User login
From Hydroplane to Ankle Pain

ANSWER
The radiograph shows an acute fracture of the medial malleolus. It is minimally displaced. The mortise joint appears intact. The patient was placed in a short leg splint for immobilization, and prompt orthopedic follow-up was arranged.
ANSWER
The radiograph shows an acute fracture of the medial malleolus. It is minimally displaced. The mortise joint appears intact. The patient was placed in a short leg splint for immobilization, and prompt orthopedic follow-up was arranged.
ANSWER
The radiograph shows an acute fracture of the medial malleolus. It is minimally displaced. The mortise joint appears intact. The patient was placed in a short leg splint for immobilization, and prompt orthopedic follow-up was arranged.

A 40-year-old woman presents to urgent care for evaluation of ankle pain following a car accident. She was a restrained driver who lost control of her vehicle while driving on wet roads. Her vehicle hit a telephone pole head on. There was no air bag deployment. Initially, she thought she was fine and declined EMS transport to a local hospital. But when she experienced severe pain bearing weight on her right foot, she opted to have it evaluated.
She denies any other complaints. Her medical history is otherwise unremarkable, and vital signs are normal. Physical examination of her right ankle demonstrates general soft-tissue swelling but no obvious deformity. She has moderate tenderness on both the medial and lateral aspects of her ankle. She has limited dorsiflexion and plantar flexion secondary to pain. Good distal pulses are palpable, and good capillary refill is noted in all of the toes.
A radiograph of the ankle is shown. What is your impression?

Nutrition expert to heart patients: ‘Eat some cheese’
NEW ORLEANS – While many Americans have been dithering over the relative health benefits of high- versus low-carbohydrate diets, various pop-culture weight loss programs, vegetarianism, gluten-free living, and other nutritional matters, a quiet revolution in mainstream scientific thinking has occurred regarding the role of full-fat dairy products.
Saturated fatty acid–rich dairy products, formerly viewed as the enemy of cardiovascular health, have gone from foe to friend, according to Arne Astrup, MD, professor and head of the department of nutrition, exercise and sports at the University of Copenhagen.

“From all I have seen, I think it’s quite safe to recommend that our diabetics and heart patients eat some cheese without being afraid of it. I don’t think there’s any harmful effect, and it could actually be very beneficial,” Dr. Astrup continued.
For example, a recent comprehensive meta-analysis of 31 prospective cohort studies found that a high dairy intake was associated with a 9% reduction in the risk of stroke, compared with low or no dairy consumption. Of note, high cheese intake was associated with an 18% lower risk of coronary heart disease (CHD) and a 13% reduction in risk of stroke (Br J Nutr. 2016;115[4]:737-50).
Dutch investigators reported based upon their meta-analysis of 18 prospective cohort studies with 8-26 years of follow-up that stroke risk fell by 7% for each 200 mL of milk consumed per day. Consumption of 25 g/day or more of cheese was associated with a 13% reduction in stroke risk and an 8% lower risk of CHD (J Am Heart Assoc. 2016 May 20;5[5]. doi: 10.1161/JAHA.115.002787).

“The totality of evidence – meta-analyses of both observational studies and randomized controlled trials – cannot find any harmful effects of cheese on body fat, metabolic syndrome, type 2 diabetes, or cardiovascular disease,” he said. “And cheese has beneficial effects on LDL cholesterol, blood pressure, and postprandial triglycerides as compared with butter containing the same amount of saturated fatty acids.”
The classic lipid hypothesis of cardiovascular disease holds that dietary saturated fat raises blood cholesterol, in turn accelerating atherosclerosis and resultant coronary heart disease. But the published literature of the past few years indicates it’s not that simple. All saturated fats are not equally harmful. They have very different biologic effects, and the food matrix in which they occur seems to be important. The saturated fatty acids found in red meat are clearly damaging. Ditto trans fats.
In contrast, the saturated fats present in milk, hard cheeses, and fermented dairy products such as yogurt have been shown in a variety of study formats to be cardioprotective. They also appear to protect against other chronic diseases as well, according to the researcher.
“If we look at all the different meta-analyses addressing the various cardiovascular risk factors, it really looks like cheese, despite its high content of sodium and saturated fat, seems to exert some beneficial effects. So I think we need to address the food matrix much more. We’ve done controlled feeding trials in humans and found that if we give subjects the same amount of saturated fat from either butter or cheese, you see following the cheese [that] the subjects do not increase their total or LDL-cholesterol as you would expect based upon their intake of saturated fat. So there’s something going on with cheese,” Dr. Astrup said.
What’s going on, he continued, is the saturated fats in cheese benefit from the company they keep. Fermented dairy products contain an arm-long list of potentially beneficial nutrients, including protein, calcium, short-chain fatty acids, bioactive peptides, and phospholipids.
Take, for example, calcium: “We’ve found the calcium content of cheese completely modifies the metabolism of the saturated fat. The calcium seems to bind the bile acids and fatty acids, resulting in increased fecal fat secretion,” according to Dr. Astrup.
Although at the AHA meeting he focused mainly on the effects of cheese and other dairy products on cardiovascular health, in a recent review article he expanded upon the scientific evidence regarding the impact of these foods on the risks of obesity, type 2 diabetes, cancer, and osteoporosis (Food Nutr Res. 2016 Nov 22;60:32527).
There is solid evidence that a diet high in dairy products reduces the risk of childhood obesity and enhances body composition in adults. It aids in weight loss by promoting satiety during periods of energy restriction. A recent meta-analysis of observational studies found an inverse relationship between consumption of fermented dairy products – yogurt and cheese – and risk of type 2 diabetes (Am J Clin Nutr. 2016 Apr;103[4]:1111-24).
Regarding cancer, the World Cancer Research Fund has issued a series of evidence reviews concluding that dairy products probably protect against colorectal, breast, gastric, and bladder cancer. The jury is still out regarding prostate cancer risk.
A wealth of evidence indicates dairy consumption has a beneficial effect on bone health in children and adolescents. However, meta-analyses haven’t shown a protective effect against osteoporosis and fractures in adults. This is consistent with the adage that osteoporosis is a pediatric disease with geriatric consequences, Dr. Astrup noted.
He reported receiving research grants from the Danish Dairy Research Foundation, the Global Dairy Platform, the Danish Agriculture and Food Council, and the European Milk Forum. He serves on advisory boards for the Dutch Beer Knowledge Institute, Suntory, Weight Watchers, and several food companies.
NEW ORLEANS – While many Americans have been dithering over the relative health benefits of high- versus low-carbohydrate diets, various pop-culture weight loss programs, vegetarianism, gluten-free living, and other nutritional matters, a quiet revolution in mainstream scientific thinking has occurred regarding the role of full-fat dairy products.
Saturated fatty acid–rich dairy products, formerly viewed as the enemy of cardiovascular health, have gone from foe to friend, according to Arne Astrup, MD, professor and head of the department of nutrition, exercise and sports at the University of Copenhagen.
“From all I have seen, I think it’s quite safe to recommend that our diabetics and heart patients eat some cheese without being afraid of it. I don’t think there’s any harmful effect, and it could actually be very beneficial,” Dr. Astrup continued.
For example, a recent comprehensive meta-analysis of 31 prospective cohort studies found that a high dairy intake was associated with a 9% reduction in the risk of stroke, compared with low or no dairy consumption. Of note, high cheese intake was associated with an 18% lower risk of coronary heart disease (CHD) and a 13% reduction in risk of stroke (Br J Nutr. 2016;115[4]:737-50).
Dutch investigators reported based upon their meta-analysis of 18 prospective cohort studies with 8-26 years of follow-up that stroke risk fell by 7% for each 200 mL of milk consumed per day. Consumption of 25 g/day or more of cheese was associated with a 13% reduction in stroke risk and an 8% lower risk of CHD (J Am Heart Assoc. 2016 May 20;5[5]. doi: 10.1161/JAHA.115.002787).
“The totality of evidence – meta-analyses of both observational studies and randomized controlled trials – cannot find any harmful effects of cheese on body fat, metabolic syndrome, type 2 diabetes, or cardiovascular disease,” he said. “And cheese has beneficial effects on LDL cholesterol, blood pressure, and postprandial triglycerides as compared with butter containing the same amount of saturated fatty acids.”
The classic lipid hypothesis of cardiovascular disease holds that dietary saturated fat raises blood cholesterol, in turn accelerating atherosclerosis and resultant coronary heart disease. But the published literature of the past few years indicates it’s not that simple. All saturated fats are not equally harmful. They have very different biologic effects, and the food matrix in which they occur seems to be important. The saturated fatty acids found in red meat are clearly damaging. Ditto trans fats.
In contrast, the saturated fats present in milk, hard cheeses, and fermented dairy products such as yogurt have been shown in a variety of study formats to be cardioprotective. They also appear to protect against other chronic diseases as well, according to the researcher.
“If we look at all the different meta-analyses addressing the various cardiovascular risk factors, it really looks like cheese, despite its high content of sodium and saturated fat, seems to exert some beneficial effects. So I think we need to address the food matrix much more. We’ve done controlled feeding trials in humans and found that if we give subjects the same amount of saturated fat from either butter or cheese, you see following the cheese [that] the subjects do not increase their total or LDL-cholesterol as you would expect based upon their intake of saturated fat. So there’s something going on with cheese,” Dr. Astrup said.
What’s going on, he continued, is the saturated fats in cheese benefit from the company they keep. Fermented dairy products contain an arm-long list of potentially beneficial nutrients, including protein, calcium, short-chain fatty acids, bioactive peptides, and phospholipids.
Take, for example, calcium: “We’ve found the calcium content of cheese completely modifies the metabolism of the saturated fat. The calcium seems to bind the bile acids and fatty acids, resulting in increased fecal fat secretion,” according to Dr. Astrup.
Although at the AHA meeting he focused mainly on the effects of cheese and other dairy products on cardiovascular health, in a recent review article he expanded upon the scientific evidence regarding the impact of these foods on the risks of obesity, type 2 diabetes, cancer, and osteoporosis (Food Nutr Res. 2016 Nov 22;60:32527).
There is solid evidence that a diet high in dairy products reduces the risk of childhood obesity and enhances body composition in adults. It aids in weight loss by promoting satiety during periods of energy restriction. A recent meta-analysis of observational studies found an inverse relationship between consumption of fermented dairy products – yogurt and cheese – and risk of type 2 diabetes (Am J Clin Nutr. 2016 Apr;103[4]:1111-24).
Regarding cancer, the World Cancer Research Fund has issued a series of evidence reviews concluding that dairy products probably protect against colorectal, breast, gastric, and bladder cancer. The jury is still out regarding prostate cancer risk.
A wealth of evidence indicates dairy consumption has a beneficial effect on bone health in children and adolescents. However, meta-analyses haven’t shown a protective effect against osteoporosis and fractures in adults. This is consistent with the adage that osteoporosis is a pediatric disease with geriatric consequences, Dr. Astrup noted.
He reported receiving research grants from the Danish Dairy Research Foundation, the Global Dairy Platform, the Danish Agriculture and Food Council, and the European Milk Forum. He serves on advisory boards for the Dutch Beer Knowledge Institute, Suntory, Weight Watchers, and several food companies.
NEW ORLEANS – While many Americans have been dithering over the relative health benefits of high- versus low-carbohydrate diets, various pop-culture weight loss programs, vegetarianism, gluten-free living, and other nutritional matters, a quiet revolution in mainstream scientific thinking has occurred regarding the role of full-fat dairy products.
Saturated fatty acid–rich dairy products, formerly viewed as the enemy of cardiovascular health, have gone from foe to friend, according to Arne Astrup, MD, professor and head of the department of nutrition, exercise and sports at the University of Copenhagen.
“From all I have seen, I think it’s quite safe to recommend that our diabetics and heart patients eat some cheese without being afraid of it. I don’t think there’s any harmful effect, and it could actually be very beneficial,” Dr. Astrup continued.
For example, a recent comprehensive meta-analysis of 31 prospective cohort studies found that a high dairy intake was associated with a 9% reduction in the risk of stroke, compared with low or no dairy consumption. Of note, high cheese intake was associated with an 18% lower risk of coronary heart disease (CHD) and a 13% reduction in risk of stroke (Br J Nutr. 2016;115[4]:737-50).
Dutch investigators reported based upon their meta-analysis of 18 prospective cohort studies with 8-26 years of follow-up that stroke risk fell by 7% for each 200 mL of milk consumed per day. Consumption of 25 g/day or more of cheese was associated with a 13% reduction in stroke risk and an 8% lower risk of CHD (J Am Heart Assoc. 2016 May 20;5[5]. doi: 10.1161/JAHA.115.002787).
“The totality of evidence – meta-analyses of both observational studies and randomized controlled trials – cannot find any harmful effects of cheese on body fat, metabolic syndrome, type 2 diabetes, or cardiovascular disease,” he said. “And cheese has beneficial effects on LDL cholesterol, blood pressure, and postprandial triglycerides as compared with butter containing the same amount of saturated fatty acids.”
The classic lipid hypothesis of cardiovascular disease holds that dietary saturated fat raises blood cholesterol, in turn accelerating atherosclerosis and resultant coronary heart disease. But the published literature of the past few years indicates it’s not that simple. All saturated fats are not equally harmful. They have very different biologic effects, and the food matrix in which they occur seems to be important. The saturated fatty acids found in red meat are clearly damaging. Ditto trans fats.
In contrast, the saturated fats present in milk, hard cheeses, and fermented dairy products such as yogurt have been shown in a variety of study formats to be cardioprotective. They also appear to protect against other chronic diseases as well, according to the researcher.
“If we look at all the different meta-analyses addressing the various cardiovascular risk factors, it really looks like cheese, despite its high content of sodium and saturated fat, seems to exert some beneficial effects. So I think we need to address the food matrix much more. We’ve done controlled feeding trials in humans and found that if we give subjects the same amount of saturated fat from either butter or cheese, you see following the cheese [that] the subjects do not increase their total or LDL-cholesterol as you would expect based upon their intake of saturated fat. So there’s something going on with cheese,” Dr. Astrup said.
What’s going on, he continued, is the saturated fats in cheese benefit from the company they keep. Fermented dairy products contain an arm-long list of potentially beneficial nutrients, including protein, calcium, short-chain fatty acids, bioactive peptides, and phospholipids.
