User login
Laparoscopic challenges: The large uterus
The authors report no financial relationships relevant to this article.
CASE: Large fibroid uterus. Is laparoscopy feasible?
A 41-year-old woman known to have uterine fibroids consults you after two other gynecologists have recommended abdominal hysterectomy. She weighs 320 lb, stands 5 ft 2 in, and is nulliparous and sexually inactive. Pelvic ultrasonography reveals multiple fibroids approximating 18 weeks’ gestational size. Although she has hypertension and reactive airway disease, these conditions are well controlled by medication. Her Pap smear and endometrial biopsy are negative.
Because her professional commitments limit her time for recovery, she hopes to bypass abdominal hysterectomy in favor of the laparoscopic approach.
Is this desire realistic?
Twenty years have passed since Reich performed the first total laparoscopic hysterectomy,1 but only a small percentage of hysterectomies performed in the United States utilize that approach. In 2003, 12% of 602,457 hysterectomies were done laparoscopically; the rest were performed using the abdominal or vaginal approach (66% and 22%, respectively).2
Yet laparoscopic hysterectomy has much to recommend it. Compared with abdominal hysterectomy, it involves a shorter hospital stay, less blood loss, a speedier return to normal activities, and fewer wound infections.3 Unlike vaginal hysterectomy, it also facilitates intra-abdominal inspection.
Although the opening case represents potentially difficult surgery because of the size of the uterus, the laparoscopic approach is feasible. When the uterus weighs more than 450 g, contains fibroids larger than 6 cm, or exceeds 12 to 14 cm in size,4-7 there is an increased risk of visceral injury, bleeding necessitating transfusion, prolonged operative time, and conversion to laparotomy. This article describes techniques that simplify laparoscopic management when the uterus exceeds 14 weeks’ size. By incorporating these techniques, we have performed laparoscopic hysterectomy in uteri as large as 22 to 24 weeks’ size without increased complications.
In Part 2 of this article, we address techniques that simplify laparoscopy when extensive intra-abdominal adhesions are present.
Why do some surgeons avoid laparoscopy?
Major complications occur in approximately 5% to 6% of women who undergo total laparoscopic hysterectomy.8,9 That is one of the reasons many surgeons who perform laparoscopic procedures revert to the more traditional vaginal or abdominal approach when faced with a potentially difficult hysterectomy. These surgeons cite uteri larger than 14 weeks’ size, extensive intra-abdominal adhesions, and morbid obesity as common indications for a more conservative approach. Others cite the limitations of working with inexperienced surgeons or residents, inadequate laparoscopic instruments, and distorted pelvic anatomy. Still others avoid laparoscopy when the patient has medical problems that preclude use of pneumoperitoneum or a steep Trendelenburg position.
In some cases, laparoscopic hysterectomy is simply not practical. In others, however, such as the presence of a large uterus, it can be achieved with attention to detail, a few key techniques, and proper counseling of the patient.
Success begins preop
All surgical decisions begin with the patient. A comprehensive preoperative discussion of pertinent management options allows both patient and surgeon to proceed with confidence. Easing the patient’s preoperative anxiety is important. It can be achieved by explaining what to expect—not only the normal recovery for laparoscopic hysterectomy, but also the expected recovery if it becomes necessary to convert to laparotomy. If the patient has clear expectations, unexpected outcomes such as conversion are better tolerated. When it comes down to a choice between the surgeon’s ego or patient safety, the patient always wins. Conversion is not failure.
Another important topic to discuss with the patient is the risk of bowel injury. Mechanical bowel preparation is not essential for every patient who undergoes laparoscopic hysterectomy, but the risk of injury to the bowel necessitating colorectal surgical assistance may be heightened in women who have a large uterus or extensive intra-abdominal adhesions. Because of this risk, mechanical bowel preparation with oral polyethylene glycol solution or sodium phosphate should be considered. Most patients prefer the latter.10
What data show about bowel preps
The literature provides conflicting messages about the effectiveness of mechanical bowel preparation in averting additional complications when bowel injury occurs. Nichols and colleagues surveyed 808 active board-certified colorectal surgeons in the United States and Canada in 1995.11 All of the 471 (58%) surgeons who responded reported using some form of mechanical bowel preparation for their elective and emergency colorectal procedures.
Zmora and associates described the difficulty of designing a multicenter study to evaluate the role of mechanical bowel preparation in patient outcome.10 Of the many variables that warrant consideration, surgical technique was the single most important factor influencing surgical outcome.
In a review of evidence supporting the need for prophylactic mechanical bowel preparation prior to elective colorectal surgery, Guenaga and colleagues concluded that this practice is unsupported by the data.12
Bottom line. Given these data, the gynecologist wanting to practice evidence-based medicine should base his or her recommendations about bowel preparation on the preferences of the general or colorectal surgeon who will be called if a bowel injury occurs.
Don’t forget the team
After preparing the patient, prepare your support team—the operating room (OR) and anesthesia staffs. The OR staff should ensure that extra sutures, instruments, and retractors are unopened, in the room, and available in case conversion is necessary. Inform the anesthesia staff of your anticipated surgical time and potential pitfalls. Let them know you will need maximum Trendelenburg position for pelvic exposure, but remain flexible if the patient has trouble with oxygenation and ventilation. Making your anesthesiologist aware of your willingness to work together will benefit both you and your patient immensely.
Preparation continues in the OR
Appropriate patient positioning is key to successful completion of difficult laparoscopic cases. Position the patient’s buttocks several inches beyond the table break to facilitate maximal uterine manipulation, which may be needed for completion of the colpotomy.
Place the patient in the dorsal lithotomy position using Allen stirrups, with the knees flexed at a 90° angle. Keep the knees level with the hips and the hips extended neutrally.
Arm position is important to maximize room for the surgeon alongside the OR table. Space is limited when the patient’s arms are positioned on arm boards. Tucking the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, improves the surgical field and secures the patient to the OR table (FIGURE 1). Protect the elbows and hands with cushions.
Place sequential compression devices (on the calf or foot) for the duration of the procedure to minimize the risk of blood stasis and clots that sometimes develop in the legs with prolonged surgical times. Many complex laparoscopic cases last longer than 2 hours.

FIGURE 1 Positioning the patient
Tuck the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, to improve the surgical field.
Maximum Trendelenburg position is a must
This positioning is essential for successful anatomic exposure in complex laparoscopic surgical cases. If the patient is positioned securely, maximum Trendelenburg position does not increase the risk of the patient sliding off the OR table, nor does it affect oxygenation in most morbidly obese patients. Rather, it allows the intestines to drop out of the pelvis into the upper abdomen, facilitating visualization and decreasing the risk of bowel injury.
Anesthesia staffers often limit the degree of Trendelenburg position unless the surgeon insists otherwise. Alternating patient position between maximum Trendelenburg for optimal surgical exposure and a less steep angle when patient oxygenation requires it allows the gynecologic surgeon and anesthesiologist to work together in the patient’s best interest.
Video monitor placement is key
It helps determine how efficiently you operate. Use of a single central monitor requires both the surgeon and assistant to turn their heads acutely during prolonged procedures, accelerating their fatigue and potentially increasing the risk of injury. Using two monitors—each placed to allow the surgeon and assistant to maintain neutral head position—minimizes fatigue and its attendant risks.
Entering the abdomen
Abdominal entry poses theoretical obstacles when the patient has a large uterus, but all types of entry remain safe as long as laparoscopic surgical principles are followed scrupulously. We have successfully used traditional Veress needle entry, open laparoscopic entry, and left upper quadrant entry.
Is entry above the umbilicus helpful?
Anecdotal reports suggest a midline port above the umbilicus when the uterus extends above the umbilicus, but we do not alter standard port placement in these cases. By tenting the abdominal wall at the umbilicus, we create adequate distance to achieve pneumoperitoneum and space for directed trocar entry to avoid injury to the uterus. The conventional umbilical primary port allows use of standard-length instruments. The cephalad uterine blood supply (infundibulopelvic ligament vessels or utero-ovarian ligament vessels) remains at or below the level of the umbilicus in almost all of these patients.
Port placement in the patient who has a large uterus is the same as it is for other laparoscopic hysterectomies in our practice. We use an 11-mm trocar at the umbilicus for a 10-mm endoscope. We use the 10-mm endoscope because the light it provides to the surgical field is superior to that of a 5-mm endoscope, and the 10-mm scope is more durable.
We place a 5-mm trocar just above the anterior iliac crest on each side, lateral to the ascending inferior epigastric vessels (FIGURE 2). We place an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port on the side of the primary surgeon. This trocar serves a dual purpose: It is the primary port for the surgeon, and removal of the trocar sleeve later in the procedure allows for easy insertion of the morcellator.
Some patients will require a fifth port on the side opposite the primary surgeon to allow better access to the uterine blood supply or to facilitate uterine manipulation.
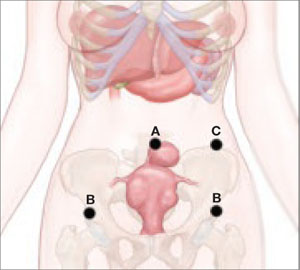
FIGURE 2 Port placement when the uterus is large
A midline umbilical port (A) is possible even when the uterus is large. Other ports include a 5-mm trocar just above the anterior iliac crest on each side (B), and an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port nearest the primary surgeon (C).
Why an angled scope is superior
Many gynecologists fear laparoscopic surgery in patients who have a large uterus. The reason? Poor visualization of the surgical field. However, the type of endoscope that is used has a bearing on visualization.
Most gynecologists are trained to use a 0° endoscope for laparoscopic surgery. However, when the uterus is large, the 0° scope yields an inadequate field of view, whether the endoscope is placed at the umbilicus or through a lateral port. Critical structures like the vascular bundles, ureters, and even the bladder may be inadequately visualized using the 0° endoscope (FIGURE 3).
Gynecologists routinely use angled scopes in hysteroscopy and cystoscopy, but tend to avoid them in laparoscopy because of difficulty orienting the surgical field. As gynecologists, we readily accept that use of an angled scope in hysteroscopy and cystoscopy requires rotation of the scope while the camera maintains its horizontal position. The same concept applies to laparoscopy.
Use of the angled scope in the abdomen is a two-step process. First, it must be rotated to achieve the desired field of view. Then, as the endoscope is held firmly to maintain this view, the camera head must be rotated on the scope to return the field to a horizontal position.
Many surgeons find this action difficult because they or the assistant are holding the camera in one hand and an instrument in the other. We solve this problem by using a mechanical scope holder to secure the camera and endoscope in the position we desire.
In some cases, the camera head does not attach securely to the eyepiece, and the scope rotates on the camera as soon as it is released. This difficulty arises when the eyepiece of the endoscope is slightly smaller than the camera attachment. The problem is easily solved by placing a small piece of surgical skin closure tape on one edge of the eyepiece, slightly increasing its diameter. The camera attachment then holds the scope securely.
Human scope holders may tire during long cases, causing field drift at critical moments. In contrast, a mechanical scope holder is easily and intermittently adjusted for field of view, producing a steady field of view and minimizing the impact of manual manipulation of the scope on surgical outcome. It also allows the surgeon and first assistant to use two hands while operating.
General surgeons and urologists often use 30° endoscopes. Gynecologists working in the pelvis see better using a 45° scope (FIGURE 3). Most ORs offer a 30° endoscope but do not always have a 45° endoscope available in the instrument room. This is regrettable. Compared with the 30° scope, the 45° instrument provides better visual access to the low lateral uterine blood supply and bladder flap, particularly when the patient has a globular uterus or large, low anterior fibroid. We include both 5-mm and 10-mm 45° endoscopes in our laparoscopic tool chest, and believe they are essential options.
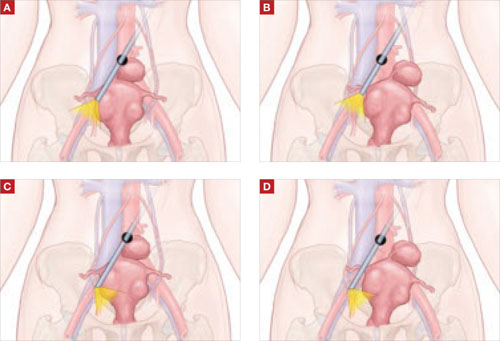
FIGURE 3 The 45° laparoscope provides better visual access
(A) 0° scope, uterus midline: Right broad ligament view obstructed. (B) 0° scope, uterus to left: Right broad ligament view still obstructed. (C) 45° scope, uterus midline: Right broad ligament view improved. (D) 45° scope, uterus to left: Right broad ligament view optimal.
Control the blood supply
Our laparoscopic approach is very similar to our technique for abdominal hysterectomy, beginning with the blood supply. The main blood supply to the uterus enters at only four points. If this blood supply is adequately controlled, morcellation of the large uterus can proceed without excessive blood loss.
Visualization of the blood supply is normally restricted because of tense, taut round ligaments that limit mobility of the large uterus. A simple step to improve mobility is to transect each round ligament in its middle position before addressing the uterine blood supply.
If the ovaries are being conserved, transect the utero-ovarian ligament and tube as close to the ovary as possible with your instrument and technique of choice (electrical or mechanical energy, etc); they all work. Stay close to the ovary to avert bleeding that might otherwise occur when the ascending uterine vascular coils are cut tangentially.
If the ovaries are being removed, transect the infundibulopelvic ligament close to the ovary, being careful not to include ovarian tissue in the pedicle. Use your method of choice, but relieve tension on the pedicle as it is being transected to minimize the risk of pedicle bleeding.
Now, 20% to 40% of the uterine blood supply is controlled, with minimal blood loss.
The key to controlling the remaining blood supply is transecting the ascending vascular bundle as low as possible on either side. The 45° endoscope provides optimal visualization for this part of the procedure. Many times the field of view attained using the 45° endoscope is all that is necessary to facilitate occlusion and transection of these vessels at the level of the internal cervical os.
We commonly use ultrasonic energy to coagulate and cut the ascending vascular bundle. Ultrasonic energy provides excellent hemostasis for this part of the procedure. Again, use the technique of your choice.
Use a laparoscopic “leash”
At times, large broad-ligament fibroids obscure the field of view and access to the ascending vascular bundle. Standard laparoscopic graspers cannot maintain a firm hold on the tissue to improve visibility or access. The solution? A laparoscopic “leash,” first described in 1999 by Tsin and colleagues.13
Giesler extended that concept with a “puppet string” variation to maximize exposure in difficult cases. To apply the “puppet string” technique, using No. 1 Prolene suture, place a large figure-of-eight suture through the tissue to be retracted (FIGURE 4). Bring the suture out of the abdomen adjacent to the trocar sleeve in a location that provides optimal traction. (First, bring the suture through the trocar sleeve. Then remove the trocar sleeve and reinsert it adjacent to the retraction suture.) This secure attachment allows better visualization and greater access to the blood supply at a lower level. It also is possible to manipulate this suture inside the abdomen using traditional graspers to provide reliable repositioning of the uterus. This degree of tissue control improves field of vision and allows the procedure to advance smoothly.
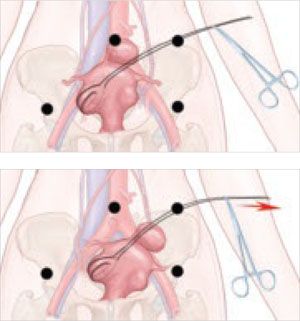
FIGURE 4 A “puppet string” improves access
This secure attachment allows better visualization and greater access to the blood supply at a lower level. Manipulation of this suture inside the abdomen using traditional graspers also helps reposition the uterus.
Morcellation techniques
Once the ascending blood supply has been managed on both sides, morcellation can be performed with minimal blood loss using one of two techniques:
- Amputate the body of the uterus above the level where the blood supply has been interrupted
- Morcellate the uterine body to a point just above the level where the blood supply has been interrupted.
Use basic principles, regardless of the technique chosen
- Hold the morcellator in one hand and a toothed grasper in the other hand to pull tissue into the morcellator. Do not push the morcellator into tissue or you may injure nonvisualized structures on the other side.
- Morcellate tissue in half-moon portions, skimming along the top of the fundus, instead of coring the uterus like an apple; it creates longer strips of tissue and is faster. This technique also allows continuous observation of the active blade, which helps avoid inadvertent injury to tissues behind the blade.
- Attempt morcellation in the anterior abdominal space to avoid injury to blood vessels, ureters, and bowel in the posterior abdominal space. The assistant feeds uterine tissue to the surgeon in the anterior space.
It is essential to control the blood supply to the tissue to be morcellated before morcellation to avoid massive hemorrhage.
Amputating the upper uterine body
Amputation of the large body of the uterus from the lower uterine segment assures complete control of the blood supply and avoids further blood loss during morcellation, but it also poses difficulties. The free uterine mass is held in position by the assistant using only one grasper. If this grasper slips, the mass can be inadvertently released while the morcellator blade is active. If the assistant is also holding the camera, there are no options for stabilizing the free uterine mass. If a mechanical scope holder or second assistant is available to hold the camera, a second trocar port can be placed on the side of the assistant to provide access for a second grasper to stabilize the uterine body during morcellation. The need for a stable uterine mass is important to minimize the risk of injury.
Once the upper body of the uterus has been removed by morcellation, the lower uterine segment and cervix must be removed—using your procedure of choice—to finish the hysterectomy.
Morcellating the upper uterine body
If the uterus remains attached to the cervix, it already has one fixed point of stability. During morcellation, the assistant has one hand available to direct the camera. Blood loss during morcellation of the uterus while it is still attached to the cervix is minimal because the ascending vascular bundles on either side have been interrupted under direct vision.
For greater control of the large uterus, a second port can be placed on the assistant’s side for a second grasper, as described above. Most of the large uterus that is still connected to the cervix can be morcellated in the anterior abdominal space in horizontal fashion, as for the free uterine mass just described.
Uterine manipulation by the assistant keeps the uterus away from critical structures as it is reduced to 8 to 10 weeks’ size. Once this size is attained, resume normal technique for total laparoscopic hysterectomy to separate the remaining tissue from the vagina.
2 types of morcellators in use today
One has a disposable 15-mm blade that attaches to a drive unit adjacent to the OR table (Gynecare-Ethicon Women’s Health and Urology). The other has a sterile, reusable drive unit with a disposable blade (Storz). Both work well on large uteri.
The reusable drive unit has more power to morcellate calcified fibroids and offers a choice between 12-mm, 15-mm, and 20-mm disposable blades for faster morcellation.
Concluding the procedure
Chips of fibroid and uterine tissue created during morcellation often remain in the pelvis after the uterus has been removed. Place them in a 10-cm specimen-collection bag and extract it through the vagina after removal of the residual uterus and cervix. This is faster and easier than recovering them one at a time with the gall bladder stone scoop through a trocar port. The value of the OR time saved with use of the specimen-collection bag is significantly greater than that of the disposable collection device.
CASE RESOLVED
You perform total laparoscopic hysterectomy and find 6-cm fibroids in both broad ligament areas and over the cervical–vaginal junction on the left. You use a “puppet string” to apply directed traction to the fibroids to simplify their extraction. The 45° endoscope allows clear visualization of the ascending vascular bundle on both sides, and the mechanical scope holder allows a fixed field of view for the meticulous dissection required to remove the broad-ligament fibroids.
You morcellate the entire 663-g uterus and remove it in pieces through the abdominal wall. The extensive morcellation required, coupled with technical issues related to the patient’s morbid obesity, prolong the procedure to more than 4 hours.
Postoperatively, the patient voids without a catheter, walks around the nursing unit, and eats half a sandwich within 4 hours. She is discharged home in less than 24 hours and is able to drive 4 days after her surgery.
1. Reich H, DeCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989;5:213-216.
2. Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091-1095.
3. Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD003677.-
4. Leonard F, Chopin N, Borghese B, et al. Total laparoscopic hysterectomy: preoperative risk factors for conversion to laparotomy. J Minim Invasive Gynecol. 2005;12:312-317.
5. Fiaccavento A, Landi S, Barbieri F, et al. Total laparoscopic hysterectomy in cases of very large uteri: a retrospective comparative study. J Minim Invasive Gynecol. 2007;14:559-563.
6. Pelosi MA, Kadar N. Laparoscopically assisted hysterectomy for uteri weighing 500 g or more. J Am Assoc Gynecol Laparosc. 1994;1:405-409.
7. Seracchioli R, Venturoli S, Vianello F, et al. Total laparoscopic hysterectomy compared with abdominal hysterectomy in the presence of a large uterus. J Am Assoc Gynecol Laparosc. 2002;9:333-338.
8. Hoffman CP, Kennedy J, Borschel L, Burchette R, Kidd A. Laparoscopic hysterectomy: the Kaiser Permanente San Diego experience. J Minim Invasive Gynecol. 2005;12:16-24.
9. Liu CY, Reich H. Complications of total laparoscopic hysterectomy in 518 cases. Gynaecol Endosc. 1994;3:203-208.
10. Zmora O, Pikarsky AJ, Wexner SD. Bowel preparation for colorectal surgery. Dis Colon Rectum. 2001;44:1537-1547.
11. Nichols RI, Smith JW, Girch RY, Waterman RS, Holmes JWC. Current practices of preoperative bowel preparation among North American colorectal surgeons. Clin Infect Dis. 1997;24:609-619.
12. Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD001544.-
13. Tsin DA, Colombero LT. Laparoscopic leash: a simple technique to prevent specimen loss during operative laparoscopy. Obstet Gynecol. 1999;94:628-629.
The authors report no financial relationships relevant to this article.
CASE: Large fibroid uterus. Is laparoscopy feasible?
A 41-year-old woman known to have uterine fibroids consults you after two other gynecologists have recommended abdominal hysterectomy. She weighs 320 lb, stands 5 ft 2 in, and is nulliparous and sexually inactive. Pelvic ultrasonography reveals multiple fibroids approximating 18 weeks’ gestational size. Although she has hypertension and reactive airway disease, these conditions are well controlled by medication. Her Pap smear and endometrial biopsy are negative.
Because her professional commitments limit her time for recovery, she hopes to bypass abdominal hysterectomy in favor of the laparoscopic approach.
Is this desire realistic?
Twenty years have passed since Reich performed the first total laparoscopic hysterectomy,1 but only a small percentage of hysterectomies performed in the United States utilize that approach. In 2003, 12% of 602,457 hysterectomies were done laparoscopically; the rest were performed using the abdominal or vaginal approach (66% and 22%, respectively).2
Yet laparoscopic hysterectomy has much to recommend it. Compared with abdominal hysterectomy, it involves a shorter hospital stay, less blood loss, a speedier return to normal activities, and fewer wound infections.3 Unlike vaginal hysterectomy, it also facilitates intra-abdominal inspection.
Although the opening case represents potentially difficult surgery because of the size of the uterus, the laparoscopic approach is feasible. When the uterus weighs more than 450 g, contains fibroids larger than 6 cm, or exceeds 12 to 14 cm in size,4-7 there is an increased risk of visceral injury, bleeding necessitating transfusion, prolonged operative time, and conversion to laparotomy. This article describes techniques that simplify laparoscopic management when the uterus exceeds 14 weeks’ size. By incorporating these techniques, we have performed laparoscopic hysterectomy in uteri as large as 22 to 24 weeks’ size without increased complications.
In Part 2 of this article, we address techniques that simplify laparoscopy when extensive intra-abdominal adhesions are present.
Why do some surgeons avoid laparoscopy?
Major complications occur in approximately 5% to 6% of women who undergo total laparoscopic hysterectomy.8,9 That is one of the reasons many surgeons who perform laparoscopic procedures revert to the more traditional vaginal or abdominal approach when faced with a potentially difficult hysterectomy. These surgeons cite uteri larger than 14 weeks’ size, extensive intra-abdominal adhesions, and morbid obesity as common indications for a more conservative approach. Others cite the limitations of working with inexperienced surgeons or residents, inadequate laparoscopic instruments, and distorted pelvic anatomy. Still others avoid laparoscopy when the patient has medical problems that preclude use of pneumoperitoneum or a steep Trendelenburg position.
In some cases, laparoscopic hysterectomy is simply not practical. In others, however, such as the presence of a large uterus, it can be achieved with attention to detail, a few key techniques, and proper counseling of the patient.
Success begins preop
All surgical decisions begin with the patient. A comprehensive preoperative discussion of pertinent management options allows both patient and surgeon to proceed with confidence. Easing the patient’s preoperative anxiety is important. It can be achieved by explaining what to expect—not only the normal recovery for laparoscopic hysterectomy, but also the expected recovery if it becomes necessary to convert to laparotomy. If the patient has clear expectations, unexpected outcomes such as conversion are better tolerated. When it comes down to a choice between the surgeon’s ego or patient safety, the patient always wins. Conversion is not failure.
