User login
Laparoscopic salpingectomy and cornual resection repurposed
I am pleased to introduce this month’s video, from the Division of Minimally Invasive Gynecologic Surgery (MIGS) at Penn State. Dr. Michelle Pacis addresses an increasingly important topic to MIGS surgeons: removal of previously hysteroscopically placed tubal occlusion devices. These devices offer a permanent alterative to laparoscopic sterilization. If women require their removal, however, whether desired or because of complications, gynecologic surgeons must be familiar with the steps involved.
The following video was produced in order to demonstrate a reproducible technique for laparoscopic removal of a device for women requesting this procedure. Key objectives of the video include:
- review of the techniques available to remove hysteroscopic tubal occlusion devices, as well as the contraindications and advantages/disadvantages of these approaches.
- discuss recommended imaging and materials required for the technique described and tips for their use.
- demonstrate salpingectomy and repair technique.
I hope that you find this month’s video helpful to your surgical practice.

Share your thoughts on this video! Send your Letter to the Editor to [email protected]
I am pleased to introduce this month’s video, from the Division of Minimally Invasive Gynecologic Surgery (MIGS) at Penn State. Dr. Michelle Pacis addresses an increasingly important topic to MIGS surgeons: removal of previously hysteroscopically placed tubal occlusion devices. These devices offer a permanent alterative to laparoscopic sterilization. If women require their removal, however, whether desired or because of complications, gynecologic surgeons must be familiar with the steps involved.
The following video was produced in order to demonstrate a reproducible technique for laparoscopic removal of a device for women requesting this procedure. Key objectives of the video include:
- review of the techniques available to remove hysteroscopic tubal occlusion devices, as well as the contraindications and advantages/disadvantages of these approaches.
- discuss recommended imaging and materials required for the technique described and tips for their use.
- demonstrate salpingectomy and repair technique.
I hope that you find this month’s video helpful to your surgical practice.
Share your thoughts on this video! Send your Letter to the Editor to [email protected]
I am pleased to introduce this month’s video, from the Division of Minimally Invasive Gynecologic Surgery (MIGS) at Penn State. Dr. Michelle Pacis addresses an increasingly important topic to MIGS surgeons: removal of previously hysteroscopically placed tubal occlusion devices. These devices offer a permanent alterative to laparoscopic sterilization. If women require their removal, however, whether desired or because of complications, gynecologic surgeons must be familiar with the steps involved.
The following video was produced in order to demonstrate a reproducible technique for laparoscopic removal of a device for women requesting this procedure. Key objectives of the video include:
- review of the techniques available to remove hysteroscopic tubal occlusion devices, as well as the contraindications and advantages/disadvantages of these approaches.
- discuss recommended imaging and materials required for the technique described and tips for their use.
- demonstrate salpingectomy and repair technique.
I hope that you find this month’s video helpful to your surgical practice.
Share your thoughts on this video! Send your Letter to the Editor to [email protected]

Team documentation—the good, the surprising
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
In this Article
- Scribing vs team documentation
- How has the physician’s role changed?

Public speaking fundamentals. Preparation: Tips that lead to a solid, engaging presentation

Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
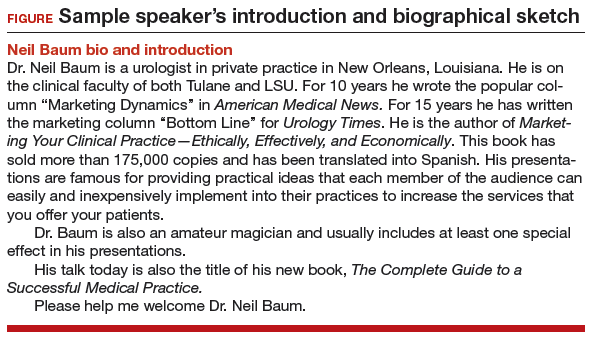
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
Mickey M. Karram, MD, and Neil H. Baum, MD

Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.

Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Mickey M. Karram, MD, and Neil H. Baum, MD
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Mickey M. Karram, MD, and Neil H. Baum, MD
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
In this Article
- Preparing a presentation
- Your speech opening
- AV equipment and support
Malaria vaccine disappoints in phase II trial
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.

“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.
“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.
“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: An investigational malaria vaccine lost efficacy over a 7-year period, and was associated with increased cases in late follow-up.
Major finding: Vaccine efficacy waned from 36% to 2.5% over 7 years, when 141 excess cases per 1,000 children were observed.
Data source: The phase II study randomized 447 children to three doses of the malaria vaccine or a control rabies vaccine.
Disclosures: The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.

