User login
What is the best empiric therapy for community-acquired cellulitis?
Case
A previously healthy 55-year-old white female presents to the ED with a three-day history of pain and erythema in her right hand. Examination reveals fluctuance as well. She is diagnosed with an abscess with surrounding cellulitis. The abscess is incised, drained, and cultured, and she is sent home on oral trimethoprim/sulfamethoxazole. The following day, her cellulitis has worsened. She is hospitalized and commenced on intravenous vancomycin. What is the best empiric therapy for community-acquired cellulitis?
Background
Cellulitis is defined as a skin and soft-tissue infection (SSTI), which develops as a result of bacterial entry via breaches in the skin barrier. Typically, it involves the dermis and subcutaneous tissue, and is associated with local tenderness, erythema, swelling and fever. Cellulitis usually affects the lower extremities, but can affect other locations resulting in diagnoses such as periorbital, abdominal wall, buccal, and perianal cellulitis.1,2
Gram-positive organisms, especially Staphylococcus aureus and beta hemolytic streptococci, are the most common causes of cellulitis. Although it is less common, cellulitis can be caused by gram-negative organisms. The recent significant increase in the prevalence of SSTIs due to community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) has led to changes in the selection of antibiotics that were most commonly utilized to empirically treat cellulitis.
The diagnosis of cellulitis is based primarily on clinical manifestations. Due to low diagnostic yields, blood cultures, needle aspiration, or punch biopsy, specimens usually are not helpful in the setting of simple cellulitis.3 Therefore, antibiotic therapy is almost universally started empirically. Starting appropriate initial antibiotic therapy improves patient outcomes by reducing mortality rates, length of stay, and inpatient costs.4
Cellulitis incidence is about two cases per 1,000 patient-years.5 This rather high incidence, coupled with escalating rates of SSTIs due to CA-MRSA, demands reliable and cost-effective treatment strategies for the management of community-acquired cellulitis.
Review of the Data
The treatment of community-acquired cellulitis was straightforward until the past decade, as physicians saw a significant increase in CA-MRSA incidence.6 MRSA was reported initially in 1961, only two years after methicillin was introduced into clinical practice.7,8 Subsequently, MRSA prevalence increased dramatically, and by the beginning of this decade, more than 50% of the Staphylococcus aureus hospital strains were resistant to methicillin.8 Furthermore, 60% to 80% of community-acquired Staphylococcus aureus strains in the U.S. are methicillin-resistant.8
The two major types of MRSA infections are healthcare-acquired (HA-MRSA) and community-acquired (CA-MRSA). The HA-MRSA infection group is further subdivided into those strains that develop during a period of hospitalization, and those that develop following contact with healthcare facilities (e.g., hospitalization or surgery within the previous year). This subgroup includes HA-MRSA infections in hemodialysis patients, residents of long-term care facilities, and individuals who have a vascular catheter or other indwelling device.9,10

CA-MRSA infections, on the other hand, occur in individuals who have not had any contact with healthcare facilities. Higher rates of CA-MRSA infection are observed in settings where individuals have close contact with each other, including military trainees, athletes involved in contact sports, patients age 65 and older, men who have sex with other men, and parenteral substance abusers.8,11-13 However, in view of the high prevalence of CA-MRSA in the U.S., most patients, including those without any apparent risk factors, are at risk.8
HA-MRSA has the ability to survive on inanimate objects for extended time periods, increasing the likelihood of transmission to persons who come into contact with those objects. Although evidence has not confirmed that CA-MRSA has a similar capacity, it seems plausible that such spread does contribute to the propagation of CA-MRSA.12
The increasing importance of CA-MRSA also is evident in hospital settings, where it is replacing HA-MRSA as the most common type of Staphylococcus aureus. Since CA-MRSA tends to be susceptible to a larger number of antibiotics than HA-MRSA is, this has led to a reduced incidence of multidrug resistance. Fortunately, unlike HA-MRSA, CA-MRSA is susceptible to non-beta-lactam antibiotics, including tetracyclines, sulfonamides, and clindamycin.9
CA-MRSA most often causes SSTIs, and a tender abscess is a typical presentation.8 Patients commonly misinterpret early skin lesions as an insect or spider bite.12,14 When cutaneous CA-MRSA presents as an abscess, an incision and drainage procedure is essential for adequate treatment of the infection. For some CA-MRSA infections, particularly those characterized by the presence of a relatively small abscess, it might be adequate to do only an incision and drainage procedure, and not administer antibiotics.8,15 However, in most instances, especially when there is an area of cellulitis around the abscess, the initiation of antibiotic therapy improves patients’ clinical outcomes.9,16
When there is no apparent drainable purulent fluid collection, which often occurs with cellulitis, antibiotics should be the mainstay of therapy. The decision about which antibiotic to start can present some challenges, because the organism causing the cellulitis usually is not identified. This is because blood cultures are positive in less than 5% of cases. Also, positive culture results from needle aspiration are only helpful from 5% to 40% of the time. Meanwhile, culture of punch biopsy specimens yields a pathogen in only 20% to 30% of cases.3,17-19
Due to increased CA-MRSA incidence, cephalexin should not be prescribed to treat cellulitis in the outpatient setting because it does not provide coverage for the pathogen.13 Instead, oral antibiotics (e.g., clindamycin or trimethoprim/sulfamethoxazole) should be prescribed. Doxycycline, minocycline, rifampin (usually prescribed in combination with fusidic acid to prevent resistance development), and linezolid are additional therapeutic options.
Trimethoprim/sulfamethoxazole and clindamycin have several advantages: good oral bioavailability, familiarity to physicians, and general affordability. A disadvantage to using both trimethoprim/sulfamethoxazole and doxycycline is that they provide inadequate coverage for group A streptococci, which are a common cause of cellulitis. Therefore, the simultaneous use of a beta-lactam antibiotic with either of these medications may improve outcomes for “nonpurulent” cellulitis.13,15 Linezolid has proven effective for skin and SSTI caused by MRSA, even though it is not bactericidal.
Excellent oral bioavailability of this drug is an attractive characteristic, as it facilitates the transition from the use of intravenous to oral antibiotic therapy later in a patient’s hospital course. Although oral linezolid has been studied in clinical trials and provides good coverage for MRSA, its use in the outpatient setting is relatively limited, largely due to its significant cost.20 In 2008, the cost of 10 days of treatment with oral linezolid was $1,286.80. In comparison, the generic trimethoprim/sulfamethox-azole cost $9.40, and generic clindamycin cost $95.10.8 The lack of routine availability in many outpatient pharmacies also hinders the widespread use of linezolid.13
To date, with the exception of linezolid, no randomized, prospective clinical trials clearly demonstrate the efficacy of the oral agents that are commonly used for the outpatient treatment of cellulitis.20
When patients require hospitalization for the optimal treatment of cellulitis, it is important to select a parenteral antibiotic that provides coverage for MRSA.8 Vancomycin, daptomycin, linezolid, and tigecycline are the most commonly used agents.6
In the inpatient setting, failure to initiate appropriate medical therapy can result in longer hospital admissions, which significantly increase inpatient costs. Inadequate antibiotic therapy creates a significant financial burden and has been associated with increased mortality.4 Historically, vancomycin is used whenever a MRSA infection is suspected. However, there is concern about the declining efficacy of vancomycin related to a gradual increase in the rate of relative resistance—a minimal inhibitory concentration (MIC) increase—in MRSA strains. This MIC creep is noted in some medical centers and can lead to a failure to respond to vancomycin.13,20
Daptomycin is rapidly bactericidal against MRSA; in some institutions, its use may be preferred over vancomycin because the former antibiotic is associated with a significantly more rapid clinical response, which may shorten the required length of hospitalization.21 The once-daily dosing requirement for daptomycin allows for ease of use in both hospital and outpatient settings, and therefore may facilitate early hospital discharge or prevent the need for hospitalization altogether. Clinical experience also suggests potential economic advantages with the use of daptomycin.22
Tigecycline is a bacteriostatic antibiotic that achieves low serum concentrations. However, it penetrates the skin well and has a similar effectiveness to combination therapy with vancomycin and aztreonam. Thus far, tigecycline is not widely used for the treatment of MRSA infections, and it has been suggested that it may be preferred for polymicrobial infections or for patients who exhibit allergies to more commonly used agents.8
When selecting an antibiotic therapy, cost considerations play an important role in the decision-making process. For intravenous agents commonly used to treat CA-MRSA infections, the 2008 cost for 10 days of treatment with generic vancomycin was $182.80; daptomycin cost $1,660.80. For tigecycline and linezolid, the same duration of treatment cost $1,362 and $1,560, respectively.8
Back to the Case
Our patient, an otherwise healthy female, presented with no apparent risk factors for developing a CA-MRSA SSTI. However, more detailed history revealed that she regularly used sports equipment at her local fitness center. Based on her clinical presentation and concerns about the high local prevalence of CA-MRSA, an incision and drainage procedure was performed, and she was started empirically on IV vancomycin. She had a positive clinical response to this treatment.
Wound culture results confirmed CA-MRSA abscess and cellulitis, susceptible to trimethoprim/sulfamethoxazole. She was discharged on the oral formulation of this antibiotic to complete a 10-day course of treatment, including the days she received intravenous antibiotics.
Few well-designed trials have compared different lengths of cellulitis therapy. Most authorities recommend five to 10 days of treatment; however, longer courses might be required for more severe or complicated diseases.
Bottom line
Because of the high prevalence of CA-MRSA, initial antibiotic therapy for the treatment of community-acquired cellulitis must provide coverage for this organism. TH
Dr. Clarke is a hospitalist and clinical instructor at Emory University School of Medicine, Atlanta. Dr. Dressler is associate professor and director of education, section of hospital medicine, and associate program director of the J. Willis Hurst Internal Medicine Residency Program. Dr. Purohit is an instructor in clinical medicine at Emory University School of Medicine.
References
- Barzilai A, Choen HA. Isolation of group A streptococci from children with perianal cellulitis and from their siblings. Pediatr Infect Dis J. 1998;17(4):358-360.
- Thorsteinsdottir B, Tleyjeh IM, Baddour LM. Abdominal wall cellulitis in the morbidly obese. Scand J Infect Dis. 2005;37(8):605-608.
- Swartz MN. Clinical practice. Cellulitis. N Engl J Med. 2004;350(9):904-912.
- Edelsberg J, Berger A, Weber DJ, et al. Clinical and economic consequences of failure of initial antibiotic therapy for hospitalized patients with complicated skin and skin-structure infections. Infect Control Hosp Epidemiol. 2008;29(2):160-169.
- McNamara DR, Tleyjeh IM, Berbari EF, et al. Incidence of lower extremity cellulitis: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 2007;82(7):817-821.
- Moellering RC. Current treatment options for community-acquired methicillin-resistant Staphylococcus aureus infection. Clin Infect Dis. 2008;46(7):1032-1037.
- Chambers HF. The changing epidemiology of Staphylococcus aureus. Emerg Infect Dis. 2001;7(2):178-182.
- Moellering RC. A 39-year-old man with a skin infection. JAMA. 2008;299(1):79-87
- Ruhe J, Smith N, Bradsher RW, Menon A. Community-onset methicillin-resistant Staphylococcus aureus skin and soft tissue infections: impact of antimicrobial therapy on outcome. Clin Infect Dis. 2007;44(6):777-784.
- David MZ, Glikman D, Crawford SE, et al. What is community-associated methicillin-resistant Staphylococcus aureus? J Infect Dis. 2008;197(9):1235-1243.
- Iyer S, Jones DH. Community-acquired methicillin-resistant Staphylococcus aureus skin infection: a retrospective analysis of clinical presentation and treatment of a local outbreak. J Am Acad Dermatol. 2004;50(6):854-858.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus skin or soft tissue infections in a state prison—Mississippi, 2000. MMWR Morb Mortal Wkly Rep. 2001;50(42):919-922.
- Daum RS. Clinical practice. Skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus. N Engl J Med. 2007;357(4):380-390.
- Dominguez TJ. It’s not a spider bite, it’s community-acquired methicillin-resistant Staphylococcus aureus. J Am Board Fam Pract. 2004;17(3):220-226.
- Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355(7):666-674.
- Jetton L. Therapy for methicillin-resistant Staphylococcus aureus. N Engl J Med. 2006;355(20):2153-2155.
- Hook EW, Hooton TM, Horton CA, et al. Microbiologic evaluation of cutaneous cellulitis in adults. Arch Intern Med. 1986;146(2):295-297.
- Duvanel T, Auckenthaler R, Rohner P, Harms M, Saurat JH. Quantitative cultures of biopsy specimens from cutaneous cellulitis. Arch Intern Med. 1989;149(2):293-296.
- Newell PM, Norden CW. Value of needle aspiration in bacteriologic diagnosis of cellulitis in adults. J Clin Microbiol. 1988; 26(3):401-404.
- Loffler CA, Macdougall C. Update on prevalence and treatment of methicillin-resistant Staphylococcus aureus infections. Expert Rev Anti Infect Ther. 2007;5(6):961-981.
- Davis SL, McKinnon PS, Hall LM, et al. Daptomycin versus vancomycin for complicated skin and skin structure infections: clinical and economic outcomes. Pharmacotherapy. 2007;27(12):1611-1618.
- Seaton RA. Daptomycin: rationale and role in the management of skin and soft tissue infections. J Antimicrob Chemother. 2008;62(Suppl 3):iii15-23.
Case
A previously healthy 55-year-old white female presents to the ED with a three-day history of pain and erythema in her right hand. Examination reveals fluctuance as well. She is diagnosed with an abscess with surrounding cellulitis. The abscess is incised, drained, and cultured, and she is sent home on oral trimethoprim/sulfamethoxazole. The following day, her cellulitis has worsened. She is hospitalized and commenced on intravenous vancomycin. What is the best empiric therapy for community-acquired cellulitis?
Background
Cellulitis is defined as a skin and soft-tissue infection (SSTI), which develops as a result of bacterial entry via breaches in the skin barrier. Typically, it involves the dermis and subcutaneous tissue, and is associated with local tenderness, erythema, swelling and fever. Cellulitis usually affects the lower extremities, but can affect other locations resulting in diagnoses such as periorbital, abdominal wall, buccal, and perianal cellulitis.1,2
Gram-positive organisms, especially Staphylococcus aureus and beta hemolytic streptococci, are the most common causes of cellulitis. Although it is less common, cellulitis can be caused by gram-negative organisms. The recent significant increase in the prevalence of SSTIs due to community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) has led to changes in the selection of antibiotics that were most commonly utilized to empirically treat cellulitis.
The diagnosis of cellulitis is based primarily on clinical manifestations. Due to low diagnostic yields, blood cultures, needle aspiration, or punch biopsy, specimens usually are not helpful in the setting of simple cellulitis.3 Therefore, antibiotic therapy is almost universally started empirically. Starting appropriate initial antibiotic therapy improves patient outcomes by reducing mortality rates, length of stay, and inpatient costs.4
Cellulitis incidence is about two cases per 1,000 patient-years.5 This rather high incidence, coupled with escalating rates of SSTIs due to CA-MRSA, demands reliable and cost-effective treatment strategies for the management of community-acquired cellulitis.
Review of the Data
The treatment of community-acquired cellulitis was straightforward until the past decade, as physicians saw a significant increase in CA-MRSA incidence.6 MRSA was reported initially in 1961, only two years after methicillin was introduced into clinical practice.7,8 Subsequently, MRSA prevalence increased dramatically, and by the beginning of this decade, more than 50% of the Staphylococcus aureus hospital strains were resistant to methicillin.8 Furthermore, 60% to 80% of community-acquired Staphylococcus aureus strains in the U.S. are methicillin-resistant.8
The two major types of MRSA infections are healthcare-acquired (HA-MRSA) and community-acquired (CA-MRSA). The HA-MRSA infection group is further subdivided into those strains that develop during a period of hospitalization, and those that develop following contact with healthcare facilities (e.g., hospitalization or surgery within the previous year). This subgroup includes HA-MRSA infections in hemodialysis patients, residents of long-term care facilities, and individuals who have a vascular catheter or other indwelling device.9,10
CA-MRSA infections, on the other hand, occur in individuals who have not had any contact with healthcare facilities. Higher rates of CA-MRSA infection are observed in settings where individuals have close contact with each other, including military trainees, athletes involved in contact sports, patients age 65 and older, men who have sex with other men, and parenteral substance abusers.8,11-13 However, in view of the high prevalence of CA-MRSA in the U.S., most patients, including those without any apparent risk factors, are at risk.8
HA-MRSA has the ability to survive on inanimate objects for extended time periods, increasing the likelihood of transmission to persons who come into contact with those objects. Although evidence has not confirmed that CA-MRSA has a similar capacity, it seems plausible that such spread does contribute to the propagation of CA-MRSA.12
The increasing importance of CA-MRSA also is evident in hospital settings, where it is replacing HA-MRSA as the most common type of Staphylococcus aureus. Since CA-MRSA tends to be susceptible to a larger number of antibiotics than HA-MRSA is, this has led to a reduced incidence of multidrug resistance. Fortunately, unlike HA-MRSA, CA-MRSA is susceptible to non-beta-lactam antibiotics, including tetracyclines, sulfonamides, and clindamycin.9
CA-MRSA most often causes SSTIs, and a tender abscess is a typical presentation.8 Patients commonly misinterpret early skin lesions as an insect or spider bite.12,14 When cutaneous CA-MRSA presents as an abscess, an incision and drainage procedure is essential for adequate treatment of the infection. For some CA-MRSA infections, particularly those characterized by the presence of a relatively small abscess, it might be adequate to do only an incision and drainage procedure, and not administer antibiotics.8,15 However, in most instances, especially when there is an area of cellulitis around the abscess, the initiation of antibiotic therapy improves patients’ clinical outcomes.9,16
When there is no apparent drainable purulent fluid collection, which often occurs with cellulitis, antibiotics should be the mainstay of therapy. The decision about which antibiotic to start can present some challenges, because the organism causing the cellulitis usually is not identified. This is because blood cultures are positive in less than 5% of cases. Also, positive culture results from needle aspiration are only helpful from 5% to 40% of the time. Meanwhile, culture of punch biopsy specimens yields a pathogen in only 20% to 30% of cases.3,17-19
Due to increased CA-MRSA incidence, cephalexin should not be prescribed to treat cellulitis in the outpatient setting because it does not provide coverage for the pathogen.13 Instead, oral antibiotics (e.g., clindamycin or trimethoprim/sulfamethoxazole) should be prescribed. Doxycycline, minocycline, rifampin (usually prescribed in combination with fusidic acid to prevent resistance development), and linezolid are additional therapeutic options.
Trimethoprim/sulfamethoxazole and clindamycin have several advantages: good oral bioavailability, familiarity to physicians, and general affordability. A disadvantage to using both trimethoprim/sulfamethoxazole and doxycycline is that they provide inadequate coverage for group A streptococci, which are a common cause of cellulitis. Therefore, the simultaneous use of a beta-lactam antibiotic with either of these medications may improve outcomes for “nonpurulent” cellulitis.13,15 Linezolid has proven effective for skin and SSTI caused by MRSA, even though it is not bactericidal.
Excellent oral bioavailability of this drug is an attractive characteristic, as it facilitates the transition from the use of intravenous to oral antibiotic therapy later in a patient’s hospital course. Although oral linezolid has been studied in clinical trials and provides good coverage for MRSA, its use in the outpatient setting is relatively limited, largely due to its significant cost.20 In 2008, the cost of 10 days of treatment with oral linezolid was $1,286.80. In comparison, the generic trimethoprim/sulfamethox-azole cost $9.40, and generic clindamycin cost $95.10.8 The lack of routine availability in many outpatient pharmacies also hinders the widespread use of linezolid.13
To date, with the exception of linezolid, no randomized, prospective clinical trials clearly demonstrate the efficacy of the oral agents that are commonly used for the outpatient treatment of cellulitis.20
When patients require hospitalization for the optimal treatment of cellulitis, it is important to select a parenteral antibiotic that provides coverage for MRSA.8 Vancomycin, daptomycin, linezolid, and tigecycline are the most commonly used agents.6
In the inpatient setting, failure to initiate appropriate medical therapy can result in longer hospital admissions, which significantly increase inpatient costs. Inadequate antibiotic therapy creates a significant financial burden and has been associated with increased mortality.4 Historically, vancomycin is used whenever a MRSA infection is suspected. However, there is concern about the declining efficacy of vancomycin related to a gradual increase in the rate of relative resistance—a minimal inhibitory concentration (MIC) increase—in MRSA strains. This MIC creep is noted in some medical centers and can lead to a failure to respond to vancomycin.13,20
Daptomycin is rapidly bactericidal against MRSA; in some institutions, its use may be preferred over vancomycin because the former antibiotic is associated with a significantly more rapid clinical response, which may shorten the required length of hospitalization.21 The once-daily dosing requirement for daptomycin allows for ease of use in both hospital and outpatient settings, and therefore may facilitate early hospital discharge or prevent the need for hospitalization altogether. Clinical experience also suggests potential economic advantages with the use of daptomycin.22
Tigecycline is a bacteriostatic antibiotic that achieves low serum concentrations. However, it penetrates the skin well and has a similar effectiveness to combination therapy with vancomycin and aztreonam. Thus far, tigecycline is not widely used for the treatment of MRSA infections, and it has been suggested that it may be preferred for polymicrobial infections or for patients who exhibit allergies to more commonly used agents.8
When selecting an antibiotic therapy, cost considerations play an important role in the decision-making process. For intravenous agents commonly used to treat CA-MRSA infections, the 2008 cost for 10 days of treatment with generic vancomycin was $182.80; daptomycin cost $1,660.80. For tigecycline and linezolid, the same duration of treatment cost $1,362 and $1,560, respectively.8
Back to the Case
Our patient, an otherwise healthy female, presented with no apparent risk factors for developing a CA-MRSA SSTI. However, more detailed history revealed that she regularly used sports equipment at her local fitness center. Based on her clinical presentation and concerns about the high local prevalence of CA-MRSA, an incision and drainage procedure was performed, and she was started empirically on IV vancomycin. She had a positive clinical response to this treatment.
Wound culture results confirmed CA-MRSA abscess and cellulitis, susceptible to trimethoprim/sulfamethoxazole. She was discharged on the oral formulation of this antibiotic to complete a 10-day course of treatment, including the days she received intravenous antibiotics.
Few well-designed trials have compared different lengths of cellulitis therapy. Most authorities recommend five to 10 days of treatment; however, longer courses might be required for more severe or complicated diseases.
Bottom line
Because of the high prevalence of CA-MRSA, initial antibiotic therapy for the treatment of community-acquired cellulitis must provide coverage for this organism. TH
Dr. Clarke is a hospitalist and clinical instructor at Emory University School of Medicine, Atlanta. Dr. Dressler is associate professor and director of education, section of hospital medicine, and associate program director of the J. Willis Hurst Internal Medicine Residency Program. Dr. Purohit is an instructor in clinical medicine at Emory University School of Medicine.
References
- Barzilai A, Choen HA. Isolation of group A streptococci from children with perianal cellulitis and from their siblings. Pediatr Infect Dis J. 1998;17(4):358-360.
- Thorsteinsdottir B, Tleyjeh IM, Baddour LM. Abdominal wall cellulitis in the morbidly obese. Scand J Infect Dis. 2005;37(8):605-608.
- Swartz MN. Clinical practice. Cellulitis. N Engl J Med. 2004;350(9):904-912.
- Edelsberg J, Berger A, Weber DJ, et al. Clinical and economic consequences of failure of initial antibiotic therapy for hospitalized patients with complicated skin and skin-structure infections. Infect Control Hosp Epidemiol. 2008;29(2):160-169.
- McNamara DR, Tleyjeh IM, Berbari EF, et al. Incidence of lower extremity cellulitis: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 2007;82(7):817-821.
- Moellering RC. Current treatment options for community-acquired methicillin-resistant Staphylococcus aureus infection. Clin Infect Dis. 2008;46(7):1032-1037.
- Chambers HF. The changing epidemiology of Staphylococcus aureus. Emerg Infect Dis. 2001;7(2):178-182.
- Moellering RC. A 39-year-old man with a skin infection. JAMA. 2008;299(1):79-87
- Ruhe J, Smith N, Bradsher RW, Menon A. Community-onset methicillin-resistant Staphylococcus aureus skin and soft tissue infections: impact of antimicrobial therapy on outcome. Clin Infect Dis. 2007;44(6):777-784.
- David MZ, Glikman D, Crawford SE, et al. What is community-associated methicillin-resistant Staphylococcus aureus? J Infect Dis. 2008;197(9):1235-1243.
- Iyer S, Jones DH. Community-acquired methicillin-resistant Staphylococcus aureus skin infection: a retrospective analysis of clinical presentation and treatment of a local outbreak. J Am Acad Dermatol. 2004;50(6):854-858.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus skin or soft tissue infections in a state prison—Mississippi, 2000. MMWR Morb Mortal Wkly Rep. 2001;50(42):919-922.
- Daum RS. Clinical practice. Skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus. N Engl J Med. 2007;357(4):380-390.
- Dominguez TJ. It’s not a spider bite, it’s community-acquired methicillin-resistant Staphylococcus aureus. J Am Board Fam Pract. 2004;17(3):220-226.
- Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355(7):666-674.
- Jetton L. Therapy for methicillin-resistant Staphylococcus aureus. N Engl J Med. 2006;355(20):2153-2155.
- Hook EW, Hooton TM, Horton CA, et al. Microbiologic evaluation of cutaneous cellulitis in adults. Arch Intern Med. 1986;146(2):295-297.
- Duvanel T, Auckenthaler R, Rohner P, Harms M, Saurat JH. Quantitative cultures of biopsy specimens from cutaneous cellulitis. Arch Intern Med. 1989;149(2):293-296.
- Newell PM, Norden CW. Value of needle aspiration in bacteriologic diagnosis of cellulitis in adults. J Clin Microbiol. 1988; 26(3):401-404.
- Loffler CA, Macdougall C. Update on prevalence and treatment of methicillin-resistant Staphylococcus aureus infections. Expert Rev Anti Infect Ther. 2007;5(6):961-981.
- Davis SL, McKinnon PS, Hall LM, et al. Daptomycin versus vancomycin for complicated skin and skin structure infections: clinical and economic outcomes. Pharmacotherapy. 2007;27(12):1611-1618.
- Seaton RA. Daptomycin: rationale and role in the management of skin and soft tissue infections. J Antimicrob Chemother. 2008;62(Suppl 3):iii15-23.
Case
A previously healthy 55-year-old white female presents to the ED with a three-day history of pain and erythema in her right hand. Examination reveals fluctuance as well. She is diagnosed with an abscess with surrounding cellulitis. The abscess is incised, drained, and cultured, and she is sent home on oral trimethoprim/sulfamethoxazole. The following day, her cellulitis has worsened. She is hospitalized and commenced on intravenous vancomycin. What is the best empiric therapy for community-acquired cellulitis?
Background
Cellulitis is defined as a skin and soft-tissue infection (SSTI), which develops as a result of bacterial entry via breaches in the skin barrier. Typically, it involves the dermis and subcutaneous tissue, and is associated with local tenderness, erythema, swelling and fever. Cellulitis usually affects the lower extremities, but can affect other locations resulting in diagnoses such as periorbital, abdominal wall, buccal, and perianal cellulitis.1,2
Gram-positive organisms, especially Staphylococcus aureus and beta hemolytic streptococci, are the most common causes of cellulitis. Although it is less common, cellulitis can be caused by gram-negative organisms. The recent significant increase in the prevalence of SSTIs due to community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) has led to changes in the selection of antibiotics that were most commonly utilized to empirically treat cellulitis.
The diagnosis of cellulitis is based primarily on clinical manifestations. Due to low diagnostic yields, blood cultures, needle aspiration, or punch biopsy, specimens usually are not helpful in the setting of simple cellulitis.3 Therefore, antibiotic therapy is almost universally started empirically. Starting appropriate initial antibiotic therapy improves patient outcomes by reducing mortality rates, length of stay, and inpatient costs.4
Cellulitis incidence is about two cases per 1,000 patient-years.5 This rather high incidence, coupled with escalating rates of SSTIs due to CA-MRSA, demands reliable and cost-effective treatment strategies for the management of community-acquired cellulitis.
Review of the Data
The treatment of community-acquired cellulitis was straightforward until the past decade, as physicians saw a significant increase in CA-MRSA incidence.6 MRSA was reported initially in 1961, only two years after methicillin was introduced into clinical practice.7,8 Subsequently, MRSA prevalence increased dramatically, and by the beginning of this decade, more than 50% of the Staphylococcus aureus hospital strains were resistant to methicillin.8 Furthermore, 60% to 80% of community-acquired Staphylococcus aureus strains in the U.S. are methicillin-resistant.8
The two major types of MRSA infections are healthcare-acquired (HA-MRSA) and community-acquired (CA-MRSA). The HA-MRSA infection group is further subdivided into those strains that develop during a period of hospitalization, and those that develop following contact with healthcare facilities (e.g., hospitalization or surgery within the previous year). This subgroup includes HA-MRSA infections in hemodialysis patients, residents of long-term care facilities, and individuals who have a vascular catheter or other indwelling device.9,10
CA-MRSA infections, on the other hand, occur in individuals who have not had any contact with healthcare facilities. Higher rates of CA-MRSA infection are observed in settings where individuals have close contact with each other, including military trainees, athletes involved in contact sports, patients age 65 and older, men who have sex with other men, and parenteral substance abusers.8,11-13 However, in view of the high prevalence of CA-MRSA in the U.S., most patients, including those without any apparent risk factors, are at risk.8
HA-MRSA has the ability to survive on inanimate objects for extended time periods, increasing the likelihood of transmission to persons who come into contact with those objects. Although evidence has not confirmed that CA-MRSA has a similar capacity, it seems plausible that such spread does contribute to the propagation of CA-MRSA.12
The increasing importance of CA-MRSA also is evident in hospital settings, where it is replacing HA-MRSA as the most common type of Staphylococcus aureus. Since CA-MRSA tends to be susceptible to a larger number of antibiotics than HA-MRSA is, this has led to a reduced incidence of multidrug resistance. Fortunately, unlike HA-MRSA, CA-MRSA is susceptible to non-beta-lactam antibiotics, including tetracyclines, sulfonamides, and clindamycin.9
CA-MRSA most often causes SSTIs, and a tender abscess is a typical presentation.8 Patients commonly misinterpret early skin lesions as an insect or spider bite.12,14 When cutaneous CA-MRSA presents as an abscess, an incision and drainage procedure is essential for adequate treatment of the infection. For some CA-MRSA infections, particularly those characterized by the presence of a relatively small abscess, it might be adequate to do only an incision and drainage procedure, and not administer antibiotics.8,15 However, in most instances, especially when there is an area of cellulitis around the abscess, the initiation of antibiotic therapy improves patients’ clinical outcomes.9,16
When there is no apparent drainable purulent fluid collection, which often occurs with cellulitis, antibiotics should be the mainstay of therapy. The decision about which antibiotic to start can present some challenges, because the organism causing the cellulitis usually is not identified. This is because blood cultures are positive in less than 5% of cases. Also, positive culture results from needle aspiration are only helpful from 5% to 40% of the time. Meanwhile, culture of punch biopsy specimens yields a pathogen in only 20% to 30% of cases.3,17-19
Due to increased CA-MRSA incidence, cephalexin should not be prescribed to treat cellulitis in the outpatient setting because it does not provide coverage for the pathogen.13 Instead, oral antibiotics (e.g., clindamycin or trimethoprim/sulfamethoxazole) should be prescribed. Doxycycline, minocycline, rifampin (usually prescribed in combination with fusidic acid to prevent resistance development), and linezolid are additional therapeutic options.
Trimethoprim/sulfamethoxazole and clindamycin have several advantages: good oral bioavailability, familiarity to physicians, and general affordability. A disadvantage to using both trimethoprim/sulfamethoxazole and doxycycline is that they provide inadequate coverage for group A streptococci, which are a common cause of cellulitis. Therefore, the simultaneous use of a beta-lactam antibiotic with either of these medications may improve outcomes for “nonpurulent” cellulitis.13,15 Linezolid has proven effective for skin and SSTI caused by MRSA, even though it is not bactericidal.
Excellent oral bioavailability of this drug is an attractive characteristic, as it facilitates the transition from the use of intravenous to oral antibiotic therapy later in a patient’s hospital course. Although oral linezolid has been studied in clinical trials and provides good coverage for MRSA, its use in the outpatient setting is relatively limited, largely due to its significant cost.20 In 2008, the cost of 10 days of treatment with oral linezolid was $1,286.80. In comparison, the generic trimethoprim/sulfamethox-azole cost $9.40, and generic clindamycin cost $95.10.8 The lack of routine availability in many outpatient pharmacies also hinders the widespread use of linezolid.13
To date, with the exception of linezolid, no randomized, prospective clinical trials clearly demonstrate the efficacy of the oral agents that are commonly used for the outpatient treatment of cellulitis.20
When patients require hospitalization for the optimal treatment of cellulitis, it is important to select a parenteral antibiotic that provides coverage for MRSA.8 Vancomycin, daptomycin, linezolid, and tigecycline are the most commonly used agents.6
In the inpatient setting, failure to initiate appropriate medical therapy can result in longer hospital admissions, which significantly increase inpatient costs. Inadequate antibiotic therapy creates a significant financial burden and has been associated with increased mortality.4 Historically, vancomycin is used whenever a MRSA infection is suspected. However, there is concern about the declining efficacy of vancomycin related to a gradual increase in the rate of relative resistance—a minimal inhibitory concentration (MIC) increase—in MRSA strains. This MIC creep is noted in some medical centers and can lead to a failure to respond to vancomycin.13,20
Daptomycin is rapidly bactericidal against MRSA; in some institutions, its use may be preferred over vancomycin because the former antibiotic is associated with a significantly more rapid clinical response, which may shorten the required length of hospitalization.21 The once-daily dosing requirement for daptomycin allows for ease of use in both hospital and outpatient settings, and therefore may facilitate early hospital discharge or prevent the need for hospitalization altogether. Clinical experience also suggests potential economic advantages with the use of daptomycin.22
Tigecycline is a bacteriostatic antibiotic that achieves low serum concentrations. However, it penetrates the skin well and has a similar effectiveness to combination therapy with vancomycin and aztreonam. Thus far, tigecycline is not widely used for the treatment of MRSA infections, and it has been suggested that it may be preferred for polymicrobial infections or for patients who exhibit allergies to more commonly used agents.8
When selecting an antibiotic therapy, cost considerations play an important role in the decision-making process. For intravenous agents commonly used to treat CA-MRSA infections, the 2008 cost for 10 days of treatment with generic vancomycin was $182.80; daptomycin cost $1,660.80. For tigecycline and linezolid, the same duration of treatment cost $1,362 and $1,560, respectively.8
Back to the Case
Our patient, an otherwise healthy female, presented with no apparent risk factors for developing a CA-MRSA SSTI. However, more detailed history revealed that she regularly used sports equipment at her local fitness center. Based on her clinical presentation and concerns about the high local prevalence of CA-MRSA, an incision and drainage procedure was performed, and she was started empirically on IV vancomycin. She had a positive clinical response to this treatment.
Wound culture results confirmed CA-MRSA abscess and cellulitis, susceptible to trimethoprim/sulfamethoxazole. She was discharged on the oral formulation of this antibiotic to complete a 10-day course of treatment, including the days she received intravenous antibiotics.
Few well-designed trials have compared different lengths of cellulitis therapy. Most authorities recommend five to 10 days of treatment; however, longer courses might be required for more severe or complicated diseases.
