User login
Comorbidities are important in psoriasis care
LAS VEGAS – Pay attention to comorbidities in your psoriasis patients because there may not be anyone else doing so.
“Many of our patients don’t have primary care physicians; many are untreated for psoriasis. They come to a clinical trial to get treated – some of them may not have insurance – so it is important for us to watch for these comorbidities,” Kristina C. Duffin, MD, said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Yet, that does not seem to be happening consistently, according to Dr. Duffin, of the department of dermatology at the University of Utah, Salt Lake City. One in five dermatologists admitted to never screening or referring their psoriasis patients for management of cardiovascular risks in a 2015 survey (J Am Acad Dermatol. 2015 doi: 10.1016/j.jaad.2015.07.029).
Often patients at the start of biologic therapy are counseled about the risk for developing tuberculosis, yet the lifetime risk for doing so in the United States is 0.3%. Similarly, patients are often counseled on the risk for developing lymphoma, even though the excess risk for developing lymphoma that can be attributed to psoriasis treatment is 7.9 per 100,000 psoriasis patients per year. That screening seems to be driven by warnings issued in direct-to-consumer advertising, Dr. Duffin suggested.
“Although psoriasis patients have an increased relative risk of lymphoma, the absolute risk attributable to psoriasis is low,” Dr. Duffin pointed out.
Some of the comorbidities she advised dermatologists to watch for are described below.
Psoriatic arthritis
Psoriatic arthritis is the most important psoriasis comorbidity, Dr. Duffin said. Between 20% and 30% of psoriasis patients will develop psoriatic arthritis.
In a study of 1,511 patients in 48 centers in Germany, 21% of psoriasis patients were diagnosed with psoriatic arthritis and of those, more than 95% had active arthritis and 53% had five or more affected joints (Br J Dermatol. 2009;160[5]:1040-7).
The GRAPPA app is an easy, free screening tool for psoriatic arthritis; patients who score 3 or more out of 5 items on the psoriasis epidemiology screening tool (PEST) are deemed positive for psoriatic arthritis, Dr. Duffin noted.
Cardiovascular disease
Psoriasis patients are at increased risk of myocardial infarction, stroke, cardiovascular death, diabetes, and chronic kidney disease, Dr. Duffin said. In fact, CV risk from severe psoriasis is similar to the risk conferred by diabetes.
She added that there is epidemiologic evidence for CV risk modification with several of the biologics approved for psoriasis.
Hypertension
Hypertension is prevalent and more severe in psoriasis patients, Dr. Duffin said, citing a 2011 case-control study of electronic medical records at the University of California, Davis. Psoriasis patients with hypertension were 5 times more likely than patients without psoriasis to be on one antihypertensive medication, 9.5 times more likely to be on two, and almost 20 times more likely to be on four antihypertensive medications (PLoS One. 2011 Mar 29;6[3]:e18227. doi: 10.1371/journal.pone.0018227).
Importantly, few primary care physicians and cardiologists are aware of the increased risk for hypertension in psoriasis patients.
Less than half (45%) of primary care physicians and 57% of cardiologists reported they were aware that psoriasis was associated with worse cardiovascular outcome, and only 43% of physicians reported screening psoriasis patients for hypertension starting at age 20 years, according to a 2012 survey of 251 physicians (J Am Acad Dermatol. 2012 Sep;67[3]:357-62).
Dr. Duffin called on dermatologists to ensure that the primary care physicians they work with understand these increased risks.
“Commit to including a comment in consultation letters or letters back to primary care physicians that talks about the cardiovascular risks of the disease,” she said.
Dr. Duffin reported that she is a consultant and has received grant or contracted research support for many companies that manufacture dermatologic therapies.
SDEF and this news organization are owned by the same parent company.
LAS VEGAS – Pay attention to comorbidities in your psoriasis patients because there may not be anyone else doing so.
“Many of our patients don’t have primary care physicians; many are untreated for psoriasis. They come to a clinical trial to get treated – some of them may not have insurance – so it is important for us to watch for these comorbidities,” Kristina C. Duffin, MD, said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Yet, that does not seem to be happening consistently, according to Dr. Duffin, of the department of dermatology at the University of Utah, Salt Lake City. One in five dermatologists admitted to never screening or referring their psoriasis patients for management of cardiovascular risks in a 2015 survey (J Am Acad Dermatol. 2015 doi: 10.1016/j.jaad.2015.07.029).
Often patients at the start of biologic therapy are counseled about the risk for developing tuberculosis, yet the lifetime risk for doing so in the United States is 0.3%. Similarly, patients are often counseled on the risk for developing lymphoma, even though the excess risk for developing lymphoma that can be attributed to psoriasis treatment is 7.9 per 100,000 psoriasis patients per year. That screening seems to be driven by warnings issued in direct-to-consumer advertising, Dr. Duffin suggested.
“Although psoriasis patients have an increased relative risk of lymphoma, the absolute risk attributable to psoriasis is low,” Dr. Duffin pointed out.
Some of the comorbidities she advised dermatologists to watch for are described below.
Psoriatic arthritis
Psoriatic arthritis is the most important psoriasis comorbidity, Dr. Duffin said. Between 20% and 30% of psoriasis patients will develop psoriatic arthritis.
In a study of 1,511 patients in 48 centers in Germany, 21% of psoriasis patients were diagnosed with psoriatic arthritis and of those, more than 95% had active arthritis and 53% had five or more affected joints (Br J Dermatol. 2009;160[5]:1040-7).
The GRAPPA app is an easy, free screening tool for psoriatic arthritis; patients who score 3 or more out of 5 items on the psoriasis epidemiology screening tool (PEST) are deemed positive for psoriatic arthritis, Dr. Duffin noted.
Cardiovascular disease
Psoriasis patients are at increased risk of myocardial infarction, stroke, cardiovascular death, diabetes, and chronic kidney disease, Dr. Duffin said. In fact, CV risk from severe psoriasis is similar to the risk conferred by diabetes.
She added that there is epidemiologic evidence for CV risk modification with several of the biologics approved for psoriasis.
Hypertension
Hypertension is prevalent and more severe in psoriasis patients, Dr. Duffin said, citing a 2011 case-control study of electronic medical records at the University of California, Davis. Psoriasis patients with hypertension were 5 times more likely than patients without psoriasis to be on one antihypertensive medication, 9.5 times more likely to be on two, and almost 20 times more likely to be on four antihypertensive medications (PLoS One. 2011 Mar 29;6[3]:e18227. doi: 10.1371/journal.pone.0018227).
Importantly, few primary care physicians and cardiologists are aware of the increased risk for hypertension in psoriasis patients.
Less than half (45%) of primary care physicians and 57% of cardiologists reported they were aware that psoriasis was associated with worse cardiovascular outcome, and only 43% of physicians reported screening psoriasis patients for hypertension starting at age 20 years, according to a 2012 survey of 251 physicians (J Am Acad Dermatol. 2012 Sep;67[3]:357-62).
Dr. Duffin called on dermatologists to ensure that the primary care physicians they work with understand these increased risks.
“Commit to including a comment in consultation letters or letters back to primary care physicians that talks about the cardiovascular risks of the disease,” she said.
Dr. Duffin reported that she is a consultant and has received grant or contracted research support for many companies that manufacture dermatologic therapies.
SDEF and this news organization are owned by the same parent company.
LAS VEGAS – Pay attention to comorbidities in your psoriasis patients because there may not be anyone else doing so.
“Many of our patients don’t have primary care physicians; many are untreated for psoriasis. They come to a clinical trial to get treated – some of them may not have insurance – so it is important for us to watch for these comorbidities,” Kristina C. Duffin, MD, said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Yet, that does not seem to be happening consistently, according to Dr. Duffin, of the department of dermatology at the University of Utah, Salt Lake City. One in five dermatologists admitted to never screening or referring their psoriasis patients for management of cardiovascular risks in a 2015 survey (J Am Acad Dermatol. 2015 doi: 10.1016/j.jaad.2015.07.029).
Often patients at the start of biologic therapy are counseled about the risk for developing tuberculosis, yet the lifetime risk for doing so in the United States is 0.3%. Similarly, patients are often counseled on the risk for developing lymphoma, even though the excess risk for developing lymphoma that can be attributed to psoriasis treatment is 7.9 per 100,000 psoriasis patients per year. That screening seems to be driven by warnings issued in direct-to-consumer advertising, Dr. Duffin suggested.
“Although psoriasis patients have an increased relative risk of lymphoma, the absolute risk attributable to psoriasis is low,” Dr. Duffin pointed out.
Some of the comorbidities she advised dermatologists to watch for are described below.
Psoriatic arthritis
Psoriatic arthritis is the most important psoriasis comorbidity, Dr. Duffin said. Between 20% and 30% of psoriasis patients will develop psoriatic arthritis.
In a study of 1,511 patients in 48 centers in Germany, 21% of psoriasis patients were diagnosed with psoriatic arthritis and of those, more than 95% had active arthritis and 53% had five or more affected joints (Br J Dermatol. 2009;160[5]:1040-7).
The GRAPPA app is an easy, free screening tool for psoriatic arthritis; patients who score 3 or more out of 5 items on the psoriasis epidemiology screening tool (PEST) are deemed positive for psoriatic arthritis, Dr. Duffin noted.
Cardiovascular disease
Psoriasis patients are at increased risk of myocardial infarction, stroke, cardiovascular death, diabetes, and chronic kidney disease, Dr. Duffin said. In fact, CV risk from severe psoriasis is similar to the risk conferred by diabetes.
She added that there is epidemiologic evidence for CV risk modification with several of the biologics approved for psoriasis.
Hypertension
Hypertension is prevalent and more severe in psoriasis patients, Dr. Duffin said, citing a 2011 case-control study of electronic medical records at the University of California, Davis. Psoriasis patients with hypertension were 5 times more likely than patients without psoriasis to be on one antihypertensive medication, 9.5 times more likely to be on two, and almost 20 times more likely to be on four antihypertensive medications (PLoS One. 2011 Mar 29;6[3]:e18227. doi: 10.1371/journal.pone.0018227).
Importantly, few primary care physicians and cardiologists are aware of the increased risk for hypertension in psoriasis patients.
Less than half (45%) of primary care physicians and 57% of cardiologists reported they were aware that psoriasis was associated with worse cardiovascular outcome, and only 43% of physicians reported screening psoriasis patients for hypertension starting at age 20 years, according to a 2012 survey of 251 physicians (J Am Acad Dermatol. 2012 Sep;67[3]:357-62).
Dr. Duffin called on dermatologists to ensure that the primary care physicians they work with understand these increased risks.
“Commit to including a comment in consultation letters or letters back to primary care physicians that talks about the cardiovascular risks of the disease,” she said.
Dr. Duffin reported that she is a consultant and has received grant or contracted research support for many companies that manufacture dermatologic therapies.
SDEF and this news organization are owned by the same parent company.
REPORTING FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
Concomitant Fibrofolliculoma and Trichodiscoma on the Abdomen
Fibrofolliculomas and trichodiscomas typically present on the head or neck as smooth, flesh-colored, dome-shaped papules. These two entities are considered to constitute two separate time points on a spectrum of histopathologic changes in mantleoma differentiation.1 Histologically, both are benign hamartomas of the pilosebaceous subunit and collectively are known as mantleomas. We present an unusual case of a concomitant fibrofolliculoma and trichodiscoma on the abdomen.
Case Report
An asymptomatic 54-year-old man presented for a routine full-body skin examination. A solitary, 2×1-cm, subcutaneous, doughy, mobile nodule was found on the left side of the abdomen with an overlying 2-mm yellow fleshy papule. The patient declined excision of the lesion, and it was recommended that he return for follow-up 3 months later.
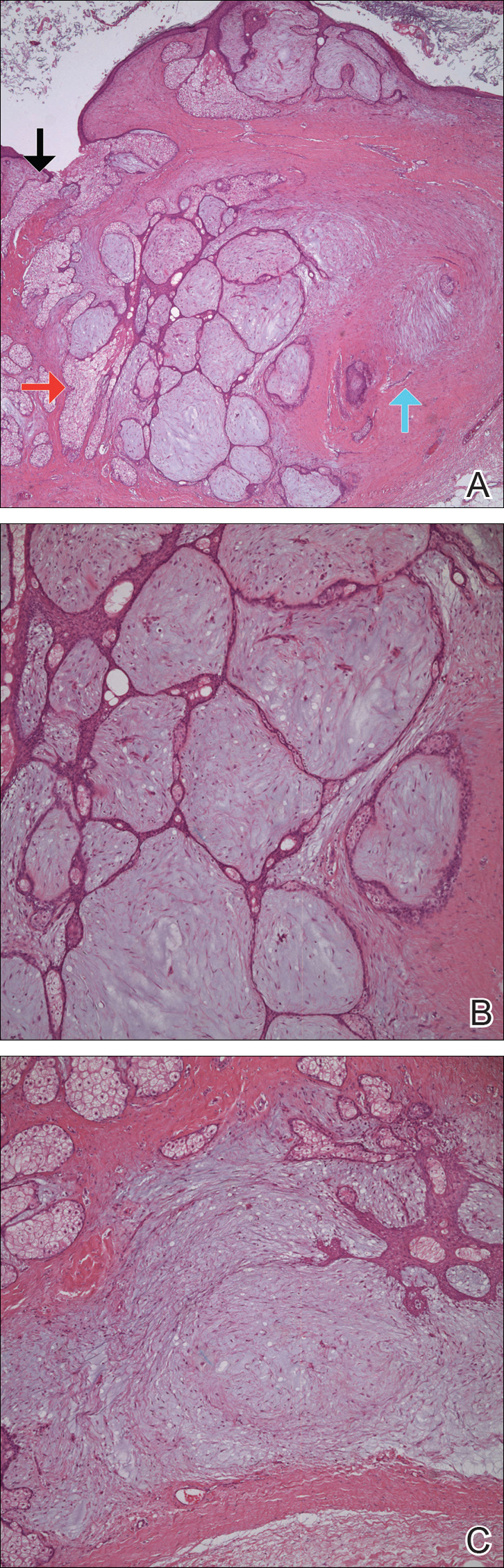
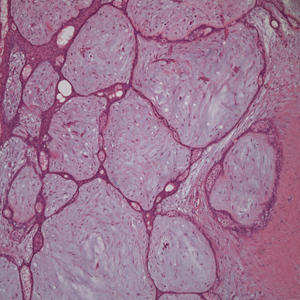
The patient did not present for follow-up until 4.5 years later, at which point the lesion had grown to 3.0×2.5 cm in size. An excision was performed, at which time the lesion was noted to be cystic, extruding an oily, yellow-white liquid. Bacterial culture was negative. Histopathologic sections showed a dome-shaped papule with connection to the overlying epidermis. Epithelial extensions from the infundibular epithelium formed a fenestrated pattern surrounding a fibrous and mucinous stroma (Figure, A and B). The differential diagnosis at this time included an epidermal inclusion cyst, fibroma, intradermal nevus, verruca, hemangioma, angiofibroma, and lipoma.2-4
The same lesion cut in a different plane of sectioning showed an expansile dermal nodule comprising clusters of sebaceous lobules surrounding a fibrous and mucinous stroma. Within the second lesion, fibrous and stromal components predominated over epithelial components (Figure, C). A diagnosis of fibrofolliculoma showing features of a trichodiscoma arising in the unusual location of the abdomen was made.