Does influenza immunization during pregnancy confer flu protection to newborns?
A recent report on data obtained from the Intermountain Healthcare facilities in Utah and Idaho suggests that maternal influenza vaccination, besides its maternal protective effect, also may benefit the newborn by protecting against influenza. I think that ObGyns generally accept the notion that influenza vaccination has defined maternal benefit. Notably, acceptance of influenza vaccine became much more widespread during and following the H1N1 flu pandemic of 2009. The fact that there may be neonatal and infant benefit as well is certainly not objectionable, especially since flu vaccine is not recommended for infants less than 6 months of age.
Details of the study
Shakib and colleagues’ goal was to compare influenza outcomes in infants younger than 6 months born to women who self-reported receiving or not receiving influenza vaccine during pregnancy. The study cohort included 245,386 women and 249,387 infants who were born between December 2005 and March 2014. The outcomes studied were influenza-like illness (ILI), laboratory-confirmed influenza, and influenza hospitalizations.
Of 866 infants younger than 6 months born to women who had received a flu shot, 32 had 1 or more ILI encounters, compared with 834 born to women who were not immunized (relative risk [RR], 0.36; 95% confidence interval [CI], 0.26–0.52; P<.001). Laboratory-confirmed influenza was identified in 658 infants; of these, 20 were born to women reporting immunization and 638 were born to unimmunized women (RR, 0.30; 95% CI, 0.19–0.46; P<.001). Finally, 151 infants with laboratory-confirmed influenza were hospitalized; 3 were born to immunized women and 148 to women who had not received a flu shot (RR, 0.19; 95% CI, 0.06–0.60; P = .005).
The authors calculated that infants born to women who reported influenza immunization during pregnancy had risk reductions of 64% for ILI, 70% for laboratory-confirmed influenza, and 81% for influenza hospitalizations.
Consider immunization benefits realistically
The authors state in their published report that “Protecting young infants from influenza through maternal immunization during pregnancy is a public health priority.” This may be overstating their case, for the following reasons. First, influenza vaccine has varying degrees of efficacy depending on the particular year and influenza strains that predominate, and it never has been shown to be entirely protective. Second, when looking only at this study’s laboratory-proven cases of influenza in newborns, infants whose mothers were vaccinated had a case rate of 0.84/1,000, while the case rate in newborns born to unvaccinated women was 2.83/1,000. While this shows a difference, the report provides no additional outcome data regarding morbidity or mortality.
In fact, although infant hospitalization rates differed (0.13/1,000 born to vaccinated women versus 0.66/1,000 born to unvaccinated women), there were no influenza-related mortalities in this cohort. The effect seems better when including “influenza-like illness,” but it is unclear why we should think that the influenza vaccine protects against infection that is not caused by influenza.
What this EVIDENCE means for practice
ObGyns should continue to promote influenza vaccination during pregnancy for the maternal protection it imparts. These new data on the potential for newborn protection, although not conclusive, may improve maternal acceptance of vaccination; from that perspective, these data are valuable.
— John T. Repke, MD
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
A recent report on data obtained from the Intermountain Healthcare facilities in Utah and Idaho suggests that maternal influenza vaccination, besides its maternal protective effect, also may benefit the newborn by protecting against influenza. I think that ObGyns generally accept the notion that influenza vaccination has defined maternal benefit. Notably, acceptance of influenza vaccine became much more widespread during and following the H1N1 flu pandemic of 2009. The fact that there may be neonatal and infant benefit as well is certainly not objectionable, especially since flu vaccine is not recommended for infants less than 6 months of age.
Details of the study
Shakib and colleagues’ goal was to compare influenza outcomes in infants younger than 6 months born to women who self-reported receiving or not receiving influenza vaccine during pregnancy. The study cohort included 245,386 women and 249,387 infants who were born between December 2005 and March 2014. The outcomes studied were influenza-like illness (ILI), laboratory-confirmed influenza, and influenza hospitalizations.
Of 866 infants younger than 6 months born to women who had received a flu shot, 32 had 1 or more ILI encounters, compared with 834 born to women who were not immunized (relative risk [RR], 0.36; 95% confidence interval [CI], 0.26–0.52; P<.001). Laboratory-confirmed influenza was identified in 658 infants; of these, 20 were born to women reporting immunization and 638 were born to unimmunized women (RR, 0.30; 95% CI, 0.19–0.46; P<.001). Finally, 151 infants with laboratory-confirmed influenza were hospitalized; 3 were born to immunized women and 148 to women who had not received a flu shot (RR, 0.19; 95% CI, 0.06–0.60; P = .005).
The authors calculated that infants born to women who reported influenza immunization during pregnancy had risk reductions of 64% for ILI, 70% for laboratory-confirmed influenza, and 81% for influenza hospitalizations.
Consider immunization benefits realistically
The authors state in their published report that “Protecting young infants from influenza through maternal immunization during pregnancy is a public health priority.” This may be overstating their case, for the following reasons. First, influenza vaccine has varying degrees of efficacy depending on the particular year and influenza strains that predominate, and it never has been shown to be entirely protective. Second, when looking only at this study’s laboratory-proven cases of influenza in newborns, infants whose mothers were vaccinated had a case rate of 0.84/1,000, while the case rate in newborns born to unvaccinated women was 2.83/1,000. While this shows a difference, the report provides no additional outcome data regarding morbidity or mortality.
In fact, although infant hospitalization rates differed (0.13/1,000 born to vaccinated women versus 0.66/1,000 born to unvaccinated women), there were no influenza-related mortalities in this cohort. The effect seems better when including “influenza-like illness,” but it is unclear why we should think that the influenza vaccine protects against infection that is not caused by influenza.
What this EVIDENCE means for practice
ObGyns should continue to promote influenza vaccination during pregnancy for the maternal protection it imparts. These new data on the potential for newborn protection, although not conclusive, may improve maternal acceptance of vaccination; from that perspective, these data are valuable.
— John T. Repke, MD
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
A recent report on data obtained from the Intermountain Healthcare facilities in Utah and Idaho suggests that maternal influenza vaccination, besides its maternal protective effect, also may benefit the newborn by protecting against influenza. I think that ObGyns generally accept the notion that influenza vaccination has defined maternal benefit. Notably, acceptance of influenza vaccine became much more widespread during and following the H1N1 flu pandemic of 2009. The fact that there may be neonatal and infant benefit as well is certainly not objectionable, especially since flu vaccine is not recommended for infants less than 6 months of age.
Details of the study
Shakib and colleagues’ goal was to compare influenza outcomes in infants younger than 6 months born to women who self-reported receiving or not receiving influenza vaccine during pregnancy. The study cohort included 245,386 women and 249,387 infants who were born between December 2005 and March 2014. The outcomes studied were influenza-like illness (ILI), laboratory-confirmed influenza, and influenza hospitalizations.
Of 866 infants younger than 6 months born to women who had received a flu shot, 32 had 1 or more ILI encounters, compared with 834 born to women who were not immunized (relative risk [RR], 0.36; 95% confidence interval [CI], 0.26–0.52; P<.001). Laboratory-confirmed influenza was identified in 658 infants; of these, 20 were born to women reporting immunization and 638 were born to unimmunized women (RR, 0.30; 95% CI, 0.19–0.46; P<.001). Finally, 151 infants with laboratory-confirmed influenza were hospitalized; 3 were born to immunized women and 148 to women who had not received a flu shot (RR, 0.19; 95% CI, 0.06–0.60; P = .005).
The authors calculated that infants born to women who reported influenza immunization during pregnancy had risk reductions of 64% for ILI, 70% for laboratory-confirmed influenza, and 81% for influenza hospitalizations.
Consider immunization benefits realistically
The authors state in their published report that “Protecting young infants from influenza through maternal immunization during pregnancy is a public health priority.” This may be overstating their case, for the following reasons. First, influenza vaccine has varying degrees of efficacy depending on the particular year and influenza strains that predominate, and it never has been shown to be entirely protective. Second, when looking only at this study’s laboratory-proven cases of influenza in newborns, infants whose mothers were vaccinated had a case rate of 0.84/1,000, while the case rate in newborns born to unvaccinated women was 2.83/1,000. While this shows a difference, the report provides no additional outcome data regarding morbidity or mortality.
In fact, although infant hospitalization rates differed (0.13/1,000 born to vaccinated women versus 0.66/1,000 born to unvaccinated women), there were no influenza-related mortalities in this cohort. The effect seems better when including “influenza-like illness,” but it is unclear why we should think that the influenza vaccine protects against infection that is not caused by influenza.
What this EVIDENCE means for practice
ObGyns should continue to promote influenza vaccination during pregnancy for the maternal protection it imparts. These new data on the potential for newborn protection, although not conclusive, may improve maternal acceptance of vaccination; from that perspective, these data are valuable.
— John T. Repke, MD
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

ObGyn salaries jumped in the last year
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim

Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim
Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim
Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
In this Article
- ACOG takes aim at burnout
- Considering salary and leadership disparities
- ObGyns’ greatest practice concerns

Failure to convert to laparotomy: $6.25M settlement
Failure to convert to laparotomy: $6.25M settlement

A 67-year-old woman with urinary incontinence underwent robot-assisted laparoscopic prolapse surgery and hysterectomy. Complications arose, including an injury to the transverse colon. Postoperatively, the patient developed sepsis and had multiple surgeries. At the time of trial, she used a colostomy bag and had a malabsorption syndrome that required frequent intravenous treatment for dehydration.
Patient's claim:
The gynecologist deviated from the standard of care by failing to convert from a laparoscopic procedure to an open procedure when complications developed.
Defendants' defense:
The procedure was properly performed.
Verdict:
A $6.25 million New Jersey settlement was reached, paid jointly by the gynecologist and the medical center.
Circumcision requires revision
A day after birth, a baby underwent circumcision performed by the mother’s ObGyn. Revision surgery was performed 2.5 years later. When the boy was age 7 years, urethral stricture developed and was treated.
Parents' claim:
Circumcision was improperly performed. Once the child was able to talk, he said that his penis constantly hurt. Pain was only relieved by revision surgery.
Physician's defense:
There was no negligence. Redundant foreskin is often left following a circumcision.
Verdict:
A Michigan defense verdict was returned.
Mother with CP has child with CP
A pregnant woman with cerebral palsy (CP) reported a prior preterm delivery at 24 weeks’ gestation to a high-risk prenatal clinic. At that time, she was offered synthetic progesterone (170HP) injections, but she declined because of the cost. She declined 170HP several times. Nine weeks after her initial visit, she declined 170HP despite ultrasonography (US) showing a shortened cervical length (25 mm) for the gestational age. In 2 weeks, when the cervical length measured 9 mm, she was hospitalized to rule out preterm labor but, before tests began, she left the hospital. Five days later, when her cervical length was 11 mm, she received the first 170HP injection. In the next month she received 4 injections, but she failed to show for the fifth injection and US. The next day, she went to the hospital with cramping. She was given steroids and medication to stop labor. US results indicated that the baby was in breech position. The mother consented to cesarean delivery, but the baby was born vaginally an hour later. The child has mild brain damage, CP, developmental delays, and learning disabilities.
Parents' claim: The mother should have been offered vaginal progesterone, which is cheaper. Given the high risk of preterm birth, steroids administered earlier would have improved fetal development. Cesarean delivery should have been performed.
Defendants' defense: Vaginal progesterone was not available at the time. Starting steroids earlier would not have improved fetal outcome. A cesarean delivery was not possible because the baby was in the birth canal.
Verdict: A $3,500,000 Michigan settlement was reached.
Fallopian tubes grow back, pregnancy
A couple decided they did not want more children and sought counseling from the woman’s ObGyn, who recommended laparoscopic tubal ligation. Several months after surgery, the patient became pregnant and gave birth to a son.
Parents' claim:
The additional child placed an economic hardship on the family, now raising 4 children. The youngest child has language delays and learning disabilities.
Physician's defense:
Regrowth of the fallopian tubes resulting in unwanted pregnancy is a known complication of tubal ligation.
Verdict:
A $397,000 Maryland verdict was returned, including funds for the cost of raising the fourth child and to cope with the child’s special needs.
Challenges in managing labor

