User login
Gap Analysis for the Conversion to Area Under the Curve Vancomycin Monitoring in a Small Rural Hospital
The use of weight-based dosing with trough-based monitoring of vancomycin has been in clinical practice for more than a decade. The American Society of Health-System Pharmacists (ASHP), the Infectious Diseases Society of America (IDSA), and the Society of Infectious Diseases Pharmacists (SIDP) published the first guidelines for vancomycin monitoring in 2009.1 Although it has been well established that area under the curve (AUC) over the minimal inhibitory concentration (MIC) ratio > 400 mg.h/L is the best predictor of clinical efficacy, obtaining this value in clinical practice was not pragmatic. Therefore, the 2009 guidelines recommended a goal vancomycin trough of 15 to 20 mcg/ml as a surrogate marker for AUC/MIC > 400 mg.hr/L. This has since become a common practice despite little data that support this recommendation.
The efficacy and safety of trough-based monitoring has been evaluated extensively over the past several years and more recent data suggest that there is wide patient variability in AUC with this method and higher trough levels are associated with more nephrotoxicity.2,3 ASHP, IDSA, SIDP, and the Pediatric Infectious Diseases Society (PIDS) updated the consensus guidelines in 2020.4 Trough-based monitoring is no longer recommended. Instead AUC24 monitoring should be implemented with a goal range of 400 to 600 mg.h/L for efficacy and safety. Given concerns for vancomycin penetration into the central nervous system (CNS), many facility protocols utilize higher targets (> 600 mg.h/L) for CNS infections.
Some hospitals have been utilizing AUC-based monitoring for years. There are strategies from tertiary care centers that drive this practice change in the medical literature.5,6 However, it is important to reproduce these implementation practices in small, rural facilities that may face unique challenges with limited resources and may be slower to implement consensus guidelines.7,8 As this is a major practice change, it is imperative to evaluate the extent of transition and identify areas of needed improvement.
Accurate therapeutic drug monitoring ensures both the safety and efficacy of vancomycin therapy. Unfortunately, research shows that inappropriate laboratory tests are common in medical facilities.9 Drug levels taken inappropriately can lead to delays in therapeutic decision-making, inappropriate dosage adjustments and create a need for repeated drug levels, which increases the overall cost of admission.
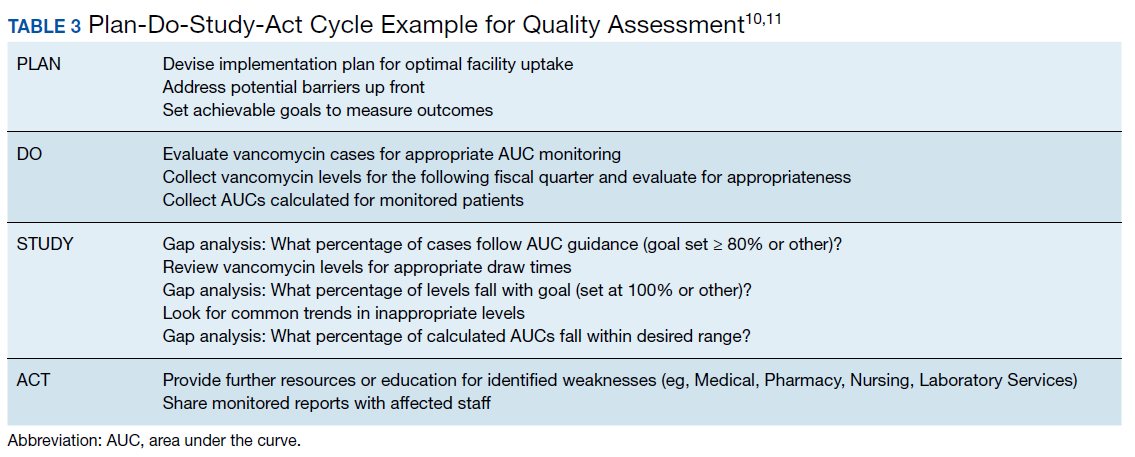
Given the multiple affected services needed to make successful practice transitions, it is paramount that facilities evaluate progress during the transition phase. The Agency for Healthcare Research and Quality and the Institute for Healthcare Improvement provide guidance in the Plan-Do-Study-Act Cycle for quality assessment and improvement of new initiatives.10,11 A gap analysis can be used as a simple tool for evaluating the transition of research into practice and to identify areas of needed improvement.
The Veterans Health Care System of the Ozarks (VHSO) in Fayetteville, Arkansas made the transition from trough-based monitoring to 2-level AUC-based monitoring on April 1, 2019. The purpose of this study was to evaluate the effectiveness of transition methods used to implement AUC-monitoring for vancomycin treated patients in a small, primary facility. A further goal of the study was to identify areas of needed improvement and education and whether the problems derived from deficiencies in knowledge and ordering (medical and pharmacy services) or execution (nursing and laboratory services).
Methods
VHSO is a 52-bed US Department of Veterans Affairs primary care hospital. The pharmacy and laboratory are staffed 24 hours each day. There is 1 clinical pharmacy specialist (CPS) available for therapeutic drug monitoring consults Monday through Friday between the hours of 7:30 AM and 4:00 PM. No partial full-time equivalent employees were added for this conversion. Pharmacy-driven vancomycin dosing and monitoring is conducted on a collaborative basis, with pharmacy managing the majority of vancomycin treated patients. Night and weekend pharmacy staff provide cross-coverage on vancomycin consultations. Laboratory orders and medication dosage adjustments fall within the CPS scope of practice. Nurses do not perform laboratory draws for therapeutic drug monitoring; this is done solely by phlebotomists. There is no infectious diseases specialist at the facility to champion antibiotic dosing initiatives.
The implementation strategy largely reflected those outlined from tertiary care centers.5,6 First, key personnel from the laboratory department met to discuss this practice change and to add vancomycin peaks to the ordering menu. A critical value was set at 40 mcg/ml. Vancomycin troughs and random levels already were orderable items. A comment field was added to all laboratory orders for further clarification. Verbiage was added to laboratory reports in the computerized medical record to assist clinicians in determining the appropriateness of the level. This was followed by an educational email to both the nursing and laboratory departments explaining the practice change and included a link to the Pharmacy Joe “Vancomycin Dosing by AUC:MIC Instead of Trough-level” podcast (www.pharmacyjoe.com episode 356).
The pharmacy department received an interactive 30-minute presentation, followed immediately by a group activity to discuss practice problems. This presentation was condensed, recorded, and emailed to all VHSO pharmacists. A shared folder contained pertinent material on AUC monitoring.
Finally, an interactive presentation was set up for hospitalists and a video teleconferencing was conducted for rotating medical residents. Both the podcast and recorded presentation were emailed to the entire medical staff with a brief introduction of the practice change. Additionally, the transition process was added as a standing item on the monthly antimicrobial stewardship meeting agenda.
The standardized pharmacokinetic model at the study facility consisted of a vancomycin volume of distribution of 0.7 mg/kg and elimination rate constant (Ke) by Matzke and colleagues for total daily dose calculations.12 Obese patients (BMI ≥ 30) undergo alternative clearance equations described by Crass and colleagues.13 Cockcroft-Gault methods using ideal body weight (or actual body weight if < ideal body weight) are used for determining creatinine clearance. In patients aged ≥ 65 years with a serum creatinine < 1.0 mg/dL, facility guidance was to round serum creatinine up to 1.0 mg/dL. Loading doses were determined on a case-by-case basis with a cap of 2,000 mg, maintenance doses were rounded to the nearest 250 mg.
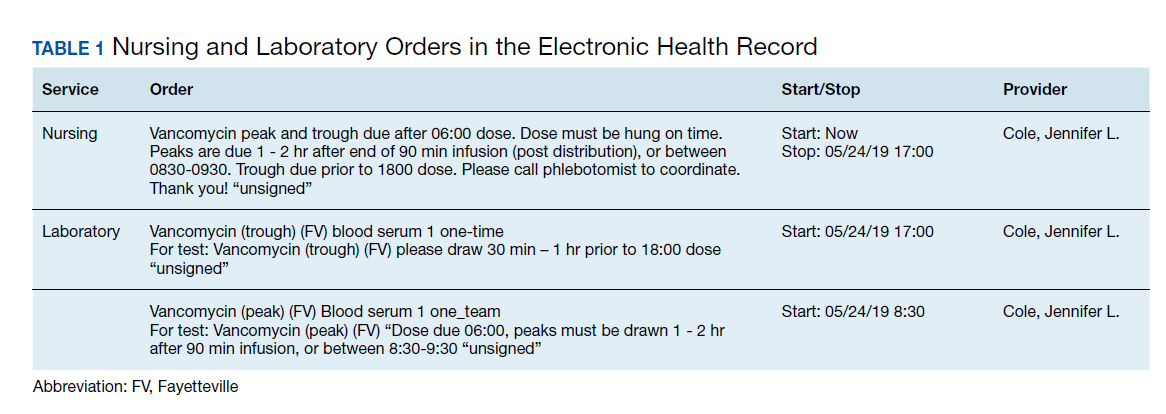
Vancomycin levels typically are drawn at steady state and analyzed using the logarithmic trapezoidal rule.14 The pharmacy and medical staff were educated to provide details on timing and coordination in nursing and laboratory orders (Table 1). Two-level AUC monitoring typically is not performed in patients with acute renal failure, expected duration of therapy < 72 hours, urinary tract infections, skin and soft tissue infections, or in renal replacement therapy.5
This gap analysis consisted of a retrospective chart review of vancomycin levels ordered after the implementation of AUC-based monitoring to determine the effectiveness of the transition. Three months of data were collected between April 2019 and June 2019. Vancomycin levels were deemed either appropriate or inappropriate based on timing and type (peak, trough, or random) of the laboratory test in relation to the previously administered vancomycin dose. Appropriate peaks were drawn within 2 hours after the end of infusion and troughs at least 1 half-life after the dose or just prior to the next dose and within the same dosing interval as the peak. Tests drawn outside of the specified time range, trough-only laboratory tests, or those drawn after vancomycin had been discontinued were considered inappropriate. Peaks and troughs drawn from separate dosing intervals also were considered inappropriate. Random levels were considered appropriate only if they fit the clinical context in acute renal failure or renal replacement therapy. An effective transition was defined as ≥ 80% of all vancomycin treated patients monitored with AUC methods rather than trough-based methods.
Inclusion criteria included all vancomycin levels ordered during the study period with no exclusions. The primary endpoint was the proportion of vancomycin levels drawn appropriately. Secondary endpoints were the proportion of AUC24 calculations within therapeutic range and a stratification of reasons for inappropriate levels. Descriptive statistics were collected to describe the scope of the project. Levels drawn from various shifts were compared (ie, day, night, or weekend). Calculated AUC24 levels between 400 and 600 mg.h/L were considered therapeutic unless treating CNS infection (600-700 mg.h/L). Given the operational outcomes (rather than clinical outcomes) and no comparator group, patient specific data were not collected.
Descriptive statistics without further analysis were used to describe proportions. The goal level for compliance was set at 100%. These methods were reviewed by the VHSO Institutional Review Board and granted nonresearch status, waiving the requirement for informed consent.
Results
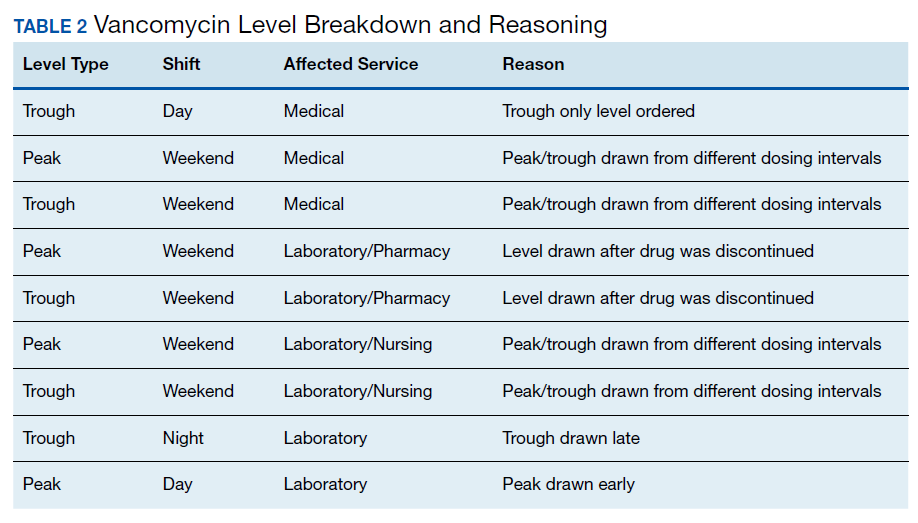
The transition was effective with 97% of all cases utilizing AUC-based methods for monitoring. A total of 65 vancomycin levels were drawn in the study period; 32 peaks, 32 troughs, and 1 random level (drawn appropriately during acute renal failure 24 hours after starting therapy). All shifts were affected proportionately; days (n = 26, 40%), nights (n = 18, 27.7%), and weekends (n = 21, 32.3%). Based on time of dosage administration and laboratory test, there were 9 levels (13.8%) deemed inappropriate, 56 levels (86.1%) were appropriate. Reasons for inappropriate levels gleaned from chart review are presented in Table 2. Four levels had to be repeated for accurate calculations.
From the peak/trough couplets drawn appropriately, calculated AUC24 fell with the desired range in 61% (n = 17) of cases. Of the 11 that fell outside of range, 8 were subtherapeutic (< 400 mg.h/L) and 3 were supratherapeutic (> 600 mg.h/L). All levels were drawn at steady state. Indications for vancomycin monitoring were osteomyelitis (n = 13, 43%), sepsis (n = 10, 33%), pneumonia (n = 6, 20%), and 1 case of meningitis (3%).
Discussion
To the author’s knowledge, this is the first report of a vancomycin AUC24 monitoring conversion in a rural facility. This study adds to the existing medical literature in that it demonstrates that: (1) implementation methods described in large, tertiary centers can be effectively utilized in primary care, rural facilities; (2) the gap analysis used can be duplicated with minimal personnel and resources to ensure effective implementation (Table 3); and (3) the reported improvement needs can serve as a model for preventative measures at other facilities. The incidence of appropriate vancomycin levels was notably better than those reported in other single center studies.15-17 However, given variations in study design and facility operating procedures, it would be difficult to compare incidence among medical facilities. As such, there are no consensus benchmarks for comparison. The majority of inappropriate levels occurred early in the study period and on weekends. Appropriateness of drug levels may have improved with continued feedback and familiarity.
The calculated AUC24 fell within predicted range in 61% of cases. For comparison, a recent study from a large academic medical center reported that 73.5% of 2-level AUC24 cases had initial values within the therapeutic range.18 Of note, the target range used was much wider (400 - 800 mg.h/L) than the present study. Another study reported dose adjustments for subtherapeutic AUC levels in 25% of cases and dose reductions for supratherapeutic levels in 33.3% of cases.19
Of the AUC24 calculations that fell outside of therapeutic range, the majority (n = 8, 73%) were subtherapeutic (< 400 mg.h/L), half of these were for patients who were obese. It was unclear in the medical record which equation was used for initial dosing (Matzke vs Crass), or whether more conservative AUCs were used for calculating the total daily dose. The VHSO policy limiting loading doses also may have played a role; indeed the updated guidelines recommend a maximum loading dose of 3,000 mg depending on the severity of infection.4 Two of the 3 supratherapeutic levels were thought to be due to accumulation with long-term therapy.
Given such a large change from long-standing practices, there was surprisingly little resistance from the various clinical services. A recent survey of academic medical centers reported that the majority (88%) of all respondents who did not currently utilize AUC24 monitoring did not plan on making this immediate transition, largely citing unfamiliarity and training requirements.20 It is conceivable that the transition to AUC monitoring in smaller facilities may have fewer barriers than those seen in tertiary care centers. There are fewer health care providers and pharmacists to educate with the primary responsibilities falling on relatively few clinicians. There is little question as to who will be conducting follow up or whom to contact for questions. A smaller patient load and lesser patient acuity may translate to fewer vancomycin cases that require monitoring.
The interactive meetings were an important element for facility implementation. Research shows that emails alone are not effective for health care provider education, and interactive methods are recommended over passive methods.21,22 Assessing and avoiding barriers up front such as unclear laboratory orders, or communication failures is paramount to successful implementation strategies.23 Additionally, the detailed written ordering communication may have contributed to a smoother transition. The educational recording proved to be helpful in educating new staff and residents. An identified logistical error was that laboratory orders entered while patients were enrolled in sham clinics for electronic workload capture (eg, Pharmacy Inpatient Clinic) created confusion on the physical location of the patient for the phlebotomists, potentially causing delays in specimen collection.
A major development that stemmed from this intervention was that the Medical Service asked that policy changes be made so that the Pharmacy Service take over all vancomycin dosing at the facility. Previously, this had been done on a collaborative basis. Similar facilities with a collaborative practice model may need to anticipate such a request as this may present a new set of challenges. Accordingly, the pharmacy department is in the process of establishing standing operating procedures, pharmacist competencies, and a facility memorandum. Future research should evaluate the safety and efficacy of vancomycin therapy after the switch to AUC-based monitoring.
Limitations
There are several limitations to consider with this study. Operating procedures and implementation processes may vary between facilities, which could limit the generalizability of these results. Given the small facility size, the overall number of laboratory tests drawn was much smaller than those seen in larger facilities. The time needed for AUC calculations is notably longer than older methods of monitoring; however, this was not objectively assessed. It is important to note that clinical outcomes were beyond the scope of this gap analysis and this is an area of future research at the study facility. Vancomycin laboratory tests that were missed due to procedures and subsequently rescheduled were occasionally observed but not accounted for in this analysis. Additionally, vancomycin courses without monitoring (appropriate or otherwise) when indicated were not assessed. However, anecdotally speaking, this would be a very unlikely occurrence.
Conclusion
Conversion to AUC-based vancomycin monitoring is feasible in primary, rural medical centers. Implementation strategies from tertiary facilities can be successfully utilized in smaller hospitals. Quality assessment strategies such as a gap analysis can be utilized with minimal resources for facility uptake of new clinical practices.
1. Rybak M, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists [published correction appears in Am J Health Syst Pharm. 2009;66(10):887]. Am J Health Syst Pharm. 2009;66(1):82‐98. doi:10.2146/ajhp080434
2. van Hal SJ, Paterson DL, Lodise TP. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob Agents Chemother. 2013;57(2):734‐744. doi:10.1128/AAC.01568-12
3. Pai MP, Neely M, Rodvold KA, Lodise TP. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv Drug Deliv Rev. 2014;77:50‐57. doi:10.1016/j.addr.2014.05.016
4. Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists [published online ahead of print, 2020 Mar 19]. Am J Health Syst Pharm. 2020;zxaa036. doi:10.1093/ajhp/zxaa036
5. Heil EL, Claeys KC, Mynatt RP, et al. Making the change to area under the curve-based vancomycin dosing. Am J Health Syst Pharm. 2018;75(24):1986‐1995. doi:10.2146/ajhp180034
6. Gregory ER, Burgess DR, Cotner SE, et al. Vancomycin area under the curve dosing and monitoring at an academic medical center: transition strategies and lessons learned [published online ahead of print, 2019 Mar 10]. J Pharm Pract. 2019;897190019834369. doi:10.1177/0897190019834369
7. Septimus EJ, Owens RC Jr. Need and potential of antimicrobial stewardship in community hospitals. Clin Infect Dis. 2011;53 Suppl 1:S8‐S14. doi:10.1093/cid/cir363
8. Goldman LE, Dudley RA. United States rural hospital quality in the Hospital Compare database-accounting for hospital characteristics. Health Policy. 2008;87(1):112‐127. doi:10.1016/j.healthpol.2008.02.002
9. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962. doi:10.1371/journal.pone.0078962
10. Institute for Healthcare Improvement. Plan-do-study-act (PDSA) worksheet. http://www.ihi.org/resources/Pages/Tools/PlanDoStudyActWorksheet.aspx. Accessed May 13, 2020.
11. Agency for Healthcare Research and Quality. Plan-do-study-act (PDSA) cycle. https://innovations.ahrq.gov/qualitytools/plan-do-study-act-pdsa-cycle. Updated April 10, 2013. Accessed May 13, 2020.
