User login
Long COVID: Advocating for Patients and Implementing Effective Techniques
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
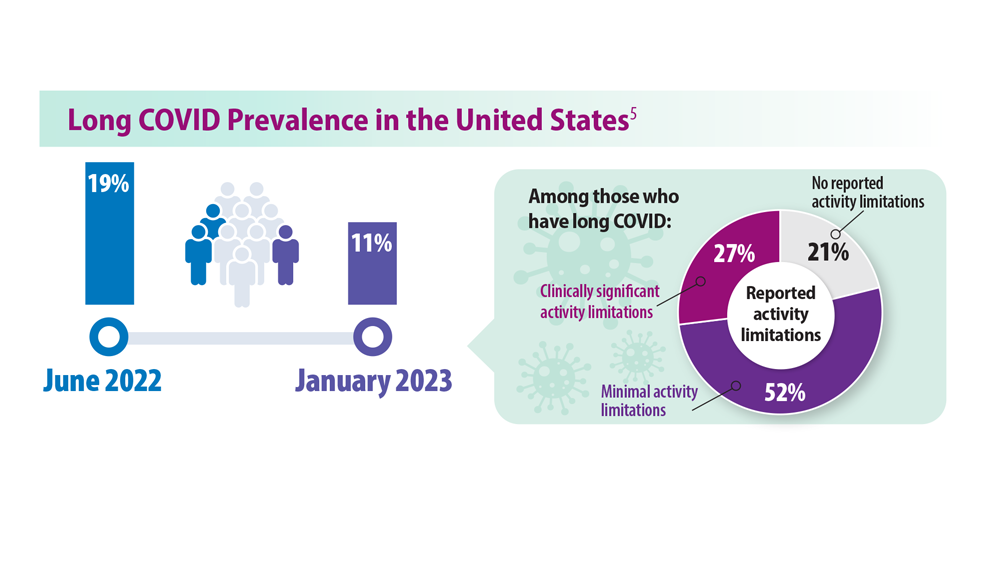
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/
1. Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
2. Davis HE et al. Nat Rev Microbiol. 2023;21(3):133-146. doi:10.1038/s41579-022-00846-2
3. Ahmed H et al. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694
4. Resources. Long COVID Physio. Accessed May 31, 2023. https://longcovid.physio/resources
5. Long COVID: What do the latest data show? KFF. Published January 26, 2023. Accessed May 31, 2023. https://www.kff.org/policy-watch/long-covid-what-do-latest-data-show/
6. Castanares-Zapatero D et al. Ann Med. 2022;54(1):1473-1487. doi:10.1080/07853890.2022.2076901
7. Mehandru S, Merad M. Nat Immunol. 2022;23(2):194-202. doi:10.1038/s41590-021-01104-y
8. Dhooria S et al. Eur Respir J. 2022;59(2):2102930. doi:10.1183/13993003.02930-2021
9. Researching COVID to enhance recovery. RECOVER. Accessed May 31, 2023. https://recovercovid.org/
Asthma Across a Woman’s Lifespan
1. Chowdhury NU et al. Eur Respir Rev. 2021;30(162):210067. doi:10.1183/16000617.0067-2021
2. Perikleous EP et al. J Pers Med. 2022;12(6):999. doi:10.3390/jpm12060999
3. Khaleva E et al. Clin Transl Allergy. 2020;10:40. doi:10.1186/s13601-020-00340-z
4. Robijn AL et al. Curr Opin Pulm Med. 2019;25(1):11-17. doi:10.1097/MCP.0000000000000538
5. Bravo-Solarte DC et al. Allergy Asthma Proc. 2023;44(1):24-34. doi:10.2500/aap.2023.44.220077
6. Wang G et al. J Matern Fetal Neonatal Med. 2014;27(9):934-942. doi:10.3109/14767058.2013.847080
7. Hough KP et al. Front Med (Lausanne). 2020;7:191. doi:10.3389/fmed.2020.00191
8. Triebner K et al. Am J Respir Crit Care Med. 2017;195(8):1058-1065. doi:10.1164/rccm.201605-0968OC
9. Bacharier LB, Jackson DJ. J Allergy Clin Immunol. 2023;151(3):581-589. doi:10.1016/j.jaci.2023.01.002
10. An amazing journey: how young lungs develop. American Lung Association. Published May 11, 2018. Accessed June 28, 2023. https://www.lung.org/blog/how-young-lungs-develop
11. Strunk RC et al. J Allergy Clin Immunol. 2006;118(5):1040-1047. doi:10.1016/j.jaci.2006.07.053
12. Kaplan A, Price D. J Asthma Allergy. 2020;13:39-49. doi:10.2147/JAA.S233268
1. Chowdhury NU et al. Eur Respir Rev. 2021;30(162):210067. doi:10.1183/16000617.0067-2021
2. Perikleous EP et al. J Pers Med. 2022;12(6):999. doi:10.3390/jpm12060999
3. Khaleva E et al. Clin Transl Allergy. 2020;10:40. doi:10.1186/s13601-020-00340-z
4. Robijn AL et al. Curr Opin Pulm Med. 2019;25(1):11-17. doi:10.1097/MCP.0000000000000538
5. Bravo-Solarte DC et al. Allergy Asthma Proc. 2023;44(1):24-34. doi:10.2500/aap.2023.44.220077
6. Wang G et al. J Matern Fetal Neonatal Med. 2014;27(9):934-942. doi:10.3109/14767058.2013.847080
7. Hough KP et al. Front Med (Lausanne). 2020;7:191. doi:10.3389/fmed.2020.00191
8. Triebner K et al. Am J Respir Crit Care Med. 2017;195(8):1058-1065. doi:10.1164/rccm.201605-0968OC
9. Bacharier LB, Jackson DJ. J Allergy Clin Immunol. 2023;151(3):581-589. doi:10.1016/j.jaci.2023.01.002
10. An amazing journey: how young lungs develop. American Lung Association. Published May 11, 2018. Accessed June 28, 2023. https://www.lung.org/blog/how-young-lungs-develop
11. Strunk RC et al. J Allergy Clin Immunol. 2006;118(5):1040-1047. doi:10.1016/j.jaci.2006.07.053
12. Kaplan A, Price D. J Asthma Allergy. 2020;13:39-49. doi:10.2147/JAA.S233268
1. Chowdhury NU et al. Eur Respir Rev. 2021;30(162):210067. doi:10.1183/16000617.0067-2021
2. Perikleous EP et al. J Pers Med. 2022;12(6):999. doi:10.3390/jpm12060999
3. Khaleva E et al. Clin Transl Allergy. 2020;10:40. doi:10.1186/s13601-020-00340-z
4. Robijn AL et al. Curr Opin Pulm Med. 2019;25(1):11-17. doi:10.1097/MCP.0000000000000538
5. Bravo-Solarte DC et al. Allergy Asthma Proc. 2023;44(1):24-34. doi:10.2500/aap.2023.44.220077
6. Wang G et al. J Matern Fetal Neonatal Med. 2014;27(9):934-942. doi:10.3109/14767058.2013.847080
7. Hough KP et al. Front Med (Lausanne). 2020;7:191. doi:10.3389/fmed.2020.00191
8. Triebner K et al. Am J Respir Crit Care Med. 2017;195(8):1058-1065. doi:10.1164/rccm.201605-0968OC
9. Bacharier LB, Jackson DJ. J Allergy Clin Immunol. 2023;151(3):581-589. doi:10.1016/j.jaci.2023.01.002
10. An amazing journey: how young lungs develop. American Lung Association. Published May 11, 2018. Accessed June 28, 2023. https://www.lung.org/blog/how-young-lungs-develop
11. Strunk RC et al. J Allergy Clin Immunol. 2006;118(5):1040-1047. doi:10.1016/j.jaci.2006.07.053
12. Kaplan A, Price D. J Asthma Allergy. 2020;13:39-49. doi:10.2147/JAA.S233268
Pulmonology Data Trends 2023 (Slideshow)

CHEST Physician presents the 2023 edition of Pulmonology Data Trends (click to read). This special issue provides updates on hot topics in pulmonology through original infographics and visual storytelling.
In this issue:
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
Burton L. Lesnick, MD, FCCP
Decreasing Pulmonary Embolism-Related Mortality
Parth Rali, MD
Addressing Physician Burnout in Pulmonology and Critical Care
Kelly Vranas, MD, MCR
Updated Guidelines for COPD Management: 2023 GOLD Strategy Report
Muhammad Adrish, MD, MBA, FCCP, FCCM
Progressive Pulmonary Fibrosis: Understanding Its Many Forms
Tejaswini Kulkarni, MD, MPH, FCCP
Sleep Apnea: Comorbidities, Racial Disparities, Weight Guidelines, and Alternatives to CPAP
Lauren Tobias, MD, FCCP
Lung Cancer Screening: A Need for Adjunctive Testing
Eric S. Edell, MD, FCCP
Asthma Across a Woman’s Lifespan
Navitha Ramesh, MD, FCCP
Tuberculosis Management: Returning to Pre-Pandemic Priorities
Patricio Escalante, MD, MSc, FCCP, and Paige K. Marty, MD
Long COVID: Advocating for Patients and Implementing Effective Techniques
Kyle B. Enfield, MD, MS, FSHEA, FCCM
CHEST Physician presents the 2023 edition of Pulmonology Data Trends (click to read). This special issue provides updates on hot topics in pulmonology through original infographics and visual storytelling.
In this issue:
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
Burton L. Lesnick, MD, FCCP
Decreasing Pulmonary Embolism-Related Mortality
Parth Rali, MD
Addressing Physician Burnout in Pulmonology and Critical Care
Kelly Vranas, MD, MCR
Updated Guidelines for COPD Management: 2023 GOLD Strategy Report
Muhammad Adrish, MD, MBA, FCCP, FCCM
Progressive Pulmonary Fibrosis: Understanding Its Many Forms
Tejaswini Kulkarni, MD, MPH, FCCP
Sleep Apnea: Comorbidities, Racial Disparities, Weight Guidelines, and Alternatives to CPAP
Lauren Tobias, MD, FCCP
Lung Cancer Screening: A Need for Adjunctive Testing
Eric S. Edell, MD, FCCP
Asthma Across a Woman’s Lifespan
Navitha Ramesh, MD, FCCP
Tuberculosis Management: Returning to Pre-Pandemic Priorities
Patricio Escalante, MD, MSc, FCCP, and Paige K. Marty, MD
Long COVID: Advocating for Patients and Implementing Effective Techniques
Kyle B. Enfield, MD, MS, FSHEA, FCCM
CHEST Physician presents the 2023 edition of Pulmonology Data Trends (click to read). This special issue provides updates on hot topics in pulmonology through original infographics and visual storytelling.
In this issue:
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
Burton L. Lesnick, MD, FCCP
Decreasing Pulmonary Embolism-Related Mortality
Parth Rali, MD
Addressing Physician Burnout in Pulmonology and Critical Care
Kelly Vranas, MD, MCR
Updated Guidelines for COPD Management: 2023 GOLD Strategy Report
Muhammad Adrish, MD, MBA, FCCP, FCCM
Progressive Pulmonary Fibrosis: Understanding Its Many Forms
Tejaswini Kulkarni, MD, MPH, FCCP
Sleep Apnea: Comorbidities, Racial Disparities, Weight Guidelines, and Alternatives to CPAP
Lauren Tobias, MD, FCCP
Lung Cancer Screening: A Need for Adjunctive Testing
Eric S. Edell, MD, FCCP
Asthma Across a Woman’s Lifespan
Navitha Ramesh, MD, FCCP
Tuberculosis Management: Returning to Pre-Pandemic Priorities
Patricio Escalante, MD, MSc, FCCP, and Paige K. Marty, MD
Long COVID: Advocating for Patients and Implementing Effective Techniques
Kyle B. Enfield, MD, MS, FSHEA, FCCM
Higher RT doses can boost lifespan, reduce risk of death in LS-SCLC patients
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
AT ASTRO 2023
CT simulation not needed in palliative radiotherapy planning
, according to a results from a randomized trial presented at the annual meeting of the American Society for Radiation Oncology.