At 37 weeks' gestation, a woman was hospitalized in labor. At 1:15 pm, she was dilated 3 cm. At 1:30 pm, she was dilated 4−5 cm with increasing contractions and a reassuring fetal heart rate (FHR). The ObGyn covering for the mother’s ObGyn ordered oxytocin augmentation, which started at 2:45 pm. Shortly thereafter, contractions became more frequent and uterine tachysystole was observed. At 4:12 pm, FHR showed multiple deep decelerations with slow recovery. The baseline dropped to a 90-bpm range and remained that way for 17 minutes. At that point, the ObGyn stopped oxytocin and administered terbutaline; the FHR returned to baseline.
After vaginal delivery, the baby’s Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Two days later, the baby had seizures and was transferred to the neonatal intensive care unit. An electroencephalogram confirmed seizure activity. Initial imaging results were normal. However, magnetic resonance imaging performed a week after delivery showed bilateral brain damage. The child has spastic displegia, is unable to ambulate, and is blind.
Parents' claim: A suit was filed against the hospital and both ObGyns. The hospital settled before trial. The case was discontinued against the primary ObGyn. The covering ObGyn allegedly made 4 departures from accepted medical practice that caused the child’s injury: ordering and administering oxytocin, failing to closely monitor the FHR, failing to timely administer terbutaline, and failing to timely respond to and correct tachysystole.
Physician's defense: The child’s injury occurred before or after labor. The pregnancy was complicated by multiple kidney infections. A week before delivery, US revealed a blood-flow abnormality. An intranatal hypoxic event did not cause the injury, proven by the fact that, after terbutaline was administered, the FHR promptly normalized.
Verdict: A $3 million New York settlement was reached with the hospital. A $134 million verdict was returned against the covering ObGyn.
Brachial plexus injury during delivery
At 37 weeks' gestation, a mother was admitted to the hospital for induction of labor. Increasing doses of oxytocin were administered. Near midnight, FHR monitoring indicated fetal distress. The ObGyn was called and he ordered cesarean delivery. Once he arrived and examined the mother, he found no fetal concerns and decided to proceed with the original birth plan. At 3:30 am, the patient was fully dilated and in active labor. The ObGyn used a vacuum extractor. Upon delivery of the baby’s head, the ObGyn encountered shoulder dystocia and called for assistance. The child was born with a near-total brachial plexus injury: avulsions of all 5 brachial plexus nerves with trauma to the cervical nerve roots at C5−C8 and T1. The child has undergone multiple nerve grafts and orthopedic operations.
Parents' claim: Fetal distress should have prompted the ObGyn to perform cesarean delivery. There was no reason to use vacuum extraction. Based on the severity of the outcome, the ObGyn must have applied excessive force and inappropriate traction during delivery maneuvers.
Physician's defense: The standard of care did not require a cesarean delivery. The vacuum extractor did not cause shoulder dystocia. The ObGyn did not apply excessive force or traction to complete the delivery. The extent of the outcome was partially due to a fetal anomaly and hypotonia.
Verdict: An Illinois defense verdict was returned.
HPV-positive pap tests results never reported
A single mother of 4 children underwent Papanicolaou (Pap) tests in 2004, 2005, and 2007 at a federally funded clinic. Each time, she tested positive for oncogenic human papillomaviruses. In 2011, the patient died of cervical cancer.
Estate's claim: The patient was never notified that the results of the 3 Pap tests were abnormal because all correspondence was sent to an outdated address although she had been treated at the same clinic for other issues during that period of time. Cervical dysplasia identified in 2004 progressed to cancer and metastasized, leading to her death 7 years later.
Defendants' defense: The case was settled during trial.
Verdict: A $4,950,000 Illinois settlement was reached.
Failure to convert to laparotomy: $6.25M settlement
A 67-year-old woman with urinary incontinence underwent robot-assisted laparoscopic prolapse surgery and hysterectomy. Complications arose, including an injury to the transverse colon. Postoperatively, the patient developed sepsis and had multiple surgeries. At the time of trial, she used a colostomy bag and had a malabsorption syndrome that required frequent intravenous treatment for dehydration.
Patient's claim:
The gynecologist deviated from the standard of care by failing to convert from a laparoscopic procedure to an open procedure when complications developed.
Defendants' defense:
The procedure was properly performed.
Verdict:
A $6.25 million New Jersey settlement was reached, paid jointly by the gynecologist and the medical center.
Circumcision requires revision
A day after birth, a baby underwent circumcision performed by the mother’s ObGyn. Revision surgery was performed 2.5 years later. When the boy was age 7 years, urethral stricture developed and was treated.
Parents' claim:
Circumcision was improperly performed. Once the child was able to talk, he said that his penis constantly hurt. Pain was only relieved by revision surgery.
Physician's defense:
There was no negligence. Redundant foreskin is often left following a circumcision.
Verdict:
A Michigan defense verdict was returned.
Mother with CP has child with CP
A pregnant woman with cerebral palsy (CP) reported a prior preterm delivery at 24 weeks’ gestation to a high-risk prenatal clinic. At that time, she was offered synthetic progesterone (170HP) injections, but she declined because of the cost. She declined 170HP several times. Nine weeks after her initial visit, she declined 170HP despite ultrasonography (US) showing a shortened cervical length (25 mm) for the gestational age. In 2 weeks, when the cervical length measured 9 mm, she was hospitalized to rule out preterm labor but, before tests began, she left the hospital. Five days later, when her cervical length was 11 mm, she received the first 170HP injection. In the next month she received 4 injections, but she failed to show for the fifth injection and US. The next day, she went to the hospital with cramping. She was given steroids and medication to stop labor. US results indicated that the baby was in breech position. The mother consented to cesarean delivery, but the baby was born vaginally an hour later. The child has mild brain damage, CP, developmental delays, and learning disabilities.
Parents' claim: The mother should have been offered vaginal progesterone, which is cheaper. Given the high risk of preterm birth, steroids administered earlier would have improved fetal development. Cesarean delivery should have been performed.
Defendants' defense: Vaginal progesterone was not available at the time. Starting steroids earlier would not have improved fetal outcome. A cesarean delivery was not possible because the baby was in the birth canal.
Verdict: A $3,500,000 Michigan settlement was reached.
Fallopian tubes grow back, pregnancy
A couple decided they did not want more children and sought counseling from the woman’s ObGyn, who recommended laparoscopic tubal ligation. Several months after surgery, the patient became pregnant and gave birth to a son.
Parents' claim:
The additional child placed an economic hardship on the family, now raising 4 children. The youngest child has language delays and learning disabilities.
Physician's defense:
Regrowth of the fallopian tubes resulting in unwanted pregnancy is a known complication of tubal ligation.
Verdict:
A $397,000 Maryland verdict was returned, including funds for the cost of raising the fourth child and to cope with the child’s special needs.
Challenges in managing labor
At 37 weeks' gestation, a woman was hospitalized in labor. At 1:15 pm, she was dilated 3 cm. At 1:30 pm, she was dilated 4−5 cm with increasing contractions and a reassuring fetal heart rate (FHR). The ObGyn covering for the mother’s ObGyn ordered oxytocin augmentation, which started at 2:45 pm. Shortly thereafter, contractions became more frequent and uterine tachysystole was observed. At 4:12 pm, FHR showed multiple deep decelerations with slow recovery. The baseline dropped to a 90-bpm range and remained that way for 17 minutes. At that point, the ObGyn stopped oxytocin and administered terbutaline; the FHR returned to baseline.
After vaginal delivery, the baby’s Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Two days later, the baby had seizures and was transferred to the neonatal intensive care unit. An electroencephalogram confirmed seizure activity. Initial imaging results were normal. However, magnetic resonance imaging performed a week after delivery showed bilateral brain damage. The child has spastic displegia, is unable to ambulate, and is blind.
Parents' claim: A suit was filed against the hospital and both ObGyns. The hospital settled before trial. The case was discontinued against the primary ObGyn. The covering ObGyn allegedly made 4 departures from accepted medical practice that caused the child’s injury: ordering and administering oxytocin, failing to closely monitor the FHR, failing to timely administer terbutaline, and failing to timely respond to and correct tachysystole.
Physician's defense: The child’s injury occurred before or after labor. The pregnancy was complicated by multiple kidney infections. A week before delivery, US revealed a blood-flow abnormality. An intranatal hypoxic event did not cause the injury, proven by the fact that, after terbutaline was administered, the FHR promptly normalized.
Verdict: A $3 million New York settlement was reached with the hospital. A $134 million verdict was returned against the covering ObGyn.
Brachial plexus injury during delivery
