User login
HM15 Offers Hospitalist Leaders Training, Encouragement
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.

“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.

Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.
“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.
Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.
“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.
Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
HM15 Speakers Urge Hospitalists to Use Technology, Teamwork, Talent

NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalist Nancy Zeitoun, MD, FHM, Seeks Better Health Outcomes
Nancy Zeitoun, MD, FHM, sees her expanding role as a leader at Long Island Jewish Medical Center in New Hyde Park, N.Y., as a chance to make a difference. As co-site director for clinical affairs in the division of hospital medicine and assistant professor at Hofstra North Shore-LIJ School of Medicine, she can introduce her “own ideas to our evolving and growing program.”
Now she’s brought that desire to share ideas to Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: I consider it among the most challenging professions, both intellectually [conceptually] and physically [tangible].
Q: How/when did you decide to become a hospitalist?
A: Ten years ago, I was entering the third year of my four-year residency with the motivation to pursue critical care medicine and with much less enthusiasm for primary care than I had anticipated. One of the junior faculty was my internal medicine teaching attending, and he described his new role as a hospitalist. He preferred inpatient care with a structured schedule, less call time, and no outpatient responsibilities that required running between the hospital and an office practice. He told me this was where the future of medicine was heading. It was the best of both worlds.
Q: Tell us about your mentor. What did she mean to you?
A: My mentor was my program director. I admired her for being a distinguished woman in medicine with an academic position. She was a natural leader with passion and vision that were electrifying. She motivated and inspired. She saw potential in her residents and gave opportunity for any willing participant to advance.

Q: You say a structured yet flexible day and multidisciplinary work appeal to you. What do you like most about being a hospitalist?
A: Hospitalists have a unique and global vantage point of a hospital’s intricate network, making them the most valuable players on the field. They see opportunity in instability and uncertainty. Hospitalists are resourceful and efficient, adhering to the business concepts of competition, sustainability, conservation, and stewardship. The challenges of the field are vast but include a balance of clinical and administrative roles, leading and implementing changes to daily practice and being the constant in a sea of subspecialists.
The flexibility of the day allows for multitasking and setting priorities, so that patient care is never compromised in an acute care setting. A clinician can spend as much time with a patient as needed without the constraints of set appointments.
Q: What do you dislike most about being a hospitalist?
A: Having to balance clinical work with administrative and committee work.
Q: What’s the best advice you ever received?
A: Be proactive and be a part of the solution, rather than wait for change to be imposed. “Change is the only constant in life.”—Heraclitus
Q: What’s the worst advice you ever received?
A: Be friends with your boss.
Q: You’ve said you’d like to see hospitalists have more impact on lobbying and legislation. Can you explain what you’d like to see, and what you would see as the benefit of that?
A: Legislative action is spearheaded by the leaders of large medical organizations speaking on behalf of all of their members. These leaders tend to be either non-clinicians or non-practicing physicians. However, differing viewpoints exist. Physicians don’t want to be politicians or lobbyists. They have a hard time agreeing on things and working as a cohesive entity. So they leave others to speak for them. Then they complain when laws are passed without their say.
Hospitalists work in and help lead such complex organizations. SHM is led by physicians in practice. Events like Hospitalists on the Hill [at SHM’s annual meeting] encourage us to be more involved in legislative advocacy.
Q: As an administrator, at least part time, why is it important for you to continue seeing patients?
A: Clinical skills directly affect ability to understand the “day to day” and target the areas that need change. It also allows you to be an effective leader when you continue to do the same work your colleagues do. You are legitimate in their eyes!
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging for you?
A: Establishing trust and confidence by first impressions.
Q: What aspect of patient care is most rewarding?
A: Patient/family appreciation.
Q: As an assistant professor, what aspect of teaching in the 21st century do you find most difficult? And, what is most enjoyable?
A: Less focus on protected/dedicated teaching time, because money drivers take precedence (i.e., length of stay, dispo, utilization, billing and documentation). The new label is “system-based practice.” This has led to decreased bedside teaching.
Most enjoyable is working with eager learners.
Q: You call your biggest professional challenge taking credit for your ideas. Why is that difficult? Do you think that’s an issue for a lot of hospitalists, particularly given the specialty focus on the multidisciplinary team?
A: Hospital medicine focuses on teamwork. Hospitalists have figured out how to step out of their silos and reach across the aisle to accomplish some daunting tasks. Clinical competence is obviously important, but the ability to work together, check egos at the door, and make individual sacrifices when necessary is the only way a team succeeds. The unintentional consequence is that they don’t take credit because it’s the collective effort that counts.
Richard Quinn is a freelance writer in New Jersey.
Nancy Zeitoun, MD, FHM, sees her expanding role as a leader at Long Island Jewish Medical Center in New Hyde Park, N.Y., as a chance to make a difference. As co-site director for clinical affairs in the division of hospital medicine and assistant professor at Hofstra North Shore-LIJ School of Medicine, she can introduce her “own ideas to our evolving and growing program.”
Now she’s brought that desire to share ideas to Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: I consider it among the most challenging professions, both intellectually [conceptually] and physically [tangible].
Q: How/when did you decide to become a hospitalist?
A: Ten years ago, I was entering the third year of my four-year residency with the motivation to pursue critical care medicine and with much less enthusiasm for primary care than I had anticipated. One of the junior faculty was my internal medicine teaching attending, and he described his new role as a hospitalist. He preferred inpatient care with a structured schedule, less call time, and no outpatient responsibilities that required running between the hospital and an office practice. He told me this was where the future of medicine was heading. It was the best of both worlds.
Q: Tell us about your mentor. What did she mean to you?
A: My mentor was my program director. I admired her for being a distinguished woman in medicine with an academic position. She was a natural leader with passion and vision that were electrifying. She motivated and inspired. She saw potential in her residents and gave opportunity for any willing participant to advance.
Q: You say a structured yet flexible day and multidisciplinary work appeal to you. What do you like most about being a hospitalist?
A: Hospitalists have a unique and global vantage point of a hospital’s intricate network, making them the most valuable players on the field. They see opportunity in instability and uncertainty. Hospitalists are resourceful and efficient, adhering to the business concepts of competition, sustainability, conservation, and stewardship. The challenges of the field are vast but include a balance of clinical and administrative roles, leading and implementing changes to daily practice and being the constant in a sea of subspecialists.
The flexibility of the day allows for multitasking and setting priorities, so that patient care is never compromised in an acute care setting. A clinician can spend as much time with a patient as needed without the constraints of set appointments.
Q: What do you dislike most about being a hospitalist?
A: Having to balance clinical work with administrative and committee work.
Q: What’s the best advice you ever received?
A: Be proactive and be a part of the solution, rather than wait for change to be imposed. “Change is the only constant in life.”—Heraclitus
Q: What’s the worst advice you ever received?
A: Be friends with your boss.
Q: You’ve said you’d like to see hospitalists have more impact on lobbying and legislation. Can you explain what you’d like to see, and what you would see as the benefit of that?
A: Legislative action is spearheaded by the leaders of large medical organizations speaking on behalf of all of their members. These leaders tend to be either non-clinicians or non-practicing physicians. However, differing viewpoints exist. Physicians don’t want to be politicians or lobbyists. They have a hard time agreeing on things and working as a cohesive entity. So they leave others to speak for them. Then they complain when laws are passed without their say.
Hospitalists work in and help lead such complex organizations. SHM is led by physicians in practice. Events like Hospitalists on the Hill [at SHM’s annual meeting] encourage us to be more involved in legislative advocacy.
Q: As an administrator, at least part time, why is it important for you to continue seeing patients?
A: Clinical skills directly affect ability to understand the “day to day” and target the areas that need change. It also allows you to be an effective leader when you continue to do the same work your colleagues do. You are legitimate in their eyes!
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging for you?
A: Establishing trust and confidence by first impressions.
Q: What aspect of patient care is most rewarding?
A: Patient/family appreciation.
Q: As an assistant professor, what aspect of teaching in the 21st century do you find most difficult? And, what is most enjoyable?
A: Less focus on protected/dedicated teaching time, because money drivers take precedence (i.e., length of stay, dispo, utilization, billing and documentation). The new label is “system-based practice.” This has led to decreased bedside teaching.
Most enjoyable is working with eager learners.
Q: You call your biggest professional challenge taking credit for your ideas. Why is that difficult? Do you think that’s an issue for a lot of hospitalists, particularly given the specialty focus on the multidisciplinary team?
A: Hospital medicine focuses on teamwork. Hospitalists have figured out how to step out of their silos and reach across the aisle to accomplish some daunting tasks. Clinical competence is obviously important, but the ability to work together, check egos at the door, and make individual sacrifices when necessary is the only way a team succeeds. The unintentional consequence is that they don’t take credit because it’s the collective effort that counts.
Richard Quinn is a freelance writer in New Jersey.
Nancy Zeitoun, MD, FHM, sees her expanding role as a leader at Long Island Jewish Medical Center in New Hyde Park, N.Y., as a chance to make a difference. As co-site director for clinical affairs in the division of hospital medicine and assistant professor at Hofstra North Shore-LIJ School of Medicine, she can introduce her “own ideas to our evolving and growing program.”
Now she’s brought that desire to share ideas to Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: I consider it among the most challenging professions, both intellectually [conceptually] and physically [tangible].
Q: How/when did you decide to become a hospitalist?
A: Ten years ago, I was entering the third year of my four-year residency with the motivation to pursue critical care medicine and with much less enthusiasm for primary care than I had anticipated. One of the junior faculty was my internal medicine teaching attending, and he described his new role as a hospitalist. He preferred inpatient care with a structured schedule, less call time, and no outpatient responsibilities that required running between the hospital and an office practice. He told me this was where the future of medicine was heading. It was the best of both worlds.
Q: Tell us about your mentor. What did she mean to you?
A: My mentor was my program director. I admired her for being a distinguished woman in medicine with an academic position. She was a natural leader with passion and vision that were electrifying. She motivated and inspired. She saw potential in her residents and gave opportunity for any willing participant to advance.
Q: You say a structured yet flexible day and multidisciplinary work appeal to you. What do you like most about being a hospitalist?
A: Hospitalists have a unique and global vantage point of a hospital’s intricate network, making them the most valuable players on the field. They see opportunity in instability and uncertainty. Hospitalists are resourceful and efficient, adhering to the business concepts of competition, sustainability, conservation, and stewardship. The challenges of the field are vast but include a balance of clinical and administrative roles, leading and implementing changes to daily practice and being the constant in a sea of subspecialists.
The flexibility of the day allows for multitasking and setting priorities, so that patient care is never compromised in an acute care setting. A clinician can spend as much time with a patient as needed without the constraints of set appointments.
Q: What do you dislike most about being a hospitalist?
A: Having to balance clinical work with administrative and committee work.
Q: What’s the best advice you ever received?
A: Be proactive and be a part of the solution, rather than wait for change to be imposed. “Change is the only constant in life.”—Heraclitus
Q: What’s the worst advice you ever received?
A: Be friends with your boss.
Q: You’ve said you’d like to see hospitalists have more impact on lobbying and legislation. Can you explain what you’d like to see, and what you would see as the benefit of that?
A: Legislative action is spearheaded by the leaders of large medical organizations speaking on behalf of all of their members. These leaders tend to be either non-clinicians or non-practicing physicians. However, differing viewpoints exist. Physicians don’t want to be politicians or lobbyists. They have a hard time agreeing on things and working as a cohesive entity. So they leave others to speak for them. Then they complain when laws are passed without their say.
Hospitalists work in and help lead such complex organizations. SHM is led by physicians in practice. Events like Hospitalists on the Hill [at SHM’s annual meeting] encourage us to be more involved in legislative advocacy.
Q: As an administrator, at least part time, why is it important for you to continue seeing patients?
A: Clinical skills directly affect ability to understand the “day to day” and target the areas that need change. It also allows you to be an effective leader when you continue to do the same work your colleagues do. You are legitimate in their eyes!
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging for you?
A: Establishing trust and confidence by first impressions.
Q: What aspect of patient care is most rewarding?
A: Patient/family appreciation.
Q: As an assistant professor, what aspect of teaching in the 21st century do you find most difficult? And, what is most enjoyable?
A: Less focus on protected/dedicated teaching time, because money drivers take precedence (i.e., length of stay, dispo, utilization, billing and documentation). The new label is “system-based practice.” This has led to decreased bedside teaching.
Most enjoyable is working with eager learners.
Q: You call your biggest professional challenge taking credit for your ideas. Why is that difficult? Do you think that’s an issue for a lot of hospitalists, particularly given the specialty focus on the multidisciplinary team?
A: Hospital medicine focuses on teamwork. Hospitalists have figured out how to step out of their silos and reach across the aisle to accomplish some daunting tasks. Clinical competence is obviously important, but the ability to work together, check egos at the door, and make individual sacrifices when necessary is the only way a team succeeds. The unintentional consequence is that they don’t take credit because it’s the collective effort that counts.
