User login
Medicare study evaluates impact of U.S. Hospital Readmissions Reduction Program
Research offers evidence against calls to curtail the program
Among Medicare beneficiaries admitted to the hospital between 2008 and 2016, there was an increase in postdischarge 30-day mortality for patients with heart failure, but not for those with acute myocardial infarction or pneumonia.

The finding comes from an effort to evaluate the use of services soon after discharge for conditions targeted in the U.S. Hospital Readmissions Reduction Program (HRRP), and patients’ outcomes.
“The announcement and implementation of the HRRP were associated with a reduction in readmissions within 30 days of discharge for heart failure, acute myocardial infarction, and pneumonia, as shown by a decrease in the overall national rate of readmissions,” first author Rohan Khera, MD, and colleagues wrote in a study published online Jan. 15, 2020, in the British Medical Journal (doi:10.1136/bmj.l6831).
“Concerns existed that pressures to reduce readmissions had led to the evolution of care patterns that may have adverse consequences through reducing access to care in appropriate settings. Therefore, determining whether patients who are seen in acute care settings, but not admitted to hospital, experience an increased risk of mortality is essential.”
Dr. Khera, a cardiologist at the University of Texas Southwestern Medical Center, Dallas, and colleagues limited the analysis to Medicare claims data from patients who were admitted to the hospital with heart failure, acute myocardial infarction (MI), or pneumonia between 2008 and 2016. Key outcomes of interest were: (1) postdischarge 30-day mortality; and (2) acute care utilization in inpatient units, observation units, and the ED during the postdischarge period.
During the study period there were 3,772,924 hospital admissions for heart failure, 1,570,113 for acute MI, and 3,131,162 for pneumonia. The greatest number of readmissions within 30 days of discharge was for heart failure patients (22.5%), followed by acute MI (17.5%), and pneumonia (17.2%).
The overall rates of observation stays were 1.7% for heart failure, 2.6% for acute MI, and 1.4% for pneumonia, while the overall rates of emergency department visits were 6.4% for heart failure, 6.8% for acute MI, and 6.3% for pneumonia. Cumulatively, about one-third of all admissions – 30.7% for heart failure, 26.9% for acute MI, and 24.8% for pneumonia – received postdischarge care in any acute care setting.
Dr. Khera and colleagues found that overall postdischarge 30-day mortality was 8.7% for heart failure, 7.3% for acute MI, and 8.4% for pneumonia. At the same time, postdischarge 30-day mortality was higher in patients with readmissions (13.2% for heart failure, 12.7% for acute MI, and 15.3% for pneumonia), compared with those who had observation stays (4.5% for heart failure, 2.7% for acute MI, and 4.6% for pneumonia), emergency department visits (9.7% for heart failure, 8.8% for acute MI, and 7.8% for pneumonia), or no postdischarge acute care (7.2% for heart failure, 6.0% for acute MI, and 6.9% for pneumonia). Risk adjusted mortality increased annually by 0.05% only for heart failure, while it decreased by 0.06% for acute MI, and did not significantly change for pneumonia.
“The study strongly suggests that the HRRP did not lead to harm through inappropriate triage of patients at high risk to observation units and the emergency department, and therefore provides evidence against calls to curtail the program owing to this theoretical concern (see JAMA 2018;320:2539-41),” the researchers concluded.
They acknowledged certain limitations of the study, including the fact that they were “unable to identify patterns of acute care during the index hospital admission that would be associated with a higher rate of postdischarge acute care in observation units and emergency departments and whether these visits represented avenues for planned postdischarge follow-up care. Moreover, the proportion of these care encounters that were preventable remains poorly understood.”
Dr. Khera disclosed that he is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. His coauthors reported having numerous disclosures.
SOURCE: Khera et al. BMJ 2020;368:l6831.
Research offers evidence against calls to curtail the program
Research offers evidence against calls to curtail the program
Among Medicare beneficiaries admitted to the hospital between 2008 and 2016, there was an increase in postdischarge 30-day mortality for patients with heart failure, but not for those with acute myocardial infarction or pneumonia.
The finding comes from an effort to evaluate the use of services soon after discharge for conditions targeted in the U.S. Hospital Readmissions Reduction Program (HRRP), and patients’ outcomes.
“The announcement and implementation of the HRRP were associated with a reduction in readmissions within 30 days of discharge for heart failure, acute myocardial infarction, and pneumonia, as shown by a decrease in the overall national rate of readmissions,” first author Rohan Khera, MD, and colleagues wrote in a study published online Jan. 15, 2020, in the British Medical Journal (doi:10.1136/bmj.l6831).
“Concerns existed that pressures to reduce readmissions had led to the evolution of care patterns that may have adverse consequences through reducing access to care in appropriate settings. Therefore, determining whether patients who are seen in acute care settings, but not admitted to hospital, experience an increased risk of mortality is essential.”
Dr. Khera, a cardiologist at the University of Texas Southwestern Medical Center, Dallas, and colleagues limited the analysis to Medicare claims data from patients who were admitted to the hospital with heart failure, acute myocardial infarction (MI), or pneumonia between 2008 and 2016. Key outcomes of interest were: (1) postdischarge 30-day mortality; and (2) acute care utilization in inpatient units, observation units, and the ED during the postdischarge period.
During the study period there were 3,772,924 hospital admissions for heart failure, 1,570,113 for acute MI, and 3,131,162 for pneumonia. The greatest number of readmissions within 30 days of discharge was for heart failure patients (22.5%), followed by acute MI (17.5%), and pneumonia (17.2%).
The overall rates of observation stays were 1.7% for heart failure, 2.6% for acute MI, and 1.4% for pneumonia, while the overall rates of emergency department visits were 6.4% for heart failure, 6.8% for acute MI, and 6.3% for pneumonia. Cumulatively, about one-third of all admissions – 30.7% for heart failure, 26.9% for acute MI, and 24.8% for pneumonia – received postdischarge care in any acute care setting.
Dr. Khera and colleagues found that overall postdischarge 30-day mortality was 8.7% for heart failure, 7.3% for acute MI, and 8.4% for pneumonia. At the same time, postdischarge 30-day mortality was higher in patients with readmissions (13.2% for heart failure, 12.7% for acute MI, and 15.3% for pneumonia), compared with those who had observation stays (4.5% for heart failure, 2.7% for acute MI, and 4.6% for pneumonia), emergency department visits (9.7% for heart failure, 8.8% for acute MI, and 7.8% for pneumonia), or no postdischarge acute care (7.2% for heart failure, 6.0% for acute MI, and 6.9% for pneumonia). Risk adjusted mortality increased annually by 0.05% only for heart failure, while it decreased by 0.06% for acute MI, and did not significantly change for pneumonia.
“The study strongly suggests that the HRRP did not lead to harm through inappropriate triage of patients at high risk to observation units and the emergency department, and therefore provides evidence against calls to curtail the program owing to this theoretical concern (see JAMA 2018;320:2539-41),” the researchers concluded.
They acknowledged certain limitations of the study, including the fact that they were “unable to identify patterns of acute care during the index hospital admission that would be associated with a higher rate of postdischarge acute care in observation units and emergency departments and whether these visits represented avenues for planned postdischarge follow-up care. Moreover, the proportion of these care encounters that were preventable remains poorly understood.”
Dr. Khera disclosed that he is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. His coauthors reported having numerous disclosures.
SOURCE: Khera et al. BMJ 2020;368:l6831.
Among Medicare beneficiaries admitted to the hospital between 2008 and 2016, there was an increase in postdischarge 30-day mortality for patients with heart failure, but not for those with acute myocardial infarction or pneumonia.
The finding comes from an effort to evaluate the use of services soon after discharge for conditions targeted in the U.S. Hospital Readmissions Reduction Program (HRRP), and patients’ outcomes.
“The announcement and implementation of the HRRP were associated with a reduction in readmissions within 30 days of discharge for heart failure, acute myocardial infarction, and pneumonia, as shown by a decrease in the overall national rate of readmissions,” first author Rohan Khera, MD, and colleagues wrote in a study published online Jan. 15, 2020, in the British Medical Journal (doi:10.1136/bmj.l6831).
“Concerns existed that pressures to reduce readmissions had led to the evolution of care patterns that may have adverse consequences through reducing access to care in appropriate settings. Therefore, determining whether patients who are seen in acute care settings, but not admitted to hospital, experience an increased risk of mortality is essential.”
Dr. Khera, a cardiologist at the University of Texas Southwestern Medical Center, Dallas, and colleagues limited the analysis to Medicare claims data from patients who were admitted to the hospital with heart failure, acute myocardial infarction (MI), or pneumonia between 2008 and 2016. Key outcomes of interest were: (1) postdischarge 30-day mortality; and (2) acute care utilization in inpatient units, observation units, and the ED during the postdischarge period.
During the study period there were 3,772,924 hospital admissions for heart failure, 1,570,113 for acute MI, and 3,131,162 for pneumonia. The greatest number of readmissions within 30 days of discharge was for heart failure patients (22.5%), followed by acute MI (17.5%), and pneumonia (17.2%).
The overall rates of observation stays were 1.7% for heart failure, 2.6% for acute MI, and 1.4% for pneumonia, while the overall rates of emergency department visits were 6.4% for heart failure, 6.8% for acute MI, and 6.3% for pneumonia. Cumulatively, about one-third of all admissions – 30.7% for heart failure, 26.9% for acute MI, and 24.8% for pneumonia – received postdischarge care in any acute care setting.
Dr. Khera and colleagues found that overall postdischarge 30-day mortality was 8.7% for heart failure, 7.3% for acute MI, and 8.4% for pneumonia. At the same time, postdischarge 30-day mortality was higher in patients with readmissions (13.2% for heart failure, 12.7% for acute MI, and 15.3% for pneumonia), compared with those who had observation stays (4.5% for heart failure, 2.7% for acute MI, and 4.6% for pneumonia), emergency department visits (9.7% for heart failure, 8.8% for acute MI, and 7.8% for pneumonia), or no postdischarge acute care (7.2% for heart failure, 6.0% for acute MI, and 6.9% for pneumonia). Risk adjusted mortality increased annually by 0.05% only for heart failure, while it decreased by 0.06% for acute MI, and did not significantly change for pneumonia.
“The study strongly suggests that the HRRP did not lead to harm through inappropriate triage of patients at high risk to observation units and the emergency department, and therefore provides evidence against calls to curtail the program owing to this theoretical concern (see JAMA 2018;320:2539-41),” the researchers concluded.
They acknowledged certain limitations of the study, including the fact that they were “unable to identify patterns of acute care during the index hospital admission that would be associated with a higher rate of postdischarge acute care in observation units and emergency departments and whether these visits represented avenues for planned postdischarge follow-up care. Moreover, the proportion of these care encounters that were preventable remains poorly understood.”
Dr. Khera disclosed that he is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. His coauthors reported having numerous disclosures.
SOURCE: Khera et al. BMJ 2020;368:l6831.
FROM BMJ
Flu activity increases for third straight week
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
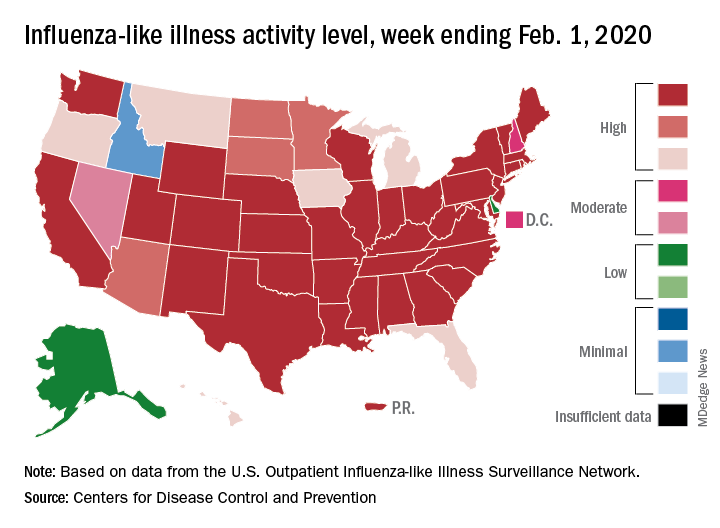
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
For the second time during the 2019-2020 flu season, activity measures have climbed into noteworthy territory.
The proportion of outpatient visits for influenza-like illness (ILI) reached its highest December level, 7.1%, since 2003 and then dropped for 2 weeks. Three weeks of increases since then, however, have the outpatient-visit rate at 6.7% for the week ending Feb. 1, 2020, the Centers for Disease Control and Prevention reported. The baseline rate for the United States is 2.4%.
That rate of 6.7% is already above the highest rates recorded in eight of the last nine flu seasons, and another increase could mean a second, separate trip above 7.0% in the 2019-2020 season – something that has not occurred since national tracking began in 1997, CDC data show.
Those same data also show that,
Another important measure on the rise, the proportion of respiratory specimens testing positive for influenza, reached a new high for the season, 29.8%, during the week of Feb. 1, the CDC’s influenza division said.
Tests at clinical laboratories also show that predominance is continuing to switch from type B (45.6%) to type A (54.4%), the influenza division noted. Overall predominance for the season, however, continues to favor type B, 59.3% to 40.7%.
The percentage of deaths caused by pneumonia and influenza, which passed the threshold for epidemic of 7.2% back in early January, has been trending downward for the last 3 weeks and was 7.1% as of Feb. 1, according to the influenza division.
