversies, and presenting challenging cases in sleep medicine. The goal of the Sleep Medicine Network has been to design content relevant to the diverse audience attending CHEST in San Antonio this year.
This goal includes topics relevant to pediatric sleep medicine. Why is this important to the larger audience at CHEST? Demand for pediatric sleep physicians significantly out paces access in many areas of this country (Phillips et al. Am J Respir Crit Care Med. 2015;192[8]:915). Adult sleep physicians may treat older children or adolescents in their practice, they may care for medically complex children when they transition to adulthood, and they may be asked for advice regarding the sleep concerns of children of their friends and colleagues. Sleep problems in children are common and may affect up to a quarter of children at some point during their lifetime (Owens. Prim Care. 2008;35[3]:533). The entire household is affected when children are not receiving adequate sleep; the sleep of their caregivers and family members is impacted. While many similarities exist between adult and pediatric sleep medicine, physicians who regularly care for children need to be aware of the important differences in the evaluation and treatment of pediatric sleep disorders.
How else can we connect with your practice? If you have an important topic you would like considered for CHEST 2019 please seek out the Sleep Medicine Network meeting in San Antonio, so we can continue to generate relevant content for your practice.
Julie Baughn, MD
Steering Committee Member
Palliative and End-of-Life Care
Patient-tailored goals-of-care discussions: Is this the new standard?
Goals-of-care discussions can be challenging conversations for even the most seasoned physicians. The challenge often is not just the timing but also knowing how to stitch together the content of the discussion. In most cases, physicians have minimal prior knowledge of patient and family preferences, and this adds to the complexity. In addition, the majority of these discussions happen in the inpatient setting (Mack et al. Ann Intern Med. 2012;156[3]:204) where the acuity of the illness adds to the barriers of effective communication (Fulmer et al. J Am Geriatr Soc. 2018;May 23. doi: 10.1111/jgs.15374. [Epub ahead of print]). Can these discussions be tailored to suit individual patient needs and can such attempts better goals-of-care communication? A recent publication by Curtis et al in JAMA Internal Medicine (2018;178[7]:930) attempts to shed light on these unanswered questions and provide physician guidance to better engage in these critical discussions. The cluster-randomized trial included both clinicians and patients. Patients were sent a survey assessing their individual preferences, and physicians were given a summary and communication tips based on these preferences (Jumpstart-Tips). This simple, cost-effective yet scalable intervention was able to improve the frequency, documentation, and patient-assessed quality of goals-of-care discussions in an outpatient setting. In addition, the delivery of goal-concordant care was increased at 3 months in the subgroup of patients with stable goals. A notable limitation of this study was the low participation among physicians. Further studies will be needed to further dissect the characteristics of participating and nonparticipating physicians. Research will also be needed to ascertain how to seamlessly integrate this into health-care delivery. But one irrefutable point is that interventions to improve communication hold the key to better end-of-life care delivery for our patients with serious illnesses. Drs. Paladino and Bernacki have aptly noted in their commentary (JAMA Intern Med. 2018;178[7]:940): “In the age of precision medicine, one can imagine a future of precision communication, where we….provide customized direction for clinicians to begin these discussions based on patient-specific needs.” One question remains. Will this be the new standard? The answer lies with us, the clinicians. My answer to this is a resounding “Yes,” and I hope early adopters will lead the way and prove me right.
Shine Raju, MD, MBBS
Steering Committee Member
Respiratory Care
Prevention of health-care professional errors in use of inhalers
Asthma affects approximately 300 million people worldwide. The 2018 Global Initiative for Asthma (GINA) guidelines recommend assessing the patient’s inhaler technique on a regular basis (www.ginasthma.org. Updated 2018. Accessed August 1, 2018).
The pressurized metered-dose inhaler (pMDI) and dry powder inhaler (DPI) are the most common aerosolized medication delivery devices.
Proper inhaler technique optimizes delivery of medication, and patients rely on a variety of their health-care providers (HCP) to teach them to use the devices. Unfortunately, evidence demonstrates patients are unable to use their inhalers properly (Sanchis et al. Chest. 2016;150[2]:394). Improper and inadequate inhaler technique is commonly associated with poor disease control, exacerbations, hospitalization stays, and need for systemic corticosteroids and antibiotic therapy (Capanoglu et al. J Asthma. 2015;52[8]:838; Levy et al. Prim Care Respir J. 2013;22:406; Westerik et al. J Asthma. 2015;53[3]:1).
Incorrect inhaler use is attributed to the design of the device, poor patient understanding, and HCPs having insufficient knowledge of the inhalers and performed the correct inhaled technique 15.5% of the time (Plaza et al. J Allergy Clin Immunol Prac. 2018;6[3]:987).
