User login
What’s Eating You? Tick Bite Alopecia
Case Report
A 44-year-old woman presented with a localized patch of hair loss on the frontal scalp of several month’s duration. She had been bitten by a tick at this site during the summer. Two months later

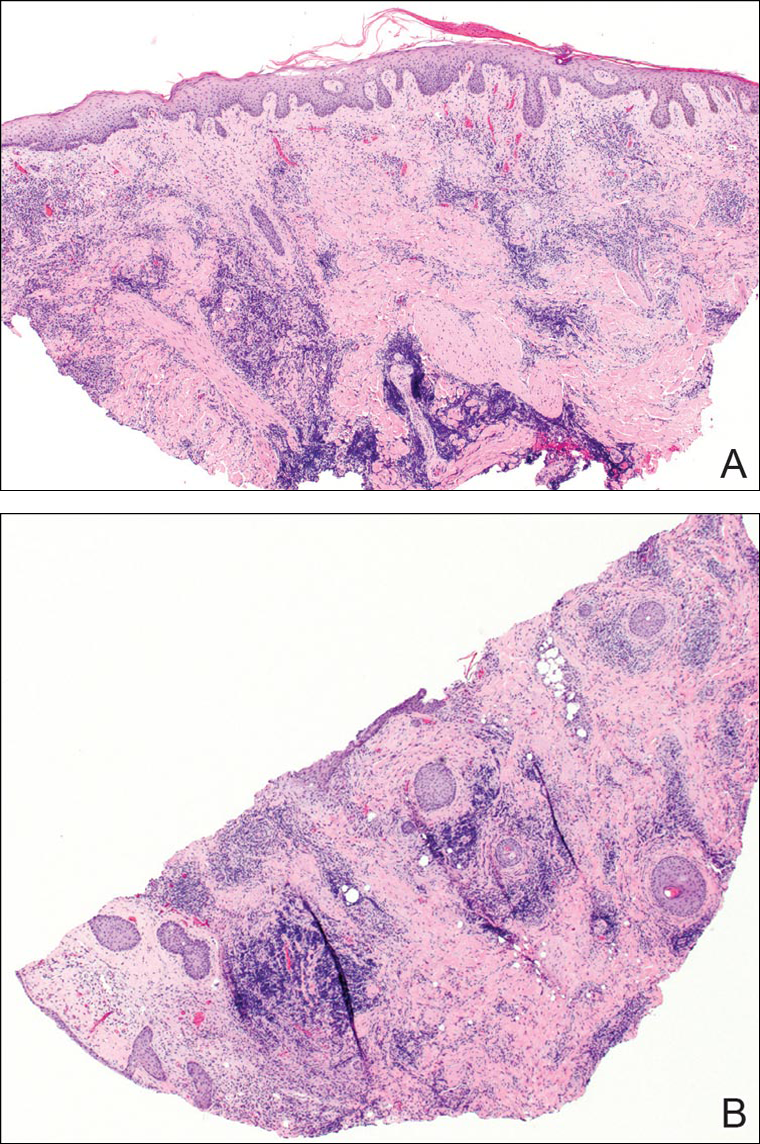
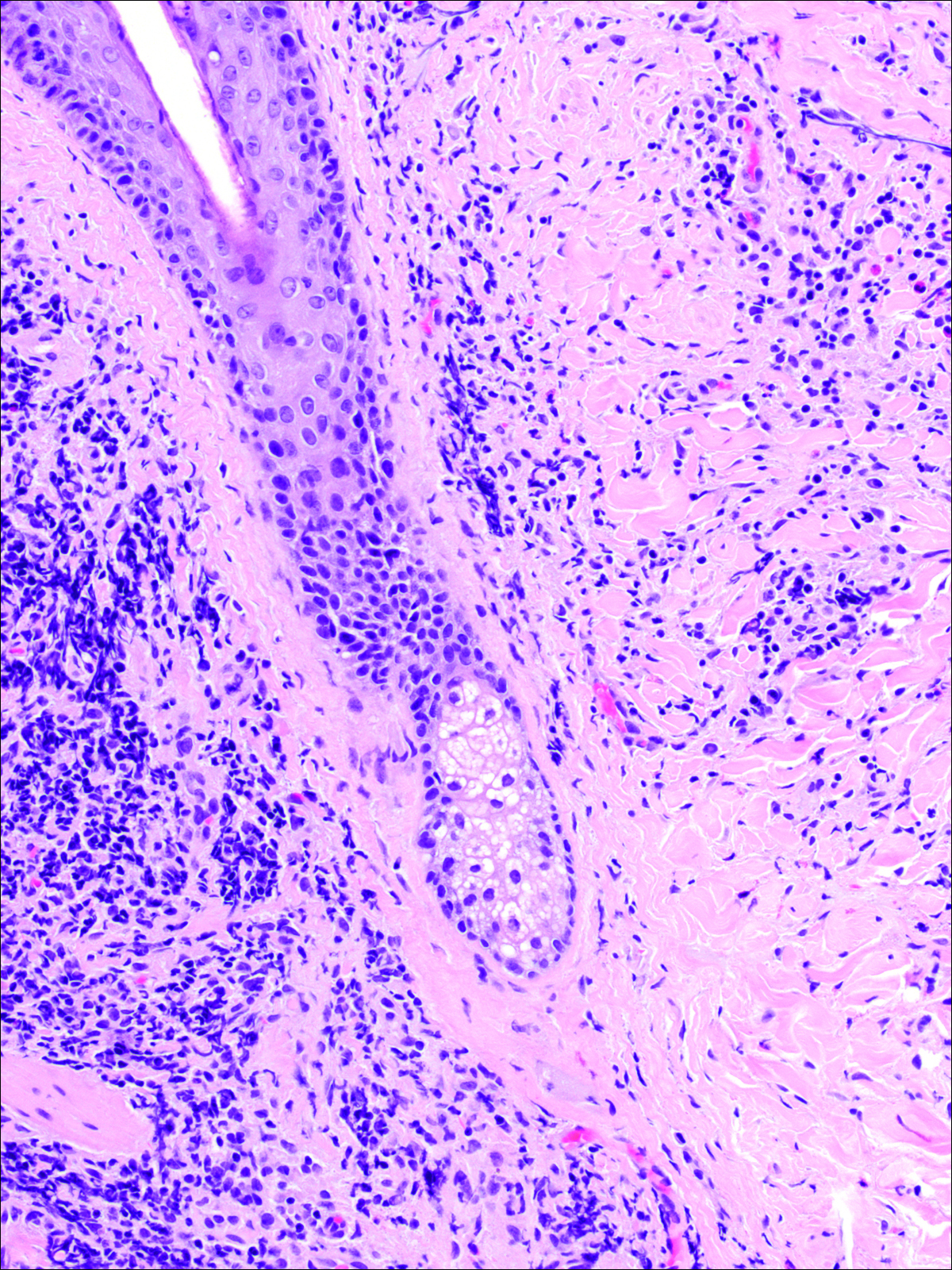
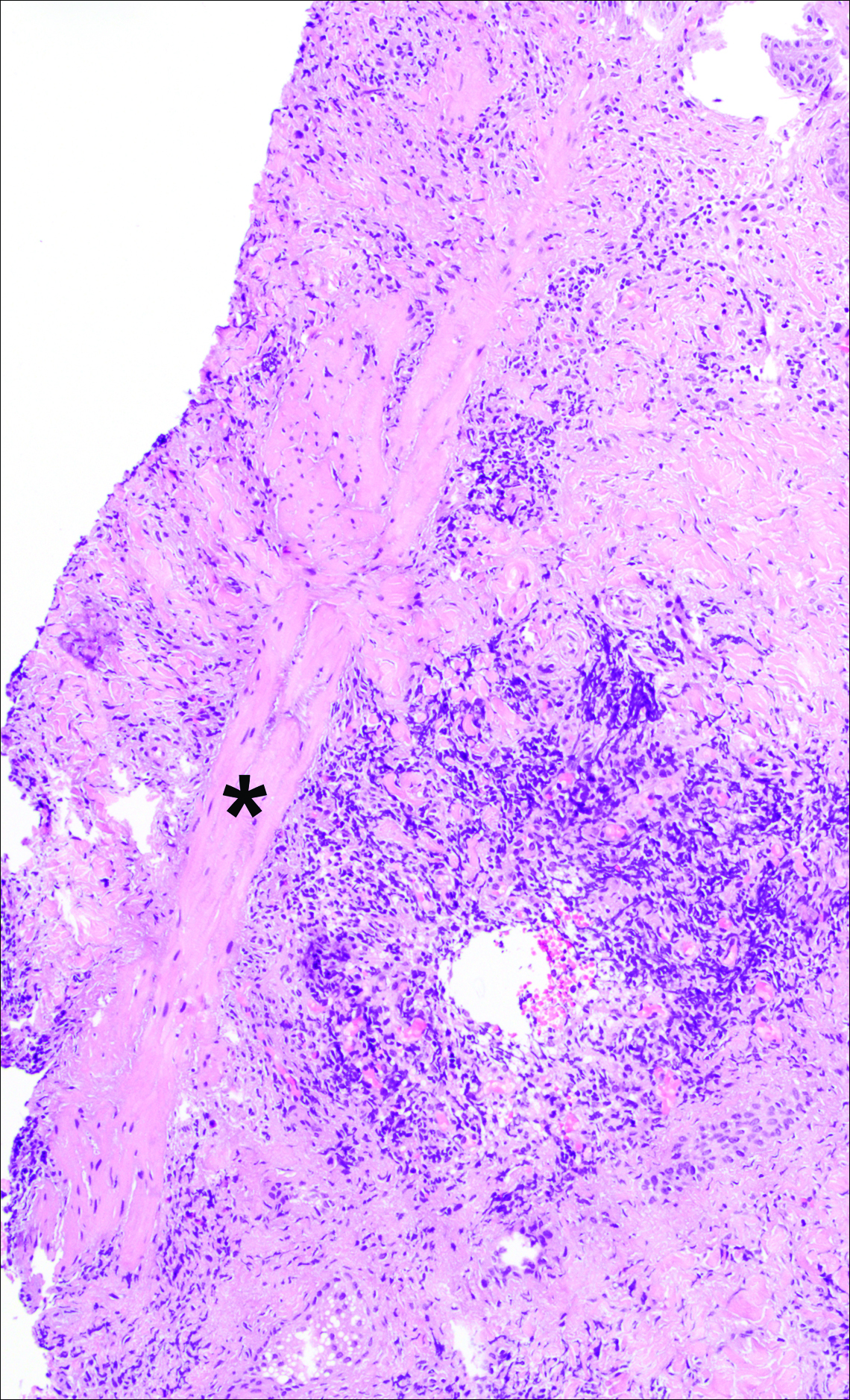
A punch biopsy was obtained from an indurated area of hyperpigmentation adjacent to the eschar. Both vertical and horizontal sections were obtained, revealing a relatively normal epidermis, a marked decrease in follicular structures with loss of sebaceous glands, and dense perifollicular lymphocytic inflammation with a few scattered eosinophils (Figures 2 and 3).