Comment
Solitary fibrofolliculomas and trichodiscomas are flesh-colored, dome-shaped papules that generally present on the face, specifically on the chin, nose, cheeks, ears, and eyebrows without considerable symptoms.2,4,5 Clinically, fibrofolliculomas are indistinguishable from trichodiscomas but demonstrate different features on biopsy.1,5
Fibrofolliculomas and trichodiscomas are well known for their association with Birt-Hogg-Dubé (BHD) syndrome when they present concomitantly and typically arise earlier in the third decade of life than solitary fibrofolliculomas; however, there have been reports of solitary fibrofolliculomas in patients aged 1 to 36 years.4,6 The triad of BHD syndrome consists of multiple fibrofolliculomas, trichodiscomas, and acrochordons, and it is acquired in an autosomal-dominant manner, unlike solitary fibrofolliculomas, which typically are not inherited. Birt-Hogg-Dubé syndrome is caused by a mutation in the FLCN gene that codes for the tumor-suppressor protein folliculin, which when mutated can cause unregulated proliferation of cells.7 Solitary fibrofolliculomas and the multiple fibrofolliculomas seen in BHD syndrome are histologically similar.
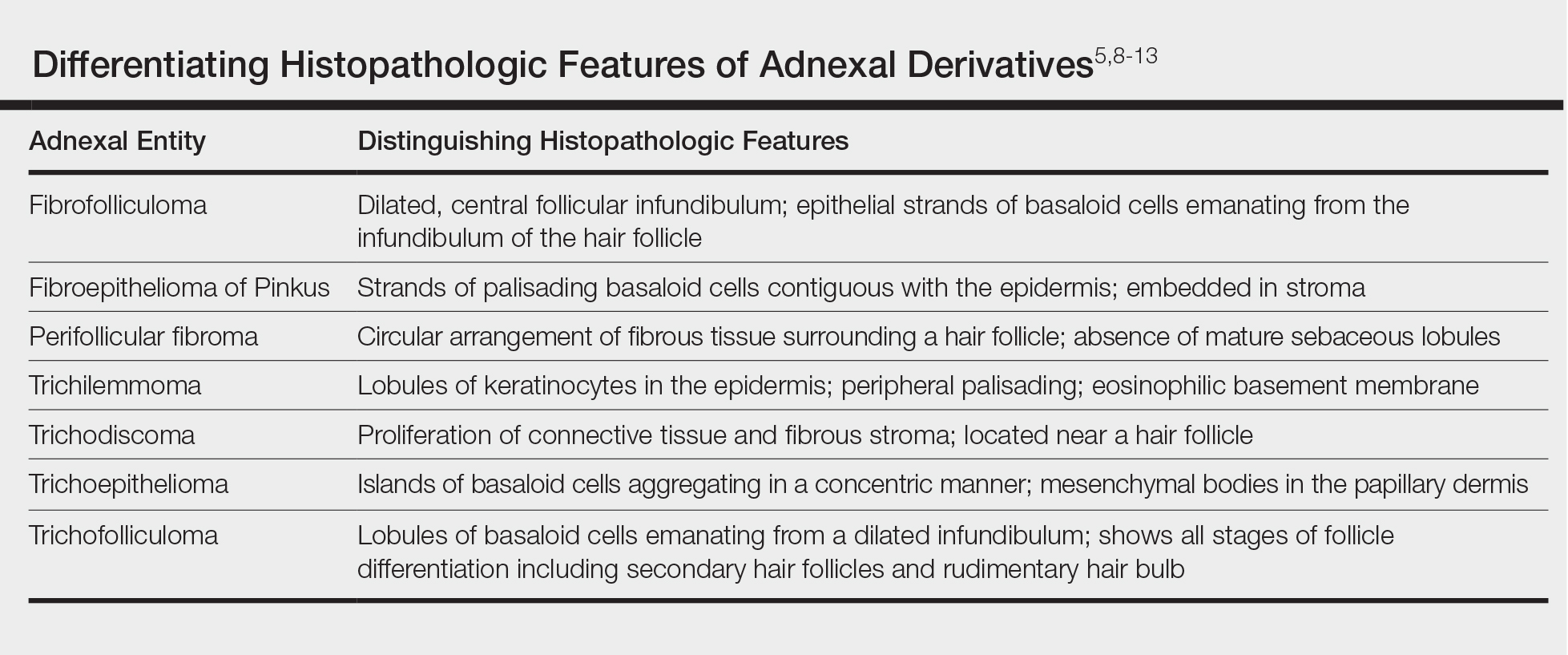
Fibrofolliculoma can be clinically indistinguishable from fibroepithelioma of Pinkus, perifollicular fibroma, trichilemmoma, trichodiscoma, trichoepithelioma, and trichofolliculoma. All typically present clinically as flesh-colored papules,1 although histologic distinction can be made (Table).5,8-13
Fibrofolliculoma is a benign hamartoma that arises from the pilosebaceous follicle and consists of an expansion of the fibrous root sheath, which typically surrounds the hair follicle along with proliferating bands or ribbons of perifollicular connective tissue. As such, the hair follicle may be dilated and filled with keratin in the expanded infundibulum.8 Follicles also may be surrounded by a myxoid stroma.2 In contrast, trichodiscoma is characterized by connective tissue with mature sebaceous lobules in the periphery. It has a myxoid stroma, as opposed to the more fibrous stroma seen in fibrofolliculomas.
Reports have examined the staining patterns of fibrofolliculomas, which show characteristics similar to those of other hair follicle hamartomas, including trichodiscomas.10 The connective tissue and epithelial components that constitute a fibrofolliculoma show different staining patterns. The connective tissue component stains positive for CD34 spindle cells, factor XIIIa, and nestin (a marker of angiogenesis). CD117 (c-kit) expression in the stroma, a marker of fibrocytes, is a feature of both fibrofolliculoma and perifollicular fibromas. The epithelial component, consisting of the hair follicle itself, stains positive for CK15. CK15 expression has been reported in undifferentiated sebocytes of the mantle and in the hair follicle.10 Immunohistochemical staining supports the notion that fibrofolliculomas contain connective tissue and epithelial components and helps to compare and contrast them to those of other hair follicle hamartomas.
Ackerman et al1 considered both fibrofolliculomas and trichodiscomas to be hamartomas of the epithelial hair follicle. The exact etiology of each of these hamartomas is unknown, but the undifferentiated epithelial strands protruding from the hair follicle in a fibrofolliculoma lie in close proximity to sebaceous glands. Furthermore, the authors postulated that fibrofolliculomas and trichodiscomas constitute a spectrum that encompasses the differentiation process of a mantleoma, with fibrofolliculoma representing the beginning of mantleoma differentiation and trichodiscoma representing the end. This end stage of follicular differentiation is one in which there is a predominant stroma and the previously undifferentiated epithelium has formed into sebaceous ducts and lobules in the stroma.1
Most cases of fibrofolliculoma and/or trichodiscoma arise in areas of dense sebaceous follicle concentration (eg, face), further supporting the hypothesis that sebaceous gland proliferation contributes to fibrofolliculoma.14 The case described here, with the fibrofolliculoma arising on the abdomen in conjunction with a trichodiscoma, is therefore worth noting because its location differs from what has been observed in previously reported cases.4
There are both surgical and medical options for treatment of fibrofolliculoma. Although surgical excision is an option for a single lesion, patients with multiple fibrofolliculomas or BHD may prefer removal with the combined CO2 laser and erbium-doped YAG laser.15
Conclusion
We present a rare case of concomitant fibrofolliculoma and trichodiscoma arising on the unusual location of the abdomen. This report highlights the histopathologic features of multiple adnexal tumors and emphasizes the importance of biopsy for differentiating fibrofolliculoma and trichodiscoma.
- Ackerman AB, Chongchitnant N, DeViragh P. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
- Scully K, Bargman H, Assaad D. Solitary fibrofolliculoma. J Am Acad Dermatol. 1984;11:361-363.
- Chang JK, Lee DC, Chang MH. A solitary fibrofolliculoma in the eyelid. Korean J Ophthalmol. 2007;21:169-171.
- Starink TM, Brownstein MH. Fibrofolliculoma: solitary and multiple types. J Am Acad Dermatol. 1987;17:493-496.
- Cho EU, Lee JD, Cho SH. A solitary fibrofolliculoma on the concha of the ear. Int J Dermatol. 2012;51:616-628.
- Mo HJ, Park CK, Yi JY. A case of solitary fibrofolliculoma. Korean J Dermatol. 2001;39:602-604.
- Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell. 2002;2:157-164.
- Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977;113:1674-1677.
- Foucar K, Rosen TH, Foucar E, et al. Fibrofolliculoma: a clinicopathologic study. Cutis. 1981;28:429-432.
- Misago NO, Kimura TE, Narisawa YU. Fibrofolliculoma/trichodiscoma and fibrous papule (perifollicular fibroma/angiofibroma): a revaluation of the histopathological and immunohistochemical features. J Cutan Pathol. 2009;36:943-951.
- Schaffer JV, Gohara MA, McNiff JM, et al. Multiple facial angiofibromas: a cutaneous manifestation of Birt-Hogg-Dubé syndrome. J Am Acad Dermatol. 2005;53(2 suppl 1):S108-S111.
- Lee Y, Su H, Chen H. Fibroepithelioma of Pinkus. a case report. Dermatologica Sinica. 2002;20:142-146.
- Nam JH, Min JH, Lee GY, et al. A case of perifollicular fibroma. Ann Dermatol. 2011:23:236-238.
- Vernooij M, Claessens T, Luijten M, et al. Birt-Hogg-Dubé syndrome and the skin. Fam Cancer. 2013;12:381-385.
- Jacob CI, Dover JS. Birt-Hogg-Dubé syndrome: treatment of cutaneous manifestations with laser skin resurfacing. Arch Dermatol. 2001;137:98-99.
Fibrofolliculomas and trichodiscomas typically present on the head or neck as smooth, flesh-colored, dome-shaped papules. These two entities are considered to constitute two separate time points on a spectrum of histopathologic changes in mantleoma differentiation.1 Histologically, both are benign hamartomas of the pilosebaceous subunit and collectively are known as mantleomas. We present an unusual case of a concomitant fibrofolliculoma and trichodiscoma on the abdomen.
Case Report
An asymptomatic 54-year-old man presented for a routine full-body skin examination. A solitary, 2×1-cm, subcutaneous, doughy, mobile nodule was found on the left side of the abdomen with an overlying 2-mm yellow fleshy papule. The patient declined excision of the lesion, and it was recommended that he return for follow-up 3 months later.
The patient did not present for follow-up until 4.5 years later, at which point the lesion had grown to 3.0×2.5 cm in size. An excision was performed, at which time the lesion was noted to be cystic, extruding an oily, yellow-white liquid. Bacterial culture was negative. Histopathologic sections showed a dome-shaped papule with connection to the overlying epidermis. Epithelial extensions from the infundibular epithelium formed a fenestrated pattern surrounding a fibrous and mucinous stroma (Figure, A and B). The differential diagnosis at this time included an epidermal inclusion cyst, fibroma, intradermal nevus, verruca, hemangioma, angiofibroma, and lipoma.2-4
The same lesion cut in a different plane of sectioning showed an expansile dermal nodule comprising clusters of sebaceous lobules surrounding a fibrous and mucinous stroma. Within the second lesion, fibrous and stromal components predominated over epithelial components (Figure, C). A diagnosis of fibrofolliculoma showing features of a trichodiscoma arising in the unusual location of the abdomen was made.
Comment
Solitary fibrofolliculomas and trichodiscomas are flesh-colored, dome-shaped papules that generally present on the face, specifically on the chin, nose, cheeks, ears, and eyebrows without considerable symptoms.2,4,5 Clinically, fibrofolliculomas are indistinguishable from trichodiscomas but demonstrate different features on biopsy.1,5
Fibrofolliculomas and trichodiscomas are well known for their association with Birt-Hogg-Dubé (BHD) syndrome when they present concomitantly and typically arise earlier in the third decade of life than solitary fibrofolliculomas; however, there have been reports of solitary fibrofolliculomas in patients aged 1 to 36 years.4,6 The triad of BHD syndrome consists of multiple fibrofolliculomas, trichodiscomas, and acrochordons, and it is acquired in an autosomal-dominant manner, unlike solitary fibrofolliculomas, which typically are not inherited. Birt-Hogg-Dubé syndrome is caused by a mutation in the FLCN gene that codes for the tumor-suppressor protein folliculin, which when mutated can cause unregulated proliferation of cells.7 Solitary fibrofolliculomas and the multiple fibrofolliculomas seen in BHD syndrome are histologically similar.
Fibrofolliculoma can be clinically indistinguishable from fibroepithelioma of Pinkus, perifollicular fibroma, trichilemmoma, trichodiscoma, trichoepithelioma, and trichofolliculoma. All typically present clinically as flesh-colored papules,1 although histologic distinction can be made (Table).5,8-13
Fibrofolliculoma is a benign hamartoma that arises from the pilosebaceous follicle and consists of an expansion of the fibrous root sheath, which typically surrounds the hair follicle along with proliferating bands or ribbons of perifollicular connective tissue. As such, the hair follicle may be dilated and filled with keratin in the expanded infundibulum.8 Follicles also may be surrounded by a myxoid stroma.2 In contrast, trichodiscoma is characterized by connective tissue with mature sebaceous lobules in the periphery. It has a myxoid stroma, as opposed to the more fibrous stroma seen in fibrofolliculomas.
Reports have examined the staining patterns of fibrofolliculomas, which show characteristics similar to those of other hair follicle hamartomas, including trichodiscomas.10 The connective tissue and epithelial components that constitute a fibrofolliculoma show different staining patterns. The connective tissue component stains positive for CD34 spindle cells, factor XIIIa, and nestin (a marker of angiogenesis). CD117 (c-kit) expression in the stroma, a marker of fibrocytes, is a feature of both fibrofolliculoma and perifollicular fibromas. The epithelial component, consisting of the hair follicle itself, stains positive for CK15. CK15 expression has been reported in undifferentiated sebocytes of the mantle and in the hair follicle.10 Immunohistochemical staining supports the notion that fibrofolliculomas contain connective tissue and epithelial components and helps to compare and contrast them to those of other hair follicle hamartomas.
Ackerman et al1 considered both fibrofolliculomas and trichodiscomas to be hamartomas of the epithelial hair follicle. The exact etiology of each of these hamartomas is unknown, but the undifferentiated epithelial strands protruding from the hair follicle in a fibrofolliculoma lie in close proximity to sebaceous glands. Furthermore, the authors postulated that fibrofolliculomas and trichodiscomas constitute a spectrum that encompasses the differentiation process of a mantleoma, with fibrofolliculoma representing the beginning of mantleoma differentiation and trichodiscoma representing the end. This end stage of follicular differentiation is one in which there is a predominant stroma and the previously undifferentiated epithelium has formed into sebaceous ducts and lobules in the stroma.1
Most cases of fibrofolliculoma and/or trichodiscoma arise in areas of dense sebaceous follicle concentration (eg, face), further supporting the hypothesis that sebaceous gland proliferation contributes to fibrofolliculoma.14 The case described here, with the fibrofolliculoma arising on the abdomen in conjunction with a trichodiscoma, is therefore worth noting because its location differs from what has been observed in previously reported cases.4
There are both surgical and medical options for treatment of fibrofolliculoma. Although surgical excision is an option for a single lesion, patients with multiple fibrofolliculomas or BHD may prefer removal with the combined CO2 laser and erbium-doped YAG laser.15
Conclusion
We present a rare case of concomitant fibrofolliculoma and trichodiscoma arising on the unusual location of the abdomen. This report highlights the histopathologic features of multiple adnexal tumors and emphasizes the importance of biopsy for differentiating fibrofolliculoma and trichodiscoma.
Fibrofolliculomas and trichodiscomas typically present on the head or neck as smooth, flesh-colored, dome-shaped papules. These two entities are considered to constitute two separate time points on a spectrum of histopathologic changes in mantleoma differentiation.1 Histologically, both are benign hamartomas of the pilosebaceous subunit and collectively are known as mantleomas. We present an unusual case of a concomitant fibrofolliculoma and trichodiscoma on the abdomen.
