User login
In-Hospital e-Alerts: A Step Toward Better Kidney Health?
TOPLINE:
METHODOLOGY:
- AKI is a common complication in hospitalized patients, leading to increased comorbidities, healthcare costs, and short- and long-term mortality, but the impact of early detection through electronic health care record systems (e-alerts) is unclear.
- Researchers conducted an updated systematic review and meta-analysis to assess the association of e-alerts for AKI with patient outcomes and clinical practice patterns.
- Overall, 13 studies involving 41,837 patients with AKI were included, comparing e-alerts for AKI with standard care or no e-alerts.
- The primary outcomes were mortality, AKI progression, dialysis events, and kidney recovery, and secondary outcomes were nephrologist consultations, post-AKI exposure to NSAIDs and other medications, and hospital length of stay and costs.
- The investigators assessed bias, the certainty of evidence, and whether the primary outcome conclusions of the meta-analysis were premature.
TAKEAWAY:
- The use of e-alerts for AKI was not associated with reduced mortality outcomes compared with no e-alerts (risk ratio [RR], 0.96; 95% CI, 0.89-1.03; 12 studies).
- E-alerts were associated with a reduced risk for AKI progression (RR, 0.91; 95% CI, 0.84-0.99; five studies); however, the results were found to be heterogeneous and possibly premature.
- E-alerts for AKI were also linked to increased nephrologist consultations (RR, 1.45; 95% CI, 1.04-2.02; 11 studies), reduced post-AKI NSAID exposure (RR, 0.75; 95% CI, 0.59-0.95; four studies), and improved AKI documentation (RR, 1.28; 95% CI, 1.04-1.58; eight studies).
- The use of e-alerts for AKI was associated with increased dialysis events (RR, 1.16; 95% CI, 1.05-1.28).
IN PRACTICE:
“We recommend that each hospital establish its own AKI e-alert system and individualized AKI management protocol tailored to its specific needs,” wrote the authors who also suggested the system be “integrated with earlier risk stratification methods, such as the renal angina index, artificial intelligence–based continuous AKI prediction, and care bundle implementation within a clinical decision support system to enhance early diagnosis and management, potentially improving outcomes.”
SOURCE:
This study was led by Jia-Jin Chen, MD, from the Kidney Research Center, Department of Nephrology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan. It was published online in JAMA Network Open.
LIMITATIONS:
The limitations included the scarcity of randomized clinical trials in the meta-analysis. Few studies examined the impact of these e-alerts on the hospital length of stay, healthcare costs, AKI stage progression, and post-AKI kidney recovery, which limited the ability to draw conclusive statements on these aspects. Major adverse kidney events at 28 and 90 days were not reported in any of the enrolled studies, so the impact of AKI e-alerts and increased dialysis events on long-term outcomes remained uncertain.
DISCLOSURES:
The study was supported by grants from the Taiwanese Ministry of Health and Welfare and Linkou Chang Gung Memorial Hospital. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- AKI is a common complication in hospitalized patients, leading to increased comorbidities, healthcare costs, and short- and long-term mortality, but the impact of early detection through electronic health care record systems (e-alerts) is unclear.
- Researchers conducted an updated systematic review and meta-analysis to assess the association of e-alerts for AKI with patient outcomes and clinical practice patterns.
- Overall, 13 studies involving 41,837 patients with AKI were included, comparing e-alerts for AKI with standard care or no e-alerts.
- The primary outcomes were mortality, AKI progression, dialysis events, and kidney recovery, and secondary outcomes were nephrologist consultations, post-AKI exposure to NSAIDs and other medications, and hospital length of stay and costs.
- The investigators assessed bias, the certainty of evidence, and whether the primary outcome conclusions of the meta-analysis were premature.
TAKEAWAY:
- The use of e-alerts for AKI was not associated with reduced mortality outcomes compared with no e-alerts (risk ratio [RR], 0.96; 95% CI, 0.89-1.03; 12 studies).
- E-alerts were associated with a reduced risk for AKI progression (RR, 0.91; 95% CI, 0.84-0.99; five studies); however, the results were found to be heterogeneous and possibly premature.
- E-alerts for AKI were also linked to increased nephrologist consultations (RR, 1.45; 95% CI, 1.04-2.02; 11 studies), reduced post-AKI NSAID exposure (RR, 0.75; 95% CI, 0.59-0.95; four studies), and improved AKI documentation (RR, 1.28; 95% CI, 1.04-1.58; eight studies).
- The use of e-alerts for AKI was associated with increased dialysis events (RR, 1.16; 95% CI, 1.05-1.28).
IN PRACTICE:
“We recommend that each hospital establish its own AKI e-alert system and individualized AKI management protocol tailored to its specific needs,” wrote the authors who also suggested the system be “integrated with earlier risk stratification methods, such as the renal angina index, artificial intelligence–based continuous AKI prediction, and care bundle implementation within a clinical decision support system to enhance early diagnosis and management, potentially improving outcomes.”
SOURCE:
This study was led by Jia-Jin Chen, MD, from the Kidney Research Center, Department of Nephrology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan. It was published online in JAMA Network Open.
LIMITATIONS:
The limitations included the scarcity of randomized clinical trials in the meta-analysis. Few studies examined the impact of these e-alerts on the hospital length of stay, healthcare costs, AKI stage progression, and post-AKI kidney recovery, which limited the ability to draw conclusive statements on these aspects. Major adverse kidney events at 28 and 90 days were not reported in any of the enrolled studies, so the impact of AKI e-alerts and increased dialysis events on long-term outcomes remained uncertain.
DISCLOSURES:
The study was supported by grants from the Taiwanese Ministry of Health and Welfare and Linkou Chang Gung Memorial Hospital. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- AKI is a common complication in hospitalized patients, leading to increased comorbidities, healthcare costs, and short- and long-term mortality, but the impact of early detection through electronic health care record systems (e-alerts) is unclear.
- Researchers conducted an updated systematic review and meta-analysis to assess the association of e-alerts for AKI with patient outcomes and clinical practice patterns.
- Overall, 13 studies involving 41,837 patients with AKI were included, comparing e-alerts for AKI with standard care or no e-alerts.
- The primary outcomes were mortality, AKI progression, dialysis events, and kidney recovery, and secondary outcomes were nephrologist consultations, post-AKI exposure to NSAIDs and other medications, and hospital length of stay and costs.
- The investigators assessed bias, the certainty of evidence, and whether the primary outcome conclusions of the meta-analysis were premature.
TAKEAWAY:
- The use of e-alerts for AKI was not associated with reduced mortality outcomes compared with no e-alerts (risk ratio [RR], 0.96; 95% CI, 0.89-1.03; 12 studies).
- E-alerts were associated with a reduced risk for AKI progression (RR, 0.91; 95% CI, 0.84-0.99; five studies); however, the results were found to be heterogeneous and possibly premature.
- E-alerts for AKI were also linked to increased nephrologist consultations (RR, 1.45; 95% CI, 1.04-2.02; 11 studies), reduced post-AKI NSAID exposure (RR, 0.75; 95% CI, 0.59-0.95; four studies), and improved AKI documentation (RR, 1.28; 95% CI, 1.04-1.58; eight studies).
- The use of e-alerts for AKI was associated with increased dialysis events (RR, 1.16; 95% CI, 1.05-1.28).
IN PRACTICE:
“We recommend that each hospital establish its own AKI e-alert system and individualized AKI management protocol tailored to its specific needs,” wrote the authors who also suggested the system be “integrated with earlier risk stratification methods, such as the renal angina index, artificial intelligence–based continuous AKI prediction, and care bundle implementation within a clinical decision support system to enhance early diagnosis and management, potentially improving outcomes.”
SOURCE:
This study was led by Jia-Jin Chen, MD, from the Kidney Research Center, Department of Nephrology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan City, Taiwan. It was published online in JAMA Network Open.
LIMITATIONS:
The limitations included the scarcity of randomized clinical trials in the meta-analysis. Few studies examined the impact of these e-alerts on the hospital length of stay, healthcare costs, AKI stage progression, and post-AKI kidney recovery, which limited the ability to draw conclusive statements on these aspects. Major adverse kidney events at 28 and 90 days were not reported in any of the enrolled studies, so the impact of AKI e-alerts and increased dialysis events on long-term outcomes remained uncertain.
DISCLOSURES:
The study was supported by grants from the Taiwanese Ministry of Health and Welfare and Linkou Chang Gung Memorial Hospital. The authors declared no conflicts of interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
As Interest From Families Wanes, Pediatricians Scale Back on COVID Shots
When pediatrician Eric Ball, MD, opened a refrigerator full of childhood vaccines, all the expected shots were there — DTaP, polio, pneumococcal vaccine — except one.
“This is where we usually store our COVID vaccines, but we don’t have any right now because they all expired at the end of last year and we had to dispose of them,” said Dr. Ball, who is part of a pediatric practice in Orange County, California.
“We thought demand would be way higher than it was.”
Providers like Dr. Ball don’t want to waste money ordering doses that won’t be used, but they need enough on hand to vaccinate vulnerable children.
The Centers for Disease Control and Prevention recommends that anyone 6 months or older get the updated COVID vaccination, but in the 2023-24 vaccination season only about 15% of eligible children in the United States got a shot.
Dr. Ball said it was difficult to let vaccines go to waste in 2023. It was the first time the federal government was no longer picking up the tab for the shots, and providers had to pay upfront for the vaccines. Parents would often skip the COVID shot, which can have a very short shelf life, compared with other vaccines.
“Watching it sitting on our shelves expiring every 30 days, that’s like throwing away $150 repeatedly every day, multiple times a month,” Dr. Ball said.
in 2024, Dr. Ball slashed his fall vaccine order to the bare minimum to avoid another costly mistake.
“We took the number of flu vaccines that we order, and then we ordered 5% of that in COVID vaccines,” Dr. Ball said. “It’s a guess.”
That small vaccine order cost more than $63,000, he said.
Pharmacists, pharmacy interns, and techs are allowed to give COVID vaccines only to children age 3 and up, meaning babies and toddlers would need to visit a doctor’s office for inoculation.
It’s difficult to predict how parents will feel about the shots this fall, said Chicago pediatrician Scott Goldstein, MD. Unlike other vaccinations, COVID shots aren’t required for kids to attend school, and parental interest seems to wane with each new formulation. For a physician-owned practice such as Dr. Goldstein’s, the upfront cost of the vaccine can be a gamble.
“The cost of vaccines, that’s far and away our biggest expense. But it’s also the most important thing we do, you could argue, is vaccinating kids,” Dr. Goldstein said.
Insurance doesn’t necessarily cover vaccine storage accidents, which can put the practice at risk of financial ruin.
“We’ve had things happen like a refrigerator gets unplugged. And then we’re all of a sudden out $80,000 overnight,” Dr. Goldstein said.
South Carolina pediatrician Deborah Greenhouse, MD, said she would order more COVID vaccines for older children if the pharmaceutical companies that she buys from had a more forgiving return policy.
“Pfizer is creating that situation. If you’re only going to let us return 30%, we’re not going to buy much,” she said. “We can’t.”
Greenhouse owns her practice, so the remaining 70% of leftover shots would come out of her pocket.
Vaccine maker Pfizer will take back all unused COVID shots for young children, but only 30% of doses for people 12 and older.
