User login
Can Endurance Exercise Be Harmful?
In 490 BC, Pheidippides (or possibly Philippides) ran from Athens to Sparta to ask for military aid against the invading Persian army, then back to Athens, then off to the battlefield of Marathon, then back to Athens to announce the army’s victory, after which he promptly died. The story, if it is to be believed (there is some doubt among historians), raises an interesting question: Are some forms of exercise dangerous?
Running a marathon is a lot of work. The “worst parade ever,” as one spectator described it, is not without its risks. As a runner myself, I know that it doesn’t take much to generate a bloody sock at the end of a long run.
But when most people think about the risks of exercise, they mean the cardiovascular risks, such as sudden deaths during marathons, probably because of the aforementioned ancient Greek’s demise. The reality is more reassuring. An analysis of 10 years’ worth of data from US marathons and half-marathons found that out of 10.9 million runners, there were 59 cardiac arrests, an incidence rate of 0.54 per 100,000 participants. Others have found incidence rates in the same range. An analysis of the annual Marine Corps and Twin Cities marathons found a sudden death rate of 0.002%.
Marathon runners do sometimes require medical attention. In the Twin Cities cohort, 25 out of every 1000 finishers required medical attention, but 90% of their problems were mild. The majority included issues such as dehydration, vasovagal syncope, hyperthermia, and exhaustion. Musculoskeletal problems and skin abrasions made up the rest. Objectively, long distance running is fairly safe.
Running and Coronary Calcium
Then a study comes around suggesting that marathon runners have more coronary artery calcium (CAC). In 2008, German researchers compared 108 healthy male marathon runners over 50 years of age with Framingham risk–matched controls. The marathoners had a higher median CAC score (36 vs 12; P =.02), but scores across the board were quite low and not all studies were in agreement. The MESA study and another from Korea found an inverse relationship between physical activity and coronary calcium, but they compared sedentary people with vigorous exercisers, not specifically marathoners.
Two later studies, published in 2017, generally corroborated that endurance exercise was associated with higher calcium — with some caveats. A group from the Netherlands looked at lifelong exercise volume and compared men who accumulated > 2000 MET-min/week with those who exercised < 1000 MET-min/week. Again, the analysis was limited to men, and CAC scores, though statistically different, were still very low (9.4 vs 0; P =.02). Importantly, in men with coronary plaques, the more active group had less mixed plaque and more calcified plaque.
A UK study of middle-aged masters-level athletes at low cardiovascular risk had similar findings. Most of the study population (70%) were men, and 77% were runners (not all were marathoners). Overall, the male athletes had not only more plaque but more calcified plaque than their sedentary peers, even though most male athletes (60%) had a CAC score of zero.
The findings from these two studies were interpreted as reassuring. They confirmed that athletes are a generally low-risk group with low calcium scores, and although they might have more plaque and coronary calcium on average, it tends to be the more benign calcified type.
Masters at Heart
But the 2023 Master@Heart study challenged that assertion. It analyzed lifelong endurance athletes, late-onset endurance athletes (those who came to the game later in life), and healthy nonathletic controls. The study also found more coronary stenoses in lifelong athletes, but the breakdown of calcified vs noncalcified vs mixed plaques was the same across groups, thus contradicting the idea that exercise exerted its protective effect by calcifying and therefore stabilizing said plaques. The silver lining was fewer vulnerable plaques in the lifelong athletes (defined via high-risk features) but these were generally rare across the entire population.
Whether Master@Heart is groundbreaking or an outlier depends on your point of view. In 2024, a study from Portugal suggested that the relationship between exercise and coronary calcification is more complicated. Among 105 male veteran athletes, a high volume of exercise was associated with more coronary atherosclerosis in those at higher cardiovascular risk, but it tended to be protective in those deemed lower risk. In fact, the high-volume exercise group had fewer individuals with a CAC score > 100 (16% vs 4%; P =.029), though again, the vast majority had low CAC scores.
A limitation of all these studies is that they had cross-sectional designs, measuring coronary calcium at a single point in time and relying on questionnaires and patient recall to determine lifelong exposure to exercise. Recall bias could have been a problem, and exercise patterns vary over time. It’s not unreasonable to wonder whether people at higher cardiovascular risk should start exercising to mitigate that risk. Granted, they might not start running marathons, but many of these studies looked only at physical activity levels. A study that measured the increase (or stability) of coronary calcium over time would be more helpful.
Prior research (in men again) showed that high levels of physical activity were associated with more coronary calcium, but not with all-cause or cardiovascular mortality. But it too looked only at a single time point. The most recent study added to the body of evidence included data on nearly 9000 men and women and found that higher exercise volume did not correlate with CAC progression over the mean follow-up of 7.8 years. The study measured physical activity of any variety and included physically taxing sports like golf (without a cart). So it was not an assessment of the dangers of endurance exercise.
Outstanding Questions and Bananas
Ultimately, many questions remain. Is the lack of risk seen in women a spurious finding because they are underrepresented in most studies, or might exercise affect men and women differently? Is it valid to combine studies on endurance exercise with those looking at physical activity more generally? How accurate are self-reports of exercise? Could endurance exercisers be using performance-enhancing drugs that are confounding the associations? Are people who engage in more physical activity healthier or just trying to mitigate a higher baseline cardiovascular risk? Why do they give out bananas at the end of marathons given that there are better sources of potassium?
We have no randomized trials on the benefits and risks of endurance exercise. Even if you could get ethics approval, one imagines there would be few volunteers. In the end, we must make do with observational data and remember that coronary calcifications are a surrogate endpoint.
When it comes to hard endpoints, an analysis of French Tour de France participants found a lower risk for both cardiovascular and cancer deaths compared with the general male population. So perhaps the most important take-home message is one that has been said many times: Beware of surrogate endpoints. And for those contemplating running a marathon, I am forced to agree with the person who wrote the sign I saw during my first race. It does seem like a lot of work for a free banana.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, Quebec, Canada. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
In 490 BC, Pheidippides (or possibly Philippides) ran from Athens to Sparta to ask for military aid against the invading Persian army, then back to Athens, then off to the battlefield of Marathon, then back to Athens to announce the army’s victory, after which he promptly died. The story, if it is to be believed (there is some doubt among historians), raises an interesting question: Are some forms of exercise dangerous?
Running a marathon is a lot of work. The “worst parade ever,” as one spectator described it, is not without its risks. As a runner myself, I know that it doesn’t take much to generate a bloody sock at the end of a long run.
But when most people think about the risks of exercise, they mean the cardiovascular risks, such as sudden deaths during marathons, probably because of the aforementioned ancient Greek’s demise. The reality is more reassuring. An analysis of 10 years’ worth of data from US marathons and half-marathons found that out of 10.9 million runners, there were 59 cardiac arrests, an incidence rate of 0.54 per 100,000 participants. Others have found incidence rates in the same range. An analysis of the annual Marine Corps and Twin Cities marathons found a sudden death rate of 0.002%.
Marathon runners do sometimes require medical attention. In the Twin Cities cohort, 25 out of every 1000 finishers required medical attention, but 90% of their problems were mild. The majority included issues such as dehydration, vasovagal syncope, hyperthermia, and exhaustion. Musculoskeletal problems and skin abrasions made up the rest. Objectively, long distance running is fairly safe.
Running and Coronary Calcium
Then a study comes around suggesting that marathon runners have more coronary artery calcium (CAC). In 2008, German researchers compared 108 healthy male marathon runners over 50 years of age with Framingham risk–matched controls. The marathoners had a higher median CAC score (36 vs 12; P =.02), but scores across the board were quite low and not all studies were in agreement. The MESA study and another from Korea found an inverse relationship between physical activity and coronary calcium, but they compared sedentary people with vigorous exercisers, not specifically marathoners.
