User login
Poison center calls for fake pot up 330% in first half of 2015
The number of telephone calls to U.S. poison centers reporting adverse health effects or concerns about possible adverse health effects related to synthetic cannabinoid use soared 330% from 349 in January 2015 to 1,501 in April 2015, newly published data from the Centers for Disease and Control and Prevention show.
Between January and May 2015, poison centers reported 3,572 calls related to synthetic cannabinoid use, a 229% increase from the 1,085 calls during the same January-May period in 2014. The number of calls spiked notably in mid-April before decreasing nearly to 2014 levels by the end of May, according to the CDC’s Morbidity and Mortality Weekly Report.

Synthetic marijuana is sold under a variety of names (such as K2, spice, or black mamba), but since manufacturers frequently change the formulation to avoid detection and regulation, chemical formulas can vary wildly, even within similar strains. The most commonly reported adverse health effects were agitation (1,262 [35.3%]), tachycardia (1,035 [29.0%]), drowsiness or lethargy (939 [26.3%]), vomiting (585 [16.4%]), and confusion (506, [14.2%]). Most of the reported use was intentional (3,310 [92.7%]) (MMWR 2015;64:618-9).
The report said that most of the calls involved males (2,882 [80.7%]), and “where age of the user was recorded, the median age was 26 years.”
“Recent outbreaks suggest a need for greater public health surveillance and awareness, targeted public health messaging, and enhanced efforts to remove these products from the market,” wrote the authors, led by Royal K. Law of the CDC.
The number of telephone calls to U.S. poison centers reporting adverse health effects or concerns about possible adverse health effects related to synthetic cannabinoid use soared 330% from 349 in January 2015 to 1,501 in April 2015, newly published data from the Centers for Disease and Control and Prevention show.
Between January and May 2015, poison centers reported 3,572 calls related to synthetic cannabinoid use, a 229% increase from the 1,085 calls during the same January-May period in 2014. The number of calls spiked notably in mid-April before decreasing nearly to 2014 levels by the end of May, according to the CDC’s Morbidity and Mortality Weekly Report.
Synthetic marijuana is sold under a variety of names (such as K2, spice, or black mamba), but since manufacturers frequently change the formulation to avoid detection and regulation, chemical formulas can vary wildly, even within similar strains. The most commonly reported adverse health effects were agitation (1,262 [35.3%]), tachycardia (1,035 [29.0%]), drowsiness or lethargy (939 [26.3%]), vomiting (585 [16.4%]), and confusion (506, [14.2%]). Most of the reported use was intentional (3,310 [92.7%]) (MMWR 2015;64:618-9).
The report said that most of the calls involved males (2,882 [80.7%]), and “where age of the user was recorded, the median age was 26 years.”
“Recent outbreaks suggest a need for greater public health surveillance and awareness, targeted public health messaging, and enhanced efforts to remove these products from the market,” wrote the authors, led by Royal K. Law of the CDC.
The number of telephone calls to U.S. poison centers reporting adverse health effects or concerns about possible adverse health effects related to synthetic cannabinoid use soared 330% from 349 in January 2015 to 1,501 in April 2015, newly published data from the Centers for Disease and Control and Prevention show.
Between January and May 2015, poison centers reported 3,572 calls related to synthetic cannabinoid use, a 229% increase from the 1,085 calls during the same January-May period in 2014. The number of calls spiked notably in mid-April before decreasing nearly to 2014 levels by the end of May, according to the CDC’s Morbidity and Mortality Weekly Report.
Synthetic marijuana is sold under a variety of names (such as K2, spice, or black mamba), but since manufacturers frequently change the formulation to avoid detection and regulation, chemical formulas can vary wildly, even within similar strains. The most commonly reported adverse health effects were agitation (1,262 [35.3%]), tachycardia (1,035 [29.0%]), drowsiness or lethargy (939 [26.3%]), vomiting (585 [16.4%]), and confusion (506, [14.2%]). Most of the reported use was intentional (3,310 [92.7%]) (MMWR 2015;64:618-9).
The report said that most of the calls involved males (2,882 [80.7%]), and “where age of the user was recorded, the median age was 26 years.”
“Recent outbreaks suggest a need for greater public health surveillance and awareness, targeted public health messaging, and enhanced efforts to remove these products from the market,” wrote the authors, led by Royal K. Law of the CDC.
FROM MMWR

VIDEO: How should you respond to a possible privacy breach?
CHICAGO – Overreact, don’t underreact, when it comes to possible health care privacy breaches, attorney Clinton Mikel advised at a conference held by the American Bar Association.
The actions that physicians take immediately following a potential data exposure will significantly impact how the Health and Human Services Department’s Office for Civil Rights (OCR) responds to the incident and whether physicians face penalties, said Mr. Mikel, who specializes in the Health Insurance Portability and Accountability Act (HIPAA) and state privacy laws.
In an interview at the conference, Mr. Mikel, who practices law in Southfield, Mich., discussed common misconceptions that physicians have about privacy breaches and the best ways in which to respond internally to possible exposures. He also offered guidance on the top mistakes to avoid when confronted with possible security breaches and shared perspective on how the OCR might address such issues in the future.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
CHICAGO – Overreact, don’t underreact, when it comes to possible health care privacy breaches, attorney Clinton Mikel advised at a conference held by the American Bar Association.
The actions that physicians take immediately following a potential data exposure will significantly impact how the Health and Human Services Department’s Office for Civil Rights (OCR) responds to the incident and whether physicians face penalties, said Mr. Mikel, who specializes in the Health Insurance Portability and Accountability Act (HIPAA) and state privacy laws.
In an interview at the conference, Mr. Mikel, who practices law in Southfield, Mich., discussed common misconceptions that physicians have about privacy breaches and the best ways in which to respond internally to possible exposures. He also offered guidance on the top mistakes to avoid when confronted with possible security breaches and shared perspective on how the OCR might address such issues in the future.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
CHICAGO – Overreact, don’t underreact, when it comes to possible health care privacy breaches, attorney Clinton Mikel advised at a conference held by the American Bar Association.
The actions that physicians take immediately following a potential data exposure will significantly impact how the Health and Human Services Department’s Office for Civil Rights (OCR) responds to the incident and whether physicians face penalties, said Mr. Mikel, who specializes in the Health Insurance Portability and Accountability Act (HIPAA) and state privacy laws.
In an interview at the conference, Mr. Mikel, who practices law in Southfield, Mich., discussed common misconceptions that physicians have about privacy breaches and the best ways in which to respond internally to possible exposures. He also offered guidance on the top mistakes to avoid when confronted with possible security breaches and shared perspective on how the OCR might address such issues in the future.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
EXPERT ANALYSIS FROM THE PHYSICIANS LEGAL ISSUES CONFERENCE

Doctor, why DO you get paid so much?
The reporter wanted to nail me, and shot me the zinger, “Doctor why do you get paid $106 to do a skin biopsy, and they only get $30 in Germany”?
I paused for minute (she was sure she had me), and then I said, “They only get $30? That stinks. You know I do get $49.”
The reporter said, “No, no, I see here in the Medicare database that doctors in the United States get paid $106.”
I explained to her that $57 of that was for equipment, staff, and supplies, and that doctors in Germany do everything in the hospital setting, where they don’t have to pay for any of that.
Oh.

This is an error that is repeated again and again, and you need to know the reason you get paid “so much.” The second year’s worth of the Medicare data were released last month, with a wrinkle: They removed the cost of medications. They floated the surgeons, oncologists, and ophthalmologists down and floated dermatology up to near the top, just under radiation oncology.
Let’s think about this for a minute. How many radiation oncologists have linear accelerators in their offices, and how many cardiologists have cath labs? How many ophthalmologists do cataract procedures in the office? The same is true for almost every other specialty. Most practitioners of procedural medicine do procedures in a hospital, where they pay no practice expenses. They may have a small office for consultations and suture removals, but for anything else they say, “Meet me at the hospital.” Often, the hospital supplies the office space for free or at a discount.
Now I don’t envy the primary care doctors, who also do everything in their offices, but guess what? Practice expense is only about 20% of the valuation of the evaluation and management codes. Think about this again. They don’t have power tables, OR lights, prep kits, sutures, hand tools, gauze, sponges, bandages, etc., to pay for, so it makes sense.
This means that most procedural physicians keep (before the huge tax bill we all are subject to) almost every Medicare dollar or insurance dollar they receive. Dermatologists’ reimbursements are 60% for practice expenses overall, with some even higher. Mohs surgery, for example, costs an average of 66% to provide. Dermatologists do almost nothing in the hospital, and instead provide more care for patients in the office setting. So, when the reporter tries to zing you about collecting $300,000 from Medicare, you explain that your dollars aren’t the same as everyone else’s dollars, and you really took $120,000 to the tax man (not that any of this is really their business anyway).
And, by the way, tell them you only get $24 for a second biopsy, which is just as much work as the first.
I think we should ask CMS to pull the practice expense out of its Medicare numbers in the next report. A dollar spent for surgical supplies is the same as a dollar spent for medications. It’s all money the doctor never sees.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The reporter wanted to nail me, and shot me the zinger, “Doctor why do you get paid $106 to do a skin biopsy, and they only get $30 in Germany”?
I paused for minute (she was sure she had me), and then I said, “They only get $30? That stinks. You know I do get $49.”
The reporter said, “No, no, I see here in the Medicare database that doctors in the United States get paid $106.”
I explained to her that $57 of that was for equipment, staff, and supplies, and that doctors in Germany do everything in the hospital setting, where they don’t have to pay for any of that.
Oh.
This is an error that is repeated again and again, and you need to know the reason you get paid “so much.” The second year’s worth of the Medicare data were released last month, with a wrinkle: They removed the cost of medications. They floated the surgeons, oncologists, and ophthalmologists down and floated dermatology up to near the top, just under radiation oncology.
Let’s think about this for a minute. How many radiation oncologists have linear accelerators in their offices, and how many cardiologists have cath labs? How many ophthalmologists do cataract procedures in the office? The same is true for almost every other specialty. Most practitioners of procedural medicine do procedures in a hospital, where they pay no practice expenses. They may have a small office for consultations and suture removals, but for anything else they say, “Meet me at the hospital.” Often, the hospital supplies the office space for free or at a discount.
Now I don’t envy the primary care doctors, who also do everything in their offices, but guess what? Practice expense is only about 20% of the valuation of the evaluation and management codes. Think about this again. They don’t have power tables, OR lights, prep kits, sutures, hand tools, gauze, sponges, bandages, etc., to pay for, so it makes sense.
This means that most procedural physicians keep (before the huge tax bill we all are subject to) almost every Medicare dollar or insurance dollar they receive. Dermatologists’ reimbursements are 60% for practice expenses overall, with some even higher. Mohs surgery, for example, costs an average of 66% to provide. Dermatologists do almost nothing in the hospital, and instead provide more care for patients in the office setting. So, when the reporter tries to zing you about collecting $300,000 from Medicare, you explain that your dollars aren’t the same as everyone else’s dollars, and you really took $120,000 to the tax man (not that any of this is really their business anyway).
And, by the way, tell them you only get $24 for a second biopsy, which is just as much work as the first.
I think we should ask CMS to pull the practice expense out of its Medicare numbers in the next report. A dollar spent for surgical supplies is the same as a dollar spent for medications. It’s all money the doctor never sees.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The reporter wanted to nail me, and shot me the zinger, “Doctor why do you get paid $106 to do a skin biopsy, and they only get $30 in Germany”?
I paused for minute (she was sure she had me), and then I said, “They only get $30? That stinks. You know I do get $49.”
The reporter said, “No, no, I see here in the Medicare database that doctors in the United States get paid $106.”
I explained to her that $57 of that was for equipment, staff, and supplies, and that doctors in Germany do everything in the hospital setting, where they don’t have to pay for any of that.
Oh.
This is an error that is repeated again and again, and you need to know the reason you get paid “so much.” The second year’s worth of the Medicare data were released last month, with a wrinkle: They removed the cost of medications. They floated the surgeons, oncologists, and ophthalmologists down and floated dermatology up to near the top, just under radiation oncology.
Let’s think about this for a minute. How many radiation oncologists have linear accelerators in their offices, and how many cardiologists have cath labs? How many ophthalmologists do cataract procedures in the office? The same is true for almost every other specialty. Most practitioners of procedural medicine do procedures in a hospital, where they pay no practice expenses. They may have a small office for consultations and suture removals, but for anything else they say, “Meet me at the hospital.” Often, the hospital supplies the office space for free or at a discount.
Now I don’t envy the primary care doctors, who also do everything in their offices, but guess what? Practice expense is only about 20% of the valuation of the evaluation and management codes. Think about this again. They don’t have power tables, OR lights, prep kits, sutures, hand tools, gauze, sponges, bandages, etc., to pay for, so it makes sense.
This means that most procedural physicians keep (before the huge tax bill we all are subject to) almost every Medicare dollar or insurance dollar they receive. Dermatologists’ reimbursements are 60% for practice expenses overall, with some even higher. Mohs surgery, for example, costs an average of 66% to provide. Dermatologists do almost nothing in the hospital, and instead provide more care for patients in the office setting. So, when the reporter tries to zing you about collecting $300,000 from Medicare, you explain that your dollars aren’t the same as everyone else’s dollars, and you really took $120,000 to the tax man (not that any of this is really their business anyway).
And, by the way, tell them you only get $24 for a second biopsy, which is just as much work as the first.
I think we should ask CMS to pull the practice expense out of its Medicare numbers in the next report. A dollar spent for surgical supplies is the same as a dollar spent for medications. It’s all money the doctor never sees.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Pathway may play key role in FLT3-ITD AML

Results of preclinical research suggest the Hedgehog signaling pathway works with FLT3-ITD mutations to accelerate the development of acute myeloid leukemia (AML).
This finding prompted investigators to look at Hedgehog signaling as a possible second target for treatment in FLT3-ITD AML.
By combining the FLT3 inhibitor sorafenib with the Hedgehog pathway inhibitor IPI-926 (saridegib), the team found they could limit AML growth in vitro and in vivo.
William Matsui, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and disclosed the results in Science Translational Medicine.
The investigators began this work with the goal of discovering why FLT3 inhibitors have fallen short in treating AML. They analyzed gene expression profiles from AML patients and found abnormally enhanced activity in the Hedgehog signaling pathway.
This pathway, which normally regulates embryonic development, is known to fuel many cancer types, but its role in AML has, thus far, remained unresolved.
