User login
Know What to Document
Hospitalists who work in teaching hospitals need to understand the teaching physician (TP) rules, to know what qualifies for payment and how to document to receive that payment. TP services are payable when they are furnished by a physician who is not a resident or a resident with a teaching physician physically present during the critical or key portions of the service.
This article will focus on the documentation guidelines for inpatient services provided by the hospitalist in a teaching setting.
Evaluation and Management Services
Teaching physicians participate in evaluation and management (E/M) services with residents in several different ways. Below, three scenarios discuss documentation requirements:
Scenario One: The Stand-Alone Service. In this scenario, the teaching physician independently performs the entire service (i.e., all required elements of the billed visit) though the resident also may have seen the patient that same day. The TP may choose to document as if the care took place in a non-teaching setting. This documentation stands alone and independently supports the reported visit level.
Alternatively, the teaching physician may use the resident’s note. He or she does this by first documenting involvement in patient management and performance of the critical or key portion(s) of the service, and then linking to the resident’s note. The teaching physician selects the visit level based on the combined documentation (i.e., that of the teaching physician and the resident).
When referencing resident documentation, the teaching physician should use Medicare-approved linkage statements. Common examples include the following:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note except the heart murmur is louder than documented, so I will obtain an echo to evaluate.”
Although all of these examples are acceptable, the last one best identifies the teaching physician’s involvement in patient management, which is a requirement of TP documentation.
Scenario Two: The Supervised Service. In this scenario, resident and teaching physician provide services simultaneously. The teaching physician either may supervise the resident’s performance of required service elements or personally perform some of them.
Documentation includes information about the teaching physician’s presence during the encounter, performance of the critical or key portions of the service and involvement in patient management, as well as a reference to the resident’s note. As in scenario one, the teaching physician selects the visit level based on the combined documentation.
Teaching physician statements associated with scenario two and accepted by Medicare reviewers include the following:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Scenario two examples contain generalized statements considered acceptable for billing under teaching physician rules. Documenting patient-specific elements of the assessment and plan, however, not only demonstrate teaching physician involvement in patient care, but also evidence better quality of care.
Scenario Three: The Shared Service. In this case, the resident performs a portion or all of the required service elements without the teaching physician present and then documents the services. The teaching physician independently performs only the critical, or key, portions of the service and, as appropriate, discusses the case with the resident. Similar to scenario two, the TP references the resident’s note and documents presence during the encounter, performance of the critical or key portions of the service and involvement in patient management.
Remember, the teaching physician can not link to a resident note that does not exist. In other words, if the resident’s note is not available when the teaching physician is documenting, the note cannot be considered for billing purposes. When documented appropriately, as in the scenarios above, the teaching physician selects the visit level based on the combined documentation.
Medicare-approved linkage statements for use by teaching physicians in this scenario include the following:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Documentation of teaching physician presence and participation provided solely by the resident is not sufficient to support the teaching physician service. Some examples of unacceptable documentation include:
- “Agree with above,” followed by legible countersignature or identity;
- “Rounded, Reviewed, Agree,” followed by legible countersignature or identity;
- “Discussed with resident. Agree,” followed by legible countersignature or identity;
- “Seen and agree,” followed by legible countersignature or identity;
- “Patient seen and evaluated,” followed by legible countersignature or identity; and
- Legible countersignature or identity alone.
Time-Based Services
Time-based E/M services require the teaching physician be present for the entire period for which the claim is made. Medical record documentation should reflect the teaching physician’s total visit time (i.e., spent on the unit/floor for inpatient services), including face-to-face time with the patient.
Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s time, nor does time the TP spends teaching activities unrelated to patient care. Examples of time-based services typically provided by hospitalists include:
- Critical-care services (CPT codes 99291-99292);
- Hospital discharge day management (CPT codes 99238-99239);
- E/M codes in which counseling and/or coordination of care dominates (more than 50% of) the encounter, and time is considered the key or controlling factor to qualify for a particular level of E/M service; and
- Prolonged services (CPT codes 99358-99359).
Surgical Services
Surgical services, which are defined as minor or major, also are subject to teaching physician rules. Teaching physician regulations identify minor procedures as those that take five minutes or less to complete and involve relatively little decision making once the need for the service is determined. Appropriate billing and payment hinges on the teaching physician’s presence for the entire procedure. Documentation should include a statement of presence, written and signed by the teaching physician.
Services that require more than five minutes are considered major surgical services, requiring teaching physician presence only during the (physician-determined) critical and key portions of the procedure. However, the teaching physician must be available to return to the procedure area during the surgery’s entirety, and not be involved in another procedure. Arrangements must be made to have another qualified physician available should the teaching physician get called away. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References:
1. Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100, www.cms.hhs.gov/manuals/downloads/clm104c12.pdf.
2. Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2, www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf.
3. Centers for Medicare & Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents, www.cms.hhs.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf.
4. Manaker, S. Teaching Physician Regulations. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008; 279-285.
5. Pohlig, C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008;57-69.
6. American Medical Association. cpt® 2008, Current Procedural Terminology Professional Edition. American Medical Association, 2007; 9-16.
Hospitalists who work in teaching hospitals need to understand the teaching physician (TP) rules, to know what qualifies for payment and how to document to receive that payment. TP services are payable when they are furnished by a physician who is not a resident or a resident with a teaching physician physically present during the critical or key portions of the service.
This article will focus on the documentation guidelines for inpatient services provided by the hospitalist in a teaching setting.
Evaluation and Management Services
Teaching physicians participate in evaluation and management (E/M) services with residents in several different ways. Below, three scenarios discuss documentation requirements:
Scenario One: The Stand-Alone Service. In this scenario, the teaching physician independently performs the entire service (i.e., all required elements of the billed visit) though the resident also may have seen the patient that same day. The TP may choose to document as if the care took place in a non-teaching setting. This documentation stands alone and independently supports the reported visit level.
Alternatively, the teaching physician may use the resident’s note. He or she does this by first documenting involvement in patient management and performance of the critical or key portion(s) of the service, and then linking to the resident’s note. The teaching physician selects the visit level based on the combined documentation (i.e., that of the teaching physician and the resident).
When referencing resident documentation, the teaching physician should use Medicare-approved linkage statements. Common examples include the following:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note except the heart murmur is louder than documented, so I will obtain an echo to evaluate.”
Although all of these examples are acceptable, the last one best identifies the teaching physician’s involvement in patient management, which is a requirement of TP documentation.
Scenario Two: The Supervised Service. In this scenario, resident and teaching physician provide services simultaneously. The teaching physician either may supervise the resident’s performance of required service elements or personally perform some of them.
Documentation includes information about the teaching physician’s presence during the encounter, performance of the critical or key portions of the service and involvement in patient management, as well as a reference to the resident’s note. As in scenario one, the teaching physician selects the visit level based on the combined documentation.
Teaching physician statements associated with scenario two and accepted by Medicare reviewers include the following:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Scenario two examples contain generalized statements considered acceptable for billing under teaching physician rules. Documenting patient-specific elements of the assessment and plan, however, not only demonstrate teaching physician involvement in patient care, but also evidence better quality of care.
Scenario Three: The Shared Service. In this case, the resident performs a portion or all of the required service elements without the teaching physician present and then documents the services. The teaching physician independently performs only the critical, or key, portions of the service and, as appropriate, discusses the case with the resident. Similar to scenario two, the TP references the resident’s note and documents presence during the encounter, performance of the critical or key portions of the service and involvement in patient management.
Remember, the teaching physician can not link to a resident note that does not exist. In other words, if the resident’s note is not available when the teaching physician is documenting, the note cannot be considered for billing purposes. When documented appropriately, as in the scenarios above, the teaching physician selects the visit level based on the combined documentation.
Medicare-approved linkage statements for use by teaching physicians in this scenario include the following:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Documentation of teaching physician presence and participation provided solely by the resident is not sufficient to support the teaching physician service. Some examples of unacceptable documentation include:
- “Agree with above,” followed by legible countersignature or identity;
- “Rounded, Reviewed, Agree,” followed by legible countersignature or identity;
- “Discussed with resident. Agree,” followed by legible countersignature or identity;
- “Seen and agree,” followed by legible countersignature or identity;
- “Patient seen and evaluated,” followed by legible countersignature or identity; and
- Legible countersignature or identity alone.
Time-Based Services
Time-based E/M services require the teaching physician be present for the entire period for which the claim is made. Medical record documentation should reflect the teaching physician’s total visit time (i.e., spent on the unit/floor for inpatient services), including face-to-face time with the patient.
Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s time, nor does time the TP spends teaching activities unrelated to patient care. Examples of time-based services typically provided by hospitalists include:
- Critical-care services (CPT codes 99291-99292);
- Hospital discharge day management (CPT codes 99238-99239);
- E/M codes in which counseling and/or coordination of care dominates (more than 50% of) the encounter, and time is considered the key or controlling factor to qualify for a particular level of E/M service; and
- Prolonged services (CPT codes 99358-99359).
Surgical Services
Surgical services, which are defined as minor or major, also are subject to teaching physician rules. Teaching physician regulations identify minor procedures as those that take five minutes or less to complete and involve relatively little decision making once the need for the service is determined. Appropriate billing and payment hinges on the teaching physician’s presence for the entire procedure. Documentation should include a statement of presence, written and signed by the teaching physician.
Services that require more than five minutes are considered major surgical services, requiring teaching physician presence only during the (physician-determined) critical and key portions of the procedure. However, the teaching physician must be available to return to the procedure area during the surgery’s entirety, and not be involved in another procedure. Arrangements must be made to have another qualified physician available should the teaching physician get called away. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References:
1. Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100, www.cms.hhs.gov/manuals/downloads/clm104c12.pdf.
2. Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2, www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf.
3. Centers for Medicare & Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents, www.cms.hhs.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf.
4. Manaker, S. Teaching Physician Regulations. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008; 279-285.
5. Pohlig, C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008;57-69.
6. American Medical Association. cpt® 2008, Current Procedural Terminology Professional Edition. American Medical Association, 2007; 9-16.
Hospitalists who work in teaching hospitals need to understand the teaching physician (TP) rules, to know what qualifies for payment and how to document to receive that payment. TP services are payable when they are furnished by a physician who is not a resident or a resident with a teaching physician physically present during the critical or key portions of the service.
This article will focus on the documentation guidelines for inpatient services provided by the hospitalist in a teaching setting.
Evaluation and Management Services
Teaching physicians participate in evaluation and management (E/M) services with residents in several different ways. Below, three scenarios discuss documentation requirements:
Scenario One: The Stand-Alone Service. In this scenario, the teaching physician independently performs the entire service (i.e., all required elements of the billed visit) though the resident also may have seen the patient that same day. The TP may choose to document as if the care took place in a non-teaching setting. This documentation stands alone and independently supports the reported visit level.
Alternatively, the teaching physician may use the resident’s note. He or she does this by first documenting involvement in patient management and performance of the critical or key portion(s) of the service, and then linking to the resident’s note. The teaching physician selects the visit level based on the combined documentation (i.e., that of the teaching physician and the resident).
When referencing resident documentation, the teaching physician should use Medicare-approved linkage statements. Common examples include the following:
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note except the heart murmur is louder than documented, so I will obtain an echo to evaluate.”
Although all of these examples are acceptable, the last one best identifies the teaching physician’s involvement in patient management, which is a requirement of TP documentation.
Scenario Two: The Supervised Service. In this scenario, resident and teaching physician provide services simultaneously. The teaching physician either may supervise the resident’s performance of required service elements or personally perform some of them.
Documentation includes information about the teaching physician’s presence during the encounter, performance of the critical or key portions of the service and involvement in patient management, as well as a reference to the resident’s note. As in scenario one, the teaching physician selects the visit level based on the combined documentation.
Teaching physician statements associated with scenario two and accepted by Medicare reviewers include the following:
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Scenario two examples contain generalized statements considered acceptable for billing under teaching physician rules. Documenting patient-specific elements of the assessment and plan, however, not only demonstrate teaching physician involvement in patient care, but also evidence better quality of care.
Scenario Three: The Shared Service. In this case, the resident performs a portion or all of the required service elements without the teaching physician present and then documents the services. The teaching physician independently performs only the critical, or key, portions of the service and, as appropriate, discusses the case with the resident. Similar to scenario two, the TP references the resident’s note and documents presence during the encounter, performance of the critical or key portions of the service and involvement in patient management.
Remember, the teaching physician can not link to a resident note that does not exist. In other words, if the resident’s note is not available when the teaching physician is documenting, the note cannot be considered for billing purposes. When documented appropriately, as in the scenarios above, the teaching physician selects the visit level based on the combined documentation.
Medicare-approved linkage statements for use by teaching physicians in this scenario include the following:
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Documentation of teaching physician presence and participation provided solely by the resident is not sufficient to support the teaching physician service. Some examples of unacceptable documentation include:
- “Agree with above,” followed by legible countersignature or identity;
- “Rounded, Reviewed, Agree,” followed by legible countersignature or identity;
- “Discussed with resident. Agree,” followed by legible countersignature or identity;
- “Seen and agree,” followed by legible countersignature or identity;
- “Patient seen and evaluated,” followed by legible countersignature or identity; and
- Legible countersignature or identity alone.
Time-Based Services
Time-based E/M services require the teaching physician be present for the entire period for which the claim is made. Medical record documentation should reflect the teaching physician’s total visit time (i.e., spent on the unit/floor for inpatient services), including face-to-face time with the patient.
Time spent by the resident without the presence of the teaching physician does not count toward the teaching physician’s time, nor does time the TP spends teaching activities unrelated to patient care. Examples of time-based services typically provided by hospitalists include:
- Critical-care services (CPT codes 99291-99292);
- Hospital discharge day management (CPT codes 99238-99239);
- E/M codes in which counseling and/or coordination of care dominates (more than 50% of) the encounter, and time is considered the key or controlling factor to qualify for a particular level of E/M service; and
- Prolonged services (CPT codes 99358-99359).
Surgical Services
Surgical services, which are defined as minor or major, also are subject to teaching physician rules. Teaching physician regulations identify minor procedures as those that take five minutes or less to complete and involve relatively little decision making once the need for the service is determined. Appropriate billing and payment hinges on the teaching physician’s presence for the entire procedure. Documentation should include a statement of presence, written and signed by the teaching physician.
Services that require more than five minutes are considered major surgical services, requiring teaching physician presence only during the (physician-determined) critical and key portions of the procedure. However, the teaching physician must be available to return to the procedure area during the surgery’s entirety, and not be involved in another procedure. Arrangements must be made to have another qualified physician available should the teaching physician get called away. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References:
1. Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100, www.cms.hhs.gov/manuals/downloads/clm104c12.pdf.
2. Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2, www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf.
3. Centers for Medicare & Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents, www.cms.hhs.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf.
4. Manaker, S. Teaching Physician Regulations. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008; 279-285.
5. Pohlig, C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008, American College of Chest Physicians, 2008;57-69.
6. American Medical Association. cpt® 2008, Current Procedural Terminology Professional Edition. American Medical Association, 2007; 9-16.
Pay-for-Reporting is Here to Stay
Congress made history in July when it passed legislation that makes Medicare’s voluntary pay-for-reporting program permanent.
The program, the Physician Quality Reporting Initiative, or PQRI, which began in 2007 as a six-month trial and was continued through 2008, rewards physicians who successfully report on specific applicable quality measures with a cash bonus. The new bill, the Medicare Improvement for Patients and Providers Act (MIPPA), extends the Centers for Medicare and Medicaid (CMS) program beyond 2010.
“PQRI is now a permanent program, even though the details have only been provided through 2010,” says Michael Rapp, MD, of the CMS Office of Clinical Standards and Quality.
Here, is a look at PQRI past, present, and future, from a hospitalist’s point of view.
Pay-for-Performance Pilot Proves Worthwhile
In August, CMS released statistics on that first pay-for-reporting period. During the trial, 101,138 physicians submitted a quality-data code. Of those, 70,207 reported on at least one measure, and 56,722 earned a bonus.
Asked about those numbers, Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee, says: “I think the folks at Medicare were pleased with that level of participation. This data helped convince them that the program should be permanent.”
What to Expect in 2009
The PQRI for 2009 is subject to revisions until the 2009 Physician Fee Schedule Final Rule is published sometime around Nov. 1. (Find the latest information on CMS Web site at www.cms.hhs.gov/pqri.) A number of proposed enhancements make it attractive and important to physicians, Dr. Torcson says.
CMS proposed 175 quality measures for physicians to report on, and MIPPA boosts payment for successful reporting of data on those measures. For 2009 and 2010, physicians who participate in the PQRI can earn an incentive payment of 2% (up from 1.5%) of their total allowed charges for Physician Fee Schedule (PFS) covered professional services.
However, except for a bigger check from CMS, hospitalists who currently report may not see much difference next year. “Overall, for hospitalists, PQRI will look pretty similar to 2007 and 2008,” Dr. Torcson warns. “The bonus is going to increase and the measures will be the same. That means that all of the background and education that SHM has provided on PQRI reporting remains relevant.”
One addition for 2009 is the use of patient registries to avoid claims systems for certain outpatient measures. “I don’t see the registry-reporting option being available to hospitalists in the short term,” Dr. Torcson says, “but it’s worth watching for the future.”
Beginning in 2009 and continuing through the next four years, Medicare also will provide incentive payments to eligible professionals who are successful electronic prescribers. (See the “Public Policy” article on p. 15 of the September 2008 The Hospitalist.) The e-prescribing measure in the 2008 PQRI will be removed for next year and used wholesale for a separate pay-for-reporting initiative pending changes from the Department of Health & Human Services. Unfortunately, none of the 2008 coding specifications for e-prescribing are available for hospitalist reporting.
“A lot of [the PQRI] measures have been created from the perspective of the cottage-industry model of an office-based private practice,” Dr. Torcson explains. “This 2008 (e-prescribing) measure was geared for an office-based physician practice—and the unforeseen consequence of the measure is that it’s not inclusive of patients being discharged from the hospital.”
Where Hospital Medicine Fits
By now, hospitalists should be resigned to the idea that many measures in PQRI don’t apply to their patients. However, SHM continues to work toward more inclusion for hospital-based physicians, by commenting on proposed rules and participating in the National Quality Forum and the American Medical Association’s Physician Consortium for Performance Improvement.
“We have been advocating for including performance measures for care processes, including transitions of care,” Dr. Torcson says. “This will probably come into play more in 2010 than 2009.”