12. Matzke GR, McGory RW, Halstenson CE, Keane WF. Pharmacokinetics of vancomycin in patients with various degrees of renal function. Antimicrob Agents Chemother. 1984;25(4):433‐437. doi:10.1128/aac.25.4.433
13. Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081‐3086. doi:10.1093/jac/dky310
14. Pai MP, Russo A, Novelli A, Venditti M, Falcone M. Simplified equations using two concentrations to calculate area under the curve for antimicrobials with concentration-dependent pharmacodynamics: daptomycin as a motivating example. Antimicrob Agents Chemother. 2014;58(6):3162‐3167. doi:10.1128/AAC.02355-14
15. Suryadevara M, Steidl KE, Probst LA, Shaw J. Inappropriate vancomycin therapeutic drug monitoring in hospitalized pediatric patients increases pediatric trauma and hospital costs. J Pediatr Pharmacol Ther. 2012;17(2):159‐165. doi:10.5863/1551-6776-17.2.159
16. Morrison AP, Melanson SE, Carty MG, Bates DW, Szumita PM, Tanasijevic MJ. What proportion of vancomycin trough levels are drawn too early?: frequency and impact on clinical actions. Am J Clin Pathol. 2012;137(3):472‐478. doi:10.1309/AJCPDSYS0DVLKFOH
17. Melanson SE, Mijailovic AS, Wright AP, Szumita PM, Bates DW, Tanasijevic MJ. An intervention to improve the timing of vancomycin levels. Am J Clin Pathol. 2013;140(6):801‐806. doi:10.1309/AJCPKQ6EAH7OYQLB
18. Meng L, Wong T, Huang S, et al. Conversion from vancomycin trough concentration-guided dosing to area under the curve-guided dosing using two sample measurements in adults: implementation at an academic medical center. Pharmacotherapy. 2019;39(4):433‐442. doi:10.1002/phar.2234
19. Stoessel AM, Hale CM, Seabury RW, Miller CD, Steele JM. The impact of AUC-based monitoring on pharmacist-directed vancomycin dose adjustments in complicated methicillin-resistant staphylococcus aureus Infection. J Pharm Pract. 2019;32(4):442‐446. doi:10.1177/0897190018764564
20. Kufel WD, Seabury RW, Mogle BT, Beccari MV, Probst LA, Steele JM. Readiness to implement vancomycin monitoring based on area under the concentration-time curve: a cross-sectional survey of a national health consortium. Am J Health Syst Pharm. 2019;76(12):889‐894. doi:10.1093/ajhp/zxz070
21. Bluestone J, Johnson P, Fullerton J, Carr C, Alderman J, BonTempo J. Effective in-service training design and delivery: evidence from an integrative literature review. Hum Resour Health. 2013;11:51. doi:10.1186/1478-4491-11-51
22. Ebben RHA, Siqeca F, Madsen UR, Vloet LCM, van Achterberg T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ Open. 2018;8(11):e017572. doi:10.1136/bmjopen-2017-017572
23. Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and Strategies in Guideline Implementation-A Scoping Review. Healthcare (Basel). 2016;4(3):36. doi:10.3390/healthcare4030036
The use of weight-based dosing with trough-based monitoring of vancomycin has been in clinical practice for more than a decade. The American Society of Health-System Pharmacists (ASHP), the Infectious Diseases Society of America (IDSA), and the Society of Infectious Diseases Pharmacists (SIDP) published the first guidelines for vancomycin monitoring in 2009.1 Although it has been well established that area under the curve (AUC) over the minimal inhibitory concentration (MIC) ratio > 400 mg.h/L is the best predictor of clinical efficacy, obtaining this value in clinical practice was not pragmatic. Therefore, the 2009 guidelines recommended a goal vancomycin trough of 15 to 20 mcg/ml as a surrogate marker for AUC/MIC > 400 mg.hr/L. This has since become a common practice despite little data that support this recommendation.
The efficacy and safety of trough-based monitoring has been evaluated extensively over the past several years and more recent data suggest that there is wide patient variability in AUC with this method and higher trough levels are associated with more nephrotoxicity.2,3 ASHP, IDSA, SIDP, and the Pediatric Infectious Diseases Society (PIDS) updated the consensus guidelines in 2020.4 Trough-based monitoring is no longer recommended. Instead AUC24 monitoring should be implemented with a goal range of 400 to 600 mg.h/L for efficacy and safety. Given concerns for vancomycin penetration into the central nervous system (CNS), many facility protocols utilize higher targets (> 600 mg.h/L) for CNS infections.
Some hospitals have been utilizing AUC-based monitoring for years. There are strategies from tertiary care centers that drive this practice change in the medical literature.5,6 However, it is important to reproduce these implementation practices in small, rural facilities that may face unique challenges with limited resources and may be slower to implement consensus guidelines.7,8 As this is a major practice change, it is imperative to evaluate the extent of transition and identify areas of needed improvement.
Accurate therapeutic drug monitoring ensures both the safety and efficacy of vancomycin therapy. Unfortunately, research shows that inappropriate laboratory tests are common in medical facilities.9 Drug levels taken inappropriately can lead to delays in therapeutic decision-making, inappropriate dosage adjustments and create a need for repeated drug levels, which increases the overall cost of admission.
Given the multiple affected services needed to make successful practice transitions, it is paramount that facilities evaluate progress during the transition phase. The Agency for Healthcare Research and Quality and the Institute for Healthcare Improvement provide guidance in the Plan-Do-Study-Act Cycle for quality assessment and improvement of new initiatives.10,11 A gap analysis can be used as a simple tool for evaluating the transition of research into practice and to identify areas of needed improvement.
The Veterans Health Care System of the Ozarks (VHSO) in Fayetteville, Arkansas made the transition from trough-based monitoring to 2-level AUC-based monitoring on April 1, 2019. The purpose of this study was to evaluate the effectiveness of transition methods used to implement AUC-monitoring for vancomycin treated patients in a small, primary facility. A further goal of the study was to identify areas of needed improvement and education and whether the problems derived from deficiencies in knowledge and ordering (medical and pharmacy services) or execution (nursing and laboratory services).
Methods
VHSO is a 52-bed US Department of Veterans Affairs primary care hospital. The pharmacy and laboratory are staffed 24 hours each day. There is 1 clinical pharmacy specialist (CPS) available for therapeutic drug monitoring consults Monday through Friday between the hours of 7:30 AM and 4:00 PM. No partial full-time equivalent employees were added for this conversion. Pharmacy-driven vancomycin dosing and monitoring is conducted on a collaborative basis, with pharmacy managing the majority of vancomycin treated patients. Night and weekend pharmacy staff provide cross-coverage on vancomycin consultations. Laboratory orders and medication dosage adjustments fall within the CPS scope of practice. Nurses do not perform laboratory draws for therapeutic drug monitoring; this is done solely by phlebotomists. There is no infectious diseases specialist at the facility to champion antibiotic dosing initiatives.
The implementation strategy largely reflected those outlined from tertiary care centers.5,6 First, key personnel from the laboratory department met to discuss this practice change and to add vancomycin peaks to the ordering menu. A critical value was set at 40 mcg/ml. Vancomycin troughs and random levels already were orderable items. A comment field was added to all laboratory orders for further clarification. Verbiage was added to laboratory reports in the computerized medical record to assist clinicians in determining the appropriateness of the level. This was followed by an educational email to both the nursing and laboratory departments explaining the practice change and included a link to the Pharmacy Joe “Vancomycin Dosing by AUC:MIC Instead of Trough-level” podcast (www.pharmacyjoe.com episode 356).
The pharmacy department received an interactive 30-minute presentation, followed immediately by a group activity to discuss practice problems. This presentation was condensed, recorded, and emailed to all VHSO pharmacists. A shared folder contained pertinent material on AUC monitoring.
Finally, an interactive presentation was set up for hospitalists and a video teleconferencing was conducted for rotating medical residents. Both the podcast and recorded presentation were emailed to the entire medical staff with a brief introduction of the practice change. Additionally, the transition process was added as a standing item on the monthly antimicrobial stewardship meeting agenda.
The standardized pharmacokinetic model at the study facility consisted of a vancomycin volume of distribution of 0.7 mg/kg and elimination rate constant (Ke) by Matzke and colleagues for total daily dose calculations.12 Obese patients (BMI ≥ 30) undergo alternative clearance equations described by Crass and colleagues.13 Cockcroft-Gault methods using ideal body weight (or actual body weight if < ideal body weight) are used for determining creatinine clearance. In patients aged ≥ 65 years with a serum creatinine < 1.0 mg/dL, facility guidance was to round serum creatinine up to 1.0 mg/dL. Loading doses were determined on a case-by-case basis with a cap of 2,000 mg, maintenance doses were rounded to the nearest 250 mg.
Vancomycin levels typically are drawn at steady state and analyzed using the logarithmic trapezoidal rule.14 The pharmacy and medical staff were educated to provide details on timing and coordination in nursing and laboratory orders (Table 1). Two-level AUC monitoring typically is not performed in patients with acute renal failure, expected duration of therapy < 72 hours, urinary tract infections, skin and soft tissue infections, or in renal replacement therapy.5
This gap analysis consisted of a retrospective chart review of vancomycin levels ordered after the implementation of AUC-based monitoring to determine the effectiveness of the transition. Three months of data were collected between April 2019 and June 2019. Vancomycin levels were deemed either appropriate or inappropriate based on timing and type (peak, trough, or random) of the laboratory test in relation to the previously administered vancomycin dose. Appropriate peaks were drawn within 2 hours after the end of infusion and troughs at least 1 half-life after the dose or just prior to the next dose and within the same dosing interval as the peak. Tests drawn outside of the specified time range, trough-only laboratory tests, or those drawn after vancomycin had been discontinued were considered inappropriate. Peaks and troughs drawn from separate dosing intervals also were considered inappropriate. Random levels were considered appropriate only if they fit the clinical context in acute renal failure or renal replacement therapy. An effective transition was defined as ≥ 80% of all vancomycin treated patients monitored with AUC methods rather than trough-based methods.
Inclusion criteria included all vancomycin levels ordered during the study period with no exclusions. The primary endpoint was the proportion of vancomycin levels drawn appropriately. Secondary endpoints were the proportion of AUC24 calculations within therapeutic range and a stratification of reasons for inappropriate levels. Descriptive statistics were collected to describe the scope of the project. Levels drawn from various shifts were compared (ie, day, night, or weekend). Calculated AUC24 levels between 400 and 600 mg.h/L were considered therapeutic unless treating CNS infection (600-700 mg.h/L). Given the operational outcomes (rather than clinical outcomes) and no comparator group, patient specific data were not collected.
Descriptive statistics without further analysis were used to describe proportions. The goal level for compliance was set at 100%. These methods were reviewed by the VHSO Institutional Review Board and granted nonresearch status, waiving the requirement for informed consent.
Results
The transition was effective with 97% of all cases utilizing AUC-based methods for monitoring. A total of 65 vancomycin levels were drawn in the study period; 32 peaks, 32 troughs, and 1 random level (drawn appropriately during acute renal failure 24 hours after starting therapy). All shifts were affected proportionately; days (n = 26, 40%), nights (n = 18, 27.7%), and weekends (n = 21, 32.3%). Based on time of dosage administration and laboratory test, there were 9 levels (13.8%) deemed inappropriate, 56 levels (86.1%) were appropriate. Reasons for inappropriate levels gleaned from chart review are presented in Table 2. Four levels had to be repeated for accurate calculations.
From the peak/trough couplets drawn appropriately, calculated AUC24 fell with the desired range in 61% (n = 17) of cases. Of the 11 that fell outside of range, 8 were subtherapeutic (< 400 mg.h/L) and 3 were supratherapeutic (> 600 mg.h/L). All levels were drawn at steady state. Indications for vancomycin monitoring were osteomyelitis (n = 13, 43%), sepsis (n = 10, 33%), pneumonia (n = 6, 20%), and 1 case of meningitis (3%).
Discussion
To the author’s knowledge, this is the first report of a vancomycin AUC24 monitoring conversion in a rural facility. This study adds to the existing medical literature in that it demonstrates that: (1) implementation methods described in large, tertiary centers can be effectively utilized in primary care, rural facilities; (2) the gap analysis used can be duplicated with minimal personnel and resources to ensure effective implementation (Table 3); and (3) the reported improvement needs can serve as a model for preventative measures at other facilities. The incidence of appropriate vancomycin levels was notably better than those reported in other single center studies.15-17 However, given variations in study design and facility operating procedures, it would be difficult to compare incidence among medical facilities. As such, there are no consensus benchmarks for comparison. The majority of inappropriate levels occurred early in the study period and on weekends. Appropriateness of drug levels may have improved with continued feedback and familiarity.
The calculated AUC24 fell within predicted range in 61% of cases. For comparison, a recent study from a large academic medical center reported that 73.5% of 2-level AUC24 cases had initial values within the therapeutic range.18 Of note, the target range used was much wider (400 - 800 mg.h/L) than the present study. Another study reported dose adjustments for subtherapeutic AUC levels in 25% of cases and dose reductions for supratherapeutic levels in 33.3% of cases.19
Of the AUC24 calculations that fell outside of therapeutic range, the majority (n = 8, 73%) were subtherapeutic (< 400 mg.h/L), half of these were for patients who were obese. It was unclear in the medical record which equation was used for initial dosing (Matzke vs Crass), or whether more conservative AUCs were used for calculating the total daily dose. The VHSO policy limiting loading doses also may have played a role; indeed the updated guidelines recommend a maximum loading dose of 3,000 mg depending on the severity of infection.4 Two of the 3 supratherapeutic levels were thought to be due to accumulation with long-term therapy.
Given such a large change from long-standing practices, there was surprisingly little resistance from the various clinical services. A recent survey of academic medical centers reported that the majority (88%) of all respondents who did not currently utilize AUC24 monitoring did not plan on making this immediate transition, largely citing unfamiliarity and training requirements.20 It is conceivable that the transition to AUC monitoring in smaller facilities may have fewer barriers than those seen in tertiary care centers. There are fewer health care providers and pharmacists to educate with the primary responsibilities falling on relatively few clinicians. There is little question as to who will be conducting follow up or whom to contact for questions. A smaller patient load and lesser patient acuity may translate to fewer vancomycin cases that require monitoring.
The interactive meetings were an important element for facility implementation. Research shows that emails alone are not effective for health care provider education, and interactive methods are recommended over passive methods.21,22 Assessing and avoiding barriers up front such as unclear laboratory orders, or communication failures is paramount to successful implementation strategies.23 Additionally, the detailed written ordering communication may have contributed to a smoother transition. The educational recording proved to be helpful in educating new staff and residents. An identified logistical error was that laboratory orders entered while patients were enrolled in sham clinics for electronic workload capture (eg, Pharmacy Inpatient Clinic) created confusion on the physical location of the patient for the phlebotomists, potentially causing delays in specimen collection.
A major development that stemmed from this intervention was that the Medical Service asked that policy changes be made so that the Pharmacy Service take over all vancomycin dosing at the facility. Previously, this had been done on a collaborative basis. Similar facilities with a collaborative practice model may need to anticipate such a request as this may present a new set of challenges. Accordingly, the pharmacy department is in the process of establishing standing operating procedures, pharmacist competencies, and a facility memorandum. Future research should evaluate the safety and efficacy of vancomycin therapy after the switch to AUC-based monitoring.
Limitations
There are several limitations to consider with this study. Operating procedures and implementation processes may vary between facilities, which could limit the generalizability of these results. Given the small facility size, the overall number of laboratory tests drawn was much smaller than those seen in larger facilities. The time needed for AUC calculations is notably longer than older methods of monitoring; however, this was not objectively assessed. It is important to note that clinical outcomes were beyond the scope of this gap analysis and this is an area of future research at the study facility. Vancomycin laboratory tests that were missed due to procedures and subsequently rescheduled were occasionally observed but not accounted for in this analysis. Additionally, vancomycin courses without monitoring (appropriate or otherwise) when indicated were not assessed. However, anecdotally speaking, this would be a very unlikely occurrence.
Conclusion
Conversion to AUC-based vancomycin monitoring is feasible in primary, rural medical centers. Implementation strategies from tertiary facilities can be successfully utilized in smaller hospitals. Quality assessment strategies such as a gap analysis can be utilized with minimal resources for facility uptake of new clinical practices.
The use of weight-based dosing with trough-based monitoring of vancomycin has been in clinical practice for more than a decade. The American Society of Health-System Pharmacists (ASHP), the Infectious Diseases Society of America (IDSA), and the Society of Infectious Diseases Pharmacists (SIDP) published the first guidelines for vancomycin monitoring in 2009.1 Although it has been well established that area under the curve (AUC) over the minimal inhibitory concentration (MIC) ratio > 400 mg.h/L is the best predictor of clinical efficacy, obtaining this value in clinical practice was not pragmatic. Therefore, the 2009 guidelines recommended a goal vancomycin trough of 15 to 20 mcg/ml as a surrogate marker for AUC/MIC > 400 mg.hr/L. This has since become a common practice despite little data that support this recommendation.
The efficacy and safety of trough-based monitoring has been evaluated extensively over the past several years and more recent data suggest that there is wide patient variability in AUC with this method and higher trough levels are associated with more nephrotoxicity.2,3 ASHP, IDSA, SIDP, and the Pediatric Infectious Diseases Society (PIDS) updated the consensus guidelines in 2020.4 Trough-based monitoring is no longer recommended. Instead AUC24 monitoring should be implemented with a goal range of 400 to 600 mg.h/L for efficacy and safety. Given concerns for vancomycin penetration into the central nervous system (CNS), many facility protocols utilize higher targets (> 600 mg.h/L) for CNS infections.
Some hospitals have been utilizing AUC-based monitoring for years. There are strategies from tertiary care centers that drive this practice change in the medical literature.5,6 However, it is important to reproduce these implementation practices in small, rural facilities that may face unique challenges with limited resources and may be slower to implement consensus guidelines.7,8 As this is a major practice change, it is imperative to evaluate the extent of transition and identify areas of needed improvement.
Accurate therapeutic drug monitoring ensures both the safety and efficacy of vancomycin therapy. Unfortunately, research shows that inappropriate laboratory tests are common in medical facilities.9 Drug levels taken inappropriately can lead to delays in therapeutic decision-making, inappropriate dosage adjustments and create a need for repeated drug levels, which increases the overall cost of admission.
Given the multiple affected services needed to make successful practice transitions, it is paramount that facilities evaluate progress during the transition phase. The Agency for Healthcare Research and Quality and the Institute for Healthcare Improvement provide guidance in the Plan-Do-Study-Act Cycle for quality assessment and improvement of new initiatives.10,11 A gap analysis can be used as a simple tool for evaluating the transition of research into practice and to identify areas of needed improvement.
The Veterans Health Care System of the Ozarks (VHSO) in Fayetteville, Arkansas made the transition from trough-based monitoring to 2-level AUC-based monitoring on April 1, 2019. The purpose of this study was to evaluate the effectiveness of transition methods used to implement AUC-monitoring for vancomycin treated patients in a small, primary facility. A further goal of the study was to identify areas of needed improvement and education and whether the problems derived from deficiencies in knowledge and ordering (medical and pharmacy services) or execution (nursing and laboratory services).
Methods
VHSO is a 52-bed US Department of Veterans Affairs primary care hospital. The pharmacy and laboratory are staffed 24 hours each day. There is 1 clinical pharmacy specialist (CPS) available for therapeutic drug monitoring consults Monday through Friday between the hours of 7:30 AM and 4:00 PM. No partial full-time equivalent employees were added for this conversion. Pharmacy-driven vancomycin dosing and monitoring is conducted on a collaborative basis, with pharmacy managing the majority of vancomycin treated patients. Night and weekend pharmacy staff provide cross-coverage on vancomycin consultations. Laboratory orders and medication dosage adjustments fall within the CPS scope of practice. Nurses do not perform laboratory draws for therapeutic drug monitoring; this is done solely by phlebotomists. There is no infectious diseases specialist at the facility to champion antibiotic dosing initiatives.
The implementation strategy largely reflected those outlined from tertiary care centers.5,6 First, key personnel from the laboratory department met to discuss this practice change and to add vancomycin peaks to the ordering menu. A critical value was set at 40 mcg/ml. Vancomycin troughs and random levels already were orderable items. A comment field was added to all laboratory orders for further clarification. Verbiage was added to laboratory reports in the computerized medical record to assist clinicians in determining the appropriateness of the level. This was followed by an educational email to both the nursing and laboratory departments explaining the practice change and included a link to the Pharmacy Joe “Vancomycin Dosing by AUC:MIC Instead of Trough-level” podcast (www.pharmacyjoe.com episode 356).
The pharmacy department received an interactive 30-minute presentation, followed immediately by a group activity to discuss practice problems. This presentation was condensed, recorded, and emailed to all VHSO pharmacists. A shared folder contained pertinent material on AUC monitoring.