The aim of this same-day CT scan, called a CT simulation scan, is to optimize radiation targeting by mimicking the conditions under which radiation is delivered using the latest information on the size and location of lesions.
But investigators reported that skipping the CT simulation scan saves patients hours in the clinic, allows patients to experience pain relief faster, and saves radiation oncologists time without compromising dosimetric coverage of cancerous lesions.
“This is huge in a symptomatic patient population,” said Melissa O’Neil, an advanced practice radiation therapist at the London, Ont., Health Sciences Centre and the lead investigator on the trial, dubbed DART (Diagnostic CT-Enabled Radiation Therapy).
“Diagnostic CT-based radiation planning substantially reduces time in the [treatment] center without a detriment in plan deliverability or quality,” Ms. O’Neil said.
In addition, patients are exposed to less radiation, and staff doesn’t have to spend as much time tending to symptomatic patients before treatment. Omitting this scan “should be considered for patients with a recent diagnostic CT scan who are undergoing simple palliative radiation,” Ms. O’Neil said.
CT simulation scans are standard of care in cases involving palliative radiation, but they create bottlenecks in the workflow. When a CT simulation is performed on the day of treatment, patients must wait hours as the results are translated into a treatment plan.
In the DART analysis, 33 patients with 42 treatment sites were randomly assigned to CT simulation planning or diagnostic CT planning.
Patients received up to 30 Gy in up to 10 fractions for bone or soft tissue metastases or primary tumor targets in the thorax, abdomen, pelvis, or proximal limbs. Single-fraction treatments were most common.
Three-quarters of the patients were men (median age, 72 years). Lung cancer was the most common type of primary tumor, followed by prostate and breast cancer.
The eight participants for whom the CT simulation approach was used waited 3-4 hours for treatment planning and overall spent a median of 4.8 hours in the cancer center on their day of treatment.
The 25 patients for whom diagnostic CT planning was used spent a median of 0.4 hours, or about 24 minutes, in the center on their day of treatment because radiation plans were completed before they arrived. The median time between their diagnostic CTs and radiation treatment was 13 days (range, 8-22 days).
Ms. O’Neil and her team found that if the original diagnostic CT was performed within 28 days, lesion anatomy would not have changed enough to warrant a new scan.
On the day of treatment, the study team used surface-guided radiation therapy techniques to ensure patients in the diagnostic CT planning group were positioned within 3 mm of where they were during their diagnostic scans, an essential step to ensure that radiation is delivered to the correct location. Ms. O’Neil noted that other investigators have used anatomic landmarks, a simpler approach, to achieve these results.
Overall, radiation oncologists rated radiation dose distribution as “acceptable” in about 80% of cases in both arms of DART and “acceptable with minor deviation” in the remaining 20% of cases.
Every radiation oncologist and medical physicists in the trial gave the workflow with diagnostic CT planning a 5 out of 5 rating for acceptability, and 90% of patients in this group rated the amount of time they spent for treatment as “acceptable.”
In contrast, only half of patients in the simulation arm said the amount of time spent was acceptable.
These findings align with several previous studies that support the diagnostic approach.
Jacob Scott, MD, a radiation oncologist at the Cleveland Clinic, said, “The comparable results using a recent diagnostic CT in place of a CT simulation for palliative radiation is an exciting step forward in radiation oncology. We may soon be in a world where we no longer need simulations.”
Dr. Scott also noted that combining diagnostic scans with cone beam or surface-guided positioning in lieu of CT simulations could further save “the health system and patients time and money.”
No external funding for the study was reported. The investigators, Ms. O’Neil, and Dr. Scott have disclosed no relevant financial relationships. One investigator reported receiving honoraria from Knight Therapeutics, AbbVie, Tersera, and Eisai and owns stock in Myovant.
A version of this article first appeared on Medscape.com.
, according to a results from a randomized trial presented at the annual meeting of the American Society for Radiation Oncology.
The aim of this same-day CT scan, called a CT simulation scan, is to optimize radiation targeting by mimicking the conditions under which radiation is delivered using the latest information on the size and location of lesions.
But investigators reported that skipping the CT simulation scan saves patients hours in the clinic, allows patients to experience pain relief faster, and saves radiation oncologists time without compromising dosimetric coverage of cancerous lesions.
“This is huge in a symptomatic patient population,” said Melissa O’Neil, an advanced practice radiation therapist at the London, Ont., Health Sciences Centre and the lead investigator on the trial, dubbed DART (Diagnostic CT-Enabled Radiation Therapy).
“Diagnostic CT-based radiation planning substantially reduces time in the [treatment] center without a detriment in plan deliverability or quality,” Ms. O’Neil said.
In addition, patients are exposed to less radiation, and staff doesn’t have to spend as much time tending to symptomatic patients before treatment. Omitting this scan “should be considered for patients with a recent diagnostic CT scan who are undergoing simple palliative radiation,” Ms. O’Neil said.
CT simulation scans are standard of care in cases involving palliative radiation, but they create bottlenecks in the workflow. When a CT simulation is performed on the day of treatment, patients must wait hours as the results are translated into a treatment plan.
In the DART analysis, 33 patients with 42 treatment sites were randomly assigned to CT simulation planning or diagnostic CT planning.
Patients received up to 30 Gy in up to 10 fractions for bone or soft tissue metastases or primary tumor targets in the thorax, abdomen, pelvis, or proximal limbs. Single-fraction treatments were most common.
Three-quarters of the patients were men (median age, 72 years). Lung cancer was the most common type of primary tumor, followed by prostate and breast cancer.
The eight participants for whom the CT simulation approach was used waited 3-4 hours for treatment planning and overall spent a median of 4.8 hours in the cancer center on their day of treatment.
The 25 patients for whom diagnostic CT planning was used spent a median of 0.4 hours, or about 24 minutes, in the center on their day of treatment because radiation plans were completed before they arrived. The median time between their diagnostic CTs and radiation treatment was 13 days (range, 8-22 days).
Ms. O’Neil and her team found that if the original diagnostic CT was performed within 28 days, lesion anatomy would not have changed enough to warrant a new scan.
On the day of treatment, the study team used surface-guided radiation therapy techniques to ensure patients in the diagnostic CT planning group were positioned within 3 mm of where they were during their diagnostic scans, an essential step to ensure that radiation is delivered to the correct location. Ms. O’Neil noted that other investigators have used anatomic landmarks, a simpler approach, to achieve these results.
Overall, radiation oncologists rated radiation dose distribution as “acceptable” in about 80% of cases in both arms of DART and “acceptable with minor deviation” in the remaining 20% of cases.
Every radiation oncologist and medical physicists in the trial gave the workflow with diagnostic CT planning a 5 out of 5 rating for acceptability, and 90% of patients in this group rated the amount of time they spent for treatment as “acceptable.”
In contrast, only half of patients in the simulation arm said the amount of time spent was acceptable.
These findings align with several previous studies that support the diagnostic approach.
Jacob Scott, MD, a radiation oncologist at the Cleveland Clinic, said, “The comparable results using a recent diagnostic CT in place of a CT simulation for palliative radiation is an exciting step forward in radiation oncology. We may soon be in a world where we no longer need simulations.”
Dr. Scott also noted that combining diagnostic scans with cone beam or surface-guided positioning in lieu of CT simulations could further save “the health system and patients time and money.”
No external funding for the study was reported. The investigators, Ms. O’Neil, and Dr. Scott have disclosed no relevant financial relationships. One investigator reported receiving honoraria from Knight Therapeutics, AbbVie, Tersera, and Eisai and owns stock in Myovant.
A version of this article first appeared on Medscape.com.
, according to a results from a randomized trial presented at the annual meeting of the American Society for Radiation Oncology.
The aim of this same-day CT scan, called a CT simulation scan, is to optimize radiation targeting by mimicking the conditions under which radiation is delivered using the latest information on the size and location of lesions.
But investigators reported that skipping the CT simulation scan saves patients hours in the clinic, allows patients to experience pain relief faster, and saves radiation oncologists time without compromising dosimetric coverage of cancerous lesions.
“This is huge in a symptomatic patient population,” said Melissa O’Neil, an advanced practice radiation therapist at the London, Ont., Health Sciences Centre and the lead investigator on the trial, dubbed DART (Diagnostic CT-Enabled Radiation Therapy).
“Diagnostic CT-based radiation planning substantially reduces time in the [treatment] center without a detriment in plan deliverability or quality,” Ms. O’Neil said.
In addition, patients are exposed to less radiation, and staff doesn’t have to spend as much time tending to symptomatic patients before treatment. Omitting this scan “should be considered for patients with a recent diagnostic CT scan who are undergoing simple palliative radiation,” Ms. O’Neil said.
CT simulation scans are standard of care in cases involving palliative radiation, but they create bottlenecks in the workflow. When a CT simulation is performed on the day of treatment, patients must wait hours as the results are translated into a treatment plan.
In the DART analysis, 33 patients with 42 treatment sites were randomly assigned to CT simulation planning or diagnostic CT planning.
Patients received up to 30 Gy in up to 10 fractions for bone or soft tissue metastases or primary tumor targets in the thorax, abdomen, pelvis, or proximal limbs. Single-fraction treatments were most common.
Three-quarters of the patients were men (median age, 72 years). Lung cancer was the most common type of primary tumor, followed by prostate and breast cancer.
The eight participants for whom the CT simulation approach was used waited 3-4 hours for treatment planning and overall spent a median of 4.8 hours in the cancer center on their day of treatment.
The 25 patients for whom diagnostic CT planning was used spent a median of 0.4 hours, or about 24 minutes, in the center on their day of treatment because radiation plans were completed before they arrived. The median time between their diagnostic CTs and radiation treatment was 13 days (range, 8-22 days).
Ms. O’Neil and her team found that if the original diagnostic CT was performed within 28 days, lesion anatomy would not have changed enough to warrant a new scan.
On the day of treatment, the study team used surface-guided radiation therapy techniques to ensure patients in the diagnostic CT planning group were positioned within 3 mm of where they were during their diagnostic scans, an essential step to ensure that radiation is delivered to the correct location. Ms. O’Neil noted that other investigators have used anatomic landmarks, a simpler approach, to achieve these results.
Overall, radiation oncologists rated radiation dose distribution as “acceptable” in about 80% of cases in both arms of DART and “acceptable with minor deviation” in the remaining 20% of cases.
Every radiation oncologist and medical physicists in the trial gave the workflow with diagnostic CT planning a 5 out of 5 rating for acceptability, and 90% of patients in this group rated the amount of time they spent for treatment as “acceptable.”
In contrast, only half of patients in the simulation arm said the amount of time spent was acceptable.
These findings align with several previous studies that support the diagnostic approach.
Jacob Scott, MD, a radiation oncologist at the Cleveland Clinic, said, “The comparable results using a recent diagnostic CT in place of a CT simulation for palliative radiation is an exciting step forward in radiation oncology. We may soon be in a world where we no longer need simulations.”
Dr. Scott also noted that combining diagnostic scans with cone beam or surface-guided positioning in lieu of CT simulations could further save “the health system and patients time and money.”