Two later studies, published in 2017, generally corroborated that endurance exercise was associated with higher calcium — with some caveats. A group from the Netherlands looked at lifelong exercise volume and compared men who accumulated > 2000 MET-min/week with those who exercised < 1000 MET-min/week. Again, the analysis was limited to men, and CAC scores, though statistically different, were still very low (9.4 vs 0; P =.02). Importantly, in men with coronary plaques, the more active group had less mixed plaque and more calcified plaque.
A UK study of middle-aged masters-level athletes at low cardiovascular risk had similar findings. Most of the study population (70%) were men, and 77% were runners (not all were marathoners). Overall, the male athletes had not only more plaque but more calcified plaque than their sedentary peers, even though most male athletes (60%) had a CAC score of zero.
The findings from these two studies were interpreted as reassuring. They confirmed that athletes are a generally low-risk group with low calcium scores, and although they might have more plaque and coronary calcium on average, it tends to be the more benign calcified type.
Masters at Heart
But the 2023 Master@Heart study challenged that assertion. It analyzed lifelong endurance athletes, late-onset endurance athletes (those who came to the game later in life), and healthy nonathletic controls. The study also found more coronary stenoses in lifelong athletes, but the breakdown of calcified vs noncalcified vs mixed plaques was the same across groups, thus contradicting the idea that exercise exerted its protective effect by calcifying and therefore stabilizing said plaques. The silver lining was fewer vulnerable plaques in the lifelong athletes (defined via high-risk features) but these were generally rare across the entire population.
Whether Master@Heart is groundbreaking or an outlier depends on your point of view. In 2024, a study from Portugal suggested that the relationship between exercise and coronary calcification is more complicated. Among 105 male veteran athletes, a high volume of exercise was associated with more coronary atherosclerosis in those at higher cardiovascular risk, but it tended to be protective in those deemed lower risk. In fact, the high-volume exercise group had fewer individuals with a CAC score > 100 (16% vs 4%; P =.029), though again, the vast majority had low CAC scores.
A limitation of all these studies is that they had cross-sectional designs, measuring coronary calcium at a single point in time and relying on questionnaires and patient recall to determine lifelong exposure to exercise. Recall bias could have been a problem, and exercise patterns vary over time. It’s not unreasonable to wonder whether people at higher cardiovascular risk should start exercising to mitigate that risk. Granted, they might not start running marathons, but many of these studies looked only at physical activity levels. A study that measured the increase (or stability) of coronary calcium over time would be more helpful.
Prior research (in men again) showed that high levels of physical activity were associated with more coronary calcium, but not with all-cause or cardiovascular mortality. But it too looked only at a single time point. The most recent study added to the body of evidence included data on nearly 9000 men and women and found that higher exercise volume did not correlate with CAC progression over the mean follow-up of 7.8 years. The study measured physical activity of any variety and included physically taxing sports like golf (without a cart). So it was not an assessment of the dangers of endurance exercise.
Outstanding Questions and Bananas
Ultimately, many questions remain. Is the lack of risk seen in women a spurious finding because they are underrepresented in most studies, or might exercise affect men and women differently? Is it valid to combine studies on endurance exercise with those looking at physical activity more generally? How accurate are self-reports of exercise? Could endurance exercisers be using performance-enhancing drugs that are confounding the associations? Are people who engage in more physical activity healthier or just trying to mitigate a higher baseline cardiovascular risk? Why do they give out bananas at the end of marathons given that there are better sources of potassium?
We have no randomized trials on the benefits and risks of endurance exercise. Even if you could get ethics approval, one imagines there would be few volunteers. In the end, we must make do with observational data and remember that coronary calcifications are a surrogate endpoint.
When it comes to hard endpoints, an analysis of French Tour de France participants found a lower risk for both cardiovascular and cancer deaths compared with the general male population. So perhaps the most important take-home message is one that has been said many times: Beware of surrogate endpoints. And for those contemplating running a marathon, I am forced to agree with the person who wrote the sign I saw during my first race. It does seem like a lot of work for a free banana.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, Quebec, Canada. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
In 490 BC, Pheidippides (or possibly Philippides) ran from Athens to Sparta to ask for military aid against the invading Persian army, then back to Athens, then off to the battlefield of Marathon, then back to Athens to announce the army’s victory, after which he promptly died. The story, if it is to be believed (there is some doubt among historians), raises an interesting question: Are some forms of exercise dangerous?
Running a marathon is a lot of work. The “worst parade ever,” as one spectator described it, is not without its risks. As a runner myself, I know that it doesn’t take much to generate a bloody sock at the end of a long run.
But when most people think about the risks of exercise, they mean the cardiovascular risks, such as sudden deaths during marathons, probably because of the aforementioned ancient Greek’s demise. The reality is more reassuring. An analysis of 10 years’ worth of data from US marathons and half-marathons found that out of 10.9 million runners, there were 59 cardiac arrests, an incidence rate of 0.54 per 100,000 participants. Others have found incidence rates in the same range. An analysis of the annual Marine Corps and Twin Cities marathons found a sudden death rate of 0.002%.
Marathon runners do sometimes require medical attention. In the Twin Cities cohort, 25 out of every 1000 finishers required medical attention, but 90% of their problems were mild. The majority included issues such as dehydration, vasovagal syncope, hyperthermia, and exhaustion. Musculoskeletal problems and skin abrasions made up the rest. Objectively, long distance running is fairly safe.
Running and Coronary Calcium
Then a study comes around suggesting that marathon runners have more coronary artery calcium (CAC). In 2008, German researchers compared 108 healthy male marathon runners over 50 years of age with Framingham risk–matched controls. The marathoners had a higher median CAC score (36 vs 12; P =.02), but scores across the board were quite low and not all studies were in agreement. The MESA study and another from Korea found an inverse relationship between physical activity and coronary calcium, but they compared sedentary people with vigorous exercisers, not specifically marathoners.
Two later studies, published in 2017, generally corroborated that endurance exercise was associated with higher calcium — with some caveats. A group from the Netherlands looked at lifelong exercise volume and compared men who accumulated > 2000 MET-min/week with those who exercised < 1000 MET-min/week. Again, the analysis was limited to men, and CAC scores, though statistically different, were still very low (9.4 vs 0; P =.02). Importantly, in men with coronary plaques, the more active group had less mixed plaque and more calcified plaque.
A UK study of middle-aged masters-level athletes at low cardiovascular risk had similar findings. Most of the study population (70%) were men, and 77% were runners (not all were marathoners). Overall, the male athletes had not only more plaque but more calcified plaque than their sedentary peers, even though most male athletes (60%) had a CAC score of zero.
The findings from these two studies were interpreted as reassuring. They confirmed that athletes are a generally low-risk group with low calcium scores, and although they might have more plaque and coronary calcium on average, it tends to be the more benign calcified type.
Masters at Heart
But the 2023 Master@Heart study challenged that assertion. It analyzed lifelong endurance athletes, late-onset endurance athletes (those who came to the game later in life), and healthy nonathletic controls. The study also found more coronary stenoses in lifelong athletes, but the breakdown of calcified vs noncalcified vs mixed plaques was the same across groups, thus contradicting the idea that exercise exerted its protective effect by calcifying and therefore stabilizing said plaques. The silver lining was fewer vulnerable plaques in the lifelong athletes (defined via high-risk features) but these were generally rare across the entire population.
Whether Master@Heart is groundbreaking or an outlier depends on your point of view. In 2024, a study from Portugal suggested that the relationship between exercise and coronary calcification is more complicated. Among 105 male veteran athletes, a high volume of exercise was associated with more coronary atherosclerosis in those at higher cardiovascular risk, but it tended to be protective in those deemed lower risk. In fact, the high-volume exercise group had fewer individuals with a CAC score > 100 (16% vs 4%; P =.029), though again, the vast majority had low CAC scores.