Finally, an interactive presentation was set up for hospitalists and a video teleconferencing was conducted for rotating medical residents. Both the podcast and recorded presentation were emailed to the entire medical staff with a brief introduction of the practice change. Additionally, the transition process was added as a standing item on the monthly antimicrobial stewardship meeting agenda.
The standardized pharmacokinetic model at the study facility consisted of a vancomycin volume of distribution of 0.7 mg/kg and elimination rate constant (Ke) by Matzke and colleagues for total daily dose calculations.12 Obese patients (BMI ≥ 30) undergo alternative clearance equations described by Crass and colleagues.13 Cockcroft-Gault methods using ideal body weight (or actual body weight if < ideal body weight) are used for determining creatinine clearance. In patients aged ≥ 65 years with a serum creatinine < 1.0 mg/dL, facility guidance was to round serum creatinine up to 1.0 mg/dL. Loading doses were determined on a case-by-case basis with a cap of 2,000 mg, maintenance doses were rounded to the nearest 250 mg.
Vancomycin levels typically are drawn at steady state and analyzed using the logarithmic trapezoidal rule.14 The pharmacy and medical staff were educated to provide details on timing and coordination in nursing and laboratory orders (Table 1). Two-level AUC monitoring typically is not performed in patients with acute renal failure, expected duration of therapy < 72 hours, urinary tract infections, skin and soft tissue infections, or in renal replacement therapy.5
This gap analysis consisted of a retrospective chart review of vancomycin levels ordered after the implementation of AUC-based monitoring to determine the effectiveness of the transition. Three months of data were collected between April 2019 and June 2019. Vancomycin levels were deemed either appropriate or inappropriate based on timing and type (peak, trough, or random) of the laboratory test in relation to the previously administered vancomycin dose. Appropriate peaks were drawn within 2 hours after the end of infusion and troughs at least 1 half-life after the dose or just prior to the next dose and within the same dosing interval as the peak. Tests drawn outside of the specified time range, trough-only laboratory tests, or those drawn after vancomycin had been discontinued were considered inappropriate. Peaks and troughs drawn from separate dosing intervals also were considered inappropriate. Random levels were considered appropriate only if they fit the clinical context in acute renal failure or renal replacement therapy. An effective transition was defined as ≥ 80% of all vancomycin treated patients monitored with AUC methods rather than trough-based methods.
Inclusion criteria included all vancomycin levels ordered during the study period with no exclusions. The primary endpoint was the proportion of vancomycin levels drawn appropriately. Secondary endpoints were the proportion of AUC24 calculations within therapeutic range and a stratification of reasons for inappropriate levels. Descriptive statistics were collected to describe the scope of the project. Levels drawn from various shifts were compared (ie, day, night, or weekend). Calculated AUC24 levels between 400 and 600 mg.h/L were considered therapeutic unless treating CNS infection (600-700 mg.h/L). Given the operational outcomes (rather than clinical outcomes) and no comparator group, patient specific data were not collected.
Descriptive statistics without further analysis were used to describe proportions. The goal level for compliance was set at 100%. These methods were reviewed by the VHSO Institutional Review Board and granted nonresearch status, waiving the requirement for informed consent.
Results
The transition was effective with 97% of all cases utilizing AUC-based methods for monitoring. A total of 65 vancomycin levels were drawn in the study period; 32 peaks, 32 troughs, and 1 random level (drawn appropriately during acute renal failure 24 hours after starting therapy). All shifts were affected proportionately; days (n = 26, 40%), nights (n = 18, 27.7%), and weekends (n = 21, 32.3%). Based on time of dosage administration and laboratory test, there were 9 levels (13.8%) deemed inappropriate, 56 levels (86.1%) were appropriate. Reasons for inappropriate levels gleaned from chart review are presented in Table 2. Four levels had to be repeated for accurate calculations.
From the peak/trough couplets drawn appropriately, calculated AUC24 fell with the desired range in 61% (n = 17) of cases. Of the 11 that fell outside of range, 8 were subtherapeutic (< 400 mg.h/L) and 3 were supratherapeutic (> 600 mg.h/L). All levels were drawn at steady state. Indications for vancomycin monitoring were osteomyelitis (n = 13, 43%), sepsis (n = 10, 33%), pneumonia (n = 6, 20%), and 1 case of meningitis (3%).
Discussion
To the author’s knowledge, this is the first report of a vancomycin AUC24 monitoring conversion in a rural facility. This study adds to the existing medical literature in that it demonstrates that: (1) implementation methods described in large, tertiary centers can be effectively utilized in primary care, rural facilities; (2) the gap analysis used can be duplicated with minimal personnel and resources to ensure effective implementation (Table 3); and (3) the reported improvement needs can serve as a model for preventative measures at other facilities. The incidence of appropriate vancomycin levels was notably better than those reported in other single center studies.15-17 However, given variations in study design and facility operating procedures, it would be difficult to compare incidence among medical facilities. As such, there are no consensus benchmarks for comparison. The majority of inappropriate levels occurred early in the study period and on weekends. Appropriateness of drug levels may have improved with continued feedback and familiarity.
The calculated AUC24 fell within predicted range in 61% of cases. For comparison, a recent study from a large academic medical center reported that 73.5% of 2-level AUC24 cases had initial values within the therapeutic range.18 Of note, the target range used was much wider (400 - 800 mg.h/L) than the present study. Another study reported dose adjustments for subtherapeutic AUC levels in 25% of cases and dose reductions for supratherapeutic levels in 33.3% of cases.19
Of the AUC24 calculations that fell outside of therapeutic range, the majority (n = 8, 73%) were subtherapeutic (< 400 mg.h/L), half of these were for patients who were obese. It was unclear in the medical record which equation was used for initial dosing (Matzke vs Crass), or whether more conservative AUCs were used for calculating the total daily dose. The VHSO policy limiting loading doses also may have played a role; indeed the updated guidelines recommend a maximum loading dose of 3,000 mg depending on the severity of infection.4 Two of the 3 supratherapeutic levels were thought to be due to accumulation with long-term therapy.
Given such a large change from long-standing practices, there was surprisingly little resistance from the various clinical services. A recent survey of academic medical centers reported that the majority (88%) of all respondents who did not currently utilize AUC24 monitoring did not plan on making this immediate transition, largely citing unfamiliarity and training requirements.20 It is conceivable that the transition to AUC monitoring in smaller facilities may have fewer barriers than those seen in tertiary care centers. There are fewer health care providers and pharmacists to educate with the primary responsibilities falling on relatively few clinicians. There is little question as to who will be conducting follow up or whom to contact for questions. A smaller patient load and lesser patient acuity may translate to fewer vancomycin cases that require monitoring.
The interactive meetings were an important element for facility implementation. Research shows that emails alone are not effective for health care provider education, and interactive methods are recommended over passive methods.21,22 Assessing and avoiding barriers up front such as unclear laboratory orders, or communication failures is paramount to successful implementation strategies.23 Additionally, the detailed written ordering communication may have contributed to a smoother transition. The educational recording proved to be helpful in educating new staff and residents. An identified logistical error was that laboratory orders entered while patients were enrolled in sham clinics for electronic workload capture (eg, Pharmacy Inpatient Clinic) created confusion on the physical location of the patient for the phlebotomists, potentially causing delays in specimen collection.
A major development that stemmed from this intervention was that the Medical Service asked that policy changes be made so that the Pharmacy Service take over all vancomycin dosing at the facility. Previously, this had been done on a collaborative basis. Similar facilities with a collaborative practice model may need to anticipate such a request as this may present a new set of challenges. Accordingly, the pharmacy department is in the process of establishing standing operating procedures, pharmacist competencies, and a facility memorandum. Future research should evaluate the safety and efficacy of vancomycin therapy after the switch to AUC-based monitoring.
Limitations
There are several limitations to consider with this study. Operating procedures and implementation processes may vary between facilities, which could limit the generalizability of these results. Given the small facility size, the overall number of laboratory tests drawn was much smaller than those seen in larger facilities. The time needed for AUC calculations is notably longer than older methods of monitoring; however, this was not objectively assessed. It is important to note that clinical outcomes were beyond the scope of this gap analysis and this is an area of future research at the study facility. Vancomycin laboratory tests that were missed due to procedures and subsequently rescheduled were occasionally observed but not accounted for in this analysis. Additionally, vancomycin courses without monitoring (appropriate or otherwise) when indicated were not assessed. However, anecdotally speaking, this would be a very unlikely occurrence.
Conclusion
Conversion to AUC-based vancomycin monitoring is feasible in primary, rural medical centers. Implementation strategies from tertiary facilities can be successfully utilized in smaller hospitals. Quality assessment strategies such as a gap analysis can be utilized with minimal resources for facility uptake of new clinical practices.
1. Rybak M, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists [published correction appears in Am J Health Syst Pharm. 2009;66(10):887]. Am J Health Syst Pharm. 2009;66(1):82‐98. doi:10.2146/ajhp080434
2. van Hal SJ, Paterson DL, Lodise TP. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob Agents Chemother. 2013;57(2):734‐744. doi:10.1128/AAC.01568-12
3. Pai MP, Neely M, Rodvold KA, Lodise TP. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv Drug Deliv Rev. 2014;77:50‐57. doi:10.1016/j.addr.2014.05.016
4. Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists [published online ahead of print, 2020 Mar 19]. Am J Health Syst Pharm. 2020;zxaa036. doi:10.1093/ajhp/zxaa036
5. Heil EL, Claeys KC, Mynatt RP, et al. Making the change to area under the curve-based vancomycin dosing. Am J Health Syst Pharm. 2018;75(24):1986‐1995. doi:10.2146/ajhp180034
6. Gregory ER, Burgess DR, Cotner SE, et al. Vancomycin area under the curve dosing and monitoring at an academic medical center: transition strategies and lessons learned [published online ahead of print, 2019 Mar 10]. J Pharm Pract. 2019;897190019834369. doi:10.1177/0897190019834369
7. Septimus EJ, Owens RC Jr. Need and potential of antimicrobial stewardship in community hospitals. Clin Infect Dis. 2011;53 Suppl 1:S8‐S14. doi:10.1093/cid/cir363
8. Goldman LE, Dudley RA. United States rural hospital quality in the Hospital Compare database-accounting for hospital characteristics. Health Policy. 2008;87(1):112‐127. doi:10.1016/j.healthpol.2008.02.002
9. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962. doi:10.1371/journal.pone.0078962
10. Institute for Healthcare Improvement. Plan-do-study-act (PDSA) worksheet. http://www.ihi.org/resources/Pages/Tools/PlanDoStudyActWorksheet.aspx. Accessed May 13, 2020.
11. Agency for Healthcare Research and Quality. Plan-do-study-act (PDSA) cycle. https://innovations.ahrq.gov/qualitytools/plan-do-study-act-pdsa-cycle. Updated April 10, 2013. Accessed May 13, 2020.
12. Matzke GR, McGory RW, Halstenson CE, Keane WF. Pharmacokinetics of vancomycin in patients with various degrees of renal function. Antimicrob Agents Chemother. 1984;25(4):433‐437. doi:10.1128/aac.25.4.433
13. Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081‐3086. doi:10.1093/jac/dky310
14. Pai MP, Russo A, Novelli A, Venditti M, Falcone M. Simplified equations using two concentrations to calculate area under the curve for antimicrobials with concentration-dependent pharmacodynamics: daptomycin as a motivating example. Antimicrob Agents Chemother. 2014;58(6):3162‐3167. doi:10.1128/AAC.02355-14
15. Suryadevara M, Steidl KE, Probst LA, Shaw J. Inappropriate vancomycin therapeutic drug monitoring in hospitalized pediatric patients increases pediatric trauma and hospital costs. J Pediatr Pharmacol Ther. 2012;17(2):159‐165. doi:10.5863/1551-6776-17.2.159
16. Morrison AP, Melanson SE, Carty MG, Bates DW, Szumita PM, Tanasijevic MJ. What proportion of vancomycin trough levels are drawn too early?: frequency and impact on clinical actions. Am J Clin Pathol. 2012;137(3):472‐478. doi:10.1309/AJCPDSYS0DVLKFOH
17. Melanson SE, Mijailovic AS, Wright AP, Szumita PM, Bates DW, Tanasijevic MJ. An intervention to improve the timing of vancomycin levels. Am J Clin Pathol. 2013;140(6):801‐806. doi:10.1309/AJCPKQ6EAH7OYQLB
18. Meng L, Wong T, Huang S, et al. Conversion from vancomycin trough concentration-guided dosing to area under the curve-guided dosing using two sample measurements in adults: implementation at an academic medical center. Pharmacotherapy. 2019;39(4):433‐442. doi:10.1002/phar.2234
19. Stoessel AM, Hale CM, Seabury RW, Miller CD, Steele JM. The impact of AUC-based monitoring on pharmacist-directed vancomycin dose adjustments in complicated methicillin-resistant staphylococcus aureus Infection. J Pharm Pract. 2019;32(4):442‐446. doi:10.1177/0897190018764564
20. Kufel WD, Seabury RW, Mogle BT, Beccari MV, Probst LA, Steele JM. Readiness to implement vancomycin monitoring based on area under the concentration-time curve: a cross-sectional survey of a national health consortium. Am J Health Syst Pharm. 2019;76(12):889‐894. doi:10.1093/ajhp/zxz070
21. Bluestone J, Johnson P, Fullerton J, Carr C, Alderman J, BonTempo J. Effective in-service training design and delivery: evidence from an integrative literature review. Hum Resour Health. 2013;11:51. doi:10.1186/1478-4491-11-51
22. Ebben RHA, Siqeca F, Madsen UR, Vloet LCM, van Achterberg T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ Open. 2018;8(11):e017572. doi:10.1136/bmjopen-2017-017572
23. Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and Strategies in Guideline Implementation-A Scoping Review. Healthcare (Basel). 2016;4(3):36. doi:10.3390/healthcare4030036
1. Rybak M, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists [published correction appears in Am J Health Syst Pharm. 2009;66(10):887]. Am J Health Syst Pharm. 2009;66(1):82‐98. doi:10.2146/ajhp080434
2. van Hal SJ, Paterson DL, Lodise TP. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob Agents Chemother. 2013;57(2):734‐744. doi:10.1128/AAC.01568-12
3. Pai MP, Neely M, Rodvold KA, Lodise TP. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv Drug Deliv Rev. 2014;77:50‐57. doi:10.1016/j.addr.2014.05.016
4. Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists [published online ahead of print, 2020 Mar 19]. Am J Health Syst Pharm. 2020;zxaa036. doi:10.1093/ajhp/zxaa036
5. Heil EL, Claeys KC, Mynatt RP, et al. Making the change to area under the curve-based vancomycin dosing. Am J Health Syst Pharm. 2018;75(24):1986‐1995. doi:10.2146/ajhp180034
6. Gregory ER, Burgess DR, Cotner SE, et al. Vancomycin area under the curve dosing and monitoring at an academic medical center: transition strategies and lessons learned [published online ahead of print, 2019 Mar 10]. J Pharm Pract. 2019;897190019834369. doi:10.1177/0897190019834369
7. Septimus EJ, Owens RC Jr. Need and potential of antimicrobial stewardship in community hospitals. Clin Infect Dis. 2011;53 Suppl 1:S8‐S14. doi:10.1093/cid/cir363
8. Goldman LE, Dudley RA. United States rural hospital quality in the Hospital Compare database-accounting for hospital characteristics. Health Policy. 2008;87(1):112‐127. doi:10.1016/j.healthpol.2008.02.002
9. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962. doi:10.1371/journal.pone.0078962
10. Institute for Healthcare Improvement. Plan-do-study-act (PDSA) worksheet. http://www.ihi.org/resources/Pages/Tools/PlanDoStudyActWorksheet.aspx. Accessed May 13, 2020.
11. Agency for Healthcare Research and Quality. Plan-do-study-act (PDSA) cycle. https://innovations.ahrq.gov/qualitytools/plan-do-study-act-pdsa-cycle. Updated April 10, 2013. Accessed May 13, 2020.
12. Matzke GR, McGory RW, Halstenson CE, Keane WF. Pharmacokinetics of vancomycin in patients with various degrees of renal function. Antimicrob Agents Chemother. 1984;25(4):433‐437. doi:10.1128/aac.25.4.433
13. Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081‐3086. doi:10.1093/jac/dky310
14. Pai MP, Russo A, Novelli A, Venditti M, Falcone M. Simplified equations using two concentrations to calculate area under the curve for antimicrobials with concentration-dependent pharmacodynamics: daptomycin as a motivating example. Antimicrob Agents Chemother. 2014;58(6):3162‐3167. doi:10.1128/AAC.02355-14
15. Suryadevara M, Steidl KE, Probst LA, Shaw J. Inappropriate vancomycin therapeutic drug monitoring in hospitalized pediatric patients increases pediatric trauma and hospital costs. J Pediatr Pharmacol Ther. 2012;17(2):159‐165. doi:10.5863/1551-6776-17.2.159
16. Morrison AP, Melanson SE, Carty MG, Bates DW, Szumita PM, Tanasijevic MJ. What proportion of vancomycin trough levels are drawn too early?: frequency and impact on clinical actions. Am J Clin Pathol. 2012;137(3):472‐478. doi:10.1309/AJCPDSYS0DVLKFOH
17. Melanson SE, Mijailovic AS, Wright AP, Szumita PM, Bates DW, Tanasijevic MJ. An intervention to improve the timing of vancomycin levels. Am J Clin Pathol. 2013;140(6):801‐806. doi:10.1309/AJCPKQ6EAH7OYQLB
18. Meng L, Wong T, Huang S, et al. Conversion from vancomycin trough concentration-guided dosing to area under the curve-guided dosing using two sample measurements in adults: implementation at an academic medical center. Pharmacotherapy. 2019;39(4):433‐442. doi:10.1002/phar.2234
19. Stoessel AM, Hale CM, Seabury RW, Miller CD, Steele JM. The impact of AUC-based monitoring on pharmacist-directed vancomycin dose adjustments in complicated methicillin-resistant staphylococcus aureus Infection. J Pharm Pract. 2019;32(4):442‐446. doi:10.1177/0897190018764564
20. Kufel WD, Seabury RW, Mogle BT, Beccari MV, Probst LA, Steele JM. Readiness to implement vancomycin monitoring based on area under the concentration-time curve: a cross-sectional survey of a national health consortium. Am J Health Syst Pharm. 2019;76(12):889‐894. doi:10.1093/ajhp/zxz070
21. Bluestone J, Johnson P, Fullerton J, Carr C, Alderman J, BonTempo J. Effective in-service training design and delivery: evidence from an integrative literature review. Hum Resour Health. 2013;11:51. doi:10.1186/1478-4491-11-51
22. Ebben RHA, Siqeca F, Madsen UR, Vloet LCM, van Achterberg T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ Open. 2018;8(11):e017572. doi:10.1136/bmjopen-2017-017572
23. Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and Strategies in Guideline Implementation-A Scoping Review. Healthcare (Basel). 2016;4(3):36. doi:10.3390/healthcare4030036
Open Clinical Trials for Patients With COVID-19
Finding effective treatment or a vaccine for COVID-19, the disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has placed significant strains on the global health care system. The National Library of Medicine database lists > 1,800 trials that are aimed at addressing COVID-19-related health care. Already, trials developed by the US Department of Veterans Affairs (VA), US Department of Defense (DoD), and the National Institute of Allergy and Infectious Diseases have provided important data on effective treatment options. The clinical trials listed below are all open as of May 31, 2020 and have trial sites at VA and DoD facilities. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Adaptive COVID-19 Treatment Trial (ACTT)
This study is an adaptive, randomized, double-blind, placebo-controlled trial to evaluate the safety and efficacy of novel therapeutic agents in hospitalized adults diagnosed with COVID-19. The study will compare different investigational therapeutic agents to a control arm. ID: NCT04280705
Sponsor: National Institute of Allergy and Infectious Diseases
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Study to Evaluate the Safety and Antiviral Activity of Remdesivir (GS-5734) in Participants With Severe Coronavirus Disease (COVID-19)
The primary objective of this study is to evaluate the efficacy of 2 remdesivir (RDV) regimens with respect to clinical status assessed by a 7-point ordinal scale on Day 11 (NCT04292730) or Day 14 (NCT04292899).
ID: NCT04292730/NCT04292899
Sponsor: Gilead Sciences
Contact: Gilead Clinical Study Information Center (833-445-3230)
Location: James J. Peters VA Medical Center, Bronx, New York
Expanded Access Remdesivir (RDV; GS-5734)
The treatment of communicable Novel Coronavirus of 2019 with Remdesivir (RDV; GS-5734) also known as severe acute respiratory syndrome coronavirus 2.