SHM also has submitted comments on the proposed e-prescribing measures. Dr. Torcson says the organization is lobbying to make e-prescribing applicable to all hospital-based physicians, including ER doctors, and for discharged patients. “We want the whole process to harmonize with a comprehensive and safe discharge process that includes medication reconciliation,” he says.
To Report or Not to Report?
Regardless of whether lobbying efforts succeed in making more reporting applicable to hospital medicine, should groups start reporting in 2009? “It’s going to be a tough decision,” Dr. Torcson admits. “There’s a pretty significant investment in time and infrastructure to set this up. For the groups I know, the return on investment was negative.” In other words, PQRI does not pay for itself in a hospital medicine setting.
He says any hospital medicine group that wants to report should have in place a computerized system, and be willing to start slowly. “I’m convinced that it’s going to take an electronic coding/documentation system, as well as designated support staff within the hospital medicine group to pull it off,” he says. “This almost requires a full-time person.”
Dr. Torcson recommends starting with the reporting of three or four measures. “If you’re using a manual process or a homegrown system,” he says, “then the fewer measures the better, in terms of doing PQRI right to reach the 80% threshold.”
If you’re interested in reporting under the 2009 PQRI, go to SHM’s Web site at www.hospitalmedicine.org/ and type “PQRI 2008” into the advanced search bar. The article, “Information on PQRI 2008,” from May 17, 2007, provides important details about the program, including which measures apply to hospitalists. TH
Jane Jerrard is a medical writer based in Chicago.
Congress made history in July when it passed legislation that makes Medicare’s voluntary pay-for-reporting program permanent.
The program, the Physician Quality Reporting Initiative, or PQRI, which began in 2007 as a six-month trial and was continued through 2008, rewards physicians who successfully report on specific applicable quality measures with a cash bonus. The new bill, the Medicare Improvement for Patients and Providers Act (MIPPA), extends the Centers for Medicare and Medicaid (CMS) program beyond 2010.
“PQRI is now a permanent program, even though the details have only been provided through 2010,” says Michael Rapp, MD, of the CMS Office of Clinical Standards and Quality.
Here, is a look at PQRI past, present, and future, from a hospitalist’s point of view.
Pay-for-Performance Pilot Proves Worthwhile
In August, CMS released statistics on that first pay-for-reporting period. During the trial, 101,138 physicians submitted a quality-data code. Of those, 70,207 reported on at least one measure, and 56,722 earned a bonus.
Asked about those numbers, Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee, says: “I think the folks at Medicare were pleased with that level of participation. This data helped convince them that the program should be permanent.”
What to Expect in 2009
The PQRI for 2009 is subject to revisions until the 2009 Physician Fee Schedule Final Rule is published sometime around Nov. 1. (Find the latest information on CMS Web site at www.cms.hhs.gov/pqri.) A number of proposed enhancements make it attractive and important to physicians, Dr. Torcson says.
CMS proposed 175 quality measures for physicians to report on, and MIPPA boosts payment for successful reporting of data on those measures. For 2009 and 2010, physicians who participate in the PQRI can earn an incentive payment of 2% (up from 1.5%) of their total allowed charges for Physician Fee Schedule (PFS) covered professional services.
However, except for a bigger check from CMS, hospitalists who currently report may not see much difference next year. “Overall, for hospitalists, PQRI will look pretty similar to 2007 and 2008,” Dr. Torcson warns. “The bonus is going to increase and the measures will be the same. That means that all of the background and education that SHM has provided on PQRI reporting remains relevant.”
One addition for 2009 is the use of patient registries to avoid claims systems for certain outpatient measures. “I don’t see the registry-reporting option being available to hospitalists in the short term,” Dr. Torcson says, “but it’s worth watching for the future.”
Beginning in 2009 and continuing through the next four years, Medicare also will provide incentive payments to eligible professionals who are successful electronic prescribers. (See the “Public Policy” article on p. 15 of the September 2008 The Hospitalist.) The e-prescribing measure in the 2008 PQRI will be removed for next year and used wholesale for a separate pay-for-reporting initiative pending changes from the Department of Health & Human Services. Unfortunately, none of the 2008 coding specifications for e-prescribing are available for hospitalist reporting.
“A lot of [the PQRI] measures have been created from the perspective of the cottage-industry model of an office-based private practice,” Dr. Torcson explains. “This 2008 (e-prescribing) measure was geared for an office-based physician practice—and the unforeseen consequence of the measure is that it’s not inclusive of patients being discharged from the hospital.”
Where Hospital Medicine Fits
By now, hospitalists should be resigned to the idea that many measures in PQRI don’t apply to their patients. However, SHM continues to work toward more inclusion for hospital-based physicians, by commenting on proposed rules and participating in the National Quality Forum and the American Medical Association’s Physician Consortium for Performance Improvement.
“We have been advocating for including performance measures for care processes, including transitions of care,” Dr. Torcson says. “This will probably come into play more in 2010 than 2009.”
SHM also has submitted comments on the proposed e-prescribing measures. Dr. Torcson says the organization is lobbying to make e-prescribing applicable to all hospital-based physicians, including ER doctors, and for discharged patients. “We want the whole process to harmonize with a comprehensive and safe discharge process that includes medication reconciliation,” he says.
To Report or Not to Report?
Regardless of whether lobbying efforts succeed in making more reporting applicable to hospital medicine, should groups start reporting in 2009? “It’s going to be a tough decision,” Dr. Torcson admits. “There’s a pretty significant investment in time and infrastructure to set this up. For the groups I know, the return on investment was negative.” In other words, PQRI does not pay for itself in a hospital medicine setting.
He says any hospital medicine group that wants to report should have in place a computerized system, and be willing to start slowly. “I’m convinced that it’s going to take an electronic coding/documentation system, as well as designated support staff within the hospital medicine group to pull it off,” he says. “This almost requires a full-time person.”
Dr. Torcson recommends starting with the reporting of three or four measures. “If you’re using a manual process or a homegrown system,” he says, “then the fewer measures the better, in terms of doing PQRI right to reach the 80% threshold.”
If you’re interested in reporting under the 2009 PQRI, go to SHM’s Web site at www.hospitalmedicine.org/ and type “PQRI 2008” into the advanced search bar. The article, “Information on PQRI 2008,” from May 17, 2007, provides important details about the program, including which measures apply to hospitalists. TH
Jane Jerrard is a medical writer based in Chicago.
Congress made history in July when it passed legislation that makes Medicare’s voluntary pay-for-reporting program permanent.
The program, the Physician Quality Reporting Initiative, or PQRI, which began in 2007 as a six-month trial and was continued through 2008, rewards physicians who successfully report on specific applicable quality measures with a cash bonus. The new bill, the Medicare Improvement for Patients and Providers Act (MIPPA), extends the Centers for Medicare and Medicaid (CMS) program beyond 2010.
“PQRI is now a permanent program, even though the details have only been provided through 2010,” says Michael Rapp, MD, of the CMS Office of Clinical Standards and Quality.
Here, is a look at PQRI past, present, and future, from a hospitalist’s point of view.
Pay-for-Performance Pilot Proves Worthwhile
In August, CMS released statistics on that first pay-for-reporting period. During the trial, 101,138 physicians submitted a quality-data code. Of those, 70,207 reported on at least one measure, and 56,722 earned a bonus.
Asked about those numbers, Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., and chair of SHM’s Performance and Standards Committee, says: “I think the folks at Medicare were pleased with that level of participation. This data helped convince them that the program should be permanent.”
What to Expect in 2009
The PQRI for 2009 is subject to revisions until the 2009 Physician Fee Schedule Final Rule is published sometime around Nov. 1. (Find the latest information on CMS Web site at www.cms.hhs.gov/pqri.) A number of proposed enhancements make it attractive and important to physicians, Dr. Torcson says.
CMS proposed 175 quality measures for physicians to report on, and MIPPA boosts payment for successful reporting of data on those measures. For 2009 and 2010, physicians who participate in the PQRI can earn an incentive payment of 2% (up from 1.5%) of their total allowed charges for Physician Fee Schedule (PFS) covered professional services.
However, except for a bigger check from CMS, hospitalists who currently report may not see much difference next year. “Overall, for hospitalists, PQRI will look pretty similar to 2007 and 2008,” Dr. Torcson warns. “The bonus is going to increase and the measures will be the same. That means that all of the background and education that SHM has provided on PQRI reporting remains relevant.”
One addition for 2009 is the use of patient registries to avoid claims systems for certain outpatient measures. “I don’t see the registry-reporting option being available to hospitalists in the short term,” Dr. Torcson says, “but it’s worth watching for the future.”
Beginning in 2009 and continuing through the next four years, Medicare also will provide incentive payments to eligible professionals who are successful electronic prescribers. (See the “Public Policy” article on p. 15 of the September 2008 The Hospitalist.) The e-prescribing measure in the 2008 PQRI will be removed for next year and used wholesale for a separate pay-for-reporting initiative pending changes from the Department of Health & Human Services. Unfortunately, none of the 2008 coding specifications for e-prescribing are available for hospitalist reporting.
“A lot of [the PQRI] measures have been created from the perspective of the cottage-industry model of an office-based private practice,” Dr. Torcson explains. “This 2008 (e-prescribing) measure was geared for an office-based physician practice—and the unforeseen consequence of the measure is that it’s not inclusive of patients being discharged from the hospital.”
Where Hospital Medicine Fits
By now, hospitalists should be resigned to the idea that many measures in PQRI don’t apply to their patients. However, SHM continues to work toward more inclusion for hospital-based physicians, by commenting on proposed rules and participating in the National Quality Forum and the American Medical Association’s Physician Consortium for Performance Improvement.
“We have been advocating for including performance measures for care processes, including transitions of care,” Dr. Torcson says. “This will probably come into play more in 2010 than 2009.”
SHM also has submitted comments on the proposed e-prescribing measures. Dr. Torcson says the organization is lobbying to make e-prescribing applicable to all hospital-based physicians, including ER doctors, and for discharged patients. “We want the whole process to harmonize with a comprehensive and safe discharge process that includes medication reconciliation,” he says.
To Report or Not to Report?
Regardless of whether lobbying efforts succeed in making more reporting applicable to hospital medicine, should groups start reporting in 2009? “It’s going to be a tough decision,” Dr. Torcson admits. “There’s a pretty significant investment in time and infrastructure to set this up. For the groups I know, the return on investment was negative.” In other words, PQRI does not pay for itself in a hospital medicine setting.
He says any hospital medicine group that wants to report should have in place a computerized system, and be willing to start slowly. “I’m convinced that it’s going to take an electronic coding/documentation system, as well as designated support staff within the hospital medicine group to pull it off,” he says. “This almost requires a full-time person.”
Dr. Torcson recommends starting with the reporting of three or four measures. “If you’re using a manual process or a homegrown system,” he says, “then the fewer measures the better, in terms of doing PQRI right to reach the 80% threshold.”
If you’re interested in reporting under the 2009 PQRI, go to SHM’s Web site at www.hospitalmedicine.org/ and type “PQRI 2008” into the advanced search bar. The article, “Information on PQRI 2008,” from May 17, 2007, provides important details about the program, including which measures apply to hospitalists. TH
Jane Jerrard is a medical writer based in Chicago.
Time to Move On?
You’re unhappy with your workload or schedule.
Your spouse has been transferred to a different state.
You simply want a change of scenery.
Regardless of the reason, you’re looking for a new job. In hospital medicine, how and when is it appropriate to give notice? To maintain good relations with your current employer now and in the future, make sure you consider your departure from both sides of the desk.
Timing is Everything
Before you start skimming classified ads and phoning friends in the field to ask about job openings, consider how much time your employer needs to fill your position.
“When you’re thinking about leaving a group, you have to realize that the timing for getting your replacement is longer than you might think,” says Heather A. Harris, MD, a hospitalist who splits her time between the University of California, San Francisco and the Palo Alto Medical Foundation. “The traditional two-week notice in other jobs is tough for most [hospital medicine] groups to handle—unless it’s a really big group or already overstaffed, which is never the case.”
Dr. Harris, who hired many hospitalists when she was director of Eden Inpatient Services, Eden Medical Center, Castro Valley, Calif., recommends giving a minimum of two months notice. “That gives your group time to figure out what to do,” she says. “Otherwise, you’re putting the entire group in a bind.”
Other physicians suggest an even longer timeframe. “My preference would be that a hospitalist give me no less than six months notification,” says Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo. “That’s a best-case scenario for finding a replacement. It could take longer than that.”
The issue is workload for the doctors left behind: “The other hospitalists are going to have to cover the slack in the meantime,” Dr. Harris points out. “Keep that in mind when you’re giving notice; you’re putting everyone else in a position where they have to cover the work.”
A lengthy timeframe actually could dovetail with your own transition. “You’ll have to get credentialed at that new hospital,” Dr. Harris says. “It’s important to realize when you get that job offer that group might want you to start the next day, but you have to wait until the credentialing process is complete.” Depending on the hospital, that could take as long as three months.
It’s important to know the specifics of your new hospital’s credential process. “You don’t want to leave a job before you have the means to enter a new job,” Dr. McCurdy warns. “Make sure you understand when you can actually start the work.”
Meanwhile, your current employer will need time to move your replacement through the same process. “Some hospitals are slower than others,” Dr. Harris says, “but even if I have a hospitalist in mind who’s available to start right away, they won’t be able to step in until the hospital’s credentialing is complete.”
—Heather A. Harris, MD, former director of Eden Inpatient Services, Eden Medical Center
Speak Up
When you decide to leave a job, tell your immediate supervisor directly and be open about your job search. “Ideally, the person who is leaving would sit down with me and tell me their intention to leave, where they intend to go, and the circumstances of their leaving,” Dr. McCurdy says. “I don’t want to hear about it third hand or through the grapevine, and I don’t want to find out that it’s some sort of negotiating tactic.”
If you want a new job because you’re unhappy with the one you have, consider whether the issues causing your discontent can be rectified. Dr. McCurdy says he would make every effort to keep a hospitalist in his group. “Obviously, there are some things I can’t help with,” he says. “I can’t change the weather, I can’t change the school systems, but I might be able to help with work issues.”
Build Bridges, Don’t Burn Them
It should go without saying that once you officially give notice, you should make every effort to maintain good relations with your employer and colleagues, by continuing to do your job well and remaining an active, positive member of your group, Dr. Harris says. This is particularly important if you stay in the same geographic area.
“There is a lot of fluidity in hospital medicine; people move from place to place,” she says. “It’s a small community and people know each other.”
If you feel comfortable doing so, offer to help your old employer find your replacement. Dr. McCurdy asks departing physicians for this favor. “I’d ask if they know someone who would be a good fit here,” he says. “The hospitalist community is small and pretty cohesive, so they may know someone.” Helping fill your position is a great way to stay connected and to show your good will toward the group.
If your employer asks you to stay a few weeks longer than you planned, consider whether you can jockey your upcoming start date to accommodate the request—but not at the price of being unhappy or risking your new job. “I might try to get someone to stay on a bit longer, but I’m not going to twist their arm if they aren’t interested,” Dr. McCurdy says. “It’s better to be without a physician than to have a disgruntled one.”
When you decide to move on to a new job, remember that you have a long career ahead of you. Be thoughtful and professional about how and when you leave. This small consideration can help maintain your reputation and connections for years to come. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You’re unhappy with your workload or schedule.
Your spouse has been transferred to a different state.
You simply want a change of scenery.
Regardless of the reason, you’re looking for a new job. In hospital medicine, how and when is it appropriate to give notice? To maintain good relations with your current employer now and in the future, make sure you consider your departure from both sides of the desk.
Timing is Everything
Before you start skimming classified ads and phoning friends in the field to ask about job openings, consider how much time your employer needs to fill your position.
“When you’re thinking about leaving a group, you have to realize that the timing for getting your replacement is longer than you might think,” says Heather A. Harris, MD, a hospitalist who splits her time between the University of California, San Francisco and the Palo Alto Medical Foundation. “The traditional two-week notice in other jobs is tough for most [hospital medicine] groups to handle—unless it’s a really big group or already overstaffed, which is never the case.”
Dr. Harris, who hired many hospitalists when she was director of Eden Inpatient Services, Eden Medical Center, Castro Valley, Calif., recommends giving a minimum of two months notice. “That gives your group time to figure out what to do,” she says. “Otherwise, you’re putting the entire group in a bind.”
Other physicians suggest an even longer timeframe. “My preference would be that a hospitalist give me no less than six months notification,” says Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo. “That’s a best-case scenario for finding a replacement. It could take longer than that.”
The issue is workload for the doctors left behind: “The other hospitalists are going to have to cover the slack in the meantime,” Dr. Harris points out. “Keep that in mind when you’re giving notice; you’re putting everyone else in a position where they have to cover the work.”
A lengthy timeframe actually could dovetail with your own transition. “You’ll have to get credentialed at that new hospital,” Dr. Harris says. “It’s important to realize when you get that job offer that group might want you to start the next day, but you have to wait until the credentialing process is complete.” Depending on the hospital, that could take as long as three months.
It’s important to know the specifics of your new hospital’s credential process. “You don’t want to leave a job before you have the means to enter a new job,” Dr. McCurdy warns. “Make sure you understand when you can actually start the work.”
Meanwhile, your current employer will need time to move your replacement through the same process. “Some hospitals are slower than others,” Dr. Harris says, “but even if I have a hospitalist in mind who’s available to start right away, they won’t be able to step in until the hospital’s credentialing is complete.”
—Heather A. Harris, MD, former director of Eden Inpatient Services, Eden Medical Center
Speak Up
When you decide to leave a job, tell your immediate supervisor directly and be open about your job search. “Ideally, the person who is leaving would sit down with me and tell me their intention to leave, where they intend to go, and the circumstances of their leaving,” Dr. McCurdy says. “I don’t want to hear about it third hand or through the grapevine, and I don’t want to find out that it’s some sort of negotiating tactic.”
If you want a new job because you’re unhappy with the one you have, consider whether the issues causing your discontent can be rectified. Dr. McCurdy says he would make every effort to keep a hospitalist in his group. “Obviously, there are some things I can’t help with,” he says. “I can’t change the weather, I can’t change the school systems, but I might be able to help with work issues.”
Build Bridges, Don’t Burn Them
It should go without saying that once you officially give notice, you should make every effort to maintain good relations with your employer and colleagues, by continuing to do your job well and remaining an active, positive member of your group, Dr. Harris says. This is particularly important if you stay in the same geographic area.
