User login
A Meal to Remember
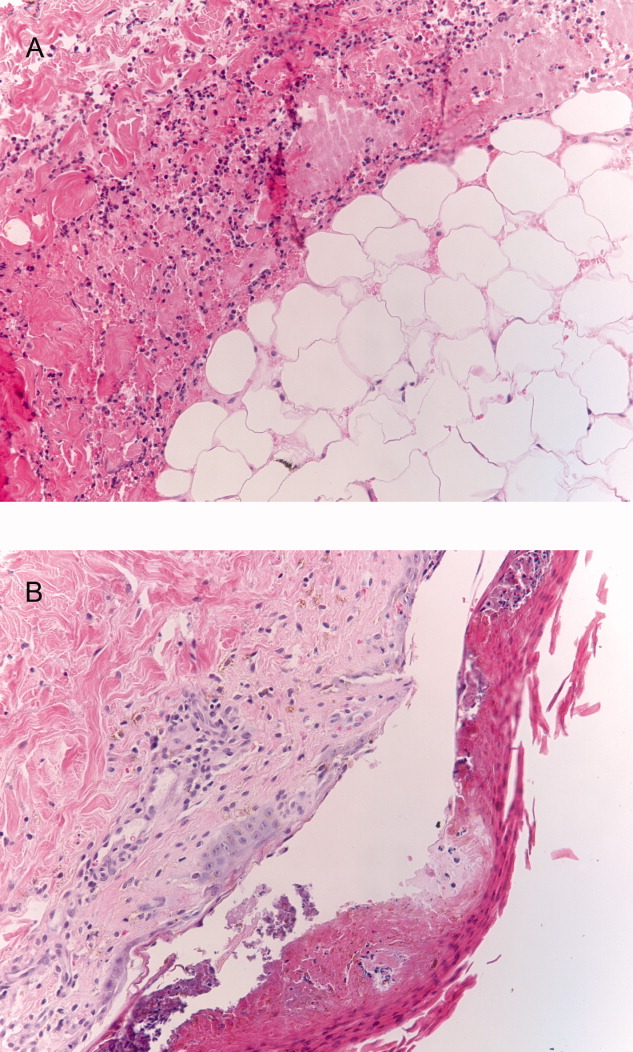
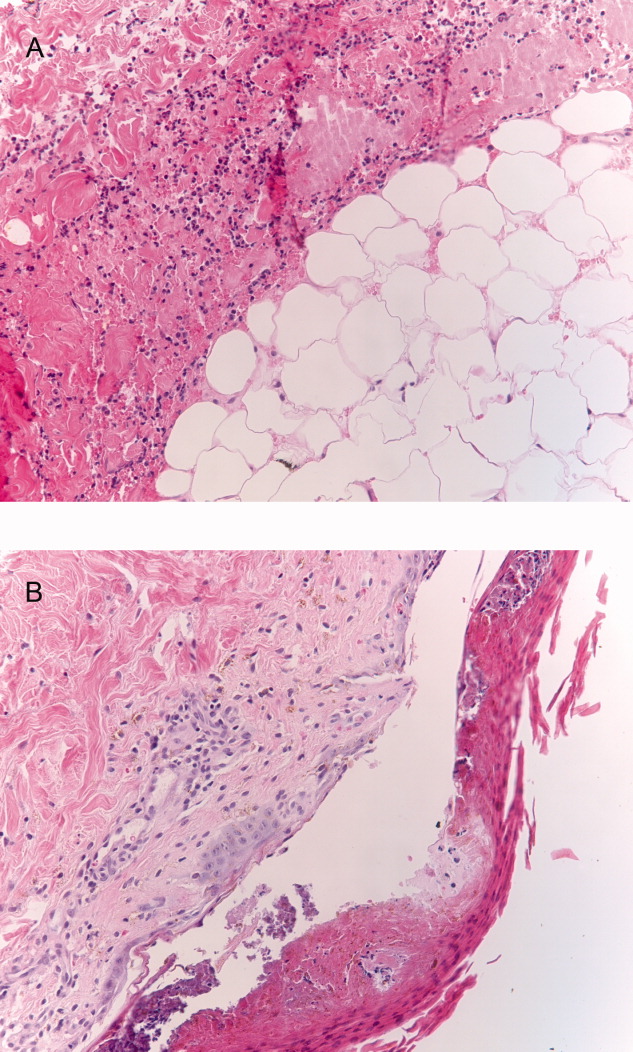
A previously healthy 50‐year‐old man was eating a meal of rigatoni and shrimp at his favorite San Francisco restaurant when he suddenly developed severe pain in his throat followed a short time later by pleuritic chest pain localized to the anterior right chest. He completed his meal and then sought medical attention in the Emergency Department. He was in mild distress secondary to pain but his physical examination was otherwise unremarkable. His laboratory studies showed a white blood cell count of 15,300/mm3 with 86% neutrophils. A chest X‐ray, electrocardiogram, cardiac enzymes, and ventilation/perfusion scan were all normal. Because there was suspicion of an ingested foreign body, an abdominal radiograph was obtained which revealed a 2‐cm trapezoidal foreign body in the right lower quadrant (Figure 1; arrow). A chest computed tomography (CT) scan revealed air in the mediastinum consistent with esophageal perforation (Figure 2). One day after admission a Hypaque esophagram showed trauma to the posterior cervical region of the esophagus, but no leak of contrast material into the mediastinum. The patient was managed conservatively with intravenous (IV) antibiotics and nothing by mouth. Stools were screened and 48 hours after admission the patient (painlessly) passed a piece of glass with a very sharp point (Figure 3) correlating in size and shape to the foreign body seen on the previous abdominal radiograph. The glass had apparently fallen into the patient's restaurant meal the night of admission. The patient did well and was discharged 6 days after admission. He asked the manager of his favorite restaurant to reimburse him the $200 copayment required for hospitalization required under his Preferred Provider Plan; the request was immediately honored.



Esophageal perforation is an emergency because of its high mortality rate. The most frequent cause is iatrogenic with instrumentation from endoscopic procedures. Other causes include foreign body ingestion (as in this case), trauma, operative injury, and tumor.1 Aggressive surgical intervention vs. conservative nonsurgical management remains a controversial topic.2 Early‐contained perforations can be managed successfully by limiting oral intake and giving parenteral antibiotics.3, 4 Any signs of sepsis, deterioration in the patient's condition, or uncontained rupture warrants immediate surgical intervention.14
- ,,, et al.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1483.
- ,,,.Esophageal perforation in adults.Ann Surg.2005;241(6):1016–1023.
- ,,.Esophageal perforation: emphasis of management.Ann Thorac Surg.1996;61:1447–1452
- ,,,.Nonoperative management of esophageal perforations.Ann Surg.1997;225(4):415–421.
A previously healthy 50‐year‐old man was eating a meal of rigatoni and shrimp at his favorite San Francisco restaurant when he suddenly developed severe pain in his throat followed a short time later by pleuritic chest pain localized to the anterior right chest. He completed his meal and then sought medical attention in the Emergency Department. He was in mild distress secondary to pain but his physical examination was otherwise unremarkable. His laboratory studies showed a white blood cell count of 15,300/mm3 with 86% neutrophils. A chest X‐ray, electrocardiogram, cardiac enzymes, and ventilation/perfusion scan were all normal. Because there was suspicion of an ingested foreign body, an abdominal radiograph was obtained which revealed a 2‐cm trapezoidal foreign body in the right lower quadrant (Figure 1; arrow). A chest computed tomography (CT) scan revealed air in the mediastinum consistent with esophageal perforation (Figure 2). One day after admission a Hypaque esophagram showed trauma to the posterior cervical region of the esophagus, but no leak of contrast material into the mediastinum. The patient was managed conservatively with intravenous (IV) antibiotics and nothing by mouth. Stools were screened and 48 hours after admission the patient (painlessly) passed a piece of glass with a very sharp point (Figure 3) correlating in size and shape to the foreign body seen on the previous abdominal radiograph. The glass had apparently fallen into the patient's restaurant meal the night of admission. The patient did well and was discharged 6 days after admission. He asked the manager of his favorite restaurant to reimburse him the $200 copayment required for hospitalization required under his Preferred Provider Plan; the request was immediately honored.
Esophageal perforation is an emergency because of its high mortality rate. The most frequent cause is iatrogenic with instrumentation from endoscopic procedures. Other causes include foreign body ingestion (as in this case), trauma, operative injury, and tumor.1 Aggressive surgical intervention vs. conservative nonsurgical management remains a controversial topic.2 Early‐contained perforations can be managed successfully by limiting oral intake and giving parenteral antibiotics.3, 4 Any signs of sepsis, deterioration in the patient's condition, or uncontained rupture warrants immediate surgical intervention.14
A previously healthy 50‐year‐old man was eating a meal of rigatoni and shrimp at his favorite San Francisco restaurant when he suddenly developed severe pain in his throat followed a short time later by pleuritic chest pain localized to the anterior right chest. He completed his meal and then sought medical attention in the Emergency Department. He was in mild distress secondary to pain but his physical examination was otherwise unremarkable. His laboratory studies showed a white blood cell count of 15,300/mm3 with 86% neutrophils. A chest X‐ray, electrocardiogram, cardiac enzymes, and ventilation/perfusion scan were all normal. Because there was suspicion of an ingested foreign body, an abdominal radiograph was obtained which revealed a 2‐cm trapezoidal foreign body in the right lower quadrant (Figure 1; arrow). A chest computed tomography (CT) scan revealed air in the mediastinum consistent with esophageal perforation (Figure 2). One day after admission a Hypaque esophagram showed trauma to the posterior cervical region of the esophagus, but no leak of contrast material into the mediastinum. The patient was managed conservatively with intravenous (IV) antibiotics and nothing by mouth. Stools were screened and 48 hours after admission the patient (painlessly) passed a piece of glass with a very sharp point (Figure 3) correlating in size and shape to the foreign body seen on the previous abdominal radiograph. The glass had apparently fallen into the patient's restaurant meal the night of admission. The patient did well and was discharged 6 days after admission. He asked the manager of his favorite restaurant to reimburse him the $200 copayment required for hospitalization required under his Preferred Provider Plan; the request was immediately honored.
Esophageal perforation is an emergency because of its high mortality rate. The most frequent cause is iatrogenic with instrumentation from endoscopic procedures. Other causes include foreign body ingestion (as in this case), trauma, operative injury, and tumor.1 Aggressive surgical intervention vs. conservative nonsurgical management remains a controversial topic.2 Early‐contained perforations can be managed successfully by limiting oral intake and giving parenteral antibiotics.3, 4 Any signs of sepsis, deterioration in the patient's condition, or uncontained rupture warrants immediate surgical intervention.14
- ,,, et al.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1483.
- ,,,.Esophageal perforation in adults.Ann Surg.2005;241(6):1016–1023.
- ,,.Esophageal perforation: emphasis of management.Ann Thorac Surg.1996;61:1447–1452
- ,,,.Nonoperative management of esophageal perforations.Ann Surg.1997;225(4):415–421.
- ,,, et al.Evolving options in the management of esophageal perforation.Ann Thorac Surg.2004;77:1475–1483.
- ,,,.Esophageal perforation in adults.Ann Surg.2005;241(6):1016–1023.
- ,,.Esophageal perforation: emphasis of management.Ann Thorac Surg.1996;61:1447–1452
- ,,,.Nonoperative management of esophageal perforations.Ann Surg.1997;225(4):415–421.

The Tip of the Iceberg
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 33‐year‐old African American man was seen in the emergency department for bilateral wrist pain and forearm swelling. He was a professional mover and had transported a piano 3 days before. Several hours after the move, he noticed wrist pain and a few small red, slightly pruritic bumps on the palmar aspect of both wrists. The following day, he developed nausea, vomiting, and watery diarrhea. His wrists and forearms became more swollen and painful.
The most distinctive aspect of the patient's symptom complex is forearm swelling. I am not certain if the primary pathology lies in the wrist or in the forearm. Examination should focus on the presence or absence of arthritis and whether the forearm swelling is simply adjacent to the wrist and rash or extends the entire length from the wrist to the elbow.
Strenuous lifting can lead to rhabdomyolysis and forearm compartment syndrome. However, transporting a piano is not an unusual task for a professional mover. More common causes of arm swelling such as fracture, cellulitis, deep vein thrombosis, and lymphatic obstruction are possible but are unexpected in this patient because of the bilateral findings. An inflammatory myopathy would not present in the distal extremities, but an infectious myositis, such as trichinosis (which can have early gastrointestinal symptoms), could.
Given the patient's age and the temporal correlation, I am inclined to pursue a unifying diagnosis between his gastrointestinal and upper extremity symptoms. The gastrointestinal symptoms could reflect vasculitis (eg, polyarteritis nodosa) or a nonspecific manifestation of systemic illness (eg, sepsis), whereas the rash could be due to infection with petechiae (eg, meningococcemia, gonococcemia, or endocarditis) or an infection with a predilection for peripheral skin lesions that progress centripetally as the illness progresses, such as Rocky Mountain spotted fever.
Although the patient had not seen spiders, he was concerned that his skin lesions might have resulted from spider bites. He had a history of atopic dermatitis but took no medications, did not smoke, and drank alcohol rarely. He lived in Denver, CO, had not traveled outside of the region, and had not visited rural areas. He was monogamous with a female partner and had no known exposures to human immunodeficiency virus. He had no family history of rheumatological disorders.
Patients and physicians frequently attribute papules, ulcers, or necrotic skin lesions to spider bites far out of proportion to their true prevalence. Bites by more innocuous arthropods such as ticks, fleas, bedbugs, or mites are much more common. The symmetry of the lesions and extensive swelling, however, make such bites unlikely.
Although the patient hails from the southwestern United States, there is no compelling evidence for endemic illness. Hantavirus infection causes a viral prodrome, but a severe pulmonary syndrome is its primary manifestation. Plague presents in bubonic, pulmonary, or septicemic forms, but other than the gastrointestinal symptoms, there is nothing to suggest such a systemic illness. The initial pulmonary infection of coccidioidomycosis is often unnoticed, and patients may present with extrapulmonary manifestations, including skin lesions and skeletal disease.
More common ailments remain on the differential. Disseminated gonococcemia must be considered in a sexually active adult with skin lesions and what may be tenosynovitis or arthritis of the distal extremities. The history of atopic dermatitis supports a diagnosis of allergic or contact dermatitis on the wrists (perhaps inoculated during the move), explaining the rash and adjacent swelling (but not the gastrointestinal symptoms).
The patient's temperature was 36.5C with a pulse of 103 beats per minute, a blood pressure of 103/67 mm Hg, and a respiratory rate of 24 breaths per minute. He appeared uncomfortable and was in moderate distress. His sclerae were injected, and his mucous membranes were dry. He had diffusely swollen fingers and firm nonpitting edema in both hands and forearms. His wrists and hands were tender and warm but had no appreciable redness. Two 1‐mm ulcerated lesions were present on his right wrist, and one 2‐mm ulcerated lesion was present on his left wrist. No lymphadenopathy was present.
The patient meets the criteria for systemic inflammatory response syndrome (SIRS), and considering his ill appearance, I am concerned that he may have an infectious process that has evolved into sepsis. The absence of cutaneous erythema rules out cellulitis, and although skin findings in necrotizing fasciitis can be modest in comparison with the underlying infection, an examination with nothing more than punctate ulcerations would be atypical. Plague and tularemia cause ulcerative skin lesions and systemic illness but usually have prominent lymphadenopathy. Cutaneous anthrax can cause intense local edema but is usually accompanied by some degree of necrosis.
I am struck by the degree of local edema. It would be a remarkable coincidence for spider bites to occur on both wrists; however, given the size of the lesions, this remains a consideration. Spider bites can cause severe local swelling and occasionally even SIRS.
The white blood cellcount was 6000/mm3 with a normal differential. The hemoglobin level was 16.6 g/dL, and the platelet count was 227,000/mm3. The serum sodium level was measured to be 135 mmol/L, the potassium level was 3.6 mmol/L, the chloride level was 94 mmol/L, and the bicarbonate level was 9 mmol/L. The urea nitrogen level was measured to be 48 mg/dL (normal, 622), and the serum creatinine level was 5.6 mg/dL (normal, 0.41.2). An arterial blood gas test on room air revealed a pH of 7.22, a partial pressure of carbon dioxide of 24 mm Hg, and a partial pressure of oxygen of 128 mm Hg. Liver enzymes were normal. The serum creatine kinase level was measured to be 194 U/L (normal, 0250). A chest radiograph revealed clear lung fields.
The anion gap is elevated and could be explained in part by renal failure, but it is quite pronounced, and I suspect that there is lactic acidosis either from SIRS and systemic hypoperfusion or from local underperfusion of the distal upper extremities (eg, compartment syndrome). Rhabdomyolysis can cause an anion gap acidosis and acute renal failure but is ruled out by a normal creatine kinase level.
Rheumatological diseases (such as polyarteritis nodosa and systemic scleroderma) can cause renal failure, gastrointestinal symptoms, and cutaneous lesions with skin ulceration but are often accompanied by hypertension. The combination of SIRS and volume depletion from nausea, vomiting, and diarrhea seems more likely, although an etiology for SIRS remains elusive. I suspect infectionmost likely of the upper extremitiesis the underlying cause in this patient despite his normal body temperature and white cell count. I would therefore start with plain films of the arms and hands. If these are unrevealing, I would proceed with an ultrasound of the arms to evaluate the soft tissues and particularly the vessels. Although imaging studies are unlikely to provide a diagnosis, they will provide guidance in choosing the next step, such as biopsy or culture.
The patient wasvolume‐resuscitated with saline and treated with clindamycin, pipercillin‐tazobactam, and vancomycin. Radiographs of the wrists and hands demonstrated edema but no subcutaneous gas and no abnormalities of the bones or joints. An ultrasound of the upper extremities was negative for superficial or deep venous thrombosis. Renal ultrasonography revealed normal‐sized kidneys and no hydronephrosis.
Short of superior vena cava thrombosis, which the ultrasound could not visualize, deep venous thrombosis can be ruled out with confidence. Superior vena cava syndrome could account for the bilateral upper extremity symptoms, but complete sparing of the face would be unusual, and the chest radiograph was normal.
Despite the bilateral nature, I doubt that this patient has an arthritis of the wrists and hands (eg, rheumatoid or psoriatic arthritis). The plain films did not show evidence of joint destruction, although that would not be expected in the first few days of most noninfectious arthropathies. Many rheumatological diseases and vasculitides have renal manifestations, but I do not find convincing evidence of such diseases yet.
Despite intravenous fluidsover the next 4 hours, the patient remained anuric. His upper extremity edema worsened, and he became increasingly tachycardic and hypotensive. Vasopressor support was required. Repeat laboratory studies demonstrated a serum creatinine level of 7.0 mg/dL, a bicarbonate level of 6 mmol/L, and a creatine kinase level of 1183 U/L. The serum lactate level was measured to be 6.5. Blood cultures obtained on admission were negative. An echocardiogram demonstrated marked impairment of left ventricular systolic dysfunction with an estimated ejection fraction of 35%. Repeat chest radiography revealed only mild pulmonary vascular congestion.
The patient has become progressively ill despite initial resuscitation. Any infection (cellulitis, fasciitis, or myositis) may progress to such a point (although to do so without fever or leukocytosis with this degree of illness is unusual) and would prompt me to ask a surgeon to explore the upper extremities for diagnostic and possibly therapeutic purposes. Among the spectrum of possible soft tissue infections, this clinical presentation is most consistent with pyomyositis (caused by Staphylococcus aureus) because of the relatively modest creatine kinase elevations that accompany it and the overall absence of cutaneous findings (save the punctuate lesions), which I would expect to be present with cellulitis or necrotizing fasciitis. A deep forearm infection and perhaps compartment syndrome leading to sepsis could explain lactic acidosis, decreased cardiac function, hypotension, and acute renal failure.
Because of the unusual characteristics noted so farparticularly the bilateral diseaseI continue to also consider systemic diseases that can cause skin lesions, cardiomyopathy, renal disease, ocular involvement (eg, keratoconjunctivitis or uveitis), and myositis. Sarcoidosis is possible, although in most of the aforementioned organs, histological disease is far more common than clinical disease, and sarcoidosis typically does not cause this degree of illness. Furthermore, over 90% of patients with sarcoidosis have pulmonary involvement. Polyarteritis nodosa could explain the multiorgan involvement and the brisk pace. If no infection is present on exploration, I would ask the surgeon to biopsy the muscle, particularly looking for granulomas or vasculitis. A progressive soft tissue infection leading to sepsis remains my leading consideration at this point.
Surgical consultation was obtained. A muscle biopsy of the left biceps and left forearm revealed group A streptococcus within the muscle and evidence of necrosis (Figure 1). Debridement of both arms and wrists was performed. The patient subsequently developed erythema of the palms and soles followed by diffuse sloughing of the skin. Streptococcal toxic shock syndrome with necrotizing myositis was diagnosed, and the antimicrobial regimen was changed to intravenous penicillin, clindamycin, and intravenous immunoglobulin G. Repeat debridement of the arms was required.
Even when a soft tissue infection is suspected, it can be challenging to preoperatively localize or characterize with precision. In retrospect, the overall severity of his illness and his previously good health status perhaps favor necrotizing myositis (and fasciitis) over pyomyositis.
I may have put undue emphasis on the absence of skin findings. Although the symmetric nature of the disease is unusual, the small skin lesions may have been portals of entry, and in retrospect, they represent the tip of the iceberg. The absence of fever and leukocytosisor hypothermia and leukopeniain a young, previously healthy patient along with the bilateral and symmetric findings made me hesitant to definitely label his illness as a deep soft tissue infection early on, but the gravity of the illness, the lack of a plausible alternative explanation, and his precipitous decline all made surgical exploration imperative.
The patient's skin sloughing progressed, and he was transferred to a regional burn unit. Three additional operations were required for debridement of both upper extremities. Despite apparent control of the initial infection, the patient continued to require significant hemodynamic and ventilator support. He subsequently developed neutropenia, thrombocytopenia, and Escherichia coli urosepsis. Necrosis of the lower extremities developed, and additional surgical debridement was recommended. After extensive discussion regarding prognosis, the family decided against further surgery and withdrew life support. The patient died shortly after extubation. The family refused an autopsy.
Commentary
Expert clinicians employ a variety of approaches to solve complex clinical problems. One of the most effective strategies is pattern recognition, in which the clinician divides the case into recognizable portions and compares these to previous cases that he or she has encountered.1, 2 If patterns from the new case appear similar or identical to those of previous cases, a diagnosis can be made quickly and without the need for unnecessary testing. However, when features of the case are unusual or atypical, pattern recognition may be disrupted. For example, although the discussant suspected a soft tissue infection, a number of features (including a normal white blood cell count, minimal skin findings, and a bilateral and symmetric distribution of swelling) did not match his illness script (a mental representation of a disease) of necrotizing fasciitis.
When pattern recognition fails, other strategies are available.3 Hypothetico‐deductive reasoning is a data‐to‐diagnosis method whereby the clinician uses the presenting information to construct a list of diagnostic possibilities.4 Additional testing and gathering of information are then used to continuously revise the diagnostic possibilities until confirmatory information is obtained and the diagnosis is established. After a pattern failed to materialize, the discussant employed this analytical strategy by noting the unusual characteristics of the case and incorporating laboratory and physiological data to revise his differential diagnosis. As a result, he requested the appropriate diagnostic test: surgical exploration of the forearms.
Necrotizing soft tissue infections are characterized by fulminant tissue destruction, rapid spread along tissue planes, and local vascular thrombosis. Mixed aerobic and anaerobic infections typically occur after penetrating skin injury or following surgery in patients with diabetes mellitus or vascular disease. In contrast, monomicrobial infections with S. aureus or group A streptococcus generally occur in healthy individuals. The prevalence of necrotizing group A streptococcal infections has increased dramatically in the last 15 to 20 years.5 Over one‐third of these cases are complicated by toxic shock syndrome.57 Mortality rates for necrotizing fasciitis with toxic shock exceed 30%, and early surgical consultation is directly associated with a reduction in morbidity and mortality.5, 8
Toxic shock is an inflammatory response syndrome caused by release of exotoxins from group A streptococcus and S. aureus.9, 10 In streptococcal toxic shock, Streptococcus pyogenes exotoxin A and Streptococcus pyogenes exotoxin B are the major toxins produced.10 These toxins activate the systemic production of inflammatory cytokines such as interleukin‐1, gamma‐interferon, and tumor necrosis factor, resulting in capillary leak, systemic hypotension, tissue hypoperfusion, and organ failure. The most common initial symptom is diffuse or localized pain that is severe and abrupt in onset and often precedes or is out of proportion to other physical findings of soft tissue infection.8 Up to 20% of individuals may also develop a viral‐like syndrome with myalgias, fever, nausea, vomiting, and diarrhea.11 Erythroderma of the skin and mucous membranes can be another early finding. The rash is diffuse, erythematous, and macular, resembling a sunburn. It involves the palms and soles but can be subtle and fleeting. Erythroderma may be particularly difficult to detect in dark‐skinned individuals.12 It is also important to consider that the absence of fever, erythroderma, or leukocytosis does not necessarily rule out the possibility of serious infection in necrotizing fasciitis patients, as the development of these signs and symptoms may occur later in the disease process.
The most common portals of entry for group A streptococcus are the skin, vagina, and pharynx. Predisposing factors include varicella infection, penetrating injuries, minor cuts, burns, splinters, and surgery. Interestingly, a portal of entry cannot be identified in 45% of cases.8 These patients in particular are at risk for developing severe necrotizing myositis or fasciitis at the site of a minor injury such as a strained muscle. Hematogenous translocation from the pharynx to the site of injury is the probable mechanism13 and would provide one scenario by which our piano mover developed bilateral and symmetric disease. An alternative explanation would be direct extension of bacteria from small breaks in the skin to adjacent areas of muscle strain. Regardless of the portal of entry, as the small skin lesions demonstrate in this patient, the smallest physical finding can represent the tip of the iceberg.
- ,,,,,.Fast and frugal models of clinical judgment in novice and expert physicians.Med Decis Making.2003;23(4):293–300.
- .What is it to be an expert? In: Chi M, Farr MJ, Glaser R, eds.The Nature of Expertise.Hillsdale, NJ:Lawrence Erlbaum;1988.
- .Clinical decision‐making: understanding how clinicians make a diagnosis. In: Saint S, Drazen JM, Solomon CG, eds.Clinical Problem‐Solving.New York, NY:McGraw‐Hill;2006.
- ,,.Medical Problem Solving: An Analysis of Clinical Reasoning.Cambridge, MA:Harvard University Press;1978.
- ,,,,.Population‐based surveillance for group A streptococcal necrotizing fasciitis: clinical features, prognostic indicators, and microbiologic analysis of seventy‐seven cases. Ontario Group A Streptococcal Study.Am J Med.1997;103(1):18–24.
- ,,, et al.Invasive group A streptococcal infections in Sweden in 1994 and 1995: epidemiology and clinical spectrum.Scand J Infect Dis.2000;32(6):609–614.
- ,,,.Reemergence of emm1 and a changed superantigen profile for group A streptococci causing invasive infections: results from a nationwide study.J Clin Microbiol.2005;43(4):1789–1796.
- ,,, et al.Severe group A streptococcal infections associated with a toxic shock‐like syndrome and scarlet fever toxin A.N Engl J Med.1989;321(1):1–7.
- ,,,.Rapidly progressive necrotizing fasciitis caused by Staphylococcus aureus.J Microbiol Immunol Infect.2005;38(5):361–364.
- ,.Streptococcal infections of skin and soft tissues.N Engl J Med.1996;334(4):240–245.
- ,.Streptococcal toxic shock syndrome after breast reconstruction.Ann Plast Surg.2005;54(5):553–556.
- ,.The influence of pigmentation and illumination on the perception of erythema.Photodermatol Photoimmunol Photomed.1992;9(2):45–47.
- .Streptococcal toxic‐shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment.Emerg Infect Dis.1995;1(3):69–78.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 33‐year‐old African American man was seen in the emergency department for bilateral wrist pain and forearm swelling. He was a professional mover and had transported a piano 3 days before. Several hours after the move, he noticed wrist pain and a few small red, slightly pruritic bumps on the palmar aspect of both wrists. The following day, he developed nausea, vomiting, and watery diarrhea. His wrists and forearms became more swollen and painful.
The most distinctive aspect of the patient's symptom complex is forearm swelling. I am not certain if the primary pathology lies in the wrist or in the forearm. Examination should focus on the presence or absence of arthritis and whether the forearm swelling is simply adjacent to the wrist and rash or extends the entire length from the wrist to the elbow.
Strenuous lifting can lead to rhabdomyolysis and forearm compartment syndrome. However, transporting a piano is not an unusual task for a professional mover. More common causes of arm swelling such as fracture, cellulitis, deep vein thrombosis, and lymphatic obstruction are possible but are unexpected in this patient because of the bilateral findings. An inflammatory myopathy would not present in the distal extremities, but an infectious myositis, such as trichinosis (which can have early gastrointestinal symptoms), could.
Given the patient's age and the temporal correlation, I am inclined to pursue a unifying diagnosis between his gastrointestinal and upper extremity symptoms. The gastrointestinal symptoms could reflect vasculitis (eg, polyarteritis nodosa) or a nonspecific manifestation of systemic illness (eg, sepsis), whereas the rash could be due to infection with petechiae (eg, meningococcemia, gonococcemia, or endocarditis) or an infection with a predilection for peripheral skin lesions that progress centripetally as the illness progresses, such as Rocky Mountain spotted fever.
Although the patient had not seen spiders, he was concerned that his skin lesions might have resulted from spider bites. He had a history of atopic dermatitis but took no medications, did not smoke, and drank alcohol rarely. He lived in Denver, CO, had not traveled outside of the region, and had not visited rural areas. He was monogamous with a female partner and had no known exposures to human immunodeficiency virus. He had no family history of rheumatological disorders.
Patients and physicians frequently attribute papules, ulcers, or necrotic skin lesions to spider bites far out of proportion to their true prevalence. Bites by more innocuous arthropods such as ticks, fleas, bedbugs, or mites are much more common. The symmetry of the lesions and extensive swelling, however, make such bites unlikely.
Although the patient hails from the southwestern United States, there is no compelling evidence for endemic illness. Hantavirus infection causes a viral prodrome, but a severe pulmonary syndrome is its primary manifestation. Plague presents in bubonic, pulmonary, or septicemic forms, but other than the gastrointestinal symptoms, there is nothing to suggest such a systemic illness. The initial pulmonary infection of coccidioidomycosis is often unnoticed, and patients may present with extrapulmonary manifestations, including skin lesions and skeletal disease.
More common ailments remain on the differential. Disseminated gonococcemia must be considered in a sexually active adult with skin lesions and what may be tenosynovitis or arthritis of the distal extremities. The history of atopic dermatitis supports a diagnosis of allergic or contact dermatitis on the wrists (perhaps inoculated during the move), explaining the rash and adjacent swelling (but not the gastrointestinal symptoms).
The patient's temperature was 36.5C with a pulse of 103 beats per minute, a blood pressure of 103/67 mm Hg, and a respiratory rate of 24 breaths per minute. He appeared uncomfortable and was in moderate distress. His sclerae were injected, and his mucous membranes were dry. He had diffusely swollen fingers and firm nonpitting edema in both hands and forearms. His wrists and hands were tender and warm but had no appreciable redness. Two 1‐mm ulcerated lesions were present on his right wrist, and one 2‐mm ulcerated lesion was present on his left wrist. No lymphadenopathy was present.
The patient meets the criteria for systemic inflammatory response syndrome (SIRS), and considering his ill appearance, I am concerned that he may have an infectious process that has evolved into sepsis. The absence of cutaneous erythema rules out cellulitis, and although skin findings in necrotizing fasciitis can be modest in comparison with the underlying infection, an examination with nothing more than punctate ulcerations would be atypical. Plague and tularemia cause ulcerative skin lesions and systemic illness but usually have prominent lymphadenopathy. Cutaneous anthrax can cause intense local edema but is usually accompanied by some degree of necrosis.
I am struck by the degree of local edema. It would be a remarkable coincidence for spider bites to occur on both wrists; however, given the size of the lesions, this remains a consideration. Spider bites can cause severe local swelling and occasionally even SIRS.
The white blood cellcount was 6000/mm3 with a normal differential. The hemoglobin level was 16.6 g/dL, and the platelet count was 227,000/mm3. The serum sodium level was measured to be 135 mmol/L, the potassium level was 3.6 mmol/L, the chloride level was 94 mmol/L, and the bicarbonate level was 9 mmol/L. The urea nitrogen level was measured to be 48 mg/dL (normal, 622), and the serum creatinine level was 5.6 mg/dL (normal, 0.41.2). An arterial blood gas test on room air revealed a pH of 7.22, a partial pressure of carbon dioxide of 24 mm Hg, and a partial pressure of oxygen of 128 mm Hg. Liver enzymes were normal. The serum creatine kinase level was measured to be 194 U/L (normal, 0250). A chest radiograph revealed clear lung fields.
The anion gap is elevated and could be explained in part by renal failure, but it is quite pronounced, and I suspect that there is lactic acidosis either from SIRS and systemic hypoperfusion or from local underperfusion of the distal upper extremities (eg, compartment syndrome). Rhabdomyolysis can cause an anion gap acidosis and acute renal failure but is ruled out by a normal creatine kinase level.
Rheumatological diseases (such as polyarteritis nodosa and systemic scleroderma) can cause renal failure, gastrointestinal symptoms, and cutaneous lesions with skin ulceration but are often accompanied by hypertension. The combination of SIRS and volume depletion from nausea, vomiting, and diarrhea seems more likely, although an etiology for SIRS remains elusive. I suspect infectionmost likely of the upper extremitiesis the underlying cause in this patient despite his normal body temperature and white cell count. I would therefore start with plain films of the arms and hands. If these are unrevealing, I would proceed with an ultrasound of the arms to evaluate the soft tissues and particularly the vessels. Although imaging studies are unlikely to provide a diagnosis, they will provide guidance in choosing the next step, such as biopsy or culture.
The patient wasvolume‐resuscitated with saline and treated with clindamycin, pipercillin‐tazobactam, and vancomycin. Radiographs of the wrists and hands demonstrated edema but no subcutaneous gas and no abnormalities of the bones or joints. An ultrasound of the upper extremities was negative for superficial or deep venous thrombosis. Renal ultrasonography revealed normal‐sized kidneys and no hydronephrosis.
Short of superior vena cava thrombosis, which the ultrasound could not visualize, deep venous thrombosis can be ruled out with confidence. Superior vena cava syndrome could account for the bilateral upper extremity symptoms, but complete sparing of the face would be unusual, and the chest radiograph was normal.
Despite the bilateral nature, I doubt that this patient has an arthritis of the wrists and hands (eg, rheumatoid or psoriatic arthritis). The plain films did not show evidence of joint destruction, although that would not be expected in the first few days of most noninfectious arthropathies. Many rheumatological diseases and vasculitides have renal manifestations, but I do not find convincing evidence of such diseases yet.
Despite intravenous fluidsover the next 4 hours, the patient remained anuric. His upper extremity edema worsened, and he became increasingly tachycardic and hypotensive. Vasopressor support was required. Repeat laboratory studies demonstrated a serum creatinine level of 7.0 mg/dL, a bicarbonate level of 6 mmol/L, and a creatine kinase level of 1183 U/L. The serum lactate level was measured to be 6.5. Blood cultures obtained on admission were negative. An echocardiogram demonstrated marked impairment of left ventricular systolic dysfunction with an estimated ejection fraction of 35%. Repeat chest radiography revealed only mild pulmonary vascular congestion.
The patient has become progressively ill despite initial resuscitation. Any infection (cellulitis, fasciitis, or myositis) may progress to such a point (although to do so without fever or leukocytosis with this degree of illness is unusual) and would prompt me to ask a surgeon to explore the upper extremities for diagnostic and possibly therapeutic purposes. Among the spectrum of possible soft tissue infections, this clinical presentation is most consistent with pyomyositis (caused by Staphylococcus aureus) because of the relatively modest creatine kinase elevations that accompany it and the overall absence of cutaneous findings (save the punctuate lesions), which I would expect to be present with cellulitis or necrotizing fasciitis. A deep forearm infection and perhaps compartment syndrome leading to sepsis could explain lactic acidosis, decreased cardiac function, hypotension, and acute renal failure.
Because of the unusual characteristics noted so farparticularly the bilateral diseaseI continue to also consider systemic diseases that can cause skin lesions, cardiomyopathy, renal disease, ocular involvement (eg, keratoconjunctivitis or uveitis), and myositis. Sarcoidosis is possible, although in most of the aforementioned organs, histological disease is far more common than clinical disease, and sarcoidosis typically does not cause this degree of illness. Furthermore, over 90% of patients with sarcoidosis have pulmonary involvement. Polyarteritis nodosa could explain the multiorgan involvement and the brisk pace. If no infection is present on exploration, I would ask the surgeon to biopsy the muscle, particularly looking for granulomas or vasculitis. A progressive soft tissue infection leading to sepsis remains my leading consideration at this point.
Surgical consultation was obtained. A muscle biopsy of the left biceps and left forearm revealed group A streptococcus within the muscle and evidence of necrosis (Figure 1). Debridement of both arms and wrists was performed. The patient subsequently developed erythema of the palms and soles followed by diffuse sloughing of the skin. Streptococcal toxic shock syndrome with necrotizing myositis was diagnosed, and the antimicrobial regimen was changed to intravenous penicillin, clindamycin, and intravenous immunoglobulin G. Repeat debridement of the arms was required.
Even when a soft tissue infection is suspected, it can be challenging to preoperatively localize or characterize with precision. In retrospect, the overall severity of his illness and his previously good health status perhaps favor necrotizing myositis (and fasciitis) over pyomyositis.
I may have put undue emphasis on the absence of skin findings. Although the symmetric nature of the disease is unusual, the small skin lesions may have been portals of entry, and in retrospect, they represent the tip of the iceberg. The absence of fever and leukocytosisor hypothermia and leukopeniain a young, previously healthy patient along with the bilateral and symmetric findings made me hesitant to definitely label his illness as a deep soft tissue infection early on, but the gravity of the illness, the lack of a plausible alternative explanation, and his precipitous decline all made surgical exploration imperative.