No external funding for the study was reported. The investigators, Ms. O’Neil, and Dr. Scott have disclosed no relevant financial relationships. One investigator reported receiving honoraria from Knight Therapeutics, AbbVie, Tersera, and Eisai and owns stock in Myovant.
A version of this article first appeared on Medscape.com.
FROM ASTRO 2023
Rheumatoid arthritis: Five things to know
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that typically presents as a symmetric inflammatory polyarthritis (synovitis) primarily affecting the hands and feet. Any joint lined by a synovial membrane may be involved; however, extraarticular involvement of various organs can be significant. RA is theorized to develop when a genetically susceptible individual experiences an external trigger (e.g., cigarette smoking, infection, trauma) that precipitates an autoimmune reaction.
Rheumatology is a rapidly advancing, but relatively young, subspecialty. An understanding of the pathophysiology, treatment, and classification of RA is still emerging. Here are five things to know about RA.
1. A healthier lifestyle is associated with a reduced risk of developing RA.
Large epidemiologic studies have identified several factors that increase the incidence of RA; these include an unhealthy diet, smoking, adiposity, low educational level, and low socioeconomic status. A patient’s response to antirheumatic medications can be affected by certain lifestyle habits, which can be associated with worse treatment outcomes; such habits include smoking, insufficient physical activity, and obesity, among others. Although methodologic problems may impede making firm conclusions regarding a causal role for these factors in the disease course and risk of developing RA, current evidence is sufficient to recommend quitting smoking, adopting a healthy diet, preventing obesity, and maintaining a high level of physical activity to support the effectiveness of current antirheumatic drugs.
In the Nurses’ Health Study, biennial questionnaires were used to collect lifestyle and medical information to determine which modifiable risk factors are associated with the risk for RA in women. Patient medical records were used to confirm incident RA and serostatus. The healthy lifestyle index score (HLIS), which includes five modifiable risk factors (smoking, alcohol consumption, body mass index, physical activity, and diet), was used to assess risk. Cox regression, which was adjusted for confounders, was used to model associations between HLIS and the incidence of RA. The study concluded that a healthier lifestyle was associated with a lower risk of developing RA, and a significant number of RA cases may be preventable if patients adopted four or more healthy lifestyle factors.
The Mediterranean diet is one current popular dietary option that appears to have promising evidence in many disease processes, including RA.
2. In pregnant women with RA, the course of the disease can change throughout pregnancy.
The course of RA often changes during pregnancy. About half of pregnant women with RA have low disease activity, and 20%-40% achieve remission by the third trimester; however, nearly 20% have worse or moderate to high disease activity during pregnancy that may require further therapeutic intervention. Postpartum flares of RA also may occur, with studies reporting rates of 39%-90%.
No specific guidelines address obstetric monitoring in patients with RA. Because few data suggest a significantly increased risk for preterm birth, preeclampsia, or fetal growth restriction, no special obstetric monitoring is indicated beyond what is performed for usual obstetric care.
Medications considered to be low risk in pregnancy include low-dose corticosteroids, antimalarial agents, sulfasalazine, and azathioprine. Certain tumor necrosis factor inhibitors are also thought to be relatively safe.
3. A well-designed exercise program can be beneficial in RA.
Regular physical activity has replaced bed rest as the recommended response to the stiffness and pain associated with RA. However, many patients who have RA do not really believe this. Lack of conviction and motivation appear to be the major factors that deter nearly half of patients with RA from moving about enough to help their situation. There is ample evidence about the benefits of physical activity in RA, but little research into why few patients with RA take advantage of it. The extreme physical inactivity of patients with RA becomes a vicious cycle in terms of health and disease progression. Thus, encouraging physical activity is an essential part of the overall treatment of RA.
Findings from randomized controlled trials show that exercise is fundamentally beneficial for patients with RA. The benefits of properly designed physical exercise programs include improved cardiorespiratory fitness and cardiovascular health, increased muscle mass, reduced adiposity, increased strength, and improved physical functioning, all achieved without exacerbation of disease activity or joint damage.
The American College of Rheumatology (ACR) has released recommendations for exercise interventions for RA. The ACR strongly recommends consistent engagement in an exercise program over no exercise. The type of exercise is open to interpretation. An exercise program for patients with rheumatic diseases aims to preserve or restore the range of motion of affected joints, increase muscle strength and endurance, and improve mood and decrease health risks associated with a sedentary lifestyle.
4. RA is a systemic disease that affects multiple organ systems.
Although synovitis is the pathologic hallmark of RA, extraarticular manifestations and comorbidities occur presumably owing to the complex, chronic, inflammatory, and autoimmune features of RA.
The most common cause of death in patients with RA is cardiovascular disease. Compared with the general population, patients with RA have two times the risk of having a myocardial infarction, and they have up to 50% greater cardiovascular mortality risk. Factors identified to play important roles in atherosclerotic damage and incident cardiovascular disease include severe and prolonged disease activity, inflammation (e.g., C-reactive protein, anti–citrullinated protein antibodies (ACPAs), cytokines, matrix-degrading enzymes), and genetics.
Respiratory disease is the second major cause of death in patients with RA; this occurs in 30%-40% of patients with RA. The lung interstitium, airways, and pleurae can all be affected by RA, but pulmonary vascular involvement is less common.
Central and peripheral nervous system involvement is typically attributed to RA-associated small-vessel vasculitis, joint damage, and/or drug toxicity. Evidence also suggests that systemic inflammation causes microvascular cerebral damage that is associated with the development of vascular dementia and Alzheimer’s disease. Finally, some observational studies have suggested that drugs commonly used to treat RA – disease-modifying antirheumatic drugs (DMARDs) and biologics – may reduce the incidence of dementia.
5. As treatment options for RA improve, many controversies have arisen.
In patients without RA symptoms but with biomarkers, experts debate whether early treatment with DMARDs could prevent irreversible joint damage.
There is no clear definition of pre-RA, but it could be defined as having positive markers for RA (e.g., positive rheumatoid factor and anti–cyclic citrullinated peptides) or having joint pain with abnormal ultrasonography findings but not having positive biomarkers. However, not all patients who have positive biomarkers progress to clinical RA, so what exactly determines this progression is unclear. Nevertheless, some clinicians do treat pre-RA. This was a major debate at the ACR’s 2022 meeting.
Studies have shown that early treatment of RA, including during the preclinical phase, can lead to better long-term outcomes. It can help reduce joint inflammation, control disease activity, and prevent or minimize irreversible joint damage. Early treatment also increases the likelihood of achieving remission or low disease activity, which improves quality of life for patients. Lifestyle interventions in these patients, including exercise, weight control, and cardiovascular health, may not prevent disease but may delay the onset of full-blown clinical RA.
The discovery of pre-RA has also underpinned the development of several clinical prevention trials in RA; specifically, the PRAIRI study demonstrated that a single dose of rituximab can delay the onset of clinically apparent RA in at-risk individuals. Additional studies are evaluating the ability of drugs, including abatacept, hydroxychloroquine, and methotrexate, to prevent or delay future RA.
Dual biologics target different pathways – ostensibly boosting efficacy – but unknowns, concerns over safety, and lack of evidence make the practice controversial.
Several randomized controlled trials have assessed the safety and efficacy of dual-biologic treatment of RA, but the results have been mixed, which has raised safety concerns. Overall, there is a paucity of data concerning the safety of the simultaneous use of more than one biologic. Dual therapy may constitute an efficacious and safe add-on treatment to biologic therapy, but properly conducted clinical investigations are needed. In the meantime, dual biologic therapy used at physicians’ discretion requires close monitoring of patients, with an emphasis on the safety profile.
Large language models (artificial intelligence [AI]) are rapidly taking hold in medicine. Many argue that they can enrich patient care, but they come with liability risks.
Large language models, such as AI chatbots or ChatGPT, can increase access to information, help with patient education, and support decision-making. Limitations include lack of personalization, clinical experience, and emotional connection. The use of large language models in health care is fraught with ethical and legal concerns.
Liability issues can arise if errors, inaccuracies, or adverse outcomes result from the use of AI chatbots. Determining liability may involve assessing factors such as the design and development of the AI system, training and deployment of the model, the communication of limitations and disclaimers to users, and the involvement of human healthcare professionals in the decision-making process.
To mitigate liability risks, AI chatbots in rheumatology must comply with applicable regulations and guidelines. Transparency in the capabilities and limitations of the system, clear communication of the boundaries of its advice, and the presence of human oversight are essential. Collaborating with legal experts and following best practices in the development and deployment of AI technologies can help to minimize liability concerns.
The benefits and risks associated with tapering DMARD therapy in patients with RA who have sustained remission of disease should be considered.
Although some patients with well-controlled RA have relapse after tapering or discontinuing DMARDs, some do not, making this treatment strategy a personal decision undertaken with a rheumatologist.
In the RETRO study, German researchers examined the effects of tapering or stopping DMARDs in patients whose RA was in sustained remission. In the phase 3 trial (n = 316), investigators randomized 303 patients with remission for ≥ 6 months who were on stable conventional synthetic or biologic DMARD treatment into three groups: (1) continuation on 100% DMARD dose, (2) tapering to 50% of the DMARD dose, and (3) 50% tapering followed by DMARD withdrawal. The proportion of patients who continued in remission at 1 year was 81.2% in group 1, 58.6% in group 2, and 43.3% in group 3. Predictors for flare-ups were female sex, longer disease duration, rheumatoid factor or ACPA positivity, and higher disease activity scores at baseline.
The abrupt cessation or reduction of DMARDs without medical supervision and guidance can exacerbate symptoms and result in disease flares.
The interplay between long COVID and RA is a recent phenomenon that needs to be considered.
RA shares similar symptoms with long COVID. Patients with a history of RA and a previous diagnosis of COVID-19 who have developed persistent joint or muscle symptoms pose a significant challenge to clinicians. Such patients may be experiencing long COVID or a flare-up of their preexisting rheumatic disease.
Immunosuppressive medications can potentially increase the risk for COVID-19, but it is not clear how they affect disease severity risk. Individuals with RA and long COVID need careful evaluation to balance the management of disease activity while considering the risks associated with immunosuppression and potential susceptibility to viral infections.
Dr. Dombrosky is a staff physician in rheumatology at Central Virginia VA Health Care System in Richmond. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that typically presents as a symmetric inflammatory polyarthritis (synovitis) primarily affecting the hands and feet. Any joint lined by a synovial membrane may be involved; however, extraarticular involvement of various organs can be significant. RA is theorized to develop when a genetically susceptible individual experiences an external trigger (e.g., cigarette smoking, infection, trauma) that precipitates an autoimmune reaction.
Rheumatology is a rapidly advancing, but relatively young, subspecialty. An understanding of the pathophysiology, treatment, and classification of RA is still emerging. Here are five things to know about RA.
1. A healthier lifestyle is associated with a reduced risk of developing RA.
Large epidemiologic studies have identified several factors that increase the incidence of RA; these include an unhealthy diet, smoking, adiposity, low educational level, and low socioeconomic status. A patient’s response to antirheumatic medications can be affected by certain lifestyle habits, which can be associated with worse treatment outcomes; such habits include smoking, insufficient physical activity, and obesity, among others. Although methodologic problems may impede making firm conclusions regarding a causal role for these factors in the disease course and risk of developing RA, current evidence is sufficient to recommend quitting smoking, adopting a healthy diet, preventing obesity, and maintaining a high level of physical activity to support the effectiveness of current antirheumatic drugs.
