User login
Reducing pediatric RSV burden is top priority
LJUBLJANA, SLOVENIA – Prevention or early effective treatment of respiratory syncytial virus (RSV) infection in infants and small children holds the promise of sharply reduced burdens of both acute otitis media (AOM) and pneumonia, Terho Heikkinen, MD, PhD, predicted in the Bill Marshall Award Lecture presented at the annual meeting of the European Society for Paediatric Infectious Diseases (ESPID).

RSV is by far the hottest virus in the world,” declared Dr. Heikkinen, professor of pediatrics at the University of Turku (Finland).
“A lot of progress is being made with respect to RSV. This increased understanding holds great promise for new interventions,” he explained. “Lots of different types of vaccines are being developed, monoclonal antibodies, antivirals. So
Today influenza is the only respiratory viral infection that’s preventable via vaccine or effectively treatable using antiviral drugs. That situation has to change, as Dr. Heikkinen demonstrated early in his career; RSV is the respiratory virus that’s most likely to invade the middle ear during AOM. It’s much more ototropic than influenza, parainfluenza, enteroviruses, or adenoviruses (N Engl J Med. 1999 Jan 28;340[4]:260-4), he noted.
The Bill Marshall Award and Lecture, ESPID’s most prestigious award, is given annually to an individual recognized as having significantly advanced the field of pediatric infectious diseases. Dr. Heikkinen was singled out for his decades of work establishing that viruses, including RSV, play a key role in AOM, which had traditionally been regarded as a bacterial infection. He and his coinvestigators demonstrated that in about two-thirds of cases, AOM is actually caused by a combination of bacteria and viruses, which explains why patients’ clinical response to antibiotic therapy for AOM often is poor. They also described the chain of events whereby viral infection of the upper airway epithelium triggers an inflammatory response in the nasopharynx, with resultant Eustachian tube dysfunction and negative middle ear pressure, which in turn encourages microbial invasion of the middle ear. Moreover, they showed that the peak incidence of AOM isn’t on day 1 after onset of upper respiratory infection symptoms, but on day 3 or 4.
“What this tells us is that, once a child has a viral respiratory infection, there is a certain window of opportunity to try to prevent the development of the complication if we have the right tools in place,” Dr. Heikkinen said.
He and his colleagues put this lesson to good use nearly a decade ago in a randomized, double-blind trial in which they showed that giving oseltamivir (Tamiflu) within 12 hours after onset of influenza symptoms in children aged 1-3 years reduced the subsequent incidence of AOM by 85%, compared with placebo (Clin Infect Dis. 2010 Oct 15;51[8]:887-94).
These observations paved the way for the ongoing intensive research effort exploring ways of preventing AOM through interventions at two different levels: by developing viral vaccines to prevent a healthy child from contracting the viral upper respiratory infection that precedes AOM and by coming up with antiviral drugs or bacterial vaccines to prevent a upper respiratory infection from evolving into AOM.
The same applies to pneumonia. Other investigators showed years ago that both respiratory viruses and bacteria were present in two-thirds of sputum samples obtained from children with community-acquired pneumonia (Clin Microbiol Infect. 2012 Mar;18[3]:300-7).
RSV is the top cause of hospitalization for acute respiratory infection – pneumonia and bronchiolitis – in infants. Worldwide, it’s estimated that RSV accounts for more than 33 million episodes of pneumonia annually, with 3.2 million hospitalizations and 118,200 deaths.
Beyond the hospital, however, Dr. Heikkinen and colleagues conducted a prospective cohort study in Turku over the course of two consecutive respiratory infection seasons in which they captured the huge burden of RSV as an outpatient illness. It hit hardest in children younger than 3 years, in whom the average annual incidence of RSV infection was 275 cases per 1,000 children. In that youngest age population, RSV upper respiratory infection was followed by AOM 58% of the time, with antibiotics prescribed in 66% of the cases of this complication of RSV illness. The mean duration of RSV illness was greatest in this young age group, at 13 days, and it was associated with parental absenteeism from work at a rate of 136 days per 100 children with RSV illness.
Moreover, while AOM occurred less frequently in children aged 3-6 years, 46% of the cases were attributed to a preceding RSV infection, which led to antibiotic treatment nearly half of the time (J Infect Dis. 2017 Jan 1;215[1]:17-23). This documentation has spurred further efforts to develop RSV vaccines and antivirals.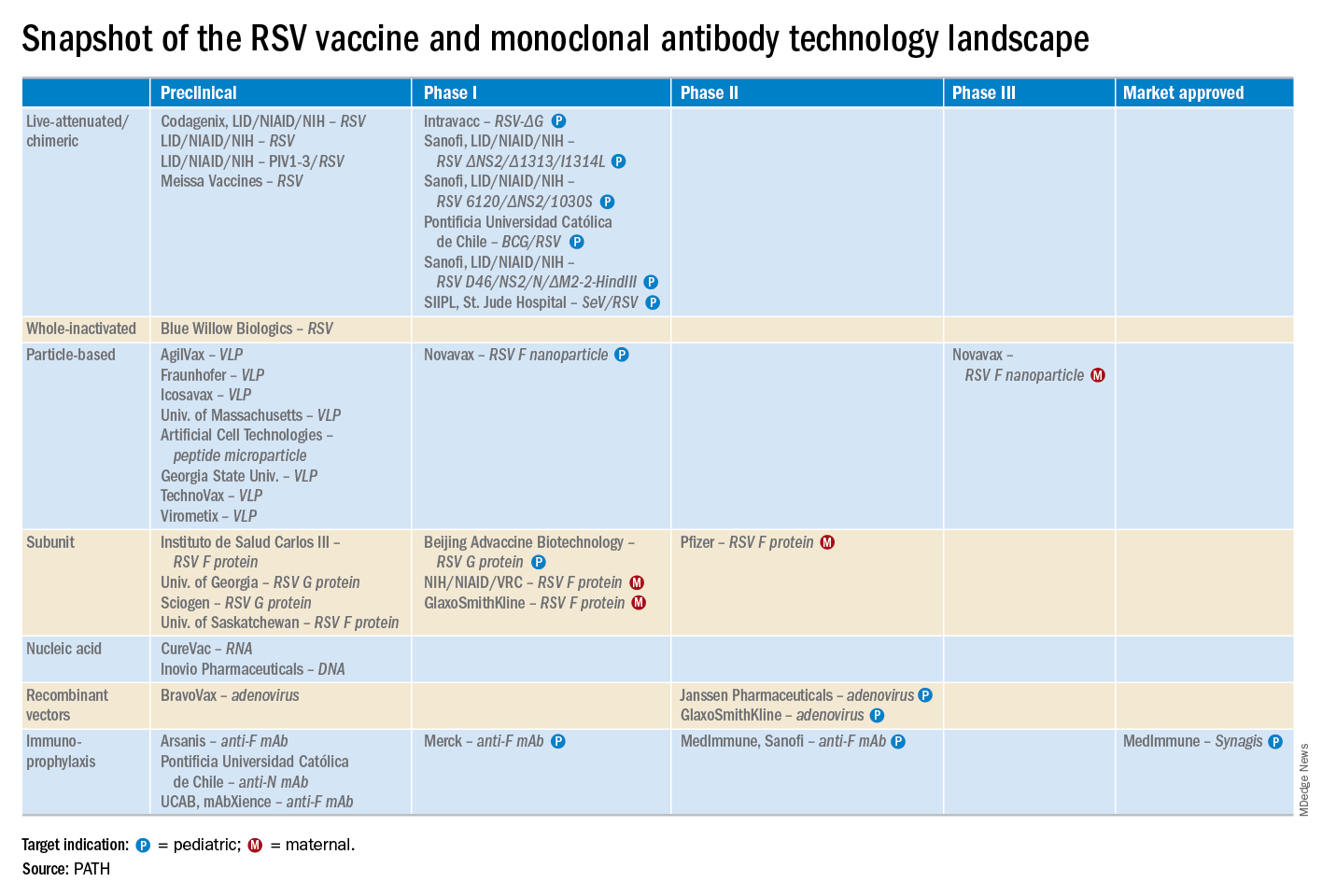
He reported serving as a consultant to a half-dozen pharmaceutical companies, as well as having received research funding from Janssen, GlaxoSmithKline, and Novavax.
LJUBLJANA, SLOVENIA – Prevention or early effective treatment of respiratory syncytial virus (RSV) infection in infants and small children holds the promise of sharply reduced burdens of both acute otitis media (AOM) and pneumonia, Terho Heikkinen, MD, PhD, predicted in the Bill Marshall Award Lecture presented at the annual meeting of the European Society for Paediatric Infectious Diseases (ESPID).
RSV is by far the hottest virus in the world,” declared Dr. Heikkinen, professor of pediatrics at the University of Turku (Finland).
“A lot of progress is being made with respect to RSV. This increased understanding holds great promise for new interventions,” he explained. “Lots of different types of vaccines are being developed, monoclonal antibodies, antivirals. So
Today influenza is the only respiratory viral infection that’s preventable via vaccine or effectively treatable using antiviral drugs. That situation has to change, as Dr. Heikkinen demonstrated early in his career; RSV is the respiratory virus that’s most likely to invade the middle ear during AOM. It’s much more ototropic than influenza, parainfluenza, enteroviruses, or adenoviruses (N Engl J Med. 1999 Jan 28;340[4]:260-4), he noted.
The Bill Marshall Award and Lecture, ESPID’s most prestigious award, is given annually to an individual recognized as having significantly advanced the field of pediatric infectious diseases. Dr. Heikkinen was singled out for his decades of work establishing that viruses, including RSV, play a key role in AOM, which had traditionally been regarded as a bacterial infection. He and his coinvestigators demonstrated that in about two-thirds of cases, AOM is actually caused by a combination of bacteria and viruses, which explains why patients’ clinical response to antibiotic therapy for AOM often is poor. They also described the chain of events whereby viral infection of the upper airway epithelium triggers an inflammatory response in the nasopharynx, with resultant Eustachian tube dysfunction and negative middle ear pressure, which in turn encourages microbial invasion of the middle ear. Moreover, they showed that the peak incidence of AOM isn’t on day 1 after onset of upper respiratory infection symptoms, but on day 3 or 4.
“What this tells us is that, once a child has a viral respiratory infection, there is a certain window of opportunity to try to prevent the development of the complication if we have the right tools in place,” Dr. Heikkinen said.
He and his colleagues put this lesson to good use nearly a decade ago in a randomized, double-blind trial in which they showed that giving oseltamivir (Tamiflu) within 12 hours after onset of influenza symptoms in children aged 1-3 years reduced the subsequent incidence of AOM by 85%, compared with placebo (Clin Infect Dis. 2010 Oct 15;51[8]:887-94).
These observations paved the way for the ongoing intensive research effort exploring ways of preventing AOM through interventions at two different levels: by developing viral vaccines to prevent a healthy child from contracting the viral upper respiratory infection that precedes AOM and by coming up with antiviral drugs or bacterial vaccines to prevent a upper respiratory infection from evolving into AOM.
The same applies to pneumonia. Other investigators showed years ago that both respiratory viruses and bacteria were present in two-thirds of sputum samples obtained from children with community-acquired pneumonia (Clin Microbiol Infect. 2012 Mar;18[3]:300-7).
RSV is the top cause of hospitalization for acute respiratory infection – pneumonia and bronchiolitis – in infants. Worldwide, it’s estimated that RSV accounts for more than 33 million episodes of pneumonia annually, with 3.2 million hospitalizations and 118,200 deaths.
Beyond the hospital, however, Dr. Heikkinen and colleagues conducted a prospective cohort study in Turku over the course of two consecutive respiratory infection seasons in which they captured the huge burden of RSV as an outpatient illness. It hit hardest in children younger than 3 years, in whom the average annual incidence of RSV infection was 275 cases per 1,000 children. In that youngest age population, RSV upper respiratory infection was followed by AOM 58% of the time, with antibiotics prescribed in 66% of the cases of this complication of RSV illness. The mean duration of RSV illness was greatest in this young age group, at 13 days, and it was associated with parental absenteeism from work at a rate of 136 days per 100 children with RSV illness.
Moreover, while AOM occurred less frequently in children aged 3-6 years, 46% of the cases were attributed to a preceding RSV infection, which led to antibiotic treatment nearly half of the time (J Infect Dis. 2017 Jan 1;215[1]:17-23). This documentation has spurred further efforts to develop RSV vaccines and antivirals.
He reported serving as a consultant to a half-dozen pharmaceutical companies, as well as having received research funding from Janssen, GlaxoSmithKline, and Novavax.
LJUBLJANA, SLOVENIA – Prevention or early effective treatment of respiratory syncytial virus (RSV) infection in infants and small children holds the promise of sharply reduced burdens of both acute otitis media (AOM) and pneumonia, Terho Heikkinen, MD, PhD, predicted in the Bill Marshall Award Lecture presented at the annual meeting of the European Society for Paediatric Infectious Diseases (ESPID).
RSV is by far the hottest virus in the world,” declared Dr. Heikkinen, professor of pediatrics at the University of Turku (Finland).
“A lot of progress is being made with respect to RSV. This increased understanding holds great promise for new interventions,” he explained. “Lots of different types of vaccines are being developed, monoclonal antibodies, antivirals. So
Today influenza is the only respiratory viral infection that’s preventable via vaccine or effectively treatable using antiviral drugs. That situation has to change, as Dr. Heikkinen demonstrated early in his career; RSV is the respiratory virus that’s most likely to invade the middle ear during AOM. It’s much more ototropic than influenza, parainfluenza, enteroviruses, or adenoviruses (N Engl J Med. 1999 Jan 28;340[4]:260-4), he noted.
The Bill Marshall Award and Lecture, ESPID’s most prestigious award, is given annually to an individual recognized as having significantly advanced the field of pediatric infectious diseases. Dr. Heikkinen was singled out for his decades of work establishing that viruses, including RSV, play a key role in AOM, which had traditionally been regarded as a bacterial infection. He and his coinvestigators demonstrated that in about two-thirds of cases, AOM is actually caused by a combination of bacteria and viruses, which explains why patients’ clinical response to antibiotic therapy for AOM often is poor. They also described the chain of events whereby viral infection of the upper airway epithelium triggers an inflammatory response in the nasopharynx, with resultant Eustachian tube dysfunction and negative middle ear pressure, which in turn encourages microbial invasion of the middle ear. Moreover, they showed that the peak incidence of AOM isn’t on day 1 after onset of upper respiratory infection symptoms, but on day 3 or 4.