ID: NCT04302766
Sponsor: US Army Medical Research and Development Command
Contact: Sandi Parriott ([email protected])
A Study to Evaluate the Safety and Efficacy of Tocilizumab in Patients With Severe COVID-19 Pneumonia (COVACTA)
This study will evaluate the efficacy, safety, pharmacodynamics, and pharmacokinetics of tocilizumab (TCZ) compared with a matching placebo in combination with standard of care (SOC) in hospitalized patients with severe COVID-19 pneumonia.
ID: NCT04320615
Sponsor: Hoffmann-La Roche
Location: James J Peters VA Medical Center, Bronx, New York
Administration of Intravenous Vitamin C in Novel Coronavirus Infection (COVID-19) and Decreased Oxygenation (AVoCaDO)
Previous research has shown that high dose intravenous vitamin C (HDIVC) may benefit patients with sepsis, acute lung injury (ALI), and the acute respiratory distress syndrome (ARDS). However, it is not known if early administration of HDIVC could prevent progression to ARDS. We hypothesize that HDIVC is safe and tolerable in COVID-19 subjects given early or late in the disease course and may reduce the risk of respiratory failure requiring mechanical ventilation and development of ARDS along with reductions in supplemental oxygen demand and inflammatory markers.
ID: NCT04357782
Sponsor: Hunter Holmes Mcguire VA Medical CenterContact: Brian Davis ([email protected])
Location: Hunter Holmes Mcguire VA Medical Center, Richmond, Virginia
Treatment Of CORONAVIRUS DISEASE 2019 (COVID-19) With Anti-Sars-CoV-2 Convalescent Plasma (ASCoV2CP)
This is an expanded access open-label, single-arm, multi-site protocol to provide convalescent plasma as a treatment for patients diagnosed with severe, or life-threatening COVID-19.
ID: NCT04360486
Sponsor: US Army Medical Research and Development Command
Contact: Andrew Cap ([email protected])
VA Remote and Equitable Access to COVID-19 Healthcare Delivery (VA-REACH TRIAL) (VA-REACH)
We propose a 3-arm randomized control trial to determine the efficacy of hydroxychloroquine or azithromycin in treating mild to moderate COVID-19 among veterans in the outpatient setting.
ID: NCT04363203
Sponsor: Salomeh Keyhani
Location: San Francisco VA Health Care System, California
A Study to Evaluate the Safety and Efficacy of MSTT1041A (Astegolimab) or UTTR1147A in Patients With Severe COVID-19 Pneumonia (COVASTIL)
This is a Phase II, randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of MSTT1041A (astegolimab) or UTTR1147A in combination with standard of care (SOC) compared with matching placebo in combination with SOC in patients hospitalized with severe coronavirus disease 2019 (COVID-19) pneumonia.
ID: NCT04386616
Sponsor: Genentech
Contact: Study ID Number: GA42469 ([email protected])
Location: Southeast Louisiana Veterans Health Care System, New Orleans
Hormonal Intervention for the Treatment in Veterans With COVID-19 Requiring Hospitalization (HITCH)
The purpose of this study is to determine if temporary androgen suppression improves the clinical outcomes of veterans who are hospitalized to an acute care ward due to COVID-19.ID: NCT04397718
Sponsor: VA Office of Research and Development
Contact: Matthew B Rettig ([email protected]), Nicholas Nickols ([email protected])
Locations: VA Greater Los Angeles Healthcare System, California; VA NY Harbor Healthcare System, New York; VA Puget Sound Health Care System, Seattle, Washington
Adaptive COVID-19 Treatment Trial 2 (ACTT-II)
ACTT-II will evaluate the combination of baricitinib and remdesivir compared to remdesivir alone. Subjects will be assessed daily while hospitalized. If the subjects are discharged from the hospital, they will have a study visit at Days 15, 22, and 29.
ID: NCT04401579
Sponsor: National Institute of Allergy and Infectious Diseases (NIAID)
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Rocky Mountain Regional Veteran Affairs Medical Center, Aurora, Colorado; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Finding effective treatment or a vaccine for COVID-19, the disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has placed significant strains on the global health care system. The National Library of Medicine database lists > 1,800 trials that are aimed at addressing COVID-19-related health care. Already, trials developed by the US Department of Veterans Affairs (VA), US Department of Defense (DoD), and the National Institute of Allergy and Infectious Diseases have provided important data on effective treatment options. The clinical trials listed below are all open as of May 31, 2020 and have trial sites at VA and DoD facilities. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Adaptive COVID-19 Treatment Trial (ACTT)
This study is an adaptive, randomized, double-blind, placebo-controlled trial to evaluate the safety and efficacy of novel therapeutic agents in hospitalized adults diagnosed with COVID-19. The study will compare different investigational therapeutic agents to a control arm. ID: NCT04280705
Sponsor: National Institute of Allergy and Infectious Diseases
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Study to Evaluate the Safety and Antiviral Activity of Remdesivir (GS-5734) in Participants With Severe Coronavirus Disease (COVID-19)
The primary objective of this study is to evaluate the efficacy of 2 remdesivir (RDV) regimens with respect to clinical status assessed by a 7-point ordinal scale on Day 11 (NCT04292730) or Day 14 (NCT04292899).
ID: NCT04292730/NCT04292899
Sponsor: Gilead Sciences
Contact: Gilead Clinical Study Information Center (833-445-3230)
Location: James J. Peters VA Medical Center, Bronx, New York
Expanded Access Remdesivir (RDV; GS-5734)
The treatment of communicable Novel Coronavirus of 2019 with Remdesivir (RDV; GS-5734) also known as severe acute respiratory syndrome coronavirus 2.
ID: NCT04302766
Sponsor: US Army Medical Research and Development Command
Contact: Sandi Parriott ([email protected])
A Study to Evaluate the Safety and Efficacy of Tocilizumab in Patients With Severe COVID-19 Pneumonia (COVACTA)
This study will evaluate the efficacy, safety, pharmacodynamics, and pharmacokinetics of tocilizumab (TCZ) compared with a matching placebo in combination with standard of care (SOC) in hospitalized patients with severe COVID-19 pneumonia.
ID: NCT04320615
Sponsor: Hoffmann-La Roche
Location: James J Peters VA Medical Center, Bronx, New York
Administration of Intravenous Vitamin C in Novel Coronavirus Infection (COVID-19) and Decreased Oxygenation (AVoCaDO)
Previous research has shown that high dose intravenous vitamin C (HDIVC) may benefit patients with sepsis, acute lung injury (ALI), and the acute respiratory distress syndrome (ARDS). However, it is not known if early administration of HDIVC could prevent progression to ARDS. We hypothesize that HDIVC is safe and tolerable in COVID-19 subjects given early or late in the disease course and may reduce the risk of respiratory failure requiring mechanical ventilation and development of ARDS along with reductions in supplemental oxygen demand and inflammatory markers.
ID: NCT04357782
Sponsor: Hunter Holmes Mcguire VA Medical CenterContact: Brian Davis ([email protected])
Location: Hunter Holmes Mcguire VA Medical Center, Richmond, Virginia
Treatment Of CORONAVIRUS DISEASE 2019 (COVID-19) With Anti-Sars-CoV-2 Convalescent Plasma (ASCoV2CP)
This is an expanded access open-label, single-arm, multi-site protocol to provide convalescent plasma as a treatment for patients diagnosed with severe, or life-threatening COVID-19.
ID: NCT04360486
Sponsor: US Army Medical Research and Development Command
Contact: Andrew Cap ([email protected])
VA Remote and Equitable Access to COVID-19 Healthcare Delivery (VA-REACH TRIAL) (VA-REACH)
We propose a 3-arm randomized control trial to determine the efficacy of hydroxychloroquine or azithromycin in treating mild to moderate COVID-19 among veterans in the outpatient setting.
ID: NCT04363203
Sponsor: Salomeh Keyhani
Location: San Francisco VA Health Care System, California
A Study to Evaluate the Safety and Efficacy of MSTT1041A (Astegolimab) or UTTR1147A in Patients With Severe COVID-19 Pneumonia (COVASTIL)
This is a Phase II, randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of MSTT1041A (astegolimab) or UTTR1147A in combination with standard of care (SOC) compared with matching placebo in combination with SOC in patients hospitalized with severe coronavirus disease 2019 (COVID-19) pneumonia.
ID: NCT04386616
Sponsor: Genentech
Contact: Study ID Number: GA42469 ([email protected])
Location: Southeast Louisiana Veterans Health Care System, New Orleans
Hormonal Intervention for the Treatment in Veterans With COVID-19 Requiring Hospitalization (HITCH)
The purpose of this study is to determine if temporary androgen suppression improves the clinical outcomes of veterans who are hospitalized to an acute care ward due to COVID-19.ID: NCT04397718
Sponsor: VA Office of Research and Development
Contact: Matthew B Rettig ([email protected]), Nicholas Nickols ([email protected])
Locations: VA Greater Los Angeles Healthcare System, California; VA NY Harbor Healthcare System, New York; VA Puget Sound Health Care System, Seattle, Washington
Adaptive COVID-19 Treatment Trial 2 (ACTT-II)
ACTT-II will evaluate the combination of baricitinib and remdesivir compared to remdesivir alone. Subjects will be assessed daily while hospitalized. If the subjects are discharged from the hospital, they will have a study visit at Days 15, 22, and 29.
ID: NCT04401579
Sponsor: National Institute of Allergy and Infectious Diseases (NIAID)
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Rocky Mountain Regional Veteran Affairs Medical Center, Aurora, Colorado; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Finding effective treatment or a vaccine for COVID-19, the disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has placed significant strains on the global health care system. The National Library of Medicine database lists > 1,800 trials that are aimed at addressing COVID-19-related health care. Already, trials developed by the US Department of Veterans Affairs (VA), US Department of Defense (DoD), and the National Institute of Allergy and Infectious Diseases have provided important data on effective treatment options. The clinical trials listed below are all open as of May 31, 2020 and have trial sites at VA and DoD facilities. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Adaptive COVID-19 Treatment Trial (ACTT)
This study is an adaptive, randomized, double-blind, placebo-controlled trial to evaluate the safety and efficacy of novel therapeutic agents in hospitalized adults diagnosed with COVID-19. The study will compare different investigational therapeutic agents to a control arm. ID: NCT04280705
Sponsor: National Institute of Allergy and Infectious Diseases
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Study to Evaluate the Safety and Antiviral Activity of Remdesivir (GS-5734) in Participants With Severe Coronavirus Disease (COVID-19)
The primary objective of this study is to evaluate the efficacy of 2 remdesivir (RDV) regimens with respect to clinical status assessed by a 7-point ordinal scale on Day 11 (NCT04292730) or Day 14 (NCT04292899).
ID: NCT04292730/NCT04292899
Sponsor: Gilead Sciences
Contact: Gilead Clinical Study Information Center (833-445-3230)
Location: James J. Peters VA Medical Center, Bronx, New York
Expanded Access Remdesivir (RDV; GS-5734)
The treatment of communicable Novel Coronavirus of 2019 with Remdesivir (RDV; GS-5734) also known as severe acute respiratory syndrome coronavirus 2.
ID: NCT04302766
Sponsor: US Army Medical Research and Development Command
Contact: Sandi Parriott ([email protected])
A Study to Evaluate the Safety and Efficacy of Tocilizumab in Patients With Severe COVID-19 Pneumonia (COVACTA)
This study will evaluate the efficacy, safety, pharmacodynamics, and pharmacokinetics of tocilizumab (TCZ) compared with a matching placebo in combination with standard of care (SOC) in hospitalized patients with severe COVID-19 pneumonia.
ID: NCT04320615
Sponsor: Hoffmann-La Roche
Location: James J Peters VA Medical Center, Bronx, New York
Administration of Intravenous Vitamin C in Novel Coronavirus Infection (COVID-19) and Decreased Oxygenation (AVoCaDO)
Previous research has shown that high dose intravenous vitamin C (HDIVC) may benefit patients with sepsis, acute lung injury (ALI), and the acute respiratory distress syndrome (ARDS). However, it is not known if early administration of HDIVC could prevent progression to ARDS. We hypothesize that HDIVC is safe and tolerable in COVID-19 subjects given early or late in the disease course and may reduce the risk of respiratory failure requiring mechanical ventilation and development of ARDS along with reductions in supplemental oxygen demand and inflammatory markers.
ID: NCT04357782
Sponsor: Hunter Holmes Mcguire VA Medical CenterContact: Brian Davis ([email protected])
Location: Hunter Holmes Mcguire VA Medical Center, Richmond, Virginia
Treatment Of CORONAVIRUS DISEASE 2019 (COVID-19) With Anti-Sars-CoV-2 Convalescent Plasma (ASCoV2CP)
This is an expanded access open-label, single-arm, multi-site protocol to provide convalescent plasma as a treatment for patients diagnosed with severe, or life-threatening COVID-19.
ID: NCT04360486
Sponsor: US Army Medical Research and Development Command
Contact: Andrew Cap ([email protected])
VA Remote and Equitable Access to COVID-19 Healthcare Delivery (VA-REACH TRIAL) (VA-REACH)
We propose a 3-arm randomized control trial to determine the efficacy of hydroxychloroquine or azithromycin in treating mild to moderate COVID-19 among veterans in the outpatient setting.
ID: NCT04363203
Sponsor: Salomeh Keyhani
Location: San Francisco VA Health Care System, California
A Study to Evaluate the Safety and Efficacy of MSTT1041A (Astegolimab) or UTTR1147A in Patients With Severe COVID-19 Pneumonia (COVASTIL)
This is a Phase II, randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of MSTT1041A (astegolimab) or UTTR1147A in combination with standard of care (SOC) compared with matching placebo in combination with SOC in patients hospitalized with severe coronavirus disease 2019 (COVID-19) pneumonia.
ID: NCT04386616
Sponsor: Genentech
Contact: Study ID Number: GA42469 ([email protected])
Location: Southeast Louisiana Veterans Health Care System, New Orleans
Hormonal Intervention for the Treatment in Veterans With COVID-19 Requiring Hospitalization (HITCH)
The purpose of this study is to determine if temporary androgen suppression improves the clinical outcomes of veterans who are hospitalized to an acute care ward due to COVID-19.ID: NCT04397718
Sponsor: VA Office of Research and Development
Contact: Matthew B Rettig ([email protected]), Nicholas Nickols ([email protected])
Locations: VA Greater Los Angeles Healthcare System, California; VA NY Harbor Healthcare System, New York; VA Puget Sound Health Care System, Seattle, Washington
Adaptive COVID-19 Treatment Trial 2 (ACTT-II)
ACTT-II will evaluate the combination of baricitinib and remdesivir compared to remdesivir alone. Subjects will be assessed daily while hospitalized. If the subjects are discharged from the hospital, they will have a study visit at Days 15, 22, and 29.
ID: NCT04401579
Sponsor: National Institute of Allergy and Infectious Diseases (NIAID)
Contact: Central Contact ([email protected])
Locations: VA Palo Alto Health Care System, California; Naval Medical Center San Diego, California; Rocky Mountain Regional Veteran Affairs Medical Center, Aurora, Colorado; Southeast Louisiana Veterans Health Care System, New Orleans; Walter Reed National Military Medical Center, Bethesda, Maryland; National Institutes of Health - Clinical Center, National Institute of Allergy and Infectious Diseases Laboratory Of Immunoregulation, Bethesda, Maryland; Brooke Army Medical Center, Fort Sam Houston, Texas; Madigan Army Medical Center, Tacoma, Washington
Preliminary evidence indicates famotidine might improve COVID-19 symptoms
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
High-dose oral famotidine might improve cardinal symptoms of COVID-19 infection, according to the findings of a small outpatient case series and a subsequent retrospective study.
After developing COVID-19 symptoms, the 10 patients in the case series began self-medicating with 60-240 mg famotidine daily over a median of 11 days. “All patients reported marked improvements of disease-related symptoms after starting famotidine,” first author Tobias Janowitz, MD, PhD, of Cold Spring Harbor Laboratory, N.Y., and associates wrote in Gut.
Improvements began within 24-48 hours of starting on the histamine-2 receptor antagonist. By 14 days after treatment initiation, all patients reported near-normalization of both respiratory and systemic symptoms, the researchers reported.
The patients were 23-71 years old. Seven tested positive for COVID-19, two had antibodies to COVID-19, and one had a clinical diagnosis of COVID-19 without laboratory confirmation. Over a median of 11 days (range, 5-21 days), six patients self-administered 80 mg famotidine three times daily and four self-administered lower amounts – from 60 to 150 mg of famotidine daily, divided into two or three doses. Patients started on famotidine between 2 and 26 days after symptom onset.
Through phone interviews and questionnaires, the researchers ascertained changes in cough, dyspnea, fatigue, headache, anosmia, and general unwellness by using a modified four-point Eastern Cooperative Oncology Group (ECOG) performance status scale. Improvements were seen across all symptom categories, and respiratory symptoms improved faster than systemic symptoms. Apart from two cases of persistent anosmia, symptoms resolved completely within 14 days of starting famotidine.
Seven patients reported no side effects of famotidine; one reported grade 1 dizziness and infrequent perceptions of tachycardia; one reported grade 1 dizziness, dry skin, and insomnia; and one reported grade 1 gastrointestinal symptoms and temporary forgetfulness. “Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine, and all side effects resolved on discontinuation of famotidine,” the investigators wrote.
While the findings are intriguing, Dr. Janowitz and associates cautioned against overinterpretation of them. Another expert agreed: “This is a preliminary study based on a hypothesized antiviral effect. It’s important to know that it doesn’t really prove it works,” said Amesh Adalja, MD, senior scholar at the Johns Hopkins University Center for Health Security, Baltimore, and a spokesperson for the Infectious Diseases Society of America, during an interview with MDedge.
These patients might have improved anyway, without self-administering famotidine, said Dr. Adalja, who was not involved in the study.
Furthermore, the mechanism by which famotidine might act on COVID-19 remains unclear. The drug “could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus,” Dr. Janowitz and associates wrote.
Dr. Adalja noted that many compounds show effects against COVID-19 that are not well understood. He called for randomized trials to evaluate the biological plausibility of famotidine use, and its potential efficacy.
“This is a cheap, over-the-counter drug, but no drug is without side effects,” he added. “We need to know whether it works.”
Based on the case series findings, researchers conducted another retrospective study of patients hospitalized with COVID-19 infection. Those who were incidentally taking famotidine before or at hospitalization had a significantly reduced risk of intubation or death, with a hazard ratio of 0.43 (Gastroenterology. 2020 May 22. doi: 10.1053/j.gastro.2020.05.053)
The National Institutes of Health provided partial support. The investigators reported having no conflicts of interest.
SOURCE: Janowitz T et al. Gut. 2020 Jun 4. doi: 10.1136/gutjnl-2020-321852.
FROM GUT
Can an app guide cancer treatment decisions during the pandemic?
Deciding which cancer patients need immediate treatment and who can safely wait is an uncomfortable assessment for cancer clinicians during the COVID-19 pandemic.
In early April, as the COVID-19 surge was bearing down on New York City, those treatment decisions were “a juggling act every single day,” Jonathan Yang, MD, PhD, a radiation oncologist from New York’s Memorial Sloan Kettering Cancer Center, told Medscape Medical News.
Eventually, a glut of guidelines, recommendations, and expert opinions aimed at helping oncologists emerged. The tools help navigate the complicated risk-benefit analysis of their patient’s risk of infection by SARS-CoV-2 and delaying therapy.
Now, a new tool, which appears to be the first of its kind, quantifies that risk-benefit analysis. But its presence immediately raises the question: can it help?
Three-Tier Systems Are Not Very Sophisticated
OncCOVID, a free tool that was launched May 26 by the University of Michigan, allows physicians to individualize risk estimates for delaying treatment of up to 25 early- to late-stage cancers. It includes more than 45 patient characteristics, such as age, location, cancer type, cancer stage, treatment plan, underlying medical conditions, and proposed length of delay in care.
Combining these personal details with data from the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) registry and the National Cancer Database, the Michigan app then estimates a patient’s 5- or 10-year survival with immediate vs delayed treatment and weighs that against their risk for COVID-19 using data from the Johns Hopkins Coronavirus Resource Center.
“We thought, isn’t it better to at least provide some evidence-based quantification, rather than a back-of-the-envelope three-tier system that is just sort of ‘made up’?“ explained one of the developers, Daniel Spratt, MD, associate professor of radiation oncology at Michigan Medicine.
Spratt explained that almost every organization, professional society, and government has created something like a three-tier system. Tier 1 represents urgent cases and patients who need immediate treatment. For tier 2, treatment can be delayed weeks or a month, and with tier 3, it can be delayed until the pandemic is over or it’s deemed safe.