In experiments with mice, the investigators found the Hedgehog pathway seemed to work together with FLT3 to accelerate AML development and earlier death.
When the team activated Hedgehog signaling in mice expressing FLT3-ITD, they observed enhanced STAT5 signaling, myeloid progenitor proliferation, and AML development.
“From our data, it appears that Hedgehog signaling is like an accelerator,” Dr Matsui said. “It facilitates the cellular events that lead to cancer, but it itself is not the driver of the whole process.”
The investigators also found that mice with both the FLT3 mutation and Hedgehog activity had a significantly shorter lifespan than mice with FLT3-ITD only—an average of 12 weeks and 40 weeks, respectively.
To build upon these findings, the team tested IPI-926 and sorafenib, both alone and in combination, in mice with AML. They found that mice treated with the combination had significantly fewer leukemic cells in the blood and bone marrow than mice treated with either drug alone.
In addition, 3 of the 5 mice treated with the combination survived past the 16 days of the experiment without any further treatment, but none of the mice treated with sorafenib or IPI-926 alone survived that long.
“When we treat mice that have leukemia with both drugs, they live longer than with either drug alone, and there is a portion of them that don’t die at all,” Dr Matsui noted.
He said it’s likely that Hedgehog signaling is involved in the progression of a number of cancers, and “this study brings home the idea that, in treating these cancers, clinicians may need to inhibit Hedgehog along with specific gene mutations.”
Dr Matsui and his colleagues have begun investigating how Hedgehog inhibitors work when combined with newer drugs that target FLT3 more precisely than sorafenib. If these tests continue to show signs that the two types of inhibitors can fight AML, the investigators think such combination therapy could move on to clinical trials. ![]()
Results of preclinical research suggest the Hedgehog signaling pathway works with FLT3-ITD mutations to accelerate the development of acute myeloid leukemia (AML).
This finding prompted investigators to look at Hedgehog signaling as a possible second target for treatment in FLT3-ITD AML.
By combining the FLT3 inhibitor sorafenib with the Hedgehog pathway inhibitor IPI-926 (saridegib), the team found they could limit AML growth in vitro and in vivo.
William Matsui, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and disclosed the results in Science Translational Medicine.
The investigators began this work with the goal of discovering why FLT3 inhibitors have fallen short in treating AML. They analyzed gene expression profiles from AML patients and found abnormally enhanced activity in the Hedgehog signaling pathway.
This pathway, which normally regulates embryonic development, is known to fuel many cancer types, but its role in AML has, thus far, remained unresolved.
In experiments with mice, the investigators found the Hedgehog pathway seemed to work together with FLT3 to accelerate AML development and earlier death.
When the team activated Hedgehog signaling in mice expressing FLT3-ITD, they observed enhanced STAT5 signaling, myeloid progenitor proliferation, and AML development.
“From our data, it appears that Hedgehog signaling is like an accelerator,” Dr Matsui said. “It facilitates the cellular events that lead to cancer, but it itself is not the driver of the whole process.”
The investigators also found that mice with both the FLT3 mutation and Hedgehog activity had a significantly shorter lifespan than mice with FLT3-ITD only—an average of 12 weeks and 40 weeks, respectively.
To build upon these findings, the team tested IPI-926 and sorafenib, both alone and in combination, in mice with AML. They found that mice treated with the combination had significantly fewer leukemic cells in the blood and bone marrow than mice treated with either drug alone.
In addition, 3 of the 5 mice treated with the combination survived past the 16 days of the experiment without any further treatment, but none of the mice treated with sorafenib or IPI-926 alone survived that long.
“When we treat mice that have leukemia with both drugs, they live longer than with either drug alone, and there is a portion of them that don’t die at all,” Dr Matsui noted.
He said it’s likely that Hedgehog signaling is involved in the progression of a number of cancers, and “this study brings home the idea that, in treating these cancers, clinicians may need to inhibit Hedgehog along with specific gene mutations.”
Dr Matsui and his colleagues have begun investigating how Hedgehog inhibitors work when combined with newer drugs that target FLT3 more precisely than sorafenib. If these tests continue to show signs that the two types of inhibitors can fight AML, the investigators think such combination therapy could move on to clinical trials. ![]()
Results of preclinical research suggest the Hedgehog signaling pathway works with FLT3-ITD mutations to accelerate the development of acute myeloid leukemia (AML).
This finding prompted investigators to look at Hedgehog signaling as a possible second target for treatment in FLT3-ITD AML.
By combining the FLT3 inhibitor sorafenib with the Hedgehog pathway inhibitor IPI-926 (saridegib), the team found they could limit AML growth in vitro and in vivo.
William Matsui, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and disclosed the results in Science Translational Medicine.
The investigators began this work with the goal of discovering why FLT3 inhibitors have fallen short in treating AML. They analyzed gene expression profiles from AML patients and found abnormally enhanced activity in the Hedgehog signaling pathway.
This pathway, which normally regulates embryonic development, is known to fuel many cancer types, but its role in AML has, thus far, remained unresolved.
In experiments with mice, the investigators found the Hedgehog pathway seemed to work together with FLT3 to accelerate AML development and earlier death.
When the team activated Hedgehog signaling in mice expressing FLT3-ITD, they observed enhanced STAT5 signaling, myeloid progenitor proliferation, and AML development.
“From our data, it appears that Hedgehog signaling is like an accelerator,” Dr Matsui said. “It facilitates the cellular events that lead to cancer, but it itself is not the driver of the whole process.”
The investigators also found that mice with both the FLT3 mutation and Hedgehog activity had a significantly shorter lifespan than mice with FLT3-ITD only—an average of 12 weeks and 40 weeks, respectively.
To build upon these findings, the team tested IPI-926 and sorafenib, both alone and in combination, in mice with AML. They found that mice treated with the combination had significantly fewer leukemic cells in the blood and bone marrow than mice treated with either drug alone.
In addition, 3 of the 5 mice treated with the combination survived past the 16 days of the experiment without any further treatment, but none of the mice treated with sorafenib or IPI-926 alone survived that long.
“When we treat mice that have leukemia with both drugs, they live longer than with either drug alone, and there is a portion of them that don’t die at all,” Dr Matsui noted.
He said it’s likely that Hedgehog signaling is involved in the progression of a number of cancers, and “this study brings home the idea that, in treating these cancers, clinicians may need to inhibit Hedgehog along with specific gene mutations.”
Dr Matsui and his colleagues have begun investigating how Hedgehog inhibitors work when combined with newer drugs that target FLT3 more precisely than sorafenib. If these tests continue to show signs that the two types of inhibitors can fight AML, the investigators think such combination therapy could move on to clinical trials. ![]()
CAR T-cell therapy seems feasible for NHL, MM

©ASCO/Rodney White
CHICAGO—The CD19-directed chimeric antigen receptor (CAR) T-cell therapy CTL019 has shown promise for treating non-Hodgkin lymphoma (NHL) and may be a feasible treatment option for multiple myeloma (MM) as well, according to researchers.
In an ongoing phase 2 trial, CTL019 has produced durable responses in patients with relapsed or refractory NHL.
And early results of a phase 1 trial suggest CTL019 can provide clinical benefit in heavily pretreated patients with MM.
Both studies were presented at the 2015 ASCO Annual Meeting. The University of Pennsylvania and Novartis have an exclusive global collaboration to research, develop, and commercialize CTL019.
CTL019 in NHL
Stephen Schuster, MD, of the Abramson Cancer Center of the University of Pennsylvania in Philadelphia, presented results of the phase 2 NHL trial (abstract 8516*).
The trial included 20 evaluable patients, 13 with diffuse large B-cell lymphoma (DLBCL) and 7 with follicular lymphoma (FL). At the time of presentation, the median follow-up was 274 days for the patients with DLBCL and 290 days for those with FL.
The overall response rate was 100% in patients with FL and 50% in those with DLBCL. Thirteen patients responded to the therapy, including 11 who achieved a complete response and 2 who experienced a partial response.
Six patients with a partial response to treatment at 3 months achieved a complete response by 6 months. Two patients with a partial response experienced disease progression at 6 and 12 months after treatment.
The researchers said toxicity appeared to be acceptable, with primarily grade 2 cytokine release syndrome (CRS). Two patients developed CRS of grade 3 or higher at peak T-cell expansion. There were no deaths from CRS.
“The results from this ongoing study of CTL019 are encouraging, as we now have data through 6 months showing that patients may have achieved durable overall response rates,” Dr Schuster said. “These data support our ongoing efforts to determine the potential role of CTL019 in improving outcomes for patients with certain types of B-cell lymphomas.”
CTL019 in MM
Alfred Garfall, MD, of the Abramson Cancer Center, presented preliminary results of an ongoing phase 1 study investigating CTL019 in patients with MM (abstract 8517*).
Dr Garfall and his colleagues hypothesized that CTL019 would exhibit efficacy in MM due to low-level CD19 expression on MM plasma cells or CD19 expression in drug-resistant, disease-propagating subsets of the MM clone.
The study included 5 patients who experienced disease progression within a year of a prior autologous stem cell transplant and were medically fit to undergo a second autologous transplant. The patients had received a median of 7.5 prior lines of therapy.
“We found potential evidence of clinical benefit in 3 of 4 patients with more than 100 days of follow-up,” Dr Garfall said.
Two patients experienced longer, deeper responses, and 1 patient experienced CRS.
The data suggest “it is safe and feasible to manufacture and administered CTL019 to refractory multiple myeloma patients,” Dr Garfall said.
*Information in the abstract differs from that presented at the meeting.
©ASCO/Rodney White
CHICAGO—The CD19-directed chimeric antigen receptor (CAR) T-cell therapy CTL019 has shown promise for treating non-Hodgkin lymphoma (NHL) and may be a feasible treatment option for multiple myeloma (MM) as well, according to researchers.
In an ongoing phase 2 trial, CTL019 has produced durable responses in patients with relapsed or refractory NHL.
And early results of a phase 1 trial suggest CTL019 can provide clinical benefit in heavily pretreated patients with MM.
Both studies were presented at the 2015 ASCO Annual Meeting. The University of Pennsylvania and Novartis have an exclusive global collaboration to research, develop, and commercialize CTL019.
CTL019 in NHL
Stephen Schuster, MD, of the Abramson Cancer Center of the University of Pennsylvania in Philadelphia, presented results of the phase 2 NHL trial (abstract 8516*).
The trial included 20 evaluable patients, 13 with diffuse large B-cell lymphoma (DLBCL) and 7 with follicular lymphoma (FL). At the time of presentation, the median follow-up was 274 days for the patients with DLBCL and 290 days for those with FL.
The overall response rate was 100% in patients with FL and 50% in those with DLBCL. Thirteen patients responded to the therapy, including 11 who achieved a complete response and 2 who experienced a partial response.
Six patients with a partial response to treatment at 3 months achieved a complete response by 6 months. Two patients with a partial response experienced disease progression at 6 and 12 months after treatment.
The researchers said toxicity appeared to be acceptable, with primarily grade 2 cytokine release syndrome (CRS). Two patients developed CRS of grade 3 or higher at peak T-cell expansion. There were no deaths from CRS.
“The results from this ongoing study of CTL019 are encouraging, as we now have data through 6 months showing that patients may have achieved durable overall response rates,” Dr Schuster said. “These data support our ongoing efforts to determine the potential role of CTL019 in improving outcomes for patients with certain types of B-cell lymphomas.”
CTL019 in MM
Alfred Garfall, MD, of the Abramson Cancer Center, presented preliminary results of an ongoing phase 1 study investigating CTL019 in patients with MM (abstract 8517*).
Dr Garfall and his colleagues hypothesized that CTL019 would exhibit efficacy in MM due to low-level CD19 expression on MM plasma cells or CD19 expression in drug-resistant, disease-propagating subsets of the MM clone.
The study included 5 patients who experienced disease progression within a year of a prior autologous stem cell transplant and were medically fit to undergo a second autologous transplant. The patients had received a median of 7.5 prior lines of therapy.
“We found potential evidence of clinical benefit in 3 of 4 patients with more than 100 days of follow-up,” Dr Garfall said.
Two patients experienced longer, deeper responses, and 1 patient experienced CRS.
The data suggest “it is safe and feasible to manufacture and administered CTL019 to refractory multiple myeloma patients,” Dr Garfall said.
*Information in the abstract differs from that presented at the meeting.
©ASCO/Rodney White
CHICAGO—The CD19-directed chimeric antigen receptor (CAR) T-cell therapy CTL019 has shown promise for treating non-Hodgkin lymphoma (NHL) and may be a feasible treatment option for multiple myeloma (MM) as well, according to researchers.
In an ongoing phase 2 trial, CTL019 has produced durable responses in patients with relapsed or refractory NHL.
And early results of a phase 1 trial suggest CTL019 can provide clinical benefit in heavily pretreated patients with MM.
Both studies were presented at the 2015 ASCO Annual Meeting. The University of Pennsylvania and Novartis have an exclusive global collaboration to research, develop, and commercialize CTL019.
CTL019 in NHL
Stephen Schuster, MD, of the Abramson Cancer Center of the University of Pennsylvania in Philadelphia, presented results of the phase 2 NHL trial (abstract 8516*).
The trial included 20 evaluable patients, 13 with diffuse large B-cell lymphoma (DLBCL) and 7 with follicular lymphoma (FL). At the time of presentation, the median follow-up was 274 days for the patients with DLBCL and 290 days for those with FL.
The overall response rate was 100% in patients with FL and 50% in those with DLBCL. Thirteen patients responded to the therapy, including 11 who achieved a complete response and 2 who experienced a partial response.
Six patients with a partial response to treatment at 3 months achieved a complete response by 6 months. Two patients with a partial response experienced disease progression at 6 and 12 months after treatment.
The researchers said toxicity appeared to be acceptable, with primarily grade 2 cytokine release syndrome (CRS). Two patients developed CRS of grade 3 or higher at peak T-cell expansion. There were no deaths from CRS.
“The results from this ongoing study of CTL019 are encouraging, as we now have data through 6 months showing that patients may have achieved durable overall response rates,” Dr Schuster said. “These data support our ongoing efforts to determine the potential role of CTL019 in improving outcomes for patients with certain types of B-cell lymphomas.”
CTL019 in MM
Alfred Garfall, MD, of the Abramson Cancer Center, presented preliminary results of an ongoing phase 1 study investigating CTL019 in patients with MM (abstract 8517*).