Another important topic to discuss with the patient is the risk of bowel injury. Mechanical bowel preparation is not essential for every patient who undergoes laparoscopic hysterectomy, but the risk of injury to the bowel necessitating colorectal surgical assistance may be heightened in women who have a large uterus or extensive intra-abdominal adhesions. Because of this risk, mechanical bowel preparation with oral polyethylene glycol solution or sodium phosphate should be considered. Most patients prefer the latter.10
What data show about bowel preps
The literature provides conflicting messages about the effectiveness of mechanical bowel preparation in averting additional complications when bowel injury occurs. Nichols and colleagues surveyed 808 active board-certified colorectal surgeons in the United States and Canada in 1995.11 All of the 471 (58%) surgeons who responded reported using some form of mechanical bowel preparation for their elective and emergency colorectal procedures.
Zmora and associates described the difficulty of designing a multicenter study to evaluate the role of mechanical bowel preparation in patient outcome.10 Of the many variables that warrant consideration, surgical technique was the single most important factor influencing surgical outcome.
In a review of evidence supporting the need for prophylactic mechanical bowel preparation prior to elective colorectal surgery, Guenaga and colleagues concluded that this practice is unsupported by the data.12
Bottom line. Given these data, the gynecologist wanting to practice evidence-based medicine should base his or her recommendations about bowel preparation on the preferences of the general or colorectal surgeon who will be called if a bowel injury occurs.
Don’t forget the team
After preparing the patient, prepare your support team—the operating room (OR) and anesthesia staffs. The OR staff should ensure that extra sutures, instruments, and retractors are unopened, in the room, and available in case conversion is necessary. Inform the anesthesia staff of your anticipated surgical time and potential pitfalls. Let them know you will need maximum Trendelenburg position for pelvic exposure, but remain flexible if the patient has trouble with oxygenation and ventilation. Making your anesthesiologist aware of your willingness to work together will benefit both you and your patient immensely.
Preparation continues in the OR
Appropriate patient positioning is key to successful completion of difficult laparoscopic cases. Position the patient’s buttocks several inches beyond the table break to facilitate maximal uterine manipulation, which may be needed for completion of the colpotomy.
Place the patient in the dorsal lithotomy position using Allen stirrups, with the knees flexed at a 90° angle. Keep the knees level with the hips and the hips extended neutrally.
Arm position is important to maximize room for the surgeon alongside the OR table. Space is limited when the patient’s arms are positioned on arm boards. Tucking the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, improves the surgical field and secures the patient to the OR table (FIGURE 1). Protect the elbows and hands with cushions.
Place sequential compression devices (on the calf or foot) for the duration of the procedure to minimize the risk of blood stasis and clots that sometimes develop in the legs with prolonged surgical times. Many complex laparoscopic cases last longer than 2 hours.
FIGURE 1 Positioning the patient
Tuck the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, to improve the surgical field.
Maximum Trendelenburg position is a must
This positioning is essential for successful anatomic exposure in complex laparoscopic surgical cases. If the patient is positioned securely, maximum Trendelenburg position does not increase the risk of the patient sliding off the OR table, nor does it affect oxygenation in most morbidly obese patients. Rather, it allows the intestines to drop out of the pelvis into the upper abdomen, facilitating visualization and decreasing the risk of bowel injury.
Anesthesia staffers often limit the degree of Trendelenburg position unless the surgeon insists otherwise. Alternating patient position between maximum Trendelenburg for optimal surgical exposure and a less steep angle when patient oxygenation requires it allows the gynecologic surgeon and anesthesiologist to work together in the patient’s best interest.
Video monitor placement is key
It helps determine how efficiently you operate. Use of a single central monitor requires both the surgeon and assistant to turn their heads acutely during prolonged procedures, accelerating their fatigue and potentially increasing the risk of injury. Using two monitors—each placed to allow the surgeon and assistant to maintain neutral head position—minimizes fatigue and its attendant risks.
Entering the abdomen
Abdominal entry poses theoretical obstacles when the patient has a large uterus, but all types of entry remain safe as long as laparoscopic surgical principles are followed scrupulously. We have successfully used traditional Veress needle entry, open laparoscopic entry, and left upper quadrant entry.
Is entry above the umbilicus helpful?
Anecdotal reports suggest a midline port above the umbilicus when the uterus extends above the umbilicus, but we do not alter standard port placement in these cases. By tenting the abdominal wall at the umbilicus, we create adequate distance to achieve pneumoperitoneum and space for directed trocar entry to avoid injury to the uterus. The conventional umbilical primary port allows use of standard-length instruments. The cephalad uterine blood supply (infundibulopelvic ligament vessels or utero-ovarian ligament vessels) remains at or below the level of the umbilicus in almost all of these patients.
Port placement in the patient who has a large uterus is the same as it is for other laparoscopic hysterectomies in our practice. We use an 11-mm trocar at the umbilicus for a 10-mm endoscope. We use the 10-mm endoscope because the light it provides to the surgical field is superior to that of a 5-mm endoscope, and the 10-mm scope is more durable.
We place a 5-mm trocar just above the anterior iliac crest on each side, lateral to the ascending inferior epigastric vessels (FIGURE 2). We place an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port on the side of the primary surgeon. This trocar serves a dual purpose: It is the primary port for the surgeon, and removal of the trocar sleeve later in the procedure allows for easy insertion of the morcellator.
Some patients will require a fifth port on the side opposite the primary surgeon to allow better access to the uterine blood supply or to facilitate uterine manipulation.
FIGURE 2 Port placement when the uterus is large
A midline umbilical port (A) is possible even when the uterus is large. Other ports include a 5-mm trocar just above the anterior iliac crest on each side (B), and an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port nearest the primary surgeon (C).
Why an angled scope is superior
Many gynecologists fear laparoscopic surgery in patients who have a large uterus. The reason? Poor visualization of the surgical field. However, the type of endoscope that is used has a bearing on visualization.
Most gynecologists are trained to use a 0° endoscope for laparoscopic surgery. However, when the uterus is large, the 0° scope yields an inadequate field of view, whether the endoscope is placed at the umbilicus or through a lateral port. Critical structures like the vascular bundles, ureters, and even the bladder may be inadequately visualized using the 0° endoscope (FIGURE 3).
Gynecologists routinely use angled scopes in hysteroscopy and cystoscopy, but tend to avoid them in laparoscopy because of difficulty orienting the surgical field. As gynecologists, we readily accept that use of an angled scope in hysteroscopy and cystoscopy requires rotation of the scope while the camera maintains its horizontal position. The same concept applies to laparoscopy.
Use of the angled scope in the abdomen is a two-step process. First, it must be rotated to achieve the desired field of view. Then, as the endoscope is held firmly to maintain this view, the camera head must be rotated on the scope to return the field to a horizontal position.
Many surgeons find this action difficult because they or the assistant are holding the camera in one hand and an instrument in the other. We solve this problem by using a mechanical scope holder to secure the camera and endoscope in the position we desire.
In some cases, the camera head does not attach securely to the eyepiece, and the scope rotates on the camera as soon as it is released. This difficulty arises when the eyepiece of the endoscope is slightly smaller than the camera attachment. The problem is easily solved by placing a small piece of surgical skin closure tape on one edge of the eyepiece, slightly increasing its diameter. The camera attachment then holds the scope securely.
Human scope holders may tire during long cases, causing field drift at critical moments. In contrast, a mechanical scope holder is easily and intermittently adjusted for field of view, producing a steady field of view and minimizing the impact of manual manipulation of the scope on surgical outcome. It also allows the surgeon and first assistant to use two hands while operating.
General surgeons and urologists often use 30° endoscopes. Gynecologists working in the pelvis see better using a 45° scope (FIGURE 3). Most ORs offer a 30° endoscope but do not always have a 45° endoscope available in the instrument room. This is regrettable. Compared with the 30° scope, the 45° instrument provides better visual access to the low lateral uterine blood supply and bladder flap, particularly when the patient has a globular uterus or large, low anterior fibroid. We include both 5-mm and 10-mm 45° endoscopes in our laparoscopic tool chest, and believe they are essential options.
FIGURE 3 The 45° laparoscope provides better visual access
(A) 0° scope, uterus midline: Right broad ligament view obstructed. (B) 0° scope, uterus to left: Right broad ligament view still obstructed. (C) 45° scope, uterus midline: Right broad ligament view improved. (D) 45° scope, uterus to left: Right broad ligament view optimal.
Control the blood supply
Our laparoscopic approach is very similar to our technique for abdominal hysterectomy, beginning with the blood supply. The main blood supply to the uterus enters at only four points. If this blood supply is adequately controlled, morcellation of the large uterus can proceed without excessive blood loss.
Visualization of the blood supply is normally restricted because of tense, taut round ligaments that limit mobility of the large uterus. A simple step to improve mobility is to transect each round ligament in its middle position before addressing the uterine blood supply.
If the ovaries are being conserved, transect the utero-ovarian ligament and tube as close to the ovary as possible with your instrument and technique of choice (electrical or mechanical energy, etc); they all work. Stay close to the ovary to avert bleeding that might otherwise occur when the ascending uterine vascular coils are cut tangentially.
If the ovaries are being removed, transect the infundibulopelvic ligament close to the ovary, being careful not to include ovarian tissue in the pedicle. Use your method of choice, but relieve tension on the pedicle as it is being transected to minimize the risk of pedicle bleeding.
Now, 20% to 40% of the uterine blood supply is controlled, with minimal blood loss.
The key to controlling the remaining blood supply is transecting the ascending vascular bundle as low as possible on either side. The 45° endoscope provides optimal visualization for this part of the procedure. Many times the field of view attained using the 45° endoscope is all that is necessary to facilitate occlusion and transection of these vessels at the level of the internal cervical os.
We commonly use ultrasonic energy to coagulate and cut the ascending vascular bundle. Ultrasonic energy provides excellent hemostasis for this part of the procedure. Again, use the technique of your choice.
Use a laparoscopic “leash”
At times, large broad-ligament fibroids obscure the field of view and access to the ascending vascular bundle. Standard laparoscopic graspers cannot maintain a firm hold on the tissue to improve visibility or access. The solution? A laparoscopic “leash,” first described in 1999 by Tsin and colleagues.13
Giesler extended that concept with a “puppet string” variation to maximize exposure in difficult cases. To apply the “puppet string” technique, using No. 1 Prolene suture, place a large figure-of-eight suture through the tissue to be retracted (FIGURE 4). Bring the suture out of the abdomen adjacent to the trocar sleeve in a location that provides optimal traction. (First, bring the suture through the trocar sleeve. Then remove the trocar sleeve and reinsert it adjacent to the retraction suture.) This secure attachment allows better visualization and greater access to the blood supply at a lower level. It also is possible to manipulate this suture inside the abdomen using traditional graspers to provide reliable repositioning of the uterus. This degree of tissue control improves field of vision and allows the procedure to advance smoothly.
FIGURE 4 A “puppet string” improves access
This secure attachment allows better visualization and greater access to the blood supply at a lower level. Manipulation of this suture inside the abdomen using traditional graspers also helps reposition the uterus.
Morcellation techniques
Once the ascending blood supply has been managed on both sides, morcellation can be performed with minimal blood loss using one of two techniques:
- Amputate the body of the uterus above the level where the blood supply has been interrupted
- Morcellate the uterine body to a point just above the level where the blood supply has been interrupted.
Use basic principles, regardless of the technique chosen
- Hold the morcellator in one hand and a toothed grasper in the other hand to pull tissue into the morcellator. Do not push the morcellator into tissue or you may injure nonvisualized structures on the other side.
- Morcellate tissue in half-moon portions, skimming along the top of the fundus, instead of coring the uterus like an apple; it creates longer strips of tissue and is faster. This technique also allows continuous observation of the active blade, which helps avoid inadvertent injury to tissues behind the blade.
- Attempt morcellation in the anterior abdominal space to avoid injury to blood vessels, ureters, and bowel in the posterior abdominal space. The assistant feeds uterine tissue to the surgeon in the anterior space.
It is essential to control the blood supply to the tissue to be morcellated before morcellation to avoid massive hemorrhage.
Amputating the upper uterine body
Amputation of the large body of the uterus from the lower uterine segment assures complete control of the blood supply and avoids further blood loss during morcellation, but it also poses difficulties. The free uterine mass is held in position by the assistant using only one grasper. If this grasper slips, the mass can be inadvertently released while the morcellator blade is active. If the assistant is also holding the camera, there are no options for stabilizing the free uterine mass. If a mechanical scope holder or second assistant is available to hold the camera, a second trocar port can be placed on the side of the assistant to provide access for a second grasper to stabilize the uterine body during morcellation. The need for a stable uterine mass is important to minimize the risk of injury.
Once the upper body of the uterus has been removed by morcellation, the lower uterine segment and cervix must be removed—using your procedure of choice—to finish the hysterectomy.
Morcellating the upper uterine body
If the uterus remains attached to the cervix, it already has one fixed point of stability. During morcellation, the assistant has one hand available to direct the camera. Blood loss during morcellation of the uterus while it is still attached to the cervix is minimal because the ascending vascular bundles on either side have been interrupted under direct vision.
For greater control of the large uterus, a second port can be placed on the assistant’s side for a second grasper, as described above. Most of the large uterus that is still connected to the cervix can be morcellated in the anterior abdominal space in horizontal fashion, as for the free uterine mass just described.
Uterine manipulation by the assistant keeps the uterus away from critical structures as it is reduced to 8 to 10 weeks’ size. Once this size is attained, resume normal technique for total laparoscopic hysterectomy to separate the remaining tissue from the vagina.
2 types of morcellators in use today
One has a disposable 15-mm blade that attaches to a drive unit adjacent to the OR table (Gynecare-Ethicon Women’s Health and Urology). The other has a sterile, reusable drive unit with a disposable blade (Storz). Both work well on large uteri.
The reusable drive unit has more power to morcellate calcified fibroids and offers a choice between 12-mm, 15-mm, and 20-mm disposable blades for faster morcellation.
Concluding the procedure
Chips of fibroid and uterine tissue created during morcellation often remain in the pelvis after the uterus has been removed. Place them in a 10-cm specimen-collection bag and extract it through the vagina after removal of the residual uterus and cervix. This is faster and easier than recovering them one at a time with the gall bladder stone scoop through a trocar port. The value of the OR time saved with use of the specimen-collection bag is significantly greater than that of the disposable collection device.
CASE RESOLVED
You perform total laparoscopic hysterectomy and find 6-cm fibroids in both broad ligament areas and over the cervical–vaginal junction on the left. You use a “puppet string” to apply directed traction to the fibroids to simplify their extraction. The 45° endoscope allows clear visualization of the ascending vascular bundle on both sides, and the mechanical scope holder allows a fixed field of view for the meticulous dissection required to remove the broad-ligament fibroids.
You morcellate the entire 663-g uterus and remove it in pieces through the abdominal wall. The extensive morcellation required, coupled with technical issues related to the patient’s morbid obesity, prolong the procedure to more than 4 hours.
Postoperatively, the patient voids without a catheter, walks around the nursing unit, and eats half a sandwich within 4 hours. She is discharged home in less than 24 hours and is able to drive 4 days after her surgery.
The authors report no financial relationships relevant to this article.
CASE: Large fibroid uterus. Is laparoscopy feasible?
A 41-year-old woman known to have uterine fibroids consults you after two other gynecologists have recommended abdominal hysterectomy. She weighs 320 lb, stands 5 ft 2 in, and is nulliparous and sexually inactive. Pelvic ultrasonography reveals multiple fibroids approximating 18 weeks’ gestational size. Although she has hypertension and reactive airway disease, these conditions are well controlled by medication. Her Pap smear and endometrial biopsy are negative.
Because her professional commitments limit her time for recovery, she hopes to bypass abdominal hysterectomy in favor of the laparoscopic approach.
Is this desire realistic?
Twenty years have passed since Reich performed the first total laparoscopic hysterectomy,1 but only a small percentage of hysterectomies performed in the United States utilize that approach. In 2003, 12% of 602,457 hysterectomies were done laparoscopically; the rest were performed using the abdominal or vaginal approach (66% and 22%, respectively).2
Yet laparoscopic hysterectomy has much to recommend it. Compared with abdominal hysterectomy, it involves a shorter hospital stay, less blood loss, a speedier return to normal activities, and fewer wound infections.3 Unlike vaginal hysterectomy, it also facilitates intra-abdominal inspection.
Although the opening case represents potentially difficult surgery because of the size of the uterus, the laparoscopic approach is feasible. When the uterus weighs more than 450 g, contains fibroids larger than 6 cm, or exceeds 12 to 14 cm in size,4-7 there is an increased risk of visceral injury, bleeding necessitating transfusion, prolonged operative time, and conversion to laparotomy. This article describes techniques that simplify laparoscopic management when the uterus exceeds 14 weeks’ size. By incorporating these techniques, we have performed laparoscopic hysterectomy in uteri as large as 22 to 24 weeks’ size without increased complications.
In Part 2 of this article, we address techniques that simplify laparoscopy when extensive intra-abdominal adhesions are present.
Why do some surgeons avoid laparoscopy?
Major complications occur in approximately 5% to 6% of women who undergo total laparoscopic hysterectomy.8,9 That is one of the reasons many surgeons who perform laparoscopic procedures revert to the more traditional vaginal or abdominal approach when faced with a potentially difficult hysterectomy. These surgeons cite uteri larger than 14 weeks’ size, extensive intra-abdominal adhesions, and morbid obesity as common indications for a more conservative approach. Others cite the limitations of working with inexperienced surgeons or residents, inadequate laparoscopic instruments, and distorted pelvic anatomy. Still others avoid laparoscopy when the patient has medical problems that preclude use of pneumoperitoneum or a steep Trendelenburg position.
In some cases, laparoscopic hysterectomy is simply not practical. In others, however, such as the presence of a large uterus, it can be achieved with attention to detail, a few key techniques, and proper counseling of the patient.
Success begins preop
All surgical decisions begin with the patient. A comprehensive preoperative discussion of pertinent management options allows both patient and surgeon to proceed with confidence. Easing the patient’s preoperative anxiety is important. It can be achieved by explaining what to expect—not only the normal recovery for laparoscopic hysterectomy, but also the expected recovery if it becomes necessary to convert to laparotomy. If the patient has clear expectations, unexpected outcomes such as conversion are better tolerated. When it comes down to a choice between the surgeon’s ego or patient safety, the patient always wins. Conversion is not failure.
Another important topic to discuss with the patient is the risk of bowel injury. Mechanical bowel preparation is not essential for every patient who undergoes laparoscopic hysterectomy, but the risk of injury to the bowel necessitating colorectal surgical assistance may be heightened in women who have a large uterus or extensive intra-abdominal adhesions. Because of this risk, mechanical bowel preparation with oral polyethylene glycol solution or sodium phosphate should be considered. Most patients prefer the latter.10
What data show about bowel preps
The literature provides conflicting messages about the effectiveness of mechanical bowel preparation in averting additional complications when bowel injury occurs. Nichols and colleagues surveyed 808 active board-certified colorectal surgeons in the United States and Canada in 1995.11 All of the 471 (58%) surgeons who responded reported using some form of mechanical bowel preparation for their elective and emergency colorectal procedures.
Zmora and associates described the difficulty of designing a multicenter study to evaluate the role of mechanical bowel preparation in patient outcome.10 Of the many variables that warrant consideration, surgical technique was the single most important factor influencing surgical outcome.
In a review of evidence supporting the need for prophylactic mechanical bowel preparation prior to elective colorectal surgery, Guenaga and colleagues concluded that this practice is unsupported by the data.12
Bottom line. Given these data, the gynecologist wanting to practice evidence-based medicine should base his or her recommendations about bowel preparation on the preferences of the general or colorectal surgeon who will be called if a bowel injury occurs.
Don’t forget the team
After preparing the patient, prepare your support team—the operating room (OR) and anesthesia staffs. The OR staff should ensure that extra sutures, instruments, and retractors are unopened, in the room, and available in case conversion is necessary. Inform the anesthesia staff of your anticipated surgical time and potential pitfalls. Let them know you will need maximum Trendelenburg position for pelvic exposure, but remain flexible if the patient has trouble with oxygenation and ventilation. Making your anesthesiologist aware of your willingness to work together will benefit both you and your patient immensely.
Preparation continues in the OR
Appropriate patient positioning is key to successful completion of difficult laparoscopic cases. Position the patient’s buttocks several inches beyond the table break to facilitate maximal uterine manipulation, which may be needed for completion of the colpotomy.
Place the patient in the dorsal lithotomy position using Allen stirrups, with the knees flexed at a 90° angle. Keep the knees level with the hips and the hips extended neutrally.
Arm position is important to maximize room for the surgeon alongside the OR table. Space is limited when the patient’s arms are positioned on arm boards. Tucking the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, improves the surgical field and secures the patient to the OR table (FIGURE 1). Protect the elbows and hands with cushions.
Place sequential compression devices (on the calf or foot) for the duration of the procedure to minimize the risk of blood stasis and clots that sometimes develop in the legs with prolonged surgical times. Many complex laparoscopic cases last longer than 2 hours.
FIGURE 1 Positioning the patient
Tuck the arms at the patient’s sides, with the antecubital fossa anterior and the palm cupping the hip, to improve the surgical field.
Maximum Trendelenburg position is a must
This positioning is essential for successful anatomic exposure in complex laparoscopic surgical cases. If the patient is positioned securely, maximum Trendelenburg position does not increase the risk of the patient sliding off the OR table, nor does it affect oxygenation in most morbidly obese patients. Rather, it allows the intestines to drop out of the pelvis into the upper abdomen, facilitating visualization and decreasing the risk of bowel injury.
Anesthesia staffers often limit the degree of Trendelenburg position unless the surgeon insists otherwise. Alternating patient position between maximum Trendelenburg for optimal surgical exposure and a less steep angle when patient oxygenation requires it allows the gynecologic surgeon and anesthesiologist to work together in the patient’s best interest.
Video monitor placement is key
It helps determine how efficiently you operate. Use of a single central monitor requires both the surgeon and assistant to turn their heads acutely during prolonged procedures, accelerating their fatigue and potentially increasing the risk of injury. Using two monitors—each placed to allow the surgeon and assistant to maintain neutral head position—minimizes fatigue and its attendant risks.
Entering the abdomen
Abdominal entry poses theoretical obstacles when the patient has a large uterus, but all types of entry remain safe as long as laparoscopic surgical principles are followed scrupulously. We have successfully used traditional Veress needle entry, open laparoscopic entry, and left upper quadrant entry.
Is entry above the umbilicus helpful?
Anecdotal reports suggest a midline port above the umbilicus when the uterus extends above the umbilicus, but we do not alter standard port placement in these cases. By tenting the abdominal wall at the umbilicus, we create adequate distance to achieve pneumoperitoneum and space for directed trocar entry to avoid injury to the uterus. The conventional umbilical primary port allows use of standard-length instruments. The cephalad uterine blood supply (infundibulopelvic ligament vessels or utero-ovarian ligament vessels) remains at or below the level of the umbilicus in almost all of these patients.
Port placement in the patient who has a large uterus is the same as it is for other laparoscopic hysterectomies in our practice. We use an 11-mm trocar at the umbilicus for a 10-mm endoscope. We use the 10-mm endoscope because the light it provides to the surgical field is superior to that of a 5-mm endoscope, and the 10-mm scope is more durable.
We place a 5-mm trocar just above the anterior iliac crest on each side, lateral to the ascending inferior epigastric vessels (FIGURE 2). We place an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port on the side of the primary surgeon. This trocar serves a dual purpose: It is the primary port for the surgeon, and removal of the trocar sleeve later in the procedure allows for easy insertion of the morcellator.
Some patients will require a fifth port on the side opposite the primary surgeon to allow better access to the uterine blood supply or to facilitate uterine manipulation.
FIGURE 2 Port placement when the uterus is large
A midline umbilical port (A) is possible even when the uterus is large. Other ports include a 5-mm trocar just above the anterior iliac crest on each side (B), and an 11-mm trocar 10 cm medial and cephalad to the lower iliac crest port nearest the primary surgeon (C).
Why an angled scope is superior
Many gynecologists fear laparoscopic surgery in patients who have a large uterus. The reason? Poor visualization of the surgical field. However, the type of endoscope that is used has a bearing on visualization.
Most gynecologists are trained to use a 0° endoscope for laparoscopic surgery. However, when the uterus is large, the 0° scope yields an inadequate field of view, whether the endoscope is placed at the umbilicus or through a lateral port. Critical structures like the vascular bundles, ureters, and even the bladder may be inadequately visualized using the 0° endoscope (FIGURE 3).
