User login
Report describes intoxication with new psychoactive substance
When evaluated at local emergency departments, lethargy and slurred speech were the most common clinical findings.

One student had mild respiratory depression with a respiratory rate of 10 breaths per minute.
“All patients had sufficient clinical improvement within 6 hours such that they could be discharged from the hospital,” according to a description of the cases that was published online in Pediatrics.
The report is the first to detail clinical toxicity from flualprazolam, and “it is likely that physicians will again encounter patients” with intoxication from this new psychoactive drug, said Adam Blumenberg, MD, of Oregon Health & Science University in Portland and colleagues.
Internet purchasing has increased rates of exposure to new psychoactive substances since the early 2000s, and law enforcement agents have seized tons of these drugs. “In the United States, the incidence of exposures to designer benzodiazepines in particular has been rising since 2014,” the authors said.
According to an addiction researcher, the COVID-19 pandemic may exacerbate abuse of designer benzodiazepines.

“This is an important paper describing what medical examiners, pathologists, and emergency rooms have been seeing recently – an increase in designer benzodiazepines,” commented Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis. “Recent increases in these drugs have started to be seen in many locations as the traditional drugs of abuse, grown and distributed in bulk, have been disrupted” by the pandemic, he said in an interview. Although it may be too early for such cases to appear in Centers for Disease Control and Prevention reports, they can be described in studies like this one and, “I suspect, sadly, in medical examiner case reports.”
Flualprazolam, known colloquially as Hulk, is structurally related to the Food and Drug Administration–approved drugs alprazolam and triazolam. During 1 week in June 2019, the patients in Oregon received the drug as a free sample from another student from their Oregon high school. They believed it was commercial Xanax (alprazolam). “The flualprazolam tablets were identical in appearance and labeling to 2-mg tablets of alprazolam,” according to the report. “This indicates an intentionally counterfeit product entering the drug supply chain.”
Five of the six patients were boys, and they ranged in age from 14 to 16 years. The patient with mild respiratory depression received 0.4-mg naloxone, which physicians gave empirically because of the unknown identity of the drug, but did not respond. Two of the six patients initially felt drowsy but were asymptomatic during the clinical evaluation.
A urine immunoassay was performed in five of the patients, and all tested positive for benzodiazepines. One patient also tested positive for cannabinoids. Analysis of a tablet fragment revealed that it contained flualprazolam.
“Although flualprazolam intoxication cannot be clinically differentiated from that of other benzodiazepines without advanced testing, patient management should be the same,” Dr. Blumenberg and coauthors said. “For mild to moderate intoxication, patients should be treated with close monitoring and supportive care until symptom resolution. The benzodiazepine antidote flumazenil may be considered a safe and effective antidote in pediatric patients with significant CNS or respiratory depression. In patients for whom there is a concern of benzodiazepine dependence and flumazenil-induced seizures, airway protection and mechanical ventilation may be considered.”
Although patients rarely die from isolated benzodiazepine toxicity, death from respiratory depression or aspiration is more common when benzodiazepine toxicity occurs “in combination with alcohol, opioids, or other sedatives,” the authors noted. In addition, counterfeit alprazolam tablets have contained adulterants such as fentanyl and the opioid U-47700, which can be deadly.
The authors had no relevant financial disclosures, and there was no external funding for the study.
SOURCE: Blumenberg A et al. Pediatrics. 2020 Jun 24. doi: 10.1542/peds.2019-2953.
When evaluated at local emergency departments, lethargy and slurred speech were the most common clinical findings.
One student had mild respiratory depression with a respiratory rate of 10 breaths per minute.
“All patients had sufficient clinical improvement within 6 hours such that they could be discharged from the hospital,” according to a description of the cases that was published online in Pediatrics.
The report is the first to detail clinical toxicity from flualprazolam, and “it is likely that physicians will again encounter patients” with intoxication from this new psychoactive drug, said Adam Blumenberg, MD, of Oregon Health & Science University in Portland and colleagues.
Internet purchasing has increased rates of exposure to new psychoactive substances since the early 2000s, and law enforcement agents have seized tons of these drugs. “In the United States, the incidence of exposures to designer benzodiazepines in particular has been rising since 2014,” the authors said.
According to an addiction researcher, the COVID-19 pandemic may exacerbate abuse of designer benzodiazepines.
“This is an important paper describing what medical examiners, pathologists, and emergency rooms have been seeing recently – an increase in designer benzodiazepines,” commented Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis. “Recent increases in these drugs have started to be seen in many locations as the traditional drugs of abuse, grown and distributed in bulk, have been disrupted” by the pandemic, he said in an interview. Although it may be too early for such cases to appear in Centers for Disease Control and Prevention reports, they can be described in studies like this one and, “I suspect, sadly, in medical examiner case reports.”
Flualprazolam, known colloquially as Hulk, is structurally related to the Food and Drug Administration–approved drugs alprazolam and triazolam. During 1 week in June 2019, the patients in Oregon received the drug as a free sample from another student from their Oregon high school. They believed it was commercial Xanax (alprazolam). “The flualprazolam tablets were identical in appearance and labeling to 2-mg tablets of alprazolam,” according to the report. “This indicates an intentionally counterfeit product entering the drug supply chain.”
Five of the six patients were boys, and they ranged in age from 14 to 16 years. The patient with mild respiratory depression received 0.4-mg naloxone, which physicians gave empirically because of the unknown identity of the drug, but did not respond. Two of the six patients initially felt drowsy but were asymptomatic during the clinical evaluation.
A urine immunoassay was performed in five of the patients, and all tested positive for benzodiazepines. One patient also tested positive for cannabinoids. Analysis of a tablet fragment revealed that it contained flualprazolam.
“Although flualprazolam intoxication cannot be clinically differentiated from that of other benzodiazepines without advanced testing, patient management should be the same,” Dr. Blumenberg and coauthors said. “For mild to moderate intoxication, patients should be treated with close monitoring and supportive care until symptom resolution. The benzodiazepine antidote flumazenil may be considered a safe and effective antidote in pediatric patients with significant CNS or respiratory depression. In patients for whom there is a concern of benzodiazepine dependence and flumazenil-induced seizures, airway protection and mechanical ventilation may be considered.”
Although patients rarely die from isolated benzodiazepine toxicity, death from respiratory depression or aspiration is more common when benzodiazepine toxicity occurs “in combination with alcohol, opioids, or other sedatives,” the authors noted. In addition, counterfeit alprazolam tablets have contained adulterants such as fentanyl and the opioid U-47700, which can be deadly.
The authors had no relevant financial disclosures, and there was no external funding for the study.
SOURCE: Blumenberg A et al. Pediatrics. 2020 Jun 24. doi: 10.1542/peds.2019-2953.
When evaluated at local emergency departments, lethargy and slurred speech were the most common clinical findings.
One student had mild respiratory depression with a respiratory rate of 10 breaths per minute.
“All patients had sufficient clinical improvement within 6 hours such that they could be discharged from the hospital,” according to a description of the cases that was published online in Pediatrics.
The report is the first to detail clinical toxicity from flualprazolam, and “it is likely that physicians will again encounter patients” with intoxication from this new psychoactive drug, said Adam Blumenberg, MD, of Oregon Health & Science University in Portland and colleagues.
Internet purchasing has increased rates of exposure to new psychoactive substances since the early 2000s, and law enforcement agents have seized tons of these drugs. “In the United States, the incidence of exposures to designer benzodiazepines in particular has been rising since 2014,” the authors said.
According to an addiction researcher, the COVID-19 pandemic may exacerbate abuse of designer benzodiazepines.
“This is an important paper describing what medical examiners, pathologists, and emergency rooms have been seeing recently – an increase in designer benzodiazepines,” commented Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis. “Recent increases in these drugs have started to be seen in many locations as the traditional drugs of abuse, grown and distributed in bulk, have been disrupted” by the pandemic, he said in an interview. Although it may be too early for such cases to appear in Centers for Disease Control and Prevention reports, they can be described in studies like this one and, “I suspect, sadly, in medical examiner case reports.”
Flualprazolam, known colloquially as Hulk, is structurally related to the Food and Drug Administration–approved drugs alprazolam and triazolam. During 1 week in June 2019, the patients in Oregon received the drug as a free sample from another student from their Oregon high school. They believed it was commercial Xanax (alprazolam). “The flualprazolam tablets were identical in appearance and labeling to 2-mg tablets of alprazolam,” according to the report. “This indicates an intentionally counterfeit product entering the drug supply chain.”
Five of the six patients were boys, and they ranged in age from 14 to 16 years. The patient with mild respiratory depression received 0.4-mg naloxone, which physicians gave empirically because of the unknown identity of the drug, but did not respond. Two of the six patients initially felt drowsy but were asymptomatic during the clinical evaluation.
A urine immunoassay was performed in five of the patients, and all tested positive for benzodiazepines. One patient also tested positive for cannabinoids. Analysis of a tablet fragment revealed that it contained flualprazolam.
“Although flualprazolam intoxication cannot be clinically differentiated from that of other benzodiazepines without advanced testing, patient management should be the same,” Dr. Blumenberg and coauthors said. “For mild to moderate intoxication, patients should be treated with close monitoring and supportive care until symptom resolution. The benzodiazepine antidote flumazenil may be considered a safe and effective antidote in pediatric patients with significant CNS or respiratory depression. In patients for whom there is a concern of benzodiazepine dependence and flumazenil-induced seizures, airway protection and mechanical ventilation may be considered.”
Although patients rarely die from isolated benzodiazepine toxicity, death from respiratory depression or aspiration is more common when benzodiazepine toxicity occurs “in combination with alcohol, opioids, or other sedatives,” the authors noted. In addition, counterfeit alprazolam tablets have contained adulterants such as fentanyl and the opioid U-47700, which can be deadly.
The authors had no relevant financial disclosures, and there was no external funding for the study.
SOURCE: Blumenberg A et al. Pediatrics. 2020 Jun 24. doi: 10.1542/peds.2019-2953.
FROM PEDIATRICS

Black women at highest risk for asthma
Women are much more likely than men to have asthma, and , according to the Centers for Disease Control and Prevention.
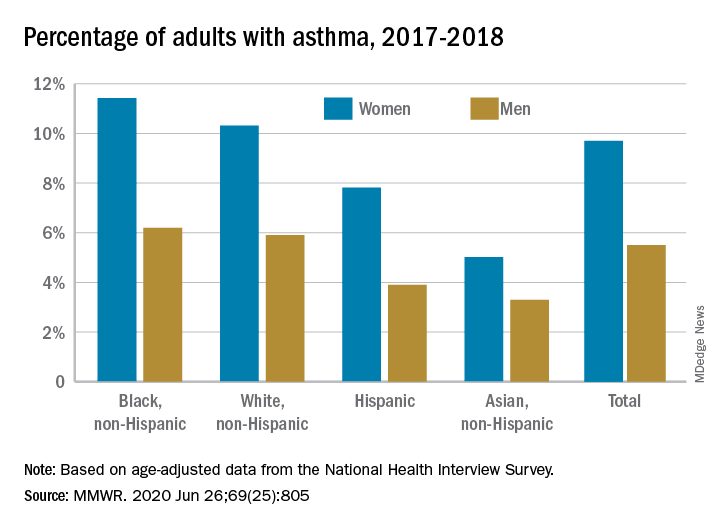
Among all women aged 18 years and older, 9.7% reported that they currently had asthma in 2017-2018, compared with 5.5% of men, based on age-adjusted data from the National Health Interview Survey.
The proportion of black, non-Hispanic women with asthma, however, was even higher, at 11.4%. White non-Hispanic women were next at 10.3%, followed by Hispanic (7.8%) and Asian (5.0%) women, the CDC reported June 26 in the Morbidity and Mortality Weekly Report.
The same pattern held for men: 6.2% of black men had asthma in 2017-2018, compared with 5.9% of whites, 3.9% of Hispanics, and 3.3% of Asian men, the CDC said.
SOURCE: MMWR. 2020 Jun 26;69(25):805.
Women are much more likely than men to have asthma, and , according to the Centers for Disease Control and Prevention.
Among all women aged 18 years and older, 9.7% reported that they currently had asthma in 2017-2018, compared with 5.5% of men, based on age-adjusted data from the National Health Interview Survey.
The proportion of black, non-Hispanic women with asthma, however, was even higher, at 11.4%. White non-Hispanic women were next at 10.3%, followed by Hispanic (7.8%) and Asian (5.0%) women, the CDC reported June 26 in the Morbidity and Mortality Weekly Report.
The same pattern held for men: 6.2% of black men had asthma in 2017-2018, compared with 5.9% of whites, 3.9% of Hispanics, and 3.3% of Asian men, the CDC said.
SOURCE: MMWR. 2020 Jun 26;69(25):805.
Women are much more likely than men to have asthma, and , according to the Centers for Disease Control and Prevention.
Among all women aged 18 years and older, 9.7% reported that they currently had asthma in 2017-2018, compared with 5.5% of men, based on age-adjusted data from the National Health Interview Survey.
The proportion of black, non-Hispanic women with asthma, however, was even higher, at 11.4%. White non-Hispanic women were next at 10.3%, followed by Hispanic (7.8%) and Asian (5.0%) women, the CDC reported June 26 in the Morbidity and Mortality Weekly Report.
The same pattern held for men: 6.2% of black men had asthma in 2017-2018, compared with 5.9% of whites, 3.9% of Hispanics, and 3.3% of Asian men, the CDC said.
SOURCE: MMWR. 2020 Jun 26;69(25):805.
FROM MMWR
Encourage parents to follow pediatric plans for vaccination
Outpatient medical care has been severely disrupted during the COVID-19 pandemic with a reduction of nearly 70% in outpatient visits since March before starting to rebound, Melinda Wharton, MD, said at the virtual meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.

Pediatrics was among the hardest hit specialties, with a 62% reduction in outpatient visits by April 5, said Dr. Wharton, director of the immunization services division at the CDC’s National Center for Immunization and Respiratory Diseases. However, visits for all pediatric age groups increased in May, compared with April, and the CDC emphasized the need to educate families about the importance of routine vaccination and well-child visits, Dr. Wharton said.