The patient's skin sloughing progressed, and he was transferred to a regional burn unit. Three additional operations were required for debridement of both upper extremities. Despite apparent control of the initial infection, the patient continued to require significant hemodynamic and ventilator support. He subsequently developed neutropenia, thrombocytopenia, and Escherichia coli urosepsis. Necrosis of the lower extremities developed, and additional surgical debridement was recommended. After extensive discussion regarding prognosis, the family decided against further surgery and withdrew life support. The patient died shortly after extubation. The family refused an autopsy.
Commentary
Expert clinicians employ a variety of approaches to solve complex clinical problems. One of the most effective strategies is pattern recognition, in which the clinician divides the case into recognizable portions and compares these to previous cases that he or she has encountered.1, 2 If patterns from the new case appear similar or identical to those of previous cases, a diagnosis can be made quickly and without the need for unnecessary testing. However, when features of the case are unusual or atypical, pattern recognition may be disrupted. For example, although the discussant suspected a soft tissue infection, a number of features (including a normal white blood cell count, minimal skin findings, and a bilateral and symmetric distribution of swelling) did not match his illness script (a mental representation of a disease) of necrotizing fasciitis.
When pattern recognition fails, other strategies are available.3 Hypothetico‐deductive reasoning is a data‐to‐diagnosis method whereby the clinician uses the presenting information to construct a list of diagnostic possibilities.4 Additional testing and gathering of information are then used to continuously revise the diagnostic possibilities until confirmatory information is obtained and the diagnosis is established. After a pattern failed to materialize, the discussant employed this analytical strategy by noting the unusual characteristics of the case and incorporating laboratory and physiological data to revise his differential diagnosis. As a result, he requested the appropriate diagnostic test: surgical exploration of the forearms.
Necrotizing soft tissue infections are characterized by fulminant tissue destruction, rapid spread along tissue planes, and local vascular thrombosis. Mixed aerobic and anaerobic infections typically occur after penetrating skin injury or following surgery in patients with diabetes mellitus or vascular disease. In contrast, monomicrobial infections with S. aureus or group A streptococcus generally occur in healthy individuals. The prevalence of necrotizing group A streptococcal infections has increased dramatically in the last 15 to 20 years.5 Over one‐third of these cases are complicated by toxic shock syndrome.57 Mortality rates for necrotizing fasciitis with toxic shock exceed 30%, and early surgical consultation is directly associated with a reduction in morbidity and mortality.5, 8
Toxic shock is an inflammatory response syndrome caused by release of exotoxins from group A streptococcus and S. aureus.9, 10 In streptococcal toxic shock, Streptococcus pyogenes exotoxin A and Streptococcus pyogenes exotoxin B are the major toxins produced.10 These toxins activate the systemic production of inflammatory cytokines such as interleukin‐1, gamma‐interferon, and tumor necrosis factor, resulting in capillary leak, systemic hypotension, tissue hypoperfusion, and organ failure. The most common initial symptom is diffuse or localized pain that is severe and abrupt in onset and often precedes or is out of proportion to other physical findings of soft tissue infection.8 Up to 20% of individuals may also develop a viral‐like syndrome with myalgias, fever, nausea, vomiting, and diarrhea.11 Erythroderma of the skin and mucous membranes can be another early finding. The rash is diffuse, erythematous, and macular, resembling a sunburn. It involves the palms and soles but can be subtle and fleeting. Erythroderma may be particularly difficult to detect in dark‐skinned individuals.12 It is also important to consider that the absence of fever, erythroderma, or leukocytosis does not necessarily rule out the possibility of serious infection in necrotizing fasciitis patients, as the development of these signs and symptoms may occur later in the disease process.
The most common portals of entry for group A streptococcus are the skin, vagina, and pharynx. Predisposing factors include varicella infection, penetrating injuries, minor cuts, burns, splinters, and surgery. Interestingly, a portal of entry cannot be identified in 45% of cases.8 These patients in particular are at risk for developing severe necrotizing myositis or fasciitis at the site of a minor injury such as a strained muscle. Hematogenous translocation from the pharynx to the site of injury is the probable mechanism13 and would provide one scenario by which our piano mover developed bilateral and symmetric disease. An alternative explanation would be direct extension of bacteria from small breaks in the skin to adjacent areas of muscle strain. Regardless of the portal of entry, as the small skin lesions demonstrate in this patient, the smallest physical finding can represent the tip of the iceberg.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 33‐year‐old African American man was seen in the emergency department for bilateral wrist pain and forearm swelling. He was a professional mover and had transported a piano 3 days before. Several hours after the move, he noticed wrist pain and a few small red, slightly pruritic bumps on the palmar aspect of both wrists. The following day, he developed nausea, vomiting, and watery diarrhea. His wrists and forearms became more swollen and painful.
The most distinctive aspect of the patient's symptom complex is forearm swelling. I am not certain if the primary pathology lies in the wrist or in the forearm. Examination should focus on the presence or absence of arthritis and whether the forearm swelling is simply adjacent to the wrist and rash or extends the entire length from the wrist to the elbow.
Strenuous lifting can lead to rhabdomyolysis and forearm compartment syndrome. However, transporting a piano is not an unusual task for a professional mover. More common causes of arm swelling such as fracture, cellulitis, deep vein thrombosis, and lymphatic obstruction are possible but are unexpected in this patient because of the bilateral findings. An inflammatory myopathy would not present in the distal extremities, but an infectious myositis, such as trichinosis (which can have early gastrointestinal symptoms), could.
Given the patient's age and the temporal correlation, I am inclined to pursue a unifying diagnosis between his gastrointestinal and upper extremity symptoms. The gastrointestinal symptoms could reflect vasculitis (eg, polyarteritis nodosa) or a nonspecific manifestation of systemic illness (eg, sepsis), whereas the rash could be due to infection with petechiae (eg, meningococcemia, gonococcemia, or endocarditis) or an infection with a predilection for peripheral skin lesions that progress centripetally as the illness progresses, such as Rocky Mountain spotted fever.
Although the patient had not seen spiders, he was concerned that his skin lesions might have resulted from spider bites. He had a history of atopic dermatitis but took no medications, did not smoke, and drank alcohol rarely. He lived in Denver, CO, had not traveled outside of the region, and had not visited rural areas. He was monogamous with a female partner and had no known exposures to human immunodeficiency virus. He had no family history of rheumatological disorders.
Patients and physicians frequently attribute papules, ulcers, or necrotic skin lesions to spider bites far out of proportion to their true prevalence. Bites by more innocuous arthropods such as ticks, fleas, bedbugs, or mites are much more common. The symmetry of the lesions and extensive swelling, however, make such bites unlikely.
Although the patient hails from the southwestern United States, there is no compelling evidence for endemic illness. Hantavirus infection causes a viral prodrome, but a severe pulmonary syndrome is its primary manifestation. Plague presents in bubonic, pulmonary, or septicemic forms, but other than the gastrointestinal symptoms, there is nothing to suggest such a systemic illness. The initial pulmonary infection of coccidioidomycosis is often unnoticed, and patients may present with extrapulmonary manifestations, including skin lesions and skeletal disease.
More common ailments remain on the differential. Disseminated gonococcemia must be considered in a sexually active adult with skin lesions and what may be tenosynovitis or arthritis of the distal extremities. The history of atopic dermatitis supports a diagnosis of allergic or contact dermatitis on the wrists (perhaps inoculated during the move), explaining the rash and adjacent swelling (but not the gastrointestinal symptoms).
The patient's temperature was 36.5C with a pulse of 103 beats per minute, a blood pressure of 103/67 mm Hg, and a respiratory rate of 24 breaths per minute. He appeared uncomfortable and was in moderate distress. His sclerae were injected, and his mucous membranes were dry. He had diffusely swollen fingers and firm nonpitting edema in both hands and forearms. His wrists and hands were tender and warm but had no appreciable redness. Two 1‐mm ulcerated lesions were present on his right wrist, and one 2‐mm ulcerated lesion was present on his left wrist. No lymphadenopathy was present.
The patient meets the criteria for systemic inflammatory response syndrome (SIRS), and considering his ill appearance, I am concerned that he may have an infectious process that has evolved into sepsis. The absence of cutaneous erythema rules out cellulitis, and although skin findings in necrotizing fasciitis can be modest in comparison with the underlying infection, an examination with nothing more than punctate ulcerations would be atypical. Plague and tularemia cause ulcerative skin lesions and systemic illness but usually have prominent lymphadenopathy. Cutaneous anthrax can cause intense local edema but is usually accompanied by some degree of necrosis.
I am struck by the degree of local edema. It would be a remarkable coincidence for spider bites to occur on both wrists; however, given the size of the lesions, this remains a consideration. Spider bites can cause severe local swelling and occasionally even SIRS.
The white blood cellcount was 6000/mm3 with a normal differential. The hemoglobin level was 16.6 g/dL, and the platelet count was 227,000/mm3. The serum sodium level was measured to be 135 mmol/L, the potassium level was 3.6 mmol/L, the chloride level was 94 mmol/L, and the bicarbonate level was 9 mmol/L. The urea nitrogen level was measured to be 48 mg/dL (normal, 622), and the serum creatinine level was 5.6 mg/dL (normal, 0.41.2). An arterial blood gas test on room air revealed a pH of 7.22, a partial pressure of carbon dioxide of 24 mm Hg, and a partial pressure of oxygen of 128 mm Hg. Liver enzymes were normal. The serum creatine kinase level was measured to be 194 U/L (normal, 0250). A chest radiograph revealed clear lung fields.
The anion gap is elevated and could be explained in part by renal failure, but it is quite pronounced, and I suspect that there is lactic acidosis either from SIRS and systemic hypoperfusion or from local underperfusion of the distal upper extremities (eg, compartment syndrome). Rhabdomyolysis can cause an anion gap acidosis and acute renal failure but is ruled out by a normal creatine kinase level.
Rheumatological diseases (such as polyarteritis nodosa and systemic scleroderma) can cause renal failure, gastrointestinal symptoms, and cutaneous lesions with skin ulceration but are often accompanied by hypertension. The combination of SIRS and volume depletion from nausea, vomiting, and diarrhea seems more likely, although an etiology for SIRS remains elusive. I suspect infectionmost likely of the upper extremitiesis the underlying cause in this patient despite his normal body temperature and white cell count. I would therefore start with plain films of the arms and hands. If these are unrevealing, I would proceed with an ultrasound of the arms to evaluate the soft tissues and particularly the vessels. Although imaging studies are unlikely to provide a diagnosis, they will provide guidance in choosing the next step, such as biopsy or culture.
The patient wasvolume‐resuscitated with saline and treated with clindamycin, pipercillin‐tazobactam, and vancomycin. Radiographs of the wrists and hands demonstrated edema but no subcutaneous gas and no abnormalities of the bones or joints. An ultrasound of the upper extremities was negative for superficial or deep venous thrombosis. Renal ultrasonography revealed normal‐sized kidneys and no hydronephrosis.
Short of superior vena cava thrombosis, which the ultrasound could not visualize, deep venous thrombosis can be ruled out with confidence. Superior vena cava syndrome could account for the bilateral upper extremity symptoms, but complete sparing of the face would be unusual, and the chest radiograph was normal.
Despite the bilateral nature, I doubt that this patient has an arthritis of the wrists and hands (eg, rheumatoid or psoriatic arthritis). The plain films did not show evidence of joint destruction, although that would not be expected in the first few days of most noninfectious arthropathies. Many rheumatological diseases and vasculitides have renal manifestations, but I do not find convincing evidence of such diseases yet.
Despite intravenous fluidsover the next 4 hours, the patient remained anuric. His upper extremity edema worsened, and he became increasingly tachycardic and hypotensive. Vasopressor support was required. Repeat laboratory studies demonstrated a serum creatinine level of 7.0 mg/dL, a bicarbonate level of 6 mmol/L, and a creatine kinase level of 1183 U/L. The serum lactate level was measured to be 6.5. Blood cultures obtained on admission were negative. An echocardiogram demonstrated marked impairment of left ventricular systolic dysfunction with an estimated ejection fraction of 35%. Repeat chest radiography revealed only mild pulmonary vascular congestion.
The patient has become progressively ill despite initial resuscitation. Any infection (cellulitis, fasciitis, or myositis) may progress to such a point (although to do so without fever or leukocytosis with this degree of illness is unusual) and would prompt me to ask a surgeon to explore the upper extremities for diagnostic and possibly therapeutic purposes. Among the spectrum of possible soft tissue infections, this clinical presentation is most consistent with pyomyositis (caused by Staphylococcus aureus) because of the relatively modest creatine kinase elevations that accompany it and the overall absence of cutaneous findings (save the punctuate lesions), which I would expect to be present with cellulitis or necrotizing fasciitis. A deep forearm infection and perhaps compartment syndrome leading to sepsis could explain lactic acidosis, decreased cardiac function, hypotension, and acute renal failure.
Because of the unusual characteristics noted so farparticularly the bilateral diseaseI continue to also consider systemic diseases that can cause skin lesions, cardiomyopathy, renal disease, ocular involvement (eg, keratoconjunctivitis or uveitis), and myositis. Sarcoidosis is possible, although in most of the aforementioned organs, histological disease is far more common than clinical disease, and sarcoidosis typically does not cause this degree of illness. Furthermore, over 90% of patients with sarcoidosis have pulmonary involvement. Polyarteritis nodosa could explain the multiorgan involvement and the brisk pace. If no infection is present on exploration, I would ask the surgeon to biopsy the muscle, particularly looking for granulomas or vasculitis. A progressive soft tissue infection leading to sepsis remains my leading consideration at this point.
Surgical consultation was obtained. A muscle biopsy of the left biceps and left forearm revealed group A streptococcus within the muscle and evidence of necrosis (Figure 1). Debridement of both arms and wrists was performed. The patient subsequently developed erythema of the palms and soles followed by diffuse sloughing of the skin. Streptococcal toxic shock syndrome with necrotizing myositis was diagnosed, and the antimicrobial regimen was changed to intravenous penicillin, clindamycin, and intravenous immunoglobulin G. Repeat debridement of the arms was required.
Even when a soft tissue infection is suspected, it can be challenging to preoperatively localize or characterize with precision. In retrospect, the overall severity of his illness and his previously good health status perhaps favor necrotizing myositis (and fasciitis) over pyomyositis.
I may have put undue emphasis on the absence of skin findings. Although the symmetric nature of the disease is unusual, the small skin lesions may have been portals of entry, and in retrospect, they represent the tip of the iceberg. The absence of fever and leukocytosisor hypothermia and leukopeniain a young, previously healthy patient along with the bilateral and symmetric findings made me hesitant to definitely label his illness as a deep soft tissue infection early on, but the gravity of the illness, the lack of a plausible alternative explanation, and his precipitous decline all made surgical exploration imperative.
The patient's skin sloughing progressed, and he was transferred to a regional burn unit. Three additional operations were required for debridement of both upper extremities. Despite apparent control of the initial infection, the patient continued to require significant hemodynamic and ventilator support. He subsequently developed neutropenia, thrombocytopenia, and Escherichia coli urosepsis. Necrosis of the lower extremities developed, and additional surgical debridement was recommended. After extensive discussion regarding prognosis, the family decided against further surgery and withdrew life support. The patient died shortly after extubation. The family refused an autopsy.
Commentary
Expert clinicians employ a variety of approaches to solve complex clinical problems. One of the most effective strategies is pattern recognition, in which the clinician divides the case into recognizable portions and compares these to previous cases that he or she has encountered.1, 2 If patterns from the new case appear similar or identical to those of previous cases, a diagnosis can be made quickly and without the need for unnecessary testing. However, when features of the case are unusual or atypical, pattern recognition may be disrupted. For example, although the discussant suspected a soft tissue infection, a number of features (including a normal white blood cell count, minimal skin findings, and a bilateral and symmetric distribution of swelling) did not match his illness script (a mental representation of a disease) of necrotizing fasciitis.
When pattern recognition fails, other strategies are available.3 Hypothetico‐deductive reasoning is a data‐to‐diagnosis method whereby the clinician uses the presenting information to construct a list of diagnostic possibilities.4 Additional testing and gathering of information are then used to continuously revise the diagnostic possibilities until confirmatory information is obtained and the diagnosis is established. After a pattern failed to materialize, the discussant employed this analytical strategy by noting the unusual characteristics of the case and incorporating laboratory and physiological data to revise his differential diagnosis. As a result, he requested the appropriate diagnostic test: surgical exploration of the forearms.
Necrotizing soft tissue infections are characterized by fulminant tissue destruction, rapid spread along tissue planes, and local vascular thrombosis. Mixed aerobic and anaerobic infections typically occur after penetrating skin injury or following surgery in patients with diabetes mellitus or vascular disease. In contrast, monomicrobial infections with S. aureus or group A streptococcus generally occur in healthy individuals. The prevalence of necrotizing group A streptococcal infections has increased dramatically in the last 15 to 20 years.5 Over one‐third of these cases are complicated by toxic shock syndrome.57 Mortality rates for necrotizing fasciitis with toxic shock exceed 30%, and early surgical consultation is directly associated with a reduction in morbidity and mortality.5, 8
Toxic shock is an inflammatory response syndrome caused by release of exotoxins from group A streptococcus and S. aureus.9, 10 In streptococcal toxic shock, Streptococcus pyogenes exotoxin A and Streptococcus pyogenes exotoxin B are the major toxins produced.10 These toxins activate the systemic production of inflammatory cytokines such as interleukin‐1, gamma‐interferon, and tumor necrosis factor, resulting in capillary leak, systemic hypotension, tissue hypoperfusion, and organ failure. The most common initial symptom is diffuse or localized pain that is severe and abrupt in onset and often precedes or is out of proportion to other physical findings of soft tissue infection.8 Up to 20% of individuals may also develop a viral‐like syndrome with myalgias, fever, nausea, vomiting, and diarrhea.11 Erythroderma of the skin and mucous membranes can be another early finding. The rash is diffuse, erythematous, and macular, resembling a sunburn. It involves the palms and soles but can be subtle and fleeting. Erythroderma may be particularly difficult to detect in dark‐skinned individuals.12 It is also important to consider that the absence of fever, erythroderma, or leukocytosis does not necessarily rule out the possibility of serious infection in necrotizing fasciitis patients, as the development of these signs and symptoms may occur later in the disease process.
The most common portals of entry for group A streptococcus are the skin, vagina, and pharynx. Predisposing factors include varicella infection, penetrating injuries, minor cuts, burns, splinters, and surgery. Interestingly, a portal of entry cannot be identified in 45% of cases.8 These patients in particular are at risk for developing severe necrotizing myositis or fasciitis at the site of a minor injury such as a strained muscle. Hematogenous translocation from the pharynx to the site of injury is the probable mechanism13 and would provide one scenario by which our piano mover developed bilateral and symmetric disease. An alternative explanation would be direct extension of bacteria from small breaks in the skin to adjacent areas of muscle strain. Regardless of the portal of entry, as the small skin lesions demonstrate in this patient, the smallest physical finding can represent the tip of the iceberg.
- ,,,,,.Fast and frugal models of clinical judgment in novice and expert physicians.Med Decis Making.2003;23(4):293–300.
- .What is it to be an expert? In: Chi M, Farr MJ, Glaser R, eds.The Nature of Expertise.Hillsdale, NJ:Lawrence Erlbaum;1988.
- .Clinical decision‐making: understanding how clinicians make a diagnosis. In: Saint S, Drazen JM, Solomon CG, eds.Clinical Problem‐Solving.New York, NY:McGraw‐Hill;2006.
- ,,.Medical Problem Solving: An Analysis of Clinical Reasoning.Cambridge, MA:Harvard University Press;1978.
- ,,,,.Population‐based surveillance for group A streptococcal necrotizing fasciitis: clinical features, prognostic indicators, and microbiologic analysis of seventy‐seven cases. Ontario Group A Streptococcal Study.Am J Med.1997;103(1):18–24.
- ,,, et al.Invasive group A streptococcal infections in Sweden in 1994 and 1995: epidemiology and clinical spectrum.Scand J Infect Dis.2000;32(6):609–614.
- ,,,.Reemergence of emm1 and a changed superantigen profile for group A streptococci causing invasive infections: results from a nationwide study.J Clin Microbiol.2005;43(4):1789–1796.
- ,,, et al.Severe group A streptococcal infections associated with a toxic shock‐like syndrome and scarlet fever toxin A.N Engl J Med.1989;321(1):1–7.
- ,,,.Rapidly progressive necrotizing fasciitis caused by Staphylococcus aureus.J Microbiol Immunol Infect.2005;38(5):361–364.
- ,.Streptococcal infections of skin and soft tissues.N Engl J Med.1996;334(4):240–245.
- ,.Streptococcal toxic shock syndrome after breast reconstruction.Ann Plast Surg.2005;54(5):553–556.
- ,.The influence of pigmentation and illumination on the perception of erythema.Photodermatol Photoimmunol Photomed.1992;9(2):45–47.
- .Streptococcal toxic‐shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment.Emerg Infect Dis.1995;1(3):69–78.
- ,,,,,.Fast and frugal models of clinical judgment in novice and expert physicians.Med Decis Making.2003;23(4):293–300.
- .What is it to be an expert? In: Chi M, Farr MJ, Glaser R, eds.The Nature of Expertise.Hillsdale, NJ:Lawrence Erlbaum;1988.
- .Clinical decision‐making: understanding how clinicians make a diagnosis. In: Saint S, Drazen JM, Solomon CG, eds.Clinical Problem‐Solving.New York, NY:McGraw‐Hill;2006.
- ,,.Medical Problem Solving: An Analysis of Clinical Reasoning.Cambridge, MA:Harvard University Press;1978.
- ,,,,.Population‐based surveillance for group A streptococcal necrotizing fasciitis: clinical features, prognostic indicators, and microbiologic analysis of seventy‐seven cases. Ontario Group A Streptococcal Study.Am J Med.1997;103(1):18–24.
- ,,, et al.Invasive group A streptococcal infections in Sweden in 1994 and 1995: epidemiology and clinical spectrum.Scand J Infect Dis.2000;32(6):609–614.
- ,,,.Reemergence of emm1 and a changed superantigen profile for group A streptococci causing invasive infections: results from a nationwide study.J Clin Microbiol.2005;43(4):1789–1796.
- ,,, et al.Severe group A streptococcal infections associated with a toxic shock‐like syndrome and scarlet fever toxin A.N Engl J Med.1989;321(1):1–7.
- ,,,.Rapidly progressive necrotizing fasciitis caused by Staphylococcus aureus.J Microbiol Immunol Infect.2005;38(5):361–364.
- ,.Streptococcal infections of skin and soft tissues.N Engl J Med.1996;334(4):240–245.
- ,.Streptococcal toxic shock syndrome after breast reconstruction.Ann Plast Surg.2005;54(5):553–556.
- ,.The influence of pigmentation and illumination on the perception of erythema.Photodermatol Photoimmunol Photomed.1992;9(2):45–47.
- .Streptococcal toxic‐shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment.Emerg Infect Dis.1995;1(3):69–78.
Medical Thromboprophylaxis
Venous thromboembolism (VTE) is a common complication of serious illness, conferring increased morbidity and mortality in hospitalized medical patients. Thromboprophylaxis has been rated the number 1 patient safety intervention for hospitalized patients by the Agency for Healthcare Research and Quality, supported by evidence of effectiveness in multiple methodologically rigorous randomized trials.1 Unfortunately, many studies have shown that suitable patients do not receive thromboprophylaxis when they should. For example, in a large teaching hospital, 44 of 245 VTE events were considered to be potentially preventable, occurring because of omitted prophylaxis, inadequate duration of prophylaxis, or incorrect type of prophylaxis.2
Medical patients appear to be at particularly high risk of not receiving thromboprophylaxis. One retrospective study of 446 medical patients in 2 hospitals revealed that only 33% had appropriate prophylaxis.3 In a large retrospective study of 29 Canadian hospitals, among 1,894 patients for whom thromboprophylaxis was considered necessary, only 23% received it.4 These findings are comparable to other practice audits512 and a large international cross‐sectional study13 showing that appropriate thromboprophylaxis is administered to only 1 of every 3 hospitalized medical patients eligible for prophylaxis. Furthermore, of patients diagnosed with VTE in a large international registry, only 33% had received heparin thromboprophylaxis prior to their event.14
The objective of this study was to understand the barriers to, and facilitators of, optimal thromboprophylaxis in hospitalized medical patients using grounded theory methods. To address our poor understanding of low rates of thromboprophylaxis on hospital medical wards, we used qualitative research, which focuses on social and interpreted, rather than natural and objectified, phenomena. Qualitative research also aims to discover, describe, and understand, rather than to test and evaluate.15 Our research question was, What do healthcare clinicians, managers and hospital administrators perceive inhibits the implementation of thromboprophylaxis for medical patients, and what do they perceive would help to optimize thromboprophylaxis?
Methods
We conducted the Qualitative Thromboprophylaxis Enquiry of Compliance (QUALITEC) survey at 3 institutions from June 2006 to September 2007. One was a university‐affiliated hospital (St. Joseph's Healthcare, Hamilton, Ontario, Canada); the other 2 were community hospitals (Joseph Brant Hospital, Burlington, Ontario, and Credit Valley Hospital, Mississauga, Ontario, Canada).
Participants included: (1) bedside nurses, nurse clinicians, and nurse educators; (2) pharmacists; (3) attending physicians; (4) nurse, pharmacy, and physician managers; (5) hospital administrators; (6)medical residents; and (7) members of the hospitals' Quality Improvement Team. Participants in groups 1 to 3 were persons who had cared for medical patients in the index hospital for at least 2 years. Participants in groups 4 and 5 were persons who had worked in the index hospital for at least 2 years. The requisite minimal duration of work on the medical ward for residents was 1 month. There were no exclusion criteria for participants based on sex, religion, ethnicity, or culture. Thus, we enrolled participants based on their a priori eligibility criteria (criterion sampling) and their ability to allow us to achieve our objectives (purposive sampling).
The Research Coordinator created a list of potential interview candidates by examining the organizational structure of each hospital to identify the names of clinicians, managers, and administrators who had responsibility for medical patients. This person identified the names of potential medical ward nurses through discussion with the nurse manager of each medical unit and identified the names of potential attending physicians, residents, and pharmacists through discussion with the physician director or designate of the medical unit (snowball sampling).
After piloting testing with 2 trial participants, the Research Coordinator conducted in‐depth, open‐ended, 1‐on‐1 interviews using a flexible interview guide. This approach allows respondents to use their own words to express ideas, and affords opportunities to probe for more information through dialog. All potential participants were provided with a brief study summary. Each interview took approximately 30 to 60 minutes. All interviews were audiotaped and transcribed verbatim. The Research Coordinator wrote field notes on the main concepts featured in the interview.
To characterize the participants, we recorded their age, sex, position, number of years in their current position, number of years in their profession, and number of years working in their hospital. For clinicians, we recorded the proportion of their professional time spent in clinical practice, the proportion of their clinical time spent caring for hospitalized medical patients (on the medical wards, doing consultations, and in the emergency department), and whether they had a formal role in a previous quality improvement project.
We transcribed each interview upon completion. As is typical for qualitative research, we began data analysis during the data collection phase. Transcripts were analyzed using the coding methods described by Strauss and Corbin.16 The main content analysis of QUALITEC consisted of line‐by‐line open coding. All transcripts were coded by 2 investigators independently who created categories and themes. The first coding process of grounded theory analysis was reduction of data to identify categories (experiences and actions that were similar or related) and to define their dimensions. We iterated between data collection and analysis, revising the interview guide to refine questions and focus on unique concepts. The qualitative data management software NVivo helped with linking codes and categories to ultimately organize ideas into a main theme and several key concepts; it also helped with retrieval of specific quotes. A third investigator reviewed the transcripts independently to identify categories. Analysis continued while the study progressed until saturation of information occurred and no new categories emerged. We invited 3 participants to review an early draft report (member checking).
Research Ethics
This study was approved by the Research Ethics Board at each participating center. Written informed consent was obtained from each participant. Participation was voluntary and confidential; participants had the opportunity to withdraw from the study without any consequences. Data were deidentified upon transcription and remained anonymized, while kept in secure password protected computerized files. Participants received a $25 gift certificate as a token of appreciation. We conducted this study according to the Guiding Ethical Principles section of the Tri‐council Policy Statement of Ethical Conduct for Research Involving Humans.17
Results
Of 39 persons we approached to participate, 36 out of 39 (92.3%) agreed. Two nurse managers at 1 community hospital declined to participate. One resident was missed due to clinical responsibilities. In Table 1, we present the characteristics of the 36 participants. When asked about the level of concern about thromboprophylaxis on the medical wards, participants stated that clinicians were generally insufficiently concerned (24/36, 68.6%) or appropriately concerned (11/36, 31.4%).
| Characteristic | Value |
|---|---|
| |
| Female, n (%) | 27 (75.0) |
| Age, mean (SD) | 39.6 (15.6) |
| Hospital, n (%) | |
| St. Joseph's Healthcare, Hamilton | 16 (44.4) |
| Joseph Brant, Burlington | 9 (25.0) |
| Credit Valley, Oakville | 11 (30.6) |
| Years in hospital, mean (SD) | 10.1 (7.4) |
| Position, n (%) | |
| Bedside nurse | 8 (22.2) |
| Charge nurse | 1 (2.8) |
| Nurse clinician | 2 (5.6) |
| Nurse educator | 2 (5.6) |
| Nurse manager | 2 (5.6) |
| Pharmacist | 3 (8.3) |
| Pharmacist manager | 3 (8.3) |
| Resident physician | 4 (11.1) |
| Attending physician | 6 (16.6) |
| Physician manager | 2 (5.6) |
| Quality improvement team member | 2 (5.6) |
| Hospital administrator | 1 (2.8) |
| Years in current position, mean (SD) | 7.3 (6.4) |
| Participated in quality improvement projects, n (%) | 20 (55.6) |
| Clinical focus (for clinicians only), mean (SD) | |
| Time spent in clinical practice (%) | 93.6 (13.4) |
| Time spent caring for medical patients (%) | 79.2 (25.1) |
Barriers
Relying on individual physicians for VTE prevention was regarded as ineffective, since medical patients often do not receive prophylaxis when they should.
It's sort of Russian roulette as to whether or not we grab a patient and it actually gets done for them. [bedside nurse]
There's a lot of mavericks out there. They do their own thing, and it has never been a problem. They're not held accountable. [quality improvement team leader]
Several different clinician groups were regarded as being involved in medical thromboprophylaxis.
Physiotherapy, occupational therapy, doctors, hopefully our clinical care educators, charge nurses . I think pretty much everybody's involved. I feel that's part of my role as care giver. [bedside nurse]
Many people in the healthcare team are involved in [deep vein thrombosis] DVT prevention at the nurse level, physiotherapy, occupational therapy (in terms of mobility of the patient) the physician, specialty services like thrombo service, hematology department. [nurse manager]
Since many clinicians implicitly or explicitly have a role in thromboprophylaxis, some participants viewed it as everyone's responsibility, or that it should be everyone's responsibility, to ensure optimal VTE prevention.
I think the responsibility should be everyone's responsibilityall across the health care professions. [ward pharmacist]
Make it so that you have a few stopgaps so that a few people are looking for the risk and make the process different so that you have a couple of stops along the way that it'll get brought up. I would create it so that it's not just one group in charge of the DVT prophylaxis decision and assessment. It has to be across the board. [nurse educator]
However, while multidisciplinary care was considered ideal to achieve optimal patient outcomes, it was also paradoxically perceived as insufficient to ensure effective thromboprophylaxis. Multidisciplinary care can lead to confusion about roles on a team, and unclear accountability, thereby becoming a potential barrier to effective prevention. Some participants thought that just one person should be ultimately responsible for thromboprophylaxis.
I think it would be crucial to identify one person responsible rather than indirectly a number of people who would be encouraged . It is probably better if you make one of those targets dependable. [physician]
[If] you assign it to one person versus having the accountability spread among [all] those peoplethen nobody takes accountability. [quality improvement team member]
Many participants reported that mobilization was important, though difficult to achieve. They also expressed uncertainty about whether, and how much, mobilization is enough.
I think the best way to prevent DVT would be to fully focus on early mobilization, regular physiotherapy, and how a patient returns to regular activities to get them up and around. [resident]
Level of mobility is a subjective matter. When it comes to the question of Well, how mobile is mobile enough?, that's not standardized to my knowledge and is very subjective as far as when to stop it. Is getting up in a chair and wiggling your toes good enough? Or are they running up and down the hall and you have to chase them? Really, what level of mobility is considered the standard for discontinuing DVT prophylaxis? That's the question that comes up repeatedly so I think that's a very large barrier. [pharmacy manager]
Several logistic barriers associated with antiembolic stockings and pneumatic compression devices were cited, including problems with fit, inconvenience, noncompliance, and cost.
I find stockings aren't always measured or worn appropriately. It's difficult; I think every nurse measures them differently. If they're too tight around the thighs they just roll them down. If anything, they really constrict any type of circulation rather than promote it. Moon boots are all right, but a little cumbersome, more expensive and are more geared to specific patients. [bedside nurse]
The patients want them off at certain times of the day. Theoretically, you only take them off to bathe them but some of them are really bothered by them. [nurse clinician]
Another key barrier was that clinicians are more focused on treating the immediate health care problem precipitating hospital admission than on preventing future complications.
It's something that we tend to forget because patients come in with giant medical problems a, b, and c, and then your DVT prophylaxis tends to fall by the wayside, as you're trying to deal with their major medical issues. [resident]
Prevention issues are a little bit different than treatment issues . We see ourselves as interventionists more than preventionists . It's the medical things we tend to deal with immediately and that's often the focus why the patient is in hospital, rightly or wrongly. Quality doesn't just include intervention, it includes prevention. [nurse manager]
Potential Solutions
To address this problem of inattention to preventive strategies, participants indicated that local data on the burden of illness and current utilization of thromboprophylaxis would be helpful. Some participants described institution‐specific information and thromboprophylaxis targets that motivate clinicians.
Give feedback to the team and physicians about what the incidence of DVT is. I don't think everybody knows. I don't even know in our hospital what it is. So give feedback to the team about what the incidence of DVT is, how many people are on DVT prophylaxis and how many people die from pulmonary embolism. If you have those numbers in front of you, then you would have something to aim for. [physician manager]
You do run charts so that you are auditing continuously and reporting the results back to the staff. And we have weekly meetings with staff members. That has been effective. And we have tip of the week via email. [quality improvement team member]
Most participants recommended redoubling efforts towards anticoagulant thromboprophylaxisa coordinated, systemwide approach across the continuum of care.
It's got to be a trigger for every patient that comes in. Does this patient need DVT prophylaxis? Is this patient a candidate for it? [physician manager]
I think if it's not tackled at the beginning it gets lost in the shuffle. I think if it's something we put into place just like we do when we're getting a history and on anything else. If we start with it [heparin] from day one we'll continue it through right to the end. [bedside nurse]
Participants suggested a variety of methods to enhance thromboprophylaxis. These included a universal, structured, dynamic risk stratification tool, and standardized order forms at the time of hospital admission, which would be reevaluated regularly, and require an enabling educational program.
Every medical patient 18 or older will be given a risk score. Risk stratifying all of our patients with just a simple little tool and considering treatment for those that are of high risk is what we need to do. Reinforcing the education and teaching required for the patients that are at low risk, because we don't need to put everyone on heparin. But anyone could potentially get a clot. [nurse educator]
It could be a standardized order sheet for every admitted patient and maybe that could help. And that would be like the first page in every chart in the whole hospital, and they can always cross it off and say I don't want to use this. [ward pharmacist]
The hospital intranet was sanctioned as a useful repository for physician orders and other tools. Computerized health records and computer decision supports were strongly endorsed.
It should be in a computerized system if it goes into a manual system, paperwork tends to get lost. I think a computerized system would be ideal. [pharmacist]
I think that having a computer health recordthat we would love, for many reasonsonce that happened, it would be a way to ensure it, because there would be prompts . You would get a prompt saying, Why are you not using it? . An electronic health record and as a back up, having a pharmacist. [physician]
Leveraging patient or family‐mediated interventions to provide reminders was also suggested, given the familiarity of the public with thrombosis.
Leave every patient a small pamphlet saying Are you getting DVT prevention? Are you getting injections? Empower people as well. [physician]
I think the absolute biggest driver from our perspective in admin is always public awareness. The demand for standard service increases the most when the public is aware of it. They ask. Patients are becoming more educated, they use the Internet, they search those things out themselves and they are knowledgeable. [hospital administrator]
Sufficient human resources to ensure mobilization and profiling thromboprophylaxis during accreditation were regarded as administrative initiatives that could help. Capitalizing on social forces in healthcare such as patient safety could also galvanize efforts to prevent VTE.
We need physio and [occupational therapy] OT. We need more rehab. We need resources. That's what we're lacking. The only physio and OT that comes to our floor is pending discharge. So it's definitely resource‐related. [bedside nurse]
From an administrative perspective, the whole concept of preventing complications reduces risk, improves patient safety, reduces length of stayall those warm fuzzy things that are attached to providing the best possible care for the patient at the right time. [nurse manager]
Discussion
In this qualitative study, participants affirmed that depending on individual physicians for VTE prevention is insufficient. Distinct from most therapeutic interventions which are understood as the responsibility of physicians, preventive interventions such as thromboprophylaxis may be more readily embraced as the charge of members of a multidisciplinary team. While every clinician group felt compelled to help with VTE prevention, reliance on multidisciplinary care was also perceived as a barrier to effective VTE prevention because it can generate confusion about roles. Participants recommended a comprehensive, systems‐approach, including screening and risk‐stratifying all patients, preprinted orders at hospital admission that are regularly reevaluated, and audit and feedback programs. Also endorsed were patient or family‐mediated reminders, and administrative interventions such as hiring more physiotherapists for mobilization and profiling thromboprophylaxis for hospital accreditation.