Case Report
An asymptomatic 54-year-old man presented for a routine full-body skin examination. A solitary, 2×1-cm, subcutaneous, doughy, mobile nodule was found on the left side of the abdomen with an overlying 2-mm yellow fleshy papule. The patient declined excision of the lesion, and it was recommended that he return for follow-up 3 months later.
The patient did not present for follow-up until 4.5 years later, at which point the lesion had grown to 3.0×2.5 cm in size. An excision was performed, at which time the lesion was noted to be cystic, extruding an oily, yellow-white liquid. Bacterial culture was negative. Histopathologic sections showed a dome-shaped papule with connection to the overlying epidermis. Epithelial extensions from the infundibular epithelium formed a fenestrated pattern surrounding a fibrous and mucinous stroma (Figure, A and B). The differential diagnosis at this time included an epidermal inclusion cyst, fibroma, intradermal nevus, verruca, hemangioma, angiofibroma, and lipoma.2-4
The same lesion cut in a different plane of sectioning showed an expansile dermal nodule comprising clusters of sebaceous lobules surrounding a fibrous and mucinous stroma. Within the second lesion, fibrous and stromal components predominated over epithelial components (Figure, C). A diagnosis of fibrofolliculoma showing features of a trichodiscoma arising in the unusual location of the abdomen was made.
Comment
Solitary fibrofolliculomas and trichodiscomas are flesh-colored, dome-shaped papules that generally present on the face, specifically on the chin, nose, cheeks, ears, and eyebrows without considerable symptoms.2,4,5 Clinically, fibrofolliculomas are indistinguishable from trichodiscomas but demonstrate different features on biopsy.1,5
Fibrofolliculomas and trichodiscomas are well known for their association with Birt-Hogg-Dubé (BHD) syndrome when they present concomitantly and typically arise earlier in the third decade of life than solitary fibrofolliculomas; however, there have been reports of solitary fibrofolliculomas in patients aged 1 to 36 years.4,6 The triad of BHD syndrome consists of multiple fibrofolliculomas, trichodiscomas, and acrochordons, and it is acquired in an autosomal-dominant manner, unlike solitary fibrofolliculomas, which typically are not inherited. Birt-Hogg-Dubé syndrome is caused by a mutation in the FLCN gene that codes for the tumor-suppressor protein folliculin, which when mutated can cause unregulated proliferation of cells.7 Solitary fibrofolliculomas and the multiple fibrofolliculomas seen in BHD syndrome are histologically similar.
Fibrofolliculoma can be clinically indistinguishable from fibroepithelioma of Pinkus, perifollicular fibroma, trichilemmoma, trichodiscoma, trichoepithelioma, and trichofolliculoma. All typically present clinically as flesh-colored papules,1 although histologic distinction can be made (Table).5,8-13
Fibrofolliculoma is a benign hamartoma that arises from the pilosebaceous follicle and consists of an expansion of the fibrous root sheath, which typically surrounds the hair follicle along with proliferating bands or ribbons of perifollicular connective tissue. As such, the hair follicle may be dilated and filled with keratin in the expanded infundibulum.8 Follicles also may be surrounded by a myxoid stroma.2 In contrast, trichodiscoma is characterized by connective tissue with mature sebaceous lobules in the periphery. It has a myxoid stroma, as opposed to the more fibrous stroma seen in fibrofolliculomas.
Reports have examined the staining patterns of fibrofolliculomas, which show characteristics similar to those of other hair follicle hamartomas, including trichodiscomas.10 The connective tissue and epithelial components that constitute a fibrofolliculoma show different staining patterns. The connective tissue component stains positive for CD34 spindle cells, factor XIIIa, and nestin (a marker of angiogenesis). CD117 (c-kit) expression in the stroma, a marker of fibrocytes, is a feature of both fibrofolliculoma and perifollicular fibromas. The epithelial component, consisting of the hair follicle itself, stains positive for CK15. CK15 expression has been reported in undifferentiated sebocytes of the mantle and in the hair follicle.10 Immunohistochemical staining supports the notion that fibrofolliculomas contain connective tissue and epithelial components and helps to compare and contrast them to those of other hair follicle hamartomas.
Ackerman et al1 considered both fibrofolliculomas and trichodiscomas to be hamartomas of the epithelial hair follicle. The exact etiology of each of these hamartomas is unknown, but the undifferentiated epithelial strands protruding from the hair follicle in a fibrofolliculoma lie in close proximity to sebaceous glands. Furthermore, the authors postulated that fibrofolliculomas and trichodiscomas constitute a spectrum that encompasses the differentiation process of a mantleoma, with fibrofolliculoma representing the beginning of mantleoma differentiation and trichodiscoma representing the end. This end stage of follicular differentiation is one in which there is a predominant stroma and the previously undifferentiated epithelium has formed into sebaceous ducts and lobules in the stroma.1
Most cases of fibrofolliculoma and/or trichodiscoma arise in areas of dense sebaceous follicle concentration (eg, face), further supporting the hypothesis that sebaceous gland proliferation contributes to fibrofolliculoma.14 The case described here, with the fibrofolliculoma arising on the abdomen in conjunction with a trichodiscoma, is therefore worth noting because its location differs from what has been observed in previously reported cases.4
There are both surgical and medical options for treatment of fibrofolliculoma. Although surgical excision is an option for a single lesion, patients with multiple fibrofolliculomas or BHD may prefer removal with the combined CO2 laser and erbium-doped YAG laser.15
Conclusion
We present a rare case of concomitant fibrofolliculoma and trichodiscoma arising on the unusual location of the abdomen. This report highlights the histopathologic features of multiple adnexal tumors and emphasizes the importance of biopsy for differentiating fibrofolliculoma and trichodiscoma.
- Ackerman AB, Chongchitnant N, DeViragh P. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
- Scully K, Bargman H, Assaad D. Solitary fibrofolliculoma. J Am Acad Dermatol. 1984;11:361-363.
- Chang JK, Lee DC, Chang MH. A solitary fibrofolliculoma in the eyelid. Korean J Ophthalmol. 2007;21:169-171.
- Starink TM, Brownstein MH. Fibrofolliculoma: solitary and multiple types. J Am Acad Dermatol. 1987;17:493-496.
- Cho EU, Lee JD, Cho SH. A solitary fibrofolliculoma on the concha of the ear. Int J Dermatol. 2012;51:616-628.
- Mo HJ, Park CK, Yi JY. A case of solitary fibrofolliculoma. Korean J Dermatol. 2001;39:602-604.
- Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell. 2002;2:157-164.
- Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977;113:1674-1677.
- Foucar K, Rosen TH, Foucar E, et al. Fibrofolliculoma: a clinicopathologic study. Cutis. 1981;28:429-432.
- Misago NO, Kimura TE, Narisawa YU. Fibrofolliculoma/trichodiscoma and fibrous papule (perifollicular fibroma/angiofibroma): a revaluation of the histopathological and immunohistochemical features. J Cutan Pathol. 2009;36:943-951.
- Schaffer JV, Gohara MA, McNiff JM, et al. Multiple facial angiofibromas: a cutaneous manifestation of Birt-Hogg-Dubé syndrome. J Am Acad Dermatol. 2005;53(2 suppl 1):S108-S111.
- Lee Y, Su H, Chen H. Fibroepithelioma of Pinkus. a case report. Dermatologica Sinica. 2002;20:142-146.
- Nam JH, Min JH, Lee GY, et al. A case of perifollicular fibroma. Ann Dermatol. 2011:23:236-238.
- Vernooij M, Claessens T, Luijten M, et al. Birt-Hogg-Dubé syndrome and the skin. Fam Cancer. 2013;12:381-385.
- Jacob CI, Dover JS. Birt-Hogg-Dubé syndrome: treatment of cutaneous manifestations with laser skin resurfacing. Arch Dermatol. 2001;137:98-99.
- Ackerman AB, Chongchitnant N, DeViragh P. Neoplasms with Follicular Differentiation. Philadelphia, PA: Lea & Febiger; 1993.
- Scully K, Bargman H, Assaad D. Solitary fibrofolliculoma. J Am Acad Dermatol. 1984;11:361-363.
- Chang JK, Lee DC, Chang MH. A solitary fibrofolliculoma in the eyelid. Korean J Ophthalmol. 2007;21:169-171.
- Starink TM, Brownstein MH. Fibrofolliculoma: solitary and multiple types. J Am Acad Dermatol. 1987;17:493-496.
- Cho EU, Lee JD, Cho SH. A solitary fibrofolliculoma on the concha of the ear. Int J Dermatol. 2012;51:616-628.
- Mo HJ, Park CK, Yi JY. A case of solitary fibrofolliculoma. Korean J Dermatol. 2001;39:602-604.
- Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell. 2002;2:157-164.
- Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977;113:1674-1677.
- Foucar K, Rosen TH, Foucar E, et al. Fibrofolliculoma: a clinicopathologic study. Cutis. 1981;28:429-432.
- Misago NO, Kimura TE, Narisawa YU. Fibrofolliculoma/trichodiscoma and fibrous papule (perifollicular fibroma/angiofibroma): a revaluation of the histopathological and immunohistochemical features. J Cutan Pathol. 2009;36:943-951.
- Schaffer JV, Gohara MA, McNiff JM, et al. Multiple facial angiofibromas: a cutaneous manifestation of Birt-Hogg-Dubé syndrome. J Am Acad Dermatol. 2005;53(2 suppl 1):S108-S111.
- Lee Y, Su H, Chen H. Fibroepithelioma of Pinkus. a case report. Dermatologica Sinica. 2002;20:142-146.
- Nam JH, Min JH, Lee GY, et al. A case of perifollicular fibroma. Ann Dermatol. 2011:23:236-238.
- Vernooij M, Claessens T, Luijten M, et al. Birt-Hogg-Dubé syndrome and the skin. Fam Cancer. 2013;12:381-385.
- Jacob CI, Dover JS. Birt-Hogg-Dubé syndrome: treatment of cutaneous manifestations with laser skin resurfacing. Arch Dermatol. 2001;137:98-99.
Practice Points
- Fibrofolliculoma and trichodiscoma are flesh-colored adnexal tumors that arise from or around hair follicles.
- It is important to recognize these entities, as they can be related to Birt-Hogg-Dubé syndrome.
Controlling Estrogen Levels May Treat Menstrual Migraine
A 20-µg decrease in dose of ethinyl estradiol may be enough to cause a migraine attack.
ASHEVILLE, NC—Menstrual-related migraine (MRM) can be particularly disabling and is difficult to treat using conventional migraine medications. To reduce the risk of MRM, a patient’s decrease in estrogen levels on the days around menses onset must be limited to 10 µg of ethinyl estradiol or less, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina and Partner and Cofounder of the Carolina Headache Institute in Durham, North Carolina.
“Most migraineurs by far are women, and as such, most migraineurs have MRM,” she said. “Nearly two-thirds of migraineurs have hormonal triggers, and it is our job to help our patients cope with them.”

Peak Times for Headache Occurrence
MRM occurrence correlates with days during a woman’s menstrual cycle, Dr. Calhoun said at the Eighth Annual Scientific Meeting of the Southern Headache Society. A study of diary data from 155 women found a 50% increased likelihood of migraine during the five days before menses, compared with all other times during the cycle.
“However, during the five days after the onset of bleeding, there was a 2.5 times increased risk of migraine,” Dr. Calhoun said. “Analysis of an even narrower time frame—two days before and after the onset of menses—shows a three to nearly five times increased migraine risk.” The pain was twice as likely to be considered severe two days before menses and more than three times as likely to be considered severe during the first three days of menstruation, she added.
Conventional migraine therapy may have limited efficacy for the treatment of MRM, Dr. Calhoun suggested. For example, one retrospective analysis examined data from two randomized trials of oral rizatriptan. In a subgroup of 335 women with MRM, 68% of women taking rizatriptan 10 mg and 70% of women taking rizatriptan 5 mg experienced pain relief, compared with 44% of women taking placebo. “However, for women who used the treatment on the day of bleeding, the response was about the same as placebo,” she said.
Hormonal Fluctuations Associated With Migraine
Fluctuations in estrogen levels are key to why migraine is more likely at certain times during a woman’s cycle, Dr. Calhoun said. She cited a study of 81 menstruating women with clinically diagnosed migraine that assessed their risk of tension-type headache and migraine with and without aura. There was a significantly elevated risk of tension-type headache and migraine without aura on the first two days of menses and a significantly higher risk of migraine without aura during the two days before menses onset. Furthermore, there was a significantly lower risk of all headache types around the time of ovulation.
“I looked at the data from this study and used the information differently,” Dr. Calhoun said. “In this same population of migraineurs, I added all their headaches together for each day and discovered that there was an increase in headache frequency when estrogen levels were low.”
When estrogen levels decrease, monoamine oxidase increases, serotonin and β-endorphin levels decrease, and serotonergic postsynaptic responsiveness and neurotransmitter uptake decrease. “In addition, there is an increase in calcitonin gene-related peptide concentrations,” Dr. Calhoun said. “This is why menstrual migraine is so much more intense than … non-MRM.”
Manipulation of Estrogen Levels
Corroborating evidence was found in a study that looked at hormone-related symptoms in 262 oral contraceptive users. Headache occurred significantly more frequently during the one-week hormone-free interval than during the three active-pill weeks, Dr. Calhoun noted. “Typical contraceptive treatment consists of a low-dose 20-µg ethinyl estradiol pill (combined with a progestin) for 21 days, followed by seven days of placebo,” she said. “A 20-µg drop in ethinyl estradiol (the estrogen in most oral contraceptives) is enough to cause a migraine, but if you limit that to a 10-µg drop, you can prevent migraine.”
Therefore, a patient on a 20-µg pill should be prescribed a 10-µg dose of ethinyl estradiol in the fourth week, Dr. Calhoun explained. If she is on a 30-µg pill, a 20-µg dose of ethinyl estradiol would be needed in the fourth week. “Continual hormonal combined contraceptives (with no placebo days) are also a good solution, so long as she does not have breakthrough bleeding,” she added.
Dr. Calhoun and colleagues examined the patient records of 229 consecutive women who were prescribed hormonal prophylaxis for MRM. Three hormonal preventive strategies were used: low-dose oral contraceptive with supplemental estrogen during the menstrual week; extended-cycle oral contraception with supplemental estrogen in the menstrual week; or a natural menstrual cycle with perimenstrual application of an estradiol patch two days beforethe expected onset of bleeding and continued for a week. In all, 168 women had resolution of MRM, 40 had persistence of MRM, and 21 refused or discontinued hormonal prophylaxis. Resolution of MRM was associated with a reversion to episodic migraine, resolution of medication overuse, and an overall decreased consumption of triptans, opioids, acute agents, and migraine preventive medication.
—Adriene Marshall
Suggested Reading
Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
Silberstein SD, Massiou H, Le Jeunne C, et al. Rizatriptan in the treatment of menstrual migraine. Obstet Gynecol. 2000;96(2):237-242.Stewart WF, Lipton RB, Chee E, et al. Menstrual cycle and headache in a population sample of migraineurs. Neurology. 2000;55(10):1517-1523.
A 20-µg decrease in dose of ethinyl estradiol may be enough to cause a migraine attack.
A 20-µg decrease in dose of ethinyl estradiol may be enough to cause a migraine attack.
ASHEVILLE, NC—Menstrual-related migraine (MRM) can be particularly disabling and is difficult to treat using conventional migraine medications. To reduce the risk of MRM, a patient’s decrease in estrogen levels on the days around menses onset must be limited to 10 µg of ethinyl estradiol or less, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina and Partner and Cofounder of the Carolina Headache Institute in Durham, North Carolina.