Pfizer said in an Aug. 20 emailed statement, “The return policy was instituted as we recognize both the importance and the complexity of pediatric vaccination and wanted to ensure that pediatric offices did not have hurdles to providing vaccine to their young patients.”
Pfizer’s return policy is similar to policies from other drugmakers for pediatric flu vaccines, also recommended during the fall season. Physicians who are worried about unwanted COVID vaccines expiring on the shelves said flu shots cost them about $20 per dose, while COVID shots cost around $150 per dose.
“We run on a very thin margin. If we get stuck holding a ton of vaccine that we cannot return, we can’t absorb that kind of cost,” Dr. Greenhouse said.
Vaccine maker Moderna will accept COVID vaccine returns, but the amount depends on the individual contract with a provider. Novavax will accept the return of only unopened vaccines and doesn’t specify the amount they’ll accept.
Dr. Greenhouse wants to vaccinate as many children as possible but said she can’t afford to stock shots with a short shelf life. Once she runs out of the doses she’s ordered, Dr. Greenhouse plans to tell families to go to a pharmacy to get older children vaccinated. If pediatricians around the country are making the same calculations, doses for very small children could be harder to find at doctors’ offices.
“Frankly, it’s not an ideal situation, but it’s what we have to do to stay in business,” she said.
Dr. Ball worries that parents’ limited interest has caused pediatricians to minimize their vaccine orders, in turn making the newest COVID shots difficult to find once they become available.
“I think there’s just a misperception that it’s less of a big deal to get COVID, but I’m still sending babies to the hospital with COVID,” Dr. Ball said. “We’re still seeing kids with long COVID. This is with us forever.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
When pediatrician Eric Ball, MD, opened a refrigerator full of childhood vaccines, all the expected shots were there — DTaP, polio, pneumococcal vaccine — except one.
“This is where we usually store our COVID vaccines, but we don’t have any right now because they all expired at the end of last year and we had to dispose of them,” said Dr. Ball, who is part of a pediatric practice in Orange County, California.
“We thought demand would be way higher than it was.”
Providers like Dr. Ball don’t want to waste money ordering doses that won’t be used, but they need enough on hand to vaccinate vulnerable children.
The Centers for Disease Control and Prevention recommends that anyone 6 months or older get the updated COVID vaccination, but in the 2023-24 vaccination season only about 15% of eligible children in the United States got a shot.
Dr. Ball said it was difficult to let vaccines go to waste in 2023. It was the first time the federal government was no longer picking up the tab for the shots, and providers had to pay upfront for the vaccines. Parents would often skip the COVID shot, which can have a very short shelf life, compared with other vaccines.
“Watching it sitting on our shelves expiring every 30 days, that’s like throwing away $150 repeatedly every day, multiple times a month,” Dr. Ball said.
in 2024, Dr. Ball slashed his fall vaccine order to the bare minimum to avoid another costly mistake.
“We took the number of flu vaccines that we order, and then we ordered 5% of that in COVID vaccines,” Dr. Ball said. “It’s a guess.”
That small vaccine order cost more than $63,000, he said.
Pharmacists, pharmacy interns, and techs are allowed to give COVID vaccines only to children age 3 and up, meaning babies and toddlers would need to visit a doctor’s office for inoculation.
It’s difficult to predict how parents will feel about the shots this fall, said Chicago pediatrician Scott Goldstein, MD. Unlike other vaccinations, COVID shots aren’t required for kids to attend school, and parental interest seems to wane with each new formulation. For a physician-owned practice such as Dr. Goldstein’s, the upfront cost of the vaccine can be a gamble.
“The cost of vaccines, that’s far and away our biggest expense. But it’s also the most important thing we do, you could argue, is vaccinating kids,” Dr. Goldstein said.
Insurance doesn’t necessarily cover vaccine storage accidents, which can put the practice at risk of financial ruin.
“We’ve had things happen like a refrigerator gets unplugged. And then we’re all of a sudden out $80,000 overnight,” Dr. Goldstein said.
South Carolina pediatrician Deborah Greenhouse, MD, said she would order more COVID vaccines for older children if the pharmaceutical companies that she buys from had a more forgiving return policy.
“Pfizer is creating that situation. If you’re only going to let us return 30%, we’re not going to buy much,” she said. “We can’t.”
Greenhouse owns her practice, so the remaining 70% of leftover shots would come out of her pocket.
Vaccine maker Pfizer will take back all unused COVID shots for young children, but only 30% of doses for people 12 and older.
Pfizer said in an Aug. 20 emailed statement, “The return policy was instituted as we recognize both the importance and the complexity of pediatric vaccination and wanted to ensure that pediatric offices did not have hurdles to providing vaccine to their young patients.”
Pfizer’s return policy is similar to policies from other drugmakers for pediatric flu vaccines, also recommended during the fall season. Physicians who are worried about unwanted COVID vaccines expiring on the shelves said flu shots cost them about $20 per dose, while COVID shots cost around $150 per dose.
“We run on a very thin margin. If we get stuck holding a ton of vaccine that we cannot return, we can’t absorb that kind of cost,” Dr. Greenhouse said.
Vaccine maker Moderna will accept COVID vaccine returns, but the amount depends on the individual contract with a provider. Novavax will accept the return of only unopened vaccines and doesn’t specify the amount they’ll accept.
Dr. Greenhouse wants to vaccinate as many children as possible but said she can’t afford to stock shots with a short shelf life. Once she runs out of the doses she’s ordered, Dr. Greenhouse plans to tell families to go to a pharmacy to get older children vaccinated. If pediatricians around the country are making the same calculations, doses for very small children could be harder to find at doctors’ offices.
“Frankly, it’s not an ideal situation, but it’s what we have to do to stay in business,” she said.
Dr. Ball worries that parents’ limited interest has caused pediatricians to minimize their vaccine orders, in turn making the newest COVID shots difficult to find once they become available.
“I think there’s just a misperception that it’s less of a big deal to get COVID, but I’m still sending babies to the hospital with COVID,” Dr. Ball said. “We’re still seeing kids with long COVID. This is with us forever.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
When pediatrician Eric Ball, MD, opened a refrigerator full of childhood vaccines, all the expected shots were there — DTaP, polio, pneumococcal vaccine — except one.
“This is where we usually store our COVID vaccines, but we don’t have any right now because they all expired at the end of last year and we had to dispose of them,” said Dr. Ball, who is part of a pediatric practice in Orange County, California.
“We thought demand would be way higher than it was.”
Providers like Dr. Ball don’t want to waste money ordering doses that won’t be used, but they need enough on hand to vaccinate vulnerable children.
The Centers for Disease Control and Prevention recommends that anyone 6 months or older get the updated COVID vaccination, but in the 2023-24 vaccination season only about 15% of eligible children in the United States got a shot.
Dr. Ball said it was difficult to let vaccines go to waste in 2023. It was the first time the federal government was no longer picking up the tab for the shots, and providers had to pay upfront for the vaccines. Parents would often skip the COVID shot, which can have a very short shelf life, compared with other vaccines.
“Watching it sitting on our shelves expiring every 30 days, that’s like throwing away $150 repeatedly every day, multiple times a month,” Dr. Ball said.
in 2024, Dr. Ball slashed his fall vaccine order to the bare minimum to avoid another costly mistake.
“We took the number of flu vaccines that we order, and then we ordered 5% of that in COVID vaccines,” Dr. Ball said. “It’s a guess.”
That small vaccine order cost more than $63,000, he said.
Pharmacists, pharmacy interns, and techs are allowed to give COVID vaccines only to children age 3 and up, meaning babies and toddlers would need to visit a doctor’s office for inoculation.
It’s difficult to predict how parents will feel about the shots this fall, said Chicago pediatrician Scott Goldstein, MD. Unlike other vaccinations, COVID shots aren’t required for kids to attend school, and parental interest seems to wane with each new formulation. For a physician-owned practice such as Dr. Goldstein’s, the upfront cost of the vaccine can be a gamble.
“The cost of vaccines, that’s far and away our biggest expense. But it’s also the most important thing we do, you could argue, is vaccinating kids,” Dr. Goldstein said.
Insurance doesn’t necessarily cover vaccine storage accidents, which can put the practice at risk of financial ruin.
“We’ve had things happen like a refrigerator gets unplugged. And then we’re all of a sudden out $80,000 overnight,” Dr. Goldstein said.
South Carolina pediatrician Deborah Greenhouse, MD, said she would order more COVID vaccines for older children if the pharmaceutical companies that she buys from had a more forgiving return policy.
“Pfizer is creating that situation. If you’re only going to let us return 30%, we’re not going to buy much,” she said. “We can’t.”
Greenhouse owns her practice, so the remaining 70% of leftover shots would come out of her pocket.
Vaccine maker Pfizer will take back all unused COVID shots for young children, but only 30% of doses for people 12 and older.
Pfizer said in an Aug. 20 emailed statement, “The return policy was instituted as we recognize both the importance and the complexity of pediatric vaccination and wanted to ensure that pediatric offices did not have hurdles to providing vaccine to their young patients.”
Pfizer’s return policy is similar to policies from other drugmakers for pediatric flu vaccines, also recommended during the fall season. Physicians who are worried about unwanted COVID vaccines expiring on the shelves said flu shots cost them about $20 per dose, while COVID shots cost around $150 per dose.
“We run on a very thin margin. If we get stuck holding a ton of vaccine that we cannot return, we can’t absorb that kind of cost,” Dr. Greenhouse said.
Vaccine maker Moderna will accept COVID vaccine returns, but the amount depends on the individual contract with a provider. Novavax will accept the return of only unopened vaccines and doesn’t specify the amount they’ll accept.
Dr. Greenhouse wants to vaccinate as many children as possible but said she can’t afford to stock shots with a short shelf life. Once she runs out of the doses she’s ordered, Dr. Greenhouse plans to tell families to go to a pharmacy to get older children vaccinated. If pediatricians around the country are making the same calculations, doses for very small children could be harder to find at doctors’ offices.
“Frankly, it’s not an ideal situation, but it’s what we have to do to stay in business,” she said.
Dr. Ball worries that parents’ limited interest has caused pediatricians to minimize their vaccine orders, in turn making the newest COVID shots difficult to find once they become available.
“I think there’s just a misperception that it’s less of a big deal to get COVID, but I’m still sending babies to the hospital with COVID,” Dr. Ball said. “We’re still seeing kids with long COVID. This is with us forever.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Vacationing Doctors Intervene After Shark Attack
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Creative Strategies Hospitals Use to Attract Nursing Talent
In a fiercely competitive healthcare landscape, hospitals are pulling out all the stops to lure top nursing talent through their doors.
As the nursing shortage intensifies, the creative recruitment approach isn’t just about the perks — it’s becoming an essential tool in the race to build a skilled nursing workforce.
Nursing vacancies are as high as 17% — more than double prepandemic levels — and hospitals scrambling to fill them need to do more than raise salaries and bolster benefits packages to entice nurses.
“I am very thankful when I hear of creative ideas that nurse administrators come up with to try to get their ultimate goal, which is enough qualified nurses to take care of patients,” said Linda Plank, dean of the Louise Herrington School of Nursing at Baylor University in Dallas, Texas.