Bottom line
Because of the high prevalence of CA-MRSA, initial antibiotic therapy for the treatment of community-acquired cellulitis must provide coverage for this organism. TH
Dr. Clarke is a hospitalist and clinical instructor at Emory University School of Medicine, Atlanta. Dr. Dressler is associate professor and director of education, section of hospital medicine, and associate program director of the J. Willis Hurst Internal Medicine Residency Program. Dr. Purohit is an instructor in clinical medicine at Emory University School of Medicine.
References
- Barzilai A, Choen HA. Isolation of group A streptococci from children with perianal cellulitis and from their siblings. Pediatr Infect Dis J. 1998;17(4):358-360.
- Thorsteinsdottir B, Tleyjeh IM, Baddour LM. Abdominal wall cellulitis in the morbidly obese. Scand J Infect Dis. 2005;37(8):605-608.
- Swartz MN. Clinical practice. Cellulitis. N Engl J Med. 2004;350(9):904-912.
- Edelsberg J, Berger A, Weber DJ, et al. Clinical and economic consequences of failure of initial antibiotic therapy for hospitalized patients with complicated skin and skin-structure infections. Infect Control Hosp Epidemiol. 2008;29(2):160-169.
- McNamara DR, Tleyjeh IM, Berbari EF, et al. Incidence of lower extremity cellulitis: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 2007;82(7):817-821.
- Moellering RC. Current treatment options for community-acquired methicillin-resistant Staphylococcus aureus infection. Clin Infect Dis. 2008;46(7):1032-1037.
- Chambers HF. The changing epidemiology of Staphylococcus aureus. Emerg Infect Dis. 2001;7(2):178-182.
- Moellering RC. A 39-year-old man with a skin infection. JAMA. 2008;299(1):79-87
- Ruhe J, Smith N, Bradsher RW, Menon A. Community-onset methicillin-resistant Staphylococcus aureus skin and soft tissue infections: impact of antimicrobial therapy on outcome. Clin Infect Dis. 2007;44(6):777-784.
- David MZ, Glikman D, Crawford SE, et al. What is community-associated methicillin-resistant Staphylococcus aureus? J Infect Dis. 2008;197(9):1235-1243.
- Iyer S, Jones DH. Community-acquired methicillin-resistant Staphylococcus aureus skin infection: a retrospective analysis of clinical presentation and treatment of a local outbreak. J Am Acad Dermatol. 2004;50(6):854-858.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus skin or soft tissue infections in a state prison—Mississippi, 2000. MMWR Morb Mortal Wkly Rep. 2001;50(42):919-922.
- Daum RS. Clinical practice. Skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus. N Engl J Med. 2007;357(4):380-390.
- Dominguez TJ. It’s not a spider bite, it’s community-acquired methicillin-resistant Staphylococcus aureus. J Am Board Fam Pract. 2004;17(3):220-226.
- Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355(7):666-674.
- Jetton L. Therapy for methicillin-resistant Staphylococcus aureus. N Engl J Med. 2006;355(20):2153-2155.
- Hook EW, Hooton TM, Horton CA, et al. Microbiologic evaluation of cutaneous cellulitis in adults. Arch Intern Med. 1986;146(2):295-297.
- Duvanel T, Auckenthaler R, Rohner P, Harms M, Saurat JH. Quantitative cultures of biopsy specimens from cutaneous cellulitis. Arch Intern Med. 1989;149(2):293-296.
- Newell PM, Norden CW. Value of needle aspiration in bacteriologic diagnosis of cellulitis in adults. J Clin Microbiol. 1988; 26(3):401-404.
- Loffler CA, Macdougall C. Update on prevalence and treatment of methicillin-resistant Staphylococcus aureus infections. Expert Rev Anti Infect Ther. 2007;5(6):961-981.
- Davis SL, McKinnon PS, Hall LM, et al. Daptomycin versus vancomycin for complicated skin and skin structure infections: clinical and economic outcomes. Pharmacotherapy. 2007;27(12):1611-1618.
- Seaton RA. Daptomycin: rationale and role in the management of skin and soft tissue infections. J Antimicrob Chemother. 2008;62(Suppl 3):iii15-23.
Increased Attention
According to the American Diabetes Association, a normal fasting plasma glucose (FPG) level is less than 100 mg/dl; impaired fasting glucose (IFG) is defined as an FPG from 100 to 125 mg/dl; and any patient with an FPG greater than or equal to 126 mg/dL carries a provisional diagnosis of diabetes.1 When the oral glucose tolerance test is used for evaluation, similar definitions exist. Patients with IFG or impaired glucose tolerance (IGT) have “pre-diabetes,” and are at a high risk for developing diabetes. Elevated blood glucose levels can have major consequences, particularly in high-risk populations.2
Macrovascular and microvascular complications, impaired wound healing, and a compromised immune system can occur in the setting of sustained, elevated blood glucose concentrations. Aside from patients with diabetes who have elevated blood glucose levels, schizophrenic patients might be predisposed to glucose intolerance and diabetes independent of treatment.3
It is not known whether IGT seen in schizophrenics is due to lifestyle risk factors (e.g., smoking, poor diet, being overweight, lack of exercise) or some genetic or biological component of the disease. However, this is complicated by the fact that many of these patients are treated with second-generation antipsychotics (SGAs), which might increase the risk of developing diabetes.4 Because of this, a warning regarding the risk of developing hyperglycemia and diabetes was mandated by the Food and Drug Administration (FDA) for SGA manufacturers.5
Hyperglycemia symptoms include polyuria, polydipsia, weight loss (sometimes with polyphagia), and blurred vision. Impairment of growth and susceptibility to certain infections might occur with chronic hyperglycemia. Hyperglycemia with ketoacidosis or the nonketotic hyperosmolar syndrome are acute, life-threatening consequences of uncontrolled diabetes. It is important for hospitalists and other healthcare professionals to be aware of drugs that can cause hyperglycemia or impair glucose tolerance. In some cases, the drug can be continued; in other cases, an alternate agent should be provided if necessary for patient management.
Certain drugs and drug classes known to cause hyperglycemia include: thiazide diuretics, glucocorticoids, oral contraceptives and sex hormones (e.g., testosterone), protease inhibitors, SGAs, thyroid hormone, phenytoin, niacin/nicotinic acid, diazoxide, and alfa-interferon.1-3,6
Limited evidence exists for some other agents/classes, including: asparaginase, beta-agonists, beta-blockers, calcium channel blockers, clonidine, cyclosporine, levodopa, lithium, minoxidil, phenothiazines, and others.7 The Seventh Report of the Joint National Committee (JNC 7) recommends thiazide diuretics as a first-line treatment for most patients with Stage 1 hypertension, alone or in combination for patients with diabetes.8 These thiazide doses tend to be smaller and, therefore, tend to have minimal effects on blood glucose levels.
In 2004, a consensus guideline was developed on antipsychotic drugs, obesity, and diabetes.9 It describes baseline and followup monitoring of patients treated with SGAs. The baseline includes personal/family history, weight/body mass index, waist circumference, blood pressure, FPG, and a fasting lipid profile. Monitoring of these parameters is then designated at specified times throughout treatment (e.g., weeks four, eight, 12, etc.). Haupt et al recently compared monitoring of lipids and glucose in a population of insured patients receiving SGAs in a retrospective cohort of patients pre- and post-guideline.10 Baseline lipid and glucose testing rates increased minimally post-guideline versus pre-guideline.
The results of this study demonstrate that even though monitoring guidelines to prevent potentially adverse outcomes in a patient population at high risk for developing adverse outcomes are available, clinicians do not always follow them. In order to improve patient outcomes, identified at-risk populations (e.g., patients receiving SGAs) need to be more closely evaluated and monitored throughout therapy to prevent IGT and/or diabetes. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2009;32:S62-S67.
- Luna B, Feinglos MN. Drug-induced hyperglycemia. JAMA. 2001;286:1945-1948.
- Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(Suppl 1):20-27.
- Tahir R. Metabolic effects of atypical antipsychotics. US Pharm. 2007;32:HS3-HS14.
- Warning about hyperglycemia and atypical antipsychotic drugs. U.S. Food & Drug Administration Web site. Available at: www.accessdata.fda.gov/scripts/cdrh/cfdocs/psn/printer.cfm?id=229. Accessed March 31, 2009.
- Kaufman MB, Simionatto C. A review of protease inhibitor-induced hyperglycemia. Pharmacotherapy. 1999;19:114-117.
- Pandit MK, Burke J, Gustafson AB, Minocha A, Peiris AN. Drug-induced disorders of glucose tolerance. Ann Intern Med. 1993;118:529-539.
- Chobanian AV, Bakris GL, Clack HR, et al. The seventh report of the joint national committee on prevention, detection, evaluations, and treatment of high blood pressure. JAMA. 2003;289:2560-2572.
- American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
- Haupt DW, Rosenblatt LC, Kim E, Baker RA, Whitehead R, Newcomer JW. Prevalence and predictors of lipid and glucose monitoring in commercially insured patients treated with second-generation antipsychotic agents. Am J Psychiatry. 2009;166:345-353.
- FDA approves generic treatment for emesis. Drug Store News Web site. Available at: www.drugstorenews.com/story.aspx?id=96143. Accessed March 6, 2009.
- Aurobindo Pharma gets tentative approval from US FDA for tenofovir disoproxil fumarate tabs. RTT News Web site. Available at: www.rttnews.com/ArticleView.aspx?id=860423. Accessed March 4, 2009.
- Teva announces approval and launch of generic Topamax tablets.Teva Web site. Available at: www.tevapharm.com/pr/2009/pr_835.asp. Accessed March 30, 2009.
- FDA approves Symbicort for chronic obstructive pulmonary disease (COPD). AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazenecaus/newsroom/all/4939997?itemId=4939997. Accessed June 5, 2009.
- Copaxone approved by the FDA for patients with a first clinical event suggestive of multiple sclerosis. Teva Web site. Available at: www.tevapharm.com/pr/2009/ pr_826.asp? Accessed June 5, 2009.
- Todoruk M. FDA approves new use for Wyeth’s Tygacil antibiotic. Available at: www.firstwordplus.com/Fws.do?articleid=CF71DE6056CE4120A295243AE2D6EC00. Accessed March 25, 2009.
- FDA Web site. Available at www.accessdata.fda.gov/drugsatfda_docs/label/2009/021821s013s017s018lbl.pdf. Accessed June 5, 2009.
- Transdermal drug patches with metallic backings. FDA Web site. Available at: www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm111493.htm. Accessed June 5, 2009.
- FDA warns about risk of wearing medicated patches during MRIs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149537.htm. Accessed March 6, 2009.
- FDA requires boxed warning and risk mitigation strategy for metoclopramide-containing drugs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149533.htm. Accessed March 4, 2009.
- Zonisamide (marketed as Zonegran, and generics). FDA Web site. Available at: www.fda.gov/ForConsumers/ConsumerUpdates/ucm095251.htm. Accessed March 4, 2009.
According to the American Diabetes Association, a normal fasting plasma glucose (FPG) level is less than 100 mg/dl; impaired fasting glucose (IFG) is defined as an FPG from 100 to 125 mg/dl; and any patient with an FPG greater than or equal to 126 mg/dL carries a provisional diagnosis of diabetes.1 When the oral glucose tolerance test is used for evaluation, similar definitions exist. Patients with IFG or impaired glucose tolerance (IGT) have “pre-diabetes,” and are at a high risk for developing diabetes. Elevated blood glucose levels can have major consequences, particularly in high-risk populations.2
Macrovascular and microvascular complications, impaired wound healing, and a compromised immune system can occur in the setting of sustained, elevated blood glucose concentrations. Aside from patients with diabetes who have elevated blood glucose levels, schizophrenic patients might be predisposed to glucose intolerance and diabetes independent of treatment.3
It is not known whether IGT seen in schizophrenics is due to lifestyle risk factors (e.g., smoking, poor diet, being overweight, lack of exercise) or some genetic or biological component of the disease. However, this is complicated by the fact that many of these patients are treated with second-generation antipsychotics (SGAs), which might increase the risk of developing diabetes.4 Because of this, a warning regarding the risk of developing hyperglycemia and diabetes was mandated by the Food and Drug Administration (FDA) for SGA manufacturers.5
Hyperglycemia symptoms include polyuria, polydipsia, weight loss (sometimes with polyphagia), and blurred vision. Impairment of growth and susceptibility to certain infections might occur with chronic hyperglycemia. Hyperglycemia with ketoacidosis or the nonketotic hyperosmolar syndrome are acute, life-threatening consequences of uncontrolled diabetes. It is important for hospitalists and other healthcare professionals to be aware of drugs that can cause hyperglycemia or impair glucose tolerance. In some cases, the drug can be continued; in other cases, an alternate agent should be provided if necessary for patient management.
Certain drugs and drug classes known to cause hyperglycemia include: thiazide diuretics, glucocorticoids, oral contraceptives and sex hormones (e.g., testosterone), protease inhibitors, SGAs, thyroid hormone, phenytoin, niacin/nicotinic acid, diazoxide, and alfa-interferon.1-3,6
Limited evidence exists for some other agents/classes, including: asparaginase, beta-agonists, beta-blockers, calcium channel blockers, clonidine, cyclosporine, levodopa, lithium, minoxidil, phenothiazines, and others.7 The Seventh Report of the Joint National Committee (JNC 7) recommends thiazide diuretics as a first-line treatment for most patients with Stage 1 hypertension, alone or in combination for patients with diabetes.8 These thiazide doses tend to be smaller and, therefore, tend to have minimal effects on blood glucose levels.
In 2004, a consensus guideline was developed on antipsychotic drugs, obesity, and diabetes.9 It describes baseline and followup monitoring of patients treated with SGAs. The baseline includes personal/family history, weight/body mass index, waist circumference, blood pressure, FPG, and a fasting lipid profile. Monitoring of these parameters is then designated at specified times throughout treatment (e.g., weeks four, eight, 12, etc.). Haupt et al recently compared monitoring of lipids and glucose in a population of insured patients receiving SGAs in a retrospective cohort of patients pre- and post-guideline.10 Baseline lipid and glucose testing rates increased minimally post-guideline versus pre-guideline.
The results of this study demonstrate that even though monitoring guidelines to prevent potentially adverse outcomes in a patient population at high risk for developing adverse outcomes are available, clinicians do not always follow them. In order to improve patient outcomes, identified at-risk populations (e.g., patients receiving SGAs) need to be more closely evaluated and monitored throughout therapy to prevent IGT and/or diabetes. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2009;32:S62-S67.
- Luna B, Feinglos MN. Drug-induced hyperglycemia. JAMA. 2001;286:1945-1948.
- Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(Suppl 1):20-27.
- Tahir R. Metabolic effects of atypical antipsychotics. US Pharm. 2007;32:HS3-HS14.
- Warning about hyperglycemia and atypical antipsychotic drugs. U.S. Food & Drug Administration Web site. Available at: www.accessdata.fda.gov/scripts/cdrh/cfdocs/psn/printer.cfm?id=229. Accessed March 31, 2009.
- Kaufman MB, Simionatto C. A review of protease inhibitor-induced hyperglycemia. Pharmacotherapy. 1999;19:114-117.
- Pandit MK, Burke J, Gustafson AB, Minocha A, Peiris AN. Drug-induced disorders of glucose tolerance. Ann Intern Med. 1993;118:529-539.
- Chobanian AV, Bakris GL, Clack HR, et al. The seventh report of the joint national committee on prevention, detection, evaluations, and treatment of high blood pressure. JAMA. 2003;289:2560-2572.
- American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
- Haupt DW, Rosenblatt LC, Kim E, Baker RA, Whitehead R, Newcomer JW. Prevalence and predictors of lipid and glucose monitoring in commercially insured patients treated with second-generation antipsychotic agents. Am J Psychiatry. 2009;166:345-353.
- FDA approves generic treatment for emesis. Drug Store News Web site. Available at: www.drugstorenews.com/story.aspx?id=96143. Accessed March 6, 2009.
- Aurobindo Pharma gets tentative approval from US FDA for tenofovir disoproxil fumarate tabs. RTT News Web site. Available at: www.rttnews.com/ArticleView.aspx?id=860423. Accessed March 4, 2009.
- Teva announces approval and launch of generic Topamax tablets.Teva Web site. Available at: www.tevapharm.com/pr/2009/pr_835.asp. Accessed March 30, 2009.
- FDA approves Symbicort for chronic obstructive pulmonary disease (COPD). AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazenecaus/newsroom/all/4939997?itemId=4939997. Accessed June 5, 2009.
- Copaxone approved by the FDA for patients with a first clinical event suggestive of multiple sclerosis. Teva Web site. Available at: www.tevapharm.com/pr/2009/ pr_826.asp? Accessed June 5, 2009.
- Todoruk M. FDA approves new use for Wyeth’s Tygacil antibiotic. Available at: www.firstwordplus.com/Fws.do?articleid=CF71DE6056CE4120A295243AE2D6EC00. Accessed March 25, 2009.
- FDA Web site. Available at www.accessdata.fda.gov/drugsatfda_docs/label/2009/021821s013s017s018lbl.pdf. Accessed June 5, 2009.
- Transdermal drug patches with metallic backings. FDA Web site. Available at: www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm111493.htm. Accessed June 5, 2009.
- FDA warns about risk of wearing medicated patches during MRIs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149537.htm. Accessed March 6, 2009.
- FDA requires boxed warning and risk mitigation strategy for metoclopramide-containing drugs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149533.htm. Accessed March 4, 2009.
- Zonisamide (marketed as Zonegran, and generics). FDA Web site. Available at: www.fda.gov/ForConsumers/ConsumerUpdates/ucm095251.htm. Accessed March 4, 2009.
According to the American Diabetes Association, a normal fasting plasma glucose (FPG) level is less than 100 mg/dl; impaired fasting glucose (IFG) is defined as an FPG from 100 to 125 mg/dl; and any patient with an FPG greater than or equal to 126 mg/dL carries a provisional diagnosis of diabetes.1 When the oral glucose tolerance test is used for evaluation, similar definitions exist. Patients with IFG or impaired glucose tolerance (IGT) have “pre-diabetes,” and are at a high risk for developing diabetes. Elevated blood glucose levels can have major consequences, particularly in high-risk populations.2
Macrovascular and microvascular complications, impaired wound healing, and a compromised immune system can occur in the setting of sustained, elevated blood glucose concentrations. Aside from patients with diabetes who have elevated blood glucose levels, schizophrenic patients might be predisposed to glucose intolerance and diabetes independent of treatment.3
It is not known whether IGT seen in schizophrenics is due to lifestyle risk factors (e.g., smoking, poor diet, being overweight, lack of exercise) or some genetic or biological component of the disease. However, this is complicated by the fact that many of these patients are treated with second-generation antipsychotics (SGAs), which might increase the risk of developing diabetes.4 Because of this, a warning regarding the risk of developing hyperglycemia and diabetes was mandated by the Food and Drug Administration (FDA) for SGA manufacturers.5
Hyperglycemia symptoms include polyuria, polydipsia, weight loss (sometimes with polyphagia), and blurred vision. Impairment of growth and susceptibility to certain infections might occur with chronic hyperglycemia. Hyperglycemia with ketoacidosis or the nonketotic hyperosmolar syndrome are acute, life-threatening consequences of uncontrolled diabetes. It is important for hospitalists and other healthcare professionals to be aware of drugs that can cause hyperglycemia or impair glucose tolerance. In some cases, the drug can be continued; in other cases, an alternate agent should be provided if necessary for patient management.
Certain drugs and drug classes known to cause hyperglycemia include: thiazide diuretics, glucocorticoids, oral contraceptives and sex hormones (e.g., testosterone), protease inhibitors, SGAs, thyroid hormone, phenytoin, niacin/nicotinic acid, diazoxide, and alfa-interferon.1-3,6
Limited evidence exists for some other agents/classes, including: asparaginase, beta-agonists, beta-blockers, calcium channel blockers, clonidine, cyclosporine, levodopa, lithium, minoxidil, phenothiazines, and others.7 The Seventh Report of the Joint National Committee (JNC 7) recommends thiazide diuretics as a first-line treatment for most patients with Stage 1 hypertension, alone or in combination for patients with diabetes.8 These thiazide doses tend to be smaller and, therefore, tend to have minimal effects on blood glucose levels.
In 2004, a consensus guideline was developed on antipsychotic drugs, obesity, and diabetes.9 It describes baseline and followup monitoring of patients treated with SGAs. The baseline includes personal/family history, weight/body mass index, waist circumference, blood pressure, FPG, and a fasting lipid profile. Monitoring of these parameters is then designated at specified times throughout treatment (e.g., weeks four, eight, 12, etc.). Haupt et al recently compared monitoring of lipids and glucose in a population of insured patients receiving SGAs in a retrospective cohort of patients pre- and post-guideline.10 Baseline lipid and glucose testing rates increased minimally post-guideline versus pre-guideline.
The results of this study demonstrate that even though monitoring guidelines to prevent potentially adverse outcomes in a patient population at high risk for developing adverse outcomes are available, clinicians do not always follow them. In order to improve patient outcomes, identified at-risk populations (e.g., patients receiving SGAs) need to be more closely evaluated and monitored throughout therapy to prevent IGT and/or diabetes. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2009;32:S62-S67.
- Luna B, Feinglos MN. Drug-induced hyperglycemia. JAMA. 2001;286:1945-1948.
- Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(Suppl 1):20-27.
- Tahir R. Metabolic effects of atypical antipsychotics. US Pharm. 2007;32:HS3-HS14.
- Warning about hyperglycemia and atypical antipsychotic drugs. U.S. Food & Drug Administration Web site. Available at: www.accessdata.fda.gov/scripts/cdrh/cfdocs/psn/printer.cfm?id=229. Accessed March 31, 2009.
- Kaufman MB, Simionatto C. A review of protease inhibitor-induced hyperglycemia. Pharmacotherapy. 1999;19:114-117.
- Pandit MK, Burke J, Gustafson AB, Minocha A, Peiris AN. Drug-induced disorders of glucose tolerance. Ann Intern Med. 1993;118:529-539.
- Chobanian AV, Bakris GL, Clack HR, et al. The seventh report of the joint national committee on prevention, detection, evaluations, and treatment of high blood pressure. JAMA. 2003;289:2560-2572.
- American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
- Haupt DW, Rosenblatt LC, Kim E, Baker RA, Whitehead R, Newcomer JW. Prevalence and predictors of lipid and glucose monitoring in commercially insured patients treated with second-generation antipsychotic agents. Am J Psychiatry. 2009;166:345-353.
- FDA approves generic treatment for emesis. Drug Store News Web site. Available at: www.drugstorenews.com/story.aspx?id=96143. Accessed March 6, 2009.
- Aurobindo Pharma gets tentative approval from US FDA for tenofovir disoproxil fumarate tabs. RTT News Web site. Available at: www.rttnews.com/ArticleView.aspx?id=860423. Accessed March 4, 2009.
- Teva announces approval and launch of generic Topamax tablets.Teva Web site. Available at: www.tevapharm.com/pr/2009/pr_835.asp. Accessed March 30, 2009.
- FDA approves Symbicort for chronic obstructive pulmonary disease (COPD). AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazenecaus/newsroom/all/4939997?itemId=4939997. Accessed June 5, 2009.
- Copaxone approved by the FDA for patients with a first clinical event suggestive of multiple sclerosis. Teva Web site. Available at: www.tevapharm.com/pr/2009/ pr_826.asp? Accessed June 5, 2009.
- Todoruk M. FDA approves new use for Wyeth’s Tygacil antibiotic. Available at: www.firstwordplus.com/Fws.do?articleid=CF71DE6056CE4120A295243AE2D6EC00. Accessed March 25, 2009.
- FDA Web site. Available at www.accessdata.fda.gov/drugsatfda_docs/label/2009/021821s013s017s018lbl.pdf. Accessed June 5, 2009.
- Transdermal drug patches with metallic backings. FDA Web site. Available at: www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm111493.htm. Accessed June 5, 2009.
- FDA warns about risk of wearing medicated patches during MRIs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149537.htm. Accessed March 6, 2009.
- FDA requires boxed warning and risk mitigation strategy for metoclopramide-containing drugs. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149533.htm. Accessed March 4, 2009.
- Zonisamide (marketed as Zonegran, and generics). FDA Web site. Available at: www.fda.gov/ForConsumers/ConsumerUpdates/ucm095251.htm. Accessed March 4, 2009.
In the Literature
In This Edition
Literature at a Glance: A guide to this month’s studies
- PPI use with clopidrogrel in ACS.
- Chlorhexidine sponge use reduces line infections.
- Extended thienopyridine use does not benefit DES patients.
- CABG is revascularization choice for severe CAD.
- Pre-treated CVC use reduces bloodstream infections.
- Hospitalist use grows in U.S.
- Sepsis order set improves outcomes.
- Admission day predicts acute PE mortality.
PEDIATRIC HM LITerature
Early Transition to Oral Therapy in Acute Osteomyelitis in Children Associated with Fewer Complications I By Mark Shen, MD
Clinical question: Can acute osteomyelitis in children be managed with early transition to oral antimicrobial therapy?
Background: Traditional treatment of acute osteomyelitis in children has involved prolonged intravenous antimicrobial therapy, typically greater than three to four weeks in duration. Small studies suggest the feasibility of a transition to prolonged oral therapy after an initial response to intravenous antimicrobial agents.
Study design: Retrospective, cohort study.
Setting: 29 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, 1,969 children were identified via ICD-9-CM codes as having been hospitalized with acute osteomyelitis—and without comorbid conditions—between January 2000 and June 2005. Rehospitalizations were reviewed for complications of both treatment failure and the treatment itself. More than half (1,021) of the children underwent central venous catheterization for prolonged intravenous (IV) therapy; 948 were assigned to the oral therapy group. No significant differences in treatment failure existed between the two groups (5% in the IV group; 4% in the oral group).
Overall, the clinical characteristics of the two groups were indistinguishable. Propensity score analysis was used to handle possible patient-level confounders; a validation study was performed to address misclassifications in assignment. No significant confounding effects were found.
Secondary findings included marked variation across hospitals in the use of oral therapy and increased treatment complications in the IV group. Although unmeasured factors not present in an administrative database may affect results, the strikingly similar groups and outcomes suggest the data are relevant.
Bottom line: Early transition to oral therapy for acute osteomyelitis in children does not increase treatment failure and is associated with fewer treatment complications.
Reference: Zaoutis T, Localio AR, Leckerman K, Saddlemire S, Bertoch D, Keren R. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics. 2009;123:636-642.

PPI Use with Clopidogrel in Acute Coronary Syndrome Is Associated with Readmissions and Mortality
Clinical question: Does concomitant use of clopidogrel and a proton pump inhibitor (PPI) following hospitalization for acute coronary syndrome (ACS) lead to adverse outcomes?
Background: Prophylactic PPIs often are prescribed with clopidogrel to reduce the risk of gastrointestinal bleeding. Mechanistic studies have shown that omeprazole decreases the platelet-inhibitory effect of clopidogrel, raising concerns that PPIs might interfere with clopidogrel’s beneficial effects. The clinical significance of this finding is unknown.
Study design: Retrospective cohort study.
Setting: 127 VA hospitals.
Synopsis: Investigators used data from the Cardiac Care Follow-up Clinical Study and VA pharmacy records to examine 8,205 male veterans who were hospitalized for ACS and treated with clopidogrel. Patients who filled prescriptions for both clopidogrel and a PPI were at significantly higher risk for death or readmission with ACS compared with those who filled prescriptions for clopidogrel only (adjusted odds ratio, 1.25; 95% confidence interval, 1.11-1.41). Patients who filled prescriptions for PPIs alone had similar risk for adverse events as those who took neither medication.
Subanalyses found similarly increased risk among patients prescribed omeprazole and rabeprazole, but those taking lanzoprazole and pantoprazole were not examined due to the small sample size. Although causality cannot be inferred from this observational study, and the risk associated with combined clopidigrel and PPI use appeared small, alternatives for gastric acid reduction exist. Thus, it may be prudent to restrict PPI use to patients who have a clear indication for their use until more definitive clinical trials can be conducted.
Bottom line: Among patients who are treated with clopidogrel for ACS, PPIs should be reserved for patients with a clear indication for gastric acid reduction and who cannot use alternative therapies.
Citation: Ho PM, Maddox TM, Wang L, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009;301(9):937-944.
Chlorhexidine-Impregnated Sponge Use Reduces Line Infections
Clinical question: Does dressing vascular catheters with chlorhexidine gluconate-impregnated sponges (CHGIS) reduce rates of catheter-related infections, and are dressing changes every seven days inferior to every three days?
Background: Process improvement strategies—including educating providers, strictly adhering to sterile technique, and promptly removing unnecessary catheters—greatly decrease catheter-related infections. It is unclear if CHGIS dressings offer additional benefit. Also uncertain is whether weekly dressing changes are as safe as changing dressings every three days.
Study design: A 2x2 factorial, assessor-blinded, randomized controlled trial.
Setting: ICUs in three university hospitals and two general hospitals in France.
Synopsis: 1,636 French adults expected to require arterial and central venous catheters for >48 hours were randomly assigned to one of four groups. Each group received either CHGIS dressings or standard dressings, and each group had dressing changes every three or seven days. Dressings were changed sooner if soiled or nonadherent. CHGIS dressings were associated with fewer catheter-related infections than standard dressings (0.6 vs. 1.4 infections per 1,000 catheter days; P=0.03). No significant difference in rates of catheter colonization existed between the three-day and seven-day dressing change strategies (10.4 vs. 11 events per 1,000 catheter days, P>0.05).
Although microbiology assessors were blinded to patients’ status, the ICU staff was not, potentially creating experimenter bias. Approximately 30% of the venous catheters and 40% of the arterial catheters were in a femoral site. Secondary analyses found higher rates of severe dermatitis among patients with CHGIS dressings but no difference in minimal bactericidal concentration (MBC) or colonizing organisms. Preliminary calculations suggested CHGIS dressings could be cost-effective.
Bottom line: Among critically ill adults, CHGIS catheter dressings may marginally reduce catheter-related infection rates, but further evaluation is needed before this technology can be adopted widely.
Citation: Timsit JF, Schwebel C, Bouadma L, et al. Chlorhexidine-impregnated sponges and less frequent dressing changes for prevention of catheter-related infections in critically-ill adults: a randomized controlled trial. JAMA. 2009;301(12):1231-1241.
Thienopyridine Use Six Months after Sirolimus-Eluting Stent Implant-ation Offers No Benefit
Clinical question: What are the relative contributions of aspirin and thienopyridine on preventing stent thrombosis in patients with sirolimus-eluting stents?
Background: There are no randomized clinical trials addressing the optimal duration, or the risks associated with discontinuation, of dual-antiplatelet therapy after drug-eluting stent (DES) implantation. Nevertheless, many patients continue to be maintained on dual-antiplatelet therapy beyond one year of their index DES implantation.
Study design: Prospective multicenter observational study.
Setting: Hospitals in Japan.
Synopsis: This study observed 10,778 Japanese patients undergoing sirolimus-eluting stent implantation. Patients discontinuing both thienopyridine and aspirin had a significantly higher rate of stent thrombosis than those who continued both medications for up to 18 months. However, discontinuation of thienopyridine alone was not associated with an excess risk of stent thrombosis. Additionally, a landmark analysis of patients who were free of events at six months showed rates of death for myocardial infarction (MI) at 24 months were 4.1% for patients taking thienopyridine and 4.1% for patients not taking thienopyridine (P=0.99). Ticlodipine was the thienopyridine used by more than 95% of patients.
Hospitalists should be aware that the role thienopyridine therapy plays in reducing stent thrombosis beyond one month after implantation has not been well addressed.
Bottom line: Discontinuation of thienopyridine therapy after six months while maintaining aspirin therapy is not associated with increased risk of stent thrombosis in patients with sirolimus-eluting stents.
Citation: Kimura T, Morimoto T, Nakagawa Y, et al. Antiplatelet therapy and stent thrombosis after sirolimus-eluting stent implantation. Circulation. 2009;119(7):987-995.
Compared with PCI, CABG Results in Lower Rates of Major Adverse Events in Severe CAD Patients
Clinical question: What is the optimal revascularization strategy for previously untreated severe coronary artery disease (CAD)?
Background: Coronary artery bypass grafting (CABG) is the treatment of choice in three-vessel and left-main CAD. However, percutaneous coronary intervention (PCI) with drug-eluting stents often is utilized despite the lack of adequately powered randomized trials.
Study design: Prospective multicenter randomized clinical trial.
Setting: 85 hospitals in Europe and the U.S.
Synopsis: 1,800 patients with an average age of 65 and previously untreated three-vessel or left-main CAD amenable to therapy with both PCI and CABG were randomized to CABG or PCI. The primary combined endpoint was a major adverse cardiac or cerebrovascular event, defined as death, stroke, MI, or repeat revascularization. PCI was associated with a significantly higher rate of major adverse cardiac or cerebrovascular events, due mostly to a higher rate of repeat revascularization (13.5% vs. 5.9%, P<0.001). At 12 months, the two groups had similar rates of death from any cause or MI, and similar rates of the combined endpoint of death from any cause, stroke, or MI; however, the rate of stroke was 1.6% higher in the CABG group.
Hospitalists should continue to favor CABG over PCI but give consideration to the risks involved with such an intervention.
Bottom line: CABG remains the revascularization choice in patients with severe CAD.
Citation: Serruys PW, Morice MC, Kappetein AP, et al. Percuta-neous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
Pre-Medicated Central Venous Catheters Reduce Risk of Catheter-Related Bloodstream Infections
Clinical question: Does pre-treating central venous catheters with anti-infective agents prevent catheter-related bloodstream infections?
Background: Use of central venous catheters (CVC) is associated with catheter-related bloodstream infection (CRBSI), with CRBSI-related mortality rates as high as 25%. Previous reviews have indicated that CVCs coated or impregnated with anti-infectives may reduce CRBSI incidence. This review integrates new trial data with information from prior reviews.
Study design: Meta-analysis of 27 randomized controlled trials.
Setting: Meta-analysis.
Synopsis: The authors report CVCs pre-treated with anti-infectives (AI-CVCs) are clinically effective in reducing the risk of CRBSI. The odds of having a CRBSI with a treated CVC versus an untreated CVC are 0.49 to 1 (95% CI, 0.37–0.64, 27 studies, fixed effects). The study also finds the use of AI-CVCs might provide a large cost savings in Great Britain. Because the findings are based on a meta-analysis, they are limited by the quality, context, and consistency of the original studies. The authors note that many of the studies had unsatisfactory descriptions of methodology. The current study is unable to separate the risk reduction attributable to AI-CVC versus that attributable to other infection control practices. Also, original data is insufficient to assess the benefits of AI-CVCs placed for longer than 12 days.
To summarize, AI-CVCs may present a means to reduce CRBSI, but more investigation of its role within infection control protocols is needed, as is investigation of longer duration of treatment.
Bottom line: Central venous catheters pre-treated with anti-infectives significantly reduce catheter-related bloodstream infections.
Citation: Hockenhull JC, Dwan KM, Smith GW, et al. The clinical effectiveness of central venous catheters treated with anti-infective agents in preventing catheter-related bloodstream infections: a systematic review. Crit Care Med. 2009;37(2):702-712.
Fivefold Increase in Hospitalists in the U.S. from 1995 to 2006
Clinical question: What is the growth rate of hospitalists and hospitalist-provided care?
Background: Survey data has shown a sharp increase in the number of hospitalists, but until now there have not been any national or population-based data on the growth of hospitalist care.
Study design: Descriptive analysis.
Setting: Medicare-enrolled patients.
Synopsis: The study is based on national Medicare data from 2.1 million admissions involving 990,785 patients in 5,800 hospitals and 120,226 general internists. It represents 5% of inpatient Medicare claims generated by general internists. The authors define “hospitalist” as a general internist who generates >90% of his or her claims from the care of hospitalized patients.