ILI-related deaths among children continue to remain high, with a total count of 78 for the season after another 10 deaths were reported during the week ending Feb. 1, the CDC reported. Comparable numbers for the last three seasons are 44 (2018-2019), 97 (2017-2018), and 35 (2016-2017).
The CDC estimates put the total number of ILIs at around 22 million for the season so far, leading to 210,000 hospitalizations. The agency said that it expects to release estimates of vaccine effectiveness later this month.
Adding ilixadencel improved outcomes in metastatic renal cell carcinoma
ORLANDO –

The confirmed overall response rate was 42.2% (19/45) in patients who received ilixadencel plus sunitinib and 24.0% (6/25) in patients who received sunitinib monotherapy. Magnus Lindskog, MD, PhD, of Uppsala (Sweden) University Hospital, reported these results at the ASCO-SITC Immuno-Oncology Symposium.
The complete response rate was 11.1% with ilixadencel plus sunitinib and 4% with sunitinib monotherapy. The confirmed complete response rates were 6.7% and 0%, respectively.
The median duration of response was 7.1 months with ilixadencel plus sunitinib and 2.9 months with sunitinib monotherapy. The median progression-free survival was 11.8 months and 11.0 months, respectively.
There was no difference in median overall survival – a coprimary endpoint – at 18 months, nor was there a difference in progression-free survival at that time. “We do find it interesting that there is a late separation of both [survival] curves like we see in many immunotherapy trials,” Dr. Lindskog said, noting that all five complete responders in the combination therapy arm were alive at 33 months, whereas the single patient with a complete response in the monotherapy group died after 41 months.
“So far, we have 54% versus 37% still alive in the ilixadencel versus sunitinib groups,” Dr. Lindskog said, adding that the observed activity of ilixadencel appears to be driven by responses in patients with intermediate risk.
The overall survival data in the intermediate-risk patients is not mature. The overall survival in poor-risk patients was 11.6 months in the combination group and 9.3 months in the monotherapy group.
MERECA study participants were adults with a mean age of 62-64 years who were considered surgical candidates. They were enrolled from eight centers in Europe and the United States between April 2014 and January 2017 and randomized 2:1 to the combination and monotherapy arms. In all, 45 patients received their assigned treatment in the combination arm, and 25 patients received their assigned treatment in the monotherapy arm.
Patients in the ilixadencel arm were injected twice, 2 weeks apart, at the primary tumor site using CT guidance. Patients in the monotherapy arm were observed until nephrectomy. Both groups received sunitinib after nephrectomy, which was performed within 6 weeks, and all were followed for 18 months.
Treatment was well tolerated. Ilixadencel did not add any clinically meaningful treatment-related grade 3-4 adverse events or serious adverse events, Dr. Lindskog said. He noted that the most common ilixadencel-related adverse event was uncomplicated pyrexia.
There were no signs of induced autoimmunity, and although 57% of patients in the combination therapy group developed ilixadencel-specific alloantibodies, this had no relationship to responses, Dr. Lindskog said.
“From this phase 2 study, we have confirmed the feasibility and safety of ilixadencel and sunitinib combined in newly diagnosed synchronous metastatic renal cell carcinoma patients,” he said.
He added that longer follow-up is needed to understand the late divergence in survival curves between the groups. Survival follow-up will continue for 5 years.
This study was funded by Immunicum. Dr. Lindskog disclosed relationships with Pfizer, Bristol-Myers Squibb, and Ipsen.
SOURCE: Lindskog M et al. ASCO-SITC 2020, Abstract 11.
ORLANDO –
The confirmed overall response rate was 42.2% (19/45) in patients who received ilixadencel plus sunitinib and 24.0% (6/25) in patients who received sunitinib monotherapy. Magnus Lindskog, MD, PhD, of Uppsala (Sweden) University Hospital, reported these results at the ASCO-SITC Immuno-Oncology Symposium.
The complete response rate was 11.1% with ilixadencel plus sunitinib and 4% with sunitinib monotherapy. The confirmed complete response rates were 6.7% and 0%, respectively.
The median duration of response was 7.1 months with ilixadencel plus sunitinib and 2.9 months with sunitinib monotherapy. The median progression-free survival was 11.8 months and 11.0 months, respectively.
There was no difference in median overall survival – a coprimary endpoint – at 18 months, nor was there a difference in progression-free survival at that time. “We do find it interesting that there is a late separation of both [survival] curves like we see in many immunotherapy trials,” Dr. Lindskog said, noting that all five complete responders in the combination therapy arm were alive at 33 months, whereas the single patient with a complete response in the monotherapy group died after 41 months.
“So far, we have 54% versus 37% still alive in the ilixadencel versus sunitinib groups,” Dr. Lindskog said, adding that the observed activity of ilixadencel appears to be driven by responses in patients with intermediate risk.
The overall survival data in the intermediate-risk patients is not mature. The overall survival in poor-risk patients was 11.6 months in the combination group and 9.3 months in the monotherapy group.
MERECA study participants were adults with a mean age of 62-64 years who were considered surgical candidates. They were enrolled from eight centers in Europe and the United States between April 2014 and January 2017 and randomized 2:1 to the combination and monotherapy arms. In all, 45 patients received their assigned treatment in the combination arm, and 25 patients received their assigned treatment in the monotherapy arm.
Patients in the ilixadencel arm were injected twice, 2 weeks apart, at the primary tumor site using CT guidance. Patients in the monotherapy arm were observed until nephrectomy. Both groups received sunitinib after nephrectomy, which was performed within 6 weeks, and all were followed for 18 months.
Treatment was well tolerated. Ilixadencel did not add any clinically meaningful treatment-related grade 3-4 adverse events or serious adverse events, Dr. Lindskog said. He noted that the most common ilixadencel-related adverse event was uncomplicated pyrexia.
There were no signs of induced autoimmunity, and although 57% of patients in the combination therapy group developed ilixadencel-specific alloantibodies, this had no relationship to responses, Dr. Lindskog said.
“From this phase 2 study, we have confirmed the feasibility and safety of ilixadencel and sunitinib combined in newly diagnosed synchronous metastatic renal cell carcinoma patients,” he said.
He added that longer follow-up is needed to understand the late divergence in survival curves between the groups. Survival follow-up will continue for 5 years.
This study was funded by Immunicum. Dr. Lindskog disclosed relationships with Pfizer, Bristol-Myers Squibb, and Ipsen.
SOURCE: Lindskog M et al. ASCO-SITC 2020, Abstract 11.
ORLANDO –
The confirmed overall response rate was 42.2% (19/45) in patients who received ilixadencel plus sunitinib and 24.0% (6/25) in patients who received sunitinib monotherapy. Magnus Lindskog, MD, PhD, of Uppsala (Sweden) University Hospital, reported these results at the ASCO-SITC Immuno-Oncology Symposium.
The complete response rate was 11.1% with ilixadencel plus sunitinib and 4% with sunitinib monotherapy. The confirmed complete response rates were 6.7% and 0%, respectively.
The median duration of response was 7.1 months with ilixadencel plus sunitinib and 2.9 months with sunitinib monotherapy. The median progression-free survival was 11.8 months and 11.0 months, respectively.
There was no difference in median overall survival – a coprimary endpoint – at 18 months, nor was there a difference in progression-free survival at that time. “We do find it interesting that there is a late separation of both [survival] curves like we see in many immunotherapy trials,” Dr. Lindskog said, noting that all five complete responders in the combination therapy arm were alive at 33 months, whereas the single patient with a complete response in the monotherapy group died after 41 months.
“So far, we have 54% versus 37% still alive in the ilixadencel versus sunitinib groups,” Dr. Lindskog said, adding that the observed activity of ilixadencel appears to be driven by responses in patients with intermediate risk.
The overall survival data in the intermediate-risk patients is not mature. The overall survival in poor-risk patients was 11.6 months in the combination group and 9.3 months in the monotherapy group.
MERECA study participants were adults with a mean age of 62-64 years who were considered surgical candidates. They were enrolled from eight centers in Europe and the United States between April 2014 and January 2017 and randomized 2:1 to the combination and monotherapy arms. In all, 45 patients received their assigned treatment in the combination arm, and 25 patients received their assigned treatment in the monotherapy arm.
Patients in the ilixadencel arm were injected twice, 2 weeks apart, at the primary tumor site using CT guidance. Patients in the monotherapy arm were observed until nephrectomy. Both groups received sunitinib after nephrectomy, which was performed within 6 weeks, and all were followed for 18 months.
Treatment was well tolerated. Ilixadencel did not add any clinically meaningful treatment-related grade 3-4 adverse events or serious adverse events, Dr. Lindskog said. He noted that the most common ilixadencel-related adverse event was uncomplicated pyrexia.
There were no signs of induced autoimmunity, and although 57% of patients in the combination therapy group developed ilixadencel-specific alloantibodies, this had no relationship to responses, Dr. Lindskog said.
“From this phase 2 study, we have confirmed the feasibility and safety of ilixadencel and sunitinib combined in newly diagnosed synchronous metastatic renal cell carcinoma patients,” he said.
He added that longer follow-up is needed to understand the late divergence in survival curves between the groups. Survival follow-up will continue for 5 years.
This study was funded by Immunicum. Dr. Lindskog disclosed relationships with Pfizer, Bristol-Myers Squibb, and Ipsen.
SOURCE: Lindskog M et al. ASCO-SITC 2020, Abstract 11.
REPORTING FROM THE CLINICAL IMMUNO-ONCOLOGY SYMPOSIUM
APOE genotype directly regulates alpha-synuclein accumulation
Apolipoprotein E epsilon 4 (APOE4) directly and independently exacerbates accumulation of alpha-synuclein in patients with Lewy body dementia, whereas APOE2 may have a protective effect, based on two recent studies involving mouse models and human patients.

These insights confirm the importance of APOE in synucleinopathies, and may lead to new treatments, according to Eliezer Masliah, MD, director of the division of neuroscience at the National Institute on Aging.
“These [studies] definitely implicate a role of APOE4,” Dr. Masliah said in an interview.
According to Dr. Masliah, previous studies linked the APOE4 genotype with cognitive decline in synucleinopathies, but underlying molecular mechanisms remained unknown.
“We [now] have more direct confirmation [based on] different experimental animal models,” Dr. Masliah said. “It also means that APOE4 could be a therapeutic target for dementia with Lewy bodies.”
The two studies were published simultaneously in Science Translational Medicine. The first study was conducted by Albert A. Davis, MD, PhD, of Washington University, St. Louis, and colleagues; the second was led by Na Zhao, MD, PhD, of the Mayo Clinic in Jacksonville, Fla.
“The studies are very synergistic, but used different techniques,” said Dr. Masliah, who was not involved in the studies.
Both studies involved mice that expressed a human variant of APOE: APOE2, APOE3, or APOE4. Three independent techniques were used to concurrently overexpress alpha-synuclein; Dr. Davis and colleagues used a transgenic approach, as well as striatal injection of alpha-synuclein preformed fibrils, whereas Dr. Zhao and colleagues turned to a viral vector. Regardless of technique, each APOE variant had a distinct impact on the level of alpha-synuclein accumulation.
“In a nutshell, [Dr. Davis and colleagues] found that those mice that have synuclein and APOE4 have a much more rapid progression of the disease,” Dr. Masliah said. “They become Parkinsonian much faster, but also, they become cognitively impaired much faster, and they have more synuclein in the brain. Remarkably, on the opposite side, those that were expressing APOE2, which we know is a protective allele, actually were far less impaired. So that’s really a remarkable finding.”
The study at the Mayo Clinic echoed these findings.
“Essentially, [Dr. Zhao and colleagues] had very similar results,” Dr. Masliah said. “[In mice expressing] APOE4, synuclein accumulation was worse and pathology was worse, and with APOE2, there was relative protection.”
Both studies found that the exacerbating effect of APOE4 translated to human patients.
Dr. Davis and colleagues evaluated data from 251 patients in the Parkinson’s Progression Markers Initiative. A multivariate model showed that patients with the APOE4 genotype had faster cognitive decline, an impact that was independent of other variables, including cerebrospinal fluid concentrations of amyloid beta and tau protein (P = .0119). This finding was further supported by additional analyses involving 177 patients with Parkinson’s disease from the Washington University Movement Disorders Center, and another 1,030 patients enrolled in the NeuroGenetics Research Consortium study.
Dr. Zhao and colleagues evaluated postmortem samples from patients with Lewy body dementia who had minimal amyloid pathology. Comparing 22 APOE4 carriers versus 22 age- and sex-matched noncarriers, they found that carriers had significantly greater accumulations of alpha-synuclein (P less than .05).
According to the investigators, these findings could have both prognostic and therapeutic implications.
“[I]t is intriguing to speculate whether APOE and other potential genetic risk or resilience genes could be useful as screening tools to stratify risk for individual patients,” Dr. Davis and colleagues wrote in their paper. They went on to suggest that APOE genotyping may one day be used to personalize treatments for patients with neurodegenerative disease.
According to Dr. Masliah, several treatment strategies are under investigation.
“There are some pharmaceutical companies and also some academic groups that have been developing antibodies against APOE4 for Alzheimer’s disease, but certainly that could also be used for dementia with Lewy bodies,” he said. “There are other ways. One could [be] to suppress the expression of APOE4 with antisense or other technologies.