The CDC strategies to support routine childhood vaccination include monitoring vaccination service delivery to inform targeted interventions, said Dr. Wharton. In addition, the CDC will continue to support providers by identifying gaps in the Vaccines For Children (VFC) program network, increasing VFC funding, developing guidance materials, and identifying policy interventions.
Many small practices have struggled during the pandemic, and financial support is available through the Provider Relief Fund, which is now available to all Medicaid and Children’s Health Insurance Program (CHIP) providers, said Dr. Wharton.
because more families may now qualify for the program because of changes in job status and income, and parents may not be aware that their children may be eligible, she said.
“Vaccination is an essential medical service for all children and adolescents, ideally in the medical home,” Dr. Wharton said. The CDC’s interim guidance for immunization during the COVID-19 pandemic calls for administering all current or overdue vaccines according to the routine immunization schedule during the same visit, and implementing strategies to get patients caught up, prioritizing newborns, infants, and children up to age 24 months. The guidance includes details on safe delivery of vaccines, including physical distance and the use of personal protective equipment.
In addition, encourage parents to return for well-child visits, and use reminder systems to help keep patients current on visits and vaccines. “Discuss the safety protocols that have been put in place,” Dr. Wharton emphasized. The CDC also offers resources for providers to help communicate with parents about routine vaccination.
Looking ahead, back-to-school vaccination requirements “provide a critical checkpoint for children’s vaccination status,” Dr. Wharton said. Catch-up vaccination during the summer will help clinical capacity manage back-to-school and influenza vaccination in the fall, she emphasized. “Influenza vaccination will be an important strategy to decrease stress on our health care system.”
Flu vaccination strategies should focus on adults at higher risk for COVID-19 infections, such as health care providers. In addition, identifying and reducing disparities will be important for future COVID-19 vaccines, as well as for the flu this season, she noted.
View the complete guidance online.
Dr. Wharton had no relevant financial disclosures.
Outpatient medical care has been severely disrupted during the COVID-19 pandemic with a reduction of nearly 70% in outpatient visits since March before starting to rebound, Melinda Wharton, MD, said at the virtual meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
Pediatrics was among the hardest hit specialties, with a 62% reduction in outpatient visits by April 5, said Dr. Wharton, director of the immunization services division at the CDC’s National Center for Immunization and Respiratory Diseases. However, visits for all pediatric age groups increased in May, compared with April, and the CDC emphasized the need to educate families about the importance of routine vaccination and well-child visits, Dr. Wharton said.
The CDC strategies to support routine childhood vaccination include monitoring vaccination service delivery to inform targeted interventions, said Dr. Wharton. In addition, the CDC will continue to support providers by identifying gaps in the Vaccines For Children (VFC) program network, increasing VFC funding, developing guidance materials, and identifying policy interventions.
Many small practices have struggled during the pandemic, and financial support is available through the Provider Relief Fund, which is now available to all Medicaid and Children’s Health Insurance Program (CHIP) providers, said Dr. Wharton.
because more families may now qualify for the program because of changes in job status and income, and parents may not be aware that their children may be eligible, she said.
“Vaccination is an essential medical service for all children and adolescents, ideally in the medical home,” Dr. Wharton said. The CDC’s interim guidance for immunization during the COVID-19 pandemic calls for administering all current or overdue vaccines according to the routine immunization schedule during the same visit, and implementing strategies to get patients caught up, prioritizing newborns, infants, and children up to age 24 months. The guidance includes details on safe delivery of vaccines, including physical distance and the use of personal protective equipment.
In addition, encourage parents to return for well-child visits, and use reminder systems to help keep patients current on visits and vaccines. “Discuss the safety protocols that have been put in place,” Dr. Wharton emphasized. The CDC also offers resources for providers to help communicate with parents about routine vaccination.
Looking ahead, back-to-school vaccination requirements “provide a critical checkpoint for children’s vaccination status,” Dr. Wharton said. Catch-up vaccination during the summer will help clinical capacity manage back-to-school and influenza vaccination in the fall, she emphasized. “Influenza vaccination will be an important strategy to decrease stress on our health care system.”
Flu vaccination strategies should focus on adults at higher risk for COVID-19 infections, such as health care providers. In addition, identifying and reducing disparities will be important for future COVID-19 vaccines, as well as for the flu this season, she noted.
View the complete guidance online.
Dr. Wharton had no relevant financial disclosures.
Outpatient medical care has been severely disrupted during the COVID-19 pandemic with a reduction of nearly 70% in outpatient visits since March before starting to rebound, Melinda Wharton, MD, said at the virtual meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
Pediatrics was among the hardest hit specialties, with a 62% reduction in outpatient visits by April 5, said Dr. Wharton, director of the immunization services division at the CDC’s National Center for Immunization and Respiratory Diseases. However, visits for all pediatric age groups increased in May, compared with April, and the CDC emphasized the need to educate families about the importance of routine vaccination and well-child visits, Dr. Wharton said.
The CDC strategies to support routine childhood vaccination include monitoring vaccination service delivery to inform targeted interventions, said Dr. Wharton. In addition, the CDC will continue to support providers by identifying gaps in the Vaccines For Children (VFC) program network, increasing VFC funding, developing guidance materials, and identifying policy interventions.
Many small practices have struggled during the pandemic, and financial support is available through the Provider Relief Fund, which is now available to all Medicaid and Children’s Health Insurance Program (CHIP) providers, said Dr. Wharton.
because more families may now qualify for the program because of changes in job status and income, and parents may not be aware that their children may be eligible, she said.
“Vaccination is an essential medical service for all children and adolescents, ideally in the medical home,” Dr. Wharton said. The CDC’s interim guidance for immunization during the COVID-19 pandemic calls for administering all current or overdue vaccines according to the routine immunization schedule during the same visit, and implementing strategies to get patients caught up, prioritizing newborns, infants, and children up to age 24 months. The guidance includes details on safe delivery of vaccines, including physical distance and the use of personal protective equipment.
In addition, encourage parents to return for well-child visits, and use reminder systems to help keep patients current on visits and vaccines. “Discuss the safety protocols that have been put in place,” Dr. Wharton emphasized. The CDC also offers resources for providers to help communicate with parents about routine vaccination.
Looking ahead, back-to-school vaccination requirements “provide a critical checkpoint for children’s vaccination status,” Dr. Wharton said. Catch-up vaccination during the summer will help clinical capacity manage back-to-school and influenza vaccination in the fall, she emphasized. “Influenza vaccination will be an important strategy to decrease stress on our health care system.”
Flu vaccination strategies should focus on adults at higher risk for COVID-19 infections, such as health care providers. In addition, identifying and reducing disparities will be important for future COVID-19 vaccines, as well as for the flu this season, she noted.
View the complete guidance online.
Dr. Wharton had no relevant financial disclosures.
Daily Recap: Higher risk of severe COVID-19 seen in pregnancy, primary care practices at risk
Here are the stories our MDedge editors across specialties think you need to know about today:
Pregnant women at higher risk for severe COVID-19
Pregnant women may be at increased risk for severe COVID-19 illness, according to a report published online June 26 in Morbidity and Mortality Weekly Report.
Among reproductive-aged women (15-44 years) infected with SARS-CoV-2, pregnancy was associated with a greater likelihood of hospitalization, admission to the intensive care unit (ICU), and mechanical ventilation, but not death. Pregnant women were 5.4 times more likely to be hospitalized, 1.5 times more likely to be admitted to the ICU, and 1.7 times more likely to need mechanical ventilation, after adjustment for age, underlying conditions, and race/ethnicity.
CDC researchers said that preventing COVID-19 infection in pregnant women should be a priority and any potential barriers to compliance with preventive measures need to be removed.
“During pregnancy, women experience immunologic and physiologic changes that could increase their risk for more severe illness from respiratory infections,” they wrote. Read more.
Going out of business: Primary care practices at risk
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. In an interview with Kenny Lin, MD, MPH, a family physician, Dr. Frieden discussed the future of primary care.
Here is a sample of Dr. Frieden’s observations:
“When I’ve looked around the United States, I’ve been extremely concerned about both the risk that primary care practitioners are subjected to in their everyday practice and the economic risk that we could lose many of our primary care practices around the country. It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.” Read more.
Surge in out-of-hospital cardiac arrests
The COVID-19 pandemic in New York City led to a surge in out-of-hospital cardiac arrests that placed a huge burden on first responders, according to a new analysis.
During the height of the pandemic in New York, there was a “dramatic increase in cardiopulmonary arrests, nearly all presented in non-shockable cardiac rhythms (> 90% fatality rate) and vulnerable patient populations were most affected,” David J. Prezant, MD, chief medical officer, Fire Department of New York (FDNY), said in an interview.
In a news release, Dr. Prezant noted that “relatively few, if any, patients were tested to confirm the presence of COVID-19,” making it impossible to distinguish between cardiac arrests as a result of COVID-19 and those that may have resulted from other health conditions.
“We also can’t rule out the possibility that some people may have died from delays in seeking or receiving treatment for non–COVID-19-related conditions. However, the dramatic increase in cardiac arrests compared to the same period in 2019 strongly indicates that the pandemic was directly or indirectly responsible for that surge in cardiac arrests and deaths,” said Dr. Prezant.
The study was published online June 19 in JAMA Cardiology.
Read more.
Fenfluramine approved for Dravet syndrome
The U.S. Food and Drug Administration has approved fenfluramine (Fintepla, Zogenix) oral solution, a Schedule IV controlled substance, for the treatment of seizures associated with Dravet syndrome in children age 2 years and older.
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy.
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Pregnant women at higher risk for severe COVID-19
Pregnant women may be at increased risk for severe COVID-19 illness, according to a report published online June 26 in Morbidity and Mortality Weekly Report.
Among reproductive-aged women (15-44 years) infected with SARS-CoV-2, pregnancy was associated with a greater likelihood of hospitalization, admission to the intensive care unit (ICU), and mechanical ventilation, but not death. Pregnant women were 5.4 times more likely to be hospitalized, 1.5 times more likely to be admitted to the ICU, and 1.7 times more likely to need mechanical ventilation, after adjustment for age, underlying conditions, and race/ethnicity.
CDC researchers said that preventing COVID-19 infection in pregnant women should be a priority and any potential barriers to compliance with preventive measures need to be removed.
“During pregnancy, women experience immunologic and physiologic changes that could increase their risk for more severe illness from respiratory infections,” they wrote. Read more.
Going out of business: Primary care practices at risk
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. In an interview with Kenny Lin, MD, MPH, a family physician, Dr. Frieden discussed the future of primary care.
Here is a sample of Dr. Frieden’s observations:
“When I’ve looked around the United States, I’ve been extremely concerned about both the risk that primary care practitioners are subjected to in their everyday practice and the economic risk that we could lose many of our primary care practices around the country. It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.” Read more.
Surge in out-of-hospital cardiac arrests
The COVID-19 pandemic in New York City led to a surge in out-of-hospital cardiac arrests that placed a huge burden on first responders, according to a new analysis.
During the height of the pandemic in New York, there was a “dramatic increase in cardiopulmonary arrests, nearly all presented in non-shockable cardiac rhythms (> 90% fatality rate) and vulnerable patient populations were most affected,” David J. Prezant, MD, chief medical officer, Fire Department of New York (FDNY), said in an interview.
In a news release, Dr. Prezant noted that “relatively few, if any, patients were tested to confirm the presence of COVID-19,” making it impossible to distinguish between cardiac arrests as a result of COVID-19 and those that may have resulted from other health conditions.
“We also can’t rule out the possibility that some people may have died from delays in seeking or receiving treatment for non–COVID-19-related conditions. However, the dramatic increase in cardiac arrests compared to the same period in 2019 strongly indicates that the pandemic was directly or indirectly responsible for that surge in cardiac arrests and deaths,” said Dr. Prezant.
The study was published online June 19 in JAMA Cardiology.
Read more.
Fenfluramine approved for Dravet syndrome
The U.S. Food and Drug Administration has approved fenfluramine (Fintepla, Zogenix) oral solution, a Schedule IV controlled substance, for the treatment of seizures associated with Dravet syndrome in children age 2 years and older.
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy.
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Pregnant women at higher risk for severe COVID-19
Pregnant women may be at increased risk for severe COVID-19 illness, according to a report published online June 26 in Morbidity and Mortality Weekly Report.
Among reproductive-aged women (15-44 years) infected with SARS-CoV-2, pregnancy was associated with a greater likelihood of hospitalization, admission to the intensive care unit (ICU), and mechanical ventilation, but not death. Pregnant women were 5.4 times more likely to be hospitalized, 1.5 times more likely to be admitted to the ICU, and 1.7 times more likely to need mechanical ventilation, after adjustment for age, underlying conditions, and race/ethnicity.
CDC researchers said that preventing COVID-19 infection in pregnant women should be a priority and any potential barriers to compliance with preventive measures need to be removed.
“During pregnancy, women experience immunologic and physiologic changes that could increase their risk for more severe illness from respiratory infections,” they wrote. Read more.
Going out of business: Primary care practices at risk
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. In an interview with Kenny Lin, MD, MPH, a family physician, Dr. Frieden discussed the future of primary care.
Here is a sample of Dr. Frieden’s observations:
“When I’ve looked around the United States, I’ve been extremely concerned about both the risk that primary care practitioners are subjected to in their everyday practice and the economic risk that we could lose many of our primary care practices around the country. It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.” Read more.
Surge in out-of-hospital cardiac arrests
The COVID-19 pandemic in New York City led to a surge in out-of-hospital cardiac arrests that placed a huge burden on first responders, according to a new analysis.
During the height of the pandemic in New York, there was a “dramatic increase in cardiopulmonary arrests, nearly all presented in non-shockable cardiac rhythms (> 90% fatality rate) and vulnerable patient populations were most affected,” David J. Prezant, MD, chief medical officer, Fire Department of New York (FDNY), said in an interview.
In a news release, Dr. Prezant noted that “relatively few, if any, patients were tested to confirm the presence of COVID-19,” making it impossible to distinguish between cardiac arrests as a result of COVID-19 and those that may have resulted from other health conditions.
