User login
Pharma Promises Price Reductions
An $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, as well as calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole.” In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and said they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
The deal includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
William D. Atchley Jr., MD, FACP, FHM, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medications from Walmart or the VA hospital pharmacy,” says Dr. Atchley, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.”
An $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, as well as calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole.” In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and said they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
The deal includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
William D. Atchley Jr., MD, FACP, FHM, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medications from Walmart or the VA hospital pharmacy,” says Dr. Atchley, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.”
An $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, as well as calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole.” In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and said they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
The deal includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
William D. Atchley Jr., MD, FACP, FHM, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medications from Walmart or the VA hospital pharmacy,” says Dr. Atchley, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.”
Bouncebacks
Mr. D is an 80-year-old gentleman who is treated in the hospital for congestive heart failure (CHF) with a question of pneumonia. He is deemed de-conditioned secondary to his medical illness and is sent to an extended care facility. He returns from the extended care facility 18 hours later with fever and shortness of breath. The emergency department (ED) attending speaks to the primary care attending who took care of him during his previous admission; the primary care physician now wants the patient on the hospitalist service.
Does this scenario sound familiar? We have all dealt with such requests during our hospitalist careers and have wondered what the potential repercussions might be.
There is a danger—always present—that the hospitalist service will be used as a receptacle for undesirable patients. The word undesirable is used loosely here to include complicated patients, patients who keep returning to the hospital with recurrent problems, patients with no insurance or poor insurance coverage, and, of course, problematic patients with problematic families.
Complicated Patients, Complicated Consequences
In the scenario described above, the patient comes back with the same diagnoses but now winds up on the hospitalist service. From an ethical perspective alone this seems objectionable. What about the legal ramifications of such a situation? Two different admissions with the same diagnoses occur within a short time frame, but different physician groups are involved in caring for the patient. Additionally, such scenarios often cause patient dissatisfaction and even hostility. Surely it doesn’t make the patient happy to hear that the primary care physician no longer wants the patient on her service.
The hospitalist service usually deals with more complicated patients than the average physician. Often, the primary physicians, who have more constraints on their time, want hospitalists to take care of the more complicated patients. This becomes a problem when a patient who was on a physician’s service is readmitted. Naturally, the primary doctors are frustrated with the recurrent admissions. A case could be made to admit to the hospitalist service when the readmitting diagnosis is different from the previous discharge diagnosis, but when the discharge and readmission diagnoses are the same, the jury is hung.
Loss of Revenue
To many physicians’ minds, a readmission occurs less than 24 hours after the previous discharge; to others, however, a readmission means something else. For example, Medicaid, considers a readmission one that occurs within fewer than seven days of the previous admission. This situation brings about an automatic readmission review, and the readmission is denied if it is perceived that the patient discharge was not appropriate or was premature.
In the case of Mr. D, the hospitalists might end up getting a denial—and suffering a loss of revenue—for a readmission that had nothing to do with them. Hospitalists are seldom cognizant of such repercussions because we are programmed to perform patient care without contemplating the financial implications.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) collects data for their core measures program. A part of this effort also involves reporting the readmission rate within 14 days—both for the same diagnosis and for a different one.
Looking again at the case of Mr. D, the core measures would have included estimation of ejection fraction, use of angiotensin-converting enzyme inhibitors, and appropriateness and timing of antibiotics in pneumonia. The hospitalists, who had no control of these indices on the first admission, might have been penalized if these particular measures were not carried out and their omission contributed to the patient’s readmission.
Resident Overflow
Another potential point of contention is the practice of admitting patients to the hospitalist service once the resident teaching service is capped. This is institution-specific. In cases where the entire resident overflow is admitted to the hospitalist service, patients seldom go back to the teaching service because ED doctors label them as belonging to the hospitalist service. Many of these patients either have no insurance (or have Medicaid); in addition, they often have multiple health problems, and noncompliance runs rife. Because unscheduled readmissions are viewed negatively under current guidelines, patients who are handed off in this manner can cause resulting penalties for the hospitalists who end up serving them.
Extended Care Readmissions
Patients with established primary care physicians often go to extended-care facilities where there is another physician of record. At readmission, the new attending is recorded as the patient’s physician. The prior primary attending might have wanted to follow the patient during the readmission. Unfortunately, the ED physician will typically call the newly assigned attending because that is the name that appears on the transfer note. If, at this time, the new attending decides to admit the patient to the hospitalist service, a misunderstanding may ensue. The original primary care attending may view this as an attempt on the part of the hospitalist service to appropriate patients, though the decision to admit to the hospitalist service is seldom made by the hospitalist.
The pitfalls of these practices are accentuated when the readmission occurs within a relatively short time frame. Another downside may arise if the new attending, who knows little of the patient’s history, orders another extensive inpatient workup. This example highlights a potential, and avoidable, cause of spiraling healthcare costs.
The Hospitalist’s Role
We practice in a milieu of increasing scrutiny. Pay for performance is gaining momentum and acceptance. Two years from now, non-compliance with specific indicators, such as readmission rates, will be met with financial penalties. Hospitals complain of decreasing reimbursements. Unscheduled readmissions to the hospital continue to be a source of lost revenue and patient dissatisfaction.
The hospitalist plays a central role in the management of the patient from a medical standpoint. Rules of admission to the hospitalist service vary widely amongst different institutions. Often, depending on patient load and available staffing, these rules are in flux even within institutions. Procedures run the gamut from the so-called “closed system,” in which only specific physicians can admit patients to the hospitalist service, to the “open system,” in which everyone is welcome, on a voluntary basis, to admit to the hospitalist service. The potential pitfalls of the open system will become more and more apparent in the years to come, and many of us will be forced to rethink our models of healthcare delivery. TH
Dr. Chabria is a hospitalist at Waterbury Hospital, Conn., and a clinical instructor at Yale University School of Medicine, New Haven, Conn.
Mr. D is an 80-year-old gentleman who is treated in the hospital for congestive heart failure (CHF) with a question of pneumonia. He is deemed de-conditioned secondary to his medical illness and is sent to an extended care facility. He returns from the extended care facility 18 hours later with fever and shortness of breath. The emergency department (ED) attending speaks to the primary care attending who took care of him during his previous admission; the primary care physician now wants the patient on the hospitalist service.
Does this scenario sound familiar? We have all dealt with such requests during our hospitalist careers and have wondered what the potential repercussions might be.
There is a danger—always present—that the hospitalist service will be used as a receptacle for undesirable patients. The word undesirable is used loosely here to include complicated patients, patients who keep returning to the hospital with recurrent problems, patients with no insurance or poor insurance coverage, and, of course, problematic patients with problematic families.
Complicated Patients, Complicated Consequences
In the scenario described above, the patient comes back with the same diagnoses but now winds up on the hospitalist service. From an ethical perspective alone this seems objectionable. What about the legal ramifications of such a situation? Two different admissions with the same diagnoses occur within a short time frame, but different physician groups are involved in caring for the patient. Additionally, such scenarios often cause patient dissatisfaction and even hostility. Surely it doesn’t make the patient happy to hear that the primary care physician no longer wants the patient on her service.
The hospitalist service usually deals with more complicated patients than the average physician. Often, the primary physicians, who have more constraints on their time, want hospitalists to take care of the more complicated patients. This becomes a problem when a patient who was on a physician’s service is readmitted. Naturally, the primary doctors are frustrated with the recurrent admissions. A case could be made to admit to the hospitalist service when the readmitting diagnosis is different from the previous discharge diagnosis, but when the discharge and readmission diagnoses are the same, the jury is hung.
Loss of Revenue
To many physicians’ minds, a readmission occurs less than 24 hours after the previous discharge; to others, however, a readmission means something else. For example, Medicaid, considers a readmission one that occurs within fewer than seven days of the previous admission. This situation brings about an automatic readmission review, and the readmission is denied if it is perceived that the patient discharge was not appropriate or was premature.
In the case of Mr. D, the hospitalists might end up getting a denial—and suffering a loss of revenue—for a readmission that had nothing to do with them. Hospitalists are seldom cognizant of such repercussions because we are programmed to perform patient care without contemplating the financial implications.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) collects data for their core measures program. A part of this effort also involves reporting the readmission rate within 14 days—both for the same diagnosis and for a different one.
Looking again at the case of Mr. D, the core measures would have included estimation of ejection fraction, use of angiotensin-converting enzyme inhibitors, and appropriateness and timing of antibiotics in pneumonia. The hospitalists, who had no control of these indices on the first admission, might have been penalized if these particular measures were not carried out and their omission contributed to the patient’s readmission.
Resident Overflow
Another potential point of contention is the practice of admitting patients to the hospitalist service once the resident teaching service is capped. This is institution-specific. In cases where the entire resident overflow is admitted to the hospitalist service, patients seldom go back to the teaching service because ED doctors label them as belonging to the hospitalist service. Many of these patients either have no insurance (or have Medicaid); in addition, they often have multiple health problems, and noncompliance runs rife. Because unscheduled readmissions are viewed negatively under current guidelines, patients who are handed off in this manner can cause resulting penalties for the hospitalists who end up serving them.
Extended Care Readmissions
Patients with established primary care physicians often go to extended-care facilities where there is another physician of record. At readmission, the new attending is recorded as the patient’s physician. The prior primary attending might have wanted to follow the patient during the readmission. Unfortunately, the ED physician will typically call the newly assigned attending because that is the name that appears on the transfer note. If, at this time, the new attending decides to admit the patient to the hospitalist service, a misunderstanding may ensue. The original primary care attending may view this as an attempt on the part of the hospitalist service to appropriate patients, though the decision to admit to the hospitalist service is seldom made by the hospitalist.
The pitfalls of these practices are accentuated when the readmission occurs within a relatively short time frame. Another downside may arise if the new attending, who knows little of the patient’s history, orders another extensive inpatient workup. This example highlights a potential, and avoidable, cause of spiraling healthcare costs.
The Hospitalist’s Role
We practice in a milieu of increasing scrutiny. Pay for performance is gaining momentum and acceptance. Two years from now, non-compliance with specific indicators, such as readmission rates, will be met with financial penalties. Hospitals complain of decreasing reimbursements. Unscheduled readmissions to the hospital continue to be a source of lost revenue and patient dissatisfaction.
The hospitalist plays a central role in the management of the patient from a medical standpoint. Rules of admission to the hospitalist service vary widely amongst different institutions. Often, depending on patient load and available staffing, these rules are in flux even within institutions. Procedures run the gamut from the so-called “closed system,” in which only specific physicians can admit patients to the hospitalist service, to the “open system,” in which everyone is welcome, on a voluntary basis, to admit to the hospitalist service. The potential pitfalls of the open system will become more and more apparent in the years to come, and many of us will be forced to rethink our models of healthcare delivery. TH
Dr. Chabria is a hospitalist at Waterbury Hospital, Conn., and a clinical instructor at Yale University School of Medicine, New Haven, Conn.
Mr. D is an 80-year-old gentleman who is treated in the hospital for congestive heart failure (CHF) with a question of pneumonia. He is deemed de-conditioned secondary to his medical illness and is sent to an extended care facility. He returns from the extended care facility 18 hours later with fever and shortness of breath. The emergency department (ED) attending speaks to the primary care attending who took care of him during his previous admission; the primary care physician now wants the patient on the hospitalist service.
Does this scenario sound familiar? We have all dealt with such requests during our hospitalist careers and have wondered what the potential repercussions might be.
There is a danger—always present—that the hospitalist service will be used as a receptacle for undesirable patients. The word undesirable is used loosely here to include complicated patients, patients who keep returning to the hospital with recurrent problems, patients with no insurance or poor insurance coverage, and, of course, problematic patients with problematic families.
Complicated Patients, Complicated Consequences
In the scenario described above, the patient comes back with the same diagnoses but now winds up on the hospitalist service. From an ethical perspective alone this seems objectionable. What about the legal ramifications of such a situation? Two different admissions with the same diagnoses occur within a short time frame, but different physician groups are involved in caring for the patient. Additionally, such scenarios often cause patient dissatisfaction and even hostility. Surely it doesn’t make the patient happy to hear that the primary care physician no longer wants the patient on her service.
The hospitalist service usually deals with more complicated patients than the average physician. Often, the primary physicians, who have more constraints on their time, want hospitalists to take care of the more complicated patients. This becomes a problem when a patient who was on a physician’s service is readmitted. Naturally, the primary doctors are frustrated with the recurrent admissions. A case could be made to admit to the hospitalist service when the readmitting diagnosis is different from the previous discharge diagnosis, but when the discharge and readmission diagnoses are the same, the jury is hung.
Loss of Revenue
To many physicians’ minds, a readmission occurs less than 24 hours after the previous discharge; to others, however, a readmission means something else. For example, Medicaid, considers a readmission one that occurs within fewer than seven days of the previous admission. This situation brings about an automatic readmission review, and the readmission is denied if it is perceived that the patient discharge was not appropriate or was premature.
In the case of Mr. D, the hospitalists might end up getting a denial—and suffering a loss of revenue—for a readmission that had nothing to do with them. Hospitalists are seldom cognizant of such repercussions because we are programmed to perform patient care without contemplating the financial implications.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) collects data for their core measures program. A part of this effort also involves reporting the readmission rate within 14 days—both for the same diagnosis and for a different one.
Looking again at the case of Mr. D, the core measures would have included estimation of ejection fraction, use of angiotensin-converting enzyme inhibitors, and appropriateness and timing of antibiotics in pneumonia. The hospitalists, who had no control of these indices on the first admission, might have been penalized if these particular measures were not carried out and their omission contributed to the patient’s readmission.
Resident Overflow
Another potential point of contention is the practice of admitting patients to the hospitalist service once the resident teaching service is capped. This is institution-specific. In cases where the entire resident overflow is admitted to the hospitalist service, patients seldom go back to the teaching service because ED doctors label them as belonging to the hospitalist service. Many of these patients either have no insurance (or have Medicaid); in addition, they often have multiple health problems, and noncompliance runs rife. Because unscheduled readmissions are viewed negatively under current guidelines, patients who are handed off in this manner can cause resulting penalties for the hospitalists who end up serving them.
