User login
Women in Hospital Medicine Have to be Ready, Willing, Proactive
Several years into her hospitalist career, committee work had satisfied Sarita Satpathy, MD’s desire to positively impact patient care. Then she attended SHM’s Leadership Academy and was inspired to do more.
“I thought, ‘I want to do something and actually have a title where I can effect change,’” says Dr. Satpathy, now the hospitalist program medical director for Cogent HMG at Seton Medical Center in Daly City, Calif.
A year and a half after starting from scratch, Dr. Satpathy’s program has improved patient-care continuity, implemented 24/7 coverage, and earned buy-in from specialists, surgeons, and hospital leaders—most of whom are men.
“There aren’t as many female physician leaders, period,” says Dr. Satpathy, speaking of Seton Medical Center.
She could be talking about medicine in general.
Despite the fact that women have made up nearly half of all medical school graduates since 2005-2006 and make up 30% of the total physician population, only 16% of MD faculty at the full professor rank are female.1,2,3 Just 11% and 13% of medical school permanent deans and department chairs are women, respectively.4
Beyond academia, results from surveys conducted by the American College of Healthcare Executives show that female healthcare executives are less likely to be CEOs and chief operating officers than their male counterparts. The results also indicate that the proportion of female CEOs remained fairly stable between surveys in 1990, 1995, 2000, and 2006; the proportion of female vice presidents actually decreased.5
This reality, experts say, undercuts America’s ability to remain at the leading edge of medical research, impedes women’s health improvements, and leaves fewer role models for future generations of physicians. In looking at why female physicians are underrepresented in leadership, key issues emerge, including unconscious bias, outdated work structures, lack of sponsorship, and conflict between the biological and professional time clocks. Although not all female doctors have faced these obstacles, many of them have and still do.
But opportunities are there—especially in HM—for female doctors to step into leadership roles. The onus is on women to seize them and on institutions to create a fertile environment for diverse leadership, physician leaders say.
Leadership Obstacles
Men often are associated with leadership by virtue of a phenomenon called unconscious bias, which posits that people identify certain genders with certain roles due to subconscious cues accumulated over time, says Hannah Valantine, MD, professor of medicine and senior associate dean for diversity and leadership at the Stanford
University School of Medicine in Palo Alto, Calif.
“These biases exist in all of us in the way we evaluate women and their work, in the way we evaluate them for leadership positions and when they’re in leadership positions, and in the thought processes that they have of their own qualifications and actions,” says Molly Carnes, MD, MS, a professor of medicine and industrial and systems engineering and co-director of the Women in Science and Engineering Leadership Institute at the University of Wisconsin at Madison.

Bias also exists in how institutions write their job announcements, performance evaluations, and grant and award applications, Dr. Carnes explains. When such terms as “aggressive” and “risk-taking” are used, women are less likely to be seen as viable candidates, she says.
What often impedes female physicians from taking leadership roles are a lack of sponsorship and obsolete work structures that don’t reflect life in the 21st century.
“There is some thought out there that women nowadays are overmentored and undersponsored,” says Dr. Valantine, a cardiologist. “By ‘sponsored,’ we mean going that extra mile to make sure a woman is promoted into the next level of leadership and into the next level of opportunities. It’s the ‘old boys’ network,’ and, unfortunately for women, there isn’t an old girls’ network that’s as well-oiled.”
Work environments are largely designed for the single breadwinner, even though most households, including physicians, have two earners. As a result, women who seek work flexibility or work part time often are labeled as “not serious about their careers,” Dr. Valantine says. This label affects women, who begin to think they can’t pursue leadership roles because they’re working less than full time, says Rachel George, MD, MBA, CPE, FHM, chief operating officer of the West and North-Central regions and chief medical officer of the West region for Nashville, Tenn.-based Cogent HMG, the largest privately held HM and critical-care company in the nation with partnerships in more than 100 hospitals.
There’s an inherent conflict between the professional and biological time clocks in that when female hospitalists are trained, working for a few years, and ready to accept new challenges, they’re also starting families, says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West region for Dallas-based EmCare, a company that provides outsourced physician services, including hospitalist care, in more than 500 hospitals in 40 states.
“Part of the problem is that we look at this as an all or none, that you have to be fully immersed in whatever leadership role it is, and be willing to give a tremendous amount of hours, but that’s really not true,” Dr. George says. “There are different levels of leadership. It’s OK to take it slow and do a little bit, whatever the reasoning may be.”
Dr. Carnes says many women who achieve leadership positions find themselves outside the behavioral norms assigned to women and, therefore, often confront negative reactions and perceptions that they’re disagreeable, arrogant, and superior-minded. Women sometimes get pushback from other women, too.
“When you talk to stay-at-home moms and part-time moms, I think they try and put the guilt trip on you all the time,” says Theresa Rohr-Kirchgraber, MD, board member of the American Women’s Medical Association and executive director of the National Center of Excellence in Women’s Health at Indiana University in Indianapolis.
That, in turn, often compounds the internal guilt many women feel, pitting their work and leadership goals against their responsibilities at home, she says. “There is still a big pull for women to be at home, and when you’re not, you feel guilty about it,” Dr. Rohr-Kirchgraber explains.
Good Things Don’t Come to Those Who Wait

—Kay Cannon, MBA, MCC
Female hospitalists who aspire to lead must take the initiative, experts say.
“Regardless of gender, those individuals who are known to get results, be proactive, and be part of a solution are the ones who gain the attention and, many times, have opportunities open up for advancement,” says Kay Cannon, MBA, MCC, an executive leadership consultant and coach who teaches advanced courses at SHM’s Leadership Academy.
Cathleen Ammann, MD, can attest to that. A year after joining the then-fledgling hospitalist program at Wentworth-Douglass Hospital in Dover, N.H., Dr. Ammann thought she could lead it in a positive direction.
“With zero leadership experience, I went to our CMO, who was basically the administrator for our group, and said, ‘I think I could do a good job with this,’” she says. The CMO concurred, and in October 2006, Dr. Ammann took over the hospitalist program, which she continues to lead today. “They really took a chance with me, and I’m glad they did.”
Dr. Bell says HM, as a whole, has more leadership opportunities than there are trained, capable physicians to do the job—something female hospitalists can take advantage of. But it’s up to women to seize the opportunity, says Mary Jo Gorman, MD, MBA, MHM, who started her career as a hospitalist and is now CEO of Advanced ICU Care, a St. Louis-based firm that connects intensivists to hospital ICU patients via telemedicine.
“Every leadership position that I’ve been in, I got there because I was trying to solve a problem,” says Dr. Gorman, a past president of SHM. “The No. 1 mistake that women make is they don’t step up to volunteer to take responsibility for things; they expect somebody to notice their good work and ask them to lead. Culturally, that’s been shown not to be what happens and not very successful.”

—Mary Jo Gorman, MD, MBA, MHM, CEO, Advanced ICU Care, St. Louis
Where There’s a Will, There’s a Way
Female hospitalists who are interested in leadership need to find an organization that values and encourages their employees to make meaningful contributions, Cannon says. Then they need to join projects and committees in order to develop some leadership qualities, Dr. Ammann says.
“Being involved in one or two committees initially that you strongly believe in, being active, voicing your opinion, and finding ways to find solutions─that’s where you get seen and known,” Dr. Satpathy says. “You actually gain credibility because it’s authentic.”

The old adage “from small beginnings come great things” applies to leadership, Dr. Gorman says.
“If you can complete things regularly and successfully, if you can do that, then the next time you go to a slightly bigger project and then a bigger project and a bigger project, until you’re directing a couple hundred people,” she says.
It’s also important for female physicians to find multiple mentors, Dr. Valantine notes. “You may need a mentor that is within your own discipline who can help guide you about planning your career, writing a grant, doing a project. You might need someone else entirely different who will help you think about when is the right time for you to consider having a family, taking sabbatical, and just integrating your work with life,” she says.
Additionally, female hospitalists pursuing leadership roles must remember that every time they say “yes” to something, they’re saying “no” to something else, Cannon says.
“Too often what I see is women are so eager to please and they’re so driven to be their best, they end up saying ‘yes’ in their career. Then, all of a sudden, they arrive at a point and they say, ‘Something is really missing,’” she says. “If you can get ahead of that and think through things, it’s really going to help your planning.”
Dr. Valantine says female physicians should “take the long view” of leadership and pace themselves.
“Look at this along the entire career path and say, ‘I may not be able to do everything right now, but there might be periods of flexing up and flexing down in my career, and that’s fine,’” she says. “The important thing is to stay in it.”
Dr. Bell and others urge hospitalists who are motivated to lead to tell people in positions of authority that they’re interested; otherwise, they’re not going to be thought of when a position opens.

Dr. Rohr-Kirchgarber has made appointments with deans, associate deans, and faculty affairs staff to introduce herself, explain her expertise, and find ways to use her skill sets in initiatives and committees that are important to the institution.
“Rather than waiting for three or four years for them to find out who I am and think about me for a committee, I need to get out there from Day One,” she says. “It’s proven to be successful.”
Drs. Ammann and Bell encourage hospitalists in community settings to approach their CMOs or other hospital administrators about their leadership aspirations. “And, of course, networking in a professional organization helps,” Dr. Satpathy says.
Meet Halfway
Female physicians can take the initiative and position themselves for leadership roles. They can acquire necessary skills by attending SHM’s Leadership Academy, management classes offered by the American College of Physicians and the American College of Physician Executives, and even adult education courses taught at business schools. But in order for them to be successful leaders, institutions must be invested in the effort.
Organizations can start by defining what they mean by “leadership.”
“‘Leader’ is actually a very abstract concept,” Dr. Carnes says. “But if you break it down into very specific activities, then I think you will get more women saying ‘yes.’ The first thing is getting women to see what leadership can allow them to do.”

—Rachel George, MBA, MCC
Men—and women—also have to acknowledge they have unconscious biases, then work to change the cultural norms, she says.
“Smoking is a really good example,” Dr. Carnes explains. “It took multilevel intervention at the individual and institutional level to change the cultural norms for smoking. You have to have a clear statement by the institution endorsed by all the institutional leaders that this is an institutional priority.” Examples of priorities include eliminating male-gendered words from job announcements and performance evaluations, and ensuring a fair and open application process for leadership positions that allow female physicians to make a case for themselves, she says.
Institutions can implement structural elements to help women—and men—better manage their careers and assume leadership roles, Dr. Valantine says. These include tenure clock extension, extended maternity and family leave, short- and long-term sabbaticals, onsite childcare, and emergency backup childcare.(Read about how Stanford University’s School of Medicine encourages women to seek leadership positions at the-hospitalist.org.)
“When I give talks to women about leadership, I tell them about all the programs we’re doing. I say to them, ‘I hope that you will go out and ask for these programs to be set up in your institutions,” she says. “But, more importantly, I tell women, ‘You have a responsibility to remain standing. It’s going to be tough sometimes, but if you don’t remain standing, we won’t have the role models that we need. It’s going to be a vicious cycle. We just won’t advance and increase the numbers of women leaders.”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 1. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170248/data/2010_table1.pdf. Accessed March 2, 2012.
- American Medical Association. Physician Characteristics and Distribution in the US. American Medical Association, 2012. 2012 ed. Chicago: American Medical Association Press; 2011.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 4A. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170254/data/2009_table04a.pdf. Accessed March 2, 2012.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Figure 5. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/179458/data/2009_figure05.pdf. Accessed March 2, 2012.
- American College of Healthcare Executives. A Comparison of the Career Attainments of Men and Women Healthcare Executives: 2006, Table 2. American College of Healthcare Executives website. Available at: http://www.ache.org/pubs/research/gender_study_full_report.pdf. Accessed March 2, 2012.
Several years into her hospitalist career, committee work had satisfied Sarita Satpathy, MD’s desire to positively impact patient care. Then she attended SHM’s Leadership Academy and was inspired to do more.
“I thought, ‘I want to do something and actually have a title where I can effect change,’” says Dr. Satpathy, now the hospitalist program medical director for Cogent HMG at Seton Medical Center in Daly City, Calif.
A year and a half after starting from scratch, Dr. Satpathy’s program has improved patient-care continuity, implemented 24/7 coverage, and earned buy-in from specialists, surgeons, and hospital leaders—most of whom are men.
“There aren’t as many female physician leaders, period,” says Dr. Satpathy, speaking of Seton Medical Center.
She could be talking about medicine in general.
Despite the fact that women have made up nearly half of all medical school graduates since 2005-2006 and make up 30% of the total physician population, only 16% of MD faculty at the full professor rank are female.1,2,3 Just 11% and 13% of medical school permanent deans and department chairs are women, respectively.4
Beyond academia, results from surveys conducted by the American College of Healthcare Executives show that female healthcare executives are less likely to be CEOs and chief operating officers than their male counterparts. The results also indicate that the proportion of female CEOs remained fairly stable between surveys in 1990, 1995, 2000, and 2006; the proportion of female vice presidents actually decreased.5
This reality, experts say, undercuts America’s ability to remain at the leading edge of medical research, impedes women’s health improvements, and leaves fewer role models for future generations of physicians. In looking at why female physicians are underrepresented in leadership, key issues emerge, including unconscious bias, outdated work structures, lack of sponsorship, and conflict between the biological and professional time clocks. Although not all female doctors have faced these obstacles, many of them have and still do.
But opportunities are there—especially in HM—for female doctors to step into leadership roles. The onus is on women to seize them and on institutions to create a fertile environment for diverse leadership, physician leaders say.
Leadership Obstacles
Men often are associated with leadership by virtue of a phenomenon called unconscious bias, which posits that people identify certain genders with certain roles due to subconscious cues accumulated over time, says Hannah Valantine, MD, professor of medicine and senior associate dean for diversity and leadership at the Stanford
University School of Medicine in Palo Alto, Calif.
“These biases exist in all of us in the way we evaluate women and their work, in the way we evaluate them for leadership positions and when they’re in leadership positions, and in the thought processes that they have of their own qualifications and actions,” says Molly Carnes, MD, MS, a professor of medicine and industrial and systems engineering and co-director of the Women in Science and Engineering Leadership Institute at the University of Wisconsin at Madison.
Bias also exists in how institutions write their job announcements, performance evaluations, and grant and award applications, Dr. Carnes explains. When such terms as “aggressive” and “risk-taking” are used, women are less likely to be seen as viable candidates, she says.
What often impedes female physicians from taking leadership roles are a lack of sponsorship and obsolete work structures that don’t reflect life in the 21st century.
“There is some thought out there that women nowadays are overmentored and undersponsored,” says Dr. Valantine, a cardiologist. “By ‘sponsored,’ we mean going that extra mile to make sure a woman is promoted into the next level of leadership and into the next level of opportunities. It’s the ‘old boys’ network,’ and, unfortunately for women, there isn’t an old girls’ network that’s as well-oiled.”
Work environments are largely designed for the single breadwinner, even though most households, including physicians, have two earners. As a result, women who seek work flexibility or work part time often are labeled as “not serious about their careers,” Dr. Valantine says. This label affects women, who begin to think they can’t pursue leadership roles because they’re working less than full time, says Rachel George, MD, MBA, CPE, FHM, chief operating officer of the West and North-Central regions and chief medical officer of the West region for Nashville, Tenn.-based Cogent HMG, the largest privately held HM and critical-care company in the nation with partnerships in more than 100 hospitals.
There’s an inherent conflict between the professional and biological time clocks in that when female hospitalists are trained, working for a few years, and ready to accept new challenges, they’re also starting families, says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West region for Dallas-based EmCare, a company that provides outsourced physician services, including hospitalist care, in more than 500 hospitals in 40 states.
“Part of the problem is that we look at this as an all or none, that you have to be fully immersed in whatever leadership role it is, and be willing to give a tremendous amount of hours, but that’s really not true,” Dr. George says. “There are different levels of leadership. It’s OK to take it slow and do a little bit, whatever the reasoning may be.”
Dr. Carnes says many women who achieve leadership positions find themselves outside the behavioral norms assigned to women and, therefore, often confront negative reactions and perceptions that they’re disagreeable, arrogant, and superior-minded. Women sometimes get pushback from other women, too.
“When you talk to stay-at-home moms and part-time moms, I think they try and put the guilt trip on you all the time,” says Theresa Rohr-Kirchgraber, MD, board member of the American Women’s Medical Association and executive director of the National Center of Excellence in Women’s Health at Indiana University in Indianapolis.
That, in turn, often compounds the internal guilt many women feel, pitting their work and leadership goals against their responsibilities at home, she says. “There is still a big pull for women to be at home, and when you’re not, you feel guilty about it,” Dr. Rohr-Kirchgraber explains.
Good Things Don’t Come to Those Who Wait
—Kay Cannon, MBA, MCC
Female hospitalists who aspire to lead must take the initiative, experts say.
“Regardless of gender, those individuals who are known to get results, be proactive, and be part of a solution are the ones who gain the attention and, many times, have opportunities open up for advancement,” says Kay Cannon, MBA, MCC, an executive leadership consultant and coach who teaches advanced courses at SHM’s Leadership Academy.
Cathleen Ammann, MD, can attest to that. A year after joining the then-fledgling hospitalist program at Wentworth-Douglass Hospital in Dover, N.H., Dr. Ammann thought she could lead it in a positive direction.
“With zero leadership experience, I went to our CMO, who was basically the administrator for our group, and said, ‘I think I could do a good job with this,’” she says. The CMO concurred, and in October 2006, Dr. Ammann took over the hospitalist program, which she continues to lead today. “They really took a chance with me, and I’m glad they did.”
Dr. Bell says HM, as a whole, has more leadership opportunities than there are trained, capable physicians to do the job—something female hospitalists can take advantage of. But it’s up to women to seize the opportunity, says Mary Jo Gorman, MD, MBA, MHM, who started her career as a hospitalist and is now CEO of Advanced ICU Care, a St. Louis-based firm that connects intensivists to hospital ICU patients via telemedicine.
“Every leadership position that I’ve been in, I got there because I was trying to solve a problem,” says Dr. Gorman, a past president of SHM. “The No. 1 mistake that women make is they don’t step up to volunteer to take responsibility for things; they expect somebody to notice their good work and ask them to lead. Culturally, that’s been shown not to be what happens and not very successful.”
—Mary Jo Gorman, MD, MBA, MHM, CEO, Advanced ICU Care, St. Louis
Where There’s a Will, There’s a Way
Female hospitalists who are interested in leadership need to find an organization that values and encourages their employees to make meaningful contributions, Cannon says. Then they need to join projects and committees in order to develop some leadership qualities, Dr. Ammann says.
“Being involved in one or two committees initially that you strongly believe in, being active, voicing your opinion, and finding ways to find solutions─that’s where you get seen and known,” Dr. Satpathy says. “You actually gain credibility because it’s authentic.”
The old adage “from small beginnings come great things” applies to leadership, Dr. Gorman says.
“If you can complete things regularly and successfully, if you can do that, then the next time you go to a slightly bigger project and then a bigger project and a bigger project, until you’re directing a couple hundred people,” she says.
It’s also important for female physicians to find multiple mentors, Dr. Valantine notes. “You may need a mentor that is within your own discipline who can help guide you about planning your career, writing a grant, doing a project. You might need someone else entirely different who will help you think about when is the right time for you to consider having a family, taking sabbatical, and just integrating your work with life,” she says.
Additionally, female hospitalists pursuing leadership roles must remember that every time they say “yes” to something, they’re saying “no” to something else, Cannon says.
“Too often what I see is women are so eager to please and they’re so driven to be their best, they end up saying ‘yes’ in their career. Then, all of a sudden, they arrive at a point and they say, ‘Something is really missing,’” she says. “If you can get ahead of that and think through things, it’s really going to help your planning.”
Dr. Valantine says female physicians should “take the long view” of leadership and pace themselves.
“Look at this along the entire career path and say, ‘I may not be able to do everything right now, but there might be periods of flexing up and flexing down in my career, and that’s fine,’” she says. “The important thing is to stay in it.”
Dr. Bell and others urge hospitalists who are motivated to lead to tell people in positions of authority that they’re interested; otherwise, they’re not going to be thought of when a position opens.
Dr. Rohr-Kirchgarber has made appointments with deans, associate deans, and faculty affairs staff to introduce herself, explain her expertise, and find ways to use her skill sets in initiatives and committees that are important to the institution.
“Rather than waiting for three or four years for them to find out who I am and think about me for a committee, I need to get out there from Day One,” she says. “It’s proven to be successful.”
Drs. Ammann and Bell encourage hospitalists in community settings to approach their CMOs or other hospital administrators about their leadership aspirations. “And, of course, networking in a professional organization helps,” Dr. Satpathy says.
Meet Halfway
Female physicians can take the initiative and position themselves for leadership roles. They can acquire necessary skills by attending SHM’s Leadership Academy, management classes offered by the American College of Physicians and the American College of Physician Executives, and even adult education courses taught at business schools. But in order for them to be successful leaders, institutions must be invested in the effort.
Organizations can start by defining what they mean by “leadership.”
“‘Leader’ is actually a very abstract concept,” Dr. Carnes says. “But if you break it down into very specific activities, then I think you will get more women saying ‘yes.’ The first thing is getting women to see what leadership can allow them to do.”
—Rachel George, MBA, MCC
Men—and women—also have to acknowledge they have unconscious biases, then work to change the cultural norms, she says.
“Smoking is a really good example,” Dr. Carnes explains. “It took multilevel intervention at the individual and institutional level to change the cultural norms for smoking. You have to have a clear statement by the institution endorsed by all the institutional leaders that this is an institutional priority.” Examples of priorities include eliminating male-gendered words from job announcements and performance evaluations, and ensuring a fair and open application process for leadership positions that allow female physicians to make a case for themselves, she says.
Institutions can implement structural elements to help women—and men—better manage their careers and assume leadership roles, Dr. Valantine says. These include tenure clock extension, extended maternity and family leave, short- and long-term sabbaticals, onsite childcare, and emergency backup childcare.(Read about how Stanford University’s School of Medicine encourages women to seek leadership positions at the-hospitalist.org.)
“When I give talks to women about leadership, I tell them about all the programs we’re doing. I say to them, ‘I hope that you will go out and ask for these programs to be set up in your institutions,” she says. “But, more importantly, I tell women, ‘You have a responsibility to remain standing. It’s going to be tough sometimes, but if you don’t remain standing, we won’t have the role models that we need. It’s going to be a vicious cycle. We just won’t advance and increase the numbers of women leaders.”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 1. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170248/data/2010_table1.pdf. Accessed March 2, 2012.
- American Medical Association. Physician Characteristics and Distribution in the US. American Medical Association, 2012. 2012 ed. Chicago: American Medical Association Press; 2011.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 4A. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170254/data/2009_table04a.pdf. Accessed March 2, 2012.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Figure 5. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/179458/data/2009_figure05.pdf. Accessed March 2, 2012.
- American College of Healthcare Executives. A Comparison of the Career Attainments of Men and Women Healthcare Executives: 2006, Table 2. American College of Healthcare Executives website. Available at: http://www.ache.org/pubs/research/gender_study_full_report.pdf. Accessed March 2, 2012.
Several years into her hospitalist career, committee work had satisfied Sarita Satpathy, MD’s desire to positively impact patient care. Then she attended SHM’s Leadership Academy and was inspired to do more.
“I thought, ‘I want to do something and actually have a title where I can effect change,’” says Dr. Satpathy, now the hospitalist program medical director for Cogent HMG at Seton Medical Center in Daly City, Calif.
A year and a half after starting from scratch, Dr. Satpathy’s program has improved patient-care continuity, implemented 24/7 coverage, and earned buy-in from specialists, surgeons, and hospital leaders—most of whom are men.
“There aren’t as many female physician leaders, period,” says Dr. Satpathy, speaking of Seton Medical Center.
She could be talking about medicine in general.
Despite the fact that women have made up nearly half of all medical school graduates since 2005-2006 and make up 30% of the total physician population, only 16% of MD faculty at the full professor rank are female.1,2,3 Just 11% and 13% of medical school permanent deans and department chairs are women, respectively.4
Beyond academia, results from surveys conducted by the American College of Healthcare Executives show that female healthcare executives are less likely to be CEOs and chief operating officers than their male counterparts. The results also indicate that the proportion of female CEOs remained fairly stable between surveys in 1990, 1995, 2000, and 2006; the proportion of female vice presidents actually decreased.5
This reality, experts say, undercuts America’s ability to remain at the leading edge of medical research, impedes women’s health improvements, and leaves fewer role models for future generations of physicians. In looking at why female physicians are underrepresented in leadership, key issues emerge, including unconscious bias, outdated work structures, lack of sponsorship, and conflict between the biological and professional time clocks. Although not all female doctors have faced these obstacles, many of them have and still do.
But opportunities are there—especially in HM—for female doctors to step into leadership roles. The onus is on women to seize them and on institutions to create a fertile environment for diverse leadership, physician leaders say.
Leadership Obstacles
Men often are associated with leadership by virtue of a phenomenon called unconscious bias, which posits that people identify certain genders with certain roles due to subconscious cues accumulated over time, says Hannah Valantine, MD, professor of medicine and senior associate dean for diversity and leadership at the Stanford
University School of Medicine in Palo Alto, Calif.
“These biases exist in all of us in the way we evaluate women and their work, in the way we evaluate them for leadership positions and when they’re in leadership positions, and in the thought processes that they have of their own qualifications and actions,” says Molly Carnes, MD, MS, a professor of medicine and industrial and systems engineering and co-director of the Women in Science and Engineering Leadership Institute at the University of Wisconsin at Madison.
Bias also exists in how institutions write their job announcements, performance evaluations, and grant and award applications, Dr. Carnes explains. When such terms as “aggressive” and “risk-taking” are used, women are less likely to be seen as viable candidates, she says.
What often impedes female physicians from taking leadership roles are a lack of sponsorship and obsolete work structures that don’t reflect life in the 21st century.
“There is some thought out there that women nowadays are overmentored and undersponsored,” says Dr. Valantine, a cardiologist. “By ‘sponsored,’ we mean going that extra mile to make sure a woman is promoted into the next level of leadership and into the next level of opportunities. It’s the ‘old boys’ network,’ and, unfortunately for women, there isn’t an old girls’ network that’s as well-oiled.”
Work environments are largely designed for the single breadwinner, even though most households, including physicians, have two earners. As a result, women who seek work flexibility or work part time often are labeled as “not serious about their careers,” Dr. Valantine says. This label affects women, who begin to think they can’t pursue leadership roles because they’re working less than full time, says Rachel George, MD, MBA, CPE, FHM, chief operating officer of the West and North-Central regions and chief medical officer of the West region for Nashville, Tenn.-based Cogent HMG, the largest privately held HM and critical-care company in the nation with partnerships in more than 100 hospitals.
There’s an inherent conflict between the professional and biological time clocks in that when female hospitalists are trained, working for a few years, and ready to accept new challenges, they’re also starting families, says Kim Bell, MD, FACP, SFHM, regional medical director of the Pacific West region for Dallas-based EmCare, a company that provides outsourced physician services, including hospitalist care, in more than 500 hospitals in 40 states.
“Part of the problem is that we look at this as an all or none, that you have to be fully immersed in whatever leadership role it is, and be willing to give a tremendous amount of hours, but that’s really not true,” Dr. George says. “There are different levels of leadership. It’s OK to take it slow and do a little bit, whatever the reasoning may be.”
Dr. Carnes says many women who achieve leadership positions find themselves outside the behavioral norms assigned to women and, therefore, often confront negative reactions and perceptions that they’re disagreeable, arrogant, and superior-minded. Women sometimes get pushback from other women, too.
“When you talk to stay-at-home moms and part-time moms, I think they try and put the guilt trip on you all the time,” says Theresa Rohr-Kirchgraber, MD, board member of the American Women’s Medical Association and executive director of the National Center of Excellence in Women’s Health at Indiana University in Indianapolis.
That, in turn, often compounds the internal guilt many women feel, pitting their work and leadership goals against their responsibilities at home, she says. “There is still a big pull for women to be at home, and when you’re not, you feel guilty about it,” Dr. Rohr-Kirchgraber explains.
Good Things Don’t Come to Those Who Wait
—Kay Cannon, MBA, MCC
Female hospitalists who aspire to lead must take the initiative, experts say.
“Regardless of gender, those individuals who are known to get results, be proactive, and be part of a solution are the ones who gain the attention and, many times, have opportunities open up for advancement,” says Kay Cannon, MBA, MCC, an executive leadership consultant and coach who teaches advanced courses at SHM’s Leadership Academy.
Cathleen Ammann, MD, can attest to that. A year after joining the then-fledgling hospitalist program at Wentworth-Douglass Hospital in Dover, N.H., Dr. Ammann thought she could lead it in a positive direction.
“With zero leadership experience, I went to our CMO, who was basically the administrator for our group, and said, ‘I think I could do a good job with this,’” she says. The CMO concurred, and in October 2006, Dr. Ammann took over the hospitalist program, which she continues to lead today. “They really took a chance with me, and I’m glad they did.”
Dr. Bell says HM, as a whole, has more leadership opportunities than there are trained, capable physicians to do the job—something female hospitalists can take advantage of. But it’s up to women to seize the opportunity, says Mary Jo Gorman, MD, MBA, MHM, who started her career as a hospitalist and is now CEO of Advanced ICU Care, a St. Louis-based firm that connects intensivists to hospital ICU patients via telemedicine.
“Every leadership position that I’ve been in, I got there because I was trying to solve a problem,” says Dr. Gorman, a past president of SHM. “The No. 1 mistake that women make is they don’t step up to volunteer to take responsibility for things; they expect somebody to notice their good work and ask them to lead. Culturally, that’s been shown not to be what happens and not very successful.”
—Mary Jo Gorman, MD, MBA, MHM, CEO, Advanced ICU Care, St. Louis
Where There’s a Will, There’s a Way
Female hospitalists who are interested in leadership need to find an organization that values and encourages their employees to make meaningful contributions, Cannon says. Then they need to join projects and committees in order to develop some leadership qualities, Dr. Ammann says.
“Being involved in one or two committees initially that you strongly believe in, being active, voicing your opinion, and finding ways to find solutions─that’s where you get seen and known,” Dr. Satpathy says. “You actually gain credibility because it’s authentic.”
The old adage “from small beginnings come great things” applies to leadership, Dr. Gorman says.
“If you can complete things regularly and successfully, if you can do that, then the next time you go to a slightly bigger project and then a bigger project and a bigger project, until you’re directing a couple hundred people,” she says.
It’s also important for female physicians to find multiple mentors, Dr. Valantine notes. “You may need a mentor that is within your own discipline who can help guide you about planning your career, writing a grant, doing a project. You might need someone else entirely different who will help you think about when is the right time for you to consider having a family, taking sabbatical, and just integrating your work with life,” she says.
Additionally, female hospitalists pursuing leadership roles must remember that every time they say “yes” to something, they’re saying “no” to something else, Cannon says.
“Too often what I see is women are so eager to please and they’re so driven to be their best, they end up saying ‘yes’ in their career. Then, all of a sudden, they arrive at a point and they say, ‘Something is really missing,’” she says. “If you can get ahead of that and think through things, it’s really going to help your planning.”
Dr. Valantine says female physicians should “take the long view” of leadership and pace themselves.
“Look at this along the entire career path and say, ‘I may not be able to do everything right now, but there might be periods of flexing up and flexing down in my career, and that’s fine,’” she says. “The important thing is to stay in it.”
Dr. Bell and others urge hospitalists who are motivated to lead to tell people in positions of authority that they’re interested; otherwise, they’re not going to be thought of when a position opens.
Dr. Rohr-Kirchgarber has made appointments with deans, associate deans, and faculty affairs staff to introduce herself, explain her expertise, and find ways to use her skill sets in initiatives and committees that are important to the institution.
“Rather than waiting for three or four years for them to find out who I am and think about me for a committee, I need to get out there from Day One,” she says. “It’s proven to be successful.”
Drs. Ammann and Bell encourage hospitalists in community settings to approach their CMOs or other hospital administrators about their leadership aspirations. “And, of course, networking in a professional organization helps,” Dr. Satpathy says.
Meet Halfway
Female physicians can take the initiative and position themselves for leadership roles. They can acquire necessary skills by attending SHM’s Leadership Academy, management classes offered by the American College of Physicians and the American College of Physician Executives, and even adult education courses taught at business schools. But in order for them to be successful leaders, institutions must be invested in the effort.
Organizations can start by defining what they mean by “leadership.”
“‘Leader’ is actually a very abstract concept,” Dr. Carnes says. “But if you break it down into very specific activities, then I think you will get more women saying ‘yes.’ The first thing is getting women to see what leadership can allow them to do.”
—Rachel George, MBA, MCC
Men—and women—also have to acknowledge they have unconscious biases, then work to change the cultural norms, she says.
“Smoking is a really good example,” Dr. Carnes explains. “It took multilevel intervention at the individual and institutional level to change the cultural norms for smoking. You have to have a clear statement by the institution endorsed by all the institutional leaders that this is an institutional priority.” Examples of priorities include eliminating male-gendered words from job announcements and performance evaluations, and ensuring a fair and open application process for leadership positions that allow female physicians to make a case for themselves, she says.
Institutions can implement structural elements to help women—and men—better manage their careers and assume leadership roles, Dr. Valantine says. These include tenure clock extension, extended maternity and family leave, short- and long-term sabbaticals, onsite childcare, and emergency backup childcare.(Read about how Stanford University’s School of Medicine encourages women to seek leadership positions at the-hospitalist.org.)
“When I give talks to women about leadership, I tell them about all the programs we’re doing. I say to them, ‘I hope that you will go out and ask for these programs to be set up in your institutions,” she says. “But, more importantly, I tell women, ‘You have a responsibility to remain standing. It’s going to be tough sometimes, but if you don’t remain standing, we won’t have the role models that we need. It’s going to be a vicious cycle. We just won’t advance and increase the numbers of women leaders.”
Lisa Ryan is a freelance writer based in New Jersey.
References
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 1. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170248/data/2010_table1.pdf. Accessed March 2, 2012.
- American Medical Association. Physician Characteristics and Distribution in the US. American Medical Association, 2012. 2012 ed. Chicago: American Medical Association Press; 2011.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Table 4A. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/170254/data/2009_table04a.pdf. Accessed March 2, 2012.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report 2009-2010, Figure 5. Association of American Medical Colleges website. Available at: https://www.aamc.org/download/179458/data/2009_figure05.pdf. Accessed March 2, 2012.
- American College of Healthcare Executives. A Comparison of the Career Attainments of Men and Women Healthcare Executives: 2006, Table 2. American College of Healthcare Executives website. Available at: http://www.ache.org/pubs/research/gender_study_full_report.pdf. Accessed March 2, 2012.
10 Things Hospitalists Should Know about Infectious Diseases