“We also can’t rule out the possibility that some people may have died from delays in seeking or receiving treatment for non–COVID-19-related conditions. However, the dramatic increase in cardiac arrests compared to the same period in 2019 strongly indicates that the pandemic was directly or indirectly responsible for that surge in cardiac arrests and deaths,” said Dr. Prezant.
The study was published online June 19 in JAMA Cardiology.
Read more.
Fenfluramine approved for Dravet syndrome
The U.S. Food and Drug Administration has approved fenfluramine (Fintepla, Zogenix) oral solution, a Schedule IV controlled substance, for the treatment of seizures associated with Dravet syndrome in children age 2 years and older.
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy.
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Injectable vs. oral antipsychotics: Which do patients prefer?
Patients with schizophrenia appear to prefer long-acting injectable (LAI) antipsychotics, compared with oral versions of these medications, primarily because injectables are more convenient and give individuals more control over their lives, new research shows.
Patients also prefer injections once every 3 months to monthly injections, citing the need for fewer doctor visits and less pain as key reasons. They also reported a preference for deltoid versus gluteal injections, as they were faster and easier to administer, and less embarrassing.
Study investigator Srihari Gopal, MD, senior director at Janssen Research and Development in Titusville, N.J., said in an interview that stigma, which is a “is a really powerful force in mental health treatment,” underlies these findings in terms of the disease itself and its management.
“It’s one of the [key] reasons that schizophrenia patients decide to abandon their drugs and not go to the doctor,” he added.
The study was scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Outdated perceptions
The investigators noted that there is limited information on patient preference with regard to LAI versus oral antipsychotics in the management of schizophrenia.
They also noted that LAIs have been shown to reduce the risk of relapse and rehospitalization because of treatment discontinuation and may help to improve to medication adherence.
However, these medications are still underutilized in clinical practice. Dr. Gopal estimated that only around 1 in 10 patients with schizophrenia in the United States take an LAI, although that figure varies considerably at a global level and is as high as 1 in 2 in Spain.
This is the result of a number of factors that act as potential barriers to LAI use, not the least of which is misconceptions among caregiver and health care professionals about the drugs.
“When I first was in medical school, this was in the 1990s ... there were really only first-generation antipsychotics available in a depot or a long-acting form, and those had very severe side effects,” said Dr. Gopal.
“They would tend to cause all sorts of movement disorders and would make patients feel really drowsy throughout the day, so they really hated taking them,” he said, noting that these depot medications were oil based, which was painful on injection and caused reactions.
While the newer generations of LAIs are water based and have a much-improved adverse effect profile, doctors “on my end of the age spectrum have all those negative connotations and memories in their minds about what these older LAIs were like, ” Dr. Gopal said
“It’s only the newer generation of doctors who were not around at the time that have a more forward-thinking attitude about the newer long-actings.”
Differences by country
To assess factors that determine patients’ medication preferences in order to better understand expectations and reduce potential barriers to treatment, the researchers analyzed data on 1,429 patients with schizophrenia who were participants in a double-blind, randomized, noninferiority study of paliperidone palmitate taken monthly versus once every 3 months.
Participants had a mean age of 38.4 years, and 55% were men. The majority (54%) were white, 8% were black or African American, and 38% were from other races. About one-eighth (12%) of the patients were from the United States.
The highest preference for LAIs was in Europe, at 88%, vs 59.1% in the United States and 70.7% in the rest of the world.
Interestingly, the preference for LAIs in the United States was comparable across different races, at 59.6% among black patients, 58.8% among whites, and 57.1% for other races.
All study participants had a confirmed diagnosis of schizophrenia and a Positive and Negative Syndrome Scale total score of between 70 and 120 at baseline, with worsening symptoms.
They completed the Medication Preference Questionnaire on day 1, day 120, and at the end of the study, with the current analysis focusing on day 1 responses, as that was the only time when patients would not have received any study medication.
Patient empowerment key
The most common reason patients cited for preferring LAIs over oral antipsychotics were that they felt healthier (57%), could get back to their favorite activities (56%), and didn’t have to think about taking their medication (54%).
In terms of their personal experiences, patients preferred LAIs to pills because they “are easier for me” (67% vs. 18%) and offered a greater sense of control and relieved them from having to think about taking medication (64% vs. 14%).
Finally, 50% of patients preferred LAI injections once every 3 months versus 38% for monthly and 3% for daily injections. Main reason cited were fewer injections (96%), less pain (84%), and fewer doctor visits (80%).
The preferred site for LAI injection was deltoid muscle over gluteal muscle, at 59%, with faster administration (63%), easier use (51%), and the location being less embarrassing (44%) cited as the primary reasons.
“Overall, patient empowerment and quality of life–related goals were important for patients who preferred LAI antipsychotics,” the investigators noted.
Logistic regression analysis indicated that only race and country were significantly associated with medication preferences, with white patients significantly more likely than others to prefer LAIs versus oral medications (adjusted odds ratio, 2.39; P < .001). U.S. patients were significantly less likely to prefer the drugs than those from other countries (aOR, 0.41; P < .001).
Dr. Gopal added that significant differences in patient preference for LAIs likely have a lot to do with the prevailing attitudes of doctors from different countries, with low LAI use corresponding to “more negative attitudes.”
“Better understanding of patients’ treatment priorities and perspective could help overcome barriers to LAI use and inform best course of personalized schizophrenia treatment for improved patient satisfaction and medication adherence,” the investigators noted.
Approached for comment, Matej Markota, MD, a psychiatrist at the Mayo Clinic in Rochester, Minn., who was not involved with the research, said that he agreed with the findings of the study.
He said in an interview that, in his clinical experience, the convenience of not having to take medications daily is an important factor that drives patient preference for LAI use over oral medications.
The study was funded by Janssen Research & Development. Dr. Gopal reports he is an employee of Janssen Research & Developmentand owns stock/equity in Johnson & Johnson. Dr. Markota has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with schizophrenia appear to prefer long-acting injectable (LAI) antipsychotics, compared with oral versions of these medications, primarily because injectables are more convenient and give individuals more control over their lives, new research shows.
Patients also prefer injections once every 3 months to monthly injections, citing the need for fewer doctor visits and less pain as key reasons. They also reported a preference for deltoid versus gluteal injections, as they were faster and easier to administer, and less embarrassing.
Study investigator Srihari Gopal, MD, senior director at Janssen Research and Development in Titusville, N.J., said in an interview that stigma, which is a “is a really powerful force in mental health treatment,” underlies these findings in terms of the disease itself and its management.
“It’s one of the [key] reasons that schizophrenia patients decide to abandon their drugs and not go to the doctor,” he added.
The study was scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Outdated perceptions
The investigators noted that there is limited information on patient preference with regard to LAI versus oral antipsychotics in the management of schizophrenia.
They also noted that LAIs have been shown to reduce the risk of relapse and rehospitalization because of treatment discontinuation and may help to improve to medication adherence.
However, these medications are still underutilized in clinical practice. Dr. Gopal estimated that only around 1 in 10 patients with schizophrenia in the United States take an LAI, although that figure varies considerably at a global level and is as high as 1 in 2 in Spain.
This is the result of a number of factors that act as potential barriers to LAI use, not the least of which is misconceptions among caregiver and health care professionals about the drugs.
“When I first was in medical school, this was in the 1990s ... there were really only first-generation antipsychotics available in a depot or a long-acting form, and those had very severe side effects,” said Dr. Gopal.
“They would tend to cause all sorts of movement disorders and would make patients feel really drowsy throughout the day, so they really hated taking them,” he said, noting that these depot medications were oil based, which was painful on injection and caused reactions.
While the newer generations of LAIs are water based and have a much-improved adverse effect profile, doctors “on my end of the age spectrum have all those negative connotations and memories in their minds about what these older LAIs were like, ” Dr. Gopal said
“It’s only the newer generation of doctors who were not around at the time that have a more forward-thinking attitude about the newer long-actings.”
Differences by country
To assess factors that determine patients’ medication preferences in order to better understand expectations and reduce potential barriers to treatment, the researchers analyzed data on 1,429 patients with schizophrenia who were participants in a double-blind, randomized, noninferiority study of paliperidone palmitate taken monthly versus once every 3 months.
Participants had a mean age of 38.4 years, and 55% were men. The majority (54%) were white, 8% were black or African American, and 38% were from other races. About one-eighth (12%) of the patients were from the United States.
The highest preference for LAIs was in Europe, at 88%, vs 59.1% in the United States and 70.7% in the rest of the world.
Interestingly, the preference for LAIs in the United States was comparable across different races, at 59.6% among black patients, 58.8% among whites, and 57.1% for other races.
All study participants had a confirmed diagnosis of schizophrenia and a Positive and Negative Syndrome Scale total score of between 70 and 120 at baseline, with worsening symptoms.
They completed the Medication Preference Questionnaire on day 1, day 120, and at the end of the study, with the current analysis focusing on day 1 responses, as that was the only time when patients would not have received any study medication.
Patient empowerment key
The most common reason patients cited for preferring LAIs over oral antipsychotics were that they felt healthier (57%), could get back to their favorite activities (56%), and didn’t have to think about taking their medication (54%).
In terms of their personal experiences, patients preferred LAIs to pills because they “are easier for me” (67% vs. 18%) and offered a greater sense of control and relieved them from having to think about taking medication (64% vs. 14%).
Finally, 50% of patients preferred LAI injections once every 3 months versus 38% for monthly and 3% for daily injections. Main reason cited were fewer injections (96%), less pain (84%), and fewer doctor visits (80%).
The preferred site for LAI injection was deltoid muscle over gluteal muscle, at 59%, with faster administration (63%), easier use (51%), and the location being less embarrassing (44%) cited as the primary reasons.
“Overall, patient empowerment and quality of life–related goals were important for patients who preferred LAI antipsychotics,” the investigators noted.
Logistic regression analysis indicated that only race and country were significantly associated with medication preferences, with white patients significantly more likely than others to prefer LAIs versus oral medications (adjusted odds ratio, 2.39; P < .001). U.S. patients were significantly less likely to prefer the drugs than those from other countries (aOR, 0.41; P < .001).
Dr. Gopal added that significant differences in patient preference for LAIs likely have a lot to do with the prevailing attitudes of doctors from different countries, with low LAI use corresponding to “more negative attitudes.”
“Better understanding of patients’ treatment priorities and perspective could help overcome barriers to LAI use and inform best course of personalized schizophrenia treatment for improved patient satisfaction and medication adherence,” the investigators noted.
Approached for comment, Matej Markota, MD, a psychiatrist at the Mayo Clinic in Rochester, Minn., who was not involved with the research, said that he agreed with the findings of the study.
He said in an interview that, in his clinical experience, the convenience of not having to take medications daily is an important factor that drives patient preference for LAI use over oral medications.
The study was funded by Janssen Research & Development. Dr. Gopal reports he is an employee of Janssen Research & Developmentand owns stock/equity in Johnson & Johnson. Dr. Markota has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with schizophrenia appear to prefer long-acting injectable (LAI) antipsychotics, compared with oral versions of these medications, primarily because injectables are more convenient and give individuals more control over their lives, new research shows.
Patients also prefer injections once every 3 months to monthly injections, citing the need for fewer doctor visits and less pain as key reasons. They also reported a preference for deltoid versus gluteal injections, as they were faster and easier to administer, and less embarrassing.
Study investigator Srihari Gopal, MD, senior director at Janssen Research and Development in Titusville, N.J., said in an interview that stigma, which is a “is a really powerful force in mental health treatment,” underlies these findings in terms of the disease itself and its management.
“It’s one of the [key] reasons that schizophrenia patients decide to abandon their drugs and not go to the doctor,” he added.
The study was scheduled to be presented at the Congress of the Schizophrenia International Research Society 2020, but the meeting was canceled because of the coronavirus pandemic.
Outdated perceptions
The investigators noted that there is limited information on patient preference with regard to LAI versus oral antipsychotics in the management of schizophrenia.
They also noted that LAIs have been shown to reduce the risk of relapse and rehospitalization because of treatment discontinuation and may help to improve to medication adherence.
However, these medications are still underutilized in clinical practice. Dr. Gopal estimated that only around 1 in 10 patients with schizophrenia in the United States take an LAI, although that figure varies considerably at a global level and is as high as 1 in 2 in Spain.
This is the result of a number of factors that act as potential barriers to LAI use, not the least of which is misconceptions among caregiver and health care professionals about the drugs.
“When I first was in medical school, this was in the 1990s ... there were really only first-generation antipsychotics available in a depot or a long-acting form, and those had very severe side effects,” said Dr. Gopal.
“They would tend to cause all sorts of movement disorders and would make patients feel really drowsy throughout the day, so they really hated taking them,” he said, noting that these depot medications were oil based, which was painful on injection and caused reactions.
While the newer generations of LAIs are water based and have a much-improved adverse effect profile, doctors “on my end of the age spectrum have all those negative connotations and memories in their minds about what these older LAIs were like, ” Dr. Gopal said
“It’s only the newer generation of doctors who were not around at the time that have a more forward-thinking attitude about the newer long-actings.”
Differences by country
To assess factors that determine patients’ medication preferences in order to better understand expectations and reduce potential barriers to treatment, the researchers analyzed data on 1,429 patients with schizophrenia who were participants in a double-blind, randomized, noninferiority study of paliperidone palmitate taken monthly versus once every 3 months.
Participants had a mean age of 38.4 years, and 55% were men. The majority (54%) were white, 8% were black or African American, and 38% were from other races. About one-eighth (12%) of the patients were from the United States.
The highest preference for LAIs was in Europe, at 88%, vs 59.1% in the United States and 70.7% in the rest of the world.
Interestingly, the preference for LAIs in the United States was comparable across different races, at 59.6% among black patients, 58.8% among whites, and 57.1% for other races.
All study participants had a confirmed diagnosis of schizophrenia and a Positive and Negative Syndrome Scale total score of between 70 and 120 at baseline, with worsening symptoms.
They completed the Medication Preference Questionnaire on day 1, day 120, and at the end of the study, with the current analysis focusing on day 1 responses, as that was the only time when patients would not have received any study medication.