At 37 weeks' gestation, a mother was admitted to the hospital for induction of labor. Increasing doses of oxytocin were administered. Near midnight, FHR monitoring indicated fetal distress. The ObGyn was called and he ordered cesarean delivery. Once he arrived and examined the mother, he found no fetal concerns and decided to proceed with the original birth plan. At 3:30 am, the patient was fully dilated and in active labor. The ObGyn used a vacuum extractor. Upon delivery of the baby’s head, the ObGyn encountered shoulder dystocia and called for assistance. The child was born with a near-total brachial plexus injury: avulsions of all 5 brachial plexus nerves with trauma to the cervical nerve roots at C5−C8 and T1. The child has undergone multiple nerve grafts and orthopedic operations.
Parents' claim: Fetal distress should have prompted the ObGyn to perform cesarean delivery. There was no reason to use vacuum extraction. Based on the severity of the outcome, the ObGyn must have applied excessive force and inappropriate traction during delivery maneuvers.
Physician's defense: The standard of care did not require a cesarean delivery. The vacuum extractor did not cause shoulder dystocia. The ObGyn did not apply excessive force or traction to complete the delivery. The extent of the outcome was partially due to a fetal anomaly and hypotonia.
Verdict: An Illinois defense verdict was returned.
HPV-positive pap tests results never reported
A single mother of 4 children underwent Papanicolaou (Pap) tests in 2004, 2005, and 2007 at a federally funded clinic. Each time, she tested positive for oncogenic human papillomaviruses. In 2011, the patient died of cervical cancer.
Estate's claim: The patient was never notified that the results of the 3 Pap tests were abnormal because all correspondence was sent to an outdated address although she had been treated at the same clinic for other issues during that period of time. Cervical dysplasia identified in 2004 progressed to cancer and metastasized, leading to her death 7 years later.
Defendants' defense: The case was settled during trial.
Verdict: A $4,950,000 Illinois settlement was reached.
Failure to convert to laparotomy: $6.25M settlement
A 67-year-old woman with urinary incontinence underwent robot-assisted laparoscopic prolapse surgery and hysterectomy. Complications arose, including an injury to the transverse colon. Postoperatively, the patient developed sepsis and had multiple surgeries. At the time of trial, she used a colostomy bag and had a malabsorption syndrome that required frequent intravenous treatment for dehydration.
Patient's claim:
The gynecologist deviated from the standard of care by failing to convert from a laparoscopic procedure to an open procedure when complications developed.
Defendants' defense:
The procedure was properly performed.
Verdict:
A $6.25 million New Jersey settlement was reached, paid jointly by the gynecologist and the medical center.
Circumcision requires revision
A day after birth, a baby underwent circumcision performed by the mother’s ObGyn. Revision surgery was performed 2.5 years later. When the boy was age 7 years, urethral stricture developed and was treated.
Parents' claim:
Circumcision was improperly performed. Once the child was able to talk, he said that his penis constantly hurt. Pain was only relieved by revision surgery.
Physician's defense:
There was no negligence. Redundant foreskin is often left following a circumcision.
Verdict:
A Michigan defense verdict was returned.
Mother with CP has child with CP
A pregnant woman with cerebral palsy (CP) reported a prior preterm delivery at 24 weeks’ gestation to a high-risk prenatal clinic. At that time, she was offered synthetic progesterone (170HP) injections, but she declined because of the cost. She declined 170HP several times. Nine weeks after her initial visit, she declined 170HP despite ultrasonography (US) showing a shortened cervical length (25 mm) for the gestational age. In 2 weeks, when the cervical length measured 9 mm, she was hospitalized to rule out preterm labor but, before tests began, she left the hospital. Five days later, when her cervical length was 11 mm, she received the first 170HP injection. In the next month she received 4 injections, but she failed to show for the fifth injection and US. The next day, she went to the hospital with cramping. She was given steroids and medication to stop labor. US results indicated that the baby was in breech position. The mother consented to cesarean delivery, but the baby was born vaginally an hour later. The child has mild brain damage, CP, developmental delays, and learning disabilities.
Parents' claim: The mother should have been offered vaginal progesterone, which is cheaper. Given the high risk of preterm birth, steroids administered earlier would have improved fetal development. Cesarean delivery should have been performed.
Defendants' defense: Vaginal progesterone was not available at the time. Starting steroids earlier would not have improved fetal outcome. A cesarean delivery was not possible because the baby was in the birth canal.
Verdict: A $3,500,000 Michigan settlement was reached.
Fallopian tubes grow back, pregnancy
A couple decided they did not want more children and sought counseling from the woman’s ObGyn, who recommended laparoscopic tubal ligation. Several months after surgery, the patient became pregnant and gave birth to a son.
Parents' claim:
The additional child placed an economic hardship on the family, now raising 4 children. The youngest child has language delays and learning disabilities.
Physician's defense:
Regrowth of the fallopian tubes resulting in unwanted pregnancy is a known complication of tubal ligation.
Verdict:
A $397,000 Maryland verdict was returned, including funds for the cost of raising the fourth child and to cope with the child’s special needs.
Challenges in managing labor
At 37 weeks' gestation, a woman was hospitalized in labor. At 1:15 pm, she was dilated 3 cm. At 1:30 pm, she was dilated 4−5 cm with increasing contractions and a reassuring fetal heart rate (FHR). The ObGyn covering for the mother’s ObGyn ordered oxytocin augmentation, which started at 2:45 pm. Shortly thereafter, contractions became more frequent and uterine tachysystole was observed. At 4:12 pm, FHR showed multiple deep decelerations with slow recovery. The baseline dropped to a 90-bpm range and remained that way for 17 minutes. At that point, the ObGyn stopped oxytocin and administered terbutaline; the FHR returned to baseline.
After vaginal delivery, the baby’s Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Two days later, the baby had seizures and was transferred to the neonatal intensive care unit. An electroencephalogram confirmed seizure activity. Initial imaging results were normal. However, magnetic resonance imaging performed a week after delivery showed bilateral brain damage. The child has spastic displegia, is unable to ambulate, and is blind.
Parents' claim: A suit was filed against the hospital and both ObGyns. The hospital settled before trial. The case was discontinued against the primary ObGyn. The covering ObGyn allegedly made 4 departures from accepted medical practice that caused the child’s injury: ordering and administering oxytocin, failing to closely monitor the FHR, failing to timely administer terbutaline, and failing to timely respond to and correct tachysystole.
Physician's defense: The child’s injury occurred before or after labor. The pregnancy was complicated by multiple kidney infections. A week before delivery, US revealed a blood-flow abnormality. An intranatal hypoxic event did not cause the injury, proven by the fact that, after terbutaline was administered, the FHR promptly normalized.
Verdict: A $3 million New York settlement was reached with the hospital. A $134 million verdict was returned against the covering ObGyn.
Brachial plexus injury during delivery
At 37 weeks' gestation, a mother was admitted to the hospital for induction of labor. Increasing doses of oxytocin were administered. Near midnight, FHR monitoring indicated fetal distress. The ObGyn was called and he ordered cesarean delivery. Once he arrived and examined the mother, he found no fetal concerns and decided to proceed with the original birth plan. At 3:30 am, the patient was fully dilated and in active labor. The ObGyn used a vacuum extractor. Upon delivery of the baby’s head, the ObGyn encountered shoulder dystocia and called for assistance. The child was born with a near-total brachial plexus injury: avulsions of all 5 brachial plexus nerves with trauma to the cervical nerve roots at C5−C8 and T1. The child has undergone multiple nerve grafts and orthopedic operations.
Parents' claim: Fetal distress should have prompted the ObGyn to perform cesarean delivery. There was no reason to use vacuum extraction. Based on the severity of the outcome, the ObGyn must have applied excessive force and inappropriate traction during delivery maneuvers.
Physician's defense: The standard of care did not require a cesarean delivery. The vacuum extractor did not cause shoulder dystocia. The ObGyn did not apply excessive force or traction to complete the delivery. The extent of the outcome was partially due to a fetal anomaly and hypotonia.
Verdict: An Illinois defense verdict was returned.
HPV-positive pap tests results never reported
A single mother of 4 children underwent Papanicolaou (Pap) tests in 2004, 2005, and 2007 at a federally funded clinic. Each time, she tested positive for oncogenic human papillomaviruses. In 2011, the patient died of cervical cancer.
Estate's claim: The patient was never notified that the results of the 3 Pap tests were abnormal because all correspondence was sent to an outdated address although she had been treated at the same clinic for other issues during that period of time. Cervical dysplasia identified in 2004 progressed to cancer and metastasized, leading to her death 7 years later.
Defendants' defense: The case was settled during trial.
Verdict: A $4,950,000 Illinois settlement was reached.
Additional Medical Verdicts
• Circumcision requires revision
• Mother with CP has child with CP
• Fallopian tubes grow back, pregnancy
• Challenges in managing labor
• Brachial plexus injury during delivery
• HPV-positive Pap tests results never reported