“There is a lot of fluidity in hospital medicine; people move from place to place,” she says. “It’s a small community and people know each other.”
If you feel comfortable doing so, offer to help your old employer find your replacement. Dr. McCurdy asks departing physicians for this favor. “I’d ask if they know someone who would be a good fit here,” he says. “The hospitalist community is small and pretty cohesive, so they may know someone.” Helping fill your position is a great way to stay connected and to show your good will toward the group.
If your employer asks you to stay a few weeks longer than you planned, consider whether you can jockey your upcoming start date to accommodate the request—but not at the price of being unhappy or risking your new job. “I might try to get someone to stay on a bit longer, but I’m not going to twist their arm if they aren’t interested,” Dr. McCurdy says. “It’s better to be without a physician than to have a disgruntled one.”
When you decide to move on to a new job, remember that you have a long career ahead of you. Be thoughtful and professional about how and when you leave. This small consideration can help maintain your reputation and connections for years to come. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You’re unhappy with your workload or schedule.
Your spouse has been transferred to a different state.
You simply want a change of scenery.
Regardless of the reason, you’re looking for a new job. In hospital medicine, how and when is it appropriate to give notice? To maintain good relations with your current employer now and in the future, make sure you consider your departure from both sides of the desk.
Timing is Everything
Before you start skimming classified ads and phoning friends in the field to ask about job openings, consider how much time your employer needs to fill your position.
“When you’re thinking about leaving a group, you have to realize that the timing for getting your replacement is longer than you might think,” says Heather A. Harris, MD, a hospitalist who splits her time between the University of California, San Francisco and the Palo Alto Medical Foundation. “The traditional two-week notice in other jobs is tough for most [hospital medicine] groups to handle—unless it’s a really big group or already overstaffed, which is never the case.”
Dr. Harris, who hired many hospitalists when she was director of Eden Inpatient Services, Eden Medical Center, Castro Valley, Calif., recommends giving a minimum of two months notice. “That gives your group time to figure out what to do,” she says. “Otherwise, you’re putting the entire group in a bind.”
Other physicians suggest an even longer timeframe. “My preference would be that a hospitalist give me no less than six months notification,” says Fred A. McCurdy, MD, PhD, MBA, associate dean for faculty development, Texas Tech University Health Sciences Center at Amarillo. “That’s a best-case scenario for finding a replacement. It could take longer than that.”
The issue is workload for the doctors left behind: “The other hospitalists are going to have to cover the slack in the meantime,” Dr. Harris points out. “Keep that in mind when you’re giving notice; you’re putting everyone else in a position where they have to cover the work.”
A lengthy timeframe actually could dovetail with your own transition. “You’ll have to get credentialed at that new hospital,” Dr. Harris says. “It’s important to realize when you get that job offer that group might want you to start the next day, but you have to wait until the credentialing process is complete.” Depending on the hospital, that could take as long as three months.
It’s important to know the specifics of your new hospital’s credential process. “You don’t want to leave a job before you have the means to enter a new job,” Dr. McCurdy warns. “Make sure you understand when you can actually start the work.”
Meanwhile, your current employer will need time to move your replacement through the same process. “Some hospitals are slower than others,” Dr. Harris says, “but even if I have a hospitalist in mind who’s available to start right away, they won’t be able to step in until the hospital’s credentialing is complete.”
—Heather A. Harris, MD, former director of Eden Inpatient Services, Eden Medical Center
Speak Up
When you decide to leave a job, tell your immediate supervisor directly and be open about your job search. “Ideally, the person who is leaving would sit down with me and tell me their intention to leave, where they intend to go, and the circumstances of their leaving,” Dr. McCurdy says. “I don’t want to hear about it third hand or through the grapevine, and I don’t want to find out that it’s some sort of negotiating tactic.”
If you want a new job because you’re unhappy with the one you have, consider whether the issues causing your discontent can be rectified. Dr. McCurdy says he would make every effort to keep a hospitalist in his group. “Obviously, there are some things I can’t help with,” he says. “I can’t change the weather, I can’t change the school systems, but I might be able to help with work issues.”
Build Bridges, Don’t Burn Them
It should go without saying that once you officially give notice, you should make every effort to maintain good relations with your employer and colleagues, by continuing to do your job well and remaining an active, positive member of your group, Dr. Harris says. This is particularly important if you stay in the same geographic area.
“There is a lot of fluidity in hospital medicine; people move from place to place,” she says. “It’s a small community and people know each other.”
If you feel comfortable doing so, offer to help your old employer find your replacement. Dr. McCurdy asks departing physicians for this favor. “I’d ask if they know someone who would be a good fit here,” he says. “The hospitalist community is small and pretty cohesive, so they may know someone.” Helping fill your position is a great way to stay connected and to show your good will toward the group.
If your employer asks you to stay a few weeks longer than you planned, consider whether you can jockey your upcoming start date to accommodate the request—but not at the price of being unhappy or risking your new job. “I might try to get someone to stay on a bit longer, but I’m not going to twist their arm if they aren’t interested,” Dr. McCurdy says. “It’s better to be without a physician than to have a disgruntled one.”
When you decide to move on to a new job, remember that you have a long career ahead of you. Be thoughtful and professional about how and when you leave. This small consideration can help maintain your reputation and connections for years to come. TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Drugs that Cause Movement Disorders
Most of us learned in our professional training that neuroleptic agents cause movement disorders, or extrapyramidal symptoms (EPS).1 Neuroleptics, the older class of antipsychotic agents, which includes dopamine receptor blocking agents (DRBA), can cause tardive dyskinesia (TD), dystonia, akathisia, and Parkinsonism.
We also learned that newer antipsychotic agents, the so-called second-generation antipsychotics, do not cause EPS. However, dose-related EPS has been associated with olanzapine and risperidone use (> 6 mg/day doses), and there have been two reported cases of aripiprazole-induced EPS.2,3
So which symptoms indicate a drug-induced movement disorder (DIMD)? Patients with DIMDs have difficulty with social functioning, motor-task performance, interpersonal communication, and activities of daily living. They also are less likely to adhere to a medication regimen, making disease relapse and rehospitalization more likely.
Some DIMDs are worse than others. Neuroleptic-induced TD, for example, is in some cases irreversible and can lead to functional impairment so severe a patient cannot feed himself, speak clearly, or breathe easily. In addition, removal of the offending agent does not always resolve TD.4
Milder forms of neuroleptic-induced TD occur in about 20% of patients. In higher risk groups, such as older patients, milder forms of neuroleptic-induced TD may exceed 50%.
DIMDs often elude diagnosis by clinicians, partially because they look like other medical conditions such as restless legs syndrome, agitation, or drug withdrawal. Clinicians who understand the most likely DIMD culprits and the effect of each can better manage their patients. It’s also crucial for clinicians to pay attention to
- Patient stress and anxiety levels, as both of these can exacerbate DIMD symptoms;
- Patient drug history; and
- Demographic information. Older women are most likely to develop tardive dyskinesia. Young men more commonly experience dystonic reactions. The elderly are at higher risk for Parkinsonism and akathisia.
Clinicians must watch for DIMD in any patient who has taken antipsychotics. Symptoms can occur within hours to days (acute), weeks (subacute) or even months to years (tardive) following exposure.
The Agents
Causative DRBAs include:
- Haloperidol;
- Thioridazine;
- Perphenazine;
- Droperidol;
- Metoclopramide;
- Prochlorperazine; and
- Promethazine.
DIMDs can also occur from:
- Lithium, which can cause tremors or chorea;
- Stimulants (e.g., amphetamines), which can cause tremor, tics, dystonia, and dyskinesia;
- Selective-serotonin reuptake inhibitors (SSRIs), which can cause tremors, akathisia, and possible dyskinesia, dystonia, and Parkinsonism;
- Tricyclic antidepressants (TCAs) (e.g., amitriptyline, nortriptyline, etc), which can cause myoclonus and tremors;
- Valproic acid, which causes tremors; and
- Cyclosporine A, which was implicated in one study as causing tremors and Parkinsonism.6
Management
For neuroleptics, withdrawal of the offending agent may lead to partial improvement in about half of patients. The outcome, of course, depends on the DIMD.
Early detection of TD is important to improve remission rates, which are inversely related to the disorder’s duration and severity. To treat, gradually taper the patient off the medication. It may take as long as two years after discontinuation for the condition to resolve itself. Continually re-evaluate how much a patient needs this agent. There may be another that’s just as effective but with a lower TD incidence. 7
Treat acute dystonic reactions with a short course of a potent antimuscarinic agent such as oral, intravenous (IV), or intramuscular benztropine, or diphenhydramine. If the patient’s reaction is life-threatening, use IV administration of an antimuscarinic agent and supportive measures. In some cases, you can use benzodiazepines in place of antimuscarinic agents. For tardive dystonia, prevention is the most important treatment since few pharmacologic treatments have proven efficacy.
Prevention also is the key to managing akathisia. To prevent this manifestation, prescribe atypical antipsychotics or use a standardized dose titration to avoid excessive dose escalation. In high-risk patients, consider prophylactic treatment with diphenhydramine or benztropine. Other potentially useful agents include benzodiazepines, propranolol, or cyproheptadine. For acute reactions, remove the causative agent.
Treat drug-induced Parkinsonism by withdrawing the causative agent or reducing the dose, switching to an atypical antipsychotic (if neuroleptic-induced), and possibly prescribing a trial of amantadine, an antimuscarinic agent, a dopamine agonist, or levodopa.
Though antiemetics and conventional antipsychotics are most commonly implicated, other agents also cause DIMDs. To prevent and treat these disorders, clinicians need to be particularly aware of the causative agents and symptoms. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
- Chen JJ. Drug-induced Movement Disorders. Journal of Pharmacy Practice. 2007; 20(6):415-429.
- Zacher JL, Hatchett AD. Aripiprazole-induced movement disorder. Am J Psychiatry. 2006;163:160-161[letter].
- Sajbel TA, Cheney EM, DeQuardo JR. Aripiprazole-associated dyskinesia. Ann Pharmacother. 2005;39:200-201[letter].
- Lee PE, Synkora K, Gill SS., et al. Antipsychotic medications and drug-induced movement disorders other than Parkinsonism: A population-based cohort study in older adults. J Am Geriatr Soc. 2005;53:1374-1379.
- Munhoz RP, Teive HAG, Germiniani FMB et al. Movement disorders secondary to long-term treatment with cyclosporine A. Arq Neuropsiquiatr. 2005;63(3-A)L592-596.
- Vernon, Gwen M. Drug-Induced & Tardive Movement Disorders. National Alliance for the Mentally Ill, July 2001.www.namiscc.org/newsletters/July01/tardive.htm
Most of us learned in our professional training that neuroleptic agents cause movement disorders, or extrapyramidal symptoms (EPS).1 Neuroleptics, the older class of antipsychotic agents, which includes dopamine receptor blocking agents (DRBA), can cause tardive dyskinesia (TD), dystonia, akathisia, and Parkinsonism.
We also learned that newer antipsychotic agents, the so-called second-generation antipsychotics, do not cause EPS. However, dose-related EPS has been associated with olanzapine and risperidone use (> 6 mg/day doses), and there have been two reported cases of aripiprazole-induced EPS.2,3
So which symptoms indicate a drug-induced movement disorder (DIMD)? Patients with DIMDs have difficulty with social functioning, motor-task performance, interpersonal communication, and activities of daily living. They also are less likely to adhere to a medication regimen, making disease relapse and rehospitalization more likely.
Some DIMDs are worse than others. Neuroleptic-induced TD, for example, is in some cases irreversible and can lead to functional impairment so severe a patient cannot feed himself, speak clearly, or breathe easily. In addition, removal of the offending agent does not always resolve TD.4
Milder forms of neuroleptic-induced TD occur in about 20% of patients. In higher risk groups, such as older patients, milder forms of neuroleptic-induced TD may exceed 50%.
DIMDs often elude diagnosis by clinicians, partially because they look like other medical conditions such as restless legs syndrome, agitation, or drug withdrawal. Clinicians who understand the most likely DIMD culprits and the effect of each can better manage their patients. It’s also crucial for clinicians to pay attention to
- Patient stress and anxiety levels, as both of these can exacerbate DIMD symptoms;
- Patient drug history; and
- Demographic information. Older women are most likely to develop tardive dyskinesia. Young men more commonly experience dystonic reactions. The elderly are at higher risk for Parkinsonism and akathisia.
Clinicians must watch for DIMD in any patient who has taken antipsychotics. Symptoms can occur within hours to days (acute), weeks (subacute) or even months to years (tardive) following exposure.
The Agents
Causative DRBAs include:
- Haloperidol;
- Thioridazine;
- Perphenazine;
- Droperidol;
- Metoclopramide;
- Prochlorperazine; and
- Promethazine.
DIMDs can also occur from:
- Lithium, which can cause tremors or chorea;
- Stimulants (e.g., amphetamines), which can cause tremor, tics, dystonia, and dyskinesia;
- Selective-serotonin reuptake inhibitors (SSRIs), which can cause tremors, akathisia, and possible dyskinesia, dystonia, and Parkinsonism;
- Tricyclic antidepressants (TCAs) (e.g., amitriptyline, nortriptyline, etc), which can cause myoclonus and tremors;
- Valproic acid, which causes tremors; and
- Cyclosporine A, which was implicated in one study as causing tremors and Parkinsonism.6
Management
For neuroleptics, withdrawal of the offending agent may lead to partial improvement in about half of patients. The outcome, of course, depends on the DIMD.
Early detection of TD is important to improve remission rates, which are inversely related to the disorder’s duration and severity. To treat, gradually taper the patient off the medication. It may take as long as two years after discontinuation for the condition to resolve itself. Continually re-evaluate how much a patient needs this agent. There may be another that’s just as effective but with a lower TD incidence. 7
Treat acute dystonic reactions with a short course of a potent antimuscarinic agent such as oral, intravenous (IV), or intramuscular benztropine, or diphenhydramine. If the patient’s reaction is life-threatening, use IV administration of an antimuscarinic agent and supportive measures. In some cases, you can use benzodiazepines in place of antimuscarinic agents. For tardive dystonia, prevention is the most important treatment since few pharmacologic treatments have proven efficacy.
Prevention also is the key to managing akathisia. To prevent this manifestation, prescribe atypical antipsychotics or use a standardized dose titration to avoid excessive dose escalation. In high-risk patients, consider prophylactic treatment with diphenhydramine or benztropine. Other potentially useful agents include benzodiazepines, propranolol, or cyproheptadine. For acute reactions, remove the causative agent.
Treat drug-induced Parkinsonism by withdrawing the causative agent or reducing the dose, switching to an atypical antipsychotic (if neuroleptic-induced), and possibly prescribing a trial of amantadine, an antimuscarinic agent, a dopamine agonist, or levodopa.
Though antiemetics and conventional antipsychotics are most commonly implicated, other agents also cause DIMDs. To prevent and treat these disorders, clinicians need to be particularly aware of the causative agents and symptoms. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
- Chen JJ. Drug-induced Movement Disorders. Journal of Pharmacy Practice. 2007; 20(6):415-429.
- Zacher JL, Hatchett AD. Aripiprazole-induced movement disorder. Am J Psychiatry. 2006;163:160-161[letter].
- Sajbel TA, Cheney EM, DeQuardo JR. Aripiprazole-associated dyskinesia. Ann Pharmacother. 2005;39:200-201[letter].
- Lee PE, Synkora K, Gill SS., et al. Antipsychotic medications and drug-induced movement disorders other than Parkinsonism: A population-based cohort study in older adults. J Am Geriatr Soc. 2005;53:1374-1379.
- Munhoz RP, Teive HAG, Germiniani FMB et al. Movement disorders secondary to long-term treatment with cyclosporine A. Arq Neuropsiquiatr. 2005;63(3-A)L592-596.
- Vernon, Gwen M. Drug-Induced & Tardive Movement Disorders. National Alliance for the Mentally Ill, July 2001.www.namiscc.org/newsletters/July01/tardive.htm
Most of us learned in our professional training that neuroleptic agents cause movement disorders, or extrapyramidal symptoms (EPS).1 Neuroleptics, the older class of antipsychotic agents, which includes dopamine receptor blocking agents (DRBA), can cause tardive dyskinesia (TD), dystonia, akathisia, and Parkinsonism.
We also learned that newer antipsychotic agents, the so-called second-generation antipsychotics, do not cause EPS. However, dose-related EPS has been associated with olanzapine and risperidone use (> 6 mg/day doses), and there have been two reported cases of aripiprazole-induced EPS.2,3
So which symptoms indicate a drug-induced movement disorder (DIMD)? Patients with DIMDs have difficulty with social functioning, motor-task performance, interpersonal communication, and activities of daily living. They also are less likely to adhere to a medication regimen, making disease relapse and rehospitalization more likely.
Some DIMDs are worse than others. Neuroleptic-induced TD, for example, is in some cases irreversible and can lead to functional impairment so severe a patient cannot feed himself, speak clearly, or breathe easily. In addition, removal of the offending agent does not always resolve TD.4
Milder forms of neuroleptic-induced TD occur in about 20% of patients. In higher risk groups, such as older patients, milder forms of neuroleptic-induced TD may exceed 50%.
DIMDs often elude diagnosis by clinicians, partially because they look like other medical conditions such as restless legs syndrome, agitation, or drug withdrawal. Clinicians who understand the most likely DIMD culprits and the effect of each can better manage their patients. It’s also crucial for clinicians to pay attention to
- Patient stress and anxiety levels, as both of these can exacerbate DIMD symptoms;
- Patient drug history; and
- Demographic information. Older women are most likely to develop tardive dyskinesia. Young men more commonly experience dystonic reactions. The elderly are at higher risk for Parkinsonism and akathisia.
Clinicians must watch for DIMD in any patient who has taken antipsychotics. Symptoms can occur within hours to days (acute), weeks (subacute) or even months to years (tardive) following exposure.
The Agents
Causative DRBAs include:
- Haloperidol;
- Thioridazine;
- Perphenazine;
- Droperidol;
- Metoclopramide;
- Prochlorperazine; and
- Promethazine.