Richard Quinn is a freelance writer in New Jersey.
D-Dimer Not Reliable Marker to Stop Anticoagulation Therapy
Clinical question: In patients with a first unprovoked VTE, is it safe to use a normalized D-dimer test to stop anticoagulation therapy?
Background: The risk of VTE recurrence after stopping anticoagulation is higher in patients who have elevated D-dimer levels after treatment. It is unknown whether we can use normalized D-dimer levels to guide the decision about whether or not to stop anticoagulation.
Study design: Prospective cohort study.
Setting: Thirteen university-affiliated centers.
Synopsis: Study authors screened 410 adult patients who had a first unprovoked VTE and completed three to seven months of anticoagulation therapy with D-dimer tests. In patients with negative D-dimer tests, anticoagulation was stopped, and D-dimer tests were repeated after a month. In those with two consecutive negative D-dimer tests, anticoagulation was stopped indefinitely; these patients were followed for an average of 2.2 years. Among those 319 patients, there was an overall recurrent VTE rate of 6.7% per patient year. Subgroup analysis was performed among men, women not on estrogen therapy, and women on estrogen therapy; recurrence rates per patient year were 9.7%, 5.4%, and 0%, respectively.
This study used a point-of-care D-dimer test that was either positive or negative; it is unclear if the results can be generalized to all D-dimer tests. Additionally, although the study found a lower recurrence VTE rate among women, the study was not powered for the subgroups.
Bottom line: The high rate of recurrent VTE among men makes the D-dimer test an unsafe marker to use in deciding whether or not to stop anticoagulation for an unprovoked VTE. Among women, D-dimer test can potentially be used to guide length of treatment, but, given the limitations of the study, more evidence is needed.
Citation: Kearon C, Spencer FA, O’Keeffe D, et al. D-Dimer testing to select patients with a first unprovoked venous thromboembolism who can stop anticoagulant therapy. Ann Intern Med. 2015;162(1):27-34.
Clinical question: In patients with a first unprovoked VTE, is it safe to use a normalized D-dimer test to stop anticoagulation therapy?
Background: The risk of VTE recurrence after stopping anticoagulation is higher in patients who have elevated D-dimer levels after treatment. It is unknown whether we can use normalized D-dimer levels to guide the decision about whether or not to stop anticoagulation.
Study design: Prospective cohort study.
Setting: Thirteen university-affiliated centers.
Synopsis: Study authors screened 410 adult patients who had a first unprovoked VTE and completed three to seven months of anticoagulation therapy with D-dimer tests. In patients with negative D-dimer tests, anticoagulation was stopped, and D-dimer tests were repeated after a month. In those with two consecutive negative D-dimer tests, anticoagulation was stopped indefinitely; these patients were followed for an average of 2.2 years. Among those 319 patients, there was an overall recurrent VTE rate of 6.7% per patient year. Subgroup analysis was performed among men, women not on estrogen therapy, and women on estrogen therapy; recurrence rates per patient year were 9.7%, 5.4%, and 0%, respectively.
This study used a point-of-care D-dimer test that was either positive or negative; it is unclear if the results can be generalized to all D-dimer tests. Additionally, although the study found a lower recurrence VTE rate among women, the study was not powered for the subgroups.
Bottom line: The high rate of recurrent VTE among men makes the D-dimer test an unsafe marker to use in deciding whether or not to stop anticoagulation for an unprovoked VTE. Among women, D-dimer test can potentially be used to guide length of treatment, but, given the limitations of the study, more evidence is needed.
Citation: Kearon C, Spencer FA, O’Keeffe D, et al. D-Dimer testing to select patients with a first unprovoked venous thromboembolism who can stop anticoagulant therapy. Ann Intern Med. 2015;162(1):27-34.
Clinical question: In patients with a first unprovoked VTE, is it safe to use a normalized D-dimer test to stop anticoagulation therapy?
Background: The risk of VTE recurrence after stopping anticoagulation is higher in patients who have elevated D-dimer levels after treatment. It is unknown whether we can use normalized D-dimer levels to guide the decision about whether or not to stop anticoagulation.
Study design: Prospective cohort study.
Setting: Thirteen university-affiliated centers.
Synopsis: Study authors screened 410 adult patients who had a first unprovoked VTE and completed three to seven months of anticoagulation therapy with D-dimer tests. In patients with negative D-dimer tests, anticoagulation was stopped, and D-dimer tests were repeated after a month. In those with two consecutive negative D-dimer tests, anticoagulation was stopped indefinitely; these patients were followed for an average of 2.2 years. Among those 319 patients, there was an overall recurrent VTE rate of 6.7% per patient year. Subgroup analysis was performed among men, women not on estrogen therapy, and women on estrogen therapy; recurrence rates per patient year were 9.7%, 5.4%, and 0%, respectively.
This study used a point-of-care D-dimer test that was either positive or negative; it is unclear if the results can be generalized to all D-dimer tests. Additionally, although the study found a lower recurrence VTE rate among women, the study was not powered for the subgroups.
Bottom line: The high rate of recurrent VTE among men makes the D-dimer test an unsafe marker to use in deciding whether or not to stop anticoagulation for an unprovoked VTE. Among women, D-dimer test can potentially be used to guide length of treatment, but, given the limitations of the study, more evidence is needed.
Citation: Kearon C, Spencer FA, O’Keeffe D, et al. D-Dimer testing to select patients with a first unprovoked venous thromboembolism who can stop anticoagulant therapy. Ann Intern Med. 2015;162(1):27-34.
Noninvasive Ventilation Improves Outcomes for COPD Inpatients
Clinical question: Do patients hospitalized with acute COPD exacerbations have improved outcomes with noninvasive ventilation (NIV) compared to those treated with invasive mechanical ventilation (IMV)?
Background: Previous studies have shown that in select patients, NIV has a mortality benefit over IMV for acute COPD exacerbations requiring hospitalization. NIV may also decrease complication rates and reduce length of stay; however, the previous prospective studies have been small.
Study design: Retrospective cohort study.
Setting: 420 structurally and geographically diverse U.S. hospitals.
Synopsis: Using the Premier Healthcare Informatics database, this study looked at 25,628 patients over 40 years old who were hospitalized with COPD exacerbations. Compared with patients who were initially treated with IMV, patients treated with NIV demonstrated lower mortality rates with an odds ratio of 0.54, lower risk of hospital-acquired pneumonia with an odds ratio of 0.53, and a 32% cost reduction. They also had shorter lengths of stay.
This was a retrospective study using a limited data set, and the authors did not have access to potentially confounding factors between the two groups, including vital signs and blood gases. Additionally, the advantages of NIV were attenuated among patients with pneumonia present on admission, patients with high burden of comorbid diseases, and patients older than 85 years.
Bottom line: Treatment of acute COPD exacerbations with NIV is associated with lower mortality, lower costs, and shorter length of stay as compared with IMV.
Citation: Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease. JAMA Intern Med. 2014;174(12):1982-1993.
Clinical question: Do patients hospitalized with acute COPD exacerbations have improved outcomes with noninvasive ventilation (NIV) compared to those treated with invasive mechanical ventilation (IMV)?
Background: Previous studies have shown that in select patients, NIV has a mortality benefit over IMV for acute COPD exacerbations requiring hospitalization. NIV may also decrease complication rates and reduce length of stay; however, the previous prospective studies have been small.
Study design: Retrospective cohort study.
Setting: 420 structurally and geographically diverse U.S. hospitals.
Synopsis: Using the Premier Healthcare Informatics database, this study looked at 25,628 patients over 40 years old who were hospitalized with COPD exacerbations. Compared with patients who were initially treated with IMV, patients treated with NIV demonstrated lower mortality rates with an odds ratio of 0.54, lower risk of hospital-acquired pneumonia with an odds ratio of 0.53, and a 32% cost reduction. They also had shorter lengths of stay.
This was a retrospective study using a limited data set, and the authors did not have access to potentially confounding factors between the two groups, including vital signs and blood gases. Additionally, the advantages of NIV were attenuated among patients with pneumonia present on admission, patients with high burden of comorbid diseases, and patients older than 85 years.
Bottom line: Treatment of acute COPD exacerbations with NIV is associated with lower mortality, lower costs, and shorter length of stay as compared with IMV.
Citation: Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease. JAMA Intern Med. 2014;174(12):1982-1993.
Clinical question: Do patients hospitalized with acute COPD exacerbations have improved outcomes with noninvasive ventilation (NIV) compared to those treated with invasive mechanical ventilation (IMV)?
Background: Previous studies have shown that in select patients, NIV has a mortality benefit over IMV for acute COPD exacerbations requiring hospitalization. NIV may also decrease complication rates and reduce length of stay; however, the previous prospective studies have been small.
Study design: Retrospective cohort study.
Setting: 420 structurally and geographically diverse U.S. hospitals.
Synopsis: Using the Premier Healthcare Informatics database, this study looked at 25,628 patients over 40 years old who were hospitalized with COPD exacerbations. Compared with patients who were initially treated with IMV, patients treated with NIV demonstrated lower mortality rates with an odds ratio of 0.54, lower risk of hospital-acquired pneumonia with an odds ratio of 0.53, and a 32% cost reduction. They also had shorter lengths of stay.
This was a retrospective study using a limited data set, and the authors did not have access to potentially confounding factors between the two groups, including vital signs and blood gases. Additionally, the advantages of NIV were attenuated among patients with pneumonia present on admission, patients with high burden of comorbid diseases, and patients older than 85 years.
Bottom line: Treatment of acute COPD exacerbations with NIV is associated with lower mortality, lower costs, and shorter length of stay as compared with IMV.
Citation: Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease. JAMA Intern Med. 2014;174(12):1982-1993.
Bova Risk Model Predicts 30-Day Pulmonary Embolism-Related Complications
Clinical question: Can the Bova risk model stratify patients with acute PE into stages of increasing risk for 30-day pulmonary embolism (PE)-related complications?
Background: The Bova score is based on four variables assessed at the time of PE diagnosis: heart rate, systolic blood pressure, cardiac troponin, and a marker of right ventricular (RV) dysfunction. In the original study, the Bova risk model was derived from 2,874 normotensive patients with PE. This study performed a retrospective validation of this model on a different cohort of patients.
Study design: Retrospective cohort study.
Setting: Academic urban ED in Madrid, Spain.
Synopsis: Investigators included 1,083 patients with normotensive PE, and the Bova risk score classified 80% into class I, 15% into class II, and 5% into class III—correlating 30-day PE-related complication rates were 4.4%, 18%, and 42%, respectively. When dichotomized into low risk (class I and II) versus intermediate to high risk (class III), the model had a specificity of 97%, a positive predictive value of 42%, and a positive likelihood ratio of 7.9 for predicting 30-day PE-related complications.
The existing risk assessment models, the pulmonary embolism severity index (PESI) and the simplified PESI (sPESI), have been extensively validated but were specifically developed to identity patients with low risk for mortality. The Bova risk model could be used in a stepwise fashion, with the PESI or sPESI model, to further assess intermediate-risk patients.
This model was derived and validated at one single center, so the results may not be generalizable. Additionally, the variables were collected prospectively, but this validation analysis was performed retrospectively.
Bottom line: The Bova risk model accurately stratifies patients with normotensive PE into stages of increasing risk for developing 30-day PE-related complications.
Citation: Fernández C, Bova C, Sanchez O, et al. Validation of a model for identification of patients at intermediate to high risk for complications associated with acute symptomatic pulmonary embolism [published online ahead of print January 29, 2015]. Chest.
Clinical question: Can the Bova risk model stratify patients with acute PE into stages of increasing risk for 30-day pulmonary embolism (PE)-related complications?
Background: The Bova score is based on four variables assessed at the time of PE diagnosis: heart rate, systolic blood pressure, cardiac troponin, and a marker of right ventricular (RV) dysfunction. In the original study, the Bova risk model was derived from 2,874 normotensive patients with PE. This study performed a retrospective validation of this model on a different cohort of patients.
Study design: Retrospective cohort study.
Setting: Academic urban ED in Madrid, Spain.
Synopsis: Investigators included 1,083 patients with normotensive PE, and the Bova risk score classified 80% into class I, 15% into class II, and 5% into class III—correlating 30-day PE-related complication rates were 4.4%, 18%, and 42%, respectively. When dichotomized into low risk (class I and II) versus intermediate to high risk (class III), the model had a specificity of 97%, a positive predictive value of 42%, and a positive likelihood ratio of 7.9 for predicting 30-day PE-related complications.
The existing risk assessment models, the pulmonary embolism severity index (PESI) and the simplified PESI (sPESI), have been extensively validated but were specifically developed to identity patients with low risk for mortality. The Bova risk model could be used in a stepwise fashion, with the PESI or sPESI model, to further assess intermediate-risk patients.