Extended Care Readmissions
Patients with established primary care physicians often go to extended-care facilities where there is another physician of record. At readmission, the new attending is recorded as the patient’s physician. The prior primary attending might have wanted to follow the patient during the readmission. Unfortunately, the ED physician will typically call the newly assigned attending because that is the name that appears on the transfer note. If, at this time, the new attending decides to admit the patient to the hospitalist service, a misunderstanding may ensue. The original primary care attending may view this as an attempt on the part of the hospitalist service to appropriate patients, though the decision to admit to the hospitalist service is seldom made by the hospitalist.
The pitfalls of these practices are accentuated when the readmission occurs within a relatively short time frame. Another downside may arise if the new attending, who knows little of the patient’s history, orders another extensive inpatient workup. This example highlights a potential, and avoidable, cause of spiraling healthcare costs.
The Hospitalist’s Role
We practice in a milieu of increasing scrutiny. Pay for performance is gaining momentum and acceptance. Two years from now, non-compliance with specific indicators, such as readmission rates, will be met with financial penalties. Hospitals complain of decreasing reimbursements. Unscheduled readmissions to the hospital continue to be a source of lost revenue and patient dissatisfaction.
The hospitalist plays a central role in the management of the patient from a medical standpoint. Rules of admission to the hospitalist service vary widely amongst different institutions. Often, depending on patient load and available staffing, these rules are in flux even within institutions. Procedures run the gamut from the so-called “closed system,” in which only specific physicians can admit patients to the hospitalist service, to the “open system,” in which everyone is welcome, on a voluntary basis, to admit to the hospitalist service. The potential pitfalls of the open system will become more and more apparent in the years to come, and many of us will be forced to rethink our models of healthcare delivery. TH
Dr. Chabria is a hospitalist at Waterbury Hospital, Conn., and a clinical instructor at Yale University School of Medicine, New Haven, Conn.
Relational Growth
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
A new survey conducted by SHM and the American Medical Association’s (AMA) Organized Medical Staff Section finds that while more than 90% of hospitalists feel an HM presence improves the quality of hospital care, less than half of primary-care physicians (PCPs) feel the same way. On the bright side, the percentage of PCPs with favorable views of HM is climbing.
“There seems to be a general trend toward improvement of how primary-care physicians view hospitalists,” says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine and chair of SHM’s Career Satisfaction Task Force. “But there are still very different views. ... It’s a narrower gap, but it’s still a gap.”
The data come from a recent survey of 874 hospitalists and 497 PCPs. The "Survey on the Growing Hospitalist Trend" is a follow-up to a similar study conducted two years ago to gauge the effects of HM on the primary-care model, and vice versa. The study also looks to define perceptions of the hospitalist model on the care of shared patients.
One key issue the survey examined was viewpoints on how well hospitalists and PCPs communicate with each other. Upon admission, the survey shows, half of hospitalists feel they communicate effectively with PCPs, but only 25% of PCPs feel the same way about hospitalists. On discharge, the disparity grows, with 70% of hospitalists saying they feel they communicate well with PCPs; however, only 35% of PCPs agree.
Still, 46% of PCPs agree or strongly agree that hospitalists have improved the overall quality of hospital care. That number is up from 40% two years ago.
“Everyone can learn from this,” says James DeNuccio, director of the AMA’s Organized Medical Staff Services and Physicians in Practice. “If the hospitalists and PCPs both can learn something from this, that helps them adjust their practice. In the end, patients will benefit.”
In the Literature: Research You Need to Know
Clinical question: Do the benefits of statin use in secondary stroke prevention apply equally to younger patients as they do elderly patients?
Background: The 2003 SPARCL trial assigned stroke patients with LDL of 100 mg/dL to 190 mg/dL to treatment with 80 mg atorvastatin or placebo. Over median of 4.9 years of followup, 13.1% of patients in the placebo group had a recurrent stroke, compared with 11.2% of patients in the atorvastatin group, resulting in a significant, 2.2% absolute reduction of stroke risk.
Study design: Secondary analysis of a randomized, double-blind, placebo-controlled trial.
Setting: Multicenter study.
Synopsis: Using data from the original SPARCL trial, 2,482 patients in the younger cohort (<65)—a mean age of 54 years—were compared with 2,249 patients in the elderly group (>65) with a mean age of 72.4 years. There was comparable reduction of LDL cholesterol in both groups and no significant differences in adverse drug events.
The magnitude of reduction in fatal or nonfatal second strokes was greater for younger patients (RRR 26%, P=0.02) than for older patients (RRR 10%, P=0.33). However, in the elderly cohort, secondary endpoints including stroke or TIA (HR 0.79, P=0.01), major coronary events (HR 0.68, P=0.035), or any coronary heart event (HR 0.61, P=0.0006) were significantly reduced by statin use. Mortality was not reduced in either group.
The authors found a lack of heterogeneity of benefit in treatment-age interaction analysis and concluded that the results support use of statins in the elderly after stroke. This study is limited by its post-hoc analysis, which might have been underpowered to detect a difference in the primary endpoint when separated into the age groups.
Bottom line: Elderly patients derive less stroke-reduction benefit from high-dose, high-potency statins compared with younger patients in the post-stroke period. Even so, statins continue to derive statistically significant reductions in other cerebrovascular and cardiac events.
Citation: Chaturvedi S, Zivin J, Breazna A, et al. Effect of atorvastatin in elderly patients with a recent stroke or transient ischemic attack. Neurology. 2009;72:688-694.
Reviewed for TH eWire by Erin A. Egan, MD, JD, Ethan Cumbler, MD, Jodie Grout, RN, MS, ANP-C, Jeannette Guerrasio, MD, Nichole Zehnder, MD, and Judy Zerzan, MD, MPH, Hospital Medicine Group, University of Colorado Denver
Clinical question: Do the benefits of statin use in secondary stroke prevention apply equally to younger patients as they do elderly patients?
Background: The 2003 SPARCL trial assigned stroke patients with LDL of 100 mg/dL to 190 mg/dL to treatment with 80 mg atorvastatin or placebo. Over median of 4.9 years of followup, 13.1% of patients in the placebo group had a recurrent stroke, compared with 11.2% of patients in the atorvastatin group, resulting in a significant, 2.2% absolute reduction of stroke risk.
Study design: Secondary analysis of a randomized, double-blind, placebo-controlled trial.
Setting: Multicenter study.
Synopsis: Using data from the original SPARCL trial, 2,482 patients in the younger cohort (<65)—a mean age of 54 years—were compared with 2,249 patients in the elderly group (>65) with a mean age of 72.4 years. There was comparable reduction of LDL cholesterol in both groups and no significant differences in adverse drug events.
The magnitude of reduction in fatal or nonfatal second strokes was greater for younger patients (RRR 26%, P=0.02) than for older patients (RRR 10%, P=0.33). However, in the elderly cohort, secondary endpoints including stroke or TIA (HR 0.79, P=0.01), major coronary events (HR 0.68, P=0.035), or any coronary heart event (HR 0.61, P=0.0006) were significantly reduced by statin use. Mortality was not reduced in either group.
The authors found a lack of heterogeneity of benefit in treatment-age interaction analysis and concluded that the results support use of statins in the elderly after stroke. This study is limited by its post-hoc analysis, which might have been underpowered to detect a difference in the primary endpoint when separated into the age groups.
Bottom line: Elderly patients derive less stroke-reduction benefit from high-dose, high-potency statins compared with younger patients in the post-stroke period. Even so, statins continue to derive statistically significant reductions in other cerebrovascular and cardiac events.
Citation: Chaturvedi S, Zivin J, Breazna A, et al. Effect of atorvastatin in elderly patients with a recent stroke or transient ischemic attack. Neurology. 2009;72:688-694.
Reviewed for TH eWire by Erin A. Egan, MD, JD, Ethan Cumbler, MD, Jodie Grout, RN, MS, ANP-C, Jeannette Guerrasio, MD, Nichole Zehnder, MD, and Judy Zerzan, MD, MPH, Hospital Medicine Group, University of Colorado Denver
Clinical question: Do the benefits of statin use in secondary stroke prevention apply equally to younger patients as they do elderly patients?
Background: The 2003 SPARCL trial assigned stroke patients with LDL of 100 mg/dL to 190 mg/dL to treatment with 80 mg atorvastatin or placebo. Over median of 4.9 years of followup, 13.1% of patients in the placebo group had a recurrent stroke, compared with 11.2% of patients in the atorvastatin group, resulting in a significant, 2.2% absolute reduction of stroke risk.
Study design: Secondary analysis of a randomized, double-blind, placebo-controlled trial.
Setting: Multicenter study.
Synopsis: Using data from the original SPARCL trial, 2,482 patients in the younger cohort (<65)—a mean age of 54 years—were compared with 2,249 patients in the elderly group (>65) with a mean age of 72.4 years. There was comparable reduction of LDL cholesterol in both groups and no significant differences in adverse drug events.
The magnitude of reduction in fatal or nonfatal second strokes was greater for younger patients (RRR 26%, P=0.02) than for older patients (RRR 10%, P=0.33). However, in the elderly cohort, secondary endpoints including stroke or TIA (HR 0.79, P=0.01), major coronary events (HR 0.68, P=0.035), or any coronary heart event (HR 0.61, P=0.0006) were significantly reduced by statin use. Mortality was not reduced in either group.
The authors found a lack of heterogeneity of benefit in treatment-age interaction analysis and concluded that the results support use of statins in the elderly after stroke. This study is limited by its post-hoc analysis, which might have been underpowered to detect a difference in the primary endpoint when separated into the age groups.
Bottom line: Elderly patients derive less stroke-reduction benefit from high-dose, high-potency statins compared with younger patients in the post-stroke period. Even so, statins continue to derive statistically significant reductions in other cerebrovascular and cardiac events.
Citation: Chaturvedi S, Zivin J, Breazna A, et al. Effect of atorvastatin in elderly patients with a recent stroke or transient ischemic attack. Neurology. 2009;72:688-694.
Reviewed for TH eWire by Erin A. Egan, MD, JD, Ethan Cumbler, MD, Jodie Grout, RN, MS, ANP-C, Jeannette Guerrasio, MD, Nichole Zehnder, MD, and Judy Zerzan, MD, MPH, Hospital Medicine Group, University of Colorado Denver
Internal Peer Review

As far as I can tell, few hospitalist groups conduct any sort of formal peer review. Most seem to rely on the hospital’s medical staff peer review to encourage quality of care and address shortcomings; the review is often coupled with a salary incentive paid for good performance on certain quality metrics. While these reviews are of some value, I think they are pretty blunt instruments. Every hospitalist practice should think about developing a more robust system of peer review for their group.
Review Categories
Assessment of each provider’s individual performance, whether they are an MD, nurse practitioner, or physician assistant, can be divided into three general categories. The first is the traditional “human resources” category of performance, which includes whether the person gets along well with others in the practice as well as other hospital staff, patients, and families. Does the person arrive at work when scheduled, manage time effectively, and work efficiently? Do nurses and other hospital staff have compliments or complaints about this doctor?
The second category of performance can encompass the hospitalist’s business and operational contributions to the practice. Do they document, code, and bill visits correctly? Do they attend and participate in meetings and serve on one or more hospital committees?
The third category assesses measurable quality of care. This could include an assessment of mortality, readmission rate, performance on such quality metrics as core measures, and performance on selected initiatives (e.g., appropriate VTE prophylaxis). Aggregate data for these measures can be difficult to attribute to a single hospitalist, so this may require a review of individual charts instead of relying on reports generated by the hospital’s data systems.
A number of metrics might apply to more than one of the three categories. For example, documenting accurate medicine reconciliation can be thought of as both a quality issue (good for patients) and a business issue (e.g., your hospital might provide a financial reward to your group for good performance). Ensuring the referring physician is “CC’d” on all dictated reports is both a quality and business issue. It really doesn’t matter which category you put these in.
The categories I have listed, and the sample items in each, are intended as examples. You should think about the unique attributes of your practice and its current priorities in order to develop the best internal peer review system for your group. You probably will want to change metrics periodically. For example, you may choose to focus on VTE prophylaxis for now, but at some point it may make sense to replace it with a new metric, such as glycemic control.
Manage the Review
There is no single right approach to conducting your own peer review. Just make sure that the process is fair and meaningful for all involved. The process probably will be more valuable if most of the data on each hospitalist can be reviewed by the whole group, or at least by a designated peer review committee. The main exceptions to such transparency are issues in the first human resources category. If a nurse or another hospitalist has specific criticisms of one hospitalist, it is best not to share that information with the whole group. But it should be fine for everyone in the group to know who is best and worst at things like documenting and coding visits or ordering VTE prophylaxis when needed. Beyond these general principles, the specific process your group uses for peer review can take many forms.
It may make sense to form a peer review committee that performs all the reviews on everyone in the group, including the members of the committee itself. Each member of the committee should have a specified term, such as one or two years. It might not make sense for some groups, especially ones with less than 10 hospitalists, to have a formal committee. In that case, every member of the group could serve as a reviewer for all other doctors except themselves.
The group should hold formal peer review sessions quarterly or semi-annually. The group for which I serve as medical director reviews about one-fourth of the doctors at a roughly two-hour meeting each quarter. Prior to each meeting, we conduct a survey (see Figure 1) using a free Web-based tool to collect opinions about the doctors under review. We use SurveyMonkey.com, though there are many other options. The tool makes it easy to send reminders to get everyone to complete the survey and to collect and analyze the results. At the beginning of the meeting, the medical director of the practice reviews the results with the doctor being surveyed; they are not shared with others.
Most of the meeting time is spent assessing 10 charts for the doctor under review. Using the billing system, we select patients the doctor saw for many consecutive days. We want to avoid pulling charts at random only to find that the doctor only made one visit and there isn’t much to review. We assess a number of measures:
- Was VTE prophylaxis addressed appropriately?
- Was the referring doctor CC’d in the dictated reports?
- Did the doctor choose the appropriate CPT code for each visit?
- Was there a good plan for transition of care at discharge?
The doctor is provided a summary of all the findings of the peer review session, and a copy is kept on file. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
As far as I can tell, few hospitalist groups conduct any sort of formal peer review. Most seem to rely on the hospital’s medical staff peer review to encourage quality of care and address shortcomings; the review is often coupled with a salary incentive paid for good performance on certain quality metrics. While these reviews are of some value, I think they are pretty blunt instruments. Every hospitalist practice should think about developing a more robust system of peer review for their group.