“There is also a very innovative technology that has been developed by the group at the Gladstone Institutes in San Francisco, which is to switch APOE4 to APOE3.” This technique, Dr. Masliah explained, is accomplished by breaking a disulfide bond in APOE4, which opens the structure into an isoform that mimics APOE3. “They have developed small molecules that actually can break that bond and essentially chemically switch APOE4 to APOE3,” he said.
Although multiple techniques are feasible, Dr. Masliah stressed that these therapeutic efforts are still in their infancy.
“We need to better understand the mechanisms as to how APOE4 and alpha-synuclein interact,” he said. “I think we need a lot more work in this area.”
The Davis study was funded by the American Academy of Neurology/American Brain Foundation, the BrightFocus Foundation, the Mary E. Groff Charitable Trust, and others; the investigators reported additional relationships with Biogen, Alector, Parabon, and others. The Zhao study was funded by the National Institutes of Health and the Lewy Body Dementia Center Without Walls; the investigators reported no competing interests. Dr. Masliah reported no conflicts of interest.
SOURCES: Davis AA et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay3069; Zhao N et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay1809.
Apolipoprotein E epsilon 4 (APOE4) directly and independently exacerbates accumulation of alpha-synuclein in patients with Lewy body dementia, whereas APOE2 may have a protective effect, based on two recent studies involving mouse models and human patients.
These insights confirm the importance of APOE in synucleinopathies, and may lead to new treatments, according to Eliezer Masliah, MD, director of the division of neuroscience at the National Institute on Aging.
“These [studies] definitely implicate a role of APOE4,” Dr. Masliah said in an interview.
According to Dr. Masliah, previous studies linked the APOE4 genotype with cognitive decline in synucleinopathies, but underlying molecular mechanisms remained unknown.
“We [now] have more direct confirmation [based on] different experimental animal models,” Dr. Masliah said. “It also means that APOE4 could be a therapeutic target for dementia with Lewy bodies.”
The two studies were published simultaneously in Science Translational Medicine. The first study was conducted by Albert A. Davis, MD, PhD, of Washington University, St. Louis, and colleagues; the second was led by Na Zhao, MD, PhD, of the Mayo Clinic in Jacksonville, Fla.
“The studies are very synergistic, but used different techniques,” said Dr. Masliah, who was not involved in the studies.
Both studies involved mice that expressed a human variant of APOE: APOE2, APOE3, or APOE4. Three independent techniques were used to concurrently overexpress alpha-synuclein; Dr. Davis and colleagues used a transgenic approach, as well as striatal injection of alpha-synuclein preformed fibrils, whereas Dr. Zhao and colleagues turned to a viral vector. Regardless of technique, each APOE variant had a distinct impact on the level of alpha-synuclein accumulation.
“In a nutshell, [Dr. Davis and colleagues] found that those mice that have synuclein and APOE4 have a much more rapid progression of the disease,” Dr. Masliah said. “They become Parkinsonian much faster, but also, they become cognitively impaired much faster, and they have more synuclein in the brain. Remarkably, on the opposite side, those that were expressing APOE2, which we know is a protective allele, actually were far less impaired. So that’s really a remarkable finding.”
The study at the Mayo Clinic echoed these findings.
“Essentially, [Dr. Zhao and colleagues] had very similar results,” Dr. Masliah said. “[In mice expressing] APOE4, synuclein accumulation was worse and pathology was worse, and with APOE2, there was relative protection.”
Both studies found that the exacerbating effect of APOE4 translated to human patients.
Dr. Davis and colleagues evaluated data from 251 patients in the Parkinson’s Progression Markers Initiative. A multivariate model showed that patients with the APOE4 genotype had faster cognitive decline, an impact that was independent of other variables, including cerebrospinal fluid concentrations of amyloid beta and tau protein (P = .0119). This finding was further supported by additional analyses involving 177 patients with Parkinson’s disease from the Washington University Movement Disorders Center, and another 1,030 patients enrolled in the NeuroGenetics Research Consortium study.
Dr. Zhao and colleagues evaluated postmortem samples from patients with Lewy body dementia who had minimal amyloid pathology. Comparing 22 APOE4 carriers versus 22 age- and sex-matched noncarriers, they found that carriers had significantly greater accumulations of alpha-synuclein (P less than .05).
According to the investigators, these findings could have both prognostic and therapeutic implications.
“[I]t is intriguing to speculate whether APOE and other potential genetic risk or resilience genes could be useful as screening tools to stratify risk for individual patients,” Dr. Davis and colleagues wrote in their paper. They went on to suggest that APOE genotyping may one day be used to personalize treatments for patients with neurodegenerative disease.
According to Dr. Masliah, several treatment strategies are under investigation.
“There are some pharmaceutical companies and also some academic groups that have been developing antibodies against APOE4 for Alzheimer’s disease, but certainly that could also be used for dementia with Lewy bodies,” he said. “There are other ways. One could [be] to suppress the expression of APOE4 with antisense or other technologies.
“There is also a very innovative technology that has been developed by the group at the Gladstone Institutes in San Francisco, which is to switch APOE4 to APOE3.” This technique, Dr. Masliah explained, is accomplished by breaking a disulfide bond in APOE4, which opens the structure into an isoform that mimics APOE3. “They have developed small molecules that actually can break that bond and essentially chemically switch APOE4 to APOE3,” he said.
Although multiple techniques are feasible, Dr. Masliah stressed that these therapeutic efforts are still in their infancy.
“We need to better understand the mechanisms as to how APOE4 and alpha-synuclein interact,” he said. “I think we need a lot more work in this area.”
The Davis study was funded by the American Academy of Neurology/American Brain Foundation, the BrightFocus Foundation, the Mary E. Groff Charitable Trust, and others; the investigators reported additional relationships with Biogen, Alector, Parabon, and others. The Zhao study was funded by the National Institutes of Health and the Lewy Body Dementia Center Without Walls; the investigators reported no competing interests. Dr. Masliah reported no conflicts of interest.
SOURCES: Davis AA et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay3069; Zhao N et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay1809.
Apolipoprotein E epsilon 4 (APOE4) directly and independently exacerbates accumulation of alpha-synuclein in patients with Lewy body dementia, whereas APOE2 may have a protective effect, based on two recent studies involving mouse models and human patients.
These insights confirm the importance of APOE in synucleinopathies, and may lead to new treatments, according to Eliezer Masliah, MD, director of the division of neuroscience at the National Institute on Aging.
“These [studies] definitely implicate a role of APOE4,” Dr. Masliah said in an interview.
According to Dr. Masliah, previous studies linked the APOE4 genotype with cognitive decline in synucleinopathies, but underlying molecular mechanisms remained unknown.
“We [now] have more direct confirmation [based on] different experimental animal models,” Dr. Masliah said. “It also means that APOE4 could be a therapeutic target for dementia with Lewy bodies.”
The two studies were published simultaneously in Science Translational Medicine. The first study was conducted by Albert A. Davis, MD, PhD, of Washington University, St. Louis, and colleagues; the second was led by Na Zhao, MD, PhD, of the Mayo Clinic in Jacksonville, Fla.
“The studies are very synergistic, but used different techniques,” said Dr. Masliah, who was not involved in the studies.
Both studies involved mice that expressed a human variant of APOE: APOE2, APOE3, or APOE4. Three independent techniques were used to concurrently overexpress alpha-synuclein; Dr. Davis and colleagues used a transgenic approach, as well as striatal injection of alpha-synuclein preformed fibrils, whereas Dr. Zhao and colleagues turned to a viral vector. Regardless of technique, each APOE variant had a distinct impact on the level of alpha-synuclein accumulation.
“In a nutshell, [Dr. Davis and colleagues] found that those mice that have synuclein and APOE4 have a much more rapid progression of the disease,” Dr. Masliah said. “They become Parkinsonian much faster, but also, they become cognitively impaired much faster, and they have more synuclein in the brain. Remarkably, on the opposite side, those that were expressing APOE2, which we know is a protective allele, actually were far less impaired. So that’s really a remarkable finding.”
The study at the Mayo Clinic echoed these findings.
“Essentially, [Dr. Zhao and colleagues] had very similar results,” Dr. Masliah said. “[In mice expressing] APOE4, synuclein accumulation was worse and pathology was worse, and with APOE2, there was relative protection.”
Both studies found that the exacerbating effect of APOE4 translated to human patients.
Dr. Davis and colleagues evaluated data from 251 patients in the Parkinson’s Progression Markers Initiative. A multivariate model showed that patients with the APOE4 genotype had faster cognitive decline, an impact that was independent of other variables, including cerebrospinal fluid concentrations of amyloid beta and tau protein (P = .0119). This finding was further supported by additional analyses involving 177 patients with Parkinson’s disease from the Washington University Movement Disorders Center, and another 1,030 patients enrolled in the NeuroGenetics Research Consortium study.
Dr. Zhao and colleagues evaluated postmortem samples from patients with Lewy body dementia who had minimal amyloid pathology. Comparing 22 APOE4 carriers versus 22 age- and sex-matched noncarriers, they found that carriers had significantly greater accumulations of alpha-synuclein (P less than .05).
According to the investigators, these findings could have both prognostic and therapeutic implications.
“[I]t is intriguing to speculate whether APOE and other potential genetic risk or resilience genes could be useful as screening tools to stratify risk for individual patients,” Dr. Davis and colleagues wrote in their paper. They went on to suggest that APOE genotyping may one day be used to personalize treatments for patients with neurodegenerative disease.
According to Dr. Masliah, several treatment strategies are under investigation.
“There are some pharmaceutical companies and also some academic groups that have been developing antibodies against APOE4 for Alzheimer’s disease, but certainly that could also be used for dementia with Lewy bodies,” he said. “There are other ways. One could [be] to suppress the expression of APOE4 with antisense or other technologies.
“There is also a very innovative technology that has been developed by the group at the Gladstone Institutes in San Francisco, which is to switch APOE4 to APOE3.” This technique, Dr. Masliah explained, is accomplished by breaking a disulfide bond in APOE4, which opens the structure into an isoform that mimics APOE3. “They have developed small molecules that actually can break that bond and essentially chemically switch APOE4 to APOE3,” he said.
Although multiple techniques are feasible, Dr. Masliah stressed that these therapeutic efforts are still in their infancy.
“We need to better understand the mechanisms as to how APOE4 and alpha-synuclein interact,” he said. “I think we need a lot more work in this area.”
The Davis study was funded by the American Academy of Neurology/American Brain Foundation, the BrightFocus Foundation, the Mary E. Groff Charitable Trust, and others; the investigators reported additional relationships with Biogen, Alector, Parabon, and others. The Zhao study was funded by the National Institutes of Health and the Lewy Body Dementia Center Without Walls; the investigators reported no competing interests. Dr. Masliah reported no conflicts of interest.
SOURCES: Davis AA et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay3069; Zhao N et al. Sci Transl Med. 2020 Feb 5. doi: 10.1126/scitranslmed.aay1809.
FROM SCIENCE TRANSLATIONAL MEDICINE
Meta-analysis eyes impact of adherence to HCQ among SLE patients
Low serum levels of hydroxychloroquine (HCQ) among patients with systemic lupus erythematosus are associated with a threefold increased likelihood of physician- and patient-reported nonadherence to the medication. In addition, routine monitoring of HCQ levels are associated with improvements in adherence and disease activity.

Those are two key findings from a systematic review and meta-analysis published in Arthritis Care & Research.
“HCQ is recommended for all patients with systemic lupus erythematosus (SLE, or lupus) to reduce disease activity and improve damage-free-survival,” the authors, led by Shivani Garg, MD, of the University of Wisconsin–Madison, wrote in the article. “Yet, up to 83% of lupus patients are nonadherent to HCQ commonly because of poor understanding of benefits of HCQ, lack of motivation to continue therapy, and inflated concerns regarding side effects from HCQ use.”
For their analysis, the researchers drew from 17 published observational and interventional studies that measured HCQ levels and assessed adherence or Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in adults with SLE. They used forest plots to compare pooled estimates of correlations between HCQ levels and reported nonadherence, or SLEDAI scores. Patient-reported nonadherence was defined as less than 80% medication adherence reported, and physician-reported adherence was estimated based on physicians’ interpretations of the previous month’s adherence as reported by patients during clinic visits.
The study population consisted of 1,223 patients. Dr. Garg and colleagues found a threefold higher odds of reported nonadherence in patients with low HCQ levels (odds ratio, 2.95; P less than .001). The mean SLEDAI score was 3.14 points higher in a group with below-threshold HCQ levels on a priori analysis (P = .053), and 1.4 points higher in a group with HCQ levels below 500 ng/mL (P = .039). Among all patients, those with HCQ levels 750 ng/mL or greater had a 58% lower risk of active disease, and their SLEDAI score was 3.2 points lower. “Our study support levels greater than or equal to 750 ng/mL to be clinically meaningful and statistically significant to identify disease flare (change in SLEDAI greater than or equal to 3 points) and predict active disease (SLEDAI greater than or equal to 6),” the authors wrote.

In an interview, Michelle A. Petri, MD, MPH, took issue with the HCQ goal of 750 ng/mL or greater recommended by the authors. “I think that was premature,” said Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore. “We presented data at last year’s ACR [which showed] that the level needs to be higher than that to prevent thrombosis. But it is important to open the discussion that HCQ blood levels are not just for nonadherence. I believe they will help us to reduce retinopathy, and also to make sure the dose remains in an efficacious range, such as what is needed to prevent thrombosis.”