Signing Bonuses, Tuition Reimbursement, and Self-Scheduling, Please
Signing bonuses were among the top perks offered to healthcare workers, with almost 18% of job openings advertising the incentive for new nurse hires; the average signing bonus for registered nurses (RNs) topped $11,000. In 2023, California-based Palomar Health made headlines when it offered eligible RNs a $100,000 signing bonus paid over a 3-year period.
“We are seeing a variety of incentives, like sign-on bonuses, that can be effective at getting the attention of potential new hires,” said Deborah Trautman, PhD, RN, FAAN, president, and CEO of the American Association of Colleges of Nursing. “With the growing competition for registered nurses, especially those prepared in baccalaureate programs, employers should consider what’s most important to nurses entering the field.”
Hospitals have also invested in benefits ranging from tuition reimbursement, student loan forgiveness, and professional development opportunities to expanded parental leave and onsite childcare. Flexible scheduling is a sought-after perk that benefits both new and experienced RNs and could also help with recruitment.
“In the past, [hospitals said], ‘our shift starts at 7 and ends at 7,’ ” Ms. Plank said. “Now, hospitals are a little bit more flexible ... and being open to flexible shifts has merit. If we’re willing to look at things differently, it could get more people involved in patient care.”
An American Nurses Foundation report found that nurses preferred variable and flexible shift lengths, flexible start times, and self-scheduling options over set schedules. In fact, 45% of nurses who left clinical practice would consider returning to work if hospitals switched to a self-scheduling model.
The Cleveland Clinic in Ohio introduced staggered shifts that start at nontraditional times, including 11 AM to 11 PM, flexible shift lengths, and split RN positions that allow clinical care nurses to divide their time between different departments. Last year, Hackensack Meridian Health in New Jersey also piloted a self-scheduling program for its nursing staff.
Hiring Outside the United States
Despite the prevalence of signing bonuses and premium perks, some hospitals still struggled to fill open positions with nurses recruited from outside the United States. Data from The Kaiser Family Foundation show that 32% of hospitals hired foreign-educated RNs in 2022 — more than double the number hired in 2010.
Jennifer Mensik Kennedy, PhD, MBA, RN, NEA-BC, FAAN, president of the American Nurses Association (ANA), is concerned about that trend. The ANA supports the International Council of Nurses and their call for “stronger codes for ethical recruitment of nurses” because international nurse recruitment practices can negatively affect the quality of healthcare in countries that are depleted of nurses.
“Recruiting international nurses as a key strategy for building core staffing is not sustainable in the long term,” Ms. Kennedy said in an interview. “We need to redirect our focus on how to retain staff through fostering healthy work environments and addressing antiquated payment models.”
Reinforcing Retention
Recruiting nurses is just one element of addressing the nursing shortage. Prioritizing job satisfaction is essential to retaining nursing staff. Currently, 33% of nurses who enter the profession quit within the first 2 years.
A growing number of hospitals have implemented programs focused on increasing retention. Lifepoint Health, a national network of 60-plus acute care hospitals, launched a Nurse Residency Program in 2023. The 12-month program, which offers training and mentorship to help recent nursing school graduates, has recruited 750 new nurses and helped them transition to clinical practice.
The Nurse Residency Program has been so successful that the hospital system plans to introduce a 2-year fellowship program in the fall of 2024 that supports the professional development of nurses who want to specialize in areas like acute care, obstetrics, or the intensive care unit.
“We are more focused than ever on increasing partnerships and alignment with our local nursing programs, expanding clinical education opportunities for nursing students, owning and driving a nursing culture, and creating an environment where employees want to work,” said Michelle Watson, MSN, RN, CENP, chief nurse executive and senior vice president of clinical operations at Lifepoint Health.
Ms. Watson also credits their facilities’ chief nursing officers as being “highly engaged and visible leaders” who spend time with RNs to learn about their career aspirations and help them understand how the organization can support their desires for ongoing professional development.
The 2022 Nurse Staffing Task Force, a collaborative initiative by the ANA and other prominent national nursing and healthcare organizations, has developed and widely disseminated a set of recommendations for hospitals focusing on investing in nurse staffing, safe and supportive work environments, and competitive wages.
In addition, the Reimagining Nursing Initiative, started by the American Nurses Foundation, is striving to help nurses feel valued and compensated by creating pilot programs that can help modernize nurses’ reimbursement structure so that they can direct bill.
In the end, attracting and retaining top nursing talent is about more than filling positions — it’s about building a healthcare system where nurses thrive. “In the United States and abroad, we owe it to nurses and the communities they serve to have sustainable and appropriate solutions to staffing and work environment challenges,” said Ms. Kennedy.
A version of this article appeared on Medscape.com.
In a fiercely competitive healthcare landscape, hospitals are pulling out all the stops to lure top nursing talent through their doors.
As the nursing shortage intensifies, the creative recruitment approach isn’t just about the perks — it’s becoming an essential tool in the race to build a skilled nursing workforce.
Nursing vacancies are as high as 17% — more than double prepandemic levels — and hospitals scrambling to fill them need to do more than raise salaries and bolster benefits packages to entice nurses.
“I am very thankful when I hear of creative ideas that nurse administrators come up with to try to get their ultimate goal, which is enough qualified nurses to take care of patients,” said Linda Plank, dean of the Louise Herrington School of Nursing at Baylor University in Dallas, Texas.
Signing Bonuses, Tuition Reimbursement, and Self-Scheduling, Please
Signing bonuses were among the top perks offered to healthcare workers, with almost 18% of job openings advertising the incentive for new nurse hires; the average signing bonus for registered nurses (RNs) topped $11,000. In 2023, California-based Palomar Health made headlines when it offered eligible RNs a $100,000 signing bonus paid over a 3-year period.
“We are seeing a variety of incentives, like sign-on bonuses, that can be effective at getting the attention of potential new hires,” said Deborah Trautman, PhD, RN, FAAN, president, and CEO of the American Association of Colleges of Nursing. “With the growing competition for registered nurses, especially those prepared in baccalaureate programs, employers should consider what’s most important to nurses entering the field.”
Hospitals have also invested in benefits ranging from tuition reimbursement, student loan forgiveness, and professional development opportunities to expanded parental leave and onsite childcare. Flexible scheduling is a sought-after perk that benefits both new and experienced RNs and could also help with recruitment.
“In the past, [hospitals said], ‘our shift starts at 7 and ends at 7,’ ” Ms. Plank said. “Now, hospitals are a little bit more flexible ... and being open to flexible shifts has merit. If we’re willing to look at things differently, it could get more people involved in patient care.”
An American Nurses Foundation report found that nurses preferred variable and flexible shift lengths, flexible start times, and self-scheduling options over set schedules. In fact, 45% of nurses who left clinical practice would consider returning to work if hospitals switched to a self-scheduling model.
The Cleveland Clinic in Ohio introduced staggered shifts that start at nontraditional times, including 11 AM to 11 PM, flexible shift lengths, and split RN positions that allow clinical care nurses to divide their time between different departments. Last year, Hackensack Meridian Health in New Jersey also piloted a self-scheduling program for its nursing staff.
Hiring Outside the United States
Despite the prevalence of signing bonuses and premium perks, some hospitals still struggled to fill open positions with nurses recruited from outside the United States. Data from The Kaiser Family Foundation show that 32% of hospitals hired foreign-educated RNs in 2022 — more than double the number hired in 2010.
Jennifer Mensik Kennedy, PhD, MBA, RN, NEA-BC, FAAN, president of the American Nurses Association (ANA), is concerned about that trend. The ANA supports the International Council of Nurses and their call for “stronger codes for ethical recruitment of nurses” because international nurse recruitment practices can negatively affect the quality of healthcare in countries that are depleted of nurses.
“Recruiting international nurses as a key strategy for building core staffing is not sustainable in the long term,” Ms. Kennedy said in an interview. “We need to redirect our focus on how to retain staff through fostering healthy work environments and addressing antiquated payment models.”
Reinforcing Retention
Recruiting nurses is just one element of addressing the nursing shortage. Prioritizing job satisfaction is essential to retaining nursing staff. Currently, 33% of nurses who enter the profession quit within the first 2 years.
A growing number of hospitals have implemented programs focused on increasing retention. Lifepoint Health, a national network of 60-plus acute care hospitals, launched a Nurse Residency Program in 2023. The 12-month program, which offers training and mentorship to help recent nursing school graduates, has recruited 750 new nurses and helped them transition to clinical practice.
The Nurse Residency Program has been so successful that the hospital system plans to introduce a 2-year fellowship program in the fall of 2024 that supports the professional development of nurses who want to specialize in areas like acute care, obstetrics, or the intensive care unit.
“We are more focused than ever on increasing partnerships and alignment with our local nursing programs, expanding clinical education opportunities for nursing students, owning and driving a nursing culture, and creating an environment where employees want to work,” said Michelle Watson, MSN, RN, CENP, chief nurse executive and senior vice president of clinical operations at Lifepoint Health.
Ms. Watson also credits their facilities’ chief nursing officers as being “highly engaged and visible leaders” who spend time with RNs to learn about their career aspirations and help them understand how the organization can support their desires for ongoing professional development.
The 2022 Nurse Staffing Task Force, a collaborative initiative by the ANA and other prominent national nursing and healthcare organizations, has developed and widely disseminated a set of recommendations for hospitals focusing on investing in nurse staffing, safe and supportive work environments, and competitive wages.
In addition, the Reimagining Nursing Initiative, started by the American Nurses Foundation, is striving to help nurses feel valued and compensated by creating pilot programs that can help modernize nurses’ reimbursement structure so that they can direct bill.
In the end, attracting and retaining top nursing talent is about more than filling positions — it’s about building a healthcare system where nurses thrive. “In the United States and abroad, we owe it to nurses and the communities they serve to have sustainable and appropriate solutions to staffing and work environment challenges,” said Ms. Kennedy.
A version of this article appeared on Medscape.com.
In a fiercely competitive healthcare landscape, hospitals are pulling out all the stops to lure top nursing talent through their doors.
As the nursing shortage intensifies, the creative recruitment approach isn’t just about the perks — it’s becoming an essential tool in the race to build a skilled nursing workforce.
Nursing vacancies are as high as 17% — more than double prepandemic levels — and hospitals scrambling to fill them need to do more than raise salaries and bolster benefits packages to entice nurses.
“I am very thankful when I hear of creative ideas that nurse administrators come up with to try to get their ultimate goal, which is enough qualified nurses to take care of patients,” said Linda Plank, dean of the Louise Herrington School of Nursing at Baylor University in Dallas, Texas.
Signing Bonuses, Tuition Reimbursement, and Self-Scheduling, Please
Signing bonuses were among the top perks offered to healthcare workers, with almost 18% of job openings advertising the incentive for new nurse hires; the average signing bonus for registered nurses (RNs) topped $11,000. In 2023, California-based Palomar Health made headlines when it offered eligible RNs a $100,000 signing bonus paid over a 3-year period.
“We are seeing a variety of incentives, like sign-on bonuses, that can be effective at getting the attention of potential new hires,” said Deborah Trautman, PhD, RN, FAAN, president, and CEO of the American Association of Colleges of Nursing. “With the growing competition for registered nurses, especially those prepared in baccalaureate programs, employers should consider what’s most important to nurses entering the field.”