Letters to the Editor: Determining fetal demise; SERMS in menopause; Aspirin for preeclampsia; Treating cesarean scar defect

Determining fetal demise
I appreciate and thank Drs. Esplin and Eller for their discussion of fetal monitoring pitfalls. I agree with their sentiment that this is an inexact science. After 40 years of looking at these strips, I am convinced there must be a better way. I look forward to some innovative approach to better determine fetal well-being in labor. This article raises a question I have asked, and sought the answer to, for years.
On occasion, I have diagnosed intrauterine fetal demise by detecting the maternal heart rate with an internal fetal scalp electrode. On one particular occasion, somewhere between the time of admission, spontaneous rupture of membranes, and applying the fetal scalp electrode, the fetus died. This case was similar to the one you describe in which early efforts with the external Doppler were unsatisfactory and fetal status was suspect. My question: “What is the time interval from the moment of fetal death and loss of fetal electrical activity until the fetus becomes an effective conduit for the conduction of the maternal cardiac signal? Is it minutes, hours, days? Clearly, this would be difficult to evaluate other than on animal models, but I have yet to find an answer.
Edward Hall, MD
Edgewood, Kentucky
Drs. Esplin and Eller respond
We are grateful for your interest in our article. Unfortunately the answer to your question about the timing between fetal demise and the appearance of maternal electrocardiac activity detected by a fetal scalp electrode after transmission through the fetal body is not clear. We are not aware of any data that would conclusively prove the time required for this to occur. It is likely that this type of information would require an animal model to elucidate. However, we are aware of at least 2 clinical cases in which fetal cardiac activity was convincingly documented at admission and for several hours intrapartum with subsequent episodic loss of signal and then delivery of a dead fetus wherein retrospective review confirmed that for a period of time the maternal heart rate was recorded and interpreted to be the fetal heart rate. From these experiences we conclude that this is possible shortly after the fetal demise, likely within minutes to hours.
Despite this uncertainty, we are confident that the information in our article will help clinicians identify and correct those instances when the maternal heart rate is being recorded instead of the fetal heart rate. Fortunately, this rarely involves a situation in which there has been an undiagnosed intrauterine fetal demise.
“SERMs” definition inaccurate
I disagree with Drs. Liu and Collins’ description of selective estrogen receptor modulators (SERMs) on page S18, in which they state, “Estrogens and SERMs are lipid-soluble steroid hormones that bind to 2 specific hormone receptors, estrogen receptor α and estrogen receptor β…” SERMs are not hormones, and they are defined improperly as such.
Gideon G. Panter, MD
New York, New York
Drs. Liu and Collins respond
Thank you for your interest in our article. SERMs are typically synthetic organic compounds that can activate estrogen receptors or modify activity of the estrogen receptor and, thus, can be considered hormones.
Stop aspirin in pregnancy?
Like many colleagues, I had been stopping low-dose aspirin prior to planned or expected delivery. Evidence suggests a bigger risk of rebound hypercoagulability than bleeding after stopping low-dose aspirin, according to an article on aspirin use in the perioperative period.1 Because of lack of benefit and increased risks of stopping aspirin, it may be time to change our practice and continue aspirin to minimize peridelivery thromboembolic risk.
Mark Jacobs, MD
Mill Valley, CA
Reference
- Gerstein NS, Schulman PM, Gerstein WH, Petersen TR, Tawil I. Should more patients continue aspirin therapy perioperatively?: clinical impact of aspirin withdrawal syndrome. Ann Surg. 2012;255:811–819.
Dr. Barbieri responds
I thank Dr. Jacobs for his advice to continue low-dose aspirin throughout pregnancy in women taking aspirin for prevention of preeclampsia. The review he references is focused on elderly patients taking aspirin for existing heart disease, which is a very different population than pregnant women. There are no high-quality data from clinical trials on whether to continue or stop low-dose aspirin in pregnant women as they approach their due date. I think obstetricians can use their best judgment in making the decision of whether to stop low-dose aspirin at 36 or 37 weeks or continue aspirin throughout the pregnancy.
Technique for preventing cesarean scar defect
I read with interest the proposed treatment options that Dr. Nezhat and colleagues suggested for cesarean scar defect. However, nowhere did I see mention of preventing this defect.
For 30 years I have been closing the hysterotomy in a fashion that I believe leaves no presence of an isthmocele and is a superior closure. I overlap the upper flap with the lower flap and, most importantly, close with chromic catgut. A cesarean scar “niche” occurs with involution of the uterus causing the suture line to bunch up. Chromic catgut has a shorter half-life and will “give;” a suture made of polypropylene will not stretch. I use a running interlocking line with sutures about 0.5 inches apart.
Donald M. Werner, MD
Binghamton, New York
Dr. Nezhat and colleagues respond
We thank Dr. Werner for his inquiry regarding the prevention of cesarean scar defects; as we all agree, the best treatment is prevention. As mentioned in our article, there are no definitive results from the studies published to date that show superiority of one surgical technique over another in regard to hysterotomy closure and prevention of cesarean scar defects. Possible risk factors for developing cesarean scar defects include low (cervical) hysterotomy, single-layer uterine wall closure, use of locking sutures, closure of hysterotomy with endometrial-sparing technique, and multiple cesarean deliveries. Although these factors may be associated with increased risk of cesarean scar defects, additional randomized controlled trials need to be performed prior to being able to offer a recommendation on a conclusive preventative measure. For additional information, I would direct you to references 3 and 4 in our article. We thank you for sharing your positive experience and eagerly await additional studies on the topic.
Share your thoughts! Send your Letter to the Editor to [email protected]
Determining fetal demise
I appreciate and thank Drs. Esplin and Eller for their discussion of fetal monitoring pitfalls. I agree with their sentiment that this is an inexact science. After 40 years of looking at these strips, I am convinced there must be a better way. I look forward to some innovative approach to better determine fetal well-being in labor. This article raises a question I have asked, and sought the answer to, for years.
On occasion, I have diagnosed intrauterine fetal demise by detecting the maternal heart rate with an internal fetal scalp electrode. On one particular occasion, somewhere between the time of admission, spontaneous rupture of membranes, and applying the fetal scalp electrode, the fetus died. This case was similar to the one you describe in which early efforts with the external Doppler were unsatisfactory and fetal status was suspect. My question: “What is the time interval from the moment of fetal death and loss of fetal electrical activity until the fetus becomes an effective conduit for the conduction of the maternal cardiac signal? Is it minutes, hours, days? Clearly, this would be difficult to evaluate other than on animal models, but I have yet to find an answer.
Edward Hall, MD
Edgewood, Kentucky
Drs. Esplin and Eller respond
We are grateful for your interest in our article. Unfortunately the answer to your question about the timing between fetal demise and the appearance of maternal electrocardiac activity detected by a fetal scalp electrode after transmission through the fetal body is not clear. We are not aware of any data that would conclusively prove the time required for this to occur. It is likely that this type of information would require an animal model to elucidate. However, we are aware of at least 2 clinical cases in which fetal cardiac activity was convincingly documented at admission and for several hours intrapartum with subsequent episodic loss of signal and then delivery of a dead fetus wherein retrospective review confirmed that for a period of time the maternal heart rate was recorded and interpreted to be the fetal heart rate. From these experiences we conclude that this is possible shortly after the fetal demise, likely within minutes to hours.
Despite this uncertainty, we are confident that the information in our article will help clinicians identify and correct those instances when the maternal heart rate is being recorded instead of the fetal heart rate. Fortunately, this rarely involves a situation in which there has been an undiagnosed intrauterine fetal demise.
“SERMs” definition inaccurate
I disagree with Drs. Liu and Collins’ description of selective estrogen receptor modulators (SERMs) on page S18, in which they state, “Estrogens and SERMs are lipid-soluble steroid hormones that bind to 2 specific hormone receptors, estrogen receptor α and estrogen receptor β…” SERMs are not hormones, and they are defined improperly as such.
Gideon G. Panter, MD
New York, New York
Drs. Liu and Collins respond
Thank you for your interest in our article. SERMs are typically synthetic organic compounds that can activate estrogen receptors or modify activity of the estrogen receptor and, thus, can be considered hormones.