This model was derived and validated at one single center, so the results may not be generalizable. Additionally, the variables were collected prospectively, but this validation analysis was performed retrospectively.
Bottom line: The Bova risk model accurately stratifies patients with normotensive PE into stages of increasing risk for developing 30-day PE-related complications.
Citation: Fernández C, Bova C, Sanchez O, et al. Validation of a model for identification of patients at intermediate to high risk for complications associated with acute symptomatic pulmonary embolism [published online ahead of print January 29, 2015]. Chest.
Clinical question: Can the Bova risk model stratify patients with acute PE into stages of increasing risk for 30-day pulmonary embolism (PE)-related complications?
Background: The Bova score is based on four variables assessed at the time of PE diagnosis: heart rate, systolic blood pressure, cardiac troponin, and a marker of right ventricular (RV) dysfunction. In the original study, the Bova risk model was derived from 2,874 normotensive patients with PE. This study performed a retrospective validation of this model on a different cohort of patients.
Study design: Retrospective cohort study.
Setting: Academic urban ED in Madrid, Spain.
Synopsis: Investigators included 1,083 patients with normotensive PE, and the Bova risk score classified 80% into class I, 15% into class II, and 5% into class III—correlating 30-day PE-related complication rates were 4.4%, 18%, and 42%, respectively. When dichotomized into low risk (class I and II) versus intermediate to high risk (class III), the model had a specificity of 97%, a positive predictive value of 42%, and a positive likelihood ratio of 7.9 for predicting 30-day PE-related complications.
The existing risk assessment models, the pulmonary embolism severity index (PESI) and the simplified PESI (sPESI), have been extensively validated but were specifically developed to identity patients with low risk for mortality. The Bova risk model could be used in a stepwise fashion, with the PESI or sPESI model, to further assess intermediate-risk patients.
This model was derived and validated at one single center, so the results may not be generalizable. Additionally, the variables were collected prospectively, but this validation analysis was performed retrospectively.
Bottom line: The Bova risk model accurately stratifies patients with normotensive PE into stages of increasing risk for developing 30-day PE-related complications.
Citation: Fernández C, Bova C, Sanchez O, et al. Validation of a model for identification of patients at intermediate to high risk for complications associated with acute symptomatic pulmonary embolism [published online ahead of print January 29, 2015]. Chest.
Intracranial Bleeding Risk for Head Injury Patients on Warfarin
Clinical question: Do minor and minimal head injuries in patients on warfarin lead to significant intracranial bleed?
Background: Warfarin use is common, and many of these patients sustain minor and minimal head injuries. When presenting to the ED, these patients pose a clinical dilemma regarding whether to obtain neuroimaging and/or admit.
Study design: Retrospective cohort study.
Setting: Two urban tertiary care EDs in Ottawa, Canada, over a two-year period.
Synopsis: Using the Canadian National Ambulatory Care Reporting System database and the associated coding data, 259 patients were identified that fit the inclusion criteria GCS ≥13 and INR >1.5. This study showed that the rate of intracranial bleeds in this group of patients was high (15.9%); for minor and minimal head injury groups, the rate was 21.9% and 4.8%, respectively. Additionally, loss of consciousness was associated with higher rates of intracranial bleeding.
The risk of intracranial bleed after a head injury while on warfarin is considerably high, particularly for those patients with minor head injury (21.9%), which is about three times the rate previously reported. Hospitalists evaluating these patients should consider obtaining neuroimaging.
Nonetheless, these rates may be overestimating the true prevalence due to the following: 1) Coding data may overlook minor and minimal head injuries in the presence of more serious injuries, and 2) patients with minimal head injuries may not seek medical care.
Bottom line: Patients sustaining minor head injury while on warfarin have a high rate of intracranial bleed.
Reference: Alrajhi KN, Perry JJ, Forster AJ. Intracranial bleeds after minor and minimal head injury in patients on warfarin. J Emer Med. 2015;48(2):137-142.
Clinical question: Do minor and minimal head injuries in patients on warfarin lead to significant intracranial bleed?
Background: Warfarin use is common, and many of these patients sustain minor and minimal head injuries. When presenting to the ED, these patients pose a clinical dilemma regarding whether to obtain neuroimaging and/or admit.
Study design: Retrospective cohort study.
Setting: Two urban tertiary care EDs in Ottawa, Canada, over a two-year period.
Synopsis: Using the Canadian National Ambulatory Care Reporting System database and the associated coding data, 259 patients were identified that fit the inclusion criteria GCS ≥13 and INR >1.5. This study showed that the rate of intracranial bleeds in this group of patients was high (15.9%); for minor and minimal head injury groups, the rate was 21.9% and 4.8%, respectively. Additionally, loss of consciousness was associated with higher rates of intracranial bleeding.
The risk of intracranial bleed after a head injury while on warfarin is considerably high, particularly for those patients with minor head injury (21.9%), which is about three times the rate previously reported. Hospitalists evaluating these patients should consider obtaining neuroimaging.
Nonetheless, these rates may be overestimating the true prevalence due to the following: 1) Coding data may overlook minor and minimal head injuries in the presence of more serious injuries, and 2) patients with minimal head injuries may not seek medical care.
Bottom line: Patients sustaining minor head injury while on warfarin have a high rate of intracranial bleed.
Reference: Alrajhi KN, Perry JJ, Forster AJ. Intracranial bleeds after minor and minimal head injury in patients on warfarin. J Emer Med. 2015;48(2):137-142.
Clinical question: Do minor and minimal head injuries in patients on warfarin lead to significant intracranial bleed?
Background: Warfarin use is common, and many of these patients sustain minor and minimal head injuries. When presenting to the ED, these patients pose a clinical dilemma regarding whether to obtain neuroimaging and/or admit.
Study design: Retrospective cohort study.
Setting: Two urban tertiary care EDs in Ottawa, Canada, over a two-year period.
Synopsis: Using the Canadian National Ambulatory Care Reporting System database and the associated coding data, 259 patients were identified that fit the inclusion criteria GCS ≥13 and INR >1.5. This study showed that the rate of intracranial bleeds in this group of patients was high (15.9%); for minor and minimal head injury groups, the rate was 21.9% and 4.8%, respectively. Additionally, loss of consciousness was associated with higher rates of intracranial bleeding.
The risk of intracranial bleed after a head injury while on warfarin is considerably high, particularly for those patients with minor head injury (21.9%), which is about three times the rate previously reported. Hospitalists evaluating these patients should consider obtaining neuroimaging.
Nonetheless, these rates may be overestimating the true prevalence due to the following: 1) Coding data may overlook minor and minimal head injuries in the presence of more serious injuries, and 2) patients with minimal head injuries may not seek medical care.
Bottom line: Patients sustaining minor head injury while on warfarin have a high rate of intracranial bleed.
Reference: Alrajhi KN, Perry JJ, Forster AJ. Intracranial bleeds after minor and minimal head injury in patients on warfarin. J Emer Med. 2015;48(2):137-142.
Enriched Nutritional Formulas Help Heal Pressure Ulcers
Clinical question: Does a high-calorie, high-protein formula enriched with supplements of arginine, zinc, and antioxidants improve pressure ulcer healing?
Background: Malnutrition is thought to be a major factor in the development and poor healing of pressure ulcers. Trials evaluating whether or not the addition of antioxidants, arginine, and zinc to nutritional formulas improves pressure ulcer healing have been small and inconsistent.
Study design: Multicenter, randomized, controlled, blinded trial.
Setting: Long-term care facilities and patients receiving home care services.
Synopsis: Two hundred patients with stage II, III, or IV pressure ulcers receiving standardized wound care were randomly assigned to a control formula or an experimental formula enriched with arginine, zinc, and antioxidants. At eight weeks, the experimental formula group had an 18.7% (CI, 5.7% to 31.8%, P=0.017) mean reduction in pressure ulcer size compared with the control formula group, although both groups showed efficacy in wound healing.
Nutrition is an important part of wound healing and should be incorporated into the plan of care for the hospitalized patient with pressure ulcers. Hospitalists should be mindful that this study was conducted in non-acute settings, with a chronically ill patient population; more research needs to be done to investigate the effect of these specific immune-modulating nutritional supplements in acutely ill hospitalized patients, given the inconclusive safety profile of certain nutrients such as arginine in severe sepsis.
Bottom line: Enhanced nutritional support with an oral nutritional formula enriched with arginine, zinc, and antioxidants improves pressure ulcer healing in malnourished patients already receiving standard wound care.
Citation: Cereda E, Klersy C, Serioli M, Crespi A, D’Andrea F, OligoElement Sore Trial Study Group. A nutritional formula enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers: a randomized trial. Ann Intern Med. 2015;162(3):167-174.
Clinical question: Does a high-calorie, high-protein formula enriched with supplements of arginine, zinc, and antioxidants improve pressure ulcer healing?
Background: Malnutrition is thought to be a major factor in the development and poor healing of pressure ulcers. Trials evaluating whether or not the addition of antioxidants, arginine, and zinc to nutritional formulas improves pressure ulcer healing have been small and inconsistent.
Study design: Multicenter, randomized, controlled, blinded trial.
Setting: Long-term care facilities and patients receiving home care services.
Synopsis: Two hundred patients with stage II, III, or IV pressure ulcers receiving standardized wound care were randomly assigned to a control formula or an experimental formula enriched with arginine, zinc, and antioxidants. At eight weeks, the experimental formula group had an 18.7% (CI, 5.7% to 31.8%, P=0.017) mean reduction in pressure ulcer size compared with the control formula group, although both groups showed efficacy in wound healing.
Nutrition is an important part of wound healing and should be incorporated into the plan of care for the hospitalized patient with pressure ulcers. Hospitalists should be mindful that this study was conducted in non-acute settings, with a chronically ill patient population; more research needs to be done to investigate the effect of these specific immune-modulating nutritional supplements in acutely ill hospitalized patients, given the inconclusive safety profile of certain nutrients such as arginine in severe sepsis.
Bottom line: Enhanced nutritional support with an oral nutritional formula enriched with arginine, zinc, and antioxidants improves pressure ulcer healing in malnourished patients already receiving standard wound care.
Citation: Cereda E, Klersy C, Serioli M, Crespi A, D’Andrea F, OligoElement Sore Trial Study Group. A nutritional formula enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers: a randomized trial. Ann Intern Med. 2015;162(3):167-174.
Clinical question: Does a high-calorie, high-protein formula enriched with supplements of arginine, zinc, and antioxidants improve pressure ulcer healing?
Background: Malnutrition is thought to be a major factor in the development and poor healing of pressure ulcers. Trials evaluating whether or not the addition of antioxidants, arginine, and zinc to nutritional formulas improves pressure ulcer healing have been small and inconsistent.
Study design: Multicenter, randomized, controlled, blinded trial.
Setting: Long-term care facilities and patients receiving home care services.
Synopsis: Two hundred patients with stage II, III, or IV pressure ulcers receiving standardized wound care were randomly assigned to a control formula or an experimental formula enriched with arginine, zinc, and antioxidants. At eight weeks, the experimental formula group had an 18.7% (CI, 5.7% to 31.8%, P=0.017) mean reduction in pressure ulcer size compared with the control formula group, although both groups showed efficacy in wound healing.
Nutrition is an important part of wound healing and should be incorporated into the plan of care for the hospitalized patient with pressure ulcers. Hospitalists should be mindful that this study was conducted in non-acute settings, with a chronically ill patient population; more research needs to be done to investigate the effect of these specific immune-modulating nutritional supplements in acutely ill hospitalized patients, given the inconclusive safety profile of certain nutrients such as arginine in severe sepsis.
Bottom line: Enhanced nutritional support with an oral nutritional formula enriched with arginine, zinc, and antioxidants improves pressure ulcer healing in malnourished patients already receiving standard wound care.
Citation: Cereda E, Klersy C, Serioli M, Crespi A, D’Andrea F, OligoElement Sore Trial Study Group. A nutritional formula enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers: a randomized trial. Ann Intern Med. 2015;162(3):167-174.
High-Volume Hospitals Have Higher Readmission Rates
Clinical question: Is there an association between hospital volume and hospital readmission rates?
Background: There is an established association between high patient volume and reduced complications or mortality after surgical procedures; however, readmission represents a different type of quality metric than mortality or complications. Studies on the association between hospital patient volume and readmission rates have been controversial.
Study design: Retrospective, cross-sectional study.
Setting: Acute care hospitals.
Synopsis: The study included 6,916,644 admissions to 4,651 hospitals, where patients were assigned to one of five cohorts: medicine, surgery/gynecology, cardiorespiratory, cardiovascular, and neurology. The hospital with the highest volume group had a hospital-wide mean standardized readmission rate of 15.9%, while the hospital with the lowest volume group had a readmission rate of 14.7%. This was a 1.2 percentage point absolute difference between the two hospitals (95% confidence interval 0.9 to 1.5). This trend continued when specialty cohorts were examined, with the exception of the procedure-heavy cardiovascular cohort.