The Hospitalist surveyed half a dozen infectious disease (ID) experts—some of whom also have experience as hospitalists—what they would tell a roomful of hospitalists who were curious about ID. Based on those discussions, we offer 10 tips that should help hospitalists treat their patients more effectively.
Hospitalists routinely care for patients with infections, or symptoms of infections, or suspected infections that might not even be infections at all. Many times, hospitalists have more than one treatment option. So which is the best to use? Is there a better option than the therapy that first comes to mind? What about that new antibiotic out there—is it really worth it?
All the while, hospitalists who want to practice conscientious medicine have to be careful they don’t overuse broad-spectrum antibiotics so that bugs’ resistance to the drugs is not speeded up unnecessarily.
In short, infectious diseases can be dicey terrain.
1. Prepare for the reality that the availability of new drugs is shrinking because of antibiotic resistance.
That grim fact might be cause for hospitalists to seek help from ID specialists at their hospitals, says John Bartlett, MD, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health in Baltimore and founding director of the Center for Civilian Biodefense Strategies. The FDA has approved just two new drugs for major infections in the last five years, he says.
“The FDA faucet is really dry,” says Dr. Bartlett, a world-renowned speaker on ID topics and a frequent speaker at SHM annual meetings. “There are no new antibiotics to speak of, no new antibiotics for resistant bacteria. And there’s not likely to be any for several years. So [hospitalists] are going to find themselves painted in a corner, and they’ll probably have to ask for help.”
Leland Allen, MD, an infectious-disease specialist at Shelby Baptist Medical Center near Birmingham, Ala., who worked as a hospitalist for nine years, says hospitalists should not hesitate to seek assistance. “It’s never a burden to do a consult,” he says. “The reality is that it’s a lot less work if you consult early rather than waiting until the patient is sick.”
Dr. Bartlett says hospitalists should brush up on the use of colistin, a drug developed in 1959 that has been little used and requires careful dosing to avoid toxicity. “We’re finding more and more patients that that’s the only thing we’ve got for them,” he says.

—John Bartlett, MD, professor of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, founding director, Center for Civilian Biodefense Strategies
2. Familiarize yourself with new technologyfor identifying bugs.
“Mass spectrometers have been used for identifying microorganisms through a computerized database, and these units are just starting to become available to large health centers,” says Robert Orenstein, DO, associate professor of medicine in infectious diseases at the Mayo Clinic in Phoenix. “This allows you potentially to identify some of these microorganisms almost immediately—if they’re in the database, which is the key.”
Dr. Bartlett says it’s important for hospitalists to pay attention to the “dramatic changes” in the technology, including the emergence of the ppolymerase chain reaction (PCR) test.
“They have to be aware that there are methods that are very sophisticated and very sensitive and specific,” he says, adding that hospitalists have to keep up with what the methods can measure and what their limitations are.
“If you’re going to practice 2012 medicine and infectious disease, you’ve got to know about the rapid movement in microbiology,” he says. “It’s very fast.”
3. Beware the nuances of Staphylococcus aureus treatment.
James Pile, MD, FACP, SFHM, an ID specialist and interim director of hospital medicine at Case Western Reserve University/MetroHealth Medical Center in Cleveland, says an important tidbit regarding S. aureus is that when it’s isolated from blood culture, it should never be considered a contaminant; it’s the real thing.
“Any of us that have practiced for any length of time can certainly recite tales of bad outcomes when even transients. aureus bacteremia was ignored or considered a contaminant, and then patients many times were subsequently readmitted with serious complications,” he says.
He also notes that beta-lactam antibiotics continue to be the clear choice for serious methicillin-sensitive S. aureus (MSSA) infections. He says doctors should not give in to the temptation to treat these patients with vancomycin, as studies have shown better outcomes and lower mortality with beta-lactams.1,2,3