Hospitals have also invested in benefits ranging from tuition reimbursement, student loan forgiveness, and professional development opportunities to expanded parental leave and onsite childcare. Flexible scheduling is a sought-after perk that benefits both new and experienced RNs and could also help with recruitment.
“In the past, [hospitals said], ‘our shift starts at 7 and ends at 7,’ ” Ms. Plank said. “Now, hospitals are a little bit more flexible ... and being open to flexible shifts has merit. If we’re willing to look at things differently, it could get more people involved in patient care.”
An American Nurses Foundation report found that nurses preferred variable and flexible shift lengths, flexible start times, and self-scheduling options over set schedules. In fact, 45% of nurses who left clinical practice would consider returning to work if hospitals switched to a self-scheduling model.
The Cleveland Clinic in Ohio introduced staggered shifts that start at nontraditional times, including 11 AM to 11 PM, flexible shift lengths, and split RN positions that allow clinical care nurses to divide their time between different departments. Last year, Hackensack Meridian Health in New Jersey also piloted a self-scheduling program for its nursing staff.
Hiring Outside the United States
Despite the prevalence of signing bonuses and premium perks, some hospitals still struggled to fill open positions with nurses recruited from outside the United States. Data from The Kaiser Family Foundation show that 32% of hospitals hired foreign-educated RNs in 2022 — more than double the number hired in 2010.
Jennifer Mensik Kennedy, PhD, MBA, RN, NEA-BC, FAAN, president of the American Nurses Association (ANA), is concerned about that trend. The ANA supports the International Council of Nurses and their call for “stronger codes for ethical recruitment of nurses” because international nurse recruitment practices can negatively affect the quality of healthcare in countries that are depleted of nurses.
“Recruiting international nurses as a key strategy for building core staffing is not sustainable in the long term,” Ms. Kennedy said in an interview. “We need to redirect our focus on how to retain staff through fostering healthy work environments and addressing antiquated payment models.”
Reinforcing Retention
Recruiting nurses is just one element of addressing the nursing shortage. Prioritizing job satisfaction is essential to retaining nursing staff. Currently, 33% of nurses who enter the profession quit within the first 2 years.
A growing number of hospitals have implemented programs focused on increasing retention. Lifepoint Health, a national network of 60-plus acute care hospitals, launched a Nurse Residency Program in 2023. The 12-month program, which offers training and mentorship to help recent nursing school graduates, has recruited 750 new nurses and helped them transition to clinical practice.
The Nurse Residency Program has been so successful that the hospital system plans to introduce a 2-year fellowship program in the fall of 2024 that supports the professional development of nurses who want to specialize in areas like acute care, obstetrics, or the intensive care unit.
“We are more focused than ever on increasing partnerships and alignment with our local nursing programs, expanding clinical education opportunities for nursing students, owning and driving a nursing culture, and creating an environment where employees want to work,” said Michelle Watson, MSN, RN, CENP, chief nurse executive and senior vice president of clinical operations at Lifepoint Health.
Ms. Watson also credits their facilities’ chief nursing officers as being “highly engaged and visible leaders” who spend time with RNs to learn about their career aspirations and help them understand how the organization can support their desires for ongoing professional development.
The 2022 Nurse Staffing Task Force, a collaborative initiative by the ANA and other prominent national nursing and healthcare organizations, has developed and widely disseminated a set of recommendations for hospitals focusing on investing in nurse staffing, safe and supportive work environments, and competitive wages.
In addition, the Reimagining Nursing Initiative, started by the American Nurses Foundation, is striving to help nurses feel valued and compensated by creating pilot programs that can help modernize nurses’ reimbursement structure so that they can direct bill.
In the end, attracting and retaining top nursing talent is about more than filling positions — it’s about building a healthcare system where nurses thrive. “In the United States and abroad, we owe it to nurses and the communities they serve to have sustainable and appropriate solutions to staffing and work environment challenges,” said Ms. Kennedy.
A version of this article appeared on Medscape.com.
Delayed Bleeding: The Silent Risk for Seniors
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
Primary Care Physicians Track an Average of 57 Quality Measures for Value-Based Care Pay
A new analysis suggests one reason doctors are wary of value-based care arrangements: Overkill.
Researchers found that primary care physicians in one large integrated health system were required to track an average of 57 different quality measures across multiple insurers that linked outcomes to payments under value-based contracts.
Medicare contracts were the most likely to pile quality measures on physicians with an average of 13.42 measures vs 10.07 for commercial insurer contracts and 5.37 for Medicaid contracts, reported Claire Boone, PhD, of the University of Chicago in Illinois and Providence Research Network, Portland, Oregon, and colleagues in JAMA Health Forum. The analysis, which may be the first of its kind, tracked 890 primary care physicians from 2020 to 2022.
The average of 57 quality measures per physician was unexpectedly high, Dr. Boone said in an interview.
“The magnitude of that number surprised us,” Dr. Boone said. “Primary care physicians and their practices have a lot on their plate. Now we know that one of those things is a very large number of different quality metrics to pay attention to, measure, report on, and implement.
Value-based care programs use quality measures to evaluate how well clinicians are doing their jobs and adjust reimbursement accordingly. A payer, for example, may raise reimbursements if a clinician has higher numbers of patients who meet quality measure standards for depression screening or blood pressure.
Dr. Boone said her research group is studying the impact of quality measures and was surprised that data showed individual primary care physicians had to deal with a high number of value-based contracts.
The researchers tracked value-based contracts for 890 physicians (58.3% women, 41.7% men) in an unidentified West Coast Health system. (Several study authors work for the Providence Health System, which serves several Western States and Texas.) The average number of patients per physician was 1309.
The physicians were part of an average of 11.18 value-based contracts (commercial insurers, 49.50%; Medicaid, 21.49%; and Medicare, 29.01%). This number grew from 9.39 in 2020 to 12.26 in 2022. Quality measure data weren’t available for 29% of contracts.
Quality measures were considered unique if they referenced different conditions.
For example, colorectal cancer screening is unique from depression screening. The researchers also considered measures for the same condition unique if the target value differed — for example, blood pressure control defined as < 140/90 vs blood pressure control defined as < 130/80, Dr. Boone said.
Dr. Boone said she expected payers to coordinate quality measures.
“The fact that they largely are not is really the main finding of this paper. Without coordination, the use of value-based contracts and quality measures at scale leads to many unique measures being used. This may reflect the fact that there are so many important tasks to do in primary care, and there’s no consensus on which ones should be included in quality-based contracts.”
Ronald N. Adler, MD, an associate professor in the Department of Family Medicine and Community Health at UMass Chan Medical School, Worcester, Massachusetts, who’s familiar with the findings but didn’t take part in the research, said the study offers something new — the quantification of quality measures.
He said in an interview that physicians deal with quality measures in different ways. Some clinicians “don’t really care,” and have an attitude of “this is not why I got into medicine.” But others “are very competitive around this, and it leads to a lot of a lot of stress. Trying to address 50-plus measures is impossible and demoralizing.”
The metrics may measure things like mammogram screening that are out of the physician’s control, Dr. Adler said. “I can recommend a mammogram, and my patient can choose not to do it. Or maybe my patient is homeless; she doesn’t have transportation, and it’s not a priority for her, even though she wants to do it.”
Patients may not take medication as prescribed, or they may be unable to afford it, he said. “Can they afford to eat healthy foods? Or is ramen all they can afford, and their sugars are through the roof? There are a lot of factors at play here that are independent of the quality of care provided by the doctor.”
As for his own approach, Dr. Adler said he worries about some measures more than others. “I’m very proactive about screening my patients for colon cancer and maybe a little less so about mammography.”
For colon cancer screening, “there are a lot of benefits and not that many harms as opposed to mammography, which has harms such as false positives and overdiagnosis of breast cancer.”
Dr. Adler is a member of the Quality Measure Alignment Taskforce in Massachusetts, which is trying to establish consensus on appropriate quality measures. But payer participation is voluntary. “Our health systems are too siloed ... so there is no readily available mechanism for enforcing such recommendations.”
Wayne Altman, MD, chair of Family Medicine at Tufts University School of Medicine, Boston, Massachusetts, is also familiar with the study findings but didn’t take part in the research. He said in an interview that clinicians shouldn’t have to deal with more than 5-10 quality measures in total.
He pointed out that many measures don’t make sense in certain populations. Titrating blood pressure to < 140/90 isn’t ideal for elderly patients because aggressive control can send their blood pressure dangerously low. “They’re going to fall down, break a hip, and likely die within a year. You have to have the right population and be aware of unintended consequences.”
Still, Dr. Adler noted, there’s an important role for quality measures in healthcare.
“We need data to inform our quality improvement activities, but they need to be the right measures. People can’t respond reasonably to improve on 50-plus measures,” he said. “They need to be consolidated and prioritized. It would be really helpful if we could have a much lower number of measures that are meaningful, safe, and connect to things that matter.”
No funding has been reported. Dr. Boone disclosed a grant from the National Institute on Aging. Dr. Adler and Dr. Altman had no disclosures.
A version of this article first appeared on Medscape.com.
A new analysis suggests one reason doctors are wary of value-based care arrangements: Overkill.
Researchers found that primary care physicians in one large integrated health system were required to track an average of 57 different quality measures across multiple insurers that linked outcomes to payments under value-based contracts.
Medicare contracts were the most likely to pile quality measures on physicians with an average of 13.42 measures vs 10.07 for commercial insurer contracts and 5.37 for Medicaid contracts, reported Claire Boone, PhD, of the University of Chicago in Illinois and Providence Research Network, Portland, Oregon, and colleagues in JAMA Health Forum. The analysis, which may be the first of its kind, tracked 890 primary care physicians from 2020 to 2022.
The average of 57 quality measures per physician was unexpectedly high, Dr. Boone said in an interview.
“The magnitude of that number surprised us,” Dr. Boone said. “Primary care physicians and their practices have a lot on their plate. Now we know that one of those things is a very large number of different quality metrics to pay attention to, measure, report on, and implement.
Value-based care programs use quality measures to evaluate how well clinicians are doing their jobs and adjust reimbursement accordingly. A payer, for example, may raise reimbursements if a clinician has higher numbers of patients who meet quality measure standards for depression screening or blood pressure.
Dr. Boone said her research group is studying the impact of quality measures and was surprised that data showed individual primary care physicians had to deal with a high number of value-based contracts.
The researchers tracked value-based contracts for 890 physicians (58.3% women, 41.7% men) in an unidentified West Coast Health system. (Several study authors work for the Providence Health System, which serves several Western States and Texas.) The average number of patients per physician was 1309.
The physicians were part of an average of 11.18 value-based contracts (commercial insurers, 49.50%; Medicaid, 21.49%; and Medicare, 29.01%). This number grew from 9.39 in 2020 to 12.26 in 2022. Quality measure data weren’t available for 29% of contracts.
Quality measures were considered unique if they referenced different conditions.
For example, colorectal cancer screening is unique from depression screening. The researchers also considered measures for the same condition unique if the target value differed — for example, blood pressure control defined as < 140/90 vs blood pressure control defined as < 130/80, Dr. Boone said.
Dr. Boone said she expected payers to coordinate quality measures.