Review Categories
Assessment of each provider’s individual performance, whether they are an MD, nurse practitioner, or physician assistant, can be divided into three general categories. The first is the traditional “human resources” category of performance, which includes whether the person gets along well with others in the practice as well as other hospital staff, patients, and families. Does the person arrive at work when scheduled, manage time effectively, and work efficiently? Do nurses and other hospital staff have compliments or complaints about this doctor?
The second category of performance can encompass the hospitalist’s business and operational contributions to the practice. Do they document, code, and bill visits correctly? Do they attend and participate in meetings and serve on one or more hospital committees?
The third category assesses measurable quality of care. This could include an assessment of mortality, readmission rate, performance on such quality metrics as core measures, and performance on selected initiatives (e.g., appropriate VTE prophylaxis). Aggregate data for these measures can be difficult to attribute to a single hospitalist, so this may require a review of individual charts instead of relying on reports generated by the hospital’s data systems.
A number of metrics might apply to more than one of the three categories. For example, documenting accurate medicine reconciliation can be thought of as both a quality issue (good for patients) and a business issue (e.g., your hospital might provide a financial reward to your group for good performance). Ensuring the referring physician is “CC’d” on all dictated reports is both a quality and business issue. It really doesn’t matter which category you put these in.
The categories I have listed, and the sample items in each, are intended as examples. You should think about the unique attributes of your practice and its current priorities in order to develop the best internal peer review system for your group. You probably will want to change metrics periodically. For example, you may choose to focus on VTE prophylaxis for now, but at some point it may make sense to replace it with a new metric, such as glycemic control.
Manage the Review
There is no single right approach to conducting your own peer review. Just make sure that the process is fair and meaningful for all involved. The process probably will be more valuable if most of the data on each hospitalist can be reviewed by the whole group, or at least by a designated peer review committee. The main exceptions to such transparency are issues in the first human resources category. If a nurse or another hospitalist has specific criticisms of one hospitalist, it is best not to share that information with the whole group. But it should be fine for everyone in the group to know who is best and worst at things like documenting and coding visits or ordering VTE prophylaxis when needed. Beyond these general principles, the specific process your group uses for peer review can take many forms.
It may make sense to form a peer review committee that performs all the reviews on everyone in the group, including the members of the committee itself. Each member of the committee should have a specified term, such as one or two years. It might not make sense for some groups, especially ones with less than 10 hospitalists, to have a formal committee. In that case, every member of the group could serve as a reviewer for all other doctors except themselves.
The group should hold formal peer review sessions quarterly or semi-annually. The group for which I serve as medical director reviews about one-fourth of the doctors at a roughly two-hour meeting each quarter. Prior to each meeting, we conduct a survey (see Figure 1) using a free Web-based tool to collect opinions about the doctors under review. We use SurveyMonkey.com, though there are many other options. The tool makes it easy to send reminders to get everyone to complete the survey and to collect and analyze the results. At the beginning of the meeting, the medical director of the practice reviews the results with the doctor being surveyed; they are not shared with others.
Most of the meeting time is spent assessing 10 charts for the doctor under review. Using the billing system, we select patients the doctor saw for many consecutive days. We want to avoid pulling charts at random only to find that the doctor only made one visit and there isn’t much to review. We assess a number of measures:
- Was VTE prophylaxis addressed appropriately?
- Was the referring doctor CC’d in the dictated reports?
- Did the doctor choose the appropriate CPT code for each visit?
- Was there a good plan for transition of care at discharge?
The doctor is provided a summary of all the findings of the peer review session, and a copy is kept on file. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
As far as I can tell, few hospitalist groups conduct any sort of formal peer review. Most seem to rely on the hospital’s medical staff peer review to encourage quality of care and address shortcomings; the review is often coupled with a salary incentive paid for good performance on certain quality metrics. While these reviews are of some value, I think they are pretty blunt instruments. Every hospitalist practice should think about developing a more robust system of peer review for their group.
Review Categories
Assessment of each provider’s individual performance, whether they are an MD, nurse practitioner, or physician assistant, can be divided into three general categories. The first is the traditional “human resources” category of performance, which includes whether the person gets along well with others in the practice as well as other hospital staff, patients, and families. Does the person arrive at work when scheduled, manage time effectively, and work efficiently? Do nurses and other hospital staff have compliments or complaints about this doctor?
The second category of performance can encompass the hospitalist’s business and operational contributions to the practice. Do they document, code, and bill visits correctly? Do they attend and participate in meetings and serve on one or more hospital committees?
The third category assesses measurable quality of care. This could include an assessment of mortality, readmission rate, performance on such quality metrics as core measures, and performance on selected initiatives (e.g., appropriate VTE prophylaxis). Aggregate data for these measures can be difficult to attribute to a single hospitalist, so this may require a review of individual charts instead of relying on reports generated by the hospital’s data systems.
A number of metrics might apply to more than one of the three categories. For example, documenting accurate medicine reconciliation can be thought of as both a quality issue (good for patients) and a business issue (e.g., your hospital might provide a financial reward to your group for good performance). Ensuring the referring physician is “CC’d” on all dictated reports is both a quality and business issue. It really doesn’t matter which category you put these in.
The categories I have listed, and the sample items in each, are intended as examples. You should think about the unique attributes of your practice and its current priorities in order to develop the best internal peer review system for your group. You probably will want to change metrics periodically. For example, you may choose to focus on VTE prophylaxis for now, but at some point it may make sense to replace it with a new metric, such as glycemic control.
Manage the Review
There is no single right approach to conducting your own peer review. Just make sure that the process is fair and meaningful for all involved. The process probably will be more valuable if most of the data on each hospitalist can be reviewed by the whole group, or at least by a designated peer review committee. The main exceptions to such transparency are issues in the first human resources category. If a nurse or another hospitalist has specific criticisms of one hospitalist, it is best not to share that information with the whole group. But it should be fine for everyone in the group to know who is best and worst at things like documenting and coding visits or ordering VTE prophylaxis when needed. Beyond these general principles, the specific process your group uses for peer review can take many forms.
It may make sense to form a peer review committee that performs all the reviews on everyone in the group, including the members of the committee itself. Each member of the committee should have a specified term, such as one or two years. It might not make sense for some groups, especially ones with less than 10 hospitalists, to have a formal committee. In that case, every member of the group could serve as a reviewer for all other doctors except themselves.
The group should hold formal peer review sessions quarterly or semi-annually. The group for which I serve as medical director reviews about one-fourth of the doctors at a roughly two-hour meeting each quarter. Prior to each meeting, we conduct a survey (see Figure 1) using a free Web-based tool to collect opinions about the doctors under review. We use SurveyMonkey.com, though there are many other options. The tool makes it easy to send reminders to get everyone to complete the survey and to collect and analyze the results. At the beginning of the meeting, the medical director of the practice reviews the results with the doctor being surveyed; they are not shared with others.
Most of the meeting time is spent assessing 10 charts for the doctor under review. Using the billing system, we select patients the doctor saw for many consecutive days. We want to avoid pulling charts at random only to find that the doctor only made one visit and there isn’t much to review. We assess a number of measures:
- Was VTE prophylaxis addressed appropriately?
- Was the referring doctor CC’d in the dictated reports?
- Did the doctor choose the appropriate CPT code for each visit?
- Was there a good plan for transition of care at discharge?
The doctor is provided a summary of all the findings of the peer review session, and a copy is kept on file. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He also is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Clarion Call

A specialty without a disease: It was a major hangup for the field of hospital medicine in the early days. We’d hurdled many of the traditional barriers to specialty status—research fellowships, textbooks, an active society, a growing body of research, and thousands of practitioners focusing their practice on the hospital setting. However, despite several examples of site-defined specialties like emergency and critical-care medicine, cynics clung to the time-honored need for a specialty to own an organ, or at least a disease.
Early SHM efforts made a strong push to make VTE our disease—both its treatment and, more importantly, its prevention. It was a laudable effort, one that has saved many thousands of lives and limbs. It made sense for hospitalists to tackle VTE; it’s an incapacitating disease that affects many, is largely preventable, and had no strong inpatient advocate. While hematologists were the obvious “owner” of this disease, they were neither available nor able to redesign the inpatient systems of care necessary to thwart this illness. Hospitalists, invested in this issue by consequence of direct care of many at-risk patients and through commitment to improving hospital systems, came to own VTE prevention.
The Next Frontier: Stroke
It is time hospitalists apply this experience to the management of an even more incapacitating, largely preventable disease looking for an inpatient steward: stroke. A stroke occurs in the U.S. every 40 seconds, with disabling sequelae that often are avoidable with rapid detection and treatment. This is especially true when we are given the clarion call of a transient ischemic attack (TIA). The problem is that most American hospitals are not kingpins of efficiency—the key ingredient of the processes necessary to improve stroke outcomes. Furthermore, while our neurologic colleagues are the obvious group to lead the deployment of stroke QI programs, there just aren’t enough of them to do so.
Hospitalists provide a significant amount of neurologic care. One study notes that TIA and stroke were among the most commonly cared-for diseases by hospitalists.1 This places us in a prime position to take the lead and own this disease in collaboration with our neurology colleagues. Just as with reliable VTE prevention, the key to effective stroke care requires effective systems engineering in conjunction with disease-specific expertise.
Rapid Care for Acute Medical Crisis
EDs are equipped with stroke pathways to efficiently evaluate, triage, scan, and intervene for patients who present with stroke symptoms. While most hospitals have a long way to go to perfect these systems, some hospitals—mostly in large, urban centers—have achieved the appropriate level of ED efficiency. These hospitals are recognized by The Joint Commission accreditation as stroke centers. As a result, patients who present to these hospitals with stroke symptoms often receive thrombolytics—a disease- and life-altering therapy—within the appropriate, but very limited, time window for benefit.
But what happens if that same patient develops those same signs and symptoms in the hospital? Will they get the same level of efficient evaluation, triage, scanning, and intervention that occurs in the ED? This is more than an academic question. Fifteen percent of all strokes are heralded by transient neurologic deficits, so many of the estimated 300,000 annual TIA patients are admitted to the hospital. What’s the reason for the admission? To facilitate the diagnostic workup, monitor for stroke symptoms and apply timely interventions should this occur.
But are we equipped to provide this kind of timely care in the hospital?
Case Study
Let’s take a 70-year-old diabetic male who presents with 45 minutes of aphasia and right-side arm weakness that resolve prior to presentation to the ED. If the patient is hypertensive on admission, the ABCD tool would suggest that he has a risk of stroke that approximates 20% in 90 days.2 Importantly, nearly half of that risk is in the first 48 hours. In other words, he has about a 10% risk of having a stroke in the next two days. Thus, we rightly admit him for monitoring in order to react quickly to any new signs and symptoms.
The problem is that most hospitals don’t have a system to efficiently manage patients who develop new stroke symptoms in the hospital. Does your hospital have an inpatient stroke pathway? That is, for a patient who has stroke onset while already in the hospital:
- Are the nurses aware of stroke signs and symptoms?
- Do nurses have a phone number to call to initiate an evaluation?
- Is there a team with stroke expertise immediately available to respond to those calls?
- Is there a priority path to get the patient promptly transported to the CT scanner for brain imaging with immediate radiology interpretation?
- How fast can thrombolytics be delivered, and is there an inpatient neurologist available 24/7 to assist?
The goal is 25 minutes from first recognition of symptoms to CT scan, and 60 minutes to complete evaluation and commencement of treatment. What percentage of your inpatient units could meet that goal? Could they do it any day of the week, at any time of the day or night?
ED systems had to be developed and implemented to ensure that appropriate candidates receive thrombolytic therapy in a timely manner. If those systems are not in place outside your hospital’s ED, then inpatient stroke cases are likely to miss the window of opportunity for thrombolytics. Ironically, they might have been better off going home and coming to the ED with any new symptoms. As a hospitalist, that is a sobering thought.
Hospitalist Ownership
It takes more than hospitalists being on-site to improve stroke outcomes. Processes need to be sharpened, roles defined, and outcomes monitored and acted upon to further sharpen the process. All of this plays to the strengths of hospitalists and should be undertaken with the vigor afforded to VTE prevention. This will take recognition that there’s a problem with the system, a dedication of resources, and a commitment to relentlessly work to improve and streamline the processes of stroke care.
In other words, it takes ownership. TH
Dr. Glasheen is associate professor of medicine and director of the hospital medicine group and hospitalist training program at the University of Colorado Denver. Ethan Cumbler, MD, contributed to this article. Dr. Cumbler is assistant professor of medicine at UC Denver and a member of the university’s Hospital Stroke Council.
This column represents the opinions of the author and is not intended to reflect an official position of SHM.
References
- Glasheen JJ, Epstein KR, Siegal E, Kutner J, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
A specialty without a disease: It was a major hangup for the field of hospital medicine in the early days. We’d hurdled many of the traditional barriers to specialty status—research fellowships, textbooks, an active society, a growing body of research, and thousands of practitioners focusing their practice on the hospital setting. However, despite several examples of site-defined specialties like emergency and critical-care medicine, cynics clung to the time-honored need for a specialty to own an organ, or at least a disease.
Early SHM efforts made a strong push to make VTE our disease—both its treatment and, more importantly, its prevention. It was a laudable effort, one that has saved many thousands of lives and limbs. It made sense for hospitalists to tackle VTE; it’s an incapacitating disease that affects many, is largely preventable, and had no strong inpatient advocate. While hematologists were the obvious “owner” of this disease, they were neither available nor able to redesign the inpatient systems of care necessary to thwart this illness. Hospitalists, invested in this issue by consequence of direct care of many at-risk patients and through commitment to improving hospital systems, came to own VTE prevention.
The Next Frontier: Stroke
It is time hospitalists apply this experience to the management of an even more incapacitating, largely preventable disease looking for an inpatient steward: stroke. A stroke occurs in the U.S. every 40 seconds, with disabling sequelae that often are avoidable with rapid detection and treatment. This is especially true when we are given the clarion call of a transient ischemic attack (TIA). The problem is that most American hospitals are not kingpins of efficiency—the key ingredient of the processes necessary to improve stroke outcomes. Furthermore, while our neurologic colleagues are the obvious group to lead the deployment of stroke QI programs, there just aren’t enough of them to do so.