A limitation of all these studies is that they had cross-sectional designs, measuring coronary calcium at a single point in time and relying on questionnaires and patient recall to determine lifelong exposure to exercise. Recall bias could have been a problem, and exercise patterns vary over time. It’s not unreasonable to wonder whether people at higher cardiovascular risk should start exercising to mitigate that risk. Granted, they might not start running marathons, but many of these studies looked only at physical activity levels. A study that measured the increase (or stability) of coronary calcium over time would be more helpful.
Prior research (in men again) showed that high levels of physical activity were associated with more coronary calcium, but not with all-cause or cardiovascular mortality. But it too looked only at a single time point. The most recent study added to the body of evidence included data on nearly 9000 men and women and found that higher exercise volume did not correlate with CAC progression over the mean follow-up of 7.8 years. The study measured physical activity of any variety and included physically taxing sports like golf (without a cart). So it was not an assessment of the dangers of endurance exercise.
Outstanding Questions and Bananas
Ultimately, many questions remain. Is the lack of risk seen in women a spurious finding because they are underrepresented in most studies, or might exercise affect men and women differently? Is it valid to combine studies on endurance exercise with those looking at physical activity more generally? How accurate are self-reports of exercise? Could endurance exercisers be using performance-enhancing drugs that are confounding the associations? Are people who engage in more physical activity healthier or just trying to mitigate a higher baseline cardiovascular risk? Why do they give out bananas at the end of marathons given that there are better sources of potassium?
We have no randomized trials on the benefits and risks of endurance exercise. Even if you could get ethics approval, one imagines there would be few volunteers. In the end, we must make do with observational data and remember that coronary calcifications are a surrogate endpoint.
When it comes to hard endpoints, an analysis of French Tour de France participants found a lower risk for both cardiovascular and cancer deaths compared with the general male population. So perhaps the most important take-home message is one that has been said many times: Beware of surrogate endpoints. And for those contemplating running a marathon, I am forced to agree with the person who wrote the sign I saw during my first race. It does seem like a lot of work for a free banana.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, Quebec, Canada. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
New AFib Guidelines Address Underlying Illness, Comorbidities
LONDON — Updated guidelines for the management of atrial fibrillation released by the European Society of Cardiology are revamping the approach to care for this complex, multifactorial disease.
, Isabelle Van Gelder, MD, PhD, professor of cardiology at the University Medical Center in Groningen, the Netherlands, explained at the European Society of Cardiology (ESC) Congress.
It is not just appropriate to place the same emphasis on the control of comorbidities as on the rhythm disturbance, it is critical, said Dr. Van Gelder, who served as chair of the ESC-AF guidelines task force.
Comorbidities are the drivers of both the onset and recurrence of atrial fibrillation, and a dynamic approach to comorbidities is “central for the success of AF management.”
Class I Recommendation
In fact, on the basis of overwhelming evidence, a class I recommendation has been issued for a large number of goals in the comorbidity and risk factor management step of atrial fibrillation management, including those for hypertension, components of heart failure, obesity, diabetes, alcohol consumption, and exercise.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors “should be offered to all patients with AF,” according to Dr. Van Gelder, who identified this as a new class I recommendation.
Patients who are not managed aggressively for the listed comorbidities ultimately face “treatment failure, poor patient outcomes, and a waste of healthcare resources,” she said.
Control of sleep apnea is also noted as a key target, although Van Gelder acknowledged that the supporting evidence only allows for a class IIb recommendation.
Control of comorbidities is not a new idea. In the 2023 joint guideline, led by a consortium of professional groups, including the American Heart Association (AHA) and the American College of Cardiology (ACC), the control of comorbidities, including most of those identified in the new ESC guidelines, was second in a list of 10 key take-home messages.
However, the new ESC guidelines have prioritized comorbidity management by listing it first in each of the specific patient-care pathways developed to define optimized care.
These pathways, defined in algorithms for newly diagnosed AF, paroxysmal AF, and persistent AF, always start with the assessment of comorbidities, followed by step A — avoiding stroke — largely with anticoagulation.
Direct oral anticoagulants should be used, “except in those with a mechanical valve or mitral stenosis,” Dr. Van Gelder said. This includes, essentially, all patients with a CHA2DS2-VASc score of 2 or greater, and it should be “considered” in those with a score of 1.
The ESC framework has been identified with the acronym AF-CARE, in which the C stands for comorbidities.
In the A step of the framework, identifying and treating all modifiable bleeding risk factors in AF patients is a class I recommendation. On the basis of a class III recommendation, she cautioned against withholding anticoagulants because of CHA2DS2-VASc risk factors alone. Rather, Dr. Van Gelder called the decision to administer or withhold anticoagulation — like all decisions — one that should be individualized in consultation with the patient.
For reducing AF symptoms and rhythm control, the specific pathways diverge for newly diagnosed AF, paroxysmal AF, and persistent AF. Like all of the guidelines, the specific options for symptom management and AF ablation are color coded, with green signifying level 1 evidence.
The evaluation and dynamic reassessment step refers to the need to periodically assess patients for new modifiable risk factors related to comorbidities, risk for stroke, risk for bleeding, and risk for AF.
The management of risk factors for AF has long been emphasized in guidelines, but a previous focus on AF with attention to comorbidities has been replaced by a focus on comorbidities with an expectation of more durable AF control. The success of this pivot is based on multidisciplinary care, chosen in collaboration with the patient, to reduce or eliminate the triggers of AF and the risks of its complications.
Pathways Are Appropriate for All Patients
A very important recommendation — and this is new — is “to treat all our patients with atrial fibrillation, whether they are young or old, men or women, Black or White, or at high or low risk, according to our patient-centered integrated AF-CARE approach,” Dr. Van Gelder said.
The changes reflect a shared appreciation for the tight relation between the control of comorbidities and the control of AF, according to José A. Joglar, MD, professor of cardiac electrophysiologic research at the University of Texas Southwestern Medical Center in Dallas. Dr. Joglar was chair of the writing committee for the joint 2023 AF guidelines released by the AHA, ACC, the American College of Clinical Pharmacy, and the Heart Rhythm Society.
“It is increasingly clear that AF in many cases is the consequence of underlying risk factors and comorbidities, which cannot be separated from AF alone,” Dr. Joglar explained in an interview.
This was placed first “to emphasize the importance of viewing AFib as a complex disease that requires a holistic, multidisciplinary approach to care, as opposed to being viewed just as a rhythm abnormality,” he said.
A version of this article first appeared on Medscape.com.
LONDON — Updated guidelines for the management of atrial fibrillation released by the European Society of Cardiology are revamping the approach to care for this complex, multifactorial disease.
, Isabelle Van Gelder, MD, PhD, professor of cardiology at the University Medical Center in Groningen, the Netherlands, explained at the European Society of Cardiology (ESC) Congress.
It is not just appropriate to place the same emphasis on the control of comorbidities as on the rhythm disturbance, it is critical, said Dr. Van Gelder, who served as chair of the ESC-AF guidelines task force.
Comorbidities are the drivers of both the onset and recurrence of atrial fibrillation, and a dynamic approach to comorbidities is “central for the success of AF management.”
Class I Recommendation
In fact, on the basis of overwhelming evidence, a class I recommendation has been issued for a large number of goals in the comorbidity and risk factor management step of atrial fibrillation management, including those for hypertension, components of heart failure, obesity, diabetes, alcohol consumption, and exercise.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors “should be offered to all patients with AF,” according to Dr. Van Gelder, who identified this as a new class I recommendation.
Patients who are not managed aggressively for the listed comorbidities ultimately face “treatment failure, poor patient outcomes, and a waste of healthcare resources,” she said.
Control of sleep apnea is also noted as a key target, although Van Gelder acknowledged that the supporting evidence only allows for a class IIb recommendation.
Control of comorbidities is not a new idea. In the 2023 joint guideline, led by a consortium of professional groups, including the American Heart Association (AHA) and the American College of Cardiology (ACC), the control of comorbidities, including most of those identified in the new ESC guidelines, was second in a list of 10 key take-home messages.