Gynecologists routinely use angled scopes in hysteroscopy and cystoscopy, but tend to avoid them in laparoscopy because of difficulty orienting the surgical field. As gynecologists, we readily accept that use of an angled scope in hysteroscopy and cystoscopy requires rotation of the scope while the camera maintains its horizontal position. The same concept applies to laparoscopy.
Use of the angled scope in the abdomen is a two-step process. First, it must be rotated to achieve the desired field of view. Then, as the endoscope is held firmly to maintain this view, the camera head must be rotated on the scope to return the field to a horizontal position.
Many surgeons find this action difficult because they or the assistant are holding the camera in one hand and an instrument in the other. We solve this problem by using a mechanical scope holder to secure the camera and endoscope in the position we desire.
In some cases, the camera head does not attach securely to the eyepiece, and the scope rotates on the camera as soon as it is released. This difficulty arises when the eyepiece of the endoscope is slightly smaller than the camera attachment. The problem is easily solved by placing a small piece of surgical skin closure tape on one edge of the eyepiece, slightly increasing its diameter. The camera attachment then holds the scope securely.
Human scope holders may tire during long cases, causing field drift at critical moments. In contrast, a mechanical scope holder is easily and intermittently adjusted for field of view, producing a steady field of view and minimizing the impact of manual manipulation of the scope on surgical outcome. It also allows the surgeon and first assistant to use two hands while operating.
General surgeons and urologists often use 30° endoscopes. Gynecologists working in the pelvis see better using a 45° scope (FIGURE 3). Most ORs offer a 30° endoscope but do not always have a 45° endoscope available in the instrument room. This is regrettable. Compared with the 30° scope, the 45° instrument provides better visual access to the low lateral uterine blood supply and bladder flap, particularly when the patient has a globular uterus or large, low anterior fibroid. We include both 5-mm and 10-mm 45° endoscopes in our laparoscopic tool chest, and believe they are essential options.
FIGURE 3 The 45° laparoscope provides better visual access
(A) 0° scope, uterus midline: Right broad ligament view obstructed. (B) 0° scope, uterus to left: Right broad ligament view still obstructed. (C) 45° scope, uterus midline: Right broad ligament view improved. (D) 45° scope, uterus to left: Right broad ligament view optimal.
Control the blood supply
Our laparoscopic approach is very similar to our technique for abdominal hysterectomy, beginning with the blood supply. The main blood supply to the uterus enters at only four points. If this blood supply is adequately controlled, morcellation of the large uterus can proceed without excessive blood loss.
Visualization of the blood supply is normally restricted because of tense, taut round ligaments that limit mobility of the large uterus. A simple step to improve mobility is to transect each round ligament in its middle position before addressing the uterine blood supply.
If the ovaries are being conserved, transect the utero-ovarian ligament and tube as close to the ovary as possible with your instrument and technique of choice (electrical or mechanical energy, etc); they all work. Stay close to the ovary to avert bleeding that might otherwise occur when the ascending uterine vascular coils are cut tangentially.
If the ovaries are being removed, transect the infundibulopelvic ligament close to the ovary, being careful not to include ovarian tissue in the pedicle. Use your method of choice, but relieve tension on the pedicle as it is being transected to minimize the risk of pedicle bleeding.
Now, 20% to 40% of the uterine blood supply is controlled, with minimal blood loss.
The key to controlling the remaining blood supply is transecting the ascending vascular bundle as low as possible on either side. The 45° endoscope provides optimal visualization for this part of the procedure. Many times the field of view attained using the 45° endoscope is all that is necessary to facilitate occlusion and transection of these vessels at the level of the internal cervical os.
We commonly use ultrasonic energy to coagulate and cut the ascending vascular bundle. Ultrasonic energy provides excellent hemostasis for this part of the procedure. Again, use the technique of your choice.
Use a laparoscopic “leash”
At times, large broad-ligament fibroids obscure the field of view and access to the ascending vascular bundle. Standard laparoscopic graspers cannot maintain a firm hold on the tissue to improve visibility or access. The solution? A laparoscopic “leash,” first described in 1999 by Tsin and colleagues.13
Giesler extended that concept with a “puppet string” variation to maximize exposure in difficult cases. To apply the “puppet string” technique, using No. 1 Prolene suture, place a large figure-of-eight suture through the tissue to be retracted (FIGURE 4). Bring the suture out of the abdomen adjacent to the trocar sleeve in a location that provides optimal traction. (First, bring the suture through the trocar sleeve. Then remove the trocar sleeve and reinsert it adjacent to the retraction suture.) This secure attachment allows better visualization and greater access to the blood supply at a lower level. It also is possible to manipulate this suture inside the abdomen using traditional graspers to provide reliable repositioning of the uterus. This degree of tissue control improves field of vision and allows the procedure to advance smoothly.
FIGURE 4 A “puppet string” improves access
This secure attachment allows better visualization and greater access to the blood supply at a lower level. Manipulation of this suture inside the abdomen using traditional graspers also helps reposition the uterus.
Morcellation techniques
Once the ascending blood supply has been managed on both sides, morcellation can be performed with minimal blood loss using one of two techniques:
- Amputate the body of the uterus above the level where the blood supply has been interrupted
- Morcellate the uterine body to a point just above the level where the blood supply has been interrupted.
Use basic principles, regardless of the technique chosen
- Hold the morcellator in one hand and a toothed grasper in the other hand to pull tissue into the morcellator. Do not push the morcellator into tissue or you may injure nonvisualized structures on the other side.
- Morcellate tissue in half-moon portions, skimming along the top of the fundus, instead of coring the uterus like an apple; it creates longer strips of tissue and is faster. This technique also allows continuous observation of the active blade, which helps avoid inadvertent injury to tissues behind the blade.
- Attempt morcellation in the anterior abdominal space to avoid injury to blood vessels, ureters, and bowel in the posterior abdominal space. The assistant feeds uterine tissue to the surgeon in the anterior space.
It is essential to control the blood supply to the tissue to be morcellated before morcellation to avoid massive hemorrhage.
Amputating the upper uterine body
Amputation of the large body of the uterus from the lower uterine segment assures complete control of the blood supply and avoids further blood loss during morcellation, but it also poses difficulties. The free uterine mass is held in position by the assistant using only one grasper. If this grasper slips, the mass can be inadvertently released while the morcellator blade is active. If the assistant is also holding the camera, there are no options for stabilizing the free uterine mass. If a mechanical scope holder or second assistant is available to hold the camera, a second trocar port can be placed on the side of the assistant to provide access for a second grasper to stabilize the uterine body during morcellation. The need for a stable uterine mass is important to minimize the risk of injury.
Once the upper body of the uterus has been removed by morcellation, the lower uterine segment and cervix must be removed—using your procedure of choice—to finish the hysterectomy.
Morcellating the upper uterine body
If the uterus remains attached to the cervix, it already has one fixed point of stability. During morcellation, the assistant has one hand available to direct the camera. Blood loss during morcellation of the uterus while it is still attached to the cervix is minimal because the ascending vascular bundles on either side have been interrupted under direct vision.
For greater control of the large uterus, a second port can be placed on the assistant’s side for a second grasper, as described above. Most of the large uterus that is still connected to the cervix can be morcellated in the anterior abdominal space in horizontal fashion, as for the free uterine mass just described.
Uterine manipulation by the assistant keeps the uterus away from critical structures as it is reduced to 8 to 10 weeks’ size. Once this size is attained, resume normal technique for total laparoscopic hysterectomy to separate the remaining tissue from the vagina.
2 types of morcellators in use today
One has a disposable 15-mm blade that attaches to a drive unit adjacent to the OR table (Gynecare-Ethicon Women’s Health and Urology). The other has a sterile, reusable drive unit with a disposable blade (Storz). Both work well on large uteri.
The reusable drive unit has more power to morcellate calcified fibroids and offers a choice between 12-mm, 15-mm, and 20-mm disposable blades for faster morcellation.
Concluding the procedure
Chips of fibroid and uterine tissue created during morcellation often remain in the pelvis after the uterus has been removed. Place them in a 10-cm specimen-collection bag and extract it through the vagina after removal of the residual uterus and cervix. This is faster and easier than recovering them one at a time with the gall bladder stone scoop through a trocar port. The value of the OR time saved with use of the specimen-collection bag is significantly greater than that of the disposable collection device.
CASE RESOLVED
You perform total laparoscopic hysterectomy and find 6-cm fibroids in both broad ligament areas and over the cervical–vaginal junction on the left. You use a “puppet string” to apply directed traction to the fibroids to simplify their extraction. The 45° endoscope allows clear visualization of the ascending vascular bundle on both sides, and the mechanical scope holder allows a fixed field of view for the meticulous dissection required to remove the broad-ligament fibroids.
You morcellate the entire 663-g uterus and remove it in pieces through the abdominal wall. The extensive morcellation required, coupled with technical issues related to the patient’s morbid obesity, prolong the procedure to more than 4 hours.
Postoperatively, the patient voids without a catheter, walks around the nursing unit, and eats half a sandwich within 4 hours. She is discharged home in less than 24 hours and is able to drive 4 days after her surgery.
1. Reich H, DeCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989;5:213-216.
2. Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091-1095.
3. Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD003677.-
4. Leonard F, Chopin N, Borghese B, et al. Total laparoscopic hysterectomy: preoperative risk factors for conversion to laparotomy. J Minim Invasive Gynecol. 2005;12:312-317.
5. Fiaccavento A, Landi S, Barbieri F, et al. Total laparoscopic hysterectomy in cases of very large uteri: a retrospective comparative study. J Minim Invasive Gynecol. 2007;14:559-563.
6. Pelosi MA, Kadar N. Laparoscopically assisted hysterectomy for uteri weighing 500 g or more. J Am Assoc Gynecol Laparosc. 1994;1:405-409.
7. Seracchioli R, Venturoli S, Vianello F, et al. Total laparoscopic hysterectomy compared with abdominal hysterectomy in the presence of a large uterus. J Am Assoc Gynecol Laparosc. 2002;9:333-338.
8. Hoffman CP, Kennedy J, Borschel L, Burchette R, Kidd A. Laparoscopic hysterectomy: the Kaiser Permanente San Diego experience. J Minim Invasive Gynecol. 2005;12:16-24.
9. Liu CY, Reich H. Complications of total laparoscopic hysterectomy in 518 cases. Gynaecol Endosc. 1994;3:203-208.
10. Zmora O, Pikarsky AJ, Wexner SD. Bowel preparation for colorectal surgery. Dis Colon Rectum. 2001;44:1537-1547.
11. Nichols RI, Smith JW, Girch RY, Waterman RS, Holmes JWC. Current practices of preoperative bowel preparation among North American colorectal surgeons. Clin Infect Dis. 1997;24:609-619.
12. Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD001544.-
13. Tsin DA, Colombero LT. Laparoscopic leash: a simple technique to prevent specimen loss during operative laparoscopy. Obstet Gynecol. 1999;94:628-629.
1. Reich H, DeCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989;5:213-216.
2. Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091-1095.
3. Johnson N, Barlow D, Lethaby A, Tavender E, Curr E, Garry R. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD003677.-
4. Leonard F, Chopin N, Borghese B, et al. Total laparoscopic hysterectomy: preoperative risk factors for conversion to laparotomy. J Minim Invasive Gynecol. 2005;12:312-317.
5. Fiaccavento A, Landi S, Barbieri F, et al. Total laparoscopic hysterectomy in cases of very large uteri: a retrospective comparative study. J Minim Invasive Gynecol. 2007;14:559-563.
6. Pelosi MA, Kadar N. Laparoscopically assisted hysterectomy for uteri weighing 500 g or more. J Am Assoc Gynecol Laparosc. 1994;1:405-409.
7. Seracchioli R, Venturoli S, Vianello F, et al. Total laparoscopic hysterectomy compared with abdominal hysterectomy in the presence of a large uterus. J Am Assoc Gynecol Laparosc. 2002;9:333-338.
8. Hoffman CP, Kennedy J, Borschel L, Burchette R, Kidd A. Laparoscopic hysterectomy: the Kaiser Permanente San Diego experience. J Minim Invasive Gynecol. 2005;12:16-24.
9. Liu CY, Reich H. Complications of total laparoscopic hysterectomy in 518 cases. Gynaecol Endosc. 1994;3:203-208.
10. Zmora O, Pikarsky AJ, Wexner SD. Bowel preparation for colorectal surgery. Dis Colon Rectum. 2001;44:1537-1547.
11. Nichols RI, Smith JW, Girch RY, Waterman RS, Holmes JWC. Current practices of preoperative bowel preparation among North American colorectal surgeons. Clin Infect Dis. 1997;24:609-619.
12. Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jørgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD001544.-
13. Tsin DA, Colombero LT. Laparoscopic leash: a simple technique to prevent specimen loss during operative laparoscopy. Obstet Gynecol. 1999;94:628-629.
June 2008 Instant Poll Results
WHAT IS THE C-SECTION RATE AT YOUR HOSPITAL?
At my hospital, the overall cesarean delivery rate is:
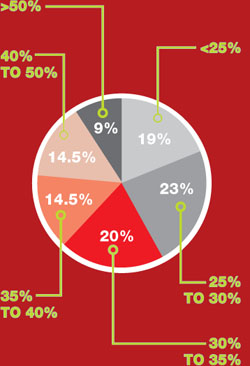
…and I think that this rate is: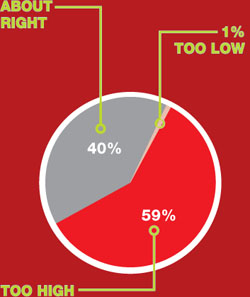
WHAT IS THE C-SECTION RATE AT YOUR HOSPITAL?
At my hospital, the overall cesarean delivery rate is:
…and I think that this rate is:
WHAT IS THE C-SECTION RATE AT YOUR HOSPITAL?
At my hospital, the overall cesarean delivery rate is:
…and I think that this rate is:
Going outside your area of expertise: How far is too far?
Dear Dr. Mossman:
I am an adult psychiatrist practicing in a geographically isolated area. I am working with the family of 10-year-old “Bobby” who is struggling with attention problems. Top notch neuropsychologic testing recommends a stimulant trial, but the local pediatrician is too busy to give Bobby adequate follow-up and attention.
I am an experienced psychopharmacologist but have not prescribed medication to children since residency. My relationship with the family is excellent, and the local pediatrician said that she would supervise me. If I choose to treat Bobby, what are the possible liability issues I should be aware of, and how can I address them?—Submitted by “Dr. F”
Dr. F’s question raises issues that come up whenever patients need treatment for conditions outside the few with which you are highly familiar. Although you can’t be an expert on every aspect of every patient’s treatment, psychiatrists shouldn’t practice outside their area of competence.
Thus, the main liability-related issue that Dr. F should ask herself is, “Can I treat Bobby competently?” Of course, whenever you decide to treat any patient, you should be able to answer “yes” to this question. When thinking about potential liability related to treating Bobby, Dr. F might also ask, “If a lawsuit occurred, how would my treatment of Bobby appear?” This article discusses key issues that arise when general psychiatrists treat children and the steps general psychiatrists can take to show that they are practicing prudently.
Problem: Not enough clinicians
Child and adolescent psychiatrists (CAPs) are in short supply.1,2 In 2001 the United States had 8.67 CAPs per 100,000 youths and 1.6 CAPs for every 1,000 youths with severe mental disorders.1 Studies suggest that the United States needs nearly twice that many CAPs.3 The shortage is especially severe in rural areas, but approximately one-half of metropolitan counties with populations of >250,000 have no CAPs.1 In much of the nation, finding CAPs who are accepting new patients is difficult, and child and adolescent psychiatric treatment often is delivered by pediatricians, family practitioners, psychiatric nurse practitioners, and general adult psychiatrists.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Children’s special medical issues
General psychiatrists know that children aren’t just little adults. CAPs develop skills and thinking styles during their 2 years of subspecialty fellowship training that are quite different from those used by their general psychiatric colleagues.
Communication. Children and adolescents who need psychiatric care often have limited verbal abilities. Working and communicating with these patients requires a different interactive style.
Information sources. CAPs learn to seek and assimilate clinically important information from many settings—especially a child’s home—where their patients interact with others.
Caution. Only a small subset of psychotropic medications that adult psychiatrists prescribe are FDA-approved for use in children (Table 1).4 Because we don’t know how psychotropic drugs affect brain development, CAPs sometimes are leery of giving kids the same medications that adult psychiatrists readily prescribe.
Table 1
FDA-approved drugs and dosages for ADHD in children and adults
| Brand name | Generic name | Drug class | Dosing forms (mg) | Dosage range | Age range |
|---|---|---|---|---|---|
| Adderall | Amphetamine-dextroamphetamine | IR stimulant | 5, 7.5, 10, 12.5, 15, 20, 30 | 5 to 40 mg | 3 to 18 years |
| Adderall XR | Amphetamine-dextroamphetamine | ER stimulant | 5, 10, 15, 20, 25, 30 | 5 to 30 mg | 3 years to adult |
| Concerta | Methylphenidate | ER stimulant | 18, 27, 36, 54 | 18 to 72 mg | 6 years to adult |
| Daytrana | Methylphenidate transdermal | Stimulant | 10, 15, 20, 30 (patch) | 10 to 30 mg | 6 to 18 years |
| Focalin | Dexmethylphenidate | IR stimulant | 2.5, 5, 10 | 2.5 to 10 mg bid | 6 to 17 years |
| Focalin XR | Dexmethylphenidate | ER stimulant | 5, 10, 15, 20 | 5 to 20 mg | 6 years to adult |
| Metadate CD | Methylphenidate | ER stimulant | 10, 20, 30, 50, 60 | 10 to 60 mg | 6 to 18 years |
| Ritalin | Methylphenidate | IR stimulant | 5, 10, 20 | 5 to 20 mg bid or tid | 6 to 18 years |
| Ritalin LA | Methylphenidate | ER stimulant | 10, 20, 30, 40 | 10 to 60 mg | 6 to 18 years |
| Strattera | Atomoxetine | SNRI | 10, 18, 25, 40, 60, 80, 100 | 10 to 100 mg | 6 years to adult |
| Vyvanse | Lisdexamfetamine dimesylate | ER stimulant (precursor) | 30, 50, 70 | 30 to 70 mg | 6 years to adult |
| LA: long acting; CD: controlled delivery; ER, XR: extended release; IR: immediate release; SNRI: selective norepinephrine reuptake inhibitor | |||||
| Source: Adapted from references 2,3 | |||||
Different drugs. Some medications commonly taken by children are not often prescribed for adults, although this is changing as attention-deficit/hyperactivity disorder (ADHD) is better recognized in adults.5,6
Dosages. Dosing psychotropics in adults is fairly standardized, but in children and adolescents dosages vary with age, body weight, and physical maturity.
Adverse effects. The side effects kids experience and the way they report them can differ markedly from adults and will vary with age and developmental maturity. Some issues related to monitoring children—such as appropriate cardiac screening before starting stimulants—are controversial and remain unsettled.7,8
Consider alternatives
Dr. F may be tempted to treat Bobby because of her preexisting, positive relationship with the child’s family and a laudable desire to help. But Dr. F needs to ask, “Is there really no other workable alternative for Bobby?” Some possibilities include:
- Refer Bobby to a CAP in another community for initiation of treatment. Dr. F or Bobby’s pediatrician might safely continue care once a CAP establishes an effective treatment regimen.
- Find another pediatrician who might have more time to provide the follow-up that Dr. F feels is necessary.
- Decline to treat Bobby. Before doing this, Dr. F should consider what effect this refusal might have on her relationship with the family and the consequences for Bobby if his problems go untreated.
- Consult a CAP from another community, describing the situation and clinical factors in detail without naming or identifying the patient, and then ask, “Is this really the best thing to do?”
From a liability standpoint, this last point may be crucial. If the CAP answers “yes,” Dr. F can document the alternatives she has considered and her consultation and discussion with the CAP colleague as evidence of prudent practice. Dr. F can also document any advice that she has received and her plans to follow it.
If you choose to treat
Presumably, Dr. F would not perform thoracic surgery or provide any treatment that is far outside a general psychiatrist’s competence except under the most dire circumstances. General psychiatrists receive child psychiatry training during residency, and treating children is within their scope of practice. Similarly, most elderly patients are treated by general psychiatrists, rather than graduates of geropsychiatry fellowships. Prescribing medication for Bobby is not grossly different from Dr. F’s other duties, and she might provide services that a pediatrician might not.
Ask yourself 4 questions to determine if you are competent to provide medical treatment outside your usual area of expertise (Table 2). In Bobby’s case, Dr. F can consider these additional questions:
- Am I comfortable doing this? Would I be comfortable with this scenario if Bobby were my child?
- How extensive was my general residency training in child psychiatry?
- How long ago was my last CAP experience?
- Have I treated ADHD in adults, and am I familiar with stimulant medications?
- What kind of supervision could I arrange, such as regular phone consultation with a CAP or pediatrician?
- How helpful are other information sources, such as recent texts, journals, and medical Web sites?
- What is my relationship with the family, and how would treating Bobby affect it?
Table 2
Should you provide treatment? 4 questions to ask yourself
| How sure am I that I know what I don’t know? |
| How will I know when I should ask for help? |
| Do I have colleagues readily available for consultation if I need help? |
| Do I have a good track record for seeking consultation when I need it? |
Advantages and benefits
So far, we’ve emphasized cautions, but Dr. F also should remember that she may offer patients services that general psychiatrists provide but that pediatricians might not do routinely. Among the possibilities:
- Performing a diagnostic assessment that incorporates biopsychosocial factors.
- Taking time to foster a strong doctor-patient relationship with the family.
- Reserving time for medication-related psychoeducation.
- Scheduling longer visits to discuss a child’s psychiatric problems and explore solutions.
- Utilizing knowledge of and existing relationships with nonphysician therapists who could provide additional psychotherapy.
1. Thomas CR, Holzer CE, III. The continuing shortage of child and adolescent psychiatrists. J Am Acad Child Adolesc Psychiatry 2006;45:1023-31.
2. U.S. Department of Health and Human Services. Mental health: a report of the Surgeon General. Rockville, MD: National Institute of Mental Health; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/home.html. Accessed August 20, 2008.
3. Levin A. Rural counties suffer from child psychiatry shortage. Psychiatr News 2006;42(14):4-41.
4. National Institute of Mental Health. Treatment of children with mental disorders. 2004. Available at: http://www.nimh.nih.gov/publicat/childqa.cfm. Accessed August 2, 2008.
5. Wilens TE, Biederman J, Spencer TJ. Attention deficit/hyperactivity disorder across the lifespan. Annu Rev Med 2002;53:113-31.
6. Greenhill LL, Pliszka S, Dulcan MK, et al. American Academy of Child and Adolescent Psychiatry. Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry. 2002;41(2 suppl):26S-49S.
7. Perrin JM, Friedman RA, Knilans TK. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics 2008;122:451-3.
8. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407-23.

Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Dear Dr. Mossman:
I am an adult psychiatrist practicing in a geographically isolated area. I am working with the family of 10-year-old “Bobby” who is struggling with attention problems. Top notch neuropsychologic testing recommends a stimulant trial, but the local pediatrician is too busy to give Bobby adequate follow-up and attention.
I am an experienced psychopharmacologist but have not prescribed medication to children since residency. My relationship with the family is excellent, and the local pediatrician said that she would supervise me. If I choose to treat Bobby, what are the possible liability issues I should be aware of, and how can I address them?—Submitted by “Dr. F”
Dr. F’s question raises issues that come up whenever patients need treatment for conditions outside the few with which you are highly familiar. Although you can’t be an expert on every aspect of every patient’s treatment, psychiatrists shouldn’t practice outside their area of competence.
Thus, the main liability-related issue that Dr. F should ask herself is, “Can I treat Bobby competently?” Of course, whenever you decide to treat any patient, you should be able to answer “yes” to this question. When thinking about potential liability related to treating Bobby, Dr. F might also ask, “If a lawsuit occurred, how would my treatment of Bobby appear?” This article discusses key issues that arise when general psychiatrists treat children and the steps general psychiatrists can take to show that they are practicing prudently.
Problem: Not enough clinicians
Child and adolescent psychiatrists (CAPs) are in short supply.1,2 In 2001 the United States had 8.67 CAPs per 100,000 youths and 1.6 CAPs for every 1,000 youths with severe mental disorders.1 Studies suggest that the United States needs nearly twice that many CAPs.3 The shortage is especially severe in rural areas, but approximately one-half of metropolitan counties with populations of >250,000 have no CAPs.1 In much of the nation, finding CAPs who are accepting new patients is difficult, and child and adolescent psychiatric treatment often is delivered by pediatricians, family practitioners, psychiatric nurse practitioners, and general adult psychiatrists.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Children’s special medical issues
General psychiatrists know that children aren’t just little adults. CAPs develop skills and thinking styles during their 2 years of subspecialty fellowship training that are quite different from those used by their general psychiatric colleagues.