Hospitalists provide a significant amount of neurologic care. One study notes that TIA and stroke were among the most commonly cared-for diseases by hospitalists.1 This places us in a prime position to take the lead and own this disease in collaboration with our neurology colleagues. Just as with reliable VTE prevention, the key to effective stroke care requires effective systems engineering in conjunction with disease-specific expertise.
Rapid Care for Acute Medical Crisis
EDs are equipped with stroke pathways to efficiently evaluate, triage, scan, and intervene for patients who present with stroke symptoms. While most hospitals have a long way to go to perfect these systems, some hospitals—mostly in large, urban centers—have achieved the appropriate level of ED efficiency. These hospitals are recognized by The Joint Commission accreditation as stroke centers. As a result, patients who present to these hospitals with stroke symptoms often receive thrombolytics—a disease- and life-altering therapy—within the appropriate, but very limited, time window for benefit.
But what happens if that same patient develops those same signs and symptoms in the hospital? Will they get the same level of efficient evaluation, triage, scanning, and intervention that occurs in the ED? This is more than an academic question. Fifteen percent of all strokes are heralded by transient neurologic deficits, so many of the estimated 300,000 annual TIA patients are admitted to the hospital. What’s the reason for the admission? To facilitate the diagnostic workup, monitor for stroke symptoms and apply timely interventions should this occur.
But are we equipped to provide this kind of timely care in the hospital?
Case Study
Let’s take a 70-year-old diabetic male who presents with 45 minutes of aphasia and right-side arm weakness that resolve prior to presentation to the ED. If the patient is hypertensive on admission, the ABCD tool would suggest that he has a risk of stroke that approximates 20% in 90 days.2 Importantly, nearly half of that risk is in the first 48 hours. In other words, he has about a 10% risk of having a stroke in the next two days. Thus, we rightly admit him for monitoring in order to react quickly to any new signs and symptoms.
The problem is that most hospitals don’t have a system to efficiently manage patients who develop new stroke symptoms in the hospital. Does your hospital have an inpatient stroke pathway? That is, for a patient who has stroke onset while already in the hospital:
- Are the nurses aware of stroke signs and symptoms?
- Do nurses have a phone number to call to initiate an evaluation?
- Is there a team with stroke expertise immediately available to respond to those calls?
- Is there a priority path to get the patient promptly transported to the CT scanner for brain imaging with immediate radiology interpretation?
- How fast can thrombolytics be delivered, and is there an inpatient neurologist available 24/7 to assist?
The goal is 25 minutes from first recognition of symptoms to CT scan, and 60 minutes to complete evaluation and commencement of treatment. What percentage of your inpatient units could meet that goal? Could they do it any day of the week, at any time of the day or night?
ED systems had to be developed and implemented to ensure that appropriate candidates receive thrombolytic therapy in a timely manner. If those systems are not in place outside your hospital’s ED, then inpatient stroke cases are likely to miss the window of opportunity for thrombolytics. Ironically, they might have been better off going home and coming to the ED with any new symptoms. As a hospitalist, that is a sobering thought.
Hospitalist Ownership
It takes more than hospitalists being on-site to improve stroke outcomes. Processes need to be sharpened, roles defined, and outcomes monitored and acted upon to further sharpen the process. All of this plays to the strengths of hospitalists and should be undertaken with the vigor afforded to VTE prevention. This will take recognition that there’s a problem with the system, a dedication of resources, and a commitment to relentlessly work to improve and streamline the processes of stroke care.
In other words, it takes ownership. TH
Dr. Glasheen is associate professor of medicine and director of the hospital medicine group and hospitalist training program at the University of Colorado Denver. Ethan Cumbler, MD, contributed to this article. Dr. Cumbler is assistant professor of medicine at UC Denver and a member of the university’s Hospital Stroke Council.
This column represents the opinions of the author and is not intended to reflect an official position of SHM.
References
- Glasheen JJ, Epstein KR, Siegal E, Kutner J, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
A specialty without a disease: It was a major hangup for the field of hospital medicine in the early days. We’d hurdled many of the traditional barriers to specialty status—research fellowships, textbooks, an active society, a growing body of research, and thousands of practitioners focusing their practice on the hospital setting. However, despite several examples of site-defined specialties like emergency and critical-care medicine, cynics clung to the time-honored need for a specialty to own an organ, or at least a disease.
Early SHM efforts made a strong push to make VTE our disease—both its treatment and, more importantly, its prevention. It was a laudable effort, one that has saved many thousands of lives and limbs. It made sense for hospitalists to tackle VTE; it’s an incapacitating disease that affects many, is largely preventable, and had no strong inpatient advocate. While hematologists were the obvious “owner” of this disease, they were neither available nor able to redesign the inpatient systems of care necessary to thwart this illness. Hospitalists, invested in this issue by consequence of direct care of many at-risk patients and through commitment to improving hospital systems, came to own VTE prevention.
The Next Frontier: Stroke
It is time hospitalists apply this experience to the management of an even more incapacitating, largely preventable disease looking for an inpatient steward: stroke. A stroke occurs in the U.S. every 40 seconds, with disabling sequelae that often are avoidable with rapid detection and treatment. This is especially true when we are given the clarion call of a transient ischemic attack (TIA). The problem is that most American hospitals are not kingpins of efficiency—the key ingredient of the processes necessary to improve stroke outcomes. Furthermore, while our neurologic colleagues are the obvious group to lead the deployment of stroke QI programs, there just aren’t enough of them to do so.
Hospitalists provide a significant amount of neurologic care. One study notes that TIA and stroke were among the most commonly cared-for diseases by hospitalists.1 This places us in a prime position to take the lead and own this disease in collaboration with our neurology colleagues. Just as with reliable VTE prevention, the key to effective stroke care requires effective systems engineering in conjunction with disease-specific expertise.
Rapid Care for Acute Medical Crisis
EDs are equipped with stroke pathways to efficiently evaluate, triage, scan, and intervene for patients who present with stroke symptoms. While most hospitals have a long way to go to perfect these systems, some hospitals—mostly in large, urban centers—have achieved the appropriate level of ED efficiency. These hospitals are recognized by The Joint Commission accreditation as stroke centers. As a result, patients who present to these hospitals with stroke symptoms often receive thrombolytics—a disease- and life-altering therapy—within the appropriate, but very limited, time window for benefit.
But what happens if that same patient develops those same signs and symptoms in the hospital? Will they get the same level of efficient evaluation, triage, scanning, and intervention that occurs in the ED? This is more than an academic question. Fifteen percent of all strokes are heralded by transient neurologic deficits, so many of the estimated 300,000 annual TIA patients are admitted to the hospital. What’s the reason for the admission? To facilitate the diagnostic workup, monitor for stroke symptoms and apply timely interventions should this occur.
But are we equipped to provide this kind of timely care in the hospital?
Case Study
Let’s take a 70-year-old diabetic male who presents with 45 minutes of aphasia and right-side arm weakness that resolve prior to presentation to the ED. If the patient is hypertensive on admission, the ABCD tool would suggest that he has a risk of stroke that approximates 20% in 90 days.2 Importantly, nearly half of that risk is in the first 48 hours. In other words, he has about a 10% risk of having a stroke in the next two days. Thus, we rightly admit him for monitoring in order to react quickly to any new signs and symptoms.
The problem is that most hospitals don’t have a system to efficiently manage patients who develop new stroke symptoms in the hospital. Does your hospital have an inpatient stroke pathway? That is, for a patient who has stroke onset while already in the hospital:
- Are the nurses aware of stroke signs and symptoms?
- Do nurses have a phone number to call to initiate an evaluation?
- Is there a team with stroke expertise immediately available to respond to those calls?
- Is there a priority path to get the patient promptly transported to the CT scanner for brain imaging with immediate radiology interpretation?
- How fast can thrombolytics be delivered, and is there an inpatient neurologist available 24/7 to assist?
The goal is 25 minutes from first recognition of symptoms to CT scan, and 60 minutes to complete evaluation and commencement of treatment. What percentage of your inpatient units could meet that goal? Could they do it any day of the week, at any time of the day or night?
ED systems had to be developed and implemented to ensure that appropriate candidates receive thrombolytic therapy in a timely manner. If those systems are not in place outside your hospital’s ED, then inpatient stroke cases are likely to miss the window of opportunity for thrombolytics. Ironically, they might have been better off going home and coming to the ED with any new symptoms. As a hospitalist, that is a sobering thought.
Hospitalist Ownership
It takes more than hospitalists being on-site to improve stroke outcomes. Processes need to be sharpened, roles defined, and outcomes monitored and acted upon to further sharpen the process. All of this plays to the strengths of hospitalists and should be undertaken with the vigor afforded to VTE prevention. This will take recognition that there’s a problem with the system, a dedication of resources, and a commitment to relentlessly work to improve and streamline the processes of stroke care.
In other words, it takes ownership. TH
Dr. Glasheen is associate professor of medicine and director of the hospital medicine group and hospitalist training program at the University of Colorado Denver. Ethan Cumbler, MD, contributed to this article. Dr. Cumbler is assistant professor of medicine at UC Denver and a member of the university’s Hospital Stroke Council.
This column represents the opinions of the author and is not intended to reflect an official position of SHM.
References
- Glasheen JJ, Epstein KR, Siegal E, Kutner J, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
Bundling Bedlam

Even if you receive your salary as an employee of your hospital or hospitalist group, you should keep a close eye on discussions taking place in Washington about reshaping the way hospital care is paid for. It seems that every 10 to 20 years, a seismic tremor starts on Capitol Hill and fundamentally shakes up the way healthcare is funded. It starts with Medicare, then quickly is adopted by private insurers; it not only changes the distribution of dollars, but the new incentives also drive the way medicine is practiced.
In the 1960s, change began with President Johnson and the development of Medicare and Medicaid. It was the first time specific populations—seniors and the poor—were “entitled” to healthcare coverage. In essence, Johnson created the largest “insurance company” in the country, and it became the tail that wagged the dog.
In the 1970s, President Nixon pushed through support for HMOs, and capitation and managed care spread well beyond the Kaisers of the world. This system incentivized controlling costs, because the total amount was capped, while maintaining an acceptable level of quality. For the first time, doing more did not generate more money.
In the 1980s, diagnosis-related groups (DRGs) changed Medicare payments to hospitals from cost-plus billings to a bundled fee for an episode of care. This motivated hospitals to work with their physicians—sometimes driven by protocols and case managers—to efficiently manage resources and length of stay (LOS). Between capitation, case rates, and DRGs, hospitals have had to refashion themselves to be leaner and more efficient.
Today, with national thought leaders like John Wennberg and Elliot Fisher at Dartmouth and Brent James at Intermountain revealing the many variations in the way healthcare is practiced—and throwing around statistics like “40% of healthcare is wasteful”—it is no wonder that as President Obama and Congress look to add 47 million uninsured persons to the system and try to reduce variation and increase accountabilities, there is every indication that radical changes will be made to the payment system.
One of these newfangled approaches is the bundling of payment for an episode of care to include both the facility charges (e.g., hospital care) and the professional charges (e.g., physician care). Bundling can be a good thing or a worrisome approach, depending on where you sit in this dialogue and how bundling is actually implemented.
Background on Bundling
The motivation of the government—and, by extension, all insurers—is that efforts to control what they pay per unit for a visit, a procedure, or even an entire hospitalization has not curbed costs or led to a satisfactory level of performance. With respect to hospitalized patients, Obama has stated that he wants to eliminate waste by reducing unnecessary readmissions to the tune of $6.8 billion annually. Furthermore, Medicare officials want to look for strategies that either keep people out of the ED post-discharge or at least eliminate Medicare’s need to pay for this care, which they feel is unnecessary and avoidable.
By bundling payment for a specific admission (e.g., decompensated heart failure or pneumonia) and including the facility and professional-care fees, both during hospitalization and for a period of time (e.g., 30 days post-discharge) and providing incentives for best performance, the insurer (i.e., Medicare) can hand off responsibility to the hospitals and the doctors to figure it all out. There is nothing like the accountability of knowing “this is all you are going to get,” or “if you want more, you have to meet these standards,” to motivate professionals to reshape their system to improve their discharge process, engage the outpatient physicians, and do the job right the first time. This can play to HM’s strengths, and SHM already has started developing and implementing change in the discharge process through Project BOOST (Better Outcomes for Older Adults through Safe Transitions, www.hospitalmedicine.org/boost).
Potential Problems
One key concern is not knowing who—or what—will control the dollars once Medicare sets the bundled payment. Right now, hospitals receive the DRG payment and physicians bill for their own professional services. In the future, will all the money flow to the hospital? How will these dollars be distributed? Who determines who will be awarded performance bonuses?
In California and other states with significant managed-care populations and large medical groups, there is real-life experience with setting up efficient physician-hospital organizations (PHOs) to solve these issues. Some take the form of independent physician associations (IPAs), which represent the physicians in PHOs. There is no reason PHOs cannot be developed to administrate these bundled funds, and hospitalists, who are seeing an increasing number of hospitalized patients on medicine and surgery, should be key leaders in such PHO arrangements.
But HM is not a monolith in this discussion. The diversity in how HM groups are organized, their relationship with their hospitals, and how hospitalists or their groups receive funding can, and will, influence the group’s perspective on this issue. Hospitalist groups that are independent from their hospitals, or those that rely on referrals from primary-care physicians (PCPs) or the ED, might be justifiably concerned about all of “their” money having to flow through the hospital. Hospitalists who are employed by a hospital might be concerned that they will need to develop new metrics to justify their salaries and bonuses. HM groups that contract with the hospital might be concerned that a change in the flow of funding from Medicare to the hospital might make their contractual arrangements more difficult.
For those who battle with hospital administration over hospital support of their HM group, they might find bundling alleviates the need for the current use of Part A dollars to support hospitalists, because the new bundling of Part A (current payments for hospital facility charges) and Part B (current payment for physicians’ professional services) can allow for a more professional discussion, based on the value hospitalists bring. The need for subsidies or support could diminish or vanish.
Change Is Coming
No matter your perspective or viewpoint, one reality is coming into focus: This president and this Congress will make sweeping changes, and it appears from our conversations with Sen. Max Baucus (D-Mont.), chair of the powerful Senate Finance Committee (see “Medicine’s Change Agent,” May 2009, p. 18), that bundling and value-based purchasing will be part of healthcare reform.