“What this tells us is that, once a child has a viral respiratory infection, there is a certain window of opportunity to try to prevent the development of the complication if we have the right tools in place,” Dr. Heikkinen said.
He and his colleagues put this lesson to good use nearly a decade ago in a randomized, double-blind trial in which they showed that giving oseltamivir (Tamiflu) within 12 hours after onset of influenza symptoms in children aged 1-3 years reduced the subsequent incidence of AOM by 85%, compared with placebo (Clin Infect Dis. 2010 Oct 15;51[8]:887-94).
These observations paved the way for the ongoing intensive research effort exploring ways of preventing AOM through interventions at two different levels: by developing viral vaccines to prevent a healthy child from contracting the viral upper respiratory infection that precedes AOM and by coming up with antiviral drugs or bacterial vaccines to prevent a upper respiratory infection from evolving into AOM.
The same applies to pneumonia. Other investigators showed years ago that both respiratory viruses and bacteria were present in two-thirds of sputum samples obtained from children with community-acquired pneumonia (Clin Microbiol Infect. 2012 Mar;18[3]:300-7).
RSV is the top cause of hospitalization for acute respiratory infection – pneumonia and bronchiolitis – in infants. Worldwide, it’s estimated that RSV accounts for more than 33 million episodes of pneumonia annually, with 3.2 million hospitalizations and 118,200 deaths.
Beyond the hospital, however, Dr. Heikkinen and colleagues conducted a prospective cohort study in Turku over the course of two consecutive respiratory infection seasons in which they captured the huge burden of RSV as an outpatient illness. It hit hardest in children younger than 3 years, in whom the average annual incidence of RSV infection was 275 cases per 1,000 children. In that youngest age population, RSV upper respiratory infection was followed by AOM 58% of the time, with antibiotics prescribed in 66% of the cases of this complication of RSV illness. The mean duration of RSV illness was greatest in this young age group, at 13 days, and it was associated with parental absenteeism from work at a rate of 136 days per 100 children with RSV illness.
Moreover, while AOM occurred less frequently in children aged 3-6 years, 46% of the cases were attributed to a preceding RSV infection, which led to antibiotic treatment nearly half of the time (J Infect Dis. 2017 Jan 1;215[1]:17-23). This documentation has spurred further efforts to develop RSV vaccines and antivirals.
He reported serving as a consultant to a half-dozen pharmaceutical companies, as well as having received research funding from Janssen, GlaxoSmithKline, and Novavax.
EXPERT ANALYSIS FROM ESPID 2019
Chronic opioid use may be common in patients with ankylosing spondylitis
About a quarter of all patients with ankylosing spondylitis, and more than half of those patients who were on Medicaid, received at least a 90-day supply of opioids in a year, based on an analysis of U.S. commercial claims data.

The findings were noted in 2012-2017 data from a cohort of 11,945 patients in the Truven Health MarketScan Research database. Of those patients given the International Classification of Diseases (ICD) code 720.0, which is specific for ankylosing spondylitis, 23.5% of patients chronically used opioids. In the broader 720.x commercial claims cohort of 79,190 patients, the proportion who chronically used opioids was 27.3%.
More than 60% of the patients who chronically used opioids had a cumulative drug supply of 270 days or more.
“Patients with ankylosing spondylitis receive opioids with disturbing frequency,” said study author Victor S. Sloan, MD, and research colleagues in the June issue of the Journal of Rheumatology. Ankylosing spondylitis treatment guidelines “specify use of an NSAID as initial pharmacotherapy, with anti-TNF [tumor necrosis factor] therapy in cases of NSAID inefficacy or intolerance. However, for many patients, prescription opioids – while not addressing the underlying inflammation – may offer an inexpensive and rapid means of achieving symptomatic relief.”
Patients who chronically used opioids were more likely to have depression (25.4% vs. 12.5%) and anxiety (20.9% vs. 11.7%) during the baseline period of the study. Patients with chronic opioid use also were more likely to receive muscle relaxants (54.4% vs. 20.2%) and oral corticosteroids (18.4% vs. 9.6%), compared with patients without chronic opioid use, reported Dr. Sloan, vice president and immunology development strategy lead for UCB Pharma and of the Rutgers Robert Wood Johnson Medical School in New Brunswick, N.J., and colleagues.
Claims for anti-TNF therapies, disease-modifying antirheumatic drugs (DMARDs), and NSAIDs were similar for patients with and without chronic opioid use.
The patients in the study had claims with the specified diagnosis codes during Jan. 1, 2013–March 31, 2016 and were enrolled in medical and pharmacy benefits for 12 months before and after the first qualifying ICD code. The study excluded patients with a history of cancer other than nonmelanoma skin cancer. Opioid claims within 7 days of a hospitalization or 2 days of an emergency department or urgent care visit were not included.
The investigators assessed patients’ demographics, clinical characteristics, comorbidities, and prior treatments during a 12-month baseline period prior to the index date. They examined opioid use and exposure to other treatments during a 12-month follow-up period after the index date. They defined chronic opioid use as at least 90 cumulative days of opioid use based on the supply value on opioid pharmacy claims. They summed the days’ supply for all opioid claims during the follow-up period.
Chronic use of opioids was most pronounced in the 917 patients with Medicaid claims with 720.0 diagnosis codes; 57.1% chronically used opioids during follow-up. Among 14,041 patients with Medicaid claims with 720.x codes, 76.7% chronically used opioids.
The data suggest that some patients may receive opioids before they receive recommended therapies. “If this is the case, there may be an opportunity to prevent chronic opioid use by intervening with recommended therapies earlier in the patient’s treatment course,” the authors wrote.
Dr. Sloan and colleagues noted that they had limited information about the timing of opioid use relative to ankylosing spondylitis diagnosis, opioid potency and dose, and the indication for which opioids were prescribed.
UCB Pharma funded the study. The authors are employees of UCB Pharma.
SOURCE: Sloan VS et al. J Rheumatol. 2019 Jan 15. doi: 10.3899/jrheum.180972.
About a quarter of all patients with ankylosing spondylitis, and more than half of those patients who were on Medicaid, received at least a 90-day supply of opioids in a year, based on an analysis of U.S. commercial claims data.
The findings were noted in 2012-2017 data from a cohort of 11,945 patients in the Truven Health MarketScan Research database. Of those patients given the International Classification of Diseases (ICD) code 720.0, which is specific for ankylosing spondylitis, 23.5% of patients chronically used opioids. In the broader 720.x commercial claims cohort of 79,190 patients, the proportion who chronically used opioids was 27.3%.
More than 60% of the patients who chronically used opioids had a cumulative drug supply of 270 days or more.
“Patients with ankylosing spondylitis receive opioids with disturbing frequency,” said study author Victor S. Sloan, MD, and research colleagues in the June issue of the Journal of Rheumatology. Ankylosing spondylitis treatment guidelines “specify use of an NSAID as initial pharmacotherapy, with anti-TNF [tumor necrosis factor] therapy in cases of NSAID inefficacy or intolerance. However, for many patients, prescription opioids – while not addressing the underlying inflammation – may offer an inexpensive and rapid means of achieving symptomatic relief.”
Patients who chronically used opioids were more likely to have depression (25.4% vs. 12.5%) and anxiety (20.9% vs. 11.7%) during the baseline period of the study. Patients with chronic opioid use also were more likely to receive muscle relaxants (54.4% vs. 20.2%) and oral corticosteroids (18.4% vs. 9.6%), compared with patients without chronic opioid use, reported Dr. Sloan, vice president and immunology development strategy lead for UCB Pharma and of the Rutgers Robert Wood Johnson Medical School in New Brunswick, N.J., and colleagues.
Claims for anti-TNF therapies, disease-modifying antirheumatic drugs (DMARDs), and NSAIDs were similar for patients with and without chronic opioid use.
The patients in the study had claims with the specified diagnosis codes during Jan. 1, 2013–March 31, 2016 and were enrolled in medical and pharmacy benefits for 12 months before and after the first qualifying ICD code. The study excluded patients with a history of cancer other than nonmelanoma skin cancer. Opioid claims within 7 days of a hospitalization or 2 days of an emergency department or urgent care visit were not included.
The investigators assessed patients’ demographics, clinical characteristics, comorbidities, and prior treatments during a 12-month baseline period prior to the index date. They examined opioid use and exposure to other treatments during a 12-month follow-up period after the index date. They defined chronic opioid use as at least 90 cumulative days of opioid use based on the supply value on opioid pharmacy claims. They summed the days’ supply for all opioid claims during the follow-up period.
Chronic use of opioids was most pronounced in the 917 patients with Medicaid claims with 720.0 diagnosis codes; 57.1% chronically used opioids during follow-up. Among 14,041 patients with Medicaid claims with 720.x codes, 76.7% chronically used opioids.
The data suggest that some patients may receive opioids before they receive recommended therapies. “If this is the case, there may be an opportunity to prevent chronic opioid use by intervening with recommended therapies earlier in the patient’s treatment course,” the authors wrote.
Dr. Sloan and colleagues noted that they had limited information about the timing of opioid use relative to ankylosing spondylitis diagnosis, opioid potency and dose, and the indication for which opioids were prescribed.
UCB Pharma funded the study. The authors are employees of UCB Pharma.
SOURCE: Sloan VS et al. J Rheumatol. 2019 Jan 15. doi: 10.3899/jrheum.180972.
About a quarter of all patients with ankylosing spondylitis, and more than half of those patients who were on Medicaid, received at least a 90-day supply of opioids in a year, based on an analysis of U.S. commercial claims data.
The findings were noted in 2012-2017 data from a cohort of 11,945 patients in the Truven Health MarketScan Research database. Of those patients given the International Classification of Diseases (ICD) code 720.0, which is specific for ankylosing spondylitis, 23.5% of patients chronically used opioids. In the broader 720.x commercial claims cohort of 79,190 patients, the proportion who chronically used opioids was 27.3%.
More than 60% of the patients who chronically used opioids had a cumulative drug supply of 270 days or more.
“Patients with ankylosing spondylitis receive opioids with disturbing frequency,” said study author Victor S. Sloan, MD, and research colleagues in the June issue of the Journal of Rheumatology. Ankylosing spondylitis treatment guidelines “specify use of an NSAID as initial pharmacotherapy, with anti-TNF [tumor necrosis factor] therapy in cases of NSAID inefficacy or intolerance. However, for many patients, prescription opioids – while not addressing the underlying inflammation – may offer an inexpensive and rapid means of achieving symptomatic relief.”
Patients who chronically used opioids were more likely to have depression (25.4% vs. 12.5%) and anxiety (20.9% vs. 11.7%) during the baseline period of the study. Patients with chronic opioid use also were more likely to receive muscle relaxants (54.4% vs. 20.2%) and oral corticosteroids (18.4% vs. 9.6%), compared with patients without chronic opioid use, reported Dr. Sloan, vice president and immunology development strategy lead for UCB Pharma and of the Rutgers Robert Wood Johnson Medical School in New Brunswick, N.J., and colleagues.
Claims for anti-TNF therapies, disease-modifying antirheumatic drugs (DMARDs), and NSAIDs were similar for patients with and without chronic opioid use.
The patients in the study had claims with the specified diagnosis codes during Jan. 1, 2013–March 31, 2016 and were enrolled in medical and pharmacy benefits for 12 months before and after the first qualifying ICD code. The study excluded patients with a history of cancer other than nonmelanoma skin cancer. Opioid claims within 7 days of a hospitalization or 2 days of an emergency department or urgent care visit were not included.
The investigators assessed patients’ demographics, clinical characteristics, comorbidities, and prior treatments during a 12-month baseline period prior to the index date. They examined opioid use and exposure to other treatments during a 12-month follow-up period after the index date. They defined chronic opioid use as at least 90 cumulative days of opioid use based on the supply value on opioid pharmacy claims. They summed the days’ supply for all opioid claims during the follow-up period.
Chronic use of opioids was most pronounced in the 917 patients with Medicaid claims with 720.0 diagnosis codes; 57.1% chronically used opioids during follow-up. Among 14,041 patients with Medicaid claims with 720.x codes, 76.7% chronically used opioids.
The data suggest that some patients may receive opioids before they receive recommended therapies. “If this is the case, there may be an opportunity to prevent chronic opioid use by intervening with recommended therapies earlier in the patient’s treatment course,” the authors wrote.
Dr. Sloan and colleagues noted that they had limited information about the timing of opioid use relative to ankylosing spondylitis diagnosis, opioid potency and dose, and the indication for which opioids were prescribed.
UCB Pharma funded the study. The authors are employees of UCB Pharma.
SOURCE: Sloan VS et al. J Rheumatol. 2019 Jan 15. doi: 10.3899/jrheum.180972.
FROM THE JOURNAL OF RHEUMATOLOGY
Nivo/ipi shrinks early NSCLC before surgery
CHICAGO – Two immune checkpoint inhibitors were better than one as neoadjuvant therapy for patients with resectable early-stage non–small cell lung cancer (NSCLC) in the phase 2 NEOSTAR trial.

Among 44 patients with stage I-IIIA NSCLC who were randomized to either a combination of nivolumab (Opdivo) and ipilimumab (Yervoy) or to nivolumab alone, the combination was associated with higher rates of the primary endpoint of major pathological response (MPR), defined as a reduction in viable tumors cells to 10% or less, reported Tina Cascone, MD, PhD, from the University of Texas MD Anderson Cancer Center in Houston.
“Nivolumab/ipilimumab induced a 44% MPR rate in resected patients, met the trial prespecified boundary with seven MPRs in the intention-to-treat population, and induced pathologic complete responses in 38% of resected patients,” she said at the annual meeting of the American Society of Clinical Oncology.
To test whether neoadjuvant monotherapy or combination therapy could improve outcomes of standard induction chemotherapy, NEOSTAR investigators enrolled patients with NSCLC stage I-IIIA, including patients with a single involved mediastinal node (N2 single station) who were eligible for surgical resection.