Results showed a trend toward decreased readmission rates in lower-volume hospitals; however, it is unclear why this trend exists. Possible reasons include different patient populations and different practitioner-to-patient ratios in low-volume hospitals.
Limitations of this study are the inclusion of only patients 65 years and older and the fact that all admissions per patient were included, which may bias the results against hospitals with many frequently admitted patients.
Bottom line: Hospitals with high patient volumes are associated with higher readmission rates, except in procedure-heavy patient groups.
Citation: Horwitz LI, Lin Z, Herrin J, et al.Association of hospital volume with readmission rates: a retrospective cross-sectional study. BMJ. 2015;350:h447.
Clinical question: Is there an association between hospital volume and hospital readmission rates?
Background: There is an established association between high patient volume and reduced complications or mortality after surgical procedures; however, readmission represents a different type of quality metric than mortality or complications. Studies on the association between hospital patient volume and readmission rates have been controversial.
Study design: Retrospective, cross-sectional study.
Setting: Acute care hospitals.
Synopsis: The study included 6,916,644 admissions to 4,651 hospitals, where patients were assigned to one of five cohorts: medicine, surgery/gynecology, cardiorespiratory, cardiovascular, and neurology. The hospital with the highest volume group had a hospital-wide mean standardized readmission rate of 15.9%, while the hospital with the lowest volume group had a readmission rate of 14.7%. This was a 1.2 percentage point absolute difference between the two hospitals (95% confidence interval 0.9 to 1.5). This trend continued when specialty cohorts were examined, with the exception of the procedure-heavy cardiovascular cohort.
Results showed a trend toward decreased readmission rates in lower-volume hospitals; however, it is unclear why this trend exists. Possible reasons include different patient populations and different practitioner-to-patient ratios in low-volume hospitals.
Limitations of this study are the inclusion of only patients 65 years and older and the fact that all admissions per patient were included, which may bias the results against hospitals with many frequently admitted patients.
Bottom line: Hospitals with high patient volumes are associated with higher readmission rates, except in procedure-heavy patient groups.
Citation: Horwitz LI, Lin Z, Herrin J, et al.Association of hospital volume with readmission rates: a retrospective cross-sectional study. BMJ. 2015;350:h447.
Clinical question: Is there an association between hospital volume and hospital readmission rates?
Background: There is an established association between high patient volume and reduced complications or mortality after surgical procedures; however, readmission represents a different type of quality metric than mortality or complications. Studies on the association between hospital patient volume and readmission rates have been controversial.
Study design: Retrospective, cross-sectional study.
Setting: Acute care hospitals.
Synopsis: The study included 6,916,644 admissions to 4,651 hospitals, where patients were assigned to one of five cohorts: medicine, surgery/gynecology, cardiorespiratory, cardiovascular, and neurology. The hospital with the highest volume group had a hospital-wide mean standardized readmission rate of 15.9%, while the hospital with the lowest volume group had a readmission rate of 14.7%. This was a 1.2 percentage point absolute difference between the two hospitals (95% confidence interval 0.9 to 1.5). This trend continued when specialty cohorts were examined, with the exception of the procedure-heavy cardiovascular cohort.
Results showed a trend toward decreased readmission rates in lower-volume hospitals; however, it is unclear why this trend exists. Possible reasons include different patient populations and different practitioner-to-patient ratios in low-volume hospitals.
Limitations of this study are the inclusion of only patients 65 years and older and the fact that all admissions per patient were included, which may bias the results against hospitals with many frequently admitted patients.
Bottom line: Hospitals with high patient volumes are associated with higher readmission rates, except in procedure-heavy patient groups.
Citation: Horwitz LI, Lin Z, Herrin J, et al.Association of hospital volume with readmission rates: a retrospective cross-sectional study. BMJ. 2015;350:h447.
Arthroscopic Treatment of Tibial Spine Malunion With Resorbable Screws
Anterior tibial spine fractures are rare, occurring with an incidence of 3 per 100,000 per year.1,2 Historically, this fracture has occurred more frequently in children,3-5 and was considered a condition of skeletal immaturity and the pediatric equivalent of an anterior cruciate ligament (ACL) rupture.6 However, recent literature indicates that this fracture is more common in the adult population than previously thought.7 The tibial spine is an attachment point for the ACL and an avulsion may produce ACL laxity,8 predisposing to further symptomatic laxity and premature osteoarthritis. Nearly 40% of these fractures are associated with concomitant injuries to surrounding structures.9
Meyers and McKeever10,11 originally classified these fractures into 3 groups on the basis of displacement. Type I fractures present with no significant displacement of the anterior margin, type II involve displacement and are hinged, while type III have complete displacement.10,11 More recently, a type IV fracture has been added, involving comminution of the displaced fragment. Nondisplaced fractures are commonly treated with immobilization in varying degrees of extension; this allows the femoral condyles to compress and to reduce the fracture while arthroscopic or open reduction is the preferred method for displaced fractures of the tibial spine.2,4,8,10
We report the case of an 11-year-old boy with a tibial spine fracture that failed conservative management. He developed a subsequent malunion with impingement anteriorly of the tibial spine on the notch, and residual instability of the ACL. The patient’s parents provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old Caucasian boy was referred to our office for evaluation of right knee injury. He sustained the injury approximately 3 months earlier, and it was determined that he had a tibial spine fracture. Conservative management with immobilization in extension and activity modification was undertaken; however, he was referred for further evaluation because of healing in a malreduced position and residual ACL laxity. Physical examination showed a grade 2A Lachman test (contralateral limb with negative Lachman examination), negative McMurray test, and pain with forced hyperextension; range-of-motion examination showed lack of the terminal 5º of extension. Magnetic resonance and computed tomography imaging from an outside facility showed a skeletally immature individual with a large tibial spine fracture that had healed in a malunited position with the fragment extended on a posterior hinge, creating a large prominence anteriorly (Figures 1A, 1B). Magnetic resonance imaging showed that the ACL fibers were likely to remain intact but would lack appropriate tension secondary to the displacement of the tibial insertion.
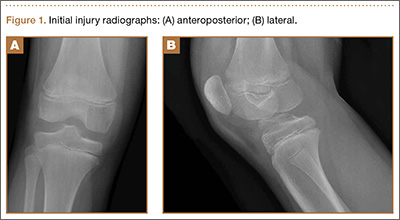
Because of healing in a displaced position, lack of terminal extension, ACL laxity, and subjective complaints of pain, we discussed surgery with the patient and his parents (Figures 2A, 2B). Four months after the initial injury, the patient underwent surgery for a right tibial spine malunion arthroscopic takedown and repair, as well as an intraoperative evaluation of the ACL. Standard arthroscopy was performed, using anterolateral and anteromedial arthroscopic portals, and an accessory medial peripatellar portal. During surgery, a large prominence was noted in the region of the anterior tibial spine (Figure 3A). The ACL fibers maintained a slack position secondary to the elevation of the tibial insertion point, and intraoperative Lachman examination showed anterior translation of the tibia on the femur as the slack was removed from the ACL. During surgery, impingement of the anterior tibial spine along the femoral notch was shown to be significant by taking the knee into near-full extension (Figure 3B). A cam-like effect was noted at the time of impingement with the posterior soft tissues relaxing to accommodate slight further extension.
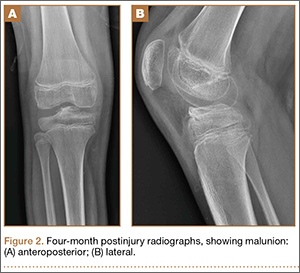
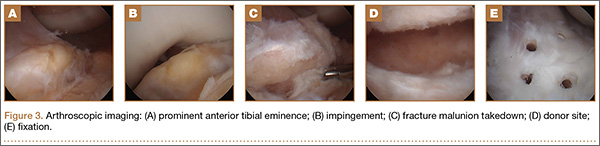
Based on these findings, we chose to take down the malunited fracture and repair it (Figure 3C). PDS suture (Ethicon, Somerville, New Jersey) was temporarily placed along the intermeniscal ligament and anterior horns of the medial and lateral menisci, using a system of spinal needles to facilitate suture passage. Surgical clamps were hung from the suture to provide traction on the sutures throughout the case, allowing the intermeniscal ligament and menisci to recede anteriorly to improve working space and aid in preventing iatrogenic injury. These sutures were removed at the conclusion of the case. Using a combination of curettes, elevator, and small shaver, we were able to meticulously remove interposed malunited callus to allow for mobilization of the displaced fragment. After removal of the excess bone formation, a typical donor site was created, allowing the displaced spine fragment to be hinged into appropriate alignment (Figure 3D). We were able to maintain a posterior cortical hinge to facilitate this process.
Then, we placed Kirschner wires (K-wires) across the fracture in an antegrade fashion, anterior to the trochlea and notch, using an accessory medial peripatellar starting point percutaneously, under direct visualization to avoid iatrogenic chondral injury. The tibial spine fragment was temporarily maintained in a reduced position with an arthroscopic probe and pinned in place with two 0.062-in K-wires. The fracture was stabilized with 8 resorbable 1.6-mm poly-L-lactic/polyglycolic acid (PLLA/PGA) nails, in varying lengths from 18 mm to 22 mm. Excellent fixation was obtained, and range of motion was tested from 0º to 80º, without movement of the fracture site (Figure 3E). Fluoroscopy with multi-axial views verified adequate fixation and reduction. Further, we examined and noted a taut ACL after fixation. The patient was placed in a long leg cast for 3 weeks at 30º, based upon intraoperative determination of the position of least tension on the fracture fragment.
At 3-week follow-up, the patient was progressing well and transitioned from a long leg cast to a hinged knee brace, to allow for early range of motion. Radiographs showed appropriate alignment of the tibial spine fracture with no significant loss of fixation (Figures 4A, 4B). Physical therapy was initiated between 0º and 30º, and flexion was progressively increased over the course of the first 3 weeks. Active and active-assist, closed-chain activities were maintained. Seven weeks postoperatively, the patient displayed continued clinical progression. Radiographs showed interval healing with slight lucency over the anterolateral aspect of the fracture fragment, likely related to the early resorptive process of healing. Physical examination showed movement between 0º and 120º, stable Lachman test, and stable anterior drawer. Crutches were discontinued and hinged knee brace was converted to an ACL brace. By the 11th week, motion had increased to 140º, and radiographs continued to show acceptable alignment and healing (Figures 5A, 5B). The patient was released to return to play as tolerated; however, an ACL brace was recommended during his initial return to provide additional support.
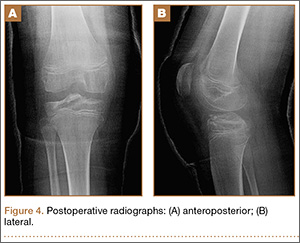
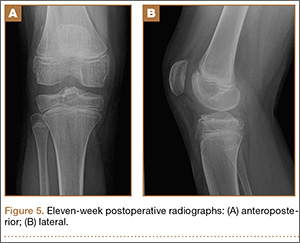
Discussion
In this report, we present an approach for arthroscopic reduction of a malunited tibial spine fracture using resorbable PLLA/PGA nails. The number of polyglycolic nails employed is individualized per case, dependent on the surface area and the quality of the bone within the fractured fragment. Preoperative templating allows for measurements from the fractured fragment to the level of the proximal tibial physis. Based on these measurements, nails are chosen to maximize fixation length and avoid the physis. Despite studies that have examined the effect of transphyseal K-wire pinning or drilling on subsequent growth, there is no consensus about optimal technique. Experiments in animal models indicate that drill injuries destroying less than 8% to 9% of the physis do not impact total bone growth.12,13 Further, temporary crossing of the physeal plate for internal fixation of dislocated joint injuries has not been shown to result in bone bridging or growth disturbance.14,15
Each nail is 1.6 mm in diameter, leaving a small footprint. The nails are used judiciously to provide effective stabilization of the fragment and to maintain a cost-conscious approach. An accessory superomedial peripatellar portal allows an appropriate angle for nail placement. This portal allows access to all regions of the fractured fragment, while an anteromedial and anterolateral portal are used as working and camera portals, respectively. Nails are placed to provide an axis perpendicular to the fracture line to allow appropriate compression. By virtue of the shape of the typical fragment in a tibial spine fracture, the nails vary in insertion angle.
The occurrence of anterior tibial spine fractures is rare, and while several techniques have been described to repair this fracture, there remains a great deal of uncertainty regarding the best course of treatment. A review of the literature finds arthroscopic and open approaches, as well as techniques employing K-wire fixation, metal screw fixation, staple fixation, absorbable fixation, and fixation with sutures passed through the tibial tunnel.16-18
Avulsion fractures of the tibial eminence were treated with open fixation until McLennan8 first reported the benefits of reduction with an arthroscope. Open reduction and internal fixation provide the benefit of direct visualization,9 while arthroscopic reduction offers decreased morbidity and an accelerated recovery of knee functions,8 despite the fact that a higher rate of range-of-motion deficits were seen in patients treated arthroscopically.19 We feel that with proper early rehabilitation to achieve range of motion, the risk of this can be minimal.