“The fact that they largely are not is really the main finding of this paper. Without coordination, the use of value-based contracts and quality measures at scale leads to many unique measures being used. This may reflect the fact that there are so many important tasks to do in primary care, and there’s no consensus on which ones should be included in quality-based contracts.”
Ronald N. Adler, MD, an associate professor in the Department of Family Medicine and Community Health at UMass Chan Medical School, Worcester, Massachusetts, who’s familiar with the findings but didn’t take part in the research, said the study offers something new — the quantification of quality measures.
He said in an interview that physicians deal with quality measures in different ways. Some clinicians “don’t really care,” and have an attitude of “this is not why I got into medicine.” But others “are very competitive around this, and it leads to a lot of a lot of stress. Trying to address 50-plus measures is impossible and demoralizing.”
The metrics may measure things like mammogram screening that are out of the physician’s control, Dr. Adler said. “I can recommend a mammogram, and my patient can choose not to do it. Or maybe my patient is homeless; she doesn’t have transportation, and it’s not a priority for her, even though she wants to do it.”
Patients may not take medication as prescribed, or they may be unable to afford it, he said. “Can they afford to eat healthy foods? Or is ramen all they can afford, and their sugars are through the roof? There are a lot of factors at play here that are independent of the quality of care provided by the doctor.”
As for his own approach, Dr. Adler said he worries about some measures more than others. “I’m very proactive about screening my patients for colon cancer and maybe a little less so about mammography.”
For colon cancer screening, “there are a lot of benefits and not that many harms as opposed to mammography, which has harms such as false positives and overdiagnosis of breast cancer.”
Dr. Adler is a member of the Quality Measure Alignment Taskforce in Massachusetts, which is trying to establish consensus on appropriate quality measures. But payer participation is voluntary. “Our health systems are too siloed ... so there is no readily available mechanism for enforcing such recommendations.”
Wayne Altman, MD, chair of Family Medicine at Tufts University School of Medicine, Boston, Massachusetts, is also familiar with the study findings but didn’t take part in the research. He said in an interview that clinicians shouldn’t have to deal with more than 5-10 quality measures in total.
He pointed out that many measures don’t make sense in certain populations. Titrating blood pressure to < 140/90 isn’t ideal for elderly patients because aggressive control can send their blood pressure dangerously low. “They’re going to fall down, break a hip, and likely die within a year. You have to have the right population and be aware of unintended consequences.”
Still, Dr. Adler noted, there’s an important role for quality measures in healthcare.
“We need data to inform our quality improvement activities, but they need to be the right measures. People can’t respond reasonably to improve on 50-plus measures,” he said. “They need to be consolidated and prioritized. It would be really helpful if we could have a much lower number of measures that are meaningful, safe, and connect to things that matter.”
No funding has been reported. Dr. Boone disclosed a grant from the National Institute on Aging. Dr. Adler and Dr. Altman had no disclosures.
A version of this article first appeared on Medscape.com.
A new analysis suggests one reason doctors are wary of value-based care arrangements: Overkill.
Researchers found that primary care physicians in one large integrated health system were required to track an average of 57 different quality measures across multiple insurers that linked outcomes to payments under value-based contracts.
Medicare contracts were the most likely to pile quality measures on physicians with an average of 13.42 measures vs 10.07 for commercial insurer contracts and 5.37 for Medicaid contracts, reported Claire Boone, PhD, of the University of Chicago in Illinois and Providence Research Network, Portland, Oregon, and colleagues in JAMA Health Forum. The analysis, which may be the first of its kind, tracked 890 primary care physicians from 2020 to 2022.
The average of 57 quality measures per physician was unexpectedly high, Dr. Boone said in an interview.
“The magnitude of that number surprised us,” Dr. Boone said. “Primary care physicians and their practices have a lot on their plate. Now we know that one of those things is a very large number of different quality metrics to pay attention to, measure, report on, and implement.
Value-based care programs use quality measures to evaluate how well clinicians are doing their jobs and adjust reimbursement accordingly. A payer, for example, may raise reimbursements if a clinician has higher numbers of patients who meet quality measure standards for depression screening or blood pressure.
Dr. Boone said her research group is studying the impact of quality measures and was surprised that data showed individual primary care physicians had to deal with a high number of value-based contracts.
The researchers tracked value-based contracts for 890 physicians (58.3% women, 41.7% men) in an unidentified West Coast Health system. (Several study authors work for the Providence Health System, which serves several Western States and Texas.) The average number of patients per physician was 1309.
The physicians were part of an average of 11.18 value-based contracts (commercial insurers, 49.50%; Medicaid, 21.49%; and Medicare, 29.01%). This number grew from 9.39 in 2020 to 12.26 in 2022. Quality measure data weren’t available for 29% of contracts.
Quality measures were considered unique if they referenced different conditions.
For example, colorectal cancer screening is unique from depression screening. The researchers also considered measures for the same condition unique if the target value differed — for example, blood pressure control defined as < 140/90 vs blood pressure control defined as < 130/80, Dr. Boone said.
Dr. Boone said she expected payers to coordinate quality measures.
“The fact that they largely are not is really the main finding of this paper. Without coordination, the use of value-based contracts and quality measures at scale leads to many unique measures being used. This may reflect the fact that there are so many important tasks to do in primary care, and there’s no consensus on which ones should be included in quality-based contracts.”
Ronald N. Adler, MD, an associate professor in the Department of Family Medicine and Community Health at UMass Chan Medical School, Worcester, Massachusetts, who’s familiar with the findings but didn’t take part in the research, said the study offers something new — the quantification of quality measures.
He said in an interview that physicians deal with quality measures in different ways. Some clinicians “don’t really care,” and have an attitude of “this is not why I got into medicine.” But others “are very competitive around this, and it leads to a lot of a lot of stress. Trying to address 50-plus measures is impossible and demoralizing.”
The metrics may measure things like mammogram screening that are out of the physician’s control, Dr. Adler said. “I can recommend a mammogram, and my patient can choose not to do it. Or maybe my patient is homeless; she doesn’t have transportation, and it’s not a priority for her, even though she wants to do it.”
Patients may not take medication as prescribed, or they may be unable to afford it, he said. “Can they afford to eat healthy foods? Or is ramen all they can afford, and their sugars are through the roof? There are a lot of factors at play here that are independent of the quality of care provided by the doctor.”
As for his own approach, Dr. Adler said he worries about some measures more than others. “I’m very proactive about screening my patients for colon cancer and maybe a little less so about mammography.”
For colon cancer screening, “there are a lot of benefits and not that many harms as opposed to mammography, which has harms such as false positives and overdiagnosis of breast cancer.”
Dr. Adler is a member of the Quality Measure Alignment Taskforce in Massachusetts, which is trying to establish consensus on appropriate quality measures. But payer participation is voluntary. “Our health systems are too siloed ... so there is no readily available mechanism for enforcing such recommendations.”
Wayne Altman, MD, chair of Family Medicine at Tufts University School of Medicine, Boston, Massachusetts, is also familiar with the study findings but didn’t take part in the research. He said in an interview that clinicians shouldn’t have to deal with more than 5-10 quality measures in total.
He pointed out that many measures don’t make sense in certain populations. Titrating blood pressure to < 140/90 isn’t ideal for elderly patients because aggressive control can send their blood pressure dangerously low. “They’re going to fall down, break a hip, and likely die within a year. You have to have the right population and be aware of unintended consequences.”
Still, Dr. Adler noted, there’s an important role for quality measures in healthcare.
“We need data to inform our quality improvement activities, but they need to be the right measures. People can’t respond reasonably to improve on 50-plus measures,” he said. “They need to be consolidated and prioritized. It would be really helpful if we could have a much lower number of measures that are meaningful, safe, and connect to things that matter.”
No funding has been reported. Dr. Boone disclosed a grant from the National Institute on Aging. Dr. Adler and Dr. Altman had no disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA HEALTH FORUM
Involuntary flashbacks
The correct diagnosis is posttraumatic stress disorder (PTSD). The patient's anxiety, irritability, sleep difficulties, and other symptoms are directly related to the recent traumatic event (car crash), and he has no significant physical injuries or neurologic abnormalities.
Generalized anxiety disorder is incorrect because it involves chronic worry about various life aspects for at least 6 months, unrelated to a specific trauma.
Postconcussion syndrome is not applicable because of the lack of concussion evidence and other symptoms, such as headaches or dizziness.
Acute stress disorder is similar to PTSD but is diagnosed when symptoms occur within 3 days to 1 month after a trauma. Because this patient's symptoms have persisted beyond 1 month, PTSD is the most likely diagnosis.
Patients with PTSD exhibit pronounced cognitive, affective, or behavioral responses to trauma reminders; these responses may include severe anxiety, dissociative episodes, flashbacks, and hyperreactive behaviors. The intensity of these symptoms and the resulting psychosocial impairment are more severe in individuals with PTSD compared with people who experience trauma without developing the disorder. To manage such heightened arousal, individuals with PTSD often engage in avoidance behaviors, leading to emotional numbing; reduced interest in daily activities; and, in severe cases, detachment from others.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals older than 6 years. These criteria include: (A) exposure to actual or threatened death, serious injury, or sexual violence; (B) the presence of one or more intrusion symptoms related to the traumatic event; (C) persistent avoidance of stimuli associated with the trauma; (D) negative alterations in cognitions and mood related to the trauma; and (E) marked alterations in arousal and reactivity, evidenced by two or more specific symptoms.
Early intervention is key in the treatment of PTSD to prevent the condition from becoming chronic. Although more empirical data are needed, especially regarding pharmacotherapy, early supportive interventions such as psychoeducation and case management have shown promise in acutely traumatized individuals.
Trauma-focused psychotherapy is recommended as the first-line treatment for most adults with PTSD. This approach, which includes exposure-based therapies, is generally preferred over other therapies or pharmacologic treatments, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors. However, in patients with comorbid conditions (eg, depression, psychosis) that impair their ability to engage in trauma-focused therapy, initial pharmacologic management is advised until symptoms stabilize, after which psychotherapy can be introduced.
Clinical trials and meta-analyses have demonstrated the efficacy of various trauma-focused therapies, including trauma-focused cognitive-behavioral therapy, prolonged exposure therapy, and eye movement desensitization and reprocessing. The treatment choice should be collaborative, based on patient presentation, preference, and therapist expertise.
For individuals with PTSD experiencing significant sleep disturbances, particularly nightmares, prazosin is suggested. Clinical studies demonstrate that prazosin effectively reduces overall PTSD symptoms, nightmares, and sleep disturbances in approximately half of the patients treated.
Medication regimens effective for PTSD should be continued for at least 6 months to 1 year to prevent relapse or recurrence. Multiple clinical trials in patients with PTSD who completed acute treatment with SSRIs have demonstrated that those who continued with SSRIs were less likely to have relapse compared with those receiving placebo.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The correct diagnosis is posttraumatic stress disorder (PTSD). The patient's anxiety, irritability, sleep difficulties, and other symptoms are directly related to the recent traumatic event (car crash), and he has no significant physical injuries or neurologic abnormalities.
Generalized anxiety disorder is incorrect because it involves chronic worry about various life aspects for at least 6 months, unrelated to a specific trauma.
Postconcussion syndrome is not applicable because of the lack of concussion evidence and other symptoms, such as headaches or dizziness.