Take, for example, calcium: “We’ve found the calcium content of cheese completely modifies the metabolism of the saturated fat. The calcium seems to bind the bile acids and fatty acids, resulting in increased fecal fat secretion,” according to Dr. Astrup.
Although at the AHA meeting he focused mainly on the effects of cheese and other dairy products on cardiovascular health, in a recent review article he expanded upon the scientific evidence regarding the impact of these foods on the risks of obesity, type 2 diabetes, cancer, and osteoporosis (Food Nutr Res. 2016 Nov 22;60:32527).
There is solid evidence that a diet high in dairy products reduces the risk of childhood obesity and enhances body composition in adults. It aids in weight loss by promoting satiety during periods of energy restriction. A recent meta-analysis of observational studies found an inverse relationship between consumption of fermented dairy products – yogurt and cheese – and risk of type 2 diabetes (Am J Clin Nutr. 2016 Apr;103[4]:1111-24).
Regarding cancer, the World Cancer Research Fund has issued a series of evidence reviews concluding that dairy products probably protect against colorectal, breast, gastric, and bladder cancer. The jury is still out regarding prostate cancer risk.
A wealth of evidence indicates dairy consumption has a beneficial effect on bone health in children and adolescents. However, meta-analyses haven’t shown a protective effect against osteoporosis and fractures in adults. This is consistent with the adage that osteoporosis is a pediatric disease with geriatric consequences, Dr. Astrup noted.
He reported receiving research grants from the Danish Dairy Research Foundation, the Global Dairy Platform, the Danish Agriculture and Food Council, and the European Milk Forum. He serves on advisory boards for the Dutch Beer Knowledge Institute, Suntory, Weight Watchers, and several food companies.
FROM THE AHA SCIENTIFIC SESSIONS
Chest-worn seizure detection device shows promise
HOUSTON – An investigative, chest-worn device shows promise for detecting a wide range of seizure types in children with epilepsy, results from a small single-center study showed.
“Our goal is for parents to have more peace of mind, not feeling like they have to watch their kids all night long,” one of the study authors, Kristin H. Gilchrist, PhD, said in an interview at the annual meeting of the American Epilepsy Society. “There are currently many wearable devices marketed for fitness [purposes], but if we can leverage some of these heart rate monitors and use them to detect seizures with specialized algorithms, that would be ideal.”
Approximately 60% of patients had a seizure during the monitoring period. Seizures without any clinical response or those lasting less than 10 seconds (such as single myoclonic jerks or clusters) were excluded from analysis, as were subjects with multiple seizures per hour because the autonomic signals often did not return to baseline, and this seizure frequency is outside of the intended use of the monitor. After exclusions, the algorithm was evaluated on 10 children with a mean age of 12 years. For additional validation, the algorithm was also evaluated with the Massachusetts Institute of Technology, Boston, PhysioNet database with ECG from five adults with partial seizures (Neurology. 1999;53:1590-2).The algorithm without motion parameters detected all seizures classified as tonic-clonic (3/3) or atonic/clonic/tonic (4/4), and 3/9 and 7/10 of focal seizures from the CNMC and MIT subjects, respectively. In the CNMC dataset, the motion algorithm detected all seizures classified as tonic-clonic (3/3), half of those categorized as atonic/clonic/tonic (2/4), and one of nine classified as focal seizures.
In the CNMC dataset, false positives averaged one per 14 hours, however, the majority of false positives occurred in a few patients with poor sensor data quality. More than half of the subjects (70%) had no false positives. One false positive occurred in the 16.8 hours of MIT data.
“In addition to an alert application, we have a technology that can be beneficial to clinic-based studies to quantify how many seizures people are having,” Dr. Gilchrist said. “Hopefully someday it will reach the commercial market.” She reported having no financial disclosures.
HOUSTON – An investigative, chest-worn device shows promise for detecting a wide range of seizure types in children with epilepsy, results from a small single-center study showed.
“Our goal is for parents to have more peace of mind, not feeling like they have to watch their kids all night long,” one of the study authors, Kristin H. Gilchrist, PhD, said in an interview at the annual meeting of the American Epilepsy Society. “There are currently many wearable devices marketed for fitness [purposes], but if we can leverage some of these heart rate monitors and use them to detect seizures with specialized algorithms, that would be ideal.”
Approximately 60% of patients had a seizure during the monitoring period. Seizures without any clinical response or those lasting less than 10 seconds (such as single myoclonic jerks or clusters) were excluded from analysis, as were subjects with multiple seizures per hour because the autonomic signals often did not return to baseline, and this seizure frequency is outside of the intended use of the monitor. After exclusions, the algorithm was evaluated on 10 children with a mean age of 12 years. For additional validation, the algorithm was also evaluated with the Massachusetts Institute of Technology, Boston, PhysioNet database with ECG from five adults with partial seizures (Neurology. 1999;53:1590-2).The algorithm without motion parameters detected all seizures classified as tonic-clonic (3/3) or atonic/clonic/tonic (4/4), and 3/9 and 7/10 of focal seizures from the CNMC and MIT subjects, respectively. In the CNMC dataset, the motion algorithm detected all seizures classified as tonic-clonic (3/3), half of those categorized as atonic/clonic/tonic (2/4), and one of nine classified as focal seizures.
In the CNMC dataset, false positives averaged one per 14 hours, however, the majority of false positives occurred in a few patients with poor sensor data quality. More than half of the subjects (70%) had no false positives. One false positive occurred in the 16.8 hours of MIT data.
“In addition to an alert application, we have a technology that can be beneficial to clinic-based studies to quantify how many seizures people are having,” Dr. Gilchrist said. “Hopefully someday it will reach the commercial market.” She reported having no financial disclosures.
HOUSTON – An investigative, chest-worn device shows promise for detecting a wide range of seizure types in children with epilepsy, results from a small single-center study showed.
“Our goal is for parents to have more peace of mind, not feeling like they have to watch their kids all night long,” one of the study authors, Kristin H. Gilchrist, PhD, said in an interview at the annual meeting of the American Epilepsy Society. “There are currently many wearable devices marketed for fitness [purposes], but if we can leverage some of these heart rate monitors and use them to detect seizures with specialized algorithms, that would be ideal.”
Approximately 60% of patients had a seizure during the monitoring period. Seizures without any clinical response or those lasting less than 10 seconds (such as single myoclonic jerks or clusters) were excluded from analysis, as were subjects with multiple seizures per hour because the autonomic signals often did not return to baseline, and this seizure frequency is outside of the intended use of the monitor. After exclusions, the algorithm was evaluated on 10 children with a mean age of 12 years. For additional validation, the algorithm was also evaluated with the Massachusetts Institute of Technology, Boston, PhysioNet database with ECG from five adults with partial seizures (Neurology. 1999;53:1590-2).The algorithm without motion parameters detected all seizures classified as tonic-clonic (3/3) or atonic/clonic/tonic (4/4), and 3/9 and 7/10 of focal seizures from the CNMC and MIT subjects, respectively. In the CNMC dataset, the motion algorithm detected all seizures classified as tonic-clonic (3/3), half of those categorized as atonic/clonic/tonic (2/4), and one of nine classified as focal seizures.
In the CNMC dataset, false positives averaged one per 14 hours, however, the majority of false positives occurred in a few patients with poor sensor data quality. More than half of the subjects (70%) had no false positives. One false positive occurred in the 16.8 hours of MIT data.
“In addition to an alert application, we have a technology that can be beneficial to clinic-based studies to quantify how many seizures people are having,” Dr. Gilchrist said. “Hopefully someday it will reach the commercial market.” She reported having no financial disclosures.
AT AES 2016
Key clinical point:
Major finding: The algorithm without motion parameters detected all seizures classified as tonic-clonic (3/3) or atonic/clonic/tonic (4/4), and 3 of 9 classified as focal seizures.
Data source: A clinic-based study of 10 epilepsy patients with a mean age of 12 years who wore an investigative device to detect seizures.
Disclosures: The study was funded by a grant from the National Institutes of Health. Dr. Gilchrist reported having no financial disclosures.
Survey: Docs see health care improvements as unlikely in 2017
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.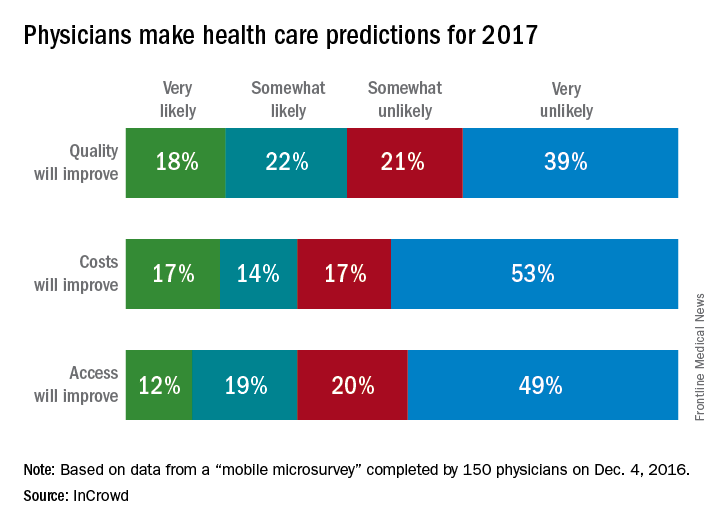
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.
Diabetes-related kidney failure down sharply in Native Americans
Kidney failure in Native Americans and Alaska Natives with diabetes has declined drastically over the last 20 years, according to new data released as part of this month’s Vital Signs report by the CDC.
“The 54 percent decline in kidney failure from diabetes followed implementation of public health and population approaches to diabetes as well as improvements in clinical care by the IHS [Indian Health Service],” said Mary L. Smith, principal deputy director of the Indian Health Service.
Of all U.S.-based populations, Native Americans are the most susceptible to diabetes and are about twice as likely as white Americans to develop diabetes. Furthermore, 69% of kidney failure deaths in Native Americans are the result of diabetes (MMWR. 2017 Jan 10. doi: 10.15585/mmwr.mm6601e1).
Since 1996, however, kidney failure has dropped more among Native Americans than any other ethnic group in the country. The 54% drop represents a decrease from 57.3 diabetes-related end-stage renal disease cases per 100,000 population in 1996 to 26.5 per 100,000 population in 2013 among U.S. adults.
“This decline is especially remarkable given the well-documented health and socioeconomic disparities in the [Native American and Alaska Natives] population, including poverty, limited health care resources, and disproportionate burden of many health problems,” wrote the authors of the Vital Signs report.
According to the report, blood sugar control among Native American populations has improved by 10%, kidney testing in diabetic Native Americans aged 65 years or older is 50% greater than Medicare diabetes patients of the same age, and the average blood pressure of Native Americans with both diabetes and hypertension was 133/76 in 2015.
“We believe these strategies can be effective in any population,” Ms. Smith stated, a sentiment that was also shared by Tom Frieden, MD, director of the CDC.
“Strong coordinated clinical care and education, community outreach and environmental changes can make a dramatic difference in reducing complications from diabetes for all Americans,” Dr. Frieden said in a statement.
Not only does diabetes persist as a significant burden on the U.S. health care system, but kidney failure in particular can be costly. Figures released by the CDC indicate that average medical costs associated with kidney failure in 2013 were as high as $82,000 per patient, with Medicare spending nearly $14 billion for kidney failure treatments in the same year.
“The findings in this report are consistent with other studies among [Native Americans and Alaska Natives] nationwide and among Pima Indians in the Southwest, which concluded that improvements in blood pressure, blood glucose, and the use of ACE inhibitors and [angiotensin II receptor blockers] played a significant role in the decline of [diabetes-related end-stage renal disease] in these populations,” the report concludes.
To ensure that kidney failure decreases continue in Native Americans, the U.S. government will continue funding diabetes screening and prevention efforts in applicable communities, assist community health care facilities to provide care for diabetes, and will establish a nationwide system for tracking chronic kidney disease. The CDC also advocates using population approaches and coordinated care to treat diabetes, advising health care professionals to “integrate kidney disease prevention and education into routine diabetes care.”
“The Indian Health Service has made tremendous progress by applying population health and team-based approaches to diabetes and kidney care,” Dr. Frieden stated.
Kidney failure in Native Americans and Alaska Natives with diabetes has declined drastically over the last 20 years, according to new data released as part of this month’s Vital Signs report by the CDC.
“The 54 percent decline in kidney failure from diabetes followed implementation of public health and population approaches to diabetes as well as improvements in clinical care by the IHS [Indian Health Service],” said Mary L. Smith, principal deputy director of the Indian Health Service.
Of all U.S.-based populations, Native Americans are the most susceptible to diabetes and are about twice as likely as white Americans to develop diabetes. Furthermore, 69% of kidney failure deaths in Native Americans are the result of diabetes (MMWR. 2017 Jan 10. doi: 10.15585/mmwr.mm6601e1).
Since 1996, however, kidney failure has dropped more among Native Americans than any other ethnic group in the country. The 54% drop represents a decrease from 57.3 diabetes-related end-stage renal disease cases per 100,000 population in 1996 to 26.5 per 100,000 population in 2013 among U.S. adults.
“This decline is especially remarkable given the well-documented health and socioeconomic disparities in the [Native American and Alaska Natives] population, including poverty, limited health care resources, and disproportionate burden of many health problems,” wrote the authors of the Vital Signs report.
According to the report, blood sugar control among Native American populations has improved by 10%, kidney testing in diabetic Native Americans aged 65 years or older is 50% greater than Medicare diabetes patients of the same age, and the average blood pressure of Native Americans with both diabetes and hypertension was 133/76 in 2015.
“We believe these strategies can be effective in any population,” Ms. Smith stated, a sentiment that was also shared by Tom Frieden, MD, director of the CDC.
“Strong coordinated clinical care and education, community outreach and environmental changes can make a dramatic difference in reducing complications from diabetes for all Americans,” Dr. Frieden said in a statement.
Not only does diabetes persist as a significant burden on the U.S. health care system, but kidney failure in particular can be costly. Figures released by the CDC indicate that average medical costs associated with kidney failure in 2013 were as high as $82,000 per patient, with Medicare spending nearly $14 billion for kidney failure treatments in the same year.