Approximately 70% of participants judged that clinicians were insufficiently concerned about thromboprophylaxis. In contrast to many commonly cited reasons for underutilization of evidence‐based interventions such as lack of awareness of (or resistance to) new information, and lack of self‐efficacy of clinicians (wondering whether the benefits observed in the research setting will be realized in the practice setting),18 participants in our study did not raise these as barriers to thromboprophylaxis. As physician and pharmacist participants indicated, because the evidentiary basis for heparin thromboprophylaxis is strong and understood (in contrast to that for mechanical prophylaxis), lack of knowledge was not considered a barrier.
Our findings are consistent with a previous qualitative study in which clinicians and managers were interviewed to learn about factors that increase beta‐blocker use following myocardial infarction; these investigators found that administrative support, use of data, and quality improvement initiatives were key.19 Detailed implementation directives to clarify clinical responsibilities for many different stakeholders were also suggested in a qualitative study on the optimal use of noninvasive ventilation.20 Extending these results, participants in our study suggested several interventions aimed at different levels of the healthcare system (eg, patient, provider, and administrator) that are either enabling or reinforcing. While just 1 implementation strategy may result in improved thromboprophylaxis,21 efficient application of multiply‐redundant strategies delivered by a multidisciplinary team may be more powerful. Such an approach has driven high level performance for the American Heart Association's Get With The Guidelines Program, resulting in lower community and hospital cardiovascular and cerebrovascular mortality in Massachusetts.22
Although our aim was to obtain multidisciplinary input, we did not focus on physicians who primarily prescribe thromboprophylaxis, thereby potentially underrepresenting their views relative to their role. We did not interview all clinicians who can influence VTE risk (eg, physiotherapists) or prescribe thromboprophylaxis (eg, family physicians). During this study, patient safety emerged as a major hospital initiative,23 which could modify participants' views on the importance of VTE prevention. Although VTE prevention may be enhanced by understanding barriers to, and solutions for, optimal thromboprophylaxis from both clinicians' and managers' perspectives, the suggestions we elicited on methods to improve VTE prevention represent participants' opinions, rather than evidence, about effective strategies. Our findings are not generalizable to settings with nurse practitioners who are dedicated to VTE prevention, nor to settings with computer decision support systems that already incorporate thromboprophylaxis.
Strengths of this study include interviewing key stakeholders representing several clinician groups and managers, to obtain perspectives on both individual and systemwide influences on thromboprophylaxis in medical patients. By eliciting the views and experiences of participants in both the community and university settings, we captured multicenter perspectives on preventive health. We used triangulation of data sources (researcher and participant) and invited participants to review an early draft of the report (member checking).24 This study highlights the merits of qualitative research which can provide insights into familiar patterns and problems, and contribute to knowledge for interdisciplinary audiences. These qualitative research results help to explain quantitative research results documenting very low rates of medical thromboprophylaxis,214 raising hypotheses to test in future studies testing systemwide interventions that may improve patient safety. One prominent publication reported the impact of electronic reminders,25 while a recent systematic review of methods to increase thromboprophylaxis outlines many potentially effective approaches.21
In summary, the findings of this qualitative study challenge the notion that either individual physician efforts or multidisciplinary care are enough to lead to optimal VTE prevention. Participants believed that while well‐functioning teams at the bedside hold great promise to deliver superior care, they may also lead to unclear role definition. Since physicians commit many errors of omission regarding thromboprophylaxis, these results raise the possibility of delegated medical acts outside the scope of conventional practice for nurses and pharmacists. Leveraging the skills and knowledge of multidisciplinary teams for medical thromboprophylaxis requires not only clear accountabilities, but also excellent interprofessional communication, and institution‐wide approaches to change prescribing behavior, potentially involving patients and administrators as well as clinicians.
Acknowledgements
The authors thank the participants of this study for sharing their experiences and views with them. The authors are grateful for the help of Laurel Raftery, Michelle Murray, Monica Owen, and Shelley Anderson for transcriptions. The authors appreciate the organizational assistance of Nancy Lloyd and the biostatistical support of Diane Heels‐Ansdell for analyzing respondent characteristics. The authors are grateful to Nancy Lloyd, Alice Huh, Barbara Young, and Gray Ellrodt for feedback on earlier versions of this report. Deborah Cook had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Appendix
Qualitec Interview Guide
Opening Statement
Thank you for your participation in this research study we are conducting with colleagues at St. Joseph's Hospital and McMaster University. Through this interview, I hope to learn how you think about DVT prevention in medical patients. When you answer the interview questions, please keep in mind that we are interested in your own thoughts and approaches.
First, I have a consent form I'd like you to read to make sure you understand the reason for this study, and to see if you have any questions about becoming involved. Please take a few minutes to read it over.
[Participant reads consent, questions about the study may or may not ensue, participant signs to indicate informed consent, the interview proceeds.]
Structured Interview Begins
Demographics
Before we begin the interview, I would like you to take a few minutes to complete this form, which consists of a few demographic questions.
[Participant completes demographic form].
Thank you. Now I'll move on to some questions about DVT prevention.
[The interviewer informs the participant that she is putting the tape recorder on].
Core Study Interview Guide
Can you tell me a bit about your own approach to DVT prevention in medical patients? For what types of patients are you concerned about DVT?
What do you find are the best ways to prevent DVT? Why?
Who else is involved in trying to prevent DVT? In general, how are DVTs are prevented at this hospital?
What are some of the barriers to preventing DVTs? (e.g., risks of prevention, disbelief that prevention really works, DVT prevention is someone else's responsibilitywhose?)
Are there other ways to ensure that DVTs are prevented in medical patients? If so, how would they work?
Can you tell me how different clinicians (such as physicians, nurses, pharmacists, and residents) could do a better job at preventing DVT? How could medical wards and departments help? How could hospital administration help?
Do you remember a patient who had a problem with DVT prevention? If so, can you tell me about this problem and how it might have been avoided?
If you could create a perfect system of DVT prevention what would it be?
Do you think people are overconcerned, appropriately concerned, or underconcerned about DVT prevention?
Is there anything else you would like to tell me?
Final Debriefing Question
How has this interview experience been for you? Thank you very much for sharing your views. We really appreciate it.
- Agency for Health Care Policy Research. Prevention of venous thromboembolism after injury. Summary, evidence report/technology assessment. Available at: http://www. ahrq.gov/clinic/epcsums/vtsumm.htm. Accessed April 2008.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of thromboprophylaxis guidelines.Chest.2001;120:1964–1971.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,, et al.,for the CURVE Study Investigators.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,.Thromboprophylaxis in an academic medical center.Cardiovasc Surg.2001;9:426–430.
- ,,.Deep venous thrombosis prophylaxis: are guidelines being followed?ANZ J Surg.2002;72:331–334.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17:788–791.
- ,.Preventing venous thromboembolism in acute medical patients.QJM.2004;97:797–801.
- ,.Venous thromboembolic prophylaxis in hospitalized medical patients.Ann Pharmacother.2004;38:36–40.
- ,,.Physicians' practice for prevention of venous thromboembolism in medical patients.J Coll Physicians Surg.2004;14:211.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill medical patients: definite need for improvement.J Intern Med.2005;257:352–357.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.,for the ENDORSE Investigators.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE Study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,, et al.,for the IMPROVE Investigators.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,for the Evidence‐Based Medicine Working Group.Users' guides to the medical literature. XXIII. Qualitative research in health care. A. Are the results of the study valid?JAMA.2000;284:357–362.
- ,.Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.2nd ed.London:Sage Publications;1998.
- Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, Social Sciences and Humanities Research Council of Canada.Tri‐Council Policy Statement: Ethical Conduct for Research Involving Humans.Ottawa, Ontario:Public Works and Government Services Canada;1998 [with 2000, 2002, and 2005 amendments].
- ,,, et al.Why don't physicians follow clinical practice guidelines?JAMA.1999;282:1458–1465.
- ,,,,,.A qualitative study of increasing β‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- ,,,.Practice guidelines as multipurpose tools: a qualitative study of noninvasive ventilation.Crit Care Med.2007;35:776–782.
- ,,, et al.A systemic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Multidisciplinary rounds: an implementation system for sustained improvement in the American Heart Association's “Get With the Guidelines” Program.Crit Pathw Cardiol.2007;6:1016–1116.
- ,,,,.Changing clinician behaviour to improve patient safety.Lancet.2004;363:1224–1230.
- ,.Papers that go beyond numbers: qualitative research.BMJ.1997;315:740–748.
- ,,,,,,.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352(10):969–977.
Venous thromboembolism (VTE) is a common complication of serious illness, conferring increased morbidity and mortality in hospitalized medical patients. Thromboprophylaxis has been rated the number 1 patient safety intervention for hospitalized patients by the Agency for Healthcare Research and Quality, supported by evidence of effectiveness in multiple methodologically rigorous randomized trials.1 Unfortunately, many studies have shown that suitable patients do not receive thromboprophylaxis when they should. For example, in a large teaching hospital, 44 of 245 VTE events were considered to be potentially preventable, occurring because of omitted prophylaxis, inadequate duration of prophylaxis, or incorrect type of prophylaxis.2
Medical patients appear to be at particularly high risk of not receiving thromboprophylaxis. One retrospective study of 446 medical patients in 2 hospitals revealed that only 33% had appropriate prophylaxis.3 In a large retrospective study of 29 Canadian hospitals, among 1,894 patients for whom thromboprophylaxis was considered necessary, only 23% received it.4 These findings are comparable to other practice audits512 and a large international cross‐sectional study13 showing that appropriate thromboprophylaxis is administered to only 1 of every 3 hospitalized medical patients eligible for prophylaxis. Furthermore, of patients diagnosed with VTE in a large international registry, only 33% had received heparin thromboprophylaxis prior to their event.14
The objective of this study was to understand the barriers to, and facilitators of, optimal thromboprophylaxis in hospitalized medical patients using grounded theory methods. To address our poor understanding of low rates of thromboprophylaxis on hospital medical wards, we used qualitative research, which focuses on social and interpreted, rather than natural and objectified, phenomena. Qualitative research also aims to discover, describe, and understand, rather than to test and evaluate.15 Our research question was, What do healthcare clinicians, managers and hospital administrators perceive inhibits the implementation of thromboprophylaxis for medical patients, and what do they perceive would help to optimize thromboprophylaxis?
Methods
We conducted the Qualitative Thromboprophylaxis Enquiry of Compliance (QUALITEC) survey at 3 institutions from June 2006 to September 2007. One was a university‐affiliated hospital (St. Joseph's Healthcare, Hamilton, Ontario, Canada); the other 2 were community hospitals (Joseph Brant Hospital, Burlington, Ontario, and Credit Valley Hospital, Mississauga, Ontario, Canada).
Participants included: (1) bedside nurses, nurse clinicians, and nurse educators; (2) pharmacists; (3) attending physicians; (4) nurse, pharmacy, and physician managers; (5) hospital administrators; (6)medical residents; and (7) members of the hospitals' Quality Improvement Team. Participants in groups 1 to 3 were persons who had cared for medical patients in the index hospital for at least 2 years. Participants in groups 4 and 5 were persons who had worked in the index hospital for at least 2 years. The requisite minimal duration of work on the medical ward for residents was 1 month. There were no exclusion criteria for participants based on sex, religion, ethnicity, or culture. Thus, we enrolled participants based on their a priori eligibility criteria (criterion sampling) and their ability to allow us to achieve our objectives (purposive sampling).
The Research Coordinator created a list of potential interview candidates by examining the organizational structure of each hospital to identify the names of clinicians, managers, and administrators who had responsibility for medical patients. This person identified the names of potential medical ward nurses through discussion with the nurse manager of each medical unit and identified the names of potential attending physicians, residents, and pharmacists through discussion with the physician director or designate of the medical unit (snowball sampling).
After piloting testing with 2 trial participants, the Research Coordinator conducted in‐depth, open‐ended, 1‐on‐1 interviews using a flexible interview guide. This approach allows respondents to use their own words to express ideas, and affords opportunities to probe for more information through dialog. All potential participants were provided with a brief study summary. Each interview took approximately 30 to 60 minutes. All interviews were audiotaped and transcribed verbatim. The Research Coordinator wrote field notes on the main concepts featured in the interview.
To characterize the participants, we recorded their age, sex, position, number of years in their current position, number of years in their profession, and number of years working in their hospital. For clinicians, we recorded the proportion of their professional time spent in clinical practice, the proportion of their clinical time spent caring for hospitalized medical patients (on the medical wards, doing consultations, and in the emergency department), and whether they had a formal role in a previous quality improvement project.
We transcribed each interview upon completion. As is typical for qualitative research, we began data analysis during the data collection phase. Transcripts were analyzed using the coding methods described by Strauss and Corbin.16 The main content analysis of QUALITEC consisted of line‐by‐line open coding. All transcripts were coded by 2 investigators independently who created categories and themes. The first coding process of grounded theory analysis was reduction of data to identify categories (experiences and actions that were similar or related) and to define their dimensions. We iterated between data collection and analysis, revising the interview guide to refine questions and focus on unique concepts. The qualitative data management software NVivo helped with linking codes and categories to ultimately organize ideas into a main theme and several key concepts; it also helped with retrieval of specific quotes. A third investigator reviewed the transcripts independently to identify categories. Analysis continued while the study progressed until saturation of information occurred and no new categories emerged. We invited 3 participants to review an early draft report (member checking).
Research Ethics
This study was approved by the Research Ethics Board at each participating center. Written informed consent was obtained from each participant. Participation was voluntary and confidential; participants had the opportunity to withdraw from the study without any consequences. Data were deidentified upon transcription and remained anonymized, while kept in secure password protected computerized files. Participants received a $25 gift certificate as a token of appreciation. We conducted this study according to the Guiding Ethical Principles section of the Tri‐council Policy Statement of Ethical Conduct for Research Involving Humans.17
Results
Of 39 persons we approached to participate, 36 out of 39 (92.3%) agreed. Two nurse managers at 1 community hospital declined to participate. One resident was missed due to clinical responsibilities. In Table 1, we present the characteristics of the 36 participants. When asked about the level of concern about thromboprophylaxis on the medical wards, participants stated that clinicians were generally insufficiently concerned (24/36, 68.6%) or appropriately concerned (11/36, 31.4%).
| Characteristic | Value |
|---|---|
| |
| Female, n (%) | 27 (75.0) |
| Age, mean (SD) | 39.6 (15.6) |
| Hospital, n (%) | |
| St. Joseph's Healthcare, Hamilton | 16 (44.4) |
| Joseph Brant, Burlington | 9 (25.0) |
| Credit Valley, Oakville | 11 (30.6) |
| Years in hospital, mean (SD) | 10.1 (7.4) |
| Position, n (%) | |
| Bedside nurse | 8 (22.2) |
| Charge nurse | 1 (2.8) |
| Nurse clinician | 2 (5.6) |
| Nurse educator | 2 (5.6) |
| Nurse manager | 2 (5.6) |
| Pharmacist | 3 (8.3) |
| Pharmacist manager | 3 (8.3) |
| Resident physician | 4 (11.1) |
| Attending physician | 6 (16.6) |
| Physician manager | 2 (5.6) |
| Quality improvement team member | 2 (5.6) |
| Hospital administrator | 1 (2.8) |
| Years in current position, mean (SD) | 7.3 (6.4) |
| Participated in quality improvement projects, n (%) | 20 (55.6) |
| Clinical focus (for clinicians only), mean (SD) | |
| Time spent in clinical practice (%) | 93.6 (13.4) |
| Time spent caring for medical patients (%) | 79.2 (25.1) |
Barriers
Relying on individual physicians for VTE prevention was regarded as ineffective, since medical patients often do not receive prophylaxis when they should.
It's sort of Russian roulette as to whether or not we grab a patient and it actually gets done for them. [bedside nurse]
There's a lot of mavericks out there. They do their own thing, and it has never been a problem. They're not held accountable. [quality improvement team leader]
Several different clinician groups were regarded as being involved in medical thromboprophylaxis.
Physiotherapy, occupational therapy, doctors, hopefully our clinical care educators, charge nurses . I think pretty much everybody's involved. I feel that's part of my role as care giver. [bedside nurse]
Many people in the healthcare team are involved in [deep vein thrombosis] DVT prevention at the nurse level, physiotherapy, occupational therapy (in terms of mobility of the patient) the physician, specialty services like thrombo service, hematology department. [nurse manager]
Since many clinicians implicitly or explicitly have a role in thromboprophylaxis, some participants viewed it as everyone's responsibility, or that it should be everyone's responsibility, to ensure optimal VTE prevention.
I think the responsibility should be everyone's responsibilityall across the health care professions. [ward pharmacist]
Make it so that you have a few stopgaps so that a few people are looking for the risk and make the process different so that you have a couple of stops along the way that it'll get brought up. I would create it so that it's not just one group in charge of the DVT prophylaxis decision and assessment. It has to be across the board. [nurse educator]
However, while multidisciplinary care was considered ideal to achieve optimal patient outcomes, it was also paradoxically perceived as insufficient to ensure effective thromboprophylaxis. Multidisciplinary care can lead to confusion about roles on a team, and unclear accountability, thereby becoming a potential barrier to effective prevention. Some participants thought that just one person should be ultimately responsible for thromboprophylaxis.
I think it would be crucial to identify one person responsible rather than indirectly a number of people who would be encouraged . It is probably better if you make one of those targets dependable. [physician]
[If] you assign it to one person versus having the accountability spread among [all] those peoplethen nobody takes accountability. [quality improvement team member]
Many participants reported that mobilization was important, though difficult to achieve. They also expressed uncertainty about whether, and how much, mobilization is enough.
I think the best way to prevent DVT would be to fully focus on early mobilization, regular physiotherapy, and how a patient returns to regular activities to get them up and around. [resident]
Level of mobility is a subjective matter. When it comes to the question of Well, how mobile is mobile enough?, that's not standardized to my knowledge and is very subjective as far as when to stop it. Is getting up in a chair and wiggling your toes good enough? Or are they running up and down the hall and you have to chase them? Really, what level of mobility is considered the standard for discontinuing DVT prophylaxis? That's the question that comes up repeatedly so I think that's a very large barrier. [pharmacy manager]
Several logistic barriers associated with antiembolic stockings and pneumatic compression devices were cited, including problems with fit, inconvenience, noncompliance, and cost.
I find stockings aren't always measured or worn appropriately. It's difficult; I think every nurse measures them differently. If they're too tight around the thighs they just roll them down. If anything, they really constrict any type of circulation rather than promote it. Moon boots are all right, but a little cumbersome, more expensive and are more geared to specific patients. [bedside nurse]
The patients want them off at certain times of the day. Theoretically, you only take them off to bathe them but some of them are really bothered by them. [nurse clinician]
Another key barrier was that clinicians are more focused on treating the immediate health care problem precipitating hospital admission than on preventing future complications.
It's something that we tend to forget because patients come in with giant medical problems a, b, and c, and then your DVT prophylaxis tends to fall by the wayside, as you're trying to deal with their major medical issues. [resident]
Prevention issues are a little bit different than treatment issues . We see ourselves as interventionists more than preventionists . It's the medical things we tend to deal with immediately and that's often the focus why the patient is in hospital, rightly or wrongly. Quality doesn't just include intervention, it includes prevention. [nurse manager]
Potential Solutions
To address this problem of inattention to preventive strategies, participants indicated that local data on the burden of illness and current utilization of thromboprophylaxis would be helpful. Some participants described institution‐specific information and thromboprophylaxis targets that motivate clinicians.
Give feedback to the team and physicians about what the incidence of DVT is. I don't think everybody knows. I don't even know in our hospital what it is. So give feedback to the team about what the incidence of DVT is, how many people are on DVT prophylaxis and how many people die from pulmonary embolism. If you have those numbers in front of you, then you would have something to aim for. [physician manager]
You do run charts so that you are auditing continuously and reporting the results back to the staff. And we have weekly meetings with staff members. That has been effective. And we have tip of the week via email. [quality improvement team member]
Most participants recommended redoubling efforts towards anticoagulant thromboprophylaxisa coordinated, systemwide approach across the continuum of care.
It's got to be a trigger for every patient that comes in. Does this patient need DVT prophylaxis? Is this patient a candidate for it? [physician manager]
I think if it's not tackled at the beginning it gets lost in the shuffle. I think if it's something we put into place just like we do when we're getting a history and on anything else. If we start with it [heparin] from day one we'll continue it through right to the end. [bedside nurse]
Participants suggested a variety of methods to enhance thromboprophylaxis. These included a universal, structured, dynamic risk stratification tool, and standardized order forms at the time of hospital admission, which would be reevaluated regularly, and require an enabling educational program.
Every medical patient 18 or older will be given a risk score. Risk stratifying all of our patients with just a simple little tool and considering treatment for those that are of high risk is what we need to do. Reinforcing the education and teaching required for the patients that are at low risk, because we don't need to put everyone on heparin. But anyone could potentially get a clot. [nurse educator]
It could be a standardized order sheet for every admitted patient and maybe that could help. And that would be like the first page in every chart in the whole hospital, and they can always cross it off and say I don't want to use this. [ward pharmacist]
The hospital intranet was sanctioned as a useful repository for physician orders and other tools. Computerized health records and computer decision supports were strongly endorsed.
It should be in a computerized system if it goes into a manual system, paperwork tends to get lost. I think a computerized system would be ideal. [pharmacist]
I think that having a computer health recordthat we would love, for many reasonsonce that happened, it would be a way to ensure it, because there would be prompts . You would get a prompt saying, Why are you not using it? . An electronic health record and as a back up, having a pharmacist. [physician]
Leveraging patient or family‐mediated interventions to provide reminders was also suggested, given the familiarity of the public with thrombosis.
Leave every patient a small pamphlet saying Are you getting DVT prevention? Are you getting injections? Empower people as well. [physician]
I think the absolute biggest driver from our perspective in admin is always public awareness. The demand for standard service increases the most when the public is aware of it. They ask. Patients are becoming more educated, they use the Internet, they search those things out themselves and they are knowledgeable. [hospital administrator]
Sufficient human resources to ensure mobilization and profiling thromboprophylaxis during accreditation were regarded as administrative initiatives that could help. Capitalizing on social forces in healthcare such as patient safety could also galvanize efforts to prevent VTE.
We need physio and [occupational therapy] OT. We need more rehab. We need resources. That's what we're lacking. The only physio and OT that comes to our floor is pending discharge. So it's definitely resource‐related. [bedside nurse]
From an administrative perspective, the whole concept of preventing complications reduces risk, improves patient safety, reduces length of stayall those warm fuzzy things that are attached to providing the best possible care for the patient at the right time. [nurse manager]
Discussion
In this qualitative study, participants affirmed that depending on individual physicians for VTE prevention is insufficient. Distinct from most therapeutic interventions which are understood as the responsibility of physicians, preventive interventions such as thromboprophylaxis may be more readily embraced as the charge of members of a multidisciplinary team. While every clinician group felt compelled to help with VTE prevention, reliance on multidisciplinary care was also perceived as a barrier to effective VTE prevention because it can generate confusion about roles. Participants recommended a comprehensive, systems‐approach, including screening and risk‐stratifying all patients, preprinted orders at hospital admission that are regularly reevaluated, and audit and feedback programs. Also endorsed were patient or family‐mediated reminders, and administrative interventions such as hiring more physiotherapists for mobilization and profiling thromboprophylaxis for hospital accreditation.
Approximately 70% of participants judged that clinicians were insufficiently concerned about thromboprophylaxis. In contrast to many commonly cited reasons for underutilization of evidence‐based interventions such as lack of awareness of (or resistance to) new information, and lack of self‐efficacy of clinicians (wondering whether the benefits observed in the research setting will be realized in the practice setting),18 participants in our study did not raise these as barriers to thromboprophylaxis. As physician and pharmacist participants indicated, because the evidentiary basis for heparin thromboprophylaxis is strong and understood (in contrast to that for mechanical prophylaxis), lack of knowledge was not considered a barrier.
Our findings are consistent with a previous qualitative study in which clinicians and managers were interviewed to learn about factors that increase beta‐blocker use following myocardial infarction; these investigators found that administrative support, use of data, and quality improvement initiatives were key.19 Detailed implementation directives to clarify clinical responsibilities for many different stakeholders were also suggested in a qualitative study on the optimal use of noninvasive ventilation.20 Extending these results, participants in our study suggested several interventions aimed at different levels of the healthcare system (eg, patient, provider, and administrator) that are either enabling or reinforcing. While just 1 implementation strategy may result in improved thromboprophylaxis,21 efficient application of multiply‐redundant strategies delivered by a multidisciplinary team may be more powerful. Such an approach has driven high level performance for the American Heart Association's Get With The Guidelines Program, resulting in lower community and hospital cardiovascular and cerebrovascular mortality in Massachusetts.22
Although our aim was to obtain multidisciplinary input, we did not focus on physicians who primarily prescribe thromboprophylaxis, thereby potentially underrepresenting their views relative to their role. We did not interview all clinicians who can influence VTE risk (eg, physiotherapists) or prescribe thromboprophylaxis (eg, family physicians). During this study, patient safety emerged as a major hospital initiative,23 which could modify participants' views on the importance of VTE prevention. Although VTE prevention may be enhanced by understanding barriers to, and solutions for, optimal thromboprophylaxis from both clinicians' and managers' perspectives, the suggestions we elicited on methods to improve VTE prevention represent participants' opinions, rather than evidence, about effective strategies. Our findings are not generalizable to settings with nurse practitioners who are dedicated to VTE prevention, nor to settings with computer decision support systems that already incorporate thromboprophylaxis.
Strengths of this study include interviewing key stakeholders representing several clinician groups and managers, to obtain perspectives on both individual and systemwide influences on thromboprophylaxis in medical patients. By eliciting the views and experiences of participants in both the community and university settings, we captured multicenter perspectives on preventive health. We used triangulation of data sources (researcher and participant) and invited participants to review an early draft of the report (member checking).24 This study highlights the merits of qualitative research which can provide insights into familiar patterns and problems, and contribute to knowledge for interdisciplinary audiences. These qualitative research results help to explain quantitative research results documenting very low rates of medical thromboprophylaxis,214 raising hypotheses to test in future studies testing systemwide interventions that may improve patient safety. One prominent publication reported the impact of electronic reminders,25 while a recent systematic review of methods to increase thromboprophylaxis outlines many potentially effective approaches.21
In summary, the findings of this qualitative study challenge the notion that either individual physician efforts or multidisciplinary care are enough to lead to optimal VTE prevention. Participants believed that while well‐functioning teams at the bedside hold great promise to deliver superior care, they may also lead to unclear role definition. Since physicians commit many errors of omission regarding thromboprophylaxis, these results raise the possibility of delegated medical acts outside the scope of conventional practice for nurses and pharmacists. Leveraging the skills and knowledge of multidisciplinary teams for medical thromboprophylaxis requires not only clear accountabilities, but also excellent interprofessional communication, and institution‐wide approaches to change prescribing behavior, potentially involving patients and administrators as well as clinicians.
Acknowledgements
The authors thank the participants of this study for sharing their experiences and views with them. The authors are grateful for the help of Laurel Raftery, Michelle Murray, Monica Owen, and Shelley Anderson for transcriptions. The authors appreciate the organizational assistance of Nancy Lloyd and the biostatistical support of Diane Heels‐Ansdell for analyzing respondent characteristics. The authors are grateful to Nancy Lloyd, Alice Huh, Barbara Young, and Gray Ellrodt for feedback on earlier versions of this report. Deborah Cook had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Appendix
Qualitec Interview Guide
Opening Statement
Thank you for your participation in this research study we are conducting with colleagues at St. Joseph's Hospital and McMaster University. Through this interview, I hope to learn how you think about DVT prevention in medical patients. When you answer the interview questions, please keep in mind that we are interested in your own thoughts and approaches.
First, I have a consent form I'd like you to read to make sure you understand the reason for this study, and to see if you have any questions about becoming involved. Please take a few minutes to read it over.
[Participant reads consent, questions about the study may or may not ensue, participant signs to indicate informed consent, the interview proceeds.]
Structured Interview Begins
Demographics
Before we begin the interview, I would like you to take a few minutes to complete this form, which consists of a few demographic questions.
[Participant completes demographic form].
Thank you. Now I'll move on to some questions about DVT prevention.
[The interviewer informs the participant that she is putting the tape recorder on].
Core Study Interview Guide
Can you tell me a bit about your own approach to DVT prevention in medical patients? For what types of patients are you concerned about DVT?
What do you find are the best ways to prevent DVT? Why?
Who else is involved in trying to prevent DVT? In general, how are DVTs are prevented at this hospital?
What are some of the barriers to preventing DVTs? (e.g., risks of prevention, disbelief that prevention really works, DVT prevention is someone else's responsibilitywhose?)
Are there other ways to ensure that DVTs are prevented in medical patients? If so, how would they work?
Can you tell me how different clinicians (such as physicians, nurses, pharmacists, and residents) could do a better job at preventing DVT? How could medical wards and departments help? How could hospital administration help?
Do you remember a patient who had a problem with DVT prevention? If so, can you tell me about this problem and how it might have been avoided?
If you could create a perfect system of DVT prevention what would it be?
Do you think people are overconcerned, appropriately concerned, or underconcerned about DVT prevention?
Is there anything else you would like to tell me?
Final Debriefing Question
How has this interview experience been for you? Thank you very much for sharing your views. We really appreciate it.
Venous thromboembolism (VTE) is a common complication of serious illness, conferring increased morbidity and mortality in hospitalized medical patients. Thromboprophylaxis has been rated the number 1 patient safety intervention for hospitalized patients by the Agency for Healthcare Research and Quality, supported by evidence of effectiveness in multiple methodologically rigorous randomized trials.1 Unfortunately, many studies have shown that suitable patients do not receive thromboprophylaxis when they should. For example, in a large teaching hospital, 44 of 245 VTE events were considered to be potentially preventable, occurring because of omitted prophylaxis, inadequate duration of prophylaxis, or incorrect type of prophylaxis.2
Medical patients appear to be at particularly high risk of not receiving thromboprophylaxis. One retrospective study of 446 medical patients in 2 hospitals revealed that only 33% had appropriate prophylaxis.3 In a large retrospective study of 29 Canadian hospitals, among 1,894 patients for whom thromboprophylaxis was considered necessary, only 23% received it.4 These findings are comparable to other practice audits512 and a large international cross‐sectional study13 showing that appropriate thromboprophylaxis is administered to only 1 of every 3 hospitalized medical patients eligible for prophylaxis. Furthermore, of patients diagnosed with VTE in a large international registry, only 33% had received heparin thromboprophylaxis prior to their event.14
The objective of this study was to understand the barriers to, and facilitators of, optimal thromboprophylaxis in hospitalized medical patients using grounded theory methods. To address our poor understanding of low rates of thromboprophylaxis on hospital medical wards, we used qualitative research, which focuses on social and interpreted, rather than natural and objectified, phenomena. Qualitative research also aims to discover, describe, and understand, rather than to test and evaluate.15 Our research question was, What do healthcare clinicians, managers and hospital administrators perceive inhibits the implementation of thromboprophylaxis for medical patients, and what do they perceive would help to optimize thromboprophylaxis?
Methods
We conducted the Qualitative Thromboprophylaxis Enquiry of Compliance (QUALITEC) survey at 3 institutions from June 2006 to September 2007. One was a university‐affiliated hospital (St. Joseph's Healthcare, Hamilton, Ontario, Canada); the other 2 were community hospitals (Joseph Brant Hospital, Burlington, Ontario, and Credit Valley Hospital, Mississauga, Ontario, Canada).
Participants included: (1) bedside nurses, nurse clinicians, and nurse educators; (2) pharmacists; (3) attending physicians; (4) nurse, pharmacy, and physician managers; (5) hospital administrators; (6)medical residents; and (7) members of the hospitals' Quality Improvement Team. Participants in groups 1 to 3 were persons who had cared for medical patients in the index hospital for at least 2 years. Participants in groups 4 and 5 were persons who had worked in the index hospital for at least 2 years. The requisite minimal duration of work on the medical ward for residents was 1 month. There were no exclusion criteria for participants based on sex, religion, ethnicity, or culture. Thus, we enrolled participants based on their a priori eligibility criteria (criterion sampling) and their ability to allow us to achieve our objectives (purposive sampling).
The Research Coordinator created a list of potential interview candidates by examining the organizational structure of each hospital to identify the names of clinicians, managers, and administrators who had responsibility for medical patients. This person identified the names of potential medical ward nurses through discussion with the nurse manager of each medical unit and identified the names of potential attending physicians, residents, and pharmacists through discussion with the physician director or designate of the medical unit (snowball sampling).
After piloting testing with 2 trial participants, the Research Coordinator conducted in‐depth, open‐ended, 1‐on‐1 interviews using a flexible interview guide. This approach allows respondents to use their own words to express ideas, and affords opportunities to probe for more information through dialog. All potential participants were provided with a brief study summary. Each interview took approximately 30 to 60 minutes. All interviews were audiotaped and transcribed verbatim. The Research Coordinator wrote field notes on the main concepts featured in the interview.
To characterize the participants, we recorded their age, sex, position, number of years in their current position, number of years in their profession, and number of years working in their hospital. For clinicians, we recorded the proportion of their professional time spent in clinical practice, the proportion of their clinical time spent caring for hospitalized medical patients (on the medical wards, doing consultations, and in the emergency department), and whether they had a formal role in a previous quality improvement project.
We transcribed each interview upon completion. As is typical for qualitative research, we began data analysis during the data collection phase. Transcripts were analyzed using the coding methods described by Strauss and Corbin.16 The main content analysis of QUALITEC consisted of line‐by‐line open coding. All transcripts were coded by 2 investigators independently who created categories and themes. The first coding process of grounded theory analysis was reduction of data to identify categories (experiences and actions that were similar or related) and to define their dimensions. We iterated between data collection and analysis, revising the interview guide to refine questions and focus on unique concepts. The qualitative data management software NVivo helped with linking codes and categories to ultimately organize ideas into a main theme and several key concepts; it also helped with retrieval of specific quotes. A third investigator reviewed the transcripts independently to identify categories. Analysis continued while the study progressed until saturation of information occurred and no new categories emerged. We invited 3 participants to review an early draft report (member checking).
Research Ethics
This study was approved by the Research Ethics Board at each participating center. Written informed consent was obtained from each participant. Participation was voluntary and confidential; participants had the opportunity to withdraw from the study without any consequences. Data were deidentified upon transcription and remained anonymized, while kept in secure password protected computerized files. Participants received a $25 gift certificate as a token of appreciation. We conducted this study according to the Guiding Ethical Principles section of the Tri‐council Policy Statement of Ethical Conduct for Research Involving Humans.17
Results
Of 39 persons we approached to participate, 36 out of 39 (92.3%) agreed. Two nurse managers at 1 community hospital declined to participate. One resident was missed due to clinical responsibilities. In Table 1, we present the characteristics of the 36 participants. When asked about the level of concern about thromboprophylaxis on the medical wards, participants stated that clinicians were generally insufficiently concerned (24/36, 68.6%) or appropriately concerned (11/36, 31.4%).
| Characteristic | Value |
|---|---|
| |
| Female, n (%) | 27 (75.0) |
| Age, mean (SD) | 39.6 (15.6) |
| Hospital, n (%) | |
| St. Joseph's Healthcare, Hamilton | 16 (44.4) |
| Joseph Brant, Burlington | 9 (25.0) |
| Credit Valley, Oakville | 11 (30.6) |
| Years in hospital, mean (SD) | 10.1 (7.4) |
| Position, n (%) | |
| Bedside nurse | 8 (22.2) |
| Charge nurse | 1 (2.8) |
| Nurse clinician | 2 (5.6) |
| Nurse educator | 2 (5.6) |
| Nurse manager | 2 (5.6) |
| Pharmacist | 3 (8.3) |
| Pharmacist manager | 3 (8.3) |
| Resident physician | 4 (11.1) |
| Attending physician | 6 (16.6) |
| Physician manager | 2 (5.6) |
| Quality improvement team member | 2 (5.6) |
| Hospital administrator | 1 (2.8) |
| Years in current position, mean (SD) | 7.3 (6.4) |
| Participated in quality improvement projects, n (%) | 20 (55.6) |
| Clinical focus (for clinicians only), mean (SD) | |
| Time spent in clinical practice (%) | 93.6 (13.4) |
| Time spent caring for medical patients (%) | 79.2 (25.1) |
Barriers
Relying on individual physicians for VTE prevention was regarded as ineffective, since medical patients often do not receive prophylaxis when they should.
It's sort of Russian roulette as to whether or not we grab a patient and it actually gets done for them. [bedside nurse]
There's a lot of mavericks out there. They do their own thing, and it has never been a problem. They're not held accountable. [quality improvement team leader]
Several different clinician groups were regarded as being involved in medical thromboprophylaxis.
Physiotherapy, occupational therapy, doctors, hopefully our clinical care educators, charge nurses . I think pretty much everybody's involved. I feel that's part of my role as care giver. [bedside nurse]
Many people in the healthcare team are involved in [deep vein thrombosis] DVT prevention at the nurse level, physiotherapy, occupational therapy (in terms of mobility of the patient) the physician, specialty services like thrombo service, hematology department. [nurse manager]
Since many clinicians implicitly or explicitly have a role in thromboprophylaxis, some participants viewed it as everyone's responsibility, or that it should be everyone's responsibility, to ensure optimal VTE prevention.
I think the responsibility should be everyone's responsibilityall across the health care professions. [ward pharmacist]
Make it so that you have a few stopgaps so that a few people are looking for the risk and make the process different so that you have a couple of stops along the way that it'll get brought up. I would create it so that it's not just one group in charge of the DVT prophylaxis decision and assessment. It has to be across the board. [nurse educator]
However, while multidisciplinary care was considered ideal to achieve optimal patient outcomes, it was also paradoxically perceived as insufficient to ensure effective thromboprophylaxis. Multidisciplinary care can lead to confusion about roles on a team, and unclear accountability, thereby becoming a potential barrier to effective prevention. Some participants thought that just one person should be ultimately responsible for thromboprophylaxis.
I think it would be crucial to identify one person responsible rather than indirectly a number of people who would be encouraged . It is probably better if you make one of those targets dependable. [physician]
[If] you assign it to one person versus having the accountability spread among [all] those peoplethen nobody takes accountability. [quality improvement team member]
Many participants reported that mobilization was important, though difficult to achieve. They also expressed uncertainty about whether, and how much, mobilization is enough.
