User login
NCCN survey shows ongoing chemo drug shortages
Although access to carboplatin and cisplatin has improved slightly since June, when 93% and 70% of 27 NCCN member institutions reported shortages of the two agents, supplies remain limited and other anticancer drugs remain scarce, an NCCN follow-up survey shows.
Of 29 institutions surveyed last month, 86% reported having difficulty obtaining at least one anticancer drug, and 72% and 59% reported ongoing shortages of carboplatin and cisplatin, respectively – drugs recommended for treating patients involved in hundreds of different cancer scenarios, according to the NCCN.
“Drug shortages aren’t new, but the widespread impact makes this one particularly alarming,” NCCN’s chief executive officer, Robert W. Carlson, MD, said in a press statement. “It is extremely concerning that this situation continues despite significant attention and effort over the past few months.”
The latest survey, conducted between Sept. 6 and 27, was sent to the 33 NCCN member institutions. Overall, most respondents reported “being able to continue treating every patient who needs carboplatin or cisplatin, despite lowered supply, primarily by implementing strict waste management strategies,” the network noted, adding that “the responses may not reflect any additional challenges experienced by smaller community practices serving rural and marginalized patients.”
In addition to carboplatin and cisplatin shortages, the survey results also revealed that centers are experiencing shortages of a host of other drugs, including methotrexate (66%), 5-flourouracil (55%), fludarabine (45%), hydrocortisone (41%), and dacarbazine (28%), according to the press release.
“These drug shortages are the result of decades of systemic challenges,” noted Alyssa Schatz, senior director of policy and advocacy for NCCN, in a press release. “We recognize that comprehensive solutions take time, and we appreciate everyone who has put forth proposals to improve investment in generics and our data infrastructure. At the same time, we have to acknowledge that the cancer drug shortage has been ongoing for months, which is unacceptable for anyone impacted by cancer today.”
Following the June survey, the NCCN called for action from the federal government, the pharmaceutical industry, providers, and payers, encouraging them “to work together to ensure quality, effective, equitable, and accessible cancer care” and has since worked with multiple stakeholders and policymaking organizations to “advocate for short- and long-term fixes.”
“These new survey results remind us that we are still in an ongoing crisis and must respond with appropriate urgency,” Ms. Shatz added.
A version of this article first appeared on Medscape.com.
Although access to carboplatin and cisplatin has improved slightly since June, when 93% and 70% of 27 NCCN member institutions reported shortages of the two agents, supplies remain limited and other anticancer drugs remain scarce, an NCCN follow-up survey shows.
Of 29 institutions surveyed last month, 86% reported having difficulty obtaining at least one anticancer drug, and 72% and 59% reported ongoing shortages of carboplatin and cisplatin, respectively – drugs recommended for treating patients involved in hundreds of different cancer scenarios, according to the NCCN.
“Drug shortages aren’t new, but the widespread impact makes this one particularly alarming,” NCCN’s chief executive officer, Robert W. Carlson, MD, said in a press statement. “It is extremely concerning that this situation continues despite significant attention and effort over the past few months.”
The latest survey, conducted between Sept. 6 and 27, was sent to the 33 NCCN member institutions. Overall, most respondents reported “being able to continue treating every patient who needs carboplatin or cisplatin, despite lowered supply, primarily by implementing strict waste management strategies,” the network noted, adding that “the responses may not reflect any additional challenges experienced by smaller community practices serving rural and marginalized patients.”
In addition to carboplatin and cisplatin shortages, the survey results also revealed that centers are experiencing shortages of a host of other drugs, including methotrexate (66%), 5-flourouracil (55%), fludarabine (45%), hydrocortisone (41%), and dacarbazine (28%), according to the press release.
“These drug shortages are the result of decades of systemic challenges,” noted Alyssa Schatz, senior director of policy and advocacy for NCCN, in a press release. “We recognize that comprehensive solutions take time, and we appreciate everyone who has put forth proposals to improve investment in generics and our data infrastructure. At the same time, we have to acknowledge that the cancer drug shortage has been ongoing for months, which is unacceptable for anyone impacted by cancer today.”
Following the June survey, the NCCN called for action from the federal government, the pharmaceutical industry, providers, and payers, encouraging them “to work together to ensure quality, effective, equitable, and accessible cancer care” and has since worked with multiple stakeholders and policymaking organizations to “advocate for short- and long-term fixes.”
“These new survey results remind us that we are still in an ongoing crisis and must respond with appropriate urgency,” Ms. Shatz added.
A version of this article first appeared on Medscape.com.
Although access to carboplatin and cisplatin has improved slightly since June, when 93% and 70% of 27 NCCN member institutions reported shortages of the two agents, supplies remain limited and other anticancer drugs remain scarce, an NCCN follow-up survey shows.
Of 29 institutions surveyed last month, 86% reported having difficulty obtaining at least one anticancer drug, and 72% and 59% reported ongoing shortages of carboplatin and cisplatin, respectively – drugs recommended for treating patients involved in hundreds of different cancer scenarios, according to the NCCN.
“Drug shortages aren’t new, but the widespread impact makes this one particularly alarming,” NCCN’s chief executive officer, Robert W. Carlson, MD, said in a press statement. “It is extremely concerning that this situation continues despite significant attention and effort over the past few months.”
The latest survey, conducted between Sept. 6 and 27, was sent to the 33 NCCN member institutions. Overall, most respondents reported “being able to continue treating every patient who needs carboplatin or cisplatin, despite lowered supply, primarily by implementing strict waste management strategies,” the network noted, adding that “the responses may not reflect any additional challenges experienced by smaller community practices serving rural and marginalized patients.”
In addition to carboplatin and cisplatin shortages, the survey results also revealed that centers are experiencing shortages of a host of other drugs, including methotrexate (66%), 5-flourouracil (55%), fludarabine (45%), hydrocortisone (41%), and dacarbazine (28%), according to the press release.
“These drug shortages are the result of decades of systemic challenges,” noted Alyssa Schatz, senior director of policy and advocacy for NCCN, in a press release. “We recognize that comprehensive solutions take time, and we appreciate everyone who has put forth proposals to improve investment in generics and our data infrastructure. At the same time, we have to acknowledge that the cancer drug shortage has been ongoing for months, which is unacceptable for anyone impacted by cancer today.”
Following the June survey, the NCCN called for action from the federal government, the pharmaceutical industry, providers, and payers, encouraging them “to work together to ensure quality, effective, equitable, and accessible cancer care” and has since worked with multiple stakeholders and policymaking organizations to “advocate for short- and long-term fixes.”
“These new survey results remind us that we are still in an ongoing crisis and must respond with appropriate urgency,” Ms. Shatz added.
A version of this article first appeared on Medscape.com.
Training more doctors should be our first priority, says ethicist
This transcript has been edited for clarity.
Recently, the Supreme Court of the United States struck down the use of affirmative action in admissions to colleges, universities, medical schools, and nursing schools. This has led to an enormous amount of worry and concern, particularly in medical school admissions in the world I’m in, where people start to say that diversity matters. Diversity is important.
I know many deans of medical schools immediately sent out messages of reassurance to their students, saying New York University or Stanford or Harvard or Minnesota or Case Western is still deeply concerned about diversity, and we’re going to do what we can to preserve attention to diversity.
I’ve served on admissions at a number of schools over the years for med school. I understand – and have been told – that diversity is important, and according to the Supreme Court, not explicitly by race. There are obviously many variables to take into account when trying to keep diversity at the forefront of admissions.
At the schools I’ve been at, including Columbia, NYU, University of Pittsburgh, University of Minnesota, and University of Pennsylvania, there are plenty of qualified students. Happily, we’ve always been engaged in some effort to try and whittle down the class to the size that we can manage and accept, and many qualified students don’t get admitted.
The first order of business for me is not to worry about how to maintain diversity. It’s to recognize that we need more doctors, nurses, and mental health care providers. I will, in a second, say a few words about diversity and where it fits into admissions, but I want to make the point clearly that what we should be doing is trying to expand the pool of students who are going to become doctors, nurses, mental health care providers, and social workers.
There are too many early retirements. We don’t have the person power we need to manage the health care challenges of an aging population. Let’s not get lost in arguing about what characteristics ought to get you into the finest medical schools. Let’s realize that we have to expand the number of schools we have.
We better be working pretty hard to expand our physician assistant programs, to make sure that we give full authority to qualified dentists and nurses who can help deliver some clinical care. We need more folks. That’s really where the battle ought to be: How do we get that done and how do we get it done quickly, not arguing about who’s in, who’s out, and why.
That said, diversity to me has never meant just race. I’m always interested in gender orientation, disability, and geographic input. Sometimes in decisions that you’re looking at, when I have students in front of me, they tell me they play a musical instrument or about the obstacles they had to overcome to get to medical school. Some of them will say they were involved in 4-H and did rodeo in high school or junior high school, which makes them a diverse potential student with characteristics that maybe some others don’t bring.
I’m not against diversity. I think having a rich set of experiences in any class – medicine, nursing, whatever it’s going to be – is beneficial to the students. They learn from each other. It is sometimes said that it’s also good for patients. I’m a little less excited about that, because I think our training goal should be to make every medical student and nursing student qualified to treat anybody.
I don’t think that, just because you’re Latinx or gay, that’s going to make a gay patient feel better. I think we should teach our students how to give care to everybody that they encounter. They shouldn’t have to match up characteristics to feel like they’re going to get quality care. That isn’t the right reason.
When you have a diverse set of providers, they can call that out and be on the alert for it, and that’s very important.
I also believe that we should think widely and broadly about diversity. Maybe race is out, but certainly other experiences related to income, background, struggle that got you to the point where you’re applying to medical school, motivation, the kinds of experiences you might have had caring for an elderly person, dealing with a disability or learning disability, and trying to overcome, let’s say, going to school in a poor area with not such a wonderful school, really help in terms of forming professionalism, empathy, and a caring point of view.
To me, the main goal is to expand our workforce. The secondary goal is to stay diverse, because we get better providers when we do so.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Recently, the Supreme Court of the United States struck down the use of affirmative action in admissions to colleges, universities, medical schools, and nursing schools. This has led to an enormous amount of worry and concern, particularly in medical school admissions in the world I’m in, where people start to say that diversity matters. Diversity is important.
I know many deans of medical schools immediately sent out messages of reassurance to their students, saying New York University or Stanford or Harvard or Minnesota or Case Western is still deeply concerned about diversity, and we’re going to do what we can to preserve attention to diversity.
I’ve served on admissions at a number of schools over the years for med school. I understand – and have been told – that diversity is important, and according to the Supreme Court, not explicitly by race. There are obviously many variables to take into account when trying to keep diversity at the forefront of admissions.
At the schools I’ve been at, including Columbia, NYU, University of Pittsburgh, University of Minnesota, and University of Pennsylvania, there are plenty of qualified students. Happily, we’ve always been engaged in some effort to try and whittle down the class to the size that we can manage and accept, and many qualified students don’t get admitted.
The first order of business for me is not to worry about how to maintain diversity. It’s to recognize that we need more doctors, nurses, and mental health care providers. I will, in a second, say a few words about diversity and where it fits into admissions, but I want to make the point clearly that what we should be doing is trying to expand the pool of students who are going to become doctors, nurses, mental health care providers, and social workers.
There are too many early retirements. We don’t have the person power we need to manage the health care challenges of an aging population. Let’s not get lost in arguing about what characteristics ought to get you into the finest medical schools. Let’s realize that we have to expand the number of schools we have.
We better be working pretty hard to expand our physician assistant programs, to make sure that we give full authority to qualified dentists and nurses who can help deliver some clinical care. We need more folks. That’s really where the battle ought to be: How do we get that done and how do we get it done quickly, not arguing about who’s in, who’s out, and why.
That said, diversity to me has never meant just race. I’m always interested in gender orientation, disability, and geographic input. Sometimes in decisions that you’re looking at, when I have students in front of me, they tell me they play a musical instrument or about the obstacles they had to overcome to get to medical school. Some of them will say they were involved in 4-H and did rodeo in high school or junior high school, which makes them a diverse potential student with characteristics that maybe some others don’t bring.
I’m not against diversity. I think having a rich set of experiences in any class – medicine, nursing, whatever it’s going to be – is beneficial to the students. They learn from each other. It is sometimes said that it’s also good for patients. I’m a little less excited about that, because I think our training goal should be to make every medical student and nursing student qualified to treat anybody.
I don’t think that, just because you’re Latinx or gay, that’s going to make a gay patient feel better. I think we should teach our students how to give care to everybody that they encounter. They shouldn’t have to match up characteristics to feel like they’re going to get quality care. That isn’t the right reason.
When you have a diverse set of providers, they can call that out and be on the alert for it, and that’s very important.
I also believe that we should think widely and broadly about diversity. Maybe race is out, but certainly other experiences related to income, background, struggle that got you to the point where you’re applying to medical school, motivation, the kinds of experiences you might have had caring for an elderly person, dealing with a disability or learning disability, and trying to overcome, let’s say, going to school in a poor area with not such a wonderful school, really help in terms of forming professionalism, empathy, and a caring point of view.
To me, the main goal is to expand our workforce. The secondary goal is to stay diverse, because we get better providers when we do so.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Recently, the Supreme Court of the United States struck down the use of affirmative action in admissions to colleges, universities, medical schools, and nursing schools. This has led to an enormous amount of worry and concern, particularly in medical school admissions in the world I’m in, where people start to say that diversity matters. Diversity is important.
I know many deans of medical schools immediately sent out messages of reassurance to their students, saying New York University or Stanford or Harvard or Minnesota or Case Western is still deeply concerned about diversity, and we’re going to do what we can to preserve attention to diversity.