—Robert Orenstein, DO, associate professor of medicinein infectious diseases, Mayo Clinic, Phoenix
As for methicillin-resistant. aureus (MRSA), vancomycin—long the “workhorse” in the fight against MRSA—might remain the best choice despite a series of newer, and more costly, drugs. The reason: a lack of persuasive data that show the new therapies are better, he notes.
Dr. Bartlett cautions that because of the growing resistance of MRSA, the rules for vancomycin use for MRSA are “totally new.”
“They have to know the rules,” he adds.
4. It’s important to continue to keep Clostridium difficile on your radar—it’s still a top threat.
Neil Gupta, MD, a former hospitalist who works as an epidemic intelligence service officer with Atlanta-based Centers for Disease Control and Prevention (CDC), emphasizes glove use and, if possible, immediately curtailing the use of other antibiotics for patients with suspected C. diff.
“Glove use has been proven to be one of the most effective measures at reducing transmission of C. diff,” he says, “and treatment for C. diff is less effective if a patient is on other antimicrobials.”
Dr. Orenstein says hospitalists should be familiar with the evidence-based guidelines for C. diff treatment—the use of metronidazole for mild to moderate cases, or vancomycin for severe cases.
“The practice that we see is all over the board,” Dr. Orenstein notes.
Dr. Pile offered another C. diff tip: If patients who are hospitalized or were recently hospitalized display an unexplained, marked elevation of their white blood cell count, it’s important to think about the possibility of a C. diff infection due to the organism’s predilection for causing striking leukocytosis. On occasion, this might precede, or occur in the absence of, diarrhea.
5. Take out unnecessary IV lines.
David Chansolme, MD, medical director of infection control for Integra Southwest Medical Center in Oklahoma City and a member of the Clinical Affairs Committee with the Infectious Diseases Society of America, explains that all too often the lines will be kept in during the transport of a patient to a skilled-nursing facility. It’s a practice that, he says, comes with a big risk.
“Leaving a line in just for blood draws is probably not OK,” Dr. Chansolme says. “Nowadays, you’re just seeing way too many of those infections.”
Patients headed for a skilled-nursing facility are at an especially high risk because there is such a high rate of multi-drug-resistant organisms, he says.
6. Be aware of urinary catheters, and use appropriate therapy for catheter-associated urinary tract infections (CAUTIs).
Physicians often are unaware when patients have urinary catheters, Dr. Gupta says, in part because they are frequently placed in the ED and documentation can be missing.
“It’s important to keep this on [hospitalists’] radar whenever they see a patient, so they can remember to remove these as soon as they can, when they’re no longer needed,” Dr. Gupta says, adding that timely removal can prevent an unnecessary risk of CAUTIs.
He also cautions that a third of antimicrobials used to treat CAUTIs are inappropriately aimed at treating asymptomatic bacteriuria, and hospitalists have to be sure that there truly is an infection.
7. A urine culture without a simultaneous urine analysis is practically worthless.
Once a catheter has been in for three or four days, most patients will have “all kinds of bacteria and fungus growing in their urine,” Dr. Allen says.
“A urinalysis lets you assess for the presence of pyuria or other signs of urinary tract inflammation,” he says. “That’s how you determine whether a germ growing in the urine is a colonizer or a true pathogen.”
8. Bactrim does not treat strep.
“If you have somebody that maybe has been in the hospital on vancomycin because they have cellulitis and are getting better and ready to go home, if you don’t know if that cellulitis is staph or strep, be careful about the agent that you choose to send them home on,” Dr. Chansolme says. “Make sure it has activity against Streptococcus.”
He frequently sees patients de-escalated to the wrong drug—trimethoprim/sulfamethoxazole (Bactrim).
“They’ll go home, and a couple days later they’ll be back because it was in fact a strep infection, not a staph infection,” he says. “If you’re not sure, it’s probably better to use something like doxycycline or clindamycin, or something along those lines, that will treat both.”
9. Be sure to take proper precautions when it comes to norovirus.
Winter is the time of year to be most concerned about norovirus outbreaks. It’s also important to realize it affects people of all ages, is especially common to closed or semi-closed communities (i.e. hospitals, long-term care facilities, cruise ships), and spreads very rapidly either by person-to-person transmission or contaminated food.
“It’s really important to understand that if a patient is suspected of having norovirus, that patient should be placed in contact precautions immediately, and preferably, when possible, in a single-occupancy room,” Dr. Gupta says. “If a healthcare provider becomes ill with sudden nausea, vomiting, or diarrhea, that’s consistent with possible norovirus. They should stay home for a minimum of 48 hours after symptom resolution before coming back to work.”
And because norovirus is so contagious, quick action has to be taken if such an outbreak is suspected.
“If there’s any concern at all in your facility,” he says, “get in touch with an infection prevention committee to make sue all appropriate measures are taken.”
10. Never swab a decubitus ulcer unless that ulcer is clearly infected.
Dr. Allen says it’s important to know that it doesn’t make sense to culture an ulcer that doesn’t have any signs of infection, such as pus or redness—although he sees it happen routinely.
“Just because a patient has a bedsore doesn’t mean it’s infected,” Dr. Allen says. “Usually, they’re not infected. But they’re going to have a dozen different germs growing in them.”
Culturing and treatment without signs of infection, he says, often leads to “inappropriate antibiotic use and probably increased length of stay."
Tom Collins is a freelance writer in South Florida
References
- Kim SH, Kim KH, Kim HB, et al. Outcome of vancomycin treatment in patients with methicillin-susceptible Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. 2008;52(1):192-197.
- González C, Rubio M, Romero-Vivas J, González M, Picazo JJ.. Bacteremic pneumonia due to Staphylococcus aureus: A comparison of disease caused by methicillin-resistant and methicillin-susceptible organisms. Clin Infect Dis. 1999;29(5):1171-1177.
- Stryjewski ME, Szczech LA, Benjamin DK Jr., et al. Use of vancomycin or first-generation cephalosporins for the treatment of hemodialysis-dependent patients with methicillin-susceptible Staphylococcus aureus bacteremia. Clin Infect Dis. 2007;44(2):190-196.
The Hospitalist surveyed half a dozen infectious disease (ID) experts—some of whom also have experience as hospitalists—what they would tell a roomful of hospitalists who were curious about ID. Based on those discussions, we offer 10 tips that should help hospitalists treat their patients more effectively.
Hospitalists routinely care for patients with infections, or symptoms of infections, or suspected infections that might not even be infections at all. Many times, hospitalists have more than one treatment option. So which is the best to use? Is there a better option than the therapy that first comes to mind? What about that new antibiotic out there—is it really worth it?
All the while, hospitalists who want to practice conscientious medicine have to be careful they don’t overuse broad-spectrum antibiotics so that bugs’ resistance to the drugs is not speeded up unnecessarily.
In short, infectious diseases can be dicey terrain.
1. Prepare for the reality that the availability of new drugs is shrinking because of antibiotic resistance.
That grim fact might be cause for hospitalists to seek help from ID specialists at their hospitals, says John Bartlett, MD, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health in Baltimore and founding director of the Center for Civilian Biodefense Strategies. The FDA has approved just two new drugs for major infections in the last five years, he says.
“The FDA faucet is really dry,” says Dr. Bartlett, a world-renowned speaker on ID topics and a frequent speaker at SHM annual meetings. “There are no new antibiotics to speak of, no new antibiotics for resistant bacteria. And there’s not likely to be any for several years. So [hospitalists] are going to find themselves painted in a corner, and they’ll probably have to ask for help.”
Leland Allen, MD, an infectious-disease specialist at Shelby Baptist Medical Center near Birmingham, Ala., who worked as a hospitalist for nine years, says hospitalists should not hesitate to seek assistance. “It’s never a burden to do a consult,” he says. “The reality is that it’s a lot less work if you consult early rather than waiting until the patient is sick.”
Dr. Bartlett says hospitalists should brush up on the use of colistin, a drug developed in 1959 that has been little used and requires careful dosing to avoid toxicity. “We’re finding more and more patients that that’s the only thing we’ve got for them,” he says.
—John Bartlett, MD, professor of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, founding director, Center for Civilian Biodefense Strategies
2. Familiarize yourself with new technologyfor identifying bugs.
“Mass spectrometers have been used for identifying microorganisms through a computerized database, and these units are just starting to become available to large health centers,” says Robert Orenstein, DO, associate professor of medicine in infectious diseases at the Mayo Clinic in Phoenix. “This allows you potentially to identify some of these microorganisms almost immediately—if they’re in the database, which is the key.”
Dr. Bartlett says it’s important for hospitalists to pay attention to the “dramatic changes” in the technology, including the emergence of the ppolymerase chain reaction (PCR) test.
“They have to be aware that there are methods that are very sophisticated and very sensitive and specific,” he says, adding that hospitalists have to keep up with what the methods can measure and what their limitations are.
“If you’re going to practice 2012 medicine and infectious disease, you’ve got to know about the rapid movement in microbiology,” he says. “It’s very fast.”
3. Beware the nuances of Staphylococcus aureus treatment.
James Pile, MD, FACP, SFHM, an ID specialist and interim director of hospital medicine at Case Western Reserve University/MetroHealth Medical Center in Cleveland, says an important tidbit regarding S. aureus is that when it’s isolated from blood culture, it should never be considered a contaminant; it’s the real thing.
“Any of us that have practiced for any length of time can certainly recite tales of bad outcomes when even transients. aureus bacteremia was ignored or considered a contaminant, and then patients many times were subsequently readmitted with serious complications,” he says.
He also notes that beta-lactam antibiotics continue to be the clear choice for serious methicillin-sensitive S. aureus (MSSA) infections. He says doctors should not give in to the temptation to treat these patients with vancomycin, as studies have shown better outcomes and lower mortality with beta-lactams.1,2,3
—Robert Orenstein, DO, associate professor of medicinein infectious diseases, Mayo Clinic, Phoenix
As for methicillin-resistant. aureus (MRSA), vancomycin—long the “workhorse” in the fight against MRSA—might remain the best choice despite a series of newer, and more costly, drugs. The reason: a lack of persuasive data that show the new therapies are better, he notes.
Dr. Bartlett cautions that because of the growing resistance of MRSA, the rules for vancomycin use for MRSA are “totally new.”
“They have to know the rules,” he adds.
4. It’s important to continue to keep Clostridium difficile on your radar—it’s still a top threat.
Neil Gupta, MD, a former hospitalist who works as an epidemic intelligence service officer with Atlanta-based Centers for Disease Control and Prevention (CDC), emphasizes glove use and, if possible, immediately curtailing the use of other antibiotics for patients with suspected C. diff.
“Glove use has been proven to be one of the most effective measures at reducing transmission of C. diff,” he says, “and treatment for C. diff is less effective if a patient is on other antimicrobials.”
Dr. Orenstein says hospitalists should be familiar with the evidence-based guidelines for C. diff treatment—the use of metronidazole for mild to moderate cases, or vancomycin for severe cases.
“The practice that we see is all over the board,” Dr. Orenstein notes.
Dr. Pile offered another C. diff tip: If patients who are hospitalized or were recently hospitalized display an unexplained, marked elevation of their white blood cell count, it’s important to think about the possibility of a C. diff infection due to the organism’s predilection for causing striking leukocytosis. On occasion, this might precede, or occur in the absence of, diarrhea.
5. Take out unnecessary IV lines.
David Chansolme, MD, medical director of infection control for Integra Southwest Medical Center in Oklahoma City and a member of the Clinical Affairs Committee with the Infectious Diseases Society of America, explains that all too often the lines will be kept in during the transport of a patient to a skilled-nursing facility. It’s a practice that, he says, comes with a big risk.
“Leaving a line in just for blood draws is probably not OK,” Dr. Chansolme says. “Nowadays, you’re just seeing way too many of those infections.”
Patients headed for a skilled-nursing facility are at an especially high risk because there is such a high rate of multi-drug-resistant organisms, he says.
6. Be aware of urinary catheters, and use appropriate therapy for catheter-associated urinary tract infections (CAUTIs).
Physicians often are unaware when patients have urinary catheters, Dr. Gupta says, in part because they are frequently placed in the ED and documentation can be missing.
“It’s important to keep this on [hospitalists’] radar whenever they see a patient, so they can remember to remove these as soon as they can, when they’re no longer needed,” Dr. Gupta says, adding that timely removal can prevent an unnecessary risk of CAUTIs.
He also cautions that a third of antimicrobials used to treat CAUTIs are inappropriately aimed at treating asymptomatic bacteriuria, and hospitalists have to be sure that there truly is an infection.
7. A urine culture without a simultaneous urine analysis is practically worthless.
Once a catheter has been in for three or four days, most patients will have “all kinds of bacteria and fungus growing in their urine,” Dr. Allen says.
“A urinalysis lets you assess for the presence of pyuria or other signs of urinary tract inflammation,” he says. “That’s how you determine whether a germ growing in the urine is a colonizer or a true pathogen.”
8. Bactrim does not treat strep.
“If you have somebody that maybe has been in the hospital on vancomycin because they have cellulitis and are getting better and ready to go home, if you don’t know if that cellulitis is staph or strep, be careful about the agent that you choose to send them home on,” Dr. Chansolme says. “Make sure it has activity against Streptococcus.”
He frequently sees patients de-escalated to the wrong drug—trimethoprim/sulfamethoxazole (Bactrim).
“They’ll go home, and a couple days later they’ll be back because it was in fact a strep infection, not a staph infection,” he says. “If you’re not sure, it’s probably better to use something like doxycycline or clindamycin, or something along those lines, that will treat both.”
9. Be sure to take proper precautions when it comes to norovirus.
Winter is the time of year to be most concerned about norovirus outbreaks. It’s also important to realize it affects people of all ages, is especially common to closed or semi-closed communities (i.e. hospitals, long-term care facilities, cruise ships), and spreads very rapidly either by person-to-person transmission or contaminated food.
“It’s really important to understand that if a patient is suspected of having norovirus, that patient should be placed in contact precautions immediately, and preferably, when possible, in a single-occupancy room,” Dr. Gupta says. “If a healthcare provider becomes ill with sudden nausea, vomiting, or diarrhea, that’s consistent with possible norovirus. They should stay home for a minimum of 48 hours after symptom resolution before coming back to work.”
And because norovirus is so contagious, quick action has to be taken if such an outbreak is suspected.
“If there’s any concern at all in your facility,” he says, “get in touch with an infection prevention committee to make sue all appropriate measures are taken.”
10. Never swab a decubitus ulcer unless that ulcer is clearly infected.
Dr. Allen says it’s important to know that it doesn’t make sense to culture an ulcer that doesn’t have any signs of infection, such as pus or redness—although he sees it happen routinely.
“Just because a patient has a bedsore doesn’t mean it’s infected,” Dr. Allen says. “Usually, they’re not infected. But they’re going to have a dozen different germs growing in them.”
Culturing and treatment without signs of infection, he says, often leads to “inappropriate antibiotic use and probably increased length of stay."
Tom Collins is a freelance writer in South Florida
References
- Kim SH, Kim KH, Kim HB, et al. Outcome of vancomycin treatment in patients with methicillin-susceptible Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. 2008;52(1):192-197.
- González C, Rubio M, Romero-Vivas J, González M, Picazo JJ.. Bacteremic pneumonia due to Staphylococcus aureus: A comparison of disease caused by methicillin-resistant and methicillin-susceptible organisms. Clin Infect Dis. 1999;29(5):1171-1177.
- Stryjewski ME, Szczech LA, Benjamin DK Jr., et al. Use of vancomycin or first-generation cephalosporins for the treatment of hemodialysis-dependent patients with methicillin-susceptible Staphylococcus aureus bacteremia. Clin Infect Dis. 2007;44(2):190-196.
The Hospitalist surveyed half a dozen infectious disease (ID) experts—some of whom also have experience as hospitalists—what they would tell a roomful of hospitalists who were curious about ID. Based on those discussions, we offer 10 tips that should help hospitalists treat their patients more effectively.
Hospitalists routinely care for patients with infections, or symptoms of infections, or suspected infections that might not even be infections at all. Many times, hospitalists have more than one treatment option. So which is the best to use? Is there a better option than the therapy that first comes to mind? What about that new antibiotic out there—is it really worth it?
All the while, hospitalists who want to practice conscientious medicine have to be careful they don’t overuse broad-spectrum antibiotics so that bugs’ resistance to the drugs is not speeded up unnecessarily.
In short, infectious diseases can be dicey terrain.
1. Prepare for the reality that the availability of new drugs is shrinking because of antibiotic resistance.
That grim fact might be cause for hospitalists to seek help from ID specialists at their hospitals, says John Bartlett, MD, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health in Baltimore and founding director of the Center for Civilian Biodefense Strategies. The FDA has approved just two new drugs for major infections in the last five years, he says.
“The FDA faucet is really dry,” says Dr. Bartlett, a world-renowned speaker on ID topics and a frequent speaker at SHM annual meetings. “There are no new antibiotics to speak of, no new antibiotics for resistant bacteria. And there’s not likely to be any for several years. So [hospitalists] are going to find themselves painted in a corner, and they’ll probably have to ask for help.”
Leland Allen, MD, an infectious-disease specialist at Shelby Baptist Medical Center near Birmingham, Ala., who worked as a hospitalist for nine years, says hospitalists should not hesitate to seek assistance. “It’s never a burden to do a consult,” he says. “The reality is that it’s a lot less work if you consult early rather than waiting until the patient is sick.”
Dr. Bartlett says hospitalists should brush up on the use of colistin, a drug developed in 1959 that has been little used and requires careful dosing to avoid toxicity. “We’re finding more and more patients that that’s the only thing we’ve got for them,” he says.
—John Bartlett, MD, professor of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, founding director, Center for Civilian Biodefense Strategies
2. Familiarize yourself with new technologyfor identifying bugs.
“Mass spectrometers have been used for identifying microorganisms through a computerized database, and these units are just starting to become available to large health centers,” says Robert Orenstein, DO, associate professor of medicine in infectious diseases at the Mayo Clinic in Phoenix. “This allows you potentially to identify some of these microorganisms almost immediately—if they’re in the database, which is the key.”
Dr. Bartlett says it’s important for hospitalists to pay attention to the “dramatic changes” in the technology, including the emergence of the ppolymerase chain reaction (PCR) test.
“They have to be aware that there are methods that are very sophisticated and very sensitive and specific,” he says, adding that hospitalists have to keep up with what the methods can measure and what their limitations are.
“If you’re going to practice 2012 medicine and infectious disease, you’ve got to know about the rapid movement in microbiology,” he says. “It’s very fast.”
3. Beware the nuances of Staphylococcus aureus treatment.
James Pile, MD, FACP, SFHM, an ID specialist and interim director of hospital medicine at Case Western Reserve University/MetroHealth Medical Center in Cleveland, says an important tidbit regarding S. aureus is that when it’s isolated from blood culture, it should never be considered a contaminant; it’s the real thing.
“Any of us that have practiced for any length of time can certainly recite tales of bad outcomes when even transients. aureus bacteremia was ignored or considered a contaminant, and then patients many times were subsequently readmitted with serious complications,” he says.
He also notes that beta-lactam antibiotics continue to be the clear choice for serious methicillin-sensitive S. aureus (MSSA) infections. He says doctors should not give in to the temptation to treat these patients with vancomycin, as studies have shown better outcomes and lower mortality with beta-lactams.1,2,3
—Robert Orenstein, DO, associate professor of medicinein infectious diseases, Mayo Clinic, Phoenix
As for methicillin-resistant. aureus (MRSA), vancomycin—long the “workhorse” in the fight against MRSA—might remain the best choice despite a series of newer, and more costly, drugs. The reason: a lack of persuasive data that show the new therapies are better, he notes.
Dr. Bartlett cautions that because of the growing resistance of MRSA, the rules for vancomycin use for MRSA are “totally new.”
“They have to know the rules,” he adds.
4. It’s important to continue to keep Clostridium difficile on your radar—it’s still a top threat.
Neil Gupta, MD, a former hospitalist who works as an epidemic intelligence service officer with Atlanta-based Centers for Disease Control and Prevention (CDC), emphasizes glove use and, if possible, immediately curtailing the use of other antibiotics for patients with suspected C. diff.
“Glove use has been proven to be one of the most effective measures at reducing transmission of C. diff,” he says, “and treatment for C. diff is less effective if a patient is on other antimicrobials.”
Dr. Orenstein says hospitalists should be familiar with the evidence-based guidelines for C. diff treatment—the use of metronidazole for mild to moderate cases, or vancomycin for severe cases.
“The practice that we see is all over the board,” Dr. Orenstein notes.
Dr. Pile offered another C. diff tip: If patients who are hospitalized or were recently hospitalized display an unexplained, marked elevation of their white blood cell count, it’s important to think about the possibility of a C. diff infection due to the organism’s predilection for causing striking leukocytosis. On occasion, this might precede, or occur in the absence of, diarrhea.
5. Take out unnecessary IV lines.
David Chansolme, MD, medical director of infection control for Integra Southwest Medical Center in Oklahoma City and a member of the Clinical Affairs Committee with the Infectious Diseases Society of America, explains that all too often the lines will be kept in during the transport of a patient to a skilled-nursing facility. It’s a practice that, he says, comes with a big risk.
“Leaving a line in just for blood draws is probably not OK,” Dr. Chansolme says. “Nowadays, you’re just seeing way too many of those infections.”
Patients headed for a skilled-nursing facility are at an especially high risk because there is such a high rate of multi-drug-resistant organisms, he says.
6. Be aware of urinary catheters, and use appropriate therapy for catheter-associated urinary tract infections (CAUTIs).
Physicians often are unaware when patients have urinary catheters, Dr. Gupta says, in part because they are frequently placed in the ED and documentation can be missing.
“It’s important to keep this on [hospitalists’] radar whenever they see a patient, so they can remember to remove these as soon as they can, when they’re no longer needed,” Dr. Gupta says, adding that timely removal can prevent an unnecessary risk of CAUTIs.
He also cautions that a third of antimicrobials used to treat CAUTIs are inappropriately aimed at treating asymptomatic bacteriuria, and hospitalists have to be sure that there truly is an infection.
7. A urine culture without a simultaneous urine analysis is practically worthless.
Once a catheter has been in for three or four days, most patients will have “all kinds of bacteria and fungus growing in their urine,” Dr. Allen says.
“A urinalysis lets you assess for the presence of pyuria or other signs of urinary tract inflammation,” he says. “That’s how you determine whether a germ growing in the urine is a colonizer or a true pathogen.”
8. Bactrim does not treat strep.
“If you have somebody that maybe has been in the hospital on vancomycin because they have cellulitis and are getting better and ready to go home, if you don’t know if that cellulitis is staph or strep, be careful about the agent that you choose to send them home on,” Dr. Chansolme says. “Make sure it has activity against Streptococcus.”
He frequently sees patients de-escalated to the wrong drug—trimethoprim/sulfamethoxazole (Bactrim).
“They’ll go home, and a couple days later they’ll be back because it was in fact a strep infection, not a staph infection,” he says. “If you’re not sure, it’s probably better to use something like doxycycline or clindamycin, or something along those lines, that will treat both.”
9. Be sure to take proper precautions when it comes to norovirus.
Winter is the time of year to be most concerned about norovirus outbreaks. It’s also important to realize it affects people of all ages, is especially common to closed or semi-closed communities (i.e. hospitals, long-term care facilities, cruise ships), and spreads very rapidly either by person-to-person transmission or contaminated food.
“It’s really important to understand that if a patient is suspected of having norovirus, that patient should be placed in contact precautions immediately, and preferably, when possible, in a single-occupancy room,” Dr. Gupta says. “If a healthcare provider becomes ill with sudden nausea, vomiting, or diarrhea, that’s consistent with possible norovirus. They should stay home for a minimum of 48 hours after symptom resolution before coming back to work.”
And because norovirus is so contagious, quick action has to be taken if such an outbreak is suspected.
“If there’s any concern at all in your facility,” he says, “get in touch with an infection prevention committee to make sue all appropriate measures are taken.”
10. Never swab a decubitus ulcer unless that ulcer is clearly infected.
Dr. Allen says it’s important to know that it doesn’t make sense to culture an ulcer that doesn’t have any signs of infection, such as pus or redness—although he sees it happen routinely.
“Just because a patient has a bedsore doesn’t mean it’s infected,” Dr. Allen says. “Usually, they’re not infected. But they’re going to have a dozen different germs growing in them.”
Culturing and treatment without signs of infection, he says, often leads to “inappropriate antibiotic use and probably increased length of stay."
Tom Collins is a freelance writer in South Florida
References
- Kim SH, Kim KH, Kim HB, et al. Outcome of vancomycin treatment in patients with methicillin-susceptible Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. 2008;52(1):192-197.
- González C, Rubio M, Romero-Vivas J, González M, Picazo JJ.. Bacteremic pneumonia due to Staphylococcus aureus: A comparison of disease caused by methicillin-resistant and methicillin-susceptible organisms. Clin Infect Dis. 1999;29(5):1171-1177.
- Stryjewski ME, Szczech LA, Benjamin DK Jr., et al. Use of vancomycin or first-generation cephalosporins for the treatment of hemodialysis-dependent patients with methicillin-susceptible Staphylococcus aureus bacteremia. Clin Infect Dis. 2007;44(2):190-196.
Society of Hospital Medicine Earns National Quality Award

—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalist Jordan Messler, MD, SFHM, has experienced SHM’s mentored-implementation program as both mentee and mentor. So when he heard that the mentored-implementation model was named the winner of the 2011 John M. Eisenberg Innovation in Patient Safety and Quality at the National Level Award, he knew it was well-earned.
“The biggest aspect of these programs has been the collegiality and the learning from others,” says Dr. Messler, medical director at Morton Plant Hospital in Clearwater, Fla. “That’s really the core of this. We’ve all felt that we’re out on an island and we’re all building these projects from the ground up. We all probably at one point in a meeting say, ‘Someone else must have solved this.’ ... These mentored-implementation programs say, ‘Yes, of course other folks have solved this.’”
SHM is the first professional society to earn the award, bestowed by the National Quality Forum (NQF) and The Joint Commission. The model has helped propel SHM’s Glycemic Control Mentored Implementation (GCMI) Program, Project BOOST (Better Outcomes for Older Adults through Safe Transitions), and the VTE Prevention Collaborative. Mentors have been put in place in more than 300 hospitals in the U.S. and Canada, according to an announcement.
“There are significant congratulations [due] to the profession and all the people at the society who have done all the work on this,” says SHM president Joseph Ming-Wah Li, MD, SFHM. “Part of what we’ve been saying all along is that quality is important. In terms of teaching quality—it’s a real team effort.”
NQF president and chief executive Janet Corrigan, PhD, MBA, says that one of the hallmarks of SHM’s program is its ability to be applied to different quality initiatives. Corrigan adds that while a professional society had never previously won the national award, SHM’s execution in creating, implementing, and providing follow-up resources helped differentiate the construct.
“We want to shed light on the kinds of things that are working and encourage others to emulate them, to build on them, and to reinvent them in new and even better ways,” Corrigan says. “It is a whole process of quality improvement.”
Dr. Li says the honor is a milestone for SHM, but the society must not rest on its laurels because it “hit a home run.” Instead, the society should use the momentum of the award to push for and apply for more QI programs. The more successful programs the society and its members launch and successfully implement, the more HM as a field will be considered a leader in quality improvement, he adds.
“We’re an absolute infant compared to many other medical organizations and other medical societies,” Dr. Li says. “Hospitalists and SHM should be very proud that NQF and The Joint Commission chose to bestow this award onto SHM. But at the end of the day, we at SHM also recognize that this is an award. We’re going to celebrate in San Diego with everybody, but once the [annual] meeting is over, we’re going to roll up our sleeves. There’s a heck of a lot more work to get done.”
Richard Quinn is a freelance writer based in New Jersey.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalist Jordan Messler, MD, SFHM, has experienced SHM’s mentored-implementation program as both mentee and mentor. So when he heard that the mentored-implementation model was named the winner of the 2011 John M. Eisenberg Innovation in Patient Safety and Quality at the National Level Award, he knew it was well-earned.
“The biggest aspect of these programs has been the collegiality and the learning from others,” says Dr. Messler, medical director at Morton Plant Hospital in Clearwater, Fla. “That’s really the core of this. We’ve all felt that we’re out on an island and we’re all building these projects from the ground up. We all probably at one point in a meeting say, ‘Someone else must have solved this.’ ... These mentored-implementation programs say, ‘Yes, of course other folks have solved this.’”
SHM is the first professional society to earn the award, bestowed by the National Quality Forum (NQF) and The Joint Commission. The model has helped propel SHM’s Glycemic Control Mentored Implementation (GCMI) Program, Project BOOST (Better Outcomes for Older Adults through Safe Transitions), and the VTE Prevention Collaborative. Mentors have been put in place in more than 300 hospitals in the U.S. and Canada, according to an announcement.
“There are significant congratulations [due] to the profession and all the people at the society who have done all the work on this,” says SHM president Joseph Ming-Wah Li, MD, SFHM. “Part of what we’ve been saying all along is that quality is important. In terms of teaching quality—it’s a real team effort.”
NQF president and chief executive Janet Corrigan, PhD, MBA, says that one of the hallmarks of SHM’s program is its ability to be applied to different quality initiatives. Corrigan adds that while a professional society had never previously won the national award, SHM’s execution in creating, implementing, and providing follow-up resources helped differentiate the construct.
“We want to shed light on the kinds of things that are working and encourage others to emulate them, to build on them, and to reinvent them in new and even better ways,” Corrigan says. “It is a whole process of quality improvement.”
Dr. Li says the honor is a milestone for SHM, but the society must not rest on its laurels because it “hit a home run.” Instead, the society should use the momentum of the award to push for and apply for more QI programs. The more successful programs the society and its members launch and successfully implement, the more HM as a field will be considered a leader in quality improvement, he adds.
“We’re an absolute infant compared to many other medical organizations and other medical societies,” Dr. Li says. “Hospitalists and SHM should be very proud that NQF and The Joint Commission chose to bestow this award onto SHM. But at the end of the day, we at SHM also recognize that this is an award. We’re going to celebrate in San Diego with everybody, but once the [annual] meeting is over, we’re going to roll up our sleeves. There’s a heck of a lot more work to get done.”
Richard Quinn is a freelance writer based in New Jersey.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalist Jordan Messler, MD, SFHM, has experienced SHM’s mentored-implementation program as both mentee and mentor. So when he heard that the mentored-implementation model was named the winner of the 2011 John M. Eisenberg Innovation in Patient Safety and Quality at the National Level Award, he knew it was well-earned.
“The biggest aspect of these programs has been the collegiality and the learning from others,” says Dr. Messler, medical director at Morton Plant Hospital in Clearwater, Fla. “That’s really the core of this. We’ve all felt that we’re out on an island and we’re all building these projects from the ground up. We all probably at one point in a meeting say, ‘Someone else must have solved this.’ ... These mentored-implementation programs say, ‘Yes, of course other folks have solved this.’”
SHM is the first professional society to earn the award, bestowed by the National Quality Forum (NQF) and The Joint Commission. The model has helped propel SHM’s Glycemic Control Mentored Implementation (GCMI) Program, Project BOOST (Better Outcomes for Older Adults through Safe Transitions), and the VTE Prevention Collaborative. Mentors have been put in place in more than 300 hospitals in the U.S. and Canada, according to an announcement.
“There are significant congratulations [due] to the profession and all the people at the society who have done all the work on this,” says SHM president Joseph Ming-Wah Li, MD, SFHM. “Part of what we’ve been saying all along is that quality is important. In terms of teaching quality—it’s a real team effort.”
NQF president and chief executive Janet Corrigan, PhD, MBA, says that one of the hallmarks of SHM’s program is its ability to be applied to different quality initiatives. Corrigan adds that while a professional society had never previously won the national award, SHM’s execution in creating, implementing, and providing follow-up resources helped differentiate the construct.
“We want to shed light on the kinds of things that are working and encourage others to emulate them, to build on them, and to reinvent them in new and even better ways,” Corrigan says. “It is a whole process of quality improvement.”
Dr. Li says the honor is a milestone for SHM, but the society must not rest on its laurels because it “hit a home run.” Instead, the society should use the momentum of the award to push for and apply for more QI programs. The more successful programs the society and its members launch and successfully implement, the more HM as a field will be considered a leader in quality improvement, he adds.
“We’re an absolute infant compared to many other medical organizations and other medical societies,” Dr. Li says. “Hospitalists and SHM should be very proud that NQF and The Joint Commission chose to bestow this award onto SHM. But at the end of the day, we at SHM also recognize that this is an award. We’re going to celebrate in San Diego with everybody, but once the [annual] meeting is over, we’re going to roll up our sleeves. There’s a heck of a lot more work to get done.”
Richard Quinn is a freelance writer based in New Jersey.
New Physician Editor of The Hospitalist Offers Broad Experience and an Eye for QI