However, the new ESC guidelines have prioritized comorbidity management by listing it first in each of the specific patient-care pathways developed to define optimized care.
These pathways, defined in algorithms for newly diagnosed AF, paroxysmal AF, and persistent AF, always start with the assessment of comorbidities, followed by step A — avoiding stroke — largely with anticoagulation.
Direct oral anticoagulants should be used, “except in those with a mechanical valve or mitral stenosis,” Dr. Van Gelder said. This includes, essentially, all patients with a CHA2DS2-VASc score of 2 or greater, and it should be “considered” in those with a score of 1.
The ESC framework has been identified with the acronym AF-CARE, in which the C stands for comorbidities.
In the A step of the framework, identifying and treating all modifiable bleeding risk factors in AF patients is a class I recommendation. On the basis of a class III recommendation, she cautioned against withholding anticoagulants because of CHA2DS2-VASc risk factors alone. Rather, Dr. Van Gelder called the decision to administer or withhold anticoagulation — like all decisions — one that should be individualized in consultation with the patient.
For reducing AF symptoms and rhythm control, the specific pathways diverge for newly diagnosed AF, paroxysmal AF, and persistent AF. Like all of the guidelines, the specific options for symptom management and AF ablation are color coded, with green signifying level 1 evidence.
The evaluation and dynamic reassessment step refers to the need to periodically assess patients for new modifiable risk factors related to comorbidities, risk for stroke, risk for bleeding, and risk for AF.
The management of risk factors for AF has long been emphasized in guidelines, but a previous focus on AF with attention to comorbidities has been replaced by a focus on comorbidities with an expectation of more durable AF control. The success of this pivot is based on multidisciplinary care, chosen in collaboration with the patient, to reduce or eliminate the triggers of AF and the risks of its complications.
Pathways Are Appropriate for All Patients
A very important recommendation — and this is new — is “to treat all our patients with atrial fibrillation, whether they are young or old, men or women, Black or White, or at high or low risk, according to our patient-centered integrated AF-CARE approach,” Dr. Van Gelder said.
The changes reflect a shared appreciation for the tight relation between the control of comorbidities and the control of AF, according to José A. Joglar, MD, professor of cardiac electrophysiologic research at the University of Texas Southwestern Medical Center in Dallas. Dr. Joglar was chair of the writing committee for the joint 2023 AF guidelines released by the AHA, ACC, the American College of Clinical Pharmacy, and the Heart Rhythm Society.
“It is increasingly clear that AF in many cases is the consequence of underlying risk factors and comorbidities, which cannot be separated from AF alone,” Dr. Joglar explained in an interview.
This was placed first “to emphasize the importance of viewing AFib as a complex disease that requires a holistic, multidisciplinary approach to care, as opposed to being viewed just as a rhythm abnormality,” he said.
A version of this article first appeared on Medscape.com.
LONDON — Updated guidelines for the management of atrial fibrillation released by the European Society of Cardiology are revamping the approach to care for this complex, multifactorial disease.
, Isabelle Van Gelder, MD, PhD, professor of cardiology at the University Medical Center in Groningen, the Netherlands, explained at the European Society of Cardiology (ESC) Congress.
It is not just appropriate to place the same emphasis on the control of comorbidities as on the rhythm disturbance, it is critical, said Dr. Van Gelder, who served as chair of the ESC-AF guidelines task force.
Comorbidities are the drivers of both the onset and recurrence of atrial fibrillation, and a dynamic approach to comorbidities is “central for the success of AF management.”
Class I Recommendation
In fact, on the basis of overwhelming evidence, a class I recommendation has been issued for a large number of goals in the comorbidity and risk factor management step of atrial fibrillation management, including those for hypertension, components of heart failure, obesity, diabetes, alcohol consumption, and exercise.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors “should be offered to all patients with AF,” according to Dr. Van Gelder, who identified this as a new class I recommendation.
Patients who are not managed aggressively for the listed comorbidities ultimately face “treatment failure, poor patient outcomes, and a waste of healthcare resources,” she said.
Control of sleep apnea is also noted as a key target, although Van Gelder acknowledged that the supporting evidence only allows for a class IIb recommendation.
Control of comorbidities is not a new idea. In the 2023 joint guideline, led by a consortium of professional groups, including the American Heart Association (AHA) and the American College of Cardiology (ACC), the control of comorbidities, including most of those identified in the new ESC guidelines, was second in a list of 10 key take-home messages.
However, the new ESC guidelines have prioritized comorbidity management by listing it first in each of the specific patient-care pathways developed to define optimized care.
These pathways, defined in algorithms for newly diagnosed AF, paroxysmal AF, and persistent AF, always start with the assessment of comorbidities, followed by step A — avoiding stroke — largely with anticoagulation.
Direct oral anticoagulants should be used, “except in those with a mechanical valve or mitral stenosis,” Dr. Van Gelder said. This includes, essentially, all patients with a CHA2DS2-VASc score of 2 or greater, and it should be “considered” in those with a score of 1.
The ESC framework has been identified with the acronym AF-CARE, in which the C stands for comorbidities.
In the A step of the framework, identifying and treating all modifiable bleeding risk factors in AF patients is a class I recommendation. On the basis of a class III recommendation, she cautioned against withholding anticoagulants because of CHA2DS2-VASc risk factors alone. Rather, Dr. Van Gelder called the decision to administer or withhold anticoagulation — like all decisions — one that should be individualized in consultation with the patient.
For reducing AF symptoms and rhythm control, the specific pathways diverge for newly diagnosed AF, paroxysmal AF, and persistent AF. Like all of the guidelines, the specific options for symptom management and AF ablation are color coded, with green signifying level 1 evidence.
The evaluation and dynamic reassessment step refers to the need to periodically assess patients for new modifiable risk factors related to comorbidities, risk for stroke, risk for bleeding, and risk for AF.
The management of risk factors for AF has long been emphasized in guidelines, but a previous focus on AF with attention to comorbidities has been replaced by a focus on comorbidities with an expectation of more durable AF control. The success of this pivot is based on multidisciplinary care, chosen in collaboration with the patient, to reduce or eliminate the triggers of AF and the risks of its complications.
Pathways Are Appropriate for All Patients
A very important recommendation — and this is new — is “to treat all our patients with atrial fibrillation, whether they are young or old, men or women, Black or White, or at high or low risk, according to our patient-centered integrated AF-CARE approach,” Dr. Van Gelder said.
The changes reflect a shared appreciation for the tight relation between the control of comorbidities and the control of AF, according to José A. Joglar, MD, professor of cardiac electrophysiologic research at the University of Texas Southwestern Medical Center in Dallas. Dr. Joglar was chair of the writing committee for the joint 2023 AF guidelines released by the AHA, ACC, the American College of Clinical Pharmacy, and the Heart Rhythm Society.
“It is increasingly clear that AF in many cases is the consequence of underlying risk factors and comorbidities, which cannot be separated from AF alone,” Dr. Joglar explained in an interview.
This was placed first “to emphasize the importance of viewing AFib as a complex disease that requires a holistic, multidisciplinary approach to care, as opposed to being viewed just as a rhythm abnormality,” he said.
A version of this article first appeared on Medscape.com.
FROM ESC 2024
New Blood Pressure Guidelines Simplified, Lower Treatment Target
LONDON — Simplified and more aggressive targets are among the significant changes to the updated hypertension guidelines released by the European Society of Cardiology.
Although the updated guidelines, presented here at the ESC Congress, continue to define hypertension as a systolic BP of at least 140 mm Hg and a diastolic BP of at least 90 mm Hg, there is a new category — elevated BP. This is defined as a systolic BP of 120 mm Hg to 139 mm Hg or a diastolic BP of 70 mm Hg to 89 mm Hg, and cardiovascular risk assessment is advised to guide treatment, particularly in patients with a BP of at least 130/80 mm Hg.