I’ve served on admissions at a number of schools over the years for med school. I understand – and have been told – that diversity is important, and according to the Supreme Court, not explicitly by race. There are obviously many variables to take into account when trying to keep diversity at the forefront of admissions.
At the schools I’ve been at, including Columbia, NYU, University of Pittsburgh, University of Minnesota, and University of Pennsylvania, there are plenty of qualified students. Happily, we’ve always been engaged in some effort to try and whittle down the class to the size that we can manage and accept, and many qualified students don’t get admitted.
The first order of business for me is not to worry about how to maintain diversity. It’s to recognize that we need more doctors, nurses, and mental health care providers. I will, in a second, say a few words about diversity and where it fits into admissions, but I want to make the point clearly that what we should be doing is trying to expand the pool of students who are going to become doctors, nurses, mental health care providers, and social workers.
There are too many early retirements. We don’t have the person power we need to manage the health care challenges of an aging population. Let’s not get lost in arguing about what characteristics ought to get you into the finest medical schools. Let’s realize that we have to expand the number of schools we have.
We better be working pretty hard to expand our physician assistant programs, to make sure that we give full authority to qualified dentists and nurses who can help deliver some clinical care. We need more folks. That’s really where the battle ought to be: How do we get that done and how do we get it done quickly, not arguing about who’s in, who’s out, and why.
That said, diversity to me has never meant just race. I’m always interested in gender orientation, disability, and geographic input. Sometimes in decisions that you’re looking at, when I have students in front of me, they tell me they play a musical instrument or about the obstacles they had to overcome to get to medical school. Some of them will say they were involved in 4-H and did rodeo in high school or junior high school, which makes them a diverse potential student with characteristics that maybe some others don’t bring.
I’m not against diversity. I think having a rich set of experiences in any class – medicine, nursing, whatever it’s going to be – is beneficial to the students. They learn from each other. It is sometimes said that it’s also good for patients. I’m a little less excited about that, because I think our training goal should be to make every medical student and nursing student qualified to treat anybody.
I don’t think that, just because you’re Latinx or gay, that’s going to make a gay patient feel better. I think we should teach our students how to give care to everybody that they encounter. They shouldn’t have to match up characteristics to feel like they’re going to get quality care. That isn’t the right reason.
When you have a diverse set of providers, they can call that out and be on the alert for it, and that’s very important.
I also believe that we should think widely and broadly about diversity. Maybe race is out, but certainly other experiences related to income, background, struggle that got you to the point where you’re applying to medical school, motivation, the kinds of experiences you might have had caring for an elderly person, dealing with a disability or learning disability, and trying to overcome, let’s say, going to school in a poor area with not such a wonderful school, really help in terms of forming professionalism, empathy, and a caring point of view.
To me, the main goal is to expand our workforce. The secondary goal is to stay diverse, because we get better providers when we do so.
A version of this article first appeared on Medscape.com.
Updated guidance from USPSTF on PrEP for HIV prevention
The US Preventive Services Task Force (USPSTF) recently released their final recommendation update on the use of antiretroviral therapy to prevent HIV infection in adolescents and adults who are at increased risk.1 The Task Force last addressed this topic in 2019; since then, 2 additional antiretroviral regimens have been approved for preexposure prophylaxis (PrEP). The update also includes revised wording on who should consider receiving PrEP.
HIV remains a significant public health problem in the United States. The Centers for Disease Control and Prevention (CDC) estimates that 1.2 million people in the United States are living with HIV, and approximately 30,000 new infections occur each year.2 Men who have sex with men account for 68% of new infections, and there are marked racial disparities in both incidence and prevalence of infection, with Black/African Americans accounting for 42% of new infections.2
PrEP decreases the risk for HIV by about 50% overall, with higher rates of protection correlated to higher adherence (close to 100% protection with daily adherence to oral regimens).3 The 3 approved regimens for PrEP are outlined in TABLE 13.

Who’s at increased risk? The USPSTF did not find any risk assessment tools with proven accuracy in identifying those at increased risk for HIV infection but did document risk factors and behaviors that can be used to predict risk. They encourage discussion about HIV prevention with all adults and adolescents who are sexually active or who inject drugs.
Those people for whom the Task Force recommends considering PrEP are listed in TABLE 21. However, the USPSTF recommends providing PrEP to anyone who requests it, as they may not want to disclose their risk factors.

What to keep in mind. Family physicians are encouraged to read the full USPSTF report and refer to CDC guidelines on prescribing PrEP, which provide details on each regimen and the routine laboratory testing that should be performed.4 The most important clinical considerations described in the USPSTF report are:
- Before starting PrEP, document a negative HIV antigen/antibody test result and continue to test for HIV every 3 months. PrEP regimens should not be used to treat HIV.
- Document a negative HIV RNA assay if the patient has taken oral PrEP in the past 3 months or injectable PrEP in the past 12 months.
- At PrEP initiation, consider ordering other recommended tests, such as those for kidney function, chronic hepatitis B infection (if using tenofovir disoproxil fumarate/emtricitabine), lipid levels (if using tenofovir alafenamide/emtricitabine), and other sexually transmitted infection (STIs).
- Encourage the use of condoms, as PrEP does not protect from other STIs.
- Follow up regularly, and at each patient visit stress the need for medication adherence to achieve maximum protection.
1. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final recommendation statement. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/recommendation/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
2. CDC. HIV surveillance report: diagnoses of HIV infection in the United States and dependent areas, 2020. Published May 2022. Accessed September 29, 2023. www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2020-updated-vol-33.pdf
3. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final evidence review. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/document/final-evidence-review/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
4. CDC. Preexposure prophylaxis for the prevention of HIV infection in the United States—2021 update: a clinical practice guideline. Accessed September 28, 2023. www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf
The US Preventive Services Task Force (USPSTF) recently released their final recommendation update on the use of antiretroviral therapy to prevent HIV infection in adolescents and adults who are at increased risk.1 The Task Force last addressed this topic in 2019; since then, 2 additional antiretroviral regimens have been approved for preexposure prophylaxis (PrEP). The update also includes revised wording on who should consider receiving PrEP.
HIV remains a significant public health problem in the United States. The Centers for Disease Control and Prevention (CDC) estimates that 1.2 million people in the United States are living with HIV, and approximately 30,000 new infections occur each year.2 Men who have sex with men account for 68% of new infections, and there are marked racial disparities in both incidence and prevalence of infection, with Black/African Americans accounting for 42% of new infections.2
PrEP decreases the risk for HIV by about 50% overall, with higher rates of protection correlated to higher adherence (close to 100% protection with daily adherence to oral regimens).3 The 3 approved regimens for PrEP are outlined in TABLE 13.
Who’s at increased risk? The USPSTF did not find any risk assessment tools with proven accuracy in identifying those at increased risk for HIV infection but did document risk factors and behaviors that can be used to predict risk. They encourage discussion about HIV prevention with all adults and adolescents who are sexually active or who inject drugs.
Those people for whom the Task Force recommends considering PrEP are listed in TABLE 21. However, the USPSTF recommends providing PrEP to anyone who requests it, as they may not want to disclose their risk factors.
What to keep in mind. Family physicians are encouraged to read the full USPSTF report and refer to CDC guidelines on prescribing PrEP, which provide details on each regimen and the routine laboratory testing that should be performed.4 The most important clinical considerations described in the USPSTF report are:
- Before starting PrEP, document a negative HIV antigen/antibody test result and continue to test for HIV every 3 months. PrEP regimens should not be used to treat HIV.
- Document a negative HIV RNA assay if the patient has taken oral PrEP in the past 3 months or injectable PrEP in the past 12 months.
- At PrEP initiation, consider ordering other recommended tests, such as those for kidney function, chronic hepatitis B infection (if using tenofovir disoproxil fumarate/emtricitabine), lipid levels (if using tenofovir alafenamide/emtricitabine), and other sexually transmitted infection (STIs).
- Encourage the use of condoms, as PrEP does not protect from other STIs.
- Follow up regularly, and at each patient visit stress the need for medication adherence to achieve maximum protection.
The US Preventive Services Task Force (USPSTF) recently released their final recommendation update on the use of antiretroviral therapy to prevent HIV infection in adolescents and adults who are at increased risk.1 The Task Force last addressed this topic in 2019; since then, 2 additional antiretroviral regimens have been approved for preexposure prophylaxis (PrEP). The update also includes revised wording on who should consider receiving PrEP.
HIV remains a significant public health problem in the United States. The Centers for Disease Control and Prevention (CDC) estimates that 1.2 million people in the United States are living with HIV, and approximately 30,000 new infections occur each year.2 Men who have sex with men account for 68% of new infections, and there are marked racial disparities in both incidence and prevalence of infection, with Black/African Americans accounting for 42% of new infections.2
PrEP decreases the risk for HIV by about 50% overall, with higher rates of protection correlated to higher adherence (close to 100% protection with daily adherence to oral regimens).3 The 3 approved regimens for PrEP are outlined in TABLE 13.
Who’s at increased risk? The USPSTF did not find any risk assessment tools with proven accuracy in identifying those at increased risk for HIV infection but did document risk factors and behaviors that can be used to predict risk. They encourage discussion about HIV prevention with all adults and adolescents who are sexually active or who inject drugs.
Those people for whom the Task Force recommends considering PrEP are listed in TABLE 21. However, the USPSTF recommends providing PrEP to anyone who requests it, as they may not want to disclose their risk factors.
What to keep in mind. Family physicians are encouraged to read the full USPSTF report and refer to CDC guidelines on prescribing PrEP, which provide details on each regimen and the routine laboratory testing that should be performed.4 The most important clinical considerations described in the USPSTF report are:
- Before starting PrEP, document a negative HIV antigen/antibody test result and continue to test for HIV every 3 months. PrEP regimens should not be used to treat HIV.
- Document a negative HIV RNA assay if the patient has taken oral PrEP in the past 3 months or injectable PrEP in the past 12 months.
- At PrEP initiation, consider ordering other recommended tests, such as those for kidney function, chronic hepatitis B infection (if using tenofovir disoproxil fumarate/emtricitabine), lipid levels (if using tenofovir alafenamide/emtricitabine), and other sexually transmitted infection (STIs).
- Encourage the use of condoms, as PrEP does not protect from other STIs.
- Follow up regularly, and at each patient visit stress the need for medication adherence to achieve maximum protection.
1. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final recommendation statement. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/recommendation/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
2. CDC. HIV surveillance report: diagnoses of HIV infection in the United States and dependent areas, 2020. Published May 2022. Accessed September 29, 2023. www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2020-updated-vol-33.pdf
3. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final evidence review. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/document/final-evidence-review/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
4. CDC. Preexposure prophylaxis for the prevention of HIV infection in the United States—2021 update: a clinical practice guideline. Accessed September 28, 2023. www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf
1. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final recommendation statement. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/recommendation/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
2. CDC. HIV surveillance report: diagnoses of HIV infection in the United States and dependent areas, 2020. Published May 2022. Accessed September 29, 2023. www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2020-updated-vol-33.pdf
3. USPSTF. Prevention of acquisition of HIV: preexposure prophylaxis. Final evidence review. Published August 22, 2023. Accessed September 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/document/final-evidence-review/prevention-of-human-immunodeficiency-virus-hiv-infection-pre-exposure-prophylaxis
4. CDC. Preexposure prophylaxis for the prevention of HIV infection in the United States—2021 update: a clinical practice guideline. Accessed September 28, 2023. www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf

The new word in liver disease: The story behind NAFLD’s rebranding as MASLD
A noteworthy shift recently occurred in the field of hepatology, but it didn’t stem from a clinical trial or medical finding. Instead, the change arose from a matter of semantics.
In a special article published online in the journal Hepatology, a diverse international consensus group introduced new terminology for one of the world’s most rapidly growing diseases.
The term nonalcoholic fatty liver disease (NAFLD) was to be officially retired, replaced with a more precise and descriptive term – metabolic dysfunction–associated steatotic liver disease (MASLD).
In addition, steatotic liver disease (SLD) would be used as an umbrella term encompassing both MASLD and a new subcategory, MetALD, for individuals with MASLD whose alcohol consumption ranges from 140 to 350 g/wk for women and from 210 to 420 g/wk for men. Nonalcoholic steatohepatitis (NASH) would be known as metabolic dysfunction-associated steatohepatitis (MASH).
said the NAFLD nomenclature consensus group’s co-lead, Mary E. Rinella, MD, professor of medicine at University of Chicago and director of the metabolic and fatty liver program at University of Chicago Hospitals.
“The only really new thing we did is identify a group of people who meet criteria for MASLD and also drink more than the allowable limit,” she said. “There are tons of these patients who were not being considered before. Now they’re in a category by themselves, where they are going to be able to be studied and better understood.”
Why make a change?
The unveiling of the new nomenclature marked the culmination of 3 years of dedicated work that was built upon decades of growing understanding about the pathophysiologic underpinnings of these disease states.
The terms NAFLD and NASH emerged in 1980 to describe patients with chronic liver disease who denied excessive alcohol consumption. However, in the past 2 decades, it became increasingly evident that the existing terminology was inadequate, the consensus group’s co-lead, Philip Newsome, PhD, said in an interview.
“There was a strong desire for a name that describes what the condition is, rather than what it isn’t; avoiding use of stigmatizing terms, such as fatty and alcoholic; and finally, a nomenclature that could recognize the coexistence of conditions,” said Dr. Newsome, former secretary general of the European Association for the Study of the Liver (EASL), and director of the Centre for Liver and Gastrointestinal Research at the University of Birmingham, England.