The patients were randomized on a 1:1 basis to receive nivolumab 3 mg/kg on days 1, 15 and 29 alone or in combination with ipilimumab delivered 1 mg/kg on day 1, followed by surgery 3-6 weeks after the last study dose and then postoperative standard-of-care chemotherapy.
Of 53 patients screened, 44 were eligible, with 23 randomized to nivolumab monotherapy and 21 randomized to nivolumab/ipilimumab. Of this group, five did not proceed to surgery (one in the monotherapy arm, four in the combination arm) because of either high surgical risk, lack of respectability, or refusal of surgery. The mean age at randomization was 65.6 years. In all, 18% were never smokers, and the remaining 82% were former or current smokers.
The MPR rate in the intention-to-treat population – the primary endpoint – was reached in four patients (17%) in the monotherapy arm and in seven patients (33%) in the combination arm. As noted, the combination arm reached the prespecified boundary of six or more patients with an MPR. All patients in each arm who had an MPR also had a pathologic complete responses.
Of the 39 patients who went on to resection, 37 were evaluable, and in these patients the respective MPR rates were 19% and 44%. Two patients on nivolumab alone and six on nivolumab plus ipilimumab had 0% viable tumor detectable at the time of surgery. Radiographic responses included one complete response in the combination arm and eight total partial responses, in five and three patients, respectively. The objective response rated was 20%. The responses, assessed by Response Evaluation Criteria in Solid Tumors (RECIST) were positively associated with MPR, Dr. Cascone said.
In 11% of patients, the investigators observed apparent radiographic progression after neoadjuvant immune checkpoint inhibitors in mediastinal and or in nonregional nodes. However, pathological assessment and evaluation of the flaring nodes did not reveal evidence of disease, but instead showed noncaseating granulomas that were not present at baseline.
“Awareness of this phenomenon, which we named the ‘nodal immune flare,’ is of critical importance, as if the clinician fails to distinguish the nodal immune flare from disease progression, potential curative surgery for these patients could be avoided,” she said.
Grade 1 or 2 treatment-related adverse events included rash, itching, fatigue, anemia, cough, and diarrhea. Grade 3 or greater treatment-related adverse events included hypoxia, pneumonia, and pneumonitis in the nivolumab monotherapy arm and diarrhea and hyponatremia in the combination group. One patient treated with nivolumab monotherapy, who had achieved 0% viable tumor, had grade 3 pneumonia and pneumonitis, which was treated with steroids that impeded the healing of a bronchopleural fistula and subsequent empyema. Other surgical complications included air leaks, which occurred in five patients in the nivolumab group and three in the nivolumab plus ipilimumab arm.
Two patients died, one in the monotherapy arm from steroid-treated pneumonitis 4.1 months after randomization and one in the combination arm who had progressive disease 2 months after randomization, and died from the disease 15 months later.
Invited discussant Maximilian Diehn, MD, PhD, from Stanford (California) University School of Medicine, commented that the choice of neoadjuvant immunotherapy was not based on molecular markers, “and I think we have a major unmet need for developing biomarkers for personalized treatment in this area.
“Ideally, the biomarkers that we would have in this setting would, A, allow us to identify which patients have micrometastatic disease and therefore are likely to benefit from the upfront systemic therapy and, secondly, also could tell us which neoadjuvant therapy they would respond to, be it immunotherapy, chemotherapy, or the combination,” he added.
The study was supported by Bristol-Myers Squibb. Dr. Cascone disclosed honoraria from the company. Dr. Diehn reported stock ownership, consulting, research funding and travel expenses from various companies.
SOURCE: Cascone T. et al. ASCO 2019, Abstract 8504.
CHICAGO – Two immune checkpoint inhibitors were better than one as neoadjuvant therapy for patients with resectable early-stage non–small cell lung cancer (NSCLC) in the phase 2 NEOSTAR trial.
Among 44 patients with stage I-IIIA NSCLC who were randomized to either a combination of nivolumab (Opdivo) and ipilimumab (Yervoy) or to nivolumab alone, the combination was associated with higher rates of the primary endpoint of major pathological response (MPR), defined as a reduction in viable tumors cells to 10% or less, reported Tina Cascone, MD, PhD, from the University of Texas MD Anderson Cancer Center in Houston.
“Nivolumab/ipilimumab induced a 44% MPR rate in resected patients, met the trial prespecified boundary with seven MPRs in the intention-to-treat population, and induced pathologic complete responses in 38% of resected patients,” she said at the annual meeting of the American Society of Clinical Oncology.
To test whether neoadjuvant monotherapy or combination therapy could improve outcomes of standard induction chemotherapy, NEOSTAR investigators enrolled patients with NSCLC stage I-IIIA, including patients with a single involved mediastinal node (N2 single station) who were eligible for surgical resection.
The patients were randomized on a 1:1 basis to receive nivolumab 3 mg/kg on days 1, 15 and 29 alone or in combination with ipilimumab delivered 1 mg/kg on day 1, followed by surgery 3-6 weeks after the last study dose and then postoperative standard-of-care chemotherapy.
Of 53 patients screened, 44 were eligible, with 23 randomized to nivolumab monotherapy and 21 randomized to nivolumab/ipilimumab. Of this group, five did not proceed to surgery (one in the monotherapy arm, four in the combination arm) because of either high surgical risk, lack of respectability, or refusal of surgery. The mean age at randomization was 65.6 years. In all, 18% were never smokers, and the remaining 82% were former or current smokers.
The MPR rate in the intention-to-treat population – the primary endpoint – was reached in four patients (17%) in the monotherapy arm and in seven patients (33%) in the combination arm. As noted, the combination arm reached the prespecified boundary of six or more patients with an MPR. All patients in each arm who had an MPR also had a pathologic complete responses.
Of the 39 patients who went on to resection, 37 were evaluable, and in these patients the respective MPR rates were 19% and 44%. Two patients on nivolumab alone and six on nivolumab plus ipilimumab had 0% viable tumor detectable at the time of surgery. Radiographic responses included one complete response in the combination arm and eight total partial responses, in five and three patients, respectively. The objective response rated was 20%. The responses, assessed by Response Evaluation Criteria in Solid Tumors (RECIST) were positively associated with MPR, Dr. Cascone said.
In 11% of patients, the investigators observed apparent radiographic progression after neoadjuvant immune checkpoint inhibitors in mediastinal and or in nonregional nodes. However, pathological assessment and evaluation of the flaring nodes did not reveal evidence of disease, but instead showed noncaseating granulomas that were not present at baseline.
“Awareness of this phenomenon, which we named the ‘nodal immune flare,’ is of critical importance, as if the clinician fails to distinguish the nodal immune flare from disease progression, potential curative surgery for these patients could be avoided,” she said.
Grade 1 or 2 treatment-related adverse events included rash, itching, fatigue, anemia, cough, and diarrhea. Grade 3 or greater treatment-related adverse events included hypoxia, pneumonia, and pneumonitis in the nivolumab monotherapy arm and diarrhea and hyponatremia in the combination group. One patient treated with nivolumab monotherapy, who had achieved 0% viable tumor, had grade 3 pneumonia and pneumonitis, which was treated with steroids that impeded the healing of a bronchopleural fistula and subsequent empyema. Other surgical complications included air leaks, which occurred in five patients in the nivolumab group and three in the nivolumab plus ipilimumab arm.
Two patients died, one in the monotherapy arm from steroid-treated pneumonitis 4.1 months after randomization and one in the combination arm who had progressive disease 2 months after randomization, and died from the disease 15 months later.
Invited discussant Maximilian Diehn, MD, PhD, from Stanford (California) University School of Medicine, commented that the choice of neoadjuvant immunotherapy was not based on molecular markers, “and I think we have a major unmet need for developing biomarkers for personalized treatment in this area.
“Ideally, the biomarkers that we would have in this setting would, A, allow us to identify which patients have micrometastatic disease and therefore are likely to benefit from the upfront systemic therapy and, secondly, also could tell us which neoadjuvant therapy they would respond to, be it immunotherapy, chemotherapy, or the combination,” he added.
The study was supported by Bristol-Myers Squibb. Dr. Cascone disclosed honoraria from the company. Dr. Diehn reported stock ownership, consulting, research funding and travel expenses from various companies.
SOURCE: Cascone T. et al. ASCO 2019, Abstract 8504.
CHICAGO – Two immune checkpoint inhibitors were better than one as neoadjuvant therapy for patients with resectable early-stage non–small cell lung cancer (NSCLC) in the phase 2 NEOSTAR trial.
Among 44 patients with stage I-IIIA NSCLC who were randomized to either a combination of nivolumab (Opdivo) and ipilimumab (Yervoy) or to nivolumab alone, the combination was associated with higher rates of the primary endpoint of major pathological response (MPR), defined as a reduction in viable tumors cells to 10% or less, reported Tina Cascone, MD, PhD, from the University of Texas MD Anderson Cancer Center in Houston.
“Nivolumab/ipilimumab induced a 44% MPR rate in resected patients, met the trial prespecified boundary with seven MPRs in the intention-to-treat population, and induced pathologic complete responses in 38% of resected patients,” she said at the annual meeting of the American Society of Clinical Oncology.
To test whether neoadjuvant monotherapy or combination therapy could improve outcomes of standard induction chemotherapy, NEOSTAR investigators enrolled patients with NSCLC stage I-IIIA, including patients with a single involved mediastinal node (N2 single station) who were eligible for surgical resection.
The patients were randomized on a 1:1 basis to receive nivolumab 3 mg/kg on days 1, 15 and 29 alone or in combination with ipilimumab delivered 1 mg/kg on day 1, followed by surgery 3-6 weeks after the last study dose and then postoperative standard-of-care chemotherapy.
Of 53 patients screened, 44 were eligible, with 23 randomized to nivolumab monotherapy and 21 randomized to nivolumab/ipilimumab. Of this group, five did not proceed to surgery (one in the monotherapy arm, four in the combination arm) because of either high surgical risk, lack of respectability, or refusal of surgery. The mean age at randomization was 65.6 years. In all, 18% were never smokers, and the remaining 82% were former or current smokers.
The MPR rate in the intention-to-treat population – the primary endpoint – was reached in four patients (17%) in the monotherapy arm and in seven patients (33%) in the combination arm. As noted, the combination arm reached the prespecified boundary of six or more patients with an MPR. All patients in each arm who had an MPR also had a pathologic complete responses.
Of the 39 patients who went on to resection, 37 were evaluable, and in these patients the respective MPR rates were 19% and 44%. Two patients on nivolumab alone and six on nivolumab plus ipilimumab had 0% viable tumor detectable at the time of surgery. Radiographic responses included one complete response in the combination arm and eight total partial responses, in five and three patients, respectively. The objective response rated was 20%. The responses, assessed by Response Evaluation Criteria in Solid Tumors (RECIST) were positively associated with MPR, Dr. Cascone said.
In 11% of patients, the investigators observed apparent radiographic progression after neoadjuvant immune checkpoint inhibitors in mediastinal and or in nonregional nodes. However, pathological assessment and evaluation of the flaring nodes did not reveal evidence of disease, but instead showed noncaseating granulomas that were not present at baseline.
“Awareness of this phenomenon, which we named the ‘nodal immune flare,’ is of critical importance, as if the clinician fails to distinguish the nodal immune flare from disease progression, potential curative surgery for these patients could be avoided,” she said.
Grade 1 or 2 treatment-related adverse events included rash, itching, fatigue, anemia, cough, and diarrhea. Grade 3 or greater treatment-related adverse events included hypoxia, pneumonia, and pneumonitis in the nivolumab monotherapy arm and diarrhea and hyponatremia in the combination group. One patient treated with nivolumab monotherapy, who had achieved 0% viable tumor, had grade 3 pneumonia and pneumonitis, which was treated with steroids that impeded the healing of a bronchopleural fistula and subsequent empyema. Other surgical complications included air leaks, which occurred in five patients in the nivolumab group and three in the nivolumab plus ipilimumab arm.
Two patients died, one in the monotherapy arm from steroid-treated pneumonitis 4.1 months after randomization and one in the combination arm who had progressive disease 2 months after randomization, and died from the disease 15 months later.
Invited discussant Maximilian Diehn, MD, PhD, from Stanford (California) University School of Medicine, commented that the choice of neoadjuvant immunotherapy was not based on molecular markers, “and I think we have a major unmet need for developing biomarkers for personalized treatment in this area.
“Ideally, the biomarkers that we would have in this setting would, A, allow us to identify which patients have micrometastatic disease and therefore are likely to benefit from the upfront systemic therapy and, secondly, also could tell us which neoadjuvant therapy they would respond to, be it immunotherapy, chemotherapy, or the combination,” he added.
The study was supported by Bristol-Myers Squibb. Dr. Cascone disclosed honoraria from the company. Dr. Diehn reported stock ownership, consulting, research funding and travel expenses from various companies.
SOURCE: Cascone T. et al. ASCO 2019, Abstract 8504.
REPORTING FROM ASCO 2019
USPSTF reaffirms HIV screening recommendations
According to the task force, screening is recommended for all patients aged 15-65 years. Screening also is recommended for adolescents and older adults at increased risk for acquiring HIV infection and for all pregnant patients, including those in labor whose HIV status is unknown (JAMA. 2019. doi: 10.1001/jama.2019.6587).
Patients who are considered at increased risk for acquiring HIV include the following: Men who have sex with men, those who inject drugs, those who have receptive sex without a condom, those with at least one partner whose HIV status is positive or unknown, those who have transactional sex, and those who request testing for sexually transmitted infection, including HIV. All recommendations are A-level, meaning the task force recommends the service,with high certainty that the net benefit is substantial.
In a systematic review created for the task force, Roger Chou, MD, of Oregon Health & Science University, Portland, and colleagues found there continued to be no studies that examined the benefits and harms of HIV screening for HIV infections, compared with no screening, but new evidence found beginning antiretroviral therapy (ART) for patients with CD4 cell counts greater than 500/mm3 who are otherwise asymptomatic was associated with a reduced risk of mortality, compared with waiting for ART in cases of CD4 cell counts less than 350/mm3 (JAMA. 2019. doi: 10.1001/jama.2019.2592).