Health-care providers who are directly responsible for managing patients with pulmonary disease must have knowledge of correct inhaler techniques to effectively teach patients and properly assess their use of these devices. The quality of the HCP instruction to the patient is key to reducing poor inhaler technique (Klijn et al. NPJ Prim Care Respir Med. 2017;;27[1]:24. doi: 10.1038/s41533-017-0022-1). Targeted inhaler technique educational programs for HCPs have been shown to improve clinical outcomes of patients with asthma (Myers. Respir Care. 2015;60[8]:1190). The Respiratory Care NetWork is developing HCP and patient handouts for each aerosol delivery device which may be available in early 2019.
De De Gardner, DrPH, RRT-NPS, FCCP
Steering Committee Member
Sleep Medicine
Pediatric Sleep Disorders
The Sleep Medicine Network has worked hard to contribute to the CHEST 2018 exciting program of events by highlighting hot topics, discussing clinical controversies, and presenting challenging cases in sleep medicine. The goal of the Sleep Medicine Network has been to design content relevant to the diverse audience attending CHEST in San Antonio this year.
This goal includes topics relevant to pediatric sleep medicine. Why is this important to the larger audience at CHEST? Demand for pediatric sleep physicians significantly out paces access in many areas of this country (Phillips et al. Am J Respir Crit Care Med. 2015;192[8]:915). Adult sleep physicians may treat older children or adolescents in their practice, they may care for medically complex children when they transition to adulthood, and they may be asked for advice regarding the sleep concerns of children of their friends and colleagues. Sleep problems in children are common and may affect up to a quarter of children at some point during their lifetime (Owens. Prim Care. 2008;35[3]:533). The entire household is affected when children are not receiving adequate sleep; the sleep of their caregivers and family members is impacted. While many similarities exist between adult and pediatric sleep medicine, physicians who regularly care for children need to be aware of the important differences in the evaluation and treatment of pediatric sleep disorders.
How else can we connect with your practice? If you have an important topic you would like considered for CHEST 2019 please seek out the Sleep Medicine Network meeting in San Antonio, so we can continue to generate relevant content for your practice.
Julie Baughn, MD
Steering Committee Member
VA Releases Spanish Version of Health Benefits Application
Nearly 1.5 million veterans and more than 500,000 already enrolled in the VA health care system identify as being Hispanic or Latino. “Our veteran population is made up of an increasingly diverse group of people,” said VA Secretary Robert Wilkie. “It’s our duty to expand the ways we communicate with all veterans, so they’re properly informed about the benefits they’ve earned.”
To that end, the VA has released a Spanish version of the application for health benefits, “to simplify and improve the health care enrollment process.” The new language version follows on the VA Advisory Committee on Minority Veterans’ recommendation.
The form is available at VA medical facilities and online at https://www.va.gov/vaforms/medical/pdf/10-10EZ_Spanish.pdf.
Nearly 1.5 million veterans and more than 500,000 already enrolled in the VA health care system identify as being Hispanic or Latino. “Our veteran population is made up of an increasingly diverse group of people,” said VA Secretary Robert Wilkie. “It’s our duty to expand the ways we communicate with all veterans, so they’re properly informed about the benefits they’ve earned.”
To that end, the VA has released a Spanish version of the application for health benefits, “to simplify and improve the health care enrollment process.” The new language version follows on the VA Advisory Committee on Minority Veterans’ recommendation.
The form is available at VA medical facilities and online at https://www.va.gov/vaforms/medical/pdf/10-10EZ_Spanish.pdf.
Nearly 1.5 million veterans and more than 500,000 already enrolled in the VA health care system identify as being Hispanic or Latino. “Our veteran population is made up of an increasingly diverse group of people,” said VA Secretary Robert Wilkie. “It’s our duty to expand the ways we communicate with all veterans, so they’re properly informed about the benefits they’ve earned.”
To that end, the VA has released a Spanish version of the application for health benefits, “to simplify and improve the health care enrollment process.” The new language version follows on the VA Advisory Committee on Minority Veterans’ recommendation.
The form is available at VA medical facilities and online at https://www.va.gov/vaforms/medical/pdf/10-10EZ_Spanish.pdf.
CHEST Keynote: Reflections of a Lifetime Practicing Chest Medicine
Dr. Richard Irwin, the Editor in Chief for the journal CHEST, and Chair of UMass Memorial Medical Center’s Department of Critical Care, has observed the way patient-focused care has evolved through the years. He will be speaking on this topic at the CHEST 2018 opening session on Sunday, October 7.
During Dr. Irwin’s early years at UMass Memorial, the then chairman of Medicine, Dr. James Dalen, a longtime CHEST member who was about to begin his term as CHEST President, strongly encouraged Dr. Irwin to join the organization. By joining the college, Dr. Irwin was able to form strong connections with other influential chest medicine professionals, such as Dr. Jack Weg, a former CHEST President, and Dr. Alfred Soffer – who was the Editor in Chief of CHEST.