These forces, combined with the recognition that NAFLD and alcohol-related liver disease shared biological processes, created momentum for change.
The idea gained traction with a 2020 article that proposed “MAFLD” as a more suitable term because it would link the disease with its known cardiometabolic risks, Dr. Rinella explained.
“We thought that paper was going to be the beginning of a conversation, but what happened instead is it became a full-court press,” Dr. Rinella said.
Dr. Rinella and Dr. Newsome then spearheaded a study to determine whether content experts and patients supported change. The process was led by three prominent international liver societies: EASL, the American Association for the Study of Liver Diseases (AASLD), and the Asociación Latinoamericana para el Estudio del Hígado. The organizations received input from 236 panelists from 56 countries, reflecting the diverse voices essential for addressing a disease with an expanding global prevalence rate.
In this globalized world, you cannot make a decision from on high and then expect everybody to just adopt it, Dr. Rinella noted.
The panel utilized a modified Delphi consensus approach, necessitating a supermajority of respondents (67%) to vote in favor of the changes. Seventy-four percent felt that the current nomenclature was sufficiently flawed to consider a name change, and 89% preferred terminology that describes the underlying cause of the disease. A supermajority felt that having “metabolic disease or dysfunction” in the name would help patients better understand their disease (72%) and help health care professionals better explain or understand the disease (80%).
The participants settled on the new terminology, and the study resulted in a conclusion: “The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification.”
It was by no means a simple or straightforward task, according to Dr. Rinella. “Anytime you have a contentious issue and you engage a broad range of stakeholders, many of which you know are in disagreement, you’re going to have a difficult time reaching consensus,” she said.
Reassuring reluctant adopters
The backing of international liver societies will be crucial to ensuring the smooth and relatively swift adoption of the new nomenclature. The AASLD announced in July that it would begin this process by holding conversations with key stakeholders, including the Food and Drug Administration, patient organizations, and pharmaceutical industry representatives.
“By engaging external groups, we have gained valuable insights into potential roadblocks or barriers that may impede the full implementation of the new MASLD nomenclature,” AASLD President Norah Terrault, MD, MPH, FAASLD, told this news organization. “Knowing the types of issues they face will allow us to build an implementation plan that will help guide the field through adoption.”
Even with buy-in from key stakeholders, implementing the changes will be no small feat. It’s a “vast undertaking” that may result in short-term frustrations for some groups, Dr. Terrault said.
“For instance, researchers whose work commenced under the old nomenclature may not be able to alter their research papers and will need to publish under the old nomenclature, which may impact which journals their research could be published in,” she said. “Some patient advocacy groups may have the old nomenclature in their names, resulting in a need to rebrand and revise their educational resources. Patient materials need to be updated. Primary care professionals need to be educated. The list goes on.”
These changes demand both patience and time, Dr. Terrault said. This applies to those tasked with persuading colleagues and patients, as well as clinicians, many of whom have already expressed some resistance to the updated terminology.
The panel anticipated pushback from clinicians who still advocate for NAFLD. However, Dr. Rinella countered that a diagnosis of MASLD requires only one cardiometabolic risk factor and has 99% overlap in most populations. In contrast, the MAFLD diagnostic criteria put forward in 2020 proposed even more restrictive cardiometabolic criteria and greater tolerance for alcohol consumption and would alter the disease natural history, she said.
Concerns have also been raised that replacing NAFLD with MASLD might complicate the value of prior research efforts. However, this should not be a cause for concern, as extensive examination across multiple populations has demonstrated near complete overlap between the two definitions, Dr. Rinella said. Biomarker development, natural history studies, and drug development research will remain unaffected, she said.
Some detractors argue that the term “fatty” is sufficiently descriptive and not stigmatizing. However, Dr. Newsome contends that the panel’s research unequivocally disproves this notion.
“Our Delphi process demonstrated very clearly that over 50% felt it was stigmatizing, and in particular, there were clear supportive views for this change from many patient groups,” he noted. “The new nomenclature empowers patients to explain what the condition means without the use of emotional language.”
An opportunity to improve care
One compelling way to persuade reluctant adopters of the new nomenclature’s value is to highlight the opportunities it presents.
The updated terminology opens avenues for research and clinical improvements for patients who meet MASLD criteria and consume alcohol at higher levels (MetALD), Dr. Newsome said.
“There are questions about the relative contribution of these two factors to liver injury, and I see this as an opportunity to explore this area further,” he said.
Hepatologists should embrace this change as a means of increasing awareness regarding the metabolic origins of the disease, Dr. Rinella said. This, in turn, will help identify more patients who require treatment but who are currently overlooked by the existing system, she noted.
“Right now, only around 1% of people with advanced disease are being identified by primary care physicians,” she said. “Hopefully, by elevating the role of metabolic disease, primary care physicians, endocrinologists, and gastroenterologists will be able to identify more patients and bring them to care before they develop cirrhosis.”
Such an outcome would signify much more than a mere semantic shift; it would represent a major advancement in the diagnosis and management of the disease.
A version of this article appeared on Medscape.com.
A noteworthy shift recently occurred in the field of hepatology, but it didn’t stem from a clinical trial or medical finding. Instead, the change arose from a matter of semantics.
In a special article published online in the journal Hepatology, a diverse international consensus group introduced new terminology for one of the world’s most rapidly growing diseases.
The term nonalcoholic fatty liver disease (NAFLD) was to be officially retired, replaced with a more precise and descriptive term – metabolic dysfunction–associated steatotic liver disease (MASLD).
In addition, steatotic liver disease (SLD) would be used as an umbrella term encompassing both MASLD and a new subcategory, MetALD, for individuals with MASLD whose alcohol consumption ranges from 140 to 350 g/wk for women and from 210 to 420 g/wk for men. Nonalcoholic steatohepatitis (NASH) would be known as metabolic dysfunction-associated steatohepatitis (MASH).
said the NAFLD nomenclature consensus group’s co-lead, Mary E. Rinella, MD, professor of medicine at University of Chicago and director of the metabolic and fatty liver program at University of Chicago Hospitals.
“The only really new thing we did is identify a group of people who meet criteria for MASLD and also drink more than the allowable limit,” she said. “There are tons of these patients who were not being considered before. Now they’re in a category by themselves, where they are going to be able to be studied and better understood.”
Why make a change?
The unveiling of the new nomenclature marked the culmination of 3 years of dedicated work that was built upon decades of growing understanding about the pathophysiologic underpinnings of these disease states.
The terms NAFLD and NASH emerged in 1980 to describe patients with chronic liver disease who denied excessive alcohol consumption. However, in the past 2 decades, it became increasingly evident that the existing terminology was inadequate, the consensus group’s co-lead, Philip Newsome, PhD, said in an interview.
“There was a strong desire for a name that describes what the condition is, rather than what it isn’t; avoiding use of stigmatizing terms, such as fatty and alcoholic; and finally, a nomenclature that could recognize the coexistence of conditions,” said Dr. Newsome, former secretary general of the European Association for the Study of the Liver (EASL), and director of the Centre for Liver and Gastrointestinal Research at the University of Birmingham, England.
These forces, combined with the recognition that NAFLD and alcohol-related liver disease shared biological processes, created momentum for change.
The idea gained traction with a 2020 article that proposed “MAFLD” as a more suitable term because it would link the disease with its known cardiometabolic risks, Dr. Rinella explained.
“We thought that paper was going to be the beginning of a conversation, but what happened instead is it became a full-court press,” Dr. Rinella said.
Dr. Rinella and Dr. Newsome then spearheaded a study to determine whether content experts and patients supported change. The process was led by three prominent international liver societies: EASL, the American Association for the Study of Liver Diseases (AASLD), and the Asociación Latinoamericana para el Estudio del Hígado. The organizations received input from 236 panelists from 56 countries, reflecting the diverse voices essential for addressing a disease with an expanding global prevalence rate.
In this globalized world, you cannot make a decision from on high and then expect everybody to just adopt it, Dr. Rinella noted.
The panel utilized a modified Delphi consensus approach, necessitating a supermajority of respondents (67%) to vote in favor of the changes. Seventy-four percent felt that the current nomenclature was sufficiently flawed to consider a name change, and 89% preferred terminology that describes the underlying cause of the disease. A supermajority felt that having “metabolic disease or dysfunction” in the name would help patients better understand their disease (72%) and help health care professionals better explain or understand the disease (80%).
The participants settled on the new terminology, and the study resulted in a conclusion: “The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification.”
It was by no means a simple or straightforward task, according to Dr. Rinella. “Anytime you have a contentious issue and you engage a broad range of stakeholders, many of which you know are in disagreement, you’re going to have a difficult time reaching consensus,” she said.
Reassuring reluctant adopters
The backing of international liver societies will be crucial to ensuring the smooth and relatively swift adoption of the new nomenclature. The AASLD announced in July that it would begin this process by holding conversations with key stakeholders, including the Food and Drug Administration, patient organizations, and pharmaceutical industry representatives.
“By engaging external groups, we have gained valuable insights into potential roadblocks or barriers that may impede the full implementation of the new MASLD nomenclature,” AASLD President Norah Terrault, MD, MPH, FAASLD, told this news organization. “Knowing the types of issues they face will allow us to build an implementation plan that will help guide the field through adoption.”
Even with buy-in from key stakeholders, implementing the changes will be no small feat. It’s a “vast undertaking” that may result in short-term frustrations for some groups, Dr. Terrault said.
“For instance, researchers whose work commenced under the old nomenclature may not be able to alter their research papers and will need to publish under the old nomenclature, which may impact which journals their research could be published in,” she said. “Some patient advocacy groups may have the old nomenclature in their names, resulting in a need to rebrand and revise their educational resources. Patient materials need to be updated. Primary care professionals need to be educated. The list goes on.”
These changes demand both patience and time, Dr. Terrault said. This applies to those tasked with persuading colleagues and patients, as well as clinicians, many of whom have already expressed some resistance to the updated terminology.
The panel anticipated pushback from clinicians who still advocate for NAFLD. However, Dr. Rinella countered that a diagnosis of MASLD requires only one cardiometabolic risk factor and has 99% overlap in most populations. In contrast, the MAFLD diagnostic criteria put forward in 2020 proposed even more restrictive cardiometabolic criteria and greater tolerance for alcohol consumption and would alter the disease natural history, she said.
Concerns have also been raised that replacing NAFLD with MASLD might complicate the value of prior research efforts. However, this should not be a cause for concern, as extensive examination across multiple populations has demonstrated near complete overlap between the two definitions, Dr. Rinella said. Biomarker development, natural history studies, and drug development research will remain unaffected, she said.
Some detractors argue that the term “fatty” is sufficiently descriptive and not stigmatizing. However, Dr. Newsome contends that the panel’s research unequivocally disproves this notion.
“Our Delphi process demonstrated very clearly that over 50% felt it was stigmatizing, and in particular, there were clear supportive views for this change from many patient groups,” he noted. “The new nomenclature empowers patients to explain what the condition means without the use of emotional language.”
An opportunity to improve care
One compelling way to persuade reluctant adopters of the new nomenclature’s value is to highlight the opportunities it presents.
The updated terminology opens avenues for research and clinical improvements for patients who meet MASLD criteria and consume alcohol at higher levels (MetALD), Dr. Newsome said.
“There are questions about the relative contribution of these two factors to liver injury, and I see this as an opportunity to explore this area further,” he said.
Hepatologists should embrace this change as a means of increasing awareness regarding the metabolic origins of the disease, Dr. Rinella said. This, in turn, will help identify more patients who require treatment but who are currently overlooked by the existing system, she noted.
“Right now, only around 1% of people with advanced disease are being identified by primary care physicians,” she said. “Hopefully, by elevating the role of metabolic disease, primary care physicians, endocrinologists, and gastroenterologists will be able to identify more patients and bring them to care before they develop cirrhosis.”
Such an outcome would signify much more than a mere semantic shift; it would represent a major advancement in the diagnosis and management of the disease.
A version of this article appeared on Medscape.com.
A noteworthy shift recently occurred in the field of hepatology, but it didn’t stem from a clinical trial or medical finding. Instead, the change arose from a matter of semantics.
In a special article published online in the journal Hepatology, a diverse international consensus group introduced new terminology for one of the world’s most rapidly growing diseases.
The term nonalcoholic fatty liver disease (NAFLD) was to be officially retired, replaced with a more precise and descriptive term – metabolic dysfunction–associated steatotic liver disease (MASLD).
In addition, steatotic liver disease (SLD) would be used as an umbrella term encompassing both MASLD and a new subcategory, MetALD, for individuals with MASLD whose alcohol consumption ranges from 140 to 350 g/wk for women and from 210 to 420 g/wk for men. Nonalcoholic steatohepatitis (NASH) would be known as metabolic dysfunction-associated steatohepatitis (MASH).
said the NAFLD nomenclature consensus group’s co-lead, Mary E. Rinella, MD, professor of medicine at University of Chicago and director of the metabolic and fatty liver program at University of Chicago Hospitals.
“The only really new thing we did is identify a group of people who meet criteria for MASLD and also drink more than the allowable limit,” she said. “There are tons of these patients who were not being considered before. Now they’re in a category by themselves, where they are going to be able to be studied and better understood.”
Why make a change?
The unveiling of the new nomenclature marked the culmination of 3 years of dedicated work that was built upon decades of growing understanding about the pathophysiologic underpinnings of these disease states.
The terms NAFLD and NASH emerged in 1980 to describe patients with chronic liver disease who denied excessive alcohol consumption. However, in the past 2 decades, it became increasingly evident that the existing terminology was inadequate, the consensus group’s co-lead, Philip Newsome, PhD, said in an interview.