A second systematic review of pregnant patients by Shelley S. Selph, MD, also of Oregon Health & Science University, Portland, and colleagues found no studies examining the effectiveness of prenatal screening on mother-to-child HIV transmission, but combination ART was significantly effective at reducing transmission between mother and child, while ART that includes a boosted protease inhibitor may result in preterm delivery (JAMA. 2019. doi: 10.1001/jama.2019.2593).
Although no studies have been conducted that compare the benefits of screening with not screening for HIV, the task force concluded with “high certainty” that early HIV detection and treatment has “substantial benefits.”
“Clinicians can make a real difference toward reducing the burden of HIV in the United States,” Douglas K. Owens, MD, task force chairman, said in a statement. “HIV screening and HIV prevention work to reduce new HIV infections and ultimately save lives.”
The USPSTF is a voluntary, independent body, with operations supported by the U.S. Agency for Healthcare Research and Quality. Task force members received travel reimbursement and an honorarium for attending meetings. Dr. Owens reports financial disclosures with relation to HIV infection screening, preexposure prophylaxis for HIV prevention, and hepatitis C screening. Other task force members reported no relevant conflicts of interest.
SOURCE: JAMA. 2019. doi: 10.1001/jama.2019.6587.
According to the task force, screening is recommended for all patients aged 15-65 years. Screening also is recommended for adolescents and older adults at increased risk for acquiring HIV infection and for all pregnant patients, including those in labor whose HIV status is unknown (JAMA. 2019. doi: 10.1001/jama.2019.6587).
Patients who are considered at increased risk for acquiring HIV include the following: Men who have sex with men, those who inject drugs, those who have receptive sex without a condom, those with at least one partner whose HIV status is positive or unknown, those who have transactional sex, and those who request testing for sexually transmitted infection, including HIV. All recommendations are A-level, meaning the task force recommends the service,with high certainty that the net benefit is substantial.
In a systematic review created for the task force, Roger Chou, MD, of Oregon Health & Science University, Portland, and colleagues found there continued to be no studies that examined the benefits and harms of HIV screening for HIV infections, compared with no screening, but new evidence found beginning antiretroviral therapy (ART) for patients with CD4 cell counts greater than 500/mm3 who are otherwise asymptomatic was associated with a reduced risk of mortality, compared with waiting for ART in cases of CD4 cell counts less than 350/mm3 (JAMA. 2019. doi: 10.1001/jama.2019.2592).
A second systematic review of pregnant patients by Shelley S. Selph, MD, also of Oregon Health & Science University, Portland, and colleagues found no studies examining the effectiveness of prenatal screening on mother-to-child HIV transmission, but combination ART was significantly effective at reducing transmission between mother and child, while ART that includes a boosted protease inhibitor may result in preterm delivery (JAMA. 2019. doi: 10.1001/jama.2019.2593).
Although no studies have been conducted that compare the benefits of screening with not screening for HIV, the task force concluded with “high certainty” that early HIV detection and treatment has “substantial benefits.”
“Clinicians can make a real difference toward reducing the burden of HIV in the United States,” Douglas K. Owens, MD, task force chairman, said in a statement. “HIV screening and HIV prevention work to reduce new HIV infections and ultimately save lives.”
The USPSTF is a voluntary, independent body, with operations supported by the U.S. Agency for Healthcare Research and Quality. Task force members received travel reimbursement and an honorarium for attending meetings. Dr. Owens reports financial disclosures with relation to HIV infection screening, preexposure prophylaxis for HIV prevention, and hepatitis C screening. Other task force members reported no relevant conflicts of interest.
SOURCE: JAMA. 2019. doi: 10.1001/jama.2019.6587.
According to the task force, screening is recommended for all patients aged 15-65 years. Screening also is recommended for adolescents and older adults at increased risk for acquiring HIV infection and for all pregnant patients, including those in labor whose HIV status is unknown (JAMA. 2019. doi: 10.1001/jama.2019.6587).
Patients who are considered at increased risk for acquiring HIV include the following: Men who have sex with men, those who inject drugs, those who have receptive sex without a condom, those with at least one partner whose HIV status is positive or unknown, those who have transactional sex, and those who request testing for sexually transmitted infection, including HIV. All recommendations are A-level, meaning the task force recommends the service,with high certainty that the net benefit is substantial.
In a systematic review created for the task force, Roger Chou, MD, of Oregon Health & Science University, Portland, and colleagues found there continued to be no studies that examined the benefits and harms of HIV screening for HIV infections, compared with no screening, but new evidence found beginning antiretroviral therapy (ART) for patients with CD4 cell counts greater than 500/mm3 who are otherwise asymptomatic was associated with a reduced risk of mortality, compared with waiting for ART in cases of CD4 cell counts less than 350/mm3 (JAMA. 2019. doi: 10.1001/jama.2019.2592).
A second systematic review of pregnant patients by Shelley S. Selph, MD, also of Oregon Health & Science University, Portland, and colleagues found no studies examining the effectiveness of prenatal screening on mother-to-child HIV transmission, but combination ART was significantly effective at reducing transmission between mother and child, while ART that includes a boosted protease inhibitor may result in preterm delivery (JAMA. 2019. doi: 10.1001/jama.2019.2593).
Although no studies have been conducted that compare the benefits of screening with not screening for HIV, the task force concluded with “high certainty” that early HIV detection and treatment has “substantial benefits.”
“Clinicians can make a real difference toward reducing the burden of HIV in the United States,” Douglas K. Owens, MD, task force chairman, said in a statement. “HIV screening and HIV prevention work to reduce new HIV infections and ultimately save lives.”
The USPSTF is a voluntary, independent body, with operations supported by the U.S. Agency for Healthcare Research and Quality. Task force members received travel reimbursement and an honorarium for attending meetings. Dr. Owens reports financial disclosures with relation to HIV infection screening, preexposure prophylaxis for HIV prevention, and hepatitis C screening. Other task force members reported no relevant conflicts of interest.
SOURCE: JAMA. 2019. doi: 10.1001/jama.2019.6587.
FROM JAMA
Screening for Endocrine Hypertension
Hypertension is one of the most common reasons for patient visits.1 According to the US Preventive Services Task Force, more than 70 million individuals older than 20 have hypertension, which is defined as a blood pressure (BP) of ≥ 130/85 mm Hg.2 Essential hypertension is the most common form of this condition; most affected patients will show improvement with evidence-based pharmacologic treatment, lifestyle modifications, and risk factor reductions.
For patients with refractory hypertension, however, identifying what steps to take in screening and diagnosis can be daunting for clinicians. It is important to identify cases of secondary hypertension, because if it is left undiagnosed and untreated, serious complications—such as cardiovascular and renal disease—are likely to occur.3,4
Secondary hypertension can be caused by myriad disease states and disorders, including endocrine disorders, renal disease, neurologic disorders, acute stress, and drug-induced hypertension.5 Endocrine hypertension is most commonly caused by adrenal gland disorders, including primary aldosteronism, Cushing syndrome, and pheochromocytoma. (Of note, Cushing syndrome is caused by glucocorticoid-secreting adrenal tumors, while Cushing disease is a condition in which there is glucocorticoid excess caused by oversecretion of pituitary adrenocorticotropic hormone.6 Cushing disease is more common than Cushing syndrome, which is rare.7) While nonadrenal endocrine disorders are not as common, they pose significant health issues, including growth hormone excess or deficiency, thyroid disorders, testosterone deficiency, obesity, insulin resistance, and metabolic syndrome.8
Understanding the endocrine causes of hypertension is a valuable resource for clinicians to have in their toolbox. Although the negative consequences of endocrine disorders are significant, these conditions are often recognizable, and pharmacologic treatment and/or surgical interventions can potentially resolve or improve hypertension and reduce risk for other comorbidities. This article summarizes screening and diagnosis guidelines for several possible causes of endocrine hypertension: primary aldosteronism, Cushing syndrome, and pheochromocytoma.
PRIMARY ALDOSTERONISM
Primary aldosteronism occurs in 5% to 10% of all hypertensive patients and is a common cause of secondary and endocrine hypertension (although in younger—particularly female—patients, it most commonly causes renal artery stenosis).9,10 Historically, primary aldosteronism was considered rare and not generally included in a differential diagnosis for patients presenting with resistant hypertension. However, clinical investigations have indicated that primary aldosteronism is more prevalent than previously thought.11
Patients develop this condition when there is increased aldosterone production independent of the renin-angiotensin system. The resulting sodium retention can lead to hypertension, hypokalemia, and high plasma aldosterone/renin ratio (ARR).12 Clinical findings and symptoms can be vague, increasing the difficulty in identifying primary aldosteronism as the diagnosis. Patients may be asymptomatic, with the only abnormal lab finding being hypokalemia (an infrequent finding, affecting < 25% of patients).13 If hypokalemia is present, symptoms can include nocturia, polyuria, muscle weakness, cramps, paresthesias, and palpitations.11
The Endocrine Society has identified 8 characteristics that increase the likelihood of primary aldosteronism. Patients require further screening if they
- Have a sustained elevated BP (≥ 150 mm Hg [systolic] and/or 100 mm Hg [diastolic])
- Have hypertension (BP > 140/90 mm Hg) that is resistant to 3 conventional antihypertensive drugs, including a diuretic
- Have controlled BP (BP < 140/90 mm Hg) with ≥ 4 antihypertensive drugs
- Have hypertension and spontaneous or diuretic-induced hypokalemia
- Have hypertension and adrenal incidentaloma
- Have hypertension and obstructive sleep apnea
- Have hypertension and a family history of early-onset hypertension or a cerebrovascular accident at a young age (< 40 years)
- Are hypertensive and a first-degree relative of a patient with primary aldosteronism.14
Continue to: The most reliable screening test...
The most reliable screening test for primary aldosterone is the ARR, although false-negative and false-positive results are possible.11 False-negative results can be caused by dietary salt restriction, hypokalemia, and use of medications including diuretics, calcium channel blockers, ACE inhibitors, and angiotensin receptor antagonists. Use of ß-adrenergic blockers, α-methyldopa, or NSAIDs can cause false-positive results.15 Patients should be encouraged to follow a liberal sodium diet before ARR testing, and efforts to correct hypokalemia should be implemented. Before ARR is measured, diuretics (specifically spironolactone) should be stopped for at least 4 weeks; other possible interfering medications should be stopped for at least 2 weeks.16
The ARR should be obtained multiple times to confirm elevated readings.16 Reference ranges vary, but generally plasma aldosterone concentrations > 20 ng/dL and plasma renin activity < 1 ng/mL/h indicate whether confirmatory testing should be completed.14 Further confirmatory testing can be achieved with efforts to suppress plasma aldosterone to < 10 ng/dL after an IV infusion of 2 L isotonic saline over 4 hours.12 Oral sodium load is used as well and usually before IV infusion.
CUSHING SYNDROME
Cushing syndrome is caused by excess circulating levels of glucocorticoids and affects < 0.1% of the world population.17 Signs and symptoms include centripetal obesity, moon facies, facial plethora, easy bruising, buffalo hump (or posterior cervical fat pad), hirsutism, and wide-purple striae.18 Up to 80% of these patients also have hypertension.19 If these patients have chronic exposure to high levels of glucocorticoid (the most common source being therapeutic administration of exogenous glucocorticoids), multiple complications can occur.6,20
The Endocrine Society Clinical Practice Guideline recommends the following patient groups be tested for Cushing syndrome:
- Young patients with unusual medical conditions, such as osteoporosis and resistant hypertension
- Patients with classic signs and symptoms, such as easy bruising, weight gain, facial plethora, and purple striae
- Children with decreasing height percentile and increasing weight
- Patients with adrenal incidentaloma compatible with adenoma.18
If Cushing syndrome is suspected, 1 of the following 3 initial tests can be completed: 24-hour, urine-free cortisol and creatinine; late-night salivary cortisol; or 1-mg overnight dexamethasone suppression test. Two of these tests must have abnormal results for confirmation before appropriate pituitary or adrenal imaging. If a patient has clinical features indicating Cushing syndrome but test results are normal, he or she should be referred to an endocrinologist. If a patient has ≥ 2 normal tests and probability of Cushing syndrome is unlikely, patients should be recommended for follow-up in 6 months to evaluate for any worsening of symptoms.18
Continue to: PHEOCHROMOCYTOMA
PHEOCHROMOCYTOMA
Pheochromocytoma is a condition in which there is secretion of excess catecholamines, epinephrine, norepinephrine, and dopamine due to a tumor of the adrenal medulla.21 This is a rare disease and accounts for only 0.2% to 0.6% of all causes of hypertension.22 Hypertension (persistent or paroxysmal) is the most common finding for patients with pheochromocytoma, with 80% to 90% presenting with this finding.23 It is important to note that approximately 10% of these patients will be normotensive. Three of the condition’s classic symptoms are headache, sweating, and palpitations.24 Additional symptoms include anxiety, sense of impending doom, fever, nausea, or vomiting.21
If left untreated, there is risk for hypertensive retinopathy, nephropathy, myocardial infarction, stroke from cerebral infarction, intracranial hemorrhage, or embolism.25 Due to the high rate of morbidity and mortality with untreated pheochromocytoma, laboratory testing should be initiated immediately upon suspicion of this diagnosis or if the patient has relevant family history.11
Patients should be screened for pheochromocytoma if they have ≥ 1 of the following factors:
- Resistant hypertension and hyperadrenergic symptoms (palpitations, perspiration, pallor, or headache)
- Family history of pheochromocytoma
- Any genetic syndrome with a known association to pheochromocytoma
- An adrenal mass that is > 4 cm, is cystic, or has hemorrhagic changes.19
Pheochromocytoma is diagnosed by identifying high concentrations of plasma-free metanephrines or 24-hour fractionated metanephrines and catecholamines. Some medications can interfere with the accuracy of lab results and therefore may need to be temporarily stopped; it is important to check the specific lab guidelines and review the patient’s medication lists before tests are ordered and conducted.25
ALWAYS SCREEN THE PATIENT
Although the causes of endocrine-related hypertension are very rare, screening for endocrine hypertension in patients who present with signs and symptoms of these conditions can greatly improve their lives. The endocrine disorders discussed in this article can be treated or controlled with appropriate diagnosis and treatment. In addition, resolving uncontrolled hypertension by addressing endocrine disorders can reduce the risk for long-term sequelae. It is important for clinicians to consider referral to an endocrine specialist if a patient has endocrine-related hypertension. In particular, patients with pheochromocytoma require quick referral due to a risk for high morbidity and mortality if left untreated.11
1. Smith MA, Schrager S, WinklerPrins V. Essentials of Family Medicine. 7th ed. Baltimore, MD: Lipincott Williams & Wilkins; 2019.