DIMDs can also occur from:
- Lithium, which can cause tremors or chorea;
- Stimulants (e.g., amphetamines), which can cause tremor, tics, dystonia, and dyskinesia;
- Selective-serotonin reuptake inhibitors (SSRIs), which can cause tremors, akathisia, and possible dyskinesia, dystonia, and Parkinsonism;
- Tricyclic antidepressants (TCAs) (e.g., amitriptyline, nortriptyline, etc), which can cause myoclonus and tremors;
- Valproic acid, which causes tremors; and
- Cyclosporine A, which was implicated in one study as causing tremors and Parkinsonism.6
Management
For neuroleptics, withdrawal of the offending agent may lead to partial improvement in about half of patients. The outcome, of course, depends on the DIMD.
Early detection of TD is important to improve remission rates, which are inversely related to the disorder’s duration and severity. To treat, gradually taper the patient off the medication. It may take as long as two years after discontinuation for the condition to resolve itself. Continually re-evaluate how much a patient needs this agent. There may be another that’s just as effective but with a lower TD incidence. 7
Treat acute dystonic reactions with a short course of a potent antimuscarinic agent such as oral, intravenous (IV), or intramuscular benztropine, or diphenhydramine. If the patient’s reaction is life-threatening, use IV administration of an antimuscarinic agent and supportive measures. In some cases, you can use benzodiazepines in place of antimuscarinic agents. For tardive dystonia, prevention is the most important treatment since few pharmacologic treatments have proven efficacy.
Prevention also is the key to managing akathisia. To prevent this manifestation, prescribe atypical antipsychotics or use a standardized dose titration to avoid excessive dose escalation. In high-risk patients, consider prophylactic treatment with diphenhydramine or benztropine. Other potentially useful agents include benzodiazepines, propranolol, or cyproheptadine. For acute reactions, remove the causative agent.
Treat drug-induced Parkinsonism by withdrawing the causative agent or reducing the dose, switching to an atypical antipsychotic (if neuroleptic-induced), and possibly prescribing a trial of amantadine, an antimuscarinic agent, a dopamine agonist, or levodopa.
Though antiemetics and conventional antipsychotics are most commonly implicated, other agents also cause DIMDs. To prevent and treat these disorders, clinicians need to be particularly aware of the causative agents and symptoms. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a registered pharmacist based in New York City.
References
- Chen JJ. Drug-induced Movement Disorders. Journal of Pharmacy Practice. 2007; 20(6):415-429.
- Zacher JL, Hatchett AD. Aripiprazole-induced movement disorder. Am J Psychiatry. 2006;163:160-161[letter].
- Sajbel TA, Cheney EM, DeQuardo JR. Aripiprazole-associated dyskinesia. Ann Pharmacother. 2005;39:200-201[letter].
- Lee PE, Synkora K, Gill SS., et al. Antipsychotic medications and drug-induced movement disorders other than Parkinsonism: A population-based cohort study in older adults. J Am Geriatr Soc. 2005;53:1374-1379.
- Munhoz RP, Teive HAG, Germiniani FMB et al. Movement disorders secondary to long-term treatment with cyclosporine A. Arq Neuropsiquiatr. 2005;63(3-A)L592-596.
- Vernon, Gwen M. Drug-Induced & Tardive Movement Disorders. National Alliance for the Mentally Ill, July 2001.www.namiscc.org/newsletters/July01/tardive.htm
The Burdens of Comanagement
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
It may be time for hospitalists to rethink their co-management relationships, says Eric Siegal, MD, chair of the Society of Hospital Medicine’s Public Policy Committee. Co-management is a mainstay of hospital medicine, but “recent, albeit limited evidence suggests hospitalist consultation and co-management may not be as effective as originally anticipated,” Dr. Siegal writes in this month’s Journal of Hospital Medicine.
He demonstrates his point with several studies, including the Hospitalist Orthopedic Team trial, which involved 526 patients who underwent elective hip or knee surgery at the Mayo Clinic. Hospitalist intervention reduced incidence of minor complications, such as urinary tract infections, but had no effect on more serious complications; it reduced adjusted length of stay (LOS) by a modest 0.5 days but did not affect actual LOS or cost per case. On the other hand, patients admitted to the Mayo Clinic for hip fractures derived a clear benefit from hospitalist co-management: Compared to the standard orthopedic service, the hospitalist team decreased time-to-surgery and lowered LOS by 2.2 days without compromising outcomes.
These and similar findings “support the common sense notion that hospitalists most benefit patients who are sick, frail, and medically or socially complex,” Dr. Siegal writes. “As a corollary, hospitalists probably offer relatively little benefit to surgical and specialty patients who are young or have compensated medical co-morbidities and/or straightforward disposition plans.”
Dr. Siegal says he wrote the article because he realized even though hospitalists share accountability and authority for patient care with other specialists, there’s rarely a clear line defining where one physician’s responsibilities end and the other’s begin. “My intention was to make people stop and think about what they were doing, rather than just doing it,” he tells The Hospitalist.
Co-management is a good example of the phenomenon known in the military as mission creep, Dr. Siegal explains. Mission creep occurs when a project originates with well-defined and perhaps limited goals, but then expands into areas for which it was never intended.
Co-management arose during California’s managed care heyday: Hospital administrators realized surgeons were having difficulty controlling patient length of stay and managing medical co-morbidities during surgery. Enter the hospitalist, charged with coordinating the care of the acutely ill in the most effective and efficient way possible. Surgeons and other specialists liked the idea of sharing responsibility with another physician, and administrators liked the effect on the bottom line.
So, little by little, co-management evolved from a strategy for managing only the most complicated cases to a routine practice at many institutions—even when hospitalists actually added little to a patient’s care. For example, a “patient with a stable GI bleed who needs little more than an endoscopy I would argue does not need co-management,” Dr. Siegal says. In fact, he points out in his paper, inserting the hospitalist into the situation above might work against the patient if it delays the gastroenterologist’s involvement and the endoscopy. A gastroenterologist who assumes a hospitalist is running the show may pay insufficient attention to the patient, Dr. Siegal writes.
Worse than that, having more than one physician involved may actually increase the risk of medical errors if the doctors give conflicting or inconsistent orders that confuse hospital staff, patients, or their families. In many cases, the specialist is simply better qualified to do the admitting, Dr. Siegal says. When a patient comes in with a cranial bleed, “if it was my mother, I wouldn’t want me admitting her,” he says.
Unnecessary co-management also can negatively affect hospitalists themselves to the extent that the process engenders burnout or unhappiness on the job, Dr. Siegal adds. Without set parameters, specialists may assume that hospitalists will conduct all patient admits. This “devalues the hospitalist,” he writes. “People start seeing us as glorified residents,” leading to “huge job dissatisfaction.”
Co-management does offer some benefits, though they vary based on situation, he says. At institutions with a limited pool of surgeons, neurologists, or other specialists, sharing duties with hospitalists can free up specialists for cases that need their specific expertise. When specialist availability isn’t a problem, however, the real—if unspoken—purpose of co-management may be to lighten the burden for superstar specialists who attract patients, prestige, and money. The result can be overworked, stressed out hospitalists who may inadvertently neglect patients requiring care.
The solution is to give hospitalists more of a say in the types of cases they co-manage, and a clearer delineation of the responsibilities of each party involved, according to Dr. Siegal. “Sit down with the specialists and revisit where you are,” he says. He also suggests calling on hospital administrators, if necessary, to mollify specialists who might dislike the idea of a change.
After all, Dr. Siegal warns, “just showing up to co-manage doesn’t mean you’re doing anything to help the patient. You should have definable outcomes that can help you say, “‘This is better.’” TH
Norra MacReady is a medical writer based in California.
In the Literature
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.
Literature at a Glance
- Drug-eluting stents decrease the need for revascularization.
- Case volume is related to hospital performance assessment.
- Prolonged QRS duration in patients with CHF is associated with increased morbidity and mortality.
- For out-of-hospital ACLS, vasopressin plus epinephrine is not better than vasopressin alone.
- Oral rivaroxaban is more efficacious than enoxaparin for VTE prophylaxis after total hip replacement.
- LMWH and UFH offer similar perioperative VTE prophylaxis benefit in patients with cancer.
- Salmeterol added to inhaled corticosteroids decreases severe asthma exacerbations.
- Early invasive strategy has unclear benefit in low-risk women with unstable angina or NSTEMI.
- Strategies to prevent contrast-induced acute kidney injury are not uniform.
- Hyperglycemia in hospitalized children is common and associated with ICU admission.
Do drug-eluting stents improve outcomes after ST-elevation myocardial infarction (STEMI)?
Background: Drug-eluting stents reduce restenosis rates compared to bare-metal stents. However, there is concern drug-eluting stents increase the risk of stent thrombosis leading to MI and death. Prior studies compared patients who received bare-metal versus those who received drug-eluting stents. Outcomes on a population level might provide new insight.
Study design: Observational study.
Setting: 100% national sample of patients 65 and older who received a coronary stent from 2002-05 enrolled in the traditional fee-for-service Medicare program.
Synopsis: 38,917 patients in the pre-drug-eluting-stent era from October 2002 to March 2003 received bare-metal stents. Nearly 62% of 28,086 patients studied from September to December 2003 received drug-eluting stents. The remaining 38.5% received bare-metal stents. Outcomes of percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), STEMI, and death were observed through December 31, 2005.
Patients in the drug-eluting-stent era had a lower two-year risk for repeat revascularization compared to patients in the bare-metal-stent era. In the drug-eluting versus bare-metal eras, repeat PCI was 17.1% versus 20.0% (p<0.001) and need for CABG was 2.7% versus 4.2% (p<0.01). Comparing adjusted outcomes for death, or STEMI, at two years, the two groups appeared similar.
The study did have limitations: the data only reflect sirolimus stents, the authors could not assess dual-antiplatelet therapy or obtain information on coronary anatomy or procedure details to account for selection bias in stent utilization, and the patients were all Medicare beneficiaries.
Bottom line: Drug-eluting stents are associated with fewer repeat revascularization procedures than bare-metal stents, but have not shown a significant improvement in the subsequent risk of STEMI or death.
Citation: Malenka DJ, Kaplan AV, Lucas FL, Sharp SM, Skinner JA. Outcomes following coronary stenting in the era of bare-metal vs. the era of drug-eluting stents. JAMA 2008;299(24):2868-2877.
Does case volume affect hospital performance for publicly reported process measures?
Background: Hospitals are increasingly graded and compared to one another. “Top medical centers” are defined as those within the top 10% of hospitals in specified performance measures. Hospitals with large and small case volumes might not be compared evenly and fairly.
Study design: Eight publicly reported process measures for acute myocardial infarction (AMI) were compared to hospital case volume, process performance, and label as “top hospital.”
Setting: Data were analyzed from the Hospital Quality Alliance for 3,761 hospitals from January to December 2005.
Synopsis: Hospitals with large case volume overall had better process performance. For example, looking at use of beta-blockers in patients with AMI on arrival to a hospital, small-volume hospitals (<10 AMI cases) averaged 72% while large volume (>100 AMI cases) averaged 80% (p<0.001). However, hospitals with small case volumes were more likely to receive “top hospital” rating even when hospitals with very low case volumes were excluded.
Hospital quality reporting that does not account for case volume is misleading to hospitals and consumers. In this study, larger-volume hospitals appeared to perform better in process measures, but were less likely to receive “top hospital” rating.
Bottom line: Hospitals with large and small case volumes can easily be compared to one another for process measures in AMI.
Citation: O’Brien SM, DeLong ER, Peterson ED. Impact of case volume on hospital performance assessment. Arch Intern Med. 2008;168(12):1277-1284.
What is the predictive value of QRS duration in patients hospitalized with worsening CHF?
Background: In outpatients, a prolonged QRS duration (greater than 120 ms) is associated with increased mortality. Its value in the inpatient setting is unclear. For patients hospitalized with CHF exacerbations, establishing the value of QRS duration may allow for tailored management.
Study design: Retrospective post hoc analysis from the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST).
Setting: 4,133 patients were enrolled from North American, South American, and European sites.
Synopsis: Of 2,962 patients included in the final post hoc analysis, 1,321 (44.6%) had a prolonged QRS duration. During a median follow up of 9.9 months, the all-cause mortality rate was 18.7% for patients with a normal baseline QRS duration and 28.1% for patients with a prolonged baseline QRS.
After adjusting for confounding variables, patients with a prolonged baseline QRS had a 24% increased risk of all-cause mortality and a 28% increased risk for a composite endpoint of cardiac mortality or hospitalization for heart failure exacerbation.
The retrospective nature of the analysis represents the major limitation of this study. In addition, most of the enrolled patients were white, which limits the studies generalizability to other ethnic groups.
Bottom Line: A prolonged QRS duration for patients admitted with decompensated left ventricular heart failure is common and may be associated with increased morbidity and mortality.
Citation: Wang NC, Maggioni AP, Konstam MA, Zannad F, Drasa HB, Burnett JC, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA. 2008;299(22):2656-2666.
For patients with out-of-hospital cardiac arrest, does the addition of vasopressin to epinephrine in a protocol for ACLS improve outcomes?
Background: The outcome for patients experiencing cardiac arrest who require vasopressors remains extremely poor. Despite disappointing data on vasopressin as an alternative treatment during cardiac arrest, a recent subgroup analysis suggested patients who received epinephrine and vasopressin together had superior clinical outcomes.
Study Design: Prospective multicenter randomized double-blind controlled trial.
Setting: 31 emergency medical service organizations in France.
Synopsis: Of the 2,894 patients, 20.7% of those receiving combination treatment (vasopressin plus epinephrine) survived to hospital admission versus 21.3% of those in the epinephrine-only group. For those same groups, 1.7% of combination and 2.3% of epinephrine-only patients survived to hospital discharge. No significant outcome differences were found in any group or subgroup analysis.
The study had lower-than-expected overall survival to hospital discharge, which may have handicapped its effort to find a true difference in treatment arms.
Bottom line: The addition of vasopressin to epinephrine in the treatment of out-of-hospital cardiac arrest does not improve outcomes.
Citation: Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien P, Mauriaucourt P, et al. Vasopressin and epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl J Med. 2008;359(1):21-30.
Is oral rivaroxaban more efficacious than subcutaneous enoxaparin in preventing VTE after hip-replacement surgery?
Background: Venous thromboembolism (VTE) prophylaxis after total hip replacement (THR) is important but can be cumbersome because the most commonly used anticoagulants are either subcutaneous or require frequent monitoring. Rivaroxaban, an oral direct inhibitor of factor Xa may provide more convenient anticoagulation postoperatively. However, its efficacy and safety are unknown.
Study design: Randomized double-blind trial.
Setting: Multicenter study performed in 27 countries.
Synopsis: Patients undergoing THR surgery were randomized to oral rivaroxaban (10mg once daily without monitoring, started six to eight hours after surgery) or subcutaneous enoxaparin (40mg once daily, started 12 hours prior to surgery). After surgery, prophylaxis was administered for 35 days. The primary outcome was a composite of asymptomatic deep venous thrombosis (DVT), symptomatic DVT or pulmonary embolism (PE), or death from any cause at 36 days after surgery.
In the enoxaparin group, 3.7% of patients experienced the primary outcome. This decreased to 1.1% in the rivaroxaban group. Approximately one-third of events were symptomatic. Major bleeding occurred in 0.1% and 0.3% (p=NS) of patients in the enoxaparin and rivaroxaban groups, respectively.
The study is limited by the exclusion of 1,388 of the 4,541 patients (30.6%) randomized, primarily due to having inadequate venography. Also, because the majority of thromboembolic events were asymptomatic, the primary outcome overemphasizes the clinical difference.
Bottom line: Oral rivaroxaban without monitoring is more efficacious than, and as safe as, subcutaneous enoxaparin when used for VTE prophylaxis for THR.
Citation: Eriksson B, Borris LC, Friedman RJ, Hass S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. 2008;358:2765-75.
Is LMWH more efficacious than UFH in preventing postoperative VTE in cancer patients?
Background: Patients with cancer are at increased risk for VTE and require prophylaxis to prevent this complication postoperatively. Low molecular weight heparin (LMWH) has proven more efficacious than subcutaneous unfractionated heparin (UFH) in other settings (e.g., DVT treatment). However, it is still unknown whether LMWH offers better prophylaxis compared to UFH for cancer patients undergoing surgery.
Study design: Systematic review and meta-analysis.
Setting: 14 randomized controlled trials.
Synopsis: Eleven trials exclusively examined patients with cancer (n=4006) and three trials reported data for cancer patients as subgroups (n=1816). There were in differences in mortality, pulmonary embolism, and symptomatic DVT rates between the two groups.
LMWH was associated with a decrease in total (asymptomatic or symptomatic) DVT (RR, 0.72; 95% CI, 0.55-0.94). Rates of major bleeding, minor bleeding, and intraoperative blood loss were similar between the two treatments.
This meta-analysis is limited because 12 remaining trials (n=3185) also enrolled cancer patients but did not provide specific data for the cancer patient subgroup. The study also is limited by the heterogeneity of the original trials, including utilizing varying LMWHs and dosing regimens, numerous types of surgeries, and a wide range of neoplasms.
Bottom line: LMWH does not decrease mortality, pulmonary embolism, or symptomatic DVT compared to UFH in cancer patients undergoing surgery.
Citation: Akl EA, Terrenato I, Barba M, Sperati F, Sempos EV, Muti P, et al. Low-molecular-weight heparin vs. unfractionated heparin for perioperative thromboprophylaxis in patients with cancer. Arch Intern Med. 2008;168:1261-9.
Does salmeterol added to inhaled corticosteroids improve severe asthma-related events?
Background: Asthma is a chronic disease causing major morbidity and mortality worldwide. Disease guidelines recommend all patients with persistent asthma be treated with inhaled corticosteroids. These same guidelines recommend adding a long-acting beta-agonist for patients whose symptoms persist. However, the safety of this practice has come under scrutiny.
Study design: Meta-analysis.
Setting: Sixty-six randomized, controlled trials conducted worldwide.
Synopsis: Analysis included 66 GlaxoSmithKline trials with a total of 20,966 patients with persistent asthma. Patients used either salmeterol (50mcg twice daily) plus inhaled corticosteroid (10,400 patients) or inhaled corticosteroid alone (10,566 patients).
Results showed no differences in asthma-related hospitalizations, asthma-related intubations, or deaths between the two groups. However, due to the low number of events, definitive conclusions are difficult to make. Severe asthma exacerbations requiring systemic corticosteroids significantly decreased in the inhaled corticosteroid plus salmeterol group.
The study is limited by it inclusion of only those trials sponsored by GlaxoSmithKline and by the short duration of most of the studies. Additionally, the studies included in the analysis used clinical outcomes as secondary endpoints.