“There was a strong desire for a name that describes what the condition is, rather than what it isn’t; avoiding use of stigmatizing terms, such as fatty and alcoholic; and finally, a nomenclature that could recognize the coexistence of conditions,” said Dr. Newsome, former secretary general of the European Association for the Study of the Liver (EASL), and director of the Centre for Liver and Gastrointestinal Research at the University of Birmingham, England.
These forces, combined with the recognition that NAFLD and alcohol-related liver disease shared biological processes, created momentum for change.
The idea gained traction with a 2020 article that proposed “MAFLD” as a more suitable term because it would link the disease with its known cardiometabolic risks, Dr. Rinella explained.
“We thought that paper was going to be the beginning of a conversation, but what happened instead is it became a full-court press,” Dr. Rinella said.
Dr. Rinella and Dr. Newsome then spearheaded a study to determine whether content experts and patients supported change. The process was led by three prominent international liver societies: EASL, the American Association for the Study of Liver Diseases (AASLD), and the Asociación Latinoamericana para el Estudio del Hígado. The organizations received input from 236 panelists from 56 countries, reflecting the diverse voices essential for addressing a disease with an expanding global prevalence rate.
In this globalized world, you cannot make a decision from on high and then expect everybody to just adopt it, Dr. Rinella noted.
The panel utilized a modified Delphi consensus approach, necessitating a supermajority of respondents (67%) to vote in favor of the changes. Seventy-four percent felt that the current nomenclature was sufficiently flawed to consider a name change, and 89% preferred terminology that describes the underlying cause of the disease. A supermajority felt that having “metabolic disease or dysfunction” in the name would help patients better understand their disease (72%) and help health care professionals better explain or understand the disease (80%).
The participants settled on the new terminology, and the study resulted in a conclusion: “The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification.”
It was by no means a simple or straightforward task, according to Dr. Rinella. “Anytime you have a contentious issue and you engage a broad range of stakeholders, many of which you know are in disagreement, you’re going to have a difficult time reaching consensus,” she said.
Reassuring reluctant adopters
The backing of international liver societies will be crucial to ensuring the smooth and relatively swift adoption of the new nomenclature. The AASLD announced in July that it would begin this process by holding conversations with key stakeholders, including the Food and Drug Administration, patient organizations, and pharmaceutical industry representatives.
“By engaging external groups, we have gained valuable insights into potential roadblocks or barriers that may impede the full implementation of the new MASLD nomenclature,” AASLD President Norah Terrault, MD, MPH, FAASLD, told this news organization. “Knowing the types of issues they face will allow us to build an implementation plan that will help guide the field through adoption.”
Even with buy-in from key stakeholders, implementing the changes will be no small feat. It’s a “vast undertaking” that may result in short-term frustrations for some groups, Dr. Terrault said.
“For instance, researchers whose work commenced under the old nomenclature may not be able to alter their research papers and will need to publish under the old nomenclature, which may impact which journals their research could be published in,” she said. “Some patient advocacy groups may have the old nomenclature in their names, resulting in a need to rebrand and revise their educational resources. Patient materials need to be updated. Primary care professionals need to be educated. The list goes on.”
These changes demand both patience and time, Dr. Terrault said. This applies to those tasked with persuading colleagues and patients, as well as clinicians, many of whom have already expressed some resistance to the updated terminology.
The panel anticipated pushback from clinicians who still advocate for NAFLD. However, Dr. Rinella countered that a diagnosis of MASLD requires only one cardiometabolic risk factor and has 99% overlap in most populations. In contrast, the MAFLD diagnostic criteria put forward in 2020 proposed even more restrictive cardiometabolic criteria and greater tolerance for alcohol consumption and would alter the disease natural history, she said.
Concerns have also been raised that replacing NAFLD with MASLD might complicate the value of prior research efforts. However, this should not be a cause for concern, as extensive examination across multiple populations has demonstrated near complete overlap between the two definitions, Dr. Rinella said. Biomarker development, natural history studies, and drug development research will remain unaffected, she said.
Some detractors argue that the term “fatty” is sufficiently descriptive and not stigmatizing. However, Dr. Newsome contends that the panel’s research unequivocally disproves this notion.
“Our Delphi process demonstrated very clearly that over 50% felt it was stigmatizing, and in particular, there were clear supportive views for this change from many patient groups,” he noted. “The new nomenclature empowers patients to explain what the condition means without the use of emotional language.”
An opportunity to improve care
One compelling way to persuade reluctant adopters of the new nomenclature’s value is to highlight the opportunities it presents.
The updated terminology opens avenues for research and clinical improvements for patients who meet MASLD criteria and consume alcohol at higher levels (MetALD), Dr. Newsome said.
“There are questions about the relative contribution of these two factors to liver injury, and I see this as an opportunity to explore this area further,” he said.
Hepatologists should embrace this change as a means of increasing awareness regarding the metabolic origins of the disease, Dr. Rinella said. This, in turn, will help identify more patients who require treatment but who are currently overlooked by the existing system, she noted.
“Right now, only around 1% of people with advanced disease are being identified by primary care physicians,” she said. “Hopefully, by elevating the role of metabolic disease, primary care physicians, endocrinologists, and gastroenterologists will be able to identify more patients and bring them to care before they develop cirrhosis.”
Such an outcome would signify much more than a mere semantic shift; it would represent a major advancement in the diagnosis and management of the disease.
A version of this article appeared on Medscape.com.
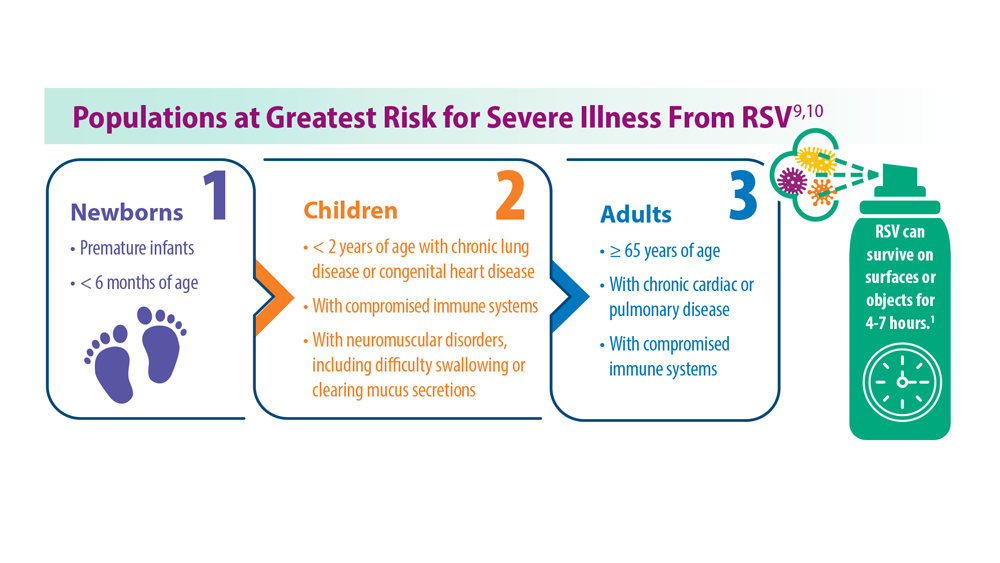
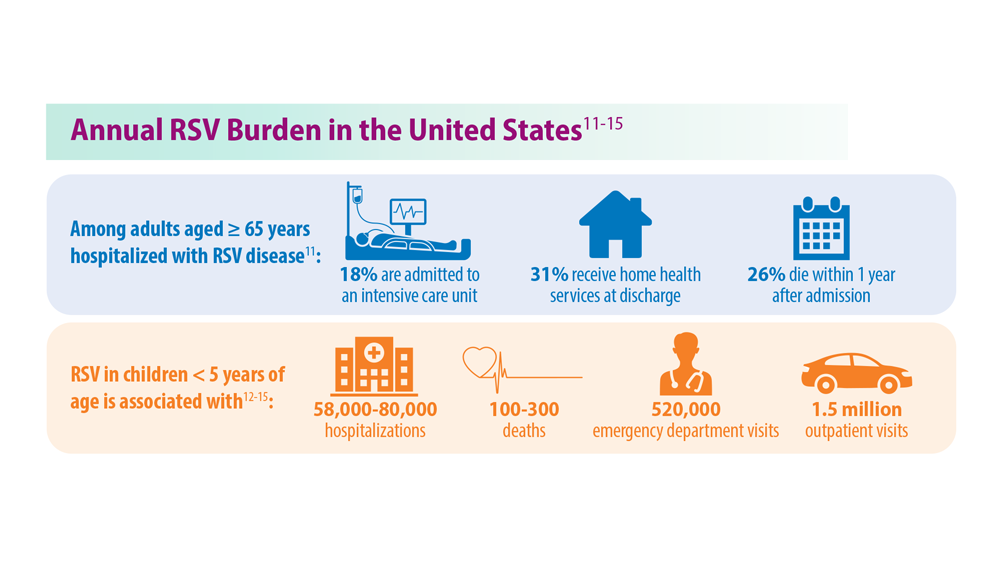
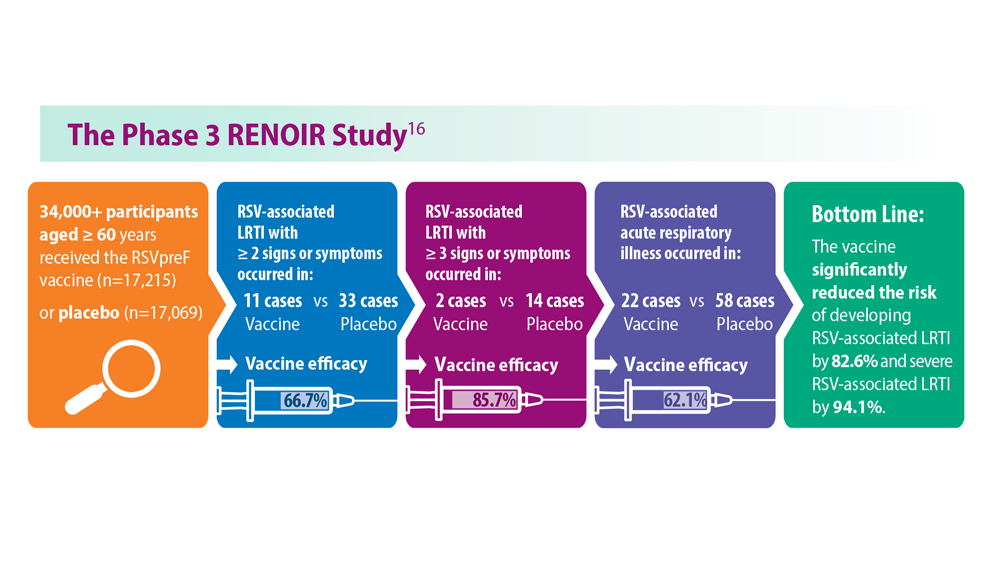
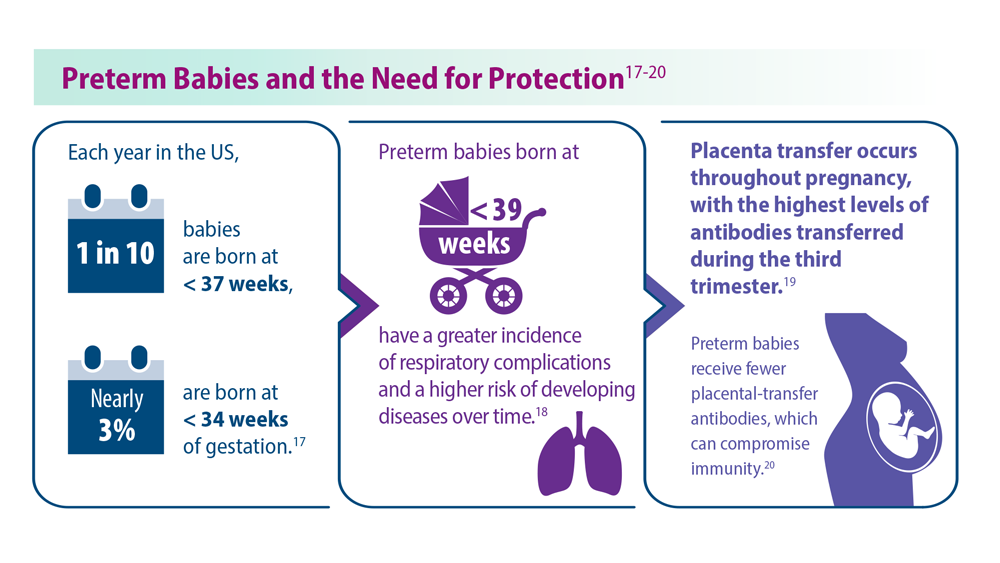
Long-Awaited RSV Vaccines Now Available for Older Adults and Pediatric Patients
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
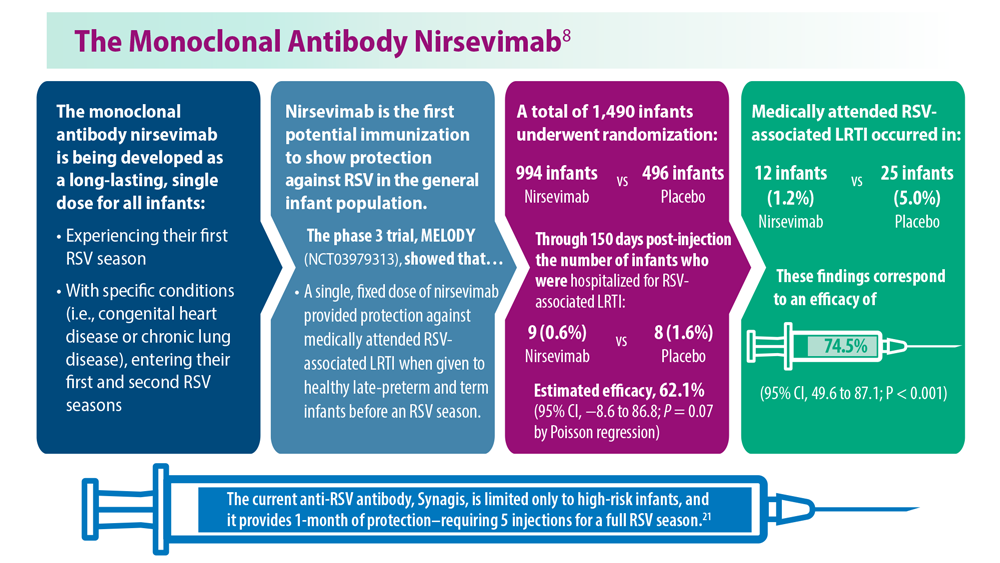
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
- Jha A et al. Respiratory syncytial virus. In: Hui DS, Rossi GA, Johnston SL, eds. Respiratory Syncytial Virus. SARS, MERS and Other Viral Lung Infections. European Respiratory Society; 2016:chap 5. Accessed May 17, 2023.