While Dr. Irwin was not yet a member of the CHEST community, the college became instrumental in focusing Dr. Irwin’s academic career because of a manuscript that he and colleagues had been working on, titled Cough. A Comprehensive Review. After submitting the early version of his manuscript to ten different journals and being rejected by each one, Dr. Irwin contacted Dr. Soffer and asked him, if he had the time, could he please read it and offer advice. Dr. Soffer, who had a reputation of being a mentor with endless generosity of his time, reviewed the manuscript and worked with Dr. Irwin on the article, leading to its publication in the Archives of Internal Medicine in 1977. Dr. Soffer’s kindness would lead to the start of Dr. Irwin’s 40-year career of studying cough.
Dr. Irwin has been very influential within the CHEST organization throughout his career. In addition to his years as the Editor in Chief of CHEST, he also served on every major CHEST committee and held the office of CHEST President in 2003-2004. “If you want to join a society that has a family-feel to it and focuses on clinical care and education, then CHEST is the place to be.”
Throughout his years as a physician, Dr. Irwin has been interested in the way physicians learn. During his formative years, he says the way he learned was to “see one, do one, teach one.” He gives the example of the flexible fiber-optic bronchoscope, which was developed in Japan in the late 1960s, arriving in the US in 1970. It was a new way of performing bronchoscopy, which led to physicians reading about it, and then putting what they read into action. Now – there are high fidelity simulation instruments and models and a lot of experiential learning prefacing the use of new technologies for patients. We have CHEST to thank for being a leader in experiential learning and an international resource for simulation training.
Dr. Richard Irwin, the Editor in Chief for the journal CHEST, and Chair of UMass Memorial Medical Center’s Department of Critical Care, has observed the way patient-focused care has evolved through the years. He will be speaking on this topic at the CHEST 2018 opening session on Sunday, October 7.
During Dr. Irwin’s early years at UMass Memorial, the then chairman of Medicine, Dr. James Dalen, a longtime CHEST member who was about to begin his term as CHEST President, strongly encouraged Dr. Irwin to join the organization. By joining the college, Dr. Irwin was able to form strong connections with other influential chest medicine professionals, such as Dr. Jack Weg, a former CHEST President, and Dr. Alfred Soffer – who was the Editor in Chief of CHEST.
While Dr. Irwin was not yet a member of the CHEST community, the college became instrumental in focusing Dr. Irwin’s academic career because of a manuscript that he and colleagues had been working on, titled Cough. A Comprehensive Review. After submitting the early version of his manuscript to ten different journals and being rejected by each one, Dr. Irwin contacted Dr. Soffer and asked him, if he had the time, could he please read it and offer advice. Dr. Soffer, who had a reputation of being a mentor with endless generosity of his time, reviewed the manuscript and worked with Dr. Irwin on the article, leading to its publication in the Archives of Internal Medicine in 1977. Dr. Soffer’s kindness would lead to the start of Dr. Irwin’s 40-year career of studying cough.
Dr. Irwin has been very influential within the CHEST organization throughout his career. In addition to his years as the Editor in Chief of CHEST, he also served on every major CHEST committee and held the office of CHEST President in 2003-2004. “If you want to join a society that has a family-feel to it and focuses on clinical care and education, then CHEST is the place to be.”
Throughout his years as a physician, Dr. Irwin has been interested in the way physicians learn. During his formative years, he says the way he learned was to “see one, do one, teach one.” He gives the example of the flexible fiber-optic bronchoscope, which was developed in Japan in the late 1960s, arriving in the US in 1970. It was a new way of performing bronchoscopy, which led to physicians reading about it, and then putting what they read into action. Now – there are high fidelity simulation instruments and models and a lot of experiential learning prefacing the use of new technologies for patients. We have CHEST to thank for being a leader in experiential learning and an international resource for simulation training.
Dr. Richard Irwin, the Editor in Chief for the journal CHEST, and Chair of UMass Memorial Medical Center’s Department of Critical Care, has observed the way patient-focused care has evolved through the years. He will be speaking on this topic at the CHEST 2018 opening session on Sunday, October 7.
During Dr. Irwin’s early years at UMass Memorial, the then chairman of Medicine, Dr. James Dalen, a longtime CHEST member who was about to begin his term as CHEST President, strongly encouraged Dr. Irwin to join the organization. By joining the college, Dr. Irwin was able to form strong connections with other influential chest medicine professionals, such as Dr. Jack Weg, a former CHEST President, and Dr. Alfred Soffer – who was the Editor in Chief of CHEST.
While Dr. Irwin was not yet a member of the CHEST community, the college became instrumental in focusing Dr. Irwin’s academic career because of a manuscript that he and colleagues had been working on, titled Cough. A Comprehensive Review. After submitting the early version of his manuscript to ten different journals and being rejected by each one, Dr. Irwin contacted Dr. Soffer and asked him, if he had the time, could he please read it and offer advice. Dr. Soffer, who had a reputation of being a mentor with endless generosity of his time, reviewed the manuscript and worked with Dr. Irwin on the article, leading to its publication in the Archives of Internal Medicine in 1977. Dr. Soffer’s kindness would lead to the start of Dr. Irwin’s 40-year career of studying cough.