Dr. Petri, who also directs the Hopkins Lupus Center, said that the study’s overall conclusions confirms the need for blood testing for HCQ to identify nonadherence. “Everyone remembers the saying of the [former] Surgeon General Dr. C. Everett Koop: ‘Drugs can’t work if patients don’t take them!’ – in particular, blood levels which represent what the patient has taken in the last month. I call blood levels the ‘lupus A1C.’ ”
She added that HCQ blood levels have utility for nonadherence, prediction of retinopathy, and prevention of thrombosis. Such tests “are now much more widely available, including by some large national laboratories such as Quest Diagnostics, as well as by Exagen. No more excuses.” LabCorp plans to start offering HCQ blood level testing by the middle of 2020, she said.
In their manuscript, the study authors acknowledged certain limitations of their analysis, including the fact that there were only four studies that measured HCQ levels and nonadherence or SLEDAI. “Second, most of the studies that examined the correlation between reported adherence and HCQ blood levels were performed in Europe, and there was only one small U.S. study,” they wrote. “Therefore, generalizability for our findings could be limited because of differences in cultural beliefs, social issues, and insurance/medical coverage in populations from diverse countries.”
The study authors reported having no disclosures. Dr. Petri disclosed that she has conducted research on HCQ that was funded by the National Institutes of Health. She has also conducted research for Exagen.
SOURCE: Garg S et al. Arthritis Care Res. 2020 Jan 31. doi: 10.1002/acr.24155.
Low serum levels of hydroxychloroquine (HCQ) among patients with systemic lupus erythematosus are associated with a threefold increased likelihood of physician- and patient-reported nonadherence to the medication. In addition, routine monitoring of HCQ levels are associated with improvements in adherence and disease activity.
Those are two key findings from a systematic review and meta-analysis published in Arthritis Care & Research.
“HCQ is recommended for all patients with systemic lupus erythematosus (SLE, or lupus) to reduce disease activity and improve damage-free-survival,” the authors, led by Shivani Garg, MD, of the University of Wisconsin–Madison, wrote in the article. “Yet, up to 83% of lupus patients are nonadherent to HCQ commonly because of poor understanding of benefits of HCQ, lack of motivation to continue therapy, and inflated concerns regarding side effects from HCQ use.”
For their analysis, the researchers drew from 17 published observational and interventional studies that measured HCQ levels and assessed adherence or Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in adults with SLE. They used forest plots to compare pooled estimates of correlations between HCQ levels and reported nonadherence, or SLEDAI scores. Patient-reported nonadherence was defined as less than 80% medication adherence reported, and physician-reported adherence was estimated based on physicians’ interpretations of the previous month’s adherence as reported by patients during clinic visits.
The study population consisted of 1,223 patients. Dr. Garg and colleagues found a threefold higher odds of reported nonadherence in patients with low HCQ levels (odds ratio, 2.95; P less than .001). The mean SLEDAI score was 3.14 points higher in a group with below-threshold HCQ levels on a priori analysis (P = .053), and 1.4 points higher in a group with HCQ levels below 500 ng/mL (P = .039). Among all patients, those with HCQ levels 750 ng/mL or greater had a 58% lower risk of active disease, and their SLEDAI score was 3.2 points lower. “Our study support levels greater than or equal to 750 ng/mL to be clinically meaningful and statistically significant to identify disease flare (change in SLEDAI greater than or equal to 3 points) and predict active disease (SLEDAI greater than or equal to 6),” the authors wrote.
In an interview, Michelle A. Petri, MD, MPH, took issue with the HCQ goal of 750 ng/mL or greater recommended by the authors. “I think that was premature,” said Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore. “We presented data at last year’s ACR [which showed] that the level needs to be higher than that to prevent thrombosis. But it is important to open the discussion that HCQ blood levels are not just for nonadherence. I believe they will help us to reduce retinopathy, and also to make sure the dose remains in an efficacious range, such as what is needed to prevent thrombosis.”
Dr. Petri, who also directs the Hopkins Lupus Center, said that the study’s overall conclusions confirms the need for blood testing for HCQ to identify nonadherence. “Everyone remembers the saying of the [former] Surgeon General Dr. C. Everett Koop: ‘Drugs can’t work if patients don’t take them!’ – in particular, blood levels which represent what the patient has taken in the last month. I call blood levels the ‘lupus A1C.’ ”
She added that HCQ blood levels have utility for nonadherence, prediction of retinopathy, and prevention of thrombosis. Such tests “are now much more widely available, including by some large national laboratories such as Quest Diagnostics, as well as by Exagen. No more excuses.” LabCorp plans to start offering HCQ blood level testing by the middle of 2020, she said.
In their manuscript, the study authors acknowledged certain limitations of their analysis, including the fact that there were only four studies that measured HCQ levels and nonadherence or SLEDAI. “Second, most of the studies that examined the correlation between reported adherence and HCQ blood levels were performed in Europe, and there was only one small U.S. study,” they wrote. “Therefore, generalizability for our findings could be limited because of differences in cultural beliefs, social issues, and insurance/medical coverage in populations from diverse countries.”
The study authors reported having no disclosures. Dr. Petri disclosed that she has conducted research on HCQ that was funded by the National Institutes of Health. She has also conducted research for Exagen.
SOURCE: Garg S et al. Arthritis Care Res. 2020 Jan 31. doi: 10.1002/acr.24155.
Low serum levels of hydroxychloroquine (HCQ) among patients with systemic lupus erythematosus are associated with a threefold increased likelihood of physician- and patient-reported nonadherence to the medication. In addition, routine monitoring of HCQ levels are associated with improvements in adherence and disease activity.
Those are two key findings from a systematic review and meta-analysis published in Arthritis Care & Research.
“HCQ is recommended for all patients with systemic lupus erythematosus (SLE, or lupus) to reduce disease activity and improve damage-free-survival,” the authors, led by Shivani Garg, MD, of the University of Wisconsin–Madison, wrote in the article. “Yet, up to 83% of lupus patients are nonadherent to HCQ commonly because of poor understanding of benefits of HCQ, lack of motivation to continue therapy, and inflated concerns regarding side effects from HCQ use.”
For their analysis, the researchers drew from 17 published observational and interventional studies that measured HCQ levels and assessed adherence or Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in adults with SLE. They used forest plots to compare pooled estimates of correlations between HCQ levels and reported nonadherence, or SLEDAI scores. Patient-reported nonadherence was defined as less than 80% medication adherence reported, and physician-reported adherence was estimated based on physicians’ interpretations of the previous month’s adherence as reported by patients during clinic visits.
The study population consisted of 1,223 patients. Dr. Garg and colleagues found a threefold higher odds of reported nonadherence in patients with low HCQ levels (odds ratio, 2.95; P less than .001). The mean SLEDAI score was 3.14 points higher in a group with below-threshold HCQ levels on a priori analysis (P = .053), and 1.4 points higher in a group with HCQ levels below 500 ng/mL (P = .039). Among all patients, those with HCQ levels 750 ng/mL or greater had a 58% lower risk of active disease, and their SLEDAI score was 3.2 points lower. “Our study support levels greater than or equal to 750 ng/mL to be clinically meaningful and statistically significant to identify disease flare (change in SLEDAI greater than or equal to 3 points) and predict active disease (SLEDAI greater than or equal to 6),” the authors wrote.
In an interview, Michelle A. Petri, MD, MPH, took issue with the HCQ goal of 750 ng/mL or greater recommended by the authors. “I think that was premature,” said Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore. “We presented data at last year’s ACR [which showed] that the level needs to be higher than that to prevent thrombosis. But it is important to open the discussion that HCQ blood levels are not just for nonadherence. I believe they will help us to reduce retinopathy, and also to make sure the dose remains in an efficacious range, such as what is needed to prevent thrombosis.”
Dr. Petri, who also directs the Hopkins Lupus Center, said that the study’s overall conclusions confirms the need for blood testing for HCQ to identify nonadherence. “Everyone remembers the saying of the [former] Surgeon General Dr. C. Everett Koop: ‘Drugs can’t work if patients don’t take them!’ – in particular, blood levels which represent what the patient has taken in the last month. I call blood levels the ‘lupus A1C.’ ”
She added that HCQ blood levels have utility for nonadherence, prediction of retinopathy, and prevention of thrombosis. Such tests “are now much more widely available, including by some large national laboratories such as Quest Diagnostics, as well as by Exagen. No more excuses.” LabCorp plans to start offering HCQ blood level testing by the middle of 2020, she said.
In their manuscript, the study authors acknowledged certain limitations of their analysis, including the fact that there were only four studies that measured HCQ levels and nonadherence or SLEDAI. “Second, most of the studies that examined the correlation between reported adherence and HCQ blood levels were performed in Europe, and there was only one small U.S. study,” they wrote. “Therefore, generalizability for our findings could be limited because of differences in cultural beliefs, social issues, and insurance/medical coverage in populations from diverse countries.”
The study authors reported having no disclosures. Dr. Petri disclosed that she has conducted research on HCQ that was funded by the National Institutes of Health. She has also conducted research for Exagen.
SOURCE: Garg S et al. Arthritis Care Res. 2020 Jan 31. doi: 10.1002/acr.24155.
FROM ARTHRITIS CARE & RESEARCH
Any dose of HPV vaccine is better than none
A single dose of the human papillomavirus vaccine is as effective as two or three doses for preventing cervical cancer in girls and women vaccinated at 15-19 years of age, based on data from a retrospective study of more than 100,000 girls and women.
The Centers for Disease Control and Prevention’s current recommendations include a two-dose vaccine schedule for the HPV vaccine for girls and boys younger than 15 years, and a three-dose schedule for girls and young women aged 16-26 years who had their first dose before turning 15.
However, rates of HPV vaccination in the United States fall short of those in other developed nations, and evidence supporting the protective value of a specific number of vaccine doses are mixed, wrote Ana M. Rodriguez, MD, MPH, of the University of Texas Medical Branch at Galveston, and colleagues. Fewer than three doses could have benefits, including easier logistics, lower costs, higher acceptance rates, and fewer side effects, they said. The study was published in Cancer.
The researchers reviewed data from 66,541 girls and women aged 9-26 years who had received at least one dose of HPV vaccine (4vHPV) between Jan. 1, 2006, and June 30, 2015, and 66,541 matched unvaccinated controls. The primary outcomes were histologically confirmed preinvasive cervical disease and high-grade cytology.
Overall, the adjusted hazard ratios for histologically confirmed preinvasive cervical disease among patients vaccinated at the ages of 15-19 years with one, two, and three doses were similar, at 0.64, 0.72, and 0.66, respectively, compared with unvaccinated individuals.
The risk of high-grade cytology was significantly lower for girls and women who received three doses at age 15-19 years, compared with unvaccinated individuals, but no difference was seen in high-grade cytology between unvaccinated individuals and those who received one or two doses. In addition, the unadjusted rate of preinvasive cervical disease at 5 years was 2.65% for unvaccinated teens aged 15-19 years, compared with 1.62%, 1.99%, and 1.86% in the one-, two- and three-dose groups, respectively.The findings were limited by several factors, including the use of billing codes to determine outcomes and the inability to determine potential vaccination through multiple insurance carriers, and the inclusion only of privately insured patients from the claims database, the researchers noted.
However, the results support findings from previous studies and show a similar level of association between varying vaccine doses and preinvasive cervical lesions in the 15- to 19-year-old population, they said.
“Efforts should focus on not only the need to initiate the HPV vaccine but also the need for beginning and continuing cervical cancer screening among young women who are vaccinated at older ages (18 years and older),” they said.
In an editorial accompanying the study, Julia M.L. Brotherton, PhD, MPH, and Karin Sundström, MD, PhD, of the University of Melbourne, Australia, and the Karolinska Institutet, Stockholm, respectively, wrote that the study’s strengths included the large numbers of girls and women who received a single dose of the HPV vaccine, compared with previous studies, as well as the adjustments for histories of sexually transmitted infections and pregnancy (Cancer. 2020 Feb 10. doi: 10.1002/cncr.32696). “Initial observational data from vaccination programs did not support equivalent one-dose protection against genital warts or cervical disease, but such data may have been confounded by potentially higher risk characteristics of women who only ever received one or two doses of an intended three-dose course i.e., women noncompliant with the vaccine program [amplified by the monitoring of outcomes among the initial catch-up populations of already infected women]) and by the inherent bias that prevalent infection/disease is more likely to become apparent coincidently with the earlier doses in a vaccine course,” they said. The study findings have implications for global goals to eliminate cervical cancer, the editorial authors noted.
“If one dose of an HPV vaccine were sufficient for effective protection, HPV vaccine implementation and scale-up would require less logistics (while being amenable to a periodic campaign approach), available doses could be extended further, and the overall cost would be lower,” they said.
The study was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health, and by the Cancer Prevention Research Institute of Texas. The researchers had no financial conflicts to disclose.
Dr. Brotherton disclosed serving as an investigator for Seqirus and Merck; Dr. Sundström disclosed research funding for her institution from Merck and MSD Sweden.
SOURCE: Rodriguez AM et al. Cancer. 2020 Feb 10. doi: 10.1002/cncr.32700.
A single dose of the human papillomavirus vaccine is as effective as two or three doses for preventing cervical cancer in girls and women vaccinated at 15-19 years of age, based on data from a retrospective study of more than 100,000 girls and women.
The Centers for Disease Control and Prevention’s current recommendations include a two-dose vaccine schedule for the HPV vaccine for girls and boys younger than 15 years, and a three-dose schedule for girls and young women aged 16-26 years who had their first dose before turning 15.