- Ginsburg SA, Srikantiah P. Lancet Glob Health. 2021;9(12):e1644-e6145. doi:10.1016/S2214-109X(21)00455-1
- US Food and Drug Administration. FDA approves first respiratory syncytial virus (RSV) vaccine [press release]. Published May 3, 2023. Accessed May 17, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine
- US Food and Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers [press release]. Published July 17, 2023. Accessed August 11, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers
- US Food and Drug Administration. FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Published August 21, 2023. Accessed August 22, 2023. https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
- Madhi SA et al. N Engl J Med. 2020;383(5):426-439. doi:10.1056/ NEJMoa1908380
- Centers for Disease Control. Advisory Committee on Immunization Practices (ACIP) Meeting recommendations, August 2023. https://www.cdc.gov/vaccines/acip/recommendations.html
- Hammit LL et al. N Engl J Med. 2022;386(9):837-846. doi:10.1056/ NEJMoa2110275
- Centers for Disease Control and Prevention. RSV in infants and young children. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/ high-risk/infants-young-children.html
- Centers for Disease Control and Prevention. RSV in older adults and adults with chronic medical conditions. Updated October 28, 2022. Accessed May 30, 2023. https://www.cdc.gov/rsv/high-risk/older-adults.html
- Widmer K et al. J Infect Dis. 2012;206(1):56-62. doi:10.1093/infdis/jis309
- Hall CB et al. N Engl J Med. 2009;360(6):588-598. doi:10.1056/NEJMoa0804877
- McLaughlin JM et al. Open Forum Infect Dis. 2022;9(7):ofac300. doi:10.1093/ofid/ofac300
- Thompson et al. JAMA. 2003;289(2):179-186. doi:10.1001/jama.289.2.179
- Hansen CL et al. JAMA Netw Open. 2022;5(2):e220527. doi:10.1001/jamanetworkopen.2022.0527
- Walsh EE et al; RENOIR Clinical Trial Group. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
- Martin JA et al. Natl Vital Stat Rep. 2019;68(13):1-47. PMID:32501202
- Townsi N et al. Eur Clin Respir J. 2018;5(1):1487214. doi:10.1080/20018525.20 18.1487214
- Malek A et al. Am J Reprod Immunol. 1994;32(1):8-14. doi:10.1111/j.1600-0897.1994.tb00873.x
- Kampmann B et al; MATISSE Study Group. N Engl J Med. 2023;388(16):1451- 1464. doi:10.1056/NEJMoa2216480
- Synagis (palivizumab) injection prescribing information. Published June 2023. Accessed August 2023. https://www.synagis.com/synagis.pdf
How exercise boosts the body’s ability to prevent cancer
That amount of exercise made the immune system more able to stamp out cancer cells, researchers at the found. The intervention was specific by design, said Eduardo Vilar-Sanchez, MD, PhD, a professor of clinical cancer prevention at the University of Texas MD Anderson Cancer Center, Houston, and the study’s lead author.
“We wanted to be very concrete on the recommendation,” he said. “People don’t adhere to vague lifestyle advice like ‘just exercise.’ We wanted to link a specific biologic effect to a very concrete intervention.”
The study was small (just 21 people), but it builds on a vast body of evidence linking regular exercise to a decreased risk of cancer, particularly colorectal cancer. But the researchers went a step further, investigating how exercise might lower cancer risk.
Exercise and the immune system
All 21 people in the study had Lynch syndrome, and they were divided into two groups. One was given a 12-month exercise program; the other was not. The scientists checked their cardio and respiratory fitness and tracked immune cells – natural killer cells and CD8+ T cells – in the blood and colon tissues.
“These are the immune cells that are in charge of attacking foreign entities like cancer cells,” Dr. Vilar-Sanchez said, “and they were more active with the participants who exercised.”
People in the exercise group also saw a drop in levels of the inflammatory marker prostaglandin E2 (PGE2). The drop was closely linked to the increase in immune cells. Both changes suggest a stronger immune response.
The researchers believe the changes relate to a boost in the body’s “immune surveillance” system for hunting down and clearing out cells that would otherwise become cancerous.
Building on prior research
Science already offers a lot of support that regular exercise can help prevent cancer. A massive 2019 systematic review of more than 45 studies and several million people found strong evidence that exercise can reduce the risk of several cancers – including bladder, breast, colorectal, and gastric cancers – by up to 20%.
But the MD Anderson study is the first to show a link between exercise and changes in immune biomarkers, the researchers said.
“One thing is having the epidemiological correlation, but it’s another thing to know the biological basis,” added Xavier Llor, MD, PhD, a professor of medicine at Yale University, New Haven, Conn, who was not involved in the study.
Two previous studies looked at exercise and inflammation markers in healthy people and in those with a history of colon polyps, but neither study produced meaningful results. This new study’s success could be caused by the higher-intensity exercise or extra colon tissue samples. But also, advances in technology now allow for more sensitive measurements, the researchers said.
Wider implications?
Dr. Vilar-Sanchez hesitated to extend the study findings beyond people with Lynch syndrome, but he’s optimistic that they may apply to the general population as well.
Dr. Llor agreed: “Exercise could be protective against other types of cancer through some of these mechanisms.”
According to the American Cancer Society, more than 15% of all cancer deaths (aside from tobacco-related cancers) in the United States are related to lifestyle factors, including physical inactivity, excess body weight, alcohol use, and poor nutrition. It recommends 150-300 minutes of moderate-intensity exercise a week to reduce cancer risk. People in the study saw a significant immune response with 135 minutes of high-intensity exercise a week.
“The public should know that engaging in any form of exercise will somehow lead to effects in cancer prevention,” Dr. Vilar-Sanchez said.
A version of this article appeared on WebMD.com.
That amount of exercise made the immune system more able to stamp out cancer cells, researchers at the found. The intervention was specific by design, said Eduardo Vilar-Sanchez, MD, PhD, a professor of clinical cancer prevention at the University of Texas MD Anderson Cancer Center, Houston, and the study’s lead author.
“We wanted to be very concrete on the recommendation,” he said. “People don’t adhere to vague lifestyle advice like ‘just exercise.’ We wanted to link a specific biologic effect to a very concrete intervention.”
The study was small (just 21 people), but it builds on a vast body of evidence linking regular exercise to a decreased risk of cancer, particularly colorectal cancer. But the researchers went a step further, investigating how exercise might lower cancer risk.
Exercise and the immune system
All 21 people in the study had Lynch syndrome, and they were divided into two groups. One was given a 12-month exercise program; the other was not. The scientists checked their cardio and respiratory fitness and tracked immune cells – natural killer cells and CD8+ T cells – in the blood and colon tissues.
“These are the immune cells that are in charge of attacking foreign entities like cancer cells,” Dr. Vilar-Sanchez said, “and they were more active with the participants who exercised.”
People in the exercise group also saw a drop in levels of the inflammatory marker prostaglandin E2 (PGE2). The drop was closely linked to the increase in immune cells. Both changes suggest a stronger immune response.
The researchers believe the changes relate to a boost in the body’s “immune surveillance” system for hunting down and clearing out cells that would otherwise become cancerous.
Building on prior research
Science already offers a lot of support that regular exercise can help prevent cancer. A massive 2019 systematic review of more than 45 studies and several million people found strong evidence that exercise can reduce the risk of several cancers – including bladder, breast, colorectal, and gastric cancers – by up to 20%.
But the MD Anderson study is the first to show a link between exercise and changes in immune biomarkers, the researchers said.
“One thing is having the epidemiological correlation, but it’s another thing to know the biological basis,” added Xavier Llor, MD, PhD, a professor of medicine at Yale University, New Haven, Conn, who was not involved in the study.
Two previous studies looked at exercise and inflammation markers in healthy people and in those with a history of colon polyps, but neither study produced meaningful results. This new study’s success could be caused by the higher-intensity exercise or extra colon tissue samples. But also, advances in technology now allow for more sensitive measurements, the researchers said.
Wider implications?
Dr. Vilar-Sanchez hesitated to extend the study findings beyond people with Lynch syndrome, but he’s optimistic that they may apply to the general population as well.
Dr. Llor agreed: “Exercise could be protective against other types of cancer through some of these mechanisms.”
According to the American Cancer Society, more than 15% of all cancer deaths (aside from tobacco-related cancers) in the United States are related to lifestyle factors, including physical inactivity, excess body weight, alcohol use, and poor nutrition. It recommends 150-300 minutes of moderate-intensity exercise a week to reduce cancer risk. People in the study saw a significant immune response with 135 minutes of high-intensity exercise a week.
“The public should know that engaging in any form of exercise will somehow lead to effects in cancer prevention,” Dr. Vilar-Sanchez said.
A version of this article appeared on WebMD.com.
That amount of exercise made the immune system more able to stamp out cancer cells, researchers at the found. The intervention was specific by design, said Eduardo Vilar-Sanchez, MD, PhD, a professor of clinical cancer prevention at the University of Texas MD Anderson Cancer Center, Houston, and the study’s lead author.
“We wanted to be very concrete on the recommendation,” he said. “People don’t adhere to vague lifestyle advice like ‘just exercise.’ We wanted to link a specific biologic effect to a very concrete intervention.”
The study was small (just 21 people), but it builds on a vast body of evidence linking regular exercise to a decreased risk of cancer, particularly colorectal cancer. But the researchers went a step further, investigating how exercise might lower cancer risk.
Exercise and the immune system
All 21 people in the study had Lynch syndrome, and they were divided into two groups. One was given a 12-month exercise program; the other was not. The scientists checked their cardio and respiratory fitness and tracked immune cells – natural killer cells and CD8+ T cells – in the blood and colon tissues.
“These are the immune cells that are in charge of attacking foreign entities like cancer cells,” Dr. Vilar-Sanchez said, “and they were more active with the participants who exercised.”
People in the exercise group also saw a drop in levels of the inflammatory marker prostaglandin E2 (PGE2). The drop was closely linked to the increase in immune cells. Both changes suggest a stronger immune response.
The researchers believe the changes relate to a boost in the body’s “immune surveillance” system for hunting down and clearing out cells that would otherwise become cancerous.
Building on prior research
Science already offers a lot of support that regular exercise can help prevent cancer. A massive 2019 systematic review of more than 45 studies and several million people found strong evidence that exercise can reduce the risk of several cancers – including bladder, breast, colorectal, and gastric cancers – by up to 20%.
But the MD Anderson study is the first to show a link between exercise and changes in immune biomarkers, the researchers said.
“One thing is having the epidemiological correlation, but it’s another thing to know the biological basis,” added Xavier Llor, MD, PhD, a professor of medicine at Yale University, New Haven, Conn, who was not involved in the study.
Two previous studies looked at exercise and inflammation markers in healthy people and in those with a history of colon polyps, but neither study produced meaningful results. This new study’s success could be caused by the higher-intensity exercise or extra colon tissue samples. But also, advances in technology now allow for more sensitive measurements, the researchers said.
Wider implications?
Dr. Vilar-Sanchez hesitated to extend the study findings beyond people with Lynch syndrome, but he’s optimistic that they may apply to the general population as well.
Dr. Llor agreed: “Exercise could be protective against other types of cancer through some of these mechanisms.”
According to the American Cancer Society, more than 15% of all cancer deaths (aside from tobacco-related cancers) in the United States are related to lifestyle factors, including physical inactivity, excess body weight, alcohol use, and poor nutrition. It recommends 150-300 minutes of moderate-intensity exercise a week to reduce cancer risk. People in the study saw a significant immune response with 135 minutes of high-intensity exercise a week.
“The public should know that engaging in any form of exercise will somehow lead to effects in cancer prevention,” Dr. Vilar-Sanchez said.
A version of this article appeared on WebMD.com.