Dr. Irwin has been very influential within the CHEST organization throughout his career. In addition to his years as the Editor in Chief of CHEST, he also served on every major CHEST committee and held the office of CHEST President in 2003-2004. “If you want to join a society that has a family-feel to it and focuses on clinical care and education, then CHEST is the place to be.”
Throughout his years as a physician, Dr. Irwin has been interested in the way physicians learn. During his formative years, he says the way he learned was to “see one, do one, teach one.” He gives the example of the flexible fiber-optic bronchoscope, which was developed in Japan in the late 1960s, arriving in the US in 1970. It was a new way of performing bronchoscopy, which led to physicians reading about it, and then putting what they read into action. Now – there are high fidelity simulation instruments and models and a lot of experiential learning prefacing the use of new technologies for patients. We have CHEST to thank for being a leader in experiential learning and an international resource for simulation training.
Doc reports ‘very encouraging’ results in penta-refractory MM

HOUSTON—Treatment with selinexor and low-dose dexamethasone can provide a “meaningful clinical benefit” in patients with penta-refractory multiple myeloma (MM), according to the principal investigator of the STORM trial.
Updated results from this phase 2 trial showed that selinexor and low-dose dexamethasone produced an overall response rate of 26.2% and a clinical benefit rate of 39.3%.
The median progression-free survival was 3.7 months, and the median overall survival was 8.6 months.
The trial’s principal investigator, Sundar Jagannath, MBBS, of the Mount Sinai School of Medicine in New York, N.Y., presented these results at the Society of Hematologic Oncology (SOHO) 2018 Annual Meeting as abstract MM-255.*
“The additional phase 2b clinical results ... are very encouraging for the patients suffering from penta-refractory multiple myeloma and their families,” Dr. Jagannath said.
“Of particular significance, for the nearly 40% of patients who had a minimal response or better, the median survival was 15.6 months, which provided the opportunity for a meaningful clinical benefit for patients on the STORM study.”
The study (NCT02336815) included 122 patients with penta-refractory MM. They had previously received bortezomib, carfilzomib, lenalidomide, pomalidomide, daratumumab, alkylating agents, and glucocorticoids. Their disease was refractory to glucocorticoids, at least one proteasome inhibitor, at least one immunomodulatory drug, daratumumab, and their most recent therapy.
The patients had received a median of 7 (range, 3-18) prior treatment regimens. Their median age was 65 (range, 40-86), 58% were male, and 53% had high-risk cytogenetics.
Patients received oral selinexor at 80 mg twice weekly plus dexamethasone at 20 mg twice weekly until disease progression.
Response and survival
Two patients (1.6%) achieved stringent complete responses. They also had minimal residual disease negativity, one at the level of 1 x 10-6 and one at 1 x 10-4.
Six patients (4.9%) had very good partial responses, 24 (19.7%) had partial responses (PRs), 16 (13.1%) had minimal responses (MRs), and 48 (39.3%) had stable disease (SD).
Sixteen patients (13.1%) had progressive disease (PD), and 10 (8.2%) were not evaluable for response.
The overall response rate (PR or better) was 26.2% (n=32), the clinical benefit rate (MR or better) was 39.3% (n=48), and the disease control rate (SD or better) was 78.7% (n=98).
The median duration of response was 4.4 months (range, <1 to 12.2 months).
The median progression-free survival was 3.7 months overall, 4.6 months in patients with an MR or better, and 1.1 months in patients who had PD or were not evaluable.
The median overall survival was 8.6 months for the entire cohort. It was 15.6 months in patients with an MR or better and 1.7 months in patients who had PD or were not evaluable (P<0.0001).
Safety
The most common non-hematologic treatment-related adverse events (AEs) were fatigue/asthenia (69.9%), nausea (69.1%), anorexia (52.0%), weight loss (47.2%), vomiting (35.0%), diarrhea (33.3%), and hyponatremia (30.9%).
Hematologic treatment-related AEs included thrombocytopenia (67.5%), anemia (48.0%), neutropenia (35.8%), leukopenia (29.3%), and lymphopenia (13.8%).
The “most important” grade 3/4 AEs, according to Dr. Jagannath, were thrombocytopenia (53.7%), anemia (29.3%), fatigue (22.8%), hyponatremia (16.3%), nausea (9.8%), diarrhea (6.5%), anorexia (3.3%), and emesis (3.3%).
Twenty-three patients (19.5%) discontinued treatment due to a related AE.
This study was sponsored by Karyopharm Therapeutics. Dr. Jagannath reported relationships with Karyopharm, Janssen, Celgene, Amgen, and GSK.
*Information in the abstract differs from the presentation.
HOUSTON—Treatment with selinexor and low-dose dexamethasone can provide a “meaningful clinical benefit” in patients with penta-refractory multiple myeloma (MM), according to the principal investigator of the STORM trial.