Stop aspirin in pregnancy?
Like many colleagues, I had been stopping low-dose aspirin prior to planned or expected delivery. Evidence suggests a bigger risk of rebound hypercoagulability than bleeding after stopping low-dose aspirin, according to an article on aspirin use in the perioperative period.1 Because of lack of benefit and increased risks of stopping aspirin, it may be time to change our practice and continue aspirin to minimize peridelivery thromboembolic risk.
Mark Jacobs, MD
Mill Valley, CA
Reference
- Gerstein NS, Schulman PM, Gerstein WH, Petersen TR, Tawil I. Should more patients continue aspirin therapy perioperatively?: clinical impact of aspirin withdrawal syndrome. Ann Surg. 2012;255:811–819.
Dr. Barbieri responds
I thank Dr. Jacobs for his advice to continue low-dose aspirin throughout pregnancy in women taking aspirin for prevention of preeclampsia. The review he references is focused on elderly patients taking aspirin for existing heart disease, which is a very different population than pregnant women. There are no high-quality data from clinical trials on whether to continue or stop low-dose aspirin in pregnant women as they approach their due date. I think obstetricians can use their best judgment in making the decision of whether to stop low-dose aspirin at 36 or 37 weeks or continue aspirin throughout the pregnancy.
Technique for preventing cesarean scar defect
I read with interest the proposed treatment options that Dr. Nezhat and colleagues suggested for cesarean scar defect. However, nowhere did I see mention of preventing this defect.
For 30 years I have been closing the hysterotomy in a fashion that I believe leaves no presence of an isthmocele and is a superior closure. I overlap the upper flap with the lower flap and, most importantly, close with chromic catgut. A cesarean scar “niche” occurs with involution of the uterus causing the suture line to bunch up. Chromic catgut has a shorter half-life and will “give;” a suture made of polypropylene will not stretch. I use a running interlocking line with sutures about 0.5 inches apart.
Donald M. Werner, MD
Binghamton, New York
Dr. Nezhat and colleagues respond
We thank Dr. Werner for his inquiry regarding the prevention of cesarean scar defects; as we all agree, the best treatment is prevention. As mentioned in our article, there are no definitive results from the studies published to date that show superiority of one surgical technique over another in regard to hysterotomy closure and prevention of cesarean scar defects. Possible risk factors for developing cesarean scar defects include low (cervical) hysterotomy, single-layer uterine wall closure, use of locking sutures, closure of hysterotomy with endometrial-sparing technique, and multiple cesarean deliveries. Although these factors may be associated with increased risk of cesarean scar defects, additional randomized controlled trials need to be performed prior to being able to offer a recommendation on a conclusive preventative measure. For additional information, I would direct you to references 3 and 4 in our article. We thank you for sharing your positive experience and eagerly await additional studies on the topic.
Share your thoughts! Send your Letter to the Editor to [email protected]
Determining fetal demise
I appreciate and thank Drs. Esplin and Eller for their discussion of fetal monitoring pitfalls. I agree with their sentiment that this is an inexact science. After 40 years of looking at these strips, I am convinced there must be a better way. I look forward to some innovative approach to better determine fetal well-being in labor. This article raises a question I have asked, and sought the answer to, for years.
On occasion, I have diagnosed intrauterine fetal demise by detecting the maternal heart rate with an internal fetal scalp electrode. On one particular occasion, somewhere between the time of admission, spontaneous rupture of membranes, and applying the fetal scalp electrode, the fetus died. This case was similar to the one you describe in which early efforts with the external Doppler were unsatisfactory and fetal status was suspect. My question: “What is the time interval from the moment of fetal death and loss of fetal electrical activity until the fetus becomes an effective conduit for the conduction of the maternal cardiac signal? Is it minutes, hours, days? Clearly, this would be difficult to evaluate other than on animal models, but I have yet to find an answer.
Edward Hall, MD
Edgewood, Kentucky
Drs. Esplin and Eller respond
We are grateful for your interest in our article. Unfortunately the answer to your question about the timing between fetal demise and the appearance of maternal electrocardiac activity detected by a fetal scalp electrode after transmission through the fetal body is not clear. We are not aware of any data that would conclusively prove the time required for this to occur. It is likely that this type of information would require an animal model to elucidate. However, we are aware of at least 2 clinical cases in which fetal cardiac activity was convincingly documented at admission and for several hours intrapartum with subsequent episodic loss of signal and then delivery of a dead fetus wherein retrospective review confirmed that for a period of time the maternal heart rate was recorded and interpreted to be the fetal heart rate. From these experiences we conclude that this is possible shortly after the fetal demise, likely within minutes to hours.
Despite this uncertainty, we are confident that the information in our article will help clinicians identify and correct those instances when the maternal heart rate is being recorded instead of the fetal heart rate. Fortunately, this rarely involves a situation in which there has been an undiagnosed intrauterine fetal demise.
“SERMs” definition inaccurate
I disagree with Drs. Liu and Collins’ description of selective estrogen receptor modulators (SERMs) on page S18, in which they state, “Estrogens and SERMs are lipid-soluble steroid hormones that bind to 2 specific hormone receptors, estrogen receptor α and estrogen receptor β…” SERMs are not hormones, and they are defined improperly as such.
Gideon G. Panter, MD
New York, New York
Drs. Liu and Collins respond
Thank you for your interest in our article. SERMs are typically synthetic organic compounds that can activate estrogen receptors or modify activity of the estrogen receptor and, thus, can be considered hormones.
Stop aspirin in pregnancy?
Like many colleagues, I had been stopping low-dose aspirin prior to planned or expected delivery. Evidence suggests a bigger risk of rebound hypercoagulability than bleeding after stopping low-dose aspirin, according to an article on aspirin use in the perioperative period.1 Because of lack of benefit and increased risks of stopping aspirin, it may be time to change our practice and continue aspirin to minimize peridelivery thromboembolic risk.
Mark Jacobs, MD
Mill Valley, CA
Reference
- Gerstein NS, Schulman PM, Gerstein WH, Petersen TR, Tawil I. Should more patients continue aspirin therapy perioperatively?: clinical impact of aspirin withdrawal syndrome. Ann Surg. 2012;255:811–819.
Dr. Barbieri responds
I thank Dr. Jacobs for his advice to continue low-dose aspirin throughout pregnancy in women taking aspirin for prevention of preeclampsia. The review he references is focused on elderly patients taking aspirin for existing heart disease, which is a very different population than pregnant women. There are no high-quality data from clinical trials on whether to continue or stop low-dose aspirin in pregnant women as they approach their due date. I think obstetricians can use their best judgment in making the decision of whether to stop low-dose aspirin at 36 or 37 weeks or continue aspirin throughout the pregnancy.
Technique for preventing cesarean scar defect
I read with interest the proposed treatment options that Dr. Nezhat and colleagues suggested for cesarean scar defect. However, nowhere did I see mention of preventing this defect.
For 30 years I have been closing the hysterotomy in a fashion that I believe leaves no presence of an isthmocele and is a superior closure. I overlap the upper flap with the lower flap and, most importantly, close with chromic catgut. A cesarean scar “niche” occurs with involution of the uterus causing the suture line to bunch up. Chromic catgut has a shorter half-life and will “give;” a suture made of polypropylene will not stretch. I use a running interlocking line with sutures about 0.5 inches apart.
Donald M. Werner, MD
Binghamton, New York
Dr. Nezhat and colleagues respond
We thank Dr. Werner for his inquiry regarding the prevention of cesarean scar defects; as we all agree, the best treatment is prevention. As mentioned in our article, there are no definitive results from the studies published to date that show superiority of one surgical technique over another in regard to hysterotomy closure and prevention of cesarean scar defects. Possible risk factors for developing cesarean scar defects include low (cervical) hysterotomy, single-layer uterine wall closure, use of locking sutures, closure of hysterotomy with endometrial-sparing technique, and multiple cesarean deliveries. Although these factors may be associated with increased risk of cesarean scar defects, additional randomized controlled trials need to be performed prior to being able to offer a recommendation on a conclusive preventative measure. For additional information, I would direct you to references 3 and 4 in our article. We thank you for sharing your positive experience and eagerly await additional studies on the topic.
Share your thoughts! Send your Letter to the Editor to [email protected]