Patient empowerment key
The most common reason patients cited for preferring LAIs over oral antipsychotics were that they felt healthier (57%), could get back to their favorite activities (56%), and didn’t have to think about taking their medication (54%).
In terms of their personal experiences, patients preferred LAIs to pills because they “are easier for me” (67% vs. 18%) and offered a greater sense of control and relieved them from having to think about taking medication (64% vs. 14%).
Finally, 50% of patients preferred LAI injections once every 3 months versus 38% for monthly and 3% for daily injections. Main reason cited were fewer injections (96%), less pain (84%), and fewer doctor visits (80%).
The preferred site for LAI injection was deltoid muscle over gluteal muscle, at 59%, with faster administration (63%), easier use (51%), and the location being less embarrassing (44%) cited as the primary reasons.
“Overall, patient empowerment and quality of life–related goals were important for patients who preferred LAI antipsychotics,” the investigators noted.
Logistic regression analysis indicated that only race and country were significantly associated with medication preferences, with white patients significantly more likely than others to prefer LAIs versus oral medications (adjusted odds ratio, 2.39; P < .001). U.S. patients were significantly less likely to prefer the drugs than those from other countries (aOR, 0.41; P < .001).
Dr. Gopal added that significant differences in patient preference for LAIs likely have a lot to do with the prevailing attitudes of doctors from different countries, with low LAI use corresponding to “more negative attitudes.”
“Better understanding of patients’ treatment priorities and perspective could help overcome barriers to LAI use and inform best course of personalized schizophrenia treatment for improved patient satisfaction and medication adherence,” the investigators noted.
Approached for comment, Matej Markota, MD, a psychiatrist at the Mayo Clinic in Rochester, Minn., who was not involved with the research, said that he agreed with the findings of the study.
He said in an interview that, in his clinical experience, the convenience of not having to take medications daily is an important factor that drives patient preference for LAI use over oral medications.
The study was funded by Janssen Research & Development. Dr. Gopal reports he is an employee of Janssen Research & Developmentand owns stock/equity in Johnson & Johnson. Dr. Markota has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SIRS 2020
Combo carboplatin/paclitaxel dubbed new standard of care for anal cancer
say experts discussing results from InterAAct, the first international prospective randomized trial in advanced anal cancer.
In the head-to-head trial, both combinations achieved a similar overall response rate — 59% for carboplatin plus paclitaxel and 57% for 5-FU plus cisplatin.
However, the 5-FU/cisplatin regimen was associated with significantly more adverse events, and there was a trend toward longer survival with carboplatin plus paclitaxel.
Median overall survival was 12.3 months for cisplatin plus 5-FU vs 20 months for carboplatin plus paclitaxel (adjusted hazard ratio [HR], 1.78; P =.059).
Serious adverse events were reported by more patients on cisplatin plus 5-FU vs carboplatin plus paclitaxel (62% vs. 36%; P =.016). The two regimens had different toxicity profiles, with more neutropenia and anemia observed in the carboplatin plus paclitaxel group, but more nausea, vomiting, mucositis, and diarrhea with cisplatin plus 5-FU.
“I think many of us were not surprised that the response rate was equivalent for the two arms but are pleasantly surprised by the difference in toxicity and the impact on survival,” said coauthor Cathy Eng, MD, chair in surgical and medical oncology at the Vanderbilt-Ingram Cancer Center in Nashville, Tennessee.
“We feel fairly confident that the carbo/taxol arm is the new arm to build upon,” she added.
“I think in comparison to the standard 5-FU/cisplatin, which was the control arm of the trial, this regimen should be considered the new standard of care,” said Eng.
Eng told Medscape Medical News that she doesn’t think that it needs further validation. “This is considered a rare cancer in the US,” she said. “The primary endpoint was feasibility of this international effort, which we established. If the response rate was equivalent, the less toxic regimen would be considered.”
“We fulfilled our primary endpoint of wanting to identify the best chemotherapy backbone to build upon,” she added.
These findings were initially presented at the European Society of Medical Oncology 2018 annual meeting, and reported by Medscape Medical News at the time. The full results were published earlier this month in the Journal of Clinical Oncology.
“The InterAAct trial has established carboplatin-paclitaxel as a new standard of care in this population in the frontline setting,” commented Sarbajit Mukherjee, MD, assistant professor of oncology at Roswell Park Comprehensive Cancer, Buffalo, New York, who was approached for an independent comment. “Clinicians should start using this regimen now, and it is also supported by the National Comprehensive Cancer Network guidelines.”
He emphasized the need for caution in interpreting the survival data because overall survival was not the primary endpoint of the study. “However, I do think that we should use this chemo regimen as a backbone for future randomized studies in this rare disease population,” said Mukherjee, who was not involved with the study.
Study Details
Anal cancer is rare, accounting for less than 3% of all gastrointestinal malignancies, but there has been a “dramatic” rise in incidence in recent decades, as previously reported by Medscape Medical News.
Most patients present with localized or locally advanced disease and are treated with chemoradiotherapy with curative intent, the authors explain. However, metastatic dissemination occurs in about 10% of these patients, whereas <10% of all anal cancer patients present with metastatic disease de novo.
For patients with metastatic disease and for those with inoperable disease, the prognosis is poor, with relative 5-year survival rates of about 30%. Palliative chemotherapy is routinely offered, but to date, there have been no randomized controlled trials to inform clinicians of the optimal chemotherapy regimen in this setting.
International guidelines have suggested a platinum agent combined with fluoropyrimidine for the first-line treatment of advanced anal cancer, but this recommendation is based on limited evidence from single-arm phase 2 studies. The International Rare Cancers Initiative Anal Cancer Working Group recognized the evidence gap in clinical decision-making for patients with advanced cancer as an area of unmet clinical need, prompting the global InterAAct trial.
The trial involved 91 patients with locally recurrent inoperable or metastatic squamous cell carcinoma of the anus from 60 sites in North America, Europe and Australia. They were randomly assigned to receive either cisplatin 60 mg/m2 (day 1) plus 5-FU 1000 mg/m2 (days 1-4) every 21 days or carboplatin (area under the curve, 5; day 1) plus paclitaxel 80 mg/m2 (days 1, 8, and 15) every 28 days. Patients were treated for 24 weeks or until disease progression, intolerable toxicity, or withdrawal of consent.
A “pick the winner” study design was used, in which the least toxic regimen would be selected as the “winner” if no significant difference in objective response rate between treatment groups was detected.
At a median follow-up of 28.6 months, the overall response rate did not differ significantly between both groups. The complete response rate was 17% with 5-FU/cisplatin and 12.8% with carboplatin-paclitaxel. Disease progression occurred in 22.9% of patients in the 5-FU/cisplatin group and 15.4% in the carboplatin-paclitaxel group.
The median progression-free survival was 5.7 months for cisplatin plus 5-FU compared with 8.1 months for carboplatin plus paclitaxel. The difference was not statistically significant. After adjusting for confounders, the HR was 1.17 (P = .564).
As already noted, there was a trend toward a significant difference in overall survival of almost 8 months favoring the carboplatin plus paclitaxel regimen. In addition, there was a significant difference in toxicity between the two regimens.
Commenting on the study, Michael Buckstein, MD, PhD, assistant professor, Department of Radiation Oncology, Icahn School of Medicine at Mount Sinai, New York City, noted that even though “this study technically did not meet its endpoint of improved objective response rate and there was only a trend toward improved overall survival, the results presented here, especially with regard to toxicity, are very encouraging for a rare disease in a challenging population.”
Buckstein, who was not associated with the current research, added: “The trial is small, had problems in accrual, very few HIV patients, and was technically negative, so it’s hard to say this should be a ‘standard of care’ but it certainly should be considered ‘standard of practice’ and strongly considered for first-line therapy.”
The next US trial to follow InterAAct will look at the addition of immunotherapy to carboplatin/paclitaxel. This is the phase 3 EA2176 trial of carboplatin/paclitaxel ± nivolumab (plus maintenance), and it will have a primary endpoint of progression-free survival. “It will likely be open this summer, if not early fall, and will enroll 208 patients,” Eng commented.
The current study was supported by Cancer Research UK, AGITG, and ECOG-ACRIN. Eng has disclosed relationships with Bayer Schering Pharma, Foundation of Medicine, Array BioPharma, and Natera. Mukherjee and Buckstein have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
say experts discussing results from InterAAct, the first international prospective randomized trial in advanced anal cancer.
In the head-to-head trial, both combinations achieved a similar overall response rate — 59% for carboplatin plus paclitaxel and 57% for 5-FU plus cisplatin.
However, the 5-FU/cisplatin regimen was associated with significantly more adverse events, and there was a trend toward longer survival with carboplatin plus paclitaxel.
Median overall survival was 12.3 months for cisplatin plus 5-FU vs 20 months for carboplatin plus paclitaxel (adjusted hazard ratio [HR], 1.78; P =.059).
Serious adverse events were reported by more patients on cisplatin plus 5-FU vs carboplatin plus paclitaxel (62% vs. 36%; P =.016). The two regimens had different toxicity profiles, with more neutropenia and anemia observed in the carboplatin plus paclitaxel group, but more nausea, vomiting, mucositis, and diarrhea with cisplatin plus 5-FU.
“I think many of us were not surprised that the response rate was equivalent for the two arms but are pleasantly surprised by the difference in toxicity and the impact on survival,” said coauthor Cathy Eng, MD, chair in surgical and medical oncology at the Vanderbilt-Ingram Cancer Center in Nashville, Tennessee.
“We feel fairly confident that the carbo/taxol arm is the new arm to build upon,” she added.
“I think in comparison to the standard 5-FU/cisplatin, which was the control arm of the trial, this regimen should be considered the new standard of care,” said Eng.
Eng told Medscape Medical News that she doesn’t think that it needs further validation. “This is considered a rare cancer in the US,” she said. “The primary endpoint was feasibility of this international effort, which we established. If the response rate was equivalent, the less toxic regimen would be considered.”
“We fulfilled our primary endpoint of wanting to identify the best chemotherapy backbone to build upon,” she added.
These findings were initially presented at the European Society of Medical Oncology 2018 annual meeting, and reported by Medscape Medical News at the time. The full results were published earlier this month in the Journal of Clinical Oncology.
“The InterAAct trial has established carboplatin-paclitaxel as a new standard of care in this population in the frontline setting,” commented Sarbajit Mukherjee, MD, assistant professor of oncology at Roswell Park Comprehensive Cancer, Buffalo, New York, who was approached for an independent comment. “Clinicians should start using this regimen now, and it is also supported by the National Comprehensive Cancer Network guidelines.”
He emphasized the need for caution in interpreting the survival data because overall survival was not the primary endpoint of the study. “However, I do think that we should use this chemo regimen as a backbone for future randomized studies in this rare disease population,” said Mukherjee, who was not involved with the study.
Study Details
Anal cancer is rare, accounting for less than 3% of all gastrointestinal malignancies, but there has been a “dramatic” rise in incidence in recent decades, as previously reported by Medscape Medical News.
Most patients present with localized or locally advanced disease and are treated with chemoradiotherapy with curative intent, the authors explain. However, metastatic dissemination occurs in about 10% of these patients, whereas <10% of all anal cancer patients present with metastatic disease de novo.
For patients with metastatic disease and for those with inoperable disease, the prognosis is poor, with relative 5-year survival rates of about 30%. Palliative chemotherapy is routinely offered, but to date, there have been no randomized controlled trials to inform clinicians of the optimal chemotherapy regimen in this setting.
International guidelines have suggested a platinum agent combined with fluoropyrimidine for the first-line treatment of advanced anal cancer, but this recommendation is based on limited evidence from single-arm phase 2 studies. The International Rare Cancers Initiative Anal Cancer Working Group recognized the evidence gap in clinical decision-making for patients with advanced cancer as an area of unmet clinical need, prompting the global InterAAct trial.
The trial involved 91 patients with locally recurrent inoperable or metastatic squamous cell carcinoma of the anus from 60 sites in North America, Europe and Australia. They were randomly assigned to receive either cisplatin 60 mg/m2 (day 1) plus 5-FU 1000 mg/m2 (days 1-4) every 21 days or carboplatin (area under the curve, 5; day 1) plus paclitaxel 80 mg/m2 (days 1, 8, and 15) every 28 days. Patients were treated for 24 weeks or until disease progression, intolerable toxicity, or withdrawal of consent.
A “pick the winner” study design was used, in which the least toxic regimen would be selected as the “winner” if no significant difference in objective response rate between treatment groups was detected.
At a median follow-up of 28.6 months, the overall response rate did not differ significantly between both groups. The complete response rate was 17% with 5-FU/cisplatin and 12.8% with carboplatin-paclitaxel. Disease progression occurred in 22.9% of patients in the 5-FU/cisplatin group and 15.4% in the carboplatin-paclitaxel group.
The median progression-free survival was 5.7 months for cisplatin plus 5-FU compared with 8.1 months for carboplatin plus paclitaxel. The difference was not statistically significant. After adjusting for confounders, the HR was 1.17 (P = .564).
As already noted, there was a trend toward a significant difference in overall survival of almost 8 months favoring the carboplatin plus paclitaxel regimen. In addition, there was a significant difference in toxicity between the two regimens.
Commenting on the study, Michael Buckstein, MD, PhD, assistant professor, Department of Radiation Oncology, Icahn School of Medicine at Mount Sinai, New York City, noted that even though “this study technically did not meet its endpoint of improved objective response rate and there was only a trend toward improved overall survival, the results presented here, especially with regard to toxicity, are very encouraging for a rare disease in a challenging population.”
Buckstein, who was not associated with the current research, added: “The trial is small, had problems in accrual, very few HIV patients, and was technically negative, so it’s hard to say this should be a ‘standard of care’ but it certainly should be considered ‘standard of practice’ and strongly considered for first-line therapy.”
The next US trial to follow InterAAct will look at the addition of immunotherapy to carboplatin/paclitaxel. This is the phase 3 EA2176 trial of carboplatin/paclitaxel ± nivolumab (plus maintenance), and it will have a primary endpoint of progression-free survival. “It will likely be open this summer, if not early fall, and will enroll 208 patients,” Eng commented.
