User login
Small practices, say hello to the VBM
While much has been written about the Center for Medicare & Medicaid Services (CMS) plan to shift its payment system away from fee for service and toward a “value-based” structure, most physicians in small and solo private settings have given little, if any, thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS plan is something called the Value-Based Payment Modifier (VBM), a component of the Affordable Care Act (ACA). The VBM has been off the radar of smaller private practices, because up until now it has applied only to groups with more than 10 providers. Starting this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBM “score.”

That score will be based on your “quality of care” (as defined by the CMS) and how much your care costs the system, compared with care provided by other physicians. The quality component will be calculated from measures reported through the Physician Quality Reporting System (PQRS). Your practice will then be “tiered” to determine whether your performance is statistically better, the same, or worse than the national mean. The CMS has not shared all the details of its “quality tiering” formula, but you can get an idea of their general criteria by reviewing the recently released “Quality Benchmarks for the 2015 Value Modifier” at CMS.org.
To calculate the cost component, the CMS will evaluate measures that include total overall costs per beneficiary, and total costs for a composite of chronic conditions, such as (for internists) chronic obstructive pulmonary disease, heart failure, coronary artery disease, and diabetes; no one has speculated on which diseases might be used for dermatology. Practitioners are eligible for a 1% bonus if their average score is in the top 25% of all scores nationwide. You can get some sense of where you stand in the national hierarchy by studying your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. Reports for the first half of 2014 were released by the CMS in April, and can be downloaded from the QRUR section of CMS.gov.
The ACA requires that the program be budget neutral – which means that all bonuses to physicians in the highest 25% must be offset by penalties – “negative adjustments” – to those in the lowest 25%. The good news is that groups with two to nine providers, and solo practitioners who report successfully for PQRS, receive only the upward or neutral adjustment for 2017, with no downward adjustments. That means you will have at least one penalty-free year to determine where you stand in the VBM pecking order – and perhaps earn a bonus.
So in summary, here is what you have to do now, in 2015, to maximize your chances of earning that upward adjustment in 2017:
• If you haven’t already, make sure your practice data are correct in the Medicare Provider Enrollment, Chain, and Ownership System (PECOS). This is where CMS will gather data for the VBM and the Physician Feedback Reports.
• Study the Quality Benchmarks and download your practice’s QRUR, as mentioned.
• Report successfully for PQRS in 2015, which will also avoid an automatic penalty of 4% in 2017.
Are there serious potential consequences inherent in this unprecedented new system? I think so. For all the talk that the transition from fee-for-service to “value-based” reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing.
In essence, the VBM establishes arbitrary practice standards and spending ceilings. It creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. Physicians who have the temerity to practice medicine as they see fit, irrespective of the costs involved, will be punished.
Patients will certainly not welcome their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs, and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
All of that said, the VBM is a reality, and can no longer be ignored if you treat Medicare patients.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters.
While much has been written about the Center for Medicare & Medicaid Services (CMS) plan to shift its payment system away from fee for service and toward a “value-based” structure, most physicians in small and solo private settings have given little, if any, thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS plan is something called the Value-Based Payment Modifier (VBM), a component of the Affordable Care Act (ACA). The VBM has been off the radar of smaller private practices, because up until now it has applied only to groups with more than 10 providers. Starting this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBM “score.”
That score will be based on your “quality of care” (as defined by the CMS) and how much your care costs the system, compared with care provided by other physicians. The quality component will be calculated from measures reported through the Physician Quality Reporting System (PQRS). Your practice will then be “tiered” to determine whether your performance is statistically better, the same, or worse than the national mean. The CMS has not shared all the details of its “quality tiering” formula, but you can get an idea of their general criteria by reviewing the recently released “Quality Benchmarks for the 2015 Value Modifier” at CMS.org.
To calculate the cost component, the CMS will evaluate measures that include total overall costs per beneficiary, and total costs for a composite of chronic conditions, such as (for internists) chronic obstructive pulmonary disease, heart failure, coronary artery disease, and diabetes; no one has speculated on which diseases might be used for dermatology. Practitioners are eligible for a 1% bonus if their average score is in the top 25% of all scores nationwide. You can get some sense of where you stand in the national hierarchy by studying your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. Reports for the first half of 2014 were released by the CMS in April, and can be downloaded from the QRUR section of CMS.gov.
The ACA requires that the program be budget neutral – which means that all bonuses to physicians in the highest 25% must be offset by penalties – “negative adjustments” – to those in the lowest 25%. The good news is that groups with two to nine providers, and solo practitioners who report successfully for PQRS, receive only the upward or neutral adjustment for 2017, with no downward adjustments. That means you will have at least one penalty-free year to determine where you stand in the VBM pecking order – and perhaps earn a bonus.
So in summary, here is what you have to do now, in 2015, to maximize your chances of earning that upward adjustment in 2017:
• If you haven’t already, make sure your practice data are correct in the Medicare Provider Enrollment, Chain, and Ownership System (PECOS). This is where CMS will gather data for the VBM and the Physician Feedback Reports.
• Study the Quality Benchmarks and download your practice’s QRUR, as mentioned.
• Report successfully for PQRS in 2015, which will also avoid an automatic penalty of 4% in 2017.
Are there serious potential consequences inherent in this unprecedented new system? I think so. For all the talk that the transition from fee-for-service to “value-based” reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing.
In essence, the VBM establishes arbitrary practice standards and spending ceilings. It creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. Physicians who have the temerity to practice medicine as they see fit, irrespective of the costs involved, will be punished.
Patients will certainly not welcome their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs, and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
All of that said, the VBM is a reality, and can no longer be ignored if you treat Medicare patients.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters.
While much has been written about the Center for Medicare & Medicaid Services (CMS) plan to shift its payment system away from fee for service and toward a “value-based” structure, most physicians in small and solo private settings have given little, if any, thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS plan is something called the Value-Based Payment Modifier (VBM), a component of the Affordable Care Act (ACA). The VBM has been off the radar of smaller private practices, because up until now it has applied only to groups with more than 10 providers. Starting this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBM “score.”
That score will be based on your “quality of care” (as defined by the CMS) and how much your care costs the system, compared with care provided by other physicians. The quality component will be calculated from measures reported through the Physician Quality Reporting System (PQRS). Your practice will then be “tiered” to determine whether your performance is statistically better, the same, or worse than the national mean. The CMS has not shared all the details of its “quality tiering” formula, but you can get an idea of their general criteria by reviewing the recently released “Quality Benchmarks for the 2015 Value Modifier” at CMS.org.
To calculate the cost component, the CMS will evaluate measures that include total overall costs per beneficiary, and total costs for a composite of chronic conditions, such as (for internists) chronic obstructive pulmonary disease, heart failure, coronary artery disease, and diabetes; no one has speculated on which diseases might be used for dermatology. Practitioners are eligible for a 1% bonus if their average score is in the top 25% of all scores nationwide. You can get some sense of where you stand in the national hierarchy by studying your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. Reports for the first half of 2014 were released by the CMS in April, and can be downloaded from the QRUR section of CMS.gov.
The ACA requires that the program be budget neutral – which means that all bonuses to physicians in the highest 25% must be offset by penalties – “negative adjustments” – to those in the lowest 25%. The good news is that groups with two to nine providers, and solo practitioners who report successfully for PQRS, receive only the upward or neutral adjustment for 2017, with no downward adjustments. That means you will have at least one penalty-free year to determine where you stand in the VBM pecking order – and perhaps earn a bonus.
So in summary, here is what you have to do now, in 2015, to maximize your chances of earning that upward adjustment in 2017:
• If you haven’t already, make sure your practice data are correct in the Medicare Provider Enrollment, Chain, and Ownership System (PECOS). This is where CMS will gather data for the VBM and the Physician Feedback Reports.
• Study the Quality Benchmarks and download your practice’s QRUR, as mentioned.
• Report successfully for PQRS in 2015, which will also avoid an automatic penalty of 4% in 2017.
Are there serious potential consequences inherent in this unprecedented new system? I think so. For all the talk that the transition from fee-for-service to “value-based” reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing.
In essence, the VBM establishes arbitrary practice standards and spending ceilings. It creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. Physicians who have the temerity to practice medicine as they see fit, irrespective of the costs involved, will be punished.
Patients will certainly not welcome their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs, and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
All of that said, the VBM is a reality, and can no longer be ignored if you treat Medicare patients.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters.

H.R. 2646 vs. H.R. 3717: The difference 2 years makes
In 2013, Rep. Tim Murphy (R-Pa.) proposed the Helping Families in Mental Health Crisis Act, H.R. 3717, as a response to the tragedy in Newtown, Conn. The legislation did not make it out of committee before the congressional session ended, and on June 4, a revised version of the bill – now H.R. 2646 – was introduced in Congress, cosponsored by Texas Democrat Rep. Eddie Bernice Johnson. The legislation is being framed as sweeping legislation “to fix America’s broken health system.” Those familiar with the original version may recall that controversial portions included a requirement for states to have legislation for outpatient civil commitment or lose funding, and allow caretakers to access information for mental health patients without patient consent. That version also proposed the shifting of funds from the Substance Abuse and Mental Health Services Administration (SAMHSA) to the National Institute of Mental Health (NIMH) to promote research.
The text of H.R. 2646 is 173 pages long, nearly 40 pages longer than the original version of the bill Even those who are well versed in these issues are having trouble deciphering the new proposals.
Let me start with a rather unusual disclaimer for someone writing about a piece of legislation: I haven’t read the bill. Instead, I read the blog of journalist/advocate Pete Earley, after he went to the effort of reading the text, soliciting the opinions of leadership at several organizations, and putting together a list of comparisons between the 2013 and 2015 versions of the proposed legislation. In a piece headlined, “Murphy Introduces Revamped Mental Health Bill: Will It Fly This Time Around?” Earley compares the new 2015 bill to the original legislation proposed in 2013.
I’m going to summarize the differences Earley noted, and I’ll add his caveat that he is not certain that his interpretations are correct; the wording of the bill is confusing, and there is not yet agreement on what the different components of the legislation mean. Because the issues around requirements for outpatient commitment have been so volatile, let me add that Earley did communicate with a staffer in Murphy’s office and confirmed that his understanding of that portion of the legislation is correct.
Earley noted eight main points:
1. Rather than removing funding from SAMHSA and shifting it to the NIMH, the new bill gives oversight for mental health care and funding to an assistant secretary for mental health and substance abuse treatment within the Department of Health and Human Services. The bill stipulates that the position must be held by a psychiatrist or psychologist.
2. In H.R. 2646, this funding would be provided only for programs recognized as evidence-based practices; it does not target specific SAMHSA programs for elimination.
3. States that implement outpatient civil commitment would receive a 2% increase in block funding grants. In the original version, states without this legislation would lose federal funding.
4. The new bill allows psychiatrists to share only specific information with caretakers without patient consent: diagnoses, treatment plans, and information about medications but not psychotherapy notes.
5. Murphy’s bill would repeal the so-called IMD (institutions for mental disease) exclusion for facilities with more than 16 beds as long as a facility kept patients less than an average of 30 days.
6. In the original version of the bill, Murphy wanted to eliminate funding to protection and advocacy agencies charged with protecting patients’ rights. The 2015 version bill would limit the powers of advocates by restricting their authority to the investigation of abuse and neglect, and would forbid these agencies from lobbying and from “counseling an individual with a serious mental illness who lacks insight into their condition on refusing medical treatment or acting against the wishes of such individual’s caregiver.”
7. The newer version eliminates the 190-day lifetime cap on inpatient psychiatric hospitalizations in Medicare.
8. H.R. 2646 encourages funding and support for peer-to-peer programs, but sets standards for peers and requires their work to be monitored by a mental health professional.
Obviously, legislation of this length includes much more, but these were the differences Earley identified in his comparison to text of the first version. His Website includes more detail and explanation of these points, and I encourage you to visit PeteEarley.com.
Days after the introduction of the bill, now known as the Murphy-Johnson Act, American Psychiatric Association President Renée Binder and CEO Saul Levin wrote a letter of support for the bill. The letter outlines some of the major issues that the legislation addresses, including increases to the psychiatric workforce. In it, they note: “This is historic legislation that would, for the first time in decades, bring systemwide reforms and improvements to care for our patients and for those who currently lack access to needed treatment.”
A hearing will be held on the bill today.
With thanks to Pete Earley who allowed me to hijack his article.
Dr. Miller is coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011). Follow Dr. Miller on Twitter @shrinkrapdinah.
In 2013, Rep. Tim Murphy (R-Pa.) proposed the Helping Families in Mental Health Crisis Act, H.R. 3717, as a response to the tragedy in Newtown, Conn. The legislation did not make it out of committee before the congressional session ended, and on June 4, a revised version of the bill – now H.R. 2646 – was introduced in Congress, cosponsored by Texas Democrat Rep. Eddie Bernice Johnson. The legislation is being framed as sweeping legislation “to fix America’s broken health system.” Those familiar with the original version may recall that controversial portions included a requirement for states to have legislation for outpatient civil commitment or lose funding, and allow caretakers to access information for mental health patients without patient consent. That version also proposed the shifting of funds from the Substance Abuse and Mental Health Services Administration (SAMHSA) to the National Institute of Mental Health (NIMH) to promote research.
The text of H.R. 2646 is 173 pages long, nearly 40 pages longer than the original version of the bill Even those who are well versed in these issues are having trouble deciphering the new proposals.
Let me start with a rather unusual disclaimer for someone writing about a piece of legislation: I haven’t read the bill. Instead, I read the blog of journalist/advocate Pete Earley, after he went to the effort of reading the text, soliciting the opinions of leadership at several organizations, and putting together a list of comparisons between the 2013 and 2015 versions of the proposed legislation. In a piece headlined, “Murphy Introduces Revamped Mental Health Bill: Will It Fly This Time Around?” Earley compares the new 2015 bill to the original legislation proposed in 2013.
I’m going to summarize the differences Earley noted, and I’ll add his caveat that he is not certain that his interpretations are correct; the wording of the bill is confusing, and there is not yet agreement on what the different components of the legislation mean. Because the issues around requirements for outpatient commitment have been so volatile, let me add that Earley did communicate with a staffer in Murphy’s office and confirmed that his understanding of that portion of the legislation is correct.
Earley noted eight main points:
1. Rather than removing funding from SAMHSA and shifting it to the NIMH, the new bill gives oversight for mental health care and funding to an assistant secretary for mental health and substance abuse treatment within the Department of Health and Human Services. The bill stipulates that the position must be held by a psychiatrist or psychologist.
2. In H.R. 2646, this funding would be provided only for programs recognized as evidence-based practices; it does not target specific SAMHSA programs for elimination.
3. States that implement outpatient civil commitment would receive a 2% increase in block funding grants. In the original version, states without this legislation would lose federal funding.
4. The new bill allows psychiatrists to share only specific information with caretakers without patient consent: diagnoses, treatment plans, and information about medications but not psychotherapy notes.
5. Murphy’s bill would repeal the so-called IMD (institutions for mental disease) exclusion for facilities with more than 16 beds as long as a facility kept patients less than an average of 30 days.
6. In the original version of the bill, Murphy wanted to eliminate funding to protection and advocacy agencies charged with protecting patients’ rights. The 2015 version bill would limit the powers of advocates by restricting their authority to the investigation of abuse and neglect, and would forbid these agencies from lobbying and from “counseling an individual with a serious mental illness who lacks insight into their condition on refusing medical treatment or acting against the wishes of such individual’s caregiver.”
7. The newer version eliminates the 190-day lifetime cap on inpatient psychiatric hospitalizations in Medicare.
8. H.R. 2646 encourages funding and support for peer-to-peer programs, but sets standards for peers and requires their work to be monitored by a mental health professional.
Obviously, legislation of this length includes much more, but these were the differences Earley identified in his comparison to text of the first version. His Website includes more detail and explanation of these points, and I encourage you to visit PeteEarley.com.
Days after the introduction of the bill, now known as the Murphy-Johnson Act, American Psychiatric Association President Renée Binder and CEO Saul Levin wrote a letter of support for the bill. The letter outlines some of the major issues that the legislation addresses, including increases to the psychiatric workforce. In it, they note: “This is historic legislation that would, for the first time in decades, bring systemwide reforms and improvements to care for our patients and for those who currently lack access to needed treatment.”
A hearing will be held on the bill today.
With thanks to Pete Earley who allowed me to hijack his article.
Dr. Miller is coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011). Follow Dr. Miller on Twitter @shrinkrapdinah.
In 2013, Rep. Tim Murphy (R-Pa.) proposed the Helping Families in Mental Health Crisis Act, H.R. 3717, as a response to the tragedy in Newtown, Conn. The legislation did not make it out of committee before the congressional session ended, and on June 4, a revised version of the bill – now H.R. 2646 – was introduced in Congress, cosponsored by Texas Democrat Rep. Eddie Bernice Johnson. The legislation is being framed as sweeping legislation “to fix America’s broken health system.” Those familiar with the original version may recall that controversial portions included a requirement for states to have legislation for outpatient civil commitment or lose funding, and allow caretakers to access information for mental health patients without patient consent. That version also proposed the shifting of funds from the Substance Abuse and Mental Health Services Administration (SAMHSA) to the National Institute of Mental Health (NIMH) to promote research.
The text of H.R. 2646 is 173 pages long, nearly 40 pages longer than the original version of the bill Even those who are well versed in these issues are having trouble deciphering the new proposals.
Let me start with a rather unusual disclaimer for someone writing about a piece of legislation: I haven’t read the bill. Instead, I read the blog of journalist/advocate Pete Earley, after he went to the effort of reading the text, soliciting the opinions of leadership at several organizations, and putting together a list of comparisons between the 2013 and 2015 versions of the proposed legislation. In a piece headlined, “Murphy Introduces Revamped Mental Health Bill: Will It Fly This Time Around?” Earley compares the new 2015 bill to the original legislation proposed in 2013.
I’m going to summarize the differences Earley noted, and I’ll add his caveat that he is not certain that his interpretations are correct; the wording of the bill is confusing, and there is not yet agreement on what the different components of the legislation mean. Because the issues around requirements for outpatient commitment have been so volatile, let me add that Earley did communicate with a staffer in Murphy’s office and confirmed that his understanding of that portion of the legislation is correct.
Earley noted eight main points:
1. Rather than removing funding from SAMHSA and shifting it to the NIMH, the new bill gives oversight for mental health care and funding to an assistant secretary for mental health and substance abuse treatment within the Department of Health and Human Services. The bill stipulates that the position must be held by a psychiatrist or psychologist.
2. In H.R. 2646, this funding would be provided only for programs recognized as evidence-based practices; it does not target specific SAMHSA programs for elimination.
3. States that implement outpatient civil commitment would receive a 2% increase in block funding grants. In the original version, states without this legislation would lose federal funding.
4. The new bill allows psychiatrists to share only specific information with caretakers without patient consent: diagnoses, treatment plans, and information about medications but not psychotherapy notes.
5. Murphy’s bill would repeal the so-called IMD (institutions for mental disease) exclusion for facilities with more than 16 beds as long as a facility kept patients less than an average of 30 days.
6. In the original version of the bill, Murphy wanted to eliminate funding to protection and advocacy agencies charged with protecting patients’ rights. The 2015 version bill would limit the powers of advocates by restricting their authority to the investigation of abuse and neglect, and would forbid these agencies from lobbying and from “counseling an individual with a serious mental illness who lacks insight into their condition on refusing medical treatment or acting against the wishes of such individual’s caregiver.”
7. The newer version eliminates the 190-day lifetime cap on inpatient psychiatric hospitalizations in Medicare.
8. H.R. 2646 encourages funding and support for peer-to-peer programs, but sets standards for peers and requires their work to be monitored by a mental health professional.
Obviously, legislation of this length includes much more, but these were the differences Earley identified in his comparison to text of the first version. His Website includes more detail and explanation of these points, and I encourage you to visit PeteEarley.com.
Days after the introduction of the bill, now known as the Murphy-Johnson Act, American Psychiatric Association President Renée Binder and CEO Saul Levin wrote a letter of support for the bill. The letter outlines some of the major issues that the legislation addresses, including increases to the psychiatric workforce. In it, they note: “This is historic legislation that would, for the first time in decades, bring systemwide reforms and improvements to care for our patients and for those who currently lack access to needed treatment.”
A hearing will be held on the bill today.
With thanks to Pete Earley who allowed me to hijack his article.
Dr. Miller is coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011). Follow Dr. Miller on Twitter @shrinkrapdinah.

Put ‘The Digital Doctor’ on your summer reading list
The last time I spoke with my 70-year-old mother in Rhode Island, I asked her how she made out at her latest dermatology appointment. She burst forth: “Don’t get me started! The doctor spent the whole time with his face in the computer screen. He hardly examined me!” It went downhill from there.
I feel both her pain and his. As a Gen-X physician, I’m in a unique position. I trained in the pre-EHR age with the Dr. Marcus Welby–type physicians my parents knew and admired. I have also embraced the digitization of medicine and the advances this affords. At Kaiser Permanente, I help run one of the country’s most robust telemedicine programs, and I answer dozens of patient e-mails each week. Yet I too experience the frustration of having to split my attention between my screens and my patients.

At conferences and in articles, it seems the chasm between physicians who eagerly embrace the new digital world of medicine and those who long for the way things used to be is expanding rather than shrinking. Too often, there is insufficient dialogue between these two groups. Dr. Robert Wachter hopes to change that.
Professor and associate chair of the department of medicine at the University of California, San Francisco, Dr. Wachter has authored six books, has developed the concept of the “hospitalist,” and has been a leader in patient safety. His latest book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age,” (McGraw-Hill, 2015) has been hailed as a “must read” for physicians and other health care practitioners. I agree.
Medicine is in the midst of profound change that is as frightening as it is exciting. Dr. Wachter captures this tension through memorable patient stories and interviews. He argues that technology has made medicine both better and worse. It has enabled clinicians to improve diagnostics and health care delivery. Consider the explosive growth of “big data” in health care and of patient empowerment (e-mailing, texting, Skyping, OpenNotes). Yet, an astute observer acknowledges technology’s shortfalls. For example, what happens when information is incorrectly entered in an EHR? What are physicians to do with the massive patient data we receive?
To illustrate his theme, Dr. Wachter examines EHRs in depth. He argues that the most brilliant engineers can create the most complex computer systems, but if they’re not implemented and funded systemically, how will they be successful? Why would private practice physicians want to relinquish their “tried-and-true paper prescription and record system for an expensive and complex EHR?” And what happens when EHRs don’t talk to one another?
Despite their obvious advantages, EHRs have several drawbacks, including poor usability, time-consuming data entry (that adversely affects the doctor-patient relationship), the high cost of implementation, and decreased satisfaction among physicians with their jobs, Dr. Wachter notes. Who has the solution to these problems? Is it Silicon Valley? Or did they create the problem? (Dr. Wachter spends a great deal of time interviewing key players from that region.) Ultimately, he determines that the EHR, despite its brilliant advantages, wasn’t designed to give both physicians and patients what they really want.
The most compelling patient story that Dr. Wachter shares concerns a teenage boy who nearly died from an overdose of an antibiotic. He shows with devastating clarity how one wrong click of the keypad can lead to tragedy. No one – physicians, nurses, nor pharmacists – caught the error (the patient was administered 38.5 tablets instead of 1 tablet). Why? Dr. Wachter blames our “blind trust” in computers, which causes us to not question when something seems wrong. Moreover, multiple warnings went unheeded by nurses, who probably suffered from “alert fatigue,” desensitization to warning alarms (think of the ubiquitous car alarms sounding and how no one reacts to them), he says.
This leads to Dr. Wachter’s dive into the “complex interface between technology and people.” At what point do computers stop assisting physicians and begin replacing them? While he clearly believes that the human component of the doctor-patient relationship is irreplaceable, he does acknowledge through interviews with people such as Vinod Khosla, cofounder of Sun Microsystems, that computers will continue to “displace” much of the physician’s diagnostic and prescription work.
As Dr. Wachter seesaws through both sides of this argument, he finds himself “stick[ing] up for my teams: humans and the subset of humans called doctors.” After all, isn’t diagnostic skill at the core of an astute clinician’s arsenal? How do we relinquish it to computers?
What about technologies like OpenNotes that empower patients? How will this affect the doctor-patient relationship? What are we to do about patients who make bad choices, opt for high copays to save money up front, or choose Minute Clinics for all their health care needs? Will patients be harmed by such openness? The jury is still out.
For those who like clear black-and-white answers, Dr. Wachter’s book will seem maddeningly gray. Yet as a practicing clinician, I found it enlightening and thought provoking, and hope you will, too. I also hope it prompts you to step away from the computer, walk next door to your colleague’s office, and start a real-life conversation.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
The last time I spoke with my 70-year-old mother in Rhode Island, I asked her how she made out at her latest dermatology appointment. She burst forth: “Don’t get me started! The doctor spent the whole time with his face in the computer screen. He hardly examined me!” It went downhill from there.
I feel both her pain and his. As a Gen-X physician, I’m in a unique position. I trained in the pre-EHR age with the Dr. Marcus Welby–type physicians my parents knew and admired. I have also embraced the digitization of medicine and the advances this affords. At Kaiser Permanente, I help run one of the country’s most robust telemedicine programs, and I answer dozens of patient e-mails each week. Yet I too experience the frustration of having to split my attention between my screens and my patients.
At conferences and in articles, it seems the chasm between physicians who eagerly embrace the new digital world of medicine and those who long for the way things used to be is expanding rather than shrinking. Too often, there is insufficient dialogue between these two groups. Dr. Robert Wachter hopes to change that.
Professor and associate chair of the department of medicine at the University of California, San Francisco, Dr. Wachter has authored six books, has developed the concept of the “hospitalist,” and has been a leader in patient safety. His latest book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age,” (McGraw-Hill, 2015) has been hailed as a “must read” for physicians and other health care practitioners. I agree.
Medicine is in the midst of profound change that is as frightening as it is exciting. Dr. Wachter captures this tension through memorable patient stories and interviews. He argues that technology has made medicine both better and worse. It has enabled clinicians to improve diagnostics and health care delivery. Consider the explosive growth of “big data” in health care and of patient empowerment (e-mailing, texting, Skyping, OpenNotes). Yet, an astute observer acknowledges technology’s shortfalls. For example, what happens when information is incorrectly entered in an EHR? What are physicians to do with the massive patient data we receive?
To illustrate his theme, Dr. Wachter examines EHRs in depth. He argues that the most brilliant engineers can create the most complex computer systems, but if they’re not implemented and funded systemically, how will they be successful? Why would private practice physicians want to relinquish their “tried-and-true paper prescription and record system for an expensive and complex EHR?” And what happens when EHRs don’t talk to one another?
Despite their obvious advantages, EHRs have several drawbacks, including poor usability, time-consuming data entry (that adversely affects the doctor-patient relationship), the high cost of implementation, and decreased satisfaction among physicians with their jobs, Dr. Wachter notes. Who has the solution to these problems? Is it Silicon Valley? Or did they create the problem? (Dr. Wachter spends a great deal of time interviewing key players from that region.) Ultimately, he determines that the EHR, despite its brilliant advantages, wasn’t designed to give both physicians and patients what they really want.
The most compelling patient story that Dr. Wachter shares concerns a teenage boy who nearly died from an overdose of an antibiotic. He shows with devastating clarity how one wrong click of the keypad can lead to tragedy. No one – physicians, nurses, nor pharmacists – caught the error (the patient was administered 38.5 tablets instead of 1 tablet). Why? Dr. Wachter blames our “blind trust” in computers, which causes us to not question when something seems wrong. Moreover, multiple warnings went unheeded by nurses, who probably suffered from “alert fatigue,” desensitization to warning alarms (think of the ubiquitous car alarms sounding and how no one reacts to them), he says.
This leads to Dr. Wachter’s dive into the “complex interface between technology and people.” At what point do computers stop assisting physicians and begin replacing them? While he clearly believes that the human component of the doctor-patient relationship is irreplaceable, he does acknowledge through interviews with people such as Vinod Khosla, cofounder of Sun Microsystems, that computers will continue to “displace” much of the physician’s diagnostic and prescription work.
As Dr. Wachter seesaws through both sides of this argument, he finds himself “stick[ing] up for my teams: humans and the subset of humans called doctors.” After all, isn’t diagnostic skill at the core of an astute clinician’s arsenal? How do we relinquish it to computers?
What about technologies like OpenNotes that empower patients? How will this affect the doctor-patient relationship? What are we to do about patients who make bad choices, opt for high copays to save money up front, or choose Minute Clinics for all their health care needs? Will patients be harmed by such openness? The jury is still out.
For those who like clear black-and-white answers, Dr. Wachter’s book will seem maddeningly gray. Yet as a practicing clinician, I found it enlightening and thought provoking, and hope you will, too. I also hope it prompts you to step away from the computer, walk next door to your colleague’s office, and start a real-life conversation.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
The last time I spoke with my 70-year-old mother in Rhode Island, I asked her how she made out at her latest dermatology appointment. She burst forth: “Don’t get me started! The doctor spent the whole time with his face in the computer screen. He hardly examined me!” It went downhill from there.
I feel both her pain and his. As a Gen-X physician, I’m in a unique position. I trained in the pre-EHR age with the Dr. Marcus Welby–type physicians my parents knew and admired. I have also embraced the digitization of medicine and the advances this affords. At Kaiser Permanente, I help run one of the country’s most robust telemedicine programs, and I answer dozens of patient e-mails each week. Yet I too experience the frustration of having to split my attention between my screens and my patients.
At conferences and in articles, it seems the chasm between physicians who eagerly embrace the new digital world of medicine and those who long for the way things used to be is expanding rather than shrinking. Too often, there is insufficient dialogue between these two groups. Dr. Robert Wachter hopes to change that.
Professor and associate chair of the department of medicine at the University of California, San Francisco, Dr. Wachter has authored six books, has developed the concept of the “hospitalist,” and has been a leader in patient safety. His latest book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age,” (McGraw-Hill, 2015) has been hailed as a “must read” for physicians and other health care practitioners. I agree.
Medicine is in the midst of profound change that is as frightening as it is exciting. Dr. Wachter captures this tension through memorable patient stories and interviews. He argues that technology has made medicine both better and worse. It has enabled clinicians to improve diagnostics and health care delivery. Consider the explosive growth of “big data” in health care and of patient empowerment (e-mailing, texting, Skyping, OpenNotes). Yet, an astute observer acknowledges technology’s shortfalls. For example, what happens when information is incorrectly entered in an EHR? What are physicians to do with the massive patient data we receive?
To illustrate his theme, Dr. Wachter examines EHRs in depth. He argues that the most brilliant engineers can create the most complex computer systems, but if they’re not implemented and funded systemically, how will they be successful? Why would private practice physicians want to relinquish their “tried-and-true paper prescription and record system for an expensive and complex EHR?” And what happens when EHRs don’t talk to one another?
Despite their obvious advantages, EHRs have several drawbacks, including poor usability, time-consuming data entry (that adversely affects the doctor-patient relationship), the high cost of implementation, and decreased satisfaction among physicians with their jobs, Dr. Wachter notes. Who has the solution to these problems? Is it Silicon Valley? Or did they create the problem? (Dr. Wachter spends a great deal of time interviewing key players from that region.) Ultimately, he determines that the EHR, despite its brilliant advantages, wasn’t designed to give both physicians and patients what they really want.
The most compelling patient story that Dr. Wachter shares concerns a teenage boy who nearly died from an overdose of an antibiotic. He shows with devastating clarity how one wrong click of the keypad can lead to tragedy. No one – physicians, nurses, nor pharmacists – caught the error (the patient was administered 38.5 tablets instead of 1 tablet). Why? Dr. Wachter blames our “blind trust” in computers, which causes us to not question when something seems wrong. Moreover, multiple warnings went unheeded by nurses, who probably suffered from “alert fatigue,” desensitization to warning alarms (think of the ubiquitous car alarms sounding and how no one reacts to them), he says.
This leads to Dr. Wachter’s dive into the “complex interface between technology and people.” At what point do computers stop assisting physicians and begin replacing them? While he clearly believes that the human component of the doctor-patient relationship is irreplaceable, he does acknowledge through interviews with people such as Vinod Khosla, cofounder of Sun Microsystems, that computers will continue to “displace” much of the physician’s diagnostic and prescription work.
As Dr. Wachter seesaws through both sides of this argument, he finds himself “stick[ing] up for my teams: humans and the subset of humans called doctors.” After all, isn’t diagnostic skill at the core of an astute clinician’s arsenal? How do we relinquish it to computers?
What about technologies like OpenNotes that empower patients? How will this affect the doctor-patient relationship? What are we to do about patients who make bad choices, opt for high copays to save money up front, or choose Minute Clinics for all their health care needs? Will patients be harmed by such openness? The jury is still out.
For those who like clear black-and-white answers, Dr. Wachter’s book will seem maddeningly gray. Yet as a practicing clinician, I found it enlightening and thought provoking, and hope you will, too. I also hope it prompts you to step away from the computer, walk next door to your colleague’s office, and start a real-life conversation.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and a volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.

VTE may cause mental health problems

Photo by Jiri Hodan
DUBROVNIK, CROATIA—Results of a large study suggest patients who develop a venous thromboembolism (VTE) may have more mental health problems than their healthy peers.
One in 5 patients in the study purchased psychotropic drugs within 5 years of developing a VTE, a rate that was more than double that of age- and sex-matched control subjects.
Anette Arbjerg Højen, of Aalborg University Hospital in Denmark, presented these findings at EuroHeartCare 2015 (abstract 22).
“We know that other chronic medical illnesses in youth can lead to emotional and behavioral problems,” Arbjerg Højen said. “However, until now, VTE has been considered an acute condition that occurs in older people. There is no follow-up of [young VTE] patients regarding their mental health, and no studies have been done on this issue.”
So she and her colleagues investigated the mental health prognosis of young VTE patients using data from 4 nationwide registries: the Danish Civil Registration System, the Danish National Patient Register, the Danish National Prescription Registry, and the Danish Medical Birth Registry.
The investigators identified 4132 patients, ages 13 to 33, who had a first VTE between 1997 and 2010. The team then matched these patients by sex and birth year to a control group of 19,292 people without VTE.
All study participants were followed for their first purchase of psychotropic drugs, including antidepressants, anti-anxiety medications, sedatives, and antipsychotics.
The researchers used the purchase of psychotropic drugs as a proxy measure for mental health status and compared the measure between the two groups. The team used regression analysis to exclude non-VTE-related causes of psychotropic drug purchase, such as postpartum depression.
Results showed the VTE patients were much more likely to purchase psychotropic drugs than control subjects. Among VTE patients, the risk of purchasing psychotropic drugs following their diagnosis was 7.1% after 1 year and 22.1% after 5 years.
The excess risk for VTE patients relative to the controls was 4.7% after 1 year and 10.8% after 5 years. When the investigators adjusted for the effect of recent pregnancy or recent provocations, the risk differences became 4.1% after 1 year and 9.6% after 5 years.
“Most of the drugs prescribed were antidepressants,” Arbjerg Højen said. “These young patients struggle a lot with the fear of VTE recurrence. They are scared that, if it strikes again, it could become a pulmonary embolism and they might die.”
“Our study only included patients who received a prescription for psychotropic drugs. There will be others who were not prescribed medication because of their young age, so the group with mental health problems could be much larger than what we found.”
“Our study looked at mental health up to 5 years and not just in the immediate period after the VTE event, suggesting that it is not just a short-term panic. We don’t know how long mental health problems in VTE patients last, but we do know that these patients will always be at high risk of recurrent VTE, so there is a possibility that their depression or anxiety could be life-long if untreated.”
“Most young VTE patients are monitored by their general practitioner for 3 to 6 months because they are on oral anticoagulant treatment, but, after that, there is generally no long-term follow up. Our study points to the need for treating VTE as a chronic condition with serious mental health consequences requiring specialist care.” ![]()
Photo by Jiri Hodan
DUBROVNIK, CROATIA—Results of a large study suggest patients who develop a venous thromboembolism (VTE) may have more mental health problems than their healthy peers.
One in 5 patients in the study purchased psychotropic drugs within 5 years of developing a VTE, a rate that was more than double that of age- and sex-matched control subjects.
Anette Arbjerg Højen, of Aalborg University Hospital in Denmark, presented these findings at EuroHeartCare 2015 (abstract 22).
“We know that other chronic medical illnesses in youth can lead to emotional and behavioral problems,” Arbjerg Højen said. “However, until now, VTE has been considered an acute condition that occurs in older people. There is no follow-up of [young VTE] patients regarding their mental health, and no studies have been done on this issue.”
So she and her colleagues investigated the mental health prognosis of young VTE patients using data from 4 nationwide registries: the Danish Civil Registration System, the Danish National Patient Register, the Danish National Prescription Registry, and the Danish Medical Birth Registry.
The investigators identified 4132 patients, ages 13 to 33, who had a first VTE between 1997 and 2010. The team then matched these patients by sex and birth year to a control group of 19,292 people without VTE.
All study participants were followed for their first purchase of psychotropic drugs, including antidepressants, anti-anxiety medications, sedatives, and antipsychotics.
The researchers used the purchase of psychotropic drugs as a proxy measure for mental health status and compared the measure between the two groups. The team used regression analysis to exclude non-VTE-related causes of psychotropic drug purchase, such as postpartum depression.
Results showed the VTE patients were much more likely to purchase psychotropic drugs than control subjects. Among VTE patients, the risk of purchasing psychotropic drugs following their diagnosis was 7.1% after 1 year and 22.1% after 5 years.
The excess risk for VTE patients relative to the controls was 4.7% after 1 year and 10.8% after 5 years. When the investigators adjusted for the effect of recent pregnancy or recent provocations, the risk differences became 4.1% after 1 year and 9.6% after 5 years.
“Most of the drugs prescribed were antidepressants,” Arbjerg Højen said. “These young patients struggle a lot with the fear of VTE recurrence. They are scared that, if it strikes again, it could become a pulmonary embolism and they might die.”
“Our study only included patients who received a prescription for psychotropic drugs. There will be others who were not prescribed medication because of their young age, so the group with mental health problems could be much larger than what we found.”
“Our study looked at mental health up to 5 years and not just in the immediate period after the VTE event, suggesting that it is not just a short-term panic. We don’t know how long mental health problems in VTE patients last, but we do know that these patients will always be at high risk of recurrent VTE, so there is a possibility that their depression or anxiety could be life-long if untreated.”
“Most young VTE patients are monitored by their general practitioner for 3 to 6 months because they are on oral anticoagulant treatment, but, after that, there is generally no long-term follow up. Our study points to the need for treating VTE as a chronic condition with serious mental health consequences requiring specialist care.” ![]()
Photo by Jiri Hodan
DUBROVNIK, CROATIA—Results of a large study suggest patients who develop a venous thromboembolism (VTE) may have more mental health problems than their healthy peers.
One in 5 patients in the study purchased psychotropic drugs within 5 years of developing a VTE, a rate that was more than double that of age- and sex-matched control subjects.
Anette Arbjerg Højen, of Aalborg University Hospital in Denmark, presented these findings at EuroHeartCare 2015 (abstract 22).
“We know that other chronic medical illnesses in youth can lead to emotional and behavioral problems,” Arbjerg Højen said. “However, until now, VTE has been considered an acute condition that occurs in older people. There is no follow-up of [young VTE] patients regarding their mental health, and no studies have been done on this issue.”
So she and her colleagues investigated the mental health prognosis of young VTE patients using data from 4 nationwide registries: the Danish Civil Registration System, the Danish National Patient Register, the Danish National Prescription Registry, and the Danish Medical Birth Registry.
The investigators identified 4132 patients, ages 13 to 33, who had a first VTE between 1997 and 2010. The team then matched these patients by sex and birth year to a control group of 19,292 people without VTE.
All study participants were followed for their first purchase of psychotropic drugs, including antidepressants, anti-anxiety medications, sedatives, and antipsychotics.
The researchers used the purchase of psychotropic drugs as a proxy measure for mental health status and compared the measure between the two groups. The team used regression analysis to exclude non-VTE-related causes of psychotropic drug purchase, such as postpartum depression.
Results showed the VTE patients were much more likely to purchase psychotropic drugs than control subjects. Among VTE patients, the risk of purchasing psychotropic drugs following their diagnosis was 7.1% after 1 year and 22.1% after 5 years.
The excess risk for VTE patients relative to the controls was 4.7% after 1 year and 10.8% after 5 years. When the investigators adjusted for the effect of recent pregnancy or recent provocations, the risk differences became 4.1% after 1 year and 9.6% after 5 years.
“Most of the drugs prescribed were antidepressants,” Arbjerg Højen said. “These young patients struggle a lot with the fear of VTE recurrence. They are scared that, if it strikes again, it could become a pulmonary embolism and they might die.”
“Our study only included patients who received a prescription for psychotropic drugs. There will be others who were not prescribed medication because of their young age, so the group with mental health problems could be much larger than what we found.”
“Our study looked at mental health up to 5 years and not just in the immediate period after the VTE event, suggesting that it is not just a short-term panic. We don’t know how long mental health problems in VTE patients last, but we do know that these patients will always be at high risk of recurrent VTE, so there is a possibility that their depression or anxiety could be life-long if untreated.”
“Most young VTE patients are monitored by their general practitioner for 3 to 6 months because they are on oral anticoagulant treatment, but, after that, there is generally no long-term follow up. Our study points to the need for treating VTE as a chronic condition with serious mental health consequences requiring specialist care.” ![]()
Treatment of Ampicillin-Resistant Enterococcus faecium Urinary Tract Infections
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
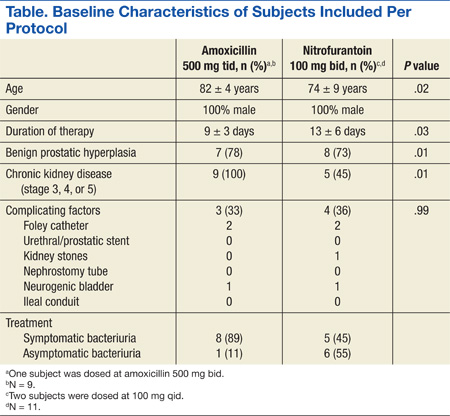
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
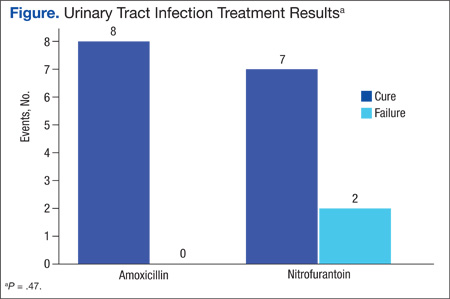
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Enterococcus species account for about 110,000 urinary tract infections (UTIs) annually in the U.S.1 The most common species isolated are Enterococcus faecalis and Enterococcus faecium (E faecium). Amoxicillin is the drug of choice for the treatment of enterococcal UTIs. Second-line therapies include vancomycin and nitrofurantoin. Alternative therapies include daptomycin and linezolid; however, these newer agents ideally would be reserved for more serious infections to preserve activity.2
Increased E faecium resistance to ampicillin and vancomycin has limited the therapeutic options. The results of a study by Zhanel and colleagues assessed the prevalence of resistant enterococcal urine isolates in North America.3 Of the 658 E faecium urine isolates, about 96% were resistant to ampicillin and 94% were resistant to vancoymcin.3 Nitrofurantoin has much lower resistance rates; however, its use is contraindicated in patients with a creatinine clearance (CrCl) < 60 mL/min.4 Data supporting the contraindication are limited, but the results of a study by Oplinger and Andrews suggested that using nitrofurantoin in patients with a CrCl ≥ 40 mL/min may be safe and effective.5 A therapeutic dilemma may occur when resistant E faecium UTIs are encountered and viable treatment options are limited due to intolerances, administration difficulties, lack of susceptibility data, or cost.
Related: Antimicrobial Stewardship in an Outpatient Parenteral Antibiotic Therapy Program
Based on the current Clinical and Laboratory Standards Institute standard, Enterococcus species with a minimal inhibitory concentration (MIC) ≥ 16 μg/mL are considered ampicillin resistant. Microbiology laboratories use the same breakpoint regardless of the site of infection.6 Amoxicillin concentrates in the urine; therefore, urinary concentrations are much higher than serum concentrations. The mean serum peak concentration after a single dose of oral amoxicillin 500 mg is 7.6 μg/mL.7 After a single dose of oral amoxicillin 500 mg, the average concentration in pooled urine collected over 6 hours was 1,100 μg/mL.8
In 2002, Williamson and colleagues analyzed 30 ampicillin- resistant E faecium urine isolates. Reported MICs were 128 μg/mL (30%), 256 μg/mL (60%), and 512 μg/mL (10%).9 A more recent retrospective analysis analyzed 234 ampicillin-resistant E faecium urine isolates. The MIC ranged from 32 to 1,024 μg/mL, with a median MIC of 256 μg/mL. Only 5 isolates had an MIC value > 1,000 μg/mL, but each of these isolates was within 1 dilution of 512 μg/mL.10 Because penicillins exhibit time-dependent killing, an optimal response will occur as long as the urine concentration is above the MIC for at least 50% of the dosing interval.11 Therefore, therapeutic doses of amoxicillin are expected to produce urine concentrations that exceed the MIC of resistant E faecium urine isolates. The purpose of this study was to determine if amoxicillin was a viable treatment option for ampicillin-resistant E faecium UTIs based on this in vitro theory.
Methods
Veterans aged ≥ 18 years with a positive urine culture for ampicillin- resistant E faecium who received antibiotic therapy for cystitis at the Jesse Brown VA Medical Center (JBVAMC) from January 1, 2005, through June 22, 2010, were evaluated in this retrospective cohort study. Exclusion criteria were the presence of any other organisms in the initial urine culture, prostatic involvement, and the presence of E faecium in a blood culture. Subjects treated with multiple antibiotics concurrently and with sequential treatment of different antibiotics with no evaluation of efficacy between courses were also excluded.
Related: Urologist Workforce Variation Across the VHA
All included subjects were evaluated for resolution of symptoms; improvement in leukocyte esterase count and white blood cell (WBC) count from urine analysis (UA); and eradication of E faecium from a repeat urine culture. The response to treatment was classified as cure, presumed cure, or failure. The criteria for cure were based on the following: resolution of symptoms if present at baseline; repeat UA indicating improvement from the initial positive UA (if obtained); and eradication of E faecium in a repeat urine culture (if obtained).
At least 1 of the aforementioned criteria must have been met to be classified as cure. If more than 1 of the aforementioned criteria was present, then each one must have been met to be classified as cure. To be evaluated for presumed cure, the subject must have had symptoms at baseline. No documentation of ongoing symptoms in subjects who had an appropriate follow-up but did not have a repeat UA or urine culture indicated presumed cure. Persistence or worsening of pretreatment symptoms, a repeat UA without improvement from the initial positive UA, or a repeat urine culture demonstrating continued presence of E faecium indicated failure. The primary endpoint for the study was to determine whether amoxicillin was effective for the management of ampicillin-resistant E faecium UTIs. This study was conducted in compliance with the University of Illinois at Chicago Institutional Review Board and JBVAMC Human Subjects Research Committee requirements.
Results
This study included 20 positive urine cultures for ampicillin-resistant E faecium in 19 subjects. Nine cases were treated with amoxicillin, and 11 cases were treated with nitrofurantoin. At baseline, the mean age was 75 years, mean duration of therapy was 14 days, and all the subjects were male. The baseline characteristics of the 2 groups were similar with the exception of an older population, shorter duration of therapy, and increased incidence of chronic kidney disease in the amoxicillin treatment group, P = .02, .03, and .01, respectively.
Symptoms were documented in 8 of 9 (89%) cases at the time of the positive culture in the amoxicillin treatment group and 5 of 11 (45%) cases in the nitrofurantoin treatment group (Table). The asymptomatic amoxicillin treatment group case and 5 of the 6 nitrofurantoin treatment group asymptomatic cases received treatment prior to a urologic procedure in accordance with the Infectious Diseases Society of America (IDSA) guidelines for the treatment of asymptomatic bacteriuria. The urologic procedures included transurethral resection of a bladder tumor, cystoscopy, urethral dilation, cystometrogram, and transurethral resection of the prostate. One asymptomatic subject in the nitrofurantoin group did not have any documentation to support an appropriate indication for treatment. All positive cultures were > 100,000 colonies/mL except for 1 culture in the nitrofurantoin treatment group, which was 45,000 colonies/mL, but because the subject was symptomatic, treatment was administered and a repeat urine culture was negative.
There were 8 cases classified as cure, 1 presumed cure, and no failures in the amoxicillin group. In the nitrofurantoin group, 7 cases were classified as cure, 1 presumed cure, and 3 failures. The presumed cures were excluded from the statistical analysis due to inability to ensure these cases were truly cured. Also excluded from the statistical analysis was one of the failures in the nitrofurantoin group, because the subject was asymptomatic with no known indication for treatment. This left 8 cases classified as cure and no failures in the amoxicillin group compared with 7 cases classified as cure and 2 failures in the nitrofurantoin group, P = .47 (Figure). Statistical analysis was performed using the Fisher exact test.
Discussion
There was no statistically significant difference between amoxicillin and nitrofurantoin for the treatment of ampicillin-resistant E faecium UTIs. There were no failures in the amoxicillin group despite all isolates displaying resistance based on current breakpoints, supporting the theory that higher urine concentrations of amoxicillin may overcome the MIC of resistant isolates.
Related: Novel Therapy for Treating Complicated UTIs
Of the 11 cases treated with nitrofurantoin, 3 were classified failures. The first failure in the nitrofurantoin group was an asymptomatic subject who did not have a repeat urine culture but had a repeat UA, which showed a persistent elevation in WBC and leukocyte esterase count. This subject was removed from the statistical analysis, as treatment was not indicated per IDSA guidelines. No reason could be identified for the second failure, as a repeat culture demonstrated continued presence of E faecium. Chronic kidney disease (CKD) contributed to the third failure in the nitrofurantoin treatment group; the subject’s CrCl was about 17 mL/min. After treatment, the subject had a repeat urine culture, which indicated the continued presence of E faecium. The subject was later successfully treated with amoxicillin. Both cultures in the same subject were included in the final analysis per protocol, as the subject had an adequate evaluation of efficacy between courses. Four additional cases with CKD were treated with nitrofurantoin; however, their CrCl ranged from 40 to 55 mL/min, and all were classified cure or presumed cure.
Limitations
There were several limitations to this study. Due to the strict inclusion and exclusion criteria, a limited number of subjects were evaluated. Given that this was a retrospective study, it is possible that symptoms were reported by a subject but not appropriately documented. Another significant limitation of this trial was that MICs were not determined due to the retrospective nature of the study. External validity was also limited due to a predominately elderly and male population. Safety data regarding different therapies were not collected, as this study evaluated only the efficacy of therapies.
Conclusion
Although this was a very small retrospective analysis, to the authors knowledge this is the first clinical study supporting the in vitro theory that amoxicillin (500 mg every 8 hours) may overcome the MIC of resistant isolates due to achievement of higher urinary concentrations. Because this was a small retrospective analysis, more prospective evidence is needed to confirm these results.
Acknowledgements
Heather Kim, biostatistician, University of Illinois at Chicago. CCTS Support: UL1RR029879.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
1. Huycke MM, Sahm DF, Gilmore MS. Multiple-drug resistant enterococci: the nature of the problem and an agenda for the future. Emerg Infect Dis. 1998;4(2):239-249.
2. Heintz BH, Halilovic J, Christensen CL. Vancomycin -resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30(11):1136-1149.
3. Zhanel GG, Laing NM, Nichol KA, et al; NAVRESS Group. Antibiotic activity against urinary tract infection (UTI) isolates of vancomycin-resistant enterococci (VRE): results from the 2002 North American Vancomycin Resistant Enterococci Susceptibility Study (NAVRESS). J Antimicrob Chemother. 2003;52(3):382-388.
4. Macrobid [package insert]. Pine Brook, NJ: Almatica Pharma; 2013.
5. Oplinger M, Andrews CO. Nitrofurantoin contraindicated in patients with a creatinine clearance below 60 mL/min: looking for the evidence. Ann Pharmacother. 2013;47(1):106-111.
6. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
7. Gordon RC, Regamey C, Kirby WM. Comparative clinical pharmacology of amoxicillin and ampicillin administered orally. Antimicrob Agents Chemother. 1972;1(6):504-507.
8. Sutherland R, Croydon EA, Rolinson GN. Amoxycillin: a new semi-synthetic penicillin. Br Med J. 1972;3(5817):13-16.
9. Williamson JC, Craft DW, Butts JD, Raasch RH. In vitro assessment of urinary isolates of ampicillin-resistant enterococci. Ann Pharmacother. 2002;36(2):246-250.
10. Dumkow LE, Perri MB, Zervos M. Time to stop using alternatives to ampicillin for enterococcal UTIs? In-vitro susceptibility trends for enterococcus urinary isolates over a one-year period in Detroit. Poster presented at: 53rd Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC); September 10-13, 2013; Denver, CO.
11. Quintiliani R. Using pharmacodynamics and pharmacokinetics concepts to optimize treatment of infectious diseases. Infect Med. 2004;21(5):219-232.
Assay could guide therapy for MM, other cancers

showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
showing multiple myeloma
Researchers say they have created a microenvironment in a dish that can be used to anticipate a multiple myeloma (MM) patient’s response to treatment.
The team developed an assay that involves co-culturing MM cells with their surrounding nontumor cells, all from the same patient, in a microscale petri dish.
The researchers then treated the tumor cells with bortezomib, and, after 3 days, they could determine whether the drug was effective or not.
The team described this research in Integrative Biology.
They compared the results of their ex vivo tests with the success or failure rates of actual MM patients who received bortezomib, and 100% of the ex vivo test results matched the patients’ results.
The researchers therefore believe this assay could save many MM patients the psychological stress of having to try multiple drugs until they find the most effective one. The assay could reduce clinicians’ need for this trial-and-error approach while lowering the cost of treatment, the team said.
Study author Chorom Pak, PhD, of the University of Toronto in Ontario, Canada, has founded a service-based company called Lynx Biosciences based on these findings. Now, she and her colleagues are planning to conduct a prospective trial in which they will use the ex vivo tests to identify responsive and nonresponsive patients.
The researchers believe this work could have wide-ranging implications for the treatment of MM and other malignancies, but their work is far from over.
“This is only one type of cancer, one particular drug, and we’re a long way from implementing this and helping patients in a widespread way,” said study author David Beebe, PhD, of the University of Wisconsin Carbone Cancer Center in Madison.
“But it’s happening. This is an exciting time in this area, and we’re definitely going to see more of this.” ![]()
New trial design accounts for patient behavior

Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Photo by Esther Dyson
New research suggests patient behavior can have a serious impact on the effectiveness of a treatment, and procedures used in double-blind randomized controlled trials (DBRCTs) may not allow researchers to assess the effects of behavior on treatment.
To solve this problem, a group of investigators has proposed a new trial design, called a two-by-two trial, that can account for behavior-treatment interactions.
They described this design in PLOS ONE.
Study rationale
The study authors pointed out that patient behaviors can directly relate to a trial. For example, a patient who believes in the drug might religiously stick to his or her treatment regimen, while someone more skeptical might skip a few doses.
Alternatively, patient behaviors may relate to how the person acts in general, such as preferences in diet, exercise, and social engagement. And in the design of today’s standard trials, these behaviors are not accounted for, said author Erik Snowberg, PhD, of the California Institute of Technology in Pasadena.
He noted that DBRCTs typically assign patients to an experimental group that receives the new treatment and a control group that does not. As the trial is double-blinded, neither the subjects nor their doctors know who falls into which group.
However, patients do know their probability of getting the treatment, and that 50% likelihood of getting the new treatment might not be enough to encourage a patient to change behaviors that could influence the efficacy of the drug, Dr Snowberg said.
For example, if a subject wants to lose weight and knows he has a high probability—a 70% chance—of being in the experimental group for a new weight loss drug, he may be more likely to take the drug as directed and to make other healthy lifestyle choices that can contribute to weight loss. As a result, he might lose more weight, boosting the apparent effectiveness of the drug.
However, if the subject knows he only has a 30% chance of being in the experimental group, he might be less motivated to both take the drug as directed and to make those other changes. As a result, he might lose less weight—even if he is in the treatment group—and the same drug would seem less effective.
“Most medical research just wants to know if a drug will work or not,” Dr Snowberg said. “We wanted to go a step further, designing new trials that would take into account the way people behave. As social scientists, we naturally turned to the mathematical tools of formal social science to do this.”
New trial design
Dr Snowberg and his colleagues found that, with the two-by-two trial, they can tease out the effects of behavior and the interaction of behavior and treatment, as well as the effects of treatment alone. The new trial design, which still randomizes treatment, also randomizes the probability of treatment, which can change a patient’s behavior.
In a two-by-two trial, instead of patients first being assigned to either the experimental or control groups, they are randomly assigned to either a “high probability of treatment” group or a “low probability of treatment” group.
The patients in the high probability group are then randomized to either the treatment or the control group, giving them a 70% chance of receiving the treatment. Patients in the low probability group are also randomized to treatment or control, and their likelihood of receiving the treatment is 30%. The patients are then informed of their probability of treatment.
By randomizing both the treatment and the probability of treatment, researchers can quantify the effects of treatment, the effects of behavior, and the effects of the interaction between treatment and behavior, Dr Snowberg said. And determining each is essential for understanding the overall efficacy of treatment.
“It’s a very small change to the design of the trial, but it’s important,” he said. “The effect of a treatment has these two constituent parts: pure treatment effect and the treatment-behavior interaction. Standard blind trials just randomize the likelihood of treatment, so you can’t see this interaction. Although you can’t just tell someone to randomize their behavior, we found a way that you can randomize the probability that a patient will get something that will change their behavior.”
Testing the design
Because it is difficult to implement new trial design changes in active trials, Dr Snowberg and his colleagues wanted to first test their idea with a meta-analysis of data from previous clinical trials. They devised a new mathematical formula that can be used to analyze DBRCT data.
The formula teases out the health outcomes resulting from treatment alone as well as outcomes resulting from an interaction between treatment and behavior.
The investigators used the formula to analyze 6 DBRCTs evaluating the antidepressants imipramine (a tricyclic antidepressant also known as Tofranil) and paroxetine (a selective serotonin reuptake inhibitor sold as Paxil).
First, the researchers wanted to see if there was evidence that patients behave differently when they have a high probability of treatment and when they have a low probability of treatment.
The trials recorded how many patients dropped out of the study, so this was the behavior Dr Snowberg and his colleagues analyzed. They found that, in trials where patients happened to have a relatively high probability of treatment—near 70%—the dropout rate was significantly lower than in trials where patients had a lower probability of treatment—around 50%.
Although the team did not have any specific behaviors to analyze, other than dropping out of the study, they also wanted to determine if behavior in general could have added to the effect of the treatments.
Using their statistical techniques, the investigators found that imipramine seemed to have a pure treatment effect but no effect from the interaction between treatment and behavior. That is, the drug seemed to work fine, regardless of any behavioral differences that may have been present.
The researchers also found that paroxetine seemed to have no effect from the treatment alone or behavior alone. However, an interaction between the treatment and behavior did effectively decrease depression.
Because this study was conducted in the past, the investigators could not determine which specific behavior was responsible for the interaction, but with the mathematical formula, they were able to tell that this behavior was necessary for the drug to be effective.
In their paper, Dr Snowberg and his colleagues speculate how a situation like this might come about.
“Maybe there is a drug, for instance, that makes people feel better in social situations, and if you’re in the high probability group, then maybe you’d be more willing to go out to parties to see if the drug helps you talk to people,” Dr Snowberg explained.
“Your behavior drives you to go to the party, and once you’re at the party, the drug helps you feel comfortable talking to people. That would be an example of an interaction effect. You couldn’t get that if people just took this drug alone at home.”
Although this specific example is just speculation, Dr Snowberg said the researchers’ actual results reveal that some behavior or set of behaviors interact with paroxetine to effectively treat depression. And, without this behavior, the drug appears to be ineffective.
“Normally, what you get when you run a standard blind trial is some sort of mishmash of the treatment effect and the treatment-behavior interaction effect,” Dr Snowberg said. “But knowing the full interaction effect is important.”
“Our work indicates that clinical trials underestimate the efficacy of a drug where behavior matters. It may be the case that 50% probability isn’t high enough for people to change any of their behaviors, especially if it’s a really uncertain new treatment. Then, it’s just going to look like the drug doesn’t work, and that isn’t the case.”
Because the meta-analysis supported the team’s hypothesis—that the interaction between treatment and behavior can have an effect on health outcomes—the next step is incorporating these new ideas into an active clinical trial.
Dr Snowberg said the best fit would be a drug trial for a condition, such as a mental health disorder or an addiction, that is known to be associated with behavior. At the very least, he hopes these results will lead the medical research community to a conversation about ways to improve the DBRCT. ![]()
Program helped reduce VTE in trauma patients

Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
Photo by Piotr Bodzek
Data from a statewide quality collaborative helped the University of Michigan Trauma Service reduce its annual rate of venous thromboembolism (VTE), according to an article published in the Journal of the American College of Surgeons.
The data suggested that changing first-line VTE prophylaxis from unfractionated heparin to enoxaparin would decrease the incidence of VTE, and it did. The annual VTE incidence fell from about 36 cases to about 14.
Researchers said this study should not be interpreted as a head-to-head comparison of unfractionated heparin and enoxaparin as VTE prophylaxis in trauma patients. Instead, it should be seen as a model of how hospitals and physicians can use quality improvement data in a real-world setting.
Existing medical evidence has shown that both heparin and enoxaparin can be effective in preventing VTE, depending on factors such as how the agents are dosed and administered.
“Based on our data, the enoxaparin regimen was more effective than heparin,” said study author David A. Machado-Aranda, MD, of the University of Michigan in Ann Arbor.
“Now, this result could be different in another institution, another collaborative, another geographical area, or another patient population based on the circumstances encountered.”
Dr Machado-Aranda and his colleagues participate in the Michigan Trauma Quality Improvement Program (MTQIP), a statewide program of 27 ACS Level 1 and 2 trauma centers.
The program showed the researchers that the rate of VTE was higher for the University of Michigan Trauma Service than the collaborative average.
A closer look at the data revealed that VTE rates among trauma patients who received unfractionated heparin were twice as high as rates for patients who received enoxaparin.
After the University of Michigan Trauma Service switched from using unfractionated heparin to enoxaparin as first-line VTE prophylaxis, the rate of VTE dropped from 6.2% to 2.6%.
“What we’ve done is to use the collaborative as our ‘mission control’ to see where we’re heading and what our trajectory is,” Dr Machado-Aranda said. “Once we saw ourselves deviating from a favorable trajectory, we used the data derived from the collaborative to investigate our problem.”
“We also accessed many different resources to review best practices, receive suggestions from other collaborative participants, and perform root-cause analysis. An action plan was formulated, approved, and implemented to get our trauma service off of an unfavorable trajectory for VTE complications.”
Dr Machado-Aranda noted that the trauma team encountered some challenges in changing the protocol for VTE prophylaxis. Hospital administration and other departments were concerned about the higher cost of enoxaparin.
In the end, “the increased costs of using enoxaparin were more than offset by savings generated by reducing the rate of venous thromboembolism complications,” he said.
The trauma surgeons also found they had to review the data with the neurosurgeons and orthopedic surgeons on staff to understand and alleviate their concerns about enoxaparin and potential higher rates of bleeding complications.
The neurosurgical group had previously published a study that showed higher rates of intracranial bleeding in patients undergoing brain tumor surgery who received enoxaparin rather than sequential compression devices alone.
“These results became extrapolated into the trauma setting, and it took us some time convincing our neurosurgeons to consider changing their practice for trauma patients,” Dr Machado-Aranda said. ![]()
HRS: Blacks show higher A fib–stroke risk than whites do
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.

The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.
The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
BOSTON – Black people with new-onset atrial fibrillation have a 60% increased risk for stroke compared with white people who have incident atrial fibrillation when not maintained on an appropriate anticlotting regimen, according to prospectively collected data from more than 56,000 subjects at a U.S. center.
But in the subgroup of new-onset atrial fibrillation (AF) patients who received appropriate treatment with aspirin or an anticoagulant, the stroke rates among white and blacks equalized. The analysis showed that 46% of the more than 3,000 people who developed AF during follow-up received aspirin if their CHA2DS2-VASc score was less than 2, or anticoagulation with warfarin or a new oral anticoagulant if their score was 2 or greater, Dr. Parin J. Patel said at the annual scientific sessions of the Heart Rhythm Society.
The majority of the followed cohort with incident atrial fibrillation did not receive this treatment, and in the total group, the relative rate of stroke among blacks exceeded that of whites by a statistically significant 60% in an analysis that adjusted for several demographic and clinical features. The excess of strokes occurred at about the same rate in black women compared with white women, and in black men compared with white men, reported Dr. Patel, an electrophysiologist at the University of Pennsylvania in Philadelphia.
The implication is that because their stroke risk is greater, blacks with AF should especially receive appropriate stroke prophylaxis and AF therapy, he said. The overall findings also highlight the substantial stroke risk faced by all AF patients.
The data came from the University of Pennsylvania Atrial Fibrillation-Free study of 91,274 people who underwent an ECG examination in the University of Pennsylvania health system during 2004-2009 along with an index clinical encounter within 30 days. Excluding patients with a prevalent AF or other arrhythmia, prevalent stroke, or incomplete data left 56,835 AF- and stroke-free people to follow for incident AF, which occurred in 3,891 patients. At the time of AF diagnosis, the average age of patients was 63 years; more than a third had hypertension; a fifth had diabetes; and a fifth had heart failure. One-third of the incident-AF group was black, 58% were white, and the remainder were from other demographic groups.
Dr. Patel and his associates defined an AF-related stroke as any that occurred within 6 months before AF diagnosis or anytime after, which occurred in 645 (17%) of the incident-AF patients. The more than 50,000 AF-free people followed in the study had a total of 3,001 strokes not related to AF during follow-up, which meant that 18% of all strokes in the entire cohort were AF related.
Among the 645 AF-related strokes, roughly half occurred during the 6 months before AF diagnosis, and the other half following AF diagnosis. An analysis that focused exclusively on strokes that occurred after AF diagnosis showed that this subset of AF-associated strokes also occurred significantly more often in blacks than in whites.
Dr. Patel had no disclosures.
On Twitter @mitchelzoler
AT HEART RHYTHM 2015
Key clinical point: Strokes associated with newly diagnosed atrial fibrillation were significantly more common in African American patients than in white patients.
Major finding: The rate of atrial fibrillation–associated stroke was 60% higher in black patients than in white patients.
Data source: A review of prospectively-collected data from 56,835 people who underwent a baseline ECG at one U.S. center during 2004-2009.
Disclosures: Dr. Patel had no disclosures.

Listen Now: Hospital Medicine Intersects with Global Patient Safety
{kind=link}
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.
Dr. Phuoc Le of the University of California at San Francisco and Dr. Bijay Achariya of Mass General Hospital in Boston, both practicing global hospitalists, share their perspectives on the US hospitalist movement, how it intersects with the global patient safety movement, and the opportunities presented for hospitalists with a global perspective to make a difference for patients everywhere.