U.S. hospitals have seen substantial growth in hospitalists over the period examined. The nation saw a 500% increase in the number of general-internist hospitalists, and a 28% increase (to 37.1% in 2006 from 9.1% in 1995) in the number of Medicare patients who received care from a hospitalist. The odds that a hospitalized Medicare patient received care from a hospitalist increased 29.2% per year from 1997 to 2006. The percentage of hospitals with at least three hospitalists rose to 47.1% in 2006 from 11.6% in 1995.
This analysis might actually have underestimated HM’s growth. Analysis of Medicare claims does not identify pediatric hospitalists and hospitalists who work exclusively within HMOs. This analysis also did not include family practitioners or internal-medicine subspecialists who are hospitalists.
Bottom line: Medicare claims data confirm survey data findings: Hospitalists and hospitalist care has grown sharply over the last decade.
Citation: Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360:1102-1012.
Standardized Order Set for Bacteremic Sepsis Improves LOS and Mortality
Clinical question: Does a standardized order set for bacteremic sepsis impact patient management and outcomes?
Background: Prompt cardiovascular resuscitation and appropriate antibiotics decrease morbidity and mortality in bacteremic sepsis. This study examined whether hospitalwide, standardized sepsis order set improved management and outcomes.
Study design: Retrospective, before-and-after study design.
Setting: 1,200-bed academic medical center.
Synopsis: Two hundred patients with bacteremic severe sepsis were randomly selected from 18 months before the order set was introduced, and 200 were selected from 18 months after the order set was introduced. Primary outcomes measured were quantity of fluid administered and appropriate initial antibiotics. Secondary outcomes measured were hospital mortality and length of stay. Patients in the “after” group received more intravenous fluid (1627±1862 ml vs. 2054±2237 ml, P=.04), more appropriate antibiotics (53.0% vs. 65.5%, P=.01), had shorter hospital stays (28.7±30.1 days vs. 22.4±20.9 days, P=.02), and decreased in-house mortality (55.0% vs. 39.5%, P =<0.01).
The retrospective design of the study limited its ability to determine causal relationship. Extensive education may have contributed to the change (Hawthorne effect). Management in the ICU and ED, not the hospital wards, was the primary reason for mortality difference.
Bottom line: A standardized order set for bacteremic sepsis was associated with increased compliance with evidence-based treatment and improved outcomes. Hospitalists should promptly treat bacteremic sepsis with appropriate fluid resuscitation and antibiotics.
Citation: Thiel SW, Asghar MF, Micek ST, Reichley RM, Doherty JA, Kollef MH. Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis. Crit Care Med. 2009;37(3):819-824.
Admission Day of the Week Predicts Mortality in Patients with Acute Pulmonary Embolus
Clinical question: Do weekend pulmonary embolus (PE) admissions have worse outcomes than weekday admissions?
Background: Studies of patients with acute cardiovascular diagnoses (e.g., stroke, cardiac arrest) have shown higher short-term mortality and longer length of stay (LOS) for weekend versus weekday admissions. PE diagnosis is complex, requiring timely testing and experienced staff who are sometimes unavailable on weekends. Optimal anticoagulation therapy also depends on provider skill.
Study design: Retrospective observational study.
Setting: 186 private Pennsylvania hospitals, January 2000 through November 2002.
Synopsis: Using the Pennsylvania Health Care Cost Containment Council database, the authors reviewed 15,531 records of patients with a primary or secondary PE diagnosis code. The primary outcome was all-cause mortality over 30 days; LOS was the secondary outcome.
Weekend admissions in the highest severity of illness risk class had higher 30-day mortality than weekday admissions. Weekend admissions were significantly more likely than weekday admissions to be clinically unstable and to have abnormal lab parameters. Adjusted for severity of illness risk class, overall mortality was 1.4% higher for weekend versus weekday admissions. All excess mortality came from the sickest group of patients. LOS did not differ.
Less-experienced caregivers or delayed diagnostic testing may play a role in poor outcomes. Patients admitted on weekends might receive delayed care from the first onset of symptoms. This is important because timely therapy has been shown to influence outcomes in acute PE. Reasons for these observed differences should be explored further to help provide more consistent PE management, regardless of admission day.
Bottom line: The sickest patients with PE admitted on weekends experienced small but significantly greater 30-day mortality compared with those admitted on weekdays.
Citation: Aujesky D, Jimenez D, Mor M, Geng M, Fine M, Ibrahim S. Weekend versus weekday admission and mortality after acute pulmonary embolism. Circulation. 2009;119:962-968. TH
In This Edition
Literature at a Glance: A guide to this month’s studies
- PPI use with clopidrogrel in ACS.
- Chlorhexidine sponge use reduces line infections.
- Extended thienopyridine use does not benefit DES patients.
- CABG is revascularization choice for severe CAD.
- Pre-treated CVC use reduces bloodstream infections.
- Hospitalist use grows in U.S.
- Sepsis order set improves outcomes.
- Admission day predicts acute PE mortality.
PEDIATRIC HM LITerature
Early Transition to Oral Therapy in Acute Osteomyelitis in Children Associated with Fewer Complications I By Mark Shen, MD
Clinical question: Can acute osteomyelitis in children be managed with early transition to oral antimicrobial therapy?
Background: Traditional treatment of acute osteomyelitis in children has involved prolonged intravenous antimicrobial therapy, typically greater than three to four weeks in duration. Small studies suggest the feasibility of a transition to prolonged oral therapy after an initial response to intravenous antimicrobial agents.
Study design: Retrospective, cohort study.
Setting: 29 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, 1,969 children were identified via ICD-9-CM codes as having been hospitalized with acute osteomyelitis—and without comorbid conditions—between January 2000 and June 2005. Rehospitalizations were reviewed for complications of both treatment failure and the treatment itself. More than half (1,021) of the children underwent central venous catheterization for prolonged intravenous (IV) therapy; 948 were assigned to the oral therapy group. No significant differences in treatment failure existed between the two groups (5% in the IV group; 4% in the oral group).
Overall, the clinical characteristics of the two groups were indistinguishable. Propensity score analysis was used to handle possible patient-level confounders; a validation study was performed to address misclassifications in assignment. No significant confounding effects were found.
Secondary findings included marked variation across hospitals in the use of oral therapy and increased treatment complications in the IV group. Although unmeasured factors not present in an administrative database may affect results, the strikingly similar groups and outcomes suggest the data are relevant.
Bottom line: Early transition to oral therapy for acute osteomyelitis in children does not increase treatment failure and is associated with fewer treatment complications.
Reference: Zaoutis T, Localio AR, Leckerman K, Saddlemire S, Bertoch D, Keren R. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics. 2009;123:636-642.
PPI Use with Clopidogrel in Acute Coronary Syndrome Is Associated with Readmissions and Mortality
Clinical question: Does concomitant use of clopidogrel and a proton pump inhibitor (PPI) following hospitalization for acute coronary syndrome (ACS) lead to adverse outcomes?
Background: Prophylactic PPIs often are prescribed with clopidogrel to reduce the risk of gastrointestinal bleeding. Mechanistic studies have shown that omeprazole decreases the platelet-inhibitory effect of clopidogrel, raising concerns that PPIs might interfere with clopidogrel’s beneficial effects. The clinical significance of this finding is unknown.
Study design: Retrospective cohort study.
Setting: 127 VA hospitals.
Synopsis: Investigators used data from the Cardiac Care Follow-up Clinical Study and VA pharmacy records to examine 8,205 male veterans who were hospitalized for ACS and treated with clopidogrel. Patients who filled prescriptions for both clopidogrel and a PPI were at significantly higher risk for death or readmission with ACS compared with those who filled prescriptions for clopidogrel only (adjusted odds ratio, 1.25; 95% confidence interval, 1.11-1.41). Patients who filled prescriptions for PPIs alone had similar risk for adverse events as those who took neither medication.
Subanalyses found similarly increased risk among patients prescribed omeprazole and rabeprazole, but those taking lanzoprazole and pantoprazole were not examined due to the small sample size. Although causality cannot be inferred from this observational study, and the risk associated with combined clopidigrel and PPI use appeared small, alternatives for gastric acid reduction exist. Thus, it may be prudent to restrict PPI use to patients who have a clear indication for their use until more definitive clinical trials can be conducted.
Bottom line: Among patients who are treated with clopidogrel for ACS, PPIs should be reserved for patients with a clear indication for gastric acid reduction and who cannot use alternative therapies.
Citation: Ho PM, Maddox TM, Wang L, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009;301(9):937-944.
Chlorhexidine-Impregnated Sponge Use Reduces Line Infections
Clinical question: Does dressing vascular catheters with chlorhexidine gluconate-impregnated sponges (CHGIS) reduce rates of catheter-related infections, and are dressing changes every seven days inferior to every three days?
Background: Process improvement strategies—including educating providers, strictly adhering to sterile technique, and promptly removing unnecessary catheters—greatly decrease catheter-related infections. It is unclear if CHGIS dressings offer additional benefit. Also uncertain is whether weekly dressing changes are as safe as changing dressings every three days.
Study design: A 2x2 factorial, assessor-blinded, randomized controlled trial.
Setting: ICUs in three university hospitals and two general hospitals in France.
Synopsis: 1,636 French adults expected to require arterial and central venous catheters for >48 hours were randomly assigned to one of four groups. Each group received either CHGIS dressings or standard dressings, and each group had dressing changes every three or seven days. Dressings were changed sooner if soiled or nonadherent. CHGIS dressings were associated with fewer catheter-related infections than standard dressings (0.6 vs. 1.4 infections per 1,000 catheter days; P=0.03). No significant difference in rates of catheter colonization existed between the three-day and seven-day dressing change strategies (10.4 vs. 11 events per 1,000 catheter days, P>0.05).
Although microbiology assessors were blinded to patients’ status, the ICU staff was not, potentially creating experimenter bias. Approximately 30% of the venous catheters and 40% of the arterial catheters were in a femoral site. Secondary analyses found higher rates of severe dermatitis among patients with CHGIS dressings but no difference in minimal bactericidal concentration (MBC) or colonizing organisms. Preliminary calculations suggested CHGIS dressings could be cost-effective.
Bottom line: Among critically ill adults, CHGIS catheter dressings may marginally reduce catheter-related infection rates, but further evaluation is needed before this technology can be adopted widely.
Citation: Timsit JF, Schwebel C, Bouadma L, et al. Chlorhexidine-impregnated sponges and less frequent dressing changes for prevention of catheter-related infections in critically-ill adults: a randomized controlled trial. JAMA. 2009;301(12):1231-1241.
Thienopyridine Use Six Months after Sirolimus-Eluting Stent Implant-ation Offers No Benefit
Clinical question: What are the relative contributions of aspirin and thienopyridine on preventing stent thrombosis in patients with sirolimus-eluting stents?
Background: There are no randomized clinical trials addressing the optimal duration, or the risks associated with discontinuation, of dual-antiplatelet therapy after drug-eluting stent (DES) implantation. Nevertheless, many patients continue to be maintained on dual-antiplatelet therapy beyond one year of their index DES implantation.
Study design: Prospective multicenter observational study.
Setting: Hospitals in Japan.
Synopsis: This study observed 10,778 Japanese patients undergoing sirolimus-eluting stent implantation. Patients discontinuing both thienopyridine and aspirin had a significantly higher rate of stent thrombosis than those who continued both medications for up to 18 months. However, discontinuation of thienopyridine alone was not associated with an excess risk of stent thrombosis. Additionally, a landmark analysis of patients who were free of events at six months showed rates of death for myocardial infarction (MI) at 24 months were 4.1% for patients taking thienopyridine and 4.1% for patients not taking thienopyridine (P=0.99). Ticlodipine was the thienopyridine used by more than 95% of patients.
Hospitalists should be aware that the role thienopyridine therapy plays in reducing stent thrombosis beyond one month after implantation has not been well addressed.
Bottom line: Discontinuation of thienopyridine therapy after six months while maintaining aspirin therapy is not associated with increased risk of stent thrombosis in patients with sirolimus-eluting stents.
Citation: Kimura T, Morimoto T, Nakagawa Y, et al. Antiplatelet therapy and stent thrombosis after sirolimus-eluting stent implantation. Circulation. 2009;119(7):987-995.
Compared with PCI, CABG Results in Lower Rates of Major Adverse Events in Severe CAD Patients
Clinical question: What is the optimal revascularization strategy for previously untreated severe coronary artery disease (CAD)?
Background: Coronary artery bypass grafting (CABG) is the treatment of choice in three-vessel and left-main CAD. However, percutaneous coronary intervention (PCI) with drug-eluting stents often is utilized despite the lack of adequately powered randomized trials.
Study design: Prospective multicenter randomized clinical trial.
Setting: 85 hospitals in Europe and the U.S.
Synopsis: 1,800 patients with an average age of 65 and previously untreated three-vessel or left-main CAD amenable to therapy with both PCI and CABG were randomized to CABG or PCI. The primary combined endpoint was a major adverse cardiac or cerebrovascular event, defined as death, stroke, MI, or repeat revascularization. PCI was associated with a significantly higher rate of major adverse cardiac or cerebrovascular events, due mostly to a higher rate of repeat revascularization (13.5% vs. 5.9%, P<0.001). At 12 months, the two groups had similar rates of death from any cause or MI, and similar rates of the combined endpoint of death from any cause, stroke, or MI; however, the rate of stroke was 1.6% higher in the CABG group.
Hospitalists should continue to favor CABG over PCI but give consideration to the risks involved with such an intervention.
Bottom line: CABG remains the revascularization choice in patients with severe CAD.
Citation: Serruys PW, Morice MC, Kappetein AP, et al. Percuta-neous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
Pre-Medicated Central Venous Catheters Reduce Risk of Catheter-Related Bloodstream Infections
Clinical question: Does pre-treating central venous catheters with anti-infective agents prevent catheter-related bloodstream infections?
Background: Use of central venous catheters (CVC) is associated with catheter-related bloodstream infection (CRBSI), with CRBSI-related mortality rates as high as 25%. Previous reviews have indicated that CVCs coated or impregnated with anti-infectives may reduce CRBSI incidence. This review integrates new trial data with information from prior reviews.
Study design: Meta-analysis of 27 randomized controlled trials.
Setting: Meta-analysis.
Synopsis: The authors report CVCs pre-treated with anti-infectives (AI-CVCs) are clinically effective in reducing the risk of CRBSI. The odds of having a CRBSI with a treated CVC versus an untreated CVC are 0.49 to 1 (95% CI, 0.37–0.64, 27 studies, fixed effects). The study also finds the use of AI-CVCs might provide a large cost savings in Great Britain. Because the findings are based on a meta-analysis, they are limited by the quality, context, and consistency of the original studies. The authors note that many of the studies had unsatisfactory descriptions of methodology. The current study is unable to separate the risk reduction attributable to AI-CVC versus that attributable to other infection control practices. Also, original data is insufficient to assess the benefits of AI-CVCs placed for longer than 12 days.
To summarize, AI-CVCs may present a means to reduce CRBSI, but more investigation of its role within infection control protocols is needed, as is investigation of longer duration of treatment.
Bottom line: Central venous catheters pre-treated with anti-infectives significantly reduce catheter-related bloodstream infections.
Citation: Hockenhull JC, Dwan KM, Smith GW, et al. The clinical effectiveness of central venous catheters treated with anti-infective agents in preventing catheter-related bloodstream infections: a systematic review. Crit Care Med. 2009;37(2):702-712.
Fivefold Increase in Hospitalists in the U.S. from 1995 to 2006
Clinical question: What is the growth rate of hospitalists and hospitalist-provided care?
Background: Survey data has shown a sharp increase in the number of hospitalists, but until now there have not been any national or population-based data on the growth of hospitalist care.
Study design: Descriptive analysis.
Setting: Medicare-enrolled patients.
Synopsis: The study is based on national Medicare data from 2.1 million admissions involving 990,785 patients in 5,800 hospitals and 120,226 general internists. It represents 5% of inpatient Medicare claims generated by general internists. The authors define “hospitalist” as a general internist who generates >90% of his or her claims from the care of hospitalized patients.
U.S. hospitals have seen substantial growth in hospitalists over the period examined. The nation saw a 500% increase in the number of general-internist hospitalists, and a 28% increase (to 37.1% in 2006 from 9.1% in 1995) in the number of Medicare patients who received care from a hospitalist. The odds that a hospitalized Medicare patient received care from a hospitalist increased 29.2% per year from 1997 to 2006. The percentage of hospitals with at least three hospitalists rose to 47.1% in 2006 from 11.6% in 1995.
This analysis might actually have underestimated HM’s growth. Analysis of Medicare claims does not identify pediatric hospitalists and hospitalists who work exclusively within HMOs. This analysis also did not include family practitioners or internal-medicine subspecialists who are hospitalists.
Bottom line: Medicare claims data confirm survey data findings: Hospitalists and hospitalist care has grown sharply over the last decade.
Citation: Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360:1102-1012.
Standardized Order Set for Bacteremic Sepsis Improves LOS and Mortality
Clinical question: Does a standardized order set for bacteremic sepsis impact patient management and outcomes?
Background: Prompt cardiovascular resuscitation and appropriate antibiotics decrease morbidity and mortality in bacteremic sepsis. This study examined whether hospitalwide, standardized sepsis order set improved management and outcomes.
Study design: Retrospective, before-and-after study design.
Setting: 1,200-bed academic medical center.
Synopsis: Two hundred patients with bacteremic severe sepsis were randomly selected from 18 months before the order set was introduced, and 200 were selected from 18 months after the order set was introduced. Primary outcomes measured were quantity of fluid administered and appropriate initial antibiotics. Secondary outcomes measured were hospital mortality and length of stay. Patients in the “after” group received more intravenous fluid (1627±1862 ml vs. 2054±2237 ml, P=.04), more appropriate antibiotics (53.0% vs. 65.5%, P=.01), had shorter hospital stays (28.7±30.1 days vs. 22.4±20.9 days, P=.02), and decreased in-house mortality (55.0% vs. 39.5%, P =<0.01).
The retrospective design of the study limited its ability to determine causal relationship. Extensive education may have contributed to the change (Hawthorne effect). Management in the ICU and ED, not the hospital wards, was the primary reason for mortality difference.
Bottom line: A standardized order set for bacteremic sepsis was associated with increased compliance with evidence-based treatment and improved outcomes. Hospitalists should promptly treat bacteremic sepsis with appropriate fluid resuscitation and antibiotics.
Citation: Thiel SW, Asghar MF, Micek ST, Reichley RM, Doherty JA, Kollef MH. Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis. Crit Care Med. 2009;37(3):819-824.
Admission Day of the Week Predicts Mortality in Patients with Acute Pulmonary Embolus
Clinical question: Do weekend pulmonary embolus (PE) admissions have worse outcomes than weekday admissions?
Background: Studies of patients with acute cardiovascular diagnoses (e.g., stroke, cardiac arrest) have shown higher short-term mortality and longer length of stay (LOS) for weekend versus weekday admissions. PE diagnosis is complex, requiring timely testing and experienced staff who are sometimes unavailable on weekends. Optimal anticoagulation therapy also depends on provider skill.
Study design: Retrospective observational study.
Setting: 186 private Pennsylvania hospitals, January 2000 through November 2002.
Synopsis: Using the Pennsylvania Health Care Cost Containment Council database, the authors reviewed 15,531 records of patients with a primary or secondary PE diagnosis code. The primary outcome was all-cause mortality over 30 days; LOS was the secondary outcome.
Weekend admissions in the highest severity of illness risk class had higher 30-day mortality than weekday admissions. Weekend admissions were significantly more likely than weekday admissions to be clinically unstable and to have abnormal lab parameters. Adjusted for severity of illness risk class, overall mortality was 1.4% higher for weekend versus weekday admissions. All excess mortality came from the sickest group of patients. LOS did not differ.
Less-experienced caregivers or delayed diagnostic testing may play a role in poor outcomes. Patients admitted on weekends might receive delayed care from the first onset of symptoms. This is important because timely therapy has been shown to influence outcomes in acute PE. Reasons for these observed differences should be explored further to help provide more consistent PE management, regardless of admission day.
Bottom line: The sickest patients with PE admitted on weekends experienced small but significantly greater 30-day mortality compared with those admitted on weekdays.
Citation: Aujesky D, Jimenez D, Mor M, Geng M, Fine M, Ibrahim S. Weekend versus weekday admission and mortality after acute pulmonary embolism. Circulation. 2009;119:962-968. TH
In This Edition
Literature at a Glance: A guide to this month’s studies
- PPI use with clopidrogrel in ACS.
- Chlorhexidine sponge use reduces line infections.
- Extended thienopyridine use does not benefit DES patients.
- CABG is revascularization choice for severe CAD.
- Pre-treated CVC use reduces bloodstream infections.
- Hospitalist use grows in U.S.
- Sepsis order set improves outcomes.
- Admission day predicts acute PE mortality.
PEDIATRIC HM LITerature
Early Transition to Oral Therapy in Acute Osteomyelitis in Children Associated with Fewer Complications I By Mark Shen, MD
Clinical question: Can acute osteomyelitis in children be managed with early transition to oral antimicrobial therapy?
Background: Traditional treatment of acute osteomyelitis in children has involved prolonged intravenous antimicrobial therapy, typically greater than three to four weeks in duration. Small studies suggest the feasibility of a transition to prolonged oral therapy after an initial response to intravenous antimicrobial agents.
Study design: Retrospective, cohort study.
Setting: 29 freestanding children’s hospitals.
Synopsis: Using the Pediatric Health Information System (PHIS) database, 1,969 children were identified via ICD-9-CM codes as having been hospitalized with acute osteomyelitis—and without comorbid conditions—between January 2000 and June 2005. Rehospitalizations were reviewed for complications of both treatment failure and the treatment itself. More than half (1,021) of the children underwent central venous catheterization for prolonged intravenous (IV) therapy; 948 were assigned to the oral therapy group. No significant differences in treatment failure existed between the two groups (5% in the IV group; 4% in the oral group).
Overall, the clinical characteristics of the two groups were indistinguishable. Propensity score analysis was used to handle possible patient-level confounders; a validation study was performed to address misclassifications in assignment. No significant confounding effects were found.
Secondary findings included marked variation across hospitals in the use of oral therapy and increased treatment complications in the IV group. Although unmeasured factors not present in an administrative database may affect results, the strikingly similar groups and outcomes suggest the data are relevant.
Bottom line: Early transition to oral therapy for acute osteomyelitis in children does not increase treatment failure and is associated with fewer treatment complications.
Reference: Zaoutis T, Localio AR, Leckerman K, Saddlemire S, Bertoch D, Keren R. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics. 2009;123:636-642.
PPI Use with Clopidogrel in Acute Coronary Syndrome Is Associated with Readmissions and Mortality
Clinical question: Does concomitant use of clopidogrel and a proton pump inhibitor (PPI) following hospitalization for acute coronary syndrome (ACS) lead to adverse outcomes?
Background: Prophylactic PPIs often are prescribed with clopidogrel to reduce the risk of gastrointestinal bleeding. Mechanistic studies have shown that omeprazole decreases the platelet-inhibitory effect of clopidogrel, raising concerns that PPIs might interfere with clopidogrel’s beneficial effects. The clinical significance of this finding is unknown.
Study design: Retrospective cohort study.
Setting: 127 VA hospitals.
Synopsis: Investigators used data from the Cardiac Care Follow-up Clinical Study and VA pharmacy records to examine 8,205 male veterans who were hospitalized for ACS and treated with clopidogrel. Patients who filled prescriptions for both clopidogrel and a PPI were at significantly higher risk for death or readmission with ACS compared with those who filled prescriptions for clopidogrel only (adjusted odds ratio, 1.25; 95% confidence interval, 1.11-1.41). Patients who filled prescriptions for PPIs alone had similar risk for adverse events as those who took neither medication.
Subanalyses found similarly increased risk among patients prescribed omeprazole and rabeprazole, but those taking lanzoprazole and pantoprazole were not examined due to the small sample size. Although causality cannot be inferred from this observational study, and the risk associated with combined clopidigrel and PPI use appeared small, alternatives for gastric acid reduction exist. Thus, it may be prudent to restrict PPI use to patients who have a clear indication for their use until more definitive clinical trials can be conducted.
Bottom line: Among patients who are treated with clopidogrel for ACS, PPIs should be reserved for patients with a clear indication for gastric acid reduction and who cannot use alternative therapies.
Citation: Ho PM, Maddox TM, Wang L, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009;301(9):937-944.
Chlorhexidine-Impregnated Sponge Use Reduces Line Infections
Clinical question: Does dressing vascular catheters with chlorhexidine gluconate-impregnated sponges (CHGIS) reduce rates of catheter-related infections, and are dressing changes every seven days inferior to every three days?
Background: Process improvement strategies—including educating providers, strictly adhering to sterile technique, and promptly removing unnecessary catheters—greatly decrease catheter-related infections. It is unclear if CHGIS dressings offer additional benefit. Also uncertain is whether weekly dressing changes are as safe as changing dressings every three days.
Study design: A 2x2 factorial, assessor-blinded, randomized controlled trial.
Setting: ICUs in three university hospitals and two general hospitals in France.
Synopsis: 1,636 French adults expected to require arterial and central venous catheters for >48 hours were randomly assigned to one of four groups. Each group received either CHGIS dressings or standard dressings, and each group had dressing changes every three or seven days. Dressings were changed sooner if soiled or nonadherent. CHGIS dressings were associated with fewer catheter-related infections than standard dressings (0.6 vs. 1.4 infections per 1,000 catheter days; P=0.03). No significant difference in rates of catheter colonization existed between the three-day and seven-day dressing change strategies (10.4 vs. 11 events per 1,000 catheter days, P>0.05).
Although microbiology assessors were blinded to patients’ status, the ICU staff was not, potentially creating experimenter bias. Approximately 30% of the venous catheters and 40% of the arterial catheters were in a femoral site. Secondary analyses found higher rates of severe dermatitis among patients with CHGIS dressings but no difference in minimal bactericidal concentration (MBC) or colonizing organisms. Preliminary calculations suggested CHGIS dressings could be cost-effective.
Bottom line: Among critically ill adults, CHGIS catheter dressings may marginally reduce catheter-related infection rates, but further evaluation is needed before this technology can be adopted widely.
Citation: Timsit JF, Schwebel C, Bouadma L, et al. Chlorhexidine-impregnated sponges and less frequent dressing changes for prevention of catheter-related infections in critically-ill adults: a randomized controlled trial. JAMA. 2009;301(12):1231-1241.
Thienopyridine Use Six Months after Sirolimus-Eluting Stent Implant-ation Offers No Benefit
Clinical question: What are the relative contributions of aspirin and thienopyridine on preventing stent thrombosis in patients with sirolimus-eluting stents?
Background: There are no randomized clinical trials addressing the optimal duration, or the risks associated with discontinuation, of dual-antiplatelet therapy after drug-eluting stent (DES) implantation. Nevertheless, many patients continue to be maintained on dual-antiplatelet therapy beyond one year of their index DES implantation.
Study design: Prospective multicenter observational study.
Setting: Hospitals in Japan.
Synopsis: This study observed 10,778 Japanese patients undergoing sirolimus-eluting stent implantation. Patients discontinuing both thienopyridine and aspirin had a significantly higher rate of stent thrombosis than those who continued both medications for up to 18 months. However, discontinuation of thienopyridine alone was not associated with an excess risk of stent thrombosis. Additionally, a landmark analysis of patients who were free of events at six months showed rates of death for myocardial infarction (MI) at 24 months were 4.1% for patients taking thienopyridine and 4.1% for patients not taking thienopyridine (P=0.99). Ticlodipine was the thienopyridine used by more than 95% of patients.
Hospitalists should be aware that the role thienopyridine therapy plays in reducing stent thrombosis beyond one month after implantation has not been well addressed.
Bottom line: Discontinuation of thienopyridine therapy after six months while maintaining aspirin therapy is not associated with increased risk of stent thrombosis in patients with sirolimus-eluting stents.
Citation: Kimura T, Morimoto T, Nakagawa Y, et al. Antiplatelet therapy and stent thrombosis after sirolimus-eluting stent implantation. Circulation. 2009;119(7):987-995.
Compared with PCI, CABG Results in Lower Rates of Major Adverse Events in Severe CAD Patients
Clinical question: What is the optimal revascularization strategy for previously untreated severe coronary artery disease (CAD)?
Background: Coronary artery bypass grafting (CABG) is the treatment of choice in three-vessel and left-main CAD. However, percutaneous coronary intervention (PCI) with drug-eluting stents often is utilized despite the lack of adequately powered randomized trials.
Study design: Prospective multicenter randomized clinical trial.
Setting: 85 hospitals in Europe and the U.S.
Synopsis: 1,800 patients with an average age of 65 and previously untreated three-vessel or left-main CAD amenable to therapy with both PCI and CABG were randomized to CABG or PCI. The primary combined endpoint was a major adverse cardiac or cerebrovascular event, defined as death, stroke, MI, or repeat revascularization. PCI was associated with a significantly higher rate of major adverse cardiac or cerebrovascular events, due mostly to a higher rate of repeat revascularization (13.5% vs. 5.9%, P<0.001). At 12 months, the two groups had similar rates of death from any cause or MI, and similar rates of the combined endpoint of death from any cause, stroke, or MI; however, the rate of stroke was 1.6% higher in the CABG group.
Hospitalists should continue to favor CABG over PCI but give consideration to the risks involved with such an intervention.
Bottom line: CABG remains the revascularization choice in patients with severe CAD.
Citation: Serruys PW, Morice MC, Kappetein AP, et al. Percuta-neous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972.
Pre-Medicated Central Venous Catheters Reduce Risk of Catheter-Related Bloodstream Infections
Clinical question: Does pre-treating central venous catheters with anti-infective agents prevent catheter-related bloodstream infections?
Background: Use of central venous catheters (CVC) is associated with catheter-related bloodstream infection (CRBSI), with CRBSI-related mortality rates as high as 25%. Previous reviews have indicated that CVCs coated or impregnated with anti-infectives may reduce CRBSI incidence. This review integrates new trial data with information from prior reviews.
Study design: Meta-analysis of 27 randomized controlled trials.
Setting: Meta-analysis.
Synopsis: The authors report CVCs pre-treated with anti-infectives (AI-CVCs) are clinically effective in reducing the risk of CRBSI. The odds of having a CRBSI with a treated CVC versus an untreated CVC are 0.49 to 1 (95% CI, 0.37–0.64, 27 studies, fixed effects). The study also finds the use of AI-CVCs might provide a large cost savings in Great Britain. Because the findings are based on a meta-analysis, they are limited by the quality, context, and consistency of the original studies. The authors note that many of the studies had unsatisfactory descriptions of methodology. The current study is unable to separate the risk reduction attributable to AI-CVC versus that attributable to other infection control practices. Also, original data is insufficient to assess the benefits of AI-CVCs placed for longer than 12 days.
To summarize, AI-CVCs may present a means to reduce CRBSI, but more investigation of its role within infection control protocols is needed, as is investigation of longer duration of treatment.
Bottom line: Central venous catheters pre-treated with anti-infectives significantly reduce catheter-related bloodstream infections.
Citation: Hockenhull JC, Dwan KM, Smith GW, et al. The clinical effectiveness of central venous catheters treated with anti-infective agents in preventing catheter-related bloodstream infections: a systematic review. Crit Care Med. 2009;37(2):702-712.
Fivefold Increase in Hospitalists in the U.S. from 1995 to 2006
Clinical question: What is the growth rate of hospitalists and hospitalist-provided care?
Background: Survey data has shown a sharp increase in the number of hospitalists, but until now there have not been any national or population-based data on the growth of hospitalist care.
Study design: Descriptive analysis.
Setting: Medicare-enrolled patients.
Synopsis: The study is based on national Medicare data from 2.1 million admissions involving 990,785 patients in 5,800 hospitals and 120,226 general internists. It represents 5% of inpatient Medicare claims generated by general internists. The authors define “hospitalist” as a general internist who generates >90% of his or her claims from the care of hospitalized patients.
U.S. hospitals have seen substantial growth in hospitalists over the period examined. The nation saw a 500% increase in the number of general-internist hospitalists, and a 28% increase (to 37.1% in 2006 from 9.1% in 1995) in the number of Medicare patients who received care from a hospitalist. The odds that a hospitalized Medicare patient received care from a hospitalist increased 29.2% per year from 1997 to 2006. The percentage of hospitals with at least three hospitalists rose to 47.1% in 2006 from 11.6% in 1995.
This analysis might actually have underestimated HM’s growth. Analysis of Medicare claims does not identify pediatric hospitalists and hospitalists who work exclusively within HMOs. This analysis also did not include family practitioners or internal-medicine subspecialists who are hospitalists.
Bottom line: Medicare claims data confirm survey data findings: Hospitalists and hospitalist care has grown sharply over the last decade.
Citation: Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360:1102-1012.
Standardized Order Set for Bacteremic Sepsis Improves LOS and Mortality
Clinical question: Does a standardized order set for bacteremic sepsis impact patient management and outcomes?
Background: Prompt cardiovascular resuscitation and appropriate antibiotics decrease morbidity and mortality in bacteremic sepsis. This study examined whether hospitalwide, standardized sepsis order set improved management and outcomes.
Study design: Retrospective, before-and-after study design.
Setting: 1,200-bed academic medical center.
Synopsis: Two hundred patients with bacteremic severe sepsis were randomly selected from 18 months before the order set was introduced, and 200 were selected from 18 months after the order set was introduced. Primary outcomes measured were quantity of fluid administered and appropriate initial antibiotics. Secondary outcomes measured were hospital mortality and length of stay. Patients in the “after” group received more intravenous fluid (1627±1862 ml vs. 2054±2237 ml, P=.04), more appropriate antibiotics (53.0% vs. 65.5%, P=.01), had shorter hospital stays (28.7±30.1 days vs. 22.4±20.9 days, P=.02), and decreased in-house mortality (55.0% vs. 39.5%, P =<0.01).
The retrospective design of the study limited its ability to determine causal relationship. Extensive education may have contributed to the change (Hawthorne effect). Management in the ICU and ED, not the hospital wards, was the primary reason for mortality difference.
Bottom line: A standardized order set for bacteremic sepsis was associated with increased compliance with evidence-based treatment and improved outcomes. Hospitalists should promptly treat bacteremic sepsis with appropriate fluid resuscitation and antibiotics.
Citation: Thiel SW, Asghar MF, Micek ST, Reichley RM, Doherty JA, Kollef MH. Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis. Crit Care Med. 2009;37(3):819-824.
Admission Day of the Week Predicts Mortality in Patients with Acute Pulmonary Embolus
Clinical question: Do weekend pulmonary embolus (PE) admissions have worse outcomes than weekday admissions?
Background: Studies of patients with acute cardiovascular diagnoses (e.g., stroke, cardiac arrest) have shown higher short-term mortality and longer length of stay (LOS) for weekend versus weekday admissions. PE diagnosis is complex, requiring timely testing and experienced staff who are sometimes unavailable on weekends. Optimal anticoagulation therapy also depends on provider skill.
Study design: Retrospective observational study.
Setting: 186 private Pennsylvania hospitals, January 2000 through November 2002.
Synopsis: Using the Pennsylvania Health Care Cost Containment Council database, the authors reviewed 15,531 records of patients with a primary or secondary PE diagnosis code. The primary outcome was all-cause mortality over 30 days; LOS was the secondary outcome.
Weekend admissions in the highest severity of illness risk class had higher 30-day mortality than weekday admissions. Weekend admissions were significantly more likely than weekday admissions to be clinically unstable and to have abnormal lab parameters. Adjusted for severity of illness risk class, overall mortality was 1.4% higher for weekend versus weekday admissions. All excess mortality came from the sickest group of patients. LOS did not differ.