—Danielle Scheurer, MD, MSCR, SFHM, physician editor, The Hospitalist
There has always been a journalist dwelling in Danielle Scheurer, MD, MSCR, SFHM. As an undergrad at Emory University, she saw TV reporting in her future.
“I was on the Katie Couric kick for a decade,” she says.
Her course eventually shifted—dramatically. But since she became a hospitalist, Dr. Scheurer, now the chief quality officer at the Medical University of South Carolina (MUSC) in Charleston, has stayed involved with a long slate of editorial projects.
Her latest: She is the new physician editor of The Hospitalist. With the appointment, the magazine gains a high-energy physician with a broad spectrum of knowledge. Colleagues say she has a knack for seeing the big picture and taking a bolus of information and conveying its relevance to hospitalists and other medical professionals.
Dr. Scheurer says that one of her aims will be to make the publication’s website—www.the-hospitalist.org—more interactive, allowing for more direct participation from readers, such as with polls and forums on topics covered.
“A lot of us in the hospital sort of struggle with the exact same things,” she says. “I think there’s some value in connecting, even if it’s in just short little snippets.”
She also would like to increase the website’s use of audio files so that doctors have more options in how they get their information.
But above all, she says, she wants to keep The Hospitalist “one of the most practical publications available to hospitalists,” a publication that is specifically tailored to deliver useful messages.
“I feel like it’s a very high-yield publication for really busy hospitalists,” she says.
Career Shuffle = Diverse Experience
Dr. Scheurer brings experience from a variety of settings, such as the small community hospital Trident Medical Center in Charleston to the large, urban medical centers that are Brigham and Women’s Hospital in Boston and MUSC.
She said some of her career moves came with some apprehension, including those that came about when her husband got a position that required her to move, too. But she says she has benefited from those experiences. Trident “gave me a window into hospital medicine that I never otherwise would have had,” she notes.
She never anticipated moving to Boston, and she admits it felt outside of her “comfort zone.” But in 2005, she found herself at Brigham. She had just earned a master’s degree in clinical research and thought she’d end up being a researcher. In Boston, she got a glimpse of what it meant to be a “hard-core, NIH-funded researcher” and decided it wasn’t for her.
While there, she took training courses in leadership and quality improvement. And QI stuck.
In 2010, she returned to MUSC and now leads QI for the whole hospital, a medium-size setting that she says is just right for promoting change.
“This is definitely my sweet spot,” she says. “If you’re going to change people’s minds, it’s a lot easer to change 200 people’s minds than 450 people’s minds.”
Chris Roy, MD, medical director of the hospitalist service at Brigham, says Dr. Scheurer was “one of the most-hard working people that I knew” and a strong leader with an “uncanny, almost photographic memory of all the hospital medicine literature.”
“Even though she was very forceful as a leader, she never irritated anyone,” he adds. “She was very skillful in managing people.”
Chris Rees, the director of quality and patient safety at MUSC, says Dr. Scheurer is adept at taking issues that evolve from the hospital and collaborating on them with other university departments. She is good at putting herself in other groups’ shoes and delivering messages succinctly, he says.
“She’s definitely not seen as just one of those white coats,” Rees says.
Highly Recommended
On top of her QI projects, Dr. Scheurer is involved as an advisor, contributor, or reviewer at 11 other publications or online venues. The Hospitalist will make it an even dozen.
“She’s just a dynamo,” Rees says. “She walks around with her MacAir book and she’s constantly writing stuff on it and sending out emails.”
Patrick Cawley, MD, MBA, MHM, the chief medical officer at MUSC who hired Dr. Scheurer when she first worked there in 2003, has seen her move from small projects to systemwide efforts.
“She did a great job and is very collaborative, very knowledgeable, [and] brings an evidence-based approach to problems,” says Dr. Cawley, a past president of SHM and recent inductee as a Master in Hospital Medicine (MHM).
She is quick to notice trends and patterns, he points out. “She’s very knowledgeable about what’s going on in the hospitalist arena,” he says, adding he anticipates she’ll be interested in “data-driven” coverage, along with QI topics.
Dr. Scheurer’s interest in disseminating information shouldn’t be a surprise—it’s a fundamental part of QI and instrumental in systemwide change. She finds it “appealing to work on a project and know that it’s going to affect the next 20,000 patients.”
“There’s no one single person that can ensure that the patient gets all of their needs met,” she says. “There has to be a system approach.”
At The Hospitalist, she will try to keep pace with all the change that hospitals are constantly trying to navigate.
“I don’t think there will ever be a deficiency of content to cover,” she says. “Something’s always brand-new.”
Tom Collins is a freelance writer in Florida.
—Danielle Scheurer, MD, MSCR, SFHM, physician editor, The Hospitalist
There has always been a journalist dwelling in Danielle Scheurer, MD, MSCR, SFHM. As an undergrad at Emory University, she saw TV reporting in her future.
“I was on the Katie Couric kick for a decade,” she says.
Her course eventually shifted—dramatically. But since she became a hospitalist, Dr. Scheurer, now the chief quality officer at the Medical University of South Carolina (MUSC) in Charleston, has stayed involved with a long slate of editorial projects.
Her latest: She is the new physician editor of The Hospitalist. With the appointment, the magazine gains a high-energy physician with a broad spectrum of knowledge. Colleagues say she has a knack for seeing the big picture and taking a bolus of information and conveying its relevance to hospitalists and other medical professionals.
Dr. Scheurer says that one of her aims will be to make the publication’s website—www.the-hospitalist.org—more interactive, allowing for more direct participation from readers, such as with polls and forums on topics covered.
“A lot of us in the hospital sort of struggle with the exact same things,” she says. “I think there’s some value in connecting, even if it’s in just short little snippets.”
She also would like to increase the website’s use of audio files so that doctors have more options in how they get their information.
But above all, she says, she wants to keep The Hospitalist “one of the most practical publications available to hospitalists,” a publication that is specifically tailored to deliver useful messages.
“I feel like it’s a very high-yield publication for really busy hospitalists,” she says.
Career Shuffle = Diverse Experience
Dr. Scheurer brings experience from a variety of settings, such as the small community hospital Trident Medical Center in Charleston to the large, urban medical centers that are Brigham and Women’s Hospital in Boston and MUSC.
She said some of her career moves came with some apprehension, including those that came about when her husband got a position that required her to move, too. But she says she has benefited from those experiences. Trident “gave me a window into hospital medicine that I never otherwise would have had,” she notes.
She never anticipated moving to Boston, and she admits it felt outside of her “comfort zone.” But in 2005, she found herself at Brigham. She had just earned a master’s degree in clinical research and thought she’d end up being a researcher. In Boston, she got a glimpse of what it meant to be a “hard-core, NIH-funded researcher” and decided it wasn’t for her.
While there, she took training courses in leadership and quality improvement. And QI stuck.
In 2010, she returned to MUSC and now leads QI for the whole hospital, a medium-size setting that she says is just right for promoting change.
“This is definitely my sweet spot,” she says. “If you’re going to change people’s minds, it’s a lot easer to change 200 people’s minds than 450 people’s minds.”
Chris Roy, MD, medical director of the hospitalist service at Brigham, says Dr. Scheurer was “one of the most-hard working people that I knew” and a strong leader with an “uncanny, almost photographic memory of all the hospital medicine literature.”
“Even though she was very forceful as a leader, she never irritated anyone,” he adds. “She was very skillful in managing people.”
Chris Rees, the director of quality and patient safety at MUSC, says Dr. Scheurer is adept at taking issues that evolve from the hospital and collaborating on them with other university departments. She is good at putting herself in other groups’ shoes and delivering messages succinctly, he says.
“She’s definitely not seen as just one of those white coats,” Rees says.
Highly Recommended
On top of her QI projects, Dr. Scheurer is involved as an advisor, contributor, or reviewer at 11 other publications or online venues. The Hospitalist will make it an even dozen.
“She’s just a dynamo,” Rees says. “She walks around with her MacAir book and she’s constantly writing stuff on it and sending out emails.”
Patrick Cawley, MD, MBA, MHM, the chief medical officer at MUSC who hired Dr. Scheurer when she first worked there in 2003, has seen her move from small projects to systemwide efforts.
“She did a great job and is very collaborative, very knowledgeable, [and] brings an evidence-based approach to problems,” says Dr. Cawley, a past president of SHM and recent inductee as a Master in Hospital Medicine (MHM).
She is quick to notice trends and patterns, he points out. “She’s very knowledgeable about what’s going on in the hospitalist arena,” he says, adding he anticipates she’ll be interested in “data-driven” coverage, along with QI topics.
Dr. Scheurer’s interest in disseminating information shouldn’t be a surprise—it’s a fundamental part of QI and instrumental in systemwide change. She finds it “appealing to work on a project and know that it’s going to affect the next 20,000 patients.”
“There’s no one single person that can ensure that the patient gets all of their needs met,” she says. “There has to be a system approach.”
At The Hospitalist, she will try to keep pace with all the change that hospitals are constantly trying to navigate.
“I don’t think there will ever be a deficiency of content to cover,” she says. “Something’s always brand-new.”
Tom Collins is a freelance writer in Florida.
—Danielle Scheurer, MD, MSCR, SFHM, physician editor, The Hospitalist
There has always been a journalist dwelling in Danielle Scheurer, MD, MSCR, SFHM. As an undergrad at Emory University, she saw TV reporting in her future.
“I was on the Katie Couric kick for a decade,” she says.
Her course eventually shifted—dramatically. But since she became a hospitalist, Dr. Scheurer, now the chief quality officer at the Medical University of South Carolina (MUSC) in Charleston, has stayed involved with a long slate of editorial projects.
Her latest: She is the new physician editor of The Hospitalist. With the appointment, the magazine gains a high-energy physician with a broad spectrum of knowledge. Colleagues say she has a knack for seeing the big picture and taking a bolus of information and conveying its relevance to hospitalists and other medical professionals.
Dr. Scheurer says that one of her aims will be to make the publication’s website—www.the-hospitalist.org—more interactive, allowing for more direct participation from readers, such as with polls and forums on topics covered.
“A lot of us in the hospital sort of struggle with the exact same things,” she says. “I think there’s some value in connecting, even if it’s in just short little snippets.”
She also would like to increase the website’s use of audio files so that doctors have more options in how they get their information.
But above all, she says, she wants to keep The Hospitalist “one of the most practical publications available to hospitalists,” a publication that is specifically tailored to deliver useful messages.
“I feel like it’s a very high-yield publication for really busy hospitalists,” she says.
Career Shuffle = Diverse Experience
Dr. Scheurer brings experience from a variety of settings, such as the small community hospital Trident Medical Center in Charleston to the large, urban medical centers that are Brigham and Women’s Hospital in Boston and MUSC.
She said some of her career moves came with some apprehension, including those that came about when her husband got a position that required her to move, too. But she says she has benefited from those experiences. Trident “gave me a window into hospital medicine that I never otherwise would have had,” she notes.
She never anticipated moving to Boston, and she admits it felt outside of her “comfort zone.” But in 2005, she found herself at Brigham. She had just earned a master’s degree in clinical research and thought she’d end up being a researcher. In Boston, she got a glimpse of what it meant to be a “hard-core, NIH-funded researcher” and decided it wasn’t for her.
While there, she took training courses in leadership and quality improvement. And QI stuck.
In 2010, she returned to MUSC and now leads QI for the whole hospital, a medium-size setting that she says is just right for promoting change.
“This is definitely my sweet spot,” she says. “If you’re going to change people’s minds, it’s a lot easer to change 200 people’s minds than 450 people’s minds.”
Chris Roy, MD, medical director of the hospitalist service at Brigham, says Dr. Scheurer was “one of the most-hard working people that I knew” and a strong leader with an “uncanny, almost photographic memory of all the hospital medicine literature.”
“Even though she was very forceful as a leader, she never irritated anyone,” he adds. “She was very skillful in managing people.”
Chris Rees, the director of quality and patient safety at MUSC, says Dr. Scheurer is adept at taking issues that evolve from the hospital and collaborating on them with other university departments. She is good at putting herself in other groups’ shoes and delivering messages succinctly, he says.
“She’s definitely not seen as just one of those white coats,” Rees says.
Highly Recommended
On top of her QI projects, Dr. Scheurer is involved as an advisor, contributor, or reviewer at 11 other publications or online venues. The Hospitalist will make it an even dozen.
“She’s just a dynamo,” Rees says. “She walks around with her MacAir book and she’s constantly writing stuff on it and sending out emails.”
Patrick Cawley, MD, MBA, MHM, the chief medical officer at MUSC who hired Dr. Scheurer when she first worked there in 2003, has seen her move from small projects to systemwide efforts.
“She did a great job and is very collaborative, very knowledgeable, [and] brings an evidence-based approach to problems,” says Dr. Cawley, a past president of SHM and recent inductee as a Master in Hospital Medicine (MHM).
She is quick to notice trends and patterns, he points out. “She’s very knowledgeable about what’s going on in the hospitalist arena,” he says, adding he anticipates she’ll be interested in “data-driven” coverage, along with QI topics.
Dr. Scheurer’s interest in disseminating information shouldn’t be a surprise—it’s a fundamental part of QI and instrumental in systemwide change. She finds it “appealing to work on a project and know that it’s going to affect the next 20,000 patients.”
“There’s no one single person that can ensure that the patient gets all of their needs met,” she says. “There has to be a system approach.”
At The Hospitalist, she will try to keep pace with all the change that hospitals are constantly trying to navigate.
“I don’t think there will ever be a deficiency of content to cover,” she says. “Something’s always brand-new.”
Tom Collins is a freelance writer in Florida.
In the Literature: Physician Reviews of HM-Related Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- IDSA/ATS guidelines for community-acquired pneumonia
- Improved asthma with IL-13 antibody
- Rivaroxaban vs. warfarin for stroke prevention in atrial fibrillation
- Apixaban vs. warfarin for stroke prevention in atrial fibrillation
- Ultrasonography more sensitive than chest radiograph for pneumothorax
- Current readmission risk models inadequate
- Optimal fluid volume for acute pancreatitis
- Low mortality in saddle pulmonary embolism
Triage Decisions for Patients with Severe Community-Acquired Pneumonia Should Be Based on IDSA/ATS Guidelines, Not Inflammatory Biomarkers
Clinical question: Can C-reactive protein levels (CRP), procalcitonin, TNF-alpha, and cytokine levels predict the need for intensive-care admission more accurately than IDSA/ATS guidelines in patients with severe community-acquired pneumonia (CAP)?
Background: Inflammatory biomarkers, such as CRP and procalcitonin, have diagnostic and prognostic utility in patients with CAP. Whether these inflammatory biomarkers can help triage patients to the appropriate level of care is unknown.
Study design: Prospective case control study.
Setting: Two university hospitals in Spain.
Synopsis: The study included 685 patients with severe CAP who did not require mechanical ventilation or vasopressor support. Serum levels of CRP, procalcitonin, TNF-alpha, IL-1, IL-6, IL-8, and IL-10, as well as Infectious Diseases Society of American/American Thoracic Society (IDSA/ATS) minor severity criteria data, were collected on admission. After controlling for age, comorbidities, and PSI risk class, serum levels of CRP and procalcitonin were found to be significantly higher in ICU patients compared with non-ICU patients. Despite this, these inflammatory biomarkers did not augment the IDSA/ATS guidelines, suggesting that patients who have three or more minor criteria be considered for ICU admission.
The study did suggest that patients with severe CAP and low levels of IL-6 and procalcitonin could potentially be managed safely outside of the ICU. However, hospitalists should be wary of applying the study results due to the small number of ICU patients in this study and the lack of real-time availability of these biomarkers at most institutions.
Bottom line: More studies of inflammatory biomarkers are needed before using them to determine the level of care required for patients with CAP. Until these data are available, physicians should use the IDSA/ATS guidelines to triage patients to the appropriate level of care.
Citation: Ramirez P, Ferrer M, Torres A, et al. Inflammatory biomarkers and prediction for intensive care unit admission pneumonia. Crit Care Med. 2011;39:2211-2217.
IL-13 Antibody Lebrikizumab Shows Promise as a New Therapy for Adults with Uncontrolled Asthma
Clinical question: Can lebrikizumab, an IL-13 antibody, improve asthma control in patients with uncontrolled asthma?
Background: Asthma is a complex disease, with varied patient response to treatment. Some patients have uncontrolled asthma despite inhaled glucocorticoids. It is postulated that IL-13 may account for this variability and that some patients with uncontrolled asthma are poorly controlled due to glucocorticoid resistance mediated by IL-13. Lebrikizumab is an IgG4 monoclonal antibody that binds to and inhibits the function of IL-13. This study was performed to see if this antibody would be effective in patients with uncontrolled asthma despite inhaled glucocorticoid therapy.
Study design: Randomized double-blinded placebo-controlled trial.
Setting: Multiple centers.
Synopsis: The study randomized 219 adult asthma patients who were inadequately controlled despite inhaled corticosteroids to a placebo or lebrikizumab. The primary outcome was improvement in prebronchodilator FEV1 from baseline. Secondary outcomes were exacerbations, use of rescue medications, and symptom scores. Patients were also stratified and analyzed based on surrogate markers for IL-13, which included serum IGE levels, eosinophil counts, and periostin levels.
In patients who were randomized to the lebrikizumab treatment, there was a statistically significant improvement in FEV1 of 5.5%, which occurred almost immediately and was sustained for the entire 32 weeks of the study. The improvement was more significant in patients who had high surrogate markers for IL-13. Despite this improvement in FEV1, there were no differences in secondary outcomes except in patients who had surrogate markers for high IL-13 levels.
Bottom line: In adults with asthma who remained uncontrolled despite inhaled corticosteroid therapy, IL-13 antagonism with lebrikizumab improved FEV1. However, the clinical relevance of these modest improvements remains unclear.
Citation: Corren J, Lemanske R, Matthews J, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365:1088-1098.
Rivaroxaban Is Noninferior to Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does rivaroxaban compare with warfarin in the prevention of stroke or systemic embolism in patients with nonvalvular atrial fibrillation?
Background: Warfarin is effective for the prevention of stroke in atrial fibrillation, but it requires close monitoring and adjustment. Rivaroxaban, an oral Xa inhibitor, may be safer, easier, and more effective than warfarin.
Study design: Multicenter, randomized, double-blind, double-dummy trial.
Setting: 1,178 sites in 45 countries.
Synopsis: The study included 14,264 patients with nonvalvular atrial fibrillation who were randomized to either fixed-dose rivaroxaban (20 mg daily or 15 mg daily for CrCl 30-49 mL/min) plus placebo or adjusted-dose warfarin (target INR 2.0 to 3.0) plus placebo. The mean CHADS2 score was 3.5. The primary endpoint (stroke or systemic embolism) occurred in 1.7% of patients per year in the rivaroxaban group and 2.2% per year in the warfarin group (hazard ratio for rivaroxaban 0.79; 95% CI: 0.66 to 0.96, P<0.001 for noninferiority). There was no difference in major or nonmajor clinically significant bleeding between the two groups (14.9% rivaroxaban vs. 14.5% warfarin, hazard ratio=1.03, 95% CI: 0.96 to 1.11, P=0.44). There were fewer intracranial hemorrhages (0.5% vs. 0.7%, P=0.02) and fatal bleeding (0.2% vs. 0.5%, P=0.003) in the rivaroxaban group.
Bottom line: In patients with atrial fibrillation, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolization, with a similar risk of major bleeding and a lower risk of intracranial hemorrhage or fatal bleeding.
Citation: Patel MR, Mahaffey K, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-891.
Apixaban More Effective and Safer than Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does the effectiveness and safety of apixaban compare with warfarin for stroke prevention in atrial fibrillation?
Background: Until recently, warfarin has been the only available oral anticoagulant for stroke prevention in patients with atrial fibrillation (AF). The oral factor Xa inhibitors have shown similar efficacy and safety, without the monitoring requirement and drug interactions associated with warfarin.
Study design: Prospective randomized double-blind controlled trial.
Setting: More than 1,000 clinical sites in 39 countries.
Synopsis: This study randomized 18,201 patients with atrial fibrillation or flutter and at least one CHADS2 risk factor for stroke to receive oral apixaban or warfarin therapy. Exclusion criteria were prosthetic valves and severe kidney disease. The median duration of follow-up was 1.8 years, and the major endpoints were incidence of stroke, systemic embolism, bleeding complications, and mortality.
Compared with warfarin, apixaban reduced the annual incidence of stroke and systemic embolism from 1.6% to 1.3% (HR 0.79, 95%: CI 0.66 to 0.95, P=0.01 for superiority), and reduced mortality (HR: 0.89, 95% CI: 0.80 to 0.998). For the combined endpoint of stroke, systemic embolism, MI, or death, the annual rate was reduced from 5.5% to 4.9% (HR: 0.88, 95% CI: 0.80 to 0.97). All measures of bleeding were less frequent with apixaban: major 2.1% vs. 3.1% (HR: 0.69, 95% CI: 0.60 to 0.80), and combined major and minor bleeding 4.1% vs. 6.0% (HR: 0.68, 95% CI: 0.61 to 0.75). The annual rate for the net outcome of stroke, embolism, or major bleeding was 3.2% with apixaban and 4.1% with warfarin (HR: 0.77, 95% CI: 0.69 to 0.86).
Bottom line: Compared with warfarin therapy, apixaban is more effective and safer for stroke prevention in patients with atrial fibrillation.
Citation: Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-992.
Ultrasonography Is Useful in Diagnosis of Pneumothorax
Clinical question: Is transthoracic ultrasonography a useful tool to diagnose pneumothorax?
Background: CT is the diagnostic gold standard for pneumothorax, but it is associated with radiation exposure and requires patient transport. Chest radiograph is easy to perform but may be too insensitive for adequate diagnosis. Ultrasonography’s diagnostic performance for detecting pneumothorax needs further evaluation.
Study design: Systematic review and meta-analysis.
Setting: Critically ill, trauma, or post-biopsy patients were identified in each of the studies.
Synopsis: The meta-analysis of 20 eligible studies found a pooled sensitivity of ultrasound for the detection of pneumothorax of 0.88 (95% CI: 0.85 to 0.91) and specificity of 0.99 (0.98 to 0.99) compared with sensitivity of 0.52 (0.49 to 0.55) and specificity of 1.00 (1.00 to 1.00) for chest radiograph. Although the overall ROC curve was not significantly different between these modalities, the accuracy of ultrasonography was highly dependent on the skill of the operator.
Bottom line: When performed by a skilled operator, transthoracic ultrasonography is as specific, and more sensitive, than chest radiograph in diagnosing pneumothorax.
Citation: Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneumothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011;140:859-866.
Risk Prediction for Hospital Readmission Remains Challenging
Clinical question: Can readmission risk assessment be used to identify which patients would benefit most from care-transition interventions, or to risk-adjust readmission rates for hospital comparison?
Background: Multiple models to predict hospital readmission have been described and validated. Identifying patients at high risk for readmission could allow for customized care-transition interventions, or could be used to risk-adjust readmission rates to compare publicly reported rates by hospital.
Study design: Systematic review with qualitative synthesis of results.
Setting: Thirty studies (23 from the U.S.) tested 26 unique readmission models.
Synopsis: Each model had been tested in both a derivation and validation cohort. Fourteen models (nine from the U.S.), using retrospective administrative data to compare risk-adjusted rates between hospitals, had poor discriminative capacity (c statistic range: 0.55 to 0.65). Seven models could be used to identify high-risk patients early in the hospitalization (c statistic range: 0.56 to 0.72) and five could be used to identify high-risk patients at discharge (c statistic range: 0.68 to 0.83), but these also had poor to moderate discriminative capacity. Multiple variables were considered in each of the models; most incorporated medical comorbidities and prior use of healthcare services.
Bottom line: Current readmission risk prediction models do not perform adequately for comparative or clinical purposes.
Citation: Kansagara D, Englander H, Salanitro A, et. al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688-1698.
Intravenous Fluids for Acute Pancreatitis: More May Be Less
Clinical question: What is the optimal volume of fluid administration for treatment of acute pancreatitis?
Background: Current guidelines for management of acute pancreatitis emphasize vigorous administration of intravenous fluids to reduce the risk of pancreatic necrosis and organ failure. This recommendation is based upon animal studies, and has not been subjected to clinical evaluation in humans.
Study design: Prospective observational cohort.
Setting: University-affiliated tertiary-care public hospital in Spain.
Synopsis: This study enrolled 247 patients admitted with acute pancreatitis to determine the association between the volume of fluid administered during the first 24 hours and the development of persistent organ failure, pancreatic fluid collection or necrosis, and mortality. The volume and rate of fluid administered were determined by the treating physician. Patients were classified into three groups: those receiving a volume <3.1 L, 3.1 to 4.1 L, or >4.1 L.
After multivariate adjustment, those receiving <3.1 L had no increased risk of necrosis or any other adverse outcome, compared with those who received the middle range of fluid volume.
Patients receiving >4.1 L had a higher risk of persistent organ failure (OR: 7.7, 95% CI: 1.5 to 38.7), particularly renal and respiratory insufficiency, and fluid collection development (OR: 1.9, 95% CI: 1 to 3.7) independent of disease severity. Pancreatic necrosis and mortality were similar in the three groups.
Bottom line: Administration of large-volume intravenous fluids (>4.1 L) in
the first 24 hours was associated with worse outcomes, although residual confounding cannot be excluded in this nonrandomized study.
Citation: de-Madaria E, Soler-Sala G, Sanchez-Paya J, et al. Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study. Am J Gastroenterol. 2011;106:1843-1850.
Clinical Outcomes in Saddle Pulmonary Embolism
Clinical question: What are the treatments used and outcomes associated with saddle pulmonary embolism?
Background: Saddle pulmonary embolism is a risk for right ventricular dysfunction and sudden hemodynamic collapse. There are limited data on the clinical presentation and outcomes in these patients.
Study design: Retrospective case review.
Setting: Single academic medical center.
Synopsis: In this retrospective review of 680 patients diagnosed with pulmonary embolism on CT at a single academic medical center from 2004 to 2009, 5.4% (37 patients) had a saddle pulmonary embolism.