FROM CLINICAL CANCER RESEARCH
Updated Guidelines for COPD Management: 2023 GOLD Strategy Report
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Published 2023. Accessed June 6, 2023. https://goldcopd.org/2023-gold-report-2/
- Celli B et al. Am J Respir Crit Care Med. 2022;206(11):1317. doi:10.1164/rccm.202204-0671PP
- Han M et al. Lancet Respir Med. 2013;1(1):43-50. doi:10.1016/S2213-2600(12)70044-9
- Klijn SL et al. NPJ Prim Care Respir Med. 2017;27(1):24. doi:10.1038/s41533-017-0022-1
- Chan AH et al. J Allergy Clin Immunol Pract. 2015;3(3):335-349.e1-e5. doi:10.1016/j.jaip.2015.01.024
- Brusselle G et al. Int J Chron Obstruct Pulmon Dis. 2015;10:2207-2217. doi:10.2147/COPD.S91694
- Salvi SS, Barnes PJ. Lancet. 2009;374(9691):733-743. doi:10.1016/S0140-6736(09)61303-9
- Trupin L et al. Eur Respir J. 2003;22(3):462-469. doi:10.1183/09031936.03.00094203
- Celli BR et al. Am J Respir Crit Care Med. 2021;204(11):1251-1258. doi:10.1164/rccm.202108-1819PP
- Barnes PJ, Celli BR. Eur Respir J. 2009;33(5):1165-1185. doi:10.1183/09031936.00128008
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Published 2023. Accessed June 6, 2023. https://goldcopd.org/2023-gold-report-2/
- Celli B et al. Am J Respir Crit Care Med. 2022;206(11):1317. doi:10.1164/rccm.202204-0671PP
- Han M et al. Lancet Respir Med. 2013;1(1):43-50. doi:10.1016/S2213-2600(12)70044-9
- Klijn SL et al. NPJ Prim Care Respir Med. 2017;27(1):24. doi:10.1038/s41533-017-0022-1
- Chan AH et al. J Allergy Clin Immunol Pract. 2015;3(3):335-349.e1-e5. doi:10.1016/j.jaip.2015.01.024
- Brusselle G et al. Int J Chron Obstruct Pulmon Dis. 2015;10:2207-2217. doi:10.2147/COPD.S91694
- Salvi SS, Barnes PJ. Lancet. 2009;374(9691):733-743. doi:10.1016/S0140-6736(09)61303-9
- Trupin L et al. Eur Respir J. 2003;22(3):462-469. doi:10.1183/09031936.03.00094203
- Celli BR et al. Am J Respir Crit Care Med. 2021;204(11):1251-1258. doi:10.1164/rccm.202108-1819PP
- Barnes PJ, Celli BR. Eur Respir J. 2009;33(5):1165-1185. doi:10.1183/09031936.00128008
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Published 2023. Accessed June 6, 2023. https://goldcopd.org/2023-gold-report-2/
- Celli B et al. Am J Respir Crit Care Med. 2022;206(11):1317. doi:10.1164/rccm.202204-0671PP
- Han M et al. Lancet Respir Med. 2013;1(1):43-50. doi:10.1016/S2213-2600(12)70044-9
- Klijn SL et al. NPJ Prim Care Respir Med. 2017;27(1):24. doi:10.1038/s41533-017-0022-1
- Chan AH et al. J Allergy Clin Immunol Pract. 2015;3(3):335-349.e1-e5. doi:10.1016/j.jaip.2015.01.024
- Brusselle G et al. Int J Chron Obstruct Pulmon Dis. 2015;10:2207-2217. doi:10.2147/COPD.S91694
- Salvi SS, Barnes PJ. Lancet. 2009;374(9691):733-743. doi:10.1016/S0140-6736(09)61303-9
- Trupin L et al. Eur Respir J. 2003;22(3):462-469. doi:10.1183/09031936.03.00094203
- Celli BR et al. Am J Respir Crit Care Med. 2021;204(11):1251-1258. doi:10.1164/rccm.202108-1819PP
- Barnes PJ, Celli BR. Eur Respir J. 2009;33(5):1165-1185. doi:10.1183/09031936.00128008
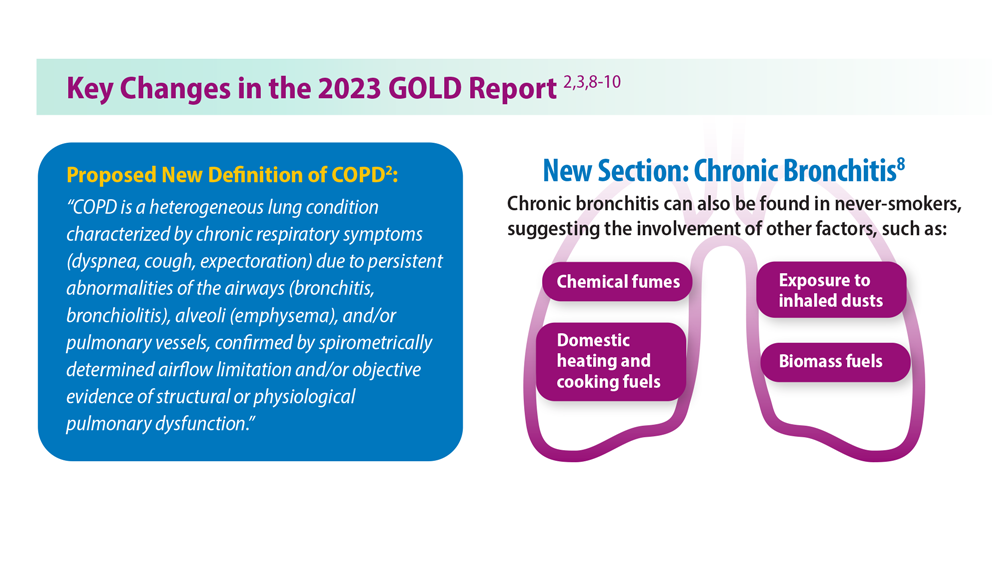
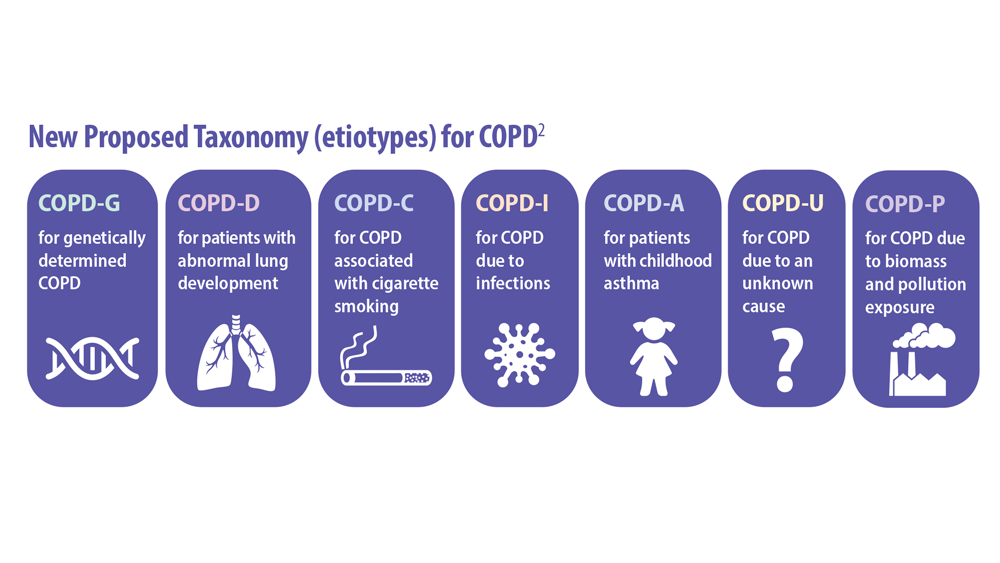
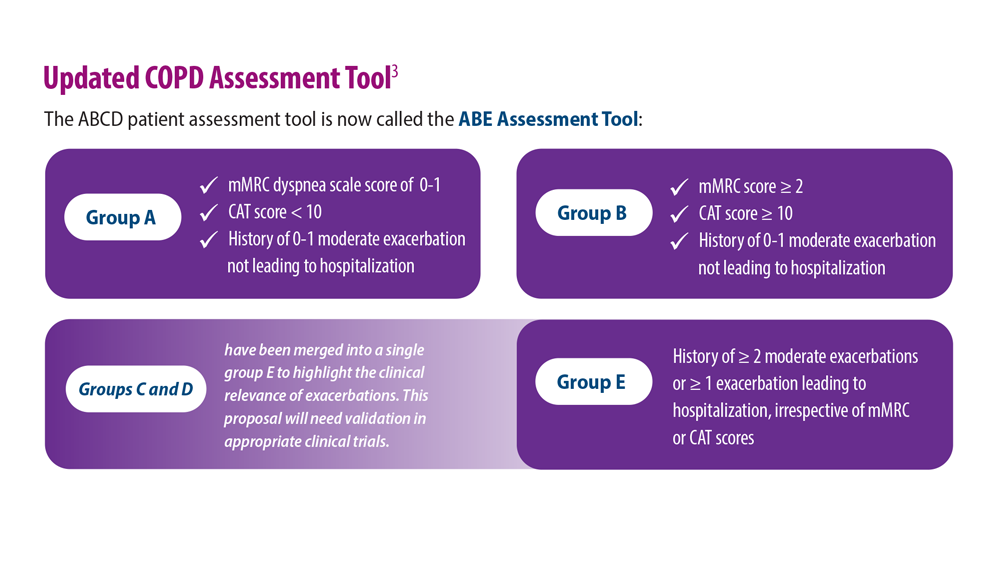
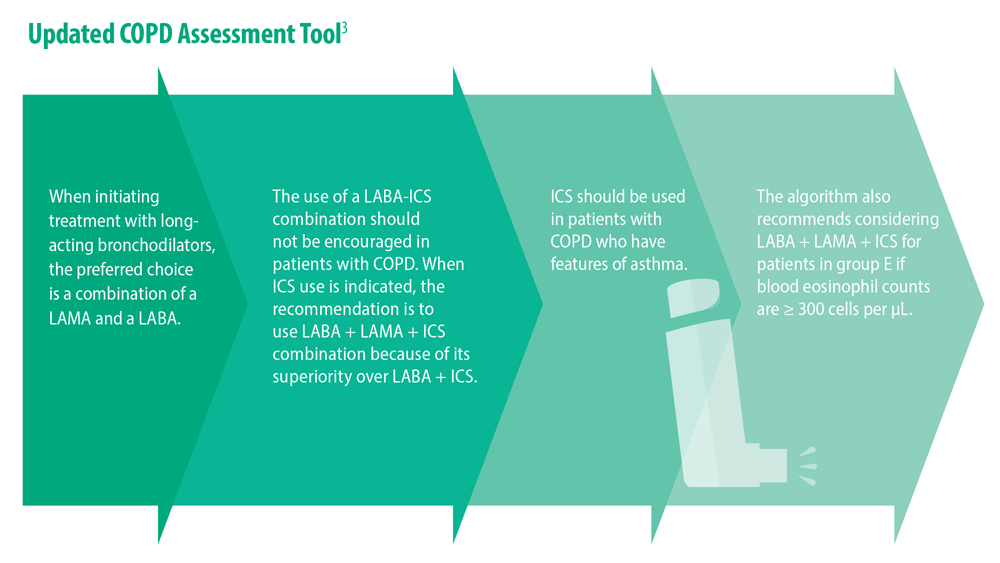
Lung Cancer Screening: A Need for Adjunctive Testing
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
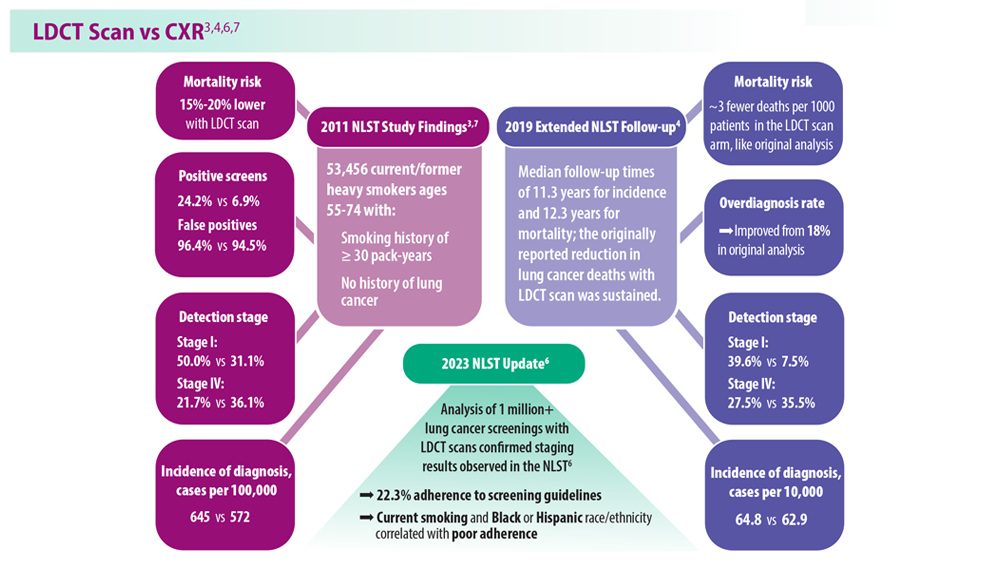
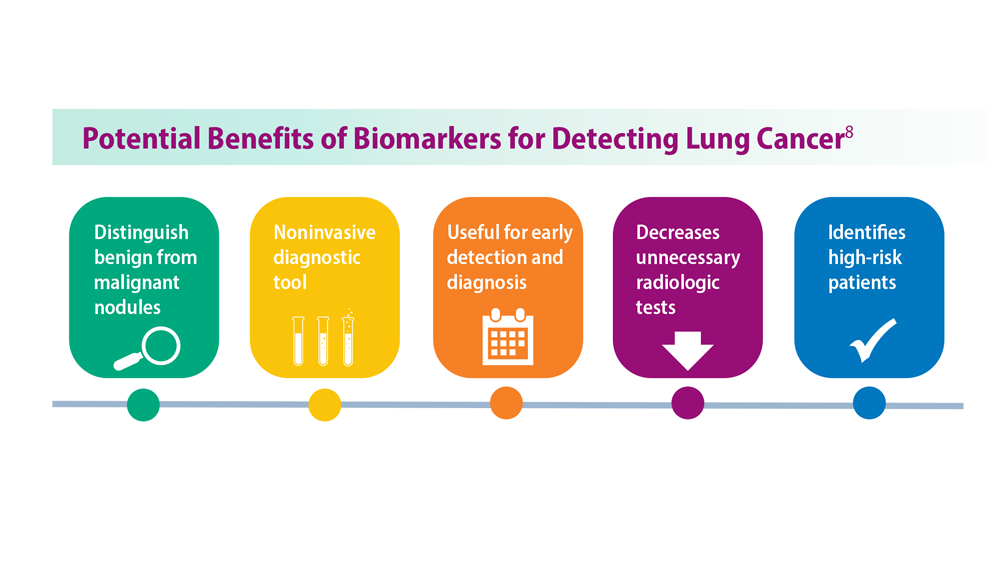
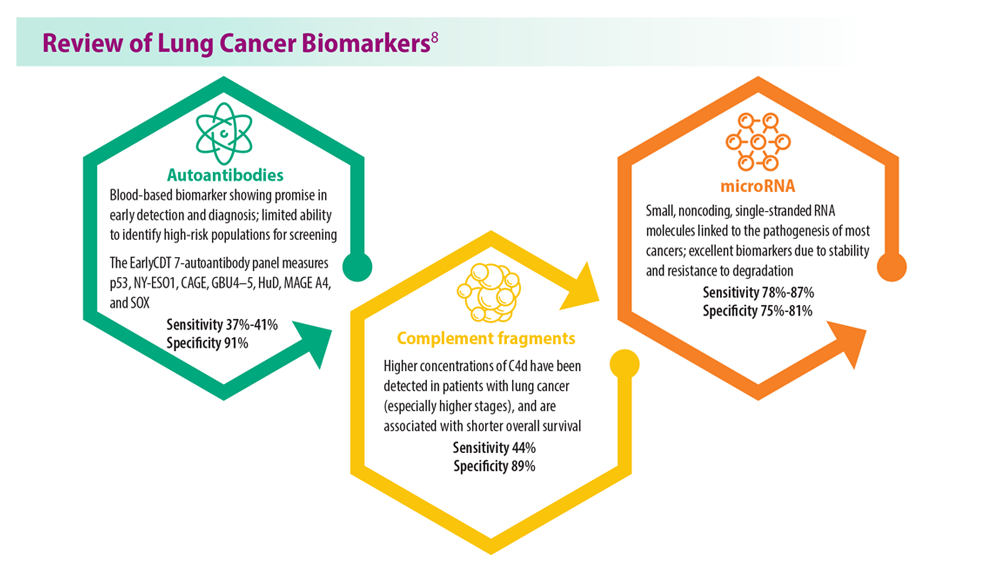
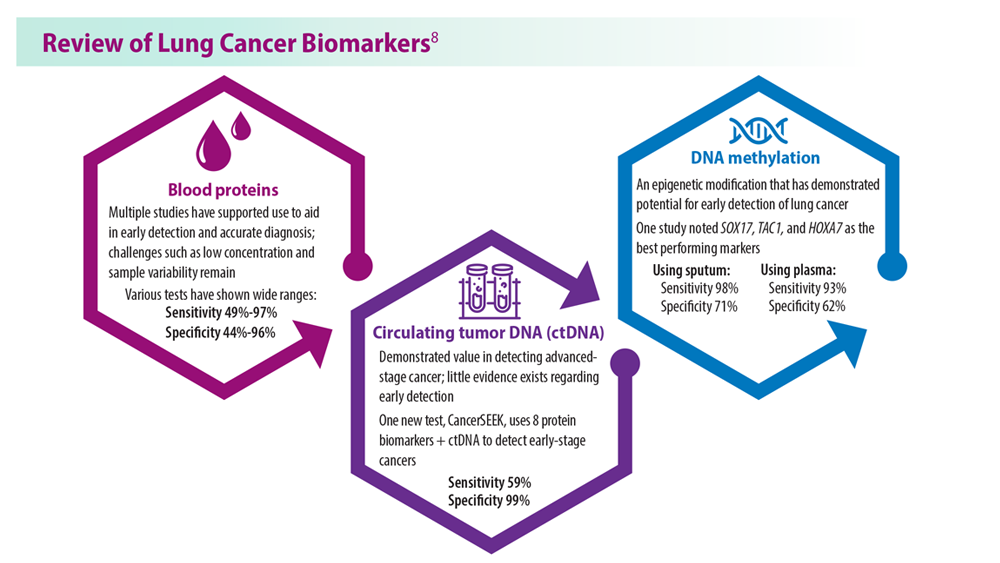
Tuberculosis Management: Returning to Pre-Pandemic Priorities
- Global tuberculosis report 2022. World Health Organization. Published October 27, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240061729
- WHO consolidated guidelines on tuberculosis. Module 4: treatment – drug-resistant tuberculosis treatment, 2022 update. World Health Organization. Published December 15, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240063129
- Migliori GB, Tiberi S. Int J Tuberc Lung Dis. 2022 ;26(7):590-591. doi:10.5588/ijtld.22.0263.
- Lange C et al. Am J Respir Crit Care Med. 2022;205(10):1142-1144. doi:10.1164/rccm.202202-0393ED
- Esmail A et al. Am J Respir Crit Care Med. 2022;205(10):1214-1227. doi:10.1164/rccm.202107-1779OC
- WHO BPaLM Accelerator Platform: to support the call to action for implementation of the shorter and more effective treatment for all people suffering from drug-resistant TB. World Health Organization. Published May 9, 2023. Accessed June 26, 2023. https://www.who.int/news-room/events/detail/2023/05/09/default-calendar/who-bpalm-accelerator-platform–to-support-the-call-to-action-for-implementation-of-the-shorter-and-moreeffective-
- Trevisi L et al. Am J Respir Crit Care Med. 2023;207(11):1525-1532. doi:10.1164/rccm.202211-2125OC
- Domínguez J et al; TBnet and RESIST-TB networks. Lancet Infect Dis. 2023;23(4):e122-e137. doi:10.1016/S1473-3099(22)00875-1
- WHO operational handbook on tuberculosis: module 3: diagnosis: rapid diagnostics for tuberculosis detection, 2021 update. World Health Organization. Published July 7, 2021. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240030589treatment-for-all-people-suffering-from-drug-resistant-tb
- Global tuberculosis report 2022. World Health Organization. Published October 27, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240061729
- WHO consolidated guidelines on tuberculosis. Module 4: treatment – drug-resistant tuberculosis treatment, 2022 update. World Health Organization. Published December 15, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240063129
- Migliori GB, Tiberi S. Int J Tuberc Lung Dis. 2022 ;26(7):590-591. doi:10.5588/ijtld.22.0263.
- Lange C et al. Am J Respir Crit Care Med. 2022;205(10):1142-1144. doi:10.1164/rccm.202202-0393ED
- Esmail A et al. Am J Respir Crit Care Med. 2022;205(10):1214-1227. doi:10.1164/rccm.202107-1779OC