Less-experienced caregivers or delayed diagnostic testing may play a role in poor outcomes. Patients admitted on weekends might receive delayed care from the first onset of symptoms. This is important because timely therapy has been shown to influence outcomes in acute PE. Reasons for these observed differences should be explored further to help provide more consistent PE management, regardless of admission day.
Bottom line: The sickest patients with PE admitted on weekends experienced small but significantly greater 30-day mortality compared with those admitted on weekdays.
Citation: Aujesky D, Jimenez D, Mor M, Geng M, Fine M, Ibrahim S. Weekend versus weekday admission and mortality after acute pulmonary embolism. Circulation. 2009;119:962-968. TH
Healthcare Trailblazers
Younger generations blaze new paths through the American economy. Fifteen years ago, Generation X was fresh out of college and flush with the unimagined potential of the Internet. They helped change the way the world shared information and conducted business. The impact of such innovation and enthusiasm for new technology is still felt today.
The healthcare sector possesses pioneers of its own, many with the same kind of drive and vision as the dot-com entrepreneurs of the 1990s. Fifteen years from now, today’s young hospitalists—shaped by ever-changing demands and healthcare hurdles—will be recognized as an authority in the new ways patient care is delivered.
—Brian Markoff, MD, FHM, associate professor of medicine, Mount Sinai Hospitalist Group, New York City
Bijo Chacko, MD, FHM, former chair of SHM’s Young Physicians Committee, sees energy in the newest generation of hospitalists. He also sees great potential from residents who are finishing their training and considering their job options. Until recently, SHM’s Young Physicians Committee operated as a task force. The group’s growth and increased young-physician representation throughout the society prompted SHM leadership to promote the task force to full committee status.
“The wonderful thing is that we have received lots of input from around the country and dramatically increased membership in the past few years,” says Dr. Chacko, hospital medicine medical director for Preferred Health Partners in New York City. “We have moved from simply gathering information about young physicians in hospital medicine to actively disseminating it, including the new Resident’s Corner [department in The Hospitalist]. It addresses the needs of residents and introduces them to the nuances and specifics of hospital medicine.”
The demand for information has spurred the launch of a young physicians section (www.hospitalmedicine.org/youngdoctor) on SHM’s Web site. Combined with SHM’s online career center (www.hospitalmedicine.org/careercenter), the new microsites provide young physicians a broad range of information about the specialty and—most importantly—HM career options.
Natural Progression
Four out of five large hospitals now use hospitalists, and as more hospitals implement HM programs, more residents will be exposed to the hospitalist model of care. For residents, the allure of an HM career is broad and deep. In many ways, HM is the logical extension of residency training. Brian Markoff, MD, FHM, a hospitalist and associate professor of medicine at Mount Sinai Hospitalist Group in New York City, was a chief resident when he founded the hospitalist program at the University of California at Davis Health System in Sacramento in 1998.
“Creating the hospitalist program at UC-Davis was pretty easy,” Dr. Markoff says. “All of the program’s founders were chief residents at the time. The people involved were warm to the idea, and we could teach without being in the fellowship program. Residents are already very comfortable treating patients in the hospital setting.”
Dr. Markoff says practicing hospitalists are a positive influence on residents who are still undecided on a career path. “If you’re a good role model, they’ll be interested in hospital medicine,” he says.
Diversity of Patients, Issues, Settings
Dr. Markoff and others caution that HM encompasses more than an expansion of a resident’s standard roles and responsibilities. “We’re not just super-residents,” he says. “We’re highly trained specialists in the care of hospitalized patients and the process of making care in hospital better.”
Medical conditions, patient issues, and administrative situations that often are outside a resident’s scope quickly come into focus for a new hospitalist. When Mona Patel, DO, associate director of hospitalist services at Staten Island University Hospital in New York, chose an HM career five years ago, the diversity in opportunities was a major draw. Like many hospitalists, she knew she would enjoy the type of care she provides to patients.
“I liked the acuity of the patients and disease processes; it was much more interesting and exciting for me than ongoing outpatient care of chronic diseases,” Dr. Patel says. “I liked the interaction with the hospital house staff and lots of consultants. If I had questions about a patient, I could easily consult with a specialist within the hospital.”
In addition to providing bedside care, new hospitalists often find themselves at the forefront of a monumental change in how healthcare is provided nationwide. Quality improvement (QI) initiatives, such as reducing preventable diseases in the hospital and reducing readmission rates, attracted Bryan Huang, MD, to hospital medicine at the University of California at San Diego.
“When I interviewed at UCSD, I was very interested in quality improvement,” says Dr. Huang, an assistant clinical professor at UCSD’s Division of Hospital Medicine. “UCSD is well known for glycemic control and VTE prophylaxis. We’re now working on quality improvement for treating delirium and hospital discharge.”
His experience as an academic hospitalist has opened up the QI world to him. “Before this job, I was almost not familiar at all with quality improvement,” Dr. Huang says. “As a resident, I did some quality-improvement work, but not much. Quality improvement was missing from residency training, but it’s getting better.”
Dr. Patel says HM’s biggest selling point is the variety of settings available to a new hospitalist. She’s been working for the past two years in an academic hospital program in a community hospital setting with 20 hospitalists. Before that, she worked in private practice as a hospitalist. Now, when she talks with residents, she talks about their options.
“It’s really important that you figure out what kind of setting you want,” Dr. Patel says. “Hospital medicine has a diversity of settings, from a small community hospital where you do a broad range of inpatient care to a larger academic teaching environment or a private practice group.”
Leadership Opportunities
The continuing demand for hospitalists affords young physicians who are considering an HM career additional freedom in the job market. In comparison to more traditional primary-care models, hospitalist jobs offer flexible hours and competitive salaries.
Dr. Chacko points to another benefit that is a direct result of the high demand for hospitalists: increased opportunities to launch management careers. The average age of a hospitalist is 37 and the average age of an HM group leader is 41, according to SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.
“That’s not that much of a difference,” Dr. Chacko says. “Early-career hospitalists find ample leadership opportunities in the specialty. There are lots of opportunities for young hospitalists.”
How to Get Started
Because most teaching hospitals have hospitalists, most residents are exposed to HM. Many hospitalists relish the opportunity to mentor and provide early-career counseling. “Sometimes, a resident will ask to grab coffee and learn more about hospital medicine,” Dr. Huang says. “I tell them what my job is like. Many ask, ‘How do I get started looking for a job?’ I tell them that connections really help. Word of mouth is very important, so I refer people to other people.”
Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco’s division of hospital medicine and a founding member of the Young Physicians Committee, recommends that residents begin with a vision and work backward. “On a broad level, if you’re a resident, you should think about where you want to be in five years,” she says. “Look around your hospital and find a few people whose job you want.”
For some young physicians, looking ahead five years could mean being part of the healthcare revolution of tomorrow. TH
Brendon Shank is a freelance writer based in Philadelphia.
Longtime leader takes SHM helm

New SHM President Scott A. Flanders, MD, FHM, has been part of HM since the beginning. Now, he’s leading the movement.
“Scott has been a major force in shaping the hospital medicine specialty into what it is today,” says Larry Wellikson, MD, FHM, CEO of SHM. “It’s only fitting that he guide our organization and its members through this time of explosive growth and unprecedented change within the healthcare sector.”
Dr. Flanders is recognized as a leader in HM’s academic community. He is professor and director of the hospitalist program at the University of Michigan in Ann Arbor. His HM resume includes dozens of peer-reviewed research articles and presentations. He has devoted countless hours of his time to SHM as a board member, committee member, editor, and leadership track faculty. “He has already been a positive influence on hundreds of practicing hospitalists in the last decade,” Dr. Wellikson says. “We look forward to helping him expand that influence as president.”
Scott A. Flanders, MD, FHM
- SHM member since 1996
- Associate professor of medicine on the clinical track, University of Michigan
- Associate division chief of general medicine for inpatient programs
- Director of the hospitalist program at the University of Michigan
- Associate director of inpatient programs, Department of Medicine, University of Michigan
- Attending physician, University of Michigan Hospitals
- Member, SHM Board of Directors
- Faculty, SHM 2006 Leadership Academy
- Deputy editor, Journal of Hospital Medicine
- Former editor, The Hospitalist
SHM elects board members
SHM has elected three new members to its Board of Directors and re-elected two members. Board members are nominated and elected by the membership and serve a three-year term.The newly elected members of the board are:



Re-elected board members:


Younger generations blaze new paths through the American economy. Fifteen years ago, Generation X was fresh out of college and flush with the unimagined potential of the Internet. They helped change the way the world shared information and conducted business. The impact of such innovation and enthusiasm for new technology is still felt today.
The healthcare sector possesses pioneers of its own, many with the same kind of drive and vision as the dot-com entrepreneurs of the 1990s. Fifteen years from now, today’s young hospitalists—shaped by ever-changing demands and healthcare hurdles—will be recognized as an authority in the new ways patient care is delivered.
—Brian Markoff, MD, FHM, associate professor of medicine, Mount Sinai Hospitalist Group, New York City
Bijo Chacko, MD, FHM, former chair of SHM’s Young Physicians Committee, sees energy in the newest generation of hospitalists. He also sees great potential from residents who are finishing their training and considering their job options. Until recently, SHM’s Young Physicians Committee operated as a task force. The group’s growth and increased young-physician representation throughout the society prompted SHM leadership to promote the task force to full committee status.
“The wonderful thing is that we have received lots of input from around the country and dramatically increased membership in the past few years,” says Dr. Chacko, hospital medicine medical director for Preferred Health Partners in New York City. “We have moved from simply gathering information about young physicians in hospital medicine to actively disseminating it, including the new Resident’s Corner [department in The Hospitalist]. It addresses the needs of residents and introduces them to the nuances and specifics of hospital medicine.”
The demand for information has spurred the launch of a young physicians section (www.hospitalmedicine.org/youngdoctor) on SHM’s Web site. Combined with SHM’s online career center (www.hospitalmedicine.org/careercenter), the new microsites provide young physicians a broad range of information about the specialty and—most importantly—HM career options.
Natural Progression
Four out of five large hospitals now use hospitalists, and as more hospitals implement HM programs, more residents will be exposed to the hospitalist model of care. For residents, the allure of an HM career is broad and deep. In many ways, HM is the logical extension of residency training. Brian Markoff, MD, FHM, a hospitalist and associate professor of medicine at Mount Sinai Hospitalist Group in New York City, was a chief resident when he founded the hospitalist program at the University of California at Davis Health System in Sacramento in 1998.
“Creating the hospitalist program at UC-Davis was pretty easy,” Dr. Markoff says. “All of the program’s founders were chief residents at the time. The people involved were warm to the idea, and we could teach without being in the fellowship program. Residents are already very comfortable treating patients in the hospital setting.”
Dr. Markoff says practicing hospitalists are a positive influence on residents who are still undecided on a career path. “If you’re a good role model, they’ll be interested in hospital medicine,” he says.
Diversity of Patients, Issues, Settings
Dr. Markoff and others caution that HM encompasses more than an expansion of a resident’s standard roles and responsibilities. “We’re not just super-residents,” he says. “We’re highly trained specialists in the care of hospitalized patients and the process of making care in hospital better.”
Medical conditions, patient issues, and administrative situations that often are outside a resident’s scope quickly come into focus for a new hospitalist. When Mona Patel, DO, associate director of hospitalist services at Staten Island University Hospital in New York, chose an HM career five years ago, the diversity in opportunities was a major draw. Like many hospitalists, she knew she would enjoy the type of care she provides to patients.
“I liked the acuity of the patients and disease processes; it was much more interesting and exciting for me than ongoing outpatient care of chronic diseases,” Dr. Patel says. “I liked the interaction with the hospital house staff and lots of consultants. If I had questions about a patient, I could easily consult with a specialist within the hospital.”
In addition to providing bedside care, new hospitalists often find themselves at the forefront of a monumental change in how healthcare is provided nationwide. Quality improvement (QI) initiatives, such as reducing preventable diseases in the hospital and reducing readmission rates, attracted Bryan Huang, MD, to hospital medicine at the University of California at San Diego.
“When I interviewed at UCSD, I was very interested in quality improvement,” says Dr. Huang, an assistant clinical professor at UCSD’s Division of Hospital Medicine. “UCSD is well known for glycemic control and VTE prophylaxis. We’re now working on quality improvement for treating delirium and hospital discharge.”
His experience as an academic hospitalist has opened up the QI world to him. “Before this job, I was almost not familiar at all with quality improvement,” Dr. Huang says. “As a resident, I did some quality-improvement work, but not much. Quality improvement was missing from residency training, but it’s getting better.”
Dr. Patel says HM’s biggest selling point is the variety of settings available to a new hospitalist. She’s been working for the past two years in an academic hospital program in a community hospital setting with 20 hospitalists. Before that, she worked in private practice as a hospitalist. Now, when she talks with residents, she talks about their options.
“It’s really important that you figure out what kind of setting you want,” Dr. Patel says. “Hospital medicine has a diversity of settings, from a small community hospital where you do a broad range of inpatient care to a larger academic teaching environment or a private practice group.”
Leadership Opportunities
The continuing demand for hospitalists affords young physicians who are considering an HM career additional freedom in the job market. In comparison to more traditional primary-care models, hospitalist jobs offer flexible hours and competitive salaries.
Dr. Chacko points to another benefit that is a direct result of the high demand for hospitalists: increased opportunities to launch management careers. The average age of a hospitalist is 37 and the average age of an HM group leader is 41, according to SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.
“That’s not that much of a difference,” Dr. Chacko says. “Early-career hospitalists find ample leadership opportunities in the specialty. There are lots of opportunities for young hospitalists.”
How to Get Started
Because most teaching hospitals have hospitalists, most residents are exposed to HM. Many hospitalists relish the opportunity to mentor and provide early-career counseling. “Sometimes, a resident will ask to grab coffee and learn more about hospital medicine,” Dr. Huang says. “I tell them what my job is like. Many ask, ‘How do I get started looking for a job?’ I tell them that connections really help. Word of mouth is very important, so I refer people to other people.”
Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco’s division of hospital medicine and a founding member of the Young Physicians Committee, recommends that residents begin with a vision and work backward. “On a broad level, if you’re a resident, you should think about where you want to be in five years,” she says. “Look around your hospital and find a few people whose job you want.”
For some young physicians, looking ahead five years could mean being part of the healthcare revolution of tomorrow. TH
Brendon Shank is a freelance writer based in Philadelphia.
Longtime leader takes SHM helm
New SHM President Scott A. Flanders, MD, FHM, has been part of HM since the beginning. Now, he’s leading the movement.
“Scott has been a major force in shaping the hospital medicine specialty into what it is today,” says Larry Wellikson, MD, FHM, CEO of SHM. “It’s only fitting that he guide our organization and its members through this time of explosive growth and unprecedented change within the healthcare sector.”
Dr. Flanders is recognized as a leader in HM’s academic community. He is professor and director of the hospitalist program at the University of Michigan in Ann Arbor. His HM resume includes dozens of peer-reviewed research articles and presentations. He has devoted countless hours of his time to SHM as a board member, committee member, editor, and leadership track faculty. “He has already been a positive influence on hundreds of practicing hospitalists in the last decade,” Dr. Wellikson says. “We look forward to helping him expand that influence as president.”
Scott A. Flanders, MD, FHM
- SHM member since 1996
- Associate professor of medicine on the clinical track, University of Michigan
- Associate division chief of general medicine for inpatient programs
- Director of the hospitalist program at the University of Michigan
- Associate director of inpatient programs, Department of Medicine, University of Michigan
- Attending physician, University of Michigan Hospitals
- Member, SHM Board of Directors
- Faculty, SHM 2006 Leadership Academy
- Deputy editor, Journal of Hospital Medicine
- Former editor, The Hospitalist
SHM elects board members
SHM has elected three new members to its Board of Directors and re-elected two members. Board members are nominated and elected by the membership and serve a three-year term.The newly elected members of the board are:
Re-elected board members:
Younger generations blaze new paths through the American economy. Fifteen years ago, Generation X was fresh out of college and flush with the unimagined potential of the Internet. They helped change the way the world shared information and conducted business. The impact of such innovation and enthusiasm for new technology is still felt today.
The healthcare sector possesses pioneers of its own, many with the same kind of drive and vision as the dot-com entrepreneurs of the 1990s. Fifteen years from now, today’s young hospitalists—shaped by ever-changing demands and healthcare hurdles—will be recognized as an authority in the new ways patient care is delivered.
—Brian Markoff, MD, FHM, associate professor of medicine, Mount Sinai Hospitalist Group, New York City
Bijo Chacko, MD, FHM, former chair of SHM’s Young Physicians Committee, sees energy in the newest generation of hospitalists. He also sees great potential from residents who are finishing their training and considering their job options. Until recently, SHM’s Young Physicians Committee operated as a task force. The group’s growth and increased young-physician representation throughout the society prompted SHM leadership to promote the task force to full committee status.
“The wonderful thing is that we have received lots of input from around the country and dramatically increased membership in the past few years,” says Dr. Chacko, hospital medicine medical director for Preferred Health Partners in New York City. “We have moved from simply gathering information about young physicians in hospital medicine to actively disseminating it, including the new Resident’s Corner [department in The Hospitalist]. It addresses the needs of residents and introduces them to the nuances and specifics of hospital medicine.”
The demand for information has spurred the launch of a young physicians section (www.hospitalmedicine.org/youngdoctor) on SHM’s Web site. Combined with SHM’s online career center (www.hospitalmedicine.org/careercenter), the new microsites provide young physicians a broad range of information about the specialty and—most importantly—HM career options.
Natural Progression
Four out of five large hospitals now use hospitalists, and as more hospitals implement HM programs, more residents will be exposed to the hospitalist model of care. For residents, the allure of an HM career is broad and deep. In many ways, HM is the logical extension of residency training. Brian Markoff, MD, FHM, a hospitalist and associate professor of medicine at Mount Sinai Hospitalist Group in New York City, was a chief resident when he founded the hospitalist program at the University of California at Davis Health System in Sacramento in 1998.
“Creating the hospitalist program at UC-Davis was pretty easy,” Dr. Markoff says. “All of the program’s founders were chief residents at the time. The people involved were warm to the idea, and we could teach without being in the fellowship program. Residents are already very comfortable treating patients in the hospital setting.”
Dr. Markoff says practicing hospitalists are a positive influence on residents who are still undecided on a career path. “If you’re a good role model, they’ll be interested in hospital medicine,” he says.
Diversity of Patients, Issues, Settings
Dr. Markoff and others caution that HM encompasses more than an expansion of a resident’s standard roles and responsibilities. “We’re not just super-residents,” he says. “We’re highly trained specialists in the care of hospitalized patients and the process of making care in hospital better.”
Medical conditions, patient issues, and administrative situations that often are outside a resident’s scope quickly come into focus for a new hospitalist. When Mona Patel, DO, associate director of hospitalist services at Staten Island University Hospital in New York, chose an HM career five years ago, the diversity in opportunities was a major draw. Like many hospitalists, she knew she would enjoy the type of care she provides to patients.
“I liked the acuity of the patients and disease processes; it was much more interesting and exciting for me than ongoing outpatient care of chronic diseases,” Dr. Patel says. “I liked the interaction with the hospital house staff and lots of consultants. If I had questions about a patient, I could easily consult with a specialist within the hospital.”
In addition to providing bedside care, new hospitalists often find themselves at the forefront of a monumental change in how healthcare is provided nationwide. Quality improvement (QI) initiatives, such as reducing preventable diseases in the hospital and reducing readmission rates, attracted Bryan Huang, MD, to hospital medicine at the University of California at San Diego.
“When I interviewed at UCSD, I was very interested in quality improvement,” says Dr. Huang, an assistant clinical professor at UCSD’s Division of Hospital Medicine. “UCSD is well known for glycemic control and VTE prophylaxis. We’re now working on quality improvement for treating delirium and hospital discharge.”
His experience as an academic hospitalist has opened up the QI world to him. “Before this job, I was almost not familiar at all with quality improvement,” Dr. Huang says. “As a resident, I did some quality-improvement work, but not much. Quality improvement was missing from residency training, but it’s getting better.”
Dr. Patel says HM’s biggest selling point is the variety of settings available to a new hospitalist. She’s been working for the past two years in an academic hospital program in a community hospital setting with 20 hospitalists. Before that, she worked in private practice as a hospitalist. Now, when she talks with residents, she talks about their options.
“It’s really important that you figure out what kind of setting you want,” Dr. Patel says. “Hospital medicine has a diversity of settings, from a small community hospital where you do a broad range of inpatient care to a larger academic teaching environment or a private practice group.”
Leadership Opportunities
The continuing demand for hospitalists affords young physicians who are considering an HM career additional freedom in the job market. In comparison to more traditional primary-care models, hospitalist jobs offer flexible hours and competitive salaries.
Dr. Chacko points to another benefit that is a direct result of the high demand for hospitalists: increased opportunities to launch management careers. The average age of a hospitalist is 37 and the average age of an HM group leader is 41, according to SHM’s 2007-2008 Bi-Annual Survey on the State of the Hospital Medicine Movement.
“That’s not that much of a difference,” Dr. Chacko says. “Early-career hospitalists find ample leadership opportunities in the specialty. There are lots of opportunities for young hospitalists.”
How to Get Started
Because most teaching hospitals have hospitalists, most residents are exposed to HM. Many hospitalists relish the opportunity to mentor and provide early-career counseling. “Sometimes, a resident will ask to grab coffee and learn more about hospital medicine,” Dr. Huang says. “I tell them what my job is like. Many ask, ‘How do I get started looking for a job?’ I tell them that connections really help. Word of mouth is very important, so I refer people to other people.”
Margaret Fang, MD, MPH, FHM, assistant professor of medicine at the University of California at San Francisco’s division of hospital medicine and a founding member of the Young Physicians Committee, recommends that residents begin with a vision and work backward. “On a broad level, if you’re a resident, you should think about where you want to be in five years,” she says. “Look around your hospital and find a few people whose job you want.”
For some young physicians, looking ahead five years could mean being part of the healthcare revolution of tomorrow. TH
Brendon Shank is a freelance writer based in Philadelphia.
Longtime leader takes SHM helm
New SHM President Scott A. Flanders, MD, FHM, has been part of HM since the beginning. Now, he’s leading the movement.
“Scott has been a major force in shaping the hospital medicine specialty into what it is today,” says Larry Wellikson, MD, FHM, CEO of SHM. “It’s only fitting that he guide our organization and its members through this time of explosive growth and unprecedented change within the healthcare sector.”
Dr. Flanders is recognized as a leader in HM’s academic community. He is professor and director of the hospitalist program at the University of Michigan in Ann Arbor. His HM resume includes dozens of peer-reviewed research articles and presentations. He has devoted countless hours of his time to SHM as a board member, committee member, editor, and leadership track faculty. “He has already been a positive influence on hundreds of practicing hospitalists in the last decade,” Dr. Wellikson says. “We look forward to helping him expand that influence as president.”
Scott A. Flanders, MD, FHM
- SHM member since 1996
- Associate professor of medicine on the clinical track, University of Michigan
- Associate division chief of general medicine for inpatient programs
- Director of the hospitalist program at the University of Michigan
- Associate director of inpatient programs, Department of Medicine, University of Michigan
- Attending physician, University of Michigan Hospitals
- Member, SHM Board of Directors
- Faculty, SHM 2006 Leadership Academy
- Deputy editor, Journal of Hospital Medicine
- Former editor, The Hospitalist
SHM elects board members
SHM has elected three new members to its Board of Directors and re-elected two members. Board members are nominated and elected by the membership and serve a three-year term.The newly elected members of the board are:
Re-elected board members:
Use Metrics to Identify Documentation and Coding Errors

Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I can remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. Determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the current as well as previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with others in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH
Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I can remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. Determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the current as well as previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with others in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH
Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I can remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. Determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the current as well as previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with others in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH
Uniquely Positioned
How can a family physician with a demanding clinical schedule juggle patient care with the grueling administrative and travel duties required of the president-elect of the American Academy of Family Physicians (AAFP)? Lori Heim, MD, FAAFP, found the perfect compromise: Give up the family practice and become a hospitalist.
She did so last November, soon after AAFP members voted her the next president of one of the nation’s largest medical organizations. In fact, she is the only hospitalist at 104-bed Scotland Memorial Hospital in Laurinburg, N.C.
“I was looking for an opportunity while I was working as president-elect and then president of the academy,” says Dr. Heim, who takes over as president of the 94,000-member AAFP in October. “Because of the heavy travel demands, it was not possible to keep my old practice.”
Although the career swap is borne of professional necessity, Dr. Heim says her transition to HM practice has been relatively easy. “I love it. [The new job] utilizes my prior training and skills,” she says. “In private practice, I was doing rounds on my own patients, then I would have to run to the office to see my other patients. I could see the advantages of using the hospitalist services. … Now, here I am on this side.”
An active AAFP member for nearly 25 years, Dr. Heim brings a unique confluence of medical training and experience to her new role. She has firsthand knowledge of the key issues intersecting primary care and hospital-based practice—care coordination, physician reimbursement, and quality improvement. She also acknowledges that walls need to be broken down when it comes to family physicians (FP) transitioning to HM careers. More complete training and improvement in hospital administrations’ understanding of an FP’s clinical capabilities will advance their entrance into hospitalist careers.

“I think it could become a large trend because of the financial constraints on family care,” Dr. Heim says, also noting the lifestyle benefits of an HM career. “FPs often cannot do both inpatient and outpatient care. Your productivity, if you are in the clinic, must make a tradeoff between rounds and office hours—and how late at night do I want to be doing rounds?”
Bumpy Road to HM
The transition from family practice to HM is working out well for Heim, but it wasn’t as smooth as one might expect for a decorated career physician.
The daughter of a military pilot, Dr. Heim earned her bachelor’s degree with honors from Portland State University and her medical degree at the Uniformed Services University of Health Sciences in Bethesda, Md. Following her residency at Andrews Air Force Base in Maryland and a fellowship in faculty development and research at the University of North Carolina at Chapel Hill, her military medical career resembled a spiral staircase. She went from staff physician to clinic chief to residency director to chief of medical staff, with a few stops in between. After 25 years of military service, she retired as an Air Force colonel and opened a private practice.
Even with decades of training and patient care under her belt, Dr. Heim wasn’t rubber-stamped into a hospitalist position. It’s an issue she hopes to address as part of her AAFP tenure. “I know of hospitals where family physicians can admit and treat their patients but not be considered for a hospitalist position. It happened to me,” she explains. “I went and found a hospital that would use my skills.”

Hospitalist Robert Harrington, MD, FHM, knows the feeling. He had a more traditional primary-care practice before entering a HM career, and he understands the intense financial and workload pressures of family practice. Now the vice president of medical affairs for Alpharetta, Ga.-based IN Compass Health Inc. and chair of SHM’s Family Medicine Task Force, he says “there are barriers to hiring because of the wide variability in family physician training.” The root of the problem is that residents in some programs get less hospital time and experience with HM-patient encounters. “In opposed programs, they compete with other specialties and get less time,” Dr. Harrington says. “In unopposed programs, they tend to get more hospital experience and more rotations in inpatient services. Those folks can transition with little to no difficulty to hospital medicine.”
SHM President Scott Flanders, MD, FHM, associate professor and director of the hospitalist program at the University of Michigan in Ann Arbor, sees great value in what FPs can bring to HM. He wants HM to be open to those interested in a career change; however, he agrees physician training and experience can be an obstacle in the recruitment process. “The training in internal medicine is more geared to hospital medicine than it is in family practice [training],” Dr. Flanders says. “FPs must make sure they have hospital training, including the ICU. Many FP programs may not have this.” He also says FPs looking at an HM career—and internists as well—need to be “up to speed” in systems-based practice.

—Lori Heim, MD, FAAFP, Scotland Memorial Hospital, Laurinburg, N.C., AAFP president-elect
Although they represent a small part of SHM’s membership, Dr. Harrington and his task force want FPs to have “representation and a voice” in the society. “They are a small but growing minority,” he says. “Four or five percent of hospitalists are family-medicine-trained by our membership rolls, but we believe it is a bigger number, as some may not be members of SHM. … We run into more problems with hospital administrators. Some of them insist on IM-trained physicians, and there just aren’t enough IMs out there.”
It’s a C-suite roadblock Dr. Heim is familiar with. “Sometimes there is a parochial view in using internists above family physicians. Why should family doctors be second? It’s a misunderstanding of the experience and what family physicians bring to the table,” she says. “They haven’t done it, so people don’t think they can. Some hospitals are underutilizing family physicians in a hospitalist role. If a physician has hospital privileges, there is no reason they should not be considered to be hired as a hospitalist.”
Tenure of Change
As AAFP president, Dr. Heim says she’ll work to improve working conditions for FPs and fight for her constituents’ rights as Washington debates national healthcare reform. The AAFP and SHM share a number of policy interests, including reimbursement reform, new technologies, and patient-safety initiatives.
“I would like to do more with the various societies to increase opportunities for family medicine,” Dr. Heim says. “In some ways, primary care is being squeezed all around. How are you going to increase the numbers of FPs when they earn less? You are not going to unless you reform the system.”
Another top priority is advancing the idea of a national network of electronic health records (EHRs). Dr. Heim says a linked EHR system would improve communication and handoffs, and help physicians limit medical errors. “That’s the key,” she says. “Until then, it is going to be a hodgepodge of solutions. As long as it requires multiple steps, there will always be slipups.
“When I was in the military, records were kept electronically, and I learned the value of having continuity of electronic records.”
Dr. Heim says she would like to partner with hospital-based physicians on QI projects. “Any doctor, it doesn’t matter who you are, has a role to play in quality improvement, either in procedures to improve outcomes in the operating room or ICU or ED. We all have a role in that,” she says. “That is one of the reasons we have supported comparative effectiveness research. Guidelines are valuable.”
As AAFP president, Dr. Heim says she won’t forget her family physician roots. Her platform is ambitious: Reform both the practice and the payment of healthcare in this country. “I think the country recognizes that the current way of paying for healthcare—built on volume and procedures rather than patient outcome—has resulted in a fragmented and disjointed process,” she says. “It’s not an even a system. … We have to look at patient experience and outcome, not ‘what procedure did we do to that patient?’
“Right now, we are paying more for lower-quality healthcare, and we are not getting the bang for our bucks. We cannot afford to continue to spend money and not get value; we really have to change this time.” TH
Carol Berczuk is a freelance writer based in New York City.
How can a family physician with a demanding clinical schedule juggle patient care with the grueling administrative and travel duties required of the president-elect of the American Academy of Family Physicians (AAFP)? Lori Heim, MD, FAAFP, found the perfect compromise: Give up the family practice and become a hospitalist.
She did so last November, soon after AAFP members voted her the next president of one of the nation’s largest medical organizations. In fact, she is the only hospitalist at 104-bed Scotland Memorial Hospital in Laurinburg, N.C.
“I was looking for an opportunity while I was working as president-elect and then president of the academy,” says Dr. Heim, who takes over as president of the 94,000-member AAFP in October. “Because of the heavy travel demands, it was not possible to keep my old practice.”
Although the career swap is borne of professional necessity, Dr. Heim says her transition to HM practice has been relatively easy. “I love it. [The new job] utilizes my prior training and skills,” she says. “In private practice, I was doing rounds on my own patients, then I would have to run to the office to see my other patients. I could see the advantages of using the hospitalist services. … Now, here I am on this side.”
An active AAFP member for nearly 25 years, Dr. Heim brings a unique confluence of medical training and experience to her new role. She has firsthand knowledge of the key issues intersecting primary care and hospital-based practice—care coordination, physician reimbursement, and quality improvement. She also acknowledges that walls need to be broken down when it comes to family physicians (FP) transitioning to HM careers. More complete training and improvement in hospital administrations’ understanding of an FP’s clinical capabilities will advance their entrance into hospitalist careers.
“I think it could become a large trend because of the financial constraints on family care,” Dr. Heim says, also noting the lifestyle benefits of an HM career. “FPs often cannot do both inpatient and outpatient care. Your productivity, if you are in the clinic, must make a tradeoff between rounds and office hours—and how late at night do I want to be doing rounds?”
Bumpy Road to HM
The transition from family practice to HM is working out well for Heim, but it wasn’t as smooth as one might expect for a decorated career physician.
The daughter of a military pilot, Dr. Heim earned her bachelor’s degree with honors from Portland State University and her medical degree at the Uniformed Services University of Health Sciences in Bethesda, Md. Following her residency at Andrews Air Force Base in Maryland and a fellowship in faculty development and research at the University of North Carolina at Chapel Hill, her military medical career resembled a spiral staircase. She went from staff physician to clinic chief to residency director to chief of medical staff, with a few stops in between. After 25 years of military service, she retired as an Air Force colonel and opened a private practice.
Even with decades of training and patient care under her belt, Dr. Heim wasn’t rubber-stamped into a hospitalist position. It’s an issue she hopes to address as part of her AAFP tenure. “I know of hospitals where family physicians can admit and treat their patients but not be considered for a hospitalist position. It happened to me,” she explains. “I went and found a hospital that would use my skills.”
Hospitalist Robert Harrington, MD, FHM, knows the feeling. He had a more traditional primary-care practice before entering a HM career, and he understands the intense financial and workload pressures of family practice. Now the vice president of medical affairs for Alpharetta, Ga.-based IN Compass Health Inc. and chair of SHM’s Family Medicine Task Force, he says “there are barriers to hiring because of the wide variability in family physician training.” The root of the problem is that residents in some programs get less hospital time and experience with HM-patient encounters. “In opposed programs, they compete with other specialties and get less time,” Dr. Harrington says. “In unopposed programs, they tend to get more hospital experience and more rotations in inpatient services. Those folks can transition with little to no difficulty to hospital medicine.”
SHM President Scott Flanders, MD, FHM, associate professor and director of the hospitalist program at the University of Michigan in Ann Arbor, sees great value in what FPs can bring to HM. He wants HM to be open to those interested in a career change; however, he agrees physician training and experience can be an obstacle in the recruitment process. “The training in internal medicine is more geared to hospital medicine than it is in family practice [training],” Dr. Flanders says. “FPs must make sure they have hospital training, including the ICU. Many FP programs may not have this.” He also says FPs looking at an HM career—and internists as well—need to be “up to speed” in systems-based practice.
—Lori Heim, MD, FAAFP, Scotland Memorial Hospital, Laurinburg, N.C., AAFP president-elect
Although they represent a small part of SHM’s membership, Dr. Harrington and his task force want FPs to have “representation and a voice” in the society. “They are a small but growing minority,” he says. “Four or five percent of hospitalists are family-medicine-trained by our membership rolls, but we believe it is a bigger number, as some may not be members of SHM. … We run into more problems with hospital administrators. Some of them insist on IM-trained physicians, and there just aren’t enough IMs out there.”
It’s a C-suite roadblock Dr. Heim is familiar with. “Sometimes there is a parochial view in using internists above family physicians. Why should family doctors be second? It’s a misunderstanding of the experience and what family physicians bring to the table,” she says. “They haven’t done it, so people don’t think they can. Some hospitals are underutilizing family physicians in a hospitalist role. If a physician has hospital privileges, there is no reason they should not be considered to be hired as a hospitalist.”
Tenure of Change
As AAFP president, Dr. Heim says she’ll work to improve working conditions for FPs and fight for her constituents’ rights as Washington debates national healthcare reform. The AAFP and SHM share a number of policy interests, including reimbursement reform, new technologies, and patient-safety initiatives.