Acute stress disorder is similar to PTSD but is diagnosed when symptoms occur within 3 days to 1 month after a trauma. Because this patient's symptoms have persisted beyond 1 month, PTSD is the most likely diagnosis.
Patients with PTSD exhibit pronounced cognitive, affective, or behavioral responses to trauma reminders; these responses may include severe anxiety, dissociative episodes, flashbacks, and hyperreactive behaviors. The intensity of these symptoms and the resulting psychosocial impairment are more severe in individuals with PTSD compared with people who experience trauma without developing the disorder. To manage such heightened arousal, individuals with PTSD often engage in avoidance behaviors, leading to emotional numbing; reduced interest in daily activities; and, in severe cases, detachment from others.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals older than 6 years. These criteria include: (A) exposure to actual or threatened death, serious injury, or sexual violence; (B) the presence of one or more intrusion symptoms related to the traumatic event; (C) persistent avoidance of stimuli associated with the trauma; (D) negative alterations in cognitions and mood related to the trauma; and (E) marked alterations in arousal and reactivity, evidenced by two or more specific symptoms.
Early intervention is key in the treatment of PTSD to prevent the condition from becoming chronic. Although more empirical data are needed, especially regarding pharmacotherapy, early supportive interventions such as psychoeducation and case management have shown promise in acutely traumatized individuals.
Trauma-focused psychotherapy is recommended as the first-line treatment for most adults with PTSD. This approach, which includes exposure-based therapies, is generally preferred over other therapies or pharmacologic treatments, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors. However, in patients with comorbid conditions (eg, depression, psychosis) that impair their ability to engage in trauma-focused therapy, initial pharmacologic management is advised until symptoms stabilize, after which psychotherapy can be introduced.
Clinical trials and meta-analyses have demonstrated the efficacy of various trauma-focused therapies, including trauma-focused cognitive-behavioral therapy, prolonged exposure therapy, and eye movement desensitization and reprocessing. The treatment choice should be collaborative, based on patient presentation, preference, and therapist expertise.
For individuals with PTSD experiencing significant sleep disturbances, particularly nightmares, prazosin is suggested. Clinical studies demonstrate that prazosin effectively reduces overall PTSD symptoms, nightmares, and sleep disturbances in approximately half of the patients treated.
Medication regimens effective for PTSD should be continued for at least 6 months to 1 year to prevent relapse or recurrence. Multiple clinical trials in patients with PTSD who completed acute treatment with SSRIs have demonstrated that those who continued with SSRIs were less likely to have relapse compared with those receiving placebo.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The correct diagnosis is posttraumatic stress disorder (PTSD). The patient's anxiety, irritability, sleep difficulties, and other symptoms are directly related to the recent traumatic event (car crash), and he has no significant physical injuries or neurologic abnormalities.
Generalized anxiety disorder is incorrect because it involves chronic worry about various life aspects for at least 6 months, unrelated to a specific trauma.
Postconcussion syndrome is not applicable because of the lack of concussion evidence and other symptoms, such as headaches or dizziness.
Acute stress disorder is similar to PTSD but is diagnosed when symptoms occur within 3 days to 1 month after a trauma. Because this patient's symptoms have persisted beyond 1 month, PTSD is the most likely diagnosis.
Patients with PTSD exhibit pronounced cognitive, affective, or behavioral responses to trauma reminders; these responses may include severe anxiety, dissociative episodes, flashbacks, and hyperreactive behaviors. The intensity of these symptoms and the resulting psychosocial impairment are more severe in individuals with PTSD compared with people who experience trauma without developing the disorder. To manage such heightened arousal, individuals with PTSD often engage in avoidance behaviors, leading to emotional numbing; reduced interest in daily activities; and, in severe cases, detachment from others.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) outlines specific criteria for diagnosing PTSD in individuals older than 6 years. These criteria include: (A) exposure to actual or threatened death, serious injury, or sexual violence; (B) the presence of one or more intrusion symptoms related to the traumatic event; (C) persistent avoidance of stimuli associated with the trauma; (D) negative alterations in cognitions and mood related to the trauma; and (E) marked alterations in arousal and reactivity, evidenced by two or more specific symptoms.
Early intervention is key in the treatment of PTSD to prevent the condition from becoming chronic. Although more empirical data are needed, especially regarding pharmacotherapy, early supportive interventions such as psychoeducation and case management have shown promise in acutely traumatized individuals.
Trauma-focused psychotherapy is recommended as the first-line treatment for most adults with PTSD. This approach, which includes exposure-based therapies, is generally preferred over other therapies or pharmacologic treatments, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors. However, in patients with comorbid conditions (eg, depression, psychosis) that impair their ability to engage in trauma-focused therapy, initial pharmacologic management is advised until symptoms stabilize, after which psychotherapy can be introduced.
Clinical trials and meta-analyses have demonstrated the efficacy of various trauma-focused therapies, including trauma-focused cognitive-behavioral therapy, prolonged exposure therapy, and eye movement desensitization and reprocessing. The treatment choice should be collaborative, based on patient presentation, preference, and therapist expertise.
For individuals with PTSD experiencing significant sleep disturbances, particularly nightmares, prazosin is suggested. Clinical studies demonstrate that prazosin effectively reduces overall PTSD symptoms, nightmares, and sleep disturbances in approximately half of the patients treated.
Medication regimens effective for PTSD should be continued for at least 6 months to 1 year to prevent relapse or recurrence. Multiple clinical trials in patients with PTSD who completed acute treatment with SSRIs have demonstrated that those who continued with SSRIs were less likely to have relapse compared with those receiving placebo.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
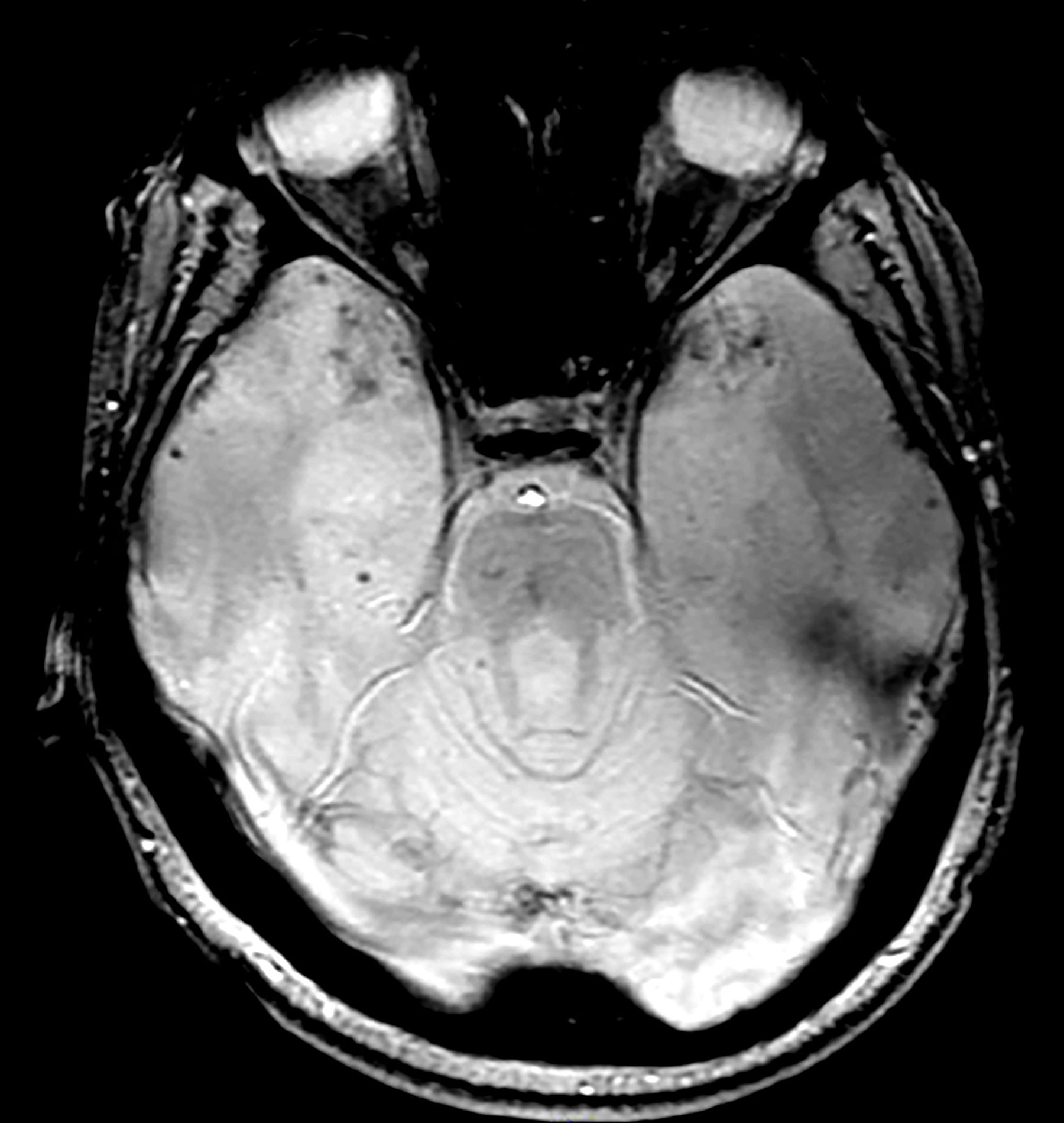
A 28-year-old man presented to the emergency department following a high-speed motor vehicle accident 2 months ago. He sustained no major physical injuries but had minor lacerations and bruising. The patient reported feeling unusually irritable and having difficulty sleeping since the accident, citing frequent flashbacks to the accident and occasional nightmares. He has started to feel more anxious and withdrawn, losing interest in hobbies such as swimming and biking that he previously enjoyed.
The patient's medical history is unremarkable, with no previous psychiatric or neurologic conditions. His neurologic examination was normal. An initial axial T2-weighted brain MRI demonstrated multiple small areas of hemorrhage, indicative of a diffuse axonal injury or shear-type injury. Despite the lack of significant physical injuries, the patient expressed ongoing distress related to the traumatic event.