The guidelines also introduce new recommendations for lifestyle options to help lower BP, including changes to exercise advice and the addition of potassium supplementation. And for the first time, the ESC guidelines provide recommendations for the use of renal denervation to treat hypertension in certain circumstances.
The guidelines were produced by an international panel, led by Bill McEvoy, MB BCh, from the University of Galway, Ireland, and Rhian Touyz, MB BCh, PhD, from McGill University in Montreal.
Three Categories of Blood Pressure
There are now three categories for BP classification — non-elevated (< 120/70 mm Hg), elevated (120 mm Hg to139 mm Hg/70 mm Hg to 89 mm Hg), and hypertension (≥ 140/90 mm Hg) — Dr. McEvoy reported during a session on the new guidelines here at ESC.
The emphasis on out-of-office BP measurement is stronger than in previous guidelines, but office measurement will still be used, he said.
All patients in the hypertension category qualify for treatment, whereas those in the new elevated BP category will be subject to cardiovascular risk stratification before a treatment decision is made.
Patients in the elevated BP category who also have moderate or severe chronic kidney disease, established cardiovascular disease, diabetes, or familial hypercholesterolemia are among those considered at increased risk for cardiovascular disease, as are patients with an estimated 10-year cardiovascular risk of 10% or higher. In such patients with a confirmed BP of at least 130/80 mm Hg, after 3 months of lifestyle intervention, pharmacologic treatment is recommended.
“This new category of elevated blood pressure recognizes that people do not go from normal blood pressure to hypertensive overnight,” Dr. McEvoy said. “It is, in most cases, a steady gradient of change, and different subgroups of patients — for example, those at a higher risk of developing cardiovascular disease — could benefit from more intensive treatment before their blood pressure reaches the traditional threshold of hypertension.”
New Lower Target
The major change in target pressures in these guidelines is based on new clinical trial data that confirm that lower pressures lead to lower cardiovascular event rates, resulting in the new systolic BP target of 120 mm Hg to 129 mm Hg for most patients receiving antihypertensive medications.
This systolic target represents a major change from previous European guidelines, Dr. McEvoy said, which have generally recommended that patients be treated to a target of less than 140/90 mm Hg and, only after that has been reached, then treated to a target of less than 130/80 mm Hg (a two-step approach).
“This change is driven by new trial evidence confirming that more intensive blood pressure treatment targets reduce cardiovascular outcomes across a broad spectrum of eligible patients,” Dr. McEvoy said.
There are, however, several caveats to this recommendation, including the requirement that treatment to this target be well tolerated; more lenient targets can be considered in people with symptomatic orthostatic hypotension, those 85 years and older, and those with moderate to severe frailty or a limited life expectancy. For these patients, the guidelines recommend a target “that is as low as reasonably achievable.”
More in Line With US Guidelines
The new European guidelines are now more in line with the American guidelines, said Eugene Yang, MD, from the University of Washington in Seattle, who is chair of the Hypertension Writing Group at the American College of Cardiology.
“These new European guidelines have thoughtfully used the latest study data to simplify recommendations for a specific lower blood pressure target. This is a step forward. There is now a greater alignment of European and US guidelines. This is good to reduce confusion and build consensus across the world,” he said.
Both sets of guidelines now recommend a BP target of less than 130/80 mm Hg for most people.
“I think the Europeans have now embraced this more aggressive target because there are many more studies now showing that these lower blood pressure levels do lead to a reduction in cardiovascular events,” Dr. Yang explained. “When the last European guidelines came out, there was only SPRINT. Now there are several more studies showing similar results.”
New Lifestyle Advice
The updated recommendation of 75 minutes of vigorous-intensity aerobic exercise per week has been added as an alternative to the previous recommendation of at least 2.5 hours per week of moderate-intensity aerobic exercise. This should be complemented with low- or moderate-intensity dynamic or isometric resistance training two to three times a week.
It is also recommended that people with hypertension, but without moderate or advanced chronic kidney disease, increase potassium intake with salt substitutes or diets rich in fruits and vegetables.
Renal Denervation Included for First Time
For the first time, the guidelines include the option of renal denervation for the treatment of hypertension — at medium- to high-volume centers — for patients with resistant hypertension that is uncontrolled despite a three-drug combination.
However, renal denervation is not recommended as a first-line treatment because of the lack of evidence of a benefit in cardiovascular outcomes. It is also not recommended for patients with highly impaired renal function or secondary causes of hypertension.
Dr. Yang said he approves of the inclusion of a frailty assessment in the new guidelines and less aggressive targets for people who are in poor health and older than age 85 years, but added that, “on the whole, they have less age-specific stratification than before, which is a significant change, and a good one in my view.”
Again, this is like the American guidelines, which have no age cutoffs and a target of less than 130/80 mm Hg for all, with the caveat that clinical judgment may be needed for individuals who are institutionalized, he added.
Dr. Yang said he was not as keen on the requirement for a cardiovascular risk assessment to guide treatment decisions for people with a systolic BP in the 130 mm Hg to 139 mm Hg range, although this is also included in the current American guidelines.
“As a clinician, I think this complicates things a bit too much and, as such, will be a barrier to treatment. In my view, blood pressure treatment recommendations need to be as simple as possible, so I think we still have some work to do there,” he said.
A version of this article first appeared on Medscape.com.
LONDON — Simplified and more aggressive targets are among the significant changes to the updated hypertension guidelines released by the European Society of Cardiology.
Although the updated guidelines, presented here at the ESC Congress, continue to define hypertension as a systolic BP of at least 140 mm Hg and a diastolic BP of at least 90 mm Hg, there is a new category — elevated BP. This is defined as a systolic BP of 120 mm Hg to 139 mm Hg or a diastolic BP of 70 mm Hg to 89 mm Hg, and cardiovascular risk assessment is advised to guide treatment, particularly in patients with a BP of at least 130/80 mm Hg.
The guidelines also introduce new recommendations for lifestyle options to help lower BP, including changes to exercise advice and the addition of potassium supplementation. And for the first time, the ESC guidelines provide recommendations for the use of renal denervation to treat hypertension in certain circumstances.
The guidelines were produced by an international panel, led by Bill McEvoy, MB BCh, from the University of Galway, Ireland, and Rhian Touyz, MB BCh, PhD, from McGill University in Montreal.
Three Categories of Blood Pressure
There are now three categories for BP classification — non-elevated (< 120/70 mm Hg), elevated (120 mm Hg to139 mm Hg/70 mm Hg to 89 mm Hg), and hypertension (≥ 140/90 mm Hg) — Dr. McEvoy reported during a session on the new guidelines here at ESC.
The emphasis on out-of-office BP measurement is stronger than in previous guidelines, but office measurement will still be used, he said.
All patients in the hypertension category qualify for treatment, whereas those in the new elevated BP category will be subject to cardiovascular risk stratification before a treatment decision is made.
Patients in the elevated BP category who also have moderate or severe chronic kidney disease, established cardiovascular disease, diabetes, or familial hypercholesterolemia are among those considered at increased risk for cardiovascular disease, as are patients with an estimated 10-year cardiovascular risk of 10% or higher. In such patients with a confirmed BP of at least 130/80 mm Hg, after 3 months of lifestyle intervention, pharmacologic treatment is recommended.
“This new category of elevated blood pressure recognizes that people do not go from normal blood pressure to hypertensive overnight,” Dr. McEvoy said. “It is, in most cases, a steady gradient of change, and different subgroups of patients — for example, those at a higher risk of developing cardiovascular disease — could benefit from more intensive treatment before their blood pressure reaches the traditional threshold of hypertension.”
New Lower Target
The major change in target pressures in these guidelines is based on new clinical trial data that confirm that lower pressures lead to lower cardiovascular event rates, resulting in the new systolic BP target of 120 mm Hg to 129 mm Hg for most patients receiving antihypertensive medications.