Historical Perspective
Tick bite alopecia was first described in the French literature in 19211 and in the English-language literature in 1955.2 A few additional cases were subsequently reported.3-5 In 2008, Castelli et al6 described the histologic and immunohistochemical features of 25 tick bite cases, a few of which resulted in alopecia. Other than these reports, little original information has been written about tick bite alopecia.
Clinical and Histologic Presentation
Tick bite alopecia is well described in the veterinary literature.7-9 It is possible that the condition is underreported in humans because the cause is often obvious or the alopecia is never discovered. The typical presentation is a roughly oval zone of alopecia that develops 1 to 2 weeks after the removal of a tick from the scalp. Often there is a small central eschar representing the site of tick attachment and the surrounding scalp may appear scaly. In one report of 2 siblings, multiple oval zones of alopecia resembling the moth-eaten alopecia of syphilis were noted in both patients, but only a single attached tick was found.2 In some reported cases, hair loss was only temporary, and at least partial if not complete regrowth of hair occurred.3,4 Follow-up on most cases is not provided, but to our knowledge permanent alopecia has not been described.
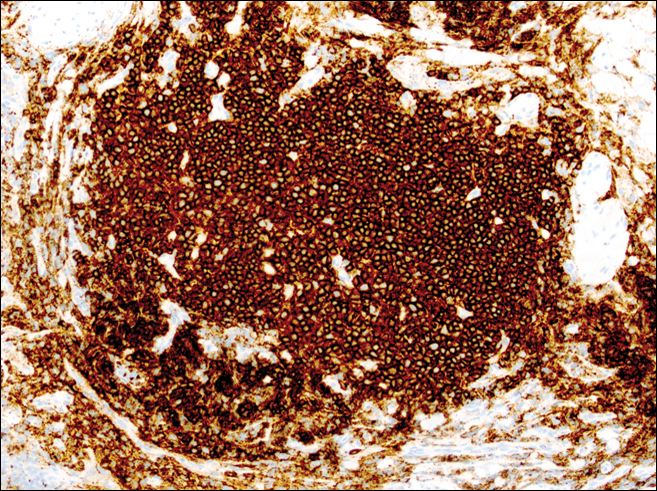
Information about the histologic findings of tick bite alopecia is particularly limited. In a report by Heyl,3 biopsies were conducted in 2 patients, but the areas selected for biopsy were the sites of tick attachment. Centrally dense, acute, and chronic inflammation was seen, as well as marked tissue necrosis of the connective tissue and hair follicles. Peripheral to the attachment zone, tissue necrosis was not found, but telogen hairs with “crumpled up hair shafts” were present.3 The histologic findings presented by Castelli et al6 were based on a single case of tick bite alopecia; however, the specimen was a generous excisional biopsy, allowing for a panoramic histologic view of the lesion. In the center of the specimen, hair follicles were absent, but residual follicular streamers and follicular remnants were surrounded by lymphocytic inflammation. Sebaceous glands were conspicuously absent, but foci with naked hairs, fibrosis, and granulomatous inflammation were seen. Peripherally, the hair follicles were thinned and miniaturized with an increased number of catagen/telogen hairs. Some follicles showed lamellar fibroplasia and perifollicular chronic inflammation. The inflammatory infiltrate consisted predominantly of helper T cells with a smaller population of B lymphocytes and a few plasma cells.6 In 2016, Lynch et al5 described a single case of tick bite alopecia and noted pseudolymphomatous inflammation with germinal center formation associated with hair miniaturization and an elevated catagen/telogen count; focal follicular mucinosis also was noted.Our histologic findings are similar to those of Castelli et al,6 except that the inflammatory infiltrate was clearly B-cell dominant, with a suggestion of germinal center formation, as noted by Lynch et al.5 This inflammatory pattern often can be encountered in a chronic tick bite lesion. Destruction of follicles and associated sebaceous glands and their replacement by follicular scars indicate that at least in the central portion of the lesion some permanent hair loss occurs. The presence of catagen/telogen hairs and miniaturized follicles indicates the potential for at least partial regrowth.
Similar to other investigators who have described tick bite alopecia, we can only speculate as to the mechanism by which clinical alopecia occurs. Given the density of the inflammatory infiltrate and perifollicular inflammation, it seems reasonable to assume that inflammation either destroys hair follicles or precipitates the catagen/telogen phase, resulting in temporary hair loss. The inflammation itself may be due to the presence of tick parts or the antigens in their saliva (or both). The delay between tick attachment and the onset of alopecia can be attributed to the time it takes follicles to cycle into the catagen/telogen phase and shed the hair shaft.
- Sauphar L. Alopecie peladoide consecutive a une piqure de tique. Bull Soc Fr Dermatol Syphiligr. 1921;28:442.
- Ross MS, Friede H. Alopecia due to tick bite. AMA Arch Derm. 1955;71:524-525.
- Heyl T. Tick bite alopecia. Clin Exp Dermatol. 1982;7:537-542.
- Marshall J. Alopecia after tick bite. S Afr Med J. 1966;40:555-556.
- Lynch MC, Milchak MA, Parnes H, et al. Tick bite alopecia: a report and review [published online April 19, 2016]. Am J Dermatopathol. doi:10.1097/DAD.0000000000000598.
- Castelli E, Caputo V, Morello V, et al. Local reactions to tick bites. Am J Dermatopathol. 2008;30:241-248.
- Nemeth NM, Ruder MG, Gerhold RW, et al. Demodectic mange, dermatophilosis, and other parasitic and bacterial dermatologic diseases in free-ranging white-tailed deer (Odocoileus virginianus) in the United States from 1975 to 2012. Vet Pathol. 2014;51:633-640.
- Welch DA, Samuel WM, Hudson RJ. Bioenergetic consequences of alopecia induced by Dermacentor albipictus (Acari: Ixodidae) on moose. J Med Entomol. 1990;27:656-660.
- Samuel WM. Locations of moose in northwestern Canada with hair loss probably caused by the winter tick, Dermacentor albipictus (Acari: Ixodidae). J Wildl Dis. 1989;25:436-439.
Case Report
A 44-year-old woman presented with a localized patch of hair loss on the frontal scalp of several month’s duration. She had been bitten by a tick at this site during the summer. Two months later
A punch biopsy was obtained from an indurated area of hyperpigmentation adjacent to the eschar. Both vertical and horizontal sections were obtained, revealing a relatively normal epidermis, a marked decrease in follicular structures with loss of sebaceous glands, and dense perifollicular lymphocytic inflammation with a few scattered eosinophils (Figures 2 and 3).
Historical Perspective
Tick bite alopecia was first described in the French literature in 19211 and in the English-language literature in 1955.2 A few additional cases were subsequently reported.3-5 In 2008, Castelli et al6 described the histologic and immunohistochemical features of 25 tick bite cases, a few of which resulted in alopecia. Other than these reports, little original information has been written about tick bite alopecia.
Clinical and Histologic Presentation
Tick bite alopecia is well described in the veterinary literature.7-9 It is possible that the condition is underreported in humans because the cause is often obvious or the alopecia is never discovered. The typical presentation is a roughly oval zone of alopecia that develops 1 to 2 weeks after the removal of a tick from the scalp. Often there is a small central eschar representing the site of tick attachment and the surrounding scalp may appear scaly. In one report of 2 siblings, multiple oval zones of alopecia resembling the moth-eaten alopecia of syphilis were noted in both patients, but only a single attached tick was found.2 In some reported cases, hair loss was only temporary, and at least partial if not complete regrowth of hair occurred.3,4 Follow-up on most cases is not provided, but to our knowledge permanent alopecia has not been described.