Dr Garfall and his colleagues hypothesized that CTL019 would exhibit efficacy in MM due to low-level CD19 expression on MM plasma cells or CD19 expression in drug-resistant, disease-propagating subsets of the MM clone.
The study included 5 patients who experienced disease progression within a year of a prior autologous stem cell transplant and were medically fit to undergo a second autologous transplant. The patients had received a median of 7.5 prior lines of therapy.
“We found potential evidence of clinical benefit in 3 of 4 patients with more than 100 days of follow-up,” Dr Garfall said.
Two patients experienced longer, deeper responses, and 1 patient experienced CRS.
The data suggest “it is safe and feasible to manufacture and administered CTL019 to refractory multiple myeloma patients,” Dr Garfall said.
*Information in the abstract differs from that presented at the meeting.
Establishing cause of death in HSCT recipients

With a new study, researchers hope to establish definitions for specific causes of death in patients who undergo allogeneic hematopoietic stem cell transplant (HSCT).
The group noted that scientists conducting clinical trials commonly use committees to review and define endpoints.
However, investigators conducting genome-wide association studies rarely do, relying instead on center-reported outcomes, which are variable.
“It is important that we accurately define outcomes in these types of genomic studies as precisely as possible,” said Lara Sucheston-Campbell, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
To that end, she and her colleagues convened a consensus panel to review specific causes of death in HSCT recipients. The panel evaluated outcome data for 1484 patients who had been treated for acute leukemia or myelodysplasia at 1 of 11 US transplant centers and died within a year of undergoing HSCT.
Dr Sucheston-Campbell and her colleagues reported the results of this evaluation in Biology of Blood and Marrow Transplantation.
In the cases where the transplant center reported disease-related mortality, the researchers found almost perfect agreement between the consensus panel and the transplant center, in terms of how those deaths were classified. The panel agreed with more than 99% of deaths that were reported as disease-related.
There was less agreement for transplant-related mortality, however. The panel agreed with about 80% of deaths reported to be transplant-related.
And the level of agreement/discordance varied depending on the specific cause of death. For example, the panel agreed with transplant centers on most of the deaths that were reportedly caused by graft-vs-host disease.
But the panel reclassified many of the deaths that reportedly resulted from organ failure, saying these deaths should be considered disease-related, a result of graft-vs-host disease, infection-related, or due to “other” causes.
These results indicate that transplant-related mortality needs to be better defined, the researchers said. They believe this study provides a mechanism for prioritizing those HSCT cases that should be reviewed.
“We need to make sure that patients who experienced similar clinical events after a transplant were consistently defined regardless of where they were treated,” said study author Theresa Hahn, PhD, also of Roswell Park Cancer Center.
“This is a difficult topic to consider, but we can’t make progress to improve transplant outcomes without these discussions.” ![]()
With a new study, researchers hope to establish definitions for specific causes of death in patients who undergo allogeneic hematopoietic stem cell transplant (HSCT).
The group noted that scientists conducting clinical trials commonly use committees to review and define endpoints.
However, investigators conducting genome-wide association studies rarely do, relying instead on center-reported outcomes, which are variable.
“It is important that we accurately define outcomes in these types of genomic studies as precisely as possible,” said Lara Sucheston-Campbell, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
To that end, she and her colleagues convened a consensus panel to review specific causes of death in HSCT recipients. The panel evaluated outcome data for 1484 patients who had been treated for acute leukemia or myelodysplasia at 1 of 11 US transplant centers and died within a year of undergoing HSCT.
Dr Sucheston-Campbell and her colleagues reported the results of this evaluation in Biology of Blood and Marrow Transplantation.
In the cases where the transplant center reported disease-related mortality, the researchers found almost perfect agreement between the consensus panel and the transplant center, in terms of how those deaths were classified. The panel agreed with more than 99% of deaths that were reported as disease-related.
There was less agreement for transplant-related mortality, however. The panel agreed with about 80% of deaths reported to be transplant-related.
And the level of agreement/discordance varied depending on the specific cause of death. For example, the panel agreed with transplant centers on most of the deaths that were reportedly caused by graft-vs-host disease.
But the panel reclassified many of the deaths that reportedly resulted from organ failure, saying these deaths should be considered disease-related, a result of graft-vs-host disease, infection-related, or due to “other” causes.
These results indicate that transplant-related mortality needs to be better defined, the researchers said. They believe this study provides a mechanism for prioritizing those HSCT cases that should be reviewed.
“We need to make sure that patients who experienced similar clinical events after a transplant were consistently defined regardless of where they were treated,” said study author Theresa Hahn, PhD, also of Roswell Park Cancer Center.
“This is a difficult topic to consider, but we can’t make progress to improve transplant outcomes without these discussions.” ![]()
With a new study, researchers hope to establish definitions for specific causes of death in patients who undergo allogeneic hematopoietic stem cell transplant (HSCT).
The group noted that scientists conducting clinical trials commonly use committees to review and define endpoints.
However, investigators conducting genome-wide association studies rarely do, relying instead on center-reported outcomes, which are variable.
“It is important that we accurately define outcomes in these types of genomic studies as precisely as possible,” said Lara Sucheston-Campbell, PhD, of Roswell Park Cancer Institute in Buffalo, New York.
To that end, she and her colleagues convened a consensus panel to review specific causes of death in HSCT recipients. The panel evaluated outcome data for 1484 patients who had been treated for acute leukemia or myelodysplasia at 1 of 11 US transplant centers and died within a year of undergoing HSCT.
Dr Sucheston-Campbell and her colleagues reported the results of this evaluation in Biology of Blood and Marrow Transplantation.
In the cases where the transplant center reported disease-related mortality, the researchers found almost perfect agreement between the consensus panel and the transplant center, in terms of how those deaths were classified. The panel agreed with more than 99% of deaths that were reported as disease-related.
There was less agreement for transplant-related mortality, however. The panel agreed with about 80% of deaths reported to be transplant-related.
And the level of agreement/discordance varied depending on the specific cause of death. For example, the panel agreed with transplant centers on most of the deaths that were reportedly caused by graft-vs-host disease.
But the panel reclassified many of the deaths that reportedly resulted from organ failure, saying these deaths should be considered disease-related, a result of graft-vs-host disease, infection-related, or due to “other” causes.
These results indicate that transplant-related mortality needs to be better defined, the researchers said. They believe this study provides a mechanism for prioritizing those HSCT cases that should be reviewed.
“We need to make sure that patients who experienced similar clinical events after a transplant were consistently defined regardless of where they were treated,” said study author Theresa Hahn, PhD, also of Roswell Park Cancer Center.
“This is a difficult topic to consider, but we can’t make progress to improve transplant outcomes without these discussions.” ![]()
Harnessing immune defense to treat Candida infection

An upset in the body’s natural balance of gut bacteria that may lead to life-threatening bloodstream infections can be reversed by enhancing an
immune response, according to research published in Nature Medicine.
Researchers found that a transcription factor known as HIF-1α works with LL-37, a naturally occurring antibiotic, to kill the infection-causing fungi Candida albicans.
And this response can be enhanced with a drug called L-mimosine.
The researchers noted that Candida albicans can be lethal if it invades the bloodstream from the gut. And stem cell transplant recipients and immunosuppressed cancer patients have a high risk for this type of infection.
“For a cancer patient with a Candida bloodstream infection, the fatality rate is about 30%, [and] Candida is the number 1 fungal pathogen,” said study author Andrew Koh, MD, of the University of Texas Southwestern Medical Center in Dallas.
With that in mind, he and his colleagues set out to determine how the body’s natural immune defense system might be enhanced to fight a Candida infection. By studying how mice infected with Candida responded in different scenarios, the team found their answer.
“The commensal bacteria stimulate gut tissue to make a transcription factor and a natural antibiotic, which then kills the Candida fungus,” Dr Koh explained.
“When we gave the mice a pharmacologic agent called L-mimosine that stimulates the transcription factor, the agent knocked down Candida 100-fold, which translated into a 50% reduction in mortality from invasive Candida infection.”
Specifically, the researchers found that enhancing the transcription factor HIF-1α with L-mimosine led to increased production of the natural antibiotic peptide LL-37, which, in turn, killed the fungi. L-mimosine is a natural product derived from seeds of the koa haole tree that is known to boost HIF-1α activity.
The study also suggested that certain gut bacteria—Clostridial Firmicutes and Bacteroidetes—may be important in producing short-chain fatty acids that help fight infection.
The researchers said more work is needed to pinpoint the optimal method of inducing the body’s gut defense system, whether through use of an agent like L-mimosine or by administering short-chain fatty acids such as vinegar.
“Can we modulate the gut system to maintain balance so that it never gets to the point of pathogens invading the bloodstream?” Dr Koh asked. “Boosting [gastrointestinal] mucosal immune effectors to reduce fungal burden may be the key to tipping the balance back toward normal and preventing invasive fungal disease.” ![]()
An upset in the body’s natural balance of gut bacteria that may lead to life-threatening bloodstream infections can be reversed by enhancing an
immune response, according to research published in Nature Medicine.
Researchers found that a transcription factor known as HIF-1α works with LL-37, a naturally occurring antibiotic, to kill the infection-causing fungi Candida albicans.
And this response can be enhanced with a drug called L-mimosine.
The researchers noted that Candida albicans can be lethal if it invades the bloodstream from the gut. And stem cell transplant recipients and immunosuppressed cancer patients have a high risk for this type of infection.
“For a cancer patient with a Candida bloodstream infection, the fatality rate is about 30%, [and] Candida is the number 1 fungal pathogen,” said study author Andrew Koh, MD, of the University of Texas Southwestern Medical Center in Dallas.
With that in mind, he and his colleagues set out to determine how the body’s natural immune defense system might be enhanced to fight a Candida infection. By studying how mice infected with Candida responded in different scenarios, the team found their answer.
“The commensal bacteria stimulate gut tissue to make a transcription factor and a natural antibiotic, which then kills the Candida fungus,” Dr Koh explained.
“When we gave the mice a pharmacologic agent called L-mimosine that stimulates the transcription factor, the agent knocked down Candida 100-fold, which translated into a 50% reduction in mortality from invasive Candida infection.”
Specifically, the researchers found that enhancing the transcription factor HIF-1α with L-mimosine led to increased production of the natural antibiotic peptide LL-37, which, in turn, killed the fungi. L-mimosine is a natural product derived from seeds of the koa haole tree that is known to boost HIF-1α activity.
The study also suggested that certain gut bacteria—Clostridial Firmicutes and Bacteroidetes—may be important in producing short-chain fatty acids that help fight infection.
The researchers said more work is needed to pinpoint the optimal method of inducing the body’s gut defense system, whether through use of an agent like L-mimosine or by administering short-chain fatty acids such as vinegar.
“Can we modulate the gut system to maintain balance so that it never gets to the point of pathogens invading the bloodstream?” Dr Koh asked. “Boosting [gastrointestinal] mucosal immune effectors to reduce fungal burden may be the key to tipping the balance back toward normal and preventing invasive fungal disease.” ![]()
An upset in the body’s natural balance of gut bacteria that may lead to life-threatening bloodstream infections can be reversed by enhancing an
immune response, according to research published in Nature Medicine.
Researchers found that a transcription factor known as HIF-1α works with LL-37, a naturally occurring antibiotic, to kill the infection-causing fungi Candida albicans.
And this response can be enhanced with a drug called L-mimosine.
The researchers noted that Candida albicans can be lethal if it invades the bloodstream from the gut. And stem cell transplant recipients and immunosuppressed cancer patients have a high risk for this type of infection.
“For a cancer patient with a Candida bloodstream infection, the fatality rate is about 30%, [and] Candida is the number 1 fungal pathogen,” said study author Andrew Koh, MD, of the University of Texas Southwestern Medical Center in Dallas.
With that in mind, he and his colleagues set out to determine how the body’s natural immune defense system might be enhanced to fight a Candida infection. By studying how mice infected with Candida responded in different scenarios, the team found their answer.
“The commensal bacteria stimulate gut tissue to make a transcription factor and a natural antibiotic, which then kills the Candida fungus,” Dr Koh explained.
“When we gave the mice a pharmacologic agent called L-mimosine that stimulates the transcription factor, the agent knocked down Candida 100-fold, which translated into a 50% reduction in mortality from invasive Candida infection.”
Specifically, the researchers found that enhancing the transcription factor HIF-1α with L-mimosine led to increased production of the natural antibiotic peptide LL-37, which, in turn, killed the fungi. L-mimosine is a natural product derived from seeds of the koa haole tree that is known to boost HIF-1α activity.
The study also suggested that certain gut bacteria—Clostridial Firmicutes and Bacteroidetes—may be important in producing short-chain fatty acids that help fight infection.
The researchers said more work is needed to pinpoint the optimal method of inducing the body’s gut defense system, whether through use of an agent like L-mimosine or by administering short-chain fatty acids such as vinegar.
“Can we modulate the gut system to maintain balance so that it never gets to the point of pathogens invading the bloodstream?” Dr Koh asked. “Boosting [gastrointestinal] mucosal immune effectors to reduce fungal burden may be the key to tipping the balance back toward normal and preventing invasive fungal disease.” ![]()
ASCO: Adjuvant denosumab halves fracture risk for breast cancer patients on AIs
CHICAGO – Adjuvant denosumab is efficacious and safe for reducing fracture risk among women taking aromatase inhibitors (AIs) as part of their treatment for early breast cancer, finds the Austrian Breast & Colorectal Cancer Study Group’s study 18 (ABCSG-18).
Compared with peers randomized to placebo in the phase III trial, women randomized to the antiresorptive monoclonal antibody at the dose typically used to treat osteoporosis were half as likely to experience a first clinical fracture, first author Dr. Michael Gnant reported at the annual meeting of the American Society of Clinical Oncology. The benefit was similar whether women had normal bone mineral density at baseline or already had osteopenia.

Patients in the denosumab group did not have a significantly higher rate of adverse events, including the much-feared complication of osteonecrosis of the jaw.
“The actual fracture risk of postmenopausal breast cancer patients on AIs is substantial and may have been underestimated until today,” commented Dr. Gnant, professor of surgery at the Medical University of Vienna. “In these patients with only a modest risk of disease recurrence, adjuvant denosumab significantly reduced the bone side effects of AI treatment. We therefore believe that denosumab 60 mg every 6 months should be considered for clinical practice.”