I think the best way to prevent DVT would be to fully focus on early mobilization, regular physiotherapy, and how a patient returns to regular activities to get them up and around. [resident]
Level of mobility is a subjective matter. When it comes to the question of Well, how mobile is mobile enough?, that's not standardized to my knowledge and is very subjective as far as when to stop it. Is getting up in a chair and wiggling your toes good enough? Or are they running up and down the hall and you have to chase them? Really, what level of mobility is considered the standard for discontinuing DVT prophylaxis? That's the question that comes up repeatedly so I think that's a very large barrier. [pharmacy manager]
Several logistic barriers associated with antiembolic stockings and pneumatic compression devices were cited, including problems with fit, inconvenience, noncompliance, and cost.
I find stockings aren't always measured or worn appropriately. It's difficult; I think every nurse measures them differently. If they're too tight around the thighs they just roll them down. If anything, they really constrict any type of circulation rather than promote it. Moon boots are all right, but a little cumbersome, more expensive and are more geared to specific patients. [bedside nurse]
The patients want them off at certain times of the day. Theoretically, you only take them off to bathe them but some of them are really bothered by them. [nurse clinician]
Another key barrier was that clinicians are more focused on treating the immediate health care problem precipitating hospital admission than on preventing future complications.
It's something that we tend to forget because patients come in with giant medical problems a, b, and c, and then your DVT prophylaxis tends to fall by the wayside, as you're trying to deal with their major medical issues. [resident]
Prevention issues are a little bit different than treatment issues . We see ourselves as interventionists more than preventionists . It's the medical things we tend to deal with immediately and that's often the focus why the patient is in hospital, rightly or wrongly. Quality doesn't just include intervention, it includes prevention. [nurse manager]
Potential Solutions
To address this problem of inattention to preventive strategies, participants indicated that local data on the burden of illness and current utilization of thromboprophylaxis would be helpful. Some participants described institution‐specific information and thromboprophylaxis targets that motivate clinicians.
Give feedback to the team and physicians about what the incidence of DVT is. I don't think everybody knows. I don't even know in our hospital what it is. So give feedback to the team about what the incidence of DVT is, how many people are on DVT prophylaxis and how many people die from pulmonary embolism. If you have those numbers in front of you, then you would have something to aim for. [physician manager]
You do run charts so that you are auditing continuously and reporting the results back to the staff. And we have weekly meetings with staff members. That has been effective. And we have tip of the week via email. [quality improvement team member]
Most participants recommended redoubling efforts towards anticoagulant thromboprophylaxisa coordinated, systemwide approach across the continuum of care.
It's got to be a trigger for every patient that comes in. Does this patient need DVT prophylaxis? Is this patient a candidate for it? [physician manager]
I think if it's not tackled at the beginning it gets lost in the shuffle. I think if it's something we put into place just like we do when we're getting a history and on anything else. If we start with it [heparin] from day one we'll continue it through right to the end. [bedside nurse]
Participants suggested a variety of methods to enhance thromboprophylaxis. These included a universal, structured, dynamic risk stratification tool, and standardized order forms at the time of hospital admission, which would be reevaluated regularly, and require an enabling educational program.
Every medical patient 18 or older will be given a risk score. Risk stratifying all of our patients with just a simple little tool and considering treatment for those that are of high risk is what we need to do. Reinforcing the education and teaching required for the patients that are at low risk, because we don't need to put everyone on heparin. But anyone could potentially get a clot. [nurse educator]
It could be a standardized order sheet for every admitted patient and maybe that could help. And that would be like the first page in every chart in the whole hospital, and they can always cross it off and say I don't want to use this. [ward pharmacist]
The hospital intranet was sanctioned as a useful repository for physician orders and other tools. Computerized health records and computer decision supports were strongly endorsed.
It should be in a computerized system if it goes into a manual system, paperwork tends to get lost. I think a computerized system would be ideal. [pharmacist]
I think that having a computer health recordthat we would love, for many reasonsonce that happened, it would be a way to ensure it, because there would be prompts . You would get a prompt saying, Why are you not using it? . An electronic health record and as a back up, having a pharmacist. [physician]
Leveraging patient or family‐mediated interventions to provide reminders was also suggested, given the familiarity of the public with thrombosis.
Leave every patient a small pamphlet saying Are you getting DVT prevention? Are you getting injections? Empower people as well. [physician]
I think the absolute biggest driver from our perspective in admin is always public awareness. The demand for standard service increases the most when the public is aware of it. They ask. Patients are becoming more educated, they use the Internet, they search those things out themselves and they are knowledgeable. [hospital administrator]
Sufficient human resources to ensure mobilization and profiling thromboprophylaxis during accreditation were regarded as administrative initiatives that could help. Capitalizing on social forces in healthcare such as patient safety could also galvanize efforts to prevent VTE.
We need physio and [occupational therapy] OT. We need more rehab. We need resources. That's what we're lacking. The only physio and OT that comes to our floor is pending discharge. So it's definitely resource‐related. [bedside nurse]
From an administrative perspective, the whole concept of preventing complications reduces risk, improves patient safety, reduces length of stayall those warm fuzzy things that are attached to providing the best possible care for the patient at the right time. [nurse manager]
Discussion
In this qualitative study, participants affirmed that depending on individual physicians for VTE prevention is insufficient. Distinct from most therapeutic interventions which are understood as the responsibility of physicians, preventive interventions such as thromboprophylaxis may be more readily embraced as the charge of members of a multidisciplinary team. While every clinician group felt compelled to help with VTE prevention, reliance on multidisciplinary care was also perceived as a barrier to effective VTE prevention because it can generate confusion about roles. Participants recommended a comprehensive, systems‐approach, including screening and risk‐stratifying all patients, preprinted orders at hospital admission that are regularly reevaluated, and audit and feedback programs. Also endorsed were patient or family‐mediated reminders, and administrative interventions such as hiring more physiotherapists for mobilization and profiling thromboprophylaxis for hospital accreditation.
Approximately 70% of participants judged that clinicians were insufficiently concerned about thromboprophylaxis. In contrast to many commonly cited reasons for underutilization of evidence‐based interventions such as lack of awareness of (or resistance to) new information, and lack of self‐efficacy of clinicians (wondering whether the benefits observed in the research setting will be realized in the practice setting),18 participants in our study did not raise these as barriers to thromboprophylaxis. As physician and pharmacist participants indicated, because the evidentiary basis for heparin thromboprophylaxis is strong and understood (in contrast to that for mechanical prophylaxis), lack of knowledge was not considered a barrier.
Our findings are consistent with a previous qualitative study in which clinicians and managers were interviewed to learn about factors that increase beta‐blocker use following myocardial infarction; these investigators found that administrative support, use of data, and quality improvement initiatives were key.19 Detailed implementation directives to clarify clinical responsibilities for many different stakeholders were also suggested in a qualitative study on the optimal use of noninvasive ventilation.20 Extending these results, participants in our study suggested several interventions aimed at different levels of the healthcare system (eg, patient, provider, and administrator) that are either enabling or reinforcing. While just 1 implementation strategy may result in improved thromboprophylaxis,21 efficient application of multiply‐redundant strategies delivered by a multidisciplinary team may be more powerful. Such an approach has driven high level performance for the American Heart Association's Get With The Guidelines Program, resulting in lower community and hospital cardiovascular and cerebrovascular mortality in Massachusetts.22
Although our aim was to obtain multidisciplinary input, we did not focus on physicians who primarily prescribe thromboprophylaxis, thereby potentially underrepresenting their views relative to their role. We did not interview all clinicians who can influence VTE risk (eg, physiotherapists) or prescribe thromboprophylaxis (eg, family physicians). During this study, patient safety emerged as a major hospital initiative,23 which could modify participants' views on the importance of VTE prevention. Although VTE prevention may be enhanced by understanding barriers to, and solutions for, optimal thromboprophylaxis from both clinicians' and managers' perspectives, the suggestions we elicited on methods to improve VTE prevention represent participants' opinions, rather than evidence, about effective strategies. Our findings are not generalizable to settings with nurse practitioners who are dedicated to VTE prevention, nor to settings with computer decision support systems that already incorporate thromboprophylaxis.
Strengths of this study include interviewing key stakeholders representing several clinician groups and managers, to obtain perspectives on both individual and systemwide influences on thromboprophylaxis in medical patients. By eliciting the views and experiences of participants in both the community and university settings, we captured multicenter perspectives on preventive health. We used triangulation of data sources (researcher and participant) and invited participants to review an early draft of the report (member checking).24 This study highlights the merits of qualitative research which can provide insights into familiar patterns and problems, and contribute to knowledge for interdisciplinary audiences. These qualitative research results help to explain quantitative research results documenting very low rates of medical thromboprophylaxis,214 raising hypotheses to test in future studies testing systemwide interventions that may improve patient safety. One prominent publication reported the impact of electronic reminders,25 while a recent systematic review of methods to increase thromboprophylaxis outlines many potentially effective approaches.21
In summary, the findings of this qualitative study challenge the notion that either individual physician efforts or multidisciplinary care are enough to lead to optimal VTE prevention. Participants believed that while well‐functioning teams at the bedside hold great promise to deliver superior care, they may also lead to unclear role definition. Since physicians commit many errors of omission regarding thromboprophylaxis, these results raise the possibility of delegated medical acts outside the scope of conventional practice for nurses and pharmacists. Leveraging the skills and knowledge of multidisciplinary teams for medical thromboprophylaxis requires not only clear accountabilities, but also excellent interprofessional communication, and institution‐wide approaches to change prescribing behavior, potentially involving patients and administrators as well as clinicians.
Acknowledgements
The authors thank the participants of this study for sharing their experiences and views with them. The authors are grateful for the help of Laurel Raftery, Michelle Murray, Monica Owen, and Shelley Anderson for transcriptions. The authors appreciate the organizational assistance of Nancy Lloyd and the biostatistical support of Diane Heels‐Ansdell for analyzing respondent characteristics. The authors are grateful to Nancy Lloyd, Alice Huh, Barbara Young, and Gray Ellrodt for feedback on earlier versions of this report. Deborah Cook had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Appendix
Qualitec Interview Guide
Opening Statement
Thank you for your participation in this research study we are conducting with colleagues at St. Joseph's Hospital and McMaster University. Through this interview, I hope to learn how you think about DVT prevention in medical patients. When you answer the interview questions, please keep in mind that we are interested in your own thoughts and approaches.
First, I have a consent form I'd like you to read to make sure you understand the reason for this study, and to see if you have any questions about becoming involved. Please take a few minutes to read it over.
[Participant reads consent, questions about the study may or may not ensue, participant signs to indicate informed consent, the interview proceeds.]
Structured Interview Begins
Demographics
Before we begin the interview, I would like you to take a few minutes to complete this form, which consists of a few demographic questions.
[Participant completes demographic form].
Thank you. Now I'll move on to some questions about DVT prevention.
[The interviewer informs the participant that she is putting the tape recorder on].
Core Study Interview Guide
Can you tell me a bit about your own approach to DVT prevention in medical patients? For what types of patients are you concerned about DVT?
What do you find are the best ways to prevent DVT? Why?
Who else is involved in trying to prevent DVT? In general, how are DVTs are prevented at this hospital?
What are some of the barriers to preventing DVTs? (e.g., risks of prevention, disbelief that prevention really works, DVT prevention is someone else's responsibilitywhose?)
Are there other ways to ensure that DVTs are prevented in medical patients? If so, how would they work?
Can you tell me how different clinicians (such as physicians, nurses, pharmacists, and residents) could do a better job at preventing DVT? How could medical wards and departments help? How could hospital administration help?
Do you remember a patient who had a problem with DVT prevention? If so, can you tell me about this problem and how it might have been avoided?
If you could create a perfect system of DVT prevention what would it be?
Do you think people are overconcerned, appropriately concerned, or underconcerned about DVT prevention?
Is there anything else you would like to tell me?
Final Debriefing Question
How has this interview experience been for you? Thank you very much for sharing your views. We really appreciate it.
- Agency for Health Care Policy Research. Prevention of venous thromboembolism after injury. Summary, evidence report/technology assessment. Available at: http://www. ahrq.gov/clinic/epcsums/vtsumm.htm. Accessed April 2008.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of thromboprophylaxis guidelines.Chest.2001;120:1964–1971.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,, et al.,for the CURVE Study Investigators.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,.Thromboprophylaxis in an academic medical center.Cardiovasc Surg.2001;9:426–430.
- ,,.Deep venous thrombosis prophylaxis: are guidelines being followed?ANZ J Surg.2002;72:331–334.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17:788–791.
- ,.Preventing venous thromboembolism in acute medical patients.QJM.2004;97:797–801.
- ,.Venous thromboembolic prophylaxis in hospitalized medical patients.Ann Pharmacother.2004;38:36–40.
- ,,.Physicians' practice for prevention of venous thromboembolism in medical patients.J Coll Physicians Surg.2004;14:211.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill medical patients: definite need for improvement.J Intern Med.2005;257:352–357.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.,for the ENDORSE Investigators.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE Study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,, et al.,for the IMPROVE Investigators.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,for the Evidence‐Based Medicine Working Group.Users' guides to the medical literature. XXIII. Qualitative research in health care. A. Are the results of the study valid?JAMA.2000;284:357–362.
- ,.Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.2nd ed.London:Sage Publications;1998.
- Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, Social Sciences and Humanities Research Council of Canada.Tri‐Council Policy Statement: Ethical Conduct for Research Involving Humans.Ottawa, Ontario:Public Works and Government Services Canada;1998 [with 2000, 2002, and 2005 amendments].
- ,,, et al.Why don't physicians follow clinical practice guidelines?JAMA.1999;282:1458–1465.
- ,,,,,.A qualitative study of increasing β‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- ,,,.Practice guidelines as multipurpose tools: a qualitative study of noninvasive ventilation.Crit Care Med.2007;35:776–782.
- ,,, et al.A systemic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Multidisciplinary rounds: an implementation system for sustained improvement in the American Heart Association's “Get With the Guidelines” Program.Crit Pathw Cardiol.2007;6:1016–1116.
- ,,,,.Changing clinician behaviour to improve patient safety.Lancet.2004;363:1224–1230.
- ,.Papers that go beyond numbers: qualitative research.BMJ.1997;315:740–748.
- ,,,,,,.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352(10):969–977.
- Agency for Health Care Policy Research. Prevention of venous thromboembolism after injury. Summary, evidence report/technology assessment. Available at: http://www. ahrq.gov/clinic/epcsums/vtsumm.htm. Accessed April 2008.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of thromboprophylaxis guidelines.Chest.2001;120:1964–1971.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,, et al.,for the CURVE Study Investigators.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,.Thromboprophylaxis in an academic medical center.Cardiovasc Surg.2001;9:426–430.
- ,,.Deep venous thrombosis prophylaxis: are guidelines being followed?ANZ J Surg.2002;72:331–334.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17:788–791.
- ,.Preventing venous thromboembolism in acute medical patients.QJM.2004;97:797–801.
- ,.Venous thromboembolic prophylaxis in hospitalized medical patients.Ann Pharmacother.2004;38:36–40.
- ,,.Physicians' practice for prevention of venous thromboembolism in medical patients.J Coll Physicians Surg.2004;14:211.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill medical patients: definite need for improvement.J Intern Med.2005;257:352–357.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.,for the ENDORSE Investigators.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE Study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,, et al.,for the IMPROVE Investigators.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,for the Evidence‐Based Medicine Working Group.Users' guides to the medical literature. XXIII. Qualitative research in health care. A. Are the results of the study valid?JAMA.2000;284:357–362.
- ,.Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.2nd ed.London:Sage Publications;1998.
- Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, Social Sciences and Humanities Research Council of Canada.Tri‐Council Policy Statement: Ethical Conduct for Research Involving Humans.Ottawa, Ontario:Public Works and Government Services Canada;1998 [with 2000, 2002, and 2005 amendments].
- ,,, et al.Why don't physicians follow clinical practice guidelines?JAMA.1999;282:1458–1465.
- ,,,,,.A qualitative study of increasing β‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- ,,,.Practice guidelines as multipurpose tools: a qualitative study of noninvasive ventilation.Crit Care Med.2007;35:776–782.
- ,,, et al.A systemic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Multidisciplinary rounds: an implementation system for sustained improvement in the American Heart Association's “Get With the Guidelines” Program.Crit Pathw Cardiol.2007;6:1016–1116.
- ,,,,.Changing clinician behaviour to improve patient safety.Lancet.2004;363:1224–1230.
- ,.Papers that go beyond numbers: qualitative research.BMJ.1997;315:740–748.
- ,,,,,,.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352(10):969–977.
Copyright © 2009 Society of Hospital Medicine
TB with Pott's Disease and Psoas Abscess
A 22‐year‐old man was referred from an outside hospital with 2 weeks of generalized weakness and difficulty ambulating. He also reported a 6‐month history of abdominal pain, right‐sided lumbar back pain, malaise, night sweats, cough, and weight loss of 30 kg. The patient was born in Mexico but had lived in the US for 10 years, working as a construction worker in northern California. He had had no prior medical care. On examination, the patient had a temperature of 40C, a heart rate of 109, and a respiratory rate of 20. His oxygen saturation was 97% on room air, and lung fields were clear bilaterally. Strength was slightly decreased in the right leg, with tenderness in the posterolateral aspect of the right thigh and thoracic lumbar spine.
Radiograph of the chest showed bilateral upper lobe reticulonodular infiltrates, cavitation, and pleural thickening (Figure 1). Computed tomography (CT) showed innumerable pulmonary nodules throughout the mid and lower lungs, a loss of disc space between L4 and L5, and a large multiloculated abscess of the right iliacus and psoas muscles that extended into the right thigh (Figure 2). Longitudinal relaxation time (T1)‐weighted magnetic resonance imaging (MRI) of the lumbar spine revealed vertebral destruction of L4 and L5 (Figure 3).

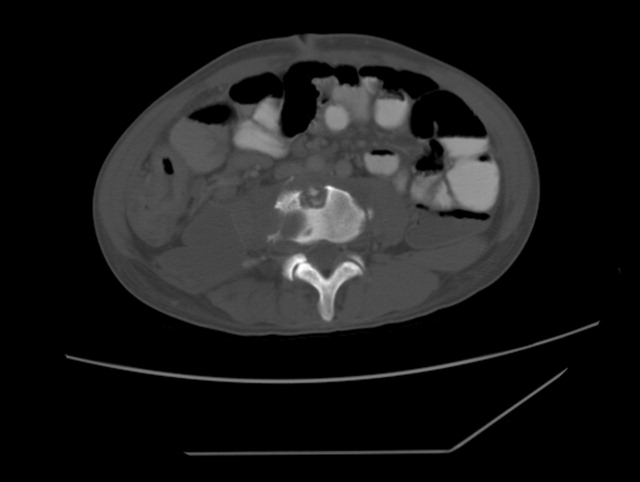
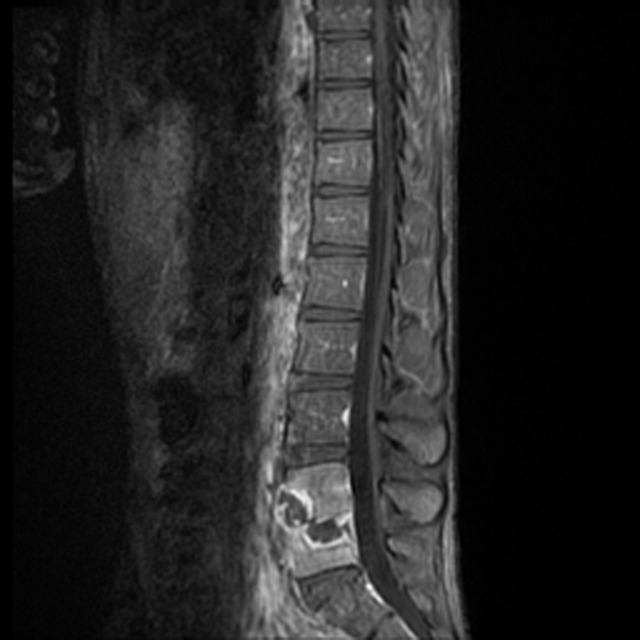
The patient underwent vertebrectomy of L4 and L5, anterior/posterior fixation and fusion from L4 to S1, and drainage of a large right‐sided psoas abscess. Acid‐fast bacilli were seen in abscess fluid and vertebral bone. Subsequently, the intraoperative cultures and 6 sequential sputum cultures all grew Mycobacterium tuberculosis. The patient was begun on rifampin, isoniazid, pyrazinamide, and ethambutol with a good clinical response, and subsequently transferred back to his referring hospital for continued medical care and rehabilitation.
Extrapulmonary manifestations of tuberculosis should be suspected in patients from a tuberculosis‐endemic country of origin. Bone and joint tuberculosis account for up to 35% of cases of extrapulmonary tuberculosis. Spinal tuberculosis (Pott's disease) most commonly involves the anteroinferior aspect of vertebral bodies in the thoracic spine. Tuberculosis is a disease with diverse manifestations and can elude even the most astute physician if it is not considered as a diagnosis.
A 22‐year‐old man was referred from an outside hospital with 2 weeks of generalized weakness and difficulty ambulating. He also reported a 6‐month history of abdominal pain, right‐sided lumbar back pain, malaise, night sweats, cough, and weight loss of 30 kg. The patient was born in Mexico but had lived in the US for 10 years, working as a construction worker in northern California. He had had no prior medical care. On examination, the patient had a temperature of 40C, a heart rate of 109, and a respiratory rate of 20. His oxygen saturation was 97% on room air, and lung fields were clear bilaterally. Strength was slightly decreased in the right leg, with tenderness in the posterolateral aspect of the right thigh and thoracic lumbar spine.
Radiograph of the chest showed bilateral upper lobe reticulonodular infiltrates, cavitation, and pleural thickening (Figure 1). Computed tomography (CT) showed innumerable pulmonary nodules throughout the mid and lower lungs, a loss of disc space between L4 and L5, and a large multiloculated abscess of the right iliacus and psoas muscles that extended into the right thigh (Figure 2). Longitudinal relaxation time (T1)‐weighted magnetic resonance imaging (MRI) of the lumbar spine revealed vertebral destruction of L4 and L5 (Figure 3).
The patient underwent vertebrectomy of L4 and L5, anterior/posterior fixation and fusion from L4 to S1, and drainage of a large right‐sided psoas abscess. Acid‐fast bacilli were seen in abscess fluid and vertebral bone. Subsequently, the intraoperative cultures and 6 sequential sputum cultures all grew Mycobacterium tuberculosis. The patient was begun on rifampin, isoniazid, pyrazinamide, and ethambutol with a good clinical response, and subsequently transferred back to his referring hospital for continued medical care and rehabilitation.
Extrapulmonary manifestations of tuberculosis should be suspected in patients from a tuberculosis‐endemic country of origin. Bone and joint tuberculosis account for up to 35% of cases of extrapulmonary tuberculosis. Spinal tuberculosis (Pott's disease) most commonly involves the anteroinferior aspect of vertebral bodies in the thoracic spine. Tuberculosis is a disease with diverse manifestations and can elude even the most astute physician if it is not considered as a diagnosis.
A 22‐year‐old man was referred from an outside hospital with 2 weeks of generalized weakness and difficulty ambulating. He also reported a 6‐month history of abdominal pain, right‐sided lumbar back pain, malaise, night sweats, cough, and weight loss of 30 kg. The patient was born in Mexico but had lived in the US for 10 years, working as a construction worker in northern California. He had had no prior medical care. On examination, the patient had a temperature of 40C, a heart rate of 109, and a respiratory rate of 20. His oxygen saturation was 97% on room air, and lung fields were clear bilaterally. Strength was slightly decreased in the right leg, with tenderness in the posterolateral aspect of the right thigh and thoracic lumbar spine.
Radiograph of the chest showed bilateral upper lobe reticulonodular infiltrates, cavitation, and pleural thickening (Figure 1). Computed tomography (CT) showed innumerable pulmonary nodules throughout the mid and lower lungs, a loss of disc space between L4 and L5, and a large multiloculated abscess of the right iliacus and psoas muscles that extended into the right thigh (Figure 2). Longitudinal relaxation time (T1)‐weighted magnetic resonance imaging (MRI) of the lumbar spine revealed vertebral destruction of L4 and L5 (Figure 3).
The patient underwent vertebrectomy of L4 and L5, anterior/posterior fixation and fusion from L4 to S1, and drainage of a large right‐sided psoas abscess. Acid‐fast bacilli were seen in abscess fluid and vertebral bone. Subsequently, the intraoperative cultures and 6 sequential sputum cultures all grew Mycobacterium tuberculosis. The patient was begun on rifampin, isoniazid, pyrazinamide, and ethambutol with a good clinical response, and subsequently transferred back to his referring hospital for continued medical care and rehabilitation.
Extrapulmonary manifestations of tuberculosis should be suspected in patients from a tuberculosis‐endemic country of origin. Bone and joint tuberculosis account for up to 35% of cases of extrapulmonary tuberculosis. Spinal tuberculosis (Pott's disease) most commonly involves the anteroinferior aspect of vertebral bodies in the thoracic spine. Tuberculosis is a disease with diverse manifestations and can elude even the most astute physician if it is not considered as a diagnosis.

Evidence for Thromboembolism Prophylaxis
Deep venous thrombosis (DVT) and pulmonary embolism (PE), collectively referred to as venous thromboembolism (VTE), are common events in hospitalized patients and result in significant morbidity and mortality. Often silent and frequently unexpected, VTE is preventable. Accordingly, the American College of Chest Physicians recommends that pharmacologic prophylaxis be given to acutely ill medical patients admitted to the hospital with congestive heart failure or severe respiratory disease, or to patients who are confined to bed who have additional risk factors, such as cancer or previous VTE.1 Three recent meta‐analyses24 demonstrated significant reductions in VTE in general medicine patients with pharmacologic prophylaxis. Recently the National Quality Forum advocated that hospitals evaluate each patient upon admission and regularly thereafter, for the risk of developing DVT/VTE and utilize clinically appropriate methods to prevent DVT/VTE.5
Despite recommendations for prophylaxis, multiple studies demonstrate utilization in <50% of at‐risk general medical patients.68 Physicians' lack of awareness may partially explain this underutilization, but other likely factors include physicians' questions about the clinical importance of the outcome (eg, some studies have shown reductions primarily in asymptomatic distal DVT), doubt regarding the best form of prophylaxis (ie, unfractionated heparin [UFH] vs. low molecular weight heparin [LMWH]), uncertainty regarding optimal dosing regimens, and comparable uncertainty regarding which patients have sufficiently high risk for VTE to outweigh the risks of anticoagulation.
We undertook the current meta‐analysis to address questions about thromboembolism prevention in general medicine patients. Does pharmacologic prophylaxis prevent clinically relevant events? Is LMWH or UFH preferable in terms of either efficacy or safety?
MATERIALS AND METHODS
Search Strategy
We conducted an extensive search that included reviewing electronic databases (MEDLINE, EMBASE, and CINAHL) through June 2008, reviewing conference proceedings, and contacting drug manufacturers. The MEDLINE search combined the key words deep venous thrombosis, thromboembolism, AND pulmonary embolism with the terms primary prevention, prophylaxis, OR prevention. We limited the search results using the filter for randomized controlled trials in PubMed. Similar strategies (available on request) were used to search EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials. We also searched the Cochrane Database of Systematic Reviews to identify previous reviews on the same topic. We obtained translations of eligible, non‐English‐language articles.
The proceedings of annual meetings from the American Thoracic Society, the American Society of Hematology, and the Society for General Internal Medicine from 1994 to 2008 were hand‐searched for reports on DVT or PE prevention published in abstract form only. (Note: the American Society of Hematology was only available through 2007). We contacted the 3 main manufacturers of LMWHPfizer (dalteparin), Aventis (enoxaparin), Glaxo Smith Kline (nadoparin)and requested information on unpublished pharmaceutical sponsored trials. First authors from the trials included in this meta‐analysis were also contacted to determine if they knew of additional published or unpublished trials.
Inclusion and Exclusion Criteria
Studies were required to be prospective randomized controlled trials comparing UFH or LMWH to mechanical prophylaxis, placebo, or no intervention. We also included randomized head‐to‐head comparisons of UFH and LMWH. Eligible studies enrolled general medical patients. Trials including predominantly intensive care unit (ICU) patients; stroke, spinal cord, or acute myocardial infarction patients were excluded. We excluded trials focused on these populations because the risk for VTE may differ from that for general medical patients and because patients in these groups already commonly receive anticoagulants as a preventive measure or as active treatment (eg, for acute myocardial infarction [MI] care). Trials assessing thrombosis in patients with long‐term central venous access/catheters were also excluded. Articles focusing on long‐term rehabilitation patients were excluded.
Studies had to employ objective criteria for diagnosing VTE. For DVT these included duplex ultrasonography, venography, fibrinogen uptake scanning, impedance plethysmography, or autopsy as a primary or secondary outcome. Studies utilizing thermographic techniques were excluded.9 Eligible diagnostic modalities for PE consisted of pulmonary arteriogram, ventilation/perfusion scan, CT angiography, and autopsy.
After an initial review of article titles and abstracts, the full texts of all articles that potentially met our inclusion criteria were independently reviewed for eligibility by 2 authors (G.M.B., M.D.). In cases of disagreement, a third author (S.F.) independently reviewed the article and adjudicated decisions.
Quantitative Data Synthesis and Statistical Analysis
For all included articles, 2 reviewers independently abstracted data on key study features (including population size, trial design, modality of VTE diagnosis, and interventions delivered to treatment and control groups), results (including the rates of all DVT, proximal DVT, symptomatic DVT, PE, and death), as well as adverse events (such as bleeding and thrombocytopenia). We accepted the endpoint of DVT when assessed by duplex ultrasonography, venography, autopsy, or when diagnosed by fibrinogen uptake scanning or impedance plethysmography. For all endpoints we abstracted event rates as number of events based on intention to treat. Each study was assessed for quality using the Jadad scale.10 The Jadad scale is a validated tool for characterizing study quality that accounts for randomization, blinding, and description of withdrawals and dropouts in individual trials. The Jadad score ranges from 0 to 5 with higher numbers identifying trials of greater methodological rigor.
The trials were divided into 4 groups based on the prophylaxis agent used and the method of comparison (UFH vs. control, LMWH vs. control, LMWH vs. UFH, and LMWH/UFH combined vs. control). After combining trials for each group, we calculated a pooled relative risk (RR) and a 95% confidence interval (CI) based on both fixed and a random effects model using the DerSimonian and Laird method. Heterogeneity of the included studies was evaluated with a chi‐square statistic. The percentage of variation in the pooled RR attributable to heterogeneity was calculated and reported using the I‐squared statistic.11 Sensitivity analyses were performed and included repeating all analyses using high‐quality studies only (Jadad score 3 or higher). Publication bias was assessed using the methods developed by Egger et al.12 and Begg and Mazumdar.13 All analyses were performed using STATA SE version 9 (Stata Corp, College Station, TX).
RESULTS
Study Identification and Selection
The computerized literature search resulted in 5284 articles. Three additional citations were found by review of bibliographies. No additional trials were identified from reviews of abstracts from national meetings. Representatives from the 3 pharmaceutical companies reported no knowledge of additional published or unpublished data. Of the 5287 studies identified by the search, 14 studies met all eligibility criteria (Figure 1).
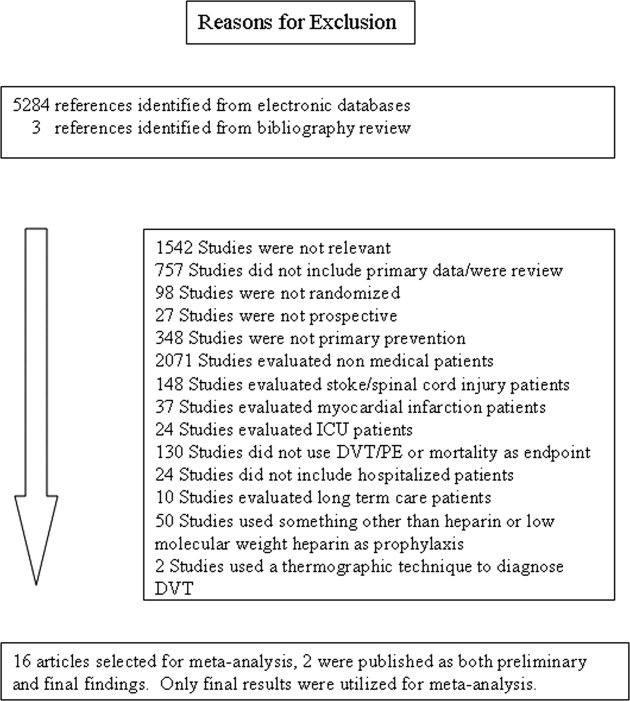
Study Characteristics
The 14 trials eligible for inclusion in the analysis consisted of 8 comparisons of UFH or LMWH vs. control (Table 1) and 6 head‐to‐head comparisons of UFH and LMWH (Table 2). The 14 studies included 8 multicenter trials and enrolled a total of 24,515 patients: 20,594 in the 8 trials that compared UFH or LMWH with placebo and 3921 in the 6 trials that compared LMWH with UFH. Two trials exclusively enrolled patients with either congestive heart failure or severe respiratory disease,14, 15 while 12 trials enrolled mixed populations. In 8 trials a period of immobility was necessary for study entry,14, 1621 while in 2 trials immobility was not required.22, 23 In the 4 remaining trials immobility was not explicitly discussed.15, 2426 One‐half of the trials required a length of stay greater than 3 days.1719, 2225
| Study (Year)Reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Belch et al. (1981)15 | 100 | 8 | Age 40‐80 years; CHF; chest infection | UFH TID | None | FUS | VQ | No | 1 |
| Dahan et al. (1986)23 | 270 | 10* | Age >65 years | Enoxaparin 60 mg | Placebo | FUS | Autopsy | Yes | 3 |
| Halkin et al. (1982)20 | 1358 | Not reported | Age >40 years; immobile | UFH BID | None | No | No | No | 1 |
| Mahe et al. (2005)16 | 2474 | 13.08 | Age >40 years; immobile | Nadroparin 7500 IU | Placebo | Autopsy | Autopsy | Yes | 5 |
| Gardlund (1996)21 | 11693 | 8.2 | Age >55 years; immobile | UFH BID | None | Autopsy | Autopsy | No | 2 |
| Samama et al. (1999)24 | 738 | 7 | Age >40 years; length of stay 6 days; CHF; respiratory failure or 1 additional risk factor | Enoxaparin 40 mg | Placebo | Venography | Composite | Yes | 4 |
| Leizorovicz et al. (2004)25 | 3681 | 12.6 | Age >40 years; length of stay 4 days; CHF; respiratory failure or 1 additional risk factor | Dalteparin 5000 IU | Placebo | DUS | Composite | Yes | 4 |
| Lederle et al. (2006)22 | 280 | 13.4 | Age >60 years; length of stay 3 days | Enoxaparin 40 mg | Placebo | DUS | Composite | Yes | 5 |
| Study (Year)reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug/Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Bergmann and Neuhart (1996)27 | 442 | 9.5 | Age >65 years; immobile | Enoxaparin 20 mg | UFH BID | FUS | Composite | Yes | 5 |
| Harenberg et al. (1990)19 | 166 | 10* | Age 40‐80 years; 1 week of bed rest | LMWH 1.500 aPTT units QD | UFH TID | IP | No | Yes | 3 |
| Kleber et al. (2003)14 | 665 | 9.8 | Age 18 years; severe CHF or respiratory disease; immobile | Enoxaparin 40 mg | UFH TID | Venography | Composite | No | 3 |
| Aquino et al. (1990)26 | 99 | Not reported | Age >70 years | Nadoparine 7500 IU | UFH BID | DUS | Composite | No | 1 |
| Harenberg et al. (1996)18 | 1590 | 10* | Age 50‐80 years; immobile + 1 additional risk factor | Nadoparine 36 mg | UFH TID | DUS | Composite | Yes | 4 |
| Lechler et al. (1996)17 | 959 | 7* | Age >18 years; immobile + 1 additional risk factor | Enoxaparin 40 mg | UFH TID | DUS | Composite | Yes | 3 |
While minimum age for study entry varied, the patient population predominantly ranged from 65 to 85 years of age. Many of the trials reported expected, not actual, treatment duration. The range of expected treatment was 7 to 21 days, with 10 days of treatment the most frequently mentioned. In the 8 trials1416, 21, 22, 24, 25, 27 that reported actual treatment duration, the range was 8 to 13.4 days. Most trials did not report number of VTE risk factors per patient, nor was there uniform acceptance of risk factors across trials.
UFH or LMWH vs. Control
DVT
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of all DVT (RR = 0.55; 95% CI: 0.36‐0.83) (Figure 2A). When stratified by methodological quality, 5 trials16, 2225 with Jadad scores of 3 or higher showed an RR reduction of 0.53 (95% CI: 0.38‐0.72) in reducing all DVT. All of the higher‐quality trials compared LMWH to placebo. Across 4 trials that reported data for symptomatic DVT there was a nonsignificant reduction in RR compared with placebo (RR = 0.73; 95% CI: 0.45‐1.16) (Figure 2B). Only 2 trials24, 25 (both LMWH trials) reported results for proximal DVT and demonstrated significant benefit of prophylaxis with a pooled RR of 0.46 (95% CI: 0.31‐0.69) (Figure 2C).