Various arthroscopic approaches that improve the accuracy of the reduction and decrease surgical invasiveness have been described. Suture and screw fixation are among the most common methods, and both have resulted in positive outcomes.20-24 Suture fixation of the tibial eminence is technically demanding but offers secure fixation without the need for follow-up hardware removal. Screw fixation results in secure fixation; however, numerous hardware-related issues may necessitate removal. Furthermore, in skeletally immature patients, screw fixation may disturb the growth plate if it crosses an open physis.9
Hunter and Willis25 retrospectively reviewed patients with tibial eminence fractures treated with either screw or suture fixation and found a 44% reoperation rate in the screw-fixation group. Removal was often recommended as a result of hardware-related issues. There was a 13% reoperation rate in the suture-fixation group, which resulted largely from stiffness.25 In a recent review, Gans and colleagues19 reviewed 6 publications comparing screw and suture fixation of tibial eminence fractures and found 82.4% of screw patients had laxity on both the anterior drawer and Lachman tests, compared with 18.8% in the suture-fixation group. This study also noted a slightly higher rate of arthrofibrosis in patients treated with suture fixation.19 Biomechanical studies indicate that suture fixation imparts greater strength under cyclic-loading conditions;26 however, there does not appear to be a difference in ultimate force required for fixation failure.27
Ultimately, both suture and screw fixation result in secure methods of fixation; however, there are often greater issues with screw fixation because of the persistent hardware. Metal has been the most popular method for fracture fixation, and while biodegradable materials have been alluring, adverse tissue reactions have slowed implementation. However, these implants have become increasingly sophisticated, thereby reducing disadvantages.28 Previous biodegradable devices were often composed of a single polymer, and many caused adverse reactions by degrading too quickly or provided no real advantages because they degraded too slowly.29 As the number of polymers approved for internal use and surgical applications continues to rise, so too will the benefits of employing this technology. Furthermore, by including multiple polymers in these implants, one is better able to control the degradation rate, limiting the tissue response.
In this study, we employed PLLA/PGA nails. Studies of PGA implants indicate this molecule degrades at a fast rate resulting in adverse tissue reactions. Adverse reactions in studies of PLLA implants are less frequent because of their slower rate of degradation.29,30 Combining these monomers results in appropriate strength and a controlled degradation rate, reducing the likelihood of adverse reactions. Furthermore, numerous studies have reported that inflammatory responses in children are rare and mild in nature.31,32 Absorbable implants have displayed efficacy in numerous orthopedic settings33-36 and are beneficial in procedures that are not suitable for repeated surgeries, such as reconstruction of the ACL.37 There is some concern about the use of absorbable implants in synovial joints. Polyglycolic acid use in synovial joints may cause foreign-body reactions and may increase the risk of intra-articular dissemination of polymeric debris;38 however, use of a multipolymer construct decreases the likelihood of this occurrence.
Polyglycolic nails confer the advantage over nonresorbable screw fixation because further procedure for hardware removal is not required. Although suture fixation has proved to be beneficial over nonresorbable screw fixation, implantation of resorbable nails appears to have several advantages. In Dr. Estes’ experience, placement of resorbable screws through an accessory superomedial portal is far less technically demanding than placement of suture through the fracture fragment. Further, as sutures are passed from the extra-articular to the intra-articular region of the joint, capsular layers of the knee may inadvertently be bound up in the fixation, predisposing to arthrofibrosis.
At the same time, biodegradable devices are often more costly than alternative forms of treatment; however, a true cost-to-benefit analysis requires consideration of other factors. One of the benefits of biodegradable hardware is that there is no need for follow-up hardware removal. Reports have indicated that up to 91% of patients thought that hardware removal was the most negative aspect of metal implants.39 It is estimated that if the removal rate for metallic implants is higher than 19% to 54%, resorbable implants would be more cost-effective.40 The cost of sutures and screws is variable, however; they are invariably less expensive than biodegradable nails. A study of fracture patients determined that biodegradable implants were cheaper on average after considering the cost of implant removal.40 Ultimately, the hardware choice depends on numerous factors, including surgeon’s discretion; however, biodegradable hardware should not be discounted for financial reasons because the difference in cost is likely negligible.
Conclusion
The approach described in this report offers efficient and secure fixation with resorbable hardware without a reduction in range of motion. Resorbable implants may prove beneficial in the treatment of tibial eminence fractures by offering robust fixation without the concerns associated with permanent hardware.
1. Hargrove R, Parsons S, Payne R. Anterior tibial spine fracture – an easy fracture to miss. Accid Emerg Nurs. 2004;12(3):173-175.
2. Aderinto J, Walmsley P, Keating JF. Fractures of the tibial spine: epidemiology and outcome. Knee. 2008;15(3):164-167.
3. Driessen MJ, Winkelman PA. Fractures of the intercondylar eminence of the tibia in childhood. Neth J Surg. 1984;36(3):69-72.
4. Zaricznyj B. Avulsion fracture of the tibial eminence: treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59(8):1111-1114.
5. Molander ML, Wallin G, Wikstad I. Fracture of the intercondylar eminence of the tibia: a review of 35 patients. J Bone Joint Surg Br. 1981;63(1):89-91.
6. Kieser DC, Gwynne-Jones D, Dreyer S. Displaced tibial intercondylar eminence fractures. J Orthop Surg. 2011;19(3):292-296.
7. Ishibashi Y, Tsuda E, Sasaki T, Toh S. Magnetic resonance imaging AIDS in detecting concomitant injuries in patients with tibial spine fractures. Clin Orthop. 2005;(434):207-212.
8. McLennan JG. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br. 1982;64(4):477-480.
9. Lafrance RM, Giordano B, Goldblatt J, Voloshin I, Maloney M. Pediatric tibial eminence fractures: evaluation and management. J Am Acad Orthop Surg. 2010;18(7):395-405.
10. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1959;41(2):209-220.
11. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970;52(8):1677-1684.
12. Garcés GL, Mugica-Garay I, López-González Coviella N, Guerado E. Growth-plate modifications after drilling. J Pediatr Orthop. 1994;14(2):225-228.
13. Janarv PM, Wikström B, Hirsch G. The influence of transphyseal drilling and tendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Orthop. 1998;18(2):149-154.
14. Boelitz R, Dallek M, Meenen NM, Jungbluth KH. Reaction of the epiphyseal groove to groove-crossing bore-wire osteosynthesis. Results of a histomorphologic small animal study. Unfallchirurgie. 1994;20(3):131-137.
15. Yung PS, Lam CY, Ng BK, Lam TP, Cheng JC. Percutaneous transphyseal intramedullary Kirschner wire pinning: a safe and effective procedure for treatment of displaced diaphyseal forearm fracture in children. J Pediatr Orthop. 2004;24(1):7-12.
16. Bong MR, Romero A, Kubiak E, et al. Suture versus screw fixation of displaced tibial eminence fractures: a biomechanical comparison. Arthroscopy. 2005;21(10):1172-1176.
17. Vega JR, Irribarra LA, Baar AK, Iñiguez M, Salgado M, Gana N. Arthroscopic fixation of displaced tibial eminence fractures: a new growth plate-sparing method. Arthroscopy. 2008;24(11):1239-1243.
18. Shepley RW. Arthroscopic treatment of type III tibial spine fractures using absorbable fixation. Orthopedics. 2004;27(7):767-769.
19. Gans I, Baldwin KD, Ganley TJ. Treatment and management outcomes of tibial eminence fractures in pediatric patients: a systematic review. Am J Sports Med. 2013;42(7):1743-1750.
20. Delcogliano A, Chiossi S, Caporaso A, Menghi A, Rinonapoli G. Tibial intercondylar eminence fractures in adults: arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc. 2003;11(4):255-259.
21. Mulhall KJ, Dowdall J, Grannell M, McCabe JP. Tibial spine fractures: an analysis of outcome in surgically treated type III injuries. Injury. 1999;30(4):289-292.
22. Geissler WB, Matthews DE. Arthroscopic suture fixation of displaced tibial eminence fractures. Orthopedics. 1993;16(3):331-333.
23. Mah JY, Otsuka NY, McLean J. An arthroscopic technique for the reduction and fixation of tibial-eminence fractures. J Pediatr Orthop. 1996;16(1):119-121.
24. Reynders P, Reynders K, Broos P. Pediatric and adolescent tibial eminence fractures: arthroscopic cannulated screw fixation. J Trauma. 2002;53(1):49-54.
25. Hunter RE, Willis JA. Arthroscopic fixation of avulsion fractures of the tibial eminence: technique and outcome. Arthroscopy. 2004;20(2):113-121.
26. Eggers AK, Becker C, Weimann A, et al. Biomechanical evaluation of different fixation methods for tibial eminence fractures. Am J Sports Med. 2007;35(3):404-410.
27. Mahar AT, Duncan D, Oka R, Lowry A, Gillingham B, Chambers H. Biomechanical comparison of four different fixation techniques for pediatric tibial eminence avulsion fractures. J Pediatr Orthop. 2008;28(2):159-162.
28. Toro C, Robiony M, Zerman N, Politi M. Resorbable plates in maxillary fixation. A 5-year experience. Minerva Stomatol. 2005;54(4):199-206.
29. Andriano KP, Pohjonen T, Törmälä P. Processing and characterization of absorbable polylactide polymers for use in surgical implants. J Appl Biomater.1994;5(2):133-140.
30. Böstman O, Pihlajamäki H. Clinical biocompatibility of biodegradable orthopaedic implants for internal fixation: a review. Biomaterials. 2000;21(24):2615-2621.
31. Rokkanen PU, Böstman O, Hirvensalo E, et al. Bioabsorbable fixation in orthopaedic surgery and traumatology. Biomaterials. 2000;21(24):2607-2613.
32. Athanasiou KA, Niederauer GG, Agrawal CM. Sterilization, toxicity, biocompatibility and clinical applications of polylactic acid/polyglycolic acid copolymers. Biomaterials. 1996;17(2):93-102.
33. Li ZH, Yu AX, Guo XP, Qi BW, Zhou M, Wang WY. Absorbable implants versus metal implants for the treatment of ankle fractures: A meta-analysis. Exp Ther Med. 2013;5(5):1531-1537.
34. Singh G, Mohammad S, Chak RK, Lepcha N, Singh N, Malkunje LR. Bio-resorbable plates as effective implant in paediatric mandibular fracture. J Maxillofac Oral Surg. 2012;11(4):400-406.
35. Sakamoto Y, Shimizu Y, Nagasao T, Kishi K. Combined use of resorbable poly-L-lactic acid-polyglycolic acid implant and bone cement for treating large orbital floor fractures. J Plast Reconstr Aesthet Surg. 2014;67(3):e88-e90.
36. Benz G, Kallieris D, Seeböck T, McIntosh A, Daum R. Bioresorbable pins and screws in paediatric traumatology. Eur J Pediatr Surg. 1994;4(2):103-107.
37. Gaweda K, Walawski J, Weglowski R, Krzyzanowski W. Comparison of bioabsorbable interference screws and posts for distal fixation in anterior cruciate ligament reconstruction. Int Orthop. 2009;33(1):123-127.
38. Böstman OM. Osteoarthritis of the ankle after foreign-body reaction to absorbable pins and screws: a three- to nine-year follow-up study. J Bone Joint Surg Br. 1998;80(2):333-338.
39. Mittal R, Morley J, Dinopoulos H, Drakoulakis EG, Vermani E, Giannoudis PV. Use of bio-resorbable implants for stabilisation of distal radius fractures: the United Kingdom patients’ perspective. Injury. 2005;36(2):333-338.
40. Böstman OM. Metallic or absorbable fracture fixation devices. A cost minimization analysis. Clin Orthop. 1996;(329):233-239.