“[This system] sounds good at first glance, but in cancer, we’re always talking about personalized medicine, and it’s mind-blowing that these tier systems are only based on urgency and prognosis,” he told Medscape Medical News.
Spratt offered an example. Consider a patient with a very aggressive brain tumor ― that patient is in tier 1 and should undergo treatment immediately. But will the treatment actually help? And how helpful would the procedure be if, say, the patient is 80 years old and, if infected, would have a 30% to 50% chance of dying from the coronavirus?
“If the model says this guy has a 5% harm and this one has 30% harm, you can use that to help prioritize,” summarized Spratt.
The app can generate risk estimates for patients living anywhere in the world and has already been accessed by people from 37 countries. However, Spratt cautions that it is primarily “designed and calibrated for the US.
“The estimates are based on very large US registries, and though it’s probably somewhat similar across much of the world, there’s probably certain cancer types that are more region specific ― especially something like stomach cancer or certain types of head and neck cancer in parts of Asia, for example,” he said.
Although the app’s COVID-19 data are specific to the county level in the United States, elsewhere in the world, it is only country specific.
“We’re using the best data we have for coronavirus, but everyone knows we still have large data gaps,” he acknowledged.
How Accurate?
Asked to comment on the app, Richard Bleicher, MD, leader of the Breast Cancer Program at Fox Chase Cancer Center, Philadelphia, praised the effort and the goal but had some concerns.
“Several questions arise, most important of which is, How accurate is this, and how has this been validated, if at all ― especially as it is too soon to see the outcomes of patients affected in this pandemic?” he told Medscape Medical News.
“We are imposing delays on a broad scale because of the coronavirus, and we are getting continuously changing data as we test more patients. But both situations are novel and may not be accurately represented by the data being pulled, because the datasets use patients from a few years ago, and confounders in these datasets may not apply to this situation,” Bleicher continued.
Although acknowledging the “value in delineating the risk of dying from cancer vs the risk of dying from the SARS-CoV-2 pandemic,” Bleicher urged caution in using the tool to make individual patient decisions.
“We need to remember that the best of modeling ... can be wildly inaccurate and needs to be validated using patients having the circumstances in question. ... This won’t be possible until long after the pandemic is completed, and so the model’s accuracy remains unknown.”
That sentiment was echoed by Giampaolo Bianchini, MD, head of the Breast Cancer Group, Department of Medical Oncology, Ospedale San Raffaele, in Milan, Italy.
“Arbitrarily postponing and modifying treatment strategies including surgery, radiation therapy, and medical therapy without properly balancing the risk/benefit ratio may lead to significantly worse cancer-related outcomes, which largely exceed the actual risks for COVID,” he wrote in an email.
“The OncCOVID app is a remarkable attempt to fill the gap between perception and estimation,” he said. The app provides side by side the COVID-19 risk estimation and the consequences of arbitrary deviation from the standard of care, observed Bianchini.
However, he pointed out weaknesses, including the fact that the “data generated in literature are not always of high quality and do not take into consideration relevant characteristics of the disease and treatment benefit. It should for sure be used, but then also interpreted with caution.”
Another Italian group responded more positively.
“In our opinion, it could be a useful tool for clinicians,” wrote colleagues Alessio Cortelinni and Giampiero Porzio, both medical oncologists at San Salvatore Hospital and the University of L’Aquila, in Italy. “This Web app might assist clinicians in balancing the risk/benefit ratio of being treated and/or access to the outpatient cancer center for each kind of patient (both early and advanced stages), in order to make a more tailored counseling,” they wrote in an email. “Importantly, the Web app might help those clinicians who work ‘alone,’ in peripheral centers, without resources, colleagues, and multidisciplinary tumor boards on whom they can rely.”
Bleicher, who was involved in the COVID-19 Breast Cancer Consortium’s recommendations for prioritizing breast cancer treatment, summarized that the app “may end up being close or accurate, but we won’t know except in hindsight.”
This article first appeared on Medscape.com.
Deciding which cancer patients need immediate treatment and who can safely wait is an uncomfortable assessment for cancer clinicians during the COVID-19 pandemic.
In early April, as the COVID-19 surge was bearing down on New York City, those treatment decisions were “a juggling act every single day,” Jonathan Yang, MD, PhD, a radiation oncologist from New York’s Memorial Sloan Kettering Cancer Center, told Medscape Medical News.
Eventually, a glut of guidelines, recommendations, and expert opinions aimed at helping oncologists emerged. The tools help navigate the complicated risk-benefit analysis of their patient’s risk of infection by SARS-CoV-2 and delaying therapy.
Now, a new tool, which appears to be the first of its kind, quantifies that risk-benefit analysis. But its presence immediately raises the question: can it help?
Three-Tier Systems Are Not Very Sophisticated
OncCOVID, a free tool that was launched May 26 by the University of Michigan, allows physicians to individualize risk estimates for delaying treatment of up to 25 early- to late-stage cancers. It includes more than 45 patient characteristics, such as age, location, cancer type, cancer stage, treatment plan, underlying medical conditions, and proposed length of delay in care.
Combining these personal details with data from the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) registry and the National Cancer Database, the Michigan app then estimates a patient’s 5- or 10-year survival with immediate vs delayed treatment and weighs that against their risk for COVID-19 using data from the Johns Hopkins Coronavirus Resource Center.
“We thought, isn’t it better to at least provide some evidence-based quantification, rather than a back-of-the-envelope three-tier system that is just sort of ‘made up’?“ explained one of the developers, Daniel Spratt, MD, associate professor of radiation oncology at Michigan Medicine.
Spratt explained that almost every organization, professional society, and government has created something like a three-tier system. Tier 1 represents urgent cases and patients who need immediate treatment. For tier 2, treatment can be delayed weeks or a month, and with tier 3, it can be delayed until the pandemic is over or it’s deemed safe.
“[This system] sounds good at first glance, but in cancer, we’re always talking about personalized medicine, and it’s mind-blowing that these tier systems are only based on urgency and prognosis,” he told Medscape Medical News.
Spratt offered an example. Consider a patient with a very aggressive brain tumor ― that patient is in tier 1 and should undergo treatment immediately. But will the treatment actually help? And how helpful would the procedure be if, say, the patient is 80 years old and, if infected, would have a 30% to 50% chance of dying from the coronavirus?
“If the model says this guy has a 5% harm and this one has 30% harm, you can use that to help prioritize,” summarized Spratt.
The app can generate risk estimates for patients living anywhere in the world and has already been accessed by people from 37 countries. However, Spratt cautions that it is primarily “designed and calibrated for the US.
“The estimates are based on very large US registries, and though it’s probably somewhat similar across much of the world, there’s probably certain cancer types that are more region specific ― especially something like stomach cancer or certain types of head and neck cancer in parts of Asia, for example,” he said.
Although the app’s COVID-19 data are specific to the county level in the United States, elsewhere in the world, it is only country specific.
“We’re using the best data we have for coronavirus, but everyone knows we still have large data gaps,” he acknowledged.
How Accurate?
Asked to comment on the app, Richard Bleicher, MD, leader of the Breast Cancer Program at Fox Chase Cancer Center, Philadelphia, praised the effort and the goal but had some concerns.
“Several questions arise, most important of which is, How accurate is this, and how has this been validated, if at all ― especially as it is too soon to see the outcomes of patients affected in this pandemic?” he told Medscape Medical News.
“We are imposing delays on a broad scale because of the coronavirus, and we are getting continuously changing data as we test more patients. But both situations are novel and may not be accurately represented by the data being pulled, because the datasets use patients from a few years ago, and confounders in these datasets may not apply to this situation,” Bleicher continued.
Although acknowledging the “value in delineating the risk of dying from cancer vs the risk of dying from the SARS-CoV-2 pandemic,” Bleicher urged caution in using the tool to make individual patient decisions.
“We need to remember that the best of modeling ... can be wildly inaccurate and needs to be validated using patients having the circumstances in question. ... This won’t be possible until long after the pandemic is completed, and so the model’s accuracy remains unknown.”
That sentiment was echoed by Giampaolo Bianchini, MD, head of the Breast Cancer Group, Department of Medical Oncology, Ospedale San Raffaele, in Milan, Italy.
“Arbitrarily postponing and modifying treatment strategies including surgery, radiation therapy, and medical therapy without properly balancing the risk/benefit ratio may lead to significantly worse cancer-related outcomes, which largely exceed the actual risks for COVID,” he wrote in an email.
“The OncCOVID app is a remarkable attempt to fill the gap between perception and estimation,” he said. The app provides side by side the COVID-19 risk estimation and the consequences of arbitrary deviation from the standard of care, observed Bianchini.
However, he pointed out weaknesses, including the fact that the “data generated in literature are not always of high quality and do not take into consideration relevant characteristics of the disease and treatment benefit. It should for sure be used, but then also interpreted with caution.”
Another Italian group responded more positively.
“In our opinion, it could be a useful tool for clinicians,” wrote colleagues Alessio Cortelinni and Giampiero Porzio, both medical oncologists at San Salvatore Hospital and the University of L’Aquila, in Italy. “This Web app might assist clinicians in balancing the risk/benefit ratio of being treated and/or access to the outpatient cancer center for each kind of patient (both early and advanced stages), in order to make a more tailored counseling,” they wrote in an email. “Importantly, the Web app might help those clinicians who work ‘alone,’ in peripheral centers, without resources, colleagues, and multidisciplinary tumor boards on whom they can rely.”
Bleicher, who was involved in the COVID-19 Breast Cancer Consortium’s recommendations for prioritizing breast cancer treatment, summarized that the app “may end up being close or accurate, but we won’t know except in hindsight.”
This article first appeared on Medscape.com.
Deciding which cancer patients need immediate treatment and who can safely wait is an uncomfortable assessment for cancer clinicians during the COVID-19 pandemic.
In early April, as the COVID-19 surge was bearing down on New York City, those treatment decisions were “a juggling act every single day,” Jonathan Yang, MD, PhD, a radiation oncologist from New York’s Memorial Sloan Kettering Cancer Center, told Medscape Medical News.
Eventually, a glut of guidelines, recommendations, and expert opinions aimed at helping oncologists emerged. The tools help navigate the complicated risk-benefit analysis of their patient’s risk of infection by SARS-CoV-2 and delaying therapy.
Now, a new tool, which appears to be the first of its kind, quantifies that risk-benefit analysis. But its presence immediately raises the question: can it help?
Three-Tier Systems Are Not Very Sophisticated
OncCOVID, a free tool that was launched May 26 by the University of Michigan, allows physicians to individualize risk estimates for delaying treatment of up to 25 early- to late-stage cancers. It includes more than 45 patient characteristics, such as age, location, cancer type, cancer stage, treatment plan, underlying medical conditions, and proposed length of delay in care.
Combining these personal details with data from the National Cancer Institute’s SEER (Surveillance, Epidemiology, and End Results) registry and the National Cancer Database, the Michigan app then estimates a patient’s 5- or 10-year survival with immediate vs delayed treatment and weighs that against their risk for COVID-19 using data from the Johns Hopkins Coronavirus Resource Center.
“We thought, isn’t it better to at least provide some evidence-based quantification, rather than a back-of-the-envelope three-tier system that is just sort of ‘made up’?“ explained one of the developers, Daniel Spratt, MD, associate professor of radiation oncology at Michigan Medicine.
Spratt explained that almost every organization, professional society, and government has created something like a three-tier system. Tier 1 represents urgent cases and patients who need immediate treatment. For tier 2, treatment can be delayed weeks or a month, and with tier 3, it can be delayed until the pandemic is over or it’s deemed safe.
“[This system] sounds good at first glance, but in cancer, we’re always talking about personalized medicine, and it’s mind-blowing that these tier systems are only based on urgency and prognosis,” he told Medscape Medical News.
Spratt offered an example. Consider a patient with a very aggressive brain tumor ― that patient is in tier 1 and should undergo treatment immediately. But will the treatment actually help? And how helpful would the procedure be if, say, the patient is 80 years old and, if infected, would have a 30% to 50% chance of dying from the coronavirus?
“If the model says this guy has a 5% harm and this one has 30% harm, you can use that to help prioritize,” summarized Spratt.
The app can generate risk estimates for patients living anywhere in the world and has already been accessed by people from 37 countries. However, Spratt cautions that it is primarily “designed and calibrated for the US.
“The estimates are based on very large US registries, and though it’s probably somewhat similar across much of the world, there’s probably certain cancer types that are more region specific ― especially something like stomach cancer or certain types of head and neck cancer in parts of Asia, for example,” he said.
Although the app’s COVID-19 data are specific to the county level in the United States, elsewhere in the world, it is only country specific.
“We’re using the best data we have for coronavirus, but everyone knows we still have large data gaps,” he acknowledged.
How Accurate?
Asked to comment on the app, Richard Bleicher, MD, leader of the Breast Cancer Program at Fox Chase Cancer Center, Philadelphia, praised the effort and the goal but had some concerns.
“Several questions arise, most important of which is, How accurate is this, and how has this been validated, if at all ― especially as it is too soon to see the outcomes of patients affected in this pandemic?” he told Medscape Medical News.
“We are imposing delays on a broad scale because of the coronavirus, and we are getting continuously changing data as we test more patients. But both situations are novel and may not be accurately represented by the data being pulled, because the datasets use patients from a few years ago, and confounders in these datasets may not apply to this situation,” Bleicher continued.
Although acknowledging the “value in delineating the risk of dying from cancer vs the risk of dying from the SARS-CoV-2 pandemic,” Bleicher urged caution in using the tool to make individual patient decisions.
“We need to remember that the best of modeling ... can be wildly inaccurate and needs to be validated using patients having the circumstances in question. ... This won’t be possible until long after the pandemic is completed, and so the model’s accuracy remains unknown.”
That sentiment was echoed by Giampaolo Bianchini, MD, head of the Breast Cancer Group, Department of Medical Oncology, Ospedale San Raffaele, in Milan, Italy.
“Arbitrarily postponing and modifying treatment strategies including surgery, radiation therapy, and medical therapy without properly balancing the risk/benefit ratio may lead to significantly worse cancer-related outcomes, which largely exceed the actual risks for COVID,” he wrote in an email.
“The OncCOVID app is a remarkable attempt to fill the gap between perception and estimation,” he said. The app provides side by side the COVID-19 risk estimation and the consequences of arbitrary deviation from the standard of care, observed Bianchini.
However, he pointed out weaknesses, including the fact that the “data generated in literature are not always of high quality and do not take into consideration relevant characteristics of the disease and treatment benefit. It should for sure be used, but then also interpreted with caution.”
Another Italian group responded more positively.
“In our opinion, it could be a useful tool for clinicians,” wrote colleagues Alessio Cortelinni and Giampiero Porzio, both medical oncologists at San Salvatore Hospital and the University of L’Aquila, in Italy. “This Web app might assist clinicians in balancing the risk/benefit ratio of being treated and/or access to the outpatient cancer center for each kind of patient (both early and advanced stages), in order to make a more tailored counseling,” they wrote in an email. “Importantly, the Web app might help those clinicians who work ‘alone,’ in peripheral centers, without resources, colleagues, and multidisciplinary tumor boards on whom they can rely.”
Bleicher, who was involved in the COVID-19 Breast Cancer Consortium’s recommendations for prioritizing breast cancer treatment, summarized that the app “may end up being close or accurate, but we won’t know except in hindsight.”
This article first appeared on Medscape.com.
Three years of imatinib may halve death rate in GIST
, phase 3 trial data suggest.
The most recent analysis of the SSGXVIII/AIO trial shows that, in about 400 patients who underwent surgery and had a high estimated risk of recurrence, there was a 50% increase in overall survival with longer treatment at 10 years on an efficacy analysis.
Moreover, there was a 30% improvement in recurrence-free survival (RFS) with 3 years vs 1 year of imatinib, with an even greater benefit seen in patients with a common tumor mutation.
The research was presented at the 2020 annual meeting of the American Society of Clinical Oncology (abstract 11503), held virtually because of the coronavirus pandemic.
Lead author Peter Reichardt, MD, Helios Klinikum Berlin-Buch, Berlin, Germany, said the results show that “3 years of adjuvant imatinib is highly superior” in terms of RFS and overall survival to 1 year of treatment.
“Overall, approximately 50% of deaths can be avoided during the first 10 years of follow-up after surgery with the longer adjuvant imatinib treatment.”
Study discussant Giovanni Grignani, MD, Division of Medical Oncology, Candiolo Cancer Institute, FPO-IRCCS, Turin, Italy, said that the “burning question” in the sarcoma space is: “Can we improve overall survival by reducing the risk of relapse with a perioperative treatment?
“We would like to able to identify patients for whom the cost of toxicity is paid off by an improvement in their outcome,” he added, noting that this is not achievable “and this is why perioperative treatment is so controversial in oncology.”
Grignani said the picture is a little different for GIST, as the relapse risk is unevenly distributed, the activity of imatinib is “extraordinary,” and the drug toxicity is “certainly bearable but not negligible.”
RFS is, however, affected by the inability of imatinib to eradicate resistant clones left behind by surgery, and replication resumes once the drug is stopped.
The current study nevertheless shows that overall survival “clearly favors 3-year imatinib therapy…with an impressive median follow-up of 119 months [10 years],” commented Patrick Leavey, MD, University of Texas Southwestern Medical Center, Dallas, in a highlights session.
He added that, in GIST, what might be considered “new progress” with the findings “is clarity over the length of imatinib therapy, which ... seems to be safe.”
Reichardt began by noting that several large randomized trials over the past decade have shown that adjuvant imatinib improves both RFS and overall survival.
However, “it is unknown whether imatinib improves overall survival after extended follow-up,” in addition to which “little is known about the long-term safety” of the drug in this setting.
To offer further insights, the protocol of SSGXVIII/AIO was amended in April 2017 to allow for a third analysis to be carried out once the last patient who entered the trial has been followed up for 10 years.
More Details
Reichardt recalled that the study, which was an open-label, multicenter phase 3 trial, involved GIST patients who were randomly assigned following surgery in a 1:1 fashion to imatinib for either 12 months or 36 months.
The patients were required to have a high-risk of recurrence, defined as at least one of the following:
- Tumor size >10 cm
- Tumor mitosis count >10/50 on high-powered microscopy (HPF)
- Tumor size >5 cm and mitosis count >5/50 HPF
- Tumor rupture, either spontaneously or at surgery.
Four hundred patients were recruited between February 2004 and September 2008, and 181 patients who were randomly assigned to 12 months of imatinib and 177 to 36 months were included in the efficacy analysis.
The median age of the patients was approximately 61 years, and half were female. The treatment groups were well-balanced in terms of their baseline characteristics.
Of note, 69% of patients in the 1-year treatment group and 71% of those given imatinib for 3 years had a detectable mutation in the KIT exon 11 site. The mean mitosis count was 10/50 and 8/50, respectively.
Over a median follow-up of 119 months (9 years, 11 months), 53% of 1-year treatment patients experienced a recurrence event, and 30% died, of whom 82% died with metastatic GIST.
In the 3-year treatment group, 44% experienced a recurrence event, and 18% died, with 83% of deaths from metastatic GIST.
On intention-to-treat analysis, RFS at 10 years was significantly higher with 3 years of imatinib than with 1 year, at 53% vs 42% (hazard ratio [HR], 0.66; P = .003).
Overall survival at 10 years was also higher with longer imatinib treatment, at 79% with 3 years of therapy vs 65% with 1 year (HR, 0.55; P = .004).
The team found on subgroup analysis that RFS was significantly better with 3-year than 1-year imatinib in patients with:
- A local mitotic count >10 (HR = 0.42)
- A central mitotic count >10 (HR = 0.50)
- A KIT exon 11 tumor mutation (HR = 0.57).
On the efficacy analysis, which included patients who signed informed consent, had GIST at pathology review, and no overt metastases at study entry, the HR for RFS with 3-year vs 1-year therapy was 0.70, whereas the HR for overall survival was 0.50.
Patients treated with imatinib for 3 years had a higher rate of any new cancer during follow-up, at 17%, vs 12% for those treated with imatinib for 1 year. Prostate cancer was the most common form of the disease in both groups.
Cardiac events were, in contrast, evenly distributed between the two groups, with 5% of 3-year patients and 6% of 1-year patients experiencing an event.
The study was funded by Novartis.
Reichardt reports honoraria from Amgen, Bayer, Lilly, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, Clinigen Group, Decipher, Lilly, Novartis, Pfizer, PharmaMar, and Roche; and receiving research funding from Novartis (Inst). Other authors report potential conflicts of interest.