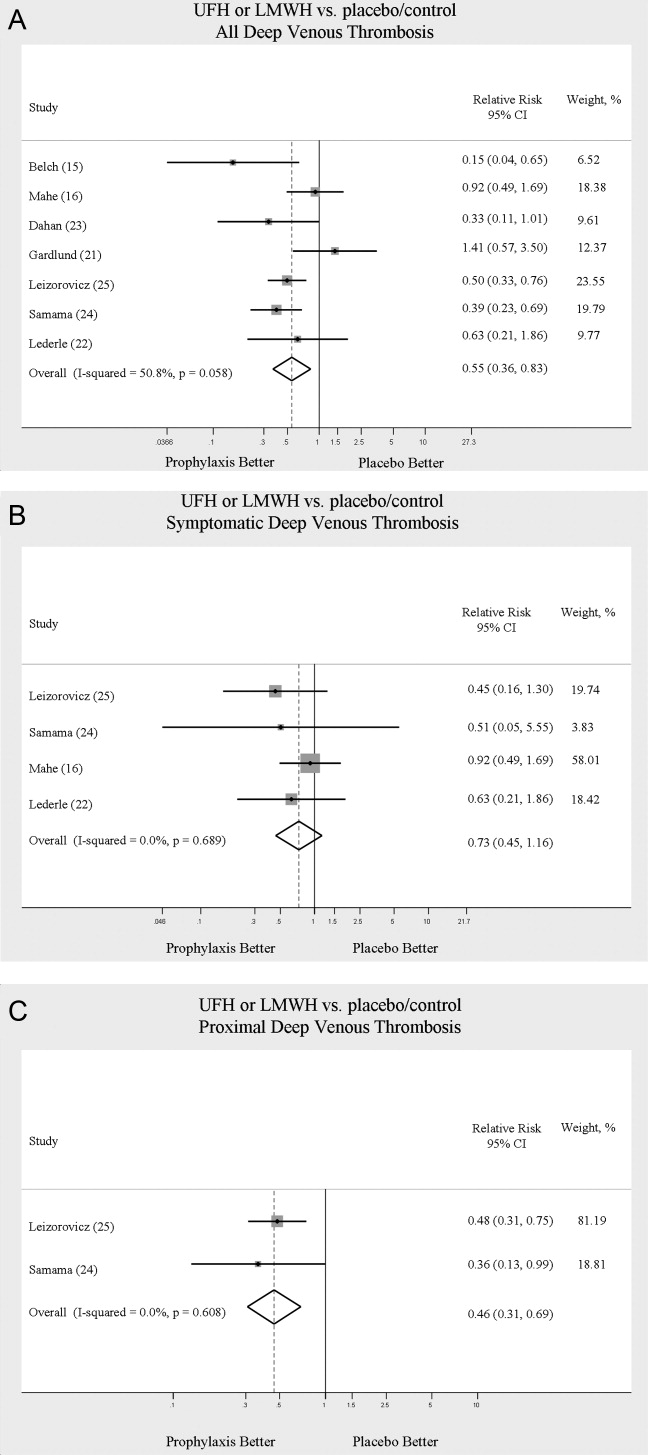
PE
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of PE (RR = 0.70; 95% CI: 0.53‐0.93) (Figure 3A). The 5 trials16, 2225 with Jadad scores of 3 or greater showed a similar relative risk reduction, but the result was no longer statistically significant (RR = 0.56; 95% CI: 0.31‐1.02). Two of the trials16, 21 relied solely on the results of autopsy to diagnose PE, which may have given rise to chance differences in detection due to generally low autopsy rates. Eliminating these 2 studies from the analysis resulted in loss of statistical significance for the reduction in risk for PE (RR = 0.48; 95% CI: 0.20‐1.15).
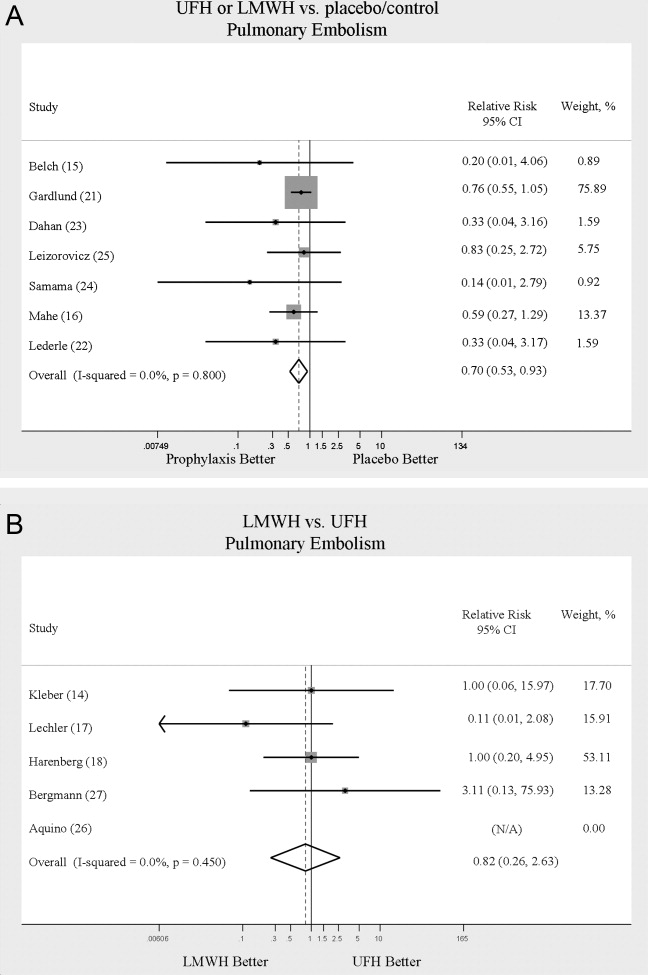
Death
Seven trials16, 2025 comparing either UFH or LMWH to control examined the impact of pharmacologic prophylaxis on death and found no significant difference between treated and untreated patients across all trials (RR = 0.92; 95% CI: 0.82‐1.03) and those limited to studies with Jadad scores of 3 or higher (RR = 0.97; 95% CI: 0.80‐1.17).
LMWH vs. UFH
DVT
In 6 trials14, 1719, 26, 27 comparing LMWH to UFH given either twice a day (BID) or 3 times a day (TID), there was no statistically significant difference in all DVT (RR = 0.90; 95% CI: 0.57‐1.43). (For all analyses RRs <1 favor LMWH, while RRs >1 favor UFH.) A total of 2 trials14, 18 reported results separately for proximal DVT with no statistically significant difference noted between UFH and LMWH (RR = 1.60; 95% CI: 0.53‐4.88). One small trial26 reported findings comparing UFH to LMWH for prevention of symptomatic DVT with no difference noted.
PE
Pooled data from the 5 trials14, 17, 18, 26, 27 comparing UFH to LMWH in the prevention of PE showed no statistically significant difference in rates of pulmonary embolism (RR = 0.82; 95% CI: 0.26‐2.63) (Figure 3B). In sensitivity analysis this result was not impacted by Jadad score.
Death
When UFH was compared to LMWH no statistically significant difference in the rate of death was found (RR = 0.96; 95% CI: 0.50‐1.85). Here again, no difference was noted when limited to studies with Jadad scores of 3 or higher.
Complications
We evaluated adverse events of heparin products used for prophylaxis and whether there were differences between UFH and LMWH. Reporting of complications was not uniform from study to study, making pooling more difficult. However, we were able to abstract data on any bleeding, major bleeding, and thrombocytopenia from several studies. In 5 studies15, 16, 2325 of either UFH or LMWH vs. control, a significantly increased risk of any bleeding (RR = 1.54; 95% CI: 1.15‐2.06) (Figure 4A) was found. When only major bleeding was evaluated, no statistically significant difference was noted (RR = 1.20; 95% CI: 0.55‐2.58) (Figure 4B). In 4 trials16, 22, 24, 25 the occurrence of thrombocytopenia was not significantly different when comparing UFH or LMWH to control (RR = 0.92; 95% CI: 0.46‐1.86).
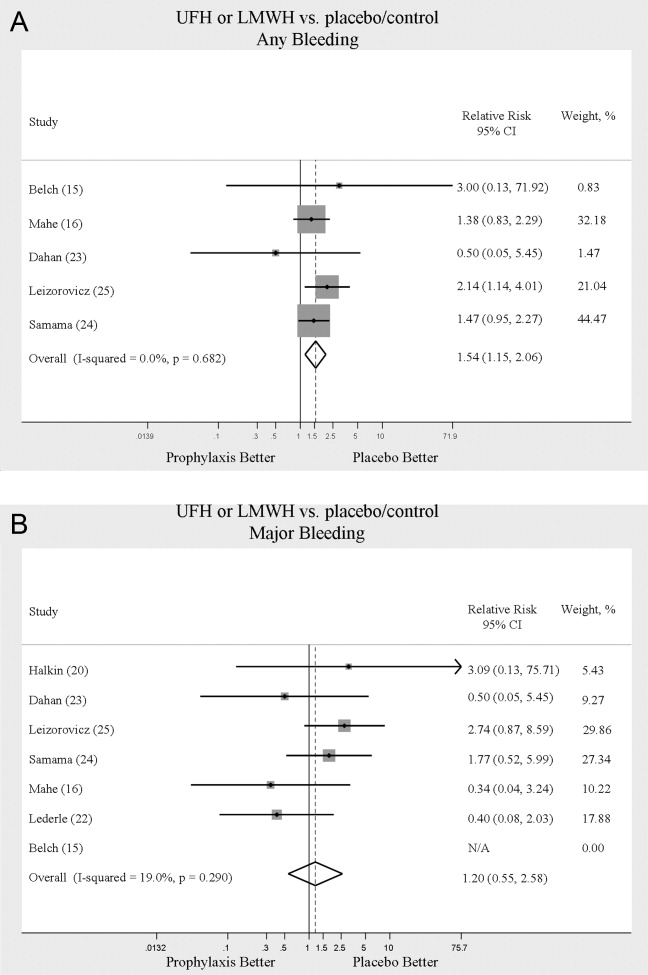
When LMWH was compared to UFH in 4 trials,14, 17, 18, 27 a nonsignificant trend toward a decrease in any bleeding was found in the LMWH group (RR = 0.72; 95% CI: 0.44‐1.16) (Figure 5A). A similar trend was seen favoring LMWH in rates of major bleeding (RR = 0.57; 95% CI: 0.25‐1.32) (Figure 5B). Neither trend was statistically significant. Three trials comparing LMWH to UFH reported on thrombocytopenia17, 18, 27 with no significant difference noted (RR = 0.52; 95% CI: 0.06‐4.18).
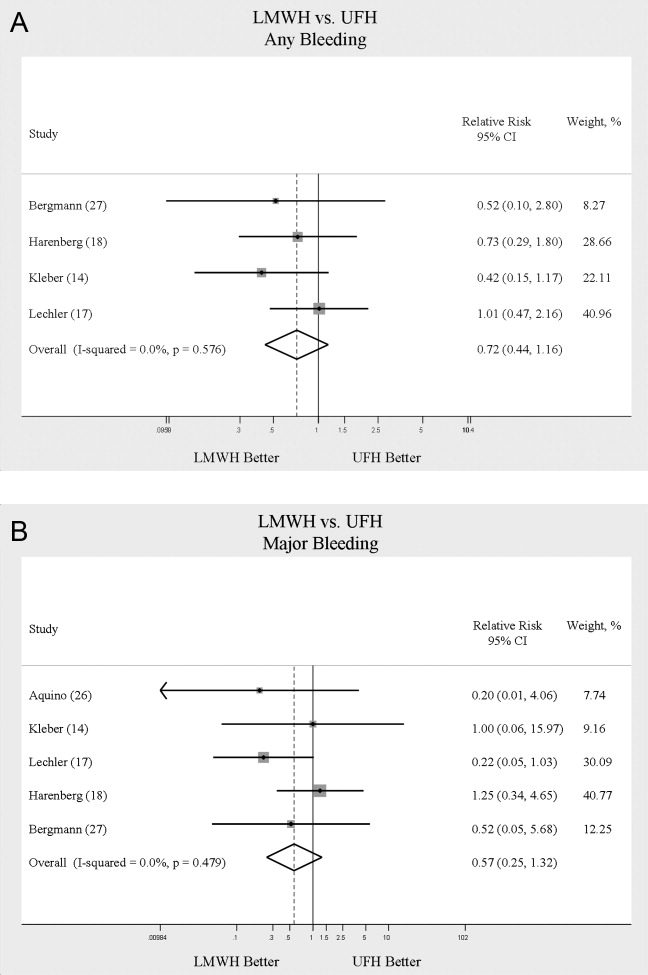
Heterogeneity and Publication Bias
No statistically significant heterogeneity was identified between trials for any outcomes. The highest I‐squared value was 54.5% (P = 0.14) for the endpoint of thrombocytopenia when UFH was compared to LMWH. In some cases, the nonsignificant results for tests of heterogeneity may have reflected small numbers of trials, but the values for I‐squared for all other endpoints were close to zero indicating that little nonrandom variation existed in the results across studies. All analyses were run using both random effects and fixed effects modeling. While we report results for random effects, no significant differences were observed using fixed effects.
We tested for publication bias using the methods developed by Egger et al.12 and Begg and Mazumdar.13 There was evidence of bias only for the outcome of PE when prophylaxis was compared to control, as the results for both tests were significant (Begg and Mazumdar:13 P = 0.035; Egger et al.:12 P = 0.010). For other outcomes tested, including all DVT (prophylaxis compared to control, and LMWH vs. UFH) as well as PE (LMWH vs. UFH), the P‐values were not significant.
DISCUSSION
When compared to control, LMWH or UFH decreased the risk of all DVT by 45% (RR = 0.55; 95% CI: 0.36‐0.83) and proximal DVT by 54% (RR = 0.46; 95% CI: 0.31‐0.69). PE was also decreased by 30% (RR = 0.70; 95% CI: 0.53‐0.93). Of note, when prophylaxis was compared with placebo all of the high‐quality studies showing a benefit were done using LMWH. The benefits of prophylaxis occurred at the cost of a 54% increased overall risk of bleeding (RR = 1.54; 95% CI 1.15‐2.06). However, the risk of major bleeding was not significantly increased. We did not find a mortality benefit to pharmacologic thromboembolism prophylaxis.
When comparing UFH to LMWH, we noted no difference in all DVT, symptomatic DVT, proximal DVT, PE, or death. While there was a trend toward less bleeding with LMWH, this was not statistically significant.
Taken in aggregate, our findings are in agreement with previous published meta‐analyses reporting net benefit for thromboembolism prophylaxis in medical patients.24, 22, 28, 29 Our meta‐analysis has several methodological strengths over the prior studies, including a comprehensive search of both the published and unpublished literature and assessment of the relationship between methodological quality of included trials and reported benefit. In contrast to previous reviews, our analysis highlights several limitations of the current evidence.
First, many of the studies are older, with predicted lengths of stay of greater than 1 week. The 8‐13‐day range of treatment duration we found in this study is longer than the average length of stay in today's hospitals. Second, there is variability in the diagnostic tests used to diagnose DVT, as well as variation in the definition of DVT among studies. Studies using fibrinogen uptake scanning reported rates of DVT as high as 26%15 while studies using venography reported DVT rates of almost 15% in the placebo arm.24 These rates are higher than most physicians' routine practice. One reason for this discrepancy is most studies did not distinguish below‐the‐knee DVT from more clinically relevant above‐the‐knee DVT. Systematic reviews of medical and surgical patients have found rates of proximal propagation from 0% to 29% in untreated patients.30, 31 Though controversial, below‐the‐knee DVT is believed less morbid than proximal DVT or symptomatic DVT. We addressed this by focusing specifically on clinically relevant endpoints of proximal and symptomatic DVT. When we restricted our analysis to proximal DVT we found a 54% RR reduction in 2 pooled trials of LMWH compared to placebo. In pooled analyses symptomatic DVT was not affected by prophylaxis. When compared head‐to‐head there were no differences between LMWH and UFH for proximal DVT or symptomatic DVT.
When considering PE, the utilization of autopsy as the sole diagnostic method in 2 large trials16, 21 is particularly problematic. In the trial by Garlund,21 the mortality rate was 5.4%, with an autopsy rate of 60.1%. Similarly, in the trial by Mahe et al.,16 the mortality rate was 10%, with an autopsy rate of 49%. Given the low absolute number of deaths and substantial proportion of decedents without autopsy, the potential for chance to produce an imbalance in detection of PE is high in these studies. When we excluded these 2 trials, we found that PE was no longer reduced to a statistically significant degree by prophylaxis. Loss of significance for PE in 2 sensitivity analyses (when excluding studies of lower quality, or using autopsy as a sole diagnostic study) is problematic and calls into question the true benefit of prophylaxis for prevention of PE.
Another limitation of the current literature centers on the variability of dosing used. We pooled trials of UFH whether given BID or TID. Given the small number of trials we did not do sensitivity analyses by dosage. A recent meta‐analysis3 found both doses are efficacious, while a recent review article32 suggested superiority of TID dosing. We believe the available literature does not clearly address this issue. Regarding comparisons of LMWH to UFH, dosing variability was also noted. The trial by Bergmann and Neuhart27 used enoxaparin 20 mg per day and found similar efficacy to UFH BID, while the Samama et al.24 trial found enoxaparin 20 mg per day no more efficacious than placebo. While the literature does not clearly define a best dose, we believe enoxaparin doses lower than 40 mg daily do not reflect the standard of care.
An additional limitation of the literature is publication bias. We assessed the possibility of publication bias by a variety of means. We did find statistical evidence of publication bias for the outcome of PE when prophylaxis was compared to control. Importantly, two meta‐analyses2, 4 on thromboembolism prophylaxis for general medicine patients suggested publication bias is present and our finding supports this conclusion. While no test for publication bias is foolproof, the best protection against publication bias, which we pursued in our study, consists of a thorough search for unpublished studies, including a search of conference proceedings, contact with experts in the field, and manufacturers of LMWH.
A final limitation of the current literature centers on risk assessment. All of the trials in this meta‐analysis included patients with an elevated level of risk. Unfortunately, risk was not clearly defined in many studies, and there was no minimum level of risk between trials. While immobility, age, and length of stay were reported for most studies, other risk factors such as personal history of thromboembolism and malignancy were not uniformly reported. Based on our analysis we are not confident our results can be extrapolated to all general medicine patients.
In conclusion, we found good evidence that pharmacologic prophylaxis significantly decreases the risk of all DVT and proximal DVT in at‐risk general medical patients. However, only LMWH was shown to prevent proximal DVT. We found inconclusive evidence that prophylaxis prevents PE. When compared directly we did not find clear superiority between UFH and LMWH, though several limitations of the current literature hamper decision‐making. Given the lower cost, it may seem justified to use UFH. However, there are other practical issues, such as the fact that LMWH is given once daily, and so potentially preferred by patients and more efficient for nurses. All of these results pertain to patients with elevated risk. While we did not find significant safety concerns with prophylaxis we do not know if these results can be extrapolated to lower‐risk patients. We believe that recommending widespread prophylaxis of all general medicine patients requires additional evidence about appropriate patient selection.
Acknowledgements
The authors thank Emmanuelle Williams, MD, for translating articles from French; Claudia Figueroa, MS, for translating articles from Spanish; Vikas Gulani, MD, for translating articles from German; and Rebecca Lee, MS, for translating articles from German, Dutch, and Italian. In addition, the authors thank Dr. Dilzer from Pfizer Global Pharmaceuticals, Kathleen E. Moigis from Aventis, and Carol McCullen from Glaxo Smith Kline for their search for unpublished pharmaceutical trials of low molecular weight heparins. Finally, the authors thank the Veterans Administration/University of Michigan Patient Safety Enhancement Program for research support.
- ,,, et al.Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126(suppl):338S–400S.
- ,,,,.Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta‐analysis of randomized controlled trials.Arch Intern Med.2007;167(14):1476–1486.
- ,,,,.Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: a metaanalysis.Chest.2007;131(2):507–516.
- ,,,,.Meta‐analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients.Ann Intern Med.2007;146(4):278–288.
- National Quality Forum. National Consensus Standards for the Prevention and Care of Venous Thromboembolism (including Deep Vein Thrombosis and Pulmonary Embolism). Available at: http://www.qualityforum.org/projects/completed/vte/index.asp. Accessed May2009.
- ,.A prospective registry of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;93(2):259–262.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371(9610):387–394.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17(10):788–791.
- ,,,.[Effectiveness of low molecular weight heparin (Fragmin) in the prevention of thromboembolism in internal medicine patients. A randomized double‐blind study].Med Klin (Munich).1988;83(7):241–245, 278.
- ,,, et al.Assessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials.1996;17(1):1–12.
- ,.Quantifying heterogeneity in a meta‐analysis.Stat Med.2002;21(11):1539–1558.
- ,,,.Bias in meta‐analysis detected by a simple, graphical test.BMJ.1997;315(7109):629–634.
- ,.Operating characteristics of a rank correlation test for publication bias.Biometrics.1994;50(4):1088–1101.
- ,,,,,.Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease.Am Heart J.2003;145(4):614–621.
- ,,,,.Prevention of deep vein thrombosis in medical patients by low‐dose heparin.Scott Med J.1981;26(2):115–117.
- ,,,,.Lack of effect of a low‐molecular‐weight heparin (nadroparin) on mortality in bedridden medical in‐patients: a prospective randomised double‐blind study.Eur J Clin Pharmacol.2005;61(5‐6):347–351.
- ,,.The venous thrombotic risk in non‐surgical patients: epidemiological data and efficacy/safety profile of a low‐molecular‐weight heparin (enoxaparin). The Prime Study Group.Haemostasis.1996;26(suppl 2):49–56.
- ,,.Subcutaneous low‐molecular‐weight heparin versus standard heparin and the prevention of thromboembolism in medical inpatients. The Heparin Study in Internal Medicine Group.Haemostasis.1996;26(3):127–139.
- ,,, et al.Randomized controlled study of heparin and low molecular weight heparin for prevention of deep‐vein thrombosis in medical patients.Thromb Res.1990;59(3):639–650.
- ,,,.Reduction of mortality in general medical in‐patients by low‐dose heparin prophylaxis.Ann Intern Med.1982;96(5):561–565.
- .Randomised, controlled trial of low‐dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group.Lancet.1996;347(9012):1357–1361.
- ,,, et al.The prophylaxis of medical patients for thromboembolism pilot study.Am J Med.2006;119(1):54–59.
- ,,, et al.Prevention of deep vein thrombosis in elderly medical in‐patients by a low molecular weight heparin: a randomized double‐blind trial.Haemostasis.1986;16(2):159–164.
- ,,, et al.A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group.N Engl J Med.1999;341(11):793–800.
- ,,,,,.Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients.Circulation.2004;110(7):874–879.
- ,,.Prevention of thromboembolic accidents in elderly subjects with Fraxiparine. In: Bounameaux H, Samama MM, Ten Cate JW, eds.Fraxiaparine. 2nd International Symposium. Recent pharmacological and clinical data.New York:Schattauer;1990:51‐54.
- ,.A multicenter randomized double‐blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in‐patients bedridden for an acute medical illness. The Enoxaparin in Medicine Study Group.Thromb Haemost.1996;76(4):529–534.
- ,,, et al.Prevention of venous thromboembolism in internal medicine with unfractionated or low‐molecular‐weight heparins: a meta‐analysis of randomised clinical trials.Thromb Haemost.2000;83(1):14–19.
- ,,,,.Meta‐analysis of venous thromboembolism prophylaxis in medically Ill patients.Clin Ther.2007;29(11):2395–2405.
- ,,,,,.Clinical relevance of distal deep vein thrombosis. Review of literature data.Thromb Haemost.2006;95(1):56–64.
- .Natural history of venous thromboembolism.Circulation.2003;107(suppl 1):I22–I30.
- .Clinical practice. Prophylaxis for thromboembolism in hospitalized medical patients.N Engl J Med.2007;356(14):1438–1444.
Deep venous thrombosis (DVT) and pulmonary embolism (PE), collectively referred to as venous thromboembolism (VTE), are common events in hospitalized patients and result in significant morbidity and mortality. Often silent and frequently unexpected, VTE is preventable. Accordingly, the American College of Chest Physicians recommends that pharmacologic prophylaxis be given to acutely ill medical patients admitted to the hospital with congestive heart failure or severe respiratory disease, or to patients who are confined to bed who have additional risk factors, such as cancer or previous VTE.1 Three recent meta‐analyses24 demonstrated significant reductions in VTE in general medicine patients with pharmacologic prophylaxis. Recently the National Quality Forum advocated that hospitals evaluate each patient upon admission and regularly thereafter, for the risk of developing DVT/VTE and utilize clinically appropriate methods to prevent DVT/VTE.5
Despite recommendations for prophylaxis, multiple studies demonstrate utilization in <50% of at‐risk general medical patients.68 Physicians' lack of awareness may partially explain this underutilization, but other likely factors include physicians' questions about the clinical importance of the outcome (eg, some studies have shown reductions primarily in asymptomatic distal DVT), doubt regarding the best form of prophylaxis (ie, unfractionated heparin [UFH] vs. low molecular weight heparin [LMWH]), uncertainty regarding optimal dosing regimens, and comparable uncertainty regarding which patients have sufficiently high risk for VTE to outweigh the risks of anticoagulation.
We undertook the current meta‐analysis to address questions about thromboembolism prevention in general medicine patients. Does pharmacologic prophylaxis prevent clinically relevant events? Is LMWH or UFH preferable in terms of either efficacy or safety?
MATERIALS AND METHODS
Search Strategy
We conducted an extensive search that included reviewing electronic databases (MEDLINE, EMBASE, and CINAHL) through June 2008, reviewing conference proceedings, and contacting drug manufacturers. The MEDLINE search combined the key words deep venous thrombosis, thromboembolism, AND pulmonary embolism with the terms primary prevention, prophylaxis, OR prevention. We limited the search results using the filter for randomized controlled trials in PubMed. Similar strategies (available on request) were used to search EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials. We also searched the Cochrane Database of Systematic Reviews to identify previous reviews on the same topic. We obtained translations of eligible, non‐English‐language articles.
The proceedings of annual meetings from the American Thoracic Society, the American Society of Hematology, and the Society for General Internal Medicine from 1994 to 2008 were hand‐searched for reports on DVT or PE prevention published in abstract form only. (Note: the American Society of Hematology was only available through 2007). We contacted the 3 main manufacturers of LMWHPfizer (dalteparin), Aventis (enoxaparin), Glaxo Smith Kline (nadoparin)and requested information on unpublished pharmaceutical sponsored trials. First authors from the trials included in this meta‐analysis were also contacted to determine if they knew of additional published or unpublished trials.
Inclusion and Exclusion Criteria
Studies were required to be prospective randomized controlled trials comparing UFH or LMWH to mechanical prophylaxis, placebo, or no intervention. We also included randomized head‐to‐head comparisons of UFH and LMWH. Eligible studies enrolled general medical patients. Trials including predominantly intensive care unit (ICU) patients; stroke, spinal cord, or acute myocardial infarction patients were excluded. We excluded trials focused on these populations because the risk for VTE may differ from that for general medical patients and because patients in these groups already commonly receive anticoagulants as a preventive measure or as active treatment (eg, for acute myocardial infarction [MI] care). Trials assessing thrombosis in patients with long‐term central venous access/catheters were also excluded. Articles focusing on long‐term rehabilitation patients were excluded.
Studies had to employ objective criteria for diagnosing VTE. For DVT these included duplex ultrasonography, venography, fibrinogen uptake scanning, impedance plethysmography, or autopsy as a primary or secondary outcome. Studies utilizing thermographic techniques were excluded.9 Eligible diagnostic modalities for PE consisted of pulmonary arteriogram, ventilation/perfusion scan, CT angiography, and autopsy.
After an initial review of article titles and abstracts, the full texts of all articles that potentially met our inclusion criteria were independently reviewed for eligibility by 2 authors (G.M.B., M.D.). In cases of disagreement, a third author (S.F.) independently reviewed the article and adjudicated decisions.
Quantitative Data Synthesis and Statistical Analysis
For all included articles, 2 reviewers independently abstracted data on key study features (including population size, trial design, modality of VTE diagnosis, and interventions delivered to treatment and control groups), results (including the rates of all DVT, proximal DVT, symptomatic DVT, PE, and death), as well as adverse events (such as bleeding and thrombocytopenia). We accepted the endpoint of DVT when assessed by duplex ultrasonography, venography, autopsy, or when diagnosed by fibrinogen uptake scanning or impedance plethysmography. For all endpoints we abstracted event rates as number of events based on intention to treat. Each study was assessed for quality using the Jadad scale.10 The Jadad scale is a validated tool for characterizing study quality that accounts for randomization, blinding, and description of withdrawals and dropouts in individual trials. The Jadad score ranges from 0 to 5 with higher numbers identifying trials of greater methodological rigor.
The trials were divided into 4 groups based on the prophylaxis agent used and the method of comparison (UFH vs. control, LMWH vs. control, LMWH vs. UFH, and LMWH/UFH combined vs. control). After combining trials for each group, we calculated a pooled relative risk (RR) and a 95% confidence interval (CI) based on both fixed and a random effects model using the DerSimonian and Laird method. Heterogeneity of the included studies was evaluated with a chi‐square statistic. The percentage of variation in the pooled RR attributable to heterogeneity was calculated and reported using the I‐squared statistic.11 Sensitivity analyses were performed and included repeating all analyses using high‐quality studies only (Jadad score 3 or higher). Publication bias was assessed using the methods developed by Egger et al.12 and Begg and Mazumdar.13 All analyses were performed using STATA SE version 9 (Stata Corp, College Station, TX).
RESULTS
Study Identification and Selection
The computerized literature search resulted in 5284 articles. Three additional citations were found by review of bibliographies. No additional trials were identified from reviews of abstracts from national meetings. Representatives from the 3 pharmaceutical companies reported no knowledge of additional published or unpublished data. Of the 5287 studies identified by the search, 14 studies met all eligibility criteria (Figure 1).
Study Characteristics
The 14 trials eligible for inclusion in the analysis consisted of 8 comparisons of UFH or LMWH vs. control (Table 1) and 6 head‐to‐head comparisons of UFH and LMWH (Table 2). The 14 studies included 8 multicenter trials and enrolled a total of 24,515 patients: 20,594 in the 8 trials that compared UFH or LMWH with placebo and 3921 in the 6 trials that compared LMWH with UFH. Two trials exclusively enrolled patients with either congestive heart failure or severe respiratory disease,14, 15 while 12 trials enrolled mixed populations. In 8 trials a period of immobility was necessary for study entry,14, 1621 while in 2 trials immobility was not required.22, 23 In the 4 remaining trials immobility was not explicitly discussed.15, 2426 One‐half of the trials required a length of stay greater than 3 days.1719, 2225
| Study (Year)Reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Belch et al. (1981)15 | 100 | 8 | Age 40‐80 years; CHF; chest infection | UFH TID | None | FUS | VQ | No | 1 |
| Dahan et al. (1986)23 | 270 | 10* | Age >65 years | Enoxaparin 60 mg | Placebo | FUS | Autopsy | Yes | 3 |
| Halkin et al. (1982)20 | 1358 | Not reported | Age >40 years; immobile | UFH BID | None | No | No | No | 1 |
| Mahe et al. (2005)16 | 2474 | 13.08 | Age >40 years; immobile | Nadroparin 7500 IU | Placebo | Autopsy | Autopsy | Yes | 5 |
| Gardlund (1996)21 | 11693 | 8.2 | Age >55 years; immobile | UFH BID | None | Autopsy | Autopsy | No | 2 |
| Samama et al. (1999)24 | 738 | 7 | Age >40 years; length of stay 6 days; CHF; respiratory failure or 1 additional risk factor | Enoxaparin 40 mg | Placebo | Venography | Composite | Yes | 4 |
| Leizorovicz et al. (2004)25 | 3681 | 12.6 | Age >40 years; length of stay 4 days; CHF; respiratory failure or 1 additional risk factor | Dalteparin 5000 IU | Placebo | DUS | Composite | Yes | 4 |
| Lederle et al. (2006)22 | 280 | 13.4 | Age >60 years; length of stay 3 days | Enoxaparin 40 mg | Placebo | DUS | Composite | Yes | 5 |
| Study (Year)reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug/Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Bergmann and Neuhart (1996)27 | 442 | 9.5 | Age >65 years; immobile | Enoxaparin 20 mg | UFH BID | FUS | Composite | Yes | 5 |
| Harenberg et al. (1990)19 | 166 | 10* | Age 40‐80 years; 1 week of bed rest | LMWH 1.500 aPTT units QD | UFH TID | IP | No | Yes | 3 |
| Kleber et al. (2003)14 | 665 | 9.8 | Age 18 years; severe CHF or respiratory disease; immobile | Enoxaparin 40 mg | UFH TID | Venography | Composite | No | 3 |
| Aquino et al. (1990)26 | 99 | Not reported | Age >70 years | Nadoparine 7500 IU | UFH BID | DUS | Composite | No | 1 |
| Harenberg et al. (1996)18 | 1590 | 10* | Age 50‐80 years; immobile + 1 additional risk factor | Nadoparine 36 mg | UFH TID | DUS | Composite | Yes | 4 |
| Lechler et al. (1996)17 | 959 | 7* | Age >18 years; immobile + 1 additional risk factor | Enoxaparin 40 mg | UFH TID | DUS | Composite | Yes | 3 |
While minimum age for study entry varied, the patient population predominantly ranged from 65 to 85 years of age. Many of the trials reported expected, not actual, treatment duration. The range of expected treatment was 7 to 21 days, with 10 days of treatment the most frequently mentioned. In the 8 trials1416, 21, 22, 24, 25, 27 that reported actual treatment duration, the range was 8 to 13.4 days. Most trials did not report number of VTE risk factors per patient, nor was there uniform acceptance of risk factors across trials.
UFH or LMWH vs. Control
DVT
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of all DVT (RR = 0.55; 95% CI: 0.36‐0.83) (Figure 2A). When stratified by methodological quality, 5 trials16, 2225 with Jadad scores of 3 or higher showed an RR reduction of 0.53 (95% CI: 0.38‐0.72) in reducing all DVT. All of the higher‐quality trials compared LMWH to placebo. Across 4 trials that reported data for symptomatic DVT there was a nonsignificant reduction in RR compared with placebo (RR = 0.73; 95% CI: 0.45‐1.16) (Figure 2B). Only 2 trials24, 25 (both LMWH trials) reported results for proximal DVT and demonstrated significant benefit of prophylaxis with a pooled RR of 0.46 (95% CI: 0.31‐0.69) (Figure 2C).
PE
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of PE (RR = 0.70; 95% CI: 0.53‐0.93) (Figure 3A). The 5 trials16, 2225 with Jadad scores of 3 or greater showed a similar relative risk reduction, but the result was no longer statistically significant (RR = 0.56; 95% CI: 0.31‐1.02). Two of the trials16, 21 relied solely on the results of autopsy to diagnose PE, which may have given rise to chance differences in detection due to generally low autopsy rates. Eliminating these 2 studies from the analysis resulted in loss of statistical significance for the reduction in risk for PE (RR = 0.48; 95% CI: 0.20‐1.15).
Death
Seven trials16, 2025 comparing either UFH or LMWH to control examined the impact of pharmacologic prophylaxis on death and found no significant difference between treated and untreated patients across all trials (RR = 0.92; 95% CI: 0.82‐1.03) and those limited to studies with Jadad scores of 3 or higher (RR = 0.97; 95% CI: 0.80‐1.17).
LMWH vs. UFH
DVT
In 6 trials14, 1719, 26, 27 comparing LMWH to UFH given either twice a day (BID) or 3 times a day (TID), there was no statistically significant difference in all DVT (RR = 0.90; 95% CI: 0.57‐1.43). (For all analyses RRs <1 favor LMWH, while RRs >1 favor UFH.) A total of 2 trials14, 18 reported results separately for proximal DVT with no statistically significant difference noted between UFH and LMWH (RR = 1.60; 95% CI: 0.53‐4.88). One small trial26 reported findings comparing UFH to LMWH for prevention of symptomatic DVT with no difference noted.
PE
Pooled data from the 5 trials14, 17, 18, 26, 27 comparing UFH to LMWH in the prevention of PE showed no statistically significant difference in rates of pulmonary embolism (RR = 0.82; 95% CI: 0.26‐2.63) (Figure 3B). In sensitivity analysis this result was not impacted by Jadad score.
Death
When UFH was compared to LMWH no statistically significant difference in the rate of death was found (RR = 0.96; 95% CI: 0.50‐1.85). Here again, no difference was noted when limited to studies with Jadad scores of 3 or higher.
Complications
We evaluated adverse events of heparin products used for prophylaxis and whether there were differences between UFH and LMWH. Reporting of complications was not uniform from study to study, making pooling more difficult. However, we were able to abstract data on any bleeding, major bleeding, and thrombocytopenia from several studies. In 5 studies15, 16, 2325 of either UFH or LMWH vs. control, a significantly increased risk of any bleeding (RR = 1.54; 95% CI: 1.15‐2.06) (Figure 4A) was found. When only major bleeding was evaluated, no statistically significant difference was noted (RR = 1.20; 95% CI: 0.55‐2.58) (Figure 4B). In 4 trials16, 22, 24, 25 the occurrence of thrombocytopenia was not significantly different when comparing UFH or LMWH to control (RR = 0.92; 95% CI: 0.46‐1.86).
When LMWH was compared to UFH in 4 trials,14, 17, 18, 27 a nonsignificant trend toward a decrease in any bleeding was found in the LMWH group (RR = 0.72; 95% CI: 0.44‐1.16) (Figure 5A). A similar trend was seen favoring LMWH in rates of major bleeding (RR = 0.57; 95% CI: 0.25‐1.32) (Figure 5B). Neither trend was statistically significant. Three trials comparing LMWH to UFH reported on thrombocytopenia17, 18, 27 with no significant difference noted (RR = 0.52; 95% CI: 0.06‐4.18).
Heterogeneity and Publication Bias
No statistically significant heterogeneity was identified between trials for any outcomes. The highest I‐squared value was 54.5% (P = 0.14) for the endpoint of thrombocytopenia when UFH was compared to LMWH. In some cases, the nonsignificant results for tests of heterogeneity may have reflected small numbers of trials, but the values for I‐squared for all other endpoints were close to zero indicating that little nonrandom variation existed in the results across studies. All analyses were run using both random effects and fixed effects modeling. While we report results for random effects, no significant differences were observed using fixed effects.
We tested for publication bias using the methods developed by Egger et al.12 and Begg and Mazumdar.13 There was evidence of bias only for the outcome of PE when prophylaxis was compared to control, as the results for both tests were significant (Begg and Mazumdar:13 P = 0.035; Egger et al.:12 P = 0.010). For other outcomes tested, including all DVT (prophylaxis compared to control, and LMWH vs. UFH) as well as PE (LMWH vs. UFH), the P‐values were not significant.