“Today, several clinical practice guidelines advocate the use of bisphosphonates for breast cancer patients receiving AIs, however, only if they are at high risk for fractures,” he further noted. However, “patients with normal baseline bone mineral density showed a similar fracture risk but also similar benefit from denosumab as compared to patients with baseline T scores below –1, indicating that DEXA scans may be an insufficient way to assess the individual patient’s fracture risk. In view of the benefits in this particular patient subgroup, we may have to rediscuss our current clinical practice guidelines.”

Invited discussant Dr. Robert E. Coleman of the University of Sheffield and Weston Park Hospital in England, said, “It’s very important to dissect out fractures related to subsequent recurrence from fractures due to poor bone health.” Most of the reduction in fracture risk in ABCSG-18 appeared to be because of prevention of fractures before any recurrence, whereas most of that in the AZURE trial (Adjuvant Zoledronic Acid to Reduce Recurrence) of an adjuvant bisphosphonate, another type of antiresorptive agent, appeared to be because of prevention of fractures from bone metastases. “So I think we are seeing something very different with denosumab to what we’ve seen to date with a bisphosphonate,” he said.
“As oncologists, we are somewhat wedded to measuring bone mineral density as the reason for giving bone-targeted therapy to protect [against] bone loss, but there are much better ways of predicting fracture with online algorithms such as FRAX [Fracture Risk Assessment Tool] and others,” Dr. Coleman further commented. “And bone mineral density is a pretty poor predictor of fracture, so it’s perhaps not surprising that the risk reductions were fairly similar” across bone mineral density subgroups.
During a question and answer period, session attendee Dr. Toru Watanabe, Hamamatsu (Japan) Oncology Center, said, “It is really clear that the osteoporosis-related fracture is prevented by denosumab at the dose usually used for the treatment of osteoporosis. That part is very clear. My question is, the same dose is being tested for modifying overall survival or progression-free survival. Don’t you think it’s necessary to conduct some kind of dose-finding trial?”
Two studies are addressing the impact of denosumab on breast cancer outcomes, according to Dr. Gnant: the investigators’ ABCSG-18 study and the Study of Denosumab as Adjuvant Treatment for Women With High-Risk Early Breast Cancer Receiving Neoadjuvant or Adjuvant Therapy (D-CARE), which is using a higher initial dose and tapering after 1 year. “So we will have that indirect comparison at least. My personal expectation would be that there is a trade-off potentially between efficacy and tolerability,” he commented.
The 3,425 postmenopausal breast cancer patients in ABCSG-18 were randomized evenly to receive 60 mg of denosumab or placebo every 6 months. Denosumab is approved by the Food and Drug Administration for the prevention and treatment of fractures due to bone metastases (brand name Xgeva) and osteoporosis after menopause (brand name Prolia), as well as other indications. The study used the dose for postmenopausal osteoporosis, which is much lower than that typically used for bone metastases (120 mg every 4 weeks), Dr. Gnant noted.
Main results showed that denosumab was highly efficacious in reducing the risk of first clinical fractures, meaning those that were clinically evident and causing symptoms (hazard ratio, 0.50; P less than .0001), according to data presented at the meeting and simultaneously published (Lancet 2015 May 31).
The estimated 6-year fracture rate was about 10% in the denosumab group and 20% in the placebo group. “Please note that the frequency of clinical fractures reported in this trial that is focusing on bone health is markedly higher than fracture rates reported in previous large AI trials. Obviously, we had a tendency to underreport them in those trials,” Dr. Gnant commented. “The true magnitude of the problem in clinical practice is likely reflected in the placebo group … with approximately one out of five patients experiencing a new clinical fracture within 5-6 years of adjuvant AI treatment.”
Benefit was similar across numerous patient subgroups studied, including the subgroups of women who had a baseline bone mineral density T-score of less than –1 and women who had a baseline bone mineral density T-score of –1 or greater.
Additionally, the denosumab group had improvements from baseline in bone mineral density of the lumbar spine, total hip, and femoral neck, whereas the placebo group had worsening at all sites (P less than .0001 between groups for each site). And at 36 months, the denosumab group had significantly lower risks of both new vertebral fractures and new or worsening vertebral fractures.
“Adjuvant denosumab at this dose and schedule is safe,” Dr. Gnant maintained. The two groups had similar rates of various adverse events, with musculoskeletal disorders and vascular disorders (including hot flashes) predominating. “This means that we are in essence reporting the side effects of the underlying adjuvant AI treatment,” he noted.
There were 31 cases of dental issues, but none met diagnostic criteria for osteonecrosis of the jaw. “We can safely say that at this dose of denosumab, 60 mg twice yearly, ONJ is not an issue,” Dr. Gnant commented. Additionally, none of the women experienced atypical fractures.
Dr. Gnant disclosed employment of an immediate family member with Sandoz; receipt of honoraria from Amgen, AstraZeneca, GlaxoSmithKline, NanoString Technologies, Novartis, and Roche Pharma AG; a consulting or advisory role with Accelsiors, AstraZeneca, and Novartis; and receipt of research funding from GlaxoSmithKline, Novartis, Pfizer, Roche Pharma AG, Sanofi, and Smiths Medical. The trial was sponsored by Amgen.
CHICAGO – Adjuvant denosumab is efficacious and safe for reducing fracture risk among women taking aromatase inhibitors (AIs) as part of their treatment for early breast cancer, finds the Austrian Breast & Colorectal Cancer Study Group’s study 18 (ABCSG-18).
Compared with peers randomized to placebo in the phase III trial, women randomized to the antiresorptive monoclonal antibody at the dose typically used to treat osteoporosis were half as likely to experience a first clinical fracture, first author Dr. Michael Gnant reported at the annual meeting of the American Society of Clinical Oncology. The benefit was similar whether women had normal bone mineral density at baseline or already had osteopenia.
Patients in the denosumab group did not have a significantly higher rate of adverse events, including the much-feared complication of osteonecrosis of the jaw.
“The actual fracture risk of postmenopausal breast cancer patients on AIs is substantial and may have been underestimated until today,” commented Dr. Gnant, professor of surgery at the Medical University of Vienna. “In these patients with only a modest risk of disease recurrence, adjuvant denosumab significantly reduced the bone side effects of AI treatment. We therefore believe that denosumab 60 mg every 6 months should be considered for clinical practice.”
“Today, several clinical practice guidelines advocate the use of bisphosphonates for breast cancer patients receiving AIs, however, only if they are at high risk for fractures,” he further noted. However, “patients with normal baseline bone mineral density showed a similar fracture risk but also similar benefit from denosumab as compared to patients with baseline T scores below –1, indicating that DEXA scans may be an insufficient way to assess the individual patient’s fracture risk. In view of the benefits in this particular patient subgroup, we may have to rediscuss our current clinical practice guidelines.”
Invited discussant Dr. Robert E. Coleman of the University of Sheffield and Weston Park Hospital in England, said, “It’s very important to dissect out fractures related to subsequent recurrence from fractures due to poor bone health.” Most of the reduction in fracture risk in ABCSG-18 appeared to be because of prevention of fractures before any recurrence, whereas most of that in the AZURE trial (Adjuvant Zoledronic Acid to Reduce Recurrence) of an adjuvant bisphosphonate, another type of antiresorptive agent, appeared to be because of prevention of fractures from bone metastases. “So I think we are seeing something very different with denosumab to what we’ve seen to date with a bisphosphonate,” he said.
“As oncologists, we are somewhat wedded to measuring bone mineral density as the reason for giving bone-targeted therapy to protect [against] bone loss, but there are much better ways of predicting fracture with online algorithms such as FRAX [Fracture Risk Assessment Tool] and others,” Dr. Coleman further commented. “And bone mineral density is a pretty poor predictor of fracture, so it’s perhaps not surprising that the risk reductions were fairly similar” across bone mineral density subgroups.
During a question and answer period, session attendee Dr. Toru Watanabe, Hamamatsu (Japan) Oncology Center, said, “It is really clear that the osteoporosis-related fracture is prevented by denosumab at the dose usually used for the treatment of osteoporosis. That part is very clear. My question is, the same dose is being tested for modifying overall survival or progression-free survival. Don’t you think it’s necessary to conduct some kind of dose-finding trial?”
Two studies are addressing the impact of denosumab on breast cancer outcomes, according to Dr. Gnant: the investigators’ ABCSG-18 study and the Study of Denosumab as Adjuvant Treatment for Women With High-Risk Early Breast Cancer Receiving Neoadjuvant or Adjuvant Therapy (D-CARE), which is using a higher initial dose and tapering after 1 year. “So we will have that indirect comparison at least. My personal expectation would be that there is a trade-off potentially between efficacy and tolerability,” he commented.
The 3,425 postmenopausal breast cancer patients in ABCSG-18 were randomized evenly to receive 60 mg of denosumab or placebo every 6 months. Denosumab is approved by the Food and Drug Administration for the prevention and treatment of fractures due to bone metastases (brand name Xgeva) and osteoporosis after menopause (brand name Prolia), as well as other indications. The study used the dose for postmenopausal osteoporosis, which is much lower than that typically used for bone metastases (120 mg every 4 weeks), Dr. Gnant noted.
Main results showed that denosumab was highly efficacious in reducing the risk of first clinical fractures, meaning those that were clinically evident and causing symptoms (hazard ratio, 0.50; P less than .0001), according to data presented at the meeting and simultaneously published (Lancet 2015 May 31).
The estimated 6-year fracture rate was about 10% in the denosumab group and 20% in the placebo group. “Please note that the frequency of clinical fractures reported in this trial that is focusing on bone health is markedly higher than fracture rates reported in previous large AI trials. Obviously, we had a tendency to underreport them in those trials,” Dr. Gnant commented. “The true magnitude of the problem in clinical practice is likely reflected in the placebo group … with approximately one out of five patients experiencing a new clinical fracture within 5-6 years of adjuvant AI treatment.”
Benefit was similar across numerous patient subgroups studied, including the subgroups of women who had a baseline bone mineral density T-score of less than –1 and women who had a baseline bone mineral density T-score of –1 or greater.
Additionally, the denosumab group had improvements from baseline in bone mineral density of the lumbar spine, total hip, and femoral neck, whereas the placebo group had worsening at all sites (P less than .0001 between groups for each site). And at 36 months, the denosumab group had significantly lower risks of both new vertebral fractures and new or worsening vertebral fractures.
“Adjuvant denosumab at this dose and schedule is safe,” Dr. Gnant maintained. The two groups had similar rates of various adverse events, with musculoskeletal disorders and vascular disorders (including hot flashes) predominating. “This means that we are in essence reporting the side effects of the underlying adjuvant AI treatment,” he noted.
There were 31 cases of dental issues, but none met diagnostic criteria for osteonecrosis of the jaw. “We can safely say that at this dose of denosumab, 60 mg twice yearly, ONJ is not an issue,” Dr. Gnant commented. Additionally, none of the women experienced atypical fractures.
Dr. Gnant disclosed employment of an immediate family member with Sandoz; receipt of honoraria from Amgen, AstraZeneca, GlaxoSmithKline, NanoString Technologies, Novartis, and Roche Pharma AG; a consulting or advisory role with Accelsiors, AstraZeneca, and Novartis; and receipt of research funding from GlaxoSmithKline, Novartis, Pfizer, Roche Pharma AG, Sanofi, and Smiths Medical. The trial was sponsored by Amgen.
CHICAGO – Adjuvant denosumab is efficacious and safe for reducing fracture risk among women taking aromatase inhibitors (AIs) as part of their treatment for early breast cancer, finds the Austrian Breast & Colorectal Cancer Study Group’s study 18 (ABCSG-18).
Compared with peers randomized to placebo in the phase III trial, women randomized to the antiresorptive monoclonal antibody at the dose typically used to treat osteoporosis were half as likely to experience a first clinical fracture, first author Dr. Michael Gnant reported at the annual meeting of the American Society of Clinical Oncology. The benefit was similar whether women had normal bone mineral density at baseline or already had osteopenia.
Patients in the denosumab group did not have a significantly higher rate of adverse events, including the much-feared complication of osteonecrosis of the jaw.
“The actual fracture risk of postmenopausal breast cancer patients on AIs is substantial and may have been underestimated until today,” commented Dr. Gnant, professor of surgery at the Medical University of Vienna. “In these patients with only a modest risk of disease recurrence, adjuvant denosumab significantly reduced the bone side effects of AI treatment. We therefore believe that denosumab 60 mg every 6 months should be considered for clinical practice.”
“Today, several clinical practice guidelines advocate the use of bisphosphonates for breast cancer patients receiving AIs, however, only if they are at high risk for fractures,” he further noted. However, “patients with normal baseline bone mineral density showed a similar fracture risk but also similar benefit from denosumab as compared to patients with baseline T scores below –1, indicating that DEXA scans may be an insufficient way to assess the individual patient’s fracture risk. In view of the benefits in this particular patient subgroup, we may have to rediscuss our current clinical practice guidelines.”
Invited discussant Dr. Robert E. Coleman of the University of Sheffield and Weston Park Hospital in England, said, “It’s very important to dissect out fractures related to subsequent recurrence from fractures due to poor bone health.” Most of the reduction in fracture risk in ABCSG-18 appeared to be because of prevention of fractures before any recurrence, whereas most of that in the AZURE trial (Adjuvant Zoledronic Acid to Reduce Recurrence) of an adjuvant bisphosphonate, another type of antiresorptive agent, appeared to be because of prevention of fractures from bone metastases. “So I think we are seeing something very different with denosumab to what we’ve seen to date with a bisphosphonate,” he said.
“As oncologists, we are somewhat wedded to measuring bone mineral density as the reason for giving bone-targeted therapy to protect [against] bone loss, but there are much better ways of predicting fracture with online algorithms such as FRAX [Fracture Risk Assessment Tool] and others,” Dr. Coleman further commented. “And bone mineral density is a pretty poor predictor of fracture, so it’s perhaps not surprising that the risk reductions were fairly similar” across bone mineral density subgroups.
During a question and answer period, session attendee Dr. Toru Watanabe, Hamamatsu (Japan) Oncology Center, said, “It is really clear that the osteoporosis-related fracture is prevented by denosumab at the dose usually used for the treatment of osteoporosis. That part is very clear. My question is, the same dose is being tested for modifying overall survival or progression-free survival. Don’t you think it’s necessary to conduct some kind of dose-finding trial?”
Two studies are addressing the impact of denosumab on breast cancer outcomes, according to Dr. Gnant: the investigators’ ABCSG-18 study and the Study of Denosumab as Adjuvant Treatment for Women With High-Risk Early Breast Cancer Receiving Neoadjuvant or Adjuvant Therapy (D-CARE), which is using a higher initial dose and tapering after 1 year. “So we will have that indirect comparison at least. My personal expectation would be that there is a trade-off potentially between efficacy and tolerability,” he commented.