“Most migraineurs by far are women, and as such, most migraineurs have MRM,” she said. “Nearly two-thirds of migraineurs have hormonal triggers, and it is our job to help our patients cope with them.”
Peak Times for Headache Occurrence
MRM occurrence correlates with days during a woman’s menstrual cycle, Dr. Calhoun said at the Eighth Annual Scientific Meeting of the Southern Headache Society. A study of diary data from 155 women found a 50% increased likelihood of migraine during the five days before menses, compared with all other times during the cycle.
“However, during the five days after the onset of bleeding, there was a 2.5 times increased risk of migraine,” Dr. Calhoun said. “Analysis of an even narrower time frame—two days before and after the onset of menses—shows a three to nearly five times increased migraine risk.” The pain was twice as likely to be considered severe two days before menses and more than three times as likely to be considered severe during the first three days of menstruation, she added.
Conventional migraine therapy may have limited efficacy for the treatment of MRM, Dr. Calhoun suggested. For example, one retrospective analysis examined data from two randomized trials of oral rizatriptan. In a subgroup of 335 women with MRM, 68% of women taking rizatriptan 10 mg and 70% of women taking rizatriptan 5 mg experienced pain relief, compared with 44% of women taking placebo. “However, for women who used the treatment on the day of bleeding, the response was about the same as placebo,” she said.
Hormonal Fluctuations Associated With Migraine
Fluctuations in estrogen levels are key to why migraine is more likely at certain times during a woman’s cycle, Dr. Calhoun said. She cited a study of 81 menstruating women with clinically diagnosed migraine that assessed their risk of tension-type headache and migraine with and without aura. There was a significantly elevated risk of tension-type headache and migraine without aura on the first two days of menses and a significantly higher risk of migraine without aura during the two days before menses onset. Furthermore, there was a significantly lower risk of all headache types around the time of ovulation.
“I looked at the data from this study and used the information differently,” Dr. Calhoun said. “In this same population of migraineurs, I added all their headaches together for each day and discovered that there was an increase in headache frequency when estrogen levels were low.”
When estrogen levels decrease, monoamine oxidase increases, serotonin and β-endorphin levels decrease, and serotonergic postsynaptic responsiveness and neurotransmitter uptake decrease. “In addition, there is an increase in calcitonin gene-related peptide concentrations,” Dr. Calhoun said. “This is why menstrual migraine is so much more intense than … non-MRM.”
Manipulation of Estrogen Levels
Corroborating evidence was found in a study that looked at hormone-related symptoms in 262 oral contraceptive users. Headache occurred significantly more frequently during the one-week hormone-free interval than during the three active-pill weeks, Dr. Calhoun noted. “Typical contraceptive treatment consists of a low-dose 20-µg ethinyl estradiol pill (combined with a progestin) for 21 days, followed by seven days of placebo,” she said. “A 20-µg drop in ethinyl estradiol (the estrogen in most oral contraceptives) is enough to cause a migraine, but if you limit that to a 10-µg drop, you can prevent migraine.”
Therefore, a patient on a 20-µg pill should be prescribed a 10-µg dose of ethinyl estradiol in the fourth week, Dr. Calhoun explained. If she is on a 30-µg pill, a 20-µg dose of ethinyl estradiol would be needed in the fourth week. “Continual hormonal combined contraceptives (with no placebo days) are also a good solution, so long as she does not have breakthrough bleeding,” she added.
Dr. Calhoun and colleagues examined the patient records of 229 consecutive women who were prescribed hormonal prophylaxis for MRM. Three hormonal preventive strategies were used: low-dose oral contraceptive with supplemental estrogen during the menstrual week; extended-cycle oral contraception with supplemental estrogen in the menstrual week; or a natural menstrual cycle with perimenstrual application of an estradiol patch two days beforethe expected onset of bleeding and continued for a week. In all, 168 women had resolution of MRM, 40 had persistence of MRM, and 21 refused or discontinued hormonal prophylaxis. Resolution of MRM was associated with a reversion to episodic migraine, resolution of medication overuse, and an overall decreased consumption of triptans, opioids, acute agents, and migraine preventive medication.
—Adriene Marshall
Suggested Reading
Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
Silberstein SD, Massiou H, Le Jeunne C, et al. Rizatriptan in the treatment of menstrual migraine. Obstet Gynecol. 2000;96(2):237-242.Stewart WF, Lipton RB, Chee E, et al. Menstrual cycle and headache in a population sample of migraineurs. Neurology. 2000;55(10):1517-1523.
ASHEVILLE, NC—Menstrual-related migraine (MRM) can be particularly disabling and is difficult to treat using conventional migraine medications. To reduce the risk of MRM, a patient’s decrease in estrogen levels on the days around menses onset must be limited to 10 µg of ethinyl estradiol or less, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina and Partner and Cofounder of the Carolina Headache Institute in Durham, North Carolina.
“Most migraineurs by far are women, and as such, most migraineurs have MRM,” she said. “Nearly two-thirds of migraineurs have hormonal triggers, and it is our job to help our patients cope with them.”
Peak Times for Headache Occurrence
MRM occurrence correlates with days during a woman’s menstrual cycle, Dr. Calhoun said at the Eighth Annual Scientific Meeting of the Southern Headache Society. A study of diary data from 155 women found a 50% increased likelihood of migraine during the five days before menses, compared with all other times during the cycle.
“However, during the five days after the onset of bleeding, there was a 2.5 times increased risk of migraine,” Dr. Calhoun said. “Analysis of an even narrower time frame—two days before and after the onset of menses—shows a three to nearly five times increased migraine risk.” The pain was twice as likely to be considered severe two days before menses and more than three times as likely to be considered severe during the first three days of menstruation, she added.
Conventional migraine therapy may have limited efficacy for the treatment of MRM, Dr. Calhoun suggested. For example, one retrospective analysis examined data from two randomized trials of oral rizatriptan. In a subgroup of 335 women with MRM, 68% of women taking rizatriptan 10 mg and 70% of women taking rizatriptan 5 mg experienced pain relief, compared with 44% of women taking placebo. “However, for women who used the treatment on the day of bleeding, the response was about the same as placebo,” she said.
Hormonal Fluctuations Associated With Migraine
Fluctuations in estrogen levels are key to why migraine is more likely at certain times during a woman’s cycle, Dr. Calhoun said. She cited a study of 81 menstruating women with clinically diagnosed migraine that assessed their risk of tension-type headache and migraine with and without aura. There was a significantly elevated risk of tension-type headache and migraine without aura on the first two days of menses and a significantly higher risk of migraine without aura during the two days before menses onset. Furthermore, there was a significantly lower risk of all headache types around the time of ovulation.
“I looked at the data from this study and used the information differently,” Dr. Calhoun said. “In this same population of migraineurs, I added all their headaches together for each day and discovered that there was an increase in headache frequency when estrogen levels were low.”
When estrogen levels decrease, monoamine oxidase increases, serotonin and β-endorphin levels decrease, and serotonergic postsynaptic responsiveness and neurotransmitter uptake decrease. “In addition, there is an increase in calcitonin gene-related peptide concentrations,” Dr. Calhoun said. “This is why menstrual migraine is so much more intense than … non-MRM.”
Manipulation of Estrogen Levels
Corroborating evidence was found in a study that looked at hormone-related symptoms in 262 oral contraceptive users. Headache occurred significantly more frequently during the one-week hormone-free interval than during the three active-pill weeks, Dr. Calhoun noted. “Typical contraceptive treatment consists of a low-dose 20-µg ethinyl estradiol pill (combined with a progestin) for 21 days, followed by seven days of placebo,” she said. “A 20-µg drop in ethinyl estradiol (the estrogen in most oral contraceptives) is enough to cause a migraine, but if you limit that to a 10-µg drop, you can prevent migraine.”
Therefore, a patient on a 20-µg pill should be prescribed a 10-µg dose of ethinyl estradiol in the fourth week, Dr. Calhoun explained. If she is on a 30-µg pill, a 20-µg dose of ethinyl estradiol would be needed in the fourth week. “Continual hormonal combined contraceptives (with no placebo days) are also a good solution, so long as she does not have breakthrough bleeding,” she added.
Dr. Calhoun and colleagues examined the patient records of 229 consecutive women who were prescribed hormonal prophylaxis for MRM. Three hormonal preventive strategies were used: low-dose oral contraceptive with supplemental estrogen during the menstrual week; extended-cycle oral contraception with supplemental estrogen in the menstrual week; or a natural menstrual cycle with perimenstrual application of an estradiol patch two days beforethe expected onset of bleeding and continued for a week. In all, 168 women had resolution of MRM, 40 had persistence of MRM, and 21 refused or discontinued hormonal prophylaxis. Resolution of MRM was associated with a reversion to episodic migraine, resolution of medication overuse, and an overall decreased consumption of triptans, opioids, acute agents, and migraine preventive medication.
—Adriene Marshall
Suggested Reading
Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48(8):1186-1193.
MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63(2):351-353.
Silberstein SD, Massiou H, Le Jeunne C, et al. Rizatriptan in the treatment of menstrual migraine. Obstet Gynecol. 2000;96(2):237-242.Stewart WF, Lipton RB, Chee E, et al. Menstrual cycle and headache in a population sample of migraineurs. Neurology. 2000;55(10):1517-1523.
Appendix linked to Parkinson’s disease in series of unexpected findings
Appendectomy has been associated with a reduced risk of Parkinson’s disease (PD), which supports the potential for a reservoir of aggregated alpha-synuclein in the appendix to affect risk of the condition, according to new epidemiologic and translational evidence from two data sets that promotes a new and emerging theory for PD etiology.

When placed into the context of other recent studies, these epidemiologic data “point to the appendix as a site of origin for Parkinson’s and provide a path forward for devising new treatment strategies,” reported senior author Viviane Labrie, PhD, of the Van Andel Research Institute (VARI) in Grand Rapids, Mich.
The epidemiologic data was the most recent step in a series of findings summarized in a newly published paper in Science Translational Medicine. As the researchers explained, it is relevant to a separate body of evidence that alpha-synuclein, a protein that serves as the hallmark of PD when it appears in Lewy bodies, can be isolated in the nerve fibers and nerve cells of the appendix.
“We have shown that alpha-synuclein proteins, including the truncated forms observed in Lewy bodies, are abundant in the appendix,” reported first author Bryan A. Killinger, PhD, also at VARI, in a press teleconference. He said this finding is likely to explain the reduced risk of PD from appendectomy.
In the largest of the epidemiologic studies, the effect of appendectomy on subsequent risk of PD was evaluated through the health records from more than 1.6 million individuals in Sweden. The incidence of PD was found to be 19.3% lower among 551,647 patients who had an appendectomy, compared with controls.
In addition, the data showed that when PD did occur after appendectomy, it was delayed on average by 3.6 years. It is notable that appendectomy was not associated with protection from PD in patients with a familial link to PD, a group they said comprises less than 10% of cases.
In patients with PD, nonmotor symptoms often include GI tract dysfunction, which can, in some cases, be part of a prodromal presentation that precedes the onset of classical PD symptoms by several years, the authors reported. However, the new research upends previous conceptions of disease. The demonstration of abundant alpha-synuclein in the appendix coupled with the protective effect of appendectomy, suggests that PD may originate in the GI tract and then spread to the central nervous system (CNS) rather than the other way around.
“The vermiform appendix was once considered to be an unnecessary organ. Although there is now good evidence that the appendix plays a major role in the regulation of the immune system, including the regulation of gut bacteria, our work suggests it is also mediates risk of Parkinson’s,” Dr. Labrie said in the teleconference.
In the paper, numerous pieces of the puzzle are brought together to suggest that alpha-synuclein in the appendix is linked to alpha-synuclein in the CNS. Many of the findings along this investigative pathway were described as surprising. For example, immunohistochemistry studies revealed high amounts of alpha-synuclein in nearly every sample of appendiceal tissue examined, including normal and inflamed tissue, tissue from individuals with PD and those without, and tissues from young and old individuals.
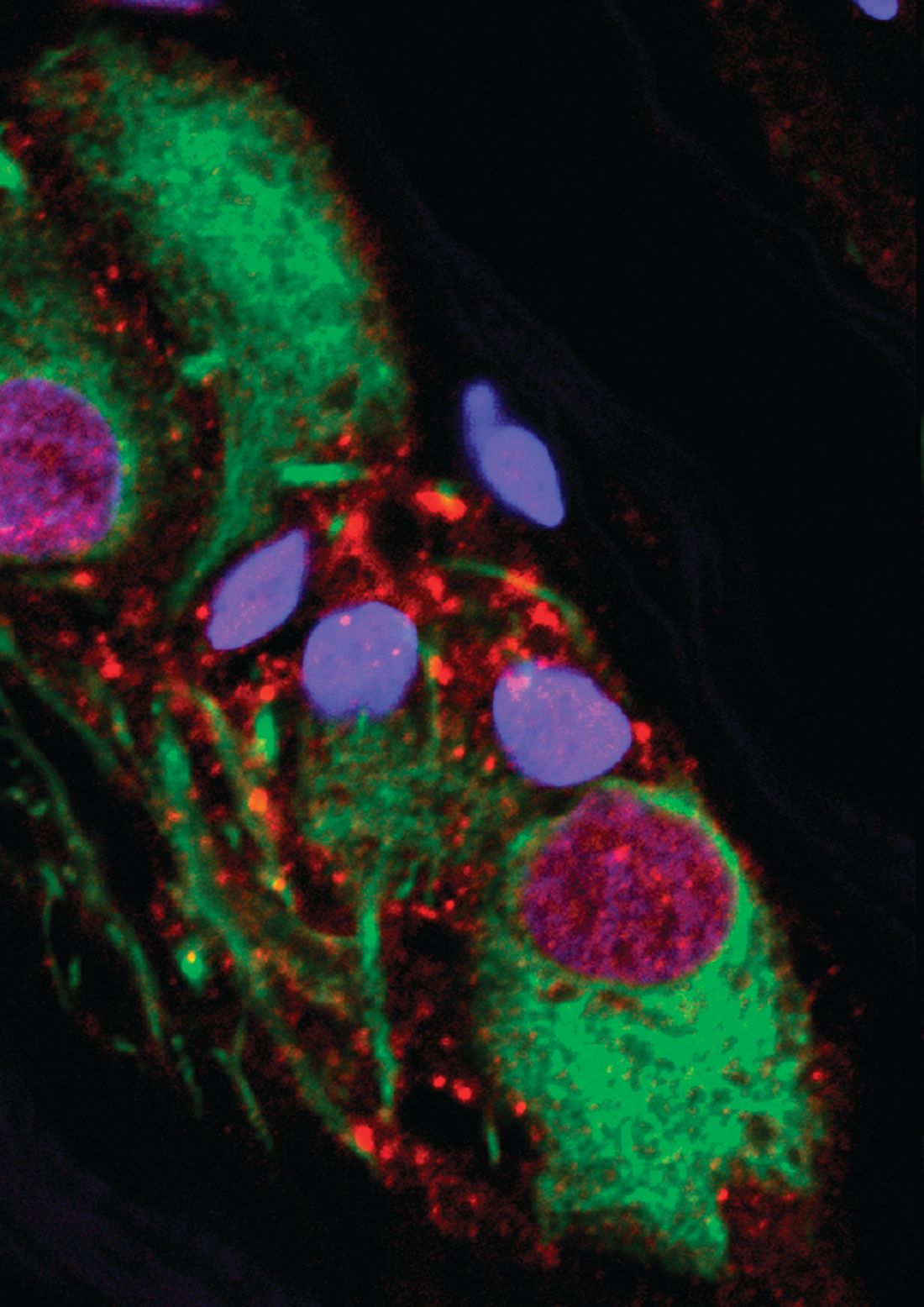
“The normal tissue, as well as appendiceal tissue from PD patients, contained high levels of alpha-synuclein in the truncated forms analogous to those seen in Lewy body pathology,” Dr. Killinger said. Based on these and other findings, he believes that alpha-synuclein in the appendix forms a reservoir for seeding the aggregates involved in the pathology of PD, although he acknowledged that it is not yet clear how the proteins in the appendix find their way to the brain.