“The findings in this report are consistent with other studies among [Native Americans and Alaska Natives] nationwide and among Pima Indians in the Southwest, which concluded that improvements in blood pressure, blood glucose, and the use of ACE inhibitors and [angiotensin II receptor blockers] played a significant role in the decline of [diabetes-related end-stage renal disease] in these populations,” the report concludes.
To ensure that kidney failure decreases continue in Native Americans, the U.S. government will continue funding diabetes screening and prevention efforts in applicable communities, assist community health care facilities to provide care for diabetes, and will establish a nationwide system for tracking chronic kidney disease. The CDC also advocates using population approaches and coordinated care to treat diabetes, advising health care professionals to “integrate kidney disease prevention and education into routine diabetes care.”
“The Indian Health Service has made tremendous progress by applying population health and team-based approaches to diabetes and kidney care,” Dr. Frieden stated.
Kidney failure in Native Americans and Alaska Natives with diabetes has declined drastically over the last 20 years, according to new data released as part of this month’s Vital Signs report by the CDC.
“The 54 percent decline in kidney failure from diabetes followed implementation of public health and population approaches to diabetes as well as improvements in clinical care by the IHS [Indian Health Service],” said Mary L. Smith, principal deputy director of the Indian Health Service.
Of all U.S.-based populations, Native Americans are the most susceptible to diabetes and are about twice as likely as white Americans to develop diabetes. Furthermore, 69% of kidney failure deaths in Native Americans are the result of diabetes (MMWR. 2017 Jan 10. doi: 10.15585/mmwr.mm6601e1).
Since 1996, however, kidney failure has dropped more among Native Americans than any other ethnic group in the country. The 54% drop represents a decrease from 57.3 diabetes-related end-stage renal disease cases per 100,000 population in 1996 to 26.5 per 100,000 population in 2013 among U.S. adults.
“This decline is especially remarkable given the well-documented health and socioeconomic disparities in the [Native American and Alaska Natives] population, including poverty, limited health care resources, and disproportionate burden of many health problems,” wrote the authors of the Vital Signs report.
According to the report, blood sugar control among Native American populations has improved by 10%, kidney testing in diabetic Native Americans aged 65 years or older is 50% greater than Medicare diabetes patients of the same age, and the average blood pressure of Native Americans with both diabetes and hypertension was 133/76 in 2015.
“We believe these strategies can be effective in any population,” Ms. Smith stated, a sentiment that was also shared by Tom Frieden, MD, director of the CDC.
“Strong coordinated clinical care and education, community outreach and environmental changes can make a dramatic difference in reducing complications from diabetes for all Americans,” Dr. Frieden said in a statement.
Not only does diabetes persist as a significant burden on the U.S. health care system, but kidney failure in particular can be costly. Figures released by the CDC indicate that average medical costs associated with kidney failure in 2013 were as high as $82,000 per patient, with Medicare spending nearly $14 billion for kidney failure treatments in the same year.
“The findings in this report are consistent with other studies among [Native Americans and Alaska Natives] nationwide and among Pima Indians in the Southwest, which concluded that improvements in blood pressure, blood glucose, and the use of ACE inhibitors and [angiotensin II receptor blockers] played a significant role in the decline of [diabetes-related end-stage renal disease] in these populations,” the report concludes.
To ensure that kidney failure decreases continue in Native Americans, the U.S. government will continue funding diabetes screening and prevention efforts in applicable communities, assist community health care facilities to provide care for diabetes, and will establish a nationwide system for tracking chronic kidney disease. The CDC also advocates using population approaches and coordinated care to treat diabetes, advising health care professionals to “integrate kidney disease prevention and education into routine diabetes care.”
“The Indian Health Service has made tremendous progress by applying population health and team-based approaches to diabetes and kidney care,” Dr. Frieden stated.
Cardiologist care for newly diagnosed A-fib improves outcomes
NEW ORLEANS – Patients who see a cardiologist for their newly diagnosed atrial fibrillation are at significantly lower subsequent risk for ischemic stroke and death than those who receive their care exclusively from primary care physicians, according to a huge Veterans Affairs study.
These superior outcomes were mediated in part by a significantly higher rate of oral anticoagulation prescription within 90 days after diagnosis of atrial fibrillation (AF) among patients who saw a cardiologist, Alexander C. Perino, MD, reported at the American Heart Association scientific sessions.

He presented results from TREAT-AF (The Retrospective Evaluation and Assessment of Therapies in AF) study, a nationwide Veterans Affairs retrospective observational cohort study including 181,161 patients with newly diagnosed AF during 2003-2012. Forty percent of them saw a cardiologist and often a primary care physician as well, while 60% received all their AF-related care in primary care clinics.
The rate of oral anticoagulant prescription within 90 days of diagnosis of AF was 70.3% in patients seen by cardiologists, compared with 58.8% in those seen by primary care physicians only.
“One way to look at this is to say, ‘Wow, look how great cardiologists are doing.’ Another way to look at it is to say, ‘What is going on here that 30% of atrial fibrillation patients seen by cardiologists are not being given an oral anticoagulant prescription? How do we increase that number?’ That needs to be looked into,” Dr. Perino said.
The incidence of ischemic stroke was 7.6 per 1,000 person-years in the cardiology group, significantly lower than the 8.8 per 1,000 in the primary care–only group.
While the two groups shared similar CHA2DS2-VASc scores, the cohort seen by cardiologists had significantly higher rates of comorbid diabetes, hypertension, coronary artery disease, prior MI, and stroke.
In a multivariate analysis adjusted for these comorbidities as well as patient demographics, distance to VA medical care, and use of medications other than oral anticoagulants, cardiology care was associated with a 9% relative risk reduction in ischemic stroke, an 11% reduction in all-cause mortality, and a 3% increase in MI, all statistically significant.
In a more sophisticated analysis featuring propensity score matching, the cardiology group had a 12% relative risk reduction in stroke and a 10% reduction in the risk of death.
The investigators determined that 17% of the improvement in outcomes seen in the cardiology group was attributable to their higher rate of early anticoagulant therapy. Another potential contributor to the outcome differences might be cardiologists’ greater use of rate and rhythm control: Rate control medication was prescribed for 90.1% of the cardiology patients, compared with 80.5% of the primary care patients. And rhythm control therapy was prescribed for 20.8% of the cardiology group versus just 11% of the primary care–only patients.
It’s also possible that cardiology care had a differential impact on non-AF conditions, although this is speculation, Dr. Perino noted.
He said it’s unrealistic to propose that all patients with newly diagnosed AF be seen by a cardiologist because the cardiology workforce isn’t big enough. But more widespread use of specialized AF clinics staffed by expert nurse practitioners and physician assistants could be a practical way for health care plans to achieve cardiologylike outcomes in patients with newly diagnosed AF, in his view.
Dr. Perino reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – Patients who see a cardiologist for their newly diagnosed atrial fibrillation are at significantly lower subsequent risk for ischemic stroke and death than those who receive their care exclusively from primary care physicians, according to a huge Veterans Affairs study.
These superior outcomes were mediated in part by a significantly higher rate of oral anticoagulation prescription within 90 days after diagnosis of atrial fibrillation (AF) among patients who saw a cardiologist, Alexander C. Perino, MD, reported at the American Heart Association scientific sessions.
He presented results from TREAT-AF (The Retrospective Evaluation and Assessment of Therapies in AF) study, a nationwide Veterans Affairs retrospective observational cohort study including 181,161 patients with newly diagnosed AF during 2003-2012. Forty percent of them saw a cardiologist and often a primary care physician as well, while 60% received all their AF-related care in primary care clinics.
The rate of oral anticoagulant prescription within 90 days of diagnosis of AF was 70.3% in patients seen by cardiologists, compared with 58.8% in those seen by primary care physicians only.
“One way to look at this is to say, ‘Wow, look how great cardiologists are doing.’ Another way to look at it is to say, ‘What is going on here that 30% of atrial fibrillation patients seen by cardiologists are not being given an oral anticoagulant prescription? How do we increase that number?’ That needs to be looked into,” Dr. Perino said.
The incidence of ischemic stroke was 7.6 per 1,000 person-years in the cardiology group, significantly lower than the 8.8 per 1,000 in the primary care–only group.
While the two groups shared similar CHA2DS2-VASc scores, the cohort seen by cardiologists had significantly higher rates of comorbid diabetes, hypertension, coronary artery disease, prior MI, and stroke.
In a multivariate analysis adjusted for these comorbidities as well as patient demographics, distance to VA medical care, and use of medications other than oral anticoagulants, cardiology care was associated with a 9% relative risk reduction in ischemic stroke, an 11% reduction in all-cause mortality, and a 3% increase in MI, all statistically significant.
In a more sophisticated analysis featuring propensity score matching, the cardiology group had a 12% relative risk reduction in stroke and a 10% reduction in the risk of death.
The investigators determined that 17% of the improvement in outcomes seen in the cardiology group was attributable to their higher rate of early anticoagulant therapy. Another potential contributor to the outcome differences might be cardiologists’ greater use of rate and rhythm control: Rate control medication was prescribed for 90.1% of the cardiology patients, compared with 80.5% of the primary care patients. And rhythm control therapy was prescribed for 20.8% of the cardiology group versus just 11% of the primary care–only patients.
It’s also possible that cardiology care had a differential impact on non-AF conditions, although this is speculation, Dr. Perino noted.
He said it’s unrealistic to propose that all patients with newly diagnosed AF be seen by a cardiologist because the cardiology workforce isn’t big enough. But more widespread use of specialized AF clinics staffed by expert nurse practitioners and physician assistants could be a practical way for health care plans to achieve cardiologylike outcomes in patients with newly diagnosed AF, in his view.
Dr. Perino reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – Patients who see a cardiologist for their newly diagnosed atrial fibrillation are at significantly lower subsequent risk for ischemic stroke and death than those who receive their care exclusively from primary care physicians, according to a huge Veterans Affairs study.
These superior outcomes were mediated in part by a significantly higher rate of oral anticoagulation prescription within 90 days after diagnosis of atrial fibrillation (AF) among patients who saw a cardiologist, Alexander C. Perino, MD, reported at the American Heart Association scientific sessions.
He presented results from TREAT-AF (The Retrospective Evaluation and Assessment of Therapies in AF) study, a nationwide Veterans Affairs retrospective observational cohort study including 181,161 patients with newly diagnosed AF during 2003-2012. Forty percent of them saw a cardiologist and often a primary care physician as well, while 60% received all their AF-related care in primary care clinics.
The rate of oral anticoagulant prescription within 90 days of diagnosis of AF was 70.3% in patients seen by cardiologists, compared with 58.8% in those seen by primary care physicians only.
“One way to look at this is to say, ‘Wow, look how great cardiologists are doing.’ Another way to look at it is to say, ‘What is going on here that 30% of atrial fibrillation patients seen by cardiologists are not being given an oral anticoagulant prescription? How do we increase that number?’ That needs to be looked into,” Dr. Perino said.
The incidence of ischemic stroke was 7.6 per 1,000 person-years in the cardiology group, significantly lower than the 8.8 per 1,000 in the primary care–only group.
While the two groups shared similar CHA2DS2-VASc scores, the cohort seen by cardiologists had significantly higher rates of comorbid diabetes, hypertension, coronary artery disease, prior MI, and stroke.
In a multivariate analysis adjusted for these comorbidities as well as patient demographics, distance to VA medical care, and use of medications other than oral anticoagulants, cardiology care was associated with a 9% relative risk reduction in ischemic stroke, an 11% reduction in all-cause mortality, and a 3% increase in MI, all statistically significant.
In a more sophisticated analysis featuring propensity score matching, the cardiology group had a 12% relative risk reduction in stroke and a 10% reduction in the risk of death.
The investigators determined that 17% of the improvement in outcomes seen in the cardiology group was attributable to their higher rate of early anticoagulant therapy. Another potential contributor to the outcome differences might be cardiologists’ greater use of rate and rhythm control: Rate control medication was prescribed for 90.1% of the cardiology patients, compared with 80.5% of the primary care patients. And rhythm control therapy was prescribed for 20.8% of the cardiology group versus just 11% of the primary care–only patients.
It’s also possible that cardiology care had a differential impact on non-AF conditions, although this is speculation, Dr. Perino noted.
He said it’s unrealistic to propose that all patients with newly diagnosed AF be seen by a cardiologist because the cardiology workforce isn’t big enough. But more widespread use of specialized AF clinics staffed by expert nurse practitioners and physician assistants could be a practical way for health care plans to achieve cardiologylike outcomes in patients with newly diagnosed AF, in his view.
Dr. Perino reported having no financial conflicts of interest regarding his study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The incidence of ischemic stroke in patients who saw a cardiologist for their newly diagnosed atrial fibrillation was 7.6 per 1,000 person-years, significantly lower than the 8.8 per 1,000 in those cared for exclusively by primary care physicians.
Data source: The TREAT-AF study was a national retrospective cohort study of 181,161 Veterans Affairs patients with newly diagnosed AF during 2003-2012.
Disclosures: The study presenter reported having no financial conflicts of interest.

Dissection of the Celiac Artery
Case
A 41-year-old man presented to our ED with a 4-day history of epigastric pain radiating to the bilateral flanks and back. His medical history was significant for hypertension, for which he was prescribed isosorbide dinitrite 30 mg four times per day; however, he reported that he did not regularly take this medication.
The patient had visited our ED 3 days earlier with the same complaint. Since his blood pressure (BP) reading at the first ED presentation was 213/141 mm Hg, he had been admitted for hypertensive urgency. The patient’s BP was controlled with antihypertensive agents during his stay, but he continued to experience epigastric pain. A basic work-up for abdominal pain was ordered, the results of which were normal. Based on these findings, the patient’s pain was attributed to gastritis, and he was discharged home with instructions to return to the ED if his pain became worse or persisted.
At both ED presentations, the patient denied experiencing any nausea, vomiting, diarrhea, or chest pain. At the second presentation, his triage BP was 158/106 mm Hg. A chest X-ray, complete blood count (CBC), basic metabolic profile (BMP), hepatic panel, and lipase evaluation were all unremarkable, with the exception of a mild increase in creatinine to 1.38 mg/dL. A point-of-care (POC) ultrasound study of the aorta was normal. 