The 3,425 postmenopausal breast cancer patients in ABCSG-18 were randomized evenly to receive 60 mg of denosumab or placebo every 6 months. Denosumab is approved by the Food and Drug Administration for the prevention and treatment of fractures due to bone metastases (brand name Xgeva) and osteoporosis after menopause (brand name Prolia), as well as other indications. The study used the dose for postmenopausal osteoporosis, which is much lower than that typically used for bone metastases (120 mg every 4 weeks), Dr. Gnant noted.
Main results showed that denosumab was highly efficacious in reducing the risk of first clinical fractures, meaning those that were clinically evident and causing symptoms (hazard ratio, 0.50; P less than .0001), according to data presented at the meeting and simultaneously published (Lancet 2015 May 31).
The estimated 6-year fracture rate was about 10% in the denosumab group and 20% in the placebo group. “Please note that the frequency of clinical fractures reported in this trial that is focusing on bone health is markedly higher than fracture rates reported in previous large AI trials. Obviously, we had a tendency to underreport them in those trials,” Dr. Gnant commented. “The true magnitude of the problem in clinical practice is likely reflected in the placebo group … with approximately one out of five patients experiencing a new clinical fracture within 5-6 years of adjuvant AI treatment.”
Benefit was similar across numerous patient subgroups studied, including the subgroups of women who had a baseline bone mineral density T-score of less than –1 and women who had a baseline bone mineral density T-score of –1 or greater.
Additionally, the denosumab group had improvements from baseline in bone mineral density of the lumbar spine, total hip, and femoral neck, whereas the placebo group had worsening at all sites (P less than .0001 between groups for each site). And at 36 months, the denosumab group had significantly lower risks of both new vertebral fractures and new or worsening vertebral fractures.
“Adjuvant denosumab at this dose and schedule is safe,” Dr. Gnant maintained. The two groups had similar rates of various adverse events, with musculoskeletal disorders and vascular disorders (including hot flashes) predominating. “This means that we are in essence reporting the side effects of the underlying adjuvant AI treatment,” he noted.
There were 31 cases of dental issues, but none met diagnostic criteria for osteonecrosis of the jaw. “We can safely say that at this dose of denosumab, 60 mg twice yearly, ONJ is not an issue,” Dr. Gnant commented. Additionally, none of the women experienced atypical fractures.
Dr. Gnant disclosed employment of an immediate family member with Sandoz; receipt of honoraria from Amgen, AstraZeneca, GlaxoSmithKline, NanoString Technologies, Novartis, and Roche Pharma AG; a consulting or advisory role with Accelsiors, AstraZeneca, and Novartis; and receipt of research funding from GlaxoSmithKline, Novartis, Pfizer, Roche Pharma AG, Sanofi, and Smiths Medical. The trial was sponsored by Amgen.
AT THE 2015 ASCO ANNUAL MEETING
Key clinical point: Denosumab reduces the risk of clinical fractures in postmenopausal women taking AIs for early breast cancer.
Major finding: The denosumab group was half as likely to have a first clinical fracture as the placebo group (HR, 0.50).
Data source: A randomized phase III trial among 3,425 postmenopausal women with early breast cancer taking AIs.
Disclosures: Dr. Gnant disclosed employment of an immediate family member with Sandoz; receipt of honoraria from Amgen, AstraZeneca, GlaxoSmithKline, NanoString Technologies, Novartis, and Roche Pharma AG; a consulting or advisory role with Accelsiors, AstraZeneca, and Novartis; and receipt of research funding from GlaxoSmithKline, Novartis, Pfizer, Roche Pharma AG, Sanofi, and Smiths Medical. The trial was sponsored by Amgen.

Coding for “Incident-to” Services
Services that physicians bill to Medicare but do not perform themselves are called “incident-to” services. These services usually are performed by nonphysician medical providers under close physician supervision. The authorization to bill for these incident-to services derives from the Social Security Act,1 which provides for Medicare coverage of services and supplies offered incident to the professional services of a physician. The underlying logic is that incident-to services are delivered as a necessary but incidental part of the physician’s professional services during diagnosis or treatment.
Eligibility Criteria
One key qualification for incident-to services is direct supervision of a nonphysician provider by a physician. When services are delivered in an office setting (place of service 11), the physician must be present in the office and immediately available to offer direction to nonphysician providers. Some states do include telecommunication in their definition of direct supervision, wherein the physician is accessible by telephone or some similar medium.
Another element necessary in the criteria for incident-to services is that initial care must be personally provided by the physician who also writes orders for ongoing care. In general, incident-to services include ongoing physician involvement in the provision of care. Importantly, the physician who first saw a patient, initiated service, or ordered a test is not the only one who can supervise subsequent incident-to visits with a nonphysician provider. In office settings where several physicians are responsible for overseeing a nonphysician provider, any of these physicians who are in clinic at the time can act as the supervising physician. In such cases, each of the other physicians should be listed in appropriate documentation as substitute physicians for the nonphysician provider.
The Centers for Medicare & Medicaid Services recognize a variety of nonphysician providers, but in dermatology these providers typically include physician assistants, certified registered nurse practitioners, or clinical nurse specialists. When services offered by these nonphysician providers are reported as incident-to services, Medicare reimburses them at 100% of the physician fee schedule; conversely, a non–incident-to service reported under a nonphysician provider’s National Provider Identifier (NPI) number is reimbursed at 85%. Only approved mid-level nonphysician providers may bill evaluation and management services with codes above 99211 under incident-to guidelines. Even then, the services delivered must be appropriate for the given nonphysician provider based on training and licensure.
Not every type of visit is eligible for coding as an incident-to service. For instance, it is not appropriate to code new patient visits or new services provided to existing patients as incident-to services. Similarly, visits with established patients that address new diagnoses or problems cannot be considered incident-to services. The only visits or services that may potentially be classified as incident to are those that address existing problems in established patients with an established care plan.
When an established patient presents with a new problem, there are at least 2 coding approaches that may be appropriate. First, the physician could choose to see the patient and code the visit as a standard physician visit under the physician’s own NPI number. Alternatively, if the supervising physician in the practice is not available to see the patient, the nonphysician provider could code the entire service, including new and old problems, under his/her own NPI number as a non–incident-to service.
Regulations by State and Payer
State regulations and rules promulgated by specific payers also must be considered to ensure incident-to coding is proper. Each state may have guidelines that define the scope of practice of particular nonphysician providers, including what services can or cannot be coded as incident-to services. Additionally, states typically regulate the number of nonphysician providers that a physician can supervise; by extension, no more than this number of nonphysician providers could bill incident-to services under a given physician’s NPI number. Private payers may have comparable rules, and specific Medicare guidelines apply to Medicare patients. When there is ambiguity regarding incident-to coding, it may be prudent to check with major payers regarding relevant guidelines. It also may be helpful to confirm when supervision via telecommunication is acceptable.
Billing Tips
Common sense also can guide appropriate use of incident-to coding. Although occasional coding errors are likely unavoidable, periodic review of billing patterns will keep these errors to a minimum. For instance, if a nonphysician provider is the only provider of any type seeing patients in the office during particular days of the week, then incident-to coding would be unlikely. In another example, the number of nonphysician providers working with a given dermatologist and billing incident-to services should not exceed the number of nonphysician providers allowed per physician in that state. An interesting twist is the case in which a dermatologist is working in an ambulatory surgery center while a nonphysician provider is seeing patients in an adjacent office suite. Even when the 2 sites of service are physically contiguous, the physician in the surgery center generally is not deemed to be in office and is not able to supervise the nonphysician provider, unless telecommunication is allowed.
Final Thoughts
Attention to correct coding for incident-to services is particularly salient, as the Office of Inspector General (OIG) for the US Department of Health & Human Services has expressed concern that these services may be routinely coded incorrectly. Specifically, the OIG work plan for the 2013 fiscal year stated, “We will review physician billing for ‘incident-to’ services to determine whether payment for such services had a higher error rate than that for non–incident-to services.” The same report also cited a 2009 OIG review that found that “unqualified nonphysicians performed 21 percent of the services that physicians did not personally perform.”2 In short, coding for incident-to services is under scrutiny, and it may be useful for dermatologists to review their internal policies regarding incident-to services.
1. Social Security Act, 42 USC §1861 (1935).
2. Work plan for fiscal year 2013. Office of Inspector General, US Department of Health & Human Services Web site. http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed May 5, 2015.
Services that physicians bill to Medicare but do not perform themselves are called “incident-to” services. These services usually are performed by nonphysician medical providers under close physician supervision. The authorization to bill for these incident-to services derives from the Social Security Act,1 which provides for Medicare coverage of services and supplies offered incident to the professional services of a physician. The underlying logic is that incident-to services are delivered as a necessary but incidental part of the physician’s professional services during diagnosis or treatment.
Eligibility Criteria
One key qualification for incident-to services is direct supervision of a nonphysician provider by a physician. When services are delivered in an office setting (place of service 11), the physician must be present in the office and immediately available to offer direction to nonphysician providers. Some states do include telecommunication in their definition of direct supervision, wherein the physician is accessible by telephone or some similar medium.
Another element necessary in the criteria for incident-to services is that initial care must be personally provided by the physician who also writes orders for ongoing care. In general, incident-to services include ongoing physician involvement in the provision of care. Importantly, the physician who first saw a patient, initiated service, or ordered a test is not the only one who can supervise subsequent incident-to visits with a nonphysician provider. In office settings where several physicians are responsible for overseeing a nonphysician provider, any of these physicians who are in clinic at the time can act as the supervising physician. In such cases, each of the other physicians should be listed in appropriate documentation as substitute physicians for the nonphysician provider.
The Centers for Medicare & Medicaid Services recognize a variety of nonphysician providers, but in dermatology these providers typically include physician assistants, certified registered nurse practitioners, or clinical nurse specialists. When services offered by these nonphysician providers are reported as incident-to services, Medicare reimburses them at 100% of the physician fee schedule; conversely, a non–incident-to service reported under a nonphysician provider’s National Provider Identifier (NPI) number is reimbursed at 85%. Only approved mid-level nonphysician providers may bill evaluation and management services with codes above 99211 under incident-to guidelines. Even then, the services delivered must be appropriate for the given nonphysician provider based on training and licensure.
Not every type of visit is eligible for coding as an incident-to service. For instance, it is not appropriate to code new patient visits or new services provided to existing patients as incident-to services. Similarly, visits with established patients that address new diagnoses or problems cannot be considered incident-to services. The only visits or services that may potentially be classified as incident to are those that address existing problems in established patients with an established care plan.
When an established patient presents with a new problem, there are at least 2 coding approaches that may be appropriate. First, the physician could choose to see the patient and code the visit as a standard physician visit under the physician’s own NPI number. Alternatively, if the supervising physician in the practice is not available to see the patient, the nonphysician provider could code the entire service, including new and old problems, under his/her own NPI number as a non–incident-to service.
Regulations by State and Payer
State regulations and rules promulgated by specific payers also must be considered to ensure incident-to coding is proper. Each state may have guidelines that define the scope of practice of particular nonphysician providers, including what services can or cannot be coded as incident-to services. Additionally, states typically regulate the number of nonphysician providers that a physician can supervise; by extension, no more than this number of nonphysician providers could bill incident-to services under a given physician’s NPI number. Private payers may have comparable rules, and specific Medicare guidelines apply to Medicare patients. When there is ambiguity regarding incident-to coding, it may be prudent to check with major payers regarding relevant guidelines. It also may be helpful to confirm when supervision via telecommunication is acceptable.
Billing Tips
Common sense also can guide appropriate use of incident-to coding. Although occasional coding errors are likely unavoidable, periodic review of billing patterns will keep these errors to a minimum. For instance, if a nonphysician provider is the only provider of any type seeing patients in the office during particular days of the week, then incident-to coding would be unlikely. In another example, the number of nonphysician providers working with a given dermatologist and billing incident-to services should not exceed the number of nonphysician providers allowed per physician in that state. An interesting twist is the case in which a dermatologist is working in an ambulatory surgery center while a nonphysician provider is seeing patients in an adjacent office suite. Even when the 2 sites of service are physically contiguous, the physician in the surgery center generally is not deemed to be in office and is not able to supervise the nonphysician provider, unless telecommunication is allowed.
Final Thoughts
Attention to correct coding for incident-to services is particularly salient, as the Office of Inspector General (OIG) for the US Department of Health & Human Services has expressed concern that these services may be routinely coded incorrectly. Specifically, the OIG work plan for the 2013 fiscal year stated, “We will review physician billing for ‘incident-to’ services to determine whether payment for such services had a higher error rate than that for non–incident-to services.” The same report also cited a 2009 OIG review that found that “unqualified nonphysicians performed 21 percent of the services that physicians did not personally perform.”2 In short, coding for incident-to services is under scrutiny, and it may be useful for dermatologists to review their internal policies regarding incident-to services.
Services that physicians bill to Medicare but do not perform themselves are called “incident-to” services. These services usually are performed by nonphysician medical providers under close physician supervision. The authorization to bill for these incident-to services derives from the Social Security Act,1 which provides for Medicare coverage of services and supplies offered incident to the professional services of a physician. The underlying logic is that incident-to services are delivered as a necessary but incidental part of the physician’s professional services during diagnosis or treatment.
Eligibility Criteria
One key qualification for incident-to services is direct supervision of a nonphysician provider by a physician. When services are delivered in an office setting (place of service 11), the physician must be present in the office and immediately available to offer direction to nonphysician providers. Some states do include telecommunication in their definition of direct supervision, wherein the physician is accessible by telephone or some similar medium.
Another element necessary in the criteria for incident-to services is that initial care must be personally provided by the physician who also writes orders for ongoing care. In general, incident-to services include ongoing physician involvement in the provision of care. Importantly, the physician who first saw a patient, initiated service, or ordered a test is not the only one who can supervise subsequent incident-to visits with a nonphysician provider. In office settings where several physicians are responsible for overseeing a nonphysician provider, any of these physicians who are in clinic at the time can act as the supervising physician. In such cases, each of the other physicians should be listed in appropriate documentation as substitute physicians for the nonphysician provider.