Updated results from this phase 2 trial showed that selinexor and low-dose dexamethasone produced an overall response rate of 26.2% and a clinical benefit rate of 39.3%.
The median progression-free survival was 3.7 months, and the median overall survival was 8.6 months.
The trial’s principal investigator, Sundar Jagannath, MBBS, of the Mount Sinai School of Medicine in New York, N.Y., presented these results at the Society of Hematologic Oncology (SOHO) 2018 Annual Meeting as abstract MM-255.*
“The additional phase 2b clinical results ... are very encouraging for the patients suffering from penta-refractory multiple myeloma and their families,” Dr. Jagannath said.
“Of particular significance, for the nearly 40% of patients who had a minimal response or better, the median survival was 15.6 months, which provided the opportunity for a meaningful clinical benefit for patients on the STORM study.”
The study (NCT02336815) included 122 patients with penta-refractory MM. They had previously received bortezomib, carfilzomib, lenalidomide, pomalidomide, daratumumab, alkylating agents, and glucocorticoids. Their disease was refractory to glucocorticoids, at least one proteasome inhibitor, at least one immunomodulatory drug, daratumumab, and their most recent therapy.
The patients had received a median of 7 (range, 3-18) prior treatment regimens. Their median age was 65 (range, 40-86), 58% were male, and 53% had high-risk cytogenetics.
Patients received oral selinexor at 80 mg twice weekly plus dexamethasone at 20 mg twice weekly until disease progression.
Response and survival
Two patients (1.6%) achieved stringent complete responses. They also had minimal residual disease negativity, one at the level of 1 x 10-6 and one at 1 x 10-4.
Six patients (4.9%) had very good partial responses, 24 (19.7%) had partial responses (PRs), 16 (13.1%) had minimal responses (MRs), and 48 (39.3%) had stable disease (SD).
Sixteen patients (13.1%) had progressive disease (PD), and 10 (8.2%) were not evaluable for response.
The overall response rate (PR or better) was 26.2% (n=32), the clinical benefit rate (MR or better) was 39.3% (n=48), and the disease control rate (SD or better) was 78.7% (n=98).
The median duration of response was 4.4 months (range, <1 to 12.2 months).
The median progression-free survival was 3.7 months overall, 4.6 months in patients with an MR or better, and 1.1 months in patients who had PD or were not evaluable.
The median overall survival was 8.6 months for the entire cohort. It was 15.6 months in patients with an MR or better and 1.7 months in patients who had PD or were not evaluable (P<0.0001).
Safety
The most common non-hematologic treatment-related adverse events (AEs) were fatigue/asthenia (69.9%), nausea (69.1%), anorexia (52.0%), weight loss (47.2%), vomiting (35.0%), diarrhea (33.3%), and hyponatremia (30.9%).
Hematologic treatment-related AEs included thrombocytopenia (67.5%), anemia (48.0%), neutropenia (35.8%), leukopenia (29.3%), and lymphopenia (13.8%).
The “most important” grade 3/4 AEs, according to Dr. Jagannath, were thrombocytopenia (53.7%), anemia (29.3%), fatigue (22.8%), hyponatremia (16.3%), nausea (9.8%), diarrhea (6.5%), anorexia (3.3%), and emesis (3.3%).
Twenty-three patients (19.5%) discontinued treatment due to a related AE.
This study was sponsored by Karyopharm Therapeutics. Dr. Jagannath reported relationships with Karyopharm, Janssen, Celgene, Amgen, and GSK.
*Information in the abstract differs from the presentation.
HOUSTON—Treatment with selinexor and low-dose dexamethasone can provide a “meaningful clinical benefit” in patients with penta-refractory multiple myeloma (MM), according to the principal investigator of the STORM trial.
Updated results from this phase 2 trial showed that selinexor and low-dose dexamethasone produced an overall response rate of 26.2% and a clinical benefit rate of 39.3%.
The median progression-free survival was 3.7 months, and the median overall survival was 8.6 months.
The trial’s principal investigator, Sundar Jagannath, MBBS, of the Mount Sinai School of Medicine in New York, N.Y., presented these results at the Society of Hematologic Oncology (SOHO) 2018 Annual Meeting as abstract MM-255.*
“The additional phase 2b clinical results ... are very encouraging for the patients suffering from penta-refractory multiple myeloma and their families,” Dr. Jagannath said.
“Of particular significance, for the nearly 40% of patients who had a minimal response or better, the median survival was 15.6 months, which provided the opportunity for a meaningful clinical benefit for patients on the STORM study.”
The study (NCT02336815) included 122 patients with penta-refractory MM. They had previously received bortezomib, carfilzomib, lenalidomide, pomalidomide, daratumumab, alkylating agents, and glucocorticoids. Their disease was refractory to glucocorticoids, at least one proteasome inhibitor, at least one immunomodulatory drug, daratumumab, and their most recent therapy.