Based on the CTA findings, a nicardipine infusion was immediately started, and the patient was admitted to the medical intensive care unit (MICU). Because his heart rate was in the range of 60 beats/min, an esmolol infusion was not required. Prior to transferring the patient to MICU, a second ultrasound study of the aorta was performed by our fellowship-trained director of emergency medicine ultrasound. 
In the MICU, the patient’s BP was stabilized on hospital day 2, and he was transitioned to oral antihypertensive medications. He was also started on a heparin infusion at the recommendation of vascular surgery services.
A repeat CTA of the abdomen taken on hospital day 3 showed an unchanged dissection in the celiac axis extending into the hepatic artery. The vascular surgeon recommended strict BP control, anticoagulation therapy, and a vascular surgery follow-up with a repeat CTA of the abdomen in 6 months.
On hospital day 6, repeat serial CBC, BMP, and hepatic panels revealed only slight increases in aspartate transaminase to 88 U/L and alanine aminotransferase to 117 U/L. The patient was transitioned to enoxaparin and discharged home on hospital day 6, and instructed to follow-up with his primary care physician for transition to warfarin. Unfortunately, this patient was lost to follow-up.
Discussion
Isolated DCA is a rare cause of abdominal pain. The first documented case of isolated DCA is often incorrectly attributed to Bauersfeld’s1 1947 case series on dissections,but that report described superior mesenteric artery dissection rather than a celiac artery dissection. Watson’s2 1956 dissection series is also incorrectly cited as the first DCA, but that series described a dissection of the splenic artery, which is a branch of the celiac artery. In a 1959 series, Foord and Lewis3 described what is most likely the first report of DCA as an incidental finding at autopsy. More frequent descriptions in recent years are thought to be due to the routine use of abdominal CTA.4
Dissection of the celiac artery is a rare occurrence, with less than 100 cases reported, and little evidence exists to guide its management.5 These dissections represent 36.8% of all visceral artery dissections,6 which themselves are less common than renal, carotid, and vertebral artery dissections.7 Dissection of visceral arteries occurs predominantly in men and more often in middle-aged patients.8 Risk factors for DCA are thought to mirror risk factors for dissection of other arteries, including atherosclerotic disease, hypertension, connective tissue disorders, trauma, vasculitis, and pregnancy.9-11
Signs and Symptoms
Patients with DCA typically present with sudden onset of epigastric, flank, and/or chest pain, though 50% of patients may be asymptomatic.12 This pain is easily overlooked because the physical examination and laboratory studies are typically unremarkable.13 Fortunately, DCA is rarely accompanied by fatal organ dysfunction due to collateral flow from other vessels.14
Diagnosis and Management
While CTA with contrast is considered the mainstay of diagnosis of DCA,15 optimal treatment for DCA has not been well established. Management options include medical management, operative repair, and endovascular embolization. Medical management is reserved for stable patients without signs of end organ dysfunction. Typical management involves anticoagulation with warfarin for 3 to 6 months and strict BP control accompanied by close surveillance for progression.10,13 Some clinicians have argued that anticoagulation therapy may be unnecessary and that risk factor modification and BP control alone may be sufficient.5,6 Others have advocated that surgical management should be favored in cases of persistent pain, development of aneurysm, or threatened or compromised flow to end organs.7
Point-of-Care Ultrasound
The American College of Emergency Physicians considers ultrasound of the abdominal aorta a core application of emergency ultrasound.16 While sensitivity and specificity of emergency ultrasound for abdominal aortic aneurysm are well established, data supporting its use for screening for dissections are less definitive. With a sensitivity of 67% to 80% and a specificity of 99% to 100% with visualization of an intimal flap, aortic dissection screening using ultrasound is less reliable than most emergency physicians (EPs) would prefer.17,18 There are no published data reporting the sensitivity or specificity of emergency ultrasound for DCA. However, the vascular surgery literature encourages color Doppler ultrasound as part of the initial diagnostic work-up for this rare entity.19 While this may seem like an area ripe for emergency ultrasound, it is important to note—as seen in our case—that the site of the dissection is not often seen. Instead, the use of Doppler allows a screening for an abnormal flow pattern suggestive of dissection.20
Conclusion
In our case, both resident EPs and an expert fellowship-trained emergency ultrasound attending physician were unable to visualize a dissection—even after knowledge of the lesion was established by CTA. This points out a limitation of emergency ultrasound. While a POC ultrasound may be able to effectively rule in dissections of the aorta and its branches, we cannot reliably rule out these lesions. As EPs continue to expand the use of ultrasound, it is important to balance the desire for efficiency and cost-effectiveness with a high index of suspicion, experience, and clinical acumen.
1. Bauersfeld SR. Dissecting aneurysm of the aorta; a presentation of 15 cases and a review of the recent literature. Ann Intern Med. 1947;26(6):873-889.
2. Watson AJ. Dissecting aneurysm of arteries other than the aorta. J Pathol. 1956;72(2):439-449. doi:10.1002/path.1700720209.
3. Foord AG, Lewis RD. Primary dissecting aneurysms of peripheral and pulmonary arteries: dissecting hemorrhage of media. Arch Pathol. 1959;68:553-577.
4. Neychev V, Krol E, Dietzek A. Unusual presentation and treatment of spontaneous celiac artery dissection. J Vasc Surg. 2013;58(2):491-495. doi:10.1016/j.jvs.2012.10.136.
5. DiMusto PD, Oberdoerster MM, Criado E. Isolated celiac artery dissection. J Vasc Surg. 2015;61(4):972-976. doi: 10.1016/j.jvs.2014.10.108.
6. Takayama T, Miyata T, Shirakawa M, Nagawa H. J Vasc Surg. 2008;48(2):329-333. doi:10.1016/j.jvs.2008.03.002.
7. Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM. Spontaneous dissection of the celiac artery. Ann Vasc Surg. 2001;15(6):687-692.
8. Patel KS, Benshar O, Vrabie R, Patel A, Adler M, Hines G. A major pain in the … back and epigastrium: an unusual case of spontaneous celiac artery dissection. J Community Hosp Intern Med Perspect. 2014;4(5):23840. doi:10.3402/jchimp.v4.23840.
9. Kang TL, Teich DL, McGillicuddy DC. Isolated, spontaneous superior mesenteric and celiac artery dissection: case report and review of literature. J Emerg Med. 2011;40(2):e21-e25. doi:10.1016/j.jemermed.2007.12.038.
10. Galastri FL, Cavalcante RN, Motta-Leal-Filho JM, et al. Evaluation and management of symptomatic isolated spontaneous celiac trunk dissection. Vasc Med. 2015;20(4):358-363. doi:10.1177/1358863X15581447.
11. Wang HC, Chen JH, Hsiao CC, Jeng CM, Chen WL. Spontaneous dissection of the celiac artery: a case report and literature review. Am J Emerg Med. 2013;31(6):1000.e3-e5. doi:10.1016/j.ajem.2013.02.007.
12. Oh S, Cho YP, Kim JH, Shin S, Kwon TW, Ko GY. Symptomatic spontaneous celiac artery dissection treated by conservative management: serial imaging findings. Abdom Imaging. 2011;36(1):79-82. doi:10.1007/s00261-010-9657-x.
13. Wang JL, Hsieh MJ, Lee CH, Chen CC, Hsieh IC. Celiac artery dissection presenting with abdominal and chest pain. Am J Emerg Med. 2010;28(1):111.e3-e5. doi:10.1016/j.ajem.2009.02.023.
14. Takayama Y, Takao M, Inoue T, Yoshimi F, Koyama K, Nagai H. Isolated spontaneous dissection of the celiac artery: report of two cases. Ann Vasc Dis. 2014;7(1):64-67. doi:10.3400/avd.cr.13-00102.
15. Rehman AU, Almanfi A, Nadella S, Sohail U. Isolated spontaneous celiac artery dissection in a 47-year-old man with von Willebrand disease. Tex Heart Inst J. 2014;41(3):344-345. doi:10.14503/THIJ-13-3404.
16. American College of Emergency Physicians. Policy statement. Ultrasound Guidelines: Emergency, Point-of-Care, and Clinical Ultrasound Guidelines in Medicine, June 2016. https://www.acep.org/Clinical---Practice-Management/Ultrasound/. Accessed November 15, 2016.
17. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99.
18. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196.
19. Woolard JD, Ammar AD. Spontaneous dissection of the celiac artery: a case report. J Vasc Surg. 2007;45(6):1256-1258.
20. Fenoglio L, Allione A, Scalabrino E, et al. Spontaneous dissection of the celiac artery: a pitfall in the diagnosis of acute abdominal pain. Presentation of two cases. Dig Dis Sci. 2004;49(7-8):1223-1227.
Case
A 41-year-old man presented to our ED with a 4-day history of epigastric pain radiating to the bilateral flanks and back. His medical history was significant for hypertension, for which he was prescribed isosorbide dinitrite 30 mg four times per day; however, he reported that he did not regularly take this medication.
The patient had visited our ED 3 days earlier with the same complaint. Since his blood pressure (BP) reading at the first ED presentation was 213/141 mm Hg, he had been admitted for hypertensive urgency. The patient’s BP was controlled with antihypertensive agents during his stay, but he continued to experience epigastric pain. A basic work-up for abdominal pain was ordered, the results of which were normal. Based on these findings, the patient’s pain was attributed to gastritis, and he was discharged home with instructions to return to the ED if his pain became worse or persisted.
At both ED presentations, the patient denied experiencing any nausea, vomiting, diarrhea, or chest pain. At the second presentation, his triage BP was 158/106 mm Hg. A chest X-ray, complete blood count (CBC), basic metabolic profile (BMP), hepatic panel, and lipase evaluation were all unremarkable, with the exception of a mild increase in creatinine to 1.38 mg/dL. A point-of-care (POC) ultrasound study of the aorta was normal.
Based on the CTA findings, a nicardipine infusion was immediately started, and the patient was admitted to the medical intensive care unit (MICU). Because his heart rate was in the range of 60 beats/min, an esmolol infusion was not required. Prior to transferring the patient to MICU, a second ultrasound study of the aorta was performed by our fellowship-trained director of emergency medicine ultrasound.
In the MICU, the patient’s BP was stabilized on hospital day 2, and he was transitioned to oral antihypertensive medications. He was also started on a heparin infusion at the recommendation of vascular surgery services.
A repeat CTA of the abdomen taken on hospital day 3 showed an unchanged dissection in the celiac axis extending into the hepatic artery. The vascular surgeon recommended strict BP control, anticoagulation therapy, and a vascular surgery follow-up with a repeat CTA of the abdomen in 6 months.
On hospital day 6, repeat serial CBC, BMP, and hepatic panels revealed only slight increases in aspartate transaminase to 88 U/L and alanine aminotransferase to 117 U/L. The patient was transitioned to enoxaparin and discharged home on hospital day 6, and instructed to follow-up with his primary care physician for transition to warfarin. Unfortunately, this patient was lost to follow-up.
Discussion
Isolated DCA is a rare cause of abdominal pain. The first documented case of isolated DCA is often incorrectly attributed to Bauersfeld’s1 1947 case series on dissections,but that report described superior mesenteric artery dissection rather than a celiac artery dissection. Watson’s2 1956 dissection series is also incorrectly cited as the first DCA, but that series described a dissection of the splenic artery, which is a branch of the celiac artery. In a 1959 series, Foord and Lewis3 described what is most likely the first report of DCA as an incidental finding at autopsy. More frequent descriptions in recent years are thought to be due to the routine use of abdominal CTA.4
Dissection of the celiac artery is a rare occurrence, with less than 100 cases reported, and little evidence exists to guide its management.5 These dissections represent 36.8% of all visceral artery dissections,6 which themselves are less common than renal, carotid, and vertebral artery dissections.7 Dissection of visceral arteries occurs predominantly in men and more often in middle-aged patients.8 Risk factors for DCA are thought to mirror risk factors for dissection of other arteries, including atherosclerotic disease, hypertension, connective tissue disorders, trauma, vasculitis, and pregnancy.9-11
Signs and Symptoms
Patients with DCA typically present with sudden onset of epigastric, flank, and/or chest pain, though 50% of patients may be asymptomatic.12 This pain is easily overlooked because the physical examination and laboratory studies are typically unremarkable.13 Fortunately, DCA is rarely accompanied by fatal organ dysfunction due to collateral flow from other vessels.14
Diagnosis and Management
While CTA with contrast is considered the mainstay of diagnosis of DCA,15 optimal treatment for DCA has not been well established. Management options include medical management, operative repair, and endovascular embolization. Medical management is reserved for stable patients without signs of end organ dysfunction. Typical management involves anticoagulation with warfarin for 3 to 6 months and strict BP control accompanied by close surveillance for progression.10,13 Some clinicians have argued that anticoagulation therapy may be unnecessary and that risk factor modification and BP control alone may be sufficient.5,6 Others have advocated that surgical management should be favored in cases of persistent pain, development of aneurysm, or threatened or compromised flow to end organs.7
Point-of-Care Ultrasound
The American College of Emergency Physicians considers ultrasound of the abdominal aorta a core application of emergency ultrasound.16 While sensitivity and specificity of emergency ultrasound for abdominal aortic aneurysm are well established, data supporting its use for screening for dissections are less definitive. With a sensitivity of 67% to 80% and a specificity of 99% to 100% with visualization of an intimal flap, aortic dissection screening using ultrasound is less reliable than most emergency physicians (EPs) would prefer.17,18 There are no published data reporting the sensitivity or specificity of emergency ultrasound for DCA. However, the vascular surgery literature encourages color Doppler ultrasound as part of the initial diagnostic work-up for this rare entity.19 While this may seem like an area ripe for emergency ultrasound, it is important to note—as seen in our case—that the site of the dissection is not often seen. Instead, the use of Doppler allows a screening for an abnormal flow pattern suggestive of dissection.20
Conclusion
In our case, both resident EPs and an expert fellowship-trained emergency ultrasound attending physician were unable to visualize a dissection—even after knowledge of the lesion was established by CTA. This points out a limitation of emergency ultrasound. While a POC ultrasound may be able to effectively rule in dissections of the aorta and its branches, we cannot reliably rule out these lesions. As EPs continue to expand the use of ultrasound, it is important to balance the desire for efficiency and cost-effectiveness with a high index of suspicion, experience, and clinical acumen.