In the Nurses’ Health Study, biennial questionnaires were used to collect lifestyle and medical information to determine which modifiable risk factors are associated with the risk for RA in women. Patient medical records were used to confirm incident RA and serostatus. The healthy lifestyle index score (HLIS), which includes five modifiable risk factors (smoking, alcohol consumption, body mass index, physical activity, and diet), was used to assess risk. Cox regression, which was adjusted for confounders, was used to model associations between HLIS and the incidence of RA. The study concluded that a healthier lifestyle was associated with a lower risk of developing RA, and a significant number of RA cases may be preventable if patients adopted four or more healthy lifestyle factors.
The Mediterranean diet is one current popular dietary option that appears to have promising evidence in many disease processes, including RA.
2. In pregnant women with RA, the course of the disease can change throughout pregnancy.
The course of RA often changes during pregnancy. About half of pregnant women with RA have low disease activity, and 20%-40% achieve remission by the third trimester; however, nearly 20% have worse or moderate to high disease activity during pregnancy that may require further therapeutic intervention. Postpartum flares of RA also may occur, with studies reporting rates of 39%-90%.
No specific guidelines address obstetric monitoring in patients with RA. Because few data suggest a significantly increased risk for preterm birth, preeclampsia, or fetal growth restriction, no special obstetric monitoring is indicated beyond what is performed for usual obstetric care.
Medications considered to be low risk in pregnancy include low-dose corticosteroids, antimalarial agents, sulfasalazine, and azathioprine. Certain tumor necrosis factor inhibitors are also thought to be relatively safe.
3. A well-designed exercise program can be beneficial in RA.
Regular physical activity has replaced bed rest as the recommended response to the stiffness and pain associated with RA. However, many patients who have RA do not really believe this. Lack of conviction and motivation appear to be the major factors that deter nearly half of patients with RA from moving about enough to help their situation. There is ample evidence about the benefits of physical activity in RA, but little research into why few patients with RA take advantage of it. The extreme physical inactivity of patients with RA becomes a vicious cycle in terms of health and disease progression. Thus, encouraging physical activity is an essential part of the overall treatment of RA.
Findings from randomized controlled trials show that exercise is fundamentally beneficial for patients with RA. The benefits of properly designed physical exercise programs include improved cardiorespiratory fitness and cardiovascular health, increased muscle mass, reduced adiposity, increased strength, and improved physical functioning, all achieved without exacerbation of disease activity or joint damage.
The American College of Rheumatology (ACR) has released recommendations for exercise interventions for RA. The ACR strongly recommends consistent engagement in an exercise program over no exercise. The type of exercise is open to interpretation. An exercise program for patients with rheumatic diseases aims to preserve or restore the range of motion of affected joints, increase muscle strength and endurance, and improve mood and decrease health risks associated with a sedentary lifestyle.
4. RA is a systemic disease that affects multiple organ systems.
Although synovitis is the pathologic hallmark of RA, extraarticular manifestations and comorbidities occur presumably owing to the complex, chronic, inflammatory, and autoimmune features of RA.
The most common cause of death in patients with RA is cardiovascular disease. Compared with the general population, patients with RA have two times the risk of having a myocardial infarction, and they have up to 50% greater cardiovascular mortality risk. Factors identified to play important roles in atherosclerotic damage and incident cardiovascular disease include severe and prolonged disease activity, inflammation (e.g., C-reactive protein, anti–citrullinated protein antibodies (ACPAs), cytokines, matrix-degrading enzymes), and genetics.
Respiratory disease is the second major cause of death in patients with RA; this occurs in 30%-40% of patients with RA. The lung interstitium, airways, and pleurae can all be affected by RA, but pulmonary vascular involvement is less common.
Central and peripheral nervous system involvement is typically attributed to RA-associated small-vessel vasculitis, joint damage, and/or drug toxicity. Evidence also suggests that systemic inflammation causes microvascular cerebral damage that is associated with the development of vascular dementia and Alzheimer’s disease. Finally, some observational studies have suggested that drugs commonly used to treat RA – disease-modifying antirheumatic drugs (DMARDs) and biologics – may reduce the incidence of dementia.
5. As treatment options for RA improve, many controversies have arisen.
In patients without RA symptoms but with biomarkers, experts debate whether early treatment with DMARDs could prevent irreversible joint damage.
There is no clear definition of pre-RA, but it could be defined as having positive markers for RA (e.g., positive rheumatoid factor and anti–cyclic citrullinated peptides) or having joint pain with abnormal ultrasonography findings but not having positive biomarkers. However, not all patients who have positive biomarkers progress to clinical RA, so what exactly determines this progression is unclear. Nevertheless, some clinicians do treat pre-RA. This was a major debate at the ACR’s 2022 meeting.
Studies have shown that early treatment of RA, including during the preclinical phase, can lead to better long-term outcomes. It can help reduce joint inflammation, control disease activity, and prevent or minimize irreversible joint damage. Early treatment also increases the likelihood of achieving remission or low disease activity, which improves quality of life for patients. Lifestyle interventions in these patients, including exercise, weight control, and cardiovascular health, may not prevent disease but may delay the onset of full-blown clinical RA.
The discovery of pre-RA has also underpinned the development of several clinical prevention trials in RA; specifically, the PRAIRI study demonstrated that a single dose of rituximab can delay the onset of clinically apparent RA in at-risk individuals. Additional studies are evaluating the ability of drugs, including abatacept, hydroxychloroquine, and methotrexate, to prevent or delay future RA.
Dual biologics target different pathways – ostensibly boosting efficacy – but unknowns, concerns over safety, and lack of evidence make the practice controversial.
Several randomized controlled trials have assessed the safety and efficacy of dual-biologic treatment of RA, but the results have been mixed, which has raised safety concerns. Overall, there is a paucity of data concerning the safety of the simultaneous use of more than one biologic. Dual therapy may constitute an efficacious and safe add-on treatment to biologic therapy, but properly conducted clinical investigations are needed. In the meantime, dual biologic therapy used at physicians’ discretion requires close monitoring of patients, with an emphasis on the safety profile.
Large language models (artificial intelligence [AI]) are rapidly taking hold in medicine. Many argue that they can enrich patient care, but they come with liability risks.
Large language models, such as AI chatbots or ChatGPT, can increase access to information, help with patient education, and support decision-making. Limitations include lack of personalization, clinical experience, and emotional connection. The use of large language models in health care is fraught with ethical and legal concerns.
Liability issues can arise if errors, inaccuracies, or adverse outcomes result from the use of AI chatbots. Determining liability may involve assessing factors such as the design and development of the AI system, training and deployment of the model, the communication of limitations and disclaimers to users, and the involvement of human healthcare professionals in the decision-making process.
To mitigate liability risks, AI chatbots in rheumatology must comply with applicable regulations and guidelines. Transparency in the capabilities and limitations of the system, clear communication of the boundaries of its advice, and the presence of human oversight are essential. Collaborating with legal experts and following best practices in the development and deployment of AI technologies can help to minimize liability concerns.
The benefits and risks associated with tapering DMARD therapy in patients with RA who have sustained remission of disease should be considered.
Although some patients with well-controlled RA have relapse after tapering or discontinuing DMARDs, some do not, making this treatment strategy a personal decision undertaken with a rheumatologist.
In the RETRO study, German researchers examined the effects of tapering or stopping DMARDs in patients whose RA was in sustained remission. In the phase 3 trial (n = 316), investigators randomized 303 patients with remission for ≥ 6 months who were on stable conventional synthetic or biologic DMARD treatment into three groups: (1) continuation on 100% DMARD dose, (2) tapering to 50% of the DMARD dose, and (3) 50% tapering followed by DMARD withdrawal. The proportion of patients who continued in remission at 1 year was 81.2% in group 1, 58.6% in group 2, and 43.3% in group 3. Predictors for flare-ups were female sex, longer disease duration, rheumatoid factor or ACPA positivity, and higher disease activity scores at baseline.
The abrupt cessation or reduction of DMARDs without medical supervision and guidance can exacerbate symptoms and result in disease flares.
The interplay between long COVID and RA is a recent phenomenon that needs to be considered.
RA shares similar symptoms with long COVID. Patients with a history of RA and a previous diagnosis of COVID-19 who have developed persistent joint or muscle symptoms pose a significant challenge to clinicians. Such patients may be experiencing long COVID or a flare-up of their preexisting rheumatic disease.
Immunosuppressive medications can potentially increase the risk for COVID-19, but it is not clear how they affect disease severity risk. Individuals with RA and long COVID need careful evaluation to balance the management of disease activity while considering the risks associated with immunosuppression and potential susceptibility to viral infections.
Dr. Dombrosky is a staff physician in rheumatology at Central Virginia VA Health Care System in Richmond. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that typically presents as a symmetric inflammatory polyarthritis (synovitis) primarily affecting the hands and feet. Any joint lined by a synovial membrane may be involved; however, extraarticular involvement of various organs can be significant. RA is theorized to develop when a genetically susceptible individual experiences an external trigger (e.g., cigarette smoking, infection, trauma) that precipitates an autoimmune reaction.
Rheumatology is a rapidly advancing, but relatively young, subspecialty. An understanding of the pathophysiology, treatment, and classification of RA is still emerging. Here are five things to know about RA.
1. A healthier lifestyle is associated with a reduced risk of developing RA.
Large epidemiologic studies have identified several factors that increase the incidence of RA; these include an unhealthy diet, smoking, adiposity, low educational level, and low socioeconomic status. A patient’s response to antirheumatic medications can be affected by certain lifestyle habits, which can be associated with worse treatment outcomes; such habits include smoking, insufficient physical activity, and obesity, among others. Although methodologic problems may impede making firm conclusions regarding a causal role for these factors in the disease course and risk of developing RA, current evidence is sufficient to recommend quitting smoking, adopting a healthy diet, preventing obesity, and maintaining a high level of physical activity to support the effectiveness of current antirheumatic drugs.
In the Nurses’ Health Study, biennial questionnaires were used to collect lifestyle and medical information to determine which modifiable risk factors are associated with the risk for RA in women. Patient medical records were used to confirm incident RA and serostatus. The healthy lifestyle index score (HLIS), which includes five modifiable risk factors (smoking, alcohol consumption, body mass index, physical activity, and diet), was used to assess risk. Cox regression, which was adjusted for confounders, was used to model associations between HLIS and the incidence of RA. The study concluded that a healthier lifestyle was associated with a lower risk of developing RA, and a significant number of RA cases may be preventable if patients adopted four or more healthy lifestyle factors.
The Mediterranean diet is one current popular dietary option that appears to have promising evidence in many disease processes, including RA.
2. In pregnant women with RA, the course of the disease can change throughout pregnancy.
The course of RA often changes during pregnancy. About half of pregnant women with RA have low disease activity, and 20%-40% achieve remission by the third trimester; however, nearly 20% have worse or moderate to high disease activity during pregnancy that may require further therapeutic intervention. Postpartum flares of RA also may occur, with studies reporting rates of 39%-90%.
No specific guidelines address obstetric monitoring in patients with RA. Because few data suggest a significantly increased risk for preterm birth, preeclampsia, or fetal growth restriction, no special obstetric monitoring is indicated beyond what is performed for usual obstetric care.
Medications considered to be low risk in pregnancy include low-dose corticosteroids, antimalarial agents, sulfasalazine, and azathioprine. Certain tumor necrosis factor inhibitors are also thought to be relatively safe.
3. A well-designed exercise program can be beneficial in RA.
Regular physical activity has replaced bed rest as the recommended response to the stiffness and pain associated with RA. However, many patients who have RA do not really believe this. Lack of conviction and motivation appear to be the major factors that deter nearly half of patients with RA from moving about enough to help their situation. There is ample evidence about the benefits of physical activity in RA, but little research into why few patients with RA take advantage of it. The extreme physical inactivity of patients with RA becomes a vicious cycle in terms of health and disease progression. Thus, encouraging physical activity is an essential part of the overall treatment of RA.