With this in mind, SHM’s Public Policy Committee is actively engaged in trying to shape bundling in a way that fits emerging changes in the care of hospitalized patients. We want a system that works for the way healthcare will be practiced in the future, not a Band-Aid on the system of the past. This is very important stuff. Hospitalists will be affected by reform because so many of our patients are on Medicare and our compensation is generated by patient care in the hospital.
SHM has created an easy-to-use, Web-based system to send a message to members of Congress through a partnership with Capwiz. Visit www.hospitalmedicine.org/beheard to get started.
While the uncertainty of healthcare reform and, more specifically, payment reform is at times frightening, mainly because it is so sweeping and at this point so undefined, HM has been forged in the cauldron of change and ambiguity. Hospitalists are positioned as well as any health professionals to seize the opportunities that a new system will provide. And SHM will do its part to help shape the new reality and assist our members in creating successful strategies in this new environment. TH
Dr. Wellikson is CEO of SHM.
Even if you receive your salary as an employee of your hospital or hospitalist group, you should keep a close eye on discussions taking place in Washington about reshaping the way hospital care is paid for. It seems that every 10 to 20 years, a seismic tremor starts on Capitol Hill and fundamentally shakes up the way healthcare is funded. It starts with Medicare, then quickly is adopted by private insurers; it not only changes the distribution of dollars, but the new incentives also drive the way medicine is practiced.
In the 1960s, change began with President Johnson and the development of Medicare and Medicaid. It was the first time specific populations—seniors and the poor—were “entitled” to healthcare coverage. In essence, Johnson created the largest “insurance company” in the country, and it became the tail that wagged the dog.
In the 1970s, President Nixon pushed through support for HMOs, and capitation and managed care spread well beyond the Kaisers of the world. This system incentivized controlling costs, because the total amount was capped, while maintaining an acceptable level of quality. For the first time, doing more did not generate more money.
In the 1980s, diagnosis-related groups (DRGs) changed Medicare payments to hospitals from cost-plus billings to a bundled fee for an episode of care. This motivated hospitals to work with their physicians—sometimes driven by protocols and case managers—to efficiently manage resources and length of stay (LOS). Between capitation, case rates, and DRGs, hospitals have had to refashion themselves to be leaner and more efficient.
Today, with national thought leaders like John Wennberg and Elliot Fisher at Dartmouth and Brent James at Intermountain revealing the many variations in the way healthcare is practiced—and throwing around statistics like “40% of healthcare is wasteful”—it is no wonder that as President Obama and Congress look to add 47 million uninsured persons to the system and try to reduce variation and increase accountabilities, there is every indication that radical changes will be made to the payment system.
One of these newfangled approaches is the bundling of payment for an episode of care to include both the facility charges (e.g., hospital care) and the professional charges (e.g., physician care). Bundling can be a good thing or a worrisome approach, depending on where you sit in this dialogue and how bundling is actually implemented.
Background on Bundling
The motivation of the government—and, by extension, all insurers—is that efforts to control what they pay per unit for a visit, a procedure, or even an entire hospitalization has not curbed costs or led to a satisfactory level of performance. With respect to hospitalized patients, Obama has stated that he wants to eliminate waste by reducing unnecessary readmissions to the tune of $6.8 billion annually. Furthermore, Medicare officials want to look for strategies that either keep people out of the ED post-discharge or at least eliminate Medicare’s need to pay for this care, which they feel is unnecessary and avoidable.
By bundling payment for a specific admission (e.g., decompensated heart failure or pneumonia) and including the facility and professional-care fees, both during hospitalization and for a period of time (e.g., 30 days post-discharge) and providing incentives for best performance, the insurer (i.e., Medicare) can hand off responsibility to the hospitals and the doctors to figure it all out. There is nothing like the accountability of knowing “this is all you are going to get,” or “if you want more, you have to meet these standards,” to motivate professionals to reshape their system to improve their discharge process, engage the outpatient physicians, and do the job right the first time. This can play to HM’s strengths, and SHM already has started developing and implementing change in the discharge process through Project BOOST (Better Outcomes for Older Adults through Safe Transitions, www.hospitalmedicine.org/boost).
Potential Problems
One key concern is not knowing who—or what—will control the dollars once Medicare sets the bundled payment. Right now, hospitals receive the DRG payment and physicians bill for their own professional services. In the future, will all the money flow to the hospital? How will these dollars be distributed? Who determines who will be awarded performance bonuses?
In California and other states with significant managed-care populations and large medical groups, there is real-life experience with setting up efficient physician-hospital organizations (PHOs) to solve these issues. Some take the form of independent physician associations (IPAs), which represent the physicians in PHOs. There is no reason PHOs cannot be developed to administrate these bundled funds, and hospitalists, who are seeing an increasing number of hospitalized patients on medicine and surgery, should be key leaders in such PHO arrangements.
But HM is not a monolith in this discussion. The diversity in how HM groups are organized, their relationship with their hospitals, and how hospitalists or their groups receive funding can, and will, influence the group’s perspective on this issue. Hospitalist groups that are independent from their hospitals, or those that rely on referrals from primary-care physicians (PCPs) or the ED, might be justifiably concerned about all of “their” money having to flow through the hospital. Hospitalists who are employed by a hospital might be concerned that they will need to develop new metrics to justify their salaries and bonuses. HM groups that contract with the hospital might be concerned that a change in the flow of funding from Medicare to the hospital might make their contractual arrangements more difficult.
For those who battle with hospital administration over hospital support of their HM group, they might find bundling alleviates the need for the current use of Part A dollars to support hospitalists, because the new bundling of Part A (current payments for hospital facility charges) and Part B (current payment for physicians’ professional services) can allow for a more professional discussion, based on the value hospitalists bring. The need for subsidies or support could diminish or vanish.
Change Is Coming
No matter your perspective or viewpoint, one reality is coming into focus: This president and this Congress will make sweeping changes, and it appears from our conversations with Sen. Max Baucus (D-Mont.), chair of the powerful Senate Finance Committee (see “Medicine’s Change Agent,” May 2009, p. 18), that bundling and value-based purchasing will be part of healthcare reform.
With this in mind, SHM’s Public Policy Committee is actively engaged in trying to shape bundling in a way that fits emerging changes in the care of hospitalized patients. We want a system that works for the way healthcare will be practiced in the future, not a Band-Aid on the system of the past. This is very important stuff. Hospitalists will be affected by reform because so many of our patients are on Medicare and our compensation is generated by patient care in the hospital.
SHM has created an easy-to-use, Web-based system to send a message to members of Congress through a partnership with Capwiz. Visit www.hospitalmedicine.org/beheard to get started.
While the uncertainty of healthcare reform and, more specifically, payment reform is at times frightening, mainly because it is so sweeping and at this point so undefined, HM has been forged in the cauldron of change and ambiguity. Hospitalists are positioned as well as any health professionals to seize the opportunities that a new system will provide. And SHM will do its part to help shape the new reality and assist our members in creating successful strategies in this new environment. TH
Dr. Wellikson is CEO of SHM.
Even if you receive your salary as an employee of your hospital or hospitalist group, you should keep a close eye on discussions taking place in Washington about reshaping the way hospital care is paid for. It seems that every 10 to 20 years, a seismic tremor starts on Capitol Hill and fundamentally shakes up the way healthcare is funded. It starts with Medicare, then quickly is adopted by private insurers; it not only changes the distribution of dollars, but the new incentives also drive the way medicine is practiced.
In the 1960s, change began with President Johnson and the development of Medicare and Medicaid. It was the first time specific populations—seniors and the poor—were “entitled” to healthcare coverage. In essence, Johnson created the largest “insurance company” in the country, and it became the tail that wagged the dog.
In the 1970s, President Nixon pushed through support for HMOs, and capitation and managed care spread well beyond the Kaisers of the world. This system incentivized controlling costs, because the total amount was capped, while maintaining an acceptable level of quality. For the first time, doing more did not generate more money.
In the 1980s, diagnosis-related groups (DRGs) changed Medicare payments to hospitals from cost-plus billings to a bundled fee for an episode of care. This motivated hospitals to work with their physicians—sometimes driven by protocols and case managers—to efficiently manage resources and length of stay (LOS). Between capitation, case rates, and DRGs, hospitals have had to refashion themselves to be leaner and more efficient.
Today, with national thought leaders like John Wennberg and Elliot Fisher at Dartmouth and Brent James at Intermountain revealing the many variations in the way healthcare is practiced—and throwing around statistics like “40% of healthcare is wasteful”—it is no wonder that as President Obama and Congress look to add 47 million uninsured persons to the system and try to reduce variation and increase accountabilities, there is every indication that radical changes will be made to the payment system.
One of these newfangled approaches is the bundling of payment for an episode of care to include both the facility charges (e.g., hospital care) and the professional charges (e.g., physician care). Bundling can be a good thing or a worrisome approach, depending on where you sit in this dialogue and how bundling is actually implemented.
Background on Bundling
The motivation of the government—and, by extension, all insurers—is that efforts to control what they pay per unit for a visit, a procedure, or even an entire hospitalization has not curbed costs or led to a satisfactory level of performance. With respect to hospitalized patients, Obama has stated that he wants to eliminate waste by reducing unnecessary readmissions to the tune of $6.8 billion annually. Furthermore, Medicare officials want to look for strategies that either keep people out of the ED post-discharge or at least eliminate Medicare’s need to pay for this care, which they feel is unnecessary and avoidable.
By bundling payment for a specific admission (e.g., decompensated heart failure or pneumonia) and including the facility and professional-care fees, both during hospitalization and for a period of time (e.g., 30 days post-discharge) and providing incentives for best performance, the insurer (i.e., Medicare) can hand off responsibility to the hospitals and the doctors to figure it all out. There is nothing like the accountability of knowing “this is all you are going to get,” or “if you want more, you have to meet these standards,” to motivate professionals to reshape their system to improve their discharge process, engage the outpatient physicians, and do the job right the first time. This can play to HM’s strengths, and SHM already has started developing and implementing change in the discharge process through Project BOOST (Better Outcomes for Older Adults through Safe Transitions, www.hospitalmedicine.org/boost).
Potential Problems
One key concern is not knowing who—or what—will control the dollars once Medicare sets the bundled payment. Right now, hospitals receive the DRG payment and physicians bill for their own professional services. In the future, will all the money flow to the hospital? How will these dollars be distributed? Who determines who will be awarded performance bonuses?
In California and other states with significant managed-care populations and large medical groups, there is real-life experience with setting up efficient physician-hospital organizations (PHOs) to solve these issues. Some take the form of independent physician associations (IPAs), which represent the physicians in PHOs. There is no reason PHOs cannot be developed to administrate these bundled funds, and hospitalists, who are seeing an increasing number of hospitalized patients on medicine and surgery, should be key leaders in such PHO arrangements.
But HM is not a monolith in this discussion. The diversity in how HM groups are organized, their relationship with their hospitals, and how hospitalists or their groups receive funding can, and will, influence the group’s perspective on this issue. Hospitalist groups that are independent from their hospitals, or those that rely on referrals from primary-care physicians (PCPs) or the ED, might be justifiably concerned about all of “their” money having to flow through the hospital. Hospitalists who are employed by a hospital might be concerned that they will need to develop new metrics to justify their salaries and bonuses. HM groups that contract with the hospital might be concerned that a change in the flow of funding from Medicare to the hospital might make their contractual arrangements more difficult.
For those who battle with hospital administration over hospital support of their HM group, they might find bundling alleviates the need for the current use of Part A dollars to support hospitalists, because the new bundling of Part A (current payments for hospital facility charges) and Part B (current payment for physicians’ professional services) can allow for a more professional discussion, based on the value hospitalists bring. The need for subsidies or support could diminish or vanish.
Change Is Coming
No matter your perspective or viewpoint, one reality is coming into focus: This president and this Congress will make sweeping changes, and it appears from our conversations with Sen. Max Baucus (D-Mont.), chair of the powerful Senate Finance Committee (see “Medicine’s Change Agent,” May 2009, p. 18), that bundling and value-based purchasing will be part of healthcare reform.
With this in mind, SHM’s Public Policy Committee is actively engaged in trying to shape bundling in a way that fits emerging changes in the care of hospitalized patients. We want a system that works for the way healthcare will be practiced in the future, not a Band-Aid on the system of the past. This is very important stuff. Hospitalists will be affected by reform because so many of our patients are on Medicare and our compensation is generated by patient care in the hospital.
SHM has created an easy-to-use, Web-based system to send a message to members of Congress through a partnership with Capwiz. Visit www.hospitalmedicine.org/beheard to get started.
While the uncertainty of healthcare reform and, more specifically, payment reform is at times frightening, mainly because it is so sweeping and at this point so undefined, HM has been forged in the cauldron of change and ambiguity. Hospitalists are positioned as well as any health professionals to seize the opportunities that a new system will provide. And SHM will do its part to help shape the new reality and assist our members in creating successful strategies in this new environment. TH
Dr. Wellikson is CEO of SHM.
Grassroots Mentorship
Indu Michael remembers the one-page medical field survey she filled out around this time last year. A pre-med student at the University of California at Los Angeles, she provided the correct job descriptions for surgeons, pediatricians, OB/GYNs, psychiatrists, and internal medicine physicians. Only one medical specialty stumped her.
“I had no idea what a hospitalist did,” says Michael, 21, a senior.
The anonymous survey was part of the application and interview process for the Undergraduate Preceptorship in Internal Medicine (UPIM), a program that was launched last summer at UCLA Medical Center. By the time Michael finished the three-week program in early September, she had a complete understanding of what hospitalists do. She also says she’s leaning toward an internal medicine (IM) career—and might become a hospitalist.
“I’m seriously thinking [Hem-Onc] may not be the direction I want to take,” Michael says. “I realized oncologists are mainly consultative doctors and it’s really the general medicine team that does the medicine.”
Those kind of comments are music to Nasim Afsar-manesh’s ear. Dr. Afsar-manesh, a hospitalist and assistant clinical professor at UCLA, developed the UPIM program from scratch as a way to expose pre-med undergrads to internal medicine. The ultimate goal, of course, is steering them toward an internist career. She is well aware of medical students’ declining interest in IM, and she believes outreach to undergrads and first-year medical students will help reverse the trend.
“Undergraduates are like sponges,” Dr. Afsar-manesh says. “They are so genuinely excited about the possibilities of getting to do this stuff. … You can appeal to their idealism.” She created the program because “the general field of medicine has become so complex that students who are thinking about making it a career don’t have a good chance to see what the day-to-day practicing of medicine is like.”