The Centers for Medicare & Medicaid Services recognize a variety of nonphysician providers, but in dermatology these providers typically include physician assistants, certified registered nurse practitioners, or clinical nurse specialists. When services offered by these nonphysician providers are reported as incident-to services, Medicare reimburses them at 100% of the physician fee schedule; conversely, a non–incident-to service reported under a nonphysician provider’s National Provider Identifier (NPI) number is reimbursed at 85%. Only approved mid-level nonphysician providers may bill evaluation and management services with codes above 99211 under incident-to guidelines. Even then, the services delivered must be appropriate for the given nonphysician provider based on training and licensure.
Not every type of visit is eligible for coding as an incident-to service. For instance, it is not appropriate to code new patient visits or new services provided to existing patients as incident-to services. Similarly, visits with established patients that address new diagnoses or problems cannot be considered incident-to services. The only visits or services that may potentially be classified as incident to are those that address existing problems in established patients with an established care plan.
When an established patient presents with a new problem, there are at least 2 coding approaches that may be appropriate. First, the physician could choose to see the patient and code the visit as a standard physician visit under the physician’s own NPI number. Alternatively, if the supervising physician in the practice is not available to see the patient, the nonphysician provider could code the entire service, including new and old problems, under his/her own NPI number as a non–incident-to service.
Regulations by State and Payer
State regulations and rules promulgated by specific payers also must be considered to ensure incident-to coding is proper. Each state may have guidelines that define the scope of practice of particular nonphysician providers, including what services can or cannot be coded as incident-to services. Additionally, states typically regulate the number of nonphysician providers that a physician can supervise; by extension, no more than this number of nonphysician providers could bill incident-to services under a given physician’s NPI number. Private payers may have comparable rules, and specific Medicare guidelines apply to Medicare patients. When there is ambiguity regarding incident-to coding, it may be prudent to check with major payers regarding relevant guidelines. It also may be helpful to confirm when supervision via telecommunication is acceptable.
Billing Tips
Common sense also can guide appropriate use of incident-to coding. Although occasional coding errors are likely unavoidable, periodic review of billing patterns will keep these errors to a minimum. For instance, if a nonphysician provider is the only provider of any type seeing patients in the office during particular days of the week, then incident-to coding would be unlikely. In another example, the number of nonphysician providers working with a given dermatologist and billing incident-to services should not exceed the number of nonphysician providers allowed per physician in that state. An interesting twist is the case in which a dermatologist is working in an ambulatory surgery center while a nonphysician provider is seeing patients in an adjacent office suite. Even when the 2 sites of service are physically contiguous, the physician in the surgery center generally is not deemed to be in office and is not able to supervise the nonphysician provider, unless telecommunication is allowed.
Final Thoughts
Attention to correct coding for incident-to services is particularly salient, as the Office of Inspector General (OIG) for the US Department of Health & Human Services has expressed concern that these services may be routinely coded incorrectly. Specifically, the OIG work plan for the 2013 fiscal year stated, “We will review physician billing for ‘incident-to’ services to determine whether payment for such services had a higher error rate than that for non–incident-to services.” The same report also cited a 2009 OIG review that found that “unqualified nonphysicians performed 21 percent of the services that physicians did not personally perform.”2 In short, coding for incident-to services is under scrutiny, and it may be useful for dermatologists to review their internal policies regarding incident-to services.
1. Social Security Act, 42 USC §1861 (1935).
2. Work plan for fiscal year 2013. Office of Inspector General, US Department of Health & Human Services Web site. http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed May 5, 2015.
1. Social Security Act, 42 USC §1861 (1935).
2. Work plan for fiscal year 2013. Office of Inspector General, US Department of Health & Human Services Web site. http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed May 5, 2015.
Practice Points
- Direct supervision of a nonphysician provider by a physician must be demonstrated for incident-to services. Not every type of visit is eligible for incident-to billing.
- Only management of established problems on established patients by nonphysician providers may qualify as incident-to services.
- Refer to state and payer regulations and rules for proper incident-to coding.

Prevalence and Impact of Health-Related Internet and Smartphone Use Among Dermatology Patients
Patients increasingly use the Internet and/or smartphone applications (apps) to seek health information and track personal health data,1,2 typically in the spirit of being a more educated consumer. However, many patients use the Internet in an attempt to self-diagnose and independently find treatment options, thus avoiding (in their opinion) the need to seek in-person medical care. Additionally, electronic access to health information has expanded beyond computers to smartphones with apps that can provide users with a simple interface to personalize the health information they seek and receive.
Prior studies have shown that seeking online health information and health-related social media is more common among women, younger patients, those with a college education, and those with a higher income.3,4 However, the prevalence of health-related Internet and smartphone use among dermatology patients as well as how patients ultimately use this information is not well studied. This information about patient behavior is important because of the potential harm that may come from patient self-diagnosis, which may delay or prevent treatment, as well as the benefits of patient self-education, which may expedite diagnosis and treatment.5 We surveyed a heterogeneous patient population at 2 dermatology offices in a major academic medical center to assess the prevalence and predictors of Internet and smartphone use to obtain both general medical and dermatologic information among dermatology patients. We also evaluated the impact that health information obtained from online sources has on a patient’s degree of concern about cutaneous disease and the likelihood of seeing a dermatologist for a skin problem.
Methods
Survey and Participants
This study was approved by the institutional review board at the University of Pittsburgh, Pennsylvania. All patients aged 18 years or older who presented to the department of dermatology at 2 offices of the University of Pittsburgh Medical Center from September 2013 through July 2014 were invited to participate in an anonymous 33-question survey regarding their use of the Internet and smartphone apps to obtain health information and make health care decisions. Patients were asked to complete the survey prior to seeing a health care provider and return it to a locked box by the front desk before leaving the office. Survey questions were designed by physicians with content expertise (J.A.W. and L.K.F.) and were reviewed by a statistician with survey expertise (D.G.W.). The survey included questions about patient demographics, Internet and smartphone use (both general and health related), and specific sources accessed. The survey also inquired about the impact of health information obtained via the Internet and smartphone apps on respondents’ degree of worry about a hypothetical skin condition or lesion using a 5-point Likert scale (1=no worry; 5=very worried). Respondents also were asked which skin conditions they previously researched online and whether their findings impacted their decision to see a dermatologist. Additionally, respondents were asked to list the smartphone apps and other online health resources they had used within the last 3 months. Prior to distribution, the survey was piloted with 10 participants and no issues with comprehensibility were noted.
Statistical Analysis
We described demographic traits (eg, age, sex, race/ethnicity, level of education, income) and factors associated with access to health care (eg, specialist co-pay, travel time from dermatology office) of respondents using proportions. We evaluated respondents’ access to and use of Internet- and smartphone-based health information using proportions and used χ² tests to quantify differences by sex and age (<50 years and ≥50 years).
We analyzed the impact of Internet and smartphone-based health information on patient worry about skin conditions by obtaining median worry on a 5-point Likert scale. Due to the nonparametric nature of the data, we used the Mann-Whitney U test to quantify differences by sex and age (<50 and ≥50 years). We used multiple logistic regression to identify factors associated with 3 outcomes: (1) using the Internet to self-diagnose a dermatologic disease, (2) using the Internet to obtain dermatology-related information within the last 3 months, (3) and previously refraining from visiting a dermatologist based on reassurance from online resources. Predictors included the aforementioned demographic and health-care access–related traits. We also categorized smartphone apps used by respondents (ie, fitness/nutrition, reference, self-help, health monitoring, diagnostic aids, electronic medical record) and calculated the proportion of respondents with 1 or more of each type of app on their smartphones. Analyses were conducted in Stata 13.1 and IBM SPSS 22.0.
Results
Of 1000 patients who were invited to participate in the study, a total of 775 respondents completed the survey, yielding a response rate of 77.5%. The majority of respondents were aged 30 to 60 years (mean age [standard deviation], 44.5 [17.2] years; median age [interquartile range], 44 [29–59] years), female (66.7%), and non-Hispanic white (83.3%)(Table 1). The majority of respondents (88.8%) had completed at least some college. Nearly all respondents had medical insurance (97.8%), but annual household income and insurance co-pay varied considerably. Only 10.8% of respondents traveled more than an hour to our offices.
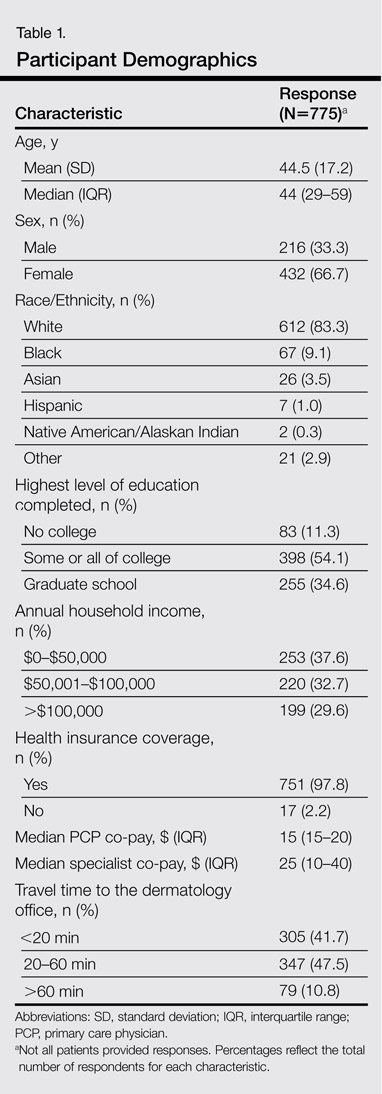
The majority of respondents had access to home Internet and owned a smartphone (Table 2). Use of the Internet to obtain health-related information in the 3 months prior to presentation was more common among females (77.9% vs 70.1%; P=.03) and respondents younger than 50 years (83.4% vs 62.5%; P<.001); the same was true for dermatology-related infor-mation (females: 43.2% vs 31.0%; P=.003; aged <50 years, 51.6% vs 22.2%; P<.001). The majority of respondents indicated that they use the Internet to obtain health-related information both before and after they see their doctor. Most respondents indicated that they sometimes discuss health-related information found on the Internet with a physician. Smartphone use to obtain health-related information was more common among respondents younger than 50 years versus those who were 50 years or older (55.5% vs 24.1%; P<.001), as was smartphone use to diagnose skin problems (20.0% vs 6.3%; P<.001).
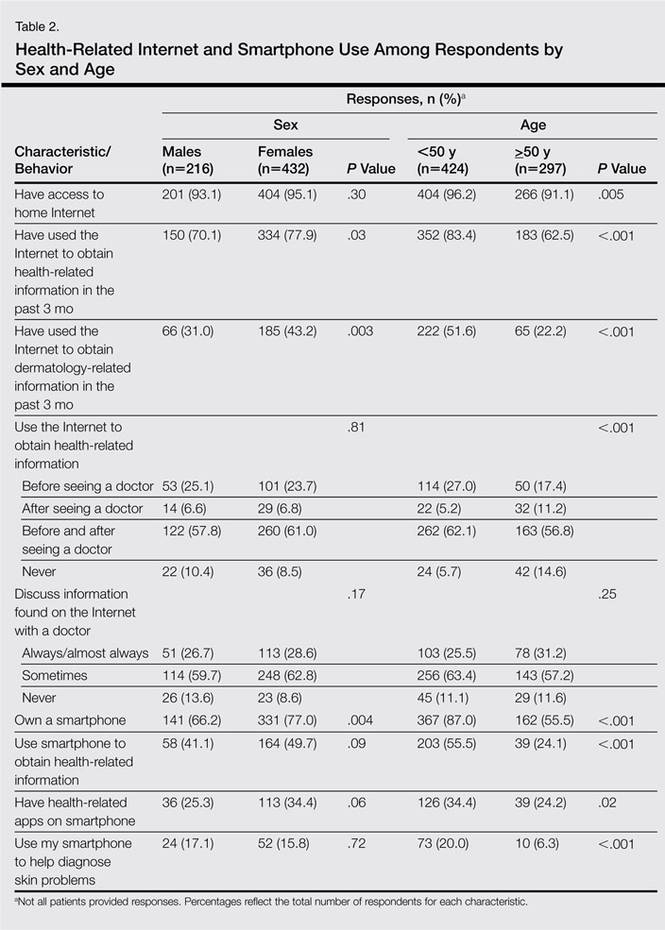
In multivariable analysis, use of the Internet or a smartphone to obtain health-related information was associated with younger age (<50 years) and a higher level of education (both P<.001). Use of the Internet to obtain dermatology-related information (P<.001) and use of a smartphone to help diagnose a skin problem (P=.001) was associated with younger age (<50 years) only. Income, sex, co-pay to see a dermatologist, and travel time to the dermatology office were not associated with use of online resources for general or dermatology-specific health-related information or assistance with diagnosing a skin problem.
Of 204 respondents who indicated that they previously attempted to self-diagnose a skin condition using the Internet, the most commonly researched condition was skin cancer/moles/unknown spots (64.7%), followed by rashes (40.7%), acne (20.6%), cosmetic issues (16.2%), psoriasis (12.7%), dermatitis (3.4%), warts (1.5%), tick bites (1.0%), and lupus (1.0%)(some respondents selected more than one condition). Only 7.0% of respondents indicated that they previously had refrained from visiting a dermatologist based on reassurance from online resources. Compared to the rest of the surveyed population, these respondents were younger (P=.001), but there were no significant differences in sex, highest level of education, household income, or travel time to the dermatology office. The most commonly researched condition among these respondents was acne (12 respondents), and 11 respondents indicated that they had attempted to self-diagnose a mole or potential cancer using online sources.
Of 557 respondents who owned a smartphone, 31.8% reported using at least 1 health-related app (mean number of health apps per respondent, 1.5). Of the apps that respondents used, 45.9% focused on fitness/nutrition, 28.7% provided reference information, 13.4% were a patient portal for receiving information from their electronic medical record, 8.6% provided a health monitoring function, 1.9% served as a diagnostic aid, and 1.5% provided coping assistance and emotional support for individuals with cognitive or emotional conditions; only 1 respondent reported using an app related to dermatology.
All respondents were asked to rate their anticipated degree of worry if the Internet or a smartphone app suggested that a skin lesion was benign versus dangerous on a 5-point scale. Overall, the median worry rating increased from 3 to 5 when information accessed via the Internet or a smartphone app suggested a lesion was dangerous rather than benign. A change in worry of 2 or more points was seen in 36.1% of females and 49.1% of males (P=.002) when information obtained via the Internet indicated a lesion was dangerous and in 47.5% of females and 58.8% of males (P=.006) when a smartphone app indicated that a lesion was dangerous. When information obtained via the Internet indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 41.8% of respondents who were younger than 50 years and in 41.1% of those who were 50 years or older (P=.93). When a smartphone app indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 50.2% of respondents who were younger than 50 years and in 52.2% of those who were 50 years or older (P=.61).