However, rates of HPV vaccination in the United States fall short of those in other developed nations, and evidence supporting the protective value of a specific number of vaccine doses are mixed, wrote Ana M. Rodriguez, MD, MPH, of the University of Texas Medical Branch at Galveston, and colleagues. Fewer than three doses could have benefits, including easier logistics, lower costs, higher acceptance rates, and fewer side effects, they said. The study was published in Cancer.
The researchers reviewed data from 66,541 girls and women aged 9-26 years who had received at least one dose of HPV vaccine (4vHPV) between Jan. 1, 2006, and June 30, 2015, and 66,541 matched unvaccinated controls. The primary outcomes were histologically confirmed preinvasive cervical disease and high-grade cytology.
Overall, the adjusted hazard ratios for histologically confirmed preinvasive cervical disease among patients vaccinated at the ages of 15-19 years with one, two, and three doses were similar, at 0.64, 0.72, and 0.66, respectively, compared with unvaccinated individuals.
The risk of high-grade cytology was significantly lower for girls and women who received three doses at age 15-19 years, compared with unvaccinated individuals, but no difference was seen in high-grade cytology between unvaccinated individuals and those who received one or two doses. In addition, the unadjusted rate of preinvasive cervical disease at 5 years was 2.65% for unvaccinated teens aged 15-19 years, compared with 1.62%, 1.99%, and 1.86% in the one-, two- and three-dose groups, respectively.The findings were limited by several factors, including the use of billing codes to determine outcomes and the inability to determine potential vaccination through multiple insurance carriers, and the inclusion only of privately insured patients from the claims database, the researchers noted.
However, the results support findings from previous studies and show a similar level of association between varying vaccine doses and preinvasive cervical lesions in the 15- to 19-year-old population, they said.
“Efforts should focus on not only the need to initiate the HPV vaccine but also the need for beginning and continuing cervical cancer screening among young women who are vaccinated at older ages (18 years and older),” they said.
In an editorial accompanying the study, Julia M.L. Brotherton, PhD, MPH, and Karin Sundström, MD, PhD, of the University of Melbourne, Australia, and the Karolinska Institutet, Stockholm, respectively, wrote that the study’s strengths included the large numbers of girls and women who received a single dose of the HPV vaccine, compared with previous studies, as well as the adjustments for histories of sexually transmitted infections and pregnancy (Cancer. 2020 Feb 10. doi: 10.1002/cncr.32696). “Initial observational data from vaccination programs did not support equivalent one-dose protection against genital warts or cervical disease, but such data may have been confounded by potentially higher risk characteristics of women who only ever received one or two doses of an intended three-dose course i.e., women noncompliant with the vaccine program [amplified by the monitoring of outcomes among the initial catch-up populations of already infected women]) and by the inherent bias that prevalent infection/disease is more likely to become apparent coincidently with the earlier doses in a vaccine course,” they said. The study findings have implications for global goals to eliminate cervical cancer, the editorial authors noted.
“If one dose of an HPV vaccine were sufficient for effective protection, HPV vaccine implementation and scale-up would require less logistics (while being amenable to a periodic campaign approach), available doses could be extended further, and the overall cost would be lower,” they said.
The study was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health, and by the Cancer Prevention Research Institute of Texas. The researchers had no financial conflicts to disclose.
Dr. Brotherton disclosed serving as an investigator for Seqirus and Merck; Dr. Sundström disclosed research funding for her institution from Merck and MSD Sweden.
SOURCE: Rodriguez AM et al. Cancer. 2020 Feb 10. doi: 10.1002/cncr.32700.
A single dose of the human papillomavirus vaccine is as effective as two or three doses for preventing cervical cancer in girls and women vaccinated at 15-19 years of age, based on data from a retrospective study of more than 100,000 girls and women.
The Centers for Disease Control and Prevention’s current recommendations include a two-dose vaccine schedule for the HPV vaccine for girls and boys younger than 15 years, and a three-dose schedule for girls and young women aged 16-26 years who had their first dose before turning 15.
However, rates of HPV vaccination in the United States fall short of those in other developed nations, and evidence supporting the protective value of a specific number of vaccine doses are mixed, wrote Ana M. Rodriguez, MD, MPH, of the University of Texas Medical Branch at Galveston, and colleagues. Fewer than three doses could have benefits, including easier logistics, lower costs, higher acceptance rates, and fewer side effects, they said. The study was published in Cancer.
The researchers reviewed data from 66,541 girls and women aged 9-26 years who had received at least one dose of HPV vaccine (4vHPV) between Jan. 1, 2006, and June 30, 2015, and 66,541 matched unvaccinated controls. The primary outcomes were histologically confirmed preinvasive cervical disease and high-grade cytology.
Overall, the adjusted hazard ratios for histologically confirmed preinvasive cervical disease among patients vaccinated at the ages of 15-19 years with one, two, and three doses were similar, at 0.64, 0.72, and 0.66, respectively, compared with unvaccinated individuals.
The risk of high-grade cytology was significantly lower for girls and women who received three doses at age 15-19 years, compared with unvaccinated individuals, but no difference was seen in high-grade cytology between unvaccinated individuals and those who received one or two doses. In addition, the unadjusted rate of preinvasive cervical disease at 5 years was 2.65% for unvaccinated teens aged 15-19 years, compared with 1.62%, 1.99%, and 1.86% in the one-, two- and three-dose groups, respectively.The findings were limited by several factors, including the use of billing codes to determine outcomes and the inability to determine potential vaccination through multiple insurance carriers, and the inclusion only of privately insured patients from the claims database, the researchers noted.
However, the results support findings from previous studies and show a similar level of association between varying vaccine doses and preinvasive cervical lesions in the 15- to 19-year-old population, they said.
“Efforts should focus on not only the need to initiate the HPV vaccine but also the need for beginning and continuing cervical cancer screening among young women who are vaccinated at older ages (18 years and older),” they said.
In an editorial accompanying the study, Julia M.L. Brotherton, PhD, MPH, and Karin Sundström, MD, PhD, of the University of Melbourne, Australia, and the Karolinska Institutet, Stockholm, respectively, wrote that the study’s strengths included the large numbers of girls and women who received a single dose of the HPV vaccine, compared with previous studies, as well as the adjustments for histories of sexually transmitted infections and pregnancy (Cancer. 2020 Feb 10. doi: 10.1002/cncr.32696). “Initial observational data from vaccination programs did not support equivalent one-dose protection against genital warts or cervical disease, but such data may have been confounded by potentially higher risk characteristics of women who only ever received one or two doses of an intended three-dose course i.e., women noncompliant with the vaccine program [amplified by the monitoring of outcomes among the initial catch-up populations of already infected women]) and by the inherent bias that prevalent infection/disease is more likely to become apparent coincidently with the earlier doses in a vaccine course,” they said. The study findings have implications for global goals to eliminate cervical cancer, the editorial authors noted.
“If one dose of an HPV vaccine were sufficient for effective protection, HPV vaccine implementation and scale-up would require less logistics (while being amenable to a periodic campaign approach), available doses could be extended further, and the overall cost would be lower,” they said.
The study was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health, and by the Cancer Prevention Research Institute of Texas. The researchers had no financial conflicts to disclose.
Dr. Brotherton disclosed serving as an investigator for Seqirus and Merck; Dr. Sundström disclosed research funding for her institution from Merck and MSD Sweden.
SOURCE: Rodriguez AM et al. Cancer. 2020 Feb 10. doi: 10.1002/cncr.32700.
FROM CANCER
Key clinical point: HPV vaccination was similarly effective for preventing cervical cancer in girls and women who received 1, 2, or 3 doses at age 15-19 years.
Major finding: The adjusted hazard ratios for preinvasive cervical disease for women vaccinated at age 15-19 years with 1, 2, and 3 doses of the HPV vaccine were 0.64, 0.72, and 0.66 respectively.
Study details: The data come from a retrospective matched cohort study of 133,082 women from the Optum Clinformatics DataMart Database.
Disclosures: The study was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the Cancer Prevention Research Institute of Texas. The researchers disclosed no financial conflicts.
Source: Rodriguez AM et al. Cancer. 2020 Feb 10. doi: 10.1002/cncr.32700.
Abbreviated MRI equals standard protocol for high-risk breast cancer screens
CHICAGO – An abbreviated magnetic resonance imaging (MRI) protocol for screening individuals at high risk for breast cancer performed as well as a standard protocol, in about half the time and with greater patient satisfaction.
The abbreviated protocol also resulted in fewer false positive findings, with 5% fewer patients receiving biopsies for benign lesions than with a standard protocol (8.4% versus 13.7%, P less than .001).
Findings from the prospective 10-month trial conducted in the province of Ontario were presented by Jean Seely, MD, professor of radiology at the University of Ottawa, at the annual meeting of the Radiological Society of North America.
“The abbreviated protocol was shown to be as effective as the standard protocol in high-risk screening breast MRI, supporting previous studies,” said Dr. Seely. The shorter protocol took 16.3 minutes on average, compared with 27 minutes for the standard MRI protocol. This difference resulted in a 50% increase in institutional capacity, or a jump from two to three patients screened per hour.
In the province of Ontario, said Dr. Seely, women assessed at being at a 25% or greater lifetime risk of breast cancer receive MRIs as part of the Ontario Breast Screening Program (OBSP), which calculates risk by using the International Breast Cancer Intervention Study model.
For high-risk patients, the OBSP model provides annual mammography and an MRI for women between the ages of 30 and 60 years. Not only is the half-hour duration of the standard protocol resource-intensive, especially in regions with limited scanner availability, but patients may either be reluctant to undergo a half-hour scan, or not tolerate a lengthy scan very well.
Dr. Seely cited previous work (J Clin Oncol. 2014 Aug 1;32[22]:2304-10) showing that an abbreviated MRI protocol has similar accuracy as the full standard protocol. With the foundation of evidence from this study, Dr. Seely and her collaborators compared outcomes for high-risk patients who were screened with an abbreviated versus a standard protocol.
The abbreviated protocol, approved by the American College of Radiology, omits a final round of image acquisition sequences at the 9-minute mark after gadolinium administration, instead performing acquisition at 1, 2, 3, and 4 minutes after contrast delivery. Total time required for this protocol is just over 13 minutes, said Dr. Seely, and additional diagnostic MRIs were not required.
The trial was constructed so that the abbreviated protocol was used for the entire OBSP cohort for 10 months in 2018. Results were compared with those from the 12 previous months, when OBSP patients’ MRIs were performed using the standard protocol.
A total of 881 patients received standard-protocol MRIs; about three quarters (651) of those patients had previous MRI screening, while the remaining 230 patients had a baseline screen via the standard protocol.
Of the 658 patients in the abbreviated protocol group, 135, or about 20%, received the briefer scans as a baseline screen; the remast of the patients in this arm had received earlier MRI screening.
In addition to tracking scanning times, Dr. Seely and her collaborators also compared cancer detection rates, Breast Imaging Reporting and Data System (BI-RADS) assessment categories, positive predictive values, and the abnormal interpretation rate – that is, how many scans fell into BI-RADS categories 0, 4, and 5.
No significant difference was found between the rates of BI-RADs 0, 3, or 5 studies between the groups. Significantly fewer abbreviated scans fell into the BI-RADS 4 category, however (9.3% vs. 14.9%; P less than .001).
Similarly, the abnormal interpretation rate was 12.5% for the abbreviated protocol, compared with 17.5% for the standard protocol (P less than .007), with a correspondingly lower biopsy rate of 8.4% for the abbreviated protocol, compared with 13.7% for the standard protocol (P less than .001). The overall cancer detection rate did not differ between groups.
She and her colleagues will continue to track outcomes for those receiving abbreviated screening within the province of Ontario to track performance over time.
Dr. Seely reported that she had no relevant conflicts of interest. She reported no funding source beyond the province of Ontario.
SOURCE: Seely J et al. RSNA 2019, Session RC-215-04.
CHICAGO – An abbreviated magnetic resonance imaging (MRI) protocol for screening individuals at high risk for breast cancer performed as well as a standard protocol, in about half the time and with greater patient satisfaction.
The abbreviated protocol also resulted in fewer false positive findings, with 5% fewer patients receiving biopsies for benign lesions than with a standard protocol (8.4% versus 13.7%, P less than .001).
Findings from the prospective 10-month trial conducted in the province of Ontario were presented by Jean Seely, MD, professor of radiology at the University of Ottawa, at the annual meeting of the Radiological Society of North America.
“The abbreviated protocol was shown to be as effective as the standard protocol in high-risk screening breast MRI, supporting previous studies,” said Dr. Seely. The shorter protocol took 16.3 minutes on average, compared with 27 minutes for the standard MRI protocol. This difference resulted in a 50% increase in institutional capacity, or a jump from two to three patients screened per hour.
In the province of Ontario, said Dr. Seely, women assessed at being at a 25% or greater lifetime risk of breast cancer receive MRIs as part of the Ontario Breast Screening Program (OBSP), which calculates risk by using the International Breast Cancer Intervention Study model.
For high-risk patients, the OBSP model provides annual mammography and an MRI for women between the ages of 30 and 60 years. Not only is the half-hour duration of the standard protocol resource-intensive, especially in regions with limited scanner availability, but patients may either be reluctant to undergo a half-hour scan, or not tolerate a lengthy scan very well.