Information about the histologic findings of tick bite alopecia is particularly limited. In a report by Heyl,3 biopsies were conducted in 2 patients, but the areas selected for biopsy were the sites of tick attachment. Centrally dense, acute, and chronic inflammation was seen, as well as marked tissue necrosis of the connective tissue and hair follicles. Peripheral to the attachment zone, tissue necrosis was not found, but telogen hairs with “crumpled up hair shafts” were present.3 The histologic findings presented by Castelli et al6 were based on a single case of tick bite alopecia; however, the specimen was a generous excisional biopsy, allowing for a panoramic histologic view of the lesion. In the center of the specimen, hair follicles were absent, but residual follicular streamers and follicular remnants were surrounded by lymphocytic inflammation. Sebaceous glands were conspicuously absent, but foci with naked hairs, fibrosis, and granulomatous inflammation were seen. Peripherally, the hair follicles were thinned and miniaturized with an increased number of catagen/telogen hairs. Some follicles showed lamellar fibroplasia and perifollicular chronic inflammation. The inflammatory infiltrate consisted predominantly of helper T cells with a smaller population of B lymphocytes and a few plasma cells.6 In 2016, Lynch et al5 described a single case of tick bite alopecia and noted pseudolymphomatous inflammation with germinal center formation associated with hair miniaturization and an elevated catagen/telogen count; focal follicular mucinosis also was noted.Our histologic findings are similar to those of Castelli et al,6 except that the inflammatory infiltrate was clearly B-cell dominant, with a suggestion of germinal center formation, as noted by Lynch et al.5 This inflammatory pattern often can be encountered in a chronic tick bite lesion. Destruction of follicles and associated sebaceous glands and their replacement by follicular scars indicate that at least in the central portion of the lesion some permanent hair loss occurs. The presence of catagen/telogen hairs and miniaturized follicles indicates the potential for at least partial regrowth.
Similar to other investigators who have described tick bite alopecia, we can only speculate as to the mechanism by which clinical alopecia occurs. Given the density of the inflammatory infiltrate and perifollicular inflammation, it seems reasonable to assume that inflammation either destroys hair follicles or precipitates the catagen/telogen phase, resulting in temporary hair loss. The inflammation itself may be due to the presence of tick parts or the antigens in their saliva (or both). The delay between tick attachment and the onset of alopecia can be attributed to the time it takes follicles to cycle into the catagen/telogen phase and shed the hair shaft.
Case Report
A 44-year-old woman presented with a localized patch of hair loss on the frontal scalp of several month’s duration. She had been bitten by a tick at this site during the summer. Two months later
A punch biopsy was obtained from an indurated area of hyperpigmentation adjacent to the eschar. Both vertical and horizontal sections were obtained, revealing a relatively normal epidermis, a marked decrease in follicular structures with loss of sebaceous glands, and dense perifollicular lymphocytic inflammation with a few scattered eosinophils (Figures 2 and 3).
Historical Perspective
Tick bite alopecia was first described in the French literature in 19211 and in the English-language literature in 1955.2 A few additional cases were subsequently reported.3-5 In 2008, Castelli et al6 described the histologic and immunohistochemical features of 25 tick bite cases, a few of which resulted in alopecia. Other than these reports, little original information has been written about tick bite alopecia.
Clinical and Histologic Presentation
Tick bite alopecia is well described in the veterinary literature.7-9 It is possible that the condition is underreported in humans because the cause is often obvious or the alopecia is never discovered. The typical presentation is a roughly oval zone of alopecia that develops 1 to 2 weeks after the removal of a tick from the scalp. Often there is a small central eschar representing the site of tick attachment and the surrounding scalp may appear scaly. In one report of 2 siblings, multiple oval zones of alopecia resembling the moth-eaten alopecia of syphilis were noted in both patients, but only a single attached tick was found.2 In some reported cases, hair loss was only temporary, and at least partial if not complete regrowth of hair occurred.3,4 Follow-up on most cases is not provided, but to our knowledge permanent alopecia has not been described.
Information about the histologic findings of tick bite alopecia is particularly limited. In a report by Heyl,3 biopsies were conducted in 2 patients, but the areas selected for biopsy were the sites of tick attachment. Centrally dense, acute, and chronic inflammation was seen, as well as marked tissue necrosis of the connective tissue and hair follicles. Peripheral to the attachment zone, tissue necrosis was not found, but telogen hairs with “crumpled up hair shafts” were present.3 The histologic findings presented by Castelli et al6 were based on a single case of tick bite alopecia; however, the specimen was a generous excisional biopsy, allowing for a panoramic histologic view of the lesion. In the center of the specimen, hair follicles were absent, but residual follicular streamers and follicular remnants were surrounded by lymphocytic inflammation. Sebaceous glands were conspicuously absent, but foci with naked hairs, fibrosis, and granulomatous inflammation were seen. Peripherally, the hair follicles were thinned and miniaturized with an increased number of catagen/telogen hairs. Some follicles showed lamellar fibroplasia and perifollicular chronic inflammation. The inflammatory infiltrate consisted predominantly of helper T cells with a smaller population of B lymphocytes and a few plasma cells.6 In 2016, Lynch et al5 described a single case of tick bite alopecia and noted pseudolymphomatous inflammation with germinal center formation associated with hair miniaturization and an elevated catagen/telogen count; focal follicular mucinosis also was noted.Our histologic findings are similar to those of Castelli et al,6 except that the inflammatory infiltrate was clearly B-cell dominant, with a suggestion of germinal center formation, as noted by Lynch et al.5 This inflammatory pattern often can be encountered in a chronic tick bite lesion. Destruction of follicles and associated sebaceous glands and their replacement by follicular scars indicate that at least in the central portion of the lesion some permanent hair loss occurs. The presence of catagen/telogen hairs and miniaturized follicles indicates the potential for at least partial regrowth.
Similar to other investigators who have described tick bite alopecia, we can only speculate as to the mechanism by which clinical alopecia occurs. Given the density of the inflammatory infiltrate and perifollicular inflammation, it seems reasonable to assume that inflammation either destroys hair follicles or precipitates the catagen/telogen phase, resulting in temporary hair loss. The inflammation itself may be due to the presence of tick parts or the antigens in their saliva (or both). The delay between tick attachment and the onset of alopecia can be attributed to the time it takes follicles to cycle into the catagen/telogen phase and shed the hair shaft.
- Sauphar L. Alopecie peladoide consecutive a une piqure de tique. Bull Soc Fr Dermatol Syphiligr. 1921;28:442.
- Ross MS, Friede H. Alopecia due to tick bite. AMA Arch Derm. 1955;71:524-525.
- Heyl T. Tick bite alopecia. Clin Exp Dermatol. 1982;7:537-542.
- Marshall J. Alopecia after tick bite. S Afr Med J. 1966;40:555-556.
- Lynch MC, Milchak MA, Parnes H, et al. Tick bite alopecia: a report and review [published online April 19, 2016]. Am J Dermatopathol. doi:10.1097/DAD.0000000000000598.
- Castelli E, Caputo V, Morello V, et al. Local reactions to tick bites. Am J Dermatopathol. 2008;30:241-248.
- Nemeth NM, Ruder MG, Gerhold RW, et al. Demodectic mange, dermatophilosis, and other parasitic and bacterial dermatologic diseases in free-ranging white-tailed deer (Odocoileus virginianus) in the United States from 1975 to 2012. Vet Pathol. 2014;51:633-640.
- Welch DA, Samuel WM, Hudson RJ. Bioenergetic consequences of alopecia induced by Dermacentor albipictus (Acari: Ixodidae) on moose. J Med Entomol. 1990;27:656-660.
- Samuel WM. Locations of moose in northwestern Canada with hair loss probably caused by the winter tick, Dermacentor albipictus (Acari: Ixodidae). J Wildl Dis. 1989;25:436-439.
- Sauphar L. Alopecie peladoide consecutive a une piqure de tique. Bull Soc Fr Dermatol Syphiligr. 1921;28:442.
- Ross MS, Friede H. Alopecia due to tick bite. AMA Arch Derm. 1955;71:524-525.
- Heyl T. Tick bite alopecia. Clin Exp Dermatol. 1982;7:537-542.
- Marshall J. Alopecia after tick bite. S Afr Med J. 1966;40:555-556.
- Lynch MC, Milchak MA, Parnes H, et al. Tick bite alopecia: a report and review [published online April 19, 2016]. Am J Dermatopathol. doi:10.1097/DAD.0000000000000598.
- Castelli E, Caputo V, Morello V, et al. Local reactions to tick bites. Am J Dermatopathol. 2008;30:241-248.
- Nemeth NM, Ruder MG, Gerhold RW, et al. Demodectic mange, dermatophilosis, and other parasitic and bacterial dermatologic diseases in free-ranging white-tailed deer (Odocoileus virginianus) in the United States from 1975 to 2012. Vet Pathol. 2014;51:633-640.
- Welch DA, Samuel WM, Hudson RJ. Bioenergetic consequences of alopecia induced by Dermacentor albipictus (Acari: Ixodidae) on moose. J Med Entomol. 1990;27:656-660.
- Samuel WM. Locations of moose in northwestern Canada with hair loss probably caused by the winter tick, Dermacentor albipictus (Acari: Ixodidae). J Wildl Dis. 1989;25:436-439.
Practice Points
- Tick bite alopecia should be included in the differential diagnosis of both solitary and moth-eaten lesions of localized hair loss.
- In most cases, hair regrowth can be expected in a lesion of tick bite alopecia.
Early Decision Deadline Approaching for Class of 2017 Fellows Application
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30. Apply now at www.hospitalmedicine.org/fellows.
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30. Apply now at www.hospitalmedicine.org/fellows.
SHM Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently 2,000 hospitalists who have earned the FHM/SFHM designation by demonstrating core values of leadership, teamwork, and quality improvement.
Apply by Sept. 15 to receive an early decision on or before Oct. 28. The regular decision application will remain open through Nov. 30. Apply now at www.hospitalmedicine.org/fellows.