“I would like to do more with the various societies to increase opportunities for family medicine,” Dr. Heim says. “In some ways, primary care is being squeezed all around. How are you going to increase the numbers of FPs when they earn less? You are not going to unless you reform the system.”
Another top priority is advancing the idea of a national network of electronic health records (EHRs). Dr. Heim says a linked EHR system would improve communication and handoffs, and help physicians limit medical errors. “That’s the key,” she says. “Until then, it is going to be a hodgepodge of solutions. As long as it requires multiple steps, there will always be slipups.
“When I was in the military, records were kept electronically, and I learned the value of having continuity of electronic records.”
Dr. Heim says she would like to partner with hospital-based physicians on QI projects. “Any doctor, it doesn’t matter who you are, has a role to play in quality improvement, either in procedures to improve outcomes in the operating room or ICU or ED. We all have a role in that,” she says. “That is one of the reasons we have supported comparative effectiveness research. Guidelines are valuable.”
As AAFP president, Dr. Heim says she won’t forget her family physician roots. Her platform is ambitious: Reform both the practice and the payment of healthcare in this country. “I think the country recognizes that the current way of paying for healthcare—built on volume and procedures rather than patient outcome—has resulted in a fragmented and disjointed process,” she says. “It’s not an even a system. … We have to look at patient experience and outcome, not ‘what procedure did we do to that patient?’
“Right now, we are paying more for lower-quality healthcare, and we are not getting the bang for our bucks. We cannot afford to continue to spend money and not get value; we really have to change this time.” TH
Carol Berczuk is a freelance writer based in New York City.
How can a family physician with a demanding clinical schedule juggle patient care with the grueling administrative and travel duties required of the president-elect of the American Academy of Family Physicians (AAFP)? Lori Heim, MD, FAAFP, found the perfect compromise: Give up the family practice and become a hospitalist.
She did so last November, soon after AAFP members voted her the next president of one of the nation’s largest medical organizations. In fact, she is the only hospitalist at 104-bed Scotland Memorial Hospital in Laurinburg, N.C.
“I was looking for an opportunity while I was working as president-elect and then president of the academy,” says Dr. Heim, who takes over as president of the 94,000-member AAFP in October. “Because of the heavy travel demands, it was not possible to keep my old practice.”
Although the career swap is borne of professional necessity, Dr. Heim says her transition to HM practice has been relatively easy. “I love it. [The new job] utilizes my prior training and skills,” she says. “In private practice, I was doing rounds on my own patients, then I would have to run to the office to see my other patients. I could see the advantages of using the hospitalist services. … Now, here I am on this side.”
An active AAFP member for nearly 25 years, Dr. Heim brings a unique confluence of medical training and experience to her new role. She has firsthand knowledge of the key issues intersecting primary care and hospital-based practice—care coordination, physician reimbursement, and quality improvement. She also acknowledges that walls need to be broken down when it comes to family physicians (FP) transitioning to HM careers. More complete training and improvement in hospital administrations’ understanding of an FP’s clinical capabilities will advance their entrance into hospitalist careers.
“I think it could become a large trend because of the financial constraints on family care,” Dr. Heim says, also noting the lifestyle benefits of an HM career. “FPs often cannot do both inpatient and outpatient care. Your productivity, if you are in the clinic, must make a tradeoff between rounds and office hours—and how late at night do I want to be doing rounds?”
Bumpy Road to HM
The transition from family practice to HM is working out well for Heim, but it wasn’t as smooth as one might expect for a decorated career physician.
The daughter of a military pilot, Dr. Heim earned her bachelor’s degree with honors from Portland State University and her medical degree at the Uniformed Services University of Health Sciences in Bethesda, Md. Following her residency at Andrews Air Force Base in Maryland and a fellowship in faculty development and research at the University of North Carolina at Chapel Hill, her military medical career resembled a spiral staircase. She went from staff physician to clinic chief to residency director to chief of medical staff, with a few stops in between. After 25 years of military service, she retired as an Air Force colonel and opened a private practice.
Even with decades of training and patient care under her belt, Dr. Heim wasn’t rubber-stamped into a hospitalist position. It’s an issue she hopes to address as part of her AAFP tenure. “I know of hospitals where family physicians can admit and treat their patients but not be considered for a hospitalist position. It happened to me,” she explains. “I went and found a hospital that would use my skills.”
Hospitalist Robert Harrington, MD, FHM, knows the feeling. He had a more traditional primary-care practice before entering a HM career, and he understands the intense financial and workload pressures of family practice. Now the vice president of medical affairs for Alpharetta, Ga.-based IN Compass Health Inc. and chair of SHM’s Family Medicine Task Force, he says “there are barriers to hiring because of the wide variability in family physician training.” The root of the problem is that residents in some programs get less hospital time and experience with HM-patient encounters. “In opposed programs, they compete with other specialties and get less time,” Dr. Harrington says. “In unopposed programs, they tend to get more hospital experience and more rotations in inpatient services. Those folks can transition with little to no difficulty to hospital medicine.”
SHM President Scott Flanders, MD, FHM, associate professor and director of the hospitalist program at the University of Michigan in Ann Arbor, sees great value in what FPs can bring to HM. He wants HM to be open to those interested in a career change; however, he agrees physician training and experience can be an obstacle in the recruitment process. “The training in internal medicine is more geared to hospital medicine than it is in family practice [training],” Dr. Flanders says. “FPs must make sure they have hospital training, including the ICU. Many FP programs may not have this.” He also says FPs looking at an HM career—and internists as well—need to be “up to speed” in systems-based practice.
—Lori Heim, MD, FAAFP, Scotland Memorial Hospital, Laurinburg, N.C., AAFP president-elect
Although they represent a small part of SHM’s membership, Dr. Harrington and his task force want FPs to have “representation and a voice” in the society. “They are a small but growing minority,” he says. “Four or five percent of hospitalists are family-medicine-trained by our membership rolls, but we believe it is a bigger number, as some may not be members of SHM. … We run into more problems with hospital administrators. Some of them insist on IM-trained physicians, and there just aren’t enough IMs out there.”
It’s a C-suite roadblock Dr. Heim is familiar with. “Sometimes there is a parochial view in using internists above family physicians. Why should family doctors be second? It’s a misunderstanding of the experience and what family physicians bring to the table,” she says. “They haven’t done it, so people don’t think they can. Some hospitals are underutilizing family physicians in a hospitalist role. If a physician has hospital privileges, there is no reason they should not be considered to be hired as a hospitalist.”
Tenure of Change
As AAFP president, Dr. Heim says she’ll work to improve working conditions for FPs and fight for her constituents’ rights as Washington debates national healthcare reform. The AAFP and SHM share a number of policy interests, including reimbursement reform, new technologies, and patient-safety initiatives.
“I would like to do more with the various societies to increase opportunities for family medicine,” Dr. Heim says. “In some ways, primary care is being squeezed all around. How are you going to increase the numbers of FPs when they earn less? You are not going to unless you reform the system.”
Another top priority is advancing the idea of a national network of electronic health records (EHRs). Dr. Heim says a linked EHR system would improve communication and handoffs, and help physicians limit medical errors. “That’s the key,” she says. “Until then, it is going to be a hodgepodge of solutions. As long as it requires multiple steps, there will always be slipups.
“When I was in the military, records were kept electronically, and I learned the value of having continuity of electronic records.”
Dr. Heim says she would like to partner with hospital-based physicians on QI projects. “Any doctor, it doesn’t matter who you are, has a role to play in quality improvement, either in procedures to improve outcomes in the operating room or ICU or ED. We all have a role in that,” she says. “That is one of the reasons we have supported comparative effectiveness research. Guidelines are valuable.”
As AAFP president, Dr. Heim says she won’t forget her family physician roots. Her platform is ambitious: Reform both the practice and the payment of healthcare in this country. “I think the country recognizes that the current way of paying for healthcare—built on volume and procedures rather than patient outcome—has resulted in a fragmented and disjointed process,” she says. “It’s not an even a system. … We have to look at patient experience and outcome, not ‘what procedure did we do to that patient?’
“Right now, we are paying more for lower-quality healthcare, and we are not getting the bang for our bucks. We cannot afford to continue to spend money and not get value; we really have to change this time.” TH
Carol Berczuk is a freelance writer based in New York City.
Financial Fallout
Not once has Vanessa Yasmin Calderón regretted her decision to go into primary care, but she admits she’s disquieted by the amount of debt she’s accumulated while attending the University of California at Los Angeles for medical school and Harvard University’s Kennedy School of Government in pursuit of a master’s degree in public policy.
“I will be 30 years old when I graduate,” says Calderón, who plans to receive her medical degree in 2010. “Right now, I have no retirement account, and I’m staring at loads of debt in a bad economy. There’s a lot to think about.”
Calderón estimates she will have more than $146,000 in loans when she graduates—a daunting sum for someone who used scholarship money and a part-time job to put herself through college. Although Calderón is committed to a career in emergency or general internal medicine (IM), she has watched many of her peers forgo primary care in favor of anesthesiology, dermatology, and surgical specialties—partly because they are worried about how they are going to pay back their education debt.
“I guarantee you that primary care is being the most affected by rising debt,” says Calderón, vice president of finances for the American Medical Student Association (AMSA).
Her personal observations correlate with more than 15 years’ worth of published medical studies that have found compensation plays a role in dissuading medical students who are facing mountains of debt from choosing primary care. That includes careers in IM and, by extension, careers in HM, as more than 82% of hospitalists consider themselves IM specialists, according to SHM’s 2007-2008 “Bi-Annual Survey on the State of the Hospital Medicine Movement.” This doesn’t bode well for the nation’s future, experts say, because primary care and IM comprise the foundation of our nation’s healthcare system.
While the steep decline in IM recruits has leveled off in recent years, the number of medical students choosing IM residency (2,632 seniors entered three-year IM residency programs in 2009) is nowhere near the high point (3,884) of the mid-1980s, says Steven E. Weinberger, MD, FACP, senior vice president for medical education and publishing for the American College of Physicians (ACP).
“If there is not a change in how we support students going through medical school, how can we be surprised when they choose a higher-paying specialty?” says Michael Rosenthal, MD, professor and vice chairman of academic programs and research in the Department of Family and Community Medicine at Thomas Jefferson University in Philadelphia.
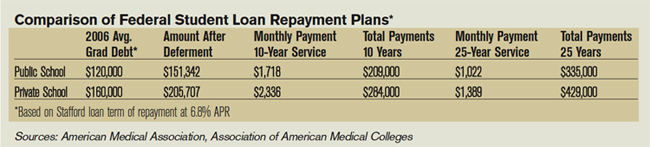
Loan Obligations
In 2006, more than 84% of medical school graduates had educational debt, with a median debt of $120,000 for graduates of public medical schools and $160,000 for graduates of private medical schools, according to a 2007 report by the Association of American Medical Colleges (AAMC). In comparison, the same report shows that, in 2001, the median debt for public and private medical school graduates was $86,000 and $120,000, respectively.
Just as the rising cost of healthcare leads to skyrocketing health insurance premiums, so, too, does it result in higher tuition and fees for medical students, says Brian Hurley, MD, MBA, president of AMSA. Public medical schools in particular are affected as state governments, which are obliged to annually balance their budgets, often pay for burgeoning healthcare expenses by cutting subsidies to higher education, he says.
“In a way, universities are balancing their squeezed budgets on the backs of their students,” says Dr. Hurley, who recently graduated from the University of Southern California’s Keck School of Medicine with $300,000 in educational debt.
There is no regulatory body in place that can moderate medical school tuition increases, he laments. But medical students are partly to blame for the spiraling tuition costs, Dr. Hurley says, because students rarely base their school selections on tuition costs. As a result, medical schools aren’t forced to decelerate tuition hikes, because students aren’t taking them to task.
“When pre-med students decide to go to medical school, they have this idea that they will have more opportunities if they can go to Harvard or some other top medical school,” Dr. Hurley says. “Students want to go to the best school they can, and they trust that everything will work itself out in the end.”
Meanwhile, escalating tuition costs and debt loads deter prospective medical students from low-income backgrounds from going to medical school, which hampers efforts to diversify the nation’s medical workforce and provide quality healthcare in poorer communities. “People tend to practice medicine where they came from,” Dr. Hurley says. “It’s not a perfect correlation, but it does match up.”
For its part, AMSA is educating pre-med students on how to select more affordable medical schools that provide a quality education. The association also focuses on teaching medical students how to manage educational debt. “The public perception is that physicians are rich, and it’s a perception we haven’t successfully been able to combat,” Dr. Hurley says. “Right now, medical student debt is not seen as a healthcare issue. We can try to work within the Higher Education Act to better subsidize medical students’ education, but lawmakers tend to focus on undergraduate education.”
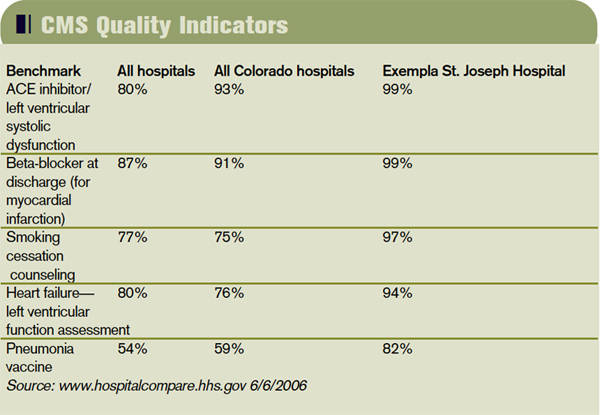
Nonprocedurals at Risk
But medical students’ rising debt is a healthcare issue, experts say. “Many students are now leaving medical school with over $200,000 in debt,” says Daniel Dressler, MD, FHM, SHM board member and education director for the HM section and associate program director for the IM residency program at Emory University’s School of Medicine in Atlanta. “As the cost of education increases each year and significantly outpaces the rate of increase in physician salaries, students may look toward specialties where they can pay that off within a more reasonable time frame while they begin their families and build their lives.”
Aside from primary care and IM, the medical fields that have been at the losing end of the bloated-educational-debt trend are nonprocedural-based IM specialties such as geriatrics, endocrinology, pulmonary/critical care, rheumatology, and infectious disease, says Jeffrey Wiese, MD, FACP, FHM, SHM president-elect and associate dean of graduate medical education and director of the IM residency program at Tulane University Hospital in New Orleans.
Doctors in nonprocedural-based IM specialties generally receive lower compensation than those in procedural-based IM specialties like cardiology, gastroenterology, and nephrology. For example, the median annual compensation for private-practice physicians in cardiology and gastroenterology is nearly $385,000; the median salary of endocrinologists and rheumatologists is $184,000; and the median salary for general internists is $166,000, according to a 2007 compensation survey by the Medical Group Management Association.
IM physician salaries always have been significantly less than the salaries of procedure-based specialists, Dr. Wiese says. “But now the workload of general internists has grown, and it hasn’t grown proportional to compensation, as compared to other specialties,” he says. “That’s compelling to students.”
Dr. Weinberger agrees the compensation disparity is disconcerting to medical students who consider IM because “they are choosing a harder lifestyle. It doesn’t help that the doctors who are practicing internal medicine complain about the hassles and the problems with reimbursement. The role models medical students look up to are not as happy as they used to be.”
—Daniel Dressler, MD, FHM, Emory University School of Medicine, Atlanta
HM Holds Its Own
Hospitalists seem to be surviving relatively well in these difficult times, according to data compiled by the American College of Physicians. In 2002, 4% of third-year IM residents surveyed said they were choosing HM. That number has risen steadily, to 10% in 2007 and 2008, Dr. Weinberger notes.
HM compensation varies widely, Dr. Wiese says; however, the mean salary for HM physicians was $196,700 in 2007, according to SHM survey data. That puts hospitalist salaries at the mid- to lower end of the scale when compared with all medical specialties but smack in the middle of IM specialties.
A 2008 study published in the Annals of Internal Medicine suggests that U.S. categorical IM residents with educational debt of $50,000 or more are more likely than those with no debt to choose a HM career, possibly because they can enter the work force right after residency training, as opposed to continuing with fellowship training for a subspecialty at substantially less compensation.1
For HM to continue gaining ground, many say the specialty has to go on the offensive and not wait for medical students and residents to decide to become hospitalists. “It will be more difficult to recruit from residency programs if there are fewer people going into internal medicine,” Dr. Dressler says. “Hospital medicine will simply be competing for a smaller pool of residents.”
Dr. Wiese says academia can contribute by providing a solid foundation in medicine and a clear path to HM careers as next-generation physicians and leaders. “Hospitalists assuming more of a teaching role are good not only for hospital medicine, but internal medicine education,” Dr. Wiese says. “The stronger the mentors, the more internal medicine students you’re going to recruit.”
The same can be said of medical practice settings, Dr. Weinberger explains. Many ambulatory settings in which medical students and residents work are among the most poorly supported and operated, even though they have the sickest patients, he says. That can be a huge turnoff for medical students. To counter that negative, students must be exposed to higher-quality ambulatory settings, Dr. Weinberger says.
Medical schools can help the cause by admitting students who show an inclination to go into primary care and IM, says Dr. Rosenthal, of Thomas Jefferson University. Those students are more likely to leave medical school in pursuit of a generalist career—especially if they’re matched with good IM mentors.
Federal and state governments should consider paying the educational loans of medical students who promise to practice primary care or IM for a certain period of time, especially in high-need communities, Dr. Rosenthal says. Fifteen years ago, he was a lead author in a study published in the Journal of the American Medical Association that found a significant number of fourth-year medical students would go into primary care, including general IM, if positive changes were made to income, hours worked, and loan repayment.2 Dr. Rosenthal says he’s not surprised physicians and researchers are writing about the same topic today.
“The article was written in the Clinton era, at a time when there was a sense the nation’s healthcare system might be reformed. But there was backlash to the plan,” Dr. Rosenthal says. “Today, we are again considering healthcare reform, except this time people are more willing to accept it because the high cost of healthcare is now affecting businesses and the economy.”
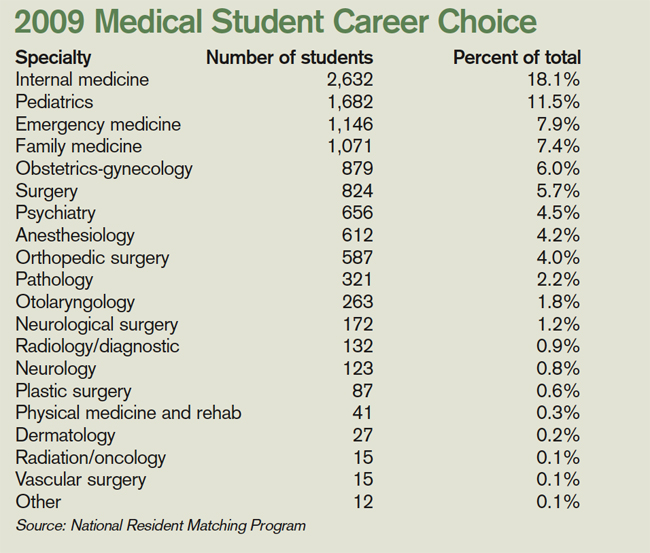
Change in Outlook
President Obama’s stated goal of extending health insurance to more Americans makes increasing the ranks of primary-care physicians, general internists, and hospitalists even more urgent, experts say. In Massachusetts, a state that is experimenting with universal health coverage for all of its residents, a shortfall in the primary-care work force is evident, Dr. Weinberger says. It is troubling news, because research consistently shows that when a primary-care physician coordinates a patient’s care, the result is fewer visits to the ED and medical specialists, he says.
“What this means is, we need more internists in the outpatient side to care for these patients longitudinally,” Dr. Dressler says. “We need more hospitalists, as the burden of inpatient care is very likely to grow as well.”
Dr. Rosenthal says more students will be attracted to medicine in part because the recession is making solid, good-paying jobs that play a vital role in communities very attractive. If better support were available for students interested in primary care, he says, he would have reason to hope more students would choose generalist careers.
“There was this expectation among people in their 20s that, if they were bright and able, they would have a nice lifestyle without having to work too hard. But the recession is having an effect on this generation’s outlook,” Dr. Rosenthal says. “I think there is a changing landscape out there.” TH
Lisa Ryan is a freelance writer based in New Jersey.
References
- McDonald FS, West CP, Popkave C, Kolars JC. Educational debt and reported career plans among internal medicine residents. Ann Intern Med. 2008;149(6): 416-420.
- Rosenthal MP, Diamond JJ, Rabinowitz HK, et al. Influence of income, hours worked, and loan repayment on medical students’ decision to pursue a primary care career. JAMA. 1994;271(12):914-917.
Not once has Vanessa Yasmin Calderón regretted her decision to go into primary care, but she admits she’s disquieted by the amount of debt she’s accumulated while attending the University of California at Los Angeles for medical school and Harvard University’s Kennedy School of Government in pursuit of a master’s degree in public policy.
“I will be 30 years old when I graduate,” says Calderón, who plans to receive her medical degree in 2010. “Right now, I have no retirement account, and I’m staring at loads of debt in a bad economy. There’s a lot to think about.”
Calderón estimates she will have more than $146,000 in loans when she graduates—a daunting sum for someone who used scholarship money and a part-time job to put herself through college. Although Calderón is committed to a career in emergency or general internal medicine (IM), she has watched many of her peers forgo primary care in favor of anesthesiology, dermatology, and surgical specialties—partly because they are worried about how they are going to pay back their education debt.
“I guarantee you that primary care is being the most affected by rising debt,” says Calderón, vice president of finances for the American Medical Student Association (AMSA).
Her personal observations correlate with more than 15 years’ worth of published medical studies that have found compensation plays a role in dissuading medical students who are facing mountains of debt from choosing primary care. That includes careers in IM and, by extension, careers in HM, as more than 82% of hospitalists consider themselves IM specialists, according to SHM’s 2007-2008 “Bi-Annual Survey on the State of the Hospital Medicine Movement.” This doesn’t bode well for the nation’s future, experts say, because primary care and IM comprise the foundation of our nation’s healthcare system.
While the steep decline in IM recruits has leveled off in recent years, the number of medical students choosing IM residency (2,632 seniors entered three-year IM residency programs in 2009) is nowhere near the high point (3,884) of the mid-1980s, says Steven E. Weinberger, MD, FACP, senior vice president for medical education and publishing for the American College of Physicians (ACP).
“If there is not a change in how we support students going through medical school, how can we be surprised when they choose a higher-paying specialty?” says Michael Rosenthal, MD, professor and vice chairman of academic programs and research in the Department of Family and Community Medicine at Thomas Jefferson University in Philadelphia.
Loan Obligations
In 2006, more than 84% of medical school graduates had educational debt, with a median debt of $120,000 for graduates of public medical schools and $160,000 for graduates of private medical schools, according to a 2007 report by the Association of American Medical Colleges (AAMC). In comparison, the same report shows that, in 2001, the median debt for public and private medical school graduates was $86,000 and $120,000, respectively.
Just as the rising cost of healthcare leads to skyrocketing health insurance premiums, so, too, does it result in higher tuition and fees for medical students, says Brian Hurley, MD, MBA, president of AMSA. Public medical schools in particular are affected as state governments, which are obliged to annually balance their budgets, often pay for burgeoning healthcare expenses by cutting subsidies to higher education, he says.
“In a way, universities are balancing their squeezed budgets on the backs of their students,” says Dr. Hurley, who recently graduated from the University of Southern California’s Keck School of Medicine with $300,000 in educational debt.
There is no regulatory body in place that can moderate medical school tuition increases, he laments. But medical students are partly to blame for the spiraling tuition costs, Dr. Hurley says, because students rarely base their school selections on tuition costs. As a result, medical schools aren’t forced to decelerate tuition hikes, because students aren’t taking them to task.
“When pre-med students decide to go to medical school, they have this idea that they will have more opportunities if they can go to Harvard or some other top medical school,” Dr. Hurley says. “Students want to go to the best school they can, and they trust that everything will work itself out in the end.”
Meanwhile, escalating tuition costs and debt loads deter prospective medical students from low-income backgrounds from going to medical school, which hampers efforts to diversify the nation’s medical workforce and provide quality healthcare in poorer communities. “People tend to practice medicine where they came from,” Dr. Hurley says. “It’s not a perfect correlation, but it does match up.”
For its part, AMSA is educating pre-med students on how to select more affordable medical schools that provide a quality education. The association also focuses on teaching medical students how to manage educational debt. “The public perception is that physicians are rich, and it’s a perception we haven’t successfully been able to combat,” Dr. Hurley says. “Right now, medical student debt is not seen as a healthcare issue. We can try to work within the Higher Education Act to better subsidize medical students’ education, but lawmakers tend to focus on undergraduate education.”
Nonprocedurals at Risk
But medical students’ rising debt is a healthcare issue, experts say. “Many students are now leaving medical school with over $200,000 in debt,” says Daniel Dressler, MD, FHM, SHM board member and education director for the HM section and associate program director for the IM residency program at Emory University’s School of Medicine in Atlanta. “As the cost of education increases each year and significantly outpaces the rate of increase in physician salaries, students may look toward specialties where they can pay that off within a more reasonable time frame while they begin their families and build their lives.”
Aside from primary care and IM, the medical fields that have been at the losing end of the bloated-educational-debt trend are nonprocedural-based IM specialties such as geriatrics, endocrinology, pulmonary/critical care, rheumatology, and infectious disease, says Jeffrey Wiese, MD, FACP, FHM, SHM president-elect and associate dean of graduate medical education and director of the IM residency program at Tulane University Hospital in New Orleans.
Doctors in nonprocedural-based IM specialties generally receive lower compensation than those in procedural-based IM specialties like cardiology, gastroenterology, and nephrology. For example, the median annual compensation for private-practice physicians in cardiology and gastroenterology is nearly $385,000; the median salary of endocrinologists and rheumatologists is $184,000; and the median salary for general internists is $166,000, according to a 2007 compensation survey by the Medical Group Management Association.
IM physician salaries always have been significantly less than the salaries of procedure-based specialists, Dr. Wiese says. “But now the workload of general internists has grown, and it hasn’t grown proportional to compensation, as compared to other specialties,” he says. “That’s compelling to students.”
Dr. Weinberger agrees the compensation disparity is disconcerting to medical students who consider IM because “they are choosing a harder lifestyle. It doesn’t help that the doctors who are practicing internal medicine complain about the hassles and the problems with reimbursement. The role models medical students look up to are not as happy as they used to be.”
—Daniel Dressler, MD, FHM, Emory University School of Medicine, Atlanta
HM Holds Its Own
Hospitalists seem to be surviving relatively well in these difficult times, according to data compiled by the American College of Physicians. In 2002, 4% of third-year IM residents surveyed said they were choosing HM. That number has risen steadily, to 10% in 2007 and 2008, Dr. Weinberger notes.
HM compensation varies widely, Dr. Wiese says; however, the mean salary for HM physicians was $196,700 in 2007, according to SHM survey data. That puts hospitalist salaries at the mid- to lower end of the scale when compared with all medical specialties but smack in the middle of IM specialties.
A 2008 study published in the Annals of Internal Medicine suggests that U.S. categorical IM residents with educational debt of $50,000 or more are more likely than those with no debt to choose a HM career, possibly because they can enter the work force right after residency training, as opposed to continuing with fellowship training for a subspecialty at substantially less compensation.1
For HM to continue gaining ground, many say the specialty has to go on the offensive and not wait for medical students and residents to decide to become hospitalists. “It will be more difficult to recruit from residency programs if there are fewer people going into internal medicine,” Dr. Dressler says. “Hospital medicine will simply be competing for a smaller pool of residents.”
Dr. Wiese says academia can contribute by providing a solid foundation in medicine and a clear path to HM careers as next-generation physicians and leaders. “Hospitalists assuming more of a teaching role are good not only for hospital medicine, but internal medicine education,” Dr. Wiese says. “The stronger the mentors, the more internal medicine students you’re going to recruit.”
The same can be said of medical practice settings, Dr. Weinberger explains. Many ambulatory settings in which medical students and residents work are among the most poorly supported and operated, even though they have the sickest patients, he says. That can be a huge turnoff for medical students. To counter that negative, students must be exposed to higher-quality ambulatory settings, Dr. Weinberger says.
Medical schools can help the cause by admitting students who show an inclination to go into primary care and IM, says Dr. Rosenthal, of Thomas Jefferson University. Those students are more likely to leave medical school in pursuit of a generalist career—especially if they’re matched with good IM mentors.
Federal and state governments should consider paying the educational loans of medical students who promise to practice primary care or IM for a certain period of time, especially in high-need communities, Dr. Rosenthal says. Fifteen years ago, he was a lead author in a study published in the Journal of the American Medical Association that found a significant number of fourth-year medical students would go into primary care, including general IM, if positive changes were made to income, hours worked, and loan repayment.2 Dr. Rosenthal says he’s not surprised physicians and researchers are writing about the same topic today.
“The article was written in the Clinton era, at a time when there was a sense the nation’s healthcare system might be reformed. But there was backlash to the plan,” Dr. Rosenthal says. “Today, we are again considering healthcare reform, except this time people are more willing to accept it because the high cost of healthcare is now affecting businesses and the economy.”
Change in Outlook
President Obama’s stated goal of extending health insurance to more Americans makes increasing the ranks of primary-care physicians, general internists, and hospitalists even more urgent, experts say. In Massachusetts, a state that is experimenting with universal health coverage for all of its residents, a shortfall in the primary-care work force is evident, Dr. Weinberger says. It is troubling news, because research consistently shows that when a primary-care physician coordinates a patient’s care, the result is fewer visits to the ED and medical specialists, he says.
“What this means is, we need more internists in the outpatient side to care for these patients longitudinally,” Dr. Dressler says. “We need more hospitalists, as the burden of inpatient care is very likely to grow as well.”
Dr. Rosenthal says more students will be attracted to medicine in part because the recession is making solid, good-paying jobs that play a vital role in communities very attractive. If better support were available for students interested in primary care, he says, he would have reason to hope more students would choose generalist careers.
“There was this expectation among people in their 20s that, if they were bright and able, they would have a nice lifestyle without having to work too hard. But the recession is having an effect on this generation’s outlook,” Dr. Rosenthal says. “I think there is a changing landscape out there.” TH
Lisa Ryan is a freelance writer based in New Jersey.
References
- McDonald FS, West CP, Popkave C, Kolars JC. Educational debt and reported career plans among internal medicine residents. Ann Intern Med. 2008;149(6): 416-420.
- Rosenthal MP, Diamond JJ, Rabinowitz HK, et al. Influence of income, hours worked, and loan repayment on medical students’ decision to pursue a primary care career. JAMA. 1994;271(12):914-917.
Not once has Vanessa Yasmin Calderón regretted her decision to go into primary care, but she admits she’s disquieted by the amount of debt she’s accumulated while attending the University of California at Los Angeles for medical school and Harvard University’s Kennedy School of Government in pursuit of a master’s degree in public policy.
“I will be 30 years old when I graduate,” says Calderón, who plans to receive her medical degree in 2010. “Right now, I have no retirement account, and I’m staring at loads of debt in a bad economy. There’s a lot to think about.”
Calderón estimates she will have more than $146,000 in loans when she graduates—a daunting sum for someone who used scholarship money and a part-time job to put herself through college. Although Calderón is committed to a career in emergency or general internal medicine (IM), she has watched many of her peers forgo primary care in favor of anesthesiology, dermatology, and surgical specialties—partly because they are worried about how they are going to pay back their education debt.
“I guarantee you that primary care is being the most affected by rising debt,” says Calderón, vice president of finances for the American Medical Student Association (AMSA).
Her personal observations correlate with more than 15 years’ worth of published medical studies that have found compensation plays a role in dissuading medical students who are facing mountains of debt from choosing primary care. That includes careers in IM and, by extension, careers in HM, as more than 82% of hospitalists consider themselves IM specialists, according to SHM’s 2007-2008 “Bi-Annual Survey on the State of the Hospital Medicine Movement.” This doesn’t bode well for the nation’s future, experts say, because primary care and IM comprise the foundation of our nation’s healthcare system.
While the steep decline in IM recruits has leveled off in recent years, the number of medical students choosing IM residency (2,632 seniors entered three-year IM residency programs in 2009) is nowhere near the high point (3,884) of the mid-1980s, says Steven E. Weinberger, MD, FACP, senior vice president for medical education and publishing for the American College of Physicians (ACP).
“If there is not a change in how we support students going through medical school, how can we be surprised when they choose a higher-paying specialty?” says Michael Rosenthal, MD, professor and vice chairman of academic programs and research in the Department of Family and Community Medicine at Thomas Jefferson University in Philadelphia.
Loan Obligations
In 2006, more than 84% of medical school graduates had educational debt, with a median debt of $120,000 for graduates of public medical schools and $160,000 for graduates of private medical schools, according to a 2007 report by the Association of American Medical Colleges (AAMC). In comparison, the same report shows that, in 2001, the median debt for public and private medical school graduates was $86,000 and $120,000, respectively.
Just as the rising cost of healthcare leads to skyrocketing health insurance premiums, so, too, does it result in higher tuition and fees for medical students, says Brian Hurley, MD, MBA, president of AMSA. Public medical schools in particular are affected as state governments, which are obliged to annually balance their budgets, often pay for burgeoning healthcare expenses by cutting subsidies to higher education, he says.
“In a way, universities are balancing their squeezed budgets on the backs of their students,” says Dr. Hurley, who recently graduated from the University of Southern California’s Keck School of Medicine with $300,000 in educational debt.
There is no regulatory body in place that can moderate medical school tuition increases, he laments. But medical students are partly to blame for the spiraling tuition costs, Dr. Hurley says, because students rarely base their school selections on tuition costs. As a result, medical schools aren’t forced to decelerate tuition hikes, because students aren’t taking them to task.
“When pre-med students decide to go to medical school, they have this idea that they will have more opportunities if they can go to Harvard or some other top medical school,” Dr. Hurley says. “Students want to go to the best school they can, and they trust that everything will work itself out in the end.”
Meanwhile, escalating tuition costs and debt loads deter prospective medical students from low-income backgrounds from going to medical school, which hampers efforts to diversify the nation’s medical workforce and provide quality healthcare in poorer communities. “People tend to practice medicine where they came from,” Dr. Hurley says. “It’s not a perfect correlation, but it does match up.”
For its part, AMSA is educating pre-med students on how to select more affordable medical schools that provide a quality education. The association also focuses on teaching medical students how to manage educational debt. “The public perception is that physicians are rich, and it’s a perception we haven’t successfully been able to combat,” Dr. Hurley says. “Right now, medical student debt is not seen as a healthcare issue. We can try to work within the Higher Education Act to better subsidize medical students’ education, but lawmakers tend to focus on undergraduate education.”
Nonprocedurals at Risk
But medical students’ rising debt is a healthcare issue, experts say. “Many students are now leaving medical school with over $200,000 in debt,” says Daniel Dressler, MD, FHM, SHM board member and education director for the HM section and associate program director for the IM residency program at Emory University’s School of Medicine in Atlanta. “As the cost of education increases each year and significantly outpaces the rate of increase in physician salaries, students may look toward specialties where they can pay that off within a more reasonable time frame while they begin their families and build their lives.”
Aside from primary care and IM, the medical fields that have been at the losing end of the bloated-educational-debt trend are nonprocedural-based IM specialties such as geriatrics, endocrinology, pulmonary/critical care, rheumatology, and infectious disease, says Jeffrey Wiese, MD, FACP, FHM, SHM president-elect and associate dean of graduate medical education and director of the IM residency program at Tulane University Hospital in New Orleans.
Doctors in nonprocedural-based IM specialties generally receive lower compensation than those in procedural-based IM specialties like cardiology, gastroenterology, and nephrology. For example, the median annual compensation for private-practice physicians in cardiology and gastroenterology is nearly $385,000; the median salary of endocrinologists and rheumatologists is $184,000; and the median salary for general internists is $166,000, according to a 2007 compensation survey by the Medical Group Management Association.