From these data, it appears that most individuals with an intact appendix have alpha-synuclein in the nerve fibers, but Dr. Labrie pointed out that the only about 1% of the population develops PD. She speculated that there is “some confluence of events,” such as an environmental trigger altering the GI microbiome, that mediates ultimate risk of PD, but she noted that these events may take place decades before signs and symptoms of PD develop. The data appear to be a substantial reorientation in understanding PD.
“We have shown that the appendix is a hub for the accumulation of clumped forms of alpha-synuclein proteins, which are implicated in Parkinson’s,” Dr. Killinger said. “This knowledge will be invaluable as we explore new prevention and treatment strategies.”
The research was funded by a variety of governmental and private grants to individual authors. Dr. Killinger and Dr. Labrie report no financial relationships relevant to this study.
SOURCE: Killinger BA et al. Sci Transl Med. 2018;10:eaar5380.
Appendectomy has been associated with a reduced risk of Parkinson’s disease (PD), which supports the potential for a reservoir of aggregated alpha-synuclein in the appendix to affect risk of the condition, according to new epidemiologic and translational evidence from two data sets that promotes a new and emerging theory for PD etiology.
When placed into the context of other recent studies, these epidemiologic data “point to the appendix as a site of origin for Parkinson’s and provide a path forward for devising new treatment strategies,” reported senior author Viviane Labrie, PhD, of the Van Andel Research Institute (VARI) in Grand Rapids, Mich.
The epidemiologic data was the most recent step in a series of findings summarized in a newly published paper in Science Translational Medicine. As the researchers explained, it is relevant to a separate body of evidence that alpha-synuclein, a protein that serves as the hallmark of PD when it appears in Lewy bodies, can be isolated in the nerve fibers and nerve cells of the appendix.
“We have shown that alpha-synuclein proteins, including the truncated forms observed in Lewy bodies, are abundant in the appendix,” reported first author Bryan A. Killinger, PhD, also at VARI, in a press teleconference. He said this finding is likely to explain the reduced risk of PD from appendectomy.
In the largest of the epidemiologic studies, the effect of appendectomy on subsequent risk of PD was evaluated through the health records from more than 1.6 million individuals in Sweden. The incidence of PD was found to be 19.3% lower among 551,647 patients who had an appendectomy, compared with controls.
In addition, the data showed that when PD did occur after appendectomy, it was delayed on average by 3.6 years. It is notable that appendectomy was not associated with protection from PD in patients with a familial link to PD, a group they said comprises less than 10% of cases.
In patients with PD, nonmotor symptoms often include GI tract dysfunction, which can, in some cases, be part of a prodromal presentation that precedes the onset of classical PD symptoms by several years, the authors reported. However, the new research upends previous conceptions of disease. The demonstration of abundant alpha-synuclein in the appendix coupled with the protective effect of appendectomy, suggests that PD may originate in the GI tract and then spread to the central nervous system (CNS) rather than the other way around.
“The vermiform appendix was once considered to be an unnecessary organ. Although there is now good evidence that the appendix plays a major role in the regulation of the immune system, including the regulation of gut bacteria, our work suggests it is also mediates risk of Parkinson’s,” Dr. Labrie said in the teleconference.
In the paper, numerous pieces of the puzzle are brought together to suggest that alpha-synuclein in the appendix is linked to alpha-synuclein in the CNS. Many of the findings along this investigative pathway were described as surprising. For example, immunohistochemistry studies revealed high amounts of alpha-synuclein in nearly every sample of appendiceal tissue examined, including normal and inflamed tissue, tissue from individuals with PD and those without, and tissues from young and old individuals.
“The normal tissue, as well as appendiceal tissue from PD patients, contained high levels of alpha-synuclein in the truncated forms analogous to those seen in Lewy body pathology,” Dr. Killinger said. Based on these and other findings, he believes that alpha-synuclein in the appendix forms a reservoir for seeding the aggregates involved in the pathology of PD, although he acknowledged that it is not yet clear how the proteins in the appendix find their way to the brain.
From these data, it appears that most individuals with an intact appendix have alpha-synuclein in the nerve fibers, but Dr. Labrie pointed out that the only about 1% of the population develops PD. She speculated that there is “some confluence of events,” such as an environmental trigger altering the GI microbiome, that mediates ultimate risk of PD, but she noted that these events may take place decades before signs and symptoms of PD develop. The data appear to be a substantial reorientation in understanding PD.
“We have shown that the appendix is a hub for the accumulation of clumped forms of alpha-synuclein proteins, which are implicated in Parkinson’s,” Dr. Killinger said. “This knowledge will be invaluable as we explore new prevention and treatment strategies.”
The research was funded by a variety of governmental and private grants to individual authors. Dr. Killinger and Dr. Labrie report no financial relationships relevant to this study.
SOURCE: Killinger BA et al. Sci Transl Med. 2018;10:eaar5380.
Appendectomy has been associated with a reduced risk of Parkinson’s disease (PD), which supports the potential for a reservoir of aggregated alpha-synuclein in the appendix to affect risk of the condition, according to new epidemiologic and translational evidence from two data sets that promotes a new and emerging theory for PD etiology.
When placed into the context of other recent studies, these epidemiologic data “point to the appendix as a site of origin for Parkinson’s and provide a path forward for devising new treatment strategies,” reported senior author Viviane Labrie, PhD, of the Van Andel Research Institute (VARI) in Grand Rapids, Mich.
The epidemiologic data was the most recent step in a series of findings summarized in a newly published paper in Science Translational Medicine. As the researchers explained, it is relevant to a separate body of evidence that alpha-synuclein, a protein that serves as the hallmark of PD when it appears in Lewy bodies, can be isolated in the nerve fibers and nerve cells of the appendix.
“We have shown that alpha-synuclein proteins, including the truncated forms observed in Lewy bodies, are abundant in the appendix,” reported first author Bryan A. Killinger, PhD, also at VARI, in a press teleconference. He said this finding is likely to explain the reduced risk of PD from appendectomy.
In the largest of the epidemiologic studies, the effect of appendectomy on subsequent risk of PD was evaluated through the health records from more than 1.6 million individuals in Sweden. The incidence of PD was found to be 19.3% lower among 551,647 patients who had an appendectomy, compared with controls.
In addition, the data showed that when PD did occur after appendectomy, it was delayed on average by 3.6 years. It is notable that appendectomy was not associated with protection from PD in patients with a familial link to PD, a group they said comprises less than 10% of cases.
In patients with PD, nonmotor symptoms often include GI tract dysfunction, which can, in some cases, be part of a prodromal presentation that precedes the onset of classical PD symptoms by several years, the authors reported. However, the new research upends previous conceptions of disease. The demonstration of abundant alpha-synuclein in the appendix coupled with the protective effect of appendectomy, suggests that PD may originate in the GI tract and then spread to the central nervous system (CNS) rather than the other way around.
“The vermiform appendix was once considered to be an unnecessary organ. Although there is now good evidence that the appendix plays a major role in the regulation of the immune system, including the regulation of gut bacteria, our work suggests it is also mediates risk of Parkinson’s,” Dr. Labrie said in the teleconference.
In the paper, numerous pieces of the puzzle are brought together to suggest that alpha-synuclein in the appendix is linked to alpha-synuclein in the CNS. Many of the findings along this investigative pathway were described as surprising. For example, immunohistochemistry studies revealed high amounts of alpha-synuclein in nearly every sample of appendiceal tissue examined, including normal and inflamed tissue, tissue from individuals with PD and those without, and tissues from young and old individuals.
“The normal tissue, as well as appendiceal tissue from PD patients, contained high levels of alpha-synuclein in the truncated forms analogous to those seen in Lewy body pathology,” Dr. Killinger said. Based on these and other findings, he believes that alpha-synuclein in the appendix forms a reservoir for seeding the aggregates involved in the pathology of PD, although he acknowledged that it is not yet clear how the proteins in the appendix find their way to the brain.
From these data, it appears that most individuals with an intact appendix have alpha-synuclein in the nerve fibers, but Dr. Labrie pointed out that the only about 1% of the population develops PD. She speculated that there is “some confluence of events,” such as an environmental trigger altering the GI microbiome, that mediates ultimate risk of PD, but she noted that these events may take place decades before signs and symptoms of PD develop. The data appear to be a substantial reorientation in understanding PD.
“We have shown that the appendix is a hub for the accumulation of clumped forms of alpha-synuclein proteins, which are implicated in Parkinson’s,” Dr. Killinger said. “This knowledge will be invaluable as we explore new prevention and treatment strategies.”
The research was funded by a variety of governmental and private grants to individual authors. Dr. Killinger and Dr. Labrie report no financial relationships relevant to this study.
SOURCE: Killinger BA et al. Sci Transl Med. 2018;10:eaar5380.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: A 19.3% reduction in risk of PD from appendectomy may relate to alpha-synuclein in the appendix.
Study details: Series of related epidemiologic and translational studies.
Disclosures: The research was funded by a variety of governmental and private grants to individual authors. Dr. Killinger and Dr. Labrie report no financial relationships relevant to this study.
Source: Killinger BA et al. Sci Transl Med. 2018;10:eaar5380.
AML relapse after HSCT linked to potentially reversible immune changes
Relapse of acute myeloid leukemia after hematopoietic stem cell transplantation appears to be related to posttransplant changes in immune function that may be reversible with interferon-gamma therapy, investigators said.
Researchers performed a comparison of acute myeloid leukemia (AML) samples taken from patients before hematopoietic stem cell transplantation (HSCT) and at the time of relapse. They found that, while the general genomic changes seen at relapse resembled changes seen when patients experience relapse after chemotherapy, HSCT was associated with changes in genes believed to control both adaptive and innate immunity.
The findings suggest that transplantation results in a dampening of immune surveillance that could potentially be reversed with interferon gamma, an immunostimulatory cytokine, reported Matthew J. Christopher, MD, PhD, from Washington University, St. Louis, and his colleagues.
“These changes appeared to be epigenetic in nature in at least some cases, which suggests that therapeutic strategies to resensitize AML cells to the graft-versus-leukemia effect may be feasible,” they wrote in the New England Journal of Medicine.
The researchers noted that, while the presence of certain AML mutations may predict risk for relapse following HSCT, “the mechanisms by which these mutations promote relapse remain unclear.”
To get a better sense of how genetic and epigenetic changes after transplantation may allow leukemic cells to avoid the graft-versus-leukemia effect – and to see whether immune-related genes are affected by HSCT – they performed enhanced exome sequencing, flow cytometry, and immunohistochemical analyses on samples from 15 patients with AML who had a relapse after receiving transplants from HLA-matched siblings, matched unrelated donors, or HLA-mismatched unrelated donors, and on paired samples from 20 patients who experienced relapses after chemotherapy.
To validate their findings, they also evaluated samples from 28 other patients with AML who had a relapse after transplantation.
They first looked for relapse-specific mutations, but found no driver mutations associated with relapse after transplantation. The mutations seen during relapse after transplantation were generally similar to those seen both before treatment and after relapse in patients who had undergone chemotherapy. The researchers could not identify any patterns of mutations related to relapse.
They then looked for, but did not find, relapse-specific mutations in genes involved in either modulation of immune checkpoints, antigen presentation, or cytokine signaling.
The researchers did, however, find evidence of epigenetic changes that were more common in the samples of patients with posttransplant relapses, compared with postchemotherapy relapses. Specifically, they found that major histocompatibility (MHC) class II genes were down-regulated 200%-1100% after transplant, compared with the pretransplant samples.
In samples from 17 of 34 patients who experienced a relapse after transplantation, both flow cytometry and immunohistochemical analyses confirmed that expression of MHC class II molecules were decreased at relapse.
To see whether this down-regulation was reversible, the researchers treated samples from three patients with posttransplant relapse with interferon gamma, which is known to up-regulate MHC class II protein on myeloid cells and other cell types.
“Culture of these cells with interferon-gamma rapidly induced MHC class II protein expression on leukemic blasts, with essentially full restoration of MHC class II protein expression in nearly all AML blasts after 72 hours,” they wrote, adding that the reversibility of down-regulation of MHC class II in these blasts “strongly suggests that this phenomenon is mediated by an epigenetic mechanism.”
The study was supported by grants to investigators from the National Institutes of Health, Leukemia & Lymphoma Society, and the Barnes-Jewish Hospital Foundation. Dr. Christopher and several coauthors reported receiving grants from the study funders but no other relevant conflicts of interest. Several coauthors reported receiving personal fees and/or research support from industry outside the submitted work.
SOURCE: Christopher MJ et al. N Engl J Med. 2018 Oct 31. doi: 10.1056/NEJMoa1808777.
Relapse of acute myeloid leukemia after hematopoietic stem cell transplantation appears to be related to posttransplant changes in immune function that may be reversible with interferon-gamma therapy, investigators said.
Researchers performed a comparison of acute myeloid leukemia (AML) samples taken from patients before hematopoietic stem cell transplantation (HSCT) and at the time of relapse. They found that, while the general genomic changes seen at relapse resembled changes seen when patients experience relapse after chemotherapy, HSCT was associated with changes in genes believed to control both adaptive and innate immunity.
The findings suggest that transplantation results in a dampening of immune surveillance that could potentially be reversed with interferon gamma, an immunostimulatory cytokine, reported Matthew J. Christopher, MD, PhD, from Washington University, St. Louis, and his colleagues.
“These changes appeared to be epigenetic in nature in at least some cases, which suggests that therapeutic strategies to resensitize AML cells to the graft-versus-leukemia effect may be feasible,” they wrote in the New England Journal of Medicine.
The researchers noted that, while the presence of certain AML mutations may predict risk for relapse following HSCT, “the mechanisms by which these mutations promote relapse remain unclear.”
To get a better sense of how genetic and epigenetic changes after transplantation may allow leukemic cells to avoid the graft-versus-leukemia effect – and to see whether immune-related genes are affected by HSCT – they performed enhanced exome sequencing, flow cytometry, and immunohistochemical analyses on samples from 15 patients with AML who had a relapse after receiving transplants from HLA-matched siblings, matched unrelated donors, or HLA-mismatched unrelated donors, and on paired samples from 20 patients who experienced relapses after chemotherapy.
To validate their findings, they also evaluated samples from 28 other patients with AML who had a relapse after transplantation.
They first looked for relapse-specific mutations, but found no driver mutations associated with relapse after transplantation. The mutations seen during relapse after transplantation were generally similar to those seen both before treatment and after relapse in patients who had undergone chemotherapy. The researchers could not identify any patterns of mutations related to relapse.
They then looked for, but did not find, relapse-specific mutations in genes involved in either modulation of immune checkpoints, antigen presentation, or cytokine signaling.
The researchers did, however, find evidence of epigenetic changes that were more common in the samples of patients with posttransplant relapses, compared with postchemotherapy relapses. Specifically, they found that major histocompatibility (MHC) class II genes were down-regulated 200%-1100% after transplant, compared with the pretransplant samples.
In samples from 17 of 34 patients who experienced a relapse after transplantation, both flow cytometry and immunohistochemical analyses confirmed that expression of MHC class II molecules were decreased at relapse.
To see whether this down-regulation was reversible, the researchers treated samples from three patients with posttransplant relapse with interferon gamma, which is known to up-regulate MHC class II protein on myeloid cells and other cell types.