Communication. Children and adolescents who need psychiatric care often have limited verbal abilities. Working and communicating with these patients requires a different interactive style.
Information sources. CAPs learn to seek and assimilate clinically important information from many settings—especially a child’s home—where their patients interact with others.
Caution. Only a small subset of psychotropic medications that adult psychiatrists prescribe are FDA-approved for use in children (Table 1).4 Because we don’t know how psychotropic drugs affect brain development, CAPs sometimes are leery of giving kids the same medications that adult psychiatrists readily prescribe.
Table 1
FDA-approved drugs and dosages for ADHD in children and adults
| Brand name | Generic name | Drug class | Dosing forms (mg) | Dosage range | Age range |
|---|---|---|---|---|---|
| Adderall | Amphetamine-dextroamphetamine | IR stimulant | 5, 7.5, 10, 12.5, 15, 20, 30 | 5 to 40 mg | 3 to 18 years |
| Adderall XR | Amphetamine-dextroamphetamine | ER stimulant | 5, 10, 15, 20, 25, 30 | 5 to 30 mg | 3 years to adult |
| Concerta | Methylphenidate | ER stimulant | 18, 27, 36, 54 | 18 to 72 mg | 6 years to adult |
| Daytrana | Methylphenidate transdermal | Stimulant | 10, 15, 20, 30 (patch) | 10 to 30 mg | 6 to 18 years |
| Focalin | Dexmethylphenidate | IR stimulant | 2.5, 5, 10 | 2.5 to 10 mg bid | 6 to 17 years |
| Focalin XR | Dexmethylphenidate | ER stimulant | 5, 10, 15, 20 | 5 to 20 mg | 6 years to adult |
| Metadate CD | Methylphenidate | ER stimulant | 10, 20, 30, 50, 60 | 10 to 60 mg | 6 to 18 years |
| Ritalin | Methylphenidate | IR stimulant | 5, 10, 20 | 5 to 20 mg bid or tid | 6 to 18 years |
| Ritalin LA | Methylphenidate | ER stimulant | 10, 20, 30, 40 | 10 to 60 mg | 6 to 18 years |
| Strattera | Atomoxetine | SNRI | 10, 18, 25, 40, 60, 80, 100 | 10 to 100 mg | 6 years to adult |
| Vyvanse | Lisdexamfetamine dimesylate | ER stimulant (precursor) | 30, 50, 70 | 30 to 70 mg | 6 years to adult |
| LA: long acting; CD: controlled delivery; ER, XR: extended release; IR: immediate release; SNRI: selective norepinephrine reuptake inhibitor | |||||
| Source: Adapted from references 2,3 | |||||
Different drugs. Some medications commonly taken by children are not often prescribed for adults, although this is changing as attention-deficit/hyperactivity disorder (ADHD) is better recognized in adults.5,6
Dosages. Dosing psychotropics in adults is fairly standardized, but in children and adolescents dosages vary with age, body weight, and physical maturity.
Adverse effects. The side effects kids experience and the way they report them can differ markedly from adults and will vary with age and developmental maturity. Some issues related to monitoring children—such as appropriate cardiac screening before starting stimulants—are controversial and remain unsettled.7,8
Consider alternatives
Dr. F may be tempted to treat Bobby because of her preexisting, positive relationship with the child’s family and a laudable desire to help. But Dr. F needs to ask, “Is there really no other workable alternative for Bobby?” Some possibilities include:
- Refer Bobby to a CAP in another community for initiation of treatment. Dr. F or Bobby’s pediatrician might safely continue care once a CAP establishes an effective treatment regimen.
- Find another pediatrician who might have more time to provide the follow-up that Dr. F feels is necessary.
- Decline to treat Bobby. Before doing this, Dr. F should consider what effect this refusal might have on her relationship with the family and the consequences for Bobby if his problems go untreated.
- Consult a CAP from another community, describing the situation and clinical factors in detail without naming or identifying the patient, and then ask, “Is this really the best thing to do?”
From a liability standpoint, this last point may be crucial. If the CAP answers “yes,” Dr. F can document the alternatives she has considered and her consultation and discussion with the CAP colleague as evidence of prudent practice. Dr. F can also document any advice that she has received and her plans to follow it.
If you choose to treat
Presumably, Dr. F would not perform thoracic surgery or provide any treatment that is far outside a general psychiatrist’s competence except under the most dire circumstances. General psychiatrists receive child psychiatry training during residency, and treating children is within their scope of practice. Similarly, most elderly patients are treated by general psychiatrists, rather than graduates of geropsychiatry fellowships. Prescribing medication for Bobby is not grossly different from Dr. F’s other duties, and she might provide services that a pediatrician might not.
Ask yourself 4 questions to determine if you are competent to provide medical treatment outside your usual area of expertise (Table 2). In Bobby’s case, Dr. F can consider these additional questions:
- Am I comfortable doing this? Would I be comfortable with this scenario if Bobby were my child?
- How extensive was my general residency training in child psychiatry?
- How long ago was my last CAP experience?
- Have I treated ADHD in adults, and am I familiar with stimulant medications?
- What kind of supervision could I arrange, such as regular phone consultation with a CAP or pediatrician?
- How helpful are other information sources, such as recent texts, journals, and medical Web sites?
- What is my relationship with the family, and how would treating Bobby affect it?
Table 2
Should you provide treatment? 4 questions to ask yourself
| How sure am I that I know what I don’t know? |
| How will I know when I should ask for help? |
| Do I have colleagues readily available for consultation if I need help? |
| Do I have a good track record for seeking consultation when I need it? |
Advantages and benefits
So far, we’ve emphasized cautions, but Dr. F also should remember that she may offer patients services that general psychiatrists provide but that pediatricians might not do routinely. Among the possibilities:
- Performing a diagnostic assessment that incorporates biopsychosocial factors.
- Taking time to foster a strong doctor-patient relationship with the family.
- Reserving time for medication-related psychoeducation.
- Scheduling longer visits to discuss a child’s psychiatric problems and explore solutions.
- Utilizing knowledge of and existing relationships with nonphysician therapists who could provide additional psychotherapy.
Dear Dr. Mossman:
I am an adult psychiatrist practicing in a geographically isolated area. I am working with the family of 10-year-old “Bobby” who is struggling with attention problems. Top notch neuropsychologic testing recommends a stimulant trial, but the local pediatrician is too busy to give Bobby adequate follow-up and attention.
I am an experienced psychopharmacologist but have not prescribed medication to children since residency. My relationship with the family is excellent, and the local pediatrician said that she would supervise me. If I choose to treat Bobby, what are the possible liability issues I should be aware of, and how can I address them?—Submitted by “Dr. F”
Dr. F’s question raises issues that come up whenever patients need treatment for conditions outside the few with which you are highly familiar. Although you can’t be an expert on every aspect of every patient’s treatment, psychiatrists shouldn’t practice outside their area of competence.
Thus, the main liability-related issue that Dr. F should ask herself is, “Can I treat Bobby competently?” Of course, whenever you decide to treat any patient, you should be able to answer “yes” to this question. When thinking about potential liability related to treating Bobby, Dr. F might also ask, “If a lawsuit occurred, how would my treatment of Bobby appear?” This article discusses key issues that arise when general psychiatrists treat children and the steps general psychiatrists can take to show that they are practicing prudently.
Problem: Not enough clinicians
Child and adolescent psychiatrists (CAPs) are in short supply.1,2 In 2001 the United States had 8.67 CAPs per 100,000 youths and 1.6 CAPs for every 1,000 youths with severe mental disorders.1 Studies suggest that the United States needs nearly twice that many CAPs.3 The shortage is especially severe in rural areas, but approximately one-half of metropolitan counties with populations of >250,000 have no CAPs.1 In much of the nation, finding CAPs who are accepting new patients is difficult, and child and adolescent psychiatric treatment often is delivered by pediatricians, family practitioners, psychiatric nurse practitioners, and general adult psychiatrists.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Children’s special medical issues
General psychiatrists know that children aren’t just little adults. CAPs develop skills and thinking styles during their 2 years of subspecialty fellowship training that are quite different from those used by their general psychiatric colleagues.
Communication. Children and adolescents who need psychiatric care often have limited verbal abilities. Working and communicating with these patients requires a different interactive style.
Information sources. CAPs learn to seek and assimilate clinically important information from many settings—especially a child’s home—where their patients interact with others.
Caution. Only a small subset of psychotropic medications that adult psychiatrists prescribe are FDA-approved for use in children (Table 1).4 Because we don’t know how psychotropic drugs affect brain development, CAPs sometimes are leery of giving kids the same medications that adult psychiatrists readily prescribe.
Table 1
FDA-approved drugs and dosages for ADHD in children and adults
| Brand name | Generic name | Drug class | Dosing forms (mg) | Dosage range | Age range |
|---|---|---|---|---|---|
| Adderall | Amphetamine-dextroamphetamine | IR stimulant | 5, 7.5, 10, 12.5, 15, 20, 30 | 5 to 40 mg | 3 to 18 years |
| Adderall XR | Amphetamine-dextroamphetamine | ER stimulant | 5, 10, 15, 20, 25, 30 | 5 to 30 mg | 3 years to adult |
| Concerta | Methylphenidate | ER stimulant | 18, 27, 36, 54 | 18 to 72 mg | 6 years to adult |
| Daytrana | Methylphenidate transdermal | Stimulant | 10, 15, 20, 30 (patch) | 10 to 30 mg | 6 to 18 years |
| Focalin | Dexmethylphenidate | IR stimulant | 2.5, 5, 10 | 2.5 to 10 mg bid | 6 to 17 years |
| Focalin XR | Dexmethylphenidate | ER stimulant | 5, 10, 15, 20 | 5 to 20 mg | 6 years to adult |
| Metadate CD | Methylphenidate | ER stimulant | 10, 20, 30, 50, 60 | 10 to 60 mg | 6 to 18 years |
| Ritalin | Methylphenidate | IR stimulant | 5, 10, 20 | 5 to 20 mg bid or tid | 6 to 18 years |
| Ritalin LA | Methylphenidate | ER stimulant | 10, 20, 30, 40 | 10 to 60 mg | 6 to 18 years |
| Strattera | Atomoxetine | SNRI | 10, 18, 25, 40, 60, 80, 100 | 10 to 100 mg | 6 years to adult |
| Vyvanse | Lisdexamfetamine dimesylate | ER stimulant (precursor) | 30, 50, 70 | 30 to 70 mg | 6 years to adult |
| LA: long acting; CD: controlled delivery; ER, XR: extended release; IR: immediate release; SNRI: selective norepinephrine reuptake inhibitor | |||||
| Source: Adapted from references 2,3 | |||||
Different drugs. Some medications commonly taken by children are not often prescribed for adults, although this is changing as attention-deficit/hyperactivity disorder (ADHD) is better recognized in adults.5,6
Dosages. Dosing psychotropics in adults is fairly standardized, but in children and adolescents dosages vary with age, body weight, and physical maturity.
Adverse effects. The side effects kids experience and the way they report them can differ markedly from adults and will vary with age and developmental maturity. Some issues related to monitoring children—such as appropriate cardiac screening before starting stimulants—are controversial and remain unsettled.7,8
Consider alternatives
Dr. F may be tempted to treat Bobby because of her preexisting, positive relationship with the child’s family and a laudable desire to help. But Dr. F needs to ask, “Is there really no other workable alternative for Bobby?” Some possibilities include:
- Refer Bobby to a CAP in another community for initiation of treatment. Dr. F or Bobby’s pediatrician might safely continue care once a CAP establishes an effective treatment regimen.
- Find another pediatrician who might have more time to provide the follow-up that Dr. F feels is necessary.
- Decline to treat Bobby. Before doing this, Dr. F should consider what effect this refusal might have on her relationship with the family and the consequences for Bobby if his problems go untreated.
- Consult a CAP from another community, describing the situation and clinical factors in detail without naming or identifying the patient, and then ask, “Is this really the best thing to do?”
From a liability standpoint, this last point may be crucial. If the CAP answers “yes,” Dr. F can document the alternatives she has considered and her consultation and discussion with the CAP colleague as evidence of prudent practice. Dr. F can also document any advice that she has received and her plans to follow it.
If you choose to treat
Presumably, Dr. F would not perform thoracic surgery or provide any treatment that is far outside a general psychiatrist’s competence except under the most dire circumstances. General psychiatrists receive child psychiatry training during residency, and treating children is within their scope of practice. Similarly, most elderly patients are treated by general psychiatrists, rather than graduates of geropsychiatry fellowships. Prescribing medication for Bobby is not grossly different from Dr. F’s other duties, and she might provide services that a pediatrician might not.
Ask yourself 4 questions to determine if you are competent to provide medical treatment outside your usual area of expertise (Table 2). In Bobby’s case, Dr. F can consider these additional questions:
- Am I comfortable doing this? Would I be comfortable with this scenario if Bobby were my child?
- How extensive was my general residency training in child psychiatry?
- How long ago was my last CAP experience?
- Have I treated ADHD in adults, and am I familiar with stimulant medications?
- What kind of supervision could I arrange, such as regular phone consultation with a CAP or pediatrician?
- How helpful are other information sources, such as recent texts, journals, and medical Web sites?
- What is my relationship with the family, and how would treating Bobby affect it?
Table 2
Should you provide treatment? 4 questions to ask yourself
| How sure am I that I know what I don’t know? |
| How will I know when I should ask for help? |
| Do I have colleagues readily available for consultation if I need help? |
| Do I have a good track record for seeking consultation when I need it? |
Advantages and benefits
So far, we’ve emphasized cautions, but Dr. F also should remember that she may offer patients services that general psychiatrists provide but that pediatricians might not do routinely. Among the possibilities:
- Performing a diagnostic assessment that incorporates biopsychosocial factors.
- Taking time to foster a strong doctor-patient relationship with the family.
- Reserving time for medication-related psychoeducation.
- Scheduling longer visits to discuss a child’s psychiatric problems and explore solutions.
- Utilizing knowledge of and existing relationships with nonphysician therapists who could provide additional psychotherapy.
1. Thomas CR, Holzer CE, III. The continuing shortage of child and adolescent psychiatrists. J Am Acad Child Adolesc Psychiatry 2006;45:1023-31.
2. U.S. Department of Health and Human Services. Mental health: a report of the Surgeon General. Rockville, MD: National Institute of Mental Health; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/home.html. Accessed August 20, 2008.
3. Levin A. Rural counties suffer from child psychiatry shortage. Psychiatr News 2006;42(14):4-41.
4. National Institute of Mental Health. Treatment of children with mental disorders. 2004. Available at: http://www.nimh.nih.gov/publicat/childqa.cfm. Accessed August 2, 2008.
5. Wilens TE, Biederman J, Spencer TJ. Attention deficit/hyperactivity disorder across the lifespan. Annu Rev Med 2002;53:113-31.
6. Greenhill LL, Pliszka S, Dulcan MK, et al. American Academy of Child and Adolescent Psychiatry. Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry. 2002;41(2 suppl):26S-49S.
7. Perrin JM, Friedman RA, Knilans TK. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics 2008;122:451-3.
8. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407-23.
1. Thomas CR, Holzer CE, III. The continuing shortage of child and adolescent psychiatrists. J Am Acad Child Adolesc Psychiatry 2006;45:1023-31.
2. U.S. Department of Health and Human Services. Mental health: a report of the Surgeon General. Rockville, MD: National Institute of Mental Health; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/home.html. Accessed August 20, 2008.
3. Levin A. Rural counties suffer from child psychiatry shortage. Psychiatr News 2006;42(14):4-41.
4. National Institute of Mental Health. Treatment of children with mental disorders. 2004. Available at: http://www.nimh.nih.gov/publicat/childqa.cfm. Accessed August 2, 2008.
5. Wilens TE, Biederman J, Spencer TJ. Attention deficit/hyperactivity disorder across the lifespan. Annu Rev Med 2002;53:113-31.
6. Greenhill LL, Pliszka S, Dulcan MK, et al. American Academy of Child and Adolescent Psychiatry. Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry. 2002;41(2 suppl):26S-49S.
7. Perrin JM, Friedman RA, Knilans TK. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics 2008;122:451-3.
8. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407-23.
Put your patients to sleep: Useful nondrug strategies for chronic insomnia
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
Ms. H, age 53, has a 20-year history of recurrent major depressive disorder. She seeks treatment for insomnia; her primary complaint is that “no medicine has really ever helped me to sleep for very long.” She reports that every night she experiences a 2-hour sleep onset delay and an average of 5 awakenings that last 10 to 60 minutes each. Her mood is stable.
After failed trials of zolpidem, mirtazapine, amitriptyline, and sertraline plus trazodone, she improves with quetiapine, 50 mg at bedtime, plus sertraline, 150 mg at bedtime. Unfortunately, over the next 6 months Ms. H gains 20 pounds and her physician becomes concerned about her fasting serum glucose levels, which suggest borderline diabetes.
After Ms. H discontinues quetiapine, onset and maintenance insomnia remain clinically significant. Polysomnography reveals moderately loud snoring, a normal respiratory disturbance index of 4.5 per hour, no periodic leg movements of sleep, 32-minute sleep onset, total sleep time of 389 minutes (6.5 hours), and a sleep efficiency of 72%. Ms. H estimates that it took her 120 minutes to fall asleep and that she slept only 270 minutes (4.5 hours) of the 540 minutes (9 hours) in bed. The sleep specialist recommends cognitive-behavioral therapy for insomnia.
For some chronic insomnia patients—such as Ms. H—pharmacotherapy is ineffective or causes intolerable side effects. In any year, >50% of adults in the general population report experiencing difficulty falling asleep, staying asleep, early awakening, or poorly restorative sleep, but these symptoms are usually time-limited and have only a small impact on daytime alertness and function. Chronic insomnia, on the other hand, lasts ≥1 month and has substantial impact on daytime alertness and attention, cognitive function, depressed and anxious mood, and focused performance (Box).1
Medications used to treat insomnia include FDA-approved drugs such as eszopiclone and zolpidem and off-label agents such as mirtazapine and trazodone. The cognitive, behavioral, and other nonpharmacologic therapies described below can be effective options, either alone or in combination with medication.
One in 10 adults in industrialized nations experiences chronic insomnia. Women are affected twice as often as men, with higher rates also reported in older patients and those in lower socioeconomic groups.
Among adults with chronic insomnia, 35% to 45% have psychiatric comorbidities, such as anxiety or mood disorders, and 15% have primary insomnia—sleep disturbance with no identifiable cause, which traditional medical literature described as conditioned or psychophysiologic insomnia.
In the remaining cases, chronic insomnia is associated with:
- medical and sleep disorders (restless legs syndrome, periodic leg movements of sleep, and sleep apnea)
- general medical disorders, particularly those that cause pain
- use of medications that disrupt normal CNS sleep mechanisms.
Source: Reference 1
Assessing insomnia
Start by performing a thorough assessment and history. I have described this process in previous reviews,1,2 as has Neubauer in Current Psychiatry.3
Before initiating therapy for insomnia, assess and address the following:
- significant ongoing depression, mania, hypomania, generalized anxiety, panic, or obsessive-compulsive symptoms that impact sleep
- primary medical disorders of sleep, including restless legs syndrome, increased motor activity during sleep such as periodic leg movements of sleep, and the snoring/snorting of sleep apnea
- prescribed or self-administered medications or substances that can disrupt sleep, such as alcohol, caffeine, stimulants, corticosteroids, or beta blockers.
Recommended nondrug therapies
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine (AASM) updated a comprehensive literature review of psychological and behavioral treatments of primary and secondary insomnia. On the basis of this peer-reviewed, graded evidence, the AASM recommended:
- stimulus control therapy
- relaxation training
- cognitive-behavioral therapy for insomnia (CBTi).4
The AASM also offered guidelines for sleep restriction therapy, multi-component therapy without cognitive therapy, paradoxical intention, and biofeedback. Evidence for sleep hygiene, imaging training, or cognitive therapy alone was insufficient, and the AASM neither recommended nor excluded these methods. Psychological and behavioral interventions were considered effective for treating insomnia in older adults and patients withdrawing from hypnotics.
Stimulus control therapy. Bootzin et al5 first evaluated stimulus control therapy for conditioned insomnia (subsequently identified as primary insomnia). This therapy’s goal is to interrupt the conditioned activation that occurs at bedtime. Patients are instructed to:
- go to bed when sleepy
- remain in bed for no more than 10 minutes (20 minutes if elderly) without sleeping
- if unable to sleep, get up, do something boring, and return to bed only when sleepy
- repeat getting up and returning as frequently as necessary until sleep onset.
For the first 2 weeks of stimulus control therapy, patients are required to self-monitor their sleep behaviors using a sleep diary. Stimulus control therapy is beneficial for primary insomnia and insomnia related to anxious preoccupation. About 70% of patients with conditioned insomnia will improve using stimulus control therapy,4 but it is not clear whether the primary effective intervention is:
- patients dissociating conditioned responses at bedtime, or
- the inevitable sleep restriction caused by getting out of bed.
Relaxation training. Progressive muscle relaxation is a common behavioral treatment of insomnia. Patients learn to tense and then relax individual muscles, beginning at the feet or head and working their way up or down the body. Patients are taught the difference between tension and relaxation to facilitate a relaxation response at bedtime. Another method is the body scanning technique, in which the patient “talks” to each body part, telling it to “relax… relax… relax.”
Relaxation training is predicated on the belief that insomnia is caused by somatized tension and psychophysiologic arousal. The greatest challenge to effective relaxation training is that patients need extensive daytime practice before they can bring the method to the bedroom.
Remind patients that “practice makes perfect.” Therapists often instruct patients to start practicing their relaxation method during the day while self-monitoring by sleep diary and restricting time in bed at night.2
CBTi is the most extensively investigated nonpharmacologic therapy for insomnia.6 It has been used to effectively manage comorbid insomnia in patients with psychiatric disorders,7,8 such as depression,9 generalized anxiety,10 and alcohol dependence,11 as well as those with breast cancer,12 traumatic brain injury,13 and fibromyalgia.14 Age does not appear to be a limitation; research trials show the technique is effective in elderly patients.15
CBTi incorporates cognitive strategies and behavioral interventions to improve sleep quality. Patient self-monitoring with sleep diaries and worksheets is essential.
CBTi commonly is provided in 5 to 8 sessions over 8 to 12 weeks, although studies have described abbreviated practices that used 2 sessions16 and CBTi delivered over the Internet.17 Highly trained clinical psychologists are at the forefront of therapy, but counselors and nurses in primary care settings have administered CBTi.18 For primary insomnia, CBTi is superior in efficacy to pharmacotherapy:
- as initial treatment19
- for long-term management4
- in assisting discontinuation of hypnotic medication.20
CASE CONTINUED: An effective approach
You refer Ms. H to a clinical psychologist who specializes in CBTi. Ms. H begins self-monitoring with a sleep diary and has 5 CBTi sessions over 8 weeks. Initial interventions reduce time in bed from 9 hours to 7 hours per night. Ms. H learns simple relaxation methods that she practices for 2 weeks before attempting to use them to sleep. The psychologist addresses her dysfunctional beliefs about sleep.
During the last 2 weeks of therapy, Ms. H’s sleep diary reveals a sleep efficiency of 92% and improvements in well being, energy, and perceived work efficiency. At a 3-month booster visit, Ms. H has sustained these gains in sleep and daytime function.
Implementing nondrug therapy
I recommend the following steps when offering psychological and behavioral treatment of chronic insomnia, such as CBTi.
Initial visit. Determine whether your patient needs treatment for depressive or anxiety symptoms. Assess the need for polysomnography. Does the patient have a history of an urge to move the legs (restless legs syndrome), increased kicking behavior at night (periodic leg movements of sleep), or loud, disruptive snoring (obstructive sleep apnea)? It is often helpful to have patients think back to when they were consistently sleeping well to identify factors that might be exacerbating poor sleep.
Session 1 (Week 0). Teach patients about normal sleep, how it changes over the life cycle, and common dysfunctional beliefs and behaviors that worsen sleep. Tell patients that every morning when they wake up they should complete a sleep diary (Table 1); you can download a sample sleep diary by visiting this article on CurrentPsychiatry.com.
Table 1
Insomnia: What to document on a sleep diary
| Daytime fatigue |
| Minutes spent napping |
| Medication use |
| Time the patient first tried to fall asleep |
| How long it took to fall asleep |
| How many times the patient woke up |
| Final waking time |
| Hours slept |
| Sleep quality rating |
| How refreshed the patient feels on awakening |
Session 2 (Week 1). Review the sleep diary. Address infractions of sleep hygiene, such as working until bedtime, using caffeine or alcohol in the evening, excessive smoking, or eating in bed. Discuss and specify mutual therapeutic goals for:
- minutes to sleep onset
- minutes of nighttime wakefulness
- number of awakenings
- improvements in sleep efficiency, morning refreshment/alertness, and daytime functioning.