SHM Nomination, Election Season Has Begun
Nominations for SHM Awards of Excellence, committees, Board of Director seats, and Masters of Hospital Medicine designations are now open. The deadline for award, committee, and board election nominations is Oct. 14. The deadline for MHM submission is Dec. 9. Make your nominations now at www.hospitalmedicine.org:
• Awards of Excellence: www.hospitalmedicine.org/awards
• Board of Directors: www.hospitalmedicine.org/boardelection
• Committee nominations: www.hospitalmedicine.org/committee
• Masters of Hospital Medicine: www.hospitalmedicine.org/masters
Nominations for SHM Awards of Excellence, committees, Board of Director seats, and Masters of Hospital Medicine designations are now open. The deadline for award, committee, and board election nominations is Oct. 14. The deadline for MHM submission is Dec. 9. Make your nominations now at www.hospitalmedicine.org:
• Awards of Excellence: www.hospitalmedicine.org/awards
• Board of Directors: www.hospitalmedicine.org/boardelection
• Committee nominations: www.hospitalmedicine.org/committee
• Masters of Hospital Medicine: www.hospitalmedicine.org/masters
Nominations for SHM Awards of Excellence, committees, Board of Director seats, and Masters of Hospital Medicine designations are now open. The deadline for award, committee, and board election nominations is Oct. 14. The deadline for MHM submission is Dec. 9. Make your nominations now at www.hospitalmedicine.org:
• Awards of Excellence: www.hospitalmedicine.org/awards
• Board of Directors: www.hospitalmedicine.org/boardelection
• Committee nominations: www.hospitalmedicine.org/committee
• Masters of Hospital Medicine: www.hospitalmedicine.org/masters
Immunotherapy conditioning proves successful in mice

Photo by Aaron Logan
Research in mice suggests it’s feasible to use an immunotherapy conditioning regimen rather than radiation or chemotherapy prior to hematopoietic stem cell transplant (HSCT).
Investigators found that combining an antibody against the HSC receptor c-Kit with a CD47-blocking therapy could eliminate host HSCs and allow for successful engraftment of donor HSCs in immunocompetent recipient mice.
Adding T-cell-depleting antibodies to the mix allowed for robust HSC engraftment in a clinically relevant model of allogeneic HSCT.
Irving Weissman, MD, of Stanford University School of Medicine in California, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers first found that ACK2, an antibody against c-Kit, successfully depleted HSCs in immune-deficient mice.
“However, this antibody alone would not be effective in immune-competent recipients, who represent a majority of potential bone marrow transplant recipients,” said study author Akanksha Chhabra, PhD, of Stanford University School of Medicine.
So the researchers sought to enhance the effectiveness of ACK2 by combining it with antibodies or biologic agents that block CD47. They found that blocking CD47—particularly with an antagonist known as CV1mb—liberated macrophages to engulf target cells.
In this way, the immune system effectively depleted host HSCs in the immunocompetent mice, clearing the way for donor HSCs to take up residence in the bone marrow.
Finally, the researchers set out to determine whether conditioning with an anti-c-Kit antibody and CD47-blocking therapy could be extended to a clinically relevant model of allogeneic HSCT, in which the donor and recipient are matched through human leukocyte antigen alleles but mismatched at minor histocompatibility complex (mHC) antigens.
So the team conditioned mice with either ACK2 and CV1mb or ACK2 and the anti-CD47 antibody MIAP410. And they achieved immune ablation with T-cell-depleting antibodies—GK1.5 (anti-CD4) and YTS169.4 (anti-CD8). The mice then received mHC-mismatched HSCs.
The researchers found that either conditioning regimen, when combined with a T-cell-depleting regimen, resulted in substantial granulocyte, B-cell, T-cell, and NK-cell chimerism, as well as HSC engraftment in the bone marrow.
The success of these techniques in mice raises the researchers’ hopes that similar techniques will succeed in humans.
“If it works in humans like it did in mice, we would expect that the risk of death from blood stem cell transplant would drop from 20% to effectively 0,” said study author Judith Shizuru, MD, PhD, of Stanford University School of Medicine.
“If and when this is accomplished, it will be a whole new era in disease treatment and regenerative medicine,” Dr Weissman said. ![]()
Photo by Aaron Logan
Research in mice suggests it’s feasible to use an immunotherapy conditioning regimen rather than radiation or chemotherapy prior to hematopoietic stem cell transplant (HSCT).
Investigators found that combining an antibody against the HSC receptor c-Kit with a CD47-blocking therapy could eliminate host HSCs and allow for successful engraftment of donor HSCs in immunocompetent recipient mice.
Adding T-cell-depleting antibodies to the mix allowed for robust HSC engraftment in a clinically relevant model of allogeneic HSCT.
Irving Weissman, MD, of Stanford University School of Medicine in California, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers first found that ACK2, an antibody against c-Kit, successfully depleted HSCs in immune-deficient mice.
“However, this antibody alone would not be effective in immune-competent recipients, who represent a majority of potential bone marrow transplant recipients,” said study author Akanksha Chhabra, PhD, of Stanford University School of Medicine.
So the researchers sought to enhance the effectiveness of ACK2 by combining it with antibodies or biologic agents that block CD47. They found that blocking CD47—particularly with an antagonist known as CV1mb—liberated macrophages to engulf target cells.
In this way, the immune system effectively depleted host HSCs in the immunocompetent mice, clearing the way for donor HSCs to take up residence in the bone marrow.
Finally, the researchers set out to determine whether conditioning with an anti-c-Kit antibody and CD47-blocking therapy could be extended to a clinically relevant model of allogeneic HSCT, in which the donor and recipient are matched through human leukocyte antigen alleles but mismatched at minor histocompatibility complex (mHC) antigens.
So the team conditioned mice with either ACK2 and CV1mb or ACK2 and the anti-CD47 antibody MIAP410. And they achieved immune ablation with T-cell-depleting antibodies—GK1.5 (anti-CD4) and YTS169.4 (anti-CD8). The mice then received mHC-mismatched HSCs.
The researchers found that either conditioning regimen, when combined with a T-cell-depleting regimen, resulted in substantial granulocyte, B-cell, T-cell, and NK-cell chimerism, as well as HSC engraftment in the bone marrow.
The success of these techniques in mice raises the researchers’ hopes that similar techniques will succeed in humans.
“If it works in humans like it did in mice, we would expect that the risk of death from blood stem cell transplant would drop from 20% to effectively 0,” said study author Judith Shizuru, MD, PhD, of Stanford University School of Medicine.
“If and when this is accomplished, it will be a whole new era in disease treatment and regenerative medicine,” Dr Weissman said. ![]()
Photo by Aaron Logan
Research in mice suggests it’s feasible to use an immunotherapy conditioning regimen rather than radiation or chemotherapy prior to hematopoietic stem cell transplant (HSCT).
Investigators found that combining an antibody against the HSC receptor c-Kit with a CD47-blocking therapy could eliminate host HSCs and allow for successful engraftment of donor HSCs in immunocompetent recipient mice.
Adding T-cell-depleting antibodies to the mix allowed for robust HSC engraftment in a clinically relevant model of allogeneic HSCT.
Irving Weissman, MD, of Stanford University School of Medicine in California, and his colleagues conducted this research and reported the results in Science Translational Medicine.
The researchers first found that ACK2, an antibody against c-Kit, successfully depleted HSCs in immune-deficient mice.
“However, this antibody alone would not be effective in immune-competent recipients, who represent a majority of potential bone marrow transplant recipients,” said study author Akanksha Chhabra, PhD, of Stanford University School of Medicine.
So the researchers sought to enhance the effectiveness of ACK2 by combining it with antibodies or biologic agents that block CD47. They found that blocking CD47—particularly with an antagonist known as CV1mb—liberated macrophages to engulf target cells.
In this way, the immune system effectively depleted host HSCs in the immunocompetent mice, clearing the way for donor HSCs to take up residence in the bone marrow.
Finally, the researchers set out to determine whether conditioning with an anti-c-Kit antibody and CD47-blocking therapy could be extended to a clinically relevant model of allogeneic HSCT, in which the donor and recipient are matched through human leukocyte antigen alleles but mismatched at minor histocompatibility complex (mHC) antigens.
So the team conditioned mice with either ACK2 and CV1mb or ACK2 and the anti-CD47 antibody MIAP410. And they achieved immune ablation with T-cell-depleting antibodies—GK1.5 (anti-CD4) and YTS169.4 (anti-CD8). The mice then received mHC-mismatched HSCs.
The researchers found that either conditioning regimen, when combined with a T-cell-depleting regimen, resulted in substantial granulocyte, B-cell, T-cell, and NK-cell chimerism, as well as HSC engraftment in the bone marrow.
The success of these techniques in mice raises the researchers’ hopes that similar techniques will succeed in humans.
“If it works in humans like it did in mice, we would expect that the risk of death from blood stem cell transplant would drop from 20% to effectively 0,” said study author Judith Shizuru, MD, PhD, of Stanford University School of Medicine.
“If and when this is accomplished, it will be a whole new era in disease treatment and regenerative medicine,” Dr Weissman said. ![]()
FDA authorizes use of Zika assay

Photo by Juan D. Alfonso
The US Food and Drug Administration (FDA) has granted emergency use authorization (EUA) for the xMAP® MultiFLEX™ Zika RNA Assay.
This multiplex nucleic acid test is designed to detect Zika virus RNA in blood serum, plasma, or urine (collected alongside a patient-matched serum or plasma specimen).
The xMAP® MultiFLEX™ Zika RNA Assay is available for purchase by laboratories that are certified under the Clinical Laboratory Improvement Amendments of 1988 (CLIA) to perform high complexity tests.
The assay uses the Luminex® 100/200™ analyzer, MAGPIX® system, or other authorized instruments to simultaneously test for 6 genetic targets of the Zika virus.
The xMAP® MultiFLEX™ Zika RNA Assay was designed by GenArraytion, Inc. and is marketed by Luminex Corporation.