The current study was supported by Cancer Research UK, AGITG, and ECOG-ACRIN. Eng has disclosed relationships with Bayer Schering Pharma, Foundation of Medicine, Array BioPharma, and Natera. Mukherjee and Buckstein have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
say experts discussing results from InterAAct, the first international prospective randomized trial in advanced anal cancer.
In the head-to-head trial, both combinations achieved a similar overall response rate — 59% for carboplatin plus paclitaxel and 57% for 5-FU plus cisplatin.
However, the 5-FU/cisplatin regimen was associated with significantly more adverse events, and there was a trend toward longer survival with carboplatin plus paclitaxel.
Median overall survival was 12.3 months for cisplatin plus 5-FU vs 20 months for carboplatin plus paclitaxel (adjusted hazard ratio [HR], 1.78; P =.059).
Serious adverse events were reported by more patients on cisplatin plus 5-FU vs carboplatin plus paclitaxel (62% vs. 36%; P =.016). The two regimens had different toxicity profiles, with more neutropenia and anemia observed in the carboplatin plus paclitaxel group, but more nausea, vomiting, mucositis, and diarrhea with cisplatin plus 5-FU.
“I think many of us were not surprised that the response rate was equivalent for the two arms but are pleasantly surprised by the difference in toxicity and the impact on survival,” said coauthor Cathy Eng, MD, chair in surgical and medical oncology at the Vanderbilt-Ingram Cancer Center in Nashville, Tennessee.
“We feel fairly confident that the carbo/taxol arm is the new arm to build upon,” she added.
“I think in comparison to the standard 5-FU/cisplatin, which was the control arm of the trial, this regimen should be considered the new standard of care,” said Eng.
Eng told Medscape Medical News that she doesn’t think that it needs further validation. “This is considered a rare cancer in the US,” she said. “The primary endpoint was feasibility of this international effort, which we established. If the response rate was equivalent, the less toxic regimen would be considered.”
“We fulfilled our primary endpoint of wanting to identify the best chemotherapy backbone to build upon,” she added.
These findings were initially presented at the European Society of Medical Oncology 2018 annual meeting, and reported by Medscape Medical News at the time. The full results were published earlier this month in the Journal of Clinical Oncology.
“The InterAAct trial has established carboplatin-paclitaxel as a new standard of care in this population in the frontline setting,” commented Sarbajit Mukherjee, MD, assistant professor of oncology at Roswell Park Comprehensive Cancer, Buffalo, New York, who was approached for an independent comment. “Clinicians should start using this regimen now, and it is also supported by the National Comprehensive Cancer Network guidelines.”
He emphasized the need for caution in interpreting the survival data because overall survival was not the primary endpoint of the study. “However, I do think that we should use this chemo regimen as a backbone for future randomized studies in this rare disease population,” said Mukherjee, who was not involved with the study.
Study Details
Anal cancer is rare, accounting for less than 3% of all gastrointestinal malignancies, but there has been a “dramatic” rise in incidence in recent decades, as previously reported by Medscape Medical News.
Most patients present with localized or locally advanced disease and are treated with chemoradiotherapy with curative intent, the authors explain. However, metastatic dissemination occurs in about 10% of these patients, whereas <10% of all anal cancer patients present with metastatic disease de novo.
For patients with metastatic disease and for those with inoperable disease, the prognosis is poor, with relative 5-year survival rates of about 30%. Palliative chemotherapy is routinely offered, but to date, there have been no randomized controlled trials to inform clinicians of the optimal chemotherapy regimen in this setting.
International guidelines have suggested a platinum agent combined with fluoropyrimidine for the first-line treatment of advanced anal cancer, but this recommendation is based on limited evidence from single-arm phase 2 studies. The International Rare Cancers Initiative Anal Cancer Working Group recognized the evidence gap in clinical decision-making for patients with advanced cancer as an area of unmet clinical need, prompting the global InterAAct trial.
The trial involved 91 patients with locally recurrent inoperable or metastatic squamous cell carcinoma of the anus from 60 sites in North America, Europe and Australia. They were randomly assigned to receive either cisplatin 60 mg/m2 (day 1) plus 5-FU 1000 mg/m2 (days 1-4) every 21 days or carboplatin (area under the curve, 5; day 1) plus paclitaxel 80 mg/m2 (days 1, 8, and 15) every 28 days. Patients were treated for 24 weeks or until disease progression, intolerable toxicity, or withdrawal of consent.
A “pick the winner” study design was used, in which the least toxic regimen would be selected as the “winner” if no significant difference in objective response rate between treatment groups was detected.
At a median follow-up of 28.6 months, the overall response rate did not differ significantly between both groups. The complete response rate was 17% with 5-FU/cisplatin and 12.8% with carboplatin-paclitaxel. Disease progression occurred in 22.9% of patients in the 5-FU/cisplatin group and 15.4% in the carboplatin-paclitaxel group.
The median progression-free survival was 5.7 months for cisplatin plus 5-FU compared with 8.1 months for carboplatin plus paclitaxel. The difference was not statistically significant. After adjusting for confounders, the HR was 1.17 (P = .564).
As already noted, there was a trend toward a significant difference in overall survival of almost 8 months favoring the carboplatin plus paclitaxel regimen. In addition, there was a significant difference in toxicity between the two regimens.
Commenting on the study, Michael Buckstein, MD, PhD, assistant professor, Department of Radiation Oncology, Icahn School of Medicine at Mount Sinai, New York City, noted that even though “this study technically did not meet its endpoint of improved objective response rate and there was only a trend toward improved overall survival, the results presented here, especially with regard to toxicity, are very encouraging for a rare disease in a challenging population.”
Buckstein, who was not associated with the current research, added: “The trial is small, had problems in accrual, very few HIV patients, and was technically negative, so it’s hard to say this should be a ‘standard of care’ but it certainly should be considered ‘standard of practice’ and strongly considered for first-line therapy.”
The next US trial to follow InterAAct will look at the addition of immunotherapy to carboplatin/paclitaxel. This is the phase 3 EA2176 trial of carboplatin/paclitaxel ± nivolumab (plus maintenance), and it will have a primary endpoint of progression-free survival. “It will likely be open this summer, if not early fall, and will enroll 208 patients,” Eng commented.
The current study was supported by Cancer Research UK, AGITG, and ECOG-ACRIN. Eng has disclosed relationships with Bayer Schering Pharma, Foundation of Medicine, Array BioPharma, and Natera. Mukherjee and Buckstein have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
PAP use associated with lower mortality
Background: OSA is a key modifiable risk factor for adverse cardiovascular outcomes and is increasingly prevalent in older populations. PAP improves OSA severity, increases oxygenation, and reduces daytime sleepiness. Its effect on major adverse cardiovascular outcomes remains uncertain.
Study design: Retrospective cohort study of the Sleep Heart Health Study.
Setting: Nine existing U.S. epidemiologic studies.
Synopsis: Of the 392 patients analyzed, 81 were prescribed PAP and 311 were not. Investigators controlled for OSA severity, history of stroke or MI, hypertension, diabetes, weight, smoking, and alcohol intake. The adjusted hazard ratio for death at mean 11 years was 42% lower for those prescribed PAP.
Bottom line: PAP markedly lowers mortality in OSA, with survival curves separating at 6-7 years.
Citation: Lisan Q et al. Association of positive airway pressure prescription with mortality in patients with obesity and severe obstructive sleep apnea. JAMA Otolaryngol Head Neck Surg. 2019 Apr 11. doi: 10.1001/jamaoto.2019.0281.
Dr. Anderson is chief, hospital medicine section, and deputy chief, medicine service, at the Veterans Affairs Eastern Colorado Health Care System, Aurora.
Background: OSA is a key modifiable risk factor for adverse cardiovascular outcomes and is increasingly prevalent in older populations. PAP improves OSA severity, increases oxygenation, and reduces daytime sleepiness. Its effect on major adverse cardiovascular outcomes remains uncertain.
Study design: Retrospective cohort study of the Sleep Heart Health Study.
Setting: Nine existing U.S. epidemiologic studies.
Synopsis: Of the 392 patients analyzed, 81 were prescribed PAP and 311 were not. Investigators controlled for OSA severity, history of stroke or MI, hypertension, diabetes, weight, smoking, and alcohol intake. The adjusted hazard ratio for death at mean 11 years was 42% lower for those prescribed PAP.
Bottom line: PAP markedly lowers mortality in OSA, with survival curves separating at 6-7 years.
Citation: Lisan Q et al. Association of positive airway pressure prescription with mortality in patients with obesity and severe obstructive sleep apnea. JAMA Otolaryngol Head Neck Surg. 2019 Apr 11. doi: 10.1001/jamaoto.2019.0281.
Dr. Anderson is chief, hospital medicine section, and deputy chief, medicine service, at the Veterans Affairs Eastern Colorado Health Care System, Aurora.
Background: OSA is a key modifiable risk factor for adverse cardiovascular outcomes and is increasingly prevalent in older populations. PAP improves OSA severity, increases oxygenation, and reduces daytime sleepiness. Its effect on major adverse cardiovascular outcomes remains uncertain.
Study design: Retrospective cohort study of the Sleep Heart Health Study.
Setting: Nine existing U.S. epidemiologic studies.
Synopsis: Of the 392 patients analyzed, 81 were prescribed PAP and 311 were not. Investigators controlled for OSA severity, history of stroke or MI, hypertension, diabetes, weight, smoking, and alcohol intake. The adjusted hazard ratio for death at mean 11 years was 42% lower for those prescribed PAP.
Bottom line: PAP markedly lowers mortality in OSA, with survival curves separating at 6-7 years.
Citation: Lisan Q et al. Association of positive airway pressure prescription with mortality in patients with obesity and severe obstructive sleep apnea. JAMA Otolaryngol Head Neck Surg. 2019 Apr 11. doi: 10.1001/jamaoto.2019.0281.
Dr. Anderson is chief, hospital medicine section, and deputy chief, medicine service, at the Veterans Affairs Eastern Colorado Health Care System, Aurora.

Combo drug improves survival in older patients with high-risk/secondary AML
The use of CPX-351, a dual-drug liposomal encapsulation of cytarabine and daunorubicin, was tied to long-term remission and survival in older patients with newly diagnosed high-risk or secondary acute myeloid leukemia (AML), according to final results of a phase 3 study.
As part of the American Society of Clinical Oncology virtual scientific program, Jeffrey E. Lancet, MD, of the Moffitt Cancer Center in Tampa, Fla., presented the 5-year final data from a trial comparing CPX-351 vs. the conventional 7+3 regimen of cytarabine and daunorubicin in more than 300 older adult patients (age 60-75 years) with newly diagnosed high-risk or secondary AML. Early mortality rates for CPX-351 vs. 7+3 were 6% vs. 11% at Day 30 and 14% vs. 21% at day 60, respectively.
The final 5-year follow-up results had a median follow-up of just greater than 60 months, and maintained the improved median overall survival previously observed in the trial with CPX-351 (153 patients), compared with 7+3 (155 patients), Dr. Lancet reported.
Allogeneic hematopoietic stem cell transplant was received by 35% of the patients in the CPX-351 arm and 25% of patients in the 7+3 arm. The median overall survival after transplant was not reached for the CPX-351 arm, compared with 10.3 months with the 7+3 treated patients.
Remission, either complete remission or complete remission with incomplete neutrophil or platelet recovery, was achieved by 48% of patients in the CPX-351 arm and 33% of patients in the 7+3 arm, according to the results of the 5-year follow-up. In addition, among all patients who achieved remission, median overall survival was longer with CPX-351 than with 7+3, and the Kaplan-Meier estimated survival rate was higher for CPX-351 at both 3 years and 5 years.
At 5 years of follow-up, 81% of patients in the CPX-351 arm and 93% of patients in the 7+3 arm had died, with similar causes cited in each arm. Progressive leukemia was the most common primary cause of death in both treatment arms, according to Dr. Lancet.
“The final 5-year follow-up results from this phase 3 study support the prior evidence that CPX-351 has the ability to produce or contribute to long-term remission and survival in older patients with newly diagnosed high-risk or secondary AML,” Dr. Lancet concluded.
CPX-351 (Vyxeos) has been approved by the Food and Drug Administration and the European Medicines Agency for the treatment of adults with newly diagnosed therapy-related AML or AML with myelodysplastic syndrome–related changes.
The study was funded by Jazz Pharmaceuticals. Dr. Lancet disclosed that he has a consulting or advisory role for Agios, Daiichi Sankyo, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Lancet JE et al. ASCO 2020, Abstract 7510.
The use of CPX-351, a dual-drug liposomal encapsulation of cytarabine and daunorubicin, was tied to long-term remission and survival in older patients with newly diagnosed high-risk or secondary acute myeloid leukemia (AML), according to final results of a phase 3 study.
As part of the American Society of Clinical Oncology virtual scientific program, Jeffrey E. Lancet, MD, of the Moffitt Cancer Center in Tampa, Fla., presented the 5-year final data from a trial comparing CPX-351 vs. the conventional 7+3 regimen of cytarabine and daunorubicin in more than 300 older adult patients (age 60-75 years) with newly diagnosed high-risk or secondary AML. Early mortality rates for CPX-351 vs. 7+3 were 6% vs. 11% at Day 30 and 14% vs. 21% at day 60, respectively.
The final 5-year follow-up results had a median follow-up of just greater than 60 months, and maintained the improved median overall survival previously observed in the trial with CPX-351 (153 patients), compared with 7+3 (155 patients), Dr. Lancet reported.
Allogeneic hematopoietic stem cell transplant was received by 35% of the patients in the CPX-351 arm and 25% of patients in the 7+3 arm. The median overall survival after transplant was not reached for the CPX-351 arm, compared with 10.3 months with the 7+3 treated patients.
Remission, either complete remission or complete remission with incomplete neutrophil or platelet recovery, was achieved by 48% of patients in the CPX-351 arm and 33% of patients in the 7+3 arm, according to the results of the 5-year follow-up. In addition, among all patients who achieved remission, median overall survival was longer with CPX-351 than with 7+3, and the Kaplan-Meier estimated survival rate was higher for CPX-351 at both 3 years and 5 years.