2. US Preventive Services Task Force. High blood pressure in adults: screening [final recommendation statement]. www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/high-blood-pressure-in-adults-screening. Accessed May 20, 2019.
3. Puar T, Mok Y, Debajyoti R, et al. Secondary hypertension in adults. Singapore Med J. 2016;57:228-232.
4. Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet. 2015;386:801-812.
5. Faselis C, Doumas M, Papademetriou V. Common secondary causes of resistant hypertension and rational for treatment. Int J Hypertens. 2010;2011: doi: 10.4061/2011/236239.
6. Else T, Hammer GD. Disorders of the Adrenal Cortex. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.
7. Nieman L, Swearingen B; the Pituitary Society. Cushing’s syndrome and Cushing’s disease: your questions answered. www.pituitarysociety.org/sites/all/pdfs/Pituitary_Society_Cushings_brochure.pdf. Accessed May 20, 2019.
8. Koch, C. Chrousos, G. Overview of endocrine hypertension. In: Feingold KR, Anawalt B, Boyce A, et al, eds. Endotext. South Dartmouth, MA: MDText.com; 2016.
9. Barlow M, Abdel-Latif A. The forgotten cause of hypertension: a case report and literature review of the prevalence, diagnosis and management of primary aldosteronism. Case Rep Intern Med. 2018;5:4-7.
10. Viera A, Neutze D. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician. 2010;82:1471-1478.
11. Young WF, Calhoun DA, Lenders JWM, et al. Screening for endocrine hypertension: an Endocrine Society scientific statement. Endocr Rev. 2017;38:103-122.
12. Kotchen TA. Hypertensive vascular disease. In: Jameson JL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 20th ed. New York, NY: McGraw-Hill Education; 2018.
13. Rossi GP, Bernini G, Caliumi C, et al; PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293-2300.
14. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889-1916.
15. Stowasser M, Taylor PJ, Pimenta E, et al. Laboratory investigation of primary aldosteronism. Clin Biochem Rev. 2010;31:39-56.
16. Stowasser M, Gordon RD. The aldosterone-renin ratio for screening for primary aldosteronism. Endocrinologist. 2004;14:267-276.
17. Newell-Price J, Bertagna X, Grossman AB, et al. Cushing’s syndrome. Lancet. 2006;367:1605-1617.
18. Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2008;93: 1526-1540.
19. Rimoldi S, Scherrer U, Messerli F. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014;35:1245-1254.
20. Kirk L, Hash R, Harold K. Cushing’s syndrome and Cushing’s disease. Am Fam Physician. 2000;62:1133-1134.
21. Thomas RM, Ruel E, Shantavasinkul PC. Endocrine hypertension: an overview on the current etiopathogenesis and management options. World J Hypertens. 2015;5:14-27.
22. Ariton M, Juan CS, AvRuskin TW. Pheochromocytoma: clinical observations from a Brooklyn tertiary hospital. Endocr Pract. 2000;6:249-252.
23. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403-1419.
24. Lenders JW, Eisenhofer G, Mannelli M, et al. Pheochromocytoma. Lancet. 2005;366:665-675.
25. Fishbein L, Else T. Disorders of the adrenal medulla. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.
Clinician Reviews in partnership with
Aimee Pragle is an Assistant Professor in the School of PA Practice, College of Medicine, Florida State University, Tallahassee.
Clinician Reviews in partnership with
Aimee Pragle is an Assistant Professor in the School of PA Practice, College of Medicine, Florida State University, Tallahassee.
Clinician Reviews in partnership with
Aimee Pragle is an Assistant Professor in the School of PA Practice, College of Medicine, Florida State University, Tallahassee.
Hypertension is one of the most common reasons for patient visits.1 According to the US Preventive Services Task Force, more than 70 million individuals older than 20 have hypertension, which is defined as a blood pressure (BP) of ≥ 130/85 mm Hg.2 Essential hypertension is the most common form of this condition; most affected patients will show improvement with evidence-based pharmacologic treatment, lifestyle modifications, and risk factor reductions.
For patients with refractory hypertension, however, identifying what steps to take in screening and diagnosis can be daunting for clinicians. It is important to identify cases of secondary hypertension, because if it is left undiagnosed and untreated, serious complications—such as cardiovascular and renal disease—are likely to occur.3,4
Secondary hypertension can be caused by myriad disease states and disorders, including endocrine disorders, renal disease, neurologic disorders, acute stress, and drug-induced hypertension.5 Endocrine hypertension is most commonly caused by adrenal gland disorders, including primary aldosteronism, Cushing syndrome, and pheochromocytoma. (Of note, Cushing syndrome is caused by glucocorticoid-secreting adrenal tumors, while Cushing disease is a condition in which there is glucocorticoid excess caused by oversecretion of pituitary adrenocorticotropic hormone.6 Cushing disease is more common than Cushing syndrome, which is rare.7) While nonadrenal endocrine disorders are not as common, they pose significant health issues, including growth hormone excess or deficiency, thyroid disorders, testosterone deficiency, obesity, insulin resistance, and metabolic syndrome.8
Understanding the endocrine causes of hypertension is a valuable resource for clinicians to have in their toolbox. Although the negative consequences of endocrine disorders are significant, these conditions are often recognizable, and pharmacologic treatment and/or surgical interventions can potentially resolve or improve hypertension and reduce risk for other comorbidities. This article summarizes screening and diagnosis guidelines for several possible causes of endocrine hypertension: primary aldosteronism, Cushing syndrome, and pheochromocytoma.
PRIMARY ALDOSTERONISM
Primary aldosteronism occurs in 5% to 10% of all hypertensive patients and is a common cause of secondary and endocrine hypertension (although in younger—particularly female—patients, it most commonly causes renal artery stenosis).9,10 Historically, primary aldosteronism was considered rare and not generally included in a differential diagnosis for patients presenting with resistant hypertension. However, clinical investigations have indicated that primary aldosteronism is more prevalent than previously thought.11
Patients develop this condition when there is increased aldosterone production independent of the renin-angiotensin system. The resulting sodium retention can lead to hypertension, hypokalemia, and high plasma aldosterone/renin ratio (ARR).12 Clinical findings and symptoms can be vague, increasing the difficulty in identifying primary aldosteronism as the diagnosis. Patients may be asymptomatic, with the only abnormal lab finding being hypokalemia (an infrequent finding, affecting < 25% of patients).13 If hypokalemia is present, symptoms can include nocturia, polyuria, muscle weakness, cramps, paresthesias, and palpitations.11
The Endocrine Society has identified 8 characteristics that increase the likelihood of primary aldosteronism. Patients require further screening if they
- Have a sustained elevated BP (≥ 150 mm Hg [systolic] and/or 100 mm Hg [diastolic])
- Have hypertension (BP > 140/90 mm Hg) that is resistant to 3 conventional antihypertensive drugs, including a diuretic
- Have controlled BP (BP < 140/90 mm Hg) with ≥ 4 antihypertensive drugs
- Have hypertension and spontaneous or diuretic-induced hypokalemia
- Have hypertension and adrenal incidentaloma
- Have hypertension and obstructive sleep apnea
- Have hypertension and a family history of early-onset hypertension or a cerebrovascular accident at a young age (< 40 years)
- Are hypertensive and a first-degree relative of a patient with primary aldosteronism.14
Continue to: The most reliable screening test...
The most reliable screening test for primary aldosterone is the ARR, although false-negative and false-positive results are possible.11 False-negative results can be caused by dietary salt restriction, hypokalemia, and use of medications including diuretics, calcium channel blockers, ACE inhibitors, and angiotensin receptor antagonists. Use of ß-adrenergic blockers, α-methyldopa, or NSAIDs can cause false-positive results.15 Patients should be encouraged to follow a liberal sodium diet before ARR testing, and efforts to correct hypokalemia should be implemented. Before ARR is measured, diuretics (specifically spironolactone) should be stopped for at least 4 weeks; other possible interfering medications should be stopped for at least 2 weeks.16
The ARR should be obtained multiple times to confirm elevated readings.16 Reference ranges vary, but generally plasma aldosterone concentrations > 20 ng/dL and plasma renin activity < 1 ng/mL/h indicate whether confirmatory testing should be completed.14 Further confirmatory testing can be achieved with efforts to suppress plasma aldosterone to < 10 ng/dL after an IV infusion of 2 L isotonic saline over 4 hours.12 Oral sodium load is used as well and usually before IV infusion.
CUSHING SYNDROME
Cushing syndrome is caused by excess circulating levels of glucocorticoids and affects < 0.1% of the world population.17 Signs and symptoms include centripetal obesity, moon facies, facial plethora, easy bruising, buffalo hump (or posterior cervical fat pad), hirsutism, and wide-purple striae.18 Up to 80% of these patients also have hypertension.19 If these patients have chronic exposure to high levels of glucocorticoid (the most common source being therapeutic administration of exogenous glucocorticoids), multiple complications can occur.6,20
The Endocrine Society Clinical Practice Guideline recommends the following patient groups be tested for Cushing syndrome:
- Young patients with unusual medical conditions, such as osteoporosis and resistant hypertension
- Patients with classic signs and symptoms, such as easy bruising, weight gain, facial plethora, and purple striae
- Children with decreasing height percentile and increasing weight
- Patients with adrenal incidentaloma compatible with adenoma.18
If Cushing syndrome is suspected, 1 of the following 3 initial tests can be completed: 24-hour, urine-free cortisol and creatinine; late-night salivary cortisol; or 1-mg overnight dexamethasone suppression test. Two of these tests must have abnormal results for confirmation before appropriate pituitary or adrenal imaging. If a patient has clinical features indicating Cushing syndrome but test results are normal, he or she should be referred to an endocrinologist. If a patient has ≥ 2 normal tests and probability of Cushing syndrome is unlikely, patients should be recommended for follow-up in 6 months to evaluate for any worsening of symptoms.18
Continue to: PHEOCHROMOCYTOMA
PHEOCHROMOCYTOMA
Pheochromocytoma is a condition in which there is secretion of excess catecholamines, epinephrine, norepinephrine, and dopamine due to a tumor of the adrenal medulla.21 This is a rare disease and accounts for only 0.2% to 0.6% of all causes of hypertension.22 Hypertension (persistent or paroxysmal) is the most common finding for patients with pheochromocytoma, with 80% to 90% presenting with this finding.23 It is important to note that approximately 10% of these patients will be normotensive. Three of the condition’s classic symptoms are headache, sweating, and palpitations.24 Additional symptoms include anxiety, sense of impending doom, fever, nausea, or vomiting.21
If left untreated, there is risk for hypertensive retinopathy, nephropathy, myocardial infarction, stroke from cerebral infarction, intracranial hemorrhage, or embolism.25 Due to the high rate of morbidity and mortality with untreated pheochromocytoma, laboratory testing should be initiated immediately upon suspicion of this diagnosis or if the patient has relevant family history.11
Patients should be screened for pheochromocytoma if they have ≥ 1 of the following factors:
- Resistant hypertension and hyperadrenergic symptoms (palpitations, perspiration, pallor, or headache)
- Family history of pheochromocytoma
- Any genetic syndrome with a known association to pheochromocytoma
- An adrenal mass that is > 4 cm, is cystic, or has hemorrhagic changes.19
Pheochromocytoma is diagnosed by identifying high concentrations of plasma-free metanephrines or 24-hour fractionated metanephrines and catecholamines. Some medications can interfere with the accuracy of lab results and therefore may need to be temporarily stopped; it is important to check the specific lab guidelines and review the patient’s medication lists before tests are ordered and conducted.25
ALWAYS SCREEN THE PATIENT
Although the causes of endocrine-related hypertension are very rare, screening for endocrine hypertension in patients who present with signs and symptoms of these conditions can greatly improve their lives. The endocrine disorders discussed in this article can be treated or controlled with appropriate diagnosis and treatment. In addition, resolving uncontrolled hypertension by addressing endocrine disorders can reduce the risk for long-term sequelae. It is important for clinicians to consider referral to an endocrine specialist if a patient has endocrine-related hypertension. In particular, patients with pheochromocytoma require quick referral due to a risk for high morbidity and mortality if left untreated.11
Hypertension is one of the most common reasons for patient visits.1 According to the US Preventive Services Task Force, more than 70 million individuals older than 20 have hypertension, which is defined as a blood pressure (BP) of ≥ 130/85 mm Hg.2 Essential hypertension is the most common form of this condition; most affected patients will show improvement with evidence-based pharmacologic treatment, lifestyle modifications, and risk factor reductions.
For patients with refractory hypertension, however, identifying what steps to take in screening and diagnosis can be daunting for clinicians. It is important to identify cases of secondary hypertension, because if it is left undiagnosed and untreated, serious complications—such as cardiovascular and renal disease—are likely to occur.3,4
Secondary hypertension can be caused by myriad disease states and disorders, including endocrine disorders, renal disease, neurologic disorders, acute stress, and drug-induced hypertension.5 Endocrine hypertension is most commonly caused by adrenal gland disorders, including primary aldosteronism, Cushing syndrome, and pheochromocytoma. (Of note, Cushing syndrome is caused by glucocorticoid-secreting adrenal tumors, while Cushing disease is a condition in which there is glucocorticoid excess caused by oversecretion of pituitary adrenocorticotropic hormone.6 Cushing disease is more common than Cushing syndrome, which is rare.7) While nonadrenal endocrine disorders are not as common, they pose significant health issues, including growth hormone excess or deficiency, thyroid disorders, testosterone deficiency, obesity, insulin resistance, and metabolic syndrome.8
Understanding the endocrine causes of hypertension is a valuable resource for clinicians to have in their toolbox. Although the negative consequences of endocrine disorders are significant, these conditions are often recognizable, and pharmacologic treatment and/or surgical interventions can potentially resolve or improve hypertension and reduce risk for other comorbidities. This article summarizes screening and diagnosis guidelines for several possible causes of endocrine hypertension: primary aldosteronism, Cushing syndrome, and pheochromocytoma.