Discussion
In this cross-sectional study, we found that health-related Internet and smartphone use among dermatology patients is common and may impact both patients’ degree of concern about a skin lesion as well as the likelihood of seeking in-person medical care if they are reassured by the results of their online findings. Age and level of education were associated with Internet and smartphone use to obtain dermatology-related health information but not factors related to health care access. More patients used the Internet or a smartphone to obtain general medical information versus dermatology-related information. Respondents who indicated that they used the Internet to obtain health-related information tended to do so before visiting their physician.
Our finding that a patient’s level of worry about a hypothetical skin condition or lesion is influenced by health information obtained via the Internet or a smartphone app is concerning. One study found that participants who used a popular search engine to look for information about vaccine safety and dangers were directed to Web sites with inaccurate information more than 50% of the time, and 65% of the information they obtained from these sites was false.6 In our study, approximately 25% of respondents had previously consulted online resources to attempt toself-diagnose a skin condition. Online sources about dermatologic conditions were consulted most frequently for information about potential skin cancers, moles, and unknown spots. A prior study showed that smartphone apps that claim to aid patients in determining whether a skin lesion is low or high risk for melanoma often are inaccurate and are associated with a high rate of missed melanomas.5 Even though we surveyed patients who did end up seeing a dermatologist, some respondents had previously opted out of seeing a dermatologist based on information they had found online. Because our study was conducted among patients who chose to seek care at a dermatology office, the problem is likely greater than estimated from our findings because we had no way of reaching individuals who decided to completely forgo a visit with a dermatologist.
Although use of the Internet to obtain health-related information was common among older adults in our population, it was nearly universal in younger adults. Health-related smartphone use was more than twice as common in younger versus older adults, which could be due to an increased comfort with technology and its integration into daily life. The fact that age and education were associated with Internet use for dermatology-related health information but not household income or travel time to the dermatology office suggests that information seeking is not due to lack of resources limiting access to dermatologic care but rather to the greater role that rapid access to online information plays in patients’ lives. Our findings are similar to another study that examined the use of online sources for general health information.7
This study has several limitations. First, there may have been some selection bias. We specifically aimed to understand the health-related Internet and smartphone use among dermatology patients, thus restricting our sample to this population. By doing so, we were unable to assess the use of such resources by the general population, particularly those individuals who chose not to see a dermatologist at all based on their own online research. Our findings may not apply to other practices and regions of the country, as we implemented our study in one geographic location and in offices of an academic practice. Although our sample size and diversity with regard to income, education, and age suggest that our results are likely generalizable to many settings, it is important to note that nearly all respondents in this study had health insurance and our findings are thus not necessarily applicable to those individuals who are uninsured.
Conclusion
Our findings suggest that the availability of online health information regarding dermatologic conditions provides dermatologists with both opportunities and challenges. Many patients consult online resources for health information, and the popularity of this practice is likely to increase with time, particularly as newer smartphones with features designed to allow users to monitor their health are developed with health-conscious consumers in mind. Most large health care systems provide patients with resources to view laboratory results and communicate with physicians online. It is important for dermatologists to be involved in the development of high-quality online content that educates the public while also emphasizing the need to seek in-person medical care, particularly in potential cases of skin cancer. It also is important for patients to be involved in the content development process to ensure that the messages they take away from online resources are the ones physicians wish to convey. Ideally, online forms of education will increase patients’ sense of self-efficacy while encouraging appropriate consultation for potentially harmful skin conditions.
1. Atkinson NL, Saperstein SL, Pleis J. Using the Internet for health-related activities: findings from a national probability sample. J Med Internet Res. 2009;11:e4.
2. Ybarra M, Suman M. Reasons, assessments and actions taken: sex and age differences in uses of Internet health information. Health Educ Res. 2008;23:512-521.
3. Bhandari N, Shi Y, Jung K. Seeking health information online: does limited healthcare access matter? J Am Med Inform Assoc. 2014;21:1113-1117.
4. Thackeray R, Crookston BT, West JH. Correlates of health-related social media use among adults. J Med Internet Res. 2013;15:e21.
5. Wolf JA, Moreau JF, Akilov O, et al. Diagnostic inaccuracy of smartphone applications for melanoma detection. JAMA Dermatol. 2013;149:422-426.
6. Kortum P, Edwards C, Richards-Kortum R. The impact of inaccurate Internet health information in a secondary school learning environment. J Med Internet Res. 2008;10:e17.
7. Mead N, Varnam R, Rogers A, et al. What predicts patients’ interest in the internet as a health resource in primary care in England? J Health Serv Res Policy. 2003;8:33-39.
Patients increasingly use the Internet and/or smartphone applications (apps) to seek health information and track personal health data,1,2 typically in the spirit of being a more educated consumer. However, many patients use the Internet in an attempt to self-diagnose and independently find treatment options, thus avoiding (in their opinion) the need to seek in-person medical care. Additionally, electronic access to health information has expanded beyond computers to smartphones with apps that can provide users with a simple interface to personalize the health information they seek and receive.
Prior studies have shown that seeking online health information and health-related social media is more common among women, younger patients, those with a college education, and those with a higher income.3,4 However, the prevalence of health-related Internet and smartphone use among dermatology patients as well as how patients ultimately use this information is not well studied. This information about patient behavior is important because of the potential harm that may come from patient self-diagnosis, which may delay or prevent treatment, as well as the benefits of patient self-education, which may expedite diagnosis and treatment.5 We surveyed a heterogeneous patient population at 2 dermatology offices in a major academic medical center to assess the prevalence and predictors of Internet and smartphone use to obtain both general medical and dermatologic information among dermatology patients. We also evaluated the impact that health information obtained from online sources has on a patient’s degree of concern about cutaneous disease and the likelihood of seeing a dermatologist for a skin problem.
Methods
Survey and Participants
This study was approved by the institutional review board at the University of Pittsburgh, Pennsylvania. All patients aged 18 years or older who presented to the department of dermatology at 2 offices of the University of Pittsburgh Medical Center from September 2013 through July 2014 were invited to participate in an anonymous 33-question survey regarding their use of the Internet and smartphone apps to obtain health information and make health care decisions. Patients were asked to complete the survey prior to seeing a health care provider and return it to a locked box by the front desk before leaving the office. Survey questions were designed by physicians with content expertise (J.A.W. and L.K.F.) and were reviewed by a statistician with survey expertise (D.G.W.). The survey included questions about patient demographics, Internet and smartphone use (both general and health related), and specific sources accessed. The survey also inquired about the impact of health information obtained via the Internet and smartphone apps on respondents’ degree of worry about a hypothetical skin condition or lesion using a 5-point Likert scale (1=no worry; 5=very worried). Respondents also were asked which skin conditions they previously researched online and whether their findings impacted their decision to see a dermatologist. Additionally, respondents were asked to list the smartphone apps and other online health resources they had used within the last 3 months. Prior to distribution, the survey was piloted with 10 participants and no issues with comprehensibility were noted.
Statistical Analysis
We described demographic traits (eg, age, sex, race/ethnicity, level of education, income) and factors associated with access to health care (eg, specialist co-pay, travel time from dermatology office) of respondents using proportions. We evaluated respondents’ access to and use of Internet- and smartphone-based health information using proportions and used χ² tests to quantify differences by sex and age (<50 years and ≥50 years).
We analyzed the impact of Internet and smartphone-based health information on patient worry about skin conditions by obtaining median worry on a 5-point Likert scale. Due to the nonparametric nature of the data, we used the Mann-Whitney U test to quantify differences by sex and age (<50 and ≥50 years). We used multiple logistic regression to identify factors associated with 3 outcomes: (1) using the Internet to self-diagnose a dermatologic disease, (2) using the Internet to obtain dermatology-related information within the last 3 months, (3) and previously refraining from visiting a dermatologist based on reassurance from online resources. Predictors included the aforementioned demographic and health-care access–related traits. We also categorized smartphone apps used by respondents (ie, fitness/nutrition, reference, self-help, health monitoring, diagnostic aids, electronic medical record) and calculated the proportion of respondents with 1 or more of each type of app on their smartphones. Analyses were conducted in Stata 13.1 and IBM SPSS 22.0.
Results
Of 1000 patients who were invited to participate in the study, a total of 775 respondents completed the survey, yielding a response rate of 77.5%. The majority of respondents were aged 30 to 60 years (mean age [standard deviation], 44.5 [17.2] years; median age [interquartile range], 44 [29–59] years), female (66.7%), and non-Hispanic white (83.3%)(Table 1). The majority of respondents (88.8%) had completed at least some college. Nearly all respondents had medical insurance (97.8%), but annual household income and insurance co-pay varied considerably. Only 10.8% of respondents traveled more than an hour to our offices.
The majority of respondents had access to home Internet and owned a smartphone (Table 2). Use of the Internet to obtain health-related information in the 3 months prior to presentation was more common among females (77.9% vs 70.1%; P=.03) and respondents younger than 50 years (83.4% vs 62.5%; P<.001); the same was true for dermatology-related infor-mation (females: 43.2% vs 31.0%; P=.003; aged <50 years, 51.6% vs 22.2%; P<.001). The majority of respondents indicated that they use the Internet to obtain health-related information both before and after they see their doctor. Most respondents indicated that they sometimes discuss health-related information found on the Internet with a physician. Smartphone use to obtain health-related information was more common among respondents younger than 50 years versus those who were 50 years or older (55.5% vs 24.1%; P<.001), as was smartphone use to diagnose skin problems (20.0% vs 6.3%; P<.001).
In multivariable analysis, use of the Internet or a smartphone to obtain health-related information was associated with younger age (<50 years) and a higher level of education (both P<.001). Use of the Internet to obtain dermatology-related information (P<.001) and use of a smartphone to help diagnose a skin problem (P=.001) was associated with younger age (<50 years) only. Income, sex, co-pay to see a dermatologist, and travel time to the dermatology office were not associated with use of online resources for general or dermatology-specific health-related information or assistance with diagnosing a skin problem.
Of 204 respondents who indicated that they previously attempted to self-diagnose a skin condition using the Internet, the most commonly researched condition was skin cancer/moles/unknown spots (64.7%), followed by rashes (40.7%), acne (20.6%), cosmetic issues (16.2%), psoriasis (12.7%), dermatitis (3.4%), warts (1.5%), tick bites (1.0%), and lupus (1.0%)(some respondents selected more than one condition). Only 7.0% of respondents indicated that they previously had refrained from visiting a dermatologist based on reassurance from online resources. Compared to the rest of the surveyed population, these respondents were younger (P=.001), but there were no significant differences in sex, highest level of education, household income, or travel time to the dermatology office. The most commonly researched condition among these respondents was acne (12 respondents), and 11 respondents indicated that they had attempted to self-diagnose a mole or potential cancer using online sources.
Of 557 respondents who owned a smartphone, 31.8% reported using at least 1 health-related app (mean number of health apps per respondent, 1.5). Of the apps that respondents used, 45.9% focused on fitness/nutrition, 28.7% provided reference information, 13.4% were a patient portal for receiving information from their electronic medical record, 8.6% provided a health monitoring function, 1.9% served as a diagnostic aid, and 1.5% provided coping assistance and emotional support for individuals with cognitive or emotional conditions; only 1 respondent reported using an app related to dermatology.
All respondents were asked to rate their anticipated degree of worry if the Internet or a smartphone app suggested that a skin lesion was benign versus dangerous on a 5-point scale. Overall, the median worry rating increased from 3 to 5 when information accessed via the Internet or a smartphone app suggested a lesion was dangerous rather than benign. A change in worry of 2 or more points was seen in 36.1% of females and 49.1% of males (P=.002) when information obtained via the Internet indicated a lesion was dangerous and in 47.5% of females and 58.8% of males (P=.006) when a smartphone app indicated that a lesion was dangerous. When information obtained via the Internet indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 41.8% of respondents who were younger than 50 years and in 41.1% of those who were 50 years or older (P=.93). When a smartphone app indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 50.2% of respondents who were younger than 50 years and in 52.2% of those who were 50 years or older (P=.61).
Discussion
In this cross-sectional study, we found that health-related Internet and smartphone use among dermatology patients is common and may impact both patients’ degree of concern about a skin lesion as well as the likelihood of seeking in-person medical care if they are reassured by the results of their online findings. Age and level of education were associated with Internet and smartphone use to obtain dermatology-related health information but not factors related to health care access. More patients used the Internet or a smartphone to obtain general medical information versus dermatology-related information. Respondents who indicated that they used the Internet to obtain health-related information tended to do so before visiting their physician.
Our finding that a patient’s level of worry about a hypothetical skin condition or lesion is influenced by health information obtained via the Internet or a smartphone app is concerning. One study found that participants who used a popular search engine to look for information about vaccine safety and dangers were directed to Web sites with inaccurate information more than 50% of the time, and 65% of the information they obtained from these sites was false.6 In our study, approximately 25% of respondents had previously consulted online resources to attempt toself-diagnose a skin condition. Online sources about dermatologic conditions were consulted most frequently for information about potential skin cancers, moles, and unknown spots. A prior study showed that smartphone apps that claim to aid patients in determining whether a skin lesion is low or high risk for melanoma often are inaccurate and are associated with a high rate of missed melanomas.5 Even though we surveyed patients who did end up seeing a dermatologist, some respondents had previously opted out of seeing a dermatologist based on information they had found online. Because our study was conducted among patients who chose to seek care at a dermatology office, the problem is likely greater than estimated from our findings because we had no way of reaching individuals who decided to completely forgo a visit with a dermatologist.
Although use of the Internet to obtain health-related information was common among older adults in our population, it was nearly universal in younger adults. Health-related smartphone use was more than twice as common in younger versus older adults, which could be due to an increased comfort with technology and its integration into daily life. The fact that age and education were associated with Internet use for dermatology-related health information but not household income or travel time to the dermatology office suggests that information seeking is not due to lack of resources limiting access to dermatologic care but rather to the greater role that rapid access to online information plays in patients’ lives. Our findings are similar to another study that examined the use of online sources for general health information.7
This study has several limitations. First, there may have been some selection bias. We specifically aimed to understand the health-related Internet and smartphone use among dermatology patients, thus restricting our sample to this population. By doing so, we were unable to assess the use of such resources by the general population, particularly those individuals who chose not to see a dermatologist at all based on their own online research. Our findings may not apply to other practices and regions of the country, as we implemented our study in one geographic location and in offices of an academic practice. Although our sample size and diversity with regard to income, education, and age suggest that our results are likely generalizable to many settings, it is important to note that nearly all respondents in this study had health insurance and our findings are thus not necessarily applicable to those individuals who are uninsured.