- WHO BPaLM Accelerator Platform: to support the call to action for implementation of the shorter and more effective treatment for all people suffering from drug-resistant TB. World Health Organization. Published May 9, 2023. Accessed June 26, 2023. https://www.who.int/news-room/events/detail/2023/05/09/default-calendar/who-bpalm-accelerator-platform–to-support-the-call-to-action-for-implementation-of-the-shorter-and-moreeffective-
- Trevisi L et al. Am J Respir Crit Care Med. 2023;207(11):1525-1532. doi:10.1164/rccm.202211-2125OC
- Domínguez J et al; TBnet and RESIST-TB networks. Lancet Infect Dis. 2023;23(4):e122-e137. doi:10.1016/S1473-3099(22)00875-1
- WHO operational handbook on tuberculosis: module 3: diagnosis: rapid diagnostics for tuberculosis detection, 2021 update. World Health Organization. Published July 7, 2021. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240030589treatment-for-all-people-suffering-from-drug-resistant-tb
- Global tuberculosis report 2022. World Health Organization. Published October 27, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240061729
- WHO consolidated guidelines on tuberculosis. Module 4: treatment – drug-resistant tuberculosis treatment, 2022 update. World Health Organization. Published December 15, 2022. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240063129
- Migliori GB, Tiberi S. Int J Tuberc Lung Dis. 2022 ;26(7):590-591. doi:10.5588/ijtld.22.0263.
- Lange C et al. Am J Respir Crit Care Med. 2022;205(10):1142-1144. doi:10.1164/rccm.202202-0393ED
- Esmail A et al. Am J Respir Crit Care Med. 2022;205(10):1214-1227. doi:10.1164/rccm.202107-1779OC
- WHO BPaLM Accelerator Platform: to support the call to action for implementation of the shorter and more effective treatment for all people suffering from drug-resistant TB. World Health Organization. Published May 9, 2023. Accessed June 26, 2023. https://www.who.int/news-room/events/detail/2023/05/09/default-calendar/who-bpalm-accelerator-platform–to-support-the-call-to-action-for-implementation-of-the-shorter-and-moreeffective-
- Trevisi L et al. Am J Respir Crit Care Med. 2023;207(11):1525-1532. doi:10.1164/rccm.202211-2125OC
- Domínguez J et al; TBnet and RESIST-TB networks. Lancet Infect Dis. 2023;23(4):e122-e137. doi:10.1016/S1473-3099(22)00875-1
- WHO operational handbook on tuberculosis: module 3: diagnosis: rapid diagnostics for tuberculosis detection, 2021 update. World Health Organization. Published July 7, 2021. Accessed June 26, 2023. https://www.who.int/publications/i/item/9789240030589treatment-for-all-people-suffering-from-drug-resistant-tb
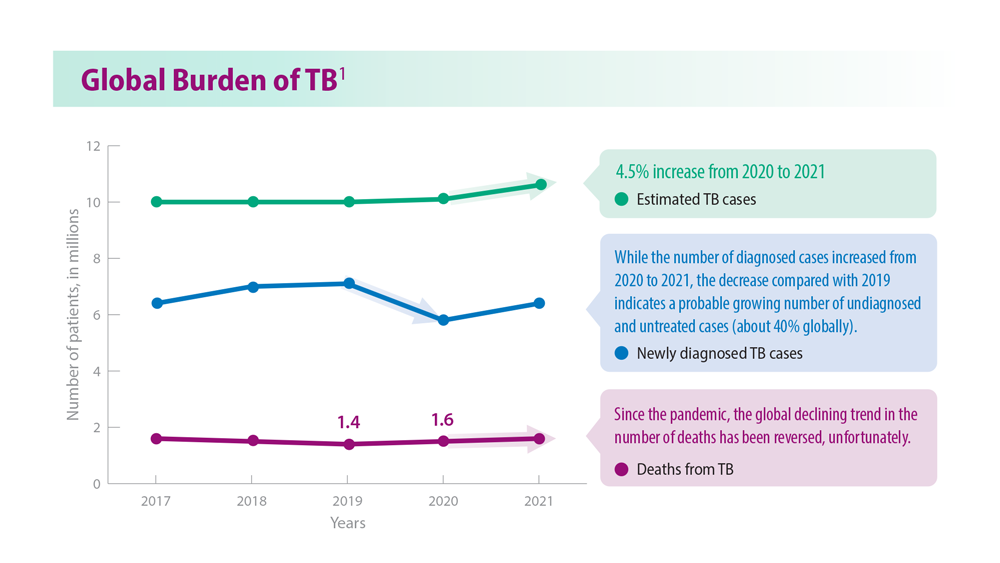
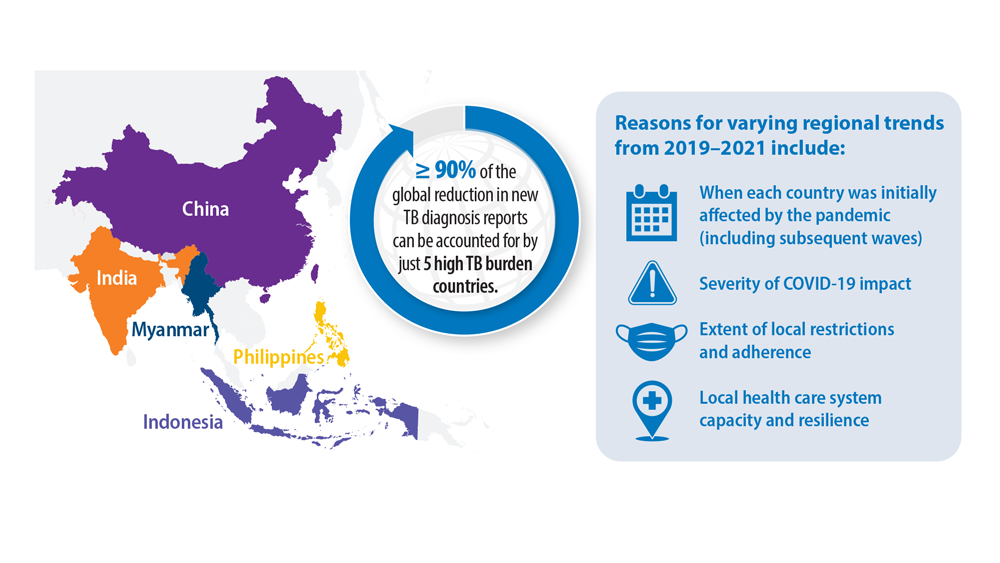
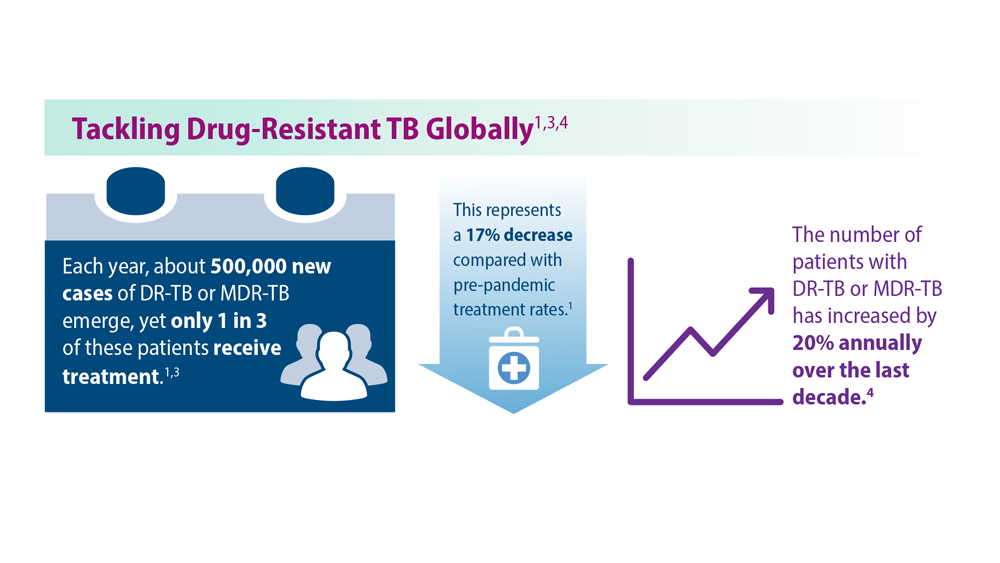
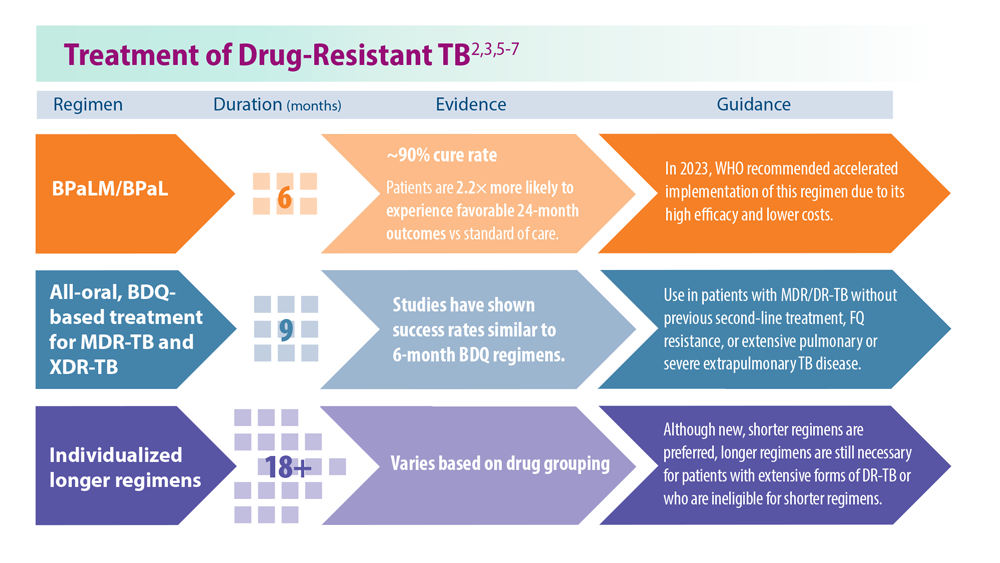
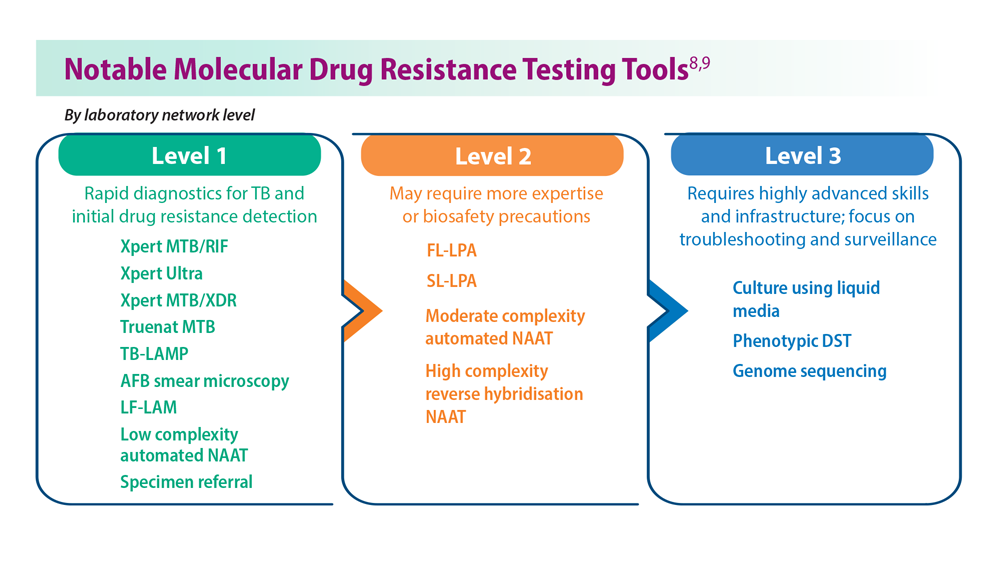
CPAP adherence curbs severe cardiovascular disease outcomes
, based on data from more than 4,000 individuals.
Obstructive sleep apnea (OSA) is associated with an increased risk of cardiovascular diseases, but the association between management of OSA with a continuous positive-airway pressure device (CPAP) and major adverse cardiac or cerebrovascular events (MACCEs) remains unclear, wrote Manuel Sánchez-de-la-Torre, PhD, of the University of Lleida, Spain, and colleagues.
In a meta-analysis published in JAMA, the researchers reviewed data from 4,186 individuals with a mean age of 61.2 years; 82.1% were men. The study population included 2,097 patients who used CPAP and 2,089 who did not. The mean apnea-hypopnea index (AHI) was 31.2 events per hour, and OSA was defined as an oxygen desaturation index of 12 events or more per hour or an AHI of 15 events or more per hour. The composite primary outcome included the first MACCE, or death from cardiovascular causes, myocardial infarction, stroke, revascularization procedure, hospital admission for heart failure, hospital admission for unstable angina, or hospital admission for transient ischemic attack. Each of these components was a secondary endpoint.
Overall, the primary outcome of MACCE was similar for CPAP and non-CPAP using patients (hazard ratio, 1.01) with a total of 349 MACCE events in the CPAP group and 342 in the non-CPAP group. The mean adherence to CPAP was 3.1 hours per day. A total of 38.5% of patients in the CPAP group met the criteria for good adherence, defined as a mean of 4 or more hours per day.
However, as defined, good adherence to CPAP significantly reduced the risk of MACCE, compared with no CPAP use (HR, 0.69), and a sensitivity analysis showed a significant risk reduction, compared with patients who did not meet the criteria for good adherence (HR, 0.55; P = .005).
“Adherence to treatment is complex to determine and there are other potential factors that could affect patient adherence, such as health education, motivation, attitude, self-efficacy, psychosocial factors, and other health care system–related features,” the researchers wrote in their discussion.
The findings were limited by several factors including the evaluation only of CPAP as a treatment for OSA, and the inability to assess separate components of the composite endpoint, the researchers noted. Other limitations included the relatively small number of female patients, reliance mainly on at-home sleep apnea tests, and the potential for selection bias, they said.
However, the results suggest that CPAP adherence is important to prevention of secondary cardiovascular outcomes in OSA patients, and that implementation of specific and personalized strategies to improve adherence to treatment should be a clinical priority, they concluded.
The study was funded by the Instituto de Salud Carlos III, the European Union and FEDER, IRBLleida–Fundació Dr Pifarré, SEPAR, ResMed Ltd. (Australia), Associació Lleidatana de Respiratori, and CIBERES. Dr Sánchez-de-la-Torre also disclosed financial support from a Ramón y Cajal grant.
, based on data from more than 4,000 individuals.