Findings from randomized controlled trials show that exercise is fundamentally beneficial for patients with RA. The benefits of properly designed physical exercise programs include improved cardiorespiratory fitness and cardiovascular health, increased muscle mass, reduced adiposity, increased strength, and improved physical functioning, all achieved without exacerbation of disease activity or joint damage.
The American College of Rheumatology (ACR) has released recommendations for exercise interventions for RA. The ACR strongly recommends consistent engagement in an exercise program over no exercise. The type of exercise is open to interpretation. An exercise program for patients with rheumatic diseases aims to preserve or restore the range of motion of affected joints, increase muscle strength and endurance, and improve mood and decrease health risks associated with a sedentary lifestyle.
4. RA is a systemic disease that affects multiple organ systems.
Although synovitis is the pathologic hallmark of RA, extraarticular manifestations and comorbidities occur presumably owing to the complex, chronic, inflammatory, and autoimmune features of RA.
The most common cause of death in patients with RA is cardiovascular disease. Compared with the general population, patients with RA have two times the risk of having a myocardial infarction, and they have up to 50% greater cardiovascular mortality risk. Factors identified to play important roles in atherosclerotic damage and incident cardiovascular disease include severe and prolonged disease activity, inflammation (e.g., C-reactive protein, anti–citrullinated protein antibodies (ACPAs), cytokines, matrix-degrading enzymes), and genetics.
Respiratory disease is the second major cause of death in patients with RA; this occurs in 30%-40% of patients with RA. The lung interstitium, airways, and pleurae can all be affected by RA, but pulmonary vascular involvement is less common.
Central and peripheral nervous system involvement is typically attributed to RA-associated small-vessel vasculitis, joint damage, and/or drug toxicity. Evidence also suggests that systemic inflammation causes microvascular cerebral damage that is associated with the development of vascular dementia and Alzheimer’s disease. Finally, some observational studies have suggested that drugs commonly used to treat RA – disease-modifying antirheumatic drugs (DMARDs) and biologics – may reduce the incidence of dementia.
5. As treatment options for RA improve, many controversies have arisen.
In patients without RA symptoms but with biomarkers, experts debate whether early treatment with DMARDs could prevent irreversible joint damage.
There is no clear definition of pre-RA, but it could be defined as having positive markers for RA (e.g., positive rheumatoid factor and anti–cyclic citrullinated peptides) or having joint pain with abnormal ultrasonography findings but not having positive biomarkers. However, not all patients who have positive biomarkers progress to clinical RA, so what exactly determines this progression is unclear. Nevertheless, some clinicians do treat pre-RA. This was a major debate at the ACR’s 2022 meeting.
Studies have shown that early treatment of RA, including during the preclinical phase, can lead to better long-term outcomes. It can help reduce joint inflammation, control disease activity, and prevent or minimize irreversible joint damage. Early treatment also increases the likelihood of achieving remission or low disease activity, which improves quality of life for patients. Lifestyle interventions in these patients, including exercise, weight control, and cardiovascular health, may not prevent disease but may delay the onset of full-blown clinical RA.
The discovery of pre-RA has also underpinned the development of several clinical prevention trials in RA; specifically, the PRAIRI study demonstrated that a single dose of rituximab can delay the onset of clinically apparent RA in at-risk individuals. Additional studies are evaluating the ability of drugs, including abatacept, hydroxychloroquine, and methotrexate, to prevent or delay future RA.
Dual biologics target different pathways – ostensibly boosting efficacy – but unknowns, concerns over safety, and lack of evidence make the practice controversial.
Several randomized controlled trials have assessed the safety and efficacy of dual-biologic treatment of RA, but the results have been mixed, which has raised safety concerns. Overall, there is a paucity of data concerning the safety of the simultaneous use of more than one biologic. Dual therapy may constitute an efficacious and safe add-on treatment to biologic therapy, but properly conducted clinical investigations are needed. In the meantime, dual biologic therapy used at physicians’ discretion requires close monitoring of patients, with an emphasis on the safety profile.
Large language models (artificial intelligence [AI]) are rapidly taking hold in medicine. Many argue that they can enrich patient care, but they come with liability risks.
Large language models, such as AI chatbots or ChatGPT, can increase access to information, help with patient education, and support decision-making. Limitations include lack of personalization, clinical experience, and emotional connection. The use of large language models in health care is fraught with ethical and legal concerns.
Liability issues can arise if errors, inaccuracies, or adverse outcomes result from the use of AI chatbots. Determining liability may involve assessing factors such as the design and development of the AI system, training and deployment of the model, the communication of limitations and disclaimers to users, and the involvement of human healthcare professionals in the decision-making process.
To mitigate liability risks, AI chatbots in rheumatology must comply with applicable regulations and guidelines. Transparency in the capabilities and limitations of the system, clear communication of the boundaries of its advice, and the presence of human oversight are essential. Collaborating with legal experts and following best practices in the development and deployment of AI technologies can help to minimize liability concerns.
The benefits and risks associated with tapering DMARD therapy in patients with RA who have sustained remission of disease should be considered.
Although some patients with well-controlled RA have relapse after tapering or discontinuing DMARDs, some do not, making this treatment strategy a personal decision undertaken with a rheumatologist.
In the RETRO study, German researchers examined the effects of tapering or stopping DMARDs in patients whose RA was in sustained remission. In the phase 3 trial (n = 316), investigators randomized 303 patients with remission for ≥ 6 months who were on stable conventional synthetic or biologic DMARD treatment into three groups: (1) continuation on 100% DMARD dose, (2) tapering to 50% of the DMARD dose, and (3) 50% tapering followed by DMARD withdrawal. The proportion of patients who continued in remission at 1 year was 81.2% in group 1, 58.6% in group 2, and 43.3% in group 3. Predictors for flare-ups were female sex, longer disease duration, rheumatoid factor or ACPA positivity, and higher disease activity scores at baseline.
The abrupt cessation or reduction of DMARDs without medical supervision and guidance can exacerbate symptoms and result in disease flares.
The interplay between long COVID and RA is a recent phenomenon that needs to be considered.
RA shares similar symptoms with long COVID. Patients with a history of RA and a previous diagnosis of COVID-19 who have developed persistent joint or muscle symptoms pose a significant challenge to clinicians. Such patients may be experiencing long COVID or a flare-up of their preexisting rheumatic disease.
Immunosuppressive medications can potentially increase the risk for COVID-19, but it is not clear how they affect disease severity risk. Individuals with RA and long COVID need careful evaluation to balance the management of disease activity while considering the risks associated with immunosuppression and potential susceptibility to viral infections.
Dr. Dombrosky is a staff physician in rheumatology at Central Virginia VA Health Care System in Richmond. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Sleep Apnea: Comorbidities, Racial Disparities, Weight Guidelines, and Alternatives to CPAP
1. Gottlieb DJ, Punjabi NM. JAMA. 2020;323(14):1389-1400. doi:10.1001/jama.2020.3514
2. Slowik JM et al. Obstructive Sleep Apnea. In: StatPearls. Treasure Island (FL): StatPearls Publishing; December 11, 2022.
3. Bonsignore MR et al. Multidiscip Respir Med. 2019;14:8. doi:10.1186/s40248-019-0172-9
4. Schwartz SW et al. Sleep Breath. 2016;20(3):947-955. doi:10.1007/s11325-016-1316-1
5. Grandner MA et al. Sleep Med. 2016;18:7-18. doi:10.1016/j.sleep.2015.01.020
6. Lee YC et al. Sleep Med. 2022;90:204-213. doi:10.1016/j.sleep.2021.11.014
7. Hudgel DW et al. Am J Respir Crit Care Med. 2018;198(6):e70-e87. doi:10.1164/rccm.201807-1326ST
8. Lloyd R et al. J Clin Sleep Med. 2022;18(11):2673-2680. doi:10.5664/jcsm.10244
9. Nokes B et al. Expert Rev Respir Med. 2022;16(8):917-929. doi:10.1080/17476348.2022.2112669
10. Pinto JA et al. Int Arch Otorhinolaryngol. 2016;20(2):145-150.doi:10.1055/s-0036-1579546
11. Georgoulis M et al. J Clin Sleep Med. 2022;18(5):1251-1261. doi:10.5664/jcsm.9834
12. Askland K et al. Cochrane Database Syst Rev. 2020;4(4):CD007736. doi:10.1002/14651858.CD007736.pub3
13. Jugé L et al. Sleep. 2022;45(6):zsac044. doi:10.1093/sleep/zsac044
14. Strollo PJ Jr et al. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
15. Fattal D et al. J Clin Sleep Med. 2022;18(12):2723-2729. doi:10.5664/jcsm.10190
16. He M et al. Otolaryngol Head Neck Surg. 2019;161(3):401-411. doi:10.1177/0194599819840356
1. Gottlieb DJ, Punjabi NM. JAMA. 2020;323(14):1389-1400. doi:10.1001/jama.2020.3514
2. Slowik JM et al. Obstructive Sleep Apnea. In: StatPearls. Treasure Island (FL): StatPearls Publishing; December 11, 2022.
3. Bonsignore MR et al. Multidiscip Respir Med. 2019;14:8. doi:10.1186/s40248-019-0172-9
4. Schwartz SW et al. Sleep Breath. 2016;20(3):947-955. doi:10.1007/s11325-016-1316-1
5. Grandner MA et al. Sleep Med. 2016;18:7-18. doi:10.1016/j.sleep.2015.01.020
6. Lee YC et al. Sleep Med. 2022;90:204-213. doi:10.1016/j.sleep.2021.11.014
7. Hudgel DW et al. Am J Respir Crit Care Med. 2018;198(6):e70-e87. doi:10.1164/rccm.201807-1326ST
8. Lloyd R et al. J Clin Sleep Med. 2022;18(11):2673-2680. doi:10.5664/jcsm.10244
9. Nokes B et al. Expert Rev Respir Med. 2022;16(8):917-929. doi:10.1080/17476348.2022.2112669
10. Pinto JA et al. Int Arch Otorhinolaryngol. 2016;20(2):145-150.doi:10.1055/s-0036-1579546
11. Georgoulis M et al. J Clin Sleep Med. 2022;18(5):1251-1261. doi:10.5664/jcsm.9834
12. Askland K et al. Cochrane Database Syst Rev. 2020;4(4):CD007736. doi:10.1002/14651858.CD007736.pub3
13. Jugé L et al. Sleep. 2022;45(6):zsac044. doi:10.1093/sleep/zsac044
14. Strollo PJ Jr et al. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
15. Fattal D et al. J Clin Sleep Med. 2022;18(12):2723-2729. doi:10.5664/jcsm.10190
16. He M et al. Otolaryngol Head Neck Surg. 2019;161(3):401-411. doi:10.1177/0194599819840356
1. Gottlieb DJ, Punjabi NM. JAMA. 2020;323(14):1389-1400. doi:10.1001/jama.2020.3514
2. Slowik JM et al. Obstructive Sleep Apnea. In: StatPearls. Treasure Island (FL): StatPearls Publishing; December 11, 2022.