Anterior tibial spine fractures are rare, occurring with an incidence of 3 per 100,000 per year.1,2 Historically, this fracture has occurred more frequently in children,3-5 and was considered a condition of skeletal immaturity and the pediatric equivalent of an anterior cruciate ligament (ACL) rupture.6 However, recent literature indicates that this fracture is more common in the adult population than previously thought.7 The tibial spine is an attachment point for the ACL and an avulsion may produce ACL laxity,8 predisposing to further symptomatic laxity and premature osteoarthritis. Nearly 40% of these fractures are associated with concomitant injuries to surrounding structures.9
Meyers and McKeever10,11 originally classified these fractures into 3 groups on the basis of displacement. Type I fractures present with no significant displacement of the anterior margin, type II involve displacement and are hinged, while type III have complete displacement.10,11 More recently, a type IV fracture has been added, involving comminution of the displaced fragment. Nondisplaced fractures are commonly treated with immobilization in varying degrees of extension; this allows the femoral condyles to compress and to reduce the fracture while arthroscopic or open reduction is the preferred method for displaced fractures of the tibial spine.2,4,8,10
We report the case of an 11-year-old boy with a tibial spine fracture that failed conservative management. He developed a subsequent malunion with impingement anteriorly of the tibial spine on the notch, and residual instability of the ACL. The patient’s parents provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old Caucasian boy was referred to our office for evaluation of right knee injury. He sustained the injury approximately 3 months earlier, and it was determined that he had a tibial spine fracture. Conservative management with immobilization in extension and activity modification was undertaken; however, he was referred for further evaluation because of healing in a malreduced position and residual ACL laxity. Physical examination showed a grade 2A Lachman test (contralateral limb with negative Lachman examination), negative McMurray test, and pain with forced hyperextension; range-of-motion examination showed lack of the terminal 5º of extension. Magnetic resonance and computed tomography imaging from an outside facility showed a skeletally immature individual with a large tibial spine fracture that had healed in a malunited position with the fragment extended on a posterior hinge, creating a large prominence anteriorly (Figures 1A, 1B). Magnetic resonance imaging showed that the ACL fibers were likely to remain intact but would lack appropriate tension secondary to the displacement of the tibial insertion.
Because of healing in a displaced position, lack of terminal extension, ACL laxity, and subjective complaints of pain, we discussed surgery with the patient and his parents (Figures 2A, 2B). Four months after the initial injury, the patient underwent surgery for a right tibial spine malunion arthroscopic takedown and repair, as well as an intraoperative evaluation of the ACL. Standard arthroscopy was performed, using anterolateral and anteromedial arthroscopic portals, and an accessory medial peripatellar portal. During surgery, a large prominence was noted in the region of the anterior tibial spine (Figure 3A). The ACL fibers maintained a slack position secondary to the elevation of the tibial insertion point, and intraoperative Lachman examination showed anterior translation of the tibia on the femur as the slack was removed from the ACL. During surgery, impingement of the anterior tibial spine along the femoral notch was shown to be significant by taking the knee into near-full extension (Figure 3B). A cam-like effect was noted at the time of impingement with the posterior soft tissues relaxing to accommodate slight further extension.
Based on these findings, we chose to take down the malunited fracture and repair it (Figure 3C). PDS suture (Ethicon, Somerville, New Jersey) was temporarily placed along the intermeniscal ligament and anterior horns of the medial and lateral menisci, using a system of spinal needles to facilitate suture passage. Surgical clamps were hung from the suture to provide traction on the sutures throughout the case, allowing the intermeniscal ligament and menisci to recede anteriorly to improve working space and aid in preventing iatrogenic injury. These sutures were removed at the conclusion of the case. Using a combination of curettes, elevator, and small shaver, we were able to meticulously remove interposed malunited callus to allow for mobilization of the displaced fragment. After removal of the excess bone formation, a typical donor site was created, allowing the displaced spine fragment to be hinged into appropriate alignment (Figure 3D). We were able to maintain a posterior cortical hinge to facilitate this process.
Then, we placed Kirschner wires (K-wires) across the fracture in an antegrade fashion, anterior to the trochlea and notch, using an accessory medial peripatellar starting point percutaneously, under direct visualization to avoid iatrogenic chondral injury. The tibial spine fragment was temporarily maintained in a reduced position with an arthroscopic probe and pinned in place with two 0.062-in K-wires. The fracture was stabilized with 8 resorbable 1.6-mm poly-L-lactic/polyglycolic acid (PLLA/PGA) nails, in varying lengths from 18 mm to 22 mm. Excellent fixation was obtained, and range of motion was tested from 0º to 80º, without movement of the fracture site (Figure 3E). Fluoroscopy with multi-axial views verified adequate fixation and reduction. Further, we examined and noted a taut ACL after fixation. The patient was placed in a long leg cast for 3 weeks at 30º, based upon intraoperative determination of the position of least tension on the fracture fragment.
At 3-week follow-up, the patient was progressing well and transitioned from a long leg cast to a hinged knee brace, to allow for early range of motion. Radiographs showed appropriate alignment of the tibial spine fracture with no significant loss of fixation (Figures 4A, 4B). Physical therapy was initiated between 0º and 30º, and flexion was progressively increased over the course of the first 3 weeks. Active and active-assist, closed-chain activities were maintained. Seven weeks postoperatively, the patient displayed continued clinical progression. Radiographs showed interval healing with slight lucency over the anterolateral aspect of the fracture fragment, likely related to the early resorptive process of healing. Physical examination showed movement between 0º and 120º, stable Lachman test, and stable anterior drawer. Crutches were discontinued and hinged knee brace was converted to an ACL brace. By the 11th week, motion had increased to 140º, and radiographs continued to show acceptable alignment and healing (Figures 5A, 5B). The patient was released to return to play as tolerated; however, an ACL brace was recommended during his initial return to provide additional support.
Discussion
In this report, we present an approach for arthroscopic reduction of a malunited tibial spine fracture using resorbable PLLA/PGA nails. The number of polyglycolic nails employed is individualized per case, dependent on the surface area and the quality of the bone within the fractured fragment. Preoperative templating allows for measurements from the fractured fragment to the level of the proximal tibial physis. Based on these measurements, nails are chosen to maximize fixation length and avoid the physis. Despite studies that have examined the effect of transphyseal K-wire pinning or drilling on subsequent growth, there is no consensus about optimal technique. Experiments in animal models indicate that drill injuries destroying less than 8% to 9% of the physis do not impact total bone growth.12,13 Further, temporary crossing of the physeal plate for internal fixation of dislocated joint injuries has not been shown to result in bone bridging or growth disturbance.14,15
Each nail is 1.6 mm in diameter, leaving a small footprint. The nails are used judiciously to provide effective stabilization of the fragment and to maintain a cost-conscious approach. An accessory superomedial peripatellar portal allows an appropriate angle for nail placement. This portal allows access to all regions of the fractured fragment, while an anteromedial and anterolateral portal are used as working and camera portals, respectively. Nails are placed to provide an axis perpendicular to the fracture line to allow appropriate compression. By virtue of the shape of the typical fragment in a tibial spine fracture, the nails vary in insertion angle.
The occurrence of anterior tibial spine fractures is rare, and while several techniques have been described to repair this fracture, there remains a great deal of uncertainty regarding the best course of treatment. A review of the literature finds arthroscopic and open approaches, as well as techniques employing K-wire fixation, metal screw fixation, staple fixation, absorbable fixation, and fixation with sutures passed through the tibial tunnel.16-18
Avulsion fractures of the tibial eminence were treated with open fixation until McLennan8 first reported the benefits of reduction with an arthroscope. Open reduction and internal fixation provide the benefit of direct visualization,9 while arthroscopic reduction offers decreased morbidity and an accelerated recovery of knee functions,8 despite the fact that a higher rate of range-of-motion deficits were seen in patients treated arthroscopically.19 We feel that with proper early rehabilitation to achieve range of motion, the risk of this can be minimal.
Various arthroscopic approaches that improve the accuracy of the reduction and decrease surgical invasiveness have been described. Suture and screw fixation are among the most common methods, and both have resulted in positive outcomes.20-24 Suture fixation of the tibial eminence is technically demanding but offers secure fixation without the need for follow-up hardware removal. Screw fixation results in secure fixation; however, numerous hardware-related issues may necessitate removal. Furthermore, in skeletally immature patients, screw fixation may disturb the growth plate if it crosses an open physis.9
Hunter and Willis25 retrospectively reviewed patients with tibial eminence fractures treated with either screw or suture fixation and found a 44% reoperation rate in the screw-fixation group. Removal was often recommended as a result of hardware-related issues. There was a 13% reoperation rate in the suture-fixation group, which resulted largely from stiffness.25 In a recent review, Gans and colleagues19 reviewed 6 publications comparing screw and suture fixation of tibial eminence fractures and found 82.4% of screw patients had laxity on both the anterior drawer and Lachman tests, compared with 18.8% in the suture-fixation group. This study also noted a slightly higher rate of arthrofibrosis in patients treated with suture fixation.19 Biomechanical studies indicate that suture fixation imparts greater strength under cyclic-loading conditions;26 however, there does not appear to be a difference in ultimate force required for fixation failure.27
Ultimately, both suture and screw fixation result in secure methods of fixation; however, there are often greater issues with screw fixation because of the persistent hardware. Metal has been the most popular method for fracture fixation, and while biodegradable materials have been alluring, adverse tissue reactions have slowed implementation. However, these implants have become increasingly sophisticated, thereby reducing disadvantages.28 Previous biodegradable devices were often composed of a single polymer, and many caused adverse reactions by degrading too quickly or provided no real advantages because they degraded too slowly.29 As the number of polymers approved for internal use and surgical applications continues to rise, so too will the benefits of employing this technology. Furthermore, by including multiple polymers in these implants, one is better able to control the degradation rate, limiting the tissue response.
In this study, we employed PLLA/PGA nails. Studies of PGA implants indicate this molecule degrades at a fast rate resulting in adverse tissue reactions. Adverse reactions in studies of PLLA implants are less frequent because of their slower rate of degradation.29,30 Combining these monomers results in appropriate strength and a controlled degradation rate, reducing the likelihood of adverse reactions. Furthermore, numerous studies have reported that inflammatory responses in children are rare and mild in nature.31,32 Absorbable implants have displayed efficacy in numerous orthopedic settings33-36 and are beneficial in procedures that are not suitable for repeated surgeries, such as reconstruction of the ACL.37 There is some concern about the use of absorbable implants in synovial joints. Polyglycolic acid use in synovial joints may cause foreign-body reactions and may increase the risk of intra-articular dissemination of polymeric debris;38 however, use of a multipolymer construct decreases the likelihood of this occurrence.
Polyglycolic nails confer the advantage over nonresorbable screw fixation because further procedure for hardware removal is not required. Although suture fixation has proved to be beneficial over nonresorbable screw fixation, implantation of resorbable nails appears to have several advantages. In Dr. Estes’ experience, placement of resorbable screws through an accessory superomedial portal is far less technically demanding than placement of suture through the fracture fragment. Further, as sutures are passed from the extra-articular to the intra-articular region of the joint, capsular layers of the knee may inadvertently be bound up in the fixation, predisposing to arthrofibrosis.
At the same time, biodegradable devices are often more costly than alternative forms of treatment; however, a true cost-to-benefit analysis requires consideration of other factors. One of the benefits of biodegradable hardware is that there is no need for follow-up hardware removal. Reports have indicated that up to 91% of patients thought that hardware removal was the most negative aspect of metal implants.39 It is estimated that if the removal rate for metallic implants is higher than 19% to 54%, resorbable implants would be more cost-effective.40 The cost of sutures and screws is variable, however; they are invariably less expensive than biodegradable nails. A study of fracture patients determined that biodegradable implants were cheaper on average after considering the cost of implant removal.40 Ultimately, the hardware choice depends on numerous factors, including surgeon’s discretion; however, biodegradable hardware should not be discounted for financial reasons because the difference in cost is likely negligible.
Conclusion
The approach described in this report offers efficient and secure fixation with resorbable hardware without a reduction in range of motion. Resorbable implants may prove beneficial in the treatment of tibial eminence fractures by offering robust fixation without the concerns associated with permanent hardware.
Anterior tibial spine fractures are rare, occurring with an incidence of 3 per 100,000 per year.1,2 Historically, this fracture has occurred more frequently in children,3-5 and was considered a condition of skeletal immaturity and the pediatric equivalent of an anterior cruciate ligament (ACL) rupture.6 However, recent literature indicates that this fracture is more common in the adult population than previously thought.7 The tibial spine is an attachment point for the ACL and an avulsion may produce ACL laxity,8 predisposing to further symptomatic laxity and premature osteoarthritis. Nearly 40% of these fractures are associated with concomitant injuries to surrounding structures.9
Meyers and McKeever10,11 originally classified these fractures into 3 groups on the basis of displacement. Type I fractures present with no significant displacement of the anterior margin, type II involve displacement and are hinged, while type III have complete displacement.10,11 More recently, a type IV fracture has been added, involving comminution of the displaced fragment. Nondisplaced fractures are commonly treated with immobilization in varying degrees of extension; this allows the femoral condyles to compress and to reduce the fracture while arthroscopic or open reduction is the preferred method for displaced fractures of the tibial spine.2,4,8,10
We report the case of an 11-year-old boy with a tibial spine fracture that failed conservative management. He developed a subsequent malunion with impingement anteriorly of the tibial spine on the notch, and residual instability of the ACL. The patient’s parents provided written informed consent for print and electronic publication of this case report.