IM physician salaries always have been significantly less than the salaries of procedure-based specialists, Dr. Wiese says. “But now the workload of general internists has grown, and it hasn’t grown proportional to compensation, as compared to other specialties,” he says. “That’s compelling to students.”
Dr. Weinberger agrees the compensation disparity is disconcerting to medical students who consider IM because “they are choosing a harder lifestyle. It doesn’t help that the doctors who are practicing internal medicine complain about the hassles and the problems with reimbursement. The role models medical students look up to are not as happy as they used to be.”
—Daniel Dressler, MD, FHM, Emory University School of Medicine, Atlanta
HM Holds Its Own
Hospitalists seem to be surviving relatively well in these difficult times, according to data compiled by the American College of Physicians. In 2002, 4% of third-year IM residents surveyed said they were choosing HM. That number has risen steadily, to 10% in 2007 and 2008, Dr. Weinberger notes.
HM compensation varies widely, Dr. Wiese says; however, the mean salary for HM physicians was $196,700 in 2007, according to SHM survey data. That puts hospitalist salaries at the mid- to lower end of the scale when compared with all medical specialties but smack in the middle of IM specialties.
A 2008 study published in the Annals of Internal Medicine suggests that U.S. categorical IM residents with educational debt of $50,000 or more are more likely than those with no debt to choose a HM career, possibly because they can enter the work force right after residency training, as opposed to continuing with fellowship training for a subspecialty at substantially less compensation.1
For HM to continue gaining ground, many say the specialty has to go on the offensive and not wait for medical students and residents to decide to become hospitalists. “It will be more difficult to recruit from residency programs if there are fewer people going into internal medicine,” Dr. Dressler says. “Hospital medicine will simply be competing for a smaller pool of residents.”
Dr. Wiese says academia can contribute by providing a solid foundation in medicine and a clear path to HM careers as next-generation physicians and leaders. “Hospitalists assuming more of a teaching role are good not only for hospital medicine, but internal medicine education,” Dr. Wiese says. “The stronger the mentors, the more internal medicine students you’re going to recruit.”
The same can be said of medical practice settings, Dr. Weinberger explains. Many ambulatory settings in which medical students and residents work are among the most poorly supported and operated, even though they have the sickest patients, he says. That can be a huge turnoff for medical students. To counter that negative, students must be exposed to higher-quality ambulatory settings, Dr. Weinberger says.
Medical schools can help the cause by admitting students who show an inclination to go into primary care and IM, says Dr. Rosenthal, of Thomas Jefferson University. Those students are more likely to leave medical school in pursuit of a generalist career—especially if they’re matched with good IM mentors.
Federal and state governments should consider paying the educational loans of medical students who promise to practice primary care or IM for a certain period of time, especially in high-need communities, Dr. Rosenthal says. Fifteen years ago, he was a lead author in a study published in the Journal of the American Medical Association that found a significant number of fourth-year medical students would go into primary care, including general IM, if positive changes were made to income, hours worked, and loan repayment.2 Dr. Rosenthal says he’s not surprised physicians and researchers are writing about the same topic today.
“The article was written in the Clinton era, at a time when there was a sense the nation’s healthcare system might be reformed. But there was backlash to the plan,” Dr. Rosenthal says. “Today, we are again considering healthcare reform, except this time people are more willing to accept it because the high cost of healthcare is now affecting businesses and the economy.”
Change in Outlook
President Obama’s stated goal of extending health insurance to more Americans makes increasing the ranks of primary-care physicians, general internists, and hospitalists even more urgent, experts say. In Massachusetts, a state that is experimenting with universal health coverage for all of its residents, a shortfall in the primary-care work force is evident, Dr. Weinberger says. It is troubling news, because research consistently shows that when a primary-care physician coordinates a patient’s care, the result is fewer visits to the ED and medical specialists, he says.
“What this means is, we need more internists in the outpatient side to care for these patients longitudinally,” Dr. Dressler says. “We need more hospitalists, as the burden of inpatient care is very likely to grow as well.”
Dr. Rosenthal says more students will be attracted to medicine in part because the recession is making solid, good-paying jobs that play a vital role in communities very attractive. If better support were available for students interested in primary care, he says, he would have reason to hope more students would choose generalist careers.
“There was this expectation among people in their 20s that, if they were bright and able, they would have a nice lifestyle without having to work too hard. But the recession is having an effect on this generation’s outlook,” Dr. Rosenthal says. “I think there is a changing landscape out there.” TH
Lisa Ryan is a freelance writer based in New Jersey.
References
- McDonald FS, West CP, Popkave C, Kolars JC. Educational debt and reported career plans among internal medicine residents. Ann Intern Med. 2008;149(6): 416-420.
- Rosenthal MP, Diamond JJ, Rabinowitz HK, et al. Influence of income, hours worked, and loan repayment on medical students’ decision to pursue a primary care career. JAMA. 1994;271(12):914-917.
The Big One
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
Tips to differentiate bipolar II disorder and borderline personality disorder
Alternative modes of mechanical ventilation: A review for the hospitalist
Technologic advances and computerized control of mechanical ventilators have made it possible to deliver ventilatory assistance in new modes. Driving these innovations is the desire to prevent ventilator-induced lung injury, improve patient comfort, and liberate the patient from mechanical ventilation as soon as possible.
We call these innovations “alternative” modes to differentiate them from the plain volume-control and pressure-control modes. Some clinicians rarely use these new modes, but in some medical centers they have become the most common ones used, or are being used unknowingly (the operator misunderstands the mode name). The information we provide on these modes of ventilation is by no means an endorsement of their use, but rather a tool to help the clinician understand their physiologic, theoretical, and clinical effects.
We focused on two goals:
- Explain what the mode does
- Briefly review the theoretical benefits and the actual evidence supporting these alternative modes of ventilation.
STANDARD NOMENCLATURE NEEDED
Since its invention, mechanical ventilation has been plagued by multiple names being used to describe the same things. For example, volume-control ventilation is also called volume-cycled ventilation, assist-control ventilation, volume-limited ventilation, and controlled mechanical ventilation. Similarly, multiple abbreviations are used, each depending on the brand of ventilator, and new acronyms have been added in recent years as new modes have been developed. The vast number of names and modes can confuse even the most seasoned critical care physician.
Efforts to establish a common nomenclature are under way.1
WHAT IS A MODE?
A mode of mechanical ventilation has three essential components:
- The control variable
- The breath sequence
- The targeting scheme.
Similar modes may require more detailed descriptions to distinguish them, but the basic function can be explained by these three components.
The control variable
In general, inspiration is an active process, driven by the patient’s effort, the ventilator, or both, while expiration is passive. For simplicity, in this article a mechanical breath means the inspiratory phase of the breath.
The machine can only control the volume (and flow) or the pressure given. The breaths can be further described on the basis of what triggers the breath, what limits it (the maximum value of a control variable), and what ends (cycles) it.
The breath sequence
There are three possible breath sequences:

- Intermittent mandatory ventilation, in which the patient can take spontaneous breaths between mandatory breaths
- Continuous spontaneous ventilation, in which all breaths are spontaneous (Table 1).
The targeting scheme
The targeting or feedback scheme refers to the ventilator settings and programming that dictate its response to the patient’s lung compliance, lung resistance, and respiratory effort. The regulation can be as simple as controlling the pressure in pressure-control mode, or it can be based on a complicated algorithm.
ADAPTIVE PRESSURE CONTROL
Other names for adaptive pressure control
- Pressure Regulated Volume Control (Maquet Servo-i, Rastatt, Germany)
- AutoFlow (Dräger Medical AG, Lübeck, Germany)
- Adaptive Pressure Ventilation (Hamilton Galileo, Hamilton Medical AG, Bonaduz, Switzerland)
- Volume Control+ (Puritan Bennett, Tyco Healthcare; Mansfield, MA)
- Volume Targeted Pressure Control, Pressure Controlled Volume Guaranteed (Engström, General Electric, Madison, WI).
What does adaptive pressure control do?
The APC mode delivers pressure-controlled breaths with an adaptive targeting scheme (Table 2).
In pressure-control ventilation, tidal volumes depend on the lung’s physiologic mechanics (compliance and resistance) and patient effort (Figure 1). Therefore, the tidal volume varies with changes in lung physiology (ie, larger or smaller tidal volumes than targeted).
To overcome this effect, a machine in APC mode adjusts the inspiratory pressure to deliver the set minimal target tidal volume. If tidal volume increases, the machine decreases the inspiratory pressure, and if tidal volume decreases, the machine increases the inspiratory pressure. However, if the patient effort is large enough, the tidal volume will increase in spite of decreasing the inspiratory pressure (Figure 2). The adjustments to the inspiratory pressure occur after the tidal volume is off-target in a number of breaths.
Common sources of confusion with adaptive pressure control
First, APC is not a volume-control mode. In volume control, the tidal volume does not change; in APC the tidal volume can increase or decrease, and the ventilator will adjust the inflation pressure to achieve the target volume. Thus, APC guarantees an average minimum tidal volume but not a maximum tidal volume.
Second, a characteristic of pressure control (and hence, APC) is that the flow of gas varies to maintain constant airway pressure (ie, maintain the set inspiratory pressure). This characteristic allows a patient who generates an inspiratory effort to receive flow as demanded, which is likely more comfortable. This is essentially different from volume control, in which flow is set by the operator and hence is fixed. Thus, if the patient effort is strong enough (Figure 1), this leads to what is called flow asynchrony, in which the patient does not get the flow asked for in a breath.
Ventilator settings in adaptive pressure control
Ventilator settings in APC are:
- Tidal volume
- Time spent in inspiration (inspiratory time)
- Frequency
- Fraction of inspired oxygen (Fio2)
- Positive end-expiratory pressure (PEEP).
Some ventilators also require setting the speed to reach the peak pressure (also known as slope percent or inspiratory rise time).
Clinical applications of adaptive pressure control
This mode is designed to maintain a consistent tidal volume during pressure-control ventilation and to promote inspiratory flow synchrony. It is a means of automatically reducing ventilatory support (ie, weaning) as the patient’s inspiratory effort becomes stronger, as in awakening from anesthesia.
APC may not be ideal for patients who have an inappropriately increased respiratory drive (eg, in severe metabolic acidosis), since the inspiratory pressure will decrease to maintain the targeted average tidal volume, inappropriately shifting the work of breathing onto the patient.
Theoretical benefits of adaptive pressure control
APC guarantees a minimum average tidal volume (unless the pressure alarm threshold is set too low, so that the target tidal volume is not delivered). Other theoretical benefits are flow synchrony, less ventilator manipulation by the operator, and automatic weaning of ventilator support.
Evidence of benefit of adaptive pressure control
Physiologic benefits. This mode has lower peak inspiratory pressures than does volume-control ventilation,3,4 which is often reported as a positive finding. However, in volume-control mode (the usual comparator), the peak inspiratory pressure is a manifestation of both resistance and compliance. Hence, peak inspiratory pressure is expected to be higher but does not reflect actual lung-distending pressures. It is the plateau pressure, a manifestation of lung compliance, that is related to lung injury.
Patient comfort. APC may increase the work of breathing when using low tidal volume ventilation and when there is increased respiratory effort (drive).5 Interestingly, APC was less comfortable than pressure support ventilation in a small trial.6
Outcomes have not been studied.7
Adaptive pressure control: Bottom line
APC is widely available and widely used, sometimes unknowingly (eg, if the operator thinks it is volume control). It is relatively easy to use and to set; however, evidence of its benefit is scant.
ADAPTIVE SUPPORT VENTILATION
Adaptive support ventilation (ASV) evolved as a form of mandatory minute ventilation implemented with adaptive pressure control. Mandatory minute ventilation is a mode that allows the operator to preset a target minute ventilation, and the ventilator then supplies mandatory breaths, either volume- or pressure-controlled, if the patient’s spontaneous breaths generate a lower minute ventilation.
ASV automatically selects the appropriate tidal volume and frequency for mandatory breaths and the appropriate tidal volume for spontaneous breaths on the basis of the respiratory system mechanics and target minute alveolar ventilation.
Described in 1994 by Laubscher et al,8,9 ASV became commercially available in 1998 in Europe and in 2007 in the United States (Hamilton Galileo ventilator, Hamilton Medical AG). This is the first commercially available ventilator that uses an “optimal” targeting scheme (see below).
What does adaptive support ventilation do?
ASV delivers pressure-controlled breaths using an adaptive (optimal) scheme (Table 2). “Optimal,” in this context, means minimizing the mechanical work of breathing: the machine selects a tidal volume and frequency that the patient’s brain would presumably select if the patient were not connected to a ventilator. This pattern is assumed to encourage the patient to generate spontaneous breaths.
The ventilator calculates the normal required minute ventilation based on the patient’s ideal weight and estimated dead space volume (ie, 2.2 mL/kg). This calculation represents 100% of minute ventilation. The clinician at the bedside sets a target percent of minute ventilation that the ventilator will support—higher than 100% if the patient has increased requirements due, eg, to sepsis or increased dead space, or less than 100% during weaning.
The ventilator initially delivers test breaths, in which it measures the expiratory time constant for the respiratory system and then uses this along with the estimated dead space and normal minute ventilation to calculate an optimal breathing frequency in terms of mechanical work.
The optimal or target tidal volume is calculated as the normal minute ventilation divided by the optimal frequency. The target tidal volume is achieved by the use of APC (see above) (Figure 2). This means that the pressure limit is automatically adjusted to achieve an average delivered tidal volume equal to the target. The ventilator continuously monitors the respiratory system mechanics and adjusts its settings accordingly.
The ventilator adjusts its breaths to avoid air trapping by allowing enough time to exhale, to avoid hypoventilation by delivering tidal volume greater than the dead space, and to avoid volutrauma by avoiding large tidal volumes.
Ventilator settings in adaptive support ventilation
Ventilator settings in ASV are:
- Patient height (to calculate the ideal body weight)
- Sex
- Percent of normal predicted minute ventilation goal
- Fio2
- PEEP.
Clinical applications of adaptive support ventilation
ASV is intended as a sole mode of ventilation, from initial support to weaning.
Theoretical benefits of adaptive support ventilation
In theory, ASV offers automatic selection of ventilator settings, automatic adaptation to changing patient lung mechanics, less need for human manipulation of the machine, improved synchrony, and automatic weaning.
Evidence of benefit of adaptive support ventilation
Physiologic benefits. Ventilator settings are adjusted automatically. ASV selects different tidal volume-respiratory rate combinations based on respiratory mechanics in passive and paralyzed patients.10–12 In actively breathing patients, there was no difference in the ventilator settings chosen by ASV for different clinical scenarios (and lung physiology).10 Compared with pressure-controlled intermittent mandatory ventilation, with ASV, the inspiratory load is less and patient-ventilator interaction is better.13
Patient-ventilator synchrony and comfort have not been studied.
Outcomes. Two trials suggest that ASV may decrease time on mechanical ventilation.14,15 However, in another trial,16 compared with a standard protocol, ASV led to fewer ventilator adjustments but achieved similar postsurgical weaning outcomes. The effect of this mode on the death rate has not been examined.17,18
Adaptive support ventilation: Bottom line
ASV is the first commercially available mode that automatically selects all the ventilator settings except PEEP and Fio2. These seem appropriate for different clinical scenarios in patients with poor respiratory effort or in paralyzed patients. Evidence of the effect in actively breathing patients and on outcomes such as length of stay or death is still lacking.
PROPORTIONAL ASSIST VENTILATION
Patients who have normal respiratory drive but who have difficulty sustaining adequate spontaneous ventilation are often subjected to pressure support ventilation (PSV), in which the ventilator generates a constant pressure throughout inspiration regardless of the intensity of the patient’s effort.
In 1992, Younes and colleagues19,20 developed proportional assist ventilation (PAV) as an alternative in which the ventilator generates pressure in proportion to the patient’s effort. PAV became commercially available in Europe in 1999 and was approved in the United States in 2006, available on the Puritan Bennett 840 ventilator (Puritan Bennett Co, Boulder, CO). PAV has also been used for noninvasive ventilation, but this is not available in the United States.
Other names for proportional assist ventilation
Proportional Pressure Support (Dräger Medical; not yet available in the United States).
What does proportional assist ventilation do?
This mode delivers pressure-controlled breaths with a servo control scheme (Table 2).
To better understand PAV, we can compare it with PSV. With PSV, the pressure applied by the ventilator rises to a preset level that is held constant (a set-point scheme) until a cycling criterion (a percent of the maximum inspiratory flow value) is reached. The inspiratory flow and tidal volume are the result of the patient’s inspiratory effort, the level of pressure applied, and the respiratory system mechanics.
In PAV, as in PSV, all breaths are spontaneous (Table 1). The patient controls the timing and size of the breath. There are no preset pressure, flow, or volume goals, but safety limits on the volume and pressure delivered can be set.
Ventilator settings in proportional assist ventilation
Ventilator settings in PAV are:
- Airway type (endotracheal tube, tracheostomy)
- Airway size (inner diameter)
- Percentage of work supported (assist range 5%–95%)
- Tidal volume limit
- Pressure limit
- Expiratory sensitivity (normally, as inspiration ends, flow should stop; this parameter tells the ventilator at what flow to end inspiration).
Caution when assessing the literature. Earlier ventilator versions, ie, Dräger and Manitoba (University of Manitoba, Winnipeg, MB, Canada), which are not available in the United States, required the repeated calculation of the respiratory system mechanics and the manual setting of flow and volume assists (amplification factors) independently. To overcome this limitation, new software automatically adjusts the flow and volume amplification to support the loads imposed by the automatically measured values of resistance and elastance (inverse of compliance) of the respiratory system.21 This software is included in the model (Puritan Bennett) available in the United States.
Clinical applications of proportional assist ventilation
The PAV mode is indicated for maximizing ventilator patient synchrony for assisted spontaneous ventilation.
PAV is contraindicated in patients with respiratory depression (bradypnea) or large air leaks (eg, bronchopleural fistulas). It should be used with caution in patients with severe hyperinflation, in which the patient may still be exhaling but the ventilator doesn’t recognize it. Another group in which PAV should be used with caution is those with high ventilatory drives, in which the ventilator overestimates respiratory system mechanics. This situation can lead to overassistance due to the “runaway phenomenon,” in which the ventilator continues to provide support even if the patient has stopped inspiration.22
Theoretical benefits of proportional assist ventilation
In theory, PAV should reduce the work of breathing, improve synchrony, automatically adapt to changing patient lung mechanics and effort, decrease the need for ventilator intervention and manipulation, decrease the need for sedation, and improve sleep.
Evidence of benefit of proportional assist ventilation
Physiologic benefits. PAV reduces the work of breathing better than PSV,21 even in the face of changing respiratory mechanics or increased respiratory demand (hypercapnia).23–25 The hemodynamic profile is similar to that in PSV. Tidal volumes are variable; however, in recent reports the tidal volumes were within the lung-protective range (6–8 mL/kg, plateau pressure < 30 cm H20).26,27
Comfort. PAV entails less patient effort and discomfort that PSV does.23,25 PAV significantly reduces asynchrony,27 which in turn may favorably affect sleep in critically ill patients. 28
Outcomes. The probability of spontaneous breathing without assistance was significantly better in critically ill patients ventilated with PAV than with PSV. No trial has reported the effect of PAV on deaths.27,29
Proportional assist ventilation: Bottom line
Extensive basic research has been done with PAV in different forms of respiratory failure, such as obstructive lung disease, acute respiratory distress syndrome (ARDS), and chronic respiratory failure. It fulfills its main goal, which is to improve patient-ventilator synchrony. Clinical experience with PAV in the United States is limited, as it was only recently approved.
AIRWAY PRESSURE-RELEASE VENTILATION AND BIPHASIC POSITIVE AIRWAY PRESSURE
Airway pressure-release ventilation (APRV) was described in 1987 by Stock et al30 as a mode for delivering ventilation in acute lung injury while avoiding high airway pressures. APRV combines high constant positive airway pressure (improving oxygenation and promoting alveolar recruitment) with intermittent releases (causing exhalation).
Other names for biphasic positive airway pressure
Other names for biphasic positive airway pressure are:
- BiLevel (Puritan Bennett)
- BIPAP (Dräger Europe)
- Bi Vent (Siemens)
- BiPhasic (Avea, Cardinal Health, Inc, Dublin, OH)
- PCV+ (Dräger Medical)
- DuoPAP (Hamilton).
Caution—name confusion. In North America, BiPAP (Respironics, Murrysville, PA) and BiLevel are used to refer to noninvasive modes of ventilation.
APRV has no other name.
What do these modes do?
These modes deliver pressure-controlled, time-triggered, and time-cycled breaths using a set-point targeting scheme (Table 2). This means that the ventilator maintains a constant pressure (set point) even in the face of spontaneous breaths.
Caution—source of confusion. The term continuous positive airway pressure (CPAP) is often used to describe this mode. However, CPAP is pressure that is applied continuously at the same level; the patient generates all the work to maintain ventilation (“pressure-controlled continuous spontaneous ventilation” in the current nomenclature). In APRV, the airway pressure is intermittently released and reapplied, generating a tidal volume that supports ventilation. In other words, this is a pressure-controlled breath with a very prolonged inspiratory time and a short expiratory time in which spontaneous ventilation is possible at any point (“pressure-controlled intermittent mandatory ventilation” in the current nomenclature).
How these modes are set in the ventilator may also be a source of confusion. To describe the time spent in high and low airway pressures, we use the terms Thigh and Tlow, respectively. By convention, the difference between APRV and biphasic mode is the duration of Tlow (< 1.5 sec for APRV).
Similarly, Phigh and Plow are used to describe the high and low airway pressure. To better understand this concept, you can create the same mode in conventional pressure-control ventilation by thinking of the Thigh as the inspiratory time, the Tlow as the expiratory time, the Phigh as inspiratory pressure, and the Plow as PEEP.
Hence, APRV is an extreme form of inverse ratio ventilation, with an inspiration-to-expiration ratio of 4:1. This means a patient spends most of the time in Phigh and Thigh, and exhalations are short (Tlow and Plow). In contrast, the biphasic mode uses conventional inspiration-expiration ratios (Figure 4).
As with any form of pressure control, the tidal volume is generated by airway pressure rising above baseline (ie, the end-expiratory value). Hence, to ensure an increase in minute ventilation, the mandatory breath rate must be increased (ie, decreasing Thigh, Tlow, or both) or the tidal volume must be increased (ie, increasing the difference between Phigh and Plow). This means that in APRV the Tlow has to happen more often (by increasing the number of breaths) or be more prolonged (allowing more air to exhale). Because unrestricted spontaneous breaths are permitted at any point of the cycle, the patient contributes to the total minute ventilation (usually 10%–40%).
In APRV and biphasic mode, the operator’s set time and pressure in inspiration and expiration will be delivered regardless of the patient’s breathing efforts—the patient’s spontaneous breath does not trigger a mechanical breath. Some ventilators have automatic adjustments to improve the trigger synchrony.
Ventilator settings in APRV and biphasic mode
These modes require the setting of two pressure levels (Phigh and Plow) and two time durations (Thigh and Tlow). One can add pressure support or automatic tube compensation to assist spontaneous breaths. The difference in Tlow generates differences in the Thigh:Tlow ratio: APRV has a short Tlow (an inspiration-expiration ratio of 4:1). Biphasic mode has a conventional inspiration-expiration ratio of 1:1 to 1:4.
Clinical applications
APRV is used in acute lung injury and ARDS. This mode should be used with caution or not at all in patients with obstructive lung disease or inappropriately increased respiratory drive.32–35
Biphasic mode is intended for both ventilation and weaning. In a patient who has poor respiratory effort or who is paralyzed, biphasic is identical to pressure-control/continuous mandatory ventilation.
Theoretical benefits of APRV and biphasic mode
Multiple benefits have been ascribed to these modes. In theory, APRV will maximize and maintain alveolar recruitment, improve oxygenation, lower inflation pressures, and decrease overinflation. Both APRV and biphasic, by preserving spontaneous breathing, will improve ventilation-perfusion matching and gas diffusion, improve the hemodynamic profile (less need for vasopressors, higher cardiac output, reduced ventricular workload, improved organ perfusion), and improve synchrony (decrease the work of breathing and the need for sedation).
Evidence of benefit of APRV and biphasic mode
APRV and biphasic are different modes. However studies evaluating their effects are combined. This is in part the result of the nomenclature confusion and different practice in different countries.36
Physiologic benefits. In studies, spontaneous breaths contributed to 10% to 40% of minute ventilation,37,38 improved ventilation of dependent areas of the lung, improved ventilation-perfusion match and recruitment,39 and improved hemodynamic profile.40
Patient comfort. These modes are thought to decrease the need for analgesia and sedation,38 but a recent trial showed no difference with pressure-controlled intermittent mandatory ventilation.41 Patient ventilator synchrony and comfort have not been studied.32,42
Outcomes. In small trials, these modes made no difference in terms of deaths, but they may decrease the length of mechanical ventilation.38,41,43,44
APRV and biphasic mode: Bottom line
Maintaining spontaneous breathing while on mechanical ventilation has hemodynamic and ventilatory benefits.
APRV and biphasic mode are not the same thing. APRV’s main goal is to maximize mean airway pressure and, hence, lung recruitment, whereas the main goal of the biphasic mode is synchrony.
There is a plethora of ventilator settings and questions related to physiologic effects.33,34,36
Although these modes are widely used in some centers, there is no evidence yet that they are superior to conventional volume- or pressure-control ventilation with low tidal volume for ARDS and acute lung injury. There is no conclusive evidence that these modes improve synchrony, time to weaning, or patient comfort.
HIGH-FREQUENCY OSCILLATORY VENTILATION
High-frequency oscillatory ventilation (HFOV) was first described and patented in 1952 by Emerson and was clinically developed in the early 1970s by Lunkenheimer.45
The goal of HFOV is to minimize lung injury; its characteristics (discussed below) make it useful in patients with severe ARDS. The US Food and Drug Administration approved it for infants in 1991 and for children in 1995. The adult model has been available since 1993, but it was not approved until 2001 (SensorMedics 3100B, Cardinal Health, Inc).
Other names for high-frequency oscillatory ventilation
While HFOV has no alternative names, the following acronyms describe similar modes:
- HFPPV (high-frequency positive pressure ventilation)
- HFJV (high-frequency jet ventilation)
- HFFI (high-frequency flow interruption)
- HFPV (high-frequency percussive ventilation)
- HFCWO (high-frequency chest wall oscillation).
All of these modes require different specialized ventilators.
What does high-frequency oscillatory ventilation do?
Conceptually, HFOV is a form of pressure-controlled intermittent mandatory ventilation with a set-point control scheme. In contrast to conventional pressure-controlled intermittent mandatory ventilation, in which relatively small spontaneous breaths may be superimposed on relatively large mandatory breaths, HFOV superimposes very small mandatory breaths (oscillations) on top of spontaneous breaths.
Adult patients are usually paralyzed or deeply sedated, since deep spontaneous breathing will trigger alarms and affect ventilator performance.
To manage ventilation (CO2 clearance), one or several of the following maneuvers can be done: decrease the oscillation frequency, increase the amplitude of the oscillations, increase the inspiratory time, or increase bias flow (while allowing an endotracheal tube cuff leak). Oxygenation adjustments are controlled by manipulating the mean airway pressure and the Fio2.
Ventilator settings in high-frequency oscillatory ventilation
Ventilator settings in HFOV are46:
- Airway pressure amplitude (delta P or power)
- Mean airway pressure
- Percent inspiration
- Inspiratory bias flow
- Fio2.
Clinical applications of high-frequency oscillatory ventilation
This mode is usually reserved for ARDS patients for whom conventional ventilation is failing. A recently published protocol46 suggests considering HFOV when there is oxygenation failure (Fio2 ≥ 0.7 and PEEP ≥ 14 cm H2O) or ventilation failure (pH < 7.25 with tidal volume ≥ 6 mL/kg predicted body weight and plateau airway pressure ≥ 30 cm H2O).
This mode is contraindicated when there is known severe airflow obstruction or intracranial hypertension.
Theoretical benefits of high-frequency oscillatory ventilation
Conceptually, HFOV can provide the highest mean airway pressure paired with the lowest tidal volume of any mode. These benefits might make HFOV the ideal lung-protective ventilation strategy.
Evidence of benefit of high-frequency oscillatory ventilation
Physiologic benefits. Animal models have shown less histologic damage and lung inflammation with HFOV than with high-tidal-volume conventional ventilation47,48 and low-tidal-volume conventional ventilation.49
Patient comfort has not been studied. However, current technology does impose undue work of breathing in spontaneously breathing patients.50
Outcomes. Several retrospective case series have described better oxygenation with HFOV as rescue therapy for severe ARDS than with conventional mechanical ventilation. Two randomized controlled trials have studied HFOV vs high-tidal-volume conventional mechanical ventilation for early severe ARDS; HFOV was safe but made no difference in terms of deaths.42,51–54
High-frequency oscillatory ventilation: Bottom line
In theory, HFOV provides all the benefits of an ideal lung-protective strategy, at least for paralyzed or deeply sedated patients. Animal studies support these concepts. In human adults, HFOV has been shown to be safe and to provide better oxygenation but no improvement in death rates compared with conventional mechanical ventilation. Currently, HFOV is better reserved for patients with severe ARDS for whom conventional mechanical ventilation is failing.
- Chatburn RL. Classification of ventilator modes: update and proposal for implementation. Respir Care 2007; 52:301–323.
- Chatburn RL. Computer control of mechanical ventilation. Respir Care 2004; 49:507–517.
- Alvarez A, Subirana M, Benito S. Decelerating flow ventilation effects in acute respiratory failure. J Crit Care 1998; 13:21–25.
- Guldager H, Nielsen SL, Carl P, Soerensen MB. A comparison of volume control and pressure regulated volume control ventilation in acute respiratory failure. Crit Care 1997; 1:75–77.
- Kallet RH, Campbell AR, Dicker RA, Katz JA, Mackersie RC. Work of breathing during lung protective ventilation in patients with acute lung injury and acute respiratory distress syndrome: a comparison between volume and pressure regulated breathing modes. Respir Care 2005; 50:1623–1631.
- Betensley AD, Khalid I, Crawford J, Pensler RA, DiGiovine B. Patient comfort during pressure support and volume controlled continuous mandatory ventilation. Respir Care 2008; 53:897–902.
- Branson RD, Chatburn RL. Controversies in the critical care setting. Should adaptive pressure control modes be utilized for virtually all patients receiving mechanical ventilation? Respir Care 2007; 52:478–485.
- Laubscher TP, Frutiger A, Fanconi S, Jutzi H, Brunner JX. Automatic selection of tidal volume, respiratory frequency and minute ventilation in intubated ICU patients as start up procedure for closed-loop controlled ventilation. Int J Clin Monit Comput 1994; 11:19–30.
- Laubscher TP, Heinrichs W, Weiler N, Hartmann G, Brunner JX. An adaptive lung ventilation controller. IEEE Trans Biomed Eng 1994; 41:51–59.
- Arnal JM, Wysocki M, Nafati C, et al. Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med 2008; 34:75–81.
- Campbell RS, Sinamban RP, Johannigman JA, et al. Clinical evaluation of a new closed loop ventilation mode: adaptive supportive ventilation (ASV). Crit Care 1999; 3( suppl 1):083.
- Belliato M, Palo A, Pasero D, Iotti GA, Mojoli F, Braschi A. Evaluation of adaptive support ventilation in paralysed patients and in a physical lung model. Int J Artif Organs 2004; 27:709–716.
- Tassaux D, Dalmas E, Gratadour P, Jolliet P. Patient ventilator interactions during partial ventilatory support: a preliminary study comparing the effects of adaptive support ventilation with synchronized intermittent mandatory ventilation plus inspiratory pressure support. Crit Care Med 2002; 30:801–807.
- Gruber PC, Gomersall CD, Leung P, et al. Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 2008; 109:81–87.
- Sulzer CF, Chiolero R, Chassot PG, et al. Adaptive support ventilation for fast tracheal extubation after cardiac surgery: a randomized controlled study. Anesthesiology 2001; 95:1339–1345.
- Petter AH, Chiolèro RL, Cassina T, Chassot PG, Müller XM, Revelly JP. Automatic “respirator/weaning” with adaptive support ventilation: the effect on duration of endotracheal intubation and patient management. Anesth Analg 2003; 97:1743–1750.
- Brunner JX, Iotti GA. Adaptive support ventilation (ASV). Minerva Anestesiol 2002; 68:365–368.
- Campbell RS, Branson RD, Johannigman JA. Adaptive support ventilation. Respir Care Clin North Am 2001; 7:425–440.
- Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145:114–120.
- Younes M, Puddy A, Roberts D, et al. Proportional assist ventilation. Results of an initial clinical trial. Am Rev Respir Dis 1992; 145:121–129.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Respiratory load compensation during mechanical ventilatio—proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med 2006; 32:692–699.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Effect of different levels of pressure support and proportional assist ventilation on breathing pattern, work of breathing and gas exchange in mechanically ventilated hypercapnic COPD patients with acute respiratory failure. Respiration 2003; 70:355–361.
- Grasso S, Puntillo F, Mascia L, et al. Compensation for increase in respiratory workload during mechanical ventilation. Pressure support versus proportional assist ventilation. Am J Respir Crit Care Med 2000; 161:819–826.
- Wrigge H, Golisch W, Zinserling J, Sydow M, Almeling G, Burchardi H. Proportional assist versus pressure support ventilation: effects on breathing pattern and respiratory work of patients with chronic obstructive pulmonary disease. Intensive Care Med 1999; 25:790–798.
- Ranieri VM, Giuliani R, Mascia L, et al. Patient ventilator interaction during acute hypercapnia: pressure support vs. proportional assist ventilation. J Appl Physiol 1996; 81:426–436.
- Kondili E, Xirouchaki N, Vaporidi K, Klimathianaki M, Georgopoulos D. Short-term cardiorespiratory effects of proportional assist and pressure support ventilation in patients with acute lung injury/acute respiratory distress syndrome. Anesthesiology 2006; 105:703–708.
- Xirouchaki N, Kondili E, Vaporidi K, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med 2008; 34:2026–2034.
- Bosma K, Ferreyra G, Ambrogio C, et al. Patient ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med 2007; 35:1048–1054.
- Sinderby C, Beck J. Proportional assist ventilation and neurally adjusted ventilatory assist—better approaches to patient ventilator synchrony? Clin Chest Med 2008; 29:329–342.
- Stock MC, Downs JB, Frolicher DA. Airway pressure release ventilation. Crit Care Med 1987; 15:462–466.
- Baum M, Benzer H, Putensen C, Koller W, Putz G. [Biphasic positive airway pressure (BIPAP)—a new form of augmented ventilation]. Anaesthesist 1989; 38:452–458.
- Seymour CW, Frazer M, Reilly PM, Fuchs BD. Airway pressure release and biphasic intermittent positive airway pressure ventilation: are they ready for prime time? J Trauma 2007; 62:1298–1308.
- Myers TR, MacIntyre NR. Respiratory controversies in the critical care setting. Does airway pressure release ventilation offer important new advantages in mechanical ventilator support? Respir Care 2007; 52:452–458.
- Neumann P, Golisch W, Strohmeyer A, Buscher H, Burchardi H, Sydow M. Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med 2002; 28:1742–1749.
- Calzia E, Lindner KH, Witt S, et al. Pressure-time product and work of breathing during biphasic continuous positive airway pressure and assisted spontaneous breathing. Am J Respir Crit Care Med 1994; 150:904–910.
- Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intensive Care Med 2008; 34:1766–1773.
- Sydow M, Burchardi H, Ephraim E, Zielmann S, Crozier TA. Longterm effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med 1994; 149:1550–1556.
- Putensen C, Zech S, Wrigge H, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med 2001; 164:43–49.
- Davis K, Johnson DJ, Branson RD, Campbell RS, Johannigman JA, Porembka D. Airway pressure release ventilation. Arch Surg 1993; 128:1348–1352.
- Kaplan LJ, Bailey H, Formosa V. Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome. Crit Care 2001; 5:221–226.
- Varpula T, Valta P, Niemi R, Takkunen O, Hynynen M, Pettilä VV. Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiol Scand 2004; 48:722–731.
- Siau C, Stewart TE. Current role of high frequency oscillatory ventilation and airway pressure release ventilation in acute lung injury and acute respiratory distress syndrome. Clin Chest Med 2008; 29:265–275.
- Rathgeber J, Schorn B, Falk V, Kazmaier S, Spiegel T, Burchardi H. The influence of controlled mandatory ventilation (CMV), intermittent mandatory ventilation (IMV) and biphasic intermittent positive airway pressure (BIPAP) on duration of intubation and consumption of analgesics and sedatives. A prospective analysis in 596 patients following adult cardiac surgery. Eur J Anaesthesiol 1997; 14:576–582.
- Habashi NM. Other approaches to open lung ventilation: airway pressure release ventilation. Crit Care Med 2005; 33 suppl 3:S228–S240.
- Hess D, Mason S, Branson R. High-frequency ventilation design and equipment issues. Respir Care Clin North Am 2001; 7:577–598.
- Fessler HE, Derdak S, Ferguson ND, et al. A protocol for high frequency oscillatory ventilation in adults: results from a roundtable discussion. Crit Care Med 2007; 35:1649–1654.
- Hamilton PP, Onayemi A, Smyth JA, et al. Comparison of conventional and high-frequency ventilation: oxygenation and lung pathology. J Appl Physiol 1983; 55:131–138.
- Sedeek KA, Takeuchi M, Suchodolski K, et al. Open-lung protective ventilation with pressure control ventilation, high-frequency oscillation, and intratracheal pulmonary ventilation results in similar gas exchange, hemodynamics, and lung mechanics. Anesthesiology 2003; 99:1102–1111.
- Imai Y, Nakagawa S, Ito Y, Kawano T, Slutsky AS, Miyasaka K. Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol 2001; 91:1836–1844.
- van Heerde M, Roubik K, Kopelent V, Plötz FB, Markhorst DG. Unloading work of breathing during high-frequency oscillatory ventilation: a bench study. Crit Care 2006; 10:R103.
- Derdak S, Mehta S, Stewart TE, et al., Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome Trial (MOAT) Study Investigators. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 2002; 166:801–808.
- Bollen CW, van Well GT, Sherry T, et al. High-frequency oscillatory ventilation compared with conventional mechanical ventilation in adult respiratory distress syndrome: a randomized controlled trial [ISRCTN24242669]. Crit Care 2005; 9:R430–R439.
- Mehta S, Granton J, MacDonald RJ, et al. High frequency oscillatory ventilation in adults: the Toronto experience. Chest 2004; 126:518–527.
- Chan KP, Stewart TE, Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest 2007; 131:1907–1916.
Technologic advances and computerized control of mechanical ventilators have made it possible to deliver ventilatory assistance in new modes. Driving these innovations is the desire to prevent ventilator-induced lung injury, improve patient comfort, and liberate the patient from mechanical ventilation as soon as possible.
We call these innovations “alternative” modes to differentiate them from the plain volume-control and pressure-control modes. Some clinicians rarely use these new modes, but in some medical centers they have become the most common ones used, or are being used unknowingly (the operator misunderstands the mode name). The information we provide on these modes of ventilation is by no means an endorsement of their use, but rather a tool to help the clinician understand their physiologic, theoretical, and clinical effects.
We focused on two goals:
- Explain what the mode does
- Briefly review the theoretical benefits and the actual evidence supporting these alternative modes of ventilation.
STANDARD NOMENCLATURE NEEDED
Since its invention, mechanical ventilation has been plagued by multiple names being used to describe the same things. For example, volume-control ventilation is also called volume-cycled ventilation, assist-control ventilation, volume-limited ventilation, and controlled mechanical ventilation. Similarly, multiple abbreviations are used, each depending on the brand of ventilator, and new acronyms have been added in recent years as new modes have been developed. The vast number of names and modes can confuse even the most seasoned critical care physician.
Efforts to establish a common nomenclature are under way.1
WHAT IS A MODE?
A mode of mechanical ventilation has three essential components:
- The control variable
- The breath sequence
- The targeting scheme.
Similar modes may require more detailed descriptions to distinguish them, but the basic function can be explained by these three components.
The control variable
In general, inspiration is an active process, driven by the patient’s effort, the ventilator, or both, while expiration is passive. For simplicity, in this article a mechanical breath means the inspiratory phase of the breath.
The machine can only control the volume (and flow) or the pressure given. The breaths can be further described on the basis of what triggers the breath, what limits it (the maximum value of a control variable), and what ends (cycles) it.
The breath sequence
There are three possible breath sequences:
- Intermittent mandatory ventilation, in which the patient can take spontaneous breaths between mandatory breaths
- Continuous spontaneous ventilation, in which all breaths are spontaneous (Table 1).
The targeting scheme
The targeting or feedback scheme refers to the ventilator settings and programming that dictate its response to the patient’s lung compliance, lung resistance, and respiratory effort. The regulation can be as simple as controlling the pressure in pressure-control mode, or it can be based on a complicated algorithm.
ADAPTIVE PRESSURE CONTROL
Other names for adaptive pressure control
- Pressure Regulated Volume Control (Maquet Servo-i, Rastatt, Germany)
- AutoFlow (Dräger Medical AG, Lübeck, Germany)
- Adaptive Pressure Ventilation (Hamilton Galileo, Hamilton Medical AG, Bonaduz, Switzerland)
- Volume Control+ (Puritan Bennett, Tyco Healthcare; Mansfield, MA)
- Volume Targeted Pressure Control, Pressure Controlled Volume Guaranteed (Engström, General Electric, Madison, WI).
What does adaptive pressure control do?
The APC mode delivers pressure-controlled breaths with an adaptive targeting scheme (Table 2).
In pressure-control ventilation, tidal volumes depend on the lung’s physiologic mechanics (compliance and resistance) and patient effort (Figure 1). Therefore, the tidal volume varies with changes in lung physiology (ie, larger or smaller tidal volumes than targeted).
To overcome this effect, a machine in APC mode adjusts the inspiratory pressure to deliver the set minimal target tidal volume. If tidal volume increases, the machine decreases the inspiratory pressure, and if tidal volume decreases, the machine increases the inspiratory pressure. However, if the patient effort is large enough, the tidal volume will increase in spite of decreasing the inspiratory pressure (Figure 2). The adjustments to the inspiratory pressure occur after the tidal volume is off-target in a number of breaths.
Common sources of confusion with adaptive pressure control
First, APC is not a volume-control mode. In volume control, the tidal volume does not change; in APC the tidal volume can increase or decrease, and the ventilator will adjust the inflation pressure to achieve the target volume. Thus, APC guarantees an average minimum tidal volume but not a maximum tidal volume.
Second, a characteristic of pressure control (and hence, APC) is that the flow of gas varies to maintain constant airway pressure (ie, maintain the set inspiratory pressure). This characteristic allows a patient who generates an inspiratory effort to receive flow as demanded, which is likely more comfortable. This is essentially different from volume control, in which flow is set by the operator and hence is fixed. Thus, if the patient effort is strong enough (Figure 1), this leads to what is called flow asynchrony, in which the patient does not get the flow asked for in a breath.
Ventilator settings in adaptive pressure control
Ventilator settings in APC are:
- Tidal volume
- Time spent in inspiration (inspiratory time)
- Frequency
- Fraction of inspired oxygen (Fio2)
- Positive end-expiratory pressure (PEEP).
Some ventilators also require setting the speed to reach the peak pressure (also known as slope percent or inspiratory rise time).
Clinical applications of adaptive pressure control
This mode is designed to maintain a consistent tidal volume during pressure-control ventilation and to promote inspiratory flow synchrony. It is a means of automatically reducing ventilatory support (ie, weaning) as the patient’s inspiratory effort becomes stronger, as in awakening from anesthesia.
APC may not be ideal for patients who have an inappropriately increased respiratory drive (eg, in severe metabolic acidosis), since the inspiratory pressure will decrease to maintain the targeted average tidal volume, inappropriately shifting the work of breathing onto the patient.
Theoretical benefits of adaptive pressure control
APC guarantees a minimum average tidal volume (unless the pressure alarm threshold is set too low, so that the target tidal volume is not delivered). Other theoretical benefits are flow synchrony, less ventilator manipulation by the operator, and automatic weaning of ventilator support.
Evidence of benefit of adaptive pressure control
Physiologic benefits. This mode has lower peak inspiratory pressures than does volume-control ventilation,3,4 which is often reported as a positive finding. However, in volume-control mode (the usual comparator), the peak inspiratory pressure is a manifestation of both resistance and compliance. Hence, peak inspiratory pressure is expected to be higher but does not reflect actual lung-distending pressures. It is the plateau pressure, a manifestation of lung compliance, that is related to lung injury.
Patient comfort. APC may increase the work of breathing when using low tidal volume ventilation and when there is increased respiratory effort (drive).5 Interestingly, APC was less comfortable than pressure support ventilation in a small trial.6
Outcomes have not been studied.7
Adaptive pressure control: Bottom line
APC is widely available and widely used, sometimes unknowingly (eg, if the operator thinks it is volume control). It is relatively easy to use and to set; however, evidence of its benefit is scant.
ADAPTIVE SUPPORT VENTILATION
Adaptive support ventilation (ASV) evolved as a form of mandatory minute ventilation implemented with adaptive pressure control. Mandatory minute ventilation is a mode that allows the operator to preset a target minute ventilation, and the ventilator then supplies mandatory breaths, either volume- or pressure-controlled, if the patient’s spontaneous breaths generate a lower minute ventilation.
ASV automatically selects the appropriate tidal volume and frequency for mandatory breaths and the appropriate tidal volume for spontaneous breaths on the basis of the respiratory system mechanics and target minute alveolar ventilation.
Described in 1994 by Laubscher et al,8,9 ASV became commercially available in 1998 in Europe and in 2007 in the United States (Hamilton Galileo ventilator, Hamilton Medical AG). This is the first commercially available ventilator that uses an “optimal” targeting scheme (see below).
What does adaptive support ventilation do?
ASV delivers pressure-controlled breaths using an adaptive (optimal) scheme (Table 2). “Optimal,” in this context, means minimizing the mechanical work of breathing: the machine selects a tidal volume and frequency that the patient’s brain would presumably select if the patient were not connected to a ventilator. This pattern is assumed to encourage the patient to generate spontaneous breaths.
The ventilator calculates the normal required minute ventilation based on the patient’s ideal weight and estimated dead space volume (ie, 2.2 mL/kg). This calculation represents 100% of minute ventilation. The clinician at the bedside sets a target percent of minute ventilation that the ventilator will support—higher than 100% if the patient has increased requirements due, eg, to sepsis or increased dead space, or less than 100% during weaning.
The ventilator initially delivers test breaths, in which it measures the expiratory time constant for the respiratory system and then uses this along with the estimated dead space and normal minute ventilation to calculate an optimal breathing frequency in terms of mechanical work.
The optimal or target tidal volume is calculated as the normal minute ventilation divided by the optimal frequency. The target tidal volume is achieved by the use of APC (see above) (Figure 2). This means that the pressure limit is automatically adjusted to achieve an average delivered tidal volume equal to the target. The ventilator continuously monitors the respiratory system mechanics and adjusts its settings accordingly.
The ventilator adjusts its breaths to avoid air trapping by allowing enough time to exhale, to avoid hypoventilation by delivering tidal volume greater than the dead space, and to avoid volutrauma by avoiding large tidal volumes.
Ventilator settings in adaptive support ventilation
Ventilator settings in ASV are:
- Patient height (to calculate the ideal body weight)
- Sex
- Percent of normal predicted minute ventilation goal
- Fio2
- PEEP.
Clinical applications of adaptive support ventilation
ASV is intended as a sole mode of ventilation, from initial support to weaning.
Theoretical benefits of adaptive support ventilation
In theory, ASV offers automatic selection of ventilator settings, automatic adaptation to changing patient lung mechanics, less need for human manipulation of the machine, improved synchrony, and automatic weaning.
Evidence of benefit of adaptive support ventilation
Physiologic benefits. Ventilator settings are adjusted automatically. ASV selects different tidal volume-respiratory rate combinations based on respiratory mechanics in passive and paralyzed patients.10–12 In actively breathing patients, there was no difference in the ventilator settings chosen by ASV for different clinical scenarios (and lung physiology).10 Compared with pressure-controlled intermittent mandatory ventilation, with ASV, the inspiratory load is less and patient-ventilator interaction is better.13
Patient-ventilator synchrony and comfort have not been studied.
Outcomes. Two trials suggest that ASV may decrease time on mechanical ventilation.14,15 However, in another trial,16 compared with a standard protocol, ASV led to fewer ventilator adjustments but achieved similar postsurgical weaning outcomes. The effect of this mode on the death rate has not been examined.17,18
Adaptive support ventilation: Bottom line
ASV is the first commercially available mode that automatically selects all the ventilator settings except PEEP and Fio2. These seem appropriate for different clinical scenarios in patients with poor respiratory effort or in paralyzed patients. Evidence of the effect in actively breathing patients and on outcomes such as length of stay or death is still lacking.
PROPORTIONAL ASSIST VENTILATION
Patients who have normal respiratory drive but who have difficulty sustaining adequate spontaneous ventilation are often subjected to pressure support ventilation (PSV), in which the ventilator generates a constant pressure throughout inspiration regardless of the intensity of the patient’s effort.
In 1992, Younes and colleagues19,20 developed proportional assist ventilation (PAV) as an alternative in which the ventilator generates pressure in proportion to the patient’s effort. PAV became commercially available in Europe in 1999 and was approved in the United States in 2006, available on the Puritan Bennett 840 ventilator (Puritan Bennett Co, Boulder, CO). PAV has also been used for noninvasive ventilation, but this is not available in the United States.
Other names for proportional assist ventilation
Proportional Pressure Support (Dräger Medical; not yet available in the United States).
What does proportional assist ventilation do?
This mode delivers pressure-controlled breaths with a servo control scheme (Table 2).
To better understand PAV, we can compare it with PSV. With PSV, the pressure applied by the ventilator rises to a preset level that is held constant (a set-point scheme) until a cycling criterion (a percent of the maximum inspiratory flow value) is reached. The inspiratory flow and tidal volume are the result of the patient’s inspiratory effort, the level of pressure applied, and the respiratory system mechanics.
In PAV, as in PSV, all breaths are spontaneous (Table 1). The patient controls the timing and size of the breath. There are no preset pressure, flow, or volume goals, but safety limits on the volume and pressure delivered can be set.
Ventilator settings in proportional assist ventilation
Ventilator settings in PAV are:
- Airway type (endotracheal tube, tracheostomy)
- Airway size (inner diameter)
- Percentage of work supported (assist range 5%–95%)
- Tidal volume limit
- Pressure limit
- Expiratory sensitivity (normally, as inspiration ends, flow should stop; this parameter tells the ventilator at what flow to end inspiration).
Caution when assessing the literature. Earlier ventilator versions, ie, Dräger and Manitoba (University of Manitoba, Winnipeg, MB, Canada), which are not available in the United States, required the repeated calculation of the respiratory system mechanics and the manual setting of flow and volume assists (amplification factors) independently. To overcome this limitation, new software automatically adjusts the flow and volume amplification to support the loads imposed by the automatically measured values of resistance and elastance (inverse of compliance) of the respiratory system.21 This software is included in the model (Puritan Bennett) available in the United States.
Clinical applications of proportional assist ventilation
The PAV mode is indicated for maximizing ventilator patient synchrony for assisted spontaneous ventilation.
PAV is contraindicated in patients with respiratory depression (bradypnea) or large air leaks (eg, bronchopleural fistulas). It should be used with caution in patients with severe hyperinflation, in which the patient may still be exhaling but the ventilator doesn’t recognize it. Another group in which PAV should be used with caution is those with high ventilatory drives, in which the ventilator overestimates respiratory system mechanics. This situation can lead to overassistance due to the “runaway phenomenon,” in which the ventilator continues to provide support even if the patient has stopped inspiration.22
Theoretical benefits of proportional assist ventilation
In theory, PAV should reduce the work of breathing, improve synchrony, automatically adapt to changing patient lung mechanics and effort, decrease the need for ventilator intervention and manipulation, decrease the need for sedation, and improve sleep.
Evidence of benefit of proportional assist ventilation
Physiologic benefits. PAV reduces the work of breathing better than PSV,21 even in the face of changing respiratory mechanics or increased respiratory demand (hypercapnia).23–25 The hemodynamic profile is similar to that in PSV. Tidal volumes are variable; however, in recent reports the tidal volumes were within the lung-protective range (6–8 mL/kg, plateau pressure < 30 cm H20).26,27
Comfort. PAV entails less patient effort and discomfort that PSV does.23,25 PAV significantly reduces asynchrony,27 which in turn may favorably affect sleep in critically ill patients. 28
Outcomes. The probability of spontaneous breathing without assistance was significantly better in critically ill patients ventilated with PAV than with PSV. No trial has reported the effect of PAV on deaths.27,29
Proportional assist ventilation: Bottom line
Extensive basic research has been done with PAV in different forms of respiratory failure, such as obstructive lung disease, acute respiratory distress syndrome (ARDS), and chronic respiratory failure. It fulfills its main goal, which is to improve patient-ventilator synchrony. Clinical experience with PAV in the United States is limited, as it was only recently approved.
AIRWAY PRESSURE-RELEASE VENTILATION AND BIPHASIC POSITIVE AIRWAY PRESSURE
Airway pressure-release ventilation (APRV) was described in 1987 by Stock et al30 as a mode for delivering ventilation in acute lung injury while avoiding high airway pressures. APRV combines high constant positive airway pressure (improving oxygenation and promoting alveolar recruitment) with intermittent releases (causing exhalation).
Other names for biphasic positive airway pressure
Other names for biphasic positive airway pressure are:
- BiLevel (Puritan Bennett)
- BIPAP (Dräger Europe)
- Bi Vent (Siemens)
- BiPhasic (Avea, Cardinal Health, Inc, Dublin, OH)
- PCV+ (Dräger Medical)
- DuoPAP (Hamilton).
Caution—name confusion. In North America, BiPAP (Respironics, Murrysville, PA) and BiLevel are used to refer to noninvasive modes of ventilation.
APRV has no other name.
What do these modes do?
These modes deliver pressure-controlled, time-triggered, and time-cycled breaths using a set-point targeting scheme (Table 2). This means that the ventilator maintains a constant pressure (set point) even in the face of spontaneous breaths.
Caution—source of confusion. The term continuous positive airway pressure (CPAP) is often used to describe this mode. However, CPAP is pressure that is applied continuously at the same level; the patient generates all the work to maintain ventilation (“pressure-controlled continuous spontaneous ventilation” in the current nomenclature). In APRV, the airway pressure is intermittently released and reapplied, generating a tidal volume that supports ventilation. In other words, this is a pressure-controlled breath with a very prolonged inspiratory time and a short expiratory time in which spontaneous ventilation is possible at any point (“pressure-controlled intermittent mandatory ventilation” in the current nomenclature).
How these modes are set in the ventilator may also be a source of confusion. To describe the time spent in high and low airway pressures, we use the terms Thigh and Tlow, respectively. By convention, the difference between APRV and biphasic mode is the duration of Tlow (< 1.5 sec for APRV).
Similarly, Phigh and Plow are used to describe the high and low airway pressure. To better understand this concept, you can create the same mode in conventional pressure-control ventilation by thinking of the Thigh as the inspiratory time, the Tlow as the expiratory time, the Phigh as inspiratory pressure, and the Plow as PEEP.
Hence, APRV is an extreme form of inverse ratio ventilation, with an inspiration-to-expiration ratio of 4:1. This means a patient spends most of the time in Phigh and Thigh, and exhalations are short (Tlow and Plow). In contrast, the biphasic mode uses conventional inspiration-expiration ratios (Figure 4).
As with any form of pressure control, the tidal volume is generated by airway pressure rising above baseline (ie, the end-expiratory value). Hence, to ensure an increase in minute ventilation, the mandatory breath rate must be increased (ie, decreasing Thigh, Tlow, or both) or the tidal volume must be increased (ie, increasing the difference between Phigh and Plow). This means that in APRV the Tlow has to happen more often (by increasing the number of breaths) or be more prolonged (allowing more air to exhale). Because unrestricted spontaneous breaths are permitted at any point of the cycle, the patient contributes to the total minute ventilation (usually 10%–40%).
In APRV and biphasic mode, the operator’s set time and pressure in inspiration and expiration will be delivered regardless of the patient’s breathing efforts—the patient’s spontaneous breath does not trigger a mechanical breath. Some ventilators have automatic adjustments to improve the trigger synchrony.
Ventilator settings in APRV and biphasic mode
These modes require the setting of two pressure levels (Phigh and Plow) and two time durations (Thigh and Tlow). One can add pressure support or automatic tube compensation to assist spontaneous breaths. The difference in Tlow generates differences in the Thigh:Tlow ratio: APRV has a short Tlow (an inspiration-expiration ratio of 4:1). Biphasic mode has a conventional inspiration-expiration ratio of 1:1 to 1:4.
Clinical applications
APRV is used in acute lung injury and ARDS. This mode should be used with caution or not at all in patients with obstructive lung disease or inappropriately increased respiratory drive.32–35
Biphasic mode is intended for both ventilation and weaning. In a patient who has poor respiratory effort or who is paralyzed, biphasic is identical to pressure-control/continuous mandatory ventilation.
Theoretical benefits of APRV and biphasic mode
Multiple benefits have been ascribed to these modes. In theory, APRV will maximize and maintain alveolar recruitment, improve oxygenation, lower inflation pressures, and decrease overinflation. Both APRV and biphasic, by preserving spontaneous breathing, will improve ventilation-perfusion matching and gas diffusion, improve the hemodynamic profile (less need for vasopressors, higher cardiac output, reduced ventricular workload, improved organ perfusion), and improve synchrony (decrease the work of breathing and the need for sedation).
Evidence of benefit of APRV and biphasic mode
APRV and biphasic are different modes. However studies evaluating their effects are combined. This is in part the result of the nomenclature confusion and different practice in different countries.36
Physiologic benefits. In studies, spontaneous breaths contributed to 10% to 40% of minute ventilation,37,38 improved ventilation of dependent areas of the lung, improved ventilation-perfusion match and recruitment,39 and improved hemodynamic profile.40
Patient comfort. These modes are thought to decrease the need for analgesia and sedation,38 but a recent trial showed no difference with pressure-controlled intermittent mandatory ventilation.41 Patient ventilator synchrony and comfort have not been studied.32,42
Outcomes. In small trials, these modes made no difference in terms of deaths, but they may decrease the length of mechanical ventilation.38,41,43,44
APRV and biphasic mode: Bottom line
Maintaining spontaneous breathing while on mechanical ventilation has hemodynamic and ventilatory benefits.
APRV and biphasic mode are not the same thing. APRV’s main goal is to maximize mean airway pressure and, hence, lung recruitment, whereas the main goal of the biphasic mode is synchrony.
There is a plethora of ventilator settings and questions related to physiologic effects.33,34,36
Although these modes are widely used in some centers, there is no evidence yet that they are superior to conventional volume- or pressure-control ventilation with low tidal volume for ARDS and acute lung injury. There is no conclusive evidence that these modes improve synchrony, time to weaning, or patient comfort.
HIGH-FREQUENCY OSCILLATORY VENTILATION
High-frequency oscillatory ventilation (HFOV) was first described and patented in 1952 by Emerson and was clinically developed in the early 1970s by Lunkenheimer.45
The goal of HFOV is to minimize lung injury; its characteristics (discussed below) make it useful in patients with severe ARDS. The US Food and Drug Administration approved it for infants in 1991 and for children in 1995. The adult model has been available since 1993, but it was not approved until 2001 (SensorMedics 3100B, Cardinal Health, Inc).
Other names for high-frequency oscillatory ventilation
While HFOV has no alternative names, the following acronyms describe similar modes:
- HFPPV (high-frequency positive pressure ventilation)
- HFJV (high-frequency jet ventilation)
- HFFI (high-frequency flow interruption)
- HFPV (high-frequency percussive ventilation)
- HFCWO (high-frequency chest wall oscillation).
All of these modes require different specialized ventilators.
What does high-frequency oscillatory ventilation do?
Conceptually, HFOV is a form of pressure-controlled intermittent mandatory ventilation with a set-point control scheme. In contrast to conventional pressure-controlled intermittent mandatory ventilation, in which relatively small spontaneous breaths may be superimposed on relatively large mandatory breaths, HFOV superimposes very small mandatory breaths (oscillations) on top of spontaneous breaths.
Adult patients are usually paralyzed or deeply sedated, since deep spontaneous breathing will trigger alarms and affect ventilator performance.
To manage ventilation (CO2 clearance), one or several of the following maneuvers can be done: decrease the oscillation frequency, increase the amplitude of the oscillations, increase the inspiratory time, or increase bias flow (while allowing an endotracheal tube cuff leak). Oxygenation adjustments are controlled by manipulating the mean airway pressure and the Fio2.
Ventilator settings in high-frequency oscillatory ventilation
Ventilator settings in HFOV are46:
- Airway pressure amplitude (delta P or power)
- Mean airway pressure
- Percent inspiration
- Inspiratory bias flow
- Fio2.
Clinical applications of high-frequency oscillatory ventilation
This mode is usually reserved for ARDS patients for whom conventional ventilation is failing. A recently published protocol46 suggests considering HFOV when there is oxygenation failure (Fio2 ≥ 0.7 and PEEP ≥ 14 cm H2O) or ventilation failure (pH < 7.25 with tidal volume ≥ 6 mL/kg predicted body weight and plateau airway pressure ≥ 30 cm H2O).
This mode is contraindicated when there is known severe airflow obstruction or intracranial hypertension.
Theoretical benefits of high-frequency oscillatory ventilation
Conceptually, HFOV can provide the highest mean airway pressure paired with the lowest tidal volume of any mode. These benefits might make HFOV the ideal lung-protective ventilation strategy.
Evidence of benefit of high-frequency oscillatory ventilation
Physiologic benefits. Animal models have shown less histologic damage and lung inflammation with HFOV than with high-tidal-volume conventional ventilation47,48 and low-tidal-volume conventional ventilation.49
Patient comfort has not been studied. However, current technology does impose undue work of breathing in spontaneously breathing patients.50
Outcomes. Several retrospective case series have described better oxygenation with HFOV as rescue therapy for severe ARDS than with conventional mechanical ventilation. Two randomized controlled trials have studied HFOV vs high-tidal-volume conventional mechanical ventilation for early severe ARDS; HFOV was safe but made no difference in terms of deaths.42,51–54
High-frequency oscillatory ventilation: Bottom line
In theory, HFOV provides all the benefits of an ideal lung-protective strategy, at least for paralyzed or deeply sedated patients. Animal studies support these concepts. In human adults, HFOV has been shown to be safe and to provide better oxygenation but no improvement in death rates compared with conventional mechanical ventilation. Currently, HFOV is better reserved for patients with severe ARDS for whom conventional mechanical ventilation is failing.
Technologic advances and computerized control of mechanical ventilators have made it possible to deliver ventilatory assistance in new modes. Driving these innovations is the desire to prevent ventilator-induced lung injury, improve patient comfort, and liberate the patient from mechanical ventilation as soon as possible.
We call these innovations “alternative” modes to differentiate them from the plain volume-control and pressure-control modes. Some clinicians rarely use these new modes, but in some medical centers they have become the most common ones used, or are being used unknowingly (the operator misunderstands the mode name). The information we provide on these modes of ventilation is by no means an endorsement of their use, but rather a tool to help the clinician understand their physiologic, theoretical, and clinical effects.
We focused on two goals:
- Explain what the mode does
- Briefly review the theoretical benefits and the actual evidence supporting these alternative modes of ventilation.
STANDARD NOMENCLATURE NEEDED
Since its invention, mechanical ventilation has been plagued by multiple names being used to describe the same things. For example, volume-control ventilation is also called volume-cycled ventilation, assist-control ventilation, volume-limited ventilation, and controlled mechanical ventilation. Similarly, multiple abbreviations are used, each depending on the brand of ventilator, and new acronyms have been added in recent years as new modes have been developed. The vast number of names and modes can confuse even the most seasoned critical care physician.
Efforts to establish a common nomenclature are under way.1
WHAT IS A MODE?
A mode of mechanical ventilation has three essential components:
- The control variable
- The breath sequence
- The targeting scheme.
Similar modes may require more detailed descriptions to distinguish them, but the basic function can be explained by these three components.
The control variable
In general, inspiration is an active process, driven by the patient’s effort, the ventilator, or both, while expiration is passive. For simplicity, in this article a mechanical breath means the inspiratory phase of the breath.
The machine can only control the volume (and flow) or the pressure given. The breaths can be further described on the basis of what triggers the breath, what limits it (the maximum value of a control variable), and what ends (cycles) it.
The breath sequence
There are three possible breath sequences:
- Intermittent mandatory ventilation, in which the patient can take spontaneous breaths between mandatory breaths
- Continuous spontaneous ventilation, in which all breaths are spontaneous (Table 1).
The targeting scheme
The targeting or feedback scheme refers to the ventilator settings and programming that dictate its response to the patient’s lung compliance, lung resistance, and respiratory effort. The regulation can be as simple as controlling the pressure in pressure-control mode, or it can be based on a complicated algorithm.
ADAPTIVE PRESSURE CONTROL
Other names for adaptive pressure control
- Pressure Regulated Volume Control (Maquet Servo-i, Rastatt, Germany)
- AutoFlow (Dräger Medical AG, Lübeck, Germany)
- Adaptive Pressure Ventilation (Hamilton Galileo, Hamilton Medical AG, Bonaduz, Switzerland)
- Volume Control+ (Puritan Bennett, Tyco Healthcare; Mansfield, MA)
- Volume Targeted Pressure Control, Pressure Controlled Volume Guaranteed (Engström, General Electric, Madison, WI).
What does adaptive pressure control do?
The APC mode delivers pressure-controlled breaths with an adaptive targeting scheme (Table 2).
In pressure-control ventilation, tidal volumes depend on the lung’s physiologic mechanics (compliance and resistance) and patient effort (Figure 1). Therefore, the tidal volume varies with changes in lung physiology (ie, larger or smaller tidal volumes than targeted).
To overcome this effect, a machine in APC mode adjusts the inspiratory pressure to deliver the set minimal target tidal volume. If tidal volume increases, the machine decreases the inspiratory pressure, and if tidal volume decreases, the machine increases the inspiratory pressure. However, if the patient effort is large enough, the tidal volume will increase in spite of decreasing the inspiratory pressure (Figure 2). The adjustments to the inspiratory pressure occur after the tidal volume is off-target in a number of breaths.
Common sources of confusion with adaptive pressure control
First, APC is not a volume-control mode. In volume control, the tidal volume does not change; in APC the tidal volume can increase or decrease, and the ventilator will adjust the inflation pressure to achieve the target volume. Thus, APC guarantees an average minimum tidal volume but not a maximum tidal volume.
Second, a characteristic of pressure control (and hence, APC) is that the flow of gas varies to maintain constant airway pressure (ie, maintain the set inspiratory pressure). This characteristic allows a patient who generates an inspiratory effort to receive flow as demanded, which is likely more comfortable. This is essentially different from volume control, in which flow is set by the operator and hence is fixed. Thus, if the patient effort is strong enough (Figure 1), this leads to what is called flow asynchrony, in which the patient does not get the flow asked for in a breath.
Ventilator settings in adaptive pressure control
Ventilator settings in APC are:
- Tidal volume
- Time spent in inspiration (inspiratory time)
- Frequency
- Fraction of inspired oxygen (Fio2)
- Positive end-expiratory pressure (PEEP).
Some ventilators also require setting the speed to reach the peak pressure (also known as slope percent or inspiratory rise time).
Clinical applications of adaptive pressure control
This mode is designed to maintain a consistent tidal volume during pressure-control ventilation and to promote inspiratory flow synchrony. It is a means of automatically reducing ventilatory support (ie, weaning) as the patient’s inspiratory effort becomes stronger, as in awakening from anesthesia.
APC may not be ideal for patients who have an inappropriately increased respiratory drive (eg, in severe metabolic acidosis), since the inspiratory pressure will decrease to maintain the targeted average tidal volume, inappropriately shifting the work of breathing onto the patient.
Theoretical benefits of adaptive pressure control
APC guarantees a minimum average tidal volume (unless the pressure alarm threshold is set too low, so that the target tidal volume is not delivered). Other theoretical benefits are flow synchrony, less ventilator manipulation by the operator, and automatic weaning of ventilator support.
Evidence of benefit of adaptive pressure control
Physiologic benefits. This mode has lower peak inspiratory pressures than does volume-control ventilation,3,4 which is often reported as a positive finding. However, in volume-control mode (the usual comparator), the peak inspiratory pressure is a manifestation of both resistance and compliance. Hence, peak inspiratory pressure is expected to be higher but does not reflect actual lung-distending pressures. It is the plateau pressure, a manifestation of lung compliance, that is related to lung injury.
Patient comfort. APC may increase the work of breathing when using low tidal volume ventilation and when there is increased respiratory effort (drive).5 Interestingly, APC was less comfortable than pressure support ventilation in a small trial.6
Outcomes have not been studied.7
Adaptive pressure control: Bottom line
APC is widely available and widely used, sometimes unknowingly (eg, if the operator thinks it is volume control). It is relatively easy to use and to set; however, evidence of its benefit is scant.
ADAPTIVE SUPPORT VENTILATION
Adaptive support ventilation (ASV) evolved as a form of mandatory minute ventilation implemented with adaptive pressure control. Mandatory minute ventilation is a mode that allows the operator to preset a target minute ventilation, and the ventilator then supplies mandatory breaths, either volume- or pressure-controlled, if the patient’s spontaneous breaths generate a lower minute ventilation.
ASV automatically selects the appropriate tidal volume and frequency for mandatory breaths and the appropriate tidal volume for spontaneous breaths on the basis of the respiratory system mechanics and target minute alveolar ventilation.
Described in 1994 by Laubscher et al,8,9 ASV became commercially available in 1998 in Europe and in 2007 in the United States (Hamilton Galileo ventilator, Hamilton Medical AG). This is the first commercially available ventilator that uses an “optimal” targeting scheme (see below).
What does adaptive support ventilation do?
ASV delivers pressure-controlled breaths using an adaptive (optimal) scheme (Table 2). “Optimal,” in this context, means minimizing the mechanical work of breathing: the machine selects a tidal volume and frequency that the patient’s brain would presumably select if the patient were not connected to a ventilator. This pattern is assumed to encourage the patient to generate spontaneous breaths.
The ventilator calculates the normal required minute ventilation based on the patient’s ideal weight and estimated dead space volume (ie, 2.2 mL/kg). This calculation represents 100% of minute ventilation. The clinician at the bedside sets a target percent of minute ventilation that the ventilator will support—higher than 100% if the patient has increased requirements due, eg, to sepsis or increased dead space, or less than 100% during weaning.
The ventilator initially delivers test breaths, in which it measures the expiratory time constant for the respiratory system and then uses this along with the estimated dead space and normal minute ventilation to calculate an optimal breathing frequency in terms of mechanical work.