Dr. Seely cited previous work (J Clin Oncol. 2014 Aug 1;32[22]:2304-10) showing that an abbreviated MRI protocol has similar accuracy as the full standard protocol. With the foundation of evidence from this study, Dr. Seely and her collaborators compared outcomes for high-risk patients who were screened with an abbreviated versus a standard protocol.
The abbreviated protocol, approved by the American College of Radiology, omits a final round of image acquisition sequences at the 9-minute mark after gadolinium administration, instead performing acquisition at 1, 2, 3, and 4 minutes after contrast delivery. Total time required for this protocol is just over 13 minutes, said Dr. Seely, and additional diagnostic MRIs were not required.
The trial was constructed so that the abbreviated protocol was used for the entire OBSP cohort for 10 months in 2018. Results were compared with those from the 12 previous months, when OBSP patients’ MRIs were performed using the standard protocol.
A total of 881 patients received standard-protocol MRIs; about three quarters (651) of those patients had previous MRI screening, while the remaining 230 patients had a baseline screen via the standard protocol.
Of the 658 patients in the abbreviated protocol group, 135, or about 20%, received the briefer scans as a baseline screen; the remast of the patients in this arm had received earlier MRI screening.
In addition to tracking scanning times, Dr. Seely and her collaborators also compared cancer detection rates, Breast Imaging Reporting and Data System (BI-RADS) assessment categories, positive predictive values, and the abnormal interpretation rate – that is, how many scans fell into BI-RADS categories 0, 4, and 5.
No significant difference was found between the rates of BI-RADs 0, 3, or 5 studies between the groups. Significantly fewer abbreviated scans fell into the BI-RADS 4 category, however (9.3% vs. 14.9%; P less than .001).
Similarly, the abnormal interpretation rate was 12.5% for the abbreviated protocol, compared with 17.5% for the standard protocol (P less than .007), with a correspondingly lower biopsy rate of 8.4% for the abbreviated protocol, compared with 13.7% for the standard protocol (P less than .001). The overall cancer detection rate did not differ between groups.
She and her colleagues will continue to track outcomes for those receiving abbreviated screening within the province of Ontario to track performance over time.
Dr. Seely reported that she had no relevant conflicts of interest. She reported no funding source beyond the province of Ontario.
SOURCE: Seely J et al. RSNA 2019, Session RC-215-04.
CHICAGO – An abbreviated magnetic resonance imaging (MRI) protocol for screening individuals at high risk for breast cancer performed as well as a standard protocol, in about half the time and with greater patient satisfaction.
The abbreviated protocol also resulted in fewer false positive findings, with 5% fewer patients receiving biopsies for benign lesions than with a standard protocol (8.4% versus 13.7%, P less than .001).
Findings from the prospective 10-month trial conducted in the province of Ontario were presented by Jean Seely, MD, professor of radiology at the University of Ottawa, at the annual meeting of the Radiological Society of North America.
“The abbreviated protocol was shown to be as effective as the standard protocol in high-risk screening breast MRI, supporting previous studies,” said Dr. Seely. The shorter protocol took 16.3 minutes on average, compared with 27 minutes for the standard MRI protocol. This difference resulted in a 50% increase in institutional capacity, or a jump from two to three patients screened per hour.
In the province of Ontario, said Dr. Seely, women assessed at being at a 25% or greater lifetime risk of breast cancer receive MRIs as part of the Ontario Breast Screening Program (OBSP), which calculates risk by using the International Breast Cancer Intervention Study model.
For high-risk patients, the OBSP model provides annual mammography and an MRI for women between the ages of 30 and 60 years. Not only is the half-hour duration of the standard protocol resource-intensive, especially in regions with limited scanner availability, but patients may either be reluctant to undergo a half-hour scan, or not tolerate a lengthy scan very well.
Dr. Seely cited previous work (J Clin Oncol. 2014 Aug 1;32[22]:2304-10) showing that an abbreviated MRI protocol has similar accuracy as the full standard protocol. With the foundation of evidence from this study, Dr. Seely and her collaborators compared outcomes for high-risk patients who were screened with an abbreviated versus a standard protocol.
The abbreviated protocol, approved by the American College of Radiology, omits a final round of image acquisition sequences at the 9-minute mark after gadolinium administration, instead performing acquisition at 1, 2, 3, and 4 minutes after contrast delivery. Total time required for this protocol is just over 13 minutes, said Dr. Seely, and additional diagnostic MRIs were not required.
The trial was constructed so that the abbreviated protocol was used for the entire OBSP cohort for 10 months in 2018. Results were compared with those from the 12 previous months, when OBSP patients’ MRIs were performed using the standard protocol.
A total of 881 patients received standard-protocol MRIs; about three quarters (651) of those patients had previous MRI screening, while the remaining 230 patients had a baseline screen via the standard protocol.
Of the 658 patients in the abbreviated protocol group, 135, or about 20%, received the briefer scans as a baseline screen; the remast of the patients in this arm had received earlier MRI screening.
In addition to tracking scanning times, Dr. Seely and her collaborators also compared cancer detection rates, Breast Imaging Reporting and Data System (BI-RADS) assessment categories, positive predictive values, and the abnormal interpretation rate – that is, how many scans fell into BI-RADS categories 0, 4, and 5.
No significant difference was found between the rates of BI-RADs 0, 3, or 5 studies between the groups. Significantly fewer abbreviated scans fell into the BI-RADS 4 category, however (9.3% vs. 14.9%; P less than .001).
Similarly, the abnormal interpretation rate was 12.5% for the abbreviated protocol, compared with 17.5% for the standard protocol (P less than .007), with a correspondingly lower biopsy rate of 8.4% for the abbreviated protocol, compared with 13.7% for the standard protocol (P less than .001). The overall cancer detection rate did not differ between groups.
She and her colleagues will continue to track outcomes for those receiving abbreviated screening within the province of Ontario to track performance over time.
Dr. Seely reported that she had no relevant conflicts of interest. She reported no funding source beyond the province of Ontario.
SOURCE: Seely J et al. RSNA 2019, Session RC-215-04.
REPORTING FROM RSNA 2019
White Hispanic Mohs patients less informed about skin cancer risks
White Hispanic adults report a lower quality of life and less knowledge of skin cancer and sun protection behaviors than white non-Hispanic adults, survey results of 175 adults with nonmelanoma skin cancer show.
“The incidence of nonmelanoma skin cancer (NMSC) is lower in Hispanics when compared to Caucasians, but a high index of suspicion is needed given ethnic differences in presentation,” wrote Ali Rajabi-Estarabadi, MD, of the University of Miami, and colleagues.
Hispanic patients with NMSC tend to be younger than non-Hispanic white patients, and their basal cell carcinomas are more likely to be pigmented, the investigators noted. Although previous research suggests ethnic disparities in NMSC, factors including sun safety knowledge and quality of life after diagnosis have not been well studied, they said.
With this in mind, the investigators conducted a survey of white Hispanics and non-Hispanics treated for NMSC. The results were published as a research letter in the Journal of the American Academy of Dermatology.
The investigators recruited 175 consecutive patients being treated for NMSC with Mohs surgery at a single center. The average age of the patients was 67 years; 58 identified as white Hispanic, 116 identified as white non-Hispanic.
White Hispanic patients had significantly lower skin cancer knowledge scores, compared with white non-Hispanics (P = .003). White Hispanics were significantly more likely than white non-Hispanics to report never wearing hats (39% vs. 12%) and never wearing sunglasses (26% vs. 9%) for sun protection.
The findings were limited by the study population that included only residents of South Florida. However, the results highlight the need for “targeted patient education initiatives to bridge ethnic disparities regarding cancer knowledge and ultimately improve [quality of life] among Hispanic skin cancer suffers,” the investigators concluded.
The study received no outside funding. The investigators declared no conflicts of interest.
SOURCE: Rajabi-Estarabadi A et al. J Am Acad Dermatol. 2020 Feb 4. doi: 10.1016/j.jaad.2020.01.063.
White Hispanic adults report a lower quality of life and less knowledge of skin cancer and sun protection behaviors than white non-Hispanic adults, survey results of 175 adults with nonmelanoma skin cancer show.
“The incidence of nonmelanoma skin cancer (NMSC) is lower in Hispanics when compared to Caucasians, but a high index of suspicion is needed given ethnic differences in presentation,” wrote Ali Rajabi-Estarabadi, MD, of the University of Miami, and colleagues.
Hispanic patients with NMSC tend to be younger than non-Hispanic white patients, and their basal cell carcinomas are more likely to be pigmented, the investigators noted. Although previous research suggests ethnic disparities in NMSC, factors including sun safety knowledge and quality of life after diagnosis have not been well studied, they said.
With this in mind, the investigators conducted a survey of white Hispanics and non-Hispanics treated for NMSC. The results were published as a research letter in the Journal of the American Academy of Dermatology.
The investigators recruited 175 consecutive patients being treated for NMSC with Mohs surgery at a single center. The average age of the patients was 67 years; 58 identified as white Hispanic, 116 identified as white non-Hispanic.
White Hispanic patients had significantly lower skin cancer knowledge scores, compared with white non-Hispanics (P = .003). White Hispanics were significantly more likely than white non-Hispanics to report never wearing hats (39% vs. 12%) and never wearing sunglasses (26% vs. 9%) for sun protection.
The findings were limited by the study population that included only residents of South Florida. However, the results highlight the need for “targeted patient education initiatives to bridge ethnic disparities regarding cancer knowledge and ultimately improve [quality of life] among Hispanic skin cancer suffers,” the investigators concluded.
The study received no outside funding. The investigators declared no conflicts of interest.
SOURCE: Rajabi-Estarabadi A et al. J Am Acad Dermatol. 2020 Feb 4. doi: 10.1016/j.jaad.2020.01.063.
White Hispanic adults report a lower quality of life and less knowledge of skin cancer and sun protection behaviors than white non-Hispanic adults, survey results of 175 adults with nonmelanoma skin cancer show.
“The incidence of nonmelanoma skin cancer (NMSC) is lower in Hispanics when compared to Caucasians, but a high index of suspicion is needed given ethnic differences in presentation,” wrote Ali Rajabi-Estarabadi, MD, of the University of Miami, and colleagues.
Hispanic patients with NMSC tend to be younger than non-Hispanic white patients, and their basal cell carcinomas are more likely to be pigmented, the investigators noted. Although previous research suggests ethnic disparities in NMSC, factors including sun safety knowledge and quality of life after diagnosis have not been well studied, they said.
With this in mind, the investigators conducted a survey of white Hispanics and non-Hispanics treated for NMSC. The results were published as a research letter in the Journal of the American Academy of Dermatology.
The investigators recruited 175 consecutive patients being treated for NMSC with Mohs surgery at a single center. The average age of the patients was 67 years; 58 identified as white Hispanic, 116 identified as white non-Hispanic.
White Hispanic patients had significantly lower skin cancer knowledge scores, compared with white non-Hispanics (P = .003). White Hispanics were significantly more likely than white non-Hispanics to report never wearing hats (39% vs. 12%) and never wearing sunglasses (26% vs. 9%) for sun protection.
The findings were limited by the study population that included only residents of South Florida. However, the results highlight the need for “targeted patient education initiatives to bridge ethnic disparities regarding cancer knowledge and ultimately improve [quality of life] among Hispanic skin cancer suffers,” the investigators concluded.
The study received no outside funding. The investigators declared no conflicts of interest.
SOURCE: Rajabi-Estarabadi A et al. J Am Acad Dermatol. 2020 Feb 4. doi: 10.1016/j.jaad.2020.01.063.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Racial disparities persist in preterm birth risk
Education, status are not protective for non-Hispanic black women
GRAPEVINE, TEX. – College education and high socioeconomic status do not erase U.S. racial disparities in birth outcomes, according to a new analysis of all U.S. live births from 2015-2017.
Very early preterm birth – birth before 28 weeks gestational age – was five times more likely to occur in non-Hispanic black women of high socioeconomic status as similarly situated white women, even after statistical adjustment for a host of potentially confounding factors.
Being of non-Hispanic black race was the single strongest predictor of preterm birth (PTB) at less than 28 weeks’ gestation. The adjusted odds ratio (aOR) of 4.99 surpassed an interpregnancy interval under 1 year (aOR, 4.47), chronic hypertension (aOR, 2.84), and prior history of preterm birth (aOR, 2.81).
“Even among college-educated women with private insurance who are not receiving (Women, Infants, and Children support), racial disparities in prematurity persist. These results suggest that factors other than sociodemographics are important in the underlying pathogenesis of PTB and in etiologies of racial disparities,” wrote Jasmine Johnson, MD, and her coauthors in the abstract accompanying the presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The analysis that Dr. Johnson and her coinvestigators used, she explained during her plenary session presentation, still found significantly elevated risks for preterm birth for non-Hispanic black women after accounting for marital status, prior history of preterm birth, tobacco use, an interpregnancy interval of fewer than 12 months, and carrying a male fetus.
“Birth certificates do not inform the lived experiences of one’s self-identified race, and how that experience – or possibly just one’s identification with a particular racial group – may positively or negatively affect their clinical risk of preterm birth,” said Dr. Johnson. “In this study, as in others, race is a social construct. It’s a surrogate for social and societal racism that disproportionately affects birth outcomes of women of color.”
Using non-Hispanic white (NHW) women as a reference, women who described themselves as non-Hispanic black (NHB) had increased odds of preterm birth at 34 and 37 weeks gestation as well. Women identifying as both NHB and NHW had numerically elevated odds for preterm birth at all time points as well, but the odds at 37 weeks didn’t reach statistical significance.