Product Update: MyoSure REACH, Counsyl, Good Clean Love, OB Complete Gold
ACCESS TO HARD-TO-REACH UTERINE CAVITY
Hologic has added the MyoSure REACH device to its tissue removal system to maximize access for resection of fibroids up to 3 cm in size. The MyoSure REACH is designed to access hard-to-reach areas, including the upper third of the uterine cavity. Hologic says that the MyoSure REACH features a shortened distance from the distal tip to the cutting window of less than 1 millimeter to allow for easier access to polyps and fibroids. When compared with the predecessor device, the new design has been shown to get 3 times closer to the uterine wall and removes 25% more tissue in a simulated bench top model. The MyoSure REACH has an outer diameter of 3 mm and working length of 32 cm, with scope compatibility with MyoSure and MyoSure XL. The blade is made of coated stainless steel with ultra-hardness and high-wear resistance.
FOR MORE INFORMATION, VISIT: www.myosure.com/hcp/myosure-reach

DNA TESTING AND GENETIC COUNSELING SERVICE
Counsyl, a DNA testing and genetic counseling service, announced expansion into the oncology market with a focus on advancing cancer risk screening and cancer prevention.
Counsyl’s Inherited Cancer Screen is a prescription-based genetic screening test available for patients to take at the physician’s office or receive via mail. Tests include on-demand genetic counseling that is in-network with most insurance providers. Inherited Cancer Screen helps physicians identify patients who may benefit from more aggressive screening procedures, changes in lifestyle or medication regimens, or preventive actions such as surgery. Inherited Cancer Screen is designed to test for up to 36 genes associated with increased risk of cancers of the breast, ovaries, pancreas, colon, prostate, and skin, with results typically delivered within 2 weeks. To help inform these decisions, Counsyl provides physicians and patients access to a team of more than 40 board-certified genetic counselors.
FirstCare is a web and mobile-friendly software tool to help physicians determine patient eligibility for genetic screening, based on factors such as family history.
Counsyl also provides prepregnancy and prenatal genetic testing. The fee for each test includes a consultation with a genetic counselor.
FOR MORE INFORMATION, VISIT: www.counsyl.com

PERSONAL LUBRICANTS AND WASH
Good Clean Love offers vaginal lubricants and a moisturizing personal wash formulated, according to the manufacturer, to match the ideal pH, salt balance, and type of lactic acid produced by healthy bacteria levels in the vagina.
Good Clean Love’s Personal Lubricants have been developed to mimic the body’s natural mucous production using certified 95% organic and natural ingredients, including aloe and agar, without chemical additives. The 2 choices are Almost Naked Organic Personal Lubricant, lightly scented with lemon and vanilla, and Cinnamon Vanilla Organic Personal Lubricant.
Bio-Match™ Restore™ Moisturizing Personal Lubricant mimics the body’s natural lubricating response, is fertility-friendly, 100% vegan, petroleum-, glycerin-, and paraben-free, and is safe for use with latex condoms and toys.
Bio-Match™ Balance™ Moisturizing Personal Wash is a moisturizing vaginal cleanser made from botanical extracts that Good Clean Love says returns genital pH and salinity to a naturally healthy balance. It is 100% vegan, and petroleum- and paraben-free.
FOR MORE INFORMATION, VISIT: http://goodcleanlove.com