3. Bonsignore MR et al. Multidiscip Respir Med. 2019;14:8. doi:10.1186/s40248-019-0172-9
4. Schwartz SW et al. Sleep Breath. 2016;20(3):947-955. doi:10.1007/s11325-016-1316-1
5. Grandner MA et al. Sleep Med. 2016;18:7-18. doi:10.1016/j.sleep.2015.01.020
6. Lee YC et al. Sleep Med. 2022;90:204-213. doi:10.1016/j.sleep.2021.11.014
7. Hudgel DW et al. Am J Respir Crit Care Med. 2018;198(6):e70-e87. doi:10.1164/rccm.201807-1326ST
8. Lloyd R et al. J Clin Sleep Med. 2022;18(11):2673-2680. doi:10.5664/jcsm.10244
9. Nokes B et al. Expert Rev Respir Med. 2022;16(8):917-929. doi:10.1080/17476348.2022.2112669
10. Pinto JA et al. Int Arch Otorhinolaryngol. 2016;20(2):145-150.doi:10.1055/s-0036-1579546
11. Georgoulis M et al. J Clin Sleep Med. 2022;18(5):1251-1261. doi:10.5664/jcsm.9834
12. Askland K et al. Cochrane Database Syst Rev. 2020;4(4):CD007736. doi:10.1002/14651858.CD007736.pub3
13. Jugé L et al. Sleep. 2022;45(6):zsac044. doi:10.1093/sleep/zsac044
14. Strollo PJ Jr et al. N Engl J Med. 2014;370(2):139-149. doi:10.1056/NEJMoa1308659
15. Fattal D et al. J Clin Sleep Med. 2022;18(12):2723-2729. doi:10.5664/jcsm.10190
16. He M et al. Otolaryngol Head Neck Surg. 2019;161(3):401-411. doi:10.1177/0194599819840356
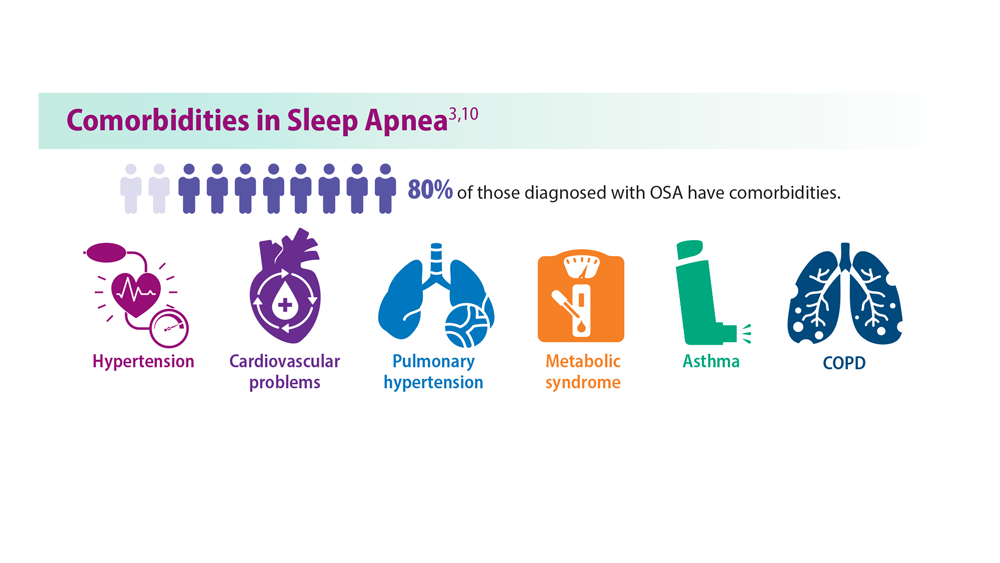
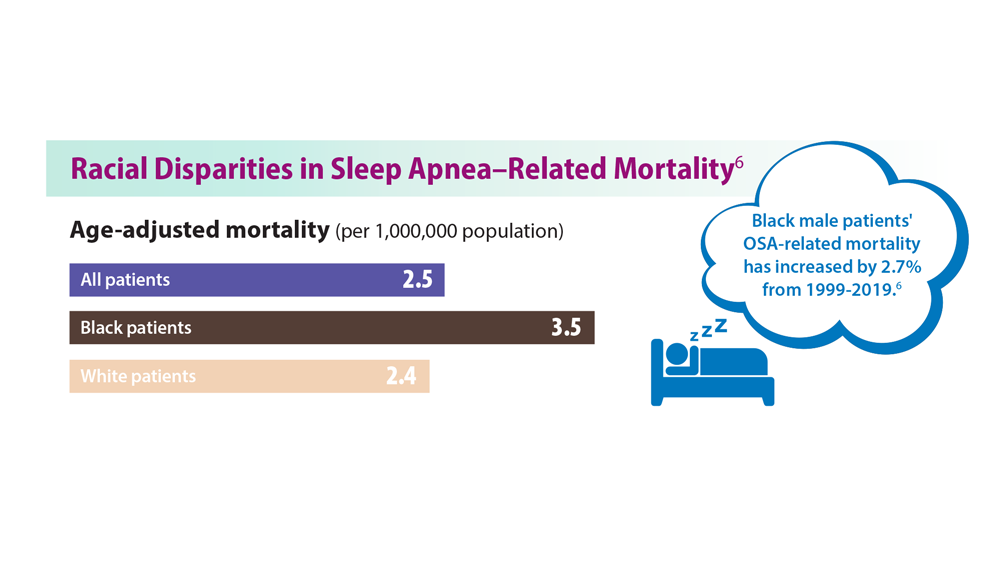
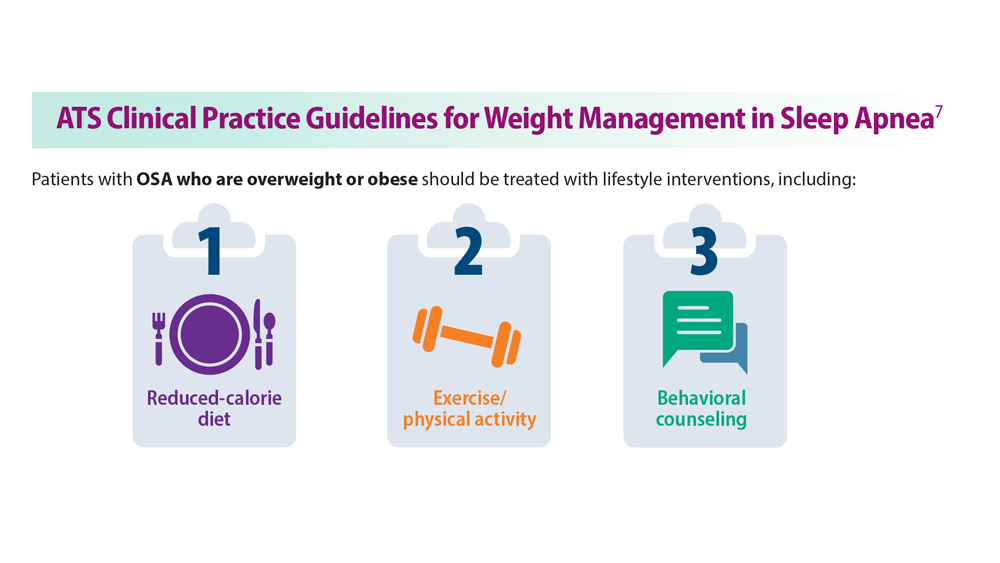
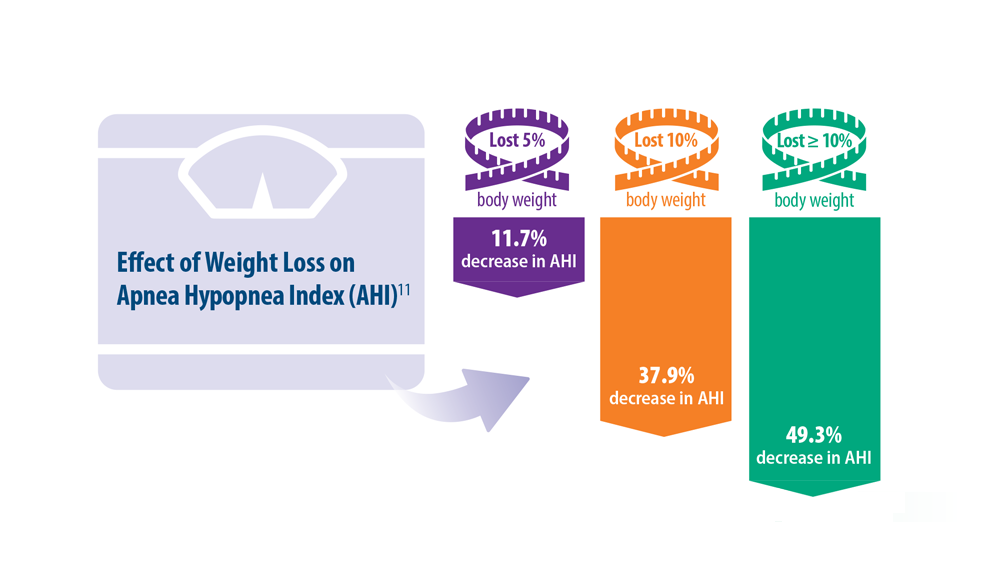
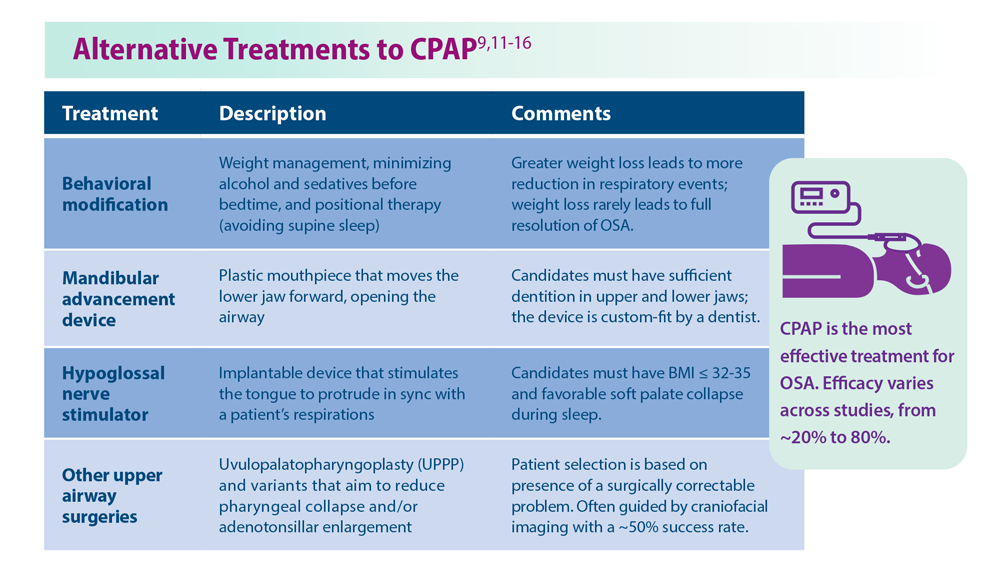
Early-onset NAFLD tied to higher cancer risk
TOPLINE:
New research shows that adults who develop nonalcoholic fatty liver disease (NAFLD) before age 45 are at increased risk of developing cancer, particularly digestive system and lung cancer.
METHODOLOGY:
- Researchers conducted a prospective age- and sex-matched cohort study of 63,696 adults (mean age, 51 years; 83% men) in China. The patients were followed for a median of 10 years; 31,848 had NAFLD, and 31,848 were control participants.
- Participants were grouped on the basis of age at the time of diagnosis of new-onset NAFLD: younger than 45, 45-54, 55-64, and 65 and older.
- Multivariable Cox models were used to analyze cancer risk by age at NAFLD onset. Population-attributable fractions were calculated to quantify cancer risk associated with age at NAFLD onset.
TAKEAWAY:
- During follow-up, 2,415 participants were diagnosed with cancer.
- NAFLD onset before age 45 was associated with highest cancer risk in comparison with the risk among control persons (average hazard ratio [AHR], 1.52). Cancer risk decreased as age at NAFLD onset increased (AHR, 1.50 for the 45-54 cohort, 1.13 for the 55-64 cohort, and 0.75 for the 65-and-older cohort).