For more information on the test, see the fact sheet for healthcare providers on the Luminex website.
About the EUA
The EUA does not mean the xMAP® MultiFLEX™ Zika RNA Assay is FDA cleared or approved.
An EUA allows for the use of unapproved medical products or unapproved uses of approved medical products in an emergency.
The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
This means the xMAP® MultiFLEX™ Zika RNA Assay is only authorized as long as circumstances exist to justify the authorization of the emergency use of in vitro diagnostics for the detection of Zika virus, unless the authorization is terminated or revoked sooner. ![]()
Photo by Juan D. Alfonso
The US Food and Drug Administration (FDA) has granted emergency use authorization (EUA) for the xMAP® MultiFLEX™ Zika RNA Assay.
This multiplex nucleic acid test is designed to detect Zika virus RNA in blood serum, plasma, or urine (collected alongside a patient-matched serum or plasma specimen).
The xMAP® MultiFLEX™ Zika RNA Assay is available for purchase by laboratories that are certified under the Clinical Laboratory Improvement Amendments of 1988 (CLIA) to perform high complexity tests.
The assay uses the Luminex® 100/200™ analyzer, MAGPIX® system, or other authorized instruments to simultaneously test for 6 genetic targets of the Zika virus.
The xMAP® MultiFLEX™ Zika RNA Assay was designed by GenArraytion, Inc. and is marketed by Luminex Corporation.
For more information on the test, see the fact sheet for healthcare providers on the Luminex website.
About the EUA
The EUA does not mean the xMAP® MultiFLEX™ Zika RNA Assay is FDA cleared or approved.
An EUA allows for the use of unapproved medical products or unapproved uses of approved medical products in an emergency.
The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
This means the xMAP® MultiFLEX™ Zika RNA Assay is only authorized as long as circumstances exist to justify the authorization of the emergency use of in vitro diagnostics for the detection of Zika virus, unless the authorization is terminated or revoked sooner. ![]()
Photo by Juan D. Alfonso
The US Food and Drug Administration (FDA) has granted emergency use authorization (EUA) for the xMAP® MultiFLEX™ Zika RNA Assay.
This multiplex nucleic acid test is designed to detect Zika virus RNA in blood serum, plasma, or urine (collected alongside a patient-matched serum or plasma specimen).
The xMAP® MultiFLEX™ Zika RNA Assay is available for purchase by laboratories that are certified under the Clinical Laboratory Improvement Amendments of 1988 (CLIA) to perform high complexity tests.
The assay uses the Luminex® 100/200™ analyzer, MAGPIX® system, or other authorized instruments to simultaneously test for 6 genetic targets of the Zika virus.
The xMAP® MultiFLEX™ Zika RNA Assay was designed by GenArraytion, Inc. and is marketed by Luminex Corporation.
For more information on the test, see the fact sheet for healthcare providers on the Luminex website.
About the EUA
The EUA does not mean the xMAP® MultiFLEX™ Zika RNA Assay is FDA cleared or approved.
An EUA allows for the use of unapproved medical products or unapproved uses of approved medical products in an emergency.
The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
This means the xMAP® MultiFLEX™ Zika RNA Assay is only authorized as long as circumstances exist to justify the authorization of the emergency use of in vitro diagnostics for the detection of Zika virus, unless the authorization is terminated or revoked sooner. ![]()
FDA approves drug for prevention of CINV

Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has approved granisetron extended-release injection (Sustol®) for the prevention of chemotherapy-induced nausea and vomiting (CINV) in adults.
Extended-release granisetron is a serotonin-3 (5-HT3) receptor antagonist that utilizes Biochronomer® polymer-based drug delivery technology to maintain therapeutic levels of granisetron for at least 5 days, covering both the acute and delayed phases of CINV.
The product is intended for use in combination with other anti-emetics to prevent acute and delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic chemotherapy (MEC) or anthracycline and cyclophosphamide (AC) combination chemotherapy regimens.
“Despite advances in the management of CINV, up to half of patients receiving chemotherapy can still experience CINV, with delayed CINV being particularly challenging to control,” said Ralph V. Boccia, MD, of the Center for Cancer and Blood Disorders in Bethesda, Maryland.
“In our experience, other 5-HT3 receptor antagonists, including palonosetron, are generally effective for 48 hours or less. Sustol, due to its extended-release profile, represents a novel option that can protect patients from CINV for a full 5 days.”
Extended-release granisetron (formerly known as APF530) is a product of Heron Therapeutics, Inc. The US commercial launch of the drug is planned for the fourth quarter of 2016.
Phase 3 trials
The global phase 3 development program of extended-release granisetron consisted of 2 large, guideline-based clinical trials of more than 2000 cancer patients.
In one trial, researchers compared extended-release granisetron to palonosetron for the prevention of acute and delayed CINV after MEC or highly emetogenic chemotherapy (HEC).
Results suggested extended-release granisetron was non-inferior to palonosetron. The most common adverse events observed in patients receiving granisetron were injection-site reactions and constipation.
In another trial, researchers compared extended-release granisetron to ondansetron for control of delayed CINV after HEC. Patients received extended-release granisetron, dexamethasone, and fosaprepitant or ondansetron, dexamethasone, and fosaprepitant.
A higher percentage of patients in the granisetron arm had delayed-phase complete response. The incidence of treatment-emergent adverse events was similar between the treatment arms.
“The Sustol clinical trial populations and results are highly representative of cancer patients in our real-world clinical practice,” said Jeffrey Vacirca, MD, of North Shore Hematology Oncology Associates in East Setauket, New York.
“Use of MEC regimens is widespread, and AC-based regimens are among the most commonly prescribed highly emetogenic chemotherapy regimens. The most significant challenge for my breast cancer patients receiving AC is chemotherapy-induced nausea and vomiting. Sustol represents a better option to manage this devastating side effect of therapy.”
For more details on the drug, access the full prescribing information at www.SUSTOL.com. ![]()
Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has approved granisetron extended-release injection (Sustol®) for the prevention of chemotherapy-induced nausea and vomiting (CINV) in adults.
Extended-release granisetron is a serotonin-3 (5-HT3) receptor antagonist that utilizes Biochronomer® polymer-based drug delivery technology to maintain therapeutic levels of granisetron for at least 5 days, covering both the acute and delayed phases of CINV.
The product is intended for use in combination with other anti-emetics to prevent acute and delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic chemotherapy (MEC) or anthracycline and cyclophosphamide (AC) combination chemotherapy regimens.
“Despite advances in the management of CINV, up to half of patients receiving chemotherapy can still experience CINV, with delayed CINV being particularly challenging to control,” said Ralph V. Boccia, MD, of the Center for Cancer and Blood Disorders in Bethesda, Maryland.
“In our experience, other 5-HT3 receptor antagonists, including palonosetron, are generally effective for 48 hours or less. Sustol, due to its extended-release profile, represents a novel option that can protect patients from CINV for a full 5 days.”
Extended-release granisetron (formerly known as APF530) is a product of Heron Therapeutics, Inc. The US commercial launch of the drug is planned for the fourth quarter of 2016.
Phase 3 trials
The global phase 3 development program of extended-release granisetron consisted of 2 large, guideline-based clinical trials of more than 2000 cancer patients.
In one trial, researchers compared extended-release granisetron to palonosetron for the prevention of acute and delayed CINV after MEC or highly emetogenic chemotherapy (HEC).
Results suggested extended-release granisetron was non-inferior to palonosetron. The most common adverse events observed in patients receiving granisetron were injection-site reactions and constipation.
In another trial, researchers compared extended-release granisetron to ondansetron for control of delayed CINV after HEC. Patients received extended-release granisetron, dexamethasone, and fosaprepitant or ondansetron, dexamethasone, and fosaprepitant.
A higher percentage of patients in the granisetron arm had delayed-phase complete response. The incidence of treatment-emergent adverse events was similar between the treatment arms.
“The Sustol clinical trial populations and results are highly representative of cancer patients in our real-world clinical practice,” said Jeffrey Vacirca, MD, of North Shore Hematology Oncology Associates in East Setauket, New York.
“Use of MEC regimens is widespread, and AC-based regimens are among the most commonly prescribed highly emetogenic chemotherapy regimens. The most significant challenge for my breast cancer patients receiving AC is chemotherapy-induced nausea and vomiting. Sustol represents a better option to manage this devastating side effect of therapy.”
For more details on the drug, access the full prescribing information at www.SUSTOL.com. ![]()
Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has approved granisetron extended-release injection (Sustol®) for the prevention of chemotherapy-induced nausea and vomiting (CINV) in adults.
Extended-release granisetron is a serotonin-3 (5-HT3) receptor antagonist that utilizes Biochronomer® polymer-based drug delivery technology to maintain therapeutic levels of granisetron for at least 5 days, covering both the acute and delayed phases of CINV.
The product is intended for use in combination with other anti-emetics to prevent acute and delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic chemotherapy (MEC) or anthracycline and cyclophosphamide (AC) combination chemotherapy regimens.
“Despite advances in the management of CINV, up to half of patients receiving chemotherapy can still experience CINV, with delayed CINV being particularly challenging to control,” said Ralph V. Boccia, MD, of the Center for Cancer and Blood Disorders in Bethesda, Maryland.
“In our experience, other 5-HT3 receptor antagonists, including palonosetron, are generally effective for 48 hours or less. Sustol, due to its extended-release profile, represents a novel option that can protect patients from CINV for a full 5 days.”
Extended-release granisetron (formerly known as APF530) is a product of Heron Therapeutics, Inc. The US commercial launch of the drug is planned for the fourth quarter of 2016.