DISCUSSION
When compared to control, LMWH or UFH decreased the risk of all DVT by 45% (RR = 0.55; 95% CI: 0.36‐0.83) and proximal DVT by 54% (RR = 0.46; 95% CI: 0.31‐0.69). PE was also decreased by 30% (RR = 0.70; 95% CI: 0.53‐0.93). Of note, when prophylaxis was compared with placebo all of the high‐quality studies showing a benefit were done using LMWH. The benefits of prophylaxis occurred at the cost of a 54% increased overall risk of bleeding (RR = 1.54; 95% CI 1.15‐2.06). However, the risk of major bleeding was not significantly increased. We did not find a mortality benefit to pharmacologic thromboembolism prophylaxis.
When comparing UFH to LMWH, we noted no difference in all DVT, symptomatic DVT, proximal DVT, PE, or death. While there was a trend toward less bleeding with LMWH, this was not statistically significant.
Taken in aggregate, our findings are in agreement with previous published meta‐analyses reporting net benefit for thromboembolism prophylaxis in medical patients.24, 22, 28, 29 Our meta‐analysis has several methodological strengths over the prior studies, including a comprehensive search of both the published and unpublished literature and assessment of the relationship between methodological quality of included trials and reported benefit. In contrast to previous reviews, our analysis highlights several limitations of the current evidence.
First, many of the studies are older, with predicted lengths of stay of greater than 1 week. The 8‐13‐day range of treatment duration we found in this study is longer than the average length of stay in today's hospitals. Second, there is variability in the diagnostic tests used to diagnose DVT, as well as variation in the definition of DVT among studies. Studies using fibrinogen uptake scanning reported rates of DVT as high as 26%15 while studies using venography reported DVT rates of almost 15% in the placebo arm.24 These rates are higher than most physicians' routine practice. One reason for this discrepancy is most studies did not distinguish below‐the‐knee DVT from more clinically relevant above‐the‐knee DVT. Systematic reviews of medical and surgical patients have found rates of proximal propagation from 0% to 29% in untreated patients.30, 31 Though controversial, below‐the‐knee DVT is believed less morbid than proximal DVT or symptomatic DVT. We addressed this by focusing specifically on clinically relevant endpoints of proximal and symptomatic DVT. When we restricted our analysis to proximal DVT we found a 54% RR reduction in 2 pooled trials of LMWH compared to placebo. In pooled analyses symptomatic DVT was not affected by prophylaxis. When compared head‐to‐head there were no differences between LMWH and UFH for proximal DVT or symptomatic DVT.
When considering PE, the utilization of autopsy as the sole diagnostic method in 2 large trials16, 21 is particularly problematic. In the trial by Garlund,21 the mortality rate was 5.4%, with an autopsy rate of 60.1%. Similarly, in the trial by Mahe et al.,16 the mortality rate was 10%, with an autopsy rate of 49%. Given the low absolute number of deaths and substantial proportion of decedents without autopsy, the potential for chance to produce an imbalance in detection of PE is high in these studies. When we excluded these 2 trials, we found that PE was no longer reduced to a statistically significant degree by prophylaxis. Loss of significance for PE in 2 sensitivity analyses (when excluding studies of lower quality, or using autopsy as a sole diagnostic study) is problematic and calls into question the true benefit of prophylaxis for prevention of PE.
Another limitation of the current literature centers on the variability of dosing used. We pooled trials of UFH whether given BID or TID. Given the small number of trials we did not do sensitivity analyses by dosage. A recent meta‐analysis3 found both doses are efficacious, while a recent review article32 suggested superiority of TID dosing. We believe the available literature does not clearly address this issue. Regarding comparisons of LMWH to UFH, dosing variability was also noted. The trial by Bergmann and Neuhart27 used enoxaparin 20 mg per day and found similar efficacy to UFH BID, while the Samama et al.24 trial found enoxaparin 20 mg per day no more efficacious than placebo. While the literature does not clearly define a best dose, we believe enoxaparin doses lower than 40 mg daily do not reflect the standard of care.
An additional limitation of the literature is publication bias. We assessed the possibility of publication bias by a variety of means. We did find statistical evidence of publication bias for the outcome of PE when prophylaxis was compared to control. Importantly, two meta‐analyses2, 4 on thromboembolism prophylaxis for general medicine patients suggested publication bias is present and our finding supports this conclusion. While no test for publication bias is foolproof, the best protection against publication bias, which we pursued in our study, consists of a thorough search for unpublished studies, including a search of conference proceedings, contact with experts in the field, and manufacturers of LMWH.
A final limitation of the current literature centers on risk assessment. All of the trials in this meta‐analysis included patients with an elevated level of risk. Unfortunately, risk was not clearly defined in many studies, and there was no minimum level of risk between trials. While immobility, age, and length of stay were reported for most studies, other risk factors such as personal history of thromboembolism and malignancy were not uniformly reported. Based on our analysis we are not confident our results can be extrapolated to all general medicine patients.
In conclusion, we found good evidence that pharmacologic prophylaxis significantly decreases the risk of all DVT and proximal DVT in at‐risk general medical patients. However, only LMWH was shown to prevent proximal DVT. We found inconclusive evidence that prophylaxis prevents PE. When compared directly we did not find clear superiority between UFH and LMWH, though several limitations of the current literature hamper decision‐making. Given the lower cost, it may seem justified to use UFH. However, there are other practical issues, such as the fact that LMWH is given once daily, and so potentially preferred by patients and more efficient for nurses. All of these results pertain to patients with elevated risk. While we did not find significant safety concerns with prophylaxis we do not know if these results can be extrapolated to lower‐risk patients. We believe that recommending widespread prophylaxis of all general medicine patients requires additional evidence about appropriate patient selection.
Acknowledgements
The authors thank Emmanuelle Williams, MD, for translating articles from French; Claudia Figueroa, MS, for translating articles from Spanish; Vikas Gulani, MD, for translating articles from German; and Rebecca Lee, MS, for translating articles from German, Dutch, and Italian. In addition, the authors thank Dr. Dilzer from Pfizer Global Pharmaceuticals, Kathleen E. Moigis from Aventis, and Carol McCullen from Glaxo Smith Kline for their search for unpublished pharmaceutical trials of low molecular weight heparins. Finally, the authors thank the Veterans Administration/University of Michigan Patient Safety Enhancement Program for research support.
Deep venous thrombosis (DVT) and pulmonary embolism (PE), collectively referred to as venous thromboembolism (VTE), are common events in hospitalized patients and result in significant morbidity and mortality. Often silent and frequently unexpected, VTE is preventable. Accordingly, the American College of Chest Physicians recommends that pharmacologic prophylaxis be given to acutely ill medical patients admitted to the hospital with congestive heart failure or severe respiratory disease, or to patients who are confined to bed who have additional risk factors, such as cancer or previous VTE.1 Three recent meta‐analyses24 demonstrated significant reductions in VTE in general medicine patients with pharmacologic prophylaxis. Recently the National Quality Forum advocated that hospitals evaluate each patient upon admission and regularly thereafter, for the risk of developing DVT/VTE and utilize clinically appropriate methods to prevent DVT/VTE.5
Despite recommendations for prophylaxis, multiple studies demonstrate utilization in <50% of at‐risk general medical patients.68 Physicians' lack of awareness may partially explain this underutilization, but other likely factors include physicians' questions about the clinical importance of the outcome (eg, some studies have shown reductions primarily in asymptomatic distal DVT), doubt regarding the best form of prophylaxis (ie, unfractionated heparin [UFH] vs. low molecular weight heparin [LMWH]), uncertainty regarding optimal dosing regimens, and comparable uncertainty regarding which patients have sufficiently high risk for VTE to outweigh the risks of anticoagulation.
We undertook the current meta‐analysis to address questions about thromboembolism prevention in general medicine patients. Does pharmacologic prophylaxis prevent clinically relevant events? Is LMWH or UFH preferable in terms of either efficacy or safety?
MATERIALS AND METHODS
Search Strategy
We conducted an extensive search that included reviewing electronic databases (MEDLINE, EMBASE, and CINAHL) through June 2008, reviewing conference proceedings, and contacting drug manufacturers. The MEDLINE search combined the key words deep venous thrombosis, thromboembolism, AND pulmonary embolism with the terms primary prevention, prophylaxis, OR prevention. We limited the search results using the filter for randomized controlled trials in PubMed. Similar strategies (available on request) were used to search EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials. We also searched the Cochrane Database of Systematic Reviews to identify previous reviews on the same topic. We obtained translations of eligible, non‐English‐language articles.
The proceedings of annual meetings from the American Thoracic Society, the American Society of Hematology, and the Society for General Internal Medicine from 1994 to 2008 were hand‐searched for reports on DVT or PE prevention published in abstract form only. (Note: the American Society of Hematology was only available through 2007). We contacted the 3 main manufacturers of LMWHPfizer (dalteparin), Aventis (enoxaparin), Glaxo Smith Kline (nadoparin)and requested information on unpublished pharmaceutical sponsored trials. First authors from the trials included in this meta‐analysis were also contacted to determine if they knew of additional published or unpublished trials.
Inclusion and Exclusion Criteria
Studies were required to be prospective randomized controlled trials comparing UFH or LMWH to mechanical prophylaxis, placebo, or no intervention. We also included randomized head‐to‐head comparisons of UFH and LMWH. Eligible studies enrolled general medical patients. Trials including predominantly intensive care unit (ICU) patients; stroke, spinal cord, or acute myocardial infarction patients were excluded. We excluded trials focused on these populations because the risk for VTE may differ from that for general medical patients and because patients in these groups already commonly receive anticoagulants as a preventive measure or as active treatment (eg, for acute myocardial infarction [MI] care). Trials assessing thrombosis in patients with long‐term central venous access/catheters were also excluded. Articles focusing on long‐term rehabilitation patients were excluded.
Studies had to employ objective criteria for diagnosing VTE. For DVT these included duplex ultrasonography, venography, fibrinogen uptake scanning, impedance plethysmography, or autopsy as a primary or secondary outcome. Studies utilizing thermographic techniques were excluded.9 Eligible diagnostic modalities for PE consisted of pulmonary arteriogram, ventilation/perfusion scan, CT angiography, and autopsy.
After an initial review of article titles and abstracts, the full texts of all articles that potentially met our inclusion criteria were independently reviewed for eligibility by 2 authors (G.M.B., M.D.). In cases of disagreement, a third author (S.F.) independently reviewed the article and adjudicated decisions.
Quantitative Data Synthesis and Statistical Analysis
For all included articles, 2 reviewers independently abstracted data on key study features (including population size, trial design, modality of VTE diagnosis, and interventions delivered to treatment and control groups), results (including the rates of all DVT, proximal DVT, symptomatic DVT, PE, and death), as well as adverse events (such as bleeding and thrombocytopenia). We accepted the endpoint of DVT when assessed by duplex ultrasonography, venography, autopsy, or when diagnosed by fibrinogen uptake scanning or impedance plethysmography. For all endpoints we abstracted event rates as number of events based on intention to treat. Each study was assessed for quality using the Jadad scale.10 The Jadad scale is a validated tool for characterizing study quality that accounts for randomization, blinding, and description of withdrawals and dropouts in individual trials. The Jadad score ranges from 0 to 5 with higher numbers identifying trials of greater methodological rigor.
The trials were divided into 4 groups based on the prophylaxis agent used and the method of comparison (UFH vs. control, LMWH vs. control, LMWH vs. UFH, and LMWH/UFH combined vs. control). After combining trials for each group, we calculated a pooled relative risk (RR) and a 95% confidence interval (CI) based on both fixed and a random effects model using the DerSimonian and Laird method. Heterogeneity of the included studies was evaluated with a chi‐square statistic. The percentage of variation in the pooled RR attributable to heterogeneity was calculated and reported using the I‐squared statistic.11 Sensitivity analyses were performed and included repeating all analyses using high‐quality studies only (Jadad score 3 or higher). Publication bias was assessed using the methods developed by Egger et al.12 and Begg and Mazumdar.13 All analyses were performed using STATA SE version 9 (Stata Corp, College Station, TX).
RESULTS
Study Identification and Selection
The computerized literature search resulted in 5284 articles. Three additional citations were found by review of bibliographies. No additional trials were identified from reviews of abstracts from national meetings. Representatives from the 3 pharmaceutical companies reported no knowledge of additional published or unpublished data. Of the 5287 studies identified by the search, 14 studies met all eligibility criteria (Figure 1).
Study Characteristics
The 14 trials eligible for inclusion in the analysis consisted of 8 comparisons of UFH or LMWH vs. control (Table 1) and 6 head‐to‐head comparisons of UFH and LMWH (Table 2). The 14 studies included 8 multicenter trials and enrolled a total of 24,515 patients: 20,594 in the 8 trials that compared UFH or LMWH with placebo and 3921 in the 6 trials that compared LMWH with UFH. Two trials exclusively enrolled patients with either congestive heart failure or severe respiratory disease,14, 15 while 12 trials enrolled mixed populations. In 8 trials a period of immobility was necessary for study entry,14, 1621 while in 2 trials immobility was not required.22, 23 In the 4 remaining trials immobility was not explicitly discussed.15, 2426 One‐half of the trials required a length of stay greater than 3 days.1719, 2225
| Study (Year)Reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Belch et al. (1981)15 | 100 | 8 | Age 40‐80 years; CHF; chest infection | UFH TID | None | FUS | VQ | No | 1 |
| Dahan et al. (1986)23 | 270 | 10* | Age >65 years | Enoxaparin 60 mg | Placebo | FUS | Autopsy | Yes | 3 |
| Halkin et al. (1982)20 | 1358 | Not reported | Age >40 years; immobile | UFH BID | None | No | No | No | 1 |
| Mahe et al. (2005)16 | 2474 | 13.08 | Age >40 years; immobile | Nadroparin 7500 IU | Placebo | Autopsy | Autopsy | Yes | 5 |
| Gardlund (1996)21 | 11693 | 8.2 | Age >55 years; immobile | UFH BID | None | Autopsy | Autopsy | No | 2 |
| Samama et al. (1999)24 | 738 | 7 | Age >40 years; length of stay 6 days; CHF; respiratory failure or 1 additional risk factor | Enoxaparin 40 mg | Placebo | Venography | Composite | Yes | 4 |
| Leizorovicz et al. (2004)25 | 3681 | 12.6 | Age >40 years; length of stay 4 days; CHF; respiratory failure or 1 additional risk factor | Dalteparin 5000 IU | Placebo | DUS | Composite | Yes | 4 |
| Lederle et al. (2006)22 | 280 | 13.4 | Age >60 years; length of stay 3 days | Enoxaparin 40 mg | Placebo | DUS | Composite | Yes | 5 |
| Study (Year)reference | Patients (n) | Duration (days) | VTE Risk Factors | Drug/Dose | Comparison | DVT Assessed | PE Assessed | Double Blind | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Bergmann and Neuhart (1996)27 | 442 | 9.5 | Age >65 years; immobile | Enoxaparin 20 mg | UFH BID | FUS | Composite | Yes | 5 |
| Harenberg et al. (1990)19 | 166 | 10* | Age 40‐80 years; 1 week of bed rest | LMWH 1.500 aPTT units QD | UFH TID | IP | No | Yes | 3 |
| Kleber et al. (2003)14 | 665 | 9.8 | Age 18 years; severe CHF or respiratory disease; immobile | Enoxaparin 40 mg | UFH TID | Venography | Composite | No | 3 |
| Aquino et al. (1990)26 | 99 | Not reported | Age >70 years | Nadoparine 7500 IU | UFH BID | DUS | Composite | No | 1 |
| Harenberg et al. (1996)18 | 1590 | 10* | Age 50‐80 years; immobile + 1 additional risk factor | Nadoparine 36 mg | UFH TID | DUS | Composite | Yes | 4 |
| Lechler et al. (1996)17 | 959 | 7* | Age >18 years; immobile + 1 additional risk factor | Enoxaparin 40 mg | UFH TID | DUS | Composite | Yes | 3 |
While minimum age for study entry varied, the patient population predominantly ranged from 65 to 85 years of age. Many of the trials reported expected, not actual, treatment duration. The range of expected treatment was 7 to 21 days, with 10 days of treatment the most frequently mentioned. In the 8 trials1416, 21, 22, 24, 25, 27 that reported actual treatment duration, the range was 8 to 13.4 days. Most trials did not report number of VTE risk factors per patient, nor was there uniform acceptance of risk factors across trials.
UFH or LMWH vs. Control
DVT
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of all DVT (RR = 0.55; 95% CI: 0.36‐0.83) (Figure 2A). When stratified by methodological quality, 5 trials16, 2225 with Jadad scores of 3 or higher showed an RR reduction of 0.53 (95% CI: 0.38‐0.72) in reducing all DVT. All of the higher‐quality trials compared LMWH to placebo. Across 4 trials that reported data for symptomatic DVT there was a nonsignificant reduction in RR compared with placebo (RR = 0.73; 95% CI: 0.45‐1.16) (Figure 2B). Only 2 trials24, 25 (both LMWH trials) reported results for proximal DVT and demonstrated significant benefit of prophylaxis with a pooled RR of 0.46 (95% CI: 0.31‐0.69) (Figure 2C).
PE
Across 7 trials comparing either UFH or LMWH to control, heparin products significantly decreased the risk of PE (RR = 0.70; 95% CI: 0.53‐0.93) (Figure 3A). The 5 trials16, 2225 with Jadad scores of 3 or greater showed a similar relative risk reduction, but the result was no longer statistically significant (RR = 0.56; 95% CI: 0.31‐1.02). Two of the trials16, 21 relied solely on the results of autopsy to diagnose PE, which may have given rise to chance differences in detection due to generally low autopsy rates. Eliminating these 2 studies from the analysis resulted in loss of statistical significance for the reduction in risk for PE (RR = 0.48; 95% CI: 0.20‐1.15).
Death
Seven trials16, 2025 comparing either UFH or LMWH to control examined the impact of pharmacologic prophylaxis on death and found no significant difference between treated and untreated patients across all trials (RR = 0.92; 95% CI: 0.82‐1.03) and those limited to studies with Jadad scores of 3 or higher (RR = 0.97; 95% CI: 0.80‐1.17).
LMWH vs. UFH
DVT
In 6 trials14, 1719, 26, 27 comparing LMWH to UFH given either twice a day (BID) or 3 times a day (TID), there was no statistically significant difference in all DVT (RR = 0.90; 95% CI: 0.57‐1.43). (For all analyses RRs <1 favor LMWH, while RRs >1 favor UFH.) A total of 2 trials14, 18 reported results separately for proximal DVT with no statistically significant difference noted between UFH and LMWH (RR = 1.60; 95% CI: 0.53‐4.88). One small trial26 reported findings comparing UFH to LMWH for prevention of symptomatic DVT with no difference noted.
PE
Pooled data from the 5 trials14, 17, 18, 26, 27 comparing UFH to LMWH in the prevention of PE showed no statistically significant difference in rates of pulmonary embolism (RR = 0.82; 95% CI: 0.26‐2.63) (Figure 3B). In sensitivity analysis this result was not impacted by Jadad score.
Death
When UFH was compared to LMWH no statistically significant difference in the rate of death was found (RR = 0.96; 95% CI: 0.50‐1.85). Here again, no difference was noted when limited to studies with Jadad scores of 3 or higher.
Complications
We evaluated adverse events of heparin products used for prophylaxis and whether there were differences between UFH and LMWH. Reporting of complications was not uniform from study to study, making pooling more difficult. However, we were able to abstract data on any bleeding, major bleeding, and thrombocytopenia from several studies. In 5 studies15, 16, 2325 of either UFH or LMWH vs. control, a significantly increased risk of any bleeding (RR = 1.54; 95% CI: 1.15‐2.06) (Figure 4A) was found. When only major bleeding was evaluated, no statistically significant difference was noted (RR = 1.20; 95% CI: 0.55‐2.58) (Figure 4B). In 4 trials16, 22, 24, 25 the occurrence of thrombocytopenia was not significantly different when comparing UFH or LMWH to control (RR = 0.92; 95% CI: 0.46‐1.86).
When LMWH was compared to UFH in 4 trials,14, 17, 18, 27 a nonsignificant trend toward a decrease in any bleeding was found in the LMWH group (RR = 0.72; 95% CI: 0.44‐1.16) (Figure 5A). A similar trend was seen favoring LMWH in rates of major bleeding (RR = 0.57; 95% CI: 0.25‐1.32) (Figure 5B). Neither trend was statistically significant. Three trials comparing LMWH to UFH reported on thrombocytopenia17, 18, 27 with no significant difference noted (RR = 0.52; 95% CI: 0.06‐4.18).
Heterogeneity and Publication Bias
No statistically significant heterogeneity was identified between trials for any outcomes. The highest I‐squared value was 54.5% (P = 0.14) for the endpoint of thrombocytopenia when UFH was compared to LMWH. In some cases, the nonsignificant results for tests of heterogeneity may have reflected small numbers of trials, but the values for I‐squared for all other endpoints were close to zero indicating that little nonrandom variation existed in the results across studies. All analyses were run using both random effects and fixed effects modeling. While we report results for random effects, no significant differences were observed using fixed effects.
We tested for publication bias using the methods developed by Egger et al.12 and Begg and Mazumdar.13 There was evidence of bias only for the outcome of PE when prophylaxis was compared to control, as the results for both tests were significant (Begg and Mazumdar:13 P = 0.035; Egger et al.:12 P = 0.010). For other outcomes tested, including all DVT (prophylaxis compared to control, and LMWH vs. UFH) as well as PE (LMWH vs. UFH), the P‐values were not significant.
DISCUSSION
When compared to control, LMWH or UFH decreased the risk of all DVT by 45% (RR = 0.55; 95% CI: 0.36‐0.83) and proximal DVT by 54% (RR = 0.46; 95% CI: 0.31‐0.69). PE was also decreased by 30% (RR = 0.70; 95% CI: 0.53‐0.93). Of note, when prophylaxis was compared with placebo all of the high‐quality studies showing a benefit were done using LMWH. The benefits of prophylaxis occurred at the cost of a 54% increased overall risk of bleeding (RR = 1.54; 95% CI 1.15‐2.06). However, the risk of major bleeding was not significantly increased. We did not find a mortality benefit to pharmacologic thromboembolism prophylaxis.
When comparing UFH to LMWH, we noted no difference in all DVT, symptomatic DVT, proximal DVT, PE, or death. While there was a trend toward less bleeding with LMWH, this was not statistically significant.
Taken in aggregate, our findings are in agreement with previous published meta‐analyses reporting net benefit for thromboembolism prophylaxis in medical patients.24, 22, 28, 29 Our meta‐analysis has several methodological strengths over the prior studies, including a comprehensive search of both the published and unpublished literature and assessment of the relationship between methodological quality of included trials and reported benefit. In contrast to previous reviews, our analysis highlights several limitations of the current evidence.
First, many of the studies are older, with predicted lengths of stay of greater than 1 week. The 8‐13‐day range of treatment duration we found in this study is longer than the average length of stay in today's hospitals. Second, there is variability in the diagnostic tests used to diagnose DVT, as well as variation in the definition of DVT among studies. Studies using fibrinogen uptake scanning reported rates of DVT as high as 26%15 while studies using venography reported DVT rates of almost 15% in the placebo arm.24 These rates are higher than most physicians' routine practice. One reason for this discrepancy is most studies did not distinguish below‐the‐knee DVT from more clinically relevant above‐the‐knee DVT. Systematic reviews of medical and surgical patients have found rates of proximal propagation from 0% to 29% in untreated patients.30, 31 Though controversial, below‐the‐knee DVT is believed less morbid than proximal DVT or symptomatic DVT. We addressed this by focusing specifically on clinically relevant endpoints of proximal and symptomatic DVT. When we restricted our analysis to proximal DVT we found a 54% RR reduction in 2 pooled trials of LMWH compared to placebo. In pooled analyses symptomatic DVT was not affected by prophylaxis. When compared head‐to‐head there were no differences between LMWH and UFH for proximal DVT or symptomatic DVT.
When considering PE, the utilization of autopsy as the sole diagnostic method in 2 large trials16, 21 is particularly problematic. In the trial by Garlund,21 the mortality rate was 5.4%, with an autopsy rate of 60.1%. Similarly, in the trial by Mahe et al.,16 the mortality rate was 10%, with an autopsy rate of 49%. Given the low absolute number of deaths and substantial proportion of decedents without autopsy, the potential for chance to produce an imbalance in detection of PE is high in these studies. When we excluded these 2 trials, we found that PE was no longer reduced to a statistically significant degree by prophylaxis. Loss of significance for PE in 2 sensitivity analyses (when excluding studies of lower quality, or using autopsy as a sole diagnostic study) is problematic and calls into question the true benefit of prophylaxis for prevention of PE.
Another limitation of the current literature centers on the variability of dosing used. We pooled trials of UFH whether given BID or TID. Given the small number of trials we did not do sensitivity analyses by dosage. A recent meta‐analysis3 found both doses are efficacious, while a recent review article32 suggested superiority of TID dosing. We believe the available literature does not clearly address this issue. Regarding comparisons of LMWH to UFH, dosing variability was also noted. The trial by Bergmann and Neuhart27 used enoxaparin 20 mg per day and found similar efficacy to UFH BID, while the Samama et al.24 trial found enoxaparin 20 mg per day no more efficacious than placebo. While the literature does not clearly define a best dose, we believe enoxaparin doses lower than 40 mg daily do not reflect the standard of care.
An additional limitation of the literature is publication bias. We assessed the possibility of publication bias by a variety of means. We did find statistical evidence of publication bias for the outcome of PE when prophylaxis was compared to control. Importantly, two meta‐analyses2, 4 on thromboembolism prophylaxis for general medicine patients suggested publication bias is present and our finding supports this conclusion. While no test for publication bias is foolproof, the best protection against publication bias, which we pursued in our study, consists of a thorough search for unpublished studies, including a search of conference proceedings, contact with experts in the field, and manufacturers of LMWH.
A final limitation of the current literature centers on risk assessment. All of the trials in this meta‐analysis included patients with an elevated level of risk. Unfortunately, risk was not clearly defined in many studies, and there was no minimum level of risk between trials. While immobility, age, and length of stay were reported for most studies, other risk factors such as personal history of thromboembolism and malignancy were not uniformly reported. Based on our analysis we are not confident our results can be extrapolated to all general medicine patients.
In conclusion, we found good evidence that pharmacologic prophylaxis significantly decreases the risk of all DVT and proximal DVT in at‐risk general medical patients. However, only LMWH was shown to prevent proximal DVT. We found inconclusive evidence that prophylaxis prevents PE. When compared directly we did not find clear superiority between UFH and LMWH, though several limitations of the current literature hamper decision‐making. Given the lower cost, it may seem justified to use UFH. However, there are other practical issues, such as the fact that LMWH is given once daily, and so potentially preferred by patients and more efficient for nurses. All of these results pertain to patients with elevated risk. While we did not find significant safety concerns with prophylaxis we do not know if these results can be extrapolated to lower‐risk patients. We believe that recommending widespread prophylaxis of all general medicine patients requires additional evidence about appropriate patient selection.
Acknowledgements
The authors thank Emmanuelle Williams, MD, for translating articles from French; Claudia Figueroa, MS, for translating articles from Spanish; Vikas Gulani, MD, for translating articles from German; and Rebecca Lee, MS, for translating articles from German, Dutch, and Italian. In addition, the authors thank Dr. Dilzer from Pfizer Global Pharmaceuticals, Kathleen E. Moigis from Aventis, and Carol McCullen from Glaxo Smith Kline for their search for unpublished pharmaceutical trials of low molecular weight heparins. Finally, the authors thank the Veterans Administration/University of Michigan Patient Safety Enhancement Program for research support.
- ,,, et al.Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126(suppl):338S–400S.
- ,,,,.Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta‐analysis of randomized controlled trials.Arch Intern Med.2007;167(14):1476–1486.
- ,,,,.Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: a metaanalysis.Chest.2007;131(2):507–516.
- ,,,,.Meta‐analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients.Ann Intern Med.2007;146(4):278–288.
- National Quality Forum. National Consensus Standards for the Prevention and Care of Venous Thromboembolism (including Deep Vein Thrombosis and Pulmonary Embolism). Available at: http://www.qualityforum.org/projects/completed/vte/index.asp. Accessed May2009.
- ,.A prospective registry of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;93(2):259–262.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371(9610):387–394.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17(10):788–791.
- ,,,.[Effectiveness of low molecular weight heparin (Fragmin) in the prevention of thromboembolism in internal medicine patients. A randomized double‐blind study].Med Klin (Munich).1988;83(7):241–245, 278.
- ,,, et al.Assessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials.1996;17(1):1–12.
- ,.Quantifying heterogeneity in a meta‐analysis.Stat Med.2002;21(11):1539–1558.
- ,,,.Bias in meta‐analysis detected by a simple, graphical test.BMJ.1997;315(7109):629–634.
- ,.Operating characteristics of a rank correlation test for publication bias.Biometrics.1994;50(4):1088–1101.
- ,,,,,.Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease.Am Heart J.2003;145(4):614–621.
- ,,,,.Prevention of deep vein thrombosis in medical patients by low‐dose heparin.Scott Med J.1981;26(2):115–117.
- ,,,,.Lack of effect of a low‐molecular‐weight heparin (nadroparin) on mortality in bedridden medical in‐patients: a prospective randomised double‐blind study.Eur J Clin Pharmacol.2005;61(5‐6):347–351.
- ,,.The venous thrombotic risk in non‐surgical patients: epidemiological data and efficacy/safety profile of a low‐molecular‐weight heparin (enoxaparin). The Prime Study Group.Haemostasis.1996;26(suppl 2):49–56.
- ,,.Subcutaneous low‐molecular‐weight heparin versus standard heparin and the prevention of thromboembolism in medical inpatients. The Heparin Study in Internal Medicine Group.Haemostasis.1996;26(3):127–139.
- ,,, et al.Randomized controlled study of heparin and low molecular weight heparin for prevention of deep‐vein thrombosis in medical patients.Thromb Res.1990;59(3):639–650.
- ,,,.Reduction of mortality in general medical in‐patients by low‐dose heparin prophylaxis.Ann Intern Med.1982;96(5):561–565.
- .Randomised, controlled trial of low‐dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group.Lancet.1996;347(9012):1357–1361.
- ,,, et al.The prophylaxis of medical patients for thromboembolism pilot study.Am J Med.2006;119(1):54–59.
- ,,, et al.Prevention of deep vein thrombosis in elderly medical in‐patients by a low molecular weight heparin: a randomized double‐blind trial.Haemostasis.1986;16(2):159–164.
- ,,, et al.A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group.N Engl J Med.1999;341(11):793–800.
- ,,,,,.Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients.Circulation.2004;110(7):874–879.
- ,,.Prevention of thromboembolic accidents in elderly subjects with Fraxiparine. In: Bounameaux H, Samama MM, Ten Cate JW, eds.Fraxiaparine. 2nd International Symposium. Recent pharmacological and clinical data.New York:Schattauer;1990:51‐54.
- ,.A multicenter randomized double‐blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in‐patients bedridden for an acute medical illness. The Enoxaparin in Medicine Study Group.Thromb Haemost.1996;76(4):529–534.
- ,,, et al.Prevention of venous thromboembolism in internal medicine with unfractionated or low‐molecular‐weight heparins: a meta‐analysis of randomised clinical trials.Thromb Haemost.2000;83(1):14–19.
- ,,,,.Meta‐analysis of venous thromboembolism prophylaxis in medically Ill patients.Clin Ther.2007;29(11):2395–2405.
- ,,,,,.Clinical relevance of distal deep vein thrombosis. Review of literature data.Thromb Haemost.2006;95(1):56–64.
- .Natural history of venous thromboembolism.Circulation.2003;107(suppl 1):I22–I30.
- .Clinical practice. Prophylaxis for thromboembolism in hospitalized medical patients.N Engl J Med.2007;356(14):1438–1444.
- ,,, et al.Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126(suppl):338S–400S.
- ,,,,.Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta‐analysis of randomized controlled trials.Arch Intern Med.2007;167(14):1476–1486.
- ,,,,.Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: a metaanalysis.Chest.2007;131(2):507–516.
- ,,,,.Meta‐analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients.Ann Intern Med.2007;146(4):278–288.
- National Quality Forum. National Consensus Standards for the Prevention and Care of Venous Thromboembolism (including Deep Vein Thrombosis and Pulmonary Embolism). Available at: http://www.qualityforum.org/projects/completed/vte/index.asp. Accessed May2009.
- ,.A prospective registry of 5,451 patients with ultrasound‐confirmed deep vein thrombosis.Am J Cardiol.2004;93(2):259–262.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371(9610):387–394.
- ,,,.Pharmacological thromboembolic prophylaxis in a medical ward: room for improvement.J Gen Intern Med.2002;17(10):788–791.
- ,,,.[Effectiveness of low molecular weight heparin (Fragmin) in the prevention of thromboembolism in internal medicine patients. A randomized double‐blind study].Med Klin (Munich).1988;83(7):241–245, 278.
- ,,, et al.Assessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials.1996;17(1):1–12.
- ,.Quantifying heterogeneity in a meta‐analysis.Stat Med.2002;21(11):1539–1558.
- ,,,.Bias in meta‐analysis detected by a simple, graphical test.BMJ.1997;315(7109):629–634.
- ,.Operating characteristics of a rank correlation test for publication bias.Biometrics.1994;50(4):1088–1101.
- ,,,,,.Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease.Am Heart J.2003;145(4):614–621.
- ,,,,.Prevention of deep vein thrombosis in medical patients by low‐dose heparin.Scott Med J.1981;26(2):115–117.
- ,,,,.Lack of effect of a low‐molecular‐weight heparin (nadroparin) on mortality in bedridden medical in‐patients: a prospective randomised double‐blind study.Eur J Clin Pharmacol.2005;61(5‐6):347–351.
- ,,.The venous thrombotic risk in non‐surgical patients: epidemiological data and efficacy/safety profile of a low‐molecular‐weight heparin (enoxaparin). The Prime Study Group.Haemostasis.1996;26(suppl 2):49–56.
- ,,.Subcutaneous low‐molecular‐weight heparin versus standard heparin and the prevention of thromboembolism in medical inpatients. The Heparin Study in Internal Medicine Group.Haemostasis.1996;26(3):127–139.
- ,,, et al.Randomized controlled study of heparin and low molecular weight heparin for prevention of deep‐vein thrombosis in medical patients.Thromb Res.1990;59(3):639–650.
- ,,,.Reduction of mortality in general medical in‐patients by low‐dose heparin prophylaxis.Ann Intern Med.1982;96(5):561–565.
- .Randomised, controlled trial of low‐dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group.Lancet.1996;347(9012):1357–1361.
- ,,, et al.The prophylaxis of medical patients for thromboembolism pilot study.Am J Med.2006;119(1):54–59.
- ,,, et al.Prevention of deep vein thrombosis in elderly medical in‐patients by a low molecular weight heparin: a randomized double‐blind trial.Haemostasis.1986;16(2):159–164.
- ,,, et al.A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group.N Engl J Med.1999;341(11):793–800.
- ,,,,,.Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients.Circulation.2004;110(7):874–879.
- ,,.Prevention of thromboembolic accidents in elderly subjects with Fraxiparine. In: Bounameaux H, Samama MM, Ten Cate JW, eds.Fraxiaparine. 2nd International Symposium. Recent pharmacological and clinical data.New York:Schattauer;1990:51‐54.
- ,.A multicenter randomized double‐blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in‐patients bedridden for an acute medical illness. The Enoxaparin in Medicine Study Group.Thromb Haemost.1996;76(4):529–534.
- ,,, et al.Prevention of venous thromboembolism in internal medicine with unfractionated or low‐molecular‐weight heparins: a meta‐analysis of randomised clinical trials.Thromb Haemost.2000;83(1):14–19.
- ,,,,.Meta‐analysis of venous thromboembolism prophylaxis in medically Ill patients.Clin Ther.2007;29(11):2395–2405.
- ,,,,,.Clinical relevance of distal deep vein thrombosis. Review of literature data.Thromb Haemost.2006;95(1):56–64.
- .Natural history of venous thromboembolism.Circulation.2003;107(suppl 1):I22–I30.
- .Clinical practice. Prophylaxis for thromboembolism in hospitalized medical patients.N Engl J Med.2007;356(14):1438–1444.
Copyright © 2009 Society of Hospital Medicine
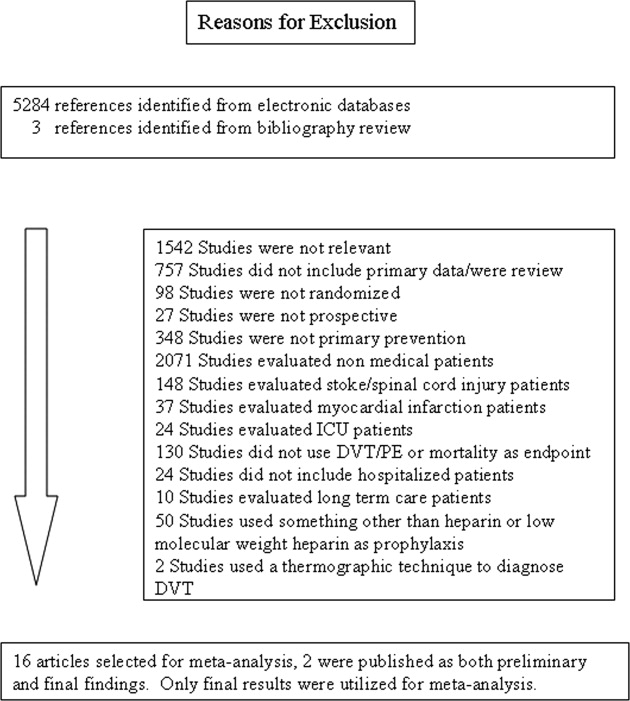
Tension Pneumocephalus as Complication of Hematoma Evacuation
A 78‐year‐old man was transferred from an outside hospital where he presented with declining mental status and a history of falls. A computed tomography (CT) scan of the brain revealed a chronic subdural hematoma with superimposed acute hemorrhage. The subdural hematoma was attributed to a fall at home approximately 5 weeks prior to admission. He was taken to the operating room for urgent craniotomy and hemorrhage evacuation and postoperatively comanaged by neurosurgery, hospitalists, and medicine residents. He tolerated the procedure and was noted to have marked improvement in mental status after the procedure. He was monitored overnight in our intensive care unit without intracranial pressure monitoring.