- Among adults younger than 45 at NAFLD onset, cancers were mainly digestive and lung cancers (AHR, 2.00 and 2.14, respectively).
- Close to 18% of the cancer risk among adults younger than 45 at NAFLD onset was attributed to their fatty liver disease.
IN PRACTICE:
“The increasing incidence of NAFLD among younger populations highlights the underestimation of harmful outcomes associated with this condition,” the authors wrote. “Our findings suggest that early control and intervention against NAFLD progression may be crucial to reduce the occurrence of NAFLD-related cancers and lessen the burden on public health.”
SOURCE:
The study, with first author Chenan Liu, MD, PhD, Beijing Shijitan Hospital, Capital Medical University, was published online in JAMA Network Open.
LIMITATIONS:
The study population was predominantly male, and NAFLD diagnosis relied on ultrasound rather than liver biopsy, potentially missing mild cases. The study lacked data on liver fibrosis elastography measurement and blood biomarkers. For some cancers, incidence rates were low.
DISCLOSURES:
The study was funded by a grant from the National Key Research and Development Program of China. The authors reported no conflicts of interest.
TOPLINE:
New research shows that adults who develop nonalcoholic fatty liver disease (NAFLD) before age 45 are at increased risk of developing cancer, particularly digestive system and lung cancer.
METHODOLOGY:
- Researchers conducted a prospective age- and sex-matched cohort study of 63,696 adults (mean age, 51 years; 83% men) in China. The patients were followed for a median of 10 years; 31,848 had NAFLD, and 31,848 were control participants.
- Participants were grouped on the basis of age at the time of diagnosis of new-onset NAFLD: younger than 45, 45-54, 55-64, and 65 and older.
- Multivariable Cox models were used to analyze cancer risk by age at NAFLD onset. Population-attributable fractions were calculated to quantify cancer risk associated with age at NAFLD onset.
TAKEAWAY:
- During follow-up, 2,415 participants were diagnosed with cancer.
- NAFLD onset before age 45 was associated with highest cancer risk in comparison with the risk among control persons (average hazard ratio [AHR], 1.52). Cancer risk decreased as age at NAFLD onset increased (AHR, 1.50 for the 45-54 cohort, 1.13 for the 55-64 cohort, and 0.75 for the 65-and-older cohort).
- Among adults younger than 45 at NAFLD onset, cancers were mainly digestive and lung cancers (AHR, 2.00 and 2.14, respectively).
- Close to 18% of the cancer risk among adults younger than 45 at NAFLD onset was attributed to their fatty liver disease.
IN PRACTICE:
“The increasing incidence of NAFLD among younger populations highlights the underestimation of harmful outcomes associated with this condition,” the authors wrote. “Our findings suggest that early control and intervention against NAFLD progression may be crucial to reduce the occurrence of NAFLD-related cancers and lessen the burden on public health.”
SOURCE:
The study, with first author Chenan Liu, MD, PhD, Beijing Shijitan Hospital, Capital Medical University, was published online in JAMA Network Open.
LIMITATIONS:
The study population was predominantly male, and NAFLD diagnosis relied on ultrasound rather than liver biopsy, potentially missing mild cases. The study lacked data on liver fibrosis elastography measurement and blood biomarkers. For some cancers, incidence rates were low.
DISCLOSURES:
The study was funded by a grant from the National Key Research and Development Program of China. The authors reported no conflicts of interest.
TOPLINE:
New research shows that adults who develop nonalcoholic fatty liver disease (NAFLD) before age 45 are at increased risk of developing cancer, particularly digestive system and lung cancer.
METHODOLOGY:
- Researchers conducted a prospective age- and sex-matched cohort study of 63,696 adults (mean age, 51 years; 83% men) in China. The patients were followed for a median of 10 years; 31,848 had NAFLD, and 31,848 were control participants.
- Participants were grouped on the basis of age at the time of diagnosis of new-onset NAFLD: younger than 45, 45-54, 55-64, and 65 and older.
- Multivariable Cox models were used to analyze cancer risk by age at NAFLD onset. Population-attributable fractions were calculated to quantify cancer risk associated with age at NAFLD onset.
TAKEAWAY:
- During follow-up, 2,415 participants were diagnosed with cancer.
- NAFLD onset before age 45 was associated with highest cancer risk in comparison with the risk among control persons (average hazard ratio [AHR], 1.52). Cancer risk decreased as age at NAFLD onset increased (AHR, 1.50 for the 45-54 cohort, 1.13 for the 55-64 cohort, and 0.75 for the 65-and-older cohort).
- Among adults younger than 45 at NAFLD onset, cancers were mainly digestive and lung cancers (AHR, 2.00 and 2.14, respectively).
- Close to 18% of the cancer risk among adults younger than 45 at NAFLD onset was attributed to their fatty liver disease.
IN PRACTICE:
“The increasing incidence of NAFLD among younger populations highlights the underestimation of harmful outcomes associated with this condition,” the authors wrote. “Our findings suggest that early control and intervention against NAFLD progression may be crucial to reduce the occurrence of NAFLD-related cancers and lessen the burden on public health.”
SOURCE:
The study, with first author Chenan Liu, MD, PhD, Beijing Shijitan Hospital, Capital Medical University, was published online in JAMA Network Open.
LIMITATIONS:
The study population was predominantly male, and NAFLD diagnosis relied on ultrasound rather than liver biopsy, potentially missing mild cases. The study lacked data on liver fibrosis elastography measurement and blood biomarkers. For some cancers, incidence rates were low.
DISCLOSURES:
The study was funded by a grant from the National Key Research and Development Program of China. The authors reported no conflicts of interest.
New insight into genetic link between schizophrenia and CVD
TOPLINE:
There is an extensive genetic overlap between schizophrenia and smoking, but there are also schizophrenia genes that may protect against obesity, illustrating the bidirectional effects of shared loci across cardiovascular disease (CVD) risk factors, results of new research suggest.
METHODOLOGY:
- Researchers obtained what they call an “unprecedentedly large” set of GWAS samples, including schizophrenia (53,386 patients and 77,258 controls) and various CVD risk factors.
- They used analytic approaches to identify genetic links between schizophrenia and CVD risk factors, including bivariate causal mixture model (MiXeR), which estimates the number of shared genetic variants between pairs of phenotypes, and conditional and conjunctional false discovery rate (condFDR and conjFDR), to identify specific genetic loci; these approaches can identify genetic overlap regardless of the effect directions.
TAKEAWAY:
- Using MiXeR, the study showed that several genetic variants underlying schizophrenia also influence CVD phenotypes, particularly risk factors of smoking and BMI.
- A total of 825 distinct loci were jointly associated with schizophrenia and CVD phenotypes at conjFDR < .05.
- Most of the loci shared with smoking were in line with positive genetic correlations; the authors noted individuals with schizophrenia are more nicotine dependent than the general population, and they experience greater reinforcing effects of nicotine and worse withdrawal symptoms during abstinence than the general population.
- The overlapping loci with BMI had effect directions consistent with negative genetic correlations, suggesting people with schizophrenia are genetically predisposed to lower BMI; this is in line with evidence of low BMI being a risk factor for schizophrenia, although obesity is more common in people with schizophrenia.
- There was a pattern of mixed effect directions among loci jointly associated with schizophrenia and lipids, blood pressure, type 2 diabetes, waist-to-hip ratio, and coronary artery disease, which may reflect variation in genetic susceptibility to CVD across subgroups of schizophrenia.
IN PRACTICE:
The new results “shed light” on biological pathways associated with comorbidity between CVD and schizophrenia, said the authors, adding future work could provide insights into mechanisms underlying the comorbidity and could facilitate development of antipsychotics with lower metabolic side effects, which could help prevent comorbid CVD, “thereby helping to mitigate a major clinical and health care problem.”
SOURCE:
The study was led by Linn Rødevand, PhD, Norwegian Center for Mental Disorders Research, Division of Mental Health and Addiction, Institute of Clinical Medicine, Oslo University Hospital, University of Oslo, and colleagues. It was published online in the American Journal of Psychiatry.
LIMITATIONS:
Methods used in the study are limited by uncertainties in translating genetic loci to causal variants, which restricts the biological interpretation of the shared genetic variants. Among other methodological limitations are that discrepancies between the linkage disequilibrium structure of the samples used for the GWAS and that of the reference panel may have biased estimates underlying MiXeR.
DISCLOSURES:
The study received support from the Research Council of Norway, Norwegian Health Association, South-East Norway Regional Health Authority, and the European Union. Dr. Rødevand reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
There is an extensive genetic overlap between schizophrenia and smoking, but there are also schizophrenia genes that may protect against obesity, illustrating the bidirectional effects of shared loci across cardiovascular disease (CVD) risk factors, results of new research suggest.
METHODOLOGY:
- Researchers obtained what they call an “unprecedentedly large” set of GWAS samples, including schizophrenia (53,386 patients and 77,258 controls) and various CVD risk factors.
- They used analytic approaches to identify genetic links between schizophrenia and CVD risk factors, including bivariate causal mixture model (MiXeR), which estimates the number of shared genetic variants between pairs of phenotypes, and conditional and conjunctional false discovery rate (condFDR and conjFDR), to identify specific genetic loci; these approaches can identify genetic overlap regardless of the effect directions.
TAKEAWAY:
- Using MiXeR, the study showed that several genetic variants underlying schizophrenia also influence CVD phenotypes, particularly risk factors of smoking and BMI.
- A total of 825 distinct loci were jointly associated with schizophrenia and CVD phenotypes at conjFDR < .05.
- Most of the loci shared with smoking were in line with positive genetic correlations; the authors noted individuals with schizophrenia are more nicotine dependent than the general population, and they experience greater reinforcing effects of nicotine and worse withdrawal symptoms during abstinence than the general population.
- The overlapping loci with BMI had effect directions consistent with negative genetic correlations, suggesting people with schizophrenia are genetically predisposed to lower BMI; this is in line with evidence of low BMI being a risk factor for schizophrenia, although obesity is more common in people with schizophrenia.
- There was a pattern of mixed effect directions among loci jointly associated with schizophrenia and lipids, blood pressure, type 2 diabetes, waist-to-hip ratio, and coronary artery disease, which may reflect variation in genetic susceptibility to CVD across subgroups of schizophrenia.
IN PRACTICE:
The new results “shed light” on biological pathways associated with comorbidity between CVD and schizophrenia, said the authors, adding future work could provide insights into mechanisms underlying the comorbidity and could facilitate development of antipsychotics with lower metabolic side effects, which could help prevent comorbid CVD, “thereby helping to mitigate a major clinical and health care problem.”
SOURCE:
The study was led by Linn Rødevand, PhD, Norwegian Center for Mental Disorders Research, Division of Mental Health and Addiction, Institute of Clinical Medicine, Oslo University Hospital, University of Oslo, and colleagues. It was published online in the American Journal of Psychiatry.
LIMITATIONS:
Methods used in the study are limited by uncertainties in translating genetic loci to causal variants, which restricts the biological interpretation of the shared genetic variants. Among other methodological limitations are that discrepancies between the linkage disequilibrium structure of the samples used for the GWAS and that of the reference panel may have biased estimates underlying MiXeR.
DISCLOSURES:
The study received support from the Research Council of Norway, Norwegian Health Association, South-East Norway Regional Health Authority, and the European Union. Dr. Rødevand reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
There is an extensive genetic overlap between schizophrenia and smoking, but there are also schizophrenia genes that may protect against obesity, illustrating the bidirectional effects of shared loci across cardiovascular disease (CVD) risk factors, results of new research suggest.