At 5 years of follow-up, 81% of patients in the CPX-351 arm and 93% of patients in the 7+3 arm had died, with similar causes cited in each arm. Progressive leukemia was the most common primary cause of death in both treatment arms, according to Dr. Lancet.
“The final 5-year follow-up results from this phase 3 study support the prior evidence that CPX-351 has the ability to produce or contribute to long-term remission and survival in older patients with newly diagnosed high-risk or secondary AML,” Dr. Lancet concluded.
CPX-351 (Vyxeos) has been approved by the Food and Drug Administration and the European Medicines Agency for the treatment of adults with newly diagnosed therapy-related AML or AML with myelodysplastic syndrome–related changes.
The study was funded by Jazz Pharmaceuticals. Dr. Lancet disclosed that he has a consulting or advisory role for Agios, Daiichi Sankyo, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Lancet JE et al. ASCO 2020, Abstract 7510.
The use of CPX-351, a dual-drug liposomal encapsulation of cytarabine and daunorubicin, was tied to long-term remission and survival in older patients with newly diagnosed high-risk or secondary acute myeloid leukemia (AML), according to final results of a phase 3 study.
As part of the American Society of Clinical Oncology virtual scientific program, Jeffrey E. Lancet, MD, of the Moffitt Cancer Center in Tampa, Fla., presented the 5-year final data from a trial comparing CPX-351 vs. the conventional 7+3 regimen of cytarabine and daunorubicin in more than 300 older adult patients (age 60-75 years) with newly diagnosed high-risk or secondary AML. Early mortality rates for CPX-351 vs. 7+3 were 6% vs. 11% at Day 30 and 14% vs. 21% at day 60, respectively.
The final 5-year follow-up results had a median follow-up of just greater than 60 months, and maintained the improved median overall survival previously observed in the trial with CPX-351 (153 patients), compared with 7+3 (155 patients), Dr. Lancet reported.
Allogeneic hematopoietic stem cell transplant was received by 35% of the patients in the CPX-351 arm and 25% of patients in the 7+3 arm. The median overall survival after transplant was not reached for the CPX-351 arm, compared with 10.3 months with the 7+3 treated patients.
Remission, either complete remission or complete remission with incomplete neutrophil or platelet recovery, was achieved by 48% of patients in the CPX-351 arm and 33% of patients in the 7+3 arm, according to the results of the 5-year follow-up. In addition, among all patients who achieved remission, median overall survival was longer with CPX-351 than with 7+3, and the Kaplan-Meier estimated survival rate was higher for CPX-351 at both 3 years and 5 years.
At 5 years of follow-up, 81% of patients in the CPX-351 arm and 93% of patients in the 7+3 arm had died, with similar causes cited in each arm. Progressive leukemia was the most common primary cause of death in both treatment arms, according to Dr. Lancet.
“The final 5-year follow-up results from this phase 3 study support the prior evidence that CPX-351 has the ability to produce or contribute to long-term remission and survival in older patients with newly diagnosed high-risk or secondary AML,” Dr. Lancet concluded.
CPX-351 (Vyxeos) has been approved by the Food and Drug Administration and the European Medicines Agency for the treatment of adults with newly diagnosed therapy-related AML or AML with myelodysplastic syndrome–related changes.
The study was funded by Jazz Pharmaceuticals. Dr. Lancet disclosed that he has a consulting or advisory role for Agios, Daiichi Sankyo, Jazz Pharmaceuticals, and Pfizer.
SOURCE: Lancet JE et al. ASCO 2020, Abstract 7510.
FROM ASCO 2020
FDA approves new treatment for Dravet syndrome
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy (SUDEP).
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The FDA approved fenfluramine for Dravet syndrome based on the results of two randomized, double-blind, placebo-controlled phase 3 trials involving children ages 2 to 18 years with Dravet syndrome.
In both studies, children treated with fenfluramine experienced significantly greater reductions in the frequency of convulsive seizures than did their peers who received placebo. These reductions occurred within 3 to 4 weeks, and remained generally consistent over the 14- to 15-week treatment periods, the FDA said.
“There remains a huge unmet need for the many Dravet syndrome patients who continue to experience frequent severe seizures even while taking one or more of the currently available antiseizure medications,” Joseph Sullivan, MD, who worked on the fenfluramine for Dravet syndrome studies, said in a news release.
Given the “profound reductions” in convulsive seizure frequency seen in the clinical trials, combined with the “ongoing, robust safety monitoring,” fenfluramine offers “an extremely important treatment option for Dravet syndrome patients,” said Dr. Sullivan, director of the Pediatric Epilepsy Center of Excellence at the University of California San Francisco (UCSF) Benioff Children’s Hospital.
Fenfluramine is an anorectic agent that was used to treat obesity until it was removed from the market in 1997 over reports of increased risk of valvular heart disease when prescribed in higher doses and most often when prescribed with phentermine. The combination of the two drugs was known as fen-phen.
In the clinical trials of Dravet syndrome, the most common adverse reactions were decreased appetite; somnolence, sedation, lethargy; diarrhea; constipation; abnormal echocardiogram; fatigue, malaise, asthenia; ataxia, balance disorder, gait disturbance; increased blood pressure; drooling, salivary hypersecretion; pyrexia; upper respiratory tract infection; vomiting; decreased weight; fall; and status epilepticus.
The Fintepla label has a boxed warning stating that the drug is associated with valvular heart disease (VHD) and pulmonary arterial hypertension (PAH). Due to these risks, patients must undergo echocardiography before treatment, every 6 months during treatment, and once 3 to 6 months after treatment is stopped.
If signs of VHD, PAH, or other cardiac abnormalities are present, clinicians should weigh the benefits and risks of continuing treatment with Fintepla, the FDA said.
Fintepla is available only through a risk evaluation and mitigation strategy (REMS) program, which requires physicians who prescribe the drug and pharmacies that dispense it to be certified in the Fintepla REMS and that patients be enrolled in the program.
As part of the REMS requirements, prescribers and patients must adhere to the required cardiac monitoring to receive the drug.
Fintepla will be available to certified prescribers in the United States in July. Zogenix is launching Zogenix Central, a comprehensive support service that will provide ongoing product assistance to patients, caregivers, and their medical teams. Further information is available online.
This article first appeared on Medscape.com.
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy (SUDEP).
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The FDA approved fenfluramine for Dravet syndrome based on the results of two randomized, double-blind, placebo-controlled phase 3 trials involving children ages 2 to 18 years with Dravet syndrome.
In both studies, children treated with fenfluramine experienced significantly greater reductions in the frequency of convulsive seizures than did their peers who received placebo. These reductions occurred within 3 to 4 weeks, and remained generally consistent over the 14- to 15-week treatment periods, the FDA said.
“There remains a huge unmet need for the many Dravet syndrome patients who continue to experience frequent severe seizures even while taking one or more of the currently available antiseizure medications,” Joseph Sullivan, MD, who worked on the fenfluramine for Dravet syndrome studies, said in a news release.
Given the “profound reductions” in convulsive seizure frequency seen in the clinical trials, combined with the “ongoing, robust safety monitoring,” fenfluramine offers “an extremely important treatment option for Dravet syndrome patients,” said Dr. Sullivan, director of the Pediatric Epilepsy Center of Excellence at the University of California San Francisco (UCSF) Benioff Children’s Hospital.
Fenfluramine is an anorectic agent that was used to treat obesity until it was removed from the market in 1997 over reports of increased risk of valvular heart disease when prescribed in higher doses and most often when prescribed with phentermine. The combination of the two drugs was known as fen-phen.
In the clinical trials of Dravet syndrome, the most common adverse reactions were decreased appetite; somnolence, sedation, lethargy; diarrhea; constipation; abnormal echocardiogram; fatigue, malaise, asthenia; ataxia, balance disorder, gait disturbance; increased blood pressure; drooling, salivary hypersecretion; pyrexia; upper respiratory tract infection; vomiting; decreased weight; fall; and status epilepticus.
The Fintepla label has a boxed warning stating that the drug is associated with valvular heart disease (VHD) and pulmonary arterial hypertension (PAH). Due to these risks, patients must undergo echocardiography before treatment, every 6 months during treatment, and once 3 to 6 months after treatment is stopped.
If signs of VHD, PAH, or other cardiac abnormalities are present, clinicians should weigh the benefits and risks of continuing treatment with Fintepla, the FDA said.
Fintepla is available only through a risk evaluation and mitigation strategy (REMS) program, which requires physicians who prescribe the drug and pharmacies that dispense it to be certified in the Fintepla REMS and that patients be enrolled in the program.
As part of the REMS requirements, prescribers and patients must adhere to the required cardiac monitoring to receive the drug.
Fintepla will be available to certified prescribers in the United States in July. Zogenix is launching Zogenix Central, a comprehensive support service that will provide ongoing product assistance to patients, caregivers, and their medical teams. Further information is available online.
This article first appeared on Medscape.com.
Dravet syndrome is a rare childhood-onset epilepsy characterized by frequent, drug-resistant convulsive seizures that may contribute to intellectual disability and impairments in motor control, behavior, and cognition, as well as an increased risk of sudden unexpected death in epilepsy (SUDEP).
Dravet syndrome takes a “tremendous toll on both patients and their families. Fintepla offers an additional effective treatment option for the treatment of seizures associated with Dravet syndrome,” Billy Dunn, MD, director, Office of Neuroscience in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The FDA approved fenfluramine for Dravet syndrome based on the results of two randomized, double-blind, placebo-controlled phase 3 trials involving children ages 2 to 18 years with Dravet syndrome.
In both studies, children treated with fenfluramine experienced significantly greater reductions in the frequency of convulsive seizures than did their peers who received placebo. These reductions occurred within 3 to 4 weeks, and remained generally consistent over the 14- to 15-week treatment periods, the FDA said.
“There remains a huge unmet need for the many Dravet syndrome patients who continue to experience frequent severe seizures even while taking one or more of the currently available antiseizure medications,” Joseph Sullivan, MD, who worked on the fenfluramine for Dravet syndrome studies, said in a news release.
Given the “profound reductions” in convulsive seizure frequency seen in the clinical trials, combined with the “ongoing, robust safety monitoring,” fenfluramine offers “an extremely important treatment option for Dravet syndrome patients,” said Dr. Sullivan, director of the Pediatric Epilepsy Center of Excellence at the University of California San Francisco (UCSF) Benioff Children’s Hospital.
Fenfluramine is an anorectic agent that was used to treat obesity until it was removed from the market in 1997 over reports of increased risk of valvular heart disease when prescribed in higher doses and most often when prescribed with phentermine. The combination of the two drugs was known as fen-phen.
In the clinical trials of Dravet syndrome, the most common adverse reactions were decreased appetite; somnolence, sedation, lethargy; diarrhea; constipation; abnormal echocardiogram; fatigue, malaise, asthenia; ataxia, balance disorder, gait disturbance; increased blood pressure; drooling, salivary hypersecretion; pyrexia; upper respiratory tract infection; vomiting; decreased weight; fall; and status epilepticus.
The Fintepla label has a boxed warning stating that the drug is associated with valvular heart disease (VHD) and pulmonary arterial hypertension (PAH). Due to these risks, patients must undergo echocardiography before treatment, every 6 months during treatment, and once 3 to 6 months after treatment is stopped.
If signs of VHD, PAH, or other cardiac abnormalities are present, clinicians should weigh the benefits and risks of continuing treatment with Fintepla, the FDA said.
Fintepla is available only through a risk evaluation and mitigation strategy (REMS) program, which requires physicians who prescribe the drug and pharmacies that dispense it to be certified in the Fintepla REMS and that patients be enrolled in the program.
As part of the REMS requirements, prescribers and patients must adhere to the required cardiac monitoring to receive the drug.
Fintepla will be available to certified prescribers in the United States in July. Zogenix is launching Zogenix Central, a comprehensive support service that will provide ongoing product assistance to patients, caregivers, and their medical teams. Further information is available online.
This article first appeared on Medscape.com.
Will primary care physicians be COVID-19’s next victims?
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. Those arguments resonated with Kenny Lin, MD, MPH, a family physician, professor at Georgetown University School of Medicine, and a regular contributor to Medscape. He spoke with Dr. Frieden about his concerns.

Dr. Lin: Why did you feel that it was important to write this piece focused on primary care?
Dr. Frieden: I’m glad you asked that question. Given all that is going on, one might ask, what is the importance of primary care? We’ve got this epidemic going on that requires public health and hospital systems. Why voice concern about primary care now?
It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.
Dr. Lin: I agree. In my own practice we haven’t had to furlough anyone, but we’ve put people on forced paid time off. We’ve been reallocating physicians to other parts of our health system. It is definitely a concern. A solo practitioner or someone in a rural practice would most likely be even much more heavily hit. You’ve argued that the neglect of our public health system on a national level has led to many preventable deaths from COVID-19. Do you feel that something similar has happened in primary care? How could a stronger, better-funded primary care infrastructure better prepare us for the next pandemic?

Dr. Frieden: All over the world, we see an overemphasis on hospital care and an underemphasis on primary care, outpatient care, family medicine. As a result, we pay more. We have larger risks, and we don’t prevent diseases that we could prevent. It’s fundamentally about the economic incentives of our health care system. Of course, that often reflects the political reality of different profit centers and cost centers of care. That won’t change with tweaking around the edges. It will only change if we change the way we pay for health care. Money talks. We need to start paying at least part of what we pay based on health outcomes.
Many years ago a colleague and I wrote an article, “Health Care as If Health Mattered.” If you step back and look at how we pay for health care, very little, if any, of our payment structure is based on how much health the care system delivers. Part of that can be addressed by going to capitated models, which I think do better. But you have also got to put into those capitated systems some quality and outcome measures that are both valid and not too burdensome to report on. That’s not easy. We could talk a lot about some of the information systems and payment systems, but I think the bottom line is that we need to be able to deal not only with health emergencies, but also with preventive care, care of chronic diseases, and behavioral health care in ways that maximize health.
One of the ways to do that is simple, monthly, capitated payments along with what I call a registry-based outcomes system.