PRIMARY ALDOSTERONISM
Primary aldosteronism occurs in 5% to 10% of all hypertensive patients and is a common cause of secondary and endocrine hypertension (although in younger—particularly female—patients, it most commonly causes renal artery stenosis).9,10 Historically, primary aldosteronism was considered rare and not generally included in a differential diagnosis for patients presenting with resistant hypertension. However, clinical investigations have indicated that primary aldosteronism is more prevalent than previously thought.11
Patients develop this condition when there is increased aldosterone production independent of the renin-angiotensin system. The resulting sodium retention can lead to hypertension, hypokalemia, and high plasma aldosterone/renin ratio (ARR).12 Clinical findings and symptoms can be vague, increasing the difficulty in identifying primary aldosteronism as the diagnosis. Patients may be asymptomatic, with the only abnormal lab finding being hypokalemia (an infrequent finding, affecting < 25% of patients).13 If hypokalemia is present, symptoms can include nocturia, polyuria, muscle weakness, cramps, paresthesias, and palpitations.11
The Endocrine Society has identified 8 characteristics that increase the likelihood of primary aldosteronism. Patients require further screening if they
- Have a sustained elevated BP (≥ 150 mm Hg [systolic] and/or 100 mm Hg [diastolic])
- Have hypertension (BP > 140/90 mm Hg) that is resistant to 3 conventional antihypertensive drugs, including a diuretic
- Have controlled BP (BP < 140/90 mm Hg) with ≥ 4 antihypertensive drugs
- Have hypertension and spontaneous or diuretic-induced hypokalemia
- Have hypertension and adrenal incidentaloma
- Have hypertension and obstructive sleep apnea
- Have hypertension and a family history of early-onset hypertension or a cerebrovascular accident at a young age (< 40 years)
- Are hypertensive and a first-degree relative of a patient with primary aldosteronism.14
Continue to: The most reliable screening test...
The most reliable screening test for primary aldosterone is the ARR, although false-negative and false-positive results are possible.11 False-negative results can be caused by dietary salt restriction, hypokalemia, and use of medications including diuretics, calcium channel blockers, ACE inhibitors, and angiotensin receptor antagonists. Use of ß-adrenergic blockers, α-methyldopa, or NSAIDs can cause false-positive results.15 Patients should be encouraged to follow a liberal sodium diet before ARR testing, and efforts to correct hypokalemia should be implemented. Before ARR is measured, diuretics (specifically spironolactone) should be stopped for at least 4 weeks; other possible interfering medications should be stopped for at least 2 weeks.16
The ARR should be obtained multiple times to confirm elevated readings.16 Reference ranges vary, but generally plasma aldosterone concentrations > 20 ng/dL and plasma renin activity < 1 ng/mL/h indicate whether confirmatory testing should be completed.14 Further confirmatory testing can be achieved with efforts to suppress plasma aldosterone to < 10 ng/dL after an IV infusion of 2 L isotonic saline over 4 hours.12 Oral sodium load is used as well and usually before IV infusion.
CUSHING SYNDROME
Cushing syndrome is caused by excess circulating levels of glucocorticoids and affects < 0.1% of the world population.17 Signs and symptoms include centripetal obesity, moon facies, facial plethora, easy bruising, buffalo hump (or posterior cervical fat pad), hirsutism, and wide-purple striae.18 Up to 80% of these patients also have hypertension.19 If these patients have chronic exposure to high levels of glucocorticoid (the most common source being therapeutic administration of exogenous glucocorticoids), multiple complications can occur.6,20
The Endocrine Society Clinical Practice Guideline recommends the following patient groups be tested for Cushing syndrome:
- Young patients with unusual medical conditions, such as osteoporosis and resistant hypertension
- Patients with classic signs and symptoms, such as easy bruising, weight gain, facial plethora, and purple striae
- Children with decreasing height percentile and increasing weight
- Patients with adrenal incidentaloma compatible with adenoma.18
If Cushing syndrome is suspected, 1 of the following 3 initial tests can be completed: 24-hour, urine-free cortisol and creatinine; late-night salivary cortisol; or 1-mg overnight dexamethasone suppression test. Two of these tests must have abnormal results for confirmation before appropriate pituitary or adrenal imaging. If a patient has clinical features indicating Cushing syndrome but test results are normal, he or she should be referred to an endocrinologist. If a patient has ≥ 2 normal tests and probability of Cushing syndrome is unlikely, patients should be recommended for follow-up in 6 months to evaluate for any worsening of symptoms.18
Continue to: PHEOCHROMOCYTOMA
PHEOCHROMOCYTOMA
Pheochromocytoma is a condition in which there is secretion of excess catecholamines, epinephrine, norepinephrine, and dopamine due to a tumor of the adrenal medulla.21 This is a rare disease and accounts for only 0.2% to 0.6% of all causes of hypertension.22 Hypertension (persistent or paroxysmal) is the most common finding for patients with pheochromocytoma, with 80% to 90% presenting with this finding.23 It is important to note that approximately 10% of these patients will be normotensive. Three of the condition’s classic symptoms are headache, sweating, and palpitations.24 Additional symptoms include anxiety, sense of impending doom, fever, nausea, or vomiting.21
If left untreated, there is risk for hypertensive retinopathy, nephropathy, myocardial infarction, stroke from cerebral infarction, intracranial hemorrhage, or embolism.25 Due to the high rate of morbidity and mortality with untreated pheochromocytoma, laboratory testing should be initiated immediately upon suspicion of this diagnosis or if the patient has relevant family history.11
Patients should be screened for pheochromocytoma if they have ≥ 1 of the following factors:
- Resistant hypertension and hyperadrenergic symptoms (palpitations, perspiration, pallor, or headache)
- Family history of pheochromocytoma
- Any genetic syndrome with a known association to pheochromocytoma
- An adrenal mass that is > 4 cm, is cystic, or has hemorrhagic changes.19
Pheochromocytoma is diagnosed by identifying high concentrations of plasma-free metanephrines or 24-hour fractionated metanephrines and catecholamines. Some medications can interfere with the accuracy of lab results and therefore may need to be temporarily stopped; it is important to check the specific lab guidelines and review the patient’s medication lists before tests are ordered and conducted.25
ALWAYS SCREEN THE PATIENT
Although the causes of endocrine-related hypertension are very rare, screening for endocrine hypertension in patients who present with signs and symptoms of these conditions can greatly improve their lives. The endocrine disorders discussed in this article can be treated or controlled with appropriate diagnosis and treatment. In addition, resolving uncontrolled hypertension by addressing endocrine disorders can reduce the risk for long-term sequelae. It is important for clinicians to consider referral to an endocrine specialist if a patient has endocrine-related hypertension. In particular, patients with pheochromocytoma require quick referral due to a risk for high morbidity and mortality if left untreated.11
1. Smith MA, Schrager S, WinklerPrins V. Essentials of Family Medicine. 7th ed. Baltimore, MD: Lipincott Williams & Wilkins; 2019.
2. US Preventive Services Task Force. High blood pressure in adults: screening [final recommendation statement]. www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/high-blood-pressure-in-adults-screening. Accessed May 20, 2019.
3. Puar T, Mok Y, Debajyoti R, et al. Secondary hypertension in adults. Singapore Med J. 2016;57:228-232.
4. Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet. 2015;386:801-812.
5. Faselis C, Doumas M, Papademetriou V. Common secondary causes of resistant hypertension and rational for treatment. Int J Hypertens. 2010;2011: doi: 10.4061/2011/236239.
6. Else T, Hammer GD. Disorders of the Adrenal Cortex. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.
7. Nieman L, Swearingen B; the Pituitary Society. Cushing’s syndrome and Cushing’s disease: your questions answered. www.pituitarysociety.org/sites/all/pdfs/Pituitary_Society_Cushings_brochure.pdf. Accessed May 20, 2019.
8. Koch, C. Chrousos, G. Overview of endocrine hypertension. In: Feingold KR, Anawalt B, Boyce A, et al, eds. Endotext. South Dartmouth, MA: MDText.com; 2016.
9. Barlow M, Abdel-Latif A. The forgotten cause of hypertension: a case report and literature review of the prevalence, diagnosis and management of primary aldosteronism. Case Rep Intern Med. 2018;5:4-7.
10. Viera A, Neutze D. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician. 2010;82:1471-1478.
11. Young WF, Calhoun DA, Lenders JWM, et al. Screening for endocrine hypertension: an Endocrine Society scientific statement. Endocr Rev. 2017;38:103-122.
12. Kotchen TA. Hypertensive vascular disease. In: Jameson JL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 20th ed. New York, NY: McGraw-Hill Education; 2018.
13. Rossi GP, Bernini G, Caliumi C, et al; PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293-2300.
14. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889-1916.
15. Stowasser M, Taylor PJ, Pimenta E, et al. Laboratory investigation of primary aldosteronism. Clin Biochem Rev. 2010;31:39-56.
16. Stowasser M, Gordon RD. The aldosterone-renin ratio for screening for primary aldosteronism. Endocrinologist. 2004;14:267-276.
17. Newell-Price J, Bertagna X, Grossman AB, et al. Cushing’s syndrome. Lancet. 2006;367:1605-1617.
18. Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2008;93: 1526-1540.
19. Rimoldi S, Scherrer U, Messerli F. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014;35:1245-1254.
20. Kirk L, Hash R, Harold K. Cushing’s syndrome and Cushing’s disease. Am Fam Physician. 2000;62:1133-1134.
21. Thomas RM, Ruel E, Shantavasinkul PC. Endocrine hypertension: an overview on the current etiopathogenesis and management options. World J Hypertens. 2015;5:14-27.
22. Ariton M, Juan CS, AvRuskin TW. Pheochromocytoma: clinical observations from a Brooklyn tertiary hospital. Endocr Pract. 2000;6:249-252.
23. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403-1419.
24. Lenders JW, Eisenhofer G, Mannelli M, et al. Pheochromocytoma. Lancet. 2005;366:665-675.
25. Fishbein L, Else T. Disorders of the adrenal medulla. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.
1. Smith MA, Schrager S, WinklerPrins V. Essentials of Family Medicine. 7th ed. Baltimore, MD: Lipincott Williams & Wilkins; 2019.
2. US Preventive Services Task Force. High blood pressure in adults: screening [final recommendation statement]. www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/high-blood-pressure-in-adults-screening. Accessed May 20, 2019.
3. Puar T, Mok Y, Debajyoti R, et al. Secondary hypertension in adults. Singapore Med J. 2016;57:228-232.
4. Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet. 2015;386:801-812.
5. Faselis C, Doumas M, Papademetriou V. Common secondary causes of resistant hypertension and rational for treatment. Int J Hypertens. 2010;2011: doi: 10.4061/2011/236239.
6. Else T, Hammer GD. Disorders of the Adrenal Cortex. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.
7. Nieman L, Swearingen B; the Pituitary Society. Cushing’s syndrome and Cushing’s disease: your questions answered. www.pituitarysociety.org/sites/all/pdfs/Pituitary_Society_Cushings_brochure.pdf. Accessed May 20, 2019.
8. Koch, C. Chrousos, G. Overview of endocrine hypertension. In: Feingold KR, Anawalt B, Boyce A, et al, eds. Endotext. South Dartmouth, MA: MDText.com; 2016.
9. Barlow M, Abdel-Latif A. The forgotten cause of hypertension: a case report and literature review of the prevalence, diagnosis and management of primary aldosteronism. Case Rep Intern Med. 2018;5:4-7.
10. Viera A, Neutze D. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician. 2010;82:1471-1478.
11. Young WF, Calhoun DA, Lenders JWM, et al. Screening for endocrine hypertension: an Endocrine Society scientific statement. Endocr Rev. 2017;38:103-122.
12. Kotchen TA. Hypertensive vascular disease. In: Jameson JL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 20th ed. New York, NY: McGraw-Hill Education; 2018.
13. Rossi GP, Bernini G, Caliumi C, et al; PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293-2300.
14. Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889-1916.
15. Stowasser M, Taylor PJ, Pimenta E, et al. Laboratory investigation of primary aldosteronism. Clin Biochem Rev. 2010;31:39-56.
16. Stowasser M, Gordon RD. The aldosterone-renin ratio for screening for primary aldosteronism. Endocrinologist. 2004;14:267-276.
17. Newell-Price J, Bertagna X, Grossman AB, et al. Cushing’s syndrome. Lancet. 2006;367:1605-1617.
18. Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2008;93: 1526-1540.
19. Rimoldi S, Scherrer U, Messerli F. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014;35:1245-1254.
20. Kirk L, Hash R, Harold K. Cushing’s syndrome and Cushing’s disease. Am Fam Physician. 2000;62:1133-1134.
21. Thomas RM, Ruel E, Shantavasinkul PC. Endocrine hypertension: an overview on the current etiopathogenesis and management options. World J Hypertens. 2015;5:14-27.
22. Ariton M, Juan CS, AvRuskin TW. Pheochromocytoma: clinical observations from a Brooklyn tertiary hospital. Endocr Pract. 2000;6:249-252.
23. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51(6):1403-1419.
24. Lenders JW, Eisenhofer G, Mannelli M, et al. Pheochromocytoma. Lancet. 2005;366:665-675.
25. Fishbein L, Else T. Disorders of the adrenal medulla. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine. 8th ed. New York, NY: McGraw-Hill; 2014.

Mutant huntingtin and neurofilament light are potential biomarkers in Huntington’s disease
PHILADELPHIA – according to an investigation presented at the annual meeting of the American Academy of Neurology. These biomarkers appear to reflect the earliest detectable changes in the natural history of Huntington’s disease, but the longitudinal prognostic value of changes in these biomarkers requires further investigation, the researchers said.
Huntington’s disease has a long prodromal phase and is associated with long survival. Investigators still need well-validated biomarkers of disease progression, prognosis, and pharmacodynamics to aid drug development, said Filipe B. Rodrigues, MD, clinical research fellow at University College London. After several years of study, Dr. Rodrigues and colleagues found mutant huntingtin and neurofilament light (NfL) to be the most promising potential biomarkers in Huntington’s disease. They sought to understand how these two biomarkers compare with each other, what their predictive ability is, and how they change longitudinally.