Therapeutic intervention: Instruct patients to reduce their total time in bed (TIB) to their estimated total sleep time, unless they report <6 hours. Insomnia patients commonly overestimate their amount of wakefulness. Because research indicates daytime performance is adversely affected when sleep falls below 6 hours per night,21 I initially limit TIB to 6 hours and further restrict TIB in future sessions as needed to improve sleep efficiency.
Session 3 (Week 2). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency (divide total minutes of reported sleep by the total minutes spent in bed). Typical goals include an average onset of 10 to 20 minutes and an average efficiency of >90%.
Therapeutic intervention: If sleep efficiency falls below 80%, further restrict TIB by 15 minutes; if sleep efficiency is >90%, increase TIB by 15 minutes (no TIB change is needed with efficiencies between 80% and 90%). Identify dysfunctional beliefs about sleep, and provide strategies to interrupt cognitive overactivation—the pressured “talking to oneself” in hopes of falling asleep.
Session 4 (Week 3). Review the sleep diary, and calculate the average time to sleep onset and sleep efficiency. Increase or decrease TIB based on sleep efficiency as described above. Determine if the patient has dysfunctional beliefs regarding sleep.
Therapeutic intervention: Reframe the patient’s dysfunctional beliefs/concepts by comparing sleep diary entries with dysfunctional beliefs (Table 2). Remind patients about strategies to address cognitive overactivation, and have them practice daily to apply the appropriate reframe response from Table 2 that improves sleep. Review progressive muscular relaxation to address somatized tension and arousal, but instruct patients to practice relaxation only during the day at this point.
Table 2
Correcting patients’ dysfunctional sleep beliefs/concepts
| Belief/concept | Reframe responses |
|---|---|
| ‘I need 8 hours sleep per night’ | 1. Nightly sleep need varies among individuals from 5 to 9 hours, particularly with aging 2. Employed adults sleep 6.5 to 7 hours per workweek night 3. For the ‘average’ person, it takes <6 hours of sleep to reduce performance |
| ‘If I don’t sleep, I can’t _____ (work, socialize, take care of the kids, etc.) or ‘If I don’t sleep tonight, I won’t be able to ____’ | 1. Every day one-third of Americans sleep <6.5 hours and yet work, socialize, and live their lives 2. ‘You told me that on ____ you had a terrible night, yet you did ____ (that presentation, meeting, activity with family, etc.)’ |
| ‘If I don’t sleep, I feel _____’ | Explore situations where the person has felt tired, irritable, angry, anxious, etc. independent from lack of sleep |
| ‘If X happens, I won’t sleep’ | Explore situations where X or something like it happened, yet sleep occurred |
| ‘I don’t sleep at all’ | 1. Explore whether a bed partner reports the patient was sleeping or snoring when the person was convinced he or she was awake 2. Tell patients that if they remain in bed for >30 minutes, it is likely they slept, particularly if anxious or frustrated (older depressed patients may be an exception) 3. Teach patients that ‘don’t at all’ statements often represent an excessive focus on wakefulness, and that self-monitoring by sleep diary is helpful |
Session 5 (Week 4). Review the sleep diary. Adjust TIB as necessary. Emphasize the patient’s mastery of dysfunctional beliefs, and highlight progress on the sleep diary. Spend much of this session helping patients improve their relaxation practice and preparing them to bring it to bedtime.
Therapeutic intervention: Tell the patient to apply the relaxation training to bedtime and nocturnal awakenings.
Session 6 (Week 6). Review the sleep diary. Emphasize progress. Address any problem areas regarding dysfunctional beliefs, maladaptive behaviors, or relaxation methods.
Therapeutic intervention: Prepare patients to maintain sleep gains on their own.
Session 7 (Week 8). Review the sleep diary. Have patients identify areas of mastery. Discuss scenarios that might be expected to result in a temporary return of insomnia—such as difficulties with work or home life, stress of job change, or medical illness—and strategies they could apply to improve sleep. Such strategies might include a “safety net” of a sedative/hypnotic agent to use after ≥2 nights of poor sleep.
‘Booster’ session. Three months later, schedule a booster session to determine whether the patient has maintained mastery of improved sleep. Patients who are doing well often cancel this session because they are satisfied with their progress.
Related resource
- American Academy of Sleep Medicine. www.aasmnet.org.
Drug brand names
- Amitriptyline • Elavil, Endep
- Eszopiclone • Lunesta
- Mirtazapine • Remeron
- Quetiapine • Seroquel
- Sertraline • Zoloft
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Becker receives research/grant support from sanofi-aventis and is a speaker for Sepracor Inc. and Takeda Pharmaceutical.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
1. Becker PM. Insomnia: prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr Clin North Am 2006;29(4):855-70.
2. Becker PM. Pharmacologic and nonpharmacologic treatments of insomnia. Neurol Clin 2005;23(4):1149-63.
3. Neubauer DN. Treatment resistant-insomnia: ask yourself 8 questions. Current Psychiatry 2007;6(12):46-54.
4. Morgenthaler T, Kramer M, Alessi C, et al. American Academy of Sleep Medicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep 2006;29(11):1415-9.
5. Bootzin RR, Perlis ML. Nonpharmacologic treatments of insomnia. J Clin Psychiatry 1992;53(suppl):37-41.
6. Morin CM, Bootzin RR, Buysse DJ, et al. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998-2004). Sleep 2006;29(11):1398-414.
7. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25(5):559-92.
8. Dopke CA, Lehner RK, Wells AM. Cognitive-behavioral group therapy for insomnia in individuals with serious mental illnesses: a preliminary evaluation. Psychiatr Rehabil J 2004;27(3):235-42.
9. Carney CE, Segal ZV, Edinger JD, Krystal AD. A comparison of rates of residual insomnia symptoms following pharmacotherapy or cognitive-behavioral therapy for major depressive disorder. J Clin Psychiatry 2007;68(2):254-60.
10. Bélanger L, Morin CM, Langlois F, Ladouceur R. Insomnia and generalized anxiety disorder: effects of cognitive behavior therapy for GAD on insomnia symptoms. J Anxiety Disord 2004;18(4):561-71.
11. Currie SR, Clark S, Hodgins DC, El-Guebaly N. Randomized controlled trial of brief cognitive-behavioural interventions for insomnia in recovering alcoholics. Addiction 2004;99(9):1121-32.
12. Epstein DR, Dirksen SR. Randomized trial of a cognitive-behavioral intervention for insomnia in breast cancer survivors. Oncol Nurs Forum 2007;34(5):E51-9.
13. Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single-case experimental design. Arch Phys Med Rehabil 2007;88(12):1581-92.
14. Edinger JD, Wohlgemuth WK, Krystal AD, Rice JR. Behavioral insomnia therapy for fibromyalgia patients: a randomized clinical trial. Arch Intern Med 2005;165(21):2527-35.
15. Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol 2006;25(1):3-14.
16. Edinger JD, Wohlgemuth WK, Radtke RA, et al. Dose-response effects of cognitive-behavioral insomnia therapy: a randomized clinical trial. Sleep 2007;30(2):203-12.
17. Ström L, Pettersson R, Andersson G. Internet-based treatment for insomnia: a controlled evaluation. J Consult Clin Psychol 2004;72(1):113-20.
18. Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep 2007;30(5):574-84.
19. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med 2004;164(17):1888-96.
20. Morin CM, Bélanger L, Bastien C, Vallières A. Long-term outcome after discontinuation of benzodiazepines for insomnia: a survival analysis of relapse. Behav Res Ther 2005;43(1):1-14.
21. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci 2008;1129:305-22.
Most effective first-line therapy for T-PLL
Washington, DC—Alemtuzumab is the most effective first-line therapy for T-cell prolymphocytic leukemia (T-PLL), according to a presentation at the Peripheral T-cell Lymphoma Forum.
Alemtuzumab is effective when administered alone or in combination with purine analogs, should be administered intravenously as opposed to subcutaneously, and is also effective as a second-line therapy in T-PLL, said Claire Dearden, MD, FRCP, FRCPATH, of The Royal Marsden Hospital.
Dr Dearden also recommended that T-PLL patients be considered for allogeneic stem cell transplant versus autologous stem cell transplant during first remission after alemtuzumab treatment to ensure long-term survival. Once patients relapse, she said, there is no second chance for transplant.
Dr Dearden discussed results she and her colleagues observed in T-PLL patients treated with alemtuzumab in the last 10 years. Some patients were previously untreated, and others underwent chemotherapy prior to receiving alemtuzumab.
In 38 previously treated patients, 62% achieved a complete response (CR). When 16 untreated patients received alemtuzumab intravenously, 88% achieved a CR. In comparison, 11% of patients achieved a CR after subcutaneous administration. This group was rescued with intravenous administration and pentastatin.
These results suggest that alemtuzumab should be administered intravenously rather than subcutaneously to achieve substantial efficacy. The use of intravenous alemtuzumab resulted in survival greater than 2 years.
Dr Dearden also communicated results in 26 T-PLL patients who received stem cell transplant following response to alemtuzumab. Fifteen patients received autograft, and 11 received allograft.
Fifty-five percent of patients who received allograft are still alive, as are 40% of patients who received autograft. Allografted patients also have a lower relapse rate than autografted patients, at 27% vs 53%, respectively. However, the rate of transplant-related mortality is higher in allografted patients, at 27% vs 14%, respectively.
Dr Dearden pointed out that allogeneic stem cell transplant is usually an attractive option. However, because patients with T-PLL tend to belong to an older age group, the procedure often involves a high morbidity and mortality rate.
Dr Dearden also discussed the cytogenetics that uniquely characterize T-PLL. She observed that 75% of cases have the same break point on chromosome 14. These include the inversion (14)(q11q32), the translocation t(14;14)(q11;q32), and the translocation t(X;14)(q28;q11).
Other recurrent changes involve chromosome 8, where 8 translocations have been noted. Significant molecular abnormalities also include the expression of ATM on 11q23, MTCP1 on Xq28, and TCL1a on 14q32.
The oncogene products, most commonly TCL1a, form stabilizing complexes with Akt. They activate Akt by complexing and inducing phosphorylation, downregulating pro-apoptotic control, and ensuring proliferation and survival of the T-PLL cell.
There is also an enrichment of deregulated genes on chromosome 8. NBS1 stimulates the Akt pathway. The gene UPD causes a loss of tumor suppressor gene regulation. ANK-1 is involved in motility and may explain the skin lesions and peritoneal involvement observed in T-PLL.
Dr Dearden suggested that many chromosomal and genetic abnormalities lead to a common upregulation of Akt. Therefore, using Akt or HSP 90 inhibitors may be viable approaches to future treatment.
The Peripheral T-cell Lymphoma Forum took place September 18-20. ![]()
Washington, DC—Alemtuzumab is the most effective first-line therapy for T-cell prolymphocytic leukemia (T-PLL), according to a presentation at the Peripheral T-cell Lymphoma Forum.
Alemtuzumab is effective when administered alone or in combination with purine analogs, should be administered intravenously as opposed to subcutaneously, and is also effective as a second-line therapy in T-PLL, said Claire Dearden, MD, FRCP, FRCPATH, of The Royal Marsden Hospital.
Dr Dearden also recommended that T-PLL patients be considered for allogeneic stem cell transplant versus autologous stem cell transplant during first remission after alemtuzumab treatment to ensure long-term survival. Once patients relapse, she said, there is no second chance for transplant.
Dr Dearden discussed results she and her colleagues observed in T-PLL patients treated with alemtuzumab in the last 10 years. Some patients were previously untreated, and others underwent chemotherapy prior to receiving alemtuzumab.
In 38 previously treated patients, 62% achieved a complete response (CR). When 16 untreated patients received alemtuzumab intravenously, 88% achieved a CR. In comparison, 11% of patients achieved a CR after subcutaneous administration. This group was rescued with intravenous administration and pentastatin.
These results suggest that alemtuzumab should be administered intravenously rather than subcutaneously to achieve substantial efficacy. The use of intravenous alemtuzumab resulted in survival greater than 2 years.
Dr Dearden also communicated results in 26 T-PLL patients who received stem cell transplant following response to alemtuzumab. Fifteen patients received autograft, and 11 received allograft.
Fifty-five percent of patients who received allograft are still alive, as are 40% of patients who received autograft. Allografted patients also have a lower relapse rate than autografted patients, at 27% vs 53%, respectively. However, the rate of transplant-related mortality is higher in allografted patients, at 27% vs 14%, respectively.
Dr Dearden pointed out that allogeneic stem cell transplant is usually an attractive option. However, because patients with T-PLL tend to belong to an older age group, the procedure often involves a high morbidity and mortality rate.
Dr Dearden also discussed the cytogenetics that uniquely characterize T-PLL. She observed that 75% of cases have the same break point on chromosome 14. These include the inversion (14)(q11q32), the translocation t(14;14)(q11;q32), and the translocation t(X;14)(q28;q11).
Other recurrent changes involve chromosome 8, where 8 translocations have been noted. Significant molecular abnormalities also include the expression of ATM on 11q23, MTCP1 on Xq28, and TCL1a on 14q32.
The oncogene products, most commonly TCL1a, form stabilizing complexes with Akt. They activate Akt by complexing and inducing phosphorylation, downregulating pro-apoptotic control, and ensuring proliferation and survival of the T-PLL cell.
There is also an enrichment of deregulated genes on chromosome 8. NBS1 stimulates the Akt pathway. The gene UPD causes a loss of tumor suppressor gene regulation. ANK-1 is involved in motility and may explain the skin lesions and peritoneal involvement observed in T-PLL.
Dr Dearden suggested that many chromosomal and genetic abnormalities lead to a common upregulation of Akt. Therefore, using Akt or HSP 90 inhibitors may be viable approaches to future treatment.
The Peripheral T-cell Lymphoma Forum took place September 18-20. ![]()
Washington, DC—Alemtuzumab is the most effective first-line therapy for T-cell prolymphocytic leukemia (T-PLL), according to a presentation at the Peripheral T-cell Lymphoma Forum.
Alemtuzumab is effective when administered alone or in combination with purine analogs, should be administered intravenously as opposed to subcutaneously, and is also effective as a second-line therapy in T-PLL, said Claire Dearden, MD, FRCP, FRCPATH, of The Royal Marsden Hospital.
Dr Dearden also recommended that T-PLL patients be considered for allogeneic stem cell transplant versus autologous stem cell transplant during first remission after alemtuzumab treatment to ensure long-term survival. Once patients relapse, she said, there is no second chance for transplant.
Dr Dearden discussed results she and her colleagues observed in T-PLL patients treated with alemtuzumab in the last 10 years. Some patients were previously untreated, and others underwent chemotherapy prior to receiving alemtuzumab.
In 38 previously treated patients, 62% achieved a complete response (CR). When 16 untreated patients received alemtuzumab intravenously, 88% achieved a CR. In comparison, 11% of patients achieved a CR after subcutaneous administration. This group was rescued with intravenous administration and pentastatin.
These results suggest that alemtuzumab should be administered intravenously rather than subcutaneously to achieve substantial efficacy. The use of intravenous alemtuzumab resulted in survival greater than 2 years.
Dr Dearden also communicated results in 26 T-PLL patients who received stem cell transplant following response to alemtuzumab. Fifteen patients received autograft, and 11 received allograft.
Fifty-five percent of patients who received allograft are still alive, as are 40% of patients who received autograft. Allografted patients also have a lower relapse rate than autografted patients, at 27% vs 53%, respectively. However, the rate of transplant-related mortality is higher in allografted patients, at 27% vs 14%, respectively.
Dr Dearden pointed out that allogeneic stem cell transplant is usually an attractive option. However, because patients with T-PLL tend to belong to an older age group, the procedure often involves a high morbidity and mortality rate.
Dr Dearden also discussed the cytogenetics that uniquely characterize T-PLL. She observed that 75% of cases have the same break point on chromosome 14. These include the inversion (14)(q11q32), the translocation t(14;14)(q11;q32), and the translocation t(X;14)(q28;q11).
Other recurrent changes involve chromosome 8, where 8 translocations have been noted. Significant molecular abnormalities also include the expression of ATM on 11q23, MTCP1 on Xq28, and TCL1a on 14q32.
The oncogene products, most commonly TCL1a, form stabilizing complexes with Akt. They activate Akt by complexing and inducing phosphorylation, downregulating pro-apoptotic control, and ensuring proliferation and survival of the T-PLL cell.
There is also an enrichment of deregulated genes on chromosome 8. NBS1 stimulates the Akt pathway. The gene UPD causes a loss of tumor suppressor gene regulation. ANK-1 is involved in motility and may explain the skin lesions and peritoneal involvement observed in T-PLL.
Dr Dearden suggested that many chromosomal and genetic abnormalities lead to a common upregulation of Akt. Therefore, using Akt or HSP 90 inhibitors may be viable approaches to future treatment.
The Peripheral T-cell Lymphoma Forum took place September 18-20. ![]()
Certification on Our Minds

Certification on Our Minds
I was wondering whether and when hospital medicine might become a board certification and distinct subspecialty?
Susan Pereira, MD
Vallejo, Calif.
Dr. Hospitalist responds: This is a question on many minds nowadays. With fewer primary care doctors providing inpatient care, new hospitalist programs are popping up all over.
Approximately 85% of this country’s more than 20,000 hospitalists are general internists. For that reason, we are seeing a divergence in the career pathways of these physicians. Some consider themselves outpatient providers; others want to offer only inpatient care. Should we call general internists who just provide inpatient care “inpatient care specialists”? The answer depends on whom you ask.
Robert M. Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco (UCSF), holder of the Lynne and Marc Benioff Endowed Chair in Hospital Medicine, chief of the Division of Hospital Medicine, and chief of the Medical Service at UCSF Medical Center, past president of SHM, member of the American Board of Internal Medicine (ABIM) board of directors, and author of “Wachter’s World” (www.wachtersworld. com) coined the term “hospitalist.” Early in the movement, he and other leaders worried that identifying individuals who worked as hospitalists would hinder the growth of hospital medicine because it would allow payers to exclude primary care providers from practicing in the hospital. Clearly that has not occurred, and the field continues to grow.
Four years ago, the SHM Board of Directors began to look at this issue of hospitalist certification. Mary Jo Gorman, MD, past president of SHM, said certifying hospitalists would allow patients, payers, and hospitals to recognize the quality of work these physicians provide. Later in 2004, the SHM Board of Directors approved a resolution outlining the need to recognize hospitalists as unique providers, and began developing a process for formally certifying hospital medicine.
In 2006, ABIM, a governing board that sets the standards and certifies the knowledge, skills, and aptitudes of U.S. physicians who practice internal medicine and its subspecialties, announced it would create a Recognition of Focused Practice (RFP) for Hospital Medicine, as part of its Maintenance of Certification (MOC) process.
The exact criteria aren’t yet finalized, but ABIM President and Chief Executive Officer Christine K. Cassel, MD, said they likely will include “a combination of significant practice focus in hospital medicine, a high knowledge level of modern, evidence-based hospital care, and a demonstrated commitment to continuously improving the quality of hospital care.”
“ABIM looks forward to working with experts in hospital medicine to develop a process and standards for recognition of this important discipline,” she says.
In my opinion, the SHM/ABIM pairing is wise for several reasons. Partnership with an established organization brings credibility to the process and speeds eventual acceptance of certification. Also, ABIM is the logical choice to start because so many hospitalists are internists. This does not, however, preclude working with the American Board of Pediatrics, the American Board of Family Medicine, or any other certifying organization. In fact, a successful SHM/ABIM partnership could establish a framework for others to follow.
One thing to keep in mind: Dr. Wachter has stressed the fact that ABIM is recognizing an area of focused practice—not expertise. Certification is not the same as fellowship. Nobody is suggesting hospitalists need fellowship training to do their jobs.
What about general internists who practice outpatient medicine? In 2007, ABIM proposed a Comprehensive Care Internal Medicine (CCIM) credential for office-based general internists. This would differentiate internists in the office setting who provide ongoing, coordinated care for a panel of patients from internists who work in urgent care or academic, administrative, or research settings.
The American College of Physicians (ACP) expressed concern about the CCIM credential, saying it would burden physicians and hurt primary care outreach efforts. “CCIM may pose another burdensome hoop that adds time, expense, and limited value, leading to fewer students choosing careers in, and fewer physicians practicing, office-based internal medicine,” wrote ACP in a review of the proposal. More work will be necessary before the larger medical community will accept the CCIM credential.
Meanwhile, the ABIM continues to move forward with the RFP in hospital medicine. For example, Jeff Wiese, MD, professor of medicine at Tulane University in New Orleans and member of SHM’s Board of Directors, became chair of the hospital medicine MOC examination committee, which aims to add hospital medicine-specific elements to the MOC process. If this rapid pace continues, it is realistic to expect examinees to sit for the first tests in 2010.
In the past, Dr. Wachter has raised important questions about this RFP. Will anybody choose to get certified in hospital medicine? What effect will it have on primary care? How will the market value this certification? Will certified hospitalists get paid more? What will happen to those who aren’t certified? Is this the start of a separate specialty with separate training?
I believe when the time comes, hospitalists will choose to get certified. They will view this as a way to distinguish themselves from physicians who work as hospitalists for one to two years between residency and fellowship. Right now, job opportunities for hospitalists abound, but at some point the market will become saturated. The more saturated the market, the greater the value of hospitalist certification. Employers will use this RFP to separate qualified candidates. I also believe it will prevent the remaining primary care physicians from providing care in the hospital. Without additional external funding, however, I doubt this will lead to separate hospitalist training. TH
Certification on Our Minds
I was wondering whether and when hospital medicine might become a board certification and distinct subspecialty?
Susan Pereira, MD
Vallejo, Calif.
Dr. Hospitalist responds: This is a question on many minds nowadays. With fewer primary care doctors providing inpatient care, new hospitalist programs are popping up all over.
Approximately 85% of this country’s more than 20,000 hospitalists are general internists. For that reason, we are seeing a divergence in the career pathways of these physicians. Some consider themselves outpatient providers; others want to offer only inpatient care. Should we call general internists who just provide inpatient care “inpatient care specialists”? The answer depends on whom you ask.
Robert M. Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco (UCSF), holder of the Lynne and Marc Benioff Endowed Chair in Hospital Medicine, chief of the Division of Hospital Medicine, and chief of the Medical Service at UCSF Medical Center, past president of SHM, member of the American Board of Internal Medicine (ABIM) board of directors, and author of “Wachter’s World” (www.wachtersworld. com) coined the term “hospitalist.” Early in the movement, he and other leaders worried that identifying individuals who worked as hospitalists would hinder the growth of hospital medicine because it would allow payers to exclude primary care providers from practicing in the hospital. Clearly that has not occurred, and the field continues to grow.
Four years ago, the SHM Board of Directors began to look at this issue of hospitalist certification. Mary Jo Gorman, MD, past president of SHM, said certifying hospitalists would allow patients, payers, and hospitals to recognize the quality of work these physicians provide. Later in 2004, the SHM Board of Directors approved a resolution outlining the need to recognize hospitalists as unique providers, and began developing a process for formally certifying hospital medicine.
In 2006, ABIM, a governing board that sets the standards and certifies the knowledge, skills, and aptitudes of U.S. physicians who practice internal medicine and its subspecialties, announced it would create a Recognition of Focused Practice (RFP) for Hospital Medicine, as part of its Maintenance of Certification (MOC) process.
The exact criteria aren’t yet finalized, but ABIM President and Chief Executive Officer Christine K. Cassel, MD, said they likely will include “a combination of significant practice focus in hospital medicine, a high knowledge level of modern, evidence-based hospital care, and a demonstrated commitment to continuously improving the quality of hospital care.”
“ABIM looks forward to working with experts in hospital medicine to develop a process and standards for recognition of this important discipline,” she says.
In my opinion, the SHM/ABIM pairing is wise for several reasons. Partnership with an established organization brings credibility to the process and speeds eventual acceptance of certification. Also, ABIM is the logical choice to start because so many hospitalists are internists. This does not, however, preclude working with the American Board of Pediatrics, the American Board of Family Medicine, or any other certifying organization. In fact, a successful SHM/ABIM partnership could establish a framework for others to follow.
One thing to keep in mind: Dr. Wachter has stressed the fact that ABIM is recognizing an area of focused practice—not expertise. Certification is not the same as fellowship. Nobody is suggesting hospitalists need fellowship training to do their jobs.