“Culture of these cells with interferon-gamma rapidly induced MHC class II protein expression on leukemic blasts, with essentially full restoration of MHC class II protein expression in nearly all AML blasts after 72 hours,” they wrote, adding that the reversibility of down-regulation of MHC class II in these blasts “strongly suggests that this phenomenon is mediated by an epigenetic mechanism.”
The study was supported by grants to investigators from the National Institutes of Health, Leukemia & Lymphoma Society, and the Barnes-Jewish Hospital Foundation. Dr. Christopher and several coauthors reported receiving grants from the study funders but no other relevant conflicts of interest. Several coauthors reported receiving personal fees and/or research support from industry outside the submitted work.
SOURCE: Christopher MJ et al. N Engl J Med. 2018 Oct 31. doi: 10.1056/NEJMoa1808777.
Relapse of acute myeloid leukemia after hematopoietic stem cell transplantation appears to be related to posttransplant changes in immune function that may be reversible with interferon-gamma therapy, investigators said.
Researchers performed a comparison of acute myeloid leukemia (AML) samples taken from patients before hematopoietic stem cell transplantation (HSCT) and at the time of relapse. They found that, while the general genomic changes seen at relapse resembled changes seen when patients experience relapse after chemotherapy, HSCT was associated with changes in genes believed to control both adaptive and innate immunity.
The findings suggest that transplantation results in a dampening of immune surveillance that could potentially be reversed with interferon gamma, an immunostimulatory cytokine, reported Matthew J. Christopher, MD, PhD, from Washington University, St. Louis, and his colleagues.
“These changes appeared to be epigenetic in nature in at least some cases, which suggests that therapeutic strategies to resensitize AML cells to the graft-versus-leukemia effect may be feasible,” they wrote in the New England Journal of Medicine.
The researchers noted that, while the presence of certain AML mutations may predict risk for relapse following HSCT, “the mechanisms by which these mutations promote relapse remain unclear.”
To get a better sense of how genetic and epigenetic changes after transplantation may allow leukemic cells to avoid the graft-versus-leukemia effect – and to see whether immune-related genes are affected by HSCT – they performed enhanced exome sequencing, flow cytometry, and immunohistochemical analyses on samples from 15 patients with AML who had a relapse after receiving transplants from HLA-matched siblings, matched unrelated donors, or HLA-mismatched unrelated donors, and on paired samples from 20 patients who experienced relapses after chemotherapy.
To validate their findings, they also evaluated samples from 28 other patients with AML who had a relapse after transplantation.
They first looked for relapse-specific mutations, but found no driver mutations associated with relapse after transplantation. The mutations seen during relapse after transplantation were generally similar to those seen both before treatment and after relapse in patients who had undergone chemotherapy. The researchers could not identify any patterns of mutations related to relapse.
They then looked for, but did not find, relapse-specific mutations in genes involved in either modulation of immune checkpoints, antigen presentation, or cytokine signaling.
The researchers did, however, find evidence of epigenetic changes that were more common in the samples of patients with posttransplant relapses, compared with postchemotherapy relapses. Specifically, they found that major histocompatibility (MHC) class II genes were down-regulated 200%-1100% after transplant, compared with the pretransplant samples.
In samples from 17 of 34 patients who experienced a relapse after transplantation, both flow cytometry and immunohistochemical analyses confirmed that expression of MHC class II molecules were decreased at relapse.
To see whether this down-regulation was reversible, the researchers treated samples from three patients with posttransplant relapse with interferon gamma, which is known to up-regulate MHC class II protein on myeloid cells and other cell types.
“Culture of these cells with interferon-gamma rapidly induced MHC class II protein expression on leukemic blasts, with essentially full restoration of MHC class II protein expression in nearly all AML blasts after 72 hours,” they wrote, adding that the reversibility of down-regulation of MHC class II in these blasts “strongly suggests that this phenomenon is mediated by an epigenetic mechanism.”
The study was supported by grants to investigators from the National Institutes of Health, Leukemia & Lymphoma Society, and the Barnes-Jewish Hospital Foundation. Dr. Christopher and several coauthors reported receiving grants from the study funders but no other relevant conflicts of interest. Several coauthors reported receiving personal fees and/or research support from industry outside the submitted work.
SOURCE: Christopher MJ et al. N Engl J Med. 2018 Oct 31. doi: 10.1056/NEJMoa1808777.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: MHC class II genes were down-regulated 200%-1100% after transplant, compared with pretransplant samples.
Study details: Analysis of genetic changes pre- and posttransplant in 15 patients with AML relapse after transplant, 20 patients with relapse after chemotherapy, and 28 patients in a validation sample.
Disclosures: The study was supported by grants to investigators from the National Institutes of Health, Leukemia & Lymphoma Society, and the Barnes-Jewish Hospital Foundation. Dr. Christopher and several coauthors reported receiving grants from the study funders but no other relevant conflicts of interest. Several coauthors reported receiving personal fees and/or research support from industry outside the submitted work.
Source: Christopher MJ et al. N Engl J Med. 2018 Oct 31. doi: 10.1056/NEJMoa1808777.
Experience – not evidence – is best guide in keloid treatment
LAS VEGAS – The first written mention of keloids in history came about 4,500 years ago. But there is still so much more to be learned about keloids, according to dermatologist Hilary E. Baldwin, MD.
Yes, there is more information about who gets keloids and where they appear on the body. “What we do not know is everything else,” Dr. Baldwin said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar. “We don’t even know which treatments work. Not a single treatment has any evidence basis behind it. It’s all fly-by-night, seat-of-your-pants, based on your knowledge and that of those who treat keloids frequently.”
. Cases show an unknown factor serves as a contributing factor, she said.
There’s no gender disparity in keloids, she said, and they’re more likely to occur after puberty than before. Family history isn’t helpful.
Also, while darker skin produces keloids more easily and consistently than other skin types, these keloids aren’t the hardest to treat, said Dr. Baldwin, medical director of the Acne Treatment and Research Center in Morristown, N.J. “From my personal experience – but not from data or papers – keloids are the most difficult to treat and recur the most when you see them in a Caucasian patient.”
Patients want the keloids to disappear forever along with any evidence that they ever existed. “Virtually every patient says ‘I want this cut off, I want it gone,’” Dr. Baldwin said. “And they want it gone yesterday. Few understand this is a long process. I tell them we’ll become extraordinarily good friends over the next 6-12 months while we get rid of this thing.” Moreover, it’s not possible to eliminate keloids without leaving a sign behind. “Most want it eradicated with normal skin,” but the skin beneath a keloid “will never look normal,” she observed.
The following are some tips for treating patients with keloids that she provided during her presentation:
- Surgery is usually not an option, and it may be necessary to convince patients about other treatment options. “Most don’t want corticosteroid injections, but that is how we treat them and keep them from coming back,” Dr. Baldwin said.
- Surgery may be appropriate in certain cases, such as keloids that are shaped like mushrooms and are attached to the skin via a stalk. Patient compliance with adjunctive therapy (injected corticosteroids) is crucial to prevent recurrence after surgery. Be aware that some patients – such as those who are afraid of needles – may refuse to return. Earlobes, a common site of keloids because of earrings, are a special case in surgery. Patients with earlobe keloids often fare well after surgery, Dr. Baldwin said, and recurrence is less common than in other parts of the body, especially when corticosteroids are added. It helps that patients are often more compliant with adjunctive therapy, she added, because the keloids are highly visible, and they want to wear earrings again.
- Ask patients what bothers them the most about the keloids. Some may want to eliminate burning, itching, or stinging, and Dr. Baldwin attempts to treat those issues. Patients may want keloids to be softer, flatter, or lighter, she said.
- Modification of the keloid’s appearance may be enough for some patients. For example, one of her patients objected to extensive keloids around his breasts because they gave him the appearance of cleavage. Another believed – accurately – that his keloid looked like male genitalia. Dr. Baldwin treated it with the keloid equivalent of castration (surgically removing its “testicles”) and circumcision of sorts (a flattening of its “glans penis” with corticosteroids). “It didn’t look pretty,” she said, “but it no longer looked offensive to him.”
- Many patients present with keloids on the chest, back, and deltoids, “which have to have been from acne, but you can’t actually see the pimples,” Dr. Baldwin said. In these cases, she may turn to isotretinoin. This is not for treatment of keloids, but is a preventive strategy to stop further lesions from appearing and causing more keloids, she explained.
- In addition to corticosteroids, other postsurgical options include freezing, interferon, pressure dressings, dextran hydrogel scaffolding, and radiation therapy.
Moving forward, researchers “are looking at biologics, TNF-alpha inhibitors, and tyrosine kinase inhibitors in hopes that we can find something that will stop the incessant forward movement of some of our keloid patients,” Dr. Baldwin noted.
Dr. Baldwin reported no relevant disclosures.
SDEF and this news organization are owned by the same parent company.
LAS VEGAS – The first written mention of keloids in history came about 4,500 years ago. But there is still so much more to be learned about keloids, according to dermatologist Hilary E. Baldwin, MD.
Yes, there is more information about who gets keloids and where they appear on the body. “What we do not know is everything else,” Dr. Baldwin said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar. “We don’t even know which treatments work. Not a single treatment has any evidence basis behind it. It’s all fly-by-night, seat-of-your-pants, based on your knowledge and that of those who treat keloids frequently.”
. Cases show an unknown factor serves as a contributing factor, she said.
There’s no gender disparity in keloids, she said, and they’re more likely to occur after puberty than before. Family history isn’t helpful.
Also, while darker skin produces keloids more easily and consistently than other skin types, these keloids aren’t the hardest to treat, said Dr. Baldwin, medical director of the Acne Treatment and Research Center in Morristown, N.J. “From my personal experience – but not from data or papers – keloids are the most difficult to treat and recur the most when you see them in a Caucasian patient.”
Patients want the keloids to disappear forever along with any evidence that they ever existed. “Virtually every patient says ‘I want this cut off, I want it gone,’” Dr. Baldwin said. “And they want it gone yesterday. Few understand this is a long process. I tell them we’ll become extraordinarily good friends over the next 6-12 months while we get rid of this thing.” Moreover, it’s not possible to eliminate keloids without leaving a sign behind. “Most want it eradicated with normal skin,” but the skin beneath a keloid “will never look normal,” she observed.
The following are some tips for treating patients with keloids that she provided during her presentation:
- Surgery is usually not an option, and it may be necessary to convince patients about other treatment options. “Most don’t want corticosteroid injections, but that is how we treat them and keep them from coming back,” Dr. Baldwin said.
- Surgery may be appropriate in certain cases, such as keloids that are shaped like mushrooms and are attached to the skin via a stalk. Patient compliance with adjunctive therapy (injected corticosteroids) is crucial to prevent recurrence after surgery. Be aware that some patients – such as those who are afraid of needles – may refuse to return. Earlobes, a common site of keloids because of earrings, are a special case in surgery. Patients with earlobe keloids often fare well after surgery, Dr. Baldwin said, and recurrence is less common than in other parts of the body, especially when corticosteroids are added. It helps that patients are often more compliant with adjunctive therapy, she added, because the keloids are highly visible, and they want to wear earrings again.
- Ask patients what bothers them the most about the keloids. Some may want to eliminate burning, itching, or stinging, and Dr. Baldwin attempts to treat those issues. Patients may want keloids to be softer, flatter, or lighter, she said.
- Modification of the keloid’s appearance may be enough for some patients. For example, one of her patients objected to extensive keloids around his breasts because they gave him the appearance of cleavage. Another believed – accurately – that his keloid looked like male genitalia. Dr. Baldwin treated it with the keloid equivalent of castration (surgically removing its “testicles”) and circumcision of sorts (a flattening of its “glans penis” with corticosteroids). “It didn’t look pretty,” she said, “but it no longer looked offensive to him.”
- Many patients present with keloids on the chest, back, and deltoids, “which have to have been from acne, but you can’t actually see the pimples,” Dr. Baldwin said. In these cases, she may turn to isotretinoin. This is not for treatment of keloids, but is a preventive strategy to stop further lesions from appearing and causing more keloids, she explained.
- In addition to corticosteroids, other postsurgical options include freezing, interferon, pressure dressings, dextran hydrogel scaffolding, and radiation therapy.
Moving forward, researchers “are looking at biologics, TNF-alpha inhibitors, and tyrosine kinase inhibitors in hopes that we can find something that will stop the incessant forward movement of some of our keloid patients,” Dr. Baldwin noted.
Dr. Baldwin reported no relevant disclosures.
SDEF and this news organization are owned by the same parent company.
LAS VEGAS – The first written mention of keloids in history came about 4,500 years ago. But there is still so much more to be learned about keloids, according to dermatologist Hilary E. Baldwin, MD.
Yes, there is more information about who gets keloids and where they appear on the body. “What we do not know is everything else,” Dr. Baldwin said at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar. “We don’t even know which treatments work. Not a single treatment has any evidence basis behind it. It’s all fly-by-night, seat-of-your-pants, based on your knowledge and that of those who treat keloids frequently.”
. Cases show an unknown factor serves as a contributing factor, she said.
There’s no gender disparity in keloids, she said, and they’re more likely to occur after puberty than before. Family history isn’t helpful.
Also, while darker skin produces keloids more easily and consistently than other skin types, these keloids aren’t the hardest to treat, said Dr. Baldwin, medical director of the Acne Treatment and Research Center in Morristown, N.J. “From my personal experience – but not from data or papers – keloids are the most difficult to treat and recur the most when you see them in a Caucasian patient.”
Patients want the keloids to disappear forever along with any evidence that they ever existed. “Virtually every patient says ‘I want this cut off, I want it gone,’” Dr. Baldwin said. “And they want it gone yesterday. Few understand this is a long process. I tell them we’ll become extraordinarily good friends over the next 6-12 months while we get rid of this thing.” Moreover, it’s not possible to eliminate keloids without leaving a sign behind. “Most want it eradicated with normal skin,” but the skin beneath a keloid “will never look normal,” she observed.
The following are some tips for treating patients with keloids that she provided during her presentation:
- Surgery is usually not an option, and it may be necessary to convince patients about other treatment options. “Most don’t want corticosteroid injections, but that is how we treat them and keep them from coming back,” Dr. Baldwin said.
- Surgery may be appropriate in certain cases, such as keloids that are shaped like mushrooms and are attached to the skin via a stalk. Patient compliance with adjunctive therapy (injected corticosteroids) is crucial to prevent recurrence after surgery. Be aware that some patients – such as those who are afraid of needles – may refuse to return. Earlobes, a common site of keloids because of earrings, are a special case in surgery. Patients with earlobe keloids often fare well after surgery, Dr. Baldwin said, and recurrence is less common than in other parts of the body, especially when corticosteroids are added. It helps that patients are often more compliant with adjunctive therapy, she added, because the keloids are highly visible, and they want to wear earrings again.
- Ask patients what bothers them the most about the keloids. Some may want to eliminate burning, itching, or stinging, and Dr. Baldwin attempts to treat those issues. Patients may want keloids to be softer, flatter, or lighter, she said.
- Modification of the keloid’s appearance may be enough for some patients. For example, one of her patients objected to extensive keloids around his breasts because they gave him the appearance of cleavage. Another believed – accurately – that his keloid looked like male genitalia. Dr. Baldwin treated it with the keloid equivalent of castration (surgically removing its “testicles”) and circumcision of sorts (a flattening of its “glans penis” with corticosteroids). “It didn’t look pretty,” she said, “but it no longer looked offensive to him.”
- Many patients present with keloids on the chest, back, and deltoids, “which have to have been from acne, but you can’t actually see the pimples,” Dr. Baldwin said. In these cases, she may turn to isotretinoin. This is not for treatment of keloids, but is a preventive strategy to stop further lesions from appearing and causing more keloids, she explained.
- In addition to corticosteroids, other postsurgical options include freezing, interferon, pressure dressings, dextran hydrogel scaffolding, and radiation therapy.