Case Report
An 11-year-old Caucasian boy was referred to our office for evaluation of right knee injury. He sustained the injury approximately 3 months earlier, and it was determined that he had a tibial spine fracture. Conservative management with immobilization in extension and activity modification was undertaken; however, he was referred for further evaluation because of healing in a malreduced position and residual ACL laxity. Physical examination showed a grade 2A Lachman test (contralateral limb with negative Lachman examination), negative McMurray test, and pain with forced hyperextension; range-of-motion examination showed lack of the terminal 5º of extension. Magnetic resonance and computed tomography imaging from an outside facility showed a skeletally immature individual with a large tibial spine fracture that had healed in a malunited position with the fragment extended on a posterior hinge, creating a large prominence anteriorly (Figures 1A, 1B). Magnetic resonance imaging showed that the ACL fibers were likely to remain intact but would lack appropriate tension secondary to the displacement of the tibial insertion.
Because of healing in a displaced position, lack of terminal extension, ACL laxity, and subjective complaints of pain, we discussed surgery with the patient and his parents (Figures 2A, 2B). Four months after the initial injury, the patient underwent surgery for a right tibial spine malunion arthroscopic takedown and repair, as well as an intraoperative evaluation of the ACL. Standard arthroscopy was performed, using anterolateral and anteromedial arthroscopic portals, and an accessory medial peripatellar portal. During surgery, a large prominence was noted in the region of the anterior tibial spine (Figure 3A). The ACL fibers maintained a slack position secondary to the elevation of the tibial insertion point, and intraoperative Lachman examination showed anterior translation of the tibia on the femur as the slack was removed from the ACL. During surgery, impingement of the anterior tibial spine along the femoral notch was shown to be significant by taking the knee into near-full extension (Figure 3B). A cam-like effect was noted at the time of impingement with the posterior soft tissues relaxing to accommodate slight further extension.
Based on these findings, we chose to take down the malunited fracture and repair it (Figure 3C). PDS suture (Ethicon, Somerville, New Jersey) was temporarily placed along the intermeniscal ligament and anterior horns of the medial and lateral menisci, using a system of spinal needles to facilitate suture passage. Surgical clamps were hung from the suture to provide traction on the sutures throughout the case, allowing the intermeniscal ligament and menisci to recede anteriorly to improve working space and aid in preventing iatrogenic injury. These sutures were removed at the conclusion of the case. Using a combination of curettes, elevator, and small shaver, we were able to meticulously remove interposed malunited callus to allow for mobilization of the displaced fragment. After removal of the excess bone formation, a typical donor site was created, allowing the displaced spine fragment to be hinged into appropriate alignment (Figure 3D). We were able to maintain a posterior cortical hinge to facilitate this process.
Then, we placed Kirschner wires (K-wires) across the fracture in an antegrade fashion, anterior to the trochlea and notch, using an accessory medial peripatellar starting point percutaneously, under direct visualization to avoid iatrogenic chondral injury. The tibial spine fragment was temporarily maintained in a reduced position with an arthroscopic probe and pinned in place with two 0.062-in K-wires. The fracture was stabilized with 8 resorbable 1.6-mm poly-L-lactic/polyglycolic acid (PLLA/PGA) nails, in varying lengths from 18 mm to 22 mm. Excellent fixation was obtained, and range of motion was tested from 0º to 80º, without movement of the fracture site (Figure 3E). Fluoroscopy with multi-axial views verified adequate fixation and reduction. Further, we examined and noted a taut ACL after fixation. The patient was placed in a long leg cast for 3 weeks at 30º, based upon intraoperative determination of the position of least tension on the fracture fragment.
At 3-week follow-up, the patient was progressing well and transitioned from a long leg cast to a hinged knee brace, to allow for early range of motion. Radiographs showed appropriate alignment of the tibial spine fracture with no significant loss of fixation (Figures 4A, 4B). Physical therapy was initiated between 0º and 30º, and flexion was progressively increased over the course of the first 3 weeks. Active and active-assist, closed-chain activities were maintained. Seven weeks postoperatively, the patient displayed continued clinical progression. Radiographs showed interval healing with slight lucency over the anterolateral aspect of the fracture fragment, likely related to the early resorptive process of healing. Physical examination showed movement between 0º and 120º, stable Lachman test, and stable anterior drawer. Crutches were discontinued and hinged knee brace was converted to an ACL brace. By the 11th week, motion had increased to 140º, and radiographs continued to show acceptable alignment and healing (Figures 5A, 5B). The patient was released to return to play as tolerated; however, an ACL brace was recommended during his initial return to provide additional support.
Discussion
In this report, we present an approach for arthroscopic reduction of a malunited tibial spine fracture using resorbable PLLA/PGA nails. The number of polyglycolic nails employed is individualized per case, dependent on the surface area and the quality of the bone within the fractured fragment. Preoperative templating allows for measurements from the fractured fragment to the level of the proximal tibial physis. Based on these measurements, nails are chosen to maximize fixation length and avoid the physis. Despite studies that have examined the effect of transphyseal K-wire pinning or drilling on subsequent growth, there is no consensus about optimal technique. Experiments in animal models indicate that drill injuries destroying less than 8% to 9% of the physis do not impact total bone growth.12,13 Further, temporary crossing of the physeal plate for internal fixation of dislocated joint injuries has not been shown to result in bone bridging or growth disturbance.14,15
Each nail is 1.6 mm in diameter, leaving a small footprint. The nails are used judiciously to provide effective stabilization of the fragment and to maintain a cost-conscious approach. An accessory superomedial peripatellar portal allows an appropriate angle for nail placement. This portal allows access to all regions of the fractured fragment, while an anteromedial and anterolateral portal are used as working and camera portals, respectively. Nails are placed to provide an axis perpendicular to the fracture line to allow appropriate compression. By virtue of the shape of the typical fragment in a tibial spine fracture, the nails vary in insertion angle.
The occurrence of anterior tibial spine fractures is rare, and while several techniques have been described to repair this fracture, there remains a great deal of uncertainty regarding the best course of treatment. A review of the literature finds arthroscopic and open approaches, as well as techniques employing K-wire fixation, metal screw fixation, staple fixation, absorbable fixation, and fixation with sutures passed through the tibial tunnel.16-18
Avulsion fractures of the tibial eminence were treated with open fixation until McLennan8 first reported the benefits of reduction with an arthroscope. Open reduction and internal fixation provide the benefit of direct visualization,9 while arthroscopic reduction offers decreased morbidity and an accelerated recovery of knee functions,8 despite the fact that a higher rate of range-of-motion deficits were seen in patients treated arthroscopically.19 We feel that with proper early rehabilitation to achieve range of motion, the risk of this can be minimal.
Various arthroscopic approaches that improve the accuracy of the reduction and decrease surgical invasiveness have been described. Suture and screw fixation are among the most common methods, and both have resulted in positive outcomes.20-24 Suture fixation of the tibial eminence is technically demanding but offers secure fixation without the need for follow-up hardware removal. Screw fixation results in secure fixation; however, numerous hardware-related issues may necessitate removal. Furthermore, in skeletally immature patients, screw fixation may disturb the growth plate if it crosses an open physis.9
Hunter and Willis25 retrospectively reviewed patients with tibial eminence fractures treated with either screw or suture fixation and found a 44% reoperation rate in the screw-fixation group. Removal was often recommended as a result of hardware-related issues. There was a 13% reoperation rate in the suture-fixation group, which resulted largely from stiffness.25 In a recent review, Gans and colleagues19 reviewed 6 publications comparing screw and suture fixation of tibial eminence fractures and found 82.4% of screw patients had laxity on both the anterior drawer and Lachman tests, compared with 18.8% in the suture-fixation group. This study also noted a slightly higher rate of arthrofibrosis in patients treated with suture fixation.19 Biomechanical studies indicate that suture fixation imparts greater strength under cyclic-loading conditions;26 however, there does not appear to be a difference in ultimate force required for fixation failure.27
Ultimately, both suture and screw fixation result in secure methods of fixation; however, there are often greater issues with screw fixation because of the persistent hardware. Metal has been the most popular method for fracture fixation, and while biodegradable materials have been alluring, adverse tissue reactions have slowed implementation. However, these implants have become increasingly sophisticated, thereby reducing disadvantages.28 Previous biodegradable devices were often composed of a single polymer, and many caused adverse reactions by degrading too quickly or provided no real advantages because they degraded too slowly.29 As the number of polymers approved for internal use and surgical applications continues to rise, so too will the benefits of employing this technology. Furthermore, by including multiple polymers in these implants, one is better able to control the degradation rate, limiting the tissue response.
In this study, we employed PLLA/PGA nails. Studies of PGA implants indicate this molecule degrades at a fast rate resulting in adverse tissue reactions. Adverse reactions in studies of PLLA implants are less frequent because of their slower rate of degradation.29,30 Combining these monomers results in appropriate strength and a controlled degradation rate, reducing the likelihood of adverse reactions. Furthermore, numerous studies have reported that inflammatory responses in children are rare and mild in nature.31,32 Absorbable implants have displayed efficacy in numerous orthopedic settings33-36 and are beneficial in procedures that are not suitable for repeated surgeries, such as reconstruction of the ACL.37 There is some concern about the use of absorbable implants in synovial joints. Polyglycolic acid use in synovial joints may cause foreign-body reactions and may increase the risk of intra-articular dissemination of polymeric debris;38 however, use of a multipolymer construct decreases the likelihood of this occurrence.
Polyglycolic nails confer the advantage over nonresorbable screw fixation because further procedure for hardware removal is not required. Although suture fixation has proved to be beneficial over nonresorbable screw fixation, implantation of resorbable nails appears to have several advantages. In Dr. Estes’ experience, placement of resorbable screws through an accessory superomedial portal is far less technically demanding than placement of suture through the fracture fragment. Further, as sutures are passed from the extra-articular to the intra-articular region of the joint, capsular layers of the knee may inadvertently be bound up in the fixation, predisposing to arthrofibrosis.
At the same time, biodegradable devices are often more costly than alternative forms of treatment; however, a true cost-to-benefit analysis requires consideration of other factors. One of the benefits of biodegradable hardware is that there is no need for follow-up hardware removal. Reports have indicated that up to 91% of patients thought that hardware removal was the most negative aspect of metal implants.39 It is estimated that if the removal rate for metallic implants is higher than 19% to 54%, resorbable implants would be more cost-effective.40 The cost of sutures and screws is variable, however; they are invariably less expensive than biodegradable nails. A study of fracture patients determined that biodegradable implants were cheaper on average after considering the cost of implant removal.40 Ultimately, the hardware choice depends on numerous factors, including surgeon’s discretion; however, biodegradable hardware should not be discounted for financial reasons because the difference in cost is likely negligible.
Conclusion
The approach described in this report offers efficient and secure fixation with resorbable hardware without a reduction in range of motion. Resorbable implants may prove beneficial in the treatment of tibial eminence fractures by offering robust fixation without the concerns associated with permanent hardware.
1. Hargrove R, Parsons S, Payne R. Anterior tibial spine fracture – an easy fracture to miss. Accid Emerg Nurs. 2004;12(3):173-175.
2. Aderinto J, Walmsley P, Keating JF. Fractures of the tibial spine: epidemiology and outcome. Knee. 2008;15(3):164-167.
3. Driessen MJ, Winkelman PA. Fractures of the intercondylar eminence of the tibia in childhood. Neth J Surg. 1984;36(3):69-72.
4. Zaricznyj B. Avulsion fracture of the tibial eminence: treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59(8):1111-1114.
5. Molander ML, Wallin G, Wikstad I. Fracture of the intercondylar eminence of the tibia: a review of 35 patients. J Bone Joint Surg Br. 1981;63(1):89-91.
6. Kieser DC, Gwynne-Jones D, Dreyer S. Displaced tibial intercondylar eminence fractures. J Orthop Surg. 2011;19(3):292-296.
7. Ishibashi Y, Tsuda E, Sasaki T, Toh S. Magnetic resonance imaging AIDS in detecting concomitant injuries in patients with tibial spine fractures. Clin Orthop. 2005;(434):207-212.
8. McLennan JG. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br. 1982;64(4):477-480.
9. Lafrance RM, Giordano B, Goldblatt J, Voloshin I, Maloney M. Pediatric tibial eminence fractures: evaluation and management. J Am Acad Orthop Surg. 2010;18(7):395-405.
10. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1959;41(2):209-220.
11. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970;52(8):1677-1684.
12. Garcés GL, Mugica-Garay I, López-González Coviella N, Guerado E. Growth-plate modifications after drilling. J Pediatr Orthop. 1994;14(2):225-228.
13. Janarv PM, Wikström B, Hirsch G. The influence of transphyseal drilling and tendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Orthop. 1998;18(2):149-154.