What about general internists who practice outpatient medicine? In 2007, ABIM proposed a Comprehensive Care Internal Medicine (CCIM) credential for office-based general internists. This would differentiate internists in the office setting who provide ongoing, coordinated care for a panel of patients from internists who work in urgent care or academic, administrative, or research settings.
The American College of Physicians (ACP) expressed concern about the CCIM credential, saying it would burden physicians and hurt primary care outreach efforts. “CCIM may pose another burdensome hoop that adds time, expense, and limited value, leading to fewer students choosing careers in, and fewer physicians practicing, office-based internal medicine,” wrote ACP in a review of the proposal. More work will be necessary before the larger medical community will accept the CCIM credential.
Meanwhile, the ABIM continues to move forward with the RFP in hospital medicine. For example, Jeff Wiese, MD, professor of medicine at Tulane University in New Orleans and member of SHM’s Board of Directors, became chair of the hospital medicine MOC examination committee, which aims to add hospital medicine-specific elements to the MOC process. If this rapid pace continues, it is realistic to expect examinees to sit for the first tests in 2010.
In the past, Dr. Wachter has raised important questions about this RFP. Will anybody choose to get certified in hospital medicine? What effect will it have on primary care? How will the market value this certification? Will certified hospitalists get paid more? What will happen to those who aren’t certified? Is this the start of a separate specialty with separate training?
I believe when the time comes, hospitalists will choose to get certified. They will view this as a way to distinguish themselves from physicians who work as hospitalists for one to two years between residency and fellowship. Right now, job opportunities for hospitalists abound, but at some point the market will become saturated. The more saturated the market, the greater the value of hospitalist certification. Employers will use this RFP to separate qualified candidates. I also believe it will prevent the remaining primary care physicians from providing care in the hospital. Without additional external funding, however, I doubt this will lead to separate hospitalist training. TH
Certification on Our Minds
I was wondering whether and when hospital medicine might become a board certification and distinct subspecialty?
Susan Pereira, MD
Vallejo, Calif.
Dr. Hospitalist responds: This is a question on many minds nowadays. With fewer primary care doctors providing inpatient care, new hospitalist programs are popping up all over.
Approximately 85% of this country’s more than 20,000 hospitalists are general internists. For that reason, we are seeing a divergence in the career pathways of these physicians. Some consider themselves outpatient providers; others want to offer only inpatient care. Should we call general internists who just provide inpatient care “inpatient care specialists”? The answer depends on whom you ask.
Robert M. Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco (UCSF), holder of the Lynne and Marc Benioff Endowed Chair in Hospital Medicine, chief of the Division of Hospital Medicine, and chief of the Medical Service at UCSF Medical Center, past president of SHM, member of the American Board of Internal Medicine (ABIM) board of directors, and author of “Wachter’s World” (www.wachtersworld. com) coined the term “hospitalist.” Early in the movement, he and other leaders worried that identifying individuals who worked as hospitalists would hinder the growth of hospital medicine because it would allow payers to exclude primary care providers from practicing in the hospital. Clearly that has not occurred, and the field continues to grow.
Four years ago, the SHM Board of Directors began to look at this issue of hospitalist certification. Mary Jo Gorman, MD, past president of SHM, said certifying hospitalists would allow patients, payers, and hospitals to recognize the quality of work these physicians provide. Later in 2004, the SHM Board of Directors approved a resolution outlining the need to recognize hospitalists as unique providers, and began developing a process for formally certifying hospital medicine.
In 2006, ABIM, a governing board that sets the standards and certifies the knowledge, skills, and aptitudes of U.S. physicians who practice internal medicine and its subspecialties, announced it would create a Recognition of Focused Practice (RFP) for Hospital Medicine, as part of its Maintenance of Certification (MOC) process.
The exact criteria aren’t yet finalized, but ABIM President and Chief Executive Officer Christine K. Cassel, MD, said they likely will include “a combination of significant practice focus in hospital medicine, a high knowledge level of modern, evidence-based hospital care, and a demonstrated commitment to continuously improving the quality of hospital care.”
“ABIM looks forward to working with experts in hospital medicine to develop a process and standards for recognition of this important discipline,” she says.
In my opinion, the SHM/ABIM pairing is wise for several reasons. Partnership with an established organization brings credibility to the process and speeds eventual acceptance of certification. Also, ABIM is the logical choice to start because so many hospitalists are internists. This does not, however, preclude working with the American Board of Pediatrics, the American Board of Family Medicine, or any other certifying organization. In fact, a successful SHM/ABIM partnership could establish a framework for others to follow.
One thing to keep in mind: Dr. Wachter has stressed the fact that ABIM is recognizing an area of focused practice—not expertise. Certification is not the same as fellowship. Nobody is suggesting hospitalists need fellowship training to do their jobs.
What about general internists who practice outpatient medicine? In 2007, ABIM proposed a Comprehensive Care Internal Medicine (CCIM) credential for office-based general internists. This would differentiate internists in the office setting who provide ongoing, coordinated care for a panel of patients from internists who work in urgent care or academic, administrative, or research settings.
The American College of Physicians (ACP) expressed concern about the CCIM credential, saying it would burden physicians and hurt primary care outreach efforts. “CCIM may pose another burdensome hoop that adds time, expense, and limited value, leading to fewer students choosing careers in, and fewer physicians practicing, office-based internal medicine,” wrote ACP in a review of the proposal. More work will be necessary before the larger medical community will accept the CCIM credential.
Meanwhile, the ABIM continues to move forward with the RFP in hospital medicine. For example, Jeff Wiese, MD, professor of medicine at Tulane University in New Orleans and member of SHM’s Board of Directors, became chair of the hospital medicine MOC examination committee, which aims to add hospital medicine-specific elements to the MOC process. If this rapid pace continues, it is realistic to expect examinees to sit for the first tests in 2010.
In the past, Dr. Wachter has raised important questions about this RFP. Will anybody choose to get certified in hospital medicine? What effect will it have on primary care? How will the market value this certification? Will certified hospitalists get paid more? What will happen to those who aren’t certified? Is this the start of a separate specialty with separate training?
I believe when the time comes, hospitalists will choose to get certified. They will view this as a way to distinguish themselves from physicians who work as hospitalists for one to two years between residency and fellowship. Right now, job opportunities for hospitalists abound, but at some point the market will become saturated. The more saturated the market, the greater the value of hospitalist certification. Employers will use this RFP to separate qualified candidates. I also believe it will prevent the remaining primary care physicians from providing care in the hospital. Without additional external funding, however, I doubt this will lead to separate hospitalist training. TH
The 4-1-1 on NPPs

I’m convinced it is smart for many hospitalist practices to include nurse practitioners and/or physician assistants. The most common problem I see is that a practice doesn’t execute this idea well. They may have the right idea to add these providers, but they fail to create the right job description, support, and management oversight.
While there are a variety of terms in common use, such as “mid-level” and “allied health professional,” I will use “non-physician provider” (NPP) to refer to both NPs and PAs.
The two most common reasons to add NPPs are a strategy to manage growth in the difficult physician recruiting environment and as a way to optimize practice value (provide the best care at the lowest provider cost).
Valuable Roles?
My anecdotal experience suggests most practices have the NPP function in ways that may not be optimal. Most commonly, the NPP works much like another hospitalist in the practice, admitting and “carrying” their own patient caseload. There is often an attempt to have the NPP care for patients that are somewhat less sick and complicated, or care for a smaller patient volume (though this varies a lot).
This is a great concept, but often proves difficult to implement well. The NPPs in such practices often say their caseload—and amount of supervision and interaction with the physician hospitalists—varies a great deal, depending on which hospitalist is on duty. At times, they may have little interaction, leading to a defacto independent practice. At other times, work done by the NPP is repeated by the physician hospitalist. In either case, the NPP is unable to contribute optimally to the practice.
NPPs in this situation often express uncertainty about their job description and who serves as their physician supervisor. If the NPPs in your practice say their job varies, depending on which doctor is on duty, you’re probably limiting the NPP’s contribution to the practice.
Some practices have the NPP manage only the discharge process (and not provide ongoing patient care), including dictation of the discharge summary, for most or all hospitalist patients. In such a system, the NPP may have had little or no involvement with the patient prior to discharge. A variation on this system is to transfer a patient to the care of the NPP (with physician oversight) a day or two before the anticipated day of discharge and when the acute illness has improved.
While reasonable people can disagree, the problem I see with an NPP dedicated to managing the discharge process is that discharge is often the most complicated visit. Managing it well requires knowing a great deal about the patient’s medical and social situation. Asking any provider, including a physician, to step in on the last day and handle this, and prepare a meaningful discharge summary, is very challenging.
While that is unavoidable in some cases, it seems to me a poor idea to create a system in which it happens routinely for all (or nearly all) patients. I worry that referring doctors may not be pleased if they routinely get discharge summaries prepared by someone who had little or no involvement with the patient prior to the day of discharge. How informative and reliable could such a summary be?
New Alternatives
A few practices have begun asking NPPs to function in less common roles, but ones that may contribute more to the practice and provide the NPP with greater satisfaction.
A common scenario is for the several, day-shift doctors to end their work around 7 p.m. when they’re replaced by a single night doctor. And the number of admissions and “crosscover” burdens tend to be greatest in the late afternoon and early night hours around this shift change. This regularly overwhelms the night doctor for the first few hours of the shift (and the ED gets backed up, and so on).
Relief in the form of an NPP functioning in a “swing shift” role—working from the mid-afternoon until around midnight—may make more sense for some practices than having a physician hospitalist work this shift. The NPP would be responsible for admitting patients (all of whom would be seen by the in-house supervising MD that night) and functioning as the first responder for all “crosscover” issues. The practice could have an NPP work this shift seven days a week, and all other patient visits could be made by the MD hospitalists (i.e., the NPP would not have their own “service” of patients to round on daily).
An NPP could also be put in charge of a consult service, such as serving as the main hospitalist consultant on orthopedic patients that need medical consultants. In this role, the NPP would work nearly all his/her time on a single floor, such as the orthopedic floor, and get to know the orthopedic physicians and nursing staff well. This close communication and working relationship would make the NPP well accepted and effective. While physician oversight would still be required, the NPP would likely take mental ownership of issues, such as response times to consult requests, rates of VTE prophylaxis, perioperative beta-blocker use, etc. This could lead to a rewarding role for the NPP and might result in better clinical performance because it would be “owned” by a single person. It is easy to envision a role like this on other units, such as psychiatry or an in-hospital skilled nursing unit.
Lastly, the NPP might be asked to own issues, such as glycemic control or CMS core measure performance for all hospitalist patients (or all patients in the hospital). He or she might see all diabetic patients daily and adjust glycemic therapy as appropriate, but all of those patients would have a separate MD hospitalist see them daily to care for all other problems.
Room for Opinions
There aren’t much data to guide decisions about the right or best role for NPPs in hospitalist practice. For various reasons including local culture, some practices may function best without including NPPs. Yet, many, or most, practices should thoughtfully consider high value roles for NPPs. I think it is important to avoid a knee-jerk response of simply adding NPPs in the role of additional hospitalists, and instead considering less traditional or novel roles. That is just my opinion (informed by considerable experience with a lot of practices) and reasonable people can see it differently. I’m interested in hearing from anyone with an opinion about optimal NPP roles within hospitalist practices.
Next month I’ll offer comments on the economics of NPPs and thoughts about patient satisfaction with NPPs. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I’m convinced it is smart for many hospitalist practices to include nurse practitioners and/or physician assistants. The most common problem I see is that a practice doesn’t execute this idea well. They may have the right idea to add these providers, but they fail to create the right job description, support, and management oversight.
While there are a variety of terms in common use, such as “mid-level” and “allied health professional,” I will use “non-physician provider” (NPP) to refer to both NPs and PAs.
The two most common reasons to add NPPs are a strategy to manage growth in the difficult physician recruiting environment and as a way to optimize practice value (provide the best care at the lowest provider cost).
Valuable Roles?
My anecdotal experience suggests most practices have the NPP function in ways that may not be optimal. Most commonly, the NPP works much like another hospitalist in the practice, admitting and “carrying” their own patient caseload. There is often an attempt to have the NPP care for patients that are somewhat less sick and complicated, or care for a smaller patient volume (though this varies a lot).
This is a great concept, but often proves difficult to implement well. The NPPs in such practices often say their caseload—and amount of supervision and interaction with the physician hospitalists—varies a great deal, depending on which hospitalist is on duty. At times, they may have little interaction, leading to a defacto independent practice. At other times, work done by the NPP is repeated by the physician hospitalist. In either case, the NPP is unable to contribute optimally to the practice.
NPPs in this situation often express uncertainty about their job description and who serves as their physician supervisor. If the NPPs in your practice say their job varies, depending on which doctor is on duty, you’re probably limiting the NPP’s contribution to the practice.
Some practices have the NPP manage only the discharge process (and not provide ongoing patient care), including dictation of the discharge summary, for most or all hospitalist patients. In such a system, the NPP may have had little or no involvement with the patient prior to discharge. A variation on this system is to transfer a patient to the care of the NPP (with physician oversight) a day or two before the anticipated day of discharge and when the acute illness has improved.
While reasonable people can disagree, the problem I see with an NPP dedicated to managing the discharge process is that discharge is often the most complicated visit. Managing it well requires knowing a great deal about the patient’s medical and social situation. Asking any provider, including a physician, to step in on the last day and handle this, and prepare a meaningful discharge summary, is very challenging.
While that is unavoidable in some cases, it seems to me a poor idea to create a system in which it happens routinely for all (or nearly all) patients. I worry that referring doctors may not be pleased if they routinely get discharge summaries prepared by someone who had little or no involvement with the patient prior to the day of discharge. How informative and reliable could such a summary be?
New Alternatives
A few practices have begun asking NPPs to function in less common roles, but ones that may contribute more to the practice and provide the NPP with greater satisfaction.
A common scenario is for the several, day-shift doctors to end their work around 7 p.m. when they’re replaced by a single night doctor. And the number of admissions and “crosscover” burdens tend to be greatest in the late afternoon and early night hours around this shift change. This regularly overwhelms the night doctor for the first few hours of the shift (and the ED gets backed up, and so on).
Relief in the form of an NPP functioning in a “swing shift” role—working from the mid-afternoon until around midnight—may make more sense for some practices than having a physician hospitalist work this shift. The NPP would be responsible for admitting patients (all of whom would be seen by the in-house supervising MD that night) and functioning as the first responder for all “crosscover” issues. The practice could have an NPP work this shift seven days a week, and all other patient visits could be made by the MD hospitalists (i.e., the NPP would not have their own “service” of patients to round on daily).
An NPP could also be put in charge of a consult service, such as serving as the main hospitalist consultant on orthopedic patients that need medical consultants. In this role, the NPP would work nearly all his/her time on a single floor, such as the orthopedic floor, and get to know the orthopedic physicians and nursing staff well. This close communication and working relationship would make the NPP well accepted and effective. While physician oversight would still be required, the NPP would likely take mental ownership of issues, such as response times to consult requests, rates of VTE prophylaxis, perioperative beta-blocker use, etc. This could lead to a rewarding role for the NPP and might result in better clinical performance because it would be “owned” by a single person. It is easy to envision a role like this on other units, such as psychiatry or an in-hospital skilled nursing unit.
Lastly, the NPP might be asked to own issues, such as glycemic control or CMS core measure performance for all hospitalist patients (or all patients in the hospital). He or she might see all diabetic patients daily and adjust glycemic therapy as appropriate, but all of those patients would have a separate MD hospitalist see them daily to care for all other problems.
Room for Opinions
There aren’t much data to guide decisions about the right or best role for NPPs in hospitalist practice. For various reasons including local culture, some practices may function best without including NPPs. Yet, many, or most, practices should thoughtfully consider high value roles for NPPs. I think it is important to avoid a knee-jerk response of simply adding NPPs in the role of additional hospitalists, and instead considering less traditional or novel roles. That is just my opinion (informed by considerable experience with a lot of practices) and reasonable people can see it differently. I’m interested in hearing from anyone with an opinion about optimal NPP roles within hospitalist practices.
Next month I’ll offer comments on the economics of NPPs and thoughts about patient satisfaction with NPPs. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I’m convinced it is smart for many hospitalist practices to include nurse practitioners and/or physician assistants. The most common problem I see is that a practice doesn’t execute this idea well. They may have the right idea to add these providers, but they fail to create the right job description, support, and management oversight.
While there are a variety of terms in common use, such as “mid-level” and “allied health professional,” I will use “non-physician provider” (NPP) to refer to both NPs and PAs.
The two most common reasons to add NPPs are a strategy to manage growth in the difficult physician recruiting environment and as a way to optimize practice value (provide the best care at the lowest provider cost).
Valuable Roles?
My anecdotal experience suggests most practices have the NPP function in ways that may not be optimal. Most commonly, the NPP works much like another hospitalist in the practice, admitting and “carrying” their own patient caseload. There is often an attempt to have the NPP care for patients that are somewhat less sick and complicated, or care for a smaller patient volume (though this varies a lot).
This is a great concept, but often proves difficult to implement well. The NPPs in such practices often say their caseload—and amount of supervision and interaction with the physician hospitalists—varies a great deal, depending on which hospitalist is on duty. At times, they may have little interaction, leading to a defacto independent practice. At other times, work done by the NPP is repeated by the physician hospitalist. In either case, the NPP is unable to contribute optimally to the practice.
NPPs in this situation often express uncertainty about their job description and who serves as their physician supervisor. If the NPPs in your practice say their job varies, depending on which doctor is on duty, you’re probably limiting the NPP’s contribution to the practice.
Some practices have the NPP manage only the discharge process (and not provide ongoing patient care), including dictation of the discharge summary, for most or all hospitalist patients. In such a system, the NPP may have had little or no involvement with the patient prior to discharge. A variation on this system is to transfer a patient to the care of the NPP (with physician oversight) a day or two before the anticipated day of discharge and when the acute illness has improved.
While reasonable people can disagree, the problem I see with an NPP dedicated to managing the discharge process is that discharge is often the most complicated visit. Managing it well requires knowing a great deal about the patient’s medical and social situation. Asking any provider, including a physician, to step in on the last day and handle this, and prepare a meaningful discharge summary, is very challenging.
While that is unavoidable in some cases, it seems to me a poor idea to create a system in which it happens routinely for all (or nearly all) patients. I worry that referring doctors may not be pleased if they routinely get discharge summaries prepared by someone who had little or no involvement with the patient prior to the day of discharge. How informative and reliable could such a summary be?
New Alternatives
A few practices have begun asking NPPs to function in less common roles, but ones that may contribute more to the practice and provide the NPP with greater satisfaction.
A common scenario is for the several, day-shift doctors to end their work around 7 p.m. when they’re replaced by a single night doctor. And the number of admissions and “crosscover” burdens tend to be greatest in the late afternoon and early night hours around this shift change. This regularly overwhelms the night doctor for the first few hours of the shift (and the ED gets backed up, and so on).
Relief in the form of an NPP functioning in a “swing shift” role—working from the mid-afternoon until around midnight—may make more sense for some practices than having a physician hospitalist work this shift. The NPP would be responsible for admitting patients (all of whom would be seen by the in-house supervising MD that night) and functioning as the first responder for all “crosscover” issues. The practice could have an NPP work this shift seven days a week, and all other patient visits could be made by the MD hospitalists (i.e., the NPP would not have their own “service” of patients to round on daily).
An NPP could also be put in charge of a consult service, such as serving as the main hospitalist consultant on orthopedic patients that need medical consultants. In this role, the NPP would work nearly all his/her time on a single floor, such as the orthopedic floor, and get to know the orthopedic physicians and nursing staff well. This close communication and working relationship would make the NPP well accepted and effective. While physician oversight would still be required, the NPP would likely take mental ownership of issues, such as response times to consult requests, rates of VTE prophylaxis, perioperative beta-blocker use, etc. This could lead to a rewarding role for the NPP and might result in better clinical performance because it would be “owned” by a single person. It is easy to envision a role like this on other units, such as psychiatry or an in-hospital skilled nursing unit.
Lastly, the NPP might be asked to own issues, such as glycemic control or CMS core measure performance for all hospitalist patients (or all patients in the hospital). He or she might see all diabetic patients daily and adjust glycemic therapy as appropriate, but all of those patients would have a separate MD hospitalist see them daily to care for all other problems.
Room for Opinions
There aren’t much data to guide decisions about the right or best role for NPPs in hospitalist practice. For various reasons including local culture, some practices may function best without including NPPs. Yet, many, or most, practices should thoughtfully consider high value roles for NPPs. I think it is important to avoid a knee-jerk response of simply adding NPPs in the role of additional hospitalists, and instead considering less traditional or novel roles. That is just my opinion (informed by considerable experience with a lot of practices) and reasonable people can see it differently. I’m interested in hearing from anyone with an opinion about optimal NPP roles within hospitalist practices.
Next month I’ll offer comments on the economics of NPPs and thoughts about patient satisfaction with NPPs. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is also part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Left Turns

Balance—that unrelenting chemistry project necessary to maintain our sanity. In its simplest form, balance means achieving harmony in work and life, job and home, career and family. However, as we move along the life continuum this straightforward linear equation can take on second, third, seemingly infinite dimensions.
Children need raising, marriages need cultivation, friendships need nurturing, lawns need mowing, books need reading, waistlines need shrinking, charities need volunteering, extended family need visiting, dogs need walking, minds need relaxing, beds need sleeping in, and so on and so forth.
Add to this concoction a full-time hospitalist job with its clinical demands, night shifts, long stretches of days, administrative or scholarly duties, and patients’ emotional needs and you have a volatile cauldron that’s nearly impossible to keep from boiling over.
Thus, the need to maintain perspective, keep even, and stay in balance. We all have our own means to maintain balance and methods to measure if we are in or out of it. For me, it all comes down to left turns.
I moved to Denver in the mid-’90s to do my residency in internal medicine. Prior to that, balance wasn’t something I thought much about. Certainly there were times when the work-life continuum strayed too far toward the former—especially during the doldrums of medical school. However, it wasn’t until residency that I began to feel the true equilibrium tug-of-war.
At the time, I wasn’t juggling nearly as many balls as I am now, but nonetheless it was easy to become discombobulated. With limitless work hours, every fourth night call with 36-plus-hour shifts, morning report preparations, and the occasional harrowing attending rounds, finding ways to let off steam became paramount. I had moved to Colorado partly to enjoy its natural bounty. With the foothills a mere 30 minutes away and the high country within an hour’s drive, I frequently recharged by heading west for a hike, snow shoe, or cross country ski. Driving north from my house in central Denver you quickly come to Interstate 70, which traverses the state of Colorado, east to west. For me, I-70 is more than just a means of transportation; it is the scale upon which I measure my life’s balance. A trip east takes me to the airport and the hospital at which I work. A trip west takes me to the mountains. Right turn = travel, work, stress. Left turn = recreation, exercise, relaxation. Reflecting on my ratio of right to left turns is a simple and sure means to gauge my level of balance.
Maintaining enough left turns is one of the key issues facing the field of hospital medicine. As a young, exciting, and rapidly growing field it’s easy to become overwhelmed in our jobs. For most of us, our first hospitalist jobs felt comfortable: basically residency with less hours and more pay. However, as it turns out, the hospitalist job’s similarity to residency is one of the biggest hurdles we face.
Studies of internal medicine residency programs have revealed that up to three-quarters of residents are burned out.1,2 This doesn’t bode well for a field that strongly recruits from this burned-out pool of applicants and shares many of the structural elements that make residents so prone to burn out. The common causes of burnout—extended workloads, limited autonomy and control over one’s work-life, ambiguous employer expectations, deficient support systems, lack of stability and predictability—are mainstays of many hospitalist systems.
The only study to systematically evaluate hospitalist burnout found 13% of hospitalists were burned out with an additional 25% at risk for burnout.3 While this is a noteworthy improvement over the residency rates, it is likely the rate has risen significantly since the study was completed in 1999. Even if it hasn’t, it’s concerning to build a hospitalist group (let alone an entire field) with about 40% of its base nearing or completely burned out. Burnout is associated with employee turnover, reduced individual and group morale, and—quite possibly—worse patient outcomes.
As such, it is incumbent upon hospitalists and hospitalist group leaders to promote healthy work environments. In most cases, this doesn’t mean making changes to reinvigorate a burned-out employee (although this may be necessary). Rather, it involves targeting the larger organizational structure to mitigate the factors that promote burnout in the first place.
A successful group must provide individuals control over its work environment to help offset the hefty demands the job levies on hospitalists. Individual hospitalists should have a voice in the group’s decision-making and scheduling process. This encourages ownership in the group’s future; ownership is inversely associated with burnout. Further, attempts should be made to reduce the unpredictability of the job as much as possible. This should include setting and maintaining clear expectations, having back-up systems to deal with unexpected spikes in volume or an ill colleague, and placing hard caps on the number of encounters per day. Finally, a group should strive to provide hospitalists with flexible scheduling so that, when necessary, they can care for a child or a sick relative, limit the number of consecutive shifts worked and ensure adequate time away from work.