Phase 3 trials
The global phase 3 development program of extended-release granisetron consisted of 2 large, guideline-based clinical trials of more than 2000 cancer patients.
In one trial, researchers compared extended-release granisetron to palonosetron for the prevention of acute and delayed CINV after MEC or highly emetogenic chemotherapy (HEC).
Results suggested extended-release granisetron was non-inferior to palonosetron. The most common adverse events observed in patients receiving granisetron were injection-site reactions and constipation.
In another trial, researchers compared extended-release granisetron to ondansetron for control of delayed CINV after HEC. Patients received extended-release granisetron, dexamethasone, and fosaprepitant or ondansetron, dexamethasone, and fosaprepitant.
A higher percentage of patients in the granisetron arm had delayed-phase complete response. The incidence of treatment-emergent adverse events was similar between the treatment arms.
“The Sustol clinical trial populations and results are highly representative of cancer patients in our real-world clinical practice,” said Jeffrey Vacirca, MD, of North Shore Hematology Oncology Associates in East Setauket, New York.
“Use of MEC regimens is widespread, and AC-based regimens are among the most commonly prescribed highly emetogenic chemotherapy regimens. The most significant challenge for my breast cancer patients receiving AC is chemotherapy-induced nausea and vomiting. Sustol represents a better option to manage this devastating side effect of therapy.”
For more details on the drug, access the full prescribing information at www.SUSTOL.com. ![]()
How procoagulant platelets develop

Image by Andre E.X. Brown
Researchers say they have determined how procoagulant platelets develop.
One of the mysteries in the field of thrombosis and hemostasis is how platelets are divided into two kinds when activated—“ordinary” platelets capable of aggregation and “super-activated,” procoagulant platelets.
The new study suggests that, to become super-activated, platelets must die. And the platelets need mitochondria to commit suicide.
Researchers were able to show how this programmed death—mitochondrial necrosis—follows a chain of events that lead to the platelets’ transition to a super-activated state.
“It was not clear before how a platelet makes the decision of what type to become,” said study author Mikhail Panteleev, of Lomonosov Moscow State University in Russia.
“We have deciphered the sequence of events: how the signal goes within the platelet and how the cell decides to die.”
Panteleev and his colleagues described these events in the Journal of Thrombosis and Haemostasis.
The team noted that platelets have many activators, but the chief among them are collagen, ADP, and thrombin.
Platelets detect different concentrations of an activator and respond with a varying frequency of calcium impulses in the cytoplasm.
The platelets’ mitochondria absorb and store the calcium, and when its concentration exceeds the critical level, the process of mitochondrial necrosis starts.
Calcium and reactive oxygen species are released from mitochondria, ATPases begin to destroy ATP instead of synthesizing it, the cell cytoskeleton collapses, and the platelets greatly increase in size.
As a result, at the outer membrane of the enlarged platelets, a lipid called phosphatidylserine appears, which is responsible for rapid blood clotting. And all this happens in seconds. ![]()
Image by Andre E.X. Brown
Researchers say they have determined how procoagulant platelets develop.
One of the mysteries in the field of thrombosis and hemostasis is how platelets are divided into two kinds when activated—“ordinary” platelets capable of aggregation and “super-activated,” procoagulant platelets.
The new study suggests that, to become super-activated, platelets must die. And the platelets need mitochondria to commit suicide.
Researchers were able to show how this programmed death—mitochondrial necrosis—follows a chain of events that lead to the platelets’ transition to a super-activated state.
“It was not clear before how a platelet makes the decision of what type to become,” said study author Mikhail Panteleev, of Lomonosov Moscow State University in Russia.
“We have deciphered the sequence of events: how the signal goes within the platelet and how the cell decides to die.”
Panteleev and his colleagues described these events in the Journal of Thrombosis and Haemostasis.
The team noted that platelets have many activators, but the chief among them are collagen, ADP, and thrombin.
Platelets detect different concentrations of an activator and respond with a varying frequency of calcium impulses in the cytoplasm.
The platelets’ mitochondria absorb and store the calcium, and when its concentration exceeds the critical level, the process of mitochondrial necrosis starts.
Calcium and reactive oxygen species are released from mitochondria, ATPases begin to destroy ATP instead of synthesizing it, the cell cytoskeleton collapses, and the platelets greatly increase in size.
As a result, at the outer membrane of the enlarged platelets, a lipid called phosphatidylserine appears, which is responsible for rapid blood clotting. And all this happens in seconds. ![]()
Image by Andre E.X. Brown
Researchers say they have determined how procoagulant platelets develop.
One of the mysteries in the field of thrombosis and hemostasis is how platelets are divided into two kinds when activated—“ordinary” platelets capable of aggregation and “super-activated,” procoagulant platelets.
The new study suggests that, to become super-activated, platelets must die. And the platelets need mitochondria to commit suicide.
Researchers were able to show how this programmed death—mitochondrial necrosis—follows a chain of events that lead to the platelets’ transition to a super-activated state.
“It was not clear before how a platelet makes the decision of what type to become,” said study author Mikhail Panteleev, of Lomonosov Moscow State University in Russia.
“We have deciphered the sequence of events: how the signal goes within the platelet and how the cell decides to die.”
Panteleev and his colleagues described these events in the Journal of Thrombosis and Haemostasis.
The team noted that platelets have many activators, but the chief among them are collagen, ADP, and thrombin.
Platelets detect different concentrations of an activator and respond with a varying frequency of calcium impulses in the cytoplasm.
The platelets’ mitochondria absorb and store the calcium, and when its concentration exceeds the critical level, the process of mitochondrial necrosis starts.
Calcium and reactive oxygen species are released from mitochondria, ATPases begin to destroy ATP instead of synthesizing it, the cell cytoskeleton collapses, and the platelets greatly increase in size.
As a result, at the outer membrane of the enlarged platelets, a lipid called phosphatidylserine appears, which is responsible for rapid blood clotting. And all this happens in seconds. ![]()
Thymectomy improves clinical outcomes for myasthenia gravis
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Landmark trial establishes effectiveness of thymectomy in myasthenia gravis
One of the many challenges of treating patients with myasthenia gravis (MG) is the fluctuating nature of symptoms and deficits. The neurologist or neuromuscular specialist must decide whether the disease is truly worsening, whether the patient is experiencing more pronounced symptoms from intercurrent illness or the effects of a medication known to affect the neuromuscular junction adversely, or whether the patient is concerned that there might be worsening disease when all objective measures indicate stability. These factors make treatment decisions more difficult in MG than for many other neuromuscular disorders.
Similarly, researchers considering a trial investigating treatment efficacy in MG face the complex issues of disease fluctuation in cohorts of individuals with the disease, varying levels of corticosteroid and immunosuppressant doses in different MG patients, and thorny ethical dilemmas in providing accepted therapies but not withholding effective treatments from those in need.
Dr. Wolfe and his colleagues demonstrate that they have navigated these treacherous waters. They have succeeded in completing a landmark controlled clinical trial which establishes the effectiveness of transsternal thymectomy with adjuvant corticosteroid therapy in nonthymomatous MG vs. oral prednisone without surgery. While this international 36-center trial managed to recruit 126 subjects over a 6-year period, using sound inclusion and exclusion criteria and a meticulous trial design, the number of patients is not sufficient to allow for as robust a subgroup analysis for age, gender, and a variety of clinical variables reflecting severity of disease as would have been hoped for by the MG community.
Nonetheless, this paper sets the use of thymectomy in nonthymomatous MG on firmer ground going forward. The investigators will doubtless be presenting further data from the trial, including clinical-pathologic correlates and other relevant novel observations. In addition, Wolfe et al. have opened the door for future trials of thymectomy in MG to address such issues as the benefits vs. risks of performing the operation via the traditional transsternal vs. alternative non–sternal splitting approaches.
Benn E. Smith, MD, is an associate professor of neurology at the Mayo Clinic in Scottsdale, Ariz. and is the director of the sensory laboratory there. Dr. Smith is on the Editorial Advisory Board of Clinical Neurology News.
End to an 80-year controversy
These findings from Wolfe et al. end an 80-year controversy over the effectiveness of thymectomy for patients with myasthenia gravis.
Perhaps the most important benefit for patients is that even when they require prednisone following the surgery, they can take lower doses, endure fewer glucocorticoid-related symptoms, and experience less distress from those symptoms than patients who don’t undergo thymectomy.
Unfortunately, the study results cannot offer further clarity regarding patient selection for thymectomy. The patient population in this trial was so small that subgroup analyses couldn’t allow conclusions regarding the relative effectiveness of thymectomy in men vs. women or younger vs. older patients.
Allan H. Ropper, MD, is in the department of neurology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston. His financial disclosures are available at NEJM.org. Dr. Ropper made these remarks in an editorial accompanying Dr. Wolfe’s report (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMe1607953).
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Thymectomy improved 3-year clinical outcomes and proved superior to medical therapy for mild to severe nonthymomatous myasthenia gravis, according to a report published online Aug. 11 in the New England Journal of Medicine.
Compared with standard prednisone therapy, thymectomy plus prednisone decreased the number and severity of symptoms, allowed the lowering of steroid doses, decreased the number and length of hospitalizations for disease exacerbations, reduced the need for immunosuppressive agents, and improved health-related quality of life in an international, randomized clinical trial, said Gil I. Wolfe, MD, of the department of neurology, State University of New York at Buffalo and his associates.
Until now, thymectomy was known to be beneficial in some cases of myasthenia gravis “but with widely varying rates of clinical improvement or remission.” And the success of immunotherapy has raised the question of whether an invasive surgery is necessary. Data from randomized, controlled studies have been sparse.