METHODOLOGY:
- Researchers obtained what they call an “unprecedentedly large” set of GWAS samples, including schizophrenia (53,386 patients and 77,258 controls) and various CVD risk factors.
- They used analytic approaches to identify genetic links between schizophrenia and CVD risk factors, including bivariate causal mixture model (MiXeR), which estimates the number of shared genetic variants between pairs of phenotypes, and conditional and conjunctional false discovery rate (condFDR and conjFDR), to identify specific genetic loci; these approaches can identify genetic overlap regardless of the effect directions.
TAKEAWAY:
- Using MiXeR, the study showed that several genetic variants underlying schizophrenia also influence CVD phenotypes, particularly risk factors of smoking and BMI.
- A total of 825 distinct loci were jointly associated with schizophrenia and CVD phenotypes at conjFDR < .05.
- Most of the loci shared with smoking were in line with positive genetic correlations; the authors noted individuals with schizophrenia are more nicotine dependent than the general population, and they experience greater reinforcing effects of nicotine and worse withdrawal symptoms during abstinence than the general population.
- The overlapping loci with BMI had effect directions consistent with negative genetic correlations, suggesting people with schizophrenia are genetically predisposed to lower BMI; this is in line with evidence of low BMI being a risk factor for schizophrenia, although obesity is more common in people with schizophrenia.
- There was a pattern of mixed effect directions among loci jointly associated with schizophrenia and lipids, blood pressure, type 2 diabetes, waist-to-hip ratio, and coronary artery disease, which may reflect variation in genetic susceptibility to CVD across subgroups of schizophrenia.
IN PRACTICE:
The new results “shed light” on biological pathways associated with comorbidity between CVD and schizophrenia, said the authors, adding future work could provide insights into mechanisms underlying the comorbidity and could facilitate development of antipsychotics with lower metabolic side effects, which could help prevent comorbid CVD, “thereby helping to mitigate a major clinical and health care problem.”
SOURCE:
The study was led by Linn Rødevand, PhD, Norwegian Center for Mental Disorders Research, Division of Mental Health and Addiction, Institute of Clinical Medicine, Oslo University Hospital, University of Oslo, and colleagues. It was published online in the American Journal of Psychiatry.
LIMITATIONS:
Methods used in the study are limited by uncertainties in translating genetic loci to causal variants, which restricts the biological interpretation of the shared genetic variants. Among other methodological limitations are that discrepancies between the linkage disequilibrium structure of the samples used for the GWAS and that of the reference panel may have biased estimates underlying MiXeR.
DISCLOSURES:
The study received support from the Research Council of Norway, Norwegian Health Association, South-East Norway Regional Health Authority, and the European Union. Dr. Rødevand reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF PSYCHIATRY
Decreasing Pulmonary Embolism-Related Mortality
- Centers for Disease Control and Prevention. Data and statistics on venous thromboembolism. Last reviewed June 28, 2023. Accessed July 18, 2023. https://www.cdc.gov/ncbddd/dvt/data.html
- Becattini C et al. Chest. 2016;149(1):192-200. doi:10.1378/chest.15-0808
- Triantafyllou GA et al. Semin Respir Crit Care Med. 2021;42(2):183-198.doi:10.1055/s-0041-1722898
- Ng ACC et al. Respiration. 2013;85(5):408-416. doi:10.1159/000342024
- Phillips AR et al. J Am Heart Assoc. 2021;10(17):e021818. doi:10.1161/JAHA.121.021818
- Wadhera RK et al. J Am Heart Assoc. 2021;10(13):e021117. doi:10.1161/JAHA.121.021117
- Bashir R et al. JACC Cardiovasc Interv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011
- Patel NJ et al. Int J Cardiol. 2019;287:116-117. doi:10.1016/j.ijcard.2019.04.029
- Li X et al. Ann Transl Med. 2021;9(10):838. doi:10.21037/atm-21-975
- Rivera-Lebron BN et al. Chest. 2021;159(1):347-355. doi:10.1016/j.chest.2020.07.065
- Noto JG, Rali P. Pulm Circ. 2022;12(1):e12021. doi:10.1002/pul2.12021
- Snyder DJ et al. Vasc Med. 2023;28(3):222-232. doi:10.1177/1358863X231157441
- Bikdeli B et al. Semin Thromb Hemost. 2023. doi:10.1055/s-0043-1764231
- Fleitas Sosa D et al. Eur Respir Rev. 2022;31(165):220023. doi:10.1183/16000617.0023-2022
- Pulmonary embolism - thrombus removal with catheter-directed therapy (PE-TRACT). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05591118
- The PEERLESS study (PEERLESS). ClinicalTrials.gov. Updated Jun 23, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05111613
- Inari Medical, Inc. Inari Medical announces Peerless II, a randomized controlled trial evaluating clinical outcomes of the FlowTriever® system vs. anticoagulation in pulmonary embolism patients [press release]. Published May 22,2023. Accessed July 18, 2023. https://ir.inarimedical.com/news-releases/news-release-details/inari-medical-announces-peerless-ii-randomized-controlled-trial
- Ultrasound-facilitated, catheter-directed, thrombolysis in intermediate-high risk pulmonary embolism (HI-PEITHO). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04790370
- Comparison of two pulmonary embolism treatments. ClinicalTrials.gov. Updated May 31, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05684796
- Pulmonary Embolism International THrOmbolysis Study-3 (PEITHO-3).ClinicalTrials.gov. Updated June 8, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04430569
- Study of the long-term safety and outcomes of treating pulmonary embolism with the Indigo Aspiration System. ClinicalTrials.gov. Updated May 11, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04798261
- Bashir R et al. J Am Coll Cardiol Intv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011
- Centers for Disease Control and Prevention. Data and statistics on venous thromboembolism. Last reviewed June 28, 2023. Accessed July 18, 2023. https://www.cdc.gov/ncbddd/dvt/data.html
- Becattini C et al. Chest. 2016;149(1):192-200. doi:10.1378/chest.15-0808
- Triantafyllou GA et al. Semin Respir Crit Care Med. 2021;42(2):183-198.doi:10.1055/s-0041-1722898
- Ng ACC et al. Respiration. 2013;85(5):408-416. doi:10.1159/000342024
- Phillips AR et al. J Am Heart Assoc. 2021;10(17):e021818. doi:10.1161/JAHA.121.021818
- Wadhera RK et al. J Am Heart Assoc. 2021;10(13):e021117. doi:10.1161/JAHA.121.021117
- Bashir R et al. JACC Cardiovasc Interv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011
- Patel NJ et al. Int J Cardiol. 2019;287:116-117. doi:10.1016/j.ijcard.2019.04.029
- Li X et al. Ann Transl Med. 2021;9(10):838. doi:10.21037/atm-21-975
- Rivera-Lebron BN et al. Chest. 2021;159(1):347-355. doi:10.1016/j.chest.2020.07.065
- Noto JG, Rali P. Pulm Circ. 2022;12(1):e12021. doi:10.1002/pul2.12021
- Snyder DJ et al. Vasc Med. 2023;28(3):222-232. doi:10.1177/1358863X231157441
- Bikdeli B et al. Semin Thromb Hemost. 2023. doi:10.1055/s-0043-1764231
- Fleitas Sosa D et al. Eur Respir Rev. 2022;31(165):220023. doi:10.1183/16000617.0023-2022
- Pulmonary embolism - thrombus removal with catheter-directed therapy (PE-TRACT). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05591118
- The PEERLESS study (PEERLESS). ClinicalTrials.gov. Updated Jun 23, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05111613
- Inari Medical, Inc. Inari Medical announces Peerless II, a randomized controlled trial evaluating clinical outcomes of the FlowTriever® system vs. anticoagulation in pulmonary embolism patients [press release]. Published May 22,2023. Accessed July 18, 2023. https://ir.inarimedical.com/news-releases/news-release-details/inari-medical-announces-peerless-ii-randomized-controlled-trial
- Ultrasound-facilitated, catheter-directed, thrombolysis in intermediate-high risk pulmonary embolism (HI-PEITHO). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04790370
- Comparison of two pulmonary embolism treatments. ClinicalTrials.gov. Updated May 31, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05684796
- Pulmonary Embolism International THrOmbolysis Study-3 (PEITHO-3).ClinicalTrials.gov. Updated June 8, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04430569
- Study of the long-term safety and outcomes of treating pulmonary embolism with the Indigo Aspiration System. ClinicalTrials.gov. Updated May 11, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04798261
- Bashir R et al. J Am Coll Cardiol Intv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011
- Centers for Disease Control and Prevention. Data and statistics on venous thromboembolism. Last reviewed June 28, 2023. Accessed July 18, 2023. https://www.cdc.gov/ncbddd/dvt/data.html
- Becattini C et al. Chest. 2016;149(1):192-200. doi:10.1378/chest.15-0808
- Triantafyllou GA et al. Semin Respir Crit Care Med. 2021;42(2):183-198.doi:10.1055/s-0041-1722898
- Ng ACC et al. Respiration. 2013;85(5):408-416. doi:10.1159/000342024
- Phillips AR et al. J Am Heart Assoc. 2021;10(17):e021818. doi:10.1161/JAHA.121.021818
- Wadhera RK et al. J Am Heart Assoc. 2021;10(13):e021117. doi:10.1161/JAHA.121.021117
- Bashir R et al. JACC Cardiovasc Interv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011
- Patel NJ et al. Int J Cardiol. 2019;287:116-117. doi:10.1016/j.ijcard.2019.04.029
- Li X et al. Ann Transl Med. 2021;9(10):838. doi:10.21037/atm-21-975
- Rivera-Lebron BN et al. Chest. 2021;159(1):347-355. doi:10.1016/j.chest.2020.07.065
- Noto JG, Rali P. Pulm Circ. 2022;12(1):e12021. doi:10.1002/pul2.12021
- Snyder DJ et al. Vasc Med. 2023;28(3):222-232. doi:10.1177/1358863X231157441
- Bikdeli B et al. Semin Thromb Hemost. 2023. doi:10.1055/s-0043-1764231
- Fleitas Sosa D et al. Eur Respir Rev. 2022;31(165):220023. doi:10.1183/16000617.0023-2022
- Pulmonary embolism - thrombus removal with catheter-directed therapy (PE-TRACT). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05591118
- The PEERLESS study (PEERLESS). ClinicalTrials.gov. Updated Jun 23, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05111613
- Inari Medical, Inc. Inari Medical announces Peerless II, a randomized controlled trial evaluating clinical outcomes of the FlowTriever® system vs. anticoagulation in pulmonary embolism patients [press release]. Published May 22,2023. Accessed July 18, 2023. https://ir.inarimedical.com/news-releases/news-release-details/inari-medical-announces-peerless-ii-randomized-controlled-trial
- Ultrasound-facilitated, catheter-directed, thrombolysis in intermediate-high risk pulmonary embolism (HI-PEITHO). ClinicalTrials.gov. Updated July 17, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04790370
- Comparison of two pulmonary embolism treatments. ClinicalTrials.gov. Updated May 31, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT05684796
- Pulmonary Embolism International THrOmbolysis Study-3 (PEITHO-3).ClinicalTrials.gov. Updated June 8, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04430569
- Study of the long-term safety and outcomes of treating pulmonary embolism with the Indigo Aspiration System. ClinicalTrials.gov. Updated May 11, 2023. Accessed July 18, 2023. https://clinicaltrials.gov/ct2/show/NCT04798261
- Bashir R et al. J Am Coll Cardiol Intv. 2022;15(23):2427-2436. doi:10.1016/j.jcin.2022.09.011