To this end, Dr. Rodrigues and colleagues designed the HD-CSF study, a prospective, observational, longitudinal cohort study with a 2-year follow-up. They recruited 20 healthy controls, 20 patients with premanifest Huntington’s disease, and 40 patients with manifest Huntington’s disease. All participants underwent regular clinical assessments and standardized collections of cerebrospinal fluid (CSF) and blood. They also had the option of undergoing brain MRI scans.
The investigators analyzed their data using multiple linear regression models, Pearson’s correlations, receiver operating characteristic curves, and sample size calculations. They used an event-based model to evaluate the temporal sequence of changes in Huntington’s disease-related biomarkers.
Dr. Rodrigues and colleagues first observed that all three biomarkers successfully distinguished between healthy controls, patients with premanifest Huntington’s disease, and patients with Huntington’s disease. Mutant huntingtin, the pathogenic agent in Huntington’s disease, discriminated perfectly between healthy controls and mutation carriers, as the researchers had expected. CSF and plasma levels of NfL also discriminated well between healthy controls and mutation carriers. These biomarkers had areas under the ROC curve greater than 0.9. NfL in plasma and CSF also distinguished well between patients with premanifest Huntington’s disease and those with manifest Huntington’s disease, with areas under the curve greater than 0.9. Their discriminative ability in this regard was significantly better than that of mutant huntingtin.
When the researchers examined the relationship between the three biomarkers, they found that CSF levels of NfL were strongly correlated in a linear fashion with plasma levels of NfL. CSF levels of mutant huntingtin were moderately associated with CSF levels of NfL.
Levels of all three biomarkers increased significantly as the disease progressed and were associated with all clinical scales and imaging measures. CSF and plasma levels of NfL had superior predictive ability for clinical and imaging measures, compared with mutant huntingtin. CSF and plasma NfL were associated with brain volume, but mutant huntingtin was not.
All three biomarkers were stable during a 6-week period. Dr. Rodrigues and colleagues calculated sample sizes for a two-arm interventional trial involving various hypothetical therapeutic effects. They found that the required sample sizes were small enough to be incorporated easily into ongoing and future clinical trials.
In silico modeling suggested among the markers measured in the HD-CSF study, the three biofluid biomarkers were the first factors to be altered in the course of Huntington’s disease. Alterations in the biomarkers were followed by changes in imaging markers, and then by changes in clinical markers (for example, motor and cognitive function).
Finally, Dr. Rodrigues and colleagues found preliminary evidence that levels of NfL in CSF and plasma increase over time at different rates in patients with Huntington’s disease, compared with healthy controls. NfL appears to be more useful than mutant huntingtin for evaluating the rate of disease progression than for gauging response to treatment, said Dr. Rodrigues. “If [we] can prove that we can assess response to treatment by measuring NfL, I think that would be great.”
The investigators are currently analyzing the longitudinal predictive value of changes in these biomarkers. They also have begun analyzing other markers such as tau and brain-derived neurotrophic factor.
This study was funded by the Medical Research Council UK, the CHDI Foundation, and F. Hoffmann-La Roche.
This article was updated 6/18/19.
SOURCE: Rodrigues FB et al. AAN 2019, Abstract S16.003.
PHILADELPHIA – according to an investigation presented at the annual meeting of the American Academy of Neurology. These biomarkers appear to reflect the earliest detectable changes in the natural history of Huntington’s disease, but the longitudinal prognostic value of changes in these biomarkers requires further investigation, the researchers said.
Huntington’s disease has a long prodromal phase and is associated with long survival. Investigators still need well-validated biomarkers of disease progression, prognosis, and pharmacodynamics to aid drug development, said Filipe B. Rodrigues, MD, clinical research fellow at University College London. After several years of study, Dr. Rodrigues and colleagues found mutant huntingtin and neurofilament light (NfL) to be the most promising potential biomarkers in Huntington’s disease. They sought to understand how these two biomarkers compare with each other, what their predictive ability is, and how they change longitudinally.
To this end, Dr. Rodrigues and colleagues designed the HD-CSF study, a prospective, observational, longitudinal cohort study with a 2-year follow-up. They recruited 20 healthy controls, 20 patients with premanifest Huntington’s disease, and 40 patients with manifest Huntington’s disease. All participants underwent regular clinical assessments and standardized collections of cerebrospinal fluid (CSF) and blood. They also had the option of undergoing brain MRI scans.
The investigators analyzed their data using multiple linear regression models, Pearson’s correlations, receiver operating characteristic curves, and sample size calculations. They used an event-based model to evaluate the temporal sequence of changes in Huntington’s disease-related biomarkers.
Dr. Rodrigues and colleagues first observed that all three biomarkers successfully distinguished between healthy controls, patients with premanifest Huntington’s disease, and patients with Huntington’s disease. Mutant huntingtin, the pathogenic agent in Huntington’s disease, discriminated perfectly between healthy controls and mutation carriers, as the researchers had expected. CSF and plasma levels of NfL also discriminated well between healthy controls and mutation carriers. These biomarkers had areas under the ROC curve greater than 0.9. NfL in plasma and CSF also distinguished well between patients with premanifest Huntington’s disease and those with manifest Huntington’s disease, with areas under the curve greater than 0.9. Their discriminative ability in this regard was significantly better than that of mutant huntingtin.
When the researchers examined the relationship between the three biomarkers, they found that CSF levels of NfL were strongly correlated in a linear fashion with plasma levels of NfL. CSF levels of mutant huntingtin were moderately associated with CSF levels of NfL.
Levels of all three biomarkers increased significantly as the disease progressed and were associated with all clinical scales and imaging measures. CSF and plasma levels of NfL had superior predictive ability for clinical and imaging measures, compared with mutant huntingtin. CSF and plasma NfL were associated with brain volume, but mutant huntingtin was not.
All three biomarkers were stable during a 6-week period. Dr. Rodrigues and colleagues calculated sample sizes for a two-arm interventional trial involving various hypothetical therapeutic effects. They found that the required sample sizes were small enough to be incorporated easily into ongoing and future clinical trials.
In silico modeling suggested among the markers measured in the HD-CSF study, the three biofluid biomarkers were the first factors to be altered in the course of Huntington’s disease. Alterations in the biomarkers were followed by changes in imaging markers, and then by changes in clinical markers (for example, motor and cognitive function).
Finally, Dr. Rodrigues and colleagues found preliminary evidence that levels of NfL in CSF and plasma increase over time at different rates in patients with Huntington’s disease, compared with healthy controls. NfL appears to be more useful than mutant huntingtin for evaluating the rate of disease progression than for gauging response to treatment, said Dr. Rodrigues. “If [we] can prove that we can assess response to treatment by measuring NfL, I think that would be great.”
The investigators are currently analyzing the longitudinal predictive value of changes in these biomarkers. They also have begun analyzing other markers such as tau and brain-derived neurotrophic factor.
This study was funded by the Medical Research Council UK, the CHDI Foundation, and F. Hoffmann-La Roche.
This article was updated 6/18/19.
SOURCE: Rodrigues FB et al. AAN 2019, Abstract S16.003.
PHILADELPHIA – according to an investigation presented at the annual meeting of the American Academy of Neurology. These biomarkers appear to reflect the earliest detectable changes in the natural history of Huntington’s disease, but the longitudinal prognostic value of changes in these biomarkers requires further investigation, the researchers said.
Huntington’s disease has a long prodromal phase and is associated with long survival. Investigators still need well-validated biomarkers of disease progression, prognosis, and pharmacodynamics to aid drug development, said Filipe B. Rodrigues, MD, clinical research fellow at University College London. After several years of study, Dr. Rodrigues and colleagues found mutant huntingtin and neurofilament light (NfL) to be the most promising potential biomarkers in Huntington’s disease. They sought to understand how these two biomarkers compare with each other, what their predictive ability is, and how they change longitudinally.
To this end, Dr. Rodrigues and colleagues designed the HD-CSF study, a prospective, observational, longitudinal cohort study with a 2-year follow-up. They recruited 20 healthy controls, 20 patients with premanifest Huntington’s disease, and 40 patients with manifest Huntington’s disease. All participants underwent regular clinical assessments and standardized collections of cerebrospinal fluid (CSF) and blood. They also had the option of undergoing brain MRI scans.
The investigators analyzed their data using multiple linear regression models, Pearson’s correlations, receiver operating characteristic curves, and sample size calculations. They used an event-based model to evaluate the temporal sequence of changes in Huntington’s disease-related biomarkers.
Dr. Rodrigues and colleagues first observed that all three biomarkers successfully distinguished between healthy controls, patients with premanifest Huntington’s disease, and patients with Huntington’s disease. Mutant huntingtin, the pathogenic agent in Huntington’s disease, discriminated perfectly between healthy controls and mutation carriers, as the researchers had expected. CSF and plasma levels of NfL also discriminated well between healthy controls and mutation carriers. These biomarkers had areas under the ROC curve greater than 0.9. NfL in plasma and CSF also distinguished well between patients with premanifest Huntington’s disease and those with manifest Huntington’s disease, with areas under the curve greater than 0.9. Their discriminative ability in this regard was significantly better than that of mutant huntingtin.
When the researchers examined the relationship between the three biomarkers, they found that CSF levels of NfL were strongly correlated in a linear fashion with plasma levels of NfL. CSF levels of mutant huntingtin were moderately associated with CSF levels of NfL.
Levels of all three biomarkers increased significantly as the disease progressed and were associated with all clinical scales and imaging measures. CSF and plasma levels of NfL had superior predictive ability for clinical and imaging measures, compared with mutant huntingtin. CSF and plasma NfL were associated with brain volume, but mutant huntingtin was not.
All three biomarkers were stable during a 6-week period. Dr. Rodrigues and colleagues calculated sample sizes for a two-arm interventional trial involving various hypothetical therapeutic effects. They found that the required sample sizes were small enough to be incorporated easily into ongoing and future clinical trials.
In silico modeling suggested among the markers measured in the HD-CSF study, the three biofluid biomarkers were the first factors to be altered in the course of Huntington’s disease. Alterations in the biomarkers were followed by changes in imaging markers, and then by changes in clinical markers (for example, motor and cognitive function).
Finally, Dr. Rodrigues and colleagues found preliminary evidence that levels of NfL in CSF and plasma increase over time at different rates in patients with Huntington’s disease, compared with healthy controls. NfL appears to be more useful than mutant huntingtin for evaluating the rate of disease progression than for gauging response to treatment, said Dr. Rodrigues. “If [we] can prove that we can assess response to treatment by measuring NfL, I think that would be great.”
The investigators are currently analyzing the longitudinal predictive value of changes in these biomarkers. They also have begun analyzing other markers such as tau and brain-derived neurotrophic factor.
This study was funded by the Medical Research Council UK, the CHDI Foundation, and F. Hoffmann-La Roche.
This article was updated 6/18/19.
SOURCE: Rodrigues FB et al. AAN 2019, Abstract S16.003.
REPORTING FROM AAN 2019
Key clinical point: Mutant huntingtin and plasma and cerebrospinal fluid levels of neurofilament light are useful potential biomarkers in Huntington’s disease.
Major finding: Levels of neurofilament light in plasma are correlated with those in cerebrospinal fluid.
Study details: A prospective, observational, longitudinal cohort study including 80 participants with and without Huntington’s disease.
Disclosures: This study was funded by the Medical Research Council UK, the CHDI Foundation, and F. Hoffmann-La Roche.
Source: Rodrigues FB et al. AAN 2019, Abstract S16.003.
Nearly two-thirds of gynecologic oncology respondents experienced sexual harassment
CHICAGO – Nearly two-thirds of more than 400 U.S.-based physician members of the Society of Gynecologic Oncology who participated in a recent survey reported experiencing sexual harassment in training or practice.
Notably, of the 255 women and 147 men who responded, 71% and 51%, respectively, reported such sexual harassment – and only 15% overall reported it to officials, Marina Stasenko, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The survey also addressed gender-based discrimination and disparities, including respondents’ views on pay disparities. In this video interview, Dr. Stasenko, a gynecologic oncology fellow at Memorial Sloan Kettering Cancer Center, New York, discusses the findings, their implications and context in this age of #MeToo and #TimesUp, and potential approaches to addressing the ongoing problem and the concerns victims have about reporting harassment.
“We need to start by setting an example, saying these things are not tolerated [and] put that into policy – really show folks how it can be reported and what is being done once that report is filed,” she said.
Dr. Stasenko reported having no disclosures.
SOURCE: Stasenko M et al. ASCO 2019, Abstract LBA10502.
CHICAGO – Nearly two-thirds of more than 400 U.S.-based physician members of the Society of Gynecologic Oncology who participated in a recent survey reported experiencing sexual harassment in training or practice.
Notably, of the 255 women and 147 men who responded, 71% and 51%, respectively, reported such sexual harassment – and only 15% overall reported it to officials, Marina Stasenko, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The survey also addressed gender-based discrimination and disparities, including respondents’ views on pay disparities. In this video interview, Dr. Stasenko, a gynecologic oncology fellow at Memorial Sloan Kettering Cancer Center, New York, discusses the findings, their implications and context in this age of #MeToo and #TimesUp, and potential approaches to addressing the ongoing problem and the concerns victims have about reporting harassment.
“We need to start by setting an example, saying these things are not tolerated [and] put that into policy – really show folks how it can be reported and what is being done once that report is filed,” she said.
Dr. Stasenko reported having no disclosures.
SOURCE: Stasenko M et al. ASCO 2019, Abstract LBA10502.
CHICAGO – Nearly two-thirds of more than 400 U.S.-based physician members of the Society of Gynecologic Oncology who participated in a recent survey reported experiencing sexual harassment in training or practice.
Notably, of the 255 women and 147 men who responded, 71% and 51%, respectively, reported such sexual harassment – and only 15% overall reported it to officials, Marina Stasenko, MD, reported at the annual meeting of the American Society of Clinical Oncology.