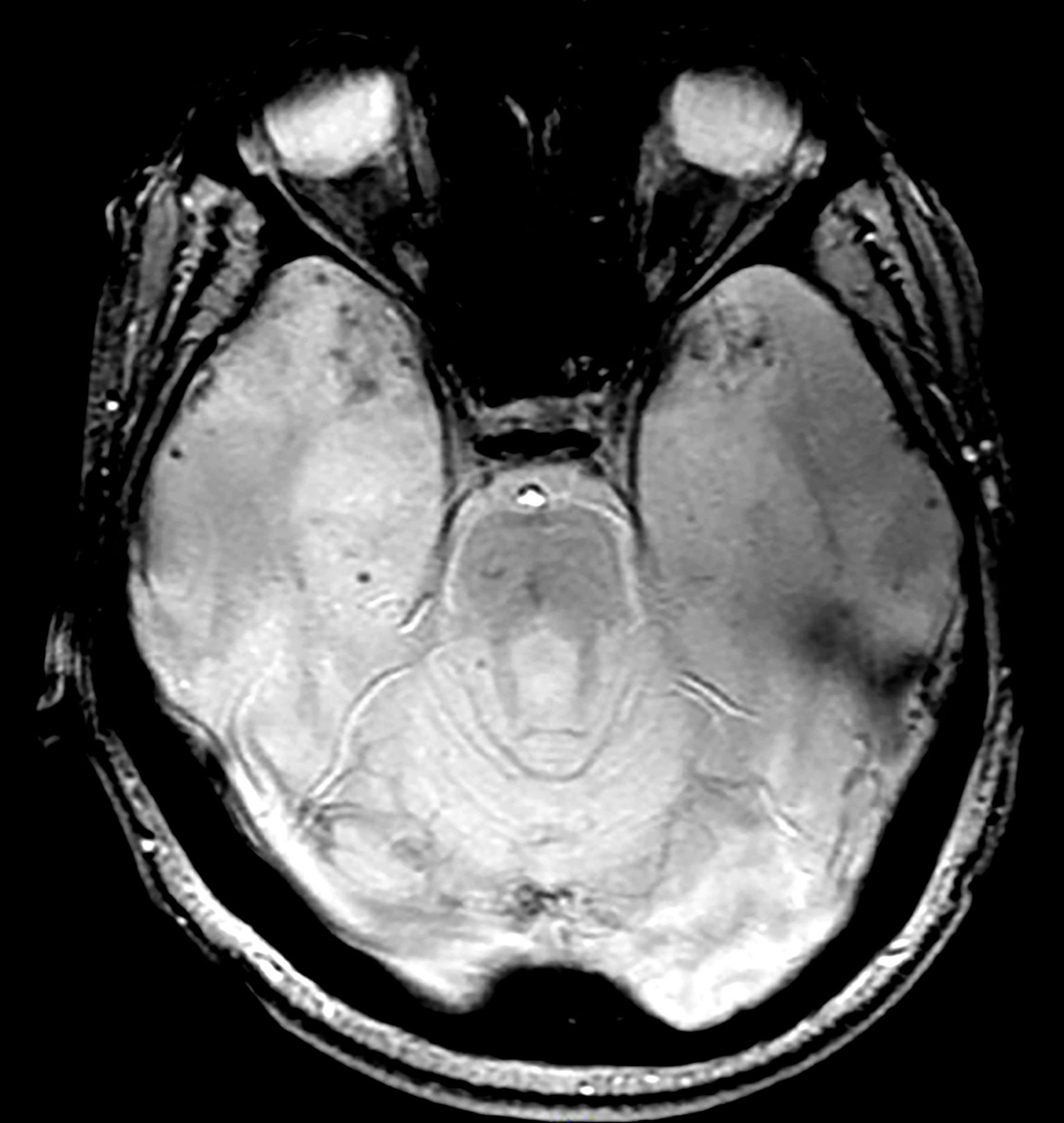
Technoference
You see it all the time. It’s the family at the table next to you in the restaurant where the two teenage children are texting away on their phones. Or the playground, where a 3-year-old is playing with his toy truck and bulldozer in the sand and his father, immersed in his laptop, hasn’t said a word to his child.
It may trouble you when you witness social situations like that in which an electronic device is preventing or certainly interfering with interpersonal interactions. Or at least I hope it troubles you. Maybe it is so ubiquitous that you have come to accept it as the norm. It’s likely you may even be a participant. But, do you have a name for it?
It’s called “technoference,” a word coined by a doctoral student in human development and family studies at Penn State a decade ago “to describe the everyday intrusions and interruptions in couple interactions that take place due to technology devices and their always-on, ever-present nature.” Although, the original research that triggered the coinage was about couples, obviously the phenomenon occurs whenever people of any age are together in social situations.

While the word may not have crept into common parlance, we all know it when we see it. Technoference may not appear in the paper’s title, but it is a subject being investigated across a broad array of disciplines. One phone tracking study found that parents of young infants spend more than 5 hours each day on their smartphones. More than a quarter of that time the infant is engaged with the parent’s digital device. Technoference has been associated with decreased parent-child interaction during early childhood. It has been associated with more negative responses to children’s behavior, as well as an increased risk of child injury.
There are numerous studies suggesting an association between parental technoference and mental health difficulties in children. I have recently reviewed one of these studies that looks at the relationship of perceived parental technoference and the mental health of children entering adolescents. The authors collected longitudinal data of more than 1300 emerging adolescents, hoping to determine if the relationship between parental distraction and mental health was bidirectional. In other words, could a child’s mental health be contributing to his parents’ perceived distraction? Or was it primarily the parents’ technoference that was playing a role in the child’s mental health problems?
What investigators found was that higher levels of parental distraction were associated with higher levels of inattention and hyperactivity in the emerging adolescents, but not vice versa. On the other hand, higher levels of adolescent anxiety was associated with higher levels of perceived parental technoference, but not vice versa.
I know this sounds a bit confusing and a bit chicken-egg-chicken-eggish. The study was not designed to determine causation in these associations. However, the authors offer some possible scenarios that may provide a bit of clarity. It could be that parents who are concerned about their anxious child respond by retreating into the cyberspace to avoid tense situations or for support or information.
On the other hand, This explanation meshes with other studies demonstrating an association between parental distraction and aggression and attention problems in early childhood.
While one could spend more time imagining other factors that could be driving these bidirectional relationships, I’m not sure that it makes a heckuva lot of difference. Whether the child’s mental illness is the primary driver or the parent’s device-associated distraction is the dominant force isn’t the point. These are bidirectional relationships. If we are interested in pointing fingers, the common denominator is the device and our failure as a society to keep it in proper perspective. We all know that smartphones, tablets, and computers create an unhealthy distraction in personal relationships. The parents know and most of the children know. It’s time for us all to demonstrate some self-discipline. And that can begin for us as health care providers as we sit behind our computers spending more time looking at the screen than we do engaging the patient with our eyes.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
You see it all the time. It’s the family at the table next to you in the restaurant where the two teenage children are texting away on their phones. Or the playground, where a 3-year-old is playing with his toy truck and bulldozer in the sand and his father, immersed in his laptop, hasn’t said a word to his child.
It may trouble you when you witness social situations like that in which an electronic device is preventing or certainly interfering with interpersonal interactions. Or at least I hope it troubles you. Maybe it is so ubiquitous that you have come to accept it as the norm. It’s likely you may even be a participant. But, do you have a name for it?
It’s called “technoference,” a word coined by a doctoral student in human development and family studies at Penn State a decade ago “to describe the everyday intrusions and interruptions in couple interactions that take place due to technology devices and their always-on, ever-present nature.” Although, the original research that triggered the coinage was about couples, obviously the phenomenon occurs whenever people of any age are together in social situations.
While the word may not have crept into common parlance, we all know it when we see it. Technoference may not appear in the paper’s title, but it is a subject being investigated across a broad array of disciplines. One phone tracking study found that parents of young infants spend more than 5 hours each day on their smartphones. More than a quarter of that time the infant is engaged with the parent’s digital device. Technoference has been associated with decreased parent-child interaction during early childhood. It has been associated with more negative responses to children’s behavior, as well as an increased risk of child injury.
There are numerous studies suggesting an association between parental technoference and mental health difficulties in children. I have recently reviewed one of these studies that looks at the relationship of perceived parental technoference and the mental health of children entering adolescents. The authors collected longitudinal data of more than 1300 emerging adolescents, hoping to determine if the relationship between parental distraction and mental health was bidirectional. In other words, could a child’s mental health be contributing to his parents’ perceived distraction? Or was it primarily the parents’ technoference that was playing a role in the child’s mental health problems?
What investigators found was that higher levels of parental distraction were associated with higher levels of inattention and hyperactivity in the emerging adolescents, but not vice versa. On the other hand, higher levels of adolescent anxiety was associated with higher levels of perceived parental technoference, but not vice versa.
I know this sounds a bit confusing and a bit chicken-egg-chicken-eggish. The study was not designed to determine causation in these associations. However, the authors offer some possible scenarios that may provide a bit of clarity. It could be that parents who are concerned about their anxious child respond by retreating into the cyberspace to avoid tense situations or for support or information.
On the other hand, This explanation meshes with other studies demonstrating an association between parental distraction and aggression and attention problems in early childhood.
While one could spend more time imagining other factors that could be driving these bidirectional relationships, I’m not sure that it makes a heckuva lot of difference. Whether the child’s mental illness is the primary driver or the parent’s device-associated distraction is the dominant force isn’t the point. These are bidirectional relationships. If we are interested in pointing fingers, the common denominator is the device and our failure as a society to keep it in proper perspective. We all know that smartphones, tablets, and computers create an unhealthy distraction in personal relationships. The parents know and most of the children know. It’s time for us all to demonstrate some self-discipline. And that can begin for us as health care providers as we sit behind our computers spending more time looking at the screen than we do engaging the patient with our eyes.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
You see it all the time. It’s the family at the table next to you in the restaurant where the two teenage children are texting away on their phones. Or the playground, where a 3-year-old is playing with his toy truck and bulldozer in the sand and his father, immersed in his laptop, hasn’t said a word to his child.
It may trouble you when you witness social situations like that in which an electronic device is preventing or certainly interfering with interpersonal interactions. Or at least I hope it troubles you. Maybe it is so ubiquitous that you have come to accept it as the norm. It’s likely you may even be a participant. But, do you have a name for it?
It’s called “technoference,” a word coined by a doctoral student in human development and family studies at Penn State a decade ago “to describe the everyday intrusions and interruptions in couple interactions that take place due to technology devices and their always-on, ever-present nature.” Although, the original research that triggered the coinage was about couples, obviously the phenomenon occurs whenever people of any age are together in social situations.
While the word may not have crept into common parlance, we all know it when we see it. Technoference may not appear in the paper’s title, but it is a subject being investigated across a broad array of disciplines. One phone tracking study found that parents of young infants spend more than 5 hours each day on their smartphones. More than a quarter of that time the infant is engaged with the parent’s digital device. Technoference has been associated with decreased parent-child interaction during early childhood. It has been associated with more negative responses to children’s behavior, as well as an increased risk of child injury.
There are numerous studies suggesting an association between parental technoference and mental health difficulties in children. I have recently reviewed one of these studies that looks at the relationship of perceived parental technoference and the mental health of children entering adolescents. The authors collected longitudinal data of more than 1300 emerging adolescents, hoping to determine if the relationship between parental distraction and mental health was bidirectional. In other words, could a child’s mental health be contributing to his parents’ perceived distraction? Or was it primarily the parents’ technoference that was playing a role in the child’s mental health problems?
What investigators found was that higher levels of parental distraction were associated with higher levels of inattention and hyperactivity in the emerging adolescents, but not vice versa. On the other hand, higher levels of adolescent anxiety was associated with higher levels of perceived parental technoference, but not vice versa.
I know this sounds a bit confusing and a bit chicken-egg-chicken-eggish. The study was not designed to determine causation in these associations. However, the authors offer some possible scenarios that may provide a bit of clarity. It could be that parents who are concerned about their anxious child respond by retreating into the cyberspace to avoid tense situations or for support or information.
On the other hand, This explanation meshes with other studies demonstrating an association between parental distraction and aggression and attention problems in early childhood.