Moving forward, researchers “are looking at biologics, TNF-alpha inhibitors, and tyrosine kinase inhibitors in hopes that we can find something that will stop the incessant forward movement of some of our keloid patients,” Dr. Baldwin noted.
Dr. Baldwin reported no relevant disclosures.
SDEF and this news organization are owned by the same parent company.
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR
Hospitals could reduce maternal mortality with four achievable steps
rate in the United States, according to a new perspective from leading obstetricians published in the New England Journal of Medicine.
The authors, including Kimberlee McKay, MD, president of the American College of Obstetricians and Gynecologists (ACOG), also call for collaboration with family physicians to increase access to obstetric care in rural areas.
The president of the American Academy of Family Physicians (AAFP), John S. Cullen, MD, in a separate statement, welcomed the opportunity for collaboration in addressing the maternal mortality crisis. However, some distance still lies between the finer points of how the two organizations see family physicians helping curb the crisis.
“Women in the United States are more likely to die from childbirth- or pregnancy-related causes than women in any other high-income country, and black women die at a rate three to four times that of white women,” noted Susan Mann, MD, along with her coauthors of the obstetric perspective, calling increasing maternal mortality a “tragedy.”
In an interview, Dr. Cullen concurred, calling the current situation “unconscionable.” One of the primary reasons he sought AAFP leadership, he said, was to bring experiences learned during his 25 years of obstetric practice in rural Alaska to bear on the current crisis.
A set of maternal care bundles created by the Alliance for Innovation on Maternal Health (AIM) provides the framework for the first action recommended by Dr. Mann and her coauthors. The AIM bundles focus on protocols that improve readiness, recognition, response, and reporting in maternal care. The protocols are institution specific. For example, the authors noted, antihypertensive medications should be readily available around the clock, because not all facilities will have a pharmacist in-house at all times, and hypertensive emergencies are among the gravest obstetric complications.
“Although management may vary from institution to institution, each unit can be required to demonstrate readiness to deal with emergencies 24/7,” said Dr. Mann, a physician in private practice in Boston, and her coauthors.

The second recommended action revolves around multidisciplinary staff meetings to perform individual assessments for each woman’s obstetric risk factors. These huddles should include assessing hemorrhage risk by using the California Maternal Quality Care Collaborative guidelines, and briefings with the full care team to “develop shared understandings of the patient and the procedure” before elective or nonurgent cesarean deliveries, said Dr. Mann and her colleagues. Patients should be informed of any safety concerns, and caregivers should use shared decision-making moving forward.
“Approximately 50% of U.S. hospitals provide care for three or fewer deliveries per day, but the need to identify women at risk is equally important for these small obstetrics services,” Dr. Mann and her coauthors noted.
Third, simulation of obstetric emergencies lets all members of the team understand the speed at which decisions must be made and actions taken when minutes, or even seconds, count. Dr. Mann and her coauthors pointed out that logistics problems come out during a well-run simulation, giving such examples as a lag in receiving blood products or a poorly placed hemorrhage cart.
Drawing an analogy to the extensive time pilots spend in flight simulators, Dr. Mann and her coauthors noted that “because severe maternity-related events are rare and often unpredictable, and because members of the care team may not know each other, it is important to train for low-probability but high-risk events.”
Using the Maternal Health Compact will help ensure that lower-resource hospitals have a relationship in place with a facility that can provide a higher level of maternal care when needed, they said.
This fourth action means that there’s a connection that “can be activated by lower-resource hospitals to get immediate consultation in the event of an unexpected obstetrical emergency whose care demands exceed their resources,” said Dr. Mann and her coauthors. When transport is necessary, it too can be facilitated if a compact is already in place.
The final, broader, recommendation from the obstetricians is that ACOG and AAFP collaborate “on an additional year of comprehensive training for family medicine physicians who are considering practicing obstetrics in rural areas.” The fourth year of training for these family physicians could help address widespread shortages of obstetricians and midwives in rural communities, Dr. Mann and her coauthors wrote. They observed that “pregnant women who live in rural areas may need to travel hundreds of miles to obtain routine prenatal care or consultation with an obstetrical specialist.”
Dr. Cullen, whose practice is in Valdez, Alaska, said he happily reciprocates the desire for collaboration. In his inaugural blog post after assuming the AAFP presidency in October, 2018, he extended warm thanks to his obstetrician and perinatologist colleagues. “The relationship between family physicians and obstetricians is vital in rural communities like mine. The training I received has saved lives and prevented catastrophe,” he wrote.

At the same time, Dr. Cullen said that he believes family physicians are the best hope for quality obstetrical care in rural communities. Dr. Cullen’s own training, he said, was structured to involve significant obstetric experience with obstetrician mentorship. “A 3-year residency left me very comfortable with fairly sophisticated obstetric management at graduation,” he added.
In his practice, Dr. Cullen said, a family physician hired a decade ago after a 3-year residency came with excellent obstetric skills, which have been further honed during the succeeding years of rural practice. During a 3-year residency, “family physicians receive training and demonstrate the skills and competencies required to deliver high-quality maternity care in any community, including those in rural settings,” he said in his statement.
“The bigger issue is really the closure of obstetric units in rural hospitals,” said Dr. Cullen. He pointed out that although obstetric services may have left a community, that rural hospital will still have miscarrying patients with hemorrhage, patients in preterm labor, and other obstetric emergencies arriving at the doorstep. These and other instances often “represent true emergencies without possibility of transfer, requiring immediate and effective response,” he wrote.
“We would encourage the authors to ensure an equal focus on improving care at all levels and in all hospitals, as well as relying on transfer as appropriate,” Dr. Cullen said in his statement.
Such mutual support can be bolstered by new technology, wrote Dr. Mann and her coauthors, because “telehealth and collaborations and consultation with clinics and regional hospitals can help increase the availability of maternity care in the United States.”
For Dr. Cullen also, the way forward is together. In his blog, he wrote: “As family physicians, we can only deliver obstetrical care to our patients with the cooperation of obstetricians and perinatologists. Conversely, obstetricians can only improve maternal and infant mortality rates, especially in rural areas, with the help of family physicians.”
SOURCE: Mann S et al. N Engl J Med 2018;379:1689-91.
rate in the United States, according to a new perspective from leading obstetricians published in the New England Journal of Medicine.
The authors, including Kimberlee McKay, MD, president of the American College of Obstetricians and Gynecologists (ACOG), also call for collaboration with family physicians to increase access to obstetric care in rural areas.
The president of the American Academy of Family Physicians (AAFP), John S. Cullen, MD, in a separate statement, welcomed the opportunity for collaboration in addressing the maternal mortality crisis. However, some distance still lies between the finer points of how the two organizations see family physicians helping curb the crisis.
“Women in the United States are more likely to die from childbirth- or pregnancy-related causes than women in any other high-income country, and black women die at a rate three to four times that of white women,” noted Susan Mann, MD, along with her coauthors of the obstetric perspective, calling increasing maternal mortality a “tragedy.”
In an interview, Dr. Cullen concurred, calling the current situation “unconscionable.” One of the primary reasons he sought AAFP leadership, he said, was to bring experiences learned during his 25 years of obstetric practice in rural Alaska to bear on the current crisis.
A set of maternal care bundles created by the Alliance for Innovation on Maternal Health (AIM) provides the framework for the first action recommended by Dr. Mann and her coauthors. The AIM bundles focus on protocols that improve readiness, recognition, response, and reporting in maternal care. The protocols are institution specific. For example, the authors noted, antihypertensive medications should be readily available around the clock, because not all facilities will have a pharmacist in-house at all times, and hypertensive emergencies are among the gravest obstetric complications.
“Although management may vary from institution to institution, each unit can be required to demonstrate readiness to deal with emergencies 24/7,” said Dr. Mann, a physician in private practice in Boston, and her coauthors.
The second recommended action revolves around multidisciplinary staff meetings to perform individual assessments for each woman’s obstetric risk factors. These huddles should include assessing hemorrhage risk by using the California Maternal Quality Care Collaborative guidelines, and briefings with the full care team to “develop shared understandings of the patient and the procedure” before elective or nonurgent cesarean deliveries, said Dr. Mann and her colleagues. Patients should be informed of any safety concerns, and caregivers should use shared decision-making moving forward.
“Approximately 50% of U.S. hospitals provide care for three or fewer deliveries per day, but the need to identify women at risk is equally important for these small obstetrics services,” Dr. Mann and her coauthors noted.
Third, simulation of obstetric emergencies lets all members of the team understand the speed at which decisions must be made and actions taken when minutes, or even seconds, count. Dr. Mann and her coauthors pointed out that logistics problems come out during a well-run simulation, giving such examples as a lag in receiving blood products or a poorly placed hemorrhage cart.
Drawing an analogy to the extensive time pilots spend in flight simulators, Dr. Mann and her coauthors noted that “because severe maternity-related events are rare and often unpredictable, and because members of the care team may not know each other, it is important to train for low-probability but high-risk events.”
Using the Maternal Health Compact will help ensure that lower-resource hospitals have a relationship in place with a facility that can provide a higher level of maternal care when needed, they said.
This fourth action means that there’s a connection that “can be activated by lower-resource hospitals to get immediate consultation in the event of an unexpected obstetrical emergency whose care demands exceed their resources,” said Dr. Mann and her coauthors. When transport is necessary, it too can be facilitated if a compact is already in place.
The final, broader, recommendation from the obstetricians is that ACOG and AAFP collaborate “on an additional year of comprehensive training for family medicine physicians who are considering practicing obstetrics in rural areas.” The fourth year of training for these family physicians could help address widespread shortages of obstetricians and midwives in rural communities, Dr. Mann and her coauthors wrote. They observed that “pregnant women who live in rural areas may need to travel hundreds of miles to obtain routine prenatal care or consultation with an obstetrical specialist.”
Dr. Cullen, whose practice is in Valdez, Alaska, said he happily reciprocates the desire for collaboration. In his inaugural blog post after assuming the AAFP presidency in October, 2018, he extended warm thanks to his obstetrician and perinatologist colleagues. “The relationship between family physicians and obstetricians is vital in rural communities like mine. The training I received has saved lives and prevented catastrophe,” he wrote.
At the same time, Dr. Cullen said that he believes family physicians are the best hope for quality obstetrical care in rural communities. Dr. Cullen’s own training, he said, was structured to involve significant obstetric experience with obstetrician mentorship. “A 3-year residency left me very comfortable with fairly sophisticated obstetric management at graduation,” he added.
In his practice, Dr. Cullen said, a family physician hired a decade ago after a 3-year residency came with excellent obstetric skills, which have been further honed during the succeeding years of rural practice. During a 3-year residency, “family physicians receive training and demonstrate the skills and competencies required to deliver high-quality maternity care in any community, including those in rural settings,” he said in his statement.
“The bigger issue is really the closure of obstetric units in rural hospitals,” said Dr. Cullen. He pointed out that although obstetric services may have left a community, that rural hospital will still have miscarrying patients with hemorrhage, patients in preterm labor, and other obstetric emergencies arriving at the doorstep. These and other instances often “represent true emergencies without possibility of transfer, requiring immediate and effective response,” he wrote.
“We would encourage the authors to ensure an equal focus on improving care at all levels and in all hospitals, as well as relying on transfer as appropriate,” Dr. Cullen said in his statement.
Such mutual support can be bolstered by new technology, wrote Dr. Mann and her coauthors, because “telehealth and collaborations and consultation with clinics and regional hospitals can help increase the availability of maternity care in the United States.”
For Dr. Cullen also, the way forward is together. In his blog, he wrote: “As family physicians, we can only deliver obstetrical care to our patients with the cooperation of obstetricians and perinatologists. Conversely, obstetricians can only improve maternal and infant mortality rates, especially in rural areas, with the help of family physicians.”
SOURCE: Mann S et al. N Engl J Med 2018;379:1689-91.
rate in the United States, according to a new perspective from leading obstetricians published in the New England Journal of Medicine.
The authors, including Kimberlee McKay, MD, president of the American College of Obstetricians and Gynecologists (ACOG), also call for collaboration with family physicians to increase access to obstetric care in rural areas.
The president of the American Academy of Family Physicians (AAFP), John S. Cullen, MD, in a separate statement, welcomed the opportunity for collaboration in addressing the maternal mortality crisis. However, some distance still lies between the finer points of how the two organizations see family physicians helping curb the crisis.
“Women in the United States are more likely to die from childbirth- or pregnancy-related causes than women in any other high-income country, and black women die at a rate three to four times that of white women,” noted Susan Mann, MD, along with her coauthors of the obstetric perspective, calling increasing maternal mortality a “tragedy.”
In an interview, Dr. Cullen concurred, calling the current situation “unconscionable.” One of the primary reasons he sought AAFP leadership, he said, was to bring experiences learned during his 25 years of obstetric practice in rural Alaska to bear on the current crisis.
A set of maternal care bundles created by the Alliance for Innovation on Maternal Health (AIM) provides the framework for the first action recommended by Dr. Mann and her coauthors. The AIM bundles focus on protocols that improve readiness, recognition, response, and reporting in maternal care. The protocols are institution specific. For example, the authors noted, antihypertensive medications should be readily available around the clock, because not all facilities will have a pharmacist in-house at all times, and hypertensive emergencies are among the gravest obstetric complications.
“Although management may vary from institution to institution, each unit can be required to demonstrate readiness to deal with emergencies 24/7,” said Dr. Mann, a physician in private practice in Boston, and her coauthors.
The second recommended action revolves around multidisciplinary staff meetings to perform individual assessments for each woman’s obstetric risk factors. These huddles should include assessing hemorrhage risk by using the California Maternal Quality Care Collaborative guidelines, and briefings with the full care team to “develop shared understandings of the patient and the procedure” before elective or nonurgent cesarean deliveries, said Dr. Mann and her colleagues. Patients should be informed of any safety concerns, and caregivers should use shared decision-making moving forward.
“Approximately 50% of U.S. hospitals provide care for three or fewer deliveries per day, but the need to identify women at risk is equally important for these small obstetrics services,” Dr. Mann and her coauthors noted.
Third, simulation of obstetric emergencies lets all members of the team understand the speed at which decisions must be made and actions taken when minutes, or even seconds, count. Dr. Mann and her coauthors pointed out that logistics problems come out during a well-run simulation, giving such examples as a lag in receiving blood products or a poorly placed hemorrhage cart.
Drawing an analogy to the extensive time pilots spend in flight simulators, Dr. Mann and her coauthors noted that “because severe maternity-related events are rare and often unpredictable, and because members of the care team may not know each other, it is important to train for low-probability but high-risk events.”
Using the Maternal Health Compact will help ensure that lower-resource hospitals have a relationship in place with a facility that can provide a higher level of maternal care when needed, they said.
This fourth action means that there’s a connection that “can be activated by lower-resource hospitals to get immediate consultation in the event of an unexpected obstetrical emergency whose care demands exceed their resources,” said Dr. Mann and her coauthors. When transport is necessary, it too can be facilitated if a compact is already in place.
The final, broader, recommendation from the obstetricians is that ACOG and AAFP collaborate “on an additional year of comprehensive training for family medicine physicians who are considering practicing obstetrics in rural areas.” The fourth year of training for these family physicians could help address widespread shortages of obstetricians and midwives in rural communities, Dr. Mann and her coauthors wrote. They observed that “pregnant women who live in rural areas may need to travel hundreds of miles to obtain routine prenatal care or consultation with an obstetrical specialist.”
Dr. Cullen, whose practice is in Valdez, Alaska, said he happily reciprocates the desire for collaboration. In his inaugural blog post after assuming the AAFP presidency in October, 2018, he extended warm thanks to his obstetrician and perinatologist colleagues. “The relationship between family physicians and obstetricians is vital in rural communities like mine. The training I received has saved lives and prevented catastrophe,” he wrote.