Obstructive sleep apnea (OSA) is associated with an increased risk of cardiovascular diseases, but the association between management of OSA with a continuous positive-airway pressure device (CPAP) and major adverse cardiac or cerebrovascular events (MACCEs) remains unclear, wrote Manuel Sánchez-de-la-Torre, PhD, of the University of Lleida, Spain, and colleagues.
In a meta-analysis published in JAMA, the researchers reviewed data from 4,186 individuals with a mean age of 61.2 years; 82.1% were men. The study population included 2,097 patients who used CPAP and 2,089 who did not. The mean apnea-hypopnea index (AHI) was 31.2 events per hour, and OSA was defined as an oxygen desaturation index of 12 events or more per hour or an AHI of 15 events or more per hour. The composite primary outcome included the first MACCE, or death from cardiovascular causes, myocardial infarction, stroke, revascularization procedure, hospital admission for heart failure, hospital admission for unstable angina, or hospital admission for transient ischemic attack. Each of these components was a secondary endpoint.
Overall, the primary outcome of MACCE was similar for CPAP and non-CPAP using patients (hazard ratio, 1.01) with a total of 349 MACCE events in the CPAP group and 342 in the non-CPAP group. The mean adherence to CPAP was 3.1 hours per day. A total of 38.5% of patients in the CPAP group met the criteria for good adherence, defined as a mean of 4 or more hours per day.
However, as defined, good adherence to CPAP significantly reduced the risk of MACCE, compared with no CPAP use (HR, 0.69), and a sensitivity analysis showed a significant risk reduction, compared with patients who did not meet the criteria for good adherence (HR, 0.55; P = .005).
“Adherence to treatment is complex to determine and there are other potential factors that could affect patient adherence, such as health education, motivation, attitude, self-efficacy, psychosocial factors, and other health care system–related features,” the researchers wrote in their discussion.
The findings were limited by several factors including the evaluation only of CPAP as a treatment for OSA, and the inability to assess separate components of the composite endpoint, the researchers noted. Other limitations included the relatively small number of female patients, reliance mainly on at-home sleep apnea tests, and the potential for selection bias, they said.
However, the results suggest that CPAP adherence is important to prevention of secondary cardiovascular outcomes in OSA patients, and that implementation of specific and personalized strategies to improve adherence to treatment should be a clinical priority, they concluded.
The study was funded by the Instituto de Salud Carlos III, the European Union and FEDER, IRBLleida–Fundació Dr Pifarré, SEPAR, ResMed Ltd. (Australia), Associació Lleidatana de Respiratori, and CIBERES. Dr Sánchez-de-la-Torre also disclosed financial support from a Ramón y Cajal grant.
, based on data from more than 4,000 individuals.
Obstructive sleep apnea (OSA) is associated with an increased risk of cardiovascular diseases, but the association between management of OSA with a continuous positive-airway pressure device (CPAP) and major adverse cardiac or cerebrovascular events (MACCEs) remains unclear, wrote Manuel Sánchez-de-la-Torre, PhD, of the University of Lleida, Spain, and colleagues.
In a meta-analysis published in JAMA, the researchers reviewed data from 4,186 individuals with a mean age of 61.2 years; 82.1% were men. The study population included 2,097 patients who used CPAP and 2,089 who did not. The mean apnea-hypopnea index (AHI) was 31.2 events per hour, and OSA was defined as an oxygen desaturation index of 12 events or more per hour or an AHI of 15 events or more per hour. The composite primary outcome included the first MACCE, or death from cardiovascular causes, myocardial infarction, stroke, revascularization procedure, hospital admission for heart failure, hospital admission for unstable angina, or hospital admission for transient ischemic attack. Each of these components was a secondary endpoint.
Overall, the primary outcome of MACCE was similar for CPAP and non-CPAP using patients (hazard ratio, 1.01) with a total of 349 MACCE events in the CPAP group and 342 in the non-CPAP group. The mean adherence to CPAP was 3.1 hours per day. A total of 38.5% of patients in the CPAP group met the criteria for good adherence, defined as a mean of 4 or more hours per day.
However, as defined, good adherence to CPAP significantly reduced the risk of MACCE, compared with no CPAP use (HR, 0.69), and a sensitivity analysis showed a significant risk reduction, compared with patients who did not meet the criteria for good adherence (HR, 0.55; P = .005).
“Adherence to treatment is complex to determine and there are other potential factors that could affect patient adherence, such as health education, motivation, attitude, self-efficacy, psychosocial factors, and other health care system–related features,” the researchers wrote in their discussion.
The findings were limited by several factors including the evaluation only of CPAP as a treatment for OSA, and the inability to assess separate components of the composite endpoint, the researchers noted. Other limitations included the relatively small number of female patients, reliance mainly on at-home sleep apnea tests, and the potential for selection bias, they said.
However, the results suggest that CPAP adherence is important to prevention of secondary cardiovascular outcomes in OSA patients, and that implementation of specific and personalized strategies to improve adherence to treatment should be a clinical priority, they concluded.
The study was funded by the Instituto de Salud Carlos III, the European Union and FEDER, IRBLleida–Fundació Dr Pifarré, SEPAR, ResMed Ltd. (Australia), Associació Lleidatana de Respiratori, and CIBERES. Dr Sánchez-de-la-Torre also disclosed financial support from a Ramón y Cajal grant.
FROM JAMA