Bottom line: Adding salmeterol to inhaled corticosteroid decreases severe asthma exacerbations and is likely safe, but does not have an effect on asthma-related hospitalization or death.
Citation: Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et.al. Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. Annals Intern Med. 2008;149:33-42.
Is an early invasive strategy effective in women with unstable angina or NSTEMI?
Background: Despite many trials showing the value of an early invasive strategy for patients with non-ST-segment elevation acute coronary syndrome (NSTE ACS), data from several trials question this benefit in women. Some trials show higher risk of death and myocardial infarction (MI) in subgroup analysis of women.
Study Design: Meta-analysis.
Setting: Eight randomized, controlled trials conducted worldwide.
Synopsis: Analysis included eight trials with 10,412 patients (3,075 women) with NSTE ACS. The invasive group (5,083 patients) was defined as those referred for coronary angiography with subsequent intervention as needed. The composite endpoint of death, MI, or rehospitalization within 12 months with ACS occurred in 21.1% of the invasive group and 25.9% of the medically managed group (OR, 0.78; CI, 0.61-0.98).
The subgroup, including only women, had a non-statistically significant OR of 0.81 (CI, 0.65-1.01), including no effect on all-cause mortality, nonfatal MI, or the composite of death and MI. However, women with high-risk features (elevated biomarkers) undergoing the invasive strategy had a significant reduction in the composite endpoint (OR, 0.67; CI, 0.50-0.88).
The study is limited by the use of subgroup analysis, secondary endpoints, heterogeneity between trials, and possible publication bias.
Bottom line: Early invasive strategy is effective in men and high-risk women with NSTE ACS, but not in low-risk women.
Citation: O’Donoghue M, Boden W, Braunwald E, Cannon CP, Clayton TC, Winter RJ, et.al. Early invasive vs. conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction. JAMA. 2008;300:71-80.
What strategies are used to prevent contrast-induced acute kidney injury?
Background: Contrast-induced acute kidney injury (CIAKI) is a condition potentially amenable to preventive care. Several trials have identified intravenous hydration, N-acetylcysteine, and withdrawal of NSAIDS as interventions that reduce the possibility of CIAKI in high-risk patients. Little is known about whether healthcare providers routinely use these strategies.
Study design: Prospective observational cohort study.
Setting: Veterans Affairs (VA) Pittsburgh Healthcare System.
Synopsis: 11,410 patients scheduled for radiographic procedures were screened. After exclusion criteria and eligibility, 660 patients with an estimated glomerular filtration rate less than 60ml/min/1.73m2 were identified. Usage of intravenous fluids, N-acetylcysteine, and discontinuation of NSAIDS were recorded. Serum creatinine (SCr) was measured 48 to 96 hours post-procedure. CIAKI was defined as relative increase in SCr from baseline (≥25%, ≥50% and ≥100%) and absolute increase in SCr levels from baseline (≥0.25, ≥0.5, and ≥1.0). CIAKI association with adverse outcomes was evaluated by tracking 30-day mortality, need for dialysis, and hospitalization.
The incidence of CIAKI was less common in patients undergoing CT scans versus those having angiograms. Adverse 30-day outcomes were uncommon. Pre- and post-procedure intravenous hydration was administered to 40% of study patients, more commonly with coronary angiogram than with computed tomography (91.2% vs. 16%, p<0.0001). N-acetylcysteine was administered to 39.2%. Only 6.8% of those taking NSAIDS reported being told to discontinue the medication.
Study limitations include the small sample size and the single site location, both limiting generalizability.
Bottom line: Clinically significant CIAKI is uncommon, and preventive care is not uniformly implemented in patients undergoing contrast-enhanced radiographic procedures.
Citation: Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Sonel AF, Fine MJ, et al. Prevention, incidence, and outcomes of contrast-induced acute kidney injury. Arch Intern Med. 2008;168(12):1325-1332.
How does hyperglycemia affect morbidity and mortality in children admitted to a community pediatric hospital?
Background: Inpatient hyperglycemia in adult patients is a predictor of poor clinical outcomes. The association of hyperglycemia and clinical outcomes in children admitted to a general community hospital has not been studied.
Study design: Retrospective observational cohort study.
Setting: A community pediatric hospital in Atlanta, Ga.
Synopsis: Review of medical records of 903 consecutive pediatric patients admitted to critical and non-critical areas took place. Of these, 542 patients constituted the study population. The study excluded 342 patients who didn’t have a blood glucose measurement. Hyperglycemia was defined as an admission or in-hospital blood glucose greater than 120mg/dl.
One-fourth of the children admitted to the hospital had hyperglycemia, most without a prior history of diabetes. The presence of hyperglycemia on admission was not associated with increased length of stay (LOS) or increased mortality. Children with hyperglycemia were more likely to be admitted to the ICU and had longer ICU LOS.
This was a retrospective study conducted at a single site whose demographics and disease spectrum may differ from those of other institutions. There were an insufficient number of deaths to make any conclusions regarding the impact of hyperglycemia on mortality. Prospective, randomized, multicenter trials are needed to better elucidate the effects of in-patient hyperglycemia.
Bottom line: Hyperglycemia is common in children with or without diabetes admitted to the hospital, and is associated with increased ICU admissions and ICU length of stay. Its connection to mortality is inconclusive.
Citation: Palaio A, Smiley D, Ceron M, Klein R, Cho IS, Mejia R, et al. Prevalence and clinical outcome of inpatient hyperglycemia in a community pediatric hospital. J Hosp Med.2008;3(3):212-217.
Neal R. Axon, MD
Ed note: This article is the second in a series of interviews with members of Team Hospitalist: 12 hospital medicine experts who are serving a two-year term as special editorial consultants to our magazine.
Ever consider working as an academic hospitalist? Here to give you the scoop on what it’s like is “Team Hospitalist” member R. Neal Axon, MD, assistant professor of internal medicine and pediatrics at the Medical University of South Carolina (MUSC) in Charleston.
Dr. Axon completed his residency at Duke University Medical Center and received his medical degree from the University of Alabama School of Medicine in 2000.
Why is it important to conduct research in hospital medicine?
We haven’t perfected medicine just yet, and until we do we have to work to make it better. Even though hospital medicine research is different from clinical medicine, we need to have people who are working to make the systems of care better.
What attracted you to academic medicine?
I love teaching residents and medical students, and I missed doing it when I entered in private practice. I just completed my master’s at MUSC in clinical research. My department was very supportive and even paid my tuition.
Is it difficult to balance research work with shift work?
It’s definitely a challenge. Fortunately for me, my group does not have shift work in the traditional sense. We do have a night shift, but it’s something we do on an infrequent basis. It would be extremely difficult to do in a seven-on, seven-off schedule that most hospitalists have.
What type of research are you working on?
I’m currently doing some work with hypertension. One of the projects is doing survey work where we access the attitudes of providers (doctors and house staff) on what to do with patients who have hypertension. My observation has been that, in many cases, when patients are admitted to a hospital, they also have high blood pressure that may equate with hypertension in the outpatient setting. It’s not clear when that should be addressed--or how. This survey would help us understand that.
What do you like about what you do?
I worry more about what the department chief thinks than what the CEO of the hospital thinks. At community and non-teaching hospitals, the focus is much more on the bottom line.
So is it impossible to do research if you work at a non-teaching hospital?
I think it’s likely to be more difficult--in that setting--to be a pure clinical researcher, but I do think there are opportunities out there for every day hospitalists to participate in research. This is one of the things I’m currently working on as a member of the SHM Research Committee. One deliverable we’re excited about is the fact that there will be sessions at the [2009] annual meeting in Chicago that will specifically address how hospitalists can do research.
Another thing I hope can evolve is practice-based research networks, which exist in the primary care setting, but not so much in hospital medicine. These networks include groups of community doctors who band together to do clinical research projects. Central leadership helps the members of the group come up with research questions. This is something I’m working on in my state to develop, but this type of setup does exist in other areas.
What advice do you have for hospitalists who are interested in research?
The most important piece of advice is to find a good mentor.
The second thing is that most medical schools have master’s degree programs that teach you the skills that will get you started in clinical research. I went to medical school, but didn’t learn anything about biostatistics or trial design. TH
Ed note: This article is the second in a series of interviews with members of Team Hospitalist: 12 hospital medicine experts who are serving a two-year term as special editorial consultants to our magazine.
Ever consider working as an academic hospitalist? Here to give you the scoop on what it’s like is “Team Hospitalist” member R. Neal Axon, MD, assistant professor of internal medicine and pediatrics at the Medical University of South Carolina (MUSC) in Charleston.
Dr. Axon completed his residency at Duke University Medical Center and received his medical degree from the University of Alabama School of Medicine in 2000.
Why is it important to conduct research in hospital medicine?
We haven’t perfected medicine just yet, and until we do we have to work to make it better. Even though hospital medicine research is different from clinical medicine, we need to have people who are working to make the systems of care better.
What attracted you to academic medicine?
I love teaching residents and medical students, and I missed doing it when I entered in private practice. I just completed my master’s at MUSC in clinical research. My department was very supportive and even paid my tuition.
Is it difficult to balance research work with shift work?
It’s definitely a challenge. Fortunately for me, my group does not have shift work in the traditional sense. We do have a night shift, but it’s something we do on an infrequent basis. It would be extremely difficult to do in a seven-on, seven-off schedule that most hospitalists have.
What type of research are you working on?
I’m currently doing some work with hypertension. One of the projects is doing survey work where we access the attitudes of providers (doctors and house staff) on what to do with patients who have hypertension. My observation has been that, in many cases, when patients are admitted to a hospital, they also have high blood pressure that may equate with hypertension in the outpatient setting. It’s not clear when that should be addressed--or how. This survey would help us understand that.
What do you like about what you do?
I worry more about what the department chief thinks than what the CEO of the hospital thinks. At community and non-teaching hospitals, the focus is much more on the bottom line.
So is it impossible to do research if you work at a non-teaching hospital?
I think it’s likely to be more difficult--in that setting--to be a pure clinical researcher, but I do think there are opportunities out there for every day hospitalists to participate in research. This is one of the things I’m currently working on as a member of the SHM Research Committee. One deliverable we’re excited about is the fact that there will be sessions at the [2009] annual meeting in Chicago that will specifically address how hospitalists can do research.
Another thing I hope can evolve is practice-based research networks, which exist in the primary care setting, but not so much in hospital medicine. These networks include groups of community doctors who band together to do clinical research projects. Central leadership helps the members of the group come up with research questions. This is something I’m working on in my state to develop, but this type of setup does exist in other areas.
What advice do you have for hospitalists who are interested in research?
The most important piece of advice is to find a good mentor.
The second thing is that most medical schools have master’s degree programs that teach you the skills that will get you started in clinical research. I went to medical school, but didn’t learn anything about biostatistics or trial design. TH
Ed note: This article is the second in a series of interviews with members of Team Hospitalist: 12 hospital medicine experts who are serving a two-year term as special editorial consultants to our magazine.
Ever consider working as an academic hospitalist? Here to give you the scoop on what it’s like is “Team Hospitalist” member R. Neal Axon, MD, assistant professor of internal medicine and pediatrics at the Medical University of South Carolina (MUSC) in Charleston.
Dr. Axon completed his residency at Duke University Medical Center and received his medical degree from the University of Alabama School of Medicine in 2000.
Why is it important to conduct research in hospital medicine?
We haven’t perfected medicine just yet, and until we do we have to work to make it better. Even though hospital medicine research is different from clinical medicine, we need to have people who are working to make the systems of care better.
What attracted you to academic medicine?
I love teaching residents and medical students, and I missed doing it when I entered in private practice. I just completed my master’s at MUSC in clinical research. My department was very supportive and even paid my tuition.
Is it difficult to balance research work with shift work?
It’s definitely a challenge. Fortunately for me, my group does not have shift work in the traditional sense. We do have a night shift, but it’s something we do on an infrequent basis. It would be extremely difficult to do in a seven-on, seven-off schedule that most hospitalists have.
What type of research are you working on?
I’m currently doing some work with hypertension. One of the projects is doing survey work where we access the attitudes of providers (doctors and house staff) on what to do with patients who have hypertension. My observation has been that, in many cases, when patients are admitted to a hospital, they also have high blood pressure that may equate with hypertension in the outpatient setting. It’s not clear when that should be addressed--or how. This survey would help us understand that.
What do you like about what you do?
I worry more about what the department chief thinks than what the CEO of the hospital thinks. At community and non-teaching hospitals, the focus is much more on the bottom line.
So is it impossible to do research if you work at a non-teaching hospital?
I think it’s likely to be more difficult--in that setting--to be a pure clinical researcher, but I do think there are opportunities out there for every day hospitalists to participate in research. This is one of the things I’m currently working on as a member of the SHM Research Committee. One deliverable we’re excited about is the fact that there will be sessions at the [2009] annual meeting in Chicago that will specifically address how hospitalists can do research.
Another thing I hope can evolve is practice-based research networks, which exist in the primary care setting, but not so much in hospital medicine. These networks include groups of community doctors who band together to do clinical research projects. Central leadership helps the members of the group come up with research questions. This is something I’m working on in my state to develop, but this type of setup does exist in other areas.
What advice do you have for hospitalists who are interested in research?
The most important piece of advice is to find a good mentor.
The second thing is that most medical schools have master’s degree programs that teach you the skills that will get you started in clinical research. I went to medical school, but didn’t learn anything about biostatistics or trial design. TH
SHM Invests in 'Champions' and SHM's Future

Not content with the status quo, SHM has taken significant steps to ensure the society’s reach grows in line with the exponential expansion of hospital medicine. These investments put SHM’s premier educational content into the hands of more hospitalists and increase the society’s ability to hear firsthand—and more quickly react to—the challenges of the field.
One key initiative is SHM’s Champions Program, which identifies hospitalists on the ground to serve as information conduits. These “champions” share feedback with SHM’s staff and leadership about the state of hospital medicine locally, and react to SHM plans and proposals. They also help SHM disseminate news and resources to hospitalists in their communities.
In the Champions Program’s short tenure, it already has proven its value. Champions in 26 key markets are engaged and providing valuable feedback in a wide variety of areas, through participation on conference calls, individual surveys, and even a private breakfast with SHM CEO Larry Wellikson.
On top of that, the program has enabled SHM to expand its pool of identified hospitalists by nearly 60%. This expansion not only means SHM’s education and quality improvement resources will reach more communities, but that the society will gain clout and credibility in all facets of healthcare from divergent groups, such as MedPAC and Congress.
Champions are leaders in their communities, dedicated to making a difference in hospital medicine. If this describes you, consider becoming a Champion. Committing to this vital program means helping to steer the course of hospital medicine locally and globally. If you aspire to become a leader within the society, the Champions Program is a great way to begin.
If you’re interested in becoming a Champion or want to suggest someone in your community who would be a good fit, call Cathy Peduzzi, SHM’s manager of membership outreach programs at (215) 351-2584 or e-mail her at [email protected].
The SHM Bi-Annual Survey on the State of the Hospital Medicine Movement has quickly become a must-have resource for hospital medicine group leaders, administrators, and hospitalists. This survey provides baseline information on topics such as hospital medicine group financial support, compensation and employment models, and productivity.
Whether you’re an experienced hospitalist or you are just starting out in the specialty, the survey has information that will benefit you. Here’s a sampling of the frequently asked questions that can be answered using information found in the survey:
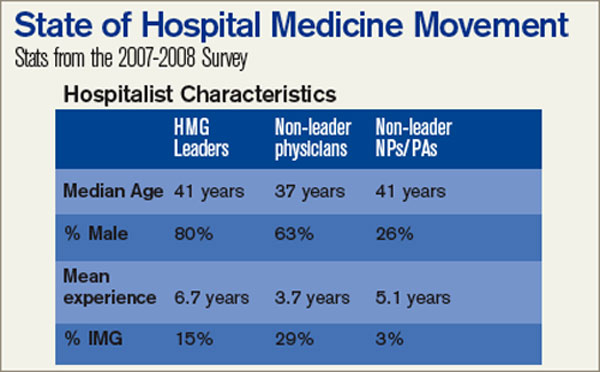
Q: I’m recruiting hospitalists for a hospital medicine group on the East Coast. What’s the average salary for a hospitalist in my area?
A: The average salary for the hospitalist on the East Coast is $189,400, compared to the national average of $193,300.
Q: As a hospital medicine group leader, should I expect financial support for my program?
A: According to the survey, 91% of HMGs receive some kind of financial backing for their program, with an average of $97,275 in support per FTE physician.
Q: How do hospital medicine groups handle night coverage?
A: Currently, 53% of HMGs have an on-site provider, 27% have a hospitalist on-call at home, 16% have a combination of on-site and on-call coverage, and 3% have no night coverage at all.
To purchase the “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement,” visit www.hospital medicine.org/survey.
Not content with the status quo, SHM has taken significant steps to ensure the society’s reach grows in line with the exponential expansion of hospital medicine. These investments put SHM’s premier educational content into the hands of more hospitalists and increase the society’s ability to hear firsthand—and more quickly react to—the challenges of the field.
One key initiative is SHM’s Champions Program, which identifies hospitalists on the ground to serve as information conduits. These “champions” share feedback with SHM’s staff and leadership about the state of hospital medicine locally, and react to SHM plans and proposals. They also help SHM disseminate news and resources to hospitalists in their communities.
In the Champions Program’s short tenure, it already has proven its value. Champions in 26 key markets are engaged and providing valuable feedback in a wide variety of areas, through participation on conference calls, individual surveys, and even a private breakfast with SHM CEO Larry Wellikson.
On top of that, the program has enabled SHM to expand its pool of identified hospitalists by nearly 60%. This expansion not only means SHM’s education and quality improvement resources will reach more communities, but that the society will gain clout and credibility in all facets of healthcare from divergent groups, such as MedPAC and Congress.
Champions are leaders in their communities, dedicated to making a difference in hospital medicine. If this describes you, consider becoming a Champion. Committing to this vital program means helping to steer the course of hospital medicine locally and globally. If you aspire to become a leader within the society, the Champions Program is a great way to begin.
If you’re interested in becoming a Champion or want to suggest someone in your community who would be a good fit, call Cathy Peduzzi, SHM’s manager of membership outreach programs at (215) 351-2584 or e-mail her at [email protected].