PRENATAL VITAMINS WITH EGG-BASED DHA
OB Complete® Gold are prescription prenatal vitamin supple-ments from Vertical Pharmaceuticals indicated for use in improving the nutritional status of women prior to conception, throughout pregnancy, and in the postnatal period for both lactating and nonlactating women. The supplement delivers gluten-free, sugar-free, and lactose-free multivitamins and minerals in a small softgel taken once a day.
OB Complete Gold prenatal vitamin supplements contain OmEGGa DHA™ (docosahexaenoic acid), an egg-based Omega 3 fatty acid that is believed to play an important role in the development of the brain, retina, and central nervous system of the fetus. According to Vertical Pharmaceuticals, this form of DHA, found naturally in the body and breast milk, is more easily absorbed, digested, and distributed to the body’s tissues than the triglyceride form of DHA developed from marine sources such as fish or algae, which can produce unwanted side effects such as bad breath, a fishy taste, and burping.
FOR MORE INFORMATION, VISIT: www.obcompletegold.com
ACCESS TO HARD-TO-REACH UTERINE CAVITY
Hologic has added the MyoSure REACH device to its tissue removal system to maximize access for resection of fibroids up to 3 cm in size. The MyoSure REACH is designed to access hard-to-reach areas, including the upper third of the uterine cavity. Hologic says that the MyoSure REACH features a shortened distance from the distal tip to the cutting window of less than 1 millimeter to allow for easier access to polyps and fibroids. When compared with the predecessor device, the new design has been shown to get 3 times closer to the uterine wall and removes 25% more tissue in a simulated bench top model. The MyoSure REACH has an outer diameter of 3 mm and working length of 32 cm, with scope compatibility with MyoSure and MyoSure XL. The blade is made of coated stainless steel with ultra-hardness and high-wear resistance.
FOR MORE INFORMATION, VISIT: www.myosure.com/hcp/myosure-reach
DNA TESTING AND GENETIC COUNSELING SERVICE
Counsyl, a DNA testing and genetic counseling service, announced expansion into the oncology market with a focus on advancing cancer risk screening and cancer prevention.
Counsyl’s Inherited Cancer Screen is a prescription-based genetic screening test available for patients to take at the physician’s office or receive via mail. Tests include on-demand genetic counseling that is in-network with most insurance providers. Inherited Cancer Screen helps physicians identify patients who may benefit from more aggressive screening procedures, changes in lifestyle or medication regimens, or preventive actions such as surgery. Inherited Cancer Screen is designed to test for up to 36 genes associated with increased risk of cancers of the breast, ovaries, pancreas, colon, prostate, and skin, with results typically delivered within 2 weeks. To help inform these decisions, Counsyl provides physicians and patients access to a team of more than 40 board-certified genetic counselors.
FirstCare is a web and mobile-friendly software tool to help physicians determine patient eligibility for genetic screening, based on factors such as family history.
Counsyl also provides prepregnancy and prenatal genetic testing. The fee for each test includes a consultation with a genetic counselor.
FOR MORE INFORMATION, VISIT: www.counsyl.com
PERSONAL LUBRICANTS AND WASH
Good Clean Love offers vaginal lubricants and a moisturizing personal wash formulated, according to the manufacturer, to match the ideal pH, salt balance, and type of lactic acid produced by healthy bacteria levels in the vagina.
Good Clean Love’s Personal Lubricants have been developed to mimic the body’s natural mucous production using certified 95% organic and natural ingredients, including aloe and agar, without chemical additives. The 2 choices are Almost Naked Organic Personal Lubricant, lightly scented with lemon and vanilla, and Cinnamon Vanilla Organic Personal Lubricant.
Bio-Match™ Restore™ Moisturizing Personal Lubricant mimics the body’s natural lubricating response, is fertility-friendly, 100% vegan, petroleum-, glycerin-, and paraben-free, and is safe for use with latex condoms and toys.
Bio-Match™ Balance™ Moisturizing Personal Wash is a moisturizing vaginal cleanser made from botanical extracts that Good Clean Love says returns genital pH and salinity to a naturally healthy balance. It is 100% vegan, and petroleum- and paraben-free.
FOR MORE INFORMATION, VISIT: http://goodcleanlove.com
PRENATAL VITAMINS WITH EGG-BASED DHA
OB Complete® Gold are prescription prenatal vitamin supple-ments from Vertical Pharmaceuticals indicated for use in improving the nutritional status of women prior to conception, throughout pregnancy, and in the postnatal period for both lactating and nonlactating women. The supplement delivers gluten-free, sugar-free, and lactose-free multivitamins and minerals in a small softgel taken once a day.
OB Complete Gold prenatal vitamin supplements contain OmEGGa DHA™ (docosahexaenoic acid), an egg-based Omega 3 fatty acid that is believed to play an important role in the development of the brain, retina, and central nervous system of the fetus. According to Vertical Pharmaceuticals, this form of DHA, found naturally in the body and breast milk, is more easily absorbed, digested, and distributed to the body’s tissues than the triglyceride form of DHA developed from marine sources such as fish or algae, which can produce unwanted side effects such as bad breath, a fishy taste, and burping.
FOR MORE INFORMATION, VISIT: www.obcompletegold.com
ACCESS TO HARD-TO-REACH UTERINE CAVITY
Hologic has added the MyoSure REACH device to its tissue removal system to maximize access for resection of fibroids up to 3 cm in size. The MyoSure REACH is designed to access hard-to-reach areas, including the upper third of the uterine cavity. Hologic says that the MyoSure REACH features a shortened distance from the distal tip to the cutting window of less than 1 millimeter to allow for easier access to polyps and fibroids. When compared with the predecessor device, the new design has been shown to get 3 times closer to the uterine wall and removes 25% more tissue in a simulated bench top model. The MyoSure REACH has an outer diameter of 3 mm and working length of 32 cm, with scope compatibility with MyoSure and MyoSure XL. The blade is made of coated stainless steel with ultra-hardness and high-wear resistance.
FOR MORE INFORMATION, VISIT: www.myosure.com/hcp/myosure-reach
DNA TESTING AND GENETIC COUNSELING SERVICE
Counsyl, a DNA testing and genetic counseling service, announced expansion into the oncology market with a focus on advancing cancer risk screening and cancer prevention.
Counsyl’s Inherited Cancer Screen is a prescription-based genetic screening test available for patients to take at the physician’s office or receive via mail. Tests include on-demand genetic counseling that is in-network with most insurance providers. Inherited Cancer Screen helps physicians identify patients who may benefit from more aggressive screening procedures, changes in lifestyle or medication regimens, or preventive actions such as surgery. Inherited Cancer Screen is designed to test for up to 36 genes associated with increased risk of cancers of the breast, ovaries, pancreas, colon, prostate, and skin, with results typically delivered within 2 weeks. To help inform these decisions, Counsyl provides physicians and patients access to a team of more than 40 board-certified genetic counselors.
FirstCare is a web and mobile-friendly software tool to help physicians determine patient eligibility for genetic screening, based on factors such as family history.
Counsyl also provides prepregnancy and prenatal genetic testing. The fee for each test includes a consultation with a genetic counselor.
FOR MORE INFORMATION, VISIT: www.counsyl.com
PERSONAL LUBRICANTS AND WASH
Good Clean Love offers vaginal lubricants and a moisturizing personal wash formulated, according to the manufacturer, to match the ideal pH, salt balance, and type of lactic acid produced by healthy bacteria levels in the vagina.
Good Clean Love’s Personal Lubricants have been developed to mimic the body’s natural mucous production using certified 95% organic and natural ingredients, including aloe and agar, without chemical additives. The 2 choices are Almost Naked Organic Personal Lubricant, lightly scented with lemon and vanilla, and Cinnamon Vanilla Organic Personal Lubricant.
Bio-Match™ Restore™ Moisturizing Personal Lubricant mimics the body’s natural lubricating response, is fertility-friendly, 100% vegan, petroleum-, glycerin-, and paraben-free, and is safe for use with latex condoms and toys.
Bio-Match™ Balance™ Moisturizing Personal Wash is a moisturizing vaginal cleanser made from botanical extracts that Good Clean Love says returns genital pH and salinity to a naturally healthy balance. It is 100% vegan, and petroleum- and paraben-free.
FOR MORE INFORMATION, VISIT: http://goodcleanlove.com
PRENATAL VITAMINS WITH EGG-BASED DHA
OB Complete® Gold are prescription prenatal vitamin supple-ments from Vertical Pharmaceuticals indicated for use in improving the nutritional status of women prior to conception, throughout pregnancy, and in the postnatal period for both lactating and nonlactating women. The supplement delivers gluten-free, sugar-free, and lactose-free multivitamins and minerals in a small softgel taken once a day.
OB Complete Gold prenatal vitamin supplements contain OmEGGa DHA™ (docosahexaenoic acid), an egg-based Omega 3 fatty acid that is believed to play an important role in the development of the brain, retina, and central nervous system of the fetus. According to Vertical Pharmaceuticals, this form of DHA, found naturally in the body and breast milk, is more easily absorbed, digested, and distributed to the body’s tissues than the triglyceride form of DHA developed from marine sources such as fish or algae, which can produce unwanted side effects such as bad breath, a fishy taste, and burping.
FOR MORE INFORMATION, VISIT: www.obcompletegold.com
Analysis Supports Daily Folate for Children With Psoriasis on Methotrexate
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.

Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.
Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.
Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
AT THE 2016 SID ANNUAL MEETING