Case
A 41-year-old man presented to our ED with a 4-day history of epigastric pain radiating to the bilateral flanks and back. His medical history was significant for hypertension, for which he was prescribed isosorbide dinitrite 30 mg four times per day; however, he reported that he did not regularly take this medication.
The patient had visited our ED 3 days earlier with the same complaint. Since his blood pressure (BP) reading at the first ED presentation was 213/141 mm Hg, he had been admitted for hypertensive urgency. The patient’s BP was controlled with antihypertensive agents during his stay, but he continued to experience epigastric pain. A basic work-up for abdominal pain was ordered, the results of which were normal. Based on these findings, the patient’s pain was attributed to gastritis, and he was discharged home with instructions to return to the ED if his pain became worse or persisted.
At both ED presentations, the patient denied experiencing any nausea, vomiting, diarrhea, or chest pain. At the second presentation, his triage BP was 158/106 mm Hg. A chest X-ray, complete blood count (CBC), basic metabolic profile (BMP), hepatic panel, and lipase evaluation were all unremarkable, with the exception of a mild increase in creatinine to 1.38 mg/dL. A point-of-care (POC) ultrasound study of the aorta was normal.
Based on the CTA findings, a nicardipine infusion was immediately started, and the patient was admitted to the medical intensive care unit (MICU). Because his heart rate was in the range of 60 beats/min, an esmolol infusion was not required. Prior to transferring the patient to MICU, a second ultrasound study of the aorta was performed by our fellowship-trained director of emergency medicine ultrasound.
In the MICU, the patient’s BP was stabilized on hospital day 2, and he was transitioned to oral antihypertensive medications. He was also started on a heparin infusion at the recommendation of vascular surgery services.
A repeat CTA of the abdomen taken on hospital day 3 showed an unchanged dissection in the celiac axis extending into the hepatic artery. The vascular surgeon recommended strict BP control, anticoagulation therapy, and a vascular surgery follow-up with a repeat CTA of the abdomen in 6 months.
On hospital day 6, repeat serial CBC, BMP, and hepatic panels revealed only slight increases in aspartate transaminase to 88 U/L and alanine aminotransferase to 117 U/L. The patient was transitioned to enoxaparin and discharged home on hospital day 6, and instructed to follow-up with his primary care physician for transition to warfarin. Unfortunately, this patient was lost to follow-up.
Discussion
Isolated DCA is a rare cause of abdominal pain. The first documented case of isolated DCA is often incorrectly attributed to Bauersfeld’s1 1947 case series on dissections,but that report described superior mesenteric artery dissection rather than a celiac artery dissection. Watson’s2 1956 dissection series is also incorrectly cited as the first DCA, but that series described a dissection of the splenic artery, which is a branch of the celiac artery. In a 1959 series, Foord and Lewis3 described what is most likely the first report of DCA as an incidental finding at autopsy. More frequent descriptions in recent years are thought to be due to the routine use of abdominal CTA.4
Dissection of the celiac artery is a rare occurrence, with less than 100 cases reported, and little evidence exists to guide its management.5 These dissections represent 36.8% of all visceral artery dissections,6 which themselves are less common than renal, carotid, and vertebral artery dissections.7 Dissection of visceral arteries occurs predominantly in men and more often in middle-aged patients.8 Risk factors for DCA are thought to mirror risk factors for dissection of other arteries, including atherosclerotic disease, hypertension, connective tissue disorders, trauma, vasculitis, and pregnancy.9-11
Signs and Symptoms
Patients with DCA typically present with sudden onset of epigastric, flank, and/or chest pain, though 50% of patients may be asymptomatic.12 This pain is easily overlooked because the physical examination and laboratory studies are typically unremarkable.13 Fortunately, DCA is rarely accompanied by fatal organ dysfunction due to collateral flow from other vessels.14
Diagnosis and Management
While CTA with contrast is considered the mainstay of diagnosis of DCA,15 optimal treatment for DCA has not been well established. Management options include medical management, operative repair, and endovascular embolization. Medical management is reserved for stable patients without signs of end organ dysfunction. Typical management involves anticoagulation with warfarin for 3 to 6 months and strict BP control accompanied by close surveillance for progression.10,13 Some clinicians have argued that anticoagulation therapy may be unnecessary and that risk factor modification and BP control alone may be sufficient.5,6 Others have advocated that surgical management should be favored in cases of persistent pain, development of aneurysm, or threatened or compromised flow to end organs.7
Point-of-Care Ultrasound
The American College of Emergency Physicians considers ultrasound of the abdominal aorta a core application of emergency ultrasound.16 While sensitivity and specificity of emergency ultrasound for abdominal aortic aneurysm are well established, data supporting its use for screening for dissections are less definitive. With a sensitivity of 67% to 80% and a specificity of 99% to 100% with visualization of an intimal flap, aortic dissection screening using ultrasound is less reliable than most emergency physicians (EPs) would prefer.17,18 There are no published data reporting the sensitivity or specificity of emergency ultrasound for DCA. However, the vascular surgery literature encourages color Doppler ultrasound as part of the initial diagnostic work-up for this rare entity.19 While this may seem like an area ripe for emergency ultrasound, it is important to note—as seen in our case—that the site of the dissection is not often seen. Instead, the use of Doppler allows a screening for an abnormal flow pattern suggestive of dissection.20
Conclusion
In our case, both resident EPs and an expert fellowship-trained emergency ultrasound attending physician were unable to visualize a dissection—even after knowledge of the lesion was established by CTA. This points out a limitation of emergency ultrasound. While a POC ultrasound may be able to effectively rule in dissections of the aorta and its branches, we cannot reliably rule out these lesions. As EPs continue to expand the use of ultrasound, it is important to balance the desire for efficiency and cost-effectiveness with a high index of suspicion, experience, and clinical acumen.
1. Bauersfeld SR. Dissecting aneurysm of the aorta; a presentation of 15 cases and a review of the recent literature. Ann Intern Med. 1947;26(6):873-889.
2. Watson AJ. Dissecting aneurysm of arteries other than the aorta. J Pathol. 1956;72(2):439-449. doi:10.1002/path.1700720209.
3. Foord AG, Lewis RD. Primary dissecting aneurysms of peripheral and pulmonary arteries: dissecting hemorrhage of media. Arch Pathol. 1959;68:553-577.
4. Neychev V, Krol E, Dietzek A. Unusual presentation and treatment of spontaneous celiac artery dissection. J Vasc Surg. 2013;58(2):491-495. doi:10.1016/j.jvs.2012.10.136.
5. DiMusto PD, Oberdoerster MM, Criado E. Isolated celiac artery dissection. J Vasc Surg. 2015;61(4):972-976. doi: 10.1016/j.jvs.2014.10.108.
6. Takayama T, Miyata T, Shirakawa M, Nagawa H. J Vasc Surg. 2008;48(2):329-333. doi:10.1016/j.jvs.2008.03.002.
7. Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM. Spontaneous dissection of the celiac artery. Ann Vasc Surg. 2001;15(6):687-692.
8. Patel KS, Benshar O, Vrabie R, Patel A, Adler M, Hines G. A major pain in the … back and epigastrium: an unusual case of spontaneous celiac artery dissection. J Community Hosp Intern Med Perspect. 2014;4(5):23840. doi:10.3402/jchimp.v4.23840.
9. Kang TL, Teich DL, McGillicuddy DC. Isolated, spontaneous superior mesenteric and celiac artery dissection: case report and review of literature. J Emerg Med. 2011;40(2):e21-e25. doi:10.1016/j.jemermed.2007.12.038.
10. Galastri FL, Cavalcante RN, Motta-Leal-Filho JM, et al. Evaluation and management of symptomatic isolated spontaneous celiac trunk dissection. Vasc Med. 2015;20(4):358-363. doi:10.1177/1358863X15581447.
11. Wang HC, Chen JH, Hsiao CC, Jeng CM, Chen WL. Spontaneous dissection of the celiac artery: a case report and literature review. Am J Emerg Med. 2013;31(6):1000.e3-e5. doi:10.1016/j.ajem.2013.02.007.
12. Oh S, Cho YP, Kim JH, Shin S, Kwon TW, Ko GY. Symptomatic spontaneous celiac artery dissection treated by conservative management: serial imaging findings. Abdom Imaging. 2011;36(1):79-82. doi:10.1007/s00261-010-9657-x.
13. Wang JL, Hsieh MJ, Lee CH, Chen CC, Hsieh IC. Celiac artery dissection presenting with abdominal and chest pain. Am J Emerg Med. 2010;28(1):111.e3-e5. doi:10.1016/j.ajem.2009.02.023.
14. Takayama Y, Takao M, Inoue T, Yoshimi F, Koyama K, Nagai H. Isolated spontaneous dissection of the celiac artery: report of two cases. Ann Vasc Dis. 2014;7(1):64-67. doi:10.3400/avd.cr.13-00102.
15. Rehman AU, Almanfi A, Nadella S, Sohail U. Isolated spontaneous celiac artery dissection in a 47-year-old man with von Willebrand disease. Tex Heart Inst J. 2014;41(3):344-345. doi:10.14503/THIJ-13-3404.
16. American College of Emergency Physicians. Policy statement. Ultrasound Guidelines: Emergency, Point-of-Care, and Clinical Ultrasound Guidelines in Medicine, June 2016. https://www.acep.org/Clinical---Practice-Management/Ultrasound/. Accessed November 15, 2016.
17. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99.
18. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196.
19. Woolard JD, Ammar AD. Spontaneous dissection of the celiac artery: a case report. J Vasc Surg. 2007;45(6):1256-1258.
20. Fenoglio L, Allione A, Scalabrino E, et al. Spontaneous dissection of the celiac artery: a pitfall in the diagnosis of acute abdominal pain. Presentation of two cases. Dig Dis Sci. 2004;49(7-8):1223-1227.
1. Bauersfeld SR. Dissecting aneurysm of the aorta; a presentation of 15 cases and a review of the recent literature. Ann Intern Med. 1947;26(6):873-889.
2. Watson AJ. Dissecting aneurysm of arteries other than the aorta. J Pathol. 1956;72(2):439-449. doi:10.1002/path.1700720209.
3. Foord AG, Lewis RD. Primary dissecting aneurysms of peripheral and pulmonary arteries: dissecting hemorrhage of media. Arch Pathol. 1959;68:553-577.
4. Neychev V, Krol E, Dietzek A. Unusual presentation and treatment of spontaneous celiac artery dissection. J Vasc Surg. 2013;58(2):491-495. doi:10.1016/j.jvs.2012.10.136.
5. DiMusto PD, Oberdoerster MM, Criado E. Isolated celiac artery dissection. J Vasc Surg. 2015;61(4):972-976. doi: 10.1016/j.jvs.2014.10.108.
6. Takayama T, Miyata T, Shirakawa M, Nagawa H. J Vasc Surg. 2008;48(2):329-333. doi:10.1016/j.jvs.2008.03.002.
7. Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM. Spontaneous dissection of the celiac artery. Ann Vasc Surg. 2001;15(6):687-692.
8. Patel KS, Benshar O, Vrabie R, Patel A, Adler M, Hines G. A major pain in the … back and epigastrium: an unusual case of spontaneous celiac artery dissection. J Community Hosp Intern Med Perspect. 2014;4(5):23840. doi:10.3402/jchimp.v4.23840.
9. Kang TL, Teich DL, McGillicuddy DC. Isolated, spontaneous superior mesenteric and celiac artery dissection: case report and review of literature. J Emerg Med. 2011;40(2):e21-e25. doi:10.1016/j.jemermed.2007.12.038.
10. Galastri FL, Cavalcante RN, Motta-Leal-Filho JM, et al. Evaluation and management of symptomatic isolated spontaneous celiac trunk dissection. Vasc Med. 2015;20(4):358-363. doi:10.1177/1358863X15581447.
11. Wang HC, Chen JH, Hsiao CC, Jeng CM, Chen WL. Spontaneous dissection of the celiac artery: a case report and literature review. Am J Emerg Med. 2013;31(6):1000.e3-e5. doi:10.1016/j.ajem.2013.02.007.
12. Oh S, Cho YP, Kim JH, Shin S, Kwon TW, Ko GY. Symptomatic spontaneous celiac artery dissection treated by conservative management: serial imaging findings. Abdom Imaging. 2011;36(1):79-82. doi:10.1007/s00261-010-9657-x.
13. Wang JL, Hsieh MJ, Lee CH, Chen CC, Hsieh IC. Celiac artery dissection presenting with abdominal and chest pain. Am J Emerg Med. 2010;28(1):111.e3-e5. doi:10.1016/j.ajem.2009.02.023.
14. Takayama Y, Takao M, Inoue T, Yoshimi F, Koyama K, Nagai H. Isolated spontaneous dissection of the celiac artery: report of two cases. Ann Vasc Dis. 2014;7(1):64-67. doi:10.3400/avd.cr.13-00102.
15. Rehman AU, Almanfi A, Nadella S, Sohail U. Isolated spontaneous celiac artery dissection in a 47-year-old man with von Willebrand disease. Tex Heart Inst J. 2014;41(3):344-345. doi:10.14503/THIJ-13-3404.
16. American College of Emergency Physicians. Policy statement. Ultrasound Guidelines: Emergency, Point-of-Care, and Clinical Ultrasound Guidelines in Medicine, June 2016. https://www.acep.org/Clinical---Practice-Management/Ultrasound/. Accessed November 15, 2016.
17. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99.
18. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196.
19. Woolard JD, Ammar AD. Spontaneous dissection of the celiac artery: a case report. J Vasc Surg. 2007;45(6):1256-1258.
20. Fenoglio L, Allione A, Scalabrino E, et al. Spontaneous dissection of the celiac artery: a pitfall in the diagnosis of acute abdominal pain. Presentation of two cases. Dig Dis Sci. 2004;49(7-8):1223-1227.