Moreover, thymectomy rarely causes adverse effects, but “the procedure can cost up to $80,000 and can be associated with operative complications that need to be weighed against benefits.” In comparison, medical therapy with glucocorticoids and other immunosuppressive agents is less invasive but is definitely associated with adverse events, including some that are life threatening, and negatively impacts quality of life, the investigators said.
To address the lack of randomized controlled trial data, they assessed 3-year outcomes in 126 patients treated at 67 medical centers in 18 countries during a 6-year period. The study participants were aged 18-65 years, had a disease duration of less than 5 years at enrollment (median duration, 1 year), and had class II (mild generalized disease) to class IV (severe generalized disease) myasthenia gravis. These patients were randomly assigned to undergo thymectomy and receive standard prednisone therapy (66 participants) or to receive standard prednisone alone (60 participants).
Thymectomy was performed using a median sternotomy “with the goal of an en bloc resection of all mediastinal tissue that could anatomically contain gross or microscopic thymus.”
At follow-up, time-weighted average scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group. Time-weighted average prednisone dose also was significantly lower, at an average alternate-day dose of 44 mg in the thymectomy group and 60 mg in the control group, Dr. Wolfe and his associates said (N Engl J Med. 2016 Aug 11. doi: 10.1056/NEJMoa1602489).
On a measure of treatment-related complications, scores favored thymectomy with regard to the number of patients with symptoms, the total number of symptoms, and the distress level related to symptoms throughout the study period. Fewer patients in the thymectomy group required hospitalization for exacerbations of myasthenia gravis (9% vs. 37%), and the mean cumulative number of hospital days was lower with thymectomy (8.4 vs. 19.2).
In addition, scores on the Myasthenia Gravis Activities of Daily Living scale favored thymectomy (2.24 vs. 3.41). Fewer patients in the thymectomy group required azathioprine (17% vs. 0.48%). And the percentage of patients who reported having minimal manifestations of the disease at 3 years was significantly higher with thymectomy (67%) than with prednisone alone (47%).
This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Thymectomy improved 3-year clinical outcomes and was superior to medical therapy for mild to severe nonthymomatous myasthenia gravis.
Major finding: Scores on the Quantitative Myasthenia Gravis scale were significantly lower by 2.85 points, indicating improved clinical status, in the thymectomy group than in the control group.
Data source: An international, randomized, medication-controlled trial involving 126 patients at 67 medical centers.
Disclosures: This study was supported by the National Institute of Neurological Disorders and Stroke, the Muscular Dystrophy Association, and the Myasthenia Gravis Foundation of America and received no commercial support. Dr. Wolfe reported ties to Alexion Pharmaceuticals, Alpha Cancer Technologies, Argenx, Baxalta, CSL Behring, Grifols, and UCB, and his associates reported ties to numerous industry sources.
Making Fillers a Success Through Technique and Patient Education
What does your patient need to know at the first visit?
In my practice, we try our best to start the education process before the patient even comes in for the first visit. If a patient is going to have a filler injection, we mail out an information packet that contains information on what to expect, how to minimize bruising, what side effects (eg, bruising, swelling) may occur, and what to avoid posttreatment. By providing them with this information prior to their visit, they can better plan their treatment around social and work obligations.
We ask patients to avoid or minimize blood-thinning agents such as aspirin, ibuprofen, fish oil, or vitamin E starting 2 weeks prior to and 1 week after the procedure. We recommend that patients take a pineapple extract such as bromelain 500 mg twice daily on an empty stomach starting 1 week prior to the treatment and for up to 1 week posttreatment. We ask that patients avoid exercise for 24 hours to reduce late-onset bruising and to avoid dental work for 2 weeks posttreatment to reduce the risk for the filler becoming infected.
What are your go-to treatments?
I use a variety of fillers depending on the area I am treating (thin vs thick skin) or the amount of lift I need (ie, G')(Restylane [Galderma Laboratories, LP] has a high G', thus it gives a lot of lift) versus the amount of water absorption I am seeking to further plump an area after the filler integrates (Juvéderm [Allergan] can absorb up to 300% its weight in water) versus the filler’s cohesiveness (Belotero [Merz Aesthetics] is highly cohesive). If I am treating a thin-faced individual, I may start with a global volumizer such as poly-L-lactic acid to get a good foundation set in the temples, cheeks, and jawline, and then after a few months, I will add a hyaluronic acid filler to focal areas that still need to be lifted (eg, nasolabial folds, tear troughs).
What are the side effects?
Side effects are divided into common and rare. Common would be bruising and swelling, which are temporary and will go away in all patients. Rare but serious side effects are infection and embolization. Both can cause notable tissue loss and risk to the patient. Every practitioner needs to know how to recognize and treat these complications should they arise.
How do you keep patients compliant?
Patients who get good results will always return, which means being up front about how much filler a patient needs and how frequently he/she will need it, and also doing everything we can to reduce bruising and swelling.
Suggested Readings
- Dayan SH, Arkins JP, Brindise R. Soft tissue fillers and biofilms. Facial Plast Surg. 2011;27:23-28.
- Orsini RA; Plastic Surgery Educational Technology Assessment Committee. Bromelain. Plast Reconstr Surg. 2006;118:1640-1644.
What does your patient need to know at the first visit?
In my practice, we try our best to start the education process before the patient even comes in for the first visit. If a patient is going to have a filler injection, we mail out an information packet that contains information on what to expect, how to minimize bruising, what side effects (eg, bruising, swelling) may occur, and what to avoid posttreatment. By providing them with this information prior to their visit, they can better plan their treatment around social and work obligations.
We ask patients to avoid or minimize blood-thinning agents such as aspirin, ibuprofen, fish oil, or vitamin E starting 2 weeks prior to and 1 week after the procedure. We recommend that patients take a pineapple extract such as bromelain 500 mg twice daily on an empty stomach starting 1 week prior to the treatment and for up to 1 week posttreatment. We ask that patients avoid exercise for 24 hours to reduce late-onset bruising and to avoid dental work for 2 weeks posttreatment to reduce the risk for the filler becoming infected.
What are your go-to treatments?
I use a variety of fillers depending on the area I am treating (thin vs thick skin) or the amount of lift I need (ie, G')(Restylane [Galderma Laboratories, LP] has a high G', thus it gives a lot of lift) versus the amount of water absorption I am seeking to further plump an area after the filler integrates (Juvéderm [Allergan] can absorb up to 300% its weight in water) versus the filler’s cohesiveness (Belotero [Merz Aesthetics] is highly cohesive). If I am treating a thin-faced individual, I may start with a global volumizer such as poly-L-lactic acid to get a good foundation set in the temples, cheeks, and jawline, and then after a few months, I will add a hyaluronic acid filler to focal areas that still need to be lifted (eg, nasolabial folds, tear troughs).
What are the side effects?
Side effects are divided into common and rare. Common would be bruising and swelling, which are temporary and will go away in all patients. Rare but serious side effects are infection and embolization. Both can cause notable tissue loss and risk to the patient. Every practitioner needs to know how to recognize and treat these complications should they arise.
How do you keep patients compliant?
Patients who get good results will always return, which means being up front about how much filler a patient needs and how frequently he/she will need it, and also doing everything we can to reduce bruising and swelling.
Suggested Readings
- Dayan SH, Arkins JP, Brindise R. Soft tissue fillers and biofilms. Facial Plast Surg. 2011;27:23-28.
- Orsini RA; Plastic Surgery Educational Technology Assessment Committee. Bromelain. Plast Reconstr Surg. 2006;118:1640-1644.
What does your patient need to know at the first visit?
In my practice, we try our best to start the education process before the patient even comes in for the first visit. If a patient is going to have a filler injection, we mail out an information packet that contains information on what to expect, how to minimize bruising, what side effects (eg, bruising, swelling) may occur, and what to avoid posttreatment. By providing them with this information prior to their visit, they can better plan their treatment around social and work obligations.
We ask patients to avoid or minimize blood-thinning agents such as aspirin, ibuprofen, fish oil, or vitamin E starting 2 weeks prior to and 1 week after the procedure. We recommend that patients take a pineapple extract such as bromelain 500 mg twice daily on an empty stomach starting 1 week prior to the treatment and for up to 1 week posttreatment. We ask that patients avoid exercise for 24 hours to reduce late-onset bruising and to avoid dental work for 2 weeks posttreatment to reduce the risk for the filler becoming infected.
What are your go-to treatments?
I use a variety of fillers depending on the area I am treating (thin vs thick skin) or the amount of lift I need (ie, G')(Restylane [Galderma Laboratories, LP] has a high G', thus it gives a lot of lift) versus the amount of water absorption I am seeking to further plump an area after the filler integrates (Juvéderm [Allergan] can absorb up to 300% its weight in water) versus the filler’s cohesiveness (Belotero [Merz Aesthetics] is highly cohesive). If I am treating a thin-faced individual, I may start with a global volumizer such as poly-L-lactic acid to get a good foundation set in the temples, cheeks, and jawline, and then after a few months, I will add a hyaluronic acid filler to focal areas that still need to be lifted (eg, nasolabial folds, tear troughs).
What are the side effects?
Side effects are divided into common and rare. Common would be bruising and swelling, which are temporary and will go away in all patients. Rare but serious side effects are infection and embolization. Both can cause notable tissue loss and risk to the patient. Every practitioner needs to know how to recognize and treat these complications should they arise.
How do you keep patients compliant?
Patients who get good results will always return, which means being up front about how much filler a patient needs and how frequently he/she will need it, and also doing everything we can to reduce bruising and swelling.
Suggested Readings
- Dayan SH, Arkins JP, Brindise R. Soft tissue fillers and biofilms. Facial Plast Surg. 2011;27:23-28.