HM Test Drive
Michael was one of seven students in the inaugural UPIM session. The program is open to UCLA undergrads who volunteer at least 80 hours at the medical center and pre-med students at the California Institute of Technology, where Dr. Afsar-manesh received her undergraduate degree. Seventeen students applied for the first session; the seven who were selected were chosen based on their motivation, maturity, and enthusiasm for medicine. The plan is simple: UPIM aims to offer an early spark of excitement that will stay with students and serve as positive reinforcement as they proceed through medical school and confront the challenges of an IM career.
UPIM participants were integrated into teams of attendings, residents, and medical school students, and they spent time on hospital units and subspecialty consult services. The undergrads observed residents in their patient evaluations, daily rounds, and discussions with patient families. They witnessed a number of procedures, including central-line placement and bone-marrow biopsies. Although the attendings and residents weren’t required to teach the undergrads, many volunteered a significant amount of their time, Dr. Afsar-manesh says. Some of the students spent night shifts at the hospital.
“The students felt they had participated in something special. They felt the experience had overshadowed anything they had previously done,” says Dr. Afsar-manesh, a member of SHM’s Young Physicians Committee. “I think it’s a program that can really quickly grow.”
Every Friday, undergrads participated in a teaching session, during which they had to present a medically, socially, or ethically challenging case from the previous week. They received lectures on common HM topics, such as coronary artery disease, hypertension, and diabetes mellitus. The sessions featured guest speakers who touched on career options in IM and HM, research careers, tips for getting into medical school, and international health issues.
“I loved the patient interaction, as well as discussing a case with fellow students. I didn’t even mind the long hours,” says Stacey Yudin, 23, a senior pre-med student at UCLA. “While on rounds, medical students and doctors took the time to explain concepts while we were scurrying from patient to patient. The program gave me the opportunity to test-drive my dream. We always test-drive a car before we hand over thousands of dollars for it. Shouldn’t future medical students be able to at least safely experience the practice of medicine?”
Round Two: Upgrade
This summer, Dr. Afsar-manesh is improving the student presentation and guest speaker component of the Friday sessions. She will add QI and patient-safety sessions. But the biggest change to the program is expansion, as she and fellow UCLA hospitalist Ed Ha, MD, will offer a summer session for medical students between their first and second years.
Dr. Afsar-manesh also is busy reaching out to other academic IM and HM programs interested in establishing a preceptorship program. So far, she’s made headway with 10 institutions, including Northwestern University, Stanford University, the University of Michigan Health System, and a handful of the campuses within the University of California system. She’s invited the institutions to participate in a research collaborative to combine their data on program results. “We ultimately need to see how many participants will go into IM and compare that to the national numbers. That will take years,” she says.
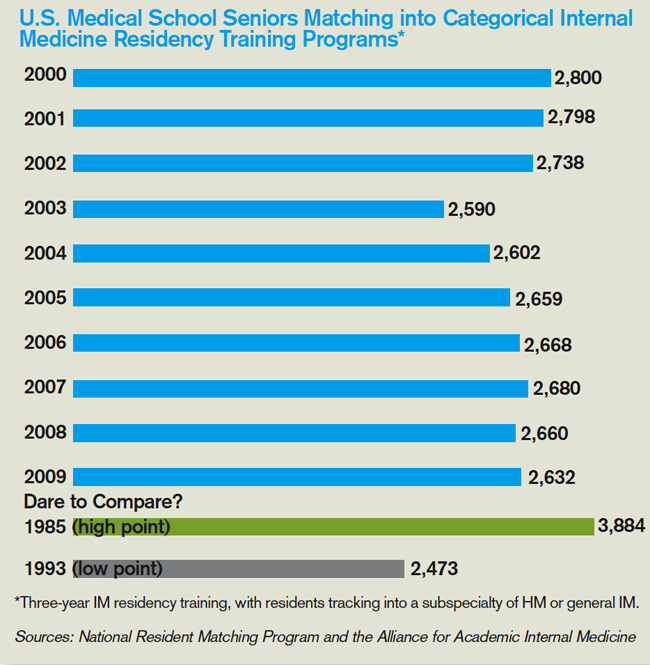
Uphill Battle
Mark Schwartz, MD, an associate professor in the division of general IM at New York University’s School of Medicine, believes UPIM and programs like it will help—even if only marginally—address the declining interest in IM careers among medical students.
“It will take more than tinkering around in the educational environment,” says Dr. Schwartz, who believes workforce planning, changes in reimbursement, and redesigning medical practices are essential to recruiting medical students to internal medicine (see “A Good Start, But Not Enough”).
Nevertheless, SHM is ready to support a combined IM/HM preceptorship program that targets medical school students in their first and second years, says Larry Wellikson, MD, FHM, CEO of SHM. The society already has assigned staff to manage the project and named Dr. Afsar-manesh as the lead physician. The plan is to track preceptorship participants as they make their way through medical school and residency, and see if the program changes their attitudes toward IM careers.
Even though the number of medical students who aspire to hospitalist careers continues to increase every year, SHM believes it must move to counteract the lackluster IM numbers, because that is where most medical students are introduced to HM, Dr. Wellikson says. “The problem of people not picking internal medicine could affect hospital medicine down the road,” he says. “We can’t sit passively by and see who picks to be a hospitalist. We believe we need to be active.”
One of the last things Dr. Afsar-manesh did at the conclusion of the inaugural UPIM program was collect the students’ e-mail addresses and phone numbers so she can stay in touch and track their career paths. The UPIM survey results give her hope: After UPIM, 100% of the students were “extremely confident” in their decision to pursue medicine; 57% indicated they were “very likely” to consider IM as a specialty; and 47% were “very likely” to think about HM.
“This program is a great way to encourage students to enter into internal medicine,” Yudin says. “I am sure that all my subsequent experiences working in a hospital will be measured against my first experience rounding with the IM department.” It seems as though the student took the words right out of the doctor’s mouth. TH
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hauer KE, Durning SJ, Kernan WN, et al. Factors associated with medical students’ career choices regarding internal medicine. JAMA. 2008;300(10):1154-1164.
Indu Michael remembers the one-page medical field survey she filled out around this time last year. A pre-med student at the University of California at Los Angeles, she provided the correct job descriptions for surgeons, pediatricians, OB/GYNs, psychiatrists, and internal medicine physicians. Only one medical specialty stumped her.
“I had no idea what a hospitalist did,” says Michael, 21, a senior.
The anonymous survey was part of the application and interview process for the Undergraduate Preceptorship in Internal Medicine (UPIM), a program that was launched last summer at UCLA Medical Center. By the time Michael finished the three-week program in early September, she had a complete understanding of what hospitalists do. She also says she’s leaning toward an internal medicine (IM) career—and might become a hospitalist.
“I’m seriously thinking [Hem-Onc] may not be the direction I want to take,” Michael says. “I realized oncologists are mainly consultative doctors and it’s really the general medicine team that does the medicine.”
Those kind of comments are music to Nasim Afsar-manesh’s ear. Dr. Afsar-manesh, a hospitalist and assistant clinical professor at UCLA, developed the UPIM program from scratch as a way to expose pre-med undergrads to internal medicine. The ultimate goal, of course, is steering them toward an internist career. She is well aware of medical students’ declining interest in IM, and she believes outreach to undergrads and first-year medical students will help reverse the trend.
“Undergraduates are like sponges,” Dr. Afsar-manesh says. “They are so genuinely excited about the possibilities of getting to do this stuff. … You can appeal to their idealism.” She created the program because “the general field of medicine has become so complex that students who are thinking about making it a career don’t have a good chance to see what the day-to-day practicing of medicine is like.”
HM Test Drive
Michael was one of seven students in the inaugural UPIM session. The program is open to UCLA undergrads who volunteer at least 80 hours at the medical center and pre-med students at the California Institute of Technology, where Dr. Afsar-manesh received her undergraduate degree. Seventeen students applied for the first session; the seven who were selected were chosen based on their motivation, maturity, and enthusiasm for medicine. The plan is simple: UPIM aims to offer an early spark of excitement that will stay with students and serve as positive reinforcement as they proceed through medical school and confront the challenges of an IM career.
UPIM participants were integrated into teams of attendings, residents, and medical school students, and they spent time on hospital units and subspecialty consult services. The undergrads observed residents in their patient evaluations, daily rounds, and discussions with patient families. They witnessed a number of procedures, including central-line placement and bone-marrow biopsies. Although the attendings and residents weren’t required to teach the undergrads, many volunteered a significant amount of their time, Dr. Afsar-manesh says. Some of the students spent night shifts at the hospital.
“The students felt they had participated in something special. They felt the experience had overshadowed anything they had previously done,” says Dr. Afsar-manesh, a member of SHM’s Young Physicians Committee. “I think it’s a program that can really quickly grow.”
Every Friday, undergrads participated in a teaching session, during which they had to present a medically, socially, or ethically challenging case from the previous week. They received lectures on common HM topics, such as coronary artery disease, hypertension, and diabetes mellitus. The sessions featured guest speakers who touched on career options in IM and HM, research careers, tips for getting into medical school, and international health issues.
“I loved the patient interaction, as well as discussing a case with fellow students. I didn’t even mind the long hours,” says Stacey Yudin, 23, a senior pre-med student at UCLA. “While on rounds, medical students and doctors took the time to explain concepts while we were scurrying from patient to patient. The program gave me the opportunity to test-drive my dream. We always test-drive a car before we hand over thousands of dollars for it. Shouldn’t future medical students be able to at least safely experience the practice of medicine?”
Round Two: Upgrade
This summer, Dr. Afsar-manesh is improving the student presentation and guest speaker component of the Friday sessions. She will add QI and patient-safety sessions. But the biggest change to the program is expansion, as she and fellow UCLA hospitalist Ed Ha, MD, will offer a summer session for medical students between their first and second years.
Dr. Afsar-manesh also is busy reaching out to other academic IM and HM programs interested in establishing a preceptorship program. So far, she’s made headway with 10 institutions, including Northwestern University, Stanford University, the University of Michigan Health System, and a handful of the campuses within the University of California system. She’s invited the institutions to participate in a research collaborative to combine their data on program results. “We ultimately need to see how many participants will go into IM and compare that to the national numbers. That will take years,” she says.
Uphill Battle
Mark Schwartz, MD, an associate professor in the division of general IM at New York University’s School of Medicine, believes UPIM and programs like it will help—even if only marginally—address the declining interest in IM careers among medical students.
“It will take more than tinkering around in the educational environment,” says Dr. Schwartz, who believes workforce planning, changes in reimbursement, and redesigning medical practices are essential to recruiting medical students to internal medicine (see “A Good Start, But Not Enough”).
Nevertheless, SHM is ready to support a combined IM/HM preceptorship program that targets medical school students in their first and second years, says Larry Wellikson, MD, FHM, CEO of SHM. The society already has assigned staff to manage the project and named Dr. Afsar-manesh as the lead physician. The plan is to track preceptorship participants as they make their way through medical school and residency, and see if the program changes their attitudes toward IM careers.
Even though the number of medical students who aspire to hospitalist careers continues to increase every year, SHM believes it must move to counteract the lackluster IM numbers, because that is where most medical students are introduced to HM, Dr. Wellikson says. “The problem of people not picking internal medicine could affect hospital medicine down the road,” he says. “We can’t sit passively by and see who picks to be a hospitalist. We believe we need to be active.”
One of the last things Dr. Afsar-manesh did at the conclusion of the inaugural UPIM program was collect the students’ e-mail addresses and phone numbers so she can stay in touch and track their career paths. The UPIM survey results give her hope: After UPIM, 100% of the students were “extremely confident” in their decision to pursue medicine; 57% indicated they were “very likely” to consider IM as a specialty; and 47% were “very likely” to think about HM.
“This program is a great way to encourage students to enter into internal medicine,” Yudin says. “I am sure that all my subsequent experiences working in a hospital will be measured against my first experience rounding with the IM department.” It seems as though the student took the words right out of the doctor’s mouth. TH
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hauer KE, Durning SJ, Kernan WN, et al. Factors associated with medical students’ career choices regarding internal medicine. JAMA. 2008;300(10):1154-1164.
Indu Michael remembers the one-page medical field survey she filled out around this time last year. A pre-med student at the University of California at Los Angeles, she provided the correct job descriptions for surgeons, pediatricians, OB/GYNs, psychiatrists, and internal medicine physicians. Only one medical specialty stumped her.
“I had no idea what a hospitalist did,” says Michael, 21, a senior.
The anonymous survey was part of the application and interview process for the Undergraduate Preceptorship in Internal Medicine (UPIM), a program that was launched last summer at UCLA Medical Center. By the time Michael finished the three-week program in early September, she had a complete understanding of what hospitalists do. She also says she’s leaning toward an internal medicine (IM) career—and might become a hospitalist.
“I’m seriously thinking [Hem-Onc] may not be the direction I want to take,” Michael says. “I realized oncologists are mainly consultative doctors and it’s really the general medicine team that does the medicine.”
Those kind of comments are music to Nasim Afsar-manesh’s ear. Dr. Afsar-manesh, a hospitalist and assistant clinical professor at UCLA, developed the UPIM program from scratch as a way to expose pre-med undergrads to internal medicine. The ultimate goal, of course, is steering them toward an internist career. She is well aware of medical students’ declining interest in IM, and she believes outreach to undergrads and first-year medical students will help reverse the trend.
“Undergraduates are like sponges,” Dr. Afsar-manesh says. “They are so genuinely excited about the possibilities of getting to do this stuff. … You can appeal to their idealism.” She created the program because “the general field of medicine has become so complex that students who are thinking about making it a career don’t have a good chance to see what the day-to-day practicing of medicine is like.”
HM Test Drive
Michael was one of seven students in the inaugural UPIM session. The program is open to UCLA undergrads who volunteer at least 80 hours at the medical center and pre-med students at the California Institute of Technology, where Dr. Afsar-manesh received her undergraduate degree. Seventeen students applied for the first session; the seven who were selected were chosen based on their motivation, maturity, and enthusiasm for medicine. The plan is simple: UPIM aims to offer an early spark of excitement that will stay with students and serve as positive reinforcement as they proceed through medical school and confront the challenges of an IM career.