Most patients with saddle pulmonary embolism were hemodynamically stable and responded to standard therapy with unfractionated heparin. The mean length of stay was nine days, 46% received an inferior vena cava filter, 41% were treated in an ICU, and 5.4% (two patients) died in the hospital. Thrombolytics were used in only 11% of patients, most of which had sustained hypotension and/or were mechanically ventilated.
Bottom line: Most patients with saddle pulmonary embolus in this single institution study did not receive thrombolytics and had overall low mortality.
Citation: Sardi A, Gluskin J, Guttentag A, Kotler MN, Braitman LE, Lippmann M. Saddle pulmonary embolism: is it as bad as it looks? A community hospital experience. Crit Care Med. 2011;39:2413-2418.
In This Edition
Literature At A Glance
A guide to this month’s studies
- IDSA/ATS guidelines for community-acquired pneumonia
- Improved asthma with IL-13 antibody
- Rivaroxaban vs. warfarin for stroke prevention in atrial fibrillation
- Apixaban vs. warfarin for stroke prevention in atrial fibrillation
- Ultrasonography more sensitive than chest radiograph for pneumothorax
- Current readmission risk models inadequate
- Optimal fluid volume for acute pancreatitis
- Low mortality in saddle pulmonary embolism
Triage Decisions for Patients with Severe Community-Acquired Pneumonia Should Be Based on IDSA/ATS Guidelines, Not Inflammatory Biomarkers
Clinical question: Can C-reactive protein levels (CRP), procalcitonin, TNF-alpha, and cytokine levels predict the need for intensive-care admission more accurately than IDSA/ATS guidelines in patients with severe community-acquired pneumonia (CAP)?
Background: Inflammatory biomarkers, such as CRP and procalcitonin, have diagnostic and prognostic utility in patients with CAP. Whether these inflammatory biomarkers can help triage patients to the appropriate level of care is unknown.
Study design: Prospective case control study.
Setting: Two university hospitals in Spain.
Synopsis: The study included 685 patients with severe CAP who did not require mechanical ventilation or vasopressor support. Serum levels of CRP, procalcitonin, TNF-alpha, IL-1, IL-6, IL-8, and IL-10, as well as Infectious Diseases Society of American/American Thoracic Society (IDSA/ATS) minor severity criteria data, were collected on admission. After controlling for age, comorbidities, and PSI risk class, serum levels of CRP and procalcitonin were found to be significantly higher in ICU patients compared with non-ICU patients. Despite this, these inflammatory biomarkers did not augment the IDSA/ATS guidelines, suggesting that patients who have three or more minor criteria be considered for ICU admission.
The study did suggest that patients with severe CAP and low levels of IL-6 and procalcitonin could potentially be managed safely outside of the ICU. However, hospitalists should be wary of applying the study results due to the small number of ICU patients in this study and the lack of real-time availability of these biomarkers at most institutions.
Bottom line: More studies of inflammatory biomarkers are needed before using them to determine the level of care required for patients with CAP. Until these data are available, physicians should use the IDSA/ATS guidelines to triage patients to the appropriate level of care.
Citation: Ramirez P, Ferrer M, Torres A, et al. Inflammatory biomarkers and prediction for intensive care unit admission pneumonia. Crit Care Med. 2011;39:2211-2217.
IL-13 Antibody Lebrikizumab Shows Promise as a New Therapy for Adults with Uncontrolled Asthma
Clinical question: Can lebrikizumab, an IL-13 antibody, improve asthma control in patients with uncontrolled asthma?
Background: Asthma is a complex disease, with varied patient response to treatment. Some patients have uncontrolled asthma despite inhaled glucocorticoids. It is postulated that IL-13 may account for this variability and that some patients with uncontrolled asthma are poorly controlled due to glucocorticoid resistance mediated by IL-13. Lebrikizumab is an IgG4 monoclonal antibody that binds to and inhibits the function of IL-13. This study was performed to see if this antibody would be effective in patients with uncontrolled asthma despite inhaled glucocorticoid therapy.
Study design: Randomized double-blinded placebo-controlled trial.
Setting: Multiple centers.
Synopsis: The study randomized 219 adult asthma patients who were inadequately controlled despite inhaled corticosteroids to a placebo or lebrikizumab. The primary outcome was improvement in prebronchodilator FEV1 from baseline. Secondary outcomes were exacerbations, use of rescue medications, and symptom scores. Patients were also stratified and analyzed based on surrogate markers for IL-13, which included serum IGE levels, eosinophil counts, and periostin levels.
In patients who were randomized to the lebrikizumab treatment, there was a statistically significant improvement in FEV1 of 5.5%, which occurred almost immediately and was sustained for the entire 32 weeks of the study. The improvement was more significant in patients who had high surrogate markers for IL-13. Despite this improvement in FEV1, there were no differences in secondary outcomes except in patients who had surrogate markers for high IL-13 levels.
Bottom line: In adults with asthma who remained uncontrolled despite inhaled corticosteroid therapy, IL-13 antagonism with lebrikizumab improved FEV1. However, the clinical relevance of these modest improvements remains unclear.
Citation: Corren J, Lemanske R, Matthews J, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365:1088-1098.
Rivaroxaban Is Noninferior to Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does rivaroxaban compare with warfarin in the prevention of stroke or systemic embolism in patients with nonvalvular atrial fibrillation?
Background: Warfarin is effective for the prevention of stroke in atrial fibrillation, but it requires close monitoring and adjustment. Rivaroxaban, an oral Xa inhibitor, may be safer, easier, and more effective than warfarin.
Study design: Multicenter, randomized, double-blind, double-dummy trial.
Setting: 1,178 sites in 45 countries.
Synopsis: The study included 14,264 patients with nonvalvular atrial fibrillation who were randomized to either fixed-dose rivaroxaban (20 mg daily or 15 mg daily for CrCl 30-49 mL/min) plus placebo or adjusted-dose warfarin (target INR 2.0 to 3.0) plus placebo. The mean CHADS2 score was 3.5. The primary endpoint (stroke or systemic embolism) occurred in 1.7% of patients per year in the rivaroxaban group and 2.2% per year in the warfarin group (hazard ratio for rivaroxaban 0.79; 95% CI: 0.66 to 0.96, P<0.001 for noninferiority). There was no difference in major or nonmajor clinically significant bleeding between the two groups (14.9% rivaroxaban vs. 14.5% warfarin, hazard ratio=1.03, 95% CI: 0.96 to 1.11, P=0.44). There were fewer intracranial hemorrhages (0.5% vs. 0.7%, P=0.02) and fatal bleeding (0.2% vs. 0.5%, P=0.003) in the rivaroxaban group.
Bottom line: In patients with atrial fibrillation, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolization, with a similar risk of major bleeding and a lower risk of intracranial hemorrhage or fatal bleeding.
Citation: Patel MR, Mahaffey K, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-891.
Apixaban More Effective and Safer than Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does the effectiveness and safety of apixaban compare with warfarin for stroke prevention in atrial fibrillation?
Background: Until recently, warfarin has been the only available oral anticoagulant for stroke prevention in patients with atrial fibrillation (AF). The oral factor Xa inhibitors have shown similar efficacy and safety, without the monitoring requirement and drug interactions associated with warfarin.
Study design: Prospective randomized double-blind controlled trial.
Setting: More than 1,000 clinical sites in 39 countries.
Synopsis: This study randomized 18,201 patients with atrial fibrillation or flutter and at least one CHADS2 risk factor for stroke to receive oral apixaban or warfarin therapy. Exclusion criteria were prosthetic valves and severe kidney disease. The median duration of follow-up was 1.8 years, and the major endpoints were incidence of stroke, systemic embolism, bleeding complications, and mortality.
Compared with warfarin, apixaban reduced the annual incidence of stroke and systemic embolism from 1.6% to 1.3% (HR 0.79, 95%: CI 0.66 to 0.95, P=0.01 for superiority), and reduced mortality (HR: 0.89, 95% CI: 0.80 to 0.998). For the combined endpoint of stroke, systemic embolism, MI, or death, the annual rate was reduced from 5.5% to 4.9% (HR: 0.88, 95% CI: 0.80 to 0.97). All measures of bleeding were less frequent with apixaban: major 2.1% vs. 3.1% (HR: 0.69, 95% CI: 0.60 to 0.80), and combined major and minor bleeding 4.1% vs. 6.0% (HR: 0.68, 95% CI: 0.61 to 0.75). The annual rate for the net outcome of stroke, embolism, or major bleeding was 3.2% with apixaban and 4.1% with warfarin (HR: 0.77, 95% CI: 0.69 to 0.86).
Bottom line: Compared with warfarin therapy, apixaban is more effective and safer for stroke prevention in patients with atrial fibrillation.
Citation: Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-992.
Ultrasonography Is Useful in Diagnosis of Pneumothorax
Clinical question: Is transthoracic ultrasonography a useful tool to diagnose pneumothorax?
Background: CT is the diagnostic gold standard for pneumothorax, but it is associated with radiation exposure and requires patient transport. Chest radiograph is easy to perform but may be too insensitive for adequate diagnosis. Ultrasonography’s diagnostic performance for detecting pneumothorax needs further evaluation.
Study design: Systematic review and meta-analysis.
Setting: Critically ill, trauma, or post-biopsy patients were identified in each of the studies.
Synopsis: The meta-analysis of 20 eligible studies found a pooled sensitivity of ultrasound for the detection of pneumothorax of 0.88 (95% CI: 0.85 to 0.91) and specificity of 0.99 (0.98 to 0.99) compared with sensitivity of 0.52 (0.49 to 0.55) and specificity of 1.00 (1.00 to 1.00) for chest radiograph. Although the overall ROC curve was not significantly different between these modalities, the accuracy of ultrasonography was highly dependent on the skill of the operator.
Bottom line: When performed by a skilled operator, transthoracic ultrasonography is as specific, and more sensitive, than chest radiograph in diagnosing pneumothorax.
Citation: Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneumothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011;140:859-866.
Risk Prediction for Hospital Readmission Remains Challenging
Clinical question: Can readmission risk assessment be used to identify which patients would benefit most from care-transition interventions, or to risk-adjust readmission rates for hospital comparison?
Background: Multiple models to predict hospital readmission have been described and validated. Identifying patients at high risk for readmission could allow for customized care-transition interventions, or could be used to risk-adjust readmission rates to compare publicly reported rates by hospital.
Study design: Systematic review with qualitative synthesis of results.
Setting: Thirty studies (23 from the U.S.) tested 26 unique readmission models.
Synopsis: Each model had been tested in both a derivation and validation cohort. Fourteen models (nine from the U.S.), using retrospective administrative data to compare risk-adjusted rates between hospitals, had poor discriminative capacity (c statistic range: 0.55 to 0.65). Seven models could be used to identify high-risk patients early in the hospitalization (c statistic range: 0.56 to 0.72) and five could be used to identify high-risk patients at discharge (c statistic range: 0.68 to 0.83), but these also had poor to moderate discriminative capacity. Multiple variables were considered in each of the models; most incorporated medical comorbidities and prior use of healthcare services.
Bottom line: Current readmission risk prediction models do not perform adequately for comparative or clinical purposes.
Citation: Kansagara D, Englander H, Salanitro A, et. al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688-1698.
Intravenous Fluids for Acute Pancreatitis: More May Be Less
Clinical question: What is the optimal volume of fluid administration for treatment of acute pancreatitis?
Background: Current guidelines for management of acute pancreatitis emphasize vigorous administration of intravenous fluids to reduce the risk of pancreatic necrosis and organ failure. This recommendation is based upon animal studies, and has not been subjected to clinical evaluation in humans.
Study design: Prospective observational cohort.
Setting: University-affiliated tertiary-care public hospital in Spain.
Synopsis: This study enrolled 247 patients admitted with acute pancreatitis to determine the association between the volume of fluid administered during the first 24 hours and the development of persistent organ failure, pancreatic fluid collection or necrosis, and mortality. The volume and rate of fluid administered were determined by the treating physician. Patients were classified into three groups: those receiving a volume <3.1 L, 3.1 to 4.1 L, or >4.1 L.
After multivariate adjustment, those receiving <3.1 L had no increased risk of necrosis or any other adverse outcome, compared with those who received the middle range of fluid volume.
Patients receiving >4.1 L had a higher risk of persistent organ failure (OR: 7.7, 95% CI: 1.5 to 38.7), particularly renal and respiratory insufficiency, and fluid collection development (OR: 1.9, 95% CI: 1 to 3.7) independent of disease severity. Pancreatic necrosis and mortality were similar in the three groups.
Bottom line: Administration of large-volume intravenous fluids (>4.1 L) in
the first 24 hours was associated with worse outcomes, although residual confounding cannot be excluded in this nonrandomized study.
Citation: de-Madaria E, Soler-Sala G, Sanchez-Paya J, et al. Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study. Am J Gastroenterol. 2011;106:1843-1850.
Clinical Outcomes in Saddle Pulmonary Embolism
Clinical question: What are the treatments used and outcomes associated with saddle pulmonary embolism?
Background: Saddle pulmonary embolism is a risk for right ventricular dysfunction and sudden hemodynamic collapse. There are limited data on the clinical presentation and outcomes in these patients.
Study design: Retrospective case review.
Setting: Single academic medical center.
Synopsis: In this retrospective review of 680 patients diagnosed with pulmonary embolism on CT at a single academic medical center from 2004 to 2009, 5.4% (37 patients) had a saddle pulmonary embolism.
Most patients with saddle pulmonary embolism were hemodynamically stable and responded to standard therapy with unfractionated heparin. The mean length of stay was nine days, 46% received an inferior vena cava filter, 41% were treated in an ICU, and 5.4% (two patients) died in the hospital. Thrombolytics were used in only 11% of patients, most of which had sustained hypotension and/or were mechanically ventilated.
Bottom line: Most patients with saddle pulmonary embolus in this single institution study did not receive thrombolytics and had overall low mortality.
Citation: Sardi A, Gluskin J, Guttentag A, Kotler MN, Braitman LE, Lippmann M. Saddle pulmonary embolism: is it as bad as it looks? A community hospital experience. Crit Care Med. 2011;39:2413-2418.
In This Edition
Literature At A Glance
A guide to this month’s studies
- IDSA/ATS guidelines for community-acquired pneumonia
- Improved asthma with IL-13 antibody
- Rivaroxaban vs. warfarin for stroke prevention in atrial fibrillation
- Apixaban vs. warfarin for stroke prevention in atrial fibrillation
- Ultrasonography more sensitive than chest radiograph for pneumothorax
- Current readmission risk models inadequate
- Optimal fluid volume for acute pancreatitis
- Low mortality in saddle pulmonary embolism
Triage Decisions for Patients with Severe Community-Acquired Pneumonia Should Be Based on IDSA/ATS Guidelines, Not Inflammatory Biomarkers
Clinical question: Can C-reactive protein levels (CRP), procalcitonin, TNF-alpha, and cytokine levels predict the need for intensive-care admission more accurately than IDSA/ATS guidelines in patients with severe community-acquired pneumonia (CAP)?
Background: Inflammatory biomarkers, such as CRP and procalcitonin, have diagnostic and prognostic utility in patients with CAP. Whether these inflammatory biomarkers can help triage patients to the appropriate level of care is unknown.
Study design: Prospective case control study.
Setting: Two university hospitals in Spain.
Synopsis: The study included 685 patients with severe CAP who did not require mechanical ventilation or vasopressor support. Serum levels of CRP, procalcitonin, TNF-alpha, IL-1, IL-6, IL-8, and IL-10, as well as Infectious Diseases Society of American/American Thoracic Society (IDSA/ATS) minor severity criteria data, were collected on admission. After controlling for age, comorbidities, and PSI risk class, serum levels of CRP and procalcitonin were found to be significantly higher in ICU patients compared with non-ICU patients. Despite this, these inflammatory biomarkers did not augment the IDSA/ATS guidelines, suggesting that patients who have three or more minor criteria be considered for ICU admission.
The study did suggest that patients with severe CAP and low levels of IL-6 and procalcitonin could potentially be managed safely outside of the ICU. However, hospitalists should be wary of applying the study results due to the small number of ICU patients in this study and the lack of real-time availability of these biomarkers at most institutions.
Bottom line: More studies of inflammatory biomarkers are needed before using them to determine the level of care required for patients with CAP. Until these data are available, physicians should use the IDSA/ATS guidelines to triage patients to the appropriate level of care.
Citation: Ramirez P, Ferrer M, Torres A, et al. Inflammatory biomarkers and prediction for intensive care unit admission pneumonia. Crit Care Med. 2011;39:2211-2217.
IL-13 Antibody Lebrikizumab Shows Promise as a New Therapy for Adults with Uncontrolled Asthma
Clinical question: Can lebrikizumab, an IL-13 antibody, improve asthma control in patients with uncontrolled asthma?
Background: Asthma is a complex disease, with varied patient response to treatment. Some patients have uncontrolled asthma despite inhaled glucocorticoids. It is postulated that IL-13 may account for this variability and that some patients with uncontrolled asthma are poorly controlled due to glucocorticoid resistance mediated by IL-13. Lebrikizumab is an IgG4 monoclonal antibody that binds to and inhibits the function of IL-13. This study was performed to see if this antibody would be effective in patients with uncontrolled asthma despite inhaled glucocorticoid therapy.
Study design: Randomized double-blinded placebo-controlled trial.
Setting: Multiple centers.
Synopsis: The study randomized 219 adult asthma patients who were inadequately controlled despite inhaled corticosteroids to a placebo or lebrikizumab. The primary outcome was improvement in prebronchodilator FEV1 from baseline. Secondary outcomes were exacerbations, use of rescue medications, and symptom scores. Patients were also stratified and analyzed based on surrogate markers for IL-13, which included serum IGE levels, eosinophil counts, and periostin levels.
In patients who were randomized to the lebrikizumab treatment, there was a statistically significant improvement in FEV1 of 5.5%, which occurred almost immediately and was sustained for the entire 32 weeks of the study. The improvement was more significant in patients who had high surrogate markers for IL-13. Despite this improvement in FEV1, there were no differences in secondary outcomes except in patients who had surrogate markers for high IL-13 levels.
Bottom line: In adults with asthma who remained uncontrolled despite inhaled corticosteroid therapy, IL-13 antagonism with lebrikizumab improved FEV1. However, the clinical relevance of these modest improvements remains unclear.
Citation: Corren J, Lemanske R, Matthews J, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365:1088-1098.
Rivaroxaban Is Noninferior to Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does rivaroxaban compare with warfarin in the prevention of stroke or systemic embolism in patients with nonvalvular atrial fibrillation?
Background: Warfarin is effective for the prevention of stroke in atrial fibrillation, but it requires close monitoring and adjustment. Rivaroxaban, an oral Xa inhibitor, may be safer, easier, and more effective than warfarin.
Study design: Multicenter, randomized, double-blind, double-dummy trial.
Setting: 1,178 sites in 45 countries.
Synopsis: The study included 14,264 patients with nonvalvular atrial fibrillation who were randomized to either fixed-dose rivaroxaban (20 mg daily or 15 mg daily for CrCl 30-49 mL/min) plus placebo or adjusted-dose warfarin (target INR 2.0 to 3.0) plus placebo. The mean CHADS2 score was 3.5. The primary endpoint (stroke or systemic embolism) occurred in 1.7% of patients per year in the rivaroxaban group and 2.2% per year in the warfarin group (hazard ratio for rivaroxaban 0.79; 95% CI: 0.66 to 0.96, P<0.001 for noninferiority). There was no difference in major or nonmajor clinically significant bleeding between the two groups (14.9% rivaroxaban vs. 14.5% warfarin, hazard ratio=1.03, 95% CI: 0.96 to 1.11, P=0.44). There were fewer intracranial hemorrhages (0.5% vs. 0.7%, P=0.02) and fatal bleeding (0.2% vs. 0.5%, P=0.003) in the rivaroxaban group.
Bottom line: In patients with atrial fibrillation, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolization, with a similar risk of major bleeding and a lower risk of intracranial hemorrhage or fatal bleeding.
Citation: Patel MR, Mahaffey K, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-891.
Apixaban More Effective and Safer than Warfarin for Stroke Prevention in Atrial Fibrillation
Clinical question: How does the effectiveness and safety of apixaban compare with warfarin for stroke prevention in atrial fibrillation?
Background: Until recently, warfarin has been the only available oral anticoagulant for stroke prevention in patients with atrial fibrillation (AF). The oral factor Xa inhibitors have shown similar efficacy and safety, without the monitoring requirement and drug interactions associated with warfarin.
Study design: Prospective randomized double-blind controlled trial.
Setting: More than 1,000 clinical sites in 39 countries.
Synopsis: This study randomized 18,201 patients with atrial fibrillation or flutter and at least one CHADS2 risk factor for stroke to receive oral apixaban or warfarin therapy. Exclusion criteria were prosthetic valves and severe kidney disease. The median duration of follow-up was 1.8 years, and the major endpoints were incidence of stroke, systemic embolism, bleeding complications, and mortality.
Compared with warfarin, apixaban reduced the annual incidence of stroke and systemic embolism from 1.6% to 1.3% (HR 0.79, 95%: CI 0.66 to 0.95, P=0.01 for superiority), and reduced mortality (HR: 0.89, 95% CI: 0.80 to 0.998). For the combined endpoint of stroke, systemic embolism, MI, or death, the annual rate was reduced from 5.5% to 4.9% (HR: 0.88, 95% CI: 0.80 to 0.97). All measures of bleeding were less frequent with apixaban: major 2.1% vs. 3.1% (HR: 0.69, 95% CI: 0.60 to 0.80), and combined major and minor bleeding 4.1% vs. 6.0% (HR: 0.68, 95% CI: 0.61 to 0.75). The annual rate for the net outcome of stroke, embolism, or major bleeding was 3.2% with apixaban and 4.1% with warfarin (HR: 0.77, 95% CI: 0.69 to 0.86).
Bottom line: Compared with warfarin therapy, apixaban is more effective and safer for stroke prevention in patients with atrial fibrillation.
Citation: Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-992.
Ultrasonography Is Useful in Diagnosis of Pneumothorax
Clinical question: Is transthoracic ultrasonography a useful tool to diagnose pneumothorax?
Background: CT is the diagnostic gold standard for pneumothorax, but it is associated with radiation exposure and requires patient transport. Chest radiograph is easy to perform but may be too insensitive for adequate diagnosis. Ultrasonography’s diagnostic performance for detecting pneumothorax needs further evaluation.
Study design: Systematic review and meta-analysis.
Setting: Critically ill, trauma, or post-biopsy patients were identified in each of the studies.
Synopsis: The meta-analysis of 20 eligible studies found a pooled sensitivity of ultrasound for the detection of pneumothorax of 0.88 (95% CI: 0.85 to 0.91) and specificity of 0.99 (0.98 to 0.99) compared with sensitivity of 0.52 (0.49 to 0.55) and specificity of 1.00 (1.00 to 1.00) for chest radiograph. Although the overall ROC curve was not significantly different between these modalities, the accuracy of ultrasonography was highly dependent on the skill of the operator.
Bottom line: When performed by a skilled operator, transthoracic ultrasonography is as specific, and more sensitive, than chest radiograph in diagnosing pneumothorax.
Citation: Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneumothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011;140:859-866.
Risk Prediction for Hospital Readmission Remains Challenging
Clinical question: Can readmission risk assessment be used to identify which patients would benefit most from care-transition interventions, or to risk-adjust readmission rates for hospital comparison?
Background: Multiple models to predict hospital readmission have been described and validated. Identifying patients at high risk for readmission could allow for customized care-transition interventions, or could be used to risk-adjust readmission rates to compare publicly reported rates by hospital.
Study design: Systematic review with qualitative synthesis of results.
Setting: Thirty studies (23 from the U.S.) tested 26 unique readmission models.
Synopsis: Each model had been tested in both a derivation and validation cohort. Fourteen models (nine from the U.S.), using retrospective administrative data to compare risk-adjusted rates between hospitals, had poor discriminative capacity (c statistic range: 0.55 to 0.65). Seven models could be used to identify high-risk patients early in the hospitalization (c statistic range: 0.56 to 0.72) and five could be used to identify high-risk patients at discharge (c statistic range: 0.68 to 0.83), but these also had poor to moderate discriminative capacity. Multiple variables were considered in each of the models; most incorporated medical comorbidities and prior use of healthcare services.
Bottom line: Current readmission risk prediction models do not perform adequately for comparative or clinical purposes.
Citation: Kansagara D, Englander H, Salanitro A, et. al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688-1698.
Intravenous Fluids for Acute Pancreatitis: More May Be Less
Clinical question: What is the optimal volume of fluid administration for treatment of acute pancreatitis?
Background: Current guidelines for management of acute pancreatitis emphasize vigorous administration of intravenous fluids to reduce the risk of pancreatic necrosis and organ failure. This recommendation is based upon animal studies, and has not been subjected to clinical evaluation in humans.
Study design: Prospective observational cohort.
Setting: University-affiliated tertiary-care public hospital in Spain.
Synopsis: This study enrolled 247 patients admitted with acute pancreatitis to determine the association between the volume of fluid administered during the first 24 hours and the development of persistent organ failure, pancreatic fluid collection or necrosis, and mortality. The volume and rate of fluid administered were determined by the treating physician. Patients were classified into three groups: those receiving a volume <3.1 L, 3.1 to 4.1 L, or >4.1 L.
After multivariate adjustment, those receiving <3.1 L had no increased risk of necrosis or any other adverse outcome, compared with those who received the middle range of fluid volume.
Patients receiving >4.1 L had a higher risk of persistent organ failure (OR: 7.7, 95% CI: 1.5 to 38.7), particularly renal and respiratory insufficiency, and fluid collection development (OR: 1.9, 95% CI: 1 to 3.7) independent of disease severity. Pancreatic necrosis and mortality were similar in the three groups.
Bottom line: Administration of large-volume intravenous fluids (>4.1 L) in
the first 24 hours was associated with worse outcomes, although residual confounding cannot be excluded in this nonrandomized study.
Citation: de-Madaria E, Soler-Sala G, Sanchez-Paya J, et al. Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study. Am J Gastroenterol. 2011;106:1843-1850.
Clinical Outcomes in Saddle Pulmonary Embolism
Clinical question: What are the treatments used and outcomes associated with saddle pulmonary embolism?
Background: Saddle pulmonary embolism is a risk for right ventricular dysfunction and sudden hemodynamic collapse. There are limited data on the clinical presentation and outcomes in these patients.
Study design: Retrospective case review.
Setting: Single academic medical center.
Synopsis: In this retrospective review of 680 patients diagnosed with pulmonary embolism on CT at a single academic medical center from 2004 to 2009, 5.4% (37 patients) had a saddle pulmonary embolism.
Most patients with saddle pulmonary embolism were hemodynamically stable and responded to standard therapy with unfractionated heparin. The mean length of stay was nine days, 46% received an inferior vena cava filter, 41% were treated in an ICU, and 5.4% (two patients) died in the hospital. Thrombolytics were used in only 11% of patients, most of which had sustained hypotension and/or were mechanically ventilated.
Bottom line: Most patients with saddle pulmonary embolus in this single institution study did not receive thrombolytics and had overall low mortality.
Citation: Sardi A, Gluskin J, Guttentag A, Kotler MN, Braitman LE, Lippmann M. Saddle pulmonary embolism: is it as bad as it looks? A community hospital experience. Crit Care Med. 2011;39:2413-2418.
Early Fluids Might Decrease Renal Morbidity in Hemolytic Uremic Syndrome