Physician Communications: Avoiding the Blame Game
A recent opinion piece in MedPage Today by an internist about poor communications between emergency physicians (EPs) and primary care physicians (PCPs) was subtitled “We’ve gotten better going from office to ER, but not the other way,” and complained about the lack of a “live, warm handoff” from EPs to PCPs of patients being discharged from EDs. Similar complaints were examined in two recent Emergency Medicine (EM) editorials (Anger Management, 2015;47[4]:149 and Broadside Journalism, 2015;47[6]:244). In the first, we noted that PCPs sometimes are angered when they are not consulted about one of their patients in the ED or about a treatment or disposition plan with which they disagree, while EPs are frustrated by the number of phone calls required to reach some PCPs or a knowledgeable covering physician.
Only 2 months later, we expressed concerns about a New York Times opinion editorial describing a young patient whose vertebral artery dissection had been “diagnosed correctly and acted on in the ED,” but then angrily criticizing an initial recommendation that the patient curtail her physical activities based on what a famous neurologist considered an erroneously interpreted vascular imaging study. (Presumably, the recommendation was by another neurologist and the interpretation by a radiologist, but all of the neurologist’s caustic criticism was directed at the EP and ED.) Although the neurologist subsequently apologized in a letter to his emergency medicine colleagues for “being quoted out of context,” few if any
We concluded the second EM editorial with the suggestion that “all physicians must be very, very careful in framing statements to the media, and should assume that their remarks will not be placed ‘in context’ or nuanced as they may have been intended....Most important, is to not disparage entire specialties or use belittling terms such as ‘ER docs’....[that] heighten...patients’ fears” of being treated in EDs.
Why another editorial about physician-to-physician miscommunications and name-calling? Because patient care is significantly affected.
The Centers for Medicare and Medicaid Services originally classified four medical specialties as “primary care” for reimbursement purposes: family medicine, internal medicine, pediatrics, and obstetrics-gynecology, and the 2010 Affordable Care Act added geriatrics. Although emergency medicine had been considered initially, it has never been categorized as a primary care specialty. That being the case, isn’t it incumbent upon us to learn as much as we can from PCPs about their ill patients en route to the ED for treatment or admission, and afterward ensure that an ED visit is part of a continuum of patient care and not an isolated episode?
In 1996, when I accepted an offer to become New York Presbyterian-Weill Cornell’s first Emergency Physician-in-Chief, I created a new position of full-time “ED follow-up nurse practitioner” to track and report test results to discharged patients and their designated PCPs. When we added a fourth unit to the ED a few years later, I designated an experienced, senior attending EP among the four on duty as the “administrative attending” (AA) who, among other tasks, took all phone calls from PCPs about patients they were sending to the ED and entered the information in the “en route” section of our electronic tracking board. In this way, important patient information, including PCP contact information, was no longer misplaced during shift changes. The AA carried a direct-dial cell phone-like device and eventually all attending EPs and the charge nurse were equipped with such phones. In a short time, most of the communications problems and complaints about incoming patients were eliminated.
But despite numerous attempts, for the reasons mentioned above, systematically ensuring effective communications with PCPs for discharged patients has proven to be a more difficult task. At present, handing off discharged patients to PCPs still depends largely on a combination of judgment, understanding, compassion, and respect.
A recent opinion piece in MedPage Today by an internist about poor communications between emergency physicians (EPs) and primary care physicians (PCPs) was subtitled “We’ve gotten better going from office to ER, but not the other way,” and complained about the lack of a “live, warm handoff” from EPs to PCPs of patients being discharged from EDs. Similar complaints were examined in two recent Emergency Medicine (EM) editorials (Anger Management, 2015;47[4]:149 and Broadside Journalism, 2015;47[6]:244). In the first, we noted that PCPs sometimes are angered when they are not consulted about one of their patients in the ED or about a treatment or disposition plan with which they disagree, while EPs are frustrated by the number of phone calls required to reach some PCPs or a knowledgeable covering physician.
Only 2 months later, we expressed concerns about a New York Times opinion editorial describing a young patient whose vertebral artery dissection had been “diagnosed correctly and acted on in the ED,” but then angrily criticizing an initial recommendation that the patient curtail her physical activities based on what a famous neurologist considered an erroneously interpreted vascular imaging study. (Presumably, the recommendation was by another neurologist and the interpretation by a radiologist, but all of the neurologist’s caustic criticism was directed at the EP and ED.) Although the neurologist subsequently apologized in a letter to his emergency medicine colleagues for “being quoted out of context,” few if any
We concluded the second EM editorial with the suggestion that “all physicians must be very, very careful in framing statements to the media, and should assume that their remarks will not be placed ‘in context’ or nuanced as they may have been intended....Most important, is to not disparage entire specialties or use belittling terms such as ‘ER docs’....[that] heighten...patients’ fears” of being treated in EDs.
Why another editorial about physician-to-physician miscommunications and name-calling? Because patient care is significantly affected.
The Centers for Medicare and Medicaid Services originally classified four medical specialties as “primary care” for reimbursement purposes: family medicine, internal medicine, pediatrics, and obstetrics-gynecology, and the 2010 Affordable Care Act added geriatrics. Although emergency medicine had been considered initially, it has never been categorized as a primary care specialty. That being the case, isn’t it incumbent upon us to learn as much as we can from PCPs about their ill patients en route to the ED for treatment or admission, and afterward ensure that an ED visit is part of a continuum of patient care and not an isolated episode?
In 1996, when I accepted an offer to become New York Presbyterian-Weill Cornell’s first Emergency Physician-in-Chief, I created a new position of full-time “ED follow-up nurse practitioner” to track and report test results to discharged patients and their designated PCPs. When we added a fourth unit to the ED a few years later, I designated an experienced, senior attending EP among the four on duty as the “administrative attending” (AA) who, among other tasks, took all phone calls from PCPs about patients they were sending to the ED and entered the information in the “en route” section of our electronic tracking board. In this way, important patient information, including PCP contact information, was no longer misplaced during shift changes. The AA carried a direct-dial cell phone-like device and eventually all attending EPs and the charge nurse were equipped with such phones. In a short time, most of the communications problems and complaints about incoming patients were eliminated.
But despite numerous attempts, for the reasons mentioned above, systematically ensuring effective communications with PCPs for discharged patients has proven to be a more difficult task. At present, handing off discharged patients to PCPs still depends largely on a combination of judgment, understanding, compassion, and respect.
A recent opinion piece in MedPage Today by an internist about poor communications between emergency physicians (EPs) and primary care physicians (PCPs) was subtitled “We’ve gotten better going from office to ER, but not the other way,” and complained about the lack of a “live, warm handoff” from EPs to PCPs of patients being discharged from EDs. Similar complaints were examined in two recent Emergency Medicine (EM) editorials (Anger Management, 2015;47[4]:149 and Broadside Journalism, 2015;47[6]:244). In the first, we noted that PCPs sometimes are angered when they are not consulted about one of their patients in the ED or about a treatment or disposition plan with which they disagree, while EPs are frustrated by the number of phone calls required to reach some PCPs or a knowledgeable covering physician.
Only 2 months later, we expressed concerns about a New York Times opinion editorial describing a young patient whose vertebral artery dissection had been “diagnosed correctly and acted on in the ED,” but then angrily criticizing an initial recommendation that the patient curtail her physical activities based on what a famous neurologist considered an erroneously interpreted vascular imaging study. (Presumably, the recommendation was by another neurologist and the interpretation by a radiologist, but all of the neurologist’s caustic criticism was directed at the EP and ED.) Although the neurologist subsequently apologized in a letter to his emergency medicine colleagues for “being quoted out of context,” few if any
We concluded the second EM editorial with the suggestion that “all physicians must be very, very careful in framing statements to the media, and should assume that their remarks will not be placed ‘in context’ or nuanced as they may have been intended....Most important, is to not disparage entire specialties or use belittling terms such as ‘ER docs’....[that] heighten...patients’ fears” of being treated in EDs.
Why another editorial about physician-to-physician miscommunications and name-calling? Because patient care is significantly affected.
The Centers for Medicare and Medicaid Services originally classified four medical specialties as “primary care” for reimbursement purposes: family medicine, internal medicine, pediatrics, and obstetrics-gynecology, and the 2010 Affordable Care Act added geriatrics. Although emergency medicine had been considered initially, it has never been categorized as a primary care specialty. That being the case, isn’t it incumbent upon us to learn as much as we can from PCPs about their ill patients en route to the ED for treatment or admission, and afterward ensure that an ED visit is part of a continuum of patient care and not an isolated episode?
In 1996, when I accepted an offer to become New York Presbyterian-Weill Cornell’s first Emergency Physician-in-Chief, I created a new position of full-time “ED follow-up nurse practitioner” to track and report test results to discharged patients and their designated PCPs. When we added a fourth unit to the ED a few years later, I designated an experienced, senior attending EP among the four on duty as the “administrative attending” (AA) who, among other tasks, took all phone calls from PCPs about patients they were sending to the ED and entered the information in the “en route” section of our electronic tracking board. In this way, important patient information, including PCP contact information, was no longer misplaced during shift changes. The AA carried a direct-dial cell phone-like device and eventually all attending EPs and the charge nurse were equipped with such phones. In a short time, most of the communications problems and complaints about incoming patients were eliminated.
But despite numerous attempts, for the reasons mentioned above, systematically ensuring effective communications with PCPs for discharged patients has proven to be a more difficult task. At present, handing off discharged patients to PCPs still depends largely on a combination of judgment, understanding, compassion, and respect.

SHM welcomes its newest members - January 2017
Justin Kimsey, Alabama
Mohammed N.Y. Shah, MD, Alaska