The SHM Bi-Annual Survey on the State of the Hospital Medicine Movement has quickly become a must-have resource for hospital medicine group leaders, administrators, and hospitalists. This survey provides baseline information on topics such as hospital medicine group financial support, compensation and employment models, and productivity.
Whether you’re an experienced hospitalist or you are just starting out in the specialty, the survey has information that will benefit you. Here’s a sampling of the frequently asked questions that can be answered using information found in the survey:
Q: I’m recruiting hospitalists for a hospital medicine group on the East Coast. What’s the average salary for a hospitalist in my area?
A: The average salary for the hospitalist on the East Coast is $189,400, compared to the national average of $193,300.
Q: As a hospital medicine group leader, should I expect financial support for my program?
A: According to the survey, 91% of HMGs receive some kind of financial backing for their program, with an average of $97,275 in support per FTE physician.
Q: How do hospital medicine groups handle night coverage?
A: Currently, 53% of HMGs have an on-site provider, 27% have a hospitalist on-call at home, 16% have a combination of on-site and on-call coverage, and 3% have no night coverage at all.
To purchase the “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement,” visit www.hospital medicine.org/survey.
Not content with the status quo, SHM has taken significant steps to ensure the society’s reach grows in line with the exponential expansion of hospital medicine. These investments put SHM’s premier educational content into the hands of more hospitalists and increase the society’s ability to hear firsthand—and more quickly react to—the challenges of the field.
One key initiative is SHM’s Champions Program, which identifies hospitalists on the ground to serve as information conduits. These “champions” share feedback with SHM’s staff and leadership about the state of hospital medicine locally, and react to SHM plans and proposals. They also help SHM disseminate news and resources to hospitalists in their communities.
In the Champions Program’s short tenure, it already has proven its value. Champions in 26 key markets are engaged and providing valuable feedback in a wide variety of areas, through participation on conference calls, individual surveys, and even a private breakfast with SHM CEO Larry Wellikson.
On top of that, the program has enabled SHM to expand its pool of identified hospitalists by nearly 60%. This expansion not only means SHM’s education and quality improvement resources will reach more communities, but that the society will gain clout and credibility in all facets of healthcare from divergent groups, such as MedPAC and Congress.
Champions are leaders in their communities, dedicated to making a difference in hospital medicine. If this describes you, consider becoming a Champion. Committing to this vital program means helping to steer the course of hospital medicine locally and globally. If you aspire to become a leader within the society, the Champions Program is a great way to begin.
If you’re interested in becoming a Champion or want to suggest someone in your community who would be a good fit, call Cathy Peduzzi, SHM’s manager of membership outreach programs at (215) 351-2584 or e-mail her at [email protected].
The SHM Bi-Annual Survey on the State of the Hospital Medicine Movement has quickly become a must-have resource for hospital medicine group leaders, administrators, and hospitalists. This survey provides baseline information on topics such as hospital medicine group financial support, compensation and employment models, and productivity.
Whether you’re an experienced hospitalist or you are just starting out in the specialty, the survey has information that will benefit you. Here’s a sampling of the frequently asked questions that can be answered using information found in the survey:
Q: I’m recruiting hospitalists for a hospital medicine group on the East Coast. What’s the average salary for a hospitalist in my area?
A: The average salary for the hospitalist on the East Coast is $189,400, compared to the national average of $193,300.
Q: As a hospital medicine group leader, should I expect financial support for my program?
A: According to the survey, 91% of HMGs receive some kind of financial backing for their program, with an average of $97,275 in support per FTE physician.
Q: How do hospital medicine groups handle night coverage?
A: Currently, 53% of HMGs have an on-site provider, 27% have a hospitalist on-call at home, 16% have a combination of on-site and on-call coverage, and 3% have no night coverage at all.
To purchase the “2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement,” visit www.hospital medicine.org/survey.
A Bumpy Bundling Road Ahead
Patrick J. Torcson, MD, MMM, FACP, laughs when he recalls his initial reaction to the proposal to bundle Medicare payments to hospitals: “If this passes legislation, I’m moving to Dubai.”
Dr. Torcson, chairman of SHM’s Performance and Standards Committee, and medical director of the hospitalist program at St. Tammany Parish Hospital in Covington, La., has since tempered his thinking. Like many physicians, he understands the need for Medicare to address growing costs. Nevertheless, he is wary about the bundling proposal in June’s Medicare Payment Advisory Commission (MedPAC) report to Congress.
Dr. Torcson’s opinion about reforming the nation’s healthcare delivery system points to the difficult dichotomy facing hospitalists and other physicians: they agree change is necessary, but worry about the consequences of bundling payments.
Under the new model, rather than pay for each service provided, Medicare would reimburse a lump sum for all treatment linked to an episode of care for conditions such as congestive heart failure, chronic obstructive pulmonary disease or cardiac bypass surgery. In addition, the Centers for Medicare & Medicaid Services (CMS) would provide hospitals and physicians with reports detailing their resource use and readmission rates for specific episodes of inpatient care. After two years, the providers’ reports would become public.
Another proposal would cut payments to hospitals with high risk-adjusted readmission rates for select conditions while urging Congress to ease gainsharing restrictions to financially reward physicians helping hospitals improve readmission rates and overall patient care.
—Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare
The switch to bundling, Dr. Torcson says, could entice hospitalists to encourage a healthcare delivery model that fosters collective accountability. He and other physicians warn the system could just as easily create imbalances in power, provide incentives for withholding care and spell disaster for rural physicians and ill-prepared networks.
“Philosophically, it’s a nice idea, but I don’t think it’s realistic and I don’t think hospitals that have a small budget will be able to survive it,” says Rachel Lovins, MD, director of the hospitalist program at Waterbury Hospital in Connecticut. Dividing a bundled payment equally amongst hospital departments “will be close to impossible,” she says, and struggling hospitals will fall further into debt. The new system also may leave providers with inadequate resources and lead to angry outpatient doctors who refuse to accept Medicare patients.
Part of the problem, according to Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare, is how little physicians know about the effects of the new plan. “Everyone understands that this is a dramatic paradigm shift,” he says. “Bundling is a really radical change. It’s going to generate all kinds of consequences—intended and unintended—and no one really has a handle on what’s going to happen.”
The Status Quo Must Change
One of few points of agreement is that the status quo is untenable. A recent summary of MedPAC’s report in The New England Journal of Medicine blamed the fee-for-service model for fueling negative aspects of the current healthcare system and warned of an escalation in Medicare spending. “Fee-for-service payment spurs spending growth, supports a fragmented and compartmentalized delivery system and does nothing to reward quality or value,” the MedPAC authors write.
Though some physicians remain cautiously optimistic about bundling, Dr. Siegal doubts the model is ready for primetime. “Bundling says, ‘Let’s create accountability for outcomes by not paying for single services but for an entire episode of care,’” he says. But many questions remain unanswered. What constitutes an episode? Who controls the allocation of the Medicare payment? If an episode is defined as 30 days from when a patient enters the hospital for a specific procedure, are other health providers accountable for addressing unrelated complaints within the same episode window?
“There are an enormous number of ways you can contort and twist this so you can create scenarios where people come out of it feeling like they have been penalized for behavior well outside their control,” Dr. Siegal says. “I think those are the big risks: imbalance of power and how do you create lines of accountability that actually make sense?”
But, he says, a system that promotes collective responsibility for patients could create a compelling incentive for more collaboration between physicians and consultants. “I think if ‘done right,’ and I say that in quotations because nobody knows what ‘done right’ means,” Dr. Siegal says, “bundling could actually be huge for hospitalists.”
Mary Dallas, MD, medical information officer at Presbyterian Healthcare Services in Albuquerque, N.M., says she’s seen first hand how collaboration among a health plan, a hospital and physicians can improve quality and balance finances. “Those efforts were really spawned out of a forced alignment between all groups in order to focus on common goals,” she says. Bundling could force a similar convergence of priorities.
Transition Troubles
If “alignment” has become the favorite watchword in bundling discussions, “gainsharing” as a concept has been greeted by far more ambivalence. “I oppose gainsharing that puts money directly into the physician’s pocket,” Dr. Dallas says. “This is something that occurs frequently in the free-market world in other industries, and to pay a few for the success that demands participation of many is just wrong in my book.”
Instead, Dr. Dallas supports the idea of directing monetary rewards toward improving infrastructure and the overall healthcare delivery process. As examples, she suggests using the money to buy time from physicians willing to be involved in pilot projects aimed at improving the delivery process, or to add more resources for better patient continuity between the hospital and the community.
Even with a more equitable distribution of resources, she and other hospitalists concede any transition to bundling could be bumpy. “If I were an independent physician, and my personal payment from Medicare was dependent on or tied to the hospital’s performance,” Dr. Dallas says, “there would be a lot of work to prepare me for this.”
As several hospitalists warn, a bundling system could trigger ratcheting down of care—and a whole new set of headaches. “The concern for everyone is that it is going to incentivize physicians to give less services,” says Jonathan Lovins, MD, director of hospitalist and midlevel practitioner services at the Hospital of Central Connecticut, and the brother of Waterbury Hospital’s Dr. Rachel Lovins.
Several hospitalists say the problem could be similar to what happened with Medicare’s capitation system, which gained traction in the 1980s and peaked in the mid-1990s before waning because of a backlash by both providers and patients. This fixed pre-payment reimbursement system, Dr. Lovins says, created an inherent conflict of interest for primary caregivers because referring patients to specialists for tests lowered profits whereas delivering fewer services did not.
Bradley Flansbaum, DO, MPH, FACP, director of hospitalist services at Lenox Hill Hospital in New York City, goes a step further, calling the bundling plan capitation on steroids, and cautions that a one-size-fits-all system is bound to fail. “Having technology and having the intellectual firepower to figure out how this system is going to manage the bundled payment is an advantage,” he says, adding that larger hospitals are more likely to have this advantage. For rural physicians or those within inefficient networks, bundling payments could be disastrous. “CMS may just say, ‘We’re turning on the lights tomorrow and tough,’ but it’s going to be a hell of a mess if they do,” he says.
A Demonstration Project
A demonstration project slated to begin in four states next year may show just how steep that learning curve is. The Acute Care Episode (ACE) Demonstration would bundle virtually all payments of certain orthopedic and cardiovascular inpatient procedures at participating hospitals in Texas, Oklahoma, New Mexico, and Colorado. Hospitals and physicians still would receive separate fee-for-service payments, but a confidential report would detail their resource use. High-resource providers would incur penalties while low-resource providers would receive bonuses.
Dr. Siegal says it makes sense to begin a bundling pilot project with procedures that have defined treatment windows, such as hip replacements or open heart surgery. Other conditions will be far more difficult to contain within a neatly defined episode. “Clearly, we’re going to have to figure out what to do with heart failure and pneumonia and stroke because those are huge consumers of dollars,” he says.
Despite all the caveats and unknowns, hospitalists still may have much to gain if bundling follows in the footsteps of the successful diagnosis-related group (DRG) payment system. “I think that enlightened hospital CEOs are going to be looking to their hospitalists as their champions to really pull this off and make this work,” Dr. Torcson says, particularly as the stakes for hospitals increase.
Medicare’s Physician Quality Reporting Initiative, established by the 2006 Tax Relief and Health Care Act, already links a 1.5% financial incentive to increased performance. With bundled payments adjusted up or down by the proposed gainsharing and penalties for higher readmission rates, Dr. Torcson says, the equivalent of 3% to 5% of DRG payments could be at risk.
“I think it could be something potentially very beneficial to those hospitalist groups that get it right,” he says. “It’s kind of like before the Ice Age comes, if you’ve got your animal skins ready, those are the tribes that survive.” TH
Gretchen Henkel is a medical writer based in California.
Patrick J. Torcson, MD, MMM, FACP, laughs when he recalls his initial reaction to the proposal to bundle Medicare payments to hospitals: “If this passes legislation, I’m moving to Dubai.”
Dr. Torcson, chairman of SHM’s Performance and Standards Committee, and medical director of the hospitalist program at St. Tammany Parish Hospital in Covington, La., has since tempered his thinking. Like many physicians, he understands the need for Medicare to address growing costs. Nevertheless, he is wary about the bundling proposal in June’s Medicare Payment Advisory Commission (MedPAC) report to Congress.
Dr. Torcson’s opinion about reforming the nation’s healthcare delivery system points to the difficult dichotomy facing hospitalists and other physicians: they agree change is necessary, but worry about the consequences of bundling payments.
Under the new model, rather than pay for each service provided, Medicare would reimburse a lump sum for all treatment linked to an episode of care for conditions such as congestive heart failure, chronic obstructive pulmonary disease or cardiac bypass surgery. In addition, the Centers for Medicare & Medicaid Services (CMS) would provide hospitals and physicians with reports detailing their resource use and readmission rates for specific episodes of inpatient care. After two years, the providers’ reports would become public.
Another proposal would cut payments to hospitals with high risk-adjusted readmission rates for select conditions while urging Congress to ease gainsharing restrictions to financially reward physicians helping hospitals improve readmission rates and overall patient care.
—Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare
The switch to bundling, Dr. Torcson says, could entice hospitalists to encourage a healthcare delivery model that fosters collective accountability. He and other physicians warn the system could just as easily create imbalances in power, provide incentives for withholding care and spell disaster for rural physicians and ill-prepared networks.
“Philosophically, it’s a nice idea, but I don’t think it’s realistic and I don’t think hospitals that have a small budget will be able to survive it,” says Rachel Lovins, MD, director of the hospitalist program at Waterbury Hospital in Connecticut. Dividing a bundled payment equally amongst hospital departments “will be close to impossible,” she says, and struggling hospitals will fall further into debt. The new system also may leave providers with inadequate resources and lead to angry outpatient doctors who refuse to accept Medicare patients.
Part of the problem, according to Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare, is how little physicians know about the effects of the new plan. “Everyone understands that this is a dramatic paradigm shift,” he says. “Bundling is a really radical change. It’s going to generate all kinds of consequences—intended and unintended—and no one really has a handle on what’s going to happen.”
The Status Quo Must Change
One of few points of agreement is that the status quo is untenable. A recent summary of MedPAC’s report in The New England Journal of Medicine blamed the fee-for-service model for fueling negative aspects of the current healthcare system and warned of an escalation in Medicare spending. “Fee-for-service payment spurs spending growth, supports a fragmented and compartmentalized delivery system and does nothing to reward quality or value,” the MedPAC authors write.
Though some physicians remain cautiously optimistic about bundling, Dr. Siegal doubts the model is ready for primetime. “Bundling says, ‘Let’s create accountability for outcomes by not paying for single services but for an entire episode of care,’” he says. But many questions remain unanswered. What constitutes an episode? Who controls the allocation of the Medicare payment? If an episode is defined as 30 days from when a patient enters the hospital for a specific procedure, are other health providers accountable for addressing unrelated complaints within the same episode window?
“There are an enormous number of ways you can contort and twist this so you can create scenarios where people come out of it feeling like they have been penalized for behavior well outside their control,” Dr. Siegal says. “I think those are the big risks: imbalance of power and how do you create lines of accountability that actually make sense?”
But, he says, a system that promotes collective responsibility for patients could create a compelling incentive for more collaboration between physicians and consultants. “I think if ‘done right,’ and I say that in quotations because nobody knows what ‘done right’ means,” Dr. Siegal says, “bundling could actually be huge for hospitalists.”
Mary Dallas, MD, medical information officer at Presbyterian Healthcare Services in Albuquerque, N.M., says she’s seen first hand how collaboration among a health plan, a hospital and physicians can improve quality and balance finances. “Those efforts were really spawned out of a forced alignment between all groups in order to focus on common goals,” she says. Bundling could force a similar convergence of priorities.
Transition Troubles
If “alignment” has become the favorite watchword in bundling discussions, “gainsharing” as a concept has been greeted by far more ambivalence. “I oppose gainsharing that puts money directly into the physician’s pocket,” Dr. Dallas says. “This is something that occurs frequently in the free-market world in other industries, and to pay a few for the success that demands participation of many is just wrong in my book.”
Instead, Dr. Dallas supports the idea of directing monetary rewards toward improving infrastructure and the overall healthcare delivery process. As examples, she suggests using the money to buy time from physicians willing to be involved in pilot projects aimed at improving the delivery process, or to add more resources for better patient continuity between the hospital and the community.
Even with a more equitable distribution of resources, she and other hospitalists concede any transition to bundling could be bumpy. “If I were an independent physician, and my personal payment from Medicare was dependent on or tied to the hospital’s performance,” Dr. Dallas says, “there would be a lot of work to prepare me for this.”
As several hospitalists warn, a bundling system could trigger ratcheting down of care—and a whole new set of headaches. “The concern for everyone is that it is going to incentivize physicians to give less services,” says Jonathan Lovins, MD, director of hospitalist and midlevel practitioner services at the Hospital of Central Connecticut, and the brother of Waterbury Hospital’s Dr. Rachel Lovins.
Several hospitalists say the problem could be similar to what happened with Medicare’s capitation system, which gained traction in the 1980s and peaked in the mid-1990s before waning because of a backlash by both providers and patients. This fixed pre-payment reimbursement system, Dr. Lovins says, created an inherent conflict of interest for primary caregivers because referring patients to specialists for tests lowered profits whereas delivering fewer services did not.
Bradley Flansbaum, DO, MPH, FACP, director of hospitalist services at Lenox Hill Hospital in New York City, goes a step further, calling the bundling plan capitation on steroids, and cautions that a one-size-fits-all system is bound to fail. “Having technology and having the intellectual firepower to figure out how this system is going to manage the bundled payment is an advantage,” he says, adding that larger hospitals are more likely to have this advantage. For rural physicians or those within inefficient networks, bundling payments could be disastrous. “CMS may just say, ‘We’re turning on the lights tomorrow and tough,’ but it’s going to be a hell of a mess if they do,” he says.
A Demonstration Project
A demonstration project slated to begin in four states next year may show just how steep that learning curve is. The Acute Care Episode (ACE) Demonstration would bundle virtually all payments of certain orthopedic and cardiovascular inpatient procedures at participating hospitals in Texas, Oklahoma, New Mexico, and Colorado. Hospitals and physicians still would receive separate fee-for-service payments, but a confidential report would detail their resource use. High-resource providers would incur penalties while low-resource providers would receive bonuses.
Dr. Siegal says it makes sense to begin a bundling pilot project with procedures that have defined treatment windows, such as hip replacements or open heart surgery. Other conditions will be far more difficult to contain within a neatly defined episode. “Clearly, we’re going to have to figure out what to do with heart failure and pneumonia and stroke because those are huge consumers of dollars,” he says.