The results were based on a retrospective population-based study of a cohort drawn from the National Vital Statistics birth certificate data of all live births in the United States between 2015 and 2017, explained Dr. Johnson, a maternal-fetal medicine fellow at the University of North Carolina, Chapel Hill. Drawing from a nationally representative sample and having a population-level design drawn were strengths of the study, she said.
Women with singleton pregnancies without anomalies who identified as NHB, NHW, or as both NHB and NHW were included if they also had high socioeconomic status. Including women who identify as both black and white was another strength of the study, Dr. Johnson added.
She explained that, for the purposes of the study, high socioeconomic status was defined as having 16 or more years of education and private insurance, and not receiving WIC benefits.
In addition to the primary outcome measure of preterm birth at fewer than 37 weeks gestation, secondary outcomes included preterm birth at fewer than 34 and fewer than 28 weeks’ gestation, as well as low birthweight (LBW) and very low birthweight (VLBW).
About 11.8 million live births occurred during the study period, and 11.3 million of those were singleton pregnancies without fetal anomaly. After excluding women who did not meet the racial self-identification or socioeconomic status inclusion criteria, the investigators arrived at the final study population of 2,170,688 individuals.
Of those, 2,017,470, or 92.9%, were non-Hispanic white, while 144,612, or 6.7%, were non-Hispanic black. The remaining 8,604 participants, or 0.4%, identified their race as non-Hispanic black and non-Hispanic white.
The groups identified in the study differed significantly in demographic characteristics, Dr. Johnson said. Women in the NHB and NHB + NHW groups were less likely to be married than NHW women – about 75% of the former two groups were married, compared with 92.5% of NHW women. This difference was statistically significant with a P value of .001, as were all the differences Dr. Johnson reported.
Pre-pregnancy body mass index (BMI) was highest in NHB women at 27.1 kg/m sq, followed by NHB = NHW women at 25.7 kg/m sq, with NHW women having the lowest BMI at 23.8 kg/m sq.
Prior preterm birth of 37 weeks’ gestation or less was more common in NHB women and NHB + NHW women, as was an interpregnancy interval of fewer than 12 months.
Chronic hypertension was more than twice as common in NHB women than in either NHB = NHW or NHW women, occurring in 3.9%, 1.8%, and 1.4% of participants, respectively.
Pregestational diabetes was about twice as common in NHB women than NHW women, occurring in 1% and 0.52% of those groups, respectively. Prevalence of pregestational diabetes was intermediate in NHB = NHW women, at 0.72%.
Tobacco use was rare overall, and less common in NHB women than NHB + NHW and NHW women.
In terms of pregnancy characteristics, though 85% of NHB women initiated prenatal care in the first trimester, they were less likely to have done so than either of the other two groups. Few women overall had no prenatal care, but 0.7% of NHB women fell into this category, more than the 0.4% and 0.3% reported for NHB + NHW and NHW women, respectively.
During their pregnancies, NHB women were more likely to develop gestational hypertension and/or pre-eclampsia as well as gestational diabetes than either of the other two groups (7.6% compared with 6% for the other two groups). Of the NHB women, 5.9% developed gestational diabetes, compared with 4.8% of NHB + NHW and 4.8% of NHW women.
Delivering a baby with a birthweight less than the 10th percentile was twice as common for NHB, compared with NHW women (7.2% versus 3.4%). The risk for NHB + NHW women was intermediate, at 4.7%.
Dr. Johnson said she and her team performed further analyses, including using initiation of prenatal care in the first trimester of pregnancy as a surrogate for high socioeconomic status; the association of race and risk for preterm birth persisted.
The study had the usual limitations of using National Vital Statistics data, such as the inability to evaluate underlying etiologies for preterm birth.
However, Dr. Johnson highlighted additional limitations that pertain to the experience of race in 21st century America. “Our definition of high socioeconomic status does not guarantee that all women in this analysis have financial stability,” she said, pointing out that the study’s definition of high socioeconomic status was insensitive to wealth accumulation. She also noted that high educational attainment does not necessarily correlate with high income. Hence, the potential burden of economic stressors could not fully be captured.
The study was supported by the National Institutes of Health. Dr. Johnson reported no conflicts of interest.
SOURCE: Johnson J et al. Obstet Gynecol. 2020 Jan;222(1):S-37-8, Abstract 44.
Education, status are not protective for non-Hispanic black women
Education, status are not protective for non-Hispanic black women
GRAPEVINE, TEX. – College education and high socioeconomic status do not erase U.S. racial disparities in birth outcomes, according to a new analysis of all U.S. live births from 2015-2017.
Very early preterm birth – birth before 28 weeks gestational age – was five times more likely to occur in non-Hispanic black women of high socioeconomic status as similarly situated white women, even after statistical adjustment for a host of potentially confounding factors.
Being of non-Hispanic black race was the single strongest predictor of preterm birth (PTB) at less than 28 weeks’ gestation. The adjusted odds ratio (aOR) of 4.99 surpassed an interpregnancy interval under 1 year (aOR, 4.47), chronic hypertension (aOR, 2.84), and prior history of preterm birth (aOR, 2.81).
“Even among college-educated women with private insurance who are not receiving (Women, Infants, and Children support), racial disparities in prematurity persist. These results suggest that factors other than sociodemographics are important in the underlying pathogenesis of PTB and in etiologies of racial disparities,” wrote Jasmine Johnson, MD, and her coauthors in the abstract accompanying the presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The analysis that Dr. Johnson and her coinvestigators used, she explained during her plenary session presentation, still found significantly elevated risks for preterm birth for non-Hispanic black women after accounting for marital status, prior history of preterm birth, tobacco use, an interpregnancy interval of fewer than 12 months, and carrying a male fetus.
“Birth certificates do not inform the lived experiences of one’s self-identified race, and how that experience – or possibly just one’s identification with a particular racial group – may positively or negatively affect their clinical risk of preterm birth,” said Dr. Johnson. “In this study, as in others, race is a social construct. It’s a surrogate for social and societal racism that disproportionately affects birth outcomes of women of color.”
Using non-Hispanic white (NHW) women as a reference, women who described themselves as non-Hispanic black (NHB) had increased odds of preterm birth at 34 and 37 weeks gestation as well. Women identifying as both NHB and NHW had numerically elevated odds for preterm birth at all time points as well, but the odds at 37 weeks didn’t reach statistical significance.
The results were based on a retrospective population-based study of a cohort drawn from the National Vital Statistics birth certificate data of all live births in the United States between 2015 and 2017, explained Dr. Johnson, a maternal-fetal medicine fellow at the University of North Carolina, Chapel Hill. Drawing from a nationally representative sample and having a population-level design drawn were strengths of the study, she said.
Women with singleton pregnancies without anomalies who identified as NHB, NHW, or as both NHB and NHW were included if they also had high socioeconomic status. Including women who identify as both black and white was another strength of the study, Dr. Johnson added.
She explained that, for the purposes of the study, high socioeconomic status was defined as having 16 or more years of education and private insurance, and not receiving WIC benefits.
In addition to the primary outcome measure of preterm birth at fewer than 37 weeks gestation, secondary outcomes included preterm birth at fewer than 34 and fewer than 28 weeks’ gestation, as well as low birthweight (LBW) and very low birthweight (VLBW).
About 11.8 million live births occurred during the study period, and 11.3 million of those were singleton pregnancies without fetal anomaly. After excluding women who did not meet the racial self-identification or socioeconomic status inclusion criteria, the investigators arrived at the final study population of 2,170,688 individuals.
Of those, 2,017,470, or 92.9%, were non-Hispanic white, while 144,612, or 6.7%, were non-Hispanic black. The remaining 8,604 participants, or 0.4%, identified their race as non-Hispanic black and non-Hispanic white.
The groups identified in the study differed significantly in demographic characteristics, Dr. Johnson said. Women in the NHB and NHB + NHW groups were less likely to be married than NHW women – about 75% of the former two groups were married, compared with 92.5% of NHW women. This difference was statistically significant with a P value of .001, as were all the differences Dr. Johnson reported.
Pre-pregnancy body mass index (BMI) was highest in NHB women at 27.1 kg/m sq, followed by NHB = NHW women at 25.7 kg/m sq, with NHW women having the lowest BMI at 23.8 kg/m sq.
Prior preterm birth of 37 weeks’ gestation or less was more common in NHB women and NHB + NHW women, as was an interpregnancy interval of fewer than 12 months.
Chronic hypertension was more than twice as common in NHB women than in either NHB = NHW or NHW women, occurring in 3.9%, 1.8%, and 1.4% of participants, respectively.
Pregestational diabetes was about twice as common in NHB women than NHW women, occurring in 1% and 0.52% of those groups, respectively. Prevalence of pregestational diabetes was intermediate in NHB = NHW women, at 0.72%.
Tobacco use was rare overall, and less common in NHB women than NHB + NHW and NHW women.
In terms of pregnancy characteristics, though 85% of NHB women initiated prenatal care in the first trimester, they were less likely to have done so than either of the other two groups. Few women overall had no prenatal care, but 0.7% of NHB women fell into this category, more than the 0.4% and 0.3% reported for NHB + NHW and NHW women, respectively.
During their pregnancies, NHB women were more likely to develop gestational hypertension and/or pre-eclampsia as well as gestational diabetes than either of the other two groups (7.6% compared with 6% for the other two groups). Of the NHB women, 5.9% developed gestational diabetes, compared with 4.8% of NHB + NHW and 4.8% of NHW women.
Delivering a baby with a birthweight less than the 10th percentile was twice as common for NHB, compared with NHW women (7.2% versus 3.4%). The risk for NHB + NHW women was intermediate, at 4.7%.
Dr. Johnson said she and her team performed further analyses, including using initiation of prenatal care in the first trimester of pregnancy as a surrogate for high socioeconomic status; the association of race and risk for preterm birth persisted.
The study had the usual limitations of using National Vital Statistics data, such as the inability to evaluate underlying etiologies for preterm birth.
However, Dr. Johnson highlighted additional limitations that pertain to the experience of race in 21st century America. “Our definition of high socioeconomic status does not guarantee that all women in this analysis have financial stability,” she said, pointing out that the study’s definition of high socioeconomic status was insensitive to wealth accumulation. She also noted that high educational attainment does not necessarily correlate with high income. Hence, the potential burden of economic stressors could not fully be captured.
The study was supported by the National Institutes of Health. Dr. Johnson reported no conflicts of interest.
SOURCE: Johnson J et al. Obstet Gynecol. 2020 Jan;222(1):S-37-8, Abstract 44.
GRAPEVINE, TEX. – College education and high socioeconomic status do not erase U.S. racial disparities in birth outcomes, according to a new analysis of all U.S. live births from 2015-2017.
Very early preterm birth – birth before 28 weeks gestational age – was five times more likely to occur in non-Hispanic black women of high socioeconomic status as similarly situated white women, even after statistical adjustment for a host of potentially confounding factors.
Being of non-Hispanic black race was the single strongest predictor of preterm birth (PTB) at less than 28 weeks’ gestation. The adjusted odds ratio (aOR) of 4.99 surpassed an interpregnancy interval under 1 year (aOR, 4.47), chronic hypertension (aOR, 2.84), and prior history of preterm birth (aOR, 2.81).
“Even among college-educated women with private insurance who are not receiving (Women, Infants, and Children support), racial disparities in prematurity persist. These results suggest that factors other than sociodemographics are important in the underlying pathogenesis of PTB and in etiologies of racial disparities,” wrote Jasmine Johnson, MD, and her coauthors in the abstract accompanying the presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine.
The analysis that Dr. Johnson and her coinvestigators used, she explained during her plenary session presentation, still found significantly elevated risks for preterm birth for non-Hispanic black women after accounting for marital status, prior history of preterm birth, tobacco use, an interpregnancy interval of fewer than 12 months, and carrying a male fetus.
“Birth certificates do not inform the lived experiences of one’s self-identified race, and how that experience – or possibly just one’s identification with a particular racial group – may positively or negatively affect their clinical risk of preterm birth,” said Dr. Johnson. “In this study, as in others, race is a social construct. It’s a surrogate for social and societal racism that disproportionately affects birth outcomes of women of color.”
Using non-Hispanic white (NHW) women as a reference, women who described themselves as non-Hispanic black (NHB) had increased odds of preterm birth at 34 and 37 weeks gestation as well. Women identifying as both NHB and NHW had numerically elevated odds for preterm birth at all time points as well, but the odds at 37 weeks didn’t reach statistical significance.
The results were based on a retrospective population-based study of a cohort drawn from the National Vital Statistics birth certificate data of all live births in the United States between 2015 and 2017, explained Dr. Johnson, a maternal-fetal medicine fellow at the University of North Carolina, Chapel Hill. Drawing from a nationally representative sample and having a population-level design drawn were strengths of the study, she said.
Women with singleton pregnancies without anomalies who identified as NHB, NHW, or as both NHB and NHW were included if they also had high socioeconomic status. Including women who identify as both black and white was another strength of the study, Dr. Johnson added.
She explained that, for the purposes of the study, high socioeconomic status was defined as having 16 or more years of education and private insurance, and not receiving WIC benefits.
In addition to the primary outcome measure of preterm birth at fewer than 37 weeks gestation, secondary outcomes included preterm birth at fewer than 34 and fewer than 28 weeks’ gestation, as well as low birthweight (LBW) and very low birthweight (VLBW).