Katharina Beeler, MD, Arizona
Khoi Nguyen, MD, Arizona
Vinay Saini, MD, Arizona
Maria Aceves, PA-C, California
Sarvenaz Alibeigi, California
Peter Cadman, MD, California
Katrina Chapman, DO, MPH, California
Cheryll Gallardo-Villena, MD, California
Sripriya Ganesan, California
Alice Gong, MD, California
Henry Kwang, MD, California
Kevin Li, California
Anthony Murphy, MD, California
Dan Nguyen, California
Daniel Oh, California
Joon Parle, California
Katie Raffel, California
Darshana Sarathchandra, MD, California
Lifang Zhang, California
Jaime Baker, MD, Colorado
Eric Johnson, PA-C, Colorado
Juan Lessing, MD, Colorado
Benjamin Ruckman, DO, Colorado
Rehaan Shaffie, MD, Colorado
Deborah Casey, MD, Connecticut
Daniel Heacock, PA-C, Connecticut
Shabana Ansari, DO, Delaware
Madhu Prattipati, MD, Delaware
Pallavi Aneja, MD, Florida
Satcha Borgella, MD, Florida
Thendrex H. Estrella, MD, Florida
Abid Hussain, MD, Florida
Daphnee Hutchinson, DO, Florida
Muhammad Jaffer, Florida
Sue Lee, ANP, Florida
Melissa Odermann, DO, Florida
Jose Guillermo Revelo Paiz, MD, Florida
Rafael J. Rolon Rivera, MD, Florida
Eleonor Rongo, Florida
Esther Roth, Florida
Shitaye Argaw, MD, Georgia
Taryn DeGrazia, Georgia
Becca Feistritzer, Georgia
Jamal Fitts, Georgia
Kristen Flint, Georgia
Zachary Hermes, Georgia
Mukesh Kumar, Georgia
Kajal Patel, Georgia
Madeline Smith, Georgia
Wade Flowers, PharmD, Idaho
Ajay Bhandare, Illinois
Kimberly Brighton, Illinois
Hristo D. Hristov, MD, Illinois
Sidney Iriana, Illinois
Aurelian Ivan, Illinois
Ming Lee, MD, Illinois
Michelle Lundholm, Illinois
Idrees Mohiuddin, MD, Illinois
Murr Murray, Illinois
Tad Nair, MD, Illinois
Shalini Reddy, MD, Illinois
Richard Rethorst, MD, Illinois
Kelly Robertshaw, Illinois
Gracelene Wegrzyn, Illinois
Evan Yates, Illinois
Lora J. Jones McClure, MD, Indiana
Carleigh Wilson, DO, Indiana
Erin Brown, ARNP, Iowa
Adam Gray, Iowa
Paul Greco, MD, Iowa
Shelly McGurk, ACNP, ARNP, Iowa
Julie Stanik-Hutt, ACNP, CNS, PhD, Iowa
Elizabeth Cozad, DO, Kansas
Roshan Pais, Kentucky
Mark Youssef, MD, Kentucky
Heather Kahn, MD, Louisiana
Danielle Parrott, PA-C, Maine
Erica Lafferty, ACNP, Maryland
Andrea Limpuangthip, Maryland
Steven Schwartz, CCM, MD, Maryland
Eisha Azhar, MBBS, Massachusetts
Badal Kalamkar, MD, MPH, Massachusetts
Bhavya Rajanna, MD, Massachusetts
Sahib Baljinder Singh, MD, Massachusetts
Kathryn Adams, Michigan
Haseeb Aslam, MD, MBBS, Michigan
Hilda Crispin, MD, Michigan
Sharmistha Dev, MD, Michigan
Tristan Feierabend, MD, Michigan
Sonal Kamalia, MD, MBBS, Michigan
Matthew Luzum, MD, Michigan
Daniel Mitzel, MD, Michigan
Richard Raad, Michigan
Mythri Ramegowda, MD, Michigan
Katie Scally, MD, Michigan
Linden Spital, MSN, NP, Michigan
Porama Koy Thanaporn, MD, Michigan
Chanteil Ulatowski, Michigan
Tingting Xiong, MD, Michigan
Adam Zahr, Michigan
Mike Beste, MD, Minnesota
Elise Haupt, PA-C, Minnesota
Lobsang Trasar, MD, Minnesota
Kari Goan, DO, Mississippi
David C. Pierre, Mississippi
Sudheer Tangella, MD, Mississippi
Tahani Atieh, Missouri
Nicholas Arnold, Missouri
Amanda Calhoun, Missouri
Jyotirmoy Das, Missouri
Umber Dube, Missouri
Daniel Gaughan, Missouri
Woojin Joo, Missouri
Khaled Jumean, MBBS, Missouri
Salma Kazmi, MBBS, MD, Missouri
Yoon Kook (Danny) Kim, Missouri
Ryan Kronen, Missouri
Alyssa Kroner, Missouri
Randy Laine, Missouri
Edward Lee, Missouri
Cerena Leung, Missouri
Patricia Lithrow, Missouri
Brandt Lydon, Missouri
Mary Morgan Scott, Missouri
Jay Patel, Missouri
Justin Porter, Missouri
Danelle Reagin, FNP-C, Missouri
Amanda Reis, Missouri
Awik Som, Missouri
Abby Sung, Missouri
Mary Sutherland, Missouri
Maggie Wang, Missouri
Noah Wasserman, Missouri
Alexis Webber, Missouri
Ryan White, Missouri
Amy Xu, Missouri
Ran Xu, Missouri
Michael Yang, Missouri
Christopher Dietrich, MD, Montana
Jason Kunz, DO, Montana
Jodi Cantrell, MD, Nebraska
Steven Hart, MD, Nebraska
Kurt Kapels, MD, Nebraska
Brian Keegan, MD, Nebraska
Shaun Jang, MD, Nevada
Gurpinder Singh, MD, New Hampshire
Pragati Banda, MD, New Jersey
Sahai Donaldson, MBBS, New Jersey
Ashesha Mechineni, MD, New Jersey
Alisa Clark, New Mexico
Prajit Arora, MBBS, New Mexico
Crystal Cardwell, New Mexico
Landon Casaus, New Mexico
Tapuwa Mupfumira, MD, New Mexico
Eric Rightley, New Mexico
David S. Anderson, New York
Joan Bosco, MD, New York
Jessica Caro, New York
Anna Dewan, New York
Amrita Dhillon, MBBS, New York
Julia Frydman, New York
Radhika Gali, MBBS, MDS, New York
Allison Guttmann, MD, New York
Aryles Hedjar, MD, New York
Peter Janes, New York
Nadine Kalavazoff, New York
Jeffrey Lach, DO, New York
Keron Lezama, MD, New York
Yingheng Liu, New York
Taimur Mirza, New York
Cyrus Nensey, MD, New York
Nekee Pandya, MD, New York
Thushara Paul, MD, New York
Yu Sung, New York
Joel Boggan, MD, North Carolina
Angela Fletcher, North Carolina
Rebecca Gimpert, PA-C, North Carolina
Samantha Levering, PA-C, North Carolina
Nancy Martin, North Carolina
Richard Sherwood, North Carolina
Kranthi K. Sitammagari, MD, North Carolina
Aaron Swedberg, MPAS, PA-C, North Carolina
Yih-Cherng Tsai, North Carolina
Richard Bakker, MD, PhD, Ohio
Matthew Broderick, MD, Ohio
Subbaraju Budharaju, MD, MS, Ohio
Steven Bumb, MD, Ohio
Ahmed Eltelbany, MD, Ohio
Tracey Hardin, MS, Ohio
Patricia Hardman, APRN, Ohio
Michael Lewis, MD, Ohio
Volodymyr Manko, Ohio
Rebecca Stone, Ohio
Chaitanya Valluri, Ohio
Holly Wierzbicki, CNP, Ohio
Jamie Yockey, APRN, CNP, Ohio
Mahdi Mussa, MD, Oklahoma
Monica Saemz, DO, Oklahoma
Peter Ganter, MD, Oregon
Bethany Roy, MD, Oregon
Mary Clare Bohnett, Oregon
Molly Rabinowitz, Oregon
Abdullateef Abdulkareem, MD, MPH, Pennsylvania
David Ahamba, MD, MPH, Pennsylvania
David Chin, MD, Pennsylvania
Thomas Conlon, Pennsylvania
Dan Giesler, MD, Pennsylvania
Umair Randhawa, MD, Pennsylvania
Syed Yusuf, MBBS, Pennsylvania
Michael Rigatti, Pennsylvania
Thaylon Barreto, Rhode Island
Jessica Cook, MD, South Carolina
Robin Malik, MD, South Carolina
John Busigin, Tennessee
Shefali Paranjape, MD, Tennessee
Thai Dang, MD, Texas
Matthew Glover, MD, Texas
Snigdha Jain, MD, Texas
David Kellenberger, Texas
Sumeet Kumar, Texas
Kyle McClendon, PA-C, Texas
Sowjanya Mohan, Texas
Akhil D. Vats, MD, Texas
Samatha Vellanki, Texas
Lee-Anna Burgess, MD, Vermont
Rick Hildebrant, MD, Vermont
Matthew Backens, MD, Virginia
Megan Coe, Virginia
Kevin Dehaan, Virginia
Stephen Fox, Virginia
Amber Inofuentes, MD, Virginia
Jessica Keiser, MD, Virginia
Joseph Perez, MD, FAAFP, MBA, Virginia
Kanwapreet S. Saini, MD, Virginia
Erin Vipler, MD, Virginia
Naveen Voore, MBBS, Virginia
Abhishek Agarwal, MD, MBBS, Washington
Robert Cooney, MD, Washington
Cynthia Horton, MD, Washington
Rich A. Kukreja, MD, Washington
Ji Young Nam, MD, Washington
Kai Wilhelm, MD, Washington
In Kyu Yoo, Washington
Temu Brown, Wisconsin
Pablo Colon Nieves, Wisconsin
Christina Evans, PAC, Wisconsin
Swetha Karturi, MBBS, Wisconsin
Mark Babcock, DO, Wyoming
Ahmad Von Schlegell, Canada
Anand Kartha, Japan
Mohamed Sadek, Qatar
Amine Rakab, MD, Qatar
Abazar Saeed, Qatar
Joao Guerra, MD
Justin Kimsey, Alabama
Mohammed N.Y. Shah, MD, Alaska
Katharina Beeler, MD, Arizona
Khoi Nguyen, MD, Arizona
Vinay Saini, MD, Arizona
Maria Aceves, PA-C, California
Sarvenaz Alibeigi, California
Peter Cadman, MD, California
Katrina Chapman, DO, MPH, California
Cheryll Gallardo-Villena, MD, California
Sripriya Ganesan, California
Alice Gong, MD, California
Henry Kwang, MD, California
Kevin Li, California
Anthony Murphy, MD, California
Dan Nguyen, California
Daniel Oh, California
Joon Parle, California
Katie Raffel, California
Darshana Sarathchandra, MD, California
Lifang Zhang, California
Jaime Baker, MD, Colorado
Eric Johnson, PA-C, Colorado
Juan Lessing, MD, Colorado
Benjamin Ruckman, DO, Colorado
Rehaan Shaffie, MD, Colorado
Deborah Casey, MD, Connecticut
Daniel Heacock, PA-C, Connecticut
Shabana Ansari, DO, Delaware
Madhu Prattipati, MD, Delaware
Pallavi Aneja, MD, Florida
Satcha Borgella, MD, Florida
Thendrex H. Estrella, MD, Florida
Abid Hussain, MD, Florida
Daphnee Hutchinson, DO, Florida
Muhammad Jaffer, Florida
Sue Lee, ANP, Florida
Melissa Odermann, DO, Florida
Jose Guillermo Revelo Paiz, MD, Florida
Rafael J. Rolon Rivera, MD, Florida
Eleonor Rongo, Florida
Esther Roth, Florida
Shitaye Argaw, MD, Georgia
Taryn DeGrazia, Georgia
Becca Feistritzer, Georgia
Jamal Fitts, Georgia
Kristen Flint, Georgia
Zachary Hermes, Georgia
Mukesh Kumar, Georgia
Kajal Patel, Georgia
Madeline Smith, Georgia
Wade Flowers, PharmD, Idaho
Ajay Bhandare, Illinois
Kimberly Brighton, Illinois
Hristo D. Hristov, MD, Illinois
Sidney Iriana, Illinois
Aurelian Ivan, Illinois
Ming Lee, MD, Illinois
Michelle Lundholm, Illinois
Idrees Mohiuddin, MD, Illinois
Murr Murray, Illinois
Tad Nair, MD, Illinois
Shalini Reddy, MD, Illinois
Richard Rethorst, MD, Illinois
Kelly Robertshaw, Illinois
Gracelene Wegrzyn, Illinois
Evan Yates, Illinois
Lora J. Jones McClure, MD, Indiana
Carleigh Wilson, DO, Indiana
Erin Brown, ARNP, Iowa
Adam Gray, Iowa
Paul Greco, MD, Iowa
Shelly McGurk, ACNP, ARNP, Iowa
Julie Stanik-Hutt, ACNP, CNS, PhD, Iowa
Elizabeth Cozad, DO, Kansas
Roshan Pais, Kentucky
Mark Youssef, MD, Kentucky
Heather Kahn, MD, Louisiana
Danielle Parrott, PA-C, Maine
Erica Lafferty, ACNP, Maryland
Andrea Limpuangthip, Maryland
Steven Schwartz, CCM, MD, Maryland
Eisha Azhar, MBBS, Massachusetts
Badal Kalamkar, MD, MPH, Massachusetts
Bhavya Rajanna, MD, Massachusetts
Sahib Baljinder Singh, MD, Massachusetts
Kathryn Adams, Michigan
Haseeb Aslam, MD, MBBS, Michigan
Hilda Crispin, MD, Michigan
Sharmistha Dev, MD, Michigan
Tristan Feierabend, MD, Michigan
Sonal Kamalia, MD, MBBS, Michigan
Matthew Luzum, MD, Michigan
Daniel Mitzel, MD, Michigan
Richard Raad, Michigan
Mythri Ramegowda, MD, Michigan
Katie Scally, MD, Michigan
Linden Spital, MSN, NP, Michigan
Porama Koy Thanaporn, MD, Michigan
Chanteil Ulatowski, Michigan
Tingting Xiong, MD, Michigan
Adam Zahr, Michigan
Mike Beste, MD, Minnesota
Elise Haupt, PA-C, Minnesota
Lobsang Trasar, MD, Minnesota
Kari Goan, DO, Mississippi
David C. Pierre, Mississippi
Sudheer Tangella, MD, Mississippi
Tahani Atieh, Missouri
Nicholas Arnold, Missouri
Amanda Calhoun, Missouri
Jyotirmoy Das, Missouri
Umber Dube, Missouri
Daniel Gaughan, Missouri
Woojin Joo, Missouri
Khaled Jumean, MBBS, Missouri
Salma Kazmi, MBBS, MD, Missouri
Yoon Kook (Danny) Kim, Missouri
Ryan Kronen, Missouri
Alyssa Kroner, Missouri
Randy Laine, Missouri
Edward Lee, Missouri
Cerena Leung, Missouri
Patricia Lithrow, Missouri
Brandt Lydon, Missouri
Mary Morgan Scott, Missouri
Jay Patel, Missouri
Justin Porter, Missouri
Danelle Reagin, FNP-C, Missouri
Amanda Reis, Missouri
Awik Som, Missouri
Abby Sung, Missouri
Mary Sutherland, Missouri
Maggie Wang, Missouri
Noah Wasserman, Missouri
Alexis Webber, Missouri
Ryan White, Missouri
Amy Xu, Missouri
Ran Xu, Missouri
Michael Yang, Missouri
Christopher Dietrich, MD, Montana
Jason Kunz, DO, Montana
Jodi Cantrell, MD, Nebraska
Steven Hart, MD, Nebraska
Kurt Kapels, MD, Nebraska
Brian Keegan, MD, Nebraska
Shaun Jang, MD, Nevada
Gurpinder Singh, MD, New Hampshire
Pragati Banda, MD, New Jersey
Sahai Donaldson, MBBS, New Jersey
Ashesha Mechineni, MD, New Jersey
Alisa Clark, New Mexico
Prajit Arora, MBBS, New Mexico
Crystal Cardwell, New Mexico
Landon Casaus, New Mexico
Tapuwa Mupfumira, MD, New Mexico
Eric Rightley, New Mexico
David S. Anderson, New York
Joan Bosco, MD, New York
Jessica Caro, New York
Anna Dewan, New York
Amrita Dhillon, MBBS, New York
Julia Frydman, New York
Radhika Gali, MBBS, MDS, New York
Allison Guttmann, MD, New York
Aryles Hedjar, MD, New York
Peter Janes, New York
Nadine Kalavazoff, New York
Jeffrey Lach, DO, New York
Keron Lezama, MD, New York
Yingheng Liu, New York
Taimur Mirza, New York
Cyrus Nensey, MD, New York
Nekee Pandya, MD, New York
Thushara Paul, MD, New York
Yu Sung, New York
Joel Boggan, MD, North Carolina
Angela Fletcher, North Carolina
Rebecca Gimpert, PA-C, North Carolina
Samantha Levering, PA-C, North Carolina
Nancy Martin, North Carolina
Richard Sherwood, North Carolina
Kranthi K. Sitammagari, MD, North Carolina
Aaron Swedberg, MPAS, PA-C, North Carolina
Yih-Cherng Tsai, North Carolina
Richard Bakker, MD, PhD, Ohio
Matthew Broderick, MD, Ohio
Subbaraju Budharaju, MD, MS, Ohio
Steven Bumb, MD, Ohio
Ahmed Eltelbany, MD, Ohio
Tracey Hardin, MS, Ohio
Patricia Hardman, APRN, Ohio
Michael Lewis, MD, Ohio