Clinical question: Does intravenous volume expansion during diarrheal illness mitigate the nephrotoxic effects of hemolytic uremic syndrome (HUS)?
Background: HUS often results in significant morbidity, particularly when oligoanuria is also present. Shiga-toxin-producing bacteria, notoriously Escherichia coli O157:H7 in the context of a diarrheal illness, are the most common cause, and worldwide outbreaks have been increasingly described. One prior report suggests that early IV fluid administration results in improved outcomes.
Study design: Prospective cohort study.
Setting: Eleven pediatric hospitals in the U.S. and Scotland.
Synopsis: Fifty children with diarrhea-associated HUS were enrolled and received clinical care at the discretion of the local provider, independent of the study. A family questionnaire (to define initial illness) and chart review were subsequently performed. Oligoanuria, defined as a urine output of less than 0.5 mL/kg/hr for at least one calendar day after HUS onset, was present in 34 (68%) patients. Oligoanuric and nonoligoanuric patients were similar at baseline; however, there was a significant association between less fluid administration in the first four days of illness and oligoanuria. Specifically, lack of IV fluids portended a 1.6 times higher likelihood of oligoanuria (95% confidence interval, 1.1-2.4; P=0.02).
The authors also suggest a dose-response relationship to their findings, which potentially strengthens their findings. However, the practical applicability of these findings appears limited. Many of the patients who did not receive IV fluids early on were also not admitted to a hospital, likely signifying mild illness without notable dehydration. Replicability of the benefits of early volume expansion in HUS will depend on the ability to accurately identify patients with Shiga-toxin-producing diarrheal illnesses at presentation. If this is feasible, it would be interesting to examine the details of oral hydration as well, particularly in those who are not dehydrated enough to require hospitalization.
Bottom line: Early IV fluids might be nephroprotective in diarrhea-associated HUS.
Citation: Hickey CA, Beattie J, Cowieson J, et al. Early volume expansion during diarrhea and relative nephroprotection during subsequent hemolytic uremic syndrome. Arch Pediatr Adolesc Med. 2011;165:884-889.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: Does intravenous volume expansion during diarrheal illness mitigate the nephrotoxic effects of hemolytic uremic syndrome (HUS)?
Background: HUS often results in significant morbidity, particularly when oligoanuria is also present. Shiga-toxin-producing bacteria, notoriously Escherichia coli O157:H7 in the context of a diarrheal illness, are the most common cause, and worldwide outbreaks have been increasingly described. One prior report suggests that early IV fluid administration results in improved outcomes.
Study design: Prospective cohort study.
Setting: Eleven pediatric hospitals in the U.S. and Scotland.
Synopsis: Fifty children with diarrhea-associated HUS were enrolled and received clinical care at the discretion of the local provider, independent of the study. A family questionnaire (to define initial illness) and chart review were subsequently performed. Oligoanuria, defined as a urine output of less than 0.5 mL/kg/hr for at least one calendar day after HUS onset, was present in 34 (68%) patients. Oligoanuric and nonoligoanuric patients were similar at baseline; however, there was a significant association between less fluid administration in the first four days of illness and oligoanuria. Specifically, lack of IV fluids portended a 1.6 times higher likelihood of oligoanuria (95% confidence interval, 1.1-2.4; P=0.02).
The authors also suggest a dose-response relationship to their findings, which potentially strengthens their findings. However, the practical applicability of these findings appears limited. Many of the patients who did not receive IV fluids early on were also not admitted to a hospital, likely signifying mild illness without notable dehydration. Replicability of the benefits of early volume expansion in HUS will depend on the ability to accurately identify patients with Shiga-toxin-producing diarrheal illnesses at presentation. If this is feasible, it would be interesting to examine the details of oral hydration as well, particularly in those who are not dehydrated enough to require hospitalization.
Bottom line: Early IV fluids might be nephroprotective in diarrhea-associated HUS.
Citation: Hickey CA, Beattie J, Cowieson J, et al. Early volume expansion during diarrhea and relative nephroprotection during subsequent hemolytic uremic syndrome. Arch Pediatr Adolesc Med. 2011;165:884-889.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: Does intravenous volume expansion during diarrheal illness mitigate the nephrotoxic effects of hemolytic uremic syndrome (HUS)?
Background: HUS often results in significant morbidity, particularly when oligoanuria is also present. Shiga-toxin-producing bacteria, notoriously Escherichia coli O157:H7 in the context of a diarrheal illness, are the most common cause, and worldwide outbreaks have been increasingly described. One prior report suggests that early IV fluid administration results in improved outcomes.
Study design: Prospective cohort study.
Setting: Eleven pediatric hospitals in the U.S. and Scotland.
Synopsis: Fifty children with diarrhea-associated HUS were enrolled and received clinical care at the discretion of the local provider, independent of the study. A family questionnaire (to define initial illness) and chart review were subsequently performed. Oligoanuria, defined as a urine output of less than 0.5 mL/kg/hr for at least one calendar day after HUS onset, was present in 34 (68%) patients. Oligoanuric and nonoligoanuric patients were similar at baseline; however, there was a significant association between less fluid administration in the first four days of illness and oligoanuria. Specifically, lack of IV fluids portended a 1.6 times higher likelihood of oligoanuria (95% confidence interval, 1.1-2.4; P=0.02).
The authors also suggest a dose-response relationship to their findings, which potentially strengthens their findings. However, the practical applicability of these findings appears limited. Many of the patients who did not receive IV fluids early on were also not admitted to a hospital, likely signifying mild illness without notable dehydration. Replicability of the benefits of early volume expansion in HUS will depend on the ability to accurately identify patients with Shiga-toxin-producing diarrheal illnesses at presentation. If this is feasible, it would be interesting to examine the details of oral hydration as well, particularly in those who are not dehydrated enough to require hospitalization.
Bottom line: Early IV fluids might be nephroprotective in diarrhea-associated HUS.
Citation: Hickey CA, Beattie J, Cowieson J, et al. Early volume expansion during diarrhea and relative nephroprotection during subsequent hemolytic uremic syndrome. Arch Pediatr Adolesc Med. 2011;165:884-889.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
What Are Common Causes of Glomerular Disease in Adults?