Early on postoperative day 1, he was awake, alert, following commands, and felt to be stable enough to be transferred to our transitional intensive care unit. However, later in the day he became progressively more confused. A follow‐up CT scan of the brain was ordered (Fig. 1) by the medicine team which revealed a large collection of air (wide arrow) and marked midline shift (thin arrow) consistent with tension pneumocephaly and subfalcine herniation (Fig. 2; arrow). Examination revealed that he was grossly obtunded with marked anisocoria, decerebrate posturing, and rigid tone. Neurosurgery was immediately contacted and recommended accessing 2 indwelling catheters left in the cerebrum as part of the normal postoperative course. Approximately 100 mL of serosanguinous fluid and air was aspirated with immediate improvement in his mental status and exam findings. Over the next few days, he remained clinically stable, and repeat CT scan showed slow resolution of the pneumocephalus and a decrease of his mass effect and midline shift. He was ultimately transferred to our skilled nursing facility for physical therapy and has done relatively well.
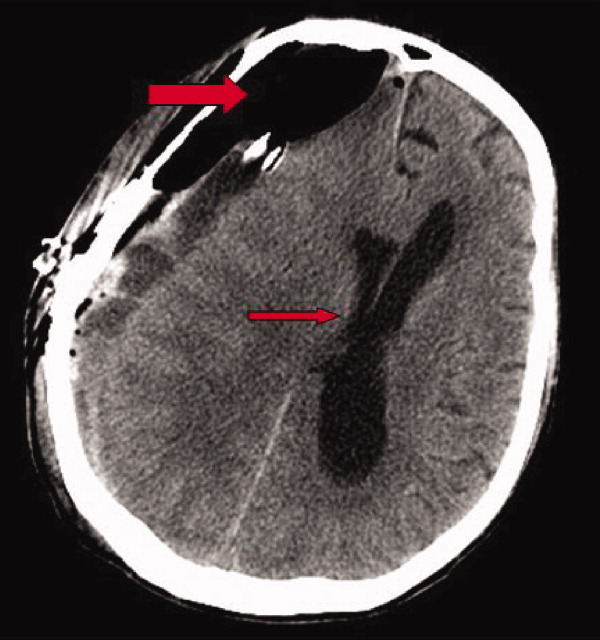
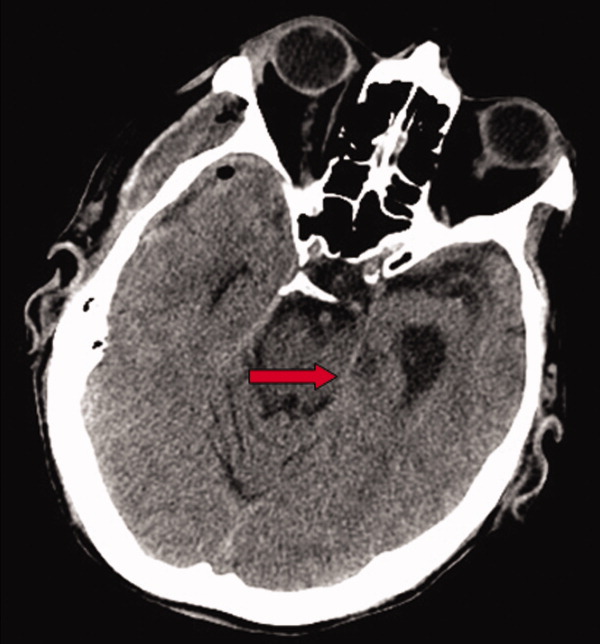
Pneumocephalus is a relatively common finding in many neurosurgical, intracranial procedures. However, tension pneumocephalus is a rare, life‐threatening form of pneumocephalus in which intracranial air causes mass effect and midline shift. In a review of 295 cases of pneumocephalus, 75% were caused by surgery, mostly intracranial and transsphenoidal, and head trauma. About 9% of cases resulted from infection with gas‐forming bacteria and rare causes include invasion of a nasopharyngeal carcinoma, frequent Valsalva maneuver, and air travel.1 Tension pneumocephalus occurs most commonly after the neurosurgical evacuation of a subdural hematoma. The prevalence of tension pneumocephalus following the evacuation of chronic subdural hematomas has been reported from 2.5% to 16%.2
There are 2 proposed mechanisms for the development of pneumocephalus; 1 proposes that air passes through a dural tear by a ball valve effect in which air can be forced into the intracranial cavity by a rapid increase in intrasinus pressure that occurs during sneezing, coughing, or straining. The air is then trapped intracranially. The second theory proposes that cerebrospinal fluid leakage permits air to enter the intracranial cavity because negative pressure is created as cerebrospinal fluid leaves the space.3 The conversion to tension physiology in either of these theories is less well understood.
- ,,,,.Pneumocephalus secondary to septic thrombosis of the superior sagittal sinus: report of a case.J Formos Med Assoc.2001;100(2):142‐144.
- ,,, et al.Subdural tension pneumocephalus following surgery for chronic subdural hematoma.J Neurosurg.1988;68:58‐61.
- ,,,.Nontraumatic tension pneumocephalus—a differential diagnosis of headache in the ED.Am J Emerg Med.2005, Vol.23, pp235‐236.
A 78‐year‐old man was transferred from an outside hospital where he presented with declining mental status and a history of falls. A computed tomography (CT) scan of the brain revealed a chronic subdural hematoma with superimposed acute hemorrhage. The subdural hematoma was attributed to a fall at home approximately 5 weeks prior to admission. He was taken to the operating room for urgent craniotomy and hemorrhage evacuation and postoperatively comanaged by neurosurgery, hospitalists, and medicine residents. He tolerated the procedure and was noted to have marked improvement in mental status after the procedure. He was monitored overnight in our intensive care unit without intracranial pressure monitoring.
Early on postoperative day 1, he was awake, alert, following commands, and felt to be stable enough to be transferred to our transitional intensive care unit. However, later in the day he became progressively more confused. A follow‐up CT scan of the brain was ordered (Fig. 1) by the medicine team which revealed a large collection of air (wide arrow) and marked midline shift (thin arrow) consistent with tension pneumocephaly and subfalcine herniation (Fig. 2; arrow). Examination revealed that he was grossly obtunded with marked anisocoria, decerebrate posturing, and rigid tone. Neurosurgery was immediately contacted and recommended accessing 2 indwelling catheters left in the cerebrum as part of the normal postoperative course. Approximately 100 mL of serosanguinous fluid and air was aspirated with immediate improvement in his mental status and exam findings. Over the next few days, he remained clinically stable, and repeat CT scan showed slow resolution of the pneumocephalus and a decrease of his mass effect and midline shift. He was ultimately transferred to our skilled nursing facility for physical therapy and has done relatively well.
Pneumocephalus is a relatively common finding in many neurosurgical, intracranial procedures. However, tension pneumocephalus is a rare, life‐threatening form of pneumocephalus in which intracranial air causes mass effect and midline shift. In a review of 295 cases of pneumocephalus, 75% were caused by surgery, mostly intracranial and transsphenoidal, and head trauma. About 9% of cases resulted from infection with gas‐forming bacteria and rare causes include invasion of a nasopharyngeal carcinoma, frequent Valsalva maneuver, and air travel.1 Tension pneumocephalus occurs most commonly after the neurosurgical evacuation of a subdural hematoma. The prevalence of tension pneumocephalus following the evacuation of chronic subdural hematomas has been reported from 2.5% to 16%.2
There are 2 proposed mechanisms for the development of pneumocephalus; 1 proposes that air passes through a dural tear by a ball valve effect in which air can be forced into the intracranial cavity by a rapid increase in intrasinus pressure that occurs during sneezing, coughing, or straining. The air is then trapped intracranially. The second theory proposes that cerebrospinal fluid leakage permits air to enter the intracranial cavity because negative pressure is created as cerebrospinal fluid leaves the space.3 The conversion to tension physiology in either of these theories is less well understood.
A 78‐year‐old man was transferred from an outside hospital where he presented with declining mental status and a history of falls. A computed tomography (CT) scan of the brain revealed a chronic subdural hematoma with superimposed acute hemorrhage. The subdural hematoma was attributed to a fall at home approximately 5 weeks prior to admission. He was taken to the operating room for urgent craniotomy and hemorrhage evacuation and postoperatively comanaged by neurosurgery, hospitalists, and medicine residents. He tolerated the procedure and was noted to have marked improvement in mental status after the procedure. He was monitored overnight in our intensive care unit without intracranial pressure monitoring.
Early on postoperative day 1, he was awake, alert, following commands, and felt to be stable enough to be transferred to our transitional intensive care unit. However, later in the day he became progressively more confused. A follow‐up CT scan of the brain was ordered (Fig. 1) by the medicine team which revealed a large collection of air (wide arrow) and marked midline shift (thin arrow) consistent with tension pneumocephaly and subfalcine herniation (Fig. 2; arrow). Examination revealed that he was grossly obtunded with marked anisocoria, decerebrate posturing, and rigid tone. Neurosurgery was immediately contacted and recommended accessing 2 indwelling catheters left in the cerebrum as part of the normal postoperative course. Approximately 100 mL of serosanguinous fluid and air was aspirated with immediate improvement in his mental status and exam findings. Over the next few days, he remained clinically stable, and repeat CT scan showed slow resolution of the pneumocephalus and a decrease of his mass effect and midline shift. He was ultimately transferred to our skilled nursing facility for physical therapy and has done relatively well.
Pneumocephalus is a relatively common finding in many neurosurgical, intracranial procedures. However, tension pneumocephalus is a rare, life‐threatening form of pneumocephalus in which intracranial air causes mass effect and midline shift. In a review of 295 cases of pneumocephalus, 75% were caused by surgery, mostly intracranial and transsphenoidal, and head trauma. About 9% of cases resulted from infection with gas‐forming bacteria and rare causes include invasion of a nasopharyngeal carcinoma, frequent Valsalva maneuver, and air travel.1 Tension pneumocephalus occurs most commonly after the neurosurgical evacuation of a subdural hematoma. The prevalence of tension pneumocephalus following the evacuation of chronic subdural hematomas has been reported from 2.5% to 16%.2
There are 2 proposed mechanisms for the development of pneumocephalus; 1 proposes that air passes through a dural tear by a ball valve effect in which air can be forced into the intracranial cavity by a rapid increase in intrasinus pressure that occurs during sneezing, coughing, or straining. The air is then trapped intracranially. The second theory proposes that cerebrospinal fluid leakage permits air to enter the intracranial cavity because negative pressure is created as cerebrospinal fluid leaves the space.3 The conversion to tension physiology in either of these theories is less well understood.
- ,,,,.Pneumocephalus secondary to septic thrombosis of the superior sagittal sinus: report of a case.J Formos Med Assoc.2001;100(2):142‐144.
- ,,, et al.Subdural tension pneumocephalus following surgery for chronic subdural hematoma.J Neurosurg.1988;68:58‐61.
- ,,,.Nontraumatic tension pneumocephalus—a differential diagnosis of headache in the ED.Am J Emerg Med.2005, Vol.23, pp235‐236.
- ,,,,.Pneumocephalus secondary to septic thrombosis of the superior sagittal sinus: report of a case.J Formos Med Assoc.2001;100(2):142‐144.
- ,,, et al.Subdural tension pneumocephalus following surgery for chronic subdural hematoma.J Neurosurg.1988;68:58‐61.
- ,,,.Nontraumatic tension pneumocephalus—a differential diagnosis of headache in the ED.Am J Emerg Med.2005, Vol.23, pp235‐236.
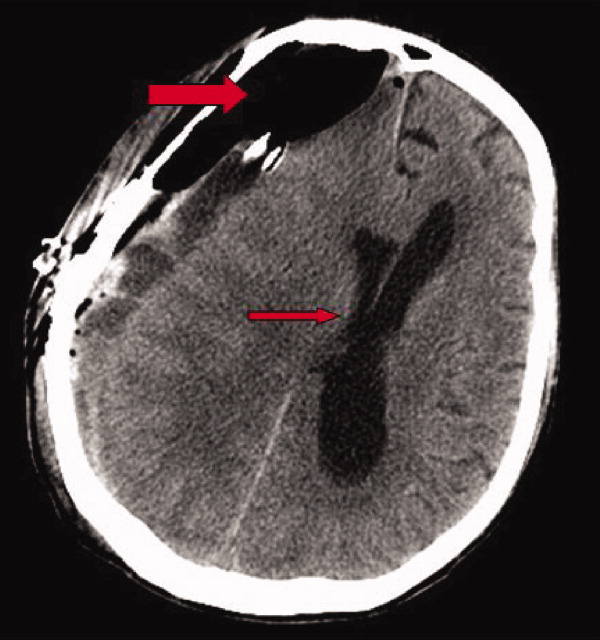
Quantification of Bedside Teaching
Bedside teaching, defined as teaching in the presence of a patient, has been an integral, respected part of medical education throughout the history of modern medicine. There is widespread concern among medical educators that bedside teaching is declining, and in particular, physical examination teaching.1‐5 Learning at the bedside accounted for 75% of clinical teaching in the 1960s and only 16% by 1978.2 Current estimates range from 8% to 19%.1
The bedside is the ideal venue for demonstrating, observing, and evaluating medical interviewing skills, physical examination techniques, and interpersonal and communication skills. Role modeling is the primary method by which clinical teachers demonstrate and teach professionalism and humanistic behavior.6 The bedside is also a place to develop clinical reasoning skills, stimulate problem‐based learning,7 and demonstrate teamwork.4 Thus, the decline in bedside teaching is of major concern for more than just the dying of a time‐honored tradition, but for the threat to the development of skills and attitudes essential for the practice of medicine.
With the rapid growth in the number of hospitalists and their presence at most major U.S. teaching hospitals, internal medicine residents and medical students in their medicine clerkships receive much of their inpatient training from attending physicians who are hospitalists.8 Little is known about the teaching practices of hospitalist attending physicians. We investigated the fraction of time hospitalist attending physicians spend at the bedside during attending teaching rounds and the frequency of the demonstration of physical examination skills at 1 academic teaching hospital.
Patients and Methods
The Brigham & Women's Hospitalist Service, a 28‐member academic hospitalist group who serve as both the teaching attendings and patient care attendings on 4 general medicine teams, was studied in a prospective, observational fashion. Internal medicine residents at Brigham & Women's Hospital rotating on the hospitalist service were identified by examining the schedule of inpatient rotations during the 2007‐2008 academic year and were asked to participate in the study via an e‐mail invitation. The Institutional Review Board of Brigham & Women's Hospital approved the study.
Teams were made up of 1 senior resident and 2 interns. Call frequency was every fourth day. Over a period of 23 sequential weekdays, medical residents and interns from each of the 4 hospitalist teams observed and reported the behavior of their attendings on rounds. Their reports captured the fraction of time spent at the bedside during rounds and the frequency of physical examination teaching. Residents and interns were asked to respond to 3 questions in a daily e‐mail. Respondents reported (1) total time spent with their hospitalist attending during attending rounds, (2) time spent inside patient rooms during attending rounds, and (3) whether or not a physical examination finding or skill was demonstrated by their hospitalist attending. When more than 1 team member responded, time reported among team members was averaged and if there was a discrepancy between whether or not a physical examination finding or skill was demonstrated, it was defaulted to the positive response. Hospitalist attendings remained unaware of the daily observations.
Hospitalist attendings were independently invited to complete a baseline needs assessment survey on bedside teaching. Surveys addressed attitudes toward bedside teaching, confidence in ability to lead bedside teaching rounds and teach the physical examination, and adequacy of their own training in these skills. Respondents were asked to comment on obstacles to bedside teaching. Residents were surveyed at the completion of a rotation with a hospitalist attending regarding the value of the time spent at the bedside and their self‐perceived improvement in physical examination skills and bedside teaching skills. The survey solicited the residents' opinion of the most valuable aspect of bedside teaching. The survey questions used a 4‐point Likert scale with response options ranging from 1 = strongly disagree to 4 = strongly agree.
The fraction of time spent at the bedside during attending hospitalist rounds was calculated from the average time spent in patient rooms and the average time of attending rounds. The frequency of physical examination teaching was expressed as a percent of all teaching encounters. Interrater reliability was calculated using the intraclass correlation coefficient with the Spearman‐Brown adjustment. Differences between groups were calculated using the Fisher's exact test for counts and the Wilcoxon rank‐sum test for continuous data. Significance was accepted for P < 0.05.
Results
Thirty‐five residents provided observations on 61 of 92 potentially observed attending rounds (66% response rate) over 23 weekdays, including observations of the rounding behavior of 12 different hospitalists. The interrater reliability was 0.91. The average patient census on each team during this time period was 12 (range 6‐19).
Residents reported that their attendings went to the bedside at least once during 37 of these 61 rounds (61%), and provided physical examination teaching during 23 of these 61 (38%) encounters. Hospitalists spent an average of 101 minutes on rounds and an average of 17 minutes (17%) of their time inside patient rooms.
Rounds that included time spent at the bedside were significantly longer on average than rounds that did not include time spent at the bedside (122 vs. 69 minutes, P < 0.001). During rounds that included bedside teaching, teams spent an average of 29 minutes (24% of the total time) in patient rooms, and rounds were significantly more likely to include teaching on physical diagnosis (23/37 rounds vs. 0/24 rounds, P < 0.001). Physical examination teaching did not significantly prolong those rounds that included bedside teaching (124 vs. 119 minutes, P = 0.56), but did significantly increase the amount of time spent at the bedside (32 vs. 22 minutes, P = 0.046).
Eighteen hospitalists (64% response) with a mean of 5.9 years of experience as attending physicians completed a needs‐assessment survey (Table 1). Fourteen of the 18 hospitalists (78%) reported that they prioritize bedside teaching and 16 (89%) requested more emphasis on bedside teaching in the residency curriculum. Twelve hospitalists (67%) indicated that they were confident in their ability to lead bedside teaching rounds; 9 (50%) were confident in their ability to teach physical examination. Eleven (61%) of the respondents felt poorly prepared to do bedside teaching after completing their residency, and 12 (67%) felt that they had received inadequate training in how to teach the physical examination. Of the obstacles to bedside teaching, time and inadequate training and skills were the most frequently noted, present in 11 and 6 of the reports, respectively. Lack of confidence and lack of role models were also cited in 4 and 2 of the reports, respectively.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| I make bedside teaching a priority | 0 | 22 | 56 | 22 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 11 | 39 | 50 |
| I feel confident in my ability to lead bedside teaching rounds | 11 | 22 | 50 | 17 |
| I was well‐prepared to do bedside teaching after residency training | 22 | 39 | 28 | 11 |
| I feel confident in my ability to teach the physical exam | 11 | 39 | 33 | 17 |
| I have received adequate training in how to teach the physical exam | 17 | 50 | 22 | 11 |
Seventeen medical residents (49% response) completed a survey regarding their general medical service rotation with a hospitalist upon its completion (Table 2). Sixteen of the respondents (94%) agreed that time spent at the bedside during hospitalist attending teaching rounds that specific rotation was valuable, and 15 (82%) of the residents sought more emphasis on bedside teaching in the residency curriculum. Four of the respondents (24%) reported that their physical examination skills improved over the rotation, 5 (29%) felt better prepared to teach the physical examination, and 9 (53%) felt better prepared to lead bedside teaching rounds. Only 3 (18%) of the respondents reported that they had received helpful feedback on their physical examination skills from their attending. Responding residents noted physical examination teaching, communication and interpersonal skills, focus on patient‐centered care, and integrating the clinical examination with diagnostic and management decisions as the most valuable aspects of bedside teaching.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| Time spent at the bedside during teaching rounds was valuable | 0 | 6 | 65 | 29 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 18 | 53 | 29 |
| I feel better prepared to lead bedside teaching rounds | 6 | 41 | 53 | 0 |
| My physical exam skills improved over the rotation | 6 | 71 | 24 | 0 |
| I feel better prepared to teach the physical exam | 6 | 65 | 29 | 0 |
| I received helpful feedback on my physical exam skills | 18 | 65 | 18 | 0 |
Discussion
Bedside teaching is highly valued by clinicians and trainees, though there is little evidence supporting its efficacy. Patients also enjoy and are accepting of bedside presentations7, 9, 10 if certain rules are adhered to (eg, avoid medical jargon) and benefit by having a better understanding of their illness.9 This study supports previous views of medical residents, students,1, 5, 7 and faculty11 of the value and need for greater emphasis on bedside teaching in medical education.
This study of rounding behavior found that hospitalists in this academic center go to the bedside most days, but 39% of attending teaching rounds did not include a bedside encounter. Physical examination teaching is infrequent. Though time spent at the bedside was only a small fraction of total teaching time (17%) in this practice, this fraction is at the high end of previous reports. Teaching rounds that did not include bedside teaching most likely occurred in the confines of a conference room.
Many factors appear to contribute to the paucity of time spent at the bedside: time constraints, shorter hospital stays, greater work demands,11 residency duty‐hour regulations,12 declining bedside teaching skills, unrealistic expectations of the encounter, and erosion of the teaching ethic.3 A decline in clinical examination skills among trainees and attending physicians leads to a growing reliance on data and technology, thereby perpetuating the cycle of declining bedside skills.4
The hospitalists in this study identify time as the most dominant obstacle to bedside teaching. On days when hospitalist attending physicians went to the bedside, rounds were on average 53 minutes longer than on those days when they did not go to the bedside. This time increase varied little whether or not physical examination teaching occurred. The difference in rounding time may be partially explained by the admitting cycle and patient census. Teaching attendings are likely to go to the bedside to see new patients on postcall days when the patient census is also the highest.
Many members of this hospitalist group indicated that they felt inadequately prepared to lead bedside teaching rounds. Of those who responded to the survey, 67% did not feel that they received adequate training in how to teach the physical examination. Consequently, only one‐half of responding hospitalists expressed confidence in their ability to teach the physical examination. Not surprisingly, physical examination skills were a component of a minority of teaching sessions and only one‐quarter of the medical residents perceived that their physical examination skills improved during the rotation with a hospitalist attending. The paucity of feedback to the house‐staff likely contributed to this stagnancy. Residents who become hospitalists ill‐prepared to lead bedside teaching and teach the physical examination will perpetuate the decline in bedside teaching.
Though a substantial portion of the hospitalists in this study lacked confidence, an overwhelming majority of medical residents found their time spent at the bedside with a hospitalist to be valuable. More than one‐half of residents reported that they were better prepared to lead bedside teaching after the rotation. Residents recognize that bedside teaching can include communication and clinical reasoning skills. Hospitalists should be made aware that a broad range of skills and content can be taught at the bedside.
Hospitalists have an increasing influence on the education of medical residents and students and are appropriate targets for faculty development programs aimed at improving bedside teaching. As a newer, growing specialty, hospitalists tend to be younger physicians, and are therefore more reliant on the education attained during residency to support their bedside activities. Many residencies have developed resident as educator programs in an attempt to create a future generation of attendings better able to teach.13
Several limitations should be acknowledged when interpreting the results of this study. The study was limited to a hospitalist group at a single academic medical center and relied on resident recall. Though the response rate to the daily e‐mails was relatively low, the interrater reliability was high, and a broad range of residents and attendings were represented. Residents with greater patient censuses may have been too busy to respond, but it is unclear in which direction this would bias the results.
Conclusions
This study provides additional evidence that bedside and physical examination teaching are in decline. Time is an increasingly precious commodity for hospitalists; though many commentators echo the sentiments of the respondents in this study that more time at the bedside is needed, the amount of time that should be optimally spent at the bedside remains unclear. Research to improve the quality of bedside learning and its influence on patient care outcomes is needed.
- ,,,.Improving bedside teaching: findings from a focus group study of learners.Acad Med.2008;83(3):257–264.
- .On bedside teaching.Ann Intern Med.1997;126(3):217–220.
- ,,,.Whither bedside teaching? A focus‐group study of clinical teachers.Acad Med.2003;78(4):384–390.
- .Bedside rounds revisited.N Engl J Med.1997;336(16):1174–1175.
- ,,,.Effect of a physical examination teaching program on the behavior of medical residents.J Gen Intern Med.2005;20(8):710–714.
- ,,,,.Role modeling humanistic behavior: learning bedside manner from the experts.Acad Med.2006;81(7):661–667.
- ,,.Student and patient perspectives on bedside teaching.Med Educ.1997;31(5):341–346.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350(19):1935–1936.
- ,,,,.The effect of bedside case presentations on patients' perceptions of their medical care.N Engl J Med.1997;336(16):1150–1155.
- ,,,.A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit.Pediatrics.2007;120(2):275–280.
- ,,.Impediments to bed‐side teaching.Med Educ.1998;32(2):159–162.
- ,,, et al.Internal medicine and general surgery residents' attitudes about the ACGME duty hours regulations: a multicenter study.Acad Med.2006;81(12):1052–1058.
- ,,.Resident as teacher: educating the educators.Mt Sinai J Med.2006;73(8):1165–1169.
Bedside teaching, defined as teaching in the presence of a patient, has been an integral, respected part of medical education throughout the history of modern medicine. There is widespread concern among medical educators that bedside teaching is declining, and in particular, physical examination teaching.1‐5 Learning at the bedside accounted for 75% of clinical teaching in the 1960s and only 16% by 1978.2 Current estimates range from 8% to 19%.1
The bedside is the ideal venue for demonstrating, observing, and evaluating medical interviewing skills, physical examination techniques, and interpersonal and communication skills. Role modeling is the primary method by which clinical teachers demonstrate and teach professionalism and humanistic behavior.6 The bedside is also a place to develop clinical reasoning skills, stimulate problem‐based learning,7 and demonstrate teamwork.4 Thus, the decline in bedside teaching is of major concern for more than just the dying of a time‐honored tradition, but for the threat to the development of skills and attitudes essential for the practice of medicine.
With the rapid growth in the number of hospitalists and their presence at most major U.S. teaching hospitals, internal medicine residents and medical students in their medicine clerkships receive much of their inpatient training from attending physicians who are hospitalists.8 Little is known about the teaching practices of hospitalist attending physicians. We investigated the fraction of time hospitalist attending physicians spend at the bedside during attending teaching rounds and the frequency of the demonstration of physical examination skills at 1 academic teaching hospital.
Patients and Methods
The Brigham & Women's Hospitalist Service, a 28‐member academic hospitalist group who serve as both the teaching attendings and patient care attendings on 4 general medicine teams, was studied in a prospective, observational fashion. Internal medicine residents at Brigham & Women's Hospital rotating on the hospitalist service were identified by examining the schedule of inpatient rotations during the 2007‐2008 academic year and were asked to participate in the study via an e‐mail invitation. The Institutional Review Board of Brigham & Women's Hospital approved the study.
Teams were made up of 1 senior resident and 2 interns. Call frequency was every fourth day. Over a period of 23 sequential weekdays, medical residents and interns from each of the 4 hospitalist teams observed and reported the behavior of their attendings on rounds. Their reports captured the fraction of time spent at the bedside during rounds and the frequency of physical examination teaching. Residents and interns were asked to respond to 3 questions in a daily e‐mail. Respondents reported (1) total time spent with their hospitalist attending during attending rounds, (2) time spent inside patient rooms during attending rounds, and (3) whether or not a physical examination finding or skill was demonstrated by their hospitalist attending. When more than 1 team member responded, time reported among team members was averaged and if there was a discrepancy between whether or not a physical examination finding or skill was demonstrated, it was defaulted to the positive response. Hospitalist attendings remained unaware of the daily observations.
Hospitalist attendings were independently invited to complete a baseline needs assessment survey on bedside teaching. Surveys addressed attitudes toward bedside teaching, confidence in ability to lead bedside teaching rounds and teach the physical examination, and adequacy of their own training in these skills. Respondents were asked to comment on obstacles to bedside teaching. Residents were surveyed at the completion of a rotation with a hospitalist attending regarding the value of the time spent at the bedside and their self‐perceived improvement in physical examination skills and bedside teaching skills. The survey solicited the residents' opinion of the most valuable aspect of bedside teaching. The survey questions used a 4‐point Likert scale with response options ranging from 1 = strongly disagree to 4 = strongly agree.
The fraction of time spent at the bedside during attending hospitalist rounds was calculated from the average time spent in patient rooms and the average time of attending rounds. The frequency of physical examination teaching was expressed as a percent of all teaching encounters. Interrater reliability was calculated using the intraclass correlation coefficient with the Spearman‐Brown adjustment. Differences between groups were calculated using the Fisher's exact test for counts and the Wilcoxon rank‐sum test for continuous data. Significance was accepted for P < 0.05.
Results
Thirty‐five residents provided observations on 61 of 92 potentially observed attending rounds (66% response rate) over 23 weekdays, including observations of the rounding behavior of 12 different hospitalists. The interrater reliability was 0.91. The average patient census on each team during this time period was 12 (range 6‐19).
Residents reported that their attendings went to the bedside at least once during 37 of these 61 rounds (61%), and provided physical examination teaching during 23 of these 61 (38%) encounters. Hospitalists spent an average of 101 minutes on rounds and an average of 17 minutes (17%) of their time inside patient rooms.
Rounds that included time spent at the bedside were significantly longer on average than rounds that did not include time spent at the bedside (122 vs. 69 minutes, P < 0.001). During rounds that included bedside teaching, teams spent an average of 29 minutes (24% of the total time) in patient rooms, and rounds were significantly more likely to include teaching on physical diagnosis (23/37 rounds vs. 0/24 rounds, P < 0.001). Physical examination teaching did not significantly prolong those rounds that included bedside teaching (124 vs. 119 minutes, P = 0.56), but did significantly increase the amount of time spent at the bedside (32 vs. 22 minutes, P = 0.046).
Eighteen hospitalists (64% response) with a mean of 5.9 years of experience as attending physicians completed a needs‐assessment survey (Table 1). Fourteen of the 18 hospitalists (78%) reported that they prioritize bedside teaching and 16 (89%) requested more emphasis on bedside teaching in the residency curriculum. Twelve hospitalists (67%) indicated that they were confident in their ability to lead bedside teaching rounds; 9 (50%) were confident in their ability to teach physical examination. Eleven (61%) of the respondents felt poorly prepared to do bedside teaching after completing their residency, and 12 (67%) felt that they had received inadequate training in how to teach the physical examination. Of the obstacles to bedside teaching, time and inadequate training and skills were the most frequently noted, present in 11 and 6 of the reports, respectively. Lack of confidence and lack of role models were also cited in 4 and 2 of the reports, respectively.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| I make bedside teaching a priority | 0 | 22 | 56 | 22 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 11 | 39 | 50 |
| I feel confident in my ability to lead bedside teaching rounds | 11 | 22 | 50 | 17 |
| I was well‐prepared to do bedside teaching after residency training | 22 | 39 | 28 | 11 |
| I feel confident in my ability to teach the physical exam | 11 | 39 | 33 | 17 |
| I have received adequate training in how to teach the physical exam | 17 | 50 | 22 | 11 |
Seventeen medical residents (49% response) completed a survey regarding their general medical service rotation with a hospitalist upon its completion (Table 2). Sixteen of the respondents (94%) agreed that time spent at the bedside during hospitalist attending teaching rounds that specific rotation was valuable, and 15 (82%) of the residents sought more emphasis on bedside teaching in the residency curriculum. Four of the respondents (24%) reported that their physical examination skills improved over the rotation, 5 (29%) felt better prepared to teach the physical examination, and 9 (53%) felt better prepared to lead bedside teaching rounds. Only 3 (18%) of the respondents reported that they had received helpful feedback on their physical examination skills from their attending. Responding residents noted physical examination teaching, communication and interpersonal skills, focus on patient‐centered care, and integrating the clinical examination with diagnostic and management decisions as the most valuable aspects of bedside teaching.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| Time spent at the bedside during teaching rounds was valuable | 0 | 6 | 65 | 29 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 18 | 53 | 29 |
| I feel better prepared to lead bedside teaching rounds | 6 | 41 | 53 | 0 |
| My physical exam skills improved over the rotation | 6 | 71 | 24 | 0 |
| I feel better prepared to teach the physical exam | 6 | 65 | 29 | 0 |
| I received helpful feedback on my physical exam skills | 18 | 65 | 18 | 0 |
Discussion
Bedside teaching is highly valued by clinicians and trainees, though there is little evidence supporting its efficacy. Patients also enjoy and are accepting of bedside presentations7, 9, 10 if certain rules are adhered to (eg, avoid medical jargon) and benefit by having a better understanding of their illness.9 This study supports previous views of medical residents, students,1, 5, 7 and faculty11 of the value and need for greater emphasis on bedside teaching in medical education.
This study of rounding behavior found that hospitalists in this academic center go to the bedside most days, but 39% of attending teaching rounds did not include a bedside encounter. Physical examination teaching is infrequent. Though time spent at the bedside was only a small fraction of total teaching time (17%) in this practice, this fraction is at the high end of previous reports. Teaching rounds that did not include bedside teaching most likely occurred in the confines of a conference room.
Many factors appear to contribute to the paucity of time spent at the bedside: time constraints, shorter hospital stays, greater work demands,11 residency duty‐hour regulations,12 declining bedside teaching skills, unrealistic expectations of the encounter, and erosion of the teaching ethic.3 A decline in clinical examination skills among trainees and attending physicians leads to a growing reliance on data and technology, thereby perpetuating the cycle of declining bedside skills.4
The hospitalists in this study identify time as the most dominant obstacle to bedside teaching. On days when hospitalist attending physicians went to the bedside, rounds were on average 53 minutes longer than on those days when they did not go to the bedside. This time increase varied little whether or not physical examination teaching occurred. The difference in rounding time may be partially explained by the admitting cycle and patient census. Teaching attendings are likely to go to the bedside to see new patients on postcall days when the patient census is also the highest.
Many members of this hospitalist group indicated that they felt inadequately prepared to lead bedside teaching rounds. Of those who responded to the survey, 67% did not feel that they received adequate training in how to teach the physical examination. Consequently, only one‐half of responding hospitalists expressed confidence in their ability to teach the physical examination. Not surprisingly, physical examination skills were a component of a minority of teaching sessions and only one‐quarter of the medical residents perceived that their physical examination skills improved during the rotation with a hospitalist attending. The paucity of feedback to the house‐staff likely contributed to this stagnancy. Residents who become hospitalists ill‐prepared to lead bedside teaching and teach the physical examination will perpetuate the decline in bedside teaching.
Though a substantial portion of the hospitalists in this study lacked confidence, an overwhelming majority of medical residents found their time spent at the bedside with a hospitalist to be valuable. More than one‐half of residents reported that they were better prepared to lead bedside teaching after the rotation. Residents recognize that bedside teaching can include communication and clinical reasoning skills. Hospitalists should be made aware that a broad range of skills and content can be taught at the bedside.
Hospitalists have an increasing influence on the education of medical residents and students and are appropriate targets for faculty development programs aimed at improving bedside teaching. As a newer, growing specialty, hospitalists tend to be younger physicians, and are therefore more reliant on the education attained during residency to support their bedside activities. Many residencies have developed resident as educator programs in an attempt to create a future generation of attendings better able to teach.13
Several limitations should be acknowledged when interpreting the results of this study. The study was limited to a hospitalist group at a single academic medical center and relied on resident recall. Though the response rate to the daily e‐mails was relatively low, the interrater reliability was high, and a broad range of residents and attendings were represented. Residents with greater patient censuses may have been too busy to respond, but it is unclear in which direction this would bias the results.
Conclusions
This study provides additional evidence that bedside and physical examination teaching are in decline. Time is an increasingly precious commodity for hospitalists; though many commentators echo the sentiments of the respondents in this study that more time at the bedside is needed, the amount of time that should be optimally spent at the bedside remains unclear. Research to improve the quality of bedside learning and its influence on patient care outcomes is needed.
Bedside teaching, defined as teaching in the presence of a patient, has been an integral, respected part of medical education throughout the history of modern medicine. There is widespread concern among medical educators that bedside teaching is declining, and in particular, physical examination teaching.1‐5 Learning at the bedside accounted for 75% of clinical teaching in the 1960s and only 16% by 1978.2 Current estimates range from 8% to 19%.1
The bedside is the ideal venue for demonstrating, observing, and evaluating medical interviewing skills, physical examination techniques, and interpersonal and communication skills. Role modeling is the primary method by which clinical teachers demonstrate and teach professionalism and humanistic behavior.6 The bedside is also a place to develop clinical reasoning skills, stimulate problem‐based learning,7 and demonstrate teamwork.4 Thus, the decline in bedside teaching is of major concern for more than just the dying of a time‐honored tradition, but for the threat to the development of skills and attitudes essential for the practice of medicine.
With the rapid growth in the number of hospitalists and their presence at most major U.S. teaching hospitals, internal medicine residents and medical students in their medicine clerkships receive much of their inpatient training from attending physicians who are hospitalists.8 Little is known about the teaching practices of hospitalist attending physicians. We investigated the fraction of time hospitalist attending physicians spend at the bedside during attending teaching rounds and the frequency of the demonstration of physical examination skills at 1 academic teaching hospital.
Patients and Methods
The Brigham & Women's Hospitalist Service, a 28‐member academic hospitalist group who serve as both the teaching attendings and patient care attendings on 4 general medicine teams, was studied in a prospective, observational fashion. Internal medicine residents at Brigham & Women's Hospital rotating on the hospitalist service were identified by examining the schedule of inpatient rotations during the 2007‐2008 academic year and were asked to participate in the study via an e‐mail invitation. The Institutional Review Board of Brigham & Women's Hospital approved the study.
Teams were made up of 1 senior resident and 2 interns. Call frequency was every fourth day. Over a period of 23 sequential weekdays, medical residents and interns from each of the 4 hospitalist teams observed and reported the behavior of their attendings on rounds. Their reports captured the fraction of time spent at the bedside during rounds and the frequency of physical examination teaching. Residents and interns were asked to respond to 3 questions in a daily e‐mail. Respondents reported (1) total time spent with their hospitalist attending during attending rounds, (2) time spent inside patient rooms during attending rounds, and (3) whether or not a physical examination finding or skill was demonstrated by their hospitalist attending. When more than 1 team member responded, time reported among team members was averaged and if there was a discrepancy between whether or not a physical examination finding or skill was demonstrated, it was defaulted to the positive response. Hospitalist attendings remained unaware of the daily observations.