The patients had received a median of 7 (range, 3-18) prior treatment regimens. Their median age was 65 (range, 40-86), 58% were male, and 53% had high-risk cytogenetics.
Patients received oral selinexor at 80 mg twice weekly plus dexamethasone at 20 mg twice weekly until disease progression.
Response and survival
Two patients (1.6%) achieved stringent complete responses. They also had minimal residual disease negativity, one at the level of 1 x 10-6 and one at 1 x 10-4.
Six patients (4.9%) had very good partial responses, 24 (19.7%) had partial responses (PRs), 16 (13.1%) had minimal responses (MRs), and 48 (39.3%) had stable disease (SD).
Sixteen patients (13.1%) had progressive disease (PD), and 10 (8.2%) were not evaluable for response.
The overall response rate (PR or better) was 26.2% (n=32), the clinical benefit rate (MR or better) was 39.3% (n=48), and the disease control rate (SD or better) was 78.7% (n=98).
The median duration of response was 4.4 months (range, <1 to 12.2 months).
The median progression-free survival was 3.7 months overall, 4.6 months in patients with an MR or better, and 1.1 months in patients who had PD or were not evaluable.
The median overall survival was 8.6 months for the entire cohort. It was 15.6 months in patients with an MR or better and 1.7 months in patients who had PD or were not evaluable (P<0.0001).
Safety
The most common non-hematologic treatment-related adverse events (AEs) were fatigue/asthenia (69.9%), nausea (69.1%), anorexia (52.0%), weight loss (47.2%), vomiting (35.0%), diarrhea (33.3%), and hyponatremia (30.9%).
Hematologic treatment-related AEs included thrombocytopenia (67.5%), anemia (48.0%), neutropenia (35.8%), leukopenia (29.3%), and lymphopenia (13.8%).
The “most important” grade 3/4 AEs, according to Dr. Jagannath, were thrombocytopenia (53.7%), anemia (29.3%), fatigue (22.8%), hyponatremia (16.3%), nausea (9.8%), diarrhea (6.5%), anorexia (3.3%), and emesis (3.3%).
Twenty-three patients (19.5%) discontinued treatment due to a related AE.
This study was sponsored by Karyopharm Therapeutics. Dr. Jagannath reported relationships with Karyopharm, Janssen, Celgene, Amgen, and GSK.
*Information in the abstract differs from the presentation.
Pediatricians fall short on transition to adult care
Many adolescent patients, both with and without special health care needs, are not receiving guidance from their physicians about transitioning to adult care, according to recent findings published in Pediatrics.

Lydie A. Lebrun-Harris, PhD, of the Maternal and Child Health Bureau at the Health Resources and Services Administration, and her colleagues examined data from 20,708 youth aged 12-17 years with and without special health care needs obtained from the 2016 National Survey of Children’s Health. The aim was to determine the current level of transition planning to adult care from a pediatric or other health care provider (HCP).
Parents and caregivers were asked whether a doctor or HCP had spent time alone with the adolescent during the last year, had discussed the transition to adult care, and had actively helped the adolescent “gain self-care skills or understand changes in health care” when they reached the age of 18 years.
Overall, 17% of youth with special health care needs and 14% of youth without met all three transition elements.
The figures were higher for individual measures. For instance, 44% of youth with special health care needs spent time alone with an HCP within the past year, 41% discussed transition to an adult provider, and 69% reported an HCP had worked with them to understand health care changes and gain self-care skills.
Youth without special health care needs were more likely to discus the shift to adult care with HCPs than those with special needs, but special needs youth were more likely to have met the other two transition measurements (P less than .001).
Being older (aged 15-17 years) were associated with an increased prevalence of meeting the overall transition measure and the individual elements among both youth with and without special health care needs.
“Findings from this study underscore the urgent need for HCPs to work with youth independently and in collaboration with their parents and/or caregivers throughout the adolescent years to improve transition planning,” Dr. Lebrun-Harris and her colleagues wrote.
The study was supported by the Health Resources and Services Administration and the National Alliance to Advance Adolescent Health. The authors reported having no relevant conflicts of interest.
SOURCE: Lebrun-Harris LA et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-0194.
While researchers and clinicians have been discussing how to improve the poor health outcomes seen in the transition from pediatric to adult care for youth with special health care needs for decades, there has been little improvement, Megumi J. Okumura, MD, wrote in an accompanying editorial.
In 2016, 41% of youth with special health care needs had a discussion about the transition from pediatric to adult care, a figure that is “largely unchanged from 2010,” she noted.
One hurdle is the lack of a gold standard for measuring an ideal transition. Is it successful scheduling of an appointment with adult provider or having a job and being able to manage one’s own disease?
“Until our health system supports pediatric providers in offering adequate transition planning, it will be difficult to expect any uptick in these measures. In addition, we still need to understand why some adolescents fail in their transition and transfer and how to develop the appropriate interventions to improve health outcomes for these patients,” Dr. Okumura wrote.