The Case
A 52-year-old man presents with abdominal pain. His temperature is 100.8°F, his blood pressure is 170/90 mm/Hg, and his pulse is 110 beats per minute. On exam, he has 2+ lower extremity edema, periorbital edema, and left-sided flank tenderness. His BUN is 42 mg/dL, his creatinine is 2.5 mg/dL, and his albumin is 1.4 g/dL. Urinalysis shows 2+ protein, large blood, and red blood cells (RBCs). What are the next steps in his diagnosis?
Overview
Glomerular diseases involve a wide spectrum of disease processes. They can result from an acute illness, such as an upper respiratory infection that self-resolves, or from chronic disease states, such as HIV. In some instances, such illnesses as systemic lupus erythematosus (SLE) can cause rapidly progressive renal failure, requiring prompt intervention. While glomerular diseases can be daunting, it is essential for hospitalists to be familiar with fundamental concepts and key features unique to each syndrome.
The approach to glomerulonephritis (GN) can be simplified by summarizing various types into the two broad categories of nephrotic and nephritic syndromes, and identifying the key clinical findings (see Table 1, p. below).
The major subtypes of nephrotic syndrome are minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), and membranoproliferative glomerulonephritis (MPGN). The clinical manifestations of nephrotic syndrome are edema, hyperlipidemia, lipiduria, and hypoalbuminemia.1 The urinalysis is significant for >3.5 g/day of proteinuria showing fatty casts or oval fat bodies.2 The loss of other proteins, such as anti-thrombin III, may put patients at higher risk for developing venous thromboses.1
The major subtypes of nephritic syndrome are post-streptococcal glomerulonephritis (PSGS), IgA nephropathy, Henoch-Schonlein Purpura (HSP), and rapidly progressive GN (RPGN types I, II, and III). The clinical manifestations of nephritic syndrome are hypertension (HTN) and hematuria.1 Nephritic syndromes may present with more rapidly progressive renal failure when compared with nephrotic syndrome.1 The urinalysis is significant for hematuria with RBC casts, and variable levels of proteinuria (typically, less than 3.5 g/day is seen in nephritic syndrome).1
Review of the Data
Nephrotic Syndromes
Minimal change disease. MCD is more common in children than adults, and only accounts for 10% to 15% of glomerular disease cases in adults.3 It is associated with Hodgkin’s lymphoma, NSAID use, and allergic conditions. There usually is an absence of hypertension (HTN). There are no glomerular basement membrane abnormalities seen on light microscopy. Electron microscopy shows effacement of podocytes. On urinalysis, oval fat bodies are seen, which are characteristic of heavy proteinuria. Complement levels are normal. Steroids are first-line treatment, but in adults with relapses or steroid resistance, immunosuppressive agents have also been used.2
Focal segment glomerlosclerosis.
FSGS is the most common primary glomerular disorder in the United States and is the most common cause of nephrotic syndrome among blacks.4,5 It is associated with HIV (collapsing variant), parvovirus B19, heroin use, sickle-cell disease, obesity, chronic vesicoureteral reflux, and HTN.4,6 Sclerosis of segmental glomeruli is seen on light microscopy.
Electron microscopy shows effacement of podocytes. Complement levels are normal. Treatment of primary idiopathic FSGS includes use of renin-angiotensin inhibitors and steroids.4 Immunosuppressives are reserved for relapses. Treatment of secondary FSGS involves identifying the underlying cause.
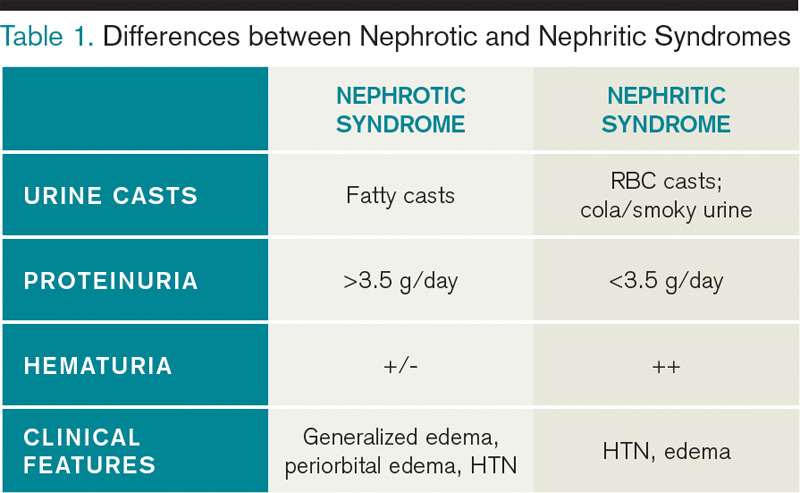
Membranous nephropathy. MN is twice as common in males as in females and is the most common cause of adult-onset idiopathic nephrotic syndrome, with the average presentation in the fifth or sixth decade of life.7,8 Aside from its idiopathic form, up to 25% of MN cases have an underlying disease process, such as solid organ tumors or hepatitis B.7,9 While nephrotic syndrome overall can increase the risk of thromboembolic complications, MN is the most common nephrotic disorder predisposing the development of renal vein thrombosis.7 Diffuse capillary wall thickening is seen on light microscopy, and electron microscopy shows sub-epithelial immune deposits. Complement levels are normal. Steroids and immunosuppressive agents are used for treatment.10
Membranoproliferative glomerulonephritis. MPGN is a nephrotic syndrome that is more common in children and young adults and can present with features of nephritic syndrome.1,11 It is associated with hepatitis C, SLE, and cryoglobulinemia.11 Light microscopy shows mesangial and endocapillary proliferation, as well as glomerular basement membrane thickening and splitting (“tram track” appearance). Electron microscopy shows subendothelial and dense deposits. It presents with reduced complement levels (C3 and C4).11 Treatment depends on the associated disease.
Nephritic Syndromes
Post-streptococcal glomerulonephritis. PSGN is seen in children and young adults and is associated with skin (impetigo) and throat infections (pharyngitis).12 Hematuria usually presents two to three weeks after a streptococcal infection. The urine is classically dark and smoky-colored. Levels of C3 and CH50 are low, but C4 levels are normal.1 In addition, there are positive antibody titers for ASO and anti-DNase. Light microscopy shows hypercellularity of glomeruli. Electron microscopy shows dome-shaped sub-endothelial deposits. Treatment is usually supportive.
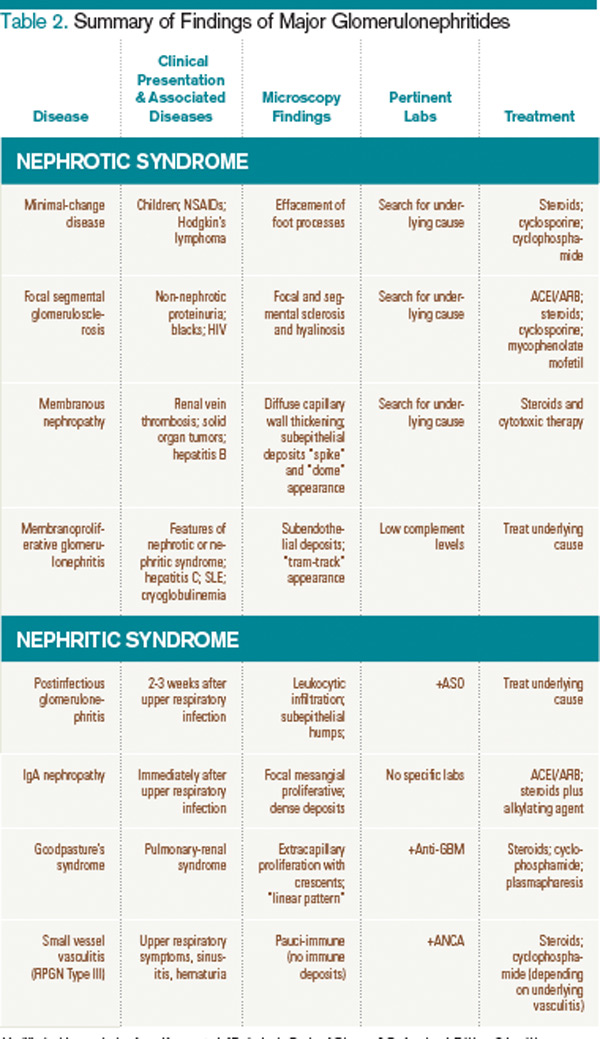
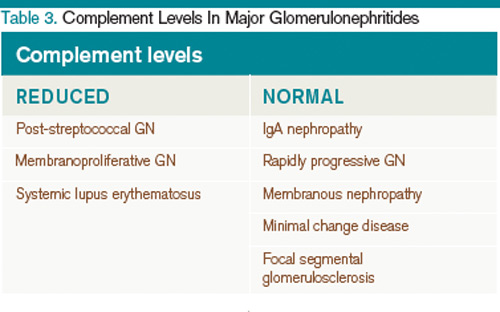
IgA nephropathy. IgA nephropathy is the most common form of glomerular disease worldwide and the most common form of glomerular-related microscopic hematuria in all age groups.2,13 It occurs in all ages but more frequently in males.14 It occurs during or immediately after an upper respiratory infection. Light microscopy shows mesangial cell proliferation and crescentic GN. Electron microscopy shows immune deposits in the mesangium. Complement levels are normal. There has been no proven therapy, but ACE inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), fish oil, steroids, and tonsillectomy have been used with some success.14 The clinical course of IgA nephropathy can be highly variable, with the potential for a benign course to rapidly progressive renal failure, with 15% to 40% of patients developing end-stage renal disease.14
Henoch-Schonlein purpura. HSP affects children more than adults and is the systemic form of IgA nephropathy.14 Most cases are idiopathic. Clinical
manifestations include: HTN; purpuric palpable rash on buttocks, ankles, and legs; bloody diarrhea with abdominal cramps; and pain in wrist, ankle, and knee joints.15 Light microscopy shows mesangial cell proliferation. Immune deposits in the mesangium are seen on electron microscopy. Complement levels are normal. Treatment is supportive.
Rapidly progressive glomerulonephritis types I, II, and III. RPGN represents a wide variety of disease states in which rapid progression to renal failure is seen within days to weeks.16 They are categorized into three sub-categories: I, II, and III.
Type I is an anti-GBM disease, an example being Goodpasture’s syndrome. This condition presents with hemoptysis, pulmonary infiltrates, and hematuria with RBC casts. Anti-GBM antibodies are classically found.1 Complement levels are normal and a linear immunofluorescence pattern is seen. Treatment is steroids, immunosuppressive agents, and plasmapheresis.17
Type II is an immune complex deposition disease, such as HSP, SLE, or post-streptococcal GN, in which granular complex deposits are seen. Treatment is directed toward treating the underlying cause.
Type III is pauci-immune (no immune deposits), showing necrotizing crescentic GN on biopsy, and is associated with a positive ANCA.1,18 They are associated with systemic small-vessel vasculitis, such as granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), microscopic polyangiitis, and Churg-Strauss syndrome, or can be limited to renal involvement.1,18 Complement levels are normal. Treatment is steroids and immunosuppressive agents, such as cyclophosphamide.
A summary of the findings found in the glomerulonephritides and how complement levels are affected are found in Table 2 and Table 3, respectively.
Secondary Causes of Nephrotic Diseases
Diabetic nephropathy. Diabetic nephropathy is the single most common cause of progressive renal failure in the United States.3 Up to 50% of patients with diabetes present with diabetic nephropathy.19 Current recommendations are to screen yearly for microalbuminuria at the time of diagnosis.3 Treatment involves use of ACE-Is or ARBs to reduce proteinuria and slow the progression of renal disease.
HIV-associated nephropathy. HIV-associated nephropathy commonly presents as the collapsing variant of FSGS. However, it can present as other forms of glomerulopathy, such as MPGN or IgA nephropathy, as well as an immune complex GN with “lupus-like” features without evidence of SLE.19,20 Therefore, HIV nephropathy has now been categorized as a separate entity.3 ACE-Is, HAART therapy, and corticosteroids are the mainstays of treatment.
Amyloidosis. Renal involvement is seen in both primary (AL) and secondary (AA) amyloidosis. Eighty percent of patients with AL have renal disease, and 25% of these patients have nephrotic syndrome.16 Diagnosis is made with Congo Red stain, which shows fibrillary amyloid deposits within the mesangium and capillary walls. Treatment is directed at the underlying process.
Systemic lupus erythematosus. SLE is divided into six classes (I-VI) based on the involvement and severity of renal disease, and steroids and immunosuppressive agents are used for treatment, also based on the severity of the disease.21
Back to the Case
Our patient presented to the hospital with abdominal pain, low-grade fever, HTN, edema, hypoalbuminemia, and new-onset renal failure with gross hematuria and proteinuria. The presence of proteinuria and hypoalbuminemia, combined with peripheral and periorbital edema, suggests glomerular loss of albumin, such as in nephrotic syndrome. His renal failure in the setting of the sudden development of gross hematuria with flank pain is concerning for a renal vein thrombosis, and an abdominal magnetic resonance venography did in fact visualize a renal vein thrombosis.
He was admitted to the hospital and was started on therapeutic intravenous heparin, and bridged to warfarin. Subsequent renal biopsy confirmed the findings of membranous nephropathy, which was suspected due to his renal vein thrombosis. Therapy was initiated with corticosteroids after the biopsy, and he responded well. Because of his risk factors for further thromboembolic events, lifelong anticoagulation therapy was recommended.
Bottom Line
For patients with glomerular disease, differentiating between nephrotic and nephritic syndromes and understanding key clinical and laboratory differences can lead to easier identification and treatment.
Drs. Khan and Smith are assistant professors of medicine, and Dr. Ansari is associate division director, in the Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
References
- Donegio RGB, Salant DJ. Nephrology: Glomerular Diseases. In: ACP Medicine. Dale D, Federman D, eds. Available at: http://www.acpmedicine.com/acpmedicine/institutional/instHtmlReader.action?readerFlag=chapt&chapId=part10_ch05. Accessed Feb. 15, 2012.
- Orth SR, Ritz E. The nephrotic syndrome. N Engl J Med. 1998;338:1202-1211.
- Lewis JB, Neilson EG. Chapter 283. Glomerular Diseases. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012.
- D’Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-23411.
- Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis. 2004;44:815-825.
- Balow JE. Nephropathy in the context of HIV infection. Kidney Int. 2005;67:1632-1633.
- Glassock RJ. Diagnosis and natural course of membranous nephropathy. Semin Nephrol. 2003;23:324-332.
- Nickolas TL, Radhakrishnan J, Appel GB. Hyperlipidemia and thrombotic complications in patients with membranous nephropathy. Semin Nephrol. 2003;23:406-411.
- Burstein DM, Korbet SM, Schwartz MM. Membranous glomerulonephritis and malignancy. Am J Kidney Dis. 1993;22:5-10.
- Hofstra JM, Wetzels JF. Management of patients with membranous nephropathy. Nephrol Dial Transplant. 2012;27:6-9.
- Alchi B, Jayne D. Membranoproliferative glomerulonephritis. Pediatr Nephrol. 2010;25:1409-1418.
- Eison TM, Ault BH, Jones DP, Chesney RW, Wyatt RJ. Post-streptococcal acute glomerulonephritis in children: clinical features and pathogenesis. Pediatr Nephrol. 2011;26:165-180.
- Cohen RA, Brown RS. Clinical practice. Microscopic hematuria. N Engl J Med. 2003;348:2330-2338.
- Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. 2002;347:738-748.
- McCarthy HJ, Tizard EJ. Clinical practice: Diagnosis and management of henoch-schonlein purpura. Eur J Pediatr. 2010169:643-650.
- Appel GB, Radhakrishnan J. Cecil Medicine: Volume 1: Chapter 123: Glomerular Disorders and Nephrotic Syndromes. MD Consult Preview website. Available at: http://www.mdconsult.com/books/page.do?eid=4-u1.0-B978-1-4377-1604-7..00123-8&isbn=978-1-4377-1604-7&uniqId=313771243-2#4-u1.0-B978-1-4377-1604-7..00123-8. Accessed Feb. 16, 2012.
- Walters G, Willis NS, Craig JC. Interventions for renal vasculitis in adults. Cochrane Database Syst Rev. 2008;(3)(3):CD003232.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164-1177.
- Falk, RJ: Medical Knowledge Self Assessment Program 14. Nephrology: 2006.
- Haas M, Kaul S, Eustace JA. HIV-associated immune complex glomerulonephritis with “lupus-like” features: a clinicopathologic study of 14 cases. Kidney Int. 2005;67:1381.
- Dooley MA, Hogan S, Jennette C, Falk R. Cyclophosphamide therapy for lupus nephritis: poor renal survival in black americans. glomerular disease collaborative network. Kidney Int. 1997;51:1188-1195.
The Case
A 52-year-old man presents with abdominal pain. His temperature is 100.8°F, his blood pressure is 170/90 mm/Hg, and his pulse is 110 beats per minute. On exam, he has 2+ lower extremity edema, periorbital edema, and left-sided flank tenderness. His BUN is 42 mg/dL, his creatinine is 2.5 mg/dL, and his albumin is 1.4 g/dL. Urinalysis shows 2+ protein, large blood, and red blood cells (RBCs). What are the next steps in his diagnosis?
Overview
Glomerular diseases involve a wide spectrum of disease processes. They can result from an acute illness, such as an upper respiratory infection that self-resolves, or from chronic disease states, such as HIV. In some instances, such illnesses as systemic lupus erythematosus (SLE) can cause rapidly progressive renal failure, requiring prompt intervention. While glomerular diseases can be daunting, it is essential for hospitalists to be familiar with fundamental concepts and key features unique to each syndrome.
The approach to glomerulonephritis (GN) can be simplified by summarizing various types into the two broad categories of nephrotic and nephritic syndromes, and identifying the key clinical findings (see Table 1, p. below).
The major subtypes of nephrotic syndrome are minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), and membranoproliferative glomerulonephritis (MPGN). The clinical manifestations of nephrotic syndrome are edema, hyperlipidemia, lipiduria, and hypoalbuminemia.1 The urinalysis is significant for >3.5 g/day of proteinuria showing fatty casts or oval fat bodies.2 The loss of other proteins, such as anti-thrombin III, may put patients at higher risk for developing venous thromboses.1
The major subtypes of nephritic syndrome are post-streptococcal glomerulonephritis (PSGS), IgA nephropathy, Henoch-Schonlein Purpura (HSP), and rapidly progressive GN (RPGN types I, II, and III). The clinical manifestations of nephritic syndrome are hypertension (HTN) and hematuria.1 Nephritic syndromes may present with more rapidly progressive renal failure when compared with nephrotic syndrome.1 The urinalysis is significant for hematuria with RBC casts, and variable levels of proteinuria (typically, less than 3.5 g/day is seen in nephritic syndrome).1
Review of the Data
Nephrotic Syndromes
Minimal change disease. MCD is more common in children than adults, and only accounts for 10% to 15% of glomerular disease cases in adults.3 It is associated with Hodgkin’s lymphoma, NSAID use, and allergic conditions. There usually is an absence of hypertension (HTN). There are no glomerular basement membrane abnormalities seen on light microscopy. Electron microscopy shows effacement of podocytes. On urinalysis, oval fat bodies are seen, which are characteristic of heavy proteinuria. Complement levels are normal. Steroids are first-line treatment, but in adults with relapses or steroid resistance, immunosuppressive agents have also been used.2
Focal segment glomerlosclerosis.
FSGS is the most common primary glomerular disorder in the United States and is the most common cause of nephrotic syndrome among blacks.4,5 It is associated with HIV (collapsing variant), parvovirus B19, heroin use, sickle-cell disease, obesity, chronic vesicoureteral reflux, and HTN.4,6 Sclerosis of segmental glomeruli is seen on light microscopy.
Electron microscopy shows effacement of podocytes. Complement levels are normal. Treatment of primary idiopathic FSGS includes use of renin-angiotensin inhibitors and steroids.4 Immunosuppressives are reserved for relapses. Treatment of secondary FSGS involves identifying the underlying cause.
Membranous nephropathy. MN is twice as common in males as in females and is the most common cause of adult-onset idiopathic nephrotic syndrome, with the average presentation in the fifth or sixth decade of life.7,8 Aside from its idiopathic form, up to 25% of MN cases have an underlying disease process, such as solid organ tumors or hepatitis B.7,9 While nephrotic syndrome overall can increase the risk of thromboembolic complications, MN is the most common nephrotic disorder predisposing the development of renal vein thrombosis.7 Diffuse capillary wall thickening is seen on light microscopy, and electron microscopy shows sub-epithelial immune deposits. Complement levels are normal. Steroids and immunosuppressive agents are used for treatment.10
Membranoproliferative glomerulonephritis. MPGN is a nephrotic syndrome that is more common in children and young adults and can present with features of nephritic syndrome.1,11 It is associated with hepatitis C, SLE, and cryoglobulinemia.11 Light microscopy shows mesangial and endocapillary proliferation, as well as glomerular basement membrane thickening and splitting (“tram track” appearance). Electron microscopy shows subendothelial and dense deposits. It presents with reduced complement levels (C3 and C4).11 Treatment depends on the associated disease.
Nephritic Syndromes
Post-streptococcal glomerulonephritis. PSGN is seen in children and young adults and is associated with skin (impetigo) and throat infections (pharyngitis).12 Hematuria usually presents two to three weeks after a streptococcal infection. The urine is classically dark and smoky-colored. Levels of C3 and CH50 are low, but C4 levels are normal.1 In addition, there are positive antibody titers for ASO and anti-DNase. Light microscopy shows hypercellularity of glomeruli. Electron microscopy shows dome-shaped sub-endothelial deposits. Treatment is usually supportive.
IgA nephropathy. IgA nephropathy is the most common form of glomerular disease worldwide and the most common form of glomerular-related microscopic hematuria in all age groups.2,13 It occurs in all ages but more frequently in males.14 It occurs during or immediately after an upper respiratory infection. Light microscopy shows mesangial cell proliferation and crescentic GN. Electron microscopy shows immune deposits in the mesangium. Complement levels are normal. There has been no proven therapy, but ACE inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), fish oil, steroids, and tonsillectomy have been used with some success.14 The clinical course of IgA nephropathy can be highly variable, with the potential for a benign course to rapidly progressive renal failure, with 15% to 40% of patients developing end-stage renal disease.14
Henoch-Schonlein purpura. HSP affects children more than adults and is the systemic form of IgA nephropathy.14 Most cases are idiopathic. Clinical
manifestations include: HTN; purpuric palpable rash on buttocks, ankles, and legs; bloody diarrhea with abdominal cramps; and pain in wrist, ankle, and knee joints.15 Light microscopy shows mesangial cell proliferation. Immune deposits in the mesangium are seen on electron microscopy. Complement levels are normal. Treatment is supportive.
Rapidly progressive glomerulonephritis types I, II, and III. RPGN represents a wide variety of disease states in which rapid progression to renal failure is seen within days to weeks.16 They are categorized into three sub-categories: I, II, and III.
Type I is an anti-GBM disease, an example being Goodpasture’s syndrome. This condition presents with hemoptysis, pulmonary infiltrates, and hematuria with RBC casts. Anti-GBM antibodies are classically found.1 Complement levels are normal and a linear immunofluorescence pattern is seen. Treatment is steroids, immunosuppressive agents, and plasmapheresis.17
Type II is an immune complex deposition disease, such as HSP, SLE, or post-streptococcal GN, in which granular complex deposits are seen. Treatment is directed toward treating the underlying cause.
Type III is pauci-immune (no immune deposits), showing necrotizing crescentic GN on biopsy, and is associated with a positive ANCA.1,18 They are associated with systemic small-vessel vasculitis, such as granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), microscopic polyangiitis, and Churg-Strauss syndrome, or can be limited to renal involvement.1,18 Complement levels are normal. Treatment is steroids and immunosuppressive agents, such as cyclophosphamide.
A summary of the findings found in the glomerulonephritides and how complement levels are affected are found in Table 2 and Table 3, respectively.
Secondary Causes of Nephrotic Diseases
Diabetic nephropathy. Diabetic nephropathy is the single most common cause of progressive renal failure in the United States.3 Up to 50% of patients with diabetes present with diabetic nephropathy.19 Current recommendations are to screen yearly for microalbuminuria at the time of diagnosis.3 Treatment involves use of ACE-Is or ARBs to reduce proteinuria and slow the progression of renal disease.
HIV-associated nephropathy. HIV-associated nephropathy commonly presents as the collapsing variant of FSGS. However, it can present as other forms of glomerulopathy, such as MPGN or IgA nephropathy, as well as an immune complex GN with “lupus-like” features without evidence of SLE.19,20 Therefore, HIV nephropathy has now been categorized as a separate entity.3 ACE-Is, HAART therapy, and corticosteroids are the mainstays of treatment.
Amyloidosis. Renal involvement is seen in both primary (AL) and secondary (AA) amyloidosis. Eighty percent of patients with AL have renal disease, and 25% of these patients have nephrotic syndrome.16 Diagnosis is made with Congo Red stain, which shows fibrillary amyloid deposits within the mesangium and capillary walls. Treatment is directed at the underlying process.
Systemic lupus erythematosus. SLE is divided into six classes (I-VI) based on the involvement and severity of renal disease, and steroids and immunosuppressive agents are used for treatment, also based on the severity of the disease.21
Back to the Case
Our patient presented to the hospital with abdominal pain, low-grade fever, HTN, edema, hypoalbuminemia, and new-onset renal failure with gross hematuria and proteinuria. The presence of proteinuria and hypoalbuminemia, combined with peripheral and periorbital edema, suggests glomerular loss of albumin, such as in nephrotic syndrome. His renal failure in the setting of the sudden development of gross hematuria with flank pain is concerning for a renal vein thrombosis, and an abdominal magnetic resonance venography did in fact visualize a renal vein thrombosis.
He was admitted to the hospital and was started on therapeutic intravenous heparin, and bridged to warfarin. Subsequent renal biopsy confirmed the findings of membranous nephropathy, which was suspected due to his renal vein thrombosis. Therapy was initiated with corticosteroids after the biopsy, and he responded well. Because of his risk factors for further thromboembolic events, lifelong anticoagulation therapy was recommended.
Bottom Line
For patients with glomerular disease, differentiating between nephrotic and nephritic syndromes and understanding key clinical and laboratory differences can lead to easier identification and treatment.
Drs. Khan and Smith are assistant professors of medicine, and Dr. Ansari is associate division director, in the Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
References
- Donegio RGB, Salant DJ. Nephrology: Glomerular Diseases. In: ACP Medicine. Dale D, Federman D, eds. Available at: http://www.acpmedicine.com/acpmedicine/institutional/instHtmlReader.action?readerFlag=chapt&chapId=part10_ch05. Accessed Feb. 15, 2012.
- Orth SR, Ritz E. The nephrotic syndrome. N Engl J Med. 1998;338:1202-1211.
- Lewis JB, Neilson EG. Chapter 283. Glomerular Diseases. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012.
- D’Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-23411.
- Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis. 2004;44:815-825.
- Balow JE. Nephropathy in the context of HIV infection. Kidney Int. 2005;67:1632-1633.
- Glassock RJ. Diagnosis and natural course of membranous nephropathy. Semin Nephrol. 2003;23:324-332.
- Nickolas TL, Radhakrishnan J, Appel GB. Hyperlipidemia and thrombotic complications in patients with membranous nephropathy. Semin Nephrol. 2003;23:406-411.
- Burstein DM, Korbet SM, Schwartz MM. Membranous glomerulonephritis and malignancy. Am J Kidney Dis. 1993;22:5-10.
- Hofstra JM, Wetzels JF. Management of patients with membranous nephropathy. Nephrol Dial Transplant. 2012;27:6-9.
- Alchi B, Jayne D. Membranoproliferative glomerulonephritis. Pediatr Nephrol. 2010;25:1409-1418.
- Eison TM, Ault BH, Jones DP, Chesney RW, Wyatt RJ. Post-streptococcal acute glomerulonephritis in children: clinical features and pathogenesis. Pediatr Nephrol. 2011;26:165-180.
- Cohen RA, Brown RS. Clinical practice. Microscopic hematuria. N Engl J Med. 2003;348:2330-2338.
- Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. 2002;347:738-748.
- McCarthy HJ, Tizard EJ. Clinical practice: Diagnosis and management of henoch-schonlein purpura. Eur J Pediatr. 2010169:643-650.
- Appel GB, Radhakrishnan J. Cecil Medicine: Volume 1: Chapter 123: Glomerular Disorders and Nephrotic Syndromes. MD Consult Preview website. Available at: http://www.mdconsult.com/books/page.do?eid=4-u1.0-B978-1-4377-1604-7..00123-8&isbn=978-1-4377-1604-7&uniqId=313771243-2#4-u1.0-B978-1-4377-1604-7..00123-8. Accessed Feb. 16, 2012.
- Walters G, Willis NS, Craig JC. Interventions for renal vasculitis in adults. Cochrane Database Syst Rev. 2008;(3)(3):CD003232.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164-1177.
- Falk, RJ: Medical Knowledge Self Assessment Program 14. Nephrology: 2006.
- Haas M, Kaul S, Eustace JA. HIV-associated immune complex glomerulonephritis with “lupus-like” features: a clinicopathologic study of 14 cases. Kidney Int. 2005;67:1381.
- Dooley MA, Hogan S, Jennette C, Falk R. Cyclophosphamide therapy for lupus nephritis: poor renal survival in black americans. glomerular disease collaborative network. Kidney Int. 1997;51:1188-1195.
The Case
A 52-year-old man presents with abdominal pain. His temperature is 100.8°F, his blood pressure is 170/90 mm/Hg, and his pulse is 110 beats per minute. On exam, he has 2+ lower extremity edema, periorbital edema, and left-sided flank tenderness. His BUN is 42 mg/dL, his creatinine is 2.5 mg/dL, and his albumin is 1.4 g/dL. Urinalysis shows 2+ protein, large blood, and red blood cells (RBCs). What are the next steps in his diagnosis?
Overview
Glomerular diseases involve a wide spectrum of disease processes. They can result from an acute illness, such as an upper respiratory infection that self-resolves, or from chronic disease states, such as HIV. In some instances, such illnesses as systemic lupus erythematosus (SLE) can cause rapidly progressive renal failure, requiring prompt intervention. While glomerular diseases can be daunting, it is essential for hospitalists to be familiar with fundamental concepts and key features unique to each syndrome.
The approach to glomerulonephritis (GN) can be simplified by summarizing various types into the two broad categories of nephrotic and nephritic syndromes, and identifying the key clinical findings (see Table 1, p. below).
The major subtypes of nephrotic syndrome are minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), and membranoproliferative glomerulonephritis (MPGN). The clinical manifestations of nephrotic syndrome are edema, hyperlipidemia, lipiduria, and hypoalbuminemia.1 The urinalysis is significant for >3.5 g/day of proteinuria showing fatty casts or oval fat bodies.2 The loss of other proteins, such as anti-thrombin III, may put patients at higher risk for developing venous thromboses.1
The major subtypes of nephritic syndrome are post-streptococcal glomerulonephritis (PSGS), IgA nephropathy, Henoch-Schonlein Purpura (HSP), and rapidly progressive GN (RPGN types I, II, and III). The clinical manifestations of nephritic syndrome are hypertension (HTN) and hematuria.1 Nephritic syndromes may present with more rapidly progressive renal failure when compared with nephrotic syndrome.1 The urinalysis is significant for hematuria with RBC casts, and variable levels of proteinuria (typically, less than 3.5 g/day is seen in nephritic syndrome).1
Review of the Data
Nephrotic Syndromes
Minimal change disease. MCD is more common in children than adults, and only accounts for 10% to 15% of glomerular disease cases in adults.3 It is associated with Hodgkin’s lymphoma, NSAID use, and allergic conditions. There usually is an absence of hypertension (HTN). There are no glomerular basement membrane abnormalities seen on light microscopy. Electron microscopy shows effacement of podocytes. On urinalysis, oval fat bodies are seen, which are characteristic of heavy proteinuria. Complement levels are normal. Steroids are first-line treatment, but in adults with relapses or steroid resistance, immunosuppressive agents have also been used.2
Focal segment glomerlosclerosis.
FSGS is the most common primary glomerular disorder in the United States and is the most common cause of nephrotic syndrome among blacks.4,5 It is associated with HIV (collapsing variant), parvovirus B19, heroin use, sickle-cell disease, obesity, chronic vesicoureteral reflux, and HTN.4,6 Sclerosis of segmental glomeruli is seen on light microscopy.
Electron microscopy shows effacement of podocytes. Complement levels are normal. Treatment of primary idiopathic FSGS includes use of renin-angiotensin inhibitors and steroids.4 Immunosuppressives are reserved for relapses. Treatment of secondary FSGS involves identifying the underlying cause.
Membranous nephropathy. MN is twice as common in males as in females and is the most common cause of adult-onset idiopathic nephrotic syndrome, with the average presentation in the fifth or sixth decade of life.7,8 Aside from its idiopathic form, up to 25% of MN cases have an underlying disease process, such as solid organ tumors or hepatitis B.7,9 While nephrotic syndrome overall can increase the risk of thromboembolic complications, MN is the most common nephrotic disorder predisposing the development of renal vein thrombosis.7 Diffuse capillary wall thickening is seen on light microscopy, and electron microscopy shows sub-epithelial immune deposits. Complement levels are normal. Steroids and immunosuppressive agents are used for treatment.10
Membranoproliferative glomerulonephritis. MPGN is a nephrotic syndrome that is more common in children and young adults and can present with features of nephritic syndrome.1,11 It is associated with hepatitis C, SLE, and cryoglobulinemia.11 Light microscopy shows mesangial and endocapillary proliferation, as well as glomerular basement membrane thickening and splitting (“tram track” appearance). Electron microscopy shows subendothelial and dense deposits. It presents with reduced complement levels (C3 and C4).11 Treatment depends on the associated disease.
Nephritic Syndromes
Post-streptococcal glomerulonephritis. PSGN is seen in children and young adults and is associated with skin (impetigo) and throat infections (pharyngitis).12 Hematuria usually presents two to three weeks after a streptococcal infection. The urine is classically dark and smoky-colored. Levels of C3 and CH50 are low, but C4 levels are normal.1 In addition, there are positive antibody titers for ASO and anti-DNase. Light microscopy shows hypercellularity of glomeruli. Electron microscopy shows dome-shaped sub-endothelial deposits. Treatment is usually supportive.
IgA nephropathy. IgA nephropathy is the most common form of glomerular disease worldwide and the most common form of glomerular-related microscopic hematuria in all age groups.2,13 It occurs in all ages but more frequently in males.14 It occurs during or immediately after an upper respiratory infection. Light microscopy shows mesangial cell proliferation and crescentic GN. Electron microscopy shows immune deposits in the mesangium. Complement levels are normal. There has been no proven therapy, but ACE inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), fish oil, steroids, and tonsillectomy have been used with some success.14 The clinical course of IgA nephropathy can be highly variable, with the potential for a benign course to rapidly progressive renal failure, with 15% to 40% of patients developing end-stage renal disease.14
Henoch-Schonlein purpura. HSP affects children more than adults and is the systemic form of IgA nephropathy.14 Most cases are idiopathic. Clinical
manifestations include: HTN; purpuric palpable rash on buttocks, ankles, and legs; bloody diarrhea with abdominal cramps; and pain in wrist, ankle, and knee joints.15 Light microscopy shows mesangial cell proliferation. Immune deposits in the mesangium are seen on electron microscopy. Complement levels are normal. Treatment is supportive.
Rapidly progressive glomerulonephritis types I, II, and III. RPGN represents a wide variety of disease states in which rapid progression to renal failure is seen within days to weeks.16 They are categorized into three sub-categories: I, II, and III.
Type I is an anti-GBM disease, an example being Goodpasture’s syndrome. This condition presents with hemoptysis, pulmonary infiltrates, and hematuria with RBC casts. Anti-GBM antibodies are classically found.1 Complement levels are normal and a linear immunofluorescence pattern is seen. Treatment is steroids, immunosuppressive agents, and plasmapheresis.17
Type II is an immune complex deposition disease, such as HSP, SLE, or post-streptococcal GN, in which granular complex deposits are seen. Treatment is directed toward treating the underlying cause.
Type III is pauci-immune (no immune deposits), showing necrotizing crescentic GN on biopsy, and is associated with a positive ANCA.1,18 They are associated with systemic small-vessel vasculitis, such as granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), microscopic polyangiitis, and Churg-Strauss syndrome, or can be limited to renal involvement.1,18 Complement levels are normal. Treatment is steroids and immunosuppressive agents, such as cyclophosphamide.
A summary of the findings found in the glomerulonephritides and how complement levels are affected are found in Table 2 and Table 3, respectively.
Secondary Causes of Nephrotic Diseases
Diabetic nephropathy. Diabetic nephropathy is the single most common cause of progressive renal failure in the United States.3 Up to 50% of patients with diabetes present with diabetic nephropathy.19 Current recommendations are to screen yearly for microalbuminuria at the time of diagnosis.3 Treatment involves use of ACE-Is or ARBs to reduce proteinuria and slow the progression of renal disease.
HIV-associated nephropathy. HIV-associated nephropathy commonly presents as the collapsing variant of FSGS. However, it can present as other forms of glomerulopathy, such as MPGN or IgA nephropathy, as well as an immune complex GN with “lupus-like” features without evidence of SLE.19,20 Therefore, HIV nephropathy has now been categorized as a separate entity.3 ACE-Is, HAART therapy, and corticosteroids are the mainstays of treatment.
Amyloidosis. Renal involvement is seen in both primary (AL) and secondary (AA) amyloidosis. Eighty percent of patients with AL have renal disease, and 25% of these patients have nephrotic syndrome.16 Diagnosis is made with Congo Red stain, which shows fibrillary amyloid deposits within the mesangium and capillary walls. Treatment is directed at the underlying process.
Systemic lupus erythematosus. SLE is divided into six classes (I-VI) based on the involvement and severity of renal disease, and steroids and immunosuppressive agents are used for treatment, also based on the severity of the disease.21
Back to the Case
Our patient presented to the hospital with abdominal pain, low-grade fever, HTN, edema, hypoalbuminemia, and new-onset renal failure with gross hematuria and proteinuria. The presence of proteinuria and hypoalbuminemia, combined with peripheral and periorbital edema, suggests glomerular loss of albumin, such as in nephrotic syndrome. His renal failure in the setting of the sudden development of gross hematuria with flank pain is concerning for a renal vein thrombosis, and an abdominal magnetic resonance venography did in fact visualize a renal vein thrombosis.
He was admitted to the hospital and was started on therapeutic intravenous heparin, and bridged to warfarin. Subsequent renal biopsy confirmed the findings of membranous nephropathy, which was suspected due to his renal vein thrombosis. Therapy was initiated with corticosteroids after the biopsy, and he responded well. Because of his risk factors for further thromboembolic events, lifelong anticoagulation therapy was recommended.
Bottom Line
For patients with glomerular disease, differentiating between nephrotic and nephritic syndromes and understanding key clinical and laboratory differences can lead to easier identification and treatment.
Drs. Khan and Smith are assistant professors of medicine, and Dr. Ansari is associate division director, in the Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
References
- Donegio RGB, Salant DJ. Nephrology: Glomerular Diseases. In: ACP Medicine. Dale D, Federman D, eds. Available at: http://www.acpmedicine.com/acpmedicine/institutional/instHtmlReader.action?readerFlag=chapt&chapId=part10_ch05. Accessed Feb. 15, 2012.
- Orth SR, Ritz E. The nephrotic syndrome. N Engl J Med. 1998;338:1202-1211.
- Lewis JB, Neilson EG. Chapter 283. Glomerular Diseases. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012.
- D’Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-23411.
- Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis. 2004;44:815-825.
- Balow JE. Nephropathy in the context of HIV infection. Kidney Int. 2005;67:1632-1633.
- Glassock RJ. Diagnosis and natural course of membranous nephropathy. Semin Nephrol. 2003;23:324-332.
- Nickolas TL, Radhakrishnan J, Appel GB. Hyperlipidemia and thrombotic complications in patients with membranous nephropathy. Semin Nephrol. 2003;23:406-411.
- Burstein DM, Korbet SM, Schwartz MM. Membranous glomerulonephritis and malignancy. Am J Kidney Dis. 1993;22:5-10.
- Hofstra JM, Wetzels JF. Management of patients with membranous nephropathy. Nephrol Dial Transplant. 2012;27:6-9.
- Alchi B, Jayne D. Membranoproliferative glomerulonephritis. Pediatr Nephrol. 2010;25:1409-1418.
- Eison TM, Ault BH, Jones DP, Chesney RW, Wyatt RJ. Post-streptococcal acute glomerulonephritis in children: clinical features and pathogenesis. Pediatr Nephrol. 2011;26:165-180.
- Cohen RA, Brown RS. Clinical practice. Microscopic hematuria. N Engl J Med. 2003;348:2330-2338.
- Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. 2002;347:738-748.
- McCarthy HJ, Tizard EJ. Clinical practice: Diagnosis and management of henoch-schonlein purpura. Eur J Pediatr. 2010169:643-650.
- Appel GB, Radhakrishnan J. Cecil Medicine: Volume 1: Chapter 123: Glomerular Disorders and Nephrotic Syndromes. MD Consult Preview website. Available at: http://www.mdconsult.com/books/page.do?eid=4-u1.0-B978-1-4377-1604-7..00123-8&isbn=978-1-4377-1604-7&uniqId=313771243-2#4-u1.0-B978-1-4377-1604-7..00123-8. Accessed Feb. 16, 2012.
- Walters G, Willis NS, Craig JC. Interventions for renal vasculitis in adults. Cochrane Database Syst Rev. 2008;(3)(3):CD003232.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164-1177.
- Falk, RJ: Medical Knowledge Self Assessment Program 14. Nephrology: 2006.
- Haas M, Kaul S, Eustace JA. HIV-associated immune complex glomerulonephritis with “lupus-like” features: a clinicopathologic study of 14 cases. Kidney Int. 2005;67:1381.
- Dooley MA, Hogan S, Jennette C, Falk R. Cyclophosphamide therapy for lupus nephritis: poor renal survival in black americans. glomerular disease collaborative network. Kidney Int. 1997;51:1188-1195.
Three Earn Master of Hospital Medicine Designation