Hospitalist attendings were independently invited to complete a baseline needs assessment survey on bedside teaching. Surveys addressed attitudes toward bedside teaching, confidence in ability to lead bedside teaching rounds and teach the physical examination, and adequacy of their own training in these skills. Respondents were asked to comment on obstacles to bedside teaching. Residents were surveyed at the completion of a rotation with a hospitalist attending regarding the value of the time spent at the bedside and their self‐perceived improvement in physical examination skills and bedside teaching skills. The survey solicited the residents' opinion of the most valuable aspect of bedside teaching. The survey questions used a 4‐point Likert scale with response options ranging from 1 = strongly disagree to 4 = strongly agree.
The fraction of time spent at the bedside during attending hospitalist rounds was calculated from the average time spent in patient rooms and the average time of attending rounds. The frequency of physical examination teaching was expressed as a percent of all teaching encounters. Interrater reliability was calculated using the intraclass correlation coefficient with the Spearman‐Brown adjustment. Differences between groups were calculated using the Fisher's exact test for counts and the Wilcoxon rank‐sum test for continuous data. Significance was accepted for P < 0.05.
Results
Thirty‐five residents provided observations on 61 of 92 potentially observed attending rounds (66% response rate) over 23 weekdays, including observations of the rounding behavior of 12 different hospitalists. The interrater reliability was 0.91. The average patient census on each team during this time period was 12 (range 6‐19).
Residents reported that their attendings went to the bedside at least once during 37 of these 61 rounds (61%), and provided physical examination teaching during 23 of these 61 (38%) encounters. Hospitalists spent an average of 101 minutes on rounds and an average of 17 minutes (17%) of their time inside patient rooms.
Rounds that included time spent at the bedside were significantly longer on average than rounds that did not include time spent at the bedside (122 vs. 69 minutes, P < 0.001). During rounds that included bedside teaching, teams spent an average of 29 minutes (24% of the total time) in patient rooms, and rounds were significantly more likely to include teaching on physical diagnosis (23/37 rounds vs. 0/24 rounds, P < 0.001). Physical examination teaching did not significantly prolong those rounds that included bedside teaching (124 vs. 119 minutes, P = 0.56), but did significantly increase the amount of time spent at the bedside (32 vs. 22 minutes, P = 0.046).
Eighteen hospitalists (64% response) with a mean of 5.9 years of experience as attending physicians completed a needs‐assessment survey (Table 1). Fourteen of the 18 hospitalists (78%) reported that they prioritize bedside teaching and 16 (89%) requested more emphasis on bedside teaching in the residency curriculum. Twelve hospitalists (67%) indicated that they were confident in their ability to lead bedside teaching rounds; 9 (50%) were confident in their ability to teach physical examination. Eleven (61%) of the respondents felt poorly prepared to do bedside teaching after completing their residency, and 12 (67%) felt that they had received inadequate training in how to teach the physical examination. Of the obstacles to bedside teaching, time and inadequate training and skills were the most frequently noted, present in 11 and 6 of the reports, respectively. Lack of confidence and lack of role models were also cited in 4 and 2 of the reports, respectively.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| I make bedside teaching a priority | 0 | 22 | 56 | 22 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 11 | 39 | 50 |
| I feel confident in my ability to lead bedside teaching rounds | 11 | 22 | 50 | 17 |
| I was well‐prepared to do bedside teaching after residency training | 22 | 39 | 28 | 11 |
| I feel confident in my ability to teach the physical exam | 11 | 39 | 33 | 17 |
| I have received adequate training in how to teach the physical exam | 17 | 50 | 22 | 11 |
Seventeen medical residents (49% response) completed a survey regarding their general medical service rotation with a hospitalist upon its completion (Table 2). Sixteen of the respondents (94%) agreed that time spent at the bedside during hospitalist attending teaching rounds that specific rotation was valuable, and 15 (82%) of the residents sought more emphasis on bedside teaching in the residency curriculum. Four of the respondents (24%) reported that their physical examination skills improved over the rotation, 5 (29%) felt better prepared to teach the physical examination, and 9 (53%) felt better prepared to lead bedside teaching rounds. Only 3 (18%) of the respondents reported that they had received helpful feedback on their physical examination skills from their attending. Responding residents noted physical examination teaching, communication and interpersonal skills, focus on patient‐centered care, and integrating the clinical examination with diagnostic and management decisions as the most valuable aspects of bedside teaching.
| Strongly Disagree (%) | Disagree (%) | Agree (%) | Strongly Agree (%) | |
|---|---|---|---|---|
| ||||
| Time spent at the bedside during teaching rounds was valuable | 0 | 6 | 65 | 29 |
| More emphasis on bedside teaching in the residency curriculum is needed | 0 | 18 | 53 | 29 |
| I feel better prepared to lead bedside teaching rounds | 6 | 41 | 53 | 0 |
| My physical exam skills improved over the rotation | 6 | 71 | 24 | 0 |
| I feel better prepared to teach the physical exam | 6 | 65 | 29 | 0 |
| I received helpful feedback on my physical exam skills | 18 | 65 | 18 | 0 |
Discussion
Bedside teaching is highly valued by clinicians and trainees, though there is little evidence supporting its efficacy. Patients also enjoy and are accepting of bedside presentations7, 9, 10 if certain rules are adhered to (eg, avoid medical jargon) and benefit by having a better understanding of their illness.9 This study supports previous views of medical residents, students,1, 5, 7 and faculty11 of the value and need for greater emphasis on bedside teaching in medical education.
This study of rounding behavior found that hospitalists in this academic center go to the bedside most days, but 39% of attending teaching rounds did not include a bedside encounter. Physical examination teaching is infrequent. Though time spent at the bedside was only a small fraction of total teaching time (17%) in this practice, this fraction is at the high end of previous reports. Teaching rounds that did not include bedside teaching most likely occurred in the confines of a conference room.
Many factors appear to contribute to the paucity of time spent at the bedside: time constraints, shorter hospital stays, greater work demands,11 residency duty‐hour regulations,12 declining bedside teaching skills, unrealistic expectations of the encounter, and erosion of the teaching ethic.3 A decline in clinical examination skills among trainees and attending physicians leads to a growing reliance on data and technology, thereby perpetuating the cycle of declining bedside skills.4
The hospitalists in this study identify time as the most dominant obstacle to bedside teaching. On days when hospitalist attending physicians went to the bedside, rounds were on average 53 minutes longer than on those days when they did not go to the bedside. This time increase varied little whether or not physical examination teaching occurred. The difference in rounding time may be partially explained by the admitting cycle and patient census. Teaching attendings are likely to go to the bedside to see new patients on postcall days when the patient census is also the highest.
Many members of this hospitalist group indicated that they felt inadequately prepared to lead bedside teaching rounds. Of those who responded to the survey, 67% did not feel that they received adequate training in how to teach the physical examination. Consequently, only one‐half of responding hospitalists expressed confidence in their ability to teach the physical examination. Not surprisingly, physical examination skills were a component of a minority of teaching sessions and only one‐quarter of the medical residents perceived that their physical examination skills improved during the rotation with a hospitalist attending. The paucity of feedback to the house‐staff likely contributed to this stagnancy. Residents who become hospitalists ill‐prepared to lead bedside teaching and teach the physical examination will perpetuate the decline in bedside teaching.
Though a substantial portion of the hospitalists in this study lacked confidence, an overwhelming majority of medical residents found their time spent at the bedside with a hospitalist to be valuable. More than one‐half of residents reported that they were better prepared to lead bedside teaching after the rotation. Residents recognize that bedside teaching can include communication and clinical reasoning skills. Hospitalists should be made aware that a broad range of skills and content can be taught at the bedside.
Hospitalists have an increasing influence on the education of medical residents and students and are appropriate targets for faculty development programs aimed at improving bedside teaching. As a newer, growing specialty, hospitalists tend to be younger physicians, and are therefore more reliant on the education attained during residency to support their bedside activities. Many residencies have developed resident as educator programs in an attempt to create a future generation of attendings better able to teach.13
Several limitations should be acknowledged when interpreting the results of this study. The study was limited to a hospitalist group at a single academic medical center and relied on resident recall. Though the response rate to the daily e‐mails was relatively low, the interrater reliability was high, and a broad range of residents and attendings were represented. Residents with greater patient censuses may have been too busy to respond, but it is unclear in which direction this would bias the results.
Conclusions
This study provides additional evidence that bedside and physical examination teaching are in decline. Time is an increasingly precious commodity for hospitalists; though many commentators echo the sentiments of the respondents in this study that more time at the bedside is needed, the amount of time that should be optimally spent at the bedside remains unclear. Research to improve the quality of bedside learning and its influence on patient care outcomes is needed.
- ,,,.Improving bedside teaching: findings from a focus group study of learners.Acad Med.2008;83(3):257–264.
- .On bedside teaching.Ann Intern Med.1997;126(3):217–220.
- ,,,.Whither bedside teaching? A focus‐group study of clinical teachers.Acad Med.2003;78(4):384–390.
- .Bedside rounds revisited.N Engl J Med.1997;336(16):1174–1175.
- ,,,.Effect of a physical examination teaching program on the behavior of medical residents.J Gen Intern Med.2005;20(8):710–714.
- ,,,,.Role modeling humanistic behavior: learning bedside manner from the experts.Acad Med.2006;81(7):661–667.
- ,,.Student and patient perspectives on bedside teaching.Med Educ.1997;31(5):341–346.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350(19):1935–1936.
- ,,,,.The effect of bedside case presentations on patients' perceptions of their medical care.N Engl J Med.1997;336(16):1150–1155.
- ,,,.A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit.Pediatrics.2007;120(2):275–280.
- ,,.Impediments to bed‐side teaching.Med Educ.1998;32(2):159–162.
- ,,, et al.Internal medicine and general surgery residents' attitudes about the ACGME duty hours regulations: a multicenter study.Acad Med.2006;81(12):1052–1058.
- ,,.Resident as teacher: educating the educators.Mt Sinai J Med.2006;73(8):1165–1169.
- ,,,.Improving bedside teaching: findings from a focus group study of learners.Acad Med.2008;83(3):257–264.
- .On bedside teaching.Ann Intern Med.1997;126(3):217–220.
- ,,,.Whither bedside teaching? A focus‐group study of clinical teachers.Acad Med.2003;78(4):384–390.
- .Bedside rounds revisited.N Engl J Med.1997;336(16):1174–1175.
- ,,,.Effect of a physical examination teaching program on the behavior of medical residents.J Gen Intern Med.2005;20(8):710–714.
- ,,,,.Role modeling humanistic behavior: learning bedside manner from the experts.Acad Med.2006;81(7):661–667.
- ,,.Student and patient perspectives on bedside teaching.Med Educ.1997;31(5):341–346.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350(19):1935–1936.
- ,,,,.The effect of bedside case presentations on patients' perceptions of their medical care.N Engl J Med.1997;336(16):1150–1155.
- ,,,.A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit.Pediatrics.2007;120(2):275–280.
- ,,.Impediments to bed‐side teaching.Med Educ.1998;32(2):159–162.
- ,,, et al.Internal medicine and general surgery residents' attitudes about the ACGME duty hours regulations: a multicenter study.Acad Med.2006;81(12):1052–1058.
- ,,.Resident as teacher: educating the educators.Mt Sinai J Med.2006;73(8):1165–1169.
Copyright © 2009 Society of Hospital Medicine
A numbered day in the life
It seemed like years had passed since he was told he had cancer. While he basked in the cool white ambiance of the examination room, Jim mentally traced his many steps up and down the nearby hospital hallways. From this room to that, he had shuffled through most of the rooms on this hospital ward. Jim had read every outdated Time and National Geographic magazine, and all of the kids' books. From sitting in waiting rooms, he had even developed a deep appreciation for Thomas the Tank Engine. As he sat there, he realized that he had only spent 8 days in this hospital ward. But in here, 8 days might as well be 11 years. Time doesn't so much pass in hospital wards as it stands perfectly still on your chest. The total isolation for those who must stay is startling. Jim had begun judging time by the movements of those lucky enough to go home. Instead of Mondays, Tuesdays, and Wednesdays, he was also measuring time by food. Days of the week had become known as Styrofoam meatloaf, highly suspect lasagna, and inedible beef Wellington; all had become units of time measurement.
When he was told about his cancerthe doctor told him it was a type of hematological neo‐something‐or‐otherJim felt strangely aroused by the news. He felt energy racing through his body as he geared for battle. His immediate response was to think about how he would volunteer for the harshest, meanest, nastiest treatment he could get the doctor to agree with. Poke him full of holes, pour poison straight in his veins, run him on treadmills while doing all of thatit didn't matter. There was nothing he would not do to beat this thing. The doctor had finished telling Jim about all those options at the very minute Jim was ready to hear them. Whatever, whatever, Doc, let's get going with this, was his response.
Then, he had gradually noticed that the pace of medicine was something a little less urgent than he had thought. On TV the doctors run everywhere, but here they walked with a brisk but awkward gait, as if afraid of falling on the floor by going too fast. While waiting for his appointments, Jim noticed that everything was about waitingwaiting for everything. Nothing happens in the hospital. There are people walking everywhere with some projected sense of purpose but it all seems so meaningless when there's a hundred people in hospital uniforms walking past a whole room of patients.
Finally, the door to the examination room burst open and in walked Dr. Day. Standing slightly less than 6 feet tall, Docas Jim called himwas one of those well‐preserved 50‐year‐olds who could be found wind‐surfing his way back to his convertible sports car during his off‐hours. Jim imagined that Doc had been the star student, the handsome rover, the jock. Age had started to claw at his youthful looks, but vanity had led the charge against age for Doc. His behavior and choices worked against his clock, and he was not going quietly into that dark night. Doc's athletic stride made it seem like his feet never touched the floor, and he wafted deep into the room before the doors had even fully opened. Doc never looked forward, but always studied the charts in front of him. He was intense; it was as if he had to truly concentrate sometimes to keep pace with his own mind. Doc was talking, but it was unclear to whom. Finally, he looked up with an expectant pause, and Jim, battered with indifference, nodded in affirmationto what, he didn't care. Doc then gave Jim the thumbs‐up, turned on his heel and headed toward the door; he spun around on the spot and looked back, Yeah, you'll need to change into a robe with nothing on underneath it. He gestured to the one wall where a shelf held neatly folded paper‐thin gowns. Jim put one on and could barely believe how sheer it was. It had the density of a paper napkin, he thought. Then again, this was hardly a cause for modesty. The cancer, he had learned, was actually lymphoma, and it had settled in his groin. At first, Jim was ashamed to have doctors and nurses poke and prod his nether regions, but after a while he became quite causal about it with the usual array of doctors and nurses who populated his monotonous life in this shiny new white palace. After the requisite 15 minutes of unexplained absence, Dr. Day returned through the doors. There was something different about him now, and in a world so dominated by sameness, predictability, and routine, change was a dark storm cloud and sudden wind in Jim's mind.
Lie down on that table please, Doc said in his usual my hand may be making a tactile map of your groin, but my mind is in Bermuda manner. As Jim hopped up on the table and shifted his diseased area closer to the end, the Doc seemed to brighten up, Stay right there, he said as he moved quickly from the room once again. Jim pondered the instruction. As opposed to going where? Jim groaned. He would go somewhere, but his treatment, eventually, would happen here. If he left, he didn't know if would ever come back.
In through the door, one more time, came Dr. Day, but this time he seemed to be leading some kind of tour. Trailing behind him in different states of interest and alertness was a team of young people, all in the little training smocks they give them that look just like the big‐boy coat that Dr. Day wore. Their smocks were more wrinkled and more ivory colored, but they still looked official. Dr. Day hardly looked toward the patient as he smoothly rolled into the side of the table nearest Jim's now‐exposed groin.
Jim looked up between his upstretched knees to see them, all of them, standing around trying to decide if they should be looking at the Doc or looking at the affected area. Jim was embarrassed. Jim was mad. Jim was embarrassed again. He tried to make eye contact with every single visitor in the room, and all he could see were eyes looking straight down under the flap of his hospital gown. Doc had broken into his whole song and dance when he stopped short and looked to Jim, almost apologetically, You're alright with this, right? These are first‐year residents and I wanted them to see this kind of tumor up close. Doc hardly took a full breath and he had turned and was back into his blather about mito, crypto, this, that, and some other bullshit. Jim felt like if he rested his head back maybe no one would ever know that he was the real fleshy cadaver that they stared at that day. He might never see any of these students again, and even if he did, none of them could bring themselves to look him anywhere near the eye anyway. Not much danger that any of them could pick him out of a police lineup, even if he did it without any pants on.
It's important to palpate the region, each of you need to feel what this is like, starting with you. Jim heard this particular instruction and snapped his head up to see exactly where the students were now headed to see and feel the thing they just had to touch. Imagine his dismay when he saw that all of them were still there, still transfixed on whatever they had found to look at studiously during this whole period of time. Doc had motioned to the smallest, frailest, most out‐of‐her‐element young woman he had ever seen. She visibly swallowed hard at the news that she would be first. Her eyes, previously fixed without distraction on some point on Jim's leg, now began to frantically search the eyes of others, possibly looking for some permission to run away. Her eyes met Jim's quite by accident, and she shared with him a look of total and complete shame. He took out his annoyance on her by fixing her with a murderous stare, while he watched as her hand inched ever closer to his leg. In a continuous, but painfully slow motion, she reached under the robe and Jim felt the slightest touch of what he assumed was her finger come to rest on the lowest part of his abdomen. She held her finger there, motionless, and then drew it away quickly while nodding to the Doc. No, no, no, you have to really feel it! Doc chided. He reached down and poked the area firmly, but with a certainty and comfort that comes only from unspoken familiarity. Doc then grabbed the poor girl's hand and guided it and proceeded, with his hand holding her wrist, to make the poking motion with her hand. She was clearly horrified and would have rather been poking through the exposed abdomen of a cadaver at that point. Jim's mood became even more annoyed at her response. It was okay to be embarrassed, but she was now acting like his groin was Elephant‐Man‐esque in its hideousness. He wondered if Doc would set up a barker stand and call to the passers‐by to see the bulbous freak, 50 cents for a viewing! Don't forget about our snack tents! Nobody should go home without candy, everybody loves candy!
After the young resident had endured all that the Doc thought she should, he motioned to the next one and repeated the same process; one after another, after another. The students instinctively formed a line that snaked around the table and spilled out through the room. Jim became callous at this point and began chatting up the students while they stood, quietly waiting their turn for the guided poking, to make them feel even more uncomfortable and intimidated. Jim spied one extremely uncomfortable‐looking male student. You know, if you like this, it doesn't make you gay, Jim shared in an almost caring tone. As the target of his comments shuffled forward, eyes never leaving the floor, Jim targeted another victim with his comments, and then another, and then another. Jim became a sniper of sarcasm, picking off helpless young residents as they stood helplessly in his aim. Doc finally reacted to Jim and shot him a scolding look. Doc leaned into Jim's ear, Fun is fun, but let's just take it easy now, ok? Jim grunted in disagreement, but complied. There was no anger left to vent, and really no need to vent it. Residents weren't the problem, but it was easy to treat them that way. Besides, Jim figured there was many more days for him to make it up to them by being a nicer patient. Today was today, but there were probably 20 more tomorrows for him here.
Finally, the last student had his moment. Jim noticed that the region was now sore from the guiding probing, and Doc had his back to him while addressing the students about what they had seen there today. Jim hopped off the table and proceeded to change back into his clothes while Doc carried on talking. Then, Doc was gone; he sped from the room with his entourage in close pursuit. Jim finished dressing and shuffled down the hallway to his room. Jim sighed under the weight of monotony. Every day was the same, and only the torturous delight he enjoyed at the expense of those residents made the day unique. It was, for the most part, emotion that broke the routine. Emotion was the only thing that Jim controlled at this point, and occasionally, selfishly, he would let it loose on the unsuspecting, simply to bookmark his day. Cancer was not killing Jim, but boredom quite possibly could. As Jim passed the drink machine around the corner from his ward, he saw nurse Janet coming in to work with her neon pink lunch kit slung over her shoulder. She smiled at Jim and asked him how he was feeling. Jim smiled, told her all was getting better, and then made his way back to his room. Janet's arrival meant it was almost supper time, and today was lasagna.
It seemed like years had passed since he was told he had cancer. While he basked in the cool white ambiance of the examination room, Jim mentally traced his many steps up and down the nearby hospital hallways. From this room to that, he had shuffled through most of the rooms on this hospital ward. Jim had read every outdated Time and National Geographic magazine, and all of the kids' books. From sitting in waiting rooms, he had even developed a deep appreciation for Thomas the Tank Engine. As he sat there, he realized that he had only spent 8 days in this hospital ward. But in here, 8 days might as well be 11 years. Time doesn't so much pass in hospital wards as it stands perfectly still on your chest. The total isolation for those who must stay is startling. Jim had begun judging time by the movements of those lucky enough to go home. Instead of Mondays, Tuesdays, and Wednesdays, he was also measuring time by food. Days of the week had become known as Styrofoam meatloaf, highly suspect lasagna, and inedible beef Wellington; all had become units of time measurement.
When he was told about his cancerthe doctor told him it was a type of hematological neo‐something‐or‐otherJim felt strangely aroused by the news. He felt energy racing through his body as he geared for battle. His immediate response was to think about how he would volunteer for the harshest, meanest, nastiest treatment he could get the doctor to agree with. Poke him full of holes, pour poison straight in his veins, run him on treadmills while doing all of thatit didn't matter. There was nothing he would not do to beat this thing. The doctor had finished telling Jim about all those options at the very minute Jim was ready to hear them. Whatever, whatever, Doc, let's get going with this, was his response.
Then, he had gradually noticed that the pace of medicine was something a little less urgent than he had thought. On TV the doctors run everywhere, but here they walked with a brisk but awkward gait, as if afraid of falling on the floor by going too fast. While waiting for his appointments, Jim noticed that everything was about waitingwaiting for everything. Nothing happens in the hospital. There are people walking everywhere with some projected sense of purpose but it all seems so meaningless when there's a hundred people in hospital uniforms walking past a whole room of patients.
Finally, the door to the examination room burst open and in walked Dr. Day. Standing slightly less than 6 feet tall, Docas Jim called himwas one of those well‐preserved 50‐year‐olds who could be found wind‐surfing his way back to his convertible sports car during his off‐hours. Jim imagined that Doc had been the star student, the handsome rover, the jock. Age had started to claw at his youthful looks, but vanity had led the charge against age for Doc. His behavior and choices worked against his clock, and he was not going quietly into that dark night. Doc's athletic stride made it seem like his feet never touched the floor, and he wafted deep into the room before the doors had even fully opened. Doc never looked forward, but always studied the charts in front of him. He was intense; it was as if he had to truly concentrate sometimes to keep pace with his own mind. Doc was talking, but it was unclear to whom. Finally, he looked up with an expectant pause, and Jim, battered with indifference, nodded in affirmationto what, he didn't care. Doc then gave Jim the thumbs‐up, turned on his heel and headed toward the door; he spun around on the spot and looked back, Yeah, you'll need to change into a robe with nothing on underneath it. He gestured to the one wall where a shelf held neatly folded paper‐thin gowns. Jim put one on and could barely believe how sheer it was. It had the density of a paper napkin, he thought. Then again, this was hardly a cause for modesty. The cancer, he had learned, was actually lymphoma, and it had settled in his groin. At first, Jim was ashamed to have doctors and nurses poke and prod his nether regions, but after a while he became quite causal about it with the usual array of doctors and nurses who populated his monotonous life in this shiny new white palace. After the requisite 15 minutes of unexplained absence, Dr. Day returned through the doors. There was something different about him now, and in a world so dominated by sameness, predictability, and routine, change was a dark storm cloud and sudden wind in Jim's mind.
Lie down on that table please, Doc said in his usual my hand may be making a tactile map of your groin, but my mind is in Bermuda manner. As Jim hopped up on the table and shifted his diseased area closer to the end, the Doc seemed to brighten up, Stay right there, he said as he moved quickly from the room once again. Jim pondered the instruction. As opposed to going where? Jim groaned. He would go somewhere, but his treatment, eventually, would happen here. If he left, he didn't know if would ever come back.
In through the door, one more time, came Dr. Day, but this time he seemed to be leading some kind of tour. Trailing behind him in different states of interest and alertness was a team of young people, all in the little training smocks they give them that look just like the big‐boy coat that Dr. Day wore. Their smocks were more wrinkled and more ivory colored, but they still looked official. Dr. Day hardly looked toward the patient as he smoothly rolled into the side of the table nearest Jim's now‐exposed groin.
Jim looked up between his upstretched knees to see them, all of them, standing around trying to decide if they should be looking at the Doc or looking at the affected area. Jim was embarrassed. Jim was mad. Jim was embarrassed again. He tried to make eye contact with every single visitor in the room, and all he could see were eyes looking straight down under the flap of his hospital gown. Doc had broken into his whole song and dance when he stopped short and looked to Jim, almost apologetically, You're alright with this, right? These are first‐year residents and I wanted them to see this kind of tumor up close. Doc hardly took a full breath and he had turned and was back into his blather about mito, crypto, this, that, and some other bullshit. Jim felt like if he rested his head back maybe no one would ever know that he was the real fleshy cadaver that they stared at that day. He might never see any of these students again, and even if he did, none of them could bring themselves to look him anywhere near the eye anyway. Not much danger that any of them could pick him out of a police lineup, even if he did it without any pants on.
It's important to palpate the region, each of you need to feel what this is like, starting with you. Jim heard this particular instruction and snapped his head up to see exactly where the students were now headed to see and feel the thing they just had to touch. Imagine his dismay when he saw that all of them were still there, still transfixed on whatever they had found to look at studiously during this whole period of time. Doc had motioned to the smallest, frailest, most out‐of‐her‐element young woman he had ever seen. She visibly swallowed hard at the news that she would be first. Her eyes, previously fixed without distraction on some point on Jim's leg, now began to frantically search the eyes of others, possibly looking for some permission to run away. Her eyes met Jim's quite by accident, and she shared with him a look of total and complete shame. He took out his annoyance on her by fixing her with a murderous stare, while he watched as her hand inched ever closer to his leg. In a continuous, but painfully slow motion, she reached under the robe and Jim felt the slightest touch of what he assumed was her finger come to rest on the lowest part of his abdomen. She held her finger there, motionless, and then drew it away quickly while nodding to the Doc. No, no, no, you have to really feel it! Doc chided. He reached down and poked the area firmly, but with a certainty and comfort that comes only from unspoken familiarity. Doc then grabbed the poor girl's hand and guided it and proceeded, with his hand holding her wrist, to make the poking motion with her hand. She was clearly horrified and would have rather been poking through the exposed abdomen of a cadaver at that point. Jim's mood became even more annoyed at her response. It was okay to be embarrassed, but she was now acting like his groin was Elephant‐Man‐esque in its hideousness. He wondered if Doc would set up a barker stand and call to the passers‐by to see the bulbous freak, 50 cents for a viewing! Don't forget about our snack tents! Nobody should go home without candy, everybody loves candy!
After the young resident had endured all that the Doc thought she should, he motioned to the next one and repeated the same process; one after another, after another. The students instinctively formed a line that snaked around the table and spilled out through the room. Jim became callous at this point and began chatting up the students while they stood, quietly waiting their turn for the guided poking, to make them feel even more uncomfortable and intimidated. Jim spied one extremely uncomfortable‐looking male student. You know, if you like this, it doesn't make you gay, Jim shared in an almost caring tone. As the target of his comments shuffled forward, eyes never leaving the floor, Jim targeted another victim with his comments, and then another, and then another. Jim became a sniper of sarcasm, picking off helpless young residents as they stood helplessly in his aim. Doc finally reacted to Jim and shot him a scolding look. Doc leaned into Jim's ear, Fun is fun, but let's just take it easy now, ok? Jim grunted in disagreement, but complied. There was no anger left to vent, and really no need to vent it. Residents weren't the problem, but it was easy to treat them that way. Besides, Jim figured there was many more days for him to make it up to them by being a nicer patient. Today was today, but there were probably 20 more tomorrows for him here.
Finally, the last student had his moment. Jim noticed that the region was now sore from the guiding probing, and Doc had his back to him while addressing the students about what they had seen there today. Jim hopped off the table and proceeded to change back into his clothes while Doc carried on talking. Then, Doc was gone; he sped from the room with his entourage in close pursuit. Jim finished dressing and shuffled down the hallway to his room. Jim sighed under the weight of monotony. Every day was the same, and only the torturous delight he enjoyed at the expense of those residents made the day unique. It was, for the most part, emotion that broke the routine. Emotion was the only thing that Jim controlled at this point, and occasionally, selfishly, he would let it loose on the unsuspecting, simply to bookmark his day. Cancer was not killing Jim, but boredom quite possibly could. As Jim passed the drink machine around the corner from his ward, he saw nurse Janet coming in to work with her neon pink lunch kit slung over her shoulder. She smiled at Jim and asked him how he was feeling. Jim smiled, told her all was getting better, and then made his way back to his room. Janet's arrival meant it was almost supper time, and today was lasagna.
It seemed like years had passed since he was told he had cancer. While he basked in the cool white ambiance of the examination room, Jim mentally traced his many steps up and down the nearby hospital hallways. From this room to that, he had shuffled through most of the rooms on this hospital ward. Jim had read every outdated Time and National Geographic magazine, and all of the kids' books. From sitting in waiting rooms, he had even developed a deep appreciation for Thomas the Tank Engine. As he sat there, he realized that he had only spent 8 days in this hospital ward. But in here, 8 days might as well be 11 years. Time doesn't so much pass in hospital wards as it stands perfectly still on your chest. The total isolation for those who must stay is startling. Jim had begun judging time by the movements of those lucky enough to go home. Instead of Mondays, Tuesdays, and Wednesdays, he was also measuring time by food. Days of the week had become known as Styrofoam meatloaf, highly suspect lasagna, and inedible beef Wellington; all had become units of time measurement.
When he was told about his cancerthe doctor told him it was a type of hematological neo‐something‐or‐otherJim felt strangely aroused by the news. He felt energy racing through his body as he geared for battle. His immediate response was to think about how he would volunteer for the harshest, meanest, nastiest treatment he could get the doctor to agree with. Poke him full of holes, pour poison straight in his veins, run him on treadmills while doing all of thatit didn't matter. There was nothing he would not do to beat this thing. The doctor had finished telling Jim about all those options at the very minute Jim was ready to hear them. Whatever, whatever, Doc, let's get going with this, was his response.
Then, he had gradually noticed that the pace of medicine was something a little less urgent than he had thought. On TV the doctors run everywhere, but here they walked with a brisk but awkward gait, as if afraid of falling on the floor by going too fast. While waiting for his appointments, Jim noticed that everything was about waitingwaiting for everything. Nothing happens in the hospital. There are people walking everywhere with some projected sense of purpose but it all seems so meaningless when there's a hundred people in hospital uniforms walking past a whole room of patients.
Finally, the door to the examination room burst open and in walked Dr. Day. Standing slightly less than 6 feet tall, Docas Jim called himwas one of those well‐preserved 50‐year‐olds who could be found wind‐surfing his way back to his convertible sports car during his off‐hours. Jim imagined that Doc had been the star student, the handsome rover, the jock. Age had started to claw at his youthful looks, but vanity had led the charge against age for Doc. His behavior and choices worked against his clock, and he was not going quietly into that dark night. Doc's athletic stride made it seem like his feet never touched the floor, and he wafted deep into the room before the doors had even fully opened. Doc never looked forward, but always studied the charts in front of him. He was intense; it was as if he had to truly concentrate sometimes to keep pace with his own mind. Doc was talking, but it was unclear to whom. Finally, he looked up with an expectant pause, and Jim, battered with indifference, nodded in affirmationto what, he didn't care. Doc then gave Jim the thumbs‐up, turned on his heel and headed toward the door; he spun around on the spot and looked back, Yeah, you'll need to change into a robe with nothing on underneath it. He gestured to the one wall where a shelf held neatly folded paper‐thin gowns. Jim put one on and could barely believe how sheer it was. It had the density of a paper napkin, he thought. Then again, this was hardly a cause for modesty. The cancer, he had learned, was actually lymphoma, and it had settled in his groin. At first, Jim was ashamed to have doctors and nurses poke and prod his nether regions, but after a while he became quite causal about it with the usual array of doctors and nurses who populated his monotonous life in this shiny new white palace. After the requisite 15 minutes of unexplained absence, Dr. Day returned through the doors. There was something different about him now, and in a world so dominated by sameness, predictability, and routine, change was a dark storm cloud and sudden wind in Jim's mind.
Lie down on that table please, Doc said in his usual my hand may be making a tactile map of your groin, but my mind is in Bermuda manner. As Jim hopped up on the table and shifted his diseased area closer to the end, the Doc seemed to brighten up, Stay right there, he said as he moved quickly from the room once again. Jim pondered the instruction. As opposed to going where? Jim groaned. He would go somewhere, but his treatment, eventually, would happen here. If he left, he didn't know if would ever come back.
In through the door, one more time, came Dr. Day, but this time he seemed to be leading some kind of tour. Trailing behind him in different states of interest and alertness was a team of young people, all in the little training smocks they give them that look just like the big‐boy coat that Dr. Day wore. Their smocks were more wrinkled and more ivory colored, but they still looked official. Dr. Day hardly looked toward the patient as he smoothly rolled into the side of the table nearest Jim's now‐exposed groin.
Jim looked up between his upstretched knees to see them, all of them, standing around trying to decide if they should be looking at the Doc or looking at the affected area. Jim was embarrassed. Jim was mad. Jim was embarrassed again. He tried to make eye contact with every single visitor in the room, and all he could see were eyes looking straight down under the flap of his hospital gown. Doc had broken into his whole song and dance when he stopped short and looked to Jim, almost apologetically, You're alright with this, right? These are first‐year residents and I wanted them to see this kind of tumor up close. Doc hardly took a full breath and he had turned and was back into his blather about mito, crypto, this, that, and some other bullshit. Jim felt like if he rested his head back maybe no one would ever know that he was the real fleshy cadaver that they stared at that day. He might never see any of these students again, and even if he did, none of them could bring themselves to look him anywhere near the eye anyway. Not much danger that any of them could pick him out of a police lineup, even if he did it without any pants on.
It's important to palpate the region, each of you need to feel what this is like, starting with you. Jim heard this particular instruction and snapped his head up to see exactly where the students were now headed to see and feel the thing they just had to touch. Imagine his dismay when he saw that all of them were still there, still transfixed on whatever they had found to look at studiously during this whole period of time. Doc had motioned to the smallest, frailest, most out‐of‐her‐element young woman he had ever seen. She visibly swallowed hard at the news that she would be first. Her eyes, previously fixed without distraction on some point on Jim's leg, now began to frantically search the eyes of others, possibly looking for some permission to run away. Her eyes met Jim's quite by accident, and she shared with him a look of total and complete shame. He took out his annoyance on her by fixing her with a murderous stare, while he watched as her hand inched ever closer to his leg. In a continuous, but painfully slow motion, she reached under the robe and Jim felt the slightest touch of what he assumed was her finger come to rest on the lowest part of his abdomen. She held her finger there, motionless, and then drew it away quickly while nodding to the Doc. No, no, no, you have to really feel it! Doc chided. He reached down and poked the area firmly, but with a certainty and comfort that comes only from unspoken familiarity. Doc then grabbed the poor girl's hand and guided it and proceeded, with his hand holding her wrist, to make the poking motion with her hand. She was clearly horrified and would have rather been poking through the exposed abdomen of a cadaver at that point. Jim's mood became even more annoyed at her response. It was okay to be embarrassed, but she was now acting like his groin was Elephant‐Man‐esque in its hideousness. He wondered if Doc would set up a barker stand and call to the passers‐by to see the bulbous freak, 50 cents for a viewing! Don't forget about our snack tents! Nobody should go home without candy, everybody loves candy!
After the young resident had endured all that the Doc thought she should, he motioned to the next one and repeated the same process; one after another, after another. The students instinctively formed a line that snaked around the table and spilled out through the room. Jim became callous at this point and began chatting up the students while they stood, quietly waiting their turn for the guided poking, to make them feel even more uncomfortable and intimidated. Jim spied one extremely uncomfortable‐looking male student. You know, if you like this, it doesn't make you gay, Jim shared in an almost caring tone. As the target of his comments shuffled forward, eyes never leaving the floor, Jim targeted another victim with his comments, and then another, and then another. Jim became a sniper of sarcasm, picking off helpless young residents as they stood helplessly in his aim. Doc finally reacted to Jim and shot him a scolding look. Doc leaned into Jim's ear, Fun is fun, but let's just take it easy now, ok? Jim grunted in disagreement, but complied. There was no anger left to vent, and really no need to vent it. Residents weren't the problem, but it was easy to treat them that way. Besides, Jim figured there was many more days for him to make it up to them by being a nicer patient. Today was today, but there were probably 20 more tomorrows for him here.
Finally, the last student had his moment. Jim noticed that the region was now sore from the guiding probing, and Doc had his back to him while addressing the students about what they had seen there today. Jim hopped off the table and proceeded to change back into his clothes while Doc carried on talking. Then, Doc was gone; he sped from the room with his entourage in close pursuit. Jim finished dressing and shuffled down the hallway to his room. Jim sighed under the weight of monotony. Every day was the same, and only the torturous delight he enjoyed at the expense of those residents made the day unique. It was, for the most part, emotion that broke the routine. Emotion was the only thing that Jim controlled at this point, and occasionally, selfishly, he would let it loose on the unsuspecting, simply to bookmark his day. Cancer was not killing Jim, but boredom quite possibly could. As Jim passed the drink machine around the corner from his ward, he saw nurse Janet coming in to work with her neon pink lunch kit slung over her shoulder. She smiled at Jim and asked him how he was feeling. Jim smiled, told her all was getting better, and then made his way back to his room. Janet's arrival meant it was almost supper time, and today was lasagna.
PRESsed for time
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).

Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).
Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).
Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
Pemetrexed
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.