Dr. Okumura is with the division of general pediatrics at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-2245). She reported having no relevant conflicts of interest.
While researchers and clinicians have been discussing how to improve the poor health outcomes seen in the transition from pediatric to adult care for youth with special health care needs for decades, there has been little improvement, Megumi J. Okumura, MD, wrote in an accompanying editorial.
In 2016, 41% of youth with special health care needs had a discussion about the transition from pediatric to adult care, a figure that is “largely unchanged from 2010,” she noted.
One hurdle is the lack of a gold standard for measuring an ideal transition. Is it successful scheduling of an appointment with adult provider or having a job and being able to manage one’s own disease?
“Until our health system supports pediatric providers in offering adequate transition planning, it will be difficult to expect any uptick in these measures. In addition, we still need to understand why some adolescents fail in their transition and transfer and how to develop the appropriate interventions to improve health outcomes for these patients,” Dr. Okumura wrote.
Dr. Okumura is with the division of general pediatrics at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-2245). She reported having no relevant conflicts of interest.
While researchers and clinicians have been discussing how to improve the poor health outcomes seen in the transition from pediatric to adult care for youth with special health care needs for decades, there has been little improvement, Megumi J. Okumura, MD, wrote in an accompanying editorial.
In 2016, 41% of youth with special health care needs had a discussion about the transition from pediatric to adult care, a figure that is “largely unchanged from 2010,” she noted.
One hurdle is the lack of a gold standard for measuring an ideal transition. Is it successful scheduling of an appointment with adult provider or having a job and being able to manage one’s own disease?
“Until our health system supports pediatric providers in offering adequate transition planning, it will be difficult to expect any uptick in these measures. In addition, we still need to understand why some adolescents fail in their transition and transfer and how to develop the appropriate interventions to improve health outcomes for these patients,” Dr. Okumura wrote.
Dr. Okumura is with the division of general pediatrics at the University of California, San Francisco. These comments are adapted from an accompanying editorial (Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-2245). She reported having no relevant conflicts of interest.
Many adolescent patients, both with and without special health care needs, are not receiving guidance from their physicians about transitioning to adult care, according to recent findings published in Pediatrics.
Lydie A. Lebrun-Harris, PhD, of the Maternal and Child Health Bureau at the Health Resources and Services Administration, and her colleagues examined data from 20,708 youth aged 12-17 years with and without special health care needs obtained from the 2016 National Survey of Children’s Health. The aim was to determine the current level of transition planning to adult care from a pediatric or other health care provider (HCP).
Parents and caregivers were asked whether a doctor or HCP had spent time alone with the adolescent during the last year, had discussed the transition to adult care, and had actively helped the adolescent “gain self-care skills or understand changes in health care” when they reached the age of 18 years.
Overall, 17% of youth with special health care needs and 14% of youth without met all three transition elements.
The figures were higher for individual measures. For instance, 44% of youth with special health care needs spent time alone with an HCP within the past year, 41% discussed transition to an adult provider, and 69% reported an HCP had worked with them to understand health care changes and gain self-care skills.
Youth without special health care needs were more likely to discus the shift to adult care with HCPs than those with special needs, but special needs youth were more likely to have met the other two transition measurements (P less than .001).
Being older (aged 15-17 years) were associated with an increased prevalence of meeting the overall transition measure and the individual elements among both youth with and without special health care needs.
“Findings from this study underscore the urgent need for HCPs to work with youth independently and in collaboration with their parents and/or caregivers throughout the adolescent years to improve transition planning,” Dr. Lebrun-Harris and her colleagues wrote.
The study was supported by the Health Resources and Services Administration and the National Alliance to Advance Adolescent Health. The authors reported having no relevant conflicts of interest.
SOURCE: Lebrun-Harris LA et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-0194.
Many adolescent patients, both with and without special health care needs, are not receiving guidance from their physicians about transitioning to adult care, according to recent findings published in Pediatrics.
Lydie A. Lebrun-Harris, PhD, of the Maternal and Child Health Bureau at the Health Resources and Services Administration, and her colleagues examined data from 20,708 youth aged 12-17 years with and without special health care needs obtained from the 2016 National Survey of Children’s Health. The aim was to determine the current level of transition planning to adult care from a pediatric or other health care provider (HCP).
Parents and caregivers were asked whether a doctor or HCP had spent time alone with the adolescent during the last year, had discussed the transition to adult care, and had actively helped the adolescent “gain self-care skills or understand changes in health care” when they reached the age of 18 years.
Overall, 17% of youth with special health care needs and 14% of youth without met all three transition elements.
The figures were higher for individual measures. For instance, 44% of youth with special health care needs spent time alone with an HCP within the past year, 41% discussed transition to an adult provider, and 69% reported an HCP had worked with them to understand health care changes and gain self-care skills.
Youth without special health care needs were more likely to discus the shift to adult care with HCPs than those with special needs, but special needs youth were more likely to have met the other two transition measurements (P less than .001).
Being older (aged 15-17 years) were associated with an increased prevalence of meeting the overall transition measure and the individual elements among both youth with and without special health care needs.
“Findings from this study underscore the urgent need for HCPs to work with youth independently and in collaboration with their parents and/or caregivers throughout the adolescent years to improve transition planning,” Dr. Lebrun-Harris and her colleagues wrote.
The study was supported by the Health Resources and Services Administration and the National Alliance to Advance Adolescent Health. The authors reported having no relevant conflicts of interest.
SOURCE: Lebrun-Harris LA et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-0194.
FROM PEDIATRICS
Key clinical point:
Major finding: In total, 17% of youth with special health care needs and 14% of youth without received support for the transition to adult care.
Study details: A nationally representative exploratory analysis of transition planning from pediatric to adult health care for 20,708 adolescents from the 2016 National Survey of Children’s Health.
Disclosures: The study was supported by the Health Resources and Services Administration and the National Alliance to Advance Adolescent Health. The authors reported having no relevant conflicts of interest.
Source: Lebrun-Harris LA et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2018-0194.
AAP guidelines emphasize gender-affirmative care
according to an American Academy of Pediatrics policy statement published in Pediatrics.

The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.

Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
FROM PEDATRICS

Decline of infant walker–related injuries continues
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.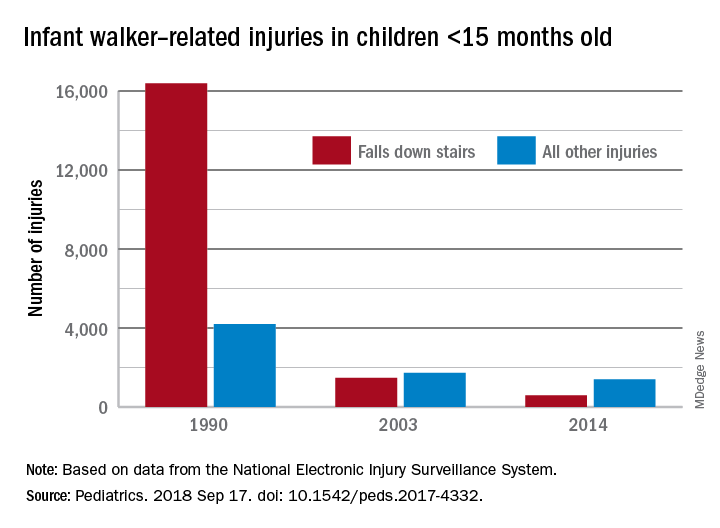
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
but most of that drop occurred before the federal mandatory safety standard went into effect in 2010, according to an analysis of a federal injury database.
In 1990, there were 20,650 walker-related injuries among children younger than 15 months, and by 2003 that number was down to 3,201 – a significant decline of 85%. In 2014, the last year for which data were available, there were 1,995 such injuries, which translates to a nonsignificant decrease of 38% from 2003 to 2014, Ariel Sims, MS, and her associates at the Center for Injury Research and Policy at Nationwide Children’s Hospital, Columbus, Ohio, wrote in Pediatrics.
During the study period from 1990 to 2014, a total of 230,676 children aged less than 15 months received treatment in emergency departments after walker-related injuries, with the majority (74%) caused by falls down stairs. That percentage did go down over time, though, with falls down stairs representing more than 80% of all such injuries during 1990-1996, 66% during 1997-2009, and 41% during 2010-2014, Ms. Sims and her associates reported based on data from the National Electronic Injury Surveillance System.
As for the 2010 federal safety standard, the annual average injury total went from 2,801 for the previous 4 years (2006-2009) to 2,165 for the 4 years after (2010-2014) – a decline of 23% (P = .019), they noted.
The federal standard may have contributed to the overall decline, Ms. Sims and her associates suggested, but the “reduction is most likely attributable to … an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the [Consumer Product Safety Commission] in 1992 to ban infant walker sales in the United States, the increasing use of stationary activity centers as an alternative to infant walkers, and improvements in the voluntary infant walker safety standard.”
In a September 2001 policy statement, the American Academy of Pediatrics recommended a ban on the manufacture and sale of mobile infant walkers (Pediatrics. 2001 Sep. doi: 10.1542/peds.108.3.790). This policy has been reaffirmed every 5 years in accordance with AAP policy.
Ms. Sims received a research stipend from the Research Institute at Nationwide Children’s Hospital and was funded by the Centers for Disease Control and Prevention and the Child Injury Prevention Alliance. The other investigators said that they have no relevant financial disclosures.
SOURCE: Sims A et al. Pediatrics. 2018 Sep 17. doi: 10.1542/peds.2017-4332.
FROM PEDIATRICS
Embracing therapeutic silence: A resident’s perspective on learning psychotherapy
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.