Despite all the caveats and unknowns, hospitalists still may have much to gain if bundling follows in the footsteps of the successful diagnosis-related group (DRG) payment system. “I think that enlightened hospital CEOs are going to be looking to their hospitalists as their champions to really pull this off and make this work,” Dr. Torcson says, particularly as the stakes for hospitals increase.
Medicare’s Physician Quality Reporting Initiative, established by the 2006 Tax Relief and Health Care Act, already links a 1.5% financial incentive to increased performance. With bundled payments adjusted up or down by the proposed gainsharing and penalties for higher readmission rates, Dr. Torcson says, the equivalent of 3% to 5% of DRG payments could be at risk.
“I think it could be something potentially very beneficial to those hospitalist groups that get it right,” he says. “It’s kind of like before the Ice Age comes, if you’ve got your animal skins ready, those are the tribes that survive.” TH
Gretchen Henkel is a medical writer based in California.
Patrick J. Torcson, MD, MMM, FACP, laughs when he recalls his initial reaction to the proposal to bundle Medicare payments to hospitals: “If this passes legislation, I’m moving to Dubai.”
Dr. Torcson, chairman of SHM’s Performance and Standards Committee, and medical director of the hospitalist program at St. Tammany Parish Hospital in Covington, La., has since tempered his thinking. Like many physicians, he understands the need for Medicare to address growing costs. Nevertheless, he is wary about the bundling proposal in June’s Medicare Payment Advisory Commission (MedPAC) report to Congress.
Dr. Torcson’s opinion about reforming the nation’s healthcare delivery system points to the difficult dichotomy facing hospitalists and other physicians: they agree change is necessary, but worry about the consequences of bundling payments.
Under the new model, rather than pay for each service provided, Medicare would reimburse a lump sum for all treatment linked to an episode of care for conditions such as congestive heart failure, chronic obstructive pulmonary disease or cardiac bypass surgery. In addition, the Centers for Medicare & Medicaid Services (CMS) would provide hospitals and physicians with reports detailing their resource use and readmission rates for specific episodes of inpatient care. After two years, the providers’ reports would become public.
Another proposal would cut payments to hospitals with high risk-adjusted readmission rates for select conditions while urging Congress to ease gainsharing restrictions to financially reward physicians helping hospitals improve readmission rates and overall patient care.
—Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare
The switch to bundling, Dr. Torcson says, could entice hospitalists to encourage a healthcare delivery model that fosters collective accountability. He and other physicians warn the system could just as easily create imbalances in power, provide incentives for withholding care and spell disaster for rural physicians and ill-prepared networks.
“Philosophically, it’s a nice idea, but I don’t think it’s realistic and I don’t think hospitals that have a small budget will be able to survive it,” says Rachel Lovins, MD, director of the hospitalist program at Waterbury Hospital in Connecticut. Dividing a bundled payment equally amongst hospital departments “will be close to impossible,” she says, and struggling hospitals will fall further into debt. The new system also may leave providers with inadequate resources and lead to angry outpatient doctors who refuse to accept Medicare patients.
Part of the problem, according to Eric Siegal, MD, chairman of SHM’s Public Policy Committee and regional medical director for Cogent Healthcare, is how little physicians know about the effects of the new plan. “Everyone understands that this is a dramatic paradigm shift,” he says. “Bundling is a really radical change. It’s going to generate all kinds of consequences—intended and unintended—and no one really has a handle on what’s going to happen.”
The Status Quo Must Change
One of few points of agreement is that the status quo is untenable. A recent summary of MedPAC’s report in The New England Journal of Medicine blamed the fee-for-service model for fueling negative aspects of the current healthcare system and warned of an escalation in Medicare spending. “Fee-for-service payment spurs spending growth, supports a fragmented and compartmentalized delivery system and does nothing to reward quality or value,” the MedPAC authors write.
Though some physicians remain cautiously optimistic about bundling, Dr. Siegal doubts the model is ready for primetime. “Bundling says, ‘Let’s create accountability for outcomes by not paying for single services but for an entire episode of care,’” he says. But many questions remain unanswered. What constitutes an episode? Who controls the allocation of the Medicare payment? If an episode is defined as 30 days from when a patient enters the hospital for a specific procedure, are other health providers accountable for addressing unrelated complaints within the same episode window?
“There are an enormous number of ways you can contort and twist this so you can create scenarios where people come out of it feeling like they have been penalized for behavior well outside their control,” Dr. Siegal says. “I think those are the big risks: imbalance of power and how do you create lines of accountability that actually make sense?”
But, he says, a system that promotes collective responsibility for patients could create a compelling incentive for more collaboration between physicians and consultants. “I think if ‘done right,’ and I say that in quotations because nobody knows what ‘done right’ means,” Dr. Siegal says, “bundling could actually be huge for hospitalists.”
Mary Dallas, MD, medical information officer at Presbyterian Healthcare Services in Albuquerque, N.M., says she’s seen first hand how collaboration among a health plan, a hospital and physicians can improve quality and balance finances. “Those efforts were really spawned out of a forced alignment between all groups in order to focus on common goals,” she says. Bundling could force a similar convergence of priorities.
Transition Troubles
If “alignment” has become the favorite watchword in bundling discussions, “gainsharing” as a concept has been greeted by far more ambivalence. “I oppose gainsharing that puts money directly into the physician’s pocket,” Dr. Dallas says. “This is something that occurs frequently in the free-market world in other industries, and to pay a few for the success that demands participation of many is just wrong in my book.”
Instead, Dr. Dallas supports the idea of directing monetary rewards toward improving infrastructure and the overall healthcare delivery process. As examples, she suggests using the money to buy time from physicians willing to be involved in pilot projects aimed at improving the delivery process, or to add more resources for better patient continuity between the hospital and the community.
Even with a more equitable distribution of resources, she and other hospitalists concede any transition to bundling could be bumpy. “If I were an independent physician, and my personal payment from Medicare was dependent on or tied to the hospital’s performance,” Dr. Dallas says, “there would be a lot of work to prepare me for this.”
As several hospitalists warn, a bundling system could trigger ratcheting down of care—and a whole new set of headaches. “The concern for everyone is that it is going to incentivize physicians to give less services,” says Jonathan Lovins, MD, director of hospitalist and midlevel practitioner services at the Hospital of Central Connecticut, and the brother of Waterbury Hospital’s Dr. Rachel Lovins.
Several hospitalists say the problem could be similar to what happened with Medicare’s capitation system, which gained traction in the 1980s and peaked in the mid-1990s before waning because of a backlash by both providers and patients. This fixed pre-payment reimbursement system, Dr. Lovins says, created an inherent conflict of interest for primary caregivers because referring patients to specialists for tests lowered profits whereas delivering fewer services did not.
Bradley Flansbaum, DO, MPH, FACP, director of hospitalist services at Lenox Hill Hospital in New York City, goes a step further, calling the bundling plan capitation on steroids, and cautions that a one-size-fits-all system is bound to fail. “Having technology and having the intellectual firepower to figure out how this system is going to manage the bundled payment is an advantage,” he says, adding that larger hospitals are more likely to have this advantage. For rural physicians or those within inefficient networks, bundling payments could be disastrous. “CMS may just say, ‘We’re turning on the lights tomorrow and tough,’ but it’s going to be a hell of a mess if they do,” he says.
A Demonstration Project
A demonstration project slated to begin in four states next year may show just how steep that learning curve is. The Acute Care Episode (ACE) Demonstration would bundle virtually all payments of certain orthopedic and cardiovascular inpatient procedures at participating hospitals in Texas, Oklahoma, New Mexico, and Colorado. Hospitals and physicians still would receive separate fee-for-service payments, but a confidential report would detail their resource use. High-resource providers would incur penalties while low-resource providers would receive bonuses.
Dr. Siegal says it makes sense to begin a bundling pilot project with procedures that have defined treatment windows, such as hip replacements or open heart surgery. Other conditions will be far more difficult to contain within a neatly defined episode. “Clearly, we’re going to have to figure out what to do with heart failure and pneumonia and stroke because those are huge consumers of dollars,” he says.
Despite all the caveats and unknowns, hospitalists still may have much to gain if bundling follows in the footsteps of the successful diagnosis-related group (DRG) payment system. “I think that enlightened hospital CEOs are going to be looking to their hospitalists as their champions to really pull this off and make this work,” Dr. Torcson says, particularly as the stakes for hospitals increase.
Medicare’s Physician Quality Reporting Initiative, established by the 2006 Tax Relief and Health Care Act, already links a 1.5% financial incentive to increased performance. With bundled payments adjusted up or down by the proposed gainsharing and penalties for higher readmission rates, Dr. Torcson says, the equivalent of 3% to 5% of DRG payments could be at risk.
“I think it could be something potentially very beneficial to those hospitalist groups that get it right,” he says. “It’s kind of like before the Ice Age comes, if you’ve got your animal skins ready, those are the tribes that survive.” TH
Gretchen Henkel is a medical writer based in California.
The New Intensivists
As critical care workforce shortages continue, and as Medicare enrollment swells—a number slated to increase an estimated 50% by 2030—hospitalists are increasingly filling in the gaps in their institutions’ intensive care units.1-2 In SHM’s 2005-06 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” for example, 75% of participants reported caring for patients in the ICU.3
The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-35% The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-25% shortfall of needed critical care physicians (also called “intensivists”) by 2030. Are hospitalists a viable option to fill the void created by the shortage of intensivists? What is the practice scope of hospitalists in the ICU? Which models work for effective co-management of ICUs and can hospitalists help to deliver round-the-clock coverage in the ICU that the Leapfrog Group safety standards have stipulated should be provided by intensivists?4 According to academic and community-based hospitalists and intensivists, much depends on local demographics and each hospital’s ICU model.
Two Models
Michael A. Gropper, MD, PhD, believes hospitalists are well suited to help manage patients in the critical care unit. At the University of California, San Francisco (UCSF), where Gropper is a professor, vice chair of the Department of Anesthesia and Perioperative Care, and the Medical Center’s director of critical care medicine, the ICU uses a co-management system.
This high-intensity model mandates an intensivist consultation for every patient. In addition, the intensivists conduct procedures, such as ventilator management, placement of central lines, and sedation. The hospital medicine service then handles patient medical management. Hospitalists write orders for antibiotics, nutrition, and fluid management. Splitting the patient management with their hospitalist colleagues allows the intensivists to care for more patients than in a completely “closed” ICU. (In “closed” systems, only intensivists are authorized to care for ICU patients.)
For this model to be effective, however, participating hospitalists should have experience and feel comfortable working in the ICU. “I don’t think you would want to pluck the average hospitalist and throw him into the ICU,” cautions Dr. Gropper. “But a hospitalist who started to consistently spend some time in the ICU would be very good. In collaboration with an intensivist, I think it’s a model that allows high-quality patient care.”
Inpatient Physician Associates, a privately owned hospital medicine group in Lincoln, Neb., headed by Brian Bossard, MD, found a slightly different way to collaborate with a group of intensivists to deliver high-quality care at the city’s two community hospitals, BryanLGH Medical Center and St. Elizabeth Regional Medical Center. Dr. Bossard and Bill Johnson, MD, a pulmonologist certified in intensive care, and director of the ICU at both hospitals, crafted an open ICU model. Although intensivists conduct multidisciplinary rounds at Bryan and St. Elizabeth, consults are not mandatory. Hospitalists provide 24/7 coverage, often placing central lines and doing other procedures. Intensivists are available for consultations and more complicated critical care procedures, such as chest tube placement, Swan-Ganz catheters, and difficult ventilator management.
This system evolved out of necessity; the hospitalist program predated the intensivist program at BryanLGH. “When I started the group, we needed docs who were comfortable in the ICU,” explains Dr. Bossard. With the open ICU model, that requirement still applies today.
When recruiting new hospitalists, Dr. Bossard looks for those who function well in the ICU environment, understand evidence-based practice, and have an aptitude for learning procedures. He also seeks out doctors comfortable with cognitive critical care.
The system seems to work.
“There are many patients who are admitted and discharged from the ICU who don’t require an intensivist’s care,” Dr. Bossard says. Hospitalists in his group cooperatively manage most patients, with intensivist consultation.
“We have a very good collaborative approach here,” says Dr. Johnson, adding that it’s difficult to have a closed ICU at a community hospital because of intensivist shortages and resistance from primary care physicians who want access to their patients. The key to the success of the program in Lincoln is that all physicians know their limits. “We don’t force ICU consults upon anybody,” Dr. Johnson says. “But I think the hospitalists do recognize when it benefits them to have the intensivist involved.”
The proof is in the proverbial pudding. Since the co-managed ICU program began in 2006 in Lincoln, the ICU mortality rate has dropped 50%, and there have been no ventilator-acquired pneumonias or central line-related infections for two years.
Ideals Versus Reality
The Leapfrog Group identified around-the-clock coverage of surgical and medical intensive care units by intensivists as one of its three safety standards.5 “In an ideal world,” says Bradley A. Sharpe, MD, associate division chief in the Division of Hospital Medicine at UCSF, “every critically ill patient would be seen, managed, or co-managed by a critical care specialist.”
David A. Hoffmann, DO, agrees certain standards in the ICU should exist, but says community hospitals will never be able to reproduce the academic model. “They don’t have the labor from residencies,” says Dr. Hoffman, medical director of Hospitalists of Franklin County, an HM group at Chambersburg Hospital, a community hospital in Chambersburg, Pa.
He says his hospitalists fill a crucial gap that intensivists can’t: “We’re the only doctors who are here in the hospital 24 hours a day—besides the ER doctors.”
Dr. Hoffman believes it’s more important to focus on outcomes than to adhere to strict Leapfrog standards. His HM group, comprised of half family medicine-trained, half internal medicine-trained hospitalists, emphasizes teamwork, evidence-based protocols, and bonuses tied to quality outcomes and patient satisfaction.
In many smaller community hospitals, HM groups must do what works to simply provide coverage. Richard Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in Cortland, N.Y, who also works as a hospitalist, says, “The people who are here around the clock are the hospitalists, so they also do the ICU management.” Last summer an intensivist who joined his hospitalist team provided ICU coverage five days a week.
Dr. Rohr believes hospitalists must acquire skills in mechanical ventilation and placement of central lines, and have high-level knowledge of infectious disease. For most ICU patients, however, this type of care is “basically internal medicine pushed to extremes,” he says.
Advantages and Disadvantages of Shared Responsibility
Under a co-managed ICU model, hospitalists can offer benefits beyond their direct time on the unit, says Hugo Quinny Cheng, MD, associate clinical professor in the Division of Hospital Medicine at the University of California at San Francisco. Dr. Cheng says his colleagues can provide more continuous care to patients because they rotate less frequently than do intensivists. In addition, hospitalists may have a broader view of hospital-wide systems and often can maximize ancillary services, such as physical therapy or nutrition, when it’s most appropriate for the patient, Dr. Sharpe adds.
One possible downside to a co-managed ICU, however, is confusion about responsibility. “In a critical care setting, ambiguity can lead to bad outcomes,” says Dr. Sharpe. To avoid this, make all ICU policies and procedures collaborative and involve all providers, including ancillary staff, in the process. “The clearer those guidelines and boundaries are, the easier it is for everyone,” he emphasizes.
For the most part, offering ICU rotations is a useful recruiting, hiring, and retention tool.
“Many hospitalists enjoy critical care and enjoy the opportunity to take care of very ill patients as part of their day-to-day practice, as long as they’re not in over their heads,” Dr. Sharpe says.
Preparation for the Future
Physicians have differing ideas about how intensivist-hospitalist relations will look in the future and what role hospitalists should play in the ICU. R. Neal Axon, MD, assistant professor in the departments of internal medicine and pediatrics at the Medical University of South Carolina in Charleston and a Team Hospitalist member, has worked in both academic and community settings. In the former, a pulmonary critical care specialist with a team of fellows, residents, and students ran the high-intensity ICU. In a local hospital where he worked as an attending, “there was no critical care team, per se. The hospitalists were the critical care team,” he says. “The difference in the care setting was pretty dramatic.”
Dr. Axon believes it might be a better long-term solution (in light of continuing critical care workforce shortages) to pursue formation of a fellowship program that combines advanced training in hospital medicine and critical care medicine.
Robert M. Wachter, MD, professor and chief of the Division of Hospital Medicine, associate chairman of the Department of Medicine, and Lynne and Marc Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco, and author of the “Wachter’s World” blog (www.the-hospitalist.org) says it’s a matter of whether hospitalists have enough intensive care training to work in the ICU.
“My own bias is that they’re probably close enough that they don’t need an extra year of training, but they’re not quite there,” he says.
As a result, UCSF’s HM division developed these strategies to augment hospitalists’ ICU skills:
- A hospitalist mini-college: a small group, hands-on experience, with one full day in the ICU, added to its annual CME course in October (www.ucsfcme. com/2009/MDM09P01A.pdf); and
- The creation of a critical care/hos-pital medicine fellowship that will launch in 2009.
By improving their ICU skills, hospitalists can form collaborative partnerships with their intensivist colleagues—both on the unit and in the critical care committees. This team approach can help their hospitals achieve the attributes of successful intensive care units.
“We have to acknowledge there’s no magic in being a hospitalist or a critical care specialist,” Dr. Axon says. “Individual decisions for individual patients, and the ways in which we all work together to systematize care, are the real differences that affect outcomes.” TH
Gretchen Henkel is a freelance writer based in California and a frequent contributor to The Hospitalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: Can we meet the requirements of an aging population? JAMA December, 2006;284(21):2762-2770.
- White J. Uses and abuses of long-term Medicare cost estimates. Health Aff (Millwood). 1999;18:63-79.
- The Society of Hospital Medicine 2005-2006 Survey: The Authoritative Source on the State of the Hospital Medicine Movement.
- Mello MM, Studdert DM, and Brennan TA. The Leapfrog Standards: Ready to jump from marketplace to courtroom? Health Aff 2003;22(2):46-59.
- Leapfrog Group, The Leapfrog Group Fact Sheet, May 2002. Available at www.leapfroggroup.org/FactSheets/LF_FactSheet.pdf. Last accessed May 28, 2008.