- Orsini RA; Plastic Surgery Educational Technology Assessment Committee. Bromelain. Plast Reconstr Surg. 2006;118:1640-1644.

Changes in HIV-related cancers reflect changes in HIV patient care
The incidence of Kaposi’s sarcoma among HIV patients has declined in the antiretroviral era, but the cancers are now presenting in older patients, after treatment starts, and in patients who have undetectable levels of HIV RNA.
Changes were also seen in the appearance of non-Hodgkin lymphoma, which is now occurring in patients with higher CD4 counts and lower HIV viral loads.
Although the findings of this large database study were largely driven by the fact that more patients are on antiretroviral therapy (ART) and in active clinical care, biological forces may also be at work, wrote Elizabeth L. Yanik, PhD, of the National Cancer Institute, Rockville, Md., and her associates (Am J Clin Oncol. 2016 Aug 9. doi: 10.1200/JCO.2016.67.6999).
“For example, cancers that develop in patients with HIV infection after immune recovery may manifest genetic or epigenetic changes that facilitate evasion from the immune system … [and] given that human herpesvirus-8 and Epstein-Barr virus are genetically heterogeneous, another possibility is that patients in whom Kaposi’s or non-Hodgkin lymphoma develops after immune reconstitution may be infected with more pathogenic strains.”
Dr. Yanik and her colleagues mined data from the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS). The 24,901 patients have been followed from 1996-2011. Among them, 446 cases of Kaposi’s sarcoma (KS) and 258 cases of non-Hodgkin lymphoma (NHL) developed. Overall, KS and NHL incidence rates decreased 5% and 8% per year, respectively.
The proportion of KS diagnosed during routine care increased significantly, from 32% to 49%, reflecting the fact that more HIV patients continue to enter active clinical settings. The diagnostic setting of NHL did not change significantly over the study period, with 64% of cases being diagnosed in routine care in the latter years. From the beginning to the end of the study period, patient median age at diagnosis increased for both KS (from 37 to 42 years) and NHL (from 40 to 46 years).
The authors said this is a direct result of changing care patterns. “The proportion of KS cases diagnosed among patients who received ART increased not because KS incidence increased in patients who received ART but because of the growing fraction of the HIV population administered ART.”
As the study period progressed, more cases of KS appeared 6 months or longer after ART initiation, from 26% in the early years to 60% in the latter years. This change didn’t occur with NHL cases; 68% of them were diagnosed at least 6 months after ART began.
The mean CD4 count at diagnosis increased with time for both KS and NHL. During 2007-2011, 15% of KS cases and 24% of NHL cases were diagnosed at CD4 counts of 500 cells/mL or more, whereas less than half were diagnosed at CD4 counts less than 200 cells/mL, the authors observed.
Both cancers began to appear during periods of decreased viral load as the study progressed, although the decrease was only significant for NHL. However, from 2007 to 2011, 29% of KS cases and 51% of NHL cases were diagnosed when HIV RNA was suppressed to 500 copies/mL or lower.
Again, the authors related this to improved clinical care. “These clinical characteristics and the changes in the underlying HIV population are inherently related. Improvements in ART access and earlier initiation lead to earlier suppression of HIV RNA and, ultimately, higher CD4 counts,” they said.
On Twitter @Alz_Gal
The incidence of Kaposi’s sarcoma among HIV patients has declined in the antiretroviral era, but the cancers are now presenting in older patients, after treatment starts, and in patients who have undetectable levels of HIV RNA.
Changes were also seen in the appearance of non-Hodgkin lymphoma, which is now occurring in patients with higher CD4 counts and lower HIV viral loads.
Although the findings of this large database study were largely driven by the fact that more patients are on antiretroviral therapy (ART) and in active clinical care, biological forces may also be at work, wrote Elizabeth L. Yanik, PhD, of the National Cancer Institute, Rockville, Md., and her associates (Am J Clin Oncol. 2016 Aug 9. doi: 10.1200/JCO.2016.67.6999).
“For example, cancers that develop in patients with HIV infection after immune recovery may manifest genetic or epigenetic changes that facilitate evasion from the immune system … [and] given that human herpesvirus-8 and Epstein-Barr virus are genetically heterogeneous, another possibility is that patients in whom Kaposi’s or non-Hodgkin lymphoma develops after immune reconstitution may be infected with more pathogenic strains.”
Dr. Yanik and her colleagues mined data from the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS). The 24,901 patients have been followed from 1996-2011. Among them, 446 cases of Kaposi’s sarcoma (KS) and 258 cases of non-Hodgkin lymphoma (NHL) developed. Overall, KS and NHL incidence rates decreased 5% and 8% per year, respectively.
The proportion of KS diagnosed during routine care increased significantly, from 32% to 49%, reflecting the fact that more HIV patients continue to enter active clinical settings. The diagnostic setting of NHL did not change significantly over the study period, with 64% of cases being diagnosed in routine care in the latter years. From the beginning to the end of the study period, patient median age at diagnosis increased for both KS (from 37 to 42 years) and NHL (from 40 to 46 years).
The authors said this is a direct result of changing care patterns. “The proportion of KS cases diagnosed among patients who received ART increased not because KS incidence increased in patients who received ART but because of the growing fraction of the HIV population administered ART.”
As the study period progressed, more cases of KS appeared 6 months or longer after ART initiation, from 26% in the early years to 60% in the latter years. This change didn’t occur with NHL cases; 68% of them were diagnosed at least 6 months after ART began.
The mean CD4 count at diagnosis increased with time for both KS and NHL. During 2007-2011, 15% of KS cases and 24% of NHL cases were diagnosed at CD4 counts of 500 cells/mL or more, whereas less than half were diagnosed at CD4 counts less than 200 cells/mL, the authors observed.
Both cancers began to appear during periods of decreased viral load as the study progressed, although the decrease was only significant for NHL. However, from 2007 to 2011, 29% of KS cases and 51% of NHL cases were diagnosed when HIV RNA was suppressed to 500 copies/mL or lower.
Again, the authors related this to improved clinical care. “These clinical characteristics and the changes in the underlying HIV population are inherently related. Improvements in ART access and earlier initiation lead to earlier suppression of HIV RNA and, ultimately, higher CD4 counts,” they said.
On Twitter @Alz_Gal
The incidence of Kaposi’s sarcoma among HIV patients has declined in the antiretroviral era, but the cancers are now presenting in older patients, after treatment starts, and in patients who have undetectable levels of HIV RNA.
Changes were also seen in the appearance of non-Hodgkin lymphoma, which is now occurring in patients with higher CD4 counts and lower HIV viral loads.
Although the findings of this large database study were largely driven by the fact that more patients are on antiretroviral therapy (ART) and in active clinical care, biological forces may also be at work, wrote Elizabeth L. Yanik, PhD, of the National Cancer Institute, Rockville, Md., and her associates (Am J Clin Oncol. 2016 Aug 9. doi: 10.1200/JCO.2016.67.6999).
“For example, cancers that develop in patients with HIV infection after immune recovery may manifest genetic or epigenetic changes that facilitate evasion from the immune system … [and] given that human herpesvirus-8 and Epstein-Barr virus are genetically heterogeneous, another possibility is that patients in whom Kaposi’s or non-Hodgkin lymphoma develops after immune reconstitution may be infected with more pathogenic strains.”
Dr. Yanik and her colleagues mined data from the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS). The 24,901 patients have been followed from 1996-2011. Among them, 446 cases of Kaposi’s sarcoma (KS) and 258 cases of non-Hodgkin lymphoma (NHL) developed. Overall, KS and NHL incidence rates decreased 5% and 8% per year, respectively.
The proportion of KS diagnosed during routine care increased significantly, from 32% to 49%, reflecting the fact that more HIV patients continue to enter active clinical settings. The diagnostic setting of NHL did not change significantly over the study period, with 64% of cases being diagnosed in routine care in the latter years. From the beginning to the end of the study period, patient median age at diagnosis increased for both KS (from 37 to 42 years) and NHL (from 40 to 46 years).
The authors said this is a direct result of changing care patterns. “The proportion of KS cases diagnosed among patients who received ART increased not because KS incidence increased in patients who received ART but because of the growing fraction of the HIV population administered ART.”
As the study period progressed, more cases of KS appeared 6 months or longer after ART initiation, from 26% in the early years to 60% in the latter years. This change didn’t occur with NHL cases; 68% of them were diagnosed at least 6 months after ART began.
The mean CD4 count at diagnosis increased with time for both KS and NHL. During 2007-2011, 15% of KS cases and 24% of NHL cases were diagnosed at CD4 counts of 500 cells/mL or more, whereas less than half were diagnosed at CD4 counts less than 200 cells/mL, the authors observed.
Both cancers began to appear during periods of decreased viral load as the study progressed, although the decrease was only significant for NHL. However, from 2007 to 2011, 29% of KS cases and 51% of NHL cases were diagnosed when HIV RNA was suppressed to 500 copies/mL or lower.
Again, the authors related this to improved clinical care. “These clinical characteristics and the changes in the underlying HIV population are inherently related. Improvements in ART access and earlier initiation lead to earlier suppression of HIV RNA and, ultimately, higher CD4 counts,” they said.
On Twitter @Alz_Gal
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Kaposi’s sarcoma and non-Hodgkin lymphoma are appearing in older, less- immunosuppressed patients.
Major finding: From 1996-2011, median patient age at diagnosis increased for both Kaposi’s sarcoma (from 37 to 42 years) and non-Hodgkin lymphoma (from 40 to 46 years).
Data source: The database study examined 446 cases of Kaposi’s sarcoma and 258 cases of non-Hodgkin lymphoma.
Disclosures: The National Cancer Institute headed the study; Dr. Yanik had no financial disclosures.