The optimal or target tidal volume is calculated as the normal minute ventilation divided by the optimal frequency. The target tidal volume is achieved by the use of APC (see above) (Figure 2). This means that the pressure limit is automatically adjusted to achieve an average delivered tidal volume equal to the target. The ventilator continuously monitors the respiratory system mechanics and adjusts its settings accordingly.
The ventilator adjusts its breaths to avoid air trapping by allowing enough time to exhale, to avoid hypoventilation by delivering tidal volume greater than the dead space, and to avoid volutrauma by avoiding large tidal volumes.
Ventilator settings in adaptive support ventilation
Ventilator settings in ASV are:
- Patient height (to calculate the ideal body weight)
- Sex
- Percent of normal predicted minute ventilation goal
- Fio2
- PEEP.
Clinical applications of adaptive support ventilation
ASV is intended as a sole mode of ventilation, from initial support to weaning.
Theoretical benefits of adaptive support ventilation
In theory, ASV offers automatic selection of ventilator settings, automatic adaptation to changing patient lung mechanics, less need for human manipulation of the machine, improved synchrony, and automatic weaning.
Evidence of benefit of adaptive support ventilation
Physiologic benefits. Ventilator settings are adjusted automatically. ASV selects different tidal volume-respiratory rate combinations based on respiratory mechanics in passive and paralyzed patients.10–12 In actively breathing patients, there was no difference in the ventilator settings chosen by ASV for different clinical scenarios (and lung physiology).10 Compared with pressure-controlled intermittent mandatory ventilation, with ASV, the inspiratory load is less and patient-ventilator interaction is better.13
Patient-ventilator synchrony and comfort have not been studied.
Outcomes. Two trials suggest that ASV may decrease time on mechanical ventilation.14,15 However, in another trial,16 compared with a standard protocol, ASV led to fewer ventilator adjustments but achieved similar postsurgical weaning outcomes. The effect of this mode on the death rate has not been examined.17,18
Adaptive support ventilation: Bottom line
ASV is the first commercially available mode that automatically selects all the ventilator settings except PEEP and Fio2. These seem appropriate for different clinical scenarios in patients with poor respiratory effort or in paralyzed patients. Evidence of the effect in actively breathing patients and on outcomes such as length of stay or death is still lacking.
PROPORTIONAL ASSIST VENTILATION
Patients who have normal respiratory drive but who have difficulty sustaining adequate spontaneous ventilation are often subjected to pressure support ventilation (PSV), in which the ventilator generates a constant pressure throughout inspiration regardless of the intensity of the patient’s effort.
In 1992, Younes and colleagues19,20 developed proportional assist ventilation (PAV) as an alternative in which the ventilator generates pressure in proportion to the patient’s effort. PAV became commercially available in Europe in 1999 and was approved in the United States in 2006, available on the Puritan Bennett 840 ventilator (Puritan Bennett Co, Boulder, CO). PAV has also been used for noninvasive ventilation, but this is not available in the United States.
Other names for proportional assist ventilation
Proportional Pressure Support (Dräger Medical; not yet available in the United States).
What does proportional assist ventilation do?
This mode delivers pressure-controlled breaths with a servo control scheme (Table 2).
To better understand PAV, we can compare it with PSV. With PSV, the pressure applied by the ventilator rises to a preset level that is held constant (a set-point scheme) until a cycling criterion (a percent of the maximum inspiratory flow value) is reached. The inspiratory flow and tidal volume are the result of the patient’s inspiratory effort, the level of pressure applied, and the respiratory system mechanics.
In PAV, as in PSV, all breaths are spontaneous (Table 1). The patient controls the timing and size of the breath. There are no preset pressure, flow, or volume goals, but safety limits on the volume and pressure delivered can be set.
Ventilator settings in proportional assist ventilation
Ventilator settings in PAV are:
- Airway type (endotracheal tube, tracheostomy)
- Airway size (inner diameter)
- Percentage of work supported (assist range 5%–95%)
- Tidal volume limit
- Pressure limit
- Expiratory sensitivity (normally, as inspiration ends, flow should stop; this parameter tells the ventilator at what flow to end inspiration).
Caution when assessing the literature. Earlier ventilator versions, ie, Dräger and Manitoba (University of Manitoba, Winnipeg, MB, Canada), which are not available in the United States, required the repeated calculation of the respiratory system mechanics and the manual setting of flow and volume assists (amplification factors) independently. To overcome this limitation, new software automatically adjusts the flow and volume amplification to support the loads imposed by the automatically measured values of resistance and elastance (inverse of compliance) of the respiratory system.21 This software is included in the model (Puritan Bennett) available in the United States.
Clinical applications of proportional assist ventilation
The PAV mode is indicated for maximizing ventilator patient synchrony for assisted spontaneous ventilation.
PAV is contraindicated in patients with respiratory depression (bradypnea) or large air leaks (eg, bronchopleural fistulas). It should be used with caution in patients with severe hyperinflation, in which the patient may still be exhaling but the ventilator doesn’t recognize it. Another group in which PAV should be used with caution is those with high ventilatory drives, in which the ventilator overestimates respiratory system mechanics. This situation can lead to overassistance due to the “runaway phenomenon,” in which the ventilator continues to provide support even if the patient has stopped inspiration.22
Theoretical benefits of proportional assist ventilation
In theory, PAV should reduce the work of breathing, improve synchrony, automatically adapt to changing patient lung mechanics and effort, decrease the need for ventilator intervention and manipulation, decrease the need for sedation, and improve sleep.
Evidence of benefit of proportional assist ventilation
Physiologic benefits. PAV reduces the work of breathing better than PSV,21 even in the face of changing respiratory mechanics or increased respiratory demand (hypercapnia).23–25 The hemodynamic profile is similar to that in PSV. Tidal volumes are variable; however, in recent reports the tidal volumes were within the lung-protective range (6–8 mL/kg, plateau pressure < 30 cm H20).26,27
Comfort. PAV entails less patient effort and discomfort that PSV does.23,25 PAV significantly reduces asynchrony,27 which in turn may favorably affect sleep in critically ill patients. 28
Outcomes. The probability of spontaneous breathing without assistance was significantly better in critically ill patients ventilated with PAV than with PSV. No trial has reported the effect of PAV on deaths.27,29
Proportional assist ventilation: Bottom line
Extensive basic research has been done with PAV in different forms of respiratory failure, such as obstructive lung disease, acute respiratory distress syndrome (ARDS), and chronic respiratory failure. It fulfills its main goal, which is to improve patient-ventilator synchrony. Clinical experience with PAV in the United States is limited, as it was only recently approved.
AIRWAY PRESSURE-RELEASE VENTILATION AND BIPHASIC POSITIVE AIRWAY PRESSURE
Airway pressure-release ventilation (APRV) was described in 1987 by Stock et al30 as a mode for delivering ventilation in acute lung injury while avoiding high airway pressures. APRV combines high constant positive airway pressure (improving oxygenation and promoting alveolar recruitment) with intermittent releases (causing exhalation).
Other names for biphasic positive airway pressure
Other names for biphasic positive airway pressure are:
- BiLevel (Puritan Bennett)
- BIPAP (Dräger Europe)
- Bi Vent (Siemens)
- BiPhasic (Avea, Cardinal Health, Inc, Dublin, OH)
- PCV+ (Dräger Medical)
- DuoPAP (Hamilton).
Caution—name confusion. In North America, BiPAP (Respironics, Murrysville, PA) and BiLevel are used to refer to noninvasive modes of ventilation.
APRV has no other name.
What do these modes do?
These modes deliver pressure-controlled, time-triggered, and time-cycled breaths using a set-point targeting scheme (Table 2). This means that the ventilator maintains a constant pressure (set point) even in the face of spontaneous breaths.
Caution—source of confusion. The term continuous positive airway pressure (CPAP) is often used to describe this mode. However, CPAP is pressure that is applied continuously at the same level; the patient generates all the work to maintain ventilation (“pressure-controlled continuous spontaneous ventilation” in the current nomenclature). In APRV, the airway pressure is intermittently released and reapplied, generating a tidal volume that supports ventilation. In other words, this is a pressure-controlled breath with a very prolonged inspiratory time and a short expiratory time in which spontaneous ventilation is possible at any point (“pressure-controlled intermittent mandatory ventilation” in the current nomenclature).
How these modes are set in the ventilator may also be a source of confusion. To describe the time spent in high and low airway pressures, we use the terms Thigh and Tlow, respectively. By convention, the difference between APRV and biphasic mode is the duration of Tlow (< 1.5 sec for APRV).
Similarly, Phigh and Plow are used to describe the high and low airway pressure. To better understand this concept, you can create the same mode in conventional pressure-control ventilation by thinking of the Thigh as the inspiratory time, the Tlow as the expiratory time, the Phigh as inspiratory pressure, and the Plow as PEEP.
Hence, APRV is an extreme form of inverse ratio ventilation, with an inspiration-to-expiration ratio of 4:1. This means a patient spends most of the time in Phigh and Thigh, and exhalations are short (Tlow and Plow). In contrast, the biphasic mode uses conventional inspiration-expiration ratios (Figure 4).
As with any form of pressure control, the tidal volume is generated by airway pressure rising above baseline (ie, the end-expiratory value). Hence, to ensure an increase in minute ventilation, the mandatory breath rate must be increased (ie, decreasing Thigh, Tlow, or both) or the tidal volume must be increased (ie, increasing the difference between Phigh and Plow). This means that in APRV the Tlow has to happen more often (by increasing the number of breaths) or be more prolonged (allowing more air to exhale). Because unrestricted spontaneous breaths are permitted at any point of the cycle, the patient contributes to the total minute ventilation (usually 10%–40%).
In APRV and biphasic mode, the operator’s set time and pressure in inspiration and expiration will be delivered regardless of the patient’s breathing efforts—the patient’s spontaneous breath does not trigger a mechanical breath. Some ventilators have automatic adjustments to improve the trigger synchrony.
Ventilator settings in APRV and biphasic mode
These modes require the setting of two pressure levels (Phigh and Plow) and two time durations (Thigh and Tlow). One can add pressure support or automatic tube compensation to assist spontaneous breaths. The difference in Tlow generates differences in the Thigh:Tlow ratio: APRV has a short Tlow (an inspiration-expiration ratio of 4:1). Biphasic mode has a conventional inspiration-expiration ratio of 1:1 to 1:4.
Clinical applications
APRV is used in acute lung injury and ARDS. This mode should be used with caution or not at all in patients with obstructive lung disease or inappropriately increased respiratory drive.32–35
Biphasic mode is intended for both ventilation and weaning. In a patient who has poor respiratory effort or who is paralyzed, biphasic is identical to pressure-control/continuous mandatory ventilation.
Theoretical benefits of APRV and biphasic mode
Multiple benefits have been ascribed to these modes. In theory, APRV will maximize and maintain alveolar recruitment, improve oxygenation, lower inflation pressures, and decrease overinflation. Both APRV and biphasic, by preserving spontaneous breathing, will improve ventilation-perfusion matching and gas diffusion, improve the hemodynamic profile (less need for vasopressors, higher cardiac output, reduced ventricular workload, improved organ perfusion), and improve synchrony (decrease the work of breathing and the need for sedation).
Evidence of benefit of APRV and biphasic mode
APRV and biphasic are different modes. However studies evaluating their effects are combined. This is in part the result of the nomenclature confusion and different practice in different countries.36
Physiologic benefits. In studies, spontaneous breaths contributed to 10% to 40% of minute ventilation,37,38 improved ventilation of dependent areas of the lung, improved ventilation-perfusion match and recruitment,39 and improved hemodynamic profile.40
Patient comfort. These modes are thought to decrease the need for analgesia and sedation,38 but a recent trial showed no difference with pressure-controlled intermittent mandatory ventilation.41 Patient ventilator synchrony and comfort have not been studied.32,42
Outcomes. In small trials, these modes made no difference in terms of deaths, but they may decrease the length of mechanical ventilation.38,41,43,44
APRV and biphasic mode: Bottom line
Maintaining spontaneous breathing while on mechanical ventilation has hemodynamic and ventilatory benefits.
APRV and biphasic mode are not the same thing. APRV’s main goal is to maximize mean airway pressure and, hence, lung recruitment, whereas the main goal of the biphasic mode is synchrony.
There is a plethora of ventilator settings and questions related to physiologic effects.33,34,36
Although these modes are widely used in some centers, there is no evidence yet that they are superior to conventional volume- or pressure-control ventilation with low tidal volume for ARDS and acute lung injury. There is no conclusive evidence that these modes improve synchrony, time to weaning, or patient comfort.
HIGH-FREQUENCY OSCILLATORY VENTILATION
High-frequency oscillatory ventilation (HFOV) was first described and patented in 1952 by Emerson and was clinically developed in the early 1970s by Lunkenheimer.45
The goal of HFOV is to minimize lung injury; its characteristics (discussed below) make it useful in patients with severe ARDS. The US Food and Drug Administration approved it for infants in 1991 and for children in 1995. The adult model has been available since 1993, but it was not approved until 2001 (SensorMedics 3100B, Cardinal Health, Inc).
Other names for high-frequency oscillatory ventilation
While HFOV has no alternative names, the following acronyms describe similar modes:
- HFPPV (high-frequency positive pressure ventilation)
- HFJV (high-frequency jet ventilation)
- HFFI (high-frequency flow interruption)
- HFPV (high-frequency percussive ventilation)
- HFCWO (high-frequency chest wall oscillation).
All of these modes require different specialized ventilators.
What does high-frequency oscillatory ventilation do?
Conceptually, HFOV is a form of pressure-controlled intermittent mandatory ventilation with a set-point control scheme. In contrast to conventional pressure-controlled intermittent mandatory ventilation, in which relatively small spontaneous breaths may be superimposed on relatively large mandatory breaths, HFOV superimposes very small mandatory breaths (oscillations) on top of spontaneous breaths.
Adult patients are usually paralyzed or deeply sedated, since deep spontaneous breathing will trigger alarms and affect ventilator performance.
To manage ventilation (CO2 clearance), one or several of the following maneuvers can be done: decrease the oscillation frequency, increase the amplitude of the oscillations, increase the inspiratory time, or increase bias flow (while allowing an endotracheal tube cuff leak). Oxygenation adjustments are controlled by manipulating the mean airway pressure and the Fio2.
Ventilator settings in high-frequency oscillatory ventilation
Ventilator settings in HFOV are46:
- Airway pressure amplitude (delta P or power)
- Mean airway pressure
- Percent inspiration
- Inspiratory bias flow
- Fio2.
Clinical applications of high-frequency oscillatory ventilation
This mode is usually reserved for ARDS patients for whom conventional ventilation is failing. A recently published protocol46 suggests considering HFOV when there is oxygenation failure (Fio2 ≥ 0.7 and PEEP ≥ 14 cm H2O) or ventilation failure (pH < 7.25 with tidal volume ≥ 6 mL/kg predicted body weight and plateau airway pressure ≥ 30 cm H2O).
This mode is contraindicated when there is known severe airflow obstruction or intracranial hypertension.
Theoretical benefits of high-frequency oscillatory ventilation
Conceptually, HFOV can provide the highest mean airway pressure paired with the lowest tidal volume of any mode. These benefits might make HFOV the ideal lung-protective ventilation strategy.
Evidence of benefit of high-frequency oscillatory ventilation
Physiologic benefits. Animal models have shown less histologic damage and lung inflammation with HFOV than with high-tidal-volume conventional ventilation47,48 and low-tidal-volume conventional ventilation.49
Patient comfort has not been studied. However, current technology does impose undue work of breathing in spontaneously breathing patients.50
Outcomes. Several retrospective case series have described better oxygenation with HFOV as rescue therapy for severe ARDS than with conventional mechanical ventilation. Two randomized controlled trials have studied HFOV vs high-tidal-volume conventional mechanical ventilation for early severe ARDS; HFOV was safe but made no difference in terms of deaths.42,51–54
High-frequency oscillatory ventilation: Bottom line
In theory, HFOV provides all the benefits of an ideal lung-protective strategy, at least for paralyzed or deeply sedated patients. Animal studies support these concepts. In human adults, HFOV has been shown to be safe and to provide better oxygenation but no improvement in death rates compared with conventional mechanical ventilation. Currently, HFOV is better reserved for patients with severe ARDS for whom conventional mechanical ventilation is failing.
- Chatburn RL. Classification of ventilator modes: update and proposal for implementation. Respir Care 2007; 52:301–323.
- Chatburn RL. Computer control of mechanical ventilation. Respir Care 2004; 49:507–517.
- Alvarez A, Subirana M, Benito S. Decelerating flow ventilation effects in acute respiratory failure. J Crit Care 1998; 13:21–25.
- Guldager H, Nielsen SL, Carl P, Soerensen MB. A comparison of volume control and pressure regulated volume control ventilation in acute respiratory failure. Crit Care 1997; 1:75–77.
- Kallet RH, Campbell AR, Dicker RA, Katz JA, Mackersie RC. Work of breathing during lung protective ventilation in patients with acute lung injury and acute respiratory distress syndrome: a comparison between volume and pressure regulated breathing modes. Respir Care 2005; 50:1623–1631.
- Betensley AD, Khalid I, Crawford J, Pensler RA, DiGiovine B. Patient comfort during pressure support and volume controlled continuous mandatory ventilation. Respir Care 2008; 53:897–902.
- Branson RD, Chatburn RL. Controversies in the critical care setting. Should adaptive pressure control modes be utilized for virtually all patients receiving mechanical ventilation? Respir Care 2007; 52:478–485.
- Laubscher TP, Frutiger A, Fanconi S, Jutzi H, Brunner JX. Automatic selection of tidal volume, respiratory frequency and minute ventilation in intubated ICU patients as start up procedure for closed-loop controlled ventilation. Int J Clin Monit Comput 1994; 11:19–30.
- Laubscher TP, Heinrichs W, Weiler N, Hartmann G, Brunner JX. An adaptive lung ventilation controller. IEEE Trans Biomed Eng 1994; 41:51–59.
- Arnal JM, Wysocki M, Nafati C, et al. Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med 2008; 34:75–81.
- Campbell RS, Sinamban RP, Johannigman JA, et al. Clinical evaluation of a new closed loop ventilation mode: adaptive supportive ventilation (ASV). Crit Care 1999; 3( suppl 1):083.
- Belliato M, Palo A, Pasero D, Iotti GA, Mojoli F, Braschi A. Evaluation of adaptive support ventilation in paralysed patients and in a physical lung model. Int J Artif Organs 2004; 27:709–716.
- Tassaux D, Dalmas E, Gratadour P, Jolliet P. Patient ventilator interactions during partial ventilatory support: a preliminary study comparing the effects of adaptive support ventilation with synchronized intermittent mandatory ventilation plus inspiratory pressure support. Crit Care Med 2002; 30:801–807.
- Gruber PC, Gomersall CD, Leung P, et al. Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 2008; 109:81–87.
- Sulzer CF, Chiolero R, Chassot PG, et al. Adaptive support ventilation for fast tracheal extubation after cardiac surgery: a randomized controlled study. Anesthesiology 2001; 95:1339–1345.
- Petter AH, Chiolèro RL, Cassina T, Chassot PG, Müller XM, Revelly JP. Automatic “respirator/weaning” with adaptive support ventilation: the effect on duration of endotracheal intubation and patient management. Anesth Analg 2003; 97:1743–1750.
- Brunner JX, Iotti GA. Adaptive support ventilation (ASV). Minerva Anestesiol 2002; 68:365–368.
- Campbell RS, Branson RD, Johannigman JA. Adaptive support ventilation. Respir Care Clin North Am 2001; 7:425–440.
- Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145:114–120.
- Younes M, Puddy A, Roberts D, et al. Proportional assist ventilation. Results of an initial clinical trial. Am Rev Respir Dis 1992; 145:121–129.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Respiratory load compensation during mechanical ventilatio—proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med 2006; 32:692–699.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Effect of different levels of pressure support and proportional assist ventilation on breathing pattern, work of breathing and gas exchange in mechanically ventilated hypercapnic COPD patients with acute respiratory failure. Respiration 2003; 70:355–361.
- Grasso S, Puntillo F, Mascia L, et al. Compensation for increase in respiratory workload during mechanical ventilation. Pressure support versus proportional assist ventilation. Am J Respir Crit Care Med 2000; 161:819–826.
- Wrigge H, Golisch W, Zinserling J, Sydow M, Almeling G, Burchardi H. Proportional assist versus pressure support ventilation: effects on breathing pattern and respiratory work of patients with chronic obstructive pulmonary disease. Intensive Care Med 1999; 25:790–798.
- Ranieri VM, Giuliani R, Mascia L, et al. Patient ventilator interaction during acute hypercapnia: pressure support vs. proportional assist ventilation. J Appl Physiol 1996; 81:426–436.
- Kondili E, Xirouchaki N, Vaporidi K, Klimathianaki M, Georgopoulos D. Short-term cardiorespiratory effects of proportional assist and pressure support ventilation in patients with acute lung injury/acute respiratory distress syndrome. Anesthesiology 2006; 105:703–708.
- Xirouchaki N, Kondili E, Vaporidi K, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med 2008; 34:2026–2034.
- Bosma K, Ferreyra G, Ambrogio C, et al. Patient ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med 2007; 35:1048–1054.
- Sinderby C, Beck J. Proportional assist ventilation and neurally adjusted ventilatory assist—better approaches to patient ventilator synchrony? Clin Chest Med 2008; 29:329–342.
- Stock MC, Downs JB, Frolicher DA. Airway pressure release ventilation. Crit Care Med 1987; 15:462–466.
- Baum M, Benzer H, Putensen C, Koller W, Putz G. [Biphasic positive airway pressure (BIPAP)—a new form of augmented ventilation]. Anaesthesist 1989; 38:452–458.
- Seymour CW, Frazer M, Reilly PM, Fuchs BD. Airway pressure release and biphasic intermittent positive airway pressure ventilation: are they ready for prime time? J Trauma 2007; 62:1298–1308.
- Myers TR, MacIntyre NR. Respiratory controversies in the critical care setting. Does airway pressure release ventilation offer important new advantages in mechanical ventilator support? Respir Care 2007; 52:452–458.
- Neumann P, Golisch W, Strohmeyer A, Buscher H, Burchardi H, Sydow M. Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med 2002; 28:1742–1749.
- Calzia E, Lindner KH, Witt S, et al. Pressure-time product and work of breathing during biphasic continuous positive airway pressure and assisted spontaneous breathing. Am J Respir Crit Care Med 1994; 150:904–910.
- Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intensive Care Med 2008; 34:1766–1773.
- Sydow M, Burchardi H, Ephraim E, Zielmann S, Crozier TA. Longterm effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med 1994; 149:1550–1556.
- Putensen C, Zech S, Wrigge H, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med 2001; 164:43–49.
- Davis K, Johnson DJ, Branson RD, Campbell RS, Johannigman JA, Porembka D. Airway pressure release ventilation. Arch Surg 1993; 128:1348–1352.
- Kaplan LJ, Bailey H, Formosa V. Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome. Crit Care 2001; 5:221–226.
- Varpula T, Valta P, Niemi R, Takkunen O, Hynynen M, Pettilä VV. Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiol Scand 2004; 48:722–731.
- Siau C, Stewart TE. Current role of high frequency oscillatory ventilation and airway pressure release ventilation in acute lung injury and acute respiratory distress syndrome. Clin Chest Med 2008; 29:265–275.
- Rathgeber J, Schorn B, Falk V, Kazmaier S, Spiegel T, Burchardi H. The influence of controlled mandatory ventilation (CMV), intermittent mandatory ventilation (IMV) and biphasic intermittent positive airway pressure (BIPAP) on duration of intubation and consumption of analgesics and sedatives. A prospective analysis in 596 patients following adult cardiac surgery. Eur J Anaesthesiol 1997; 14:576–582.
- Habashi NM. Other approaches to open lung ventilation: airway pressure release ventilation. Crit Care Med 2005; 33 suppl 3:S228–S240.
- Hess D, Mason S, Branson R. High-frequency ventilation design and equipment issues. Respir Care Clin North Am 2001; 7:577–598.
- Fessler HE, Derdak S, Ferguson ND, et al. A protocol for high frequency oscillatory ventilation in adults: results from a roundtable discussion. Crit Care Med 2007; 35:1649–1654.
- Hamilton PP, Onayemi A, Smyth JA, et al. Comparison of conventional and high-frequency ventilation: oxygenation and lung pathology. J Appl Physiol 1983; 55:131–138.
- Sedeek KA, Takeuchi M, Suchodolski K, et al. Open-lung protective ventilation with pressure control ventilation, high-frequency oscillation, and intratracheal pulmonary ventilation results in similar gas exchange, hemodynamics, and lung mechanics. Anesthesiology 2003; 99:1102–1111.
- Imai Y, Nakagawa S, Ito Y, Kawano T, Slutsky AS, Miyasaka K. Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol 2001; 91:1836–1844.
- van Heerde M, Roubik K, Kopelent V, Plötz FB, Markhorst DG. Unloading work of breathing during high-frequency oscillatory ventilation: a bench study. Crit Care 2006; 10:R103.
- Derdak S, Mehta S, Stewart TE, et al., Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome Trial (MOAT) Study Investigators. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 2002; 166:801–808.
- Bollen CW, van Well GT, Sherry T, et al. High-frequency oscillatory ventilation compared with conventional mechanical ventilation in adult respiratory distress syndrome: a randomized controlled trial [ISRCTN24242669]. Crit Care 2005; 9:R430–R439.
- Mehta S, Granton J, MacDonald RJ, et al. High frequency oscillatory ventilation in adults: the Toronto experience. Chest 2004; 126:518–527.
- Chan KP, Stewart TE, Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest 2007; 131:1907–1916.
- Chatburn RL. Classification of ventilator modes: update and proposal for implementation. Respir Care 2007; 52:301–323.
- Chatburn RL. Computer control of mechanical ventilation. Respir Care 2004; 49:507–517.
- Alvarez A, Subirana M, Benito S. Decelerating flow ventilation effects in acute respiratory failure. J Crit Care 1998; 13:21–25.
- Guldager H, Nielsen SL, Carl P, Soerensen MB. A comparison of volume control and pressure regulated volume control ventilation in acute respiratory failure. Crit Care 1997; 1:75–77.
- Kallet RH, Campbell AR, Dicker RA, Katz JA, Mackersie RC. Work of breathing during lung protective ventilation in patients with acute lung injury and acute respiratory distress syndrome: a comparison between volume and pressure regulated breathing modes. Respir Care 2005; 50:1623–1631.
- Betensley AD, Khalid I, Crawford J, Pensler RA, DiGiovine B. Patient comfort during pressure support and volume controlled continuous mandatory ventilation. Respir Care 2008; 53:897–902.
- Branson RD, Chatburn RL. Controversies in the critical care setting. Should adaptive pressure control modes be utilized for virtually all patients receiving mechanical ventilation? Respir Care 2007; 52:478–485.
- Laubscher TP, Frutiger A, Fanconi S, Jutzi H, Brunner JX. Automatic selection of tidal volume, respiratory frequency and minute ventilation in intubated ICU patients as start up procedure for closed-loop controlled ventilation. Int J Clin Monit Comput 1994; 11:19–30.
- Laubscher TP, Heinrichs W, Weiler N, Hartmann G, Brunner JX. An adaptive lung ventilation controller. IEEE Trans Biomed Eng 1994; 41:51–59.
- Arnal JM, Wysocki M, Nafati C, et al. Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med 2008; 34:75–81.
- Campbell RS, Sinamban RP, Johannigman JA, et al. Clinical evaluation of a new closed loop ventilation mode: adaptive supportive ventilation (ASV). Crit Care 1999; 3( suppl 1):083.
- Belliato M, Palo A, Pasero D, Iotti GA, Mojoli F, Braschi A. Evaluation of adaptive support ventilation in paralysed patients and in a physical lung model. Int J Artif Organs 2004; 27:709–716.
- Tassaux D, Dalmas E, Gratadour P, Jolliet P. Patient ventilator interactions during partial ventilatory support: a preliminary study comparing the effects of adaptive support ventilation with synchronized intermittent mandatory ventilation plus inspiratory pressure support. Crit Care Med 2002; 30:801–807.
- Gruber PC, Gomersall CD, Leung P, et al. Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 2008; 109:81–87.
- Sulzer CF, Chiolero R, Chassot PG, et al. Adaptive support ventilation for fast tracheal extubation after cardiac surgery: a randomized controlled study. Anesthesiology 2001; 95:1339–1345.
- Petter AH, Chiolèro RL, Cassina T, Chassot PG, Müller XM, Revelly JP. Automatic “respirator/weaning” with adaptive support ventilation: the effect on duration of endotracheal intubation and patient management. Anesth Analg 2003; 97:1743–1750.
- Brunner JX, Iotti GA. Adaptive support ventilation (ASV). Minerva Anestesiol 2002; 68:365–368.
- Campbell RS, Branson RD, Johannigman JA. Adaptive support ventilation. Respir Care Clin North Am 2001; 7:425–440.
- Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145:114–120.
- Younes M, Puddy A, Roberts D, et al. Proportional assist ventilation. Results of an initial clinical trial. Am Rev Respir Dis 1992; 145:121–129.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Respiratory load compensation during mechanical ventilatio—proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med 2006; 32:692–699.
- Kondili E, Prinianakis G, Alexopoulou C, Vakouti E, Klimathianaki M, Georgopoulos D. Effect of different levels of pressure support and proportional assist ventilation on breathing pattern, work of breathing and gas exchange in mechanically ventilated hypercapnic COPD patients with acute respiratory failure. Respiration 2003; 70:355–361.
- Grasso S, Puntillo F, Mascia L, et al. Compensation for increase in respiratory workload during mechanical ventilation. Pressure support versus proportional assist ventilation. Am J Respir Crit Care Med 2000; 161:819–826.
- Wrigge H, Golisch W, Zinserling J, Sydow M, Almeling G, Burchardi H. Proportional assist versus pressure support ventilation: effects on breathing pattern and respiratory work of patients with chronic obstructive pulmonary disease. Intensive Care Med 1999; 25:790–798.
- Ranieri VM, Giuliani R, Mascia L, et al. Patient ventilator interaction during acute hypercapnia: pressure support vs. proportional assist ventilation. J Appl Physiol 1996; 81:426–436.
- Kondili E, Xirouchaki N, Vaporidi K, Klimathianaki M, Georgopoulos D. Short-term cardiorespiratory effects of proportional assist and pressure support ventilation in patients with acute lung injury/acute respiratory distress syndrome. Anesthesiology 2006; 105:703–708.
- Xirouchaki N, Kondili E, Vaporidi K, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med 2008; 34:2026–2034.
- Bosma K, Ferreyra G, Ambrogio C, et al. Patient ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med 2007; 35:1048–1054.
- Sinderby C, Beck J. Proportional assist ventilation and neurally adjusted ventilatory assist—better approaches to patient ventilator synchrony? Clin Chest Med 2008; 29:329–342.
- Stock MC, Downs JB, Frolicher DA. Airway pressure release ventilation. Crit Care Med 1987; 15:462–466.
- Baum M, Benzer H, Putensen C, Koller W, Putz G. [Biphasic positive airway pressure (BIPAP)—a new form of augmented ventilation]. Anaesthesist 1989; 38:452–458.
- Seymour CW, Frazer M, Reilly PM, Fuchs BD. Airway pressure release and biphasic intermittent positive airway pressure ventilation: are they ready for prime time? J Trauma 2007; 62:1298–1308.
- Myers TR, MacIntyre NR. Respiratory controversies in the critical care setting. Does airway pressure release ventilation offer important new advantages in mechanical ventilator support? Respir Care 2007; 52:452–458.
- Neumann P, Golisch W, Strohmeyer A, Buscher H, Burchardi H, Sydow M. Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med 2002; 28:1742–1749.
- Calzia E, Lindner KH, Witt S, et al. Pressure-time product and work of breathing during biphasic continuous positive airway pressure and assisted spontaneous breathing. Am J Respir Crit Care Med 1994; 150:904–910.
- Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intensive Care Med 2008; 34:1766–1773.
- Sydow M, Burchardi H, Ephraim E, Zielmann S, Crozier TA. Longterm effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med 1994; 149:1550–1556.
- Putensen C, Zech S, Wrigge H, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med 2001; 164:43–49.
- Davis K, Johnson DJ, Branson RD, Campbell RS, Johannigman JA, Porembka D. Airway pressure release ventilation. Arch Surg 1993; 128:1348–1352.
- Kaplan LJ, Bailey H, Formosa V. Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome. Crit Care 2001; 5:221–226.
- Varpula T, Valta P, Niemi R, Takkunen O, Hynynen M, Pettilä VV. Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiol Scand 2004; 48:722–731.
- Siau C, Stewart TE. Current role of high frequency oscillatory ventilation and airway pressure release ventilation in acute lung injury and acute respiratory distress syndrome. Clin Chest Med 2008; 29:265–275.
- Rathgeber J, Schorn B, Falk V, Kazmaier S, Spiegel T, Burchardi H. The influence of controlled mandatory ventilation (CMV), intermittent mandatory ventilation (IMV) and biphasic intermittent positive airway pressure (BIPAP) on duration of intubation and consumption of analgesics and sedatives. A prospective analysis in 596 patients following adult cardiac surgery. Eur J Anaesthesiol 1997; 14:576–582.
- Habashi NM. Other approaches to open lung ventilation: airway pressure release ventilation. Crit Care Med 2005; 33 suppl 3:S228–S240.
- Hess D, Mason S, Branson R. High-frequency ventilation design and equipment issues. Respir Care Clin North Am 2001; 7:577–598.
- Fessler HE, Derdak S, Ferguson ND, et al. A protocol for high frequency oscillatory ventilation in adults: results from a roundtable discussion. Crit Care Med 2007; 35:1649–1654.
- Hamilton PP, Onayemi A, Smyth JA, et al. Comparison of conventional and high-frequency ventilation: oxygenation and lung pathology. J Appl Physiol 1983; 55:131–138.
- Sedeek KA, Takeuchi M, Suchodolski K, et al. Open-lung protective ventilation with pressure control ventilation, high-frequency oscillation, and intratracheal pulmonary ventilation results in similar gas exchange, hemodynamics, and lung mechanics. Anesthesiology 2003; 99:1102–1111.
- Imai Y, Nakagawa S, Ito Y, Kawano T, Slutsky AS, Miyasaka K. Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol 2001; 91:1836–1844.
- van Heerde M, Roubik K, Kopelent V, Plötz FB, Markhorst DG. Unloading work of breathing during high-frequency oscillatory ventilation: a bench study. Crit Care 2006; 10:R103.
- Derdak S, Mehta S, Stewart TE, et al., Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome Trial (MOAT) Study Investigators. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 2002; 166:801–808.
- Bollen CW, van Well GT, Sherry T, et al. High-frequency oscillatory ventilation compared with conventional mechanical ventilation in adult respiratory distress syndrome: a randomized controlled trial [ISRCTN24242669]. Crit Care 2005; 9:R430–R439.
- Mehta S, Granton J, MacDonald RJ, et al. High frequency oscillatory ventilation in adults: the Toronto experience. Chest 2004; 126:518–527.
- Chan KP, Stewart TE, Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest 2007; 131:1907–1916.
KEY POINTS
- The alternative modes of ventilation were developed to prevent lung injury and asynchrony, promote better oxygenation and faster weaning, and be easier to use. However, evidence of their benefit is scant.
- Until now, we have lacked a standard nomenclature for mechanical ventilation, leading to confusion.
- Regardless of the mode used, the goals are to avoid lung injury, keep the patient comfortable, and wean the patient from mechanical ventilation as soon as possible.