About 11.8 million live births occurred during the study period, and 11.3 million of those were singleton pregnancies without fetal anomaly. After excluding women who did not meet the racial self-identification or socioeconomic status inclusion criteria, the investigators arrived at the final study population of 2,170,688 individuals.
Of those, 2,017,470, or 92.9%, were non-Hispanic white, while 144,612, or 6.7%, were non-Hispanic black. The remaining 8,604 participants, or 0.4%, identified their race as non-Hispanic black and non-Hispanic white.
The groups identified in the study differed significantly in demographic characteristics, Dr. Johnson said. Women in the NHB and NHB + NHW groups were less likely to be married than NHW women – about 75% of the former two groups were married, compared with 92.5% of NHW women. This difference was statistically significant with a P value of .001, as were all the differences Dr. Johnson reported.
Pre-pregnancy body mass index (BMI) was highest in NHB women at 27.1 kg/m sq, followed by NHB = NHW women at 25.7 kg/m sq, with NHW women having the lowest BMI at 23.8 kg/m sq.
Prior preterm birth of 37 weeks’ gestation or less was more common in NHB women and NHB + NHW women, as was an interpregnancy interval of fewer than 12 months.
Chronic hypertension was more than twice as common in NHB women than in either NHB = NHW or NHW women, occurring in 3.9%, 1.8%, and 1.4% of participants, respectively.
Pregestational diabetes was about twice as common in NHB women than NHW women, occurring in 1% and 0.52% of those groups, respectively. Prevalence of pregestational diabetes was intermediate in NHB = NHW women, at 0.72%.
Tobacco use was rare overall, and less common in NHB women than NHB + NHW and NHW women.
In terms of pregnancy characteristics, though 85% of NHB women initiated prenatal care in the first trimester, they were less likely to have done so than either of the other two groups. Few women overall had no prenatal care, but 0.7% of NHB women fell into this category, more than the 0.4% and 0.3% reported for NHB + NHW and NHW women, respectively.
During their pregnancies, NHB women were more likely to develop gestational hypertension and/or pre-eclampsia as well as gestational diabetes than either of the other two groups (7.6% compared with 6% for the other two groups). Of the NHB women, 5.9% developed gestational diabetes, compared with 4.8% of NHB + NHW and 4.8% of NHW women.
Delivering a baby with a birthweight less than the 10th percentile was twice as common for NHB, compared with NHW women (7.2% versus 3.4%). The risk for NHB + NHW women was intermediate, at 4.7%.
Dr. Johnson said she and her team performed further analyses, including using initiation of prenatal care in the first trimester of pregnancy as a surrogate for high socioeconomic status; the association of race and risk for preterm birth persisted.
The study had the usual limitations of using National Vital Statistics data, such as the inability to evaluate underlying etiologies for preterm birth.
However, Dr. Johnson highlighted additional limitations that pertain to the experience of race in 21st century America. “Our definition of high socioeconomic status does not guarantee that all women in this analysis have financial stability,” she said, pointing out that the study’s definition of high socioeconomic status was insensitive to wealth accumulation. She also noted that high educational attainment does not necessarily correlate with high income. Hence, the potential burden of economic stressors could not fully be captured.
The study was supported by the National Institutes of Health. Dr. Johnson reported no conflicts of interest.
SOURCE: Johnson J et al. Obstet Gynecol. 2020 Jan;222(1):S-37-8, Abstract 44.
AT THE PREGNANCY MEETING
Glioma trials should track living well, not just longer
Neuro-oncology working group backs focus on how patients feel, function
Glioma treatment goals traditionally have focused on tumor shrinkage or prolonging survival, but it’s time for those endpoints to be supplemented by clinical outcomes that are meaningful to the patient, according to a recently published report from a neuro-oncology working group.
The group, which includes representatives of previous oncology working groups, the Food and Drug Administration, and observers from the European Medicines Agency, has established a core set of symptoms and functional points that they say could be used in clinical trials and clinical care for patients with high-grade gliomas.
“Patients want to live longer, but they also want to continue to function as well as possible for as long as possible,” said Terri S. Armstrong, PhD, of the National Cancer Institute (NCI), and coauthors in a report that sums up the work to date of the Fast Track COA Group.
That work, while specific to gliomas, echoes results from broader initiatives that seek to standardize patient-reported outcomes in oncology trials, Dr. Armstrong and coauthors wrote. The report was published in the Lancet Oncology.
The core set of symptom constructs and functional issues identified by the work group are represented already in patient-reported outcome measures, according to the authors.
The symptoms worth measuring fall into five categories, including pain, difficulty communicating, perceived cognition, seizures, and symptomatic adverse events. The functional issues were divided into two categories, physical functioning, including weakness or walking, and role functioning, which they defined as the ability to work or participate in social or leisure activities.
Some of those outcomes can be challenging or cumbersome to track, Dr. Armstrong and coauthors said.
Pain has “many dimensions“ and is important to track, the group wrote. Likewise, patients’ concerns related to language function also are important, but are very “noisy“ as a variable and can be specific to tumor location.
Collecting data on seizure frequency and severity is important yet complicated, because of the variability in seizures and considerable difference between focal and generalized seizures. Assessment of cognitive functioning can be lengthy and burdensome to patients.
Adverse events of relevance will vary, depending on the drug used, its mechanism of action, and available data, though some allowance needs to be made for the possibility of “overlap“ with disease-related symptoms, the report said.
Physical functioning, including walking and weakness, should be evaluated. It also would be useful to distinguish the duration of time that patients have deficits in physical functioning in the later stages of their disease progression, authors said.
Role and social functioning should be assessed in most patients with high-grade gliomas, who will have symptoms and deficits that prevent returning to a job. “Patients might spend a substantial portion of their lives feeling ill, unable to do usual activities, or meet occupational, social, financial, and family obligations,” said Dr. Armstrong and coauthors in the report.
The scales and tools used to measure symptoms and functional concerns need to be those that best fit a particular clinical trial or clinical practice scenario. Several instruments that would be appropriate are discussed in the report, including the NCI Patient-Reported Outcome of the Common Toxicity Criteria Adverse Events (NCI PRO-CTCAE) and symptom and function scales or items in the Patient-Reported Outcomes Measurement System (PROMIS).
, such as time to recurrence or survival.
“Strategies for introducing these constructs to clinical trial cooperative groups and sponsors will be necessary,” they concluded.
Dr. Armstrong reported employment as a senior investigator and deputy chief of the neuro-oncology branch of the Center for Cancer Research at the NCI. His coauthors reported disclosures related to several companies and interests, including AbbVie, AstraZeneca, Bristol-Myers Squibb, Genentech, Merck, Taiho, and Tocagen.
SOURCE: Armstrong TS et al. Lancet Oncol. 2020;21(2):e97-103.
Neuro-oncology working group backs focus on how patients feel, function
Neuro-oncology working group backs focus on how patients feel, function
Glioma treatment goals traditionally have focused on tumor shrinkage or prolonging survival, but it’s time for those endpoints to be supplemented by clinical outcomes that are meaningful to the patient, according to a recently published report from a neuro-oncology working group.
The group, which includes representatives of previous oncology working groups, the Food and Drug Administration, and observers from the European Medicines Agency, has established a core set of symptoms and functional points that they say could be used in clinical trials and clinical care for patients with high-grade gliomas.
“Patients want to live longer, but they also want to continue to function as well as possible for as long as possible,” said Terri S. Armstrong, PhD, of the National Cancer Institute (NCI), and coauthors in a report that sums up the work to date of the Fast Track COA Group.
That work, while specific to gliomas, echoes results from broader initiatives that seek to standardize patient-reported outcomes in oncology trials, Dr. Armstrong and coauthors wrote. The report was published in the Lancet Oncology.
The core set of symptom constructs and functional issues identified by the work group are represented already in patient-reported outcome measures, according to the authors.
The symptoms worth measuring fall into five categories, including pain, difficulty communicating, perceived cognition, seizures, and symptomatic adverse events. The functional issues were divided into two categories, physical functioning, including weakness or walking, and role functioning, which they defined as the ability to work or participate in social or leisure activities.
Some of those outcomes can be challenging or cumbersome to track, Dr. Armstrong and coauthors said.
Pain has “many dimensions“ and is important to track, the group wrote. Likewise, patients’ concerns related to language function also are important, but are very “noisy“ as a variable and can be specific to tumor location.
Collecting data on seizure frequency and severity is important yet complicated, because of the variability in seizures and considerable difference between focal and generalized seizures. Assessment of cognitive functioning can be lengthy and burdensome to patients.
Adverse events of relevance will vary, depending on the drug used, its mechanism of action, and available data, though some allowance needs to be made for the possibility of “overlap“ with disease-related symptoms, the report said.
Physical functioning, including walking and weakness, should be evaluated. It also would be useful to distinguish the duration of time that patients have deficits in physical functioning in the later stages of their disease progression, authors said.
Role and social functioning should be assessed in most patients with high-grade gliomas, who will have symptoms and deficits that prevent returning to a job. “Patients might spend a substantial portion of their lives feeling ill, unable to do usual activities, or meet occupational, social, financial, and family obligations,” said Dr. Armstrong and coauthors in the report.
The scales and tools used to measure symptoms and functional concerns need to be those that best fit a particular clinical trial or clinical practice scenario. Several instruments that would be appropriate are discussed in the report, including the NCI Patient-Reported Outcome of the Common Toxicity Criteria Adverse Events (NCI PRO-CTCAE) and symptom and function scales or items in the Patient-Reported Outcomes Measurement System (PROMIS).
, such as time to recurrence or survival.
“Strategies for introducing these constructs to clinical trial cooperative groups and sponsors will be necessary,” they concluded.
Dr. Armstrong reported employment as a senior investigator and deputy chief of the neuro-oncology branch of the Center for Cancer Research at the NCI. His coauthors reported disclosures related to several companies and interests, including AbbVie, AstraZeneca, Bristol-Myers Squibb, Genentech, Merck, Taiho, and Tocagen.
SOURCE: Armstrong TS et al. Lancet Oncol. 2020;21(2):e97-103.
Glioma treatment goals traditionally have focused on tumor shrinkage or prolonging survival, but it’s time for those endpoints to be supplemented by clinical outcomes that are meaningful to the patient, according to a recently published report from a neuro-oncology working group.
The group, which includes representatives of previous oncology working groups, the Food and Drug Administration, and observers from the European Medicines Agency, has established a core set of symptoms and functional points that they say could be used in clinical trials and clinical care for patients with high-grade gliomas.
“Patients want to live longer, but they also want to continue to function as well as possible for as long as possible,” said Terri S. Armstrong, PhD, of the National Cancer Institute (NCI), and coauthors in a report that sums up the work to date of the Fast Track COA Group.
That work, while specific to gliomas, echoes results from broader initiatives that seek to standardize patient-reported outcomes in oncology trials, Dr. Armstrong and coauthors wrote. The report was published in the Lancet Oncology.
The core set of symptom constructs and functional issues identified by the work group are represented already in patient-reported outcome measures, according to the authors.
The symptoms worth measuring fall into five categories, including pain, difficulty communicating, perceived cognition, seizures, and symptomatic adverse events. The functional issues were divided into two categories, physical functioning, including weakness or walking, and role functioning, which they defined as the ability to work or participate in social or leisure activities.
Some of those outcomes can be challenging or cumbersome to track, Dr. Armstrong and coauthors said.
Pain has “many dimensions“ and is important to track, the group wrote. Likewise, patients’ concerns related to language function also are important, but are very “noisy“ as a variable and can be specific to tumor location.
Collecting data on seizure frequency and severity is important yet complicated, because of the variability in seizures and considerable difference between focal and generalized seizures. Assessment of cognitive functioning can be lengthy and burdensome to patients.
Adverse events of relevance will vary, depending on the drug used, its mechanism of action, and available data, though some allowance needs to be made for the possibility of “overlap“ with disease-related symptoms, the report said.
Physical functioning, including walking and weakness, should be evaluated. It also would be useful to distinguish the duration of time that patients have deficits in physical functioning in the later stages of their disease progression, authors said.
Role and social functioning should be assessed in most patients with high-grade gliomas, who will have symptoms and deficits that prevent returning to a job. “Patients might spend a substantial portion of their lives feeling ill, unable to do usual activities, or meet occupational, social, financial, and family obligations,” said Dr. Armstrong and coauthors in the report.
The scales and tools used to measure symptoms and functional concerns need to be those that best fit a particular clinical trial or clinical practice scenario. Several instruments that would be appropriate are discussed in the report, including the NCI Patient-Reported Outcome of the Common Toxicity Criteria Adverse Events (NCI PRO-CTCAE) and symptom and function scales or items in the Patient-Reported Outcomes Measurement System (PROMIS).
, such as time to recurrence or survival.
“Strategies for introducing these constructs to clinical trial cooperative groups and sponsors will be necessary,” they concluded.
Dr. Armstrong reported employment as a senior investigator and deputy chief of the neuro-oncology branch of the Center for Cancer Research at the NCI. His coauthors reported disclosures related to several companies and interests, including AbbVie, AstraZeneca, Bristol-Myers Squibb, Genentech, Merck, Taiho, and Tocagen.
SOURCE: Armstrong TS et al. Lancet Oncol. 2020;21(2):e97-103.
FROM THE LANCET ONCOLOGY