UPIM participants were integrated into teams of attendings, residents, and medical school students, and they spent time on hospital units and subspecialty consult services. The undergrads observed residents in their patient evaluations, daily rounds, and discussions with patient families. They witnessed a number of procedures, including central-line placement and bone-marrow biopsies. Although the attendings and residents weren’t required to teach the undergrads, many volunteered a significant amount of their time, Dr. Afsar-manesh says. Some of the students spent night shifts at the hospital.
“The students felt they had participated in something special. They felt the experience had overshadowed anything they had previously done,” says Dr. Afsar-manesh, a member of SHM’s Young Physicians Committee. “I think it’s a program that can really quickly grow.”
Every Friday, undergrads participated in a teaching session, during which they had to present a medically, socially, or ethically challenging case from the previous week. They received lectures on common HM topics, such as coronary artery disease, hypertension, and diabetes mellitus. The sessions featured guest speakers who touched on career options in IM and HM, research careers, tips for getting into medical school, and international health issues.
“I loved the patient interaction, as well as discussing a case with fellow students. I didn’t even mind the long hours,” says Stacey Yudin, 23, a senior pre-med student at UCLA. “While on rounds, medical students and doctors took the time to explain concepts while we were scurrying from patient to patient. The program gave me the opportunity to test-drive my dream. We always test-drive a car before we hand over thousands of dollars for it. Shouldn’t future medical students be able to at least safely experience the practice of medicine?”
Round Two: Upgrade
This summer, Dr. Afsar-manesh is improving the student presentation and guest speaker component of the Friday sessions. She will add QI and patient-safety sessions. But the biggest change to the program is expansion, as she and fellow UCLA hospitalist Ed Ha, MD, will offer a summer session for medical students between their first and second years.
Dr. Afsar-manesh also is busy reaching out to other academic IM and HM programs interested in establishing a preceptorship program. So far, she’s made headway with 10 institutions, including Northwestern University, Stanford University, the University of Michigan Health System, and a handful of the campuses within the University of California system. She’s invited the institutions to participate in a research collaborative to combine their data on program results. “We ultimately need to see how many participants will go into IM and compare that to the national numbers. That will take years,” she says.
Uphill Battle
Mark Schwartz, MD, an associate professor in the division of general IM at New York University’s School of Medicine, believes UPIM and programs like it will help—even if only marginally—address the declining interest in IM careers among medical students.
“It will take more than tinkering around in the educational environment,” says Dr. Schwartz, who believes workforce planning, changes in reimbursement, and redesigning medical practices are essential to recruiting medical students to internal medicine (see “A Good Start, But Not Enough”).
Nevertheless, SHM is ready to support a combined IM/HM preceptorship program that targets medical school students in their first and second years, says Larry Wellikson, MD, FHM, CEO of SHM. The society already has assigned staff to manage the project and named Dr. Afsar-manesh as the lead physician. The plan is to track preceptorship participants as they make their way through medical school and residency, and see if the program changes their attitudes toward IM careers.
Even though the number of medical students who aspire to hospitalist careers continues to increase every year, SHM believes it must move to counteract the lackluster IM numbers, because that is where most medical students are introduced to HM, Dr. Wellikson says. “The problem of people not picking internal medicine could affect hospital medicine down the road,” he says. “We can’t sit passively by and see who picks to be a hospitalist. We believe we need to be active.”
One of the last things Dr. Afsar-manesh did at the conclusion of the inaugural UPIM program was collect the students’ e-mail addresses and phone numbers so she can stay in touch and track their career paths. The UPIM survey results give her hope: After UPIM, 100% of the students were “extremely confident” in their decision to pursue medicine; 57% indicated they were “very likely” to consider IM as a specialty; and 47% were “very likely” to think about HM.
“This program is a great way to encourage students to enter into internal medicine,” Yudin says. “I am sure that all my subsequent experiences working in a hospital will be measured against my first experience rounding with the IM department.” It seems as though the student took the words right out of the doctor’s mouth. TH
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hauer KE, Durning SJ, Kernan WN, et al. Factors associated with medical students’ career choices regarding internal medicine. JAMA. 2008;300(10):1154-1164.
Code Correctly
A hospitalist who scrutinizes claims might notice a payment denial related to “unbundling” issues. Line-item rejections might state the service is “mutually exclusive,” “incidental to another procedure,” or “payment was received as part of another service/procedure.” Unbundling refers to the practice of reporting each component of a service or procedure instead of reporting the single, comprehensive code. Two types of practices lead to unbundling: unintentional reporting resulting from a basic misunderstanding of correct coding, and intentional reporting to improperly maximize payment of otherwise bundled Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) codes.1
The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) for implementation and application to physician claims (e.g., Medicare Part B) with dates of service on or after Jan. 1, 1996. The rationale for these edits is a culmination of:
- Coding standards identified in the American Medical Association’s (AMA) CPT manual;
- National and local coverage determinations developed by CMS and local Medicare contractors;
- Coding standards set forth by national medical organizations and specialty societies;
- Appropriate standards of medical and surgical care; and
- Current coding practices identified through claim analysis, pre- and post-payment documentation reviews, and other forms of payor-initiated audit.
The initial NCCI goal was to promote correct coding methodologies and to control improper coding, which led to inappropriate payment in Part B claims.2 It later expanded to include corresponding NCCI edits in the outpatient code editor (OCE) for both outpatient hospital providers and therapy providers. Therapy providers encompass skilled nursing facilities (SNFs), comprehensive outpatient rehabilitation facilities (CORFs), outpatient physical therapy (OPTs) and speech-language pathology providers, and home health agencies (HHAs).
Fact-Check
The NCCI recognizes two edit types: Column One/Column Two Correct Coding edits and Mutually Exclusive edits. Each of these edit categories lists code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When applying Column One/Column Two editing logic to physician claims, the Column One code represents the more comprehensive code of the pair being reported. The Column Two code (the component service that is bundled into the comprehensive service) will be denied. This is not to say a code that appears in Column Two of the NCCI cannot be paid when reported by itself on any given date. The denial occurs only when the component service is reported on the same date as the more comprehensive service.
For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) is considered comprehensive to codes 36000 (introduction of needle or intracatheter, vein) and 36410 (venipuncture, age 3 years or older, necessitating physician’s skill [separate procedure], for diagnostic or therapeutic purposes). These code combinations should not be reported together on the same date when performed as part of the same procedure by the same physician or physicians of the same practice group. If this occurs, the payor will reimburse the initial service and deny the subsequent service. As a result, the first code received by the payor, on the same or separate claims, is reimbursed, even if that code represents the lesser of the two services.
Mutually Exclusive edits occur with less frequency than Column One/Column Two edits. Mutually Exclusive edits prevent reporting of two services or procedures that are highly unlikely to be performed together on the same patient, at the same session or encounter, by the same physician or physicians of the same specialty in a provider group. For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) would not be reported on the same day as 36555 (insertion of nontunneled centrally inserted central venous catheter, younger than 5 years of age).
CMS publishes the National Correct Coding Initiative Coding Policy Manual for Medicare Services (www.cms.hhs.gov/NationalCorrectCodInitEd) and encourages local Medicare contractors and fiscal intermediaries to use it as a reference for claims-processing edits. The manual is updated annually, and the NCCI edits are updated quarterly. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
References
- National correct coding initiative edits. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd. Accessed March 10, 2009.
- Medicare claims processing manual. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 10, 2009.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press, 2008;477-481.
- Modifier 59 article. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd/Downloads/modifier59.pdf. Accessed March 10, 2009.
- French K. Coding for Chest Medicine 2009. Northbrook, IL: American College of Chest Physicians. 2008;283-287.
A hospitalist who scrutinizes claims might notice a payment denial related to “unbundling” issues. Line-item rejections might state the service is “mutually exclusive,” “incidental to another procedure,” or “payment was received as part of another service/procedure.” Unbundling refers to the practice of reporting each component of a service or procedure instead of reporting the single, comprehensive code. Two types of practices lead to unbundling: unintentional reporting resulting from a basic misunderstanding of correct coding, and intentional reporting to improperly maximize payment of otherwise bundled Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) codes.1
The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) for implementation and application to physician claims (e.g., Medicare Part B) with dates of service on or after Jan. 1, 1996. The rationale for these edits is a culmination of:
- Coding standards identified in the American Medical Association’s (AMA) CPT manual;
- National and local coverage determinations developed by CMS and local Medicare contractors;
- Coding standards set forth by national medical organizations and specialty societies;
- Appropriate standards of medical and surgical care; and
- Current coding practices identified through claim analysis, pre- and post-payment documentation reviews, and other forms of payor-initiated audit.
The initial NCCI goal was to promote correct coding methodologies and to control improper coding, which led to inappropriate payment in Part B claims.2 It later expanded to include corresponding NCCI edits in the outpatient code editor (OCE) for both outpatient hospital providers and therapy providers. Therapy providers encompass skilled nursing facilities (SNFs), comprehensive outpatient rehabilitation facilities (CORFs), outpatient physical therapy (OPTs) and speech-language pathology providers, and home health agencies (HHAs).
Fact-Check
The NCCI recognizes two edit types: Column One/Column Two Correct Coding edits and Mutually Exclusive edits. Each of these edit categories lists code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When applying Column One/Column Two editing logic to physician claims, the Column One code represents the more comprehensive code of the pair being reported. The Column Two code (the component service that is bundled into the comprehensive service) will be denied. This is not to say a code that appears in Column Two of the NCCI cannot be paid when reported by itself on any given date. The denial occurs only when the component service is reported on the same date as the more comprehensive service.
For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) is considered comprehensive to codes 36000 (introduction of needle or intracatheter, vein) and 36410 (venipuncture, age 3 years or older, necessitating physician’s skill [separate procedure], for diagnostic or therapeutic purposes). These code combinations should not be reported together on the same date when performed as part of the same procedure by the same physician or physicians of the same practice group. If this occurs, the payor will reimburse the initial service and deny the subsequent service. As a result, the first code received by the payor, on the same or separate claims, is reimbursed, even if that code represents the lesser of the two services.
Mutually Exclusive edits occur with less frequency than Column One/Column Two edits. Mutually Exclusive edits prevent reporting of two services or procedures that are highly unlikely to be performed together on the same patient, at the same session or encounter, by the same physician or physicians of the same specialty in a provider group. For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) would not be reported on the same day as 36555 (insertion of nontunneled centrally inserted central venous catheter, younger than 5 years of age).
CMS publishes the National Correct Coding Initiative Coding Policy Manual for Medicare Services (www.cms.hhs.gov/NationalCorrectCodInitEd) and encourages local Medicare contractors and fiscal intermediaries to use it as a reference for claims-processing edits. The manual is updated annually, and the NCCI edits are updated quarterly. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
References
- National correct coding initiative edits. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd. Accessed March 10, 2009.
- Medicare claims processing manual. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 10, 2009.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press, 2008;477-481.
- Modifier 59 article. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd/Downloads/modifier59.pdf. Accessed March 10, 2009.
- French K. Coding for Chest Medicine 2009. Northbrook, IL: American College of Chest Physicians. 2008;283-287.
A hospitalist who scrutinizes claims might notice a payment denial related to “unbundling” issues. Line-item rejections might state the service is “mutually exclusive,” “incidental to another procedure,” or “payment was received as part of another service/procedure.” Unbundling refers to the practice of reporting each component of a service or procedure instead of reporting the single, comprehensive code. Two types of practices lead to unbundling: unintentional reporting resulting from a basic misunderstanding of correct coding, and intentional reporting to improperly maximize payment of otherwise bundled Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) codes.1
The Centers for Medicare and Medicaid Services (CMS) developed the National Correct Coding Initiative (NCCI) for implementation and application to physician claims (e.g., Medicare Part B) with dates of service on or after Jan. 1, 1996. The rationale for these edits is a culmination of:
- Coding standards identified in the American Medical Association’s (AMA) CPT manual;
- National and local coverage determinations developed by CMS and local Medicare contractors;
- Coding standards set forth by national medical organizations and specialty societies;
- Appropriate standards of medical and surgical care; and
- Current coding practices identified through claim analysis, pre- and post-payment documentation reviews, and other forms of payor-initiated audit.
The initial NCCI goal was to promote correct coding methodologies and to control improper coding, which led to inappropriate payment in Part B claims.2 It later expanded to include corresponding NCCI edits in the outpatient code editor (OCE) for both outpatient hospital providers and therapy providers. Therapy providers encompass skilled nursing facilities (SNFs), comprehensive outpatient rehabilitation facilities (CORFs), outpatient physical therapy (OPTs) and speech-language pathology providers, and home health agencies (HHAs).
Fact-Check
The NCCI recognizes two edit types: Column One/Column Two Correct Coding edits and Mutually Exclusive edits. Each of these edit categories lists code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When applying Column One/Column Two editing logic to physician claims, the Column One code represents the more comprehensive code of the pair being reported. The Column Two code (the component service that is bundled into the comprehensive service) will be denied. This is not to say a code that appears in Column Two of the NCCI cannot be paid when reported by itself on any given date. The denial occurs only when the component service is reported on the same date as the more comprehensive service.
For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) is considered comprehensive to codes 36000 (introduction of needle or intracatheter, vein) and 36410 (venipuncture, age 3 years or older, necessitating physician’s skill [separate procedure], for diagnostic or therapeutic purposes). These code combinations should not be reported together on the same date when performed as part of the same procedure by the same physician or physicians of the same practice group. If this occurs, the payor will reimburse the initial service and deny the subsequent service. As a result, the first code received by the payor, on the same or separate claims, is reimbursed, even if that code represents the lesser of the two services.
Mutually Exclusive edits occur with less frequency than Column One/Column Two edits. Mutually Exclusive edits prevent reporting of two services or procedures that are highly unlikely to be performed together on the same patient, at the same session or encounter, by the same physician or physicians of the same specialty in a provider group. For example, CPT code 36556 (insertion of nontunneled centrally inserted central venous catheter, age 5 years or older) would not be reported on the same day as 36555 (insertion of nontunneled centrally inserted central venous catheter, younger than 5 years of age).
CMS publishes the National Correct Coding Initiative Coding Policy Manual for Medicare Services (www.cms.hhs.gov/NationalCorrectCodInitEd) and encourages local Medicare contractors and fiscal intermediaries to use it as a reference for claims-processing edits. The manual is updated annually, and the NCCI edits are updated quarterly. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
References
- National correct coding initiative edits. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd. Accessed March 10, 2009.