—Joseph Ming-Wah Li, MD, SFHM, SHM president
If the SHM Award of Excellence winners are the MVPs of HM, then the specialty’s new Masters in Hospital Medicine are this year’s Hall of Famers.
SHM is proud to announce that Patrick J. Cawley, MD, MBA, MHM, Peter K. Lindenauer, MD, MSc, FACP, MHM, and Mark V. Williams, MD, FACP, MHM, have earned the Master in Hospital Medicine designation. They are the eighth, ninth, and 10th SHM members to receive the exclusive designation. In addition to being honored at HM12, they have earned the right to use the “MHM” credential.
“Hospitalists of all stripes owe our new Masters in Hospital Medicine a great debt for their commitment to the specialty, to their patients, and to healthcare,” says Joseph Ming Wah Li, MD, SFHM, SHM president. “Their innovation, leadership, and vision have helped grow the influence and credibility of the hospital medicine specialty.”

Dr. Cawley is a charter member and past president of SHM who has served on the Ethics and Public Policy committees. He is a frequent speaker at the society’s annual meetings. Dr. Cawley received his medical degree from Georgetown University School of Medicine and trained as a resident at Duke University Medical Center, where he also served as an assistant chief resident. He has been a contributing writer to The Hospitalist and several other journals and books.
Dr. Lindenauer is a board-certified internist and founding SHM board member. His research focuses on measuring the quality and outcomes of hospital care for patients with common medical conditions. He is supported by grants from the Agency for Healthcare Research and Quality and the NIH’s National Heart Lung and Blood Institute. His research has appeared in the New England Journal of Medicine, JAMA, Annals of Internal Medicine, Health Affairs, Medical Care, and other general internal medicine and subspecialty journals.
Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. He is the principal investigator for SHM’s Project BOOST and is a former SHM president and board member. He has served in numerous leadership roles since the society’s establishment in 1996. In 1998, Dr. Williams established the first hospitalist program at a public hospital, Grady Memorial Hospital in Atlanta.
Drs. Cawley, Lindenauer, and Williams represent the third year of the Masters program. This marks the first year that nominations could be submitted to the SHM Masters Selection committee.
Joining the new masters in earning a new designation are 120 new Fellows in Hospital Medicine (FHM) and 52 Senior Fellows in Hospital Medicine (SFHM). The new members push the fellows program totals to 947 FHMs, 243 SFHMs, and 10 MHMs.
Brendon Shank is SHM’s associate vice president of communications.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
If the SHM Award of Excellence winners are the MVPs of HM, then the specialty’s new Masters in Hospital Medicine are this year’s Hall of Famers.
SHM is proud to announce that Patrick J. Cawley, MD, MBA, MHM, Peter K. Lindenauer, MD, MSc, FACP, MHM, and Mark V. Williams, MD, FACP, MHM, have earned the Master in Hospital Medicine designation. They are the eighth, ninth, and 10th SHM members to receive the exclusive designation. In addition to being honored at HM12, they have earned the right to use the “MHM” credential.
“Hospitalists of all stripes owe our new Masters in Hospital Medicine a great debt for their commitment to the specialty, to their patients, and to healthcare,” says Joseph Ming Wah Li, MD, SFHM, SHM president. “Their innovation, leadership, and vision have helped grow the influence and credibility of the hospital medicine specialty.”
Dr. Cawley is a charter member and past president of SHM who has served on the Ethics and Public Policy committees. He is a frequent speaker at the society’s annual meetings. Dr. Cawley received his medical degree from Georgetown University School of Medicine and trained as a resident at Duke University Medical Center, where he also served as an assistant chief resident. He has been a contributing writer to The Hospitalist and several other journals and books.
Dr. Lindenauer is a board-certified internist and founding SHM board member. His research focuses on measuring the quality and outcomes of hospital care for patients with common medical conditions. He is supported by grants from the Agency for Healthcare Research and Quality and the NIH’s National Heart Lung and Blood Institute. His research has appeared in the New England Journal of Medicine, JAMA, Annals of Internal Medicine, Health Affairs, Medical Care, and other general internal medicine and subspecialty journals.
Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. He is the principal investigator for SHM’s Project BOOST and is a former SHM president and board member. He has served in numerous leadership roles since the society’s establishment in 1996. In 1998, Dr. Williams established the first hospitalist program at a public hospital, Grady Memorial Hospital in Atlanta.
Drs. Cawley, Lindenauer, and Williams represent the third year of the Masters program. This marks the first year that nominations could be submitted to the SHM Masters Selection committee.
Joining the new masters in earning a new designation are 120 new Fellows in Hospital Medicine (FHM) and 52 Senior Fellows in Hospital Medicine (SFHM). The new members push the fellows program totals to 947 FHMs, 243 SFHMs, and 10 MHMs.
Brendon Shank is SHM’s associate vice president of communications.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
If the SHM Award of Excellence winners are the MVPs of HM, then the specialty’s new Masters in Hospital Medicine are this year’s Hall of Famers.
SHM is proud to announce that Patrick J. Cawley, MD, MBA, MHM, Peter K. Lindenauer, MD, MSc, FACP, MHM, and Mark V. Williams, MD, FACP, MHM, have earned the Master in Hospital Medicine designation. They are the eighth, ninth, and 10th SHM members to receive the exclusive designation. In addition to being honored at HM12, they have earned the right to use the “MHM” credential.
“Hospitalists of all stripes owe our new Masters in Hospital Medicine a great debt for their commitment to the specialty, to their patients, and to healthcare,” says Joseph Ming Wah Li, MD, SFHM, SHM president. “Their innovation, leadership, and vision have helped grow the influence and credibility of the hospital medicine specialty.”
Dr. Cawley is a charter member and past president of SHM who has served on the Ethics and Public Policy committees. He is a frequent speaker at the society’s annual meetings. Dr. Cawley received his medical degree from Georgetown University School of Medicine and trained as a resident at Duke University Medical Center, where he also served as an assistant chief resident. He has been a contributing writer to The Hospitalist and several other journals and books.
Dr. Lindenauer is a board-certified internist and founding SHM board member. His research focuses on measuring the quality and outcomes of hospital care for patients with common medical conditions. He is supported by grants from the Agency for Healthcare Research and Quality and the NIH’s National Heart Lung and Blood Institute. His research has appeared in the New England Journal of Medicine, JAMA, Annals of Internal Medicine, Health Affairs, Medical Care, and other general internal medicine and subspecialty journals.
Dr. Williams is professor and chief of the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine in Chicago. He is the principal investigator for SHM’s Project BOOST and is a former SHM president and board member. He has served in numerous leadership roles since the society’s establishment in 1996. In 1998, Dr. Williams established the first hospitalist program at a public hospital, Grady Memorial Hospital in Atlanta.
Drs. Cawley, Lindenauer, and Williams represent the third year of the Masters program. This marks the first year that nominations could be submitted to the SHM Masters Selection committee.
Joining the new masters in earning a new designation are 120 new Fellows in Hospital Medicine (FHM) and 52 Senior Fellows in Hospital Medicine (SFHM). The new members push the fellows program totals to 947 FHMs, 243 SFHMs, and 10 MHMs.
Brendon Shank is SHM’s associate vice president of communications.
Society of Hospital Medicine's Award of Excellence Winners Lead the Way
—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalists across the country are taking the lead—leading their HM groups, leading care teams, and leading quality-improvement (QI) efforts.
With this year’s annual SHM Awards of Excellence, thousands of hospitalists at HM12 saluted the leaders in the specialty. Five individuals and one team were recognized at the San Diego Convention Center for their efforts to transform healthcare and revolutionize patient care.
In addition to being recognized at HM12, the honorees were the subjects of a video presented at HM12 and posted on SHM’s YouTube channel.
Brendon Shank is associate vice president of communications at SHM
The 2012 SHM Award of Excellence winners are:
Excellence in Teamwork and Quality Improvement
The In-Hospital Stroke QI Team at the University of Colorado Hospital, led by Ethan Cumbler, MD, FACP, associate professor of medicine and hospitalist at University of Colorado Hospital, was recognized for exemplary quality improvement initiatives in hospital medicine that engage the full patient care team.
Excellence in Hospital Medicine for Non-Physicians
Jina Saltzman, physician assistant, University of Chicago.
Outstanding Service in Hospital Medicine
William D. Atchley Jr., MD, FACP, SFHM, regional senior medical director, Eagle Hospital Physicians.
Excellence in Teaching
Jeff Barsuk, MD, MS, FHM, associate professor of medicine, Northwestern University Feinberg School of Medicine, Chicago.
Clinical Excellence
Douglas W. Carlson, MD, SFHM, professor of pediatrics and director of the Division of Pediatric Hospital Medicine at Washington University and St. Louis Children’s Hospital.
Excellence in Research
Ron Keren, MD, MPH, associate professor of pediatrics and epidemiology, The Children’s Hospital of Philadelphia, and the University of Pennsylvania School of Medicine.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalists across the country are taking the lead—leading their HM groups, leading care teams, and leading quality-improvement (QI) efforts.
With this year’s annual SHM Awards of Excellence, thousands of hospitalists at HM12 saluted the leaders in the specialty. Five individuals and one team were recognized at the San Diego Convention Center for their efforts to transform healthcare and revolutionize patient care.
In addition to being recognized at HM12, the honorees were the subjects of a video presented at HM12 and posted on SHM’s YouTube channel.
Brendon Shank is associate vice president of communications at SHM
The 2012 SHM Award of Excellence winners are:
Excellence in Teamwork and Quality Improvement
The In-Hospital Stroke QI Team at the University of Colorado Hospital, led by Ethan Cumbler, MD, FACP, associate professor of medicine and hospitalist at University of Colorado Hospital, was recognized for exemplary quality improvement initiatives in hospital medicine that engage the full patient care team.
Excellence in Hospital Medicine for Non-Physicians
Jina Saltzman, physician assistant, University of Chicago.
Outstanding Service in Hospital Medicine
William D. Atchley Jr., MD, FACP, SFHM, regional senior medical director, Eagle Hospital Physicians.
Excellence in Teaching
Jeff Barsuk, MD, MS, FHM, associate professor of medicine, Northwestern University Feinberg School of Medicine, Chicago.
Clinical Excellence
Douglas W. Carlson, MD, SFHM, professor of pediatrics and director of the Division of Pediatric Hospital Medicine at Washington University and St. Louis Children’s Hospital.
Excellence in Research
Ron Keren, MD, MPH, associate professor of pediatrics and epidemiology, The Children’s Hospital of Philadelphia, and the University of Pennsylvania School of Medicine.
—Joseph Ming-Wah Li, MD, SFHM, SHM president
Hospitalists across the country are taking the lead—leading their HM groups, leading care teams, and leading quality-improvement (QI) efforts.
With this year’s annual SHM Awards of Excellence, thousands of hospitalists at HM12 saluted the leaders in the specialty. Five individuals and one team were recognized at the San Diego Convention Center for their efforts to transform healthcare and revolutionize patient care.
In addition to being recognized at HM12, the honorees were the subjects of a video presented at HM12 and posted on SHM’s YouTube channel.
Brendon Shank is associate vice president of communications at SHM
The 2012 SHM Award of Excellence winners are:
Excellence in Teamwork and Quality Improvement
The In-Hospital Stroke QI Team at the University of Colorado Hospital, led by Ethan Cumbler, MD, FACP, associate professor of medicine and hospitalist at University of Colorado Hospital, was recognized for exemplary quality improvement initiatives in hospital medicine that engage the full patient care team.
Excellence in Hospital Medicine for Non-Physicians
Jina Saltzman, physician assistant, University of Chicago.
Outstanding Service in Hospital Medicine
William D. Atchley Jr., MD, FACP, SFHM, regional senior medical director, Eagle Hospital Physicians.
Excellence in Teaching
Jeff Barsuk, MD, MS, FHM, associate professor of medicine, Northwestern University Feinberg School of Medicine, Chicago.
Clinical Excellence
Douglas W. Carlson, MD, SFHM, professor of pediatrics and director of the Division of Pediatric Hospital Medicine at Washington University and St. Louis Children’s Hospital.
Excellence in Research
Ron Keren, MD, MPH, associate professor of pediatrics and epidemiology, The Children’s Hospital of Philadelphia, and the University of Pennsylvania School of Medicine.
Complex Medically Ill Patients: A Challenge for PCPs and Hospitalists
Every year, primary-care physicians (PCPs) and hospitalists struggle to manage care for complex medically ill patients, according to a new survey conducted by SHM and QuantiaMD.
Complex medically ill patients have two or more concurrent chronic conditions that require ongoing medical attention or limit activities of daily living. These 4 million patients, which make up 10% of the Medicare population, consume a disproportionate amount of acute healthcare resources, accounting for up to 20% of ED visits, and have significantly higher likelihood of hospital admission and readmission, according to the survey.1 This presents a challenge to both inpatient and outpatient providers charged with coordinating their care.
SHM, in partnership with QuantiaMD, conducted a survey of nearly 4,000 physicians about this topic, which has resulted in a white paper and online expert series to outline opportunities and feature innovative examples to improve patient care of the complex medically ill.
“Communication greatly impacts quality of care and the ability to prevent excess hospital admissions and readmissions,” says Michael Radzienda, MD, SFHM, principal investigator for the Medically Complex Ill Project. “Findings from the study identified barriers to timely and effective communication on the health team who care for the medically complex ill and opportunities to implement the latest innovations to improve patient care and safety.”
A new expert practice series in the reducing readmissions special-interest group from SHM and QuantiaMD, “Innovations in Care Coordination for the Complex Medically Ill,” grew from the study and provides best practices, and also features actual case studies of existing care-coordination efforts. This online interactive forum is the first of its kind, providing resources to address care-coordination challenges that have plagued patient care over the past decade. The series includes nine presentations on topics including patient-centered medical homes, telemedicine, and post-discharge clinics.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Every year, primary-care physicians (PCPs) and hospitalists struggle to manage care for complex medically ill patients, according to a new survey conducted by SHM and QuantiaMD.
Complex medically ill patients have two or more concurrent chronic conditions that require ongoing medical attention or limit activities of daily living. These 4 million patients, which make up 10% of the Medicare population, consume a disproportionate amount of acute healthcare resources, accounting for up to 20% of ED visits, and have significantly higher likelihood of hospital admission and readmission, according to the survey.1 This presents a challenge to both inpatient and outpatient providers charged with coordinating their care.
SHM, in partnership with QuantiaMD, conducted a survey of nearly 4,000 physicians about this topic, which has resulted in a white paper and online expert series to outline opportunities and feature innovative examples to improve patient care of the complex medically ill.
“Communication greatly impacts quality of care and the ability to prevent excess hospital admissions and readmissions,” says Michael Radzienda, MD, SFHM, principal investigator for the Medically Complex Ill Project. “Findings from the study identified barriers to timely and effective communication on the health team who care for the medically complex ill and opportunities to implement the latest innovations to improve patient care and safety.”
A new expert practice series in the reducing readmissions special-interest group from SHM and QuantiaMD, “Innovations in Care Coordination for the Complex Medically Ill,” grew from the study and provides best practices, and also features actual case studies of existing care-coordination efforts. This online interactive forum is the first of its kind, providing resources to address care-coordination challenges that have plagued patient care over the past decade. The series includes nine presentations on topics including patient-centered medical homes, telemedicine, and post-discharge clinics.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Every year, primary-care physicians (PCPs) and hospitalists struggle to manage care for complex medically ill patients, according to a new survey conducted by SHM and QuantiaMD.
Complex medically ill patients have two or more concurrent chronic conditions that require ongoing medical attention or limit activities of daily living. These 4 million patients, which make up 10% of the Medicare population, consume a disproportionate amount of acute healthcare resources, accounting for up to 20% of ED visits, and have significantly higher likelihood of hospital admission and readmission, according to the survey.1 This presents a challenge to both inpatient and outpatient providers charged with coordinating their care.
SHM, in partnership with QuantiaMD, conducted a survey of nearly 4,000 physicians about this topic, which has resulted in a white paper and online expert series to outline opportunities and feature innovative examples to improve patient care of the complex medically ill.
“Communication greatly impacts quality of care and the ability to prevent excess hospital admissions and readmissions,” says Michael Radzienda, MD, SFHM, principal investigator for the Medically Complex Ill Project. “Findings from the study identified barriers to timely and effective communication on the health team who care for the medically complex ill and opportunities to implement the latest innovations to improve patient care and safety.”
A new expert practice series in the reducing readmissions special-interest group from SHM and QuantiaMD, “Innovations in Care Coordination for the Complex Medically Ill,” grew from the study and provides best practices, and also features actual case studies of existing care-coordination efforts. This online interactive forum is the first of its kind, providing resources to address care-coordination challenges that have plagued patient care over the past decade. The series includes nine presentations on topics including patient-centered medical homes, telemedicine, and post-discharge clinics.
Reference
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.