The survey also addressed gender-based discrimination and disparities, including respondents’ views on pay disparities. In this video interview, Dr. Stasenko, a gynecologic oncology fellow at Memorial Sloan Kettering Cancer Center, New York, discusses the findings, their implications and context in this age of #MeToo and #TimesUp, and potential approaches to addressing the ongoing problem and the concerns victims have about reporting harassment.
“We need to start by setting an example, saying these things are not tolerated [and] put that into policy – really show folks how it can be reported and what is being done once that report is filed,” she said.
Dr. Stasenko reported having no disclosures.
SOURCE: Stasenko M et al. ASCO 2019, Abstract LBA10502.
REPORTING FROM ASCO 2019

Pivotal trial shows HFrEF benefits from baroreceptor stimulation
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.

The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.

Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.
Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.
Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.
The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.
The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
REPORTING FROM HEART RHYTHM 2019
Cumulative smoking affects skin manifestations of SLE
SAN FRANCISCO – Nnenna Ezeh reported at an international congress on systemic lupus erythematosus.

“We saw in our study a suggestion of a dose-response relationship. If we tell patients, ‘The more you smoke, the more likely you are to have chronic skin disease or skin damage that’s permanent,’ it could be a way to trigger more smoking cessation strategies in their mind,” said Ms. Ezeh, of the University of Wisconsin, Madison. “We know that skin manifestations of lupus have a major negative impact on a patient’s quality of life, so this could be a way to decrease smoking by saying, ‘Not only does smoking impact your heart and put you at risk for cardiovascular disease, it also affects your skin.’ It’s a way to bridge the priorities that physicians have with the priorities that patients have.”
She presented a retrospective study of the medical records of 632 consecutive SLE patients seen at the university medical center’s ambulatory rheumatology clinic. Slightly more than 60% of them were never smokers; 8.7% had a history of low smoking exposure, defined as less than 5 pack-years; 5.8% had a medium-smoking history of 5-10 pack-years; 15% had a high-smoking history, with more than 10 pack-years; and the smoking history of 10% of the patients was unrecorded.
In a multivariate analysis adjusted for age, sex, and race, the low-smoking group was ninefold more likely than never smokers to develop any mucocutaneous manifestations of SLE, including a malar or discoid rash, mucosal ulcers, photosensitivity, alopecia, or scarring. They were also 3.7 times more likely to meet any Systemic Lupus International Collaborating Clinics (SLICC) cutaneous criteria and twofold more likely than never smokers to meet any of the American College of Rheumatology cutaneous criteria. Patients with an intermediate smoking exposure history of 5-10 pack-years were 2.3-fold more likely to meet any SLICC cutaneous criteria.
The risks of meeting SLICC chronic cutaneous criteria and SLICC Damage Index skin damage criteria rose in a linear fashion with the number of pack-years of smoking. Those SLE patients with more than a 10 pack-year smoking history were 4.2-fold more likely than never smokers to fulfill any SLICC Damage Index skin damage criteria, which consist of scarring alopecia, extensive scarring, or skin ulcers. The heaviest smokers were also at 2.1-fold increased risk of discoid lupus and 2.2-fold more likely to meet SLICC chronic cutaneous criteria, according to Ms. Ezeh.
Patients of color, who comprised 18% of the study population, were significantly more likely to smoke than white patients. Independent of their smoking history, however, they had significantly increased risks of chronic cutaneous manifestations of lupus and of irreversible skin damage.
Ms. Ezeh reported having no financial conflicts regarding her study, supported by a grant from the Rheumatology Research Foundation.
SAN FRANCISCO – Nnenna Ezeh reported at an international congress on systemic lupus erythematosus.
“We saw in our study a suggestion of a dose-response relationship. If we tell patients, ‘The more you smoke, the more likely you are to have chronic skin disease or skin damage that’s permanent,’ it could be a way to trigger more smoking cessation strategies in their mind,” said Ms. Ezeh, of the University of Wisconsin, Madison. “We know that skin manifestations of lupus have a major negative impact on a patient’s quality of life, so this could be a way to decrease smoking by saying, ‘Not only does smoking impact your heart and put you at risk for cardiovascular disease, it also affects your skin.’ It’s a way to bridge the priorities that physicians have with the priorities that patients have.”
She presented a retrospective study of the medical records of 632 consecutive SLE patients seen at the university medical center’s ambulatory rheumatology clinic. Slightly more than 60% of them were never smokers; 8.7% had a history of low smoking exposure, defined as less than 5 pack-years; 5.8% had a medium-smoking history of 5-10 pack-years; 15% had a high-smoking history, with more than 10 pack-years; and the smoking history of 10% of the patients was unrecorded.
In a multivariate analysis adjusted for age, sex, and race, the low-smoking group was ninefold more likely than never smokers to develop any mucocutaneous manifestations of SLE, including a malar or discoid rash, mucosal ulcers, photosensitivity, alopecia, or scarring. They were also 3.7 times more likely to meet any Systemic Lupus International Collaborating Clinics (SLICC) cutaneous criteria and twofold more likely than never smokers to meet any of the American College of Rheumatology cutaneous criteria. Patients with an intermediate smoking exposure history of 5-10 pack-years were 2.3-fold more likely to meet any SLICC cutaneous criteria.
The risks of meeting SLICC chronic cutaneous criteria and SLICC Damage Index skin damage criteria rose in a linear fashion with the number of pack-years of smoking. Those SLE patients with more than a 10 pack-year smoking history were 4.2-fold more likely than never smokers to fulfill any SLICC Damage Index skin damage criteria, which consist of scarring alopecia, extensive scarring, or skin ulcers. The heaviest smokers were also at 2.1-fold increased risk of discoid lupus and 2.2-fold more likely to meet SLICC chronic cutaneous criteria, according to Ms. Ezeh.
Patients of color, who comprised 18% of the study population, were significantly more likely to smoke than white patients. Independent of their smoking history, however, they had significantly increased risks of chronic cutaneous manifestations of lupus and of irreversible skin damage.
Ms. Ezeh reported having no financial conflicts regarding her study, supported by a grant from the Rheumatology Research Foundation.
SAN FRANCISCO – Nnenna Ezeh reported at an international congress on systemic lupus erythematosus.
“We saw in our study a suggestion of a dose-response relationship. If we tell patients, ‘The more you smoke, the more likely you are to have chronic skin disease or skin damage that’s permanent,’ it could be a way to trigger more smoking cessation strategies in their mind,” said Ms. Ezeh, of the University of Wisconsin, Madison. “We know that skin manifestations of lupus have a major negative impact on a patient’s quality of life, so this could be a way to decrease smoking by saying, ‘Not only does smoking impact your heart and put you at risk for cardiovascular disease, it also affects your skin.’ It’s a way to bridge the priorities that physicians have with the priorities that patients have.”
She presented a retrospective study of the medical records of 632 consecutive SLE patients seen at the university medical center’s ambulatory rheumatology clinic. Slightly more than 60% of them were never smokers; 8.7% had a history of low smoking exposure, defined as less than 5 pack-years; 5.8% had a medium-smoking history of 5-10 pack-years; 15% had a high-smoking history, with more than 10 pack-years; and the smoking history of 10% of the patients was unrecorded.
In a multivariate analysis adjusted for age, sex, and race, the low-smoking group was ninefold more likely than never smokers to develop any mucocutaneous manifestations of SLE, including a malar or discoid rash, mucosal ulcers, photosensitivity, alopecia, or scarring. They were also 3.7 times more likely to meet any Systemic Lupus International Collaborating Clinics (SLICC) cutaneous criteria and twofold more likely than never smokers to meet any of the American College of Rheumatology cutaneous criteria. Patients with an intermediate smoking exposure history of 5-10 pack-years were 2.3-fold more likely to meet any SLICC cutaneous criteria.
The risks of meeting SLICC chronic cutaneous criteria and SLICC Damage Index skin damage criteria rose in a linear fashion with the number of pack-years of smoking. Those SLE patients with more than a 10 pack-year smoking history were 4.2-fold more likely than never smokers to fulfill any SLICC Damage Index skin damage criteria, which consist of scarring alopecia, extensive scarring, or skin ulcers. The heaviest smokers were also at 2.1-fold increased risk of discoid lupus and 2.2-fold more likely to meet SLICC chronic cutaneous criteria, according to Ms. Ezeh.
Patients of color, who comprised 18% of the study population, were significantly more likely to smoke than white patients. Independent of their smoking history, however, they had significantly increased risks of chronic cutaneous manifestations of lupus and of irreversible skin damage.
Ms. Ezeh reported having no financial conflicts regarding her study, supported by a grant from the Rheumatology Research Foundation.
REPORTING FROM LUPUS 2019
FDA approves Keytruda for metastatic HNSCC
The Food and Drug Administration has approved pembrolizumab (Keytruda) for the first-line treatment of patients with metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC).

FDA approval was based on results of the randomized, multicenter, three-arm, open‑label, active‑controlled KEYNOTE-048 trial. The 882 patients in the trial had metastatic HNSCC, and they received either single-agent pembrolizumab; pembrolizumab, carboplatin or cisplatin, and platinum and fluorouracil; or cetuximab, carboplatin or cisplatin, and platinum and fluorouracil.
Patients who received pembrolizumab plus chemotherapy had a mean overall survival of 13.0 months, compared with 10.7 months in the cetuximab plus chemotherapy group (hazard ratio, 0.77; 95% CI, 0.63-0.93; P = .0067).
In the patient subgroups that received single-agent pembrolizumab, overall survival was 12.3 months in patients with a Combined Positive Score of at least 1, compared with 10.3 months for the cetuximab plus chemotherapy group (HR, 0.78; 95% CI, 0.64-0.96; P = .0171). In patients with a Combined Positive Score of at least 20, overall survival was 14.9 months in the pembrolizumab-only group and 10.7 months in the cetuximab plus chemotherapy group (HR, 0.61; 95% CI, 0.45-0.83; P = .0015).
The most common adverse events in patients who received single-agent pembrolizumab were fatigue, constipation, and rash. In patients who received pembrolizumab plus chemotherapy, the most common adverse events were nausea, fatigue, constipation, vomiting, mucosal inflammation, diarrhea, decreased appetite, stomatitis, and cough.
Pembrolizumab is approved for use in combination with platinum and fluorouracil for all patients and as a single agent for patients whose tumors express programmed death–ligand 1, the FDA said.
The FDA also expanded the intended use for the PD-L1 IHC 22C3 pharmDx kit to include use as a companion diagnostic device for selecting patients with HNSCC for treatment with pembrolizumab as a single agent.
Find the full press release on the FDA website.
The Food and Drug Administration has approved pembrolizumab (Keytruda) for the first-line treatment of patients with metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC).
FDA approval was based on results of the randomized, multicenter, three-arm, open‑label, active‑controlled KEYNOTE-048 trial. The 882 patients in the trial had metastatic HNSCC, and they received either single-agent pembrolizumab; pembrolizumab, carboplatin or cisplatin, and platinum and fluorouracil; or cetuximab, carboplatin or cisplatin, and platinum and fluorouracil.
Patients who received pembrolizumab plus chemotherapy had a mean overall survival of 13.0 months, compared with 10.7 months in the cetuximab plus chemotherapy group (hazard ratio, 0.77; 95% CI, 0.63-0.93; P = .0067).
In the patient subgroups that received single-agent pembrolizumab, overall survival was 12.3 months in patients with a Combined Positive Score of at least 1, compared with 10.3 months for the cetuximab plus chemotherapy group (HR, 0.78; 95% CI, 0.64-0.96; P = .0171). In patients with a Combined Positive Score of at least 20, overall survival was 14.9 months in the pembrolizumab-only group and 10.7 months in the cetuximab plus chemotherapy group (HR, 0.61; 95% CI, 0.45-0.83; P = .0015).
The most common adverse events in patients who received single-agent pembrolizumab were fatigue, constipation, and rash. In patients who received pembrolizumab plus chemotherapy, the most common adverse events were nausea, fatigue, constipation, vomiting, mucosal inflammation, diarrhea, decreased appetite, stomatitis, and cough.
Pembrolizumab is approved for use in combination with platinum and fluorouracil for all patients and as a single agent for patients whose tumors express programmed death–ligand 1, the FDA said.
The FDA also expanded the intended use for the PD-L1 IHC 22C3 pharmDx kit to include use as a companion diagnostic device for selecting patients with HNSCC for treatment with pembrolizumab as a single agent.
Find the full press release on the FDA website.
The Food and Drug Administration has approved pembrolizumab (Keytruda) for the first-line treatment of patients with metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC).
FDA approval was based on results of the randomized, multicenter, three-arm, open‑label, active‑controlled KEYNOTE-048 trial. The 882 patients in the trial had metastatic HNSCC, and they received either single-agent pembrolizumab; pembrolizumab, carboplatin or cisplatin, and platinum and fluorouracil; or cetuximab, carboplatin or cisplatin, and platinum and fluorouracil.
Patients who received pembrolizumab plus chemotherapy had a mean overall survival of 13.0 months, compared with 10.7 months in the cetuximab plus chemotherapy group (hazard ratio, 0.77; 95% CI, 0.63-0.93; P = .0067).
In the patient subgroups that received single-agent pembrolizumab, overall survival was 12.3 months in patients with a Combined Positive Score of at least 1, compared with 10.3 months for the cetuximab plus chemotherapy group (HR, 0.78; 95% CI, 0.64-0.96; P = .0171). In patients with a Combined Positive Score of at least 20, overall survival was 14.9 months in the pembrolizumab-only group and 10.7 months in the cetuximab plus chemotherapy group (HR, 0.61; 95% CI, 0.45-0.83; P = .0015).
The most common adverse events in patients who received single-agent pembrolizumab were fatigue, constipation, and rash. In patients who received pembrolizumab plus chemotherapy, the most common adverse events were nausea, fatigue, constipation, vomiting, mucosal inflammation, diarrhea, decreased appetite, stomatitis, and cough.
Pembrolizumab is approved for use in combination with platinum and fluorouracil for all patients and as a single agent for patients whose tumors express programmed death–ligand 1, the FDA said.
The FDA also expanded the intended use for the PD-L1 IHC 22C3 pharmDx kit to include use as a companion diagnostic device for selecting patients with HNSCC for treatment with pembrolizumab as a single agent.
Find the full press release on the FDA website.