This systolic target represents a major change from previous European guidelines, Dr. McEvoy said, which have generally recommended that patients be treated to a target of less than 140/90 mm Hg and, only after that has been reached, then treated to a target of less than 130/80 mm Hg (a two-step approach).
“This change is driven by new trial evidence confirming that more intensive blood pressure treatment targets reduce cardiovascular outcomes across a broad spectrum of eligible patients,” Dr. McEvoy said.
There are, however, several caveats to this recommendation, including the requirement that treatment to this target be well tolerated; more lenient targets can be considered in people with symptomatic orthostatic hypotension, those 85 years and older, and those with moderate to severe frailty or a limited life expectancy. For these patients, the guidelines recommend a target “that is as low as reasonably achievable.”
More in Line With US Guidelines
The new European guidelines are now more in line with the American guidelines, said Eugene Yang, MD, from the University of Washington in Seattle, who is chair of the Hypertension Writing Group at the American College of Cardiology.
“These new European guidelines have thoughtfully used the latest study data to simplify recommendations for a specific lower blood pressure target. This is a step forward. There is now a greater alignment of European and US guidelines. This is good to reduce confusion and build consensus across the world,” he said.
Both sets of guidelines now recommend a BP target of less than 130/80 mm Hg for most people.
“I think the Europeans have now embraced this more aggressive target because there are many more studies now showing that these lower blood pressure levels do lead to a reduction in cardiovascular events,” Dr. Yang explained. “When the last European guidelines came out, there was only SPRINT. Now there are several more studies showing similar results.”
New Lifestyle Advice
The updated recommendation of 75 minutes of vigorous-intensity aerobic exercise per week has been added as an alternative to the previous recommendation of at least 2.5 hours per week of moderate-intensity aerobic exercise. This should be complemented with low- or moderate-intensity dynamic or isometric resistance training two to three times a week.
It is also recommended that people with hypertension, but without moderate or advanced chronic kidney disease, increase potassium intake with salt substitutes or diets rich in fruits and vegetables.
Renal Denervation Included for First Time
For the first time, the guidelines include the option of renal denervation for the treatment of hypertension — at medium- to high-volume centers — for patients with resistant hypertension that is uncontrolled despite a three-drug combination.
However, renal denervation is not recommended as a first-line treatment because of the lack of evidence of a benefit in cardiovascular outcomes. It is also not recommended for patients with highly impaired renal function or secondary causes of hypertension.
Dr. Yang said he approves of the inclusion of a frailty assessment in the new guidelines and less aggressive targets for people who are in poor health and older than age 85 years, but added that, “on the whole, they have less age-specific stratification than before, which is a significant change, and a good one in my view.”
Again, this is like the American guidelines, which have no age cutoffs and a target of less than 130/80 mm Hg for all, with the caveat that clinical judgment may be needed for individuals who are institutionalized, he added.
Dr. Yang said he was not as keen on the requirement for a cardiovascular risk assessment to guide treatment decisions for people with a systolic BP in the 130 mm Hg to 139 mm Hg range, although this is also included in the current American guidelines.
“As a clinician, I think this complicates things a bit too much and, as such, will be a barrier to treatment. In my view, blood pressure treatment recommendations need to be as simple as possible, so I think we still have some work to do there,” he said.
A version of this article first appeared on Medscape.com.
LONDON — Simplified and more aggressive targets are among the significant changes to the updated hypertension guidelines released by the European Society of Cardiology.
Although the updated guidelines, presented here at the ESC Congress, continue to define hypertension as a systolic BP of at least 140 mm Hg and a diastolic BP of at least 90 mm Hg, there is a new category — elevated BP. This is defined as a systolic BP of 120 mm Hg to 139 mm Hg or a diastolic BP of 70 mm Hg to 89 mm Hg, and cardiovascular risk assessment is advised to guide treatment, particularly in patients with a BP of at least 130/80 mm Hg.
The guidelines also introduce new recommendations for lifestyle options to help lower BP, including changes to exercise advice and the addition of potassium supplementation. And for the first time, the ESC guidelines provide recommendations for the use of renal denervation to treat hypertension in certain circumstances.
The guidelines were produced by an international panel, led by Bill McEvoy, MB BCh, from the University of Galway, Ireland, and Rhian Touyz, MB BCh, PhD, from McGill University in Montreal.
Three Categories of Blood Pressure
There are now three categories for BP classification — non-elevated (< 120/70 mm Hg), elevated (120 mm Hg to139 mm Hg/70 mm Hg to 89 mm Hg), and hypertension (≥ 140/90 mm Hg) — Dr. McEvoy reported during a session on the new guidelines here at ESC.
The emphasis on out-of-office BP measurement is stronger than in previous guidelines, but office measurement will still be used, he said.
All patients in the hypertension category qualify for treatment, whereas those in the new elevated BP category will be subject to cardiovascular risk stratification before a treatment decision is made.
Patients in the elevated BP category who also have moderate or severe chronic kidney disease, established cardiovascular disease, diabetes, or familial hypercholesterolemia are among those considered at increased risk for cardiovascular disease, as are patients with an estimated 10-year cardiovascular risk of 10% or higher. In such patients with a confirmed BP of at least 130/80 mm Hg, after 3 months of lifestyle intervention, pharmacologic treatment is recommended.
“This new category of elevated blood pressure recognizes that people do not go from normal blood pressure to hypertensive overnight,” Dr. McEvoy said. “It is, in most cases, a steady gradient of change, and different subgroups of patients — for example, those at a higher risk of developing cardiovascular disease — could benefit from more intensive treatment before their blood pressure reaches the traditional threshold of hypertension.”
New Lower Target
The major change in target pressures in these guidelines is based on new clinical trial data that confirm that lower pressures lead to lower cardiovascular event rates, resulting in the new systolic BP target of 120 mm Hg to 129 mm Hg for most patients receiving antihypertensive medications.
This systolic target represents a major change from previous European guidelines, Dr. McEvoy said, which have generally recommended that patients be treated to a target of less than 140/90 mm Hg and, only after that has been reached, then treated to a target of less than 130/80 mm Hg (a two-step approach).
“This change is driven by new trial evidence confirming that more intensive blood pressure treatment targets reduce cardiovascular outcomes across a broad spectrum of eligible patients,” Dr. McEvoy said.
There are, however, several caveats to this recommendation, including the requirement that treatment to this target be well tolerated; more lenient targets can be considered in people with symptomatic orthostatic hypotension, those 85 years and older, and those with moderate to severe frailty or a limited life expectancy. For these patients, the guidelines recommend a target “that is as low as reasonably achievable.”
More in Line With US Guidelines
The new European guidelines are now more in line with the American guidelines, said Eugene Yang, MD, from the University of Washington in Seattle, who is chair of the Hypertension Writing Group at the American College of Cardiology.
“These new European guidelines have thoughtfully used the latest study data to simplify recommendations for a specific lower blood pressure target. This is a step forward. There is now a greater alignment of European and US guidelines. This is good to reduce confusion and build consensus across the world,” he said.
Both sets of guidelines now recommend a BP target of less than 130/80 mm Hg for most people.
“I think the Europeans have now embraced this more aggressive target because there are many more studies now showing that these lower blood pressure levels do lead to a reduction in cardiovascular events,” Dr. Yang explained. “When the last European guidelines came out, there was only SPRINT. Now there are several more studies showing similar results.”
New Lifestyle Advice
The updated recommendation of 75 minutes of vigorous-intensity aerobic exercise per week has been added as an alternative to the previous recommendation of at least 2.5 hours per week of moderate-intensity aerobic exercise. This should be complemented with low- or moderate-intensity dynamic or isometric resistance training two to three times a week.
It is also recommended that people with hypertension, but without moderate or advanced chronic kidney disease, increase potassium intake with salt substitutes or diets rich in fruits and vegetables.