Grignani reports honoraria from Bayer, EISAI, Lilly, Merck Serono, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, EISAI, and PharmaMar; receiving research funding from PharmaMar (Inst); and travel, accommodations, expenses from PharmaMar and Tesaro.
Leavey reports receiving research funding from Elison Pharmaceuticals (Inst).
This article first appeared on Medscape.com.
, phase 3 trial data suggest.
The most recent analysis of the SSGXVIII/AIO trial shows that, in about 400 patients who underwent surgery and had a high estimated risk of recurrence, there was a 50% increase in overall survival with longer treatment at 10 years on an efficacy analysis.
Moreover, there was a 30% improvement in recurrence-free survival (RFS) with 3 years vs 1 year of imatinib, with an even greater benefit seen in patients with a common tumor mutation.
The research was presented at the 2020 annual meeting of the American Society of Clinical Oncology (abstract 11503), held virtually because of the coronavirus pandemic.
Lead author Peter Reichardt, MD, Helios Klinikum Berlin-Buch, Berlin, Germany, said the results show that “3 years of adjuvant imatinib is highly superior” in terms of RFS and overall survival to 1 year of treatment.
“Overall, approximately 50% of deaths can be avoided during the first 10 years of follow-up after surgery with the longer adjuvant imatinib treatment.”
Study discussant Giovanni Grignani, MD, Division of Medical Oncology, Candiolo Cancer Institute, FPO-IRCCS, Turin, Italy, said that the “burning question” in the sarcoma space is: “Can we improve overall survival by reducing the risk of relapse with a perioperative treatment?
“We would like to able to identify patients for whom the cost of toxicity is paid off by an improvement in their outcome,” he added, noting that this is not achievable “and this is why perioperative treatment is so controversial in oncology.”
Grignani said the picture is a little different for GIST, as the relapse risk is unevenly distributed, the activity of imatinib is “extraordinary,” and the drug toxicity is “certainly bearable but not negligible.”
RFS is, however, affected by the inability of imatinib to eradicate resistant clones left behind by surgery, and replication resumes once the drug is stopped.
The current study nevertheless shows that overall survival “clearly favors 3-year imatinib therapy…with an impressive median follow-up of 119 months [10 years],” commented Patrick Leavey, MD, University of Texas Southwestern Medical Center, Dallas, in a highlights session.
He added that, in GIST, what might be considered “new progress” with the findings “is clarity over the length of imatinib therapy, which ... seems to be safe.”
Reichardt began by noting that several large randomized trials over the past decade have shown that adjuvant imatinib improves both RFS and overall survival.
However, “it is unknown whether imatinib improves overall survival after extended follow-up,” in addition to which “little is known about the long-term safety” of the drug in this setting.
To offer further insights, the protocol of SSGXVIII/AIO was amended in April 2017 to allow for a third analysis to be carried out once the last patient who entered the trial has been followed up for 10 years.
More Details
Reichardt recalled that the study, which was an open-label, multicenter phase 3 trial, involved GIST patients who were randomly assigned following surgery in a 1:1 fashion to imatinib for either 12 months or 36 months.
The patients were required to have a high-risk of recurrence, defined as at least one of the following:
- Tumor size >10 cm
- Tumor mitosis count >10/50 on high-powered microscopy (HPF)
- Tumor size >5 cm and mitosis count >5/50 HPF
- Tumor rupture, either spontaneously or at surgery.
Four hundred patients were recruited between February 2004 and September 2008, and 181 patients who were randomly assigned to 12 months of imatinib and 177 to 36 months were included in the efficacy analysis.
The median age of the patients was approximately 61 years, and half were female. The treatment groups were well-balanced in terms of their baseline characteristics.
Of note, 69% of patients in the 1-year treatment group and 71% of those given imatinib for 3 years had a detectable mutation in the KIT exon 11 site. The mean mitosis count was 10/50 and 8/50, respectively.
Over a median follow-up of 119 months (9 years, 11 months), 53% of 1-year treatment patients experienced a recurrence event, and 30% died, of whom 82% died with metastatic GIST.
In the 3-year treatment group, 44% experienced a recurrence event, and 18% died, with 83% of deaths from metastatic GIST.
On intention-to-treat analysis, RFS at 10 years was significantly higher with 3 years of imatinib than with 1 year, at 53% vs 42% (hazard ratio [HR], 0.66; P = .003).
Overall survival at 10 years was also higher with longer imatinib treatment, at 79% with 3 years of therapy vs 65% with 1 year (HR, 0.55; P = .004).
The team found on subgroup analysis that RFS was significantly better with 3-year than 1-year imatinib in patients with:
- A local mitotic count >10 (HR = 0.42)
- A central mitotic count >10 (HR = 0.50)
- A KIT exon 11 tumor mutation (HR = 0.57).
On the efficacy analysis, which included patients who signed informed consent, had GIST at pathology review, and no overt metastases at study entry, the HR for RFS with 3-year vs 1-year therapy was 0.70, whereas the HR for overall survival was 0.50.
Patients treated with imatinib for 3 years had a higher rate of any new cancer during follow-up, at 17%, vs 12% for those treated with imatinib for 1 year. Prostate cancer was the most common form of the disease in both groups.
Cardiac events were, in contrast, evenly distributed between the two groups, with 5% of 3-year patients and 6% of 1-year patients experiencing an event.
The study was funded by Novartis.
Reichardt reports honoraria from Amgen, Bayer, Lilly, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, Clinigen Group, Decipher, Lilly, Novartis, Pfizer, PharmaMar, and Roche; and receiving research funding from Novartis (Inst). Other authors report potential conflicts of interest.
Grignani reports honoraria from Bayer, EISAI, Lilly, Merck Serono, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, EISAI, and PharmaMar; receiving research funding from PharmaMar (Inst); and travel, accommodations, expenses from PharmaMar and Tesaro.
Leavey reports receiving research funding from Elison Pharmaceuticals (Inst).
This article first appeared on Medscape.com.
, phase 3 trial data suggest.
The most recent analysis of the SSGXVIII/AIO trial shows that, in about 400 patients who underwent surgery and had a high estimated risk of recurrence, there was a 50% increase in overall survival with longer treatment at 10 years on an efficacy analysis.
Moreover, there was a 30% improvement in recurrence-free survival (RFS) with 3 years vs 1 year of imatinib, with an even greater benefit seen in patients with a common tumor mutation.
The research was presented at the 2020 annual meeting of the American Society of Clinical Oncology (abstract 11503), held virtually because of the coronavirus pandemic.
Lead author Peter Reichardt, MD, Helios Klinikum Berlin-Buch, Berlin, Germany, said the results show that “3 years of adjuvant imatinib is highly superior” in terms of RFS and overall survival to 1 year of treatment.
“Overall, approximately 50% of deaths can be avoided during the first 10 years of follow-up after surgery with the longer adjuvant imatinib treatment.”
Study discussant Giovanni Grignani, MD, Division of Medical Oncology, Candiolo Cancer Institute, FPO-IRCCS, Turin, Italy, said that the “burning question” in the sarcoma space is: “Can we improve overall survival by reducing the risk of relapse with a perioperative treatment?
“We would like to able to identify patients for whom the cost of toxicity is paid off by an improvement in their outcome,” he added, noting that this is not achievable “and this is why perioperative treatment is so controversial in oncology.”
Grignani said the picture is a little different for GIST, as the relapse risk is unevenly distributed, the activity of imatinib is “extraordinary,” and the drug toxicity is “certainly bearable but not negligible.”
RFS is, however, affected by the inability of imatinib to eradicate resistant clones left behind by surgery, and replication resumes once the drug is stopped.
The current study nevertheless shows that overall survival “clearly favors 3-year imatinib therapy…with an impressive median follow-up of 119 months [10 years],” commented Patrick Leavey, MD, University of Texas Southwestern Medical Center, Dallas, in a highlights session.
He added that, in GIST, what might be considered “new progress” with the findings “is clarity over the length of imatinib therapy, which ... seems to be safe.”
Reichardt began by noting that several large randomized trials over the past decade have shown that adjuvant imatinib improves both RFS and overall survival.
However, “it is unknown whether imatinib improves overall survival after extended follow-up,” in addition to which “little is known about the long-term safety” of the drug in this setting.
To offer further insights, the protocol of SSGXVIII/AIO was amended in April 2017 to allow for a third analysis to be carried out once the last patient who entered the trial has been followed up for 10 years.
More Details
Reichardt recalled that the study, which was an open-label, multicenter phase 3 trial, involved GIST patients who were randomly assigned following surgery in a 1:1 fashion to imatinib for either 12 months or 36 months.
The patients were required to have a high-risk of recurrence, defined as at least one of the following:
- Tumor size >10 cm
- Tumor mitosis count >10/50 on high-powered microscopy (HPF)
- Tumor size >5 cm and mitosis count >5/50 HPF
- Tumor rupture, either spontaneously or at surgery.
Four hundred patients were recruited between February 2004 and September 2008, and 181 patients who were randomly assigned to 12 months of imatinib and 177 to 36 months were included in the efficacy analysis.
The median age of the patients was approximately 61 years, and half were female. The treatment groups were well-balanced in terms of their baseline characteristics.
Of note, 69% of patients in the 1-year treatment group and 71% of those given imatinib for 3 years had a detectable mutation in the KIT exon 11 site. The mean mitosis count was 10/50 and 8/50, respectively.
Over a median follow-up of 119 months (9 years, 11 months), 53% of 1-year treatment patients experienced a recurrence event, and 30% died, of whom 82% died with metastatic GIST.
In the 3-year treatment group, 44% experienced a recurrence event, and 18% died, with 83% of deaths from metastatic GIST.
On intention-to-treat analysis, RFS at 10 years was significantly higher with 3 years of imatinib than with 1 year, at 53% vs 42% (hazard ratio [HR], 0.66; P = .003).
Overall survival at 10 years was also higher with longer imatinib treatment, at 79% with 3 years of therapy vs 65% with 1 year (HR, 0.55; P = .004).
The team found on subgroup analysis that RFS was significantly better with 3-year than 1-year imatinib in patients with:
- A local mitotic count >10 (HR = 0.42)
- A central mitotic count >10 (HR = 0.50)
- A KIT exon 11 tumor mutation (HR = 0.57).
On the efficacy analysis, which included patients who signed informed consent, had GIST at pathology review, and no overt metastases at study entry, the HR for RFS with 3-year vs 1-year therapy was 0.70, whereas the HR for overall survival was 0.50.
Patients treated with imatinib for 3 years had a higher rate of any new cancer during follow-up, at 17%, vs 12% for those treated with imatinib for 1 year. Prostate cancer was the most common form of the disease in both groups.
Cardiac events were, in contrast, evenly distributed between the two groups, with 5% of 3-year patients and 6% of 1-year patients experiencing an event.
The study was funded by Novartis.
Reichardt reports honoraria from Amgen, Bayer, Lilly, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, Clinigen Group, Decipher, Lilly, Novartis, Pfizer, PharmaMar, and Roche; and receiving research funding from Novartis (Inst). Other authors report potential conflicts of interest.
Grignani reports honoraria from Bayer, EISAI, Lilly, Merck Serono, Novartis, Pfizer, and PharmaMar; serving in a consulting or advisory role with Bayer, EISAI, and PharmaMar; receiving research funding from PharmaMar (Inst); and travel, accommodations, expenses from PharmaMar and Tesaro.
Leavey reports receiving research funding from Elison Pharmaceuticals (Inst).
This article first appeared on Medscape.com.
FROM ASCO 2020
Virtual ADA Scientific Sessions to offer full program
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
TKI plus SBRT tops TKI alone for oligometastatic EGFRm NSCLC
Adding aggressive local radiotherapy to treatment with tyrosine kinase inhibitor (TKI) significantly improved progression-free and overall survival in patients with previously untreated, EGFR-mutated, oligometastatic non–small cell lung cancer (NSCLC) in a phase 3 trial presented as part of the American Society of Clinical Oncology virtual scientific program.
Sixty-eight patients were randomized at diagnosis to receive a first-generation TKI plus stereotactic body radiation therapy (SBRT) to all disease sites. The other 68 patients were randomized to receive a TKI alone, but 3 patients were lost follow-up and not included in the analysis. The TKIs used were gefitinib, erlotinib, and icotinib.
At baseline, patients had a maximum of two lesions in any one organ and no more than five metastases overall. Patients with brain metastases were excluded.
The median progression-free survival was 20.2 months in the SBRT arm and 12.5 months in the TKI-only arm (hazard ratio, 0.618; P < .001). The median overall survival was 25.5 months and 17.4 months, respectively (HR, 0.682; P < .001).
There were no grade 4/5 adverse events nor any statistically significant between-group differences in grade 3 events.
‘Compelling’ data with caveats
The study results suggest that “aggressive local therapy to sites at diagnosis should be explored further in large cohort phase 3 trials as a standard treatment option in this clinical scenario,” said investigator Xiao-shan Wang, MD, PhD, of the University of Electronic Science and Technology of China and Sichuan Provincial People’s Hospital in Chengdu.
“The data are compelling,” Dr. Wang added. “As we attempt to maximize the benefits of EGFR-directed targeted therapies, we are likely going to be moving away from a sequentially administered approach to treatment and considering combinations.”
The new findings, combined with prior phase 2 results, support “incorporation of upfront SBRT with TKI into practice for selected patients with oligometastatic disease, with the open question remaining of how many metastases are too many,” said study discussant Rachel Sanborn, MD, of Providence Cancer Institute Franz Clinic in Portland, Ore.
However, “it’s important to make note of the baseline characteristics of the patients enrolled,” she said.
Twelve percent of patients in the control arm and 4% of those in the SBRT group had EGFR exon 20 insertions. This “imbalance could have negatively impacted the outcomes in the TKI-alone arm,” Dr. Sanborn said.
Also, a higher proportion of patients in the TKI-alone arm received gefitinib, and “there was no information offered on second-line therapies in the study, which might have also affected outcomes,” Dr. Sanborn added.
Additional details
The study (NCT02893332) enrolled NSCLC patients with a life expectancy of at least 6 months and an Eastern Cooperative Oncology Group performance status score of 0-2. NSCLC was confirmed by pathology and EGFR mutations by gene sequencing.
The radiation dose was 25-40 Gy in five fractions. Gefitinib was used in 47% of patients in the SBRT arm and 58% of the control group. Erlotinib was used in 44% of the SBRT arm and 35% of controls. Icotinib was used by less than 10% of patients in each group.
Grade 3 skin rash occurred in 50% of patients in the SBRT arm and 62% of those in the TKI-alone arm. Grade 3 pneumonitis occurred in 30% and 15%, respectively. Grade 3 esophagitis occurred in 15% of patients in both arms.
One patient in the TKI arm had severe liver injury. One patient in the SBRT arm fractured a rib, which was considered probably related to the radiation.
Multivariate analysis revealed that, in addition to SBRT, lower baseline performance status score (0 vs. 1-2) and fewer metastases (<2 vs. ≥3) were protective for progression-free survival. Lower performance scores, fewer metastases, lower T stage (T1-2 vs. T3-4), and exon 19 versus exon 20 and 21 mutations were protective for overall survival.
The study arms were well balanced at baseline. The mean patient age was 66.9 years in the SBRT arm and 63.32 years in the TKI-only arm. In both arms, most patients were women (63% and 60%, respectively).
The study was sponsored by Sichuan Provincial People’s Hospital. The investigators and Dr. Sanborn have no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 9508.
Adding aggressive local radiotherapy to treatment with tyrosine kinase inhibitor (TKI) significantly improved progression-free and overall survival in patients with previously untreated, EGFR-mutated, oligometastatic non–small cell lung cancer (NSCLC) in a phase 3 trial presented as part of the American Society of Clinical Oncology virtual scientific program.
Sixty-eight patients were randomized at diagnosis to receive a first-generation TKI plus stereotactic body radiation therapy (SBRT) to all disease sites. The other 68 patients were randomized to receive a TKI alone, but 3 patients were lost follow-up and not included in the analysis. The TKIs used were gefitinib, erlotinib, and icotinib.
At baseline, patients had a maximum of two lesions in any one organ and no more than five metastases overall. Patients with brain metastases were excluded.
The median progression-free survival was 20.2 months in the SBRT arm and 12.5 months in the TKI-only arm (hazard ratio, 0.618; P < .001). The median overall survival was 25.5 months and 17.4 months, respectively (HR, 0.682; P < .001).
There were no grade 4/5 adverse events nor any statistically significant between-group differences in grade 3 events.
‘Compelling’ data with caveats
The study results suggest that “aggressive local therapy to sites at diagnosis should be explored further in large cohort phase 3 trials as a standard treatment option in this clinical scenario,” said investigator Xiao-shan Wang, MD, PhD, of the University of Electronic Science and Technology of China and Sichuan Provincial People’s Hospital in Chengdu.
“The data are compelling,” Dr. Wang added. “As we attempt to maximize the benefits of EGFR-directed targeted therapies, we are likely going to be moving away from a sequentially administered approach to treatment and considering combinations.”
The new findings, combined with prior phase 2 results, support “incorporation of upfront SBRT with TKI into practice for selected patients with oligometastatic disease, with the open question remaining of how many metastases are too many,” said study discussant Rachel Sanborn, MD, of Providence Cancer Institute Franz Clinic in Portland, Ore.
However, “it’s important to make note of the baseline characteristics of the patients enrolled,” she said.
Twelve percent of patients in the control arm and 4% of those in the SBRT group had EGFR exon 20 insertions. This “imbalance could have negatively impacted the outcomes in the TKI-alone arm,” Dr. Sanborn said.
Also, a higher proportion of patients in the TKI-alone arm received gefitinib, and “there was no information offered on second-line therapies in the study, which might have also affected outcomes,” Dr. Sanborn added.
Additional details
The study (NCT02893332) enrolled NSCLC patients with a life expectancy of at least 6 months and an Eastern Cooperative Oncology Group performance status score of 0-2. NSCLC was confirmed by pathology and EGFR mutations by gene sequencing.
The radiation dose was 25-40 Gy in five fractions. Gefitinib was used in 47% of patients in the SBRT arm and 58% of the control group. Erlotinib was used in 44% of the SBRT arm and 35% of controls. Icotinib was used by less than 10% of patients in each group.
Grade 3 skin rash occurred in 50% of patients in the SBRT arm and 62% of those in the TKI-alone arm. Grade 3 pneumonitis occurred in 30% and 15%, respectively. Grade 3 esophagitis occurred in 15% of patients in both arms.
One patient in the TKI arm had severe liver injury. One patient in the SBRT arm fractured a rib, which was considered probably related to the radiation.
Multivariate analysis revealed that, in addition to SBRT, lower baseline performance status score (0 vs. 1-2) and fewer metastases (<2 vs. ≥3) were protective for progression-free survival. Lower performance scores, fewer metastases, lower T stage (T1-2 vs. T3-4), and exon 19 versus exon 20 and 21 mutations were protective for overall survival.
The study arms were well balanced at baseline. The mean patient age was 66.9 years in the SBRT arm and 63.32 years in the TKI-only arm. In both arms, most patients were women (63% and 60%, respectively).
The study was sponsored by Sichuan Provincial People’s Hospital. The investigators and Dr. Sanborn have no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 9508.
Adding aggressive local radiotherapy to treatment with tyrosine kinase inhibitor (TKI) significantly improved progression-free and overall survival in patients with previously untreated, EGFR-mutated, oligometastatic non–small cell lung cancer (NSCLC) in a phase 3 trial presented as part of the American Society of Clinical Oncology virtual scientific program.
Sixty-eight patients were randomized at diagnosis to receive a first-generation TKI plus stereotactic body radiation therapy (SBRT) to all disease sites. The other 68 patients were randomized to receive a TKI alone, but 3 patients were lost follow-up and not included in the analysis. The TKIs used were gefitinib, erlotinib, and icotinib.
At baseline, patients had a maximum of two lesions in any one organ and no more than five metastases overall. Patients with brain metastases were excluded.
The median progression-free survival was 20.2 months in the SBRT arm and 12.5 months in the TKI-only arm (hazard ratio, 0.618; P < .001). The median overall survival was 25.5 months and 17.4 months, respectively (HR, 0.682; P < .001).
There were no grade 4/5 adverse events nor any statistically significant between-group differences in grade 3 events.
‘Compelling’ data with caveats
The study results suggest that “aggressive local therapy to sites at diagnosis should be explored further in large cohort phase 3 trials as a standard treatment option in this clinical scenario,” said investigator Xiao-shan Wang, MD, PhD, of the University of Electronic Science and Technology of China and Sichuan Provincial People’s Hospital in Chengdu.