- Medicare claims processing manual. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 10, 2009.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press, 2008;477-481.
- Modifier 59 article. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/NationalCorrectCodInitEd/Downloads/modifier59.pdf. Accessed March 10, 2009.
- French K. Coding for Chest Medicine 2009. Northbrook, IL: American College of Chest Physicians. 2008;283-287.
Medicare: Enroll Early
Some healthcare providers probably missed an important change buried within the 2009 Medicare Physician Fee Schedule: New rules for physician enrollment have drastically reduced the period for retroactive billing. Effective April 1, physicians enrolling or re-enrolling with Medicare can only submit a bill for services provided up to 30 days prior to the effective date, rather than for the prior 27 months.
Those who miss this deadline will be denied reimbursement for services to Medicare patients seen before the deadline. And those who move to a new job (“change of location,” in Medicare parlance) and fail to update their address within 30 days risk a two-year suspension from receiving Medicare payments.
What It Means
Essentially, HM group leaders must make sure they are ready to credential a new hire long before they start working. Before now, groups had months to get new hires enrolled in the Medicare system; now, with just 30 days to enroll, you need to start your credentialing and enrollment process early—before the physician’s start date, if possible.
“In a nutshell, groups are going to have to be more proactive than ever before in getting paperwork submitted for new providers,” says Derise Woods, operations project manager for Knoxville, Tenn.-based TeamHealth. “The situation we often face is that the provider is found and placed, and sometimes the paperwork does not get submitted right away. The natural focus is to get them on board and then get them up and running.”
If that is the case in your group, you should create a checklist for enrollment in Medicare and for other payors. Then, as soon as your new hire signs the contract, require them to submit all available information (e.g., DEA number and proof of board certification).
Woods says the rule states that “retroactive billing can start from the provider’s start date or from the date the enrollment is received at [Medicare], whichever is later.”
Even if you don’t capture all the necessary information, enroll the new physician as soon as possible. According to the Centers for Medicare & Medicaid Services (CMS), incomplete applications will be denied, but the date of the original filing will be preserved. So if a hospitalist begins working for your group Sept. 1, and you submit the enrollment application Sept. 7, the hospitalist can bill retroactively starting Sept. 7, even if that application is kicked back to you for more information and doesn’t get resolved for several weeks.
—Derise Woods, TeamHealth, Knoxville, Tenn.
Large and Small Groups
Missing the new enrollment deadline means reimbursement losses. Hospitalists provide services to a significant number of Medicare patients, so cutting back on retroactive billing could hurt the bottom line. “In most [HM] instances where Medicare is a large portion of income, this has potential to disrupt a practice,” Woods says, noting TeamHealth has yet to see the impact of the new enrollment rules.
Which entity incurs the loss of Medicare payments depends on your program’s payment structure. “For instance, TeamHealth contracts with our providers and pays them an hourly rate,” says Woods, explaining that the third-party contractor will suffer any loss of fees. “In a hospital-based program, the hospital might bill for the provider—and that provider may not get paid.”
Smaller HM groups might not have as much experience with these changes simply because they don’t hire physicians as often. “I did not know about this,” says Heidi Tessler, MD, president of the Colorado Hospitalist Company in Denver. “We contract with a billing company [for physician enrollments], and we would have been caught flat-footed with our next hire.”
Small groups could end up scrambling when they need to fill a position, especially if it’s a quick turnover. Groups that outsource their recruiting and billing should plan to communicate with those companies to expedite the enrollment process, Woods says.
TeamHealth, the largest provider of hospital-based clinical outsourcing in the U.S., has made numerous changes to accommodate the new enrollment rules, all the way up to a new business development group. “They now take this new rule into consideration when we are planning to start providing service,” Woods says. “Our recruiters are helping. They are ensuring that new providers fill out their paperwork and get it in. Understandably, physicians can let paperwork sit for a number of days.”
The good news is CMS has made it easier—and faster—to enroll through a Web-based portal called PECOS (Provider Enrollment, Chain, and Ownership System), which can be accessed at www.cms.hhs.gov/MedicareProviderSupEnroll/.
Central Source
SHM has consolidated essential sources on the new rules to include:
- Medicare’s all-inclusive Web section on provider enrollment is www.cms.hhs.gov/medicareprovidersupenroll.
- The CMS manual on enrollment is at www.cms.hhs.gov. Click on “manuals,” then “Internet-only manuals”; select “Publication 100-08, Program Integrity Manual,” then “Chapter 10.”
- AMA provides an overview on its Web site, and, with the Medical Group Management Association (MGMA), has developed a toolkit to guide physicians through the new rules. “The toolkit is probably the best resource available,” says Leslie Flores, principal in Nelson/Flores Associates, a national hospitalist management consulting firm and director of SHM’s Practice Management Institute. AMA and MGMA members can access the toolkit at www.mgma.com/policy/default.aspx?id=5712.
“SHM wants to make sure we communicate these new rules to our members,” says Flores, “and provide direction to resources they can use.” Check www.hospitalmedicine.org for the latest links and information. TH
Jane Jerrard is a freelance writer based in Chicago.
Some healthcare providers probably missed an important change buried within the 2009 Medicare Physician Fee Schedule: New rules for physician enrollment have drastically reduced the period for retroactive billing. Effective April 1, physicians enrolling or re-enrolling with Medicare can only submit a bill for services provided up to 30 days prior to the effective date, rather than for the prior 27 months.
Those who miss this deadline will be denied reimbursement for services to Medicare patients seen before the deadline. And those who move to a new job (“change of location,” in Medicare parlance) and fail to update their address within 30 days risk a two-year suspension from receiving Medicare payments.
What It Means
Essentially, HM group leaders must make sure they are ready to credential a new hire long before they start working. Before now, groups had months to get new hires enrolled in the Medicare system; now, with just 30 days to enroll, you need to start your credentialing and enrollment process early—before the physician’s start date, if possible.
“In a nutshell, groups are going to have to be more proactive than ever before in getting paperwork submitted for new providers,” says Derise Woods, operations project manager for Knoxville, Tenn.-based TeamHealth. “The situation we often face is that the provider is found and placed, and sometimes the paperwork does not get submitted right away. The natural focus is to get them on board and then get them up and running.”
If that is the case in your group, you should create a checklist for enrollment in Medicare and for other payors. Then, as soon as your new hire signs the contract, require them to submit all available information (e.g., DEA number and proof of board certification).
Woods says the rule states that “retroactive billing can start from the provider’s start date or from the date the enrollment is received at [Medicare], whichever is later.”
Even if you don’t capture all the necessary information, enroll the new physician as soon as possible. According to the Centers for Medicare & Medicaid Services (CMS), incomplete applications will be denied, but the date of the original filing will be preserved. So if a hospitalist begins working for your group Sept. 1, and you submit the enrollment application Sept. 7, the hospitalist can bill retroactively starting Sept. 7, even if that application is kicked back to you for more information and doesn’t get resolved for several weeks.
—Derise Woods, TeamHealth, Knoxville, Tenn.
Large and Small Groups
Missing the new enrollment deadline means reimbursement losses. Hospitalists provide services to a significant number of Medicare patients, so cutting back on retroactive billing could hurt the bottom line. “In most [HM] instances where Medicare is a large portion of income, this has potential to disrupt a practice,” Woods says, noting TeamHealth has yet to see the impact of the new enrollment rules.
Which entity incurs the loss of Medicare payments depends on your program’s payment structure. “For instance, TeamHealth contracts with our providers and pays them an hourly rate,” says Woods, explaining that the third-party contractor will suffer any loss of fees. “In a hospital-based program, the hospital might bill for the provider—and that provider may not get paid.”
Smaller HM groups might not have as much experience with these changes simply because they don’t hire physicians as often. “I did not know about this,” says Heidi Tessler, MD, president of the Colorado Hospitalist Company in Denver. “We contract with a billing company [for physician enrollments], and we would have been caught flat-footed with our next hire.”
Small groups could end up scrambling when they need to fill a position, especially if it’s a quick turnover. Groups that outsource their recruiting and billing should plan to communicate with those companies to expedite the enrollment process, Woods says.
TeamHealth, the largest provider of hospital-based clinical outsourcing in the U.S., has made numerous changes to accommodate the new enrollment rules, all the way up to a new business development group. “They now take this new rule into consideration when we are planning to start providing service,” Woods says. “Our recruiters are helping. They are ensuring that new providers fill out their paperwork and get it in. Understandably, physicians can let paperwork sit for a number of days.”
The good news is CMS has made it easier—and faster—to enroll through a Web-based portal called PECOS (Provider Enrollment, Chain, and Ownership System), which can be accessed at www.cms.hhs.gov/MedicareProviderSupEnroll/.
Central Source
SHM has consolidated essential sources on the new rules to include:
- Medicare’s all-inclusive Web section on provider enrollment is www.cms.hhs.gov/medicareprovidersupenroll.
- The CMS manual on enrollment is at www.cms.hhs.gov. Click on “manuals,” then “Internet-only manuals”; select “Publication 100-08, Program Integrity Manual,” then “Chapter 10.”
- AMA provides an overview on its Web site, and, with the Medical Group Management Association (MGMA), has developed a toolkit to guide physicians through the new rules. “The toolkit is probably the best resource available,” says Leslie Flores, principal in Nelson/Flores Associates, a national hospitalist management consulting firm and director of SHM’s Practice Management Institute. AMA and MGMA members can access the toolkit at www.mgma.com/policy/default.aspx?id=5712.
“SHM wants to make sure we communicate these new rules to our members,” says Flores, “and provide direction to resources they can use.” Check www.hospitalmedicine.org for the latest links and information. TH
Jane Jerrard is a freelance writer based in Chicago.
Some healthcare providers probably missed an important change buried within the 2009 Medicare Physician Fee Schedule: New rules for physician enrollment have drastically reduced the period for retroactive billing. Effective April 1, physicians enrolling or re-enrolling with Medicare can only submit a bill for services provided up to 30 days prior to the effective date, rather than for the prior 27 months.
Those who miss this deadline will be denied reimbursement for services to Medicare patients seen before the deadline. And those who move to a new job (“change of location,” in Medicare parlance) and fail to update their address within 30 days risk a two-year suspension from receiving Medicare payments.
What It Means
Essentially, HM group leaders must make sure they are ready to credential a new hire long before they start working. Before now, groups had months to get new hires enrolled in the Medicare system; now, with just 30 days to enroll, you need to start your credentialing and enrollment process early—before the physician’s start date, if possible.
“In a nutshell, groups are going to have to be more proactive than ever before in getting paperwork submitted for new providers,” says Derise Woods, operations project manager for Knoxville, Tenn.-based TeamHealth. “The situation we often face is that the provider is found and placed, and sometimes the paperwork does not get submitted right away. The natural focus is to get them on board and then get them up and running.”
If that is the case in your group, you should create a checklist for enrollment in Medicare and for other payors. Then, as soon as your new hire signs the contract, require them to submit all available information (e.g., DEA number and proof of board certification).
Woods says the rule states that “retroactive billing can start from the provider’s start date or from the date the enrollment is received at [Medicare], whichever is later.”
Even if you don’t capture all the necessary information, enroll the new physician as soon as possible. According to the Centers for Medicare & Medicaid Services (CMS), incomplete applications will be denied, but the date of the original filing will be preserved. So if a hospitalist begins working for your group Sept. 1, and you submit the enrollment application Sept. 7, the hospitalist can bill retroactively starting Sept. 7, even if that application is kicked back to you for more information and doesn’t get resolved for several weeks.
—Derise Woods, TeamHealth, Knoxville, Tenn.
Large and Small Groups
Missing the new enrollment deadline means reimbursement losses. Hospitalists provide services to a significant number of Medicare patients, so cutting back on retroactive billing could hurt the bottom line. “In most [HM] instances where Medicare is a large portion of income, this has potential to disrupt a practice,” Woods says, noting TeamHealth has yet to see the impact of the new enrollment rules.
Which entity incurs the loss of Medicare payments depends on your program’s payment structure. “For instance, TeamHealth contracts with our providers and pays them an hourly rate,” says Woods, explaining that the third-party contractor will suffer any loss of fees. “In a hospital-based program, the hospital might bill for the provider—and that provider may not get paid.”
Smaller HM groups might not have as much experience with these changes simply because they don’t hire physicians as often. “I did not know about this,” says Heidi Tessler, MD, president of the Colorado Hospitalist Company in Denver. “We contract with a billing company [for physician enrollments], and we would have been caught flat-footed with our next hire.”
Small groups could end up scrambling when they need to fill a position, especially if it’s a quick turnover. Groups that outsource their recruiting and billing should plan to communicate with those companies to expedite the enrollment process, Woods says.
TeamHealth, the largest provider of hospital-based clinical outsourcing in the U.S., has made numerous changes to accommodate the new enrollment rules, all the way up to a new business development group. “They now take this new rule into consideration when we are planning to start providing service,” Woods says. “Our recruiters are helping. They are ensuring that new providers fill out their paperwork and get it in. Understandably, physicians can let paperwork sit for a number of days.”
The good news is CMS has made it easier—and faster—to enroll through a Web-based portal called PECOS (Provider Enrollment, Chain, and Ownership System), which can be accessed at www.cms.hhs.gov/MedicareProviderSupEnroll/.
Central Source
SHM has consolidated essential sources on the new rules to include:
- Medicare’s all-inclusive Web section on provider enrollment is www.cms.hhs.gov/medicareprovidersupenroll.
- The CMS manual on enrollment is at www.cms.hhs.gov. Click on “manuals,” then “Internet-only manuals”; select “Publication 100-08, Program Integrity Manual,” then “Chapter 10.”
- AMA provides an overview on its Web site, and, with the Medical Group Management Association (MGMA), has developed a toolkit to guide physicians through the new rules. “The toolkit is probably the best resource available,” says Leslie Flores, principal in Nelson/Flores Associates, a national hospitalist management consulting firm and director of SHM’s Practice Management Institute. AMA and MGMA members can access the toolkit at www.mgma.com/policy/default.aspx?id=5712.
“SHM wants to make sure we communicate these new rules to our members,” says Flores, “and provide direction to resources they can use.” Check www.hospitalmedicine.org for the latest links and information. TH
Jane Jerrard is a freelance writer based in Chicago.