Which brings us back to balance.
It ultimately falls to each of us to ensure that we remain on kilter. As the summer draws to a close, take a quick biopsy of your level of balance. If you’re a bit out of whack, make an effort to realign. Take some extra time with your kids, spend a night alone with your spouse, go to bed early and read by yourself. Take a left turn. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado, Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Gopal R, Glasheen JJ, Miyoshi T, Prochazka AV. Burnout and internal medicine resident work-hour restrictions. Arch Intern Med. 2005;165:2595-2600.
- Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Arch Intern Med. 2002;136(5):358-67
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91
Balance—that unrelenting chemistry project necessary to maintain our sanity. In its simplest form, balance means achieving harmony in work and life, job and home, career and family. However, as we move along the life continuum this straightforward linear equation can take on second, third, seemingly infinite dimensions.
Children need raising, marriages need cultivation, friendships need nurturing, lawns need mowing, books need reading, waistlines need shrinking, charities need volunteering, extended family need visiting, dogs need walking, minds need relaxing, beds need sleeping in, and so on and so forth.
Add to this concoction a full-time hospitalist job with its clinical demands, night shifts, long stretches of days, administrative or scholarly duties, and patients’ emotional needs and you have a volatile cauldron that’s nearly impossible to keep from boiling over.
Thus, the need to maintain perspective, keep even, and stay in balance. We all have our own means to maintain balance and methods to measure if we are in or out of it. For me, it all comes down to left turns.
I moved to Denver in the mid-’90s to do my residency in internal medicine. Prior to that, balance wasn’t something I thought much about. Certainly there were times when the work-life continuum strayed too far toward the former—especially during the doldrums of medical school. However, it wasn’t until residency that I began to feel the true equilibrium tug-of-war.
At the time, I wasn’t juggling nearly as many balls as I am now, but nonetheless it was easy to become discombobulated. With limitless work hours, every fourth night call with 36-plus-hour shifts, morning report preparations, and the occasional harrowing attending rounds, finding ways to let off steam became paramount. I had moved to Colorado partly to enjoy its natural bounty. With the foothills a mere 30 minutes away and the high country within an hour’s drive, I frequently recharged by heading west for a hike, snow shoe, or cross country ski. Driving north from my house in central Denver you quickly come to Interstate 70, which traverses the state of Colorado, east to west. For me, I-70 is more than just a means of transportation; it is the scale upon which I measure my life’s balance. A trip east takes me to the airport and the hospital at which I work. A trip west takes me to the mountains. Right turn = travel, work, stress. Left turn = recreation, exercise, relaxation. Reflecting on my ratio of right to left turns is a simple and sure means to gauge my level of balance.
Maintaining enough left turns is one of the key issues facing the field of hospital medicine. As a young, exciting, and rapidly growing field it’s easy to become overwhelmed in our jobs. For most of us, our first hospitalist jobs felt comfortable: basically residency with less hours and more pay. However, as it turns out, the hospitalist job’s similarity to residency is one of the biggest hurdles we face.
Studies of internal medicine residency programs have revealed that up to three-quarters of residents are burned out.1,2 This doesn’t bode well for a field that strongly recruits from this burned-out pool of applicants and shares many of the structural elements that make residents so prone to burn out. The common causes of burnout—extended workloads, limited autonomy and control over one’s work-life, ambiguous employer expectations, deficient support systems, lack of stability and predictability—are mainstays of many hospitalist systems.
The only study to systematically evaluate hospitalist burnout found 13% of hospitalists were burned out with an additional 25% at risk for burnout.3 While this is a noteworthy improvement over the residency rates, it is likely the rate has risen significantly since the study was completed in 1999. Even if it hasn’t, it’s concerning to build a hospitalist group (let alone an entire field) with about 40% of its base nearing or completely burned out. Burnout is associated with employee turnover, reduced individual and group morale, and—quite possibly—worse patient outcomes.
As such, it is incumbent upon hospitalists and hospitalist group leaders to promote healthy work environments. In most cases, this doesn’t mean making changes to reinvigorate a burned-out employee (although this may be necessary). Rather, it involves targeting the larger organizational structure to mitigate the factors that promote burnout in the first place.
A successful group must provide individuals control over its work environment to help offset the hefty demands the job levies on hospitalists. Individual hospitalists should have a voice in the group’s decision-making and scheduling process. This encourages ownership in the group’s future; ownership is inversely associated with burnout. Further, attempts should be made to reduce the unpredictability of the job as much as possible. This should include setting and maintaining clear expectations, having back-up systems to deal with unexpected spikes in volume or an ill colleague, and placing hard caps on the number of encounters per day. Finally, a group should strive to provide hospitalists with flexible scheduling so that, when necessary, they can care for a child or a sick relative, limit the number of consecutive shifts worked and ensure adequate time away from work.
Which brings us back to balance.
It ultimately falls to each of us to ensure that we remain on kilter. As the summer draws to a close, take a quick biopsy of your level of balance. If you’re a bit out of whack, make an effort to realign. Take some extra time with your kids, spend a night alone with your spouse, go to bed early and read by yourself. Take a left turn. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado, Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Gopal R, Glasheen JJ, Miyoshi T, Prochazka AV. Burnout and internal medicine resident work-hour restrictions. Arch Intern Med. 2005;165:2595-2600.
- Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Arch Intern Med. 2002;136(5):358-67
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91
Balance—that unrelenting chemistry project necessary to maintain our sanity. In its simplest form, balance means achieving harmony in work and life, job and home, career and family. However, as we move along the life continuum this straightforward linear equation can take on second, third, seemingly infinite dimensions.
Children need raising, marriages need cultivation, friendships need nurturing, lawns need mowing, books need reading, waistlines need shrinking, charities need volunteering, extended family need visiting, dogs need walking, minds need relaxing, beds need sleeping in, and so on and so forth.
Add to this concoction a full-time hospitalist job with its clinical demands, night shifts, long stretches of days, administrative or scholarly duties, and patients’ emotional needs and you have a volatile cauldron that’s nearly impossible to keep from boiling over.
Thus, the need to maintain perspective, keep even, and stay in balance. We all have our own means to maintain balance and methods to measure if we are in or out of it. For me, it all comes down to left turns.
I moved to Denver in the mid-’90s to do my residency in internal medicine. Prior to that, balance wasn’t something I thought much about. Certainly there were times when the work-life continuum strayed too far toward the former—especially during the doldrums of medical school. However, it wasn’t until residency that I began to feel the true equilibrium tug-of-war.
At the time, I wasn’t juggling nearly as many balls as I am now, but nonetheless it was easy to become discombobulated. With limitless work hours, every fourth night call with 36-plus-hour shifts, morning report preparations, and the occasional harrowing attending rounds, finding ways to let off steam became paramount. I had moved to Colorado partly to enjoy its natural bounty. With the foothills a mere 30 minutes away and the high country within an hour’s drive, I frequently recharged by heading west for a hike, snow shoe, or cross country ski. Driving north from my house in central Denver you quickly come to Interstate 70, which traverses the state of Colorado, east to west. For me, I-70 is more than just a means of transportation; it is the scale upon which I measure my life’s balance. A trip east takes me to the airport and the hospital at which I work. A trip west takes me to the mountains. Right turn = travel, work, stress. Left turn = recreation, exercise, relaxation. Reflecting on my ratio of right to left turns is a simple and sure means to gauge my level of balance.
Maintaining enough left turns is one of the key issues facing the field of hospital medicine. As a young, exciting, and rapidly growing field it’s easy to become overwhelmed in our jobs. For most of us, our first hospitalist jobs felt comfortable: basically residency with less hours and more pay. However, as it turns out, the hospitalist job’s similarity to residency is one of the biggest hurdles we face.
Studies of internal medicine residency programs have revealed that up to three-quarters of residents are burned out.1,2 This doesn’t bode well for a field that strongly recruits from this burned-out pool of applicants and shares many of the structural elements that make residents so prone to burn out. The common causes of burnout—extended workloads, limited autonomy and control over one’s work-life, ambiguous employer expectations, deficient support systems, lack of stability and predictability—are mainstays of many hospitalist systems.
The only study to systematically evaluate hospitalist burnout found 13% of hospitalists were burned out with an additional 25% at risk for burnout.3 While this is a noteworthy improvement over the residency rates, it is likely the rate has risen significantly since the study was completed in 1999. Even if it hasn’t, it’s concerning to build a hospitalist group (let alone an entire field) with about 40% of its base nearing or completely burned out. Burnout is associated with employee turnover, reduced individual and group morale, and—quite possibly—worse patient outcomes.
As such, it is incumbent upon hospitalists and hospitalist group leaders to promote healthy work environments. In most cases, this doesn’t mean making changes to reinvigorate a burned-out employee (although this may be necessary). Rather, it involves targeting the larger organizational structure to mitigate the factors that promote burnout in the first place.
A successful group must provide individuals control over its work environment to help offset the hefty demands the job levies on hospitalists. Individual hospitalists should have a voice in the group’s decision-making and scheduling process. This encourages ownership in the group’s future; ownership is inversely associated with burnout. Further, attempts should be made to reduce the unpredictability of the job as much as possible. This should include setting and maintaining clear expectations, having back-up systems to deal with unexpected spikes in volume or an ill colleague, and placing hard caps on the number of encounters per day. Finally, a group should strive to provide hospitalists with flexible scheduling so that, when necessary, they can care for a child or a sick relative, limit the number of consecutive shifts worked and ensure adequate time away from work.
Which brings us back to balance.
It ultimately falls to each of us to ensure that we remain on kilter. As the summer draws to a close, take a quick biopsy of your level of balance. If you’re a bit out of whack, make an effort to realign. Take some extra time with your kids, spend a night alone with your spouse, go to bed early and read by yourself. Take a left turn. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado, Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Gopal R, Glasheen JJ, Miyoshi T, Prochazka AV. Burnout and internal medicine resident work-hour restrictions. Arch Intern Med. 2005;165:2595-2600.
- Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Arch Intern Med. 2002;136(5):358-67
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91
PCPs Come Home

Hospitalists have been concerned about the entire continuum of care from the early days of the hospital medicine movement. We have tried to look at the system of healthcare from the patients’ viewpoint, where an admission to the hospital is rare in the larger scheme of their healthcare and their interaction with a variety of physicians and health professionals.
Hospitalists will always need to rely on our professional relationships with surgeons and specialists, as well as with the primary care physicians (PCPs) who refer their patients for admission to the hospital and who partner with us to resume patient care at discharge.
With this fundamental backdrop, two interesting trends in the PCP world—the patient-centered medical home (PCMH) and PCPs’ use of performance measurements to drive referrals to hospitals and specialists—will have a profound effect on hospitalists, the patients we treat, and the systems of care in which we work.
PCMH and Hospitalists
For many years, the problems in primary care have been virtually ignored and dismissed by the insurance industry—and even by most of organized medicine. As if a light has suddenly been turned on, everyone now wants to “do something” to save primary care.
One of the latest “solutions’ is the PCMH. As we all know, ideas without funding are just ideas. It’s time to take note of PCMH. Why? Because insurance companies and Medicare are paying for a variety of pilot and demonstration projects to see how PCMH might play out in real-life interactions among patients and physicians.
The main new characteristics in the PCMH (as opposed to the traditional PCP) are a more robust information system and the commitment of personnel and organization within the PCP practice to allow proactive coordination of the patient’s care. The hope on the performance side is that patients will receive better care that will lead to better patient satisfaction and better outcomes. On the payment side, the PCP must receive significant monetary support to pay for the staff and equipment to coordinate and manage their patient’s journey through an increasingly complex series of tests, referrals, and treatments.
Accountability
SHM has tried to raise the issues of how the PCMH would relate to hospitalists at key junctures in the hospitalization continuum. Hopefully this will lead to a dialogue with the PCP community about how PCMH proposals would meet the goals of defining accountability and responsibility for the PCMH and for hospitalists. In turn this would lead to a better, safer system for our patients.
While discussions have specifically focused on the PCMH-hospitalist interface, many of the same tenets of accountability, responsibility, timeliness, and information transfer would apply to the PCMH-specialist interfaces.
Time of Admission
Accurate, timely information is crucial at the time of acute illness. It would be expected that at the time of the patient’s arrival at the hospital the following set of data elements would be available to the hospitalist (and/or emergency department physician or specialist). These elements are lifted directly from the joint SHM-ACP-SGIM Transitions of Care Consensus document from 2007 (available at www.hospitalmedicine.org): principle diagnosis and problem list; medication list (reconciliation), including over-the-counter and herbal products, allergies, and drug interactions; emergency plan and contact number and person; treatment and diagnostic plan; prognosis and goals of care; test results/pending results; clearly identifies medical home and/or transferring coordinating physician/institution; patient’s cognitive status; advance directives, power of attorney, consent; planned interventions, durable medical equipment, wound care; and assessment of caregiver status.
Time of Discharge
While it is clear that the hospitalist is responsible for overseeing the patient’s care while hospitalized, it is essential for patients and their families to know who will be accountable at the time of discharge. SHM proposes that the PCMH:
- Assume the primary role of caring for the patient as of the time of discharge from the hospital;
- Provide a timely first post-discharge office visit consistent with the acute illness as documented in the discharge summary; and
- Ensure a handoff formally confirmed and documented by the hospitalist and PCMH.
The hospitalist should provide to the PCMH:
- An accurate and timely discharge summary; and
- The availability to the PCMH to answer questions about the hospitalization.
Further, discharge summaries should include:
- Primary and secondary diagnoses;
- Pertinent history and physical findings;
- Dates of hospitalization, treatment provided, brief hospital course;
- Results of procedures and abnormal laboratory tests;
- Recommendations of any subspecialty consultants;
- Information given to the patient and family;
- The patient’s condition or functional status at discharge;
- Reconciled discharge medication regimen, with reasons for any changes and indications for newly prescribed medications;
- Details of follow-up arrangements made;
- Specific follow-up needs, including appointments or procedures to be scheduled, and tests pending at the time of discharge; and
- Name and contact information of the responsible hospital physician.1
Other Considerations
Obviously other aspects of the PCMH-hospitalist relationship must be considered, including when the PCMH would like to be informed (or involved) during their patient’s hospitalization, as well as how to manage the handoff of responsibilities and information when the patient leaves the hospital but does not go directly home (e.g., when they are sent to a skilled nursing facility or rehabilitation center). If we continue to look at solutions from the patient’s and family’s points of view, we can come up with a workable solution.
Performance-driven Referral
Part of the result of the growth of the hospital medicine movement is that, increasingly, PCPs are not directly managing their patients for acute illnesses. That said, the PCP still has a significant role in determining whether their patients get the best care available—even if other physicians (e.g., hospitalists, surgeons, subspecialists) deliver the actual care.
We are just at the beginning of performance measurement and reporting. Today, PCPs and their patients can log on to www.hospitalcompare.hhs.gov and look at any hospital’s performance for pneumonia, acute coronary syndrome, and heart failure. The era of disease-specific and institution-specific—even physician-specific—reporting grows on a seemingly monthly basis.
Armed with this information, the PCP’s role shifts from managing the acute illnesses of their patients to understanding the report cards on their local hospitals and specialists and using this information to direct their patients to the hospitals and physicians who have the best outcomes. The expanding role of the PCP as the informed guide for their patients further will drive hospitals and all physicians who rely on referrals to improve their feedback and communication with PCPs.
We will begin to see that best-of-breed hospitals not only will have excellent clinical outcomes but will be pushed to have better patient-satisfaction and PCP-satisfaction scores. This is an opportunity for enlightened PCPs to use their medical background and hands-on understanding of local healthcare to be a vital resource to their patients.
By the same token, this is an opportunity for product differentiation for hospitals and their hospitalists to reshape a healthcare referral world traditionally built more on geography and familiarity than on information and performance, and replace it with strong communication and better outcomes. The best thing about this approach is the patient wins. TH
Dr. Wellikson is the CEO of SHM
Reference
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007 Feb 28;297(8):831-841.
Hospitalists have been concerned about the entire continuum of care from the early days of the hospital medicine movement. We have tried to look at the system of healthcare from the patients’ viewpoint, where an admission to the hospital is rare in the larger scheme of their healthcare and their interaction with a variety of physicians and health professionals.
Hospitalists will always need to rely on our professional relationships with surgeons and specialists, as well as with the primary care physicians (PCPs) who refer their patients for admission to the hospital and who partner with us to resume patient care at discharge.
With this fundamental backdrop, two interesting trends in the PCP world—the patient-centered medical home (PCMH) and PCPs’ use of performance measurements to drive referrals to hospitals and specialists—will have a profound effect on hospitalists, the patients we treat, and the systems of care in which we work.
PCMH and Hospitalists
For many years, the problems in primary care have been virtually ignored and dismissed by the insurance industry—and even by most of organized medicine. As if a light has suddenly been turned on, everyone now wants to “do something” to save primary care.
One of the latest “solutions’ is the PCMH. As we all know, ideas without funding are just ideas. It’s time to take note of PCMH. Why? Because insurance companies and Medicare are paying for a variety of pilot and demonstration projects to see how PCMH might play out in real-life interactions among patients and physicians.
The main new characteristics in the PCMH (as opposed to the traditional PCP) are a more robust information system and the commitment of personnel and organization within the PCP practice to allow proactive coordination of the patient’s care. The hope on the performance side is that patients will receive better care that will lead to better patient satisfaction and better outcomes. On the payment side, the PCP must receive significant monetary support to pay for the staff and equipment to coordinate and manage their patient’s journey through an increasingly complex series of tests, referrals, and treatments.
Accountability
SHM has tried to raise the issues of how the PCMH would relate to hospitalists at key junctures in the hospitalization continuum. Hopefully this will lead to a dialogue with the PCP community about how PCMH proposals would meet the goals of defining accountability and responsibility for the PCMH and for hospitalists. In turn this would lead to a better, safer system for our patients.
While discussions have specifically focused on the PCMH-hospitalist interface, many of the same tenets of accountability, responsibility, timeliness, and information transfer would apply to the PCMH-specialist interfaces.
Time of Admission
Accurate, timely information is crucial at the time of acute illness. It would be expected that at the time of the patient’s arrival at the hospital the following set of data elements would be available to the hospitalist (and/or emergency department physician or specialist). These elements are lifted directly from the joint SHM-ACP-SGIM Transitions of Care Consensus document from 2007 (available at www.hospitalmedicine.org): principle diagnosis and problem list; medication list (reconciliation), including over-the-counter and herbal products, allergies, and drug interactions; emergency plan and contact number and person; treatment and diagnostic plan; prognosis and goals of care; test results/pending results; clearly identifies medical home and/or transferring coordinating physician/institution; patient’s cognitive status; advance directives, power of attorney, consent; planned interventions, durable medical equipment, wound care; and assessment of caregiver status.
Time of Discharge
While it is clear that the hospitalist is responsible for overseeing the patient’s care while hospitalized, it is essential for patients and their families to know who will be accountable at the time of discharge. SHM proposes that the PCMH:
- Assume the primary role of caring for the patient as of the time of discharge from the hospital;
- Provide a timely first post-discharge office visit consistent with the acute illness as documented in the discharge summary; and
- Ensure a handoff formally confirmed and documented by the hospitalist and PCMH.
The hospitalist should provide to the PCMH:
- An accurate and timely discharge summary; and
- The availability to the PCMH to answer questions about the hospitalization.
Further, discharge summaries should include:
- Primary and secondary diagnoses;
- Pertinent history and physical findings;
- Dates of hospitalization, treatment provided, brief hospital course;
- Results of procedures and abnormal laboratory tests;
- Recommendations of any subspecialty consultants;
- Information given to the patient and family;
- The patient’s condition or functional status at discharge;
- Reconciled discharge medication regimen, with reasons for any changes and indications for newly prescribed medications;
- Details of follow-up arrangements made;
- Specific follow-up needs, including appointments or procedures to be scheduled, and tests pending at the time of discharge; and
- Name and contact information of the responsible hospital physician.1
Other Considerations
Obviously other aspects of the PCMH-hospitalist relationship must be considered, including when the PCMH would like to be informed (or involved) during their patient’s hospitalization, as well as how to manage the handoff of responsibilities and information when the patient leaves the hospital but does not go directly home (e.g., when they are sent to a skilled nursing facility or rehabilitation center). If we continue to look at solutions from the patient’s and family’s points of view, we can come up with a workable solution.
Performance-driven Referral
Part of the result of the growth of the hospital medicine movement is that, increasingly, PCPs are not directly managing their patients for acute illnesses. That said, the PCP still has a significant role in determining whether their patients get the best care available—even if other physicians (e.g., hospitalists, surgeons, subspecialists) deliver the actual care.
We are just at the beginning of performance measurement and reporting. Today, PCPs and their patients can log on to www.hospitalcompare.hhs.gov and look at any hospital’s performance for pneumonia, acute coronary syndrome, and heart failure. The era of disease-specific and institution-specific—even physician-specific—reporting grows on a seemingly monthly basis.
Armed with this information, the PCP’s role shifts from managing the acute illnesses of their patients to understanding the report cards on their local hospitals and specialists and using this information to direct their patients to the hospitals and physicians who have the best outcomes. The expanding role of the PCP as the informed guide for their patients further will drive hospitals and all physicians who rely on referrals to improve their feedback and communication with PCPs.
We will begin to see that best-of-breed hospitals not only will have excellent clinical outcomes but will be pushed to have better patient-satisfaction and PCP-satisfaction scores. This is an opportunity for enlightened PCPs to use their medical background and hands-on understanding of local healthcare to be a vital resource to their patients.
By the same token, this is an opportunity for product differentiation for hospitals and their hospitalists to reshape a healthcare referral world traditionally built more on geography and familiarity than on information and performance, and replace it with strong communication and better outcomes. The best thing about this approach is the patient wins. TH
Dr. Wellikson is the CEO of SHM
Reference
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007 Feb 28;297(8):831-841.
Hospitalists have been concerned about the entire continuum of care from the early days of the hospital medicine movement. We have tried to look at the system of healthcare from the patients’ viewpoint, where an admission to the hospital is rare in the larger scheme of their healthcare and their interaction with a variety of physicians and health professionals.
Hospitalists will always need to rely on our professional relationships with surgeons and specialists, as well as with the primary care physicians (PCPs) who refer their patients for admission to the hospital and who partner with us to resume patient care at discharge.
With this fundamental backdrop, two interesting trends in the PCP world—the patient-centered medical home (PCMH) and PCPs’ use of performance measurements to drive referrals to hospitals and specialists—will have a profound effect on hospitalists, the patients we treat, and the systems of care in which we work.
PCMH and Hospitalists
For many years, the problems in primary care have been virtually ignored and dismissed by the insurance industry—and even by most of organized medicine. As if a light has suddenly been turned on, everyone now wants to “do something” to save primary care.
One of the latest “solutions’ is the PCMH. As we all know, ideas without funding are just ideas. It’s time to take note of PCMH. Why? Because insurance companies and Medicare are paying for a variety of pilot and demonstration projects to see how PCMH might play out in real-life interactions among patients and physicians.
The main new characteristics in the PCMH (as opposed to the traditional PCP) are a more robust information system and the commitment of personnel and organization within the PCP practice to allow proactive coordination of the patient’s care. The hope on the performance side is that patients will receive better care that will lead to better patient satisfaction and better outcomes. On the payment side, the PCP must receive significant monetary support to pay for the staff and equipment to coordinate and manage their patient’s journey through an increasingly complex series of tests, referrals, and treatments.
Accountability
SHM has tried to raise the issues of how the PCMH would relate to hospitalists at key junctures in the hospitalization continuum. Hopefully this will lead to a dialogue with the PCP community about how PCMH proposals would meet the goals of defining accountability and responsibility for the PCMH and for hospitalists. In turn this would lead to a better, safer system for our patients.
While discussions have specifically focused on the PCMH-hospitalist interface, many of the same tenets of accountability, responsibility, timeliness, and information transfer would apply to the PCMH-specialist interfaces.
Time of Admission
Accurate, timely information is crucial at the time of acute illness. It would be expected that at the time of the patient’s arrival at the hospital the following set of data elements would be available to the hospitalist (and/or emergency department physician or specialist). These elements are lifted directly from the joint SHM-ACP-SGIM Transitions of Care Consensus document from 2007 (available at www.hospitalmedicine.org): principle diagnosis and problem list; medication list (reconciliation), including over-the-counter and herbal products, allergies, and drug interactions; emergency plan and contact number and person; treatment and diagnostic plan; prognosis and goals of care; test results/pending results; clearly identifies medical home and/or transferring coordinating physician/institution; patient’s cognitive status; advance directives, power of attorney, consent; planned interventions, durable medical equipment, wound care; and assessment of caregiver status.