14. Boelitz R, Dallek M, Meenen NM, Jungbluth KH. Reaction of the epiphyseal groove to groove-crossing bore-wire osteosynthesis. Results of a histomorphologic small animal study. Unfallchirurgie. 1994;20(3):131-137.
15. Yung PS, Lam CY, Ng BK, Lam TP, Cheng JC. Percutaneous transphyseal intramedullary Kirschner wire pinning: a safe and effective procedure for treatment of displaced diaphyseal forearm fracture in children. J Pediatr Orthop. 2004;24(1):7-12.
16. Bong MR, Romero A, Kubiak E, et al. Suture versus screw fixation of displaced tibial eminence fractures: a biomechanical comparison. Arthroscopy. 2005;21(10):1172-1176.
17. Vega JR, Irribarra LA, Baar AK, Iñiguez M, Salgado M, Gana N. Arthroscopic fixation of displaced tibial eminence fractures: a new growth plate-sparing method. Arthroscopy. 2008;24(11):1239-1243.
18. Shepley RW. Arthroscopic treatment of type III tibial spine fractures using absorbable fixation. Orthopedics. 2004;27(7):767-769.
19. Gans I, Baldwin KD, Ganley TJ. Treatment and management outcomes of tibial eminence fractures in pediatric patients: a systematic review. Am J Sports Med. 2013;42(7):1743-1750.
20. Delcogliano A, Chiossi S, Caporaso A, Menghi A, Rinonapoli G. Tibial intercondylar eminence fractures in adults: arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc. 2003;11(4):255-259.
21. Mulhall KJ, Dowdall J, Grannell M, McCabe JP. Tibial spine fractures: an analysis of outcome in surgically treated type III injuries. Injury. 1999;30(4):289-292.
22. Geissler WB, Matthews DE. Arthroscopic suture fixation of displaced tibial eminence fractures. Orthopedics. 1993;16(3):331-333.
23. Mah JY, Otsuka NY, McLean J. An arthroscopic technique for the reduction and fixation of tibial-eminence fractures. J Pediatr Orthop. 1996;16(1):119-121.
24. Reynders P, Reynders K, Broos P. Pediatric and adolescent tibial eminence fractures: arthroscopic cannulated screw fixation. J Trauma. 2002;53(1):49-54.
25. Hunter RE, Willis JA. Arthroscopic fixation of avulsion fractures of the tibial eminence: technique and outcome. Arthroscopy. 2004;20(2):113-121.
26. Eggers AK, Becker C, Weimann A, et al. Biomechanical evaluation of different fixation methods for tibial eminence fractures. Am J Sports Med. 2007;35(3):404-410.
27. Mahar AT, Duncan D, Oka R, Lowry A, Gillingham B, Chambers H. Biomechanical comparison of four different fixation techniques for pediatric tibial eminence avulsion fractures. J Pediatr Orthop. 2008;28(2):159-162.
28. Toro C, Robiony M, Zerman N, Politi M. Resorbable plates in maxillary fixation. A 5-year experience. Minerva Stomatol. 2005;54(4):199-206.
29. Andriano KP, Pohjonen T, Törmälä P. Processing and characterization of absorbable polylactide polymers for use in surgical implants. J Appl Biomater.1994;5(2):133-140.
30. Böstman O, Pihlajamäki H. Clinical biocompatibility of biodegradable orthopaedic implants for internal fixation: a review. Biomaterials. 2000;21(24):2615-2621.
31. Rokkanen PU, Böstman O, Hirvensalo E, et al. Bioabsorbable fixation in orthopaedic surgery and traumatology. Biomaterials. 2000;21(24):2607-2613.
32. Athanasiou KA, Niederauer GG, Agrawal CM. Sterilization, toxicity, biocompatibility and clinical applications of polylactic acid/polyglycolic acid copolymers. Biomaterials. 1996;17(2):93-102.
33. Li ZH, Yu AX, Guo XP, Qi BW, Zhou M, Wang WY. Absorbable implants versus metal implants for the treatment of ankle fractures: A meta-analysis. Exp Ther Med. 2013;5(5):1531-1537.
34. Singh G, Mohammad S, Chak RK, Lepcha N, Singh N, Malkunje LR. Bio-resorbable plates as effective implant in paediatric mandibular fracture. J Maxillofac Oral Surg. 2012;11(4):400-406.
35. Sakamoto Y, Shimizu Y, Nagasao T, Kishi K. Combined use of resorbable poly-L-lactic acid-polyglycolic acid implant and bone cement for treating large orbital floor fractures. J Plast Reconstr Aesthet Surg. 2014;67(3):e88-e90.
36. Benz G, Kallieris D, Seeböck T, McIntosh A, Daum R. Bioresorbable pins and screws in paediatric traumatology. Eur J Pediatr Surg. 1994;4(2):103-107.
37. Gaweda K, Walawski J, Weglowski R, Krzyzanowski W. Comparison of bioabsorbable interference screws and posts for distal fixation in anterior cruciate ligament reconstruction. Int Orthop. 2009;33(1):123-127.
38. Böstman OM. Osteoarthritis of the ankle after foreign-body reaction to absorbable pins and screws: a three- to nine-year follow-up study. J Bone Joint Surg Br. 1998;80(2):333-338.
39. Mittal R, Morley J, Dinopoulos H, Drakoulakis EG, Vermani E, Giannoudis PV. Use of bio-resorbable implants for stabilisation of distal radius fractures: the United Kingdom patients’ perspective. Injury. 2005;36(2):333-338.
40. Böstman OM. Metallic or absorbable fracture fixation devices. A cost minimization analysis. Clin Orthop. 1996;(329):233-239.
1. Hargrove R, Parsons S, Payne R. Anterior tibial spine fracture – an easy fracture to miss. Accid Emerg Nurs. 2004;12(3):173-175.
2. Aderinto J, Walmsley P, Keating JF. Fractures of the tibial spine: epidemiology and outcome. Knee. 2008;15(3):164-167.
3. Driessen MJ, Winkelman PA. Fractures of the intercondylar eminence of the tibia in childhood. Neth J Surg. 1984;36(3):69-72.
4. Zaricznyj B. Avulsion fracture of the tibial eminence: treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59(8):1111-1114.
5. Molander ML, Wallin G, Wikstad I. Fracture of the intercondylar eminence of the tibia: a review of 35 patients. J Bone Joint Surg Br. 1981;63(1):89-91.
6. Kieser DC, Gwynne-Jones D, Dreyer S. Displaced tibial intercondylar eminence fractures. J Orthop Surg. 2011;19(3):292-296.
7. Ishibashi Y, Tsuda E, Sasaki T, Toh S. Magnetic resonance imaging AIDS in detecting concomitant injuries in patients with tibial spine fractures. Clin Orthop. 2005;(434):207-212.
8. McLennan JG. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br. 1982;64(4):477-480.
9. Lafrance RM, Giordano B, Goldblatt J, Voloshin I, Maloney M. Pediatric tibial eminence fractures: evaluation and management. J Am Acad Orthop Surg. 2010;18(7):395-405.
10. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1959;41(2):209-220.
11. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970;52(8):1677-1684.
12. Garcés GL, Mugica-Garay I, López-González Coviella N, Guerado E. Growth-plate modifications after drilling. J Pediatr Orthop. 1994;14(2):225-228.
13. Janarv PM, Wikström B, Hirsch G. The influence of transphyseal drilling and tendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Orthop. 1998;18(2):149-154.
14. Boelitz R, Dallek M, Meenen NM, Jungbluth KH. Reaction of the epiphyseal groove to groove-crossing bore-wire osteosynthesis. Results of a histomorphologic small animal study. Unfallchirurgie. 1994;20(3):131-137.
15. Yung PS, Lam CY, Ng BK, Lam TP, Cheng JC. Percutaneous transphyseal intramedullary Kirschner wire pinning: a safe and effective procedure for treatment of displaced diaphyseal forearm fracture in children. J Pediatr Orthop. 2004;24(1):7-12.
16. Bong MR, Romero A, Kubiak E, et al. Suture versus screw fixation of displaced tibial eminence fractures: a biomechanical comparison. Arthroscopy. 2005;21(10):1172-1176.
17. Vega JR, Irribarra LA, Baar AK, Iñiguez M, Salgado M, Gana N. Arthroscopic fixation of displaced tibial eminence fractures: a new growth plate-sparing method. Arthroscopy. 2008;24(11):1239-1243.
18. Shepley RW. Arthroscopic treatment of type III tibial spine fractures using absorbable fixation. Orthopedics. 2004;27(7):767-769.
19. Gans I, Baldwin KD, Ganley TJ. Treatment and management outcomes of tibial eminence fractures in pediatric patients: a systematic review. Am J Sports Med. 2013;42(7):1743-1750.
20. Delcogliano A, Chiossi S, Caporaso A, Menghi A, Rinonapoli G. Tibial intercondylar eminence fractures in adults: arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc. 2003;11(4):255-259.
21. Mulhall KJ, Dowdall J, Grannell M, McCabe JP. Tibial spine fractures: an analysis of outcome in surgically treated type III injuries. Injury. 1999;30(4):289-292.
22. Geissler WB, Matthews DE. Arthroscopic suture fixation of displaced tibial eminence fractures. Orthopedics. 1993;16(3):331-333.
23. Mah JY, Otsuka NY, McLean J. An arthroscopic technique for the reduction and fixation of tibial-eminence fractures. J Pediatr Orthop. 1996;16(1):119-121.
24. Reynders P, Reynders K, Broos P. Pediatric and adolescent tibial eminence fractures: arthroscopic cannulated screw fixation. J Trauma. 2002;53(1):49-54.
25. Hunter RE, Willis JA. Arthroscopic fixation of avulsion fractures of the tibial eminence: technique and outcome. Arthroscopy. 2004;20(2):113-121.
26. Eggers AK, Becker C, Weimann A, et al. Biomechanical evaluation of different fixation methods for tibial eminence fractures. Am J Sports Med. 2007;35(3):404-410.
27. Mahar AT, Duncan D, Oka R, Lowry A, Gillingham B, Chambers H. Biomechanical comparison of four different fixation techniques for pediatric tibial eminence avulsion fractures. J Pediatr Orthop. 2008;28(2):159-162.
28. Toro C, Robiony M, Zerman N, Politi M. Resorbable plates in maxillary fixation. A 5-year experience. Minerva Stomatol. 2005;54(4):199-206.
29. Andriano KP, Pohjonen T, Törmälä P. Processing and characterization of absorbable polylactide polymers for use in surgical implants. J Appl Biomater.1994;5(2):133-140.
30. Böstman O, Pihlajamäki H. Clinical biocompatibility of biodegradable orthopaedic implants for internal fixation: a review. Biomaterials. 2000;21(24):2615-2621.
31. Rokkanen PU, Böstman O, Hirvensalo E, et al. Bioabsorbable fixation in orthopaedic surgery and traumatology. Biomaterials. 2000;21(24):2607-2613.
32. Athanasiou KA, Niederauer GG, Agrawal CM. Sterilization, toxicity, biocompatibility and clinical applications of polylactic acid/polyglycolic acid copolymers. Biomaterials. 1996;17(2):93-102.
33. Li ZH, Yu AX, Guo XP, Qi BW, Zhou M, Wang WY. Absorbable implants versus metal implants for the treatment of ankle fractures: A meta-analysis. Exp Ther Med. 2013;5(5):1531-1537.
34. Singh G, Mohammad S, Chak RK, Lepcha N, Singh N, Malkunje LR. Bio-resorbable plates as effective implant in paediatric mandibular fracture. J Maxillofac Oral Surg. 2012;11(4):400-406.
35. Sakamoto Y, Shimizu Y, Nagasao T, Kishi K. Combined use of resorbable poly-L-lactic acid-polyglycolic acid implant and bone cement for treating large orbital floor fractures. J Plast Reconstr Aesthet Surg. 2014;67(3):e88-e90.
36. Benz G, Kallieris D, Seeböck T, McIntosh A, Daum R. Bioresorbable pins and screws in paediatric traumatology. Eur J Pediatr Surg. 1994;4(2):103-107.
37. Gaweda K, Walawski J, Weglowski R, Krzyzanowski W. Comparison of bioabsorbable interference screws and posts for distal fixation in anterior cruciate ligament reconstruction. Int Orthop. 2009;33(1):123-127.
38. Böstman OM. Osteoarthritis of the ankle after foreign-body reaction to absorbable pins and screws: a three- to nine-year follow-up study. J Bone Joint Surg Br. 1998;80(2):333-338.
39. Mittal R, Morley J, Dinopoulos H, Drakoulakis EG, Vermani E, Giannoudis PV. Use of bio-resorbable implants for stabilisation of distal radius fractures: the United Kingdom patients’ perspective. Injury. 2005;36(2):333-338.
40. Böstman OM. Metallic or absorbable fracture fixation devices. A cost minimization analysis. Clin Orthop. 1996;(329):233-239.