“The data are compelling,” Dr. Wang added. “As we attempt to maximize the benefits of EGFR-directed targeted therapies, we are likely going to be moving away from a sequentially administered approach to treatment and considering combinations.”
The new findings, combined with prior phase 2 results, support “incorporation of upfront SBRT with TKI into practice for selected patients with oligometastatic disease, with the open question remaining of how many metastases are too many,” said study discussant Rachel Sanborn, MD, of Providence Cancer Institute Franz Clinic in Portland, Ore.
However, “it’s important to make note of the baseline characteristics of the patients enrolled,” she said.
Twelve percent of patients in the control arm and 4% of those in the SBRT group had EGFR exon 20 insertions. This “imbalance could have negatively impacted the outcomes in the TKI-alone arm,” Dr. Sanborn said.
Also, a higher proportion of patients in the TKI-alone arm received gefitinib, and “there was no information offered on second-line therapies in the study, which might have also affected outcomes,” Dr. Sanborn added.
Additional details
The study (NCT02893332) enrolled NSCLC patients with a life expectancy of at least 6 months and an Eastern Cooperative Oncology Group performance status score of 0-2. NSCLC was confirmed by pathology and EGFR mutations by gene sequencing.
The radiation dose was 25-40 Gy in five fractions. Gefitinib was used in 47% of patients in the SBRT arm and 58% of the control group. Erlotinib was used in 44% of the SBRT arm and 35% of controls. Icotinib was used by less than 10% of patients in each group.
Grade 3 skin rash occurred in 50% of patients in the SBRT arm and 62% of those in the TKI-alone arm. Grade 3 pneumonitis occurred in 30% and 15%, respectively. Grade 3 esophagitis occurred in 15% of patients in both arms.
One patient in the TKI arm had severe liver injury. One patient in the SBRT arm fractured a rib, which was considered probably related to the radiation.
Multivariate analysis revealed that, in addition to SBRT, lower baseline performance status score (0 vs. 1-2) and fewer metastases (<2 vs. ≥3) were protective for progression-free survival. Lower performance scores, fewer metastases, lower T stage (T1-2 vs. T3-4), and exon 19 versus exon 20 and 21 mutations were protective for overall survival.
The study arms were well balanced at baseline. The mean patient age was 66.9 years in the SBRT arm and 63.32 years in the TKI-only arm. In both arms, most patients were women (63% and 60%, respectively).
The study was sponsored by Sichuan Provincial People’s Hospital. The investigators and Dr. Sanborn have no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 9508.
FROM ASCO 2020
Cannabis misconceptions still common among MS clinicians
experts say.

“There is evidence of a ‘clinical void,’ with clinicians on one side and people with MS and other conditions on the other that doesn’t usually exist regarding therapies that people with MS are using,” said Allen C. Bowling, MD, PhD, director of the NeuroHealth Institute and clinical professor of neurology at the University of Colorado, in Aurora. His presentation was part of the virtual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
While approximately 8% of the general population uses cannabis, evidence shows that the proportion of people with MS who do so ranges from 9% to 38%, for an average of about 20%, Dr. Bowling noted. Yet, according to research, only about 20% of those actually discuss their cannabis use with their clinicians, which could have potentially adverse implications in the management of the disease.
As an example, Dr. Bowling described a case of his own involving a stroke syndrome associated with cannabis use – reversible cerebral vasoconstriction syndrome (RCVS), which he mistook for an MS flare-up. “I had a patient who developed RCVS, but because it appeared to be an MS attack, I was treating her with corticosteroids, and she kept getting worse,” he said. “It’s very important for MS clinicians to be aware of this stroke syndrome that can mimic an MS attack. The way to rule it out is with CT angiography.”
Misconceptions common among clinicians
Studies underscore that such misconceptions could be common. One recent study showed that as many as 90% of residents and fellows did not feel prepared to recommend or answer questions on cannabis use, and in fact, most states do not even require physicians to have training in medical uses of cannabis, Dr. Bowling noted.
Other research shows that the rates of clinicians with high knowledge in medical cannabis use are in the single digits, while many have no cannabis training at all.
In a survey of 556 physicians taken as recently as January 2020, 47% gave incorrect responses regarding tetrahydrocannabinol (THC), while 33% reported being familiar with “nano-cannabinoids” – which don’t even exist, and the term was created for the sake of the survey.
Clinicians’ misconceptions about the regulation of cannabis was especially eyebrow raising, Dr. Bowling indicated. “The part that concerns me the most is regarding dispensary cannabis products – 17% of respondents thought the products were Food and Drug Administration–controlled and 25% said they thought that dispensary products were FDA approved,” he said.
There are, meanwhile, no formal clinical studies evaluating the medical efficacy of any products sold in U.S. cannabis dispensaries, much less FDA regulation, Dr. Bowling said.
Among the most recent research of cannabis use among MS patients is a real-world study of more than 2,000 patients with MS in Denmark. Said to be the most comprehensive survey of cannabis use among MS patients to date, the researchers found that 21% of patients reported cannabis use in the past year, with only 21% of those having a prescription to use the drug legally because of strict regulations in Denmark.
Respondents reported that the primary reasons for use in MS were to alleviate pain (61%), spasticity (52%), and sleep disturbances (46%). The most common adverse effects were drowsiness (30%), feeling quiet/subdued (23%), and dizziness (13%), with effects that were mild to moderate.
And a 2019 study of electronic medical record data for 561 patients with multiple sclerosis in British Columbia, Canada, showed that 19% reported using cannabis, with 71% reporting use for alleviation of pain, 71% for sleep, 44% for mood, and 40% for spasticity.
Dr. Bowling said the findings are consistent with his clinical experience in treating patients in Colorado, where medical cannabis has been legal for about 2 decades. “It seems that people who benefit most are those who use small amounts and typically use it for alleviation of pain and/or spasticity that interferes with sleep,” he said.
However, with a lack of regulation about the true components in dispensary products, there are many uncertainties about what works or doesn’t. “Very anecdotally, preparations that are high in cannabidiol (CBD) and low in tetrahydrocannabinol (THC, the main psychoactive compound in cannabis) seem the most helpful. Pure CBD preparations (i.e., with no THC) seem less effective,” Dr. Bowling noted.
Other recent evidence on cannabis use in MS, however, suggests important benefits once patients abstain from its use.
However, the exceptionally wide array of components in unregulated cannabis accounts for substantial variety in potency, benefits, and side effects, Dr. Bowling said.
He pointed out one recent study looking mainly at patients with MS who regularly smoked cannabis and showed cognitive improvements upon abstaining. The study included 40 MS patients who reported smoking cannabis regularly – at least 4 days per week for multiple years – who were randomized to continue their cannabis use or withdraw.
While there were no cognitive differences among the patients at baseline, after 28 days, the abstinence group showed significant improvements on functional MRI in every cognitive index (P < .0001 for all). On the Symbol Digit Modalities Test at day 28, the withdrawal group completed more trials correctly (P < .012) and had a faster reaction time (P < .002) that was associated with significantly increased activation in brain regions known to be associated with performance of the test, including the bilateral inferior frontal gyri, caudate, and declive/cerebellum (P < .001 for all regions), the authors said.
“These results reveal that patients with multiple sclerosis who are frequent, long-term cannabis users can show significant improvements in memory, processing speed, and executive function after 28 days of drug abstinence,” the authors reported.
Addiction, distinguishing cannabis from MS symptoms
Dr. Bowling said that, while the findings are consistent with his own clinical observations, abstinence isn’t always easy. “I’ve seen patients with cognitive impairment whose cognition and overall day-to-day function have improved with discontinuation of cannabis,” he said. “For some of these patients, however, it was a long-term challenge to discontinue cannabis because they were addicted.”
Addiction to cannabis in MS in fact may be more common than many realize, and comes with a host of other adverse effects, Dr. Bowling said. “In my practice, I have definitely seen many cases of addiction. I think that it’s very underdiagnosed. In addition to cognitive dysfunction, it can worsen anxiety and depression and decrease balance, leading to falls.”
The RCVS risk is another concern, and changes in liver enzymes should also raise a red flag when MS patients are cannabis users, Bowling added.
“I’ve seen in multiple patients where the liver enzymes went up and I thought it was because of the disease-modifying therapy, but it turned out to have been because the patient had started CBD, so you need to be aware of potential hepatotoxicity.”
“The bottom line is that we don’t have strong data in this area and herbs are extremely complex with many unknown constituents.”
Dr. Bowling noted that pure CBD or CBD-enriched products would be expected to produce less cognitive dysfunction than does regular cannabis smoking, “however, it’s important to keep in mind that a ‘CBD-enriched’ product could have low but still significant THC content,” he said.
Dr. Bowling reported relationships with Bristol-Myers Squibb, EMD Serono, Genentech, Genzyme, Greenwich Biosciences, and Novartis, and he received royalties from Springer Publishing.
A version of this article originally appeared on Medscape.com.
experts say.
“There is evidence of a ‘clinical void,’ with clinicians on one side and people with MS and other conditions on the other that doesn’t usually exist regarding therapies that people with MS are using,” said Allen C. Bowling, MD, PhD, director of the NeuroHealth Institute and clinical professor of neurology at the University of Colorado, in Aurora. His presentation was part of the virtual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
While approximately 8% of the general population uses cannabis, evidence shows that the proportion of people with MS who do so ranges from 9% to 38%, for an average of about 20%, Dr. Bowling noted. Yet, according to research, only about 20% of those actually discuss their cannabis use with their clinicians, which could have potentially adverse implications in the management of the disease.
As an example, Dr. Bowling described a case of his own involving a stroke syndrome associated with cannabis use – reversible cerebral vasoconstriction syndrome (RCVS), which he mistook for an MS flare-up. “I had a patient who developed RCVS, but because it appeared to be an MS attack, I was treating her with corticosteroids, and she kept getting worse,” he said. “It’s very important for MS clinicians to be aware of this stroke syndrome that can mimic an MS attack. The way to rule it out is with CT angiography.”
Misconceptions common among clinicians
Studies underscore that such misconceptions could be common. One recent study showed that as many as 90% of residents and fellows did not feel prepared to recommend or answer questions on cannabis use, and in fact, most states do not even require physicians to have training in medical uses of cannabis, Dr. Bowling noted.
Other research shows that the rates of clinicians with high knowledge in medical cannabis use are in the single digits, while many have no cannabis training at all.
In a survey of 556 physicians taken as recently as January 2020, 47% gave incorrect responses regarding tetrahydrocannabinol (THC), while 33% reported being familiar with “nano-cannabinoids” – which don’t even exist, and the term was created for the sake of the survey.
Clinicians’ misconceptions about the regulation of cannabis was especially eyebrow raising, Dr. Bowling indicated. “The part that concerns me the most is regarding dispensary cannabis products – 17% of respondents thought the products were Food and Drug Administration–controlled and 25% said they thought that dispensary products were FDA approved,” he said.
There are, meanwhile, no formal clinical studies evaluating the medical efficacy of any products sold in U.S. cannabis dispensaries, much less FDA regulation, Dr. Bowling said.
Among the most recent research of cannabis use among MS patients is a real-world study of more than 2,000 patients with MS in Denmark. Said to be the most comprehensive survey of cannabis use among MS patients to date, the researchers found that 21% of patients reported cannabis use in the past year, with only 21% of those having a prescription to use the drug legally because of strict regulations in Denmark.
Respondents reported that the primary reasons for use in MS were to alleviate pain (61%), spasticity (52%), and sleep disturbances (46%). The most common adverse effects were drowsiness (30%), feeling quiet/subdued (23%), and dizziness (13%), with effects that were mild to moderate.
And a 2019 study of electronic medical record data for 561 patients with multiple sclerosis in British Columbia, Canada, showed that 19% reported using cannabis, with 71% reporting use for alleviation of pain, 71% for sleep, 44% for mood, and 40% for spasticity.
Dr. Bowling said the findings are consistent with his clinical experience in treating patients in Colorado, where medical cannabis has been legal for about 2 decades. “It seems that people who benefit most are those who use small amounts and typically use it for alleviation of pain and/or spasticity that interferes with sleep,” he said.
However, with a lack of regulation about the true components in dispensary products, there are many uncertainties about what works or doesn’t. “Very anecdotally, preparations that are high in cannabidiol (CBD) and low in tetrahydrocannabinol (THC, the main psychoactive compound in cannabis) seem the most helpful. Pure CBD preparations (i.e., with no THC) seem less effective,” Dr. Bowling noted.
Other recent evidence on cannabis use in MS, however, suggests important benefits once patients abstain from its use.
However, the exceptionally wide array of components in unregulated cannabis accounts for substantial variety in potency, benefits, and side effects, Dr. Bowling said.
He pointed out one recent study looking mainly at patients with MS who regularly smoked cannabis and showed cognitive improvements upon abstaining. The study included 40 MS patients who reported smoking cannabis regularly – at least 4 days per week for multiple years – who were randomized to continue their cannabis use or withdraw.
While there were no cognitive differences among the patients at baseline, after 28 days, the abstinence group showed significant improvements on functional MRI in every cognitive index (P < .0001 for all). On the Symbol Digit Modalities Test at day 28, the withdrawal group completed more trials correctly (P < .012) and had a faster reaction time (P < .002) that was associated with significantly increased activation in brain regions known to be associated with performance of the test, including the bilateral inferior frontal gyri, caudate, and declive/cerebellum (P < .001 for all regions), the authors said.
“These results reveal that patients with multiple sclerosis who are frequent, long-term cannabis users can show significant improvements in memory, processing speed, and executive function after 28 days of drug abstinence,” the authors reported.
Addiction, distinguishing cannabis from MS symptoms
Dr. Bowling said that, while the findings are consistent with his own clinical observations, abstinence isn’t always easy. “I’ve seen patients with cognitive impairment whose cognition and overall day-to-day function have improved with discontinuation of cannabis,” he said. “For some of these patients, however, it was a long-term challenge to discontinue cannabis because they were addicted.”
Addiction to cannabis in MS in fact may be more common than many realize, and comes with a host of other adverse effects, Dr. Bowling said. “In my practice, I have definitely seen many cases of addiction. I think that it’s very underdiagnosed. In addition to cognitive dysfunction, it can worsen anxiety and depression and decrease balance, leading to falls.”
The RCVS risk is another concern, and changes in liver enzymes should also raise a red flag when MS patients are cannabis users, Bowling added.
“I’ve seen in multiple patients where the liver enzymes went up and I thought it was because of the disease-modifying therapy, but it turned out to have been because the patient had started CBD, so you need to be aware of potential hepatotoxicity.”
“The bottom line is that we don’t have strong data in this area and herbs are extremely complex with many unknown constituents.”
Dr. Bowling noted that pure CBD or CBD-enriched products would be expected to produce less cognitive dysfunction than does regular cannabis smoking, “however, it’s important to keep in mind that a ‘CBD-enriched’ product could have low but still significant THC content,” he said.
Dr. Bowling reported relationships with Bristol-Myers Squibb, EMD Serono, Genentech, Genzyme, Greenwich Biosciences, and Novartis, and he received royalties from Springer Publishing.
A version of this article originally appeared on Medscape.com.
experts say.
“There is evidence of a ‘clinical void,’ with clinicians on one side and people with MS and other conditions on the other that doesn’t usually exist regarding therapies that people with MS are using,” said Allen C. Bowling, MD, PhD, director of the NeuroHealth Institute and clinical professor of neurology at the University of Colorado, in Aurora. His presentation was part of the virtual meeting of the Consortium of Multiple Sclerosis Centers (CMSC).
While approximately 8% of the general population uses cannabis, evidence shows that the proportion of people with MS who do so ranges from 9% to 38%, for an average of about 20%, Dr. Bowling noted. Yet, according to research, only about 20% of those actually discuss their cannabis use with their clinicians, which could have potentially adverse implications in the management of the disease.
As an example, Dr. Bowling described a case of his own involving a stroke syndrome associated with cannabis use – reversible cerebral vasoconstriction syndrome (RCVS), which he mistook for an MS flare-up. “I had a patient who developed RCVS, but because it appeared to be an MS attack, I was treating her with corticosteroids, and she kept getting worse,” he said. “It’s very important for MS clinicians to be aware of this stroke syndrome that can mimic an MS attack. The way to rule it out is with CT angiography.”
Misconceptions common among clinicians
Studies underscore that such misconceptions could be common. One recent study showed that as many as 90% of residents and fellows did not feel prepared to recommend or answer questions on cannabis use, and in fact, most states do not even require physicians to have training in medical uses of cannabis, Dr. Bowling noted.
Other research shows that the rates of clinicians with high knowledge in medical cannabis use are in the single digits, while many have no cannabis training at all.
In a survey of 556 physicians taken as recently as January 2020, 47% gave incorrect responses regarding tetrahydrocannabinol (THC), while 33% reported being familiar with “nano-cannabinoids” – which don’t even exist, and the term was created for the sake of the survey.
Clinicians’ misconceptions about the regulation of cannabis was especially eyebrow raising, Dr. Bowling indicated. “The part that concerns me the most is regarding dispensary cannabis products – 17% of respondents thought the products were Food and Drug Administration–controlled and 25% said they thought that dispensary products were FDA approved,” he said.
There are, meanwhile, no formal clinical studies evaluating the medical efficacy of any products sold in U.S. cannabis dispensaries, much less FDA regulation, Dr. Bowling said.
Among the most recent research of cannabis use among MS patients is a real-world study of more than 2,000 patients with MS in Denmark. Said to be the most comprehensive survey of cannabis use among MS patients to date, the researchers found that 21% of patients reported cannabis use in the past year, with only 21% of those having a prescription to use the drug legally because of strict regulations in Denmark.
Respondents reported that the primary reasons for use in MS were to alleviate pain (61%), spasticity (52%), and sleep disturbances (46%). The most common adverse effects were drowsiness (30%), feeling quiet/subdued (23%), and dizziness (13%), with effects that were mild to moderate.
And a 2019 study of electronic medical record data for 561 patients with multiple sclerosis in British Columbia, Canada, showed that 19% reported using cannabis, with 71% reporting use for alleviation of pain, 71% for sleep, 44% for mood, and 40% for spasticity.
Dr. Bowling said the findings are consistent with his clinical experience in treating patients in Colorado, where medical cannabis has been legal for about 2 decades. “It seems that people who benefit most are those who use small amounts and typically use it for alleviation of pain and/or spasticity that interferes with sleep,” he said.
However, with a lack of regulation about the true components in dispensary products, there are many uncertainties about what works or doesn’t. “Very anecdotally, preparations that are high in cannabidiol (CBD) and low in tetrahydrocannabinol (THC, the main psychoactive compound in cannabis) seem the most helpful. Pure CBD preparations (i.e., with no THC) seem less effective,” Dr. Bowling noted.
Other recent evidence on cannabis use in MS, however, suggests important benefits once patients abstain from its use.
However, the exceptionally wide array of components in unregulated cannabis accounts for substantial variety in potency, benefits, and side effects, Dr. Bowling said.
He pointed out one recent study looking mainly at patients with MS who regularly smoked cannabis and showed cognitive improvements upon abstaining. The study included 40 MS patients who reported smoking cannabis regularly – at least 4 days per week for multiple years – who were randomized to continue their cannabis use or withdraw.
While there were no cognitive differences among the patients at baseline, after 28 days, the abstinence group showed significant improvements on functional MRI in every cognitive index (P < .0001 for all). On the Symbol Digit Modalities Test at day 28, the withdrawal group completed more trials correctly (P < .012) and had a faster reaction time (P < .002) that was associated with significantly increased activation in brain regions known to be associated with performance of the test, including the bilateral inferior frontal gyri, caudate, and declive/cerebellum (P < .001 for all regions), the authors said.
“These results reveal that patients with multiple sclerosis who are frequent, long-term cannabis users can show significant improvements in memory, processing speed, and executive function after 28 days of drug abstinence,” the authors reported.
Addiction, distinguishing cannabis from MS symptoms
Dr. Bowling said that, while the findings are consistent with his own clinical observations, abstinence isn’t always easy. “I’ve seen patients with cognitive impairment whose cognition and overall day-to-day function have improved with discontinuation of cannabis,” he said. “For some of these patients, however, it was a long-term challenge to discontinue cannabis because they were addicted.”
Addiction to cannabis in MS in fact may be more common than many realize, and comes with a host of other adverse effects, Dr. Bowling said. “In my practice, I have definitely seen many cases of addiction. I think that it’s very underdiagnosed. In addition to cognitive dysfunction, it can worsen anxiety and depression and decrease balance, leading to falls.”
The RCVS risk is another concern, and changes in liver enzymes should also raise a red flag when MS patients are cannabis users, Bowling added.
“I’ve seen in multiple patients where the liver enzymes went up and I thought it was because of the disease-modifying therapy, but it turned out to have been because the patient had started CBD, so you need to be aware of potential hepatotoxicity.”
“The bottom line is that we don’t have strong data in this area and herbs are extremely complex with many unknown constituents.”
Dr. Bowling noted that pure CBD or CBD-enriched products would be expected to produce less cognitive dysfunction than does regular cannabis smoking, “however, it’s important to keep in mind that a ‘CBD-enriched’ product could have low but still significant THC content,” he said.
Dr. Bowling reported relationships with Bristol-Myers Squibb, EMD Serono, Genentech, Genzyme, Greenwich Biosciences, and Novartis, and he received royalties from Springer Publishing.
A version of this article originally appeared on Medscape.com.
From CMSC 2020
Today’s Top News Highlights: Your coding questions answered, biologics and melanoma, and more
Here are the stories our MDedge editors across specialties think you need to know about today:
Answers to your top telehealth coding questions
How long can we continue using telehealth? How do I select a level of office visit? How do I bill for behavioral health services if I am not able to conduct in-person visits?
Our coding expert has fielded these and other questions from physicians ever since the Centers for Medicare & Medicaid Services expanded use of telehealth during the COVID-19 emergency. Find the answers to these questions and get more expert tips on how to code properly to miximize reimbursement.
Read more.
Asymptomatic COVID-19 spread
A WHO official has stated that it appears to be “rare” that an asymptomatic individual can pass SARS-CoV-2 to someone else.
“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,” Maria Van Kerkhove, PhD, WHO’s COVID-19 technical lead and an infectious disease epidemiologist, said June 8 at a news briefing from the agency’s Geneva headquarters.
This announcement came on the heels of the publication of an analysis in the Annals of Internal Medicine, which suggested that as many as 40-45% of COVID-19 cases may be asymptomatic. In this paper, the authors, Daniel P. Oran, AM, and Eric J. Topol, MD, of the Scripps Research Translational Institute in La Jolla, Calif stated: “The likelihood that approximately 40%-45% of those infected with SARS-CoV-2 will remain asymptomatic suggests that the virus might have greater potential than previously estimated to spread silently and deeply through human populations.” Read more.
Biologics and melanoma risk
New data suggest patients taking biologics for inflammatory bowel disease, rheumatoid arthritis, or psoriasis may have an increased risk of melanoma, but the association was not statistically significant in a systematic review and meta-analysis.
The study, published in JAMA Dermatology, assessed melanoma risk in 34,029 patients receiving biologics and 135,370 patients receiving conventional systemic therapy for IBD, RA, or psoriasis, using data from seven cohort studies.
The researchers analyzed the pooled relative risk across all studies. Compared with patients who received conventional systemic therapy, there was a nonsignificant association with risk of melanoma in patients with psoriasis (hazard ratio, 1.57), RA (pooled relative risk, 1.20), and IBD (pRR, 1.20).
Previous studies that have found an increased risk of melanoma in patients on biologics for these three conditions have “typically used the general population as the comparator,” the investigators noted. There is a large amount of evidence that has established short-term efficacy and safety of biologics, compared with conventional systemic treatments, but concerns about longer-term cancer risk associated with biologics remains a concern. “We advocate for more large, well-designed studies of this issue to be performed to help improve certainty,” the researchers said.
Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Answers to your top telehealth coding questions
How long can we continue using telehealth? How do I select a level of office visit? How do I bill for behavioral health services if I am not able to conduct in-person visits?
Our coding expert has fielded these and other questions from physicians ever since the Centers for Medicare & Medicaid Services expanded use of telehealth during the COVID-19 emergency. Find the answers to these questions and get more expert tips on how to code properly to miximize reimbursement.
Read more.
Asymptomatic COVID-19 spread
A WHO official has stated that it appears to be “rare” that an asymptomatic individual can pass SARS-CoV-2 to someone else.
“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,” Maria Van Kerkhove, PhD, WHO’s COVID-19 technical lead and an infectious disease epidemiologist, said June 8 at a news briefing from the agency’s Geneva headquarters.
This announcement came on the heels of the publication of an analysis in the Annals of Internal Medicine, which suggested that as many as 40-45% of COVID-19 cases may be asymptomatic. In this paper, the authors, Daniel P. Oran, AM, and Eric J. Topol, MD, of the Scripps Research Translational Institute in La Jolla, Calif stated: “The likelihood that approximately 40%-45% of those infected with SARS-CoV-2 will remain asymptomatic suggests that the virus might have greater potential than previously estimated to spread silently and deeply through human populations.” Read more.
Biologics and melanoma risk
New data suggest patients taking biologics for inflammatory bowel disease, rheumatoid arthritis, or psoriasis may have an increased risk of melanoma, but the association was not statistically significant in a systematic review and meta-analysis.
The study, published in JAMA Dermatology, assessed melanoma risk in 34,029 patients receiving biologics and 135,370 patients receiving conventional systemic therapy for IBD, RA, or psoriasis, using data from seven cohort studies.
The researchers analyzed the pooled relative risk across all studies. Compared with patients who received conventional systemic therapy, there was a nonsignificant association with risk of melanoma in patients with psoriasis (hazard ratio, 1.57), RA (pooled relative risk, 1.20), and IBD (pRR, 1.20).
Previous studies that have found an increased risk of melanoma in patients on biologics for these three conditions have “typically used the general population as the comparator,” the investigators noted. There is a large amount of evidence that has established short-term efficacy and safety of biologics, compared with conventional systemic treatments, but concerns about longer-term cancer risk associated with biologics remains a concern. “We advocate for more large, well-designed studies of this issue to be performed to help improve certainty,” the researchers said.
Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Answers to your top telehealth coding questions
How long can we continue using telehealth? How do I select a level of office visit? How do I bill for behavioral health services if I am not able to conduct in-person visits?
Our coding expert has fielded these and other questions from physicians ever since the Centers for Medicare & Medicaid Services expanded use of telehealth during the COVID-19 emergency. Find the answers to these questions and get more expert tips on how to code properly to miximize reimbursement.
Read more.
Asymptomatic COVID-19 spread
A WHO official has stated that it appears to be “rare” that an asymptomatic individual can pass SARS-CoV-2 to someone else.
“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,” Maria Van Kerkhove, PhD, WHO’s COVID-19 technical lead and an infectious disease epidemiologist, said June 8 at a news briefing from the agency’s Geneva headquarters.
This announcement came on the heels of the publication of an analysis in the Annals of Internal Medicine, which suggested that as many as 40-45% of COVID-19 cases may be asymptomatic. In this paper, the authors, Daniel P. Oran, AM, and Eric J. Topol, MD, of the Scripps Research Translational Institute in La Jolla, Calif stated: “The likelihood that approximately 40%-45% of those infected with SARS-CoV-2 will remain asymptomatic suggests that the virus might have greater potential than previously estimated to spread silently and deeply through human populations.” Read more.
Biologics and melanoma risk
New data suggest patients taking biologics for inflammatory bowel disease, rheumatoid arthritis, or psoriasis may have an increased risk of melanoma, but the association was not statistically significant in a systematic review and meta-analysis.
The study, published in JAMA Dermatology, assessed melanoma risk in 34,029 patients receiving biologics and 135,370 patients receiving conventional systemic therapy for IBD, RA, or psoriasis, using data from seven cohort studies.
The researchers analyzed the pooled relative risk across all studies. Compared with patients who received conventional systemic therapy, there was a nonsignificant association with risk of melanoma in patients with psoriasis (hazard ratio, 1.57), RA (pooled relative risk, 1.20), and IBD (pRR, 1.20).
Previous studies that have found an increased risk of melanoma in patients on biologics for these three conditions have “typically used the general population as the comparator,” the investigators noted. There is a large amount of evidence that has established short-term efficacy and safety of biologics, compared with conventional systemic treatments, but concerns about longer-term cancer risk associated with biologics remains a concern. “We advocate for more large, well-designed studies of this issue to be performed to help improve certainty,” the researchers said.
Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Doctors’ top telehealth coding questions answered
The coding expert answers your questions
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it here.
Telehealth: Frequently asked questions
Since the Centers for Medicare & Medicaid Services (CMS) expanded use of telehealth during the COVID-19 emergency, I’ve seen various follow-up questions coming from physicians. Here are the most common ones received and some guidance.
Q: How long can we continue using telehealth?
A: Private payers will set their own rules for the end date. For Medicare, telehealth is allowed until the end of the public health emergency. Department of Health & Human Services Secretary Alex M. Azar II renewed the status of the public health emergency, effective April 26, 2020, for an additional 90 days.
Q: Can I bill Medicare annual wellness visits via telehealth?
A: Yes, you can bill the initial and subsequent Medicare wellness visits (G0438, G0439) via telehealth, but the Welcome to Medicare visit (G0402) is not on the list of telehealth services.
In fact, the wellness visits mentioned above may be billed with audio-only communications because of the expansion of telehealth services, although these visits require height, weight, BMI calculation, and blood pressure, and CMS has not issued guidance about whether the patient’s self-reported measurements are sufficient or whether they can be deferred.
Q: Can I bill an office visit via telehealth?
A: Yes, you may bill new and established patient visits 99201-99215 via telehealth, but for Medicare, these still require the use of real-time, audio-visual communications equipment.
Q: Can I bill an office visit conducted via telephone only?
A: For Medicare patients, you may not bill office visit codes for audio only communication. If there is audio only, use phone call codes 99441-99443. In order to bill an office visit, with codes 99201-99215 to a Medicare patient, audio and visual, real time communication is required. Some state Medicaid programs and private insurers allow office visits to be billed with audio equipment only, so check your state requirements.
Q: How do I select a level of office visit?
A: CMS’s announcement on March 31 relaxed the rules for practitioners to select a level of service for office and other patient services (99201-99215). CMS stated that clinicians could use either total time or medical decision-making to select a code.
If using time, count the practitioner’s total time for the visit, both face to face and non–face to face. It does not need to be greater than 50% in counseling. If using medical decision-making, history and exam are not needed to select the level of service. Medical decision-making alone can be used to select the code.
Q: Can I count the time it takes my medical assistant to set up the audio-visual communication with a patient?
A: No, you cannot count staff time in coding and billing a patient visit in this manner.
Q: Is there a code for a registered nurse to use for making phone calls with patients?
A: No, unfortunately.
Q: How do I know if a service can be billed with phone only?
A: These are indicated as “yes” on CMS’s list of covered telehealth services as allowed via audio only.
Providing mental health services during COVID-19
Q: I am a mental health provider who finds himself trying to provide the best care for my patients during this pandemic. How do I bill for behavioral health services if I am not able to conduct in-person visits?
A: Psychiatrists and behavioral health professionals can perform psychiatric diagnostic evaluations and psychotherapy over the phone during the public health emergency.
The use of real-time, audio-visual communication equipment is not required. This is one of the many changes CMS made in its interim final rule regarding COVID-19, released April 30.
Not only did CMS update the list of Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes that could be reported via real-time, audio-visual communication, but it also added a column to guidance on covered telehealth services: “Can Audio-only Interaction Meet the Requirements?” The codes for psychiatric diagnostic evaluations and psychotherapy are indicated as “yes.”
In addition to psychiatric diagnostic evaluations and time-based psychotherapy codes, psychotherapy for crisis, family, and group psychotherapy can be done with audio-only technology.
CMS has issued multiple waivers and two major rules that greatly expand the ability of medical practices to treat patients without requiring an in-person visit. This latest change, allowing some services to be performed with audio equipment only, is remarkable.
For Medicare patients, report the place of service that would have been used if the patient was seen in person. This could be office (POS 11), outpatient department (POS 19, 21), or community mental health center (POS 53).
Some private payers require the place of service for telehealth (02). The lack of consistency between payers is difficult for practices. Append modifier 95 to the CPT code for all payers. The definition of modifier 95 is “synchronous telemedicine service using audio and visual communication.” However, as CMS added these services to the telehealth list, use modifier 95.
Have a coding question? Send it in and it may be answered in a future column. (Please be sure to note your specialty in the text of the question.)
Betsy Nicoletti, MS, is a consultant, author, and speaker, as well as the founder of CodingIntel.com, a library of medical practice coding resources.
A version of this article originally appeared on Medscape.com.
The coding expert answers your questions
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it here.
Telehealth: Frequently asked questions
Since the Centers for Medicare & Medicaid Services (CMS) expanded use of telehealth during the COVID-19 emergency, I’ve seen various follow-up questions coming from physicians. Here are the most common ones received and some guidance.
Q: How long can we continue using telehealth?
A: Private payers will set their own rules for the end date. For Medicare, telehealth is allowed until the end of the public health emergency. Department of Health & Human Services Secretary Alex M. Azar II renewed the status of the public health emergency, effective April 26, 2020, for an additional 90 days.
Q: Can I bill Medicare annual wellness visits via telehealth?
A: Yes, you can bill the initial and subsequent Medicare wellness visits (G0438, G0439) via telehealth, but the Welcome to Medicare visit (G0402) is not on the list of telehealth services.
In fact, the wellness visits mentioned above may be billed with audio-only communications because of the expansion of telehealth services, although these visits require height, weight, BMI calculation, and blood pressure, and CMS has not issued guidance about whether the patient’s self-reported measurements are sufficient or whether they can be deferred.
Q: Can I bill an office visit via telehealth?
A: Yes, you may bill new and established patient visits 99201-99215 via telehealth, but for Medicare, these still require the use of real-time, audio-visual communications equipment.
Q: Can I bill an office visit conducted via telephone only?
A: For Medicare patients, you may not bill office visit codes for audio only communication. If there is audio only, use phone call codes 99441-99443. In order to bill an office visit, with codes 99201-99215 to a Medicare patient, audio and visual, real time communication is required. Some state Medicaid programs and private insurers allow office visits to be billed with audio equipment only, so check your state requirements.
Q: How do I select a level of office visit?
A: CMS’s announcement on March 31 relaxed the rules for practitioners to select a level of service for office and other patient services (99201-99215). CMS stated that clinicians could use either total time or medical decision-making to select a code.
If using time, count the practitioner’s total time for the visit, both face to face and non–face to face. It does not need to be greater than 50% in counseling. If using medical decision-making, history and exam are not needed to select the level of service. Medical decision-making alone can be used to select the code.
Q: Can I count the time it takes my medical assistant to set up the audio-visual communication with a patient?
A: No, you cannot count staff time in coding and billing a patient visit in this manner.
Q: Is there a code for a registered nurse to use for making phone calls with patients?
A: No, unfortunately.
Q: How do I know if a service can be billed with phone only?
A: These are indicated as “yes” on CMS’s list of covered telehealth services as allowed via audio only.
Providing mental health services during COVID-19
Q: I am a mental health provider who finds himself trying to provide the best care for my patients during this pandemic. How do I bill for behavioral health services if I am not able to conduct in-person visits?
A: Psychiatrists and behavioral health professionals can perform psychiatric diagnostic evaluations and psychotherapy over the phone during the public health emergency.
The use of real-time, audio-visual communication equipment is not required. This is one of the many changes CMS made in its interim final rule regarding COVID-19, released April 30.
Not only did CMS update the list of Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes that could be reported via real-time, audio-visual communication, but it also added a column to guidance on covered telehealth services: “Can Audio-only Interaction Meet the Requirements?” The codes for psychiatric diagnostic evaluations and psychotherapy are indicated as “yes.”
In addition to psychiatric diagnostic evaluations and time-based psychotherapy codes, psychotherapy for crisis, family, and group psychotherapy can be done with audio-only technology.
CMS has issued multiple waivers and two major rules that greatly expand the ability of medical practices to treat patients without requiring an in-person visit. This latest change, allowing some services to be performed with audio equipment only, is remarkable.
For Medicare patients, report the place of service that would have been used if the patient was seen in person. This could be office (POS 11), outpatient department (POS 19, 21), or community mental health center (POS 53).
Some private payers require the place of service for telehealth (02). The lack of consistency between payers is difficult for practices. Append modifier 95 to the CPT code for all payers. The definition of modifier 95 is “synchronous telemedicine service using audio and visual communication.” However, as CMS added these services to the telehealth list, use modifier 95.
Have a coding question? Send it in and it may be answered in a future column. (Please be sure to note your specialty in the text of the question.)
Betsy Nicoletti, MS, is a consultant, author, and speaker, as well as the founder of CodingIntel.com, a library of medical practice coding resources.
A version of this article originally appeared on Medscape.com.
The coding expert answers your questions
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it here.
Telehealth: Frequently asked questions
Since the Centers for Medicare & Medicaid Services (CMS) expanded use of telehealth during the COVID-19 emergency, I’ve seen various follow-up questions coming from physicians. Here are the most common ones received and some guidance.
Q: How long can we continue using telehealth?
A: Private payers will set their own rules for the end date. For Medicare, telehealth is allowed until the end of the public health emergency. Department of Health & Human Services Secretary Alex M. Azar II renewed the status of the public health emergency, effective April 26, 2020, for an additional 90 days.
Q: Can I bill Medicare annual wellness visits via telehealth?
A: Yes, you can bill the initial and subsequent Medicare wellness visits (G0438, G0439) via telehealth, but the Welcome to Medicare visit (G0402) is not on the list of telehealth services.
In fact, the wellness visits mentioned above may be billed with audio-only communications because of the expansion of telehealth services, although these visits require height, weight, BMI calculation, and blood pressure, and CMS has not issued guidance about whether the patient’s self-reported measurements are sufficient or whether they can be deferred.
Q: Can I bill an office visit via telehealth?
A: Yes, you may bill new and established patient visits 99201-99215 via telehealth, but for Medicare, these still require the use of real-time, audio-visual communications equipment.
Q: Can I bill an office visit conducted via telephone only?
A: For Medicare patients, you may not bill office visit codes for audio only communication. If there is audio only, use phone call codes 99441-99443. In order to bill an office visit, with codes 99201-99215 to a Medicare patient, audio and visual, real time communication is required. Some state Medicaid programs and private insurers allow office visits to be billed with audio equipment only, so check your state requirements.
Q: How do I select a level of office visit?
A: CMS’s announcement on March 31 relaxed the rules for practitioners to select a level of service for office and other patient services (99201-99215). CMS stated that clinicians could use either total time or medical decision-making to select a code.
If using time, count the practitioner’s total time for the visit, both face to face and non–face to face. It does not need to be greater than 50% in counseling. If using medical decision-making, history and exam are not needed to select the level of service. Medical decision-making alone can be used to select the code.
Q: Can I count the time it takes my medical assistant to set up the audio-visual communication with a patient?
A: No, you cannot count staff time in coding and billing a patient visit in this manner.
Q: Is there a code for a registered nurse to use for making phone calls with patients?
A: No, unfortunately.
Q: How do I know if a service can be billed with phone only?
A: These are indicated as “yes” on CMS’s list of covered telehealth services as allowed via audio only.
Providing mental health services during COVID-19
Q: I am a mental health provider who finds himself trying to provide the best care for my patients during this pandemic. How do I bill for behavioral health services if I am not able to conduct in-person visits?
A: Psychiatrists and behavioral health professionals can perform psychiatric diagnostic evaluations and psychotherapy over the phone during the public health emergency.
The use of real-time, audio-visual communication equipment is not required. This is one of the many changes CMS made in its interim final rule regarding COVID-19, released April 30.
Not only did CMS update the list of Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes that could be reported via real-time, audio-visual communication, but it also added a column to guidance on covered telehealth services: “Can Audio-only Interaction Meet the Requirements?” The codes for psychiatric diagnostic evaluations and psychotherapy are indicated as “yes.”
In addition to psychiatric diagnostic evaluations and time-based psychotherapy codes, psychotherapy for crisis, family, and group psychotherapy can be done with audio-only technology.
CMS has issued multiple waivers and two major rules that greatly expand the ability of medical practices to treat patients without requiring an in-person visit. This latest change, allowing some services to be performed with audio equipment only, is remarkable.
For Medicare patients, report the place of service that would have been used if the patient was seen in person. This could be office (POS 11), outpatient department (POS 19, 21), or community mental health center (POS 53).
Some private payers require the place of service for telehealth (02). The lack of consistency between payers is difficult for practices. Append modifier 95 to the CPT code for all payers. The definition of modifier 95 is “synchronous telemedicine service using audio and visual communication.” However, as CMS added these services to the telehealth list, use modifier 95.
Have a coding question? Send it in and it may be answered in a future column. (Please be sure to note your specialty in the text of the question.)
Betsy Nicoletti, MS, is a consultant, author, and speaker, as well as the founder of CodingIntel.com, a library of medical practice coding resources.
A version of this article originally appeared on Medscape.com.