Volodymyr Manko, Ohio
Rebecca Stone, Ohio
Chaitanya Valluri, Ohio
Holly Wierzbicki, CNP, Ohio
Jamie Yockey, APRN, CNP, Ohio
Mahdi Mussa, MD, Oklahoma
Monica Saemz, DO, Oklahoma
Peter Ganter, MD, Oregon
Bethany Roy, MD, Oregon
Mary Clare Bohnett, Oregon
Molly Rabinowitz, Oregon
Abdullateef Abdulkareem, MD, MPH, Pennsylvania
David Ahamba, MD, MPH, Pennsylvania
David Chin, MD, Pennsylvania
Thomas Conlon, Pennsylvania
Dan Giesler, MD, Pennsylvania
Umair Randhawa, MD, Pennsylvania
Syed Yusuf, MBBS, Pennsylvania
Michael Rigatti, Pennsylvania
Thaylon Barreto, Rhode Island
Jessica Cook, MD, South Carolina
Robin Malik, MD, South Carolina
John Busigin, Tennessee
Shefali Paranjape, MD, Tennessee
Thai Dang, MD, Texas
Matthew Glover, MD, Texas
Snigdha Jain, MD, Texas
David Kellenberger, Texas
Sumeet Kumar, Texas
Kyle McClendon, PA-C, Texas
Sowjanya Mohan, Texas
Akhil D. Vats, MD, Texas
Samatha Vellanki, Texas
Lee-Anna Burgess, MD, Vermont
Rick Hildebrant, MD, Vermont
Matthew Backens, MD, Virginia
Megan Coe, Virginia
Kevin Dehaan, Virginia
Stephen Fox, Virginia
Amber Inofuentes, MD, Virginia
Jessica Keiser, MD, Virginia
Joseph Perez, MD, FAAFP, MBA, Virginia
Kanwapreet S. Saini, MD, Virginia
Erin Vipler, MD, Virginia
Naveen Voore, MBBS, Virginia
Abhishek Agarwal, MD, MBBS, Washington
Robert Cooney, MD, Washington
Cynthia Horton, MD, Washington
Rich A. Kukreja, MD, Washington
Ji Young Nam, MD, Washington
Kai Wilhelm, MD, Washington
In Kyu Yoo, Washington
Temu Brown, Wisconsin
Pablo Colon Nieves, Wisconsin
Christina Evans, PAC, Wisconsin
Swetha Karturi, MBBS, Wisconsin
Mark Babcock, DO, Wyoming
Ahmad Von Schlegell, Canada
Anand Kartha, Japan
Mohamed Sadek, Qatar
Amine Rakab, MD, Qatar
Abazar Saeed, Qatar
Joao Guerra, MD
Justin Kimsey, Alabama
Mohammed N.Y. Shah, MD, Alaska
Katharina Beeler, MD, Arizona
Khoi Nguyen, MD, Arizona
Vinay Saini, MD, Arizona
Maria Aceves, PA-C, California
Sarvenaz Alibeigi, California
Peter Cadman, MD, California
Katrina Chapman, DO, MPH, California
Cheryll Gallardo-Villena, MD, California
Sripriya Ganesan, California
Alice Gong, MD, California
Henry Kwang, MD, California
Kevin Li, California
Anthony Murphy, MD, California
Dan Nguyen, California
Daniel Oh, California
Joon Parle, California
Katie Raffel, California
Darshana Sarathchandra, MD, California
Lifang Zhang, California
Jaime Baker, MD, Colorado
Eric Johnson, PA-C, Colorado
Juan Lessing, MD, Colorado
Benjamin Ruckman, DO, Colorado
Rehaan Shaffie, MD, Colorado
Deborah Casey, MD, Connecticut
Daniel Heacock, PA-C, Connecticut
Shabana Ansari, DO, Delaware
Madhu Prattipati, MD, Delaware
Pallavi Aneja, MD, Florida
Satcha Borgella, MD, Florida
Thendrex H. Estrella, MD, Florida
Abid Hussain, MD, Florida
Daphnee Hutchinson, DO, Florida
Muhammad Jaffer, Florida
Sue Lee, ANP, Florida
Melissa Odermann, DO, Florida
Jose Guillermo Revelo Paiz, MD, Florida
Rafael J. Rolon Rivera, MD, Florida
Eleonor Rongo, Florida
Esther Roth, Florida
Shitaye Argaw, MD, Georgia
Taryn DeGrazia, Georgia
Becca Feistritzer, Georgia
Jamal Fitts, Georgia
Kristen Flint, Georgia
Zachary Hermes, Georgia
Mukesh Kumar, Georgia
Kajal Patel, Georgia
Madeline Smith, Georgia
Wade Flowers, PharmD, Idaho
Ajay Bhandare, Illinois
Kimberly Brighton, Illinois
Hristo D. Hristov, MD, Illinois
Sidney Iriana, Illinois
Aurelian Ivan, Illinois
Ming Lee, MD, Illinois
Michelle Lundholm, Illinois
Idrees Mohiuddin, MD, Illinois
Murr Murray, Illinois
Tad Nair, MD, Illinois
Shalini Reddy, MD, Illinois
Richard Rethorst, MD, Illinois
Kelly Robertshaw, Illinois
Gracelene Wegrzyn, Illinois
Evan Yates, Illinois
Lora J. Jones McClure, MD, Indiana
Carleigh Wilson, DO, Indiana
Erin Brown, ARNP, Iowa
Adam Gray, Iowa
Paul Greco, MD, Iowa
Shelly McGurk, ACNP, ARNP, Iowa
Julie Stanik-Hutt, ACNP, CNS, PhD, Iowa
Elizabeth Cozad, DO, Kansas
Roshan Pais, Kentucky
Mark Youssef, MD, Kentucky
Heather Kahn, MD, Louisiana
Danielle Parrott, PA-C, Maine
Erica Lafferty, ACNP, Maryland
Andrea Limpuangthip, Maryland
Steven Schwartz, CCM, MD, Maryland
Eisha Azhar, MBBS, Massachusetts
Badal Kalamkar, MD, MPH, Massachusetts
Bhavya Rajanna, MD, Massachusetts
Sahib Baljinder Singh, MD, Massachusetts
Kathryn Adams, Michigan
Haseeb Aslam, MD, MBBS, Michigan
Hilda Crispin, MD, Michigan
Sharmistha Dev, MD, Michigan
Tristan Feierabend, MD, Michigan
Sonal Kamalia, MD, MBBS, Michigan
Matthew Luzum, MD, Michigan
Daniel Mitzel, MD, Michigan
Richard Raad, Michigan
Mythri Ramegowda, MD, Michigan
Katie Scally, MD, Michigan
Linden Spital, MSN, NP, Michigan
Porama Koy Thanaporn, MD, Michigan
Chanteil Ulatowski, Michigan
Tingting Xiong, MD, Michigan
Adam Zahr, Michigan
Mike Beste, MD, Minnesota
Elise Haupt, PA-C, Minnesota
Lobsang Trasar, MD, Minnesota
Kari Goan, DO, Mississippi
David C. Pierre, Mississippi
Sudheer Tangella, MD, Mississippi
Tahani Atieh, Missouri
Nicholas Arnold, Missouri
Amanda Calhoun, Missouri
Jyotirmoy Das, Missouri
Umber Dube, Missouri
Daniel Gaughan, Missouri
Woojin Joo, Missouri
Khaled Jumean, MBBS, Missouri
Salma Kazmi, MBBS, MD, Missouri
Yoon Kook (Danny) Kim, Missouri
Ryan Kronen, Missouri
Alyssa Kroner, Missouri
Randy Laine, Missouri
Edward Lee, Missouri
Cerena Leung, Missouri
Patricia Lithrow, Missouri
Brandt Lydon, Missouri
Mary Morgan Scott, Missouri
Jay Patel, Missouri
Justin Porter, Missouri
Danelle Reagin, FNP-C, Missouri
Amanda Reis, Missouri
Awik Som, Missouri
Abby Sung, Missouri
Mary Sutherland, Missouri
Maggie Wang, Missouri
Noah Wasserman, Missouri
Alexis Webber, Missouri
Ryan White, Missouri
Amy Xu, Missouri
Ran Xu, Missouri
Michael Yang, Missouri
Christopher Dietrich, MD, Montana
Jason Kunz, DO, Montana
Jodi Cantrell, MD, Nebraska
Steven Hart, MD, Nebraska
Kurt Kapels, MD, Nebraska
Brian Keegan, MD, Nebraska
Shaun Jang, MD, Nevada
Gurpinder Singh, MD, New Hampshire
Pragati Banda, MD, New Jersey
Sahai Donaldson, MBBS, New Jersey
Ashesha Mechineni, MD, New Jersey
Alisa Clark, New Mexico
Prajit Arora, MBBS, New Mexico
Crystal Cardwell, New Mexico
Landon Casaus, New Mexico
Tapuwa Mupfumira, MD, New Mexico
Eric Rightley, New Mexico
David S. Anderson, New York
Joan Bosco, MD, New York
Jessica Caro, New York
Anna Dewan, New York
Amrita Dhillon, MBBS, New York
Julia Frydman, New York
Radhika Gali, MBBS, MDS, New York
Allison Guttmann, MD, New York
Aryles Hedjar, MD, New York
Peter Janes, New York
Nadine Kalavazoff, New York
Jeffrey Lach, DO, New York
Keron Lezama, MD, New York
Yingheng Liu, New York
Taimur Mirza, New York
Cyrus Nensey, MD, New York
Nekee Pandya, MD, New York
Thushara Paul, MD, New York
Yu Sung, New York
Joel Boggan, MD, North Carolina
Angela Fletcher, North Carolina
Rebecca Gimpert, PA-C, North Carolina
Samantha Levering, PA-C, North Carolina
Nancy Martin, North Carolina
Richard Sherwood, North Carolina
Kranthi K. Sitammagari, MD, North Carolina
Aaron Swedberg, MPAS, PA-C, North Carolina
Yih-Cherng Tsai, North Carolina
Richard Bakker, MD, PhD, Ohio
Matthew Broderick, MD, Ohio
Subbaraju Budharaju, MD, MS, Ohio
Steven Bumb, MD, Ohio
Ahmed Eltelbany, MD, Ohio
Tracey Hardin, MS, Ohio
Patricia Hardman, APRN, Ohio
Michael Lewis, MD, Ohio
Volodymyr Manko, Ohio
Rebecca Stone, Ohio
Chaitanya Valluri, Ohio
Holly Wierzbicki, CNP, Ohio
Jamie Yockey, APRN, CNP, Ohio
Mahdi Mussa, MD, Oklahoma
Monica Saemz, DO, Oklahoma
Peter Ganter, MD, Oregon
Bethany Roy, MD, Oregon
Mary Clare Bohnett, Oregon
Molly Rabinowitz, Oregon
Abdullateef Abdulkareem, MD, MPH, Pennsylvania
David Ahamba, MD, MPH, Pennsylvania
David Chin, MD, Pennsylvania
Thomas Conlon, Pennsylvania
Dan Giesler, MD, Pennsylvania
Umair Randhawa, MD, Pennsylvania
Syed Yusuf, MBBS, Pennsylvania
Michael Rigatti, Pennsylvania
Thaylon Barreto, Rhode Island
Jessica Cook, MD, South Carolina
Robin Malik, MD, South Carolina
John Busigin, Tennessee
Shefali Paranjape, MD, Tennessee
Thai Dang, MD, Texas
Matthew Glover, MD, Texas
Snigdha Jain, MD, Texas
David Kellenberger, Texas
Sumeet Kumar, Texas
Kyle McClendon, PA-C, Texas
Sowjanya Mohan, Texas
Akhil D. Vats, MD, Texas
Samatha Vellanki, Texas
Lee-Anna Burgess, MD, Vermont
Rick Hildebrant, MD, Vermont
Matthew Backens, MD, Virginia
Megan Coe, Virginia
Kevin Dehaan, Virginia
Stephen Fox, Virginia
Amber Inofuentes, MD, Virginia
Jessica Keiser, MD, Virginia
Joseph Perez, MD, FAAFP, MBA, Virginia
Kanwapreet S. Saini, MD, Virginia
Erin Vipler, MD, Virginia
Naveen Voore, MBBS, Virginia
Abhishek Agarwal, MD, MBBS, Washington
Robert Cooney, MD, Washington
Cynthia Horton, MD, Washington
Rich A. Kukreja, MD, Washington
Ji Young Nam, MD, Washington
Kai Wilhelm, MD, Washington
In Kyu Yoo, Washington
Temu Brown, Wisconsin
Pablo Colon Nieves, Wisconsin
Christina Evans, PAC, Wisconsin
Swetha Karturi, MBBS, Wisconsin
Mark Babcock, DO, Wyoming
Ahmad Von Schlegell, Canada
Anand Kartha, Japan
Mohamed Sadek, Qatar
Amine Rakab, MD, Qatar
Abazar Saeed, Qatar
Joao Guerra, MD
VIDEO: HIV PrEP effective, but adoption lags among high-risk patients
NEW ORLEANS – The adoption and use of HIV preexposure prophylaxis (PrEP) continues to lag behind studies showing its effectiveness in the high-risk population of men who have sex with men, says a clinician who works with these patients.
John Krotchko, MD, a family practitioner at Denver Health and Hospital Authority, has studied the impact of a community outreach program – targeting HIV-negative men who have sex with men – that educates about HIV PrEP and offers HIV testing. He and his colleagues have examined the effectiveness of this approach, how comfortable participants are discussing their behaviors, and have tried to determine whether availability of HIV PrEP increases high-risk behaviors.
Dr. Krotchko and his colleagues also studied overall trends in awareness about PrEP over time, as well as the acceptability of participants to take a once-daily emtricitabine/tenofovir pill. He explained in a video interview why he believes it’s important to manage these patients in a primary care setting. The interview took place at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Dr. Krotchko had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – The adoption and use of HIV preexposure prophylaxis (PrEP) continues to lag behind studies showing its effectiveness in the high-risk population of men who have sex with men, says a clinician who works with these patients.
John Krotchko, MD, a family practitioner at Denver Health and Hospital Authority, has studied the impact of a community outreach program – targeting HIV-negative men who have sex with men – that educates about HIV PrEP and offers HIV testing. He and his colleagues have examined the effectiveness of this approach, how comfortable participants are discussing their behaviors, and have tried to determine whether availability of HIV PrEP increases high-risk behaviors.
Dr. Krotchko and his colleagues also studied overall trends in awareness about PrEP over time, as well as the acceptability of participants to take a once-daily emtricitabine/tenofovir pill. He explained in a video interview why he believes it’s important to manage these patients in a primary care setting. The interview took place at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Dr. Krotchko had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – The adoption and use of HIV preexposure prophylaxis (PrEP) continues to lag behind studies showing its effectiveness in the high-risk population of men who have sex with men, says a clinician who works with these patients.
John Krotchko, MD, a family practitioner at Denver Health and Hospital Authority, has studied the impact of a community outreach program – targeting HIV-negative men who have sex with men – that educates about HIV PrEP and offers HIV testing. He and his colleagues have examined the effectiveness of this approach, how comfortable participants are discussing their behaviors, and have tried to determine whether availability of HIV PrEP increases high-risk behaviors.
Dr. Krotchko and his colleagues also studied overall trends in awareness about PrEP over time, as well as the acceptability of participants to take a once-daily emtricitabine/tenofovir pill. He explained in a video interview why he believes it’s important to manage these patients in a primary care setting. The interview took place at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Dr. Krotchko had no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT IDWEEK 2016