I’m a tuberculosis specialist by training. In tuberculosis there really is a great information system. We track every single patient who has been diagnosed, and we hold every clinician accountable for whether or not they’ve successfully treated that patient. An optimal health care system should do the same with treatment of hypertension, diabetes, seizure disorder, and other common conditions in which treatment makes a really big difference. Preventive care, especially vaccine delivery, is another example.
I understand that physicians will point out that patients may not come in for that care, or they’re hard to deal with, or they refuse recommended treatment. We don’t expect 100%. But we should expect that, if we’re paying for health care, we should get health.
To do that, I think we need much more support for primary care, both in terms of the absolute amount of dollars going in and the administrative support. Some of our systems are so complicated that you can’t manage them without a billing department. How does a one- or two-physician practice deal with systems that will take dozens of hours a week to manage? You have to deal with the administrative complexity, the structure of the incentives, and the structure of care.
I think these are all things that we have to address. But for a minute, let’s helicopter up and look at the big picture. Without additional help from Congress, tens of thousands of primary care physicians could go out of business in the coming weeks. This is a crisis, and this will be very hard to rebuild. We don’t have a strong, resilient primary care infrastructure today, and if we’re not careful it’ll be even weaker as we try to rebuild.
It has been encouraging to see some of the care innovations that have occurred in response to the pandemic. I’m particularly encouraged by the widespread interest in and support for telemedicine. Telemedicine is a very important way of making care safer, more accessible, less expensive, more efficient. There have been a lot of restrictions on it, not just in the United States but globally, for many years. It’s really interesting to see those restrictions rapidly change. I give credit to the Centers for Medicare & Medicaid Services for quick changes in this area.
Now, telemedicine isn’t a cure-all. There are lots of things you can’t do from a distance. It’s a pale reflection of reality, compared with an in-person first visit with a patient. But it’s a whole lot better than nothing. If we look at some of the best health systems in the United States, they’ve gone to as much as 80% of clinical visits done by telemedicine. I don’t think we’re going to go back. Even if COVID is no longer the threat that it is today, if you can do things more quickly, more efficiently, and more conveniently for both patients and doctors, do them. Obviously, it won’t be all visits, but it could be a large proportion of visits and an important part of strengthening our primary care system.
My initiative, Resolve to Save Lives, which is part of the global health organization Vital Strategies, has done work in the area of public health around the world. I am really struck by how weak primary care systems are in so many countries. Strong primary care systems are the exception rather than the rule, but they’re also a best buy in health care. They’re crucially important, and they’re going to work differently in different countries, in different states, in different communities. We need to do a better job of supporting primary care, building primary care, and paying for primary care.
Dr. Lin: You’ve identified two needs. The immediate need is that primary care practices need revenue now to not have to close in the immediate aftermath or the ongoing COVID epidemic, but also there’s the long term, the percentage of health care dollars that are going to primary care in the long term. You pointed out in your article that currently 5% or less of health care spending is in primary care, which is a lot less percentage-wise than in many other countries. I think the question always comes up is that we want to increase that share, but the money has to come from somewhere. Where is that extra money going to come from? Dr. Frieden: I’m not an expert in health care finance, but one thing I’ve learned over the years is that one person’s waste, fraud, and abuse is somebody else’s profit center. It’s not going to be easy. On the one hand, we do need to think about more efficient ways to organize primary care; on the other hand, we have to figure out a way to internalize some of the savings. If you give good primary care and, therefore, someone doesn’t get hospitalized, you can actually lose money in the current system, whereas you’re saving the system a lot of money by preventing that hospitalization.
I think our health system does have significant inefficiencies in terms of the number of tests and interventions that are done that are really not proven to help patients. It has been demonstrated for decades now that the usual economic incentives don’t operate in health care. In health care, supply often generates demand. The number of gallbladder operations is proportional not to population but to the number of gallbladder surgeons. That’s a problem, and it’s a problem that we’re going to have to assess. “Gatekeeper” is an unpleasant word, but if a primary care practitioner could be the advocate for patients so that we’re not pushing for patients to get more care or to get less care but to get the right care, we have the potential to reduce costs while improving quality.
Dr. Lin: You accurately point out that the fee-for-service payment system has been the major culprit in the declining revenues of primary care practices since the start of the pandemic. But for the majority of primary care physicians, including myself, fee-for-service is all that we’ve ever known. Do you think that primary care is ready for such an abrupt financing change, particularly in a very short period of time?Dr. Frieden: You’re certainly accurate in saying that nothing about health care finance is easy. Trying to address these problems at the national or state level has been extremely difficult. I think that the pilot programs in Medicare are very important. Medicaid is a particular challenge because it’s a state-based program and many of the costs are driven by nursing home and long-term care. When you take those costs out, the actual funding per patient or per provider is quite low in most places.
It’s hard enough to reorganize if you’ve got ample resources, but to reorganize when they are insufficient is particularly hard. I would say only that there are no quick and simple answers to this question, but there is a widespread understanding that what we’re doing now doesn’t make sense. We pay top dollar and we get – despite fantastic doctors and fantastic hospitals – lousy outcomes. I’m a public health physician. I’m an internal medicine and infectious disease specialist. Fundamentally, I look at the data. If you think of our health care system as a patient, the patient is not doing well. We’re not functional to the degree we need to be, particularly when you think of what an enormous outlier our per capita expenditures are [compared with other developed countries] – almost twice the average upper-income country and 25% more than any other upper-income country.
Now, anyone who tells you that change is going to be pain-free is not leveling with you. In addition to things like telemedicine, we have to make much more use of team-based care and task sharing. There are lots of things that doctors are doing these days that they really shouldn’t.
Dr. Lin: In your recent op-ed, you noted the pivot to telehealth that primary care practices have made very quickly in response to the pandemic. That certainly was the experience for my practice. But what are some other strategies that you think are important to support the goal of better care delivery in our primary care practices?Dr. Frieden: Another really important innovation is team-based care. There are lots of things that doctors are doing today that nurses, nurse practitioners, physician assistants, and community health workers can do better and for less money. Frankly, I think that should increase the job satisfaction of physicians, to be doing work that is specific to the physician, requiring either more patient interaction or advanced reasoning or experience.
In my own field of tuberculosis control, I learned how to treat tuberculosis because the nurse at the TB clinic kept correcting me because that’s all she did. She did tuberculosis care, so she had seen everything. Even though I’d finished an infectious disease fellowship and internal medicine residency, the public health nurse knew TB a whole lot better than I did.
Similarly, as we work on hypertension control, you can protocolize most of this care and do a much better job. That’s been proven for more than 40 years, and yet we still don’t do it.
One of the big parts of being able to do more with the same or fewer resources is going to be more team-based care. That’s really a task-sharing approach. I think of that as a triple win: You get better care for lower costs with more employment. What’s not to like?
Dr. Lin: I’m hopeful, as you are, that many of these innovations that have been made by necessity will persist beyond the duration of COVID-19. As you said, the health care system has been really difficult to change, and it often takes something like this to galvanize enough consensus that things need to change.
Dr. Frieden: I think the bottom line here is that we should pay our primary health care providers to keep us healthy and ensure that we have a payment system that lets them do that without risking bankruptcy. That’s not too much to ask of our system. It’s important for our health. It’s important for our economy. It’s important for our communities.
Dr. Lin teaches family medicine, preventive medicine, and health policy at Georgetown University School of Medicine. He is deputy editor of the journal American Family Physician. Follow him on Twitter. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for MedStar Georgetown University Hospital and received income in an amount equal to or greater than $250 from UpToDate, Wiley-Blackwell, and American Academy of Family Physicians.
Dr. Frieden is a physician with advanced training in internal medicine, infectious disease, public health, and epidemiology. He has served as director of the Centers for Disease Control and Prevention and as commissioner of the New York City Health Department. Currently he is president and CEO of Resolve to Save Lives. Follow him on Twitter. Thomas R. Frieden, MD, MPH, has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. Those arguments resonated with Kenny Lin, MD, MPH, a family physician, professor at Georgetown University School of Medicine, and a regular contributor to Medscape. He spoke with Dr. Frieden about his concerns.
Dr. Lin: Why did you feel that it was important to write this piece focused on primary care?
Dr. Frieden: I’m glad you asked that question. Given all that is going on, one might ask, what is the importance of primary care? We’ve got this epidemic going on that requires public health and hospital systems. Why voice concern about primary care now?
It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.
Dr. Lin: I agree. In my own practice we haven’t had to furlough anyone, but we’ve put people on forced paid time off. We’ve been reallocating physicians to other parts of our health system. It is definitely a concern. A solo practitioner or someone in a rural practice would most likely be even much more heavily hit. You’ve argued that the neglect of our public health system on a national level has led to many preventable deaths from COVID-19. Do you feel that something similar has happened in primary care? How could a stronger, better-funded primary care infrastructure better prepare us for the next pandemic?
Dr. Frieden: All over the world, we see an overemphasis on hospital care and an underemphasis on primary care, outpatient care, family medicine. As a result, we pay more. We have larger risks, and we don’t prevent diseases that we could prevent. It’s fundamentally about the economic incentives of our health care system. Of course, that often reflects the political reality of different profit centers and cost centers of care. That won’t change with tweaking around the edges. It will only change if we change the way we pay for health care. Money talks. We need to start paying at least part of what we pay based on health outcomes.
Many years ago a colleague and I wrote an article, “Health Care as If Health Mattered.” If you step back and look at how we pay for health care, very little, if any, of our payment structure is based on how much health the care system delivers. Part of that can be addressed by going to capitated models, which I think do better. But you have also got to put into those capitated systems some quality and outcome measures that are both valid and not too burdensome to report on. That’s not easy. We could talk a lot about some of the information systems and payment systems, but I think the bottom line is that we need to be able to deal not only with health emergencies, but also with preventive care, care of chronic diseases, and behavioral health care in ways that maximize health.
One of the ways to do that is simple, monthly, capitated payments along with what I call a registry-based outcomes system.
I’m a tuberculosis specialist by training. In tuberculosis there really is a great information system. We track every single patient who has been diagnosed, and we hold every clinician accountable for whether or not they’ve successfully treated that patient. An optimal health care system should do the same with treatment of hypertension, diabetes, seizure disorder, and other common conditions in which treatment makes a really big difference. Preventive care, especially vaccine delivery, is another example.
I understand that physicians will point out that patients may not come in for that care, or they’re hard to deal with, or they refuse recommended treatment. We don’t expect 100%. But we should expect that, if we’re paying for health care, we should get health.
To do that, I think we need much more support for primary care, both in terms of the absolute amount of dollars going in and the administrative support. Some of our systems are so complicated that you can’t manage them without a billing department. How does a one- or two-physician practice deal with systems that will take dozens of hours a week to manage? You have to deal with the administrative complexity, the structure of the incentives, and the structure of care.
I think these are all things that we have to address. But for a minute, let’s helicopter up and look at the big picture. Without additional help from Congress, tens of thousands of primary care physicians could go out of business in the coming weeks. This is a crisis, and this will be very hard to rebuild. We don’t have a strong, resilient primary care infrastructure today, and if we’re not careful it’ll be even weaker as we try to rebuild.
It has been encouraging to see some of the care innovations that have occurred in response to the pandemic. I’m particularly encouraged by the widespread interest in and support for telemedicine. Telemedicine is a very important way of making care safer, more accessible, less expensive, more efficient. There have been a lot of restrictions on it, not just in the United States but globally, for many years. It’s really interesting to see those restrictions rapidly change. I give credit to the Centers for Medicare & Medicaid Services for quick changes in this area.
Now, telemedicine isn’t a cure-all. There are lots of things you can’t do from a distance. It’s a pale reflection of reality, compared with an in-person first visit with a patient. But it’s a whole lot better than nothing. If we look at some of the best health systems in the United States, they’ve gone to as much as 80% of clinical visits done by telemedicine. I don’t think we’re going to go back. Even if COVID is no longer the threat that it is today, if you can do things more quickly, more efficiently, and more conveniently for both patients and doctors, do them. Obviously, it won’t be all visits, but it could be a large proportion of visits and an important part of strengthening our primary care system.
My initiative, Resolve to Save Lives, which is part of the global health organization Vital Strategies, has done work in the area of public health around the world. I am really struck by how weak primary care systems are in so many countries. Strong primary care systems are the exception rather than the rule, but they’re also a best buy in health care. They’re crucially important, and they’re going to work differently in different countries, in different states, in different communities. We need to do a better job of supporting primary care, building primary care, and paying for primary care.
Dr. Lin: You’ve identified two needs. The immediate need is that primary care practices need revenue now to not have to close in the immediate aftermath or the ongoing COVID epidemic, but also there’s the long term, the percentage of health care dollars that are going to primary care in the long term. You pointed out in your article that currently 5% or less of health care spending is in primary care, which is a lot less percentage-wise than in many other countries. I think the question always comes up is that we want to increase that share, but the money has to come from somewhere. Where is that extra money going to come from? Dr. Frieden: I’m not an expert in health care finance, but one thing I’ve learned over the years is that one person’s waste, fraud, and abuse is somebody else’s profit center. It’s not going to be easy. On the one hand, we do need to think about more efficient ways to organize primary care; on the other hand, we have to figure out a way to internalize some of the savings. If you give good primary care and, therefore, someone doesn’t get hospitalized, you can actually lose money in the current system, whereas you’re saving the system a lot of money by preventing that hospitalization.
I think our health system does have significant inefficiencies in terms of the number of tests and interventions that are done that are really not proven to help patients. It has been demonstrated for decades now that the usual economic incentives don’t operate in health care. In health care, supply often generates demand. The number of gallbladder operations is proportional not to population but to the number of gallbladder surgeons. That’s a problem, and it’s a problem that we’re going to have to assess. “Gatekeeper” is an unpleasant word, but if a primary care practitioner could be the advocate for patients so that we’re not pushing for patients to get more care or to get less care but to get the right care, we have the potential to reduce costs while improving quality.