While one could spend more time imagining other factors that could be driving these bidirectional relationships, I’m not sure that it makes a heckuva lot of difference. Whether the child’s mental illness is the primary driver or the parent’s device-associated distraction is the dominant force isn’t the point. These are bidirectional relationships. If we are interested in pointing fingers, the common denominator is the device and our failure as a society to keep it in proper perspective. We all know that smartphones, tablets, and computers create an unhealthy distraction in personal relationships. The parents know and most of the children know. It’s time for us all to demonstrate some self-discipline. And that can begin for us as health care providers as we sit behind our computers spending more time looking at the screen than we do engaging the patient with our eyes.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Closing the GAP in Idiopathic Pulmonary Fibrosis
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
5 things you should know about IPF. American Lung Association. April 12, 2023. Accessed June 21, 2024. https://www.lung.org/blog/idiopathic-pulmonary-fibrosis-things-to-know
Raghu G, Chen SY, Yeh WS, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med. 2014;2(7):566-572. doi:10.1016/S2213-2600(14)70101-8
Morrow T. Improving outcomes and managing costs in idiopathic pulmonary fibrosis. Am J Manag Care. 2019;25(11 suppl):S204-S209. PMID: 31419090
Man RK, Gogikar A, Nanda A, et al. A comparison of the effectiveness of nintedanib and pirfenidone in treating idiopathic pulmonary fibrosis: a systematic review. Cureus. 2024;16(2):e54268. doi:10.7759/cureus.54268
Ley B, Ryerson CJ, Vittinghoff E, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684-691. doi:10.7326/0003-4819-156-10-201205150-00004
Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44-e68. doi:10.1164/rccm.201807-1255ST
Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation of idiopathic pulmonary fibrosis. An International Working Group report. Am J Respir Crit Care Med. 2016;194(3):265-275. doi:10.1164/rccm.201604-0801CI
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360. doi:10.7759/cureus.15360
Lee JH, Jang JH, Jang HJ, et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front Med (Lausanne). 2023;10:1052129. doi:10.3389/fmed.2023.1052129
Chandel A, Pastre J, Valery S, King CS, Nathan SD. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax. 2023;78(4):368-375. doi:10.1136/thoraxjnl-2021-218440
Chandel A, King CS, Ignacio RV, et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023;9(3):00124-2023. doi:10.1183/23120541.00124-2023
Suzuki Y, Mori K, Aono Y, et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci Rep. 2021;11(1):18579. doi:10.1038/s41598-021-98161-y
Lacedonia D, De Pace CC, Rea G, et al. Machine learning and BMI improve the prognostic value of GAP index in treated IPF patients. Bioengineering (Basel). 2023;10(2):251. doi:10.3390/bioengineering10020251
Fujii H, Hara Y, Saigusa Y, et al. ILD-GAP combined with the Charlson Comorbidity Index score (ILD-GAPC) as a prognostic prediction model in patients with interstitial lung disease. Can Respir J. 2023;2023:5088207. doi:10.1155/2023/5088207
Ley B, Bradford WZ, Weycker D, Vittinghoff E, du Bois RM, Collard HR. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1374-1381. doi:10.1183/09031936.00146314
Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74-81. doi:10.1164/rccm.202003-0669OC
Kreuter M, Lee JS, Tzouvelekis A, et al. A modified blood cell GAP (cGAP) to prognosticate outcomes in IPF. Poster presented at: European Respiratory Society International Congress; September 4-6, 2022. https://medically.gene.com/global/en/unrestricted/respiratory/ERS-2022/ers-2022-poster-kreuter-a-modified-blood-cell-gap.html
Nishikiori H, Chiba H, Lee SH, et al. A modified GAP model for East-Asian populations with idiopathic pulmonary fibrosis. Respir Investig. 2020;58(5):395-402. doi:10.1016/j.resinv.2020.04.001
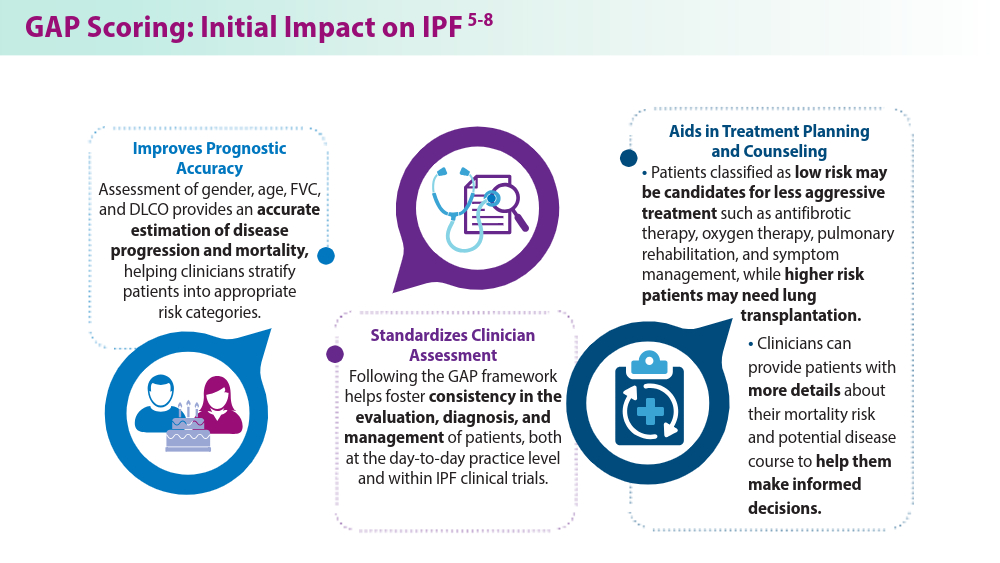
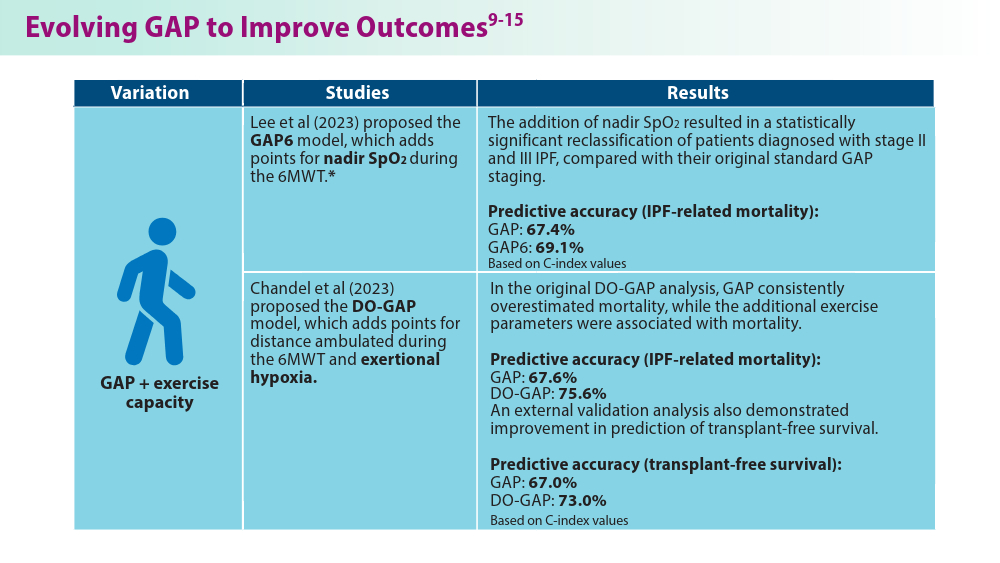
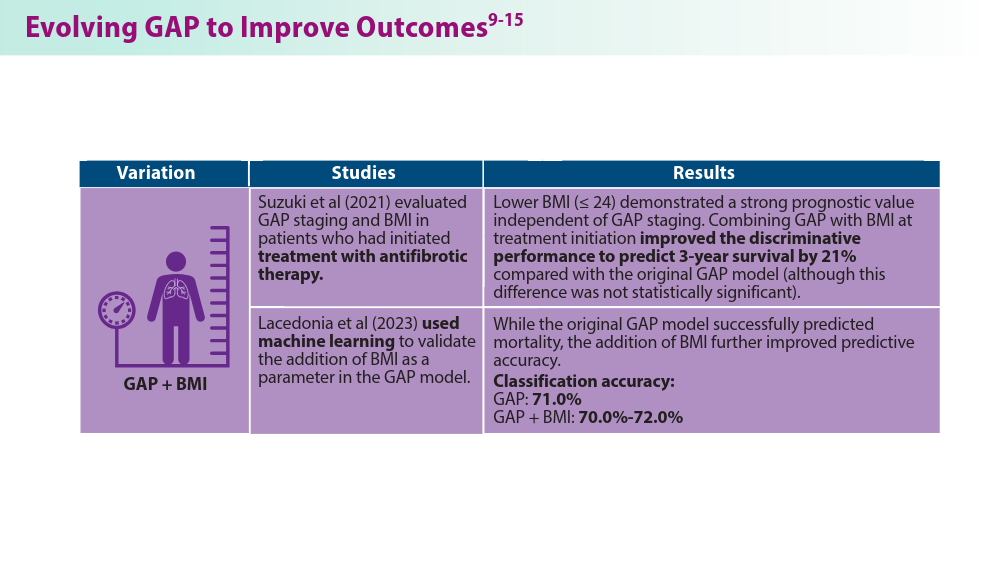
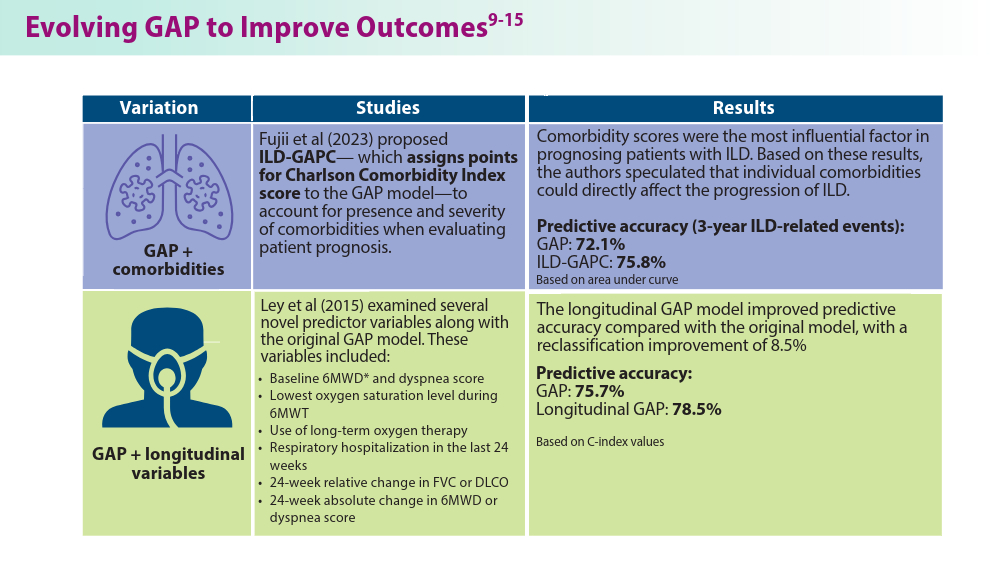
Pulmonology Data Trends 2024
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:

Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP