User login
FDA lifts partial clinical hold on pidilizumab

The US Food and Drug Administration (FDA) has lifted the partial clinical hold on the investigational new drug (IND) application for pidilizumab (MDV9300) in hematologic malignancies.
This means the phase 2 trial of pidilizumab in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), as well as other studies that cross-reference the IND for the drug, may now proceed.
The partial clinical hold on pidilizumab was not related to any safety concerns.
The FDA placed the hold because the company developing pidilizumab, Medivation Inc., determined that the drug is not an inhibitor of PD-1, as researchers previously thought.
The phase 2 trial of pidilizumab in DLBCL was launched in late 2015 but had not enrolled any patients before the FDA placed the partial clinical hold.
Patients who were receiving pidilizumab through investigator-sponsored trials have continued to receive treatment despite the hold, and those investigators have been told to update their protocols and informed consent documents to reflect that pidilizumab is not an anti-PD-1 antibody.
Medivation has likewise revised the investigator brochure, protocols, and informed consent documents related to the phase 2 trial of DLBCL patients.
The company said it is still trying to determine pidilizumab’s mechanism of action.
“We are delighted that the FDA has lifted the partial clinical hold and that we may proceed with our potentially pivotal trial in this area of high unmet medical need,” said David Hung, MD, founder, president, and chief executive officer of Medivation.
“As we move forward, we also are working to determine the compound’s exact binding mechanism which, we believe, modulates the body’s innate immune response and differentiates it from the heavily crowded immuno-oncology space that targets the adaptive side of immunity.”
Medivation said it intends to submit an amendment to the Chemistry, Manufacturing, and Controls section of the IND for pidilizumab to provide for larger manufacturing lot sizes to better support the current and planned clinical activities for the drug.
The company also said it plans to resume the phase 2 trial of pidilizumab in DLBLCL in the second half of this year.
The trial is expected to enroll approximately 180 patients who had an incomplete response to salvage therapy or autologous stem cell transplant for relapsed or refractory CD20+ DLBCL, transformed indolent lymphoma, or primary mediastinal B-cell lymphoma.
The patients will be assessed in 2 parallel cohorts of approximately 90 patients each. One cohort will enroll patients who have received an autologous stem cell transplant, and the other will enroll patients who have received salvage chemotherapy but are ineligible for transplant.
Pidilizumab will be given at a dose of 200 mg by intravenous infusion. The primary endpoint of the trial is best overall response rate. ![]()
The US Food and Drug Administration (FDA) has lifted the partial clinical hold on the investigational new drug (IND) application for pidilizumab (MDV9300) in hematologic malignancies.
This means the phase 2 trial of pidilizumab in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), as well as other studies that cross-reference the IND for the drug, may now proceed.
The partial clinical hold on pidilizumab was not related to any safety concerns.
The FDA placed the hold because the company developing pidilizumab, Medivation Inc., determined that the drug is not an inhibitor of PD-1, as researchers previously thought.
The phase 2 trial of pidilizumab in DLBCL was launched in late 2015 but had not enrolled any patients before the FDA placed the partial clinical hold.
Patients who were receiving pidilizumab through investigator-sponsored trials have continued to receive treatment despite the hold, and those investigators have been told to update their protocols and informed consent documents to reflect that pidilizumab is not an anti-PD-1 antibody.
Medivation has likewise revised the investigator brochure, protocols, and informed consent documents related to the phase 2 trial of DLBCL patients.
The company said it is still trying to determine pidilizumab’s mechanism of action.
“We are delighted that the FDA has lifted the partial clinical hold and that we may proceed with our potentially pivotal trial in this area of high unmet medical need,” said David Hung, MD, founder, president, and chief executive officer of Medivation.
“As we move forward, we also are working to determine the compound’s exact binding mechanism which, we believe, modulates the body’s innate immune response and differentiates it from the heavily crowded immuno-oncology space that targets the adaptive side of immunity.”
Medivation said it intends to submit an amendment to the Chemistry, Manufacturing, and Controls section of the IND for pidilizumab to provide for larger manufacturing lot sizes to better support the current and planned clinical activities for the drug.
The company also said it plans to resume the phase 2 trial of pidilizumab in DLBLCL in the second half of this year.
The trial is expected to enroll approximately 180 patients who had an incomplete response to salvage therapy or autologous stem cell transplant for relapsed or refractory CD20+ DLBCL, transformed indolent lymphoma, or primary mediastinal B-cell lymphoma.
The patients will be assessed in 2 parallel cohorts of approximately 90 patients each. One cohort will enroll patients who have received an autologous stem cell transplant, and the other will enroll patients who have received salvage chemotherapy but are ineligible for transplant.
Pidilizumab will be given at a dose of 200 mg by intravenous infusion. The primary endpoint of the trial is best overall response rate. ![]()
The US Food and Drug Administration (FDA) has lifted the partial clinical hold on the investigational new drug (IND) application for pidilizumab (MDV9300) in hematologic malignancies.
This means the phase 2 trial of pidilizumab in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), as well as other studies that cross-reference the IND for the drug, may now proceed.
The partial clinical hold on pidilizumab was not related to any safety concerns.
The FDA placed the hold because the company developing pidilizumab, Medivation Inc., determined that the drug is not an inhibitor of PD-1, as researchers previously thought.
The phase 2 trial of pidilizumab in DLBCL was launched in late 2015 but had not enrolled any patients before the FDA placed the partial clinical hold.
Patients who were receiving pidilizumab through investigator-sponsored trials have continued to receive treatment despite the hold, and those investigators have been told to update their protocols and informed consent documents to reflect that pidilizumab is not an anti-PD-1 antibody.
Medivation has likewise revised the investigator brochure, protocols, and informed consent documents related to the phase 2 trial of DLBCL patients.
The company said it is still trying to determine pidilizumab’s mechanism of action.
“We are delighted that the FDA has lifted the partial clinical hold and that we may proceed with our potentially pivotal trial in this area of high unmet medical need,” said David Hung, MD, founder, president, and chief executive officer of Medivation.
“As we move forward, we also are working to determine the compound’s exact binding mechanism which, we believe, modulates the body’s innate immune response and differentiates it from the heavily crowded immuno-oncology space that targets the adaptive side of immunity.”
Medivation said it intends to submit an amendment to the Chemistry, Manufacturing, and Controls section of the IND for pidilizumab to provide for larger manufacturing lot sizes to better support the current and planned clinical activities for the drug.
The company also said it plans to resume the phase 2 trial of pidilizumab in DLBLCL in the second half of this year.
The trial is expected to enroll approximately 180 patients who had an incomplete response to salvage therapy or autologous stem cell transplant for relapsed or refractory CD20+ DLBCL, transformed indolent lymphoma, or primary mediastinal B-cell lymphoma.
The patients will be assessed in 2 parallel cohorts of approximately 90 patients each. One cohort will enroll patients who have received an autologous stem cell transplant, and the other will enroll patients who have received salvage chemotherapy but are ineligible for transplant.
Pidilizumab will be given at a dose of 200 mg by intravenous infusion. The primary endpoint of the trial is best overall response rate. ![]()
Introducing the Hospitalist Morale Index
Explosive growth in hospital medicine has led to hospitalists having the option to change jobs easily. Annual turnover for all physicians is 6.8%, whereas that of hospitalists exceeds 14.8%.[1] Losing a single physician has significant financial and operational implications, with estimates of $20,000 to $120,000 in recruiting costs, and up to $500,000 in lost revenue that may take years to recoup due to the time required for new physician assimilation.[2, 3] In 2006, the Society of Hospital Medicine (SHM) appointed a career task force to develop retention recommendations, 1 of which includes monitoring hospitalists' job satisfaction.[4]
Studies examining physician satisfaction have demonstrated that high physician job satisfaction is associated with lower physician turnover.[5] However, surveys of hospitalists, including SHM's Hospital Medicine Physician Worklife Survey (HMPWS), have reported high job satisfaction among hospitalists,[6, 7, 8, 9, 10] suggesting that high job satisfaction may not be enough to overcome forces that pull hospitalists toward other opportunities.
Morale, a more complex construct related to an individual's contentment and happiness, might provide insight into reducing hospitalist turnover. Morale has been defined as the emotional or mental condition with respect to cheerfulness, confidence, or zeal and is especially relevant in the face of opposition or hardship.[11] Job satisfaction is 1 element that contributes to morale, but alone does not equate morale.[12] Morale, more than satisfaction, relates to how people see themselves within the group and may be closely tied to the concept of esprit de corps. To illustrate, workers may feel satisfied with the content of their job, but frustration with the organization may result in low morale.[13] Efforts focused on assessing provider morale may provide deeper understanding of hospitalists' professional needs and garner insight for retention strategies.
The construct of hospitalist morale and its underlying drivers has not been explored in the literature. Using literature within and outside of healthcare,[1, 12, 14, 15, 16, 17, 18, 19, 20, 21, 22] and our own prior work,[23] we sought to characterize elements that contribute to hospitalist morale and develop a metric to measure it. The HMPWS found that job satisfaction factors vary across hospitalist groups.[9] We suspected that the same would hold true for factors important to morale at the individual level. This study describes the development and validation of the Hospitalist Morale Index (HMI), and explores the relationship between morale and intent to leave due to unhappiness.
METHODS
2009 Pilot Survey
To establish content validity, after reviewing employee morale literature, and examining qualitative comments from our 2007 and 2008 morale surveys, our expert panel, consisting of practicing hospitalists, hospitalist leaders, and administrative staff, identified 46 potential drivers of hospitalist morale. In May 2009, all hospitalists, including physicians, nurse practitioners (NPs), and physician assistants (PAs) from a single hospitalist group received invitations to complete the pilot survey. We asked hospitalists to assess on 5‐point Likert scales the importance of (not at all to tremendously) and contentment with (extremely discontent to extremely content) each of the 46 items as it relates to their work morale. Also included were demographic questions and general morale questions (including rating participants' own morale), investment, long‐term career plans, and intent to leave due to unhappiness.
Data Collection
To maintain anonymity and limit social desirability bias, a database manager, working outside the Division of Hospital Medicine and otherwise not associated with the research team, used Survey Monkey to coordinate survey distribution and data collection. Each respondent had a unique identifier code that was unrelated to the respondent's name and email address. Personal identifiers were maintained in a secure database accessible only to the database manager.
Establishing Internal Structure Validity Evidence
Response frequency to each question was examined for irregularities in distribution. For continuous variables, descriptive statistics were examined for evidence of skewness, outliers, and non‐normality to ensure appropriate use of parametric statistical tests. Upon ranking importance ratings by mode, 15 of 46 items were judged to be of low importance by almost all participants and removed from further consideration.
Stata 13.1 (StataCorp, College Station, TX) was used for exploratory factor analysis (EFA) of the importance responses for all 31 remaining items by principal components factoring. Eigenvalues >1 were designated as a cutoff point for inclusion in varimax rotation. Factor loading of 0.50 was the threshold for inclusion in a factor.
The 31 items loaded across 10 factors; however, 3 factors included 1 item each. After reviewing the scree plot and considering their face value, these items/factors were omitted. Repeating the factor analysis resulted in a 28‐item, 7‐factor solution that accounted for 75% variance. All items were considered informative as demonstrated by low uniqueness scores (0.050.38). Using standard validation procedures, all 7 factors were found to have acceptable factor loadings (0.460.98) and face validity. Cronbach's quantified internal reliability of the 7 factors with scores ranging from 0.68 to 0.92. We named the resultant solution the Hospitalist Morale Index (HMI).
Establishing Response Process Validity Evidence
In developing the HMI, we asked respondents to rate the importance of and their contentment with each variable as related to their work morale. From pilot testing, which included discussions with respondents immediately after completing the survey, we learned that the 2‐part consideration of each variable resulted in thoughtful reflection about their morale. Further, by multiplying the contentment score for each item (scaled from 15) by the corresponding importance score (scaled 01), we quantified the relative contribution and contentment of each item for each hospitalist. Scaling importance scores from 0 to 1 insured that items that were not considered important to the respondent did not affect the respondent's personal morale score. Averaging resultant item scores that were greater than 0 resulted in a personal morale score for each hospitalist. Averaging item scores >0 that constituted each factor resulted in factor scores.
May 2011 Survey
The refined survey was distributed in May 2011 to a convenience sample of 5 hospitalist programs at separate hospitals (3 community hospitals, 2 academic hospitals) encompassing 108 hospitalists in 3 different states. Responses to the 2011 survey were used to complete confirmatory factor analyses (CFA) and establish further validity and reliability evidence.
Based on the 28‐item, 7‐factor solution developed from the pilot study, we developed the theoretical model of factors constituting hospitalist morale. We used the structural equation modeling command in Stata 13 to perform CFA. Factor loading of 0.50 was the threshold for inclusion of an item in a factor. To measure internal consistency, we considered Cronbach's score of 0.60 acceptable. Iterative models were reviewed to find the optimal solution for the data. Four items did not fit into any of the 5 resulting factors and were evaluated in terms of mean importance score and face value. Three items were considered important enough to warrant being stand‐alone items, whereas 1 was omitted. Two additional items had borderline factor loadings (0.48, 0.49) and were included in the model as stand‐alone items due to their overall relevance. The resultant solution was a 5‐factor model with 5 additional stand‐alone items (Table 1).
| Factor | Cronbach's | |||||
|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | ||
| How much does the following item contribute to your morale? | ||||||
| Paperwork | 0.72 | 0.89 | ||||
| Relationship with patients | 0.69 | 0.90 | ||||
| Electronic medical system | 0.60 | 0.90 | ||||
| Intellectual stimulation | 0.59 | 0.90 | ||||
| Variety of cases | 0.58 | 0.90 | ||||
| Relationship with consultants | 0.51 | 0.89 | ||||
| No. of night shifts | 0.74 | 0.89 | ||||
| Patient census | 0.61 | 0.90 | ||||
| No. of shifts | 0.52 | 0.90 | ||||
| Fairness of leadership | 0.82 | 0.89 | ||||
| Effectiveness of leadership | 0.82 | 0.89 | ||||
| Leadership's receptiveness to my thoughts and suggestions | 0.78 | 0.89 | ||||
| Leadership as advocate for my needs | 0.77 | 0.89 | ||||
| Approachability of leadership | 0.77 | 0.89 | ||||
| Accessibility of leadership | 0.69 | 0.89 | ||||
| Alignment of the group's goals with my goals | 0.50 | 0.89 | ||||
| Recognition within the group | 0.82 | 0.89 | ||||
| Feeling valued within the institution | 0.73 | 0.89 | ||||
| Feeling valued within the group | 0.73 | 0.89 | ||||
| Feedback | 0.52 | 0.89 | ||||
| Pay | 0.99 | 0.90 | ||||
| Benefits | 0.56 | 0.89 | ||||
| Cronbach's | 0.78 | 0.65 | 0.89 | 0.78 | 0.71 | |
| How much does the following item contribute to your morale? | Single item indicators | |||||
| Family time | 0.90 | |||||
| Job security | 0.90 | |||||
| Institutional climate | 0.89 | |||||
| Opportunities for professional growth | 0.90 | |||||
| Autonomy | 0.89 | |||||
| Cronbach's | 0.90 | |||||
Establishing Convergent, Concurrent, and Discriminant Validity Evidence
To establish convergent, concurrent, and discriminant validity, linear and logistic regression models were examined for continuous and categorical data accordingly.
Self‐perceived overall work morale and perceived group morale, as assessed by 6‐point Likert questions with response options from terrible to excellent, were modeled as predictors for personal morale as calculated by the HMI.
Personal morale scores were modeled as predictors of professional growth, stress, investment in the group, and intent to leave due to unhappiness. While completing the HMI, hospitalists simultaneously completed a validated professional growth scale[24] and Cohen stress scale.[25] We hypothesized that those with higher morale would have more professional growth. Stress, although an important issue in the workplace, is a distinct construct from morale, and we did not expect a significant relationship between personal morale and stress. We used Pearson's r to assess the strength of association between the HMI and these scales. Participants' level of investment in their group was assessed on a 5‐point Likert scale. To simplify presentation, highly invested represents those claiming to be very or tremendously invested in the success of their current hospitalist group. Intent to leave due to unhappiness was assessed on a 5‐point Likert scale, I have had serious thoughts about leaving my current hospitalist group because I am unhappy, with responses from strongly disagree (1) to strongly agree (5). To simplify presentation, responses higher than 2 are considered to be consistent with intending to leave due to unhappiness.
Our institutional review board approved the study.
RESULTS
Respondents
In May 2009, 30 of the 33 (91%) invited hospitalists completed the original pilot morale survey; 19 (63%) were women. Eleven hospitalists (37%) had been part of the group 1 year or less, whereas 4 (13%) had been with the group for more than 5 years.
In May 2011, 93 of the 108 (86%) hospitalists from 5 hospitals completed the demographic and global parts of the survey. Fifty (53%) were from community hospitals; 47 (51%) were women. Thirty‐seven (40%) physicians and 6 (60%) NPs/PAs were from academic hospitals. Thirty‐nine hospitalists (42%) had been with their current group 1 year or less. Ten hospitalists (11%) had been with their current group over 5 years. Sixty‐three respondents (68%) considered themselves career hospitalists, whereas 5 (5%) did not; the rest were undecided.
Internal Structure Validity Evidence
The final CFA from the 2011 survey resulted in a 5‐factor plus 5stand‐alone‐items HMI. The solution with item‐level and factor‐level Cronbach's scores (range, 0.890.90 and range, 0.650.89, respectively) are shown in Table 1.
Personal Morale Scores and Factor Scores
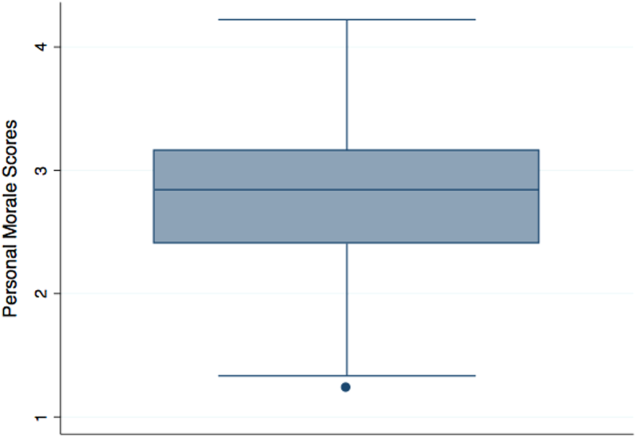
Personal morale scores were normally distributed (mean = 2.79; standard deviation [SD] = 0.58), ranging from 1.23 to 4.22, with a theoretical low of 0 and high of 5 (Figure 1). Mean personal morale scores across hospitalist groups ranged from 2.70 to 2.99 (P > 0.05). Personal morale scores, factor sores and item scores for NPs and PAs did not significantly differ from those of physicians (P > 0.05 for all analyses). Personal morale scores were lower for those in their first 3 years with their current group, compared to those with greater institutional longevity. For every categorical increase in a participant's response to seeing oneself as a career hospitalist, the personal morale score rose 0.23 points (P < 0.001).
Factor scores for material reward and mean item scores for professional growth were significantly different across the 5 hospitalist groups (P = 0.03 and P < 0.001, respectively). Community hospitalists had significantly higher factor scores, despite having similar importance scores, for material rewards than academic hospitalists (diff. = 0.44, P = 0.02). Academic hospitalists had significantly higher scores for professional growth (diff. = 0.94, P < 0.001) (Table 2). Professional growth had the highest importance score for academic hospitalists (mean = 0.87, SD = 0.18) and the lowest importance score for community hospitalists (mean = 0.65, SD = 0.24, P < 0.001).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | |||
| ||||||||||||
| All participants | Mean | 2.79 | 2.54 | 2.78 | 3.18 | 2.58 | 2.48 | 3.05 | 2.67 | 2.92 | 3.00 | 2.76 |
| SD | 0.58 | 0.63 | 0.70 | 0.95 | 0.86 | 0.85 | 1.15 | 0.97 | 1.11 | 1.10 | 1.21 | |
| Academic A | Mean | 2.77 | 2.43 | 2.92 | 3.10 | 2.54 | 2.28 | 3.16 | 2.70 | 3.06 | 3.20 | 3.08 |
| SD | 0.57 | 0.62 | 0.64 | 0.92 | 0.84 | 0.77 | 1.19 | 0.95 | 1.08 | 1.12 | 1.24 | |
| Academic B | Mean | 2.99 | 2.58 | 2.99 | 3.88 | 2.69 | 2.00 | 2.58 | 2.13 | 1.65 | 3.29 | 4.33 |
| SD | 0.36 | 0.70 | 0.80 | 0.29 | 0.80 | 0.35 | 0.92 | 0.88 | 0.78 | 1.01 | 0.82 | |
| Community A | Mean | 2.86 | 2.61 | 2.51 | 3.23 | 2.73 | 3.03 | 2.88 | 2.84 | 2.95 | 3.23 | 2.66 |
| SD | 0.75 | 0.79 | 0.68 | 1.21 | 1.11 | 1.14 | 1.37 | 1.17 | 0.98 | 1.24 | 1.15 | |
| Community B | Mean | 2.86 | 2.74 | 2.97 | 3.37 | 2.67 | 2.44 | 3.28 | 2.35 | 2.70 | 2.50 | 2.25 |
| SD | 0.67 | 0.55 | 0.86 | 1.04 | 0.94 | 0.87 | 1.00 | 1.15 | 1.40 | 0.72 | 1.26 | |
| Community C | Mean | 2.70 | 2.56 | 2.64 | 2.99 | 2.47 | 2.53 | 3.03 | 2.79 | 3.07 | 2.68 | 2.15 |
| SD | 0.49 | 0.53 | 0.67 | 0.85 | 0.73 | 0.64 | 1.08 | 0.76 | 1.05 | 1.07 | 0.71 | |
| Academic combined | Mean | 2.80 | 2.45 | 2.93 | 3.22 | 2.56 | 2.24 | 3.07 | 2.62 | 2.88 | 3.21 | 3.28 |
| SD | 0.54 | 0.63 | 0.66 | 0.89 | 0.82 | 0.72 | 1.16 | 0.95 | 1.14 | 1.10 | 1.26 | |
| Community combined | Mean | 2.79 | 2.61 | 2.66 | 3.14 | 2.60 | 2.68 | 3.03 | 2.72 | 2.95 | 2.82 | 2.34 |
| SD | 0.62 | 0.62 | 0.72 | 1.01 | 0.90 | 0.90 | 1.15 | 0.99 | 1.09 | 1.09 | 1.00 | |
| P value | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | 0.02 | >0.05 | >0.05 | >0.05 | >0.05 | <0.001 | |
Convergent, Concurrent, and Discriminant Validity Evidence
For every categorical increase on the question assessing overall morale, the personal morale score was 0.23 points higher (P < 0.001). For every categorical increase in a participant's perception of the group's morale, the personal morale score was 0.29 points higher (P < 0.001).
For every 1‐point increase in personal morale score, the odds of being highly invested in the group increased by 5 times (odds ratio [OR]: 5.23, 95% confidence interval [CI]: 1.91‐14.35, P = 0.001). The mean personal morale score for highly invested hospitalists was 2.92, whereas that of those less invested was 2.43 (diff. = 0.49, P < 0.001) (Table 3). Highly invested hospitalists had significantly higher importance factor scores for leadership (diff. = 0.08, P = 0.03) as well as appreciation and acknowledgement (diff. = 0.08, P = 0.02).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | ||
| |||||||||||
| Highly invested in success of current hospitalist group | |||||||||||
| Mean | 2.92 | 2.61 | 2.89 | 3.38 | 2.78 | 2.45 | 3.21 | 2.78 | 2.86 | 3.10 | 2.95 |
| SD | 0.55 | 0.59 | 0.68 | 0.92 | 0.88 | 0.77 | 1.11 | 1.00 | 1.09 | 1.06 | 1.25 |
| Less invested in success of current hospitalist group | |||||||||||
| Mean | 2.43 | 2.34 | 2.48 | 2.60 | 2.02 | 2.57 | 2.60 | 2.38 | 3.08 | 2.69 | 2.24 |
| SD | 0.52 | 0.69 | 0.69 | 0.81 | 0.49 | 1.04 | 1.17 | 0.83 | 1.18 | 1.19 | 0.94 |
| P value | <0.001 | >0.05 | 0.02 | 0.001 | <0.001 | >0.05 | 0.03 | >0.05 | >0.05 | >0.05 | 0.02 |
| Not intending to leave because unhappy | |||||||||||
| Mean | 2.97 | 2.67 | 2.89 | 3.48 | 2.77 | 2.52 | 3.24 | 2.85 | 3.05 | 3.06 | 3.01 |
| SD | 0.51 | 0.54 | 0.61 | 0.91 | 0.89 | 0.78 | 1.03 | 0.99 | 1.10 | 1.07 | 1.25 |
| Intending to leave current group because unhappy | |||||||||||
| Mean | 2.45 | 2.30 | 2.59 | 2.59 | 2.21 | 2.40 | 2.68 | 2.33 | 2.67 | 2.88 | 2.28 |
| SD | 0.56 | 0.72 | 0.82 | 0.74 | 0.68 | 0.97 | 1.29 | 0.83 | 1.11 | 1.17 | 0.97 |
| P value | <0.001 | 0.01 | >0.05 | <0.001 | 0.003 | >0.05 | 0.03 | 0.01 | >0.05 | >0.05 | 0.01 |
Every 1‐point increase in personal morale was associated with a rise of 2.27 on the professional growth scale (P = 0.01). The correlation between these 2 scales was 0.26 (P = 0.01). Every 1‐point increase in personal morale was associated with a 2.21 point decrease on the Cohen stress scale (P > 0.05). The correlation between these 2 scales was 0.21 (P > 0.05).
Morale and Intent to Leave Due to Unhappiness
Sixteen (37%) academic and 18 (36%) community hospitalists reported having thoughts of leaving their current hospitalist program due to unhappiness. The mean personal morale score for hospitalists with no intent to leave their current group was 2.97, whereas that of those with intent to leave was 2.45 (diff. = 0.53, P < 0.001). Each 1‐point increase in the personal morale score was associated with an 85% decrease (OR: 0.15, 95% CI: 0.05‐0.41, P < 0.001) in the odds of leaving because of unhappiness. Holding self‐perception of being a career hospitalist constant, each 1‐point increase in the personal morale score was associated with an 83% decrease (OR: 0.17, 95% CI: 0.05‐0.51, P = 0.002) in the odds of leaving because of unhappiness. Hospitalists who reported intent to leave had significantly lower factor scores for all factors and items except workload, material reward, and autonomy than those who did not report intent to leave (Table 3). Within the academic groups, those who reported intent to leave had significantly lower scores for professional growth (diff. = 1.08, P = 0.01). For community groups, those who reported intent to leave had significantly lower scores for clinical work (diff. = 0.54, P = 0.003), workload (diff. = 0.50, P = 0.02), leadership (diff. = 1.19, P < 0.001), feeling appreciated and acknowledged (diff. = 0.68, P = 0.01), job security (diff. = 0.70, P = 0.03), and institutional climate (diff. = 0.67, P = 0.02) than those who did not report intent to leave.
DISCUSSION
The HMI is a validated tool that objectively measures and quantifies hospitalist morale. The HMI's capacity to comprehensively assess morale comes from its breadth and depth in uncovering work‐related areas that may be sources of contentment or displeasure. Furthermore, the fact that HMI scores varied among groups of individuals, including those who are thinking about leaving their hospitalist group because they are unhappy and those who are highly invested in their hospitalist group, speaks to its ability to highlight and account for what is most important to hospitalist providers.
Low employee morale has been associated with decreased productivity, increased absenteeism, increased turnover, and decreased patient satisfaction.[2, 26, 27, 28] A few frustrated workers can breed group discontentment and lower the entire group's morale.[28] In addition to its financial impact, departures due to low morale can be sudden and devastating, leading to loss of team cohesiveness, increased work burden on the remaining workforce, burnout, and cascades of more turnover.[2] In contrast, when morale is high, workers more commonly go the extra mile, are more committed to the organization's mission, and are more supportive of their coworkers.[28]
While we asked the informants about plans to leave their job, there are many factors that drive an individual's intent and ultimate decision to make changes in his or her employment. Some factors are outside the control of the employer or practice leaders, such as change in an individual's family life or desire and opportunity to pursue fellowship training. Others variables, however, are more directly tied to the job or practice environment. In a specialty where providers are relatively mobile and turnover is high, it is important for hospitalist practices to cultivate a climate in which the sacrifices associated with leaving outweigh the promised benefits.[29]
Results from the HMPWS suggested the need to address climate and fairness issues in hospitalist programs to improve satisfaction and retention.[9] Two large healthcare systems achieved success by investing in multipronged physician retention strategies including recruiting advisors, sign‐on bonuses, extensive onboarding, family support, and the promotion of ongoing effective communication.[3, 30]
Our findings suggest that morale for hospitalists is a complex amalgam of contentment and importance, and that there may not be a one size fits all solution to improving morale for all. While we did not find a difference in personal morale scores across individual hospitalist groups, or even between academic and community groups, each group had a unique profile with variability in the dynamics between importance and contentment of different factors. If practice group leaders review HMI data for their providers and use the information to facilitate meaningful dialogue with them about the factors influencing their morale, such leaders will have great insight into allocating resources for the best return on investment.
While we believe that the HMI is providing unique perspective compared to other commonly used metrics, it may be best to employ HMI data as complementary measures alongside that of some of the benchmarked scales that explore job satisfaction, job fit, and burnout among hospitalists.[6, 9, 10, 31, 32, 33, 34, 35] Aggregate HMI data at the group level may allow for the identification of factors that are highly important to morale but scored low in contentment. Such factors deserve priority and attention such that the subgroups within a practice can collaborate to come to consensus on strategies for amelioration. Because the HMI generates a score and profile for each provider, we can imagine effective leaders using the HMI with individuals as part of an annual review to facilitate discussion about maximizing contentment at work. Being fully transparent and sharing an honest nonanonymous version of the HMI with a superior would require a special relationship founded on trust and mutual respect.
Several limitations of this study should be considered. First, the initial item reduction and EFA were based on a single‐site survey, and our overall sample size was relatively small. We plan on expanding our sample size in the future for further validation of our exploratory findings. Second, the data were collected at 2 specific times several years ago. In continuing to analyze the data from subsequent years, validity and reliability results remain stable, thereby minimizing the likelihood of significant historical bias. Third, there may have been some recall bias, in that respondents may have overlooked the good and perseverated over variables that disappointed them. Fourth, although intention to leave does not necessarily equate actual employee turnover, intention has been found to be a strong predictor of quitting a job.[36, 37] Finally, while we had high response rates, response bias may have existed wherein those with lower morale may have elected not to complete the survey or became apathetic in their responses.
The HMI is a validated instrument that evaluates hospitalist morale by incorporating each provider's characterization of the importance of and contentment with 27 variables. By accounting for the multidimensional and dynamic nature of morale, the HMI may help program leaders tailor retention and engagement strategies specific to their own group. Future studies may explore trends in contributors to morale and examine whether interventions to augment low morale can result in improved morale and hospitalist retention.
Acknowledgements
The authors are indebted to the hospitalists who were willing to share their perspectives about their work, and grateful to Ms. Lisa Roberts, Ms. Barbara Brigade, and Ms. Regina Landis for insuring confidentiality in managing the survey database.
Disclosures: Dr. Chandra had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Dr. Wright is a Miller‐Coulson Family Scholar through the Johns Hopkins Center for Innovative Medicine. Ethical approval has been granted for studies involving human subjects by a Johns Hopkins University School of Medicine institutional review board. The authors report no conflicts of interest.
- 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
- , , . A review of physician turnover: rates, causes, and consequences. Am J Med Qual. 2004;19(2):56–66.
- . Physician retention plans help reduce costs and optimize revenues. Healthc Financ Manage. 1998;52(1):75–77.
- SHM Career Satisfaction Task Force. A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.; 2006. Available at: www.hospitalmedicine.org. Accessed February 28, 2009.
- , . Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119–139.
- , , , , . Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851–858.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- . Physician satisfaction and communication. National findings and best practices. Available at: http://www.pressganey.com/files/clark_cox_acpe_apr06.pdf. Accessed October 10, 2010.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Available at: http://dictionary.reference.com/browse/morale. Accessed June 5, 2014.
- . Morale and satisfaction: a study in past‐future time perspective. Adm Sci Q. 1958:195–209.
- . Men and Women of the Corporation. 2nd ed. New York, NY: Basic Books; 1993.
- . The relation of morale to turnover among teachers. Am Educ Res J. 1965:163–173.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1982;61:1088.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000:34–59.
- . Factors influencing employee morale. Harv Bus Rev. 1950;28(1):61–73.
- . Dimensions of teacher morale. Am Educ Res J. 1970;7(2):221.
- , . The definition and measurement of employee morale. Adm Sci Q. 1958:157–184.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1983;61(4):1088–1108.
- . Morale and its measurement. Am J Sociol. 1941;47(3):406–414.
- , , , . Following morale over time within an academic hospitalist division. J Clin Outcomes Manag. 2011;18(1):21–26.
- , , , et al. Personal growth and its correlates during residency training. Med Educ. 2006;40(8):737–745.
- , , . A global measure of perceived stress. J Health Soc Behav. 1983:385–396.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000;71(1):34–59.
- , . Faculty members' morale and their intention to leave: a multilevel explanation. J Higher Educ. 2002;73(4):518–542.
- , . Employee Morale. New York, NY: Palgrave Macmillan; 2009.
- , , , , . Silence Kills. Silence Kills: The Seven Crucial Conversations® for Healthcare. VitalSmarts™ in association with the American Association of Critical Care Nurses, USA. 2005. Accessed October 10, 2014.
- , , . The lifelong iterative process of physician retention. J Healthc Manag. 2009;54(4):220–226.
- . Physicians' burnout. Rev Prat. 2004;54(7):753–754.
- , , , , , . Work stress and health in primary health care physicians and hospital physicians. Occup Environ Med. 2008;65(5):364–366.
- , , , et al. Understanding physicians' intentions to withdraw from practice: the role of job satisfaction, job stress, mental and physical health. 2001. Health Care Manage Rev. 2010;35(2):105–115.
- , , , , , . Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358–1367.
- , . Burnout and Hospitalists: Etiology and Prevention. In: What Exactly Does A Hospitalist Do? Best of the Best Hospital Medicine 2005: Strategies for Success. Society of Hospital Medicine; 2005:5.
- , . Using job involvement and organizational commitment interactively to predict turnover. J Manage. 1989;15(1):115–127.
- , , , et al. Nurse turnover: a literature review. Int J Nurs Stud. 2006;43(2):237–263.
Explosive growth in hospital medicine has led to hospitalists having the option to change jobs easily. Annual turnover for all physicians is 6.8%, whereas that of hospitalists exceeds 14.8%.[1] Losing a single physician has significant financial and operational implications, with estimates of $20,000 to $120,000 in recruiting costs, and up to $500,000 in lost revenue that may take years to recoup due to the time required for new physician assimilation.[2, 3] In 2006, the Society of Hospital Medicine (SHM) appointed a career task force to develop retention recommendations, 1 of which includes monitoring hospitalists' job satisfaction.[4]
Studies examining physician satisfaction have demonstrated that high physician job satisfaction is associated with lower physician turnover.[5] However, surveys of hospitalists, including SHM's Hospital Medicine Physician Worklife Survey (HMPWS), have reported high job satisfaction among hospitalists,[6, 7, 8, 9, 10] suggesting that high job satisfaction may not be enough to overcome forces that pull hospitalists toward other opportunities.
Morale, a more complex construct related to an individual's contentment and happiness, might provide insight into reducing hospitalist turnover. Morale has been defined as the emotional or mental condition with respect to cheerfulness, confidence, or zeal and is especially relevant in the face of opposition or hardship.[11] Job satisfaction is 1 element that contributes to morale, but alone does not equate morale.[12] Morale, more than satisfaction, relates to how people see themselves within the group and may be closely tied to the concept of esprit de corps. To illustrate, workers may feel satisfied with the content of their job, but frustration with the organization may result in low morale.[13] Efforts focused on assessing provider morale may provide deeper understanding of hospitalists' professional needs and garner insight for retention strategies.
The construct of hospitalist morale and its underlying drivers has not been explored in the literature. Using literature within and outside of healthcare,[1, 12, 14, 15, 16, 17, 18, 19, 20, 21, 22] and our own prior work,[23] we sought to characterize elements that contribute to hospitalist morale and develop a metric to measure it. The HMPWS found that job satisfaction factors vary across hospitalist groups.[9] We suspected that the same would hold true for factors important to morale at the individual level. This study describes the development and validation of the Hospitalist Morale Index (HMI), and explores the relationship between morale and intent to leave due to unhappiness.
METHODS
2009 Pilot Survey
To establish content validity, after reviewing employee morale literature, and examining qualitative comments from our 2007 and 2008 morale surveys, our expert panel, consisting of practicing hospitalists, hospitalist leaders, and administrative staff, identified 46 potential drivers of hospitalist morale. In May 2009, all hospitalists, including physicians, nurse practitioners (NPs), and physician assistants (PAs) from a single hospitalist group received invitations to complete the pilot survey. We asked hospitalists to assess on 5‐point Likert scales the importance of (not at all to tremendously) and contentment with (extremely discontent to extremely content) each of the 46 items as it relates to their work morale. Also included were demographic questions and general morale questions (including rating participants' own morale), investment, long‐term career plans, and intent to leave due to unhappiness.
Data Collection
To maintain anonymity and limit social desirability bias, a database manager, working outside the Division of Hospital Medicine and otherwise not associated with the research team, used Survey Monkey to coordinate survey distribution and data collection. Each respondent had a unique identifier code that was unrelated to the respondent's name and email address. Personal identifiers were maintained in a secure database accessible only to the database manager.
Establishing Internal Structure Validity Evidence
Response frequency to each question was examined for irregularities in distribution. For continuous variables, descriptive statistics were examined for evidence of skewness, outliers, and non‐normality to ensure appropriate use of parametric statistical tests. Upon ranking importance ratings by mode, 15 of 46 items were judged to be of low importance by almost all participants and removed from further consideration.
Stata 13.1 (StataCorp, College Station, TX) was used for exploratory factor analysis (EFA) of the importance responses for all 31 remaining items by principal components factoring. Eigenvalues >1 were designated as a cutoff point for inclusion in varimax rotation. Factor loading of 0.50 was the threshold for inclusion in a factor.
The 31 items loaded across 10 factors; however, 3 factors included 1 item each. After reviewing the scree plot and considering their face value, these items/factors were omitted. Repeating the factor analysis resulted in a 28‐item, 7‐factor solution that accounted for 75% variance. All items were considered informative as demonstrated by low uniqueness scores (0.050.38). Using standard validation procedures, all 7 factors were found to have acceptable factor loadings (0.460.98) and face validity. Cronbach's quantified internal reliability of the 7 factors with scores ranging from 0.68 to 0.92. We named the resultant solution the Hospitalist Morale Index (HMI).
Establishing Response Process Validity Evidence
In developing the HMI, we asked respondents to rate the importance of and their contentment with each variable as related to their work morale. From pilot testing, which included discussions with respondents immediately after completing the survey, we learned that the 2‐part consideration of each variable resulted in thoughtful reflection about their morale. Further, by multiplying the contentment score for each item (scaled from 15) by the corresponding importance score (scaled 01), we quantified the relative contribution and contentment of each item for each hospitalist. Scaling importance scores from 0 to 1 insured that items that were not considered important to the respondent did not affect the respondent's personal morale score. Averaging resultant item scores that were greater than 0 resulted in a personal morale score for each hospitalist. Averaging item scores >0 that constituted each factor resulted in factor scores.
May 2011 Survey
The refined survey was distributed in May 2011 to a convenience sample of 5 hospitalist programs at separate hospitals (3 community hospitals, 2 academic hospitals) encompassing 108 hospitalists in 3 different states. Responses to the 2011 survey were used to complete confirmatory factor analyses (CFA) and establish further validity and reliability evidence.
Based on the 28‐item, 7‐factor solution developed from the pilot study, we developed the theoretical model of factors constituting hospitalist morale. We used the structural equation modeling command in Stata 13 to perform CFA. Factor loading of 0.50 was the threshold for inclusion of an item in a factor. To measure internal consistency, we considered Cronbach's score of 0.60 acceptable. Iterative models were reviewed to find the optimal solution for the data. Four items did not fit into any of the 5 resulting factors and were evaluated in terms of mean importance score and face value. Three items were considered important enough to warrant being stand‐alone items, whereas 1 was omitted. Two additional items had borderline factor loadings (0.48, 0.49) and were included in the model as stand‐alone items due to their overall relevance. The resultant solution was a 5‐factor model with 5 additional stand‐alone items (Table 1).
| Factor | Cronbach's | |||||
|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | ||
| How much does the following item contribute to your morale? | ||||||
| Paperwork | 0.72 | 0.89 | ||||
| Relationship with patients | 0.69 | 0.90 | ||||
| Electronic medical system | 0.60 | 0.90 | ||||
| Intellectual stimulation | 0.59 | 0.90 | ||||
| Variety of cases | 0.58 | 0.90 | ||||
| Relationship with consultants | 0.51 | 0.89 | ||||
| No. of night shifts | 0.74 | 0.89 | ||||
| Patient census | 0.61 | 0.90 | ||||
| No. of shifts | 0.52 | 0.90 | ||||
| Fairness of leadership | 0.82 | 0.89 | ||||
| Effectiveness of leadership | 0.82 | 0.89 | ||||
| Leadership's receptiveness to my thoughts and suggestions | 0.78 | 0.89 | ||||
| Leadership as advocate for my needs | 0.77 | 0.89 | ||||
| Approachability of leadership | 0.77 | 0.89 | ||||
| Accessibility of leadership | 0.69 | 0.89 | ||||
| Alignment of the group's goals with my goals | 0.50 | 0.89 | ||||
| Recognition within the group | 0.82 | 0.89 | ||||
| Feeling valued within the institution | 0.73 | 0.89 | ||||
| Feeling valued within the group | 0.73 | 0.89 | ||||
| Feedback | 0.52 | 0.89 | ||||
| Pay | 0.99 | 0.90 | ||||
| Benefits | 0.56 | 0.89 | ||||
| Cronbach's | 0.78 | 0.65 | 0.89 | 0.78 | 0.71 | |
| How much does the following item contribute to your morale? | Single item indicators | |||||
| Family time | 0.90 | |||||
| Job security | 0.90 | |||||
| Institutional climate | 0.89 | |||||
| Opportunities for professional growth | 0.90 | |||||
| Autonomy | 0.89 | |||||
| Cronbach's | 0.90 | |||||
Establishing Convergent, Concurrent, and Discriminant Validity Evidence
To establish convergent, concurrent, and discriminant validity, linear and logistic regression models were examined for continuous and categorical data accordingly.
Self‐perceived overall work morale and perceived group morale, as assessed by 6‐point Likert questions with response options from terrible to excellent, were modeled as predictors for personal morale as calculated by the HMI.
Personal morale scores were modeled as predictors of professional growth, stress, investment in the group, and intent to leave due to unhappiness. While completing the HMI, hospitalists simultaneously completed a validated professional growth scale[24] and Cohen stress scale.[25] We hypothesized that those with higher morale would have more professional growth. Stress, although an important issue in the workplace, is a distinct construct from morale, and we did not expect a significant relationship between personal morale and stress. We used Pearson's r to assess the strength of association between the HMI and these scales. Participants' level of investment in their group was assessed on a 5‐point Likert scale. To simplify presentation, highly invested represents those claiming to be very or tremendously invested in the success of their current hospitalist group. Intent to leave due to unhappiness was assessed on a 5‐point Likert scale, I have had serious thoughts about leaving my current hospitalist group because I am unhappy, with responses from strongly disagree (1) to strongly agree (5). To simplify presentation, responses higher than 2 are considered to be consistent with intending to leave due to unhappiness.
Our institutional review board approved the study.
RESULTS
Respondents
In May 2009, 30 of the 33 (91%) invited hospitalists completed the original pilot morale survey; 19 (63%) were women. Eleven hospitalists (37%) had been part of the group 1 year or less, whereas 4 (13%) had been with the group for more than 5 years.
In May 2011, 93 of the 108 (86%) hospitalists from 5 hospitals completed the demographic and global parts of the survey. Fifty (53%) were from community hospitals; 47 (51%) were women. Thirty‐seven (40%) physicians and 6 (60%) NPs/PAs were from academic hospitals. Thirty‐nine hospitalists (42%) had been with their current group 1 year or less. Ten hospitalists (11%) had been with their current group over 5 years. Sixty‐three respondents (68%) considered themselves career hospitalists, whereas 5 (5%) did not; the rest were undecided.
Internal Structure Validity Evidence
The final CFA from the 2011 survey resulted in a 5‐factor plus 5stand‐alone‐items HMI. The solution with item‐level and factor‐level Cronbach's scores (range, 0.890.90 and range, 0.650.89, respectively) are shown in Table 1.
Personal Morale Scores and Factor Scores
Personal morale scores were normally distributed (mean = 2.79; standard deviation [SD] = 0.58), ranging from 1.23 to 4.22, with a theoretical low of 0 and high of 5 (Figure 1). Mean personal morale scores across hospitalist groups ranged from 2.70 to 2.99 (P > 0.05). Personal morale scores, factor sores and item scores for NPs and PAs did not significantly differ from those of physicians (P > 0.05 for all analyses). Personal morale scores were lower for those in their first 3 years with their current group, compared to those with greater institutional longevity. For every categorical increase in a participant's response to seeing oneself as a career hospitalist, the personal morale score rose 0.23 points (P < 0.001).
Factor scores for material reward and mean item scores for professional growth were significantly different across the 5 hospitalist groups (P = 0.03 and P < 0.001, respectively). Community hospitalists had significantly higher factor scores, despite having similar importance scores, for material rewards than academic hospitalists (diff. = 0.44, P = 0.02). Academic hospitalists had significantly higher scores for professional growth (diff. = 0.94, P < 0.001) (Table 2). Professional growth had the highest importance score for academic hospitalists (mean = 0.87, SD = 0.18) and the lowest importance score for community hospitalists (mean = 0.65, SD = 0.24, P < 0.001).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | |||
| ||||||||||||
| All participants | Mean | 2.79 | 2.54 | 2.78 | 3.18 | 2.58 | 2.48 | 3.05 | 2.67 | 2.92 | 3.00 | 2.76 |
| SD | 0.58 | 0.63 | 0.70 | 0.95 | 0.86 | 0.85 | 1.15 | 0.97 | 1.11 | 1.10 | 1.21 | |
| Academic A | Mean | 2.77 | 2.43 | 2.92 | 3.10 | 2.54 | 2.28 | 3.16 | 2.70 | 3.06 | 3.20 | 3.08 |
| SD | 0.57 | 0.62 | 0.64 | 0.92 | 0.84 | 0.77 | 1.19 | 0.95 | 1.08 | 1.12 | 1.24 | |
| Academic B | Mean | 2.99 | 2.58 | 2.99 | 3.88 | 2.69 | 2.00 | 2.58 | 2.13 | 1.65 | 3.29 | 4.33 |
| SD | 0.36 | 0.70 | 0.80 | 0.29 | 0.80 | 0.35 | 0.92 | 0.88 | 0.78 | 1.01 | 0.82 | |
| Community A | Mean | 2.86 | 2.61 | 2.51 | 3.23 | 2.73 | 3.03 | 2.88 | 2.84 | 2.95 | 3.23 | 2.66 |
| SD | 0.75 | 0.79 | 0.68 | 1.21 | 1.11 | 1.14 | 1.37 | 1.17 | 0.98 | 1.24 | 1.15 | |
| Community B | Mean | 2.86 | 2.74 | 2.97 | 3.37 | 2.67 | 2.44 | 3.28 | 2.35 | 2.70 | 2.50 | 2.25 |
| SD | 0.67 | 0.55 | 0.86 | 1.04 | 0.94 | 0.87 | 1.00 | 1.15 | 1.40 | 0.72 | 1.26 | |
| Community C | Mean | 2.70 | 2.56 | 2.64 | 2.99 | 2.47 | 2.53 | 3.03 | 2.79 | 3.07 | 2.68 | 2.15 |
| SD | 0.49 | 0.53 | 0.67 | 0.85 | 0.73 | 0.64 | 1.08 | 0.76 | 1.05 | 1.07 | 0.71 | |
| Academic combined | Mean | 2.80 | 2.45 | 2.93 | 3.22 | 2.56 | 2.24 | 3.07 | 2.62 | 2.88 | 3.21 | 3.28 |
| SD | 0.54 | 0.63 | 0.66 | 0.89 | 0.82 | 0.72 | 1.16 | 0.95 | 1.14 | 1.10 | 1.26 | |
| Community combined | Mean | 2.79 | 2.61 | 2.66 | 3.14 | 2.60 | 2.68 | 3.03 | 2.72 | 2.95 | 2.82 | 2.34 |
| SD | 0.62 | 0.62 | 0.72 | 1.01 | 0.90 | 0.90 | 1.15 | 0.99 | 1.09 | 1.09 | 1.00 | |
| P value | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | 0.02 | >0.05 | >0.05 | >0.05 | >0.05 | <0.001 | |
Convergent, Concurrent, and Discriminant Validity Evidence
For every categorical increase on the question assessing overall morale, the personal morale score was 0.23 points higher (P < 0.001). For every categorical increase in a participant's perception of the group's morale, the personal morale score was 0.29 points higher (P < 0.001).
For every 1‐point increase in personal morale score, the odds of being highly invested in the group increased by 5 times (odds ratio [OR]: 5.23, 95% confidence interval [CI]: 1.91‐14.35, P = 0.001). The mean personal morale score for highly invested hospitalists was 2.92, whereas that of those less invested was 2.43 (diff. = 0.49, P < 0.001) (Table 3). Highly invested hospitalists had significantly higher importance factor scores for leadership (diff. = 0.08, P = 0.03) as well as appreciation and acknowledgement (diff. = 0.08, P = 0.02).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | ||
| |||||||||||
| Highly invested in success of current hospitalist group | |||||||||||
| Mean | 2.92 | 2.61 | 2.89 | 3.38 | 2.78 | 2.45 | 3.21 | 2.78 | 2.86 | 3.10 | 2.95 |
| SD | 0.55 | 0.59 | 0.68 | 0.92 | 0.88 | 0.77 | 1.11 | 1.00 | 1.09 | 1.06 | 1.25 |
| Less invested in success of current hospitalist group | |||||||||||
| Mean | 2.43 | 2.34 | 2.48 | 2.60 | 2.02 | 2.57 | 2.60 | 2.38 | 3.08 | 2.69 | 2.24 |
| SD | 0.52 | 0.69 | 0.69 | 0.81 | 0.49 | 1.04 | 1.17 | 0.83 | 1.18 | 1.19 | 0.94 |
| P value | <0.001 | >0.05 | 0.02 | 0.001 | <0.001 | >0.05 | 0.03 | >0.05 | >0.05 | >0.05 | 0.02 |
| Not intending to leave because unhappy | |||||||||||
| Mean | 2.97 | 2.67 | 2.89 | 3.48 | 2.77 | 2.52 | 3.24 | 2.85 | 3.05 | 3.06 | 3.01 |
| SD | 0.51 | 0.54 | 0.61 | 0.91 | 0.89 | 0.78 | 1.03 | 0.99 | 1.10 | 1.07 | 1.25 |
| Intending to leave current group because unhappy | |||||||||||
| Mean | 2.45 | 2.30 | 2.59 | 2.59 | 2.21 | 2.40 | 2.68 | 2.33 | 2.67 | 2.88 | 2.28 |
| SD | 0.56 | 0.72 | 0.82 | 0.74 | 0.68 | 0.97 | 1.29 | 0.83 | 1.11 | 1.17 | 0.97 |
| P value | <0.001 | 0.01 | >0.05 | <0.001 | 0.003 | >0.05 | 0.03 | 0.01 | >0.05 | >0.05 | 0.01 |
Every 1‐point increase in personal morale was associated with a rise of 2.27 on the professional growth scale (P = 0.01). The correlation between these 2 scales was 0.26 (P = 0.01). Every 1‐point increase in personal morale was associated with a 2.21 point decrease on the Cohen stress scale (P > 0.05). The correlation between these 2 scales was 0.21 (P > 0.05).
Morale and Intent to Leave Due to Unhappiness
Sixteen (37%) academic and 18 (36%) community hospitalists reported having thoughts of leaving their current hospitalist program due to unhappiness. The mean personal morale score for hospitalists with no intent to leave their current group was 2.97, whereas that of those with intent to leave was 2.45 (diff. = 0.53, P < 0.001). Each 1‐point increase in the personal morale score was associated with an 85% decrease (OR: 0.15, 95% CI: 0.05‐0.41, P < 0.001) in the odds of leaving because of unhappiness. Holding self‐perception of being a career hospitalist constant, each 1‐point increase in the personal morale score was associated with an 83% decrease (OR: 0.17, 95% CI: 0.05‐0.51, P = 0.002) in the odds of leaving because of unhappiness. Hospitalists who reported intent to leave had significantly lower factor scores for all factors and items except workload, material reward, and autonomy than those who did not report intent to leave (Table 3). Within the academic groups, those who reported intent to leave had significantly lower scores for professional growth (diff. = 1.08, P = 0.01). For community groups, those who reported intent to leave had significantly lower scores for clinical work (diff. = 0.54, P = 0.003), workload (diff. = 0.50, P = 0.02), leadership (diff. = 1.19, P < 0.001), feeling appreciated and acknowledged (diff. = 0.68, P = 0.01), job security (diff. = 0.70, P = 0.03), and institutional climate (diff. = 0.67, P = 0.02) than those who did not report intent to leave.
DISCUSSION
The HMI is a validated tool that objectively measures and quantifies hospitalist morale. The HMI's capacity to comprehensively assess morale comes from its breadth and depth in uncovering work‐related areas that may be sources of contentment or displeasure. Furthermore, the fact that HMI scores varied among groups of individuals, including those who are thinking about leaving their hospitalist group because they are unhappy and those who are highly invested in their hospitalist group, speaks to its ability to highlight and account for what is most important to hospitalist providers.
Low employee morale has been associated with decreased productivity, increased absenteeism, increased turnover, and decreased patient satisfaction.[2, 26, 27, 28] A few frustrated workers can breed group discontentment and lower the entire group's morale.[28] In addition to its financial impact, departures due to low morale can be sudden and devastating, leading to loss of team cohesiveness, increased work burden on the remaining workforce, burnout, and cascades of more turnover.[2] In contrast, when morale is high, workers more commonly go the extra mile, are more committed to the organization's mission, and are more supportive of their coworkers.[28]
While we asked the informants about plans to leave their job, there are many factors that drive an individual's intent and ultimate decision to make changes in his or her employment. Some factors are outside the control of the employer or practice leaders, such as change in an individual's family life or desire and opportunity to pursue fellowship training. Others variables, however, are more directly tied to the job or practice environment. In a specialty where providers are relatively mobile and turnover is high, it is important for hospitalist practices to cultivate a climate in which the sacrifices associated with leaving outweigh the promised benefits.[29]
Results from the HMPWS suggested the need to address climate and fairness issues in hospitalist programs to improve satisfaction and retention.[9] Two large healthcare systems achieved success by investing in multipronged physician retention strategies including recruiting advisors, sign‐on bonuses, extensive onboarding, family support, and the promotion of ongoing effective communication.[3, 30]
Our findings suggest that morale for hospitalists is a complex amalgam of contentment and importance, and that there may not be a one size fits all solution to improving morale for all. While we did not find a difference in personal morale scores across individual hospitalist groups, or even between academic and community groups, each group had a unique profile with variability in the dynamics between importance and contentment of different factors. If practice group leaders review HMI data for their providers and use the information to facilitate meaningful dialogue with them about the factors influencing their morale, such leaders will have great insight into allocating resources for the best return on investment.
While we believe that the HMI is providing unique perspective compared to other commonly used metrics, it may be best to employ HMI data as complementary measures alongside that of some of the benchmarked scales that explore job satisfaction, job fit, and burnout among hospitalists.[6, 9, 10, 31, 32, 33, 34, 35] Aggregate HMI data at the group level may allow for the identification of factors that are highly important to morale but scored low in contentment. Such factors deserve priority and attention such that the subgroups within a practice can collaborate to come to consensus on strategies for amelioration. Because the HMI generates a score and profile for each provider, we can imagine effective leaders using the HMI with individuals as part of an annual review to facilitate discussion about maximizing contentment at work. Being fully transparent and sharing an honest nonanonymous version of the HMI with a superior would require a special relationship founded on trust and mutual respect.
Several limitations of this study should be considered. First, the initial item reduction and EFA were based on a single‐site survey, and our overall sample size was relatively small. We plan on expanding our sample size in the future for further validation of our exploratory findings. Second, the data were collected at 2 specific times several years ago. In continuing to analyze the data from subsequent years, validity and reliability results remain stable, thereby minimizing the likelihood of significant historical bias. Third, there may have been some recall bias, in that respondents may have overlooked the good and perseverated over variables that disappointed them. Fourth, although intention to leave does not necessarily equate actual employee turnover, intention has been found to be a strong predictor of quitting a job.[36, 37] Finally, while we had high response rates, response bias may have existed wherein those with lower morale may have elected not to complete the survey or became apathetic in their responses.
The HMI is a validated instrument that evaluates hospitalist morale by incorporating each provider's characterization of the importance of and contentment with 27 variables. By accounting for the multidimensional and dynamic nature of morale, the HMI may help program leaders tailor retention and engagement strategies specific to their own group. Future studies may explore trends in contributors to morale and examine whether interventions to augment low morale can result in improved morale and hospitalist retention.
Acknowledgements
The authors are indebted to the hospitalists who were willing to share their perspectives about their work, and grateful to Ms. Lisa Roberts, Ms. Barbara Brigade, and Ms. Regina Landis for insuring confidentiality in managing the survey database.
Disclosures: Dr. Chandra had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Dr. Wright is a Miller‐Coulson Family Scholar through the Johns Hopkins Center for Innovative Medicine. Ethical approval has been granted for studies involving human subjects by a Johns Hopkins University School of Medicine institutional review board. The authors report no conflicts of interest.
Explosive growth in hospital medicine has led to hospitalists having the option to change jobs easily. Annual turnover for all physicians is 6.8%, whereas that of hospitalists exceeds 14.8%.[1] Losing a single physician has significant financial and operational implications, with estimates of $20,000 to $120,000 in recruiting costs, and up to $500,000 in lost revenue that may take years to recoup due to the time required for new physician assimilation.[2, 3] In 2006, the Society of Hospital Medicine (SHM) appointed a career task force to develop retention recommendations, 1 of which includes monitoring hospitalists' job satisfaction.[4]
Studies examining physician satisfaction have demonstrated that high physician job satisfaction is associated with lower physician turnover.[5] However, surveys of hospitalists, including SHM's Hospital Medicine Physician Worklife Survey (HMPWS), have reported high job satisfaction among hospitalists,[6, 7, 8, 9, 10] suggesting that high job satisfaction may not be enough to overcome forces that pull hospitalists toward other opportunities.
Morale, a more complex construct related to an individual's contentment and happiness, might provide insight into reducing hospitalist turnover. Morale has been defined as the emotional or mental condition with respect to cheerfulness, confidence, or zeal and is especially relevant in the face of opposition or hardship.[11] Job satisfaction is 1 element that contributes to morale, but alone does not equate morale.[12] Morale, more than satisfaction, relates to how people see themselves within the group and may be closely tied to the concept of esprit de corps. To illustrate, workers may feel satisfied with the content of their job, but frustration with the organization may result in low morale.[13] Efforts focused on assessing provider morale may provide deeper understanding of hospitalists' professional needs and garner insight for retention strategies.
The construct of hospitalist morale and its underlying drivers has not been explored in the literature. Using literature within and outside of healthcare,[1, 12, 14, 15, 16, 17, 18, 19, 20, 21, 22] and our own prior work,[23] we sought to characterize elements that contribute to hospitalist morale and develop a metric to measure it. The HMPWS found that job satisfaction factors vary across hospitalist groups.[9] We suspected that the same would hold true for factors important to morale at the individual level. This study describes the development and validation of the Hospitalist Morale Index (HMI), and explores the relationship between morale and intent to leave due to unhappiness.
METHODS
2009 Pilot Survey
To establish content validity, after reviewing employee morale literature, and examining qualitative comments from our 2007 and 2008 morale surveys, our expert panel, consisting of practicing hospitalists, hospitalist leaders, and administrative staff, identified 46 potential drivers of hospitalist morale. In May 2009, all hospitalists, including physicians, nurse practitioners (NPs), and physician assistants (PAs) from a single hospitalist group received invitations to complete the pilot survey. We asked hospitalists to assess on 5‐point Likert scales the importance of (not at all to tremendously) and contentment with (extremely discontent to extremely content) each of the 46 items as it relates to their work morale. Also included were demographic questions and general morale questions (including rating participants' own morale), investment, long‐term career plans, and intent to leave due to unhappiness.
Data Collection
To maintain anonymity and limit social desirability bias, a database manager, working outside the Division of Hospital Medicine and otherwise not associated with the research team, used Survey Monkey to coordinate survey distribution and data collection. Each respondent had a unique identifier code that was unrelated to the respondent's name and email address. Personal identifiers were maintained in a secure database accessible only to the database manager.
Establishing Internal Structure Validity Evidence
Response frequency to each question was examined for irregularities in distribution. For continuous variables, descriptive statistics were examined for evidence of skewness, outliers, and non‐normality to ensure appropriate use of parametric statistical tests. Upon ranking importance ratings by mode, 15 of 46 items were judged to be of low importance by almost all participants and removed from further consideration.
Stata 13.1 (StataCorp, College Station, TX) was used for exploratory factor analysis (EFA) of the importance responses for all 31 remaining items by principal components factoring. Eigenvalues >1 were designated as a cutoff point for inclusion in varimax rotation. Factor loading of 0.50 was the threshold for inclusion in a factor.
The 31 items loaded across 10 factors; however, 3 factors included 1 item each. After reviewing the scree plot and considering their face value, these items/factors were omitted. Repeating the factor analysis resulted in a 28‐item, 7‐factor solution that accounted for 75% variance. All items were considered informative as demonstrated by low uniqueness scores (0.050.38). Using standard validation procedures, all 7 factors were found to have acceptable factor loadings (0.460.98) and face validity. Cronbach's quantified internal reliability of the 7 factors with scores ranging from 0.68 to 0.92. We named the resultant solution the Hospitalist Morale Index (HMI).
Establishing Response Process Validity Evidence
In developing the HMI, we asked respondents to rate the importance of and their contentment with each variable as related to their work morale. From pilot testing, which included discussions with respondents immediately after completing the survey, we learned that the 2‐part consideration of each variable resulted in thoughtful reflection about their morale. Further, by multiplying the contentment score for each item (scaled from 15) by the corresponding importance score (scaled 01), we quantified the relative contribution and contentment of each item for each hospitalist. Scaling importance scores from 0 to 1 insured that items that were not considered important to the respondent did not affect the respondent's personal morale score. Averaging resultant item scores that were greater than 0 resulted in a personal morale score for each hospitalist. Averaging item scores >0 that constituted each factor resulted in factor scores.
May 2011 Survey
The refined survey was distributed in May 2011 to a convenience sample of 5 hospitalist programs at separate hospitals (3 community hospitals, 2 academic hospitals) encompassing 108 hospitalists in 3 different states. Responses to the 2011 survey were used to complete confirmatory factor analyses (CFA) and establish further validity and reliability evidence.
Based on the 28‐item, 7‐factor solution developed from the pilot study, we developed the theoretical model of factors constituting hospitalist morale. We used the structural equation modeling command in Stata 13 to perform CFA. Factor loading of 0.50 was the threshold for inclusion of an item in a factor. To measure internal consistency, we considered Cronbach's score of 0.60 acceptable. Iterative models were reviewed to find the optimal solution for the data. Four items did not fit into any of the 5 resulting factors and were evaluated in terms of mean importance score and face value. Three items were considered important enough to warrant being stand‐alone items, whereas 1 was omitted. Two additional items had borderline factor loadings (0.48, 0.49) and were included in the model as stand‐alone items due to their overall relevance. The resultant solution was a 5‐factor model with 5 additional stand‐alone items (Table 1).
| Factor | Cronbach's | |||||
|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | ||
| How much does the following item contribute to your morale? | ||||||
| Paperwork | 0.72 | 0.89 | ||||
| Relationship with patients | 0.69 | 0.90 | ||||
| Electronic medical system | 0.60 | 0.90 | ||||
| Intellectual stimulation | 0.59 | 0.90 | ||||
| Variety of cases | 0.58 | 0.90 | ||||
| Relationship with consultants | 0.51 | 0.89 | ||||
| No. of night shifts | 0.74 | 0.89 | ||||
| Patient census | 0.61 | 0.90 | ||||
| No. of shifts | 0.52 | 0.90 | ||||
| Fairness of leadership | 0.82 | 0.89 | ||||
| Effectiveness of leadership | 0.82 | 0.89 | ||||
| Leadership's receptiveness to my thoughts and suggestions | 0.78 | 0.89 | ||||
| Leadership as advocate for my needs | 0.77 | 0.89 | ||||
| Approachability of leadership | 0.77 | 0.89 | ||||
| Accessibility of leadership | 0.69 | 0.89 | ||||
| Alignment of the group's goals with my goals | 0.50 | 0.89 | ||||
| Recognition within the group | 0.82 | 0.89 | ||||
| Feeling valued within the institution | 0.73 | 0.89 | ||||
| Feeling valued within the group | 0.73 | 0.89 | ||||
| Feedback | 0.52 | 0.89 | ||||
| Pay | 0.99 | 0.90 | ||||
| Benefits | 0.56 | 0.89 | ||||
| Cronbach's | 0.78 | 0.65 | 0.89 | 0.78 | 0.71 | |
| How much does the following item contribute to your morale? | Single item indicators | |||||
| Family time | 0.90 | |||||
| Job security | 0.90 | |||||
| Institutional climate | 0.89 | |||||
| Opportunities for professional growth | 0.90 | |||||
| Autonomy | 0.89 | |||||
| Cronbach's | 0.90 | |||||
Establishing Convergent, Concurrent, and Discriminant Validity Evidence
To establish convergent, concurrent, and discriminant validity, linear and logistic regression models were examined for continuous and categorical data accordingly.
Self‐perceived overall work morale and perceived group morale, as assessed by 6‐point Likert questions with response options from terrible to excellent, were modeled as predictors for personal morale as calculated by the HMI.
Personal morale scores were modeled as predictors of professional growth, stress, investment in the group, and intent to leave due to unhappiness. While completing the HMI, hospitalists simultaneously completed a validated professional growth scale[24] and Cohen stress scale.[25] We hypothesized that those with higher morale would have more professional growth. Stress, although an important issue in the workplace, is a distinct construct from morale, and we did not expect a significant relationship between personal morale and stress. We used Pearson's r to assess the strength of association between the HMI and these scales. Participants' level of investment in their group was assessed on a 5‐point Likert scale. To simplify presentation, highly invested represents those claiming to be very or tremendously invested in the success of their current hospitalist group. Intent to leave due to unhappiness was assessed on a 5‐point Likert scale, I have had serious thoughts about leaving my current hospitalist group because I am unhappy, with responses from strongly disagree (1) to strongly agree (5). To simplify presentation, responses higher than 2 are considered to be consistent with intending to leave due to unhappiness.
Our institutional review board approved the study.
RESULTS
Respondents
In May 2009, 30 of the 33 (91%) invited hospitalists completed the original pilot morale survey; 19 (63%) were women. Eleven hospitalists (37%) had been part of the group 1 year or less, whereas 4 (13%) had been with the group for more than 5 years.
In May 2011, 93 of the 108 (86%) hospitalists from 5 hospitals completed the demographic and global parts of the survey. Fifty (53%) were from community hospitals; 47 (51%) were women. Thirty‐seven (40%) physicians and 6 (60%) NPs/PAs were from academic hospitals. Thirty‐nine hospitalists (42%) had been with their current group 1 year or less. Ten hospitalists (11%) had been with their current group over 5 years. Sixty‐three respondents (68%) considered themselves career hospitalists, whereas 5 (5%) did not; the rest were undecided.
Internal Structure Validity Evidence
The final CFA from the 2011 survey resulted in a 5‐factor plus 5stand‐alone‐items HMI. The solution with item‐level and factor‐level Cronbach's scores (range, 0.890.90 and range, 0.650.89, respectively) are shown in Table 1.
Personal Morale Scores and Factor Scores
Personal morale scores were normally distributed (mean = 2.79; standard deviation [SD] = 0.58), ranging from 1.23 to 4.22, with a theoretical low of 0 and high of 5 (Figure 1). Mean personal morale scores across hospitalist groups ranged from 2.70 to 2.99 (P > 0.05). Personal morale scores, factor sores and item scores for NPs and PAs did not significantly differ from those of physicians (P > 0.05 for all analyses). Personal morale scores were lower for those in their first 3 years with their current group, compared to those with greater institutional longevity. For every categorical increase in a participant's response to seeing oneself as a career hospitalist, the personal morale score rose 0.23 points (P < 0.001).
Factor scores for material reward and mean item scores for professional growth were significantly different across the 5 hospitalist groups (P = 0.03 and P < 0.001, respectively). Community hospitalists had significantly higher factor scores, despite having similar importance scores, for material rewards than academic hospitalists (diff. = 0.44, P = 0.02). Academic hospitalists had significantly higher scores for professional growth (diff. = 0.94, P < 0.001) (Table 2). Professional growth had the highest importance score for academic hospitalists (mean = 0.87, SD = 0.18) and the lowest importance score for community hospitalists (mean = 0.65, SD = 0.24, P < 0.001).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | |||
| ||||||||||||
| All participants | Mean | 2.79 | 2.54 | 2.78 | 3.18 | 2.58 | 2.48 | 3.05 | 2.67 | 2.92 | 3.00 | 2.76 |
| SD | 0.58 | 0.63 | 0.70 | 0.95 | 0.86 | 0.85 | 1.15 | 0.97 | 1.11 | 1.10 | 1.21 | |
| Academic A | Mean | 2.77 | 2.43 | 2.92 | 3.10 | 2.54 | 2.28 | 3.16 | 2.70 | 3.06 | 3.20 | 3.08 |
| SD | 0.57 | 0.62 | 0.64 | 0.92 | 0.84 | 0.77 | 1.19 | 0.95 | 1.08 | 1.12 | 1.24 | |
| Academic B | Mean | 2.99 | 2.58 | 2.99 | 3.88 | 2.69 | 2.00 | 2.58 | 2.13 | 1.65 | 3.29 | 4.33 |
| SD | 0.36 | 0.70 | 0.80 | 0.29 | 0.80 | 0.35 | 0.92 | 0.88 | 0.78 | 1.01 | 0.82 | |
| Community A | Mean | 2.86 | 2.61 | 2.51 | 3.23 | 2.73 | 3.03 | 2.88 | 2.84 | 2.95 | 3.23 | 2.66 |
| SD | 0.75 | 0.79 | 0.68 | 1.21 | 1.11 | 1.14 | 1.37 | 1.17 | 0.98 | 1.24 | 1.15 | |
| Community B | Mean | 2.86 | 2.74 | 2.97 | 3.37 | 2.67 | 2.44 | 3.28 | 2.35 | 2.70 | 2.50 | 2.25 |
| SD | 0.67 | 0.55 | 0.86 | 1.04 | 0.94 | 0.87 | 1.00 | 1.15 | 1.40 | 0.72 | 1.26 | |
| Community C | Mean | 2.70 | 2.56 | 2.64 | 2.99 | 2.47 | 2.53 | 3.03 | 2.79 | 3.07 | 2.68 | 2.15 |
| SD | 0.49 | 0.53 | 0.67 | 0.85 | 0.73 | 0.64 | 1.08 | 0.76 | 1.05 | 1.07 | 0.71 | |
| Academic combined | Mean | 2.80 | 2.45 | 2.93 | 3.22 | 2.56 | 2.24 | 3.07 | 2.62 | 2.88 | 3.21 | 3.28 |
| SD | 0.54 | 0.63 | 0.66 | 0.89 | 0.82 | 0.72 | 1.16 | 0.95 | 1.14 | 1.10 | 1.26 | |
| Community combined | Mean | 2.79 | 2.61 | 2.66 | 3.14 | 2.60 | 2.68 | 3.03 | 2.72 | 2.95 | 2.82 | 2.34 |
| SD | 0.62 | 0.62 | 0.72 | 1.01 | 0.90 | 0.90 | 1.15 | 0.99 | 1.09 | 1.09 | 1.00 | |
| P value | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | 0.02 | >0.05 | >0.05 | >0.05 | >0.05 | <0.001 | |
Convergent, Concurrent, and Discriminant Validity Evidence
For every categorical increase on the question assessing overall morale, the personal morale score was 0.23 points higher (P < 0.001). For every categorical increase in a participant's perception of the group's morale, the personal morale score was 0.29 points higher (P < 0.001).
For every 1‐point increase in personal morale score, the odds of being highly invested in the group increased by 5 times (odds ratio [OR]: 5.23, 95% confidence interval [CI]: 1.91‐14.35, P = 0.001). The mean personal morale score for highly invested hospitalists was 2.92, whereas that of those less invested was 2.43 (diff. = 0.49, P < 0.001) (Table 3). Highly invested hospitalists had significantly higher importance factor scores for leadership (diff. = 0.08, P = 0.03) as well as appreciation and acknowledgement (diff. = 0.08, P = 0.02).
| Personal Morale Score | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Clinical | Workload | Leadership | Appreciation and Acknowledgement | Material Rewards | Family Time | Institutional Climate | Job Security | Autonomy | Professional Growth | ||
| |||||||||||
| Highly invested in success of current hospitalist group | |||||||||||
| Mean | 2.92 | 2.61 | 2.89 | 3.38 | 2.78 | 2.45 | 3.21 | 2.78 | 2.86 | 3.10 | 2.95 |
| SD | 0.55 | 0.59 | 0.68 | 0.92 | 0.88 | 0.77 | 1.11 | 1.00 | 1.09 | 1.06 | 1.25 |
| Less invested in success of current hospitalist group | |||||||||||
| Mean | 2.43 | 2.34 | 2.48 | 2.60 | 2.02 | 2.57 | 2.60 | 2.38 | 3.08 | 2.69 | 2.24 |
| SD | 0.52 | 0.69 | 0.69 | 0.81 | 0.49 | 1.04 | 1.17 | 0.83 | 1.18 | 1.19 | 0.94 |
| P value | <0.001 | >0.05 | 0.02 | 0.001 | <0.001 | >0.05 | 0.03 | >0.05 | >0.05 | >0.05 | 0.02 |
| Not intending to leave because unhappy | |||||||||||
| Mean | 2.97 | 2.67 | 2.89 | 3.48 | 2.77 | 2.52 | 3.24 | 2.85 | 3.05 | 3.06 | 3.01 |
| SD | 0.51 | 0.54 | 0.61 | 0.91 | 0.89 | 0.78 | 1.03 | 0.99 | 1.10 | 1.07 | 1.25 |
| Intending to leave current group because unhappy | |||||||||||
| Mean | 2.45 | 2.30 | 2.59 | 2.59 | 2.21 | 2.40 | 2.68 | 2.33 | 2.67 | 2.88 | 2.28 |
| SD | 0.56 | 0.72 | 0.82 | 0.74 | 0.68 | 0.97 | 1.29 | 0.83 | 1.11 | 1.17 | 0.97 |
| P value | <0.001 | 0.01 | >0.05 | <0.001 | 0.003 | >0.05 | 0.03 | 0.01 | >0.05 | >0.05 | 0.01 |
Every 1‐point increase in personal morale was associated with a rise of 2.27 on the professional growth scale (P = 0.01). The correlation between these 2 scales was 0.26 (P = 0.01). Every 1‐point increase in personal morale was associated with a 2.21 point decrease on the Cohen stress scale (P > 0.05). The correlation between these 2 scales was 0.21 (P > 0.05).
Morale and Intent to Leave Due to Unhappiness
Sixteen (37%) academic and 18 (36%) community hospitalists reported having thoughts of leaving their current hospitalist program due to unhappiness. The mean personal morale score for hospitalists with no intent to leave their current group was 2.97, whereas that of those with intent to leave was 2.45 (diff. = 0.53, P < 0.001). Each 1‐point increase in the personal morale score was associated with an 85% decrease (OR: 0.15, 95% CI: 0.05‐0.41, P < 0.001) in the odds of leaving because of unhappiness. Holding self‐perception of being a career hospitalist constant, each 1‐point increase in the personal morale score was associated with an 83% decrease (OR: 0.17, 95% CI: 0.05‐0.51, P = 0.002) in the odds of leaving because of unhappiness. Hospitalists who reported intent to leave had significantly lower factor scores for all factors and items except workload, material reward, and autonomy than those who did not report intent to leave (Table 3). Within the academic groups, those who reported intent to leave had significantly lower scores for professional growth (diff. = 1.08, P = 0.01). For community groups, those who reported intent to leave had significantly lower scores for clinical work (diff. = 0.54, P = 0.003), workload (diff. = 0.50, P = 0.02), leadership (diff. = 1.19, P < 0.001), feeling appreciated and acknowledged (diff. = 0.68, P = 0.01), job security (diff. = 0.70, P = 0.03), and institutional climate (diff. = 0.67, P = 0.02) than those who did not report intent to leave.
DISCUSSION
The HMI is a validated tool that objectively measures and quantifies hospitalist morale. The HMI's capacity to comprehensively assess morale comes from its breadth and depth in uncovering work‐related areas that may be sources of contentment or displeasure. Furthermore, the fact that HMI scores varied among groups of individuals, including those who are thinking about leaving their hospitalist group because they are unhappy and those who are highly invested in their hospitalist group, speaks to its ability to highlight and account for what is most important to hospitalist providers.
Low employee morale has been associated with decreased productivity, increased absenteeism, increased turnover, and decreased patient satisfaction.[2, 26, 27, 28] A few frustrated workers can breed group discontentment and lower the entire group's morale.[28] In addition to its financial impact, departures due to low morale can be sudden and devastating, leading to loss of team cohesiveness, increased work burden on the remaining workforce, burnout, and cascades of more turnover.[2] In contrast, when morale is high, workers more commonly go the extra mile, are more committed to the organization's mission, and are more supportive of their coworkers.[28]
While we asked the informants about plans to leave their job, there are many factors that drive an individual's intent and ultimate decision to make changes in his or her employment. Some factors are outside the control of the employer or practice leaders, such as change in an individual's family life or desire and opportunity to pursue fellowship training. Others variables, however, are more directly tied to the job or practice environment. In a specialty where providers are relatively mobile and turnover is high, it is important for hospitalist practices to cultivate a climate in which the sacrifices associated with leaving outweigh the promised benefits.[29]
Results from the HMPWS suggested the need to address climate and fairness issues in hospitalist programs to improve satisfaction and retention.[9] Two large healthcare systems achieved success by investing in multipronged physician retention strategies including recruiting advisors, sign‐on bonuses, extensive onboarding, family support, and the promotion of ongoing effective communication.[3, 30]
Our findings suggest that morale for hospitalists is a complex amalgam of contentment and importance, and that there may not be a one size fits all solution to improving morale for all. While we did not find a difference in personal morale scores across individual hospitalist groups, or even between academic and community groups, each group had a unique profile with variability in the dynamics between importance and contentment of different factors. If practice group leaders review HMI data for their providers and use the information to facilitate meaningful dialogue with them about the factors influencing their morale, such leaders will have great insight into allocating resources for the best return on investment.
While we believe that the HMI is providing unique perspective compared to other commonly used metrics, it may be best to employ HMI data as complementary measures alongside that of some of the benchmarked scales that explore job satisfaction, job fit, and burnout among hospitalists.[6, 9, 10, 31, 32, 33, 34, 35] Aggregate HMI data at the group level may allow for the identification of factors that are highly important to morale but scored low in contentment. Such factors deserve priority and attention such that the subgroups within a practice can collaborate to come to consensus on strategies for amelioration. Because the HMI generates a score and profile for each provider, we can imagine effective leaders using the HMI with individuals as part of an annual review to facilitate discussion about maximizing contentment at work. Being fully transparent and sharing an honest nonanonymous version of the HMI with a superior would require a special relationship founded on trust and mutual respect.
Several limitations of this study should be considered. First, the initial item reduction and EFA were based on a single‐site survey, and our overall sample size was relatively small. We plan on expanding our sample size in the future for further validation of our exploratory findings. Second, the data were collected at 2 specific times several years ago. In continuing to analyze the data from subsequent years, validity and reliability results remain stable, thereby minimizing the likelihood of significant historical bias. Third, there may have been some recall bias, in that respondents may have overlooked the good and perseverated over variables that disappointed them. Fourth, although intention to leave does not necessarily equate actual employee turnover, intention has been found to be a strong predictor of quitting a job.[36, 37] Finally, while we had high response rates, response bias may have existed wherein those with lower morale may have elected not to complete the survey or became apathetic in their responses.
The HMI is a validated instrument that evaluates hospitalist morale by incorporating each provider's characterization of the importance of and contentment with 27 variables. By accounting for the multidimensional and dynamic nature of morale, the HMI may help program leaders tailor retention and engagement strategies specific to their own group. Future studies may explore trends in contributors to morale and examine whether interventions to augment low morale can result in improved morale and hospitalist retention.
Acknowledgements
The authors are indebted to the hospitalists who were willing to share their perspectives about their work, and grateful to Ms. Lisa Roberts, Ms. Barbara Brigade, and Ms. Regina Landis for insuring confidentiality in managing the survey database.
Disclosures: Dr. Chandra had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Dr. Wright is a Miller‐Coulson Family Scholar through the Johns Hopkins Center for Innovative Medicine. Ethical approval has been granted for studies involving human subjects by a Johns Hopkins University School of Medicine institutional review board. The authors report no conflicts of interest.
- 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
- , , . A review of physician turnover: rates, causes, and consequences. Am J Med Qual. 2004;19(2):56–66.
- . Physician retention plans help reduce costs and optimize revenues. Healthc Financ Manage. 1998;52(1):75–77.
- SHM Career Satisfaction Task Force. A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.; 2006. Available at: www.hospitalmedicine.org. Accessed February 28, 2009.
- , . Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119–139.
- , , , , . Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851–858.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- . Physician satisfaction and communication. National findings and best practices. Available at: http://www.pressganey.com/files/clark_cox_acpe_apr06.pdf. Accessed October 10, 2010.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Available at: http://dictionary.reference.com/browse/morale. Accessed June 5, 2014.
- . Morale and satisfaction: a study in past‐future time perspective. Adm Sci Q. 1958:195–209.
- . Men and Women of the Corporation. 2nd ed. New York, NY: Basic Books; 1993.
- . The relation of morale to turnover among teachers. Am Educ Res J. 1965:163–173.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1982;61:1088.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000:34–59.
- . Factors influencing employee morale. Harv Bus Rev. 1950;28(1):61–73.
- . Dimensions of teacher morale. Am Educ Res J. 1970;7(2):221.
- , . The definition and measurement of employee morale. Adm Sci Q. 1958:157–184.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1983;61(4):1088–1108.
- . Morale and its measurement. Am J Sociol. 1941;47(3):406–414.
- , , , . Following morale over time within an academic hospitalist division. J Clin Outcomes Manag. 2011;18(1):21–26.
- , , , et al. Personal growth and its correlates during residency training. Med Educ. 2006;40(8):737–745.
- , , . A global measure of perceived stress. J Health Soc Behav. 1983:385–396.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000;71(1):34–59.
- , . Faculty members' morale and their intention to leave: a multilevel explanation. J Higher Educ. 2002;73(4):518–542.
- , . Employee Morale. New York, NY: Palgrave Macmillan; 2009.
- , , , , . Silence Kills. Silence Kills: The Seven Crucial Conversations® for Healthcare. VitalSmarts™ in association with the American Association of Critical Care Nurses, USA. 2005. Accessed October 10, 2014.
- , , . The lifelong iterative process of physician retention. J Healthc Manag. 2009;54(4):220–226.
- . Physicians' burnout. Rev Prat. 2004;54(7):753–754.
- , , , , , . Work stress and health in primary health care physicians and hospital physicians. Occup Environ Med. 2008;65(5):364–366.
- , , , et al. Understanding physicians' intentions to withdraw from practice: the role of job satisfaction, job stress, mental and physical health. 2001. Health Care Manage Rev. 2010;35(2):105–115.
- , , , , , . Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358–1367.
- , . Burnout and Hospitalists: Etiology and Prevention. In: What Exactly Does A Hospitalist Do? Best of the Best Hospital Medicine 2005: Strategies for Success. Society of Hospital Medicine; 2005:5.
- , . Using job involvement and organizational commitment interactively to predict turnover. J Manage. 1989;15(1):115–127.
- , , , et al. Nurse turnover: a literature review. Int J Nurs Stud. 2006;43(2):237–263.
- 2014 State of Hospital Medicine Report. Philadelphia, PA: Society of Hospital Medicine; 2014.
- , , . A review of physician turnover: rates, causes, and consequences. Am J Med Qual. 2004;19(2):56–66.
- . Physician retention plans help reduce costs and optimize revenues. Healthc Financ Manage. 1998;52(1):75–77.
- SHM Career Satisfaction Task Force. A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction.; 2006. Available at: www.hospitalmedicine.org. Accessed February 28, 2009.
- , . Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003;28(2):119–139.
- , , , , . Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851–858.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41(3):301–315.
- . Physician satisfaction and communication. National findings and best practices. Available at: http://www.pressganey.com/files/clark_cox_acpe_apr06.pdf. Accessed October 10, 2010.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- , , , , ; Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Morale | Define Morale at Dictionary.com. Available at: http://dictionary.reference.com/browse/morale. Accessed June 5, 2014.
- . Morale and satisfaction: a study in past‐future time perspective. Adm Sci Q. 1958:195–209.
- . Men and Women of the Corporation. 2nd ed. New York, NY: Basic Books; 1993.
- . The relation of morale to turnover among teachers. Am Educ Res J. 1965:163–173.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1982;61:1088.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000:34–59.
- . Factors influencing employee morale. Harv Bus Rev. 1950;28(1):61–73.
- . Dimensions of teacher morale. Am Educ Res J. 1970;7(2):221.
- , . The definition and measurement of employee morale. Adm Sci Q. 1958:157–184.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- . Structural and individual determinants of organization morale and satisfaction. Soc Forces. 1983;61(4):1088–1108.
- . Morale and its measurement. Am J Sociol. 1941;47(3):406–414.
- , , , . Following morale over time within an academic hospitalist division. J Clin Outcomes Manag. 2011;18(1):21–26.
- , , , et al. Personal growth and its correlates during residency training. Med Educ. 2006;40(8):737–745.
- , , . A global measure of perceived stress. J Health Soc Behav. 1983:385–396.
- , , . Morale matters: midlevel administrators and their intent to leave. J Higher Educ. 2000;71(1):34–59.
- , . Faculty members' morale and their intention to leave: a multilevel explanation. J Higher Educ. 2002;73(4):518–542.
- , . Employee Morale. New York, NY: Palgrave Macmillan; 2009.
- , , , , . Silence Kills. Silence Kills: The Seven Crucial Conversations® for Healthcare. VitalSmarts™ in association with the American Association of Critical Care Nurses, USA. 2005. Accessed October 10, 2014.
- , , . The lifelong iterative process of physician retention. J Healthc Manag. 2009;54(4):220–226.
- . Physicians' burnout. Rev Prat. 2004;54(7):753–754.
- , , , , , . Work stress and health in primary health care physicians and hospital physicians. Occup Environ Med. 2008;65(5):364–366.
- , , , et al. Understanding physicians' intentions to withdraw from practice: the role of job satisfaction, job stress, mental and physical health. 2001. Health Care Manage Rev. 2010;35(2):105–115.
- , , , , , . Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358–1367.
- , . Burnout and Hospitalists: Etiology and Prevention. In: What Exactly Does A Hospitalist Do? Best of the Best Hospital Medicine 2005: Strategies for Success. Society of Hospital Medicine; 2005:5.
- , . Using job involvement and organizational commitment interactively to predict turnover. J Manage. 1989;15(1):115–127.
- , , , et al. Nurse turnover: a literature review. Int J Nurs Stud. 2006;43(2):237–263.
© 2016 Society of Hospital Medicine
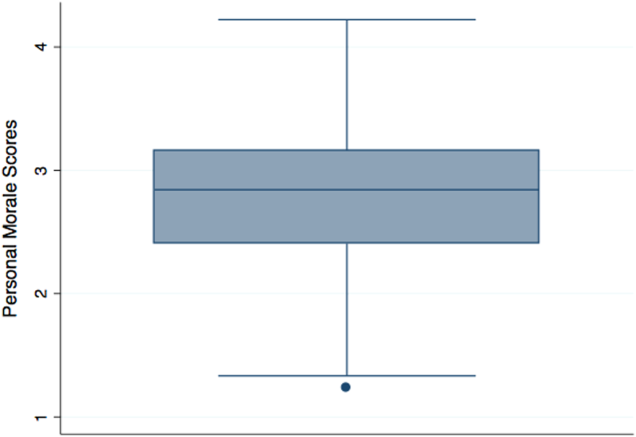
Historic Cleveland Clinic uterus transplant fails
Surgeons at the Cleveland Clinic had to remove the transplanted uterus of a 26-year-old woman who was the first patient in a groundbreaking U.S.-based study aimed at achieving pregnancy in women with uterine factor infertility.
Removal of the uterus, which was announced March 9, came after the patient experienced a sudden complication. The study was originally slated to include 10 women and is still ongoing, according to a statement from the Cleveland Clinic.
“At this time, the circumstance of the complication is under review and more information will be shared as it becomes available,” according to a statement. “There is a known risk in solid organ transplantation that the transplanted organ may have to be removed should a complication arise. The medical team took all necessary precautions and measures to ensure the safety of our patient.”
On Feb. 24, a transplant team at the Cleveland Clinic made history by performing the first uterus transplant in the United States. Prior to that, there had been nine successful uterus transplants performed at the University of Gothenburg in Sweden, with the first posttransplant baby born in 2014.
The Cleveland Clinic transplant recipient, known as “Lindsey” to protect her privacy, was selected from more than 250 applicants to undergo the 9-hour procedure involving transplantation of a uterus from a deceased organ donor of reproductive age.
If the transplant had been a successful, Lindsey was set to undergo a year of antirejection treatment followed by in vitro fertilization. Under the study protocol, the uterus transplant would be temporary and the uterus would be removed after a patient had delivered one or two babies.
Officials at the Cleveland Clinic said Lindsey was doing well and recovering after the removal of the transplanted uterus.
“I just wanted to take a moment to express my gratitude toward all of my doctors,” Lindsey and her husband said in a statement. “They acted very quickly to ensure my health and safety. Unfortunately, I did lose the uterus to complications. However, I am doing okay and appreciate all of your prayers and good thoughts.”
On Twitter @maryellenny
Surgeons at the Cleveland Clinic had to remove the transplanted uterus of a 26-year-old woman who was the first patient in a groundbreaking U.S.-based study aimed at achieving pregnancy in women with uterine factor infertility.
Removal of the uterus, which was announced March 9, came after the patient experienced a sudden complication. The study was originally slated to include 10 women and is still ongoing, according to a statement from the Cleveland Clinic.
“At this time, the circumstance of the complication is under review and more information will be shared as it becomes available,” according to a statement. “There is a known risk in solid organ transplantation that the transplanted organ may have to be removed should a complication arise. The medical team took all necessary precautions and measures to ensure the safety of our patient.”
On Feb. 24, a transplant team at the Cleveland Clinic made history by performing the first uterus transplant in the United States. Prior to that, there had been nine successful uterus transplants performed at the University of Gothenburg in Sweden, with the first posttransplant baby born in 2014.
The Cleveland Clinic transplant recipient, known as “Lindsey” to protect her privacy, was selected from more than 250 applicants to undergo the 9-hour procedure involving transplantation of a uterus from a deceased organ donor of reproductive age.
If the transplant had been a successful, Lindsey was set to undergo a year of antirejection treatment followed by in vitro fertilization. Under the study protocol, the uterus transplant would be temporary and the uterus would be removed after a patient had delivered one or two babies.
Officials at the Cleveland Clinic said Lindsey was doing well and recovering after the removal of the transplanted uterus.
“I just wanted to take a moment to express my gratitude toward all of my doctors,” Lindsey and her husband said in a statement. “They acted very quickly to ensure my health and safety. Unfortunately, I did lose the uterus to complications. However, I am doing okay and appreciate all of your prayers and good thoughts.”
On Twitter @maryellenny
Surgeons at the Cleveland Clinic had to remove the transplanted uterus of a 26-year-old woman who was the first patient in a groundbreaking U.S.-based study aimed at achieving pregnancy in women with uterine factor infertility.
Removal of the uterus, which was announced March 9, came after the patient experienced a sudden complication. The study was originally slated to include 10 women and is still ongoing, according to a statement from the Cleveland Clinic.
“At this time, the circumstance of the complication is under review and more information will be shared as it becomes available,” according to a statement. “There is a known risk in solid organ transplantation that the transplanted organ may have to be removed should a complication arise. The medical team took all necessary precautions and measures to ensure the safety of our patient.”
On Feb. 24, a transplant team at the Cleveland Clinic made history by performing the first uterus transplant in the United States. Prior to that, there had been nine successful uterus transplants performed at the University of Gothenburg in Sweden, with the first posttransplant baby born in 2014.
The Cleveland Clinic transplant recipient, known as “Lindsey” to protect her privacy, was selected from more than 250 applicants to undergo the 9-hour procedure involving transplantation of a uterus from a deceased organ donor of reproductive age.
If the transplant had been a successful, Lindsey was set to undergo a year of antirejection treatment followed by in vitro fertilization. Under the study protocol, the uterus transplant would be temporary and the uterus would be removed after a patient had delivered one or two babies.
Officials at the Cleveland Clinic said Lindsey was doing well and recovering after the removal of the transplanted uterus.
“I just wanted to take a moment to express my gratitude toward all of my doctors,” Lindsey and her husband said in a statement. “They acted very quickly to ensure my health and safety. Unfortunately, I did lose the uterus to complications. However, I am doing okay and appreciate all of your prayers and good thoughts.”
On Twitter @maryellenny
Insurance status affects treatment, outcomes for patients with head and neck cancer
SCOTTSDALE, ARIZ. – Patients with head and neck cancer have substantial disparities in presentation, treatment, and outcomes according to their health insurance status, suggest results of a cohort study reported at the Multidisciplinary Head and Neck Cancer Symposium.
The analysis of more than 50,000 patients from the Surveillance, Epidemiology, and End Results (SEER) registry found that relative to counterparts with insurance, those with Medicaid or no insurance had more advanced disease at presentation.
Additionally, the Medicaid and uninsured patients were 23% and 32% less likely, respectively, to receive radiation therapy, and the uninsured were 23% less to receive surgery, according to data reported in a session and related press briefing.
Both overall and cancer-specific survival were worse for these two groups as well. And when compared with each other, the Medicaid patients actually had poorer overall survival than the uninsured, and similar cause-specific survival.

“We noted important disparities among Medicaid and uninsured cancer patients with head and neck malignancies in the United States,” said lead author Dr. Thomas M. Churilla of the Fox Chase Cancer Center in Philadelphia. “We hypothesize that lack of access to primary care and dental providers may be one of the reasons why patients are presenting with more locally advanced disease.”
The Patient Protection and Affordable Care Act aims to address lack of insurance in part by expanding Medicaid, he noted. However, “given the excess in cancer mortality seen in the Medicaid group and striking similarity with the uninsured group, expansions in Medicaid may have limited effect on outcomes among head and neck cancer patients without further study into figuring out which patient, provider, and health care system factors may be underlying these differences.”
Press briefing moderator Dr. Randall J. Kimple of the University of Wisconsin–Madison, asked, “In your data set, do you have any information on the length of insurance coverage? We see a fair number of patients who come in with no insurance but ultimately get enrolled in Medicaid. Would they have been included in the Medicaid group or the insured group in this study?”
The SEER database does not provide that information, Dr. Churilla said. “The inability to tell the length of insurance coverage is an important limitation of our study, and it may limit our inferences to tell the difference between these two groups,” he acknowledged, adding that the database also lacks information about other important potential confounders, including systemic therapies; risk factors such as smoking, alcohol intake, and human papillomavirus status; and the size, type, and experience of the treating center.

A session attendee said, “You showed that uninsured patients did better than Medicaid patients. Is this possibly due to the uninsured getting free care rather than [clinicians] needing to follow Medicaid-approved treatment?”
“We are scratching our heads a little bit with this one as well, but I think some of the difference may be due in part to the age differences,” Dr. Churilla replied. “The Medicaid patients on average were older than uninsured patients, so perhaps more competing causes of death leading to a difference in overall survival yet similar cancer-specific survival.”
For the study, the investigators analyzed outcomes among 53,848 patients who had primary squamous cell carcinoma of the oral cavity, pharynx, or larynx diagnosed during 2007-2012. Overall, 80% were insured (through private insurance or Medicare), 15% had Medicaid, and 5% were uninsured.
Results showed that patients with Medicaid or no insurance had more advanced cancer at presentation than insured peers. For example, 56% and 59% of patients with Medicaid and no insurance, respectively, had stage 4 disease, compared with 43% of insured patients.
In multivariate analyses adjusted for socioeconomic characteristics, clinical factors (including stage), and treatments, the likelihood of receiving external-beam radiation therapy was lower for the Medicaid group (hazard ratio, 0.77; P less than .001) and the uninsured group (HR, 0.68; P less than .001). Additionally, the uninsured were less likely to receive cancer-directed surgery, defined as at least a wide local excision (HR, 0.77; P less than .001).
In addition, both Medicaid and uninsured patients had poorer overall survival (HRs, 1.54 and 1.49) and cancer-specific survival (HRs, 1.59 and 1.66) relative to insured counterparts.
Findings were generally the same after propensity score weighting and in a sensitivity analysis that excluded all patients aged 65 or older because of their Medicare eligibility.
Addressing the observed disparities for the uninsured patients will require action on both the clinician and policy levels, Dr. Churilla said.
“One of the first steps is awareness among both dental and medical communities and trying to provide social services and financial counseling to help these patients enroll in certain programs such as Medicaid that they may be eligible for,” he elaborated. “And then I think the rest of it really lies with national policy – how do we expand coverage to help get these people the health care that they need and the appropriate services that they require.”
SCOTTSDALE, ARIZ. – Patients with head and neck cancer have substantial disparities in presentation, treatment, and outcomes according to their health insurance status, suggest results of a cohort study reported at the Multidisciplinary Head and Neck Cancer Symposium.
The analysis of more than 50,000 patients from the Surveillance, Epidemiology, and End Results (SEER) registry found that relative to counterparts with insurance, those with Medicaid or no insurance had more advanced disease at presentation.
Additionally, the Medicaid and uninsured patients were 23% and 32% less likely, respectively, to receive radiation therapy, and the uninsured were 23% less to receive surgery, according to data reported in a session and related press briefing.
Both overall and cancer-specific survival were worse for these two groups as well. And when compared with each other, the Medicaid patients actually had poorer overall survival than the uninsured, and similar cause-specific survival.
“We noted important disparities among Medicaid and uninsured cancer patients with head and neck malignancies in the United States,” said lead author Dr. Thomas M. Churilla of the Fox Chase Cancer Center in Philadelphia. “We hypothesize that lack of access to primary care and dental providers may be one of the reasons why patients are presenting with more locally advanced disease.”
The Patient Protection and Affordable Care Act aims to address lack of insurance in part by expanding Medicaid, he noted. However, “given the excess in cancer mortality seen in the Medicaid group and striking similarity with the uninsured group, expansions in Medicaid may have limited effect on outcomes among head and neck cancer patients without further study into figuring out which patient, provider, and health care system factors may be underlying these differences.”
Press briefing moderator Dr. Randall J. Kimple of the University of Wisconsin–Madison, asked, “In your data set, do you have any information on the length of insurance coverage? We see a fair number of patients who come in with no insurance but ultimately get enrolled in Medicaid. Would they have been included in the Medicaid group or the insured group in this study?”
The SEER database does not provide that information, Dr. Churilla said. “The inability to tell the length of insurance coverage is an important limitation of our study, and it may limit our inferences to tell the difference between these two groups,” he acknowledged, adding that the database also lacks information about other important potential confounders, including systemic therapies; risk factors such as smoking, alcohol intake, and human papillomavirus status; and the size, type, and experience of the treating center.
A session attendee said, “You showed that uninsured patients did better than Medicaid patients. Is this possibly due to the uninsured getting free care rather than [clinicians] needing to follow Medicaid-approved treatment?”
“We are scratching our heads a little bit with this one as well, but I think some of the difference may be due in part to the age differences,” Dr. Churilla replied. “The Medicaid patients on average were older than uninsured patients, so perhaps more competing causes of death leading to a difference in overall survival yet similar cancer-specific survival.”
For the study, the investigators analyzed outcomes among 53,848 patients who had primary squamous cell carcinoma of the oral cavity, pharynx, or larynx diagnosed during 2007-2012. Overall, 80% were insured (through private insurance or Medicare), 15% had Medicaid, and 5% were uninsured.
Results showed that patients with Medicaid or no insurance had more advanced cancer at presentation than insured peers. For example, 56% and 59% of patients with Medicaid and no insurance, respectively, had stage 4 disease, compared with 43% of insured patients.
In multivariate analyses adjusted for socioeconomic characteristics, clinical factors (including stage), and treatments, the likelihood of receiving external-beam radiation therapy was lower for the Medicaid group (hazard ratio, 0.77; P less than .001) and the uninsured group (HR, 0.68; P less than .001). Additionally, the uninsured were less likely to receive cancer-directed surgery, defined as at least a wide local excision (HR, 0.77; P less than .001).
In addition, both Medicaid and uninsured patients had poorer overall survival (HRs, 1.54 and 1.49) and cancer-specific survival (HRs, 1.59 and 1.66) relative to insured counterparts.
Findings were generally the same after propensity score weighting and in a sensitivity analysis that excluded all patients aged 65 or older because of their Medicare eligibility.
Addressing the observed disparities for the uninsured patients will require action on both the clinician and policy levels, Dr. Churilla said.
“One of the first steps is awareness among both dental and medical communities and trying to provide social services and financial counseling to help these patients enroll in certain programs such as Medicaid that they may be eligible for,” he elaborated. “And then I think the rest of it really lies with national policy – how do we expand coverage to help get these people the health care that they need and the appropriate services that they require.”
SCOTTSDALE, ARIZ. – Patients with head and neck cancer have substantial disparities in presentation, treatment, and outcomes according to their health insurance status, suggest results of a cohort study reported at the Multidisciplinary Head and Neck Cancer Symposium.
The analysis of more than 50,000 patients from the Surveillance, Epidemiology, and End Results (SEER) registry found that relative to counterparts with insurance, those with Medicaid or no insurance had more advanced disease at presentation.
Additionally, the Medicaid and uninsured patients were 23% and 32% less likely, respectively, to receive radiation therapy, and the uninsured were 23% less to receive surgery, according to data reported in a session and related press briefing.
Both overall and cancer-specific survival were worse for these two groups as well. And when compared with each other, the Medicaid patients actually had poorer overall survival than the uninsured, and similar cause-specific survival.
“We noted important disparities among Medicaid and uninsured cancer patients with head and neck malignancies in the United States,” said lead author Dr. Thomas M. Churilla of the Fox Chase Cancer Center in Philadelphia. “We hypothesize that lack of access to primary care and dental providers may be one of the reasons why patients are presenting with more locally advanced disease.”
The Patient Protection and Affordable Care Act aims to address lack of insurance in part by expanding Medicaid, he noted. However, “given the excess in cancer mortality seen in the Medicaid group and striking similarity with the uninsured group, expansions in Medicaid may have limited effect on outcomes among head and neck cancer patients without further study into figuring out which patient, provider, and health care system factors may be underlying these differences.”
Press briefing moderator Dr. Randall J. Kimple of the University of Wisconsin–Madison, asked, “In your data set, do you have any information on the length of insurance coverage? We see a fair number of patients who come in with no insurance but ultimately get enrolled in Medicaid. Would they have been included in the Medicaid group or the insured group in this study?”
The SEER database does not provide that information, Dr. Churilla said. “The inability to tell the length of insurance coverage is an important limitation of our study, and it may limit our inferences to tell the difference between these two groups,” he acknowledged, adding that the database also lacks information about other important potential confounders, including systemic therapies; risk factors such as smoking, alcohol intake, and human papillomavirus status; and the size, type, and experience of the treating center.
A session attendee said, “You showed that uninsured patients did better than Medicaid patients. Is this possibly due to the uninsured getting free care rather than [clinicians] needing to follow Medicaid-approved treatment?”
“We are scratching our heads a little bit with this one as well, but I think some of the difference may be due in part to the age differences,” Dr. Churilla replied. “The Medicaid patients on average were older than uninsured patients, so perhaps more competing causes of death leading to a difference in overall survival yet similar cancer-specific survival.”
For the study, the investigators analyzed outcomes among 53,848 patients who had primary squamous cell carcinoma of the oral cavity, pharynx, or larynx diagnosed during 2007-2012. Overall, 80% were insured (through private insurance or Medicare), 15% had Medicaid, and 5% were uninsured.
Results showed that patients with Medicaid or no insurance had more advanced cancer at presentation than insured peers. For example, 56% and 59% of patients with Medicaid and no insurance, respectively, had stage 4 disease, compared with 43% of insured patients.
In multivariate analyses adjusted for socioeconomic characteristics, clinical factors (including stage), and treatments, the likelihood of receiving external-beam radiation therapy was lower for the Medicaid group (hazard ratio, 0.77; P less than .001) and the uninsured group (HR, 0.68; P less than .001). Additionally, the uninsured were less likely to receive cancer-directed surgery, defined as at least a wide local excision (HR, 0.77; P less than .001).
In addition, both Medicaid and uninsured patients had poorer overall survival (HRs, 1.54 and 1.49) and cancer-specific survival (HRs, 1.59 and 1.66) relative to insured counterparts.
Findings were generally the same after propensity score weighting and in a sensitivity analysis that excluded all patients aged 65 or older because of their Medicare eligibility.
Addressing the observed disparities for the uninsured patients will require action on both the clinician and policy levels, Dr. Churilla said.
“One of the first steps is awareness among both dental and medical communities and trying to provide social services and financial counseling to help these patients enroll in certain programs such as Medicaid that they may be eligible for,” he elaborated. “And then I think the rest of it really lies with national policy – how do we expand coverage to help get these people the health care that they need and the appropriate services that they require.”
AT THE HEAD AND NECK CANCER SYMPOSIUM
Key clinical point: Patients with Medicaid or no insurance are less likely to receive certain treatments and more likely to die.
Major finding: Compared with insured counterparts, Medicaid and uninsured patients were 23%-32% less likely to receive radiation therapy, and the uninsured were also 23% less likely to receive surgery.
Data source: A cohort study of 53,848 patients from the SEER database treated for head and neck cancer.
Disclosures: Dr. Churilla disclosed that he had no relevant conflicts of interest.

Maximizing bang in topical onychomycosis therapy
WAIKOLOA, HAWAII – Two recent studies highlight several key points regarding topical therapy for onychomycosis: Treat it early for best results, and if concomitant tinea pedis is present, be sure to treat that, too, Dr. Theodore Rosen said at the Hawaii Dermatology Seminar.
The studies were separate secondary analyses of the pooled results of two large, double blind, vehicle-controlled, 48-week, phase III randomized trials of efinaconazole 10% topical solution (Jublia) for onychomycosis. But the same lessons probably apply to any topical antifungal, according to Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Early treatment: This makes a big difference in outcome, as demonstrated in Dr. Phoebe Rich’s analysis of 1,655 patients in the phase III studies. Dr. Rich, director of the nail disorders clinic at Oregon Health and Science University, Portland, divided participants into three groups based upon disease duration: less than a year, 1-5 years, or more than 5 years. The complete cure rate was much better in the group with less than 1 year of onychomycosis, even though the extent of nail involvement of the target toenail didn’t differ significantly between the three groups (J Drugs Dermatol. 2015;Jan 14[1]:58-62).
“Now we have data: Don’t wait to treat until it has been there for 35 years. It’s easier to treat if it’s early,” Dr. Rosen commented at the seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
When onychomycosis and tinea pedis coexist, treat both: Dr. Leon H. Kircik of Indiana University, Indianapolis, and associates reported in a poster at the Hawaii Dermatology Seminar that one in five participants in the two phase III trials had tinea pedis as well as onychomycosis, and nearly half of them were treated for their athlete’s foot using their physician’s choice of topical antifungals.
The primary endpoint in the two trials was the week 53 complete cure rate, defined as no clinical involvement of the target toenail, a negative potassium hydroxide exam, and a negative fungal culture. Among subjects with concomitant onychomycosis and tinea pedis, the onychomycosis complete cure rate was 28.2% if they received efinaconazole for their onychomycosis and got treatment for their tinea pedis, compared with 20.9% if they got efinaconazole but no treatment for their tinea pedis. The complete/almost complete cure rate was 35.5% with dual therapy versus 29.6% if they only received efinaconazole. Both differences were significant.
“Doesn’t that make logical sense? If you leave the fungus on the foot or between the toes, it’s going to say, ‘Wow, that’s steak up there on the nail. That’s real food. I’m just going to crawl back onto the nail because all my brothers up there are dead and there’s wide-open space,” Dr. Rosen explained.
He added that the reverse is also true: if a patient presents seeking treatment for athlete’s foot but also has onychomycosis, the best treatment results for the tinea pedis are obtained by also treating the nail infection.
Dr. Rosen offered a money-saving tip for effective OTC therapy for tinea pedis. Two words: Lotrimin Ultra. That’s the brand name for butenafine cream 1%, not to be confused with plain old Lotrimin, which is clotrimazole.
“Clotrimazole has been around since the dawn of man, and it’s not very effective. Many of the fungi are actually resistant to it. But they’re not resistant to butenafine, which is a very good topical antifungal now available over the counter. It costs $9 or $10 dollars for a tube the size of a baseball bat. It’s a good, effective, cheap way of treating concomitant tinea pedis,” he said.
Dr. Rosen reported serving on scientific advisory boards for Anacor, Merz, and Valeant.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Two recent studies highlight several key points regarding topical therapy for onychomycosis: Treat it early for best results, and if concomitant tinea pedis is present, be sure to treat that, too, Dr. Theodore Rosen said at the Hawaii Dermatology Seminar.
The studies were separate secondary analyses of the pooled results of two large, double blind, vehicle-controlled, 48-week, phase III randomized trials of efinaconazole 10% topical solution (Jublia) for onychomycosis. But the same lessons probably apply to any topical antifungal, according to Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Early treatment: This makes a big difference in outcome, as demonstrated in Dr. Phoebe Rich’s analysis of 1,655 patients in the phase III studies. Dr. Rich, director of the nail disorders clinic at Oregon Health and Science University, Portland, divided participants into three groups based upon disease duration: less than a year, 1-5 years, or more than 5 years. The complete cure rate was much better in the group with less than 1 year of onychomycosis, even though the extent of nail involvement of the target toenail didn’t differ significantly between the three groups (J Drugs Dermatol. 2015;Jan 14[1]:58-62).
“Now we have data: Don’t wait to treat until it has been there for 35 years. It’s easier to treat if it’s early,” Dr. Rosen commented at the seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
When onychomycosis and tinea pedis coexist, treat both: Dr. Leon H. Kircik of Indiana University, Indianapolis, and associates reported in a poster at the Hawaii Dermatology Seminar that one in five participants in the two phase III trials had tinea pedis as well as onychomycosis, and nearly half of them were treated for their athlete’s foot using their physician’s choice of topical antifungals.
The primary endpoint in the two trials was the week 53 complete cure rate, defined as no clinical involvement of the target toenail, a negative potassium hydroxide exam, and a negative fungal culture. Among subjects with concomitant onychomycosis and tinea pedis, the onychomycosis complete cure rate was 28.2% if they received efinaconazole for their onychomycosis and got treatment for their tinea pedis, compared with 20.9% if they got efinaconazole but no treatment for their tinea pedis. The complete/almost complete cure rate was 35.5% with dual therapy versus 29.6% if they only received efinaconazole. Both differences were significant.
“Doesn’t that make logical sense? If you leave the fungus on the foot or between the toes, it’s going to say, ‘Wow, that’s steak up there on the nail. That’s real food. I’m just going to crawl back onto the nail because all my brothers up there are dead and there’s wide-open space,” Dr. Rosen explained.
He added that the reverse is also true: if a patient presents seeking treatment for athlete’s foot but also has onychomycosis, the best treatment results for the tinea pedis are obtained by also treating the nail infection.
Dr. Rosen offered a money-saving tip for effective OTC therapy for tinea pedis. Two words: Lotrimin Ultra. That’s the brand name for butenafine cream 1%, not to be confused with plain old Lotrimin, which is clotrimazole.
“Clotrimazole has been around since the dawn of man, and it’s not very effective. Many of the fungi are actually resistant to it. But they’re not resistant to butenafine, which is a very good topical antifungal now available over the counter. It costs $9 or $10 dollars for a tube the size of a baseball bat. It’s a good, effective, cheap way of treating concomitant tinea pedis,” he said.
Dr. Rosen reported serving on scientific advisory boards for Anacor, Merz, and Valeant.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Two recent studies highlight several key points regarding topical therapy for onychomycosis: Treat it early for best results, and if concomitant tinea pedis is present, be sure to treat that, too, Dr. Theodore Rosen said at the Hawaii Dermatology Seminar.
The studies were separate secondary analyses of the pooled results of two large, double blind, vehicle-controlled, 48-week, phase III randomized trials of efinaconazole 10% topical solution (Jublia) for onychomycosis. But the same lessons probably apply to any topical antifungal, according to Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Early treatment: This makes a big difference in outcome, as demonstrated in Dr. Phoebe Rich’s analysis of 1,655 patients in the phase III studies. Dr. Rich, director of the nail disorders clinic at Oregon Health and Science University, Portland, divided participants into three groups based upon disease duration: less than a year, 1-5 years, or more than 5 years. The complete cure rate was much better in the group with less than 1 year of onychomycosis, even though the extent of nail involvement of the target toenail didn’t differ significantly between the three groups (J Drugs Dermatol. 2015;Jan 14[1]:58-62).
“Now we have data: Don’t wait to treat until it has been there for 35 years. It’s easier to treat if it’s early,” Dr. Rosen commented at the seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
When onychomycosis and tinea pedis coexist, treat both: Dr. Leon H. Kircik of Indiana University, Indianapolis, and associates reported in a poster at the Hawaii Dermatology Seminar that one in five participants in the two phase III trials had tinea pedis as well as onychomycosis, and nearly half of them were treated for their athlete’s foot using their physician’s choice of topical antifungals.
The primary endpoint in the two trials was the week 53 complete cure rate, defined as no clinical involvement of the target toenail, a negative potassium hydroxide exam, and a negative fungal culture. Among subjects with concomitant onychomycosis and tinea pedis, the onychomycosis complete cure rate was 28.2% if they received efinaconazole for their onychomycosis and got treatment for their tinea pedis, compared with 20.9% if they got efinaconazole but no treatment for their tinea pedis. The complete/almost complete cure rate was 35.5% with dual therapy versus 29.6% if they only received efinaconazole. Both differences were significant.
“Doesn’t that make logical sense? If you leave the fungus on the foot or between the toes, it’s going to say, ‘Wow, that’s steak up there on the nail. That’s real food. I’m just going to crawl back onto the nail because all my brothers up there are dead and there’s wide-open space,” Dr. Rosen explained.
He added that the reverse is also true: if a patient presents seeking treatment for athlete’s foot but also has onychomycosis, the best treatment results for the tinea pedis are obtained by also treating the nail infection.
Dr. Rosen offered a money-saving tip for effective OTC therapy for tinea pedis. Two words: Lotrimin Ultra. That’s the brand name for butenafine cream 1%, not to be confused with plain old Lotrimin, which is clotrimazole.
“Clotrimazole has been around since the dawn of man, and it’s not very effective. Many of the fungi are actually resistant to it. But they’re not resistant to butenafine, which is a very good topical antifungal now available over the counter. It costs $9 or $10 dollars for a tube the size of a baseball bat. It’s a good, effective, cheap way of treating concomitant tinea pedis,” he said.
Dr. Rosen reported serving on scientific advisory boards for Anacor, Merz, and Valeant.
SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Gait speed hones risk stratification of elderly heart failure patients
Gait speed was independently associated with hospitalization and death and aided in risk stratification of elderly patients with heart failure in a study reported online March 9 in JACC Heart Failure.
Optimal clinical management of heart failure is dependent on accurate prognostic stratification, Dr. Giovanni Pulignano and his coinvestigators wrote. Geriatric conditions such as frailty, cognitive impairment, and disability impact prognosis along with comorbidities and cardiac disease. Further, gait speed is a marker of frailty and is predictive of adverse health events in older patients, including mortality. However, there is limited research on the impact of geriatric conditions in heart failure studies.

Dr. Pulignano of San Camillo Hospital in Rome and colleagues sought to examine the relationship between gait speed in older patients with heart failure and the risk of hospitalization and death.
The investigators calculated the predicted all-cause mortality using the Cardiac and Comorbid Conditions Heart Failure (3C-HF) score. Variables included in the 3C-HF score are left ventricular ejection fraction of less than 20%, New York Heart Association class III-IV heart failure, no renin-angiotensin inhibitor treatment, no beta-blocker treatment, severe valvular heart disease, diabetes with macro- or microangiopathy, atrial fibrillation, hypertension, anemia, renal dysfunction, and older age.
Participants were at least 70 years old, with clinically stable heart failure with normal or reduced left ventricular ejection fraction and a previous hospitalization necessitating intravenous inotropes, diuretics, and/or vasodilators for heart failure.
Exclusion criteria included a condition that would decrease their walking speed, valvular heart disease with surgery planned, long-term intravenous inotrope treatment, or living in a nursing home.
Gait speed was assessed over 4 meters and grouped into groups of slow walkers (up to 0.65 m/s), intermediate walkers (0.66-0.99 m/s), and fast walkers (at least 1.0 m/s). Participants were allowed to use a walker or cane as a walking aid.
Data were analyzed on 331 patients (mean age 78 years, 43% women) with clinically stable and optimized chronic heart failure (mean NYHA class 2.7, mean left ventricular ejection fraction 35%). The mean 3C-HF score was 19.7 points.
The mean gait speed was 0.74 m/s, with 35% (115 patients) demonstrating severely reduced (less than or equal to 0.65 m/s) gait speed.
After 1 year of follow-up, they found a significant association between the measured gait speed and 1-year mortality, with 9.1%, 21.9%, and 38.3% for the high, intermediate, and low tertiles, respectively (P less than .001). A similar relationship was found for gait speed and heart failure–related hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002) and all-cause hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002).
Multivariate analysis revealed an independent association between gait speed and lower risk of all-cause death (hazard ratio, 0.62; P = .008). Gait speed was also associated with a lower risk for all-cause hospitalizations (HR, 0.74; P = .002) and heart failure–related hospitalizations (HR, 0.69; P = .004).
Finally, when gait speed was included in the 3C-HF risk score, accuracy of risk stratification for all-cause death (net reclassification improvement, 0.49; P less than .001) and heart failure admissions (NRI, 0.37; P less than .001) was improved (JCHF. 2016 Mar 9. doi:10.1016/j.jchf.2015.12.017).
“Gait speed, in combination with a validated clinical risk score, improves prognosis prediction in older HF patients,” the investigators concluded. “Frailty assessment using gait speed is simple and inexpensive and suggests new strategies for intervention. Its measurement should be incorporated in the routine clinical evaluation of older patients with HF.”
The study was supported by the ADRIANO-Italian Association for Research on Cardiac Disease in Older Patients. The authors had no disclosures.
Gait speed was independently associated with hospitalization and death and aided in risk stratification of elderly patients with heart failure in a study reported online March 9 in JACC Heart Failure.
Optimal clinical management of heart failure is dependent on accurate prognostic stratification, Dr. Giovanni Pulignano and his coinvestigators wrote. Geriatric conditions such as frailty, cognitive impairment, and disability impact prognosis along with comorbidities and cardiac disease. Further, gait speed is a marker of frailty and is predictive of adverse health events in older patients, including mortality. However, there is limited research on the impact of geriatric conditions in heart failure studies.
Dr. Pulignano of San Camillo Hospital in Rome and colleagues sought to examine the relationship between gait speed in older patients with heart failure and the risk of hospitalization and death.
The investigators calculated the predicted all-cause mortality using the Cardiac and Comorbid Conditions Heart Failure (3C-HF) score. Variables included in the 3C-HF score are left ventricular ejection fraction of less than 20%, New York Heart Association class III-IV heart failure, no renin-angiotensin inhibitor treatment, no beta-blocker treatment, severe valvular heart disease, diabetes with macro- or microangiopathy, atrial fibrillation, hypertension, anemia, renal dysfunction, and older age.
Participants were at least 70 years old, with clinically stable heart failure with normal or reduced left ventricular ejection fraction and a previous hospitalization necessitating intravenous inotropes, diuretics, and/or vasodilators for heart failure.
Exclusion criteria included a condition that would decrease their walking speed, valvular heart disease with surgery planned, long-term intravenous inotrope treatment, or living in a nursing home.
Gait speed was assessed over 4 meters and grouped into groups of slow walkers (up to 0.65 m/s), intermediate walkers (0.66-0.99 m/s), and fast walkers (at least 1.0 m/s). Participants were allowed to use a walker or cane as a walking aid.
Data were analyzed on 331 patients (mean age 78 years, 43% women) with clinically stable and optimized chronic heart failure (mean NYHA class 2.7, mean left ventricular ejection fraction 35%). The mean 3C-HF score was 19.7 points.
The mean gait speed was 0.74 m/s, with 35% (115 patients) demonstrating severely reduced (less than or equal to 0.65 m/s) gait speed.
After 1 year of follow-up, they found a significant association between the measured gait speed and 1-year mortality, with 9.1%, 21.9%, and 38.3% for the high, intermediate, and low tertiles, respectively (P less than .001). A similar relationship was found for gait speed and heart failure–related hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002) and all-cause hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002).
Multivariate analysis revealed an independent association between gait speed and lower risk of all-cause death (hazard ratio, 0.62; P = .008). Gait speed was also associated with a lower risk for all-cause hospitalizations (HR, 0.74; P = .002) and heart failure–related hospitalizations (HR, 0.69; P = .004).
Finally, when gait speed was included in the 3C-HF risk score, accuracy of risk stratification for all-cause death (net reclassification improvement, 0.49; P less than .001) and heart failure admissions (NRI, 0.37; P less than .001) was improved (JCHF. 2016 Mar 9. doi:10.1016/j.jchf.2015.12.017).
“Gait speed, in combination with a validated clinical risk score, improves prognosis prediction in older HF patients,” the investigators concluded. “Frailty assessment using gait speed is simple and inexpensive and suggests new strategies for intervention. Its measurement should be incorporated in the routine clinical evaluation of older patients with HF.”
The study was supported by the ADRIANO-Italian Association for Research on Cardiac Disease in Older Patients. The authors had no disclosures.
Gait speed was independently associated with hospitalization and death and aided in risk stratification of elderly patients with heart failure in a study reported online March 9 in JACC Heart Failure.
Optimal clinical management of heart failure is dependent on accurate prognostic stratification, Dr. Giovanni Pulignano and his coinvestigators wrote. Geriatric conditions such as frailty, cognitive impairment, and disability impact prognosis along with comorbidities and cardiac disease. Further, gait speed is a marker of frailty and is predictive of adverse health events in older patients, including mortality. However, there is limited research on the impact of geriatric conditions in heart failure studies.
Dr. Pulignano of San Camillo Hospital in Rome and colleagues sought to examine the relationship between gait speed in older patients with heart failure and the risk of hospitalization and death.
The investigators calculated the predicted all-cause mortality using the Cardiac and Comorbid Conditions Heart Failure (3C-HF) score. Variables included in the 3C-HF score are left ventricular ejection fraction of less than 20%, New York Heart Association class III-IV heart failure, no renin-angiotensin inhibitor treatment, no beta-blocker treatment, severe valvular heart disease, diabetes with macro- or microangiopathy, atrial fibrillation, hypertension, anemia, renal dysfunction, and older age.
Participants were at least 70 years old, with clinically stable heart failure with normal or reduced left ventricular ejection fraction and a previous hospitalization necessitating intravenous inotropes, diuretics, and/or vasodilators for heart failure.
Exclusion criteria included a condition that would decrease their walking speed, valvular heart disease with surgery planned, long-term intravenous inotrope treatment, or living in a nursing home.
Gait speed was assessed over 4 meters and grouped into groups of slow walkers (up to 0.65 m/s), intermediate walkers (0.66-0.99 m/s), and fast walkers (at least 1.0 m/s). Participants were allowed to use a walker or cane as a walking aid.
Data were analyzed on 331 patients (mean age 78 years, 43% women) with clinically stable and optimized chronic heart failure (mean NYHA class 2.7, mean left ventricular ejection fraction 35%). The mean 3C-HF score was 19.7 points.
The mean gait speed was 0.74 m/s, with 35% (115 patients) demonstrating severely reduced (less than or equal to 0.65 m/s) gait speed.
After 1 year of follow-up, they found a significant association between the measured gait speed and 1-year mortality, with 9.1%, 21.9%, and 38.3% for the high, intermediate, and low tertiles, respectively (P less than .001). A similar relationship was found for gait speed and heart failure–related hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002) and all-cause hospitalization (26.6%, 58.6%, and 71.3%, respectively; P = .002).
Multivariate analysis revealed an independent association between gait speed and lower risk of all-cause death (hazard ratio, 0.62; P = .008). Gait speed was also associated with a lower risk for all-cause hospitalizations (HR, 0.74; P = .002) and heart failure–related hospitalizations (HR, 0.69; P = .004).
Finally, when gait speed was included in the 3C-HF risk score, accuracy of risk stratification for all-cause death (net reclassification improvement, 0.49; P less than .001) and heart failure admissions (NRI, 0.37; P less than .001) was improved (JCHF. 2016 Mar 9. doi:10.1016/j.jchf.2015.12.017).
“Gait speed, in combination with a validated clinical risk score, improves prognosis prediction in older HF patients,” the investigators concluded. “Frailty assessment using gait speed is simple and inexpensive and suggests new strategies for intervention. Its measurement should be incorporated in the routine clinical evaluation of older patients with HF.”
The study was supported by the ADRIANO-Italian Association for Research on Cardiac Disease in Older Patients. The authors had no disclosures.
JACC HEART FAILURE
Key clinical point: Gait speed was independently associated with hospitalization and death, and aided in risk stratification of elderly patients with heart failure.
Major finding: When gait speed was included in the 3C-HF risk score, accuracy of risk stratification for all-cause death (net reclassification improvement, 0.49) and heart failure admissions (NRI, 0.37) was improved significantly.
Data source: Gait speed was tested in 331 elderly patients with clinically stable heart failure who were prospectively followed for 1 year to assess mortality and hospitalization rate.
Disclosures: The study was supported by the ADRIANO-Italian Association for Research on Cardiac Disease in Older Patients. The authors report no disclosures.

Elective CRC resections increase with universal insurance
BOSTON – Expanding access to health insurance for low- and moderate-income families has apparently improved colorectal cancer care in Massachusetts, and may do the same for other states that participate in Medicaid expansion under the Affordable Care Act.
That assertion comes from investigators at Massachusetts General Hospital in Boston. They found that following the introduction in 2006 of a universal health insurance law in the Bay State – the law that would serve as a model for the Affordable Care Act – the rate of elective colorectal resections increased while the rate of emergent resections decreased.
In contrast, in three states used as controls, the opposite occurred.

“This could be due to a variety of different factors, including earlier diagnosis, presenting with disease more amenable to surgical resection. It could also be due to increased referrals from primary care providers or GI doctors,” said Dr. Andrew P. Loehrer from the Massachusetts General Hospital Department of Surgery, at the annual Society of Surgical Oncology Cancer Symposium.
He acknowledged, however, that the administrative dataset he and his colleagues used in the study lacks information about clinical staging or use of neoadjuvant therapy, making it difficult to determine whether insured patients actually present at an earlier, more readily treatable disease stage.
Nonetheless, “from a cancer standpoint, my study provides early, hopeful evidence. In order to definitively say that this improves care, we need to have some more of the cancer-specific variables, but with this study, combined with some other work that we and other groups have done, we see that patients in Massachusetts are presenting with earlier stage disease, whether it’s acute disease or cancer, and they’re getting more appropriate care in a more timely fashion,” he said in an interview.
Role model
Dr. Loehrer noted that disparities in access to health care have been shown in previous studies to be associated with the likelihood of unfavorable outcomes for patients with colorectal cancer. For example, a 2008 study (Lancet Oncol. 2008 Mar;9:222-31) showed that uninsured patients with colorectal cancer had a twofold greater risk for presenting with advanced disease than privately insured patients. Additionally, a 2004 study (Br J Surg. 91:605-9) showed that patients who presented with colorectal cancer requiring emergent resection had significantly lower 5-year overall survival than patients who underwent elective resection.
Massachusetts implemented its pioneering health insurance reform law in 2006. The law increased eligibility for persons with incomes up to 150% of the Federal Poverty Level, created government-subsidized insurance for those with incomes from 150% to 300% of the poverty line, mandated that all Bay State residents have some form of health insurance, and allowed young adults up to the age of 26 to remain on their parents’ plans.
To see whether insurance reform could have a salutary effect on cancer care, the investigators drew on Agency for Health Research and Quality (AHRQ) State Inpatient Databases for Massachusetts and for Florida, New Jersey, and New York as control states. They used ICD-9 diagnosis codes to identify patients with colorectal cancer, including those who underwent resection.
To establish procedure rates, they used U.S. Census Bureau data to establish the population of denominators, which included all adults 18-54 years of age who were insured either through Medicaid, Commonwealth Care (in Massachusetts), or were listed as uninsured or self-pay. Medicare-insured patients were not included, as they were not directly affected by the reform law.
They identified 18,598 patients admitted to Massachusetts hospitals for colorectal cancer from 2001 through 2011, and 147,482 admitted during the same period to hospitals in the control states.
The authors created Poisson difference-in-differences models which compare changes in the selected outcomes in Massachusetts with changes in the control states. The models were adjusted for age, sex, race, hospital type, and secular trends.
They found that admission rates for colorectal cancer increased over time in Massachusetts by 13.3 per 100,000 residents per quarter, compared with 8.3/100,000 in the control states, translating into an adjusted rate ratio (ARR) of 1.13. Resection rates for cancer, the primary study outcome, also grew by a significantly larger margin in Massachusetts, by 5.5/100,000, compared with 0.5/100,000 in control states, with an ARR of 1.37 (P less than .001 for both comparisons).
For the secondary outcome of changes in emergent and elective resections after admission, they found that emergent surgeries in Massachusetts declined by 2.7/100,000, but increased by 4.4/100,000 in the states without insurance reform. Similarly, elective resections after admission increased in the Bay State by 7.4/100,000, but decreased by 1.8/100,000 in control states.
Relative to controls, the adjusted probability that a patient with colorectal cancer in Massachusetts would have emergent surgery after admission declined by 6.1% (P = .014) and the probability that he or she would have elective resection increased by 7.8% (P = .005).
An analysis of the odds ratio of resection during admission, adjusted for age, race, presentation with metastatic disease, hospital type, and secular trends, showed that prior to reform uninsured patients in both Massachusetts and control states were significantly less likely than privately insured patients to have resections (odds ratio, 0.42 in Mass.; 0.45 in control states).
However, after the implementation of reform the gap between previously uninsured and privately insured in Massachusetts narrowed (OR, 0.63) but remained the same in control states (OR, 0.44).
Dr. Loehrer acknowledged in an interview that Massachusetts differs from other states in some regards, including in concentrations of health providers and in requirements for insurance coverage that were in place even before the 2006 reforms, but is optimistic that improvements in colorectal cancer care can occur in states that have embraced the Affordable Care Act.
“There are a lot of services that were available and we had high colonoscopy rates prior to all of this, but that said, the mechanism is exactly the same, there are still vulnerable populations, and at this point I think it’s hopeful and promising that we will see similar results in other states,” he said.
BOSTON – Expanding access to health insurance for low- and moderate-income families has apparently improved colorectal cancer care in Massachusetts, and may do the same for other states that participate in Medicaid expansion under the Affordable Care Act.
That assertion comes from investigators at Massachusetts General Hospital in Boston. They found that following the introduction in 2006 of a universal health insurance law in the Bay State – the law that would serve as a model for the Affordable Care Act – the rate of elective colorectal resections increased while the rate of emergent resections decreased.
In contrast, in three states used as controls, the opposite occurred.
“This could be due to a variety of different factors, including earlier diagnosis, presenting with disease more amenable to surgical resection. It could also be due to increased referrals from primary care providers or GI doctors,” said Dr. Andrew P. Loehrer from the Massachusetts General Hospital Department of Surgery, at the annual Society of Surgical Oncology Cancer Symposium.
He acknowledged, however, that the administrative dataset he and his colleagues used in the study lacks information about clinical staging or use of neoadjuvant therapy, making it difficult to determine whether insured patients actually present at an earlier, more readily treatable disease stage.
Nonetheless, “from a cancer standpoint, my study provides early, hopeful evidence. In order to definitively say that this improves care, we need to have some more of the cancer-specific variables, but with this study, combined with some other work that we and other groups have done, we see that patients in Massachusetts are presenting with earlier stage disease, whether it’s acute disease or cancer, and they’re getting more appropriate care in a more timely fashion,” he said in an interview.
Role model
Dr. Loehrer noted that disparities in access to health care have been shown in previous studies to be associated with the likelihood of unfavorable outcomes for patients with colorectal cancer. For example, a 2008 study (Lancet Oncol. 2008 Mar;9:222-31) showed that uninsured patients with colorectal cancer had a twofold greater risk for presenting with advanced disease than privately insured patients. Additionally, a 2004 study (Br J Surg. 91:605-9) showed that patients who presented with colorectal cancer requiring emergent resection had significantly lower 5-year overall survival than patients who underwent elective resection.
Massachusetts implemented its pioneering health insurance reform law in 2006. The law increased eligibility for persons with incomes up to 150% of the Federal Poverty Level, created government-subsidized insurance for those with incomes from 150% to 300% of the poverty line, mandated that all Bay State residents have some form of health insurance, and allowed young adults up to the age of 26 to remain on their parents’ plans.
To see whether insurance reform could have a salutary effect on cancer care, the investigators drew on Agency for Health Research and Quality (AHRQ) State Inpatient Databases for Massachusetts and for Florida, New Jersey, and New York as control states. They used ICD-9 diagnosis codes to identify patients with colorectal cancer, including those who underwent resection.
To establish procedure rates, they used U.S. Census Bureau data to establish the population of denominators, which included all adults 18-54 years of age who were insured either through Medicaid, Commonwealth Care (in Massachusetts), or were listed as uninsured or self-pay. Medicare-insured patients were not included, as they were not directly affected by the reform law.
They identified 18,598 patients admitted to Massachusetts hospitals for colorectal cancer from 2001 through 2011, and 147,482 admitted during the same period to hospitals in the control states.
The authors created Poisson difference-in-differences models which compare changes in the selected outcomes in Massachusetts with changes in the control states. The models were adjusted for age, sex, race, hospital type, and secular trends.
They found that admission rates for colorectal cancer increased over time in Massachusetts by 13.3 per 100,000 residents per quarter, compared with 8.3/100,000 in the control states, translating into an adjusted rate ratio (ARR) of 1.13. Resection rates for cancer, the primary study outcome, also grew by a significantly larger margin in Massachusetts, by 5.5/100,000, compared with 0.5/100,000 in control states, with an ARR of 1.37 (P less than .001 for both comparisons).
For the secondary outcome of changes in emergent and elective resections after admission, they found that emergent surgeries in Massachusetts declined by 2.7/100,000, but increased by 4.4/100,000 in the states without insurance reform. Similarly, elective resections after admission increased in the Bay State by 7.4/100,000, but decreased by 1.8/100,000 in control states.
Relative to controls, the adjusted probability that a patient with colorectal cancer in Massachusetts would have emergent surgery after admission declined by 6.1% (P = .014) and the probability that he or she would have elective resection increased by 7.8% (P = .005).
An analysis of the odds ratio of resection during admission, adjusted for age, race, presentation with metastatic disease, hospital type, and secular trends, showed that prior to reform uninsured patients in both Massachusetts and control states were significantly less likely than privately insured patients to have resections (odds ratio, 0.42 in Mass.; 0.45 in control states).
However, after the implementation of reform the gap between previously uninsured and privately insured in Massachusetts narrowed (OR, 0.63) but remained the same in control states (OR, 0.44).
Dr. Loehrer acknowledged in an interview that Massachusetts differs from other states in some regards, including in concentrations of health providers and in requirements for insurance coverage that were in place even before the 2006 reforms, but is optimistic that improvements in colorectal cancer care can occur in states that have embraced the Affordable Care Act.
“There are a lot of services that were available and we had high colonoscopy rates prior to all of this, but that said, the mechanism is exactly the same, there are still vulnerable populations, and at this point I think it’s hopeful and promising that we will see similar results in other states,” he said.
BOSTON – Expanding access to health insurance for low- and moderate-income families has apparently improved colorectal cancer care in Massachusetts, and may do the same for other states that participate in Medicaid expansion under the Affordable Care Act.
That assertion comes from investigators at Massachusetts General Hospital in Boston. They found that following the introduction in 2006 of a universal health insurance law in the Bay State – the law that would serve as a model for the Affordable Care Act – the rate of elective colorectal resections increased while the rate of emergent resections decreased.
In contrast, in three states used as controls, the opposite occurred.
“This could be due to a variety of different factors, including earlier diagnosis, presenting with disease more amenable to surgical resection. It could also be due to increased referrals from primary care providers or GI doctors,” said Dr. Andrew P. Loehrer from the Massachusetts General Hospital Department of Surgery, at the annual Society of Surgical Oncology Cancer Symposium.
He acknowledged, however, that the administrative dataset he and his colleagues used in the study lacks information about clinical staging or use of neoadjuvant therapy, making it difficult to determine whether insured patients actually present at an earlier, more readily treatable disease stage.
Nonetheless, “from a cancer standpoint, my study provides early, hopeful evidence. In order to definitively say that this improves care, we need to have some more of the cancer-specific variables, but with this study, combined with some other work that we and other groups have done, we see that patients in Massachusetts are presenting with earlier stage disease, whether it’s acute disease or cancer, and they’re getting more appropriate care in a more timely fashion,” he said in an interview.
Role model
Dr. Loehrer noted that disparities in access to health care have been shown in previous studies to be associated with the likelihood of unfavorable outcomes for patients with colorectal cancer. For example, a 2008 study (Lancet Oncol. 2008 Mar;9:222-31) showed that uninsured patients with colorectal cancer had a twofold greater risk for presenting with advanced disease than privately insured patients. Additionally, a 2004 study (Br J Surg. 91:605-9) showed that patients who presented with colorectal cancer requiring emergent resection had significantly lower 5-year overall survival than patients who underwent elective resection.
Massachusetts implemented its pioneering health insurance reform law in 2006. The law increased eligibility for persons with incomes up to 150% of the Federal Poverty Level, created government-subsidized insurance for those with incomes from 150% to 300% of the poverty line, mandated that all Bay State residents have some form of health insurance, and allowed young adults up to the age of 26 to remain on their parents’ plans.
To see whether insurance reform could have a salutary effect on cancer care, the investigators drew on Agency for Health Research and Quality (AHRQ) State Inpatient Databases for Massachusetts and for Florida, New Jersey, and New York as control states. They used ICD-9 diagnosis codes to identify patients with colorectal cancer, including those who underwent resection.
To establish procedure rates, they used U.S. Census Bureau data to establish the population of denominators, which included all adults 18-54 years of age who were insured either through Medicaid, Commonwealth Care (in Massachusetts), or were listed as uninsured or self-pay. Medicare-insured patients were not included, as they were not directly affected by the reform law.
They identified 18,598 patients admitted to Massachusetts hospitals for colorectal cancer from 2001 through 2011, and 147,482 admitted during the same period to hospitals in the control states.
The authors created Poisson difference-in-differences models which compare changes in the selected outcomes in Massachusetts with changes in the control states. The models were adjusted for age, sex, race, hospital type, and secular trends.
They found that admission rates for colorectal cancer increased over time in Massachusetts by 13.3 per 100,000 residents per quarter, compared with 8.3/100,000 in the control states, translating into an adjusted rate ratio (ARR) of 1.13. Resection rates for cancer, the primary study outcome, also grew by a significantly larger margin in Massachusetts, by 5.5/100,000, compared with 0.5/100,000 in control states, with an ARR of 1.37 (P less than .001 for both comparisons).
For the secondary outcome of changes in emergent and elective resections after admission, they found that emergent surgeries in Massachusetts declined by 2.7/100,000, but increased by 4.4/100,000 in the states without insurance reform. Similarly, elective resections after admission increased in the Bay State by 7.4/100,000, but decreased by 1.8/100,000 in control states.
Relative to controls, the adjusted probability that a patient with colorectal cancer in Massachusetts would have emergent surgery after admission declined by 6.1% (P = .014) and the probability that he or she would have elective resection increased by 7.8% (P = .005).
An analysis of the odds ratio of resection during admission, adjusted for age, race, presentation with metastatic disease, hospital type, and secular trends, showed that prior to reform uninsured patients in both Massachusetts and control states were significantly less likely than privately insured patients to have resections (odds ratio, 0.42 in Mass.; 0.45 in control states).
However, after the implementation of reform the gap between previously uninsured and privately insured in Massachusetts narrowed (OR, 0.63) but remained the same in control states (OR, 0.44).
Dr. Loehrer acknowledged in an interview that Massachusetts differs from other states in some regards, including in concentrations of health providers and in requirements for insurance coverage that were in place even before the 2006 reforms, but is optimistic that improvements in colorectal cancer care can occur in states that have embraced the Affordable Care Act.
“There are a lot of services that were available and we had high colonoscopy rates prior to all of this, but that said, the mechanism is exactly the same, there are still vulnerable populations, and at this point I think it’s hopeful and promising that we will see similar results in other states,” he said.
FROM SSO 2016
Key clinical point: Outcomes for patients with colorectal cancer (CRC) who undergo elective resection are better than for those who require emergent resections.
Major finding: Elective CRC resection rates increased and emergent resections decreased after universal insurance was instituted in Massachusetts in 2006.
Data source: Retrospective study comparing differences over time between CRC resection rates in Massachusetts vs. those in Florida, New Jersey, and New York.
Disclosures: The study was supported in part by a grant from the National Institute on Aging. Dr. Loehrer and his coauthors reported no conflicts of interest.

AAAAI: Albuterol dry powder inhaler offers simplified approach for young kids
LOS ANGELES – Young asthmatic children on bronchodilator therapy may soon gain access to a novel albuterol multidose dry powder inhaler that’s already proved popular with teen and adult patients with reversible obstructive airway disease because of its ease of use.
A phase III randomized, double-blind multicenter trial of the albuterol multidose dry powder inhaler (MDPI) versus placebo in 184 asthmatic children aged 4-11 years not on systemic corticosteroids met its primary and secondary lung function endpoints, with safety and tolerability similar to placebo, Dr. Tushar P. Shah reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

The albuterol MDPI is already marketed by Teva Pharmaceuticals as the ProAir RespiClick in patients aged 12 and older. The purpose of this phase III clinical trial was to obtain an expanded indication in 4- to 11-year-olds. The company has submitted its request to the Food and Drug Administration and anticipates smooth sailing based upon the new data, according to Dr. Shah, senior vice president for global respiratory research and development at Teva in Frazer, Pa.
The albuterol MDPI fills an unmet need for a simplified approach to rescue medication, the allergist said in an interview.
“This is a breath-actuated inhaler. Many patients – especially kids – have a hard time coordinating a conventional multidose inhaler actuation with inhalation. They have trouble getting the timing right, so the drug doesn’t get to the distal lung. That’s why this albuterol MDPI has been very well received in adults. For kids, I think it’s going to be even better because this is a very simple and intuitive device. All they do is open the cap, inhale, [and] close the cap,” he explained.
The young study participants used the albuterol MDPI at two inhalations four times daily, with a total daily albuterol dose of 720 mcg.
The primary study endpoint was the short-term improvement in lung function seen during testing performed after the very first study dose and again after the final dose of medication 3 weeks later. This was expressed as the area under the baseline-adjusted percent-predicted forced expiratory volume in 1 second effect-time curve from predose to 6 hours post dose. On both occasions, a sharp jump in opening of the airways was demonstrated within 5 minutes of dosing, with the effect remaining significantly better than with placebo for more than 2 hours.
Moreover, the maximum change from baseline in peak expiratory flow rate seen within 2 hours after dosing was a 26% increase with the albuterol MDPI, a significantly better result than the 14% increase with placebo.
No adverse events attributable to the study drug were seen.
The study was sponsored by Teva Pharmaceuticals. The presenter is a senior company employee.
LOS ANGELES – Young asthmatic children on bronchodilator therapy may soon gain access to a novel albuterol multidose dry powder inhaler that’s already proved popular with teen and adult patients with reversible obstructive airway disease because of its ease of use.
A phase III randomized, double-blind multicenter trial of the albuterol multidose dry powder inhaler (MDPI) versus placebo in 184 asthmatic children aged 4-11 years not on systemic corticosteroids met its primary and secondary lung function endpoints, with safety and tolerability similar to placebo, Dr. Tushar P. Shah reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The albuterol MDPI is already marketed by Teva Pharmaceuticals as the ProAir RespiClick in patients aged 12 and older. The purpose of this phase III clinical trial was to obtain an expanded indication in 4- to 11-year-olds. The company has submitted its request to the Food and Drug Administration and anticipates smooth sailing based upon the new data, according to Dr. Shah, senior vice president for global respiratory research and development at Teva in Frazer, Pa.
The albuterol MDPI fills an unmet need for a simplified approach to rescue medication, the allergist said in an interview.
“This is a breath-actuated inhaler. Many patients – especially kids – have a hard time coordinating a conventional multidose inhaler actuation with inhalation. They have trouble getting the timing right, so the drug doesn’t get to the distal lung. That’s why this albuterol MDPI has been very well received in adults. For kids, I think it’s going to be even better because this is a very simple and intuitive device. All they do is open the cap, inhale, [and] close the cap,” he explained.
The young study participants used the albuterol MDPI at two inhalations four times daily, with a total daily albuterol dose of 720 mcg.
The primary study endpoint was the short-term improvement in lung function seen during testing performed after the very first study dose and again after the final dose of medication 3 weeks later. This was expressed as the area under the baseline-adjusted percent-predicted forced expiratory volume in 1 second effect-time curve from predose to 6 hours post dose. On both occasions, a sharp jump in opening of the airways was demonstrated within 5 minutes of dosing, with the effect remaining significantly better than with placebo for more than 2 hours.
Moreover, the maximum change from baseline in peak expiratory flow rate seen within 2 hours after dosing was a 26% increase with the albuterol MDPI, a significantly better result than the 14% increase with placebo.
No adverse events attributable to the study drug were seen.
The study was sponsored by Teva Pharmaceuticals. The presenter is a senior company employee.
LOS ANGELES – Young asthmatic children on bronchodilator therapy may soon gain access to a novel albuterol multidose dry powder inhaler that’s already proved popular with teen and adult patients with reversible obstructive airway disease because of its ease of use.
A phase III randomized, double-blind multicenter trial of the albuterol multidose dry powder inhaler (MDPI) versus placebo in 184 asthmatic children aged 4-11 years not on systemic corticosteroids met its primary and secondary lung function endpoints, with safety and tolerability similar to placebo, Dr. Tushar P. Shah reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The albuterol MDPI is already marketed by Teva Pharmaceuticals as the ProAir RespiClick in patients aged 12 and older. The purpose of this phase III clinical trial was to obtain an expanded indication in 4- to 11-year-olds. The company has submitted its request to the Food and Drug Administration and anticipates smooth sailing based upon the new data, according to Dr. Shah, senior vice president for global respiratory research and development at Teva in Frazer, Pa.
The albuterol MDPI fills an unmet need for a simplified approach to rescue medication, the allergist said in an interview.
“This is a breath-actuated inhaler. Many patients – especially kids – have a hard time coordinating a conventional multidose inhaler actuation with inhalation. They have trouble getting the timing right, so the drug doesn’t get to the distal lung. That’s why this albuterol MDPI has been very well received in adults. For kids, I think it’s going to be even better because this is a very simple and intuitive device. All they do is open the cap, inhale, [and] close the cap,” he explained.
The young study participants used the albuterol MDPI at two inhalations four times daily, with a total daily albuterol dose of 720 mcg.
The primary study endpoint was the short-term improvement in lung function seen during testing performed after the very first study dose and again after the final dose of medication 3 weeks later. This was expressed as the area under the baseline-adjusted percent-predicted forced expiratory volume in 1 second effect-time curve from predose to 6 hours post dose. On both occasions, a sharp jump in opening of the airways was demonstrated within 5 minutes of dosing, with the effect remaining significantly better than with placebo for more than 2 hours.
Moreover, the maximum change from baseline in peak expiratory flow rate seen within 2 hours after dosing was a 26% increase with the albuterol MDPI, a significantly better result than the 14% increase with placebo.
No adverse events attributable to the study drug were seen.
The study was sponsored by Teva Pharmaceuticals. The presenter is a senior company employee.
AT 2016 AAAAI ANNUAL MEETING
Key clinical point: The albuterol multidose dry powder inhaler that’s now indicated for asthma patients aged 12 years and older may become available to those aged 4-11 years.
Major finding: Lung function measurements improved sharply within 5 minutes after dosing with this bronchodilator used for acute symptom relief, with the effect lasting for longer than 2 hours.
Data source: A phase III, double-blind, multicenter, placebo-controlled randomized trial involving 184 asthmatic children aged 4-11 years.
Disclosures: The study was sponsored by Teva Pharmaceuticals. The presenter is a senior company employee.

HM16 Session Analysis: Update in Pulmonary Medicine
Presenter: Daniel D. Dressler, MD, MSc, SFHM
Summary: This presentation focused on pulmonary updates specific to hospitalist practice, from end of 2014 to early 2016.
New research on community-acquired pneumonia suggest that only 38% of cases a presumptive pathogen will be isolated. Virus account for 23%, bacteria 11% (including S. pneumonia, S. Aureus and Enterobacteriaceae), both (virus and bacteria) 3%, and fungus or mycobacterium 1%. It is important to notice no recent data on etiology was available since mid-1990.
There is also a new pragmatic trial suggesting that B-lactam monotherapy is not inferior to either B-lactam in combination with macrolides or fluoroquinolones. The study reported an 11%, 90-day mortality with B-lactam monotherapy compared with 11% when combined with macrolides and 8.8% when using quinolones monotherapy.
Update evidence supports the use of corticosteroids for hospitalized patients with community-acquired pneumonia, at a dose of 20-60 mg day for 5-7 days. The study showed decreased mortality in patients with clinical criteria for severe pneumonia with NNT 7; it also showed decrease need for mechanical ventilation and development of ARDS.
An additional, interesting finding was a decrease in length of stay (LOS) in the steroid group. In patients with acute hypoxemic respiratory failure, high flow nasal cannula reduced mortality and likely reduces intubation in severely hypoxemic patients when compared to NPPV.
In patients with first unprovoked VTE, extending anticoagulation to two years or adding aspirin after initial anticoagulation might reduce recurrent VTE without significant increasing in risk for major bleeding.
Key Takeaways:
- B-lactam monotherapy for hospitalized non-ICU CAP might be reasonable choice.
- Moderate short course of steroids in CAP, reduce ARDS, intubation, LOS in all hospitalized patients (and mortality on severe CAP)
- A trial of high flow NC is indicated in acute hypoxemic respiratory failure
- Aspirin prophylaxis following anticoagulation (most benefit first year), or extended anticoagulation for 2 years reduce recurrent VTE without much additional bleeding risk.
Dr. Villagra is a hospitalist in Batesville, Ark., and a member of Team Hospitalist.
Presenter: Daniel D. Dressler, MD, MSc, SFHM
Summary: This presentation focused on pulmonary updates specific to hospitalist practice, from end of 2014 to early 2016.
New research on community-acquired pneumonia suggest that only 38% of cases a presumptive pathogen will be isolated. Virus account for 23%, bacteria 11% (including S. pneumonia, S. Aureus and Enterobacteriaceae), both (virus and bacteria) 3%, and fungus or mycobacterium 1%. It is important to notice no recent data on etiology was available since mid-1990.
There is also a new pragmatic trial suggesting that B-lactam monotherapy is not inferior to either B-lactam in combination with macrolides or fluoroquinolones. The study reported an 11%, 90-day mortality with B-lactam monotherapy compared with 11% when combined with macrolides and 8.8% when using quinolones monotherapy.
Update evidence supports the use of corticosteroids for hospitalized patients with community-acquired pneumonia, at a dose of 20-60 mg day for 5-7 days. The study showed decreased mortality in patients with clinical criteria for severe pneumonia with NNT 7; it also showed decrease need for mechanical ventilation and development of ARDS.
An additional, interesting finding was a decrease in length of stay (LOS) in the steroid group. In patients with acute hypoxemic respiratory failure, high flow nasal cannula reduced mortality and likely reduces intubation in severely hypoxemic patients when compared to NPPV.
In patients with first unprovoked VTE, extending anticoagulation to two years or adding aspirin after initial anticoagulation might reduce recurrent VTE without significant increasing in risk for major bleeding.
Key Takeaways:
- B-lactam monotherapy for hospitalized non-ICU CAP might be reasonable choice.
- Moderate short course of steroids in CAP, reduce ARDS, intubation, LOS in all hospitalized patients (and mortality on severe CAP)
- A trial of high flow NC is indicated in acute hypoxemic respiratory failure
- Aspirin prophylaxis following anticoagulation (most benefit first year), or extended anticoagulation for 2 years reduce recurrent VTE without much additional bleeding risk.
Dr. Villagra is a hospitalist in Batesville, Ark., and a member of Team Hospitalist.
Presenter: Daniel D. Dressler, MD, MSc, SFHM
Summary: This presentation focused on pulmonary updates specific to hospitalist practice, from end of 2014 to early 2016.
New research on community-acquired pneumonia suggest that only 38% of cases a presumptive pathogen will be isolated. Virus account for 23%, bacteria 11% (including S. pneumonia, S. Aureus and Enterobacteriaceae), both (virus and bacteria) 3%, and fungus or mycobacterium 1%. It is important to notice no recent data on etiology was available since mid-1990.
There is also a new pragmatic trial suggesting that B-lactam monotherapy is not inferior to either B-lactam in combination with macrolides or fluoroquinolones. The study reported an 11%, 90-day mortality with B-lactam monotherapy compared with 11% when combined with macrolides and 8.8% when using quinolones monotherapy.
Update evidence supports the use of corticosteroids for hospitalized patients with community-acquired pneumonia, at a dose of 20-60 mg day for 5-7 days. The study showed decreased mortality in patients with clinical criteria for severe pneumonia with NNT 7; it also showed decrease need for mechanical ventilation and development of ARDS.
An additional, interesting finding was a decrease in length of stay (LOS) in the steroid group. In patients with acute hypoxemic respiratory failure, high flow nasal cannula reduced mortality and likely reduces intubation in severely hypoxemic patients when compared to NPPV.
In patients with first unprovoked VTE, extending anticoagulation to two years or adding aspirin after initial anticoagulation might reduce recurrent VTE without significant increasing in risk for major bleeding.
Key Takeaways:
- B-lactam monotherapy for hospitalized non-ICU CAP might be reasonable choice.
- Moderate short course of steroids in CAP, reduce ARDS, intubation, LOS in all hospitalized patients (and mortality on severe CAP)
- A trial of high flow NC is indicated in acute hypoxemic respiratory failure
- Aspirin prophylaxis following anticoagulation (most benefit first year), or extended anticoagulation for 2 years reduce recurrent VTE without much additional bleeding risk.
Dr. Villagra is a hospitalist in Batesville, Ark., and a member of Team Hospitalist.
WATCH: It's All in Your Hospitalist Contract
Steve Harris, Esq., legal columnist for The Hospitalist, explains the ins and outs of a hospitalist contract.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Steve Harris, Esq., legal columnist for The Hospitalist, explains the ins and outs of a hospitalist contract.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Steve Harris, Esq., legal columnist for The Hospitalist, explains the ins and outs of a hospitalist contract.