Renal Denervation Included for First Time
For the first time, the guidelines include the option of renal denervation for the treatment of hypertension — at medium- to high-volume centers — for patients with resistant hypertension that is uncontrolled despite a three-drug combination.
However, renal denervation is not recommended as a first-line treatment because of the lack of evidence of a benefit in cardiovascular outcomes. It is also not recommended for patients with highly impaired renal function or secondary causes of hypertension.
Dr. Yang said he approves of the inclusion of a frailty assessment in the new guidelines and less aggressive targets for people who are in poor health and older than age 85 years, but added that, “on the whole, they have less age-specific stratification than before, which is a significant change, and a good one in my view.”
Again, this is like the American guidelines, which have no age cutoffs and a target of less than 130/80 mm Hg for all, with the caveat that clinical judgment may be needed for individuals who are institutionalized, he added.
Dr. Yang said he was not as keen on the requirement for a cardiovascular risk assessment to guide treatment decisions for people with a systolic BP in the 130 mm Hg to 139 mm Hg range, although this is also included in the current American guidelines.
“As a clinician, I think this complicates things a bit too much and, as such, will be a barrier to treatment. In my view, blood pressure treatment recommendations need to be as simple as possible, so I think we still have some work to do there,” he said.
A version of this article first appeared on Medscape.com.
FROM ESC 2024
Acute Tender Papules on the Arms and Legs
The Diagnosis: Erythema Nodosum Leprosum
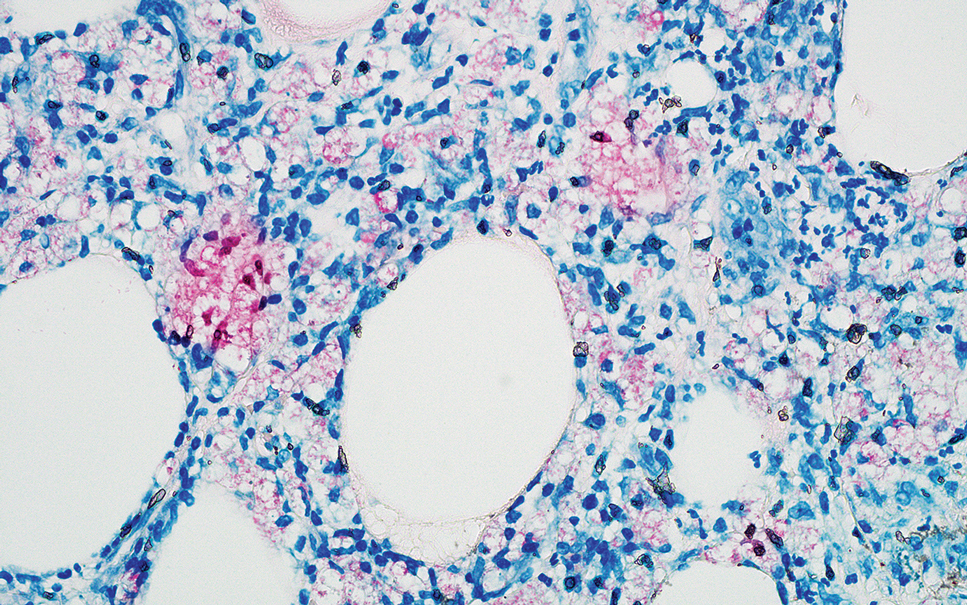
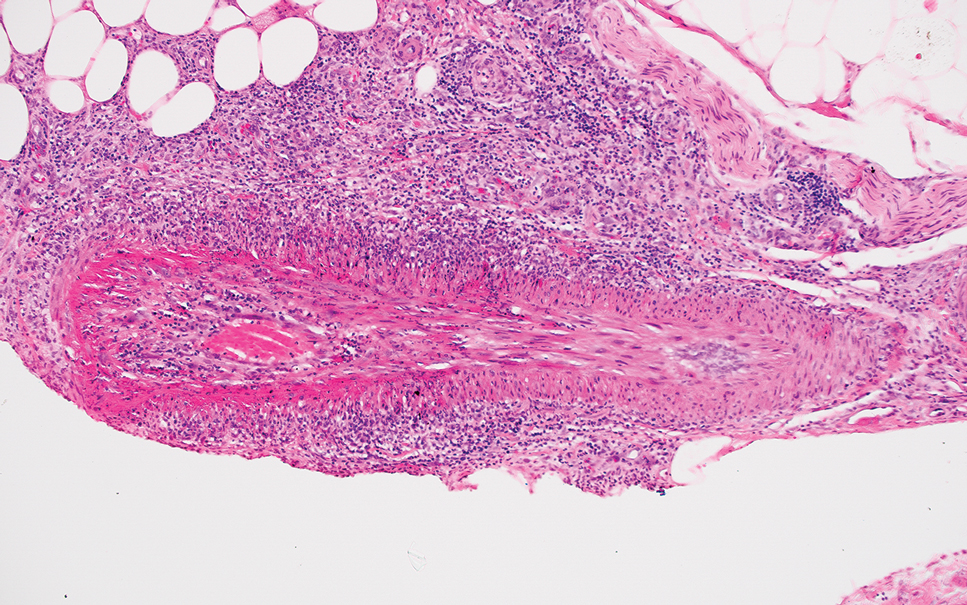
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