Conclusion
Our findings suggest that the availability of online health information regarding dermatologic conditions provides dermatologists with both opportunities and challenges. Many patients consult online resources for health information, and the popularity of this practice is likely to increase with time, particularly as newer smartphones with features designed to allow users to monitor their health are developed with health-conscious consumers in mind. Most large health care systems provide patients with resources to view laboratory results and communicate with physicians online. It is important for dermatologists to be involved in the development of high-quality online content that educates the public while also emphasizing the need to seek in-person medical care, particularly in potential cases of skin cancer. It also is important for patients to be involved in the content development process to ensure that the messages they take away from online resources are the ones physicians wish to convey. Ideally, online forms of education will increase patients’ sense of self-efficacy while encouraging appropriate consultation for potentially harmful skin conditions.
Patients increasingly use the Internet and/or smartphone applications (apps) to seek health information and track personal health data,1,2 typically in the spirit of being a more educated consumer. However, many patients use the Internet in an attempt to self-diagnose and independently find treatment options, thus avoiding (in their opinion) the need to seek in-person medical care. Additionally, electronic access to health information has expanded beyond computers to smartphones with apps that can provide users with a simple interface to personalize the health information they seek and receive.
Prior studies have shown that seeking online health information and health-related social media is more common among women, younger patients, those with a college education, and those with a higher income.3,4 However, the prevalence of health-related Internet and smartphone use among dermatology patients as well as how patients ultimately use this information is not well studied. This information about patient behavior is important because of the potential harm that may come from patient self-diagnosis, which may delay or prevent treatment, as well as the benefits of patient self-education, which may expedite diagnosis and treatment.5 We surveyed a heterogeneous patient population at 2 dermatology offices in a major academic medical center to assess the prevalence and predictors of Internet and smartphone use to obtain both general medical and dermatologic information among dermatology patients. We also evaluated the impact that health information obtained from online sources has on a patient’s degree of concern about cutaneous disease and the likelihood of seeing a dermatologist for a skin problem.
Methods
Survey and Participants
This study was approved by the institutional review board at the University of Pittsburgh, Pennsylvania. All patients aged 18 years or older who presented to the department of dermatology at 2 offices of the University of Pittsburgh Medical Center from September 2013 through July 2014 were invited to participate in an anonymous 33-question survey regarding their use of the Internet and smartphone apps to obtain health information and make health care decisions. Patients were asked to complete the survey prior to seeing a health care provider and return it to a locked box by the front desk before leaving the office. Survey questions were designed by physicians with content expertise (J.A.W. and L.K.F.) and were reviewed by a statistician with survey expertise (D.G.W.). The survey included questions about patient demographics, Internet and smartphone use (both general and health related), and specific sources accessed. The survey also inquired about the impact of health information obtained via the Internet and smartphone apps on respondents’ degree of worry about a hypothetical skin condition or lesion using a 5-point Likert scale (1=no worry; 5=very worried). Respondents also were asked which skin conditions they previously researched online and whether their findings impacted their decision to see a dermatologist. Additionally, respondents were asked to list the smartphone apps and other online health resources they had used within the last 3 months. Prior to distribution, the survey was piloted with 10 participants and no issues with comprehensibility were noted.
Statistical Analysis
We described demographic traits (eg, age, sex, race/ethnicity, level of education, income) and factors associated with access to health care (eg, specialist co-pay, travel time from dermatology office) of respondents using proportions. We evaluated respondents’ access to and use of Internet- and smartphone-based health information using proportions and used χ² tests to quantify differences by sex and age (<50 years and ≥50 years).
We analyzed the impact of Internet and smartphone-based health information on patient worry about skin conditions by obtaining median worry on a 5-point Likert scale. Due to the nonparametric nature of the data, we used the Mann-Whitney U test to quantify differences by sex and age (<50 and ≥50 years). We used multiple logistic regression to identify factors associated with 3 outcomes: (1) using the Internet to self-diagnose a dermatologic disease, (2) using the Internet to obtain dermatology-related information within the last 3 months, (3) and previously refraining from visiting a dermatologist based on reassurance from online resources. Predictors included the aforementioned demographic and health-care access–related traits. We also categorized smartphone apps used by respondents (ie, fitness/nutrition, reference, self-help, health monitoring, diagnostic aids, electronic medical record) and calculated the proportion of respondents with 1 or more of each type of app on their smartphones. Analyses were conducted in Stata 13.1 and IBM SPSS 22.0.
Results
Of 1000 patients who were invited to participate in the study, a total of 775 respondents completed the survey, yielding a response rate of 77.5%. The majority of respondents were aged 30 to 60 years (mean age [standard deviation], 44.5 [17.2] years; median age [interquartile range], 44 [29–59] years), female (66.7%), and non-Hispanic white (83.3%)(Table 1). The majority of respondents (88.8%) had completed at least some college. Nearly all respondents had medical insurance (97.8%), but annual household income and insurance co-pay varied considerably. Only 10.8% of respondents traveled more than an hour to our offices.
The majority of respondents had access to home Internet and owned a smartphone (Table 2). Use of the Internet to obtain health-related information in the 3 months prior to presentation was more common among females (77.9% vs 70.1%; P=.03) and respondents younger than 50 years (83.4% vs 62.5%; P<.001); the same was true for dermatology-related infor-mation (females: 43.2% vs 31.0%; P=.003; aged <50 years, 51.6% vs 22.2%; P<.001). The majority of respondents indicated that they use the Internet to obtain health-related information both before and after they see their doctor. Most respondents indicated that they sometimes discuss health-related information found on the Internet with a physician. Smartphone use to obtain health-related information was more common among respondents younger than 50 years versus those who were 50 years or older (55.5% vs 24.1%; P<.001), as was smartphone use to diagnose skin problems (20.0% vs 6.3%; P<.001).
In multivariable analysis, use of the Internet or a smartphone to obtain health-related information was associated with younger age (<50 years) and a higher level of education (both P<.001). Use of the Internet to obtain dermatology-related information (P<.001) and use of a smartphone to help diagnose a skin problem (P=.001) was associated with younger age (<50 years) only. Income, sex, co-pay to see a dermatologist, and travel time to the dermatology office were not associated with use of online resources for general or dermatology-specific health-related information or assistance with diagnosing a skin problem.
Of 204 respondents who indicated that they previously attempted to self-diagnose a skin condition using the Internet, the most commonly researched condition was skin cancer/moles/unknown spots (64.7%), followed by rashes (40.7%), acne (20.6%), cosmetic issues (16.2%), psoriasis (12.7%), dermatitis (3.4%), warts (1.5%), tick bites (1.0%), and lupus (1.0%)(some respondents selected more than one condition). Only 7.0% of respondents indicated that they previously had refrained from visiting a dermatologist based on reassurance from online resources. Compared to the rest of the surveyed population, these respondents were younger (P=.001), but there were no significant differences in sex, highest level of education, household income, or travel time to the dermatology office. The most commonly researched condition among these respondents was acne (12 respondents), and 11 respondents indicated that they had attempted to self-diagnose a mole or potential cancer using online sources.
Of 557 respondents who owned a smartphone, 31.8% reported using at least 1 health-related app (mean number of health apps per respondent, 1.5). Of the apps that respondents used, 45.9% focused on fitness/nutrition, 28.7% provided reference information, 13.4% were a patient portal for receiving information from their electronic medical record, 8.6% provided a health monitoring function, 1.9% served as a diagnostic aid, and 1.5% provided coping assistance and emotional support for individuals with cognitive or emotional conditions; only 1 respondent reported using an app related to dermatology.
All respondents were asked to rate their anticipated degree of worry if the Internet or a smartphone app suggested that a skin lesion was benign versus dangerous on a 5-point scale. Overall, the median worry rating increased from 3 to 5 when information accessed via the Internet or a smartphone app suggested a lesion was dangerous rather than benign. A change in worry of 2 or more points was seen in 36.1% of females and 49.1% of males (P=.002) when information obtained via the Internet indicated a lesion was dangerous and in 47.5% of females and 58.8% of males (P=.006) when a smartphone app indicated that a lesion was dangerous. When information obtained via the Internet indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 41.8% of respondents who were younger than 50 years and in 41.1% of those who were 50 years or older (P=.93). When a smartphone app indicated a lesion was dangerous, a change in worry of 2 or more points was seen in 50.2% of respondents who were younger than 50 years and in 52.2% of those who were 50 years or older (P=.61).
Discussion
In this cross-sectional study, we found that health-related Internet and smartphone use among dermatology patients is common and may impact both patients’ degree of concern about a skin lesion as well as the likelihood of seeking in-person medical care if they are reassured by the results of their online findings. Age and level of education were associated with Internet and smartphone use to obtain dermatology-related health information but not factors related to health care access. More patients used the Internet or a smartphone to obtain general medical information versus dermatology-related information. Respondents who indicated that they used the Internet to obtain health-related information tended to do so before visiting their physician.
Our finding that a patient’s level of worry about a hypothetical skin condition or lesion is influenced by health information obtained via the Internet or a smartphone app is concerning. One study found that participants who used a popular search engine to look for information about vaccine safety and dangers were directed to Web sites with inaccurate information more than 50% of the time, and 65% of the information they obtained from these sites was false.6 In our study, approximately 25% of respondents had previously consulted online resources to attempt toself-diagnose a skin condition. Online sources about dermatologic conditions were consulted most frequently for information about potential skin cancers, moles, and unknown spots. A prior study showed that smartphone apps that claim to aid patients in determining whether a skin lesion is low or high risk for melanoma often are inaccurate and are associated with a high rate of missed melanomas.5 Even though we surveyed patients who did end up seeing a dermatologist, some respondents had previously opted out of seeing a dermatologist based on information they had found online. Because our study was conducted among patients who chose to seek care at a dermatology office, the problem is likely greater than estimated from our findings because we had no way of reaching individuals who decided to completely forgo a visit with a dermatologist.
Although use of the Internet to obtain health-related information was common among older adults in our population, it was nearly universal in younger adults. Health-related smartphone use was more than twice as common in younger versus older adults, which could be due to an increased comfort with technology and its integration into daily life. The fact that age and education were associated with Internet use for dermatology-related health information but not household income or travel time to the dermatology office suggests that information seeking is not due to lack of resources limiting access to dermatologic care but rather to the greater role that rapid access to online information plays in patients’ lives. Our findings are similar to another study that examined the use of online sources for general health information.7
This study has several limitations. First, there may have been some selection bias. We specifically aimed to understand the health-related Internet and smartphone use among dermatology patients, thus restricting our sample to this population. By doing so, we were unable to assess the use of such resources by the general population, particularly those individuals who chose not to see a dermatologist at all based on their own online research. Our findings may not apply to other practices and regions of the country, as we implemented our study in one geographic location and in offices of an academic practice. Although our sample size and diversity with regard to income, education, and age suggest that our results are likely generalizable to many settings, it is important to note that nearly all respondents in this study had health insurance and our findings are thus not necessarily applicable to those individuals who are uninsured.
Conclusion
Our findings suggest that the availability of online health information regarding dermatologic conditions provides dermatologists with both opportunities and challenges. Many patients consult online resources for health information, and the popularity of this practice is likely to increase with time, particularly as newer smartphones with features designed to allow users to monitor their health are developed with health-conscious consumers in mind. Most large health care systems provide patients with resources to view laboratory results and communicate with physicians online. It is important for dermatologists to be involved in the development of high-quality online content that educates the public while also emphasizing the need to seek in-person medical care, particularly in potential cases of skin cancer. It also is important for patients to be involved in the content development process to ensure that the messages they take away from online resources are the ones physicians wish to convey. Ideally, online forms of education will increase patients’ sense of self-efficacy while encouraging appropriate consultation for potentially harmful skin conditions.
1. Atkinson NL, Saperstein SL, Pleis J. Using the Internet for health-related activities: findings from a national probability sample. J Med Internet Res. 2009;11:e4.
2. Ybarra M, Suman M. Reasons, assessments and actions taken: sex and age differences in uses of Internet health information. Health Educ Res. 2008;23:512-521.
3. Bhandari N, Shi Y, Jung K. Seeking health information online: does limited healthcare access matter? J Am Med Inform Assoc. 2014;21:1113-1117.
4. Thackeray R, Crookston BT, West JH. Correlates of health-related social media use among adults. J Med Internet Res. 2013;15:e21.
5. Wolf JA, Moreau JF, Akilov O, et al. Diagnostic inaccuracy of smartphone applications for melanoma detection. JAMA Dermatol. 2013;149:422-426.
6. Kortum P, Edwards C, Richards-Kortum R. The impact of inaccurate Internet health information in a secondary school learning environment. J Med Internet Res. 2008;10:e17.
7. Mead N, Varnam R, Rogers A, et al. What predicts patients’ interest in the internet as a health resource in primary care in England? J Health Serv Res Policy. 2003;8:33-39.
1. Atkinson NL, Saperstein SL, Pleis J. Using the Internet for health-related activities: findings from a national probability sample. J Med Internet Res. 2009;11:e4.
2. Ybarra M, Suman M. Reasons, assessments and actions taken: sex and age differences in uses of Internet health information. Health Educ Res. 2008;23:512-521.
3. Bhandari N, Shi Y, Jung K. Seeking health information online: does limited healthcare access matter? J Am Med Inform Assoc. 2014;21:1113-1117.
4. Thackeray R, Crookston BT, West JH. Correlates of health-related social media use among adults. J Med Internet Res. 2013;15:e21.
5. Wolf JA, Moreau JF, Akilov O, et al. Diagnostic inaccuracy of smartphone applications for melanoma detection. JAMA Dermatol. 2013;149:422-426.
6. Kortum P, Edwards C, Richards-Kortum R. The impact of inaccurate Internet health information in a secondary school learning environment. J Med Internet Res. 2008;10:e17.
7. Mead N, Varnam R, Rogers A, et al. What predicts patients’ interest in the internet as a health resource in primary care in England? J Health Serv Res Policy. 2003;8:33-39.