Dr. Lin: You accurately point out that the fee-for-service payment system has been the major culprit in the declining revenues of primary care practices since the start of the pandemic. But for the majority of primary care physicians, including myself, fee-for-service is all that we’ve ever known. Do you think that primary care is ready for such an abrupt financing change, particularly in a very short period of time?Dr. Frieden: You’re certainly accurate in saying that nothing about health care finance is easy. Trying to address these problems at the national or state level has been extremely difficult. I think that the pilot programs in Medicare are very important. Medicaid is a particular challenge because it’s a state-based program and many of the costs are driven by nursing home and long-term care. When you take those costs out, the actual funding per patient or per provider is quite low in most places.
It’s hard enough to reorganize if you’ve got ample resources, but to reorganize when they are insufficient is particularly hard. I would say only that there are no quick and simple answers to this question, but there is a widespread understanding that what we’re doing now doesn’t make sense. We pay top dollar and we get – despite fantastic doctors and fantastic hospitals – lousy outcomes. I’m a public health physician. I’m an internal medicine and infectious disease specialist. Fundamentally, I look at the data. If you think of our health care system as a patient, the patient is not doing well. We’re not functional to the degree we need to be, particularly when you think of what an enormous outlier our per capita expenditures are [compared with other developed countries] – almost twice the average upper-income country and 25% more than any other upper-income country.
Now, anyone who tells you that change is going to be pain-free is not leveling with you. In addition to things like telemedicine, we have to make much more use of team-based care and task sharing. There are lots of things that doctors are doing these days that they really shouldn’t.
Dr. Lin: In your recent op-ed, you noted the pivot to telehealth that primary care practices have made very quickly in response to the pandemic. That certainly was the experience for my practice. But what are some other strategies that you think are important to support the goal of better care delivery in our primary care practices?Dr. Frieden: Another really important innovation is team-based care. There are lots of things that doctors are doing today that nurses, nurse practitioners, physician assistants, and community health workers can do better and for less money. Frankly, I think that should increase the job satisfaction of physicians, to be doing work that is specific to the physician, requiring either more patient interaction or advanced reasoning or experience.
In my own field of tuberculosis control, I learned how to treat tuberculosis because the nurse at the TB clinic kept correcting me because that’s all she did. She did tuberculosis care, so she had seen everything. Even though I’d finished an infectious disease fellowship and internal medicine residency, the public health nurse knew TB a whole lot better than I did.
Similarly, as we work on hypertension control, you can protocolize most of this care and do a much better job. That’s been proven for more than 40 years, and yet we still don’t do it.
One of the big parts of being able to do more with the same or fewer resources is going to be more team-based care. That’s really a task-sharing approach. I think of that as a triple win: You get better care for lower costs with more employment. What’s not to like?
Dr. Lin: I’m hopeful, as you are, that many of these innovations that have been made by necessity will persist beyond the duration of COVID-19. As you said, the health care system has been really difficult to change, and it often takes something like this to galvanize enough consensus that things need to change.
Dr. Frieden: I think the bottom line here is that we should pay our primary health care providers to keep us healthy and ensure that we have a payment system that lets them do that without risking bankruptcy. That’s not too much to ask of our system. It’s important for our health. It’s important for our economy. It’s important for our communities.
Dr. Lin teaches family medicine, preventive medicine, and health policy at Georgetown University School of Medicine. He is deputy editor of the journal American Family Physician. Follow him on Twitter. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for MedStar Georgetown University Hospital and received income in an amount equal to or greater than $250 from UpToDate, Wiley-Blackwell, and American Academy of Family Physicians.
Dr. Frieden is a physician with advanced training in internal medicine, infectious disease, public health, and epidemiology. He has served as director of the Centers for Disease Control and Prevention and as commissioner of the New York City Health Department. Currently he is president and CEO of Resolve to Save Lives. Follow him on Twitter. Thomas R. Frieden, MD, MPH, has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In a recently published editorial, Tom Frieden, MD, MPH, former head of the Centers for Disease Control and Prevention, argued that primary care is in deep trouble, its long-standing financial problems exacerbated by the fallout from the COVID-19 pandemic. Those arguments resonated with Kenny Lin, MD, MPH, a family physician, professor at Georgetown University School of Medicine, and a regular contributor to Medscape. He spoke with Dr. Frieden about his concerns.
Dr. Lin: Why did you feel that it was important to write this piece focused on primary care?
Dr. Frieden: I’m glad you asked that question. Given all that is going on, one might ask, what is the importance of primary care? We’ve got this epidemic going on that requires public health and hospital systems. Why voice concern about primary care now?
It’s really striking to see that the number of visits has plummeted. Because of our payment structure, that means incomes have plummeted. We’re hearing about doctors’ offices getting boarded up and shuttering. As I write in the piece, it’s one thing for a theater or a restaurant or another important community entity to shut because of economic downturn, and these are real losses, but to lose their only primary care practice or one of the few in an area really is a matter of life and death for many communities.
Dr. Lin: I agree. In my own practice we haven’t had to furlough anyone, but we’ve put people on forced paid time off. We’ve been reallocating physicians to other parts of our health system. It is definitely a concern. A solo practitioner or someone in a rural practice would most likely be even much more heavily hit. You’ve argued that the neglect of our public health system on a national level has led to many preventable deaths from COVID-19. Do you feel that something similar has happened in primary care? How could a stronger, better-funded primary care infrastructure better prepare us for the next pandemic?
Dr. Frieden: All over the world, we see an overemphasis on hospital care and an underemphasis on primary care, outpatient care, family medicine. As a result, we pay more. We have larger risks, and we don’t prevent diseases that we could prevent. It’s fundamentally about the economic incentives of our health care system. Of course, that often reflects the political reality of different profit centers and cost centers of care. That won’t change with tweaking around the edges. It will only change if we change the way we pay for health care. Money talks. We need to start paying at least part of what we pay based on health outcomes.
Many years ago a colleague and I wrote an article, “Health Care as If Health Mattered.” If you step back and look at how we pay for health care, very little, if any, of our payment structure is based on how much health the care system delivers. Part of that can be addressed by going to capitated models, which I think do better. But you have also got to put into those capitated systems some quality and outcome measures that are both valid and not too burdensome to report on. That’s not easy. We could talk a lot about some of the information systems and payment systems, but I think the bottom line is that we need to be able to deal not only with health emergencies, but also with preventive care, care of chronic diseases, and behavioral health care in ways that maximize health.
One of the ways to do that is simple, monthly, capitated payments along with what I call a registry-based outcomes system.
I’m a tuberculosis specialist by training. In tuberculosis there really is a great information system. We track every single patient who has been diagnosed, and we hold every clinician accountable for whether or not they’ve successfully treated that patient. An optimal health care system should do the same with treatment of hypertension, diabetes, seizure disorder, and other common conditions in which treatment makes a really big difference. Preventive care, especially vaccine delivery, is another example.
I understand that physicians will point out that patients may not come in for that care, or they’re hard to deal with, or they refuse recommended treatment. We don’t expect 100%. But we should expect that, if we’re paying for health care, we should get health.
To do that, I think we need much more support for primary care, both in terms of the absolute amount of dollars going in and the administrative support. Some of our systems are so complicated that you can’t manage them without a billing department. How does a one- or two-physician practice deal with systems that will take dozens of hours a week to manage? You have to deal with the administrative complexity, the structure of the incentives, and the structure of care.
I think these are all things that we have to address. But for a minute, let’s helicopter up and look at the big picture. Without additional help from Congress, tens of thousands of primary care physicians could go out of business in the coming weeks. This is a crisis, and this will be very hard to rebuild. We don’t have a strong, resilient primary care infrastructure today, and if we’re not careful it’ll be even weaker as we try to rebuild.
It has been encouraging to see some of the care innovations that have occurred in response to the pandemic. I’m particularly encouraged by the widespread interest in and support for telemedicine. Telemedicine is a very important way of making care safer, more accessible, less expensive, more efficient. There have been a lot of restrictions on it, not just in the United States but globally, for many years. It’s really interesting to see those restrictions rapidly change. I give credit to the Centers for Medicare & Medicaid Services for quick changes in this area.
Now, telemedicine isn’t a cure-all. There are lots of things you can’t do from a distance. It’s a pale reflection of reality, compared with an in-person first visit with a patient. But it’s a whole lot better than nothing. If we look at some of the best health systems in the United States, they’ve gone to as much as 80% of clinical visits done by telemedicine. I don’t think we’re going to go back. Even if COVID is no longer the threat that it is today, if you can do things more quickly, more efficiently, and more conveniently for both patients and doctors, do them. Obviously, it won’t be all visits, but it could be a large proportion of visits and an important part of strengthening our primary care system.
My initiative, Resolve to Save Lives, which is part of the global health organization Vital Strategies, has done work in the area of public health around the world. I am really struck by how weak primary care systems are in so many countries. Strong primary care systems are the exception rather than the rule, but they’re also a best buy in health care. They’re crucially important, and they’re going to work differently in different countries, in different states, in different communities. We need to do a better job of supporting primary care, building primary care, and paying for primary care.
Dr. Lin: You’ve identified two needs. The immediate need is that primary care practices need revenue now to not have to close in the immediate aftermath or the ongoing COVID epidemic, but also there’s the long term, the percentage of health care dollars that are going to primary care in the long term. You pointed out in your article that currently 5% or less of health care spending is in primary care, which is a lot less percentage-wise than in many other countries. I think the question always comes up is that we want to increase that share, but the money has to come from somewhere. Where is that extra money going to come from? Dr. Frieden: I’m not an expert in health care finance, but one thing I’ve learned over the years is that one person’s waste, fraud, and abuse is somebody else’s profit center. It’s not going to be easy. On the one hand, we do need to think about more efficient ways to organize primary care; on the other hand, we have to figure out a way to internalize some of the savings. If you give good primary care and, therefore, someone doesn’t get hospitalized, you can actually lose money in the current system, whereas you’re saving the system a lot of money by preventing that hospitalization.
I think our health system does have significant inefficiencies in terms of the number of tests and interventions that are done that are really not proven to help patients. It has been demonstrated for decades now that the usual economic incentives don’t operate in health care. In health care, supply often generates demand. The number of gallbladder operations is proportional not to population but to the number of gallbladder surgeons. That’s a problem, and it’s a problem that we’re going to have to assess. “Gatekeeper” is an unpleasant word, but if a primary care practitioner could be the advocate for patients so that we’re not pushing for patients to get more care or to get less care but to get the right care, we have the potential to reduce costs while improving quality.
Dr. Lin: You accurately point out that the fee-for-service payment system has been the major culprit in the declining revenues of primary care practices since the start of the pandemic. But for the majority of primary care physicians, including myself, fee-for-service is all that we’ve ever known. Do you think that primary care is ready for such an abrupt financing change, particularly in a very short period of time?Dr. Frieden: You’re certainly accurate in saying that nothing about health care finance is easy. Trying to address these problems at the national or state level has been extremely difficult. I think that the pilot programs in Medicare are very important. Medicaid is a particular challenge because it’s a state-based program and many of the costs are driven by nursing home and long-term care. When you take those costs out, the actual funding per patient or per provider is quite low in most places.
It’s hard enough to reorganize if you’ve got ample resources, but to reorganize when they are insufficient is particularly hard. I would say only that there are no quick and simple answers to this question, but there is a widespread understanding that what we’re doing now doesn’t make sense. We pay top dollar and we get – despite fantastic doctors and fantastic hospitals – lousy outcomes. I’m a public health physician. I’m an internal medicine and infectious disease specialist. Fundamentally, I look at the data. If you think of our health care system as a patient, the patient is not doing well. We’re not functional to the degree we need to be, particularly when you think of what an enormous outlier our per capita expenditures are [compared with other developed countries] – almost twice the average upper-income country and 25% more than any other upper-income country.
Now, anyone who tells you that change is going to be pain-free is not leveling with you. In addition to things like telemedicine, we have to make much more use of team-based care and task sharing. There are lots of things that doctors are doing these days that they really shouldn’t.
Dr. Lin: In your recent op-ed, you noted the pivot to telehealth that primary care practices have made very quickly in response to the pandemic. That certainly was the experience for my practice. But what are some other strategies that you think are important to support the goal of better care delivery in our primary care practices?Dr. Frieden: Another really important innovation is team-based care. There are lots of things that doctors are doing today that nurses, nurse practitioners, physician assistants, and community health workers can do better and for less money. Frankly, I think that should increase the job satisfaction of physicians, to be doing work that is specific to the physician, requiring either more patient interaction or advanced reasoning or experience.
In my own field of tuberculosis control, I learned how to treat tuberculosis because the nurse at the TB clinic kept correcting me because that’s all she did. She did tuberculosis care, so she had seen everything. Even though I’d finished an infectious disease fellowship and internal medicine residency, the public health nurse knew TB a whole lot better than I did.
Similarly, as we work on hypertension control, you can protocolize most of this care and do a much better job. That’s been proven for more than 40 years, and yet we still don’t do it.
One of the big parts of being able to do more with the same or fewer resources is going to be more team-based care. That’s really a task-sharing approach. I think of that as a triple win: You get better care for lower costs with more employment. What’s not to like?
Dr. Lin: I’m hopeful, as you are, that many of these innovations that have been made by necessity will persist beyond the duration of COVID-19. As you said, the health care system has been really difficult to change, and it often takes something like this to galvanize enough consensus that things need to change.
Dr. Frieden: I think the bottom line here is that we should pay our primary health care providers to keep us healthy and ensure that we have a payment system that lets them do that without risking bankruptcy. That’s not too much to ask of our system. It’s important for our health. It’s important for our economy. It’s important for our communities.
Dr. Lin teaches family medicine, preventive medicine, and health policy at Georgetown University School of Medicine. He is deputy editor of the journal American Family Physician. Follow him on Twitter. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for MedStar Georgetown University Hospital and received income in an amount equal to or greater than $250 from UpToDate, Wiley-Blackwell, and American Academy of Family Physicians.
Dr. Frieden is a physician with advanced training in internal medicine, infectious disease, public health, and epidemiology. He has served as director of the Centers for Disease Control and Prevention and as commissioner of the New York City Health Department. Currently he is president and CEO of Resolve to Save Lives. Follow him on Twitter. Thomas R. Frieden, MD, MPH, has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.