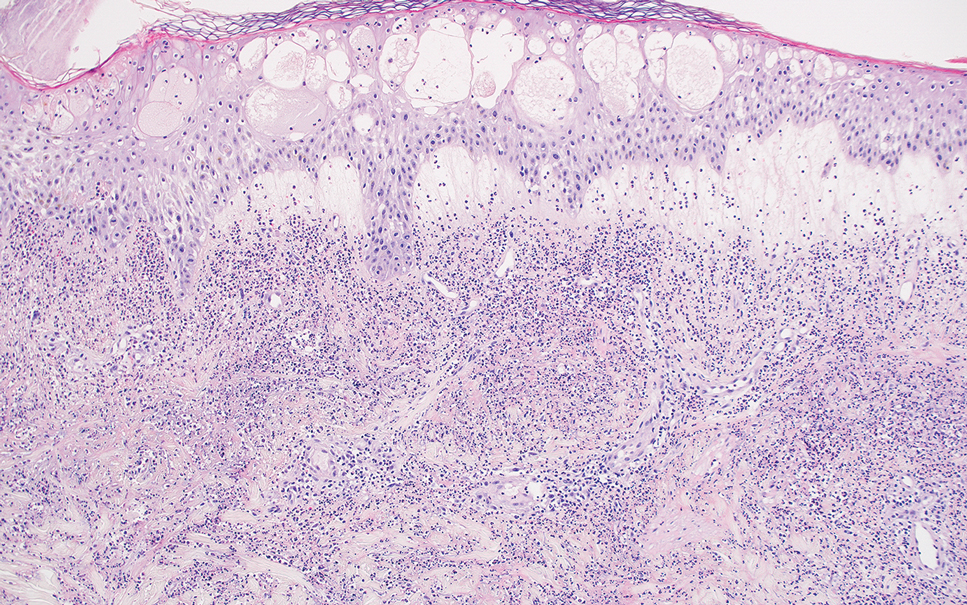
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
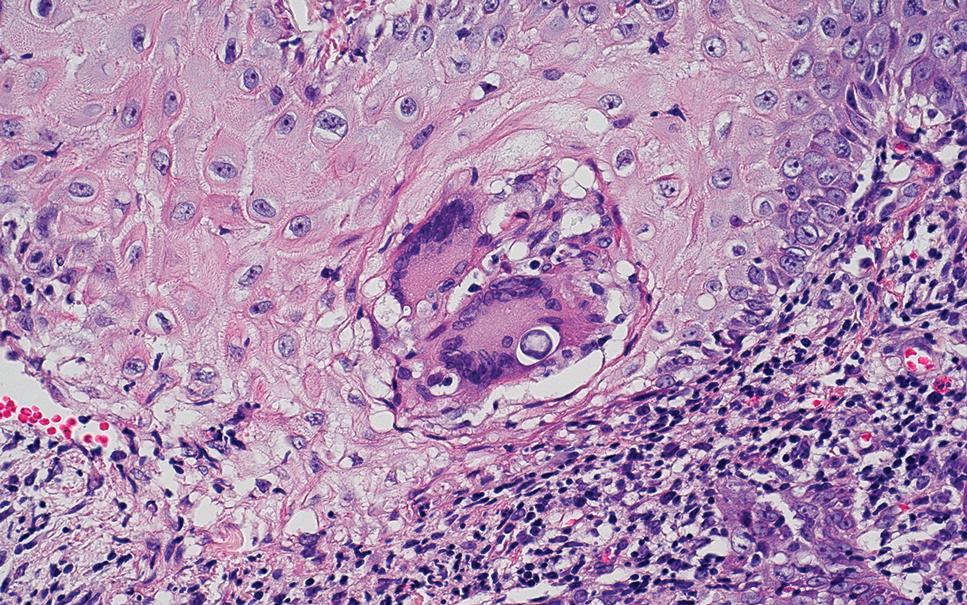
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
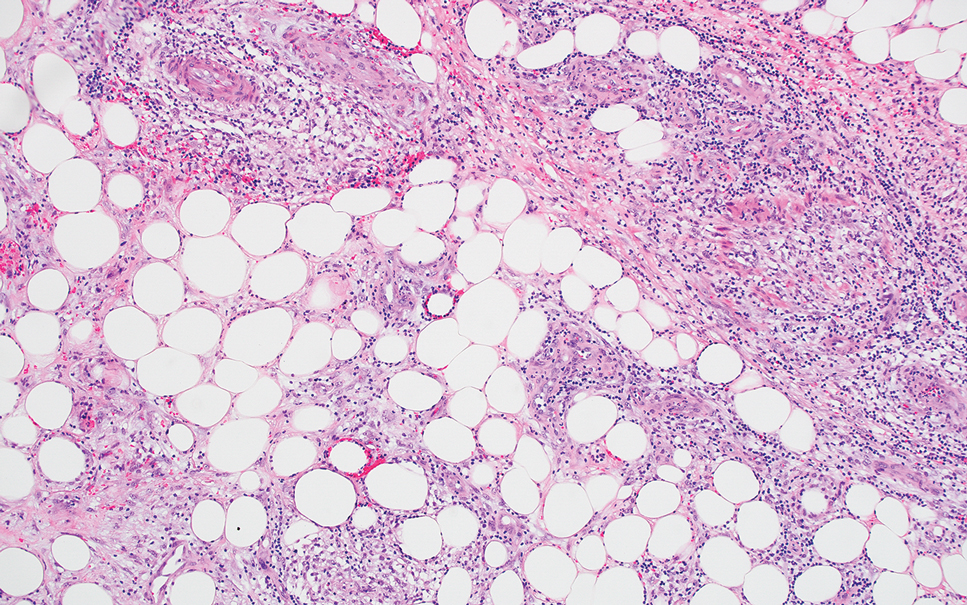
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
The Diagnosis: Erythema Nodosum Leprosum
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
The Diagnosis: Erythema Nodosum Leprosum
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
A 66-year-old man presented with new tender erythematous papules scattered over the arms and legs. A biopsy of a lesion on the left thigh was performed.
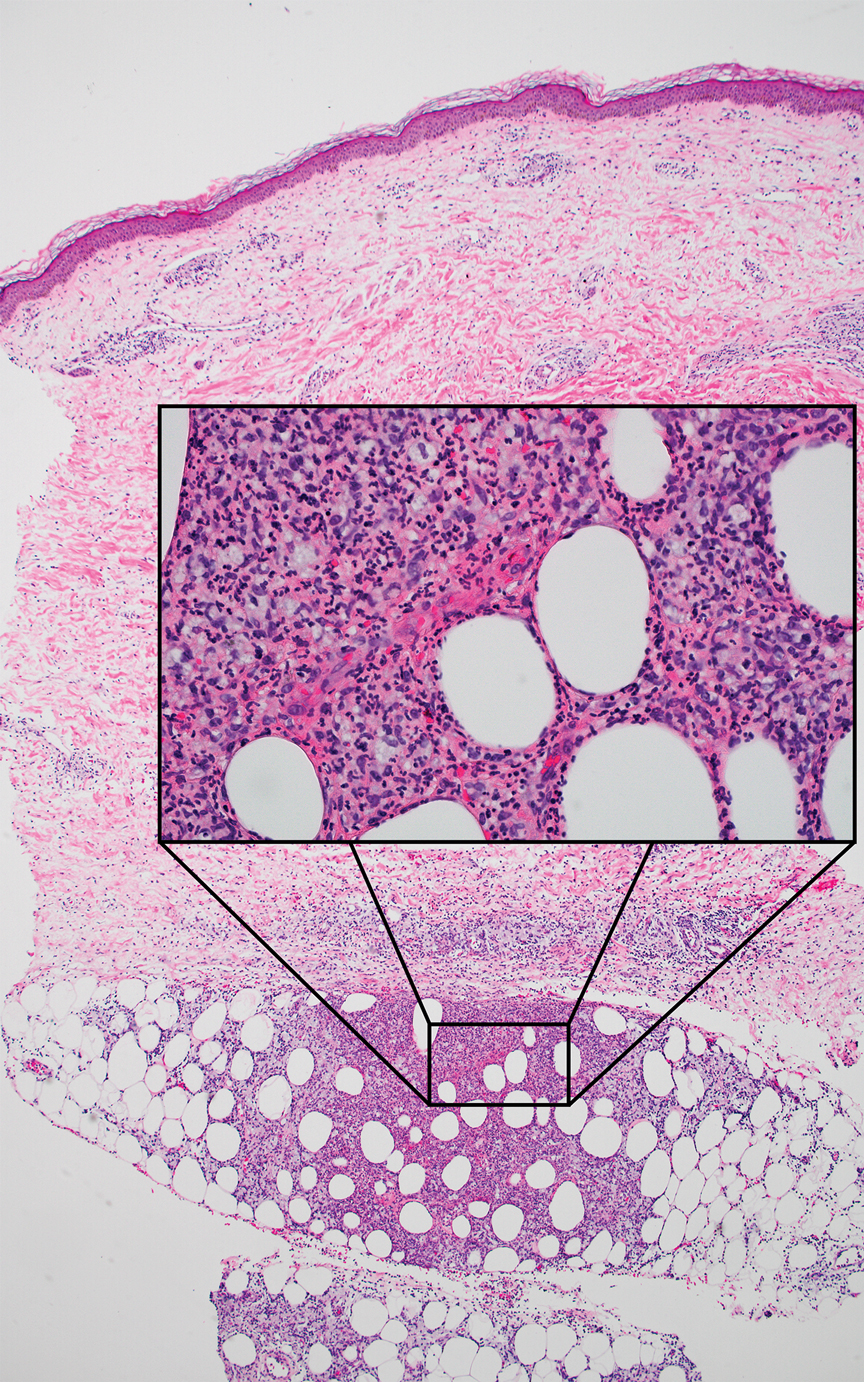
Diet Rich in Processed Foods Linked to Elevated Risk for Colorectal Cancer
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Systemic Sclerosis Without Scleroderma Has Unique Severity, Prognosis
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
GIST Rates Rise, With Black Patients Facing Higher Mortality
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Adjuvant Everolimus Offers No Survival Benefit in Non–Clear Cell RCC
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
A New Era of Obesity Medicine
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Alternative Paths to Recertification
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.

We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.

As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.

Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.
We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.
As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.
Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.
We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.
As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.
Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.