At the same time, Dr. Cullen said that he believes family physicians are the best hope for quality obstetrical care in rural communities. Dr. Cullen’s own training, he said, was structured to involve significant obstetric experience with obstetrician mentorship. “A 3-year residency left me very comfortable with fairly sophisticated obstetric management at graduation,” he added.
In his practice, Dr. Cullen said, a family physician hired a decade ago after a 3-year residency came with excellent obstetric skills, which have been further honed during the succeeding years of rural practice. During a 3-year residency, “family physicians receive training and demonstrate the skills and competencies required to deliver high-quality maternity care in any community, including those in rural settings,” he said in his statement.
“The bigger issue is really the closure of obstetric units in rural hospitals,” said Dr. Cullen. He pointed out that although obstetric services may have left a community, that rural hospital will still have miscarrying patients with hemorrhage, patients in preterm labor, and other obstetric emergencies arriving at the doorstep. These and other instances often “represent true emergencies without possibility of transfer, requiring immediate and effective response,” he wrote.
“We would encourage the authors to ensure an equal focus on improving care at all levels and in all hospitals, as well as relying on transfer as appropriate,” Dr. Cullen said in his statement.
Such mutual support can be bolstered by new technology, wrote Dr. Mann and her coauthors, because “telehealth and collaborations and consultation with clinics and regional hospitals can help increase the availability of maternity care in the United States.”
For Dr. Cullen also, the way forward is together. In his blog, he wrote: “As family physicians, we can only deliver obstetrical care to our patients with the cooperation of obstetricians and perinatologists. Conversely, obstetricians can only improve maternal and infant mortality rates, especially in rural areas, with the help of family physicians.”
SOURCE: Mann S et al. N Engl J Med 2018;379:1689-91.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Focus on patient experience to cut readmission rates
Incorporate patient-reported quality measures
Hospitalists have focused much attention on reducing 30-day readmission rates, at a time when 15-20% of health care dollars spent on those readmissions is considered potentially preventable.
But until very recently, no study has explored patient perceptions of the likelihood of readmission during index admission. Now, that’s changed.

“Our objective was to examine associations between patient perceptions of care during index hospital admission and 30-day readmission,” says Jocelyn Carter, MD, of Massachusetts General Hospital, Boston, and lead author of November 2017 study in BMJ Quality & Safety.
Enrolled in the study were 846 patients at two inpatient adult medicine units at Massachusetts General, Boston; 201 (23.8%) of these patients were readmitted within 30 days. In multivariable models adjusting for baseline differences, respondents who reported being “very satisfied” with the care received during the index hospitalization were less likely to be readmitted; participants reporting that doctors “always listened to them carefully” also were less likely to be readmitted.
“These findings are important since they suggest that engaging patients in an assessment of communication quality, unmet needs, concerns, and overall experience during admission may help to identify issues that might not be captured in standard postdischarge surveys when the appropriate time for quality improvement interventions has passed,” Dr. Carter said. “Incorporating patient-reported measures during index hospitalizations may improve readmission rates and help predict which patients are more likely to be readmitted.”
Reference
Carter J et al. The association between patient experience factors and likelihood of 30-day readmission: A prospective cohort study. BMJ Qual Saf. 16 Nov 2017. Accessed Feb 2, 2018.
Incorporate patient-reported quality measures
Incorporate patient-reported quality measures
Hospitalists have focused much attention on reducing 30-day readmission rates, at a time when 15-20% of health care dollars spent on those readmissions is considered potentially preventable.
But until very recently, no study has explored patient perceptions of the likelihood of readmission during index admission. Now, that’s changed.
“Our objective was to examine associations between patient perceptions of care during index hospital admission and 30-day readmission,” says Jocelyn Carter, MD, of Massachusetts General Hospital, Boston, and lead author of November 2017 study in BMJ Quality & Safety.
Enrolled in the study were 846 patients at two inpatient adult medicine units at Massachusetts General, Boston; 201 (23.8%) of these patients were readmitted within 30 days. In multivariable models adjusting for baseline differences, respondents who reported being “very satisfied” with the care received during the index hospitalization were less likely to be readmitted; participants reporting that doctors “always listened to them carefully” also were less likely to be readmitted.
“These findings are important since they suggest that engaging patients in an assessment of communication quality, unmet needs, concerns, and overall experience during admission may help to identify issues that might not be captured in standard postdischarge surveys when the appropriate time for quality improvement interventions has passed,” Dr. Carter said. “Incorporating patient-reported measures during index hospitalizations may improve readmission rates and help predict which patients are more likely to be readmitted.”
Reference
Carter J et al. The association between patient experience factors and likelihood of 30-day readmission: A prospective cohort study. BMJ Qual Saf. 16 Nov 2017. Accessed Feb 2, 2018.
Hospitalists have focused much attention on reducing 30-day readmission rates, at a time when 15-20% of health care dollars spent on those readmissions is considered potentially preventable.
But until very recently, no study has explored patient perceptions of the likelihood of readmission during index admission. Now, that’s changed.
“Our objective was to examine associations between patient perceptions of care during index hospital admission and 30-day readmission,” says Jocelyn Carter, MD, of Massachusetts General Hospital, Boston, and lead author of November 2017 study in BMJ Quality & Safety.
Enrolled in the study were 846 patients at two inpatient adult medicine units at Massachusetts General, Boston; 201 (23.8%) of these patients were readmitted within 30 days. In multivariable models adjusting for baseline differences, respondents who reported being “very satisfied” with the care received during the index hospitalization were less likely to be readmitted; participants reporting that doctors “always listened to them carefully” also were less likely to be readmitted.
“These findings are important since they suggest that engaging patients in an assessment of communication quality, unmet needs, concerns, and overall experience during admission may help to identify issues that might not be captured in standard postdischarge surveys when the appropriate time for quality improvement interventions has passed,” Dr. Carter said. “Incorporating patient-reported measures during index hospitalizations may improve readmission rates and help predict which patients are more likely to be readmitted.”
Reference
Carter J et al. The association between patient experience factors and likelihood of 30-day readmission: A prospective cohort study. BMJ Qual Saf. 16 Nov 2017. Accessed Feb 2, 2018.
Pediatric indications appear in one-third of orphan drug approvals
WASHINGTON – Pediatric indications appeared in approximately 36% of orphan drug approvals between 2000 and 2017, according to data from the Food and Drug Administration.
“Given the impact of rare disease on children, it is of particular interest to better understand where new drug approvals and advances are occurring, through the lens of pediatrics,” said Kathleen L. Miller, Ph.D., and Michael Lanthier of the Food and Drug Administration in Silver Spring, Md. They presented their findings in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
Overall, 31% of 314 orphan drug approvals by the FDA between 2000 and 2017 had a pediatric and adult indication, 5% had pediatric-only indications, and 64% had adult-only indications.
For the 112 pediatric indication approvals, 14% were for inherited blood disorders, 14% for inherited metabolic disorders, 13% for rare cancers, 10% for antidotes and medical countermeasures, 9% for infectious diseases, 8% for auto-inflammatory diseases, 7% for neurologic disorders, and 25% for other conditions.
Approximately 63% of the total orphan drug approvals during the study period were for rare cancers or genetic disorders (138 approvals and 59 approvals, respectively). Although 90% of the rare cancer approvals were for adults only, 84% of genetic disorder drug approvals had pediatric indications, Dr. Miller and Mr. Lanthier noted.
When analyzed by submission type, pediatric indications were included in 52% of new orphan formulations, 35% of orphan secondary indication approvals, and 32% of new molecular entity approvals.
Although more research is needed, the results suggest that “pediatric indications represent a sizable proportion of orphan drug approvals in both a range of therapeutic areas and in a range of approval types,” the investigators concluded.
The researchers are employed by the FDA, which sponsored the study. They had no financial conflicts to disclose.
WASHINGTON – Pediatric indications appeared in approximately 36% of orphan drug approvals between 2000 and 2017, according to data from the Food and Drug Administration.
“Given the impact of rare disease on children, it is of particular interest to better understand where new drug approvals and advances are occurring, through the lens of pediatrics,” said Kathleen L. Miller, Ph.D., and Michael Lanthier of the Food and Drug Administration in Silver Spring, Md. They presented their findings in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
Overall, 31% of 314 orphan drug approvals by the FDA between 2000 and 2017 had a pediatric and adult indication, 5% had pediatric-only indications, and 64% had adult-only indications.
For the 112 pediatric indication approvals, 14% were for inherited blood disorders, 14% for inherited metabolic disorders, 13% for rare cancers, 10% for antidotes and medical countermeasures, 9% for infectious diseases, 8% for auto-inflammatory diseases, 7% for neurologic disorders, and 25% for other conditions.
Approximately 63% of the total orphan drug approvals during the study period were for rare cancers or genetic disorders (138 approvals and 59 approvals, respectively). Although 90% of the rare cancer approvals were for adults only, 84% of genetic disorder drug approvals had pediatric indications, Dr. Miller and Mr. Lanthier noted.
When analyzed by submission type, pediatric indications were included in 52% of new orphan formulations, 35% of orphan secondary indication approvals, and 32% of new molecular entity approvals.
Although more research is needed, the results suggest that “pediatric indications represent a sizable proportion of orphan drug approvals in both a range of therapeutic areas and in a range of approval types,” the investigators concluded.
The researchers are employed by the FDA, which sponsored the study. They had no financial conflicts to disclose.
WASHINGTON – Pediatric indications appeared in approximately 36% of orphan drug approvals between 2000 and 2017, according to data from the Food and Drug Administration.
“Given the impact of rare disease on children, it is of particular interest to better understand where new drug approvals and advances are occurring, through the lens of pediatrics,” said Kathleen L. Miller, Ph.D., and Michael Lanthier of the Food and Drug Administration in Silver Spring, Md. They presented their findings in a poster at the NORD Rare Summit, held by the National Organization for Rare Disorders.
Overall, 31% of 314 orphan drug approvals by the FDA between 2000 and 2017 had a pediatric and adult indication, 5% had pediatric-only indications, and 64% had adult-only indications.
For the 112 pediatric indication approvals, 14% were for inherited blood disorders, 14% for inherited metabolic disorders, 13% for rare cancers, 10% for antidotes and medical countermeasures, 9% for infectious diseases, 8% for auto-inflammatory diseases, 7% for neurologic disorders, and 25% for other conditions.
Approximately 63% of the total orphan drug approvals during the study period were for rare cancers or genetic disorders (138 approvals and 59 approvals, respectively). Although 90% of the rare cancer approvals were for adults only, 84% of genetic disorder drug approvals had pediatric indications, Dr. Miller and Mr. Lanthier noted.
When analyzed by submission type, pediatric indications were included in 52% of new orphan formulations, 35% of orphan secondary indication approvals, and 32% of new molecular entity approvals.
Although more research is needed, the results suggest that “pediatric indications represent a sizable proportion of orphan drug approvals in both a range of therapeutic areas and in a range of approval types,” the investigators concluded.
The researchers are employed by the FDA, which sponsored the study. They had no financial conflicts to disclose.
REPORTING FROM NORD SUMMIT 2018
Key clinical point:
Major finding: A total of 112 orphan drug approvals between 2000 and 2017 included a pediatric indication.
Study details: The data come from a review of 314 orphan drug approvals by the FDA between 2000 and 2017.
Disclosures: The researchers are employed by the Food and Drug Administration, which sponsored the study. They had no financial conflicts to disclose.
Funding for NIH BRAIN Initiative reaches new heights
The National Institutes of Health’s Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative will finish 2018 with its largest round of grant funding ever, giving $220 million to more than 200 research awards, and bringing this year’s total to more than $400 million, according to an announcement from the agency.
The BRAIN Initiative began in 2013 with the objective of revolutionizing our understanding of the human brain by accelerating the development and application of innovative technologies that will allow researchers to show how individual cells and complex neural circuits interact in both time and space and thereby seek new ways to treat, cure, and prevent brain disorders.
In the current round of funding that was authorized by Congress through the regular appropriations process and the 21st Century Cures Act, new projects include the creation of a wireless optical tomography cap for scanning human brain activity; the development of a noninvasive brain-computer interface system for improving the lives of paralysis patients; and the testing of noninvasive brain stimulation devices for treating schizophrenia, attention deficit disorders, and other brain diseases; the development of self-growing biological electrodes for recording brain activity; and the creation of an indestructible hydrogel system to help map neural circuits, according to the announcement.
Not all of the research involves technological advancement. In fact, one line of funding involves neuroethics. For instance, for epilepsy syndromes in the latest round of funding for 2018, researchers aim to explore ethical issues confronting families and clinicians when considering new treatment options for drug-resistant epilepsy in children.
The NIH is also leveraging some of the BRAIN Initiative funding toward finding new, nonaddictive pain treatments as part of the its HEAL (Helping to End Addiction Long-term) Initiative, such as support for research on the fundamental neurobiology of endogenous opioid systems.
The National Institutes of Health’s Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative will finish 2018 with its largest round of grant funding ever, giving $220 million to more than 200 research awards, and bringing this year’s total to more than $400 million, according to an announcement from the agency.
The BRAIN Initiative began in 2013 with the objective of revolutionizing our understanding of the human brain by accelerating the development and application of innovative technologies that will allow researchers to show how individual cells and complex neural circuits interact in both time and space and thereby seek new ways to treat, cure, and prevent brain disorders.
In the current round of funding that was authorized by Congress through the regular appropriations process and the 21st Century Cures Act, new projects include the creation of a wireless optical tomography cap for scanning human brain activity; the development of a noninvasive brain-computer interface system for improving the lives of paralysis patients; and the testing of noninvasive brain stimulation devices for treating schizophrenia, attention deficit disorders, and other brain diseases; the development of self-growing biological electrodes for recording brain activity; and the creation of an indestructible hydrogel system to help map neural circuits, according to the announcement.
Not all of the research involves technological advancement. In fact, one line of funding involves neuroethics. For instance, for epilepsy syndromes in the latest round of funding for 2018, researchers aim to explore ethical issues confronting families and clinicians when considering new treatment options for drug-resistant epilepsy in children.
The NIH is also leveraging some of the BRAIN Initiative funding toward finding new, nonaddictive pain treatments as part of the its HEAL (Helping to End Addiction Long-term) Initiative, such as support for research on the fundamental neurobiology of endogenous opioid systems.
The National Institutes of Health’s Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative will finish 2018 with its largest round of grant funding ever, giving $220 million to more than 200 research awards, and bringing this year’s total to more than $400 million, according to an announcement from the agency.
The BRAIN Initiative began in 2013 with the objective of revolutionizing our understanding of the human brain by accelerating the development and application of innovative technologies that will allow researchers to show how individual cells and complex neural circuits interact in both time and space and thereby seek new ways to treat, cure, and prevent brain disorders.
In the current round of funding that was authorized by Congress through the regular appropriations process and the 21st Century Cures Act, new projects include the creation of a wireless optical tomography cap for scanning human brain activity; the development of a noninvasive brain-computer interface system for improving the lives of paralysis patients; and the testing of noninvasive brain stimulation devices for treating schizophrenia, attention deficit disorders, and other brain diseases; the development of self-growing biological electrodes for recording brain activity; and the creation of an indestructible hydrogel system to help map neural circuits, according to the announcement.
Not all of the research involves technological advancement. In fact, one line of funding involves neuroethics. For instance, for epilepsy syndromes in the latest round of funding for 2018, researchers aim to explore ethical issues confronting families and clinicians when considering new treatment options for drug-resistant epilepsy in children.
The NIH is also leveraging some of the BRAIN Initiative funding toward finding new, nonaddictive pain treatments as part of the its HEAL (Helping to End Addiction Long-term) Initiative, such as support for research on the fundamental neurobiology of endogenous opioid systems.