Time of Discharge
While it is clear that the hospitalist is responsible for overseeing the patient’s care while hospitalized, it is essential for patients and their families to know who will be accountable at the time of discharge. SHM proposes that the PCMH:
- Assume the primary role of caring for the patient as of the time of discharge from the hospital;
- Provide a timely first post-discharge office visit consistent with the acute illness as documented in the discharge summary; and
- Ensure a handoff formally confirmed and documented by the hospitalist and PCMH.
The hospitalist should provide to the PCMH:
- An accurate and timely discharge summary; and
- The availability to the PCMH to answer questions about the hospitalization.
Further, discharge summaries should include:
- Primary and secondary diagnoses;
- Pertinent history and physical findings;
- Dates of hospitalization, treatment provided, brief hospital course;
- Results of procedures and abnormal laboratory tests;
- Recommendations of any subspecialty consultants;
- Information given to the patient and family;
- The patient’s condition or functional status at discharge;
- Reconciled discharge medication regimen, with reasons for any changes and indications for newly prescribed medications;
- Details of follow-up arrangements made;
- Specific follow-up needs, including appointments or procedures to be scheduled, and tests pending at the time of discharge; and
- Name and contact information of the responsible hospital physician.1
Other Considerations
Obviously other aspects of the PCMH-hospitalist relationship must be considered, including when the PCMH would like to be informed (or involved) during their patient’s hospitalization, as well as how to manage the handoff of responsibilities and information when the patient leaves the hospital but does not go directly home (e.g., when they are sent to a skilled nursing facility or rehabilitation center). If we continue to look at solutions from the patient’s and family’s points of view, we can come up with a workable solution.
Performance-driven Referral
Part of the result of the growth of the hospital medicine movement is that, increasingly, PCPs are not directly managing their patients for acute illnesses. That said, the PCP still has a significant role in determining whether their patients get the best care available—even if other physicians (e.g., hospitalists, surgeons, subspecialists) deliver the actual care.
We are just at the beginning of performance measurement and reporting. Today, PCPs and their patients can log on to www.hospitalcompare.hhs.gov and look at any hospital’s performance for pneumonia, acute coronary syndrome, and heart failure. The era of disease-specific and institution-specific—even physician-specific—reporting grows on a seemingly monthly basis.
Armed with this information, the PCP’s role shifts from managing the acute illnesses of their patients to understanding the report cards on their local hospitals and specialists and using this information to direct their patients to the hospitals and physicians who have the best outcomes. The expanding role of the PCP as the informed guide for their patients further will drive hospitals and all physicians who rely on referrals to improve their feedback and communication with PCPs.
We will begin to see that best-of-breed hospitals not only will have excellent clinical outcomes but will be pushed to have better patient-satisfaction and PCP-satisfaction scores. This is an opportunity for enlightened PCPs to use their medical background and hands-on understanding of local healthcare to be a vital resource to their patients.
By the same token, this is an opportunity for product differentiation for hospitals and their hospitalists to reshape a healthcare referral world traditionally built more on geography and familiarity than on information and performance, and replace it with strong communication and better outcomes. The best thing about this approach is the patient wins. TH
Dr. Wellikson is the CEO of SHM
Reference
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007 Feb 28;297(8):831-841.
Round Up Staff for Better Rounds
There is almost universal agreement that conducting multidisciplinary rounds is a good idea. It’s putting them into practice that has some hospitalists scratching their heads and wondering if the payoff is worth the effort.
Multidisciplinary rounds, in a perfect world, would bring together all care providers every morning to discuss each patient’s condition and the occurrences of the past 24 hours while collaboratively planning for the day ahead. Physicians, nurses, case managers, social workers, respiratory, physical and occupational therapists, pharmacists, and the patient’s family would join in face-to-face communication and share decision-making.
In practice, many hospitals are redefining the term by bringing together only a core group of caregivers or rounding on a selected group of patients each day. Even this seems more likely to happen in hospitals that geographically segregate patients by condition, level of care, or attending physician.
“The term, multidisciplinary rounds, is vague and can even be used to refer to any two types of caregivers talking to each other on a regular basis, which almost all hospitalists regularly do,” says John Nelson, MD, medical director of the hospitalist group at Overlake Hospital Medical Center in Bellevue, Wash., and a consultant to hospitalist practices across the country. “But there are few places that bring together a larger group.”
Real-World Examples
At the minimum, multidisciplinary rounds should include physicians, bedside nurses and case managers, and ideally, everyone involved in a patient’s care, says Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and assistant professor of medicine at the Harvard Medical School. Dr. Li, also a member of SHM’s Board of Directors, has been doing multidisciplinary rounds on his teaching service for more than seven years and on his non-teaching service for almost three years. “I am a huge advocate of multidisciplinary rounds, and I think that all hospitalists should do them,” Dr. Li says. “They are not an option for me because they are one of the ways hospitalists can improve patient care.”
—Ethan Cumbler, MD, director of the acute care for the elderly service, University of Colorado Hospital
Dr. Li’s rounds are done early in the day on weekdays, with hospitalists, nurses, and case managers always involved and other providers when they are available. His team discusses all patients on a 40-bed unit in a little more than half an hour by sticking to a clearly defined script with a checklist he developed. Bedside nurses attend only for the time it takes to discuss their patients. Each floor schedules rounds at different times in the morning so physicians can attend multiple rounds if they have patients on different floors. Dr. Li says the rounds are “a work in progress” because they are continually refined.
At the University of Colorado Hospital in Denver, multidisciplinary rounds are done within the acute care for the elderly service. They are conducted weekdays by all providers caring for patients on the service. This includes four physicians, four nurses plus a charge nurse, case manager, pharmacist, and physical or occupational therapist, with the addition of a pet therapist once a week. A typical meeting covers five to six patients and lasts about 15 minutes, according to Ethan Cumbler, MD, director of the service.
Dr. Cumbler calls the current incarnation of multidisciplinary rounds “2.0.” The previous version didn’t work because elderly patients were spread throughout the hospital. “We scrapped that version and worked on getting most of our patients assigned to the same floor and began again with more success.”
Scheduling staff seems to be the biggest stumbling block for hospitalists who would like to do multidisciplinary rounds but have given up. “Although our intensive care unit does multidisciplinary rounds, we can’t find a way to make it work on our medical floors,” says Matthew Szvetecz, MD, CPE, division of internal medicine director, Kadlec Medical Associates, Richland, Wash. “When you have five geographic units, four rounding physicians, and many nurses and ancillary service providers, you’ve added more levels of scheduling complexity. Try as we might, even in our relatively small hospital, we can’t figure out how to make it work.”
Tricky Logistics
Committing so much of a providers’ time to meetings makes Dr. Nelson skeptical of whether multidisciplinary rounds are worth the effort. “If you have 20 people sitting around in a room for an hour, you’re losing 20 hours of healthcare time. You could take those people and redirect their efforts and get a better result, I suspect,” he says.
Yet, Dr. Nelson agrees multidisciplinary rounds are a good idea and says they have tried to do them at Overlake Hospital. “We’ve done it in fits and starts, but we really don’t have a meaningful model.”
Dr. Li notes that multidisciplinary rounds can be a time-saver, not a time waster. “I view rounds as an investment, and as with any wise investment, it pays off in time savings,” he says. If rounds are effective, hospitalists don’t get as many pages, nor are nurses interrupted by physicians afterward. “Everyone leaves knowing the care plan and is ready to carry it out,” he concludes.
Dr. Nelson believes adapting rounds for patients with common issues may be more effective—for example, rounds on patients age 70 and older with the goal of reducing falls. “Set up multidisciplinary rounds to address the things you know improve care that may be missed during regular caregiver rounds,” he suggests.
Although Dr. Szvetecz believes “nothing is a substitute for face-to-face communication,” he is working on a technological “rounding” system he hopes will come close. He envisions an interactive digital document containing a communication checklist that could be accessed by all caregivers. Information that would have been discussed at multidisciplinary rounds would be entered into the database and each morning caregivers would take action on the items.
“You might still be losing 25% to 50% of the information transfer in face-to-face communication, but if it’s not feasible to do multidisciplinary rounds, this might be the next best thing,” he suggests.
Advocates note that studies have credited multidisciplinary rounds with improving patient care, reducing length of stay, minimizing unneeded services, reducing bounce-back rates, and preventing gaps and delays in care. Some hospitals report that multidisciplinary rounds are a key to developing a culture of collaboration and improvement.
For those considering implementing them, Dr. Cumbler says it’s important to have champions who embrace cultural change and value communication. “People in hospitals aren’t rewarded for communication, so sometimes it’s hard getting everyone to agree to give it a try.”
After his pilot program, nurses reported they were more satisfied with their jobs and saw patient care improve in a direct and immediate way. The hospital awarded a quality improvement grant to track their effect on outcomes such as reduced falls, restraint use, and length of stay. Dr. Cumbler hopes the results will encourage the hospital to implement multidisciplinary rounds hospitalwide.
Dr. Nelson says measurement is critical: “Start with a goal in mind, then go back and measure to make sure multidisciplinary rounds are moving the quality needle on those things.”
Dr. Li says people give up on multidisciplinary rounds when team members fail to show up on time, stray off the topic at hand, and are unprepared to speak. At first, rounds can be too physician-centered, discouraging others to participate.
Dr. Cumbler solves this problem by putting his hand on the shoulder of the presenting physician if he talks for more than 40 seconds. Dr. Li recommends doing rounds standing to encourage people to be quick and to the point.
Dr. Li says caregivers learn to be more effective if they are given a script and encouraged to role play. “We have a checklist of what we need to talk about for each patient,” he says. “It’s like a play. The best way to learn your part is to practice and have a script.” He points out that as staff members change, new ones have to be taught. “It’s always a work in progress,” he notes.
Dr. Li also has found bedside nurses are critical for effective multidisciplinary rounds. “There’s no way a charge nurse can bring the same information as a bedside nurse,” he asserts.
Advocates go on to say that multidisciplinary rounds are the future of hospital medical care because they reflect attitude changes toward more cooperation and teamwork. “Physicians writing orders in isolation breaks down in the light of how sick hospitalized patients are and how complex their treatment has become,” Dr. Cumbler points out.
Perhaps the best argument for multidisciplinary rounds comes with experience. “Once you pilot it, support builds and everyone sees patient care improving,” Dr. Cumbler says. “Then they become self-sustaining.” TH
Barbara Dillard is a medical journalist based in Chicago.
There is almost universal agreement that conducting multidisciplinary rounds is a good idea. It’s putting them into practice that has some hospitalists scratching their heads and wondering if the payoff is worth the effort.
Multidisciplinary rounds, in a perfect world, would bring together all care providers every morning to discuss each patient’s condition and the occurrences of the past 24 hours while collaboratively planning for the day ahead. Physicians, nurses, case managers, social workers, respiratory, physical and occupational therapists, pharmacists, and the patient’s family would join in face-to-face communication and share decision-making.
In practice, many hospitals are redefining the term by bringing together only a core group of caregivers or rounding on a selected group of patients each day. Even this seems more likely to happen in hospitals that geographically segregate patients by condition, level of care, or attending physician.
“The term, multidisciplinary rounds, is vague and can even be used to refer to any two types of caregivers talking to each other on a regular basis, which almost all hospitalists regularly do,” says John Nelson, MD, medical director of the hospitalist group at Overlake Hospital Medical Center in Bellevue, Wash., and a consultant to hospitalist practices across the country. “But there are few places that bring together a larger group.”
Real-World Examples
At the minimum, multidisciplinary rounds should include physicians, bedside nurses and case managers, and ideally, everyone involved in a patient’s care, says Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and assistant professor of medicine at the Harvard Medical School. Dr. Li, also a member of SHM’s Board of Directors, has been doing multidisciplinary rounds on his teaching service for more than seven years and on his non-teaching service for almost three years. “I am a huge advocate of multidisciplinary rounds, and I think that all hospitalists should do them,” Dr. Li says. “They are not an option for me because they are one of the ways hospitalists can improve patient care.”
—Ethan Cumbler, MD, director of the acute care for the elderly service, University of Colorado Hospital
Dr. Li’s rounds are done early in the day on weekdays, with hospitalists, nurses, and case managers always involved and other providers when they are available. His team discusses all patients on a 40-bed unit in a little more than half an hour by sticking to a clearly defined script with a checklist he developed. Bedside nurses attend only for the time it takes to discuss their patients. Each floor schedules rounds at different times in the morning so physicians can attend multiple rounds if they have patients on different floors. Dr. Li says the rounds are “a work in progress” because they are continually refined.
At the University of Colorado Hospital in Denver, multidisciplinary rounds are done within the acute care for the elderly service. They are conducted weekdays by all providers caring for patients on the service. This includes four physicians, four nurses plus a charge nurse, case manager, pharmacist, and physical or occupational therapist, with the addition of a pet therapist once a week. A typical meeting covers five to six patients and lasts about 15 minutes, according to Ethan Cumbler, MD, director of the service.
Dr. Cumbler calls the current incarnation of multidisciplinary rounds “2.0.” The previous version didn’t work because elderly patients were spread throughout the hospital. “We scrapped that version and worked on getting most of our patients assigned to the same floor and began again with more success.”
Scheduling staff seems to be the biggest stumbling block for hospitalists who would like to do multidisciplinary rounds but have given up. “Although our intensive care unit does multidisciplinary rounds, we can’t find a way to make it work on our medical floors,” says Matthew Szvetecz, MD, CPE, division of internal medicine director, Kadlec Medical Associates, Richland, Wash. “When you have five geographic units, four rounding physicians, and many nurses and ancillary service providers, you’ve added more levels of scheduling complexity. Try as we might, even in our relatively small hospital, we can’t figure out how to make it work.”
Tricky Logistics
Committing so much of a providers’ time to meetings makes Dr. Nelson skeptical of whether multidisciplinary rounds are worth the effort. “If you have 20 people sitting around in a room for an hour, you’re losing 20 hours of healthcare time. You could take those people and redirect their efforts and get a better result, I suspect,” he says.
Yet, Dr. Nelson agrees multidisciplinary rounds are a good idea and says they have tried to do them at Overlake Hospital. “We’ve done it in fits and starts, but we really don’t have a meaningful model.”
Dr. Li notes that multidisciplinary rounds can be a time-saver, not a time waster. “I view rounds as an investment, and as with any wise investment, it pays off in time savings,” he says. If rounds are effective, hospitalists don’t get as many pages, nor are nurses interrupted by physicians afterward. “Everyone leaves knowing the care plan and is ready to carry it out,” he concludes.
Dr. Nelson believes adapting rounds for patients with common issues may be more effective—for example, rounds on patients age 70 and older with the goal of reducing falls. “Set up multidisciplinary rounds to address the things you know improve care that may be missed during regular caregiver rounds,” he suggests.
Although Dr. Szvetecz believes “nothing is a substitute for face-to-face communication,” he is working on a technological “rounding” system he hopes will come close. He envisions an interactive digital document containing a communication checklist that could be accessed by all caregivers. Information that would have been discussed at multidisciplinary rounds would be entered into the database and each morning caregivers would take action on the items.
“You might still be losing 25% to 50% of the information transfer in face-to-face communication, but if it’s not feasible to do multidisciplinary rounds, this might be the next best thing,” he suggests.
Advocates note that studies have credited multidisciplinary rounds with improving patient care, reducing length of stay, minimizing unneeded services, reducing bounce-back rates, and preventing gaps and delays in care. Some hospitals report that multidisciplinary rounds are a key to developing a culture of collaboration and improvement.
For those considering implementing them, Dr. Cumbler says it’s important to have champions who embrace cultural change and value communication. “People in hospitals aren’t rewarded for communication, so sometimes it’s hard getting everyone to agree to give it a try.”
After his pilot program, nurses reported they were more satisfied with their jobs and saw patient care improve in a direct and immediate way. The hospital awarded a quality improvement grant to track their effect on outcomes such as reduced falls, restraint use, and length of stay. Dr. Cumbler hopes the results will encourage the hospital to implement multidisciplinary rounds hospitalwide.
Dr. Nelson says measurement is critical: “Start with a goal in mind, then go back and measure to make sure multidisciplinary rounds are moving the quality needle on those things.”
Dr. Li says people give up on multidisciplinary rounds when team members fail to show up on time, stray off the topic at hand, and are unprepared to speak. At first, rounds can be too physician-centered, discouraging others to participate.
Dr. Cumbler solves this problem by putting his hand on the shoulder of the presenting physician if he talks for more than 40 seconds. Dr. Li recommends doing rounds standing to encourage people to be quick and to the point.
Dr. Li says caregivers learn to be more effective if they are given a script and encouraged to role play. “We have a checklist of what we need to talk about for each patient,” he says. “It’s like a play. The best way to learn your part is to practice and have a script.” He points out that as staff members change, new ones have to be taught. “It’s always a work in progress,” he notes.
Dr. Li also has found bedside nurses are critical for effective multidisciplinary rounds. “There’s no way a charge nurse can bring the same information as a bedside nurse,” he asserts.
Advocates go on to say that multidisciplinary rounds are the future of hospital medical care because they reflect attitude changes toward more cooperation and teamwork. “Physicians writing orders in isolation breaks down in the light of how sick hospitalized patients are and how complex their treatment has become,” Dr. Cumbler points out.
Perhaps the best argument for multidisciplinary rounds comes with experience. “Once you pilot it, support builds and everyone sees patient care improving,” Dr. Cumbler says. “Then they become self-sustaining.” TH
Barbara Dillard is a medical journalist based in Chicago.
There is almost universal agreement that conducting multidisciplinary rounds is a good idea. It’s putting them into practice that has some hospitalists scratching their heads and wondering if the payoff is worth the effort.
Multidisciplinary rounds, in a perfect world, would bring together all care providers every morning to discuss each patient’s condition and the occurrences of the past 24 hours while collaboratively planning for the day ahead. Physicians, nurses, case managers, social workers, respiratory, physical and occupational therapists, pharmacists, and the patient’s family would join in face-to-face communication and share decision-making.
In practice, many hospitals are redefining the term by bringing together only a core group of caregivers or rounding on a selected group of patients each day. Even this seems more likely to happen in hospitals that geographically segregate patients by condition, level of care, or attending physician.
“The term, multidisciplinary rounds, is vague and can even be used to refer to any two types of caregivers talking to each other on a regular basis, which almost all hospitalists regularly do,” says John Nelson, MD, medical director of the hospitalist group at Overlake Hospital Medical Center in Bellevue, Wash., and a consultant to hospitalist practices across the country. “But there are few places that bring together a larger group.”
Real-World Examples
At the minimum, multidisciplinary rounds should include physicians, bedside nurses and case managers, and ideally, everyone involved in a patient’s care, says Joseph Li, MD, director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and assistant professor of medicine at the Harvard Medical School. Dr. Li, also a member of SHM’s Board of Directors, has been doing multidisciplinary rounds on his teaching service for more than seven years and on his non-teaching service for almost three years. “I am a huge advocate of multidisciplinary rounds, and I think that all hospitalists should do them,” Dr. Li says. “They are not an option for me because they are one of the ways hospitalists can improve patient care.”
—Ethan Cumbler, MD, director of the acute care for the elderly service, University of Colorado Hospital
Dr. Li’s rounds are done early in the day on weekdays, with hospitalists, nurses, and case managers always involved and other providers when they are available. His team discusses all patients on a 40-bed unit in a little more than half an hour by sticking to a clearly defined script with a checklist he developed. Bedside nurses attend only for the time it takes to discuss their patients. Each floor schedules rounds at different times in the morning so physicians can attend multiple rounds if they have patients on different floors. Dr. Li says the rounds are “a work in progress” because they are continually refined.
At the University of Colorado Hospital in Denver, multidisciplinary rounds are done within the acute care for the elderly service. They are conducted weekdays by all providers caring for patients on the service. This includes four physicians, four nurses plus a charge nurse, case manager, pharmacist, and physical or occupational therapist, with the addition of a pet therapist once a week. A typical meeting covers five to six patients and lasts about 15 minutes, according to Ethan Cumbler, MD, director of the service.
Dr. Cumbler calls the current incarnation of multidisciplinary rounds “2.0.” The previous version didn’t work because elderly patients were spread throughout the hospital. “We scrapped that version and worked on getting most of our patients assigned to the same floor and began again with more success.”
Scheduling staff seems to be the biggest stumbling block for hospitalists who would like to do multidisciplinary rounds but have given up. “Although our intensive care unit does multidisciplinary rounds, we can’t find a way to make it work on our medical floors,” says Matthew Szvetecz, MD, CPE, division of internal medicine director, Kadlec Medical Associates, Richland, Wash. “When you have five geographic units, four rounding physicians, and many nurses and ancillary service providers, you’ve added more levels of scheduling complexity. Try as we might, even in our relatively small hospital, we can’t figure out how to make it work.”
Tricky Logistics
Committing so much of a providers’ time to meetings makes Dr. Nelson skeptical of whether multidisciplinary rounds are worth the effort. “If you have 20 people sitting around in a room for an hour, you’re losing 20 hours of healthcare time. You could take those people and redirect their efforts and get a better result, I suspect,” he says.
Yet, Dr. Nelson agrees multidisciplinary rounds are a good idea and says they have tried to do them at Overlake Hospital. “We’ve done it in fits and starts, but we really don’t have a meaningful model.”
Dr. Li notes that multidisciplinary rounds can be a time-saver, not a time waster. “I view rounds as an investment, and as with any wise investment, it pays off in time savings,” he says. If rounds are effective, hospitalists don’t get as many pages, nor are nurses interrupted by physicians afterward. “Everyone leaves knowing the care plan and is ready to carry it out,” he concludes.
Dr. Nelson believes adapting rounds for patients with common issues may be more effective—for example, rounds on patients age 70 and older with the goal of reducing falls. “Set up multidisciplinary rounds to address the things you know improve care that may be missed during regular caregiver rounds,” he suggests.
Although Dr. Szvetecz believes “nothing is a substitute for face-to-face communication,” he is working on a technological “rounding” system he hopes will come close. He envisions an interactive digital document containing a communication checklist that could be accessed by all caregivers. Information that would have been discussed at multidisciplinary rounds would be entered into the database and each morning caregivers would take action on the items.
“You might still be losing 25% to 50% of the information transfer in face-to-face communication, but if it’s not feasible to do multidisciplinary rounds, this might be the next best thing,” he suggests.
Advocates note that studies have credited multidisciplinary rounds with improving patient care, reducing length of stay, minimizing unneeded services, reducing bounce-back rates, and preventing gaps and delays in care. Some hospitals report that multidisciplinary rounds are a key to developing a culture of collaboration and improvement.
For those considering implementing them, Dr. Cumbler says it’s important to have champions who embrace cultural change and value communication. “People in hospitals aren’t rewarded for communication, so sometimes it’s hard getting everyone to agree to give it a try.”
After his pilot program, nurses reported they were more satisfied with their jobs and saw patient care improve in a direct and immediate way. The hospital awarded a quality improvement grant to track their effect on outcomes such as reduced falls, restraint use, and length of stay. Dr. Cumbler hopes the results will encourage the hospital to implement multidisciplinary rounds hospitalwide.
Dr. Nelson says measurement is critical: “Start with a goal in mind, then go back and measure to make sure multidisciplinary rounds are moving the quality needle on those things.”
Dr. Li says people give up on multidisciplinary rounds when team members fail to show up on time, stray off the topic at hand, and are unprepared to speak. At first, rounds can be too physician-centered, discouraging others to participate.
Dr. Cumbler solves this problem by putting his hand on the shoulder of the presenting physician if he talks for more than 40 seconds. Dr. Li recommends doing rounds standing to encourage people to be quick and to the point.
Dr. Li says caregivers learn to be more effective if they are given a script and encouraged to role play. “We have a checklist of what we need to talk about for each patient,” he says. “It’s like a play. The best way to learn your part is to practice and have a script.” He points out that as staff members change, new ones have to be taught. “It’s always a work in progress,” he notes.
Dr. Li also has found bedside nurses are critical for effective multidisciplinary rounds. “There’s no way a charge nurse can bring the same information as a bedside nurse,” he asserts.
Advocates go on to say that multidisciplinary rounds are the future of hospital medical care because they reflect attitude changes toward more cooperation and teamwork. “Physicians writing orders in isolation breaks down in the light of how sick hospitalized patients are and how complex their treatment has become,” Dr. Cumbler points out.
Perhaps the best argument for multidisciplinary rounds comes with experience. “Once you pilot it, support builds and everyone sees patient care improving,” Dr. Cumbler says. “Then they become self-sustaining.” TH
Barbara Dillard is a medical journalist based in Chicago.