As critical care workforce shortages continue, and as Medicare enrollment swells—a number slated to increase an estimated 50% by 2030—hospitalists are increasingly filling in the gaps in their institutions’ intensive care units.1-2 In SHM’s 2005-06 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” for example, 75% of participants reported caring for patients in the ICU.3
The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-35% The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-25% shortfall of needed critical care physicians (also called “intensivists”) by 2030. Are hospitalists a viable option to fill the void created by the shortage of intensivists? What is the practice scope of hospitalists in the ICU? Which models work for effective co-management of ICUs and can hospitalists help to deliver round-the-clock coverage in the ICU that the Leapfrog Group safety standards have stipulated should be provided by intensivists?4 According to academic and community-based hospitalists and intensivists, much depends on local demographics and each hospital’s ICU model.
Two Models
Michael A. Gropper, MD, PhD, believes hospitalists are well suited to help manage patients in the critical care unit. At the University of California, San Francisco (UCSF), where Gropper is a professor, vice chair of the Department of Anesthesia and Perioperative Care, and the Medical Center’s director of critical care medicine, the ICU uses a co-management system.
This high-intensity model mandates an intensivist consultation for every patient. In addition, the intensivists conduct procedures, such as ventilator management, placement of central lines, and sedation. The hospital medicine service then handles patient medical management. Hospitalists write orders for antibiotics, nutrition, and fluid management. Splitting the patient management with their hospitalist colleagues allows the intensivists to care for more patients than in a completely “closed” ICU. (In “closed” systems, only intensivists are authorized to care for ICU patients.)
For this model to be effective, however, participating hospitalists should have experience and feel comfortable working in the ICU. “I don’t think you would want to pluck the average hospitalist and throw him into the ICU,” cautions Dr. Gropper. “But a hospitalist who started to consistently spend some time in the ICU would be very good. In collaboration with an intensivist, I think it’s a model that allows high-quality patient care.”
Inpatient Physician Associates, a privately owned hospital medicine group in Lincoln, Neb., headed by Brian Bossard, MD, found a slightly different way to collaborate with a group of intensivists to deliver high-quality care at the city’s two community hospitals, BryanLGH Medical Center and St. Elizabeth Regional Medical Center. Dr. Bossard and Bill Johnson, MD, a pulmonologist certified in intensive care, and director of the ICU at both hospitals, crafted an open ICU model. Although intensivists conduct multidisciplinary rounds at Bryan and St. Elizabeth, consults are not mandatory. Hospitalists provide 24/7 coverage, often placing central lines and doing other procedures. Intensivists are available for consultations and more complicated critical care procedures, such as chest tube placement, Swan-Ganz catheters, and difficult ventilator management.
This system evolved out of necessity; the hospitalist program predated the intensivist program at BryanLGH. “When I started the group, we needed docs who were comfortable in the ICU,” explains Dr. Bossard. With the open ICU model, that requirement still applies today.
When recruiting new hospitalists, Dr. Bossard looks for those who function well in the ICU environment, understand evidence-based practice, and have an aptitude for learning procedures. He also seeks out doctors comfortable with cognitive critical care.
The system seems to work.
“There are many patients who are admitted and discharged from the ICU who don’t require an intensivist’s care,” Dr. Bossard says. Hospitalists in his group cooperatively manage most patients, with intensivist consultation.
“We have a very good collaborative approach here,” says Dr. Johnson, adding that it’s difficult to have a closed ICU at a community hospital because of intensivist shortages and resistance from primary care physicians who want access to their patients. The key to the success of the program in Lincoln is that all physicians know their limits. “We don’t force ICU consults upon anybody,” Dr. Johnson says. “But I think the hospitalists do recognize when it benefits them to have the intensivist involved.”
The proof is in the proverbial pudding. Since the co-managed ICU program began in 2006 in Lincoln, the ICU mortality rate has dropped 50%, and there have been no ventilator-acquired pneumonias or central line-related infections for two years.
Ideals Versus Reality
The Leapfrog Group identified around-the-clock coverage of surgical and medical intensive care units by intensivists as one of its three safety standards.5 “In an ideal world,” says Bradley A. Sharpe, MD, associate division chief in the Division of Hospital Medicine at UCSF, “every critically ill patient would be seen, managed, or co-managed by a critical care specialist.”
David A. Hoffmann, DO, agrees certain standards in the ICU should exist, but says community hospitals will never be able to reproduce the academic model. “They don’t have the labor from residencies,” says Dr. Hoffman, medical director of Hospitalists of Franklin County, an HM group at Chambersburg Hospital, a community hospital in Chambersburg, Pa.
He says his hospitalists fill a crucial gap that intensivists can’t: “We’re the only doctors who are here in the hospital 24 hours a day—besides the ER doctors.”
Dr. Hoffman believes it’s more important to focus on outcomes than to adhere to strict Leapfrog standards. His HM group, comprised of half family medicine-trained, half internal medicine-trained hospitalists, emphasizes teamwork, evidence-based protocols, and bonuses tied to quality outcomes and patient satisfaction.
In many smaller community hospitals, HM groups must do what works to simply provide coverage. Richard Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in Cortland, N.Y, who also works as a hospitalist, says, “The people who are here around the clock are the hospitalists, so they also do the ICU management.” Last summer an intensivist who joined his hospitalist team provided ICU coverage five days a week.
Dr. Rohr believes hospitalists must acquire skills in mechanical ventilation and placement of central lines, and have high-level knowledge of infectious disease. For most ICU patients, however, this type of care is “basically internal medicine pushed to extremes,” he says.
Advantages and Disadvantages of Shared Responsibility
Under a co-managed ICU model, hospitalists can offer benefits beyond their direct time on the unit, says Hugo Quinny Cheng, MD, associate clinical professor in the Division of Hospital Medicine at the University of California at San Francisco. Dr. Cheng says his colleagues can provide more continuous care to patients because they rotate less frequently than do intensivists. In addition, hospitalists may have a broader view of hospital-wide systems and often can maximize ancillary services, such as physical therapy or nutrition, when it’s most appropriate for the patient, Dr. Sharpe adds.
One possible downside to a co-managed ICU, however, is confusion about responsibility. “In a critical care setting, ambiguity can lead to bad outcomes,” says Dr. Sharpe. To avoid this, make all ICU policies and procedures collaborative and involve all providers, including ancillary staff, in the process. “The clearer those guidelines and boundaries are, the easier it is for everyone,” he emphasizes.
For the most part, offering ICU rotations is a useful recruiting, hiring, and retention tool.
“Many hospitalists enjoy critical care and enjoy the opportunity to take care of very ill patients as part of their day-to-day practice, as long as they’re not in over their heads,” Dr. Sharpe says.
Preparation for the Future
Physicians have differing ideas about how intensivist-hospitalist relations will look in the future and what role hospitalists should play in the ICU. R. Neal Axon, MD, assistant professor in the departments of internal medicine and pediatrics at the Medical University of South Carolina in Charleston and a Team Hospitalist member, has worked in both academic and community settings. In the former, a pulmonary critical care specialist with a team of fellows, residents, and students ran the high-intensity ICU. In a local hospital where he worked as an attending, “there was no critical care team, per se. The hospitalists were the critical care team,” he says. “The difference in the care setting was pretty dramatic.”
Dr. Axon believes it might be a better long-term solution (in light of continuing critical care workforce shortages) to pursue formation of a fellowship program that combines advanced training in hospital medicine and critical care medicine.
Robert M. Wachter, MD, professor and chief of the Division of Hospital Medicine, associate chairman of the Department of Medicine, and Lynne and Marc Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco, and author of the “Wachter’s World” blog (www.the-hospitalist.org) says it’s a matter of whether hospitalists have enough intensive care training to work in the ICU.
“My own bias is that they’re probably close enough that they don’t need an extra year of training, but they’re not quite there,” he says.
As a result, UCSF’s HM division developed these strategies to augment hospitalists’ ICU skills:
- A hospitalist mini-college: a small group, hands-on experience, with one full day in the ICU, added to its annual CME course in October (www.ucsfcme. com/2009/MDM09P01A.pdf); and
- The creation of a critical care/hos-pital medicine fellowship that will launch in 2009.
By improving their ICU skills, hospitalists can form collaborative partnerships with their intensivist colleagues—both on the unit and in the critical care committees. This team approach can help their hospitals achieve the attributes of successful intensive care units.
“We have to acknowledge there’s no magic in being a hospitalist or a critical care specialist,” Dr. Axon says. “Individual decisions for individual patients, and the ways in which we all work together to systematize care, are the real differences that affect outcomes.” TH
Gretchen Henkel is a freelance writer based in California and a frequent contributor to The Hospitalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: Can we meet the requirements of an aging population? JAMA December, 2006;284(21):2762-2770.
- White J. Uses and abuses of long-term Medicare cost estimates. Health Aff (Millwood). 1999;18:63-79.
- The Society of Hospital Medicine 2005-2006 Survey: The Authoritative Source on the State of the Hospital Medicine Movement.
- Mello MM, Studdert DM, and Brennan TA. The Leapfrog Standards: Ready to jump from marketplace to courtroom? Health Aff 2003;22(2):46-59.
- Leapfrog Group, The Leapfrog Group Fact Sheet, May 2002. Available at www.leapfroggroup.org/FactSheets/LF_FactSheet.pdf. Last accessed May 28, 2008.
As critical care workforce shortages continue, and as Medicare enrollment swells—a number slated to increase an estimated 50% by 2030—hospitalists are increasingly filling in the gaps in their institutions’ intensive care units.1-2 In SHM’s 2005-06 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” for example, 75% of participants reported caring for patients in the ICU.3
The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-35% The Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) has predicted a 22-25% shortfall of needed critical care physicians (also called “intensivists”) by 2030. Are hospitalists a viable option to fill the void created by the shortage of intensivists? What is the practice scope of hospitalists in the ICU? Which models work for effective co-management of ICUs and can hospitalists help to deliver round-the-clock coverage in the ICU that the Leapfrog Group safety standards have stipulated should be provided by intensivists?4 According to academic and community-based hospitalists and intensivists, much depends on local demographics and each hospital’s ICU model.
Two Models
Michael A. Gropper, MD, PhD, believes hospitalists are well suited to help manage patients in the critical care unit. At the University of California, San Francisco (UCSF), where Gropper is a professor, vice chair of the Department of Anesthesia and Perioperative Care, and the Medical Center’s director of critical care medicine, the ICU uses a co-management system.
This high-intensity model mandates an intensivist consultation for every patient. In addition, the intensivists conduct procedures, such as ventilator management, placement of central lines, and sedation. The hospital medicine service then handles patient medical management. Hospitalists write orders for antibiotics, nutrition, and fluid management. Splitting the patient management with their hospitalist colleagues allows the intensivists to care for more patients than in a completely “closed” ICU. (In “closed” systems, only intensivists are authorized to care for ICU patients.)
For this model to be effective, however, participating hospitalists should have experience and feel comfortable working in the ICU. “I don’t think you would want to pluck the average hospitalist and throw him into the ICU,” cautions Dr. Gropper. “But a hospitalist who started to consistently spend some time in the ICU would be very good. In collaboration with an intensivist, I think it’s a model that allows high-quality patient care.”
Inpatient Physician Associates, a privately owned hospital medicine group in Lincoln, Neb., headed by Brian Bossard, MD, found a slightly different way to collaborate with a group of intensivists to deliver high-quality care at the city’s two community hospitals, BryanLGH Medical Center and St. Elizabeth Regional Medical Center. Dr. Bossard and Bill Johnson, MD, a pulmonologist certified in intensive care, and director of the ICU at both hospitals, crafted an open ICU model. Although intensivists conduct multidisciplinary rounds at Bryan and St. Elizabeth, consults are not mandatory. Hospitalists provide 24/7 coverage, often placing central lines and doing other procedures. Intensivists are available for consultations and more complicated critical care procedures, such as chest tube placement, Swan-Ganz catheters, and difficult ventilator management.
This system evolved out of necessity; the hospitalist program predated the intensivist program at BryanLGH. “When I started the group, we needed docs who were comfortable in the ICU,” explains Dr. Bossard. With the open ICU model, that requirement still applies today.
When recruiting new hospitalists, Dr. Bossard looks for those who function well in the ICU environment, understand evidence-based practice, and have an aptitude for learning procedures. He also seeks out doctors comfortable with cognitive critical care.
The system seems to work.
“There are many patients who are admitted and discharged from the ICU who don’t require an intensivist’s care,” Dr. Bossard says. Hospitalists in his group cooperatively manage most patients, with intensivist consultation.
“We have a very good collaborative approach here,” says Dr. Johnson, adding that it’s difficult to have a closed ICU at a community hospital because of intensivist shortages and resistance from primary care physicians who want access to their patients. The key to the success of the program in Lincoln is that all physicians know their limits. “We don’t force ICU consults upon anybody,” Dr. Johnson says. “But I think the hospitalists do recognize when it benefits them to have the intensivist involved.”
The proof is in the proverbial pudding. Since the co-managed ICU program began in 2006 in Lincoln, the ICU mortality rate has dropped 50%, and there have been no ventilator-acquired pneumonias or central line-related infections for two years.
Ideals Versus Reality
The Leapfrog Group identified around-the-clock coverage of surgical and medical intensive care units by intensivists as one of its three safety standards.5 “In an ideal world,” says Bradley A. Sharpe, MD, associate division chief in the Division of Hospital Medicine at UCSF, “every critically ill patient would be seen, managed, or co-managed by a critical care specialist.”
David A. Hoffmann, DO, agrees certain standards in the ICU should exist, but says community hospitals will never be able to reproduce the academic model. “They don’t have the labor from residencies,” says Dr. Hoffman, medical director of Hospitalists of Franklin County, an HM group at Chambersburg Hospital, a community hospital in Chambersburg, Pa.
He says his hospitalists fill a crucial gap that intensivists can’t: “We’re the only doctors who are here in the hospital 24 hours a day—besides the ER doctors.”
Dr. Hoffman believes it’s more important to focus on outcomes than to adhere to strict Leapfrog standards. His HM group, comprised of half family medicine-trained, half internal medicine-trained hospitalists, emphasizes teamwork, evidence-based protocols, and bonuses tied to quality outcomes and patient satisfaction.
In many smaller community hospitals, HM groups must do what works to simply provide coverage. Richard Rohr, MD, vice president for medical affairs at Cortland Regional Medical Center in Cortland, N.Y, who also works as a hospitalist, says, “The people who are here around the clock are the hospitalists, so they also do the ICU management.” Last summer an intensivist who joined his hospitalist team provided ICU coverage five days a week.
Dr. Rohr believes hospitalists must acquire skills in mechanical ventilation and placement of central lines, and have high-level knowledge of infectious disease. For most ICU patients, however, this type of care is “basically internal medicine pushed to extremes,” he says.
Advantages and Disadvantages of Shared Responsibility
Under a co-managed ICU model, hospitalists can offer benefits beyond their direct time on the unit, says Hugo Quinny Cheng, MD, associate clinical professor in the Division of Hospital Medicine at the University of California at San Francisco. Dr. Cheng says his colleagues can provide more continuous care to patients because they rotate less frequently than do intensivists. In addition, hospitalists may have a broader view of hospital-wide systems and often can maximize ancillary services, such as physical therapy or nutrition, when it’s most appropriate for the patient, Dr. Sharpe adds.
One possible downside to a co-managed ICU, however, is confusion about responsibility. “In a critical care setting, ambiguity can lead to bad outcomes,” says Dr. Sharpe. To avoid this, make all ICU policies and procedures collaborative and involve all providers, including ancillary staff, in the process. “The clearer those guidelines and boundaries are, the easier it is for everyone,” he emphasizes.
For the most part, offering ICU rotations is a useful recruiting, hiring, and retention tool.
“Many hospitalists enjoy critical care and enjoy the opportunity to take care of very ill patients as part of their day-to-day practice, as long as they’re not in over their heads,” Dr. Sharpe says.
Preparation for the Future
Physicians have differing ideas about how intensivist-hospitalist relations will look in the future and what role hospitalists should play in the ICU. R. Neal Axon, MD, assistant professor in the departments of internal medicine and pediatrics at the Medical University of South Carolina in Charleston and a Team Hospitalist member, has worked in both academic and community settings. In the former, a pulmonary critical care specialist with a team of fellows, residents, and students ran the high-intensity ICU. In a local hospital where he worked as an attending, “there was no critical care team, per se. The hospitalists were the critical care team,” he says. “The difference in the care setting was pretty dramatic.”
Dr. Axon believes it might be a better long-term solution (in light of continuing critical care workforce shortages) to pursue formation of a fellowship program that combines advanced training in hospital medicine and critical care medicine.
Robert M. Wachter, MD, professor and chief of the Division of Hospital Medicine, associate chairman of the Department of Medicine, and Lynne and Marc Benioff Endowed Chair in Hospital Medicine at the University of California at San Francisco, and author of the “Wachter’s World” blog (www.the-hospitalist.org) says it’s a matter of whether hospitalists have enough intensive care training to work in the ICU.
“My own bias is that they’re probably close enough that they don’t need an extra year of training, but they’re not quite there,” he says.
As a result, UCSF’s HM division developed these strategies to augment hospitalists’ ICU skills:
- A hospitalist mini-college: a small group, hands-on experience, with one full day in the ICU, added to its annual CME course in October (www.ucsfcme. com/2009/MDM09P01A.pdf); and
- The creation of a critical care/hos-pital medicine fellowship that will launch in 2009.
By improving their ICU skills, hospitalists can form collaborative partnerships with their intensivist colleagues—both on the unit and in the critical care committees. This team approach can help their hospitals achieve the attributes of successful intensive care units.
“We have to acknowledge there’s no magic in being a hospitalist or a critical care specialist,” Dr. Axon says. “Individual decisions for individual patients, and the ways in which we all work together to systematize care, are the real differences that affect outcomes.” TH
Gretchen Henkel is a freelance writer based in California and a frequent contributor to The Hospitalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: Can we meet the requirements of an aging population? JAMA December, 2006;284(21):2762-2770.
- White J. Uses and abuses of long-term Medicare cost estimates. Health Aff (Millwood). 1999;18:63-79.
- The Society of Hospital Medicine 2005-2006 Survey: The Authoritative Source on the State of the Hospital Medicine Movement.
- Mello MM, Studdert DM, and Brennan TA. The Leapfrog Standards: Ready to jump from marketplace to courtroom? Health Aff 2003;22(2):46-59.
- Leapfrog Group, The Leapfrog Group Fact Sheet, May 2002. Available at www.leapfroggroup.org/FactSheets/LF_FactSheet.pdf. Last accessed May 28, 2008.